
Abstract
Introduction
Norwegian Stroke in the Young Study (NOR-SYS) is a three-generation research program of young ischaemic stroke. In this study, we assessed ischaemic stroke incidence, education and work status among young stroke patients. Furthermore, we evaluated the participation of family members for future validated information on hereditary cardiovascular events.
Patients and methods
Patients aged 15–60 years with radiologically verified acute ischaemic stroke, admitted to Haukeland University Hospital in Bergen, Norway from 2010 to 2015, were included. Patients’ partners, common offspring ≥ 18 years and biological parents of patients and partners were invited to participate. Ischaemic stroke incidence was analysed with respect to year, age and sex using multiple logistic regression.
Results
A total of 385 patients, 260 partners (80.0%) and 414 offspring (74.6%) were clinically examined. The mean annual ischaemic stroke incidence rate was 30.2 per 100,000. Incidence was higher in men, and the difference was accentuated with increasing age (p = 0.008). There was no sex difference in educational status (p = 0.104) in contrast to work status (p < 0.001) for patients. In all, 84.1% of men worked, and of these, 80.3% are fulltime. In all, 74.4% of women worked, and of these, 52.9% are fulltime. Parents participated by returning a questionnaire. For patients, 91 fathers (55.2%) and 142 mothers (57.3%) participated. For partners, 48 fathers (38.4%) and 68 mothers (40.2%) participated.
Conclusion
The mean annual incidence rate of young stroke was 30.2 per 100,000, and the incidence rate was higher in men. Work status was high among both sexes. Active participation rates were high for patients, partners and offspring.
Introduction
Stroke incidence increases with age and hence is lower in young adults. It is roughly estimated that approximately 10% of ischaemic stroke occurs in individuals under the age of 50 years. 1 Stroke has devastating consequences, especially in young adults, due to potentially serious sequelae such as physical disability, loss of vision fields, cognitive impairment and fatigue that may affect driving and physical mobility, social life and quality of life. Furthermore, stroke has a considerable socioeconomic impact due to loss of working years and high health-care costs. 2
Although the incidence of stroke is decreasing in older adults, epidemiological studies indicate increasing incidence among young adults.1–8 The annual incidence rate is reported as 7–17 per 100,000 for populations ≤45 years or ≤49 years old.4,7–10 There are notable sex differences in the occurrence of young stroke. Generally, the incidence rate is lower in women than in men below the age of 75 years. 11 However, some studies have shown that women outnumber men under the age of 30, 35 or 44 years.2,4,7,8,10,12,13
Norwegian Stroke in the Young Study (NOR-SYS) is the first comprehensive and prospective family study of young ischaemic stroke, and patients aged 15–60 years were included. We aimed to assess incidence, pre-stroke education and work status of young ischaemic stroke.
Participation of partners, adult offspring and parents was also evaluated in order to get more validated information about family cardiovascular events and to contribute to increase the knowledge of heredity in future studies.
Patients and methods
Study protocol
NOR–SYS is a hospital- and population-based, single centre, three-generation, prospective, long-term observational study for which methods and rationale have been described previously. 14 Patients aged 15–60 years with acute ischaemic stroke were enrolled from 1 September 2010 to 31 August 2015 and family members were enrolled to 31 December 2015. Acute ischaemic stroke was documented by magnetic resonance imaging (MRI) in 98.5% of cases and by computer tomography (CT) if there were contra-indications. 15 We examined participating patients, partners, ex-partners and adult offspring ≥18 years by standard operating procedures, including a detailed ultrasound protocol. 14
The Department of Neurology at Haukeland University Hospital has traditional local and regional function for stroke patients at age 15–60 years in a catchment area consisting of the city of Bergen and 23 surrounding communities with almost 266,000 inhabitants in the same age group as our patients.
Patients with post-traumatic stroke, stroke caused by sinus venous thrombosis, septicaemia, intracerebral haemorrhage, procedure-related cerebral infarction, serious co-morbidity (advanced cancer or multiple sclerosis) or otherwise limited co-operation (non-native speakers or patients with severe psychiatric illness) were excluded from the study.
Patients consented to contact their biological parents, partners or ex-partners and adult offspring. Partners and ex-partners consented to contact their biological parents. Parents participated by returning a questionnaire. There were 23 patients with limited cooperation due to stroke consequences such as unconsciousness, aphasia or writing difficulties, and four patients were aged <18 years. For youngest patients, parents gave their additional written consent, and for the adult patients, written informed consent was obtained from patients’ next-of-kin, usually a partner, or parents or an adult offspring. These family members were then directly informed about NOR–SYS as a three-generation family research program and were invited into the study.
