
Abstract
Purpose
There appears to be an association between poor oral hygiene and increased risk of aspiration pneumonia – a leading cause of mortality post-stroke. We aim to synthesise what is known about oral care after stroke, identify knowledge gaps and outline priorities for research that will provide evidence to inform best practice.
Methods
A narrative review from a multidisciplinary perspective, drawing on evidence from systematic reviews, literature, expert and lay opinion to scrutinise current practice in oral care after a stroke and seek consensus on research priorities.
Discussion
Oral health after a stroke is important from a social as well as physical health perspective, yet tends to be neglected. Multidisciplinary research is needed to improve understanding of the complexities associated with delivering good oral care for stroke patients. Also to provide the evidence for practice that will improve wellbeing and may reduce risk of aspiration pneumonia and other serious sequelae.
Conclusion
Although there is evidence of an association, there is only weak evidence about whether improving oral care reduces risk of pneumonia or mortality after a stroke. Clinically relevant, feasible, cost-effective, evidence-based oral care interventions to improve patient outcomes in stroke care are urgently needed.
Introduction
Poor oral care after a stroke can have serious physical, psychological and social consequences and adversely affect quality of life.1–3
Aspiration pneumonia causes the highest attributable mortality of all medical complications following stroke and its prevention is therefore of paramount importance.4,5 There is a growing body of evidence to indicate that poor oral hygiene increases the risk of pneumonia.6,7 It would be rational to expect good oral hygiene and plaque control in the early stages after a stroke to reduce risk, but evidence for this is weak.8–10
Dysphagia and loss of sensation affects up to 78% of patients who have recently had a stroke and can cause stasis of saliva and food in the oral cavity.11–13 Reduced tongue pressure and altered lateral movements result in increased risk of aspiration as well as causing food to pool in the sulci of the oral cavity resulting in denture problems and stomatitis.14–16 There also appears to be a higher than normal pathogenic bacterial and yeast count in the oral cavity in the acute phase of stroke.17,18 This combination increases the risk of aspiration pneumonia.9,19–24 Approximately 10,000 microbial phylotypes have been identified in the human oral microflora. 25 There is a huge diversity of bacterial organisms in the oral cavity of stroke patients. The balance between organisms may be as important for containing risk of aspiration pneumonia as the presence or the absence of any particular bacteria in the oral cavity. 26
Whilst stroke can affect people of all ages, the average is 71 years. 27 In many low and middle-income countries, the incidence of stroke is increasing but even in many European countries where it is decreasing, the size of the problem, based on the actual number of new strokes is rising because of the ageing population. 27 Figure 1 shows the improving pattern of dentition between 1978 and 2009 in England. Although considerably more people are surviving into old age with some natural teeth, very few have excellent oral health. Most have periodontal disease, a sizeable number of restorations (fillings and implants) and need help to maintain their oral health.28,29
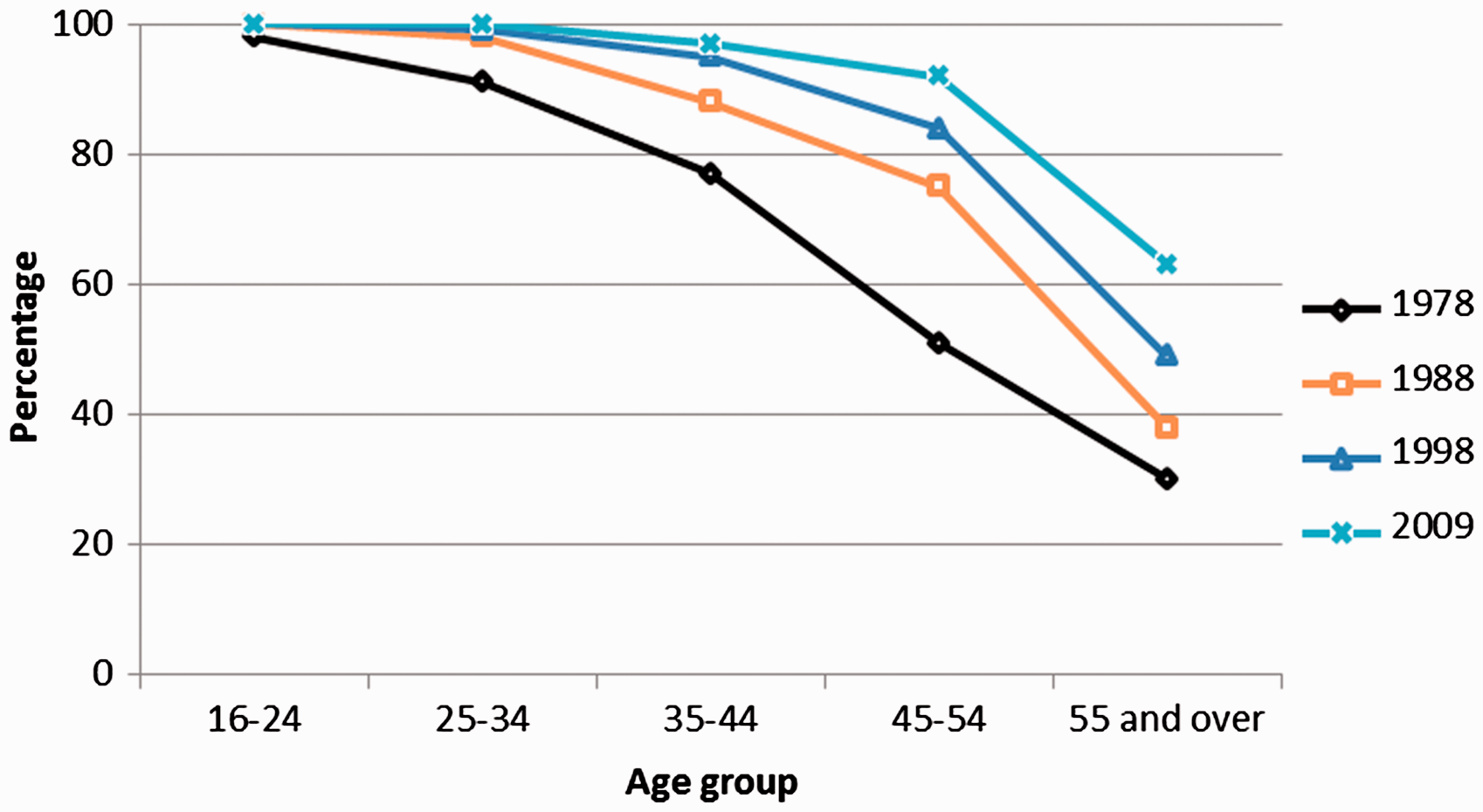
