
Abstract
Purpose
The microbiological aetiology of pneumonia complicating stroke is poorly characterised. In this second Pneumonia in Stroke ConsEnsuS statement, we propose a standardised approach to empirical antibiotic therapy in pneumonia complicating stroke, based on likely microbiological aetiology, to improve antibiotic stewardship.
Methods
Systematic literature searches of multiple databases were undertaken. An evidence review and a round of consensus consultation were completed prior to a final multi-disciplinary consensus meeting in September 2017, held in Barcelona, Spain. Consensus was approached using a modified Delphi technique and defined a priori as 75% agreement between the consensus group members.
Discussion
Consensus recommendations for antibiotic treatment of the spectrum of pneumonia complicating stroke are proposed. However, there was limited evidence available to formulate consensus on choice of specific antibiotic class for pneumonia complicating stroke.
Conclusion
Further studies are required to inform evidence-based treatment of stroke-associated pneumonia including randomised trials of antibiotics and validation of candidate biomarkers.
Introduction
Pneumonia is a serious and common complication of stroke which is associated with significantly increased healthcare costs, poor functional outcome and mortality.1–3 The Pneumonia in Stroke ConsEnSuS (PISCES) group was formed as a multi-disciplinary initiative to address uncertainties in the diagnosis, prevention and treatment of pneumonia complicating stroke, and to identify key research priorities. The first PISCES consensus focused on terminology and diagnostic criteria for the spectrum of lower respiratory tract infections, including the proposed definition and operational criteria for stroke-associated pneumonia (SAP). 4
In clinical practice, immediate treatment of pneumonia complicating stroke is recommended once suspected or diagnosed.5,6 Initial choice of antibiotics is often broad spectrum, being either clinician dependent or guided by various international guidelines for community-acquired pneumonia (CAP), hospital-acquired pneumonia (HAP) or aspiration pneumonia.5–7 There is, however, substantial variation in antibiotic prescription practices across healthcare systems, 7 which could have implications for clinical outcomes. Determining microbiological aetiology in pneumonia complicating stroke is challenging given the difficulty in obtaining sputum samples in non-ventilated stroke patients and poor diagnostic sensitivity of other available culture specimens, which may limit definitive antibiotic treatment based on microbial sensitivities. 8 Antibiotics commonly used to treat pneumonia complicating stroke vary in their spectrum of antimicrobial activity, and patterns of antibacterial resistance also vary around the globe, which are important considerations in empirical treatment. Transient immune suppression induced by acute stroke, involving both innate and adaptive responses, is a well-recognised phenomenon 9 and might also impact on the effectiveness of antibiotics. 10 Different antibiotic classes may also potentially influence outcomes by mechanisms independent of their antimicrobial coverage, for example anti-inflammatory and immunomodulatory effects. 11
Choice of antibiotics for treatment of pneumonia complicating stroke may therefore have important implications for antibiotic stewardship and clinical outcomes in clinical practice. In this second PISCES group consensus process (PISCES-2), we aimed to formulate antibiotic treatment recommendations for pneumonia complicating stroke, and to identify areas for future research.
Methods
Membership of the PISCES group and protocol development
The PISCES group was originally convened by the Chair (C.J.S) based on collective multidisciplinary expertise across the spectrum of SAP, pneumonia, respiratory medicine, stroke neurology, stroke unit and neurocritical care management, infectious diseases, clinical microbiology, systematic review, and clinical guidelines. For this consensus process, the PISCES group included 18 clinicians with representation from the UK, Germany, Spain, Italy, Netherlands and Switzerland. The protocol for the present study was drafted by the chair in conjunction with the co-chairs (A.M and J.M) and reviewed by the group to further define the objectives, methodology, and statements for consensus. The authors declare that all supporting data are available within the article [and its online supplementary files].
Systematic literature searches
An evidence review to inform the consensus development and process was undertaken as follows. As a first step, a systematic review and meta-analysis of microbiological aetiologies implicated in pneumonia complicating stroke was undertaken and has been reported previously. 8 A second systematic literature search sought to identify randomised controlled trials (RCTs) of antibiotic treatment for pneumonia complicating stroke (Table I in the online-only Data Supplement) in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 12 Briefly, published studies of ischemic stroke, intracerebral haemorrhage (ICH), or both, involving antibiotic treatment of pneumonia were independently screened for eligibility (Table II in the online-only Data Supplement) by A.K.K and C.J.S using the study title and abstract. Online trials registries (ISRCTN Registry, ClinicalTrials.gov, ICTRP Portal) were also searched for registered ongoing or recently completed, unpublished RCTs. A summary of currently available antibiotic classes in clinical practice, antimicrobial activities and antibiotic stewardship issues (including antibiotic resistance) was provided by the study microbiologist (A.R.J). Review of specialist societal recommendations for CAP, HAP and aspiration pneumonia was also undertaken, with reference to antibiotic classes used, led by A.K.K and the study infectious diseases specialist (J.G).
Summary of PISCES-2 consensus recommendation for antibiotic treatment of pneumonia complicating stroke.
