
Abstract
Introduction:
Armenia is an upper-middle-income country with a population of nearly 3 million. Stroke is one of its major public health problems and ranks as the sixth leading cause of death, with a mortality of 75.5 per 100,000.
Methods and results:
Until recently, modern stroke care was not available in Armenia. During the past 8 years substantial advances have been made in building medical infrastructure and delivering acute stroke care. This manuscript describes contributors to this progress, including extensive and long-term collaboration with international stroke experts, the development of hospital-based stroke teams, and a funding commitment for stroke care by the government.
Conclusion:
The results of acute stroke revascularization procedures during the past 3 years are reviewed and found to meet international standards. Future directions are discussed including the immediate need to expand acute stroke care to underserved parts of the country by adding primary and comprehensive stroke centers. An active educational program for nurses and physicians and the TeleStroke system development will help support this expansion.
Keywords
Introduction
Armenia is considered an upper-middle-income country with a population of nearly 3 million. 1 Its population is aging.1,2 As of 2020, stroke was the sixth leading cause of death in Armenia, with a mortality of 75.5 per 100,000 population. 3 Advances in stroke prevention, therapeutic interventions for acute stroke, the development of stroke centers, and national organizations advocating for stroke care have lowered stroke incidence, morbidity, and mortality in high-income countries. 4 During the last four decades, while stroke incidence declined by 50% in high-income countries, it doubled in low- and middle-income countries, including Armenia. 5 Until recently, modern stroke therapies such as thrombolysis and mechanical thrombectomy were not available in Armenia. The existing stroke care was not organized as a national network. Significant steps have been taken in stroke care during the last 8 years to reflect state-of-the-art evidence-based practices. Their greatest impact has been on acute stroke treatment. Public education and primary and secondary prevention of stroke remain major challenges to be addressed. In this manuscript, we present the epidemiological data pertinent to stroke and summarize the recent advances, the current state, and plans for the future of stroke care in Armenia.
Stroke epidemiology in Armenia
Compared to high-income countries, Armenia has a relatively younger population. 6 Nearly 15% of its population is over 60 years of age, while the same age segment is 22% in high-income countries. 6 In 2019, life expectancy at birth was 75 years for the general population, 71.3 years for males, and 78.5 for females. Over the last two decades, the average life expectancy has improved by approximately 4 years. 7
The combined ischemic and hemorrhagic stroke incidence was 240.2/100,000, and the prevalence was 828/100,000 in 2020. 3 The ischemic stroke incidence was 185.3/100,000. 3 Ischemic strokes accounted for 78.9% of all stroke-related hospital admissions, while 16.4% were hemorrhagic strokes and 4.7% were subarachnoid hemorrhages. 3 When combined, cardiovascular and cerebrovascular causes were the leading cause of mortality in 2020, which has not improved over the last 5 years. 3 In 2020, 4180 patients with ischemic stroke, 865 with brain hemorrhage, and 252 with subarachnoid hemorrhage received medical care (Figure 1). 3
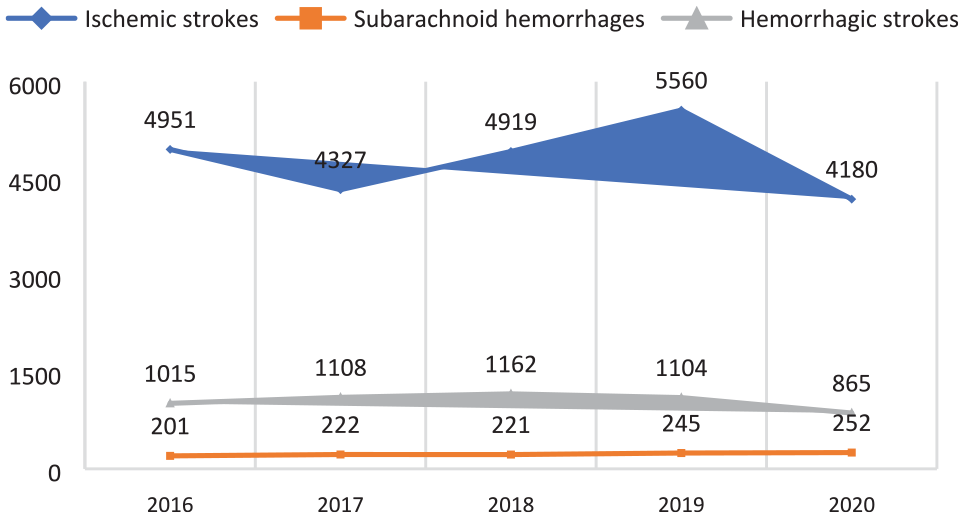
The number of patients received medical care in hospital (2016–2020).
