
Abstract
Purpose
Practical suggestions on clinical decisions about vascular disease management in patients with cognitive impairment are proposed.
Methods
The document was produced by the Dementia Committee of the European Stroke Organisation (ESO) based on the evidence from the literature where available and on the clinical experience of the Committee members. This paper was endorsed by the ESO.
Findings
Vascular risk factors and cerebrovascular disease are frequent in patients with cognitive impairment. While acute stroke treatment has evolved substantially in last decades, evidence of management of cerebrovascular pathology beyond stroke in patients with cognitive impairment and dementia is quite limited. Additionally, trials to test some daily-life clinical decisions are likely to be complex, difficult to undertake and take many years to provide sufficient evidence to produce recommendations. This document was conceived to provide some suggestions until data from field trials are available. It was conceived for the use of clinicians from memory clinics or involved specifically in cognitive disorders, addressing practical aspects on diagnostic tools, vascular risk management and suggestions on some therapeutic options.
Discussion and conclusions
The authors did not aim to do an exhaustive or systematic review or to cover all current evidence. The document approach in a very practical way frequent issues concerning cerebrovascular disease in patients with known cognitive impairment.
Introduction
Dementia and stroke share several modifiable vascular risk factors and are risk factors for each other.1–3 Hence, patients with cognitive impairment (CI) who are seen at memory clinics frequently present with vascular risk factors and cerebrovascular disease. Furthermore, cerebrovascular disease contributes to clinical symptoms that may aggravate or anticipate the clinical expression of underlying degenerative brain pathology There is a lack of evidence on the treatment of cerebrovascular disease in patients with CI.4,5 Uncertainty about management of vascular risk factors and cerebrovascular disease in people affected by CI might lead to heterogeneity in the treatment of those patients. In addition, professionals from memory clinics may have less experience in the recognition and in the appropriate management of cerebrovascular disease. The aim of this paper is to help reducing this potential knowledge gap, while waiting for appropriate field trials.
Methods
This document is a white paper produced by the Dementia Committee members, and endorsed by the European Stroke Organization, aiming to give practical clinical suggestions for the management and treatment of cerebrovascular disease in patients with cognitive disorders. It was meant for the use of professionals involved in the management of patients with CI, including medical specialists, general practitioners, but also non-medical professionals interested in CI and dementia, in order to help clinical decisions. Content is not a result of a systematic review, but rather based on relevant literature and on the clinical experience of the authors
In this paper an effort was made to incorporate differences of approach and access to ancillary investigations, keeping in mind the standard usual best practice from a cerebrovascular disease perspective. For a practical use, cognitive impairment (CI) include patients with objective cognitive impairment regardless of having or not criteria for dementia. Subjective cognitive impairment refers to subjective complaints of decline in cognition without confirmation of decline on objective cognitive assessment.
Findings
Clinical expression of cerebrovascular contribution in CI
Cognitive and behavioral manifestations
Once a patient is seen in a memory clinic and the diagnosis of CI has been confirmed, the possible presence, coexistence, or relevance of a cerebrovascular component in the etiology of CI should be considered. Identification of cerebrovascular disease through neuroimaging is quite straightforward (see below). However, identification of symptoms and signs of cerebrovascular disease on clinical grounds might be less obvious. A synthetic approach is given in Text Box 1. Over the last years, there has been much discussion about the potential role of neuropsychology in order to differentiate the vascular from the degenerative component of CI.
6
Although there is consensus that compromise of some cognitive domains (such as memory) may be more prominent in Alzheimer disease (AD) than in cerebrovascular diseases,
7
and executive dysfunctions are thought to be more typical of cerebrovascular pathology, in fact all major cognitive domains are affected in small vessel disease
8
and neuropsychological testing cannot per se differentiate between vascular CI and AD at the individual level,
9
nor clearly outline the presence of a vascular contribution in patients with CI of degenerative origin.
