
Abstract
Background:
Current studies on the role of sex in the prognosis of acute vertebrobasilar artery occlusion (VBAO) are limited. We aimed to explore whether there are sex differences on outcomes in patients treated with endovascular therapy (EVT) for VBAO.
Methods:
Patients from December 2015 to December 2018 with acute VBAO within 24 h of the estimated occlusion time in 21 stroke centers in China were retrospectively analyzed. Baseline data between sexes were compared in the total population cohort and propensity score (PS)-matched cohort. Multivariate logistic regression and ordinal regression were used to analyze the association of sex with outcomes. Mixed-effects regression model was performed for changes in modified Rankin Scale (mRS) scores in men and women from 90 days to 1 year after discharge.
Results:
A total of 577 patients (28.4% women) were finally included. Multivariate logistic regression showed that women had a lower probability of favorable outcome (mRS score 0–3 at 90 days; OR 0.544; 95% CI 0.329–0.899) and functional independence (mRS score 0–2 at 90 days; OR 0.391; 95% CI 0.228–0.670) as well as a higher possibility of shifting to worse mRS (OR 1.484; 95% CI 1.020–2.158) than men. After PS matching, 391 patients (39.4% women) were analyzed, confirming the same results regarding favorable outcome (OR 0.580; 95% CI 0.344–0.977), functional independence (OR 0.394; 95% CI 0.218–0.712), and shift mRS (OR 1.504; 95% CI 1.023–2.210). However, the results of repeated ANOVA showed that men and women had a comparable functional recovery from 90 days to 1 year.
Conclusions:
Stroke due to VBAO treated with EVT is associated with worse outcomes in women than in men. However, men and women showed similar long-term improvement trends.
Introduction
Vertebrobasilar artery occlusion (VBAO) is a fatal neurological disease with high mortality, and severe disability, which accounts for 1% of all strokes and 5% of large vessel occlusions. 1 Previous large randomized controlled trials confirmed that endovascular therapy (EVT) was not superior to standard medical therapy.2,3 However, several recent studies have indicated the efficacy and safety of EVT in patients with VBAO.4,5 Thus, EVT has become the primary treatment for patients with VBAO in the real world.
Sex differences in stroke have received extensive attention. Previous studies have demonstrated significant sex differences in the incidence, clinical manifestations, treatment, and prognosis of stroke. 6 Vascular risk factors differ between men and women, with women being more likely to have atrial fibrillation and men being more likely to smoke and drink alcohol. 7 Symptoms at onset are more often atypical in women, and the time interval, such as onset-to-first medical contact, is longer in women than in men.8,9 Due to atrial fibrillation, women are more susceptible to thromboembolic events, particularly cardioembolic strokes. 10
There is growing knowledge in many stroke areas, however, in the field of EVT, especially in VBAO patients, knowledge about sex differences is limited. In addition, VBAO patients have atypical onset symptoms, untimely recognition of symptoms, increased likelihood of stroke mimics, delayed acute imaging, and a longer time interval between symptom onset and consultation and initiation of treatment.11,12 However, these conditions are in particular evident in women. Based on this, we hypothesize that women with VBAO have a worse outcome after EVT.
The current studies on the role of sex in the prognosis of acute anterior circulation large vessel occlusion remain controversial.13–15 However, sex differences in outcomes after EVT in VBAO patients have yet to be investigated in detail. A better understanding of sex differences in outcomes following EVT, as well as how these differences are related to other risk factors, is necessary for managing patients with VBAO with tailored strategies.
Therefore, our study aims to explore whether there are sex differences on the prognosis of patients with VBAO treated with EVT and determine whether progression of functional status from 90-day to 1-year follow-up beyond discharge is associated with the sex of the patients.
Methods
Study population
Consecutive patients in the posterior circulation ischemic stroke registry (PERSIST, ChiCTR2000033211) database from December 2015 to December 2018 were retrospectively included. PERSIST is a multicenter registry study at 21 stroke centers in 13 provinces of China that recruited patients with acute, symptomatic, radiologically confirmed VBAO treated with EVT. Patients were eligible for inclusion if they met the following criteria: (1) age ⩾18 years; (2) acute symptomatic VBAO confirmed by computed tomographic angiography, magnetic resonance angiography, or digital subtracted angiography; (3) treated with EVT; and (4) treatment was initiated (groin puncture) within 24 h of estimated occlusion time. Patients were excluded if they (1) had a pre-stroke modified Rankin Scale (mRS) score ⩾3; (2) were diagnosed with combined anterior stroke, aneurysm, or arteriovenous malformation; (3) were pregnant or lactating; (4) participated in a clinical trial; or (5) had incomplete baseline critical data and imaging. Details of the PERSIST study have been described elsewhere.11,16,17 The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (USTC) in Hefei, China. Patient consent was waived due to its retrospective nature.
