
Abstract
Objective:
This 2-year observational study aimed to test the feasibility of implementing a pediatric stroke triage-setup that connected frontline providers with vascular neurologists and to examine final diagnoses in children triaged for suspected stroke.
Methods:
Prospective, consecutive registration of children with suspected stroke triaged by a team of vascular neurologists from Jan 1st, 2020 and through Dec 2021, Eastern Denmark (census 530,000 children). Based on the provided clinical information, the children were triaged to either assessment at the Comprehensive Stroke Center (CSC) in Copenhagen or to a pediatric department. All included children were retrospectively followed-up for clinical presentations and final diagnosis.
Results:
A total of 163 children with 166 suspected stroke events were triaged by the vascular neurologists. Cerebrovascular disease was present in 15 (9.0%) suspected stroke events; one child had intracerebral hemorrhage, one had subarachnoid hemorrhage, two children presented with three TIA events and nine children presented with 10 ischemic stroke events. Two children with ischemic stroke were eligible for acute revascularization treatment of which both were triaged to the CSC. The sensitivity of the triage by acute revascularization indication was 1.00 (95% confidence interval (95% CI): 0.15–1.00) and specificity 0.65 (95% CI: 0.57–0.73). Non-stroke neurological emergencies were present in 34 (20.5%) children, including seizures in 18 (10.8%) and acute demyelinating disorders in 7 (4.2%).
Conclusion:
Implementing regional triage-setup that connected frontline providers to vascular neurologists was feasible; this system was activated for the majority of children with ischemic stroke according to an expected incidence and led to identification of children eligible for revascularization treatments.
Introduction
Acute ischemic stroke (AIS) is a rare but significant cause of morbidity in children, with neurological sequelae in up to 80% and long-term social and financial effects.1–3 Acute revascularization treatments, as intravenous thrombolysis (IV-tPA) and mechanical thrombectomy (MT), have the potential to improve outcome.4–6 However, the implementation of these treatments requires timely diagnosis of stroke which have proved challenging in children; the median time from symptom onset to diagnosis of pediatric AIS is more than 20 h.7–10
Over the past decade, there has been increasing interest in developing pediatric stroke pathways to facilitate a fast evaluation of children with stroke.11–14 According to a recent statement from the American Heart and American Stroke Organization (AHA/ASA) it is recommended to establish referral networks that connect community hospitals and frontline providers to tertiary care pediatric stroke centers with specifically trained experts in vascular neurology, neuroimaging, and neurocritical care. 15 To achieve this, we integrated a 24/7 pediatric stroke triage-setup into existing adult stroke-services at the Comprehensive Stroke Center (CSC) in Copenhagen. This setup covered all of Eastern Denmark with a pediatric population (<18 years) of 530,000 individuals. Triage was done by an experienced team of vascular neurologists with the purpose of identifying pediatric patients eligible for acute revascularization treatments.
The aims of this study were:
(1) To test the feasibility of implementing a pediatric stroke triage setup that connected frontline providers with vascular neurologists and
(2) To examine final diagnoses in children triaged for suspected stroke.
Methods
Patients included in this study were a consecutive cohort of children (>1 month and <18 years) assessed according to a 24/7 pediatric stroke triage-setup at the CSC, University Hospital Rigshospitalet, Copenhagen. This triage-setup was developed in collaboration between pediatricians and neurologists at the CSC. The setup covered a geographical area of 9.764 km2 with a pediatric population of 530,000 children (census 4th quarter 2021). Eleven vascular neurologists with a background in adult neurology were responsible for the triage.
Patients
Patients were identified by consecutive registration of telephone referrals to the vascular neurologists on children with suspected stroke; (1) pre-hospital referrals from ambulance staff, (2) pre-hospital referrals from primary care doctors or primary care pediatricians, and (3) referrals from physicians in pediatric departments. The inclusion period was from January 1st 2020 until December 31st 2021.
All children referred to the vascular neurologists were triaged to either assessment at the CSC or assessment in one of seven general pediatric departments in Eastern Denmark. Triage directly to the CSC was provided for children meeting all of the following triage-criteria: (1) focal neurological deficits, including motor-deficits (unilateral paresis, facial palsy, difficulty walking), visual deficits (vision loss or double vision), speech deficits (aphasia or dysarthria), sensory deficits, balance problems or a focal epileptic seizure in a child with no prior history of focal epilepsy; (2) Sudden appearance or worsening of symptoms; (3) Potential option for acute revascularization treatment defined as symptom duration for less than 24 h and moderate to severe stroke symptoms corresponding to an estimated Pediatric National Institute of Health Stroke Scale ⩾4, Figure 1.
