
Abstract
Introduction:
Oily fish intake may reduce the progression of white matter hyperintensities (WMH) of presumed vascular origin due to their high content of omega-3 polyunsaturated fatty acids and other nutrients. However, information on this relationship is limited. We aimed to assess the association between oily fish intake and WMH progression in older adults living in rural coastal Ecuador.
Methods:
Participants of the Atahualpa Project Cohort received baseline clinical interviews and brain MRIs. Oily fish intake was calculated at every annual door-to-door survey from enrollment to the end of the study. Individuals who also received a follow-up brain MRI were included. Poisson regression models were fitted to assess the incidence rate ratio (IRR) of WMH progression according to the amount of oily fish intake, after adjusting for demographics, level of education and traditional vascular risk factors.
Results:
The study included 263 individuals of Amerindian ancestry aged ⩾60 years (mean age: 65.7 ± 6.2 years; 57% women). The mean oily fish intake was 8.3 ± 4 servings per week. Follow-up MRIs demonstrated WMH progression in 103 (39%) individuals after a median follow-up of 6.5 years. A multivariate Poisson regression model showed an inverse relationship between oily fish intake and WMH progression (IRR: 0.89; 95% CI: 0.84–0.95; p < 0.001). A similar model also revealed an inverse relationship between tertiles of oily fish intake and probabilities of WMH progression, which became significant when individuals allocated to the third tertile were compared to those in the first and second tertiles.
Conclusion:
Study results show an inverse relationship between the amount of oily fish intake and WMH progression in frequent fish consumers of Amerindian ancestry.
Keywords
Introduction
White matter hyperintensities (WMH) of presumed vascular origin – a reliable biomarker of cerebral small vessel disease (cSVD) – have been associated with an increased risk of stroke and cognitive decline. 1 Recognition of risk factors that are in the path of WMH progression are important for the implementation of intervention strategies aimed at reducing the morbidities associated with cSVD. 2 Identification of protective factors for WMH progression would be beneficial for preventive measures. However, information on this subject is limited. WMH have been related to inflammatory mechanisms that lead to endothelial damage. 3 Therefore, factors that regulate inflammation and stabilize the endothelium of intracranial arterioles may reduce WMH progression. Marine omega-3 polyunsaturated fatty acids (ω-3 PUFAs) have been shown to improve these factors. 4 It is conceivable that a diet rich in oily fish or the ingestion of fish oils supplements will reduce the occurrence of WMH and its progression. A cross-sectional study by our group demonstrated an inverse association between oily fish intake and WMH severity among frequent fish consumers living in rural Ecuador. 5 Using the same population, this longitudinal prospective study aimed to assess whether increased amounts of oily fish intake resulted in lower rates of WMH progression after more than 6 years of follow-up.
Patients and methods
Study population
The study was conducted in community-dwellers aged ⩾60 years living in Atahualpa, a rural village of coastal Ecuador, where previous studies on correlates of oily fish intake have been conducted.6–8 The population of Atahualpa is homogeneous regarding ethnicity (Amerindian ancestry with little evidence of cross-breeding), low levels of education, socio-economic status, living conditions, and dietary habits. 9 The diet is ancestrally rich in oily fish, fruits and carbohydrates, but limited in other types of meat, dairy products, and highly processed foods. Due to both high prices and lack of awareness of their importance, consumption of other foods rich in ω-3 PUFAs, or the use of fish oils supplements, is virtually nonexistent in the village.
Study design
Study participants were identified by means of door-to-door surveys. 9 Following a longitudinal prospective design, individuals aged ⩾60 years who had a baseline brain MRI, evaluation of vascular risk factors, interviews for evaluation of dietary oily fish intake determinations between 2012 and 2019, and were actively participating in the Atahualpa Project Cohort as of May 2021, were invited to receive a follow-up brain MRI. Participants signed comprehensive informed consent at enrollment, as well as before the practice of follow-up MRIs. The study was approved by the Ethics Committee of Hospital-Clínica Kennedy, Guayaquil (FWA 00030727). WMH progression at the end of follow-up was evaluated according to the mean amount of oily fish intake (evaluated at baseline and periodically over the study years), after adjusting for demographics, level of education, and vascular risk factors.
