
Abstract
Abstract
Purpose
Acute vestibular syndrome – vertigo, nausea/vomiting, nystagmus and gait unsteadiness – is common, and differentiating posterior circulation stroke from a peripheral cause can be challenging. The National Institute of Health Stroke Scale (NIHSS) does not include acute vestibular syndrome, and early computed tomography scanning cannot rule out acute ischaemia. A positive Head Impulse–Nystagmus–Test of Skew (HINTS) test suggests posterior circulation stroke in acute vestibular syndrome when any of three signs are present: normal horizontal head impulse, gaze-direction nystagmus or eye skew deviation. This systematic review examined the accuracy of positive HINTS in identifying posterior circulation stroke in acute vestibular syndrome patients.
Methods
We searched MEDLINE (1966 to 21 December 2017), EMBASE (1980 to December 2017), Web of Science and scanned bibliographies. Two authors independently screened relevant articles and extracted data. We included studies where HINTS was used to identify posterior circulation stroke with diagnosis confirmed using magnetic resonance imaging.
Findings
Six studies (n = 644 patients) were identified. Acute stroke was confirmed in 200 (31.1%) patients. There was a 15-fold increased risk of posterior circulation stroke in patients with positive HINTS test compared to those with no abnormality (RR: 15.84, 95% CI: 5.25–47.79). For any stroke, the pooled sensitivity was 95.5% (95% CI: 92.6–98.4%) and specificity was 71.2% (95% CI: 67.0–75.4%).
Discussion and Conclusion
The data suggest that the HINTS test as one element of clinical evaluation is useful to differentiate posterior circulation stroke from peripheral causes in acute vestibular syndrome. Further studies are needed to validate HINTS as a clinical prediction tool in emergency department settings and selection of patients for reperfusion treatment.
Introduction
About 25% of all strokes affect the posterior circulation and a large proportion of patients attend emergency departments. 1 Patients often present with a variety of symptoms, often with few clinical signs, 2 making the diagnosis challenging. Ongoing dizziness, nystagmus, nausea/vomiting, head motion intolerance or poor balance, collectively termed acute vestibular syndrome (AVS), 3 are common, 4 and a substantial number have a cerebrovascular cause.2,5 Up to 35% of strokes in such patients can be missed, 5 and unrecognised cerebellar stroke on initial assessment is associated with an 8-fold increase risk of death. 2 Reperfusion therapy options require rapid diagnosis, and secondary prevention is important, as recurrent stroke and complications of posterior circulation stroke (POCS) are reported to be as high as strokes affecting the anterior circulation. 6 Thus, there is need for a clinical tool to diagnose acute POCS in AVS.
The Face Arm and Speech test (FAST) is not sensitive for the posterior circulation ischaemia, 7 and the National Institutes of Health Stroke Scale (NIHSS) does not include dizziness or vertigo as a manifestation of stroke or TIA. Computed tomography (CT) scans are widely used but may miss up to 60% of early posterior circulation ischaemia. 8 Cerebral magnetic resonance imaging (MRI) is reported to be more sensitive, 9 but may not be available acutely in many hospitals.
The Head Impulse–Nystagmus–Test of Skew (HINTS) test can be performed by the bedside where the presence of any of three oculomotor signs: normal horizontal head impulse, gaze-direction nystagmus or skew deviation suggests a central cause, including stroke in AVS. 10 We performed a systematic review to evaluate the effectiveness of HINTS in diagnosing POCS in AVS.
Methods
Study selection
We searched MEDLINE (1966 to 21 December 2017), EMBASE (1980 to December 2017) and Web of Science to identify studies on clinical features and diagnostic evaluation. Two authors (KK and KB) independently screened titles and selected articles. No language restrictions were applied. Details of the search strategy are listed in the online supplementary Appendix.
Data extraction and management
We included patients with AVS in whom HINTS was performed primarily to identify POCS and where diagnosis (infarction or haemorrhage) was confirmed using cerebral MRI. We included patients with symptoms lasting 1 h or more to focus on utility in emergency settings and generalisability of results in clinical practice.
