
Abstract

Official Welcome & Large Clinical Trials
AS03-034
RIVAROXABAN FOR SECONDARY STROKE PREVENTION AFTER EMBOLIC STROKE OF UNDETERMINED SOURCE: MAIN RESULTS OF THE NAVIGATE ESUS TRIAL
1McMaster University, Medicine Neurology, Hamilton, Canada
Background and Aims
Embolic strokes of undetermined source (ESUS) represent up to 20% of ischemic strokes and have a high rate of stroke recurrence. We hypothesized that anticoagulant treatment with rivaroxaban, an oral factor Xa inhibitor, would reduce the risk of recurrent stroke compared with antiplatelet therapy with aspirin.
Method
The international NAVIGATE ESUS double-blind, randomized trial assessed the efficacy and safety of rivaroxaban 15mg once daily versus aspirin 100mg once daily for secondary stroke prevention in patients with ESUS. The primary efficacy outcome was all recurrent strokes and systemic embolism; the primary safety outcome was major bleeding.
Results
7214 participants were enrolled from 459 sites in 31 countries and were followed for a mean of 11 months before early trial termination at the recommendation of the independent data monitoring committee. Mean participant age was 67 years, 38% were women, and the median interval from qualifying stroke to randomization was 37 days. Study close-out is almost complete, and final results will be presented
Conclusion
Rivaroxaban was not superior to aspirin for preventing recurrent stroke in patients with ESUS.
Trial registration number
NCT02313909
AS01-017
THE DABIGATRAN FOLLOWING ACUTE TRANSIENT ISCHEMIC ATTACK AND MINOR STROKE TRIAL: FINAL RESULTS.
1University of Alberta, Medicine, Edmonton, Canada
2Population Health Research Institute- McMaster University, Medicine, Hamilton, Canada
3University of British Columbia, Medicine, Vancouver, Canada
4University of Calgary, Neurosciences, Calgary, Canada
5Centre Hospitalier de l'Université de Montréal, Medicine, Montreal, Canada
Background and Aims
Anticoagulation in acute stroke has been shown to reduce early recurrent events, but also results in excess hemorrhagic transformation (HT). The direct thrombin inhibitor dabigatran is associated with lower intracranial hemorrhage rates, relative to warfarin, but data are lacking in acute stroke. We tested the hypothesis that symptomatic HT rates in dabigatran treated patients are comparable to those treated with ASA.
Method
We conducted a multi-centre randomized, open label blinded endpoint trial. Participants (n = 300) with non-cardioembolic TIA/ischemic stroke (NIHSS score <9) and MRI DWI volumes <25 ml were randomized within 72 hours of symptom onset to ASA 81 mg OD or dabigatran 150/110 mg BID for 30 days. Standardized MRIs were obtained at baseline and day 30 and read by blinded readers for HT and incident DWI lesions. The primary outcome was the proportion with symptomatic HT at 30 days defined as a parenchymal hematoma >30% of the infarcted area, with substantial space-occupying effect, associated with clinical worsening (≥4 point increase in National Institutes of Health Stroke Scale (NIHSS) score) within 5 weeks of randomization. Standardized clinical assessments were completed at day 30 and 90.
Results
As of Jan 20, 2018 284 participants were randomized at 6 centres. Mean age was 66 ± 13 years (38% female). Mean time from onset to randomization was 42.2 ± 17.2 hours. Acute DWI lesions were present in 79% of cases prior to randomization. Follow-up visits and MRI analysis are being completed.
Conclusion
DATAS II will provide evidence for the safety of early anticoagulation in ischemic stroke.
Trial registration number
NCT02295826 (clinicaltrials.gov)
AS01-022
RESULTS FROM THE TRANEXAMIC ACID FOR PRIMARY INTRACEREBRAL HAEMORRHAGE-2 (TICH-2) TRIAL
1University of Nottingham, Stroke- division of clinical neuroscience, Nottingham, United Kingdom
Background and Aims
Haematoma expansion leads to worse outcome in intracerebral haemorrhage (ICH). Tranexamic acid (TXA) is a promising haemostatic agent to prevent haematoma expansion and improve outcome after ICH.
Method
TICH-2 is a multicentre prospective double blind randomised controlled trial, which recruited patients presenting within 8 hours of primary ICH to receive intravenous TXA or placebo. Primary outcome is modified Rankin Scale at day 90 and will be analysed using ordinal logistic regression, adjusted for minimisation criteria. Secondary outcomes will be analysed using adjusted binary logistic regression and multiple linear regression; these include haematoma expansion at 24 hours, day 7 National Institute of Health Stroke Scale (NIHSS), day 90 Barthel Index, quality of life, cognition and mood.
Results
A total of 2325 patients were recruited between 14th March 2013 and 30th September 2017, from 12 countries: United Kingdom (n = 1910), Italy, Georgia, Switzerland, Malaysia, Hungary, Poland, Ireland, Turkey, Sweden, Denmark and Spain. Randomisation characteristics included: age 68.9 (13.8) years; male 1301 (56.0%); time from onset to randomisation 3.6 hours [2.6, 5.0]; NIHSS 13 (7.5); Glasgow coma scale 13.4 (2.1); systolic blood pressure 172.6 (27.2) mmHg; intraventricular haemorrhage 745 (32.0%) and prior antiplatelet use 610 (26.2%).
Conclusion
TICH-2 is the largest trial of TXA in spontaneous ICH and recruited over its original target of 2000 patients. The results will be available in May 2018 and will inform whether TXA should be recommended for the treatment of acute spontaneous ICH.
Trial registration number
ISRCTN93732214
AS04-003
A TRIAL TO EVALUATE AN EXTENDED REHABILITATION SERVICE FOR STROKE PATIENTS (EXTRAS): MAIN RESULTS
1Newcastle University and Newcastle upon Tyne Hospitals NHS Foundation Trust, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
2Newcastle University, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
3Newcastle University, Institute of Health and Society, Newcastle upon Tyne, United Kingdom
4Lay member, Lay member, Lay member, United Kingdom
5Nottingham University, Faculty of Medicine and Health Sciences, Nottingham, United Kingdom
6Oxford University, Medical Sciences Division, Oxford, United Kingdom
7University of Leeds, Academic Unit of Elderly Care and Rehabilitation, Leeds, United Kingdom
8Northumbria Healthcare NHS Foundation Trust, Stroke Northumbria, Newcastle upon Tyne, United Kingdom
9Kings College London, Department of Public Health Sciences, London, United Kingdom
10Northumbria University, Faculty of Health and Life Sciences, Newcastle upon Tyne, United Kingdom
Background and Aims
Development of longer term stroke rehabilitation services is limited by lack of evidence of effectiveness for specific interventions and service models.
Method
Study design: Multicentre randomised controlled trial with health economic and process evaluations.
Participants: Adults with a new stroke (and carer if appropriate) discharged from hospital under the care of an Early Supported Discharge (ESD) team.
Intervention: An extended stroke rehabilitation service for 18 months following completion of routine ESD. The extended rehabilitation service involves regular contact (usually by telephone) with a senior ESD team member who leads and coordinates further rehabilitation.
Control: Usual care post ESD.
Randomisation: Central independent web based service.
Primary outcome: Nottingham Extended Activities of Daily Living (NEADL) Scale at 24 months.
Secondary outcomes: For patients: health status, quality of life, mood and experience of services at 12 and 24 months. For carers: quality of life, experience of services and carer stress at 12 and 24 months. Resource use and adverse events were also collected.
Process evaluation: Semi-structured interviews with participants and staff to gain insight into perceptions and experience of study treatments.
Sample size: Allowing for 25% attrition, 510 participants provide 90% power to detect a difference in mean NEADL score of 6 with a 5% significance level.
Results
From November 2012 to June 2015, 573 participants from 19 centres were randomised. Intervention delivery was completed in March 2017 and final follow up data were collected in September 2017. The main results will be available for presentation at ESOC in 2018.
Conclusion
The main results will be available for presentation at ESOC in 2018.
Trial registration number
ISRCTN45203373
AS02-007
ECASS-4:EXTEND: EUROPEAN COOPERATIVE ACUTE STROKE STUDY-4 - EXTENDING THE TIME FOR THROMBOLYSIS IN EMERGENCY NEUROLOGICAL DEFICITS
1University hospital Heidelberg, Department of Neuroradiology, Heidelberg, Germany
2National Stroke Research Institute, National Stroke Research Institute, Heidelberg Heigths VIC 3081, Australia
3University hospital Heidelberg, Department of Neurology, Heidelberg, Germany
4Hospital Universitari Vall d´Hebron, Department of Neurosciences, Barcelona, Spain
5Hopital Roger Salengro, Service de neurologie et pathologie neurovasculaire, Lille Cedex, France
6Johannes Wesseling Klinikum, Department of Neurology, Minden, Germany
7University hospital Erlangen, Department of Neurology, Erlangen, Germany
8Hospital Policlinico Umberto I, Department of Neurology, Roma, Italy
9Karolinska University Hospital, Emergency Department Stroke Unit, Emergency Department Stroke Unit, Sweden
Background and Aims
Systemic rtPA treatment is safe and effective within 4.5 hours after onset ischemic stroke. We investigated whether patients with unknown time window or seen between 4.5 and 9 hours after onset and with significant penumbral mismatch on MRI, have better outcomes after rtPA.
Method
ECASS-4:ExTEND is an investigator driven, phase 3, randomized, multi-center, double-blind, placebo-controlled study. Inclusion criteria included time window 4.5–9h after onset or unknown time of onset, NIHSS 4–26, premorbid mRS 0–1, infarct core volume <100ml, perfusion lesion: infarct core mismatch ratio >1.2 and perfusion lesion minimum volume of 20ml. The common exclusion criteria for thrombolytic therapy were applied.
The primary outcome measure is the categorical shift in the mRS at day 90. The most important safety endpoints were rate of symptomatic intracranial hemorrhage and death.
Results
The study was stopped early after inclusion of 120 patients for futility reasons mainly because of slow recruitment due to an increasing number of potentially eligible patients being treated with mechanical thrombectomy. There were no safety concerns. Detailed data analysis is ongoing and primary results will be presented.
Conclusion
ECASS 4 might was designed to establish safety and efficacy of intravenous rtPA treatment in patients outside the approved time-window together with the still ongoing Australian Start-Extend study and Wake-Up study. Further and joint analyses are planned.
Trial registration number
EudraCT-Number: 2012-003609-80
AS02-009
INTRAVENOUS THROMBOLYSIS IN STROKE PATIENTS WITH UNKNOWN TIME OF SYMPTOM ONSET – RESULTS OF THE RANDOMIZED CONTROLLED WAKE-UP TRIAL
1University Medical Center Hamburg-Eppendorf, Neurology, Hamburg, Germany
2Aarhus University Hospital, Neurology, Aarhus, Denmark
3Hospices Civils de Lyon, Service de Biostatistique, Lyon, France
4Hospices Civils de Lyon, Neurology, Lyon, France
5Medical Park Berlin, Neurology, Berlin, Germany
6Charité - Universitätsmedizin Berlin, Neurology, Berlin, Germany
7University Medical Center Hamburg-Eppendorf, Neuroradiology, Hamburg, Germany
8University of Glasgow, Robertson Center for Biostatistics, Glasgow, United Kingdom
9University Hospitals Leuven, Neurology, Leuven, Belgium
10University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
11Hospital Dr Josep Trueta- Institut d’Investgació Biomèdica de Girona IDIBGI, Radiology, Girona, Spain
12Florey Institute of Neuroscience and Mental Health, Neurology, Heidelberg, Australia
Background and Aims
Patients with unknown time of symptom onset are excluded from thombolysis according to licensing criteria and guideline recommendations. MRI with a mismatch between the acute ischemic lesion visible on diffusion weighted imaging (DWI) but not on fluid-attenuated inversion recovery (FLAIR) imaging was suggested to identify patients ≤4.5 h from symptom onset. WAKE-UP (Efficacy and safety of MRI-based thrombolysis in wake-up stroke: a randomised, double-blind, placebo-controlled trial) aimed to test the efficacy and safety of MRI-guided thrombolysis with rtPA in ischemic stroke patients with unknown time of symptom onset.
Method
WAKE-UP was an investigator initiated, European, multicentre, randomized, double-blind, placebo-controlled clinical trial. Patients with unknown time of symptom onset were studied by MRI. Patients with DWI-FLAIR-mismatch were randomised to either treatment with rtPA or placebo. The primary efficacy endpoint was favourable outcome as defined by modified Rankin Scale 0–1 at day 90. The primary safety outcome measures were mortality and death or dependency as defined by modified Rankin Scale 4–6 at 90 days.
Results
A total of 503 patients were randomized in the trial. Main results of the the trial will be presented.
Conclusion
WAKE-UP is an innovative clinical trial applying novel MRI criteria to identify stroke patients with unknown time of symptom onset likely to benefit from thrombolysis based on the estimation of lesion age. Trial results will be discussed.
Trial registration number
WAKE-UP is registered with the EU Clinical Trials Register (EudraCT No. 2011-005906-32) and ClinicalTrials.gov (ClinicalTrials.gov Identifier NCT01525290). Trial results wil be discussed.
AS03-012
PRIMARY RESULTS OF THE PLATELET-ORIENTED INHIBITION IN NEW TIA AND MINOR ISCHEMIC STROKE (POINT) TRIAL
1The University of Texas at Austin, Dell Medical School, Austin, USA
2University of California- San Francisco, Neurology, San Francisco, USA
3University of Michigan Health System, Emergency Medicine, Ann Arbor, USA
4National Institute of Neurological Disorders, Office of Clinical Research, Bethesda, USA
5Medical University of South Carolina, Data Coordination Unit- Department of Public Health Services, Charleston, USA
6The EMMES Corporation, Statistics, Rockville, USA
Background and Aims
The risk of stroke and other ischemic events is high in the first 3 months after minor ischemic stroke and transient ischemic attack (TIA). Aggressive antiplatelet therapy may be particularly effective in this setting.
Methods
POINT was a randomized, double-blind trial (NCT00991029) of patients with minor ischemic stroke (NIHSS score ≤3) or high-risk TIA (defined as an ABCD2 score ≥4). Subjects were randomized to clopidogrel (600-mg loading dose on day 1 followed by 75 mg daily for days 2–90) or placebo, and all subjects also received open-label aspirin (50-325 mg/day, with a dose of 150-200 mg daily for 5 days followed by 75-100 mg daily strongly recommended). Randomization had to occur within 12 hours of event onset. The primary efficacy endpoint was the composite of new ischemic events (ischemic stroke, myocardial infarction, or ischemic vascular death) during 90-day follow-up. Major hemorrhage was the primary safety endpoint.
Results
Prior to planned enrollment of 5840 subjects, the trial’s DSMB halted further randomization. A total of 4,890 patients were randomized from 269 sites in North America, Europe, and Australia/New Zealand. Median age was 65 years and 45% were women. The index event was ischemic stroke in 57% and TIA in 43%. Database lock will occur in April 2018. Primary results will be presented with simultaneous publication anticipated.
Conclusions
The POINT trial addresses an important clinical question for patients presenting acutely after minor ischemic stroke and TIA, by comparing clopidogrel-aspirin to aspirin alone for reducing the risk of subsequent ischemic events.
Trial registration number
NCT00991029
Presidential Symposium - Awards & Trials
AS03-011
CEREBRAL MICROBLEEDS AND INTRACRANIAL HAEMORRHAGE RISK IN PATIENTS WITH ATRIAL FIBRILLATION AFTER ACUTE ISCHAEMIC STROKE OR TRANSIENT ISCHAEMIC ATTACK: OBSERVATIONAL MULTICENTRE PROSPECTIVE COHORT STUDY
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3Harvard Medical School, Hemorrhagic Stroke Research Program- Department of Neurology, Boston, USA
4University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
5University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
6University College London Hospital, Haemostasis Research Unit- Department of Haematology, London, United Kingdom
7Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
8Institute of Neurology, Lysholm Department of Neuroradiology and the Neuroradiological Academic Unit, London, United Kingdom
9University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
Cerebral microbleeds (CMBs) are a potential imaging biomarker of bleeding-prone cerebral small vessel diseases that might identify patients with ischaemic stroke or transient ischaemic attack (TIA) at high risk of intracranial haemorrhage (ICrH) when treated with oral anticoagulants.
Method
Our observational, multi-centre, prospective inception cohort study (CROMIS-2; NCT02513316) recruited adult patients with non-valvular atrial fibrillation (AF) and acute ischaemic stroke or TIA, treated with oral anticoagulation (warfarin or a direct oral anticoagulant) at 79 UK hospitals. We followed patients over 2 years for sICrH, ischaemic stroke, intracerebral haemorrhage and death. We used multivariable Cox regression to investigate CMBs and other factors associated with sICrH, and developed risk prediction models, validated with 1000-sample bootstrapping, and using penalised regression lasso models to avoid model over fitting.
Results
We included 1490 patients, with 97% complete follow up over a mean period of 850 days (SD 373 days). The mean age was 76 years; 631 (42%) were female. The absolute sICrH rate in patients with CMBs was 10 per 1000 patient-years (95% CI 4–20) compared to 3 per 1000 patient-years (95% CI 1–5) in those without CMBs (relative adjusted risk for sICrH 3.67 (95% CI 1.27-10.60). Compared to HASBLED alone (C-index 0.41 95% CI 0.29-0.53), a risk prediction model incorporating CMBs and HASBLED (C-index 0.68; 95% CI 0.56-0.81) predicted sICH significantly better (c-index (diff): 0.27 (0.11-0.43), p < 0.001).
Conclusion
CMBs are independently associated with increased sICrH risk, and improve the predictive performance of clinical risk scores.
Trial registration number
NCT02513316
AS02-037
THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE BEYOND 6 HOURS FROM TIME LAST KNOWN WELL: PRIMARY RESULTS OF AURORA (INDIVIDUAL PATIENT LEVEL POOLED-ANALYSIS FROM FIVE RANDOMIZED TRIALS)
1University of Pittsburgh Medical Center, Stroke Institute- Department of Neurology, Pittsburgh, USA
2Stanford University Stroke Center, Neurology, Palo Alto, USA
3Hotchkiss Brain Institute, Clinical Neuroscience, Calgary, Canada
4University of Calgary, Radiology, Calgary, Canada
5Mount Sinai Health System, Neurologcal Surgery, Pittsburgh, USA
6Medical University of South Carolina, Radiology, Charleston, USA
7Hospital Germans Trias y Pujol, Neurology, Barcelona, Spain
8Stanford University, Neurology, Palo Alto, USA
9Grady Memorial Hospital- Emory University, Neurology, Atlanta, USA
Background and Aims
Two recently published randomized trials (DAWN and DEFUSE 3) have demonstrated the efficacy of endovascular treatment for anterior circulation acute ischemic stroke due to proximal large vessel occlusion in patients randomized beyond 6 hours from Time Last Seen Well. One other randomized trial (POSITIVE) has included patients who could be randomized beyond 6 hours and has recently stopped enrollment ahead of reaching the planned sample size. Two other completed randomized trials (ESCAPE and REVASCAT) allowed inclusion up to 12 hours and 8 hours, and thus enrolled some patients randomized beyond 6 hours. Three of the trials (DAWN, DEFUSE 3 and POSITIVE) required advanced imaging (MRI or CT perfusion) for patient selection. All trials used effective thrombectomy devices (stent retrievers mainly and primary aspiration).
Method
Pre-specified patient-level meta-analysis (
Results
Will be available at the time of the presentation.
Conclusion
N/A
Trial registration number
N/A
AS02-026
KEY SUBGROUP ANALYSES FROM THE DEFUSE 3 STUDY
1Stanford University Medical Center, Stanford Stroke Center, Stanford, USA
Background and Aims
DEFUSE 3 was an NIH-funded, multicenter, randomized, trial of thrombectomy in patients 6 to 16 hours after they were last known to be well who had remaining ischemic brain tissue that was not yet infarcted (penumbral imaging selection). The aim of this abstract is to assess which factors modify the treatment effect in DEFUSE 3. Key subgroup analyses will be presented at ESOC.
Method
Potentially important effect modifiers include time-to-treatment, baseline infarct volume, age, and CT vs MRI selection, and general anesthesia vs conscious sedation. The interactions between endovascular therapy and these co-variates on clinical outcomes were assessed with multivariable regression analyses. The primary clinical outcome is an ordinal analysis of modified Rankin Scale score at day 90.
Results
Of the 182 patients randomized to thrombectomy vs medical therapy in the DEFUSE 3 study, 72.6% were selected using multimodal CT imaging and 26.8% using MR. Median age was 70.5 (IQR 59 - 80), median NIHSS 16 (IQR 11-21), median ischemic core volume 10 mL (IQR 2.7-25.6 mL), and median time from stroke to randomization was 10h 48m (IQR 8h 43m – 12h 42m; range 6h 5m – 15h 54m). Outcome data are currently under embargo.
Conclusion
Wide inclusion criteria in the DEFUSE 3 trial resulted in a patient population that varies broadly in terms of age, baseline clinical and radiological severity, and time from symptom onset to randomization. This heterogeneity will allows us to compare the effect of endovascular treatment across a wide range of subgroups.
Trial registration number
NCT02586415
AS02-011
EFFECTS OF ALTEPLASE FOR ACUTE STROKE AMONG PREDEFINED SUBGROUPS: INDIVIDUAL-PATIENT-DATA META-ANALYSIS OF RANDOMISED TRIALS
1University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
Background and Aims
The proportional benefit of iv alteplase for acute ischaemic stroke is modified by delay in treatment initiation but not by age or stroke severity. We investigated the influence of other prespecified baseline factors on treatment response.
Method
We used trial-stratified logistic regression of patient-level-data from nine RCT of alteplase in acute ischaemic stroke to estimate any influence on the proportional effects of alteplase by blood pressure, diabetes, sex, hypertension, prior stroke, aspirin use or Konig’s prognostic score. Prespecified outcomes were good function (mRS 0–1), SICH, mortality and mRS distribution. We adjusted p-values for multiplicity of factors but not of outcomes. Post hoc sensitivity analyses included favourable outcome (mRS 0–2) and stratification by EU-approval date.
Results
Data were available for 6,756 patients. The adjusted OR for good outcome (mRS 0–1) fell below unity in 2 subgroups: in 1078 patients with diabetes (aOR 0.93, 95%CI 0.69-1.27) and in 1243 patients with prior stroke (aOR 0.95, 95%CI 0.71-1.27), whilst the aOR for any upwards shift in mRS fell below unity only for patients with diabetes (aOR 0.93, 95%CI 0.75-1.15); (prior stroke aOR 1.04, 95%CI 0.85-1.27). Tests for heterogeneity in treatment effect on the main pre-specified outcomes were significant for neither of these subgroups, nor any other subgroup examined. Sensitivity analyses did not support treatment response modification by prior stroke, nor by diabetes (though less conclusive for this).
Conclusion
The RCT data do not demonstrate modification of treatment response by blood pressure, sex, hypertension, prior stroke, aspirin use or prognostic score but are inconclusive for diabetes.
Trial registration number
N/A
AS01-010
STROKE123: RESULTS FROM A MULTICENTRE, CONTROLLED BEFORE-AND-AFTER STUDY TO IMPROVE ACUTE STROKE CARE IN AUSTRALIA
1Monash University, Department of Medicine- School of Clinical Sciences at Monash Health, Clayton, Australia
2Florey Institute of Neuroscience and Mental Health, Public Health and Health Services Research Group- Stroke Division, Melbourne, Australia
3Monash University, Department of Medicine- Peninsula Health, Frankston, Australia
4National Stroke Foundation, Guidelines Program, Melbourne, Australia
5La Trobe University, School of Allied Health- La Trobe University- Bundoora- Victoria- Australia, Bundoora, Australia
6Alfred Health, Department of Occupational Therapy, Prahran, Australia
7The George Institute for Global Health, Faculty of Medicine, Sydney, Australia
8Royal Prince Alfred Hospital, Neurology, Sydney, Australia
9The George Institute for Global Health China, Peking University Health Science Center, Beijing, China
10University of Newcastle, Neurology- John Hunter Hospital, Newcastle, Australia
11St Vincent's Hospital, Rehabilitation Medicine, Sydney, Australia
12Australian Catholic University, Faculty of Health Sciences, Sydney, Australia
13Queensland Health, Statewide Stroke Clinical Network, Brisbane, Australia
14Queensland Health, Clinical Excellence Division, Brisbane, Australia
15University of Queensland, Sunshine Coast Clinical School, Sunshine Coast, Australia
Background
Variation from evidence-based care contributes to increased deaths and disability after stroke.
Aims
To determine whether iterative quality improvement interventions (individually and collectively) change clinical practice and improve stroke care.
Method
Before-and-after design comparing 20 self-selected Queensland hospitals across four time-points:
Results
Patient characteristics were similar across time-points (45-47% female, median age 73-75 years) in 23,800 Queensland patients (11,894 [T0]; 4781 [T3]); and n = 20,484 from comparator hospitals (5,903 [T0]; 5,188 [T3]). Primary outcome: 18% absolute improvement in composite score (coeff 0.18 95% CI 0.15, 0.21) compared to no change in comparator hospitals (95%CI -0.03, 0.03). Overall, 6/8 individual processes improved e.g. stroke unit admission odds ratio [OR] 1.57, intravenous thrombolysis if ischaemic stroke OR 1.41; mobilised during admission OR 2.19. Hospitals developing action plans had greater improvements in composite score (coeff 0.23 95%CI 0.09, 0.37).
Conclusion
In Queensland hospitals positive changes in clinician practice were achieved from quality improvement interventions implemented during the Stroke123 study. Application in other settings is encouraged.
Trial registration number
N/A
AS01-009
THERAPEUTIC INDUCED HYPERTENSION IN ACUTE STROKE PATIENTS WITH NON-CARDIOEMBOLIC STROKE: A MULTICENTER, RANDOMIZED CONTROLLED TRIAL
1Samsung Medical Center, Neurology, Seoul, Republic of Korea
2Gyeongsang National University Hospital, Neurology, Jinju, Republic of Korea
3Hana General Hospital, Neurology, Cheongju, Republic of Korea
4Kyungbook National University Medical Center, Neurology, Daegu, Republic of Korea
5Wonkwang University Hospital, Neurology, Jeonju, Republic of Korea
6Pusan National University Hospital, Neurology, Busan, Republic of Korea
7Busan Paik Hospital, Neurology, Busan, Republic of Korea
8Keimyung University School of Medicine, Neurology, Daegu, Republic of Korea
9Seoul National University Bun-Dang Hospital, Neurology, Seongnam, Republic of Korea
Background and Aims
Collateral enhancing strategies are important ways to restore blood flow within ischemic regions, particularly in patients who are ineligible for revascularization therapy, such as those outside the therapeutic time window for IVT or EVT, or those having poor collaterals in whom unfavorable response to revascularization therapy is expected.
Method
The Safety and Efficacy of Therapeutic INduced Hypertension in Acute Non-cardioembolic Ischemic Stroke (SETIN-HYPERTENSION) trial is a multicenter prospective, randomized, open-label, blinded-endpoint designed trial. Total of 163 patients were enrolled from June 2012 through December 2017, at eight sites in South Korea to receive standard medical treatment or induced-hypertension. Patients with acute ischemic stroke within 24 hours of symptom onset with baseline NIH stroke scale (NIHSS) score 4–18 points or symptom worsening (defined by a 2-point or more increase in NIHSS score) were enrolled in this study. Patients underwent recanalization therapy, systolic blood pressure (SBP) >170 mmHg at baseline, with history of hemorrhagic stroke, and with significant arrhythmia were excluded. Induced hypertension was initiated with phenylephrine 10 cc/h and were increased 10 cc/h to reach SBP threshold for neurologic improvement or SBP of 200 mmHg. The primary endpoint was 2 points improvement in NIHSS between days 0 and 7. The secondary endpoint was proportion of good functional outcome (mRS 0–2) at 90-days. For safety measures, symptomatic hemorrhagic transformation or cerebral edema, myocardial infarction, and death from any cause were captured.
Results
placeholder for late-breaking clinical trial
Conclusion
placeholder for late-breaking clinical trial
Trial registration number
ClinicalTrials.gov: NCT01600235
AS29-015
MULTI-ANCESTRY GENOME-WIDE ASSOCIATION STUDY OF > 521,000 SUBJECTS IDENTIFIES 22 NOVEL LOCI ASSOCIATED WITH STROKE AND STROKE SUBTYPES
1Institute for Stroke and Dementia Research, Ludwig-Maximilians-University, München, Germany
2Indian Institute of Science IISc, Centre for Brain Research, Bangalore, India
3University of Cambridge, Division of Clinical Neurosciences- Stroke Research Group, Cambridge, United Kingdom
4INSERM U1219 Bordeaux Population Health Research Center- Bordeaux, INSERM U1219 Bordeaux Population Health Research Center- Bordeaux, Bordeaux, France
5RIKEN Center for Integrative Medical Sciences, Laboratory for Statistical Analysis- RIKEN Center for Integrative Medical Sciences, Yokohama, Japan
6University of Cincinnati College of Medicine, University of Cincinnati College of Medicine, Cincinnati, USA
7Massachusetts General Hospital MGH, Center for Genomic Medicine, Boston, USA
8McMaster University, Population Health Research Institute, Hamilton, Canada
9University of Oxford, Clinical Trial Service Unit and Epidemiological Studies Unit- Nuffield Department of Population Health, Oxford, United Kingdom
10University of Pennsylvania, Department of Genetics- Perelman School of Medicine, Philadelphia, USA
11University of Virginia School of Medicine, Departments of Neurology and Public Health Sciences, Charlottesville, USA
12University of Maryland School of Medicine and Baltimore, Department of Neurology, Baltimore, USA
13Boston University School of Medicine, Department of Neurology, Boston, USA
14University of Texas Health Science Center at Houston, Brown Foundation Institute of Molecular Medicine, Houston, USA
15University of Cambridge, Stroke Research Group- Division of Clinical Neurosciences, Cambridge, United Kingdom
16University of Cambridge, MRC/BHF Cardiovascular Epidemiology Unit- Department of Public Health and Primary Care, Cambridge, United Kingdom
Background and Aims
Stroke has multiple etiologies but the underlying genes and pathways remain largely elusive.
Method
We conducted a genome-wide association meta-analysis in >521,000 individuals (>67,000 cases and >454,000 controls) of European, East Asian, African, South Asian, Mixed Asian, and Latin American Ancestry collected through 29 studies genotyped with genome-wide genotyping arrays and imputed to 1000 Genomes.
Results
We found 32 genome-wide significant risk loci, 22 of which are novel. We demonstrate shared genetic variation with vascular risk factors (blood pressure primarily, to a lesser extent blood lipids), cardiac traits (coronary artery disease, atrial fibrillation), and venous thromboembolism at individual loci, and employing genetic risk scores and LD score regression. Several risk loci showed distinct association and pleiotropy patterns for etiological stroke subtypes providing mechanistic insight. Eleven of the novel loci point to mechanisms not previously implicated in stroke pathophysiology. The 32 stroke risk loci were significantly enriched in drug targets for antithrombotic therapy, one for an approved thrombolytic drug and the other for an antiplatelet agent approved for stroke prevention in Asia thus emphasizing the potential for drug discovery. Incorporation of extensive functional datasets and bioinformatics analyses enabled a prioritization of specific risk variants and genes as a resource for further functional follow-up.
Conclusion
This study more than triples the number of stroke risk loci, demonstrates shared genetic variation with multiple related vascular traits, and provides novel mechanistic insights. Our findings offer a framework for further experimental studies and prospects for the development of novel therapeutic approaches.
Trial registration number
N/A
Large Clinical Trials 2
AS03-004
5-YEAR RISK OF TIA AND MINOR ISCHEMIC STROKE : THE TIAREGISTRY.ORG FINAL RESULTS
1Paris-Diderot- Sorbonne University, Neurology and Stroke Center- Bichat hospital, Paris, France
Background and Aims
Little is known about the long-term risk of TIA and minor ischemic stroke. The one-year results have been reported [N Engl J Med. 2016 ;374 :1533]. We now report the 5-year risk, final results.
Method
It was an investigator-driven, web-based, TIA clinic based, real-world registry of patients enrolled with a TIA or a minor ischemic stroke performed in 21 countries, 61 centers and 4,583 enrolled patients. 42 centers participated in the 5-year follow-up (n = 3,847 patients) with a face-to-face or a telephone visit with the patient or a relative or its primary care physician. The primary end-point was a composite of stroke, myocardial infarction or vascular death.
Results
The median percentage of follow-up per center was 92.3% [IQR 83.4-97.8%]. 77.2% were evaluated by a stroke specialist within 24 hours of symptom onset. At baseline, 67.1% had a Rankin 0 and 31.5% Rankin 1 ; 72.5% had NIHSS = 0, 16.8% had NIHSS 1–3; 67.7% had an ABCD2 score ≥4 ; 97.4% had a brain imaging (35.1% had a brain infarction), 91.9% had extracranial artery imaging (15.7% ≥50% stenosis or occlusion), 84.6% had intracranial artery imaging (13.9% ≥50% stenosis or occlusion), 94.3% had an ECG (9.6% atrial fibrillation), and 63.1% had cardiac echography (4.8% with significant abnormality). At the time of database extraction (August 16, 2017), patients had been followed for a median of 5.01 years (interquartile range 4.62-5.23).
Conclusion
The primary end-point at 5 years, and risks by baseline ABCD2 score, presence of brain infarction and by underlying cause will be presented at the meeting.
Trial registration number
N/A
AS06-079
BLOOD PRESSURE AND FUNCTIONAL OUTCOME AFTER ENDOVASCULAR TREATMENT: RESULTS FROM THE MR CLEAN REGISTRY
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
3Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
4Erasmus MC University Medical Center, Radiology and Nuclear Medicine, Rotterdam, The Netherlands
5University Medical Center Utrecht, Brain Center Rudolf Magnus- Neurology, Utrecht, The Netherlands
Background and Aims
High systolic blood pressure (SBP) in the acute phase of ischaemic stroke is associated with an increased risk of symptomatic intracranial haemorrhage (sICH) and poor outcome. It is not well known to what extent SBP affects outcome after endovascular treatment (EVT) in daily clinical practice.
Method
MR CLEAN Registry is an observational, prospective, multicentre study of EVT in routine clinical practice in the Netherlands. The relation between SBP before EVT and collateral grade, reperfusion, sICH and 90-day functional outcome (mRS score) was assessed with logistic and ordinal regression. Odds ratios (ORs) and 95% confidence intervals (CIs) are given per 10 mmHg increase in SBP.
Results
Of 1488 patients included between March 2014 and June 2016, SBP was available in 1446 patients. The relation between SBP and poor functional outcome was U-shaped, with the highest chance of good outcome (mRS 0–2) for SBPs 110 to 119 mmHg. In patients with a SBP ≥ 115 mmHg, a higher SBP increased the risk of poor functional outcome (acOR 0.94, 95% CI 0.89 – 0.98). Higher SBP was associated with a worse collateral grade (acOR 0.95, 95% CI 0.91 – 0.99), less reperfusion (extended Thrombolysis in Cerebral Infarction score 2b-3: aOR 0.92, 95% CI 0.88 – 0.97) and higher occurrence of sICH (aOR 1.11 95% CI 1.01 – 1.22).
Conclusion
In this large phase IV cohort of patients with acute ischaemic stroke treated with EVT, both low and high SBPs were associated with poor outcome, and high SBP with a greater risk of sICH.
Trial registration number
N/A
AS02-036
TIME TO TREATMENT AND OUTCOMES IN THROMBECTOMY AT THE EXTENDED TIME WINDOW IN AURORA: POOLED ANALYSIS OF THE DAWN, DEFUSE-3, POSITIVE, ESCAPE AND REVASCAT TRIALS
1Grady Memorial Hospital- Emory University School of Medicine, Department of Neurology, Atlanta, USA
2University of Pittsburgh Medical Center, Neurology, Pittsburgh, USA
3Stanford University, Neurology, Palo Alto, USA
4University of Calgary, Radiology, Calgary, Canada
5University of Calgary, Neurology, Calgary, Canada
6State University of New York at Buffalo, Neurosurgery, Buffalo, USA
7State University of New York at Stony Brook, Radiology, Stony Brook, USA
8Hospital Germans Trias, Neurology, Barcelona, Spain
Background and Aims
It is well-established that, within 0–6 hours, the benefit of thrombectomy rapidly decays over time. The DAWN and DEFUSE-3 trials have demonstrated that, in the presence of clinical-core mismatch or perfusion-imaging mismatch, respectively, thrombectomy remains beneficial within 6–24 hours. We aim to assess the effect of time to randomization on outcomes in the trials that enrolled patients in the 6–24-hour treatment window.
Method
In AURORA (
Results
Although the data are currently under embargo, we will present the results of the analyses described above at the meeting.
Conclusion
We will present the conclusion of the analyses described above at the meeting.
Trial registration number
N/A
AS03-033
RECURRENT CLINICAL ISCHEMIC STROKES IN THE GORE REDUCE TRIAL OF PFO CLOSURE
1University of Pennsylvania, Neurology, Philadelphia, USA
2Medical University of South Carolina, Neurology, Charleston, USA
3Boston University, Neurology, Boston, USA
4University of Wisconsin, Radiology, Madison, USA
5Aarhus University Hospital and Faculty of Heath- Aarhus University, Neurology, Aarhus, Denmark
6Rigshospitalet- University of Copenhagen, Neurology, Copenhagen, Denmark
7Houston Methodist, Neurology, Houston, USA
8Rigshospitalet, Cardiology, Copenhagen, Denmark
9Medical University of South Carolina, Cardiology, Charleston, USA
10Karolinska University Hospital, Neurology and Clinical Neuroscience, Stockholm, Sweden
Background and Aims
The Gore REDUCE trial demonstrated lower stroke risk with PFO closure compared to antiplatelet therapy alone. We aimed to further characterize these strokes in terms of size, location, etiology, and severity/outcome, to emphasize the pathophysiology and clinical importance of stroke prevention in this population.
Method
In this multinational trial, we randomly assigned patients with cryptogenic stroke and PFO in a 2:1 ratio to closure plus antiplatelet therapy or to antiplatelet therapy alone. The first co-primary endpoint was freedom from clinical ischemic stroke through at least 2 years. All adjudicated strokes were characterized for etiology (TOAST and ASCOD) and severity/outcome (NIHSS/mRS) by the clinical endpoint committee while infarct size and location was determined by the imaging core lab; all were blinded to treatment allocation.
Results
We enrolled 664 patients with mean age 45.2 years, 81% with moderate or large inter-atrial shunts, and had a median follow-up of 3.2 years. There were 6 (1.4%) recurrent strokes in the closure group and 12 (5.4%) strokes in the antiplatelet therapy group (HR 0.23; 95%CI:0.09-0.62). Final blinded detailed characterization of these events is underway and results will be presented.
Conclusion
The majority of recurrent strokes in patients with cryptogenic stroke and PFO are expected to be embolic and cryptogenic. PFO closure reduces the risk of recurrent ischemic stroke, and the impact on large or disabling stroke is expected to support both the pathophysiological effect of closure and the clinical importance in this population.
Trial registration number
ClinicalTrials.gov Identifier: NCT00738894
AS04-037
GOTHENBURG VERY EARLY SUPPORTED DISCHARGE: A BLOCK-RANDOMIZED TRIAL WITH SUPERIORITY DESIGN OF VERY EARLY SUPPORTED DISCHARGE FOR PATIENTS WITH STROKE
1Neuroscience and Physiology, Physiotherapy, Gothenburg, Sweden
Background
Early supported discharge (ESD) has shown to be efficient yet not implemented everywhere.
Aim
To assess if very early supported discharge (VESD) is useful.
Method
A block randomized controlled trial comparing VESD with ordinary discharge. Inclusion: confirmed stroke, >18 years, living ≤ 30 min from the hospital, National institute of health stroke scale (NIHSS) 0–16 and Barthel Index (BI) 50–100 on day 2, with BI 100 the Montreal Cognitive Assessment (MoCA) < 26. Exclusion: life expectancy < 1 year, inability to speak or to communicate in Swedish. Intention to treat analyses were made. Chi-square was used for group differences.
Primary outcome: anxiety assessed with Hospital Anxiety and Depression Scale (HADS-A). Secondary outcomes: function with modifies Ranking Scale (mRS) activities of daily living with Barthel Index (BI).
Results
Of 140 included patient 54% were woman. Median age was 74 years. The median length of stay was 12 days in the VESD and 15 days in the controls. Thirty two patients were lost before start of intervention. There was no significant shift regarding HADS-A between admittance, 3 months or one year post stroke. The mRS was significant lower in the VESD three months post stroke (p = 0.004). There was a significant shift in proportions in mRs between admittance, 3 months post stroke and one year post stroke in both groups.
Conclusion
The VESD were discharged 3 days earlier than the control group. The mRS at 3 months was better in the VESD group but at 12 months, there were no significant differences left.
Trial registration number
NCT01622205
AS01-024
DOES TRANEXAMIC ACID LEAD TO INCREASED DWI HYPERINTENSE LESION PREVALENCE IN PATIENTS WITH SPONTANEOUS INTRACEREBRAL HAEMORRHAGE? RESULTS OF THE TICH-2 MRI SUB-STUDY
1University of Nottingham, Clinical Neuroscience, Nottingham, United Kingdom
2University Hospitals of Leicester NHS Trust, Neuroradiology, Leicester, United Kingdom
3Nottingham University Hospitals NHS Trust, Medical Physics and Clinical Engineering, Nottingham, United Kingdom
4London School of Hygiene & Tropical Medicine, Clinical Trials Unit, London, United Kingdom
5University College London, Stroke Research Centre, London, United Kingdom
6University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
7University of Nottingham, Medical Sciences & GEM, Derby, United Kingdom
Background and Aims
Diffusion weighted imaging (DWI) hyperintense lesions (HL), thought to indicate foci of cerebral ischaemia, are observed on MRI scans of people with recent spontaneous intracerebral haemorrhage (SICH) with a prevalence of 8–35%. Tranexamic acid (TXA), an antifibrinolytic agent under evaluation as a treatment for acute SICH, could theoretically potentiate this risk. We hypothesise that prevalence of DWIHL will be greater in people with SICH five days after treatment with TXA compared to placebo.
Method
MRI sub-study nested within the international multi-centre double-blind randomised controlled Tranexamic Acid for Hyperacute Primary Intracerebral Haemorrhage (TICH-2) trial which tests the hypothesis that intravenous TXA reduces death and disability when given within 8 hours of ICH onset. Eligible adults in TICH-2 underwent MRI including DWI at day 5 (range day 2–14) after randomisation. Two neuroradiologists identified DWIHL independently; a third neuroradiologist adjudicated discrepancies. We compared presence of DWIHL after SICH between treatment groups using binary logistic regression with adjustment for baseline covariates.
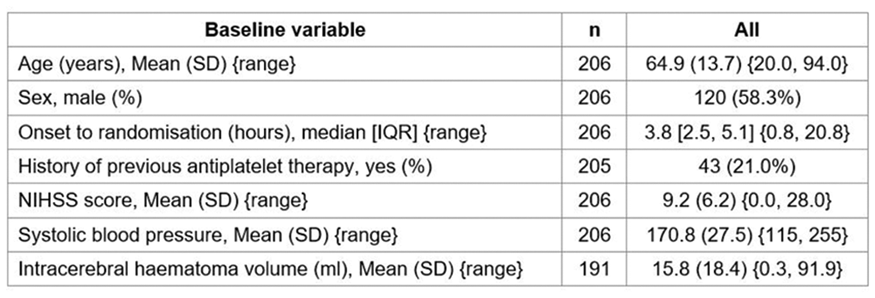
Results
Full results will be available in May 2018. Preliminary analysis of the TICH-2 MRI sub-study dataset includes 206 participants from 44 centres with baseline characteristics (Table).
Conclusion
Comparison of between-group differences in DWIHL prevalence in the TICH-2 MRI sub-study dataset will be presented. This is the first study to address this question, providing important safety data to inform clinical practice.
Trial registration number
ISRCTN93732214
AS03-025
RIVAROXABAN OR ASPIRIN FOR PATENT FORAMEN OVALE: PRESPECIFIED SUBGROUP ANALYSIS FROM THE NAVIGATE ESUS TRIAL
1University of Pennsylvania, Neurology, Philadelphia, USA
2NAVIGATE ESUS Steering Committee and Investigators, NAVIGATE ESUS Steering Committee and Investigators, NAVIGATE ESUS Steering Committee and Investigators, Canada
Background and Aims
Patent foramen ovale (PFO) is a contributor to embolic stroke of undetermined source (ESUS). Subgroup analyses from PFO closure trials suggest that anticoagulation may have comparable efficacy to closure, which is superior to antiplatelet therapy. We hypothesized that anticoagulant treatment with rivaroxaban, an oral factor Xa inhibitor, would reduce the risk of recurrent stroke compared with antiplatelet therapy with aspirin among patients with PFO enrolled in the NAVIGATE-ESUS trial.
Method
The NAVIGATE-ESUS double-blind, randomized trial assessed the efficacy and safety of rivaroxaban 15mg versus aspirin 100mg once daily for secondary stroke prevention in patients with ESUS. The primary efficacy outcome was all recurrent strokes and systemic embolism, and there was no difference in the primary outcome among all participants. Echocardiography was required for all subjects, and cCohorts with and without PFO were defined based on extent of diagnostic testing, including transthoracic (TTE) and/or transesophageal echocardiography (TEE). Agitated saline contrast (“bubble”) studies were not required.
Results
7214 participants were enrolled from 459 sites in 31 countries and were followed for a mean of 11 months. PFO was detected in 313/5993 (5%) of patients with TTE and in 370/1356 (27%) with TEE. Final results will be presented.
Conclusion
PFO is common in patients with ESUS when assessed by TEE. Results of this pre-specified subgroup analysis will be presented on the rate of ischemic strokes in PFO patients assigned to rivaroxaban versus aspirin.
Trial registration number
ClinicalTrials.gov number, NCT02313909
Scientific Communications -Service Organisation
AS24-032
BETWEEN-CENTER AND BETWEEN-COUNTRY DIFFERENCES IN OUTCOME AFTER ANEURYSMAL SUBARACHNOID HEMORRHAGE IN THE SUBARACHNOID HEMORRHAGE INTERNATIONAL TRIALISTS (SAHIT) REPOSITORY
1Erasmus University Medical Center, Public Health, Rotterdam, The Netherlands
2Li Ka Shing Knowledge Institute- St. Michael's Hospital- University of Toronto, Neuroscience Research Program, Toronto, Canada
3Erasmus University Medical Center, Intensive Care, Rotterdam, The Netherlands
4Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
5Leiden University Medical Center, Biomedical Data Sciences, Leiden, The Netherlands
6Keenan Research Center- Li Ka Shing Knowledge Institute- St. Michael's Hospital- University of Toronto, Surgery, Toronto, Canada
Background and Aims
Differences in outcome among different settings are common in many diseases and may reflect differences in quality of care. We aimed to quantify between-center and between-country differences in outcome after aneurysmal subarachnoid hemorrhage (aSAH).
Method
We analyzed data from 5530 aSAH patients from three randomized clinical trials including 170 centers and 22 countries. We used random-effects logistic regression adjusted for patient characteristics to estimate between-center and between-country differences in unfavorable outcome, defined as Glasgow Outcome Scale 1–3 (severe disability, vegetative state or death) or modified Rankin Scale 4–6 (moderately severe disability, severe disability or death) at three months. Between-center and between-country differences were quantified with the median odds ratio (MOR), which is based on the variance of the random effects and can be interpreted as the odds ratio for unfavorable outcome between two randomly selected centers or countries. We analyzed the total database and performed subgroup analysis stratified for continent (Europe, North America and Oceania).
Results
The proportion of patients with unfavorable outcome was 27%. We found substantial between-center differences (MOR = 1.26), which were not explained by patient characteristics (adjusted MOR = 1.30). Between-country differences were also found (adjusted MOR = 1.41). Between-center differences were absent in Oceania and North America (adjusted MOR = 1.00), but were present in Europe (adjusted MOR = 1.51).
Conclusion
Outcome after aSAH differs between centers and countries, especially in Europe. Since these differences could not be explained by patient characteristics, future research should focus on explanations regarding differential treatment policies and quality of care.
Trial registration number
N/A
AS12-071
SECONDARY TRANSFER OF STROKE PATIENTS FOR THROMBECTOMY BY AIR AMBULANCE IN ENGLAND: A COST-EFFECTIVESS ANALYSIS
1Newcastle University, Institute of Health and Society, Newcastle upon Tyne, United Kingdom
2Northumbria University, School of Health- Community and Education Studies, Newcastle upon Tyne, United Kingdom
3Newcastle University, Institute of Neuroscience Stroke Research Group, Newcastle upon Tyne, United Kingdom
4Clinical Research Network North East and North Cumbria, North East and North Cumbria Stroke Patient & Carer Panel, Newcastle upon Tyne, United Kingdom
5University of Oxford, Centre for Evidence Based Medicine, Oxford, United Kingdom
6Great North Air Ambulance, Northumberland Wing- The Imperial Centre, Darlington, United Kingdom
Background and Aims
Helicopter Emergency Medical Services (HEMS) for secondary transfer of stroke patients eligible for thrombectomy could have a significant impact on outcomes for patients residing in areas remote from a thrombectomy centre (TC). Remote units cannot sustain a 24/7 thrombectomy service locally and transfer to a TC is necessary. There are few data on cost-effectiveness of secondary transfer via HEMS to inform commissioning decisions. We are evaluating the cost-effectiveness of HEMS versus ground-based ambulance (GBA) for stroke thrombectomy in England.
Method
Using Geographic Information
Results
Annual stroke incidence of 3,860 at unavoidably remote hospitals (≥75km transfer distance), of which 508 patients would be transferred by HEMS. Ongoing survey of HEMS to establish operational parameters and costs to inform cost effectiveness model is ongoing and will be presented with the health economic data.
Conclusion
HEMS is an option for secondary transfer of patients eligible for thrombectomy from unavoidably “small” and remote hospitals. Estimates of HEMS cost-effectiveness will be presented to inform the optimal organisation of thrombectomy service delivery.
Trial registration number
N/A
AS12-072
VIDEO SUPPORT IN THE PREHOSPITAL STROKE CHAIN
1University of Borås, Swedish School of Library and Information Science- Prehospen Centre for Prehospital Research, Boras, Sweden
2Chalmers University of Technology, Department of Electrical Engineering, Gothenburg, Sweden
3Sahlgrenska University Hospital, MedTech West, Gothenburg, Sweden
4University of Borås, Prehospen Centre for Prehospital Research, Boras, Sweden
5Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
6the Sahlgrenska Academy at University of Gothenburg, Institute of Neuroscience and Physiology- Department of Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
Video-consultations between hospital and ambulance/EMS clinicians have the potential to increase precision of decisions regarding stroke patient assessment, management and transport. The aim of this study was to evaluate feasibility and impact of real-time video for neurologist–-EMS clinician consultation.
Method
The study used full-scale prehospital simulations including on-scene EMS clinicians, simulated patients, and remote neurologists at a tertiary stroke center. Video-consultation was used for remote assessment of cases exhibiting 1)severe, and 2)mild stroke symptoms, to determine appropriate management and transport based on geographical location (proximity to local hospital and stroke center) and NIHSS score.
Results
Three video-cameras were installed inside an ambulance. The remote neurologists were presented with a picture-in-picture layout including three views of the patient: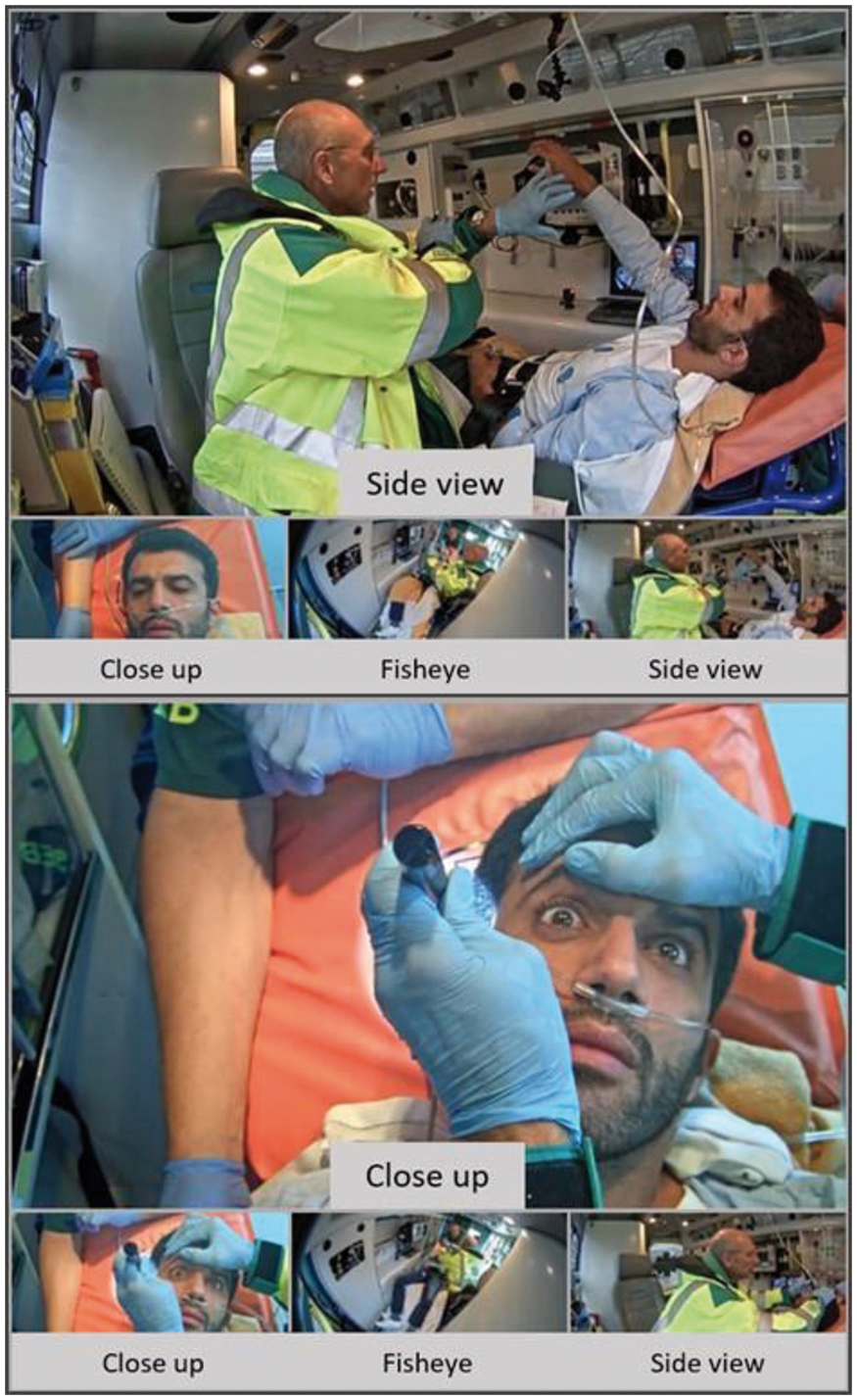
Conclusion
Video is a feasible tool for remote stroke assessment even under realistic, time-critical work conditions. The results suggest that it will lead to safer and higher quality of care, and that the procedure now is ready for next step towards real clinical implementation.
Trial registration number
N/A
AS12-060
ELIGIBILITY FOR ENDOVASCULAR THERAPY IN A LATE TIME WINDOW IN A POPULATION-BASED STUDY
1Germans Trias i Pujol Hospital, Neuroscience, Badalona, Spain
Background and Aims
Thrombectomy has recently shown to be effective in patients with ischemic stroke within 6 to 24 hours selected by clinical/infarct mismatch. We aimed to determine endovascular therapy (EVT) eligibility in stroke code patients presenting in a late time window
Method
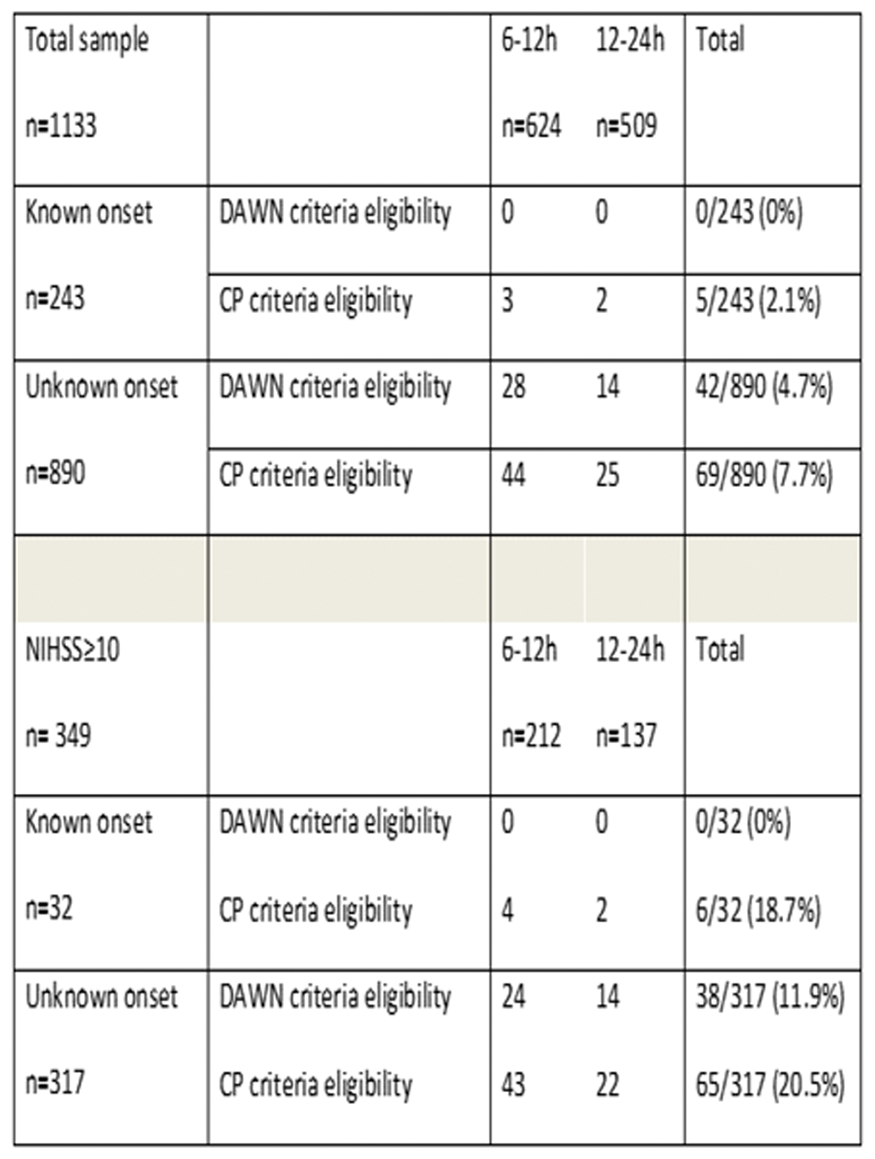
From a prospective collected data of patients with suspicion of acute stroke attended at a single comprehensive stroke center covering a population of 850.000 inhabitants (6-year period), we analyzed patients admitted within 6 to 24 hours from last time seen well. Patients were classified in known (KN) and unknown (UKN) onset of symptoms and according to the time frame (6–12h, 12-24h). DAWN criteria (M1/TICA occlusion, NIHSS≥10, ASPECTS≥6 and mRS 0–1) and clinical practice (CP) criteria (M1/M2/TICA/Tandem occlusion, NIHSS≥6, ASPECTS≥6 and mRS 0–2) were assessed in each group.
Results
Of 3511 patients, 1133(32.3%) were admitted within 6 to 24h, 243(6.9%)/ 890(25.4%) patients with KN/UKN onset, respectively. DAWN criteria fulfilled in 42/1133(3.7%) patients whereas CP criteria in 74/1133(6.5%) patients. KN patients were scarcely eligible for EVT in contrast to UKN patients (see table). Considering patients with NIHSS≥10 (n = 349), EVT eligibility increased to 10.8%/20.3% according to DAWN/CP criteria.
Conclusion
Up to 7% of patients with suspected stroke within 6–24 hours are eligible for EVT, basically those with unknown onset of symptoms. Stroke Code systems should consider including patients with unknown onset up to 24 hours, especially when a prehospital clinical scale detects severe symptoms
Trial registration number
N/A
AS12-068
REAL WORLD HOSPITAL TRANSFER TIMES AND LOSS OF BRAINTISSUE MEASURED WITH E-ASPECTS UNDERLINES IMPORTANCE OF IMPROVEMENT OF STROKE CARE DELIVERY
1Heidelberg University Hospital, Neurology, Heidelberg, Germany
2Heidelberg University Hospital, Neuroradiology, Heidelberg, Germany
Background and Aims
As thrombectomy is only available at stroke centers, there is an ongoing debate whether acute ischemic stroke patients benefit from direct referral vs. secondary transportation. We aimed to analyze the brain tissue loss in a real-world drip & ship model of acute anterior circulation stroke patients.
Method
We analyzed consecutive hospital transfer times between 2013 and 2016 for patients transported as potential candidates for thrombectomy with middle cerebral artery infarct from regional hospitals to our stroke center. All patients underwent external as well as in house emergency CT-imaging, and Alberta Stroke Program Early Computed Tomography Scores were automatically calculated using the Brainomix® e-ASPECTS software. Furthermore, weighted acute ischemia volumes were equally calculated.
Results
Of 87 patients with available e-ASPECTS, median image-to-image time was 2:36 h (IQR, 1:59–3:13). Hospital transfer was associated with a decrease in e-ASPECTS of 1 (0–2) points (first imaging 9 [7–10], secondary imaging 8 [6–9], p = 0.02). e-ASPECTS decrease was inversely associated with infarct size growth (total weighted acute ischemia lesion 5.0 ml [2.3–10.78] vs. 7.2 ml [3.7–12.9; p = 0.005]). Transfer time correlated with discharge NIHSS, with longer transport times being correlated with worse neurological status (p = 0.04).
Conclusion
Longer-image to image time is associated with a decrease in e-ASPECTS score and an increase in infarct volume, as well as a less favorable outcome. Our data underscore the need for faster hospital transfer systems as well as evaluation of prehospital triage concepts including direct referrals to stroke centers.
Trial registration number
N/A
AS12-031
ASSOCIATION BETWEEN INDIVIDUAL ADHERENCE TO QUALITY INDICATORS AND EARLY MORTALITY AFTER ISCHEMIC STROKE: THE GERMAN STROKE REGISTERS STUDY GROUP (ADSR)
1University of Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany
2Bavarian Permanent Working Party for Quality Assurance, Bavarian Permanent Working Party for Quality Assurance, Munich, Germany
3Institute of Quality Assurance Hesse GQH, Institute of Quality Assurance Hesse GQH, Eschborn, Germany
4University of Münster, Quality Assurance Project “Stroke Register Northwest Germany”- Institute of Epidemiology and Social Medicine, Münster, Germany
5Asklepios Klinik Nord Hamburg, Department of Neurology, Hamburg, Germany
6Medical Association North Rhine, Quality Assurance in Stroke Management in North Rhine-Westphalia, Düsseldorf, Germany
7Baden-Wuerttembergische Hospital Association, Office for Quality Assurance in Hospitals GeQiK®-, Stuttgart, Germany
8Institute of Quality Assurance Rhineland-Palatinate/SQMed, Institute of Quality Assurance Rhineland-Palatinate/SQMed, Mainz, Germany
9University of Lübeck, Quality Association for Acute Stroke Treatment Schleswig-Holstein QugSS- Institute of Social Medicine and Epidemiology, Lübeck, Germany
10Vivantes Klinikum im Friedrichshain Berlin, Klinik für Neurologie mit Stroke Unit, Berlin, Germany
11University Hospital Würzburg, Clinical Trial Center Würzburg, Würzburg, Germany
12University of Würzburg, Comprehensive Heart Failure Center, Würzburg, Germany
Background and Aims
Quality indicators (QI) are an accepted tool to measure performance in routine clinical care. We investigated the association between adherence to evidence-based QIs of acute stroke care and early outcome in Germany.
Method
Consecutive patients with ischemic stroke (IS) admitted to one of the hospitals cooperating within the German Stroke Register Study Group (ADSR) between 2015 and 2016 were analysed. The ADSR is a voluntary network of 9 regional stroke registers monitoring quality of acute stroke care across 750 hospitals in Germany. On patient level the association between adherences to a predefined set of 11 evidence-based indicators of process of stroke care with 7-day in-hospital-mortality was assessed a) for each single QI by multivariable logistic regression and b) for the proportion of QIs fulfilled from the number of potential QIs the individual patient was eligible for by generalized linear mixed model analysis adjusted for age, sex, NIHSS and living will with hospital as random effect.
Results
375,899 patients with IS and complete information were analysed. Adherence to QIs ranged between 41.0% (thrombolysis of eligible patients) and 95.2% (physiotherapy); adherence to 9 out of the 11 QIs showed a statistical significant association with short term survival. The proportion of QIs fulfilled from the number of potential QIs the individual patient was eligible for was median 0.90 (IQR 0.75-1.00). In multivariable analysis, a linear association between overall adherence to quality indicators and 7-day in-hospital-mortality was observed (p < 0.001).
Conclusion
Adherence to evidence-based QIs of acute stroke care is associated with lower 7-day in-hospital-mortality in clinical routine.
Trial registration number
N/A
AS06-031
STROKE NURSE INVOLVEMENT ON CODE STROKE MANAGEMENT IMPROVES REPERFUSION METRICS
1Vall d'Hebrón hospital, Stroke Unit, Barcelona, Spain
Background and Aims
Shortening door-to-needle (DTN) and door-to-groin (DTG) times without compromising safety is one of the major goals of reperfusion therapy. A pre-hospital Stroke Code (SC) activation leading to a direct transfer of patients to CT(CT-SC) or Angio-suit (Angio-SC), bypassing emergency room (ER) in selected patients, has been implemented in our center. To ensure quality and continuous care in this hyperacute process, an expert stroke nurse from the stroke unit is recruited in direct SC transfers.We aimed to assess the impact of the presence of an expert stroke nurse in reperfusion treatment parameters and the safety and feasibility of leaving the Stroke Unit to take care of the SC.
Method
When information is unclear the patient is evaluated in ER before CT(ER-SC). Direct transfers are performed when the arriving patient is stable and symptoms are<6h.Expert stroke nurse is notified only in direct SC transfers.
Results
During 2016, 816 patients were transferred to our center by SC activation. 290 patients (35,5%) underwent reperfusion treatment, ER-SC 101 (34.8%), CT-SC 146(50,3%), Angio-SC 43(14,8). Expert nurse was recruited to attend 138SC patients who received reperfusion in direct transfers (n = 189), which means a 73% of the CT/Angio-SC patients.Our mean DTN was 28+/-17min and DTG 41+/-50min in this period. DTN and DTG times were significantly lower in direct transfers compared with ER-SC(DTN 26,2min vs 37,5min p = 0.003 and DTG 41,4min vs 79,2min p < 0.001).When the expert nurse was present, those times where even lower (DTN 24,3 and DTG 17,6).
Conclusion
Expert stroke nurse recruitment from the Stroke Unit is feasible and safely helps to improve time indicators in acute stroke reperfusion treatment.
Trial registration number
N/A
AS12-069
IMPROVING WORKFLOW FOR ENDOVASCULAR THROMBECTOMY: EXPERIENCE FROM THE GREATER AMSTERDAM AREA
1Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
2Academic Medical Center, Neurology, Amsterdam, The Netherlands
3Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, The Netherlands
Background and Aims
Time to treatment is one of the most important prognostic parameters for EVT in acute ischemic stroke (AIS). We studied the effect of workflow improvements on treatment times in our high-volume comprehensive stroke center.
Method
We performed a prospective sequential comparison study: period I (before workflow improvements, April 2014–December 2016) vs. period II (after workflow improvements, January 2017–December 2017). We included consecutive AIS patients treated with EVT at our tertiary neuro-intervention center, with referrals from 13 surrounding primary stroke hospitals. Workflow improvements included optimization of transfers through a regional protocol (StrokeNet), direct referral without consultation, digital image transfer, parallel one stop CT-CT angiography and administration of IVT, and preparation of the angiosuite prior to patient arrival. Primary endpoint was the door-to-groin time (DGT, door of first hospital).
Results
We included 479 patients, 278 (58%) in period I and 201 (42%) in period II. The proportion of drip-and-ship patients was stable across the two periods (68% period I vs. 73% period II, P = 0.27). During period II, patients less often received IVT (87% vs. 74%, P<0.001). The median DGT was 30 minutes shorter in period II compared to period I (145 minutes vs. 115 minutes, P<0.001). This improvement was consistent for both mothership (109 minutes vs. 68 minutes, P<0.001) and drip-and-ship patients (163 minutes vs. 125 minutes, P<0.001).
Conclusion
Innovations to improve workflow for patients receiving EVT lead to substantially shorter door to groin times. In part, this effect may have been driven by increased experience with EVT.
Trial registration number
N/A
AS13-018
DETERMINANTS OF NON-RECOGNITION OF STROKE BY EMERGENCY MEDICAL SERVICES (EMS)
1Auckland University of Technology, Department of Paramedicine, Auckland, New Zealand
2Auckland University of Technology, National Institute for Stroke and Applied Neurosciences, Auckland, New Zealand
3University of Otago, Department of Medicine, Christchurch, New Zealand
Background and Aims
Recognition of stroke by the EMS is imperative for optimal dispatch of mobile stroke units and activation of in-hospital stroke pathways prior to arrival, testing for large vessel occlusion and by-passing the closest hospital in preference for a specialist stroke centre. Previous studies report conflicting results on the sensitivity of recognition by EMS. We aimed to determine the sensitivity of call-taker and paramedic stroke recognition and identify factors predicting paramedic non-recognition.
Method
This population-based study of confirmed stroke/TIA patients linked operational and clinical EMS data with data from patient interviews and medical records. Independent predictors of non-recognition were determined by logistic regression analysis.
Results
Call-takers correctly identified 44% and paramedics 70% of cases. Paramedic non-recognition was associated with six factors: when the callout was not classified by the dispatcher as a stroke (aOR, 0.15, 95% CI, 0.09-0.24); the patient had no known family history of stroke (0.51, 0.34-0.76); the paramedic evaluated the patient’s severity as minor compared to moderate (0.20, 0.04-0.89), serious (0.08, 0.02-0.35) or critical (0.07, 0.01-0.39); the paramedic did not record a FAST assessment compared to a negative (0.38, 0.19-0.75) or positive test result (0.02, 0.01-0.04) or exclusion (0.24, 0.12-0.51); the final diagnosis was an intracerebral haemorrhage (2.66, 1.25-5.69) or ischaemic stroke (2.57, 1.41-4.66) compared to a TIA; the patient met posterior rather than lacunar cerebral infarct criteria (2.41, 1.32-4.41).
Conclusion
An understanding of the factors associated with non-recognition of stroke by paramedics could be used to design EMS education programmes to improve stroke recognition.
Trial registration number
N/A
Scientific Communications -Prevention Non- Trials
AS01-016
INTENSIVE STATIN TREATMENT IN ACUTE ISCHEMIC STROKE PATIENTS WITH INTRACRANIAL ATHEROSCLEROSIS - HIGH-RESOLUTION MAGNETIC RESONANCE IMAGING STUDY (STAMINA-MRI STUDY)
1Samsung Medical Center, Neurology, Seoul, Republic of Korea
2Hana General Hospital, Neurology, Cheongju, Republic of Korea
3Kyungbook National University Medical Center, Neurology, Daegu, Republic of Korea
Background and Aims
Intracranial atherosclerosis is a common condition consisting over 20% of ischemic stroke etiology in Asian population. Besides lowering blood cholesterol levels statin also stabilize atherosclerotic plaque and eventually lower the risk of ischemic stroke. However, little evidence resides on the effect of statin treatment on intracranial atherosclerosis.
Method
The STAMINA-MRI trial is a single-arm, prospective, observational study, monitoring imaging and clinical outcomes of high-dose statin (atorvastatin 40-80mg and rosuvastatin 20mg) treatment among patients with acute ischemic stroke caused by symptomatic intracranial atherosclerosis. Seventy-seven statin-naïve acute ischemic stroke patients with symptomatic intracranial artery (middle cerebral and basilar artery) stenosis (above 30%) were included. The primary outcome was changes in vascular remodeling and plaque characteristics before and after 6-months statin treatment measured by high-resolution magnetic resonance imaging (HR-MRI).
Results
The mean age of the patients were 62.6 ± 13.7 years and median interval between initial and follow up HR-MRI was 180 [162–190] days. Low-density lipoprotein cholesterol levels (mg/dL) at initial and follow up were 125.81 ± 35.69 and 60.95 ± 19.28 respectively. Overall, statin treatment significantly decreased degree of stenosis (%, 76.47 ± 20.23 Vs. 64.05 ± 21.29, P<0.001) and enhancement plaque volume (mm3, 32.07 ± 39.15 Vs. 17.06 ± 34.53, P = 0.013). Treatment with rosuvastatin, longer statin treatment duration, and symptomatic basilar artery stenosis were associated with decreased enhancement volume after statin treatment. However, about 20% patients showed increased enhancement volume and stenosis degree after statin treatment.
Conclusion
High-dose statin treatment effectively stabilized symptomatic intracranial atherosclerotic plaque. Future investigations are needed to determine genetic factors associated with poor statin response and alternative therapeutic option such as PCSK9 Inhibitor.
Trial registration number
ClinicalTrials.gov: NCT02458755
AS20-036
ANTIPLATELET TREATMENT AFTER TIA AND ISCHAEMIC STROKE IN PATIENTS WITH CEREBRAL MICROBLEEDS IN TWO LARGE COHORTS
1The University of Hong Kong, Department of Medicine, Hong Kong, Hong Kong S.A.R
2University of Oxford, Centre for Prevention of Stroke and Dementia- Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
3The University of Hong Kong, Department of Diagnostic Radiology, Hong Kong, Hong Kong S.A.R
Background and Aims
In TIA/ischaemic stroke patients, microbleed-burden predicts intracerebral haemorrhage (ICH), and ischaemic stroke, but implications for antiplatelet-treatment are uncertain.
Method
In two independent prospective cohorts with TIA/ischaemic stroke (Oxford Vascular Study/mainly Caucasian; University of Hong Kong/mainly Chinese), antiplatelet-treatment was started routinely irrespective of microbleed-burden. Risks, time-course and outcome of ICH, extracranial bleeds, and recurrent ischaemic events, were determined and stratified by microbleed-burden (0 vs. 1, 2–4 and ≥5), adjusting for age, sex and vascular risk factors.
Results
Microbleeds were more frequent in the Chinese cohort (450/1003 vs. 158/1080; p < 0.0001), but risk associations were similar during 7433patient-years of follow-up. Among 1811patients on antiplatelet drugs, risk of major extracranial bleeds was unrelated to microbleed-burden (ptrend = 0.87), but the 5-year risk of ICH was steeply related (ptrend<0.0001), with 73% of ICH in 7.7% patients with ≥5microbleeds. However, risk of ischaemic stroke also increased with microbleed-burden (ptrend = 0.013), such that risk of ischaemic stroke and coronary events exceeded ICH and major extracranial bleeds during the first-year, even amongst patients with ≥5microbleeds (11.7% vs. 3.7%). However, this ratio changed over time (time-course pinteraction = 0.034), with risk of haemorrhage matching that of ischaemic events after one-year (11.0% vs. 10.5%). Moreover, whereas the association between microbleed-burden and risk of ischaemic stroke was due mainly to non-disabling events (ptrend = 0.007), the association with ICH was accounted for (ptrend < 0.0001) by disabling/fatal events (≥5microbleeds: 82% disabling/fatal ICH vs. 40% ischaemic stroke; p = 0.035).
Conclusion
In Caucasian and Chinese patients with ≥5 microbleeds, withholding antiplatelet drugs during the first-year after TIA/ischaemic stroke may be inappropriate. However, the risk of ICH may outweigh any benefit thereafter.
Trial registration number
N/A
AS09-035
FREQUENCY, RISK AND OUTCOME OF ANTIPLATELET WITHDRAWAL AFTER NON-FATAL BLEEDING IN PATIENTS WITH KNOWN VASCULAR DISEASE: POPULATION-BASED STUDY
1Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Although a randomised trial of withdrawal versus continuation of antiplatelet treatment in acute GI-bleeding showed that withdrawal is hazardous, antiplatelets are still often stopped after a bleeding event in routine practice. In the absence of trial data in patients at high-risk of ischaemic events, we performed an observational comparison of withdrawal versus continuation in secondary prevention.
Method
In a population-based study (OXVASC/2002-2012) of patients with a first TIA/ischaemic stroke/myocardial infarction treated with antiplatelet drugs, all bleeding events requiring medical attention were identified by multiple sources, including face-to-face follow-up. We determined the frequency, 30-day risk of recurrent events (stroke/TIA/MI) and outcome (disability - mRS ≥3 or increased by ≥1 point if premorbid mRS ≥3) of antiplatelet withdrawal versus continuation after bleeding.
Results
3166 eligible patients (1582 aged≥75y) had 350 non-fatal bleeding events on antiplatelet treatment during 13,509 patient-years of follow-up. Among 331 (94.6%) patients with available information, antiplatelet treatment was stopped after the bleeds in 110 (33.2%; 77 GI bleeding, 12 intracranial, 21 other), most commonly in patients≥75 years (44.3% -78/176 vs. 20.6% - 32/155 <75y, p < 0.0001). Antiplatelet withdrawal was associated with an increased risk of recurrent events (0–30days: n = 7/6.7% vs. 3/1.4% on continuation; p = 0.01) and with greater bleed-related disability (OR = 5.39, 95%CI 2.92-9.96, p < 0.0001), although this association was attenuated after adjustment for age, premorbid disability and bleeding severity (1.91, 0.92-3.98, p = 0.08).
Conclusion
In patients on antiplatelet treatment for secondary prevention, sudden discontinuation of antiplatelet treatment after non-fatal bleeding events may be hazardous, possibly reflecting the prothrombotic response to recent bleeding.
Trial registration number
N/A
AS12-015
HEALTHCARE RESOURCE USE AND COSTS ASSOCIATED WITH BLEEDING ON LONG-TERM ANTIPLATELET TREATMENT IN SECONDARY PREVENTION AFTER VASCULAR EVENTS: POPULATION-BASED COHORT STUDY
1Centre for the Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Although a large proportion of adults aged ≥75 years take antiplatelet drugs for secondary prevention, little is known about the long-term cost consequences of antiplatelet-related bleeds, especially for upper-gastrointestinal (GI) bleeding, and hence the likely cost savings from routine co-prescription with proton-pump inhibitors (PPI).
Method
In a prospective population-based cohort study of TIA, ischaemic stroke, and myocardial infarction treated with antiplatelet drugs (without routine PPI use), we evaluated hospital costs associated with treatment of major bleeding during 10-year follow-up, averaged across all patients and compared with the cost of routine co-prescription of PPI (lansoprazole 15mg daily).
Results
Among 3166 patients with 405 first bleeding events (187 major; 45 intracranial, 97 upper-GI, 16 lower-GI and 29 other sites) during 13,509 patient-years of follow-up, the average cost for upper-GI and intracranial bleeds was similar (£8,252 vs £11,365, p = 0.235), although the total population cost for upper-GI bleeds was higher (£800,444 vs £511,425). Averaged across all patients, the 10-year cost of major bleeding was £579 (95% CI: 470-696), half (£284) due to upper-GI bleeding, the cost of which increased from £121 in those aged <75 years to £481 at age ≥75 years (p < 0.0001). Corresponding costs of routine life-long co-prescription of PPI were £59 (58-61) and £38 (36-40).
Conclusion
In secondary prevention with antiplatelet treatment without routine PPI use, the long-term costs of upper-GI bleeding at age ≥75 years are much higher than at younger ages, and are at least 10-fold greater than the drug cost of routine co-prescription of PPI.
Trial registration number
N/A
AS11-014
CENTRALLY OBSERVED HOME TELEMETRIC MONITORING OF BLOOD PRESSURE TO MANAGE INTENSIVE TREATMENT (COMMIT) AFTER TIA AND STROKE: CEREBRAL HEMODYNAMICS SUBSTUDY
1University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
There is no evidence of benefit from lowering blood pressure (BP) acutely after major ischaemic stroke, but effects of intensive treatment of hypertension in the acute phase after TIA and minor stroke are uncertain. As part of the COMMIT study, we assessed middle cerebral artery (MCA) blood flow velocities before and after treatment of hypertension in the acute phase after TIA and minor stroke.
Methods
Consecutive TIA/stroke clinic patients included in the COMMIT study from 2011-2018 underwent transcranial Doppler sonography (TCD) with bilateral MCA flow velocities at baseline and 1-month follow-up visits, together with baseline MRI/MRA. Where appropriate, BP-lowering (ACE-inhibitor and thiazide, with a calcium channel blocker if required) was started immediately and titrated on subsequent days with telemetric home BP-monitoring.
Results
In the 803 patients with TCD repeated at 1-month, mean/SD SBP fell from 147.1/22.3 mmHg at baseline to 135.1/18.7 at 1-month (p < 0.001), which was associated with an increase in MCA End Diastolic Velocity (EDV; p = 0.001), and a decrease in Pulsatility Index (PI; p < 0.009). Absolute changes were largest in the 158 patients with SBP≥160 mmHg at baseline, with mean (SD) reduction in SBP of 29.7 (21.8) mmHg and mean (SD) increase in EDV of 2.2 (7.7) cm/sec. Haemodynamic changes were unrelated to age, gender or the presence of an acute DWI-lesion.
Conclusion
Intensive early BP-lowering after TIA and minor stroke had no adverse effects on TCD indices of cerebral perfusion. Rather, EDV increased after BP-lowering, suggesting that distal vascular resistance had fallen and perfusion increased.
Trial registration number
N/A
AS30-031
STATIN-BASED LIPID LOWERING THERAPY FOR THE PRIMARY AND SECONDARY PREVENTION OF ISCHEMIC STROKE: A CRITICAL OVERVIEW AND META-ANALYSIS
1School of Medicine- University of Ioannina, Internal Medicine, Ioannina, Greece
2School of Medicine- University of Thessaly, Department of Internal Medicine-, Larissa, Greece
3Eginitio Hospital- University of Athens, First Department of Neurology, Athens, Greece
4Centre Cérébrovasculaire- Service de Neurologie, Dé partement des Neurosciences Cliniques, Lausanne, Switzerland
5Hellenic Stroke Organization, Hellenic Stroke Organization, Athens, Greece
Background and Aims
We scrutinized the effect of statin-based lipid-lowering therapy on ischemic stroke in primary and secondary prevention trials with regard to achieved levels of low-density lipoprotein (LDL)-cholesterol in view of the availability of novel potent hypolipidemic agents.
Method
English literature was searched (up to December 2017) for publications restricted to trials (with a minimum enrolment of 1,000 and 500 subjects for primary and secondary prevention, respectively) meeting the following criteria: adult population, randomized controlled design, and recorded outcome data on ischemic stroke events. Data were meta-analyzed while curve-estimation procedure was applied to estimate regression statistics and produce related plots.
Results
Four primary prevention trials and four secondary prevention trials fulfilled the eligibility criteria. Lipid-lowering therapy was associated with a lower risk of ischemic stroke in primary (Risk Ratio, RR 0.70, 95% Confidence Interval, CI, 0.60-0.82; p < 0.001) and in the secondary prevention setting (RR 0.80, 95%CI 0.70-0.90; p < 0.001). Curve-estimation procedure revealed a linear relationship between the absolute risk reduction (ARR) of ischemic stroke and active treatment-achieved LDL-cholesterol levels in the secondary prevention (adjusted R-square 0.90) in support of “the lower the better” hypothesis for stroke survivors. On the other hand, the cubic model followed the observed data well in primary prevention (adjusted R-square 0.98), indicating greater ARR in high-risk cardiovascular disease-free individuals.
Conclusion
Statin-based lipid-lowering is warranted both for primary and secondary prevention of ischemic stroke. Most benefit derives by targeting disease-free individuals at high cardiovascular risk and by achieving low treatment targets for LDL-cholesterol in stroke survivors.
Trial registration number
N/A
AS18-039
SEVERE CONTRALATERAL CAROTID STENOSIS OR OCCLUSION IS ASSOCIATED WITH HIGHER RISK OF STROKE AFTER CAROTID ENDARTERECTOMY FOR ASYMPTOMATIC STENOSIS IN ACST-1
1Medical Research Council Population Health Research Unit, Nuffield Department of Population Health- University of Oxford, Oxford, United Kingdom
2Nuffield Department of Surgical Sciences, University of Oxford, Oxford, United Kingdom
Background and Aims
In the first Asymptomatic Carotid Surgery Trial (ACST-1), successful carotid endarterectomy (CEA) significantly reduced 10-year stroke risk. Contralateral carotid stenosis (at least 70%) and occlusion may be an important factor influencing future stroke risk.
Method
In ACST-1, 3120 asymptomatic patients were followed up for a median (IQR) 9.0 (6.1-11.1) years. Information collected on each patient included gender, date of birth, details of any CEA, current stenosis, medication, blood pressure, comorbidity, stroke and death. In the 1686 asymptomatic patients with CEA, we analysed the effect of severe contralateral carotid stenosis or occlusion on absolute risk of stroke. We used competing risk regression models, adjusting for other risk factors, death from non-stroke causes and second CEA as competing risks.
Results
Mean patient age at surgery was 69 years and two-thirds were men. At surgery or during follow-up, 26% had or developed contralateral carotid stenosis and occlusion (CSO) and these patients had a higher risk of stroke. The risk of stroke if CSO was present vs absent was 4.5 vs 3.3% (ipsilateral), 5.9 vs 2.4% (contralateral) and 10.8 vs 6.5% (any stroke). Comparing patients with CSO present vs absent, after adjustment for age at surgery, gender and other risk factors, the hazard ratio (95% CI) was 1.35 (0.64-2.88, p = 0.43) for ipsilateral stroke, 2.55 (1.25-5.17, p = 0.01) for contralateral stroke and 1.70 (1.05-2.74, p = 0.03) for any stroke.
Conclusion
Although carotid endarterectomy for asymptomatic stenosis reduces 10-year stroke risk, patients who have, or develop, severe contralateral stenosis or occlusion are at markedly increased long-term risk of stroke.
Trial registration number
ISRCTN26156392
AS07-009
HYPERPERFUSION SYNDROME POST- CAROTID ANGIOPLASTY AND STENTING (HISPANIAS STUDY): RESULTS FROM A NATIONAL PROSPECTIVE MULTICENTER STUDY
1Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Neurology/Interventional Neurorradiology, Seville, Spain
2Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Neurology, Seville, Spain
3Hospital Vall d´Hebron, Interventional Neurorradiology, Barcelona, Spain
4Hospital Vall d´Hebron, Neurology, Barcelona, Spain
5Hospital Reina Sofía, Interventional Neurorradiology, Córdoba, Spain
6Hospital Reina Sofía, Neurology, Córdoba, Spain
7Hospital Universitario de Salamanca, Interventional Neurorradiology, Salamanca, Spain
8Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
9Hospital Virgen de la Arrixaca, Interventional Neurorradiology, Murcia, Spain
10Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
11Hospital Universitario Central de Asturias, Interventional Neurorradiology, Oviedo, Spain
12Hospital Clínico de Valencia, Interventional Neurorradiology, Valencia, Spain
13Hospital Clínico de Valencia, Neurology, Valencia, Spain
14Hospital Universitario de Cruces, Neurology, Bilbao, Spain
15Hospital Universitario de Cruces, Interventional Neurorradiology, Bilbao, Spain
16Instituto de Biomedicina de Sevilla. Hospital Unversitario Virgen Macarena, Neurology, Sevilla, Spain
17Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Interventional Neurorradiology, Seville, Spain
Background and Aims
Cerebral hyperperfusion syndrome (CHS) is defined by the presence of symptoms in addition to the demonstration of an increase in cerebral blood flow (CBF) more than 100% compared with baseline values. The aim of the project is to develop a clinical and biological (panel of genes) predictive model for hyper-perfusion syndrome after carotid artery stenting (CAS).
Method
HISPANIAS is a national prospective multicenter study with fourteen recruiting hospitals. Transcranial Doppler sonography (TDS) before and after CAS was recorded. Follow-up was done to detect CHS up to 30 days after carotid artery stenting (CAS). CHS was classified like mild (only cephalea) and moderate-severe (impaired level of consciousness and/or neurological deficit).
Results
A total of 757 CAS were included. Median age was 70.7 yo, 80.3% were men and 81.2% were symptomatic stenosis (mean stenosis: 81.2% ). Any stroke (2.4%) and mortality (0.8%) were 2.9%. Symptomatic CHSs occurred in 22 patients (2.9%), 6 patients had mild CHS (0.8%), and 16 had moderate-severe CHS (2.1%). Five patients had intracranial hemorrhage (0.7%). Baseline preoperative predictors of moderate-severe CHS in multivariate analysis were female gender (OR, 3.243; 95% CI,1.111-9.468; P = .031), left internal carotid artery symptomatic stenosis (OR,4.133;95% CI;1.109-15.402;P = 0.035), older patients (OR, 1.088;95% CI;1.014 -1.169;P = 0.020) and renal insufficiency (OR, 6.288; 95% CI; 1.752-22.569, P = 0.005). AUC of mentioned predictive model for moderate-severe CHS was 0.865 (CI;0.812-0.919).
Conclusion
HISPANIAS study will give some light about the real incidence, outcome and pathophysiology of CHS, and will permit identifying those at highest risk of suffering this complication
Trial registration number
N/A
AS30-001
STATINS AND THE RISK OF INTRACEREBRAL HAEMORRHAGE IN STROKE PATIENTS: SYSTEMATIC REVIEW AND META-ANALYSIS
1UCL Institute of Neurology, Brain Repair and Rehabilitation, London, United Kingdom
2UCL Institute of Neurology, Statistical Science, London, United Kingdom
Background and Aims
Whether statins increase the risk of intracerebral haemorrhage in patients with a previous stroke, especially due to intracerebral haemorrhage, remains controversial. We assessed the impact of statins in patients with previous intracerebral haemorrhage or ischaemic stroke.
Method
Using a comprehensive literature search of MEDLINE, EMBASE, and the Cochrane Library, we systematically reviewed randomised and observational studies (PROSPERO:CRD42017079863). The primary outcome (intracerebral haemorrhage) and secondary outcomes (ischaemic stroke, any-stroke, mortality and function) were meta-analysed using random effects modelling according to stroke-subtype.
Results
Meta-analysis included 43 studies, with a combined total of 317,291 patient-years of follow-up. Statin-users had more diabetes, hypertension and hyperlipidaemia and greater use of anti-coagulant and anti-platelet drugs. In patients with previous intracerebral haemorrhage, compared to control, statins had no significant impact on recurrent intracerebral haemorrhage (RR 1.04, 95%CI 0.86-1.25), ischaemic stroke (1.60, 0.28-9.14) or any-stroke (2.67, 0.90-7.90); however statins were associated with lower risks of mortality (0.49, 0.36-0.67) and poor functional outcome (0.71, 0.67-0.75). In patients with previous ischaemic stroke, statins were associated with a non-significant increase in intracerebral haemorrhage (1.36, 0.96-1.91), but significantly lower risks of recurrent ischaemic stroke (0.74, 0.66-0.83), any-stroke (0.82, 0.67-0.99), mortality (0.68, 0.50-0.92) and poor functional outcome (0.83, 0.76-0.91).
Conclusion
In survivors of intracerebral haemorrhage, statins are not associated with recurrence. In patients with previous ischaemic stroke, although statins were associated with a non-significant increase in intracerebral haemorrhage, they significantly reduced ischaemic stroke recurrence. Irrespective of stroke-subtype, statins significantly improved mortality and functional outcome. Our findings do not support withholding statins after intracerebral haemorrhage.
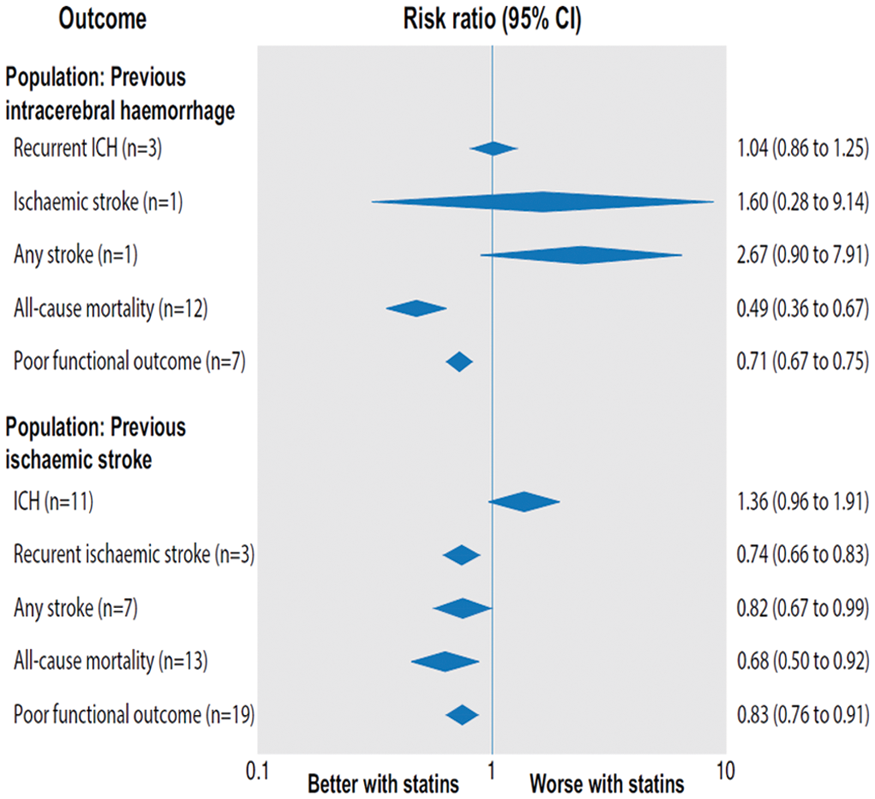
Trial registration number
N/A
Scientific Communications- Reperfusion I
AS06-012
SIMULATION TRAINING IN STROKE THROMBOLYSIS: REDUCING MEDIAN DOOR-TO-NEEDLE TIME TO 13 MINUTES
1Faculty of Health Sciences- University of Stavanger, Department of Neurology- Stavanger University Hospital, Stavanger, Norway
2Neuroscience Research Group- Stavanger University Hospital, Department of Neurology- Østfold Hospital- Kalnes, Fredrikstad, Norway
3Radiological Research Group- Stavanger University Hospital, Department of Radiology- Stavanger University Hospital, Stavanger, Norway
4The Regional Centre for Emergency Medical Research and Development, Department of Anesthesiology and Intensive Care- Stavanger University Hospital, Stavanger, Norway
5No affiliation, Stavanger Acute Foundation for Education and Research, Stavanger, Norway
6Faculty of Health Sciences- University of Stavanger, Department of Anesthesiology and Intensive Care- Stavanger University Hospital, Stavanger, Norway
7Neuroscience Research Group- Stavanger University Hospital, Department of Neurology- Stavanger University Hospital, Stavanger, Norway
Background and Aims
Stroke is a major cause of morbidity and mortality worldwide. In eligible patients with acute ischemic stroke, rapid treatment with thrombolysis is crucial for a good patient outcome. Our primary aim was to assess the effects of a quality improvement project, introducing a new treatment protocol in combination with weekly in-situ simulation-based team training, on door-to-needle times in our stroke unit.
Method
We conducted a survey amongst all stakeholders regarding our preexisting treatment protocol. A panel of experts reviewed responses and suggested changes to streamline the protocol. We introduced the revised protocol together with weekly videotaped in-situ simulation-based team training in February 2017. Our primary outcome measure was the median door-to-needle time. We enrolled 478 patients with suspected acute ischemic stroke treated with intravenous thrombolysis in our analyses, of these 78 patients were treated according to our revised protocol.
Results
Median door-to-needle time was reduced from 27 (IQR 19-41) to 13 minutes (IQR 9–21), p < 0,001) in the 6 months after our intervention. Results remained significant regardless of admission time. There were no significant changes in the rates of stroke mimics, fatal intracranial hemorrhage or prehospital times.
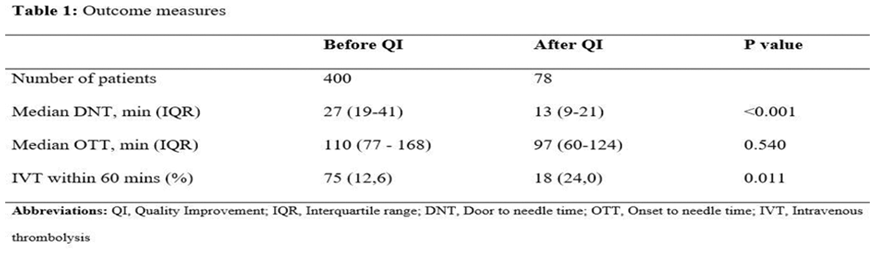
Figure 1: Individual door-to-needle times with group medians before and after quality improvement
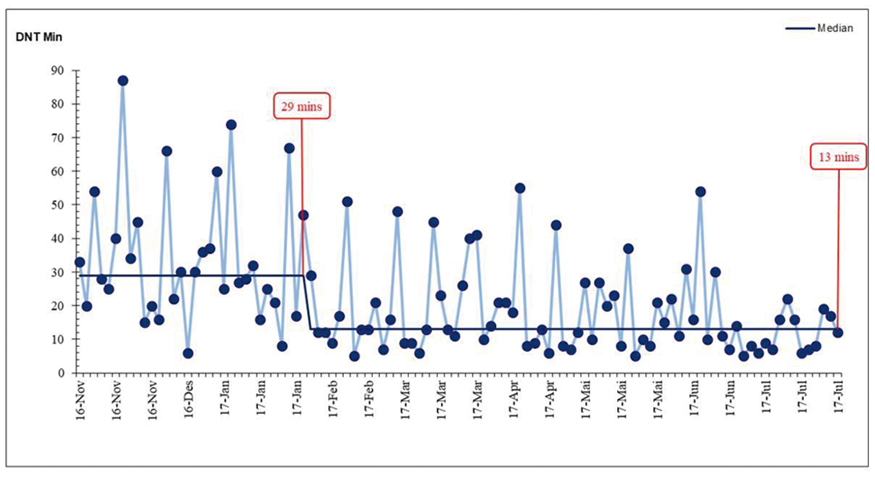
Conclusion
A revised treatment protocol in combination with weekly in-situ simulation-based team training led to a rapid and considerable reduction of median door-to-needle time. In our view, combining protocol change with simulation training is a promising method for reducing door-to-needle times in stroke thrombolysis.
Trial registration number
N/A
AS05-023
EFFECT OF HAEMOGLOBIN LEVELS ON OUTCOME IN IVT-TREATED STROKE PATIENTS
1University Hospital Basel and University of Basel, Stroke Center and Department of Neurology, Basel, Switzerland
2Helsinki University Hospital, Department of Neurology, Helsinki, Finland
3University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
4Centre Hospitalier Universitaire Vaudois and University of Lausanne, Department of Neurology, Lausanne, Switzerland
5Academic Medical Center Amsterdam, Stroke Center and Department of Neurology, Amsterdam, The Netherlands
6Inselspital- Bern University Hospital and University of Bern, Department of Neurology, Bern, Switzerland
7Ospedale Civile S. Agostino-Estense- Modena University Hospital, Stroke Unit- Department of Neuroscience, Modena, Italy
8Clinical Centre of Serbia, Neurology Clinic, Belgrade, Serbia
9Kantonsspital St. Gallen, Department of Neurology, St. Gallen, Switzerland
10Neurology Clinic- University of Brescia, Department of Clinical and Experimental Sciences, Brescia, Italy
11Klinikum der Universität München- Ludwig-Maximilians-University, Department of Neurology, München, Germany
12University of Basel and University Center for Medicine of Aging and Rehabilitation- Felix Platter Hospital, Neurorehabilitation Unit, Basel, Switzerland
Background and Aims
To study the effect of hemoglobin levels (HL) on functional outcome, mortality and bleeding risk in stroke patients treated with IV-thrombolysis (IVT).
Method
In this prospective multicenter, IVT-register based study, we compared HL with 3-month poor outcome (modified Rankin Scale 3–6), mortality and symptomatic intracranial hemorrhage (sICH;ECASS-II-criteria). HL was used as continuous and categorical variable distinguishing anemia (female:<12g/dl; male:<13g/dl) and polyglobulia (female:>15.5g/dl; male:>17g/dl). Anemia was subdivided into mild and severe (female/male:<10g/dl). Normal HL (female:12.0-15.5g/dl, male:13.0-17.0 g/dl) served as reference group. Unadjusted and adjusted odds ratios with 95% confidence intervals (OR[95%-CI]) from the logistic regression models were calculated.
Results
Among 6866 IVT-treated stroke patients, 5448 (79.3%) had normal HL, 1232 (17.9%) anemia – of those 1115 (16.2%) had mild and 117 (1.7%) severe anemia - and 186 (2.7%) polyglobulia. Decreasing HL (by 1g/dl) independently predicted poor outcome (ORadjusted 1.07[1.02-1.11]) and mortality (ORadjusted 1.08[1.02-1.15]). Anemia was associated with poor outcome (ORadjusted 1.25[1.05-1.48]) and mortality (ORadjusted 1.58[1.27-1.95]). However, in anemia subgroups, only severe anemia independently predicted poor outcome (ORadjusted 2.83[1.75-4.59]) but not mild anemia. The odds for mortality were higher in patients with severe (ORadjusted 2.50[1.56-4.02]) than with mild anemia (ORadjusted 1.50[1.12-1.86]. Neither a significant association between anemia and occurrence of sICH was found nor between polyglobulia and any outcome.
Conclusion
Anemia was independently associated with poor outcome and mortality in IVT-treated stroke patients. The more severe the anemia, the higher the probability of poor outcome and death. Severe anemia might be a target for interventions in the hyperacute setting of stroke.
Trial registration number
N/A
AS05-028
ALTEPLASE DOSE FOR ACUTE ISCHAEMIC STROKE: HIGHER ABSOLUTE DOSES ARE ASSOCIATED WITH FAVOURABLE FUNCTIONAL OUTCOMES AND SURVIVAL
1University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
2University of Glasgow, Institute of Neuroscience and Psychology, Glasgow, United Kingdom
3St Anne’s Hospital and Masaryk University, International Clinical Research Centre Neurology Department, Brno, Czech Republic
4Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden
Background and Aims
The optimal safe and efficacious dose of IV alteplase has recently been questioned despite failure of ENCHANTED to confirm non-inferiority of a lower dose. We studied the relation between alteplase dose and stroke outcomes in independent data.
Method
We analysed SITS-International thrombolysis registry data on alteplase-treated patients enrolled 2003-2016, using logistic regression models to examine trends in outcomes across the available range of total alteplase doses within 90mg, compared to a 90mg dose. We adjusted for variables known to influence outcome or found significant in univariate analyses (p < 0.05). Principal outcomes were ordinal day-90 mRS, mortality and SITS-MOST symptomatic ICH (SICH).
Results
57,480 patients were included. The adjusted models showed significant associations between higher doses of alteplase and favourable functional outcomes (p = 0.01 for better day-90 mRS in ordinal analysis) and reduced day-90 mortality (p = 0.03). 1254 patients (69.6%) of 1802 patients who received 85-89.9mg were mRS 0–2 at day-90, compared to 3020 patients (56.2%) of 5374 patients who received 50-54.9mg. The adjusted odds ratio for better day-90 mRS at 85-89.9mg was 1.14 (95% CI 1.03-1.26, p = 0.01), whereas the OR at 50-54.9 mg was 1.00 (0.92-1.07, p = 0.90).
The adjusted OR for survival at 85-89.9mg was 1.36 (95% CI 1.06-1.73, p = 0.02), whereas the OR at 50-54.9mg was 1.04 (0.89-1.22, p = 0.65). There was no association between alteplase dose and SICH (p = 0.82).
Conclusion
Notwithstanding potential confounders, favourable functional outcomes and survival among patients who received higher absolute doses of alteplase, with no effect on SICH, militate against advocating lower doses without robustly supportive RCT evidence.
Trial registration number
N/A
AS05-030
COMPREHENSIVE ANALYSIS ON RATES AND QUALITY OF PRE-INTERVENTIONAL REPERFUSION IN PATIENTS WITH IMMEDIATE ACCESS TO ENDOVASCULAR TREATMENT: PREVALENCE AND PREDICTORS
1Inselspital- University of Bern, Neuroradiology, Bern, Switzerland
2Inselspital- University of Bern, Neurology, Bern, Switzerland
Background and Aims
Pre-interventional reperfusion before endovascular treatment (ET) is a benefit of the bridging approach. However, detailed data on reperfusion quality and rates of obviating ET in a large cohort of patients with immediate access to ET is lacking.
Method
All mothership patients (n = 627) from a prospective registry subjected to angiography with an intention to perform ET were reviewed. Pre-interventional change of occlusion site (COS) was categorized into COS with TICI0/1, COS with TICI≥2a, COS with TICI≥2b, and COS with perfusion worsening. Predictors and clinical relevance were evaluated using multivariate regression.
Results
Prevalence of COS in all patients was 10.7%, subdividing into 2.7% COS with TICI0/1, 6.2% COS with ≥TICI2a (2.9% with TICI≥2b), and 1.8% COS with perfusion worsening. Factors related to COS with ≥TICI2a were IV-tPA (aOR 11.98, 95%-CI 4.5-31.6), cardioembolic thrombus (aOR 2.3, 95%-CI 1.1-4.6) and thrombus length (1mm aOR 0.926, 95%-CI 0.87-0.99). Additional ET was performed despite COS with ≥TICI2a in 51.3%. COS with ≥TICI2a showed a tendency for favorable outcomes (modified Rankin Scale≤2, aOR 2.65, 95%-CI 0.98-7.17). Rates of COS with ≥TICI2a were particularly low in ICA and proximal M1 occlusions (2.2%, 95%-CI 0.9-5%), where tPA was associated with perfusion worsening (aOR 4.33, 95%-CI 1.12-16.80).
Conclusion
Prevalence of pre-interventional reperfusion is non-negligible in patients with direct access to ET and is clearly favored by IV-tPA treatment. However, it is often incomplete, and often requires additional ET. Pre-interventional reperfusion of ICA and proximal M1 occlusions is rare and usually of low quality, where IV-tPA may also promote perfusion worsening.
Trial registration number
N/A
AS05-027
IV THROMBOLYSIS IN STROKE MIMICS - RESULTS FROM THE SITS INTERNATIONAL STROKE THROMBOLYSIS REGISTER (SITS-ISTR)
1Karolinska University Hospital and Karolinska Institutet, Department of Neurology and Department of Clinical Neuroscience, Stockholm, Sweden
2AZ Sint-Jan Brugge-Oostende, Department of Neurology, Brugge, Belgium
3San Giuseppe Hospital, Department of Neurology and Stroke Unit, Milan, Italy
4Iazzolino Hospital, Department of Neurology, Vibo Valentia, Italy
5University of Modena and Reggio Emilia and AOU of Modena, Department of Clinical Neurosciences, Modena, Italy
6UCL St Luc, Unité neuro-vasculaire, Brussels, Belgium
7University Medical School and Hospital, Department of Neurology, Olomouc, Czech Republic
8Nuovo Ospedale Civile S. Agostina Estense di Modena, Department of Neuroscience, Modena, Italy
Background
IV thrombolysis (IVT) is the only approved medical therapy for acute ischemic stroke within 4,5 hours from onset. Stroke mimics, non-stroke patients with stroke-like symptoms, may risk harm if treated with IVT. Current guidelines state low risk of intracranial haemorrhage based on studies comprising a total of <400 mimics.
Aim
To evaluate safety and outcomes following IVT in stroke mimic patients.
Method
We included IVT-treated patients in the SITS International Stroke Thrombolysis Registry (SITS-ISTR) 2003–2017, examined with MRI 22-36 hours after treatment. Baseline characteristics and outcomes were compared between stroke patients and mimics. The primary outcome measure was intracerebral parenchymal hematoma (PH) on any imaging during in-hospital care. Secondary outcomes were symptomatic intracerebral haemorrhage (SICH) per SITS-MOST and ECASS-II, death, and modified Rankin Scale (mRS) 0–1 at 3 months.
Results
Of 10435 patients, 428 mimics (4,1%) were identified. The most common types were functional (30,8%), migraine (17,5%), and seizure (14,3%). Mimics had fewer cerebrovascular risk factors and lower median NIHSS: 7 (IQR 5–10) vs 8 (IQR 5–14), (p < 0,001). Among mimics versus stroke patients, 5 (1,2%) vs 508 (5,1%) had PH (p < 0,001); 2 (0,5%) vs 212 (2,1%) had SICH ECASS-II (p = 0,02); and 0 vs 52 (0,5%) had SICH SITS-MOST, (p = 0,13). mRS 0–1 at 3 months was 84,4% vs 56,7% (p < 0,001), while death within 3 months occurred in 2,6% vs 5,4% (p = 0,03) in mimics and stroke patients respectively.
Conclusion
This large observational study indicates that PH and SICH following IVT in stroke mimics is an uncommon occurrence.
Trial registration number
N/A
AS07-003
SIMPLIFIED MISMATCH CRITERIA FOR PATIENTS WITH LONGER OR UNKNOWN TIME TO TREATMENT PREDICT GOOD OUTCOME AFTER MECHANICAL THROMBECTOMY
1University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
2University Hospital Heidelberg, Department of Neuroradiology, Heidelberg, Germany
Background and Aims
In the recent DAWN trial patients with mismatch between deficit and infarct size and 6 to 24 hours after last seen well benefitted from mechanical thrombectomy (MT). However, the inclusion was based on a sophisticated selection algorithm. We aimed to identify simpler selection criteria.
Method
Within the Heidelberg Recanalisation Registry (HeiReKa) between 2014 to 2016, patients with large vessel occlusion in the anterior circulation that underwent MT within 6 to 24 hours or unknown time from symptom onset were included. Successful recanalization was defined as Thrombolysis in cerebral infarction scale (TICI) >/=2b and good outcome on day 90 as modified Rankin scale (mRS) 0–2. Safety outcomes were mortality on day 90 and symptomatic intracranial hemorrhage (sICH). Modified mismatch criteria were defined as mDAWN (or mHERMES): premorbid mRS 0–1, National Institute of Health Stroke Scale (NIHSS) >/=10 (6) and Alberta Stroke Program Early CT Score (ASPECTS) >/=8 (6).
Results
Of 553 patients, 145 were identified. Median age was 76 years (min-max: 15-95), NIHSS: 15.5 (0–38), ASPECTS: 8 (4–10). In 79.3% of patients time of stroke onset was unknown. Successful recanalization was achieved in 77.2% of patients. In mDAWN patients (n = 35) good outcome (mortality, sICH) was observed in 42.9% (17.1%, 8.6%) in mHERMES patients (n = 69) rates of 40.6%, 17.4% and 5.8% respectively, were observed. The odds ratios (95% confidence interval) for good outcome were 2.3 (1.04-5.1) for mDAWN and 3.02 (1.4-6.4) for mHERMES patients.
Conclusion
Simplified mismatch selection criteria for MT in patients with unwitnessed or wake-up strokes predict good outcome in clinical practice.
Trial registration number
N/A
AS05-024
FACTORS ASSOCIATED WITH SUCCESSFUL RECANALIZATION AFTER IVTPA INITIATED AT LOCAL CENTERS IN ACUTE STROKE PATIENTS WITH LVO TRANSFERRED TO ENDOVASCULAR CENTERS
1Hospital Universitari Germans Trias i Pujol, Neurology- Stroke Unit, Badalona, Spain
2Hospital Vall d'Hebrón, Stroke Unit- Neurology, Barcelona, Spain
3Hospital Germans Trias i Pujol, Stroke Unit- Neurology, Badalona, Spain
4Hospital Bellvitge, Stroke Unit- Neurology, Barcelona, Spain
5Hospital Clínic, Stroke Unit- Neurology, Barcelona, Spain
6Hospital Arnau Vilanova, Stroke Unit- Neurology, Lleida, Spain
7Hospital Josep Trueta, Stroke Unit- Neurology, Girona, Spain
8Hospital Verge de la Cinta, Neurolgy, Tortosa, Spain
9Hospital Parc Taulí, Neurology, Sabadell, Spain
10Hospital Mútua de Terrassa, Neurology, Terrassa, Spain
11Hospital Joan XXIII, Neurology, Tarragona, Spain
12Hospital General de Granollers, Neurology, Granollers, Spain
13Hospital Mataró, Neurology, Mataró, Spain
14Hospital Moisés Broggi, Neurology, Barcelona, Spain
15Agència de Qualitat i Avaluació Sanitàries de Catalunya AQuAS, Pla Director Malaltia Vascular Cerebral de Catalunya, Barcelona, Spain
16Hospital Germans Trias i Pujol, Neurosciences, Badalona, Spain
Background and Aims
To assess the likelihood of and factors associated to successful recanalization after ivtPA of acute stroke patients with large vessel occlusion (LVO) admitted at local stroke centers and secondarily transferred to endovascular centers.
Method
We used data from a government-mandated, prospective registry of Stroke Code activations in Catalonia from 2016 (CICAT). Patients with evidence of LVO using non-invasive techniques at the local center were included in this analysis. Vascular risk factors, stroke severity (NIHSS) and onset-to-treatment time (OTT) were recorded at the local center. Recanalization (absence of LVO on CTA, MRA or angiography) was assessed upon arrival at the endovascular center before EVT decision-making.
Results
Recanalization during transfer was observed in 50 (21%) out of 235 patients with LVO treated with ivtPA at the local center. Recanalization was associated with lower stroke severity (NIHSS<15 35%; NIHSS 15-19 18%; NIHSS>19 11%), faster treatment (OTT<90min 25%; 90-180min 22%; >180min 15%) and site of occlusion (TICA 19%, M1 15%, M2 36%, BAO 38%). Recanalization rate was maximal (>40%) for patients with NIHSS<15 treated within 90min, whereas it was almost absent for patients with combinations of NIHSS 15-19 treated beyond 180min or patients with NIHSS>19 treated beyond 90min (Figure).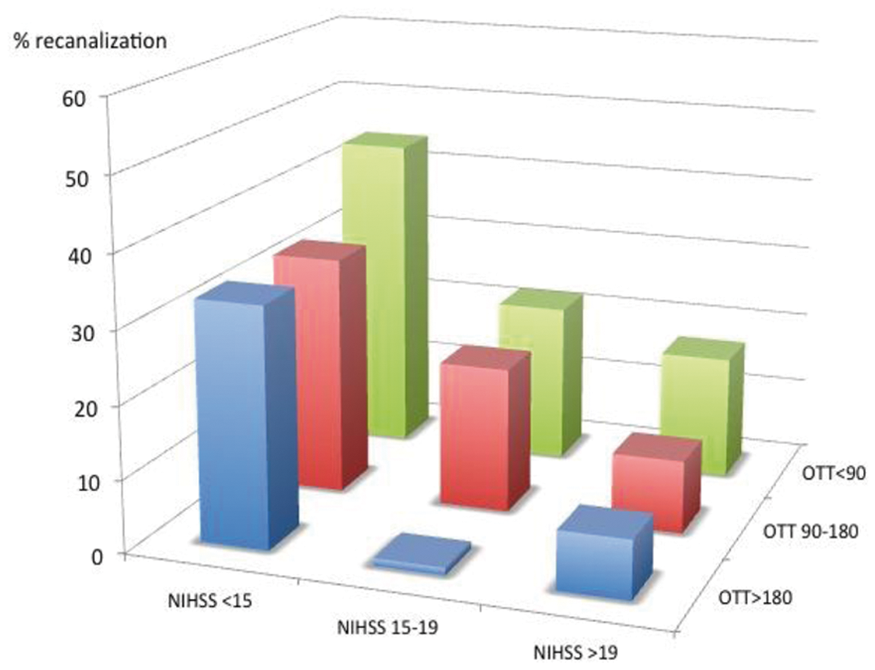
Conclusion
Stroke severity combined with the estimated time from onset to treatment influences the chances of recanalization with ivtPA and should be considered when designing transfer protocols.