10
Nevertheless, the combination of the information driven by neuropsychological testing (and remaining clinical evaluation) with brain imaging is the best clue to support a likely cerebrovascular contribution. Text Box 1. Clinical symptoms/signs which should raise possibility of concomitant cerebrovascular disease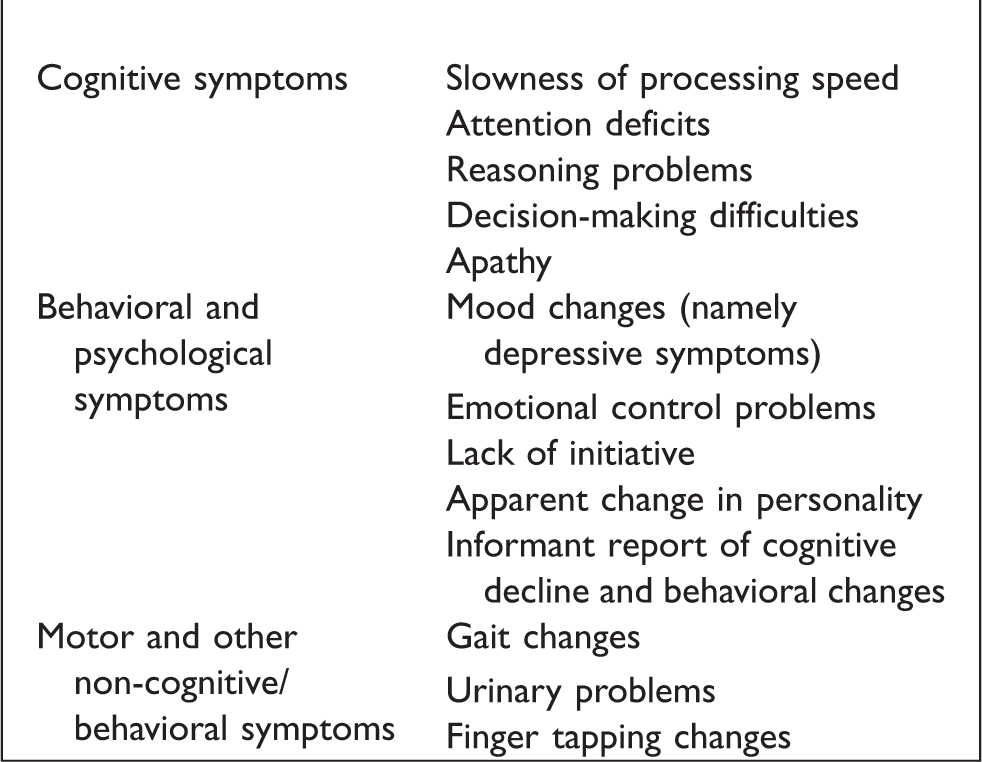
Behavioral and psychological symptoms are highly frequent among cerebrovascular disease manifestations11,12 and might be different according to the nature of cerebrovascular lesions. 13 Those symptoms might be undervalued by relatives (and interpreted for instance as due to ageing) or overlooked due to other concomitant cognitive symptoms. Depressive symptoms, lack of emotion expression control and emotionalism, apathy and lack of initiative and change in personality traits are among those symptoms. There is no ideal short battery for the identification of deficits in patients with cerebrovascular disease. We should keep in mind that less exhaustive neuropsychological study might fail to put in evidence few cognitive deficits and behavioral changes 14
Evolution over time
Apart from detailed evaluation of cognitive testing, there might be other clinical hints that suggest the presence of a vascular component in a patient with CI.
Historically, one clinical tool to differentiate the vascular component of the cognitive decline is to apply the so-called ischemic score published by Hachinski and co-authors, aiming to differentiate AD from multi-infarct dementia. 15 The score is today considered partly out-of-date and is more rarely used than in the past; however, it may serve to outline and discuss some aspects. According to the original paper, a few characteristics of the clinical course of the cognitive deterioration may indicate the presence of a vascular component (or cause); these are the abrupt onset, the stepwise deterioration, and a fluctuating course. However, it should be kept in mind that the original paper was referring to patients with multiple strokes. Today, we know that a good proportion of patients whose CI recognizes a vascular cause - or at least a vascular component of it -, have small vessel disease (SVD), 16 and the course of their cognitive decline is not usually stepwise but rather progressive and with insidious onset. Other items of the original scale, given the current knowledge, appear of limited utility as they are scarcely discriminative and are also a risk factor for AD (more information concerning Hachinski’s score is provided in supplementary material).
