
Abstract
Introduction:
Stroke etiology may affect the prognosis of acute basilar artery occlusion (BAO). This study aimed to estimate the efficacy and safety of endovascular treatment (EVT) in BAO strokes due to the underlying stroke etiologies of large artery atherosclerosis (LAA) and cardioembolism (CE).
Patients and methods:
Patients with LAA and CE subtypes from the registry EVT for Acute Basilar Artery Occlusion Study (BASILAR) were selected for this analysis. We estimated the EVT treatment effect relative to standard medical treatment (SMT) in these patients by using a propensity score approach with inverse probability of treatment weighted estimation. Outcomes included 90-day favorable functional outcomes (modified Rankin scale (mRS) 0–3), functional independence (mRS 0–2), all-cause mortality, and symptomatic intracranial hemorrhage (sICH).
Results:
A total of 744 patients were included in the final analysis. After weighting with inverse probability of treatment estimation, the patients who, based on their characteristics, were treated with EVT rather than SMT, demonstrated higher rates of favorable functional outcomes in both the LAA (29.2% vs 11.7%, adjusted OR with 95% CI: 4.34 [2.15–8.78], p < 0.001) and the CE subtype (36.0% vs 8.1%, adjusted OR with 95% CI: 9.14 [1.96–42.55], p = 0.005). A similar finding was also observed for functional independence. EVT patients also demonstrated lower rates of mortality than SMT. Among EVT patients, no significant difference was observed in mortality or sICH between LAA and CE groups, but LAA patients had lower rates of favorable functional outcome and functional independence (29.2% vs 37% and 24.2% vs 32.9%, respectively), where the latter remained significant after adjustment for imbalances in baseline data (p = 0.04).
Conclusions:
In acute BAO strokes, both LAA and CE patients who, based on their characteristics, were treated with EVT rather than SMT, demonstrated better outcomes. Among EVT patients, LAA and CE subtypes displayed important baseline and treatment differences, and LAA patients were less likely to achieve functional independence at 3 months, but mortality and sICH were similar between LAA or CE subtypes. These results need to be confirmed in future clinical trials.
Introduction
Acute basilar artery occlusion (BAO) is a devastating stroke subtype, and nearly 80% of patients with BAO have poor outcomes if not recanalized. 1 Endovascular therapy (EVT) has become the current guideline-recommended standard treatment for both anterior-circulation large vessel occlusion (LVO) strokes and BAO strokes2,3 despite of limited evidence in treating BAO strokes.1,4,5 Nevertheless, a recent large-scale, prospective, multicenter cohort demonstrated the benefit of EVT for BAO in clinical practice. 6
Large artery atherosclerosis (LAA) and cardioembolism (CE) are the most common etiologies of posterior circulation strokes of LVO subtype.7,8 Because the underlying mechanism of BAO varies, the outcome might be different. Several studies have estimated the effects of causes of BAO strokes and outcomes, but the results were inconsistent. Some studies showed that after EVT, patients with BAO from embolism (from cardiac or large arteries) had a better outcome than those from intracranial atherosclerotic disease or in situ atherosclerotic thrombosis. Other studies showed that the outcomes were similar.9–14 Overall, these studies were limited due to their retrospective nature and small sample sizes, and inconsistent etiology classification. Moreover, these studies did not compare EVT to standard medical treatment (SMT), or explore whether stroke etiology might modify the effect of EVT.
In this study, we investigated the efficacy and safety of EVT compared with SMT in patients with BAO from LAA or CE. Furthermore, we identified the association between stroke etiology and outcomes in patients with acute BAO who received EVT.
Patients and methods
Study design
The BASILAR was a multicentre, prospective, registry study conducted in 47 comprehensive stroke centers across 15 provinces in China from January 2014 to May 2019. Consecutive patients >18 years old who presented with an acute BAO stroke within 24 h from the onset were recruited into two groups: treatment with EVT plus SMT or SMT alone. Details on the rationale, design, and major results of the BASILAR study have been published previously. 6 The study protocol was approved by the ethics committee of Xinqiao Hospital, Army Medical University, Chongqing, China, and each subcenter. All patients or their legally authorized representatives signed the informed consent. The trial was registered at http://www.chictr.org.cn, and the registration number was ChiCTR1800014759.
Treatments
Patients in the SMT group received intravenous (IV) recombinant tissue plasminogen activator (rt-PA) or urokinase if appropriate and antithrombosis drugs in accordance to the guidelines of acute ischaemic stroke (AIS) management. 15 Patients in the EVT group received treatment with stent retrievers, thromboaspiration, balloon angioplasty, stenting, intra-arterial thrombolysis, or various combinations of these approaches. Balloon angioplasty and stenting were regarded as rescue treatments if recanalization was not achieved after multiple attempts with stent retrievers, thromboaspiration, or intra-arterial thrombolysis. In a minority of cases, angioplasty or stenting was the first strategy.
