
Abstract
Introduction:
Establishment of a prospective stroke registry may promote the documentation and improvement of acute stroke care. We present the status of stroke management in Greece using the Registry of Stroke Care Quality (RES-Q) dataset.
Methods:
Consecutive patients with acute stroke were prospectively registered in RES-Q registry by contributing sites in Greece during the years 2017–2021. Demographic and baseline characteristics, acute management, and clinical outcomes at discharge were recorded. Stroke quality metrics, with a specific interest in the association between acute reperfusion therapies and functional recovery in ischemic stroke patients are presented.
Results:
A total of 3590 acute stroke patients were treated in 20 Greek sites (61% men, median age 64 years; median baseline NIHSS 4; 74% ischemic stroke). Acute reperfusion therapies were administered in almost 20% of acute ischemic stroke patients, with a door to needle and door to groin puncture times of 40 and 64 min, respectively. After adjustment for contributing sites, the rates of acute reperfusion therapies were higher during the time epoch 2020–2021 compared to 2017–2019 (adjusted OR 1.31; 95% CI 1.04–1.64; p < 0.022; Cochran-Mantel-Haenszel test). After propensity-score-matching, acute reperfusion therapies administration was independently associated with higher odds of reduced disability (one point reduction across all mRS scores) at hospital discharge (common OR 1.93; 95% CI 1.45–2.58; p < 0.001).
Conclusions:
Implementation and maintenance of a nationwide stroke registry in Greece may guide the stroke management planning, so that prompt patient transportation, acute reperfusion therapies, and stroke unit hospitalization become more widely accessible, improving the functional outcomes of stroke patients.
Introduction
Stroke is a major cause of mortality and disability worldwide, presenting an increasing incidence during the last decades. 1 In Greece, the incidence of stroke, as extrapolated from a prospective population-based study in North Eastern Greece, has been calculated to more than 530 strokes per 100,000 person-years, which is one of the highest rates in South-Eastern Europe. 2 Furthermore, all-cause mortality at 1-year post-stroke was reported at 34.7%, while the stroke recurrence at 1-year was also significant (6.7%). 3 However, nowadays, effective treatments, regarding both acute management and secondary prevention therapies, exist and continue to expand, and should become readily available for stroke patients. 4 Prompt patient transportation to a stroke-ready center, 5 delivery of acute reperfusion therapies in cases of acute ischemic stroke (AIS), 6 hospitalization in dedicated stroke units, 7 early rehabilitation assessment, 8 and thorough patient evaluation regarding the etiopathogenetic stroke mechanism shall be all provided with the aim of post-stroke functional recovery. Nationwide implementation of a stroke management plan becomes even more important when considering the rapid aging of the Greek population 9 and the potential further increase of stroke incidence, stroke-associated dependency, and societal costs. 10
To facilitate the efforts toward stroke management implementation in Greece, the development and maintenance of national stroke registries may help understand the current status of stroke care by providing objective quality metrics and identifying any potential implementation gaps. 11 Establishment of a web-based, prospective registry system for acute stroke care quality surveillance seems feasible and may promote the documentation and improvement of early treatment and care of acute stroke.12,13 To that aim, the European Stroke Organisation – Enhancing and Accelerating Stroke Treatment (ESO-EAST) program has developed a platform for data collection and established a stroke quality registry for use primarily in Eastern Europe (but later worldwide, as well), which was launched in 2016; the Registry of Stroke Care Quality (RES-Q) registry. 14
Greece has been participating in RES-Q registry since 2017, registering stroke patients during a 5-year time period. Using these prospectively collected data, we aim to characterize the status of stroke management in Greece by retrospectively analyzing and presenting stroke quality metrics, with a specific interest in confirming the association between acute reperfusion treatment delivery and functional recovery in AIS patients.
Methods
Consecutive patients with acute stroke were prospectively registered in the RES-Q registry by contributing sites in Greece during the years 2017–2021. Participation and data completion in the RES-Q registry were available through an online platform which was free for noncommercial use and was developed as an initiative of the ESO-EAST Project. 15 The study was approved by the local Ethics Committee of “Attikon” University Hospital (decision number EBΔ37) which was the coordinating center of the RES-Q registry in Greece; signed informed consent was obtained from the patients or their legal representatives before enrollment in all cases.
Patient inclusion
Patients presenting with any type of acute stroke, including AIS, intracerebral hemorrhage (ICH), transient ischemic attack (TIA), subarachnoid hemorrhage (SAH), or cerebral venous thrombosis (CVT), that were evaluated at the emergency department (ER) of each site and were admitted for further management, were considered eligible. Exclusion criteria were patients younger than 18 years old, diagnosis at discharge other than stroke (i.e. stroke mimics), and lack of informed consent.
Data collection
Demographic characteristics (age, gender) were collected for all included patients. Furthermore, the baseline characteristics of the index event were also recorded, including stroke type, date and time of stroke onset, hospital admission, and initial stroke severity, as assessed by certified neurologists using the National Institute of Health Stroke Scale (NIHSS) score. 16 Acute management at the ER was registered, including prompt imaging evaluation (defined as a CT/MRI brain imaging within 1 h from ER admission) and acute reperfusion therapy in cases of AIS. All patients were treated according to the standard of care.17–20 Specifically, in cases of AIS, intravenous thrombolysis (IVT), endovascular treatment (EVT), or bridging therapy (i.e. combination of IVT and EVT) was offered according to current guidelines and site availability.21–23 Time metrics, such as door to needle (DTN) time and door to groin puncture (DTG) time, were registered in the cases that acute reperfusion treatment was performed.
Subacute management and further assessment during hospital admission were also recorded. Hospitalization in a stroke unit or intensive care unit (ICU), need for mechanical ventilation, rehabilitation assessment and screening for dysphagia, atrial fibrillation (AF), and carotid arteries stenosis were among the included variables in the registry. Status regarding Coronavirus Disease 2019 (COVID-19) during the years of the pandemic (2020–2021) was also recorded. Discharge destination and medical instructions at discharge, including drug prescriptions (anithrombotics, statins, antihypertensives), smoking cessation, and scheduled follow-up appointments were collected.