The study was registered in ClinicalTrials.gov NCT01597453 and approved by the Regional Committee for Medical and Health Research Ethics, western Norway (REK-Vest 2010/74). Written informed consent was obtained from all active participants and/or their next-of-kin relative. REK–VEST also approved the inclusion of patients aged 15–17 years with additional parental consent and verification of cardiovascular events in hospital records of deceased parents with patient’s, partner’s or ex-partner’s consent.
NOR–SYS included patients up to 60 years, due to high life-expectancy, 16 and active work life up to 67 years with quite equal working conditions for both sexes in Norway. We considered pupils and students as unpaid full-time workers, adequate to working conditions of their age. It is most decisive for pupils and students as for the payed workers, whether or not they can return to their previous social life, studies or work because this is a key goal in recovery from stroke. However, previous studies have excluded non-payed participants.1,17–21
We analysed age as a continuous variable, but for comparison with literature and a previous local study, 12 we also dichotomised patients into young (15–49 years) and middle-aged (50–60 years). We did not search for non-hospitalised stroke patients, as a former study with intensified search among general practitioners for stroke patients below age 74 years did not reveal additional cases. 22
Statistical analysis
Incidence rates were calculated based on the number of patients aged 15–60 years and the population in our region of the same age. Incidence rates were analysed by year of inclusion, age and sex. Multiple logistic regression analysis was performed to relate incidence to these variables, and interactions were tested in a forward stepwise manner. The results are reported as odds ratios (OR) and 95% confidence intervals. Chi-square test was performed to compare education and work status for both sexes. The level of significance was set at 0.05. Statistical analyses were performed using IBM SPSS Statistics version 24 and Stata 15.1.
Results
Participation of patients
After non-inclusion and exclusion of some patients, NOR–SYS included a total of 385 patients with mean age 49.5 years and a male-female ratio of 2.2:1 (Table 1). Four patients were non-Caucasians.
Demographic data of all participant groups in the Norwegian stroke in the young study 2010–2015.
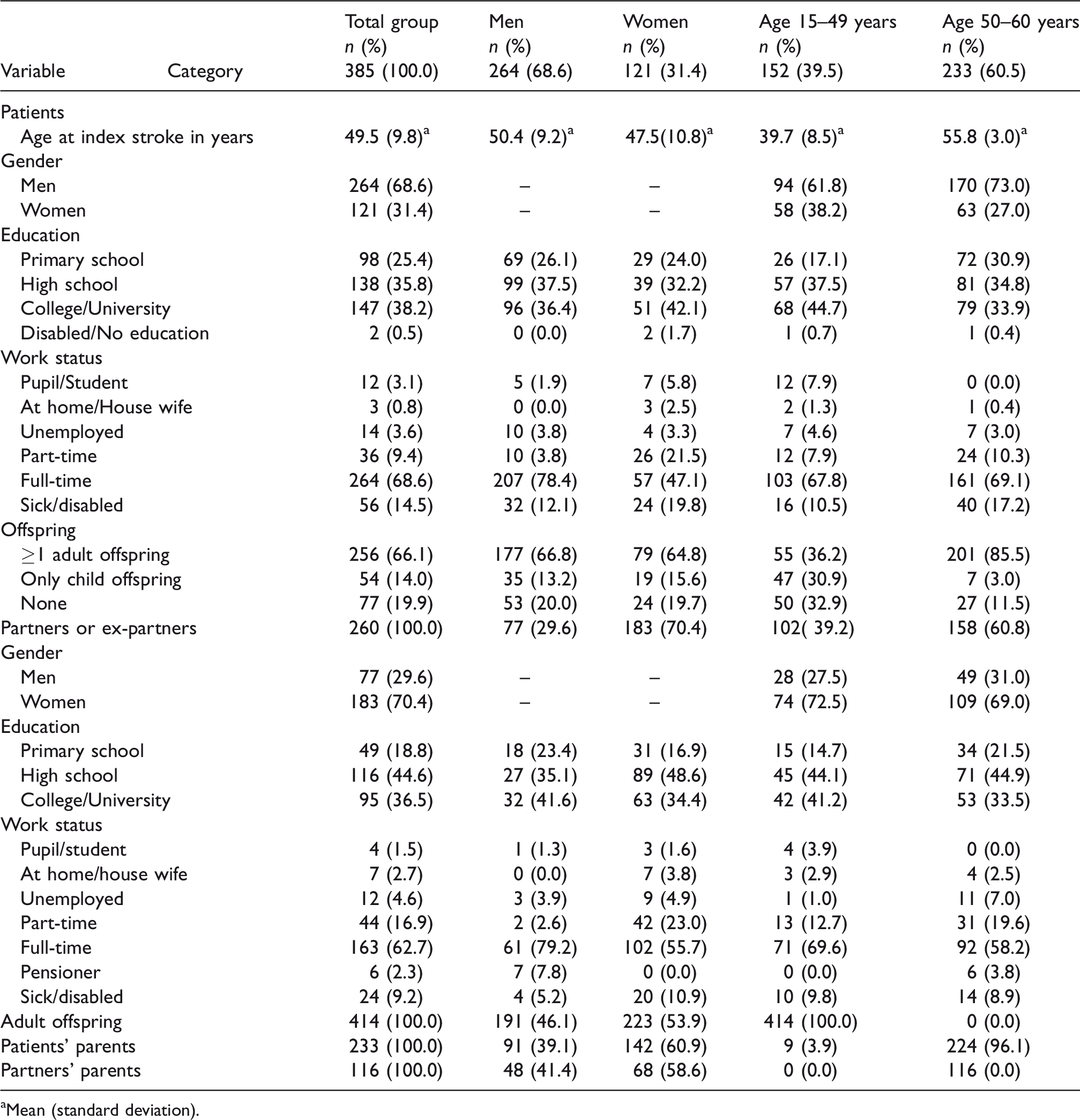
aMean (standard deviation).
Fourteen patients (3.5%) that met the inclusion criteria were not included due to refusal to consent (four patients), non-invitation because of serious psychiatric disease (seven patients) and three patients, all admitted unconscious, died early from basilar artery occlusion without written consent from family members. However, these 14 patients were included for incidence calculations in order to compare the results to our previous retrospective study. 12
