
Abstract
Introduction
Spontaneous blood pressure drop within the first 24 h has been reported following arterial recanalisation in ischaemic stroke patients. We aimed to assess if spontaneous blood pressure drop within the first hour after mechanical thrombectomy is a marker of early neurological recovery.
Patients and methods
Retrospective observational single-centre study including ischaemic stroke patients treated with mechanical thrombectomy. Blood pressure parameters from admission, mechanical thrombectomy start, mechanical thrombectomy end and hourly within 24 h after mechanical thrombectomy were reviewed. Primary outcome was early dramatic neurological recovery (8-point-reduction in NIHSS or NIHSS ≤ 2 at 24 h). Secondary outcome was functional independence at 90 days (mRankin 0–2).
Results
We included 458 patients in our analysis. Two-hundred (43.7%) patients achieved dramatic neurological recovery following mechanical thrombectomy. One hour after mechanical thrombectomy end, median systolic blood pressure was significantly different between outcome groups (129 vs. 138 mmHg, p = 0.005) and a higher drop in median systolic blood pressure was seen in the dramatic neurological recovery group (15 vs. 9 mmHg). Optimal cut-off for predicting dramatic neurological recovery was a systolic blood pressure drop of 10.5 mmHg (sensitivity 0.54, specificity 0.55, AUC 0.55). On multivariate analysis, spontaneous systolic blood pressure drop was associated with higher odds of achieving dramatic neurological recovery (OR for 10 mmHg blood pressure drop 1.14, 95% CI 1.01–1.29, p = 0.04). No significative association between any blood pressure parameter drop and functional independence at 90 days was found.
Discussion
We hypothesised that spontaneous systolic blood pressure drop is a marker of successful reperfusion and, therefore, a marker of improvement of cerebral autoregulation due to the reduced final ischaemic core.
Conclusion
Spontaneous systolic blood pressure drop after mechanical thrombectomy is an early predictor of dramatic neurological recovery.
Introduction
Between 60% and 80% of acute ischaemic stroke patients have elevated blood pressure (BP) values at presentation. 1 It is hypothesised that this increased BP could represent compensatory response to ensure cerebral blood flow to the ischaemic penumbra. 2 Ischaemic stroke patients with successful recanalisation demonstrate a linear relationship with BP, with more favourable outcomes occurring at lower BP. 3 Few studies have demonstrated a spontaneous rapid normalisation of BP measurement following arterial recanalisation in patients with intravenous tissue plasminogen activator (IV-tPA) and mechanical thrombectomy (MT).4–6 Therefore, we hypothesise that earlier normalisation of BP after recanalisation may correlate with earlier reperfusion of ischaemic penumbra. There are few known clinical predictors of early recovery and good outcome after MT besides clinical neurological recovery within the first 30 min after MT 7 which can be difficult to evaluate due to the anaesthetic and sedative medication usually administered during the procedure.
We aimed to assess whether this spontaneous BP drop within the first hour after MT is an immediate surrogate marker of early neurological recovery.
Methods
Patient population
We performed a retrospective study of a continuously acquired prospective single-centre database of acute ischaemic stroke patients due to large vessel occlusion and treated with mechanical thrombectomy between January 2017 and February 2019. All MT procedures were performed using endovascular devices comprising stent retrievers, aspiration catheters or both. After MT, patients were admitted to a stroke unit and had their neurological status monitored or were admitted in the intensive care unit when necessary due to intubation before or during procedure. Patients admitted to the stroke unit in this centre had hourly BP measurements within the first 24 h after the procedure.
Only patients admitted to the stroke unit with at least one BP measurement before EVT and one BP measurement within 1 h after EVT end were included. We excluded patients admitted to the intensive care unit as individual BP measurements after MT could not be retrospectively reviewed in those cases. BP was monitored non-invasively using electronic monitoring devices.
Primary and secondary outcome
Our primary outcome was dramatic neurological recovery, defined as a National Institute of Health Stroke Scale (NIHSS) of 2 or less at 24 h after thrombectomy or a decrease of at least 8 points from baseline NIHSS within 24 h. The secondary outcome was functional independence at 90 days defined by a modified Rankin scale (mRS) 0–2.
BP parameters
Systolic (SBP) and diastolic blood pressure (DBP) were measured at admission, at MT start (in the angio suite, before arterial puncture), after the best possible angiography outcome was reached (MT end) and then hourly for the first 24 h. Median SBP, median DBP and median MAP (mean arterial pressure) were calculated and compared between dramatic neurological recovery and no-dramatic neurological recovery group. As our hypothesis was that spontaneous early blood pressure drop after MT would predict a better outcome, we focused on the variability in median SBP, median DBP and median MAP within the first hour after MT. Therefore, we calculated median differences of SBP, DBP and MAP between MT start and end as well as between MT start and 1 h after MT end.