Quantification of dietary oily fish intake
Study participants were requested to quantify their habitual consumption of oily fish at every annual door-to-door survey, and the mean of servings per week was used for analysis. The number of servings was calculated by dividing the average intake of each fish by 140 g. In Atahualpa, fresh wild-caught fish are acquired at the local market. As previously detailed, our personnel visited the market (before the study) to weight edible parts of available fish and create a list with commonly consumed species; fish ingested by Atahualpa residents are among the species with the highest content of ω-3 PUFAs (1.3–2.5 g per serving).5–7 We also inquired about the way fish is prepared and only included in the analysis those served broiled or cooked as a soup (oily fish is rarely fried by villagers). Intake of white fish was not taken into account.
Neuroimaging studies
Both baseline and follow-up MRIs were performed with the same equipment (Philips Intera 1.5T; Philips Medical Systems, Eindhoven, the Netherlands) following previously described standards. 10 Interest focused on the presence and severity of WMH, which were defined as lesions appearing hyperintense on T2-weighted images that remained bright on FLAIR (without cavitation) and were graded in three degrees of severity (mild, moderate, and severe) according to the modified Fazekas scale. 11 Mild WMH refers to the presence of periventricular caps or thin lesions and punctate hyperintensities in subcortical white matter. In moderate WMH, there is a smooth periventricular halo and subcortical foci begin to merge. Severe WMH is characterized by extension of periventricular lesions into the subcortical white matter and large confluent subcortical foci. All MRIs were independently read by one neuroradiologist and one neurologist blinded to clinical information. Kappa coefficients for interrater agreement of WMH severity were 0.91 at baseline and 0.93 at follow-up; discrepancies were resolved by consensus. WMH progression was defined as the increase in at least one grade of the Fazekas scale in the follow-up MRI.
Covariates investigated
Demographics, level of education, and vascular risk factors were recorded at baseline. Interviews and procedures for determining vascular risk factors followed the recommendations proposed by the American Heart Association (AHA), which stratifies each of the following risk factors in the poor range according to well-defined cutoffs, including: (1) Poor smoking status if the subject is a current smoker or quitted <1 year; (2) Poor body mass index if ⩾30 kg/m2; (3) Poor physical activity if there is no moderate and vigorous activity; (4) Poor blood pressure if ⩾140/90 mmHg; (5) Poor fasting glucose if ⩾126 mg/dL; and (6) Poor total cholesterol blood levels if ⩾240 mg/dL. 12 Unhealthy diet, also used by the AHA as a vascular risk factors, was not included as a covariate in this study to avoid collinearity (since fish intake is a component of the AHA diet).
Statistical analysis
Data analyses were carried out by using STATA version 17 (College Station, TX, USA). In unadjusted analyses, continuous variables were compared by linear models and categorical variables by the chi-square or Fisher exact test as appropriate. To compute person-years of follow-up, we considered the time from baseline to follow-up MRIs (last censoring date). Multivariate Poisson regression models were fitted to estimate the incidence rate ratio (IRR) of WMH progression according to the amount of oily fish intake, after adjusting for demographics, level of education, and vascular risk factors. These models take into account the effect of time on WMH progression. Smoking was not included as a covariate in any of these models because of collinearity with other predictors.
Results
Overall, 478 individuals aged ⩾60 years were enrolled in the Atahualpa Project cohort between 2012 and 2019. Of them, 403 (84%) received a baseline brain MRI, clinical interviews, and dietary oily fish intake assessment. Among the 75 excluded individuals, 36 died or emigrated before the MRI, 19 declined consent, 17 were severely disabled or had contraindications for MRI, and three had missing clinical information. Of 403 eligible candidates, 263 (65%) had a follow-up brain MRI and were included in the study. Ninety of the 140 non-included participants died, and the remaining 50 either declined further consent, became disabled over the study years, or emigrated between baseline and follow-up MRI. Follow-up time between baseline and follow-up brain MRIs was 1711 person-years (95% CI: 1665–1757 years), and the median follow-up was 6.5 years (interquartile range: 2.3–7.8 years).
