
Abstract
Introduction
Despite the availability of prevention and therapies of stroke, their implementation in clinical practice, even of low-cost ones, remains poor. In 2015, the European Stroke Organisation (ESO) initiated the ESO Enhancing and Accelerating Stroke Treatment (EAST) program, which aims to improve stroke care quality, primarily in Eastern Europe. Here, we describe its methods and milestones.
Patients and methods
The ESO EAST program is using an implementation strategy based on a ‘detecting-understanding-reducing disparities’ conceptual framework: stroke care quality is first measured (after developing a platform for data collection), gaps are identified in the current service delivery, and ultimately feedback is provided to participating hospitals, followed by the application of interventions to reduce disparities. The ESO EAST program is carried out by establishing a stroke quality registry, stroke management infrastructure, and creating education and training opportunities for healthcare professionals.
Results
Program management and leadership infrastructure has been established in 19 countries (Country Representatives in 22 countries, National Steering Committee in 19 countries). A software platform for data collection and analysis:
Discussion
ESO EAST is the first pan-Eastern European (and beyond) multifaceted quality improvement intervention putting evidence-informed policies into practice. Continuous monitoring of stroke care quality allows hospital-to-hospital and country-to-country benchmarking and identification of the gaps and needs in health care.
Introduction
Effective interventions to prevent and treat stroke exist; however, their implementation into clinical practice has proven to be challenging. There are well-documented examples of poor translation from standard stroke treatment guidelines to clinical practice, including treatment of acute stroke with intravenous thrombolysis or secondary prevention of stroke using oral anticoagulants in patients with atrial fibrillation.1–6
Identifying and quantifying the implementation gap could lead to understanding of the magnitude and source of the problem, and finally to developing strategies to improve the access to evidence-based stroke treatments. Participation in quality monitoring and improvement programs has improved adherence to performance measures.4,7 Moreover, improving adherence to such key performance indicators has also been shown to be associated with better outcomes after stroke.5,6,8–11 Therefore, participation in quality monitoring is highly desirable and the most recent international stroke care guidelines support quality monitoring becoming a routine part of clinical care.4,12
Based on a recent systematic review, some quality control for stroke care has been established in 26 countries, primarily in Western Europe, the United States, and Canada, although it was found that in most countries nation-wide coverage was missing. 13 To address the issue of stroke care quality in Eastern Europe, in 2015 the European Stroke Organisation (ESO) developed “European Stroke Organisation – Enhancing and Accelerating Stroke Treatment” (ESO EAST) 14 to improve the implementation of evidence-based stroke treatments, as guideline adherence was expected to be lower in Eastern European countries than in Western European countries. Here we describe the methods and milestones for the first four years of ESO EAST’s existence.
Methods
ESO EAST is a quality improvement program of ESO to improve translation of knowledge from clinical studies and international guidelines into everyday clinical practice. The ultimate goal is to measurably improve stroke care at both hospital, and national levels. ESO EAST uses audit and feedback as part of multifaceted interventions which have previously been shown to be effective in improving uptake of evidence-based stroke treatments. 15 Scalable information technology (IT) solutions are an integral part of the program allowing extensive quality improvement processes.
Overall goals of the ESO EAST Project
Improve patient outcomes after stroke, through evidence-based treatments. Decrease disparities in stroke care, focusing on Eastern European countries compared to Western European countries. Develop a method of stroke care quality improvement, scalable beyond ESO EAST countries.
The ESO EAST method is presented below as: (I) what is implemented, (II) who should implement the program, and (III) how the program is implemented.
(I) What is implemented
ESO EAST aims to improve the quality of stroke care, which is delivered from the admission of a patient through to his/her discharge from that hospital. Quality of stroke care relates to imaging, acute care, prevention of complications, secondary prevention and rehabilitation.
At this stage, primary prevention has not been a focus of the project. Pre-hospital care, including Emergency Medical Services monitoring and improvement has also not yet been addressed; however, this is included in future directions for ESO EAST.