Trial registration number
N/A
AS05-013
EARLY RECANALIZATION IN TENECTEPLASE VERSUS ALTEPLASE-TREATED DRIP-AND-SHIP PATIENTS REFERRED FOR THROMBECTOMY
1Centre Hospitalier Sainte Anne, Neurology, Paris, France
2Kremlin-Bicêtre Hospital, Interventional neuroradiology, Kremlin-Bicêtre, France
3Centre Hospitalier du Sud Francilien, Neurology, Corbeil Essonne, France
4Kremlin-Bicêtre Hospital, Neurology, Kremlin-Bicêtre, France
5Fondation Ophtalmologique Adolphe de Rothschild, Interventional neuroradiology, Paris, France
6Foch Hospital, Neurology, Suresnes, France
7Roger Salengro Hospital, Neuroradiology, Lille, France
8Gui de Chauliac Hospital, Neurology, Montpellier, France
9Hospices Civils de Lyon, Stroke Unit, Lyon, France
10Tours Hospital, Neuroradiology, Tours, France
11Nancy Hospital, Neurology, Nancy, France
12Sainte-Anne Hospital, Neuroradiology, Paris, France
Background and Aims
Bridging therapy, i.e., intravenous thrombolysis (IVT) followed by mechanical thrombectomy (MT), is new standard-of-care for acute stroke with large vessel occlusion (LVO). However, delays to recanalization are frequent, particularly in IVT-treated patients transferred for MT from a non MT-capable centre (‘drip-and-ship’ paradigm). Accordingly, it would be of major importance to enhance early recanalization (ER) rate following IVT in the latter scenario. We studied whether tenecteplase 0.25mg/kg, as compared to alteplase 0.9mg/kg, improved pre-MT ER rate in drip-and-ship patients.
Method
Retrospective multicenter cohort study comparing IVT-induced ER rate with tenecteplase 0.25mg/kg vs. alteplase 0.9mg/kg in LVO patients transferred for MT as per the drip-and-ship paradigm. Propensity-score matching was used to reduce the effects of main potential confounders. ER was identified within 3hrs of IVT start on first angiographic run or non-invasive vascular imaging.
Results
816 patients were included (n = 160 and 656 tenecteplase and alteplase-treated patients, respectively). In the propensity score-matched cohort (n = 131 per group), the main confounders for ER were well balanced. ER occurred in 21.4% (95%CI: 15.2-29.2) vs. 18.3% (12.6-25.8) patients in the tenecteplase- and alteplase-treated propensity-adjusted cohorts, respectively (OR = 1.25, 95%CI: 0.65-2.41, P = 0.51). Complementary analyses on the entire cohort found similar results. There was no heterogeneity in treatment effect size in key subgroups.
Conclusion
We found that ER rate following IVT with tenecteplase 0.25mg/kg or alteplase 0.9mg/kg did not differ in stroke patients with LVO intended for MT as per the drip-and-ship paradigm. Considering the practical convenience of tenecteplase, however, RCTs testing the non-inferiority of tenecteplase on clinical outcome are now warranted.
Trial registration number
N/A
AS05-018
OUTCOMES OF INTRAVENOUS THROMBOLYSIS FOR ACUTE ISCHEMIC STROKE IN PATIENTS ON DUAL ANTIPLATELET THERAPY PRIOR TO STROKE ONSET: A PROPENSITY SCORE MATCHED ANALYSIS
1“Attikon University Hospital”- National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece
2University of Tennessee Health Science Center, Department of Neurology, Memphis, USA
3University of Ioannina School of Medicine, Department of Neurology, Ioannina, Greece
4University of Ioannina, Department of Primary Education, Ioannina, Greece
5P.J. Šafárik University- Faculty of Medicine, Department of Neurology, Košice, Slovak Republic
6Institute of Psychiatry and Neurology, Second Department of Neurology, Warsaw, Poland
7University of Aberdeen, Division of Applied Medicine, Foresterhill, United Kingdom
8Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
9Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
10Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden
Background and Aims
We assessed the outcomes of intravenous thrombolysis (IVT) in acute ischemic stroke (AIS) patients on dual antiplatelet therapy prior (DAPP) to stroke onset.
Method
We analyzed prospectively collected data from the SITS International Stroke Thrombolysis Register (SITS-ISTR) on consecutive AIS patients treated with IVT using tissue-plasminogen-activator (tPA) during a seven-year period (2010-2017). In propensity-score-matched (PSM) groups of patients with DAPP (DAPP+) and no antiplatelet pretreatment we compared: 1) SICH rates, according to SITS-MOST, ECASS II and NINDS definitions, 2) 3-month mortality, 3) 3-month favorable functional outcome (FFO; mRS-score:0-1), 4) 3-month functional independence (FI; mRS-score:0-2) and 5) distribution of the 3-month mRS scores. DAPP was defined as all possible combinations between aspirin, clopidogrel, dipyridamole or any other antiplatelet therapy.
Results
PSM resulted in two groups of 1043 patients each, balanced for all baseline characteristics. In PSM analysis DAPP+ patients had higher SICH rates according to the SITS-MOST definition compared to DAPP- patients (2.9% vs. 1.5%, p = 0.037) , while no significant differences between the two groups were found according to ECASS II (5.2% vs. 4.4%, p = 0.354) or NINDS definitions (7.7% vs. 6.6%, p = 0.318). No differences in the 3-month mortality (16.6% vs. 17.9%, p = 0.417), FFO (45.6% vs. 46.0%, p = 0.860), FI rates (59.2% vs. 60.7%, p = 0.503) or the distribution in 3-month mRS-scores (p = 0.683) were documented.
Conclusion
Although DAPP is associated with higher risk of SICH in AIS patients treated with IVT, three-month mortality and functional outcomes are not affected. DAPP history should not be used as a reason to withhold IVT in otherwise eligible AIS patients.
Trial registration number
N/A
Scientific Communications Epidemiology
AS15-035
TEMPORAL TRENDS OF STROKE EPIDEMIOLOGY IN SOUTHERN SWEDEN - A POPULATION-BASED STUDY ON STROKE INCIDENCE AND EARLY CASE-FATALITY
1Lund university, Department of Clinical Sciences- Neurology, Lund, Sweden
Background and Aims
Up-to-date epidemiological stroke studies are important for healthcare planning and evaluating prevention strategies. This population-based study investigates temporal trends in stroke incidence and case-fatality in southern Sweden.
Method
First-ever stroke cases in the local catchment area of Skåne University Hospital in Lund, Sweden, between March, 2015 and February, 2016, were included from several sources, including two prospective hospital-based registers, retrospective screening of primary care visits, and autopsy registers. Stroke incidence and 28-day case-fatality rates were compared with corresponding data from this area obtained using similar methodology between March, 2001 and February, 2002.
Results
Altogether, 456 and 413 first-ever stroke patients were identified during the earlier and later time periods, respectively. The age- and sex-standardized stroke incidence rates decreased from 246 (95% CI: 224-270) to 165 (95% CI: 149-182) per 100 000 person-years. However, the incidence remained unaltered among those <65 years. Incidence rates of ischemic stroke decreased from 197 (95% CI: 177-218) to 134 (95% CI: 120-149) per 100 000 person-years, whereas rates of intracerebral and subarachnoid hemorrhage remained unchanged. Early case-fatality decreased from 14% to 11% (p = 0.165).
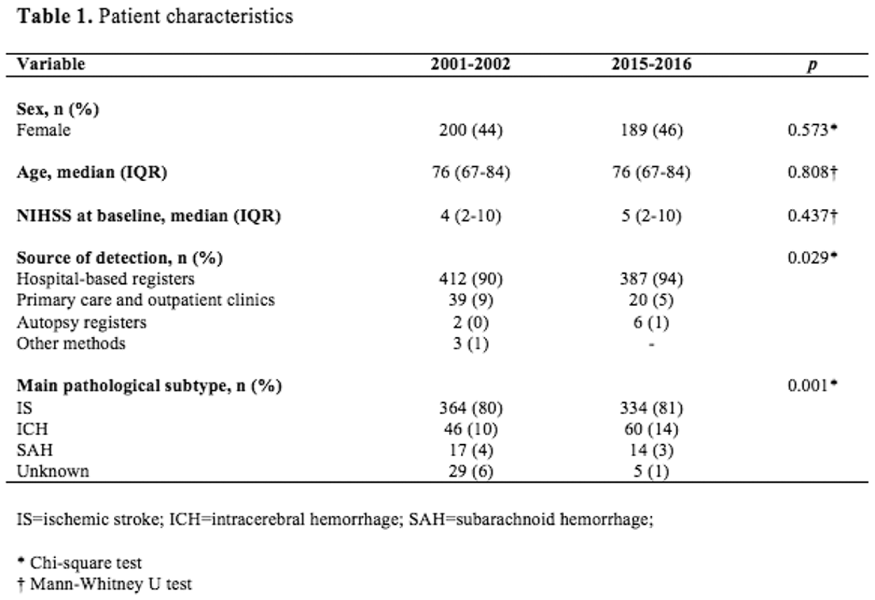
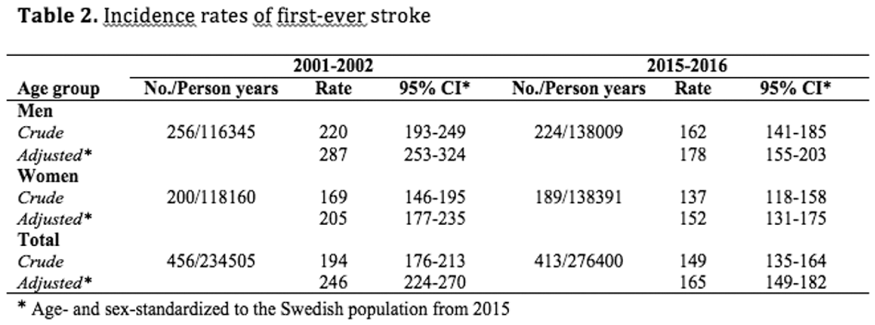
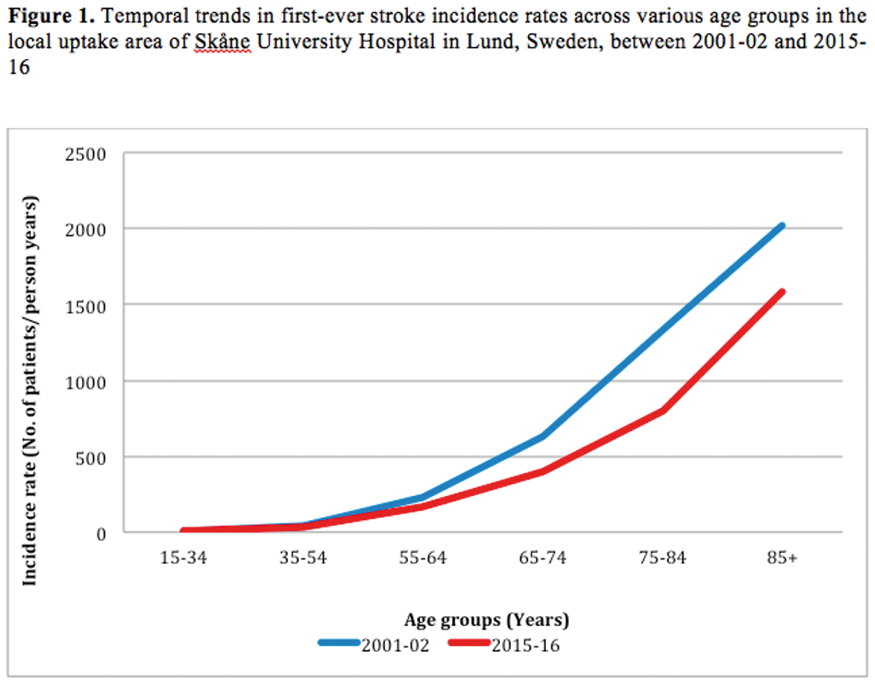
Conclusion
First-ever stroke incidence in southern Sweden has decreased with 33% since the beginning of this millennium. Stroke incidence rates have decreased among the elderly but remain unchanged among younger age groups. Ischemic stroke rates have decreased while rates of intracerebral and subarachnoid hemorrhage have remained static. Our findings warrant further studies on trends in risk factor profiles and effects of prevention strategies in the population, and heightened focus on stroke in the young.
Trial registration number
N/A
AS15-049
RISK FACTORS OF STROKE IN YOUNG ADULTS FROM A WORLDWIDE PERSPECTIVE. THE GLOBAL OUTCOME AFTER STROKE AT YOUNG AGE (GOAL)-INITIATIVE
1Radboudumc, Neurology, Nijmegen, The Netherlands
2University Lille Nord de France, Neurology, Lille, France
3University of Bordeaux- Inserm- Bordeaux Population Health Research Center- team VINTAGE- UMR, Neurology, Bordeaux, France
4Hospital Egas Moniz- Centro Hospitalar Lisboa Ocidental., Neurology, Lisbon, Portugal
5University of Bern- Kantonsspital Aarau, Neurology, Bern, Switzerland
6Veterans Affairs Maryland Health Care System- University of Maryland School of Medicine, Neurology, Baltimore, USA
7Stroke Center- University of South Florida, Neurology, Tampa, USA
8Hospital Civil de Guadalajara Fray Antonio Alcalde, Neurology, Guadalajara, Mexico
9National Institute of Neurology and Neurosurgery of Mexico- Manuel Velasco Suárez, Neurology, Mexico city, Mexico
10Chang Gung Memorial Hospital- LinKou Medical Center, Neurology, Tao-Yuan, Taiwan R.O.C
11Haukeland University Hospital, Neurology, Bergen, Norway
12University of Malaya Medical Centre, Neurology, Kuala Lumpur, Malaysia
13Helsinki University Central Hospital, Neurology, Helsinki, Finland
14University of Brescia, Neurology, Brescia, Italy
15G.B. Pant Hospital, New Delhi, India
16Nelson R. Mandela School of Medicine, Inkosi Albert Luthuli Central Hospital, Mayville, South-Africa
17Istanbul Faculty of Medicine, Istanbul University, Turkey
18Medical University of Graz, Austria
19Christchurch Hospital, New-Zealand
20Vrije Universiteit Brussel, ZorgSaam Hospital Terneuzen, Belgium
21University of AdelaideQueen Elizabeth Hospital, Adelaide, SA Queen Elizabeth Hospital, Adelaide, SA Queen Elizabeth Hospital, Adelaide, SA, Australia
22University of Adelaide, Australia
23Hanyang University, College of Medicine, Seoul, South-Korea
24SARAH Hospital of Rehabilitation, Asa Sul, Brasilia
25Ashford and St Peter's Hospitals NHS Foundation Trust, Surrey, United Kingdom
26Sheba Medical Center, Sagol Neuroscience Centre, Tel-Hashomer, Israel
27Ernst Moritz Arndt University, Greifswald, Germany
28University of Tartu, Estonia
29University of Toronto, Sunnybrook Health Sciences Centre, Canada
Background and Aims
Two million patients suffer a stroke at age 18 to 50 years each year, with geographical variation in prevalence. Little is known about risk factors and etiology underlying this difference.
Method
The GOAL initiative aims to investigate risk factors, etiology and prognosis after stroke in young adults from patients of all continents. Inclusion criteria were: age < 50 years with a first-ever stroke (both ischemic and hemorrhagic). Risk factors and etiology were defined according to diagnostic criteria. We analyzed baseline characteristics, risk factors by geographical location (Table 1), recurrent vascular events and mortality.
Results
8913 patients (405 TIA patients, 122 intracerebral hemorrhage patients and 8386 ischemic stroke patients) were included from 13 countries in 6 continents. 54.5% of patients were men. Mean age was 39.4 years old (SD 8.1 years). There were 1078 patients without any vascular risk factor. There was huge variation in the prevalence of vascular risk factors, which were less prevalent in South-America and South-Europe and most prevalent in Oceania. 10.2% of 5738 patients got a recurrent stroke, whereas 16.4% of 4239 patients got any recurrent vascular event during a mean follow-up period of 83.7 months (SD 74.5 months). Mortality was highest after intracerebral hemorrhage (36.2%; n = 94), whereas 9.0% (n = 5816) died after a TIA/ischemic stroke.
Conclusion
Stroke at young age occurs worldwide and has high mortality, especially intracerebral hemorrhage. Cardiovascular risk factors are highly prevalent among young age already, though with huge variability worldwide. Future studies will unravel geographical differences in the etiology of young stroke.
Trial registration number
N/A
AS16-114
PROGNOSTIC IMPLICATIONS OF ADDITIONAL POST-STROKE DISABILITY IN PATIENTS WITH PRE-MORBID DISABILITY: POPULATION-BASED COHORT STUDY
1University of Oxford, Centre for Prevention of Stroke and Dementia- Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
2University of Oxford, Health Economics Research Centre- Nuffield Department of Population Health, Oxford, United Kingdom
Background and Aims
Patients with pre-morbid disability (generally defined as modified Rankin Scale score (mRS) ≥2) are often excluded from trials of intervention in acute stroke. However, increased disability in patients who already have some pre-morbid disability may well impact on long-term outcomes if treatments are withheld in routine clinical practice. We assessed the extent to which increased disability post-stroke influences 5-year mortality and institutionalization in pre-morbidly disabled patients.
Method
In a population-based, prospective cohort of ischaemic stroke patients (Oxford Vascular Study, 2002-2014), we tracked mortality and institutionalization (nursing or residential care-home admission) during follow-up. We used Cox regressions (adjusted for age/sex/initial NIHSS) to compare 5-year mortality and/or new post-stroke institutionalization in 3-month survivors with pre-morbid mRS of 2–4 (excluding extreme disability, mRS = 5), based on degree of change in mRS (ΔmRS) from pre-stroke to 3-months post-stroke.
Results
Among 1,607 patients, 530 (33.0%) had pre-morbid mRS = 2-4. Only 2 pre-morbidly disabled patients received thrombolysis, but 421 (79.4%) were alive at 3-months. ΔmRS predicted 5-year mortality/institutionalization (aHR for ΔmRS 1 vs 0: 1.59, 1.20-2.11; ΔmRS 2: 2.39, 1.62-3.53; ΔmRS 3: 4.12, 1.98-8.60, p < 0.001). Results were similar in patients with pre-morbid mRS 2, 3, and 4 separately (e.g. 5-year mortality/institutionalization aHR for pre-morbid mRS 3 with ΔmRS 1: 1.60, 1.06-2.42, p = 0.027; ΔmRS 2: 3.20, 1.85-5.54, p < 0.001).
Conclusion
Stroke patients with pre-morbid disability have greater mortality and institutionalization if they accumulate additional disability due to the stroke. Trials should ideally include patients with mild-moderate pre-stroke disability, and pre-morbid disability should not in itself preclude acute interventions in practice.
Trial registration number
NA
AS15-043
SERUM CHOLESTEROL PROFILES AND NEW PROGRESSION OF CAROTID PLAQUE IN THE GENERAL JAPANESE POPULATION: THE SUITA STUDY
1National Cerebral and Cardiovascular Center, Preventive Cardiology, Suita, Japan
Background and Aims
We first showed that the new progression of incident carotid plaque is a risk factor for cardiovascular disease (CVD), but no prospective study on the association between serum cholesterol levels and carotid plaque progression in a general population was available.
Method
We studied 4,724 Japanese individuals (mean age 59.7 years) without CVD whose intima-media thickness (IMT) underwent carotid ultrasonography on both sides of the entire carotid artery areas during April 1994 to August 2001. We excluded carotid plaque (n = 1,044), lost to follow-up (n = 167), and missing data (n = 2). Carotid plaque was defined as: common carotid artery's maximum IMT >1.1 mm. Carotid ultrasonographic follow-ups for 3,511 subjects were performed every two years until March 2016. Cardiovascular-risk adjusted Cox proportional hazard regression models were used to determine the carotid plaque risk based on cholesterol levels.
Results
During 38,454 person-years of follow-up, 1,771 instances of carotid plaque progression occurred. Compared to subjects with total cholesterol <160 mg/dL, the adjusted hazard ratios (HRs, 95%CI) for incident carotid plaque were 1.28 (1.02-1.60), 1.54 (1.19-1.98), and 2.06 (1.39-3.07) in subjects with 160-239, 240-279, and >280mg/dL, respectively. Compared to the HDL cholesterol=35-49mg/dL group, the corresponding values were were 1.58 (1.15-2.16) and 0.84 (0.73-0.95) in the <35 and >60mg/dL groups, respectively. Low non-HDL (<130mg/dL) and LDL (<100mg/dL) cholesterol levels were inversely associated with incident carotid plaque.
Conclusion
This is the first demonstration that total, LDL, and non-HDL cholesterol were positively and HDL cholesterol was inversely associated with incident carotid plaque in a general population.
Trial registration number
n/a
AS15-042
EMBOLIC STROKES OF UNDETERMINED SOURCE IN THE SOUTH LONDON STROKE REGISTER: A POPULATION BASED COHORT STUDY
1King's College London, School of Population Health & Environmental Sciences, London, United Kingdom
2St Thomas' Hospital- Kings College London, Stroke Unit, London, United Kingdom
Background and Aims
Embolic stroke of undetermined source (ESUS) is a recent clinical construct with limited information available on long-term prognosis.
Method
Data were collected from the population-based South London Stroke Register of first-ever strokes in an inner London area. ESUS were defined according to the Cryptogenic Stroke/ESUS International Working Group criteria.
Results
2,835 patients registered between 1/01/2000 and 31/12/2016. 252 (8.9%, 95%CI 7.9%-9.0%) were ESUS, mean age for this group 60y ± 17.1; 61% [55.0%-67.0%] were male; 60.5% [53.4%-65.4%] were white. ESUS were younger and had lower prevalence of hypertension than Large Artery Atherotrhombotic (LAA), Cardioembolic (CE), and Small vessel occlusion (SVO). Compared to CE, ESUS were more common in black ethnic groups and had lower prevalence of atrial fibrillation and ischaemic heart disease. ESUS had milder strokes (median NIHSS 6, IQR 2–11), compared to LAA (7, 3–13, p = 0.01) and CE (8, 4–18, p < 0.001), but more severe than SVO (4, 3–6, p < 0.001). Median follow-up was 4.6 years (range: 0–16). After adjustment for demographic, clinical and treatment covariates, no difference was found on functional outcome at 1 or 5 years and ESUS experienced lower all-cause mortality than LAA (HR 0.62 95%CI 0.45-0.87) and CE (HR 0.53 95%CI 0.40-0.71), but no significant difference in number of recurrences or time to first recurrence was found.
Conclusion
ESUS patients were younger, more commonly male, had similar functional outcomes to other subtypes, and had lower mortality than LAA and CE.
Trial registration number
N/A
AS15-053
IMPACT OF EXERCISE BLOOD PRESSURE ON STROKE RISK IN PHYSICALLY FIT AND UNFIT MEN RESULTS FROM 35 YEARS FOLLOW-UP OF HEALTHY MIDDLE-AGED MEN
1Oslo University Hospital Ullevål, Department of Cardiology, Oslo, Norway
2University of Oslo, Department of Informatics, Oslo, Norway
3University of Oslo, Department of Medicine, Oslo, Norway
Background and Aims
Resting blood pressure is a major risk factor for stroke and exercise blood pressure (BP) has been shown to be a strong independent predictor of stroke in our cohort . In the present study we investigate if maximal systolic BP’s ability to predict stroke is influenced by cardiorespiratory fitness (CRF).
Method
2014 healthy men, aged 40-59 years were enrolled between 1972-75. Baseline examination included a maximal exercise test. All men were followed for 35 years. They were grouped according to high or low fitness (above/below age-adjusted median), and further for quartiles of maximal BP. Multi-adjusted Cox regression analyses (also adjusted for resting BP) were used to estimate risks for stroke.
Results
During follow-up 316 first-time strokes occurred and no participants were lost. Among men with high CRF, the highest quartile of maximal BP had a higher risk of stroke than the lowest quartile (hazard ratio 1.75, confidence interval 1.06-2.94, p = 0.03). Among men with low CRF, the highest quartile of maximal systolic BP had a non-significantly higher risk of stroke than the lowest quartile (HR 1.50, CI 0.91-2.63, p = 0.11).
Conclusion
In healthy middle-aged men, maximal systolic BP predicted stroke in men with high cardiorespiratory fitness, independently of resting systolic BP. In men with low CRF the association was not significant, but there was no evidence of a qualitative different effect in this subgroup.
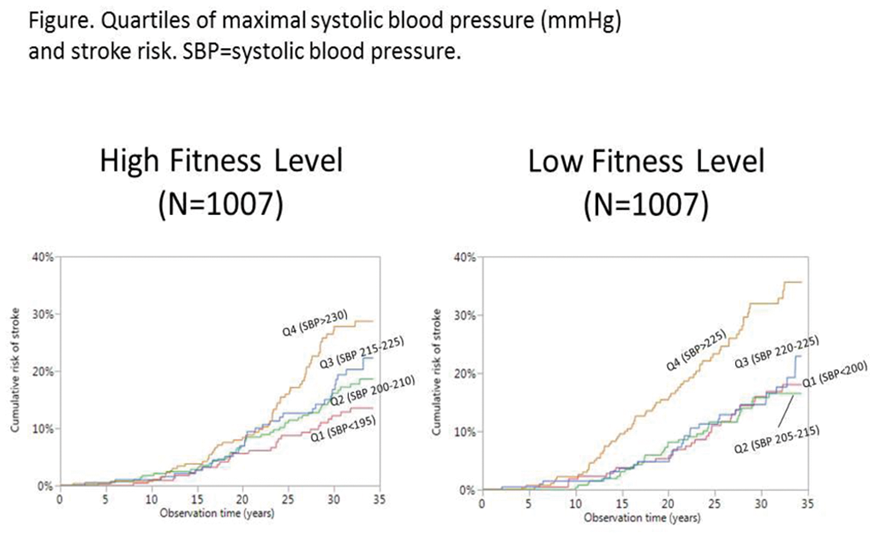
Trial registration number
N/A
AS15-016
RESOURCES USE AND COSTS BEFORE AND AFTER ISCHEMIC STROKE. A POPULATION-BASED STUDY USING ADMINISTRATIVE DATASETS
1University Hospital Vall d'Hebron, Cardiovascular Epidemiology Unit, Barcelona, Spain
2Information and Knowledge Unit, Catalan Health Service, Barcelona, Spain
3Agency for Health Quality and Assessment of Catalonia, Department of Health, Barcelona, Spain
4Stroke Programme, Agency for Health Quality and Assessment of Catalonia, Barcelona, Spain
Background and Aims
Despite improved survival rates, stroke accounts for increasing health and socioeconomic burden. We compared resources use and costs one year before and three years after stroke in a population-based dataset.
Method
Using administrative datasets contained in the Catalan Health Service Surveillance System, we identified patients with ischaemic strokes occurred between Jan 2012 and Dec 2016. For each patient, information from one year before the episode and up to three years post-stroke was linked across databases.
Results
36,058 ischaemic stroke patients were identified with mean age (SD) of 74.4 (13.3). At three years 62% of patients survived. Average cost per patient was €4,121 the year before, €14,536 the first year after the event, €4,942 the second year, and €4,641 the third year post-stroke. Major drivers of cost were acute hospitalisations within the first year (including index hospitalization), representing 46% of the excess costs following stroke (vs pre stroke), and convalescence and rehabilitation services, representing 31% of excess costs. After the first year, the major excess cost was driven by new hospital admissions and higher drug treatment needs. (Figure)
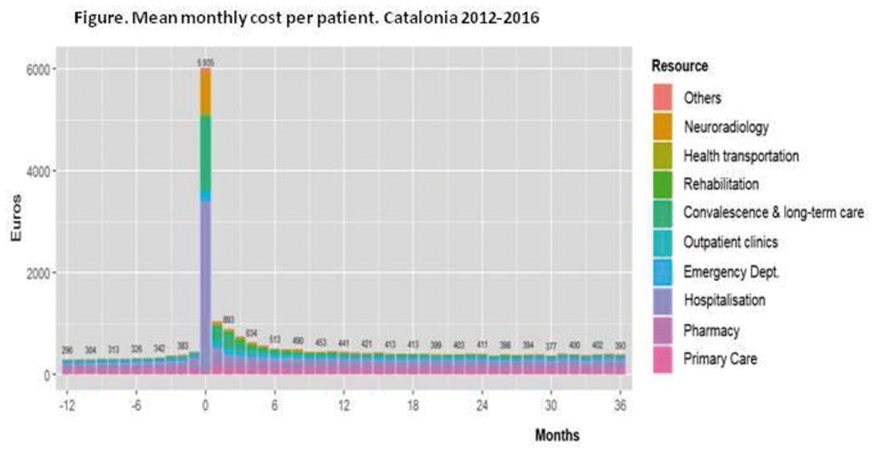
Conclusion
After stroke, healthcare costs increase primarily because of initial hospitalization. Beyond the first year, the cost decreases but remains above baseline values. Such information might be used for a better planning of stroke services.
Trial registration number
N/A
AS20-045
TEMPORAL TRENDS IN INTRACEREBRAL HEMORRHAGE - A CALL FOR ACTION. EVIDENCE FROM THE AUSTRIAN STROKE REGISTRY
1Krankenanstalt Rudolfstiftung, Department of Radiology, Vienna, Austria
2Danube University Krems, Department for Clinical Neurosciences and Preventive Medicine, Krems, Austria
3Hospital of St. John of God, Department of Neurology, Vienna, Austria
4Sigmund Freud University Vienna, Medical Faculty, Vienna, Austria
5Hospital of St. John of God, Department of Neurology, Eisenstadt, Austria
Background and Aims
Data on temporal trends in intracerebral hemorrhage (ICH) are scarce. We aimed to assess changes in incidence, severity, complications, therapy and outcome of intracerebral hemorrhage in patients treated on stroke units in Austria.
Method
Eight-year collective data of 6707 cases of ICH including age, risk factors, pre-stroke modified Rankin Score (mRS), baseline stroke severity (NIHSS), complications, therapy, functional outcome and mortality were extracted from the Austrian Stroke Registry. Multivariate regularised logistic regression models were used for statistical and time trending analyses. Bonferroni correction was applied to correct for multiple testing.
Results
Between 2008 and 2016, the relative frequency of ICH admissions to stroke units in Austria declined, with a shift among affected patients towards older age (>70 years, p = 0.005). While no significant time trends in risk factors, admission NIHSS, pre-stroke mRS and complications were observed, therapeutic interventions (e.g., continuous i.v. therapy, low dose heparin, nasogastric intubation, urinary catheterisation) declined (p < 0.001). Three-month mortality increased over the years independently (p = 0.002).
Conclusion
Despite declining incidence and unaltered clinical severity of ICH we observed a clear increase in three-month mortality. The effect seems to be independent of predictors including age, admission NIHSS, premorbid MRS or clinical complications. This observation underlines an urgent call for action in the therapy of ICH.
Trial registration number
N/A
AS15-009
LONG-TERM TRENDS IN INCIDENCE AND RISK FACTORS OF ISCHAEMIC STROKE TOAST SUBTYPES: THE SOUTH LONDON STROKE REGISTER (SLSR)
1King's College London, Populaiton Health and Environmental Sciences, London, United Kingdom
2Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, NIHR Biomedical Research Centre, London, United Kingdom
Background and Aims
To estimate long-term trends in incidence, risk factors, and preventive treatments for ischaemic stroke aetiological subtypes.
Method
Data from the South London Stroke Register (SLSR) between 2000 and 2015 were studied. Ischaemic strokes (IS) were classified based on Trial of Org 10172 in Acute Stroke Treatment (TOAST) into large artery atherosclerosis (LAA), cardio-embolism (CE), small vessel occlusion (SVO), or other causes. After calculation of the annual and quadrennial age-, sex-, and ethnicity-specific incidence rates by subtype for the 16-year period, we analysed the trends using Cochran-Armitage tests, Poisson regression models, and locally estimated scatterplot smoothers (loess). Multiple logistic regressions were performed to further investigate the changes in pre-stroke risk factors.
Results
A total of 3088 patients with IS were registered. Between 2000-03 and 2012-15, IS incidence decreased by 43% from 137·3 to 78·4 /100,000/year (relative incidence 0·57, 95% CI 0·5-0·64). Significant declines were observed in all subtypes, particularly in SVO (37·4–18; p < 0·0001) and less in CE (39·3–25; p < 0·0001). Reductions were significant in males, females, and white people, but not in black groups (144·6–116·2; p = 0·31). Despite the increasing prevalence of hypertension and atrial fibrillation, preventive use of antihypertensive and antiplatelet drugs was declining. On the other hand, a fourfold increase in prior use of cholesterol-lowering agents was found (adjusted odds ratio 3·96, 95% CI 2·98-5·29).
Conclusion
Incidence rates have declined over time among ischaemic stroke subtypes, but not in black groups. Life style changes and the increasing use of cholesterol-lowering agents may have contributed to the observed trends.
Trial registration number
N/A
Scientific Communications Rare Causes and Stroke in the Young
AS19-024
STROKE IN YOUNG ADULTS: CANCER IN DISGUISE?
1Radboud University Medical Center- Donders Institute for Brain- Cognition and Behavior, Neurology, Nijmegen, The Netherlands
2Elisabeth-TweeSteden Hospital, Neurology, Tilburg, The Netherlands
3Julius Center for Health Sciences and Primary Care- University Medical Center Utrecht, Cardiovascular Epidemiology, Utrecht, The Netherlands
Background and Aims
An association between stroke and malignancy has been established. Underlying mechanisms include direct infiltration, a hypercoagulable state, and non-bacterial thrombotic endocarditis. Malignancy may follow stroke when these mechanisms prove to be true, especially in young adults, where one third of ischemic strokes remain cryptogenic. We therefore investigated the cumulative risk of developing cancer post-stroke.
Method
We created a cohort of first-ever stroke patients from 1998 to 2010 using data from Statistics Netherlands. Information on stroke and malignancy was extracted using ICD-9 and ICD-10 codes. We calculated post-stroke cancer incidence among patients without prior cancer. Subsequently, we obtained standardized incidence ratios (SIR) by comparing this to cancer incidence in the general population based on the Dutch Cancer Registry, particularly in young adults aged 15-49.
Results
Of all young stroke patients, 2.6% was diagnosed with post-stroke cancer over a median follow-up of 9.5 (IQR 6.1-13.2) years. Over the course of 13 years, 219,636 people without history of cancer suffered a first-ever stroke, 6.8% of which were young adults (median age 44 ± 7.2; 53.1% women). Overall SIR was 3.1 for all stroke patients and 4.8 for young stroke patients specifically, where SIR was 5.8 one year post-stroke and 3.3 five years post-stroke.
Conclusion
Young stroke patients are almost five times more likely to receive a cancer diagnosis than their age-matched controls of the general population during the same time period. The risk is highest within the first year after index stroke, suggesting a role for previously undetected cancer in stroke etiology.
Trial registration number
N/A
AS19-028
IS REACTIVATION OF LATENT HSV-1 THE CAUSE OF MOST FIBROMUSCULAR DYSPLASIA (FMD)?
1University of Colorado School of Medicine, Neurology, Aurora, USA
Background and Aims
Fibromuscular Dysplasia (FMD) is an enigmatic disorder primarily of women in their childbearing years. The etiology and pathophysiology of FMD are unknown although hormonal and viral factors are suspected to play a role. FMD changes may be non-specific, making categorization problematic. Recent interest in latent virus reactivation, especially herpes simplex virus type 1 (HSV-1) and varicella zoster virus (VZV) as causes of arteriopathy and stroke may explain some pediatric and young adult strokes
Method
Patient with non-atherosclerotic cerebrovascular arteriopathy and FMD-like changes were reviewed along with other non-FMD arteriopathies (Moya-Moya, RCVS, CNS Vasculitis, other). Those with FMD-like changes from Genetic Disorders were grouped separately. This included two patients with EDS, one with PHASE, and a Loeys-Dietz Type III. The FMD patients were divided into those with an acute symptomatic diagnosis, and those found incidentally.
Results
Of the 17 with FMD, all 11 of the incidental diagnosis group have convincing remote HSV-1 reactivation evidence, and the 7 with acute symptomatic FMD all have serological or clinical evidence of current HSV-1 reactivation. Of patients with FMD-like changes from genetic disorders. Only 1 of 4 has convincing HSV-1 activity. Of the 8 with non-FMD non-atherosclerotic arteriopathy who had serological studies, only 4 had HSV-1 evidence, and 2 HSV-2.
Conclusion
For cerebrovascular FMD, HSV-1 is an ideal candidate virus to pursue as the etiology of FMD. Characterization of FMD into Genetic and/or Viral arteriopathy can be a first step in better understanding the pathophysiology. Further, reactivation of latent herpesviruses is treatable.
Trial registration number
N/A
AS23-021
CHRONIC COGNITIVE ALTERATIONS AND THEIR LINKS WITH BRAIN ATROPHY IN SUSAC SYNDROME
1Hôpital Lariboisière, Neurology, Paris, France
2Clinique Alleray-Labrouste, Imaging Department, Paris, France
3Bichat Hospital, Internal Medicine, Paris, France
Background and Aims
Susac syndrome is a very rare endotheliopathy affecting small vessels of the brain, retina and cochlea, characterized by relapsing episodes of encephalopathy in young patients. We aimed at determining the profile of chronic cognitive alterations and their relationship with brain atrophy in this disorder.
Method
We included 19 patients evaluated prospectively in the French referral centre for Susac syndrome in Bichat hospital in Paris. In 2017, they were evaluated remote to the last relapse with a specific neuropsychological battery. We used validated techniques to obtain brain volume and corpus callosum area from 3D-T1 MRI sequences, and test their outcome overtime. We used linear regression models to test the links between cognitive performances and atrophy measures.
Results
The 19 patients were aged 37.5 ± 10.5 years at inclusion. After a mean follow-up of 2.6 ± 1.3 years during which they underwent 5.8 ± 2.2 MRI scans, their mean MOCA score was 25.1 ± 3.6, but they showed clear processing speed slowing (Trail Making Test version A: 43.1 ± 16.2 seconds; version B: 84.1 ± 47.9 seconds; reaction time: 314.6 ± 79.6 milliseconds). Brain and corpus callosum atrophy were obvious and linearly related with time (2.1 ± 1.4% per year and 4.9 ± 7.7% per year respectively). No relationship was found between cognitive performances and brain volume or corpus callosum area.
Conclusion
Patients with Susac syndrome show largely preserved global cognitive functions but prominent processing speed slowing. While brain and corpus callosum area atrophy are of the highest amplitude, we did not find any relationship with cognitive performances, which questions the links between neuronal loss and cognitive disturbances in this disorder.
Trial registration number
N/A
AS19-032
ASSOCIATION BETWEEN CEREBRAL VENOUS THROMBOSIS AND DURAL ARTERIOVENOUS FISTULAS
1Sahlgrenska Academy at University of Gothenburg, Institute of Neuroscience and Physiology- Department of Clinical Neuroscience, Gothenburg, Sweden
2Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
3Instituto Nacional de Neurología and Neurocirugía Manuel Velasco Suárez, Stroke Clinic, Mexico City, Mexico
4Sahlgrenska University Hospital, Diagnostic and Interventional Neuroradiology, Gothenburg, Sweden
5Helsinki University Hospital, Department of Neurology, Helsinki, Finland
6University Hospital Bern, Deptartment of Neurology, Bern, Switzerland
7Academic Medical Center, Department of neurology, Amsterdam, The Netherlands
8Royal Adelaide Hospital, Department of stroke and neurology, Adelaide, Australia
9Hamedan University of Medial Science, Department of Neurology, Hamedan, Iran
10University Hospital of Toulouse, Department of Neuroradiology- Service de Neuroradiologie Diagnostique et Thérapeutique du CHU de Toulouse, Toulouse, France
Background and Aims
Several case reports observed the occurrence of dural arteriovenous fistulas (dAVF) prior to, simultaneously, or subsequently to the diagnosis of cerebral venous thrombosis (CVT). We aimed to investigate the association between dAVF and CVT in a multi-center setting.
Method
Consecutive adult patients diagnosed with CVT were included retrospectively from seven academic hospitals. The prevalence of dAVF was determined in the study population. Clinical features and imaging characteristics were obtained from medical records. Poor outcome was defined as modified Rankin Scale (mRS) score ≥3 at last follow-up. We are presenting unadjusted data calculated using Chi² or Fisher’s test.
Results
Among 1052 CVT patients, (median 42y, IQR 29-54y, 67.3% female), 32 patients (3.0%) were diagnosed with dAVF. Median follow-up time was 254 days (IQR = 178-366). dAVF patients were older (median 52.5y vs 41y, p = 0.004) and less frequently female (14 females and 18 males, p = 0.004). Chronic clinical onset (>30 days) was more frequent in the dAVF group (29% vs 7.3%, p < 0.001) and dAVF patients had more often history of any previous venous thrombosis (25.0% vs 9.0%, p = 0.002). At admission, dAVF patients had less often decreased consciousness (GCS<15 6.3% vs 30.2%, p = 0.002). No patients with straight sinus thrombosis developed dAVF (0.0% vs 17.3%, p = 0.01). Clinical outcome at last follow-up did not differ between the two groups.
Conclusion
Among CVT patients, dAVF occurs in 3.0% of patients and is associated with increased age, male sex, chronic clinical onset and previous venous thrombosis.
Trial registration number
N/A
AS19-042
THROMBOLYSIS USE AND OUTCOMES IN YOUNG PATIENTS (16-29 YEARS) WITH ISCHAEMIC STROKE IN ENGLAND, WALES AND NORTHERN IRELAND. DATA FROM NATIONAL STROKE REGISTRY
1Guy's and St Thomas' NHS Foundation Trust, Stroke Medicine, London, United Kingdom
2Royal College of Physicians, Stroke Programme, London, United Kingdom
3King's College- London, Division of Health and Social Care Research, London, United Kingdom
4Guy's and St Thomas' NHS Foundation Trust, National Institute for Health Research Comprehensive Biomedical Research Centre, London, United Kingdom
Background and Aims
Alteplase is licensed for patients 18-80 years across Europe. No patients under 18 years and few under 30 years are reported or participated in the randomised control trials in the cochrane review.
Method
Data were extracted from the national stroke register (Sentinel Stroke National Audit Programme (SSNAP)) of adults with acute ischaemic stroke treated in all hospitals in England and Wales from July 2013-November 2017.
Results
Conclusion
The treatment of younger patients with IV-tPA appears safe, with no reported symptomatic intracranial haemorrhage in the 1460 patients less than 30 years receiving treatment. Improvement in NIHSS 24 hours after treatment was comparable to those over 30 years. (data not presented). Despite no randomised control trial evidence these data suggest that, where appropriate, IV-tPA should not be withheld for patients under 18 years.
Trial registration number
N/A
AS11-003
IVY SIGN PREDICTS ISCHEMIC STROKE RECURRENCE IN ADULT MOYAMOYA PATIENTS RECEIVING MEDICAL TREATMENT
1Seoul National University Hospital, Neurology, Seoul, Republic of Korea
2Seoul National University Hospital, Neurosurgery, Seoul, Republic of Korea
3Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Department of Neurology, Seoul, Republic of Korea
4Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Department of Radiology, Seoul, Republic of Korea
5Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Department of Neurosurgery, Seoul, Republic of Korea
Background and Aims
To evaluate the relationship between an ipsilateral ivy sign and ischemic stroke recurrence in adult Moyamoya disease (MMD) patients receiving medical treatment.
Method
We included consecutive MMD patients receiving medical treatment between 2006 and 2014. The ivy sign was defined as a linear or focal high-signal intensity on FLAIR images, and the burdens of ivy sign were rated in each hemisphere.
Results
Conclusion
Ivy sign is associated with ischemic recurrence in adult MMD patients in a dose-response manner. It would be helpful for selecting high-risk patients who need revascularization surgery.
Trial registration number
N/A
AS22-027
PREVALENCE AND SHORT-TERM CHANGES OF COGNITIVE DYSFUNCTION IN YOUNG STROKE PATIENTS
1Medical University of Graz, Department of Neurology, Graz, Austria
2Medical University of Graz, Institute for Medical Informatics- Statistics and Documentation, Graz, Austria
3Medical University of Graz, Department of Neuroradiology- Vascular and Interventional Neuroradiology, Graz, Austria
Background and Aims
Studies assessing the prevalence and course of post-stroke cognitive deficits in young stroke patients are rare. We therefore assessed cognitive function in a sample of young stroke patients (18 to 55 years) within the first week after hospital admission (baseline, BL) and at three months follow-up (FU).
Method
In this prospective single-center study, patients underwent a comprehensive clinical and cognitive assessment, examining general cognitive function, processing speed, attention, executive function and word fluency twice.
Results
From February 2016 to December 2017, we consecutively examined 130 young stroke patients (54% males; mean age: 43.7 years). Within this period, 68 patients attended the FU assessment (52% males; mean age: 42.1 +/− 10.4 years). At BL (N = 130), deficits (defined by 1.5 standard deviations below standardized mean) were seen in general cognitive function (41.7%), processing speed (55.0%), attention (45.2%), executive function (48.4%) and word fluency (40.7%). 27% showed impairment in four or more domains. A similar frequency of deficits was present in the subgroup with FU assessment which significantly improved in most domains of cognitive performance within three months, except for word fluency. Nevertheless, considerable cognitive deficits were still present three months after stroke in almost one third of patients (processing speed: 30.9%, executive function: 28.4%; word fluency: 43.6%). Eight (12%) patients suffered from depression at FU.
Conclusion
Our study indicates a high prevalence of cognitive deficits in young stroke patients which underscores the importance of post-stroke cognitive assessment. Potential implications of these deficits (e.g. difficulties to return to work) deserve further investigations.
Trial registration number
N/A
AS19-020
ISCHEMIC STROKES IN ADOLESCENTS
1APHP- Bicêtre hospital, Neurology, Le Kremlin Bicêtre, France
2APHP- Necker Enfants Malades Hospital, Pediatric neurology, Paris, France
3APHP- Bicêtre hospital, Pediatric neurology, Le Kremlin Bicêtre, France
4Foch hospital, Department of Neurology- Stroke Center, Suresnes, France
5APHP- Lariboisière Hospital, Neurology, Paris, France
6Mignot Hospital, Neurology, Le Chesnay, France
7Centre hospitalier sud francilien, Neurology and Stroke Center, Corbeille-Essonnes, France
8Saint Joseph Hospital, Neurology, Paris, France
9Sainte Anne Hospital, Neurology, Paris, France
10APHP-Pitie Salpétrière Hospital, Cerebrovascular Emergency Department, Paris, France
11Dijon University Hospital, Neurology, Dijon, France
Background and Aims
Adolescents have unique health issues and physiology. However, only limited information exists about stroke characteristics in this population. Our aim was to describe the clinical and neuroradiological features, etiologies, initial management, treatments and functional outcome of ischemic stroke in adolescents.
Method
We conducted a retrospective cohort study evaluating all consecutive patients aged from 10 to 18 years old with a first ever ischemic stroke hospitalized between 2007 and 2016 in one of our 10 French university centers (adult and pediatric departments) representing a total catching population of 10 million people.
Results
Sixty patients (53% male) were included (mean age of 15.1 y-o). Stroke involved anterior circulation in 54% cases, posterior circulation in 41% and both in 5%. The diagnosis at first medical contact was mistaken in 36% cases, with more mistakes in strokes involving posterior circulation (65% vs 20%, OR 4.64 CI 95%[1.2124 ; 19.846]). The most common etiologies were cardioembolism (15%), systemic vasculitis (5%), cervical dissection (5%) and intracranial dissection (5%).There was no atherosclerosis or small vessel disease. Stroke remained cryptogenic despite complete workup in 50% cases. Functional outcome was favorable (modified Rankin scale 0–2 at 90 days) in 80% cases. Recurrent ischemic cerebrovascular event occurred in 12% cases (mean follow up = 23 months). Recurrence rate was 0% in patients with cryptogenic stroke and 50% in patients with identified vasculopathy.
Conclusion
Ischemic strokes in adolescents have prognostic and causes which differ from the ones expected both in young adults and in younger children, emphasizing the need for an adapted etiological workup.
Trial registration number
N/A
AS19-005
ADHERENCE TO ANTIHYPERTENSIVE MEDICATION AFTER ISCHEMIC STROKE IN YOUNG ADULTS AND ITS ASSOCIATION WITH LONG-TERM OUTCOME
1Radboud University Medical Center, Neurology, Nijmegen, The Netherlands
2Helsinki University Hospital, Neurology, Helsinki, Finland
3Helsinki University Hospital, Neurology- Cardiology- Clinical Physiology and Nuclear Medicine, Helsinki, Finland
4Helsinki University Hospital, Cardiology, Helsinki, Finland
5Sahlgrenska University Hospital, Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
There is limited knowledge of the adherence to secondary prevention medication in young adults after stroke. We studied the adherence to antihypertensive medication and its association with subsequent vascular events in young adults with ischemic stroke.
Method
We included 936 first-ever ischemic stroke 30-day survivors aged 15-49, enrolled in the Helsinki Young Stroke Registry, 1994-2007. Follow-up data until 2012 came from Finnish Care Register, Statistics Finland, and Social Insurance Institution of Finland. Adherence to antihypertensive medication was defined as (1) nonusers, (2) low (prescription coverage <30%), intermediate (30-80%), and (3) high adherence (>80%). Adjusted Cox regression allowed assessing the association of adherence with all-cause mortality, recurrent stroke or TIA, and other vascular events.
Results
Of our patients, 40.5% were non-users, 7.8% had low adherence, 11.8% intermediate adherence, and 40.0% high adherence. Higher age, vascular comorbidities and older-onset stroke causes (atherosclerosis, small-vessel occlusion, high-risk source of cardioembolism) were associated with larger proportions of high adherence. Median follow-up was 8.3 years. Compared to non-users, exhibited risk of mortality and recurrent stroke or TIA was lower for patients with low-intermediate (HR 0.41, 95% CI 0.25-0.69; HR 0.37, 95% CI 0.22-0.63) and high adherence (HR 0.34, 95% CI 0.21-0.54; HR 0.44, 95% CI 0.27-0.70), after adjustment for pre-existing hypertension and other confounders. The association between adherence and recurrent events was modulated by stroke subtype.
Conclusion
Adherence to antihypertensive medication was suboptimal (low or intermediate) in one third of all users. Rates of recurrent events and all-cause mortality were dependent of adherence and affected by stroke subtype.
Trial registration number
N/A
Scientific Communications Prognosis and Outcome
AS16-024
SUBGROUPS OF TIA AND ISCHAEMIC STROKE PATIENTS WITH A HIGH RESIDUAL RISK OF CORONARY EVENTS: POPULATION-BASED COHORT STUDY
1INSERM U1237 PhIND, Neurology, Caen, France
2University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Trials of new lipid-lowering therapies in addition to statins report reductions in risk of coronary events in patients with atherosclerotic disease but treatment is costly. Data on long-term risk of coronary events in TIA or ischaemic stroke patients on current standard management would facilitate estimation of cost-effectiveness in subgroups at high residual risk.
Method
In a population-based cohort of consecutive patients with TIA or ischaemic stroke (2002-2014), we determined risk of follow-up coronary events until 30/09/2016. To identify subgroups with 5-year risk ≥10%, we stratified by number of atherosclerotic risk factors, diabetes, peripheral artery disease (PVD) and stroke aetiology (TOAST classification), in patients with and without prior coronary artery disease (CAD).
Results
Among 2555 patients (13,071 patient-years), there were 161 coronary events, with 5-year risk (6.4%, 95%CI = 5.2-7.5) ranging from 4.5% (3.5-5.6) in patients without CAD to 14.1% (10.4-17.6) in those with CAD. Among patients with CAD, 5-year risk remained ≥10% irrespective of number of atherosclerotic risk factors, diabetes, PVD and TOAST subtypes. In the absence of CAD, the only single variable subgroup with a risk ≥10% was patients with PVD (12.9%, 9.1-25.8). Patients with prior CAD or PVD accounted for 25% of the cohort but had 51% of follow-up coronary events. After adjustment for age and sex, increased risk of coronary events remained associated with history of hypertension, diabetes, hypercholesterolemia, smoking, and large artery disease.
Conclusion
Although 5-year risk of coronary events after TIA or ischaemic stroke averages<10%, higher risk subgroups, in whom more intensive treatment might be justified, are readily identifiable.
Trial registration number
N/A
AS16-132
MULTIVARIABLE OUTCOME PREDICTION AFTER ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE: DEVELOPMENT OF A PROGNOSTIC MODEL IN DATA FROM THE HERMES COLLABORATION
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, The Netherlands
2Erasmus MC University Medical Center, Department of Radiology & Nuclear Medicine, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Department of Public Health, Rotterdam, The Netherlands
4Altair Biostatistics, Department of Biostatistics, St. Louis Park- MN, USA
5Hotchkiss Brain Institute- Cummings School of Medicine- University of Calgary, Departments of Clinical Neuroscience and Radiology, Calgary, Canada
6University of Glasgow- Queen Elizabeth University Hospital, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
7Hospital Germans Trias y Pujol, Department of Neuroscience, Barcelona, Spain
8Royal Melbourne Hospital- University of Melbourne, Department of Radiology, Melbourne, Australia
9University of Lorraine and University Hospital of Nancy, Department of Diagnostic and Interventional Neuroradiology, Nancy, France
10Newcastle University, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
11Melbourne Brain Centre Royal Melbourne Hospital- University of Melbourne, Department of Medicine and Neurology, Melbourne, Australia
12University of Lorraine and University Hospital, Department of Clinical Epidemiology- Inserm, Nancy, France
13David Geffen School of Medicine- University of Los Angeles, Department of Neurology and Comprehensive Stroke Center, Los Angeles- CA, USA
14University of Pittsburgh Medical Center Stroke Institute- Presbyterian University Hospital, Stroke Institute- Department of Neurology, Pittsburgh- PA, USA
Background and Aims
Even when the revascularization and clinical status of a patient after endovascular treatment (EVT) for acute ischemic stroke is known, outcome is still highly variable and difficult to predict. We aimed to develop a prognostic model that can be applied within one day after EVT to predict functional outcome at three months.
Method
We used data from patients in the treatment arms of seven randomized controlled trials within the HERMES collaboration (MR CLEAN, ESCAPE, REVASCAT, SWIFT-PRIME, EXTEND-IA, THRACE, and PISTE). Primary outcome was the ordinal modified Rankin Scale (mRS) score three months after EVT. Pre- and post-procedural variables, assessed within one day after EVT, were analyzed with multivariable ordinal logistic regression analysis with stepwise backward selection. From this model, predicted probabilities of functional independence (mRS 0–2) and survival (mRS 0–5) were derived. Internal validation was performed by bootstrapping. Model performance was quantified with a c-statistic, corrected for optimism.
Results
The final model, based on 781 patients, included nine variables and explained 62.4% of the variance in outcome. The post-treatment National Institutes of Health Stroke Scale score was the strongest predictor (53.9% explained variance). The internally validated c-statistic was 0.83 for prediction of the ordinal mRS, 0.89 for functional independence, and 0.80 for survival, indicating very good model performance.
Conclusion
This model, which can be applied within one day after EVT, accurately predicts functional outcome at three months. It may provide physicians, patients, and family members with improved outcome expectations and could guide physicians in personalizing the patients’ treatment and rehabilitation plan.
Trial registration number
N/A
AS16-070
REFINING PREDICTION OF MAJOR BLEEDING ON ANTIPLATELET TREATMENT AFTER NONCARDIOEMBOLIC STROKE OR TIA
1UMC Utrecht, Julius Center/Neurology - Str 6.131, Utrecht, The Netherlands
2John Radcliffe Hospital- University of Oxford, Centre for Prevention of Stroke and Dementia- Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
3University Medical Center Utrecht, Department of Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, The Netherlands
Background and Aims
Risk scores may help to identify patients at high risk of bleeding following a TIA or ischaemic stroke, but performance of currently available scores is modest. We aimed to refine prediction of major bleeding by assessing the added value of new predictors to the existing S2TOP-BLEED score.
Method
We used Cox regression analysis to study the association between candidate predictors and major bleeding among 2,072 patients with a TIA or ischaemic stroke in the Oxford Vascular Study (OXVASC). An updated model was proposed and validated in 1,094 patients with a myocardial infarction in OXVASC. Models were compared with c-statistics, calibration plots, net reclassification improvement (NRI) and integrated discrimination improvement (IDI).
Results
Independent predictors for major bleeding on top of S2TOP-BLEED variables were peptic ulcer (HR 1.72; 1.04-2.86), cancer (HR 2.40; 1.57-3.68), anaemia (HR 1.55; 0.99-2.44) and renal failure (HR 2.20; 1.57-4.28). Addition of those variables improved discriminatory performance from 0.69 (0.64-0.73) to 0.73 (0.69-0.78) in the TIA/stroke cohort. Three-year risk of major bleeding ranged from 0.6 to 14% across quartiles of predicted risk with the new model, compared with 0.8 to 11.6% according to the original score. Net reclassification improved over the entire range of the score (NRI 0.56; 0.36-0.76). In the validation cohort, discrimination improved from 0.68 (0.62-0.74) to 0.70 (0.64-0.76).
Conclusion
Peptic ulcer, cancer, anaemia and renal failure improve predictive performance of the S2TOP-BLEED score for major bleeding after stroke. Future external validation studies are required to confirm the value of the S2TOP-BLEED+ score in TIA/stroke patients.
Trial registration number
N/A
AS24-023
PREDICTION OF FUNCTIONAL OUTCOME AFTER ANEURYSMAL SUBARACHNOID HAEMORRHAGE – DEVELOPMENT AND VALIDATION OF A SIMPLE RISK SCORE (ABC2)
1Stroke Research Centre, Institute of Neurology- University College London, London, United Kingdom
2Department of Statistical Science, University College London, London, United Kingdom
3Neurocritical Care Unit, Department of Neurosurgery- University Hospital Zurich, Zurich, Switzerland
4Critical Care, The James Cook University Hospital, Middlesbrough, United Kingdom
5Department of Neurosurgery, King’s College Hospital NHS Foundation Trust, London, United Kingdom
6Department of Neurosurgery, University Hospital Southampton NHS Foundation Trust, Southampton, United Kingdom
7Department of Neurosurgery, The National Hospital of Neurology and Neurosurgery, London, United Kingdom
8Neurogenetics Laboratory, The National Hospital of Neurology and Neurosurgery, London, United Kingdom
Background and Aims
The aim of this study was to develop a model to predict functional outcome (Glasgow Outcome Scale (GOS)) after aneurysmal subarachnoid haemorrhage (aSAH), and externally validate it in an independent external cohort.
Method
We recruited 1729 patients with aSAH at 22 UK hospitals (mean age 53.18 years; 70.27% females, 29.73% males). We developed a risk model including simple baseline clinical and radiological predictors of unfavourable outcome (GOS 1–3) using logistic regression. The model was internally validated using bootstrapping, and then externally validated in a prospective cohort of 548 patients with acute aSAH from Zurich, Switzerland, by calculating measures of discrimination (AUC) and calibration (calibration slope).
Results
Four independent predictors from the multivariable logistic regression analysis were included into the final model and risk score: Age, Fisher score, Glasgow Coma Scale (GCS) and smoking, creating the ABC2 score (A = Age, B = blood, C2 = conscious level and cigarette smoking). The model’s prediction of GOS demonstrated good discrimination in both internal and external validation (AUC = 0.76 and 0.73, respectively).
Conclusion
We developed and validated a simple easy to use prediction model to accurately predict functional outcome after aSAH. Although we externally validated our risk score, the two cohorts came from different populations and further testing in other cohorts will ensure generalisability.
Trial registration number
N/A
AS09-021
DEVELOPMENT AND VALIDATION OF A RISK PREDICTION ALGORITHM FOR POST-STROKE DEPRESSION USING THE SOUTH LONDON STROKE REGISTER
1King’s College London, School of Population Health and Environmental Sciences, London, United Kingdom
2NIHR Biomedical Research Centre, Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, London, United Kingdom
Background and Aims
Approximately one third of patients develop depression after stroke, and it is strongly associated with high mortality, disability and long length of hospital stay. Although depression is a treatable condition, there is no clinical predictive tool that could support the clinical decision for early intervention. We aimed to develop and validate a predictive analytic model for early screening of post-stroke depression.
Method
5876 patients with first-ever stroke from the South London Stroke Register from 1995 to 2016 were included in the study. The patients were split into development cohort (2,927 patients from 1995-2007) for fitting the models and validation cohort’ with 2,949 patients (2008-2016). Patients were assessed for depression using the Hospital Anxiety and Depression Scale (HADS). Multivariable logistic regression models were fitted to drive a predictive analytic algorithm. Performance of the model was expressed by discrimination using Area Under receiver operating Curve, and calibration using Hosmer-Lemeshow test.
Results
The optimal model to predict 3 months depression after stroke incorporated six variables including age, living condition, physical function before stroke, stroke severity and physical function at stroke onset. The model had an acceptable discrimination, 74% (95% Confidence interval [72.0-76.0]) and calibration in the internal validation. The discrimination in the temporal cohort was also acceptable 73% (95% CI [70.1-75.1]), however, poor calibration (overfitting) was observed.
Conclusion
It is possible to develop a predictive clinical tool of post-stroke depression for clinical decision support. The change of the prevalence of depression between populations limits its utility and applicability.
Trial registration number
N/A
AS06-007
SOCIOECONOMIC DISPARITIES IN PREHOSPITAL STROKE CARE IN SWEDEN?
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience- The Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden
2Centre for Prehospital Research in Western Sweden, University of Borås, Borås, Sweden
Background and Aims
Recent studies have shown socioeconomic disparities in stroke outcomes. Here, we investigated whether the prehospital stroke care differs with respect to socioeconomic status (SES).
Method
Consecutive stroke and TIA patients (n = 3006) admitted to Stroke Units at the Sahlgrenska University Hospital, Gothenburg, Sweden, November 1, 2014 to July 31, 2016 were included. Data on prehospital care was obtained from a local stroke register. Socioeconomic status was classified according to the average level of income and education within each patient’s neighborhood (postcode area).
Results
The median delay from calling the emergency medical communication center (EMCC) to brain computer tomography was performed at hospital arrival was 3 h 49 min (95% confidence interval (CI) 3 h 10 min to 4 h 35 min) for patients within the lowest SES tertile and 3 h 24 min (95% CI 2 h 48 min to 4 h 8 min) for the highest tertile (p < 0.05). Patients with lower SES were less likely to receive the highest priority in the ambulance (p < 0.05), were more often down-prioritized in the ambulance compared to the EMCC-priority (p < 0.05), and had lower rates of prehospital recognition of stroke/TIA (p < 0.05) than those with high SES. No inequities were found concerning EMCC-prioritization, the probability of ambulance transport or in the ambulance nurses’ performance of stroke specific actions once stroke/TIA was recognized.
Conclusion
We found socioeconomic inequities in prehospital stroke care which could affect the efficacy of acute stroke treatments. The ambulance nurses’ limited ability to recognize stroke/TIA may partly explain the observed inequities.
Trial registration number
N/A
AS03-039
MICROALBUMINURIA COULD IMPROVE RISK PREDICTION OF STROKE IN PATIENTS WITH TIA AND MINOR STROKE: THE PROGNOSTIC MARKERS OF TIA EVOLUTION (PROMOTE) STUDY
1University of Exeter, Diabetes and Vascular Research Centre, Exeter, United Kingdom
2Royal Devon & Exeter Hospital, Academic Department of Healthcare for Elderly, Exeter, United Kingdom
Background and Aims
Current stroke prediction risk scores lack optimal sensitivity and specificity. Elevated urinary albumin:creatinine ratio (ACR) predicts cardiovascular disease, stroke and mortality in hypertension, diabetes and the general population. We explored the role of ACR in improving risk prediction in patients with TIA and minor stroke.
Method
Basic demographics was recorded in 2,400 patients attending 12 daily stroke clinics in the UK with TIA or minor stroke. Urinary ACR was measured on a spot sample using a bench-top analyser. Patients were followed up at day 7, 30 and 90 to determine recurrent stroke, cardiovascular events, urgent endarterectomy or death.
Results
2,262 were included in the final analysis. 287 (12.7%) patients had an outcome event. Participants with events were older (72.9 vs 70.8 years; p = 0.003) but otherwise similar. ACR was higher in those with events compared to those without (2.4(95% CI 2.1-2.7) vs 1.9(1.8-1.9)mg/mmol respectively, p = 0.001) independent of age and sex. An ABCD2 score of >4 (traditionally regarded as high risk) was associated with higher ACR; 2.4(2.2-2.6) vs 1.7(1.6-1.8)mg/mmol, p < 0.001, yet was not associated with having an event (odds ratio 1.07(0.83-1.39) p = 0.58). Contrary to ABCD2, ACR was strongly associated with recurrent events (OR: 1.22(1.10-1.36) p < 0.001), including after adjustment for age, sex, and ABCD2 (OR: 1.20(1.07-1.34) p = 0.002).
Conclusion
After TIA or minor stroke, ACR was significantly higher in those who progressed to vascular events within 90 days. Incorporating urinary ACR from a single sample in the acute setting could improve the performance of predictive risk scores.
Trial registration number
Observational study
AS16-160
ASSOCIATIONS BETWEEN THROMBUS IMAGING CHARACTERISTICS AND PATIENT OUTCOMES AFTER ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Academic Medical Center, Department of Radiology and Department of Biomedical Engineering and Physics, Amsterdam, The Netherlands
2Academic Medical Center, Department of Radiology, Amsterdam, The Netherlands
3Texas Stroke Institute, Department of Radiology, Dallas Fort Worth, USA
4Erasmus Medical Center, Department of Neurology, Rotterdam, The Netherlands
5Academic Hospital Maastricht, Department of Radiology, Rotterdam, The Netherlands
6Academic Hospital Maastricht, Department of Neurology, Maastricht, The Netherlands
7Erasmus Medical Center, Department of Public Health, Rotterdam, The Netherlands
8Erasmus Medical Center, Department of Radiology, Rotterdam, The Netherlands
9Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
Background and Aims
Studies have shown associations of thrombus imaging characteristics with functional outcome and recanalization after intravenous thrombolysis. We aim to evaluate associations between thrombus imaging characteristics and outcomes after endovascular treatment (EVT).
Method
We included 409 MR CLEAN Registry patients that were treated with EVT and had thin slice baseline NCCT and CTA, acquired less than 30 minutes apart. The association between thrombus characteristics and outcomes was assessed with multivariable ordinal and linear regression models. Thrombus imaging characteristics considered in the model include thrombus location, length and perviousness, clot burden score (CBS), absolute and relative thrombus attenuation, and distance from the terminus of internal carotid artery to the thrombus. Thrombus location was classified as proximal occlusion in the internal carotid artery (cervical and ICA-T), middle cerebral artery (M1 and M2 and anterior cerebral artery (A1 and A2). Primary outcome was the modified Rankin Scale score at 90 days, and secondary outcomes were eTICI score and duration of EVT.
Results
Statistically significant results are shown in Table 1. More proximal occlusions, longer thrombi and higher CBS were associated with worse functional outcome and less successful reperfusion. More distal occlusions, lower CBS and longer thrombi were associated with longer duration of EVT.
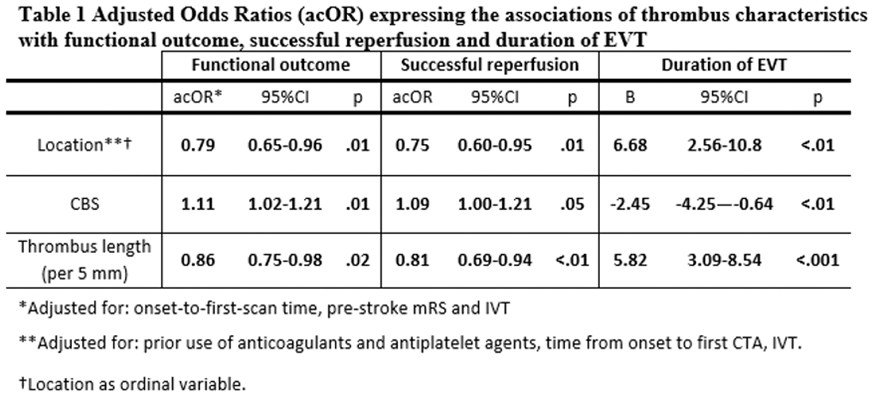
Conclusion
Thrombus location, length and CBS were independently associated with functional outcome and successful reperfusion after EVT and the duration of EVT.
Trial registration number
N/A
AS09-017
SHORT AND LONG-TERM RISKS OF STROKE AFTER ORTHODOX-DEFINITION TRANSIENT ISCHAEMIC ATTACK VERSUS DISQUALIFIED MONOSYMPTOMATIC EVENTS: POPULATION-BASED COHORT STUDY
1Oxford University, Nuffield Department of Clinical Neuroscience, Oxford, United Kingdom
Background and Aims
Medical treatment is indicated after transient ischaemic attack (TIA) and antiplatelet treatment is highly effective in preventing early recurrent stroke. Diagnosis of TIA based on the National Institute of Neurological Disorders and Stroke (NINDS) criteria, disqualifies many monosymptomatic events with sudden-onset, non-progressive focal symptoms (e.g. diplopia, dysarthria). Patients with these NINDS-excluded events are often not investigated or treated, but reliable data on prognosis are lacking. We studied stroke risk after NINDS-TIAs, NINDS-excluded events and minor ischaemic stroke (MIS).
Method
Patients seeking medical attention after transient neurological symptoms or MIS were ascertained prospectively in a population of 92,728 in Oxfordshire, UK from 2002-14. Transient events were classified at baseline as NINDS-TIA, NINDS-excluded events, or other diagnosis. Patients with NINDS-TIA and MIS were treated strictly according to secondary prevention guidelines. NINDS-excluded events had treatment according to physician judgment. 90-day and 10-year risks of stroke were determined by face-to-face follow-up.
Results
Among 3116 patients, 1002 had a MIS, 665 had NINDS-TIA, 382 had NINDS-excluded events and 1057 other diagnoses. NINDS-TIAs had a similar 90-day stroke risk to MIS (8.9%,6.7-11.1 vs 7.8%,6.0-9.6). Although the NINDS-excluded events had a lower risk (4.2%,2.4-5.2) it was considerably higher than the expected background risk (RR:28.6; p = 0.009). The stroke risk from 90-days to 10-year follow-up in NINDS-excluded events was similar to that in NINDS-TIA (11.7%,7.0-16.4 vs 10.9%,7.4-14.4; p = 0.84).
Conclusion
NINDS-excluded events account for over a third of all TIAs, have a high long-term risk of stroke, and require urgent antiplatelet treatment. Diagnostic criteria for TIA should be broadened to include these disqualified events.
Trial registration number
N/A
Scientific Communications- AF and Cardioembolism
AS03-017
BRIDGING THERAPY WITH LOW-MOLECULAR WEIGHT HEPARIN IN PATIENTS WITH ACUTE ISCHEMIC STROKE AND ATRIAL FIBRILLATION: RESULTS FROM THE RAF AND RAF-NOACS STUDIES
1Ospedale S. Maria della Misericordia- PG, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
Background and Aims
Patients with stroke and nonvalvular atrial fibrillation (NVAF) should not be “bridged” with low molecular weight heparin (LMWH) at full dose before starting oral anticoagulation (OAC). However, this practice is still common in clinical settings. This analysis of RAF and RAF-NOACs studies aimed to evaluate 1) clinical profile of patients who were treated by bridging therapy; 2) differences in outcomes 3) difference in outcome in different types of OAC (vitamin k antagonists or non-vitamin k antagonists).
Method
We analyzed data of patients from the prospective RAF and RAF NOAC studies. The primary outcome was the composite of stroke, TIA, symptomatic systemic embolism, symptomatic cerebral bleeding and major extra-cerebral bleeding at 90 days.
Results
Of 1,810 patients treated with OAC (1,219 with vitamin-k antagonists and 561 with non-vitamin k antagonists), 371 were “bridged” with LMWH. Younger age, male sex, large anterior circulation lesions and leukoaraiosis were inversely correlated with the use of bridging therapy; 42 bridged patients (11.3%) reached the combined outcome vs 72 of the non-bridged patients (5.0%) (p = 0.0001). At multivariable analysis, bridging therapy was correlated with combined (OR 2.88; 95% CI 1.87-4.43, p < 0.0001), ischemic (OR 3.08; 95% CI 1.83-5.19, p < 0.0001) and hemorrhagic (R = 2.86; 95% CI 1.52-5.37, p = 0.0001) outcomes. No differences for type of OACs were observed.
Conclusion
Our findings suggest that the use of LMWH is associated to a higher risk of early ischemic recurrence and hemorrhagic transformation, independently from the type of OAC.
Trial registration number
N/A
AS14-046
STROKE RISK ANALYSIS. A NOVEL AUTOMATIC SYSTEM WITH A HIGH DETECTION RATE OF PAROXYSMAL ATRIAL FIBRILLATION IN THE ACUTE PHASE OF STROKE
1Hospital Universitari Germans Trias i Pujol, Neurosciences, Badalona- Barcelona, Spain
2Hospital Arnau de Vilanova, Neurology, Lleida, Spain
3Hospital de Bellvitge, Neurology, Hospitalet del LLobregat- Barcelona, Spain
4Hospital de Mar, Neurology, Barcelona, Spain
5Hospital de Sant Pau, Neurology, Barcelona, Spain
6Hospital Vall d'Hebrón, Neurology, Barcelona, Spain
7Hospital Doctor Josep Trueta, Neurology, Girona, Spain
8Evina Health Solutions, Management, Bilthoven, The Netherlands
Background and Aims
The Stroke Risk Analysis (SRA) allows automated analysis of continuous ECG monitoring (CEM) enabling the detection of paroxysmal atrial fibrillation (pxAF) and risk of pxAF (RoAF). Our aims were to compare the rate of documented pxAF by SRA and by standard CEM in patients with acute ischemic stroke (AIS) or TIA and to identify whether RoAF during the first cycle of recording was associated with the detection of pxAF during the whole CEM time.
Method
514 consecutive eligible patients (median age, 72; 60% male; AIS 93%, TIA 7%) with neither history of AF nor AF in admission ECG received 2-channel Holter CEM combined with automated SRA of CEM prolonged up to a total time of 7 days. Investigators were blinded to SRA data during CEM unless pxAF was detected on SRA.
Results
Among 457 patients with CEM available for > 65 hours (median CEM time 141 hours, IQR 96-167), AF was documented by SRA in 78 patients (17,1%) compared to 22 patients (4.8%) by standard CEM in the stroke unit (stay 96 hours; IQR 53-161) (p < 0.001). SRA detected RoAF in 89 patients within the first cycle of CEM (11,5hours; 3,8-22,0), 31 of them showing an episode of AF during full time of CEM. Predictive values for AF were sensitivity 55%, specificity 85%, PPV 35% and NPV 93%.
Conclusion
Automated analysis of CEM by using SRA technology improves pxAF detection in patients with stroke compared with standard CEM. The predictive value of RoAF during the first few hours after admission deserves further investigation.
Trial registration number
N/A
AS09-037
SAFETY AND EFFECTIVENESS OF DABIGATRAN IN PATIENTS WITH ATRIAL FIBRILLATION WITH AND WITHOUT PRIOR STROKE: DATA FROM THE GLORIA-AF REGISTRY PROGRAM
1University Hospital Essen, Department of Neurology, Essen, Germany
2Boehringer Ingelheim International GmbH, Medicine TA Cardiology, Ingelheim, Germany
3Leiden University Medical Center, Department of General Internal Medicine, Leiden, Netherlands Antilles
4Clinica y Maternidad Suizo Argentina, Arrhythmias And Electrophysiology Service, Buenos Aires, Argentina
5Beijing An Zhen Hospital, National Clinical Research Center for Cardiovascular Diseases, Beijing, China
6RTI Health Solutions, Research, North Carolina, USA
7Boehringer Ingelheim Pharmaceuticals- Inc., Biostatistics & Data Sciences, Ridgefield- CT, USA
8Boehringer Ingelheim Ltd., Department of Medicine, Burlington- Ontario, Canada
9McMaster University, Department of Health Research Methods- Evidence- and Impact, Hamilton- Ontario, Canada
10Boehringer Ingelheim International GmbH, Global Epidemiology Department, Ingelheim, USA
11Mount Sinai School of Medicine, Cardiology, New York, USA
12University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
Background and Aims
Patients with atrial fibrillation (AF) and prior stroke are at a very high risk of recurrent stroke. The safety and effectiveness of dabigatran etexilate (dabigatran) for stroke prevention in AF has been shown in randomized trials and numerous database studies. Prospective, long-term data on secondary stroke prevention from clinical practice are less available. This analysis from GLORIA-AF describes outcomes of DE for up to 2 years in patients with or without prior stroke.
Method
GLORIA-AF is a prospective, global registry of patients with newly diagnosed AF. This analysis describes baseline characteristics, clinical outcomes and event rates in dabigatran patients with and without prior stroke.
Results
Overall, 4873 patients were prescribed dabigatran and 4859 received it, for an average of 18.3 months. Of these, 4288 patients had no history of stroke, while 579 had prior stroke (for 6 prior stroke status was unknown). Compared with patients without prior stroke, patients with prior stroke were older (mean age 72.9 vs 69.8 years), had higher CHA2DS2VASc (mean 5.0 vs 3.0) and HAS-BLED scores (mean 2.3 vs 1.1), but similar frequency of concurrent antiplatelet therapy (13.8% vs 12.6%). Among patients with prior stroke, the rate of recurrent stroke was 1.53 and major bleeding, 1.05, per 100 patient-years. For patients without a stroke history the rate of stroke was 0.52 and major bleeding 0.95 per 100 patient-years.
Conclusion
In clinical practice, rates of major bleeding and stroke were low with dabigatran, even among patients with prior stroke, confirming the long-term safety and effectiveness of dabigatran.
Trial registration number
N/A
AS14-045
VALUE OF CARDIAC CT-ANGIOGRAPHY IN THE DIAGNOSTIC WORKUP OF PATIENTS WITH TIA AND ACUTE ISCHAEMIC STROKE: PREVALENCE OF CARDIOEMBOLIC RISK SOURCES AND THERAPEUTIC IMPLICATIONS
1Leiden University Medical Center, Radiology, Leiden, The Netherlands
2Leiden University Medical Center, Neurology, Leiden, The Netherlands
3Leiden University Medical Center, Cardiology, Leiden, The Netherlands
Background and Aims
To evaluate the yield and the implications for therapeutic management of cardiac CTA in the diagnostic work up of patients presenting with TIA or acute ischaemic stroke (IS).
Method
Patients presenting with TIA or IS were prospectively included in the Leiden University Medical Centre (the Netherlands). Cardiac CTA was implemented as part of routine diagnostic work up. Occurrence of cardio embolic (CE) risk sources (high vs. medium/low risk) and complex plaques of the aorta, defined as plaque ≥4 mm in thickness or ulceration, were assessed. Implications of cardiac CTA for therapeutic management were assessed.
Results
Sixty-eight patients were included (TIA n = 40, IS n = 28) with a mean age of 67.7 years (SD 8.3 years) and median NIHSS of 0 (interquartile range 0–2). In total, 26 CE risk sources were detected in 21 (31%) patients. High risk CE source was present in 2 patients (TIA 0%, IS 7%), both being an intracardiac thrombus. Complex aortic plaque was identified in 7 patients (10%). Medium/low CE risk sources included filling defects in the left atrium or left atrial appendage (3%), mitral annular calcification (6%), aortic valve calcification (9%) and patent foramen ovale (7%). The intracardiac thrombi were confirmed by transoesophageal echocardiography and changed therapeutic management from antiplatelets to oral anticoagulants.
Conclusion
Our results indicate a high yield of 31% of cardiac CTA for detection of CE risk sources in the diagnostic work up of TIA/IS patients. Furthermore, early cardiac CTA changed therapeutic management in 7% of ischaemic stroke patients.
Trial registration number
N/A
AS18-053
BOTH, PFO-RELATED AND -UNRELATED FACTORS DRIVE THE RISK OF STROKE RECURRENCE IN PATIENTS WITH CRYPTOGENIC STROKE AND PFO
1Cantonal Hospital Aarau, Neurology, Aarau, Switzerland
2University Hospital of Lausanne, Neurology, Lausanne, Switzerland
3Municipal Hospital of Zurich Triemli, Cardiology, Zurich, Switzerland
4Azienda Unità Sanitaria Locale - IRCCS- Reggio Emilia, Neurology, Reggio Emilia, Italy
5University of Basel, Clinical Trials Unit, Basel, Switzerland
6University Hospital of Leuven, Neurology, Leuven, Belgium
7Florey Institute of Neuroscience and Mental Health- University of Melbourne, Stroke Division, Victoria, Australia
8Alfried-Krupp Krankenhaus Essen, Neurology, Essen, Germany
9University Hospital of Basel, Neurology, Basel, Switzerland
10Felix-Plattner Hospital, Neurology, Basel, Switzerland
11University Hospital of Girona, Neurology, Girona, Spain
12University Hospital of Essen, Neurology, Essen, Germany
13Klinikum Worms, Neurology, Worms, Germany
14University Hospital of Zurich, Neurology, Zurich, Switzerland
15University Hospital of Ghent, Neurology, Ghent, Belgium
16Tufts Medical Center of Boston, Neurology, Boston- MA, USA
17AZ Sint Blasius Dendermonde, Neurology, Dendermonde, Belgium
18University Hospital of Geneva, Neurology, Geneva, Switzerland
19University Hospital of Bern, Cardiology, Bern, Switzerland
20University Hospital of Bern, Neurology, Bern, Switzerland
Background and Aims
Patent foramen ovale (PFO) represents a known risk factor for recurrent ischemic stroke. The aim of this study was to identify PFO-related and -unrelated risk factors associated with stroke recurrence in patients with cryptogenic stroke and PFO. Furthermore, we assessed the population attributable risk (PAR) for the factors associated with prior stroke.
Method
We studied baseline data of 427 patients with first-ever and 62 patients with prior stroke from the International PFO Consortium Study (NCT00859885). Each group was analyzed for an association with PFO-related (right-to-left shunt at rest, atrial septal aneurysm, deep venous thrombosis, pulmonary embolism, and Valsalva maneuver) and PFO-unrelated factors (age, sex, hypertension, diabetes mellitus, hypercholesterolemia, smoking, self-reported migraine, coronary artery disease, family and personal history of stroke) by means of mixed-effects logistic regression and backward model selection based on Akaike’s information criterion. For the selected predictors, we estimated adjusted PAR.
Results
Age (OR = 1.04, 95%CI 1.02-1.06, P<0.001), coronary artery disease (OR = 3.24, 95%CI 1.28-8.20, P = 0.013), diabetes mellitus (OR = 2.47, 95%CI 1.04-5.85, P = 0.040), and right-to-left shunt (RLS) at rest (OR = 2.07, 95%CI 1.09-3.93, P = 0.026) were associated with prior stroke. The adjusted PAR for age was 88%, RLS at rest 20%, atrial septal aneurysm 19%, coronary artery disease 11%, diabetes 9%, and deep vein thrombosis 5%, respectively.
Conclusion
In patients with cryptogenic stroke and PFO, the recurrence risk is driven by both PFO-related and -unrelated factors. Among all independent predictors of stroke recurrence, age, RLS at rest, and atrial septal aneurysm bear the highest population attributable risk.
Trial registration number
N/A
AS30-032
CLOSURE, ANTICOAGULATION OR ANTIPLATELET THERAPY FOR STROKE WITH PATENT FORAMEN OVALE: SYSTEMATIC REVIEW OF RANDOMIZED TRIALS, SEQUENTIAL META-ANALYSIS AND NEW INSIGHTS FROM THE CLOSE TRIAL
1Hôpital Sainte Anne- Université Paris Descartes- INSERM U894- Paris- France, Neurology, Paris, France
2INSERM UMR 915- Institut du Thorax- Nantes- FranceCentre Hospitalier Universitaire de Nantes- Institut du thorax- Nantes- France, Cardiology, Nantes, France
3Cochin Hospital- APHP- Paris- France, Cardiology, Paris, France
4Epidemiology and Clinical Research Unit- Georges Pompidou European Hospital- APHP- INSERM CIC 1418, Epidemiology, Paris, France
Background and Aims
We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing either patent foramen ovale (PFO) closure, anticoagulation or antiplatelet therapy to prevent stroke recurrence in patients with PFO-associated cryptogenic stroke.
Method
We searched Medline, Cochrane Library and Embase through October 2017. The primary outcome was stroke recurrence. Pooled incidences, hazard ratios (HRs), and risk ratios (RRs) were calculated in random-effects meta-analyses.
Results
PFO closure was associated with a lower risk of recurrent stroke compared with antithrombotic therapy (3431 patients from 5 RCTs; HR = 0.40, 95%CI:0.20-0.82; I2=54%) or with antiplatelet therapy alone (1137 patients from 2 RCTs; HR = 0.18, 95%CI:0.05-0.63; I2=12%). These results were confirmed in trial sequential analysis. The incidence of stroke per 100 person-years was 0.37 (95%CI:0.07-0.89; I2=86%) in the PFO closure group and 1.19 (95%CI:0.91-1.50; I2=8%) in the antithrombotic therapy group. Major complications occurred in 2.37% (95%CI:0.95-4.36; I2=81%) of PFO closure procedures. New-onset atrial fibrillation was more frequent in patients randomized to PFO closure versus antithrombotic therapy (RR = 4.54, 95%CI:2.26-9.11; I2=31%). In patients randomized to PFO closure versus anticoagulation, the risk of recurrent stroke was not significantly different (353 patients from 1 RCT; HR = 0.14, 95%CI 0.00-1.45). Three RCTs compared anticoagulation versus antiplatelet therapy, none showing a statistically significant difference.
Conclusion
PFO closure is superior to antithrombotic therapy to prevent stroke recurrence after cryptogenic stroke. The annual absolute risk of stroke was low, but it has to be tempered by an extended period of risk in those young and middle-aged patients. PFO closure was safe despite an increased risk of atrial fibrillation.
Trial registration number
N/A
AS21-025
THE NEUROLOGIST’S APPROACH TO CEREBRAL INFARCT AND TRANSIENT ISCHEMIC ATTACK IN PATIENTS RECEIVING ANTICOAGULANT TREATMENT FOR NONVALVULAR ATRIAL FIBRILLATION. ANITA-FA STUDY
1University Hospital of La Princesa, Stroke Unit, Madrid, Spain
2Hospital General Universitario Gregorio Marañón, Stroke Unit, Madrid, Spain
3Hospital Universitario de Donostia, Stroke Unit, Donostia, Spain
4Hospital Universitari de Bellvitge, Stroke Unit, L’Hospitalet de Llobregat, Spain
5Hospital de Basurto, Stroke Unit, Bilbao, Spain
6Hospital Universitari Clinic, Stroke Unit, Barcelona, Spain
7Hospital Universitario Ramón y Cajal, Stroke Unit, Madrid, Spain
8Hospital Central de Oviedo, Stroke Unit, Oviedo, Spain
9Complejo Hospitalario Universitario A Coruña, Stroke Unit, A Coruña, Spain
10Hospital Clínico Universitario San Carlos, Stroke Unit, Madrid, Spain
11Hospital Universitario Dr. Josep Trueta, Stroke Unit, Girona, Spain
Background and Aims
In this study, we describe the epidemiological and clinical characteristics of patients receiving OACs for atrial fibrillation (AF) who experience AIS and compare those receiving vitamin K antagonists (AIS-VKAs) with those receiving direct-acting OACs (AIS-DOACs).
Method
We performed a national, multicenter, observational, descriptive, retrospective study of all adult patients presenting with AIS and previous anticoagulation therapy due to AF that were admitted to the neurology department over a 1-year period. The study population was divided into 2 groups (AIS-DOACs and AIS-VKA). Epidemiological, clinical, radiological, and therapy-related variables, as well as functional outcome at 3 months, were compared.
Results
A total of 1240 cases were included (80,4% AIS-AVK y 19,6% AIS-DOACs). AIS-DOACs more often presented as TIA (18,1% vs 10,8%; p = 0,001), with less symptomatic hemorrhagic transformation (1,6% vs 4,6%; p = 0,035), and shorter hospital stay (median 6 vs 7 days; p = 0,03) than AIS-VKA. Patients with AIS-VKA were more often treated with thrombolysis (9,2% vs 1,6%; p < 0,001) and there were no differences in the rate of mechanical thrombectomy in both groups (AIS-DOACs 10,9% vs AIS-VKA 12,3%; n.s.). Functional outcome and mortality at 3 months were not statistically different between groups. 54% of the patients were receiving DOACs as antithrombotic treatment at 3-month-follow-up.
Conclusion
AIS-DOACs in patients with AF are more often transient and have less symptomatic hemorrhagic transformation rate and shorter hospital day than those with AIS-VKA. In Spanish neurology departments, most patients previously anticoagulated that presented with AIS are treated long-term with DOACs.
Trial registration number
N/A
AS09-030
POPULATION-BASED STUDY AND SYSTEMATIC REVIEW OF TIME-TRENDS IN AF-RELATED STROKE AND PREMORBID ANTICOAGULATION: CONTINUING CHALLENGE FOR STROKE PREVENTION
1University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Incidence of AF-related stroke is increasing but the proportion of this burden that could be attributed to under-treatment remains uncertain. We did a population-based study and systematic review of time trends in AF prevalence in stroke incidence studies and in premorbid anticoagulation.
Method
All studies published to November 2017 of prospective, population based stroke incidence that reported rates of AF were included, along with unpublished data from the Oxford Vascular Study (OXVASC). Pooled rates of premorbid or total AF and prior anticoagulation among incident strokes were calculated by Mantel Haenszel methods.
Results
Of 1928 patients with incident ischaemic stroke in OXVASC, 629 (32.6%) were AF-associated, consistent with the pooled estimate from all available data (8-studies; 25.2%, 95%CI 21.6-28.9; studies completed after 2005 - 31.9%, 30.9-32.9, phet = 0.75). Data on known prior AF in incident stroke (31 reports) yielded a pooled rate of 18.6% (16.8-20.3, phet<0.0001), with age of population, study period, country and ethnicity accounting for 64% of heterogeneity. However, although rates of premorbid anticoagulation increased over time (p = 0.002), evidence of substantial under-treatment remained (2001-2015 - 25.7% anticoagulated, 21.1-30.3), even in the most recent period (≥2010 – 27.5%, 18.4-36.6).
Conclusion
In OXVASC and in other studies worldwide, 1-in-3 incident ischaemic strokes are AF-related, due partly to continuing low rates of pre-morbid anticoagulation for known prior AF, which therefore represents a major public health opportunity to reduce the burden of stroke.
Trial registration number
N/A
Scientific Communications Prevention Trials
AS03-006
ESTIMATED TREATMENT EFFECT OF TICAGRELOR VERSUS ASPIRIN BY INVESTIGATOR-ASSESSED EVENTS COMPARED WITH JUDGMENT BY AN INDEPENDENT EVENT ADJUDICATION COMMITTEE IN THE SOCRATES TRIAL
1Sandler Neurosciences Center, UCSF Department of Neurology, San Francisco, USA
2AstraZeneca, Research and Development, Gothenburg, Sweden
3Paris Diderot University, Department of Neurology and Stroke Centre, Paris, France
4Stanford University, Stanford Stroke Center, Stanford, USA
5Harvard University, Department of Biostatistics, Boston, USA
6National Cerebral and Cardiovascular Center, Research Institute, Osaka, Japan
7Hospital Vall d’Hebron, Vall d´Hebron Stroke Unit, Barcelona, Spain
8Beijing Tiantan Hospital, Neurology Department, Beijing, China
9Chinese University of Hong Kong, SH Ho Centre for Cardiovascular Disease & Stroke Faculty of Medicine, Shatin, Hong Kong S.A.R
10University of Texas at Austin, Dell Medical School, Austin, USA
Background and Aims
Adjudication of end points is standard in cardiovascular clinical trials, yet several studies indicate that the benefit of adjudication in estimating treatment effect may be limited, particularly with double-blind treatment, common clinical end points, and assessments made by investigators trained in the disease area.
Method
SOCRATES (NCT01994720) compared ticagrelor and aspirin in 13,199 patients with high-risk transient ischaemic attack (TIA) or acute minor stroke. The primary composite end point was stroke (ischaemic or haemorrhagic), myocardial infarction, or death. Stroke was the major component of the primary end point and a secondary end point. The end points were adjudicated by an independent blinded committee. In this analysis, we compared the treatment effect on the primary end point and stroke, and major bleeding events, based on the investigatorś and adjudicators’ assessments.
Results
The hazard ratios (HRs) (95% confidence interval [CI]) for ticagrelor versus aspirin therapy for the primary end point were 0.89 (0.78–1.01) when calculated on adjudicated events and 0.88 (0.78–1.00) for investigator-assessed events. The HRs (95% CIs) for stroke were 0.86 (0.75–0.99) based on the adjudicators’ diagnoses and 0.85 (0.75–0.97) based on the investigators’ diagnoses. The agreement between adjudicated and investigator-diagnosed stroke was 91%, and for major bleeds was 88%.
Conclusion
There was no clinically meaningful difference in the estimated treatment effect, on either the primary end point or stroke, by using investigator- or adjudicator-assessed events. Double-blinded outcome studies with stroke end points may not benefit from adjudication.
Trial registration number
SOCRATES (NCT01994720)
AS03-008
BENEFIT-RISK ASSESSMENT USING NOVEL METHODOLOGIES: TICAGRELOR VS ASPIRIN IN ACUTE STROKE OR TRANSIENT ISCHEMIC ATTACK IN THE SOCRATES TRIAL
1Harvard T.H. Chan School of Public Health, CBAR/Department of Biostatistics, Boston, USA
2AstraZeneca, Research and Development, Gothenburg, Sweden
3University of Texas at Austin, Dell Medical School, Austin, USA
4Paris Diderot University, Department of Neurology and Stroke Centre, Paris, France
5Stanford University, Stanford Stroke Center, Stanford, USA
6University of California, Department of Neurology, San Francisco, USA
7National Cerebral and Cardiovascular Center, Research Institute, Osaka, Japan
8Hospital Vall d’Hebron, Vall d´Hebron Stroke Unit, Barcelona, Spain
9Beijing Tiantan Hospital, Neurology Department, Beijing, China
10Chinese University of Hong Kong, SH Ho Centre for Cardiovascular Disease & Stroke Faculty of Medicine, Shatin, Hong Kong S.A.R
Background and Aims
Traditional benefit-risk evaluations in cardiovascular trials are generally limited to evaluating time to the first event. This ignores potentially valuable information that can be derived from the differential impact of the events of interest, the cumulative nature of multiple events, the association between events, and competing risks. The benefit-risk profile of ticagrelor in SOCRATES (NCT01994720; N = 13,199) (Johnston et al. NEJM 2016;375:35–43) was assessed using methodologies addressing these issues.
Method
The desirability of outcome ranking (DOOR) classified global patient outcomes into one of five mutually-exclusive categories ordered by desirability (Table). The win ratio (relative frequency that a patient randomised to ticagrelor has a more desirable DOOR compared with a patient randomised to aspirin) and DOOR probability (probability of a patient randomised to ticagrelor having a better DOOR than a patient randomised to aspirin) were estimated based on pairwise patient comparisons.
Table: DOOR by randomised treatment
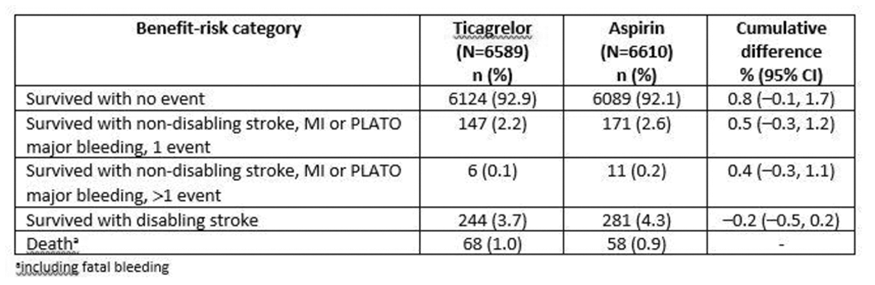
Results
The Table summarises the DOOR distribution by randomised treatment. The estimated win ratio was 1.11 (95% CI 0.98–1.26, p = 0.096), and the DOOR probability was 0.504 (95% CI 0.499–0.508, p = 0.096).
Conclusion
Results of these exploratory benefit-risk analyses were consistent with previously reported SOCRATES results, in which the hazard ratio for time-to-first event of the composite of stroke, myocardial infarction, death and fatal/life-threatening bleeding was 0.90 (95% CI 0.79–1.02). (Funding: AstraZeneca)
Trial registration number
SOCRATES (NCT01994720)
AS09-023
BALANCING BENEFITS AND RISKS OF LONG-TERM ANTIPLATELET THERAPY IN PATIENTS WITH A TIA OR NONCARDIOEMBOLIC ISCHAEMIC STROKE: AN INDIVIDUAL PATIENT DATA META-ANALYSIS
1UMC Utrecht, Julius Center/Neurology - Str 6.131, Utrecht, The Netherlands
2UMC Utrecht, Department of Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, The Netherlands
3University Hospital Essen, Department of Neurology, Essen, Germany
4University of Nottingham, Stroke Trials Unit- Division of Clinical Neuroscience, Nottingham, United Kingdom
5University of Debrecen Medical and Health Science Center, Department of Neurology, Debrecen, Hungary
6University of Heidelberg, Department of Neurology, Heidelberg, Germany
7Erasmus Medical Center, Department of Neurology, Rotterdam, The Netherlands
8University of Lille, Department of Neurology, Lille, France
9Hôpital Sainte-Anne- Université Paris Descartes, Department of Neurology, Paris, France
10Miller School of Medicine- University of Miami-, Department of Neurology, Miami, USA
Background and Aims
Bleeding complications may offset the benefit of antiplatelet drugs in patients at increased risk of bleeding and low risk of recurrent ischaemic events following a TIA or ischaemic stroke. We aimed to investigate net benefit of antiplatelet treatment according to an individuals’ bleeding risk.
Method
We pooled individual patient data from six trials (CAPRIE, ESPS-2, MATCH, CHARISMA, ESPRIT and PRoFESS) investigating antiplatelet therapy in secondary stroke prevention. Patients were stratified into quintiles according to their predicted risk of major bleeding with the S2TOP-BLEED score. The annual risk of major bleeding and ischaemic events was assessed per quintile and net benefit was compared for three scenarios: 1) aspirin versus no antiplatelet treatment, 2) aspirin+clopidogrel versus aspirin or clopidogrel monotherapy and 3) aspirin+dipyridamole versus clopidogrel.
Results
37,087 patients were included in the analyses. Both risk of major bleeding and recurrent ischaemic events increased over quintiles of predicted bleeding risk, but risk of ischaemic events was consistently higher. The net benefit was positive for aspirin versus no antiplatelet treatment irrespective of baseline bleeding risk. Treatment with aspirin+clopidogrel led to more major bleedings than it reduced ischaemic events (Figure). There was no preference for either aspirin+dipyridamole or clopidogrel according to baseline bleeding risk (Figure).
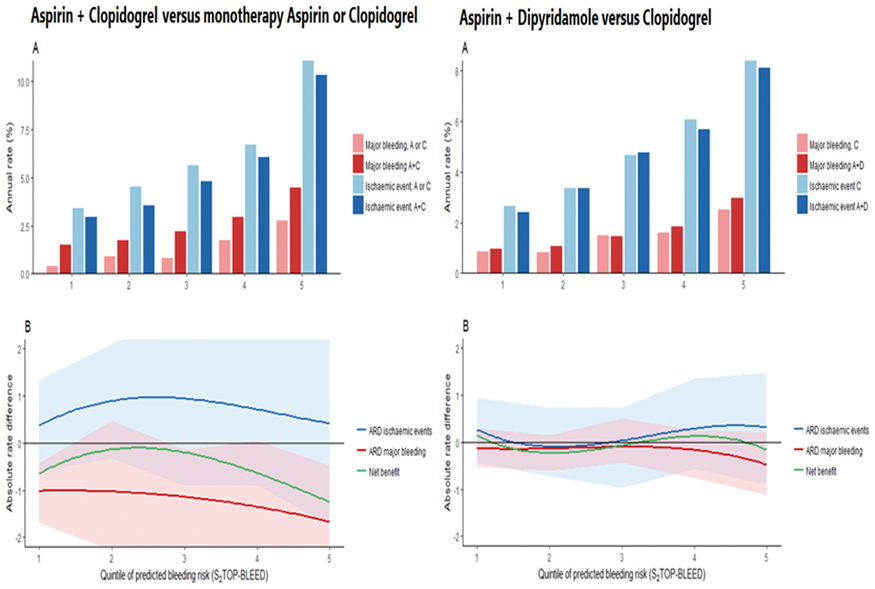
Conclusion
Risk of ischaemic events and major bleeding increase in parallel. Decisions for long-term antiplatelet treatment should not be individualized based on bleeding risk.
Trial registration number
N/A
AS04-014
EFFECT ON SEVEN YEAR SURVIVAL OF A MULTIFACTORIAL VASCULAR RISK FACTOR INTERVENTION FIRST YEAR AFTER STROKE OR TIA
1Bærum Hospital- Vestre Viken Hospital Trust, Department of Internal Medicine, Oslo, Norway
2The Norwegian Knowledge Centre for the Health Services, Medical, Oslo, Norway
3Oslo University Hospital, Department of Neurology, Oslo, Norway
4Akershus University Hospital, Department of Neurology, Oslo, Norway
5Oslo University Hospital and Dept of Informatics- University of Oslo, Bioinformatics core facility- Inst for Cancer Research, Oslo, Norway
6Oslo University Hospital and Institute of Clinical Medicine- University of Oslo, Department of Geriatric Medicine, Oslo, Norway
7Bærum Hospital- Vestre Viken Hospital Trust, Department of Medical Research, Oslo, Norway
Background and Aims
Stroke and coronary heart disease share the same risk factors, and a multifactorial intervention post stroke may potentially result in the same reduction in cardiovascular mortality as seen after coronary events. Some small studies have shown promising results, but long-term follow up is missing.
We aimed to evaluate the effect on survival seven years after a one-year multifactorial risk factor intervention, and identify clinical predictors for long-term survival in a hospital-based cohort of patients with first ever stroke or transient ischemic attack (TIA).
Method
Between February 2007 and July 2008, patients were randomized on day 7–10 to outpatient intensive risk factor intervention versus usual care the first year post stroke. From February 2014 to July 2016, the stroke survivors were invited to a follow-up. Examination at baseline, one year and seven years follow-up included extensive assessment of vascular risk factors and cognitive assessments.
Results
195 patients were randomized. Mean age 71.6, standard deviation (SD) 12.5, 53.3 % were male, mean Body Mass Index (BMI) 25.6 (SD 4.1). Kaplan-Meier survival curves show no significant difference in intention to treat (ITT) population and complete case (CC) population (log rank p = 0.293 vs log rank p = 0.065). Age and BMI are independent predictors for long term survival (HR 1,08 (CI 1,05-1.11), HR 0.91 (CI 0,85-0.97) ).
Conclusion
There was a nonsignificant trend toward better long-term survival seven years after a multidomain vascular risk factor intervention the first year post stroke. BMI is an independent predictor for long-term survival after first-ever stroke and TIA.
Trial registration number
NCT00506818
AS03-037
EFFECTS OF CANAGLIFLOZIN ON STROKE IN THE CANVAS PROGRAM
1The George Institute for Global Health and University of Sydney, Neurological & Mental Health Division, Sydney, Australia
2The George Institute for Global Health- University of New South Wales, Neurological & Mental Health Division, Sydney, Australia
3Shanghai Jiao Tong University, Department of Radiology- Ren Ji Hospital- School of Medicine, Shanghai, China
4The George Institute for Global Health- University of New South Wales, n/a, Sydney, Australia
5Linköping University, Division of Community Medicine- Primary Care- Department of Medicine and Health Sciences- Faculty of Health Sciences- Department of Local Care West- County Council of Östergötland, Linköping, Sweden
6North Shore Vertigo & Neurology Clinic, n/a, St. Leonards, Australia
7Sydney Medical School and University of Sydney, Sydney Adventist Hospital Clinical School, Sydney, Australia
8University of Oxford, Oxford Centre for Diabetes- Endocrinology and Metabolism and Harris Manchester College, Oxford, United Kingdom
9The Royal North Shore Hospital and University of Sydney, n/a, Sydney, Australia
10University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
11Stanford University School of Medicine, Stanford Center for Clinical Research- Department of Medicine, Stanford, USA
12Janssen Research & Development- LLC, n/a, Raritan, USA
13University of New South Wales, Faculty of Medicine, Sydney, Australia
14University of Sydney, The Charles Perkins Centre, Sydney, Australia
15Imperial College London, n/a, London, United Kingdom
Background and Aims
The sodium glucose co-transporter 2 inhibitor (SGLT2i) canagliflozin reduces the risk of total cardiovascular events but there is uncertainty about the effect of SGLT2i on stroke. We report the detailed stroke outcomes from the CANVAS Program.
Method
The CANVAS Program includes 10,142 participants with type 2 diabetes and high cardiovascular risk. Participants were randomly assigned to canagliflozin or placebo and followed for a mean of 188 weeks. In the intent-to-treat analysis set, stroke outcomes were determined by an endpoint adjudication committee.
Results
There were 309 strokes recorded during follow-up, at a rate of 7.93/1000 patient-years amongst those assigned canagliflozin and 9.62/1000 patient-years amongst placebo (hazard ratio [HR] 0.87, 95% CI 0.69 to 1.09). A significant reduction was observed for the small number of haemorrhagic strokes recorded (n = 30, HR 0.43, 95% CI 0.20 to 0.89) but no clear effect was apparent for the larger number of ischaemic strokes (n = 253, HR 0.95, 95% CI 0.74 to 1.22) or undetermined strokes (n = 29, HR 1.04, 95% CI 0.48 to 2.22). Effects on other cardiovascular outcomes were comparable amongst patients with (n = 1958, 19%) and without a history of cerebrovascular disease at baseline.
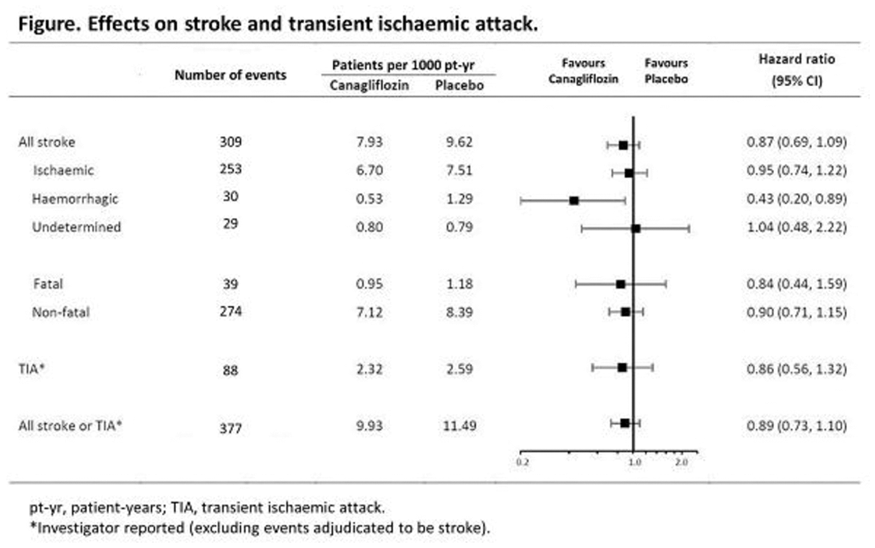
Conclusion
Statistically, there was no overall effect on stroke risk. The reduction in haemorrhagic stroke was based on small numbers of events and has a wide confidence interval.
Trial registration number
ClinicalTrials.gov identifiers: NCT01032629 and NCT01989754
AS21-006
DIRECT ORAL ANTICOAGULANTS VERSUS VITAMIN K ANTAGONISTS AFTER A RECENT ISCHEMIC STROKE - A POOLED INDIVIDUAL PATIENT DATA ANALYSIS
1University Hospital and University Basel, Neurology and Stroke Center, Basel, Switzerland
2UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Stroke Research Center- Department of Brain Repair and Rehabilitation, London, United Kingdom
3University of Perugia, Stroke Unit and Devision of Cardivascular Medicine, Perugia, Italy
4UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Stroke Research Group- Departement of Brain repair and Rehabilitation, London, United Kingdom
5National Cerebral and Cardiovascular Center, Devision of Stroke Care Unit, Osaka, Japan
6University of Erlangen-Nuremberg, Departement of Neurology, Erlangen, Germany
7Azienda Ospedaliera Universitaria Integrata, USD Stroke Unit- DAI di Neuroscienze-, Verona, Italy
8University Hospital Basel, Clinical Trial Unit, Basel, Switzerland
9National & Kapodistrian University of Athens School of Medicine- “Attikon” University Hospital, Second Department of Neurology, Athens, Greece
Background and Aims
We compared the clinical benefit of direct oral anticoagulants (DOAC) and Vitamin-K antagonists (VKA) in patients having atrial fibrillation (AF) with a recent (<3month) ischemic stroke or TIA.
Method
We conducted an individual patient data analysis of 7 prospective studies and analyzed the association between type of anticoagulation (DOAC vs. VKA) with a composite endpoint [recurrent ischemic stroke (AIS), intracerebral hemorrhage (ICH) or mortality] using mixed effects Cox proportional hazards regression models and calculating adjusted hazard ratios (HRadj) with 95% confidence intervals (95%CI).
Results
Of 4912 patients [median age 78years (IQR71-84); 2331 (47.5%) female; 4739 (96.5%) ischemic stroke as index event, median NIHSS-at-onset 5 (IQR 2–12)], 2256 (45.9%) patients received VKA and 2656 (54.1%) received DOAC after the index stroke. The median time from index stroke to start of oral anticoagulation was 5 days (IQR 2–14) for VKA and 5 days (IQR 2–11) for DOAC (p = 0.53). There were 262 AIS (4.4%/year), 71 ICH (1.2%/year) and 439 deaths (7.4%/year) during the total follow-up of 5970 patient years. DOAC treatment reduced the risk of the composite endpoint (HRadj 0.78, CI95% 0.64-0.94, p = 0.01). In a secondary analysis, DOAC reduced the risk of ICH (HRadj 0.34, CI95% 0.16-0.71, p = 0.01) and mortality (HRadj 0.71, CI95% 0.56-0.90, p < 0.01) while the risk of recurrent AIS did not differ (HRadj 0.98, 95%CI 0.72-1.35, p = 0.91).
Conclusion
In patients with AF, DOACs commenced in a median of 5 days after stroke seem to have a clinical benefit compared to treatment with VKA, mainly due to a lower risk for ICH and mortality.
Trial registration number
N/A
AS01-015
PREDICTION OF MAJOR BLEEDING WITH S2TOP-BLEED SCORE IN ACUTE ISCHAEMIC STROKE OR TIA PATIENTS: A SUB-STUDY OF THE TARDIS TRIAL
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Antiplatelet therapy is widely used in secondary prevention after cerebral ischaemia, but is associated with increased bleeding. The S2TOP-BLEED score predicts major bleeding with chronic antiplatelet therapy and is tested here in acute stroke using data from the TARDIS trial.
Method
The international TARDIS trial assessed the safety and efficacy of intensive (combined aspirin, dipyridamole and clopidogrel) versus guideline (aspirin/dipyridamole, or clopidogrel alone) antiplatelets given for one month in 3096 patients with acute stroke or TIA. The S2TOP-BLEED score was derived from age; sex; ethnicity; premorbid modified Rankin Scale (mRS); history of smoking, prior stroke, diabetes or hypertension; weight; and antiplatelet regime. Triple antiplatelet therapy was scored as for combined aspirin and clopidogrel. Data are number (%), median [interquartile range], or mean (standard deviation).
Results
S2TOP-BLEED scores were available for 2893 (93.4%) patients: mean age 68.9 (10.1) years, male 1886 (63.2%), Caucasian 2834 (95.0%), smoking 770 (25.8%), prior stroke 338 (11.3%), diabetes 563 (18.9%), hypertension 1753 (58.8%), premorbid mRS ≥3 2 (0.1%), estimated weight 75.4 (16.6) kg. 1493 patients were randomised to triple antiplatelet therapy, and 1490 to guideline: 817 (54.8%) clopidogrel and 673 (45.2%) aspirin/dipyridamole. S2TOP-BLEED scores ranged from 2 to 24, mean 11.8 (3.8), median 12 [9-14]. Major bleeding (54, 1.8% patients by day 90) increased with S2TOP-BLEED score: 0–5, 0 (0%); 6–10, 11 (1.2%); 11-15, 30 (2.1%); >15, 13 (2.8%); p = 0.0057 for trend.
Conclusion
The S2TOP-BLEED score appears to predict major bleeding by day 90 in patients on antiplatelets after acute non-cardioembolic cerebral ischaemia.
Trial registration number
ISRCTN47823388
AS01-014
CHARACTERISTICS AND OUTCOMES OF PATIENTS WITH OR WITHOUT A BLEEDING EVENT: RESULTS FROM THE TRIPLE ANTIPLATELETS FOR REDUCING DEPENDENCY IN ISCHAEMIC STROKE (TARDIS) TRIAL
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Intensive antiplatelet therapy following acute cerebral ischaemia was associated with increased bleeding in the TARDIS trial of intensive antiplatelet therapy. We compared the characteristics and outcomes of patients with or without bleeding events in the TARDIS trial.
Method
TARDIS compared one month of intensive antiplatelet therapy with guideline in patients with acute non-cardioembolic ischaemic stroke or transient ischaemic attack. Information on bleeding events and functional outcome by day 90 were assessed centrally blinded to treatment assignment. Outcomes were analysed using adjusted ordinal logistic regression and multiple regression.