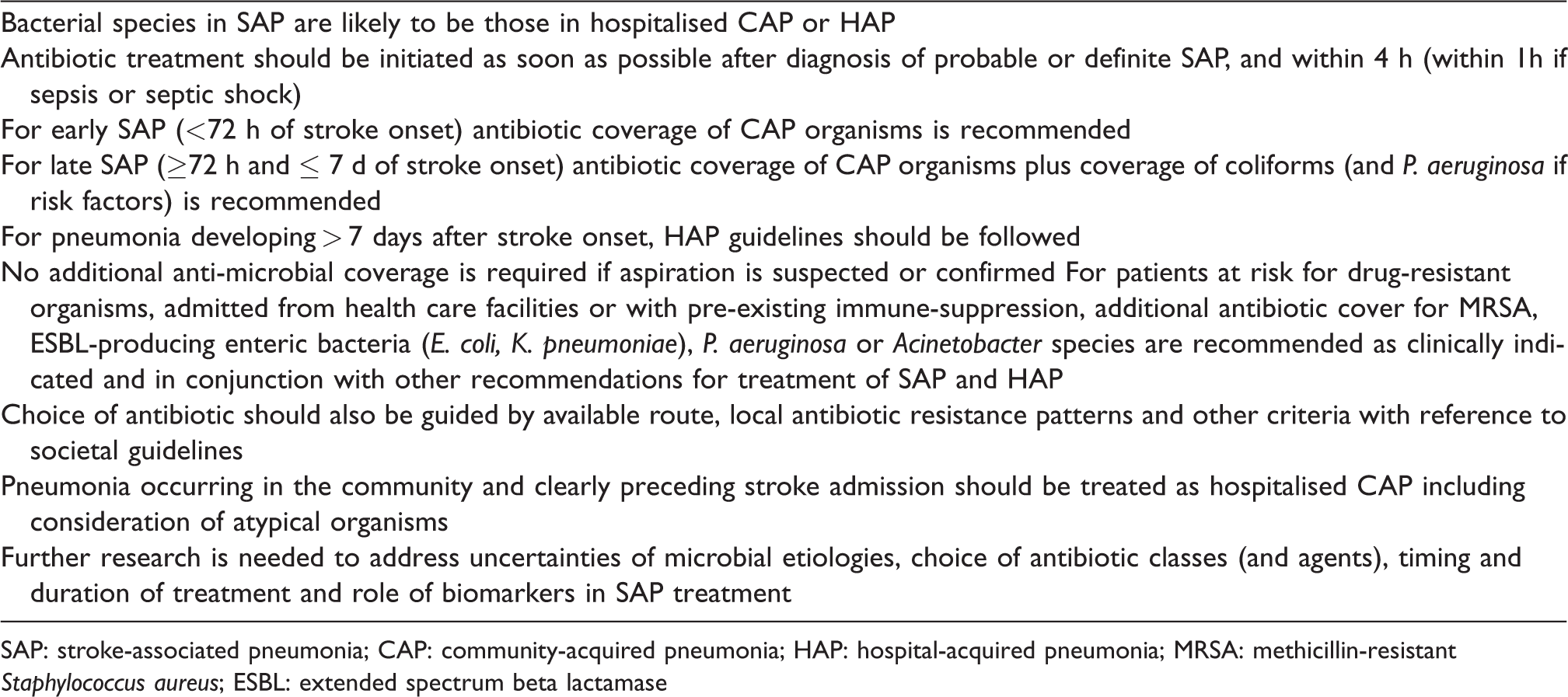
SAP: stroke-associated pneumonia; CAP: community-acquired pneumonia; HAP: hospital-acquired pneumonia; MRSA: methicillin-resistant Staphylococcus aureus; ESBL: extended spectrum beta lactamase
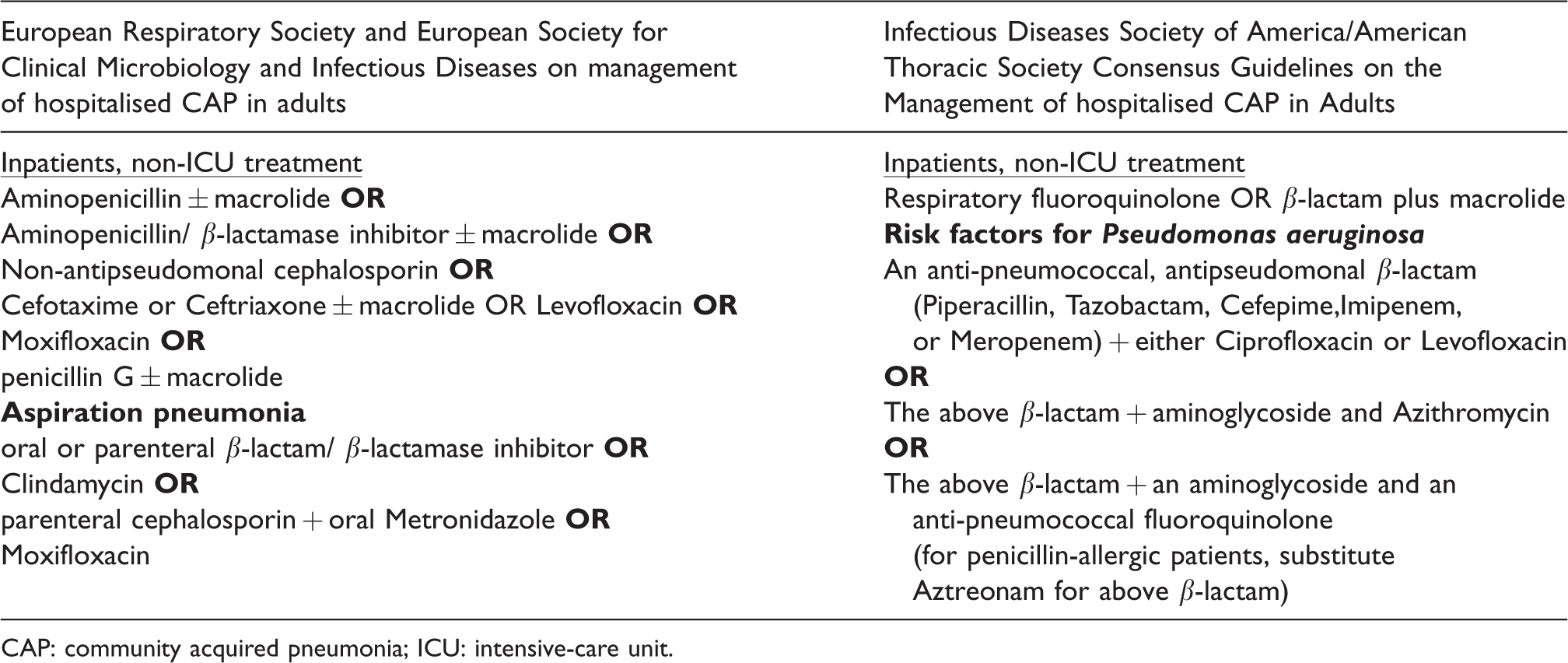
CAP: community acquired pneumonia; ICU: intensive-care unit.