Clinical parameters
Demographic and clinical data (sex, age, previous mRS ≤ 2, hypertension, dyslipidaemia, diabetes mellitus, smoking habits, atrial fibrillation, previous stroke, ischaemic heart disease, NIHSS at admission, occlusion site, ASPECTS – Alberta stroke programme early CT score, anaesthesia technique, IV-tPA administration, TICI – thrombolysis in cerebral infarction, and time of symptom onset to recanalisation) were collected (Table 1). Administration of any vasoactive treatment (labetalol, urapidil, fluid replacement therapy, noradrenaline or arterial nimodipine, before, during and after EVT procedure) was performed at the discretion of the treating physicians, according to international guidelines, 8 and was also recorded. Successful recanalisation was deemed as TICI ≥ 2 b. Haemorrhagic transformation of ischaemic infarct was evaluated at the 24 h CT and classified according to European Co-operative Acute Stroke Study-II (ECASS-II) criteria.
Clinical and demographic characteristics, per outcome group.
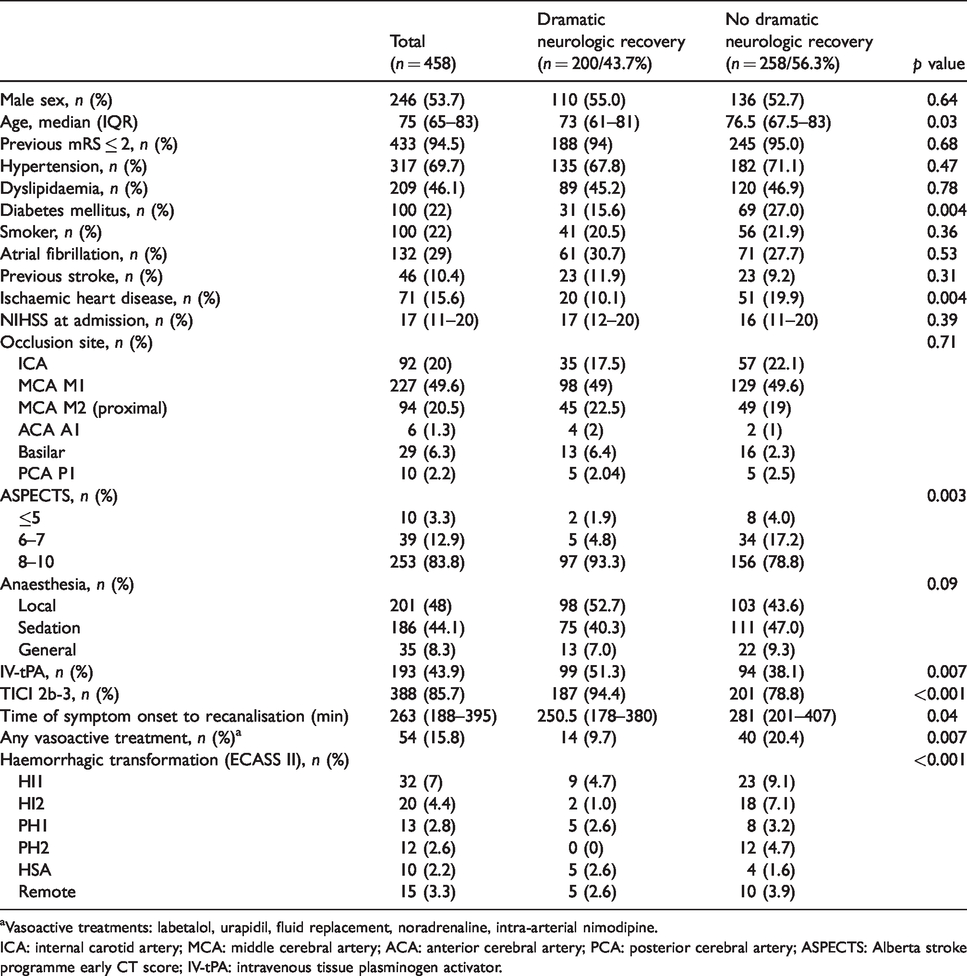
aVasoactive treatments: labetalol, urapidil, fluid replacement, noradrenaline, intra-arterial nimodipine.