Results
Bleeding event data are available for 3072/3096 (99.2%) patients, of whom 444 (14.5%) suffered a bleed. Compared to the rest, patients with a bleed were more likely to: be female (43.0% vs. 36.0%, p = 0.005); have presented with sensory loss (39.4% vs. 33.7%, p = 0.019); have a higher pre-morbid modified Rankin Scale score (>0: 19.8% vs. 15.2%, p = 0.014) and have had a qualifying event of ischaemic stroke (73.0% vs. 71.5%, p = 0.009). Patients with a bleed were also less likely to have been taking either aspirin (22.5% vs 27.1%, p = 0.043) or combined aspirin and dipyridamole (1.4% vs. 3.0%, p = 0.049) prior to their qualifying event. By day 90, patients with a bleed were more dependent (mRS, p = 0.002), disabled (Barthel Index, p < 0.001), cognitively impaired (t-MMSE, p = 0.027) and had a poorer quality of life (EQ-5D-HSUV, p = 0.007) and mood (Zung depression scale, p = 0.001).
Conclusion
Patients with a bleeding event were more dependent at baseline and had a poorer outcome by day 90.
Trial registration number
ISRCTN47823388
Scientific Communications -Genetics, Omics and Biomarkers
AS29-026
A GENOME-WIDE ASSOCIATION STUDY IDENTIFIED A CANDIDATE LOCUS ASSOCIATED WITH RTPA-INDUCED HEMORRHAGIC TRANSFORMATION
1Vall d'Hebron Institute of Research VHIR, Neurovascular Research Laboratory, Barcelona, Spain
2Fundació Docència i Recerca Mutua Terrassa- Hospital Universitari Mútua de Terrassa, Stroke pharmacogenomics and genetics, Terrassa, Spain
3Hospital Universitario Central de Asturias HUCA, Neurology Department- Stroke Unit, Oviedo, Spain
4Hospital Germans Trias i Pujol- Universitat Autònoma de Barcelona, Department of Neuroscience, Badalona, Spain
5Hospital Universitari Vall d'Hebron, Stroke Unit- Department of Neurology, Barcelona, Spain
6Fundaciò de Investigació Sanitaria de les Illes Baleares FISIB, Neuroscience Laboratory, Palma de Mallorca, Spain
7Hospital Clínic i Provincial de Barcelona, Department of Neurology, Barcelona, Spain
8University Hospital of Albacete, Department of Neurology, Albacete, Spain
9Hospital de la Santa Creu i Sant Pau, Stroke Unit- Department of Neurology, Barcelona, Spain
10Washington University School of Medicine, Division of Emergency Medicine, Saint Louis, USA
11Washington University School of Medicine, Department of Psychiatry, Saint Louis, USA
12IMIM-Hospital del Mar, Neurovascular Research Group. Department of Neurology, Barcelona, Spain
13Hospital Universitario Virgen Macarena, University of Seville & Department of Neurology, Seville, Spain
14Institute de Biomedicine of Seville IBIS, Hospital Universitario Virgen del Rocío, Seville, Spain
15Washington University School of Medicine, Department of Neurology, Saint Louis, USA
16Hospital de la Santa Creu i Sant Pau, Stroke Pharmacogenomics and Genetics, Barcelona, Spain
Background and Aims
Hemorrhagic transformation (HT) is a feared complication after tissue-plasminogen activator (rt-PA) treatment in ischemic stroke and appears to be genetically modulated. We aimed to identify genetic risk factors associated with rt-PA-induced HT in stroke patients.
Method
A four-cohort GWAs meta-analysis was performed. Ischemic stroke patients within 6 hours of symptoms onset treated with intravenous rt-PA were recruited in Spanish hospitals. Blood samples were genotyped with Omniquad 2.5M, Human Core Exome (Illumina) and Axiom Biobank (Affymetrix). Quality controls, 1000G imputation, association analysis and fixed-effect metanalysis were performed following previous recommendations. Patients with any type of HT were defined as cases by ECASS criteria. Gene expression was evaluated by Genotype-Tissue Expression (GTEx) portal.
Results
A total of 7,048,546 SNPs (minor allele frequency >1%) and 1,385 ischemic stroke patients were analyzed. HT was present in 239 patients (17.3%); cases included 135 hemorrhagic infarcts (9.74%) and 104 parenchymal hematomas (7.5%). A locus at 6p22 with genome-wide significant association (p-value 2.92 × 10-08; OR: 2.08, 95%CI:1.60-2.69) was found associated with HT. Furthermore, robust association was reached (p-value 5.25 × 10-03; OR: 1.58, 95%CI:1.15-2.20) when the top SNP was evaluated with parenchymal hematoma. In-silico GTEx identified an association between the top SNP and the expression of the nearest gene in blood tissue (p-value 2.3x10-03). The candidate gene was previously reported modulating immune response and increasing metalloproteinases levels after cerebral ischemia.
Conclusion
GWAs meta-analysis in rt-PA treated patients revealed a locus at 6p22 associated with HT and the most severe hemorrhagic event, parenchymal hematoma. Replication and functional analysis are needed to confirm the results.
Trial registration number
N/A
AS29-004
ELEVATED ENDOTHELIAL AND LEUCOCYTIC MICROVESICLE LEVELS ARE RELATED TO ADVERSE LONG-TERM CARDIOVASCULAR OUTCOME AFTER MILD TO MODERATE ISCHEMIC STROKE
1Center for Stroke Research Berlin CSB, Charité - Universitätsmedizin Berlin, Berlin, Germany
2Campus Benjamin Franklin - Department of Cardiology, Charité - Universitätsmedizin Berlin, Berlin, Germany
3Deutsches Zentrum für Herz-Kreislauf-Forschung DZHK, Charité - Universitätsmedizin Berlin, Berlin, Germany
4Department of Neurology, Charité - Universitätsmedizin Berlin, Berlin, Germany
5Institute of Public Health, Charité - Universitätsmedizin Berlin, Berlin, Germany
6Institute of Biometry and Clinical Epidemiology, Charité - Universitätsmedizin Berlin, Berlin, Germany
7German Center for Neurodegenerative Disease DZNE, Charité - Universitätsmedizin Berlin, Berlin, Germany
8Excellence Cluster Neurocure, Charité - Universitätsmedizin Berlin, Berlin, Germany
9Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands
Background and Aims
Microvesicles (MV) are extracellular vesicles formed during cell activation and apoptosis. In ischemic stroke patients, they are known to be elevated compared to healthy controls and related to short-term outcomes. Their relevance as acute phase biomarkers for long-term cardiovascular outcomes after stroke remains unknown.
Method
In the PROSpective Cohort with Incident Stroke Berlin (PROSCIS-B), patients with mild to moderate ischemic stroke were followed for 3 years. The predefined combined endpoint included recurrent stroke, myocardial infarction and all-cause death. Blood samples were taken between days 1–7 after admission. Levels of endothelial (EMV: AnnexinV+, CD45-, CD41-, CD31+/CD144+/CD146+), leucocytic (LMV: AnnexinV+, CD45+, CD41-), monocytic (MMV: AnnexinV+, CD41-, CD14+) and platelet-derived MV(PMV: AnnexinV+, CD41-) were measured using fluorescence-activated cell sorting (FACS). We tested for the difference in survival between patients with high and low MV levels (log-rank) and calculated hazard ratios (HR) adjusted for potential confounders in three different Cox regression models. Dose-response was assessed in quartiles.
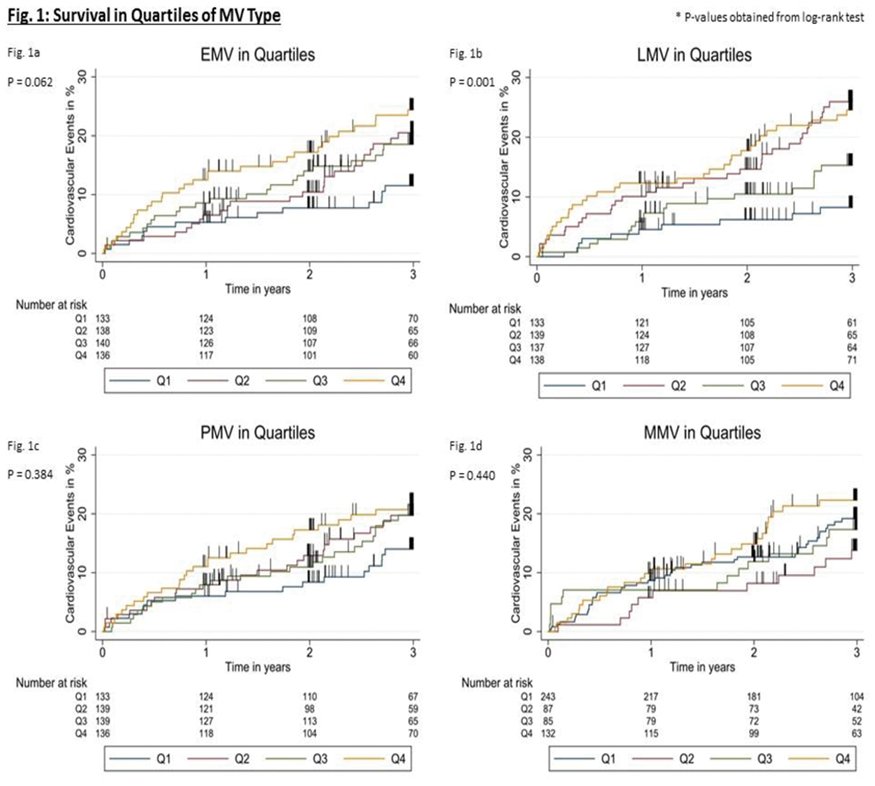
Results
We included 571 patients (median age 69y, 39% female, median NIHSS2 IQR1-4). In total, 42 recurrent strokes, 6 myocardial infarctions and 48 deaths were recorded. Cardiovascular risk was increased in patients with high levels of EMV(Q4v.Q1, HR = 2.5, 95%CI1.2-4.9) and LMV(HR = 3.1, 95%CI1.4-6.8). A minor difference was shown for PMV(HR = 1.7, 95%CI0.9-3.2) and none for MMV(HR = 1.1, 95%CI0.6-1.8).
Conclusion
High levels of EMV and LMV in the acute phase after ischemic stroke are associated with increased long-term cardiovascular risk.
Trial registration number
NCT01364168
AS29-022
BRAIN ARTERIAL DILATATION AND MIDREGIONAL PRO-ATRIAL NATRIURETIC PEPTIDE AS MARKERS OF HEMODYNAMIC DYSFUNCTION: THE NORTHERN MANHATTAN STUDY
1Columbia University, Neurology, New York, USA
2University Hospital of Zurich, Neurology, Zurich, Switzerland
3University of Miami, Neurology, Miami, USA
4National Institutes of Health, The National Institute of Neurological Disorders and Stroke, Bethesda, USA
Background and Aims
Brain arterial dilatation is a core characteristic of dolichoectasia, and is associated with higher risk of stroke. The role of systemic hemodynamic dysfunction in causing vascular dilatation is unknown, and can be estimated by circulating levels of Midregional-atrial-natriuretic peptide (MRproANP).
Method
We measured blood levels of MRproANP in 950 participants (mean age 70 ± 9 years, 40% men, 67% Hispanic) of the Northern Manhattan Study who underwent brain time-of-flight MRA. Brain arterial luminal diameters were normalized and averaged to obtain a measure of dilatation (the Brain Arterial Remodeling (BAR) score). Generalized additive models were used to assess for non-linear associations. Models were adjusted for demographics, head size, vessel-collateral status, and vascular risk factors and further stratified by sex.
Results
In the univariate analysis, there was a persistent non-linear association between log MRproANP with the BAR score (χ2 for the spline regression = 9.67, p = 0.02, figure 1).
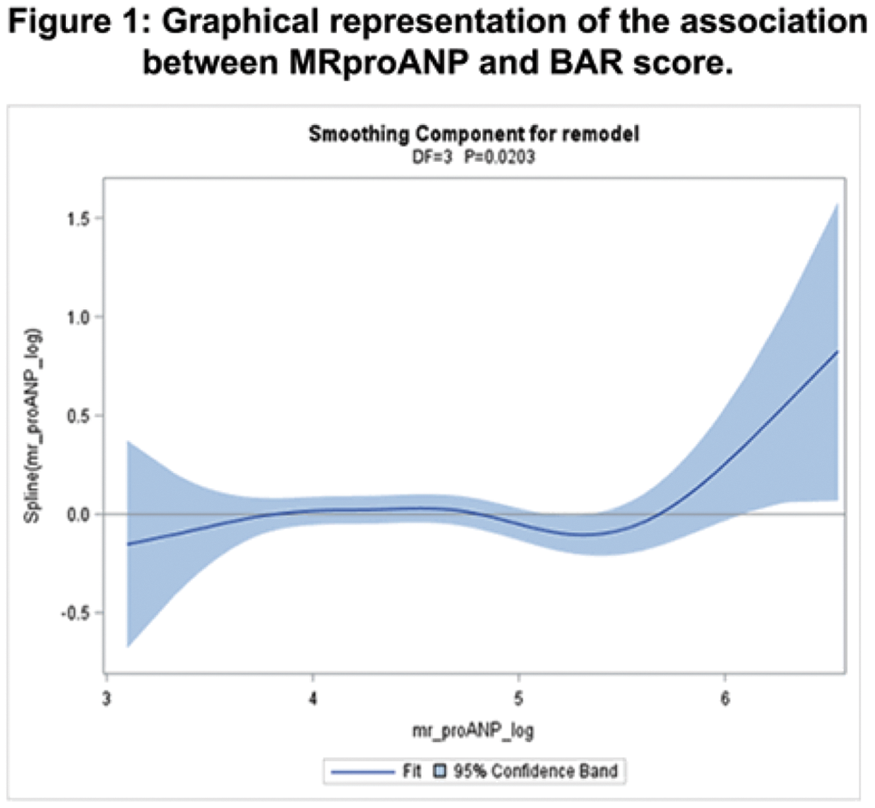
Using a threshold of log MRproANP > 5.9 derived from the spline graph (which equals an MRproANP value > 365 pmol/L), there was a significant association between high MRproANP and a larger BAR score and this association did not change after adjustment (β = 0.68 ± 0.31, p = 0.03) but was greater in women (β = 1.10 ± 0.55, p = 0.04) than in men (β = 0.34 ± 0.38, p = 0.36).
Conclusion
Among individuals with higher levels of MRproANP, a biomarker of hemodynamic dysfunction, brain arteries had larger diameters. Increased intravascular volume may play a role in brain dilatative arteriopathy, and if confirmed mechanistically, may offer targets for intervention. But larger studies with more participants at the extremes of BAR scores are needed.
Trial registration number
N/A
AS29-024
GENOME-WIDE ASSOCIATION STUDY OF FUNCTIONAL OUTCOME AFTER ISCHEMIC STROKE
1Department of Clinical Sciences Malmö, Lund University, Lund, Sweden
2Department of Neurology and Rehabilitation Medicine-, Skane University Hospital, Lund and Malmö, Sweden
3Institute of Biomedicine, Department of Pathology and Genetics, Gothenburg, Sweden
4Bioinformatics Core Facility, University of Gothenburg, Gothenburg, Sweden
5School of Life Sciences, University of Lincoln, Lincoln, United Kingdom
6Department of Neurology, .Institut Hospital del Mar d’Investigació Mèdica IMIM, Barcelona, Spain
7Universitat Autònoma de Barcelona, Barcelona, Barcelona, Spain
8Department of Neurology, Washington University School of Medicine, St. Louis MO, USA
9Department of Neurosciences, Experimental Neurology- KU Leuven – University of Leuven, Leuven, Belgium
10Department of Neurology, University Hospitals Leuven, Leuven, Belgium
11Center for Brain & Disease Research, Laboratory of Neurobiology- VIB, Leuven, Belgium
12Department of Clinical Sciences Lund, Neurology- Lund University, Lund, Sweden
13Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom
14Department of Neurology, Massachusetts General Hospital- Harvard Medical School, Boston MA, USA
15Stroke Prevention Research Unit, Nuffield Department of Clinical Neurosciences- University of Oxford, Oxford, United Kingdom
16School of Biomedical Sciences and Pharmacy, Faculty of Health and Medicine, Newcastle, Australia
17Hunter Medical Research Institute, University of Newcastle, Newcastle, Australia
18Department of Neurology, Helsinki University Hospital, Helsinki, Finland
19Department of Neurology and Rehabilitation, University of Cincinnati College of Medicine, Cincinnati OH, USA
20Departments of Neurology and Health Evaluation Sciences, University of Virginia, Charlottesville VA, USA
21Priority Research Centre for Stroke and Traumatic Brain Injury, University of Newcastle, Newcastle, Australia
22Faculty of Health and Medicine, Newcastle, Newcastle, Australia
Background and Aims
There is large variation in outcomes after ischemic stroke and genetic factors may account for part of this variation. The Genetics of Ischaemic Stroke Functional outcome (GISCOME) network aims to discover genetic variants associated with post-stroke outcomes. We present the first results of genome-wide association (GWA) analyses from GISCOME.
Method
6,165 patients with ischemic stroke from 17 cohorts in Europe, US and Australia were included. The primary outcome was modified Rankin Scale (mRS) after 60-190 days, evaluated as two dichotomous variables (0–1 versus 2–6 and 0–2 versus 3–6). We also performed ordinal analysis of mRS scores. GWA analyses were performed in each cohort independently and results were meta-analyzed. Analyses were adjusted for age, sex, stroke severity (baseline NIHSS), and the five first principal components. The significance level was P<5x10-8.
Results
We identified an intronic variant (rs1842681) in the LOC105372028 gene, which was associated with outcome defined as mRS 0–2 vs 3–6 (P = 6.8x10-9). LOC105372028 is highly expressed in the brain, but its function remains to be elucidated. We also found several variants suggestively associated with outcome (P<10-5). For example, in ordinal analysis, a suggestive (P = 1x10-6) intronic variant (rs78734480) was detected in NTN4, a gene reported to influence post-stroke functional recovery in mice.
Conclusion
We performed the largest GWA study on stroke outcome to date, and identified one significant locus and some suggestive variants with potential mechanisms in stroke outcomes. Effect sizes of genetic variants may be small for stroke outcomes, and future studies should include larger samples, enabling subgroup analyses.
Trial registration number
n/a
AS29-023
SERUM NEUROFILAMENT LIGHT PREDICTS SHORT- AND LONG-TERM OUTCOMES IN ISCHEMIC STROKE
1Institute of Biomedicine, Department of Pathology and Genetics, Göteborg, Sweden
2Department of Mathematical Statistics, Chalmers University of Technology, Gothenburg, Sweden
3Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
4Institute of Neuroscience and Physiology, Department of Psychiatry and Neurochemistry, Gothenburg, Sweden
5Clinical Neurochemistry Laboratory, Sahlgrenska University Hospital, Mölndal, Sweden
6UK Dementia Research Institute at UCL, London, London, United Kingdom
7Department of Molecular Neuroscience, UCL Institute of Neurology- Queen Square, London, United Kingdom
Background and Aims
Serum neurofilament light chain (NFL) has emerged as a biomarker of neuronal damage. We hypothesized that NFL predicts post-stroke outcomes.
Method
Serum samples from the Sahlgrenska Academy Study on Ischemic Stroke (SAHLSIS) were available from 489 cases at baseline (median day 4), 546 at 3 months post-stroke, and 595 age- and sex-matched controls. 221 cases participated in a 7-year follow-up. NFL was measured using ultrasensitive single molecule array technology. Patients were scored by NIH stroke scale (NIHSS) at baseline, and by NIHSS and modified Rankin Scale (mRS) at 3 months and 7 years.
Results
Median NFL concentrations were 60.2 pg/mL (interquartile range 28.3–190) at baseline, 90.6 (41.8–230) at 3 months, 18.1 (11.5–35.5) at 7 years, and 14.2 (9.0–21.0) in controls. NFL baseline and 3-month concentrations showed an independent association to case-control status. Three-month NFL showed highest correlation to baseline NIHSS (rp = 0.56,) and was associated to NIHSS and mRS at 3 months and 7 years, after adjustment for age, previous stroke and baseline NIHSS (p < 0.001 throughout). The c-statistic for poor outcome (mRS>2) at 7 years with NFL as predictor was 0.72 (in line with baseline NIHSS, 0.73) and increased slightly to 0.80 (i.e., a strong model) when adding age, previous stroke and NIHSS.
Conclusion
Serum NFL concentrations after an ischemic stroke independently predict neurological and functional outcomes, making NFL a candidate biomarker with multiple potential applications. However, the time profile for NFL post-stroke needs to be established to identify the optimal time for measurement.
Trial registration number
N/A
AS29-012
METALLOPROTEINASE-9, BOTH ACTIVITY AND ANTIGEN ACUTE CHANGES, PREDICTS HEMORRHAGIC TRANSFORMATION IN ISCHEMIC STROKE PATIENTS TREATED WITH THROMBOLYSIS
1Careggi University Hospital, Stroke Unit, Florence, Italy
2Institute of Neuroscience, Italian National Research Council, Florence, Italy
3Careggi University Hospital, Atherothrombotic Diseases Center, Florence, Italy
4Universisty of Florence, Department of Neurosciences- Psychology- Drug Research and Child Health, Florence, Italy
5University of Florence, Department of Neurosciences- Psychology- Drug Research and Child Health, Florence, Italy
Background and Aims
Circulating level variations of metalloproteinase-9 (MMP9) have been associated with poor outcomes in acute ischemic stroke (AIS) treated with tissue plasminogen activator (tPA). We aimed to corroborate the role of MMPs activities with antigen measurement in this clinical setting
Method
Blood was taken before and 24-hours after tPA from 327 AIS patients (mean age 68 years, median NIHSS 11). Activity of MMP2 and MMP9 at baseline and Delta median values of MMPs activity [(post tPA MMP activity - baseline MMP activity)/(baseline MMP activity)] were analyzed related to symptomatic intracranial hemorrhage (sICH), and 3-month death. We used backward selection algorithm including major clinical confounders and MMP9 and MMP2 antigen levels to test the independent associations of MMPs activities with outcomes
Results
1) baseline MMP9 activity levels were correlated with MMP9 antigen level (rho = 0.335), as well as delta MMP9 activity levels were significantly related to delta MMP9 antigen levels (rho=0.388); 2) delta MMP9 activity was significantly associated with sICH both at univariate and multivariate logistic regression analysis [OR (95% CI): 1.33 (1.06-1.68), p = 0.014 and 1.39 (1.01–1.90)], p = 0.035); 3) significantly higher baseline MMP2 activity was found in patients who died than in survivors (p = 0.02). This association was not confirmed in the multiple regression model.
Conclusion
These data refine our knowledge about the role of MMPs in tPA treated stroke patients. Specific targets for MMP inhibition need to be identified and then attacked by selective agents during the most appropriate time point.
Trial registration number
N/A
AS29-007
RABEP2 (RAB GTPASE-EFFECTOR BINDING PROTEIN-2) IS ASSOCIATED WITH ISCHEMIC STROKE PHENOTYPES: A TRANSLATIONAL REPLICATION STUDY
1Massachusetts General Hospital, Neurology, Boston, USA
2University of Virginia, Neurology, Charlottesville, USA
3Klinikum der Universität München, Institute for Stroke and Dementia Research, Munich, Germany
4Lund University, Neurology, Lund, Sweden
5Lund University, Neuroradiology, Lund, Sweden
6Massachusetts General Hospital, Radiology, Boston, USA
7University of North Carolina, Department of Cell Biology and Physiology- McAllister Heart Institute, Chapel Hill, USA
Background and Aims
Recruitment of collaterals following large-vessel occlusion (LVO) is a crucial predictor of tissue survival. Variation of anatomic collaterals has recently been linked to genetic background in mice. We tested association between ischemic stroke (IS) and the novel murine “collateral gene” RABEP2.
Method
We examined all SNPs within RABEP2 and 13 known angiogenic genes using VEGAS (Versatile Gene-based Association Study) in 532 acute IS (AIS) patients of European ancestry with genome-wide genotyping and DWI volume (DWIv) (GASROS cohort). Linear regression of natural log-transformed DWIv and SNPs was adjusted for age, sex and relevant principal components. Association between RABEP2 and IS risk was tested in METASTROKE (1700 IS patients versus 7900 non-stroke controls, 283 SNPs tested among 21 genes). Thresholds were per Bonferroni correction.
Results
RABEP2 emerged with nominal significance (P = 0.09) in association with DWIv in GASROS (age: 66 ± 14.9y, sex: 63.4% male, DWIv: 2.2cm3 (IQR: 0.6-11.7cm3), top SNP (P = 0.004, rs11645302)). In METASTROKE, two SNPs in RABEP2 had the lowest (P = 0.0004, rs35979293) and second lowest (P = 0.0012, rs4072401) nominal P-values for cardioembolic IS versus non-stroke, with a RABEP2 gene-wise P = 0.0083. The top GASROS SNP is in high-LD with the above 2 METASTROKE SNPs (D’ = 0.94EU, D’ = 1.0AF). In GASROS, rs35979293 was associated with DWIv (G/T, OR 0.2589, P = 0.04834), with differential effect in LVO versus non-LVO cases.
Conclusion
Common variants in RABEP2 appear to impact acute infarct size in AIS patients, highlighting further the role of genetic contribution to collateral circulation status and the need for future investigations using collateral-specific endophenotypes in this emerging field.
Trial registration number
METASTROKE Collaboration of the ISGC
AS19-006
A NEW, CLINICALLY AVAILABLE, TARGETED SEQUENCING PANEL TO SCREEN FOR MONOGENIC CAUSES OF SMALL VESSEL STROKE: EVALUATION IN 993 YOUNGER ONSET LACUNAR STROKE PATIENTS
1University of Cambridge, Stroke Research Group - Department of Clinical Neurosciences, Cambridge, United Kingdom
2University of Cambridge, Stroke Research Group- Department of Clinical Neurosciences, Cambridge, United Kingdom
3University of Cambridge, Department of Haematology, Cambridge, United Kingdom
4University of Cambridge, Division of Respiratory Medicine - Department of Medicine, Cambridge, United Kingdom
Background and Aims
Cerebral small vessel disease (SVD) is the most common genetic form of stroke. The most common type is Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) caused by mutations in the NOTCH3 gene, but other monogenic forms have been identified including autosomal recessive and dominant HTRA1 mutations, and dominant COL4A1/A2, TREX1 and FOXC1 mutations. Testing for these using traditional Sanger sequencing is time-consuming and expensive. Targeted multi-gene arrays allow quicker and more cost-effective testing.
Method
We designed a custom array capturing 6 candidate genes: NOTCH3, HTRA1, COL4A1, COL4A2, TREX1 and FOXC1. We sequenced 993 TOAST-classified and MRI-confirmed early-onset (≤70 years) lacunar stroke cases on this platform.
Results
Eleven patients (1.1%) had typical cysteine-altering, CADASIL-causing NOTCH3 mutations. Twelve had single copies of 9 different HTRA1 variants, 2 variants in 2 patients (0.2%) were previously associated with autosomal dominant HTRA1 disease. Nine COL4A1 variants were identified in 10 individuals; one had been previously reported in intracerebral haemorrhage. Five TREX1 variants were found in 5 individuals, one was previously reported in Aicardi-Goutieres Syndrome. Novel variants were identified in COL4A2 (9 variants, 9 individuals) and FOXC1 (2 variants, 2 individuals).
Conclusion
In this large, well characterised cohort of MRI-confirmed lacunar stroke, we found previously described pathogenic heterozygous mutations associated with monogenic forms of SVD in 13 cases (1.3%). Most of these were CADASIL-causing, but two were HTRA1-related SVD. In addition, we found 30 potentially pathogenic novel variants in 34 individuals (3.4%). Family segregation and functional data are required to confirm the pathogenicity of these variants.
Trial registration number
N/A
AS29-006
SERUM NEUROFILAMENT LIGHT: A BIOMARKER OF NEUROAXONAL INJURY AFTER ISCHEMIC STROKE
1Institute for Stroke and Dementia Research, University Hospital- LMU Munich, Munich, Germany
2Munich Cluster for Systems Neurology SyNergy, SyNergy, Munich, Germany
3Graduate School of Systemic Neurosciences, LMU Munich, Munich, Germany
4Neurologic Clinic and Policlinic- Departments of Medicine- Biomedicine and Clinical Research, University Hospital Basel- University of Basel, Basel, Switzerland
5German Center for Neurodegenerative Diseases DZNE, DZNE Bonn, Bonn, Germany
6Department of Neurology, University Hospital Bonn, Bonn, Germany
7Department of Neurology, University Hospital- LMU Munich, Munich, Germany
8Department of Neuroradiology, University Hospital- LMU Munich, Munich, Germany
9Department of Radiology, University Hospital- LMU Munich, Munich, Germany
10Department of Neurology, University of Magdeburg- University Hospital, Magdeburg, Germany
11German Center for Neurodegenerative Diseases DZNE, DZNE Magdeburg, Magdeburg, Germany
12Stroke Center and Department of Neurology, University Hospital Basel, Basel, Switzerland
13German Center for Neurodegenerative Diseases DZNE, DZNE Munich, Munich, Germany
Background and Aims
Serum neurofilament light chain (sNfL) recently gained attention as a circulating marker for neuroaxonal injury. We explored the utility of sNfL as a biomarker for primary and secondary neuroaxonal injury after ischemic stroke (IS) and assessed its value for the prediction of functional outcome.
Method
We employed a single-molecule assay to quantify sNfL levels in healthy controls (HC) and two independent cohorts of patients with IS: (i) with serial serum sampling at hospital arrival (N = 196), at days 2, 3, and 7 (N = 89), and up to 6 months post-stroke; (ii) with standardized MRI at both baseline and 6 months post-stroke, and with serum sampling at 6 months (N = 95). We determined the temporal profile of sNfL, its association with imaging markers of neuroaxonal injury, and with functional outcome.
Results
IS patients had higher sNfL levels compared with HC starting from admission until 6 months post-stroke. sNfL levels peaked at day 7 and correlated with infarct volumes (day 7: R2 = 0.57, p < 2×10−16). 6 months post-stroke sNfL levels were higher in patients with recurrent ischemic lesions on MRI (N = 19) compared to those without new lesions (N = 76, p = 0.002). sNfL levels 6 months post-stroke further correlated with a quantitative measure of secondary neurodegeneration obtained from diffusion tensor imaging MRI (R2 = 0.13, p = 0.001). sNfL levels within the first week post-stroke independently predicted modified Rankin scale scores 3 months post-stroke (cumulative OR = 2.34; p = 0.001).
Conclusion
sNfL is a sensitive biomarker for monitoring primary and secondary neuroaxonal injury after IS and adds to the prediction of functional outcome after IS.
Trial registration number
N/A
Scientific Communications - Large Vessel Disease
AS11-026
MR-DETECTED CAROTID INTRA-PLAQUE HAEMORRHAGE AND RISK OF STROKE IN PATIENTS WITH SYMPTOMATIC AND ASYMPTOMATIC CAROTID STENOSIS: AN INDIVIDUAL PATIENT-DATA META-ANALYSIS
1University Hospital Basel, Neurology, Basel, Switzerland
2University Hospital- LMU Munich, Department of Radiology, Munich, Germany
3University of Nottingham, Radiological Sciences- Division of Clinical Neuroscience, Nottingham, United Kingdom
4Technische Universität München, Department of Neurology, Munich, Germany
5Sunnybrook Health Sciences Centre- University of Toronto, Department of Medical Imaging, Toronto, Canada
6Zuyderland Medical Center, Department of Radiology, Heerlen, The Netherlands
7Kurashiki Central Hospital, Department of Neurosurgery, Okayama, Japan
8Graduate school of Medicine- Kyoto University, Department of Neurosurgery, Kyoto, Japan
9Sunnybrook Health Sciences Centre- University of Toronto, Depatment of Vascular Surgery, Toronto, Canada
10CARIM School for Cardiovascular Diseases- Maastricht University Medical Center, Department of Radiology and Nuclear Medicine, Maastricht, The Netherlands
11University of Nottingham, Radiological Sciences- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Intra-plaque hemorrhage (IPH) on MRI increases the risk for cerebrovascular events in patients with carotid stenosis. Previous studies were too small to provide reliable estimates for stroke risk and to demonstrate if IPH predicts stroke independently of clinical risk factors.
Method
We pooled individual patient data from seven studies including 696 patients (80.5% with symptomatic stenosis) examined with MRI for IPH and followed for a mean duration of 19 months. Hazard ratios (HR) and risks for ipsilateral ischemic stroke were estimated with Cox regression and Kaplan-Meier statistics.
Results
IPH was present at baseline in 51.6% and 29.4% of patients with symptomatic and asymptomatic stenosis, respectively. 66 ipsilateral strokes occurred. IPH increased stroke risk both in symptomatic (HR 10.2, 95% CI 4.6-22.5, p < 0.0001; figure), and asymptomatic patients (HR7.9, 1.3-47.6, p = 0.01). Cumulative 2-year risks were 28.5% in IPH+ vs. 1.9% in IPH- patients with symptomatic stenosis, and 13.0% vs. 1.1% in patients with asymptomatic stenosis. In multivariate analysis including patients with symptomatic stenosis, only IPH (HR 11.0, 4.8–25.1; p < 0.0001) and severe degree of stenosis (HR 3.3, 1.4–7.8; p < 0.01) predicted stroke, while sex, age, type of qualifying event, hypertension, and diabetes did not.
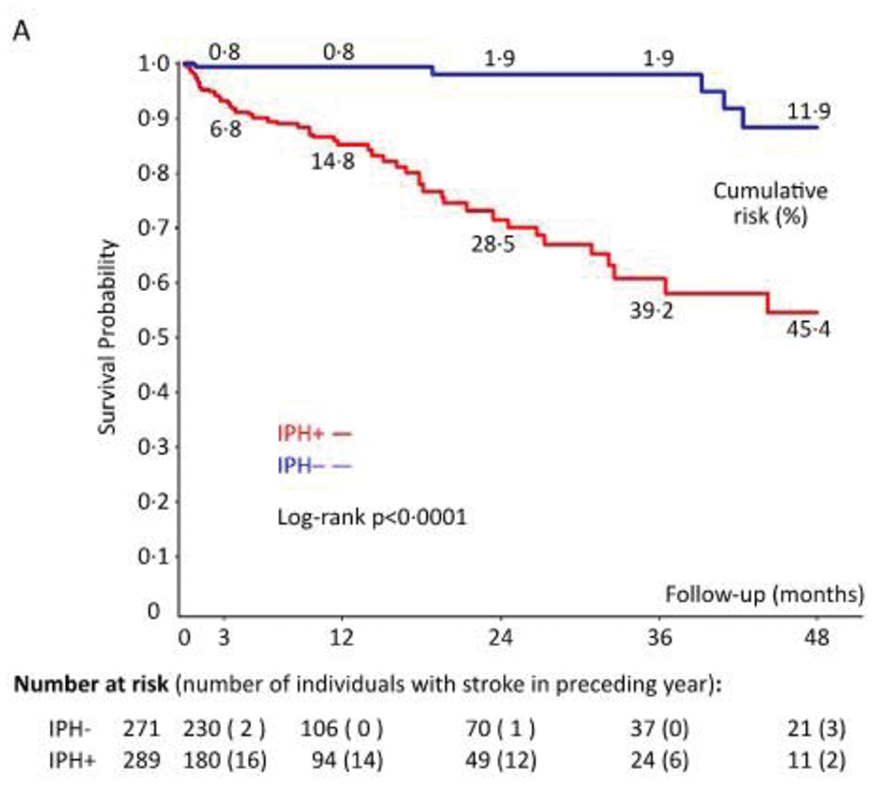
Conclusion
Carotid IPH is a strong and independent predictor of stroke risk among patients with carotid stenosis. Our findings warrant clinical trials selecting subjects for treatment on the basis of plaque MRI.
Trial registration number
N/A
AS09-032
RISK OF DEATH AND STROKE IN 19,000 PATIENTS UNDERGOING CAROTID ENDARTERECTOMY OR STENTING: AN ANALYSIS OF THE DR FOSTER GLOBAL COMPARATORS’ DATASET
1Medical Research Council Population Health Research Unit- Oxford University, Clinical Trials Service Unit- Nuffield Department of Population Health, Oxford, United Kingdom
Background and Aims
Randomised clinical trials (RCTs) show that carotid endarterectomy (CEA) and stenting (CAS) reduce long-term stroke risk. However, procedural risks in historical RCTs may not generalise to the 2010s. Large administrative datasets could provide a more reliable estimate of contemporary risk. We studied the rates of major complications following carotid intervention in an international, benchmarking, collaborative dataset, which includes 18,997 patients admitted to 28 hospitals across 7 countries.
Method
Symptomatic and asymptomatic patients undergoing CEA (n = 16,220) and CAS (n = 2777) between 2011–2015 were studied. The primary outcome was in-hospital death within seven days. The secondary outcome was use of CT head scan within two days of intervention as a proxy for suspected or actual stroke.
Results
In symptomatic patients, mortality following CEA was 0.2% [5/2118] (95% CI: 0.1-0.5) and 3.3% [10/307] (1.3-5.2) after CAS. In asymptomatic patients, mortality following CEA was 0.2% [21/14,102] (0.1-0.2) and 0.7% [18/2470] (0.4-1.1) after CAS. CT scanning was performed in 8.1% [89/1101] (6.5-9.7) of symptomatic patients after CEA and 7.1% [16/224] (4.0-10.7) after CAS. For asymptomatic patients, CT rates were 2.1% [207/10,039] (1.8-2.3) following CEA and 3.3% [71/2187] (2.5-4.0) after CAS.
Conclusion
Death and suspected stroke following carotid intervention were commoner in symptomatic than asymptomatic patients. CAS was associated with increased risk of death compared to CEA, especially in symptomatic patients. This may be partly explained by reverse causation, where sicker patients are preferentially treated with CAS. RCTs remain the standard for comparing interventions but administrative data demonstrate comparable results, making them a useful adjunct in examining patient outcomes.
Trial registration number
N/A
AS09-015
12 MONTHS RISK OF RECURRENT STROKE IN PATIENTS WITH SYMPTOMATIC CAROTID NEAR-OCCLUSION. RESULTS FROM CAOS, A MULTICENTER REGISTRY STUDY
1Hospital General Universitario Gregorio Marañón, Neurology- Stroke Unit, Madrid, Spain
2Hospital Universitario Infanta Cristina, Neurology, Badajoz, Spain
3Complejo Asistencial Universitario de León-, Neurology, León, Spain
4Hospital Universitario Virgen del Rocío, Neurology, Sevilla, Spain
5Hospital San Pedro Alcántara, Neurology, Cáceres, Spain
6Hospital Universitario La Paz, Neurology, Madrid, Spain
7Hospital Universitario Virgen Macarena, Neurology, Sevilla, Spain
8Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
9Corporació Sanitária Parc Taulí, Neurology, Sabadell, Spain
10Hospital Universitario de Getafe, Neurology, Getafe- Madrid, Spain
11Hospital Universitari i Politècnic La Fe, Neurology, Valencia, Spain
12Hospital Universitario Donostia, Neurology, Donostia, Spain
13Hospital Clínico Universitario de Valladolid, Neurology, Valladolid, Spain
14Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
15Hospital General Universitario de Alicante, Neurology, Alicante, Spain
16Hospital Universitario La Princesa, Neurology, Madrid, Spain
17Complejo Asistencial Universitario de Burgos, Neurology, Burgos, Spain
Background and Aims
The risk of recurrent stroke among patients with symptomatic carotid near-occlusion (SCNO) is not well established, and its management remains controversial. Our objective is to describe the recurrence and occlusion rate at 12 months in patients with SCNO.
Method
We performed a multicenter, nationwide, prospective study from January 2010 to May 2016. Patients with angiography-confirmed SCNO were included. We collected information on treatment modalities, recurrence (defined as ipsilateral ischemic stroke or transient ischemic attack) and evolution to complete carotid occlusion at 12 months.
Results
A total of 141 patients were included. 70 patients (49.6%) were treated with revascularization (stenting=47, endarterectomy=23). Periprocedural stroke or death occurred in 5.7%. Overall recurrence rate at 12 months was 14.6% (95% CI, 8.7-20.5), 17% in the medical treatment group and 12% in the revascularization group, log rank p = 0.425. Hemodynamically compromised patients (with a reduced or exhausted cerebral vascular reserve and/or borderline infarcts) presented a higher risk of recurrence (Hazard ratio: 2.98, [95% CI, 1.10–8.07]). Progression to complete carotid occlusion occurred in 25% of patients (40.9% in the medical treatment group and 9.1% in the revascularization group, p <0.001). Only 21.2% of patients who progressed to complete occlusion suffered ipsilateral symptoms.
Conclusion
Patients with SCNO have an increased risk of ipsilateral recurrent stroke. The risk of recurrence appears to be higher in hemodynamically compromised patients, while revascularization does not seem to reduce it. The majority of patients with SCNO who evolved to complete occlusion did so without suffering ipsilateral symptoms.
Trial registration number
N/A
AS11-056
SPONTANEOUS REGRESSION OF RECURRENT STENOSIS FROM NEOINTIMAL HYPERPLASIA IN LONG-TERM FOLLOW-UP AFTER CAROTID PATCH ENDARTERECTOMY
1Otto-von-Guericke-University, Neurology, Magdeburg, Germany
2Otto-von-Guericke-University, General- visceral- vascular and transplant surgery, Magdeburg, Germany
Background and Aims
To assess the long-term course of postoperative neointimal hyperplasia after carotid patch endarterectomy (CEA).
Method
Between 01/2005 and 12/2015, 1160 CEA patients underwent routine color duplex follow-up examinations 4 days, 6 weeks, 3 months after CEA and thereafter every 6 months to detect restenosis. Neointimal hyperplasia was defined as low echogenic arterial wall thickening, detected first not before 6 weeks follow-up and not later than 18 months after CEA. Patients with additional sources of stenosis (e.g. recurrent or residual atherosclerotic plaque, thrombus, dissection) were excluded.
Results
123 patients (10.6%; 85 men, mean age 67.0 years, SD 9.0) demonstrated neointimal hyperplasia. In these 123 patients, stenosis progressed to a median stenotic degree of 20%, resulting in 50% stenosis in 25 patients and in 70% stenosis in 12 patients. Progression was most frequent at 6 months and could be detected after 4 years only in single patients. Regression was first detected at the 1 year follow-up and its frequency reached a plateau after 1.5 years lasting up to 6 years with a decrease in 38 patients of up to 30% (median 20%). Regression was more likely to be found in women (p = 0.025 Chi-square test) and in Dacron®-patch rather than in PTFE or in bovine pericard patch (p = 0.036 Chi-square test).
Conclusion
Regression of neointimal hyperplasia can be detected up to 6 years after CEA in a substantial number of patients.
Trial registration number
N/A
AS09-024
LONG-TERM OUTCOME AFTER CAROTID ENDARTERECTOMY
1Danderyds sjukhus, Department of Clinical Sciences, Stockholm, Sweden
2Södersjukhuset, Department of Clinical Sciences, Stockholm, Sweden
Background and Aims
Introduction
In Sweden, 25,000 people suffer from stroke annually and another 10,000 suffer from TIA. Of these, about 15 percent are due to large artery disease, chiefly in the internal carotid artery.
Aim
To evaluate if the long-term outcome for patients that have undergone Carotid endarterectomy (CEA) has changed the last two decades. Specifically, we asked how many suffer from recurrent stroke or death.
Method
Swedvasc is a national register with high validity. All vascular interventions are registered which makes it possible to identify patients that have undergone CEA. Riksstroke is a national quality register for stroke care. By conducting a crossmatch between Swedvasc and Riksstroke, patients with recurrent stroke after intervention can be identified.
Results
During the examined years, 8,390 patients underwent CEA. Of these, 675 suffered from recurrent stroke and 1,618 had died. Survival was equal between men and women. At the time of follow-up, 8 percent had suffered from recurrent stroke which can be compared to 29.4 percent in previous studies during the 1990’s. Further, the 30-day risk of stroke after CEA has decreased to 3 percent compared to about 7 percent compared to earlier studies.
Conclusion
CEA is effective in preventing recurrent stroke. The risk of recurrent stroke has drastically decreased compared to previous studies in the 1990’s. This is likely due to improved pharmacological secondary prevention and substantial decrease in smoking. Mortality rates have not changed. However, patients are on average 6 years older today compared to when previous studies were conducted.
Trial registration number
N/A
AS11-047
VALUE OF TRANSCRANIAL DOPPLER SONOGRAPHY IN HYPERPERFUSION SYNDROME POST- CAROTID ANGIOPLASTY AND STENTING (HISPANIAS STUDY): RESULTS FROM A NATIONWIDE PROSPECTIVE STUDY
1Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBIS, Neurology, Sevilla, Spain
2Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBIS, Neurology/Interventional Neurorradiology, Sevilla, Spain
3Instituto de Biomedicina de Sevilla IBIS, Neurology, Sevilla, Spain
4Hospital Vall d´Hebron, Interventional Neurorradiology, Barcelona, Spain
5Hospital Vall d´Hebron, Neurology, Barcelona, Spain
6Hospital Reina Sofía, Interventional Neurorradiology, Cordoba, Spain
7Hospital Reina Sofía, Neurology, Cordoba, Spain
8Hospital Virgen de la Arrixaca, Interventional Neurorradiology, Murcia, Spain
9Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
10Hospital Universitario Central de Asturias, Interventional Neurorradiology, Oviedo, Spain
11Hospital Clínico de Valencia, Interventional Neurorradiology, Valencia, Spain
12Hospital Clínico de Valencia, Neurology, Valencia, Spain
13Hospital Universitario de Cruces, Neurology, Bilbao, Spain
14Hospital Universitario de Cruces, Interventional Neurorradiology, Bilbao, Spain
15Hospital Universitario Juan Canalejo, Interventional Neurorradiology, A Coruña, Spain
16Hospital Universitario Virgen Macarena/Instituto de Biomedicina de Sevilla IBIS, Neurology, Sevilla, Spain
17Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBIS, Interventional Neurorradiology, Sevilla, Spain
Background and Aims
Cerebral hyperperfusion syndrome (CHS) is characterized by ipsilateral headache, hypertension, seizures, and focal neurological deficits in addition to the demonstration of an increase in cerebral blood flow (CBF) compared with baseline values. The aim of the study was to evaluate the value of Transcranial Doppler (TCD) in CHS after carotid artery stenting (CAS).
Method
HISPANIAS is a national prospective multicenter study with fourteen recruiting hospitals. TCD before and after CAS was recorded, evaluating middle-cerebral-artery peak of systolic velocity (PSV), pulsatility index (PI), and cerebrovascular reactivity. Follow-up was done to detect CHS up to 30 days after CAS. CHS was classified as mild (only cephalea) or moderate-severe (impaired level of consciousness or neurological deficit or brain edema or hemorrhage).
Results
Of a total of 757 CAS, pre- and post-CAS TCD was performed in 599 patients and included in this analysis. Symptomatic CHS occurred in 21 patients (3.5%), 6 patients had mild CHS and 15 had moderate-severe CHS. In CHS there was a significant increase in PSV and PI values after CAS compared to non-CHS (73.52%[20.0%-132.1%] vs 21.89%[6.3%-47.5%], p < 0.001; 46.97%[18.9%-83.8%] vs 17.14%[0%-40.1%], p = 0.003; respectively). An increase of 49.2% in PSV had 73.7% sensitivity and 77.2% specificity for predicting CHS. Using a cut-off value of an increase of 100% in PSV, sensitivity was 47.4% and specificity 93.9%.
Conclusion
Although TCD is a useful tool for CHS in CAS patients, the evidence of hyperperfusion greater than 100% compared to baseline values as a cut-off point for CHS diagnosis, has a low sensitivity and should be revised.
Trial registration number
N/A
AS03-029
ASSOCIATIONS BETWEEN STENT DESIGN, RESTENOSIS AND RECURRENT STROKE AFTER CAROTID ARTERY STENTING IN THE INTERNATIONAL CAROTID STENTING STUDY (ICSS)
1University Hospital Basel, Department of Neurology and Stroke Center, Basel, Switzerland
2London School of Hygiene and Tropical Medicine, Department of Medical Statistics, London, United Kingdom
3The Adelaide and Meath Hospital, Department of Neurology, Dublin, Ireland
4UCL Institute of Neurology, Department of Clinical Neurosciences, London, United Kingdom
5Academic Medical Center Amsterdam, Department of Neurology, Amsterdam, The Netherlands
6University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, The Netherlands
7University Medical Center Utrecht, Department of Vascular Surgery, Utrecht, The Netherlands
8Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield Vascular Institute, Sheffield, United Kingdom
9University Hospital Basel, Department of Vascular Surgery, Basel, Switzerland
10UCL Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom
Background and Aims
Open-cell carotid artery stents (CAS) are associated with a higher procedural stroke risk than closed-cell stents but the effect of stent design on long-term durability is unknown. We compared the long-term risk of restenosis and ipsilateral stroke between patients treated with open-cell stents versus closed-cell stents in the International Carotid Stenting Study (ICSS).
Method
Patients with symptomatic carotid stenosis were randomized to CAS or endarterectomy and followed with duplex ultrasound for a median of 4.0 years. We analysed all patients with completed CAS procedures, known stent design, and available ultrasound follow-up. Restenosis was defined as any narrowing of ≥50% defined as peak systolic velocity >1.3m/s on ultrasound or occlusion of the treated artery, and analysed with interval-censored models.
Results
855 patients were allocated to CAS. 714 patients with completed CAS and known stent design were included. Restenosis ≥50% occurred more often in patients treated with closed-cell stents (n = 154) compared to patients treated with open-cell stents (n = 113; 5-year risks 46% vs. 35.5%, unadjusted hazard ratio 0.68, 95% confidence interval 0.53-0.88). There was no statistically significant difference in severe restenosis (≥70%), occurring in 27 patients with open-cell stents and in 43 patients with closed-cell stents (5-year risks 8.6% vs. 12.7%), nor in the occurrence of ipsilateral stroke beyond 30 days after treatment.
Conclusion
Restenosis occurred more often in patients treated with closed-cell stents than in those treated with open-cell stents. Both stent designs were equally effective in preventing recurrent stroke.
Trial registration number
ISRCTN 25337470
AS09-008
SAFETY OF URGENT ENDARTERECTOMY PERFORMED WITHIN TWO DAYS FROM THE INDEX EVENT IN PATIENTS WITH SYMPTOMATIC CAROTID ARTERY STENOSIS: AN INTERNATIONAL MULTICENTER STUDY
1“Attikon” University Hospital- University of Athens, Second Department of Neurology, Athens, Greece
2St. Josef-Hospital- Ruhr University, Department of Neurology, Bochum, Germany
3“Attikon” University Hospital- University of Athens, Department of Vascular Surgery, Athens, Greece
4Democritus University of Thrace- School of Medicine, Department of Vascular Surgery, Alexandroupolis, Greece
5St. Anne's University Hospital- Masaryk University, Department of Neurology, Brno, Czech Republic
6St. Josef-Hospital- Ruhr University, Department of Vascular Surgery, Bochum, Germany
Background and Aims
International recommendations advocate that carotid endarterctomy (CEA) should be performed within two weeks from the index event in symptomatic carotid artery stenosis (sCAS) patients. However, there are relatively limited and controversial data regarding the safety of urgent CEA performed during the first two days of ictus. The aim of this international, multicenter study was to prospectively evaluate the safety of urgent CEA in comparison to early (3–14 days of ictus) CEA in patients with sCAS.
Method
Consecutive patients with non-disabling (mRS≤2) acute ischemic stroke (AIS) or Transient Ischemic Attack (TIA) due to sCAS (≥70%) underwent early (≤14 days) CEA at five tertiary-care stroke-centers during a six-year period. The primary outcome events included stroke, myocardial infarction (MI) or death occurring during the 30-day follow-up period and were defined according to the International Carotid Stenting Study criteria.
Results
A total of 307 patients with sCAS [mean age 69 ± 11years; 74% men; 58% AIS; 9% crescendo TIAs] underwent urgent (n = 61, 20%) and early (n = 246, 80%) CEA. The primary outcome of 30-day stroke did not differ (p = 0.329) between patients with urgent (8.2%; 95%CI: 3.2%-18.2%) and early (4.5%; 95% CI: 2.4%-7.9%) CEA. The rates of MI did not differ between urgent (0%) and early (0.8%) CEA. The documented rates of 1-month mortality were similar between the two groups (0% vs 0.4%).
Conclusion
Our findings highlight that the safety profile of urgent CEA performed within two days from the index event appears to be acceptable and comparable to early carotid surgery performed within 3–14 days from symptom onset.
Trial registration number
AS03-010
SHORT-TERM SAFETY OF CAROTID REVASCULARISATION IN PATIENTS WITH A HISTORY OF CORONARY HEART DISEASE
1UMC Utrecht, University Department of Neurology and Neurosurgery- Brain Centre Rudolf Magnus, Utrecht, The Netherlands
2UMC Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, The Netherlands
3Hopital Privé Paul D’Egine, l'Institut Vasculaire Paris Est, Champigny 94500, France
4University College London, Department of Brain Repair and Rehabilitation- UCL Institute of Neurology, London, United Kingdom
5University of Oxford, MRC Population Health Research Unit- Clinical Trial Service Unit and Epidemiological Studies Unit- Nuffield Department of Population Health, Oxford, United Kingdom
6Hôpital Sainte-Anne- Université Paris-Descartes- DHU Neurovasc Sorbonne Paris Cité, Department of Neurology, INSERM U894- Paris, France
7Klinikum rechts der Isar- Technical University Munich, Department of Vascular and Endovascular Surgery/Vascular Centre, Munich, Germany
8Medical University of Innsbruck, Department of Vascular Surgery, Innsbruck, Austria
9London School for Hygiene and Tropical Medicine, Department of Medical Statistics, London, United Kingdom
10John Radcliffe Hospital, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
11University Medical Centre Utrecht, Department of Radiology, Utrecht, The Netherlands
12UAB School of Public Health, Department of Biostatistics, Birmingham- AL, USA
13UKSH Campus Kiel, Clinic for Radiology and Neuroradiology, Kiel, Germany
14Cardiovascular Associates of the Southeast, Cardiovascular Associates of the Southeast, Birmingham- AL, USA
15Mayo Clinic, Department of Neurology, Jacksonville- FL, USA
16University Hospital Basel, Department of Neurology and Stroke Centre, Basel, Switzerland
17University of Heidelberg Medical School, Department of Neurology, Heidelberg, Germany
Background and Aims
We investigated whether procedural risk of carotid artery stenting (CAS) compared with carotid endarterectomy (CEA) is different in patients with and without coronary heart disease (CHD) history, and whether the treatment-specific impact of age differs.
Method
We combined individual patient data of 4,486 patients with symptomatic carotid stenosis from four randomized trials (EVA-3S, SPACE, ICSS, and CREST). Procedural risk was defined as any stroke or death ≤30 days after treatment. We compared procedural risk between both treatments in per-protocol Cox regression analysis, stratified by CHD history and age (<70, 70-74, ≥75 years).
Results
1,255 (28%) patients had CHD history. The procedural risk was consistently higher in patients treated with CAS compared with CEA, both in patients with (8.3% CAS vs. 4.6% CEA; HR 1.96, 95%CI 0.67-5.73) as in those without CHD history (6.9% vs. 3.6%; 1.93, 1.40-2.65; pinteraction = 0.89). In patients with CHD history, procedural risk was substantially higher after CAS compared with CEA in patients aged ≥75 years (CAS-CEA HR 2.78, 95%CI 1.32-5.85), but there was no difference in patients aged <70 years (1.71, 0.79-3.71) and in patients aged 70-74 years (1.09, 0.45-2.65).
Conclusion
Procedural stroke or death risk of CAS compared with CEA did not differ between patients with and without CHD history. However, CAS was only clearly inferior to CEA in patients with CHD history aged ≥75 years.
Trial registration number
N/A
Scientific Communications- Small Vessel Disease
AS23-024
SMALL VESSEL DISEASE AND CLINICAL OUTCOMES AFTER ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE
1AOU Careggi, Stroke Unit and Neurology, Florence, Italy
2University of Florence, NEUROFARBA Department, Florence, Italy
3AOU Careggi, Neurovascular Interventional Unit, Florence, Italy
4Italian National Research Council, Institute of Neuroscience, Florence, Italy
Background
Pre-existing small vessel disease (SVD) has been associated with worse functional outcomes in patients with acute stroke treated with intravenous thrombolysis, however, there are scarce data in patients treated with endovascular thrombectomy. We aimed to investigate the associations between SVD and clinical outcomes in patients with ischemic stroke treated with endovascular therapy.
Methods
We retrospectively evaluated consecutive patients with acute ischemic stroke in the anterior circulation receiving endovascular treatment at a single academic centre. We assessed SVD markers (leukoaraiosis, lacunes, brain atrophy) on plain CT with visual scales and evaluated global SVD. Early outcomes included any 24-hours hemorrhagic transformation and 7-days (or discharge) stroke severity, late outcomes included modified Rankin Scale (mRS) 90 days after stroke. To investigate independent associations, we used logistic and ordinal regression models adjusted for age, sex, stroke severity, time-to-groin puncture time.
Results
A total of 175 patients were included in the study, mean ( ± SD) age 72.3 ( ± 12.4) years, 90 (51%) males; 62 (35%) patients had at least one marker of SVD rated as severe. SVD features were not associated with 24-hours hemorrhage. Among single SVD features, only brain atrophy was associated with 7-days stroke severity (OR = 2.28;95%CI = 1.11-4.68) and with worse mRS at 90 days (OR = 2.72;95%CI = 1.25-5.91). The SVD score was associated with worse mRS at 90 days (OR = 1.63;95%CI = 1.01-2.62) but not with 7-days stroke severity.
Conclusions
Pre-existing SVD burden, mainly driven by brain atrophy, was not associated with hemorrhagic transformation but negatively affected early and late clinical outcomes in anterior circulation ischemic stroke treated with endovascular therapy.
Trial registration number
N/A
AS23-033
CHILDHOOD IQ, EDUCATION AND CHILDHOOD SOCIOECONOMIC STATUS AND LATE LIFE BURDEN OF CEREBRAL SMALL VESSEL DISEASE IN 4 COHORT STUDIES
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Edinburgh, Geriatric Medicine- Department of Clinical and Surgical Sciences, Edinburgh, United Kingdom
3University of Edinburgh, Centre for Cogntiive Ageing and Cogntiive Epidemiology, Edinburgh, United Kingdom
4University of Aberdeen, Institute of Medical Sciences, Aberdeen, United Kingdom
5University of Amsterdam, Clinical Epidemiology- Biostatistics and Bioinformatics, Amsterdam, The Netherlands
Background and Aims
Development of cerebral small vessel disease (cSVD), a major cause of stroke and dementia, may be influenced by early life factors. Meta-analysis found that lower levels of childhood IQ, childhood socioeconomic status (SES) and education increased the risk of cSVD in later life but was unclear if these relationships persist after adjustment for vascular risk factors or adult SES.
Method
We analysed data from community dwelling participants from 4 cohort studies: STRADL (n = 280), The Dutch Famine Birth cohort (n = 118), the Lothian Birth Cohort 1936 (n = 617) and the Simpson cohort (n = 110). Presence of each cSVD feature was analysed individually and then summed to form a total “cSVD score” (range 1–4). Data were adjusted for vascular risk factors and adult SES, analysed separately for each cohort and then meta-analysed.
Results
Across 3 cohorts (n = 1125) higher childhood IQ was associated with lower WMH burden (OR 0.99, 95%CI 0.98-0.998, p = 0.03), fewer infarcts (OR 0.98, 95%CI 0.97-0.998, p = 0.03), fewer lacunes (OR 0.98, 95%CI 0.97-0.999, p = 0.04) and lower total cSVD burden (OR 0.98, 95%CI 0.96-0.999, p = 0.04). Childhood IQ was not available for the Dutch Famine Birth cohort. Across all cohorts low education level was associated with more micro-bleeds (OR 1.65, 95%CI 1.06-2.56, p = 0.03). Manual childhood SES was not associated with cSVD.
Conclusion
Childhood IQ is associated with cSVD in later life independent of vascular risk factors. The findings may be used to inform future interventions and changes in social policy to improve brain health and deserve further study.
Trial registration number
N/A
AS23-042
NEW CEREBRAL MICROBLEEDS AFTER INTRAVENOUS THROMBOLYSIS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Charité - Universitätsmedizin Berlin, Department of Neurology, Berlin, Germany
2Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
3Hôpital Sainte-Anne - Université Paris Descartes, Department of Neurology, Paris, France
Background and Aims
Cerebral microbleeds (CMB) are a common incidental magnetic resonance imaging (MRI) finding, especially in patients with cerebrovascular diseases. Currently, data on new CMBs occurring early after thrombolysis in acute ischemic stroke patients are scarce.
Method
We conducted an observational study including stroke patients who received MRI (3-Tesla)-based intravenous thrombolysis and underwent follow-up MRI the following day (n = 395). T2*-weighted MRIs were co-registered. The endpoints included occurrence, number and distribution of new CMBs after thrombolysis. Distribution of CMBs was categorized as strictly lobar, deep, infratentorial or mixed. Additionally, we performed a meta-analysis including our own data and other studies reporting on new CMBs after thrombolysis.
Results
Out of 395 patients, new CMBs after thrombolysis occurred in sixteen patients (4.1%). Distribution of new CMB was strictly lobar in 13/16 patients (81.3%). Patients with a strictly lobar CMB distribution on pretreatment MRI had significantly more often new CMBs after thrombolysis compared to all other patients (31% vs. 11%, p = 0.015). In random-effects meta-analysis (n = 740), presence of >2 CMBs on pretreatment MRI was associated with new CMBs after thrombolysis (odds ratio [OR] 3.6, 95% confidence interval [CI] 1.3–10.3). Patients with new CMBs after thrombolysis were more likely to develop remote parenchymal hemorrhage (OR 28.7, 95%CI 8.6–96.2).
Conclusion
In patients with an acute ischemic stroke, new CMBs following thrombolysis usually have a strictly lobar distribution. CMBs with a strictly lobar distribution on pretreatment MRI are associated with new CMBs after thrombolysis. Therefore, new CMBs occurring early after thrombolysis may indicate underlying cerebral amyloid angiopathy.
Trial registration number
N/A
AS19-014
CADASIL ENCEPHALOPATHY IN A LARGE COHORT OF BRITISH CADASIL PATIENTS
1Stroke Research Group- Department of Clinical Neurosciences- University of Cambridge- Cambridge- UK, Department of Clinical Neurosciences- University of Cambridge- Cambridge- UK, Cambridge, United Kingdom
2Cambridge University Hospital NHS Foundation Trust- Cambridge- UK, Department of Clinical Radiology, Cambridge, United Kingdom
Background and Aims
CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) is the most common monogenic form of stroke. It usually presents with migraines with aura, lacunar infarcts and cognitive impairment. A less recognised presentation is an acute encephalopathy. Clinical and imaging features of this presentation have been poorly described and little is known about its risk factors and pathogenesis.
Method
Data collected prospectively from 342 consecutively recruited symptomatic patients with diagnosis of CADASIL seen in British National CADASIL clinic was reviewed and original clinical records and imaging obtained. Clinical characteristics, risk factors and outcome of encephalopathic presentations were studied.
Results
35 of 342(10.2%) participants had a history of 50 encephalopathic events constituting the first hospital presentation of CADASIL in 33(94.3%) patients. Most commonly reported features during episodes were visual hallucinations (44%), seizures (22%) and focal neurological deficits (60%). Complete recovery within 3 months was reported in 48(96%) episodes.
In 62% of episodes there was a history of migraine or migraine aura directly preceding the encephalopathy. History of migraine was independently associated with history of encephalopathy (OR = 2.5[95%CI 0.9,5.4], p = 0.015).In 2 of 15 cases where MRI during episodes was available, unilateral focal cortical swelling was seen.
Conclusion
In up to 10% of CADASIL patients a reversible encephalopathy is the first presentation leading to diagnosis. The strong association with migraine suggests a shared pathogenesis. Cortical spreading depression, which is increased in animal models of CADASIL, may play a role. Focal cortical swelling may be seen on MRI during the acute episode.
Trial registration number
N/A
AS23-026
BASAL GANGLIA ATROPHY IN CEREBRAL AMYLOID ANGIOPATHY
1Massachusetts General Hospital, Neurology, Boston, USA
Background and Aims
Cerebral Amyloid Angiopathy (CAA) is associated with cortical and white matter atrophy. We hypothesized that atrophy in CAA extended into the subcortical grey matter.
Method
We compared multimodal MRIs from 80 non-demented patients with CAA, to 80 Healthy Controls (HC) and 80 patients with Alzheimer’s Disease (AD). FreeSurfer algorithms were used to calculate structural markers of interest, and neurocognitive evaluations were performed. A visual basal ganglia atrophy scale was also developed to assess atrophy in 93 patients with CAA-related intracerebral haemorrhage (CAA-ICH) and 93 age-matched patients diagnosed with Hypertensive Arteriopathy-related ICH (HTN-ICH).
Results
Patients with CAA had significantly lower basal ganglia volumes (BGV:1.16% ± 0.14) when compared to both age-matched HC (1.30% ± 0.13; p < 0.0001) and AD (1.23% ± 0.12; p = 0.003). Within the CAA cohort, there was a positive association between BGV and cortical grey matter volume (r = 0.45; p < 0.0001), a negative association between BGV and regional fractional anisotropy (r = −0.36; p = 0.001), and positive associations between BGV and verbal memory (r = 0.26; p = 0.034) as well as language processing (r = 0.35; p = 0.003) z-scores. For the clinical cohorts, patients diagnosed with CAA-ICH displayed significantly lower visually rated BGV when compared to age-matched patients with HTN-ICH (scale: 7.23 ± 0.92 vs 8.15 ± 1.07; p < 0.0001).
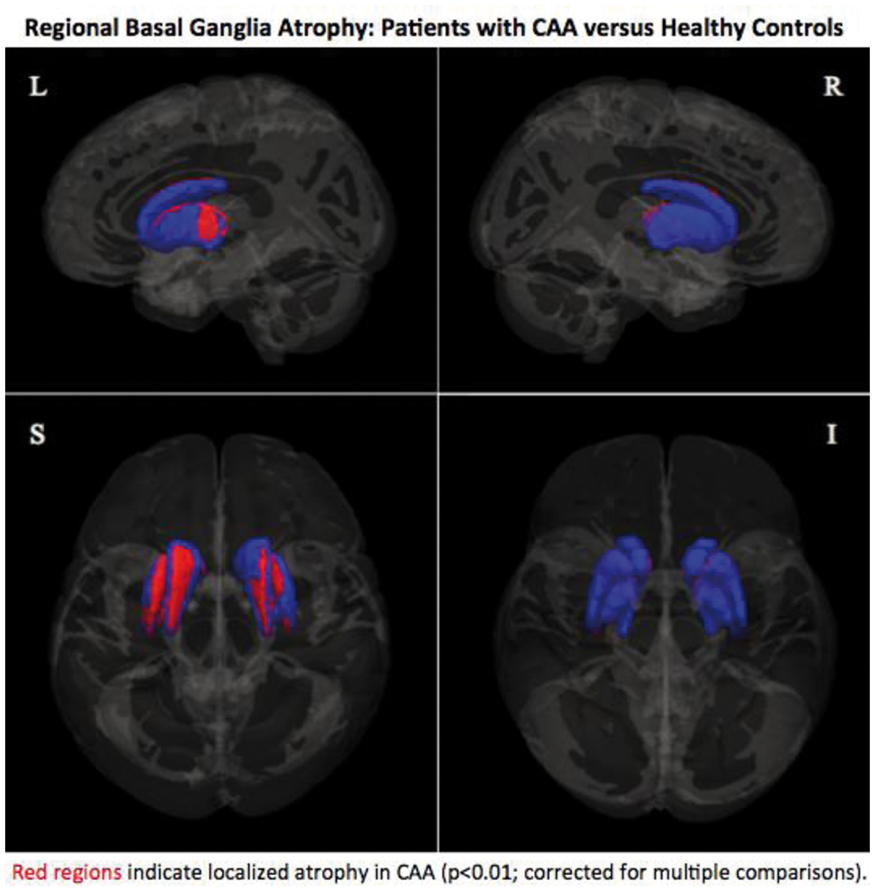
Conclusion
Patients with CAA displayed substantial atrophy in the basal ganglia when compared to various control cohorts. Within the CAA cohort, greater basal ganglia atrophy was independently correlated with greater cortical atrophy, increases in basal ganglia anisotropy, and cognitive impairment.
Trial registration number
N/A
AS23-020
CLINICAL CORRELATES OF LONGITUDINAL MRI CHANGES IN CADASIL
1Hôpital Lariboisière- APHP, neurologie, PARIS, France
2Huashan Hospital- Fudan University, Neurology, Shanghai, China
3Université Paris Denis Diderot and DHU NeuroVasc Sorbonne Paris-Cité, Department of Neurology, Paris, France
4Klinikum der Universität München- Ludwig-Maximilians-University, Institute for Stroke and Dementia Research, Munich, Germany
5Hôpital Lariboisière- APHP, neuroradiology, Paris, France
Background and Aims
This study aims to determine how the longitudinal change of markers of small vessel disease on conventional MRI are associated with clinical worsening over a 3-year period in patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL).
Method
One hundred sixty NOTCH3 mutation carriers (mean age ± SD, 49.8 ± 10.9 years) were followed over 3 years. Validated methods were used to determine the percent brain volume change (PBVC), number of incident lacunes, change of volume of white matter hyperintensities and change of number of cerebral microbleeds. Multivariable logistic regression analyses were performed to assess the independent association between changes of these MRI markers and incident clinical events. Mixed-effect multiple linear regression analyses were used to assess their association with changes of clinical scales.
Results
Over a mean period of 3.1 ± 0.2 years, incident lacunes are found independently associated with incident stroke and change of Trail Making Test Part B. PBVC is independently associated with all incident events and clinical scale changes except the modified Rankin Scale at 3 years.
Conclusion
Our results suggest that, on conventional MRI, PBVC and the number of incident lacunes are the most sensitive and independent correlates of clinical worsening over 3 years in CADASIL.
Trial registration number
N/A
AS19-041
INTRACRANIAL HEMORRHAGE IN CADASIL
1CHU Poitiers, Department of Neurology, Poitiers, France
2CHU Poitiers, Department of Clinical Genetics, Poitiers, France
3CH de Saint Nazaire, Department of Neurology, Saint Nazaire, France
Background and Aims
Intracerebral hemorrhage (ICH) has been reported in few cases of Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leucoencephalopathy (CADASIL), mostly in hypertensive patients.
We aimed to assess clinical and radiological characteristics of patients with CADASIL who presented ICH.
Method
A retrospective analysis of all neuroimaging exams of CADASIL patients hospitalized in our academic neurology department for acute cerebrovascular events was performed to find ICH. Literature search was run on this topic.
Results
A total number of 30 cases of CADASIL and symptomatic ICH (mean age: 53 years, SD 13, median age: 52 years, min-max 29-86, 73% male) were reported. Intracerebral hemorrhages were mainly deep (18 subjects), followed by lobar (6 subjects), cerebellar (3 subjects), mixed lobar and deep (2 subjects), while one patient had a subarachnoid hemorrhage. Twelve patients were taking antithrombotic medication, while in four patients medical treatment was not detailed. In the whole group, neuroimaging showed extensive FLAIR hyperintensities and cerebral microbleeds in all CADASIL subjects with ICH, and lacunar infarction in 70% of those with available information.
Conclusion
Intracerebral hemorrhage represents a possible yet uncommon manifestation of CADASIL and should be considered in patients with ICH associated with leucoencephalopathy and microbleeds, even in the absence of other clinical symptoms or in the absence of family history. Caution should be taken in aspirin prescription, and strict pressure control would appear meaningful in this category of patients, particularly in the presence of cerebral microbleeds.
Trial registration number
N/A
AS23-031
ARE ACUTE INCIDENTAL INFARCTS THE CAUSE OF CEREBRAL SMALL VESSEL DISEASE? A HIGH-FREQUENCY SERIAL IMAGING STUDY
1Donders Institute for Brain- Cognition and Behaviour- Center for Medical Neuroscience, Department of Neurology, Nijmegen, The Netherlands
2Institute for Stroke and Dementia Research ISD, University Hospital LMU, Munich, Germany
3Donders Institute for Brain- Cognition and Behaviour- Centre for Cognitive Neuroimaging, Radboud University Nijmegen, Nijmegen, The Netherlands
4Image Sciences Institute, University Medical Center Utrecht, Utrecht, The Netherlands
5Department of Neurology, Medical University of Graz, Graz, Austria
Background and Aims
Recent imaging evidence suggests a role for acute incidental infarcts on diffusion-weighted imaging (DWI) in the origin of cerebral small vessel disease (CSVD), including white matter hyperintensities (WMH), lacunes and microbleeds. We investigated the incidence and evolution of acute incidental infarcts in an unprecedented high-frequency serial imaging study, the RUN DMC – InTENse study.
Method
54 non-demented individuals with CSVD and no other presumed cause of acute stroke (mean age 70.2[SD6.5] years, 63% male), were retrieved from the RUNDMC study. Participants underwent 10 consecutive monthly 3T MRI scans, including DWI, FLAIR, T1 and susceptibility-weighted imaging (SWI). DWI scans were screened for acute infarcts and their evolution on follow-up FLAIR, T1 and SWI was assessed.
Results
Seven individuals (13%) developed 31 acute infarcts (location: cortex:n = 18; white matter: n = 5; both: n = 2; thalamus: n = 1; cerebellum: n = 5). Individuals with any acute infarct were older (mean age[SD] 76.1[8.8] vs. 69.3[5.7] years, p = .035) and more often had a microbleed at baseline (86% vs. 30%, p = .008) compared to individuals without acute infarcts. Acute infarcts gave rise to the development of WMH (n = 3), a lacune (n = 1) and microbleeds (n = 2). However, the majority of acute infarcts disappeared on follow-up FLAIR and T1.
Conclusion
Acute incidental infarcts are a common finding in individuals with CSVD and are associated with older age and the presence of microbleeds. Acute infarcts contribute to a spectrum of CSVD imaging findings, but probably are not the only source for CSVD progression. A large number of acute infarcts go completely unnoticed when not scanning on a high-frequent temporal scale.
Trial registration number
N/A
AS22-013
CONVERSION INTO WHITE MATTER HYPERINTENSITIES PRECEDED BY HETEROGENEITY AND DECLINE OF WHITE MATTER MICROSTRUCTURAL INTEGRITY OVER TIME
1Radboudumc - Donders institute for Brain - Cognition and Behaviour, Neurology, Nijmegen, The Netherlands
2Radboud University Medical Center- Diagnostic Image Analysis Group, Department of Radiology and Nuclear Medicine, Nijmegen, The Netherlands
3Jeroen Bosch Ziekenhuis, Department of Neurology, ’s-Hertogenbosch, The Netherlands
4Radboud University- Donders Institute for Brain- Cognition and Behaviour, Centre for Cognitive Neuroimaging, Nijmegen, The Netherlands
Background and Aims
White matter hyperintensities (WMH) are associated with cognitive decline and dementia. Temporal dynamics of conversion of normal appearing white matter (NAWM) into WMH remains unknown. We examined whether and when changes in DTI values preceded WMH progression, taking baseline WMH severity into account.
Method
From 266 participants of the RUNDMC study we semi-automatically segmented WMH at 3 time-points over 9 years. Images were registered to standard-space through a subject-template. We analyzed differences in mean diffusivity (MD) between 4 regions: NAWM, incident WMH in first and second time-period and WMH (Fig.A).
Results
Mean age was 62.5 (SD7.8) years, 59.0% was male and median WMH progression was 2.0 ml (IQR0.92–5.4) over 8.7 years (0.24ml/yr). Baseline NAWM converting into WMH during first and second follow-up showed higher MD than remaining NAWM (Fig.B). Baseline MD values in early converting NAWM were similar to MD in WMH. Participants with severe WMH had higher MD, in all areas including WMH (Fig.B). MD values continuously increased over time, both in incident and persistent WMH (p < 0.05; Fig.C).
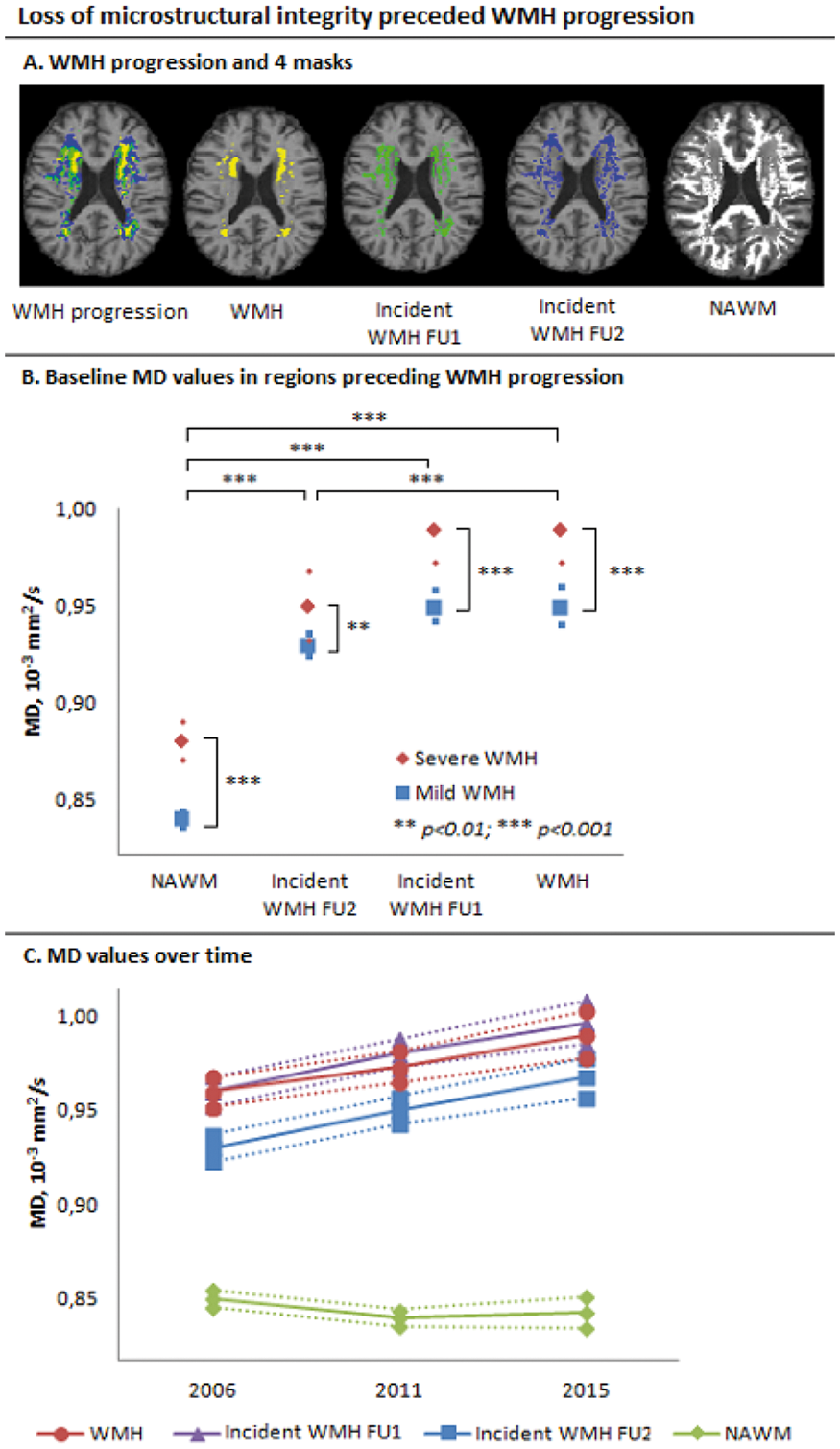
Conclusion
Impaired microstructural integrity preceded conversion into WMH and continuously declined over time, suggesting a continuous process of WM integrity loss that can be detected using DTI years before WMH become visible on conventional neuroimaging. Heterogeneity of microstructural integrity within WMH might explain variances in cognitive deficits in patients with similar SVD severity.
Trial registration number
N/A
Scientific Communications- Rehabilitation and Recovery
AS13-024
A PILOT STEPPED-WEDGE, CLUSTER RANDOMISED-CONTROLLED-TRIAL (RCT) OF THE EFFECTIVENESS OF AN ORAL HEALTH CARE (OHC) INTERVENTION COMPARED TO STANDARD CARE IN STROKE WARDS (SOCLE II)
1Glasgow Caledonian University, Nursing- Midwifery and Allied Health Professions Research Unit, Glasgow, United Kingdom
2University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
3Royal National Institute of Blind People, Royal National Institute of Blind People, Edinburgh, United Kingdom
4University of Glasgow, Dental School, Glasgow, United Kingdom
5University of Edinburgh, Edinburgh Clinical Trials Unit, Edinburgh, United Kingdom
6Glasgow Caledonian University, Yunis Centre for Social and Business Health, Glasgow, United Kingdom
7Stroke Survivor, Not applicable, Glasgow, United Kingdom
8Carer representative, not applicable, Glasgow, United Kingdom
9Glasgow Caledonian University, Yunis Centre for Social Business and Health, Glasgow, United Kingdom
Background and Aims
Stroke survivors with stroke-associated pneumonia (SAP) experience poorer outcomes (length-of-stay, dependency at discharge, healthcare costs and risk of death). High quality, OHC may reduce the incidence of pneumonia and improve patients’ oral health. We aimed to pilot a pragmatic, stepped-wedge, cluster RCT of clinical effectiveness of an enhanced OHC plan versus usual OHC in stroke wards.
Method
Four stroke rehabilitation wards (clusters) were randomly allocated to receive the OHC intervention at specific time-points. All patients admitted and nursing staff (registered nurses, nursing assistants and student nurses) were eligible for inclusion. We evaluated our intervention (training, tools, protocol, assessment, equipment, costs), recruitment, adherence, record linkage, sampling methodologies and sample size calculations. We considered the relationship between SAP, dental plaque and site diversity.
Results
Part-time researchers screened 1548/2613 patient admissions and 123 nurses. They recruited 325 patients (243 post-stroke) and 112 nurses. Data from usual care (patients =135; staff =108) and enhanced care periods (patients =147; staff =83) indicated our intervention was viable. The observed SAP rate (7% across sites) impacted on our ability to establish the association between dental/denture plaque and SAP and failed to meet predetermined (literature-based) rate for progression to full trial (10%). Our pilot logistic regression generalised linear mixed model analyses found no evidence of a difference in SAP rate between patients that received usual versus enhanced OHC (p = 0.62, OR 0.61 CI (0.08 to 4.42).
Conclusion
Our stepped-wedge cluster pilot RCT accommodated marked diversity between sites. We did not meet our predetermined criteria for progression to a definitive trial.
Trial registration number
NCT01954212
AS04-036
TRANSCUTANEOUS ELECTRICAL STIMULATION IMPROVES THE SWALLOW SAFETY AND REDUCES THE NEED OF FLUID THICKENING IN PATIENTS WITH CHRONIC POST-STROKE OROPHARYNGEAL DYSPHAGIA
1Hospital de Mataró. CSdM, GI Motility Lab, Mataró, Spain
2Centro de Investigación Biomédica en Red para enfermedades hepáticas y digestivas, GI Motility Lab. Hospital de Mataró, Mataró, Spain
3Hospital de Mataró. CSdM, Research unit, Mataró, Spain
4Hospital de Mataró. CSdM, Neurology unit, Mataró, Spain
Background and Aims
Chronic post-stroke oropharyngeal dysphagia (CPSOD) is associated with impaired pharyngeal sensory and motor function. We performed a randomized control trial to assess the therapeutic effect of transcutaneous electrical stimulation at two levels of intensity (sensory vs motor) in CPSOD.
Method
Ninety post-stroke patients (74.13 ± 11.45 years) with CPSOD were randomly assigned to a) a control group with compensatory treatment: fluid and solid bolus adaptation and posture recommendations; b) A sensory electrical stimulation group (SES): compensatory treatment plus SES (thyro-hyoid electrode placement); c) A motor neurostimulation group (NMES): compensatory treatment plus NMES, supra-hyoid electrode placement). Patients received 15 sessions of 1 hour stimulation over two weeks. A videofluoroscopy was performed before and after treatment and the Penetration-Aspiration Scale scores and swallow response timing were assessed.
Results
The control group did not present any changes following treatment. Patients having SES and NMES treatment presented a significant reduction in the prevalence of aspirations and penetrations (from 23.85% to 11.40% in SES and from 21.40% to 13.64% in NMES, both p < 0.0001) through the shortening of the laryngeal vestibule closure time (-13.51% in SES, -16.32% in NMES). This clinical improvement allowed fluid thickening to be reduced (from 96.7% to 62.0%, p < 0.001 in SES and from 90% to 65.5%, p = 0.023 in NMES). No major adverse effects were observed.
Conclusion
Transcutaneous electrical stimulation is a safe and effective therapy for post-stroke OD. Both SES and NMES greatly improved the safety of swallow and reduced the need for fluid thickening in these patients.
Trial registration number
NCT02379182
AS08-042
THE EFFECTS OF MIRROR AND NON-MIRROR VISUAL FEEDBACK CONDITIONS DURING UNILATERAL EXERCISE TRAINING ON CONTRALATERAL STRENGTH AND PASSIVE JOINT POSITION SENSE
1Bezmialem Vakif University, Department of Physiotherapy and Rehabilitation, Istanbul, Turkey
Background and Aims
Unilateral exercise training strengthens not only the muscles on the trained side but also the homologous muscles on the untrained side; however the magnitude of this interlimb cross-transfer is modest. The hypothesis of our study is that enhanced sensory feedback by mirror viewing the exercising hand would increase the contralateral strength gain and passive joint position sense.
Method
Healthy adults were randomized into a mirror visiual feedback group (MVFG, n = 11) and a non-mirror visiual feedback group (NMVFG, n = 9) and performed 300 shortening muscle contractions of the right hand grip with maximum performance with an exercise ball for only one session. Maximal hand grip (HGS) and pinch strength (PS) were assessed by using handgrip dynamometer and pinchmeter. The wrist passive joint position sense (PJPS) were evaluated via goniometer at 45° and 60° wrist extension.
Results
Untrained hand HGS and PS statistically increased after the sessions in MVFG (respectively p = 0.007, p = 0.018). The outcome scores did not not change in NMVFG (p>0.05). For all groups, error scores of PJPS decreased but it is not statistically significant (p>0.05).
Conclusion
Zult et all (2016) presented that long-term strength training with mirror-visual feedback increased cross-education effect. Reissig et all (2015) revealed that one session ballistic exercise didn’t augment cross-limb transfer. In conclusion, our study provide an evidence that one session unilateral exercise training did not change strength of contralateral homologous muscle but unilateral strength training with mirror visiual feedback to influence contralateral homologous muscle strength only in one session.
Trial registration number
N/A
AS08-048
INTERNATIONAL CONSENSUS RECOMMENDATIONS FOR OUTCOME MEASURE USE IN STROKE UPPER LIMB REHABILITATION TRIALS: DEVELOPMENT OF THE STANDARDISING MEASUREMENTS IN ARM REHABILITATION TRIALS (SMART) TOOLBOX
1Glasgow Caledonian University, NMAHP Research Unit, Glasgow, United Kingdom
2Glasgow Caledonian University, School of Health and Life Sciences, Glasgow, United Kingdom
Background and Aims
Randomised controlled trials (RCTs) of stroke upper limb (UL) rehabilitation interventions use numerous outcome measures, hindering comparison and pooled analyses. We developed international consensus recommendations (the SMART Toolbox), to support informed selection of outcome measures for use in future RCTs. Recommendations considered feasibility, psychometrics, outcomes captured by the measure, and the International Classification of Functioning, Disability and Health domain (s) addressed.
Method
Phase 1: Systematic identification of outcome measures from RCTs within the Cochrane Overview of stroke UL rehabilitation.
Phase 2: Focus groups and interviews with stroke survivors, carers and clinicians to identify important outcomes related to life with UL impairment. Systematic identification of where these important outcomes were captured by existing measures.
Phase 3: International e-Delphi with stroke UL rehabilitation researchers and subsequent consensus meeting with stakeholders to select measures for inclusion in the SMART toolbox.
Results
Phase 1 identified 144 measures from 243 RCTs. Phase 2 participants (n = 53 stroke survivors and carers; n = 58 clinicians) identified 66 important outcomes. Phase 3 e-Delphi participants (n = 55; n = 17 countries) identified 28 measures for discussion at the meeting. Meeting participants (n = 16) selected the Visual Analogue Scale for pain/0-10 Numeric Pain Rating Scale; Dynamometry; Action Research Arm Test; Fugl-Meyer Assessment (UL-section); Wolf Motor Function Test; Barthel Index; Modified Rankin Scale; Motricity Index (UL-section); Box and Block; Motor Activity Log 14; Nine Hole Peg Test; Functional Independence Measure; EQ-5D and Canadian Occupational Performance Measure.
Conclusion
Selection from the agreed measures in the SMART toolbox in future stroke UL RCTs will facilitate data comparability and aggregation for efficacy analyses.
Trial registration number
N/A
AS04-042
DYNAMIC LYCRA ORTHOSIS AS AN ADJUNCT TO UPPER LIMB REHABILITATION AFTER STROKE: A FEASIBILITY RANDOMISED CONTROLLED TRIAL
1University of Dundee, School of Nursing and Health Sciences, Dundee, United Kingdom
2Glasgow Caledonian University, NMAHP Research Unit, Glasgow, United Kingdom
Background and Aims
Upper Limb (UL) recovery after stroke at six months is incomplete in up to 66% of cases. Recovery requires high dose repetitive task training that is challenging to achieve. Dynamic Lycra® Orthoses (DLO) are lycra garments designed to provide dynamic support and sensory feedback and may optimise task practice conditions. Often used in rehabilitation, evidence of effects in stroke is scant. The aim of this study was to examine feasibility of conducting a randomised controlled trial of DLO in stroke rehabilitation
Method
Design
Randomised controlled feasibility trial
Participants
Stroke survivors with UL activity limitation, admitted to two stroke units 2–4 weeks following stroke onset, randomised 2:1 to intervention or control groups.
Intervention
After provision of individually tailored dynamic lycra orthosis (DLO), participants wore the DLO for eight hours per day over eight weeks. The control group received usual care. Feasibility outcomes were recruitment and retention rates, recorded adherence, withdrawal and completion, missing data, adverse events. Changes in Action Research Arm Test, Nine Hole Peg Test, Nottingham Sensory Assessment, Motor Assessment Log, Motricity Index, Modified Tardieu were assessed at eight weeks.
Results
Recruitment was complete on 30/12/17. Of 43 participants, 25 received the DLO. Outcome assessment is ongoing with completion by 28/2/18. To date, non-completion of assessment occurred with eight intervention group participants, four because of issues with the DLO, and with four control group participants.
Conclusion
This study provides an assessment of feasibility of DLO as an adjunct to rehabilitation after stroke. Results will be reported in May 2018.
Trial registration number
Registration No:NCT03063970
AS16-103
RECOVERY OF DEXTERITY AFTER STROKE: A LONGITUDINAL STUDY OF PRECISION GRIP FORCE CONTROL AND RELATION TO BRAIN LESION LOCATION
1Karolinska Institutet, Department of Clinical Sciences- Danderyd Hospital- Division of Rehabilitation Medicine, Stockholm, Sweden
2Inserm U894, Centre de Psychiatrie et Neurosciences, Paris, France
Background and Aims
Impaired precision grip control is common after stroke but not well characterized. The Strength-dexterity test permits quantification of the dynamic regulation of fingertip forces during precision grip. Longitudinal changes in the capacity to generate and control precision grip force were explored in individuals with stroke using the Strength-dexterity test, and the relation between precision grip impairments and stroke lesion location was studied.
Method
80 first ever stroke patients with varying degrees of weakness were evaluated at 3 weeks, 3 and 6 months after injury. Strength-dexterity test was performed on the affected and contralateral less-affected hands. Compression force was measured with springs of varying length (longer springs increase the requirements of strength and dexterity). Dexterity-score and correlation between index finger and thumb forces (CorrForce) were calculated. Conventional clinical measures included pinch strength, Box and Block test and upper limb Fugl-Meyer Assessment. Anatomical MRI was used to calculate weighted corticospinal tract lesion load (wCST-LL) and to perform voxel‐based lesion-symptom mapping (VLSM).
Results
Preliminary findings showed reduced ability to compress longer springs and lower pinch strength, dexterity score and correlation of forces in the affected hand compared to the contralateral less-affected hand. Pinch strength values of affected hand represented approximately 61.5%, 77% and 84.5% of the less-affected hand for each time point, respectively. The values improved by ca. 25% at 3 months and again by 10% at 6 months. The length of spring compressed with the affected hand correlated significantly and negatively with the amplitude of pinch force, with FM-UE motor function and FM-UE wrist/hand subscale (p < 0.01). All measures improved significantly over time. There was in fact a significant effect of time on maximum voluntary pinch strength and spring number successfully compressed [F(2, 38) = 10.114, p < 0.001 and F(1.293, 29.750) = 8.925, p < 0.005]. wCST-LL correlated with pinch strength, spring length (rs= 0.602, p = 0.01), and CorrForce (rs= -0.386, p = 0.05) and VLSM revealed a relation between lesion to CST and compression force control.
Conclusion
The Strength-dexterity test allows detection of impaired precision grip control after stroke which likely contributes to activity limitations. Degree of lesion to the CST is a key predictor of poor grip control.
Trial registration number
ClinicalTrials.gov Identifier: NCT02878304
(ProHand study)
AS04-040
SAFETY OF EARLY USE ABOBOTULINUMTOXINA (DYSPORT) IN ADULTS WITH POST-STROKE SPASTICITY: RESULTS FROM THE ONTIME AND ABCDE-S STUDIES
1Metropolitan Medical Centre, Centre for Neurodiagnostic and Therapeutic Services CNS, Manila, Philippines
2University of Santo Tomas, Department of Neurology & Psychiatry- Faculty of Medicine and Surgery, Manila, Philippines
3Tan Tock Seng Hospital, Department of Rehabilitation Medicine, Novena, Singapore
4Siriraj Hospital- Mahidol University, Department of Rehabilitation Medicine- Faculty of Medicine, Bangkok, Thailand
5University of Malaya Medical Centre, Department of Rehabilitation Medicine, Kuala Lumpur, Malaysia
6Ipsen Group, Medical Affairs, Boulogne-Billancourt, France
7University of Malaya Medical Centre, Division of Neurology- Department of Medicine, Kuala Lumpur, Malaysia
Background and Aims
Botulinum toxin-A (BoNT-A) is an effective and well-tolerated treatment for upper limb spasticity (ULS), reducing muscle tone and improving function. Most studies assessed treatment in patients >6 months post-stroke. Initial increase in muscle tone may be apparent within 6 weeks, and even days, post-stroke. The ONTIME and ABCDE-S studies assessed efficacy and safety of early use (2–12 weeks post-stroke) abobotulinumtoxinA (aboBoNT-A; Dysport®) in ULS patients; here we report the safety data.
Method
ABCDE-S (NCT00234546; 2008): 24-week, randomised study comparing single injection of aboBoNT–A 500U (n = 80) versus placebo (n = 83), 2–12 weeks following first stroke in patients with Modified Ashworth Scale (MAS) score >1+. ONTIME (NCT02321436; 2016): 28-week, randomised study (aboBoNT–A 500U, n = 28; placebo, n = 14) in patients with MAS score ≥2 treated 2–12 weeks post-stroke. All observed or volunteered adverse events (AEs) were recorded in the case report form.
Results
AboBoNT-A was well tolerated, with no clinically significant differences in AE distribution between aboBoNT-A and placebo (Table 1). Most AEs were mild–moderate in intensity. Six patients had at least one AE considered treatment-related: two in placebo groups (dysuria and complex regional pain syndrome), and four in aboBoNT-A groups (fatigue [n = 2], pyrexia, muscular weakness). No serious AEs or deaths were considered treatment-related.
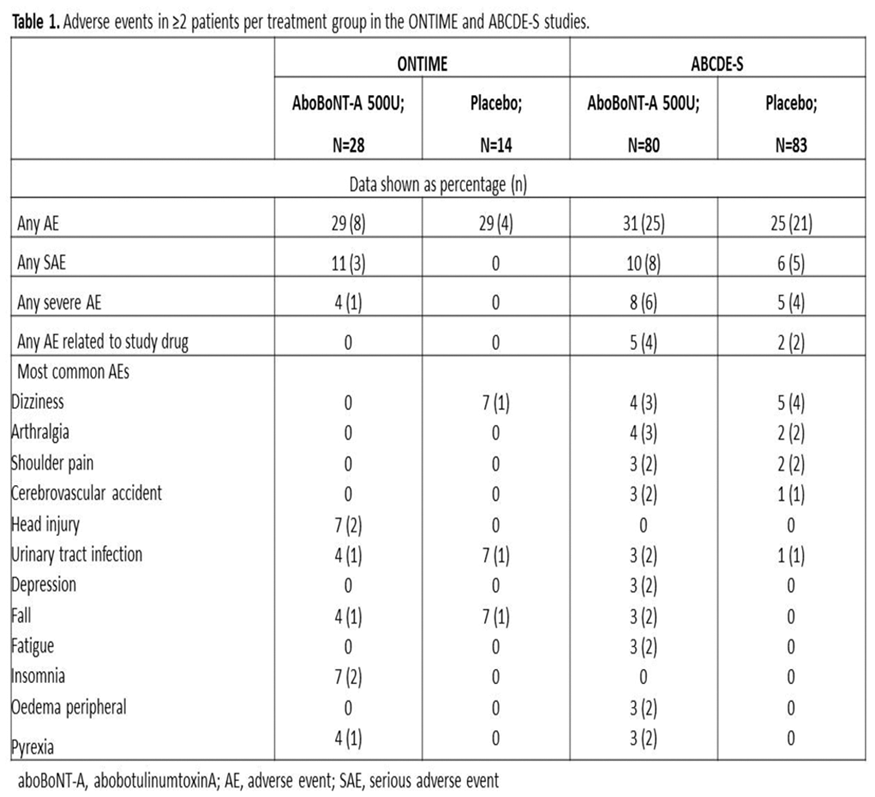
Conclusion
Both studies suggest aboBoNT-A is well tolerated in patients with ULS when administered early (2–12 weeks) post–stroke.
Trial registration number
ABCDE-S (NCT00234546; 2008); ONTIME (NCT02321436; 2016)
AS04-046
RESULTS OF LARGE CLINICAL TRIAL “DEVELOPMENT OF MEDICAL REHABILITATION IN RUSSIA”: PATIENT-ORIENTED, MULTIDISCIPLINARY AND PROBLEM-FOCUSED MODEL OF REHABILITATION PATIENTS WITH STROKE OR CEREBRAL HEMORRHAGE
1Pirogov Russian National Medical Research University, Rehabilitation, Moscow, Russia
2Pirogov Russian National Medical Research University, Neurology, Moscow, Russia
3First Saint-Petersburg I.P.Pavlov State Medical University, Department of physical methods of treatment and sports medicine, St. Petersburg, Russia
4Ural State Medical University Russian Ministry of Health, Stroke unit, Ekaterinburg, Russia
5Kazan State Medical University Russian Ministry of Health, Neurology, Kazan, Russia
6Voino-Yasenetsky V.F. Krasnoyarsk State Medical University, Neurology, Krasnoyrsk, Russia
7Kazan State Medical University Russian Ministry of Health, Rehabilitaton, Kazan, Russia
8First Saint-Petersburg I.P.Pavlov State Medical University, Department of physical methods of treatment and sports medicine, St.Petersburg, Russia
9First Saint-Petersburg I.P.Pavlov State Medical University, Department statistics, St. Petersburg, Russia
Background and Aims
Our aim: to compare “old” and “new patient-oriented, multidisciplinary and problem-focused” model of rehabilitation patients with stroke or cerebral hemorrhage in large clinical trial “Development Of MEdical rehabilitation in Russia” (DOME).
Method
Methods
Study characteristics: open, multicenter, sequential trial design. The study was registered on clinicaltrials.gov (ID: NCT02793934). In the 1st phase (n = 498) of the study the staff of the medical organizations continued to work in the traditional («outdated”) “old" scheme, but using the set of scales. In the 2nd phase (n = 523), medical organizations were start to work on a new model with the implementation of problem-oriented multidisciplinary approach and the use of modern rehabilitation technologies. Software «ICF-reader” was used for data collection. Primary Outcome Measures: modified Renkin scale (mRS) at the end of first (stroke unit) (rehabilitation centers) stages and duration of rehabilitation.
Results
Patients with stroke, who received rehabilitation at the “New Model" (0–2 points – 63%), had significantly (p < 0.0001) lower degree of disability than patients rehabilitated by “Old Model" (0–2 points – 45%). Patients spent less time (p < 0.0001) in the clinic during the second phase (28 ± 2.8 bed days) of the study compared with the first (17.7 ± 0.8 bed days).
Conclusion
“New patient-oriented, multidisciplinary and problem-focused” model of rehabilitation patients with stroke or cerebral hemorrhage is more efficient and economical than “old” model.
Trial registration number
N/A
Scientific Communications- Sex Influences and Stroke
AS26-002
SEX DIFFERENCES IN TRAJECTORIES OF DEPRESSION SYMPTOMS AND ASSOCIATIONS WITH 10 YEARS MORTALITY IN STROKE PATIENTS: THE SOUTH LONDON STROKE REGISTER
1King's College London, School of Population Health & Environmental Sciences, London, United Kingdom
2St. Thomas’ Hospital. London- UK, Stroke Unit- Guy’s and St. Thomas’ NHS Foundation Trust, London, United Kingdom
3Blizard Institute. Queen Mary University of London, Centre for Primary Care and Public HealthBarts and The London School of Medicine and Dentistry, London, United Kingdom
4School of Population Health & Environmental Sciences- King’s College London, National Institute for Health Research Biomedical Research Centre- Guy's and St Thomas' NHS Foundation Trust- and the National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care- South London, London, United Kingdom
Background and Aims
Methods that assume individuals belong to a single population overlooked patients’ heterogeneity and the varying developmental profiles of depression after stroke. We examined such profiles and their associations with mortality.
Method
Data on 1275 men and 1038 women, from South London Stroke Register (1998-2013) were investigated. Patients were screened by the Hospital Anxiety and Depression scale (HADs) at 3 months after stroke then annually. Similar developmental patterns (Trajectories) of depression symptoms were identified using group based trajectory modelling (GBTM). Kaplan-Meier and Cox regression methods were used to study survival.
Results
Three depression trajectories were identified for men: I-M (42.12%), low symptoms, predicted mean score 2.03, standard error (SE = 0.2); II-M (46.51%) moderate, mean 6.04 (SE = 0.27), and III-M (11.37%) severe, mean 12.44 (SE = 0.33), and four (I-F to IV-F) in women, means: 2.52 (SE = 0.20), 6.16 (SE = 0.24), 10.26 (SE = 0.40) and 15.16 (SE = 0.50) comprising 29.09%, 49.81%, 16.28%, and 4.82% respectively. Age adjusted hazard ratios were 2.62 (1.97 – 3.48) in group III-M, and 2.81 (1.90 – 4.16) in IV-F, significantly higher than groups I-M and I-F. Patients with severe and moderate depression symptoms have increased mortality risks. (Figure1)
Figure 1.
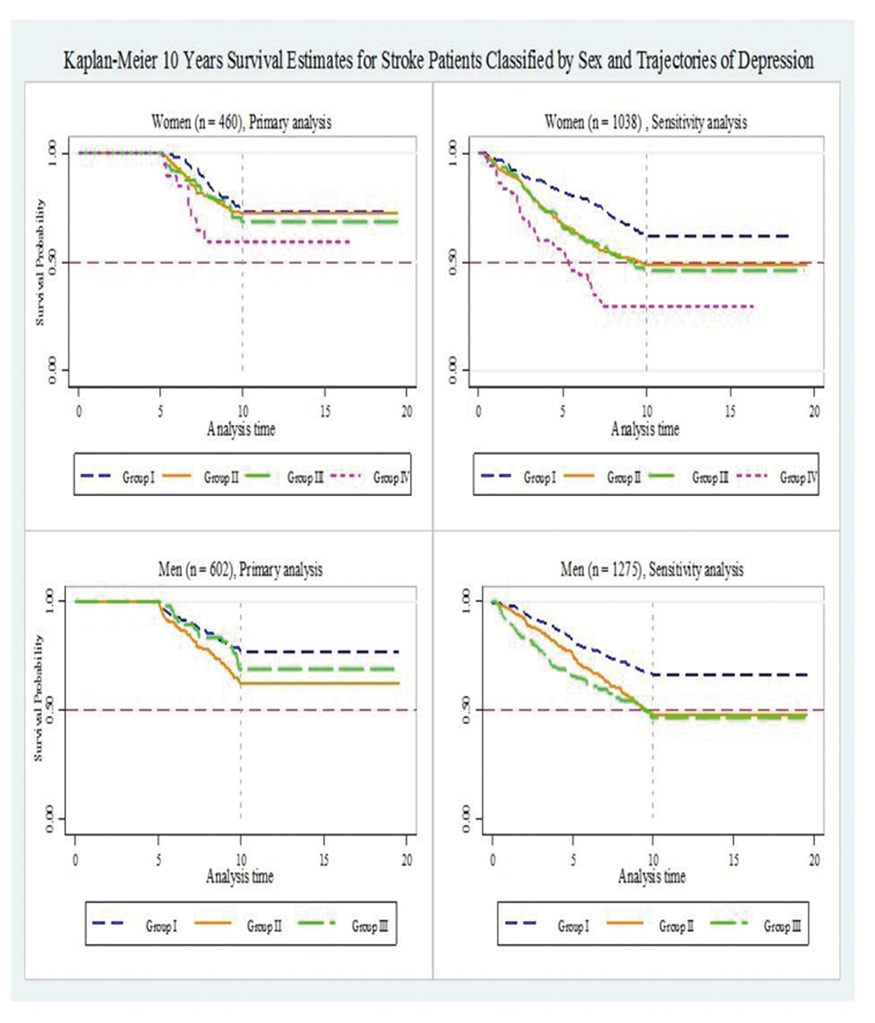
Conclusion
Depression trajectories varied between sex and within sex. The risk of severe symptoms in women is doubled that in men. Recognition of different profiles of depression symptoms is necessary for prevention and for better care provision.
Trial registration number
N/A
AS26-023
SEX DIFFERENCES IN PREVALENCE OF POST-STROKE DEPRESSION
1University of Michigan School of Public Health, Epidemiology, Ann Arbor, USA
2University of Michigan School of Public Health, Biostatistics, Ann Arbor, USA
3University of Michigan Medical School, Neurology, Ann Arbor, USA
Background and Aims
Evidence for sex differences in post-stroke depression (PSD) from population-based studies is lacking. This study investigated the sex differences in the prevalence of PSD at 90 days after first-ever stroke.
Method
The study sample consisted of 613 first-ever stroke cases identified from the Brain Attack Surveillance in Corpus Christi Project from 2011 to 2015, a population-based stroke surveillance study in south Texas, United States. PSD was assessed by the Patient Health Questionnaire-8, and pre-stroke depression was based on self-report. Logistic regression with inverse probability weighting and multiple imputation was used to examine the association between sex and PSD and whether this association was modified by pre-stroke depression.
Results
Prevalence of PSD at 90 days was 24.6% for men (95% Confidence Interval [CI]=19.6%-29.7%), and 29.2% for women (95% CI = 23.9%-34.6%). The age-adjusted odds ratio (OR) of PSD comparing women to men was 1.34 (95% CI = 0.92-1.94), but was attenuated after adjustment for pre-stroke depression (OR = 0.93, 95% CI = 0.62-1.38). Results suggested effect modification of the association between sex and PSD by pre-stroke depression (Table 1).

Conclusion
Overall, women have a higher prevalence of PSD at 90 days than men. Elevated odds of PSD in women compared with men were present in those with a past history of depression, whereas among those on antidepressants at stroke onset women were protected from PSD compared with men.
Trial registration number
N/A
AS26-014
DO WOMEN RECEIVE EQUIVALENT ACUTE STROKE CARE TO MEN? A NATIONAL STROKE REGISTRY STUDY
1Royal College of Physicians, Cqid, London, United Kingdom
2University College London, Farr Institute of Health Informatics Research, London, United Kingdom
3Royal Devon and Exeter NHS Foundation Trust, Royal Devon and Exeter NHS Foundation Trust, Exeter, United Kingdom
4King's College London, Division of Health and Social Care Research, London, United Kingdom
Background and Aims
Analysis of a national register of stroke was undertaken to determine whether quality of care differs by gender.
Method
12 quality measures (representative of whole stroke pathway) were analysed using 2016/17 Sentinel Stroke National Audit Programme (SSNAP) data, a national quality register for England, Wales and Northern Ireland. Adjustment was made for age, stroke onset while in-patient, stroke type, modified Rankin Scale score, hypertension, atrial-fibrillation (AF), diabetes, previous stroke/TIA and NIHSS-on-admission.
Results
Using data for 83,484 patients between April 2016-March 2017 admitted to hospital with acute stroke, small differences were identified for whether patient attended a stroke unit within 4hrs (adjusted odds ratio 1.04, 95% CI 1.01-1.07), swallow screen within 4hrs (aOR 1.05, CI 1.01-1.10), received Early Supported Discharge (aOR 1.05, CI 1.01-1.08).
More marked differences were present for receiving thrombolysis (aOR 1.10, CI 1.05-1.15), door-to-needle time within 60min (aOR 1.15, CI 1.05-1.25), physiotherapy within 72hrs (aOR 1.11, CI 1.03-1.19).
No evidence of differences in care by gender were found for brain scanning within 1 hour, admitted on an anticoagulant if in AF, seen by stroke nurse within 24hrs, assessed by occupational therapist within 72hrs, swallow assessment within 72hrs, seen by speech and language therapist within 72hrs.
Conclusion
Many aspects of care did not show differences between genders, however small differences were identified for the management of thrombolysis and access to physiotherapy. It is unclear why such differences might exist and care quality should be monitored to ensure that inequalities are identified and overcome. The possibility of incomplete adjustment for confounding requires further exploration.
Trial registration number
N/A
AS26-016
SEX DIFFERENCES IN THE OUTCOMES AFTER MECHANICAL THROMBECTOMY AND THROMBOLYSIS - META-ANALYSIS BY THE STROKE IN WOMEN GUIDELINE MODULE
1Skåne University Hospital- Department of Clinical Sciences Lund University, Neurology, Malmö, Sweden
2Cardiovascular Medical Science- University of Glasgow, Neurology, Glasgow, United Kingdom
3Sapienza University of Rome, Neurology and Psychiatry, Rome, Italy
4European Stroke Organization, Neurology, Basel, Switzerland
5University Hospital Dijon- University of Burgundy, Neurology, Dijon, France
6Hospital Frankfurt Höchst, Neurology, Frankfurt, Germany
7Triemli Hospital Zuerich, Neurology, Zuerich, Switzerland
8Santa Maria Misericordia Hospital- University of Perugia, Stroke Unit, Perugia, Italy
Background and Aims
Whether outcome of stroke patients treated with IV thrombolysis or mechanical thrombectomy may differ between women and men aged > 80 year is unknown.
Method
A systematic review and meta-analysis involving 4 databases of the effect of thrombectomy and thrombolysis in men and women is being conducted. We assessed whether functional outcome (mRS) at 90 days, mortality and symptomatic intracranial haemorrhage (sICH) differed between men and women, specifically in those >80 years.
Results
The preliminary results indicate no significant differences in the effect of mechanical thrombectomy on revascularization, mortality, and sICH in women and men. Intraarterial thrombolysis also showed no significant difference in mRS 4/5 between women and men. Meta-analyses of IV thrombolysis showed a significant decrease in good outcomes in women compared to men, Odds Ratio (OR) 0.89, 95% CI 0.81-0.97; p = 0.01 (9 studies, involving 8,666 patients); no significant differences in mortality, OR 0.93, 95% CI 0.82-1.05 (7 studies involving 13,742 patients) and ICH between women and men (OR 0.69, 95% CI 0.69-1.08) (9 studies involving 10,462 patients). There was no significant difference in mRS 2 or less between women and men aged 80 and higher with IV thrombolysis.
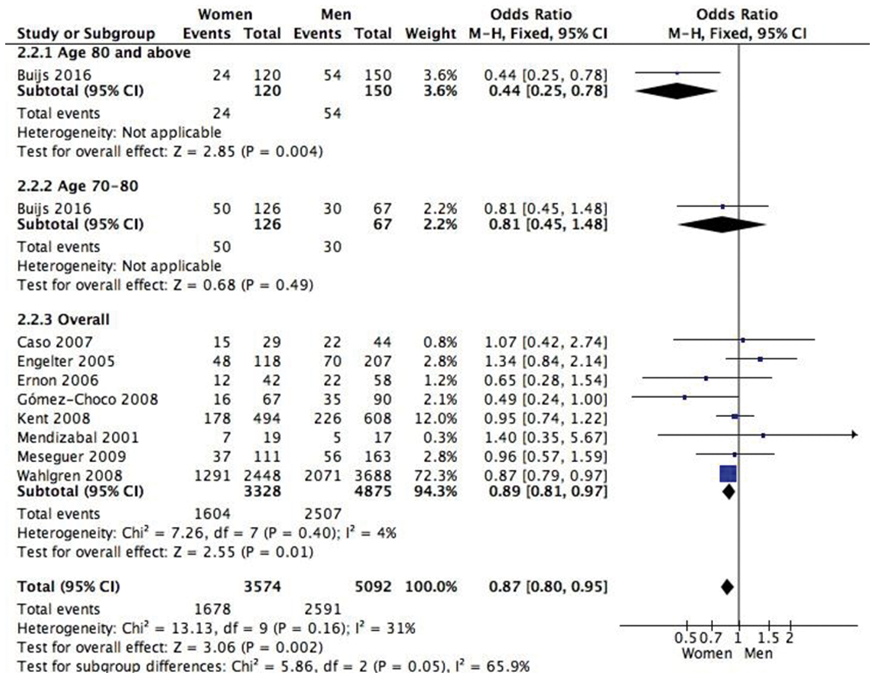
Conclusion
In this preliminary analysis we saw no difference between men and women aged ≥80 years following thrombectomy, while there was no difference in outcome for thrombolysis. Analysis of all eligible studies will be completed by ESOC 2018.
Trial registration number
N/A
AS07-075
ENDOVASCULAR THERAPY AND GENDER DISPARITIES IN STROKE OUTCOMES
1Grady Memorial Hospital- Emory University School of Medicine, Marcus Stroke Center- Department of Neurology, Atlanta, USA
Background and Aims
The burden of ischemic stroke for women is considerable: women live longer, may experience more strokes and may benefit less from specific therapies as compared to men. A few studies highlight the importance of gender peculiarities towards cerebrovascular pathologies and suggest women might benefit less from AIS thrombectomy.