Information from each extracted article included study type, number of patients, demographics, risk factors, inclusion criteria, stroke type (ischaemic or haemorrhagic) and proportion with positive and negative HINTS test results. We excluded studies with incomplete data, patients not evaluated in the acute phase (≤7 days), where HINTS was not performed, those that failed to confirm stroke on imaging or report on diagnostic accuracy. We resolved discrepancies through discussion.
Data synthesis
We defined the presence of any of three components suggestive of acute stroke on HINTS examination as positive: normal horizontal head impulse, nystagmus that changes direction with gaze and skew deviation of the eyes. We reported the results as risk ratio (that is, the likelihood of stroke among test-positive patients to those who were negative) with 95% confidence intervals using random-effects model. We calculated pooled sensitivity, specificity, positive and negative likelihood ratios. A p-value ≤0.05 was considered significant.
Heterogeneity
We considered an I2 greater than 50% to infer significant heterogeneity.
Results
Our search identified 26,837 citations from which we found 2562 articles. After screening 11 relevant articles, 6 studies met the inclusion criteria. Figure 1 shows the flow chart of the included studies.
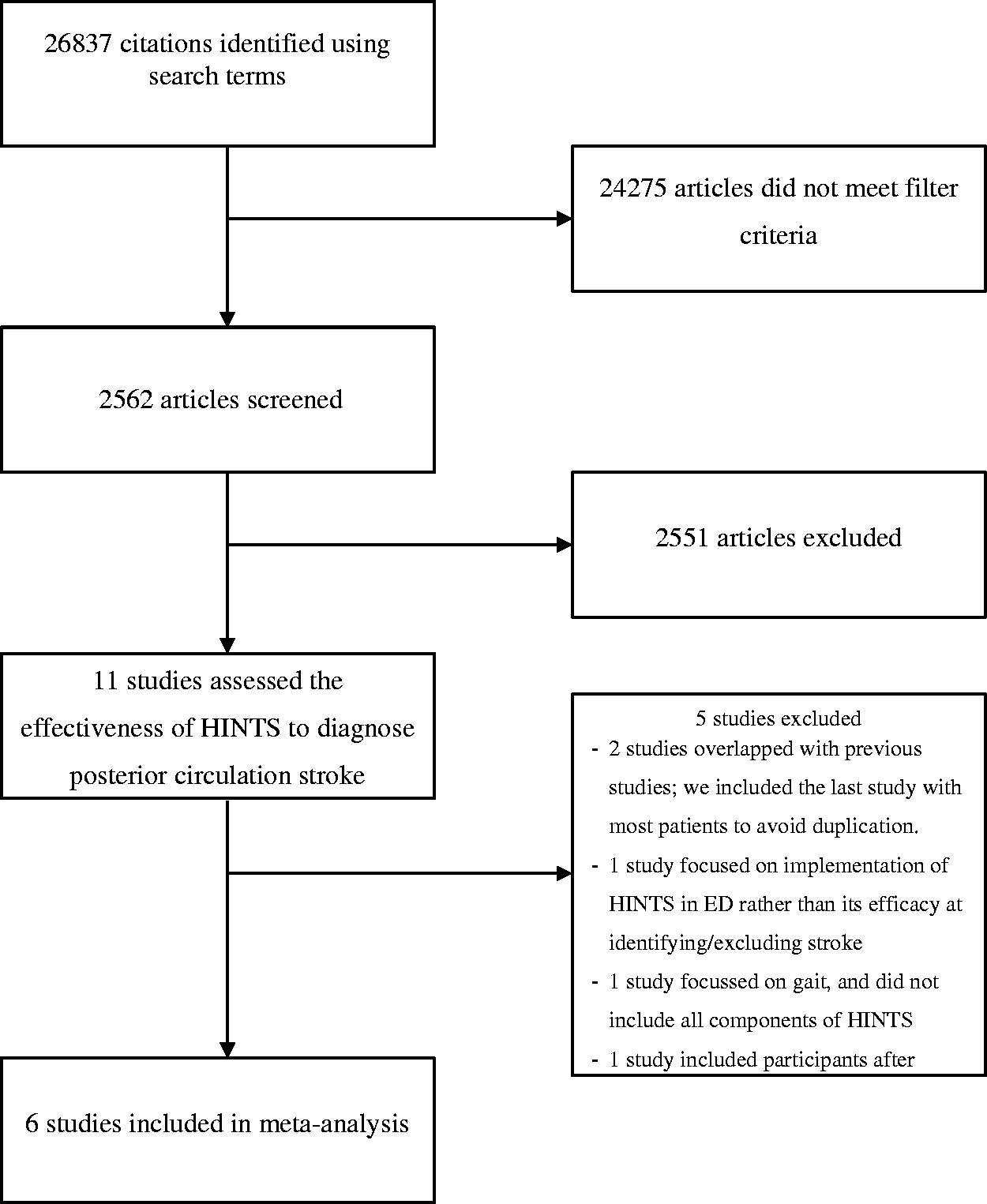
Flow diagram of searches.
