
Abstract
Introduction:
The very elderly (⩾80 years) are under-represented in randomised endovascular thrombectomy (EVT) clinical trials for acute ischaemic stroke. Rates of independent outcome in this group are generally lower than the less-old patients but the comparisons may be biased by an imbalance of non-age related baseline characteristics, treatment related metrics and medical risk factors.
Patients and methods:
We compared outcomes between very elderly (⩾80) and the less-old (<80 years) using retrospective data from consecutive patients receiving EVT from four comprehensive stroke centres in New Zealand and Australia. We used propensity score matching or multivariable logistic regression to account for confounders.
Results:
We included 600 patients (300 in each age cohort) after propensity score matching from an initial group of 1270 patients. The median baseline National Institutes of Health Stroke Scale was 16 (11–21), with 455 (75.8%) having symptom free pre-stroke independent function, and 268 (44.7%) receiving intravenous thrombolysis. Good functional outcome (90-day modified Rankin Scale 0–2) was achieved in 282 (46.8%), with very elderly patients having less proportion of good outcome compared to the less-old (118 (39.3%) vs 163 (54.3%), p < 0.01). There was no difference between the very elderly and the less-old in the proportion of patients who returned to baseline function at 90 days (56 (18.7%) vs 62 (20.7%), p = 0.54). All-cause 90-day mortality was higher in the very elderly (75 (25%) vs 49 (16.3%), p < 0.01), without a difference in symptomatic haemorrhage (very elderly 11 (3.7%) vs 6 (2.0%), p = 0.33). In the multivariable logistic regression models, the very elderly were significantly associated with reduced odds of good 90-day outcome (OR 0.49, 95% CI 0.34–0.69, p < 0.01) but not with return to baseline function (OR 0.85, 90% CI 0.54–1.29, p = 0.45) after adjusting for confounders.
Conclusion:
Endovascular thrombectomy can be successfully and safely performed in the very elderly. Despite an increase in all-cause 90-day mortality, selected very elderly patients are as likely as younger patients with similar baseline characteristics to return to baseline function following EVT.
Introduction
Endovascular thrombectomy (EVT) is a powerful intervention for ischaemic stroke caused by intracranial large vessel occlusion (LVO).1–5 Treatment is highly effective for appropriately selected patients within 24 h of stroke onset if the stroke is disabling and if salvageable brain tissue can be demonstrated.6–8 Very elderly patients (⩾80 years) are under-represented in randomised EVT clinical trials despite approximately one-third of all ischaemic strokes occurring in this age group. 9 Only 198 (15.4%) patients in the Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials (HERMES) individual patient meta-analysis were aged 80 or older, yet, EVT was highly effective in this subgroup (cOR 3.68 (1.95–6.92) for independent outcome compared with medical therapy).10,11 Even fewer patients of this age group were included in the late time-window EVT trials.12,13
A limited number of observational studies have reported real world experience on outcome after EVT in the very elderly, with rates of good functional outcome (90-day modified Rankin Scale (mRS) score 0–2) reported in larger multicentre series to be between 20% and 43% of treated patients.14–21 The rates of independent outcome are generally lower than the less-old patients but the comparisons may be biased by an imbalance of non-age related baseline characteristics such as stroke severity, treatment related metrics and medical risk factors.
Using data from four comprehensive stroke centres in New Zealand and Australia, we aimed to review the association between the very elderly and functional outcome after EVT accounting for these inherent biases. We hypothesised that functional outcomes are similar between patients 80 years or older, and those aged less than 80 years, when imbalances in baseline demographic, clinical characteristic and EVT related metrics are matched.
Methods
Study population
We performed a retrospective analysis of patient data from consecutive EVT patients treated for occlusion of the internal carotid (including tandem occlusions), proximal segments (1 and 2) of the middle cerebral and basilar artery at four comprehensive stroke centres in New Zealand (Christchurch, Auckland, Wellington hospitals) and Australia (John Hunter Hospital) between 1st January 2017 and 31st December 2020. All New Zealand data were derived from the national New Zealand reperfusion registry 22 with additional data sources. 23 Data for John Hunter Hospital was collected prospectively as part of the International Stroke Perfusion Imaging Registry (INSPIRE). 24 Collectively the included centres cover a population catchment of nearly 6 million people and include provision of services to regional centres. All centres used Computed Tomography (CT) imaging as the screening modality and have access to perfusion imaging. All centres offer EVT to four different regional networks of primary stroke centres.