The in-hospital case-fatality rate (Figure 2) was also very high at almost 16.0% for ischemic stroke and 41.7% and 40.2% for subarachnoid and intracerebral hemorrhage. 3 Overall, the in-hospital case-fatality rate for all cerebrovascular disorders was 21.0% in 2020. The average length of stay for patients with ischemic stroke was approximately 7 days. 3
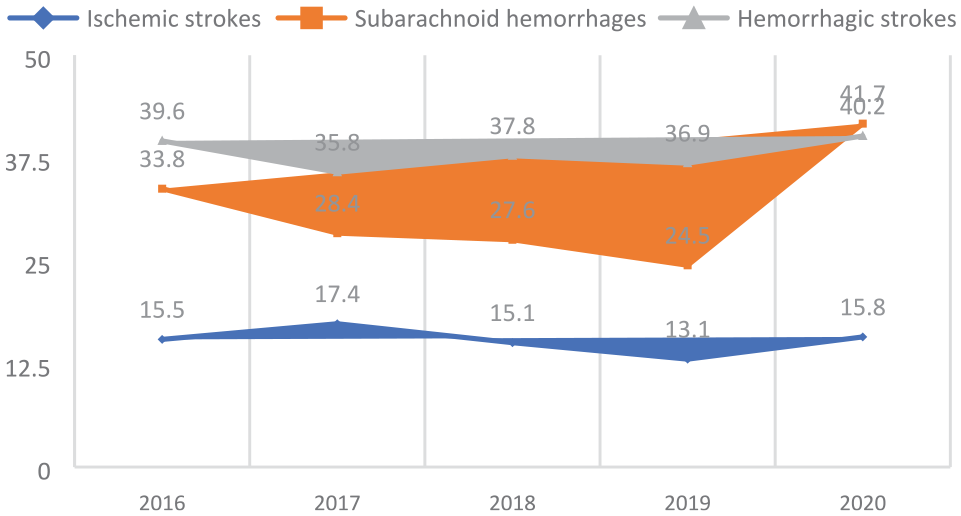
In-hospital case-fatality in Armenia (2016–2020).