(II) Who participates in the quality improvement program
The implementation team and purveyors conduct the implementation process of the stroke care quality program (Table 1). The ESO EAST program was initiated by the ESO; it comprises the ESO EAST Steering Committee, and the management and Registry of Stroke Care Quality (RES-Q) teams. The RES-Q team is focused on developing the registry platform, and handling communications pertaining to data analysis. RES-Q is a web-based platform used to collect stroke quality of care metrics, and provide reports, feedback and benchmarking at both hospital and national levels. The RES-Q platform is discussed in more detail in section A.2 of Results. The Country Representatives create National Steering Committees to implement the ESO EAST program, which is customised to country specific goals. The involvement of stakeholders such as national professional societies and Ministries of Health is usually needed. A diagram illustrating the organisational structure of the program can be found in Figure S1 of the Supplement. The main strategy is to build on the existing leadership structure in each country or encourage developing one if it is missing, and to coordinate actions between these National Steering Committees. This strategy is supported by the ANGELS Initiative 16 which is a non-promotional quality improvement program by Boehringer Ingelheim, endorsed by ESO, and providing extensive support for ESO EAST such as training and funding through ESO grants. The ANGELS Initiative employs consultants who provide support at a hospital level, including strategies to improve stroke care through standardisation and improved logistics, and motivational tools such as awards for meeting performance thresholds.
Implementation team and purveyors.
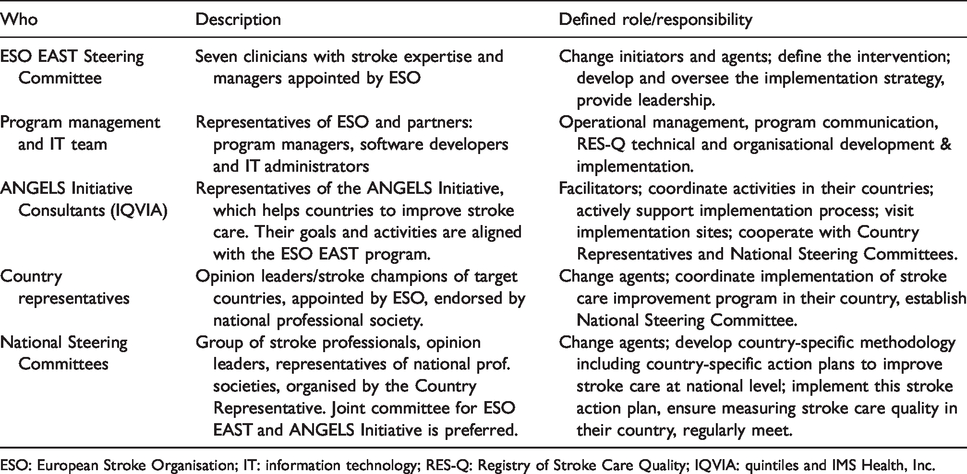
ESO: European Stroke Organisation; IT: information technology; RES-Q: Registry of Stroke Care Quality; IQVIA: quintiles and IMS Health, Inc.
ESO EAST is focused on target groups of stakeholders, described in Table 2.
Target audience and implementation sites.