Data collection
The following data were retrospectively collected from the electronic medical records: demographic characteristics, medical history (hypertension, diabetes, hyperlipidemia, atrial fibrillation, coronary heart disease), Glasgow Coma Scale (GCS) score, National Institute of Health Stroke Scale (NIHSS) score, intravenous thrombolytic (IVT), infarct site, and site of occlusion. The occlusion sites were divided into proximal, middle, and distal of basilar artery, and V4 segment of vertebral artery. The posterior circulation Alberta Stroke Program Early CT Score (pc-ASPECTS) was assessed on non-contrast CT. The modified Thrombolysis In Cerebral Infarction (mTICI) scale was used to evaluate the reperfusion status. Successful reperfusion was defined as mTICI score of 2b-3. An assessment of collateral status in the posterior circulation was performed by the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASTIN/SIR) Grading System. This system assigns a grade to collaterals ranging from 0 to 4, with 4 signifying complete and fast collateral blood flow to the region distal to the stenosis. Collaterals were graded as poor (grades 0 and 1), moderate (grade 2), or good (grades 3 or 4) for this analysis. All angiographic measurements were performed blind to neuroimaging and patient outcomes. Time parameters, including time from estimated occlusion to groin puncture and groin puncture to reperfusion, were also recorded. The core laboratory in the First Affiliated Hospital of USTC received all the neuroimaging data, which were then examined in a blinded manner by two skilled neuroradiologists. If there was any disagreement, a consensus was used to affirm the final assessment.
Treatment
Endovascular treatment included mechanical thrombectomy with stent retrievers and/or thrombo-aspiration, balloon angioplasty, stenting, intra-arterial thrombolysis, or a combination of these approaches. In each institution, specific endovascular therapeutic treatment was left to the discretion of the neurointerventionists and neurologists according to a comprehensive assessment and the intentions of patients or their legal representatives.
Outcome measures
Functional outcomes were assessed by the mRS score at 90 days and 1 year. The primary outcome was a favorable outcome (mRS 0–3) at 90 days. The secondary outcomes were functional independence (mRS 0–2) and shift mRS at 90 days. Safety endpoints included symptomatic intracerebral hemorrhage (sICH), all-cause mortality in hospital and at 90 days. Causes of death included ischemic stroke and its complications, cardiac causes, and other causes. All patients were evaluated by CT for intracranial hemorrhage within 48 h after EVT. A deterioration of the NIHSS score of 4 or more/2 or more for each item with evidence of any intracerebral hemorrhage on follow-up imaging was categorized as sICH according to the Heidelberg Bleeding Classification. 16 The difference between functional outcomes at 90 days and at 1-year follow-up as measured by mRS was also evaluated.
Statistical analysis