We collected basic patient demographics (age, sex, pre-stroke functional status), clinical risk factors, stroke related clinical variables including baseline National Institutes of Health Stroke Scale (NIHSS), treatment metrics (intravenous thrombolysis, relevant metrics related to EVT including final thrombolysis in cerebral infarction (TICI) score) and mRS data at 90 days. Thrombectomy was considered in the extended time window if reperfusion was achieved >6 h from onset or last known well time. Outcome data at 90 days was collected prospectively by either phone call or in-person assessment as part of the stroke reperfusion registries by a member of the clinical team. The outcome endpoints assessed in this study were good functional outcome (defined as 90-day modified Rankin Scale (mRS) 0–2) and return to baseline function (same 90-day mRS as baseline). Patients treated with medium or distal vessel thrombectomy (distal middle cerebral, anterior cerebral or posterior cerebral artery), with missing relevant data such as stroke or treatment related information and functional outcome were excluded. The Alberta Stroke Program Early CT score (ASPECTS) was also not available as this variable was not routinely collected at the participating centres. All data were collected as part of standard care and assessment of radiological and clinical outcomes were not performed centrally.
Statistical analysis
We used standard descriptive statistics to compare the baseline characteristics, stroke and EVT related metrics, and outcomes variables between the very elderly patients (⩾80 years) and the less-old patients. Differences were assessed with univariate analysis using X2 or Fisher’s exact test for categorical variables, and Mann-Whitney test for continuous variables. Data were reported as median (± interquartile range) or n (%). We performed propensity score matching by estimating the propensity score for baseline demographic and clinical characteristics, the main EVT related metrics and for presence of parenchymal haemorrhage on follow up imaging. Propensity score matching (ratio 1:1) was performed to the nearest neighbour with callipers set at 0.2 SD of the logit of the propensity scores. We reported the baseline characteristics between the two groups for the initial cohort and after propensity score matching.
We then constructed a multivariate logistic regression model in the matched cohort and assessed the associations with functional outcomes. The primary outcome was good functional outcome, defined as 90-day mRS 0–2, and the secondary outcome was return to baseline function defined as same mRS at 90-day as pre-stroke. The association between the very elderly and outcome endpoints was assessed in multivariable logistic regression model. The association was adjusted for male sex, baseline NIHSS, administration of intravenous thrombolysis, outside transfer, location of vessel occlusion (anterior vs posterior circulation), time to reperfusion in minutes, successful reperfusion (TICI 2B-3) and presence of parenchymal haematoma (type I and II) on repeat imaging. An a priori sample size calculation was not performed, instead we used a convenience sample of patients treated during the study period. All analyses were defined a priori. Propensity score matching was performed using R 3.1.0. MatchIt package and all other statistical analyses were performed on SPSS 27 (ABM, Armonk, NY).
Results
Of the 1314 patients available during the study period, 44 were excluded (missing variables (16), non-proximal vessel thrombectomy (28)), leaving an unmatched cohort of 1270 (Figure 1). Within this initial cohort there were 324 very elderly and 946 less-old patients with significant imbalances in baseline characteristics and stroke related factors (Table 1). The very elderly were less likely to be male (153 (47.2%) vs 557 (58.9%)), less likely to have full pre-stroke independence (baseline mRS 0, 224 (69.1%) vs 853 (90.2%)), site of vessel occlusion was more likely to be middle cerebral artery (244 (75.3%) vs 627 (66.3%)) and less likely to have been transferred from primary stroke centres (137 (42.3%) vs 485 (51.3%)). The very elderly generally had more vascular risk factors with more atrial fibrillation (65.4% vs 41.5%), hypertension (77.5% vs 57.5%), hyperlipidaemia (44.1% vs 37.5%), previous stroke (14.8% vs 12.3%) and were less likely to be a current smoker (9.9% vs 26.4%) or have diabetes mellitus (11.4% vs 19.6%) (Table 1).