Trends in percentage of adults with 21 or more natural teeth by age, England 1978–2009.
The cost of dental care in the European Union is expected to rise from €54 billion in 2000 to €93 billion in 2020. 30 A significant proportion of this relates to the provision of oral care for the growing number of dependent older people – including those who have had a stroke.31,32
People who have a stroke tend to have worse oral health than the rest of the population but a cause and effect relationship cannot be assumed and the relative importance of specific risk factors such as smoking, poor nutrition and diabetes that stroke and poor oral health have in common is unclear. 33 A scoping review of oral care post stroke found that stroke survivors aged 50 to 70 years have fewer natural teeth and are more likely to wear dentures than a control group of a similar age who had not had a stroke.19,34 A systematic review found that patients with stroke had a poorer clinical oral health status across a range of parameters (tooth loss, dental caries experience and periodontal status). 20 Other reviews have demonstrated an association between periodontal disease and stroke.33,35
What is to follow
In this paper, we review the latest research on oral health in people who have had a stroke and the care dilemmas this creates. We reflect on what people who have had a stroke and their carers think about the oral care patients receive and investigate the challenges of its provision in this population. We identify gaps in knowledge about optimum oral care for stroke patients and areas where further research is needed to provide the evidence to support best practice.
Method
This is a narrative review, based on findings from systematic reviews, primary research, other published literature combined with expert and lay opinion. It provides a holistic interpretation of the current situation in relation to oral care in stroke patients.
Consensus on knowledge gaps for optimum oral care and research priorities was reached after a series of discussions with stroke survivors, carers, clinical and academic experts in dental care, health economics, physical medicine, speech and language therapy, medical imaging, public health and nursing. It takes account of the pluralities and diversities of the disciplines involved. An iterative process to synthesise the main issues and their implications, identify gaps and directions for future research was undertaken through a series of meetings and discussions. The manuscript was drafted and revised by all authors.
Findings
A prompt oral examination and assessment in patients who have had a stroke is important because it determines oral hygiene needs, informs an oral care plan and identifies problems that may affect recovery. 36 Available oral assessment protocols score features such as saliva, soft tissues and odour; with dental plaque, oral function, swallowing, voice quality and hard tissue assessment suggested in some. However, few oral assessment tools exist, and those that do, are not specifically developed for, or validated in patients with stroke and are rarely used.19,37 Nurses are best placed to conduct the initial oral assessment and can also be trained to identify patients who may need referral to a dental specialist. 38
Dependent stroke survivors rely on nursing staff to help them, but without evidence based pathways, adequate knowledge, skills, confidence and support from senior staff and dental professionals, nurses cannot provide effective, good quality oral care.