Baseline characteristics, treatment profiles, and outcomes were compared between sexes. Normally distributed data are expressed as the mean (SD), nonnormally distributed data are expressed as the median and interquartile range (IQR), and categorical variables are expressed as numbers (%). Comparisons between groups were performed using independent sample t tests, Mann–Whitney U tests or χ 2 tests.
K-nearest neighbor imputation was used for the missing covariates before propensity score (PS) matching. Details of missing data are shown in Table 1.
Baseline characteristics according to sex in VBAO patients treated with EVT before and after propensity score matching.
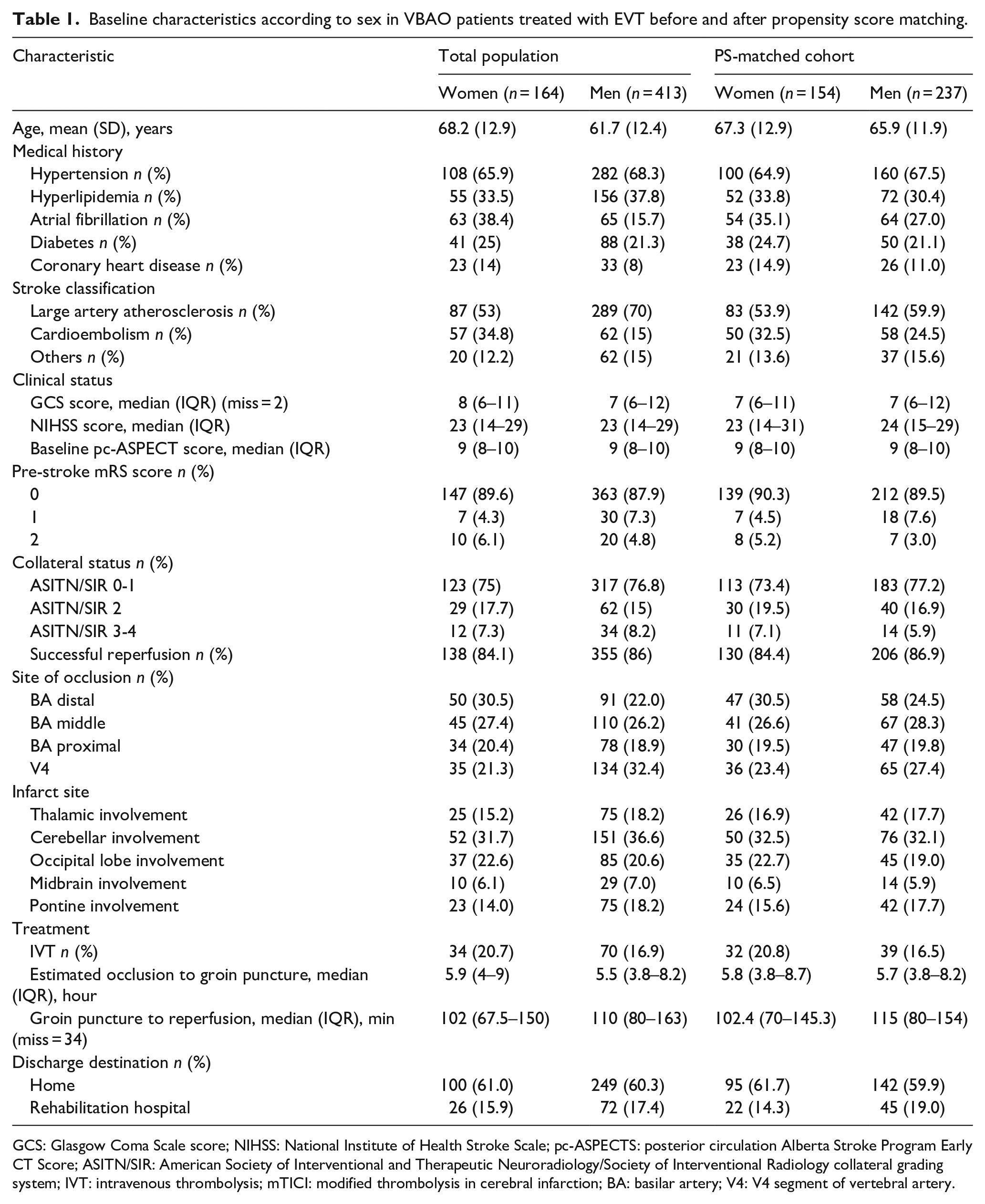
GCS: Glasgow Coma Scale score; NIHSS: National Institute of Health Stroke Scale; pc-ASPECTS: posterior circulation Alberta Stroke Program Early CT Score; ASITN/SIR: American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology collateral grading system; IVT: intravenous thrombolysis; mTICI: modified thrombolysis in cerebral infarction; BA: basilar artery; V4: V4 segment of vertebral artery.
A propensity-matched analysis was performed using age, atrial fibrillation history, occlusion location, time from estimated occlusion to groin puncture, GCS score, stroke classification, and prestroke mRS score to ensure a balanced 2:1 nearest neighbor match with a caliper width of 0.1.
Multivariable logistic regression analysis was performed both in total population cohort and PS-matched cohort adjusted for age, sex, prestroke mRS, hypertension, diabetes, hyperlipidemia, coronary heart disease, atrial fibrillation, baseline NIHSS, GCS, pc-ASPECTS, stroke classification, collateral status, reperfusion status, intravenous thrombolysis, the infarct site, time from estimated occlusion to groin puncture, time from puncture to reperfusion, site of occlusion, and discharge destination to compare outcomes and safety endpoints. The ordinal logistic regression adjusted for the above variables was applied for shifts in scores over the entire range of mRS, and the proportional odds assumption was tested. The change of mRS measures from 90 days to 1 year were analyzed by using a repeated-measure, mixed-effects regression model with a linear approximation of mRS scores.
Furthermore, we conducted a subgroup analysis to determine whether there was any possibility for sex-related outcome heterogeneity based on treatment (bridging therapy vs EVT alone) and estimated occlusion time (EOT > 6 h vs EOT ⩽6 h). Statistical analyses were performed with SPSS software, version 26.0, and R, version 3.1.3. Two-sided p values <0.05 represent significant differences.
Results
Baseline characteristics before and after matching
A total of 609 VBAO patients treated with EVT were screened in this study, and 577 patients (28.4% women) met the selection criteria and were eligible for analysis (Figure 1). The baseline characteristics of the total patient population and of the PS-matched cohort are displayed in Table 1.
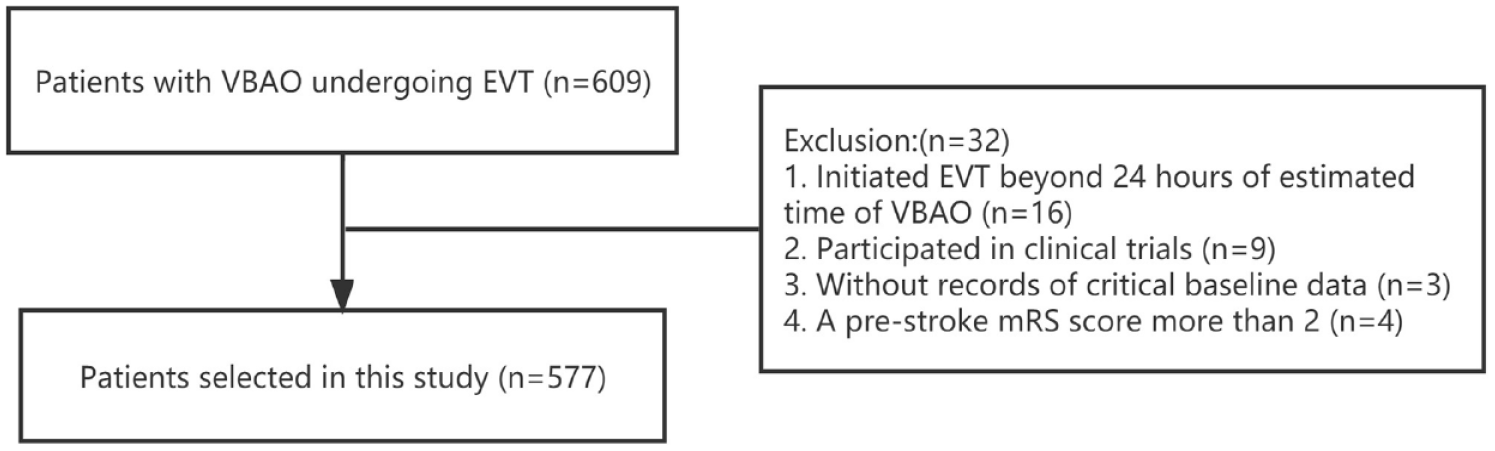
Flow chart.