Clinical characteristics and EVT related metrics of the study cohort with comparisons between the elderly and the younger patients.
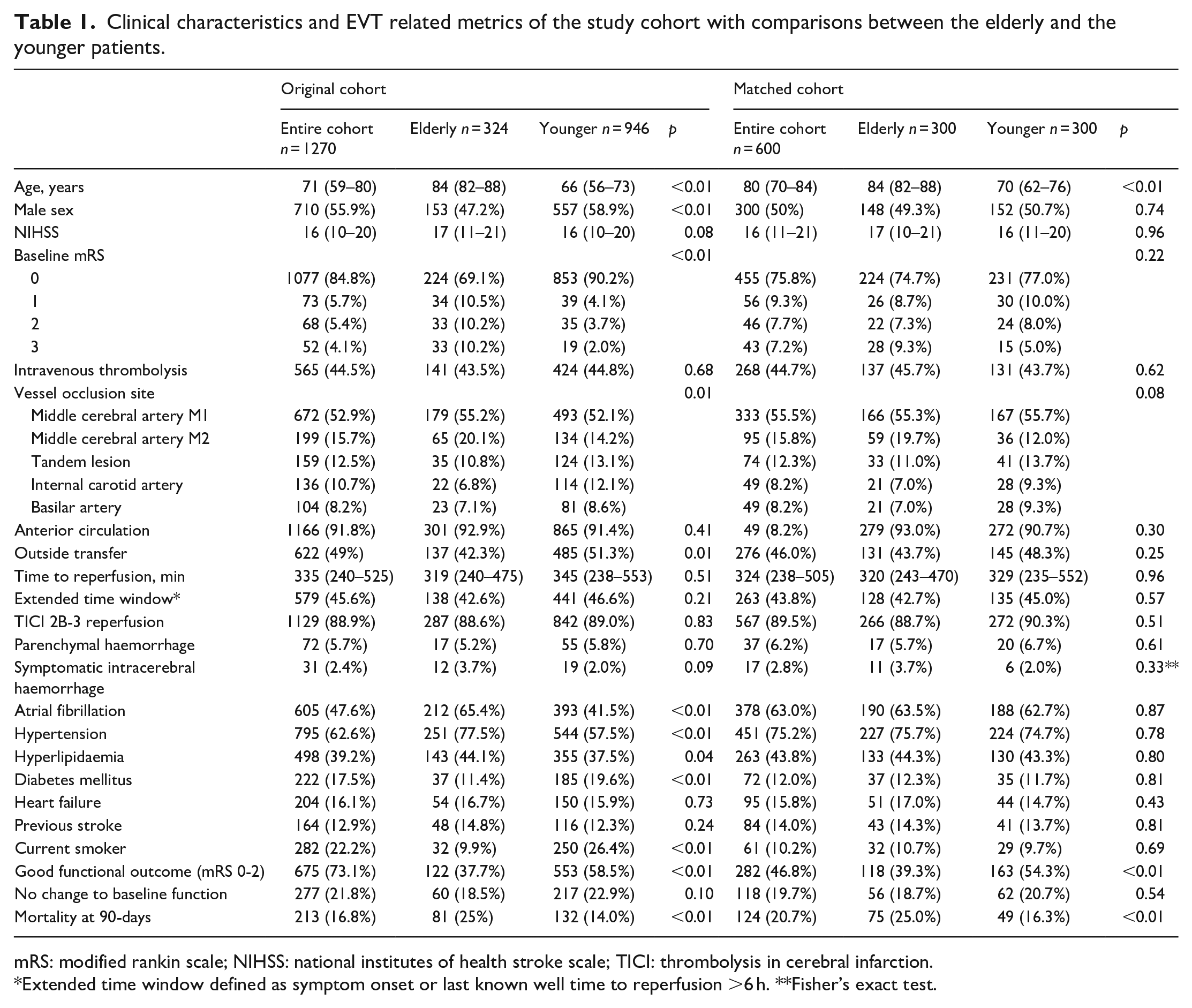
mRS: modified rankin scale; NIHSS: national institutes of health stroke scale; TICI: thrombolysis in cerebral infarction.
