
Abstract
In Turkey, the incidence of acute stroke is increasing, obviously with the contribution of the aging population. With the publication of “Directive on Health Services to be Provided to Patients with Acute Stroke” on July 18, 2019 and its entry into force in March 2021, an important period of catching up and updating has begun in the management of acute stroke patients in our country. During this period, 57 comprehensive stroke centers and 51 primary stroke centers were certified. These units have covered approximately 85% of the country’s population. In addition, around 50 interventional neurologists were trained and became the directors of many of these centers. In the following 2 years, the “inme.org.tr campaign” was launched. This campaign, aimed at increasing the public’s knowledge and awareness about stroke, continued unabated during the pandemic period. Now is the time to continue the efforts to ensure homogeneous quality metrics and to develop and continuously improve the established system.
Stroke epidemiology in Turkey
Turkey’s population is approximately 86 million, corresponding to almost 1% of the world’s population. It is appropriate to add the immigrants, mainly from Syria and Afghanistan exceeding 5 million, to this number. Three quarters of the population live in cities, and approximately 7.5% of them are 65 years or older. Average life expectancy is 75.6 years for men and 81.2 for women. 1 With the development of the welfare level in Turkey, life expectancy has been getting longer in recent years. With the contribution of this, the frequency of stroke has been increasing gradually. In Turkey, the incidence of ischemic stroke is 93.2–108.6 per hundred thousand, intracerebral hemorrhage is 31.5–39.7, and total stroke is 141.7–158. 2 In Turkey, there were 435,941 deaths in 2019. The most common cause for mortality was cardiovascular diseases (36.8%), and stroke ranks second place (22.2%) after coronary syndromes in this subgroup. Stroke is the third most common cause of mortality in women and fourth in men. From 2002 to 2017, stroke mortality increased by 56%. 3
Directive on health services to be provided to patients with acute stroke: Publication and entry into force in Turkey