The outcomes of interest were the clinical outcomes at discharge, which were assessed and recorded using the modified Rankin scale (mRS). 24 An excellent clinical outcome was defined as an mRS score of 0 or 1 and a good clinical outcome (FI) was defined as an mRS score between 0 and 2.25,26
Statistical analyses
Categorical variables are presented as number of patients with the corresponding percentages. Continuous variables are presented as mean ± standard deviation (normal distribution) and as median with interquartile range (IQR, skewed distribution). Statistical comparisons between categorical variables were performed using χ2 test, or in case of small expected frequencies, Fisher’s exact test. Continuous variables were compared using the unpaired t-test or Mann–Whitney U test, as indicated. Acute reperfusion treatment rates in AIS patients were compared between two specified time epochs (2020–2021 vs 2017–2019), after adjustment for contributing sites, using the Cochran-Mantel-Haenszel test and generating an adjusted odds ratio (OR) with corresponding 95% confidence intervals (CI).
A propensity score matching (PSM) analysis was applied for the assessment of reperfusion treatment and clinical outcomes at discharge specifically for the AIS patients. 27 After dichotomization according to receiving acute reperfusion treatment, patients in the treatment group (patients receiving reperfusion treatment) were matched to control group patients (patients not receiving reperfusion treatment). For matching, a propensity score model was used, including all baseline characteristics, initial stroke severity, and site of admission. The corresponding propensity score of the treatment variable (acute reperfusion treatment) was calculated for each subject and a nearest neighbor matching algorithm with a 1:1 allocation was subsequently implemented to match eligible patients in the treatment group to patients in the control group. 28 To determine whether the propensity score matching approach achieved balance in all potential confounders, we compared all baseline characteristics of patients in the treatment group to their control patients, before and after propensity score matching.29,30 In the propensity score matched groups, the ORs with corresponding 95% CIs were calculated for the following outcome events of interest: (1) excellent clinical outcome rates at discharge; (2) good clinical outcome rates at discharge; and (3) functional improvement at discharge quantified by the distribution of 3-month mRS scores between the two groups using ordinal logistic regression analysis.
Statistical significance was achieved if the p value was ⩽0.05. Statistical analyses were performed with the Statistical Package for Social Science (SPSS Inc, Armonk, NY, US; version 23.0 for Windows) and RStudio: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria), with the use of the “MatchIt” package (matching software for causal inference) for matching patients across the two groups.
Data availability statement
All data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Results
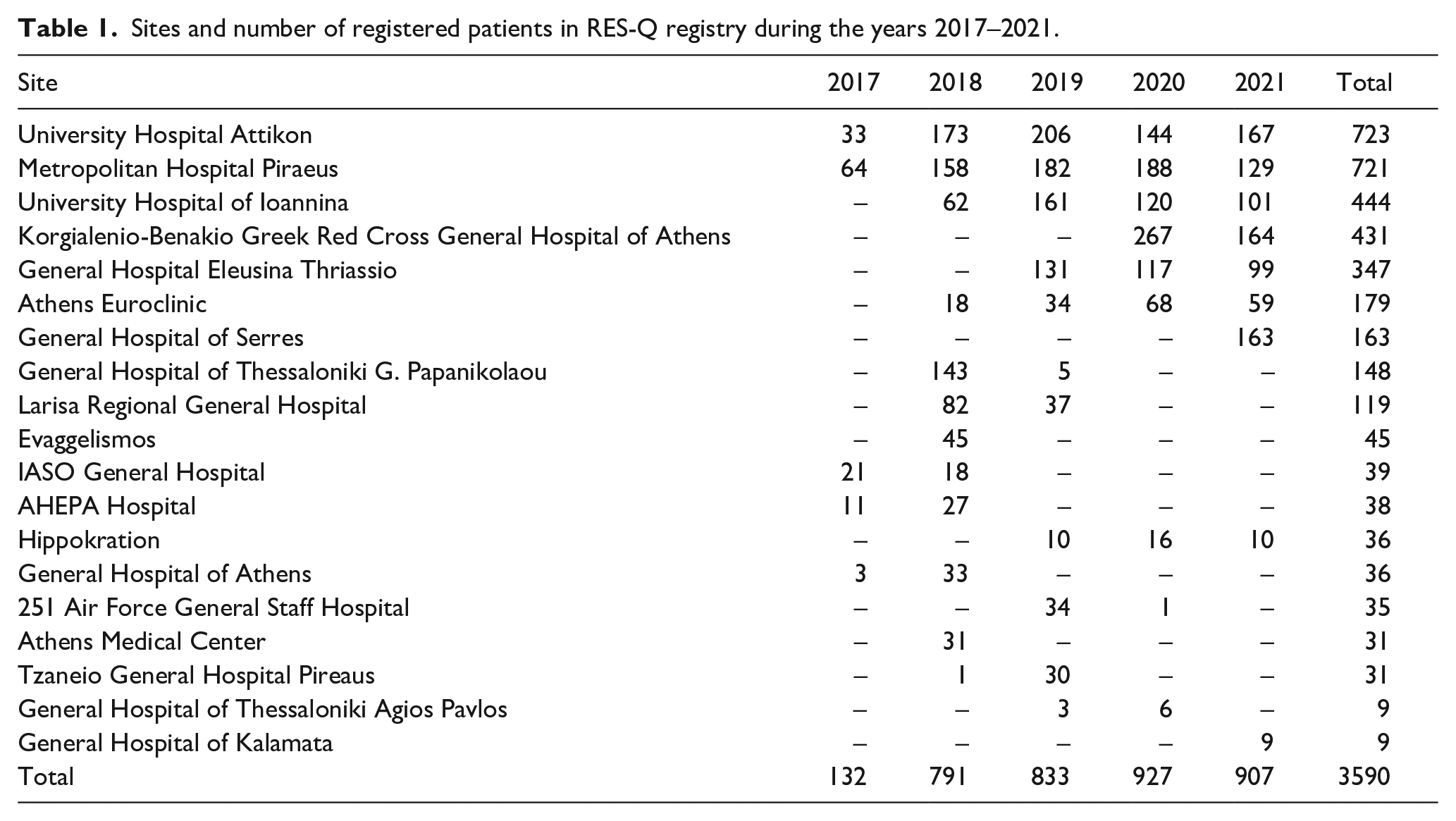
Twenty sites in Greece (Figure 1) that are responsible for the management of stroke patients in the acute setting have contributed with data in the RES-Q registry during the years 2017–2021. Two centers (University Hospital “Attikon” and Metropolitan Hospital Peiraeus) have maintained patient registration throughout a 5-year duration. Three centers registered patients for 4 years, while the rest continued patient registration for 3 years or less. However, the absolute number of patient registration has remained stable throughout those years (Table 1).
