
Abstract
Background: It is unknown if race/ethnicity modifies the response to blood pressure (BP) lowering treatment after intracerebral hemorrhage (ICH). We aimed to examine the race/ethnicity differences in the response to BP lowering treatment after ICH. Methods: This is a post hoc analysis of the Antihypertensive Treatment of Acute Cerebral Hemorrhage II (ATACH-2) trial. The primary outcome is good outcome, defined as 90-day modified Rankin Scale 0–3. The primary predictor is race/ethnicity for which we included non-Hispanic categories of White, Black, Asian, and the category of Hispanic. We fit adjusted logistic regression models with the predictor of race/ethnicity and models with the interaction term of treatment*race/ethnicity. Results: We included a total of 953 patients in our analysis (White = 213, Black = 112, Asian = 554, and Hispanic = 74). In the models with the interaction between race/ethnicity and treatment, we found that White patients assigned to the intensive treatment arm had lower predicted probability of good outcome than those assigned to the standard treatment arm (Model 1: 56.2% vs. 68.1%, p = .027; Model 2: 53.4% vs. 68.3%, p = .009). When divided into White and non-White groups, intensive treatment was associated with higher odds of serious adverse events in White group but not in the non-White group. In addition, there was an association between intensive treatment and higher risk of hematoma expansion in White patients and lower risk of hematoma expansion in non-White patients. Conclusions: In the ATACH-2, there was an interaction between race/ethnicity and response to BP lowering treatment after ICH, with White patients having an association between intensive blood pressure reduction and worse outcome.
Introduction
The benefit of blood pressure (BP) lowering treatment after intracerebral hemorrhage (ICH) remains uncertain.1–4 The Antihypertensive Treatment of Acute Cerebral Hemorrhage II (ATACH-2) trial demonstrated no benefit of intensive BP lowering treatment after ICH. 2 A subsequent meta-analysis of randomized trials suggested a potential benefit of BP reduction after intracerebral hemorrhage. 3 Considering the available evidence, the European Stroke Organization (ESO) guidelines recommend lowering systolic BP to less than 140 mmHg in patients with intracerebral hemorrhage presenting within 6 h of symptoms onset (weak recommendation). 4
Previous studies suggested racial/ethnic variation in ambulatory BP trajectories, and response to antihypertensive medications.5–9 However, it is still unknown whether the response to BP lowering treatment after acute ICH differs according to race/ethnicity. In this post hoc analysis of the ATACH trial, we examined race/ethnicity differences and their relationship to BP lowering treatment after ICH.