ICA: internal carotid artery; MCA: middle cerebral artery; ACA: anterior cerebral artery; PCA: posterior cerebral artery; ASPECTS: Alberta stroke programme early CT score; IV-tPA: intravenous tissue plasminogen activator.
Statistical analysis
We presented the numerical variables as medians and interquartile ranges (IQR). Categorical variables were presented as frequencies and percentages. Significance of intergroup differences was assessed using the Mann–Whitney U test and Fisher exact test, as appropriate. For the primary outcome, logistic regression was used to predict odds of dramatic neurological recovery for each BP parameter. For each BP parameter, optimal cut-off values for variability (drops) were estimated using the receiver operating characteristic (ROC) curves and defined as the point closest to sensitivity = 1 and specificity = 1 (corresponding to the maximum Liu index). Independent predictors of dramatic neurological recovery after MT were determined using multivariate logistic regression. Variables with a p value < 0.05 were used in the subsequent multivariate analysis. A model was computed for each BP parameter of interest. Odds ratio (OR), confidence intervals and p-values were reported for significant predictors. Standard analyses of excessive collinearity diagnostics were performed, including computation of pairwise correlation coefficients to assess interdependence of causal variables, as well as measures of multicollinearity, including variance inflation factors, to determine whether there was a linear association between ≥2 predictor variables. For the secondary outcome, logistic regression models for each BP parameter were computed to predict odds of independent functional outcome at 90 days (mRS ≤ 2). Statistical analyses were performed using SPSS MP14 (IBM Corporation, NY).
Results
From the 1993 patients admitted with acute ischaemic stroke during the study period, 494 (24.7%) patients were treated with mechanical thrombectomy. We excluded 19 patients in whom BP measurements before or within 1 h after MT were unavailable and 7 patients in whom 24 h NIHSS data were unavailable (patients admitted to the intensive care unit). Therefore, 458 patients were included in the final analysis. Baseline demographic and clinical characteristics of dramatic neurological recovery and no dramatic neurological recovery groups are described in Table 1. More than two-fifths (n = 200, 43.7%) of patients achieved dramatic neurological recovery following treatment with MT. Patients who achieved dramatic neurological recovery were younger (73.0 vs. 76.5 years old, p = 0.03), had less often diabetes mellitus (15.6 vs. 27.0%) and ischaemic heart disease (10.1 vs. 19.9%), had higher admission CT-ASPECTS (10 vs. 9, p = 0.004) and were more likely to have received treatment with IV-tPA (51.3 vs. 38.1, p = 0.007). Furthermore, successful recanalisation (TICI 2 b-3) was achieved more often (94.4 vs. 78.8%, p = 0.001) and earlier (median, 30.5 minutes earlier, p = 0.04) in this group. Patients who needed vasoactive treatment (including antihypertensive medication) after admission less frequently achieved dramatic neurological recovery (9.7 vs. 20.4%, p = 0.007). Median SBP at admission in patients who needed vasoactive treatment was higher (186 mmHg vs. 144 mmHg, p < 0.001). There were no significant differences in median SBP on admission (144 vs. 147 mmHg, p = 0.31), at MT start (143 vs. 139 mmHg, p = 0.10) and at MT end (138 vs. 134 mmHg, p = 0.07) between the dramatic neurological recovery and no-dramatic neurological recovery group, respectively. Median DBP (75 vs. 72 mmHg, p = 0.06) and median MAP (97 vs. 95 mmHg, p = 0.04) were higher in the dramatic neurological recovery group at MT start but no significant differences were found on median DBP and median MAP at admission and at MT end. One hour after MT end, median SBP was significantly different between outcome groups (129 vs. 138 mmHg, p = 0.005) and a higher spontaneous drop in median SBP was seen in the dramatic neurological recovery group (15 vs. 9 mmHg). Median MAP was also significantly lower in the dramatic neurological recovery patients (90 vs. 96 mmHg, p = 0.007) and a trend toward lower DBP was also detected (70 vs. 74 mmHg, p = 0.06). Median SBP and median MAP were the BP parameters that consistently continued to decrease in patients achieving dramatic neurological recovery until 12 h after MT end. Table 1 of Supplementary Material summarises the BP parameters trends by dramatic neurological recovery and no-dramatic neurological recovery groups, from admission to 24 h after MT end. Figure 1 shows overall median SBPs at MT start and 1 h after per achieved recanalisation degree. Figure 2 shows overall median SBPs at MT start and after 1 h, per achieved recanalisation degree and neurological outcome. Interestingly, in patients who did not achieve successful recanalisation (TICI 0-2a), spontaneous SBP drop occurred in a non-significantly higher proportion of patients with dramatic neurological recovery (n = 7, 28% vs. n = 3, 11.5%, p = 0.17). We did not find any significative association between functional independence at 90 days and spontaneous SBP drop (OR 1.00, CI 0.99–1.00, p = 0.46), spontaneous DBP drop (OR 1.00, CI 0.99–1.01, p = 0.76) or spontaneous MAP drop (OR 1.00, CI 0.99–1.01, p = 0.62).