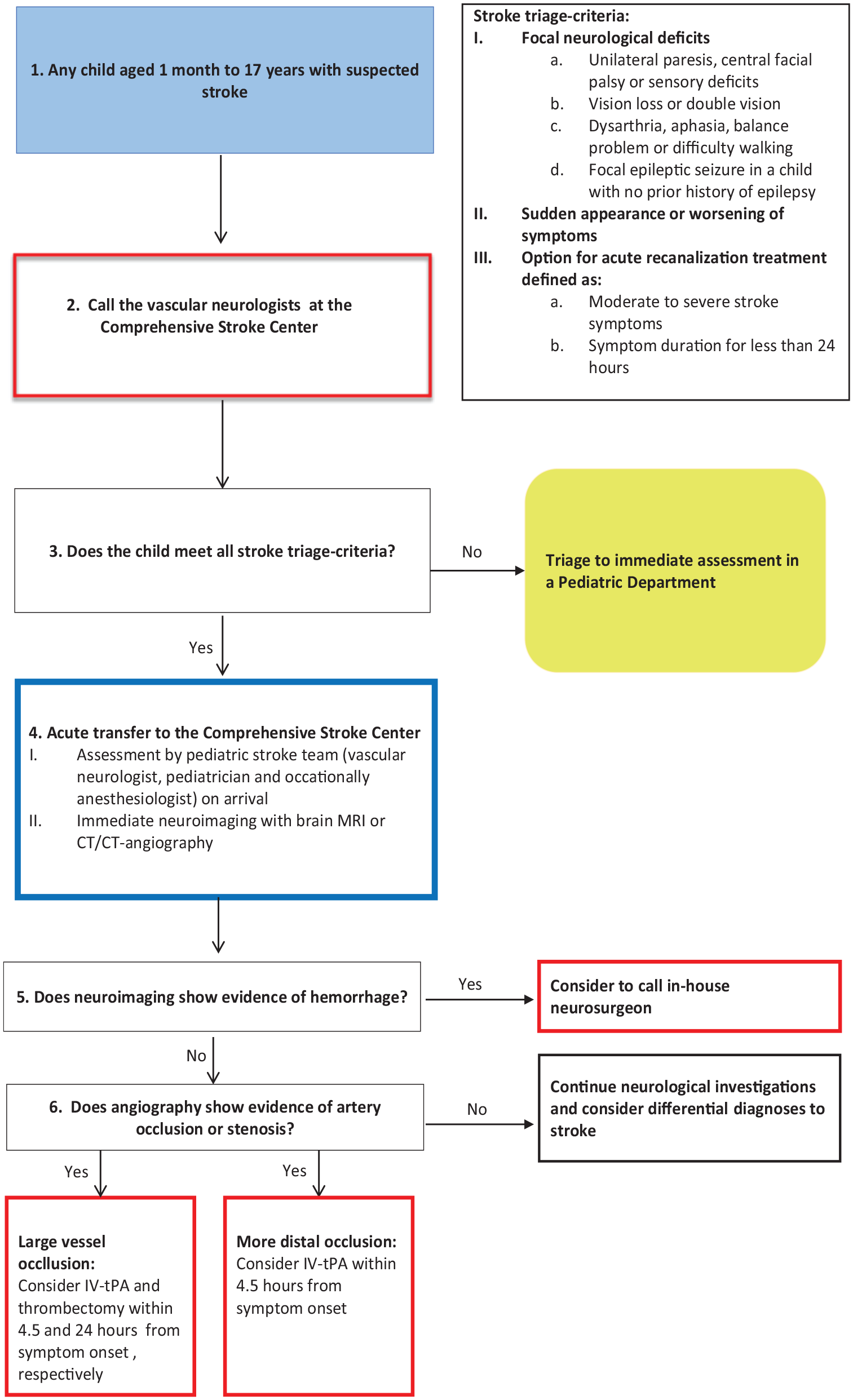
Algorithm for triage and acute evaluation of children with suspected stroke in Eastern Denmark.
Children triaged to the CSC were evaluated by a vascular neurologist and a pediatrician on arrival to the hospital. When history and clinical findings were compatible with stroke, urgent MRI or CT/CT-angiography was obtained, Figure 1. Revascularization treatment was considered for children where angiography demonstrated a vessel occlusion compatible with the clinical presentation. In children with large vessel occlusions, IV-tPA and MT were considered up to 4.5 and 24 h from symptom onset, respectively. IV-tPA was also considered for children with more distal occlusions presenting within 4.5 h from symptom onset.