Consensus process
A preliminary conference call formulated the remit, scope, themes and statements for consensus. Statements for consensus and an accompanying evidence review were circulated to the group by e-mail and a single round of provisional anonymised consensus and feedback was undertaken. The results were collated, presented and discussed at a final consensus group meeting along with summaries of antibiotic classes, sensitivities, resistance and societal recommendations for CAP, HAP and aspiration pneumonia in Barcelona, Spain on 27 September 2017. Consensus was approached using a modified Delphi technique and defined a priori as 75% agreement between the consensus group members. 13
Findings
The main recommendations of the consensus process are summarised in Table 1 and Figure 1. The consensus statements considered, including the online survey results and final consensus opinions are summarised in Table III in the online-only supplement.
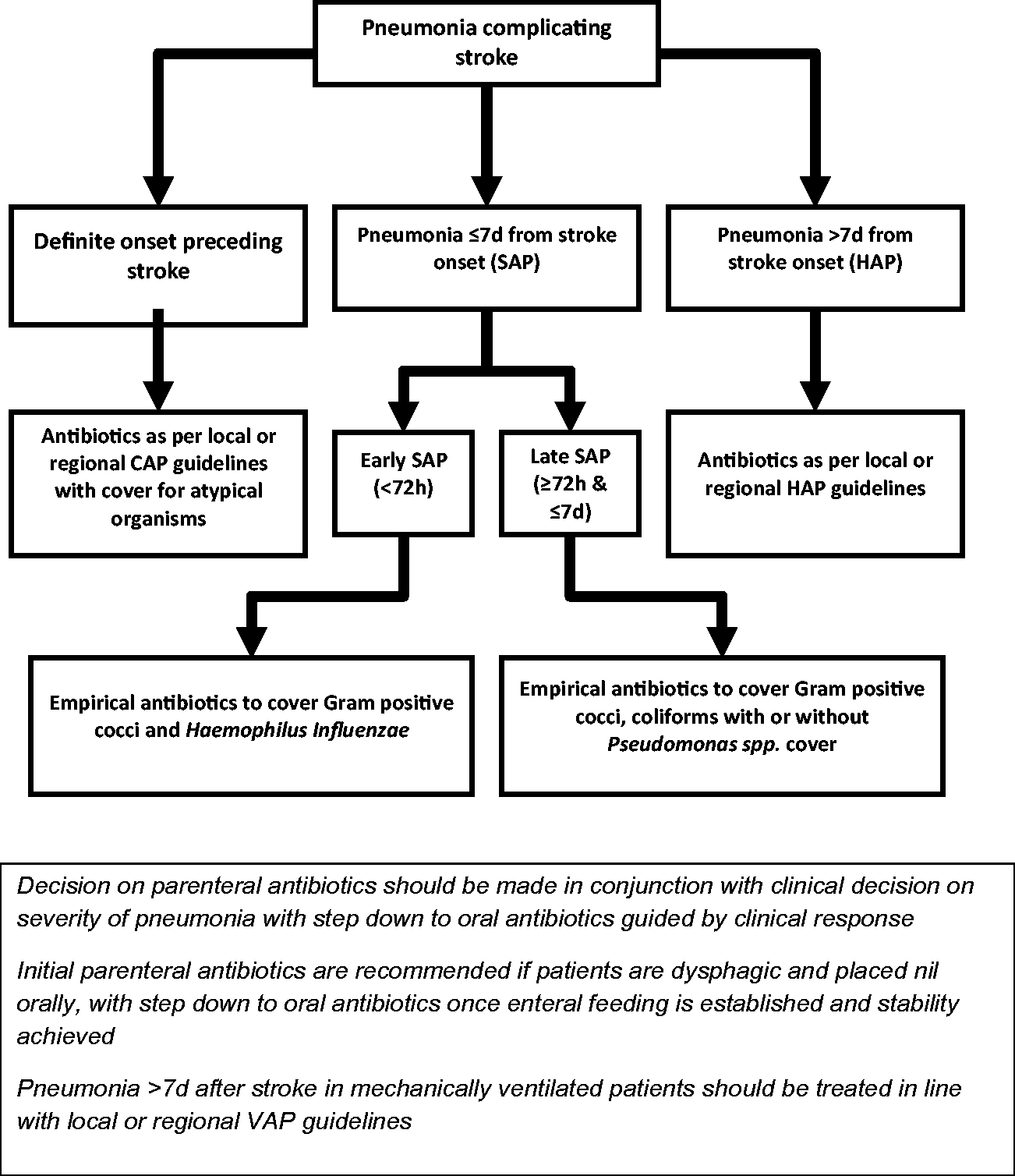
Flow chart summarising approach to antibiotic treatment of pneumonia complicating stroke (SAP: stroke-associated pneumonia; HAP: hospital-acquired pneumonia; CAP: community-acquired pneumonia).