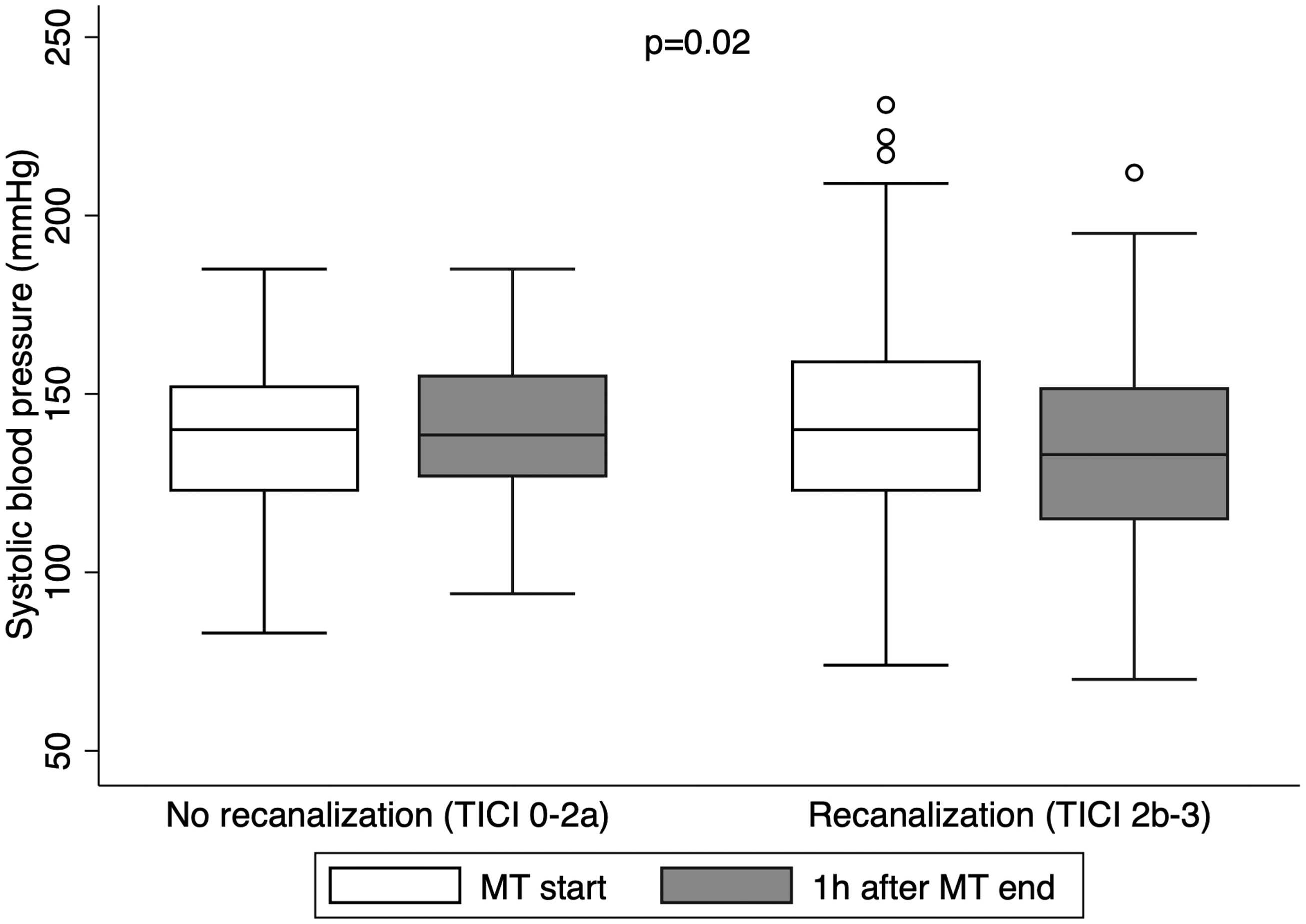
Median systolic blood pressure (SBP) at mechanical thrombectomy start (MT) and 1 h after MT end, per achieved recanalisation degree.