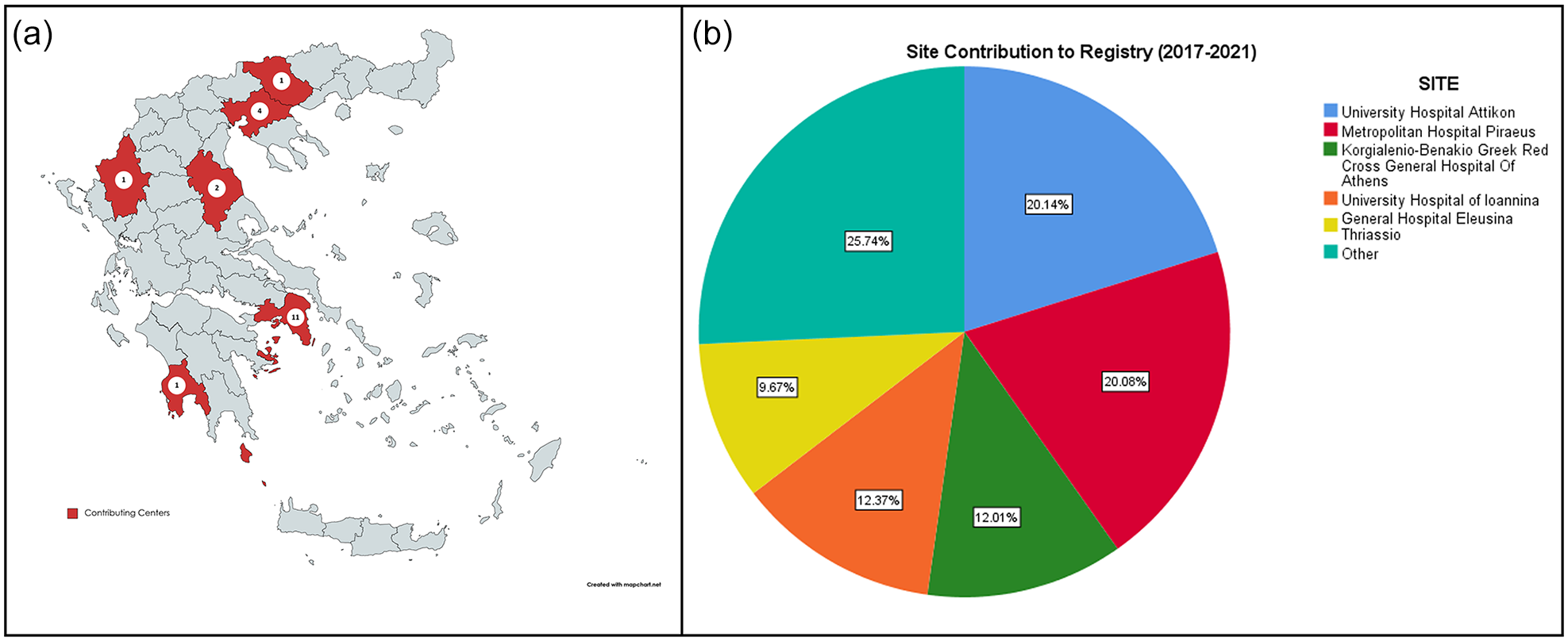
Geographical distribution of the Greek sites participating in the RES-Q registry. The majority of participating sites are located within the prefecture of Attica (n = 11; Panel (a)). Pie chart presenting the percent of registered patients for each site. Sites contributing with less than 5% of patients were collapsed. Five sites have contributed with almost 3/4 of the total registered population (Panel (b)).
Sites and number of registered patients in RES-Q registry during the years 2017–2021.
Overall, 3590 patients were prospectively registered (61% men, median age 64 years (IQR 55–74)). 74% of patients had an AIS (n = 2668), 12% presented with TIA and another 12% with ICH. About 1% and 0.5% had SAH and CVT, respectively. Stroke type remained undetermined in only five cases (0.1%). Almost 13% of the included patients had a history of prior stroke. In-hospital stroke was observed in 3.2% of cases.
During initial management in the emergency department, 90% of the patients underwent neuroimaging (brain CT or MRI) within 1 h after admission, while NIHSS evaluation was performed in 76% of the patients. Median NIHSS on admission was 4 (IQR 2–10).
Acute reperfusion treatment was offered in 20% (n = 525) of AIS patients. Among cases receiving reperfusion treatment, 80% were treated with intravenous thrombolysis (IVT) only, 8% received bridging therapy, and 12% received endovascular therapy (EVT) only. All sites except one (General Hospital of Kalamata, which contributed only eight patients overall) were administering IVT, while EVT was available and performed by eight sites. Regarding the patients receiving IVT, DTN time was 40 min (IQR 7–58), and for those undergoing EVT, DTG time was 64 min (IQR 16–116). Shortening of DTN time was observed in sites that maintained patients’ registration for 5 years with more than 85% of patients receiving IVT within 60 min compared to sites that included patients in the registry for less than 5 years (76%, p < 0.001). DTG time was not associated with the duration of registry participation (p = 0.480), possibly due to the small number of procedures. Continuous registry participation was not shown to correlate with the rates of acute reperfusion treatment administration (p = 0.152). However, when adjusted for contributing sites, the rates of acute reperfusion therapies were higher during the time epoch 2020–2021 compared to the time epoch 2017–2019, despite the COVID-19 pandemic (adjusted OR 1.31; 95% CI 1.04–1.64; p < 0.022; Cochran-Mantel-Haenszel test).
