
Abstract
Purpose
Translating research evidence into clinical practice often uses key performance indicators to monitor quality of care. We conducted a systematic review to identify the stroke key performance indicators used in large registries, and to estimate their association with patient outcomes.
Method
We sought publications of recent (January 2000–May 2017) national or regional stroke registers reporting the association of key performance indicators with patient outcome (adjusting for age and stroke severity). We searched Ovid Medline, EMBASE and PubMed and screened references from bibliographies. We used an inverse variance random effects meta-analysis to estimate associations (odds ratio; 95% confidence interval) with death or poor outcome (death or disability) at the end of follow-up.
Findings
We identified 30 eligible studies (324,409 patients). The commonest key performance indicators were swallowing/nutritional assessment, stroke unit admission, antiplatelet use for ischaemic stroke, brain imaging and anticoagulant use for ischaemic stroke with atrial fibrillation, lipid management, deep vein thrombosis prophylaxis and early physiotherapy/mobilisation. Lower case fatality was associated with stroke unit admission (odds ratio 0.79; 0.72–0.87), swallow/nutritional assessment (odds ratio 0.78; 0.66–0.92) and antiplatelet use for ischaemic stroke (odds ratio 0.61; 0.50–0.74) or anticoagulant use for ischaemic stroke with atrial fibrillation (odds ratio 0.51; 0.43–0.64), lipid management (odds ratio 0.52; 0.38–0.71) and early physiotherapy or mobilisation (odds ratio 0.78; 0.67–0.91). Reduced poor outcome was associated with adherence to swallowing/nutritional assessment (odds ratio 0.58; 0.43–0.78) and stroke unit admission (odds ratio 0.83; 0.77–0.89). Adherence with several key performance indicators appeared to have an additive benefit.
Discussion
Adherence with common key performance indicators was consistently associated with a lower risk of death or disability after stroke.
Conclusion
Policy makers and health care professionals should implement and monitor those key performance indicators supported by good evidence.
Introduction
In recent years, there have been concerted efforts to develop and implement clinical practice guidelines for the management of patients with acute stroke. 1 Clinical guidelines are written to promote diagnostic or therapeutic interventions applicable to the majority of patients in most circumstances. However, the use of guideline recommendations for individual patients has traditionally been left to the discretion of individual clinicians. 2 A recognised approach to assist the translation of research evidence into clinical practice is to monitor the quality of care using standardised performance indicators 3 also called quality indicators, process of care measures or key performance indicators (KPIs). Performance indicators are standards of care which imply that health care professionals are providing inadequate care if eligible patients do not receive that standard of care. Performance indicators can be used to monitor the adherence to current guidelines, and support the transfer of new evidence into everyday clinical practice. 4
There are now numerous stroke interventions that have been shown to improve patient outcomes in research trials; admission to specialised stroke units, use of intravenous thrombolysis, mechanical thrombectomy, antiplatelet drugs, anticoagulants and management of fever, hyperglycaemia and swallowing dysfunction for selected patient groups.5–9 However, application into routine practice is challenging and regular monitoring is important. 10 Ideally, implementation of clinical evidence can be demonstrated using a range of stroke KPIs, which offer proxy measures for ideal care being delivered. In turn, this would lead to evidence of better patient outcomes. 11
In a previous systematic review of the association between stroke quality (performance) indicators and patient-centred outcomes, out of 14 studies that met the eligibility criteria; 9 had mostly positive associations, whereas 5 reported little or no association with a lower risk for mortality, disability, medical complications, stroke recurrence or patient dissatisfaction. 12 A limitation of this review was the exclusion of stroke unit care as a performance indicator. With the ongoing developments in clinical guidelines and quality indicators for monitoring the application of these guidelines,10,13 we believe that there is a need for up-to date comprehensive information on KPIs for stroke care.
We aimed to conduct a systematic literature review to identify the KPIs that have been described in stroke care and to summarise their association with patient outcomes. We intend that information gathered from this review will provide decision makers and health care professionals with information on reliable and meaningful KPIs that can be implemented to improve outcomes post stroke.
Methods
This review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 This review was registered in Prospero Database (CRD42016050798).
Search strategy
Searching sources were Ovid Medline, Embase and PubMed databases, and relevant references from screening the bibliographies of the initial articles included in the search.
We used Medical Subject Headings (MeSH) and all subheading terms including ‘stroke’, ‘cerebrovascular accident’, ‘cerebrovascular disease’, ‘cerebrovascular disorders’, ‘brain hemorrhage’, ‘intracranial hemorrhages’, ‘brain infarction’, ‘subarachnoid hemorrhage’, ‘health care quality’, ‘quality of health care’, ‘quality indicators, health care’, ‘quality assurance, health care’, ‘quality control’, ‘quality indicator’, ‘performance indicator’, ‘register’, ‘registries’, ‘clinical audit’, ‘treatment outcome’, ‘case fatality rate’, ‘mortality’, ‘survival’, ‘disability’, ‘functional status’, ‘hospitalization’, ‘cost’, ‘quality of life’, ‘complication’, ‘hospital discharge’ and ‘stroke recurrence’. Our search was restricted to full-text manuscripts published in English from 1 January 2000 to 24 May 2017.
