
Abstract
Objective:
The aim of this analysis was to estimate 1 year and long-term cost and quality of life of ischaemic stroke patients in Croatia. In addition, we aimed to identify and estimate key categories of costs and outcomes driving the burden of stroke in Croatian healthcare system.
Methods:
Data were derived from analysis of the RES-Q Registry for Croatia in 2018 and supplemented with clinical expert opinion and relevant medical, clinical and economic literature to estimate the course of the disease and treatment patterns in Croatian healthcare system. The health economic model was comprised of a one-year discrete event simulation (DES) mapping real life patient experience and a 10-year Markov model built on existing literature. Cost and health resources use were obtained using Croatian tariffs. Health utilities were mapped to EQ5D from the Barthel Index utilising previously published studies.
Results:
The key aspects determining costs and quality of life were rehabilitation, discharge to residential care (currently 13% of patients in Croatia) and recurrent stroke. Total 1 year cost per patient was 18,221 EUR having 0.372 QALYs.
Conclusion:
Direct costing structure of ischaemic stroke in Croatia is above the value of upper-middle income countries. Our study showed that post stroke rehabilitation seems to be a strong modifier of future post-stroke costs and further research into various models of post-stroke care and rehabilitation could be the answer into more successful rehabilitation that could increase QALY and reduce the economic burden of stroke. Further investment in rehabilitation research and provision might bring promising opportunities to improve long term patient outcomes.
Introduction
Stroke is the leading cause of disability worldwide.1,2 Despite the reduction in mortality rates over the last two decades, stroke related burden has been rising, especially in developing countries. Stroke is the second largest contributor after ischaemic heart disease globally and in developing countries and the third largest contributor to disability-adjusted life-years (DALY) in developed countries. 3 Changes in healthcare provision, risk awareness, data collection and analysis over the recent decade has revolutionised healthcare decision making and understanding towards the best outcomes for stroke patients. 4
These changes represent a good response to increasing incidence as between 1990 and 1999 stroke incidence in Croatia increased almost two-fold and has been one of the leading mortality causes.5,6 Croatia has a public health care system with a single universal coverage insurer, Croatian Health Insurance Fund, based on Beveridge-Bismarck financing for taxes and contributions. 7 All of the costs (acute care and rehabilitation) are reimbursed by National Health Insurance Fund, which is using Diagnostic-Related Group (DRG) system. 7
As in many European countries, Croatia measure quality of stroke care through the Registry for Stroke Care Quality (RES-Q) – a registry tool for evaluating stroke care quality indices.8,9 RES-Q was developed, and launched in 2016, and has been used to collect data from over 90,000 patients from >750 hospitals and 56 countries between September 2016 and May 2019. It contained questions related to 28 metrics for ischaemic stroke, intracerebral haemorrhage, subarachnoid haemorrhage and cerebral venous thrombosis. 8 This registry may be used for outcome valuation and quality improvement. 8 However, the registry does not measure health care costs nor are such registries designed to measure the value provided by the health care system.
The aim of this analysis was to estimate 1 year and long-term cost and quality of life of ischaemic stroke patients in Croatia. In addition we aimed to identify and estimate key categories of costs and outcomes driving the burden of stroke in Croatian healthcare system.
Methods
The analysis was performed in three stages. First, the health economic model was constructed form clinical opinion and literature to map a care pathway for stroke patients. Then, the data from the RES-Q and literature was used to populate the probabilities and the data from the DRG codes and health care tariffs was used to populate costs. Further, mapping of the Barthel Index to the QALY (Quality Adjusted Life Year) index was performed to include quality of life data in the model via previously published studies.10,11
The health economic model is comprised of a one-year discrete event simulation (DES) mapping the patient experience with the Croatian health care system, built from a combination of expert opinion, Croatian health care data and a 10-year long term Markov model building on existing literature. Recurrent stroke cycles places patients back into the DES model. This is in line with previous similar studies which have used 90 days and 5 year DES modelling and patient registry analysis to construct similar outcome models.12,13 For this study, the first year following a stroke event was chosen as the period for the first stage of the model; this greatly simplifies the analysis as by the end of the first year all patients can be categorised into one of just a few states.