Less than 1/3 (31%) of the patients were admitted in a dedicated stroke unit or ICU, while the majority (67%) were hospitalized in standard beds in neurological wards or other general wards. Acute reperfusion therapies were associated with higher odds of admission in Stroke Unit/ICU (OR 2.67; 95% CI 2.42–2.95; p < 0.001), with almost 2/3 (63%) of the patients receiving IVT, EVT, or bridging therapy being hospitalized in Stroke Units/ICUs. Furthermore, hospitalization in Stroke Unit/ICU was also related with the maintenance of stroke registry by the contributing sites, with higher rates of admission in Stroke Unit/ICU for sites that continued patients’ registration for 5 years (54%) compared to sites that withdrew from the registry during the 5-year period (16%, p < 0.001). Dysphagia screening test was performed within the first 24 h of hospitalization in almost 80% of patients, while 3.8% of patients needed mechanical ventilation during hospitalization.
Screening for atrial fibrillation (AF) was performed in 84.9% of AIS and TIA patients, leading to the detection of AF in 7.2% of patients, either at admission or during hospitalization. Prior history of AF was present in 12.2%, while the presence of AF was not investigated in 15.1% of the patients. Screening for AF significantly varied across the contributing sites (p < 0.01; χ2 test), with four sites registering more than half of their patients as unknown AF status. Carotid arteries imaging within 7 days of the index event was performed in 83.4% of AIS and TIA patients, out of whom 9.2% displayed a hemodynamically significant carotid stenosis (>50%). Carotid endarterectomy or angioplasty/stenting was performed during the acute phase (within the first 2 weeks after stroke onset) in 28.1% of the patients with symptomatic carotid stenosis, while another 5.9% was referred to another center for acute management. Finally, rehabilitation evaluation was performed in 57.6% of patients within the first 72 h post-stroke.
Eleven centers presented data regarding the COVID-19 status of their patients during the first 2 years of the pandemic (2020–2021). In early 2020, screening for COVID-19 was restricted to patients that presented COVID-19-associated symptoms due to testing capacity limits, leading to an unknown status of COVID-19 in 60% of the hospitalized stroke patients. However, in 2021, a massive screening program for all inpatients was implemented and more than 92% (n = 786) of the stroke patients were tested, out of whom 1.7% (n = 14) tested positive for COVID-19.
After a median of 5 days of hospitalization (IQR 7), 78% of patients were discharged home, while 17.5% were transferred to another department or to a social care facility, for further rehabilitation. Antithrombotics were prescribed in 95.8% of AIS or TIA patients, while statin treatment was initiated in 79.2% of them. Among patients with AF-related AIS or TIA, 73% were prescribed anticoagulants, 12.5% of them were treated with vitamin-K antagonists, 80.7% were treated with direct oral anticoagulants, and 6.8% received low molecular weight heparin at therapeutic dose. Antihypertensive treatment was prescribed in 66.8% of stroke patients. Smoking cessation was recommended in 81.1% of stroke patients that had history of smoking. Upon discharge, follow-up appointment with a cerebrovascular expert was scheduled in 63.7% of patients.
Median mRS score at discharge was 1 (IQR 0–3). An excellent clinical outcome at discharge was achieved in 60.1% of patients and a good clinical outcome at discharge was noted in 71.3%. In-hospital mortality was 3.1%. Baseline characteristics, management, and clinical outcomes at discharge are summarized in Table 2.
Baseline characteristics, management, and clinical outcomes at discharge of the study population (n = 3590).
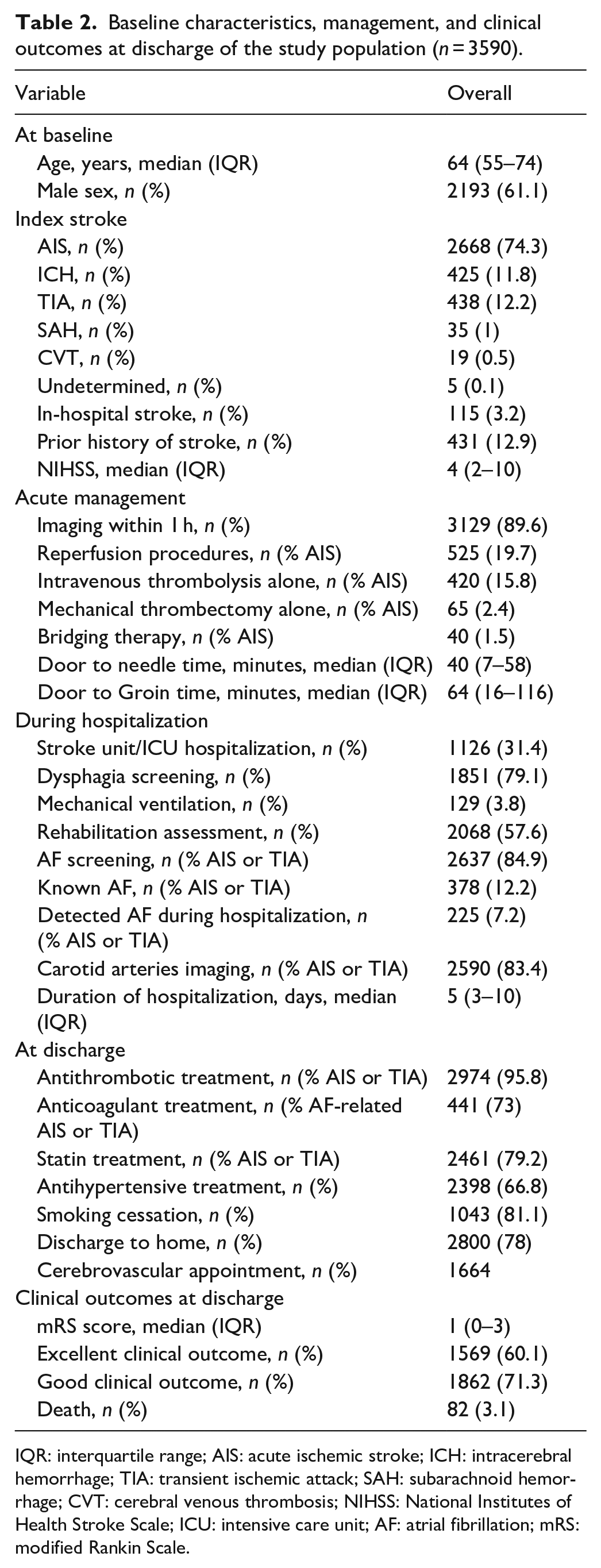
IQR: interquartile range; AIS: acute ischemic stroke; ICH: intracerebral hemorrhage; TIA: transient ischemic attack; SAH: subarachnoid hemorrhage; CVT: cerebral venous thrombosis; NIHSS: National Institutes of Health Stroke Scale; ICU: intensive care unit; AF: atrial fibrillation; mRS: modified Rankin Scale.