Methods
This is an exploratory non-prespecified analysis of ATACH-2, a randomized trial of patients with non-traumatic ICH to determine if an intensive antihypertensive goal (goal SBP of 110–139 mm Hg) was superior to a standard goal (goal SBP of 140–179 mm Hg). 2 The anonymized ATACH-2 dataset, received with a local IRB waiver, is available through NINDS at https://www.ninds.nih.gov. The primary outcome is good outcome, defined as 90-day modified Rankin Scale (mRS) score of 0–3. Additional outcomes included neurologic deterioration, hematoma expansion, serious adverse events within 3 months, and withdrawal of care. Neurological deterioration was defined as a decrease from baseline of two or more points in Glasgow Coma Scale score or an increase of four or more points in the National Institutes of Health Stroke Scale score that was not associated with sedation or hypnotic agent use and was sustained for at least 8 h within the 24 h after randomization. Hematoma expansion was defined as an increase of 33% or more in the hematoma volume from baseline to 24 h 2
The primary predictor is race/ethnicity for which we included non-Hispanic categories of White, Black, Asian, and the category of Hispanic. We fit logistic regression models to our outcome and adjusted for 1) Model 1: covariates selected with a restricted LASSO methodology 10 including patient age, intubation, baseline NIH Stroke Scale, and baseline intraparenchymal and intraventricular hemorrhage volume; and 2) Model 2: a priori for patient age, sex, baseline Glasgow Coma Scale, baseline ICH score, hemorrhage location, hemisphere, intubation, surgical intervention, and baseline intraparenchymal and intraventricular hemorrhage volume. We verified the models were not multicollinear by confirming the variance inflation factor was <10. To show the impact of the ATACH-2 intervention of intensive in race categories, we included the interaction of treatment-race/ethnicity in the models and used marginal effects to derive the predicted probability of good outcome by race categories. We also stratified patient by White versus non-White. In a sensitivity analysis, we excluded patients who had withdrawal of care. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Baseline demographics by race/ethnicity category. a
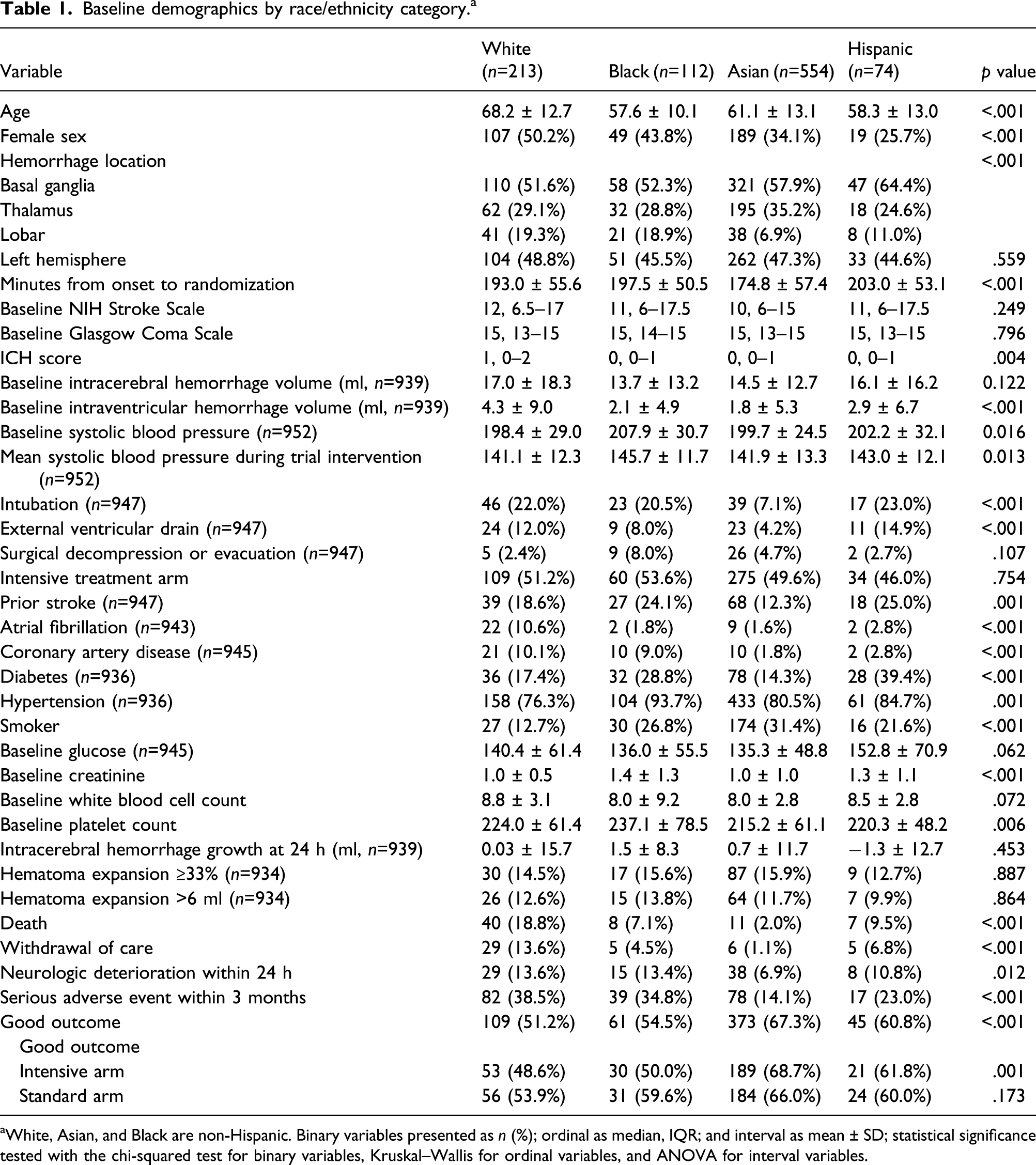
aWhite, Asian, and Black are non-Hispanic. Binary variables presented as n (%); ordinal as median, IQR; and interval as mean ± SD; statistical significance tested with the chi-squared test for binary variables, Kruskal–Wallis for ordinal variables, and ANOVA for interval variables.