Input parameters for the first year of stroke were derived from analysis of the RES-Q for Croatia entered during 2018 (578 stroke patients during 2018) by Budinčević et al. 14 Data on demographics, stroke care pathway, specific acute treatment issues, stroke prevention issues in all acute stroke admissions in Croatia were analysed in the study. Thirteen out of twenty-three acute hospitals with stroke units which provide stroke treatment recruited 578 patients for 2018 year. Most of the hospitals entered data during March, two hospitals entered data during February and March, and a hospital entered data for November and December. 14 The registry data were analysed in close collaboration with the clinicians involved to support the design of our health economic model. The model follows a natural course of disease and treatment patterns in Croatian health care system for ischaemic stroke. The identified patient pathways were then matched to Croatian DRG codes (the DRG codes represent costing system based on events of hospitalisation) to provide for the costs of first year. 12
Results
In total, 17 distinct paths of patient care were identified. All of which begin with ischaemic stroke followed by admission at the emergency unit and ended with patients returning home, entering rehabilitation or residential care, or dying. The final patient pathways are presented in Figure 1.
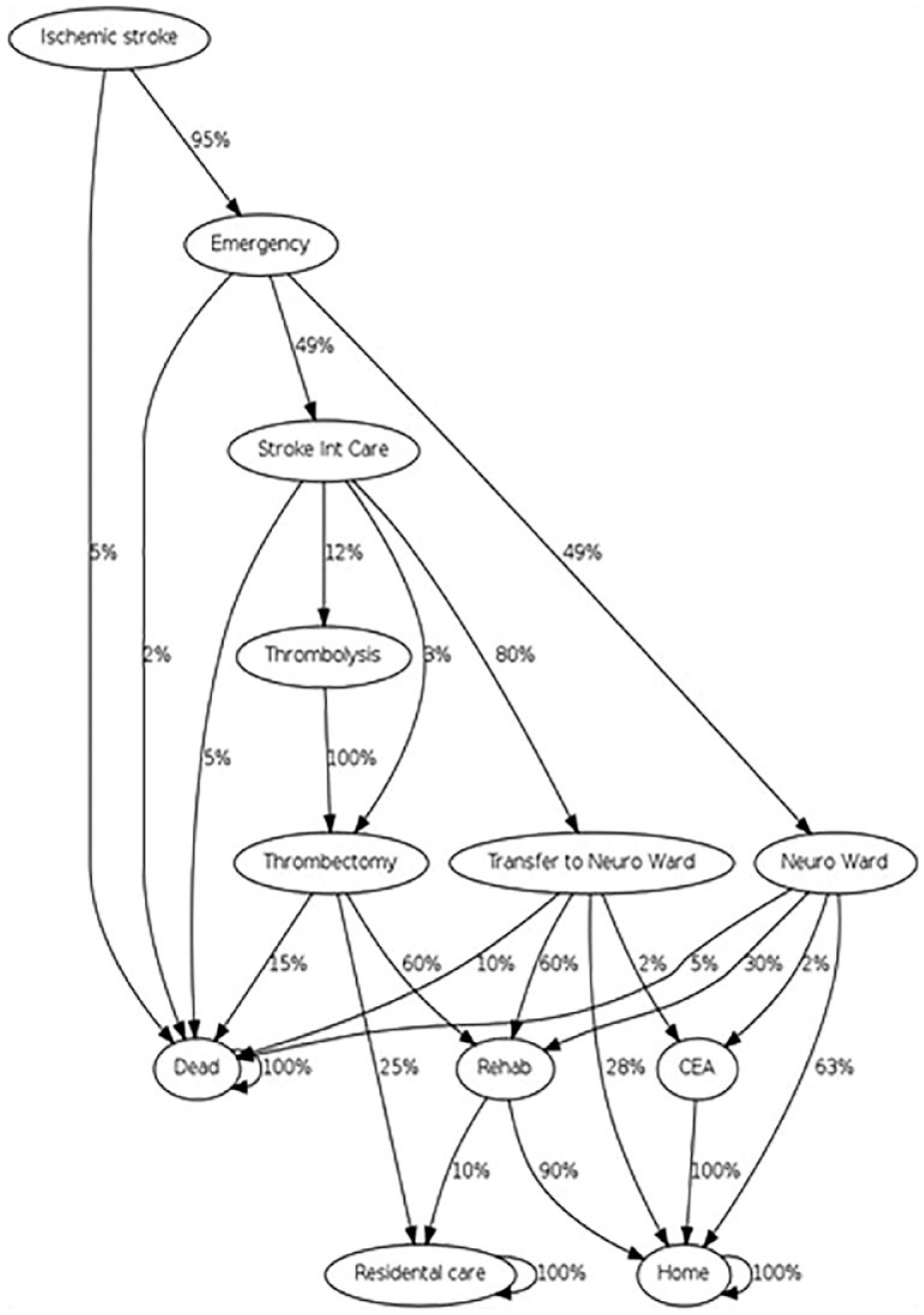
Patient pathways.