The search strategies for different databases are detailed in the Online Supplement.
Inclusion criteria
We included national or regional registers that recorded the independent association (after adjusting for at least age and a measure of stroke severity) between the KPIs and stroke patient outcomes, and involved patients from at least three hospitals.
Exclusion criteria
We excluded reports that were reviews or did not provide odds ratio (OR), hazard ratio (HR) or rate ratio (RR) data.
Screening and quality assessment
One author (GU) reviewed each title and excluded obviously irrelevant studies. Articles identified as potentially relevant underwent a full review by two authors (GU and PL) to determine if they met the inclusion criteria. In cases of disagreement, final determination was by discussion and consensus.
Data extraction
We used a standardised form to record information on country, main inclusion or exclusion criteria for the recruitment of participants, sample size, stroke severity measure, KPIs and outcome(s) reported, and reported results (and 95% confidence interval (CI)).
Data analysis
Initially, the identified KPIs and their association with the patient outcomes were categorised on whether the authors reported a significant association between the KPI and patient outcome. There was then a further quantitative analysis (meta-analysis) of the relationship (adjusted for at least age and stroke severity) between the KPIs identified and patient outcomes. Some checking of the consistency of KPIs and outcomes was required with grouping of similar KPIs. For the meta-analysis, we sought information on case fatality and poor outcome (death and disability or requiring support) after stroke.
The meta-analysis was done using the Review Manager (version 5.3) software. Log ORs were combined using an inverse variance analysis (random effects model). First, we assumed that HRs and RRs approximate the ORs and performed the primary meta-analysis including all studies reporting on association of KPIs with case fatality and poor outcome. Second, we performed sensitivity meta-analysis by excluding studies that used HR or RR as measures of association.
Results
The review profile is shown in Figure 1. We identified 3606 references from which 30 studies15–44 were eligible for the qualitative review. Among these, only 22 were eligible for the meta-analysis.
Review profile showing selection of studies. HR: hazard ratio; KPI: key performance indicator; OR: odds ratio.
Included studies
Studies eligible for the systematic literature review.
Organised stroke care included wards which encompassed multidisciplinary team-working, a physician with an interest in stroke, as well as taking into account the proportion of time spent (>50% of their length of stay) in such an environment. The wards that encompassed organised stroke care included neurology, elderly care, stroke specific unit and intensive care unit.
The complications that were considered in the analysis included pneumonia, urinary tract infection, pressure ulcer, falls, venous thromboembolism and constipation.
OCI is a summary score based on the presence of occupational therapy or physiotherapy, stroke team assessment and admission to a stroke unit. A score of zero indicates that stroke patients received none of these services, and higher scores indicate access to more services. The ‘organised care’ index was classified as having received 0, 1, 2 or 3 services.
n indicates number of applicable PoC; i, number of PoC adhered to.
The 15 processes of care consisted of CT scan < 24 h since admission, swallow < 24 h since admission, allied health < 24 h since admission, incontinence addressed, discharged on antiplatelet agent, fever > 38.5 managed, documented premorbid function, documented discharge needs, regular neurology observations for the first 24 h of admission, physiotherapist within 24 h, occupational therapist within 24 h, speech pathologist within 24 h, enteric feeding if nil by mouth > 48 h, aspiration avoidance and DVT prophylaxis if not ambulant.
Secondary prevention included deep vein thrombosis prophylaxis, discharged on lipid-lowering medication, discharged on blood-pressure–lowering medication and discharged on antithrombotics.
Education to patients consisted of lifestyle advice, information on sexuality poststroke, information about peer support, information on self-management programs, carer training and providing contact to patient.
ACE: angiotensin-converting enzyme; ADLs: Activities of Daily Living; AF: atrial fibrillation; BI: Barthel Index; CNS: Canadian neurological scale; CT: computerised tomography; MRI: magnetic resonance imaging; CI: confidence interval; DVT: deep vein thrombosis; FIM: functional independence measure; GCS: Glasgow coma scale; HR, hazard ratio; IS: ischaemic stroke; LoS: length of hospital stay; mRS: modified Rankin Scale; NIHSS: national institute of health stroke scale; PT: physiotherapy; OR: odds ratio; OT: occupational therapy; RR: rate ratio; SAH: subarachnoid haemorrhage; SSS: Scandinavian stroke scale; SSV: six simple variable; OCI: organised care index; PoC: processes of care.