In the total population, women were older (68.2 (12.9) vs 61.7 (12.4), p < 0.001) and more likely to have atrial fibrillation (38.4% vs 15.7%, p < 0.001), cardioembolic stroke (34.8% vs 15%, p < 0.001), and distal basilar artery occlusion (30.5% vs 22%, p = 0.007), and less likely to have large artery atherosclerosis stroke (53% vs 70%, p < 0.001), V4 segment of vertebral artery occlusion (21.3% vs 32.4%, p = 0.007) than men. There was no significant difference between the other variables.
After matching (39.4% women), the baseline characteristics were well balanced between men and women (Table 1).
Outcome measures before and after matching
The clinical outcomes are shown in Table 2. The distribution of mRS scores in VBAO patients treated with EVT according to sex is displayed in Figure 2. In the total population, we found that women were less likely to have a favorable outcome (OR 0.544, 95% CI 0.329–0.899) and functional independence (OR 0.391, 95% CI 0.228–0.670) and more likely to shift to worse mRS score (OR 1.484, 95% CI 1.020–2.158) after adjusted the confounders. After PS matching, the same results regarding favorable outcome (OR 0.580; 95% CI 0.344–0.977), functional independence (OR 0.394; 95% CI 0.218–0.712), and shift to worse mRS score (OR 1.504; 95% CI 1.023–2.210) were presented. Women were not associated with sICH, in-hospital mortality, or mortality at 90 days both in total population and PS-matched cohort.
Clinical outcomes in VBAO patients treated with endovascular treatment.
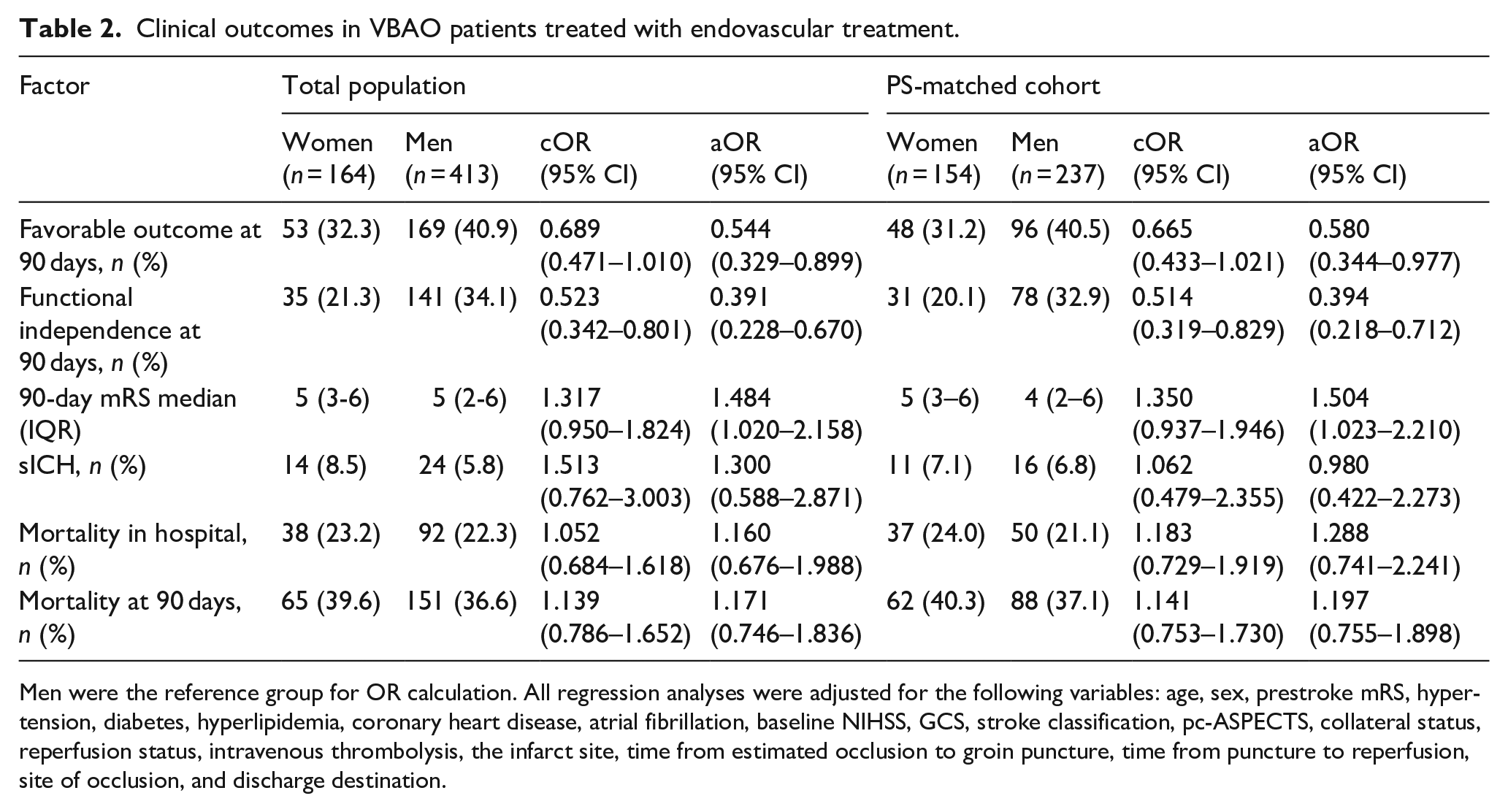
Men were the reference group for OR calculation. All regression analyses were adjusted for the following variables: age, sex, prestroke mRS, hypertension, diabetes, hyperlipidemia, coronary heart disease, atrial fibrillation, baseline NIHSS, GCS, stroke classification, pc-ASPECTS, collateral status, reperfusion status, intravenous thrombolysis, the infarct site, time from estimated occlusion to groin puncture, time from puncture to reperfusion, site of occlusion, and discharge destination.