A total of 825 patients were identified but we included 644 patients: 63 patients were excluded as their symptoms had resolved by the time of examination, 11 48 patients did not have MRI whilst 70 patients were not tested with HINTS12 (Table 1). Five studies were single-centre, prospective and observational, whilst one study was retrospective. All patients were evaluated in emergency departments and one study 12 also included outpatients and admissions.
Characteristics of included studies.
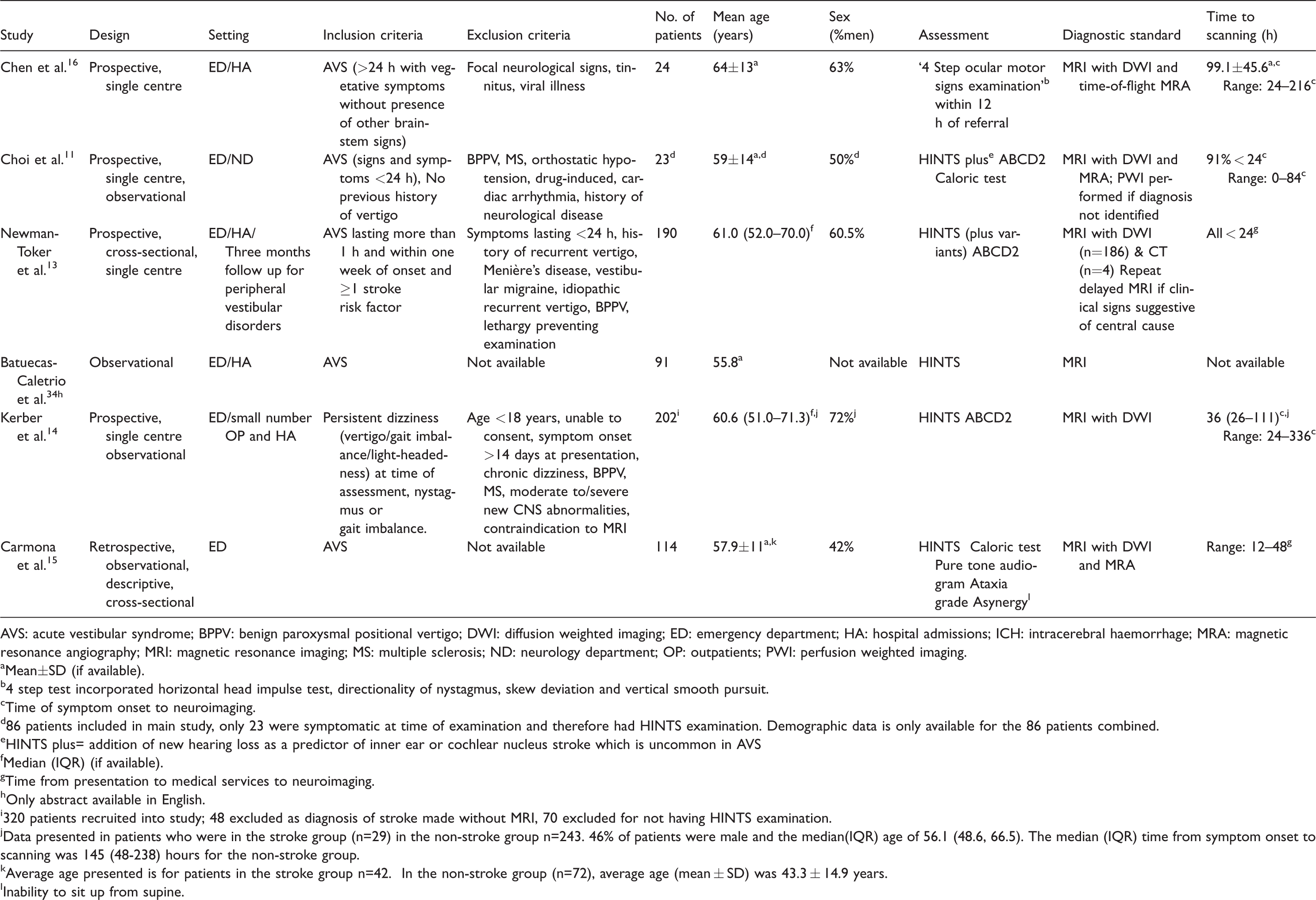
AVS: acute vestibular syndrome; BPPV: benign paroxysmal positional vertigo; DWI: diffusion weighted imaging; ED: emergency department; HA: hospital admissions; ICH: intracerebral haemorrhage; MRA: magnetic resonance angiography; MRI: magnetic resonance imaging; MS: multiple sclerosis; ND: neurology department; OP: outpatients; PWI: perfusion weighted imaging.
aMean±SD (if available).
b4 step test incorporated horizontal head impulse test, directionality of nystagmus, skew deviation and vertical smooth pursuit.
cTime of symptom onset to neuroimaging.
d86 patients included in main study, only 23 were symptomatic at time of examination and therefore had HINTS examination. Demographic data is only available for the 86 patients combined.