The majority (23/30) of the included studies used prospective recruitment while the rest25,26,28–30,35,37 consisted of retrospective audits. Thirteen16,19,20,23,24,29,30,32,34,35,40,41,43 included only patients with ischaemic stroke, and two33,42 included only patients with intracerebral haemorrhage. The remainder included both ischaemic and haemorrhagic stroke. Among those studies that included both types of stroke, six15,17,18,22,28,36 excluded patients with subarachnoid haemorrhage.
For the association between KPIs and patient outcomes, the majority 22 of the included studies used OR, six studies16,19,23,29,38,40 used HR while the remaining two17,18 used rate RR. The included studies also used different measures for stroke severity as a case mix variable for adjustment to estimate the independent association between a KPI and a patient outcome. Twenty of the included studies used validated tools including National Institute of Health Stroke Scale,28,30,40–44 Scandinavian Stroke Scale,16–21,29 Canadian Neurological Scale,32–34 Six Simple Variables25,26 and Glasgow Coma Scale, 36 while the remainder used stroke severity proxies such as level of consciousness, incontinence, dysphagia, dysphasia, paralysis and disability.
Reporting of published KPIs
As there were some variations in data definitions and analysis methods, several assumptions were made to allow easy comparison between the studies:
Swallow/nutritional assessment – This single KPI comprised an assessment of swallowing, dysphagia and/or nutritional risk. If separate data for both swallow and nutritional risk assessment18,21 were reported, we preferentially included data for swallow assessment. Antiplatelet drugs for ischaemic stroke (IS) – Aspirin administration reported in two studies25,43 was combined with a KPI for antiplatelet drugs for ischaemic stroke reported in seven studies.17,18,21,23,24,28,40 Early nurse/rehabilitation assessment – This combined indicator of early assessment by a nurse
24
and early assessment of rehabilitation needs.
28
Early physiotherapy/mobilisation – This combined five reports of early mobilisation18,21,28,30 with one
17
about early physiotherapy assessment.
Selection of outcome measures
As there were minor variations in the approach to outcome analysis adjustments were made to the reported OR, HR, RR and CI to allow comparisons between the studies. The online supplement Table S1 provides a summary of the adjustments made.
Data reported in terms of poor outcome,33,39,43 disability,15,22,41,44 death or disability17,30 or not returning home 27 post stroke were all combined as a ‘poor outcome’ post stroke. Finally, the results on the association between KPIs and stroke case fatality were categorised at the end of scheduled follow-up although the timing of follow-up was included in sensitivity analyses.
KPIs
There were 25 reported KPIs in total. The KPIs that were reported by at least a quarter of the eligible studies were swallow/nutritional assessment, stroke unit admission and antiplatelets for ischaemic stroke.
Stroke unit admission was variably defined across the related studies.15,17,18,21,22,24–27,43 Two Danish studies17,18 defined a ‘stroke unit’ as a hospital department/unit that exclusively or primarily is dedicated to patients with stroke and which is characterised by multidisciplinary teams, a staff with a specific interest in stroke, involvement of relatives and continuous education of the staff. In the Italian study, 27 stroke unit was defined as a hospital ward with dedicated beds (at least 80% stroke admission) and with a dedicated stroke staff (at least one physician and one nurse) who work exclusively in the care of stroke patients.
Reported KPIs and their association patient outcomes.
ADLs: activities of daily living; AF: atrial fibrillation; CT: computerised tomography; MRI: magnetic resonance imaging; CI: confidence interval; DVT: deep vein thrombosis; HR: hazard ratio; IS: ischaemic stroke; KPI: key performance indicator; LoS: length of hospital stay; OR: odds ratio; RR: rate ratio.
Association between individual KPIs and lower risk for case fatality at the end of scheduled follow-up
The median time of scheduled follow-up for the studies reporting on the association between individual KPIs and case fatality was 1 year; range from 1 month to 10 years. Significant reductions in case fatality were observed across multiple studies for stroke unit admission,15,17,22,25–27 swallow/nutritional assessment,17,24 antiplatelets for ischaemic stroke,17,40,24,25 anticoagulants for ischaemic stroke with atrial fibrillation,16,17,23 lipid management,23,29,33,41,42 early nurse/rehabilitation assessment24,28 and early physiotherapy/mobilisation.17,28 In addition, significant associations within single studies were observed for DVT prophylaxis 32 and blood pressure lowering therapy. 28
In contrast, several studies reported wide CIs and no statistically significant association between the reported KPIs and stroke case fatality; stroke unit admission, 24 swallow/nutritional assessment,25,28,35 antiplatelets for ischaemic stroke,23,28 anticoagulants for ischaemic stroke with atrial fibrillation, lipid management, 28 DVT prophylaxis 28 and blood pressure lowering therapy. 23 In one study, 17 the CT/MRI brain imaging was associated with increased risk of early case fatality (RR: 1.35, 95% CI: 1.24–1.46), while in other studies,15,24,25,28 no evidence for an association of CT/MRI brain imaging and stroke case fatality was found.