Three patients were excluded retrospectively due to final non-stroke diagnosis.
Incidence of young ischaemic stroke
The annual incidence rate for young and middle-aged ischaemic stroke at age 15–60 years was 25.0–34.7 per 100,000 with a mean annual incidence rate of 30.2 per 100,000 (Figure 1). For patients aged 15–49 years, the annual incidence rate was 8.5–20.0 per 100,000 with a mean annual incidence rate of 15.0 per 100,000. For patients aged 50–60 years, the annual incidence rate was 78.4–100.0 per 100,000 with a mean annual incidence rate of 87.4 per 100,000. Adjusted for sex and age, the odds for incident ischaemic stroke decreased by 7% per year in the period from 2010 to 2015 (p = 0.040 in Table 2 and Figure 2). Ischaemic stroke incidence was higher in men, except in very young women aged < 25 years, and the difference was accentuated with increasing age (p = 0.008). At age 25 years, the OR was 1.02 (men vs. women); for 45 years, the OR was 1.83 and for 60 years, the OR was 2.82 (Table 3).
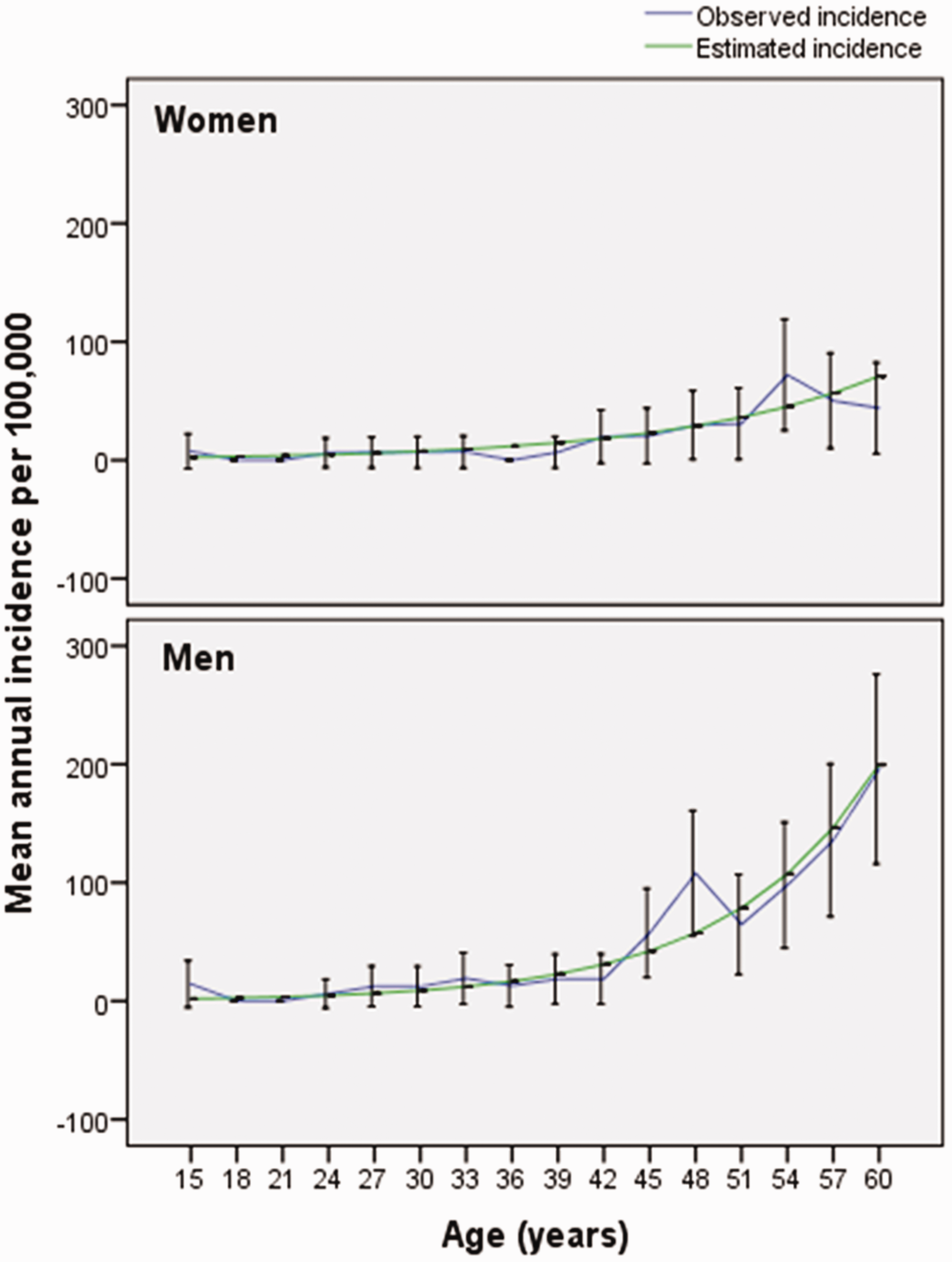
Observed and estimated (Note: from the logistic regression model given in Table 2.) mean annual incidence (Note: 95% confidence intervals (CI) are given for the incidence rates.) of ischaemic stroke at age 15–60 years per 100,000 inhabitants in Bergen and 23 surrounding