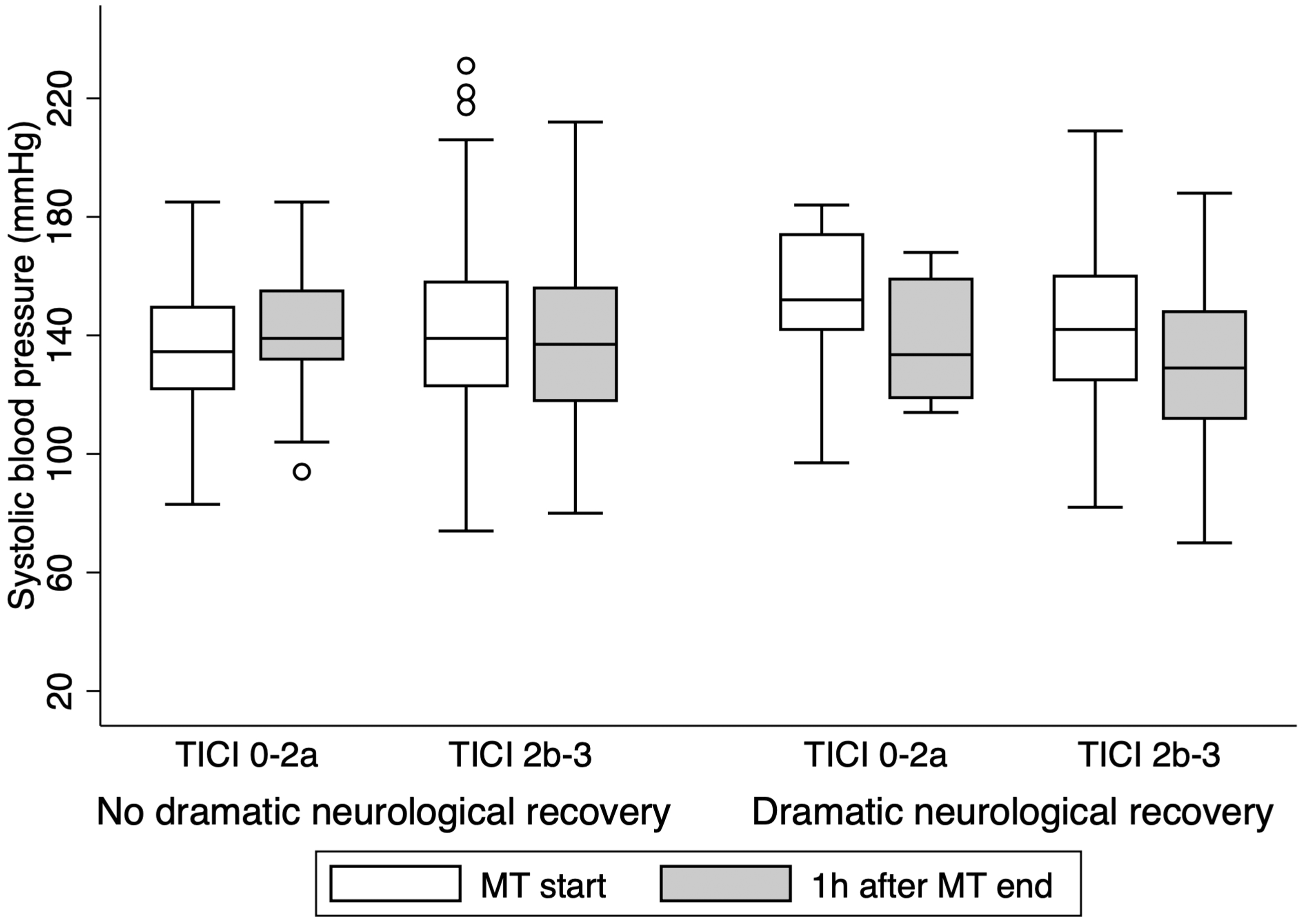
Median systolic blood pressure (SBP) at mechanical thrombectomy (MT) start and 1 h after MT end, per achieved recanalisation degree and neurological outcome.
For each BP parameter, the optimal cut-off of blood pressure drop for prediction of dramatic neurological recovery was 10.5 mmHg for SBP (sensitivity 0.54; specificity 0.55, area under ROC curve 0.55), 10.5 mmHg for DBP (sensitivity 0.38, specificity 0.70, area under ROC curve 0.54) and 8 mmHg for MAP (sensitivity 0.51, specificity 0.56, area under ROC curve 0.54). On multivariate analysis, after adjustment (Table 2), SBP drop remained as an independent predictor of achieving dramatic neurological recovery (OR 1.14 per 10 mmHg, 95% CI 1.01–1.29, p = 0.04). Figure 3 shows the ROC curve of this logistic model (area under the curve 0.79, sensitivity 0.67, specificity 0.79, positive predictive value 0.70, negative predictive value 0.76).