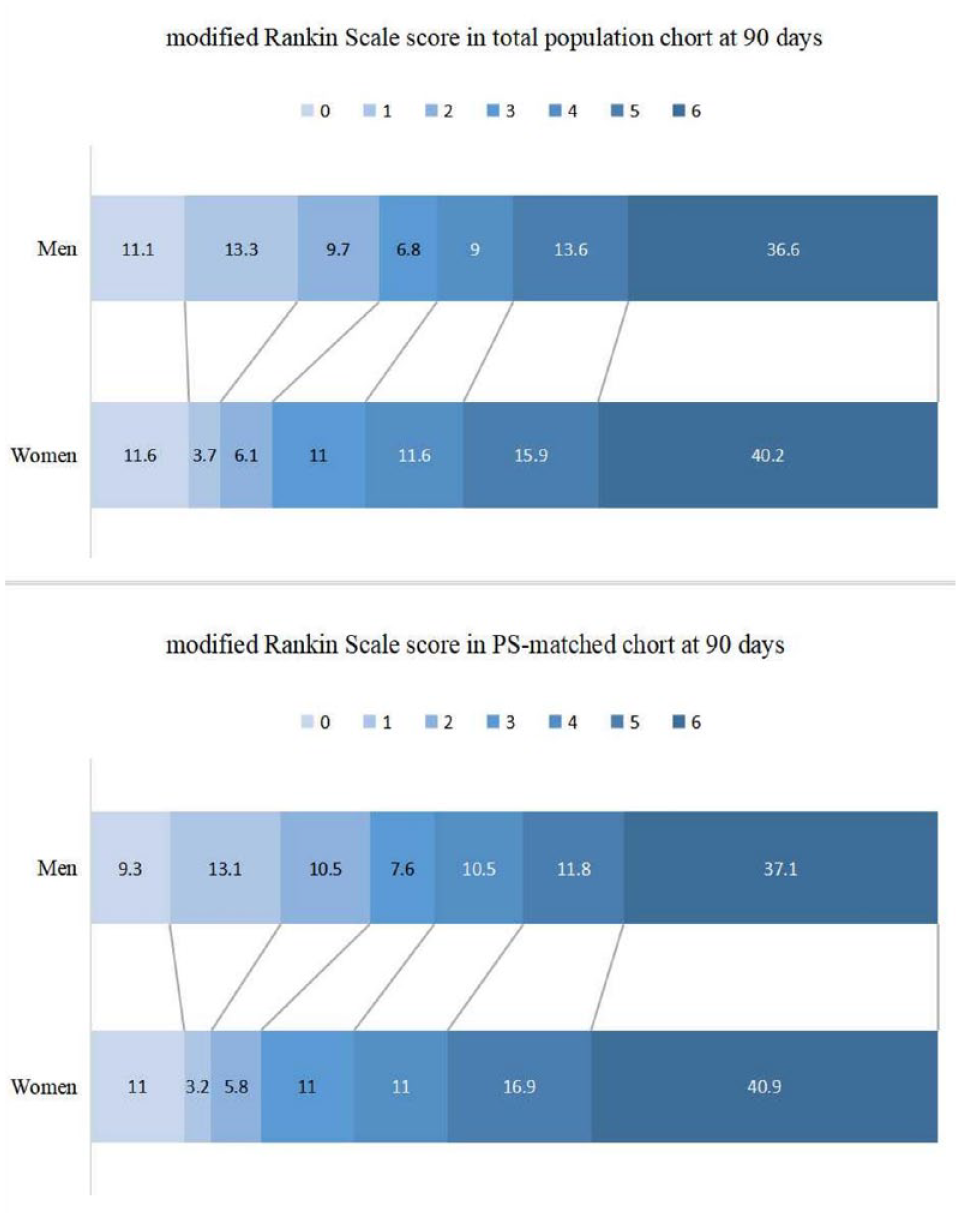
Represents the distribution of modified Rankin Scale scores in the total population and PS-matched cohort in VBAO patients treated with EVT according to sex.