communities, western Norway (Note: The total average population at age 15–60 years from 2010 to 2015 consisted of 266,000 inhabitants.) from September 2010 through August 2015 differentiated by age and gender and based on data from the Norwegian Stroke in the Young Study.
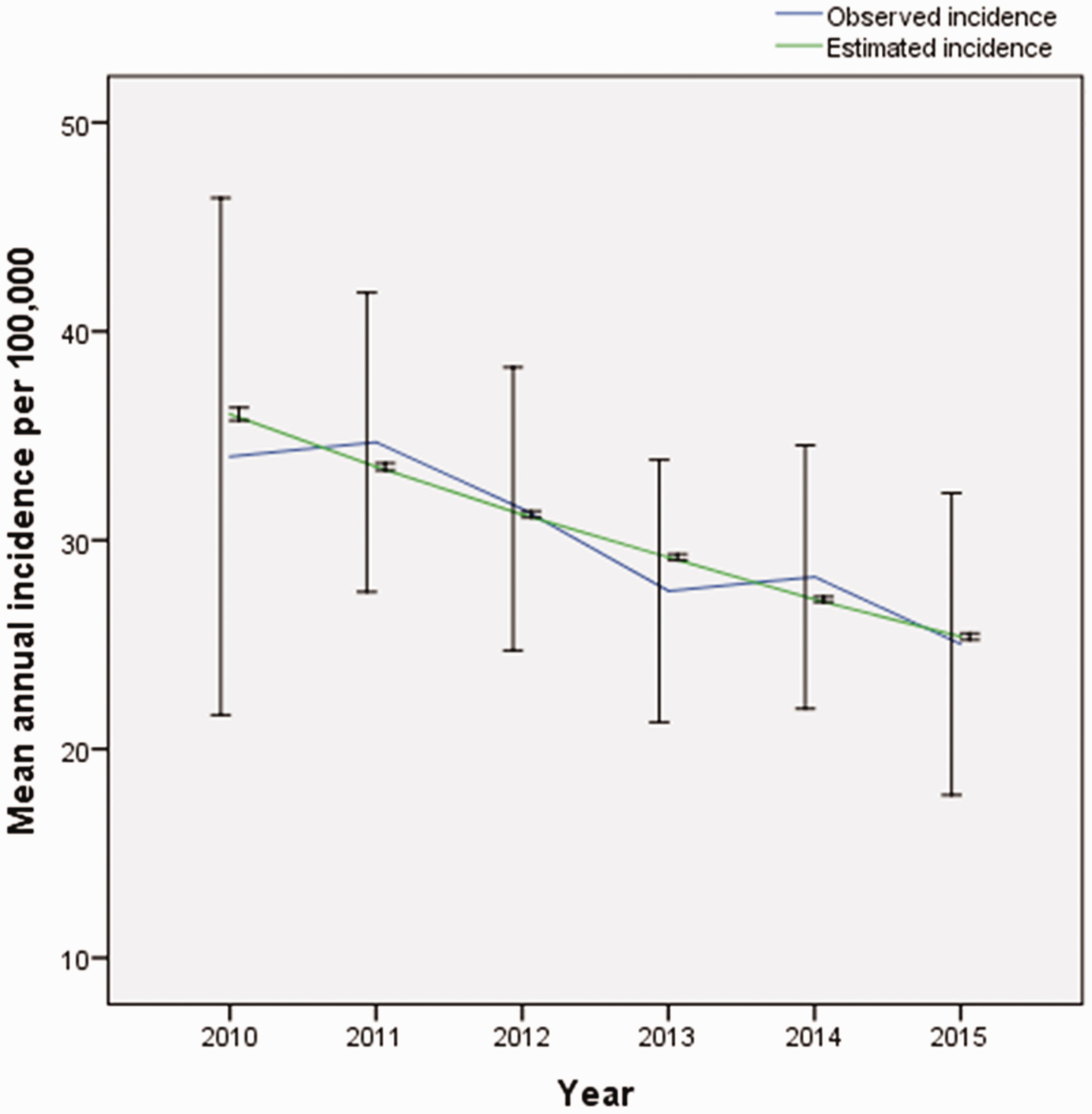
Observed and estimated (Note: From the logistic regression model given in Table 2.) mean annual incidence (Note: 95% confidence intervals (CI) are given for the incidence rates.) of ischaemic stroke at age 15–60 years per 100,000 inhabitants in Bergen and 23 surrounding communities, western Norway (Note: The total average population at age 15–60 years from 2010 to 2015 consisted of 266,000 inhabitants.) for each year from 2010 to 2015.
Results from multiple logistic regression analysis of the incidence of ischaemic stroke in the city of Bergen and 23 surrounding communities, western Norwaya from September 2010 through August 2015.
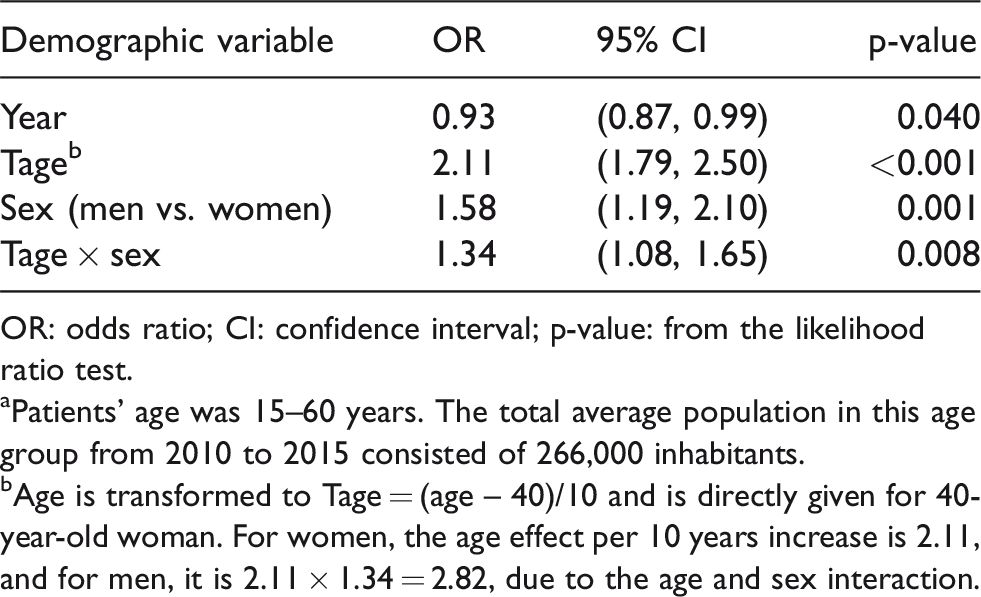
OR: odds ratio; CI: confidence interval; p-value: from the likelihood ratio test.
aPatients’ age was 15–60 years. The total average population in this age group from 2010 to 2015 consisted of 266,000 inhabitants.
bAge is transformed to Tage = (age – 40)/10 and is directly given for 40-year-old woman. For women, the age effect per 10 years increase is 2.11, and for men, it is 2.11 × 1.34 = 2.82, due to the age and sex interaction.