Motor and non-motor manifestations
More relevant in this sense are the history of strokes and the presence of focal neurological symptoms and signs. These latter should be always searched for, systematically, as they are highly indicative of a cerebrovascular contribution.
CI phenotype usually reflects more than one pathological mechanism. Biomarkers (namely imaging for vascular pathology) are able to put in evidence cerebrovascular disease. The knowledge of the clinical expression of vascular pathology leads to the possibility of addressing better the specific trigger for CI in a specific person. Some neurological signs may help in the identification of the etiology of the clinical picture. One relevant aspect to be outlined is the possibility to suspect a vascular component of CI by assessing physical performance with simple and clinically friendly tools. 17 Patients with cerebrovascular disease have frequently gait disturbances with balance difficulties, small steps, and bradykinesia. Besides those affected by the sequelae of previous stroke such as hemiparesis, patients with SVD have typically a slowed, short-stepped, wide-based gait. These patients also have an increased rate of falls. More sophisticated tools for assessing gait performance maybe better but also difficult to implement in memory clinics on a large scale. 18
Finally, there have been data supporting that changes in other non-cognitive symptoms (as for instance urinary troubles early in the course of the disease) since these are common in patients with vascular contributions to CI and have an adverse effect on their daily lives. Cerebral SVD is associated with urinary problems 19 and also with abnormalities on neurological examination, such as slowness of finger tapping. 20 Despite the possibility that these features might direct the attention of the treating physician towards the presence of a vascular contribution, other degenerative pathologies may present with similar findings21,22 . It might be reasonable however to search for all these aspects in each patient arriving at a memory clinic.
Subjective cognitive impairment