Predictors of dramatic neurological recovery after MT.
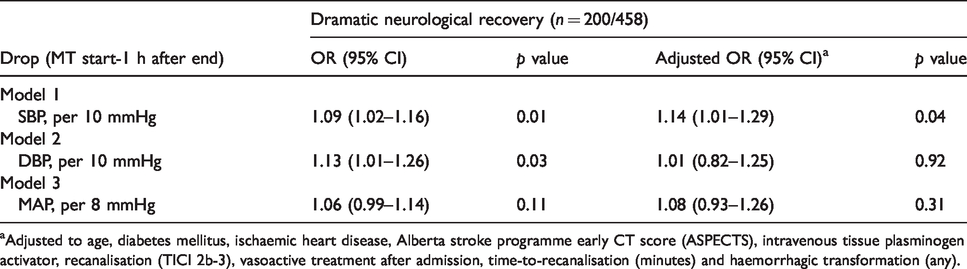
aAdjusted to age, diabetes mellitus, ischaemic heart disease, Alberta stroke programme early CT score (ASPECTS), intravenous tissue plasminogen activator, recanalisation (TICI 2b-3), vasoactive treatment after admission, time-to-recanalisation (minutes) and haemorrhagic transformation (any).
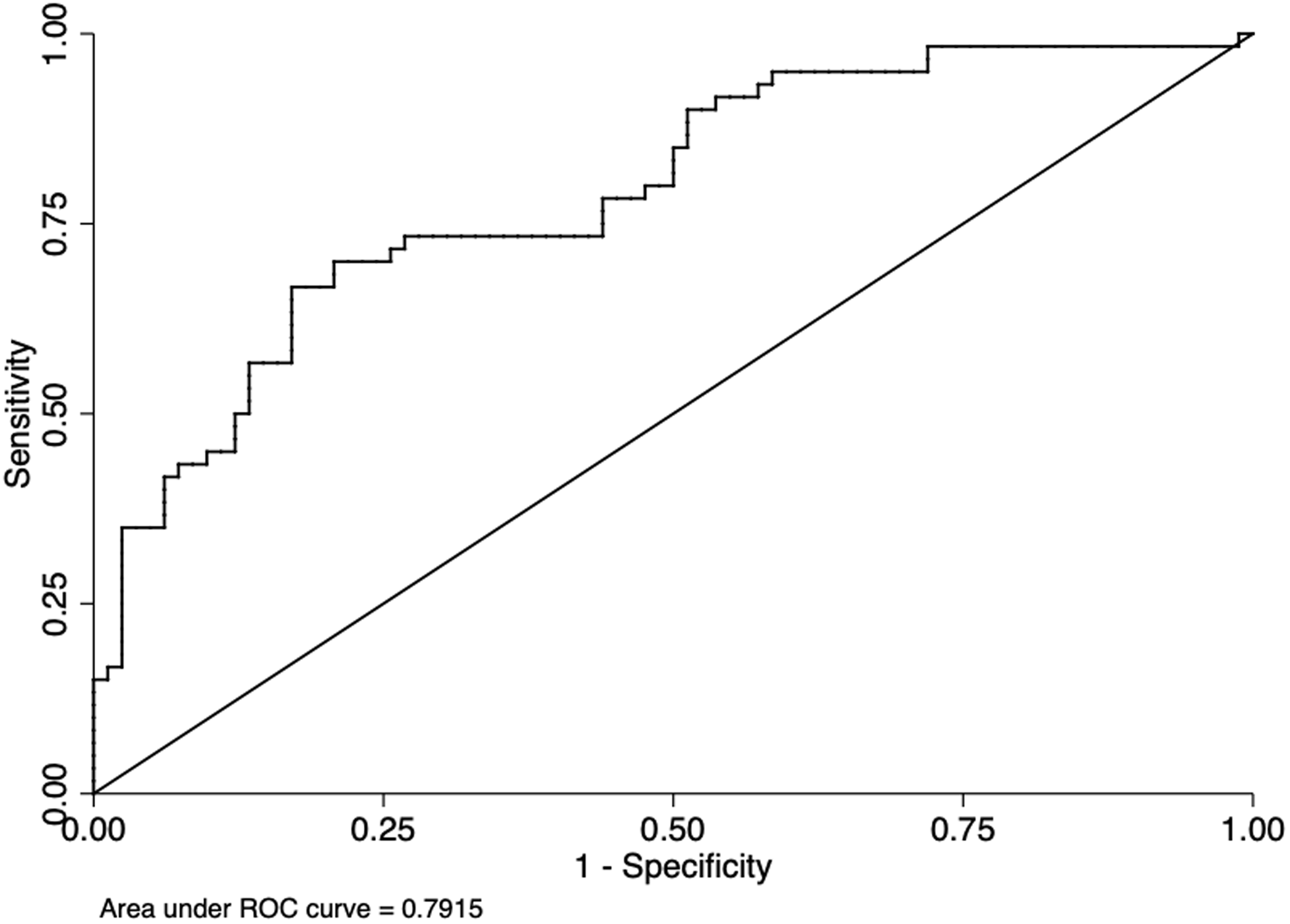
ROC curve of the multivariate logistic model for prediction of dramatic neurological recovery including SBP (drop per 10 mmHg) as an independent predictor. The area under the curve (0.79) indicates good discrimination ability. Sensitivity 0.67, specificity 0.79, positive predictive value (PPV) 0.70, negative predictive value (NPV) 0.76.