The mean age of 263 study participants at baseline was 65.7 ± 6.2 years (median age: 63.9 years), 149 (57%) were women, and 192 (73%) had primary school education only. Individual vascular risk factors in the poor range included: smoking status: 11 (4%); body mass index: 63 (24%); physical activity: 12 (5%); blood pressure: 104 (40%); fasting glucose: 72 (27%); and total cholesterol blood levels: 41 (16%). The mean amount of dietary oily fish intake was 8.3 ± 4 servings per week. On baseline MRI, 90 (34%) participants did not have WMH, 131 (50%) had mild, 33 (13%) had moderate, and nine (3%) had severe WMH. At follow-up, 52 (20%) individuals did not have WMH, 112 (43%) had mild, 67 (25%) had moderate, and 32 (12%) had severe WMH. Overall, 103 (39%) individuals had MRI evidence of WMH progression (Figure 1). Progression from none-to-mild WMH was noticed in 33 cases, from none-to-moderate in five, from mild-to-moderate in 42, from mild-to-severe in 10, and from moderate-to-severe in 13.
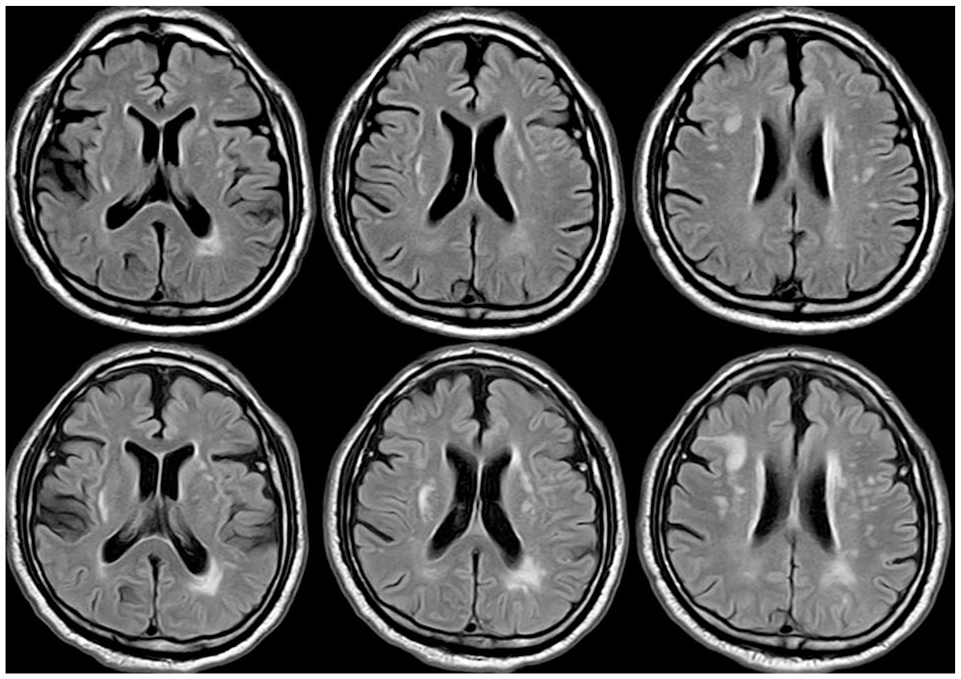
Fluid-attenuated inversion recovery MRI of a 65 years-old man allocated to the first tertile of dietary oily fish intake (less than 6.58 fish servings per week) showing progression of white matter hyperintensities from baseline MRI performed in June 2015 (upper row), to follow-up MRI performed in June 2021 (lower row).