Children who were not considered eligible for revascularization treatment could still undergo urgent imaging at the discretion of the responsible pediatrician.
Definition of stroke and transient ischemic attack
Stroke and transient ischemic attack (TIA) were defined according to the definitions by the American Heart Association/American Stroke Association (AHA/ASA). Stroke was defined as any objective evidence of permanent brain cell death due to a vascular cause based upon pathological or imaging evidence with or without the presence of clinical symptoms. 16 TIA was defined as an episode of transient neurological deficit caused by focal cerebral ischemia, without acute infarction on imaging. 17
Recurrence of stroke or TIA was defined as any subsequent event meeting the AHA/ASA stroke or TIA-definition more than 24 h after the incident event, irrespective of vascular territory.
Data collection
Review of medical records for all children triaged by the vascular neurologists was conducted by three investigators (JB, CHH, TT) using a pre-defined data-collection instrument. Discrepancies were resolved through discussions and final consensus. Demographic and clinical information was extracted, including sex, age at the time of admission, pertinent pre-existing comorbidity, clinical symptoms, neurological findings at admission, result of triage (triage to a pediatric department or to the CSC, respectively), neuroimaging modality, and final diagnoses (ICD-10-diagnoses). Pertinent pre-existing comorbidity was defined as any of the following; cardiac disease, arteriopathy, infectious disease, malignancy, genetic disorder, psychiatric disorder, trauma or recent surgery, and neurological disease (migraine, epilepsy, and previous stroke or TIA). The study was approved by the Danish Data Protection Agency (J.no.: P-2020-451) and the Danish Patient Safety Authority (J.no.: 31-1521-203).
Feasibility assessment
The feasibility of implementing our pediatric stroke triage-setup was tested based on:
(1) The number of pediatric ischemic stroke events assessed through the triage setup compared to the number of expected AIS events in our catchment area. Based on a previous Danish incidence study, 18 we estimated that 12 children (1 month–17 years) would get AIS during our study-period.
(2) The sensitivity of the triage for identification of children eligible for revascularization treatment.
Statistics
Data on all children triaged by the vascular neurologists were included for statistical analyses. The data were expressed as median and interquartile range (IQR) for quantitative variables, and as absolute and relative frequencies for categorical variables. Comparison between children triaged to the CSC and children triaged to a pediatric department were made using independent samples T-Test for quantitative variables and Fishers exact test for categorical variables. The sensitivity, specificity, positive and negative predictive value of triage by revascularization indication was calculated and reported with 95% confidence interval (95% CI) to indicate statistical precision. Statistical significance was set at p < 0.05 for test of all hypotheses. All statistical analysis was performed using SPSS software for Windows version 28.0.0.0.
Results
Between January 2020 and December 2021, 163 children with 166 suspected stroke events were referred to the vascular neurologists; 58 were triaged to an acute stroke assessment at the CSC and 108 were triaged to a general pediatric department. Median age at referral was 12 years (IQR 8–15) and 105 (64.4%) were girls, Table 1. The most common pre-existing comorbidity was psychiatric disorders present in 24 (14.5%) children and migraine present in 8 (4.8%) children.
Demographic and clinical characteristics in children triaged by the vascular neurologists (n = 163). Data presented according to first-time admission for suspected stroke.