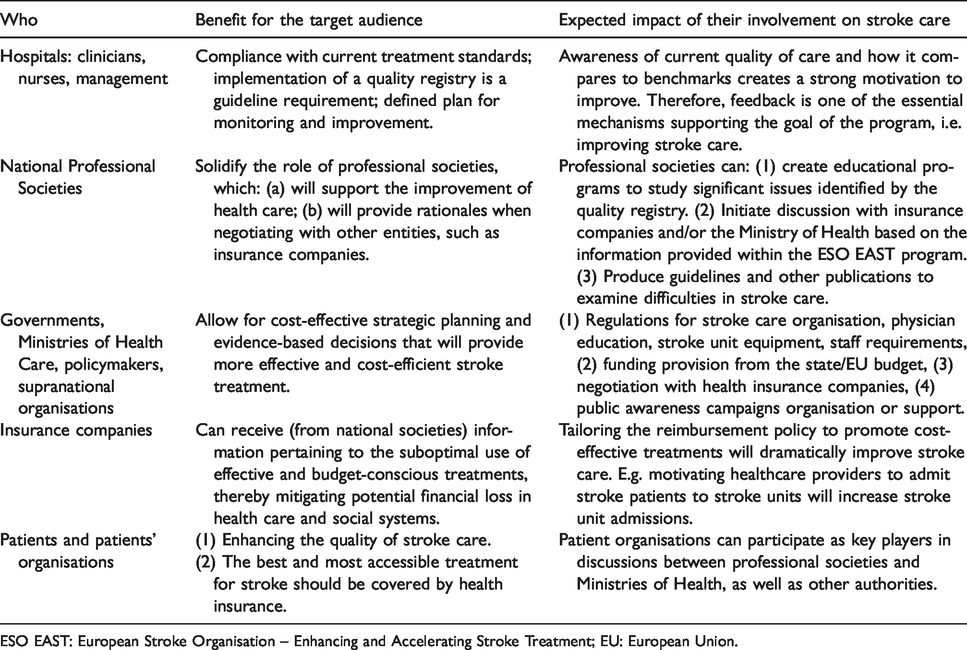
ESO EAST: European Stroke Organisation – Enhancing and Accelerating Stroke Treatment; EU: European Union.
(III) How evidence-based stroke treatments are implemented
The overall implementation strategy is based on a ‘detecting-understanding-reducing disparities’ conceptual framework. 17 This framework focuses on evaluating and improving healthcare systems, as opposed to frameworks focused on community or societal determinants as part of a public health perspective.17,18 Consistent with the framework, we considered the primary barrier to improving the uptake of evidence-based treatments to be the lack of knowledge of the current level of quality of stroke care. If gaps are not systematically monitored, including their severity, a lack of understanding of the underlying mechanisms will make it impossible to design effective (e.g. country and hospital specific) quality improvement interventions. Monitoring the quality of stroke care also allows for the establishment of an ‘audit and feedback’ mechanism as the initial motivation strategy for healthcare professionals, both to improve stroke care and provide data. 15 ‘Audit and feedback’ requires reporting of results back to hospitals, therefore provision of reports must be integrated into the project at an early stage. The logical model of implementation is described in Figure 1. Recognition of champion stroke centres through awards based on performance is used as another motivation tool through the ANGELS Initiative. 16
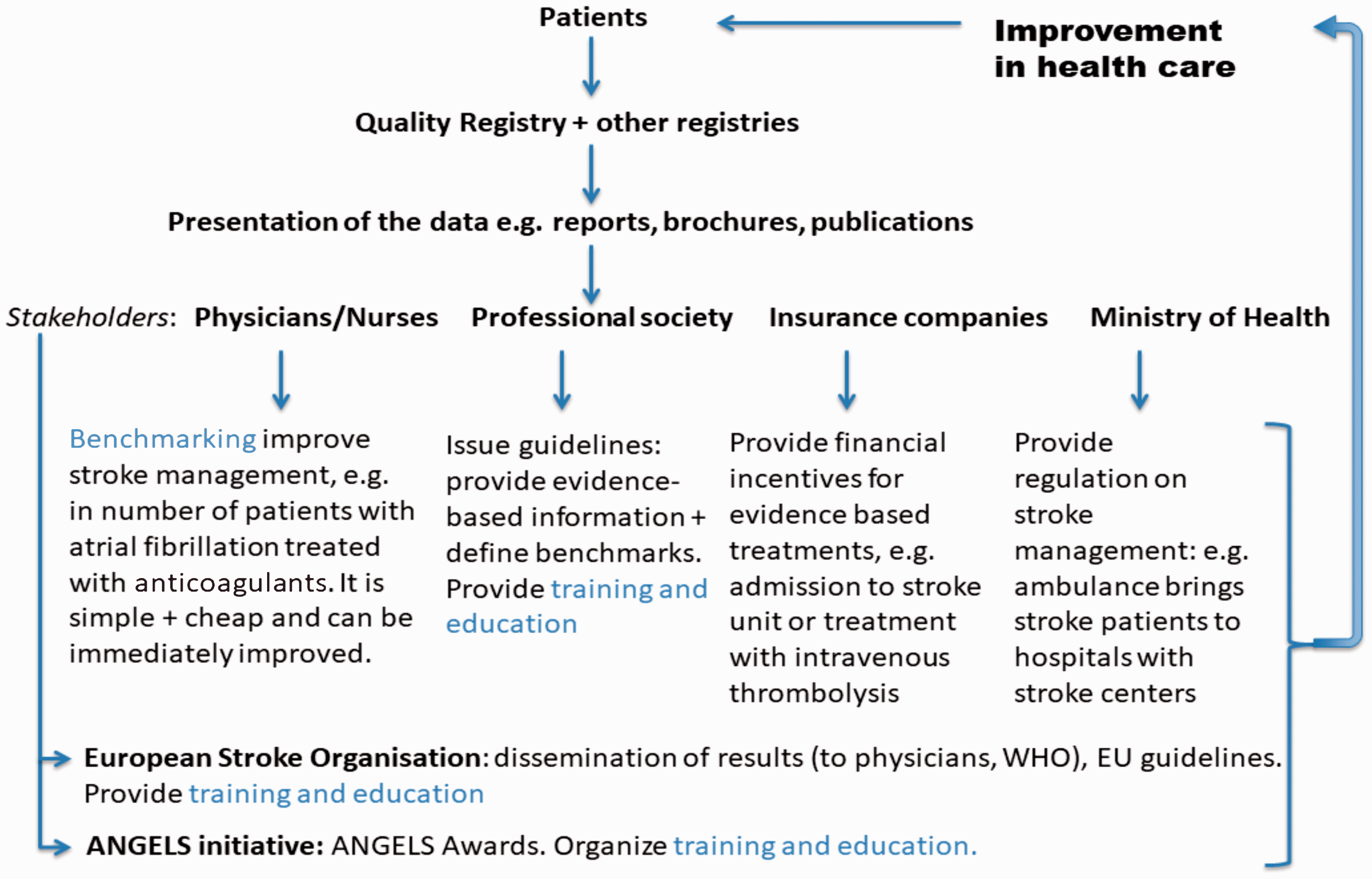
Logical model. The logical model describes how improvement in stroke care will be achieved. As mentioned above, ‘audit and feedback’ is the primary mechanism of intervention. Once gaps in stroke care are identified, additional interventions are planned.
Obtaining knowledge about the quality of stroke care has three components: (A) Stroke quality registry, (B) stroke management infrastructure which organises and performs the acquisition of quality metrics to implement programs for stroke care improvement, and (C) education and training.