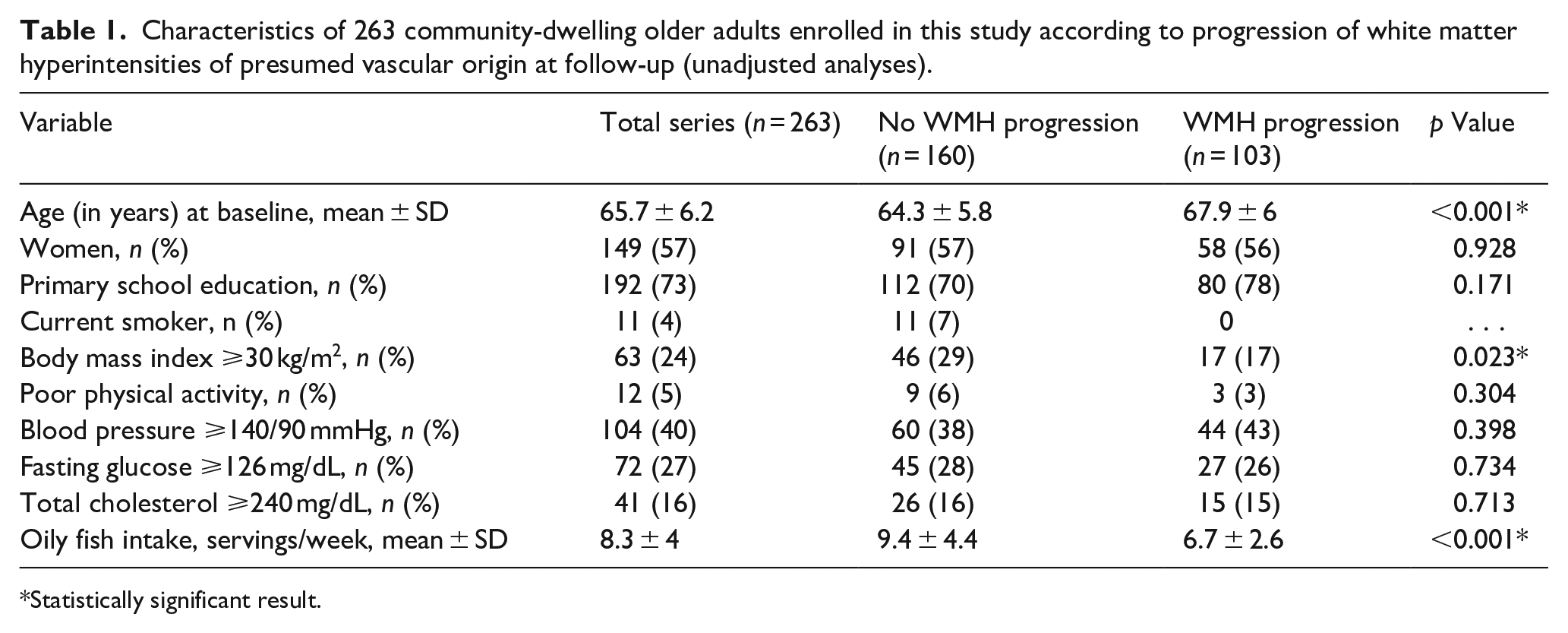
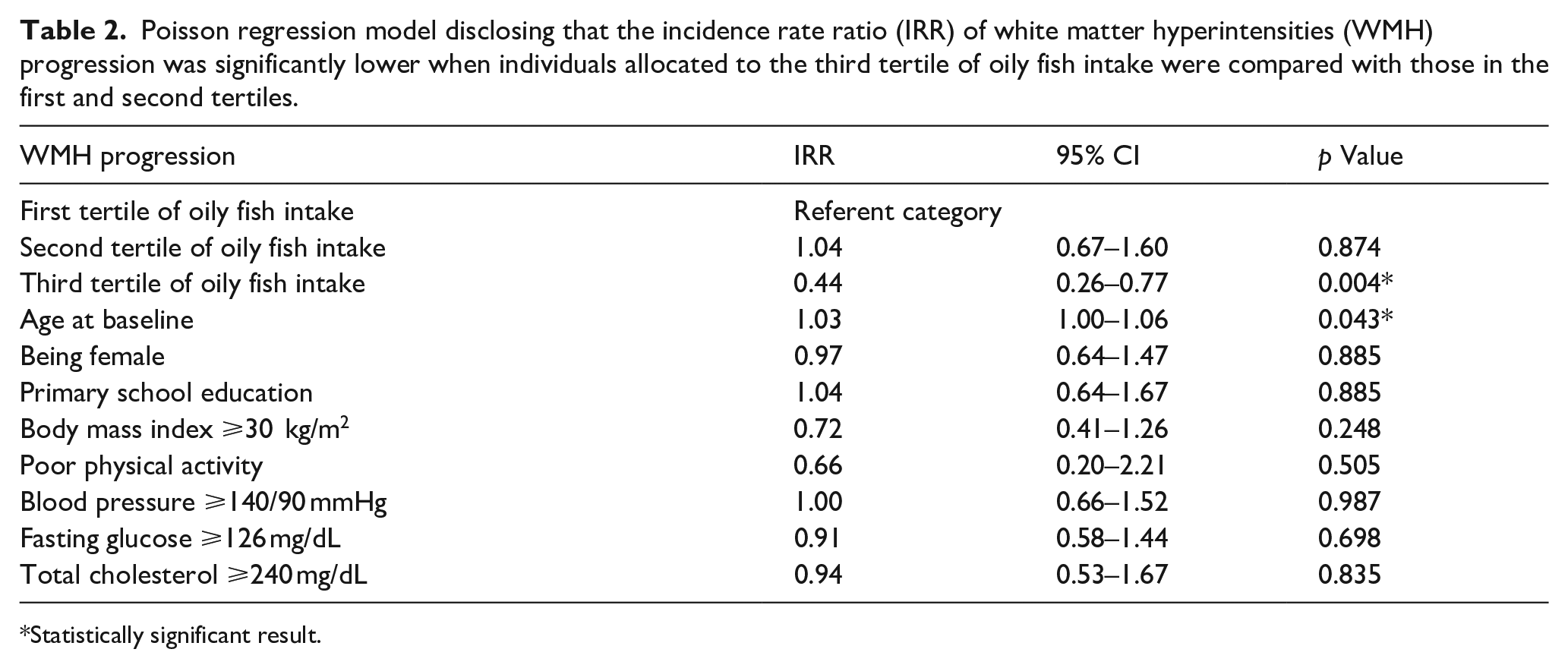
In unadjusted analysis, the mean value of dietary oily fish intake was lower among individuals who had WMH progression. In addition, people who had WMH progression were older and were less often obese than those who did not; otherwise, there were no significant differences in clinical characteristics across groups (Table 1). A Poisson regression model, considering fish servings per week as an independent continuous variable, showed that WMH progression rate was 21% lower for every serving of oily fish. The model disclosed a significantly inverse association between the amount of oily fish intake and WMH progression, after adjusting for demographics, level of education and vascular risk factors (IRR: 0.89; 95% CI: 0.84–0.95; p < 0.001). None of the investigated covariates remained independently significant in this model. A separate Poisson regression model, with the amount of fish servings per week stratified in tertiles (0.57–6.58, 6.6–8.7, and 8.8–23.3 servings) disclosed a significant reduction in the IRR of WMH progression when individuals in the third tertile were compared with those in the first and second tertiles; in this model, only increasing age remained independently significant (Table 2). Predictive margins revealed an inverse relationship between tertiles of oily fish intake and WMH progression, which became significant (no overlapping 95% CI) when the first tertile was compared with the third tertile (Figure 2).
Characteristics of 263 community-dwelling older adults enrolled in this study according to progression of white matter hyperintensities of presumed vascular origin at follow-up (unadjusted analyses).
Statistically significant result.
Poisson regression model disclosing that the incidence rate ratio (IRR) of white matter hyperintensities (WMH) progression was significantly lower when individuals allocated to the third tertile of oily fish intake were compared with those in the first and second tertiles.
Statistically significant result.