The fact that acute stroke is treated with intravenous tissue plasminogen activator (IV tPA) and/or neurointerventional methods, which can only be applicable within a certain period of time, requires a referral and management system that should cover the majority of the country. On the basis of this reality, the “Directive on Health Services to be Provided to Patients with Acute Stroke” was published by Turkish Ministry of Health on July 18, 2019. 4 While it was expected to take effect a year later, it was postponed to March 2021 due to the pandemic. Afterward, 57 comprehensive stroke centers (named as “Stroke Center”) and 51 primary stroke centers (named as “Stroke Unit”) were certified in the approximately 1-year period from March 2021. The distribution of centers within the country is shown in Figure 1.
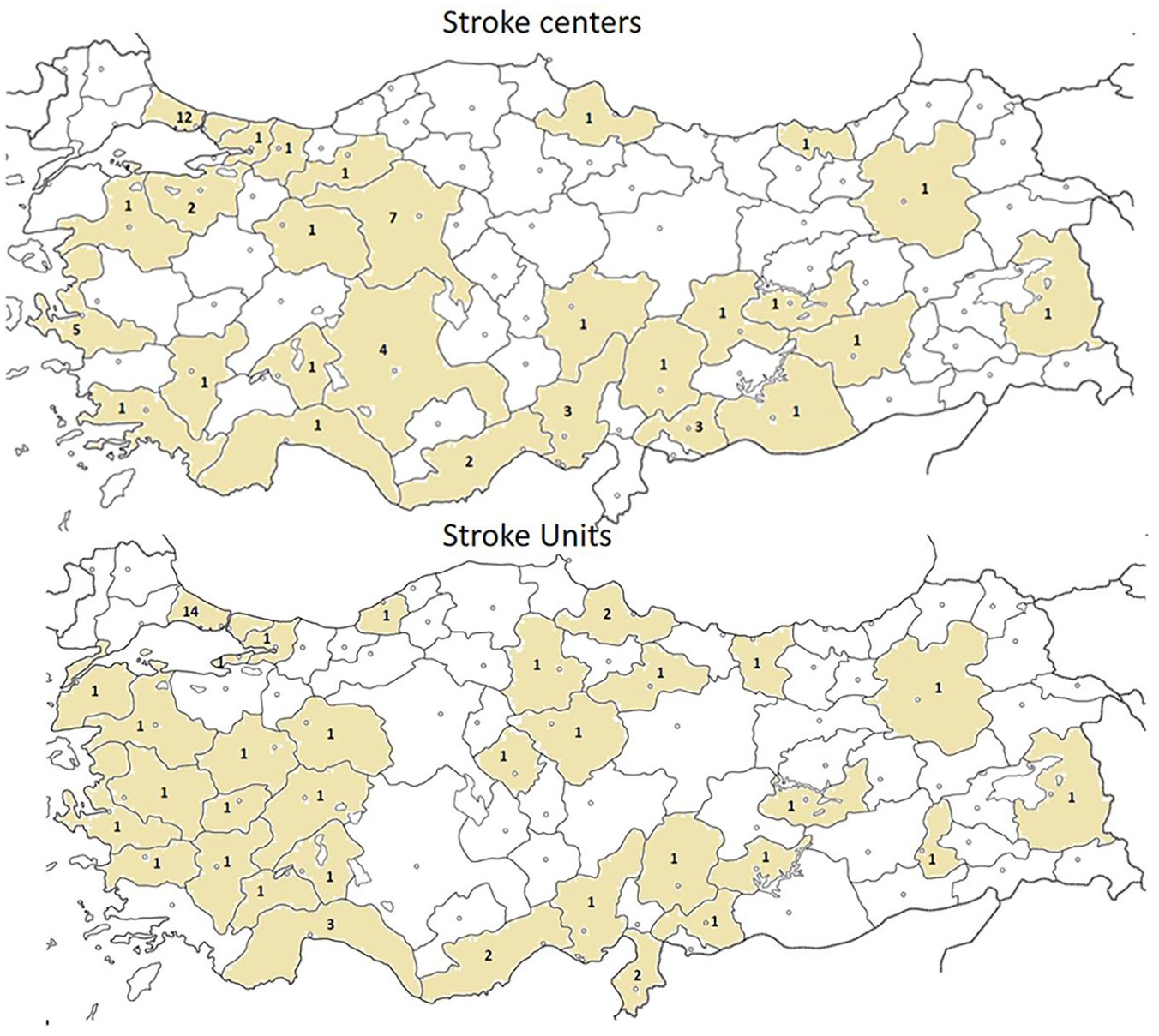
Distribution of stroke centers and units. Distribution of stroke centers (top) and stroke units (bottom) in Turkey. According to the provincial population-based analysis, stroke units covered 60.3% of Turkey’s population (84.7 million as of 13.03.2022), and stroke centers 70.5%. The total population of the provinces without stroke units and centers is around 13 million, which corresponds to 15.4%.
Organization of stroke system of care in Turkey
In the Annex-1 of this directive, hospitals involved in in acute stroke system of care in Turkey are organized in two categories as “stroke units” and “stroke centers.”
“Stroke units” are an adaptation of “the primary stroke centers” for our country. These hospitals are generally located in small settlements where IV tPA can be administered and patients who do not need critical and advanced neurological management methods can be hospitalized. The in-patient units of these hospitals must contain a minimum of four dedicated beds. The hospital should be capable of performing 7/24 of computed tomography (CT) and CT angiography. Stroke units are expected to operate in coordination with the stroke center on a regional basis. Provincial health directorates usually take a position in the creation of this regional system of acute stoke care.
Stroke centers include neurology intensive care units, angiography suits where all kinds of neurointerventional procedures can be performed, as well as advanced imaging, operation, care and monitoring utilities/facilities available on 24/7 basis. Acute ischemic stroke cases with major cerebral vascular occlusion and requiring neurological intensive care, and almost all acute intracerebral and subarachnoid hemorrhages are managed in stroke centers (Table 1).
Stroke units/centers minimum requirements.