eHINTS plus= addition of new hearing loss as a predictor of inner ear or cochlear nucleus stroke which is uncommon in AVS
fMedian (IQR) (if available).
gTime from presentation to medical services to neuroimaging.
hOnly abstract available in English.
i320 patients recruited into study; 48 excluded as diagnosis of stroke made without MRI, 70 excluded for not having HINTS examination.
jData presented in patients who were in the stroke group (n=29) in the non-stroke group n=243. 46% of patients were male and the median(IQR) age of 56.1 (48.6, 66.5). The median (IQR) time from symptom onset to scanning was 145 (48-238) hours for the non-stroke group.
kAverage age presented is for patients in the stroke group n=42. In the non-stroke group (n=72), average age (mean ± SD) was 43.3 ± 14.9 years.
lInability to sit up from supine.
The inclusion criteria differed between studies: one study included patients with more than one risk factor for stroke whilst another included patients with various neurological disorders, excluding only those with known multiple sclerosis, postural hypotension or trauma. 11 Hearing loss as an additional symptom of stroke in AVS was examined in two studies.11,13 Heterogeneity was apparent between studies (I2 = 58%) (Figure 2), and therefore we assessed for potential causes using the QUADAS-2 tool 14 (Table S1 and Figure 1 in the supplementary document online).