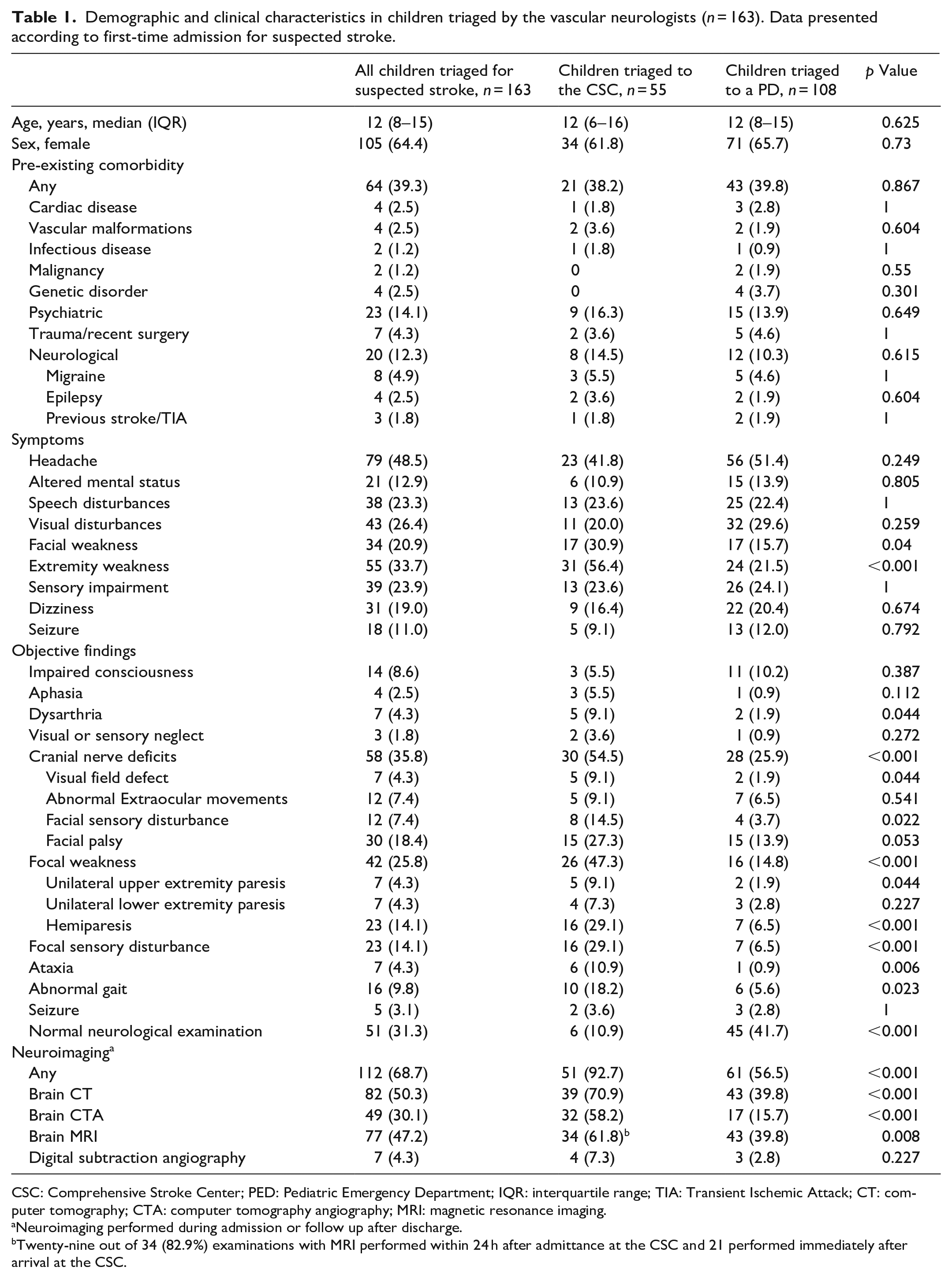
CSC: Comprehensive Stroke Center; PED: Pediatric Emergency Department; IQR: interquartile range; TIA: Transient Ischemic Attack; CT: computer tomography; CTA: computer tomography angiography; MRI: magnetic resonance imaging.
Neuroimaging performed during admission or follow up after discharge.
Twenty-nine out of 34 (82.9%) examinations with MRI performed within 24 h after admittance at the CSC and 21 performed immediately after arrival at the CSC.
Clinical presentation
The most frequent symptoms among children referred to the vascular neurologists, were headache (n = 79, 48.5%), extremity weakness (n = 55, 33.7%), and visual disturbances (n = 43, 26.4%). The most common objective findings were unilateral paresis (n = 42, 25.8%) and cranial nerve deficits (n = 58, 35.8%) with facial palsy being the most common (n = 30, 18.4), Table 1. Seven (4.3%) children had isolated peripheral facial palsy and 51 (31.3%) had a normal neurological examination on hospital admission, including 37 (22%) children who had normal examination at the time of referral to the vascular neurologists.
Children triaged directly to the CSC had significantly more often unilateral paresis, cranial nerve deficits, ataxia, dysarthria, sensory loss, or abnormal gait compared to children triaged to a pediatric department, Table 1.
Final diagnoses
Cerebrovascular disease was the final diagnosis in 15 (9.0%) suspected stroke events. One child had intracerebral hemorrhage, one had subarachnoid hemorrhage and two children presented with a total of three TIA events. Additionally, nine children presented with 10 AIS events corresponding to 75% of the expected number of first-time AIS events in our catchment area. The most common cause of AIS was artery dissection present in six children, Table 3.