Good outcome was achieved in 51.2%, 54.5%, 67.3%, and 60.8% in Whites, Blacks, Asians, and Hispanics, respectively (Table 1). The mean variance inflation factor for Model 1 was 3.17 and for Model 2 was 8.67, indicating acceptable multicollinearity. In Model 1, the predicted probability of good outcome by race category was 62.0%, 52.5%, 63.4%, and 63.7% in Whites, Blacks, Asians, and Hispanics, respectively.
Because the adjusted probability of good outcome was lower for Black patients, we compared Black patients to all other race categories and found their odds ratio for good outcome in Model 1 was 0.50 (95% CI 0.29–0.84, p = .009) and in Model 2 was 0.46 (95% CI 0.27–0.75, p = .002).
Predicted probability of good outcome with the interaction between race and treatment arm.
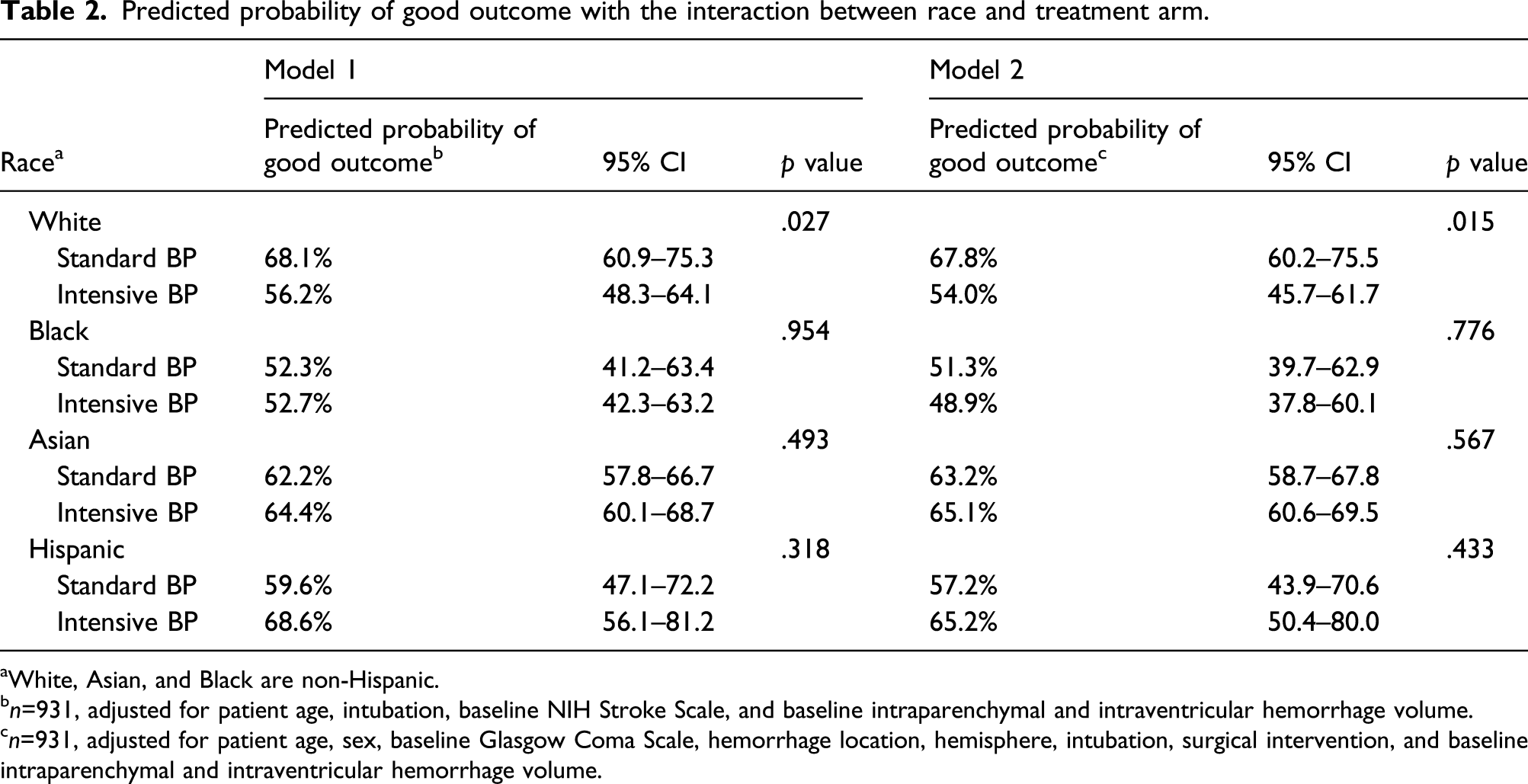
aWhite, Asian, and Black are non-Hispanic.