One last word concerning subjective CI, that usually is associated with higher risk of dementia, usually of the Alzheimer type (and not with SVD). 12 However, among community cohorts, may represent an increase in the relative risk risk for, particularly, CI of vascular origin. 23 Clinicians should keep in mind that patients with subjective complaints living in the community are an opportunity to identify vascular risk factors in people otherwise well, and reinforce preventive actions concerning those vascular risk factors.
What investigation/complementary investigation(s) are important?
Patients presenting to memory clinics should have brain imaging that includes assessment for vascular and neurodegenerative or other brain lesions. They should be assessed for common modifiable vascular and lifestyle risk factors to minimize their impact on brain and general health (Table 1).
Investigations to avoid missing modifiable vascular risk factors.
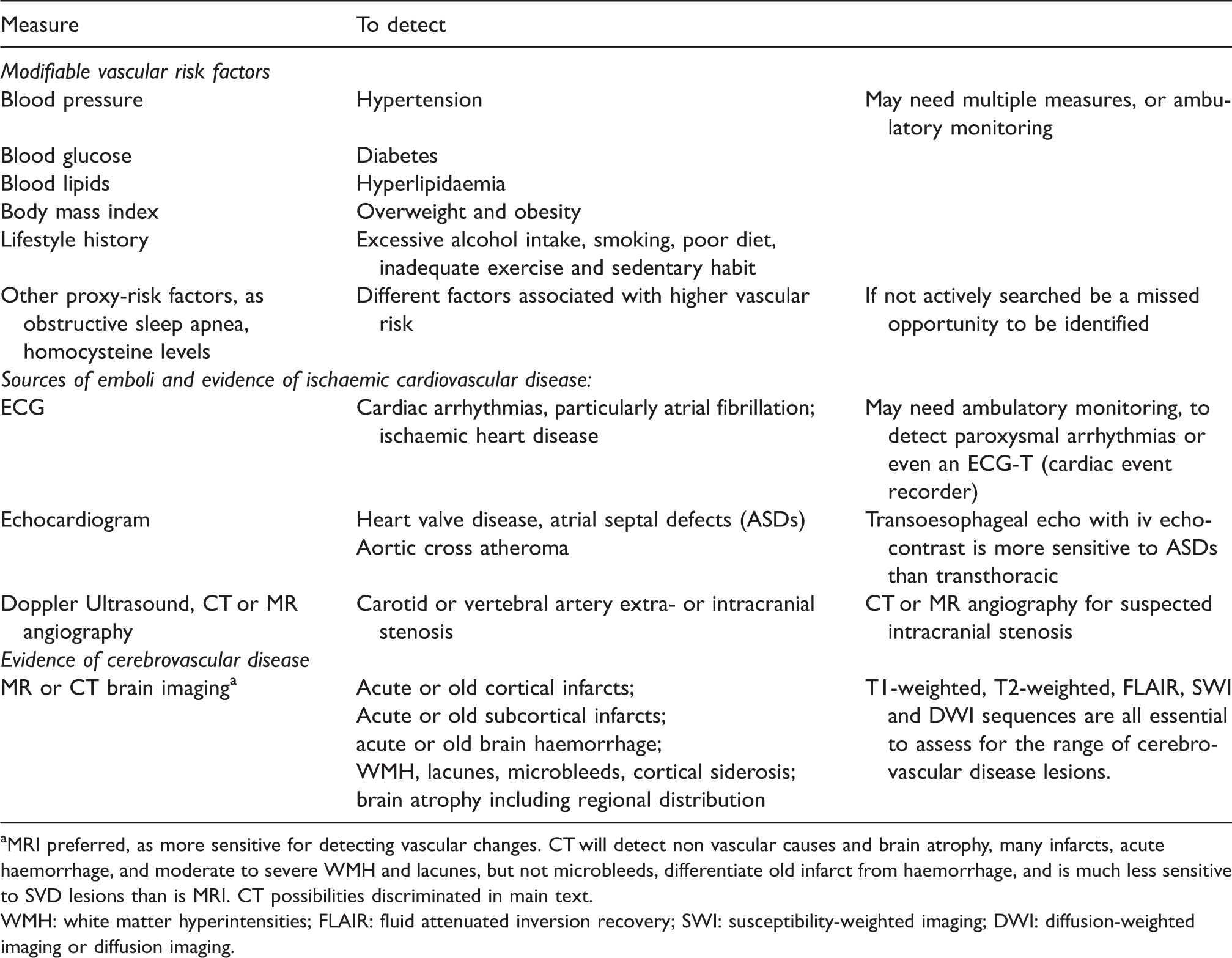
aMRI preferred, as more sensitive for detecting vascular changes. CT will detect non vascular causes and brain atrophy, many infarcts, acute haemorrhage, and moderate to severe WMH and lacunes, but not microbleeds, differentiate old infarct from haemorrhage, and is much less sensitive to SVD lesions than is MRI. CT possibilities discriminated in main text.
WMH: white matter hyperintensities; FLAIR: fluid attenuated inversion recovery; SWI: susceptibility-weighted imaging; DWI: diffusion-weighted imaging or diffusion imaging.
Neuroimaging
General considerations
On neuroimaging, vascular lesions include cortical or subcortical infarcts or old haemorrhages, signs of SVD including white matter hyperintensities (WMH), lacunes and microbleeds, and cortical superficial siderosis (cSS). 24 Perivascular spaces are common in cerebrovascular disease, but their clinical relevance is currently less clear.25,26 Brain atrophy occurs in the common neurodegenerative dementias including AD (particularly of medial temporal lobes), fronto-temporal dementia (of frontal and temporal lobes), dementia with Lewy Bodies (of parietal lobes), but also occurs diffusely in SVD 27 and focally after infarcts and haemorrhages. The pattern of atrophy may provide clues of the dementia type, but many patients have global brain atrophy, so in practice, atrophy patterns may have limited specificity.