Extended time window defined as symptom onset or last known well time to reperfusion >6 h. **Fisher’s exact test.
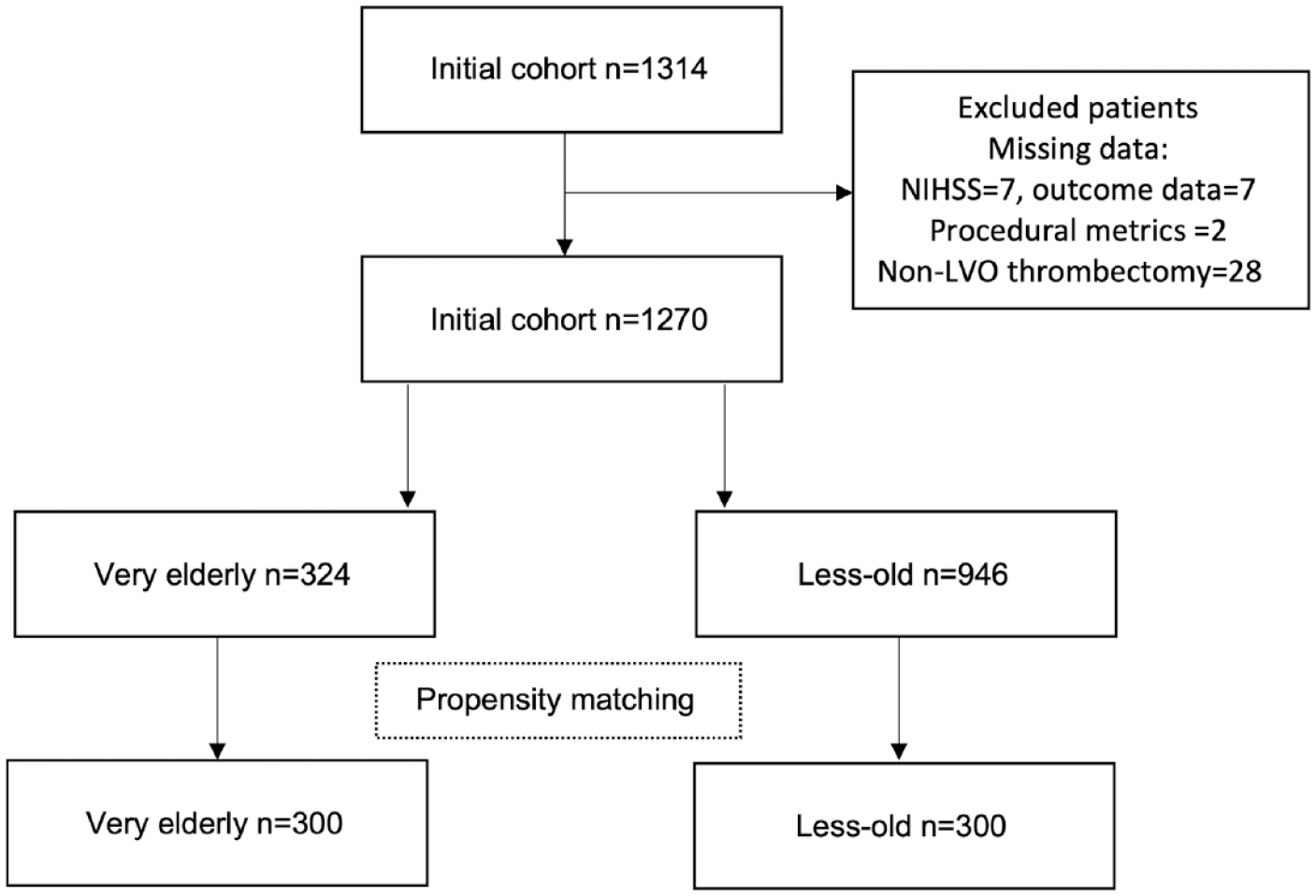
Study flow chart.