Epidemiology of stroke risk factors
Reliable statistics regarding common vascular risk factors for stroke are lacking in Armenia, and available figures seem to be underestimations. However, major behavioral risk factors such as tobacco use, high salt intake, low physical activity, and other treatable risk factors such as high blood pressure, elevated cholesterol, obesity, and diabetes remain highly prevalent. 8 Among adults aged 18–69 years, the prevalence of high blood pressure is 38%, and of those diagnosed with hypertension, only 64% receive treatment. Blood pressure is controlled in only 16% of those receiving treatment. 9 The prevalence of hyperlipidemia and diabetes is 24% and 6%, respectively. Nearly half of adults (48%) are overweight (BMI ⩾ 25 kg/m2), and one-fifth (20%) are obese (BMI ⩾ 30 kg/m2). 9 Smoking remains a substantial modifiable risk factor. About 28% of Armenians in the 18–69 age group smoke, and nearly all smoke daily. 9 Almost 52% of men and 2% of women smoke, and secondhand smoke exposure is between 21% and 58%. 9 Average daily salt consumption is 9.8 g, 9 exceeding the World Health Organization (WHO) recommendations. 10 One fifth of adults (21%) report insufficient moderate-intensity physical activity, and the majority (78%) are not involved in vigorous-intensity activity.9,11
Evolution of stroke care in Armenia
The health system in transition
After the fall of the Soviet Union and the subsequent dissolution of the Soviet economic model, a quasi-privatization process was implemented in several socioeconomic sectors in Armenia, including healthcare. 12 In the early 2000s a new healthcare funding model was gradually introduced with only a few most essential health care costs covered by the state. In addition, several hospitals were transferred to private ownership, but many remained under the state’s ownership and governance. 12 Economic difficulties during the immediate post-Soviet era and the lack of political will emerged as major obstacles preventing the implementation of modern standards of care, including stroke care. The greatest difficulty was securing funding for costly interventions for acute stroke, including thrombolysis and thrombectomy. Although by 2016, thrombolytic therapy and mechanical thrombectomy were available in Yerevan, the capital, access to these interventions was limited only to those patients who could privately cover the costs. A fortuitous and productive collaboration, as detailed below, resulted in free and universal access to acute stroke care. In February of 2019, the National Stroke Program (NSP) was launched by the Government of Armenia. Initially, two hospitals, the Erebouni Medical Center (EMC) and the Yerevan State Medical University (YSMU) Hospital, both with experienced staff and technological capability, including Computed Tomography/CT Angiography, CT Perfusion, Magnetic Resonance Imaging/Angiography, conventional digital subtraction angiography for diagnostic and neurovascular intervention applications, were chosen as comprehensive stroke centers by the Ministry of Health (MOH). Currently, there are four stroke centers in Armenia, two of which are privately owned. The state currently funds acute stroke care whether the patient is seen at a private or a government-owned facility.
International collaboration
Dynamic and long-lasting academic collaborations were established in 2014 among an international faculty of stroke experts, EMC and YSMU. Stroke conferences in Armenia and abroad, regular lecture series, stroke case discussions, bedside teaching during hospital and clinical visits, international observership opportunities, joint sessions to develop stroke care pathways, and protocols suitable to local realities proved valuable tools for transferring knowledge. As a result of international collaboration, a stroke unit was opened at the EMC in May of 2014. The development of stroke care was further invigorated when Armenia joined the European Stroke Organization (ESO) in 2016. The Registry of Stroke Care Quality (RES-Q) program was activated that year. Several neurologists participated in the Angels program, which offers training for acute stroke care through case simulations. 13 This program is of great value and provides a unique experience to neurologists who are in the process of forming a stroke team. In 2017 the Stroke Advisory Task Force for Armenia (SIATA) was founded by stroke experts from Canada, France, Russia, and the US, to advance stroke education and care in Armenia by facilitating the transfer of scientific evidence and with a spirit of public service. Since its founding, SIATA has continued to serve its mission by advising and consulting with the network of stroke centers in Armenia. The Armenia Stroke Council (ASC) was founded by ministerial order in July of 2019 as a collaborative international scientific advisory and educational organization populated by several members of SIATA and a selected group of neurologists and neurosurgeons from Armenia with a proven track record in stroke care and education. Although established by order of MOH, the autonomy of ASC is fully respected by all stakeholders. The first task of the ASC was to update acute stroke treatment protocols and develop accreditation guidelines and procedures for existing and future stroke centers. Based on these guidelines, there are three comprehensive stroke centers in Yerevan, and one recently activated thrombectomy-ready center in Gyumri, the second largest city in Armenia.