MRI and CT scan applications
Brain imaging can be performed with computerized tomography (CT) scanning or magnetic resonance imaging (MRI). MRI might not always be available, or not applicable for every patient, so clear knowledge about limitations and advantages of each technique is needed. Moreover, CT is of quick realization, which is quite relevant for instance in patients with behavioral changes, fear of closed environments or with MRI contraindications (pacemaker or some prostheses, for instance). CT is equally accurate as MRI for pathologies such as brain tumours, subdural haematomas, many larger infarcts, acute haemorrhages, and can show brain atrophy, moderate to severe white matter lesions (leukoaraiosis), and lacunes. 28 Nevertheless, differentiation of old haemorrhages from old infarcts, identification of microbleeds and cSS and some small acute infarcts is not reliable on CT. MRI is much more sensitive to vascular lesions, particularly WMH, microbleeds and cSS. MRI is also better for detecting and differentiating sporadic vascular lesions from multiple sclerosis, vasculitis, some infections and familial genetic causes of dementia and cerebrovascular disease such as CADASIL. However, when using MRI, the correct MRI sequences are required to identify key vascular pathologies. Many memory clinics use MRI protocols including 3 D T1 and T2, which detect brain atrophy, some cortical infarcts, lacunes and can exclude tumours and subdural haematomas, for instance. However, to detect key vascular lesions, a fluid attenuated inversion recovery (FLAIR) sequence is required for WMH and small cortical infarcts, a susceptibility-weighted imaging (SWI or Gradient Echo or T2*) sequence is essential to detect microbleeds, cSS, and old macrohaemorrhages, and diffusion-weighted imaging (DWI) is important to detect small acute infarcts.
Specific hints from neuroimaging
WMH, lacunes, microbleeds and atrophy all increase with age.24,25 However, a higher than expected burden of WMH for age, and any lacunes or microbleeds, should trigger a search for modifiable risk factors. 29 Smith et al. provided a practical schema of WMH severities according to age groups, based on MRI, in a recent publication (see Figure 7 in). 29 Large numbers of WMH and lacunes in a young patient should raise the possibility of a monogenic SVD such as CADASIL. Multiple cortical infarcts especially in multiple arterial territories, should trigger a search for proximal embolic sources. Microbleeds are associated with hypertension, where they typically occur mainly in deep grey and white matter, and commonly found in patients with cerebral amyloid angiopathy (CAA) where they typically have a lobar distribution and are seen at the cortical-subcortical junction, although mixed distributions of microbleeds are common. Microbleeds plus cSS are likely to indicate CAA. 30
Vascular risk management
Vascular risk factors assessment
The main modifiable vascular risk factors are hypertension, hyperlipidemia, diabetes, and sources of emboli or altered cerebral perfusion such as atrial fibrillation or other cardiac arrhythmias, heart valve disease, and atheromatous internal carotid artery stenosis. Modifiable lifestyle risk factors include tobacco smoking, lack of regular physical exercise and poor diet including excess dietary sodium and alcohol.
All patients attending memory clinics should have their blood pressure measured using an approved and well maintained sphygmomanometer device. Blood pressure should be assessed sitting after at least five minutes of rest, and in both arms to avoid falsely low reading due to a subclavian artery stenosis. More detailed repeated measures of BP in clinic or home monitoring may be required but this is out of scope for this paper. Loss of adherence to hypertension treatment should be prevented (namely patients might stop medication when values get normal due to treatment), hence, any attendance at a clinic is a good opportunity to check that vascular risk management is under control. Patients should also have their blood glucose and blood lipids (cholesterol, LDL, HDL) measured if these have not been performed recently elsewhere, and appropriate management implemented whenever necessary. 31
Ancillary investigations concerning vascular risk factors
As cholinesterase inhibitors may delay atrial-ventricular conduction, an electrocardiogram (ECG) is usually requested in memory clinics. When there is evidence of cerebrovascular disease, an ECG will be helpful to identify arrhythmias, and signs of ischaemic heart disease or left or right chamber hypertrophy. Special attention must be given to patients with recent focal neurological symptoms or evidence of cerebrovascular lesions on scanning, especially if in multiple vascular territories: in those patients, ambulatory monitoring may be required to detect paroxysmal arrhythmias and further investigations such as echocardiography, and neck or intracranial artery imaging e.g. with Doppler ultrasound, CT or MR angiography 32 may be needed. Patients with more complex cerebrovascular disease as recurrent strokes despite adequate management and adequate secondary prevention, rare causes of stroke (as genetic diseases as CADASIL) and patients with recent acute stroke or suspected TIA should be considered for referral to a stroke clinic.