Discussion
The main finding of our study is that spontaneous SBP drop early after MT is an independent predictor of early dramatic neurological recovery. There are several studies demonstrating that recanalisation is not equal to reperfusion, being the latter a better predictor of good outcome.9–12 Furthermore, there are reports of absence of reperfusion in recanalised patients (due to severe damaged microcirculation) and reperfusion in up to 30% of non-recanalised patients (due to collateral circulation). 11 A recent study using transcranial Doppler performed immediately after MT found early postprocedural changes of cerebral haemodynamics after recanalisation and suggested that other factors besides recanalisation can have impact in clinical recovery. 13 We hypothesised that early (1 h after recanalisation) spontaneous SBP drop is a marker of successful reperfusion and, therefore, a marker of improvement of cerebral autoregulation due to the reduced final ischaemic core.
Our results are in line with previous studies that report a correlation between recanalisation degree and BP decline after successful recanalisation.4–6 Also, studies that have evaluated changes in BP 24 h after MT 3 report an inverse correlation of BP and good outcome (mRankin ≤ 2 after 90 days) in successfully recanalised patients. The most relevant finding of this work is that we have identified that SBP drop early after MT is a clinical biomarker of early recovery. This finding is also supported by the fact that lower SBPs from the 1st until the 24th hour after MT were associated with better outcome in this cohort (Table 1 of Supplementary Material).
Previous studies have reported association of BP variability after MT with poor outcome14,15 but this association was only verified in patients without successful recanalisation or with successful recanalisation but poor collaterals. If recanalisation is not achieved, the ischaemic area is more susceptible to BP changes due to the impaired cerebral autoregulation. Furthermore, one additional hypothesis could be that, in these patients, large infarct cores with disturbed cerebral autoregulation induce dysfunctional BP changes. Additionally, we found that a subgroup of patients without successful recanalisation and dramatic neurological recovery presented SBP drop 1 h after mechanical thrombectomy. Our hypothesis is that these patients have good collaterals, which would be associated with fast effective reperfusion and small infarct core, leading to an earlier haemodynamic normalisation. Unfortunately, we do not have data of collateral circulation status from our patients to confirm this hypothesis.
We could not find any association of BP drop with three months functional outcome at 90 days (mRS). After the initial effect of reperfusion, there may be several factors that influence three months outcome (including rehabilitation outcomes, complications and recurrences) which may obscure the effect of the SBP drop.
To remark, the association of SBP drop with good outcome was only seen from 1 h after the end of the MT and not immediately after MT. Our hypothesis is that the latter rather reflects BP drop during the MT, which can impair perfusion of the penumbra core before recanalisation and, instead, be associated with poor outcome.11–14 Therefore, a delay in recovery of autoregulation in stroke patients of at least 1 h after reperfusion may occur. However, we should acknowledge that this can be apparent sooner, but we are not able to demonstrate it because we do not have systematic BP measurements before 1 h after MT. Although we do believe that the BP drop results from the re-establishment of cerebral autoregulation, we cannot fully exclude a reverse causal relation, in which the dramatic neurological recovery would be a result of the reduced blood pressure.