Data collection
Baseline data were collected as follows: demographics, medical history, clinical measures, stroke severity, imaging profiles, and treatment features. According to the Trial of ORG10172 in Acute Stroke Treatment (TOAST) criteria, 16 only those strokes with a presumed causative mechanism of LAA and CE were included in this study. The LAA subtype was defined as acute in situ atherosclerotic thrombo-occlusion in the basilar artery or the V4 segment of the vertebral artery after excluding cardiac source or other etiologies. The existence of multiple or diffuse atherosclerotic lesions in the other large arteries further supported the diagnosis. Distal embolism due to severe stenosis of the proximal vertebral artery was also considered as LAA. The CE subtype manifests an abrupt obstruction with obvious evidence of embolism from cardiac sources detected by cardiac examination: atrial fibrillation, valvular heart disease, cardiac mural thrombus, cardiomyopathy, intracardiac tumors, etc. The baseline ischemic changes were assessed according to the posterior circulation Acute Stroke Prognosis Early Computed Tomography Score (pc-ASPECTS) on CT imaging. 17 Neurological deficits were evaluated by the National Institutes of Health Stroke Scale (NIHSS). Stroke severity at baseline was dichotomized into severe or mild to moderate as described previously. 6 Collateral status was assessed using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) collateral grading system and classified into scores of 0–1, 2, and 3–4.18,19 Recanalization status was assessed by the modified Thrombolysis in Cerebral Infarction (mTICI) and classified from no perfusion (grade 0) to complete perfusion (grade 3). Grade 2b/3 was generally regarded as successful reperfusion. 20
Outcome assessment
The primary efficacy outcome was favorable functional outcome defined as 0–3 on the mRS at 90 days. The secondary efficacy outcome was functional independence (mRS score of 0–2) at 90 days. Safety outcomes included all-cause mortality within 90 days, intracranial hemorrhages (ICH) and symptomatic ICH (sICH) within 48 h confirmed by CT scans or magnetic resonance imaging. ICH was evaluated according to the Heidelberg Bleeding Classification, 21 and sICH was defined as a new ICH with an increase in NIHSS score of ⩾4, or an NIHSS score of ⩾2 points in one category or deterioration that led to intubation, hemicraniectomy, external ventricular drain placement, or any other major interventions.
Statistical analysis
The baseline variables were compared between groups using the χ2 test or Fisher exact test for categorical variables and the Mann–Whitney U test for continuous variables. Continuous variables are expressed as medians and interquartile ranges (IQRs), and categorical data are presented as frequencies and proportions. Moreover, baseline variables were compared using standardized mean difference (SMD). In this study, we used a propensity score approach to estimate the treatment effect. According to the previous evidence and guideline recommendations,2,22,23 ASPECTS and occlusion sites were the important factors that related to the decision of whether to undergo EVT or not and considered as a part of treatment group “features.” Based on this assumption, ASPECTS and occlusion sites would not be included as adjustment covariates. The propensity score for the EVT group was generated for each patient regardless of the outcome by using a nonparsimonious multivariable logistic regression model with all covariates in Table 1 except for ASPECTS score and occlusion sites included in the model. The spread of propensity score for each of the subgroups was calculated and expressed as mean ± SD (Supplemental Table 1), and the histogram of propensity score was shown in Supplemental Figure 1. Inverse probability of treatment weighted estimation was then defined as the inverse of the estimated propensity score for EVT patients, and the inverse of one minus the estimated propensity score for those with SMT. The association of treatment modality with clinical outcomes in LAA and CE subgroups were assessed using a logistic regression model with inverse probability of treatment weighting. The estimates of odds ratios (ORs) and 95% confidence intervals (CIs) were reported. The heterogeneity of the EVT effect across LAA and CE subgroups was estimated by introducing an interaction term between treatment modality and stroke etiology (LAA vs CE) into the model.
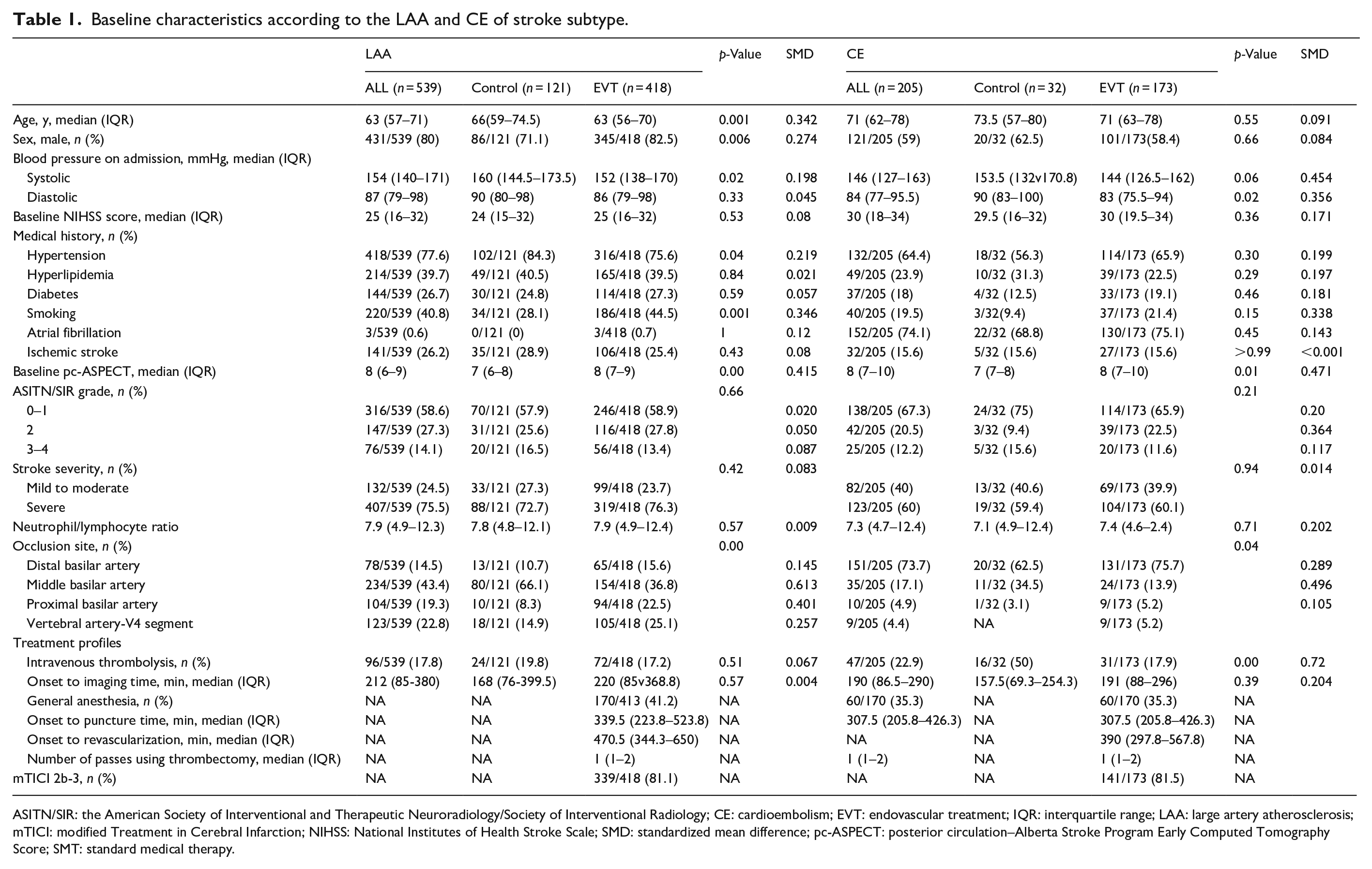
Baseline characteristics according to the LAA and CE of stroke subtype.