Figure 3 depicts the variance in mRS scores in men and women from the 90-day to 1-year follow-up. In comparison to men, women had a comparable functional recovery in both the total population cohort (p = 0.071) and the PS-matched cohort (p = 0.100). There is no interaction between sex and time in total population cohort (p = 0.738) or in PS-matched cohort (p = 0.813).
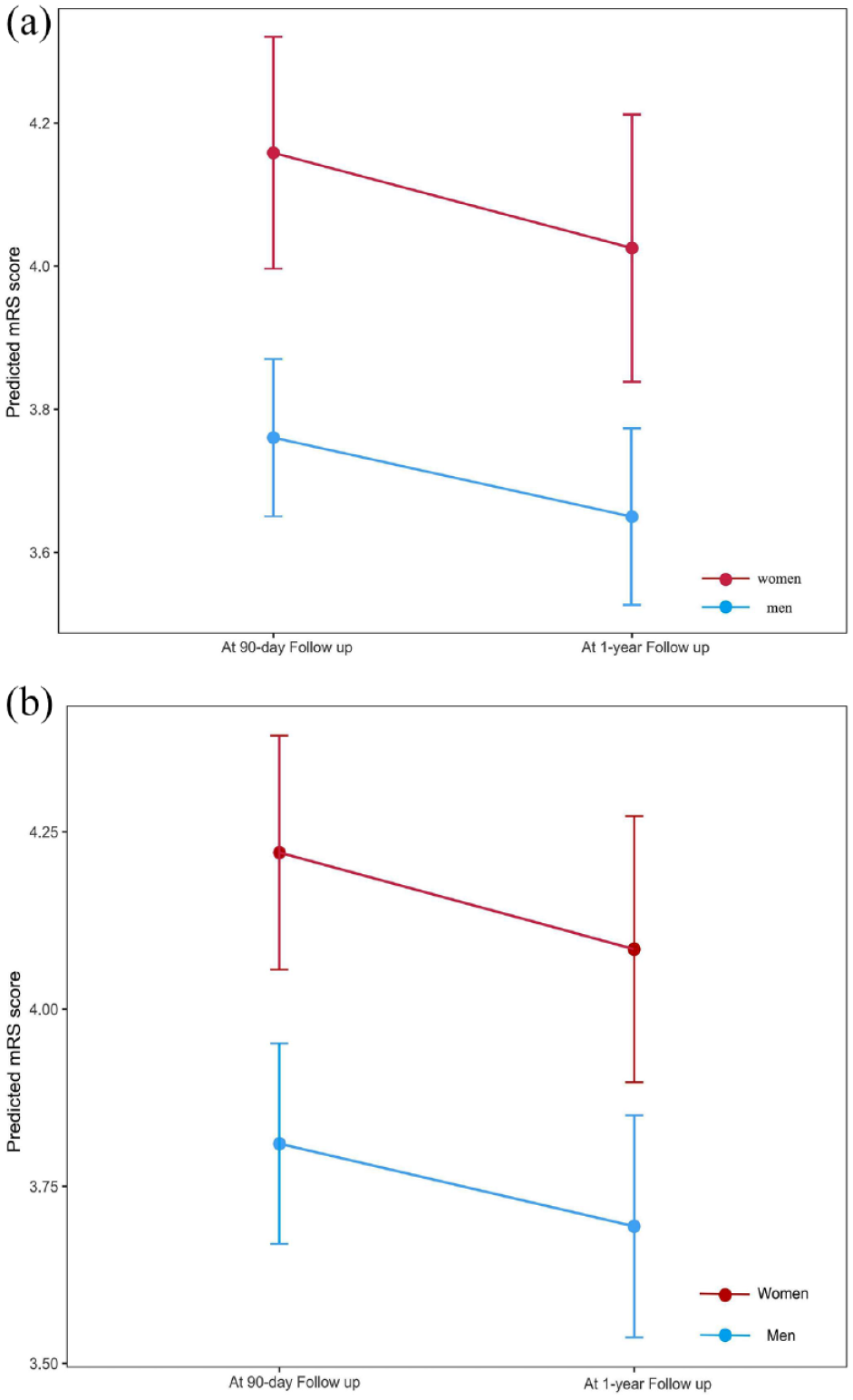
Represents variation in modified Rankin Scale (mRS) scores from 90 days to 1 year: comparisons between men and women in the total population (a) and in the PS-matched cohort (b).
Subgroup analysis
In the subgroup analysis (Table 3), 18% of patients received intravenous thrombolysis and 43.8% of patients had more than 6 h of EOT. We found that women treated with EVT alone were associated with a lower probability of favorable outcome (OR 0.463; 95% CI 0.262–0.818) and functional independence (OR 0.338; 95% CI 0.182–0.627) and more likely to shift to worse mRS score (OR 1.575, 95% CI 1.034–2.399).
Sex comparisons in outcome of total population patients based on treatment and estimated occlusion time.