Not all pathways had the required data to estimate the probabilities associated with a particular outcome. Unknown probabilities were solved using a simple genetic algorithm approach, such that the proportion of patients travelling down each pathway matched the distribution of patients in the appropriate DRG group recorded by the hospital and public data and discharge destination recorded in the registry, the results of this calculation can be seen in Table 1.
Stroke related DRG QALY and cost categories.
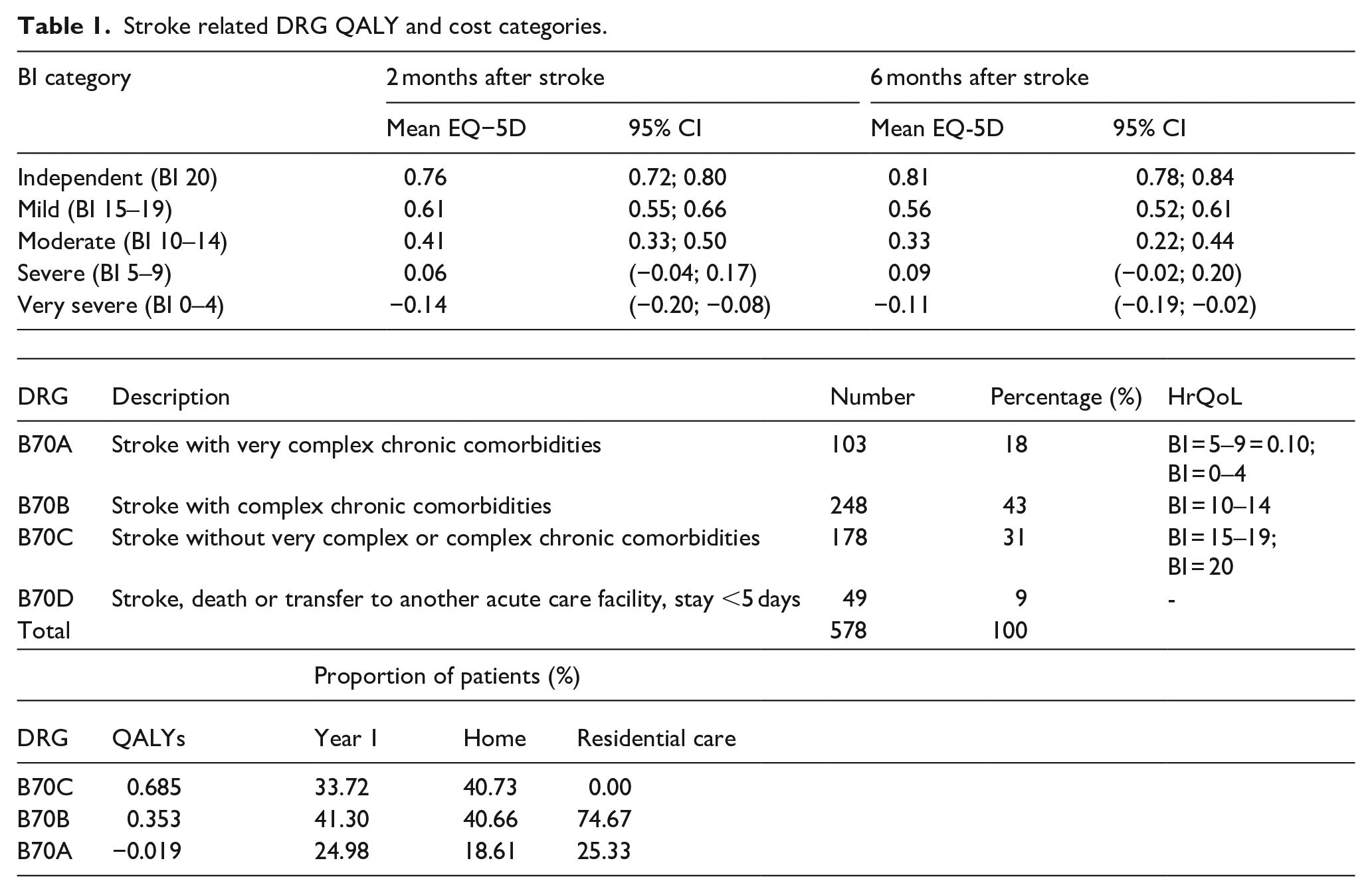
Croatian hospitals use four discrete DRG codes, no HrQoL data was included in the registry. Previous HrQoL research has already established the relationship between various stroke outcomes, the Barthel Index and EQ5D.10,11 The DRG codes were matched to Barthel Index categories according to their descriptions can be seen in Table 1, for example, a stroke without very complex or complex chronic comorbidities was matched to Barthel Index patients’ groups 15–19 and 20, with an expected quality of life of 0.685.