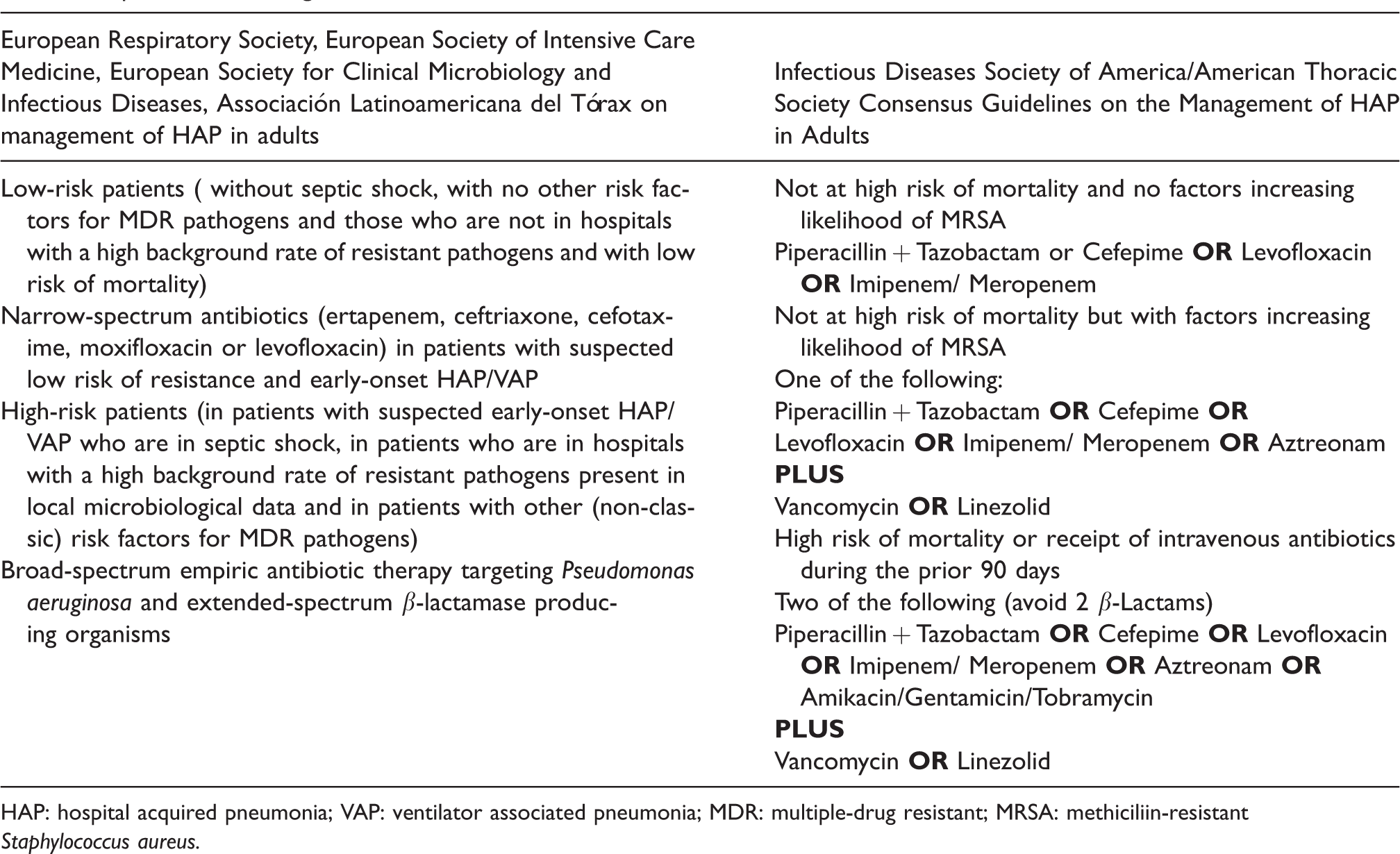
HAP: hospital acquired pneumonia; VAP: ventilator associated pneumonia; MDR: multiple-drug resistant; MRSA: methiciliin-resistant Staphylococcus aureus.