Figure 2 summarises the primary meta-analysis results regarding the associations between individual KPIs and stroke case fatality at the end of follow-up. The KPIs that were associated with lower risk for case fatality include stroke unit admission (OR: 0.79, 95% CI: 0.72–0.87), swallow/nutritional assessment (OR: 0.78, 95% CI: 0.66–0.92), antiplatelets for ischaemic stroke (OR: 0.61, 95% CI: 0.50–0.74), anticoagulants for ischaemic stroke with atrial fibrillation (OR: 0.51, 95% CI: 0.43–0.61), lipid management (OR: 0.52, 95% CI: 0.38–0.71) and early physiotherapy/mobilisation (OR: 0.78, 95% CI: 0.67–0.91). However, the significant associations of stroke unit admission, swallow/nutritional assessment, antiplatelets for ischaemic stroke and lipid management were complicated by substantial heterogeneity (I2 > 50%). When analysed at a fixed time point, swallow/nutritional assessment (OR: 0.72, 95% CI: 0.66–0.79), antiplatelets for ischaemic stroke (OR: 0.64, 95% CI: 0.44–0.93) and lipid management (OR: 0.64, 95% CI: 0.42–0.97) were associated with a lower risk for early case fatality (up to 3 months post stroke), but the heterogeneity was reduced for swallow/nutritional assessment (I2 = 1%) only. Stroke unit admission (OR: 0.77, 95% CI: 0.71–0.82), antiplatelets for ischaemic stroke (OR: 0.57, 95% CI: 0.45–0.72) and lipid management (OR: 0.45, 95% CI: 0.27–0.74) were associated with lower risk for late case fatality (beyond 3 months post stroke), but the heterogeneity was reduced for antiplatelets for ischaemic stroke (I2 = 34%) only.
Association between individual KPIs and lower risk for case fatality. AF: atrial fibrillation; CT: computerised tomography; MRI: magnetic resonance imaging; CI: confidence interval; DVT: deep vein thrombosis; I2: heterogeneity; IS: ischaemic stroke; IV: inverse variance; KPI: key performance indicator; N: number of.
The meta-analysis showed no evidence for the association between the stroke case fatality and DVT prophylaxis, blood pressure lowering therapy, early nurse/rehabilitation assessment and CT/MRI brain imaging.
The sensitivity analysis excluding those that used HR or RR produced results that were similar to those in Figure 2 (data not shown): stroke unit admission (OR: 0.79, 95% CI: 0.71–0.89), swallow/nutritional assessment (OR: 0.82, 95% CI: 0.69–0.98), antiplatelets for ischaemic stroke (OR: 0.53, 95% CI: 0.44–0.63) and lipid management (OR: 0.47, 95% CI: 0.30–0.74) remained associated with lower risk for case fatality, and there was no evidence for the association between the stroke case fatality and DVT prophylaxis, early nurse/rehabilitation assessment and CT/MRI brain imaging.
Significant associations within single studies were observed for thrombolysis, 19 early medical assessment, 24 OT assessment 17 and antidepressant therapy, 20 but there was no evidence for the association between stroke case fatality and hyperthermia management, 28 and neurological assessment. 35
Association between individual KPIs and the risk for poor outcome
For studies reporting on the association between individual KPIs and poor outcome, the available follow-up periods were between 4 days and 2 years, with a mean of 282 days.
KPIs that were reported to be associated with the lower risk for poor outcome included thrombolysis,43,44 stroke unit admission,22,26,27,43 swallowing/nutritional assessment,30,43 antiplatelets for ischaemic stroke, 40 DVT prophylaxis, 30 and lipid management management.33,42 However, some studies found no evidence of an association with poor outcome and stroke unit admission 15 ; swallowing/nutritional assessment, 39 antiplatelets for ischaemic stroke, 43 DVT prophylaxis 37 and lipid management. 41
As summarised in Figure 3, the meta-analysis showed that the KPIs associated with the lower risk for poor outcome were stroke unit admission (OR: 0.83, 95% CI: 0.77–0.89) and swallowing/nutritional assessment (OR: 0.58, 95% CI: 0.43–0.78), while there was no evidence for the association with poor outcome for thrombolysis, antiplatelets for ischaemic stroke, DVT prophylaxis and lipid management.