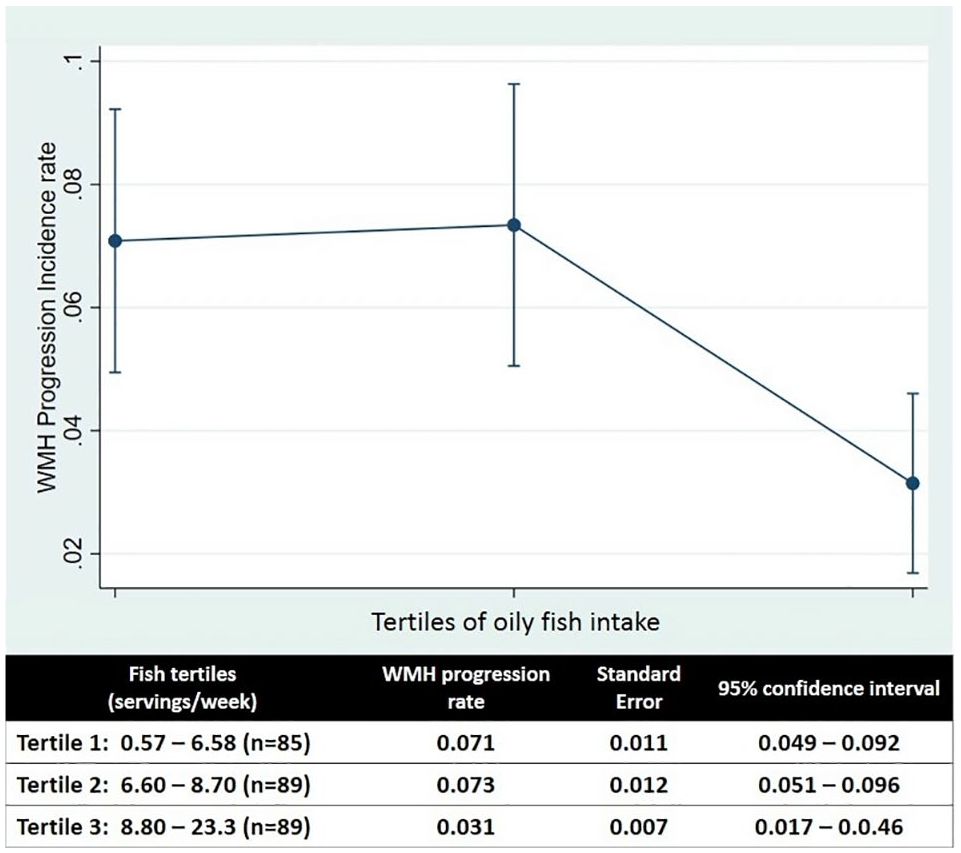
Graph plot showing an inverse relationship between tertiles of oily fish intake (servings per week) and probabilities of white matter hyperintensities (WMH) progression, which became significant (no overlapping 95% confidence intervals) when the third tertile were compared with the first and second tertiles.
Discussion
This population-based prospective study, conducted in a cohort of community-dwelling older adults living in rural Ecuador, shows an inverse relationship between the amount of dietary oily fish intake and WMH progression. None of the investigated covariates tempered the significance of the above-mentioned relationship, suggesting that the beneficial impact of fish intake on WMH progression exceeds that of demographics, level of education and traditional vascular risk factors.
Findings of the present study are mainly related to a significant reduction in the number of individuals with WMH progression among those eating 8.8 or more servings per week, when compared to those eating less than this amount. It should be noted that the usual recommended amount of dietary oily fish intake (1–2 servings per week), 13 may not be adequate to achieve the significance observed in the investigated relationship. At the same time, there are potentially adverse consequences of high consumption of oily fish as some species carry elevated levels of methylmercury which, in turn, may foster cardiac and cerebrovascular events. 14 However, fish consumed in Atahualpa are caught near the coastal border and due to their relatively small size the content of methylmercury is presumably low. 6
As previously mentioned, data linking oily fish intake with WMH severity and progression are limited. Cross-sectional studies exhibit heterogeneous results regarding the association between oily fish intake and WMH severity, but most of the variation can be attributed to differences in study designs. Consumption of baked or broiled tuna/other fish ⩾3 times per week was associated with better WMH scores when compared to <1 time per month in a cohort of older adults. 15 Other studies focused on the association between plasma levels of ω-PUFAs and WMH severity and found that higher concentrations of these nutrients were associated with lower grades of WMH severity.16–18 However, not all studies confirmed the above-mentioned inverse association. 19 Nevertheless, two cross-sectional studies (one of them conducted among Atahualpa residents) do demonstrate a significant inverse association between amounts of dietary oily fish intake and the presence of diffuse subcortical damage of vascular origin.5,20
Studies showing the beneficial effect of the Mediterranean diet on white matter integrity are not comparable to the aforementioned studies as this diet is also rich in non-marine sources of ω-3 PUFAs and other nutrients (vegetables, fruits, Greek yogurt, whole grains, seeds, olive oil). 21 It is also possible that people who adhere to the Mediterranean diet elect for a healthier lifestyle and study results may have been biased. This is not the case of individuals enrolled in the present study who do not choose to eat oily fish as a part of a healthy diet or lifestyle, but as the most affordable option to get energy from food, dismissing the above-mentioned potential bias.