Method
We reviewed our prospectively collected endovascular database at a tertiary care academic institution, between Sep 2010-Oct 2017. All patients that underwent endovascular therapy for large vessel occlusion were included and grouped by gender. Baseline, procedural, and radiological characteristics, as well as outcome variables were compared.
Results
We found 1364 patients qualified for the study, of which 636 (46.6%) were female. Women were older (67.4 ± 15.4 vs 62.5 ± 13.8, p < 0.001), had less dyslipidemia (31.4% vs 40.2% p = <0.001), less frequent smokers (14.6% vs 23.6%, p = <0.001), but with higher rates of atrial fibrillation (38.8% vs 31.3%, p = 0.02). Other baseline characteristics including NIHSS, ASPECTS, LKN-puncture times and procedural parameters were similar. Both groups had similar rates of successful reperfusion (mTICI 2b-3) (89.4 vs 92.4%, p = 0.07), parenchymal hematomas (9 vs 9.7%, p = 0.69), 90-day good outcomes (mRS 0–2) (46.9 vs 43.9%, p = 0.32) and mortality (23.9% vs 25.4%, p = 0.53). After adjusting for potential confounders, gender had no influence on good outcome. However, gender was an independent predictor of mortality: (Male, OR 1.39, CI 1.04-1.85, p = 0.024).
Conclusion
Our study shows that despite common belief and unique baseline characteristics, Women with LVO undergoing thrombectomy have lower mortality rates as compared to men.
Trial registration number
N/A
AS26-011
SEX-RELATED DIFFERENCES IN CLINICAL CHARACTERISTICS, TREATMENT AND OUTCOMES IN PATIENTS WITH ATRIAL FIBRILLATION AND SECONDARY STROKE PREVENTION WITH NOACS: RESULTS FROM THE RAF-NOACS STUDY
1Santa Maria della Misericordia Hospital- Perugia, Stroke Unit and Cardivascular Medicine Department, Perugia, Italy
Background and Aims
Less than 40% of the NOAC (Non–Vitamin-K Oral Anticoagulants) RCT populations were females. The aim of this study was to evaluate sex-differences in clinical characteristics, outcome (recurrence of ischaemic event, haemorrhagic complications, disability) and timing of anticoagulation with NOACs in secondary stroke prevention.
Method
Data were collected from the “Early Recurrence and Major Bleeding in Patients With Acute Ischemic Stroke and Atrial Fibrillation Treated With NOACs (RAF-NOACs) Study”, a prospective observational multicenter study that evaluated the rates of early recurrence, major bleeding and their timing, with a 90-days follow-up, in patients with acute ischemic stroke and AF who received NOACs for secondary prevention. Disability was measured by mRS.
Results
Out of 1,165 patients enrolled, 622 were females (53.39%), older (mean age 77.64 ± 9.11 vs 73.20 ± 10.32, p < 0.001) compared to males. No significant difference was observed in treatment before index stroke (antiplatelet 38.26% vs 41.44%, anticoagulant 20.6% vs 22.65%, p = ns). Females had more severe stroke at onset (mean NIHSS 8.11 ± 6.34 vs 7.13 ± 5.97, p < 0.008). There was no differences in NOAC timing (mean 12.17 ± 12.12 days vs 12.64 ± 13.51 days, p = ns). No differences in all specified outcomes were observed (ischaemic outcome, 2.25% vs 3.13% p = ns; haemorragic outcome 2.09% vs 2.58%, p = ns; disability (3.70% vs 3.68%, p = ns; combined endpoint, 4.18% vs 5.52% p = ns).
Conclusion
We did not observe sex-differences in our population regarding timing of NOAC treatments and outcomes after stroke
Trial registration number
N/A
AS26-001
SEX DIFFERENCES IN INTRACRANIAL AND EXTRACRANIAL ATHEROSCLEROSIS IN PATIENTS WITH ACUTE ISCHAEMIC STROKE
1LUMC, Neurology, Leiden, The Netherlands
2LUMC, Radiology, Leiden, The Netherlands
3UMC Utrecht, Radiology, Utrecht, The Netherlands
4UMC Utrecht, Neurology, Utrecht, The Netherlands
5UMC Utrecht, Cardiovascular Epidemiology, Utrecht, The Netherlands
Background and Aims
To investigate sex differences in presence and location of atherosclerosis in a large population of acute ischaemic stroke patients.
Method
Participants were included from the Dutch acute Stroke study (DUST), a large prospective multicentre cohort study. All patients received CT/CT-angiography within 9 hours of stroke onset. We assessed any sign of atherosclerosis in the intra- and extracranial circulation and measured intracranial atherosclerosis burden by quantifying intracranial internal carotid artery (ICA) calcifications to obtain calcium volumes. Relative risks between women and men were calculated with Poisson regression analysis adjusted (aRR) for potential confounders including age, hypertension, hyperlipidemia, diabetes, smoking and alcohol use.
Results
We included 1397 patients with a mean age of 67 years, 600 (43%) were women. Any sign of atherosclerosis in intracranial vessel segments was found as frequently in women as in men (71% versus 72%, aRR 0.95; 95%CI 0.89-1.01). Also, intracranial ICA calcium volume did not differ between women and men (median volume 124 mm3, IQR 35.5-304.5 in women and 112 mm3, IQR 33.0-276.5 in men, tertile largest volume 37% in women and 33% in men, aRR 1.00; 95% CI 0.95-1.05). Extracranial atherosclerosis was less common in women than in men (74% vs 81%, aRR 0.86; 95%CI 0.81-0.92).
Conclusion
In patients with acute ischemic stroke the prevalence of intracranial atherosclerosis does not differ between women and men, while extracranial atherosclerosis is less often present in women compared with men.
Trial registration number
N/A
AS26-018
DIFFERENCES BETWEEN MEN AND WOMEN WITH ISCHEMIC STROKE WITH AND WITHOUT PRE-STROKE DEMENTIA
1Karolinska Institutet, Department of Neurobiology- Care Sciences and Society- Center for Alzheimer Research, Huddinge, Sweden
2Jönköping University, Institute of Gerontology- School of Health and Welfare- Aging Research Network-Jönköping, Jönköping, Sweden
3University Medical Centre- Ljubljana, Department of Neurology, Ljubljana, Slovenia
4Lund University, Skane University Hospital- Department of Clinical Sciences Lund, Lund, Sweden
5Karolinska Institut, Medicine Solna and Clinical Science and Education- Södersjukhuset, Stockholm, Sweden
Background and Aims
To compare reperfusion treatment and outcomes in men and women with dementia and acute ischemic stroke (AIS) to non-dementia stroke controls.
Method
Patients with dementia who suffered AIS 2010-2014 (n = 1356) were compared with matched non-dementia subjects (n = 6755) in this longitudinal cohort study using data from the Swedish Dementia and Stroke Registries. Reperfusion treatment, death at one year, and living conditions and modified Rankin Scale score (mRS) at three months were compared and odds ratios (ORs) calculated using logistic and ordinal logistic regressions.
Results
764 women and 592 men with dementia and 3838 women and 2917 men without pre-stroke dementia were included. There were no differences in level of consciousness at arrival or reperfusion rate in men and women with or without dementia. Of those surviving hospitalization, more women with pre-stroke dementia had a poor outcome, had institutional care or home help (p < 0.001). When adjusting for age, dementia, and stroke severity (determined by level of consciousness) OR was higher for women for mRS 3–6 at 3 months (OR 1.60, 95%CI 1.42-1.81) and assisted living (OR 1.30, 95%CI 1.15-1.47) but lower for death 1 year post-stroke (OR 0.876, 95%CI 0.78-0.98). For death 1 year post-stroke there was no difference between men and women if dementia was not included in the analysis while higher level of assisted living and poor functional level remained in women in this partially-adjusted analysis.
Conclusion
Women both with and without pre-stroke dementia have a higher level of assisted living and poorer functional outcomes at three months after acute ischemis stroke.
Trial registration number
N/A
AS26-022
GENDER DIFFERENCES IN POST-STROKE DEPRESSION: A LONGITUDINAL ANALYSIS
1Humboldt University, Department of Psychology, Berlin, Germany
2Ernst von Bergmann Hospital, Neurology, Potsdam, Germany
Background and Aims
Depression affects affects one in three patients with cerebral stroke. Whereas the risk of depressive disorders in the general population is known to be higher in females, research is divided regarding a gender-specific risk of post-stroke depressio (PSD). Most studies are cross-sectional, and do not consider possible gender differences in depression onset. The present study used a longitudinal design to examine possible gender differences in depression risk at different time points.
Method
Participants (N = 174) were recruited in two inpatient rehabilitation centres and assessed for depression seven weeks (baseline interview), 8 and 15 months (follow-ups) after stroke. In addition to the clinical interview, established risk factors such as stroke severity, ADL, cognitive status, premorbid depression and social support were assessed. Regression analyses were conducted, which allows to control for baseline differences of other known risk factors of depression.
Results
Depressive disorders were during inpatient rehabilitation more frequent in women (48.2%) than in men (28.3%). However, gender differences disappeared in the follow-up examinations. Independent of gender, the severity of depressive symptoms was associated with low ADL functions and low social support.
Conclusion
Our analyses support previous studies reporting an equal prevalence of PSD for male and female patients within the first 15 months after stroke, and an association with the same risk factors. However, our longitudinal analyses provided evidence for different time patterns in the emergence of PSD, with an initially higher prevalence in females that evens out within the first 15 months after stroke.
Trial registration number
N/A
Scientific Communications -Risk Factors in Stroke
AS18-031
IMPORTANCE OF BLOOD PRESSURE VARIABILITY FOR THE EFFECT OF VALSARTAN VERSUS AMLODIPINE ON CARDIOVASCULAR EVENTS AND DEATH
1Oslo University Hospital, Department of Geriatric Medicine, Oslo, Norway
2Institute of Clinical Medicine, University of Oslo, Oslo, Norway
3University of Oslo, Department of Informatics, Oslo, Norway
4Oslo University Hospital, Department of Cardiology, Oslo, Norway
5University of Michigan, Division of Cardiovascular Medicine, Ann Arbor- Michigan, USA
6Novartis Pharmaceuticals Corporation, East Hanover, New Jersey, USA
7Stroke Prevention Research Unit, Nuffield Department of Clinical Neuroscience- University of Oxford, Oxford, United Kingdom
8University of Milano-Bicocca, St Gerardo Hospital, Monza, Italy
9Istituto Auxologico Italiano, Department of Cardiovascular- Neural and Metabolic Sciences- S. Luca Hospital- IRCCS- Department of Medicine and Surgery- University of Milano-Bicocca, Milan, Italy
10State University of New York- Downstate College of Medicine, Department of Cardiovascular Medicine, New York, USA
Background and Aims
Blood pressure variability is associated with increased cardiovascular risk, and drug classes affect blood pressure variability differently. We used data from the VALUE trial to study the effects of valsartan vs. amlodipine on visit-to-visit systolic blood pressure variability and risk of cardiovascular events and death.
Method
The VALUE trial was a randomised-controlled trial of valsartan vs. amlodipine in hypertensive patients at high cardiovascular risk. Target blood pressure was 140/90 mmHg, and mean follow-up time was 4.2 years. Blood pressure was measured three times at each visit, monthly during the first 6 months and thereafter every 6 months. Visit-to-visit blood pressure variability was expressed as the standard deviation (SD) of mean blood pressures from all visits. We used Cox regression to assess the treatment effect on risk of cardiovascular events and death, adjusted for mean blood pressure and blood pressure variability.
Results
15.245 patients were included. Mean baseline blood pressure was around 154/88 mmHg in both groups. During follow-up, mean systolic blood pressure was around 2.0 mmHg higher, and mean systolic blood pressure variability was also higher in the valsartan group (mean difference in SD 1.46, 95 % Cl 1.28-1.63). Analyses of effects on cardiovascular events and death will be presented at the conference.
Conclusion
The VALUE trial offers a unique opportunity to compare directly the effects of angiotensin receptor blockers vs. calcium channel blockers on cardiovascular events and death, adjusted for differences in mean blood pressure and blood pressure variability.
Trial registration number
N/A
AS15-032
STROKE INCIDENCE AND RISK FACTORS OVER 44-YEARS - THE PROSPECTIVE POPULATION STUDY OF WOMEN IN GOTHENBURG
1Institute of Medicine/The Sahlgrenska Academy at University of Gothenburg, Department of Public Health and Community Medicine/Primary Health Care, Gothenburg, Sweden
2Institute of Neuroscience and Physiology/The Sahlgenska Academy at University of Gothenburg, Section of Clinical Neuroscience/Neurology, Gothenburg, Sweden
Background and Aims
The Population Study of Women started 1968-69, is a unique long-term study with few participants lost to follow-up. Our aim was to study incidence of first-ever stroke during 44-years and associations with risk factors.
Method
Incidence for total stroke (TS) and specified subtypes, ischemic (IS), haemorrhagic (HS) fatal stroke (FS), was calculated. Smoking, BMI, WHR, blood pressure, preeclampsia, lipids, physical inactivity, perceived stress, socioeconomic factors, low education were baseline risk factors. Survival time free from stroke was calculated for diabetes, myocardial infarction, atrial fibrillation and hypertension.
Results
Of the 1460 women 337 (23%) suffered from first ever stroke. The distribution was: 262 (78%) IS, 39(12%) HS, 36 (10%) non-specified; 66 (20%) were fatal (FS). In multivariate analysis systolic pressure, grade 3 (≥180 mmgHg) was significantly associated with HS, FS and TS. Grade 2 (≥160-179 mmHg) was associated with IS and TS. For IS, BMI < 18 (OR 2.42 CI 0.99-5.96), WHR >0.80 (OR1.78 CI 1.25—2.54), triglycerides (OR 1.14 CI 1.04-1.25), low physical activity (OR 1.40 CI 1.02-1.92) and low education (OR 1.49 CI1.10-2.01), showed association. HS was associated with BMI<18 (OR3.88 CI 0.93-16.29). TS was associated with BMI < 18 (OR2.40 CI1.23-4.70), WHR>0.80 (OR1.76 CI 1.28-2.43), physical inactivity (OR1.45 CI1.10-1.90), triglycerides (OR1.11 CI1.01-1.23), low education (OR1.32 CI1.02-1.70) and smoking (OR1.28 CI1.01-1.62). FS was associated with WHR>0.80 (OR 3.50 CI1.90-6.47) and smoking (OR2.27 CI1.35-3.81).
Conclusion
Systolic hypertension, WHR >0.80, triglycerides and low education were most significant risk factors while history of preeclampsia only showed borderline significance.
Trial registration number
N/A
AS09-043
BLOOD PRESSURE TRAITS DIFFERENTIALLY AFFECT RISK OF DIFFERENT ISCHAEMIC STROKE SUBTYPES
1Imperial College London, Epidemiology and Biostatistics, London, United Kingdom
Background and Aims
Although blood pressure is an established risk factor for ischaemic stroke, its effect on different disease subtypes is not known. Observational studies in this area are limited by confounding, and randomized controlled trials are often unfeasible. Such limitations can be overcome using Mendelian randomization (MR), which employs genetic variants as proxies for the effect of different blood pressure traits. The aim of this study was to use MR to measure the causal effect of systolic, diastolic and pulse pressure of risk of different ischaemic stroke subtypes.
Method
A two-sample MR approach was used. Instruments and genetic association estimates for blood pressure taken from a genetic association study in over one million people of European ancestry. Genetic association estimates for ischaemic stroke subtypes were taken from a genetic association study of approximately 16,851 stroke cases and 32,473 controls. Appropriate statistical sensitivity analyses were used to explore and adjust for any pleiotropic effect of the genetic variants on risk of stroke risk through pathways independent of blood pressure.
Results
For risk of large artery stroke and small vessel stroke, MR evidence supported a causal effect of systolic, diastolic and pulse pressure. This was greater in magnitude than that observed for coronary artery disease. In contrast, no causal effect on risk of cardio-embolic stroke was identified for any blood pressure trait.
Conclusion
Blood pressure traits have a causal effect on the large artery and small vessel subtypes of ischaemic stroke and should be targeted in these diseases.
Trial registration number
N/A
AS30-011
SELECTIVE SEROTONIN REUPTAKE INHIBITORS AND RISK OF INTRACEREBRAL HAEMORRHAGE
1University College London- Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
Background and Aims
Selective serotonin reuptake inhibitor (SSRI) prescriptions are increasing yet recent observational studies have suggested increased risk of intracerebral haemorrhage (ICH). We sought to clarify the impact of SSRI on ICH, accounting for study methodology and prescription biases.
Method
Using a comprehensive search of Medline, Embase, the Cochrane Library, reference lists and ongoing studies from 1960 to December 2017, we systematically reviewed studies comparing SSRI with control (placebo or no treatment). First-ever ICH and recurrent ICH were meta-analysed using a random-effects model and the review was prospectively registered (PROSPERO: CRD42017084513). Unadjusted and adjusted data were pooled and study quality was assessed with the RoBANS checklist.
Results
26 observational studies, but no randomised trials, were available for meta-analysis, consisting of a combined total of 5,736,694 patient-years of follow-up. Those treated with SSRI were more likely to have depression (p < 0.001), be female (p = 0.05), and have greater use of non-steroidal anti-inflammatory drugs (p = 0.04). Compared to control, SSRI were significantly associated with first-ever ICH (RR 1.29, 95% CI 1.14-1.46); however, in survivors of ICH there was no association between SSRI and recurrence (0.95, 0.83-1.09). Meta-regression confirmed that studies with higher risk of bias were more likely to report an association of SSRI and ICH (p = 0.006).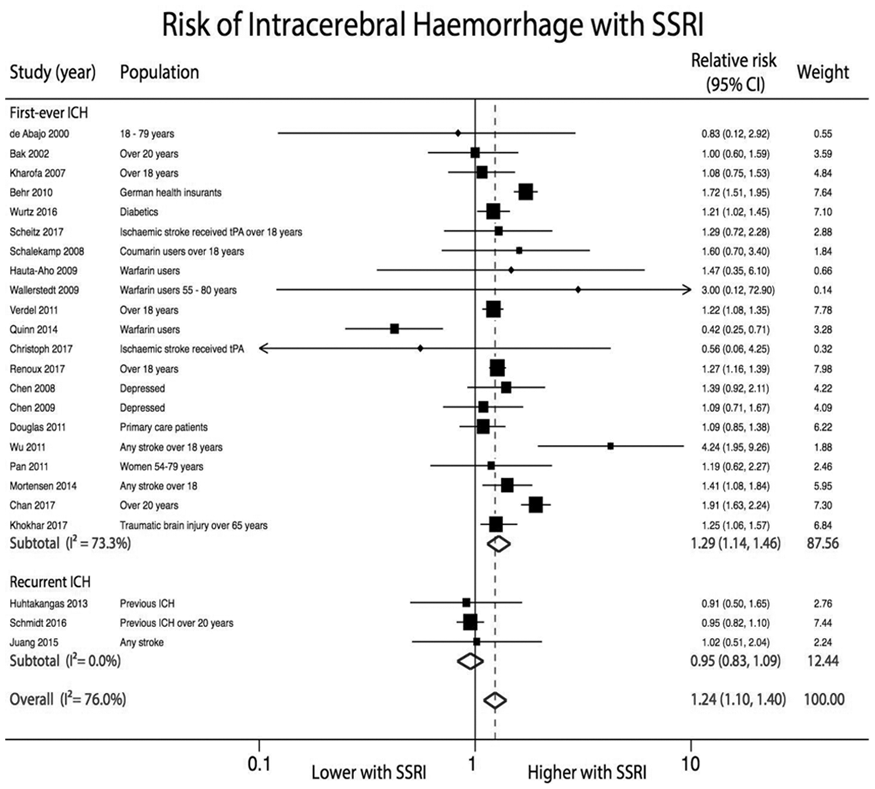
Conclusion
SSRI are associated with increased risk of first-ever ICH, but not with recurrent ICH. These findings, based solely on observational data, should be taken with caution due to fundamental differences in patients receiving treatment. To avoid prescription biases, future randomised trials are crucial to accurately estimate the risk of ICH with SSRI.
Trial registration number
N/A
AS14-053
POPULATION-BASED STUDY OF PREVALENCE AND PROGNOSTIC VALUE OF NOCTURNAL BP DIPPING PATTERNS IN TIA/STROKE SUBTYPES
1Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neuroscience, Oxford, United Kingdom
Background and Aims
In previous studies of hypertensive populations, diminished nocturnal SBP fall (non-dipping) was associated with increased risk of cardiovascular events. However, it is unclear whether abnormal diurnal BP pattern predicts recurrent events after TIA/ischaemic stroke and whether any prognostic value differs according to aetiological subtype.
Method
In a population-based incidence cohort (Oxford Vascular Study), consecutive patients with TIA or non-disabling stroke had 24-hour ambulatory BP-monitoring (ABPM) at one-month follow-up after treatment of any initial hypertension. Dipping pattern was classified in relation to mean nighttime vs daytime SBP according to standard definitions (reverse dipping <0% fall; non-dipping ≥0% but <10%; dipping ≥10% but <20%; extreme dipping ≥20% fall). Dipping pattern was related to risk of recurrent stroke on follow-up, stratified by TOAST subtype of the initial event after adjustment for age and sex.
Results
Among 1035 patients (mean/SD age 68.67/12.74) with ABPM, 139 (13.6%) were reverse dippers, 335 (32.8%) non-dippers, 416 (40.7%) dippers and 131 (12.8%) extreme dippers. Compared to normal dippers, reverse dippers had an increased risk of recurrent stroke after lacunar TIA/stroke (n = 106, HR = 5.31, 95%CI:1.33-21.1, p = 0.02) but not (pinteraction<0.01) after other subtypes (HR = 0.50, 95%CI:0.20-1.22, p = 0.13). Extreme dipping was not predictive of stroke in any aetiological subtype, but was associated with increased mortality after cardioembolic events (n = 133, HR = 5.73, 1.72-19.1, p = 0.005).
Conclusion
The prognostic significance of BP-dipping patterns may depend on the aetiological subtype of TIA/stroke and research in more general hypertension populations may not be generalisable.
Trial registration number
N/A
AS23-009
CAUSAL IMPACT OF TYPE 2 DIABETES ON CEREBRAL SMALL VESSEL DISEASE: A MENDELIAN RANDOMIZATION ANALYSIS
1Department of Neurology - West China Hospital, Neurology, Chengdu, China
2Population Health Sciences- Sigmund-Freud-Straße, German Center for Neurodegenerative diseases, Bonn, Germany
3University of Cambridge- Cambridge Biomedical Campus, Department of Clinical Neurosciences, Cambridge, United Kingdom
Background and Aims
The relationship between Type 2 diabetes (T2D) and Cerebral Small Vessel Disease (CSVD) was unclear. We aimed to examine the causal effect of T2D, fasting glucose levels and higher insulin resistance on CSVD using Mendelian randomization (MR).
Method
Five CSVD phenotypes were studied; two were clinical outcomes associated with CSVD (lacunar stroke:N = 2191/27297 and intracerebral haemorrhage:N = 2254/8195 (ICH; deep and lobar)), while three were radiological markers of CSVD(white matter hyperintensities (WMH): N = 8429, fractional anisotropy (FA): N = 8357, and mean diffusivity (MD): N = 8357). We applied two complementary analyses to evaluate the association of T2D with CSVD. First, we used summarized data from genome-wide association study to calculate the effects of T2D-related SNPs on CSVD with inverse-variance weighted and weighted median approaches. Secondly, we performed a genetic risk score approach to test the effects of T2D-associated variants on WMH, FA and MD using individual level data in UK Biobank.
Results
T2D was associated with higher risk of lacunar stroke (odds ratio[OR],1.15; 95% confidence interval[CI],1.04-1.28;P = 0.007) and lower mean FA(OR,0.78;95%CI,0.66–0.92;P = 0.004), but not WMH volume (OR,1.01;95%CI,0.97-1.04;P = 0.626), higher mean MD(OR,1.04;95%CI,0.89-1.23;P = 0.612), ICH(OR,1.07;95%CI,0.95-1.20;P = 0.269), lobar ICH(OR,1.07;95%CI,0.89-1.28;P = 0.466), or deep ICH(OR,1.16;95%CI,0.99-1.36;P = 0.074). Weighted median and penalized median weighted analysis showed similar effect estimates of T2D on lacunar stroke and FA, but with wider CIs, meaning they were not significant. The genetic score on individual level data was significantly associated with FA (OR, 0.63;95%CI,0.45-0.89;P = 0.008) after adjusting potential confounders. Genetically predicted fasting glucose and insulin was not associated with any type of CSVD.
Conclusion
Our MR study provides evidence that T2D may be causally associated with CSVD, in particular with lacunar stroke and FA.
Trial registration number
N/A
AS18-035
THE BARCELONA-ASYMPTOMATIC INTRACRANIAL ATHEROSCLEROSIS (ASIA) STUDY: INTRACRANIAL ATHEROSCLEROSIS AS PREDICTOR OF LONG-TERM VASCULAR EVENTS
1Hospital Universitario Central de Asturias, Neurology, Asturias, Spain
2Hospital Universitari Germans Trias i Pujol- Badalona, Neurology, Barcelona, Spain
3Hospital de Manresa, Neurology, Manresa, Spain
4Hospital del Mar, Neurology, Barcelona, Spain
5ABS Riu Nord-Riu Sud- Santa Coloma de Gramenet, Primary Care, Barcelona, Spain
6USR Metropolitana Nord, Primary Care, Barcelona, Spain
7Hospital Universitario Valladolid, Neurology, Valladolid, Spain
8Hospital Universitari Germans Trias i Pujol, Neurology, Barcelona, Spain
Background and Aims
Symptomatic intracranial atherosclerosis is associated with a high risk of stroke recurrence and other vascular events. We aimed to study the prognosis impact of intracranial atherosclerosis (ICAS) from its asymptomatic stage
Method
Barcelona-Asymptomatic Intracranial Atherosclerosis (AsIA) Study is a population-based study that included a random sample of 933 Caucasian subjects (mean age 66 years, 64% males) with a moderate-high vascular risk (REGICOR>5) and without history of stroke or coronary disease. Carotid and intracranial atherosclerosis were screened by color-coded duplex ultrasound, being moderate-severe stenosis confirmed by magnetic resonance imaging. Subjects were prospectively followed-up to assess the incidence of vascular events (stroke, acute coronary syndrome and/or vascular death).
Results
At baseline, 80 of the 933 subjects had asymptomatic ICAS (8.6%) of whom 31 (3.3%) had moderate-severe stenosis. After 7.16 years [6.91-7.75] of follow-up, there were 51 strokes (16 transient ischemic attacks, 27 ischemic, 8 hemorrhagic), 63 coronary events and 23 vascular deaths. After multivariate Cox regression analyses adjusted by age, sex, vascular risk (REGICOR) and presence of carotid plaques, intracranial stenosis was an independent predictor for overall vascular events (HR 1.92, 95% CI [1.16-3.17], p = 0.01), and moderate-severe intracranial stenosis was also an independent predictor for stroke (HR 3.30, 95% CI [1.35-8.02], p = 0.009).
Conclusion
Asymptomatic ICAS is independently associated with the occurrence of future vascular events in our population. These findings might have important implications in the development of primary prevention strategies.
Trial registration number
N/A
AS20-058
RISK FACTORS FOR SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1Lund University, Department of Clinical Sciences, Malmö, Sweden
Background and Aims
Results from prior studies of risk factors for intracerebral hemorrhage (ICH) are inconsistent. Few studies have investigated risk factors measured before the event and separately for different locations of ICH. We investigated risk factors for incident ICH in the population-based Malmö Diet and Cancer cohort.
Method
Baseline information, assessed by a questionnaire and in a physical examination, was gathered from 28,416 subjects without a history of ICH. ICH cases (n = 333) were identified using local and national patient registers during follow-up (mean follow-up time 18.4 years), validated by review of hospital records, and classified as lobar or non-lobar. Potential risk factors were studied using Cox regression.
Results
The following factors were significantly (p < 0.05) associated with increased incidence of ICH adjusting for age and sex: systolic and diastolic blood pressure, use of oral anticoagulants, smoking, high alcohol intake, and living alone. In a multivariable analysis, levels of apolipoprotein B were, in addition, inversely associated with ICH risk, whereas high alcohol intake was not significantly associated with ICH. Smoking was a risk factor for lobar but not non-lobar ICH. Diabetes mellitus was associated with increased risk of non-lobar but not lobar ICH. Body mass index, waist circumference, physical activity and educational level were not associated with incidence of ICH.
Conclusion
In this population-based study, hypertension, smoking, use of oral anticoagulants, and living alone were independent risk factors for ICH. Apolipoprotein B was inversely associated with incidence of ICH. Smoking was associated with lobar ICH. Diabetes was a risk factor only for non-lobar ICH.
Trial registration number
N/A
AS19-017
THE ASSOCIATIONS OF STROKE AND CANCER USING REGISTRY-BASED DATA
1Duke-NUS Medical School, Neurology, Singapore, Singapore
2National Neuroscience Institute - Singapore General Hospital, Neurology, Singapore, Singapore
Background and Aims
Associations between ischemic stroke (IS) and cancer have been reported, with IS being a complication of a known malignancy or the first manifestation of an occult one. However, there are limited data from nation-wide databases, especially in ethnic Asian populations. With the age-standardized incidence rate for cancer being 0.2 per 100 person-years in Singapore, we aimed to determine the prevalence and epidemiology of cancer-related stroke and investigate differences in vascular risk profile of IS patients with and without concomitant cancer.
Method
This was a case-control study using national registries of mandatorily reported data. Cases were IS patients with concomitant cancer, defined as cancer diagnoses up to 2 years before and after IS. Univariate and multivariate logistic regression were used to identify differences in vascular risk factors.
Results
Among the 21,068 IS patients studied (mean age 68.7years), the prevalence of concomitant cancer in IS patients was 6.3% (1330), 30.0% (395) of whom had cancer diagnoses within 2 years of IS. The top 4 cancers in IS patients were lower gastrointestinal (19.7%), lung (13.8%), genitourinary (11.5%) and hepatopancreaticobiliary (10.8%). Older age [OR = 1.02 (1.01-1.02) per year] and a lower likelihood of hypertension [OR = 0.84 (0.73-0.97)] and hyperlipidemia [OR = 0.53 (0.45-0.62)] were independently associated with cancer-related IS.
Conclusion
In a large ethnic Asian sample, 4 per 100 IS patients had prior cancer diagnosis and 2 per 100 had incident cancer over 2 years after IS. These findings highlight the need for an index of suspicion for malignancies in IS patients, especially in the absence of vascular risk factors.
Trial registration number
N/A
Scientific Communications- Reperfusion 2
AS02-017
VALIDATION OF THE CLINICAL/CORE MISMATCH AND PERFUSION/CORE MISMATCH SELECTION CRITERIA FOR LATE WINDOW THROMBECTOMY: POOLED ANALYSIS OF DEFUSE 3 AND DAWN
1Stanford University Medical Center, Stanford Stroke Center, Stanford, USA
2Emory University School of Medicine, Neurology, Atlanta, USA
3UPMC, Neurology, Pittsburgh, USA
Background and Aims
Two recently published late window thrombectomy trials (DAWN and DEFUSE 3) randomly assigned patients with proximal middle-cerebral-artery or internal-carotid-artery occlusions to treatment with endovascular thrombectomy vs. standard medical therapy alone in an extended time window. These studies used different clinical and imaging strategies to identify eligible candidates. We hypothesized that DEFUSE 3 data will validate the Clinical/Core mismatch selection criteria and that DAWN data will validate the Perfusion/Core mismatch selection criteria.
Method
Both studies installed RAPID software at all sites to standardize the assessment of ischemic lesion volumes. DAWN (N = 206) selected patients based on a mismatch between the severity of the clinical deficit and the initial infarct volume (ischemic core), with mismatch criteria defined according to age and NIHSS score. DEFUSE 3 (N = 182) selected patients with an initial infarct size of less than 70 ml, and a ratio of the volume of ischemic tissue on perfusion imaging to early infarct volume of 1.8 or more. The primary outcome is the ordinal score on the modified Rankin scale at day 90 (Wilcoxon rank-sum test); adjusted treatment effects are calculated with the use of ordinal regression on the full modified Rankin scale and stratified Cochran–Mantel–Haenszel tests. Secondary outcomes are the rate ratio for mRS 0–2 and mRS 5–6 at day 90. The primary safety outcomes are symptomatic ICH and death
Results
The results are under embargo.
Conclusion
We will present the results of the analyses described above at the meeting.
Trial registration number
DEFUSE 3: NCT02586415
DAWN: NCT02142283
AS06-050
PERFORMANCE OF THE MADRID-DIRECT (DIRECT REFERRAL TO ENDOVASCULAR CENTER) PREHOSPITAL SCALE IN IDENTIFYING POTENTIAL THROMBECTOMY CANDIDATES. ANALYSIS OF 620 CONSECUTIVE PATIENTS
1University Hospital La Paz, Neurology, Madrid, Spain
2Madrid Medical Emergency Service SUMMA-112, Stroke Code Coordination Centre, Madrid, Spain
3Puerta de Hierro-Majadahonda University Hospital, Neurology, Madrid, Spain
412 de Octubre University Hospital, Neurology, Madrid, Spain
5San Carlos University Hospital, Neurology, Madrid, Spain
6Gregorio Marañón University Hospital, Neurology, Madrid, Spain
7Ramón y Cajal University Hospital, Neurology, Madrid, Spain
8La Princesa University Hospital, Neurology, Madrid, Spain
Background and Aims
Benefits of direct transportation of patients with large vessel occlusion (LVO) to Stroke Centers (SC) providing Endovascular Treatment (ET) are clear. However, prehospital identification of potential thrombectomy candidates remains challenging as current prehospital scales demonstrate a moderate accuracy detecting LVO (70-79%), but its ability to predict actual ET is uncertain. Our aim is to evaluate the MADRID-DIRECT scale performance in a prehospital setting.
Method
The MADRID-DIRECT scale was defined as a simplification of the previously published DIRECT criteria that includes severe limb paresis, aphasia or hemineglect, gaze deviation, blood pressure and age. MADRID-DIRECT scale was prospectively performed and registered for stroke codes attended by the SUMMA-112 emergency service. Patients with a score ≥2 points were directly transferred to a SC providing ET. Patients with <2 points were transferred to the nearest stroke unit, and eventually transferred to proper SC if considered suitable for ET. Data on the first 4 months of implementation are presented.
Results
Data on the MADRID-DIRECT scores and treatments received were available for 620/652 patients (95%), mean age 69 ± 16 years. Final diagnoses were ischemic stroke (436), hemorraghic stroke (80), stroke mimics (104). MADRID-DIRECT was ≥2 points in 190 cases (31%). 125 patients (20%) received ET. Of them, 101 (81%) were directly transferred to the SC providing ET. Prehospital performance of the MADRID-DIRECT showed 64% Sensitivity, 78% Specificity, and 75% global accuracy for ET.
Conclusion
MADRID-DIRECT demonstrates a high adherence on emergency services and increases significantly the direct transfers for ET. Further results will be presented at the conference.
Trial registration number
N/A
AS10-053
IMPACT OF BASELINE ALBERTA STROKE PROGRAM EARLY CT SCORE ON CLINICAL OUTCOMES OF ENDOVASCULAR TREATMENT
1Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
2Texas Stroke Institute, Radiology, Dallas-Fort Worth- Texas, USA
3Erasmus Medical Center, Neurology, Rotterdam, The Netherlands
4Rijnstate Hospital, Radiology, Arnhem, The Netherlands
5Maastricht University Medical Center, Radiology, Maastricht, The Netherlands
6Erasmus Medical Center, Public Health and Epidemiology, Rotterdam, The Netherlands
Background and Aims
We aimed to investigate results of endovascular thrombectomy (EVT) for acute ischaemic stroke in patients with low Alberta Stroke Program Early CT Score (ASPECTS).
Method
The current study reports on MR CLEAN Registry patients with available baseline ASPECTS (N = 1459). ASPECTS was trichotomised in 0–4, 5 and 6–10. Primary outcome was modified Rankin Scale score (mRS) at 90 days. Secondary outcomes were symptomatic intracranial haemorrhage (sICH) and mortality. The effect of reperfusion (defined as extended thrombolysis in cerebral infarction [eTICI] score 2B-3) on mRS was assessed by multivariable ordinal logistic regression analysis, with interaction between reperfusion and ASPECTS, and expressed as an adjusted common odds ratio (acOR).
Results
Higher ASPECTS was associated with improved ordinal mRS (acOR 1.09, 95%CI 1.03-1.15). In the ASPECTS 0–4 subgroup (n = 95), successful reperfusion was not significantly associated with improved mRS (acOR 1.00, 95%CI 0.79-1.27). ASPECTS 5 (n = 65) and ASPECTS 6–10 subgroups (n = 1299) did show significant benefit of reperfusion (acOR 1.60, 95%CI 1.14-2.40; acOR 1.41, 95%CI 1.33-1.51, respectively, p for interaction = 0.048) (Fig.1). Patients with ASPECTS 5 had no increased risk of sICH (p = 0.71) or mortality (p = 0.70) compared to ASPECTS 6–10. ASPECTS 0–4 patients had a higher risk of mortality (p = 0.05), but not sICH (p = 0.82).
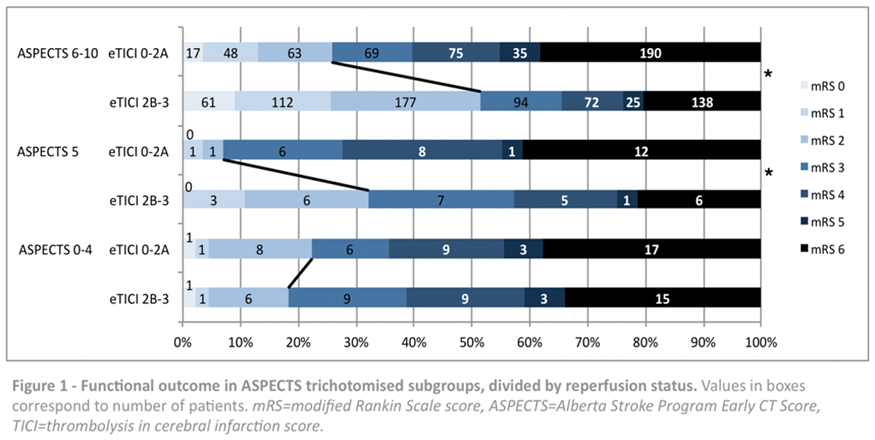
Conclusion
This study demonstrates a significant benefit of reperfusion after EVT in patients with ASPECTS 5 and 6–10. No significant benefit was seen in ASPECTS 0–4.
Trial registration number
N/A
AS07-067
VESSEL WALL ENHANCEMENT ON CONTRAST-ENHANCED MAGNETIC RESONANCE IMAGING AFTER THROMBECTOMY IN ACUTE ISCHEMIC STROKE: ROLE OF DIFERENT THROMBECTOMY TECHNIQUES
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
In preclinical models, vessel-wall damage is relatively frequent after mechanical thrombectomy (MT), especially after the use of stentrievers in comparison with aspiration techniques. Herein, we aimed to compare the effect of stentriever and aspiration techniques on vessel-wall damage after MT.
Method
A prospective cohort of 94 acute stroke patients (median NIHSS = 19) with proximal occlusions in the carotid territory treated with MT within median (IQR) 190 (125-340) minutes was analyzed. Vessel-wall damage was identified as gadolinium vessel-wall enhancement (VWE) in a 24-48 hour follow-up contrast-enhanced 3mm-thick FLAIR sequences (1.5T) by two treatment-blinded evaluators.
Results
Stentrievers were used alone or in combination with aspiration in 79 (84%) and 5 (5%) patients respectively, and aspiration alone was used in 10 (11%). VWE was observed in 41 (44%) subjects and varied significantly according to thrombectomy technique. None of the subjects treated with aspiration alone had VWE, whereas it was observed in 41 (49%) of those treated with stentrievers (p = 0.004). The rate of VWE increased significantly when aspiration devices where used in addition to stentrievers (n = 5/5, 100%) in comparison with stentriever use alone (n = 36/79, 46%; p = 0.024), along with a higher number of device passes (p < 0.001). Recanalization, post-treatment hemorrhagic complications or clinical outcome did not differ according to thrombectomy technique.
Conclusion
VWE is frequently found after stentriever use and increases in parallel with a higher mechanical load or when combination with aspiration technique is required for clot removal. The clinical relevance of direct vessel damage after MT is controversial and deserves further study.
Trial registration number
N/A
AS06-057
ELIGIBILITY FOR LATE THROMBECTOMY USING STRICT (DAWN) AND LIBERAL SELECTION CRITERIA IN A PRIMARY AND COMPREHENSIVE STROKE CENTER
1Lausanne University Hospital, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
2Lausanne University Hospital, Neuroradiological Unit- Service of Diagnostic and Interventional Radiology, Lausanne, Switzerland
3Stanford University and Medical Center, Department of Radiology- Neuroradiology Division, Standford, USA
Background and Aims
DAWN has shown efficacy of late endovascular thrombectomy (EVT) in selected, anterior proximal occlusive stroke. We aimed to identify the eligibility for late EVT (treatable 6–24h after last proof of good health) at an endovascular-capable center using DAWN and more liberal clinical-imaging mismatch criteria.
Method
All consecutive patients from ASTRAL (Lausanne, 2003-2017) were selected if they had all necessary DAWN eligibility data. A second sample with more liberal criteria was extracted adding pre-stroke Rankin 2, proximal M2 and basilar occlusions, ASPECTS-based core estimation and lower NIHSS cut-offs.
Results
Of 1’707 patients arriving between 5–23h (23% outside referrals), 551 had sufficient data for DAWN-analysis, and 1’181 for liberal criteria. Proportion of EVT eligible patients varied from 1%-10% according to criteria and referral pattern (see Table). Since 2003, late-EVT was effectively performed in 60 patients (mostly following liberal criteria). The proportion of effective late EVT increased from 6% during the 5 years before to 21% since the DAWN results (+250%).
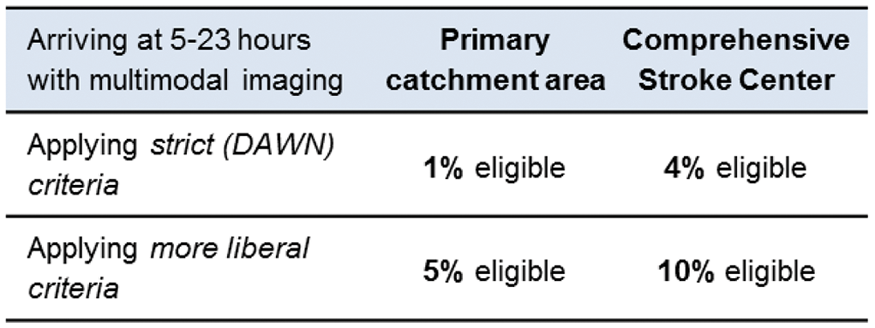
Conclusion
Of late arriving stroke patients over 15 years, only 1% from the primary catchment area are eligible for thrombectomy according to DAWN criteria. With more liberal clinical-imaging mismatch criteria, the eligibility proportion reaches 10% of all patients at a comprehensive stroke center. The observed increase of 250% effectively treated patients at our center after the DAWN results suggests an important potential of treatable patients.
Trial registration number
N/A
AS07-096
ENDOVASCULAR THERAPY IN PATIENTS WITH HIGH BASELINE DISABILITY: A TREVO REGISTRY ANALYSIS
1Grady Memorial Hospital- Emory University School of Medicine, Department of Neurology, Atlanta, USA
2EmoryUniversity/Grady Memorial Hopsital, Neurology, Atlanta, USA
3Drexel Neurosciences Institute, Neurology, Philadelphia, USA
4CHUV, Neurology, Lausanne, Switzerland
5Erlanger, Neurology, Chattanooga, USA
6Riverside Methodist Hospital/Ohio Health Research Institute, Neurology, Columbus, USA
7California Pacific Medical Center, Neurology, San Francisco, USA
8Wellstar, Neurology, Atlanta, USA
9faculty of Medicine in Hradec Kralove, Radiology, Hradec Kralove, Czech Republic
10Stryker, Neuroscience, New York, USA
11UCLA, neurology, Los Angeles, USA
Background and Aims
Patient with significant baseline disability have been historically from endovascular therapy clinical trials as there are often thought not to benefit from treatment .
Method
The Trevo registry prospectively enrolled 2010 patients with a broad inclusion criteria requiring only the utilization of the Trevo device as a first pass device. Patients were dichotomized into 2 groups according to their baseline mRS: (G1) Patients with significant baseline disability (mRS 2–5) and (G2) those without significant baseline disability (mRS 0–1). The primary endpoint was the growth in the weighted mRS scores (defined as 90-day w-mRS – baseline w-mRS).Secondary outcomes included the linear growth in the standard mRS scores (defined by 90-day mRS – baseline mRS), rates of mTICI 2b-3, sICH, and mortality.Sensitivity analysis was performed for patients with mRS 1–5 versus those with a mRS 0.
Results
1351 patients were included of which 199 (14.7%) had a significant disability at baseline.These were older (p < 0.001) had more comorbidities. They also had higher NIHSS (p < 0.001) and lower rates of IV t-PA(p < 0.001) .
There was no difference in the growth of w-mRS (-3.3(-6.5-0) for G1vs-1.5(-3.5-0), p = 0.139) as well as linear growth in mRS (11(5–19)vs5(2–12), p = 0.124), rates of mTICI 2b-3 (p = 0.08) and sICH (p = 0.39) between groups, while patients with mRS2-5 had higher rates of mortality (p = 0.008). Sensitivity analysis comparing patients with a baseline mRS 0 vs those with an mRS 1–5 yielded similar results.
Conclusion
Patients with significant disability may equally benefit from stroke Thrombectomy as those without disability and shouldnot be excluded from treatment based on that criteria alone.
Trial registration number
N/A
AS07-080
ENDOVASCULAR TREATMENT 6 TO 24 HOURS AFTER STROKE: OUTCOMES OF PATIENTS FULFILLING DAWN OR DEFUSE-3 CRITERIA COMPARED WITH PATIENTS TREATED OUT OF CLINICAL TRIALS CRITERIA
1Hospital Germans Trias i Pujol, Neurology, Badalona, Spain
2Hospital Germans Trias i Pujol, Neuroradiology, Badalona, Spain
Background and Aims
To compare efficacy and safety of endovascular thrombectomy (EVT) 6–24h after stroke between patients selected according to recent clinical trials criteria (DAWN, DEFUSE-3) and patients who were not (OUT).
Method
We studied consecutive patients treated with EVT 6–24 hours after stroke from 2009 to 2017. Core infarct volume was measured using RAPID software in patients with available multimodal neuroimaging (71%). Based on baseline variables (age, NIHSS, occlusion site, neuroimaging), patients were classified following DAWN and DEFUSE-3 criteria. Adjusted logistic regression was used to compare good outcome (mRS 0–2) and mortality at 3 months between DAWN and DEFUSE-3 vs.OUT groups.
Results
From a total of 174 patients, 61 met DAWN criteria (mean age, 66; median NIHSS, 19; time last seen normal, TLSN, 555 min), 80 met DEFUSE-3 criteria (age, 65; NIHSS, 17; TLSN, 505) and 81 none of them (OUT) (age, 68; NIHSS, 17; TLSN, 480). OUT patients were more frequently selected using no multimodal neuroimaging (61%) and had more frequently MCA-M2 occlusion (14%). There was a trend towards higher rate of SICH in OUT patients (DAWN, 0%; DEFUSE-3, 1.3%; OUT, 7.4%). Compared to DAWN and DEFUSE-3, OUT-group showed non-significant odds of poorer functional outcome and higher mortality (Figure).
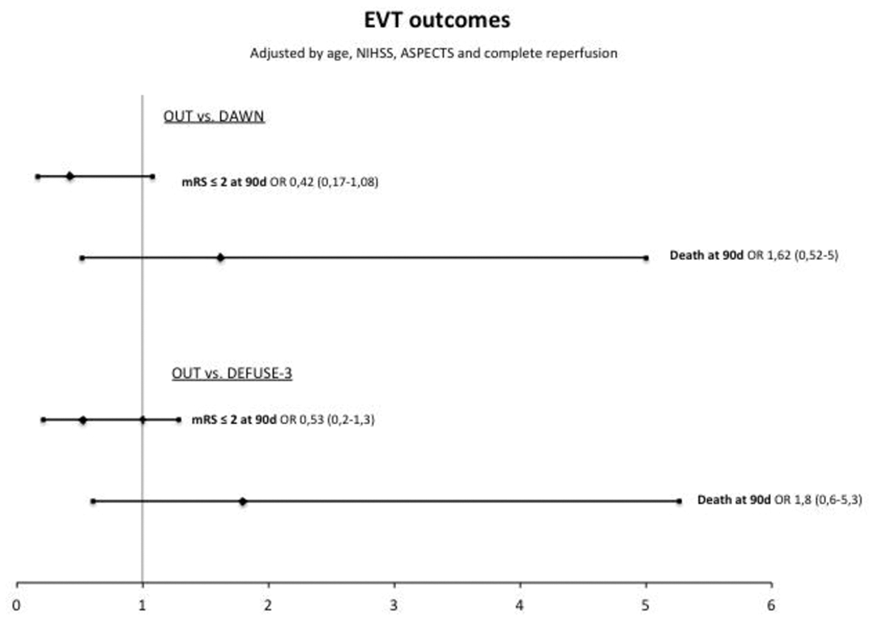
Conclusion
Selecting patients for thrombectomy 6–24h after stroke by less restrictive criteria might result in worst outcomes than using clinical trials criteria.
Trial registration number
N/A
AS02-025
REAL WORLD IMAGING SELECTION FOR ENDOVASCULAR THROMBECTOMY IN EARLY AND LATE TIME WINDOWS: A COMPARISON OF SIMPLE VERSUS ADVANCED PERFUSION IMAGES IN THE TREVO REGISTRY
1University of Texas at Houston, Neurology, Houston, USA
2University of Texas Health Science Center - San Antonio, Neurology and Radiology, San Antonio, USA
3La Foundation Rothschild, Radiology, Paris, France
4University Hospital Hradec Kralove, Neurology, Hradec Kralove, Czech Republic
5Drexel Neurosciences Institute, Neurology, Philadelphia, USA
6California Pacific Medical Center, Neurology, San Francisco, USA
7University of California Los Angeles, Neurology, Los Angeles, USA
8Grady Memorial Hospital, Neurology, Atlanta, USA
9Erlanger Medical Center, Radiology, Chattanooga, USA
10Riverside Methodist Hospital, Radiology, Columbus, USA
11Methodist Riverside Ohio, Neurology, Columbus, USA
12Rush Medical College, Neurosurgery, Chicago, USA
13Stryker, Biostatistics, Kalamazoo, USA
14St. Mary's Medical Center, Neurology, West Palm Beach, USA
15WellStar Health System, Neurosurgery, Marietta, USA
Background and Aims
DAWN and DEFUSE3 trials utilized advanced perfusion imaging (CTP/MRI) to prove thrombectomy effectiveness beyond 6hrs. We evaluated simple (non-contrast CT-NCCT) vs advanced imaging as selection methods in a large cohort outside RCTs stringent criteria.
Method
Patients with (ICA, MCA/M1-M2) occlusion from the TREVO prospective, multicenter, international registry were divided into early (0–6hrs) and late (6–24hrs) last-seen-normal (LSN) to groin-puncture (GP). We stratified patients based on imaging selection into NCCT-only vs. NCCT-plus-CTP/MRI and assessed imaging correlation with 90day good outcome (mRS = 0-2) across early and late windows.
Results
1720 patients were included (overall N = 2008, November/2013-March/2017); 1259≤6hrs and 461>6-24hrs. Median age/years (71vs.69, P = 0.04), median ASPECTS (8vs.8, p = 0.9), median/IQR NIHSS = 16(12-20) and 15(10-20),(P = 0.07), median/IQR LSN-to-GP/hr = 3.5(2.6-4.5) and 9.6(7.3-13.9) early and late windows respectively. IV tPA rates were (68%vs.24%, P<0.001).
In early window, NCCT was the only imaging in:17%, CTP:70%, and MRI:13%. In late window, NCCT only:16%, CTP:70%, and MRI:14%.
In early window, 53% of NCCT and 58% of CTP/MRI had good outcome (P = 0.2). Beyond 6hrs, good outcome was achieved in 57% of NCCT and 50% of CTP/MRI (P = 0.3). In a multivariate analysis, the addition of advanced imaging beyond NCCT, (CTP/MRI), did not confer higher correlation with good outcome in either early or late window (aOR = 0.09,95%CI = 0.00-1.67, p = 0.1 and aOR = 0.78,95%CI = 0.49-1.24, p = 0.3) (Figure:1).
In the late window, 55% of patients with ASPECTS≥6 and 56% with good perfusion profile (core-volume<50cc, mismatch-volume≥10cc and mismatch/ratio>1.2) had good outcome.
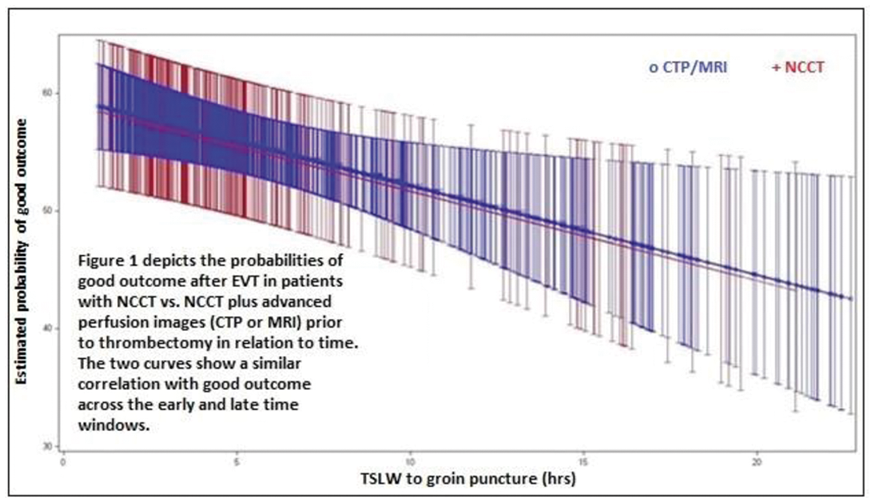
Conclusion
Both CT and advanced perfusion imaging identifies patients who may benefit from thrombectomy equally in the early or late windows in our real world registry. These findings can have implications towards more widespread adoption of thrombectomy.
Trial registration number
NCT02040259
AS07-044
LARGE-SCALE ANALYSIS OF OUTCOMES AFTER ENDOVASCULAR STROKE THERAPY OVER A 10-YEAR PERIOD IN HIGH VERSUS LOW VOLUME CENTERS
1Wayne State University, Neurology, Detroit, USA
2UT Health McGovern School of Medicine, Neurology, Houston, USA
3UT Health McGovern School of Medicine, Neurosurgery, Houston, USA
4Texas Stroke Institute, Neurology, Dallas, USA
Background and Aims
Given the time-sensitivity of endovascular stroke therapy (EST), the dissemination of these treatments to lower volume hospitals may improve outcomes. Here, we assess outcomes and complications at a population level by EST procedural volume.
Method
Using administrative data on all discharges from hospitals in California (2005-2011) and Florida (2005-2014), we identified patients with acute stroke treated with EST. Primary endpoint was intracranial hemorrhage and mortality. Higher volume was defined as >15 EST procedures per year. Logistic regression assessed factors associated with outcomes, and results are presented as OR [95% CI] or median [IQR].
Results
Among 3047 patients (at 120 hospitals) treated with EST, median age was 72[60-80], 51% were female, and 64% white. 57% received IV tPA. Post-procedure in-hospital death or ICH occurred in 760 (25%; (18% death, 8.6% ICH)). We observed a 10% annual decline (p < .001) in the risk of combined outcome, with a sharp drop after 2012 (2013 OR 0.62[0.41-0.94]; 2014 OR 0.52[0.36-0.79]). Adjusting for age and comorbidities, EST in high-volume hospitals was associated with lower risk (OR 0.8 [0.65-0.98]). This trend continued throughout the studied time period, including recent years (Figure).
Conclusion
In this cohort of over 3000 patients with EST, we demonstrate continuous improvements in clinical outcome over time, with a significant drop coinciding with the release of stent-retrievers in 2012. Higher volume centers performed better than lower volume centers, a finding that persisted despite the overall trend towards improvement.
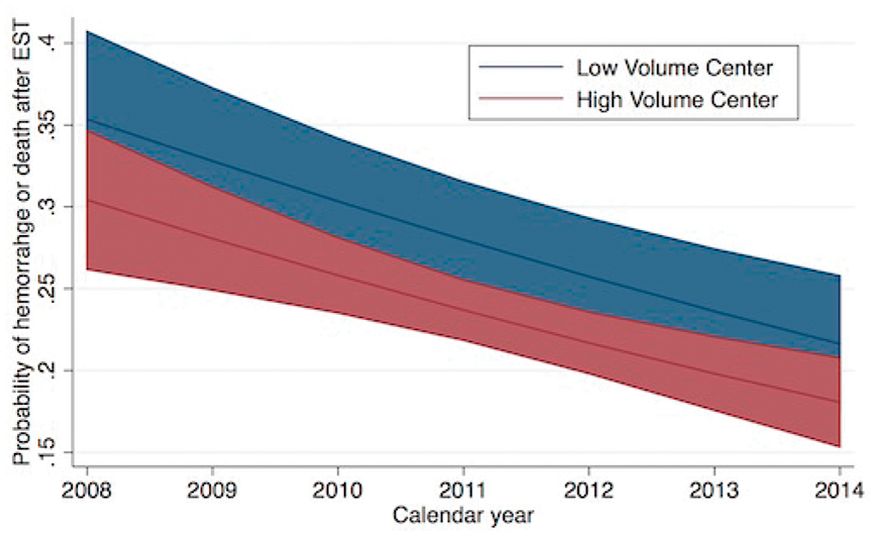
Trial registration number
N/A
Scientific Communications- Acute Non-Reperfusion Trials
AS01-027
TITLE: LABETALOL INFUSION TO REDUCE BLOOD PRESSURE VARIABILITY AND HEMATOMA EXPANSION: A RANDOMIZED CONTROL STUDY
1Christian Medical College, Neurology, LUDHIANA, India
2Christian Medical College, Radiology, Ludhiana, India
3Christian Medical College, Physiology, Ludhiana, India
Background and Aims
Blood pressure variability (BPV) is independently associated with early hematoma growth and death in patients with Intracerebral hemorrhage (ICH). However, no strategies are available to target BPV. We tested the hypothesis that labetalol infusion will reduce 24 h BPV compared to labetalol boluses in patients with acute ICH.
Method
All patients with ICH presenting within 6 h of symptom onset were screened. Patients with hematoma volume <90ml and systolic BP >140 mm Hg were randomized (1:1) to either intravenous labetalol infusion (infusion group) for a period of 24 h or intravenous labetalol bolus injections (10-40 mg) (bolus group) for a period of 24 h. Computerized Tomography head was repeated at 24 h.
Results
A total of 126 patients were screened and 76 patients were randomized. The mean ± SD age of ICH patients was 58 ± 14.6 years and 54 ± 13.1 years in infusion group and bolus group respectively (p = 0.364). The median (IQR) baseline hematoma volume was 10.24 (4.5-29.1) ml in infusion group and 16.9 (5.9-33.0) ml in bolus group (p = 0.503). The systolic blood pressure (SBP) at randomization was 194 ± 22.7 mmHg in infusion group and 193 ± 28.2 mmHg in bolus group. At 24 h, the mean SBP was 149.4 mmHg and 156.6 mmHg among infusion and bolus group respectively (p = 0.003). BPV as assessed by standard deviation (SD) was similar, 19.6 ± 6.6 in infusion group and 19.3 ± 8.2 in bolus group (p = 0.625).
Conclusion
There was no difference in 24 h BPV among patients treated with labetalol infusion in comparison to bolus injections. Novel strategies are needed to reduce BPV.
Trial registration number
ctri.nic.in:CTRI/2017/09/009619
AS06-076
STROKE ETIOLOGY CAN BE PREDICTED BY THROMBUS PERMEABILITY IN ADMISSION CT IMAGING
1Klinikum rechts der Isar- TU Muenchen, Neuroradiology, Munich, Germany
2University Hospital Bern, Neuroradiology, Bern, Switzerland
3Klinikum rechts der Isar- TU Muenchen, Neurology, Munich, Germany
Background and Aims
Intracranial thrombi can be characterized according to their permeability, as measured by penetration of contrast agent. Thrombus permeability is supposed to influence functional outcomes. We aimed to explore the factors underlying the diversity in thrombus permeability and to find a possible correlation to stroke etiology.
Method
Thrombus densities were measured in thin-slice non-contrast CT and automatically aligned CT-angiography images of 75 patients with acute M1-occlusions. Thrombus attenuation increase (Δ) and corrected void fraction (ε, attenuation increase corrected by the contralateral artery) were calculated. These thrombus permeability measures were correlated with histological components such as fractions of fibrin-platelet accumulation (F/P) and fractions of red blood cells (RBC) within the thrombus. Additionally, association with TOAST criteria was evaluated.
Results
Correlation with both thrombus permeability estimates was significant positive for F/P (Δ: r = 0.43, p = 0.016/ε: r = 0.45, p = 0.01) and inverse for RBC (Δ: r = −0.46, p = 0.01/ε: r = −0.49, p = 0.006), measured in a subgroup (n = 32). A binary logistic regression model showed a significant association between dichotomized TOAST criteria (mainly cardioembolic vs. non-cardioembolic) and Δ (β = 0.14, p = 0.002) as well as ε (β = 25.1, p = 0.003).
Conclusion
Permeable thrombi showed a strong correlation to lower fractions of RBC and more F/P conglomerations as well as an association to cardioembolic origin. This knowledge could further establish thrombus permeability in admission imaging as an imaging biomarker for the acute management of ischemic stroke patients and for identifying cardioembolic origin.
Trial registration number
N/A
AS06-021
MELBOURNE MOBILE STROKE UNIT INITIAL COMMENCEMENT ACTIVITY AND EFFECT
1Royal Melbourne Hospital, Melbourne Brain Centre, Parkville, Australia
2Royal Melbourne Hospital, Radiology, Parkville, Australia
3Ambulance Victoria, Clinical Services, Doncaster, Australia
4Ambulance Victoria, Research, Doncaster, Australia
5Ambulance Victoria, Executive Services, Doncaster, Australia
6The Florey Institute of Neuroscience and Mental health, Neuroscience and Mental Health, Parkville, Australia
Background and Aims
Stroke patients benefit from early intervention. The Melbourne Mobile Stroke Unit (MSU) aims to improve prehospital triage, treat patients earlier and provide rapid access to comprehensive stroke centres.
Method
The Melbourne MSU is staffed by 2 paramedics, a radiographer, stroke nurse and neurologist. Data, including time metrics, were prospectively collected on all MSU dispatches, and compared to national standards.
Results
The MSU launched 20/November/2017 and operates within a 20km radius of The Royal Melbourne Hospital, Australia, delivering patients to 8 stroke centres across the city. Data on the first 5 months will be available for ESOC. In the first six weeks, the MSU was dispatched to 158 code stroke calls. 74(47%) cases were attended while 84(53%) cases were cancelled pre-arrival after initial paramedic assessment. Of attended calls, 35(47%) patients had intracerebral haemorrhage, ischaemic stroke or transient ischaemic attack, while 39(53%) cases were stroke mimics. 31(42%) of attended patients received a non-contrast CT scan. 7(44% ischaemic stroke<4.5hr) patients were thrombolysed (median scene-to-CT time of 20min [range 5–34], scene-to-needle 31min [range 23-65], onset-to-needle 149min [range 64-238]), substantially faster than the Australian average of 27min, 72min, 156min respectively. 2 MSU patients received thrombolysis who would otherwise have arrived in hospital >4.5hr. The MSU has reduced inter-hospital transfers by diagnosing large vessel occlusions and neurosurgery candidates.
Conclusion
The Melbourne MSU is achieving thrombolysis workflow consistent with comprehensive stroke centres. It has reduced onset-to-needle time and allowed additional patients to receive thrombolysis. Pre-hospital triage has removed transport delays from inter-hospital transfers.
Trial registration number
N/A
AS01-019
SAFETY AND EFFICACY OF SP-8203 IN PATIENTS WITH ACUTE ISCHEMIC STROKE REQUIRING TPA STANDARD OF CARE: A MULTICENTER, RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED PHASE 2A STUDY
1University of Ulsan- Asan Medical Center, Department of Neurology, Seoul, Republic of Korea
2Soonchunhyang University School of Medicine, Department of Neurology, Seoul, Republic of Korea
3Seonam University Myongji Hospital, Department of Neurology, Goyang, Republic of Korea
4Pusan National University Hospital, Department of Neurology, Busan, Republic of Korea
5Korea University Guro Hospital, Department of Neurology, Seoul, Republic of Korea
6Inje University Busan Paik Hospital, Department of Neurology, Busan, Republic of Korea
7Kyung Hee University Hospital, Department of Neurology, Seoul, Republic of Korea
8Kyungpook National University School of Medicine and Hospital, Department of Neurology, Daegu, Republic of Korea
9Korea University College of Medicine, Department of Neuroscience, Seoul, Republic of Korea
10Shin Poong Pharm. Co. Ltd., Research Headquarters, Seoul, Republic of Korea
11Shin Poong Pharm. Co. Ltd., R&D Section, Seoul, Republic of Korea
Background and Aims
Intravenous administration of SP-8203, a multipotent neuroprotectant inhibiting matrix metalloprotease activity, significantly reduces infarct volume and tPA-induced hemorrhages in animal models. In this phase 2 study, we assessed the safety and efficacy of SP-8203 in acute stroke patients receiving tPA.
Method
In this double-blind, randomized, placebo controlled study, SP-8203 was administered immediately after tPA, which was repeated 6 times at 12-hour intervals. Patients (aged 19–80 years) were randomly assigned (1:1:1) to low-dose (40 mg bid), high-dose (80 mg bid), and placebo groups. The primary endpoint was the incidence of parenchymal hematoma (PH) at Day 1. Secondary endpoints were: frequency of adverse events, mortality, mRS and NIHSS changes.
Results
We enrolled 69 patients (24 in placebo, 24 in low-dose, 21 in high-dose groups) from 8 Korean centers. The PH incidence did not significantly differ among groups (0 of 22 patients in placebo and low dose groups, 1 of 21 in the high-dose group; difference 4.76%[90%CI -20.21–29.06]). There were no difference in mortality or adverse events. The functional outcome was significantly different between low-dose and placebo groups (ordinal analysis of 90-day mRS, OR6.77, 95%CI 1.25–36.61, p = 0.026). Multivariate analysis showed significant differences in mRS (0–2/3–6) over time between placebo and intervention groups (OR1250.5 for low-dose, p = 0.003; OR52.2 for high-dose groups, p = 0.034) and in NIHSS (0/1–15/16–42) of patients receiving thrombectomy (OR15.09 for low-dose group, 95%CI 1.65–138.42, p = 0.016).
Conclusion
The addition of 40 mg SP-8203 in patients receiving tPA was safe and significantly improved functional outcome, suggesting a potential therapeutic strategy. Further larger trials are warranted.
Trial registration number
clinicaltrials.gov#NCT02787278
AS06-068
NEW FALCON IS A SIMPLE AND POWERFUL TRIAGE SCORE TO IDENTIFY LARGE VESSEL OCCLUSION IN ACUTE ISCHEMIC STROKE
1Kantonsspital Aarau, Neurology, Aarau, Switzerland
2Kantonsspital Aarau, Neuroradiology, Aarau, Switzerland
Background and Aims
Early restoration of cerebral blood flow is crucial in preventing persistent brain damage in acute ischemic stroke. Mechanical thrombectomy in patients with large vessel occlusion (LVO) is highly effective and direct transfer to endovascular capable stroke centers may be considered in these patients. Although several scores for prehospital triage have been proposed, there is still a big need for simpler and more reliable tools. We here present the new 4-item FALCON score and compared it to previously published scores in the same stroke cohort.
Method
We included all consecutive ischemic stroke patients admitted to our comprehensive stroke center from January 2014 to June 2015 with symptom onset <24h and complete in-house emergent imaging. We assessed the association of single NIHSS items with the presence of LVO. The FALCON score derived from this analysis and its performance in predicting LVO was compared to previously published prehospital scores in this cohort.
Results
We identified 492 patients fulfilling all inclusion criteria. LVO was present in 184 (37%).
Conclusion
The new 4-item FALCON score is a simple and powerful triage tool to predict LVO in acute ischemic stroke. Paramedics might easily use it in the prehospital setting avoiding dangerous delays in effective treatment.
Trial registration number
N/A
AS02-033
RELEVANCE OF COLLATERALS FOR THE SUCCESS OF NEUROPROTECTIVE THERAPIES IN ACUTE ISCHEMIC STROKE: INSIGHTS FROM THE URICO-ICTUS STUDY
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
Background and Aims
Collateral circulation may modify the effect of neuroprotective therapies. We report a post-hoc analysis of the URICO-ICTUS trial (NCT00860366) assessing the effect of pretreatment collaterals on the efficacy of uric acid (UA) compared with placebo to improve clinical outcome.
Method
URICO-ICTUS was a double-blind, placebo-controlled, phase-2b trial where 411 alteplase-treated patients were randomized to receive UA 1000 mg (n = 211) or placebo (n = 200) before the end of alteplase infusion. Herein, we included a subset of 84 patients (Placebo=40, UA =44) who had a pretreatment CT-angiography showing a proximal arterial occlusion in the carotid territory. The collateral score was assessed on CT-angiography according to a validated grading system and excellent collaterals were defined as 100% collateral supply. Logistic regression models adjusted for baseline severity assessed the interaction between therapy and excellent collaterals on the ordinal distribution of the modified Rankin Scale (mRS, categories 5–6 collapsed) at 90 days.
Results
Excellent collaterals were found in 17/84 (20%) patients (n = 8/40 (20%) in the placebo group, n = 9/44 (21%) in the UA group). There was a significant interaction between UA therapy and pretreatment collaterals in the prediction of better ordinal mRS shift (P = 0.017). UA administration improved outcome in patients with excellent collaterals (aOR = 9.3; 95%CI = 1.24-70.01, p = 0.030), but not in those with non-excellent collaterals (aOR = 0.7; 95%CI = 0.29-1.64, p = 0.406).
Conclusion
UA therapy may improve clinical outcome after acute stroke in thrombolysed patients who have excellent collaterals. Collateral status may modify the magnitude of neuroprotection through the facilitation of drug arrival to its molecular targets.
Trial registration number
URICO-ICTUS trial (NCT00860366)
AS30-004
REDUCING BODY TEMPERATURE (COOLING) IN ACUTE STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CONTROLLED TRIALS
1University of Oxford, Centre for Evidence-Based Medicine- Department for Continuing Education, Oxford, United Kingdom
Background and Aims
Reducing body temperature (cooling) is a powerful neuroprotective intervention. Several techniques for cooling in an acute stroke have been studied but the effect is unclear. Cooling can be successfully induced to normothermic levels using medications (pharmacological cooling) or to moderately hypothermic levels using cooling catheters, fluids or external pads (physical cooling) but the results to date have been conflicting. We have conducted the most up-to-date and rigorous systematic review and meta-analysis examining cooling in acute stroke.
Method
Results
Eleven studies met the inclusion criteria (n = 2198). We used the random-effects model to combine the data. No statistically significant difference was found between cooling therapy and standard stroke care in reducing the risk of disability or mortality (RR 0.97, 95% CI 0.89-1.05, RR 0.92, 95% CI 0.76-1.12, respectively). Complications were more common in the intervention group but were not significant on the pooled analysis (RR 1.23, 95% CI 0.88-1.70). No significant statistical heterogeneity was identified.
Conclusion
We did not find any evidence to support the use of cooling in reducing mortality or morbidity in an acute stroke, however complications were more common.
Trial registration number
N/A
AS16-031
DOES CLASS OF ANTIBIOTIC USED TO TREAT POST-STROKE INFECTIONS INFLUENCE CLINICAL OUTCOMES? AN INDIVIDUAL PARTICIPANT DATA POOLED ANALYSES OF VISTA-ACUTE
1Salford Royal NHS Foundation Trust, Greater Manchester Comprehensive Stroke Centre and University of Manchester Division of Cardiovascular Sciences, Manchester, United Kingdom
2University of Manchester, Centre for Biostatistics, Manchester, United Kingdom
3Salford Royal NHS Foundation Trust, Department of Microbiology, Manchester, United Kingdom
4University of Amsterdam, Department of Neurology, Amsterdam, The Netherlands
5King's College Hospital NHS Foundation Trust, Clinical Neurosciences, London, United Kingdom
6Hospital Vall d'Hebron, Laboratorio de Investigacion Neurovascular, Barcelona, Spain
7Manchester University NHS Foundation Trust, Department of Respiratory Medicine, Manchester, United Kingdom
8Charite Universitaetsmedizin Berlin, Department of Neurology, Berlin, Germany
Background and Aims
Treatment of post-stroke infections is empirical. We hypothesised that choice of antibiotic class was associated with outcome after post-stroke infection due to differing antimicrobial activities and anti-inflammatory effects.
Method
We undertook a retrospective pooled analysis of anonymized individual participant data from the Virtual International Stroke Trials Archive (VISTA)-Acute. Trial participants with an infection treated with systemic antibiotic therapy during the first two weeks after stroke onset were eligible. Antibiotics were grouped into eight classes, according to antimicrobial mechanism and prevalence of use. Our primary analysis investigated whether antibiotic class for any infection, or for pneumonia, was independently associated with a shift in three month modified Rankin Scale (mRS) using ordinal logistic regression. The most prevalent antibiotic class was used as the reference group. Secondary analyses included three month Barthel Index (BI) and National Institutes of Health Stroke Scale (NIHSS) using multiple linear regression.
Results
2909 patients met the eligibility criteria (median age [IQR]=74 [65 to 80] y; 49% female; median [IQR] NIHSS score=15 [11 to 19]). Pneumonia occurred in 37%. Treatment with macrolides (5% of any infections; 8% of pneumonias) was independently associated with more favourable mRS distribution for any infection (adjusted OR (95% CI) = 0.61(0.42 to 0.89), p = 0.01) or pneumonia (aOR (95% CI) = 0.56 (0.33 to 0.94), p = 0.03), versus penicillin plus β-lactamase inhibitor. Macrolides were also independently associated with more favourable three month BI for any infection or for pneumonia, but were not associated with NIHSS.
Conclusion
These cautious associations justify prospective evaluation of the impact of antibiotic class on treatment of post-stroke infections.
Trial registration number
N/A
Scientific Communications- Haemorrhagic Stroke
AS20-051
CHARACTERISTICS AND OUTCOMES OF PATIENTS WITH HYPERGLYCAEMIA IN INTRACEREBRAL HAEMORRHAGE: DATA FROM THE TRANEXAMIC ACID FOR INTRACEREBRAL HAEMORRHAGE-2 (TICH-2) TRIAL
1University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom
2National University of Malaysia, Department of Medicine, Kuala Lumpur, Malaysia
3Nottingham University Hospitals NHS Trust, Stroke Services, Nottingham, United Kingdom
4University of Nottingham, Radiological Sciences Research Group, Nottingham, United Kingdom
Background and Aims
Several studies showed that hyperglycaemia is associated with poorer prognosis in intracerebral haemorrhage. We explored the characteristics and outcomes of patients with hyperglycaemia in the Tranexamic acid in IntraCerebral Haemorrhage-2 (TICH-2) trial.
Method
Of the 2325 patients recruited, 2028 with available baseline glucose levels were included for analysis. Baseline characteristics, radiological and clinical outcomes were compared between patients with admission glucose levels of <7.8 and ≥7.8 mmol/L (hyperglycaemia).
Results
545 (26.9%) patients had hyperglycaemia and did not differ from normoglycaemic patients in age (69.3 vs 68.7 years) and sex (female: 246, 45.1% vs 641, 43.2%). Hyperglycaemic patients were more likely to be diabetic (187, 34.3% vs 94, 6.3%), have worse NIHSS (13.8 ± 7.7 vs 12.1 ± 7.1), larger baseline haematoma (30.2 ± 31.5 mL vs 21.2 ± 24.3 mL) and perihaematomal oedema volumes (15.8 ± 18.1 mL vs 11.7 ± 14.1 mL). There were no significant differences in haematoma expansion and increase in oedema volume between the two groups (table). Hyperglycaemia did not increase the risk of death or worse modified Rankin Scale at day 90 after adjusting for covariates including baseline haematoma volume.
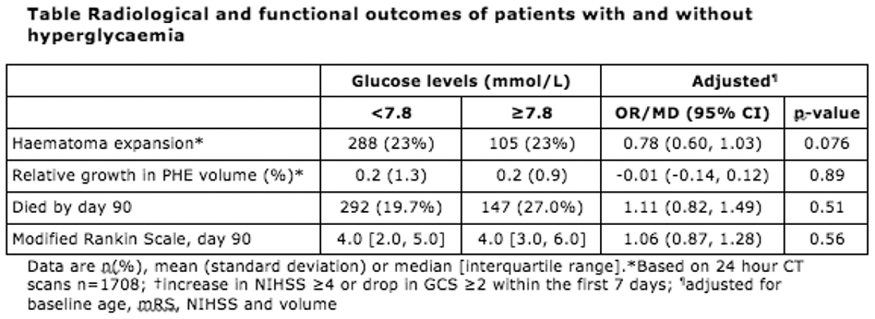
Conclusion
Hyperglycaemia was associated with larger haematomas and more severe stroke on admission but did not result in worse outcomes after accounting for baseline haematoma volume.
Trial registration number
ISRCTN93732214
AS20-031
CLINICAL RELEVANCE OF MICROBLEEDS IN PATIENTS WITH CARDIEMBOLIC STROKE WHO START LONG-TERM ORAL ANTICOAGULATION: FOLLOW-UP OF PATIENTS FROM THE HERO STUDY
1Hospital de la Santa Creu i Sant Pau- IIB Sant Pau Biomedical Research, Neurology, Barcelona, Spain
2Hospital Germans Trias i Pujol, Unitat RM IDI, Badalona, Spain
3Hospital del Mar- Parc de Salut Mar, Radiology, Barcelona, Spain
4Hospital de Navarra, Neurology, Pamplona, Spain
5Hospital Son Espases, Neurology, Palma de Mallorca, Spain
6Arcispedale Santa Maria Nuova IRCCS, Neurology, Reggio Emilia, Italy
7Hospital de Sant Joan Despí Moises Broggi, Neurology, Sant Joan Despí, Spain
8Hospital de León, Neurology, León, Spain
9Hospital de Valladolid, Neurology, Valladolid, Spain
10Hospital de Burgos, Neurology, Burgos, Spain
11Hospital Parc Taulí, Neurology, Sabadell, Spain
12Hospital Clínic, Neurology, Barcelona, Spain
13Hospital San Pedro de Alcántara, Neurology, Cáceres, Spain
14Hospital de Donostia, Neurology, Donostia, Spain
15Hospital Germans Trias i Pujol, Neurology, Badalona, Spain
16Hospital de Basurto, Neurology, Bilbao, Spain
Background and Aims
We tested the hypothesis that the presence of microbleeds (MB) increases the risk of intracranial hemorrhage (ICH) in ischemic stroke (IS) patients with a cardioembolic source who start treatment with oral anticoagulants (OA).
Method
Patients were participants of a multicenter observational study (HERO study, NCT02238470). Participants were older than 65y, had ischemic stroke (IS) attributed to cardiac embolism, and were new users of OA. A baseline magnetic resonance was performed within 1 month after the index IS. Two neuroradiologists, who were blinded to clinical data, evaluated the presence, number and distribution of MB on T2*-GRE and/or SWI sequences. During follow-up we recorded ICH, recurrent IS and vascular death. Statistics: Bivariate analyses, Kaplan-Meier survival curves, Cox regression analysis.
Results
We studied 871 patients (age 77.6 ± 6.6 y, 47.8% were men). MB were detected in 197 (22.6%) patients (46.6% with 1MB, 16% with ≥5 MB). MB distribution was lobar in 52.8%, deep in 26.9% and mixed in 20.3% patients. After a mean follow-up of 23 ± 6.7 months, 18 (2.1%) patients suffered an ICH, 31 (3.6%) a recurrent IS and 48 (5.5%) a vascular death. MBs were associated with the occurrence of ICH (HR 3.4, 95% CI 1.3-8.7). Burden of MB was not associated to ICH risk. Deep-located MB was associated with an increased risk of ICH (p = 0.002) in bivariate analysis but not in multivariate analyses.
Conclusion
Presence of MB is associated with a more than a 3-fold increase in the risk of ICH in OA users. This result may help in risk stratification when prescribing OA.
Trial registration number
NCT02238470
AS20-006
PREDICTING INTRACEREBRAL HEMORRHAGE EXPANSION WITH NON-CONTRAST CT: THE BAT SCORE
1C. Mondino National Neurological Institute, Stroke Unit, Pavia, Italy
2University of Ottawa- Ottawa Hospital Research Institute- Ottawa- Canada, Department of Medicine Neurology, Ottawa, Canada
3Université Paris Descartes- INSERM S894- DHU Neurovasc- Centre Hospitalier Sainte-Anne- Paris- France, Department of Neuroradiology, Paris, France
4Hotchkiss Brain Institute- University of Calgary- Calgary- Canada, Department of Clinical Neurosciences- Department of Radiology-, Calgary, Canada
5Sunnybrook Health Sciences Centre- University of Toronto- Toronto- Canada, Division of Neuroradiology and Department of Medical Imaging, Toronto, Canada
6Massachusetts General Hospital- Harvard Medical School- Boston, Department of Medicine-, Boston, USA
7Massachusetts General Hospital- Harvard Medical School- Boston., J. P. Kistler Stroke Research Center, Boston, USA
8Massachusetts General Hospital- Harvard Medical School- Boston, Neuroradiology Service- Department of Radiology, Boston, USA
9Massachusetts General Hospital- Harvard Medical School- Boston, J. P. Kistler Stroke Research Center, Boston, USA
10University of Minnesota- Minneapolis, Zeenat Qureshi Stroke Research Center, Minneapolis, USA
11Massachusetts General Hospital- Harvard Medical School- Boston, Department of Emergency Medicine, Boston, USA
Background and Aims
While the CT angiography (CTA) spot sign performs well as a biomarker for hematoma expansion, CTA is not routinely performed in the emergency setting. We developed and validated a score to predict hematoma expansion based on non-contrast CT (NCCT) findings in acute intracerebral hemorrhage (ICH).
Method
After developing the score in a single center cohort of ICH patients (n = 344), we validated it in a large clinical trial population (n = 954) and in a multicenter ICH cohort (n = 241). The following NCCT markers of ICH expansion were analyzed: hypodensities, blend sign, hematoma shape and density, and fluid level. ICH expansion was defined as hematoma growth>6 mL or>33%.The score was created using the estimates from multivariable logistic regression after final predictors were selected from bootstrap samples.
Results
Presence of blend sign (odds ratio (OR) 3.09,95% confidence interval (CI) 1.49-6.40, p = 0.002), any intrahematoma hypodensity (OR 4.54,95% CI 2.44-8.43, p < 0.0001) and time from onset to NCCT<2.5 h (OR 3.73,95% CI 1.86-7.51, p = 0.0002) were predictors of ICH expansion. A 5–point score was created (BAT score:1 point for Blend sign, 2 points for Any hypodensity and 2 points for Timing of NCCT<2.5h). The c statistic was 0.77 in the development population, 0.65 and 0.70 in the validation cohorts. A dichotomized score (BAT score>3) predicted hematoma growth with 0.50 sensitivity, 0.89 specificity and 0.82 accuracy.
Conclusion
An easy to use 5-point prediction score can identify subjects at high risk of ICH expansion with good specificity and accuracy. This tool requires just a baseline NCCT scan and may help select ICH patients for anti-expansion clinical trials.
Trial registration number
N/A
AS20-078
INFLAME-ICH: EVALUATION OF THE CENTRAL AND PERIPHERAL INFLAMMATORY RESPONSE TO INTRACEREBRAL HAEMORRHAGE IN MISTIE-III TRIAL PARTICIPANTS
1University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
2Johns Hopkins Medical Institutions, Division of Brain Injury Outcomes, Baltimore, USA
3Salford Royal Hospital, Salford Royal Biomedical Facility, Salford, United Kingdom
4University of Cincinnati, Department of Neurosurgery, Cincinnati, USA
5University of Chicago, Department of Neurological Surgery, Chicago, USA
6Yale University School of Medicine, Department of Neurology, New Haven, USA
Background and Aims
Inflammation exacerbates early damage in experimental intracerebral haemorrhage (ICH) but little is known about inflammation in human ICH. MISTIE-III is a phase 3 randomised controlled trial comparing standard care with tPA-augmented minimally invasive haematoma drainage. We established a sub-study of MISTIE-III (INFLAME-ICH), using cerebral haematoma aspirate and drain fluid to investigate inflammation and test for associations with imaging markers and peripheral blood inflammatory mediators.
Method
Surgical patients had haematoma aspirate and daily haematoma fluid collected until drain removal. All patients had up to 5 daily peripheral blood samples collected. Key pro- and anti-inflammatory mediators were measured by immunoassay. CT scans were analysed using semi-automated segmentation for haematoma and perihaematomal oedema (PHO) volumes. We used linear regression to test for associations between peak inflammatory mediator concentrations, imaging markers, and tPA doses.
Results
89 patients were recruited (47 surgical, 42 medical). High peak haematoma concentrations of key pro-inflammatory (interleukin (IL)-1β:mean = 117.6 pg/ml, SD = 166.3 pg/ml; tumour necrosis factor-α:mean = 275.0 pg/ml, SD = 677.3 pg/ml; IL-6:mean = 50401.8 pg/ml, SD = 39517.7 pg/ml) and anti-inflammatory (IL-10:mean = 54.8 pg/ml, SD = 39.4 pg/ml) mediators were detected. Higher IL-6 (p = 0.035) was associated with lower haematoma volume at end-of-treatment. No mediators were associated with baseline haematoma volume, PHO, or number of tPA doses. Analyses of peripheral blood samples are nearing completion and the association between peripheral and central mediators will be tested.
Conclusion
Our study confirms that an intense cerebral inflammatory response occurs in acute clinical ICH. Proof-of-concept clinical trials of immune-modulating agents are required to test potential therapeutic benefit, either combined with minimally-invasive surgery and/or as a stand-alone treatment.
Trial registration number
ISRCTN81927110
AS20-052
DOES THE ABC ACUTE CARE BUNDLE FOR INTRACEREBRAL HAEMORRHAGE LEAD TO SUSTAINED IMPROVEMENTS IN MORTALITY AND WHICH ASPECTS OF TREATMENT ARE IMPORTANT?
1University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
2University of Manchester, Centre for Health Informatics, Manchester, United Kingdom
3Salford Royal NHS Foundation Trust, Greater Manchester Neurosciences Centre, Salford, United Kingdom
4University of Manchester, Centre for Biostatistics, Manchester, United Kingdom
5University College London, Farr Institute of Health Informatics, London, United Kingdom
Background and Aims
Our ‘ABC’ intracerebral haemorrhage (ICH) care bundle consists of (A):rapid anticoagulant reversal, (B):optimal blood pressure (BP) management, and (C):a care pathway for access to neurosurgery. Implementation at our centre from June 2015 was associated with a 33% relative reduction in 30-day case-fatality. We sought to test if this improvement was sustained, compare mortality rate to national trends, and determine which factors explain the increased survival.
Method
We analysed prospective audit data for consecutive ICH patients before (01/07/13-31/05/15), during (01/06/15-31/05/16), and after (01/06/16-31/01/17) bundle implementation and determined factors associated with survival using a Cox regression model. Key process measures were added to the model to test for mediation. Difference-in-difference analysis compared our centre with the rest of England & Wales using data from the Sentinel Stroke National Audit Programme (SSNAP).
Results
810 patients were admitted during our data collection period. Admission during (HR:0.46; 95%CI:0.27-0.77; p = 0.003) and after (HR:0.33; 95%CI:0.17-0.64; p = 0.001) bundle implementation (vs. before) was associated with a reduced hazard of death. The statistically significant mediating components were a reduction in acute (<24h) do-not-resuscitate (DNR) orders (mediating 50.6% of association), and undergoing neurosurgery (mediating 19.6% of association). 30-day case fatality was 1.4 percentage points (pp) above national averages pre-implementation, but fell to 8.9pp below post-implementation (difference-in-difference -10.3pp; 95%CI -2.9 to -17.7pp; p = 0.009).
Conclusion
Our ABC bundle is associated with a sustained reduction in 30-day ICH case fatality at our centre and is not accounted for by national trends. Reduced DNR orders and neurosurgery partially mediate this association. Further evaluation in a cluster-randomised trial is planned.
Trial registration number
N/A
AS01-008
CLINICAL AND HEMATOMA OUTCOMES AND RENAL ADVERSE EVENTS DEPENDING ON ACHIEVED ACUTE BLOOD PRESSURE LEVELS AFTER INTRACEREBRAL HEMORRHAGE: THE ATACH-2 TRIAL
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita- Osaka, Japan
2Johns Hopkins University, Division of Brain Injury Outcomes, Baltimore, USA
3Medical University of South Carolina, Department of Public Health Sciences, Charleston, USA
4University of Minnesota, Zeenat Qureshi Stroke Research Center, Minneapolis, USA
Background and Aims
To determine clinical and hematoma outcomes, as well as renal complications, depending on achieved acute systolic blood pressure (SBP) levels after intracerebral hemorrhage (ICH) in the ATACH-2.
Method
One thousand patients (mean 61.9 years of age, 380 women, 562 Asians) started to receive intravenous nicardipine within 4.5 hours after onset of spontaneous supratentorial ICH for 24 hours. Patients were divided into 5 groups by mean hourly minimum SBP levels between 2 and 24 hours after randomization. The outcome measures were (1) 90-day mRS 4–6, (2) hematoma expansion defined as an increase of ≥6 mL from baseline to 24- hour CT, and (3) any renal adverse events within 7 days.
Results
Patients with 5 groups (SBP levels <120 mmHg, 199 patients; 120-130, 301; 130-140, 140; 140-150, 220; ≥150, 135) had similar baseline characteristics and hematoma features. 90-day mRS was 4–6 in 38, 36, 42, 39, and 38%, respectively, without significant intergroup differences (adjusted OR for ‘120-130’ as the reference: 0.96, 1, 1.71, 1.85, 1.02, respectively). Hematoma expansion was identified in 14, 11, 18, 19, and 25%, respectively; ‘140-150’ (crude OR 1.75, 95% CI 1.04-2.96) and ‘≥150’ (2.40, 1.36-4.22) showed higher frequency than ‘120-130’. Renal events occurred in 7, 10, 4, 5, and 4%, respectively; ‘130-140’ (crude OR 0.40, 0.16-0.99) and ‘140-150’ (0.43, 0.21-0.90) showed lower frequency than ‘120-130’.
Conclusion
Clinical outcomes at 3 months did not differ among 5 groups by achieved acute SBP levels. Protective tendency of intensive SBP lowering against hematoma expansion seemed to be offset by renal complications.
Trial registration number
ClinicalTrials.gov Identifier: NCT01176565
AS20-038
PROGNOSTIC SIGNIFICANCE OF ABNORMAL PHYSIOLOGICAL VARIABLES CLUSTER IN ACUTE ICH: INTERACT2 STUDY
1The George Institute for Global Health, Neurological and Mental Health, Sydney, Australia
2Xuzhou Central Hospital, Department of Neurology, Xuzhou, China
3Oslo University Hospital, Department of Neurology, Oslo, Norway
4Ruijin Hospital, Shanghai Institute of Hypertension, Shanghai, China
5University of Leicester, Department of Cardiovascular Sciences and NIHR Leicester Biomedical Research Centre, Leicester, United Kingdom
6The George Institute for Global Health, Professional Unit, Sydney, Australia
Background and Aims
Several physiological variables predict outcome in acute intracerebral hemorrhage (ICH). We aimed to determine the prognostic significance of a cluster of four baseline variables – blood pressure, glucose, temperature, and antithrombotic use – on adverse outcomes in ICH.
Method
Post-hoc analysis of INTERACT2, a large-scale multicenter randomized trial of intensive blood pressure (BP) reduction (target SBP <140mmHg vs. <180mmHg) in patients with acute ICH (onset <6hr) and hypertension (SBP 150-220mmHg). Scores were assigned for baseline levels of defined variables: 0 to 6 per 10mmHg SBP increase (range 150-220mmHg); and 0 or 1 for glucose (≤6.5 vs. >6.5 mmol/L), body temperature ≤37.5 vs. >37.5), and antithrombotic use (no vs. yes). Multivariable logistic regression was used to determine association of total scores and poor 90-day functional outcome (mRS 3–6) and death; reported with odds ratio (OR) and 95% confidence interval (CI).
Results
Distribution of total score was 0 (7.1%), 1 (14.5%), 2 (19%), 3 (18.5%), 4 (16%), 5 (12.1%), 6 (9.1%), 7 (3.4%), and 8 (0.2%). After adjusting for baseline severity and other confounders, a higher baseline score was significantly associated with poor functional outcome (per point increase: OR 1.08, 95% CI 1.03-1.14) and death (OR 1.10, 95% CI 1.02-1.19).
Conclusion
A care bundle targeting early rapid physiological control (BP lowering, glycemic control, treatment of pyrexia, and reversal of anticoagulation) may improve functional outcome in acute ICH. This is the rationale for the new INTERACT3 clinical trial (ClinicalTrials.gov: NCT03209258), which has commenced in China.
Trial registration number
NCT03209258
AS20-007
PROGNOSTIC RELEVANCE OF CORTICAL SUPERFICIAL SIDEROSIS IN CEREBRAL AMYLOID ANGIOPATHY
1Institute for Stroke and Dementia Research ISD, Neurology, Munich, Germany
2SLK Kliniken, Neurology, Heilbronn, Germany
3IRCCS-Arcispedale Santa Maria Nuova- Reggio Emilia- Italy, Neurology, Reggio Emilia, Italy
4Serviço de Neurologia- Centro Hospitalar do Porto - Hospital de Santo António- Porto- Portugal, Neurology, Porto, Portugal
5Hospital de la Santa Creu i Sant Pau- Biomedical Research Institute Sant Pau- IIB Sant Pau- Spain, Neurology, Barcelona, Spain
6Institut und Poliklinik für Neuroradiologie- Universitätsklinikum Carl Gustav Carus-Dresden- Germany, Neuroradiology, Dresden, Germany
Background and Aims
To determine the prognostic relevance of cortical superficial siderosis (cSS) in patients with cerebral amyloid angiopathy (CAA).
Method
302 patients meeting the modified Boston criteria for probable or possible CAA were enrolled into a prospective, multicenter cohort-study and followed for 6 months. cSS was assessed on T2*/SWI MRI. The predefined primary composite endpoint was incident stroke or death in patients with cSS compared to those without. Secondary analyses included cerebrovascular events and functional outcome measured by the modified Rankin scale (mRS). Multiple regression analysis was used to adjust for possible confounders.
Results
cSS prevalence was 40%. The primary endpoint occurred more frequently in patients with cSS (14%, 17/121) compared to those without (6%, 10/181, p = 0.0064). Presence of cSS was associated with the primary endpoint (odds ratio [OR] 3.18, 95% CI 1.2-8.46, p = 0.02), incident intracranial hemorrhage (OR 4.82, 95% CI 1.41-16.54, p = 0.01) and a less favorable outcome as assessed by the mRS (common OR 2.58, 95% CI 1.53-4.34, p = 0.00036). The primary endpoint was reached more frequently in patients with disseminated cSS compared to focal cSS (OR 9.097, 95% CI 1.02-80.96, p = 0.048).
Conclusion
Patients with cSS and suspected CAA are at high risk for incident intracranial hemorrhage and poor functional outcome. Both the presence and extent of cSS have prognostic relevance and may influence clinical decision making.
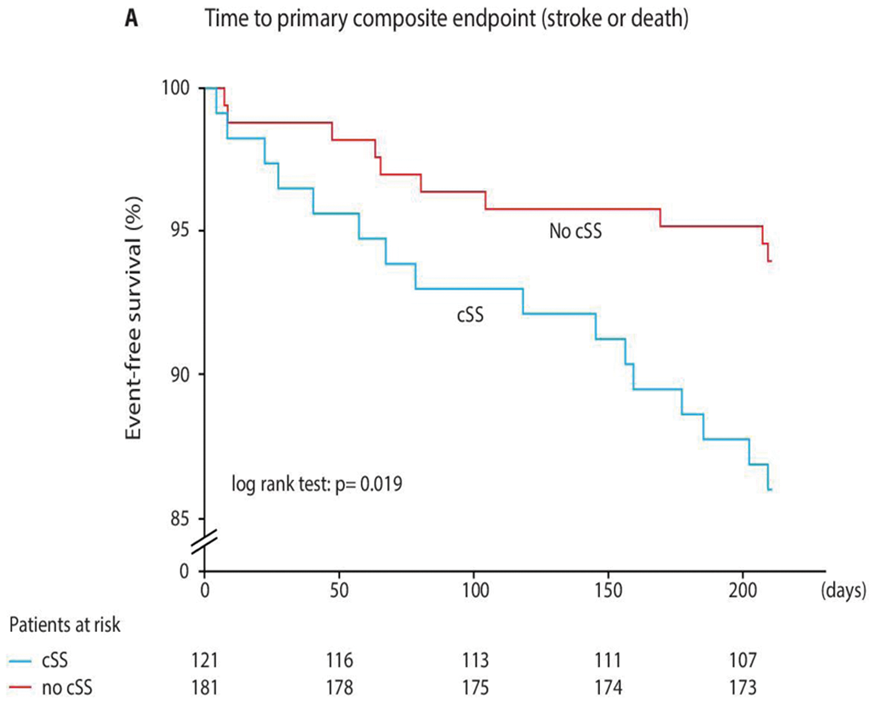
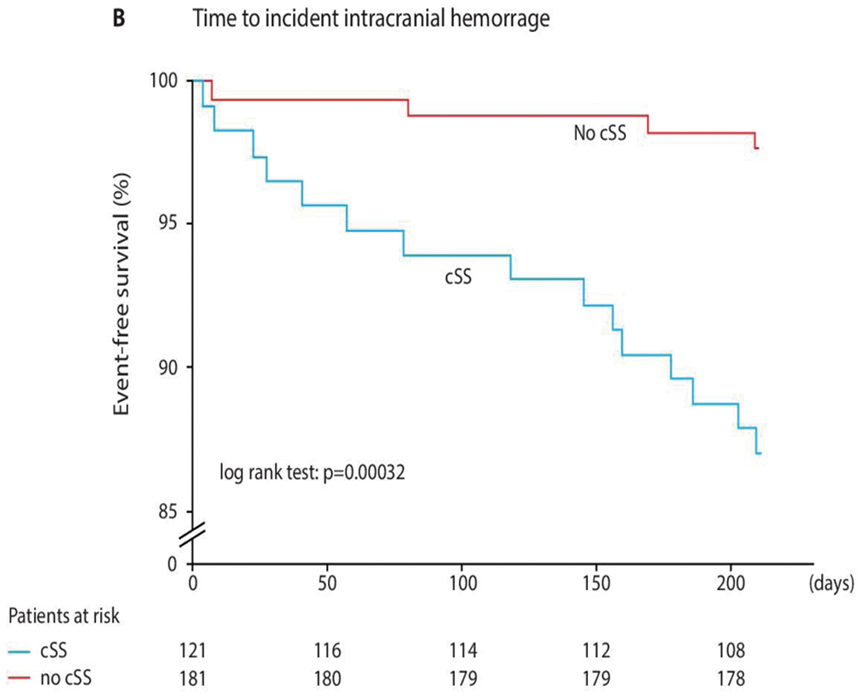
Trial registration number
ClinicalTrials.gov: NCT01856699
AS01-006
DIFFERENTIAL DETERMINANTS OF EARLY VS DELAYED NEUROLOGICAL DETERIORATION IN INTRACEREBRAL HEMORRHAGE: INTERACT2 STUDY
1the Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou, China
2University of New South Wales, The George Institute for Global Health, Sydney, Australia
3Royal Prince Alfred Hospital, Department of Neurology, Sydney, Australia
4National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
5West China Hospital, Department of Neurology, Chengdu, China
6the First Affiliated Hospital of Chengdu Medical College, Department of Neurology, Chengdu, China
Background and Aims
We elucidated factors associated with early and delayed neurological deterioration (END and DND, respectively) after intracerebral hemorrhage (ICH) in the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT2) dataset.
Method
INTERACT2 was a randomized controlled trial of early intensive vs. guideline-recommended blood pressure (BP) lowering in ‘hypertensive’ ICH (<6 hrs) patients. END and DND were defined as an increase from baseline to 24 hours, or from 24 hours to 7 days of ≥ 4 points on the NIHSS (or decrease of ≥2 points on GCS), respectively.
Results
Of 2598 participants, 450 (17.3%) had END or DND. In multivariable analysis, non-China recruitment, higher systolic BP, large baseline hematoma volume (BHV), left hemisphere ICH, intraventricular hemorrhage (IVH), heterogeneous ICH density, and associated cerebral white matter lesions were significant predictors of END (all P ≤0.02) Older age, higher glucose, large BHV, presence of IVH and heterogeneous ICH density were significant predictors of DND (all P≤0.03). END and DND were both associated with death, death or major disability (modified Rankin Scale score ≥3) at 90 days after adjusting for confounders (all P ≤0.005).
Conclusion
Overlapping variables determine END and DND in ICH patients, which has prognostic significance in terms of early mortality and functional recovery.
Trial registration number
N/A
Scientific Communications - Pathophysiology and Mechanisms
AS17-005
POST-STROKE INFLAMMATORY RESPONSE IS LINKED TO CEREBRAL VOLUME LOSS IN CONTRALATERAL HEMISPHERE FOLLOWING ISCHEMIC STROKE
1Hacettepe University Faculty of Medicine, Department of Neurology, Ankara, Turkey
2Hacettepe University, Institute of Neurological Sciences and Psychiatry, Ankara, Turkey
3Hacettepe University Faculty of Medicine, Department of Radiology, Ankara, Turkey
Background and Aims
The CNS and immune system are in a two-way relationship with a delicate homeostatic balance. The systemic immune-depressive response triggered by cerebral ischemia, suppresses the immune response directed towards neuroglial tissue as a protective reaction, while inadvertently creating an infection-prone state in stroke patients. In this study, we sought to identify whether cerebral volume loss occurs in the unaffected contralateral hemisphere after stroke, and determine the contribution of these intimate cascades of inflammation, immune-depression and infection to this loss.
Method
Thirty-one patients with ischemic stroke involving the MCA territory were enrolled into the study. Information related to clinical features, laboratory parameters (CBC, ESR, CRP, procalcitonin), heart rate variability, and infectious complications following stroke were prospectively collected. Contralateral hemisphere volume was determined by voxel-based morphometry on admission and follow-up MRI.
Results
The contralateral hemisphere volume decreased by a median (IQR) of 2.53% (0.63-5.72) after a follow-up duration of 73 (52-114) days (p < 0.001); the monthly volume reduction was 1.26% (0.00-2.53). Admission NIHSS score, infarct volume, neutrophil count, neutrophil/lymphocyte ratio, and development of pneumonia or urinary tract infections during hospitalization were significantly associated with monthly volume loss (p < 0.05). Stroke severity (NIHSS score or infarct volume) and inflammation related parameters (neutrophil/lymphocyte ratio or systemic infections) remained independently associated with monthly volume loss when assessed in multivariate regression models.
Conclusion
These findings suggest that cerebral volume loss is not limited to the symptomatic hemisphere in ischemic stroke patients. Stroke severity and impaired CNS-immune system homeostasis are critical players of neuroglial loss in the intact hemisphere.
Trial registration number
N/A
AS17-036
ULTRASTRUCTURAL AND IMMUNOHISTOLOGICAL CHARACTERIZATION OF AIS THROMBI
1Inserm 1148 - LVTS, Inserm, Paris, France
Background and Aims
The development of endovascular therapy (EVT) in acute ischemic stroke (AIS) provides an opportunity to study thrombi in order to develop new therapeutic strategies. The aim of this study is to assess the ultrastructural organization and composition of thrombi retrieved from AIS patients by EVT, and to determine their impact on t-PA-induced thrombolysis.
Method
EVT-retrieved AIS thrombi were randomly used in ex vivo lysis assay or fixed in paraformaldehyde and/or glutaraldehyde for immunohistological or scanning electron microscopy (SEM) analysis.
Results
A total of 164 thrombi are analyzed by immunohistology. Seventeen thrombi are analyzed by SEM. Both methods reveal that, although AIS thrombus organization is heterogeneous and shows some variability, a common remarkable structural feature can be found consistently among all AIS thrombi. In fact, in the vast majority of thrombi analyzed, either by immunohistology or SEM, a compact outer shell (panels A and B) made of various agglomerated thrombus components (fibrin (ogen), von Willebrand factor, platelets, neutrophil extracellular traps, RBC membrane remnants) surrounding a RBC- and fibrin-rich core (panels A and C) is observed.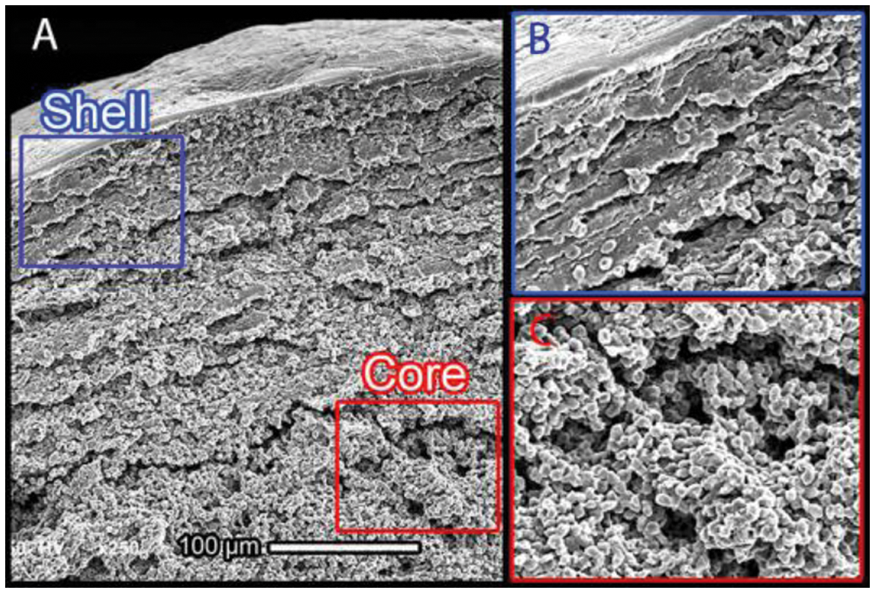
Conclusion
The majority of AIS thrombi retrieved during EVT present a RBC-rich core surrounded by a compact shell-like structure, which could participate in thrombolysis resistance.
Trial registration number
N/A
AS17-014
REDUCED TOTAL BRAIN PERFUSION AND THE RISK OF STROKE AND TRANSIENT ISCHEMIC ATTACK IN THE GENERAL POPULATION: THE ROTTERDAM STUDY
1Erasmus MC, Epidemiology, Rotterdam, The Netherlands
2Erasmus MC, Radiology and Nuclear Medicine, Rotterdam, The Netherlands
3Erasmus MC, Neurology, Rotterdam, The Netherlands
Background and Aims
Impaired brain perfusion causes inadequate nutritional flow to the brain. We examined the association of total brain perfusion with risk of stroke and transient ischemic attack (TIA) in the general population.
Method
Within the population-based Rotterdam Study, we performed 2D phase-contrast magnetic resonance imaging between 2005-2015 for cerebral blood flow (mL blood/min) measurements in stroke-free persons aged 46-98 years. We assessed associations between total brain perfusion (mL blood/100mL brain/minute) and risk of stroke and TIA with Cox regression models, adjusted for age, sex, cohort and cardiovascular risk factors. We furthermore tested interactions between total brain perfusion and MRI markers of small vessel disease (white matter lesions and lacunar infarcts), retinal vessel diameters and markers of large vessel disease (carotid stenosis and intima media thickness).
Results
Of 5289 participants (55.6% women) with a median follow-up of 7.2 years, 274 participants developed any stroke or TIA (144 TIA). Lower total brain perfusion was associated with higher risk of stroke or TIA (fully adjusted hazard ratio, 95% confidence interval, per standard deviation decrease: 1.18, 1.03–1.34), similar in ischemic stroke or TIA. For the risk of TIA alone, a hazard ratio of 1.29, 1.07–1.55 was found, compared to a hazard ratio of 1.06, 0.87–1.30 for the risk of ischemic stroke. Within wider retinal calibers, brain perfusion showed stronger associations with TIA, whereas no such effect was found with ischemic stroke.
Conclusion
This study suggests a different pathophysiology underlying TIA and stroke, with TIA being possibly caused by a less perfused brain in combination with failing autoregulation.
Trial registration number
N/A
AS17-015
INITIAL FINDINGS FROM THE CURAM AND MAYO CLINIC INTERNATIONAL ACUTE ISCHEMIC STROKE CLOT REGISTRY
1National University of Ireland Galway, CÚRAM–Centre for Research in Medical Devices, Galway, Ireland
2Mayo Clinic, Department of Radiology, Rochester MN, USA
3National University of Ireland Galway, Department of Physiology, Galway, Ireland
4University of Massachusetts Medical School, New England Center for Stroke Research. Department of Radiology, Worcester MA, USA
Background and Aims
Poor recanalization outcomes in acute ischemic stroke (AIS) persist, at least partly, because the impact of clot histological and physical characteristics in revascularization outcomes is relatively unknown. This large international study aims to investigate the relationships between histological composition, imaging data and clinical outcome in AIS patients.
Method
This multi-center international study is HIPAA compliant and institutional review board approved. Prior to endovascular treatment, each patient has a non-contrast computed tomography (CT) scan. Histopathological analysis of the AIS clots removed by mechanical embolectomy was performed and clot composition was quantified using Machine Learning (Orbital Image Analysis, Actelion Ltd.). Correlations with clinical data were assessed using linear regression and correlation coefficient analysis.
Results
In this preliminary study with fifty patients, Orbit machine learning software was validated for histological characterization of clots, correlating strongly with independent pathologist composition analysis. No significant correlation was seen between number of passes to remove the clot and suspected etiology of the clot. The final TICI score also did not correlate significantly with the etiology of the clot or with individual components (red blood cells, white blood cells, fibrin). However, trends were evident, most notably a trend towards cardioembolic versus large artery clots correlating with a Hyperdense Artery Sign (≥50HU) on non-contrast CT (ρ=0.273, p = 0.085, n = 41).
Conclusion
Initial findings suggest that non-contrast CT may provide valuable information indicative of histological characteristics of AIS clots. Analysis of 1,000 samples in this international study will allow strong conclusions to be drawn.
Acknowledgements: Science Foundation Ireland (Grant Number 13/RC/2073) and Industrial partners Cerenovus.
Trial registration number
N/A
AS17-008
VULNERABLE INTRACRANIAL ATHEROSCLEROTIC PLAQUES: A MORPHOLOGY STUDY BY 3-DIMENSIONAL ROTATIONAL ANGIOGRAPHY
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, Hong Kong S.A.R
2The Chinese University of Hong Kong, Department of Imaging & Interventional Radiology, Hong Kong, Hong Kong S.A.R
Background and Aims
Intracranial atherosclerotic disease (ICAD) is a major ischemic stroke subtype. Understanding the morphology of acute symptomatic plaques may identify vulnerable lesions and guide treatment.
Method
We performed 3-dimensional rotational angiography (3DRA) in 173 patients (median age = 60 years) within 4 weeks from an acute ischemic stroke or transient ischemic attack attributed to high-grade ICAD (>60% stenosis). We reviewed the infarct topography in DWI and FLAIR/T2 MRI brain over the corresponding vascular territory, and investigated if plaque morphology might differ in patients with or without DWI/FLAIR/T2 lesions.
Results
Among the 173 culprit lesions distributing in middle cerebral artery (MCA)-M1 (n = 127); intracranial internal carotid artery (ICA)-C6/7 (n = 26); across both MCA and ICA (n = 5); basilar artery (n = 13); and vertebral artery-V4 (n = 2), the median luminal stenosis over the thickest plaque region was 75%. In terms of surface lining, the plaques were smooth, irregular, or ulcerative in 51 (29.5%), 95 (54.9%), and 27 (15.6%). Ulcerative plaques were thicker (p = 0.002), more eccentric (p = 0.043), of a steeper upstream shoulder (p < 0.001), and were significantly associated with adjacent branch atheromatous disease (p = 0.026) compared with smooth or irregular plaques. Patients harboring ulcerative plaques had more concurrent acute and chronic infarcts in the corresponding watershed regions than those with smooth plaques (odds ratio=5.82; p = 0.006).
Conclusion
Ulcerative plaques in cerebral arteries were associated with a higher plaque burden and vulnerable geometric features. The presence of more old-and-new infarcts with ulcerated plaques might represent recurrent artery-to-artery thrombo-embolism.
Trial registration number
N/A
AS18-023
INCREASED PLATELET COUNT AND RETICULATED PLATELETS IN RECENTLY SYMPTOMATIC VERSUS ASYMPTOMATIC CAROTID ARTERY STENOSIS AND IN CEREBRAL MICROEMBOLIC SIGNAL-NEGATIVE PATIENT SUBGROUPS: RESULTS FROM HEIST STUDY
1The Adelaide and Meath Hospital, Department of Neurology, Dublin, Ireland
2St Vincent’s University Hospital- University College Dublin, Department of Neurology, Dublin, Ireland
3The Adelaide and Meath Hospital, Department of Haematology, Dublin, Ireland
4The Adelaide and Meath Hospital, Departments of Neurology- Vascular Neurology Research Foundation and Stroke Service, Dublin, Ireland
Background and Aims
The pathophysiological mechanisms responsible for the disparity in stroke risk between asymptomatic and symptomatic carotid stenosis are not fully understood. The functionally-important reticulated platelet fraction (%RPF) and reticulocytes could play a role.
Our aims were to compare full blood count parameters and platelet production/turnover/activation markers in asymptomatic versus recently symptomatic moderate (≥50–69%) or severe (≥70-99%) carotid stenosis patients.
Method
Data from 34 asymptomatic patients were compared with 43 symptomatic patients in the ‘early phase’ (≤4 weeks) and 37 patients in the ‘late phase’ (≥3 months) after TIA/ischaemic stroke in this prospective, multi-centre, observational-analytical study. Reticulated platelets were quantified by whole-blood flow cytometry and reticulated platelets and reticulocytes by ‘automated assays’ (Sysmex XE-2100™). Bilateral simultaneous transcranial Doppler ultrasound monitoring classified patients as micro-embolic signal (MES)+ve or MES-ve.