Hospitalisation, reduced food and drink intake, increased exposure to antibiotics and dependency can affect stroke patients’ ability to maintain oral hygiene effectively.14,19 Dehydration and xerostomia can be a particular problem because of oxygen therapy, mouth breathing, side-effects of medications and reduced food and fluid intake.39,40 In these circumstances, oral care can be challenging and is often given low priority by nurses. 41
Oral care can be further complicated where swallow safety is compromised, as patients may be unable to keep any food residue, toothpaste or rinsing fluids from entering their airway.
There is currently neither evidence nor consensus guidance for best practice in assessment of need, equipment, procedure or how frequently oral care should be provided. Practice in different locations varies widely and staff feel insufficiently trained to deliver oral care effectively.19,42–44 The current lack of appropriate training and failure to prioritise oral care within the stroke care pathway has the biggest impact on patients with greatest need who are at high risk of complications. 10
Patient, carer and professionals’ perspectives
For those who survive a stroke, life often changes dramatically as they and their families learn to live with the disabling consequences such as paralysis, muscle weakness, cognitive impairment, fatigue, anxiety and depression.45,46 Stroke patients often experience oral discomfort and pain, oral infections (especially oral candidiasis) and difficulties in denture wearing.2,3,14,47 Normal daily activities that affect oral hygiene such as eating, drinking and tooth brushing can be severely disrupted. 48
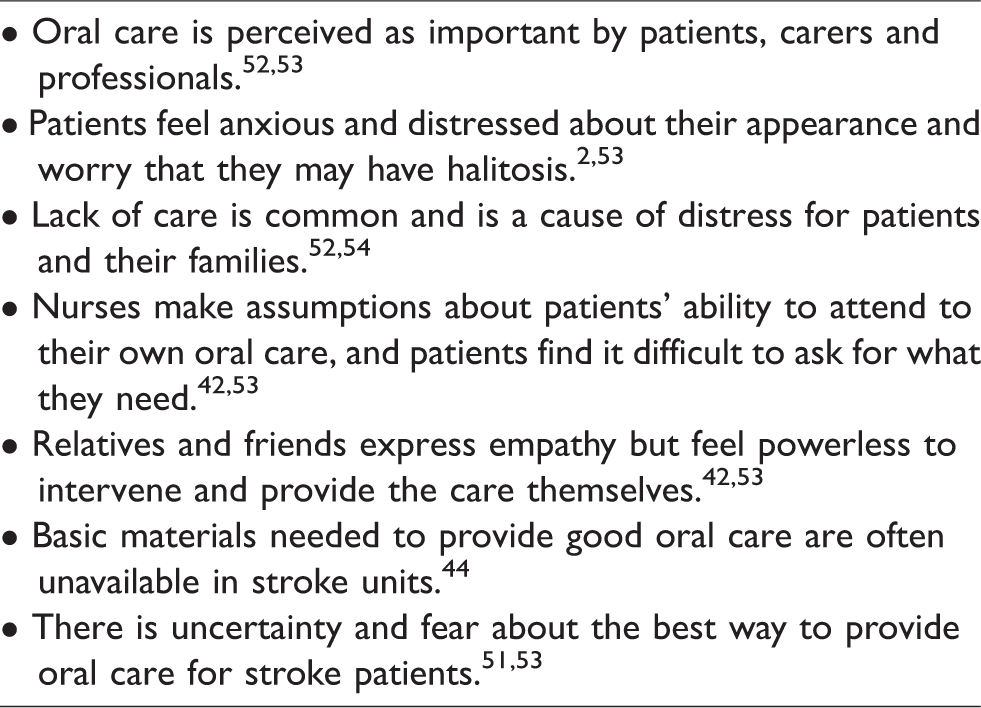
Table 1 summarises findings from studies exploring stroke patients, carers and professionals experience of oral care. Barriers such as fear of possibly causing harm, lack of knowledge, skill or ability, lack of time, low priority, inadequate resources and lack of guidance are the main explanations provided by carers and professionals for inadequate oral care provision in stroke patients.1,49–51
Key points.