Several pathogenetic mechanisms explain the inverse association between marine ω-3 PUFAs intake and WMH severity, the most relevant being inflammation regulation and stabilization of the endothelium.16–18 It is also possible that the effects of oily fish intake on white matter integrity is mediated by a reduction in arterial stiffness, another factor that is in the path of WMH progression. 22
This study has some limitations. The SARS-CoV-2 struck Atahualpa from the start of the pandemic, resulting in a high mortality rate among older adults. 23 In addition, several individuals left the village or declined consent for follow-up MRI because of fears related to the pandemic. These events probably contributed to a small amount of selection bias. We relied on the self-reported number of oily fish servings per week rather than ω-3 PUFAs concentrations in the blood or adipose tissues. The study population was limited to individuals of Amerindian ancestry. As a result, our findings may not be generalizable to other races/ethnic groups, particularly in light of studies showing that beneficial effects of oily fish intake are most often observed in certain ethnic groups, particularly in the Inuit and their Amerindian descendants. 24 It is also possible that some unmeasured confounders may be responsible for at least part of the findings from the present study. WMH were visually rated and this may be another limitation of this study, given that the modified Fazekas visual scale may be less reliable than volumetry for assessing slight changes in the follow-up MRI. 25 This may explain why WMH regression was not identified in any subjects. 26 In addition, the study aim was determined after the results obtained in a cross-sectional study conducted in the same population. 5 Despite these limitations, the study has several strengths including its population-based cohort design, the homogeneity of the study population, the systematic assessment of vascular risk factors and dietary oily fish intake by means of uniform standardized protocols, and the practice of baseline and follow-up MRIs using the same equipment and protocols.
Conclusion
In summary, this study provides evidence that dietary oily fish intake is related to a lower incidence of WMH progression. The present study suggests that high amounts of oily fish for long periods are needed to accomplish this goal. This is difficult to sustain in persons who are not frequent fish consumers. In other populations, the use of commercially available fish oil preparations may be more practical. In that situation, it would also be important to add supplements of vitamin D and selenium, since the effect of oily fish on WMH severity may not be exclusively related to their content of ω-PUFAs. 27 This study opens new avenues of research for assessing the preventive role of dietary oily fish intake in the development of diffuse subcortical damage of vascular origin.
Footnotes
Author contributions
O.H.D.: study design, imaging readings, manuscript drafting; R.M.M.: statistical analysis of data; V.J.D.: Imaging readings, significant intellectual contribution to manuscript content; B.Y.R.: study coordinator; D.A.R.: data collection and interpretation; M.J.S.: Significant intellectual contribution to manuscript content. All authors read and approved the final version of the submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study supported by Universidad Espíritu Santo – Ecuador. The sponsor had no role in the design of the study, nor in data collection or analyses, or in the decision to submit this work for publication.
Informed consent
All individuals enrolled in the Atahualpa Project signed a comprehensive informed consent and were informed about the use of their anonymized data for publication.
Ethical approval
The Institutional Review Board of Hospital Clínica Kennedy, Guayaquil, Ecuador (FWA: 00030727), approved the study. The study protocol has been registered at ClinicalTrials.gov, and the unique identifier number is NCT04123171.
Guarantor
The corresponding author (OHD) takes full responsibility for the data, the analyses and interpretation, and the conduct of the research, and has full access to all of the data and the right to publish any and all data.