Estimated ORs for men versus women from the multiple regression analysis of incident ischaemic stroke in Bergen and 23 surrounding communities, western Norway a from September 2010 through August 2015.
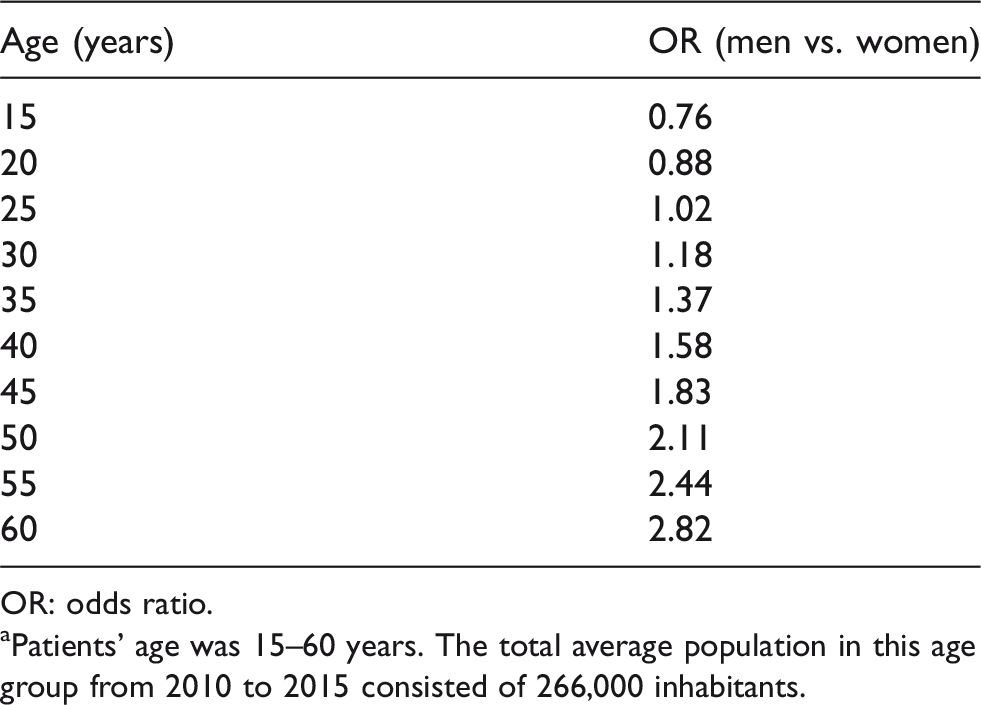
OR: odds ratio.
aPatients’ age was 15–60 years. The total average population in this age group from 2010 to 2015 consisted of 266,000 inhabitants.
Education and work status among patients
Results for education and work status are presented in Table 1. There were 74% of patients who had graduated from high school or university/college, and there was no sex difference (p = 0.104). Work status showed that 68.6% of patients worked payed fulltime. In addition, 3.1% were full-time pupils or students. There was an association between work status and sex (p < 0.001). Men predominated with full-time work (80.3% vs. women 52.9%), whereas more women worked part-time (21.5% vs. men 3.8%).
Participation of partners and ex-partners
In total, 260 partners and ex-partners were included in the study. Among partners, 223 were current partners (85.8%). Four partners were non-Caucasians.
Participation of other family members
Adult offspring and parents of 388 patients were included. Family members of the three retrospectively excluded patients remained in the study as they were also examined by the standardised ultrasound protocol and will function as controls in future studies.
Among 256 patients with adult offspring, offspring of 201 patients (78.5%) participated. In total, 414 adult offspring (74.6%) participated.
Of patients’ parents, 142 mothers (36.6%) and 91 fathers (23.5%) participated, while 53 mothers (13.7%) and 30 fathers (7.7%) did not respond to study-invitation. Furthermore, 53 mothers (13.7%) and 44 fathers (11.3%) were not eligible for inclusion due to patients’ refusal of consent due to serious health conditions, dementia, personal reasons or adoption. The number of deceased patients’ parents was 140 (36.0%) for mothers and 223 (57.5%) for fathers.