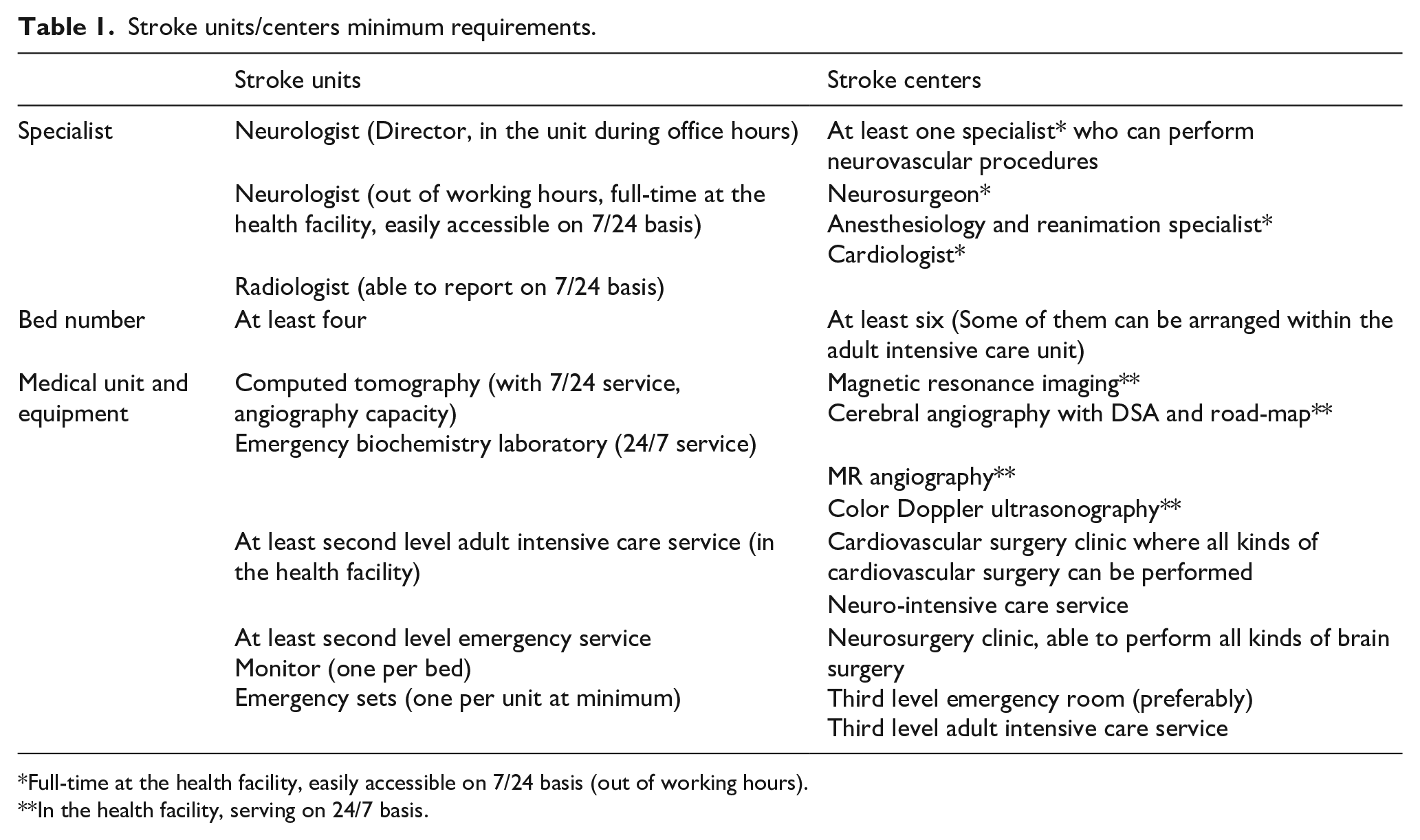
Full-time at the health facility, easily accessible on 7/24 basis (out of working hours).
In the health facility, serving on 24/7 basis.
The stroke directive has also implemented several key rules that are critical to the functioning of these two types of centers. The first, all kinds of medical management procedures of acute stroke patients will be carried out under the responsibility of the neurologist appointed as the stroke unit and stroke center director. The second, neuro-interventional procedures can be performed by neurology, cardiology, radiology, and neurosurgery specialists who meet defined competency requirements. Specialist physicians who will perform neurointerventions must have done at least 100 intracranial neurointerventions. At least 10 of these intracranial interventions should include mechanical thrombectomy or thromboaspiration. Specialists who will perform neurointerventions must have performed at least 20 extracranial neuroendovascular therapeutic interventions (such as Carotid stent) in the head and neck region. The list of neurointerventions is given in Table 2. It is mandatory to document the protocol number of the cases in which these neurointerventional procedures were performed, together with the angiography reports and, if requested, video recordings of the procedure. The validity of the documents is evaluated by the national scientific commission. The capacity and technical standards of the angiography suites in stroke centers are also clearly stated in the directive (Table 1). The third, stroke centers and units where interventional procedures are performed are first registered with local certification and then central certification by the national acute stroke science board. Finally, each stroke unit and center takes place in the management network or in a system linked to it, which is planned to operate at the country level. 4
List of neurointerventional processes*.