Results
Mean platelet count was higher in early (216 x109/L) and late symptomatic (219 x109/L) than asymptomatic patients (194 x109/L; P = 0.04). Mean platelet volume was higher in early symptomatic than asymptomatic patients (10.8 vs. 10.45fl; P = 0.045). Automated assays revealed higher %RPF in early (5.78%) and late symptomatic (5.11%) than asymptomatic patients (3.48%; P≤0.01). Reticulocyte counts were lower in early (0.92%) and late symptomatic (0.93%) than asymptomatic patients (1.07%, P≤0.036). The automated %RPF was higher in early symptomatic than asymptomatic MES-ve patients (5.7% vs. 3.55%; P = 0.001).
Conclusion
Increased platelet counts and a shift towards production of a population of larger, young, reticulated platelets could contribute to a higher risk of cerebrovascular events in recently symptomatic versus asymptomatic carotid stenosis patients, including those who are MES-ve.
Trial registration number
N/A
AS28-011
SINGLE CHAIN (SC-) VERSUS TWO CHAIN (TC-) TISSUE PLASMINOGEN ACTIVATOR (TPA) IN A MODEL OF THROMBOEMBOLIC STROKE AND REPERFUSION IN MICE
1University of Caen, UMR-S U1237 “Physiopathology and Imaging of Neurological Disorders” - PhIND - INSERM/EFS/Univ. Caen-Normandie Team “tPA and neurovascular disorders” Centre CYCERON, Caen, France
Background and Aims
Tissue type Plasminogen Activator (tPA) is the only pharmacological treatment approved by the authorities at the acute phase of ischemic stroke. Interestingly, tPA-contained in Actilyse® or Alteplase® is under two forms (singe chain (sc) and two chains (tc)) both displaying a same thrombolytic activity in the presence of fibrin. However, only the sc-tPA is capable to promote the NMDA receptor signaling and subsequent excitotoxicity. A recent report, made from a cohort of 1004 stroke patients all treated with Actilyse® revealed that patients receiving more tc-tPA than sc-tPA displayed an increased risk of symptomatic intracerebral hemorrhages and that patients receiving more sc-tPA than tc-tPA displayed an increased number of seizures during the first 7 days post-stroke onset.
Method
In the present study, we further investigated the differential effects of sc-and tc- tPA in an experimental model of thromboembolic stroke reproducing the clinical features.
Results
The data obtained in a randomized population of mice divided into 3 groups (control, sc-tPA, tc-tPA, treated 20 minutes after stroke onset) demonstrate that sc-tPA led to an improved reperfusion when compared to tc-tPA treated animals and non-treated animals, associated with a higher reduction of the ischemic lesion size compared to tc-tPA treated animals and control group. Functional assessment using strength test support these results showing better functional outcome in the sc-tPA treated group compared to the tc-tPA treated group.
Conclusion
This is the first pre-clinical study revealing a differential effect of sc- and tc- tPA in the context of thromboembolic stroke and fibrinolysis.
Trial registration number
N/A
AS17-031
CEREBRAL THROMBI RETRIEVED BY MECHANICAL THROMBECTOMY ARE HETEROGENEOUS AND THEIR COMPOSITION CORRELATES WITH THE DENSITY OF THE OCCLUDED VESSEL ON CT SCAN
1San Raffaele Hospital, Neurology Department- Stroke Unit, Milan, Italy
2San Raffaele Hospital, Institute of Experimental Neurology INSPE, Milan, Italy
3San Raffaele Hospital, Neuroradiology Department, Milan, Italy
Background and Aims
Mechanical thrombectomy has been shown to be able to recanalyse large occluded vessels with benefit in terms of disability and mortality. Thus, the introduction of endovascular procedures has allowed the availability of human thrombus material for histopathologic analysis, opening a wide area of research on the thrombus.
Method
We aimed to perform a systematic histological analysis of cerebral thrombi retrieved in acute ischemic stroke patients by endovascular approaches to unravel their composition and to detect possible correlations with imaging biomarkers. We investigated the clot composition, in terms of structural components, in particular in its composition of fibrin, platelets, red blood cells, von Willebrand Factor.
Results
Histological analysis of 27 human thrombi retrieved by angiography in acute stroke patients has been performed. We found that cerebral thrombi are macroscopically heterogeneous in terms of consistence, dimensions, color and gross appearance (Fig. 1). Even in their structural composition, all clots presented a heterogeneous pattern of red blood cells, platelets, fibrin and vWF. Fibrin was the most represented component within the retrieved thrombi (Fig.2). Moreover, we found that the “Hyperdensity Artery Sign” of the occluded vessel on the CT scan strongly correlates with the erythrocyte composition of the thrombus (Fig. 3).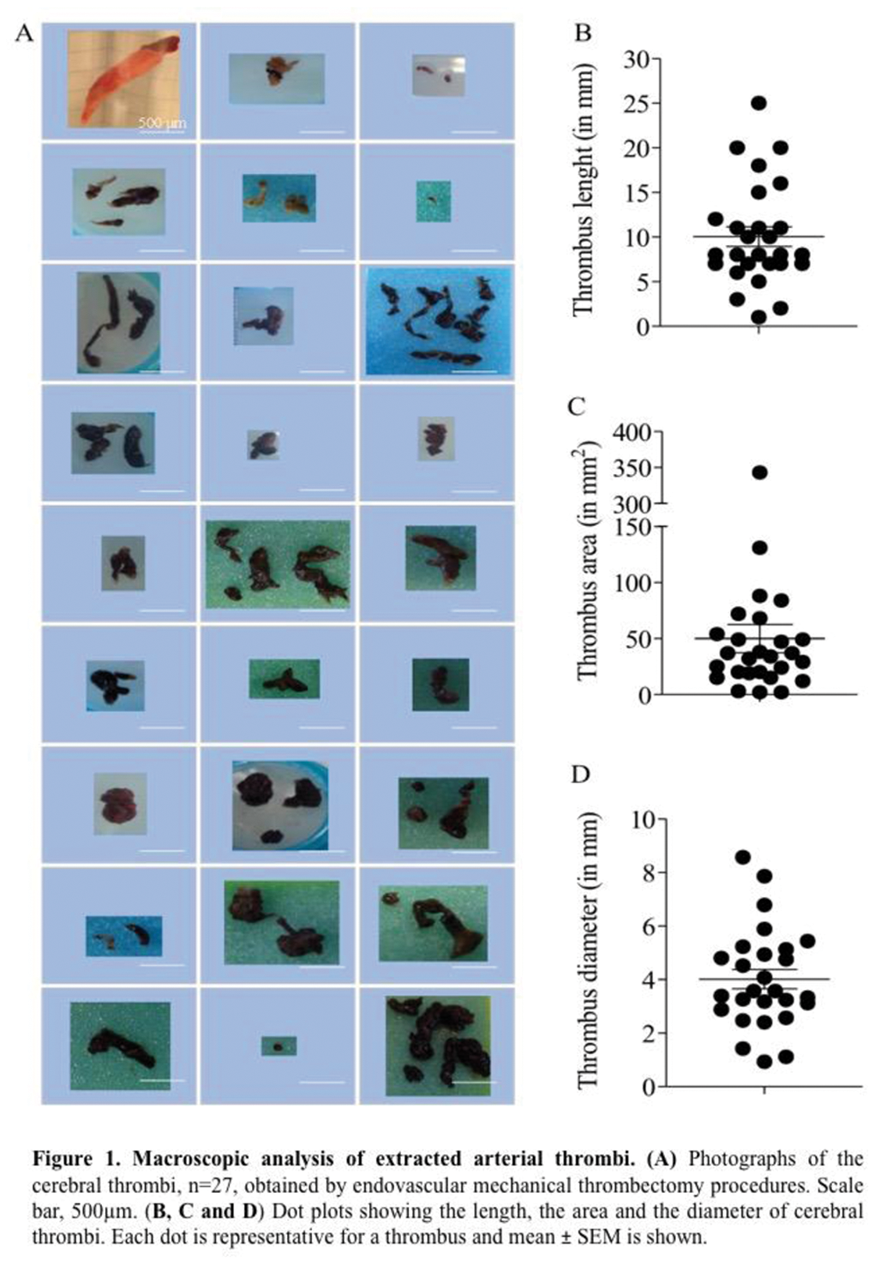
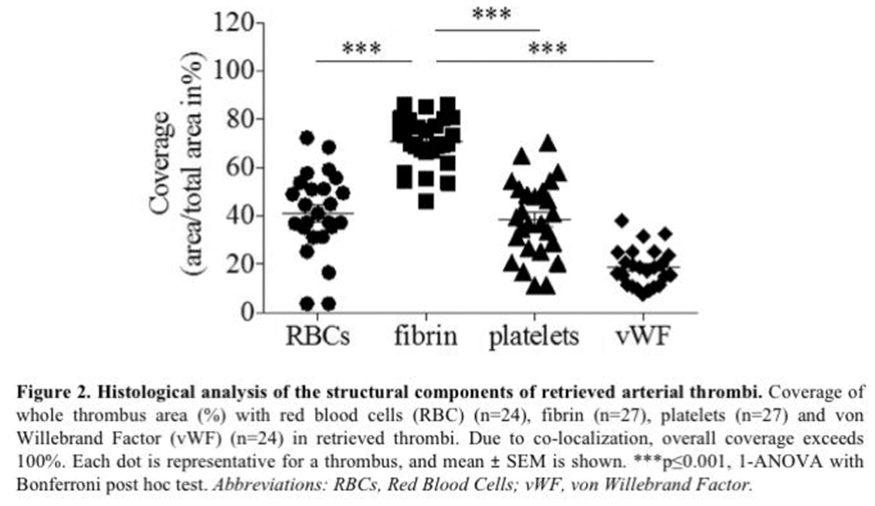
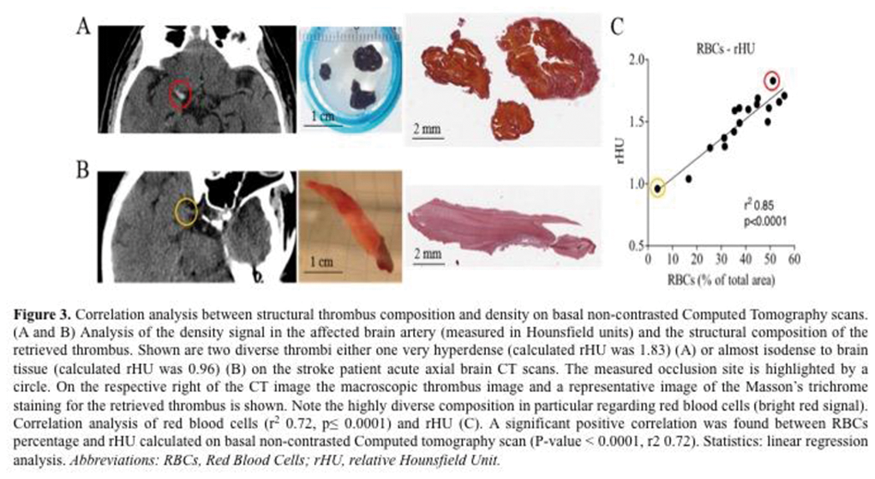
Conclusion
Arterial cerebral thrombi are widely heterogeneous and their composition correlates with the density of the occluded vessel on CT scan. Our pilot study supports the importance of the analysis of thrombus composition as a possible future tool for understanding the mechanisms underlying stroke and improve stroke care.
Trial registration number
N/A
AS17-018
EARLY CEREBRAL ISCHEMIC EVENTS IN SYPTOMATIC CAROTID STENOSIS ARE RELATED TO PLAQUE INFLAMMATION
1National University of Singapore, Neurology, Singapore, Singapore
2National University Hospital, Neurology, Singapore, Singapore
3National University Hospital, Diagnostic Imaging, Singapore, Singapore
Background and Aims
Severity of symptomatic carotid stenosis often determines the treatment approach. However, severity explains only the regional hypoperfusion as the mechanism of cerebral ischemia. Artery-to-artery embolisation remains an important pathogenic mechanism in patients with high-risk carotid plaques. Inflammation is considered as the initiating event for plaque rupture and cerebral embolism. Using 18F-fluorodeoxyglucose positron-emission tomography (FDG-PET)/computed tomography (CT) and high-resolution magnetic resonance imaging (HR-MRI), we investigated the role of plaque imaging in stroke recurrence in our patients with recently symptomatic carotid stenosis.
Method
This prospective study included consecutive patients within 30-days of recent stroke and ipsilateral carotid stenosis (≥50%). FDG uptake was quantified as mean standardized uptake values (SUV, g/ml). The ratio of T1 hyperintensity of carotid plaque to the ipsilateral sternocleidomastoid muscle (SCM) was recorded on T1-weighted fat suppressed HR-MRI. Patients were followed-up for stroke recurrence within 90-days.
Results
Of the 85 patients included in the study, 12 (14%) suffered from recurrent cerebral ischemic event in the stenosed carotid territory within 90-days. Compared to patients who remained asymptomatic, patients with recurrent cerebral ischemia showed higher mean T1 carotid-SCM ratio (2.16 versus 1.42; p < 0.0001) and higher mean SUV value in the carotid plaque (3.12g/ml versus 1.39g/ml; p < 0.0001). Higher T1 carotid-SCM ratio on HR-MRI (OR 3.625, 95%CI 1.416-5.334; p < 0.0001) and higher mean SUV on FDG-PET (OR 3.328, 95%CI 3.014-8.172; p = 0.005) were independent predictors of recurrent cerebral ischemia.
Conclusion
FDG-PET/CT and HR-MRI of carotid stenosis are useful tools for risk stratification and may aid in better therapeutic decision-making.
Trial registration number
NA
Scientific Communications- Imaging
AS10-014
REDEFINING THE ISCHEMIC CORE THRESHOLD FOR THROMBECTOMY A CASE CONTROL STUDY
1University of Melbourne, Medicine, Melbourne, Australia
2Royal Adelaide Hospital, Neurology, Adelaide, Australia
3John Hunter Hospital, Neurology, Newcastle, Australia
4University of Alberta, Neurology, Alberta, Canada
5University of Newcastle, Health and Medicine, Newcastle, Australia
6Royal Melbourne Hospital, Neurology, Melbourne, Australia
Background and Aims
We aimed to identify if ischemic stroke patients treated with thrombectomy had the same baseline CTP ischemic core threshold as patients treated with alteplase.
Method
Patients who underwent thrombectomy were matched to patients with similar clinical and imaging characteristics (occlusion location, perfusion lesion volume) who were treated with alteplase alone from the INSPIRE Registry. A pixel-based analysis of CT perfusion (CTP) and 24 hour diffusion-weighted imaging (DWI) was undertaken to define the optimum CTP thresholds for the ischemic core. Only patients who had complete occlusion pre-treatment and complete recanalization post-thrombectomy, or at 24 hour vascular imaging post IV alteplase were included.
Results
There were 132 eligible thrombectomy patients and 132 matched controls treated with alteplase alone. Baseline NIHSS (median 15, IQR 11-19) and age (median 65, IQR 59 - 80) were well-matched. Despite similar baseline CTP ischemic core volumes (median 21 and IQR 15-38 for combined group) using the previously validated measure (CBF<30%), thrombectomy patients had a smaller median 24 hour DWI infarct core of 17.3mL (IQR 11.3-32.8mL versus 24.3 mL IQR 16.7-42.2mL, p = 0.011) than alteplase-treated controls. The optimal threshold to define the ischemic core in thrombectomy patients was CBF<20% (AUC 0.89, 95% CI: 0.84, 0.94), while in alteplase controls the optimal ischemic core threshold remained CBF<30% (AUC 0.83, 95% CI: 0.77, 0.85)
Conclusion
Thrombectomy salvages tissue with a lower CBF than does alteplase, likely due to more effective and earlier reperfusion. The definition for ischemic core with CTP needs to be modified in patients being considered for thrombectomy.
Trial registration number
N/A
AS16-112
CAROTID PLAQUE INFLAMMATION MEASURED WITH 18-FLUORODEOXYGLUCOSE POSITRON-EMISSION TOMOGRAPHY PREDICTS EARLY STROKE RECURRENCE IN PATIENTS WITH ATHEROTHROMBOTIC STROKE
1Hospital De La Santa Creu I Sant Pau, Neurology, Barcelona, Spain
2Hospital De La Santa Creu I Sant Pau, Nuclear Medicine, Barcelona, Spain
Background and Aims
Inflammation is a key factor for carotid plaque destabilization. A prior study demonstrated that inflammation on 18fluorodeoxyglucose positron-emission tomography (18FDG-PET) might predict early stroke recurrence. We aimed to confirm the role of 18FDG-PET in predicting stroke recurrences in patients with carotid atherosclerosis.
Method
Prospective study of consecutive patients (2015-2017) with an acute anterior circulation stroke and at least one atherosclerotic plaque in the internal carotid artery (ICA) ipsilateral to the stroke symptoms (NCT03218527). We excluded cardioembolic strokes. We recorded demographic data and vascular risk factors at admission. All patients underwent an 18FDG-PET within three weeks from the index stroke and we determined the Standardized Uptake Value (SUV) and the Target-to-Background Ratio (TBR) in both ICAs. We recorded stroke recurrences at three months of follow-up and performed a predictive multivariable logistic regression analysis.
Results
We included 50 patients with a mean age of 74.4 ± 10.6y, 37 (74%) were men. There were 31 patients (62%) with a carotid stenosis ≥50% classified as atherothrombotic and 19 patients with a stenosis <50% (two lacunar and 17 cryptogenic). Seven patients underwent carotid revascularization after the 18FDG-PET. There were 12 recurrences (24%), all in the atherothrombotic group. In the multivariable regression analysis 18FDG uptake on PET was independently associated with the risk of stroke recurrence measured either with TBR (OR for 0.1 increase =1.33 95%CI 1.09-1.64) or SUV (OR for 0.1 increase =1.18 95%CI 1.04-1.34), after adjusting for the degree of stenosis.
Conclusion
In atherothrombotic stroke patients, plaque inflammation assessed with 18FDG-PET was independently associated with stroke recurrence.
Trial registration number
N/A
AS10-037
THROMBUS PERVIOUSNESS AS A POTENTIAL PATIENT SELECTION TOOL FOR INTRAVENOUS AND ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE
1Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
2Academic Medical Center, Radiology and Nuclear Medicine- Biomedical Engineering and Physics, Amsterdam, The Netherlands
3Altair, Biostatistics, St Louis Park- Minnesota, USA
4University of Glasgow- Queen Elizabeth University Hospital, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
5Academic Medical Center, Neurology, Amsterdam, The Netherlands
6David Geffen School of Medicine- University of California, Department of Neurology and Comprehensive Stroke Center, Los Angeles- California, USA
7University of Calgary, Clinical Neurosciences, Calgary- Alberta, Canada
8University of Pittsburgh Medical Center, Neurology, Pittsburgh- Pennsylvania, USA
9University of Lorraine and University Hospital of Nancy, Diagnostic and Interventional Neuroradiology, Nancy, France
10Royal Melbourne Hospital, Neurology, Parkville, Australia
11Erasmus Medical Center, Radiology, Rotterdam, The Netherlands
12Institute of Neuroscience, Newcastle University, Newcastle upon Tyne, United Kingdom
13Erasmus Medical Center, Neurology, Rotterdam, The Netherlands
14Royal Melbourne Hospital, Radiology, Parkville, Australia
15University of Calgary, Radiology, Calgary- Alberta, Canada
Background and Aims
Thrombus perviousness estimates residual blood flow through a clot based on radiological images. We aimed to investigate possible treatment modification effect of thrombus perviousness in the pooled HERMES-collaboration dataset.
Method
We included 393 patients with thin-slice non-contrast CT (NCCT) and CT angiography (CTA) available. We calculated thrombus attenuation increase (TAI) using NCCT and CTA. Control arm patients received intravenous tissue plasminogen activator (IV-tPA) if eligible; intervention consisted of additional endovascular treatment (EVT). We compared both arms. Multivariable regression analyses with multiplicative interaction terms were performed to determine treatment effect modification and association of TAI with functional outcome (modified Rankin scale score; mRS), favorable outcome (mRS 0–2), reperfusion (mTICI-score 2b-3), and final infarct volume (FIV).
Results
Increased TAI was associated with improved ordinal mRS, with significant treatment effect modification (p = 0.005). For control patients, aOR for 1-step mRS improvement was 1.22 (95%CI 1.11-1.35) per 5HU TAI increase. In the intervention arm no significant association was found. Among controls, increased perviousness was associated with higher chance of favorable outcome (aOR 1.33; 95%CI 1.14-1.56; Fig.1) and 13% FIV decrease (95%CI 7–18) per 5HU TAI increase. For intervention patients, perviousness was not significantly associated with favorable functional outcome, reperfusion, and FIV.
Conclusion
Thrombus perviousness measured on acute-phase NCCT and CTA is associated with improved functional outcome, mortality, and FIV after IV-tPA. For EVT, no significant associations were found.
Trial registration number
N/A
AS10-047
ALADIN STUDY: AUTOMATED LARGE ARTERY OCCLUSION DETECTION IN STROKE IMAGING STUDY - A MULTI-CENTER EXPERIENCE
1Grady Memorial Hospital- Emory University School of Medicine, Marcus Stroke Center- Department of Neurology, Atlanta, USA
2Vanderbilt University, Vanderbilt Department of Neurology, Nashville, USA
3Erlanger, Department of Radiology, Chattanooga, USA
Background and Aims
Prompt clinical recognition of Large Vessel Occlusion (LVO) for Acute Ischemic Stroke is a key point to guide reperfusion therapies. Clinical surmise, multimodal neuroimaging and referrals to stroke comprehensive centers are crucial for best patient care. Medical field faces the rise of artificial intelligence, with better computer vision. We bring an artificial-intelligence-based algorithm for AIS-related LVO detection.
Method
We performed multi-center retrospective analysis of CTAs, randomly picked from prospective cohort of AIS patients, with and without LVOs, admitted at stroke centers, from 2014-2017. Experienced stroke neurologists graded CTAs for presence and site of occlusion. Concurrently, studies were analyzed by Viz-AI-Algorithm® v3.04–a Convolutional Neural Network programed to detect MCA-M1 and/or ICA-T occlusions. Our primary analysis included ICA-T and/or MCA-M1 LVOs versus non-LVOs/more distal occlusions. Our secondary analysis also included proximal MCA-M2 vs non-LVOs.
Results
we analyzed 875 patients including 49.5% males, bNIHSS 15[IQR 10-20], bASPECTS 10[8-10] including 45.9% LVOs. Baseline characteristics were similar among groups. Primary and secondary analysis showed an accuracy of 86% and 81.8%, sensitivity of 90.1% and 81.4%, specificity of 82.5 and 82.2%, PPV of 81.8 and 83.6% and NPV of 90.6 and 79.1%, respectively; AUC 86.3% (IC95%0.83-0.90, p = <0.001) and 81.8% (IC95%0.78-0.85, p = <0.001), and ICC 84.1% (IC95%0.81-0.86; p = <0.001), and 77.6%(IC95%0.73-0.80, p < 0.001), respectively. Maximal running time of the algorithm was under five minutes.
Conclusion
Viz-AI-Algorithm shows a remarkable performance for proximal intracranial LVOs. Endeavors to optimize detection of the MCA-M2 and all intracranial ICA occlusions have been enforced. To the best of our knowledge, this is the first AI-algorithm for detecting intracranial LVOs.
Trial registration number
N/A
AS10-001
CLINICAL UTILITY OF E-ASPECTS SOFTWARE IN THE ENCHANTED TRIAL DATABASE
1University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
2The George Institute for Global Health, Neurological and Mental Health Division, Sydney, Australia
3University of Leicester, Dept. of Cardiovascular Sciences and NIHR Leicester Biomedical Research Centre, Leicester, United Kingdom
4The George Institute China at Peking University Health Science Center, The George Institute China at Peking University Health Science Center, Beijing, China
Background and Aims
Clinical utility of electronic Alberta Stroke Program Early CT Score (e-ASPECTS), an automated system for quantifying signs of infarction, was evaluated in a large database of thrombolysed acute ischemic stroke (AIS) patients.
Method
All baseline non-contrast CT scans of patients with anterior circulation AIS who participated in the alteplase-dose arm of the randomised controlled trial Enhanced Control of Hypertension and Thrombolysis Stroke Study (ENCHANTED), were reviewed; poor quality and large (>6 mm) slice thickness were excluded. Included scans had e-ASPECTS scores correlated with baseline neurological severity (National Institutes of Health stroke scale [NIHSS] scores) and 90-day disability outcomes (modified Rankin scale [mRS] scores). Multivariable logistic regression models were used to determine the predictive ability of e-ASPECTS for disability outcomes and symptomatic intracranial hemorrhage (sICH).
Results
Of 2426 available CT images, 1480 (61%) were included in analyses of e-ASPECTS scores (median 9 [IQR 8–10], 77% with ‘good’ [range 8–10] scores]. Lower e-ASPECTS scores (per 1 point decrease) were significantly associated with increasing baseline NIHSS scores (r -0.31; p < 0.0001) and 90-day poor outcome (mRS scores 2–6, r -0.27; p < 0.001). Adjusted odds ratios (OR) and 95% confidence intervals (CI) for 90-day outcomes were: death or disability (mRS 2–6, 0.91 [0.85-0.97]), death and major disability (mRS 3–6, 0.89 [0.83-0.95]), and death 0.86 [0.79-0.95]); and for sICH according to the Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria was 0.87 (0.72-1.05).
Conclusion
Scores on e-ASPECTS are highly correlated with baseline neurological severity and independently predict functional recovery and adverse outcomes in AIS.
Trial registration number
The trial is registered with ClinicalTrials.gov (NCT01422616).
AS10-012
EVALUATION OF INTRACRANIAL COLLATERALS BY A FULLY AUTOMATED COMPUTER BASED ALGORITHM COMPARED TO HUMAN READERS
1Heidelberg University Hospital, Neuroradiology, Heidelberg, Germany
2Heidelberg University Hospital, Neurology, Heidelberg, Germany
Background and Aims
Assessment of intracranial collaterals is pivotal in acute ischemic stroke but prone to interrater variability. We compared the performance of a computer based algorithm with those of experienced neuroradiologists.
Method
Single-phase CT angiography scans of acute ischemic stroke patients were retrospectively scored by the algorithm, two blinded neuroradiologists and two expert readers with full access to clinical and additional imaging information, providing the ground truth. Intracranial collaterals were scored according to Tan et al. and additionally for each cortical ASPECTS region (M1-6 & insula) on a three-point scale: no collaterals (=0) vs. 0–50% (=1) vs. > 50% (=2), compared to the contralateral side, respectively, resulting in a score between 0 and 14 (“full collaterals”). We also derived a two-point scale by merging previous categories 0 and 1 resulting in a 7-point score (“good collaterals”). Intra-class-correlation-coefficients (ICC) were calculated.
Results
235 patients with Carotid-T, M1- or M2-occlusion were analyzed. Median Tan score was 2 for all raters and ICC values between the algorithm and readers vs. ground truth were 0.793, 0.829 and 0.798 (all p < 0.001). Median “full collateral” and “good collateral” scores were similar among human readers and the algorithm (11, 8 and 9, respectively 4, 2 and 3). ICC between readers and the algorithm vs. ground truth were 0.859, 0.868 and 0.819 for “full collaterals” and 0.853, 0.824 and 0.826 for “good collaterals” (all p < 0.001).
Conclusion
Fully automated evaluation of intracranial collaterals in acute ischemic stroke patients was in excellent agreement with human readers and the ground truth.
Trial registration number
N/A
AS11-001
SPONTANEOUS DILATATION OF STENTS AFTER CAROTID ARTERY STENTING, CAS, WITHOUT POST-CAS BALLOON DILATATION FOR HIGH SIGNAL LESIONS ON MR BLACK-BLOOD IMAGES
1Shonan Kamakura general hospital, Dept of Stroke Treatment, Kamakura, Japan
Background and Aims
Introduction
Lesions showing MRI-T1WI black blood high intensity (T1BBHI) look more vulnerable and softer.
Hypothesis
Stents spontaneously dilate more significantly in lesions showing T1BBHI than in lesions without T1BBHI, when patients underwent carotid artery stenting (CAS) without post-CAS balloon dilatation.
Method
We included in our analysis patients 1) who underwent elective CAS without post-CAS balloon dilatation from May 2012 to March 2017, 2) who underwent conventional angiography at 3 months after CAS. Patients’ baseline characteristics, the presence or absence of T1WIBBHI, carotid artery % stenosis according to the NASCET criteria before and just after CAS and 3 months after CAS were evaluated. In lesions with and without T1BBHI, we compared % stenosis before, just after and 3 months after CAS. We performed CAS with distal protection of filter devices, pre-CAS balloon dilatation with a 3.0-mm balloon for lesions with T1BBHI and 4.0-mm balloon for lesions without T1BBHI, 10-mm diameter self-expandable stents of Carotidwallstent, Precise or Protégé.
Results
One hundred ten lesions were analyzed. Symptomatic lesions were sixty-two. Carotid artery % stenosis before, just after CAS, at three months after CAS was 72.7%, 33.2% (p < 0.0001) and 21.1% (p < 0.0001). In lesions with and without T1BBHI, carotid artery % stenosis was 73.3% and 71.7% before CAS (n.s.), 37.1% and 28.3% (p < 0.05) just after CAS, 24.4% and 21.9% (n.s.) 3 months after CAS, respectively, and change of % stenosis was -10.39% and -7.76% (p < 0.05). Stents were dilated spontaneously in both lesions.
Conclusion
Stents dilated spontaneously without post-CAS balloon dilatation particularly in lesions showing T1BBHI more significantly.
Trial registration number
N/A
AS11-006
HIGHER PREVALENCE OF DWI-POSITIVE LESIONS IS ASSOCIATED WITH HIGHER SEVERITY OF CEREBRAL SMALL VESSEL DISEASE AMONG STROKE IN YOUNG ADULTS; THE FUTURE STUDY
1Radboud University Medical Center- Donders Institute for Brain- Cognition and Behaviour, Neurology, Nijmegen, The Netherlands
2Luzern State Hospital, Center for Neurology and Neurorehabilitation, Luzern, Switzerland
3German Center for Neurodegenerative Diseases DZNE, Population Health Sciences, Bonn, Germany
Background and Aims
Chronic hypoperfusion is thought to play a major role in the etiology of small vessel disease (SVD). However, recent studies in individuals aged 60 years or over suggest that acute infarcts, which as detected as diffusion weighted imaging (DWI) positive (DWI+), play an important role in the pathogenesis SVD. We previously reported that young stroke patients (18-50 years) have a higher burden of SVD than controls. As the cause of SVD in the young may be different or much more heterogeneous than in elderly, we investigated if acute infarcts are involved in the etiology of SVD in young stroke patients.
Method
Prospective cohort study of 337 patients with a first-ever ischemic stroke or TIA, aged 18-50 years, and 90 controls matched on age and gender who all underwent MRI. Prevalence of DWI+ lesions and other markers of SVD in young stroke patients were compared to healthy controls by Fischer’s exact test.
Results
DWI-positive lesions were identified in 6 out of 337 young stroke patients (1.8%, 95% CI 0.6-3.3). No DWI+ lesions were identified among controls (0%, 95% CI 0–3.3) (P = 0.350). Patients with DWI-positive lesions had higher WMH volume (median 6.1 mL [interquartile range (IQR) 4.3-50.8] vs 0.5 mL [IQR 0.0-2.5], P < 0.001), more lacunes (2 (50.0%) vs 0, P < 0.05) and more microbleeds (3 (75.0%) vs 1 (6.3%), P < 0.05) compared to matched controls.
Conclusion
This study suggests that acute ischemia may also play a role in the etiology of SVD among young stroke patients.
Trial registration number
N/A
AS11-048
AORTIC ATHEROMA AND VASCULAR STIFFNESS – ASSESSMENT OF REGIONAL PULSE WAVE VELOCITY USING 4D FLOW MRI IN STROKE PATIENTS AND CONTROLS
1Medical Center – University of Freiburg, Department of Neurology and Clinical Neurophysiology, Freiburg, Germany
2Siemens, Siemens Healthcare UK, Frimley, United Kingdom
3Medical Center – University of Freiburg, Department of Diagnostic Radiology – Medical Physics, Freiburg, Germany
4Charité – Universitätsmedizin Berlin, Institute for Imaging Science and Computational Modelling in Cardiovascular Medicine, Berlin, Germany
Background and Aims
Increased vascular stiffness is regarded as a surrogate of microvascular damage and associated with a higher risk of cardiovascular events including stroke. Our purpose was to test whether increased regional aortic stiffness measured using pulse-wave velocity (PWV) is associated with presence of aortic plaques in cryptogenic stroke patients and controls.
Method
100 patients (40 acute stroke and 60 ophthalmic patients matched for age, sex, and presence of hypertension) underwent a new 3D multicontrast MRI protocol for characterization of aortic plaques (T1w bright blood, T2w and PDw black blood) and 4D flow MRI. The aorta was scrutinized for plaques which were graded according to the American Heart Association classification. Individual PWV was calculated from 4D flow MRI data using the time-to-foot of the pulse waveform in the proximal thoracic aorta (i.e. ascending aorta and aortic arch) and in the distal aorta (i.e. descending aorta behind the outlet of the left subclavian artery).
Results
Aortic atherosclerosis was found in 23(57.5%) stroke patients and 33(55.0%) controls (p = 0.81). 22(55.0%) stroke patients and 10(16.7%) controls had plaques ≥4mm (p < 0.001). Plaque presence was associated with increased PWV in the respective segment [F(2,90) = 13.29, p < 0.001] which resulted in overall higher PWV in stroke patients as compared to controls (6.55 ± 1.76m/s vs. 5.44 ± 1.12m/s; p < 0.001) and in the distal aorta where plaque prevalence was higher as compared to the proximal aorta (6.53 ± 1.93m/s vs. 5.54 ± 1.51m/s; p < 0.001).
Conclusion
Aortic stiffness was significantly higher in cryptogenic stroke patients compared to matched ophthalmic controls, which is most likely due to more advanced aortic atherosclerosis.
Trial registration number
Clinical-Trial-Registration-URL: https://drks-neu.uniklinik-freiburg.de/drks_web/setLocale_EN.do; Unique identifier:DRKS00006234
Scientific Communications- Reperfusion 3
AS07-077
INTRACRANIAL HEMORRHAGE AFTER ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE: PREDICTORS AND OUTCOME IN THE NORDICTUS REGISTRY
1H.U.Donostia, Neurology, San Sebastian, Spain
2H. U. Valdecilla, Santander, Spain
3H.U. Valladolid, Valladolid, Spain
4H.U. Oviedo, Oviedo, Spain
5H.U. Alava, Neurology Department, Vitoria, Spain
6CHUSantiago, Neurology Department, Santiago, Spain
7H.Galdakao, Galdakao, Spain
8H.U.Burgos, Neurology, Burgos, Spain
9H.U. Miguel Servet, Neurology, Zaragoza, Spain
10H.U.Basurto, Neurology, Bilbao, Spain
11H.Leon, Neurology, Leon, Spain
12H.U. Vigo, Neurology, Vigo, Spain
13H.U. A Coruña, Neurology, A Coruña, Spain
Background and Aims
Intracranial hemorrhage (ICH) is a feared complication after endovascular therapy (EVT) for acute ischemic stroke (AIS). The aim of this study is to identify predictors and determine the clinical relevance of symptomatic and asymptomatic ICH after EVT.
Method
Retrospective analysis of the prospective multicenter reperfusion registry in NORDICTUS, a research network of stroke centers in Northern Spain serving an area of 11.5 M people. AIS patients who received EVT during 2015-2016 in 13 NORDICTUS centers were included. Univariate and multivariate analysis were conducted to identify predictors of ICH and the impact on the clinical outcome of asymptomatic and symptomatic ICH.
Results
The study included 831 patients (mean age 70 years, median NIHSS score16, anterior circulation 86%); 238 (29%) suffered any form of ICH (Hemorrhagic infarction HI = 104, parenchymal hematoma PH = 124) and 71 (8%) were symptomatic. Independent predictors of ICH included anterior circulation occlusion (OR 4.2 (1.6-10.6) p = 0.003), combined stent retriever and aspiration thrombectomy (OR 1.70 (1.08-2.67) p = 0.021), longer time to treatment (OR 1.076 (1.002-1.16), p = 0.044) and lower ASPECTS score on basal CT (OR 1.13 (1.001-1.279), p = 0.047). Globally, ICH predicted poor functional outcome (OR 3.2 (2.2-4.7), p < 0.001), and so did symptomatic ICH (OR 14.7 (6.0-35.7), p < 0.001) and also asymptomatic ICH (OR 2.13 (1.4-3.2) p < 0.001). Regarding radiological classification, only PH predicted poor functional outcome (OR 5.51 (3.22-9.42), p < 0.001).
Conclusion
Both symptomatic and also asymptomatic ICH predict long-term poor functional outcome in AIS patients treated with EVT. Predictors of ICH should be considered on risk assessment for AIS endovascular therapy
Trial registration number
N/A
AS06-071
IS GENERAL ANESTHESIA ASSOCIATED WITH WORSE OUTCOMES AFTER ENDOVASCULAR THERAPY IN ANY SUBGROUP OF STROKE PATIENTS? THE NORDICTUS REGISTRY
1Hospital Clínico Universitario de Valladolid, Stroke Unit. Neurology Department, Valladolid, Spain
2Hospital Clínico Universitario de Valladolid, Neuroradiology. Radiology Department, Valladolid, Spain
3Hospital Universitario Marqués de Valdecilla, Stroke Unit. Neurology Department, Santander, Spain
4Hospital Universitario Donostia, Stroke Unit. Neurology Department, San Sebastián, Spain
5Hospital Universitario Central de Asturias, Stroke Unit. Neurology Department, Oviedo, Spain
6Hospital Universitario de Áraba y Vitoria, Stroke Unit. Neurology Department, Vitoria, Spain
7Complejo Hospitalario Universitario de Santiago de Compostela, Stroke Unit. Neurology Department, Santiago de Compostela, Spain
8Hospital de Galdakao, Stroke Unit. Neurology Department, Galdakao. Bizkaia, Spain
9Hospital Universitario de Burgos, Stroke Unit. Neurology Department, Burgos, Spain
10Hospital Universitario Miguel Servet, Stroke Unit. Neurology Department, Zaragoza, Spain
11Hospital de Basurto, Stroke Unit. Neurology Department, Bilbao, Spain
12Hospital Universitario de León, Stroke Unit. Neurology Department, León, Spain
13Complejo Hospitalario Universitario de Vigo, Stroke Unit. Neurology Department, Vigo, Spain
14Complejo Hospitalario Universitario de A Coruña, Stoke Unit. Neurology Department, A Coruña, Spain
Background and Aims
We tested the hypothesis that general anesthesia would be associated with differences in outcome after endovascular therapy (EVT) for acute ischemic stroke (AIS) in the following patient subgroups: older age, more severe strokes, and distal vs. proximal arterial occlusions.
Method
Retrospective analysis of the prospective multicenter reperfusion registry in NORDICTUS, a research network of stroke centers in Northern Spain serving an area of 11.5 M people. AIS patients who received EVT during 2015-2016 in 13 NORDICTUS centers were included. The use of general anesthesia (GA) during EVT was registered. Poor outcome was defined as a mRS> 2 at day 90. Age groups were ≤80 and >80. In anterior circulation AIS patients, M2 & M3 segments were considered distal occlusions.
Results
We included 884 AIS patients treated with EVT, with a mean age of 72, 448 (51%) women, median baseline NIHSS 16. EVT was performed under GA in 535 (61%) patients. The use of GA was associated with higher baseline NIHSS (p = 0.004), shorter groin-to-reperfusion times (p = 0.03) and more frequent use of thromboaspiration (p < 0.001). Multivariable-adjusted regression models identified interaction terms GA-NIHSS (OR 1.03, [1.01-1.05], p < 0.001) and GA-age>80 (OR 4.3, [1.2-9.6], p < 0.001) as predictors of poor outcome after EVT. No significant interaction was found for distal occlusions.
Conclusion
NGeneral anesthesia may be associated with worse outcomes after EVT in AIS patients with advanced age (>80) and more severe strokes. These observations need to be confirmed in prospective & randomized studies.
Trial registration number
N/A
AS07-015
SAFETY AND OUTCOME OF ENDOVASCULAR TREATMENT IN PRE-STROKE FUNCTIONALLY DEPENDENT PATIENTS: RESULTS FROM THE MR CLEAN REGISTRY
1Maastricht University Medical Center+, Neurology, Maastricht, The Netherlands
2Haaglanden Medical Center, Neurology, The Hague, The Netherlands
3Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
4Erasmus MC University Medical Center, Radiology, Rotterdam, The Netherlands
5Erasmus MC University Medical Center, Public Health, Rotterdam, The Netherlands
6Academic Medical Center, Neurology, Amsterdam, The Netherlands
7Academic Medical Center, Radiology, Amsterdam, The Netherlands
8Sint Antonius Hospital, Radiology, Nieuwegein, The Netherlands
9Leiden University Medical Center, Neurology, Leiden, The Netherlands
10Haaglanden Medical Center, Radiology, The Hague, The Netherlands
Background and Aims
Pre-stroke dependence is an exclusion criterion in most trials of endovascular treatment (EVT) for acute ischemic stroke. Little data have been reported on outcomes after EVT in these patients. We compared outcome and safety of EVT pre-stroke dependent and independent patients.
Method
We report patients with an anterior circulation occlusion who were included between March 2014 and June 2016 in the MR CLEAN Registry, a prospective, multicenter, observational study for stroke intervention centers in the Netherlands. Pre-stroke dependence was defined as modified Rankin Scale (mRS) score 3–5 before onset of current stroke. Primary outcome was the mRS score at 90 days. Favorable outcome was defined as mRS 0–2 or not worsening of the mRS score. Secondary outcomes included NIHSS score post intervention, reperfusion grade, and safety outcomes. Logistic regression analyses (adjusted for age, baseline NIHSS score, collaterals, time to EVT, and intravenous thrombolysis prior to EVT) were used to assess the association between pre-stroke dependence and outcomes.
Results
1441 patients were included in the present study, of whom 157 (11%) were pre-stroke dependent. Favorable outcome was seen in 27% pre-stroke dependent patients, compared to 42% pre-stroke independent patients. Pre-stroke dependence was associated with less favorable outcome (ORadjusted 0.90; 95% CI 0.58-1.39). The occurrence of symptomatic intracranial hemorrhage was similar in the groups.
Conclusion
A substantial proportion of pre-stroke dependent patients will reach pre-stroke mRS scores after EVT, and the intervention-related complication rate is comparable to pre-stroke independent patients. Therefore, pre-stroke dependent patients should not be routinely excluded from EVT.
Trial registration number
N/A
AS07-066
META-ANALYSIS ON OUTCOME DIFFERENCES AMONG PATIENTS WITH TICI2B VERSUS TICI3 REPERFUSIONS: SUCCESS REVISITED
1Inselspital- University of Bern, Neuroradiology, Bern, Switzerland
2Inselspital- University of Bern, Neurology, Bern, Switzerland
3Inselspital- University of Bern, Pediatric Neurology, Bern, Switzerland
Background and Aims
A reperfusion quality of Thrombolysis in Cerebral Infarction (TICI) ≥2b has been set as the therapeutic angiography target for interventions in acute ischaemic stroke patients. This study addresses whether the distinction between TICI2b and TICI3 reperfusion shows a clinically relevant difference on functional outcome.
Method
A systematic literature review and meta-analysis was carried out and presented in conformity with the PRISMA criteria to test the primary hypothesis that TICI2b and TICI3 reperfusion are associated with different rates of modified Rankin Scale (mRS) ≤2 at day 90. Secondary endpoints included rates of haemorrhagic transformations, mortality and excellent functional outcome (mRS≤1). Summary estimates of odds ratios (sOR) with 95% confidence intervals (95%CI) were calculated using the inverse variance heterogeneity model accounting for multiple true effect sizes.
Results
Thirteen studies on 2379 successfully reperfused patients were included (1131 TICI3, 1248 TICI2b). TICI3 reperfusions were associated with higher rates of functional independence (1.74, 95%CI 1.44-2.10) and excellent functional outcomes (2.01, 95%CI 1.60-2.53), also after including adjusted estimates. The safety profile of patients with TICI3 was superior, as demonstrated by lower rates of mortality (sOR 0.59, 95%CI 0.37-0.92) and symptomatic intracranial haemorrhages (sOR 0.42, 95%CI 0.25-0.71).
Conclusion
TICI 3 reperfusions are associated with superior outcome and better safety profiles than TICI2b reperfusions. This effect seem to be independent of time and collaterals. As reperfusion quality is the most important modifiable predictor of patients’ outcome, a more conservative definition of successful therapy and further evaluation of treatment approaches geared towards achieving TICI3 reperfusions are desirable.
Trial registration number
N/A
AS07-011
MECHANICAL THROMBECTOMY PRIOR TO ACUTE CAROTID ARTERY STENTING IN TANDEM OCCLUSIONS: ORDER OF TREATMENT HAS AN IMPACT ON CLINICAL OUTCOME
1University Medical Center Göttingen, Neuroradiology, Göttingen, Germany
2University Hospital Cologne, Radiology, Cologne, Germany
3University Medical Center Göttingen, Neuroradiology, Göttingen, Germany
4Karolinska University Hospital, Neuroradiology, Stockholm, Sweden
5National University Health System Singapore, Neurology, Singapore, Singapore
6University Hospital Heidelberg, Neuroradiology, Heidelberg, Germany
7Charite, Neuroradiology, Berlin, Germany
8University Hospital Cologne, Neurology, Cologne, Germany
9University Hospital Aachen, Neuroradiology, Aachen, Germany
Background and Aims
Endovascular treatment of acute ischemic stroke due to tandem occlusions comprises intracranial thrombecomty and acute extracranial carotid artery stenting. The impact of treatment order upon clinical outcome remains unclear in this stroke type. Accordingly, to date no standardized recommendations regarding treatment order exist.
Method
Retrospective analysis was performed of data prospectively collected in 4 international stroke centers between 2013 and 2017. One hundred sixty-five patients with anterior tandem occlusion were treated by endovascular therapy. Clinical (including demographics and NIHSS) and procedural data were evaluated. Favorable clinical outcome was defined as mRS ≤2 at 90 days. Propensity score matching was performed for the different treatment strategies.
Results
Patients’ mean age was 65 ± 11 years and 118 were male (69%). Median admission NIHSS was 15 (IQR 8). In 59% of the patients (n = 101) the antegrade strategy (first stenting, than thrombectomy) was performed, in 41% (n = 70) retrograde treatment (first thrombectomy, than stenting). Successful reperfusion (mTICI ≥2b) was achieved in 128 patients (75%). Fifty-nine patients (39%) showed a favorable clinical outcome after 90 days. After propensity score matching, data of 100 patients could be analyzed. Analysis revealed that the retrograde strategy yielded a significantly higher rate of successful reperfusion compared to the antegrade strategy (92% vs. 56%; p < 0.001). Consistently, the rate of favorable clinical outcome after 90 days (mRS ≤2) was higher (44% vs. 30%; p < 0.05) in the retrograde strategy group.
Conclusion
Mechanical thrombectomy prior to acute carotid artery stenting in tandem occlusion is a predictive factor for favorable clinical outcome.
Trial registration number
N/A
AS02-043
ENDOVASCULAR THERAPY IN THE DISTAL NEUROVASCULAR TERRITORY: RESULTS OF A LARGE PROSPECTIVE REGISTRY
1Grady Memorial Hospital- Emory University School of Medicine, Department of Neurology, Atlanta, USA
2Drexel Neurosciences Institute, Neurosurgery, Philladelphia, USA
3Wellstar Neurosurgery, Neurosurgery, Atlanta, USA
4CPMC, Neurology, San Francisco, USA
5Erlanger Medical Center, Radiology, Chattanooga, USA
6Riverside Medical Center, Radiology, Columbus, USA
7University Hospital Hradec Králové, Radiology, Prague, Czech Republic
8CHUV- Lausanne, Radiology, Lausanne, Switzerland
Background and Aims
Thrombectomy in the distal territory might be associated with higher risk to benefit profile. The purpose of this study is to evaluate the efficacy and safety of thrombectomy in patients with distal arterial occlusions (DAO).
Method
The Trevo Registry (TR) is the largest multicenter prospective endovascular registry to date including a total of 2,010 patients. We categorized the TR patients into: Proximal Arterial Occlusion (PAO): intracranial ICA, and MCA-M1, and (2) DAO: distal-MCA-M2 (occlusion distal to the posterior aspect of the insula), MCA-M3, ACA, and PCA. Baseline and outcome variables were compared. The primary efficacy endpoint: 90-day 0–2; secondary endpoint: mTICI 2b-3 reperfusion. Safety endpoints: sICH and 90-day mortality.
Results
There were 429 DAOs including 360(83.9%) distal-M2, 23(5.4%) M3,17(4%) ACA, and 29(6.8%) PCA occlusions vs 1439 PAO (332, 23.1% ICA; 1107, 76.9% MCA-M1). Baseline NIHSS was lower in DAO (median13[8-18] vs 16[12-20], p < 0.001). There were no differences in terms of age (68.2vs68.5 years), gender (female, 50.6%vs53%), IV tPA use (53%vs54%), major co-morbidities, or time from last know well to groin puncture across DAO vs PAO. No differences in post-procedure mTICI 2b-3(93% in both) or SICH (1.9%vs1.6%). The rate of 90-day mRS0-2 was higher in DAO(62.1%vs52.9%, p < 0.001). 90-day mortality was similar across groups (16.8%vs13.1%). There were no differences in terms of vessel perforation, dissection, or early neurological deterioration.
Conclusion
Endovascular therapy can be safely performed in the distal cerebrovascular bed. Future randomized trials will hopefully more precisely clarify the benefits on thrombectomy in DAO.
Trial registration number
N/A
AS06-018
INCIDENCE AND PREDICTORS OF EARLY RECANALIZATION AFTER THROMBOLYSIS IN CANDIDATES FOR THROMBECTOMY, AND DEVELOPMENT OF A CLINICAL SCORE
1Centre Hospitalier Sainte Anne- INSERM U894, Neurology, Paris, France
2Centre Hospitalier Sainte Anne, Neuroradiology, Paris, France
3Roger Salengro Hospital, Neurology, Lille, France
4Fondation Ophtalmologique A. de Rothschild, Interventional neuroradiology, Paris, France
5Gui de Chauliac Hospital, Neurology, Montpellier, France
6Hospices civils de Lyon, Stroke Unit, Lyon, France
7Tours Hospital, Neuroradiology, Tours, France
8Foch Hospital, Neurology, Suresnes, France
9Nancy Hospital, Neurology, Nancy, France
10Roger Salengro Hospital, Neuroradiology, Lille, France
11Gui de Chauliac Hospital, Neuroradiology, Montpellier, France
12Hospices civils de Lyon, Neuroradiology, Lyon, France
13Tours Hospital, Neurology, Tours, France
14Foch Hospital, Neuroradiology, Suresnes, France
15Nancy Hospital, Neuroradiology, Nancy, France
Background and Aims
Whether all acute stroke patients with large-vessel occlusion (LVO) need to undergo both intravenous thrombolysis (IVT) and mechanical thrombectomy (MT) is currently debated as i) those who enjoy post-IVT early recanalization (ER) represent futile transfers for MT, while ii) those who do not might be harmed by IVT. However, the incidence and predictors of post-IVT ER in patients referred for MT are poorly known, while an ER prediction score for clinical use is lacking.
Method
The registries of 4 MT-capable centres gathering patients referred for MT who received IVT either on site (mothership) or in a non MT-capable centre (drip-and-ship) following MR- or CT-based admission imaging between 2015 and 2017 were available. Similar registries from 4 additional MT-capable centres were used as validation cohort. ER was identified within 3hrs of IVT start on first angiographic run or on non-invasive vascular imaging.
Results
In the derivation cohort (n = 633), ER occurrence was ∼20%, and no-ER was independently predicted by long thrombi, proximal occlusion site and mothership paradigm. The derived six-point score showed strong discriminative power for no-ER, and was replicated in the validation cohort (n = 474). A similar score obviating thrombus length was also developed, again showing high discriminative power. In both, highest scores predicted no-ER with >90% specificity, while lowest scores did not reliably predicted ER.
Conclusion
The substantial ER rate found here underlines IVT-related benefits in current stroke care. Both prediction scores afforded high specificity for no-ER, but not for ER, which has strong implications for trial design and ultimately for personalized medicine.
Trial registration number
N/A
AS05-053
INFLUENCE OF THE ADMINISTRATION OF IV-RTPA ON DISTAL THROMBUS MIGRATION OR RESOLUTION IN STROKE PATIENTS UNDERGOING ENDOVASCULAR TREATMENT
1Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
2Irmandade Santa Casa de Misericordia de Sao Paulo, Radiology, Sao Paolo, Brazil
3Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, The Netherlands
4Texas Stroke Institute, Radiology, Plano- TX, USA
5Catharina Hospital, Radiology, Eindhoven, The Netherlands
6Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
7The Hague Medical Center, Neurology, The Hague, The Netherlands
8St. Antonius Hospital, Radiology, Nieuwegein, The Netherlands
9Academic Medical Center, Neurology, Amsterdam, The Netherlands
10St. Antonius Hospital, Neurology, Nieuwegein, The Netherlands
11The Hague Medical Center, Radiology, The Hague, The Netherlands
12Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
Background and Aims
In patients undergoing endovascular treatment (EVT) for stroke caused by anterior circulation large vessel occlusions (LVO), occlusion location observed on initial DSA can differ from the recent admission CTA. We assessed the frequency of distal thrombus migration or resolution, and whether intravenous administration of rtPA prior to EVT is associated with its occurrence.
Method
We report patients with LVO, included between March 2014 and June 2016 in the MR CLEAN Registry, a prospective, multicenter, observational study for stroke intervention centers in the Netherlands. Patients with intracranial ICA, M1 or M2 occlusions on baseline CTA were included. Primary A1/2 or extracranial ICA occlusions on DSA were excluded. The association of rtPA administration before EVT with distal thrombus migration or radiological resolution was assessed with binary logistic regression.
Results
Of 1275 cases included in this analysis, 977 (77%) received intravenous rtPA before EVT. Migration or resolution was observed in 313 cases (25%). Resolution occurred in 32 cases (2.5%). Migration was observed in 41%, 17% and 10% of ICA, M1 or M2 occlusions respectively. The most common migration endpoints for initial ICA, M1 and M2 occlusions were M1 (82%), M2 (79%) and M3 (65%) respectively. Migration or resolution occurred more often after rtPA administration (aOR 1.81, 95%CI 1.19-2.76).
Conclusion
Distal thrombus migration or resolution between CTA and DSA imaging occurred in 25% of patients with LVO and was associated with rtPA administration before EVT. This proportion does not account for the patients who were excluded from EVT based on dramatic clinical improvement.
Trial registration number
N/A
AS07-014
DIFFERENCES IN PROCEDURES AND OUTCOMES FOR MECHANICAL THROMBECTOMY IN ACUTE POSTERIOR VERSUS ANTERIOR CIRCULATION STROKE IN THE GERMAN REVASK REGISTRY
1Alfried Krupp Krankenhaus Essen, Department of Neurology, Essen, Germany
2University Hospital Münster, Department of Neurology, Münster, Germany
3Alfried Krupp Krankenhaus Essen, Department of Neuroradiology, Essen, Germany
4Klinikum Dortmund, Department of Neurology, Dortmund, Germany
5Ruhr University Bochum, Department of Neurology, Bochum, Germany
6St. Josef-Hospital Ruhr University Bochum, Department of Neurology, Bochum, Germany
7University of Münster, Institute of Epidemiology and Social Medicine, Münster, Germany
Background and Aims
In contrast to anterior circulation stroke (ACS), there is no evidence from randomized trials that mechanical thrombectomy (MT) with modern stent retrievers or thromboaspiration is safe and effective in posterior circulation stroke (PCS).
Method
The present analysis was based on the prospective multicenter Register on Revascularization in Ischemic Stroke Patients (REVASK) in Germany. We compared demographic data, periprocedural times and complications, recanalization rate, and functional outcome at discharge and after 3 months of 139 consecutive patients with PCS (84.9% basilar artery, 16.5% vertebral artery, 4.3% posterior cerebral artery occlusion) with 961 patients with ACS treated by MT ± intravenous thrombolysis.
Results
As compared with patients suffering ACS, patients with PCS were significantly younger (65.4 versus 69.0 years, p = 0.021) and had a lower median NIHSS score at baseline (12 versus 15, p = 0.024). Patients with PCS had a significantly longer time elapse between symptom onset and start of MT procedure. Successful recanalization (71.6% vs. 76.0%, p = 0.233) as well as number of thrombectomy passes did not differ significantly between both groups. None of the patients treated with MT for PCS experienced a symptomatic intracranial hemorrhage compared with 3.0% in ACS (p = 0.010). The median NIHSS score at discharge was 3 in PCS and 4 in ACS. Favourable functional long term outcome (mRS ≤ 2; 38.0% vs. 42.6%, p = 0.392) and mortality (33.7% vs. 30.8%, p = 0.539) did not differ significantly.
Conclusion
Our study suggests that MT in PCS has a lower risk of symptomatic intracranial hemorrhage and a similar favourable short and long term outcome as compared with ACS.
Trial registration number
N/A
Scientific Communications -Reperfusion Trials
AS05-015
A COMPARISON OF CLINICAL AND IMAGING MISMATCH RESULTS IN RANDOMISED TRIALS OF TENECTEPLASE VERSUS ALTEPLASE FOR ISCHAEMIC STROKE
1University of Newcastle, Medicine, Newcastle, Australia
2Queen Elizabeth University Hospital, Neurology, Glasgow, United Kingdom
3John Hunter Hospital, Neurology, Newcastle, Australia
4Royal Melbourne Hospital, Neurology, Melbourne, Australia
5University of Melbourne, Florey Institute of Neuroscience and Mental Health, Melbourne, Australia
Background and Aims
We sought to compare clinical and imaging mismatch treatment selection criteria in a pooled cohort from randomised trials of intravenous tenecteplase vs alteplase where CTP was performed prior to treatment.
Method
Patients baseline clinical and imaging scores were used to categorise patients as meeting either the DAWN mismatch (baseline NIHSS =>10, and age cut offs for ischemic core volume) or DEFUSE 2 mismatch criteria (mismatch volume >15mL, mismatch ratio >1.8 and ischemic core <70mL). We then investigated if tenecteplase treated patients had a favourable odds ratio on the modified Rankin scale (mRS) compared to those treated with alteplase for clinical and imaging mismatch classifications respectively.
Results
From 146 pooled patients, 71 received alteplase and 75 received tenecteplase. The overall pooled group did not show improved patient outcomes when treated with tenecteplase (mRS 0–1 OR 1.77, 95% CI 0.89-3.51, p = 0.102) compared with alteplase therapy. A total of 39 patients met both the clinical and imaging mismatch criteria, 25 patients met the only the imaging criteria, 36 met only the clinical mismatch criteria and finally 46 did not meet either of the imaging or mismatch criteria. Patients treated with tenecteplase had more favourable outcomes when they met the imaging mismatch (mRS 0–1, OR 2.33, 95% CI 1.13-5.94, p = 0.032) or the clinical mismatch criteria (mRS 0–1, OR 2.15, 95% CI 1.1428.732, p = 0.027).
Conclusion
Both selection criteria identified patients more likely to benefit from the improved reperfusion from tenecteplase, but there were considerable differences in patient classification between clinical and imaging mismatch.
Trial registration number
N/A
AS06-013
FIRST-LINE CONTACT ASPIRATION VERSUS STENT RETRIEVER THROMBECTOMY IN ISCHAEMIC STROKE PATIENTS WITH LARGE VESSEL OCCLUSION: SYSTEMATIC REVIEW AND META-ANALYSIS
1Normandie UNICAEN University - Inserm U1237, Department of Neurology, Caen, France
2University Versailles Saint-Quentin en Yvelines - Foch Hospital, Department of Neurology, Suresnes, France
3Hospices Civils de Lyon, Department of Interventional Neuroradiology, Lyon, France
4Rothschild Foundation, Department of Interventional Neuroradiology, Paris, France
5CHRU Nancy, Department of Diagnostic and Interventional Neuroradiology, Nancy, France
Background and Aims
First-line contact aspiration is reported to achieve high reperfusion rates at a lower cost than stent retriever thrombectomy for acute ischaemic stroke due to large vessel occlusion. However, whether the former is as efficient and safe as stent retrievers remains uncertain. We aimed to compare efficacy and safety of first-line contact aspiration and stent retriever thrombectomy in acute ischaemic stroke patients.
Method
We undertook a systematic review and meta-analysis of studies of patients with proximal anterior circulation occlusion who were intra-arterially treated within 6 hours of stroke onset, with the latest devices of contact aspiration or stent retrievers. Differential effects in the rates of final successful reperfusion (modified Thrombolysis in Cerebral Infarction [mTICI] ≥2b), periprocedural complications and functional outcomes at 90 days between the two strategies were determined using meta-regression random effect meta-analyses. Reperfusion was assessed with the mTICI score, ranging from 0 (no reperfusion) to 3 (complete reperfusion) and functional outcomes with the modified Rankin Scale, ranging from 0 (no symptoms) to 6 (death).
Results
Fifteen studies (1919 patients) were included. Final successful reperfusion was higher with contact aspiration (87.9%, 95% Confidence Interval [CI] 83.7-90.5) than stent retriever thrombectomy (73.7%, 95%CI 67.8-78.8, Pint<0.001). Periprocedural complications, favorable clinical outcome (modified Rankin Score 0–2) and death at 90 days did not significantly differ between the two techniques.
Conclusion
Although final successful reperfusion occurs more frequently after first-line contact aspiration than after stent retriever use, the two strategies are associated with comparable clinical outcomes in acute stroke patients with large vessel occlusion.
Trial registration number
N/A
AS02-005
MODIFIED TICI2C/TICI 3 REPERFUSION SHOULD BE THE AIM OF MECHANICAL THROMBECTOMY: INSIGHTS FROM THE ASTER TRIAL
1Montpellier University Hospital CHRU34, Neuroradiology, Montpellier, France
2Rothschild Foundation, Interventional Neuroradiology, Paris, France
3Lille Universitary Hospital, EA 2694–Santé Publique: Epidémiologie et Qualité des Soins, Lille, France
4Foch Hospital, Neurology, Suresnes, France
Background and Aims
Studies have shown that mTICI 2B patients had poorer functional outcomes than TICI 3 patients. An mTICI 2C category has been recently introduced for patients with near-complete perfusion after MT. Aim of this study was to evaluate the difference in functional outcome between patients achieving successful reperfusion (ie mTICI 2B, mTICI 2C and TICI 3 scores).
Method
Ancillary study from the ASTER prospective multicenter blinded-endpoint trial. Reperfusion results are reported as the mTICI score, including the mTICI 2C grade. Primary outcome was the percentage of patients with favorable outcome defined as a 90-day mRS score of 0–2.
Results
290 patients with successful reperfusion, harboring ischemic stroke secondary to occlusion of the anterior circulation within 6 hours of onset of symptoms, undergoing MT were included.
Favorable outcome did not differ significantly between the 3 reperfusion grades, with a similar positive effect of 2C (OR, 1.71, 95%CI, 0.98 to 3.00) and 3 (OR, 1.73; 95%CI, 0.88 to 3.41) grades compared to 2B grade. After combining grades 2C and 3, patients had a significantly higher rate of favorable outcome than patients with 2B (OR, 1.72; 95%CI, 1.01 to 2.90; p = 0.043). Favorable outcome rate decreased with increasing onset to reperfusion time (ORT), with no significant interaction between mTICI 2C/3 grade and ORT on favorable outcome.
Conclusion
Combining mTICI 2C and TICI 3 grades helps to determine a subgroup of patients who achieve better functional outcomes than mTICI 2B patients. Achieving mTICI 2C/3 reperfusion rather than mTICI 2B should be the new aim of MT for anterior circulation LVO.
Trial registration number
N/A
AS02-016
REPERFUSION WITH ADAPT TECHNIQUE USING ACE68 AND ACE64 IS SAFE AND EFFECTIVE IN LARGE VESSEL OCCLUSIONS OF THE ANTERIOR CIRCULATION – PROMISE STUDY RESULTS
1Universitätsklinikum Hamburg-Eppendorf- Hamburg- Germany, Department of Neuroradiology, Hamburg, Germany
2Universitätsklinikum Schleswig-Holstein, Department of Neuroradiology, Lübeck, Germany
3Hospital Universitario Donostia- San Sebastian, Department of Neuroradiology, Guipúzcoa, Spain
4A.O.U. Policlinico, Department of Neuroradiology, Messina, Italy
5Hospital Clínico Universitario Virgen de la Arrixaca, Department of Neuroradiology, Murcia, Spain
6Vall d'Hebron Hospital, Department of Neuroradiology, Barcelona, Spain
7Universitätsklinikum Knappschaftskrankenhaus Bochum, Department of Neuroradiology, Bochum, Germany
8Centre Hospitalier Universitaire Vaudoi, Department of Neuroradiology, Lausanne, Switzerland
9University of Toronto- Toronto Western Hospital, Department of Neuroradiology, Toronto, Canada
10Hôpital Maison Blanche, Department of Neuroradiology, Reims, France
11nselspital- Universitätsinstitut für Diagnostische und Interventionelle Neuroradiologie, Department of Neuroradiology, Bern, Switzerland
12IRCCS Centro Neurolesi Bonino Pulejo - Piemonte Hospital, Department of Neuroradiology, Messina, Italy
13University Medical Center Utrecht, Department of Neuroradiology, Utrecht, Netherlands Antilles
Background and Aims
PROMISE study aimed to observe safety and effectiveness of Penumbra System (PS) Reperfusion Catheters (ACE68/64) in patients with acute ischemic stroke (AIS) from large vessel occlusion (LVO), treated with ADAPT (A Direct Aspiration First Pass Technique) as frontline treatment.
Method
This was a prospective, single-arm, multi-center study across 20 European centers. Inclusion criteria were anterior circulation LVO ≤ 6 hours from ictus onset; NIHSS ≥ 2; CT-ASPECTS ≥ 6 or MR-ASPECTS ≥ 5. Primary endpoints included revascularization success (mTICI 2b-3), and day-90 clinical independence (mRS 0–2). Secondary endpoints included safety events, functional improvement at 7–10 days, procedural metrics and quality of life. Primary and secondary endpoints were adjudicated by core laboratory and clinical events committee.
Results
A total of 204 patients were enrolled. Median age was 74 [IQR 65-80] and median baseline NIHSS was 16 [IQR 11-20]. Median baseline CT ASPECT score was 9 [IQR 8–10]. Prior to procedure, IV rtPA was administered in 61.8% (126/204). Median time to achieve mTICI 2b-3 was 31 minutes [IQR 20-53]. Final revascularization (mTICI 2b-3) was achieved in 93.1% (190/204). Day-90 mRS 0–2 was achieved in 61.0% (122/200). Reduction of ≥10 points or 7–10 day NIHSS 0–1 was achieved in 67.9% (127/187). The safety rates were favorable (sICH = 2.9% and ENT = 1.5%). All cause-mortality observed in 7.5% (15/200). No deaths were device-related.
Conclusion
PROMISE study demonstrated safety and efficacy with latest generation of PS Reperfusion Catheters (ACE68/64) in patients with AIS from LVO, using ADAPT as frontline treatment.
Trial registration number
N/A
AS02-023
SAFETY OF THROMBOLYSIS WITH TENECTEPLASE IN STROKE MIMICS – RESULTS FROM THE NORWEGIAN TENECTEPLASE STROKE TRIAL (NOR-TEST)
1Haukeland University Hospital, Neurology, Bergen, Norway
Background and Aims
Stroke mimics (SMs) are regularly treated with thrombolysis in clinical practice and thrombolytic trials. Although alteplase in SMs appears to be safe, safety of tenecteplase in SMs has not been assessed in an ischemic stroke study setting. We aimed to assess safety of SMs treated with tenecteplase in the Norwegian Tenecteplase Stroke Trial (NOR-TEST). We also aimed to identify predictors of SMs as compared to patients with acute cerebral ischemia (ACI).
Method
NOR-TEST was a phase-3 trial investigating safety and efficacy of tenecteplase vs. alteplase in patients with suspected ACI. Two groups were defined based on diagnose at discharge: patients with a different diagnose than ischemic stroke or TIA (SMs group) and patients diagnosed with ischemic stroke or TIA (ACI group). Logistic regression analyses were performed with SMs vs. ACI as dependent variable to identify predictors of SMs.
Results
Of 1091 randomized patients, 181 (16.6%) were SMs of which 96 received tenecteplase. There was no symptomatic ICH in the SMs group. Rates of asymptomatic ICH and mortality were lower in SMs as compared to the ACI group. There were no differences in adverse events between SMs receiving tenecteplase vs. alteplase. SMs were independently associated with age ≤60 years, female sex, no history of myocardial infarction, systolic BP ≤150 mm Hg, NIHSS ≤6 points, sensory loss and no facial paresis on admission.
Conclusion
Thrombolysis with tenecteplase seems to be safe in SMs. Predictors were identified for SMs which may contribute to differentiate SMs from ACI in future stroke trials.
Trial registration number
NOR-TEST was registered with EudraCT No 2011-005793-33 and in ClinicalTrials.gov (NCT01949948).
AS02-010
INTRAVENOUS THROMBOLYSIS IN ACUTE CENTRAL RETINAL ARTERY OCCLUSION – A PROSPECTIVE INTERVENTIONAL CASE SERIES
1University Hospital Tuebingen, Neurology & Stroke, Tuebingen, Germany
2University Medical Center Hamburg-Eppendorf, Ophthalmology, Hamburg, Germany
3University Medical Center Goettingen, Ophthalmology, Goettingen, Germany
4University of Oxford, Experimental Psychology, Oxford, United Kingdom
5University Hospital Heidelberg, Coordination Center for Clinical Trials, Heidelberg, Germany
6University Hospital Heidelberg, Neurology, Heidelberg, Germany
7University of Tuebingen, University Eye Hospital Tuebingen, Tuebingen, Germany
Background and Aims
No evidence-based therapy exists for non-arteritic central retinal artery occlusion (NA-CRAO). Retinal ischemic tolerance is low; according to preclinical experiments, irreversible damage occurs within four hours of NA-CRAO. In previous randomized trials evaluating intra-arterial or intravenous thrombolysis (IVT) in NA-CRAO, only one patient was treated this early. In December 2013, we decided to treat patients using IVT within 4.5 hours of NA-CRAO, the therapeutic window established for ischemic stroke.
Method
Consecutive NA-CRAO patients with severe visual loss and no known contraindications received IVT. Follow-up was conducted at day 5 and day 30. Visual outcomes were compared to the conservative standard treatment (CST) arm of the European Assessment Group for Lysis in the Eye (EAGLE) study.
Results
Until August 2016, 20 patients received IVT within 4.5 hours after NA-CRAO with a mean onset-to-treatment time of 184 ± 62 minutes (standard deviation). Visual acuity improved from baseline mean logarithm of the minimum angle of resolution 2.46 ± 0.33 to 1.52 ± 1.09 at day 5 (p = 0.002) and 1.60 ± 1.08 at day 30. Compared to the EAGLE CST-arm, functional recovery to reading ability occurred more frequently after IVT: 6/20 (30%) versus 1/39 (3%) at day 5 (p = 0.005) and at day 30 5/20 (25%) versus 2/37 (5%) (p = 0.045). Two patients experienced serious adverse events (one angioedema and one bleeding from an abdominal aortic aneurysm) but recovered without sequelae.
Conclusion
IVT within 4.5 hours after symptom onset may represent an effective treatment of NA-CRAO. Randomized trials are warranted to evaluate efficacy and safety of early IVT in acute NA-CRAO.
Trial registration number
N/A
AS16-120
IMPROVING SELECTION OF PATIENTS FOR ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE: EXTERNAL VALIDATION OF A CLINICAL DECISION TOOL IN DATA FROM THE HERMES COLLABORATION
1Erasmus MC University Medical Center, Public Health, Rotterdam, The Netherlands
2Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Radiology & Nuclear Medicine, Rotterdam, The Netherlands
4Altair Biostatistics, Biostatistics, St Louis Park, USA
5Academic Medical Center, Radiology, Amsterdam, The Netherlands
6Hotchkiss Brain Institute- Cummings School of Medicine- University of Calgary, Clinical Neuroscience and Radiology, Calgary, Canada
7University of Glasgow- Queen Elizabeth University Hospital, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
8Hospital Germans Trias y Pujol, Neuroscience, Barcelona, Spain
9Royal Melbourne Hospital- University of Melbourne, Radiology, Melbourne, Australia
10University of Lorraine and University Hospital, Diagnostic and Interventional Neuroradiology, Nancy, France
11Newcastle University, Institute of Neuroscience, Newcastle upon Tyne, United Kingdom
12Melbourne Brain Centre- Royal Melbourne Hospital- University of Melbourne, Medicine & Neurology, Melbourne, Australia
13University of Lorraine and University Hospital, Clinical Epidemiology- Inserm, Nancy, France
14David Geffen School of Medicine- University of Los Angeles, Neurology and Comprehensive Stroke Center, Los Angeles, USA
15University of Pittsburgh Medical Center Stroke Institute- Presbyterian University Hospital, Neurology, Pittsburgh, USA
Background and Aims
Benefit of endovascular treatment (EVT) varies between individual patients with acute ischemic stroke. The MR PREDICTS decision tool, previously developed in the MR CLEAN trial, predicts outcome with and without EVT based on baseline patient characteristics. We externally validated this model with data from recent EVT trials.
Method
Individual patient data was derived from the six other randomized controlled trials within the HERMES collaboration (ESCAPE, REVASCAT, SWIFT-PRIME, EXTEND-IA, THRACE and PISTE). Outcome of the ordinal logistic regression model was the modified Rankin Scale (mRS) at 90 days after stroke. Discriminative performance was measured with the c-statistic, which ranges from 0.5 to 1.0. Model coefficients were updated after calibration.
Results
We included 1243 patients (633 assigned to EVT, 610 assigned to control). The observed probability of functional independence (mRS 0–2) was higher than predicted for treated patients (35% vs 26%) and controls (54% vs 40%), but the observed treatment benefit was comparable. The c-statistic was 0.67 (95%CI 0.65-0.69) for the ordinal mRS and 0.73 (95%CI 0.70-0.76) for functional independence , similar to previous performance. Figure 1 shows a screenshot of the decision tool for use in clinical practice.
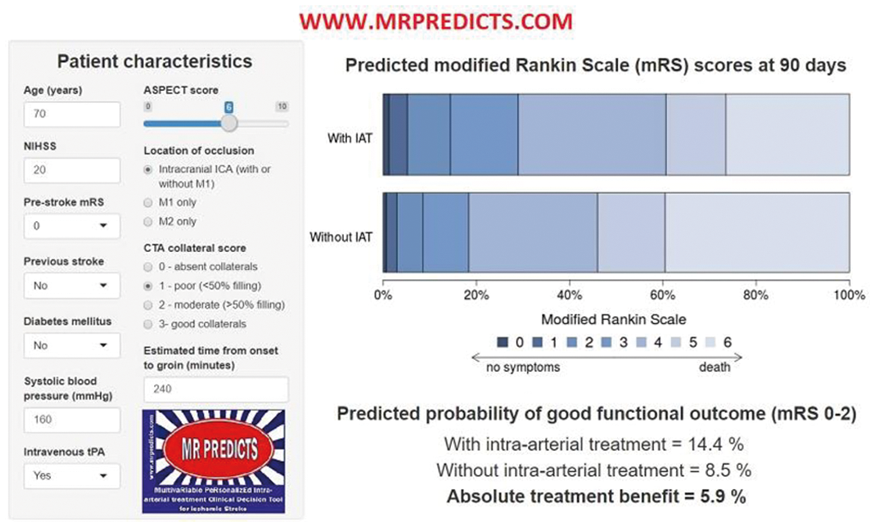
Conclusion
MR PREDICTS predicted outcome in a large heterogeneous trial population with discriminative value comparable to other well-known prediction tools. The updated model might be used to support clinical judgment in selection of patients for EVT.
Trial registration number
N/A
AS02-022
DS-1040 ASSENT STUDY: A SINGLE ASCENDING-DOSE SAFETY STUDY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Daiichi Sankyo- Inc., Clinical Development- Cardiovascular and Metabolism Therapeutic Area, Basking Ridge, USA
2Daiichi Sankyo- Inc, Clinical Operations, Basking Ridge, USA
3Daiichi Sankyo- Inc., Biostatistics and Data Management, Basking Ridge, USA
4Daiichi Sankyo UK Ltd., Clinical Safety & Pharmacovigilance, Gerrards Cross, United Kingdom
5Daiichi Sankyo- Inc., Clinical Supply Operations, Basking Ridge, USA
6Daiichi Sankyo- Inc., CMC Management and Operations, Basking Ridge, USA
7Daiichi Sankyo- Inc., Regulatory Affairs, Basking Ridge, USA
8Daiichi Sankyo- Inc., Quantitative Clinical Pharmacology and Translational Sciences, Basking Ridge, USA
9Daiichi Sankyo- Inc., Quantitative Clinical Pharmacology & Translational Sciences, Basking Ridge, USA
10Daiichi Sankyo- Inc., Clinical Biomarkers- Translational Medicine and Clinical Pharmacology, Basking Ridge, USA
Background and Aims
DS-1040 inhibits enzymatic activity of thrombin-activatable fibrinolysis inhibitor (TAFI) and enhances endogenous tissue plasminogen activator (tPA)-triggered fibrinolysis. Intravenous (IV) DS-1040 is being developed for the treatment of acute ischemic stroke (AIS). Here we describe the design and initial safety results of a randomized, placebo-controlled, single-blinded, ascending-dose multicenter study (ASSENT; NCT02586233) conducted to assess the safety of IV DS-1040 in patients with AIS.
Method
The study is currently enrolling adult patients diagnosed with AIS who presented with stroke symptoms within 4.5–12 hours of stroke onset; have National Institutes of Health Stroke Scale ≥2; Alberta Stroke Program Early CT Score >6; and have not been treated with, or are ineligible for, recombinant tPA or intra-arterial thrombectomy. Patients are randomized 3:1 to receive ascending doses of DS-1040 (0.6 to 9.6 mg), given as 0.5-hour loading dose infusion (25% of total dose) followed by a continuous 5.5-hour maintenance dose infusion (75% of total dose), or placebo. Brain hemorrhage events and recanalization of any occluded cerebral vessels are centrally adjudicated by blinded independent reviewers. Symptomatic intracranial hemorrhage (ICH) and non-ICH major bleeding are the key stopping criteria for dose escalation.
Results
Fifty-six patients have received placebo or DS-1040 in 4 sequential dose cohorts: 0.6 mg (n = 9), 1.2 mg (n = 8), 2.4 mg (n = 16), and 4.8 mg (n = 23); 55 patients completed treatment and 1 discontinued due to an adverse event. Overall, study treatment is well tolerated with no symptomatic ICH reported to date.
Conclusion
Preliminary safety results for the first 4 cohorts will be presented.
Trial registration number
NCT02586233
Scientific Communications- Reperfusion 4
AS07-061
SAFETY AND EFFICACY OF ROUTINE ENDOVASCULAR THROMBECTOMY IN ACUTE OCCLUSIVE STROKE RECORDED IN THE SITS INTERNATIONAL THROMBECTOMY REGISTER - AN OBSERVATIONAL STUDY
1Karolinska Institutet and Karolinska University Hospital, Department of Clinical Neuroscience and Department of Neurology, Stockholm, Sweden
2Centro Hospitalar Lisboa Central- Lisbon, Stroke Unit, Lisbon, Portugal
3Azienda Ospedaliera Universitaria Senese- Policlinico “Santa Maria alle Scotte”- Siena, Stroke Unit- Department of Neurological and Sensorineural Sciences, Siena, Italy
4Hospital Clínico San Carlos. Madrid, Stroke Unit. Departmento of Neurology., Madrid, Spain
5Modena University Hospital- Modena- Italy, Stroke Unit- Department of Clinical Neuroscience, Modena, Italy
6University of Modena and Reggio Emilia/AOU Modena- Modena- Italy, Department of Clinical Neuroscience, Modena, Italy
7North Estonia Medical Centre, Department of Neurology, Tallinn, Estonia
8Regional hospital Liberec- Liberec, Neurocentre, Liberec, Czech Republic
9Helsinki University Central Hospital, Department of Neurology, Helsinki, Finland
10Hospital Universitari Germans Trias i Pujol Titular de Neurologia- Universitat Autònoma de Barcelona, Departament de Neurociències, Barcelona, Spain
11Institute of Cardiovascular and Medical Sciences- University of Glasgow, Cardiovascular and Medical Sciences, Glasgow, United Kingdom
12Hospital Policlinico Umberto I ‘Sapienza’ University Viale del Policlinico- Rome- Italy, Dept. of Neurology and Psychiatry, Rome, Italy
13St. Anne’s University Hospital in Brno- Brno- Czech Republic, International Clinical Research Centre- Neurology Department-, Brno, Czech Republic
14Karolinska University Hospital and Karolinska Institutet- Stockholm, Department of Neuroradiology and Department of Clinical Neuroscience, Stockholm, Sweden
Background and Aims
Endovascular thrombectomy (EVT) significantly improved functional outcomes among patients with anterior circulation acute ischemic stroke (ACIS) due to large artery occlusions (LAO) over medical therapy. We aimed to evaluate the safety and efficacy of EVT in ACIS recorded in the SITS International Thrombectomy Register (TBYR) and compared to patients in the EVT arms of pooled randomized controlled trials (RCTs).
Method
We identified centres recording >=10 consecutive patients in the SITS-TBYR with at least 70% of available modified Rankin Scale (mRS) at 3-month during 2014 to 2017. We analysed LAO as intracranial ICA, M1, M2, A1, A2 treated with thrombectomy with or without prior IVT given within 4.5 hours of stroke onset. Primary efficacy outcome was functional independence (mRS score 0–2) at 3 months and safety outcomes were symptomatic intracranial haemorrhage (SICH) per modified SITS-MOST (any haemorrhagic transformation on 22-36h imaging scans and worsening of >=4p on NIHSS within 24h) and death within 3 months.
Results
In total, 2780 (89% with available 3-month outcomes) patients from 24 centres were treated with thrombectomy: 1751 (63%) with prior IVT, 1029 (37%) without. Median age was 72 (61-80), vs. 68 (57-77) years; baseline NIHSS score was 17 (12-21) vs. 17 (14-20) in SITS-EVT vs. RCTs. Functional independence at 3 months was 45,9% (95% CI: 43.9-47.9), vs. 46.0% (42.0-50.0) and death 18,2% (16.7-19.7) vs. 15.3% (12.7-18.4), SICH 4.8% (4.1-5.7) vs. 4.4% (3.0-6.4) in SITS-EVT vs. RCTs.
Conclusion
Our results demonstrated that thrombectomy is safe and effective in routine clinical use in ACIS with LAO
Trial registration number
N/A
AS06-064
SAFETY AND EFFICACY OF DISTAL ASPIRATION FOR ENDOVASCULAR TREATMENT OF ANTERIOR ACUTE ISCHEMIC STROKE
1University Hospital Virgen del Rocío, Department of Neurology, Sevilla Spain, Spain
2University Hospital Virgen del Rocío, Department of Radiology, Sevilla Spain, Spain
3Health Unit- Health Management Area South of Seville, Health Unit- Health Management Area South of Seville, Seville, Spain
4Hospital Universitario Virgen Macarena, Department of Neurology, Seville, Spain
Background and Aims
SOFIA® catheter was developed as a single lumen flexible catheter, but its suitability for mechanical thrombectomy had not been properly evaluated. The aim of this study is to describe preliminary results of its use in a thrombectomy reference center.
Method
A prospective descriptive study was made during 2017 including stroke patients with acute occlusion in anterior circulation treated using Sofia® catheter as first choice. Primary outcome was Thrombolysis in Cerebral Infarction (TICI) 2b/3 revascularization rate, number of required passes and time from puncture to recanalization. Secondary outcomes included complication rates and discharge NIHSS scores and mRS at discharge and 3 months.
Results
170 patients (58.2% men, mean age of 69 yo) were treated with SOFIA® catheter. Average NIHSS at arrival was 15.7 ± 6.6. Intravenous fibrinolysis was used in 57.1% of patients. Vessel occlusion involved M1 (48.5%), TICA (13.8%), M2 (14.3%) and tandem occlusion (23.8%). Thrombus aspiration using SOFIA ® catheter was successful (TICI2b/3) in 80.6% cases. With additional use of stent retrievers (Solumbra technique) recanalization rate was 92.9%. Median procedure time was 30 min (IQR 15-55). The number of passes was 2 (IQR 1–3). No catheter-related complications such as dissections were observed. Symptomatic hemorrhage was 7.9%. Median NIHSS at discharge was 3 (1–12). Discharge and 3 months mRs 0–2 was achieved in 49.8% and 61.8% respectively. After 3 months, mortality rate was 16.2%.
Conclusion
Mechanical and aspiration thrombectomy with SOFIA® is safe and effective. Thrombus aspiration using the SOFIA® Plus catheter results in high revascularization rates in a very short procedure time.
Trial registration number
N/A
AS06-061
MECHANICAL THROMBECTOMY VERSUS COMBINED THERAPY WITH THROMBOLYSIS IN ACUTE ISCHEMIC STROKE: OUTCOME DATA FROM THE NORDICTUS REGISTRY
1INIBIC/CHUAC, Department of Neurology, A Coruña, Spain
2Hospital Marqués de Valdecilla, Department of Neurology, Santander, Spain
3Hospital Clinico Universitario Valladolid, Department of Neurology, Valladolid, Spain
4Hospital de Donostia, Department of Neurology, Donostia, Spain
5Hospital Central de Asturias, Department of Neurology, Oviedo, Spain
6Hospital de Vitoria, Department of Neurology, Vitoria, Spain
7Complejo Hospitalario Universitario Santiago de Compostela, Department of Neurology, Santiago de Compostela, Spain
8Hospital de Galdakao, Department of Neurology, Bizkaia, Spain
9Hospital Universitario de Burgos, Department of Neurology, Burgos, Spain
10Hospital Universitario Miguel Servet, Department of Neurology, Zaragoza, Spain
11Hospital de Basurto, Department of Neurology, Bilbao, Spain
12Hospital de León, Department of Neurology, León, Spain
13Complejo Hospitalario Universitario Vigo, Complejo Hospitalario Universitario Vigo, Vigo, Spain
14Hospital Clínico Universitario Valladolid, Department of Neurology, Valladolid, Spain
Background and Aims
Whether the administration of prior thrombolysis provides additional benefit to patients undergoing mechanical thrombectomy (MT) is still a matter of controversy. We wanted to compare efficacy and safety outcomes in a multicenter series of patients with acute ischemic stroke treated with combined intravenous thrombolisis (ivT) vs. thrombectomy alone.
Method
We retrospectively analyzed data from patients undergoing MT following current acute stroke guidelines recommendations who were prospectively treated in a period of 2 years in 13 hospitals belonging to the NORDICTUS spanish stroke research network and serving an area of 11.5 M people. Successful recanalization ( TICI2b/3 after MT), functional independence (modified Rankin Scale –mRS- ≤ 2) at 3 months, mortality at 3 months, and symptomatic hemorrhagic transformation (sHT) were compared between patients having MT with and without previous ivT.
Results
Of the 681 patients included in the analysis, 402 (59%) underwent MT+ivT and 279 (41%) underwent MT alone. ASPECT score at baseline, time from symptom onset to groin puncture and number of passes were similar in both groups. Successful recanalization rate was higher in patients having ivT+MT (57% vs 43%, p = 0.037) and mortality rate was lower in this group of patients (14 vs 21%, p = 0.020). No differences were found neither in the percentage of functional independence at 3 months nor in the frequency of sHT between both groups.
Conclusion
Our data shows that administration of ivT before MT is a safe procedure but does not improve functional outcome, in spite of increasing recanalization rates and decreasing mortality.
Trial registration number
N/A
AS07-051
BALLOON GUIDE CATHETER IN ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Maastricht University Medical Center, Department of Neurology, Maastricht, The Netherlands
2Cardiovascular Research Institute Maastricht CARIM, Department of Neurology, Maastricht, The Netherlands
3Academic Medical Center, Department of Radiology and Nuclear Medicine, Amsterdam, The Netherlands
4Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
5Erasmus MC - University Medical Center, Department of Neurology, Rotterdam, The Netherlands
6Erasmus MC - University Medical Center, Department of Radiology, Rotterdam, The Netherlands
7Sint Antonius Hospital, Department of Radiology, Nieuwegein, The Netherlands
8Haaglanden Medical Center, Department of Neurology, The Hague, The Netherlands
9Maastricht University Medical Center, Department of Radiology, Maastricht, The Netherlands
10Cardiovascular Research Institute Maastricht CARIM, Department of Radiology, Maastricht, The Netherlands
Background and Aims
A balloon guide catheter (BGC) can be used in endovascular treatment (EVT) for acute ischemic stroke to enhance retrograde flow during clot removal. Previous studies show that this could prevent distal emboli and improve clinical outcome. However, use of a BGC is not fully implemented in current practice. The aim of this study is to compare functional and procedural outcome of EVT for acute ischemic stroke with and without BGC.
Method
We report patients with an anterior circulation occlusion, included between March 2014 and June 2016 in the MR CLEAN Registry, a prospective, multicentre, observational study for stroke intervention centers in the Netherlands. Patients with an EVT attempt were divided into two groups: BGC and non-BGC. Primary outcome was the modified Rankin Scale (mRS) score at 90 days. Secondary outcomes included successful reperfusion (eTICI>2B) and safety outcomes. Outcomes were compared with (ordinal) logistic regression analyses adjusted for potential confounders.
Results
Of 1488 patients, we excluded 208 in whom no EVT attempt was performed, and 260 because the use of a BGC was unknown. Of 1020 patients, a BGC was used in 66% and a non-BGC in 34%. Functional outcome on the mRS was not different between groups (aOR 1.00; 95% CI 0.79-1.28). Use of a BGC resulted more frequently in successful reperfusion (aOR 1.34; 95% CI 1.03-1.76). Complication rates were similar.
Conclusion
Use of a BGC in EVT for acute ischemic stroke was not associated with a difference in functional outcome, despite more frequent successful reperfusion.
Trial registration number
N/A
AS07-016
ANAESTHETIC MANAGEMENT DURING ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Maastricht University Medical Center+, Neurology, Maastricht, The Netherlands
2Rijnstate Hospital, Radiology, Arnhem, The Netherlands
3Rijnstate Hospital, Neurology, Arnhem, The Netherlands
4Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
5Erasmus MC University Medical Center, Radiology, Rotterdam, The Netherlands
6Academic Medical Center, Neurology, Amsterdam, The Netherlands
7Academic Medical Center, Radiology, Amsterdam, The Netherlands
8Sint Antonius Hospital, Radiology, Nieuwegein, The Netherlands
9Haaglanden Medical Center, Neurology, The Hague, The Netherlands
10Maastricht University Medical Center+, Radiology, Maastricht, The Netherlands
Background and Aims
Anaesthetic management during endovascular treatment (EVT) of acute ischemic stroke may have influence on functional outcome. We compared outcomes of three approaches in anaesthetic management in routine clinical practice: general anaesthesia (GA), conscious sedation (CS), and local anaesthesia only (LA).
Method
We report patients with an anterior circulation occlusion, included between March 2014 and June 2016 in the MR CLEAN Registry, a prospective, multicenter, observational study for stroke intervention centers in the Netherlands. Anaesthetic management was divided into three groups according to local protocol: GA, CS, or LA. Based on individual patient characteristics and practical feasibility, interventionists could deviate from their local protocol. Primary outcome was the modified Rankin Scale (mRS) score at 90 days. Secondary outcomes were reperfusion grade, and safety outcomes. Outcomes were compared in logistic regression analyses adjusted for baseline characteristics.
Results
1488 patients were included. The protocol for anaesthetic management was GA in 301 patients (20%), CS in 218 patients (15%), LA in 916 patients (61%), and unknown in 53 patients (4%). With LA and CS, the approach was converted to general anaesthesia in 8% of the patients. GA was associated with worse functional outcome on the mRS compared to LA (ORadjusted 0.87; 95% CI 0.68-1.12). CS was associated with worse functional outcome on the mRS compared to both LA (ORadjusted 0.64; 95% CI 0.48-0.85), and GA (ORadjusted 0.70; 95% CI 0.49-0.99).
Conclusion
Local anaesthesia only was associated with better functional outcome compared to general anaesthesia, and conscious sedation, in patients who underwent EVT for acute ischemic stroke.
Trial registration number
N/A
AS06-063
ENDOVASCULAR TREATMENT IN ELDERLY PATIENTS WITH ACUTE ISCHEMIC STROKE IN THE MR CLEAN REGISTRY
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Erasmus MC University Medical Center, Public Health, Rotterdam, The Netherlands
4Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
5Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
6Erasmus MC University Medical Center, Radiology and Nuclear Medicine, Rotterdam, The Netherlands
7Sint Antonius hospital Nieuwegein, Neurology, Nieuwegein, The Netherlands
8Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, The Netherlands
Background and Aims
Randomized trials on endovascular thrombectomy (EVT) for acute ischemic stroke (AIS) included a limited – and probably selected – number of elderly patients. We examined outcomes in elderly patients undergoing EVT in routine clinical practice.
Method
From the MR CLEAN Registry, we included consecutive patients (2014-2016) with an anterior circulation occlusion undergoing EVT. We compared patients in the upper age quartile vs. lower three quartiles. Endpoints were modified Rankin Scale score (mRS) and mortality at 90 days, symptomatic intracerebral hemorrhage (sICH), and reperfusion rate. We performed ordinal and logistic regression, adjusting for prognostic factors.
Results
Data of 1526 patients were included. The cut-off for the upper age quartile was 80 years (n = 380, 25%). Older patients were less often male (39% vs. 58%, P<0.001), had a higher median baseline NIHSS (17 vs. 15, P = 0.009), and more often had pre-stroke disability (mRS>1: 65% vs. 86%, P<0.001). Older age was associated with a substantially worse functional outcome (Figure 1) and increased mortality (aOR 3.4, 95% CI 2.6 – 4.5). Nineteen percent of elderly were functionally independent (mRS 0–2) at follow-up. There were no differences in sICH and reperfusion rates between groups.
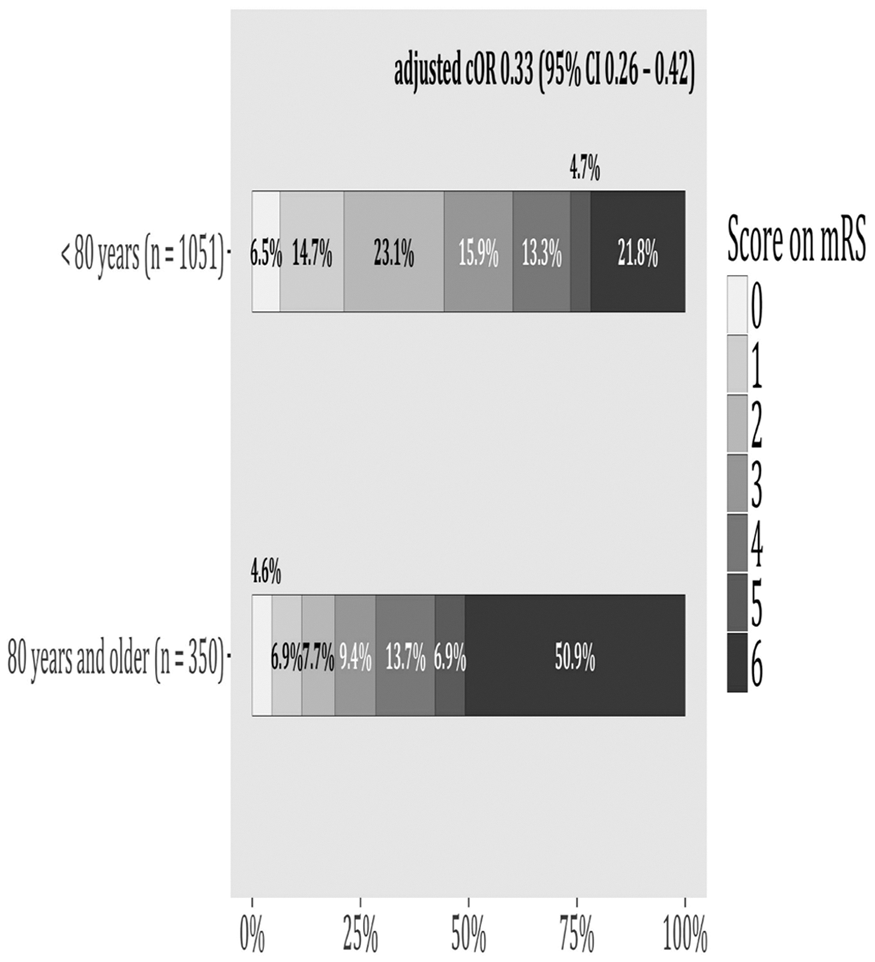
Conclusion
In routine clinical practice, the majority of elderly patients undergoing EVT had a poor clinical outcome. Further analysis of prognostic variables that can help clinical decision making for EVT in elderly is required
Trial registration number
N/A
AS07-037
SAFETY AND EFFICACY OF THROMBECTOMY IN PATIENTS WITH MILD SYMPTOMS OR LARGE INFARCT CORE: DATA FROM THE BEYOND-SWIFT REGISTRY
1Inselspital- University of Bern, Neuroradiology, Bern, Switzerland
2Inselspital- University of Bern, Neurology, Bern, Switzerland
3Klinikum rechts der Isar- Technical University Munich, Neuroradiology, Munich, Germany
4Universitat Autonoma de Barcelona, Neurovascular Unit Hospital Vall d'Hebron, Barcelona, Spain
5CHUV Centre hospitalier universitaire vaudois, Département des Neurosciences, Lausanne, Switzerland
6CHUV Centre hospitalier universitaire vaudois, Département des Neurosciences Cliniques-, Lausanne, Switzerland
7Toronto Western Hospital, Dept of Medical Imaging, Toronto, Canada
8Centre Hospitalier Universitaire de Montpellier, Neuro-radiologie Interventionnelle et clinique, Montpellier, France
Background and Aims
Stroke patients with low NIHSS or low Alberta Stroke Program Early CT Score (ASPECTS) were underrepresented in recent pivotal thrombectomy trials. Hence, safety and efficacy of mechanical reperfusion in these cohorts remains to be determined.
Method
Data from the multi-center consecutive patient
Results
Of 1311 patients with anterior circulation stroke and available ASPECTS, 145 patients were treated with an ASPECTS≤5 and 80 with NIHSS≤5. In patients with ASPECTS≤5, successful reperfusion (TICI2b/3) was an independent predictor of 3 month functional independence (mRS≤2, aOR 10.45, 95%-CI 1.98-55.01) and was independently associated with lower risk of symptomatic intracerebral hemorrhage (aOR 0.11, 95%-CI 0.02-0.56) and 3 month mortality (aOR 0.24, 95%-CI 0.09-0.64) after adjusting for relevant confounders. In patients with NIHSS≤5, successful reperfusion favored excellent functional outcomes (mRS≤1, aOR 21.41, 95%-CI 2.19-209.77) and 3 month independence (mRS≤2, aOR 13.83, 95%-CI 2.07-92.67).Complication rates did not differ between patients treated within current guidelines and patients presenting with NIHSS≤5 or ASPECTS≤5.
Conclusion
Indirect evidence from a large registry supports the notion that successful mechanical revascularization is associated with a favorable clinical course also in LVO patients with minor neurological deficits or large infarct core. Randomized-controlled trials assessing thrombectomy versus best medical care in these patients are warranted.
Trial registration number
N/A
AS06-041
AREA-WIDE IMPLEMENTATION OF MECHANICAL THROMBECTOMY IN GERMANY - ANALYSIS OF ADMINISTRATIVE DATA FROM 2010 TO 2016
1Alfried-Krupp-Krankenhaus, Neurology, Essen, Germany
2Klinikum Dortmund, Neurology, Dortmund, Germany
3Ruhr University Bochum, Neurology- Bergmannsheil, Bochum, Germany
4drg market, drg market, Osnabrück, Germany
5University Hospital Essen, Neurology, Essen, Germany
6University of Heidelberg, Neurology, Heidelberg, Germany
7Ruhr University Bochum, Neurology- St. Josef-Hospital, Bochum, Germany
Background and Aims
Since 2015, mechanical thrombectomy (MT) is an evidence-based treatment option for large vessel occlusion in the anterior brain circulation. Using comprehensive administrative data from Germany, we analysed the development of intravenous thrombolysis and MT in Germany between 2010 and 2016.
Method
We considered all documented cases with a main diagnosis of the ICD-10-GM code I63 (ischemic stroke, total of 1,698,083 cases between 2010 and 2016) and identified specific stroke recanalization therapy by using the corresponding Operating and Procedure Key for systemic thrombolysis and mechanical thrombectomy. Regional analyses were done by data aggregation into the 413 German administrative districts and cities.
Results
Ischemic strokes increased by 12.3% from 2010 (n = 229.798) to 2016 (n = 257.972) with a stable mean age of 75 years. The rate of IVT continuously increased from 8.0% in 2010 to 13.2% in 2016 and the rate of MT increased from 0.7% in 2010 to 4.1% in 2016, with a strong increase in 2015 and 2016 and a high regional variability (between 0 and 11.2% in 2016). Mean age increased from 67.8 years in 2010 to 73.3 years in 2016 and almost reached the mean age of IVT treated patients (74.4 years).
Conclusion
While the rate of IVT in acute ischemic stroke in Germany continues to increase, an even more important increase of MT procedures could be detected especially after publication of positive study results. However, there is still a high regional variability with significant lower MT rates in rural areas.
Trial registration number
N/A
AS06-067
RAPIDLY IMPROVING SYMPTOMS IN STROKE PATIENTS WITH LARGE VESSEL OCCLUSION PRIOR TO ENDOVASCULAR TREATMENT
1AMC, Neurology, Amsterdam, The Netherlands
2OLVG, Neurology, Amsterdam, The Netherlands
Background and Aims
A subset of patients with ischemic stroke and a large vessel occlusion (LVO) have mild or rapidly improving symptoms, resulting in withholding of endovascular treatment (EVT). We examined the frequency of secondary clinical deterioration in these patients.
Method
Retrospective analysis of a prospective, single centre stroke registry (2016-2017). We analysed patients with a LVO of the anterior circulation on initial imaging who did not receive EVT because of improving symptoms. Secondary deterioration was defined as increase in NIHSS score of 3 or more after initial improvement.
Results
34/360 (9%) patients (mean age 68) with a LVO did not receive EVT because of improving symptoms. Median NIHSS scores initially improved from 9 (range 2–20) to 2 (range 0–8). Location of occlusion was M1 (62%), M2 (35%), and ICA (3%). 28/34 patients (82%) received intravenous thrombolysis and 27 (79%) were drip-and-ship patients. After improvement, repeat CTA showed reperfusion in 13/34 (38%) patients and none of these patients had secondary deterioration. Of the remaining 21 patients, 8 (38%) had secondary deterioration (median NIHSS increase 4, range 3–6) within 1–48 hours after initial presentation. In 2 of these patients CTA was repeated before deterioration and both had a persistent occlusion. Two patients underwent EVT after deterioration.
Conclusion
Secondary clinical deterioration did not occur in patients with proven reperfusion, while in those in whom reperfusion was not demonstrated, one-third of patients deteriorated within two days. A repeat CTA should be considered in patients with a LVO and rapidly improving symptoms.
Trial registration number
N/A
Scientific Communications- Vascular Cognitive Impairment
AS22-014
DOMAIN-SPECIFIC CHARACTERISATION OF EARLY COGNITIVE IMPAIRMENT FOLLOWING SPONTANEOUS INTRACEREBRAL HAEMORRHAGE
1UCL Institute of Neurology, Stroke Research Centre, London, United Kingdom
2National Hospital for Neurology and Neurosurgery, Department of Neuropsychology, London, United Kingdom
3Massachusetts General Hospital and Harvard Medical School, Hemorrhagic Stroke Research Group, Boston, USA
4Università degli Studi di Palermo, Dipartimento di Scienze Psicologiche- Pedagogiche e della Formazione, Palermo, Italy
Background and Aims
Cognitive deficits after spontaneous intracerebral haemorrhage (ICH) are common and result in functional impairment, but few studies have examined deficits across cognitive domains in the subacute phase. This study aims to describe the cognitive profile following acute ICH and explore how cerebral amyloid angiopathy (CAA) may impact performance.
Method
We retrospectively reviewed 187 consecutive patients with ICH with available imaging and neuropsychological data (median 12 days after stroke).
Results
In our cohort, 84% (n = 158) were impaired in at least one cognitive domain and 65% (n = 122) in two or more domains. Deficits in non-verbal IQ (76.6%), information processing speed (62.4%) and executive functions (58.1%) were most common. Patients with lobar ICH (n = 92) had more deficits in naming and visual perception than those with non-lobar ICH, but not in adjusted analyses. Patients with probable CAA (n = 21) had more deficits in verbal IQ, visual perception and executive functions than those without probable CAA; in adjusted analyses, probable CAA predicted impairment in verbal IQ (OR 38.6, 95% CI 3.2 to 465.4, p = 0.004) and executive function (OR 3.4, 95% CI 1.0 to 11.7, p = 0.050).
Conclusion
We conclude that cognitive deficits following ICH are common across domains, and that those with CAA appear to have a different cognitive profile. Replication of this work in larger cohorts will be important for confirming and further quantifying these observations.
Trial registration number
N/A
AS22-015
RADIOLOGICAL AND PROGNOSTIC ASSOCIATIONS OF PRE-EXISTING COGNITIVE IMPAIRMENT IN PATIENTS WITH CARDIOEMBOLIC ISCHAEMIC STROKE OR TIA
1UCL Institute of Neurology, Stroke Research Centre, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3National Hospital for Neurology and Neurosurgery, Department of Neuropsychology, London, United Kingdom
4University College London, Department of Haematology, London, United Kingdom
5UCL Institute of Neurology, Lysholm Department of Neuroradiology and the Neuroradiological Academic Unit, London, United Kingdom
6University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
7City Hospital, University of Birmingham Institute of Cardiovascular Sciences, Birmingham, United Kingdom
8University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
A significant proportion of cognitive impairment identified following an ischaemic event may reflect unidentified pre-existing deficits. We investigated the radiological and prognostic associations of pre-existing cognitive impairment in patients with cardioembolic ischaemic stroke or transient ischaemic attack (TIA).
Method
We included 1085 patients from the prospective multicentre CROMIS-2 AF study. Pre-existing cognitive impairment was identified using the 16-item IQCODE (Informant Questionnaire for Cognitive Decline in the Elderly). Cognitive performance immediately post-event and functional outcome were measured using the Montreal Cognitive Assessment (MoCA) and the modified Rankin scale (mRS) respectively.
Results
Pre-existing cognitive impairment was common (n = 268, 24.7%). The presence of lacunes (OR 1.51, p = 0.034), higher grades of periventricular and deep white matter hyperintensity (reference group grade 0: periventricular grade 1 OR 1.38, grade 2 OR 2.00, grade 3 OR 2.48, p = 0.003, and deep grade 1 OR 1.53, grade 2 OR 1.29, grade 3 OR 2.16, p = 0.042) and medial temporal atrophy (reference group grade 0: grade 1 OR 1.81, grade 2 OR 2.06, grade 3 OR 4.84, grade 4 OR 8.93, p < 0.00001) were associated with pre-existing cognitive impairment in adjusted analyses. IQCODE-defined pre-existing cognitive impairment was associated with abnormal MoCA scores (OR 2.98, p = 0.001) and with worse functional outcome at 24 months (mRS > 2; adjusted OR 2.62, 95% CI 1.52 to 4.53, p = 0.001).
Conclusion
Pre-existing cognitive impairment in patients presenting with cardioembolic ischaemic stroke or TIA is common and associated with imaging markers of cerebral small vessel disease and neurodegeneration, as well as post-event cognitive performance and functional outcome.
Trial registration number
N/A
AS22-008
COGNITIVE RESERVE PROTECTS AGAINST DEMENTIA DUE TO CEREBRAL SMALL VESSEL DISEASE: DATA FROM A 5 YEAR FOLLOW-UP STUDY
1University of Cambridge, Clinical Neurosciences, Cambridge, United Kingdom
2St George’s- University of London, Neuroscience Research Centre, London, United Kingdom
3King’s College London, Division of Health & Social Care Research- Faculty of Life Sciences & Medicine, London, United Kingdom
Background and Aims
An important consequence of cerebral small vessel disease (SVD) is vascular cognitive impairment; but why do some patients show less cognitive decline than others with similar levels of disease on MRI? One potential explanation is the mitigating effect of cognitive reserve (CR), thought to be related to increased neural organisation. In Alzheimer’s disease, CR has been shown to be protective, but there is little evidence as to whether it protects against dementia in SVD. Furthermore, data from cross-sectional studies linking CR measures to dementia incidence cannot prove causality. The most powerful evidence comes from longitudinal studies, of which there are few in SVD.
Method
We determined CR (from a measure of pre-morbid IQ), SVD disease burden (from MRI markers) and cognition in 115 patients with MRI confirmed symptomatic lacunar stroke (the SCANS cohort), followed up for 5 years with repeat MRI, cognition and recording of conversion to dementia.
Results
Cross-sectional analysis of baseline data revealed MRI disease burden explained 29% of variance in cognitive test scores. The addition of CR increased this to 62%. Longitudinal analyses supported this finding and higher CR significantly predicted less conversion to dementia, when age and MRI disease burden were accounted for (X2(1) = 4.91, p = .027). The study found no mediation or moderation effects, suggesting an independent contribution of CR to cognition in patients with SVD.
Conclusion
The results suggest that CR plays an important role in mitigating the effects of SVD. IQ and education are strongly related to CR and may therefore protect against dementia in SVD.
Trial registration number
na
AS22-029
BARCELONA-ASIA STUDY: SUBCLINICAL CERVICO-CEREBRAL ATHEROSCLEROSIS AND PULSATILITY INDEX AS PREDICTORS OF LONG-TERM COGNITIVE IMPAIRMENT
1Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
2Hospital del Mar - Parc de Salut del Mar-, Neurology, Barcelona, Spain
3Hospital Universitari Germans Trias i Pujol, Neurology, Barcelona, Spain
4Hospital de Manresa, Neurology, Manresa, Spain
5Hospital Clinic de Barcelona, Neurology, Barcelona, Spain
6Hospital Clinico de Valladolid, Neurology, Valladolid, Spain
Background and Aims
Subclinical cervico-cerebral atherosclerosis has been poorly studied in our environment as a predictor of cognitive impairment.
Method
Barcelona-Asymptomatic Intracranial Atherosclerosis (AsIA) Study is a population-based study that included a random sample of 933 Caucasian subjects (mean age 66 years, 64% males) with a moderate-high vascular risk (REGICOR>5) and without history of stroke, coronary disease or dementia at baseline. Carotid and intracranial atherosclerosis were screened by color-coded duplex ultrasound, being moderate-severe stenosis confirmed by MRA. Pulsatility index (PI) in the MCA was measured bilaterally. Subjects were followed-up to determine the incidence of mild cognitive impairment (MCI) and/or dementia.
Results
After a median of 7.16 [6.91-7.75] years of follow-up, 91 subjects (9.7%) were diagnosed of MCI (27 subjects) or dementia (64 subjects). Diagnosis of MCI/dementia was significantly higher among subjects with extra and/or intracranial stenosis (21.4% vs 9%) and among those with an PI>1 (13.5% vs 7.4%) in baseline neurosonological study. In Cox regression analyses adjusted for vascular risk (REGICOR), sex and educational level, the presence of extra and/or intracranial stenosis (2.07 [1.11-3.88]) and an PI>1 (1.60 [1.02-2.49]) were independently associated with the diagnosis of MCI/dementia.
Conclusion
Presence of subclinical cervicocerebral atherosclerosis and the pulsatility index behaved as non-invasive neurosonological markers of long-term cognitive impairment in our population. These findings are important in the development of primary prevention strategies.
Trial registration number
N/A
AS03-038
A RANDOMISED CONTROLLED TRIAL OF AEROBIC EXERCISE AFTER TRANSIENT ISCHAEMIC ATTACK OR MINOR STROKE TO PREVENT COGNITIVE DECLINE: THE MOVEIT STUDY
1OLVG, Neurology, Amsterdam, The Netherlands
2Vrije Universiteit, Faculty of Behavioural and Movement Sciences- Clinical Neuropsychology, Amsterdam, The Netherlands
3OLVG, Pulmonology, Amsterdam, The Netherlands
4OLVG, Cardiology, Amsterdam, The Netherlands
5VU Medical Center- Amsterdam, Department of Rehabilitation Medicine- Move Research Institute Amsterdam, Amsterdam, The Netherlands
Background and Aims
Patients with TIA or stroke are at risk for cognitive impairment and dementia. Currently, there is no known effective strategy to prevent this cognitive decline. The aim of the present study was twofold: to investigate whether an early started physical exercise programme can prevent cognitive decline and to investigate the effect on cardiorespiratory fitness and the attainment of secondary prevention targets.
Method
A single-blinded randomised controlled trial was conducted in 120 patients with TIA or minor ischemic stroke recruited within 30 days post-stroke. The intervention consisted of a 3-month exercise programme followed by a 9-month coaching program administered by a specialized physiotherapist. The control group received usual care. Outcome measures were assessed at baseline, 1- and 2-year follow-up. The primary outcome was global cognitive functioning measured with the MoCA test. Secondary outcomes included maximal exercise capacity (Vo2max) and secondary prevention targets.
Results
We found no effect on global cognitive functioning after 2-years (MoCA-score: intervention 25.5 ± 3.2 to 25.7 ± 2.8, control 25.5 ± 2.9 to 26.0 ± 3.1, p = 0.66). There were no between-group differences for maximal exercise capacity, systolic and diastolic blood pressure, and LDL cholesterol.
Conclusion
The applied physical exercise programme did not affect global cognitive functioning after 2 years. Cardiorespiratory fitness was low. The neutral results of our trial are in line with previous studies and will be discussed at the conference.
Trial registration number
The Nederlands Trial Register: NTR 3884
AS22-010
WHO SHOULD UNDERGO A COMPREHENSIVE COGNITIVE ASSESSMENT AFTER A STROKE? THE GRECOGVASC COGNITIVE RISK SCORE
1Amiens University hospital, Neurology, Amiens, France
2Val-de-Grâce Hospital, Neurology, Paris, France
3La Rochelle Hospital, Neurology, La Rochelle, France
4Saint-Étienne University Hospital, Neurology, Saint-Étienne, France
5Saint Anne Hospital, Neurology, Paris, France
Background and Aims
To validate the ability of a specifically developed cognitive risk score to identify patients at risk of post-stroke neurocognitive disorders (NCD) and who are eligible for a comprehensive cognitive assessment.