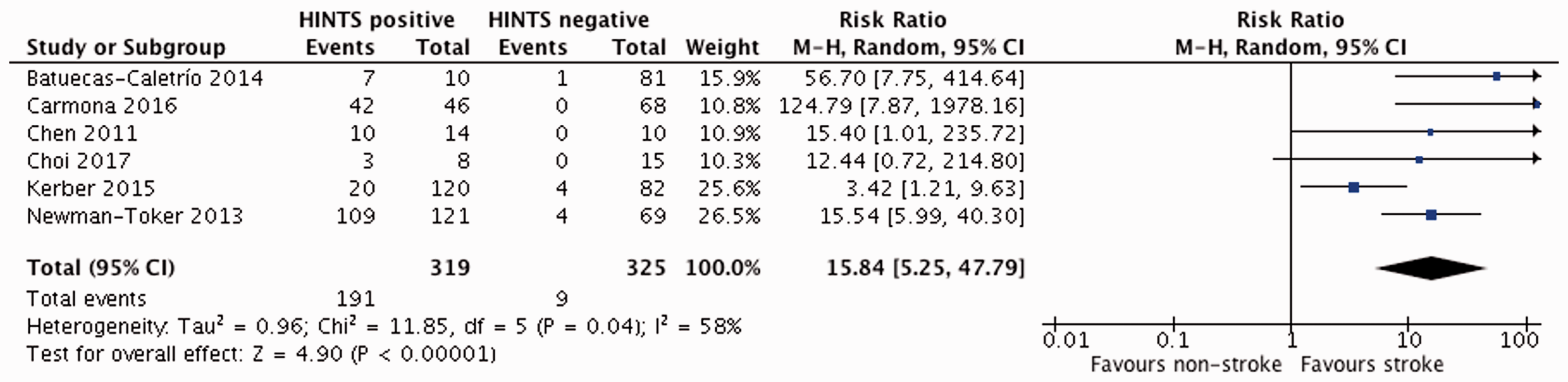
Forest-plot of studies.
Clinical features
Dizziness and vertigo, the most common symptoms in POCS, were present in all patients (Table 1). Ataxia was defined as the inability to walk 10 steps in tandem without a side step after two attempts in one study 12 and another used an ordinal three-step scale based on severity (grade 1: mild to moderate imbalance when walking independently; grade 2: severe imbalance when standing and unable to walk without support; grade 3: falling when upright). 15
Neuroimaging
Cerebral MRI scanning with diffusion-weighted imaging (DWI) was used in all studies. In the Kerber study, patients underwent a research MRI when a clinical scan was not performed. MR cerebral angiography was performed in three studies, and in the Choi et al.’s study, 11 perfusion scanning was undertaken if the diagnosis of acute stroke remained unclear.
MRI scanning was performed at different time intervals:
In one study, repeat MRI was performed in 15 AVS patients with positive HINTS in whom initial scans were normal. 13
Outcomes
From the available data (n = 644), just over half of all patients were male and the mean age was 58 years. In two studies where ABCD2 was reported, the median score was 4 (range 2–7). A positive HINTS test was found in 319 patients, and acute POCS was confirmed in 200 patients (31.1%). Data on stroke type were available from four studies (n = 150 patients): 139 ischaemic and 11 intracerebral haemorrhages. In one study, 14% of patients had an initial MRI scan which was negative but were found to have an infarction on repeat imaging.
Lesion location was reported in 35 patients; the most common site was cerebellum followed by pons. The posterior inferior cerebellar artery was most commonly affected, followed by the anterior inferior cerebellar artery.
There was a 15-fold increased risk of POCS in patients with a positive HINTS test compared to those who were negative (RR: 15.84, 95% CI: 5.25–47.79; p < 0.0001) (Figure 2). For any stroke, the pooled sensitivity using HINTS was 95.5% (95% CI: 92.6–98.4%) and specificity 71.2% (95% CI: 67.0–75.4%). The overall positive predictive value was 59.9% (95% CI: 54.5–65.3%) and negative predictive value was 97.2% (95% CI: 95.4–99.0%).
Discussion
This systematic review found that the HINTS test appears reliable and effective in differentiating acute POCS from peripheral vestibular causes in symptomatic patients with AVS. The majority of strokes were ischaemic, suggesting that HINTS could be useful for early identification of potentially eligible patients for reperfusion therapy.