Other life-style and global measures
Tobacco smoking 33 and excess alcohol consumption damage the brain, 34 so cessation of those habits should be suggested. Exercise helps to maintain brain vascular health, 35 and a well-balanced diet including recommended amounts of fruit and vegetables, 36 avoiding excess sodium 37 and processed meats, is advisable. Lifestyle advice encourages patient awareness of their vascular risk and is part of comprehensive risk management.
A synopsis of suggested investigations is given in Table 1, and a summary of relevant suggestions in Text Box 2. Text Box 2. Summary of suggestions for the management of cerebrovascular disease in patients with CI.
Treatment
Primary and secondary prevention of stroke
Prevention of new vascular events in people with symptomatic cardiovascular disease is one of the real success stories of preventive medicine. In patients who experienced a ischaemic stroke, or transient ischaemic attack, the risk of future vascular events can be reduced by 30–50% through guideline-based treatments and lifestyle recommendations. 38 Of note, the evidence on which these guidelines are built is largely derived from studies on atherosclerotic (large artery) disease. By comparison, the available evidence specifically concerning treatment of cerebral SVD, the commonest form of vascular brain injury encountered in people with CI, is quite limited.29,39
There clearly is an important potential for vascular prevention strategies in patients with CI. Yet, physicians should be careful to apply guidelines for secondary prevention after stroke to people with CI and so-called “silent cerebrovascular disease”. In this setting, some treatments that are cornerstones in secondary prevention, in particular antithrombotic agents, may be ineffective, or sometimes even harmful. Although some recommendations are published, 29 we try to summarize few practical points in the next lines.
In all patients with CI and vascular brain injury, guidelines for primary prevention of cardiovascular disease apply. 40 This includes lifestyle recommendations, and encouraging cessation of smoking, if applicable, as mentioned above. To determine if additional treatment is needed, or existing treatments should be modified, a pragmatic approach is the following:
First, determine if the patient had a previous ischaemic vascular event or other ischemic vascular disease elsewhere in the body. If this is the case, this previous cardiovascular disease generally determines the choice of antithrombotic agents and blood pressure and cholesterol targets, according to available guidelines.38,40 Nevertheless, the memory clinic visit should be taken as an opportunity to double check if this treatment is appropriately installed.
Next, determine the nature of the vascular brain injury. Asses the different lesion types and burden as indicators of risk of future vascular injury. Of note, lesions that are typically considered to be ischemic, such as WMH and lacunes, not only convey an increased risk of future ischemic stroke, but also of intracerebral haemorrhage (ICH).
41
Similarly, lesions that are typically considered to be haemorrhagic, in particular, microbleeds, also convey an increased risk of ischaemic stroke. For example, in patients who previously experienced a TIA or ischaemic stroke it has been established that presence of multiple microbleeds is associated with a much higher relative hazard ratio for future ICH than for ischaemic stroke.
42
Yet, because the overall rate of ischaemic stroke in these patients is several fold higher than that of ICH, even in patients with multiple microbleeds the absolute risk of ischaemic stroke is higher than that of ICH.
42
These observations illustrate how difficult it can be to base indications for antithrombotic agents on patients with these lesions. Practical hints are given in Text Box 3. Text Box 3. Practical suggestions concerning treatment of cerebrovascular disease in patients with CI.