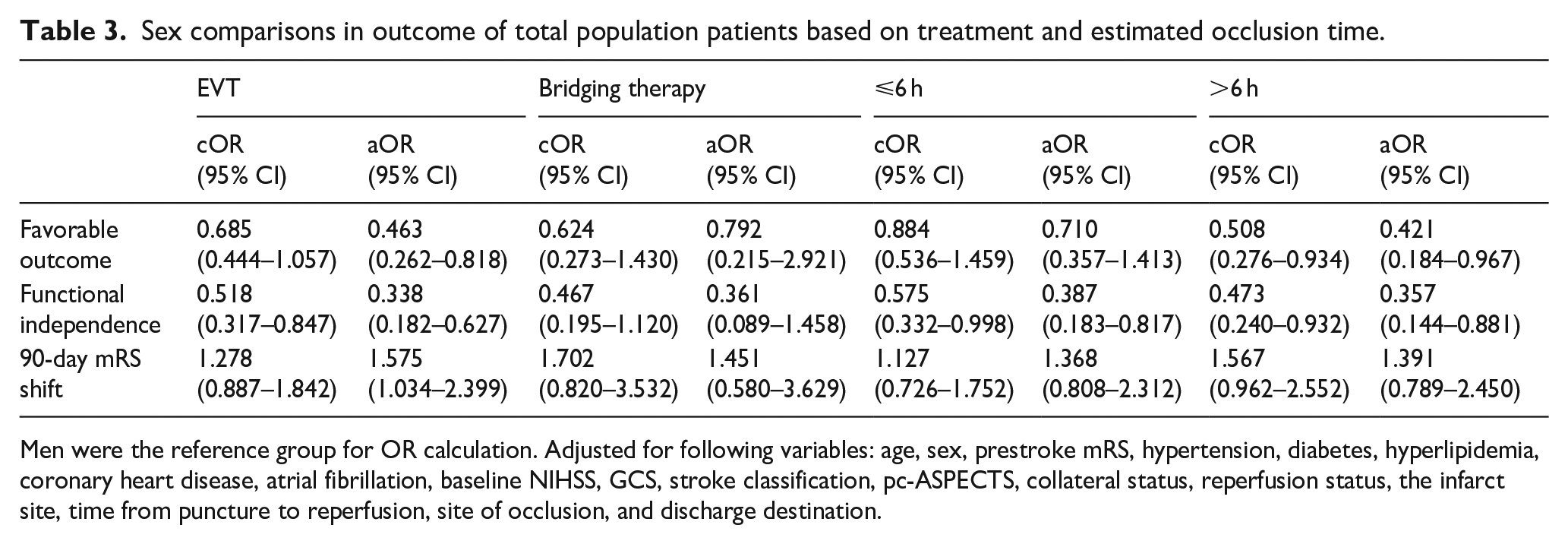
Men were the reference group for OR calculation. Adjusted for following variables: age, sex, prestroke mRS, hypertension, diabetes, hyperlipidemia, coronary heart disease, atrial fibrillation, baseline NIHSS, GCS, stroke classification, pc-ASPECTS, collateral status, reperfusion status, the infarct site, time from puncture to reperfusion, site of occlusion, and discharge destination.
In EOT > 6 h, women were associated with favorable outcome (OR 0.421; 95% CI 0.184–0.967) and functional independence (OR 0.357; 95% CI 0.144–0.881). In EOT ⩽ 6 h, women were associated with functional independence (OR 0.387; 95% CI 0.183–0.817).
Discussion
In our study, we found that clinical outcomes at 90 days were worse in women than in men among VBAO patients treated with EVT. However, in terms of improvement in functional outcomes from 90 days to 1 year, women had a comparable recovery to that of men. In the subgroup analysis, we found that, women treated with EVT alone were less likely to have a good prognosis compared to men. Whereas, it seemed that the prognosis of women was worse than that of men no matter the time onset.
The incidence of acute ischemic stroke with large vessel occlusion (LVO) has been found to be higher in men than in women. 18 Furthermore, in a series of studies on posterior circulation, no matter in the ATTENTION 4 or the BAOCHE 5 registry, the proportion of men was much higher than that of women, and this was also the case in our study. Thus, we performed 2:1 PS matching, not the usual 1:1 PS matching, to avoid excessive loss of sample size. Studies suggested that the baseline NIHSS score is less sensitive in predicting large vessel occlusion in the posterior circulation.19,20 It was difficult to match the clinical severity at presentation for VBAO based on NIHSS which has relatively poor discrimination for posterior circulation infarction. Thus, GCS score was used to match the clinical severity of VBAO patients.