Brief information on these three components is provided below, and more information is in the Supplement.
A stroke quality registry (A) requires: (A.1) selection from recognised quality metrics based on previously published data,8,13 development of definitions and of the data collection form and (A.2) a software solution including development of a web-based platform.
Creation of effective stroke management infrastructure (B) is a complex task in countries where there are no organised professional societies or where societies do not have effective power to implement systematic changes in stroke care. There are four components necessary for building an effective project management structure: (B.1) human infrastructure, (B.2) leadership, (B.3) communication and (B.4) planning, including progress measurement. Project management infrastructure effectiveness is measured by: the number of hospitals recruited for a quality improvement program, the number of cases enrolled into the quality registry database, and in the future by the improvement in stroke care quality as evidenced by results at different time points.
Several types of education and training (C) were identified as pivotal (and complementary to existing education, e.g. ESO summer or winter schools). Research skills (C.1), which are not part of medical education in Eastern Europe, are important for e.g. data analysis or interpreting results from registries.
Additional educational activities were added, addressing two specific needs in improving uptake of evidence-based treatments: (C.2) improving stroke team members’ skills in intravenous thrombolysis treatment using simulations and (C.3) nurse skills. All activities from sections (A), (B), and (C) here, as well as phases and timelines of ESO EAST are detailed in the Supplement.
Results
(A) Stroke quality registry
A.1 Selection and/or definition of quality metrics and development of the data collection form: the initial form was finalised in 2016, and revised in 2017. It contained questions related to 28 metrics for ischemic stroke, intracerebral haemorrhage, subarachnoid haemorrhage and cerebral venous thrombosis. The full collection form is in Supplemental Table S1.