Non-stroke neurological emergencies were present in 34 (20.5%) children, including seizures in 18 (10.8%), acute demyelinating disorders in 7 (4.2%), and CNS infections in 4 (2.4%), Table 2. The most common stroke mimics were migraine present in 46 children and conversion disorders present in 15 children, Table 2. Among the 46 children with migraine, six had a medical history of migraine prior to referral to the vascular neurologists. In the 15 children with conversion disorders, four had a pre-existing psychiatric disorder.
Final diagnoses in children with suspected stroke events, n = 166.
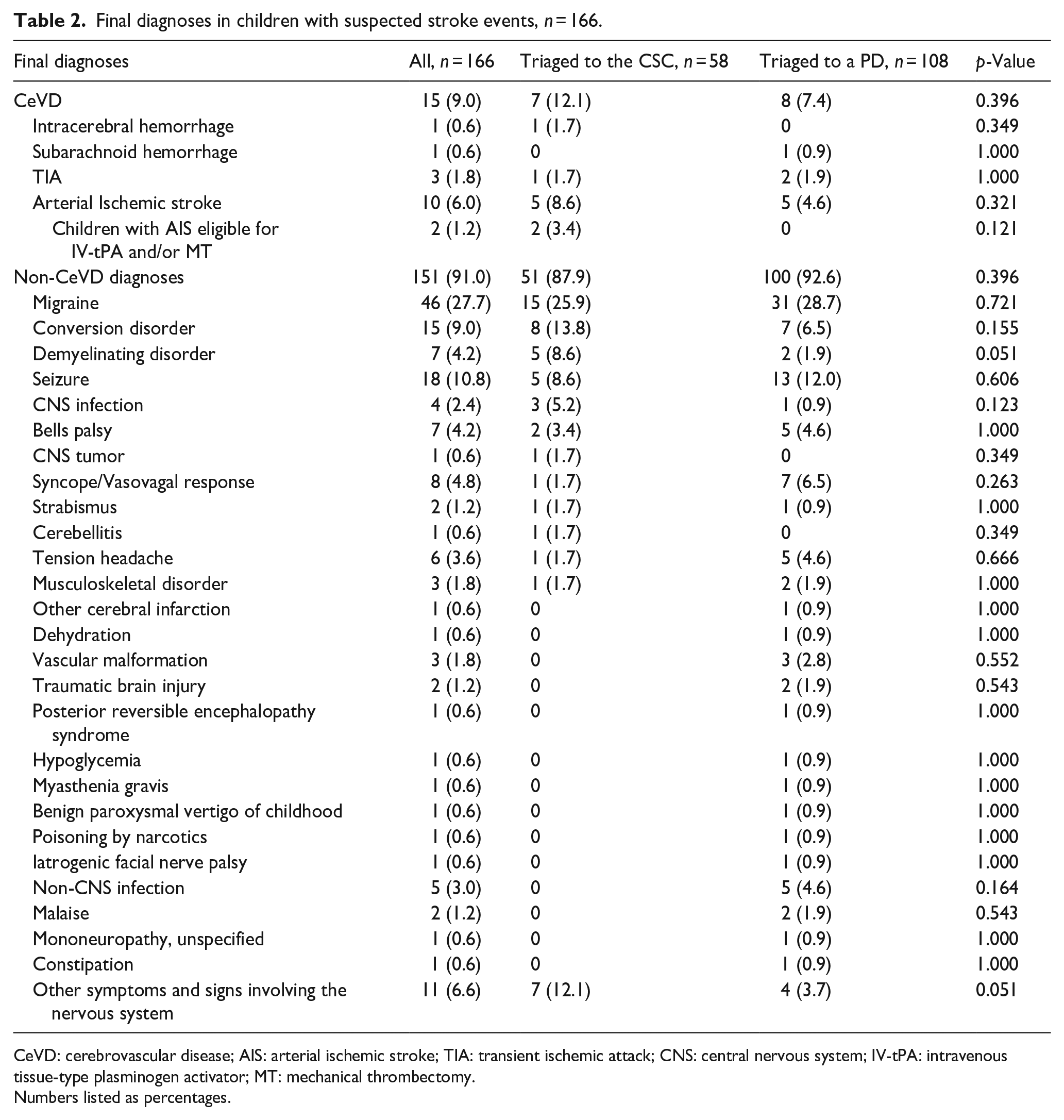
CeVD: cerebrovascular disease; AIS: arterial ischemic stroke; TIA: transient ischemic attack; CNS: central nervous system; IV-tPA: intravenous tissue-type plasminogen activator; MT: mechanical thrombectomy.
Numbers listed as percentages.