Evidence
There are few evidence-based assessment tools, guidelines and protocols for oral care in the stroke population.19,55,56 A Cochrane systematic review on staff-led interventions for improving oral hygiene following a stroke was updated in 2011. 1 The review included three trials. Gosney et al. 57 found high carriage of and colonisation by aerobic Gram-negative bacteria in stroke patients. In this randomised controlled trial, the use of an oral decontaminating gel reduced the presence of bacteria and documented episodes of pneumonia, but mortality remained unchanged. Frenkel et al. 58 found that education can improve caregivers’ knowledge, attitudes and oral care performance. Fields 59 found that the ventilator associated pneumonia rate in an intensive care unit that included, but was not specific to, stroke patients dropped to zero in the intervention group within a week of beginning a tooth-brushing regime. After six months, the control group was dropped, and all intubated patients’ teeth were brushed every 8 hours, maintaining a zero rate of ventilator-associated pneumonia until the end of the two-year study. Lack of adequate data meant that the findings were not included in the meta-analysis.
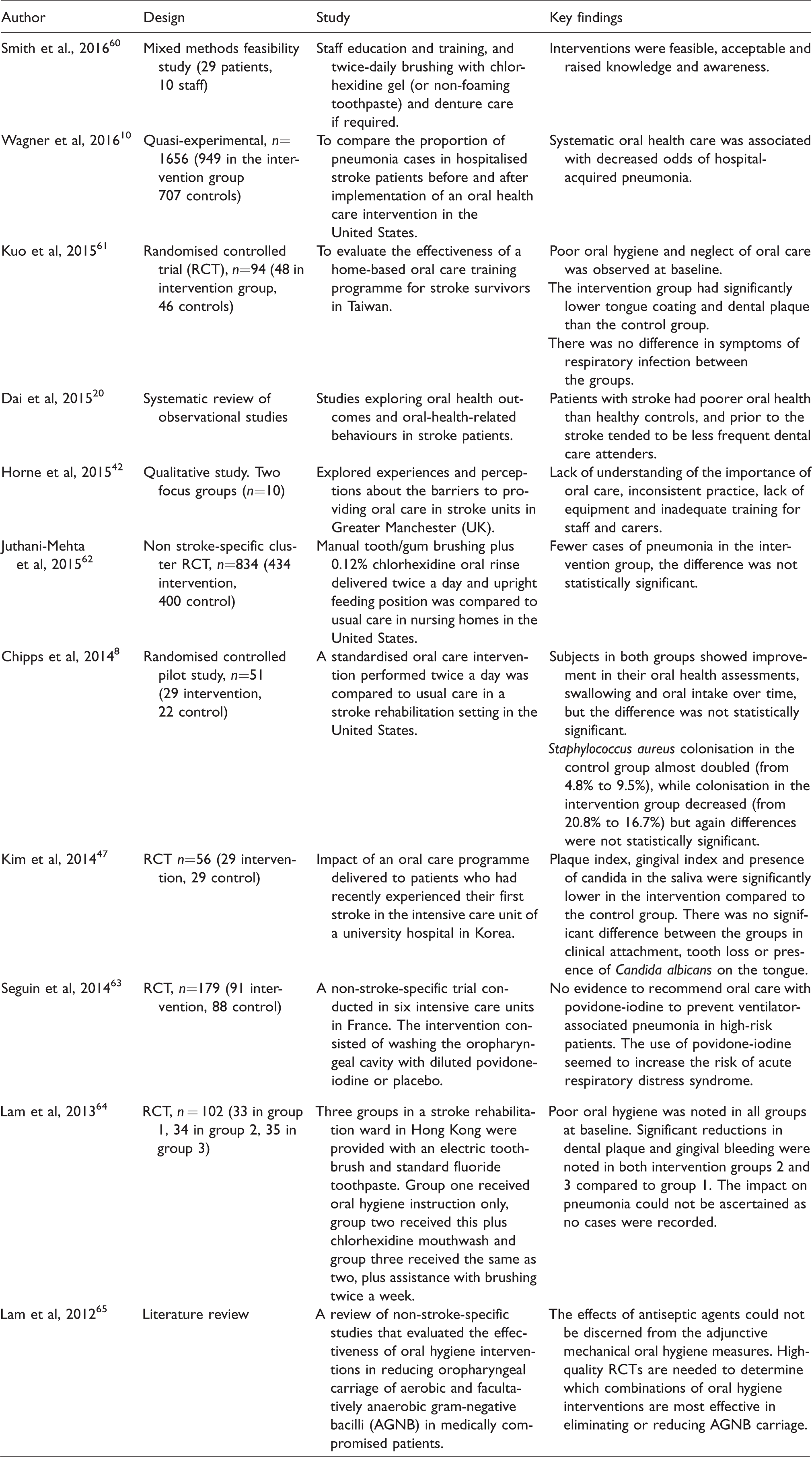
The Cochrane review concluded that provision of training in oral care interventions can improve staff knowledge and attitudes, cleanliness of patients' dentures and reduce incidence of pneumonia. However, evidence was weak and improvements in the cleanliness of patients’ teeth were not observed. Table 2 provides an overview of the relevant research published on oral care in stroke patients since the 2011 Cochrane review update.