Sex disparities in prognosis are a contentious topic. However, there are few reports on the effect of sex on the prognosis of VBAO patients. In this study, we found that in patients with VBAO treated with EVT, women had a worse prognosis than men even by applying propensity score matching. We consider that this may be related to the following reasons: (1) Women are reported to be more susceptible to some unmeasured negative health outcomes. 21 For example, musculoskeletal comorbidities such as arthritis and osteoporosis, that may lead to less compliance to rehabilitation and thus, worse outcomes. 22 (2) Women are more likely to have higher rates of social isolation, with negative consequences for outcomes, may have contributed to women having worse outcomes after a stroke.9,23 Studies have shown that women are also at a higher risk of widowhood, which may contribute to worse outcomes. 24 (3) Poststroke depression is also a common complication in women, and some evidence suggests that poststroke mood disorders result in worse mRS scores. 25 Unfortunately, due to the retrospective nature of the study, the depression screenings were not applied in all of the patients. (4) Sex hormones also affect coagulation patterns and cerebrovascular physiology. 26 It is reported in previous data that estrogen has a neuroprotective effect on ischemic stroke. 27 However, the level of menopause and estrogen decline rapidly in elder women It has been demonstrated from epidemiological studies that the majority of strokes in post-menopausal women are more severe, lead to poorer psychological outcomes, and result in higher rates of disability. 28
A recent study of the effect of sex on the outcome of mechanical thrombectomy in basilar artery occlusion (BAO) showed that women achieved comparable functional outcomes compared with men after undergoing mechanical thrombectomy. 29 However, this is not consistent with our findings. This may involve differences in population, economy, medical level, and other aspects. The countries and regions included in the previous study were developed countries and regions. The inconsistencies are as follows: (1) Different populations, including race, income, and disease conditions. Particularly in relation to differences between disease conditions, we included the common absence of basilar artery flow due to vertebral artery occlusion in the analysis. This was more representative of posterior circulation stroke. (2) The longer time from onset to procedure and longer operative time may be more representative of reality in most developing countries. (3) The adjusted baseline situation is more adequate in our study.
Recently, whether to administer intravenous thrombolysis before EVT in acute stroke patients has become a hot issue in clinical practice. Therefore, in the subgroup analysis, we further explored the relationship between treatment and sex. We found that women treated with EVT alone were less likely to have a good prognosis. Based on this result, we hypothesized that the negative prognostic sex impact might be neutralized by thrombolysis. However, the results of recent RCT studies30,31 do not support this result. Therefore, the exact mechanism may need to be further explored
Moreover, EVT is highly time-dependent. Thus, we also investigated the association between EOT and sex, it seemed that the prognosis of women were worse than that of men no matter the time onset. It is possible that the underlying driver of that men had more combined occlusions, which could lead to already established small collateral pathways in large artery atherosclerosis. However, the higher incidence of cardio-embolic stroke and the greater probability of large infarcts in women, thus causing women had worse outcomes no matter the time onset.
Few studies have examined trends in long-term prognosis according to sex. In this study, mixed regression model was applied to further analyze the improvement in mRS scores between sexes from 90 days to 1 year. We found that although women had poorer outcomes at both 90 days and 1 year, there was no significant difference in the improvement in mRS scores between sexes. Despite their older age, women appear to recover at the same rate as men. We suspect that they have a strong relationship with rehabilitation therapy and discharge destination after stroke.
Our study has several advantages. This was a multicenter study, and the sample size was a strength. Moreover, propensity score matching was employed in this study to construct populations of women and men with balanced baseline characteristics. We then followed up for 1 year, taking into account changes in mRS from 90 days to 1 year.
Our study has the following limitations. First, there are inherent defects because this is a retrospective study. Second, even though PS matching was applied, unmeasured confounding variables may exist, and hidden biases owing to uncontrolled variables may persist. Thus, the results should be interpreted with caution. Third, we lacked information about social, behavioral, socioeconomic, psychological factors that may have contributed to variations in outcomes We also did not look at how infarct volume affected potential post-discharge progression. Fourth, the under-representation of women as study participants might limit the generalizability of our results. Further prospective studies are needed to verify our findings in the future.
Conclusions
In conclusion, our study found that women with VBAO who received EVT had a worse outcome no matter at 90 days or 1 year. However, the long-term improvement trend present in men and women was comparable.
Supplemental Material
sj-docx-1-eso-10.1177_23969873221151142 – Supplemental material for Sex differences in outcomes after endovascular treatment of patients with vertebrobasilar artery occlusion
Supplemental material, sj-docx-1-eso-10.1177_23969873221151142 for Sex differences in outcomes after endovascular treatment of patients with vertebrobasilar artery occlusion by Pan Zhang, Hao Li, Jinjing Wang, Feng Zhang, Lulu Xiao, Yirong Fang, Dingyi Yan, Guoqiang Xu, Chaolai Liu, Zhixin Huang, Mengmeng Gu, Hanhong Zhang and Wen Sun in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from Key Research and Development Plan Projects of Anhui Province (No. 202104j07020049) and Natural Science Foundation of Anhui Province (No. 2108085MH271), and partially supported by the Science and Technology Program of Guangzhou, China (202201020359).
Informed consent
Informed consent was not sought for the present study because its retrospective nature.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of the First Affiliated Hospital of the University of Science and Technology of China (USTC) in Hefei, China.
Guarantor
WS
Contributorship
The study was conceived by PZ, HL, HZ, and WS. PZ and HL prepared the initial draft of the manuscript. PZ and HL carried out the statistical analysis. HZ and WS revised the manuscript. All authors participated in the data collection, analysis, and interpretation. The final version of the manuscript was reviewed approved by all authors.
Trial registration
Name of trial registry: ChiCTR2000033211
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.