HINTS is quick, non-invasive and can be performed at the bedside. Although based on well-established neuroscientific concepts, the test is underutilised in emergency settings.17,18 The head-impulse component examines the connections between vestibular pathways and the brainstem. 19 The presence of direction changing nystagmus suggests damage to gaze circuits in the brainstem and cerebellum 20 ; skew deviation of the eyes indicates injury to the central otolithic connections to the brainstem. 21 Although we were unable to estimate the sensitivity of HINTS for each vascular territory, evidence suggests better yield in strokes involving posterior inferior cerebellar artery stroke compared to anterior inferior cerebellar artery. 2
Using HINTS has its own limitations: it may be difficult to perform in very sick, nauseous patients, those with severe functional disability, under the influence of drugs or alcohol.2,22 Although the test is useful to identify stroke, a positive HINTS might also indicate other central causes in AVS. The presence of nystagmus, which improves with visual fixation or positive Dix-Hallpike manoeuvre, might indicate a vestibular disorder. It is suggested that the predictive value for diagnosing stroke could be improved by using Frenzel’s glasses, opthalmoscopy, video nystagmography, Doppler ultrasound and brain perfusion scanning, but these methods need validation in future studies.23–26
Two studies in this review categorised patients as ‘peripheral’ AVS who had ‘early’ normal MRI and this may not have been appropriate. Evidence suggests that early MRI may not be sensitive in acute POCS, 27 and studies have shown that up to 50% of lacunar infarctions can be missed within 48 h of symptom onset.27–29 One explanation could be that the structural changes visible on MRI images are delayed compared to clinical manifestations of brain dysfunction. It is possible that small infarcts cause reduced blood flow just enough to cause symptoms, but not enough to cause changes on MRI.13,30
Although isolated dizziness or vertigo, transient or persistent are common symptoms of POCS, such patients have been excluded in randomised controlled trials.31–33 The studies included in this review varied in design and diagnostic standard. Patient numbers were small, considering that POCS accounts for 25% of all strokes. The patients were highly selected and tested in single centres by experienced neurologists, which raises the issue of generalisability. Four studies in this review identified patients by referral from the emergency department, indications being uncertain diagnosis, presence of vascular risk factors and failure of symptom improvement. This may represent selection bias, as patients with mild strokes or without vascular risk factors may have been discharged without further evaluation.
In all except one study, there was no information on the time interval between AVS onset to time of assessment, which is highly relevant as the benefit of reperfusion therapies is highly time dependent. The effect of such interventions in AVS patients need further exploration since the risk of poor outcome after acute POCS is reported to be similar to that for the anterior circulation. 6
Future research
This systematic review has raised several questions for future research: the average age of patients was 58 years, and little is known about the accuracy of HINTS in older patients who comprise the largest proportion of stroke patients. The numbers are only likely to increase with an ageing population. More research is needed on the inter-rater reliability of HINTS, differences between specialists and non-specialists, training, patient cultural and language differences. Future studies should also address questions such as when to scan patients with AVS and how these impact resources between stroke services.
Conclusion
This systematic review suggests that the HINTS test as one element of clinical evaluation is useful to differentiate POCS from peripheral cause in patients presenting with AVS. Further studies are needed to validate HINTS as a clinical prediction tool in an emergency department setting and selection of patients for reperfusion treatment.
Supplemental Material
Supplemental material for Posterior circulation stroke diagnosis using HINTS in patients presenting with acute vestibular syndrome: A systematic review
Supplemental Material for Posterior circulation stroke diagnosis using HINTS in patients presenting with acute vestibular syndrome: A systematic review by Kailash Krishnan, Kerolos Bassilious, Erik Eriksen, Philip M Bath, Nikola Sprigg, Sigrun Kierulf Brækken, Hege Ihle-Hansen, Morten Andreas Horn and Else Charlotte Sandset in European Stroke Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Ethical approval
Not applicable.
Guarantor
ECS.
Contributorship
KK and ECS conceived the study. KK and KB performed literature search and extracted data. EE was involved in data checking. KK wrote the first version of the article. All authors have reviewed and edited the article, approved the final version to be submitted and agree to be accountable for all aspects undertaken in this work.
Acknowledgements
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.