Remit and scope of the consensus
The requirement for consensus-based guidelines for the empirical antibiotic treatment of pneumonia complicating stroke (ischaemic stroke and ICH) was agreed by preliminary consensus. Agreement was also reached by preliminary consensus that the main focus of these recommendations should be SAP, defined in a previous publication as pneumonia within seven days of stroke symptom onset including those receiving mechanical ventilation. 4 Consensus was reached that beyond seven days after stroke onset, published societal guidelines for HAP should be applied.14–16 For the purpose of the present recommendations, a distinction was made between the well-documented phenomenon of stroke-induced transient immune suppression and that of pre-existing immune suppression (e.g. secondary to immune suppressant therapy) referred to in other societal guidelines of antibiotic treatment.9,14–16
Recommendations
The guidelines apply mainly to SAP (pneumonia ≤ 7 days after stroke onset). Other specialist societal guidelines for HAP 11 , 12 should be applied beyond seven days after stroke onset.
Microbiological aetiology of SAP and microbiological testing
A systematic review of 15 studies of patients with pneumonia complicating stroke suggested that aerobic Gram negative bacilli (38%) and Gram positive cocci (16%) were most frequently isolated among positive cultures. 8 Commonly isolated bacterial species included Enterobacteriaceae (21.8%: Klebsiella pneumoniae, 12.8% and Escherichia coli, 9%), Staphylococcus aureus (10.1%), Pseudomonas aeruginosa (6%), Acinetobacter baumanii (4.6%) and Streptococcus pneumoniae (3.5%). Reported frequency of positive culture data (15% to 88%) varied considerably between studies. Sputum was most commonly used to identify pathogens, in isolation (40%) or in conjunction with tracheal aspirate (15%) or blood culture (20%). Although the bacterial species identified appeared to be more closely related to HAP than ventilator-associated pneumonia (VAP) or hospitalised CAP, there were several limitations, including significant heterogeneity and inability to separate causal from commensal bacteria. There were insufficient data to identify the relative contributions of particular bacteria in relation to the timing of onset of SAP. Anaerobes, often thought to be one of the primary bacterial groups causing aspiration pneumonia, were either not detected or reported in any of the studies. None of the studies in the review used modern molecular diagnostic techniques such as multiplex polymerase chain reaction (PCR) platforms to detect multiple bacterial species, respiratory viruses or atypical organisms. Difficulty in consistently obtaining sputum culture samples in non-ventilated stroke patients was acknowledged. Consensus was reached that bacterial species implicated in SAP may overlap with those associated with either CAP or HAP. It was acknowledged that evidence from other reviews on microbiological aetiology for hospitalised CAP or HAP should also be considered when recommending antibiotic treatment guidelines.5,6,14,15
Recommendations
Although routine microbiological testing is not necessary prior to commencing empirical antibiotic treatment, attempts to obtain microbiological cultures (for example, sputum cultures) should be made where feasible in stroke patients for targeted antibiotic treatment.
Antibiotic treatment considerations for SAP based on presumed microbial aetiology
Based on the available evidence for bacterial species, 8 consensus was reached that antibiotics for SAP should cover Gram positive cocci, coliforms and, when risk factors are present, Pseudomonas (see below). Empirical antibiotic treatment for early SAP (<72 h of stroke onset) to cover CAP pathogens was recommended and additional cover for Gram negative bacilli was agreed from ≥ 72 h and ≤ 7 days (late SAP) of stroke symptom onset. Consensus was reached that in cases of SAP where pneumonia was diagnosed in the community preceding stroke onset, then it would be reasonable to treat for CAP with antibiotics including cover for atypical organisms. The available literature for microbial aetiology of aspiration pneumonia was considered. 17 Aspiration pneumonia has previously been regarded as being predominantly due to anaerobes (e.g. Bacteroides spp., Fusobacterium spp.) but more recent studies have reported less contribution from anaerobes (<20%) with greater prevalence of S. aureus, Gram negative bacilli and aerobic organisms.18–20 This has been reflected by specialist societal antibiotic recommendations for aspiration pneumonia (Table 2).
Recommendations
For patients with pneumonia manifesting after admission and < 72 h of stroke onset (Early SAP) and without special circumstances (see below), empirical antibiotics to cover typical CAP pathogens i.e. Gram positive cocci in addition to Haemophilus influenzae and Moraxella catarrhalis are recommended.
For patients with pneumonia manifesting ≥ 72 h, but before seven days of stroke onset (Late SAP) and without special circumstances (see below), empirical antibiotics to cover coliforms (with or without coverage of P. aeruginosa, if risk factors*) in addition to covering pathogens for CAP are recommended.
No additional anti-microbial coverage is required if aspiration is suspected or confirmed.
When SAP occurs with a diagnosis of pneumonia in the community clearly preceding stroke onset, antibiotic treatment to cover CAP including atypical organisms is recommended.
*Risk factors for P. aeruginosa: pre-existing immune suppression (e.g. HIV infection, transplant recipients, severe burns), pre-existing pulmonary disease (e.g. cystic fibrosis, chronic obstructive pulmonary disease, bronchiectasis), mechanical ventilation, prior antibiotic therapy. 6
Special circumstances
Special circumstances, including patients with pre-existing immune suppression, at risk from multidrug-resistant organisms* 21 or patients admitted from other healthcare facilities or institutions were considered. In these circumstances, additional cover for Methicillin-resistant S. aureus (MRSA) in addition to antibiotic coverage of other Gram negative bacteria (such as P. aeruginosa) should be used in conjunction with the above recommendations. Consensus was reached that local or societal guidelines for VAP be followed for pneumonia after seven days of stroke onset in mechanically ventilated patients.14,15 As dysphagia is a common complication of stroke, parenteral antibiotics were suggested as initial cover for SAP if patients were placed nil orally. Early step-down to appropriate oral antibiotics should be considered once enteral feeding is secured and the patient has achieved stability. Patients who develop recurrent pneumonia in hospital following an initial antibiotic course for SAP or HAP should be treated with antibiotics to cover HAP organisms based on liaison with local microbiology or infectious diseases expertise and policy.