Triage
Acute revascularization treatment was indicated in two children with AIS of which both were triaged to an acute stroke assessment at the CSC, Table 3. The sensitivity of our triage-setup was 1.00 (95% CI 0.16–1.00) and the specificity was 0.66 (95% CI 0.58–0.73). The positive predictive value was 0.03 (95% CI 0.03–0.04), Supplemental Material 1. Among the remaining 13 stroke events, five were triaged to the CSC and 8 were triaged to a pediatric department, including five children with AIS, Table 2. Revascularization treatment was not indicated in any of the five AIS events triaged to a pediatric department. This was due to delayed diagnosis in three children, minor stroke symptoms in one child, and an incidental finding of an asymptomatic acute infarction in one child examined for other reasons than suspicion of stroke.
Cerebrovascular events in children triaged by the vascular neurologists.
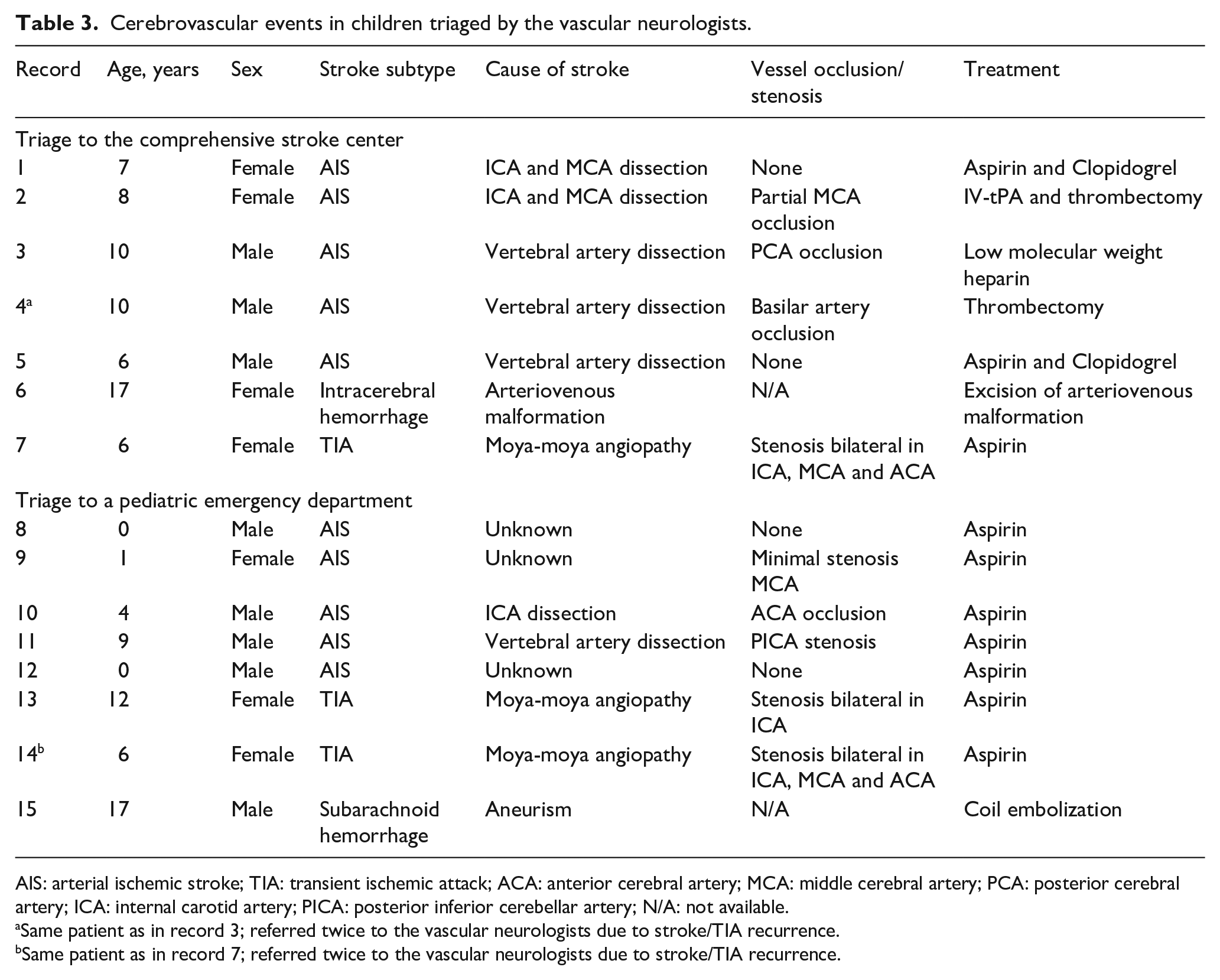
AIS: arterial ischemic stroke; TIA: transient ischemic attack; ACA: anterior cerebral artery; MCA: middle cerebral artery; PCA: posterior cerebral artery; ICA: internal carotid artery; PICA: posterior inferior cerebellar artery; N/A: not available.