Association between individual KPIs and lower risk for poor outcome. ADLs: activities of daily living; CT: computerised tomography; MRI: magnetic resonance imaging; CI: confidence interval; DVT: deep vein thrombosis; I2: heterogeneity; IS: ischaemic stroke; IV: inverse variance; KPI: key performance indicator; N: number of.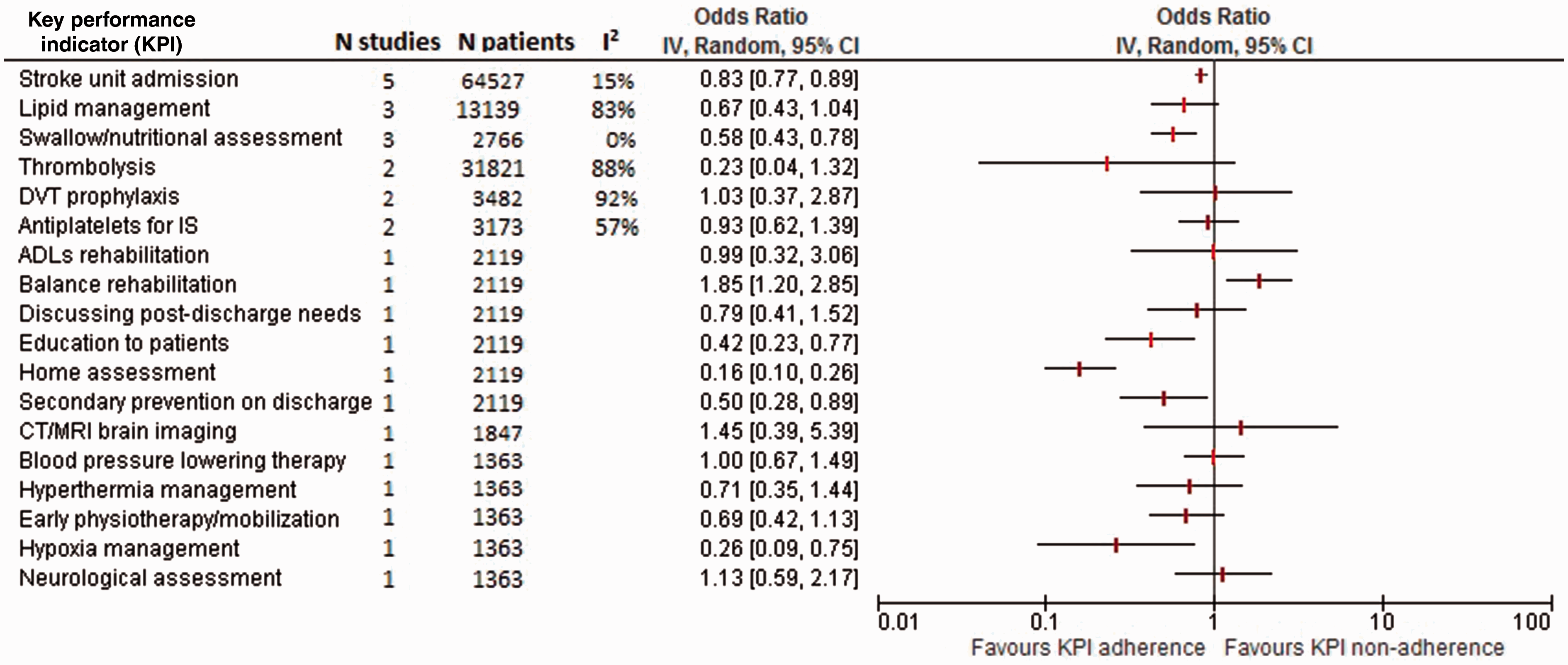
Several individual studies reported significant associations between lower risk for poor outcome and hypoxia management 30 ; home assessment, secondary prevention on discharge and education to patients. 37 No association with poor outcome was found for CT/MRI brain imaging 15 ; neurological assessment, blood pressure lowering therapy, hyperthermia management and early physiotherapy/mobilisation 30 ; ADLs rehabilitation, balance rehabilitation and discussing post-discharge needs with patients. 37
All the studies included for the primary meta-analysis about the association of KPIs with poor outcome used ORs, except one Chinese study. 40 After excluding that study, antiplatelets for ischaemic stroke remained with a single study, 43 which showed no association with poor outcome (OR: 1.25, 95% CI: 0.73–2.14).
Association between individual KPIs and relative length of hospital stay
A single Danish study 18 reported that a shorter relative length of hospital stay was associated with stroke unit admission, antiplatelets and anticoagulants for ischaemic stroke with atrial fibrillation, CT/MRI brain imaging, early physiotherapy/mobilisation, occupational therapy assessment, swallowing/nutritional assessment and DVT prophylaxis, with rate ratio ranging from 0.67 (0.61–0.73) for early physiotherapy/mobilisation to 0.85 (0.80–0.91) for occupational therapy assessment.