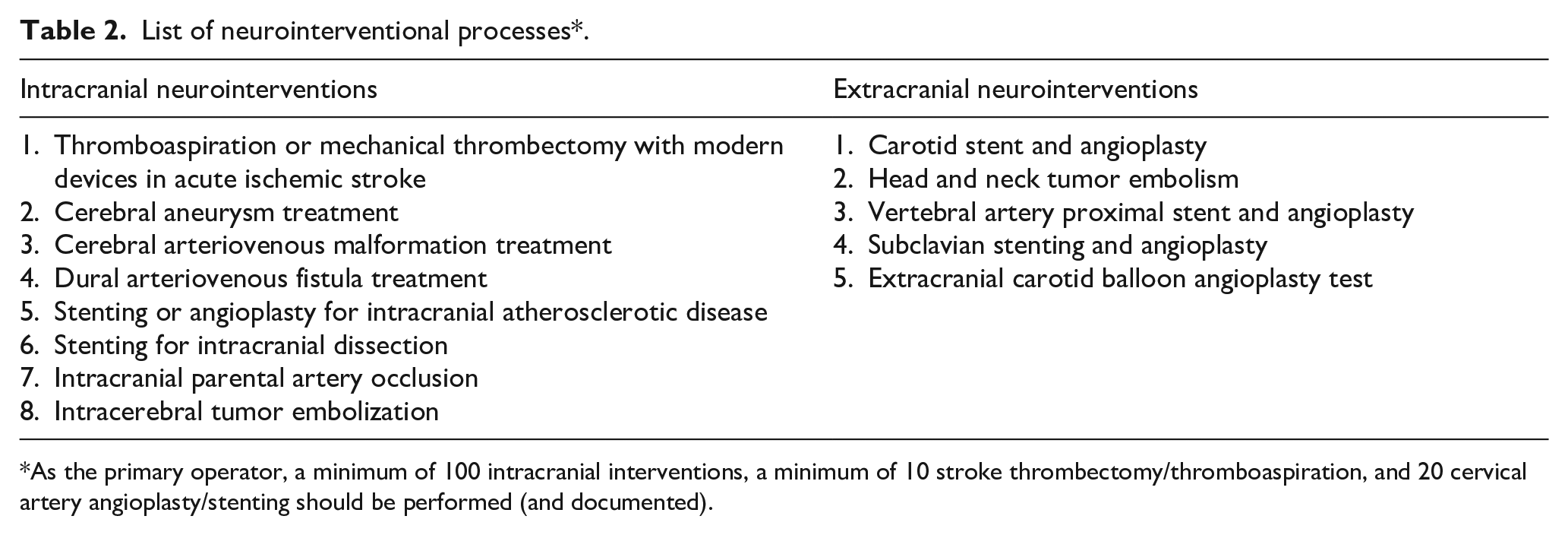
As the primary operator, a minimum of 100 intracranial interventions, a minimum of 10 stroke thrombectomy/thromboaspiration, and 20 cervical artery angioplasty/stenting should be performed (and documented).