Stroke education
Educating the general public and health professionals in medical and nursing schools or during post-graduate training are essential strategies to steer stroke-related statistics to more favorable outcomes. 14 Medical and nursing school curricula regarding stroke education appear to need significant modification. However, with the introduction of stroke protocols, the neurology residents rotating at stroke centers now have extended practical and didactic exposure to stroke. As a result, stroke training at the residency level has greatly improved during the last 2 years. Despite this progress, there still is much room for improvement in the training programs. There were no medical or surgical fellowship training programs in Armenia that taught up-to-date stroke care until recently. To close this gap, a Stroke Fellowship Program (SFP) has been developed by the Department of Neurology and Neurosurgery at the Armenia National Institute of Health (ANIH), which functions under the umbrella of the MOH. The SFP will be implemented in two phases. The first phase, the Bridging Fellowship Program (BFP), is a one-time, 6-month, didactic, and practical program tailored mainly to already practicing neurologists. Its goal is to provide additional training in stroke care expediently and adequately. The BFP was launched in March 2022 at the EMC. The EMC’s large number of stroke admissions, experienced staff, and neuroimaging capabilities make it an effective learning venue. The second phase of the SFP is designed as a 1-year program, mainly tailored to graduating neurology residents. It will eventually replace the BFP, providing more comprehensive training. The curriculum of SFP reflects current scientific concepts and clinical and interventional practices, and it is prepared by an international faculty. It is approved by the Department of Education of the ANIH and endorsed by the ASC. Clinical research and participation in multicenter trials are considered integral to the training program. The SFP will train physicians from all regions of Armenia to staff the additional stroke centers projected for the rest of the country. Along with the TeleStroke program, these steps will mitigate geographic and socioeconomic disparities in stroke care. The scope of stroke nursing practice remains very limited in Armenia, limiting nursing involvement in direct patient care. In collaboration with an international faculty, a lecture series was delivered for stroke nursing in January 2022. Substantial improvements are still needed in nursing education and practice to meet modern standards of stroke care, including ongoing monitoring and stroke scale administration.
Public education and stroke advocacy
Public education regarding many aspects of stroke, from prevention to prompt recognition of symptoms to the availability of acute stroke treatments, is considered paramount in staying ahead of the race against stroke. 15 Television and print and electronic media are being used to raise public awareness regarding stroke, and an enlarging segment of the population is making more informed decisions. However, more needs to be done in public education for stroke symptoms and modifiable risk factor recognition. Starting from primary schools, “healthy living messages” should be taken to all segments of society.
In Armenia, the concept and practice of community-based health advocacy groups or societies communicating with governmental bodies or local authorities are in their infancy. These activities are mainly carried out by the members of academic faculty members, stroke physicians, hospital administrators, professional medical organizations, SIATA, and ASC. However, increasingly, heightened public awareness is bolstering stroke advocacy.
Prehospital care
Emergency medical systems (EMS) play a key but highly varied role in stroke care globally, given differential stages of EMS development in each country. Armenia adheres to the Franco-German model of pre-hospital care with ambulances staffed by a physician, a nurse, and a driver in the capital city and the regions. 12 Ambulance physicians have not been consistently trained regarding rapid stroke rating systems. There are no well delineated geographic zones and guidelines in Yerevan to direct the transfer of patients to the nearest stroke center. This uncertainty carries the risk of “cherry-picking.” Although the MOH covers the cost of ambulance calls, many patients still choose transport by private car, further delaying diagnosis and care and accurate referral to a designated stroke center. Outside of Yerevan, suspected stroke cases are taken to the nearest regional hospital. The patients are often transferred to the EMC by ground or air transport if diagnosed with acute stroke.
The ambulance service is not under the direction of the MOH but is administered by local authorities. Keeping it outside of the governance of the MOH introduces a potential disruption in the creation of a seamless operation of stroke protocols from the patient’s home to the hospital. The ASC has voiced concerns regarding this arrangement. Thus, prehospital emergency care remains a weak link in stroke care in Armenia, and there are undoubtedly many opportunities for improvement in pre-hospital patterns of practice.
It is important to note that currently, there is little hospital-based emergency room care. When patients arrive at the hospital triage area, they are frequently seen by a non-emergency-trained on-duty physician. Stroke training of triaging physicians remains inadequate and inconsistent. Stroke team members are frequently called for patients who have not been screened for possible stroke by on-duty physicians.