Association between individual KPIs and the risk for medical complications and stroke recurrence
Stroke unit admission, anticoagulants for ischaemic stroke with atrial fibrillation and early physiotherapy/mobilisation, 21 as well as swallow/nutritional assessment 31 were found to be associated with lower risk for medical complications (OR: 0.79; 0.68–0.92; 0.59, 0.45–0.76 and 0.43, 0.35–0.53; 0.47, 0.38–0.57, respectively). By contrast, CT/MRI brain imaging was associated with a greater risk for medical complications with (1.52, 1.35–1.72). 21 Other studies with wide CIs did not show evidence for the association between the occurrence of medical complications and neurological assessment 35 ; swallow/nutritional assessment21,35; antiplatelets for ischaemic stroke, occupational therapy assessment 21 ; and thrombolysis. 19
KPIs that were reported to be associated with lower recurrence rate for stroke included antiplatelets for ischaemic stroke, 40 anticoagulants for ischaemic stroke with atrial fibrillation and DVT prophylaxis 44 and lipid management. 29 However, in one study, 21 evidence for the association between lipid management and stroke recurrence was not found, 44 and there was no evidence of an association with thrombolysis. 19
Association between adherence to groups of KPIs and the risk for case fatality
Association between the number of KPIs achieved and patient outcomes.
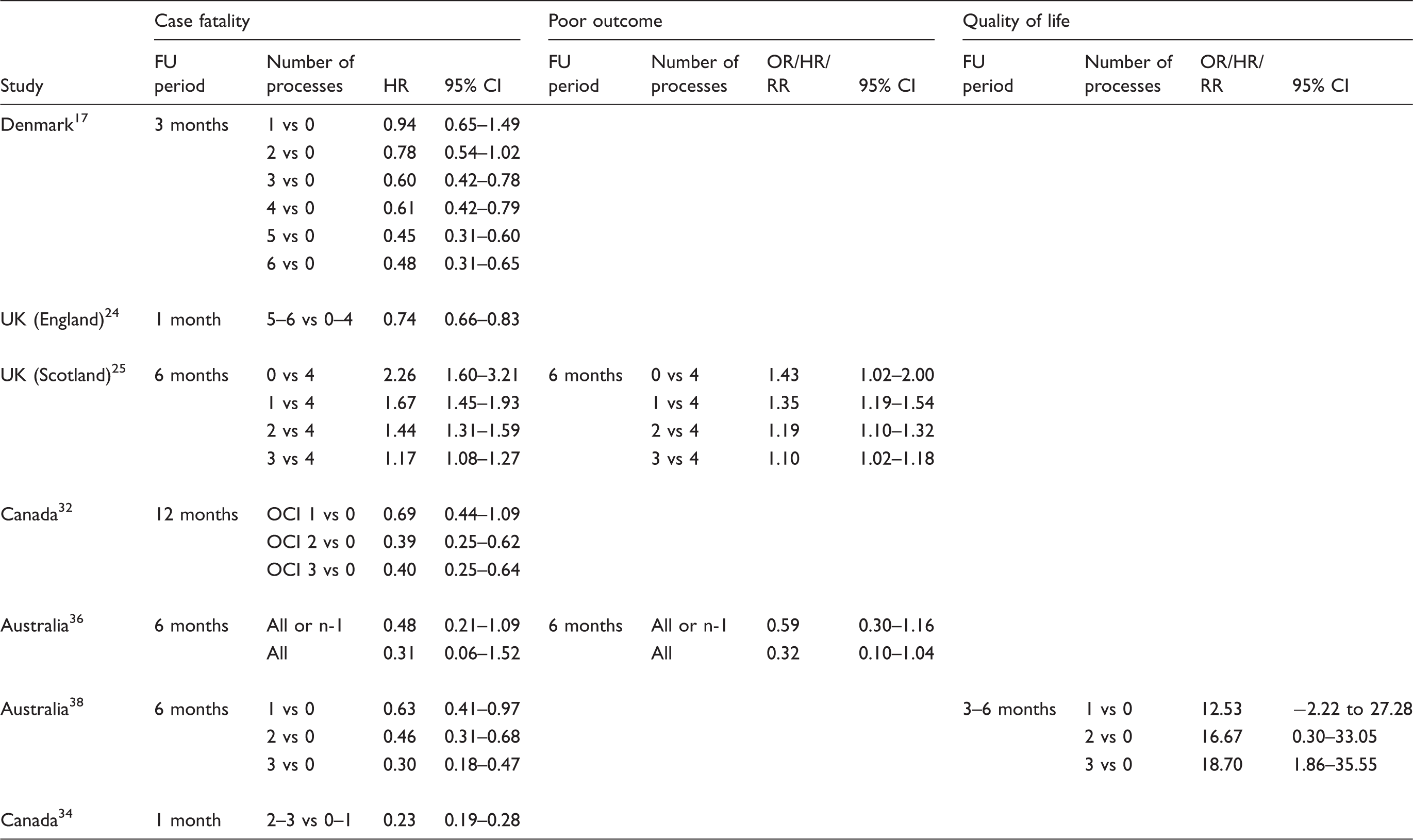
CI: confidence interval; FU: follow-up; HR: hazard ratio; n: number of applicable processes of care; OCI: organised care index; OR: odds ratio; RR: rate ratio.