A.2 A software platform for data collection: RES-Q was developed; pilot tested in 2016 and has been used to collect data since 2017. 19 Software pipelines for data processing: to support ESO EAST member hospitals with limited data processing and analysis resources, the RES-Q platform was extended to provide descriptive reporting at both the hospital and national level. Custom data processing software was created to automatically generate data reports and presentations quarterly, which are made available to all hospitals and country representatives online. Descriptive statistics are available through an online ‘dashboard’ interface, which provides graphical representations of data updated hourly, and provides a secure portal for downloading all reports. Examples of the dashboards can be found in Figure 2.
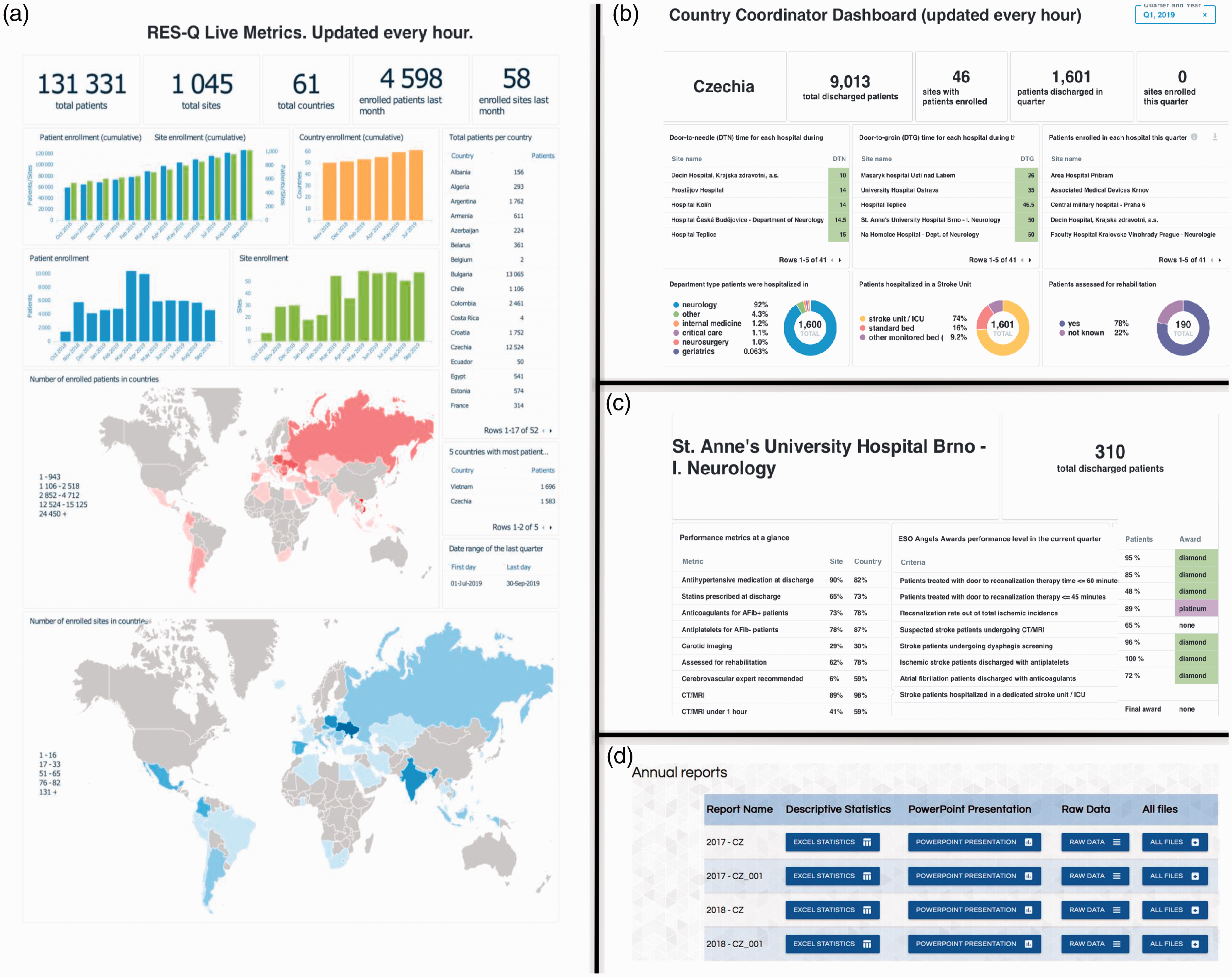
Functionalities of RES-Q website. (a) The live metrics page documents the number of patients enrolled altogether, and per country (available at www.qualityregistry.eu without log in). (b) provides an overview of results of stroke care quality for the whole country. (c) is a hospital dashboard allowing hospitals to view their results and benchmark against national results and the ANGELS award criteria. (d) is the download function allowing hospitals to download data in different formats including as a PowerPoint presentation of the results.