Same patient as in record 3; referred twice to the vascular neurologists due to stroke/TIA recurrence.
Same patient as in record 7; referred twice to the vascular neurologists due to stroke/TIA recurrence.
Among the 34 children with non-stroke neurological emergencies, 14 were triaged to an acute stroke assessment at the CSC and 20 were triaged to a pediatric department.
Discussion
Among children triaged for suspected stroke, one in 10 had a final diagnosis of stroke or TIA. Another 20% had non-stroke neurological emergencies, including seizures, acute demyelinating disorders, and CNS-infections. Our findings highlight importance of a specialized and acute evaluation of children with suspected stroke.
Due to the frequent diagnostic delay in children with stroke, it has been recommended to establish referral networks that connect frontline providers to centers with trained experts in vascular neurology. 15 The present study demonstrates the feasibility of implementing such setup in a European context. Our triage-setup was activated in a total of 15 stroke and TIA events and led to identification of all children eligible for revascularization treatments. Based on a previous Danish incidence study, 18 we estimated that 12 children would get AIS in our catchment area during our study-period. With a total of 10 AIS events identified, we expect that only few children with AIS were missed by our triage-setup.
While our triage aimed to identify children eligible for acute recanalization treatments, only two children qualified for these treatments during our 2-year study period. In the remaining children with AIS, recanalization treatment was contraindicated for different reasons, including delayed diagnosis of stroke and minor symptoms. However, when revascularization treatments are not indicated, children with stroke may still benefit from a specialized assessment and early initiation of treatment, including fluid management, antithrombotic treatment, and treatment of secondary stroke complications. 19 Therefore, triage-setups similar to ours necessitate supplementary systems for acute assessment of the children with suspected stroke where revascularization treatment is not indicated.
Non-stroke conditions were present in nine out of 10 children referred by frontline providers to the vascular neurologists. More-over, the specificity and PPV of our triage-setup were low (0.66 and 0.03, respectively) since the vast majority of children triaged to the CSC were ineligible for revascularization treatments. These findings likely result from a priority of our triage-setup of not missing a potentially eligible child. More-over, our findings are consistent with those of other pediatric stroke teams demonstrating that differentiating pediatric stroke from its mimics can be challenging.11,14,20 Several tools have been developed to improve prehospital identification of adults with stroke and thereby decrease the time to diagnosis and treatment. While these tools have demonstrated a moderate to high sensitivity in children,21,22 their specificity are low due to the high frequency of stroke mimics. A study from Australia found that the sensitivity for recognition of AIS was 62% for the Cincinnati Prehospital Stroke Scale and 67% for Recognition of Stroke in the Emergency Room (ROSIER). 22 In a study from the United States, it was demonstrated that the Central Ohio Trauma System Scale tool was insufficient to distinguish children with stroke from those with mimics. 21 Both studies concluded that prehospital stroke recognition tools developed for adults, were insufficient for children.21,22
In our study, most children referred to the vascular neurologists had symptoms compatible with stroke, including hemiparesis, dysarthria, and seizures. However, one out of four children had symptoms which were not suggestive of stroke, including 37 (22%) children who had a normal neurological examination and 7 (4.3%) children who had isolated peripheral facial palsy at the time of referral. Lehman et al. 23 outlined a number of opportunities for improving acute pediatric stroke management, including development of pediatric stroke recognition tools and education of healthcare providers about stroke symptoms in children. Our findings support these recommendations.
Similar to other studies, we found the most children with AIS had arteriopathies.24–26 However, unlike previous studies,24,25 no children with AIS were diagnosed with focal cerebral arteriopathy (FCA). As suggested by Wintermark et al., 27 FCA may be defined as a unifocal and unilateral stenosis of the large intracranial arteries of the anterior circulation. Accordingly, FCA is subdivided into FCA of inflammation type, FCA of dissection type, and FCA of undetermined type. 27 Three children diagnosed with dissection in our study, would meet the definition of FCA of dissection type. However, no cases of FCA of inflammation type was found. This may be related to a reduced incidence of FCA-associated infections during the COVID-19 pandemic 28 or a chance finding due to the number of observations. Our finding is unlikely associated with the symptom-based triage set-up.