Overall (see Online Supplement Table 3), only stroke unit admission, swallow/nutritional assessment, antiplatelets for ischaemic stroke, anticoagulants for ischaemic stroke with atrial fibrillation, lipid management and early physiotherapy/mobilisation were found to be significantly associated with improved outcomes after a meta-analysis of two or more studies. Thrombolysis results were associated with reduced poor outcome in two studies, but the combined analysis was not significant due to substantial heterogeneity. Data were very limited for the outcomes of length of stay, stroke recurrence or medical complications.
Discussion
The publications we have reviewed provide a large and diverse body of evidence on whether quality of care, as measured by adherence with a KPI, is associated with improved clinical outcomes in patients hospitalised with stroke. Our primary meta-analysis indicated that several KPIs including stroke unit admission, swallowing/nutritional risk assessment, antiplatelets for ischaemic stroke, anticoagulants for ischaemic stroke with atrial fibrillation, lipid management and early physiotherapy/mobilisation were associated with a reduction in case fatality or poor outcome. However, although our meta-analysis showed significant associations between lower risk for case fatality and several individual KPs at the end of scheduled follow-up, there was substantial heterogeneity (I2 > 50%) for stroke unit admission, swallowing/nutritional risk assessment, antiplatelets for ischaemic stroke and lipid management. Therefore, our meta-analysis results need to be interpreted with caution.
The strong association of stroke unit care with improved outcomes could be anticipated from a substantial number of RCTs. 45 Our review confirms this across a range of studies in routine care. Given the evidence for specialised multidisciplinary stroke unit care in stroke, 45 one might also expect to see benefits associated with early nurse or rehabilitation assessment and early medical assessment, 24 as well as occupational therapy assessment. 17 These indicators lack direct evidence from randomised trials, but may possibly be markers for admission to a stroke unit and multidisciplinary stroke care. However, there were no comparable data from many studies about early medical assessment, early nurse or rehabilitation assessment or early occupational therapy assessment for our review.
Our finding of a reduced risk of case fatality after early physiotherapy/mobilisation was in accordance with the literature about stroke unit care, 45 and some small RCTs 46 but not consistent with recent RCTs of very early mobilisation. 47 However, the recent AVERT trial tested mobilisation at an earlier stage than in routine care, so the optimal timing of mobilisation remains unclear, and very early intensive mobilisation within 24 h may carry some hazard. 47
Our meta-analysis showed that swallow or nutritional assessment was associated with lower risk for both mortality and disability post stroke. This finding was consistent with a randomised controlled trial, 9 which found that reinforcement of multidisciplinary management of swallowing dysfunction was significantly associated with lower risk for death or dependency. Thus, swallowing or nutritional assessment may be of paramount importance. The current meta-analysis also showed that early antiplatelet use for ischaemic stroke was associated with reduction in case fatality, and this was consistent with the results from a previous systematic review 48 of eight randomised trials. It showed that early antiplatelet therapy was associated with mortality reduction at a final follow-up between 1 and 6 months. However, our review showed greater apparent benefit than the 8% reduction in case fatality that was reported in the review of randomised trials. 48 However, a recent individual patient data meta-analysis of aspirin trials 49 confirms an important short-term benefit of aspirin therapy in preventing recurrent cerebral ischemia and that benefits may be greater than previously estimated. Our meta-analysis finding of a reduced risk of stroke case fatality associated with lipid management was consistent with the results from a meta-analysis 50 of 42 randomised trials.
One major disagreement with the RCTs is that our meta-analysis also showed that early anticoagulant use for ischaemic stroke with atrial fibrillation was associated with a reduction in early and late case fatality. However, this finding was not supported by a review 51 of 24 randomised clinical trials. This disagreement may be explained by the participants’ inclusion criteria. In fact, while the randomised trials included in the review 51 recruited patients with presumed or confirmed ischaemic stroke, the studies included in our review considered only patients with ischaemic stroke and atrial fibrillation. Additionally, as the studies included in our review were neither randomised nor blinded, the apparent effects of antiplatelets and anticoagulants for ischaemic stroke may have been overestimated due to selection bias and incomplete adjustment for confounders. Alternatively, KPIs may also reflect other important and unmeasured aspects of care, which would not be tested in a well-designed RCT. Additionally, the duration of follow-up for the studies included in our meta-analysis varied between 3 and 48 months (mean: 16.5 ± 21.4 months) while the duration of follow-up in the trials was generally shorter. This short-term follow-up may lead to missing a significant proportion of deaths that occur after 1 month, and disability is best assessed between 3 to 6 months when most of the recovery has taken place. 51
Our review has also identified some areas with inconsistent evidence of the association of KPIs with outcome. Deep vein thrombosis (DVT) prophylaxis was found to be associated with significant benefits in studies in Canada 32 and the USA 30 but not in Spain. 28 However, a meta-analysis of RCTs has failed to show improvements in survival or independence. 51
Regarding thrombolysis, in two studies included for our review,43,44 thrombolysis was associated with a lower risk for poor functional outcome, and this was consistent with the systematic review of the RCTs. 52 However, because of high heterogeneity (I2 = 88%) between the two studies reviewed, the summary effect was not statistically significant.