The first-year model was segmented into two time periods, the first 90 days following treatment, at which point all patients are either dead, in rehabilitation, in residential care or returned home. Patients that are sent to rehabilitation centres are discharged to residential care or home by the end of the year.
A total of 578 patients (age median 76 years (67.5–80) were analysed in the RES-Q it was assumed that 10% of patients in the long-term model have had a second stroke within 12 months, falling to 5% in each subsequent year. At the end the end of the first year, 65.4% of patients in the RES-Q Registry were discharged home, 8.2% to residential care and 16.3% had died, and 10% had a recurrent stroke. 14 A wide variety of discharge location per healthcare centre was observed from the registry data. 14 Prices in Croatian Kuna were converted to Euros at a rate of 0.13 Euros per Kuna.
Longer term, patients are cycled through a straightforward Markov model consistent with recent research by Fulop et al. 12 differentiating between a subsequent stroke at home and a subsequent stroke in residential care. This can be seen in Figure 2. The long-term model combines the costs and outcomes. Figure 3 shows discharge destinations according to RES-Q registry data for Croatia during 2018. 14
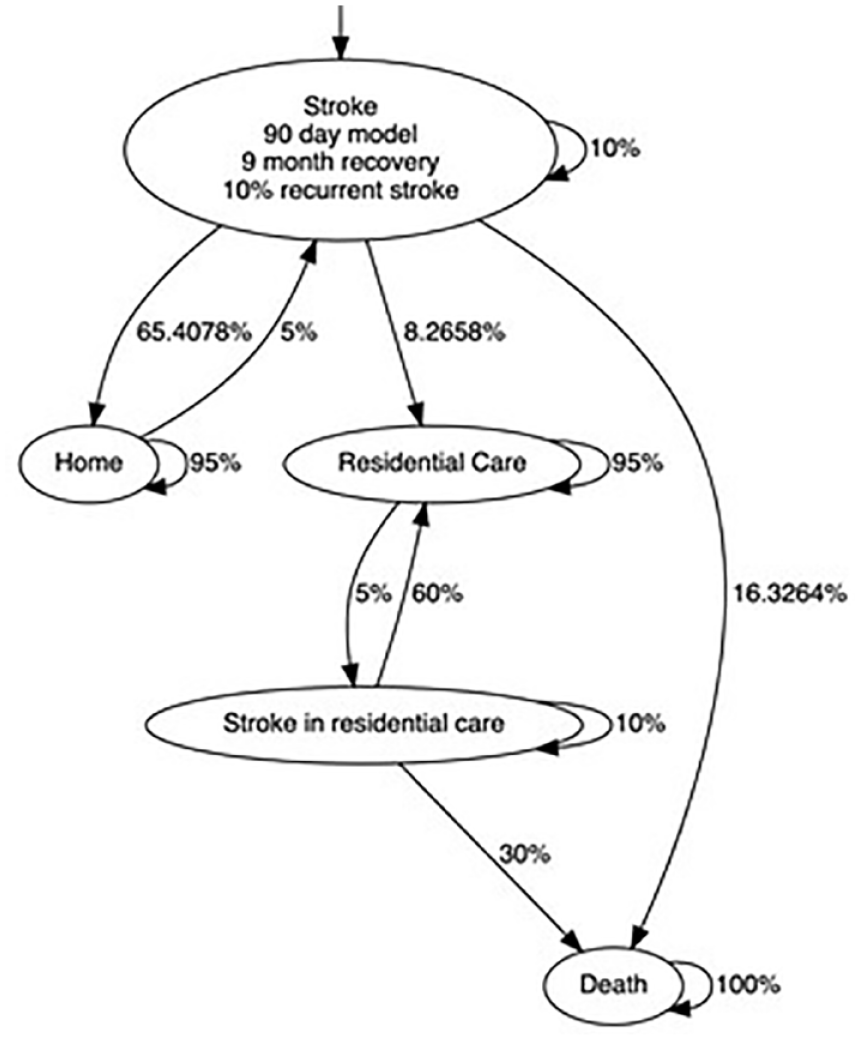
Longer term patient pathways.