Outcomes of the Armenian National Stroke Program
The Armenia NSP was launched in February of 2019. During the first 36 months of the program, 1230 patients received treatment for acute ischemic stroke. Of those, 486/1230 (39.5%) received intravenous thrombolysis (IVT) only, 546/1230 (44.4%) endovascular thrombectomy (EVT) only, and 184/1230 (15%) had both IVT and EVT. Data were missing for 1.1% (14/1230) of cases. Most patients received treatment at the EMC (1029/1230; 83.7%). Among non-thrombolysed patients the most frequent reasons for non-thrombolysis were admission delays, stroke severity (mostly mild), and advanced age; frequently non-thrombolysed patients had more than one exclusion criteria. However, the percentage of acutely treated patients was growing with every year (6.8% (377/5560) in 2019; 8.9% (372/4180) in 2020; and 8.7% (481/5554) in 2021) and was not largely affected by COVID situation. Table 1 summarizes patient and treatment-related data.
Outcomes of acute ischemic stroke revascularization therapy in Armenia from 2019 to 2021.
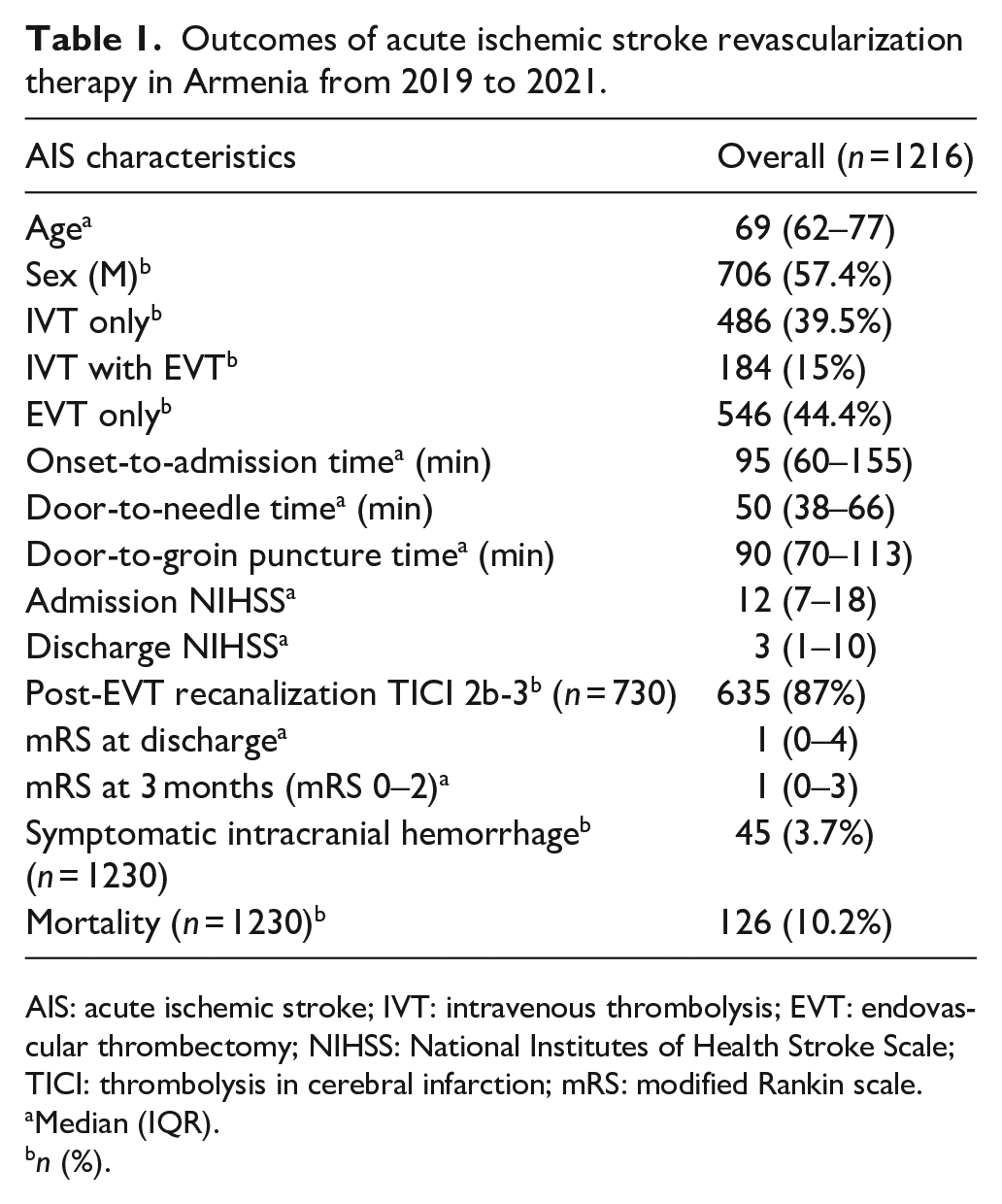
AIS: acute ischemic stroke; IVT: intravenous thrombolysis; EVT: endovascular thrombectomy; NIHSS: National Institutes of Health Stroke Scale; TICI: thrombolysis in cerebral infarction; mRS: modified Rankin scale.