Although this study was not designed to assess the effect of vasoactive medication administration after admission (including during MT), we found a significant negative association between administration of vasoactive medication and dramatic neurological recovery at 24 h. Most of these patients were treated with labetalol or urapidil to meet the recommended BP intervals before IV-tPa or MT and after recanalisation. The worse prognosis could be explained by a deleterious effect of the drugs themselves, but also by a higher rate of symptomatic haemorrhagic transformation or, in line with our results, by a persistent high BP (above guidelines thresholds) which is correlated with worse outcome. Also, it could be related to the BP variability during the procedure, which has been proposed in several studies as a marker of worse outcome.16–19 Our logistic regression was adjusted for vasoactive medication administration, thereby reducing the potential bias of this confounder. Furthermore, our data does not support the benefit of drug-induced BP lowering after MT, because in our patients the BP drop was spontaneous.
One of the major strengths of this study is that most of the patients were not submitted to general anaesthesia during procedure, reducing the potential bias of the effect of anaesthetic medication on BP. Another strength is the fact that the measuring and registering of BP hourly for the first 24 h in these patients are a standard protocol which improves the quality of the collected data.
Our study has some limitations. It is a retrospective study, although data were collected from a prospectively created stroke registry of all patients treated with MT in a comprehensive stroke centre. Patients admitted to the intensive care unit after MT were excluded due to of lack of available data, creating a potential selection bias. Although these patients are usually the most severely affected and haemodynamically instable, they were scarce in this cohort and we believe that it does not significantly influence our results. We did not access for the potential effect of anaesthetics on BP, the percentage of patients submitted to general anaesthesia was not significantly different between the compared groups and protocol used to perform general anaesthesia is usually the same in all the patients at this centre. Also, data on collateral status were not analysed. The results of this study are based on non-invasive BP measurements that may be less accurate that invasive BP measurements not routinely performed at this centre.
In our study, some established worse outcome predictors, such as older age, diabetes and lower ASPECTS, were associated with less probability of achieving dramatic neurological recovery. Although we adjusted for these confounders in the multivariate logistic regression models, persistent confounding by other non-measured variables, as collateral status, cannot be excluded.
Conclusion
Spontaneous SBP drop 1 h after mechanical thrombectomy is an early and independent predictor of good outcome.
Supplemental Material
sj-pdf-1-eso-10.1177_2396987320933384 - Supplemental material for Spontaneous systolic blood pressure drop early after mechanical thrombectomy predicts dramatic neurological recovery in ischaemic stroke patients
Supplemental material, sj-pdf-1-eso-10.1177_2396987320933384 for Spontaneous systolic blood pressure drop early after mechanical thrombectomy predicts dramatic neurological recovery in ischaemic stroke patients by Mariana Carvalho Dias, Denis Gabriel, Marlene Saraiva, Daniel Campos, Manuel Requena, Álvaro García-Tornel, Marian Muchada, Sandra Boned, David Rodriguez-Luna, Noelia Rodriguez-Villatoro, Jorge Pagola, Jesus Juega, Matías Deck, Marc Ribo, Alejandro Tomasello, Carlos A Molina and Marta Rubiera in European Stroke Journal
Supplemental Material
sj-pdf-2-eso-10.1177_2396987320933384 - Supplemental material for Spontaneous systolic blood pressure drop early after mechanical thrombectomy predicts dramatic neurological recovery in ischaemic stroke patients
Supplemental material, sj-pdf-2-eso-10.1177_2396987320933384 for Spontaneous systolic blood pressure drop early after mechanical thrombectomy predicts dramatic neurological recovery in ischaemic stroke patients by Mariana Carvalho Dias, Denis Gabriel, Marlene Saraiva, Daniel Campos, Manuel Requena, Álvaro García-Tornel, Marian Muchada, Sandra Boned, David Rodriguez-Luna, Noelia Rodriguez-Villatoro, Jorge Pagola, Jesus Juega, Matías Deck, Marc Ribo, Alejandro Tomasello, Carlos A Molina and Marta Rubiera in European Stroke Journal
Footnotes
Trial registration
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because it is a retrospective observational study with data collected from an anonymised database, and at this centre the patients routinely sign a consent form agreeing to participate on the registries and observational studies performed at the centre.
Informed consent
Informed consent was not sought for the present study because it is a retrospective observational study with data collected from an anonymised database, and at this centre the patients routinely sign a consent form agreeing to participate on the registries and observational studies performed at the centre.
Guarantor
MR.
Contributorship
MCD, DG, MS and MR researched literature and conceived the study, collected the data and performed the data analysis. MCD, DG and MR wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Acknowledgements
None.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.