Propensity score matching resulted in a final cohort of 600 (Figure 1), with 300 very elderly patients matched to 300 less-old controls who were well-balanced for sex, clinical and EVT related characteristics (Table 1). The median (IQR) baseline NIHSS in the final cohort was 16 (11–21), with 455 (75.8%) having symptom free pre-stroke independence, and 268 (44.7%) receiving thrombolysis. The main target vessel was proximal segment of the middle cerebral artery (M1, 333 (55.5%)) with basilar artery (49 (8.2%)) being the least common occlusion. The median time from onset or last known well time to reperfusion was 324 min (230–505) and successful reperfusion was achieved in 567 (89.5%) of the patients. Good functional outcome was achieved in 282 (46.8%) of the cohort, with very elderly patients having less proportion of good outcome compared to the less-old (118 (39.3%) vs 163 (54.3%), p < 0.01). Nearly 20% of the cohort had return to baseline function at 90-days with no difference between the very elderly and the less-old patients (56 (18.7%) vs 62 (20.7%), p = 0.54).
Parenchymal haemorrhage occurred in 37 (6.2%), while 17 (2.8%) had symptomatic intracerebral haemorrhage. The rates of parenchymal haemorrhage (17 (5.7%) vs 20 (6.7%), p = 0.61) and symptomatic intracerebral haemorrhage (11 (3.7%) vs 6 (2.0%), p = 0.33) were similar between the very elderly and the less-old. The 90-day mortality was higher in the very elderly (25% vs 16.3%, p < 0.01).
For the very elderly patients there was no difference in rates of good outcome (39% vs 39.8%, p = 0.88) and return to baseline function (17.4% vs 20.3%, p = 0.53) regardless of whether EVT was performed in early or extended time window (>6 h from onset to reperfusion).
In the multivariable logistic regression models, the very elderly were significantly associated with reduced odds of good 90-day outcome (OR 0.49, 95% CI 0.34–0.69, p < 0.01) but not with return to baseline function (OR 0.85, 90% CI 0.54–1.29, p = 0.45) after adjusting for baseline NIHSS, male sex, intravenous thrombolysis, outside transfer, anterior circulation target, successful reperfusion, time to reperfusion and parenchymal haemorrhage (Table 2).