ASITN/SIR: the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology; CE: cardioembolism; EVT: endovascular treatment; IQR: interquartile range; LAA: large artery atherosclerosis; mTICI: modified Treatment in Cerebral Infarction; NIHSS: National Institutes of Health Stroke Scale; SMD: standardized mean difference; pc-ASPECT: posterior circulation–Alberta Stroke Program Early Computed Tomography Score; SMT: standard medical therapy.
Second, we investigated the associations between stroke etiology and outcomes in patients treated with EVT through multivariable logistic regression, with the previously recognized variables adjusted, including age, medical history of diabetes and ischemic stroke, baseline NIHSS, pc-ASPECT, IV thrombolysis, neutrophil/ lymphocyte ratio, and onset to recanalization time.10,12 The efficacy and safety outcomes of rescue therapy were also assessed among EVT-patients with LAA subtype using χ2 test. If a statistically significant difference between three groups was observed, then a pairwise comparison between two groups was performed with Bonferroni correction for multiple comparisons.
All p-values were two-tailed, and significance was set at p < 0.05. Statistical analysis was performed using SPSS 23.0 (IBM Corporation, Armonk, NY, USA) and R version 4.0.5 (R Foundation for Statistical Computing).
Results
Patients’ characteristics
Among 829 patients in the BASILAR study, 85 patients were excluded because of different stroke subtypes. The remaining 744 patients were included in this subgroup analysis (Figure 1). Among them, 539 patients had the LAA subtype (121 patients in SMT and 418 in EVT), and 205 were CE in origin (32 in SMT and 173 in EVT).
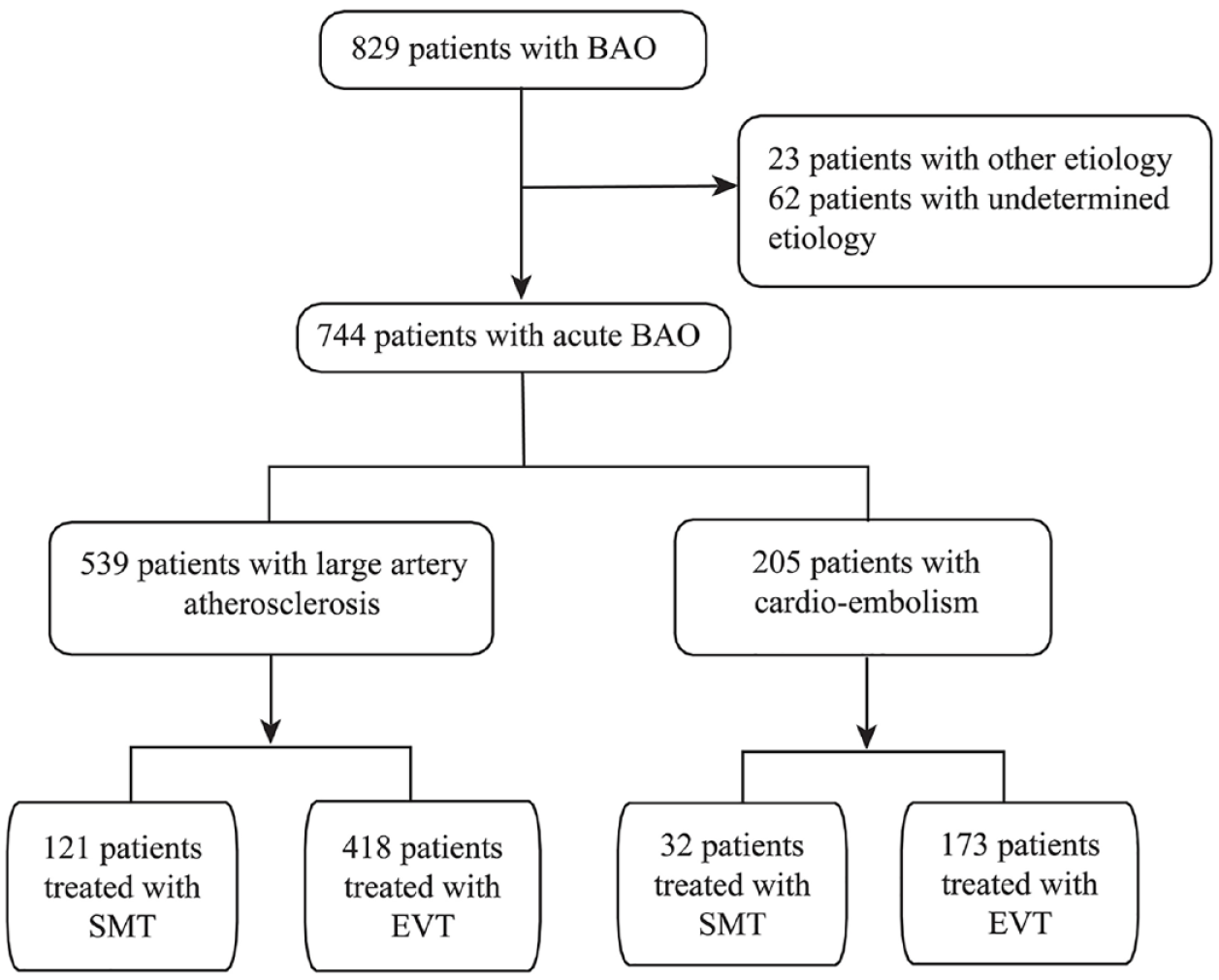
Flow diagram of the patient selection process.