Specific issues in the use of antithrombotic therapy
It is also important to consider if the vascular brain injury, as seen on the scan, provides an indication to initiate or modify antithrombotic therapy. As a general principle “silent” ischemic lesions, in particular WMH, do not provide a clear indication for prescription of antithrombotic agents. 29 By contrast, it is also questionable if presence of a few microbleeds should be a reason to withhold antithrombotic agents in patients in whom such agents are otherwise indicated for presence of symptomatic ischaemic vascular disease. An exception may be people with high (e.g. >10) numbers of microbleeds and also people with cSS, particularly if disseminated (detected in more than 3 sulci). cSS is an indicator of CAA and conveys an absolute risk of future ICH of 11% per year when disseminated.43,44
In all cases, particularly for prescribing or discontinuing antithrombotic agents, an individualized approach is needed. Where possible this should be based on weighing the patients estimated absolute risk (and not relative risk which might often be misleading) of both future ischaemic and haemorrhagic events. The challenge is that such estimates are still imprecise and are largely derived from studies that did not specifically include patients from memory clinics. This clearly is an area for further study.
Conclusion and suggestions for future research
The interplay between vascular and neurodegenerative pathologies in patients with CI and dementia remains an active area of research. In recent years, the notion of potentially significant vascular contributions to CI and dementia in different patient settings is becoming better appreciated by clinicians. However, the mechanisms of how cerebrovascular pathophysiology reciprocally interacts with neurodegeneration in producing or contributing to cognitive symptoms and decline are complex and currently elusive. For example, there are many strong epidemiological links between traditional vascular risk factors and CI, and also a plethora of theoretical pathophysiologic crosstalk mechanisms between brain vessels pathologies and β-amyloid, a hallmark of neurodegeneration pathobiology. Often, age-related CI and dementia represent really a mix of neurodegenerative and vascular pathologies. Despite the details and trajectories being largely unknown, this realization gives a reason for hope, in that more contributions to CI in patients translates to more targets and opportunities to intervene. Such targets might include protection of the endothelium, the blood-brain barrier, other components of the neurovascular unit, or targeting CAA. It will also be of interest to assess the independent benefit on cognition of commonly used medications for primary and secondary stroke prevention, including antithrombotics in different stroke patient cohorts.
Ongoing and future research should focus on human- and animal-based studies of these interactions and on multidisciplinary consortia exploring potential biomarkers and clinical targets for intervention. Another relevant issue is the need to learn how to best evaluate and qualify cognitive performance as to outline cognitive components that are more specific of the vascular contribution 45 and whether this approach would be clinically meaningful. In the meanwhile, it is reasonable for all patients being assessed or managed for CI, to also be assessed for vascular brain injury and risk for it, and follow relevant published guidelines for primary or secondary prevention of cardio-cerebrovascular disease as applicable.
Supplemental Material
sj-pdf-1-eso-10.1177_2396987321994294 - Supplemental material for Cerebrovascular disease in patients with cognitive impairment: A white paper from the ESO dementia committee – A practical point of view with suggestions for the management of cerebrovascular diseases in memory clinics
Supplemental material, sj-pdf-1-eso-10.1177_2396987321994294 for Cerebrovascular disease in patients with cognitive impairment: A white paper from the ESO dementia committee – A practical point of view with suggestions for the management of cerebrovascular diseases in memory clinics by Ana Verdelho, Geert Jan Biessels, Hugues Chabriat, Andreas Charidimou, Marco Duering, Olivier Godefroy, Leonardo Pantoni, Aleksandra Pavlovic and Joanna Wardlaw in European Stroke Journal
Footnotes
Acknowledgements
We thank Professor Franz Fazekas, from the Medical University of Graz, Austria, for his contribution on this paper and we thank the European Stroke Organisation for supporting and for endorsing this initiative.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Olivier Godefroy during the last five years has served on scientific advisory boards and speaker (Biogen, Astra Zeneca, Novartis) and received funding for travel and meetings from Bristol-Myers Squibb, Roche, Biogen, Teva-santé, Boehringer-Ingelheim, Covidien, Ipsen. The remaining authors declare that there are no conflict of interest concerning the paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent is not applicable to this manuscript.
Ethical approval
Ethical approval is not applicable for this manuscript.
Guarantor
AV.
Contributorship
All authors contributed equally to conceive the manuscript, the structure of paper, literature research and writing of the manuscript. All authors contributed to the different stages of the manuscript, reviewed and edited and finally approved the final version of the manuscript.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.