Recommendations
For stroke patients at risk for drug-resistant organisms*, admitted from health care facilities or with pre-existing immune-suppression, additional antibiotic cover for MRSA, Extended Spectrum Beta Lactamase (ESBL)-producing enteric bacteria (E. coli, K. pneumoniae), P. aeruginosa or Acinetobacter species should be considered as clinically indicated and in conjunction with local patterns of antibiotic resistance and other recommendations for treatment of SAP and HAP.
Pneumonia in stroke patients complicated by mechanical ventilation should follow guidelines for SAP (pneumonia ≤ 7 days of stroke onset) or VAP (>7 days after stroke onset) guidelines, respectively.
Initial parenteral antibiotics are recommended in dysphagic patients with SAP placed nil orally, with step-down to suitable oral antibiotics once enteral feeding or normal oral intake has been established, and clinical stability achieved.
Recurrent pneumonia following an initial course of antibiotics for SAP or HAP should be treated in line with local HAP guidance.
*At risk for drug-resistant organisms: intravenous antibiotics within the preceding 90 days (and additionally if VAP: ≥5 days of prior hospitalisation, preceding acute respiratory distress syndrome, preceding acute renal replacement, septic shock). 21
Pneumonia severity and timing of initiation of antibiotics
There is currently no evidence to support the routine use of prophylactic antibiotics to prevent development of SAP, either in unselected stroke populations or those considered at higher risk placed nil orally. 22 Furthermore, the STRoke Adverse outcome is associated WIth NoSocomial Infections (STRAWINSKI) study did not support the use of procalcitonin-guided antibiotic initiation for pneumonia or other infections complicating stroke. 23 The appropriate timing of initiation of antibiotics in probable or definite SAP4 therefore remains uncertain although immediate antibiotic treatment (and within 4 h, or within 1 h if septic shock) was considered acceptable and agreed in line with recommendations from the European Respiratory Society and National Institute of Clinical Excellence (NICE) guidelines.5,14,16 The group acknowledged that there were currently no published severity scores derived and validated in patients with SAP. Consensus was reached that the utility of pneumonia severity scores developed in CAP (for example CURB -65 and Pneumonia Severity Index [PSI]) requires evaluation in patients with SAP.5,6
Recommendations
Start antibiotic therapy as soon as possible and certainly within 4 h (within 1 h if sepsis or septic shock) in all patients with probable or definite SAP.
4
There are currently no validated severity scores for SAP and existing pneumonia severity scores for (e.g. CURB-65or PSI) require evaluation in patients with SAP.
Which antibiotics should be used in SAP and for how long?
Evidence was considered regarding currently available antibiotic classes and mechanism of action, antibiotic resistance issues, and spectrum of antibiotic cover used in treatment of hospitalised CAP and HAP in existing guidelines (Tables 2 and 3). The available evidence for using any particular class of antibiotic or individual antibiotic agent(s) in the treatment of SAP was also considered. Our systematic literature search found that there were no ongoing, completed or published trials comparing different antibiotic classes for treatment of SAP, or pneumonia complicating later stages of stroke (Figure 2 and Table IV in the online-only supplement). In our recent systematic review, 8 the choice of antibiotics used to treat pneumonia complicating stroke was documented in only four (24%) studies and was determined by local hospital policy. Antibiotics commonly included β-lactam antibiotics (including ureidopenicillin and 2nd/3rd generation cephalosporins), with or without β-lactamase inhibitors and 2nd/3rd generation fluoroquinolones and were always initiated prior to obtaining antibiotic sensitivities.