For partners’ parents, 68 mothers (26.2%) and 48 fathers (18.5%) participated. The number of deceased partners’ parents was 91 (35.0%) for mothers and 135 (51.9%) for fathers. Figure 3 presents a graphic overview of all seven participant groups.
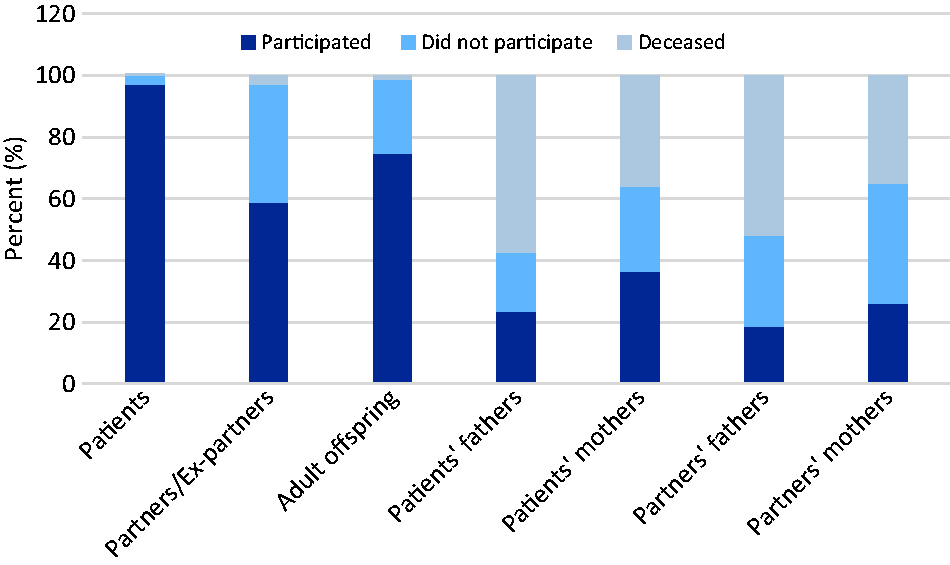
Participation rates of all participant groups in the Norwegian Stroke in the Young Study for 385 incident cases of ischaemic stroke 2010–2015.
Discussion
The incidence of stroke in our study decreased with 7% per year during the inclusion period from 2010 to 2015. However, since our study has small numbers of annually included patients, and the inclusion time of five years is relatively short, it is not possible to draw conclusions from falling incidence during the inclusion period, and it is a limitation of our study.
In our previous study from Hordaland county from 1988 to 1997, the annual incidence was 11.4 per 100,000. 12 Now, we find an increased annual incidence of 15.0 per 100,000 for patients <50 years. However, NOR–SYS results are not directly comparable with the Hordaland study due to the facts that our catchment area has most inhabitants, but does not cover Hordaland County, and because our imaging diagnostics differ. While patients in the NOR–SYS study were mainly selected with MRI verified stroke, the Hordaland study was based on Baltimore–Washington criteria 23 and diagnosed stroke mainly by CT. In addition, the Hordaland study included patients with first-ever stroke, while NOR–SYS included any patient with acute ischemic stroke. NOR–SYS included patients independent from earlier stroke history and also independent from time of admittance to hospital, as some patients were admitted delayed after MRI documentation of acute stroke, when for example working abroad or during vacation.
Several studies have reported an increasing stroke incidence.1–8 However, a recent Norwegian registry study from 2010 to 2015 reported that the stroke incidence was stationary across patients aged 15–44 years and declining across patients aged 45–54. 24 This study reported annual incidence rate as 20.7 per 100,000 across patients aged 15–49 years, higher than in our prospective, clinical study, and a decline of stroke incidence in the period 2010–2015 for patients aged 15–54 years. We expect, however, that the results of the national registry study are in line with our results as methods are different, and our ischaemic stroke diagnosis was solely based on clinical and radiological documentation with MRI performed for 98.5% of our patients. 15
Several factors may contribute to the trend with increasing young stroke incidence. Improved stroke detection with advanced neuroimaging technology, particularly MRI, results in more patients with minor stroke or rapidly regressive symptoms being identified.2,4,5,8 Furthermore, the stroke definition has changed over time. Earlier, stroke was defined clinically by the duration of neurological symptoms lasting >24 h. 25 Today, MRI also detects infarctions among patients with symptoms lasting <24 h as diffusion-weighted imaging combined with apparent diffusion coefficient image has a better sensitivity and accuracy than CT in the identification of early ischaemia. 26 In addition, the prevalence of cardiovascular risk factors has changed over time. There is increased prevalence of hypertension, diabetes mellitus, dyslipidaemia and obesity and increased use of alcohol and illicit drugs in the younger population.1–4,8,10,13,27–30 In Norway, the proportion of daily smokers has declined, as presented in the Tromsø Study from 1995 to 2012, 31 but the daily use of snuff-tobacco particular to Nordic countries has increased steadily since 2002. 32 Furthermore, the awareness of stroke occurring among young people has increased, so general practitioners more likely refer suspected young patients to hospitals.4,5 Further, we observe changes in working conditions. High efficiency and long periods of concentration are required, and manual labour has become less usual. More ‘multitasking and detailed brain work’ contribute to that minor symptoms of impaired functioning are more readily detected.