A number of studies have described the implementation of pediatric stroke pathways and triage-setups in North America.11–14,29,30 In contrast, our study is one of the first to demonstrate the feasibility of implementing a pediatric stroke triage-setup in a European context. 5 Regional differences in healthcare systems and infrastructure are important to consider in the organization of these setups. In the Danish healthcare system, neurological assessment and treatment of children is organized across several pediatric departments at different hospitals, including seven hospitals in our region (census 530,000 children). Due to the rarity of pediatric stroke, we decided to centralize triage to a single institution and thereby aim for a patient volume that was sufficient for the vascular neurologists to gain routine with the triage of children with suspected stroke. Our triage time-interval was up to 24 h from symptom onset. While there may be patients with salvageable tissue beyond 24 h, the effect and safety of MT at this late phase is unknown. 31 Therefore, we decided to apply the 24 h time-window in accordance with adult trials32,33 and a recent study with pediatric AIS patients. 34 Prior to the implementation of our triage-setup, none of the pediatric departments in our region provided a 24/7 neurological or neuropediatric coverage. Therefore, this was achieved by integrating our triage-setup into existing adult stroke services with vascular neurologists being responsible for the triage. The vascular neurologists had no certified training in clinical evaluation of pediatric patients. However, this was addressed by performing neurological assessment of children triaged to the CSC in a collaboration between the vascular neurologists and the pediatrician on call. More-over, in accordance with the AHA/ASA recommendations, our in-hospital pediatric stroke management enabled additional assessments from vascular neurosurgeons, neuroradiologists, neurointerventionalists, and neurocritical care intensivists. 15
We believe that the organization of our triage-setup may be useful in other healthcare systems similar to that of Denmark.
Strength and limitations
The main strengths of this study include the consecutive, observational study design, and completeness of data with no loss to follow-up. The Danish hospital system is public with no direct expenses to the patients ensuring that economic capacity is not a bias for referral. More-over, our triage-setup covered a large population of 530,000 children <18 years.
However, our study has some limitations. Although the children included in our study were consecutively enrolled, clinical data were collected retrospectively which may have limited information available for analysis. In addition, due to the infrequency of pediatric stroke, evaluation of the feasibility of implementation of our triage-setup was based on a small number of stroke events.
Finally, our data collection depended on consecutively registrations done by individual vascular neurologists. Thus, we cannot rule out the possibility that some patients might have been missed by the registration. However, we sought to avoid this through regular meeting and reminders to the vascular neurologists on the data collection. More-over, the number of registered stroke events was the same in the first and second year of our study-period, indicating a good adherence to the data collection.
Conclusion
Implementing a regional triage-setup that connected frontline providers to vascular neurologists was feasible in a European context; this system was activated for the majority of children with AIS according to an expected incidence and led to identification of children eligible for revascularization treatments. Among children triaged for suspected stroke, 29% had either stroke, TIA or another non-stroke neurological emergency. Our findings highlight importance of a specialized and acute evaluation of children with suspected stroke.
Supplemental Material
sj-docx-1-eso-10.1177_23969873231161381 – Supplemental material for Acute triage of childhood stroke in Denmark
Supplemental material, sj-docx-1-eso-10.1177_23969873231161381 for Acute triage of childhood stroke in Denmark by Julie Brix Bindslev, Klaus Hansen, Nicolaj Groenbaek Laugesen, Goetz Benndorf, Christina Engel Hoei-Hansen and Thomas Truelsen in European Stroke Journal
Footnotes
Acknowledgements
The authors would like to thank the vascular neurologists at the Comprehensive Stroke Center in Copenhagen for their consecutive registration of children triaged for suspected stroke.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Novo Nordisk Foundation (0065517), the Elsass Foundation (21-B01-1477), and the Institute of Clinical Medicine, Copenhagen University. The funders had no role in the design and conduct of the study; in the collection, analysis and interpretation of data; or in the preparation or approval of the manuscript.
Ethical approval
This study was approved by the Danish Data Protection Agency (J.no.: P-2020-451) and the Danish Patient Safety Authority (J.no.: 31-1521-203). This study was considered equivalent to a register-based study and thus exempted from approval by the Danish Ethics Committee.
Informed consent
Not applicable.
Guarantor
JB and TT
Contributorship
Conceptualization, JB, KH, CHH, TT; methodology, JB, KH, CHH, TT; Formal analysis, JB, NL; investigation, JB; writing – original draft preparation, JB; writing – review and editing, KH, NL, GB, CHH, TT; supervision, KH, GB, CHH, TT; project administration, JB. All authors have read and agreed to the published version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.