(B) Project management infrastructure
B.1 Human infrastructure: Six ESO EAST Steering Committee members oversee the program and 22 Country Representatives, which were selected to drive its national implementation. Based on the Annual Country Reports (April 2018), 19 countries have already established a National Steering Committee (see Table S4 in Supplement). Twelve countries have involved the ANGELS Initiative in the National Steering Committee.
B.2 Leadership building: Leadership building at national level was encouraged by: mentoring by international experts; participation of the ESO EAST Steering Committee members at >25 local and national meetings and conferences between 2015 and 2018; national strategy documents (Action Plans) development by Country Representatives; a lecture on leadership at the ESO EAST Annual Meeting in 2018.
B.3 Communication: Several communication tools were used: full day ESO EAST Annual Meetings and online resource sharing tools (ESO EAST webpage as part of the ESO website, 14 Facebook, Twitter, LinkedIn). For detailed information see Supplemental results.
B.4 Planning and measuring progress: Quality monitoring was established in 19 out of 22 countries and 395 hospitals by the end of 2018. More than 200 national reports and 3000 hospital reports on stroke care quality have been created. Seventeen posters on stroke care quality in ESO EAST countries based on RES-Q data were presented at the 2018 ESO Conference and another 14 at the 2019 ESO Conference. Data from over 95,000 patients from >750 hospitals and 56 countries have been collected between September 2016 and May 2019. RES-Q has increased participation from the initial 21 countries of ESO EAST to include hospitals in Western Europe, Southeast Asia, Latin America and the Middle East and North Africa regions. Based on the Annual Country Reports (April 2018), provided by 19 countries of 22, 16 countries defined the network of hospitals where the improvement program should be implemented, and 15 countries defined goals for improvement in their country. A timeline representing ESO EAST project implementation and progress can be found in Figure S2 of the Supplement.
(C) Education and training
C.1 Science education: In 2015, a one-week workshop for participants from ESO EAST countries took place in Brno, Czech Republic. Eighteen physicians from 16 countries were selected based on their commitment to publish a scientific paper in one year. The delegates were trained in research design and basic statistics, provided with a list of relevant publications, software licenses and offered mentoring.
C.2 Stroke team members’ skills: Simulation training. The stroke simulation training program aims to improve acute stroke management and thrombolysis treatment. It has been provided since 2016 at St. Anne’s University Hospital Brno, Czech Republic for ∼450 health professionals from eight ESO EAST countries. This work was also supported by staff from the ANGELS Initiative who frequently followed up with in-situ simulation in other participating stroke centres. Subsequently two stroke simulation centres were established based on the Brno model, in Russia and in Ukraine.
C.3 Nurse skills: In 2016, the Stroke Unit Nursing Education Project was initiated and nurses from 12 countries participated in a three-day course.
Discussion
Initiation of this multifaceted program across Central and Eastern European countries is a major achievement of ESO EAST. This achievement is documented by establishing International and National Steering Committees, recruitment of number of hospitals and enrolment of a large number of patients into the newly developed stroke quality registry, RES-Q. RES-Q has been rapidly adopted in over 750 hospitals in 56 countries by April 2019 (∼50 hospitals per month), with more than half of the participation coming from outside of the initial ESO EAST member countries. The establishment of leadership groups and organised collection of data on current stroke care quality have created a platform for driving future change in the stroke practice across the region.