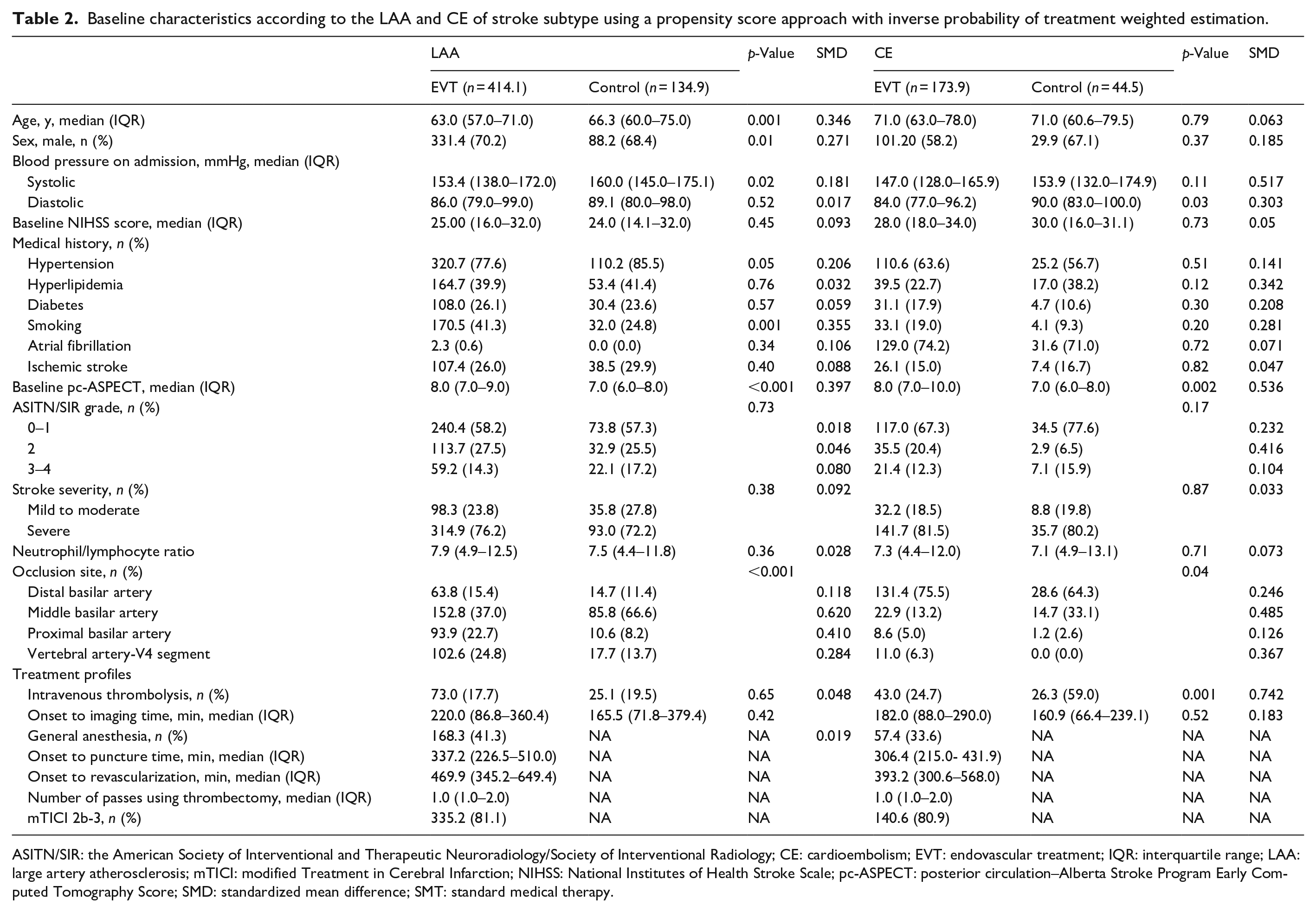
The baseline characteristics of the BAO patients are shown in Tables 1 and 2. The median age (IQR) of these patients was 63 (57–71) years and 71 (62–78) in the LAA and CE subgroups, respectively. In the LAA subgroup, the median (IQR) baseline NIHSS was 25 (16–32), pc-ASPECT was 8 (6–9), and onset to imaging time was 212 (85–380) min. In the CE group, the median (IQR) baseline NIHSS was 30 (18–34), pc-ASPECT was 8 (7–10), and onset to imaging time was 190 (86.5–290) min. In the LAA subgroup, EVT patients were younger, more often male, had less hypertension and higher baseline pc-ASPECTS, compared with SMT patients. In the CE subgroup, EVT patients had lower diastolic blood pressure, lower rate of intravenous thrombolysis, and higher baseline pc-ASPECTS, compared with SMT patients. Additionally, the occlusion site between the SMT and EVT groups was different in both the LAA and CE subgroups. When using a propensity score approach with inverse probability of treatment weighted estimation, some of the baseline characteristics were still imbalanced between EVT and SMT in both LAA and CE subtypes (Table 2).