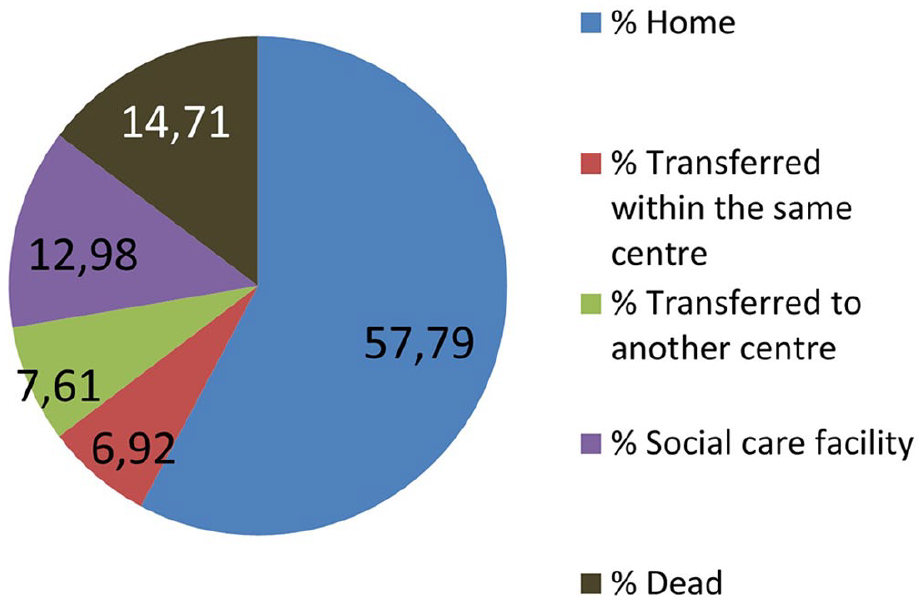
Discharge destinations according to RES-Q registry data.
Average first year cost for all patients was 18,221 EUR having 0372 QALYs.
Post-discharge rehabilitation and related care costs may often be underestimated and can depend on acute stroke treatment. Having in mind that a shift post-stroke from in-hospital to home-based rehabilitation might bring better treatment and costing efficiency, we have shown data from Res-Q on discharge location in Croatia
Discussion
Our study provides a snapshot of the economic consequences posed by stroke to Croatia where decreasing stroke burden is one of the state priorities. Moreover, it is one of the priorities of the EU where the burden of stroke is projected to increase due to demographic changes, mostly due ageing and better treatment options. 15 Despite improved diagnostic and treatment options the Central and Eastern European countries have not so far achieved the substantial decrease stroke incidence and mortality and DALYs lost which have been achieved in Western European countries. 16 The difference was primarily caused by low efficacy of stroke prevention programmes in Central and more expressed in Eastern European countries. 16 The improvement in stroke prevention might be achieved by improved targetting of common and well-known risk factors such as arterial hypertension, hyperlipidaemia, diabetes mellitus, atrial fibrillation, stress and depression, smoking, alcohol consumption, physical inactivity and inadequate diet which already have shown in improvement of stroke incidence and DALYs in high-income countries.3,17,18 By addressing these risk factors the vast majority of stroke could be prevented – up to 90% of strokes. 17 The burden of stroke shows significant regional variation.3,18 Due to these disparities regarding epidemiology and treatment through Europe, European Stroke Organisation has prepared and started to implement Stroke Action Plan for Europe where these challenges are pointed out. 15
A 30-year projection was based on current trends and there is an estimated 3% increase in the incidence of stroke along with an 27% increase in prevalence, however there is also a projected 17% decrease in mortality and 33% decrease in DALY. 19 As seen in Figure 1, there are different paths that patients can go through, even though stroke severity and response time are the determining factors in patient management, 20 pre-morbid modified Rankin scale (mRS) is a strong predictor of discharge destination, as had previously been shown in a paper that used machine learning to predict discharge destination based on multiple variables at admission. 21 Mees et al. 22 found that the main predictor of other than home discharge after stroke were: functional dependence/comorbidities, neurocognitive disfunction and previous living circumstances/marital status, furthermore medium and large infarcts were associated with institutionalisation.