Method
After assessing 404 patients (infarct: 91.3%) and 1003 healthy controls in the GRECogVASC cohort with the NINDS-CSN battery 6 months post-stroke, we used multivariable logistic regression and bootstrap analyses to determine factors associated with NCD. Independent, internally validated factors were included in a cognitive risk score.
Results
Cognitive impairment was present in 170 of the 320 patients with a Rankin score ≥1. The backward logistic regression selected 4 factors (≥73% of the permutations): NIHSS score on admission≥7 (OR [95% CI] = 2.73 [1.29-4.3]; p = 0.005), multiple strokes (3.78 [1.6-8]; p = 0.002), adjusted MMSE score (MMSEadj) ≤27 (6.69 [3.9-11.6]; p = 0.0001) and Fazekas score ≥2 (2.34 [1.3-4.2]; p = 0.004). The cognitive risk score computed using these four factors provided good calibration, discrimination (over-optimism corrected C =0.793) and goodness of fit (Hosmer-Lemeshow test: p = 0.99). A combination of Rankin score≥1, cognitive risk score ≥1 and MMSEadj ≥21 selected 230 (56.9%) of the 404 patients for a comprehensive assessment. This strategy yielded good sensitivity (96.5%) and moderate specificity (43%; PPV: 0.66; NPV: 0.91), and was more accurate than the sole use of screening tests (MMSEadj: p = 0.03; raw MMSE score: p = 0.0001; MoCA score: p = 0.008).
Conclusion
The GRECogVASC cognitive risk score comprises four easily documented factors; this strategy helps to identify patients at risk of post-stroke NCD and who must therefore undergo a comprehensive assessment.
Trial registration number
NCT 01339195
AS15-015
COGNITION AND PHYSICAL FUNCTIONING IN RELATION TO INCIDENT STROKE
1Erasmus MC, Epidemiology and Neurology, Rottedam, The Netherlands
2Erasmus MC, Epidemiology, Rottedam, The Netherlands
3Erasmus MC, Neurology, Rottedam, The Netherlands
Background and Aims
Patients, who suffer a stroke, are subsequently at increased risk of cognitive and physical impairment. In contrast, it remains unknown whether persons with poorer cognitive and physical impairment are at an increased risk of stroke.
Method
From the population-based Rotterdam Study, 8519 stroke-free non-demented participants underwent assessment of cognition and physical functioning between 2002–2005 using Mini-Mental State Examination, Verbal fluency test, 15-Word learning test, Letter-digit substitution test, Stroop test, Purdue pegboard test and questionnaires on basic and instrumental activities of daily living (BADL and IADL). Global cognition (G-factor) was derived using principal component analysis. Incident stroke was assessed through continuous monitoring of medical records until 01-01-2016. Cox proportional–hazards models were constructed to estimate hazards ratios for incidence stroke (any stroke, hemorrhagic, ischemic or unspecified) per unit decrease in a cognitive or physical test. We adjusted for age, sex, cardiovascular risk factors and apolipoprotein ε4 carriership.
Results
Among 8519 persons (mean age 66.0 years; 57.8% women), 489 suffered a stroke during mean follow-up of 8.7 years. Per SD decrease in G-factor was associated with a higher risk of stroke (HR 1.22, 95% CI:1.08–1.37). Worse scores on IADL (HR 1.11, 95% CI: 1.02–1.20), BADL (HR 1.18, 95% CI:1.07–1.29) and 15-Word learning test, Stroop reading and color naming task and Purdue pegboard test were significantly associated with a higher risk of stroke.
Conclusion
Worse cognition and physical functioning are associated with a higher risk of stroke, suggesting that both vascular and neurodegenerative pathologies are involved in the development of stroke.
Trial registration number
NTR6831
AS08-036
DOES POST-STROKE COGNITIVE IMPAIRMENT IMPROVE? SYSTEMATIC REVIEW AND META-ANALYSIS
1NHS Lothian, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom
2Glasgow University, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
3University of Edinburgh, Stroke and Elderly Care medicine, Edinburgh, United Kingdom
4University of Edinburgh, Neuroimaging Sciences and Edinburgh Imaging, Edinburgh, United Kingdom
5Southland Hospital, Medicine, Invercargill, New Zealand
Background and Aims
Little information has been available on the prognosis of post-stroke cognitive impairment, and which factors are associated with improvement. We conducted a systematic review of longitudinal studies that had measured cognition on more than one occasional after stroke.
Method
We searched longitudinal studies of ischaemic stroke which had measured post-stroke cognition at least twice. We extracted details of recruitment, testing and the numbers of patients tested, and impaired at each time-point, and which potential associated factors were measured.
We calculated a pooled proportion of the patients with cognitive impairment at different time points after stroke.
Results
We screened 429 citations, of which 33 were reviewed and 18 (n = 9803) included cognitive decline was associated with stroke severity, right hemisphere lesion, multiple infarcts, recurrent stroke/TIA, vascular risk factors, heart disease, smoking, lower socio-economic status, and baseline cognitive impairment.
Data was available for meta-analysis from 7 studies (n = 3903) at 3 months post-stroke for, 5(n = 1817) at 12 months and 4(n = 1130) 24 months.
The proportion with cognitive impairment was 16% (95% CI 4–35%) at 3 months, 26%(95% CI 15-39%) at 12 months and 17(95% CI 15-19%)at 24 months. There was a high degree of heterogeneity (I2 99%). Attrition was 10% at 12 months (95% CI 2–24%), but 33% at 24 months (95% CI 18-49%).
Conclusion
The limited data available suggests that cognition does not improve after stroke. Attrition is a potential confounding factor.
As recurrent stroke and vascular risk factors were associated with worsening cognition, secondary prevention should be prioritized.
Trial registration number
NA
AS03-031
LIFETIME RISK OF DEMENTIA IN PATIENTS WITH SEVERE CAROTID STENOSIS: EXTENDED POST-TRIAL FOLLOW-UP OF PATIENTS IN THE FIRST ASYMPTOMATIC CAROTID SURGERY TRIAL (ACST-1)
1University of Oxford, Nuffield Dept. Surgical Sciences, Oxford, United Kingdom
2University of Oxford, Medical Research Council Population Health Research Unit- Nuffield Dept.of Population Health, Oxford, United Kingdom
3University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
4University of Oxford, Nuffield Dept. of Clinical Neurosciences, Oxford, United Kingdom
5University of Uppsala, Dept. of Vascular Surgery, Uppsala, Sweden
6University of Lund, Clinical Vascular Disease Research, Lund, Sweden
Background and Aims
Observational studies suggest a strong association between carotid stenosis and dementia but, since both conditions share common risk factors, this may not be causal. Between 1993 and 2003, ACST-1 randomised 3120 participants with asymptomatic carotid stenosis to carotid endarterectomy plus medical treatment versus medical treatment alone. Whilst surgery halved the risk of stroke at 5 & 10 years, effects on dementia were not assessed. The aim of this extended follow-up is to determine the risk of developing dementia in patients with carotid stenosis and, more importantly, to see if surgery reduces this risk.
Method
Electronic data linkage of health records (NHS digital-UK, Socialstyrelsen-Sweden), dementia registries and cause-specific mortality were available for 1601 ACST-1 participants from the UK (1069) and Sweden (532). This was supplemented with a detailed review (blind to treatment allocation) of ACST-1 participant records for reports of dementia.
Results
Mean age at randomisation was 69 years (42-87), 64% were male and (due to minimisation) both groups were well matched for important baseline characteristics. We will report incident dementia rates amongst those originally allocated to endarterectomy versus medical treatment (intention-to-treat analyses). Preliminary results suggest that around three quarters have died and that rates of incident dementia are high (> 200 cases of dementia anticipated) in this trial population with established cerebrovascular disease.
Conclusion
Evidence from randomised trials is required to reliably assess the effects of carotid surgery on dementia risk, and long-term follow-up of ACST-1 provides a unique opportunity to help answer this important question.
Trial registration number
ISRCTN26156392
Young Stroke Physicians & Researchers
AS27-017
PREHOSPITAL NIHSS IN CONVENTIONAL AMBULANCE SERVICE IDENTIFIES ACUTE STROKE PATIENTS
1The Norwegian Air Ambulance Foundation, Research and Development, Oslo, Norway
Background and Aims
Acute stroke treatment depends on early notification and direct triage to treatment. Prehospital notification is known to reduce time from symptom onset to reperfusion therapy, and several prehospital stroke scales have been tested. By using scales designed to identify patients with large vessel occlusion, we risk under-triage and transfer of patients to insufficient level of care. The Norwegian Acute Stroke Prehospital Project (NASPP) study group showed that the National Institute of Health Stroke Scale (NIHSS) may be used in the prehospital setting by prehospital critical care physicians. In the present study, we aim to introduce NIHSS in the conventional ambulance service.
Method
The Para-NASPP study is a stepped-wedge cluster randomized controlled trial in the ambulance service in Oslo, Norway. The study will include 400 patients over a two year study period. The sequentially implemented training in prehospital NIHSS is based on specifically designed videos, electronic text presentation and a purpose built NIHSS-app. Feasibility will be assessed by inter-rater agreement (Bland Altman) between prehospital NIHSS and NIHSS by on-call neurologist. Efficiency will be tested by the proportion of patients receiving reperfusion therapy and symptom onset to treatment times. A ROC analyses will establish a prehospital NIHSS cut-off value for direct triage to interventional therapy.
Results
PARA-NASPP will explore the feasibility of using NIHSS in a conventional ambulance service.
Conclusion
If successful, prehospital NIHSS implemented in the ambulance service may result in more patients treated with reperfusion therapies and reduce symptom onset to treatment time.
Trial registration number
N/A
AS27-005
FEASIBILITY OF IMPROVING CEREBRAL AUTOREGULATION IN ACUTE INTRACEREBRAL HAEMORRHAGE (BREATHE-ICH) STUDY: AN EXPERIMENTAL INTERVENTIONAL STUDY
1Cerebral Haemodynamics in Ageing and Stroke Medicine CHiASM Research Group, Department of Cardiovascular Sciences- University of Leicester, Leicester, United Kingdom
2National Institute for Health Research Leicester Biomedical Research Centre, Department of Cardiovascular Sciences- University of Leicester, Leicester, United Kingdom
3University Hospitals of Leicester NHS Trust, Department of Radiology, Leicester, United Kingdom
Background and Aims
Cerebral autoregulation (CA) is crucial in patients with spontaneous intracerebral haemorrhage (ICH) to maintaining cerebral blood velocity (CBV) constant during changes in blood pressure (BP). CA is impaired up to 12 days post-ICH and is associated with larger ICH volume, lower Glasgow Coma Score and increased dependence. Hypocapnia generated via a hyperventilatory maneouvre improves CA despite concerns over lower CBV and consequent ischaemic risk. BREATHE-ICH (NCT03324321) is the first CA-targeted interventional study in acute ICH using a simple bed-side respiratory manoeuvre.
Method
Forty-five patients with acute ICH will be studied within 48 hours and 14 days after ictus. CBV (transcranial Doppler), BP (Finometer) and end-tidal CO2 (capnography) will be measured at baseline, and in response to hypocapnia achieved via hyperventilation for 90-seconds. Autoregulation Index (ARI) calculation in a minimum of 40 patients provides 80% power at ɑ error of 0.05. End-points associated with this before and after interventional study include 14-day NIHSS and mRS.
Results
Currently, 24% (11/45) have been recruited with protocol acceptability. Interim analyses of five individuals demonstrates mean (SD) age 67.8 years (12.6 years), NIHSS 3 (2.1), admission systolic BP 164mmHg (23mmHg) and haematoma volume (ABC/2 score) 1.63cm3 (1.62cm3) with regular shaped thalamic haemorrhage without intraventricular extension predominating.
Conclusion
This study has considerable potential to improve acute ICH outcome by modifying impaired CA in a highly vulnerable neurological state. Importantly, initial data analysis of the BREATHE-ICH study suggests the intervention is acceptable with a clearly defined cohort of patients completing the study protocol (milder haemorrhages with elevated BP).
Trial registration number
ClinicalTrials.gov: NCT03324321
AS27-016
REPERFUSION INJURY AFTER ISCHEMIC STROKE STUDY (RISKS): AN “IN VIVO" STUDY USING CIRCULATING AND NEURO-IMAGING MARKERS - RESULTS FROM THE INTERIM ANALYSIS
1University of Florence, NEUROFARBA Department- Neuroscience Section, Florence, Italy
2Careggi University Hospital, Stroke Unit and Neurology, Florence, Italy
3Careggi University Hospital, Atherothrombotic Diseases Center, Florence, Italy
4Careggi University Hospital, Interventional Neuroradiology Unit, Florence, Italy
5University of Florence, Department of Experimental and Clinical Biomedical Sciences, Florence, Italy
Background and Aims
Revascularization treatments for acute ischemic stroke (AIS) may result futile or even detrimental due to the reperfusion injury (RI). However, the physiopathological process involving blood brain barrier (BBB) disruption is poorly elucidated. Our aim is to evaluate the effect of circulating and imaging markers in relation to RI in a prospective cohort of AIS patients.
Method
We included AIS patients in the anterior circulation with admission NIHSS≥7, treated with systemic thrombolysis and/or endovascular treatment. BBB disruption was qualitatively assessed on pre-treatment perfusion-CT (PCT) using permeability maps. A large panel of circulating biomarkers was measured at baseline and after 24 hours. RI was defined as either hemorrhagic transformation or cerebral edema at 24 hours.
Results
From October 2015 to March 2017, 75 patients were included. Mean age ( ± SD) was 74.3 (±13.2) years and median admission NIHSS was 18 (12-22). RI occurred in 26 (35%) patients. After adjustment for major clinical confounders, increased permeability on PCT (OR = 2.29; 95%CI = 1.19-4.42) was independently associated with RI. At univariate analysis, 24 hours matrix metalloproteinase-9 (MMP-9) levels were significantly associated with RI (p = 0.04). This association was not confirmed in multivariate analysis. Among radiological variables, lower ASPECTS (OR = 0,68; 95%CI = 0,47-0,99), lower clot burden score (OR = 0,74; 95%CI = 0,60-0,91) and poor collaterals (OR = 2,87; 95%CI = 1,35-6,08) were independent predictors of RI.
Conclusion
Our results suggest that BBB permeability measurements on PCT might be useful to predict RI after acute stroke treatments. Among circulating biomarkers, MMP-9 activity could play a key role in the pathophysiology of RI. Final results are expected by the end of 2018.
Trial registration number
NCT03041753
AS27-015
SHORTENING SCAN TIMES FOR NON-INVASIVE ASSESSMENT OF HYPOPERFUSION USING BOLD DELAY
1Charité - Universitätsmedizin Berlin, Center for Stroke Research, Berlin, Germany
2Max Planck Institute for Human Cognitive and Brain Sciences, Department of Neurology, Leipzig, Germany
3Humboldt-Universität zu Berlin, Berlin School of Mind and Brain, Berlin, Germany
Background and Aims
Temporal delays in resting state blood oxygenation level-dependent (BOLD) signal fluctuations occur in hypoperfused tissue in acute and subacute stroke. Time-shift analysis (TSA) detects these lags and has recently been validated. However, scan times are known to vary a lot, and it is unclear how much data should be acquired to provide reliable results. This study investigates the implementation of a multiband echo planar imaging (EPI) sequence for assessing BOLD-delay and the plausibility of shortened scan times for detecting hypoperfusion.
Method
63 patients with acute stroke (<24 hours) received a resting-state multiband EPI scan in addition to a standard stroke MRI protocol. rsfMRI data of these patients were divided into 5 segments of various lengths (68s, 136s, 204s, 272s, 340s), preprocessed, and TSA maps of these segments were calculated. A Bland-Altman analysis will be performed to compare the hypoperfusion lesion volumes in various scan lengths. In addition, a spatial comparison of the shortened segments to the full segment will be done using the Dice similarity coefficient and a ROC analysis.
Results
Based on pilot data showing that about 80s of scan time may be sufficient to reliably visualize hypoperfusion , we expect the degree of agreement between shorter scans and full-scan across patients to be adequate to recommend shortening the scan times.
Conclusion
Multiband EPI has several advantages, including a more effective separation of low-frequency oscillations from cardiac and respiratory signals. Using this sequence to shorten BOLD delay scan times would potentially make it more applicable in a routine clinical setting.
Trial registration number
N/A
Posters
CLINICAL TRIAL RESULTS – ACUTE MANAGEMENT – NEITHER THROMBOLYSIS NOR THROMBECTOMY
AS01-001
REMOTE ISCHEMIC POST CONDITIONING (BAIPC) PLAYS A PROTECTIVE ROLE TO STROKE BY SUPRESSING PERIPHERAL IMMUNITY
1Jilin University, Neurology, changchun, China
Background and Aims
Studies suggest that peripheral immune supression might lead to a protective role through reducing inflammatory injury in the stroke infarct area.
Method
75 stroke patients, 31 in BAIPC group and 44 in controls. Patients are treated in 72 hours after stroke. The RBAIPC treatment consisted of 5 cycles of bilateral upper limb ischemia for 5 minutes followed by reperfusion for another 5 minutes, twice a day.The samples were collected before treatment, 24 hours after treatment and 7d after treatment to analyze the level of cytokines and Th cells.
Results
① The decrease of NIHSS in RBAIPC group is higher than that in controls (P<0.05) ② RBAIPC patients have lower IL-4 (P<0.05) level at 24 hours and higher IL-2 (P<0.05) and IFN-γ (P<0.05) levels at 7 days. ③ After RBAIPC, the Th1 and Th2 cells frequencies are increased relatively at 24hours. ④ The increase of IL-4 levels is correlated with the decrease of NIHSS after 7 days (R = 0.563, P = 0.002).
Conclusion
① RBAIPC have beneficial effect on the recovery of neurological functions. ② RBAIPC could limit the inflammation after stroke through increase the level of anti-inflammatory cytokines IL-4 and decrease the level of pro-inflammatory cytokines including IL-2 and IFN-γ. ③ RBAIPC could promote the differentiation of Th cells to IFN-γ+T (Th1) cells and IL-4+(Th2) cells, the increase of IL-4+ T cells might play a protective role through secreting IL-4 while the role of IFN-γ+ T cells needs works to identify.
Trial registration number
NCT03335111
AS01-003
PREDICTING THE SYMPTOMATIC INTRACEREBRAL HEMORRHAGE RISK AND PROGNOSIS AFTER A THERAPY WITH RT-PA USING SEDAN AND HAT SCORES IN A MONOCENTER STUDY
1University of Lübeck, Neurology, Luebeck, Germany
Background and Aims
The occurrence of symptomatic intracerebral hemorrhage (sICH) after a treatment with recombinant tissue-plasminogen activator (rt-PA) is a feared complication and associated with poor outcomes.
Several clinical models were developed to estimate the risk of intracerebral hemorrhage and prognosis after rt-PA therapy.
The aims of the study were to predict the risk of sICH after a therapy with rt-PA and outcomes using SEDAN and HAT score in patients with acute ischemic stroke in a monocenter study.
Method
During a 6-year period (2009-2014), 697 consecutive stroke patients (mean age, 73 ± 3 years; 51% women; median NIHSS score, 11) treated with IV thrombolysis were included in a monocenter study.
Results
A total of 60 patients (8.6%) experienced sICH after thrombolysis treatment. During a mean hospitalization of 11 days, 64 patients (9.2%) died. The risk of sICH after a treatment with rt-PA and in-hospital mortality were increased with incrementing SEDAN and HAT score. During a mean follow up period of one year, 140 (20%) patients died and 153 of 351 surviving patients were found to be disabled [the disability defined as mRS 3-£5]. The one-year mortality and disability rates among survivors were associated with increasing SEDAN and HAT scores too (Table 1).
Conclusion
The SEDAN as well as the HAT score seem to be useful tools to predict symptomatic intracerebral hemorrhage as well as prognosis after a treatment with rt-PA in acute stroke patients.
Trial registration number
N/A
AS01-004
ARE TELESTROKE WARDS AS EFFICIENT AS STROKE WARDS FOR PATIENTS NOT TREATED BY THROMBOLYSIS OR THROMBECTOMY?
1CHRU Besançon, Neurology 2, Besancon, France
2CHRU Besancon, Neurology 2, Besancon, France
3CHRU, Centre de Méthodologie Clinique, Besancon, France
Background and Aims
Stroke units (SU) improve the prognosis of stroke patients. However they are too few in French rural areas. Telemedicine has proven efficency and safety for thrombolysis but little is known about the outcome of patients admitted in neurological departement linked by telemedicine to a stroke unit (telestroke ward) but not thrombolysed. Three Telestroke wards (TSU) were deployed through Franche Comté. A telestroke unit is a department of neurology, nurses are certified in neurovascular pathology and neurovascular expertise can be done by telemedicine 7/24.The aim of this non-inferiority study was to evaluate the outcome of patients admitted in telestroke units while non reperfused.
Method
We carried out a retrospective two center study (TSU/SU) comparing the outcome of patients admitted from May 2015 to December 2016 for stroke and not thrombolysed. Patients were matched according to their age, stroke subtype and stroke severity. Primary endpoint was death or disability. National quality management criteria were also compared.
Results
Two hundred and thirty one patients were compared in both group. Mean age was 73.3. Fourty four percent were males. 66.7% suffered infarctions, 6% hemorrahagic strokes and 27.3 % TIA. Among strokes, 71,2% had a minor stroke (NIHSS<5). Death or disability were significantly different (14.5% in SU versus 19.7 in TSU). 80.31%of SU patients and 85.5 % of TSU (p:0.176) were independant at 3 months. Moreover, national quality management criteria were neither significantly different except for speech therapists assessment.
Conclusion
Outcome and management of patients admitted in TSU are not worse than those in SU.
Trial registration number
DE-2017-123
AS01-005
THE IMPACT OF PRIOR USE OF ANTITHROMBOTIC AGENTS ON SEVERITY AND OUTCOME IN STROKE PATIENTS WITH ARTERIAL FIBRILLATION. THE JAPAN STROKE DATA BANK
1National Cerebral and Cardiovascular Center, Department of Stroke Care Unit, Suita- Osaka, Japan
2National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita- Osaka, Japan
3National Cerebral and Cardiovascular Center, Center for Cerebral and Cardiovascular Disease Information, Suita- Osaka, Japan
4Shimane University, School of Medicine, Matsue- Shimane, Japan
Background and Aims
The effectiveness of oral antithrombotic agents for patients with atrial fibrillation [Af] and acute ischemic stroke [AIS] is established, but its impact on severity and outcome after AIS remains unclear.
Method
We studied AIS patients with Af admitted to 103 hospitals participating in the Japan Stroke Data Bank from 2001 to 2015. We examined annual frequencies of prior use of vitamin K-antagonist [VKA], direct oral anticoagulants [DOAC], antiplatelet agents [AP], combination of anticoagulants and AP [AP+AC] and none [N], and its associations with NIHSS score on admission and poor outcome (modified Rankin Scale of 3–6) at discharge using multivariable models.
Results
Among 65,966 AIS patients, 16,778 had Af (women, 45.3%; and age, 72.5 ± 12.1 years). VKA peaked at 27% in 2011, and then decreased. DOAC increased up to 6% after launched. AP and N declined constantly. NIHSS score was lower in VKA (median 9), DOAC (4), AP (9) and AC+AP (6) as compared with N (10). The difference remained significant after adjustment by potential confounders. Proportions of poor outcome were 60.7%, 46.4%, 60.6%, 52.8% and 60.8% in VKA, DOAC, AP, AC+AP and N, respectively. In multivariate analysis, DOAC (adjusted odds ratio [aOR] 0.53; 95% confidence interval [CI] 0.32-0.88; P = 0.015) and AC+AP (aOR 0.75; 95% CI 0.62-0.91; P = 0.004) reduced the risk of poor outcome as compared with N group.
Conclusion
In this cohort, prior use of antithrombotic agents, especially DOAC, was increased and might reduce severity and poor outcome in patients with AIS and Af.
Trial registration number
N/A
AS01-007
SURGICAL CEREBRAL REVASCULARIZATION IN ACUTE PERIOD OF ISCHEMIC STROKE (IS)
1Sklifosovsky Research Institute of Emergency care, neurosurgery, Moscow, Russia
Background and Aims
to estimate of surgical revascularization outcomes at patients with ischemic stroke (IS).
Method
160 patients with acute IS were operated on from 01.01.2014 till 01.10.2017, among them 101 (63,1%) – with ICA stenosis or tortuosity, 22 (13,8%) – with ICA occlusion, 37 (22,5%) – with acute ICA thrombosis. Carotid endarterectomy (CEE) or ICA stenting was performed at patients with ICA stenosis during first 14 days of IS, STA-MCA bypass – for patients with ICA occlusion or acute thrombosis, emergent thrombintimectomy – at patients with floating ICA thrombosis or ICA total thrombosis with preserved blood flow via intracranial segments of ICA.
Results
The postoperative step-by-step regress of neurological deficit from 2,19 till 1,64 scores by NIHSS was observed at 82,6% (N = 48) patients with minor stroke and TIAs while neurological signs regressed from 7,5 till 3,5 scores by NIHSS at 88% (N = 37) of patients with completed stroke. Patients with ICA occlusion demonstrated the restoration of neurological functions from 4,5 till 2,1 scores by NIHSS in 86,4% (N = 19) of cases as well as at 93,9% (N = 31) of patients with ICA thrombosis with positive dynamics by NIHSS from 7 till 3,02 scores. Ischemic complications were observed at 3,8% (N = 6), hemorrhagic complications – 0,6% (N = 1), lethality – 1,9% (N = 3). Repeated IS before operation was seen at 4,4% (N = 7) of patients. The best outcomes were obtained at patients with cerebral perfusion growth and decrease of penumbra area.s.
Conclusion
Cerebral revascularization in acute period of IS is safety and effective therapeutic and preventive procedure at accurately selected patients.
Trial registration number
N/A
AS01-011
INTER-RATER RELIABILITY BETWEEN PARAMEDICS AND NEUROLOGISTS IN ASSESSMENT OF HEMIPLEGIA IN ACUTE STROKE DID NOT IMPROVE AFTER RE-EDUCATION
1Comprehensive Stroke Centre- University Hospital Ostrava, Department of Neurology, Ostrava, Czech Republic
2Emergency Medical Service, Emergency, Moravian-Silesian Region, Czech Republic
3Comenius University in Bratislava, Jessenius Faculty of Medicine in Martin, Bratislava, Slovak Republic
4St. Annés University Hospital and Faculty of Medicine- Masaryk University, Department of Neurology, Brno, Czech Republic
5Faculty of Medicine- Ostrava University, Department of Neurology and Psychiatry, Ostrava, Czech Republic
6Ostrava Vitkovice Hospital, Agel Research and Training Institute, Ostrava, Czech Republic
7Primary Stroke Centre- City Hospital Ostrava, Department of Neurology, Ostrava, Czech Republic
8International Clinical Research Centre- St. Annés University Hospital, Neurology Department, Brno, Czech Republic
Background and Aims
Mechanical thrombectomy demands reliable pre-hospital triage by paramedics. Although optimal score has not been established, it is not clear what level of competency exists between paramedics for diagnosis of major neurological deficits. The aim of our study was to define inter-rater reliability between paramedics and stroke neurologists for the presence of severe hemiparesis.
Method
Prospective, double phase, multicentre study. During the first phase (April- October2016), paramedics were educated to diagnose mild or severe hemiparesis via Internet e-learning. Their participation in the training was voluntary. During the second phase (August-October 2017) paramedics were re-educated via webinars and examined straight after. Agreement for degree of hemiparesis [NIHSS, item 4 and 5, scoring 0–2 (none or mild) versus3-4 (severe)] between paramedics (assessed during pre-hospital) and neurologists (assessed immediately after stroke centre admission) was analyzed using the unweighted Kappa index.
Results
During the first phase consecutive 435 (47% of all) patients (215 men [51%], average age 73 and during the second phase 71 patients (51%) (35 men [50%], average age 74 were evaluated for the presence of hemiparesis by both paramedics and neurologists. In both phases the agreement between the paramedics and neurologists was moderate - in the first one kappa 0.54 (95%CI 0.46-0.62) in the second kappa 0.43 (95% CI 0.27-0.63).
Conclusion
In our study, reliability of assessment of hemiplegia by paramedics was only moderate and was not improved by repeated training. More effective trainings of paramedics are needed especially with the prospect of clinical need for pre-hospital triage for mechanical thrombectomy.
Trial registration number
N/A
AS01-012
HEAD POSITION AFFECTS CEREBRAL AUTOREGULATION IN ISCHAEMIC STROKE
1University of Leicester, Department of Cardiovascular Sciences, Leicester, United Kingdom
2University of Leicester, National Institute for Health Research Leicester Biomedical Research Centre, Leicester, United Kingdom
Background and Aims
Acute ischaemic stroke (AIS) patients are routinely nursed with head elevation (≥ 30°). However, little is known on how cerebral autoregulation (CA), a physiological mechanism to maintain cerebral blood flow (CBF) in response to change of cerebral perfusion pressure (CPP), and associated haemodynamic parameters, respond to gradual transitions in head positioning.
Method
16 controls (8 female, age 57 ± 17 years) and 15 AIS (8 female, age 70 ± 8 years), were assessed at two (12 ± 8 days) and three visits (13.3 ± 6.9 hrs, 4.8 ± 3.2 days and 93.9 ± 11.5 days of stroke symptom onset), respectively. Cerebral blood velocity (Transcranial Doppler), beat to beat blood pressure (BP, Finometer) and end tidal carbon dioxide (ETCO2, capnography) were recorded with lying flat (0°) and sitting up (30°) head positions.
Results
Compared to controls, baseline BP was higher in AIS (visit 1 and visit 2: p <0.001), ETCO2 was lower (all 3 visits), and critical closing pressure (CrCP) was increased (all 3 visits), in both affected and non-affected hemispheres (p = 0.004 and 0.005, respectively). In the sitting position (30°), CA (autoregulation index, ARI) was reduced in AIS (affected hemisphere, p = 0.001), but not in the unaffected hemisphere, compared to lying flat (0°).
Conclusion
Head positioning can have significant effects on the cerebral haemodynamics of AIS patients. Further investigation is needed to ensure appropriate head position for the individualised care of AIS, aiming to optimise patient recovery and outcome.
Trial registration number
NCT02932540
AS01-013
IMPACT OF ATRIAL FIBRILLATION DIAGNOSIS OR CAROTID ENDARTERECTOMY REQUIREMENT ON OUTCOME IN PATIENTS FROM THE TRIPLE ANTIPLATELETS FOR REDUCING DEPENDENCY AFTER ISCHAEMIC STROKE (TARDIS) TRIAL
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2University of Nottingham, Radiological Sciences- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Carotid stenosis and atrial fibrillation (AF) are common causes of ischaemic stroke (IS) and transient ischaemic attack (TIA), and require carotid endarterectomy (CEA) and anticoagulation respectively to reduce recurrence risk. We assessed whether these interventions improve outcome using data from the TARDIS trial.
Method
TARDIS assessed one month of intensive antiplatelet therapy versus guideline in 3,096 patients with acute non-cardioembolic IS or TIA. Information regarding CEA requirement, AF diagnosis, recurrence and functional outcome was assessed centrally blinded to treatment assignment. Data are unadjusted odds ratio (OR) or mean difference (MD) with 95% confidence interval (CI) relative to no AF/CEA.
Results
118 patients were diagnosed with AF and 84 required a CEA. In comparison with others, AF and CEA patients were older (4.2 and 2.4 years respectively) and AF patients were more likely to have been enrolled with stroke than TIA (p < 0.001). AF patients were more likely to have a stroke/TIA recurrence (OR 2.31, 95% CI 1.30-4.10; 7 before diagnosis, 9 afterwards), and have a shift to more dependency (modified Rankin Scale, OR 1.50, 95% CI 1.07-2.10) and disability (Barthel Index, MD -6.5, 95% CI -10.0 to -3.1). Outcomes of CEA patients were not significantly different from patients who did not require CEA.
Conclusion
Recurrence was more common in patients with AF than in other TARDIS patients; patients with AF also had worse functional outcomes. There was no difference in recurrence or functional outcomes between patients who did and did not require CEA.
Trial registration number
ISRCTN47823388
AS01-018
SURGICAL TREATMENT OF MALIGNANT CEREBELLAR INFARCTION
1A.I. Yevdokimov Moscow State University of Medicine and Dentistry, Neurosurgery, Moscow, Russia
2N.V. Sklifosovsky Federal Research Institute of Emergency Medicine, Neurosurgery, Moskow, Russia
3Moscow City Clinical Hospital after V.V. Veresaev, Neurosurgery, Moskow, Russia
4Moscow City Clinical Hospital after S.S. Yudin, Neurosurgery, Moskow, Russia
5Moscow City Clinical Hospital after V.M. Buyanov, Neurosurgery, Moskow, Russia
Background and Aims
Malignant cerebellar infarction (MCI) results in expressed edema of the infarction zone. Mass effect leads to development of acute occlusive hydrocephalus and damage of brainstem. Mortality rate with conservative therapy goes for 80%.
Aim is to determine the effectiveness of surgical treatment of MCI.
Results
Fifteen patients underwent isolated ventriculostomy. The recovery of consciousness level was observed in 7 patients on 13 day in average. The restoration of IV ventricle configuration was observed on 11 postoperative day in average. The efficacy was 46%.
Five patients underwent only suboccipital decompression craniotomy (SDC) with additional external ventricular drainage (EVD) in 2 patients as second operation. The efficacy was 40%.
SDC with simultaneous EVD was performed at 10 patients. The recovery of consciousness was observed on 4 day as well as the restoration of basal cisterns and IV ventricle were noted during 1st day in this group. The efficacy was 70 %.
Conclusion
The SDC with simultaneous EVD is indicated for all patients suffered from MCI if they have decrease of consciousness ≤ GSC 13 scores and CT signs of occlusive hydrocephalus or compression of the brainstem.
Trial registration number
N/A
AS01-020
FACTORS ASSOCIATED WITH STROKE MISDIAGNOSIS IN THE EMERGENCY DEPARTMENT (ED): A RETROSPECTIVE CASE-CONTROL STUDY
1Liverpool Hospital, Neurophysiology, Sydney, Australia
2Liverpool Hospital, Neurology, Sydney, Australia
Background and Aims
Failure to recognise acute stroke may result in worse outcomes due to missed opportunity to implement acute stroke therapies. Our study examines factors associated with stroke misdiagnosis in patients admitted to a large comprehensive stroke centre.
Method
Retrospective review comparing 156 consecutive patients with a final diagnosis of stroke who were initially misdiagnosed in ED with 156 randomly selected accurately diagnosed stroke controls matched for age, gender, language spoken (English v non-English) and subtype (infarct v haemorrhage)[2014-2016].
Results
There were 141 ischaemic and 15 haemorrhagic misdiagnosed strokes. Median age: 77 years, M:F = 1.3:1. Misdiagnosed patients were more likely to be triaged into a lower ED category (62%v42%, p = 0.001), be FAST-negative (78%v22%, p < 0.001) and undergo a delayed CT brain (median 4.1v1.5h, p < 0.001). ED diagnoses were typically nonspecific: syncope/collapse/loss of consciousness (16%), falls/reduced mobility/unsteadiness (13%), dizziness (10%), unspecified weakness (9%), vomiting (4%) and confusion (4%). Symptom resolution, altered mental status, nausea/vomiting, dizziness and vertigo favoured misdiagnosis (p < 0.05). Hemiparesis and dysarthria favoured an accurate diagnosis (p < 0.05). Vascular risk factors were similar. Misdiagnosed patients were more likely to have posterior circulation stroke (40%v21%, p = 0.01) and be admitted under non-neurological services (35%v11%, p < 0.001). 17% of accurately diagnosed ischaemic stroke patients received acute stroke therapies compared to 0% of misdiagnosed patients. Length of stay (median 10v8 days), discharge mRS 0–2 (45%v42%) and mortality (8%v11%) were similar.
Conclusion
Patients with stroke misdiagnosis commonly presented with FAST-negative and nonspecific symptoms often associated with posterior circulation stroke. Improved diagnostic accuracy may increase access to acute stroke therapies and thereby improve outcomes.
Trial registration number
N/A
AS01-021
RELATIONS BETWEEN ECHOCARDIOGRAPHY FINDINGS AND INFARCT SIZE IN PATIENTS WITH ESUS
1Tokyo Women's Medical University, Neurology, Tokyo, Japan
2Tokyo Women's Medical University, Cardiology, Tokyo, Japan
Background and Aims
The aim of this study is to examine the associations between the size of cerebral infarct and echocardiography findings in patients with embolic stroke of undetermined source (ESUS).
Method
This hospital-based study included 42 consecutive patients (mean age 60.8 years; male 71.4%) with ESUS who underwent both transthoracic and transesophageal echocardiography examinations during hospitalization. We classified the infarct size on MRI into three groups; small infarct was defined as ≤15 mm in size, large infarct as ≥1/3 of the cerebral hemisphere, and medium infarct as intermediate in size between small and large infarcts. Echocardiographic findings were compared between patients with small and medium/large infarcts.
Results
Of 42 patients, 22 (52.3%) and 20 (47.6%) had small and medium/large infarct, respectively. Patients with small infarct and medium/large infarct showed significant differences in left atrial appendage flow velocity (57.2 cm/s vs. 70.5 cm/s, P < 0.05). Patients with small infarct more often had left atrial diameter enlargement (>3.8cm) (38.1% vs. 30.0%, P = 0.58) and a high E/e’ ratio (≥15) (26.3% vs. 15.8%, P = 0.42) than those with medium/large infarct. On the other hand, patients with medium/large infarct had complex aortic atheroma (either of ≥4 mm in thickness, ulceration or mobile plaque) more frequently than those with small infarct (37.5% vs. 25.0%, P = 0.62).
Conclusion
In ESUS patients, small infarct was more associated with cardioembolic pathologies, whereas medium/large infarct was related to atherosclerosis.
Trial registration number
N/A
AS01-023
THERAPEUTIC HYPOTHERMIA IN STROKE PATIENTS WITH USE OF CRANIOCEREBRAL HYPOTHERMIA HELMET: FUNCTIONAL OUTCOME AND MORTALITY
1FSBI “Presidential hospital №1”, Stroke Unit, Moscow, Russia
2FSBI “Presidential hospital №1”, Scientific Director, Moscow, Russia
3“Central state medical Academy”, Neurology, Moscow, Russia
4RUDN University, Neurology, Moscow, Russia
5A.I. Yevdokimov Moscow State University of Medicine and Dentistry, Neurology, Moscow, Russia
Background and Aims
Craniocerebral hypothermia helmet (CCH) is a non invasive method of hypothermia with preferential the brain cooling. Purpose of the work is to submit functional outcome and mortality in acute stroke patients treated with application of CCH.
Method
We have 2 groups of acute stroke patients: CCH with standard management, and control group standard management without CCH. Inclusion criteria was acute ischemic stroke 72-hours onset. Exclusion criteria was bradycardia.
First group with applications craniocerebral hypothermia helmet consisted of 87 acute stroke patients (mean age 69,7 ± 12,9, NIHSS15,4 ± 7,1 points) were treated CCH and standard protocol. Second group consisted of 20 acute stroke patients (mean age 77,2 ± 6,2, NIHSS 12,8 ± 5,7 points) were treated standard protocol, without CCH.
We used CCH for therapeutic hypothermia induction during 24 hours. We calculated Neurological status (NIHSS) before treatment, after 24 hours and after 7days, modified Rankin Scale points in 14day and mortality in 21day after stroke onset.
Results
Hypothermia group: NIHSS after 24 hours was10,6 ± 7,9, after 7days was 8,1 ± 8,2. mRS 2,59 ± 1,92points. In control group: NIHSS after 24 hours was 12,9 ± 5,9, after 7days was 12,5 ± 6,8. mRS 4,25 ± 1,62points.
There was a statistic significant difference of better NIHSS after 7 days (p = 0,028), better functional outcome mRS in 14days (p = 0,0005) in hypothermia group.
Mortality rate 9,1% in hypothermia group, in control group 25%.
Conclusion
We revealed the tendency for better regress of neurological deficit and functional outcome at the patients with CCH. Also, it reduces the rate of disability of patients. ССН could further improve functional outcome and reduce mortality.
Trial registration number
N/A
AS01-025
ANALYSIS OF BIOMARKERS IN OCTOGENARIANS WITH ISCHEMIC STROKE TREATED BY ENDOVASCULAR MECHANICAL RECANALIZATION
12nd School of Medicine - Charles University and University Hospital Motol, Neurology, Prague, Czech Republic
Background and Aims
Recent clinical trials have shown clinical benefit of thrombectomy in acute ischemic stroke also in group of patients over 80 years old. However octogenarians have a lower chance of good clinical outcome and a higher mortality rate despite successful recanalization. The aim of the study was to define biomarkers associated with good or poor clinical outcome.
Method
The design was a single comprehensive stroke centre retrospective study analyzing data of octogenarians treated with thrombectomy from January 2014 to December 2017. Patients were clinically assessed at admission and after 3 months. Good functional outcome was defined as modified Rankin Scale 0–2.
Following biomarkers were compared in relation with either good or poor clinical outcome: time to recanalization, hypertension, diabetes mellitus, Ischemic heart disease, Atrial fibrillation and levels of creatinine, troponin, glycosilated hemoglobin and N-terminal brain-type natriuretic peptide (NTproBNP).
Results
39 patients, 16(41%) men, mean age 84(80-93) years were included. Mean NIHSS on admission was 17.6(SD 7.8), mean ASPECTS was 8(5–10) points, bridging thrombolysis was given to 31(79.5%). Mean time to recanalization was 97.4(SD45.8) minutes. Good outcome occurred in 9(23.1%) patients. Mortality was 21(53.8%). Mean NTproBNP in patients with good outcome (1624.3 ± 634.2) was lower than in the patients with poor outcome with a statistically significant difference of 5468.0(95% CI, 855.1-10080.8, t(27) = 2.458, p = 0.022). Other followed biomarkers were nonsignificant.
Conclusion
The only significant biomarker able to distinguish good and poor outcome in our study was the NTproBNP, suggesting that octogenarians with severe heart failure have poor outcome even with succesfull trombectomy.
Trial registration number
N/A
AS01-026
EARLY REMOTE ISCHAEMIC CONDITIONING IN ACUTE STROKE (ERICS)
1Christian Medical College- Ludhiana, Neurology, Ludhiana, India
2Christian Medical College- Ludhiana, Radio Diagnosis and Interventional Radiology, Ludhiana, India
3University of Alberta, Medicine, Edmonton, Canada
4Medical College of Georgia- Augusta University, Neurology, Augusta, USA
Background and Aims
Despite best medical management, transient ischaemic attack (TIA) and acute ischaemic strokes have high risk of early neurological deterioration, recurrent strokes and death, particularly in first 12 weeks. Remote ischaemic conditioning (RIC) is a low-cost intervention that may improve cerebral perfusion and prevent recurrent stroke. We tested the hypothesis that self or caregiver delivered early RIC in acute ischaemic stroke for the first 12 weeks is feasible and safe.
Method
Adult TIA and ischaemic stroke patients presenting within first 48 h of symptom onset were screened. Patients with a MRI evidence of acute infarct were randomized (1:1) to receive either 4 or 6-cycles of RIC therapy sessions two times daily in both arms for 12 weeks. All patients underwent MRI, CT perfusion, Endothelial dependent flow mediated dilation assessment and Ankle brachial index at baseline, 7 days and 12 weeks.
Results
A total of 60 patients with mean ± SD age of 59.4 ± 12.4years were randomised to either 4-cycles group (n = 29) or 6-cycles group (n = 31). The median (IQR) baseline NIHSS was 5 (3–8) in the 4-cycles group and 3.5(2–7) in the 6-cycles group. Transeint capillary fragility was noted in 2 patients each with 4-cycles and 6-cycles groups. Eighty percent patients in 4-cycles group and 90% in 6-cycles completed 12 weeks of RIC therapy delivered by themselves or by the caregiver.
Conclusion
Short-term self or caregiver delivered RIC therapy is safe and feasible in acute ischaemic stroke patients. A randomised control is needed to prove the efficacy of RIC therapy to reduce infarct growth and recurrent stroke.
Trial registration number
ctri.nic.in:CTRI/2016/11/007495
AS01-028
POINT-OF-CARE TESTING OF COAGULATION IN PATIENTS TREATED WITH THE DIRECT ORAL ANTICOAGULANT EDOXABAN
1University Hospital Tübingen, Department of Neurology & Stroke, Tübingen, Germany
2Ruhr University - Heart and Diabetes Centre, Institute for Laboratory & Transfusion Medicine, Bad Oeynhausen, Germany
3University Hospital Tübingen, Department of Internal Medicine IV - Division of Clinical Chemistry and Pathobiochemistry, Tübingen, Germany
4Charité, Department of Internal Medicine and Cardiology, Berlin, Germany
Background and Aims
Edoxaban, alongside other direct oral anticoagulants (DOAC), is increasingly used for stroke prevention in atrial fibrillation. Despite treatment, stroke rate in these patients remains 1–2% per year. In this growing population of edoxaban/DOAC-treated stroke patients, rapid assessment of coagulation would be useful to guide thrombolysis or reversal therapy. However, no data exists on the effect of edoxaban on available point-of-care test (POCT) systems.
Hypothesis: Test assays of the commercially available CoaguChek (CC) and Hemochron (HC) devices are able to detect clinically relevant concentrations of edoxaban in a blood sample.
Method
We studied patients receiving a first dose of edoxaban. Subjects receiving other anticoagulants were excluded. Six blood samples were collected from each patient: before drug intake, 30min, 1, 2, and 8h after intake, and before the next dose. Coagulation-POCT and mass-spectrometry for edoxaban concentrations were performed at each time-point.
Results
120 blood samples from 20 edoxaban-treated patients were analyzed. Edoxaban concentrations ranged from 0 to 302ng/mL. Pearson’s correlation coefficient illustrated significant correlation between HC-INR , HC-ACT+, CC-INR and edoxaban-concentrations (R² = 0.86/0.59/0.53). Edoxaban concentrations >30ng/mL (threshold for thrombolysis according to the European Stroke Organisation) were detected by HC-INR >1.5 with 99% sensitivity and 98% specificity, by HC-ACT+ >118 seconds with 96% sensitivity and 62% specificity and by CC-INR >1.0 with 96% sensitivity and 44% specificity.
Conclusion
Our study represents the first systematic evaluation of coagulation POCT in edoxaban-treated patients. Available POCT devices may be able to reliably detect clinically relevant edoxaban concentrations in blood samples of stroke patients.
Trial registration number
NCT02825394
AS01-029
THE ISRAEL EMS STROKE PRE-NOTIFICATION SMARTPHONE APP A NEW TOOL TO INVESTIGATE PREHOSPITAL TRIAGE ACCURACY
1Shaare-Zedek Medical Center, Stroke Unit, Jerusalem, Israel
2Shaare-Zedek Medical Center, Interventional Neurradiological Unit, Jerusalem, Israel
Background and Aims
The Face Arm Speech Test (FAST) is the the most important stroke triage tool today for Emergency Medical Services (EMS) .But it is unclear what is the contribution of each part of FAST to identify stroke in the prehospital setting, and if other parameters could be of help to improve the triage of paramedics.We attempted to investigate the FAST triage accuracy by using the newly developed Stroke Pre-notification Smartphone App (SPSA) of the Israeli national EMS.
Method
We analyzed retrospectively our institutional stroke registry between 07/2016 07/2017 for all patients arriving for suspected stroke to our hospital. We compared, in all patient arriving with prior use of SPSA, the accuracy of clinical parameters like Mean Arterial Pressure (MAP), pulse, breathing, forced eye deviation and each part of the FAST to be able to distinguish between AS patients and those with other final diagnosis.
Results
During the analyzed time period 478 patients were admitted to our hospital with AS. 114 Patients were admitted with suspected AS using the SPSA. Only 50%(n = 57) were finally diagnosed as AS patients. MAP (p = 0.003), Arm Weakness (p = 0.004), Speech (p = 0.0016) difficulties were found to be able to distinguish between the AS patients and the AS mimickers. Face Asymmetry and forced eye deviation were not helpful to differentiate between AS and other conditions.
Conclusion
The use of SPSA can investigate triage accuracy of the classical FAST triage system and each component, and shows the need of subtracting and adding other clinical features to make the prehospital stroke triage more accurate.
Trial registration number
N/A
AS01-030
CAN TELEMEDICINE BE USEFUL IN HEALTH EMERGENCIES
1CHRU, Neurology 2, Besancon, France
2Hospital Andrée ROSEMON, Neurology, Cayenne, French Guiana
3emosist, emosist, besancon, France
Background and Aims
French Guiana is an overseas French territory with a low population density, but where stroke incidence is higher than in metropolitan France. In March 2017, there was a complete absence of neurologists throughout the entire country. The National Health Organization asked the RUN-FC stroke network to help local doctors. Within three weeks, technical issues had been resolved.
The aim of the study was to evaluate the use of the system by this new spoke.
Method
Data was gathered by RUN-FC’s registry. Parameters analysed were the number of calls, the reason for each call and the number of thrombolyses carried out from May 1 to December 31 2017. Technical problems were also analysed and subjective evaluations of the doctors involved in the network were collected.
Results
One hundred and thirty-eight patients underwent teleconsultation during the period studied, 80% of whom were admitted for stroke. Seven thrombolyses were carried out. Although the rate of thrombolysis was lower than in Franche-Comté (5% versus 13.8%), without this telestroke network, these patients would not have been thrombolysed.
The main limitations for doctors were not being used to using the system and the lack of knowledge of local health organisations (no neurosurgery on site, etc.)
Conclusion
A routine telestroke network can be useful in cases of sanitary emergency. Nevertheless, doctors need to be aware of local health organisations in order to improve the quality of patient management.
Trial registration number
N/A
AS01-031
ACUTE ISCHEMIC STROKE: A NOVEL DIAGNOSTIC ALGORITHM BASED ON TRANSCRANIAL DOPPLER CURVATURE AND VELOCITY ASYMMETRY ASSESSMENT OF THE MIDDLE CEREBRAL ARTERIES
1Neural Analytics- Inc., Data Science, Los Angeles, USA
2Erlanger Medical Center, Neurology, Chattanooga- TN, USA
Background and Aims
Previous work suggests Large Vessel Occlusions (LVO) can be associated with asymmetric inter-hemispheric cerebral blood flow velocity. Recent work by our group has shown a curvature metric to be an effective indicator of LVO. Here, we introduce a novel diagnostic algorithm for LVO detection incorporating both curvature and velocity asymmetry and assess performance relative to computed tomography angiography (CTA).
Method
33 LVO patients with CTA confirmed occlusion of the Middle Cerebral or Internal Carotid Arteries were evaluated while awaiting treatment, along with 33 non-LVO in-hospital controls (IHC), and 41 additional out-of-hospital controls (OHC). TCD scans of the Left/Right MCA were recorded in 30 sec intervals across multiple depths. Recordings from each side with the highest mean velocities were identified and used to extract curvature and velocity asymmetry metrics for analysis.
Results
Fig. 1 depicts the decision algorithm in tree form. For each patient, TCD flow curvature is first evaluated. If curvature is sufficiently low, the patient is classified as LVO. Otherwise, velocity asymmetry is assessed. The patient is then classified as LVO if asymmetry is sufficiently low. For the current data set, the algorithm demonstrated sensitivity and specificity at 97%, 88%, respectively.
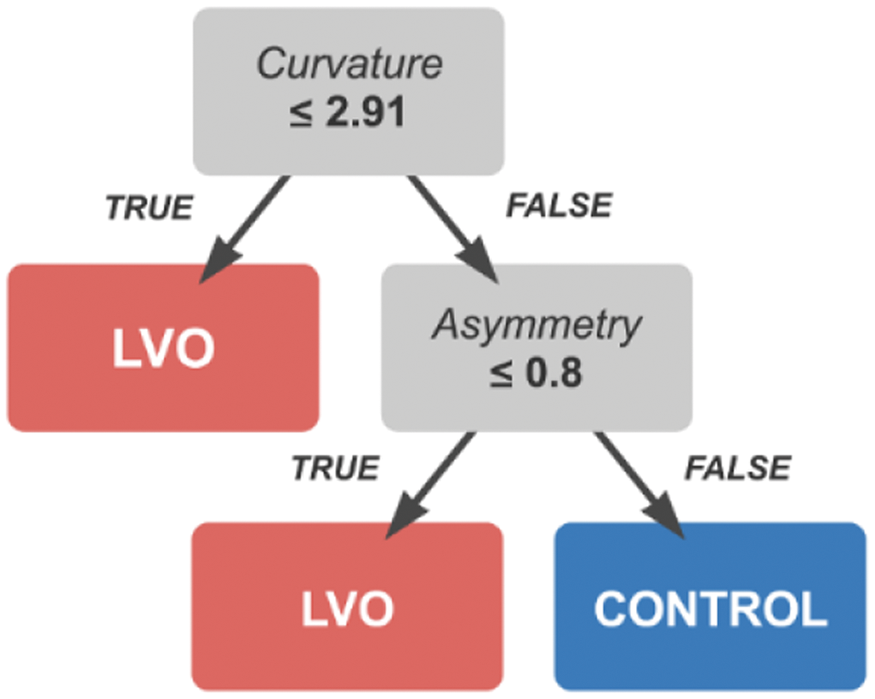
Conclusion
The current results suggest that curvature and velocity asymmetry metrics possess complimentary information concerning the presence of LVO, which together constitute a robust diagnostic.
Trial registration number
N/A
AS01-032
EFFECT AND SAFETY OF TENECTEPLASE IN STROKE PATIENTS WITH ATRIAL FIBRILLATION. THE NOR-TEST STUDY
1Oslo University Hospital Rikshospitalet, Neurology, Oslo, Norway
2Haukeland University Hospital, Neurology, Bergen, Norway
3Stavanger University Hospital, Neurology, Stavanger, Norway
Background and Aims
The purpose of study was to assess the effect and safety of intravenous tenecteplase versus alteplase in patients with acute ischemic stroke and atrial fibrillation (AF) and to assess the outcome in stroke patients with AF compared to patients with sinus rhythm.
Method
The Norwegian Tenecteplase Stroke Trial (NOR-TEST) was a multi-centre, prospective, randomized, open-label, blinded endpoint, phase 3 study including 1.100 patients with suspected ischemic stroke. The patients were randomized to receive either tenecteplase at a dose of 0.4mg/kg or alteplase at a dose of 0.9 mg/kg. AF was defined as documented paroxysmal or chronic AF prior to the ischemic stroke or documented AF during the hospital stay. Patients with AF were compared to patients without AF.
Results
183 patients (16.6 %) in the NOR-TEST population were diagnosed with AF. Compared to patients with sinus rhythm, the patients with AF were older, had more serious strokes and higher mRS score at 7 days and 3 months. There were no major differences in outcome between the tenecteplase and alteplase group in the subgroup of patients with AF. However, male sex, lower age and NIHSS was associated with better outcome.
Conclusion
This is the first randomized controlled study to report the effect and safety of tenecteplase in acute ischemic stroke in relation to AF. There were no major differences in outcome between the tenecteplase and alteplase group in the subgroup of patients with AF although female sex was associated with more serious strokes and less effect of tenecteplase.
Trial registration number
EudraCT 2011-005793-33
AS01-033
AUTOMATED COLLATERAL SCORING IN ACUTE STROKE CORRELATES WELL WITH EXPERTS AND REDUCES THEIR VARIABILITY: RESULTS FROM THE CATS STUDY
1Anglia Ruskin University, Neuroscience, Chelmsford, United Kingdom
2Hospital Bremen, Neuroradiology, Bremen, Germany
3Winnipeg University Hospital, Radiology, Winnipeg, Canada
4Brainomix, Algorithm Research and Development, Oxford, United Kingdom
5University of Oxford, Centre for Statistics in Medicine, Oxford, United Kingdom
6Southend University Hospital, Stroke, Southend-on-Sea, United Kingdom
7Saarland University Hospital, Neuroradiology, Homburg-Saar, Germany
Background and Aims
The objective of this study was to carry out a validation of the Brainomix e-CTA software for automated scoring of collaterals on CT-Angiography in acute ischaemic stroke.
Method
One hundred subjects were recruited across two sites. Three neuroradiological experts gave a Tan score for each subject, initially blinded, and then again with assistance from the e-CTA software. Following this the three experts derived a consensus score for each subject. Each of these were compared to the automated score from the e-CTA software.
Results were tabulated, and agreement assessed using the intra-class correlation (ICC).
Results
The primary outcome showed that the automated score had a very high agreement with the expert consensus score, ICC = 0.93 (0.90, 0.95). Furthermore we also found that when the experts were assisted by the software their inter-rater variability reduced, and hence the ICC increased from 0.58 to 0.77, a statistically significant difference of 0.19 (0.09, 0.31), p-value = 0.003.
Conclusion
The results show that all experts have good agreement with the automated score. The ICCs show that there is good agreement between each pair of experts.
Trial registration number
N/A
AS01-034
TRANSCRANIAL DOPPLER WAVEFORM MORPHOLOGY ASSOCIATED WITH LARGE VESSEL OCCLUSION
1Neural Analytics- Inc., Data Science, Los Angeles, USA
2Erlanger Medical Center, Neurology, Chattanooga- TN, USA
Background and Aims
Prior work suggests large vessel occlusions (LVO) can be associated with specific pathological transcranial Doppler (TCD) waveforms. Here, we seek to validate these categories by comparing the prevalence of such waveforms in a population of patients experiencing LVO relative to a population of non-LVO control patients.
Method
TCD scans of the Left/Right Middle Cerebral Arteries (MCA) were recorded in 30 second intervals across multiple depths from 33 patients with CTA confirmed LVO, and 33 non-LVO in-hospital controls (IHC). Individual beats from each interval were aligned/averaged, and dynamic time warping distances computed between all average waveforms. Individual averaged waveforms were manually classified as blunted, minimal, or dampened, according to an internally developed morphological heuristic.
Results
Fig. 1 depicts three resultant groups corresponding to “blunted”, “normal”, and “dampened” signals along with group averaged waveforms. Blunted waveforms are characterized by increased velocity and delayed/flattened peak systolic complexes while dampened waveforms by depressed velocity relative to normal. Waveform morphology of LVO patients were the majority pathologically blunted and dampened clusters, with a minority in the normal cluster.
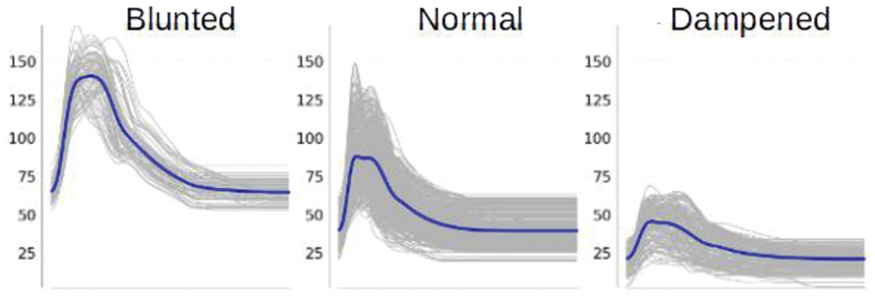
Conclusion
These results illustrate the rich diagnostic information available from non-invasive TCD waveform morphology.
Trial registration number
N/A
CLINICAL TRIAL RESULTS – ACUTE MANAGEMENT – THROMBOLYSIS OR THROMBECTOMY
AS02-001
PREDICTIVE VALUES OF T LYMPHOCYTE SUBSETS IN STROKE-ASSOCIATED PNEUMONIA
1Baotou Central Hospital, Department of Neurology, baotoushi, China
2Baotou Eight Hospital, Department of Cardiology, Baotou, China
Background and Aims
To analyze the relationship between T lymphocyte subsets and the occurrence of stroke-associated pneumonia (SAP) at early stage, and to investigate the predictive values of T lymphocyte subset changes in SAP.
Method
57 patients were admitted to the Intensive Care Unit of Neurology Department within 24h after cerebral stroke. Patients were divided into SAP group, non-SAP and control group. Peripheral venous blood was extracted to detect T lymphocyte subsets. Univariate and multivariate logistic regression analyses were used to investigate independent predictors of SAP, and the receiver operating characteristic curve was used to assess its predictive values in SAP. Moreover, dynamic trend of T lymphocyte subsets in SAP group and non-SAP group was analyzed.
Results
24h after onset, CD3 +, CD4 + and CD4+/CD8+ T lymphocytes were significantly lower, while CD8+ T lymphocytes were significantly higher in SAP and non-SAP group compared to the control group (P<0.05); CD3+, CD4+ and CD4+/CD8+ T lymphocyte levels in SAP group were lower compared non-SAP group (P<0.05) . Furthermore, levels of CD3 +, CD4 + and CD4+/CD8+ T lymphocytes 7days after stroke were higher than those measured within 24h (P<0.05).
Conclusion
CD4+ T lymphocyte count had predictive value for SAP at the early stage after cerebral stroke. In addition, CD3+T and CD4+T counts, and CD4+/CD8+T decreased in the acute stage of cerebral stroke, while CD8+T count increased, leading to decrease of cellular immune function of the body, thereby inducing pulmonary infection.
Trial registration number
N/A
AS02-002
ANALYSIS OF THE COMPLICATIONS OF MECHANICAL THROMBECTOMY IN THE TREATMENT OF ACUTE CEREBRAL ARTERY OCCLUSION
1Baotou Central Hospital, Department of Neurology, baotoushi, China
2Baotou Eight Hospital, Department of Cardiology, baotoushi, China
Background and Aims
The present study analyzed the causes of complications in mechanical thrombectomy (MT) to improve surgical safety.
Method
Medical records of the 115 patients with acute cerebrovascular occlusion who underwent MT with Solitaire AB stent were collected. Population characteristics, distribution of NIHSS scores, characteristics of the therapeutic window from onset to interventional therapy, and the types of complications and distribution sites of cerebral vessels were statistically analyzed. Statistical comparison was performed for the difference in complications of thrombectomy in different cerebral vessels, as well as, the complications in MT alone and combined thrombectomy. The occurrence of complications and mortality in MT were compared and analyzed statistically.
Results
35.65% patients with MT, suffered from complications. (1) A correlation was noted between the history of TIA disease and the occurrence of complications (P<0.05). (2) No significant difference was observed in the incidence of complications in thrombectomy among different occlusive blood vessels (P>0.05). (3) The incidence of complications in MT alone was 35% and 36%in combined thrombectomy without significant differences (P>0.05). (4) The incidences of complications in MT in different years were 66.7% in 2013, 71.43% in 2014, 25.93% in 2015, and 28.79% in 2016, which varied significantly (P<0.05).
Conclusion
(1) The probability of complications in thrombectomy was large if the patients had a history of TIA disease. (2) The improved experiences and techniques reduced the incidence of complications and mortality in MT.
Trial registration number
N/A
AS02-003
AN INDIVIDUALIZED DECISION MAKING TOOL FOR USE OF STANDARD VERSUS LOW DOSE ALTEPLASE IN ACUTE ISCHEMIC STROKE
1The George Institute for Global Health, Neurological and Mental Health, Sydney, Australia
2The George Institute for Global Health, Statistical division, Sydney, Australia
3The George Institute for Global Health, Professional Unit, Sydney, Australia
Background and Aims
Controversy persists over the net benefits of low- versus standard-dose intravenous alteplase for the treatment of acute ischemic stroke (AIS). We sought to create a practical risk-benefit tool to guide decision-making over the dose of alteplase for individualizing treatment.
Method
Observational study using data from the ENCHANTED, an international, randomized trial that assessed low-dose (0·6mg/kg) versus standard-dose (0·9mg/kg) alteplase in AIS. Logistic regression models were used to estimate the benefit of good functional outcome (scores 0 or 1 on the modified Rankin scale [mRS] at 90-days) and risk (death or symptomatic intracerebral hemorrhage [sICH]), under both regimens for individual patients. The net advantage for low-dose, relative to standard-dose, alteplase was calculated according to excess benefit minus excess risk, and by giving variable weight to risk, as opposed to benefit, a range of values for average overall net advantage were produced.
Results
Overall, 43% of the patients (weighted range 31-80%) had a positive net advantage, and could be recommended for low-dose alteplase. These patients were more likely to have lower systolic blood pressure, less severe neurological disorder, more co-morbidities of atrial fibrillation and diabetes mellitus, and pre-morbid disability.
Conclusion
Taking account of variable risk-benefit effects according to patient characteristics, the estimated net advantage of low-dose alteplase was positive in many AIS patients, either for those at high risk of sICH from co-morbidity or with mild neurological deficit. A practical tool was produced to inform treatment decisions and allow clinicians to provide their own weights to risk and benefit in an individual AIS patient.
Trial registration number
NCT01422616
AS02-004
TIME LOST, BRAIN LOST:OBSERVATIONAL PILOT STUDY OF THE OUTCOME OF POST THROMBOLYSIS IN ACUTE ISCHEMIC STROKE PATIENTS USING RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR IN TERTIARY HOSPITAL
1Corazon Locsin Montelibano Memorial Regional Hospital, Internal Medicine, Bacolod City, Philippines
Background and Aims
Background
Stroke ranked second in the top ten causes of mortality in the Philippines. Corazon Locsin Montelibano Memorial Regional Hospital (CLMMRH), is one of the selected government hospitals in the Philippines and the only tertiary hospital in Negros Island subsidized by Department of Health with recombinant tissue plasminogen activator (rTPA) to be given for FREE.
Objectives
To determine the neurological outcomes of patients with cerebrovascular disease after undergoing thrombolysis.
Method
Methodology: This study included all patients who underwent rTPA therapy within the window period of 0 to 4.5 hours, from December 2016 to June 2017 in CLMMRH. The researchers identified the age, gender, risk factors and comorbidities such as Hypertension, Diabetes mellitus, cardiovascular diseases, previous ischemic stroke, smoking, alcohol intake, dyslipidemia and the clinical features such as the BMI, blood pressure, oxygenation, CBG, prothrombin time, platelet, sodium, potassium and number of hospital day. National Institute of Health Stroke Scale (NIHSS) pre and post thrombolysis and MRS prior to discharge were compared.
Results
85% were discharged well with an improved neurological status and a
Conclusion
There is a significant difference (p-value=0.033)of neurological status of patients who were given a recombinant tissue plasminogen activator within a period of 0 to 4.5 hours.
Trial registration number
N/A
AS02-006
POINT-OF-CARE COAGULATION TESTING FOR REDUCING IN-HOSPITAL DELAY IN THROMBOLYSIS
1Asan Medical Center, Nursing, Seoul, Republic of Korea
2Asan Medical Center, Laboratory Medicine, Seoul, Republic of Korea
3Asan Medical Cetner, Nursing, Seoul, Republic of Korea
4Asan Medical Center, Medicine, Seoul, Republic of Korea
Background and Aims
The confirmation of prothrombin time international normalized ratio (INR) by central laboratory (CL-INR) often delays intravenous thrombolysis in acute ischemic stroke. We aim to investigate the feasibility, reliability, and usefulness of point-of-care testing for the prothrombin time INR (POC-INR) in stroke thrombolysis.
Method
Of 312 patients with ischemic stroke, 202 patients who arrived an emergency room within 4.5 hr of stroke onset were considered for the study. Patients who lost orders for POC-INR or CL-INR (n = 47) were excluded. We compared INR values and the time interval from arrival to reports of test results (door-to-INR time) between POC-INR and CL-INR. In patients who underwent thrombolysis, we also compared the time interval from an arrival to thrombolysis (door-to-needle time) between the current study population and historic cohort of our center.
Results
Of the 155 finally included patients, the median door-to-INR time was 9.0 min (5.0–12.0) in POC-INR and 46.0 min (38.0–55.0) in CL-INR (p < 0.001). The intraclass correlation coefficient between POC-INR and CL-INR was 0.975 (95% CI: 0.966–0.982). Forty-nine out of 155 patients underwent intravenous thrombolysis. The door-to-needle time was significantly decreased after implementation of POC-INR (median, 23.0 min; IQR, 16.0-29.8 vs. median, 46.0 min; IQR, 33.5–50.5 min).
Conclusion
Utilization of POC-INR was feasible in the management of patients with acute ischemic stroke. POC-INR was quick and reliable and had a pivotal role in expediting thrombolysis.
Trial registration number
N/A
AS02-008
RELATIONSHIP OF SYSTOLIC BLOOD PRESSURE DURING 24 HOURS AFTER THROMBOLYSIS TO CLINICAL OUTCOME IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1National Cerebral and Cardiovascular Center, Department of Neurology, Osaka, Japan
2National Cerebral and Cardiovascular Center, Division of Stroke Care Unit, Osaka, Japan
3National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
Background and Aims
The optimal management of blood pressure (BP) in acute ischemic stroke (AIS) patients receiving thrombolysis remains unclear. The present study examines the association between several BP parameters, including variability and clinical outcomes in patients with AIS who received intravenous low-dose (0.6 mg/kg) alteplase therapy.
Method
Data of AIS patients receiving thrombolysis were extracted from the National Cerebral and Cardiovascular Center Stroke Registry (ClinicalTrials.gov: NCT02251665). Systolic BP (SBP) was measured 7 times after thrombolysis during initial 24 hours. SBP variability was determined as ΔBP (maximum-minimum), standard deviation, coefficient of variation, and successive variation. Poor clinical outcome was defined as modified Rankin Scale score 3–6 at 90 days and CT-verified symptomatic intracranial hemorrhage (sICH) as any neurological deterioration within 36 hours after thrombolysis.
Results
Among 720 patients (74 ± 13 years; 270 women), 380 (53%) had poor clinical outcome and 26 (4%) sICH. In multivariable analyses, maximum (adjusted odds ratio per 10 mmHg 1.13, 95% confidence interval, 1.04 - 1.24), minimum (1.27, 1.14 - 1.42), and mean SBP (1.54, 1.35 - 1.77) were independently associated with poor clinical outcome. These parameters were not associated with sICH. Variability profiles were not associated with poor clinical outcome or sICH.
Conclusion
SBP during initial 24 hours after intravenous low-dose alteplase therapy was associated with poor clinical outcome.
Trial registration number
N/A
AS02-013
PRELIMINARY RESULTS ON SAFETY AND EFFICACY OF INTRAVENOUS TIROFIBAN BEFORE ENDOVASCULAR THROMBECTOMY FOR PATIENTS WITH ACUTE ISCHEMIC STROKE CAUSED BY LARGE ARTERY ARTHEROSCLEROSIS
1Da-Ping Hospital - The Army Medical University, ncu, Chongqing, China
2Yitu Healthcare, Yitu Healthcare, Shanghai, China
3OSF Saint Francis Medical Center, csc, San Francisco, USA
Background and Aims
Quickly achieving good reperfusion by endovascular therapy (ET) in patients with acute ischemic stroke (AIS) caused by large artery artherosclerosis (LAA) is challenging. In patients not eligible for intravenous (IV) alteplase, we investigated whether administration of tirofiban before ET (pre-ET) was safe and more effective than during ET (in-ET).
Method
Eligible patients from 1/2015 to 9/2017 were retrospectively investigated. In pre-ET group, IV tirofiban was given prior to and during ET, IA bolus tirofiban also added during the procedure if necessary. The patients of in-ET group were matched based on their gender, admission NIHSS and onset to groin puncture time. In both groups, IV tirofiban continued for 24 hours if no intracerebral hemorrhage (ICH) postoperatively. The effective outcomes included the number of thrombectomy maneuvers (NTM), 90-day modified Rankin scores (mRS). The safety outcomes included symptomatic ICH (sICH), systematic bleeding and mortality.
Results
Nineteen patients were enrolled in each group. No difference was found in the safety outcomes. The rate of sICH in Pre-ET group was 5.3%, similar to those reported undergoing ET without tirofiban. More patients in the pre-ET group achieved good reperfusion (TICI ≥2b) in ≤ 1 maneuvers compared with those in in-ET group (73.7% vs. 26.3%, P = 0.004, adjusted OR = 9.25, 95% CI 1.94-44.01), and had favorable outcome (mRS 0–2) at 90 days (42.1% vs 78.9%, P = 0.02, OR = 5.26, 95% CI 0.05-0.81).
Conclusion
Early initiation of IV tirofiban before ET appeared to be safe and potentially more effective in reperfusion procedures for AIS patients with LAA.
Trial registration number
N/A
AS02-014
THROMBOLYSIS IN STROKE WITH UNKNOWN ONSET BASED ON NON-CONTRAST CT (TRUST CT). PRELIMINARY RESULTS FROM A MULTICENTER, REGISTRY-BASED STUDY
1St. Johns Hospital Vienna, Dept. of Neurology, Vienna, Austria
2Comenius University, Dept. of Neurology, Bratislava, Slovak Republic
3Stroke Center- Lausanne University Hospital, Stroke Center- Lausanne University Hospital- Switzerland, Lausanne, Switzerland
4Institute of Cardiovascular and Medical Sciences, University Glasgow, Glasgow, United Kingdom
5University Tuebingen, Dept. of Neurology, Tuebingen, Germany
Background and Aims
Thrombolysis in wake-up stroke (WUS) or unknown onset stroke (OUS) is still considered an off-label indication contributing to low thrombolysis rates. Radiological criteria traditionally include MR- or CT-Perfusion imaging. However, in many thrombolyzing centers advanced imaging is not available 24/7. We initiated a pragmatic study to examine the safety and potential efficacy of WUS/OUS thrombolysis based on non-contrast CT (NCCT) only.
Method
TRUST-CT is a prospective multicenter registry-based study. Patients undergoing thrombolysis due to WUS/OUS with NIHSS ≥4 and initial NCCT ASPECTS ≥7 are included and compared to a propensity score matched non-thrombolyzed control group. The primary endpoint is symptomatic ICH according to ECASS3. Secondary endpoints include 24h NIHSS change of ≥4, any parenchymal ICH and modified Rankin Score (mRS) at 90 days.
Results
Currently 48 patients with WUS/OUS who were treated with NCCT-based thrombolysis were enrolled and analyzed. The median admission NIHSS was 8 and median ASPECTS was 9. No ECASS3 hemorrhage was observed. A decrease of ≥4 NIHSS points was present in 50% of the thrombolyzed patients as compared to 17% in the control group (p = 0.001). mRS 0–1 at 90 days was achieved in 42.1% of the thrombolyzed and 33.3% of the control patients (p = 0.5).
Conclusion
In an ongoing prospective multicenter registry of NCCT-based thrombolysis in WUS/OUS, preliminary results indicate possible safety and efficacy of this approach.
Trial registration number
N/A
AS02-015
MODELLING LENGTH OF STAY FOR THROMBECTOMY IN A COMPRHENSIVE UK STROKE UNIT
1Addenbrooke's hospital, Stroke, Cambridge, United Kingdom
Background and Aims
Since Mr CLEAN and 5 other trials demonstrating benefit of endovascular therapy, discussion continues around optimal service delivery across the UK. Modelling the reduction in length of stay (LOS) outside of a trial setting is required, to calculate beds days to deliver a comprehensive regional service. The NHS (UK) is working at capacity, accurate costs are central to building effective services. Locally we deliver a 9–5 service, expanding to 24/7 regional service as resources are available.
Method
We conducted a seven month retrospective audit of LOS in 2017: Patient receiving thrombectomy versus those suitable for thrombectomy but out of service hours, including both catchment and satellite hospital patients. National guideline criteria was used. All included patients received thrombolysis.
Results
There was no statistical difference in age or severity between the groups. Mean LOS for catchment thrombectomy patients: nine days. For suitable patient without thromectomy: mean LOS 34.5 days. Patients repatriated to our satellite hospital thrombectomy = five days, no thrombectomy = six days (table1).
This data demonstrates large cost savings in LOS in a non-trial setting, enabling services to invest and rapidly recoup costs, alongside improved patient outcome. Acknowledged bias: only thrombolysed patients were included.
Conclusion
Bed availability should not delay service delivery, as capacity will delivered by shorter LOS, improved patient outcome and large cost savings to health economy.
Trial registration number
N/A
AS02-018
EARLY CEREBROVASCULAR ULTRASONOGRAPHY AS A PREDICTOR OF HEMORRHAGIC TRANSFORMATION AFTER THROMBECTOMY
1Coimbra University and Hospital Centre, Neurology Department, Coimbra, Portugal
2Coimbra University and Hospital Centre, Neuroradiology Department, Coimbra, Portugal
3Coimbra University and Hospital Centre, Internal Medicine Department, Coimbra, Portugal
Background and Aims
Acute recanalization of a large vessel occlusion has a dramatic clinical impact in functional recovery. However, it increases the possibility of reperfusion lesion and hemorrhagic transformation. Reperfusion injury is initially an hemodynamic phenomenon, which through its persistency might increase tissue lesion. Transcranial Color Doppler (TCCD) might be a useful tool for early diagnosis, though its diagnostic acuity has not yet been assessed.
Method
Retrospective cohort study including consecutive patients from a 33 month period showing anterior circulation ischemic stroke with large vessel occlusion who achieved arterial recanalization after thrombectomy (final TICI 2b or 3) and had TCCD in the first 24 hours. Values included mean velocity from M1 segment of symptomatic and asymptomatic MCA and symptomatic/asymptomatic MCA ratio (RaMCA). Hemorrhagic transformation was quantified by Head CT-Scan at 24 hours.
Results
We included 101 patients, mean age of 67.99 years (SD:13.86), being 59 (58.4%) men. Mean velocity on symptomatic MCA was 59.51cm/sec (SD:20.21), while mean RaMCA was 1.06 (SD:0.36). Mean velocity for symptomatic MCA was not statistically different on patients who showed hemorrhagic transformation: 66.43cm/sec (11.17) vs. 58.78cm/sec (20.93), p = 0.072. RaMCA was higher on patients with hemorrhagic transformation: 1.32(0.39) vs. 1.02(0.34), p = 0.01. In a multivariable analysis, RaMCA remained an independent predictor of hemorrhagic transformation: OR: 6.84 (1.19-39.17) p = 0.031.
Conclusion
Early evalution of RaMCA through TCCD in the first 24 hours after ischemic stroke on patients submitted to thrombectomy is an independent predictor of hemorrhagic transformation.
Trial registration number
N/A
AS02-019
SHOULD WE RECANALIZE POSTERIOR CEREBRAL ARTERY OCCLUSIONS? INSIGHTS FROM THE TREVO REGISTRY
1Pitié-Salpêtrière Hospital, Neuroradiology, Paris, France
2Pitié-Salpêtrière Hospital, Vascular Neurology, Paris, France
3Lausanne University Hospital, Neuroradiology, Lausanne, Switzerland
4Drexel Neurosciences Institute, Endovascular Neurosurgery, Philadelphia, USA
5Riverside Methodist Hospital/ Ohio Health Research Institute, Interventional Neuroradiology, Columbus, USA
6California Pacific Medical Center, Interventional Neurology, San Francisco, USA
7Erlanger, Interventional Neuroradiology, Chattanooga, USA
8UCLA, Vascular Neurology and Neuroimaging Core Lab, Los Angeles, USA
9University Hospital Hradec Kralove, Interventional Neuroradiology, Hradec Kralove, Czech Republic
10Wellstar Health System, Interventional Neurology, Atlanta, USA
11Grady Memorial Hospital/ Emory University, Interventional Neuroradiology, Atlanta, USA
Background and Aims
The purpose of this study was to evaluate the safety and effectiveness of mechanical thrombectomy (MT) in patients with acute ischemic stroke (AIS) related to posterior cerebral artery (PCA) occlusions among the patients enrolled in the multicentre post-market Trevo Registry.
Method
Among the 2008 patients enrolled in the Trevo Registry with AIS due to large vessel occlusion treated by MT, 27 (1.3%) (14 females [51.9%], mean age: 66.7 ± 14.7 y [range 28-91]) had a PCA occlusion (15 P1 occlusions [56%], 6 P1-P2 junction occlusions [22%] and 6 P2 occlusions [22%]). Recanalization after the first Trevo (Stryker, Fremont, CA) pass and at the end of the procedure was rated using the TICI score. Procedure-related complications (i.e.: perforation, symptomatic hemorrhage, embolus in a new territory) were also recorded. mRS at 90 days was assessed.
Results
Median NIHSS at admission was 11.5 (Q1-Q3: 6–16). Stroke etiology was cardio-embolic in 74.1% of cases. 15/27 patients (55.6%) received IV tPA. 51.9% of the patients were treated under general anesthesia. Reperfusion (i.e.: TICI2b or 3) after first pass was obtained in 56% of cases. Final TICI2b-3 reperfusion was obtained in 96.3% of the cases. Only one (3.7%) procedure-related complication was recorded (puncture site). At 90-day follow-up, mRS 0–2 was obtained in 55.6% of the patients and death rate was 14.8%. The multivariate analysis showed that the only predictors for poor clinical outcome were an increased body mass index and a high initial NIHSS score.
Conclusion
MT for PCA occlusions is safe (< 4% procedure-related complications) and effective.
Trial registration number
N/A
AS02-020
STROKE THROMBOLYSIS IN THE PHILIPPINES
1Jose R. Reyes Memorial Medical Center, Department of Neurology, Manila, Philippines
2St. Luke's Medical Center - Quezon City, Department of Neurology, Manila, Philippines
3The Medical City, Department of Neurology, Manila, Philippines
4Philippine General Hospital, Department of Neurosciences, Manila, Philippines
5Baguio General Hospital, Department of Neurology, Baguio City, Philippines
6Northern Mindanao Medical Center, Department of Neurology, Cotabato, Philippines
7Zamboanga Medical Center, Department of Internal Medicine, Zamboanga City, Philippines
8St. Lukes Medical Center, Department of Neurology, Manila, Philippines
Background and Aims
Currently there is limited intervention of acute ischemic stroke. Recombinant tissue plasminogen activator (rTPA) has been approved for immediate recanalization after a steno-occlusive lesion of cerebral vessels. rTPA has shown its efficacy and safety from several clinical trials. The present study reports our experience with intravenous rTPA from several centers in the Philippines.
Method
This is a retrospective cohort study consisting of 157 patients who qualified to receive rTPA following the NINDS trial inclusion and exclusion criteria. The primary outcome is in-hospital and 3-months mortality. Other outcome measures were determined: intracranial hemorrhage secondary to hemorrhagic conversion and functional outcome as measured by modified Rankin Scale. Additionally, standard dose (0.9mg/kg) was compared to low dose (0.6mg/kg) of rTPA in terms of mortality, intracranial bleeding and functional outcome.
Results
The in-hospital mortality was seen in 23 (14.6%) and total death within 3 months was 18.3%. Independent patient (mRS 0–2) was seen in 69 (51.1%) at discharge and 95 (73.1%) at 3 months. Intracranial bleeding due to asymptomatic hemorrhagic transformation occurred in 39 (24.8%) and symptomatic hemorrhagic transformation was seen in 19 (12.1%).
Conclusion
Comparing our results with SITS-MOST and Cochrane collaborations, our data showed that we have more independent patients however death and intracranial bleeding was noted to be high in our cohort of patients.
Trial registration number
N/A
AS02-021
TENECTEPLASE IN WAKE-UP STROKE – RESULTS OF THE NOR-TEST STUDY
1Stavanger University Hospital, Neurology, Sola, Norway
2Haukeland University Hospital, Neurology, Bergen, Norway
3Haukeland University Hosapital, Neurology, Bergen, Norway
4Oslo University Hospital, Neurology, Oslo, Norway
5Stavanger University Hospital, Neurology, Stavanger, Norway
Background and Aims
Tenecteplase is a newer thrombolytic agent with some pharmacological advantages over Alteplase. The Norwegian Tenecteplase Stroke Study (NOR-TEST) showed that Tenecteplase has similar efficacy and safety compared to Alteplase. As there are no data about Tenecteplase in wake-up stroke (WUPS), we investigated the safety and efficacy of Tenecteplase versus Alteplase in the WUPS patients included in NOR-TEST.
Method
Patients eligible for thrombolysis were randomly assigned (1:1) to receive intravenous Tenecteplase 0.4 mg/kg (to a maximum of 40 mg) or Alteplase 0.9 mg/kg (to a maximum of 90 mg). WUPS patients were included if admission MRI showed mismatch between DWI-MRI and FLAIR-MRI. The clinical outcome was measured at 24 hours by the National Institutes of Health Stroke Scale (NIHSS), and at 90 days by the modified Rankin Scale at 90 days (mRS). MRI/CT was performed at 24-48 to rule out intracranial hemorrhage (ICH).
Results
Of 1107 patients included in NOR-TEST, 46 were WUPS patients (4.2%). Of these patients 24 were treated with Alteplase (52%). There was no difference in the NIHSS score measured at 24 hours between the two groups (NIHSS 1, IQR 0–9, p = 0.98). Neither was there any difference in the mRS score at day 90 (mRS 1, IQR 0–4, p = 0.68).
In none of the treatment groups ICH was detected on MRI/CT 24-28 hours after thrombolysis.
Conclusion
Compared to Alteplase, Tenecteplase appears to have similar efficacy and safety profile in WUPS patients selected by DWI-FLAIR mismatch at admission MRI.
Trial registration number
N/A
AS02-024
THROMBECTOMY IN THE ELDERLY; GOOD INITIAL NEUROLOGICAL RECOVERY DOES NOT TRANSLATE INTO LONG TERM OUTCOME
1Stavanger University Hospital, Neurology, Stavanger, Norway
2Stavanger University Hospital, Radiology, Stavanger, Norway
3Stavanger University Hospital, Biostatistics, Stavanger, Norway
Background and Aims
Endovascular treatment (EVT) is the gold standard treatment for acute ischemic stroke caused by large vessel occlusions (LVO). However, the role of EVT in the elderly remains uncertain. Our aims were to compare the initial neurological recovery and the longterm clinical outcomes between younger and elderly patients and to identify prognostic factors associated.
Method
165 patients were treated with EVT for LVO in the anterior circulation (70.3 % were < 80 years and 29.7 % > 80 years). The re-vascularization rate and clinical outcome was assessed using the modified Thrombolysis in Cerebral Infarction and National Institutes of Health Stroke Scale (NIHSS). Long term outcomes were appraised by the modified Rankin scale.
Results
Despite comparable initial neurological improvement in the elderly, only 23% achieved a good clinical outcome at 3 months as compared to 46% in the younger patients. Younger age, higher NIHSS at admission, shorter re-perfusion time, lower glucose levels at admission, and pre-EVT intravenous thrombolysis were associated with better longterm clinical outcome in the younger patients. However, none of these factors were associated with good long term clinical outcomes in the elderly.
Conclusion
Both, younger and elderly patients achieve a good and comparable initial clinical recovery in adjunct to EVT. Yet, this initial recovery does not translate into a likewise good long-term clinical outcome in the elderly. Prognostic factors predicting good clinical outcome seem to differ in the two patient groups.
Trial registration number
N/A
AS02-027
COMBINATION THERAPY OF THROMBECTOMY AND THERAPEUTIC HYPOTHERMIA IN ACUTE ISCHEMIC STROKE – A CASE SERIES
1Klinikum Darmstadt, Klinik für Neurologie und Neurointensivmedizin, Darmstadt, Germany
Background and Aims
Therapeutic hypothermia (TH) is an ideal candidate for combination with thrombectomy (TE) in acute ischemic stroke. While TH is very difficult to apply in awake stroke patients, its application in sedated and ventilated patients is more feasible. We report first data of our institutional protocol in which stroke patients receive TH, only if they are intubated and mechanically ventilated for TE.
Method
Patients receive rapid infusion of 2l of ice cold saline during TE. After admission to the neuro intensive care unit (NICU), patients remain ventilated. TH is maintained with a feed-back regulated surface cooling device at a target body core temperature of 35°C for 12 hours followed by controlled rewarming of 0.1°C per hour. So far, we have treated n = 14 patients (mean age 77 years). 9 patients received combination therapy with rt-PA. All patients reached the target temperature and remained at the desired plateau phase for the intended time.
Results
Patients could be extubated after 3.7days and remained at the NICU for a mean of 12 days. The mean NIHSS score was 16 points before treatment and significantly improved in the surviving patients. 6 patients died because of therapy limitation. 50% developed pneumonia. Mean onset of symptoms before hospitalization was 2hrs. rtPa was given after 31minutes. Mean door-to-puncture time was 176 min (22 min - 654 min), Door-to-reperfusion time was 254,1 min (118 min - 704 min).
Conclusion
Since TH could be performed in all patients without major complications, it is a candidate for a future randomized trial.
Trial registration number
N/A
AS02-028
FACTORS ASSOCIATED WITH GOOD FUNCTIONAL OUTCOME DESPITE LARGE POST-TREATMENT INFARCT VOLUME IN THE ESCAPE RANDOMIZED CONTROLLED TRIAL
1University of Calgary, Calgary Stroke Program- Department of Clinical Neurosciences, Calgary, Canada
2University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences- Radiology- Community Health Sciences- Medicine- and Hotchkiss Brain Institute, Calgary, Canada
3University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences and Radiology, Calgary, Canada
4University of Calgary, Calgary Stroke Program- Department of Radiology- Hotchkiss Brain Institute, Calgary, Canada
5King Faisal Specialist Hospital & Research Centre, Department of Neurosciences, Riyadh, Saudi Arabia
6University of Alberta, Department of Radiology, Edmonton, Canada
7University of Tennessee, Department of Radiology- Erlanger Hospital, Chattanooga, USA
8Beaumont Hospital and the Royal College of Surgeons in Ireland, Department of Neuroradiology, Dublin, Ireland
9University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences and Radiology- Hotchkiss Brain Institute, Calgary, Canada
Background and Aims
Improved outcomes after endovascular thrombectomy (EVT) are associated with smaller infarct volumes. However, some patients with large post-treatment infarct volume (PIV) fare well. We explored factors potentially associated with large PIV and good outcome.
Method
We identified ESCAPE patients (EVT/control) with PIV≥75th percentile, per 24-48-hour CT/MRI. We compared “discrepant cases”– 90-day modified Rankin Scale (mRS)≤2 despite high PIV – against “non-discrepant cases”(mRS≥3), examining imaging modality, ASPECTS locations, NIHSS, complications, demographics, and comorbidities using Fisher’s exact for binary variables and Wilcoxon rank-sum for continuous variables. Multi-variable logistic regression was used to evaluate factors independently associated with large-PIV/good-outcome.
Results
Median PIV was 21mL(IQR 7–72mL, n = 315). 80 patients had PIV≥72mL; 12(15.0%) were discrepant cases (mRS≤2). Compared to non-discrepant cases, discrepant cases had lower baseline/24-hour/48-hour NIHSS (mean 24-hour: 6.3,4.9-7.7 vs 19.9,18.4-21.4, p < 0.0001), with no differences in EVT use (33.3% vs 40.3%, p = 0.76) or CT versus MRI volume ascertainment (75.0% vs 87.9%, p = 0.36). On imaging, discrepant cases had higher ASPECTS at follow-up scanning (median 6 vs 2, p < 0.0001), less frequent lentiform involvement (25.0% vs 71.6%, p = 0.003), but no significant difference in laterality (25.0% left vs 49.3%, p = 0.21). They had lower systolic blood-pressure (134.7,124.2-145.1 vs 152.7,145.1-160.2, p = 0.03) and less frequently had cardiovascular risk-factors (58.3% vs 92.4%, p = 0.006), post-stroke complications (8.3% vs 58.2%, p = 0.001), or malignant MCA infarctions (0 vs 25.4%, p = 0.06). On multi-variable regression, lentiform involvement (p = 0.02), 24-hour NIHSS(p = 0.006), and absence of cardiovascular risk-factors (p = 0.001) or malignant infarction (perfect) were independently associated with large-PIV/good-outcome.
Conclusion
Good outcome despite large PIV is associated with absence of cardiovascular risk-factors or malignant infarction, lower NIHSS, and sparing of lentiform nucleus, the eloquence of which merits further study.
Trial registration number
NCT01778335
AS02-029
SAFETY AND OUTCOME OF ENDOVASCULAR TREATMENT IN PATIENTS WITH WAKE UP STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Leiden University Medical Center, Department of Neurology, Leiden, The Netherlands
2Erasmus MC University Medical Center, Department of Public Health, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Department of Neurology, Rotterdam, The Netherlands
4Maastricht University Medical Center, Department of Neurology, Maastricht, The Netherlands
5University Hospitals Leuven, Department of Neurology, Leuven, Belgium
6University of Leuven, Department of Neurosciences- Experimental Neurology and Leuven Research Institute for Neuroscience and Disease LIND, Leuven, Belgium
7Vesalius Research Center, Laboratory of Neurobiology, Leuven, Belgium
8Haaglanden Medical Center, Department of Neurology, The Hague, The Netherlands
9Haaglanden Medical Center, Department of Radiology, The Hague, The Netherlands
10Maastricht University Medical Center, Department of Radiology, Maastricht, The Netherlands
11Erasmus MC University Medical Center, Department of Radiology, Rotterdam, The Netherlands
12Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
13Academic Medical Center, Department of Radiology, Amsterdam, The Netherlands
Background and Aims
We assessed characteristics and outcome of WUS patients treated with endovascular treatment (EVT) in clinical practice.
Method
We used data from the MR CLEAN Registry, a prospective, multicenter, observational study, which includes all patients with anterior circulation stroke who received EVT between March 2014 and June 2016 in the Netherlands. Ordinal logistic regression was used after 1:2 propensity score matching of WUS and non-WUS patients on baseline characteristics. Primary outcome was the 3-month modified Rankin Scale (mRS) score.
Results
Ninety-two (6.0%) of 1526 treated patients were WUS. WUS patients were younger (64.9 vs. 68.8 years, p = 0.01) and less frequently received intravenous thrombolysis (47.8% vs. 78.6%, p < 0.01). WUS patients also had a longer mean time from LSW than onset to treatment (359 vs. 214 minutes, p < 0.01). After matching, there was no difference between WUS and non-WUS in 3-month mRS (adjusted common odds ratio 1.22, 95%CI 0.55-1.88), good functional outcome (mRS 0–2; 37.5% vs. 41.5%, 95%CI 0.50-1.68), successful reperfusion (eTICI≥2B; 56.8% vs. 56.3%), or mortality (20.5% vs. 21.0%). Good functional outcome rate of 38 WUS patients treated later than 6 hours after LSW was comparable to WUS patients treated within 6 hours (45.7% vs. 39.2%, p = 0.55).
Conclusion
In the MR CLEAN Registry, outcomes are comparable in WUS and non-WUS patients treated with EVT. Our findings suggest that selected WUS patients may be suitable candidates for EVT even >6 hours after LSW. A pragmatic randomized trial with lenient inclusion criteria in WUS patients is warranted.
Trial registration number
n/a
AS02-030
OPERATOR MTICI VS CORE LAB MTICI SCORES IN THE MR CLEAN REGISTRY
1the First Affiliated Hospital of Harbin Medical University, Department of Neurosurgery, Harbin, China
2Academic Medical Center, Department of Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Erasmus MC University Medical Center, Department of Radiology, Rotterdam, The Netherlands
4Academic Medical Center, Department of Biomedical Engineering, Amsterdam, The Netherlands
5University Medical Center Groningen, Department of Neurology, Groningen, The Netherlands
6Texas Stroke Institute, Division of Neurointervention, Texas, USA
7Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
8St. Antonius Hospital, Radiology, Nieuwegein, The Netherlands
9MC Haaglanden, Radiology, the Hague, The Netherlands
10Maastricht University Medical Center, Radiology, Maastricht, The Netherlands
11Erasmus MC University Medical Center, Department of Neurology, Rotterdam, The Netherlands
Background and Aims
The mTICI score is the standard method to quantify the degree of reperfusion for treatment success after EVT, and is assessed by the local interventionist after the procedure. In clinical trials, mTICI is often evaluated by an imaging core lab. The aim of this study was to compare operator mTICI with core-lab mTICI scores in patients included in the MRCLEAN Registry.
Method
Operators were asked to fill out a standard form directly after the procedure. Neuroradiologists from core lab were blinded for clinical characteristics and assessed intervention DSA in one session. Patients with an intracranial carotid artery (ICA, ICA-T) or middle cerebral artery (M1, M2, M3) occlusion with anteroposterior and lateral DSA runs were included. The overall proportion of agreement of mTICI score was estimated.
Results
1182 patients were included (occlusion site: ICA, n = 250; M1, n = 639; M2, n = 201; M3, n = 21; None, n = 71). The overall proportion of agreement was 59.0%(95%CI: 56.0%, 61.8%). In 26.9% (95% CI: 24.4%, 29.5%) the mTICI score was overestimated by operators compared to core-lab assessment and in 14.1% (95% CI: 12.2%, 16.7%) underestimated. Overall, 158 (40.9%) of the 386 patients with core lab scores 0–2a were overestimated to 2b-3 by the local site.
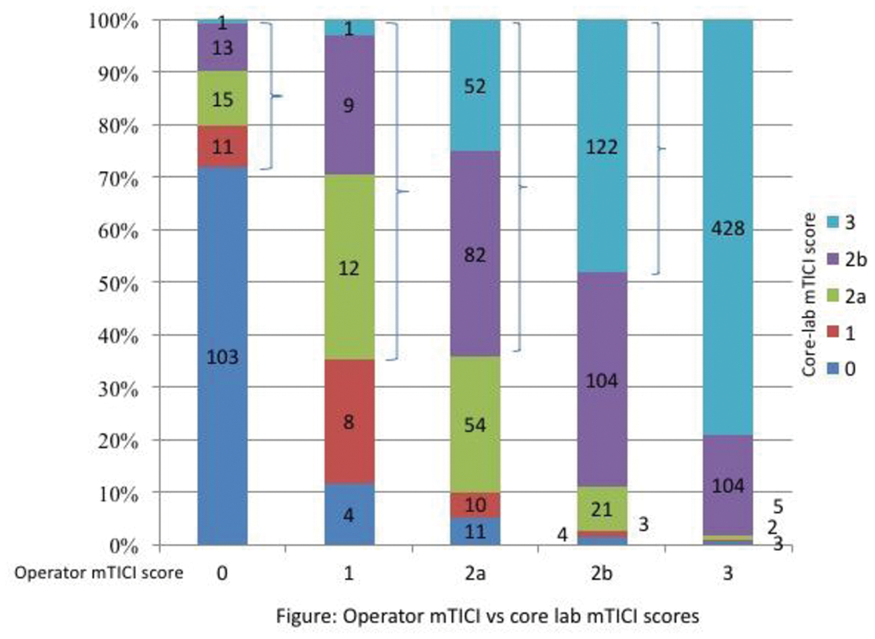
Conclusion
Masked, central core-lab assessment of DSA images is crucial for proper evaluation of intervention results in RCTs and registries of EVT.
Trial registration number
N/A
AS02-031
FACTORS ASSOCIATED WITH POOR FUNCTIONAL OUTCOME DESPITE LOW POST-TREATMENT INFARCT VOLUME IN THE ESCAPE RANDOMIZED CONTROLLED TRIAL
1University of Calgary, Calgary Stroke Program- Department of Clinical Neurosciences, Calgary, Canada
2University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences- Radiology- Community Health Sciences- Medicine- and Hotchkiss Brain Institute- Calgary- Canada., Calgary, Canada
3University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences and Radiology, Calgary, Canada
4University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences and Radiology- and Hotchkiss Brain Institute, Calgary, Canada
5King Faisal Specialist Hospital & Research Centre, Department of Neurosciences, Riyadh, Saudi Arabia
6University of Alberta, Department of Radiology, Edmonton, Canada
7University of Tennessee, Department of Radiology- Erlanger Hospital, Chattanooga, USA
8Beaumont Hospital and the Royal College of Surgeons in Ireland, Department of Neuroradiology, Dublin, Ireland
9University of Calgary, Calgary Stroke Program- Departments of Clinical Neurosciences- Radiology- Community Health Sciences- Medicine- and Hotchkiss Brain Institute, Calgary, Canada
Background and Aims
Improved outcomes after endovascular thrombectomy (EVT) are associated with smaller infarcts. However, patients with small post-treatment infarct volumes (PIV) sometimes fare poorly. We explored factors potentially associated with low PIV and poor outcome, hypothesizing differences in comorbidities and/or post-stroke complications.
Method
We identified ESCAPE patients (EVT/control) with PIV≤25th percentile, per 24-48-hour CT/MRI. We compared “discrepant cases”– 90-day modified Rankin Scale (mRS) score≥3 despite low PIV – against “non-discrepant cases”(mRS 0–2), examining imaging modality, other outcomes (Barthel Index[BI], EQ-5D), ASPECTS locations, NIHSS, post-stroke complications, demographics, and comorbidities using Fisher’s exact for binary variables and Wilcoxon rank-sum for continuous variables. Multi-variable logistic regression was used to evaluate factors independently associated with low-PIV/poor-outcome.
Results
Median PIV was 21mL (IQR 7–72mL, n = 315). 79 had PIV≤7mL; 27(34.2%) were discrepant cases (mRS≥3). Compared to non-discrepant cases with PIV≤7mL, discrepant cases had worse 90-day BI and EQ-5D (e.g. mean BI 44.6, 95%CI 27.1-62.1 vs 98.9,97.4-99.9, p < 0.001), with no significant differences in EVT use (53.9% vs 69.2%, p = 0.22) or CT versus MRI for volume ascertainment (84.6% vs 75.0%, p = 0.39). However, discrepant cases had higher 24-hour/48-hour NIHSS (mean 24-hour 8.0,5.6-10.4 vs 3.1,2.2-4.1, p = 0.0002), were older (mean age 78.1,73.5-82.7 vs 69.4,65.7-73.2, p = 0.007), more frequently had cancer (15.4% vs 0%, p = 0.01), and post-stroke complications (42.3% vs 5.7%, p < 0.0001), especially pneumonia (11.5% vs 0%, p = 0.03). On multi-variable regression, age (p = 0.025), 24-/48-hour NIHSS(p = 0.015), post-stroke complications (p = 0.007) or cancer (perfect) were independently associated with low-PIV/poor-outcome.
Conclusion
Poor outcome despite low PIV is not explained by discrepancies in imaging modality or outcome assessment, but is associated with older age, 24-/48-hour NIHSS, comorbidities (cancer), and post-stroke complications. Preventing complications may mitigate discrepant outcomes.
Trial registration number
NCT01778335
AS02-032
ACUTE ISCHEMIC STROKE IN PATIENTS ON TREATMENT WITH NON-VITAMIN K ORAL ANTICOAGULANTS - SAFETY AND EFFICACY OF NOAC PLASMA-LEVEL-GUIDED THERAPY
1University Hospital Erlangen, Neurology, Erlangen, Germany
Background and Aims
The management of patients with acute ischemic stroke during treatment with non-vitamin K oral anticoagulants (NOAC) is challenging. Functional NOAC-plasma-levels measured on admission could guide decisions on recanalization therapies.
Method
A standard operating procedure for intravenous thrombolysis (IVT) was established based on a plasma-level-guided approach: Patients with a plasma level below 50 ng/mL were considered eligible for IVT, while levels above 100 ng/mL constituted an exclusion criterion. Levels between 50 to 100 ng/mL allowed an individual decision. For patients on vitamin-K antagonists (VKA), a cutoff for IVT was set at INR 1.7. Mechanical recanalization of a large vessel occlusion was indicated independently from coagulation testing. Consecutive patients were included in an observational registry starting in January 2014.
Results
479 patients (237 on NOAC and 242 on VKA) were included. The functional NOAC-plasma level was assessed in a total of 184 (77.6%) patients who were treated with NOAC within 48 hours prior to admission. According to the SOP, 43 (17.8%) of the VKA patients and 37 (15.6%) of the NOAC patients underwent a recanalization therapy with IVT and/or endovascular therapy. Among them, there were no significant differences in functional outcome, nor in rates of major intracranial hemorrhage, which occurred in 2 (4.7%) VKA and 2 (5.4%) NOAC patients.
Conclusion
The assessment of functional NOAC-plasma levels is feasible to support decisions on recanalization therapies. Under consideration of defined thresholds, this approach does not show higher complication rates when compared to established guidelines for patients under VKA.
Trial registration number
N/A
WITHDRAWN: AS02-034
A COMPARISON OF DIRECT ASPIRATION VS. STENT RETRIEVER AS A FIRST APPROACH (“COMPASS”): A RANDOMIZED TRIAL
1Medical University of South Carolina, Neurosurgery, Charleston, USA
2Mt Sinai Hospital, Neurosurgery, New York, USA
3University at Buffalso, Department of Neurosurgery, Buffalo, USA
Background and Aims
Stent retriever thrombectomy of large vessel occlusion results in better outcomes than medical therapy alone. A recent European study designed to evaluate superior angiographic outcomes with aspiration first pass approach failed to show superiority but suggested similar clinical outcomes. COMPASS is designed to evaluate whether patients treated with a direct aspiration first pass (ADAPT) approach have non-inferior functional outcomes to those treated with a stent retriever as first-line (SRFL) approach.
Method
270 patients were enrolled into this prospective randomized open label, blinded outcome assessment and core lab adjudicated trial. Randomization was 1:1 to treatment with either ADAPT or SRFL thrombectomy. Primary outcome is non-inferiority of clinical outcome at 90d measured by the percentage of patients achieving mRS of 0–2. Secondary outcomes include angiographic outcome, procedural time, mortality and cost analyses.
Results
COMPASS completed enrollment on 07/05/17 and final Data Lock was completed on 10/31/17. Preliminary demographic and presentation-imaging analyses show excellent balance between cohorts (Table 1). COMPASS has achieved successful collection of 96% of 90d mRS for enrolled patients and 100% of imaging data. Limited preliminary results will be made available for presentation at ISC 2018. Complete data results will be made at ESOC.
Conclusion
COMPASS is the first prospective randomized open label, blinded outcome assessment and core lab adjudicated trial of patients treated with either ADAPT or SRFL approaches specifically designed to determine non-inferiority in functional outcome. Current indicators demonstrate COMPASS has achieved an extremely low loss-to-follow-up rate. These data will provide substantial insight into the appropriateness of aspiration thrombectomy.
Trial registration number
NCT02466893
AS02-035
ERASER: FIRST THROMBECTOMY STUDY WITH PREDICTIVE ANALYTICS ENDPOINT
1University Medical Center Hamburg-Eppendorf, Neuroradiology, Hamburg, Germany
2Heidelberg University, Neuroradiology, Heidelberg, Germany
3University Medical Center Hamburg-Eppendorf, Neurology, Hamburg, Germany
4Hotchkiss Brain Institute, Neuroradiology, Toronto, Canada
Background and Aims
Using a new study design we investigated whether next-generation mechanical thrombectomy (MT) methods improve clinical outcome in acute ischemic stroke (AIS) patients vs. IV tPA alone.
Method
ERASER was an investigator-initiated, prospective single-arm, multi-center study to analyze the effectiveness of a new recanalization device together with a specific intermedium catheter (ERIC/SOFIA, Microvention, USA) in AIS patients with ICA and/or MCA occlusions. Key inclusion criteria was AIS with NIH-SS score of 8–25 within 4.5h after symptom onset. The primary endpoint was the volume of saved tissue (VOST), defined as patient-individual difference of observed infarct volume and infarct volume predicted by a high-level machine-learning model trained with data from a historical IV tPA treated patient cohort with same inclusion criteria.
Results
Eighty-one patients were enrolled. Median NIH-SS score was 14 (IQR 12-17). 84% patients received intravenous tPA prior to endovascular therapy. The volume of the observed infarct volume was smaller than predicted with the IV tPA model (p < 0.0001) with a median VOST of 50 mL (IQR 19-103). Good clinical outcome (mRS 0–2 at 90 days) was observed in 77% of the patients. The rate of good recanalization (TICI 2b/3) was 93%.
Conclusion
The next-generation MT method resulted in significantly smaller infarct volumes than predicted after IV tPA therapy alone. This favorable observation is supported by the high rate of good clinical outcome and the high recanalisation rate. ERASER is the first MT study primary endpoint based on predictive analytics enabling a comparison with a historical control on the level of individual subjects.
Trial registration number
NCT02534701
AS02-038
PATIENTS WITH BRAIN TUMORS PERFORMED THROMBOLYSIS THERAPY FOR ISCHEMIC STROKE
1Tashkent medical academy, Neurology, Tashkent, Uzbekistan
2TMA, Neurology, Tashkent, Uzbekistan
Background and Aims
Thrombolysis is the most successful therapy in acute ischemic stroke. Limitations comprise strict eligibility criteria including many contraindications for thrombolysis, and in particular clinical situations lack of evidence-based data resulting in recommendations based on single experiences. Therefore, the risk-benefit effect of thrombolysis in the presence of brain tumor is unknown.
Method
We conducted a systematic literature research of electronic databases (MEDLINE) covering the period from 1990 to 2012 including search terms “thrombolysis,” “stroke,” “brain tumor,” and “intracranial neoplasm.” In addition, we report 1 new case of a 71-year-old patient with a large right frontal meningioma who fully recovered with thrombolysis from a severe ischemic stroke.
Results
Our literature research retrieved 12 patients with different brain tumors who were treated with thrombolysis for different reasons. Intracerebral hemorrhage occurred in 1 patient (8.3%) with a glioblastoma, and in the other 11 patients (91.7%), no hemorrhage was documented. In the subgroup of 8 stroke patients, both patients with a glioblastoma had no stroke but rather a focal seizure. Two of 3 patients with meningiomas showed a very good benefit from thrombolysis.
Conclusion
In summary, very limited data exist about thrombolysis in patients with brain tumors. Differentiation of tumor by additional neuroimaging before thrombolysis in ischemic stroke is recommended as thrombolysis might be considered in extra-axial benign appearing neoplasms (eg, meningioma) but is not advisable in intra-axial primary or metastatic neoplasm. Further reporting of thrombolysis in patients with brain tumors is recommended.
Trial registration number
671013
AS02-039
UZBEKISTAN TRENDS IN THROMBOLYSIS FOR OLDER ADULTS WITH ACUTE ISCHEMIC STROKE
1Tashkent medical academy, Neurology, Tashkent, Uzbekistan
2tma, Neurology, Tashkent, Uzbekistan
Background and Aims
Thrombolysis for ischemic stroke has been increasing in the United States. We sought to investigate recent trends in thrombolysis use in older adults.
Method
A retrospective, observational analysis of hospitalization data from the Nationwide Inpatient Sample (NIS) in 2005-2010 was performed. Older adults (≥65 years) admitted with a primary diagnosis of acute ischemic stroke were included. Trends in the population-based rates of thrombolysis and outcomes from the NIS were evaluated using the Cochran-Armitage test.
Results
Thrombolysis in older adult stroke patients increased from 1.7% to 5.4% (2005-2010; trend P<0.001). Large increases were observed among urban patients, urban hospitals, and high volume facilities. Individuals ≥85 years were less likely to receive thrombolysisthan younger ages throughout the study period, although there was an increase from an odds ratio of 0.50 (95% CI: 0.44-0.57) to 0.75 (95% CI: 0.69-0.81) from 2005-2006 to 2009-2010 when compared to 65-74 year olds. For those receiving thrombolysis, no change was observed in intracerebral hemorrhage over time. In-hospital mortality rates did not change significantly over the study period for age subgroups and length of stay declined from 2005 to 2010 for the thrombolysis group (7.6 vs 7.0 days; trend P<0.001).
Conclusion
Rates of thrombolysis in older adults progressively increased, especially in the oldest old. Increases were largely driven by urban and high volume hospitals.
Trial registration number
671014
AS02-040
CUTTING THE PREHOSPITAL ON-SCENE TIME OF STROKE THROMBOLYSIS IN TASHKENT: A PROSPECTIVE INTERVENTIONAL STUDY
1Tashkent Pediatric Medical Institute, Neurology, Tashkent, Uzbekistan
2Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
Background and Aims
Significant portion of the prehospital delay consists of minutes spent on the scene with the patient. We implemented a training program for the emergency medical services personnel with the aim to optimize the on-scene time (OST) and to study the impact of different elements of prehospital practice to the OST duration.
Method
In this prospective interventional study, key operational emergency medical service performance variables were analyzed from all thrombolysis candidates transported to the Tashkent hospital emergency department. The catchment period was 4 months before and 4 months after the implementation.
Results
One hundred and forty-one patients were managed as thrombolysis candidates before and 148 patients after the training program implementation. The OST duration for the groups was 25 (20.5-31) and 22.5 (18-28.5) minutes, respectively (P<0.001). Physician consultations via telephone were associated with a longer (odds ratio 0.546 [0.333-0.893]) and advanced life support training with a shorter OST (odds ration 1.760 [1.070-2.895]).
Conclusion
Implementation of the emergency medical services training program successfully decreased the OST of thrombolysiscandidates by 10%. Higher expertise level of the ambulance crew was associated with shorter OST, and decisions to consult a physician via telephone were reflected by longer OST.
Trial registration number
880712
AS02-042
ADMISSION HYPERGLYCEMIA AND IMAGING OUTCOMES IN PATIENTS WITH ACUTE ISCHAEMIC STROKE UNDERGOING ENDOVASCULAR TREATMENT
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Leiden University Medical Center, Neurology, Leiden, The Netherlands
Background and Aims
Admission hyperglycemia is a risk factor for poor outcome after acute ischemic stroke (AIS) and this association also appears to apply to patients undergoing endovascular treatment (EVT). We examined whether the association between hyperglycemia and poor outcome can be attributed to poor imaging outcomes after EVT.
Method
We used data from the MR CLEAN Registry, an ongoing, prospective, observational study performed at EVT centers in the Netherlands. We excluded patients with missing admission glucose levels. Hyperglycemia was defined as a glucose concentration ≥ 7.8 mmol/L. Endpoints were succesful reperfusion (eTICI≥2B), rate of symptomatic intracerebral hemorrhage (sICH), and good intracranial collaterals (collateral score ≥ 2). We used logistic regression analysis to adjust for confounders.
Results
We included 1316 patients, of whom 392 (30%) had admission hyperglycemia. Hyperglycemic patients were older (70 vs 68 years, p = 0.008) and more often had pre-existing diabetes (39% vs 8%, p < 0.001) than normoglycemic patients. sICH occured more often in hyperglycemic patients (8% vs 5%, p = 0.01). There was no difference in frequency in good collaterals (57% vs 62%, p = 0.14) or succesful reperfusion (57% vs 59%, p = 0.44). After adjustment, admission hyperglycemia was associated with an increased risk of sICH (aOR 1.81;95% Cl 1.12-2.91). There was a trend towards a lower chance of good collaterals in hyperglycemic patients (aOR 0.80; Cl 0.63-1.03).
Conclusion
Hyperglycemia increased the risk of sICH after endovascular treatment in patients with acute ischemic stroke, which may partly explain the association between hyperglycemia and poor clinical oucome.