Baseline characteristics according to the LAA and CE of stroke subtype using a propensity score approach with inverse probability of treatment weighted estimation.
ASITN/SIR: the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology; CE: cardioembolism; EVT: endovascular treatment; IQR: interquartile range; LAA: large artery atherosclerosis; mTICI: modified Treatment in Cerebral Infarction; NIHSS: National Institutes of Health Stroke Scale; pc-ASPECT: posterior circulation–Alberta Stroke Program Early Computed Tomography Score; SMD: standardized mean difference; SMT: standard medical therapy.
Outcomes of EVT versus SMT in the LAA and CE subgroups
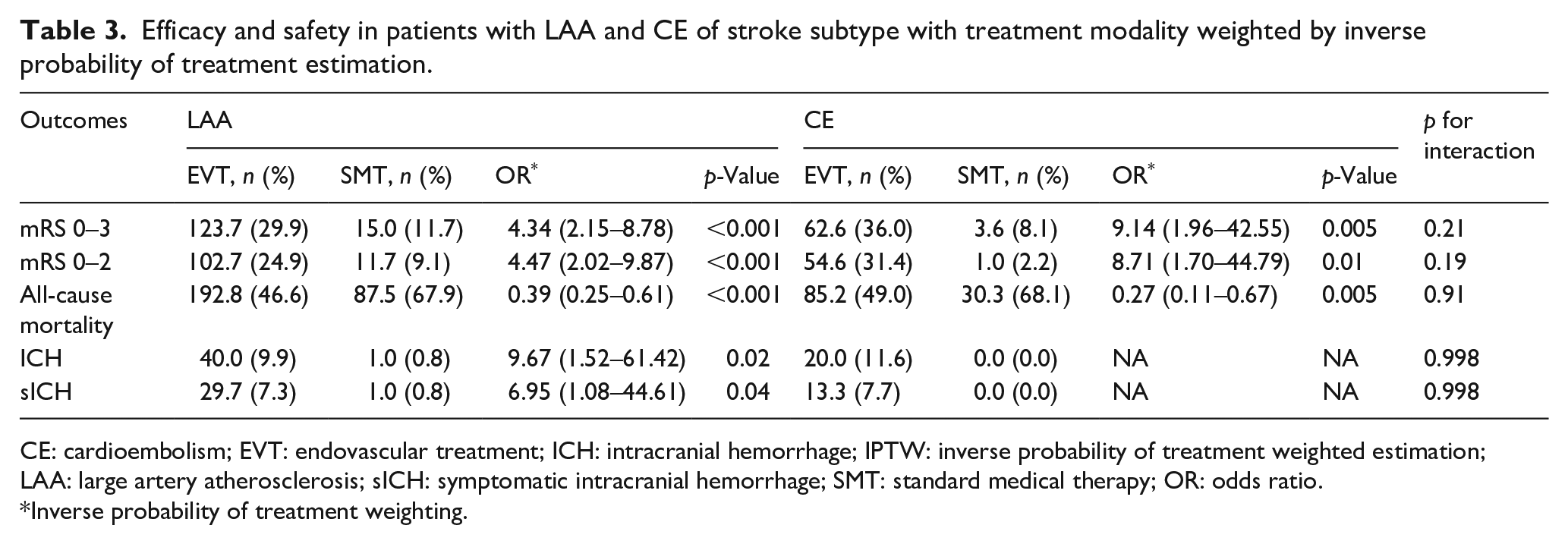
The distribution of mRS according to the treatment modality in the LAA and CE subgroups is shown in Supplemental Figure 2. After weighting with inverse probability of treatment estimation, the patients who, based on their characteristics, were treated with EVT rather than SMT, demonstrated higher rates of favorable functional outcomes in both the LAA (29.2% vs 11.7%, adjusted OR with 95% CI: 4.34 [2.15–8.78], p < 0.001) and the CE subtype (36.0% vs 8.1%, adjusted OR with 95% CI: 9.14 [1.96–42.55], p = 0.005) (Table 3). The interaction between stroke etiology and treatment effect was not significant (interaction for p value = 0.21). A similar result was found for functional independence in both the LAA and CE subgroups. Compared with SMT, EVT also demonstrated a lower incidence rate of mortality in both the LAA subgroup and the CE subgroup. In LAA subtype, the increased risks of ICH and sICH for EVT than SMT were observed (9.9% vs 0.8%, p = 0.02; and 7.3% vs 0.8%, p = 0.04, respectively). There was no ICH and sICH among SMT patients in the CE subgroup.