Up to 4% of total health care expenditures in Western countries are spent on stroke management.18,23 Generally, overall (inpatient and outpatient) poststroke care per month cost from 752 USD in Australia to 4850 USD in the US – where rehabilitation services represent the main cost driver. 24 The systematic review by Rajsic et al. 24 have found that the outpatient poststroke care varies between 192 USD (in Malaysia) to 883 USD per month (in the United Kingdom). Hospital and nursing home costs contribute to most of total cost of stroke in Australia, whereas inpatient rehabilitation accounts for cca 27% of total first-year costs. 24
In our study, the key aspects determining costs and quality of life were rehabilitation, discharge to residential care (currently 13% of patients in Croatia) and recurrent stroke. Recent analysis by Patel et al. 25 found that the mean cost of new-onset stroke is £ 45,409 (53958.83 euros) in the first year and £ 24,778 in subsequent years, what exceeded previous cost estimates. The largest compound of total costs is related to unpaid care (61%) and interventions at rehabilitation and reducing new and recurrent stroke may yield substantial benefit to carers and cost saving to society. 25 Post-discharge rehabilitation and care costs are often underestimated and can depend on acute stroke treatment. Another possible way to reduce the cost of stroke is to shift post-stroke rehabilitation from in-hospital to home-based rehabilitation, previous cost estimates by Anderson et al. 26 had shown that for every six patients that had received in-hospital rehabilitation another patient could have received rehabilitation if it had been done at home, furthermore the same practice would allow more patients to be treated using the same number of hospital beds. Rasmussen et al. 27 have shown that early home-based rehabilitation improved life-quality and reduced disability while being cost effective. Two trials tracked patients that had undergone early home-based rehabilitation and compared them to a control group that had undergone standard rehabilitation and both trials found no convincing difference in disability while being the lower-cost option.27,28 Early home-based rehabilitation shows promise as a low-cost alternative to classical in-hospital rehabilitation while allowing for less burden on hospital stays and the quality-of-life improvement of familiar surroundings.27,28
However, not all countries can afford interdisciplinary medical teams who visit people in their own homes, thus an alternative is needed that could be found in telerehabilitation. 29 A meta-analysis done by Tchero et al. 30 found that telerehabilitation has results comparable to standard rehabilitation practices. Lloréns et al. 31 in their trial managed to achieve comparable results while cutting the cost of rehabilitation by $645. 30 Another point in favour of telerehabilitation is that it can be done with very little infrastructure, some models can be accomplished via smartphone, although such models raise complex equity issues for patients from low-income backgrounds. 32
Post discharge stroke costs can vary vastly and are the greatest during the first 6 months. It has been shown there are significant direct, costs that occur when the patient is confronted with everyday tasks and mobility, and thus need wheelchairs, home modifications, drugs, diapers, transportation and new drugs. Most stroke survivors also need physiotherapy, speech therapy, nursing services and occupational therapy that also directly increase the cost of stroke. In the Italian study the average direct cost of a stroke was estimated to $3710. 33 One of the main driving factors of the cost of stroke and post-stroke rehabilitation is the residual neurological deficit after stroke. Angerova et al. 34 in their study measured the cost of rehabilitation, based on the severity of the deficit and found that the cost for the most severely disabled group was 2.4-fold greater than the self-sufficient group, furthermore the least disabled group had benefitted the most from the rehabilitation. However, in Chien et al. 35 study on Taiwanese population calculated that patient that had been transferred to a rehabilitation ward had higher 10-year medical costs and longer life expectancy than those that had no rehabilitation or had rehabilitation outside the rehabilitation ward. Nevertheless, their per day cost effectiveness was greater, possibly related to better quality of life, good function recovery and longer life expectancy.