In the process leading up to the stroke directive, “the national Stroke clinical protocol” 5 and “Stroke diagnosis and treatment guideline” 6 were published by the Turkish Ministry of Health with high degree academic cooperation of Turkish Society of Cerebrovascular Diseases and Turkish Neurology Society. In addition, these two societies supported the directive by publishing guidelines and algorithms such as “Use of IV tPA in acute stroke,”7,8 “Nursing care and hospital processes in stroke,” 9 “Non-vitamin-K oral anticoagulant (NOAC) use,” 10 “Cerebral edema and treatment in acute stroke,” 11 “Guidelines for the treatment of acute stroke in the COVID pandemic.” 12
IV tPA and neurointerventional treatment in Turkey: A short story and current situation
Intravenous tissue plasminogen activator (IV tPA) was approved by the Ministry of Health of the Republic of Turkey in March 2006, approximately 10 years after Europe. 13 The drug is covered in full reimbursement. Estimated utilization rate in acute stroke patients is about 3%. A national database does not exist. The use of tPA in stroke meets contemporary quality criteria, as demonstrated in the Turkish National Intravenous Thrombolysis Registry 14 and a meta-analysis compiling published local case series. 15 In the latter, an analysis of 2349 cases in 21 publications documented that the mean age was 65 years, the mean symptom-to-needle time was 111 min; pre-tPA National Institutes of Health Stroke Scale (NIHSS) score was 13.8, mean good prognosis at 3 months (Modified Rankin’s score-mRS ⩽ 2) 59.6%, mortality 16.5%, and symptomatic IV tPA-related intracerebral hemorrhage 5.6%. 15 In the recently published Turkish Endovascular Stroke Registry, where 975 patients were analyzed, the mean age was 65 years, the mean NIHSS 16, the good prognosis at 3 months (mRS ⩽ 2) was 43%, the mortality was 24%, and symptomatic bleeding was 13.6%. 16
In order to increase the use of IV tPA by neurologists in acute ischemic stroke, 19 certified courses were held in 17 provinces in 3 years between 2017 and 2019 in cooperation with the Turkish Society of Neurology and the Turkish Society of Cerebrovascular Diseases. Nearly 500 neurologists completed this training program where more than 50 trainers took a role. In addition, 16 neurologists received short-term IV tPA scholarship for comprehensive stroke centers in 2017–2018 with a program managed by the Turkish Neurological Society. In this context, the Turkish Neurological Society published the first edition of the Acute Stroke IV tPA user manual in 2017 and its second edition in 2019. The society-endorsed informed consent forms of IV tPA usage and drip-and-ship procedures are also included in this handbook.
The results of the MR CLEAN study, 17 which opened a new era in acute ischemic stroke, were announced at the ninth World Stroke Congress held in Istanbul on October 25, 2014. 18 Following this event which had taken place in our country, a high-degree neurointerventional training campaign sparkled among neurologists in Turkey. By the end of 2021, almost 50 neurologists had completed neurointerventional training under the structural program that was certified by Turkish Neurological Society and Turkish Cerebrovascular Disease Society and started working in stroke centers. What is pleasing is that almost all of these centers are newly introduced centers. In 2021, neurologists directly performed more than half of acute stroke thrombectomies in the country. Turkish interventional Neurology training campaign was conducted by Prof. A. Özcan Özdemir working in Eskisehir Osmangazi University Stroke Center. In the following years, neuroendovascular training centers were opened in Gaziantep and Istanbul.
“Inme.org.tr” campaign and population-level awareness
The Turkish Society of Cerebrovascular Diseases run a nation-wide campaign to overcome the obstacles preventing acute stroke patients from reaching treatment, and work in a non-stop manner to raise social awareness about acute stroke to the higher level. 19 Starting from 29 October 2020, the World Stroke Day, in the 2020–2021 pandemic period, this effort has been carried to a further dimension with introduction of website named as “www.inme.org.tr.” The motto of this campaign is “stroke cure = early intervention.” (Figure 2). In this campaign, informative announcements and news were made on radio and television programs, on our websites and on other social media facilities without any interruption. News and information about stroke were published in the newspapers. Educational posters were placed on billboards in the subways, buses, common areas, municipal facilities, parks, and squares in the cities. Our banners took place at the national football league matches. Stroke patient handbooks, t-shirts, masks, name badges and badges were prepared for clinics and distributed free of charge. The short film competition titled “Are you aware?” was an important stage of this campaign. In these activities, it is always aimed to inform the population with short and clear messages and to change the lifestyle.
English version of one of the posters used in the campaign.
Near future expectations
The time has come to establish an integrative organization of stroke units and centers, a nationwide management network, and develop a quality-based acute stroke system. And, it is the time for official definition of the personal rights of stroke nurses, physiotherapists, and language-speech therapists and other disciplines who will take part in the team headed by the neurologist directing management and care in the neurological intensive care and stroke units and angiography suits. The workforce of neurologists who can manage neurological and neurointerventional treatments to a desired level should be increased in a short time. These neurologists will adopt and implement the modern stroke system of care, drawn in the directive in our country, provide scientific stroke management uninterrupted. It is our effort and expectation that all of them will be implemented in the near future. The European Stroke Organization (ESO) and the Stroke Alliance for Europe (SAFE) will be our indispensable stakeholders in this regard.
Footnotes
Author contributions
MAT and AOO researched literature, conceived the study, and were involved in data collection. MAT wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
It is a review and not a study involving patients.
Ethical approval
Ethical approval was not obtained because it was a review type article.
Guarantor
Mehmet Akif Topcuoglu