Trial registration number
N/A
CLINICAL TRIAL RESULTS – PREVENTION
AS03-001
THE EFFICIENCY OF FLAIR IMAGES FOR HEMODYNAMIC CHANGE AFTER STA-MCA BYPASS WITH MOYAMOYA DISEASE AND SYMPTOMATIC STENO-OCCLUSIVE DISEASE
1Eulji University Hospital, Neurosurgery, Daejeon, Republic of Korea
Background and Aims
MR perfusion and SPECT are well known imaging to evaluate hemodynamic change after STA-MCA bypass. But their side effects and invasiveness make discomfort to patients. We evaluated “Ivy sign” and “spaghetti sign” on MR FLAIR in adult patients with Moyamoya disease and steno-occlusive disease performed STA-MCA bypass and compared it with result of SPECT and MR perfusion.
Method
We enrolled 49 patients and we compare the Ivy sign and spaghetti sign score on preoperative and postoperative MR FLAIR. The correlations between FLAIR images and hemodynamic status measured by and MR perfusion were evaluated.
Results
Among 49 patients, 17 were treated with Moyamoya disease, and 32 were symptomatic steno-occlusive disease. Minimal and Positive Ivy and Spaghetti sign was seen in all. In Moyamoya group, Ivy signs score on MR FLAIR were improved (10 preoperative and 5 postoperative in ACA territory, 17 and 5 in anterior MCA territory, and 24 and 11 in the posterior MCA territory). In symptomatic steno-occlusive disease group, Spaghetti signs score on MR FLAIR were also improved. (12 preoperative and 7 postoperative in ACA territory, 23 and 10 in anterior MCA territory, 7 and 4 in posterior MCA territory). Like this result, CVR on SPECT was significantly increased in the sum of CVR in same regions after STA-MCA bypass.
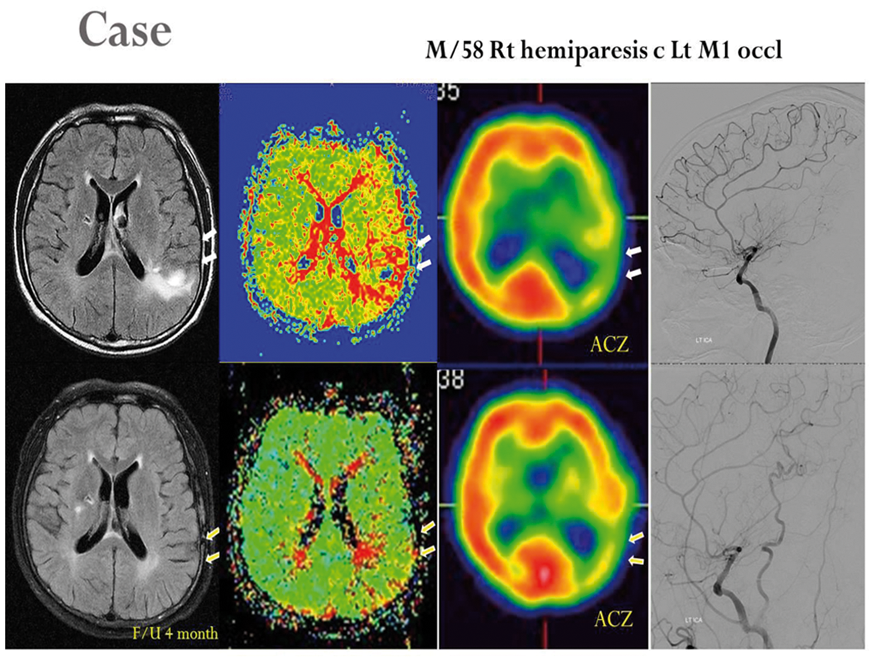
Conclusion
As compared with conventional diagnostic modalities such as SPECT and MR perfusion images, Ivy sign and Spaghetti sign on MR FLAIR is considered as a useful indicator in detecting brain hemodynamic changes between preoperatively and postoperatively after STA-MCA bypass.
Trial registration number
N/A
AS03-003
CHARACTERISTICS AND TEN-YEAR PROGNOSIS OF PATIENTS TREATED WITH ASPIRIN PRIOR TO A FIRST-EVER ACUTE ISCHEMIC STROKE. DATA FROM THE ‘ATHENS STROKE OUTCOME PROJECT’
1School of Medicine - University of Ioannina, Internal Medicine, Ioannina, Greece
2School of Medicine-University of Thessaly, Internal Medicine, Larisa, Greece
3National and Kapodistrian University of Athens, First Department of Neurology, Athens, Greece
4Leeds Teaching Hospitals NHS Trust and School of Medicine- Faculty of Medicine and Health- University of Leeds, Stroke Service- Department of Neurosciences, Leeds, United Kingdom
5Hellenic Stroke Organization, Hellenic Stroke Organization, Athens, Greece
Background and Aims
To assess the clinical characteristics and the ten-year prognosis of patients treated with aspirin prior to a first-ever acute ischemic non-cardioembolic stroke (AINCS).
Method
This was a retrospective study involving a total of 1,782 patients hospitalized due to a first-ever AINCS; of those, 14% (n = 257) were treated with aspirin (ASA group) for elective purposes, while 1,525 patients received no antiplatelets (non-ASA group) prior to the index event. Primary endpoints included: time to stroke recurrence, composite cardiovascular event (stroke recurrence, myocardial infarction, unstable angina, coronary revascularization, peripheral atherosclerotic artery diseases, or sudden death), and all-cause mortality.
Results
Subjects pre-treated with aspirin had higher composite cardiovascular event-free survival (log rank test: 4.79, p = 0.029) and 10-year mortality (log rank test: 6.8, p = 0.012) compared with the non-ASA group, while there was no difference in time to stroke recurrence (log-rank test: 0.039, p = 0.84). Age (hazard ratio, HR 1.07; 95%CI: 1.04-1.09, p < 0.001), stroke severity on admission (HR: 1.05; 95%CI: 1.03-1.08, p < 0.001), heart failure (HR 2.32; 95%CI: 1.24-4.36, p < 0.01) and peripheral artery disease (HR 2.25; 95%CI: 1.15-4.39, p < 0.05) were associated with higher 10-year mortality in the ASA group. Of note, the rate of cardiovascular events were higher among male patients (HR 2.27; 95%CI: 1.04-4.98, p <0.05) but lower among those treated for dyslipidemia prior to the index stroke (HR 0.58; 95% CI: 0.36-0.93, p <0.05).
Conclusion
This study indicates that elective treatment with aspirin prior to an AINCS does not affect long-term stroke recurrence but increases mortality and cardiovascular morbidity.
Trial registration number
N/A
AS03-009
THE METABOLIC SYNDROME AND THE RISK OF CEREBRAL VENOUS AND SINUS THROMBOSIS: A CASE–CONTROL STUDY
1Isfahan Neurosciences Research center- Isfahan University of Medical Sciences, Neurology- Alzahra Hospital, Isfahan, Iran
2Tehran University of Medical sciences, Neurology, Tehran, Iran
3Hypertension Research Center- Isfahan Cardiovascular Research Institute- Isfahan University of Medical Sciences- Isfahan- Iran., cardiology, Isfahan, Iran
Background and Aims
There is no data about the significance of the metabolic syndrome (MeS) for the development of cerebral venous and sinus thrombosis (CVST). We investigated the association of the metabolic syndrome in a consecutive series of patients with CVST in comparison to control subjects.
Method
In a case–control study, consecutive patients with confirmed CVST and control subjects underwent clinical assessment for the presence of the MeS according to the National Cholesterol Education Program criteria. The prevalence of the MeS was compared between patients with CVST and controls.
Results
We enrolled 58 patients with a first episode of CVST and 129 controls. In univariate analysis, MeS was significantly more common in CVST patients than in controls [28 (48.3%), (28) 21.7%; odds ratio (OR) 3.36; 95% confidence interval (CI) 1.77, 6.53, p < 0.001]. After adjustment for age, sex, MeS, OCP usage, we found OCP usage (OR 22.7; 95% CI 7.75, 66.66, p < 0.001) and the metabolic syndrome (OR 3.26; 95% CI 1.15, 9.25, p = 0.02) to be independently associated with CVST. When coexistence of OCP usage and MeS was considered as a variant in univariate analysis comparing CVST patients and controls, we found independently association with CVST with higher OR (OR 47.6; 95% CI 5.91, 333.3, P< 0.001).
Conclusion
In conclusion, patients with CVST have a significantly higher prevalence of the metabolic syndrome than controls. CVST is a disease with multiple risk factors and coexistence of metabolic syndrome OCP usage can potentiate the risk of CVST occurrence.
Trial registration number
N/A
AS03-013
A PERSONALIZED, DIGITAL COACHING PROGRAM AFTER STROKE (BEROERTECOACH.BE): PATIENTS AND CAREGIVERS VIEW ON USABILITY AND APPLICABILITY
1Antwerp University Hospital, Neurology, Antwerpen, Belgium
2AZ Sint- Lucas, Neurology, Bruges, Belgium
3AZ Sint- Jan, Neurology, Bruges, Belgium
4AZ Groeninge, Neurology, Kortrijk, Belgium
5Trendhuis, Trendhuis, Mechelen, Belgium
Background and Aims
A pilot project consisting of a stroke coach and a digital platform was enrolled in four Belgian hospitals with the aim of improving secondary prevention after stroke.
Method
The participating centers recruited 147 patients for a follow- up period of 6 months. The stroke coach provided at least one educational session during hospitalization. After discharge, the patient received individualized tips and tricks concerning a healthy life style through the platform. The stroke nurse overviewed recorded parameters and set up either a video-appointment or a phone interview through the platform at regular intervals.
Questionnaires about utility of the stroke coach and usability of the platform were obtained from patients and caregivers. 73 patients and 14 neurologists completed the evaluation.
Results
96% of patients would recommend the stroke coach and digital platform to others. Advantages reported by the patients were the early follow- up, additional support and easy access to the coach through the platform. 84% of the patients felt they had enough information about stroke. However 55% still prefer regular appointments with his/her neurologist instead of a predominantly online- based follow- up.
Neurologists agree that additional follow- up of their patients through the stroke coach and the platform is an added value for their patients and increases patient compliance. In daily practice there was no perceived time gain with follow- up through the platform.
Conclusion
Both patients and caregivers believe the stroke coach and the digital platform provide added value to patient follow- up after stroke.
Trial registration number
NCT03038685
AS03-014
EVALUATION OF INFLAMMATORY MARKERS IN CHRONIC STROKE PATIENTS FOR THE SELECTING DRUG THERAPY FOR THE PURPOSE OF SECONDARY PREVENTION OF STROKE
1FGBOU VO Russian National Medical Research University NI Pirogova, Neurology, Moscow, Russia
Background and Aims
The purpose of this research is to study the endothelial dysfunction process in chronic stroke patients by measuring the levels of endothelial inflammation markers such as myeloperoxidase (MPO), E-selectin, intercellular adhesion molecule-1 (ICAM-1), determined by the ELISA method.
Method
The research included 53 patients with atherothrombotic stroke. Group 1 – stroke from 1 to 6 months (n = 35), group 2 – from 7 to 12 months (n = 18).
Results
All the post-stroke patients had significantly higher MPO and sICAM-1 levels and unexpectedly significantly lower sE-selectin concentration than healthy controls. The comparison of two groups of post-stroke patients did not reveal significant differences in the MPO level, however the level of sICAM-1 was significantly higher in the group 2. According to the literature data the sICAM-1 level increases in patients with type 2 diabetes mellitus. After the exclusion of the patients with diabetes the correlation for sICAM-1 remained the same.
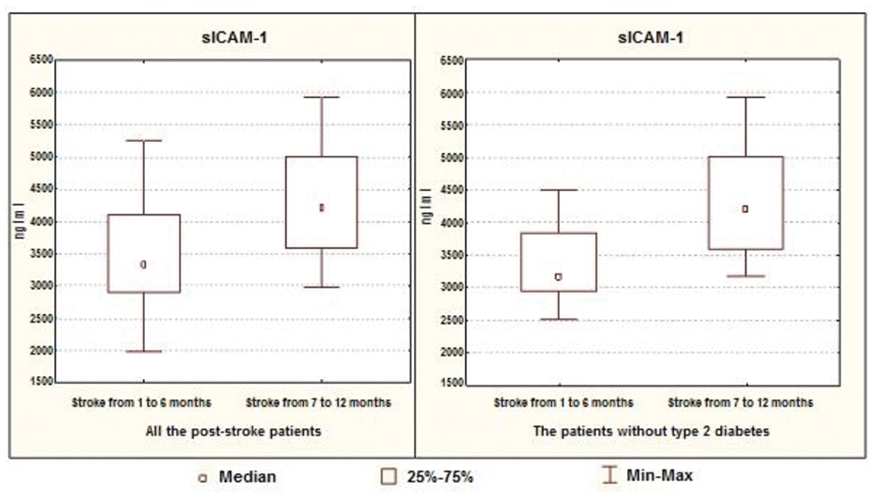
Conclusion
The obtained results indicate the progression of immune inflammation in post-stroke patients, associated with endothelial dysfunction on the cerebral ischemia background, which persists probably because of the prolonged activity of inflammatory process and the depletion of anti-inflammatory mechanisms. This chronic endothelial inflammation should be corrected in post-stroke patients using the drugs affecting the cell adhesion and endothelial dysfunction to improve cerebral circulation, to improve the disease prognosis, to provide secondary prevention of stroke.
Trial registration number
N/A
AS03-015
COMPARISON OF THE EFFECT ON BLOOD PRESSURE VARIABILITY IN ACUTE ISCHEMIC STROKE: FIMASARTAN VS. VALSARTAN
1Gachon University Gil Medical Center, Department of Neurology, Incheon, Republic of Korea
2Gachon University of Medicine and Science, Department of biomedical engineering, Incheon, Republic of Korea
Background and Aims
Increased blood pressure (BP) variability is associated with evidence of increased target organ damage in the elderly and hypertensive populations and increased cardiovascular morbidity and mortality. This randomized controlled study conducted to compare the effect on BP variability between valsartan and fimasartan (Boryung Pharm. Co., Ltd., Seoul, Republic of Korea) in acute ischemic stroke patients.
Method
We enrolled 65 patients with acute ischemic stroke prospectively. Sixteen patients were dropped out. Patients were randomly assigned to receive either valsartan (n = 24) or fimasartan (n = 25) after 7 days from stroke onset for 8 weeks. We measured 24 hours BP data at before and after 8 weeks starting BP medication. We calculated several index such as standard deviation (SD), weighted 24-hour BP SD (wSD), coefficient of variation (CV), average real variability (ARV), and smoothness index (SI) to assess BP variability and compared the indexes of BP variability between two drugs.
Results
SD of systolic BP in daytime and nighttime of patients after 8 weeks receiving fimasartan showed significant lower than valsartan . In paired t-test, wSD, CV of systolic BP and diastolic BP were significantly increased after 8 weeks and day and night pulse pressure were significantly decreased in patients receiving valsartan. However, SD of day and night systolic BP and day and night pulse pressure were significantly decreased and SI of systolic BP was significantly increased in patients receiving fimasartan.
Conclusion
Our study showed that fimasartan has the better effect for reducing BP variability after acute ischemic stroke than valsartan.
Trial registration number
N/A
AS03-016
A PERSONALIZED, DIGITAL COACHING PROGRAM AFTER STROKE (BEROERTECOACH.BE): PRELIMINARY RESULTS
1Antwerp University Hospital, Neurology, Antwerpen, Belgium
2AZ Sint- Lucas, Neurology, Bruges, Belgium
3AZ Sint- Jan, Neurology, Bruges, Belgium
4AZ Groeninge, Neurology, Kortrijk, Belgium
5Trendhuis, Trendhuis, Mechelen, Belgium
6University of Leuven, Public Health, Leuven, Belgium
Background and Aims
A pilot project consisting of a stroke coach and digital platform was enrolled in four Belgian hospitals with the aim of improving secondary prevention after stroke.
Method
The participating centers recruited 147 patients for a follow- up period of 6 months. The stroke coach provided at least one educational session during hospitalization. After discharge, the patient received individualized tips and tricks concerning a healthy life style through the customized platform. The stroke nurse overviewed recorded parameters and set up video-appointments through the platform at regular intervals. Risk factor control, measured by calculation of the SCORE © risk of this group at 6 months will be compared with a historical control group (n = 70) who received standard care.
Results
To date, we can present the first preliminary results. For now, we have complete baseline data of 97 patients in the intervention group. 77% of them are men with a mean age of 64.9 years (SD = 10.3). 78% had a prestroke mRS of 0 or 1. Stroke severity is mild with a mean NIHSS of 2 (SD = 5). SCORE of 39 patients is known at baseline and at 3 months. At baseline the mean SCORE is 13.2 (SD = 13.3) with a significant reduction of 3.973 (t36 = 3.52, p = 0.0012) at 3 months. All patients finish their coaching program before May 2018.
Conclusion
Our preliminary data suggest a potential benefit of the stroke coach and digital platform in secondary prevention after ischemic stroke. However we await further data and hope to present our definitive results at the ESOC .
Trial registration number
NCT03038685
AS03-018
SLEEP APNOEA SYNDROME AS A CAUSE OF POOR BLOOD PRESSURE CONTROL IN A DUBLIN STROKE UNIT – A PROSPECTIVE ANALYTICAL STUDY
1Connolly Hospital, Medicine for the Elderly, Dublin, Ireland
Background and Aims
The incidence of Stroke is closely related to systolic blood pressure (SBP)levels. Sleep apnoea syndrome (SAS) is underdiagnosed and raises nighttime SBP . We aim to evaluate BP from ward measurements and ABPM measurements and relate it to overnight pulse oximetry as an indicator of SAS.
Method
We selected a sample of 14 participants from our acute stroke ward. The variables were average BP value on the ward on the day of assessment, ABP measurements and presence of SAS criteria by pulse oximetry. The status of “dipper”(n = 8) was given to those with a ≥10%fall , “nondippers”(n = 6) with ≥0% but <10% fall; and “reverse-dippers”(n = 0)with <0% fall in the day time average BP.
Results
The prevalence of uncontrolled BP was 21% on ward evaluation and 86% on ABPM. This higher rate of pickup of hypertension was statistically significant as per Fisher exact test (p = 0.0018). It was found that 71% had daytime hypertension, 71% had nocturnal hypertension and 42% had a non-dipper profile. The prevalence of SAS was 28.5%. We found a statistically significant association between SAS and non-dipper profile (p = 0.015) however associations between SAS and day time and nocturnal hypertension were not statistically significant.
Conclusion
ABPM showed a 65% increased sensitivity compared to ward BP values at detecting poor BP control. SAS is strongly associated with the “non dipper” profile. Our findings indicate that SAS is a significant cause secondary cause of hypertension in these patients which can be quickly screened for in a non-specialist setting.
Trial registration number
N/A
AS03-019
SAFETY, PHARMACOKINETICS, AND PHARMACODYNAMICS OF AN ORAL FORMULATION OF DS-1040, AN INHIBITOR OF THE ACTIVATED FORM OF THROMBIN-ACTIVATABLE FIBRINOLYSIS INHIBITOR (TAFIA), IN HEALTHY SUBJECTS
1Daiichi Sankyo- Inc., Clinical Development- Cardiovascular and Metabolism Therapeutic Area, Basking Ridge, USA
2Daiichi Sankyo- Inc., Quantitative Clinical Pharmacology and Translational Sciences, Basking Ridge, USA
3Daiichi Sankyo- Inc., DSI Clinical Development Operations, Basking Ridge, USA
4Worldwide Clinical Trials, Clinical Trials, San Antonio, USA
5Daiichi Sankyo- Inc., Clinical Biomarkers- Translational Medicine and Clinical Pharmacology, Basking Ridge, USA
6Daiichi Sankyo- Inc., Quantitative Clinical Pharmacology & Translational Sciences, Basking Ridge, USA
7Daiichi Sankyo- Inc., Biostatistics and Data Management, Basking Ridge, USA
8Daiichi Sankyo- Inc., Early Development Operations, Basking Ridge, USA
Background and Aims
This randomized, placebo-controlled, phase 1 study evaluated the safety, pharmacokinetics (PK), and pharmacodynamics (PD) of an oral formulation of DS-1040—the activated form of thrombin-activatable fibrinolysis inhibitor (TAFIa)—in healthy subjects.
Method
Healthy adults (aged 20–45 years; N = 56) were randomized 1:3 to receive placebo or DS-1040 administered as single ascending oral doses (50, 100, 200, or 400 mg; part A) or multiple ascending oral doses (100 mg once daily, 200 mg once daily, or 150 mg twice daily, for 14 days; part B). Safety and PK/PD parameters were assessed.
Results
All doses of DS-1040 were well tolerated; no serious/severe adverse events (AEs) or discontinuations due to AEs occurred. At the dose regimens tested, DS-1040 had no effect on coagulation parameters, and no treatment-related trends in the mean bleeding time were observed. Mean half-life ranged from 17.2–24.9 hours. There was a dose-proportional increase in exposure (Cmax and AUC) of DS-1040 following the ascending single and multiple DS-1040 doses. Minimal accumulation was observed with multiple dosing (accumulation ratio ranged from 1.15–1.25). Approximately 9% of the highest multiple oral dose of DS-1040 (150 mg twice daily) was recovered in urine as the intact parent drug (24-hour collection on day 14). A dose-dependent inhibition of total TAFIa activity was observed following single and multiple doses of oral DS-1040. Increased D-dimer levels following DS-1040 administration were evident in some subjects.
Conclusion
Safety and PK/PD profiles demonstrated with oral DS-1040 in healthy subjects support further clinical development.
Trial registration number
phase 1
AS03-020
THROMBUS HISTOPATHOLOGY FROM THROMBECTOMY, AN IMPORTANT SECONDARY PREVENTION TOOL?
1ULB-Hôpital Erasme, Neurology, BRUXELLES, Belgium
2ULB-Hôpital Erasme, Anatomo-pathology, Bruxelles, Belgium
3ULB-Hôpital Erasme, Neurointerventional radiology, Bruxelles, Belgium
Background and Aims
Atrial fibrillation (AF) is responsible for substantial proportion ischemic strokes (IS) and need in some cases a prolonged cardiac heart rate monitoring to be detected, sometimes months after stroke index. However, optimal secondary prevention for cardioembolic (CE) stroke requires early initiation of anticoagulant therapy. We aimed in this study to assess if thrombus histopathology (TH) was reliable enough to base early specific stroke secondary prevention therapy upon its results.
Method
28 patients who had underwent thrombectomy for IS due to proximal occlusion and TH examination were included. Stroke etiologies based on TOAST classification at hospital discharge after ECG, 24h-telemetry and cardiac echography, and at follow-up after ambulatory 24h-ECG were compared to TH diagnosis. Positive and negative predictive values of TH for CE strokes were calculated.
Results
Of the 28 thrombi analyzed, 20 had a CE histology. Among these 20 patients, 13 early-proved AF based on the initial ECG/24h-telemetry were found and the follow-up 24h-ECG allowed to record AF in 3 more patients. 8 TH were classified as unknown or atherothrombotic, of those follow-up disclosed CE stroke in 4.TH has positive and negative predictive values of 85 % and 50% for CE strokes, respectively.
Conclusion
TH may be useful to identify earlier patients with a CE stroke, help giving a more accurate secondary prevention treatment in a substantial proportion of patients and prevent foreseeable recurrences. Further studies including more patients are needed to strongly demonstrate the TH reliability to base the stroke secondary prevention treatment early decision.
Trial registration number
N/A
AS03-021
RISK FACTORS FOR UNFAVORABLE OUTCOMES AND COMPLICATIONS IN PATIENTS WITH BILATERAL ATHEROSCLEROTIC OCCLUSIVE-STENOTIC DISEASE OF ICA
1Sklifosovsky Research Institute of Emergency Care, Neurosurgical department, Moscow, Russia
2MSUMD n.a. A.I. Evdokimov, department of neurosurgery and neurointensive care, Moscow, Russia
Background and Aims
To determine the risk factors for unfavorable outcomes and complications in patients with bilateral atherosclerotic disease of ICA.
Method
1463 patients with ICA atherosclerotic disease were operated on from 01.01.2010 till 31.12.2017, among them 82 (5,6%) patients (study group) were selected for retrospective analysis according to inclusion criteria. Bilateral ICA stenosis was seen in 73,2%(n = 60), combination of ICA stenosis and ICA occlusion – 23,2%(n = 19), bilateral ICA occlusion – 3,6%(n = 3). The surgical procedures included: 1)138 carotid endarterectomies, among them 42%(n = 58) – on «symptomatic» side; 2) 25 STA-MCA bypasses with 100% patency.Symptomatic ICA occlusions (73%) and stenosis (69,5%) were operated as first step, interval between operations varied from 6 till 902 (Ме=105) days. Control group included 590 patients with isolated ICA atherosclerotic disease, 27,1% (n = 160) had ICA occlusion.
Results
All patients with «symptomatic» ICA atherosclerotic disease demonstrated the improvement in neurological status (in average on 1,2 scores (NIHSS), 0,3 scores (mRs) and 2,1 scores (Rivermead mobility index)) and in cerebral perfusion measurements. Combined parameter «stroke + lethality from stroke» was 6,1% in study group comparing with 5,4% in control group (p>0,05). The only significant risk factor for unfavorable outcomes and complications in study group was interoperational interval<21 days (р<0,05).
Conclusion
«Symptomatic» side should be operated first with the interoperational interval not less than 3 weeks before second procedure in patients with bilateral ICA atherosclerotic pathology. The frequency of perioperative ischemic complications was not related to type of arteriotomy suturing, time of arteries cross-clamping and usage of temporal intraluminal shunt.
Trial registration number
N/A
AS03-022
HIGH RISK FOR FUTURE VASCULAR EVENTS IN NON-EMBOLIC ISCHEMIC STROKE WITH AN ANKLE-BRACHIAL INDEX LESS THAN 0.9
1Saint Joseph University, Neurology, Beirut, Lebanon
2Bichat University Hospital, Department of Neurology and Stroke Center, Paris, France
3National Institute of Neurology, National Institute of Neurology, Mexico City-, Mexico
4Groote Schuur Hospital- University of Cape Town, Division of Neurology and Stroke Unit, Cape Town, South Africa
5Clinica Alemana de Santiago- Universidad del Desarrollo and Department of Neurological Sciences, Neurology Service- Department of Medicine, Santiago, Chile
6São Paolo university, Neurologia, São Paolo, Brazil
7Clinica de Marly, Neurologia, Bogota, Colombia
8American University of Beirut Medical Center, Department of Neurology, Beirut, Lebanon
9Bichat University Hospital, Department of Cardiology, Paris, France
10Fernand Widal Hospital- Denis Diderot University – Paris VII, Department of Biostatistics, Paris, France
Background and Aims
Low ankle-brachial index (ABI) identifies a stroke subgroup with high risk of recurrent stroke, cardiovascular events and death. We evaluated the prevalence of ABI ≤ 0.90 in non-embolic stroke patients or transient ischemic attack from low and middle-income countries and assessed the correlation of low ABI with stroke risk factors and recurrent vascular events and death
Method
3.487 patients were enrolled from over 17 low and middle income countries.
Results
Only 93 patients had missing ABI. Abnormal ABI (< 0.9) was present in 22.3 % of patients. Patients with an ABI of ≤0.9 were more likely (p < 0.05) to be male, older and have a history of PAD, hypertension and diabetes.During the two-year follow-up, the rate of major cardiovascular event was higher in those with ABI<0.9 than those with ABI≥0.9 (Kaplan-Meier estimates, 22.5%; 95% CI [19.6-25.8] vs. 13.7% [21.4-15.1], p < 0.001) and when patients were distributed in 4 ABI groups (≤0.6 ; 0.6-0.9; 0.9-1; 1–1.4), the rate of major cardiovascular event was higher in those with ABI≤0.6 than the other groups (Kaplan-Meier estimates, 32.6% 95% IC [21.0-48.3] for ABI≤0.6 vs 21.7% 95% IC [18.8-25.0] for ABI 0.6-0.9 vs 14.3%, 95% IC [12.4-16.6] for ABI 0.9-1 vs 13.3%, 95% IC [11.6-15.2] for ABI 1–1.4, p < 0.001)
Conclusion
Patients with non-embolic ischemic stroke or TIA and a low ABI had a higher rate of vascular events and death. Screening for ABI in stroke patients may help to identify patients at high risk of future vascular events.
Trial registration number
N/A
AS03-023
THE ASSESSMENT OF BLOOD FLOW IN THE SUPRATROCHLEAR ARTERY TO DETERMINE THE SURGICAL TREATMENT STRATEGY IN PATIENTS WITH CRITICAL STENOSIS AND ICA OCCLUSION
1Scientific Research Institute of Emergency Care n.a. N.V. Sklifosovskiy, Neurosurgical department, Moscow, Russia
2MSUMD n.a. A.I. Evdokimov, department of neurosurgery and neurointensive care, Moscow, Russia
Background and Aims
to estimate hemodynamic changes after cerebral revascularization in patients with occlusion and critical stenosis of internal carotid artery (ICA).
Method
223 patients (men: women = 3:1, age from 42 to 78 years old (Me = 62,3)) were operated on from 01.01.17 till 31.12.17, 147 patients underwent carotid endarterectomies (CEE), 48 – bypass between superficial temporal artery and cortical branch of middle cerebral artery (STA-MCA bypass).
Dopplerography of supratrochlear artery (StrA) with estimation of linear blood velocity and direction of blood flow was performed in 12 patients with symptomatic critical stenosis of ICA and in 27 patients with symptomatic ICA occlusion. All patients (n = 39) had retrograde blood flow in в StrA preoperatively. The significant preoperative decrease of cerebral perfusion in ipsilateral cerebral hemisphere till 23 ± 3,1 ml/min/100g was observed in all patients, five patients with ICA occlusion had perfusion steal syndrome. Patients’ status was assessed using NIHSS, modified Rankin scale (mRs) and Rivermead mobility index.
Results
There were no ischemic complications in postoperative period and no lethal outcomes. Blood flow direction in StrA changed from retrograde to anterograde in 35 patients. Postoperative single-photon emission computerized tomography showed the increase of cerebral perfusion on 11 ± 2,7 ml/min/100g (20 ± 3,7%), neurological status improved in average on 1,1 scores (NIHSS), 0,8 scores (mRs) and 2,3 scores (Rivermead mobility index) in all patients before discharge.
Conclusion
The direction of blood flow in StrA may evident the insufficient cerebrovascular cerebrovascular reserve in patients with critical stenosis or occlusion of ICA and indicate the necessity of revascularization surgery.
Trial registration number
N/A
AS03-024
PLASMATIC CHANGES OF INFLAMMATORY BIOMARKERS BEFORE AND AFTER ENDARTERECTOMY
1Geneva University Hospital, neurology, Geneva, Switzerland
2Geneva University Hospital, vascular surgery, Geneva, Switzerland
Background and Aims
To determine whether there is a significant change of the plasmatic levels of several inflammatory biomarkers related to carotid endarterectomy
Method
Consecutive patients with recently symptomatic moderate to severe carotid stenosis and candidates for endarterectomy were evaluated. In all patients blood samples were collected before endarterectomy and within 3–6 months after. The following plasmatic biomarkers were studied : adiponectine, vWF, sVCAM-1, sICAM-1, E-selectin, P-selectin, thrombomodulin, hs CRP, serum amyloid A, IL-1b, IL-2, IL-6, IL-8, IL-10, IL-12, and TNF-alpha, lipoprotein-associated phospholipase A(2) (Lp-PLA2), MMP-, MMP-2, MMP-3, MMP-8, MMP-9, myeloperoxydase (MPO), pentraxin 3 (PTX3), Rantes, metalloprotease inhibitor TIMP-1 and TIMP-2.
Results
Twenty one patients were included. In 8 patients a bilateral carotid stenosis was documented. There was a significant decrease of the median value of the following biomarkers after surgery.
IL-6, p = 0.01; IL-8, p = 0.018; P-Selectin, p < 0.0001; Rantes, p = 0.001; MPO, p = 0.03, SAA, p = 0.04, hs CRP, p = 0.006, MMP-8, p = 0.04; vWF, p = 0.04, pentraxin3, p = 0.009 and TIMP-1, p = 0.02.When considering only those patients with unilateral carotid stenosis (n = 13) operated, a significant difference remained only for the following biomarkers: IL-6, p = 0.02; P-Selectin, p = 0.008; hsCRP, p = 0.019 and Pentraxine 3, p = 0.008. None of those patients with bilateral stenosis showed a siginificant decrease of any of the biomarkers tested after surgery.
Conclusion
Our results suggest a positive effect of endarterectomy on various biomarkers of inflammation. This effect is only observed in patients with unilateral stenosis. These results further highlight the potentially predominant role of certain biomarkers in the process of symptomatic carotid disease.
Trial registration number
N/A
AS03-026
CEREBRAL MICROBLEEDS IN PATIENTS WITH CEREBRAL ISCHEMIC, HEMORRHAGIC STROKE AND TRAUMATIC BRAIN INJURY
1Ilsan Paik Hospital - College of Medicine -Inje University, Neurological Surgery, Ilsan, Republic of Korea
Background and Aims
Cerebral microbleeds (CMBs) are small and round perivascular hemosiderin deposits detected on the T2*-weighted gradient echo (GRE) magnetic resonance imaging. CMBs are common among patients with hypertension, cerebral ischemia. In this article, we compared the CMBs between cerebral ischemic stroke, cerebral hemorrhagic strok, and traumatic cerebral hemorrhage.
Method
We analyzed T2*-weightedmagneci resonance images for the number, location, and topography of CMBs, as well as patients' demographic and clinical information of cerebral ischemic stroke, cerebral hemorrhagic strok, and traumatic cerebral hemorrhage in each 100 patients in a year period, retrospectively.
Results
A total of 300 patients with available brain MRI and clinical dataa were included. Using Cox propotional hazards model, we related CMBs presence to three different kinds of cerebral injuries. Multivariable models were adjusted for age, sex, medications, smoking, and other medical histories. There was significant different numbers of CBMs between three groups (64%/ 18%/ 8% in cerebral hemorrhagic strok, cerebral ischemic stroke, and traumatic cerebral hemorrhage, p < 0.05). The only significant risk factors was uncontrolled hypertension.
Conclusion
Ftom this retrouspective study, we obtatined the findings that CMBs were highly associated with cerebral hemorrhage stroke and CMBs were the results of long time hypertension without medication.
Trial registration number
N/A
AS03-028
SECONDARY STROKE PROPHYLAXIS WITH CLOPIDOGREL PRODUCES SUFFICIENT ANTIPLATELET RESPONSES IN MEDICATION-ADHERENT PATIENTS
1Zealand University Hospital- University of Copenhagen, Neurology, Roskilde, Denmark
2Rigshospitalet- University of Copenhagen, Clinical biochemestry, Glostrup, Denmark
Background and Purpose
Antiplatelet therapy is a cornerstone prevention strategy for secondary ischemic stroke (IS) and transient ischemic attack (TIA). Yet, a proportion of patients who receive antiplatelet therapy experience recurrent ischemic cerebrovascular events. A recent meta-analysis found an increased risk of recurrent stroke in clopidogrel- or aspirin-treated patients with IS who had high on-treatment platelet reactivity (HTPR). Few studies have focused specifically on clopidogrel HTPR. Therefore, the aim of this study was to examine the relationship between clopidogrel HTPR and recurrent ischemic events in a population of patients with IS.
Methods
We performed a prospective double-blinded observational follow-up study to evaluate the relationship between HTPR defined as platelet reaction units > 208 and a composite primary endpoint of recurrent stroke, TIA, acute myocardial infarction (AMI), or vascular death over a 2-year follow-up period
Results
A total of 142 patients were included in the final statistical analysis, but only 3 patients (2.1%) demonstrated clopidogrel HTPR. The median time of on-treatment platelet testing was 75 days (interquartile range, 21–50). Recurrent IS, TIA, AMI, or vascular death occurred in 14 patients (10%). Of these, 1 new ischemic event (AMI) occurred in a HTPR patient. There was no significant difference in the frequency of new ischemic events between the HTPR and non-HTPR groups (p = 0.27); moreover, the number of patients with HTPR was too small for statistical analysis.
Conclusions
Medication non-adherence may be a larger contributor to recurrent ischemic events than medication HTPR.
Trial registration number
clinicaltrials.gov number: NCT02093299
AS03-030
CYP2C19*2 AND *17 INFLUENCE IN VITRO PLATELET INHIBITION BUT NOT CLOPIDOGREL RESPONDER-STATUS IN DANISH STROKE PATIENTS
1Zealand University Hospital- University of Copenhagen, Neurology, Roskilde, Denmark
2Rigshospitalet- University of Copenhagen, Clinical biochemistry, Glostrup, Denmark
Background and Aims
Clopidogrel is a cornerstone in secondary stroke prevention. Being a pro-drug, clopidogrel requires hepatic transformation to reach its active metabolite. Enzymes involved in this process and several single nucleotide polymorphisms (SNPs) in these enzymes or the target receptor on the platelet surface might play a role in the clopidogrel mediated platelet inhibition.
Aim
To explore if there is an association between carrying certain single nucleotide polymorphisms and platelet response, and if so, will increased dosage of clopidogrel overcome previous lack of platelet inhibition.
Method
An observational study in ischemic stroke and transients ischemic attack patients receiving clopidogrel 75 mg/day. VerifyNow was used to determine platelet reactivity and if platelet reaction Unit (PRU) >208, clopidogrel dosage was increased and PRU re-measured. Simultaneously genotypes for 8 different SNPs in CYP2C19, CYP3A4, NR1I2 and the P2Y12 receptor were examined.
Results
103 patients were included. 30.7% carried the CYP2C19*2 allele and they had higher PRU values but no patients had PRU higher than 208. Carriers of the *17 allele had higher platelet inhibition, but no difference in PRU-values compared to non-carriers. The remaining examined SNPs had no impact on neither PRU nor platelet inhibition.
Conclusion
In conclusion, genetic analysis seem futile in determining the patient’s phenotypic clopidogrel resistance.
Trial registration number
clinicaltrials.gov number: NCT03385538
AS03-032
PLASMA LP-PLA2 ACTIVITY IN RECENTLY SYMPTOMATIC SEVERE CAROTID STENOSIS: RELATIONSHIPS WITH PLAQUE HISTOPATHOLOGY
1Centre de Psychiatrie et de Neurosciences, Department of Neurology, Paris, France
2Hôpital Européen Georges Pompidou, Department of Pathology, Paris, France
3Hôpital Sainte-Anne, Department of Biology, Paris, France
4Hôpital Européen Georges Pompidou, Department of Vascular Surgery, Paris, France
5Normandie Université- Unicaen- CHU Caen Normandie- INSERM U1237, Department of Neurology, Caen, France
Background and Aims
Lipoprotein-associated phospholipase A2 (Lp-PLA2) is secreted by inflammatory cells of atherosclerotic plaques and as such may allow identification of patients at high risk of ipsilateral ischemic stroke. This prospective pilot study evaluated whether plasma Lp-PLA2 activity could be a biomarker of histopathologically-defined carotid plaque instability.
Method
We included 25 patients with recently symptomatic carotid stenosis scheduled for surgery (carotid group) and 25 age- and sex-matched patients with recent ischemic stroke not related to atherosclerosis (control group). Plasma Lp-PLA2 activity was assayed at inclusion in both groups and at 3-month follow-up in the carotid group. Carotid plaques were assessed histopathologically using of a semi-quantitative predefined scoring of the characteristics of unstable plaques such as fibrous cap rupture/thin cap fibroatheroma, intraplaque hemorrhage and inflammation.
Results
Baseline Lp-PLA2 activity did not differ between groups (p = 0.81). In the carotid group, Lp-PLA2 activity at 3 months was lower than at inclusion (156.1 vs., 179.3 nmol/min/ml, respectively; p = 0.003). Lp-PLA2 activity was not significantly associated with plaque characteristics (intraplaque hemorrhage: p = 0.39; inflammation: p = 0.25; fibrous cap thickness: p = 0.72).
Conclusion
Our study suggests that plasma Lp-PLA2 activity may not be a useful marker for identifying patients with high-risk carotid plaque.
Trial registration number
N/A
AS03-035
DISEASE KNOWLEDGE EVOLUTION AMONG ADMITTED STROKE PATIENTS
1Hospital Universitari Arnau de Vilanova, Neurology, Lleida, Spain
Background and Aims
To determine the evolution and factors of stroke knowledge among subjects who are admitted for this reason
Method
We compare the grade of knowledge of the terminology, the risk factors, the symptoms and the attitude towards cerebrovascular disease (CVD) among patients admitted for this disease in Lleida (Catalonia) in two periods of time: Phase 1 (n = 289), from January 2011 to December 2013 and phase 2 (n = 331), January 2015 to December 2016. A closed questionnaire was used.
Results
Significant differences were observed both in the knowledge of terms (4.1 [SD 2.0] versus 4.8 [SD 1.7] p <0.001), and in the good knowledge of symptoms (more than three factors and less than two distractors) (56.6% versus 69.8% p <0.001). Likewise, calls to 112 were significantly higher in stage 2 (17.3% vs. 24.6% p = 0.003) although this proportion was still below the optimum. The term 'stroke' was more recognized in stage 2 (51.9% vs. 74.5%, p <0.001). There were no differences in the degree of knowledge factors. Unfortunately, the improvement in stroke knowledge did not translate into a decrease in the delay between the onset of symptoms and the arrival at the hospital.
Conclusion
Knowledge of the terms and symptoms of CVD has improved over time. However, the attitude towards CVD should still be improved in order to optimise the speed until arrival at the hospital. For this reason, programs must be developed to highlight the urgency of contacting 112 and going to the Hospital
Trial registration number
N/A
AS03-040
THE EFFECT OF 3 MONTH ACE-I THERAPY ON THE VESSEL WALL, ARTERIAL STIFFNESS AND COGNITION OF ASYMPTOMATIC HYPERTENSIVE PATIENTS
1Debrecen University, Neurology, Debrecen, Hungary
2Debrecen University, Behaviour Sciences, Debrecen, Hungary
3Debrecen University, Internal Medicine, Debrecen, Hungary
4Kenezy Hospital, Contract Statistician, Debrecen, Hungary
Background and Aims
The non-treated hypertension (a strong stroke risk factor) results in worsening of carotid intima-media-thickness, arterial stiffness and cognition. Our aim was to investigate whether a short (3 month) anti-hypertensive therapy has any positive effect on vessel morphology, arterial stiffness and cognition.
Method
After a screening procedure (more than 100 pts. with ABPM) the group of symptom-free hypertensive males and females (between 40-50 years) were investigated with carotid ultrasound, pulse wave velocity, augmentation index, flow-mediated dilation and neuropsychological testing (attention, short and long term memory, reaction time etc.) We also investigated the severity of anxiety and depression. All hypertensive patients received exclusively ACE-inhibitor therapy for 3 months.
Results
The intima-media thickness (0.55 ± 0.1 before therapy), the arterial stiffness (pulsed wave velocity, 9.3 ± 2.4 before therapy, augmentation index -17.5 ± 34.4 before therapy) the flow mediated dilation (7.5 ± 2.21% before therapy) did not show significant improvements. On contrary, significant improvements could be detected in some cognitive tests: 5-Point Test, p = 0.009, Stroop Test Victoria Version, p = 0.01) while a non-significant improvement in others (Trail Making Test, p = 0.06) and selective reaction time (p = 0.052). Executive functions improved significantly (unadjusted p = 0.001) especially in patients with medium to high baseline MAP and a decrease thereof during follow-up
Conclusion
Although a short (3 mo) ACE-I therapy had no positive effect on vessel wall morphology and arterial stiffness, the improvement of cognition could be already detected especially in patients with medium to high baseline MAP.
Trial registration number
N/A
AS03-041
EFFECT OF CILOSTAZOL AND ISOSORBIDE MONONITRATE ON CEREBROVASCULAR REACTIVITY IN LACUNAR STROKE: THE LACI-1 TRIAL
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Nottingham, Stroke Trials Unit- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Small vessel disease (SVD), including lacunar stroke, is associated with alterations in cerebrovascular function. Cilostazol and isosorbide mononitrate (ISMN) have multiple actions that may improve cerebrovascular function and slow or prevent SVD. LACI-1 tested their ability to improve cerebrovascular reactivity (CVR).
Method
LACI-1 randomised patients with lacunar ischaemic stroke to cilostazol alone (100mg bd), ISMN alone (25mg bd) or both drugs immediate or 3 week delayed start (the initial 3 week drug-free period providing a ‘no drug control’). We compared the median change in CVR, measured using hypercapnic BOLD MRI, between the baseline visit and after 8 weeks of treatment, or at end of ‘no drug’ period in the delayed start group.
Results
We randomised 26 participants (mean age 68.5yrs, range 53-83; 44% female). In patients allocated ISMN (n = 6) and cilostazol (n = 5) CVR increased in the white matter (ISMN +49.5%; Cilostazol +23.6% relative increases) and the grey matter (ISMN +19.5%; Cilostazol +15.2% ). In the both drug and no drug groups CVR declined in white matter (both drugs -14.1%; no drugs -5.8% relative difference) and grey matter (both drugs -6.8%; no drugs -12.3%). Lower both drugs compliance may be obscuring a treatment effect. There were no significant differences between treatment groups. Further analyses, including by treatment compliance will be performed in time for ESOC.
Conclusion
LACI-1 suggests that pharmacological intervention can improve tissue-level CVR. larger studies are warranted to confirm this finding; the ongoing LACI-2 trial will assess if improved CVR translates to clinical improvements.
Trial registration number
ISRCTN12580546
EudraCT (2015-001953-33)
CLINICAL TRIAL RESULTS – REHABILITATION & RECOVERY
AS04-001
THE EFFECTIVENESS OF MECHANICAL LUNG VENTILATION IN ACUTE CEREBROVASCULAR DISEASES IN ELDERLY PATIENTS
1Irkutsk State Medical Academy of Postgraduate Education, anesthesiology and intensive care, Irkutsk, Russia
Background and Aims
Cerebrovascular diseases (CVD) are a heavy economic burden for global health. Age of patients older than 65 years in combination with mechanical lung ventilation (MVL) for more than 3 days is considered an independent predictor of the lethal outcome within two months from the onset of the disease
Aim
to evaluate the effectiveness of MVL in elderly patients with CVD.
Method
A retrospective analysis of 520 patients with CVD, which required MVL, was conducted. The age of 30.5% was more than 70 years. Subgroups of persons older than 75 years (79% of the sample) and older than 80 (36%) were singled out separately.
Results
MVL effectiveness was assessed by us from the standpoint of patient survival and the degree of neurological deficit (using the Glasgow Outcome Scale-GOS). The effectiveness of MVL in people over 70 years should be considered unsatisfactory. The lethal outcome is from 62 to 76%. Among the survivors in 70-80% there was a severe disability (3–5 points GOS), and a good outcome is the recovery to 6–7 points GOS in only 20%.
The effectiveness of MVL in elderly patients 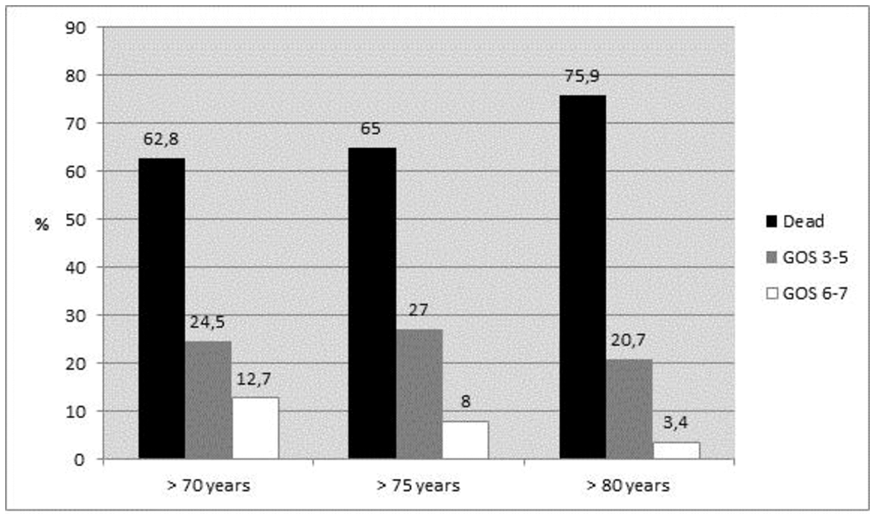
Conclusion
The effectiveness of MVL in elderly patients is reduced, which is manifested as an increase in lethality (61.9% in patients over 60, 75.9% in patients older than 80 years) and in deep disability of surviving patients, which excludes the possibility of self-service and complicating (77-80%). It is necessary to carefully select elderly patients with CVD for intensive care, and a selective approach is necessary if there is a need for MVL.
Trial registration number
N/A
AS04-002
THE EFFECTS OF COMPUTER BASED COGNITIVE REHABILITATION IN PATIENTS WITH SYMPTOMS OF VISUOSPATIAL NEGLECT OR HEMIANOPSIA AFTER STROKE: A RANDOMIZED, CONTROLLED, UNBLINDED CROSS-OVER PILOT-STUDY
1Bispebjerg Hospital, Department of neurology, Copenhagen, Denmark
Background and Aims
To address the effects of Computer Based Cognitive Rehabilitation (CBCR) in patients with visuospatial neglect and/or hemianopia in the subacute phase after stroke.
Method
CBCR was delivered by a commercially available program: ‘Scientific Braintraining PRO’ designed to train visuospatial attention and mental rotation. Fourteen patients were randomly assigned to early or late CBCR intervention targeting visuospatial symptoms in a cross-over design. All patients were included within 40 days of stroke onset. The early intervention group (EI group) received CBCR starting immediately after inclusion for three weeks, and the late intervention group (LI group) started a 3-week CBCR intervention 3 weeks after inclusion. Attention was assessed by the CABPad Butterfly test at baseline, 3 weeks and 6 weeks.
Results
Groups were balanced on baseline characteristics. The EI group showed a significant reduction in neglect score between baseline and after training (p = 0.018), while the neglect score did not change significantly in the LI group, neither during the waiting list period nor during training, though an insignificant trend in this direction was observed The LI group did not improve during their no-training period (p = 0.237) nor during their CBCR intervention period (p = 0.116). The difference in improvement during training periods was not significant between the EI and LI group (p = 0.259).
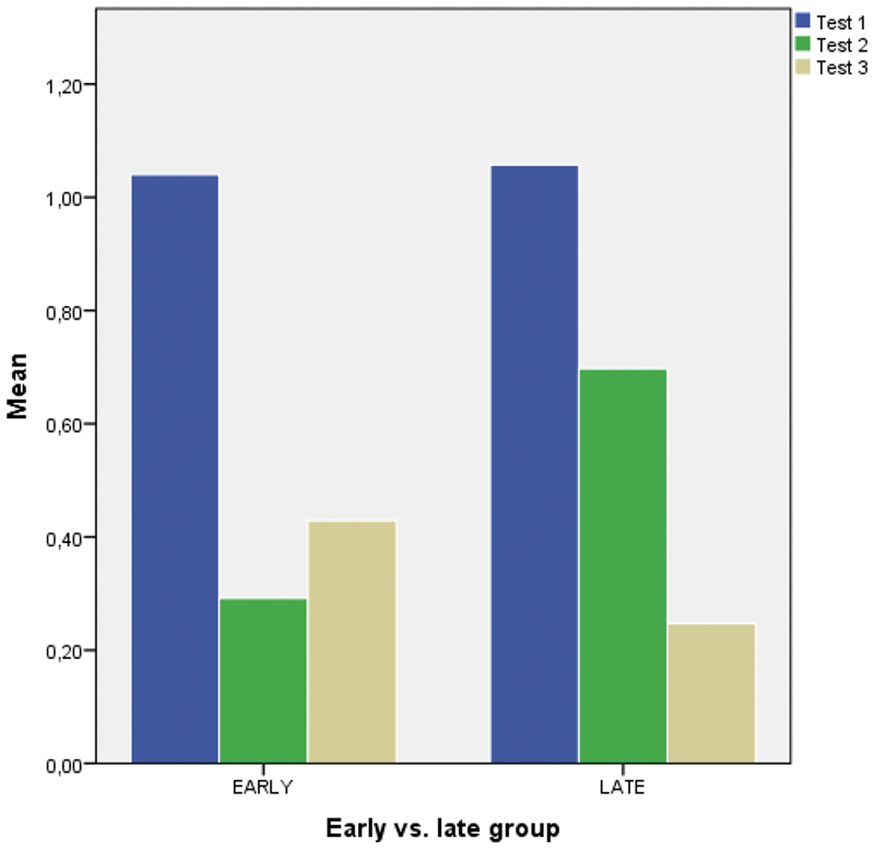
Conclusion
CBCR improved visuospatial symptoms after stroke significantly, especially when administered early in the subacute phase after stroke. The study was small and confirmation is needed.
Trial registration number
H-15005153
AS04-004
LONG TERM SYNERGISTIC EFFECT OF COMBINING MLC601 AND REHABILITATION ON POST-STROKE RECOVERY -THE CHIMES-E STUDY
1National University of Singapore, Department of Pharmacology, Singapore, Singapore
2Chulalongkorn University, Neurology, Bangkok, Thailand
3University of Hong Kong, School of Public Health, Hong Kong, Hong Kong S.A.R
4Changi General Hospital, Rehabilitation Medicine, Singapore, Singapore
5National Neuroscience Institute - Tan Tock Seng Campus, Neurology, Singapore, Singapore
6Davao Medical School Foundation Hospital, Neurology, Davao City, Philippines
7Jose Reyes Memorial Medical Center, Neurology, Manila, Philippines
8National Neuroscience Institute - Singapore General Hospital Campus, Neurology, Singapore, Singapore
9West Visayas State University Medical Center, Neurology, Iloilo City, Philippines
10Thammasat University, Neurology, Pathum Thani, Thailand
11National University Health System, Neurology, Singapore, Singapore
12University of Philippines- Philippines General Hospital, Neuroscience, Manila, Philippines
13University of Kelaniya, Pharmacology, Ragama-, Sri Lanka
14University of Kelaniya, Pharmacology, Ragama, Philippines
15Baguio General Hospital and Medical Center, Neurology, Baguio City, Philippines
16Chinese University of Hong Kong- Prince of Wales Hospital, Neurology, Shatin- New Territories, Hong Kong S.A.R
17Siriraj Hospital, Neurology, Bangkok, Thailand
18Penang Hospital, Neurology, Penang, Malaysia
19Raffles Neuroscience Centre, Raffles Hospital, Singaopore, Singapore
Background and Aims
MLC601 enhances natural neuro-repair mechanisms after stroke and may facilitate rehabilitation-stimulated recovery processes. We aimed to assess the effect of MLC601 and concomitant rehabilitation on stroke recovery in the CHIMES-E study.
Method
The CHIMES-E study recruited 880 subjects aged ≥18 years with acute ischemic stroke (AIS), National Institute of Health Stroke Scale (NIHSS) 6–14, and pre-stroke modified Rankin Scale (mRS) ≤1 in a planned double-blind extension study of CHIMES trial. MLC601 or placebo was given for 3 months plus standard stroke care and rehabilitation. mRS was compared between MLC601 and placebo from month (M) 3 to M24.
Results
The mean age was 61.8 ± 11.3 years with 318 (36%) women. Data on rehabilitation and mRS at M3 were available in 807 (91.7%) subjects. Treatment groups were balanced in baseline characteristics except for NIHSS mean score being higher in the rehabilitation group (p = 0.013). Subjects stratified according to rehabilitation status within the first three months showed a higher treatment effect of MLC601 on both mRS shift and dichotomy (0–1 vs 2–6) from M3 to M24 in the rehabilitation group, after adjusting for baseline differences and poorer prognosis factors. In the rehabilitation group, the adjusted odds of functional independence (mRS of ≤1) increased significantly for MLC601 from M3 to M24, with the highest OR at M12 of 2.42 (95% CI 1.53-3.81).
Conclusion
Combining MLC601 and rehabilitation within the first 3 months of AIS improves functional recovery over 2 years, supporting synergistic effect on brain neuro-repair processes, with more subjects improving to functional independence compared to placebo.
Trial registration number
NCT00554723
AS04-005
TIME DEPENDENT BENEFIT IN HOSPITAL ATTENTION FOR STROKE PATIENTS NOT RECEIVING REPERFUSION THERAPIES
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine - Nursery, Denia, Spain
4Hospital General La Mancha Centro, Neurology - Nursery, Alcázar de San Juan, Spain
5Hospital de Tomelloso, Neurology, Tomelloso, Spain
Background and Aims
Trials and metanalyses have all shown a time-dependent benefit of reperfusion therapies. However the role of prehospital delay (PD) in the prognosis of patients who don’t qualify for reperfusion therapies has rarely been addressed. We conducted a study to investigate if a sooner hospital arrival (PD < 3 hours) favors functional independency (mRS < 2) three months after stroke.
Method
284 Patients with acute stroke (TIA excluded) who didn’t receive thrombolysis nor thrombectomy were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors were collected, as well as data on PD. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency three months after stroke.
Results
A PD of three hours or less increased the chance of achieving a mRS of 2 or less three months after stroke onset (OR 5,478; CI 95% 1,998-15,018; p = 0,001) as did higher serum triglycerides level (OR 1,010;CI 95% 1,001-1,019; p = 0,044). Inhospital infectious comorbidities (OR 0,132;CI 95% 0,042-0,416; p = 0,001), active smoking (OR 0,182;CI 95% 0,050-0,658; p = 0,009), female gender (OR 0,374;CI 95% 0,154-0,911; p = 0,030), and higher scores on previous mRS (OR 0,226;CI 95% 0,150-0,342;p < 0,001) and initial NIHSS (OR 0,829;CI 95% 0,755-0,910;p < 0,001) predicted dependency.
Conclusion
Time is a key prognostic factor for patients undergoing reperfusion therapies as well as for those who don’t qualify for them. Future interventions should be directed towards increasing the number of patients with a PD ≤ 3 hours, which would increase thrombolysis and thrombectomy rates, but also help achieving functional independency three months after stroke.
Trial registration number
N/A
AS04-006
MELODIC INTONATION THERAPY IMPROVES COMMUNICATION IN POST-STROKE NON-FLUENT APHASIA. A PILOT RANDOMIZED TRIAL
1School of Medicine. Autonoma Madrid University, Doctoral Program, Madrid, Spain
2La Paz University Hospital. Autonoma Madrid University. IdiPAZ Health Research Institute, Neurology and Stroke Center, Madrid, Spain
3La Paz University Hospital. Autonoma Madrid University. IdiPAZ Health Research Institute, Biostatistics, Madrid, Spain
Background and Aims
The evidence of the efficacy of the Melodic intonation therapy (MIT) to improve aphasia after stroke is still scarce. Our aim is to evaluate the efficacy of Melodic intonation therapy (MIT) on post-stroke aphasia.
Method
We conducted a randomized, crossover, and interventional pilot study including stroke survivors with post-stroke non-fluent aphasia (more than 6 months prior study inclusion). Patients were randomly allocated to two groups: Group 1, MIT to start within the first three months after inclusion in the study, with a washout period of three months, then serving as controls for the second phase of the study; and Group 2, MIT to start between three and six months after their inclusion in the study, serving as waitlist controls for the first phase and as active intervention group in the second phase. A neuropsychologist blinded to the allocation group evaluated the Communicative Activity Log (CAL) questionnaire and the Boston Diagnostic Aphasia Examination (BDAE).
Results
20 patients were included. No differences in baseline characteristics neither in neuropsychological evaluations scores between study groups were found. MIT therapy showed significant higher values in the CAL test, with no differences in any of the BDAE sections. The fixed effect lineal regression models for CAL evaluation showed no significant interaction (P = .193) but with clear treatment (P = .043) and period effects (P = .019).
Conclusion
MIT therapy has positive effects on the communication skills in post-stroke non-fluent aphasia. This effect appears early after the therapy administration remaining at least 3 months after the stop of the treatment.
Trial registration number
N/A
AS04-008
HEMORRHAGIC STROKE AND PREDICTION OF LONG-TERM SURVIVAL. DESIGN AND VALIDATION OF A MODEL IN PRIMARY CARE (ICH-AP)
1Institut Catala Salut, Primary Care, Tortosa, Spain
2Institut Universitari d’Investigació en Atenció Primària IDIAP Jordi Gol, Primary Care, Barcelona, Spain
3Universidad Miguel Hernandez, Primary Care, Elche, Spain
Background and Aims
Different scales predict mortality, but most make a prediction in the short term and are mainly coming from hospital files that are not available in the area of primary care. To build a predictive tool of longterm survival within the context of the primary health care.
Method
Multicentric and retrospective study of ICH cohort (2006-2011) followed up to 2016 and collected from the government-run healthcare in Terres Ebre land, Catalonia (Spain).The primary outcome was death with all causes occurring within the 5-year follow-up after the ICH episode based on Cox proportional-hazard regression and Kaplan–Meier method, Log-Rank test, ROC curves and the AUC to assess the ability of the ICH_AP index to stratify patients prognosis.
Results
262 cases (58% men), aged 75.13 ± 12.62 years. The overall mortality was 62.2%. The prognostic factors were: age ≥80 years [HR 2.10 (CI95% 1.48–2.99, p <0.001)], cognitive impairment [HR 2.04 (CI95% 1.24–3.36, p <0.005)], disability at hospital discharge [HR 3.84 (CI95% 2.51–5.88, p <0.001)], HAS-BLED score [HR 1.23 (CI95% 1.05–1.44, p <0.008)] and non-treatment with statins [HR 1.47 (CI95% 1.03–2.10, p < 0.032)]. Cases were stratified into three risk groups. For each of the levels of risk, the value AUC was low risk, 0.97 (95%CI 0.92–1), intermediate risk, 0.83 (95%CI 0.75–0.92) and high risk, 0.85 (95%CI 0.76–0.93). The comparative analysis of the survival of the three risk groups shows Log-Rank p <0.0001.
Conclusion
The ICH-AP tool at hospital discharge is a strong predictor of long-term mortality in primary care after an episode of ICH.
Trial registration number
ClinicalTrials.gov ID: NCT03247049
AS04-009
THE ASSOCIATION OF STROKE SEVERITY WITH DISCRIMINATIVE POWER OF SELECTED ENDPOINTS IN CLINICAL TRIALS
1“Iuliu Hatieganu” University of Medicine and Pharmacy- Cluj-Napoca- Romania, Neurosciences, Cluj Napoca, Romania
2the Institute for Data Analysis and Study Planning, Multidimensional Department, Krailing, Germany
Background and Aims
Using the results of two identical stroke studies with highly deviating baseline severity the discriminative power of common clinical outcome scales is evaluated in a meta-analytic framework in order to learn for future study designs and to avoid unnecessary loss of test power.
Method
Both studies had a prospective, randomized, double-blind, placebo-controlled design. Treatment with 30ml Cerebrolysin once daily for three weeks was started 24-72 hours after stroke onset. In addition, patients participated in a standardized rehabilitation program for 21 days that was initiated within 72 hours after stroke onset.
Results
Outcome at day 90 shows considerable heterogeneity due to marked ceiling effects in the population with mild baseline severity, while the analysis of early benefit (day 14, day 21) by means of the National Institutes of Health Stroke Scale, which is regarded as most sensitive to early improvements, showed high discriminative power in both study populations despite different baseline severity levels.
Conclusion
These new results strongly support the earlier findings of DeGraba (1999) who highlighted the importance of baseline stroke severity in stroke trials for discriminative power at different selected points in time. Despite heterogeneity of study populations the meta-analysis was able to well demonstrate beneficial effects of Cerebrolysin on motor function and neurological status in early rehabilitation patients after acute ischemic stroke.
Trial registration number
N/A
AS04-011
ELECTRICAL SOMATOSENSORY STIMULATION IN EARLY REHABILITATION OF ARM PARESIS FOLLOWING ACUTE STROKE: A RANDOMIZED ASSESSOR-BLINDED CONTROLLED TRIAL
1Bispebjerg Hospital, Department of Physical and Occupational Therapy, Copenhagen NV, Denmark
2University of Copenhagen, Faculty of Health and Medical Sciences, Copenhagen, Denmark
3University of Copenhagen, Center for Healthy Aging- Faculty of Health and Medical Sciences, Copenhagen, Denmark
4Bispebjerg Hospital, Institute of Sports Medicine- Department of Orthopaedic Surgery M, Copenhagen, Denmark
5University of Copenhagen, The Research Unit for General Practice and Section of General Practice- Department of Public Health, Copenhagen, Denmark
6Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark
Background and Aims
Upper limb motor deficits are reported in 48–77% of patients after acute stroke and complete functional recovery is reported in 12–34% of patients. Although the recovery of arm functioning is most pronounced during the first 4 weeks post-stroke, few studies have investigated the effects of motor rehabilitation interventions during this period. This trial investigated the effect of electrical somatosensory stimulation (ESS) during early rehabilitation post-stroke on the recovery of arm functioning.
Method
102 patients with arm paresis were randomized to the intervention or the control group within 7 days post-stroke according to our sample-size estimation. The intervention group received 1-hour suprasensory ESS-treatment to the paretic arm daily during hospitalization immediately followed by minimum 15-minutes task-oriented arm training which was considered a component of the usual rehabilitation. The control group received a sham ESS-treatment followed by identical training. Primary outcome was hand dexterity (Box and Block Test); secondary outcomes were: Fugl-Meyer Assessment, hand grip strength, pinch strength, perceptual threshold of touch, pain and modified Rankin Scale; all recorded at baseline, post-intervention and at 6 months post-stroke.
Results
There were no differences between the intervention and the control group for any outcome measure at any time points. Patients received on average 30-minutes task-oriented arm training daily. Clinically significant remission was observed in both groups.
Conclusion
ESS in addition to usual arm training in early rehabilitation does not improve outcome after stroke. More trials are needed to identify effective interventions to improve arm functioning after stroke.
Trial registration number
ClinicalTrials.gov (NCT02250365)
AS04-016
THE OUTCOMES OF A STRUCTURAL REFORM IN HAAPSALU NEUROLOGICAL REHABILITATION CENTRE (ESTONIA) BETWEEN 2016 AND 2017
1Haapsalu Neurological Rehabilitation Centre, Neurorehabilitation, Haapsalu, Estonia
2Centre of Excellence in Health Promotion and Rehabilitation, Rehabilitation, Haapsalu, Estonia
Background and Aims
The aim of the study was to determine the influence of the structural reform in Haapsalu Neurological Rehabilitation Center (HNRC) in Estonia between 2016 and 2017.
During the reform, interdisciplinary teams were formed while patient selection and planning tasks were decentralized with a goal of increasing the number of acute phase patient cases and patientś involvement in active therapies.
Method
The study was held in the Department of Neurorehabilitation of HNRC, where there are 38 inpatient beds mainly for stroke but also traumatic brain injury (TBI) patients. The data was collected from the medical database of HNRC, comparing the cases of acute phase patients whose rehabilitation period was longer than 12 days. In Estonia, acute phase is considered 6 months post stroke and 18 months after TBI.
Results
The number of acute phase cases in the Department of Neurorehabilitation increased from 171 to 245 between 2016 an 2017, by 43,27%.
The number of hospital bed days increased by 57,27% from 3021 to 4751 respectively.
In 2016, the patients were involved in active therapies on average of 123,94 minutes per day, including the weekends, in 2017 the active time was increased to 131,83 minutes per day. Active therapies include physiotherapy, occupational therapy, speech and language therapy and psychotherapy.
Conclusion
Based on the results above, the structural reform has had a positive influence on the management of the hospital, resulting in increased number of acute phase patient cases, hospital bed days and patientś involvement in active therapies.
Trial registration number
N/A
AS04-018
PARTICIPANTS’ EXPERIENCES FROM MULTIMODAL REHABILITATION PROGRAMS LATE AFTER STROKE – A QUALITATIVE INVESTIGATION OF HORSEBACK RIDING AND RHYTHM-AND-MUSIC BASED PROGRAMS
1Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden
2Sahlgrenska Academy at University of Gothenburg, Department of Health and Rehabilitation, Gothenburg, Sweden
3University of Newcastle, Hunter Medical Research Institute, Newcastle, Australia
Background and Aims
Multimodal stimulating therapy programs combining physical, social, sensory, and cognitively challenging activities have the potential to profoundly affect neuroplastic processes beyond spontaneous recovery after stroke. Our research group recently evaluated two such integrative group-based programs delivered twice weekly during 12 weeks including 123 participants, showing significant long-term improvements in several domains. Here we present results based on individual interviews with representatives from both groups: a horseback riding group and a rhythm-and-music group.
Method
Qualitative design with an inductive approach was used in order to identify components that were associated with positive or negative experiences from taking part in the two programs. Thirty-three community-dwelling individuals with stroke took part in this qualitative study. The time elapsed since the stroke insult ranged from 18 months to 9.9 years. Eighteen participants represented the horseback riding intervention, and 15 represented the rhythm-and-music intervention. Semi-structured individual interviews were conducted and transcribed verbatim. Qualitative content analysis was used for data analysis.
Results
Taking part in a multimodal stimulating program seemed to have an impact on stroke survivors’ cognitive and motor skills, as well as emotional wellbeing and enhanced self-confidence. Similarities and dissimilarities across participants’ experiences both within and between groups were identified.
Conclusion
Rehabilitative activities based on principles of multimodal stimulation may provide enriching experiences impacting on the emotional and physical state of individuals in late phase of stroke.
Trial registration number
The study was registered on ClinicalTrials.gov, identification number NCT01372059.
AS04-019
DOES CARDIAC REHABILITATION CHANGE PHYSICAL ACTIVITY AND SEDENTARY BEHAVIOUR FOR PEOPLE WITH MILD-TO-MODERATE STROKE IN THE SUB-ACUTE PHASE OF RECOVERY?
1University Hospital of Leicester NHS Trust, Centre for Exercise and Rehabilitation Science, Leicester, United Kingdom
2University of Leicester, Physiotherapy Department- College of Life Sciences, Leicester, United Kingdom
3University of Leicester, Department of Cardiovascular Sciences- College of Life Sciences, Leicester, United Kingdom
Background and Aims
It is unclear whether cardiac rehabilitation (CR) increases the physical activity (PA) of people post-stroke in the sub-acute stage of recovery (<6 months). This study examined the effectiveness of a six-week adapted CR programme on PA and sedentary behaviour for people post-stroke in the sub-acute recovery stage.
Method
26 individuals who completed CR wore an accelerometer for 7 days before and after the programme. Step count; stationary time (ST); and light (LPA) and moderate-to-vigorous (MVPA) PA per day were compared pre- and post-CR.
Results
24 participants (63.1 ± 14.6yr, 58% male, NIHSS 2.6 ± 1.9) provided valid PA data (≥1 day of ≥8 waking hours) at both time points. Following CR, patients took significantly more steps (3255 ± 2864 vs. 3908 ± 3399steps/day, p = 0.004) and bouts of MVPA lasting ≥5min and ≥10min (0.7 ± 1.4 vs. 1.2 ± 1.8bouts/day, p = 0.008 and 0.3 ± 0.8 vs. 0.6 ± 1.1bouts/day, p = 0.021, respectively) compared to baseline (Table 1). LPA (+2.0%) and MVPA (+0.7%) increased at the expense of a significant reduction in ST (-2.7%, Figure 1).
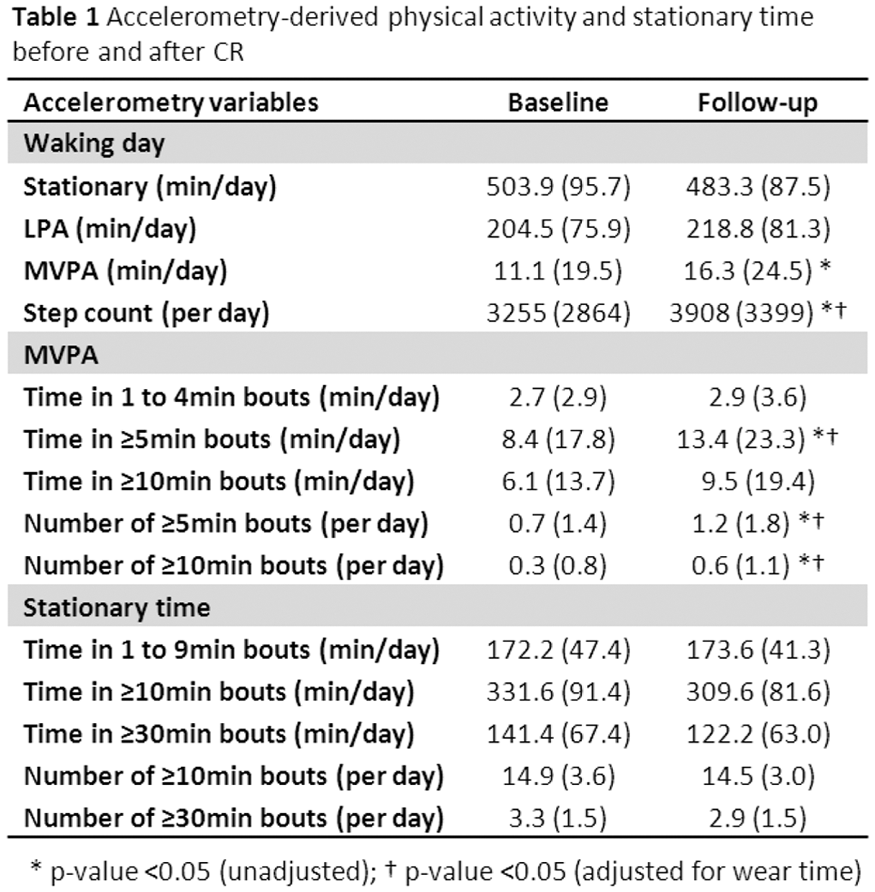
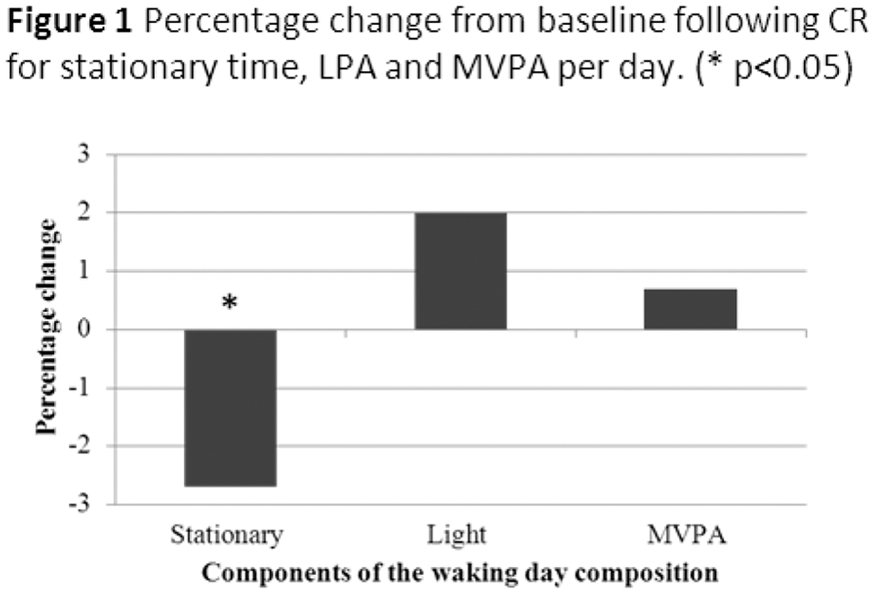
Conclusion
Physical activity of people in the sub-acute phase of stroke recovery is well below international recommendations. CR has the potential to increase steps and MVPA and reduce the sedentary behaviour of these individuals.
Trial registration number
ISRCTN14861846
AS04-020
BIOPSYCHOSOCIAL INTERVENTION FOR STROKE CARERS (BISC): RESULTS OF A FEASIBILITY RANDOMISED CONTROLLED TRIAL
1University of Nottingham, School of Medicine, Nottingham, United Kingdom
2Derbyshire Healthcare NHS Foundation Trust, Psychology, Derby, United Kingdom
3Lay Member, School of Medicine, Nottingham, United Kingdom
Background and Aims
We developed an intervention for carers of stroke survivors which combined education about the biological, psychological and social effects of stroke with strategies and techniques focussing on adjustment to stroke. Our aim was to determine whether it was feasible to deliver the intervention in a randomised controlled trial.
Method
Carers of stroke survivors were randomised to intervention or usual care control. The intervention was delivered by a research psychologist in groups of up to five carers, or one-to-one for those unable to attend groups. It was structured in two-hour sessions over six consecutive weeks. Outcomes at six months included: health-related quality of life (EQ5D-5L); anxiety and depression (HADS); carer burden (Caregiver Burden Scale).
Results
257 carers were approached and 41 consented at a median of 65 days post-stroke. 14/18 intervention participants agreed to attend the groups and four on a one-to-one basis. Participants attended a mean of 3.4(2.0) group and 5.8(0.5) one-to-one sessions. Thirty participants were followed-up. There were improvements from baseline on all outcome measures in both the intervention and control groups.
Conclusion
There were recruitment difficulties with carers stating they were too busy to take part, reporting that they had needed psychological support earlier, or that they did not need the intervention. It was possible to deliver the intervention in a group format although attendance was low due to carers’ other commitments. Attendance at one-to-one sessions was higher.
Conclusion
Further exploratory and feasibility work is needed to identify the optimum timing for recruitment and the format for intervention delivery.
Trial registration number
ISRCTN15643456
AS04-021
CORRELATION BETWEEN NEURONAL REGENERATION AND MACROPHAGE MIGRATION INHIBITORY FACTOR (MIF) AFTER ISCHEMIC RAT BRAIN
1Asan Medical Center- University of Ulsan College of Medicine, Department of Rehabilitation Medicine, Seoul, Republic of Korea
Background and Aims
The aim of this study was to investigate the neuroprotective effects of exercise and the expression levels of the macrophage migration inhibitory factor (MIF) and brain-derived neurotrophic factor (BDNF) in treadmill-exercise-induced neuronal regeneration in the ischemic penumbra of rat brains.
Method
Rats were assigned to four groups: ischemia and exercise group (Ex , n = 10) , ischemia and sedentary group (St , n = 10) , sham-surgery and exercise group (Con-Ex, n = 10), sham-surgery and sedentary group (Con-St, n = 10). Rats in the ischemia groups underwent middle cerebral artery occlusion (MCAO). Rats ran on a treadmill for 30 min once a day at a speed of 20m/min for 5days a week. Magnetic resonance imaging (MRI) and diffusion weighted image (DTI) were then acquired 24h, 7days after reperfusion (n = 20). The total infarction volume was measured in T2WI and behavioral test was evaluated at 24h, 7days after reperfusion. Then the expression level of MIF and BDNF were observed by immunohistochemistry.
Results
To compare a behavioral ability, MCAO models showed a statistical significant difference (p < 0.05) between the treadmill exercise and sedentary state. BDNF and MIF expression level between exercised and sedentary groups in penumbra region, in the MCAO models showed a statistical significant difference (p < 0.05) between the treadmill exercise and sedentary state. Correlation between immunohistochemistry (IHC) and relative fractional anisotropy (rFA), were showed a statistical significant correlation (p < 0.05).
Conclusion
Treadmill exercise helped a regeneration of the corticospinal tract and induced increasing expression levels of MIF and BDNF after ischemic stroke. MIF is an important role for the neuronal regeneration.
Trial registration number
N/A
AS04-022
THE EFFECT OF MORNING WALK (END-EFFECTOR TYPE ROBOT) TRAINING FOR PATIENTS WITH HEMIPARESIS DUE TO STROKE
1Asan Medical Center- University of Ulsan College of Medicine, Department of Rehabilitation Medicine, Seoul, Republic of Korea
Background and Aims
To investigate the effect of the Morning walk assisted gait training for subacute stroke patients.
Method
Intervention
Patients were randomized into two groups: twenty eight patients (MW group) were treated with Morning walk in 30 minutes together with one hour of conventional physiotherapy, and thirty patients (control group) received only conventional physiotherapy of one and a half hour. Both groups received treatment 5 times a week for 3 weeks.
Results
After training, all outcome measures of both groups were significantly improved. MW group showed greater improvement than control group in MI-affected limb (p = .034) and BBS(p = .047). Degree of improvement of the patients with baseline FAC below three showed greater improvement than those with FAC three or more in MBI(p = .011).
Conclusion
Morning walk assisted gait training together with conventional physiotherapy resulted in better motricity of affected limb and balance in subacute hemiparetic stroke patients, compared with conventional physiotherapy alone. Our finding suggests that Morning walk therapy is a promising intervention for gait rehabilitation.
Trial registration number
N/A
AS04-024
A RANDOMIZED TRIAL OF A SOCIAL WORKER LED HOME-BASED CASE MANAGEMENT TO IMPROVE OUTCOMES FOR CAREGIVERS OF ACUTE STROKE PATIENTS DURING THE TRANSITION PERIOD
1Michigan State University, Epidemiology and Biostatistics, East Lansing, USA
Background and Aims
Navigating the transition after returning home following a stroke is associated with substantial challenges for some caregivers. The Michigan Stroke Transitions Trial (MISTT) tested the efficacy of a social work case management (SWCM) program, and an informational website to improve caregiver outcomes.
Method
MISTT is a randomized, open, 3-group parallel designed trial conducted in 3 Michigan hospitals. Caregivers were consented shortly after the stroke patient was enrolled. Subjects were randomized to either: 1) usual care, 2) SWCM only, or 3) SWCM plus website. Interventions concluded after 90-days. Follow-up data were collected by telephone at 7- and 90-days. Primary outcomes were Bakas Caregiving Outcomes Scale (BCOS) and PHQ-9 collected at 90-days. ANCOVA was used to compare mean group differences.
Results
Among 265 randomized stroke patients, 169 (64%) had a consented caregiver. Mean caregiver age was 58 years, 77% female, 19% non-white, 60% spouses, 76% lived with the patient. Between 7- and 90-days the mean BCOS score was essentially unchanged (59.9 and 61.6, respectively, paired t p-value 0.15); at 90-days there were no statistically significant differences in mean BCOS scores between treatment groups (ANCOVA F = 1.21, p = 0.30).
Between 7- and 90-days the mean PHQ-9 declined from 3.6 to 2.7 (paired t p-value 0.01), but at 90-days there were no statistically significant differences in mean PHQ-9 scores between treatment groups (ANCOVA F = 0.40, p = 0.67).
Conclusion
An intervention that combined social worker led case management with access to an online website did not result in less stress or depression scores among caregivers.
Trial registration number
ClinicalTrials.gov: NCT02653170
AS04-025
PREDICTORS OF PNEUMONIA COMPLICATION IN PATIENTS WITH ACUTE STROKE REQUIRING ASSISTANCE FOR MOBILITY
1Saiseikai Central Hospital, Dementia Center, Minato-ku, Japan
2Tokyo Metropolitan University, Graduate School of Human Health Sciences, Arakawa-ku, Japan
3St Marianna University School of Medicine- Toyoko Hospital, Department of Rehabilitation, Kawasaki, Japan
4Saiseikai Central Hospital, Department of Rehabilitation, Minato-ku, Japan
5Saiseikai Central Hospital, Department of Neurology, Minato-ku, Japan
Background and Aims
The purpose of this study was to identify early predictors of pneumonia complications in patients with acute stroke requiring assistance for mobility.
Method
We included 111 patients who suffered acute stroke (63 with cerebral infarction and 48 with cerebral hemorrhage). We retrospectively collected data from medical records to analyze their baseline and medical characteristics at admission, the presence or absence of pneumonia complication during their hospitalization, the status of physical therapy interventions, physical function at initial ambulation and discharge, and outcomes at discharge. We performed logistic regression analysis of factors with a significance level of <0.2 as independent variables for the comparison between the two groups (presence or absence of pneumonia complication). In addition, cutoff value was calculated using receiver operating characteristic (ROC) curves.
Results
There were 17 patients (15.3%) with pneumonia complications. In logistic regression analysis, the NIHSS at admission (OR 1.066, P = 0.024), a history of orthopedic disease (OR 4.212, P = 0.025), and the presence of dementia (OR 6.697, P = 0.026) were identified as predictors of pneumonia complications. The cutoff value of pneumonia complications with ROC curves was NIHSS 12.5 points at admission (sensitivity 58.8%, specificity 66.0%).
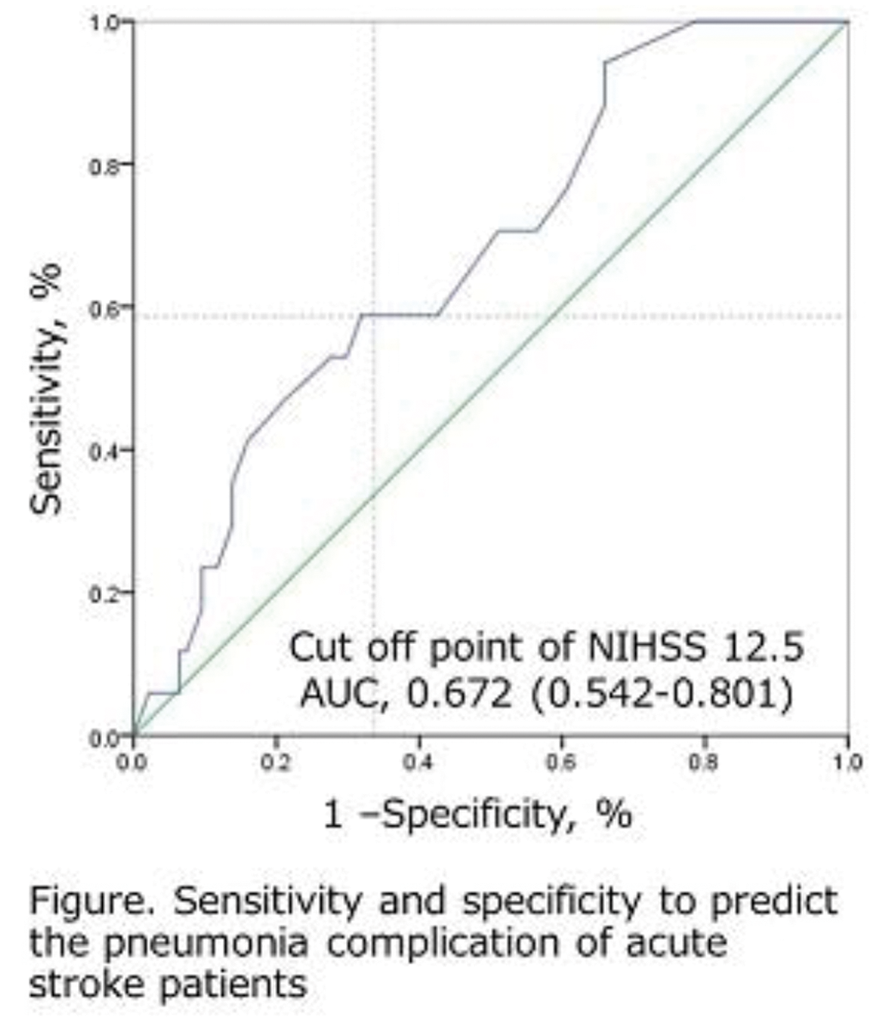
Conclusion
Concomitant diseases, such as orthopedic diseases and dementia, are important factors in addition to the severity of stroke and may predict pneumonia complications in patients requiring assistance with basic mobility immediately after admission.
Trial registration number
N/A
AS04-026
LONG-TERM INTENSIVE LOCOMOTION TRAINING WITH WEARABLE HIP-ASSIST ROBOT IN STROKE PATIENTS: A PRELIMINARY STUDY
1Samsung Medical Center- Sungkyunkwan University School of Medicine- Seoul- Korea, Department of Physical and Rehabilitation Medicine- Center for Prevention and Rehabilitation- Heart Vascular Stroke Institute, Seoul, Republic of Korea
2Sungkyunkwan University- Seoul- Korea, Department of Health Sciences and Technology- Samsung Advanced Institute for Health Science and Technology SAIHST, Seoul, Republic of Korea
3Samsung Electronics, Samsung Advanced Institute of Technology, Suwon, Republic of Korea
4Samsung Medical Center- Sungkyunkwan University School of Medicine, Department of Neurology- Neuroscience Center, Seoul, Republic of Korea
5Samsung Medical Center- Sungkyunkwan University, Office of Biomechanical science- Research Center for Future Medicine, Seoul, Republic of Korea
Background and Aims
The purpose of this study was to investigate the long-term training effect of wearable hip-assist robot on locomotion function in stroke patients.
Method
Seven stroke patients (age means: 43 ± 17.49, 5 males) were recruited. The Gait Enhancing Mechatronics System (GEMS, Samsung Electronic Co., Ltd., Korea), which functions as a wearable hip-assist robot was used. All participants received 45-minute gait training with GEMS in various overground environments for 24-sessions during the consecutive 8 weeks. Muscle efforts were acquired and analyzed using the 12-channel surface electromyography (sEMG) system (Desktop DTS system, Noraxon, USA) at preferred speed. Spatio-temporal parameters of gait were determined by 3D motion capture system (Motion Analysis Corporation, USA). In addition, cardiopulmonary metabolic energy consumption measurements were obtained during 6 minutes of treadmill walking using portable cardiopulmonary metabolic system (COSMED K4B2, Rome, IT).
Results
The 24-sessions of long-term intensive locomotion training with GEMS significantly improved gait function and gait symmetry of stroke patients (P < 0.05). Furthermore, metabolic energy consumption during 6 minutes treadmill walking was significantly lower after 24-sessions training (P < 0.05). These gains were maintained for 4 weeks after the cessation of training (P < 0.05).
Conclusion
The results of this preliminary study suggest that long-term intensive locomotion rehabilitation with the GEMS were tolerable and effective for improving gait function, gait symmetry, and cardiopulmonary metabolic efficiency during walking in the stroke survivors. Randomized controlled trial with larger participants is invited in near future.
Trial registration number
Trial registration: NCT03326011
This study was supported by the Samsung Medical Center (PHO0171341) and by a grant from the NRF (NRF-2016R1A6A3A11930931 and NRF-2017M3A9G5083690), which is funded by the Korean government.
AS04-027
WEARABLE HIP-ASSIST ROBOT MODULATE CORTICAL ACTIVATION DURING GAIT IN STROKE PATIENTS
1Samsung Medical Center, Department of Physical and Rehabilitation Medicine- Center for Prevention and Rehabilitation- Heart Vascular Stroke Institute, Seoul, Republic of Korea
2Sungkyunkwan University, Department of Health Sciences and Technology- Samsung Advanced Institute for Health Science and Technology SAIHST, Seoul, Republic of Korea
3Samsung Medical Center, Department of Neurology- Neuroscience Center, Seoul, Republic of Korea
4Samsung Medical Center, Office of Biomechanical science- Research Center for Future Medicine, Seoul, Republic of Korea
Background and Aims
The purpose of this study was to investigate the modulating effect of hip-assist robot on cortical activation during gait in stroke patients.
Method
Twenty stroke patients participated in this study. A wearable type hip-assist robot, Gait Enhancing Mechatronic System (GEMS, Samsung Electronics Co., Ltd., Korea), was used. Each patient performed randomly assigned two sets of treadmill walking sessions at self-selected speed with assistance of GEMS(GEMS) and without assistance of GEMS(NoGEMS). An experimental session began with a fixed standing condition (60s), followed by one of the 2 walking conditions (60s) and then a resting condition (60s) for five repetitions. Cerebral oxygenation was measured by oxyhemoglobin (OxyHb) concentration using the 49 channels of functional near infrared spectroscopy (fNIRS) imaging system (NIRScout, NIRx Medical Technology, LLC, Germany) covering bilateral prefrontal cortices (PFC), premotor cortices (PMC), supplemental motor areas (SMA), and lower limb sensorimotor cortices (SMC).
Results
We observed less OxyHb concentration over the lower limb SMC, SMA and PMC regions in the late phase of gait, between 31 and 60seconds after initiating walking task, with GEMS than NoGEMS conditions.
Conclusion
Human possesses a central pattern generator (CPG) for generating the rhythmic and repetitive locomotor pattern via supraspinal regulation of cerebral neural networks. Specific damages of supraspinal structures result in specific alterations of human locomotion, as evident in subjects with brain injuries such as stroke. Less activation in the lower limb SMC, PMC and SMA in the late phase of walking with GEMS may indicate that GEMS helps producing rhythmic and symmetric hip flexion and extension movement and allows more coordinated gait pattern.
Trial registration number
NCT03048968
This study was supported by the Samsung Medical Center (PHO0171341) and by a grant from the NRF (NRF-2016R1A6A3A11930931 and NRF-2017M3A9G5083690), which is funded by the Korean government.
AS04-028
STROKE CLINICAL RESEARCH – TOWARDS NEW PARADIGMS OF STUDY DESIGN
1IDV Data Analysis and Study Planning, Biometry and Clinical Research, Muenchen, Germany
2Shaare Zedek Medical Center- Jerusalem- and Sackler Faculty of Medicine- Tel Aviv University- Tel Aviv- Israel, Neurology, Jerusalem, Israel
3“Iuliu Hatieganu” University of Medicine and Pharmacy- Cluj-Napoca- Romania, Neurosciences, Cluj-Napoca, Romania
Background and Aims
Is stroke clinical research stifled by backward oriented designs? An evaluation of neuroprotection intervention studies conducted in the last 30 years shows that methodological design flaws may be among the major reasons why pharmacological agents fail to demonstrate efficacy.
Method
Many inconclusive studies used a single outcome measure approach based on dichotomization of the modified Rankin scale (mRS). As highlighted by leading researchers and methodologists, dichotomization of a full scale is burdened with loss of power and arbitrary choice of cutoffs, allowing only limited statements on treatment effects. The result of the ECASS II trial provides an excellent example for the associated risk of bias: while dichotomization using mRS 0–1 resulted in P = 0.277, dichotomization using mRS 0–2 resulted in P = 0.024, i.e. in two opposite conclusions on evidence. Another common trap is focus on mortality only. This approach cannot capture clinical relevant information in the many survivors of stroke and is bound to risk of bias by neglecting important aspects of patient rehabilitation. Another example is the Initial stroke severity, playing an important role for assay sensitivity at final outcome. Neglect may condemn clinical trials to fail.
Results
Selected examples from the literature and current study designs are discussed in order to enhance the awareness of most common traps in stroke research and to help improving the quality and assay sensitivity of future study designs.
Conclusion
Appropriate full scale analyses, multidimensional approaches, meta-analytic pooling across baseline severity strata represent promising pathways to improve assay sensitivity of clinical stroke trials.
Trial registration number
N/A
AS04-029
THE HYBRID ASSISTIVE LIMB (HAL) EXOSKELETON FOR INDIVIDUALIZED, INTENSIVE TRAINING OF GAIT DURING INPATIENT STROKE REHABILITATION – A PROSPECTIVE RANDOMIZED OPEN BLINDED END-POINT (PROBE) STUDY
1Karolinska Institutet, Department of Clinical Sciences- Danderyd Hospital, Stockholm, Sweden
Background and Aims
Impaired gait after hemiparetic stroke remains a challenge and may be approached by use of novel technology. The Hybrid Assistive Limb (HAL) is an exoskeleton allowing both autonomous and a voluntary mode of action. Our aim was to explore the added value of gait training with HAL in terms of: 1) independence in walking, 2) walking speed and endurance, 3) balance and 4) movement-related functions.
Method
This PROBE study included 32 patients with severely impaired gait function <8 weeks after stroke. Patients were randomized to:
1) Conventional training (including gait practice, individualized and followed current evidence and best practice (approximately 30-60 min/day, 5 days/week) or to
2) HAL-training in addition to the conventional training (1 session/day, 4 days/week during 4 weeks).
Blinded assessments before intervention, after intervention and at 6 months post stroke were performed using the Functional Ambulation Categories (primary outcome), the 2 Minute Walk Test, the Berg Balance Scale and the Fugl-Meyer Assessment for lower extremity.
Results
Patient characteristics are presented in Table 1. Data analysis is ongoing. Between group differences in outcome over time will be presented.
Conclusion
To our knowledge this is the first blinded, randomized controlled study after conventional training compared to additional HAL training in the sub-acute stage after stroke. Our findings will be valuable to guide both clinical praxis and further studies of robotic gait training.
Trial registration number
ClinicalTrials.gov: NCT02410915
AS04-030
MUSCLE MECHANICAL PROPERTIES ALTERNATION AFTER NEUROMUSCULAR ELECTRICAL STIMULATION COMBINED CYCLING TRAINING IN CHRONIC STROKE SURVIVORS
1First Affiliated Hospital- Sun Yat-sen University, Rehabilitation Medicine, Guangzhou, China
Background and Aims
The mechanical properties of muscles such as tone, elasticity, and stiffness are often affected in patients with stroke. The aim of this study is to examine the alternation of muscle mechanical properties after neuromuscular electrical stimulation combined cycling Training on the lower limb muscles of chronic stroke survivors.
Method
Eight chronic stroke patients (2 male, 6 female, average age=59.1) accepted one-hour per day cycling training at the most tolerated stimulation intensity for 20 sections. There were 3 training days per week. The stimulated muscles included rectus femoris, tibialis anterior, hamstrings and medial head of gastrocnemius. Muscle mechanical properties were assessed by a myotonometer before training, and after finishing 20-section training.
Results
The results showed there was significant decrease in muscle tone at rest state (p = 0.038) and dynamic stiffness (p = 0.045) in the affected side of biceps femoris than that of the unaffected side. After 20-section training, mechanical stress relaxation time (p = 0.034) and gradual elongation of muscle over time (p = 0.024) of paretic rectus femoris increased.
Conclusion
Compared with the unaffected side, the assessment of muscle mechanical properties at affected side of stroke reveals decreased muscle tone, which might lead to weak muscle contraction. Muscle viscoelasticity is related to mechanical stress relaxation time and gradual elongation of muscle over time, and the increase of viscosity might contribute to muscle fiber sliding and changes in the intra- and extracellular matrix of muscles after training.
Trial registration number
Our study has registered on Chinese Clinical Trial Registry, registration number: ChiCTR-IOR-17012299
AS04-031
GASTROCNEMIUS MUSCLE SPASTICITY AND ITS ASSOCIATION WITH GAIT SPEED, BALANCE, AND QUALITY OF LIFE IN STROKE
1Istanbul Aydın University- Faculty of Health Sciences, Division of Physiotherapy and Rehabilitation, Istanbul, Turkey
2Istanbul University-Faculty of Health Science- Division of Physiotherapy and Rehabilitation, Department of Neurological Physiotherapy and Rehabilitation, Istanbul, Turkey
3Istanbul University- Faculty of Health Sciences- Division of Physiotherapy and Rehabilitation, Department of Physiotherapy and Rehabilitation, Istanbul, Turkey
4Istanbul Physical Medicine and Rehabilitation Training Hospital, PMR Clinic, Istanbul, Turkey
Background and Aims
There is no consensus concerning the relationship between spasticity and gait speed, balance and quality of life in stroke patients. Therefore, the aim of the present study was to investigate spasticity and its association with balance, gait speed and quality of life.
Method
Fifty one stroke patients who can cooperate and have 3 or higher grade in Functional Ambulation Scale were included in the study. Gastrocnemius muscle spasticity by the Modified Ashworth Scale (MAS), gait speed by the 10-meter Comfortable and Fast Gait Speed Tests (CGST-FGST), balance by the Single Leg Stance Test (SLST) and Timed Up and Go Test (TUG), and quality of life by the Stroke Specific Quality of Life Scale (SS-QOL) were assessed. P ≤0.05 was considered statistically significant.
Results
The MAS score of gastrocnemius muscle was 2.87 ± 1.03. Significant correlations were found between the MAS score and the 10-meter FGST (r = 0.31; p = 0.002), and the affected limb SLST (r = −0.43; p = 0.004). There were no statistically significant correlations between the MAS score and 10-meter CGST(r = 0.23; p = 0.129), TUG (r = 0.28; p = 0.071), and SS-QOL(r = −0.02; p = 0.852).
Conclusion
The results indicated that the gastrocnemius muscle spasticity may contribute to impairment of fast gait speed and static balance in stroke patients. To increase ambulatory skills of stroke patients, gastrocnemius muscle spasticity should be aimed in rehabilitation programme.
Trial registration number
N/A
AS04-033
SAFETY AND CLINICAL OUTCOME OF INTRA-ARTERIAL INFUSION OF BONE MARROW DERIVED MONONUCLEAR CELLS IN SUBACUTE ISCHEMIC STROKE:RANDOMIZED OPEN LABELED BLINDED END POINT CLINICAL PILOT TRIAL
1PGIMER, Neurology, Chandigarh, India
2PGIMER, Transfusion Medicine, Chandigarh, India
3PGIMER, Radiology, Chandigarh, India
Background
Worldwide, 15 million people suffer a stroke each year; one-third die and one-third is left permanently disabled.A major unmet need exists for treatments that can reduce tissue injury progression and enhance functional recovery in patients with stroke
Aim
To assess safety and clinical outcome of intra-arterial infusion of bone marrow derived mononuclear cells in subacute ischemic stroke patients
Method
This was a single center; prospective randomized open labeled blinded end point assessment that included five cases and ten controls. Subjects with subacute ischemic stroke were randomly assigned to the arm that received intra-arterial infusion of autologous BMSCs or to the control arm.Coprimary clinical effcacy outcomes were Barthel Index score and modified Rankin scale at day 30, 90 and 180 days. Secondary outcomes were change in infarct volume, National Institute of Health Stroke Scale (NIHSS) at day 30, 90 and 180. Main safety outcome was adverse events
Results
Five subjects received a mean of 4.16x107 CD34 + BMSCs at median of 26.2 ± 14.89 days after stroke onset.There was no signifcant difference between BMSCs arm and control arm in the modifed Rankin scale at 180 days (p value- 0.267), NIHSS score (7.33 versus 6.0; p value-0.534), change in infarct volume (-3.3 versus −3.37; p value-0.95) at day 180.No adverse events were reported in two arms.
Conclusion
This is the first randomized controlled trial for using intra-arterial BM-MNCs for treatment of subacute moderate to severe ischemic stroke. The present study concludes that intra-arterial infusion of BMSCs is safe, but without benefcial effect on treatment of stroke outcome.
Trial registration number
REF/2015/12/010300
AS04-034
FOOT PLACEMENT EFFECTS THE PROPORTION OF MAXIMAL KNEE EXTENSOR MOMENT PRODUCED IN SIT TO STAND AND STAND TO SIT ACTIVITIES
1IZMIR KATIP CELEBI UNIVERSITY, Physiotherapy and Rehabilitation, IZMIR, Turkey
2Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Izmir, Turkey
Background and Aims
To identify the effects of foot placement on generated moments during sit-to-stand and stand-to-sit activities.
Method
Two healthy adults (1M, 1F) volunteered for the study. Isokinetic measurements were conducted by use of Cybex (Cybex, Inc., Ronkonkoma, NY, USA) dynamometer. Sit-to-stand performance has been analysed using CODAmpx30 (Charnwood Dynamics, Barrow on Soar, Leicestershire, England). AMTI (Advanced Mechanical Technology, Inc. [AMTI], Watertown, MA, USA) has been used to measure the force and moment components of foot. The data from sit-to-stand activity has been compared with concentric peak knee extensor moments and the data from stand-to-sit task has been compared with eccentric peak extensor moments. Peak knee extensor moments from Cybex™ represent maximal achievable force. Knee moments recorded by CODA™ has been converted to a proportion of this maximum.
Results
Participants had greater peak knee extensor moments in dominant side comparing to non-dominant side in symmetrical and left foot forward positions during the sit-to-stand task. When right foot placed forward non-dominant side had greater peak knee extensor moments than the dominant side. Similar to findings from sit-to-stand tasks, participants had greater peak knee moments on dominant side during feet symmetrical and left foot forward positions during stand-to-sit task performance.
Conclusion
This study confirms the generation of a knee extensor moment as a key component for an appropriate sit-to-stand performance. During sit-to-stand, right and left sides produce different amount of torque and before a sit-to-stand, positioning the stronger side forward results in an increase in peak knee extensor moment on the weaker side.
Trial registration number
N/A
AS04-035
A HEART FOR RUNNING – SAFETY CONSIDERATIONS ON AEROBIC EXERCISE IN THE SUBACUTE PHASE OF STROKE – DATA FROM THE PHYS-STROKE TRIAL
1Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
2Charite Universitätsmedizin Berlin, NeuroCure Clinical Research Center, Berlin, Germany
3Charite Universiätsmedizin Berlin, Klinik und Hochschulambulanz für Neurologie, Berlin, Germany
4German Center for Cardiovascular Research, partner site Berlin, Berlin, Germany
5Charité ‐ Universitätsmedizin Berlin, Institute of Biometry and Clinical Epidemiology, Berlin, Germany
6German Center for Neurodegenerative Diseases, partner site Berlin, Berlin, Germany
7Medical Park Berlin Humboldtmuehle, Neurology, Berlin, Germany
8University Medicine Greifswald, University Medicine Greifswald, Greifswald, Germany
Background and Aims
Within the subacute phase of stroke aerobic exercise including treadmill training is a promising rehabilitative therapy (Saunders et al, 2016) to improve walking abilities and minimize physical deterioration but its safety still needs to be further analyzed.
Method
Data are drawn from the German investigator initiated, multicenter, randomized clinical trial ‘Physical Activity in Subacute Stroke (PHYS-Stroke)’ (Flöel et al, 2014). In this trial 200 patients in the early subacute phase of stroke (day 5–45 after stroke) were recruited from seven rehabilitation clinics in and around Berlin. Patients were randomized to receive 25 minutes of either treadmill-based, aerobic physical exercise (study intervention) or relaxation sessions (control intervention) five times per week for four weeks, in addition to standard rehabilitative therapy. Safety endpoints were recorded until 6 months post stroke and comprised recurrent fatal or no-fatal cardiovascular event including stroke, hospital re-admissions, and death.
Results
Safety analyzes are on the basis of 200 patients who were randomized in the trial (end of recruitment: April 30th, 2017; Database closed: Nov 10th, 2017). Adverse events and incidence rate ratios with 95% confidence intervals will be presented, as well as medical characterization of patients who experienced an event, including biomarker response of the intervention.
Conclusion
Detailed description of patients undergoing an aerobic exercise such as treadmill training in the subacute phase of stroke will improve safety considerations for implementing such interventions in future trials as well as into standard care.
Trial registration number
ClinicalTrials.gov number, NCT01953549
AS04-038
THERAPY FOR POST STROKE DEPRESSION- A COMPARATIVE STUDY
1Amrita Institute of Medical Sciences, Stroke Medicine, Kochi, India
2Amrita Institute of Medical Sciences, Pharmacy Practice, Kochi, India
Background and Aims
Post stroke depression (PSD) has long been recognized as a neuropsychiatric complication of stroke but often remains masked owing to its challenging diagnosis.We intended to study the prevalence of PSD and to compare Fluoxetine and Venlafaxine for safety, efficacy profiles in post stroke depression patients
Method
Non-experimental, comparative, prospective study was carried out in the Department of Stroke Medicine for a period of 8 months.60 patients of the total patients screened for depression using Hamilton Depression Rating Scale (HDRS) satisfying the inclusion criteria were selected and 30 of them treated with fluoxetine and others with venlafaxine.Baseline values of HDRS were taken at the time of diagnosis and 2,4 and 8 weeks follow-up respectively and comparison of clinical outcome and adverse events of the two drugs were done by a 6 month follow up.
Results
Of the 60 subjects participated in the study, 40 were males, and the mean age of the sample was found to be 62.13 ± 11.14.The prevalence of PSD was found to be 22.4%.Hypertension (90%)followed by diabetes mellitus (50%), CAD (28.33%), dyslipidemia (26.57%)were the common comorbidities found in the sample population .When the ADRs of both the drugs were compared graphically, Fluoxetine group showed a higher incidence of ADRs (61.54%) than Venlafaxine group (38.46%).Statistical analysis showed a significant difference in the effectiveness of both the drugs.The results of this study suggests that venlafaxine is more effective than fluoxetine in the treatment of PSD
Conclusion
Depression following stroke can hamper the progress of the patient both physically and socially and hence should be given proper attention and management.
Trial registration number
N/A
AS04-039
TRANSCRANIAL RANDOM NOISE STIMULATION COMBINED WITH GRADED REPETITIVE ARM SUPPLEMENTARY PROGRAM (GRASP) IN MOTOR REHABILITATION OF THE UPPER LIMB IN SUBACUTE ISCHEMIC STROKE PATIENTS
1University of Palermo, Biomedical Department of Internal and Specialistic Medicine- DIBIMIS- University of Palermo- Italy, Palermo, Italy
2University of Palermo, Department of Experimental Biomedicine and Clinical Neurosciences- University of Palermo, Palermo, Italy
Background and Aims
Upper limb impairment is a common outcome after stroke. New rehabilitative interventions partially failed to show a superior effect compared to standard therapy. The present study focuses on the effect of tNRS in the sub-acute stage after stroke. The primary aim is to evaluate the combined use of TRNS with the GRASP in subacute ischemic stroke patients.
Method
A double-blind RCT, approved by local committee, was performed. Patients with upper-limb impairment were recruited 1 to 6 weeks after stroke. Participants were randomly allocated to two groups: GRASP+tRNS and GRASP+Sham stimulation. Each patient underwent 5 session (1 session/day). Fugl-Meyer Assessment Upper extremity (FMA-UE) was performed to evaluate upper limb impairment before treatment (T0) at the end (T1) and after a month (T2). Clinical and demographic characteristics and changes between baseline data and follow-up were compared between groups with the t tests and the chi-square test for the continuous and categorical variables. Anova was used to evaluate the differences among groups ( level of significance of 95% (p <0.05).
Results
11 men and 13 women were recruited, (age range from 55 to 92 years). FMA-UE, (T0), (T1) and (T2) average scores were 43,08, 48,46 and 60,62 respectively (42,42; 48,17 ; 56,18 for TRNs and 43,75; 48,75 and 53,58 for sham). TRNS group reported a significant improvement in FMA-UE score after treatment.
Conclusion
The additional use of tRNS to GRASP seems to have a significant beneficial effect . These results should be verified by additional confirmatory studies.
Trial registration number
N/A
AS04-041
FEASIBILITY OF DELIVERING ADDITIONAL TRUNK TRAINING DURING POST STROKE REHABILITATION TO PROMOTE 6 MONTHS’ MOBILITY OUTCOMES IN SEVERE STROKE
1King's College London, Academic Dept. of Physiotherapy- School of Population Health & Environmental Sciences- Faculty of Life Sciences & Medicine-, London, United Kingdom
2King's College London, School of Population Health & Environmental Sciences- Faculty of Life Sciences & Medicine-, London, United Kingdom
3Guy's and St Thomas' NHS Foundation Trust, Care of Elderly, London, United Kingdom
Background and Aims
Previous studies have found up to 40% of stroke survivors do not regain independence in walking ability at 6 months. Recent meta-analyses have shown benefits of additional trunk training (ATT) on trunk performance, balance and mobility outcomes post stroke. This study explored the acceptability and feasibility of ATT in patients with severe stroke.
Method
Twenty-one (21) adults with severe trunk impairments were recruited within the first 3–7 days after stroke. They were given up to 16 hours of ATT in addition to usual stroke rehabilitation during in-hospital stay. Feasibility outcomes of eligibility and recruitment rates, intervention delivery and completeness of outcome measures were assessed. Outcome measures of Trunk Impairment Scale (TIS), Modified Rivermead Mobility Index (MRMI), Stroke Specific Quality of Life (SSQOL), Euroqol (EQ-5D) were completed at baseline, end of ATT and 6 months post stroke.
Results
A total 578 patients were screened, 22.7% had severe trunk deficits, of which 31 were eligible for recruitment, implying an eligibility rate of 5.4%. 68% of these eligible participants consented to participate. A total of 8.1 ± 5.6 hours of ATT was delivered over an average of 5.6 weeks (range 1 -15 weeks). Mean changes (SD) in outcome measures post treatment were 7.9 ± 7.1 (TIS); 12.4 ± 9.6 (MRMI); 26.4 ± 19.7 (SSQOL) and at 6 months follow-up were: 6.9 ± 7.1 (TIS); 18 ± 13.5 (MRMI); 31.3 ± 37.0 (SSQOL); 13.6 ± 43.0 (EQ5D-VAS). Attrition was less than 10%.
Conclusion
ATT is acceptable and feasible to deliver during early rehabilitation in this population of stroke survivors.
Trial registration number
ISRCTN 12137158
AS04-043
INTERRELATION BETWEEN CONCENTRATION OF HEMOGLOBIN AND DINAMIC OF FUNCTIONAL RECOVERY OF PATIENTS WITH ISHEMIC STROKE
1Tashkent medical academy, Neurology, Tashkent, Uzbekistan
Background and Aims
Anemia is a background disease among older people who have high risk of stroke. It is very importance to estimate functional recovery of patients with ischemic stroke, depending on the concentration of hemoglobin within 1 month after debut of stroke.
Method
studied 50 patients with stroke, which devided into two groups. The first group (control 25 patients) with a hemoglobin level of 129,52 ± 6,72 g/l and the second group (anemia 25 patients) with 89,28 ± 6,80 g/l (p < 0,001). On the 1st and 10th days of ischemic stroke severity was assess by National Institute of Health Stoke Scale (NIHSS), on the 10th and 30th days patients’ functional recovery was assess by Barthel scale. Patients with anemia didn't receive iron suplementation.
Results
The estimation of control and anemia groups by NIHSS for 1st day of stroke had made 12,12 ± 1,96 and 12,32 ± 1,77 points (p>0,05), that shows relatively identical stroke severity in both groups. However, on the10th day 9,2 ± 1,95 and 9,96 ± 1,81 by NIHSS (p>0,05), indicating the divergence of results. On the same day patient's functional recovery results by Barthel scale in control group were 33,2 ± 4,39, anemia group 27 ± 5,2 points (p <0,01). Finally, on the 30th day the indecates were 73,6 ± 4,59 and 63,6 ± 5,57 points (p <0,001). Although, both groups are in the same range by Barthel scale results of 30th day, it was detect that the rates are lower in anemia group.
Conclusion
the results showed slowdown dynamic of functional recovery of patients with ischemic stroke with reduced hemoglobin and the deterioration quality of their life.
Trial registration number
N/A
AS04-044
PARTICIPATION AND AUTONOMY FIVE YEARS AFTER STROKE: A LONGITUDINAL OBSERVATIONAL STUDY; USING THE IMPACT ON PARTICIPATION AND AUTONOMY QUESTIONNAIRE
1Institute of Neuroscience and Physiology- the Sahlgrenska Academy, Department of Clinical Neuroscience, Gothenburg, Sweden
2Department of Clinical Neuroscience- Institute of Neuroscience and Physiology- the Sahlgrenska Academy, Department of Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
To regain participation and autonomy in life and in society for stroke survivors are of major importance. Assessments of self-perceived participation and autonomy can provide knowledge about the need for rehabilitation strategies aimed to optimize rehabilitation and support reintegration into society.
To evaluate self-perceived participation and autonomy for stroke survivors, five years after stroke, and to explore potential factors associated with perceived restrictions in participation and autonomy.
Method
People diagnosed with first time stroke during 2009-2010, in Gothenburg, were eligible in the 5 year follow-up study. The Impact on participation and autonomy-questionnaire were used as well as the “12 month follow up questions with added items”. Statistical methods involved descriptive analysis and logistic regressions.