With respect to AIS patients, a propensity score matched (PSM) analysis was performed, in order to balance for baseline differences that could influence the likelihood of receiving acute reperfusion therapy. After PSM analysis, 296 patients that received reperfusion therapy were matched to 296 controls, resulting in no differences regarding demographic factors (age, gender), baseline characteristics (in-hospital stroke, recurrent stroke, initial stroke severity), and contributing site (Table 3). In this matched population, reperfusion therapy was positively associated with both excellent clinical outcomes (OR 1.88; 95% CI 1.35–2.61; p < 0.001) and good clinical outcomes at discharge (OR 1.95; 95% CI 1.40–2.72; p < 0.001; Figure 2). After propensity score matching, acute reperfusion therapies were independently associated with higher odds of reduced disability (one point reduction across all mRS scores) at hospital discharge (common OR 1.93; 95% CI 1.45–2.58; p < 0.001; Figure 3). Finally, delivery of acute reperfusion therapy was not associated with in-hospital mortality (OR 0.87; 95% CI 0.31–2.44; p = 0.794).
Baseline characteristics of patients with acute ischemic stroke who received acute reperfusion treatment versus controls before and after propensity-score matching (PSM).
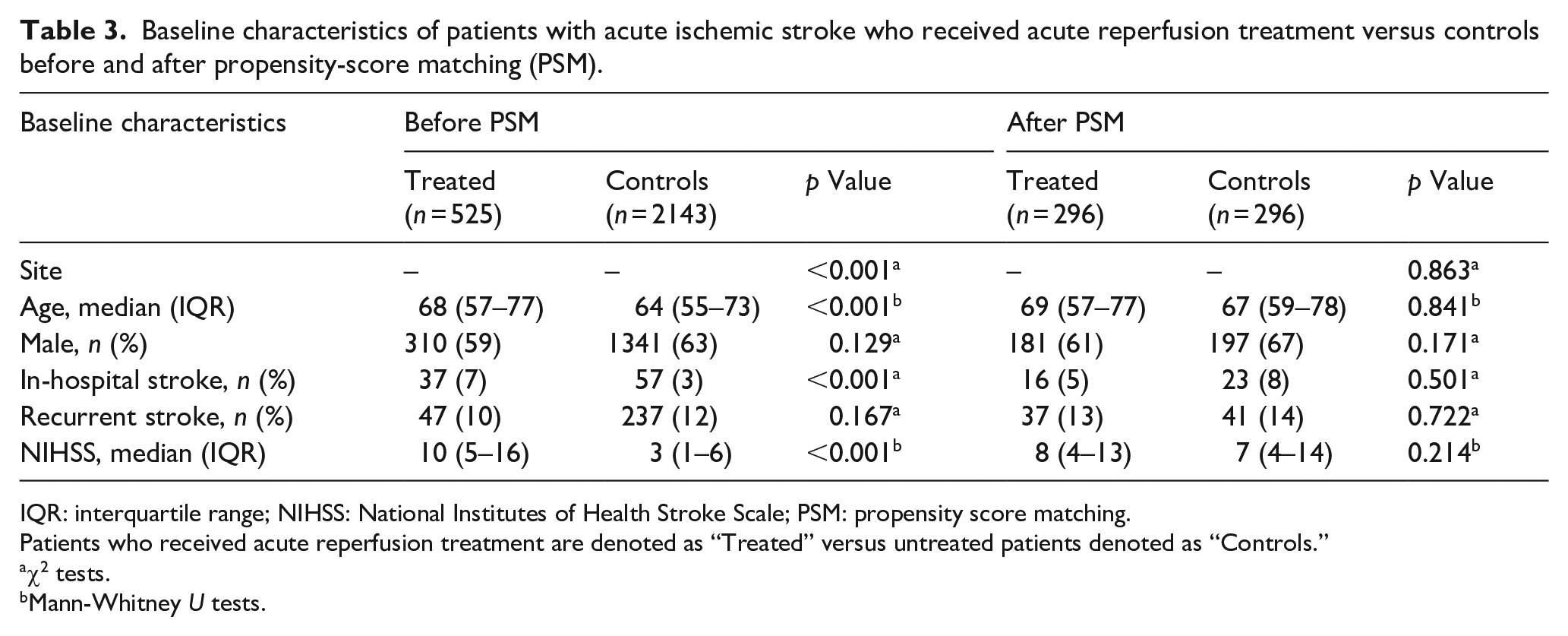
IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; PSM: propensity score matching.
Patients who received acute reperfusion treatment are denoted as “Treated” versus untreated patients denoted as “Controls.”
χ2 tests.
Mann-Whitney U tests.