In 2018, ESO conducted a survey in 44 European countries on the delivery of acute stroke services, whereby large inequalities in acute stroke care were reported disadvantaging the Eastern European region, and thus further underscoring the need for a multifaceted quality improvement program such as ESO EAST. 20 The evaluation of stroke care quality, the first step of ESO EAST, is lagging behind many Western European countries, such as the United Kingdom and Spain, which have been auditing stroke performance for 10 years.21,22 Other countries, including Sweden, the USA, Denmark, Austria, and the Netherlands have established quality registries to monitor performance.5,23–26 Australia provides a national registry and audit program for stroke, along with structured quality improvement programs. 7 ESO EAST has similar goals to these programs, with emphasis on using modern technologies to provide online feedback and benchmarking. Most established programs are national programs, whereas ESO EAST has succeeded in achieving international adoption. ESO EAST also differs in that it is focused on creating quality improvement initiatives, which can be implemented in low-resource health systems across heterogenous economic and political regions. The ESO EAST tools are made available at no cost with the main funding being provided by ESO, and the Stroke program in St. Anne’s University Hospital in Brno, Czech Republic (i.e. RES-Q developer).
RES-Q, as a central quality registry, seemed to be an appropriate solution for middle- and lower-income countries due to: cost savings, the possibility of sharing expertise, and the potential to use country-to-country benchmarking, which could provide stakeholders in healthcare guidance to defining stroke healthcare priorities. RES-Q’s adoption and utilisation have been facilitated by several factors; multiple translations of the RES-Q form, availability of training materials (both downloadable documents and online videos), and finally by the onsite presence of ANGELS Initiative representatives in many countries.
For the future, it needs to be documented that feedback to stroke centres based on monitoring performance indicators will improve adherence to guidelines and translation of evidence into routine clinical practice. 23 For countries with limited resources, it is crucial to demonstrate that improved adherence does not necessarily result in an increase in costs. Many improvements, such as streamlining logistics, reducing complications, and providing the proper medication (not necessarily more medication), do not require more resources; only better utilisation of existing ones. RES-Q established the opportunity for country specific interventions to be targeted at underserved areas in stroke care, and the ability to monitor improvements over time.
Central and Eastern Europe is a heterogeneous region in terms of stroke care quality. For example, in the Czech Republic (and in the Slovak Republic), there is a long history of managing stroke care at the national level, with national stroke conferences having been organised for 46 years (as of 2018), all citizens have health insurance, healthcare is provided for minimal cost, and a network of 45 certified stroke unit exists. In contrast, in many Eastern European countries major steps for stroke improvement need to still be undertaken and include: (1) certification of stroke hospitals, (2) increased stroke awareness of major stakeholders such as the Ministry of Health, and (3) strengthening the role of stroke professional societies as important drivers of high quality stroke care.
There are still significant limitations and challenges related to data collection and analysis. So far there is low comparability for several metrics, which could be improved, e.g. using stricter definitions for metrics. However, using stricter definitions, for e.g. stroke unit in countries with reduced resources may limit benchmarking and also deter participants who already exhausted utilisation of the resources, which could optimally be available to them in their socio-economical setting. Similarly, emphasising control of data quality through on-site auditing, or double data entry improves comparability, but may hamper data representativeness due to lower overall participation, as countries do not have resources for an increased workload. The data sharing and research cultures in many Central and Eastern European countries are different compared to Western European countries and will continue to pose a challenge for obtaining comparable and representative national data. For the future, funding may also pose a challenge.