Multivariable logistic regression models assessing the associations with functional outcomes after thrombectomy, n = 600.
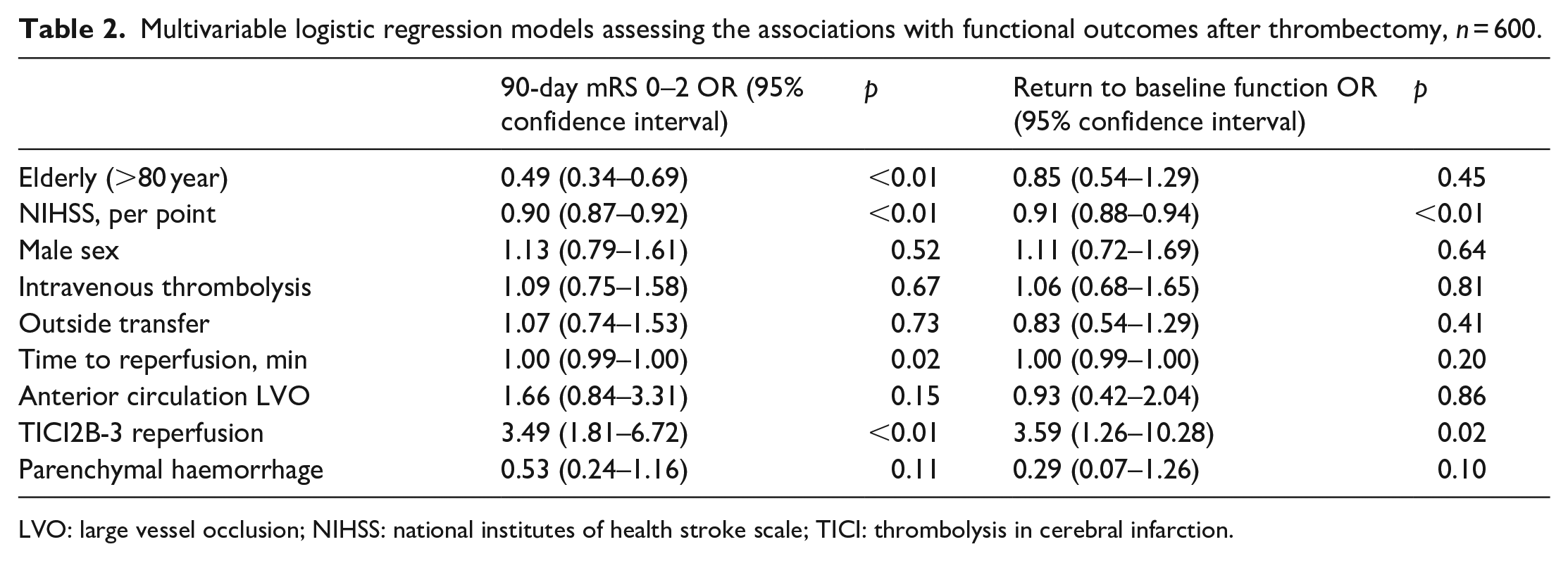
LVO: large vessel occlusion; NIHSS: national institutes of health stroke scale; TICI: thrombolysis in cerebral infarction.
Discussion
In this multicentre cohort of EVT treated patients, we demonstrated that successful reperfusion (~90% of current cohort) is feasible and could result in good functional outcome in a clinically significant number of very elderly patients. Although the very elderly were less likely to achieve a good functional outcome after EVT than the less old patients, good recovery was still achieved in ~40% at 90 days. Furthermore, our results suggest that the very elderly patients were as likely to return to baseline function as the less-old patients with nearly 20% achieving this outcome. There was however an increased rate of mortality in the very elderly compared to the less-old patients (25% vs 16%) without an increased risk of parenchymal haemorrhage.
The very elderly have been under-represented in the trials of EVT in both early and extended time window trials. However, the treatment effect of EVT appears to be maintained at least in the early time window. 10 In the Analysis Of Pooled data From Randomised Studies of Thrombectomy More Than 6 h After Last Known Well (Aurora) collaboration, only 180 very elderly patients were included but EVT was effective in improving functional outcome when compared with medical therapy (adjust common OR 2.60 (1.23–5.51), p = 0.01). 13 The current best practice guidelines recommendations have also not excluded the very elderly from EVT treatment. 8 Our data is consistent with the limited published data with 90-day functional outcome from large cohorts in North America and Europe showing EVT is safe and effective in the very elderly (Table 3).
Summary of the published large (n > 100) thrombectomy cohorts with 90-day outcome in the elderly.