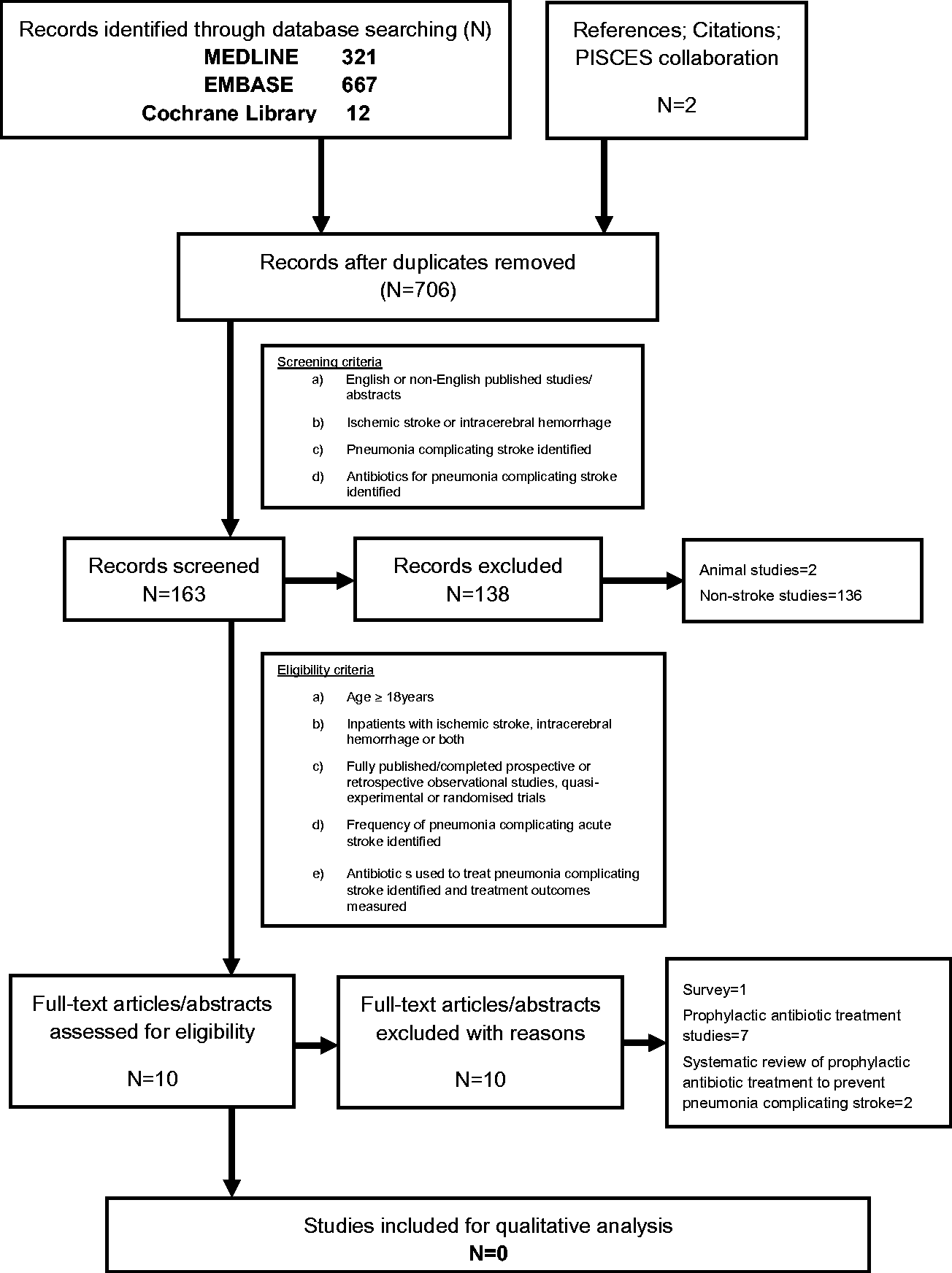
Flow diagram of systematic search methodology.
Consensus was reached that there was insufficient evidence to recommend any particular antibiotic agent(s) or classes of antibiotic for treatment of SAP, and that evaluation of antibiotic treatment of SAP was a research priority. Penicillin plus β-lactamase inhibitors were preferred by the majority of the group for patients with SAP, aspiration pneumonia and recurrent pneumonia complicating stroke. Local patterns of antimicrobial resistance should be considered when determining appropriate empirical therapy. Consensus was also achieved for recommending that duration of antibiotic treatment should be guided by clinical response and should be for at least seven days. It was acknowledged that the role of biomarkers to guide treatment duration was unknown and further research was needed in this regard.
Recommendations
Choice of initial empirical antibiotics for early SAP (predominantly Gram positive cocci) may commonly include β-lactams and macrolides or respiratory fluoroquinolones.
Choice of initial empirical antibiotic therapy for late SAP should additionally cover Gram negative bacteria, with or without Pseudomonas cover, and may commonly include β-lactams (e.g. penicillin plus β-lactamase inhibitor, 3rd or 4th generation cephalosporins, monobactams), fluoroquinolones or aminoglycosides.
Local patterns of antimicrobial resistance should be considered when determining appropriate empirical therapy.
Antibiotic treatment should be for at least seven days and guided by clinical response, in the absence of validated biomarkers.
Discussion
SAP is a significant problem worldwide and optimising antibiotic management when initiating treatment is of paramount importance. In England and Wales, there were 21,623 episodes of SAP treated with antibiotics recorded in the last three years of the Sentinel Stroke National Audit Programme. 24 As empirical antibiotic therapy is the cornerstone of the initial treatment of SAP, a standardised approach for clinicians initiating antibiotics could be a crucial component of antibiotic stewardship and improving clinical outcomes.
While there are existing specialist societal guidelines available for CAP and HAP, these do not necessarily translate directly to SAP. For example, in SAP, there is a relative lack of robust microbiological data, frequent concern regarding aspiration, transient peripheral immune-suppression induced by stroke, a lack of validated severity scores or biomarkers to inform treatment decisions and no randomised trials to inform use of specific antibiotic agent(s) or classes. For the purpose of these consensus recommendations, we further divided SAP into early and late based on likely microbiological aetiology and anticipated antimicrobial coverage. Pneumonia preceding stroke onset is common 25 and when triggering, stroke onset may subsequently manifest as pneumonia soon after admission to hospital. While S. pneumoniae, the most frequent pathogen in CAP worldwide, 26 was detected infrequently in pneumonia complicating stroke in our recent systematic review, this likely reflects heterogeneity across the included studies (including bias towards sampling beyond the first 72 h after stroke onset) plus absence of use of non-culture dependent methodologies, e.g. detection of bacterial antigens or genome. 8 By contrast, organisms usually implicated in HAP were identified most frequently in patients with pneumonia complicating stroke, particularly S. aureus, Enterobacteriaceae and P. aeruginosa. 8 While data to specifically determine the timing of SAP onset relative to organisms cultured are at best sparse, our consensus on antibiotic coverage was based on the concept that organisms in early SAP would overlap most with those that of CAP and those of late SAP would also include those of HAP.