Median (IQR).
n (%).
Funding of acute stroke care in Armenia
Stroke care is an expensive proposition for low- and middle-income countries.16,17 In Armenia, the median recombinant tissue plasminogen activator (rtPA) cost for a 50 mg vial is over seven times the allocated annual per capita health expenditure. 16 These economic realities have imposed financial restraints on health care funding. Approximately 5.7% of the Government’s yearly budget has been allocated to health care in recent years. 18 As of 2020, nearly 12% of the country’s gross domestic product (GDP) was allotted to health care, while public health expenditure constituted 2.4% of GDP. 1 These figures are much lower than in high-income countries, and they indicate that a large portion of the health care expenses is funded privately by patients and their families. Private health insurance programs remain underdeveloped, and the available programs are affordable only for a few.
To mitigate the financial burden of health-related expenses on the families, a state-sponsored program, the “co-payment,” was introduced in 2011. During subsequent years, the state’s contribution incrementally increased. The program covered significant expenses accrued for the treatment of subacute stroke, but it did not cover the costs of acute stroke treatment. The introduction of the Armenia National Stroke Program (NSP) by the MOH in 2019 was a significant undertaking as it provided funding for thrombolytic therapy and thrombectomy for acute stroke. Despite economic strains, the collaboration between the scientific advisory bodies, such as SIATA and ASC, and the MOH have allowed estimates to secure sufficient funding for acute stroke treatments in Armenia.
TeleStroke service and stroke care expansion program
The NSP described in the preceding paragraphs is centered mainly around resources in the capital city of Yerevan, home to approximately one-third of the country’s population. The geographic disparity in access to acute stroke treatment remains a significant problem for patients in the provinces. Unpublished data indicated that only 8% of the patients from distant provinces received treatment for acute stroke in 2019–2020. Expansion of the NSP is in progress. In March 2022, the first stroke center outside of Yerevan was opened in Gyumri, the second largest city in Armenia. The Gyumri Medical Center will serve a population of nearly 250,000. 19 Plans are underway to link it with a primary stroke center in another city 1 h away to expand its catchment area further. Telemedicine is part of acute stroke treatment programs in many parts of the world.20,21 ASC recommended the implementation of TeleStroke network to link peripheral and regional hospitals with the comprehensive stroke centers. In collaboration with ArMed, the national eHealth operator, the initial steps have been taken to set up a TeleStroke service between the Gyumri Medical Center and the EMC. This link will serve as a model for expanding the TeleStroke service throughout Armenia.