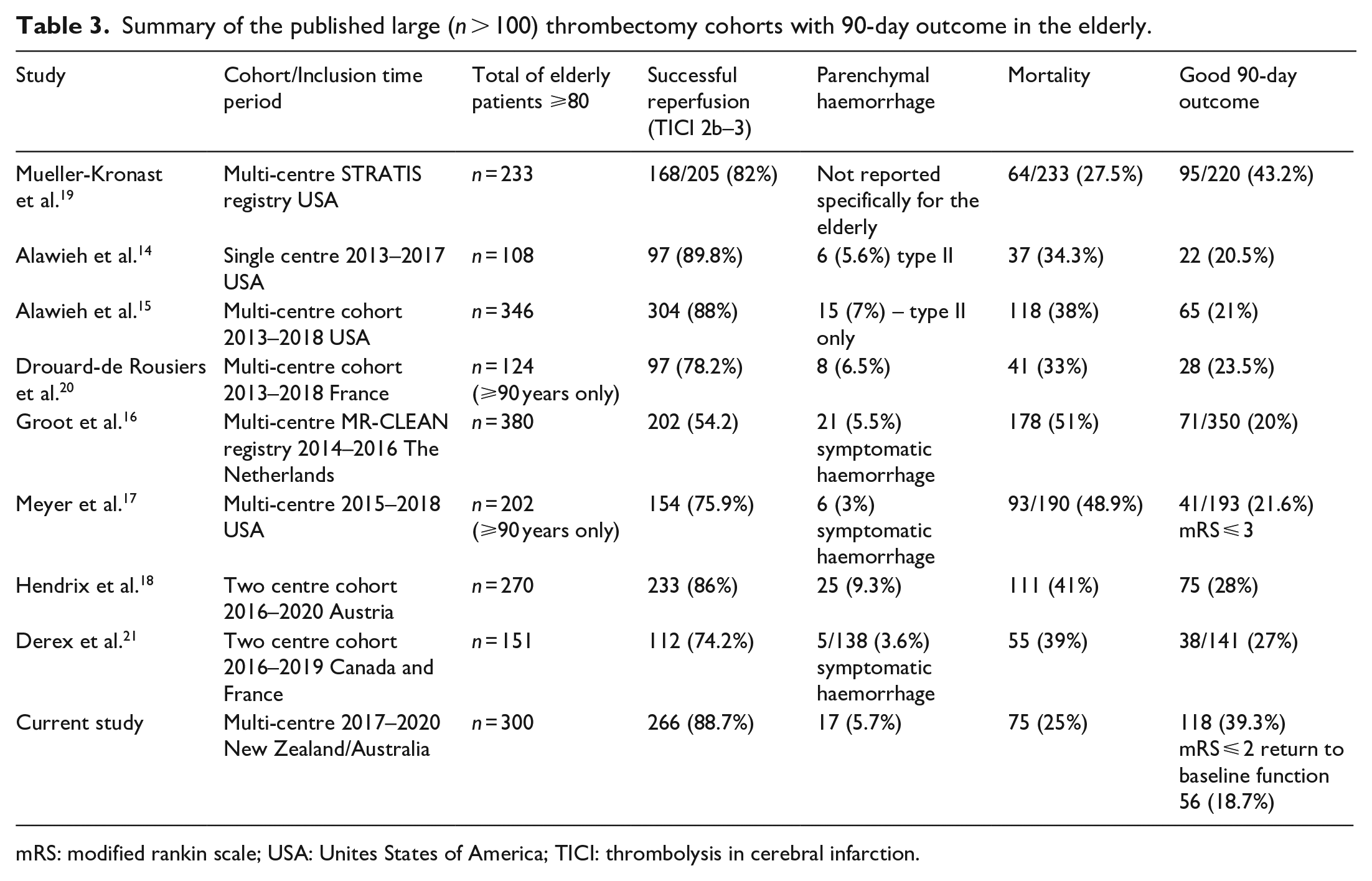
mRS: modified rankin scale; USA: Unites States of America; TICI: thrombolysis in cerebral infarction.
In contrast with most other studies we report a higher rate (39%) of good outcome in the very elderly compared to that reported in other larger cohorts of patients (20%–28%, Table 3), and also higher than the ~30% rate reported in a recent meta-analysis that included smaller studies. 25 However, our results are in line with that reported in the multicentre STRATIS registry where 43% had a 90-day mRS 0–2. One limitation of STRATIS was that it only included patients with no/minimal pre-stroke symptoms (mRS ⩽ 1), 19 whereas the present study included 16.6% of patients with mRS > 1. The observed differences in rates of good outcome in the current study to that reported in other cohorts may reflect differences in resourcing, access to EVT and practices in selection for treatment between geographic regions. The differences may also reflect a more contemporary cohort associated with improved workflow and patient selection. Most published series included patients from time periods prior to widespread implementation of extended time window EVT, suggesting a potential bias towards EVT performed in the early time window where selection for treatment is unlikely to have been augmented by modern perfusion imaging. It is also unclear in the published cohorts whether modern perfusion imaging was used for patient selection. Modern imaging with CT perfusion forms an intrinsic part of selection consideration for most patients included in this cohort where this modality is available.