Efficacy and safety in patients with LAA and CE of stroke subtype with treatment modality weighted by inverse probability of treatment estimation.
CE: cardioembolism; EVT: endovascular treatment; ICH: intracranial hemorrhage; IPTW: inverse probability of treatment weighted estimation; LAA: large artery atherosclerosis; sICH: symptomatic intracranial hemorrhage; SMT: standard medical therapy; OR: odds ratio.
Inverse probability of treatment weighting.
Outcomes of LAA versus CE after EVT
The baseline characteristics of LAA versus CE in patients treated with EVT were shown in Supplemental Table S2. BAO patients with CE subtype were older and more often female, and had lower systolic blood pressure, higher baseline NIHSS, and pc-ASPECTS. Additionally, the time from onset to puncture, from puncture to recanalization, and from onset to recanalization was shorter in patients with the CE subtype than in patients with LAA. The most common occlusion site was the middle section of the basilar artery in patients with LAA, but the distal basilar artery was the most common site in patients with CE. The assignment of rescue therapy (including balloon dilatation and stenting) to patients in the LAA subgroup was significantly higher than that in the CE subgroup (63.5% vs 12.8%). However, the rate of successful reperfusion did not differ between the two subgroups.
Table 4 shows that there were numerically higher rates of favorable outcomes (64/173 (37.0%) vs 122/418 (29.2%), p = 0.06) and functional independence (57/173 (32.9%) vs 101/418 (24.2%), p = 0.03) after EVT in patients with CE than in those with LAA. After adjustment for potential confounding factors, the CE subgroup had better odds of functional independence than LAA (adjusted OR with 95% CI: 1.96 [1.04–3.72], p = 0.04). For safety outcomes, the risks of all-cause mortality, ICH, and sICH after EVT were similar between LAA and CE patients.
Efficacy and safety of CE versus LAA in BAO patients treated with EVT.
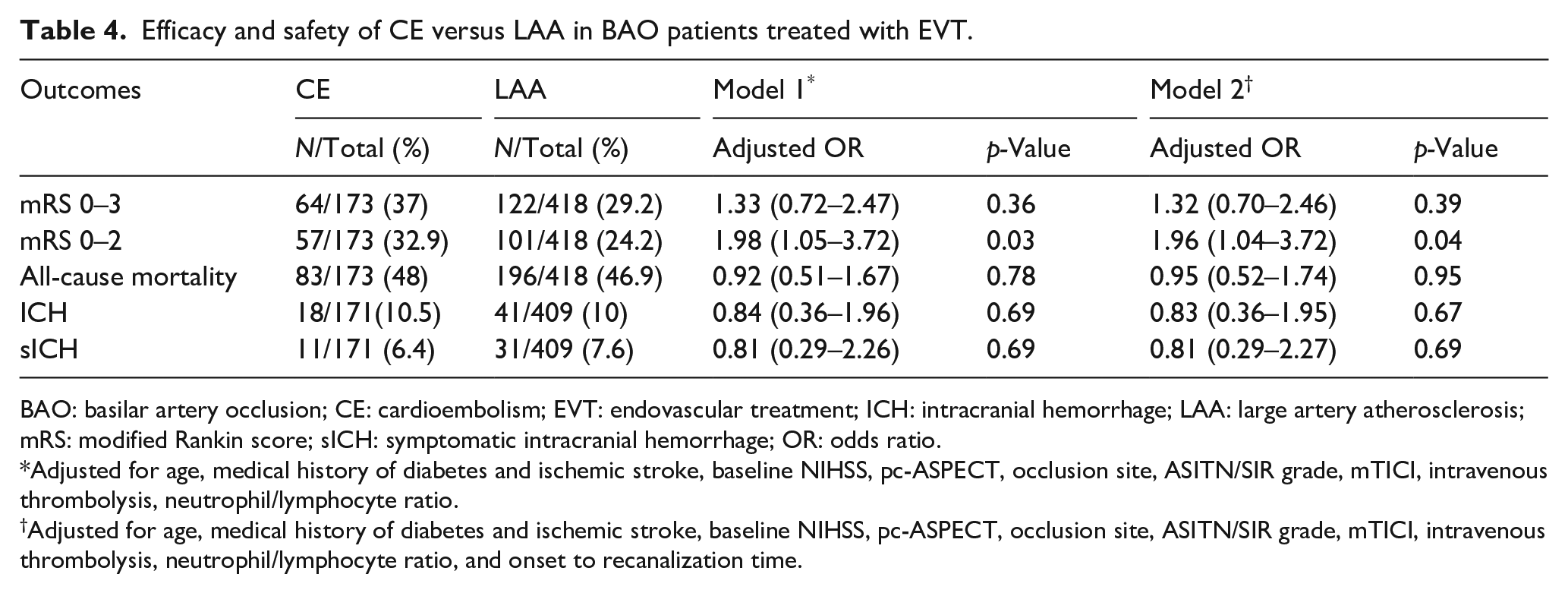
BAO: basilar artery occlusion; CE: cardioembolism; EVT: endovascular treatment; ICH: intracranial hemorrhage; LAA: large artery atherosclerosis; mRS: modified Rankin score; sICH: symptomatic intracranial hemorrhage; OR: odds ratio.
Adjusted for age, medical history of diabetes and ischemic stroke, baseline NIHSS, pc-ASPECT, occlusion site, ASITN/SIR grade, mTICI, intravenous thrombolysis, neutrophil/lymphocyte ratio.