Discussion
The introduction of state-of-the-art acute stroke treatment was delayed in Armenia, but the last 8 years have witnessed rapid advances. The results of the acute stroke revascularization procedures presented in Table 1 are encouraging and meet international standards. Contributors to this progress consist of extensive collaboration between local and international stroke experts facilitating knowledge transfer and development of hospital stroke teams, a pre-existing solid cadre of motivated physicians, the decision of the MOH to initiate the NSP, and the willingness of the private sector to make substantial investments, particularly in neuroradiological equipment, such as magnetic resonance imaging (MRI) and computerized tomography angiography (CTA), and stroke ward development. Major hurdles remain. Although the medical culture of Armenian health care professionals is changing, it needs more time to evolve. Pre-hospital EMS care and hospital-based emergency room care, and stroke referral network development present opportunities for improvement. As in many post-Soviet countries, stroke risk factors remain highly prevalent and are not optimally mitigated. Furthermore, financial constraints remain key determinants for individual choices in seeking treatment. Available medical data are also not consistently solid. For example, epidemiological data are often incomplete and probably under-estimate prevalence and incidence because of incomplete and retrospective recording. The need for a prospective national stroke database is recognized, and there are early plans to organize it in the near future. These challenges are unlikely to change rapidly and will require long-term planning.
Conclusion and future directions for stroke care in Armenia
The past 5 years have witnessed substantial advances in building the medical infrastructure and delivering acute stroke care in Armenia. Active stroke centers now exist in the country’s two largest cities, and care is provided to the population irrespective of their ability to pay. These substantial successes have geographical limitations with a significant divide between urban and rural populations. The immediate need is to expand acute stroke care to underserved parts of the country by adding TeleStroke capability and additional primary and comprehensive stroke centers. The program is expected to evolve to meet the population’s needs and to optimize care. The long-term plan is five-fold: first, public education regarding the management of stroke risk factors, a collaborative effort between the MOH, ASC, and the larger medical and nursing community; second, the monitoring of the quality of care provided and outcomes at the different stroke centers. This requires establishing quality of care standards and monitoring the centers’ results at regular intervals. Because it funds the majority of the acute stroke treatments, the MOH has access to quality measures, and the ASC provides the expertise to assess them. Third, the continuous education and further development of physicians, nurses, and healthcare professionals in cerebrovascular diseases, particularly in areas of advanced expertise, such as neuroradiology, that are not well developed. As indicated in the preceding paragraphs, courses geared toward nurses and neurologists have already been organized by the ASC, the EMC, and the plan is to continue with them. Fourth, is expansion of the NSP to hemorrhagic stroke. Fifth, is the establishment of outpatient stroke clinics at the major acute stroke centers. This presents another cultural change in medical care, as outpatient stroke clinics do not yet exist in Armenia. The goal can be achieved in the context of the NSP initiative, which we believe can serve as a model for countries in transition, many of which may face challenges similar to those encountered in Armenia.
Footnotes
Acknowledgements
We would like to thank Members of The Armenia Stroke Council: Dr. Aghajanyan Armine, Dr. Aghasaryan Manvel, Dr. Babikian Viken Levon, Dr. Badalyan Sevak, Dr. Baghdasaryan Zhora, Dr. Chekijian Sharon, Dr. Fanarjyan Ruben, Dr. Grigoryan Arthur, Dr. Grigoryan Mikayel, Dr. Hovhannesyan Gurgen, Dr. Hovhannisyan Yekaterina, Dr. Khachatryan Samson, Dr. Muratoglu Mikael Skon, Dr. Sahakyan David, Dr. Sanossian Nerses, Dr. Soghoyan Armine, Dr. Tanashyan Marine, Dr. Yeghiazaryan Nune, Dr. Zubalova Lina for their assistance and guidance in this research. We also would like to thank prof. Valeria Caso for motivation, encouragement, and for external review of the manuscript.
Contributorship
NY, AI, and SC wrote the first draft of manuscript, LZ, YH, GS, and MA did data collection, data entry and analysis. SK, MM, VB provided critical edits and guidance in drafting the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Data have been obtained from an anonymized official reports of individual comprehensive stroke hospitals, therefore, there was no need for specific informed consent.
Ethical approval
Data have been obtained from an anonymized official reports of individual comprehensive stroke hospitals, approval of Ethics Committees for data collection was not required, but patients or their representatives were informed of anonymous data collection and offered the possibility to withdraw.
Guarantor
NY.