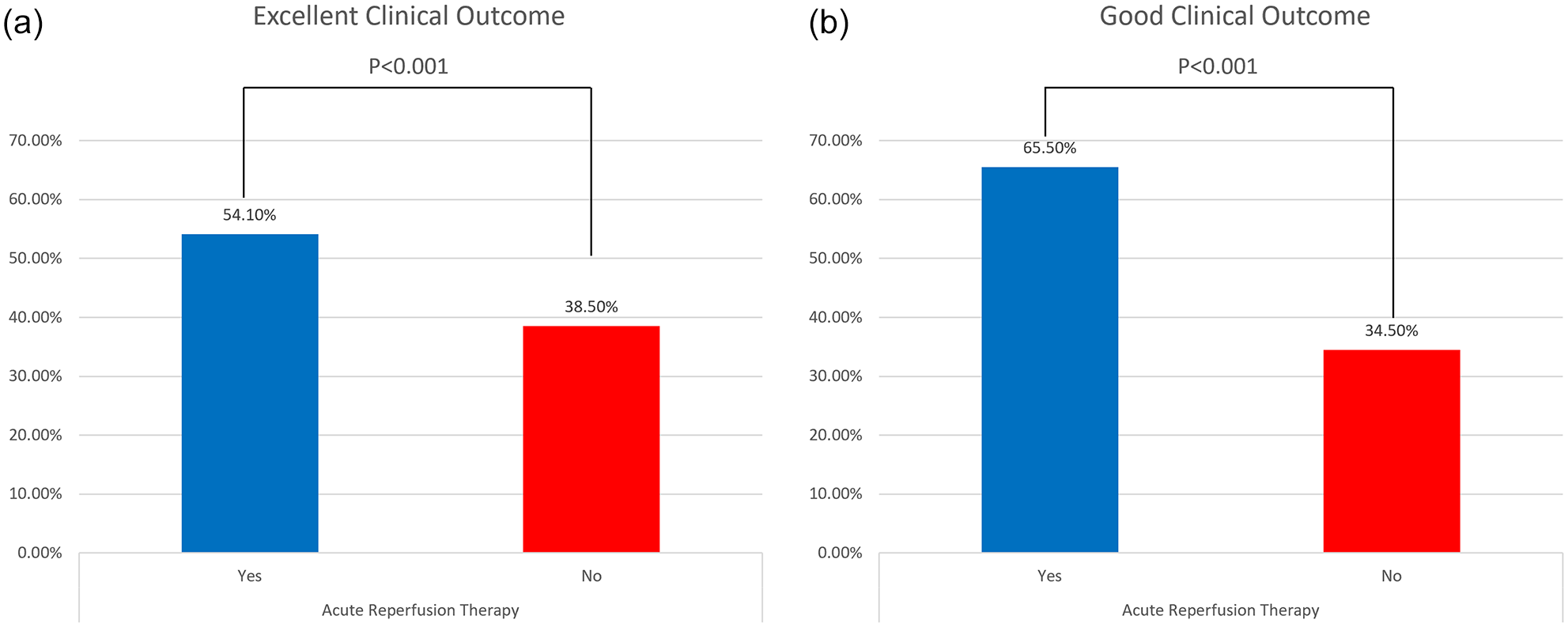
Bar chart depicting the association of acute reperfusion treatment and excellent clinical outcome at discharge of acute ischemic stroke patients in Greece (OR 1.88; 95% CI 1.35–2.61; p < 0.001; Panel (a)). Bar chart depicting the association of acute reperfusion treatment and good clinical outcome at discharge of acute ischemic stroke patients in Greece (OR 1.95; 95% CI 1.40–2.72; p < 0.001; Panel (b)).
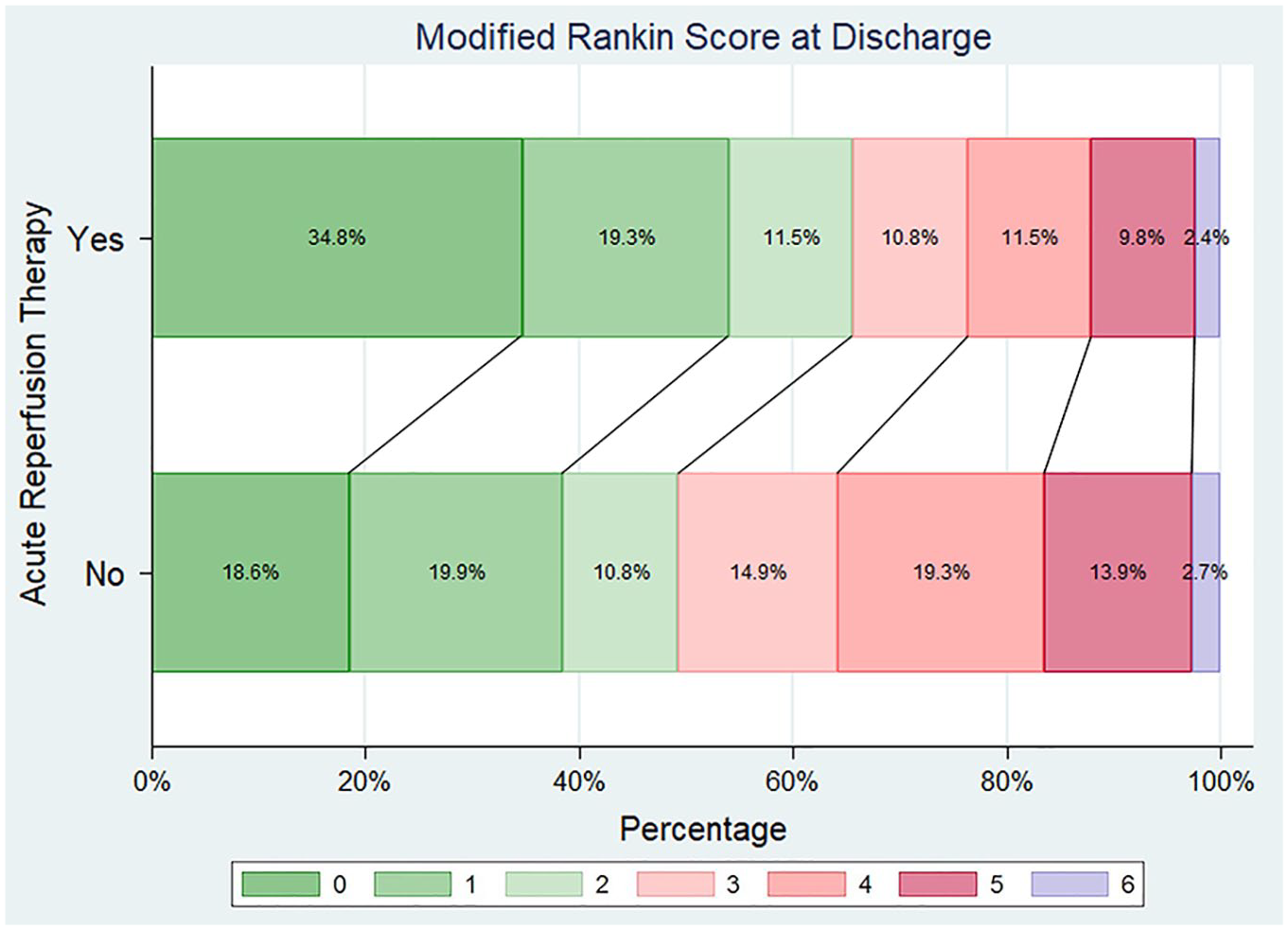
Distribution of modified Rankin Scale scores at discharge (Grotta bars) in the two treatment groups. Acute reperfusion therapies were independently associated with higher odds of reduced disability (one point reduction across all mRS scores) at hospital discharge (common OR 1.93; 95% CI 1.45–2.58; p < 0.001).