Our review showed that CT/MRI brain imaging and neurological assessment were not associated with any reported patient outcomes. This may be due to several reasons. First, the assessment itself, if not combined with adequate care, is unlikely to show any difference in outcome. For instance, once ischaemic stroke is diagnosed with brain imaging, further management by intravenous tissue plasminogen activator was found to be effective. It was however recently reported that only 3% of low-income, 19% of lower-middle-income, 33% of upper-middle-income and 50% of high-income-countries use it. 53 Second, the increased risk of early case fatality 17 and medical complications 21 that were reported after early CT/MRI brain imaging in two Danish studies was most likely due to reverse causality; patients who deteriorated during the first hours after hospitalisation were more likely to receive an early CT/MRI brain imaging, and also had a greater risk of death or medical complications. 21 Third, some of the analyses of data may have been hampered by small sample sizes, and lack of statistical power to show the differential benefit.
Adherence to an individual measure in isolation may not have a clinically detectable impact on outcomes, making determination of an effect more difficult. 54 However, adherence to several KPIs was always associated with improved outcomes.
Strengths and weaknesses
Our systematic review has several strengths including searching a wide range of databases using standardised methodology. Furthermore, the review report was based on the PRISMA guidelines. The studies that were included in our review involved large sample sizes in general, allowing sufficient statistical power and enhancing the external validity of the results. One study 15 was multinational, and 12 studies16,17,19,22,23,27,37,38,41–44 involved nationwide datasets. The remaining studies were conducted regionally with the recruitment of participants from between three 39 to 222 hospitals. 31 Additionally, we only conducted analyses using data from studies that corrected for patient casemix (age and stroke severity). Our approach to meta-analysis has used a conservative random-effects approach to acknowledge the diversity of studies identified. Finally, we performed a sensitivity analysis to evaluate the robustness of our findings.
We must acknowledge some weaknesses. We did not use any scoring system to assess risk of bias in included studies, but simply included large register studies reporting independent association of KPIs with patient outcomes after adjusting at least two variables including age and stroke severity. Second, the review was based on data from observational studies with different follow-up time periods and designs. Third, although we have only included data that used a multivariable analysis to correct for patient casemix, there remains the possibility that the patient outcomes were influenced by unmeasured or residual confounding factors such as indication bias or factors related to the nonrandomised study design rather than the reported KPIs themselves. Fourth, our review could be subject to publication bias because our search strategy was limited to electronic databases and references known to the authors, and manuscripts published in English only. Fifth, there is a potential concern about combining results from studies from different settings and using different research methodologies. For instance, there were different measures for stroke severity for case mix adjustment, different models of stroke unit and different models of implementing or measuring the KPIs. Finally, we were limited to a few studies reporting data on important outcomes such as the length of hospital stay and quality of life, and none of the studies considered the cost of care, which is clearly important in a disabling condition such as stroke.
Conclusion
Our review found that the most frequently reported KPIs for stroke care were swallow/nutritional assessment, stroke unit admission, antiplatelets for ischaemic stroke, CT/MRI brain imaging, anticoagulants for ischaemic stroke with atrial fibrillation, lipid management, DVT prophylaxis and early physiotherapy/mobilisation. Stroke unit admission and early interventions including swallowing/nutritional risk assessment, antiplatelets for ischaemic stroke, anticoagulants for ischaemic stroke with atrial fibrillation, lipid management and early physiotherapy/mobilisation were all associated with better patient outcomes. Achieving a combination of several KPIs was always associated with a better outcome. Both policy makers and health care professionals should be encouraged to implement the KPIs for stroke management that are reliable and meaningful for regularly monitoring the quality of stroke care. Future research could focus on novel stroke care quality indicators, particularly in the post-acute period.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DAC holds a Research Fellowship from the National Health and Medical Research Council (1063761 co-funded Heart Foundation), and has received educational grants from Boehringer Ingeheim for unrelated work.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
GU and PL.
Contributorship
GU and PL conceived the study, researched literature, analysed data and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.