Recent oral care research.
Discussion
Adequate oral care improves patients’ oral health, comfort and quality of life, but definitive evidence of its ability to reduce the risk of pneumonia is lacking. 55 Two non-stroke specific nursing home based studies, one from Japan (2002) and the second from the United States (2008) evaluated the impact of an oral care intervention in a setting where there were a number of stroke patients.6,66 Both studies reported fewer cases of pneumonia (or related death) amongst residents that received oral health care but the Japanese trial excluded incapacitated, dysphagic, unstable and unconscious residents. 6 Unfortunately, in many trials the challenges associated with gaining informed consent result in patients who are most dependent for oral care being excluded.
Several guidelines refer to oral care following a stroke (See Supplementary Appendix 1 which will be available online with this article, http://journals.sagepub.com/doi/full/10.1177/2396987318775206). Many refer to the lack of evidence to support detailed guidance. Answers to basic questions about whether it is best to use an electric or manual toothbrush, size and type of head, which – if any toothpaste, how frequently care should be given, etc. are not provided. No guidelines contain information or advice to alleviate nurses’ anxieties about how best to reduce risk of choking when delivering oral care for dysphagic stroke patients.
It is a limitation of this study that there is little evidence about oral care practice in stroke units across Europe, hence most of the included studies are from elsewhere.
Future considerations
Emerging evidence supports the rationale for developing best practice guidelines for oral care in stroke care units. 19 High-quality evidence is needed to inform improvements in staff training and delivery of consistent oral care. Protocols need to be developed that focus on maintenance of dentition and a quality of life associated with having acceptable oral function. Protocols need to describe simple preventative measures at every stage in the care pathway, combined with early diagnosis and management of significant dental pathology. Several oral hygiene interventions appear to be feasible and well-tolerated in early-stage studies.47,55,59,60,63,64
Research is needed to inform the spectrum and variation in existing ‘usual’ care and service provision (including the role of specialist dental services) as well as optimal oral assessment tool(s), including for patients who are intubated as well as later during the rehabilitation phase.
Safety, acceptability and resources required to deliver high-quality oral care assessments and protocols needs to be established.
Clarity is needed about the multi-disciplinary team support required, especially around optimisation of effective staff education and training, including from dental specialists.
Ultimately, large phase three randomised trials supported by realistic recruitment and clinically relevant strategies, economic evaluation and implementation strategies are required. They need to produce practical clinical outcomes that address barriers and facilitators to change and adoption of evidence into policy and practice.
Priority should be given to research that provides evidence to inform standards for oral care delivery, and guidelines for each patient with individualised care plans that illustrate the safest, most efficient equipment to use.
Conclusions
There is a lack of knowledge about how and what oral care is currently provided as well as inadequate research to inform best practice in acute stroke care, rehabilitation and nursing home settings.
Staff feel inadequately prepared to provide oral care, especially when dysphagia or other problems are present and it tends to be given low priority. This review provides an objective platform to encourage health and care services to incorporate oral care into future stroke pathways, whilst stimulating greater engagement with this under-researched area.
Supplemental Material
Appendix 1 -Supplemental material for Oral care after stroke: Where are we now?
Supplemental material, Appendix 1 for Oral care after stroke: Where are we now? by Mary Lyons, Craig Smith, Elizabeth Boaden, Marian C Brady, Paul Brocklehurst, Hazel Dickinson, Shaheen Hamdy, Susan Higham, Peter Langhorne, Catherine Lightbody, Giles McCracken, Antonieta Medina-Lara, Lise Sproson, Angus Walls and Dame Caroline Watkins in European Stroke Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a NIHR CRN/British Association of Stroke Physicians stroke writing group grant.
Informed consent
Not applicable as this is a review article.
Ethical approval
Not applicable as this is a review article and contains no primary research.
Guarantor
CLW.
Contributorship
CW and CS devised the conceptual framework. CS, EB, MCB, HD, ShH, SH, ML and GMcC contributed sections to this paper. ML synthesised contributions with support from PL, CL, AM-L, LP, AW and CW. All authors reviewed, edited and approved the final version of the paper.
Acknowledgements
Mary Harrington, Head of Speech & Language Therapy, Hull & East Yorkshire Hospitals NHS Trust reviewed and commented on the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.