Adjusted for age, medical history of diabetes and ischemic stroke, baseline NIHSS, pc-ASPECT, occlusion site, ASITN/SIR grade, mTICI, intravenous thrombolysis, neutrophil/lymphocyte ratio, and onset to recanalization time.
Angioplasty/stenting for failed mechanical thrombectomy in LAA
After mechanical thrombectomy (MT) in the LAA subtype, 265 (63.5%) patients received angioplasty and/or stenting. We further tested whether rescue angioplasty/stenting (RAS) improved clinical outcomes in patients with failed recanalization from MT.
We divided EVT-patients with the LAA subtype into recanalization success by MT alone group, rescue angioplasty/stenting group (RAS), and no rescue angioplasty/stenting group (non-RAS) after MT failed. Outcomes between these groups are shown in Table 5. We found that patients with successful recanalization by MT alone had the highest rates of favorable outcome (44/109, 40.0%) and lowest rate of mortality (38/109, 34.9%). In MT failed patients, compared with the non-RAS group, patients with RAS had higher rates of 90-day favorable functional outcome (71/265 (26.8%) vs 7/44 (15.9%)) and functional independence (61/265 (23.0%) vs 6/44 (13.6%)), although the differences were not significant. In addition, the RAS group had significantly lower mortality than the non-RAS group with no difference in the rate of sICH.
Comparisons of outcomes among patients with recanalization success by mechanical thrombectomy alone, patients with rescue angioplasty/stenting and patients without angioplasty/stenting after failed mechanical thrombectomy in the LAA subtype.
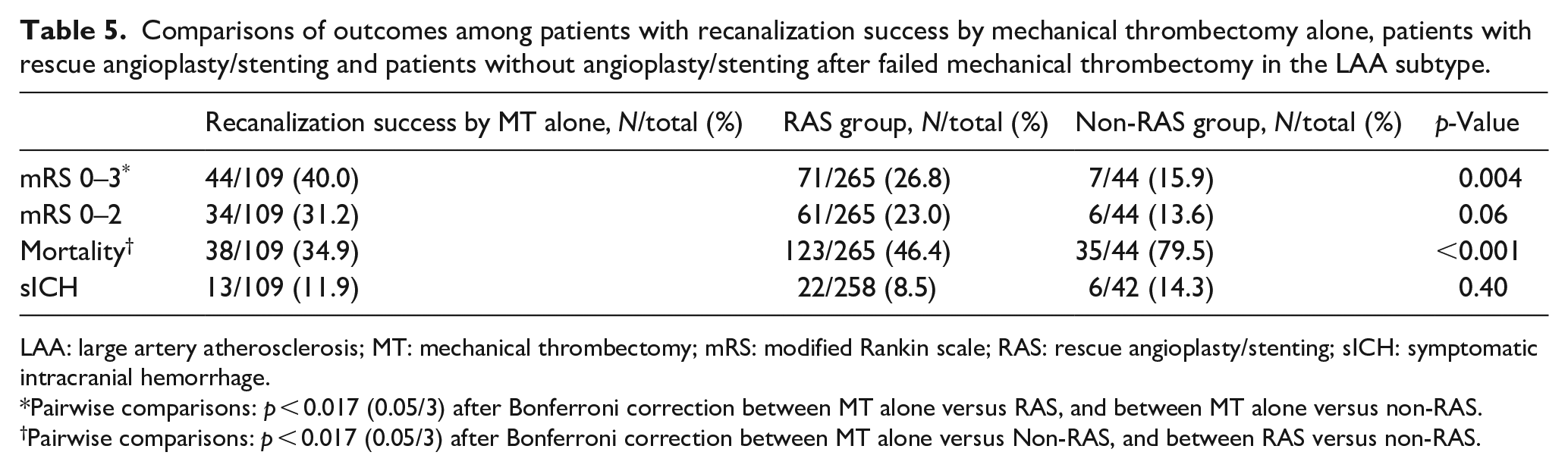
LAA: large artery atherosclerosis; MT: mechanical thrombectomy; mRS: modified Rankin scale; RAS: rescue angioplasty/stenting; sICH: symptomatic intracranial hemorrhage.
Pairwise comparisons: p < 0.017 (0.05/3) after Bonferroni correction between MT alone versus RAS, and between MT alone versus non-RAS.
Pairwise comparisons: p < 0.017 (0.05/3) after Bonferroni correction between MT alone versus Non-RAS, and between RAS versus non-RAS.
Discussion
In this study, we found that both LAA and CE patients in BAO strokes, who, based on their characteristics, were treated with EVT rather than SMT, demonstrated better outcomes. In the EVT group, despite of equal rate of recanalization, patients with BAO caused by LAA had a lower rate of favorable functional outcome at 90 days compared with patients with cardioembolic origin in unadjusted data, but with no differences in mortality rate or sICH. The two groups displayed with important differences in both baseline and treatment characteristics, both affecting prognosis. After careful statistical adjustment, the OR of achieving functional independence, but not favorable functional outcome, remained significantly higher for CE-BAO (OR 1.96).
Our findings could be related to several factors. Patients with CE were older and had more severe neurological deficits, while patients with LAA had more risk factors for atherosclerosis, such as a higher proportion of hypertension, diabetes, hyperlipidemia, and smoking. The imaging characteristics between the two subtypes were also different: more often distal basilar artery occlusion in CE, but more occlusion of the proximal and middle basilar artery in LAA. Occlusion of the proximal and middle basilar artery is related to ischemia of the pons, leading to a catastrophic status, such as locked-in syndrome. 24 Patients with the LAA subtype were associated with more rescue therapy and longer procedure time indicative of a more complicated treatment process. Prior studies have shown that a longer procedure time was an independent predictor of poor functional dependence.14,25 Overall, these specific characteristics may result in different efficacy outcomes between CE and LAA subtypes after EVT.