bn=931, adjusted for patient age, intubation, baseline NIH Stroke Scale, and baseline intraparenchymal and intraventricular hemorrhage volume.
cn=931, adjusted for patient age, sex, baseline Glasgow Coma Scale, hemorrhage location, hemisphere, intubation, surgical intervention, and baseline intraparenchymal and intraventricular hemorrhage volume.
Outcomes in white and non-white patients, according to treatment groups.
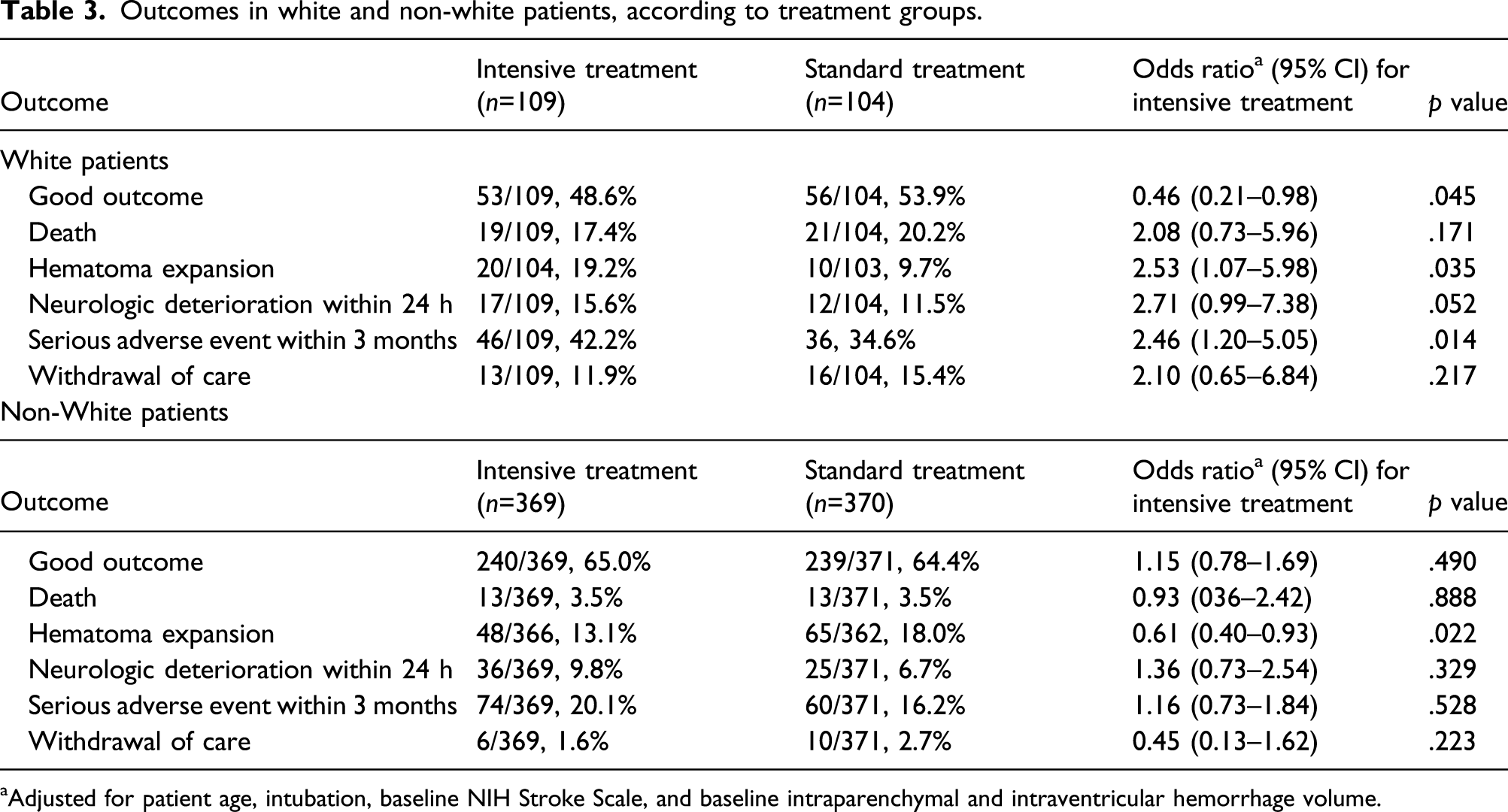
aAdjusted for patient age, intubation, baseline NIH Stroke Scale, and baseline intraparenchymal and intraventricular hemorrhage volume.