Discussion
The total number of patient registrations in RES-Q registry remained stable throughout the years 2017–2021 in Greece, with more than 3500 included patients in total. However, not all sites maintained the registry utilization throughout this 5-year period, with a median of 9 out of 20 sites (IQR 2) being active each year. Excessive workload of the medical personnel, who is most commonly involved in patient registries completion, may have accounted for the temporal dropouts of the sites in data collection for the registry of several sites. COVID-19 pandemic may have additionally contributed to discontinuation of ongoing clinical research, including continuing registrations in databases.31,32 On the other hand, harmonization to one nationwide registry may offer additional advantages, such as acknowledging potential gaps regarding stroke care quality in one site compared to others, providing clinical data and information that are derived from a larger proportion of the Greek population, directing efforts toward future stroke action plans based on nationally representative data with the aim to become applicable in different sites and areas of Greece.33,34
The geographical features of Greece, consisting of numerous islands covering the 16.7% of the total country area and a rather mountainous mainland, should also be considered. 35 Such a particular terrain complicates prompt patient accessibility to primary or comprehensive stroke centers and this may have significant implications for efficient stroke management, 36 especially when considering that older population predominantly lives in rural areas. 37 Measuring accessibility and addressing potential disparities in stroke care between urban and rural territories is a highly important step for designing a successful stroke management infrastructure. 38 However, representation of different prefectures of Greece in the registry is poor, as shown in Figure 1, with more than half of participating centers being located within the prefecture of Attica, which covers approximately 40% of Greek population. Therefore, no firm evidence exists regarding stroke care quality in the rural areas, highlighting the need for increased awareness in the smaller, peripheral, stroke-ready centers to utilize a nationwide registry and to become an active part of the stroke action plan. 39 Nowadays, involvement of stroke-ready hospitals in stroke management might be further supported by the use of telemedicine, 40 which appears to be a promising tool in Greece, 41 and has been increasingly utilized since the COVID-19 pandemic. 42
Acute reperfusion treatment was offered in almost 20% of AIS cases, which is comparable with other European cohorts during similar time periods. 43 As evident by time metrics (DTN and DTG times), acute reperfusion treatment was administered quite promptly, suggesting an accelerated triage and effective acute management once the patient has arrived at the hospital. Specifically for IVT, DTN time in our cohort during the period 2017–2021 decreased compared to a previously published Greek cohort from the Safe Implementation of Thrombolysis in Stroke: International Stroke Thrombolysis Register (SITS-ISTR) registry during the time epoch 2002–2017 (40 (IQR 50) vs 67 (IQR 42) minutes, respectively). 44 Furthermore, more patients received IVT within the golden hour in sites that maintained registry participation during the 5-year period, confirming that stroke registries implementation may improve time metrics in stroke care. 34 Certainly, there is still room for improvement, in order to further reduce time delays in treatment administration and achieve shorter targets for DTN and DTG.43,45 Importantly, the odds of receiving acute reperfusion therapies increased by 30% in the time epoch 2020–2021 compared to the time epoch 2017–2019, pointing toward a wider implementation of acute stroke pathways allowing for prompt treatment delivery, despite COVID-19-associated restrictions to the healthcare system and persistent declines of acute stroke hospitalizations during both the first and the second wave of the pandemic in Greece.46,47 Notably, when massive COVID-19 screening became available, COVID-19 was diagnosed in 1.7% of acute stroke patients; a rate which is in accordance with previous studies and further implies the association between COVID-19 and cerebrovascular events.48,49
Baseline stroke severity, as measured by the NIHSS-score, was higher in AIS patients that received acute reperfusion therapies compared to those that did not (median NIHSS 10 points (IQR 5–16) vs 3 points (IQR 1–6)). This finding may indicate that clinicians tend to treat with IVT and/or EVT patients with more severe AIS, while they are more conservative and refrain from offering reperfusion therapies in milder strokes. However, IVT has been associated with improved clinical outcomes both at discharge and at 3-month follow-up among AIS patients with mild stroke severity (NIHSS-score 0–5).50,51 Furthermore, several deficits, that are perceived as mild or cannot be even captured with the NIHSS, may have an important impact on everyday functionality and lead to substantial disability of patients. 52 Therefore, clinicians should be more critical and avoid a priory excluding AIS patients with milder strokes from IVT. Data regarding endovascular treatment for mild AIS due to large vessel occlusion are less conclusive, with several cohorts providing conflicting results.53–55 An individualized approach may be considered based on the degree of disability, perfusion mismatch, and collateral circulation status, 56 at least until ongoing randomized controlled clinical trials in this field provide more definitive results.57,58
When baseline characteristics, including stroke severity, were balanced among patients treated and not treated with acute reperfusion therapies using propensity score matching, we documented an independent association between IVT and/or EVT with improved clinical outcomes at discharge. This finding confirms that delivery of acute reperfusion therapies is safe and effective in real-world evidence settings in a Southern European country like Greece. This observation also highlights that further actions should be undertaken to increase the availability of acute reperfusion therapies across the whole Greek territory.