In our study, 12% of patients were admitted to the intensive care unit/ward, mostly for the revascularisation therapy – intravenous thrombolysis (IVT) and/or mechanical thrombectomy (MT). Despite the high costs of mechanical thrombectomy and intravenous thrombolysis, they are cost-effective, shortening hospital stay and improving functional outcome for patients.36,37 IVT and MT are the only currently approved recanalisation treatment of stroke, their rates are increasing, and they are the base of future stroke treatments that could further reduce the burden of stroke. 38 Inpatient hospital costs for acute stroke accounts for 70% of first year post-stroke care-.18,23 However, the severe strokes cost is twice that of mild strokes.18,23 The cost of haemorrhagic stroke is generally higher.18,23 The per year per patient cost of stroke varies depending on the country a patient lives in and is higher in higher income countries, per patient per year cost varies from $2100 in low-income countries to $27,702 in high-income countries. 39
When comparing our results to the prices in other countries according to the systematic review done by Strilciuc et al. 39 on Romanian population, our value of 18,221 EUR, which is roughly equivalent to $20,125 USD according to the current exchange rate, places Croatia above the value of upper-middle income countries ($14,478) and well above the value of low-middle income countries (6850 USD). This value is comparable to Italy’s 19,200 USD and higher than Denmark’s 11,625 USD, where the beforementioned direct cost of 3710 USD is the direct cost that the patient has to spend, without the cost covered by the healthcare system. The highest per year cost was in the USA (59,900 USD) which could partially be due to their specific organisation of the healthcare system, Sweden (52,725 USD) is a country with a much more comparable system to Croatia, at least considering the model of the healthcare system, however the living standard in Sweden is significantly higher thus the difference in per year per patient price.33,39 The average cost per case during first 12 months and over the lifetime in Australia was 14,361 USD and 33,658 USD respectively. 40 The economic burden of stroke report for Europe estimated in 2017 total stroke costs of 27 billion euros (18.5 for direct medical costs and 8.5 for indirect costs), with total stroke cost of 60 billion. 41 Similarly, American Heart Association projected increase of total stroke costs from 105.2 billion dollars in 2012 to 240.7 billion dollars in 2030. 42
Strengths and limitations
One of the key strengths of this study is that for the first time in the region, registry data was accompanied with estimations of costs and quality of life. The real-world data that was available to us from the RES-Q registry provided a solid base for a detailed model design. However, the study has several limitations. The major limitations are that the study was based on approximation of registry data which did not cover the whole country and whole calendar year. This model did not consider the societal perspective such as costs to patients or family members which are reflected as loss of income/informal care, too. As much as we would like to include patient costs, they are not available publicly without undertaking primary exploratory research. The QALY mapping to DRGs may not reflect the real-world picture for several reasons such as miscoding and the fact that utilities were not measured locally. In Croatian Health Care System DRG codes are not adjusted as often as they should, the last revision was not related to real life costing change, which also influenced the calculation of the costs. Available rehabilitation options vary from short inpatient procedures to dedicated rehabilitation facilities, contributing a wide variation in costs and uncertainty around longer term outcomes. Cost estimation was used equally regardless of the patient age, although in the real-world younger patients are typically less severe and incur less costs. Since this study is not interventional there is of course a set of limitations that goes with the methodological approach including estimations for many inputs such as monitoring frequency, drug consumption per specific type of patient etc.
Conclusion
The cost of stroke is a potentially underestimated factor in healthcare cost, and along with post-stroke disability has a crucial impact on life of stroke survivors and the healthcare system that cares for them. Direct costing structure of ischaemic stroke in Croatia is above the value of upper-middle income countries. The post-stroke rehabilitation seems to be a strong modifier of future post-stroke costs and further research into various models of post-stroke care and rehabilitation could be the answer into more successful rehabilitation that could increase QALY and reduce the economic burden of stroke. Further investment in rehabilitation research and provision might bring promising opportunities to improve long term patient outcomes
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VB expressed views strictly from the personal point of view which does not reflect the position of Novartis Croatia where she acts as an employee. VB is not included in selling or promoting any of Novartis drugs. TN and MP have no financial conflict of interest nor are they included in selling or promoting any drugs or medicinal devices. HB received speaker fees from Bayer, Berlin Chemie Menarini, Bohringer-Ingelheim and Pfizer. HB was supported by project No. CA18118, IRENE COST Action funded by COST Association, and ESO EAST project. AM declare that there is no conflict of interest
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable. Data analyses were carried out using fully anonymised data from previously published literature.
Informed consent
Not applicable
Guarantor
HB
Contributorship
VB and HB were involved in protocol development. VB wrote the first draft of the manuscript. HB and AM researched literature. TN and MP were involved in data analysis. All authors reviewed and edited the manuscript and approved the final version of the manuscript