Discussion
In this post hoc analysis of the ATACH trial, we found race-related differences in the functional outcome after ICH and in response to BP lowering treatment. In adjusted models, Black patients had the lowest probability of good outcome compared to other race/ethnic groups. When we examined the treatment*race interaction, we found that White patients who received intensive BP treatment had lower predicted probability of good outcome compared to standard treatment. Otherwise, there were no differences in the functional outcome between both treatment arms in other groups.
There are race/ethnic-related disparities in presentation, risk factors, and outcome after ICH.11–15 Analysis of the Virtual International Stroke Trials Archive and Efficacy of Nitric Oxide in Stroke trial demonstrated no difference in 90-day mRS between Black, Asian, and White patients. The results were echoed in a subsequent analysis of the Ethnic/Racial Variations of Intracerebral Hemorrhage study which also demonstrated no race/ethnic differences in 3-month functional outcome after ICH. 14 However, an analysis of the Get With The Guidelines-Stroke (GWTG-Stroke) registry found that Black race was associated with lower odds of good outcome after ICH which is in accordance with our findings. 15 The inconsistency in these results may be attributed to differences in study design and inclusion criteria. For example, previous studies included both supratentorial and infratentorial ICH, unlike the present study which only included supratentorial hemorrhage.
Interestingly, the interaction between treatment and race/ethnicity was only significant in White patients, who had lower probability of good outcome when receiving intensive BP reduction. In addition, intensive treatment was associated with a higher risk of serious adverse events in White patients but not in non-White patients. Surprisingly intensive treatment was also associated with a higher risk of hematoma expansion in White patients and a lower risk of hematoma expansion in non-White patients. The reason for the difference in response to BP lowering treatment between White and non-White is not clear and requires further investigation. It is possible that the differences in hemorrhagic stroke etiology, risk factors, and response to antihypertensive medications between White and non-White patients mediated the difference in response to BP lowering treatment. For example, White patients in our cohort were older, and more likely to have atrial fibrillation and cardiac ischemic disease which could have potentially made them more prone to serious adverse events with BP lowering treatment.
Future studies are needed to understand the differences in BP trajectories, autoregulation physiology, and response to BP lowering treatment after acute stroke among different race/ethnicity groups. Moreover, our study highlights that Black patient were underrepresented in trials that investigated BP management strategies after intracerebral hemorrhage and future studies focused on Black patients may be warranted.
Limitations
Despite the large sample size and the prospective nature of the study, our study has multiple limitations that need to be taken into account. First, our analysis was exploratory analyses and prone to chance findings. Second, despite the large sample size of the overall study cohort, the sample size of each race/ethnic group is modest. Finally, our results cannot be applied to patients with infratentorial hemorrhage.
Conclusion
In the ATACH-2, Black patients had a lower probability of good outcome in adjusted models. In addition, there was an interaction between race/ethnicity and response to BP lowering treatment after ICH, with White patients having an association between intensive blood pressure reduction and worse outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr de Havenon reports investigator-initiated funding from AMAG and Regeneron pharmaceuticals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr de Havenon is supported by NIH-NINDS K23NS105924.
Ethical approval
The anonymized ATACH-2 dataset, received with a local IRB waiver
Informed consent
All participants or their legally authorized representative provided written informed consent before randomization