ESO EAST actions are in line with other strategic plans, quality improvement efforts and initiatives. Firstly, public health experts from Eastern Europe recommended four priorities for public health actions: (a) implementing registries and monitoring systems, (b) developing best practice interventions, (c) creating a scientific base for public health interventions, and (d) engaging the public. 27 ESO EAST has included the first three of these recommendations in its quality improvement program. Secondly, the recently published Action Plan for Stroke in Europe 2018–2030 provides support to many ESO EAST activities, including assessment of the quality of stroke services. 28 Thirdly, closer collaboration of Eastern European countries is a recommendation within previous strategic documents on public health. 27
In conclusion, ESO EAST aims to improve stroke care using a ‘detecting-understanding-reducing disparities’ conceptual framework. To our knowledge this is the first, non-remunerative, pan-Eastern European (and beyond) multifaceted intervention used across a large number of countries that aims to improve access to evidence-informed policies and practices in real-world services. Actions are structured according to a bottom-up process framework that empowers health personnel, highlights unmet patient needs, and facilitates leadership development at local, regional, national and international levels. Educational activities are tailored based on the results and needs of local stroke professionals, including allied healthcare. It contributes significantly to the European knowledge base and language on stroke care through stroke experts’ community empowerment.
Supplemental Material
ESO897156 Supplemental material - Supplemental material for Enhancing and accelerating stroke treatment in Eastern European region: Methods and achievement of the ESO EAST program
Supplemental material, ESO897156 Supplemental material for Enhancing and accelerating stroke treatment in Eastern European region: Methods and achievement of the ESO EAST program by Robert Mikulík, Valeria Caso, Natan M Bornstein, Veronika Svobodová, Francesca Romana Pezzella, Andreea Grecu, Steven Simsic, Zuzana Gdovinova, Anna Członkowska, Tamara S Mishchenko, Yuriy Flomin, Ivan G Milanov, Silva Andonova, Cristina Tiu, Anita Arsovska, Hrvoje Budinčević, Stanislav A Groppa, Daniel Bereczki, Janika Kõrv, Tatiana Kharitonova and Milan R Vosko in European Stroke Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RM, ZG, JK, HB, CT and YF have received speaker’s fee from Boehringer Ingelheim. ZG has also received grant from Boehringer Ingelheim, and speaker’s fee from Pfizer, MSD and Bayer. JK has received travel grant from Boehringer Ingelheim, and JK and HB have also received speaker’s fee from Pfizer and Bayer. YF has also received speaker’s fees and support for attending at international meetings from Pfizer, Sanofi Genzyme, Bayer, Merz, Ipsen and Octapharma. TSM has received speaker’s fee from Bayer. AC has as received speaker’s fee from Ever Pharma.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is financed by unrestricted grants from European Stroke Organization and national grants of the St. Anne’s University Hospital Brno, Czech Republic. European Stroke Organization received funding for ESO-EAST from Boehringer Ingelheim International GmbH and Ever-Pharma. RM and VS were supported by the project no. LQ1605 from the National Program of Sustainability II (MEYS CR) and RM by Ministry of Education, Youth and Sports of the Czech Republic project no. LTV17018 (INTER-EXCELLENCE). The Stroke Unit Nursing Education Project (SUNEP) was supported by the ESO courtesy of an unrestricted grant provided by Boehringer Ingelheim.
Informed consent
Not applicable.
Ethical approval
Not applicable.
Guarantor
RM.
Contributorship
(1) RM, MV, VS, AG, SS made a substantial contribution to the concept and design of the work; RM, AG, SS acquitted, analyzed and interpreted the data, (2) RM, MV, VS, AG, SS drafted the article, all authors revised it critically for important intellectual content, (3) all authors approved the version to be published, (4) each author participated sufficiently in the work to take public responsibility for appropriate portions of the content. All country representatives substantially contributed on to the design of the work; acquisition, interpretation of data, revised manuscript critically for important intellectual content, and approved the version to be published.
Acknowledgements
We would like to thank the European Stroke Organisation, national stroke societies, Country Representatives and other ESO-EAST country delegates, physicians, nurses, as well as technical staff and IT system developers from the International Clinical Research Center of St. Anne’s University Hospital Brno, Czech Republic, for assistance and guidance in this project. ESO-EAST project highly benefited with synergistic quality improvement project Angeles.
ORCID iDs
Robert Mikulík https://orcid.org/0000-0002-7458-5166 Cristina Tiu ![]()
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.