In Greece, hospitalization in dedicated stroke units with close monitoring of patients was mostly reserved for those receiving acute reperfusion treatments. However, the rates of stroke unit admission increased in sites that continuously utilized the RES-Q registry and had access to data for stroke care quality evaluation. Stroke unit hospitalization has been associated with better clinical outcomes for all stroke patients7,59 and thus, direct admission and spending at least 90% of the hospitalization in a stroke unit is recommended. 60 Acute interventions, thorough patient evaluation, and secondary prevention institution may be more accessible and offered by clinicians with specialist training and expertise in stroke in the setting of a stroke unit.61,62 Ideally, all acute stroke patients, including TIA patients, should be hospitalized in such settings.17,63 Establishment of stroke units in strategic locations across Greece is an important step for a comprehensive and successful stroke management plan and should be considered during infrastructure formation by policymakers.
Limitations
This is a retrospective study of prospectively collected data in a voluntary, web-based registry, and inherent limitations should be acknowledged. First, possibly selection bias in registering patients cannot be excluded; for example, two sites presented unusually high rates of reperfusion therapy (Athens Medical Center and AHEPA Hospital presenting a reperfusion rate of 58% and 47%, respectively), implying that there may have been a preference of inclusion for patients receiving acute reperfusion therapies. However, the contribution of these sites in the overall study population was small (0.9% and 1.1%, respectively) and confounding of the results is considered unlikely. Moreover, the need for signed informed consent may also have been a source of selection bias during registry inclusion, since patients with severe stroke or speech disorder may have not been able to consent. In such cases, the legal representatives were asked to provide informed consent for participation. COVID-19 pandemic-associated restrictions may have limited patient participation considering that legal representatives and/or family member may have not been allowed escorting stroke patients in certain hospitals. Nevertheless, the number of registered patients has not been reduced during the COVID-19 pandemic.
Furthermore, as we have already mentioned, not all institutions in Greece treating acute stroke patients have participated in the RES-Q registry, and the data captured may not be representative for the entire Greek population, especially when urban and rural areas are compared. Given the high incidence of stroke in Greece, the number of total registered patients throughout the 5-year period is low. It should be highlighted, though, that registry participation for stroke centers in Greece has been investigator-initiated and voluntary, while there are no stakeholders involved to support this initiative. Registry maintenance has been challenging and temporal dropouts were noticed during the 5-year period in all but two sites, that managed to include more than 95% of the discharged stroke patients in the RES-Q registry. Mandatory reporting of quality indicators and the introduction of a benchmarking system providing continuous feedback among participating centers have been shown to promote stroke care in other health systems, 34 and have also been a matter of discussion between the stroke scientific community and the policy makers for future implementation in Greece. Importantly, as part of the national stroke action plan and re-organization, the minimal requirements for dedicated stroke centers regarding healthcare personnel and technical equipment are being set and are expected to be adopted and periodically audited by national authorities.
Another shortcoming is that data regarding symptomatic ICH after receiving reperfusion therapy were not collected in RES-Q registry; thus, safety outcomes reporting was limited to in-hospital mortality, which did not differ between treated versus not treated AIS cases. Finally, RES-Q registry is based on self-reporting by the participants, and impact of missing data and possible reporting bias cannot be ignored. Nevertheless, to our knowledge, this is the first study that presents the overall management of acute stroke patients in multiple centers across all Greece. The real-world data provided in our study confirm the efficacy of acute reperfusion therapies in AIS in Greece and further highlight the need for development of stroke infrastructure that will accommodate the prompt delivery of acute treatment in stroke patients improving the clinical outcomes at discharge. Therefore, despite potential limitations, the importance of our study lies in informing and further guiding future actions to be undertaken in order to optimize stroke management in Greece.
Conclusions
Participation in a nationwide stroke registry should be encouraged for all sites managing patients with acute stroke in Greece, including primary and comprehensive stroke centers and stroke-ready hospitals across the whole country. Broader implementation through incentives provided by stakeholders, quality benchmarking between participating centers that is encouraged by national authorities and further expansion of the RES-Q registry in collecting additional quality metrics will guide the stroke management planning to widen the availability of swift patient transportation, delivery of acute reperfusion therapies, and stroke unit hospitalization.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local Ethics Committee of “Attikon” University Hospital (decision number EBΔ37) which was the coordinating center of the RES-Q registry in Greece.
Informed consent
Signed informed consent was obtained from the patients or their legal representatives before enrollment in all cases.
Guarantor
Georgios Tsivgoulis, MD.
Contributorship
LP and GT contributed to conception and study design. LP, OK, AHK, AK, EB, AK, VZ, KN, GP, AT, CZ, AS, KP, EN, PP, GK, AM, MK, CL, IK, VG, AS, AR, GK, PP, SP, MG, AT, DK, TK, GM, SG, and GT contributed to acquisition and analysis of data. LP, OK, AHK, and GT contributed to drafting a significant portion of the manuscript or figures. EB, AK, VZ, KN, GP, AT, CZ, AS, KP, EN, PP, GK, AM, MK, CL, IK, VG, AS, AR, GK, PP, SP, MG, AT, DK, TK, GM, and SG contributed with critical comments during manuscript revision. All authors approved the submitted manuscript.
ORCID iDs
Data availability
The data that support the findings of this study are available from the corresponding author (LP), upon reasonable request.