Pneumonia complicating stroke has conventionally been regarded as aspiration pneumonia in the setting of dysphagia and oro-pharyngeal aspiration and may be labelled as “aspiration pneumonia” in the stroke literature. 3 The microbial aetiology and potential antibiotic coverage of aspiration pneumonia are therefore of interest to clinicians treating pneumonia in dysphagic stroke patients. Micro-aspiration is in fact the primary pathophysiological process in both CAP and HAP with the latter characterised by micro-aspiration of colonised organisms in the hospital environment. 17 In recent years, the microbial aetiology of hospitalised aspiration pneumonia appears to be less dominated by anaerobes, and broad-spectrum antibiotics such as fluoroquinolones or β-lactams (e.g. carbapenems or penicillins plus β-lactamase inhibitors) are typically recommended for empirical treatment rather than targeted coverage of anaerobes. 17
In adults hospitalised with CAP, fast antigen detection methods and real-time multibacterial and multiviral PCR platforms can increase the pathogen detection yield in sputum or endotracheal aspirate compared to conventional culture methods and could be used to better inform pathogen-directed antibiotic therapy. 27 Despite the recognised issue of reduced sputum availability in stroke patients, prospective studies of patients with suspected SAP employing more rigorous sampling, such as fiberoptic bronchoscopes in selected patients, and multiplex PCR are needed to further characterise microbial aetiology and validate empirical antibiotic recommendations. To our knowledge, viral pathogens have not been tested for in SAP or acute lower-respiratory tract syndromes complicating acute stroke, which may relate to availability of requisite molecular technology or perception that viral pneumonia does not align with the traditional paradigm of “aspiration” pneumonia in patients with stroke.
We were unable to make definitive recommendations for specific antibiotic classes (or antibiotic agents) for the treatment of SAP and could only make consensus recommendations for empirical antibiotic coverage based on limited knowledge of microbial aetiology. Indeed, the wide variation in rates of antibacterial resistance in different parts of the world necessitates that local resistance patterns should be considered when determining appropriate empirical therapy. Likewise, there were insufficient data to make recommendations regarding antibiotic dose or duration of treatment. Choice of antibiotic class or agent may be important in SAP as antibiotics have varying antimicrobial coverage and pleiotropic effects independent of their bactericidal or bacteriostatic effects. Several antibiotics (e.g. macrolides, cephalosporins, fluoroquinolones) commonly used to treat SAP have protective or deleterious effects in experimental middle cerebral artery occlusion28–31 often via anti-inflammatory and immunomodulatory effects.
Our consensus statement proposes practical recommendations on antibiotic use in pneumonia complicating stroke, by experts within the PISCES group, using a modified Delphi approach. Our recommendations were not commissioned guidelines and hence should not be considered as a clinical guideline as this would not only require an adapted methodology (for example, PICO questionnaire framework and/or Levels of quality/expression of strength of recommendations) but would also need to cover other preventative and therapeutic strategies relevant to pneumonia complicating stroke, which is beyond the scope of the present work. However, this consensus provides the framework for a SAP guideline, which is in line with previous work from the PISCES group dealing with SAP.3,4
Conclusion
Consensus opinion is proposed on antibiotic treatment for the spectrum of pneumonia complicating stroke. However, large-scale RCTs are required to evaluate the efficacy and cost-effectiveness of specific antibiotic regimens for SAP, preferably with standardised diagnostic algorithms, rigorous microbiological testing and validation of severity scores and candidate biomarker panels to guide treatment initiation and cessation. Such RCTs will inevitably be challenging when considering the logistics around organisation of stroke services, regional and local site considerations (antibiotic costs, availability, susceptibility and resistance patterns, implementation issues) but are essential for informing evidence-based treatment for SAP and advancing our commitment to antibiotic stewardship in stroke unit care.
Supplemental Material
Supplemental material for Antibiotic treatment for pneumonia complicating stroke: Recommendations from the pneumonia in stroke consensus (PISCES) group
Supplemental material, Supplemental Material for Antibiotic treatment for pneumonia complicating stroke: Recommendations from the pneumonia in stroke consensus (PISCES) group by Amit K Kishore, Adam R Jeans, Javier Garau, Alejandro Bustamante, Lalit Kalra, Peter Langhorne, Angel Chamorro, Xabier Urra, Mira Katan, Mario Di Napoli, Willeke Westendorp, Paul J Nederkoorn, Diederik van de Beek, Christine Roffe, Mark Woodhead, Joan Montaner, Andreas Meisel and Craig J Smith in European Stroke Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The consensus meet was supported by a grant (EUIN2013-51119) from Ministerio de Economía y Competitividad (MINECO) from Spain. AB is supported by a Juan Rodés research contract (JR16/00008) from Instituto de Salud Carlos III. MK is supported by Swiss National Science Foundation (PZ00P3_142422), Swiss Heart Foundation.
Ethical approval
Not applicable
Informed consent
Not applicable
Guarantor
Amit K Kishore and Craig J Smith
Contributorship
CJS, AM, and JM developed the consensus protocol. AKK and CJS researched literature and performed the systematic reviews. AKK and CJS produced first draft of the manuscript. All authors were involved in the consensus process and in the production of the submitted manuscript.
Acknowledgements
None
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.