Our study showed higher ORs for ischaemic stroke among men apart from patients younger than 25 years (Table 3). However, there were only 12 (3.1%) patients at this young age in our study, and therefore we found it difficult to draw a conclusion. The Hordaland study also reported higher incidence among women aged <30 years about 20 years ago. 12 Ischaemic stroke among young women is particularly pronounced due to gender-specific risk factors such as pregnancy, puerperium, use of oral contraceptives, higher incidence of migraine with aura and autoimmune disorders, such as antiphospholipid syndrome.2,4,7,8,13,33 However, for the whole group of young patients, other studies support our findings with higher incidence rates in men.11,34,35 A major reason may be that men have increased prevalence of cardiovascular risk factors36–38 and earlier development of cardiovascular disease. 39 This is in line with our study showing that the highest rate of deceased persons was among patient’s fathers.
Education and work status were high among both sexes. The majority of patients had graduated from high school or college/university and worked fulltime. Education status for both sexes did not differ in contrast to full-time work status. More women had part-time work and a few were housewives. The inclusion period of NOR–SYS was conducted in years with very low unemployment rates around 3.7% in Norway. 40
NOR–SYS is, to our knowledge, the first detailed family study of young ischaemic stroke. In general, the study participation rate was excellent among patients, and good among partners and adult offspring, and it reflected indirectly the family structure and composition. The highest participation rate of partners was noted among families with current partners. Furthermore, the majority of families had adult offspring, and the participation rate of adult offspring was also high. The third generation cohort of the Framingham Heart Study also reported a high recruitment rate among family members of the third generation. 41
Patients’ parents had higher participation rates than partners’ or ex-partners’ parents, as expected. There was a high number of deceased parents and especially deceased fathers. This is in line with longer life expectancy among women and earlier development of cardiovascular disease in men.16,39
Our study is a hospital-based study of acute ischaemic stroke. However, we consider our study also as population-based. Haukeland University Hospital has both local and regional function for young, acute stroke patients in the well-defined region of Bergen and close communities. In addition to young stroke diagnostics and treatment, our hospital has had for decades a traditionally regional function for cardiovascular intervention of the heart, the aorta and peripheral arteries. Transport by car to closest other university hospitals is about 4 h to Stavanger and 8–9 h to Oslo, respectively, and we therefore exclude in our case a special selection-bias that may generally occur for university hospital-based studies.
For future studies, NOR–SYS may provide useful information about the socio-economic burden of stroke at working ages. High participation rates among first degree family members and hospital information about cardiovascular events among deceased parents may contribute to increased knowledge of important factors for inheritance and ischaemic stroke.
Conclusion
The mean annual incidence rate of ischaemic stroke at age 15–60 years was 30.2 per 100.000 and 15.0 per 100.000 at age 15–49 years. Men were more prone to suffer ischaemic stroke at young age. Work status was high among both sexes. Since Norway has stable economics and an active working life up to 67 years, NOR–SYS has the future ability to show the socio-economic burden of young stroke. Active participating rates were excellent for patients and high for partners and offspring.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Western Norway Health Trust, which had no influence on the study design, data collection and presentation or the conclusions made.
Informed consent
Written informed consent was obtained from all subjects before the study.
Ethical approval
Ethical approval for this study was obtained from the Regional Committee for Medical and Health Research Ethics, western Norway (REK-VEST 2010/74).
Trial registration
The study was registered in ClinicalTrials.gov NCT01597453
Guarantor
UWA
Contributorship
UWA – conceived the study and was involved in protocol development and gaining ethical approval. Data collection was done by BN, AF, HØ, KMS and UWA. BN did literature search and wrote the first draft of the manuscript. Statistical analysis was done by BN and GEE. All authors reviewed and edited the manuscript and approved the final version.
Acknowlegdements
We would like to thank the study nurses Linn Elin Rødal, Maria Sætveit Stokkan, Toril Synnøve Bjørgo and Jeanette Haveland Antoniazzi for their assistance and guidance in this research.