The results from previous studies investigating the effect of the underlying mechanisms of BAO on prognosis after EVT were inconsistent, and different definitions of stroke mechanism was an important reason. Some studies showed that embolic strokes without vertebrobasilar artery stenosis had a better rate of recanalization and prognosis,10,26 but in situ atherosclerotic thrombosis or embolism from tandem VA steno-occlusion would do poorly. 13 Without discerning the source of embolism, Lee et al. 12 showed that BAO patients with embolism predicted a higher rate of 90-day functional independence than those with in situ atherosclerotic thrombosis. In our study, we used TOAST classification to define the potential etiology, and embolism from tandem VA steno-occlusion was categorized as LAA subtype. Our results were consistent with another study using TOAST classification for etiological determination. 18 There are limitations in making direct comparisons between these studies, which suggests the importance of establishing a standardized classification of stroke mechanisms for patients with BAO.
Different from previous studies demonstrating lower rates of successful recanalization in BAO patients with a LAA subtype,10,12,27 our results showed that the rate of successful recanalization after EVT was similar between LAA and CE subtypes. The difference was likely related to the more aggressive rescue treatment for patients with the LAA subtype in our study, with about 63.5% of patients received stent implantation or balloon dilatation.
In our study, we also found that rescue treatment may be effective for MT-failed patients, with an increased rate of favorable outcome by 10% and reduced rate of mortality by 30%. These results suggested that aggressive recanalization may be reasonable for BAO patients if reperfusion was not sustained after MT. Our results are consistent with previous studies showing that the combination of MT with angioplasty/stenting increased the rate of successful recanalization and better clinical outcome.9,27,28 Therefore, successful reperfusion might be the most important factor for prognosis regardless of recanalization tools used, as demonstrated in treating strokes in the anterior circulation. 29
Although our study was based on the largest prospective, multicentre, cohort study to date with the most important confounders adjusted in the analysis, there are still some limitations that should be considered. First, the nonrandomized nature of the BASILAR registry would have all the observational drawbacks. Second, although LAA and CE were the most common etiologies in BAO patients, other causative and unknown etiologies might also be related to the outcomes. However, the number of such patients in the BASILAR trial was too small to be analyzed. Third, other factors, such as the time from onset to puncture and to recanalization time, the procedure time, and the thrombectomy device, were not further analyzed in different stroke subtypes due to the limited sample sizes. Further studies are needed to verify these factors.
Conclusions
In conclusion, in acute BAO strokes, both LAA and CE patients who, based on their characteristics, were treated with EVT rather than SMT, demonstrated better outcomes. Among EVT patients, those with LAA might be less likely to achieve functional independence at 3 months, but mortality and sICH did not differ between LAA or CE groups. Future studies are still needed to further define the subgroups of patients with acute BAO who may benefit from individualized recanalization or reperfusion strategies.
Supplemental Material
sj-docx-2-eso-10.1177_23969873221101285 – Supplemental material for Endovascular treatment for acute basilar artery occlusion due to different stroke etiologies of large artery atherosclerosis and cardioembolism
Supplemental material, sj-docx-2-eso-10.1177_23969873221101285 for Endovascular treatment for acute basilar artery occlusion due to different stroke etiologies of large artery atherosclerosis and cardioembolism by Huihui Liu, Guoyong Zeng, Hongliang Zeng, Yang Yu, Feixue Yue, Yingbing Ke, Zhizhong Yan, Jie Pu, Jun Zhang, Wan Wei, Dengke He, Yupeng Wu, Xianjun Huang and Peiyang Zhou in European Stroke Journal
Supplemental Material
sj-pptx-1-eso-10.1177_23969873221101285 – Supplemental material for Endovascular treatment for acute basilar artery occlusion due to different stroke etiologies of large artery atherosclerosis and cardioembolism
Supplemental material, sj-pptx-1-eso-10.1177_23969873221101285 for Endovascular treatment for acute basilar artery occlusion due to different stroke etiologies of large artery atherosclerosis and cardioembolism by Huihui Liu, Guoyong Zeng, Hongliang Zeng, Yang Yu, Feixue Yue, Yingbing Ke, Zhizhong Yan, Jie Pu, Jun Zhang, Wan Wei, Dengke He, Yupeng Wu, Xianjun Huang and Peiyang Zhou in European Stroke Journal
Footnotes
Acknowledgements
We thank all the coinvestigators of BASILAR (The EVT for Acute Basilar Artery Occlusion Study) for their dedication to the study.
Correction (July 2023):
Article updated online to correct the affiliations for Xianjun Huang and Peiyang Zhou.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from National Natural Science Foundation of China (81901236, 82071310).
Informed consent
Informed consent was obtained from all subjects or their legal representatives before the study.
Ethical approval
The study was approved by the ethics committee of Xinqiao Hospital, Army Medical University, Chongqing, China, and each subcenter.
Guarantor
PZ.
Contributorship
HL and PZ conceived and designed the study, conducted data interpretation. GZ and XH carried out data acquisition and conducted the data analysis. HL wrote the first draft of the manuscript. HZ, YY, FX, YK, ZY, JP, JZ, WW, DH, and YW were involved in the subject recruitment and monitored the gathering of clinical data. GZ, XH, and PZ acquired data and critically revised the manuscript. All authors read and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.