The 39% rate of good outcome in the very elderly however is still 16% lower than the less-old in our study despite matching for risk factors, stroke severity and pre-morbid functional status. The difference is likely due to unmeasured factors such as clinical frailty which is more prevalent with advancing age, and not represented by standard functional scoring system. Reports utilising clinical frailty scores have associated increased frailty with reduced likelihood of good outcome after EVT, and it is plausible that this unmeasured factor26,27 accounts for the difference in outcome between the two groups in this study and other published cohorts (Table 3).
The very elderly patients also achieved a similar return to baseline function as the less-old patients (OR 0.85 95% CI 0.54–1.29, p = 0.45) despite increased mortality. This suggests that EVT benefits some elderly patients who would ‘hold their own’ and maintain their baseline function, while others who do not benefit are more likely to die after their stroke. The increased mortality risk may also be due to unmeasured frailties.26,27 Similar discrepancy in outcome has been observed in published cohorts of patients with pre-existing mild-moderate disability (mRS 2–3)28,29 undergoing EVT, and a return to baseline function has been proposed as a metric to determine benefit of EVT in these patients. The rates of pre-stroke disability are expected to be higher in the elderly population and the concept of return to baseline function may also be a more appropriate endpoint in the very elderly than the conventional definition of good outcome (mRS 0–2). Future studies involving the very elderly should consider utilising this concept as an endpoint assessment.
There are limitations associated with this study. The retrospective nature and lack of centralised assessment of radiological and clinical endpoints would predispose our data to intrinsic bias. However, our data is the first large cohort to examine outcome in the very elderly outside of Europe and America and provides robust real-world data. EVT practices are also similar between New Zealand and Australia with the same certification process for interventionalists and neurologists, thus providing internal consistency. Secondly, we do not have consistent availability of baseline radiological metrics in relation to ischaemic core volume (non-contrast CT ASPECTS and CT perfusion core volumes) to enable adjustment for this important predictor of outcome. However, we have accounted for other important mediators of outcome including baseline NIHSS, time to reperfusion and successful reperfusion. Thirdly, our study was not designed to investigate whether a less advanced method for patient selection without CT perfusion imaging would result in similar outcomes. Further studies, including the results of recently completed MR CLEAN-LATE randomised clinical trial would provide further insight into this matter. 30 Fourthly, we do not have cost effective analysis, but our data suggest nearly one in two elderly patients will regain functional independence with ~20% returning to baseline function, likely translating into reduction in societal costs associated with dependence. Furthermore, healthcare costs for stroke are higher in more severe strokes and in the very elderly. 31 The number of people aged 80 years or older is expected to triple between 2020 and 2050 making this a clear focus for healthcare. Finally, we do not have data for non-EVT controls at the participating registries but clinical trial data suggest LVO patients not managed with EVT are expected to have lower rates of good outcome (mRS 0–2) than reported in this study at ~27% and ~19% in the early and extended time windows respectively.10,13
The study also has strengths. This report is one of the largest real world cohorts assessing impact of EVT on outcome in the very elderly and the first to account for imbalances between baseline characteristics using statistical matching. The multicentre nature of our cohort from two countries also make our findings more generalisable. Our results substantially expand the body of data on EVT outcome in the very elderly and provides strong evidence that real world outcomes in this group are at least as good as reported in the limited randomised clinical data.
Conclusion
Selected very elderly patients benefit from EVT in acute ischaemic stroke and are as likely as the less-old patients to achieve a return to baseline function. Further studies are required to determine the optimal strategy for patient selection for EVT in the very elderly.
Footnotes
Acknowledgements
None
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This retrospective observation study has approval from each local research office. The data processing centre has ethics approval from the Health and Disability Ethics Committee (approval number 17/CEN/84) to perform this analysis.
Informed consent
As all data were collected as part of routine care, patient consent was not required as per local legislation.
Guarantor
TYW
Contributorship
TYW, AR, JNF, PAB conceived and designed the study. TYW led the data analysis and interpretation and act as the guarantor of this work. TYW, HD and DW prepared the manuscript. All authors contributed to data collection, interpretation of results and final manuscript preparation.