Results
A modest impact on perceived restrictions in participation and autonomy could be seen. The domains Autonomy Outdoors, Work and Education and Social Life and Relationship were most affected in terms of perceived participation restrictions. An increase in stroke severity and older age predicted the outcome in most of the domains. Depression explained perceived participation restrictions in present time. The categories 'mobility', 'leisure' and 'helping other people' were perceived as most problematic in terms of participation restrictions. Older age, an increase in stroke severity predicted the outcome in all of the categories.
Conclusion
5 years after stroke, the result showed a relatively low impact on perceived participation restrictions. Life domains that require a certain level of physical, cognitive and social ability were most affected.
Trial registration number
N/A
AS04-045
IMPLEMENTATION OF THE INTERNATIONAL CLASSIFICATION OF FUNCTIONING FOR MANAGEMENT A MULTIDISCIPLINARY REHABILITATION TEAM WORK IN STROKE UNIT
1First Saint-Petersburg I.P.Pavlov State Medical University, Department of physical methods of treatment and sports medicine, St.Petersburg, Russia
2First Saint-Petersburg I.P.Pavlov State Medical University, Neurology, St. Petersburg, Russia
3City Hospital #26, Stroke unit, St. Petersburg, Russia
4First Saint-Petersburg I.P.Pavlov State Medical University, Department of Pedagogics and Psychology, St. Petersburg, Russia
5First Saint-Petersburg I.P.Pavlov State Medical University, Department of physical methods of treatment and sports medicine, St. Petersburg, Russia
Background and Aims
Purpose
evaluate the effectiveness of a «new» model of rehabilitation for acute stroke patients using the International Classification of Functioning, Disability and Health (ICF) to manage a multidisciplinary rehabilitation team.
Methods
The project is registered in the ClinicalTrials.gov register under the title: «The Pilot Project Development of the MEdical Rehabilitation System in Russian Federation (DOME)». The design of the study was consecutive. In the 1st phase doctors worked according to the traditional «old» scheme of rehabilitation (n = 130) for Russia. In the second phase, medical organizations worked on a «new» model implementing a problem-oriented multidisciplinary approach (n = 130) and using a rehabilitation diagnosis in the ICF categories, which was installed using software «ICF-reader». The study analyzed the quantitative and qualitative characteristics of rehabilitation diagnoses.
Results
The total number of identified problems (domains) in the rehabilitation diagnosis decreased (p < 0.001) in a «new» model group. Implementation of the multidisciplinary principle of the team and the use of the software «ICF-reader» leads to a reduction in working time in the rehabilitation process (p < 0.001). Using software «ICF-reader» facilitates the elaboration of rehabilitation goals and objectives. The level of disability estimated by the Rankin scale was lower in the group where the ICF was used.
Conclusions
The introduction of the ICF to form a diagnosis results in better recognition of the patient’s problems and better results of stroke rehabilitation.
Trial registration number
N/A
AS04-047
COMBINATION OF CEREBROLYSIN AND OCCUPATIONAL THERAPY FOR MEN WITH POST-STROKE DEPRESSION
1First Saint-Petersburg I.P.Pavlov State Medical University, Department of physical methods of treatment and sports medicine, St.Petersburg, Russia
2First Saint-Petersburg I.P.Pavlov State Medical University, Department of Pedagogics and Psychology, St.Petersburg, Russia
Background and Aims
Purpose
to evaluate the effectiveness combination therapy of Cerebrolysin and ergotherapeutic correction for men with post-stroke depression.
Method
The study included 24 male patients aged 47 to 67 years with lacunar stroke 5–7 months before the start of the study, who had no motor and speech disorders. The criterion for inclusion in the study was the presence of depressive disorders and disadaptation. The Beck Depression Inventory (BDI) was applied to assess the severity of the depressive disorder. The Canadian Occupational Performance Measure (COPM) was applying for assessment of activity and social adaptation. In the main group, during the first 14 days of training, Cerebrolysin was administered: intravenously, 10 ml daily, once a day. In the control group, a placebo preparation was administered in the same manner. The course of ergotherapy lasted for 3 months.
Results
In patients receiving Cerebrolysin was a significant decrease in the depression level estimated by BDI in comparison with the placebo group (p = 0.0000007 and p = 0.00002, respectively) in all end points. In the Cerebrolysin group was a faster and more complete recovery of activity in the social environment (shopping) and productive activities (work for money and cooking) of the COPM-rated performance and satisfaction compared with the placebo group after end of infusion and on the 90th day.
Conclusion
Combination of Cerebrolysin infusions and the course of occupational correction in patients with post-stroke depression are more effective for depression and social disadaptation than for a separate course of occupational therapy without drug support.
Trial registration number
N/A
AS04-048
MAPPING OF PHYSICAL ACTIVITY OF STROKE PATIENTS IN A STROKE UNIT
1Neuroscience and Physiology, Clinical Neuroscience, Göteborg, Sweden
Background and Aims
In the aftermath of stroke, physical inactivity is often seen among the patients as a complication to neurological damage and disability. Physical inactivity has been shown to be associated with ill health and prolonged rehabilitation. Organized inpatient stroke unit treatment is now recommended for stroke patients in Sweden as a means to facilitate early mobilization of the patients.
Method
Twenty-five persons at age 27-90 in Gothenburg were included. On day 2 after admission to hospital, patients were observed at the stroke unit Sahlgrenska University Hospital for 1 min every 10 min between 08.00-17.00. The patient’s highest level of activity, location and people present were recorded according to National Stroke Research Institute (Australia) case report form.
Results
Mean age of stroke patients was 72.4 years old and 52% were female. 68% of the patients had a mild stroke (NIHSS <4). On average the patients spent 51.5% of the day in alone.
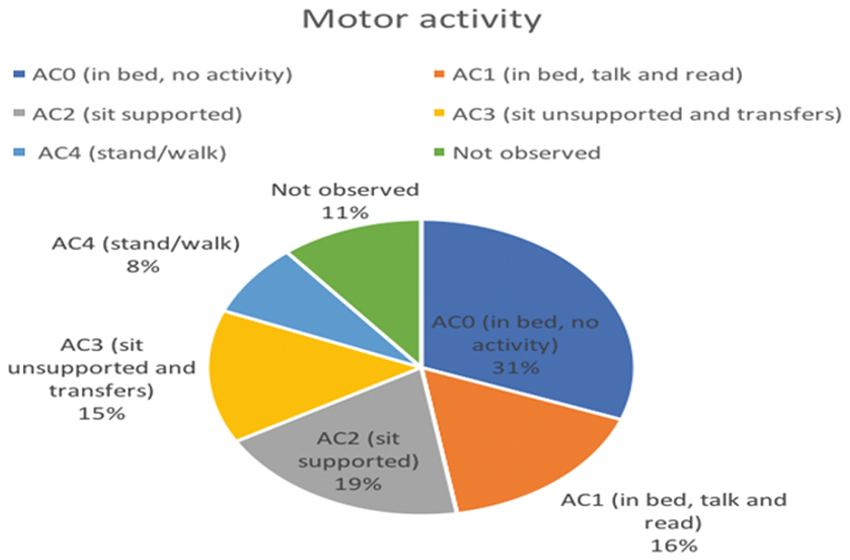
Conclusion
The results show that patients spent almost half of their day physically inactive and in bed. A majority of the patients’ days were also spent alone. This suggests room for improvement in the organization of care in the stroke unit, regarding both physical activity as well as social interactions.
Trial registration number
N/A
AS04-050
PROSPECTIVE OBSERVATIONAL STUDY OF THE EFFECTS OF SERTRALINE ON NEUROLOGICAL RECOVERY FROM ACUTE ISCHEMIC STROKE
1Universitätsklinikum Carl Gustav Carus Dresden, Department of Neurology, Dresden, Germany
Background and Aims
Fluoxetine, a selective serotonin reuptake inhibitor (SSRI), has shown to improve recovery of functional outcomes after acute ischemic stroke (AIS). We hypothesize that sertraline, which is characterized by less severe adverse effects and more stable pharmacokinetics than classic SSRIs, may also improve recovery from AIS.
Method
We present interim data of a prospective one-year single center observational study which is undertaken in AIS patients who had no disability pre-stroke (mRS 0–1). Patients receiving sertraline for depression or improvement of recovery are included as well as those not receiving SSRI. Favorable functional outcome (mRS 0–2 after three months) is the primary outcome. Patients undergo detailed cardiovascular phenotyping and assessment for neurological (NIHSS), affective (Beck’s depression inventory) and autonomic (SCOPA-AUT) symptoms at baseline and after three months.
Results
We present data from 56 patients (72.5 [21] years, median [IQR] (24 females, 41 receiving sertraline post-stroke). Of these, 40 completed the 3-month follow up. Groups did not differ in cardiovascular characteristics neither at baseline nor follow up (p = ns) except for hyperlipidemia (p < 0.05). While autonomic, neurological and affective symptoms also showed no baseline differences, sertraline treated patients showed a tendency toward less severe dysautonomia at follow up than untreated patients (p = 0.06). Favorable functional outcome was achieved by 64.5% in the sertraline group and 33.3% in the untreated group.
Conclusion
Our interim analysis indicates a tendency toward improved functional recovery from acute ischemic stroke in patients treated with sertraline. Although limited by its observational nature, our data might form the basis for a confirmatory phase II RCT.
Trial registration number
N/A
AS04-051
STROKE REHABILITATION SERVICES IN UZBEKISTAN: A SURVEY OF SERVICE CONFIGURATION, CAPACITY AND GUIDELINE ADHERENCE
1Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
Background and Aims
To provide an up-to-date account of stroke rehabilitation services in all District Health Boards (DHB) in Uzbekistan in 2016.
Method
An online survey was completed by clinicians at all 38 facilities in Uzbekistan providing rehabilitation services following acute stroke.
Results
There was some evidence of stroke rehabilitation specialisation, particularly in larger DHBs (seven of eight large DHBs provided a dedicated stroke rehabilitation unit or designated beds). Capacity was generally satisfactory with units accommodating all (68% of units) or most (further 29%) of stroke patients needing rehabilitation. Most units had guidelines for the management of common problems following stroke, apart from depression screening (7%), but intensity of therapy input remains below recommended levels. Post-discharge rehabilitationservices are available in the majority of areas but significant delays (mean 14 days) are common in accessing these services. The results for New Zealand stroke rehabilitation services are broadly comparable with those from the recent Australian stroke rehabilitation service audit.
Conclusion
Compared to previous surveys, New Zealand stroke rehabilitation services have shown progress. To maximise outcomes for stroke patients, improvements are still needed in provision of dedicated stroke rehabilitation units, rehabilitation intensity and access to prompt community rehabilitation in the community.
Trial registration number
271210
AS04-053
PATIENTS’ EXPERIENCES WITH VERY EARLY SUPPORTED DISCHARGE AFTER STROKE
1Neuroscience and Physiology, Clinical Neuroscience, Gothenburg, Sweden
2Institute of Health and Care Sciences, Institute of Health and Care Sciences, Gothenburg, Sweden
Background and Aims
An Early Supported Discharge and rehabilitation at home is recommended for patients with mild to moderate stroke, and implies an accelerated discharge from hospital. Beneficial long-term effects, such as reduced dependency and improved ADL ability, has been reported. There are limited knowledge about patients’ early experiences of returning home and going through rehabilitation. The aim was to explore patients’ experiences with very early supported discharge after stroke.
Method
This was an interview study, nested within a randomized controlled trial; Gothenburg very early supported discharge (GOTVED), comparing very early supported discharge, containing team based home rehabilitation, to conventional care. A consecutive sample of 12 participants with mild to moderate stroke were recruited from the intervention group in GOTVED. Interviews were performed on average 12 days after discharge, transcribed verbatim and analyzed with thematic analysis.
Results
The initial analysis showed that the participants’ confidence in their ability grew by recovering and going through rehabilitation at home, and the team played an important role in this process. At home, they discovered the stroke consequences and tried to adapt to the new situation. But, unfulfilled needs of information and for cognitive and emotional support were reported, as well as a lack of verification of their post-stroke experiences. Also, the very early discharge raised uncertainty whether they would manage at home and about their recovery and rehabilitation.
Conclusion
The preliminary conclusion suggests that the intervention increased confidence and responsibility for recovery and rehabilitation. But, early homecoming also highlighted the vulnerable situation for patients after stroke.
Trial registration number
N/A
THROMBOLYSIS – EXCLUDING CLINICAL TRIAL RESULTS
AS05-002
ACUTE ISCHEMIC STROKE IN THE YONGER POPULATION…ARE THEY BEING TREATED FAST ENOUGH
1Providence Holy Cross Medical Center, Stroke/Neurology, Stevenson Ranch, USA
2Prov St Vincent Medical Center, Prog Mgr Quality/Research- Program, Portland, USA
3Prov St Vincent Medical Center, Dir-Scientific Prog Svcs- Program, Portland, USA
4Prov St Vincent Medical Center, Biostatistician- Program, Portland, USA
Background and Aims
Thrombolysis in acute ischemic stroke (AIS) should be given to eligible patients emergently to prevent disability. AIS in young adults accounts for 10%-14% of strokes, however there is insufficient literature evaluating door to needle (DTN) time and treatment rates (TR) in this population. We assessed whether young patients were evaluated and treated appropriately when presenting with stroke symptoms by measuring TR and DTN times.
Method
A stroke registry was utilized to obtain data for patients presenting with AIS from 23 hospitals between January, 2012 and October, 2017. Patients were categorized into two age groups; 18-44 or 45 and older. Outcomes included TR and DTN times for patients receiving thrombolysis. To compare by age group, a chi squared test was used for TR. Wilcoxon rank sum for DTN, and a generalized estimating equation with an identity link for the log of DTN time, adjusting for covariates.
Results
There were 27,131 patients of which 3.8% (n = 1,031) were 18-44. TR was higher in the 18-44 group (19% vs. 12%; p < 0.001). The median DTN was 57 minutes for patients 18-44 and 53 minutes for those 45 and older (p = 0.018). After adjustment, patients aged 18-44 had a 6% longer DTN compared to 45 or older patients (p = 0.047).
Conclusion
While AIS can occur at any age, retrospective analysis comparing TR and DTN times in older versus younger patents showed that younger patients were given thrombolysis more often than older patients, however DTN times were longer for younger patients.
Trial registration number
N/A
AS05-003
SAFE AND VERY EFFECTIVE INTRAVENOUS THROMBOLYSIS AFTER IDARUCIZUMAB APPLICATION IN STROKE PATIENTS ON DABIGATRAN THERAPY; A CASE SERIES FROM DEPARTMENT OF VASCULAR NEUROLOGY, UMC LJUBLJANA
1University Clinical Centre Ljubljana, Department of vascular neurology, Ljubljana, Slovenia
Background and Aims
Idarucizumab is indicated when rapid reversal of dabigatran anticoagulant effects is required for emergency surgery or urgent procedures and in life-threatening or uncontrolled bleeding. Intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rt-PA) is well established urgent procedure and recommended therapy for acute ischemic stroke according to guidelines. The administration of rt-PA in ischemic stroke requires absence of effective anticoagulation proven by appropriate laboratory tests. University Medical Centre (UMC) Ljubljana provides neurological care and hospitalization to aprox.1 million persons who live in central Slovenia.
To report the safety and the effectiveness of intravenous thrombolysis in dabigatran-treated patients receiving idarucizumab at Department of vascular neurology, UMC Ljubljana.
Method
Retrospective data about all consecutive stroke patients treated with idarucizumab before IVT at our Department were collected from June 2016 till June 2017.
Results
Five (60 % female) acute stroke patients on dabigatran treatment received IVT following idarucizumab application. Time between infusion of idarucizumab and IVT ranged between 10 to 20 minutes. All patients benefited significantly from IVT (National Institutes of Health Stroke Scale: 8 vs. 3, modified Rankin Score (mRS): 4 vs.1) and they all had a mRS of ≤2 at discharge. Only one of the patients had a minor haemorrhagic transformation without clinical relevance. Oral anticoagulation was restarted in all patients (4 patients dabigatran, 3 patients warfarin).
Conclusion
Our data shows that administration of rt-PA after reversing dabigatran activity with idarucizumab in cases of acute ischemic stroke is feasible, easy to manage, effective and appears to be safe.
Trial registration number
N/A
AS05-004
REDUCING DOOR-TO-NEEDLE TIMES ACROSS 11 RURAL HOSPITALS IN CANADA
1University of Calgary, Clinical Neurosciences, Calgary, Canada
2University of Alberta, Neurology, Edmonton, Canada
3Alberta Health Services, Cardiovascular Health & Stroke - Strategic Clinical Network, Edmonton, Canada
Background and Aims
Improvements in door-to-needle times (DNT) have been reported at large urban hospitals, but not in small rural hospitals that have no staff neurologists. QuICR (Quality Improvement and Clinical Research) aimed to reduce DNT to a median of 30 minutes across the Canadian province of Alberta, which includes 11 rural Primary Stroke Centres (PSC). These hospitals have no staff neurology.
Method
We used the Improvement Collaborative Methodology from January 2015 to September 2016 with participation from all 11 rural PSCs. This methodology included 4 face-to-face workshops, site visits, webinars, data collection/feedback, and process improvements. We analyzed annual trends, and we compared data from 2009-2014 to Oct2016-Dec2017. Data from Jan2015-Sep2016 (the intervention period) were excluded in the pre-post comparison.
Results
There were 379 treated cases from 2009-2017 at these 11 PSCs. The trend shows that the annual median DNT improved from 70-96 minutes (2009-2014) to 55 minutes (2017), and the annual number of treated patients increased from 9–38 to 72 (Figure1). In the pre-post comparison, the median DNT dropped from 81 minutes (IQR:64-99min, n = 194) to 54 minutes (IQR:44-70min, n = 95) (p < 0.001) (Figure2).
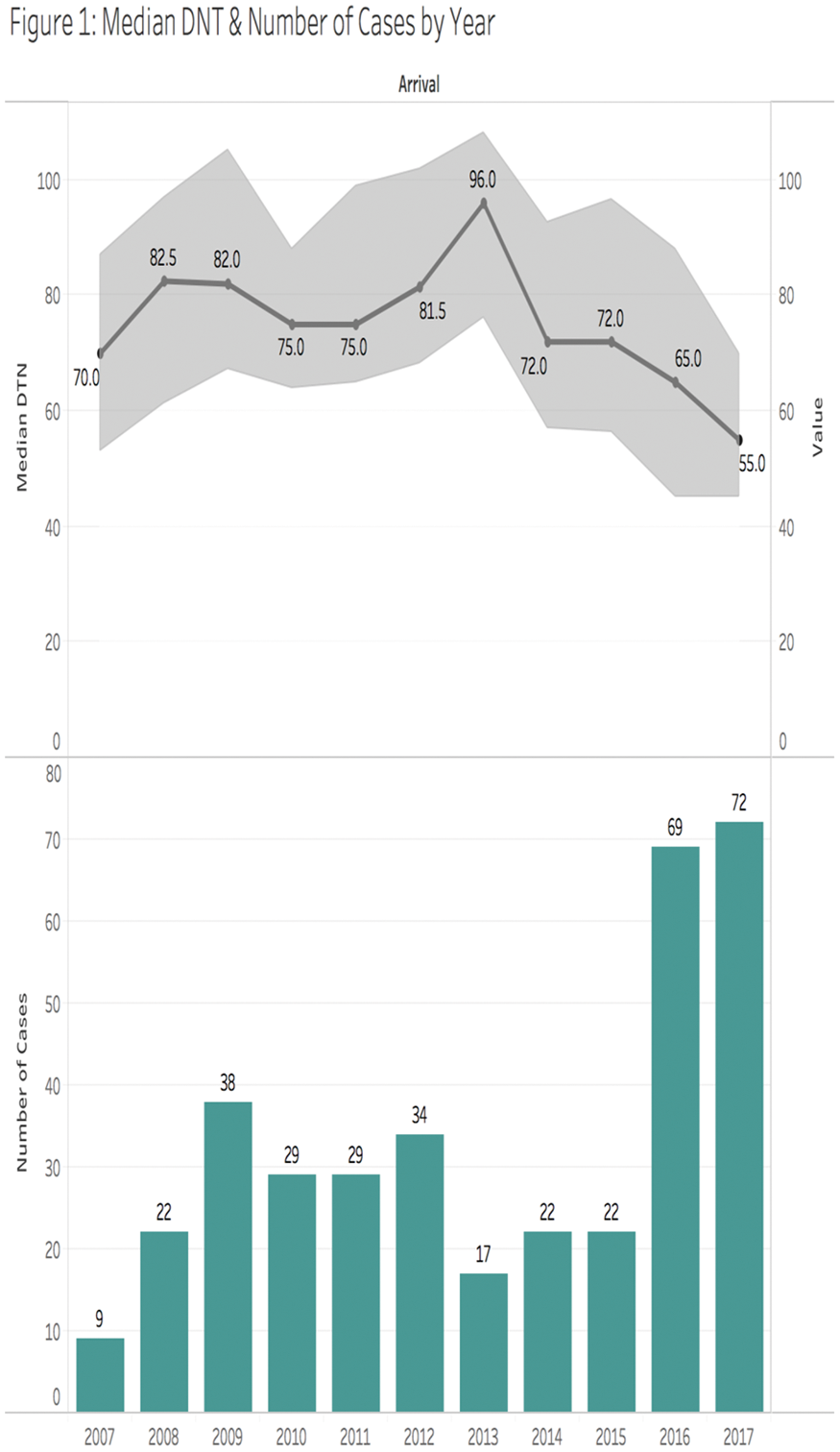
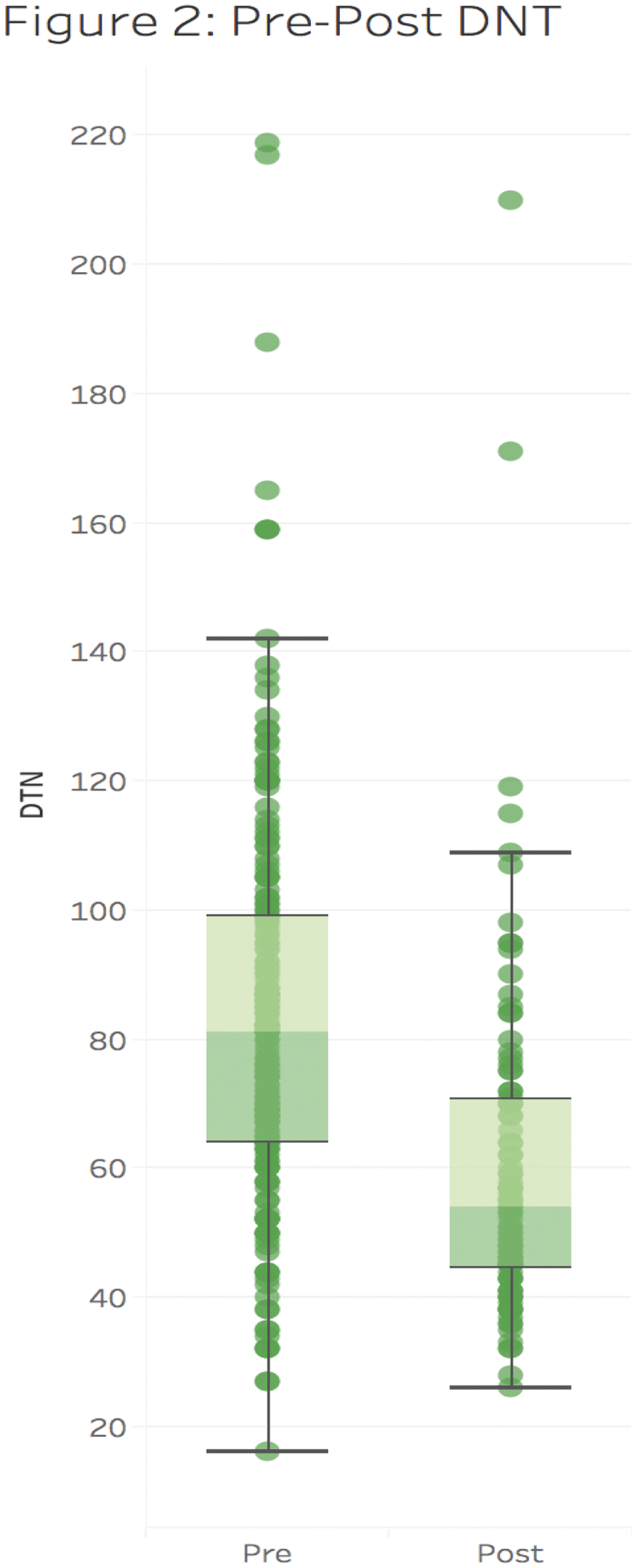
Conclusion
A targeted improvement collaborative can be an effective intervention to reduce DNT and increase utilization of thrombolysis at rural hospitals.
Trial registration number
N/A
AS05-006
SYMPTOMATIC INTRACRANIAL HEMORRHAGE RELATED TO ESTIMATED VERSUS MEASURED BODY WEIGHT IN INTRAVENOUS THROMBOLYSIS
1Leiden University Medical Center, Neurology, Amsterdam, The Netherlands
2Academic Medical Center, Neurology, Amsterdam, The Netherlands
3Medical Spectrum Twente, Neurology, Twente, The Netherlands
4Onze Lieve Vrouwe Gasthuis, Neurology, Amsterdam, The Netherlands
Background and Aims
In patients with acute ischemic stroke, under- or overestimation of body weight can lead to dosing errors of recombinant tissue plasminogen activator (rt-PA) with consequent reduced efficacy or increased risk of hemorrhagic complications. Measurement of body weight (MBW) rather than estimation of body weight (EBW) is more accurate but potentially leads to longer door-to-needle times (DNT) in intravenous thrombolysis (IVT) eligible patients. We assessed if weight modality is associated with (i) symptomatic intracranial hemorrhage (sICH) rate (ii) clinical outcome and (iii) DNT.
Method
Consecutive patients treated with IVT between 2009-2016 from 14 hospitals were included. Baseline characteristics and outcome parameters were retrieved from medical records. Clinical outcome at three months was assessed with the modified Rankin Scale (mRS). The association of weight modality and outcome parameters was estimated with regression analyses.
Results
A total of 4801 patients were included. Five hospitals used MBW (n = 1753), six hospitals EBW (n = 2325) and three hospitals changed from EBW (n = 428) to MBW (n = 295) during the study period. In 2048 of the patients (43%) MBW was used and in 2753 (57%) EBW. Estimation of body weight was not associated with increased risk of sICH (adjusted OR = 1.16; 95% CI 0.83–1.62), favorable outcome (adjusted OR = 0.91; 95% CI 0.76–1.24), or with DNT (adjusted B = −0.35; 95% CI -2.36–1.66).
Conclusion
Both EBW and MBW are acceptable methods to determine the dose of rt-PA in IVT eligible patients.
Trial registration number
N/A
AS05-008
OUTCOME DIFFERENCES AMONG PATIENTS WITH ACUTE ISCHEMIC STROKE RECEIVING THROMBOLYTIC TREATMENT VIA DIRECT ARRIVAL AT THE COMPREHENSIVE STROKE CENTER, DRIP-AND-SHIP, AND SHIP-AND-DRIP PARADIGMS
1Chulalongkorn Stroke Center, King Chulalongkorn Memorial Hospital- Thai Red Cross Society, Bangkok, Thailand
2Division of Neurology, Department of Medicine- Faculty of Medicine- Chulalongkorn University, Bangkok, Thailand
Background and Aims
Chulalongkorn Stroke Center is the comprehensive stroke center (CSC) located in Bangkok, Thailand. Our stroke network consists of different levels of spoke hospitals, ranging from community hospitals where thrombolytic treatment is not available, to those capable of onsite thrombolytic therapy.
This study aimed to assess the time to treatment and outcomes among acute ischemic stroke patients who received thrombolytic treatment in the Chulalongkorn Stroke Network by 1.) direct arrival at the CSC (direct CSC) 2.) telestroke-assisted thrombolytic treatment with secondary transferred to the CSC (drip-and-ship) 3.) referral from community hospital to the CSC for thrombolytic treatment (ship-and-drip).
Method
Acute ischemic stroke patients who received thrombolytic treatment during January 2016-June 2017 under the Chulalongkorn Stroke Network were studied. Time to treatment and clinical outcomes were compared among treatment groups.
Results
There were 179 patients in the study including 109, 39, and 31 patients in direct CSC, drip-and-ship, and ship-and-drip paradigms respectively. The DTN and OTN time were significantly longest in ship-and-drip group (127.5 ± 59.25/205 ± 44.09 mins) compared to direct CSC (38 ± 20.5/158.4 ± 62.03 mins) and drip-and-ship (60.5 ± 57.5/169.6 ± 58.43 mins), P<0.05. There was no significant difference regarding functional independence defined by modified Rankin Scale (mRS) ≤ 2 at 3 months (P = 0.22), in-hospital mortality (P = 0.91), mortality at 3 months (P = 0.73), and symptomatic intracerebral hemorrhage (P = 0.29) among groups.
Conclusion
Thrombolytic treatment with drip and ship method under teleconsultation is feasible in Thailand. There was no difference of clinical outcome among the 3 treatment paradigms. However, DTN time and OTN time were longest in the ship-and-drip paradigm.
Trial registration number
N/A
AS05-009
GENDER DIFFERENCES IN LONG-TERM SURVIVAL OUTCOME FROM STROKE IN THROMBOLYTIC THERAPY AND PHARMACOLOGY
1Institut Catala Salut, Primary Care, Tortosa, Spain
2Agència de Qualitat i Avaluació Sanitàries de Catalunya AQuAS, Departament de Salut - Generalitat de Catalunya, Barcelona, Spain
Background and Aims
There are gender differences in benefits of thrombolysis. We sought to examine the relationship between pharmacology and outcome after thrombolytic therapy.
Method
Cohort study based on the retrospective registry of ischemic stroke patients from January 2011-December 2012 in Catalonia, Spain captured through Programa PADRIS, registry population-based and managed by the Stroke Program, Agency for Health Quality and Assessment of Catalonia. The probability of survival was estimated by the Kaplan-Meier method and the hazard ratio was obtained by using Cox proportional hazard regression model for active prescriptions.
Results
Were included 14,368 people (W50.1%). Men were (p < 0.001) younger (74.22 ± 11.10 vs 80.03 ± 10.16). Thrombolysis alone (n 941) with better survival among men (p 0.023).Thrombolysis and/or thrombectomy (n 376) significantly higher (p 0.011) among men (56.1%), but better survival among women (p 0.053). With medical therapy alone there was higher survival (p <0.001) among women under 80 year-old. The regression model got the independent outcome variables: anticoagulant HR 1.53 (CI95% 1.44-1.63, p < 0.001), diuretics HR 1.71 (CI95% 1.63-1.79, p < 0.001), antiaggregant HR 1.49 (CI95% 1.42-1.56, p < 0.001), statins HR 0.73 (CI95% 0.70-0.77, p < 0.001), A-IIRA HR 0.93 (CI95% 0.89-0.98, p 0.008) and Thrombolytic therapy HR 0.88 (CI95% 0.81-0.97, p 0.009) with different benefit of beta-blockers among women and antidiabetics among men (p <0.001).
Conclusion
The overall benefit on survival with thrombolysis should be avaluated with the cardiovascular comorbidities and their treatment and severity. The challenge is whether these data can achieve better health outcomes through the selection of patients with a more favorable risk versus thrombolytic profile.
Trial registration number
ClinicalTrials.gov number, NCT03247036
AS05-010
TEMPORARY TRENDS IN DOOR-TO-NEEDLE TIME AND OUTCOME BETWEEN 2010-2017: NATION-WIDE STUDY
1St. Annés University Hospital Brno, International Clinical Research Centre and Dpt of Neurology, Brno, Czech Republic
2University Hospital Ostrava, Neurology, Ostrava, Czech Republic
3St. Annés University Hospital Brno, International Clinical Research Centre - Biostatistics, Brno, Czech Republic
4Charles University and University Hospital in Hradec Kralove, Faculty of Medicine and Dpt of Neurology and Comprehensive Stroke Center, Hradec Kralove, Czech Republic
5County Hospital Chomutov, Dpt of Neurology and Stroke Centre, Chomutov, Czech Republic
6Palacky University Hospital, Comprehensive Stroke Centre and Dpt of Neurology, Olomouc, Czech Republic
7Hospital Jihlava and University Hospital Kralovske Vinohrady and Charles University, Neurology and 3rd Faculty of Medicine, Jihlava and Praha, Czech Republic
8University Hospital Motol and Charles University, Neurology and 2nd Faculty of Medicine, Prague, Czech Republic
9Hospital Ostrava Vitkovice, Neurology, Ostrava, Czech Republic
Background and Aims
Shorter door-to-needle time (DNT) was associated with improved outcome after intravenous thrombolysis in clinical studies. Here, we present temporary trends in DNT at population level and outcome after intravenous thrombolysis.
Method
Czech Stroke Society established quality improvement program to shorten DNT which includes monthly monitoring on DNT in all stroke centers, simulation training in some stroke centers and video-records of real thrombolytic cases. To document DNT and outcome, prospectively collected data from the Safe Implementation of Treatments in Stroke registry (SITS) between January 2010 and July 2017 were analyzed. Hierarchical generalized linear model was used to identify association between year and outcome independently from pre-specified baseline variables. Two outcome measures were used: mRS 0 or 1 and any parenchymal hemorrhage.
Results
Of 18691 patients enrolled, 14832 (79%) had available data: age 70 ± 13, NIHSS-baseline median 7. Mean DNT dropped from 78 (95%CI:75-81) minutes in 2010 to 39 (95%CI:36-42) minutes in 2017 (see figure). In the same time period proportion of patients with mRS 0–1 increased from 387 (36%) to 851 (58%) and parenchymal hemorrhages dropped from 99 (7.8%) to 76 (3.8%), respectively. Year was independently associated with mRS 0–1 and parenchymal hemorrhage.
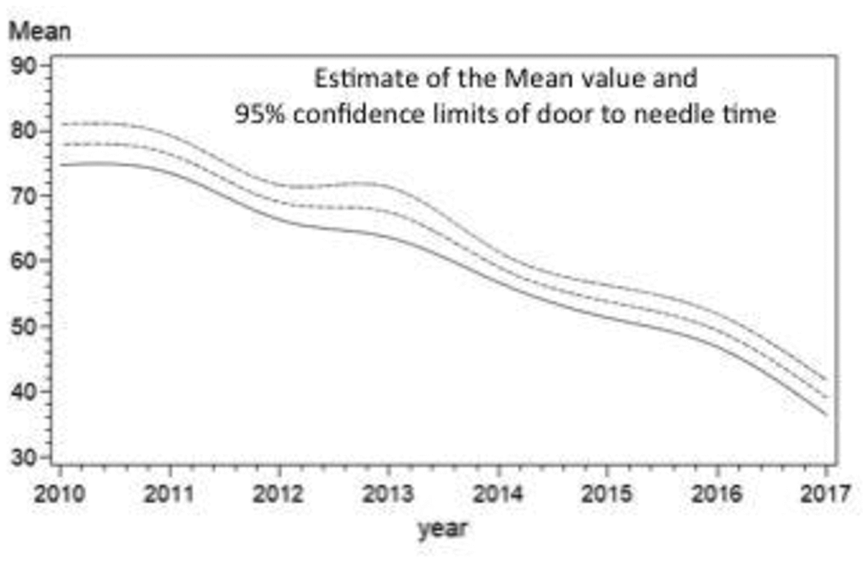
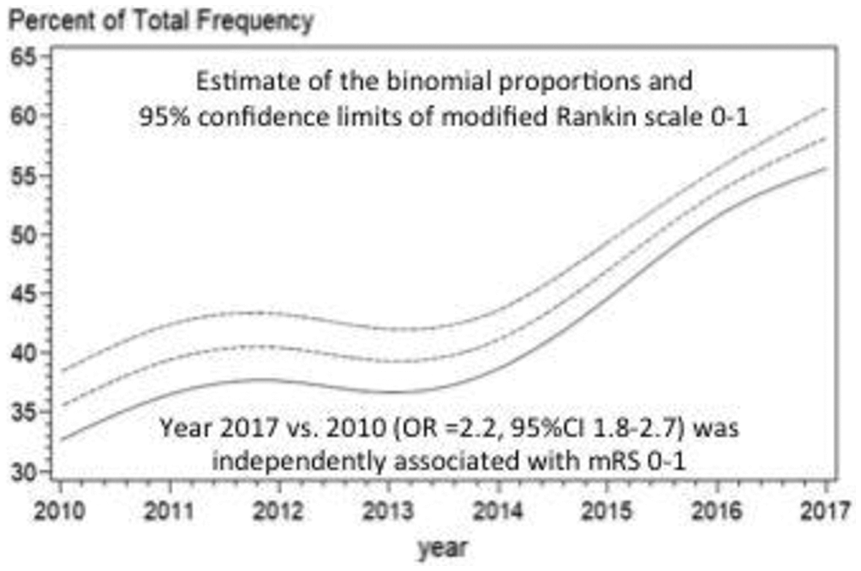
Conclusion
At population level, thrombolysis is performed faster in recent years and outcome after intravenous thrombolysis better which may be partly due to less intracerebral hemorrhages.
Trial registration number
N/A
AS05-011
INTRAVENOUS THROMBOLYSIS IN ACUTE ISCHEMIC STROKE AFTER A REVERSAL OF DABIGATRAN ANTICOAGULATION WITH IDARUCIZUMAB: A REAL-WORLD CLINICAL EXPERIENCE
1University Hospital Olomouc, Comprehensive Stroke Center- Department of Neurology, Olomouc, Czech Republic
2St. Anne's University Hospital, International Clinical Research Center and Department of Neurology, Brno, Czech Republic
3Masaryk Hospital Ústí nad Labem- KZ a.s, Comprehensive Stroke Center- Department of Neurology, Usti nad Labem, Czech Republic
4Charles University Faculty of Medicine and University Hospital, Comprehensive Stroke Center- Department of Neurology, Hradec Kralove, Czech Republic
5Hospital Ceske Budejovice, Comprehensive Stroke Center- Department of Neurology, Ceske Budejovice, Czech Republic
6Faculty of Medicine in Plzen- Charles University in Prague and Faculty Hospital Plzen, Comprehensive Stroke Center- Department of Neurology, Plzen, Czech Republic
Background and Aims
Intravenous thrombolysis (IVT) is contradicted in acute ischemic stroke (AIS) patients using oral anticoagulants. Specific human monoclonal antibody was introduced to reverse immediately anticoagulation effect of direct inhibitor of thrombin – dabigatran. Until now, mostly individual cases presenting successful IVT after reversal of dabigatran anticoagulation in AIS patients were published. Thus, we aimed to report real-world data from clinical practice.
Method
AIS patients on dabigatran treated with IVT after antidote reversal were enrolled in the retrospective national-wide study. Neurological deficit was scored using National Institutes of Health Stroke Scale (NIHSS) and 90day clinical outcome using modified Rankin scale (mRS) with a score 0–2 for a good outcome. Intracerebral hemorrhage (ICH) was defined as a presence of any sign of bleeding on control imaging after IVT and symptomatic ICH (SICH) was assessed according to the SITS-MOST criteria.
Results
In total, 12 patients (7 males, mean age 69 ± 8.4 years) with a median of admission NIHSS 7 points were analyzed. 67% of patients used 300 mg daily dose of dabigatran. Antidote was administrated 438 ± 241 min after last intake of dabigatran with mean activated prothrombin time 34 ± 19 s and thrombin time 72 ± 53 s. ICH occurred in 17%, SICH in 8% of patients and no other bleeding complications were observed. Recurrent IS occurred in two (17%) patients. 83% of patients had good 3-month clinical outcome.
Conclusion
Presented data support safety and efficacy of IVT after reversal of anticoagulation effect of dabigatran with antidote also in a real-world clinical practice.
Trial registration number
N/A
AS05-012
SURVEY ON MANAGEMENT OF POST THROMBOLYSIS SYMPTOMATIC INTRA CEREBRAL HAEMORRHAGE
1University Hospital of North Midland NHS Trust, Stroke Medicine, Stoke on Trent, United Kingdom
Background and Aims
Symptomatic intra-cerebral haemorrhage (SICH) is potentially a fatal complication of thrombolysis when treating acute ischemic stroke. The incidence and mortality of the post-thrombolysis SICH is 3.3% and 52.3% respectively. We aimed to explore how SICH are treated worldwide and which treatment option yields the greatest success.
Method
A 12-question survey was devised using SurveyMonkey. The survey was distributed electronically to members of the European Stoke Society and World Stroke Organisation in December 2017 and remained open for 12 days. The responses were analysed using descriptive statistics and qualitative comments to open-ended questions were analysed through thematic analysis.
Results
There were 64 responses in total with the majority from stroke physicians. The responses were mostly from Europe. The three most common risk factors identified for SICH following thrombolysis were stroke severity, uncontrolled hypertension and previous anti-platelets and/or anti-thrombotics use (45%, 40% and 16% respectively). The SICH incident in most hospitals was between 3–6%. The most commonly used management included fresh frozen plasma (41%) and cryoprecipitate (24%). Less commonly used treatment included vitamin K (9%), aminocaproic acid (6%), tranexamic acid (6%) and platelet transfusion (6%). However the majority of the individual answers highlighted that no particular management option yielded the best result, but all had similar outcomes. 75% of the respondent felt that the SICH associated mortality was <50% whilst 20% found mortality around 80%.
Conclusion
Overall all the respondents agree that SICH associated mortality is very high. Urgent research should be undertaken with newer agents to improve the outcome of the patients.
Trial registration number
N/A
AS05-014
THROMBOLYSIS OVER 80 YEARS IN THE LATER TIME WINDOW. A HOSPITAL-BASED STUDY
1Semmelweis University, Department Of Neurology, Budapest, Hungary
2Semmelweis University, János Szentágothai Doctoral School of Neurosciences, Budapest, Hungary
3Medical Centre Hungarian Defence Forces, Department of Neurology, Budapest, Hungary
Background and Aims
About 30% of ischemic stroke patients are over 80 years old. Large portion of these elderly patients are possible candidates for intravenous thrombolysis (IVT). However, regulations and recommendations regarding IVT in this population are controversial. The aim of our retrospective study to analyze the rates of intracerebral hemorrhage (ICH), symptomatic ICH (SICH), mortality and functional outcome of IVT in patients over 80 years with acute ischemic stroke (AIS) treated within 3 hours compared to 3–4,5 hours.
Method
We evaluated all the AIS patients over 80 years who went through IVT at our hospital between 01/01/2015 and 31/10/2017. National Institutes of Health Stroke Scale (NIHSS), rates of ICH and SICH, mortality, modified Rankin Scale (mRS) at 3 moths and radiographic description of ICH according to Heidelberg classification were compared between the groups treated within 3 hours and 3–4,5 hours.
Results
Majority of ICHs were classified as Heidelberg class 1a (33,3%) and class 2 (33,3%) in the early time window and as class 2 (57,1%) in the later time window.
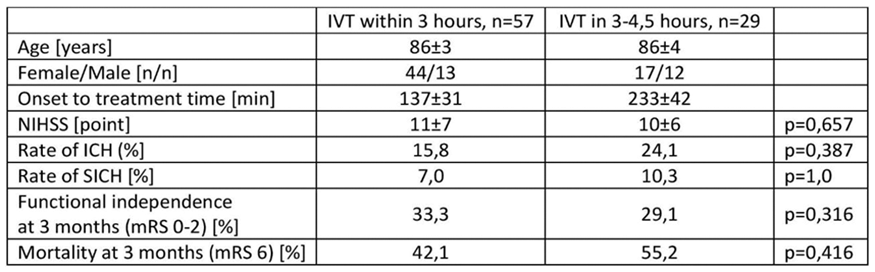
Conclusion
AIS patients over 80 years treated with IVT at 3–4,5 hours compared within 3 hours do not differ significantly in the rates of ICH, SICH, mortality and functional independence at 3 months. Our results suggest that elderly patients should not be denied IVT in the later time window solely beause of age.
Trial registration number
N/A
AS05-016
THROMBOLYTIC TREATMENT IN ISCHEMIC STROKE IN A REMOTE AREA. ELBA ISLAND EXPERIENCE
1Azienda USL Toscana Nord Ovest, Neurological, Portoferraio, Italy
2Azienda USL Toscana Nord Ovest, Emergency, Portoferraio, Italy
3Azienda USL Toscana Nord Ovest, Radiology, Piombino, Italy
4Azienda USL Toscana Nord Ovest, Emergency, Livorno, Italy
5Azienda USL Toscana Nord Ovest, Neurological, Livorno, Italy
6Azienda USL Toscana Nord Ovest, Radiology, Portoferraio, Italy
7Azienda USL Toscana Nord Ovest, Emergengy, Portoferraio, Italy
Background and Aims
Stroke is the leading cause of disability among adults in Italy, the second cause of dementia and the third cause of mortality. There are many implications for public health, health service and socioeconomic status associated with Stroke survivors. Thrombolytic treatment and endovascular thrombectomy may change patient’s quality of life.
Elba is the third largest Island in Italy with a total population of about 30,000 inhabitants with a considerably increase of up 300,000 people during the summer. It represents a geographically disadvantaged area because the patients transfer depends on the helicopter’s availability and weather conditions.
Method
From 2012 to 2017 Thrombolytic treatment was performed on 28 patients (out of a total of 291 Ischemic Stroke), 1 patient received the Thrombolytic treatment and secondary Endovascular thrombectomy (*), 1 patient received a primary Endovascular thrombectomy (*) * with drip and ship model.Patient outcome was valutated with Rankin score in the next three months following a Stroke
Results
From 2012 (our activity beginning) to 2017 the percentage of patients treated has definitely improved and in the last year arrive at 22,7%. Telemedicine and and close cooperation improve percentage of treatment.
Conclusion
Close cooperation is required between different specialists since patient selection for treatment is complex. Interventionists need close collaboration with stroke neurologists.. Telemedicine is also discussed as it has been shown to be advantageous for augmenting thrombolytic administration for acute ischemic stroke. The government needs to be involved as this treatment mandates structural changes which will incur more manpower and financial resources.
Trial registration number
N/A
AS05-017
MONOPARESIS SECONDARY TO CERVICAL EPIDURAL HEMATOMA: UNUSUAL PRESENTATION OF A HAZARDOUS STROKE MIMIC
1Hospital Universitario Central de Asturias, Neurology, Gijón, Spain
2Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
Background and Aims
Safety of intravenous thrombolysis in stroke mimics is a current issue. Some conditions such as cervical epidural hematoma (EH) deserve special attention due to the potential harm in these patients.
Method
Case 1: A 71-year old male with atrial fibrillation (AF) treated with warfarin presented with sudden right arm paresis. He had not dysarthria, face asymmetry or sensory loss. Brain CT was normal and angiography confirmed atherosclerosis in the left common carotid artery. INR was 1,2. He was not considered candidate for rTPA because of NIHSS of 2. He later referred shoulder and neck pain developed 24 hours prior to admission. Cranial MRI was normal. Cervical MRI revealed a subacute C1-C3 EH.
Case 2: A 83-year old woman was admitted because of sudden right arm paresis. She had AF treated with warfarin. Multimodal brain CT performed for suspected stroke was normal. The INR 2.5 was an absolute contraindication to rTPA. As she concomitantly reported severe posterior neck pain, an urgent cervical MRI was performed and showed an acute C3-C7 EH.
Results
In both cases, cervical EH presented as acute onset monoparesis characteristically accompanied by severe neck pain in patients taking anticoagulation drugs. We wish to emphasize that monoparesis is an alternative presentation of cervical EH that may be easily mistaken with an acute ischemic stroke.
Conclusion
The diagnosis of cervical EH should be borne in mind when neck pain accompanies a neurological deficit, even if it does not fit the classical medullary syndroms, in order to avoid deleterious complications of cerebral reperfusion therapies.
Trial registration number
N/A
AS05-019
LEFT VENTRICULAR FUNCTION DISTURBANCES IN PATIENTS WITH ACUTE ISCHEMIC STROKE: PROGNOSTIC AND THERAPEUTIC IMPLICATIONS
1University Hospital Erlangen, Department of Neurology, Erlangen, Germany
Background and Aims
Disturbances of systolic left ventricular function (DLV) in ischemic stroke constitute a source of detrimental pathophysiologic cascades, including prothrombotic and proinflammatory states, worsening of cerebral tissue oxygenation as well as hemodynamic impairment. In addition, DLV may affect the safety and efficacy of intravenous thrombolysis.
Method
Clinical cohort study among patients with ischemic stroke and acute recanalising therapies between 2006 and 2016 at a universitary stroke center.
Results
1418 patients were included. 25% had systolic DLV on echocardiography. In 67% this was established as an initial diagnosis. Neurologic deficits in patient with DLV were more sever on admission (NIHSS 11 versus 9.5) and discharge (4 versus 3, p < 0.001), mortality rate within 90 days was higher (20% vs. 13%, p < 0.01) and functional outcome was worse.
Patients with DLV did not have a higher risk of intracerebral bleeding complications following thrombolysis and the effect of treatment on the recanalization rate of occluded vessels and clinical improvement was not different.
Conclusion
DLV is highly prevalent and associated with stroke severity and outcome. Safety and efficacy of intravenous thrombolysis was not impaired.
Trial registration number
N/A
AS05-020
THE EFFECT OF EARLY AND DELAYED TREATMENT WITH MAGNESIUM SULFATE IN DELAYED TISSUE PLASMINOGEN ACTIVATOR TREATMENT IN EXPERIMENTAL MODEL OF ISCHEMIC STROKE WITH RATS
1Konya Training and Research Hospital, Neurology, Konya, Turkey
2Selcuk University- Faculty of Medicine, Neurology, Konya, Turkey
3Selcuk University- Faculty of Medicine, Pharmacology, Konya, Turkey
4Selcuk University- Faculty of Medicine, Pathology, Konya, Turkey
5Selcuk University- Faculty of Medicine, Biochemistry, Konya, Turkey
Background and Aims
The primary treatment of ischemic stroke is recanalization of occluded vascular structure with the recombinant tissue plasminogen activator (r-tPA) and/or interventional treatments. The rate of patients can be treated with tPA is only about 5% because of late admission. This experimental study was planned to evaluate the efficacy of magnesium sulfate (MgSO4) treatment before delayed thrombolytic therapy.
Method
52 rats were randomly divided to six groups. Group 1 (Control group). Group 2 (Sham group): paratracheal muscles were dissected and carotid artery was reached. Group 3: tPA (10 mg/kg) was started 345th minutes after carotid clamp occlusion. Group 4: MgSO4 (90 mg/kg) was started 120th minutes, tPA at 345th minutes after occlusion. Group 5: MgSO4 was started 300th minutes, tPA at 345th minutes after occlusion. Group 6: MgSO4 was started 120th and 300th minutes, tPA at 345th minutes after occlusion. Reperfusion was provided after 360th minutes. At 24th hours, neurological examinations of all rats were performed, blood and tissue specimens were taken. S100 beta, neuron-specific enolase (NSE), ischemia-modified albümin were analyzed from blood. Brain tissue was stained with hematoxylin-eosin and CD34(+) antibody.
Results
Mortality reduction was 17,8% in group 4, 10% in group 5 and 28,9% in group 6. Functional disability of group 6 was the least (p:0,04). There was 23,6% reduction of degenerated neurons in group 6 (p:0,005). NSE is the most effective biomarker in evaluating, functional and histopathological treatment efficacy (p:0,05).
Conclusion
Early onset and long-standing MgSO4 have the beneficial functional and histopathological results in delayed thrombolytic treatment.
Trial registration number
N/A
AS05-021
CONFOCAL DUAL- PULSE ELECTROHYDRAULIC SHOCK WAVE THERAPY REDUCE MIDDLE CEREBRAL ARTERY THROMBOEMBOLISM WITHOUT ANTI- COAGULANT DRUGS: MONITORED BY TRANSCRANIAL DOPPLER ULTRASOUND AND HISTOPATHOLOGY
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Tabriz University of Medical Sciences- Neurosciences Research Center, Department of Neurosciences, Tabriz, Iran
3Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
A plaque may rupture with high risk of subsequent thrombus mediated acute clinical events such as stroke. The efficacy of intravenous anti- anticoagulant drugs is limited owing to a relatively poor recanalization rate and incomplete function recovery in the majority of treated patients. The data in experimental and clinical settings in the arteries suggested that thrombus-rich lesions may be the ideal type of lesion to be treated by shock wave therapy. In this study, we developed an experimental confocal dual- pulse electrohydraulic shock wave generator (8 Kv, 2 Hz and 12Kv, 0.5 Hz), and investigated its effectiveness on thrombus reduction in the rabbit middle cerebral artery
Method
Male New Zealand white rabbits were randomly divided into two groups, a tPA (0.6 mg/kg) group and a confocal dual- pulse electrohydraulic shock wave therapy group without tPA administration. The middle cerebral artery (MCA) was occluded by injecting autologous blood clots through the carotid artery. Hemodynamic changes in the two groups, were monitored by transcranial Doppler ultrasound (TCD) from before until 15 minutes after confocal dual- pulse electrohydraulic shock wave thrombolysis.
Results
Results from transcranial Doppler ultrasound (TCD), showed a significant increase in the mean value for recanalization rate in the confocal dual- pulse electrohydraulic shock wave therapy group compared with the tPA group (respectively 73.5% and 57.3%, P<0.05). Histopathological examination revealed no cerebral hemorrhage in either group.
Conclusion
Enhanced inertial cavitation effect- induced by transcranial confocal dual- pulse electrohydraulic shock wave therapy can cause to reduce middle cerebral artery thromboembolism without anti- coagulant drugs.
Trial registration number
N/A
AS05-022
MULTIDISCIPLINARY STROKE THROMBOLYSIS SIMULATION TRAINING UTILISING REAL PATIENTS
1Musgrove Park Hospital, Care of the Older Person, Taunton, United Kingdom
2Yeovil District General Hospital, Department of Stroke Medicine, Yeovil, United Kingdom
3Weston General Hospital, Department for Care of the Elderly, Weston Super-Mare, United Kingdom
Background and Aims
Healthcare simulation training has rapidly become a powerful learning tool for medical education. Our project introduced a regular stroke thrombolysis simulation course available to any staff member involved in stroke care, utilising post-stroke patients with varying neurology.
Method
We conducted 6 stroke thrombolysis simulation courses over 6 months. Candidates completed self-assessment pre-and post-course questionnaires. Scores were compared using Wilcoxon paired rank tests.
Results
38 healthcare professionals participated during the study period (Table 1). Tables 2 & 3 outline results comparing pre- and post-assessment scores. All results are presented as medians.
Scale: 0 = Strongly Disagree; 10 = Strongly Agree, *p = <0.05
Scale: 0 = Unable; 5 = Excellent, * p = 0.05
Conclusion
To our knowledge this is the first simulation course that involves real post stroke patients. It has demonstrated clear benefits to candidate’s confidence and clinical skills in addition to the requirement of NIHSS certification.
Trial registration number
N/A
AS05-025
SHOCK WAVE- PHOTOMECHANIC COMBINATION THERAPY OF CAROTID ARTERY ATHEROTHROMBOSIS ACCOMPANIED BY PLGA- BASED ENCAPSULATED TPA NANOPARTICLES ADMINISTRATION
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Italian National Research Council, Institute of Translational Pharmacology- IFT, Rome, Italy
3Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
A plaque may rupture with high risk of subsequent thrombus mediated acute clinical events such as myocardial infarction and stroke. Catheter-based lasers have been extensively studied as an effective method to treat thrombosis. Low- level focused- electrohydraulic shock wave therapy is one of the non- invasive methods to treat thrombosis, but in shock wave therapy, which is used for thrombolysis, thrombosis destruction rates are very low. The aim of this study was to generate a rabbit model of carotid artery atherothrombotic occlusion and the subsequent investigating the feasibility of shock wave- photomechanic combination thrombolytic therapy accompanied by PLGA- based encapsulated tPA nanoparticles administration in this model.
Method
Briefly, New Zealand white rabbits were submitted to carotid artery atherothrombotic occlusion by primary balloon injury followed 1.5% cholesterol- rich diet injury for 12 weeks and finally perivascular severe cold injury. Then treatment group underwent catheter- based Q-switched Nd:YAG laser (30 W, 5 ns) and extracorporeal Low- level focused- electrohydraulic shock wave (10Kv, 0.3 Hz) combination thrombolytic therapy accompanied by PLGA - based encapsulated tPA nanoparticles administration (0.8 mg/kg).
Results
Results from B-mode ultrasonography and histopathology, showed a significant reduction in the mean value for atherothrombosis content at the stenotic region in the treatment group compared with the other groups (P<0.05).
Conclusion
Enhanced inertial cavitation effect of PLGA capsules- induced by shock wave- photomechanic combination therapy can cause to enhance anti- thrombotic effect of tPA, reduce the thrombus content and significantly dilate the luminal cross-sectional area of stenosis and lower treatment time.
Trial registration number
N/A
AS05-026
THE PREDICTIVE RISK SCORE OF INTRACEREBRAL HEMORRHAGE IN ACUTE ISCHEMIC STROKE PATIENTS RECEIVING INTRAVENOUS RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR (IV RT-PA) : A RETROSPECTIVE STUDY
1Prince of Songkla University, Medicine, Songkhla, Thailand
2Prince of Songkla University, Radiology, Songkhla, Thailand
Background and Aims
Acute ischemic stroke (AIS) is the most common neurological disorder causing neurological disability. Intravenous recombinant tissue-type plasminogen activator (IV rt-PA), an approved treatment of AIS by the FDA, is found to significantly increase the risk of intracerebral hemorrhage (ICH). This retrospective study is aimed to find the predictive score of ICH after IV rt-PA.
Method
Patients with AIS who were administered IV rt-PA in Songklanagarind Hospital during January, 2010 to June 2017 were eligible. The predictive risk scores were analyzed by multivariated logistic regression and generated Receiver operating characteristic curve (ROC curve).
Results
After univariate analysis, significant predictors of ICH occurrence after IV rt-PA included National Institute of Health Stroke Score (NIHSS) at arrival, systolic blood pressure before given rt-PA, history of old cerebrovascular disease (CVA), the history of atrial fibrillation and platelet count (p value <0.05). Four independent factors found including NIHSS at arrival, systolic blood pressure (SBP), history of old CVA and platelet count were used to calculate the predictive risk score. The predictive risk scores were [2x (SBP)] +[9x (NIHSS)] +[174x (old CVA)]. The AUC of a ROC curve of the sum of predictive risk score was 0.71 with a cutoff score of >370, the sensitivity and specificity were 0.84 and 0.30, respectively.
Conclusion
The predictive risk score of ICH after thrombolysis is an easily practical tool to facilitate clinical decision and consider an intensive monitoring program in high-risk AIS patients after receiving IV rt-PA.
Trial registration number
N/A
AS05-029
OUTCOME OF PATIENTS WITH NON OCCLUSIVE THROMBUS ON CT ANGIOGRAPHY TREATED WITH INTRAVENOUS THROMBOLYSIS
1Hospital Universitario Ramón y Cajal, Neurology. Stroke Unit, Madrid, Spain
2Hospital Universitario Ramón y Cajal, Department Of Radiology, Madrid, Spain
Background and Aims
Efficacy of tissue-type plasminogen activator in Ischemic stroke patients with non occlusive arterial thrombus on vascular imaging remains unknown and speculative
Method
We performed a prospective and observational single center study to collect data of patients who presented during a 4-year period with ischemic stroke and non occlusive thrombus on CT angiography. Intracranial stenosis and wall calcifications were excluded. Patients were divided into 2 groups: those who received thrombolytic therapy (TT) and those who did not (NT). Primary outcome data was excellent clinical outcome defined as mRS of 0–1 at 3 months. Safety outcomes measures were incidence of symptomatic hemorrhage and poor functional outcome or death (mRS 3–6)
Results
A total of 49 patients were registered, 25 with TT (51%) and 24 without (49%). There were no significant differences in demographic variables and risk factors. In 19 patients of the NT group (79%) tPa was not administered because of the time-window treatment. In 3 patients (TT) endovascular treatment was considered, but only in 1 patient, aspiration had to be performed. Most patients had excellent clinical outcome in both groups (68.% in the TT group vs 79% in the NT group P = .51). Only 1 patient died on the TT group (4%) and 1 patient had a symptomatic hemorrhage in the TT group (4%) with no differences
Conclusion
This study provides data that most patients with ischemic stroke and non occlusive thrombus on CTA imaging at presentation have a good clinical outcome at 90 days. TT did not result in greater improvement
Trial registration number
N/A
AS05-031
FAULTY ESTIMATES OF PATIENTS’ BODY-WEIGHT AFFECT DOSE OF INTRAVENOUS ALTEPLASE WITHOUT ANY IMPACT ON OUTCOME
1Zydus Hospital- Ahmedabad, Neurology, Ahmedabad, India
2B J Medical College - Civil Hospital, Neurology, Ahmedabad, India
3National University Health System, Division of Neurology, Singapore, Singapore
4Yashoda Hospital- Hyderabad, Neurology, Hyderabad, India
5Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
Background and Aims
Intravenously administered tissue plasminogen activator (IV-tPA) remains the main treatment for acute ischemic stroke (AIS). Since early initiation of IV-tPA results in better functional outcome, treatment is initiated, based on the estimated or last-known body-weight of the patient. This approach may result in underdosing or overdosing of tPA and affect the outcome. In this multicenter retrospective study, we evaluated the extent of error in our AIS cohort and its impact on functional outcome and symptomatic intracranial hemorrhage (SICH)
Method
Consecutive AIS patients thrombolysed on the basis of estimated body-weight at 3 tertiary centers between January-to-December 2016 were included. Collected data included information about demographics, cardiovascular risk factors, stroke subtype and National Institute of Health Stroke Scale (NIHSS) scores. Estimated and measured body-weights were recorded. Functional outcome was assessed at 3-months by modified Rankin scale (mRS), the score of 0–1 defined good outcome
Results
The study included 150 patients. Median age was 64-years (IQR 55-75) with male preponderance (67%) and median NIHSS score of 9-points (IQR 6–17). Cardioembolism was the commonest stroke subtype (30.7%). Median difference between actual and estimated body-weight was 3-kg (IQR 1.5-6). Difference was more than 10% in 35(23.3%) patients. Good functional outcome was achieved by 74(49.3%) patients and 10 (6.8%) developed SICH. NIHSS (OR 1.288; 95% CI 1.157-1.435, p < 0.001) and large artery atherosclerosis (OR 5.878; 95% CI 1.929-17.910, p = 0.002) were independent predictors of unfavorable functional outcome
Conclusion
Significant difference occurs between estimated and actual body-weight in a considerable proportion of thrombolysed AIS patients. However, this discrepancy may not affect functional outcome or the risk of SICH
Trial registration number
N/A
AS05-032
EX-VIVO GENERATION OF PLASMIN FROM PATIENTS WITH ACUTE ISCHAEMIC STROKE IS PREDICTIVE OF SUCCESSFUL THROMBOLYSIS
1Monash University, Australian Centre for Blood Diseases, Melbourne, Australia
2John Hunter Hospital, Department of Neurology-, Newcastle, Australia
3Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia
4Calvary Mater Hospital., Haematology, Newcastle, Australia
5University of Melbourne, Medicine, Melbourne, Australia
6University of Newcastle, School of Medicine and Public Health, Newcastle, Australia
7University of Technology, School of Nursing-, Sydney, Australia
Background and Aims
Thrombolysis with recombinant tissue-type plasminogen activator (rt-PA) fails in more than 60% of patients with acute ischaemic stroke (AIS). Conversely, symptomatic intracranial haemorrhage (sICH) can also occur in up to 10% of patients who do recanalize. While thrombus location, aetiology and infarct size can affect outcome, the factors distinguishing patients who recanalize from those who don’t have yet to be fully elucidated. The ability of rtPA to promote thrombolysis is dependent upon its capacity to generate plasmin. We hypothesised that patients with low plasmin generating capacity are less likely to recanalize following rtPA treatment.
Method
Plasma was obtained from 90 AIS patients up to 1-hour before thrombolysis and screened for baseline levels of plasminogen, antiplasmin, and plasmin-antiplasmin (PAP) complexes. The degree of inducible plasmin generation was determined using amidolytic assays following ex-vivo addition of rtPA for 1h. ELISA assays were also used to quantitate the fold-increase in PAP complex levels after rtPA treatment.
Results
rtPA-inducible PAP levels varied dramatically between patients. The ratio of post-thrombolysis PAP to pre-thrombolysis PAP ranged from 3.4 to 105.9. Multivariate regression analyses revealed that each fold increase in PAP levels was associated with a 4.2% increase in the odds of recanalization (p = 0,035) when corrected for blood glucose levels.
Conclusion
This is the first report of ex vivo-inducible plasmin generation as a predictor of thrombolysis. The predictive power of this screening assay for sICH is still under investigation.
Trial registration number
N/A
AS05-033
IDENTIFICATION OF STROKE MIMICS BASED ON CLINICAL CRITERIA AND CT MAY UNDERESTIMATE THE TRUE STROKE MIMIC RATE
1Charité - Campus Benjamin Franklin, Department of Neurology, Berlin, Germany
2Berlin Institute of Health BIH, Berlin Institute of Health BIH, Berlin, Germany
3Charité - Universitätsmedizin Berlin, Center for Stroke Research, Berlin, Germany
Background and Aims
The frequency of stroke mimics in patients treated with thrombolytic therapy differs considerably in the literature. We aimed to assess the impact of imaging-mode on estimation of rate of stroke mimics in patients without acute ischemic lesions in follow-up imaging (neuroimaging-negative patients).
Method
We performed a retrospective analysis of our prospective registry of all patients receiving systemic thrombolytic therapy at our tertiary care center from January 2006 to December 2016. Only patients with CT-based thrombolysis were included. We compared the likelihood of a diagnosis of stroke mimic in neuroimaging-negative patients receiving follow-up MRI vs follow-up CT in multiple logistic regression analysis.
Results
Of all 1044 treated patients (581 with follow-up MRI and 463 with follow-up CT), 191 (18%) had negative follow-up imaging. Among all 191 neuroimaging-negative patients, the rate of stroke mimics was significantly higher in patients with follow-up MRI compared to follow-up CT (65/97, 67% vs 28/94, 30%; p < 0.001). After adjusting for other factors discriminating stroke from stroke mimics (age, sex, NIHSS on admission, systolic blood pressure on admission), the likelihood of a diagnosis of stroke mimic in neuroimaging-negative patients was significantly higher in patients with follow-up MRI vs follow-up CT (aOR 4.8, 95% CI 2.3–10.0, p < 0.001).
Conclusion
Identification of stroke mimics based on clinical criteria and CT alone may yield a considerably lower estimation of stroke mimics compared to identification based on clinical criteria and MRI. Further research is needed to identify patients in whom follow-up MRI may avoid misdiagnosis of stroke and patients in whom MRI may be false-negative.
Trial registration number
N/A
AS05-034
OUT COME OF ACUTE ISCHEMIC STROKE PATIENTS TREATED WITH INTRAVENOUS RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR IN COASTAL ANDHRA PRADESH, INDIA
1Dr Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Neurology, Guntur, India
2Dr. Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Neurology, Vijayawada, India
3Dr Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Neurology, Vijayawada, India
4Dr Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Cardiology, Vijayawada, India
5Dr Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Radiology, Guntur, India
Background and Aims
Thrombolysis with intravenous (IV) tissue plasminogen activator (rtPA) decreases disability in acute ischemic stroke (AIS) when given within 4.5 hours. This study analysed outcomes of thrombolysed patients with rtPA(Actilyse) in coastal Andhra Pradesh, india where data is sparse.
Method
In this retrospective hospital based observational study, consecutive thrombolysed patients of AIS were studied over 4 years. Statistical analysis system (SAS) was used to analyse data on demography, assessment NIHSS score, comorbidities, onset to needle time (ONT) and outcome at 1,3and 6 months. Outcome was stratified as good (mRS 0–2) and bad (mRS 3–6).
Results
Eighty one patients were analysed. There were 59 males and 22 females with mean ages 58.23 and 66.59 years respectively. Sixty three patients improved (79%). NIHSSscore correlated well with outcome (95% CI 0.9999, p = 0.0001). No univariate correlation existed with age, sex, ischemic heart disease, stroke, hypertension, Diabetes Mellitus (DM), atrial fibrillation, smoking, alcohol, hyperlipedemia and ONT. Multivariate correlation of age and NIHSSscore showed significance in the middle aged (CI 0.9987, p = 0.0026) as was ONT with NIHSS in the 3 to 4.5 hours group (CI 1.000, p <0.0001)and hypertension with NIHSS (CI 0.9966, p = 0.0069). Hypertension alone had better outcome than with stroke and DM (CI 0.998, p = 0.0004). ASPECTS correlated positively with outcome (p = 0.0114) as was MRI volume on diffusion weighted imaging (CI 0.998, p = 0.0004).
Conclusion
AIS patients improve with thrombolysis at all ages especially middle age. NIHSS score with/without hypertension or ONT correlate with outcome. Hypertension alone had better outcome than with stroke and DM. ASPECTS and MRI volume correlate with outcome.
Trial registration number
N/A
AS05-035
TIMING OF CT-ANGIOGRAPHY DOES NOT AFFECT DOOR-TO-NEEDLE TIMES IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1OLVG West, Neurology, Amsterdam, The Netherlands
2AMC, Neurology, Amsterdam, The Netherlands
3AMC, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
Background and Aims
Since the introduction of intra-arterial treatment (IAT) for patients with acute ischemic stroke caused by a proximal intracranial occlusion of the anterior circulation, CT-angiography (CTA) is included in the emergency stroke workup. Currently, it is unclear whether CTA could best be timed before or after start of intravenous thrombolysis (IVT). Acquisition of CTA before IVT could result in prolonged door-to-needle times (DNT) while acquisition after IVT could prolong door-to-groin times (DGT) in IAT eligible patients.
Method
We performed a before (CTA following start IVT, period I) versus after (CTA prior to IVT, period II) study, consisting of two periods of one year. This study is based on a prospective registry of consecutive patients treated with IVT in two high volume stroke centers (mothership model). The primary outcome was DNT. Secondary outcomes included door-to-CT time, CT-to-needle time and DGT.
Results
In total, 533 patients received IVT during the study period (246 period I, 274 period II). Median DNT was shorter in period II (22 minutes, IQR 17-30) compared to period I (24 minutes (IQR 18-32) p = 0.04). Median door-to-CT was also shorter in period II (12 versus 10 minutes, p = 0.02). We found no difference in CT-to-needle time between the two study periods. Median DGT was non-significant shorter in periode II (89 versus 109 minutes, p = 0.09).
Conclusion
CTA acquisition prior to start of IVT did not adversely affect door-to-needle or CT-to-needle times. Hence, it might be beneficial to perform CTA before IVT, to avoid treatment delay in patients eligible for IAT.
Trial registration number
N/A
AS05-036
OPTIMIZING ACUTE STROKE CARE ORGANIZATION: A SIMULATION STUDY TO IDENTIFY GAINS AND HURDLES TO OVERCOME
1University Medical Center Groningen, Epidemiology, Groningen, The Netherlands
2Faculty of Economics & Business- University of Groningen., Operations, Groningen, The Netherlands
3University of Groningen- University Medical Center Groningen., Neurology, Groningen, The Netherlands
4Health Technology Assessment- University of Groningen- University Medical Center Groningen., Epidemiology, Groningen, The Netherlands
Background and Aims
Intravenous thrombolysis (IVT) is an effective treatment for ischemic stroke, yet it is substantially underused. The aim of this study was to estimate the expected increase in IVT rates given particular interventions in this pathway.
Method
Ischemic stroke patients were prospectively collected at four hospitals from February to August 2010 part of a centralized organizational model. Simulation modeling was used to compare performance of the current pathway, best practice based on literature review and an optimized model. Interventions investigated included patient response and mode of referral, prehospital treatment and intra-hospital delays. Primary outcome measure was thrombolysis utilization. Secondary measures were Onset-Treatment-Time (OTT) and the proportion with excellent functional outcome (mRS 0–1) at 90 days.
Results
Of 280 patients with ischemic stroke, 125 (44.6%) arrived at the hospital within 4.5 hours and 61 (21.8%) received IVT. The largest improvements were observed when minimizing patient response to 15 minutes, door-to-needle time to 20 minutes and increase 911 calls to 60%. IVT rates increased by 5.8%, 4.1%, and 2.9%, respectively. The OTT decreased by 6, 23, and 2 minutes. The proportion of patients with mRS 0–1 increased by 0.2%, 2.7%, and 0.2%. Taking all potential improvements together, IVT rates increased by 19.6% and OTT was reduced by 56 minutes.
Conclusion
Improving IVT rates above 30% is possible given implementation of known best practices. Educating people to seek immediate medical attention by calling 911 and expedite intrahospital times should be components of system-wide interventions to improve IVT utilization in our setting.
Trial registration number
N/A
AS05-037
INTRAVENOUS THROMBOLYSIS OF ACUTE CENTRAL RETINAL ARTERY OCCLUSION
1Turku University Hospital, Clinical neurosciences, Turku, Finland
Background and Aims
Acute loss of vision due to central retinal artery occlusion (CRAO) is a rare condition with variable treatment approaches. A recent meta-analysis found that patients with CRAO are likely to benefit from intravenous thrombolysis (IVT) with a number needed to treat (NNT) of 4, and that conservative treatments, including ocular massage, front chamber paracentesis or hemodilution, may be even harmful. Furthermore, as the diameter of central retinal artery is comparable to that of M3 segment with a recanalization rate of 52% with IVT, it would seem reasonable to treat eligible CRAO patients with tPA, even in the absence of randomized controlled trials.
Method
Between the years 2004-2014, there was only one IVT-treated patient with CRAO according to the Care Register for Health Care (CRHC), a database for all hospital discharges in Finland. Since 2016, all patients with sudden monocular vision loss have been evaluated as CRAO and IVT candidates in Turku University Hospital. Here, we report all CRAO patients treated with IVT (N = 6) in Turku University Hospital between 1 January 2016 and 31 December 2017.
Results
Four out of six patients treated with IVT experienced improvement or even complete normalization of the vision in the affected eye. There were no complications related to IVT-treatment.
Conclusion
IVT-treatment of CRAO was feasible and safe. Majority of the patients treated with rTPA benefitted from the treatment. Sudden monocular loss of vision due to CRAO should be evaluated as a stroke equivalent and thrombolysis should be considered in these patients.
Trial registration number
N/A
AS05-038
EARLY THROMBOLYSIS IN STROKE: CHARACTERISTICS OF PATIENTS AND THEIR MANAGEMENT
1Danube University Krems, Clinical Neurosciences and Preventive Medicine, Krems, Austria
2Hospital Barmherzige Brüder Wien, Neurology, Vienna, Austria
Background and Aims
The aim of this study was to look for predictors and potentially improvable factors associated with early thrombolysis of acute ischemic stroke.
Method
Data from thrombolysed patients entered in the Austrian Stroke Unit Registry between 2003 and September 2017 were analysed.
Results
3029 (21.7%) of 13937 patients were treated within 90 minutes, 687 (5.3%) within 60 minutes. Patients in the 0–90 min group had a significantly lower rate of indirect admissions to the stroke unit (SU) from other hospitals than patients treated later (7.3% in 0–90 min, vs. 9.8% in 91-180 min vs. 17.9% in 181-270 min group), shorter mean door-to needle-times (DTN) (31 vs. 49 vs. 60 min for 0–90 min resp. 81-180 min and 181-270 min group) and shorter mean admission-to-first-brain-imaging-times (15 vs. 20 vs. 23 min for 0–90 min resp. 81-180 min and 181-270 min group). They had a significantly higher NIHSS at admission, were more likely to present with a total anterior circulation syndrome and less likely with a lacunar or posterior circulation syndrome.
Multiple logistic regression analysis showed that the odds for good functional outcome (mRS 0–2) at discharge from SU were significantly higher for treatment within 90 min.
Conclusion
Early thrombolysis can be achieved in significant numbers by guidance for direct admissions to SUs and optimization of intra-hospital procedures to shorten DTN. Educational efforts to improve recognition of and rapid reaction to minor anterior and posterior stroke syndromes are recommended to further increase the rate of early thrombolysis.
Trial registration number
N/A
AS05-039
THE INFLUENCE OF HOSPITAL ARRIVAL TIME ON THE DOOR-TO-PUNCTURE TIME OF ENDOVASCULAR TREATMENT: CRCS-K (CLINICAL RESEARCH COLLABORATION FOR STROKE IN KOREA) REGISTRY
1Ilsan Paik Hospital, Neurolgy, Goyang, Republic of Korea
2Eulji General Hospital- Eulji University, Neurology, Seoul, Republic of Korea
3Soonchunhyang University College of Medicine, Neurology, Seoul, Republic of Korea
4Clinical Research Center- Asan Medical Center, Biostatistics, Seoul, Republic of Korea
5Seoul Medical Center, Neurology, Seoul, Republic of Korea
6Dong-A University Hospital, Neurology, Pusan, Republic of Korea
7Eulji University Hospital- Eulji University School of Medicine, Neurology, Daejeon, Republic of Korea
8Yeungnam University Medical Center, Neurology, Daegu, Republic of Korea
9Chonnam National University Hospital, Neurology, Gwangju, Republic of Korea
10Dongguk University Ilsan Hospital, Neurology, Goyang, Republic of Korea
11Hallym University Sacred Heart Hospital, Neurology, Anyang, Republic of Korea
12Jeju National University Hospital, Neurology, Jeju, Republic of Korea
13Korea University College of Medicine, Biostatistics, Seoul, Republic of Korea
14Seoul National University Bundang Hospital, Neurology, Seongnam, Republic of Korea
Background and Aims
Endovascular treatment (ET) requires specialized neurointerventional team. Therefore the application of ET may be different according to the patients’ arrival time at hospital due to the different level of available resources.
Method
In this prospective stroke registry, all consecutive patients, who admitted via emergency room of 12 participating centers nationwide from 2009/11 to 2016/5, were identified. All patients were presented within 6 hours from symptom onset defined as last known normal time and had relevant ischemic lesions on brain imaging. We categorized hospital arrival time into 4 groups, such as early morning (EM, 0 to 6), late morning (LM, 6 to 12), afternoon (AF, 12 to 18), and evening (EV, 18 to 24 o’clock).
Results
Among 10901 patients included, thrombolytic therapy was underwent in 4096 (37.6%) [2621 (24.0%) in intravenous thrombolysis (IVT) only, 985 (9.0%) in combined IVT and ET, 490 (4.5%) in ET only]. In patients arriving in EM, the number was 999 (9.2% vs. 26.2%, 35.9%, and 28.7%), age (mean) was 64.8 years (vs. 68.3, 68.3, and 67.6, p < 0.001), initial NIHSS (median) was 5 (vs. 5, 4, and 4, p < 0.001), the rates of ET was 11.9% (vs. 16.4%, 13.6%, and 11.3%, p < 0.001), and DTP time (mean, min) was 167 (vs. 135, 114, and 130, p = 0.004) compared to LM, AF, and EV, respectively.
Conclusion
Patients arriving at hospital in EM showed highest DTP time and lower rate of ET compared to the other times of day. Availability of neurointerventional team in EM should be improved to solve those discrepancies of endovascular treatment.
Trial registration number
N/A
AS05-040
ELEVATED FACTOR VIII AND VON WILLEBRAND FACTOR LEVELS PREDICT UNFAVOURABLE OUTCOME IN STROKE PATIENTS TREATED WITH INTRAVENOUS THROMBOLYSIS
1University of Debrecen Faculty of Medicine, Division of Clinical Laboratory Sciences, Debrecen, Hungary
2University of Debrecen Faculty of Medicine, Department of Neurology, Debrecen, Hungary
3University of Debrecen Faculty of Medicine, Department of Laboratory Medicine, Debrecen, Hungary
4University of Debrecen Faculty of Medicine, Department of Radiology, Debrecen, Hungary
Background and Aims
Factor VIII (FVIII) and von Willebrand factor (VWF) levels have been associated with arterial thrombus formation and linked to outcomes following thrombolysis in acute myocardial infarction patients. Here we aimed to investigate FVIII and VWF levels during thrombolysis in acute ischemic stroke (AIS) patients and to find out whether they predict outcomes.
Method
Study population included 131 consecutive AIS patients who underwent intravenous thrombolysis with recombinant tissue plasminogen activator (rt-PA). Blood samples were taken on admission, 1 h and 24 h after rt-PA administration to measure FVIII activity and VWF antigen levels. Neurological deficit of patients was determined according to NIHSS. ASPECTS were assessed using CT images taken before and 24 h after thrombolysis. Long-term functional outcome was determined at 90 days post- event by the modified Rankin scale (mRS).
Results
VWF levels on admission showed a gradual increase in case of more severe AIS (median: NIHSS<6:189.6%; NIHSS 6–16:199.6%; NIHSS>16:247.8%; p = 0.013). FVIII and VWF levels correlated well on admission (r = 0.748, p < 0.001) but no significant correlation was found immediately after thrombolysis, most probably due to plasmin-mediated FVIII degradation. VWF and FVIII levels were significantly associated with worse 24 h post-lysis ASPECTS. In a binary backward logistic regression analysis including age, gender, hsCRP, active smoking, diabetes and NIHSS>5 on admission, elevated FVIII and VWF levels after thrombolysis were independently associated with poor functional outcomes (mRS≥3) at 90 days (FVIII: OR:7.10, 95%CI:1.77-28.38, p = 0.006, VWF: OR:6.31, 95%CI:1.83-21.73, p = 0.003).
Conclusion
Elevated FVIII and VWF levels post-lysis have independent prognostic values regarding poor functional outcomes at 90 days.
Funding: OTKAPD111929
Trial registration number
N/A
AS05-041
DELAYED ACCESS TO ACUTE STROKE THROMBOLYSIS: IS THERE EVIDENCE FOR A “WEEKEND EFFECT”?
1Royal Group of Hospitals, Neurology, Belfast, Ireland
2Altnagelvin Hospital, Neurology, Derry, Ireland
3Royal Group of Hospitals, Audit Department, Belfast, Ireland
4Royal Group of Hospitals, Stroke Unit, Belfast, Ireland
5Craigavon Area Hospital, Stroke Unit, Portadown, Ireland
6Ulster Hospital, Stroke Unit, Dundonald, Ireland
7Antrim Area Hospital, Stroke Unit, Antrim, Ireland
8Southwest Acute Hospital, Stroke Unit, Enniskillen, Ireland
9HSCB, Stroke, Belfast, Ireland
10Queens university, statistics, belfast, Ireland
Background and Aims
Poor clinical outcomes and increased mortality have been linked to day of hospital admission in the UK National Health Service, but the association is not certain. Shorter Door to needle (DTN) times are associated with improved chance of recovery. The national impact of weekend admission on DTN in acute ischemic stroke (AIS) was examined.
Method
All patients treated with intravenous tissue plasminogen activator (iv-tPA) were recorded prospectively in a single country over 4 consecutive years. DTN time in AIS at weekends was compared to patients admitted during Monday to Friday
Results
1201 patients were treated with iv-tPA over 4 years. Median DTN time was 54 minutes (IQR 36-77). Patients admitted at weekends had significantly longer DTN time than those admitted Monday-Friday (Median=63mins, IQR 47-81 and 49mins, IQR 33-75, P<0.0001). Patients treated at weekends had similar treatment times to those treated overnight during Monday-Friday (Median 62 mins IQR 42-90, P = 0.844).
Conclusion
Weekend stroke admissions are associated with significantly longer DTN times that admissions which occur from Monday to Friday. Staffing levels and team members have substantial differences between these times. As treatment delay Is associated with increased disability after AIS, efforts to reduced DTN time through service reconfiguration must focus specifically on patients admitted at unsocial hours including weekends to improve service delivery and outcome for all stroke patients.
Trial registration number
n/a
AS05-042
TELESTROKE-GUIDED DELIVERY OF INTRAVENOUS THROMBOLYSIS IN THE EXPANDED 3–4.5-HOUR TIME-WINDOW
1University Hospital Dresden, Neurology, Dresden, Germany
2University Hospital Dresden, Neuroradiology, Dresden, Germany
Background and Aims
While intravenous thrombolysis (IVT) can be safely delivered through telestroke networks in the 3-hour time-window, there is paucity of safety data in the 3–4.5-hour time-window. Thus, we aimed to explore the safety of telestroke-guided IVT in the expanded time window.
Method
We abstracted data from consecutive ischemic stroke patients treated with IVT in the Stroke East Saxony hub-and-spoke network (SOS-Net) from 01/2014 to 12/2015. Rates of post-treatment sICH (ie, ECASS-II), in-hospital mortality and favorable functional outcome (ie, mRS 0–2) at discharge were compared between patients treated at spoke hospitals and the hub site.
Results
During the 2-years study period, 142 ischemic stroke patients received IVT in the expanded time-window: median age 76 (IQR, 15) years, 50% men, median NIHSS score 7 (8) points, median onset-to-treatment time 212 (50) minutes. Of these patients, 48 (35%) were treated at hub site and 94 (66%) at spoke hospitals. Aside from longer onset-to-treatment time (228 vs. 210 minutes, p = .022) in patients treated at the hub site, no differences were present regarding age (p = .35), admission NIHSS score (p = .39), admission serum glucose (p = .92) and pre-treatment systolic blood pressure (p = .14), when compared to telestroke patients. Telestroke patients had similar rates of sICH (6.3% vs. 4.3%, p = .69) and in-hospital mortality (8.3% vs. 8.5%, p = .1) as those treated at hub site. Rates of favorable functional outcome at discharge did not differ between the two groups (39.6% vs. 44.6%, p = .84).
Conclusion
Our data point to safe delivery of IVT via telestroke in the expanded 3–4.5-hour time-window.
Trial registration number
N/A
AS05-043
THE ROLE OF PLASMINOGEN ACTIVATOR INHIBITOR-1 (PAI-1) LEVELS AND PAI-1 4G/5G POLYMORPHISM IN THE OUTCOME OF INTRAVENOUS THROMBOLYTIC THERAPY IN ISCHEMIC STROKE PATIENTS
1University of Debrecen- Faculty of Medicine, Department of Neurology, Debrecen, Hungary
2University of Debrecen- Faculty of Medicine, Division of Clinical Laboratory Sciences, Debrecen, Hungary
3University of Debrecen- Faculty of Public Health, Department of Preventive Medicine, Debrecen, Hungary
4University of Debrecen- Faculty of Medicine, Department of Radiology, Debrecen, Hungary
Background and Aims
Thrombolysis by recombinant tissue plasminogen activator (rtPA) is the main pharmacological therapy in acute ischemic stroke (IS), however, it is only effective in a subset of patients. Here we aimed to investigate the role of plasminogen activator inhibitor-1 (PAI-1), an effective inhibitor of tPA, and its major polymorphism (PAI-1 4G/5G) in the outcome of therapy.
Method
Study population included 132 consecutive IS patients who all underwent thrombolysis. Blood samples were taken on admission, 1 and 24 h after rtPA infusion. PAI-1 activity and antigen levels were measured from all blood samples and the PAI-1 4G/5G polymorphism was determined. Clinical data of patients including NIHSS were registered at admission, day 1 and 7 after therapy. ASPECTS was assessed using CT images taken before and 24 h after thrombolysis. Intracranial hemorrhage (IC) was classified according to ECASS II. Long-term outcome was defined 3 months post-event by the modified Rankin Scale.
Results
PAI-1 activity levels dropped transiently after thrombolysis, while PAI-1 antigen levels remained unchanged. PAI-1 4G/5G polymorphism had no effect on PAI-1 levels and did not influence stroke severity. PAI-1 activity/antigen levels as measured on admission were significantly elevated in patients presenting with worse 24 h ASPECTS (7–0). In a backward binary logistic regression analysis including age, sex, NIHSS on admission, the presence of 4G allele conferred a significant protective effect against IC (OR:0.30, 95%CI:0.09-0.99, p = 0.048). PAI-1 levels and PAI-1 4G/5G polymorphism had no influence on long-term outcomes.
Conclusion
PAI-1 4G allele is associated with a significant protection against IC in post-lysis stroke patients.
Funding: OTKAPD111929
Trial registration number
N/A
AS05-044
INTRAVENOUS THROMBOLYSIS IN MECHANICAL THROMBECTOMY: GLOBAL REAL-LIFE DATA FROM SITS CENTERS
1Ludwigs-Maximilians-Universität, Neurology, München, Germany
2Institute for Stroke and Dementia Research, Neurology, Munich, Germany
3Karolinska University Hospital- and Department of Clinical Neurosciences- Karolinska Institut, Department of Neurology, Stockholm, Sweden
Background and Aims
Mechanical thrombectomy (MT) is now evidence-based treatment and standard of care in acute stroke patients with large vessel occlusion (LVO). Intravenous thrombolysis (IVT) within 4.5 h of symptom onset is also standard of care in acute ischemic stroke patients. We aimed to analyze how management of IVT in case of MT is done in clinical Routine.
Method
We conduct a worldwide survey consists of 29 questions which was send out in 10/2017 to all stroke-centers actively participating in the Safe Implementation of Treatment (SITS) International Stroke Registry (n = 476).
Results
We received 103 answers from 29 countries until 01/2018. Most replies came from Neurologist (n = 92). About half of the replies were received from comprehensive stroke centers (n = 51) and from primary stroke centers (n = 47). About 77% (79/103) give IVT as a standard treatment before MT and withhold only in individual cases. 23% stated to withhold regularly or often before MT. About 34% give a portion of tissue- plasminogen-activator (tPA) intra-arterial as a standard or as an individual decision. Dose of tPA given intra-arterial ranged from 2 to 30% of the iv-dose. In drip-and ship model 94% considered IVT before MT as important or very important and 88% in the mothership model. 22% are uncertain about national and international guideline-recommendations regarding IVT in case of MT.
Conclusion
This survey showed that evidence from clinical trials regarding IVT in MT is implemented in the majority of cases. However, IVT-management in the context of MT is still divers and requires more prospective data.
Trial registration number
N/A
AS05-045
REDUCING DOOR-TO-NEEDLE TIME IN ACUTE ISCHEMIC STROKE PATIENTS TREATED WITH INTRAVENOUS THROMBOLYSIS IN THE NETHERLANDS
1Academic Medical Centre Amsterdam, Neurology, Oegstgeest, The Netherlands
2Erasmus MC, Epidemiology, Rotterdam, The Netherlands
3OLVG, Neurology, Amsterdam, The Netherlands
4Radboud UMC, Neurology, Nijmegen, The Netherlands
Background and Aims
The effect of intravenous thrombolysis (IVT) in acute ischemic stroke (AIS) patients is largely time-dependent. Lowering the door-to-needle time (DTNT) is an important goal for quality improvement in acute stroke care. The aim of this study was to evaluate DTNT in the Netherlands, identify factors related to DTNT and assess the effect of DTNT on in-hospital mortality.
Method
The Dutch Acute Stroke Audit (DASA) is a national, quality registry-based, prospective cohort containing stroke patients in the Netherlands. For this study, we include AIS patients who received IVT from 2014 up to and including 2016. Linear regression was used to identify factors associated with DTNT. Logistic regression was used to assess the association of DTNT and in-hospital mortality, adjusted for identified factors.
Results
In total 13.978 patients are included in this cohort. The median DTNT decreased from 28 minutes (IQR 20-40) in 2014 to 25 minutes (IQR 19-35) in 2016 (p = 0.000) and in-hospital mortality reduced from 7.2% in 2014 to 5.8% in 2016 (p = 0.05). Female sex (beta= 1.048, p = 0.00), admission at IAT center (beta=1.051, p = 0.00), and admission during off-hours (beta=1.051, p = 0.00), were identified as factors associated with delay in DTNT. Increase in DTNT was only mildly related to in-hospital mortality (adjusted OR 1.01 per minute, p = 0.00).
Conclusion
Both DTNT and mortality decreased significantly in the Netherlands since the start of the DASA in 2014. We observed only a small effect of DTNT, suggesting also a role of other improvements in acute stroke care.
Trial registration number
N/A
AS05-046
HOW DO OUTCOMES DIFFER BETWEEN PATIENTS WITH MILD STROKE, MORE SEVERE STROKE AND A FINAL NON-STROKE DIAGNOSIS WHO ARE THROMBOLYSED? A RETROSPECTIVE DATA ANALYSIS
1University of Aberdeen, Institute of Applied Health Sciences, Aberdeen, United Kingdom
2Unversity of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
3University of Aberdeen, School of Medicine- Medical Science and Nutrition, Aberdeen, United Kingdom
Background and Aims
Thrombolysis in minor ischaemic stroke is controversial. We explored the effect of stroke severity and a final non-stroke diagnosis on outcomes following thrombolysis.
Method
Data was extracted from the Scottish Stroke Care Audit (SSCA) and linked to deaths recorded by National Records Scotland (NRS) for all patients thrombolysed between 2010-2015. Outcomes were compared between mild stroke, more severe stroke and non-stroke.
Results
3116 patients were included in the analysis. 492 (15.8%) had minor stroke, 2569 (82.4%) had more severe stroke and 55 (1.8%) non-stroke.
Less than 5% of mild strokes had haemorrhage on repeat imaging compared with 13.9% for more severe strokes and 19.6% for non-strokes.
In the whole population there were < 0.3% deaths at 7 days and < 0.4% deaths at 30 days from haemorrhagic stroke. The percentages across each of the three patient groups were similar.
Conclusion
In this population based study thrombolysis outcomes compare favourably to published data. Milder strokes are less likely to have post-thrombolysis haemorrhage and the risk of stroke related death is low. Further work is required to explore the diagnoses underlying the presentation of patients who are thrombolysed and have a non-stroke final diagnosis.
Trial registration number
N/A
AS05-047
LARGE VESSEL OCCLUSION IN ANTERIOR CIRCULATION IN PATIENTS WITH MINOR NEUROLOGICAL DEFICITS: THROMBOLYSIS AND/OR ENDOVASCULAR TREATMENT OR CONSERVATIVE MANAGEMENT
1Inselspital- University Hospital of Bern, Department of Neurology, Bern, Switzerland
2Inselspital- University Hospital of Bern, Department of Neurology and Diagnostic and Interventional Neuroradiology, Bern, Switzerland
3Inselspital- University Hospital of Bern, Diagnostic and Interventional Neuroradiology, Bern, Switzerland
Background and Aims
Thrombolysis and/or endovascular treatment in patients with minor neurological deficits and large vessel occlusion remains a matter of debate.
Method
In this retrospective study (01/2004-04/2017) of our prospective Bernese Stroke database, we compared MR-imaging and outcome of consecutive patients with low NIHSS score and large vessel occlusion between non-treated and (thrombolysed and/or endovascularly) treated patients.
Results
Among 153 patients (42% women, median age 66.8 y, 46.6% with occlusion of the main stem of the middle cerebral artery, 53.4% of the internal carotid artery) 70/45.8% received intravenous thrombolysis, endovascular treatment or both. Neurological deterioration (increase/decrease of ≥1 vs. ≤1 NIHSS score point compared to baseline) was observed in 33.9% vs. [61.1%]17.9%/43.5% vs. [22.2%]76.1% of non-treated vs. [non-hyperacute after neurological deterioration] treated patients (p < 0.0001). At 3 months, modified Rankin Scores (mRS 0–2: 75.4% vs. 61%; p = 0.003), secondary vessel occlusions (14.8% vs. 4.3%; p = 0.025) and secondary increased infarct volumes (66.7% vs. 47.8%; p = 0.021) differed between non-treated vs. treated patients, but not survival (91.4% vs. 90%; p = 0.495) and symptomatic intracerebral haemorrhage (0% vs. 4.3%; p = 0.097). Persistent large vessel occlusion was more often observed in non-treated than in treated patients (88.1% vs. 21.2%;p < 0.0001), showing higher risk (log-rank-p=0.009) and earlier occurrence (median 15.7 vs. 26.5 hours; p = 0.02) of neurological deterioration during 13’770 patient-days of follow-up. Persistent large vessel occlusion was associated with neurological deterioration (70.1% vs. 39.4%;HR 3.62,95%CI 1.76-7.42;p < 0.0001), as was decrease (compared to baseline) of haemoglobin (median -14g/L vs. -7g/L;HR1.05,95%CI 1.01-1.09; p = 0.008).
Conclusion
These data suggest:Hyperacute treatment is safe and effective in the analysed patient group and persistently blocked large vessels are detrimental.
Trial registration number
N/A
AS05-048
PREDICTION OF HEMORRHAGIC TRANSFORMATION WITH BLOOD BIOMARKERS IN THE ERA OF MECHANICAL THROMBECTOMY
1Institut de Recerca- Hospital Universitari Vall d'Hebron- Universitat Auntónoma, Neurovascular Research Laboratory, Barcelona, Spain
2Hospital Universitari Vall d'Hebrón, Stroke Unit, Barcelona, Spain
3Institut de Recerca- Hospital Universitari Vall d'Hebron- Universitat Auntónoma, Molecular Biology and Biochemistry Research Center for Nanomedicine Cibbim-Nanomedicine, Barcelona, Spain
4Hospital Universitari Germans Trias i Pujol, Stroke Unit, Barelona, Spain
5Parc Sanitari de Sant Joan de Déu, Unitat d'Aguts- Subaguts- Hospitalització Parcial- Urgències psiquiàtriques i TEC, Sant Boi de Llobregat- Barcelona, Spain
6Hospital del Mar, Stroke Unit, Barcelona, Spain
7Fundació Docència i Recerca Mutua Terrassa- Hospital Universitari Mútua de Terrassa, Stroke pharmacogenomics and genetics, Terrassa- Barcelona, Spain
Background and Aims
After more than two decades of experience with intravenous tissue-type plasminogen activator (IV-tPA), hemorrhagic transformation (HT) has reduced dramatically. We aimed to test whether blood biomarkers of HT after IV-tPA are still useful in the era of mechanical thrombectomy (MT).
Method
From August-2012 to August-2015, patients with suspected stroke of <6 hours were enrolled in the emergency department of Vall d’Hebron Hospital (Barcelona). Blood samples were collected before treatment. Patients treated with IV-tPA were selected to measure matrix metalloproteinase-9 (MMP-9), cellular fibronectin (cFn), vascular adhesion protein-1 (VAP-1), nuclear receptor related-1 protein (NURR-1) and carcinoembrionary antigen cell adhesion molecule-1 (CEACAM-1) by ELISA. Primary outcome was parenchymal hemorrhage (PH)-type HT. Secondary outcomes were any HT and symptomatic intracerebral hemorrhage (sICH).
Results
From 1,018 patients with suspected stroke, 214 were treated with IV-tPA (55 also received MT). 46 patients had any HT, 14 were PH-type and 11 sICH. From the evaluated biomarkers, just CEACAM-1 was associated with PH-type HT after adjustment by clinical predictors (diabetes), OR = 2.57(95%CI 1.10-5.99), p = 0.028. However this trend was lost when patients treated with MT were included. Similar negative results were found for all HT and sICH.
Conclusion
Biomarkers previously associated with HT were not replicated in this prospective cohort. Very low rates of HT and different mechanisms in endovascular procedures might be responsible for that. It is unclear whether prediction of HT after IV-tPA in the era of MT still makes sense. Its use in other indications such as recanalization after IV-tPA or futile recanalization after MT seems more promising.
Trial registration number
N/A
AS05-049
POSTPARTUM STROKE AND SYSTEMIC THROMBOLYSIS
1Ospedale Santo Stefano Prato, Ospedale Santo Stefano Prato, FIRENZE, Italy
Background and Aims
Introduction
There are very few previously published cases about intravenously applied recombinant tissue plasminogen activator in acute ischemic stroke during puerperium.
Method
Case Presentation:
We report a 42-year-old woman with postpartum acute ischemic stroke caused by carotid artery dissections treated by systemic thrombolysis.A right-handed woman who was 2 weeks postpartum was admitted to the hospital due to migraine with aura mimic symptoms. In the emergency room, her National Institutes of Health stroke scale was 19 with points received for sudden onset of right-sided weakness and global aphasia. Computed tomography of the brain was negative for hemorrhage and she was given intravenous systemic thrombolysis after fifteen minutes after onset of symptoms. CT angiography of the head and neck showed extracranial dissection.
Results
One day later she was asymptomatic and MRI showed ischemic stroke in the caudate, centrum semiovale and subcortical temporal left hemisphere. She was discharged home without physical therapy.
Conclusion
Discussion
There are only limited data regarding thrombolytic treatment in acute stroke during pregnancy and puerperium. Current acute stroke treatment guidelines–while considering pregnancy as a relative exclusion criterion–do not deal with the postpartum state.
Conclusion
As the condition is rare, randomized controlled trials are not feasible, therefore further reports on similar cases could eventually help us suggest guidelines or at least propose recommendations for the acute thrombolytic treatment of strokes occurring in pregnancy and puerperium.
Trial registration number
No
AS05-050
DIRECT VERSUS BRIDGING MECHANICAL THROMBECTOMY IN ISCHEMIC STROKES OF UNKNOWN ONSET: A MULTICENTER STUDY IN THE NORTH OF SPAIN (NORDICTUS)
1Miguel Servet University Hospital, Neurology, Zaragoza, Spain
2Miguel Servet University Hospital, Neuroradiology, Zaragoza, Spain
3Hospital Universitario Marqués de Valdecilla, Neurology, Santander, Spain
4Hospital Clínico Universitario de Valladolid, Neurology, Valladolid, Spain
5Hospital Universitario Donostia, Neurology, Donostia, Spain
6Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
7Hospital Universitario Araba, Neurology, Vitoria, Spain
8Complejo Hospitalario Universitario de Santiago, Neurology, Santiago de Compostela, Spain
9Hospital de Galdakao, Neurology, Galdakao, Spain
10Hospital Universitario de Burgos, Neurology, Burgos, Spain
11Hospital de Basurto, Neurology, Bilbao, Spain
12Hospital Universitario de León, Neurology, León, Spain
13Complejo Hospitalario Universitario de Vigo, Neurology, Vigo, Spain
14Complejo Hospitalario Universitario A Coruña, Neurology, A Coruña, Spain
Background and Aims
NORDICTUS is a stroke research network in Northern Spain, integrated by stroke centers serving a catchment area of 11.500.000 inhabitants. In 46% of these hospitals, endovascular treatment of unknown-onset strokes (UOS) is routinely performed after administration of off-label intravenous thrombolysis (bridging therapy). The aim of this study is to examine the safety and efficacy of bridging thrombolysis (BT) compared with mechanical thrombectomy alone (MTa) in the treatment of UOS.
Method
This is a retrospective follow-up study in which we compared radiological and clinical outcomes at 90 days in patients receiving MTa with those receiving BT for endovascular treatment of large-vessel occlusion anterior circulation UOS in NORDICTUS (2015-2016).
Results
Of 884 patients treated with mechanical thrombectomy, 198 were UOS. Of them, 117(59.1%) underwent BT and 81(40.9%) MTa. Regarding baseline variables, median ASPECTS in plain CT was lower in the MTa group (8vs9, p = 0.004), and the use of perfusion imaging was similar in both groups (74.3% vs 78.8%, p = 0.479). Safety: no differences were found in the rate of symptomatic (7.5% vs 9.4%, p = 0.64) or parenchymal-hematoma type 2(6.3% vs 10.3%, p = 0.44) hemorrhagic transformations. Efficacy: although a higher mTICI3 rate was observed in the MTa group (72.8vs51.7%, p = 0.003), there were not significant differences neither in good long-term outcome (53.4%vs49.1%, p = 0.56) nor in mortality (8.2%vs14%, p = 0.22) between both groups in univariate or multivariate analysis.
Conclusion
Off-label BT in UOS appears to be safe although not associated with improved outcomes. This observation may be of interest especially in the drip & ship context.
Trial registration number
N/A
AS05-051
TIME-DEPENDENT INFLUENCE OF CLINICAL AND DEMOGRAPHIC CHARACTERISTICS ON IV-THROMBOLYSIS IN THE AUSTRIAN STROKE-UNIT REGISTRY
1Medical University of Vienna, Neurology, Vienna, Austria
2Danube University Krems, Gesundheit Österreich GmbH/BIQG, Vienna, Austria
3KH Barmherzige Brüder Wien, Neurology, Vienna, Austria
4Krankenanstalt Rudolfstiftung, Neurology, Vienna, Austria
Background and Aims
Rates of iv-thrombolysis as an established treatment in acute ischemic stroke are increasing over time. We evaluated the influence of clinical and demographic factors on rtPA-treatment over time in an Austrian cohort of stroke-patients.
Method
We analysed data of patients with acute ischemic stroke from 2005-2017 in the Austrian Stroke Unit Registry (ASUR). A time-dependent logistic regression analysis was conducted to describe changes of associations of clinical and demographic factors with rtPA-treatment over time.
Results
Overall 96.173 patients were enrolled in the ASUR between 2005 and 2017 of which 16.581 (17.2%) received iv-tPA.
We detected lower odds of receiving rtPA-treatment in patients with atrial fibrillation over time (2005-2009: OR = 0.93; 2010-2017: OR = 0.64, p for interaction of AF and time as independent predictors of rtPA-treatment <0.001). The odds of receiving rtPA-treatment in patients with posterior circulation stroke (PCS) and in patients with an onset-to-door-time (ODT) >180min increased over time (PCS: 2005-2009: OR = 0.41, 2010-2017: OR 0.77, p for interaction<0.001; ODT>180min: OR 0.07 vs. OR 0.14, p for interaction=0.004). Age >80years, stroke severity, ODT 120-180min, premorbid mRS and previous stroke were significantly associated with tPA-treatment across both time periods.
Conclusion
We observed decreasing odds of rtPA-treatment in patients with AF over the last 7 years. Conversly, in patients with ODT>180min and those with PCS, likelihood of receiving rtPA-treatment increased over the last years.
Trial registration number
N/A
AS05-052
NO EFFECT ON OUTCOME DESPITE ALTEPLASE BOLUS-INFUSION DELAYS
1Addenbrooke's hospital, Neurology, Cambridge, United Kingdom
Background and Aims
Efficacy of alteplase in acute ischaemic stroke (AIS) is known to depend on time to treatment onset. There is limited literature regarding how delays between administration of the alteplase bolus and infusion may affect clinical outcomes. We investigated the extent of bolus-infusion delays in AIS and the relationship between delays and outcome.
Method
We reviewed 300 consecutive patient records who underwent thrombolysis for AIS between 2014 and 2017. The timings of alteplase administration were recorded along with the admission and post-thrombolysis NIHSS and mRS at discharge. Records were excluded where complete data was not obtainable (n = 50). As in previous studies the bolus-infusion time was dichotomised at 8 minutes; twice the plasma half-life of alteplase.
Results
The median time between bolus and infusion was 16 minutes (IQR 15). Only 24% of patients received their infusion within eight minutes. There was no correlation between the bolus-infusion delay and the change in NIHSS at 24hrs (r = -0.00097; p = 0.99) or the mRS at discharge (r = 0.062; p = 0.35). When subsetting the group to those who received their infusion within and 8 minutes or longer, the median time delay, mean change in NIHSS and mean change in mRS was 5 minutes, -5.3 and 1.86 and 20 minutes, -4.4 and 1.83 respectively.
Conclusion
We have identified that whilst there are potentially concerning bolus-infusion delays at our centre however they are not associated with adverse outcomes.
Trial registration number
NA
AS05-056
WHITE MATTER HYPERINTENSITY SEVERITY PREDICTS DEVELOPMENT OF CEREBRAL OEDEMA IN PATIENTS WITH ISCHEMIC STROKE TREATED WITH IV THROMBOLYSIS: IMPLICATIONS FOR INFARCT GROWTH AND FUNCTIONAL OUTCOME
1Sapienza University of Rome, Department of Neurology and Psychiatry, Rome, Italy
Background and Aims
Increased white matter hyperintensity (WMH) burden may be associated with chronic endothelial injury, impaired cerebrovascular reactivity, blood-brain barrier (BBB) disruption, and chronic hypoperfusion.The aim of this study was to evaluate whether in patients with acute ischemic stroke (AIS) treated with IV thrombolysis moderate to severe WMH predicts development of cerebral oedema (CE) with consequent implications for infarct growth (IG) and functional outcome.
Method
We analyzed data of patients treated with IV rt-PA at the Sapienza University of Rome and included in the SITS-ISTR.WMH was measured by modified Fazekas scale on baseline FLAIR-MRI mainly on the contralateral hemisphere. CE was measured by a visual score on baseline FLAIR-MRI performed within 24 hrs of symptom onset.Outcome measures were IG and modified Rankin Scale (mRS) score (3–6 as poor outcome) at 90 days.
Results
Overall, 440 patients were included (mean age[SD] 69.3[13.6]; 41.4% women; median[IQR] NIHSS 8[4-15]);84 (22.6%) patients had moderate/severe WMH. CE was observed in 121(36.8%) patients.In univariate analyses, moderate/severe WMH was significantly associated with the development of CE (p = 0.005).Patients with CE at baseline were more likely to have early neurological deterioration, symptomatic intracerebral hemorrhage, IG, and mortality (p < 0.05 each).Both WMH and CE resulted significantly associated with 90-day poor functional outcome (p < 0.01).In multivariate analysis, after adjusting for confounding variables, moderate/severe WMH independently predicts development of CE(OR 5.52, 95%CI 2.08-14.62, p = 0.001).
Conclusion
In AIS patients treated with IV thrombolysis, WMH severity, as potential sign of chronic microvascular dysfunction and increase of BBB permeability, predicts the development of CE. Individuation of specific quantitative WMH volume cutoffs may have implication for improving infarct growth and functional outcome prediction.
Trial registration number
N/A
HYPERACUTE MANAGEMENT – EXCLUDING CLINICAL TRIAL RESULTS
AS06-001
MELATONIN ATTENUATES AUTOPHAGY-LIKE CELL DEATH THROUGH ANTIOXIDANT ENZYMES IN CEREBELLAR PURKINJE CELLS FOLLOWING ASPHYXIAL CARDIAC ARREST
1Kangwon National University School of Medicine, Emergency Medicine, Chuncheon-si, Republic of Korea
2Kangwon National University School of Medicine, Neurobiology, Chuncheon-si, Republic of Korea
Background and Aims
Although a large number ofmultiple reports using animal models have confirmed that melatonin appears to promote neuroprotective effects following ischemia/reperfusion-induced brain injury, the relationship between its protective effects and the activation of autophagy in cerebellar Purkinje cells following aphyxial cardiac arrest and cardiopulmonary resuscitation (CA/CPR) is not clearremains unclear.
Method
Animals used in this study were randomly assigned to 6 groups.
Results
Our results demonstrate that melatonin (10 mg/kg, ip, 3 times after aphyxial CA) significantly improved the survival rates and neurological deficits compared with the vehicle-treated aphyxial CA/CPR rats (survival rates ≥ 40% vs 10%). We also demonstrated that melatonin exhibits a protective effect against aphyxial CA/CPR-induced cerebellar Purkinje cell death in rats. The protective effecteffects of melatonin in the Purkinje cell death of aphyxial CA/CPR-induced rats paralleled a dramatic reduction in superoxide anion radical, intensely intense enhancement of CuZn superoxide dismutase (SOD1) and MnSOD (SOD2) expression, and as well as a remarkable attenuation of autophagic activation (LC3 and Beclin-1), which is MT2 melatonin receptor-associated.
Conclusion
This study shows that melatonin conferred neuroprotection against aphyxial CA/CPR-induced cerebellar Purkinje cell death by inhibiting autophagic activation via bothby reducing the expression of reactive oxygen species, while and increasing the expression of antioxidative enmzymes, and suggestssuggesting that MT2 is involved in the neuroprotective effects of melatonin in this aphyxial CA/CPR-induced cerebellar Purkinje cell death induced by aphyxial CA/CPR.
Trial registration number
N/A
AS06-002
DOWN-REGULATION OF CDK5 BY ISCHEMIC PRECONDITIONING ATTENUATES P53-DEPENDENT APOPTOSIS OF HIPPOCAMPAL CA1 NEURONS FOLLOWING A SUBSEQUENT TRANSIENT CEREBRAL ISCHEMIA
1Kangwon National University School of Medicine, Emergency Medicine, Chuncheon-si, Republic of Korea
2Kangwon National University School of Medicine, Neurobiology, Chuncheon-si, Republic of Korea
Background and Aims
Deregulation of cyclin-dependent kinase 5 (Cdk5) is related to pathological conditions. Ischemic preconditioning (IPC) provides neuroprotective effects against subsequent ischemic insults.
Method
We examined effects of IPC (2-min transient cerebral ischemia) on expressions of molecules related with Cdk5 in the hippocampus following 5-min subsequent transient cerebral ischemia (TCI) in gerbils.
Results
Pyramidal neurons in the hippocampal CA1 area were dead at 5 days post-TCI; however, IPC and roscovitine treatment (inhibitor of Cdks) protected the neurons from TCI. Cdk5, p25 and phospho (p)-p53 expressions increased in nuclei of the pyramidal neurons 1 and 2 days after TCI. However, IPC and/or roscovitine treatment decreased Cdk5, p25 and p-p53 expressions in the pyramidal neurons following TCI, in particular, Cdk5 and p-p53 immunoreactivities in their nuclei decreased. Furthermore, TUNEL-positive pyramidal neurons were detected 5 days after TCI with increases of Bax, PUMA and activated caspase-3 expressions, and TUNEL-positive cells and the increased molecules were cut off by IPC and roscovitine treatment.
Conclusion
Briefly, IPC protected CA1 pyramidal neurons from TCI through down-regulating Cdk5, p25 and p-p53. Thus, we suggest that the down-regulation of Cdk5 by IPC might be a key factor in attenuation of p53-dependent apoptosis in CA1 pyramidal neurons against ischemic insults.
Trial registration number
N/A
AS06-003
NEURONAL LOSS AND GLIOSIS IN THE RAT STRIATUM SUBJECTED TO 15 AND 30 MINUTES OF MIDDLE CEREBRAL ARTERY OCCLUSION
1Kangwon National University School of Medicine, Emergency Medicine, Chuncheon-si, Republic of Korea
2Kangwon National University School of Medicine, Neurobiology, Chuncheon-si, Republic of Korea
Background and Aims
Selective neuronal death or loss in certain brain regions has been well characterized in animal models of transient global cerebral ischemia. However, selective neuronal death in transient focal cerebral ischemia needs more investigation.
Method
Therefore, in this study, we studied selective neuronal death in the striatum (caudate putamen) of rats subjected to 15 or 30 min middle cerebral artery occlusion (MCAO). Neuronal death occurred in the dorsolateral field, not in the medial field in 30 min, not 15 min, MCAO-operated rats 5 days after MCAO using neuronal nuclear antigen immunohistochemistry and Fluoro-Jade B histofluorescence staining.
Results
In this group, immunoreactivity of glial fibrillary acidic protein in astrocytes was hardly shown in the dorsolateral field, although the immunoreactivity increased in the medial field. In addition, immunoreactivity of ionized calcium binding adapter molecule 1 in microglia was dramatically increased in the dorsolateral, not in the medial, field only in 30 min MCAO-operated rats. Briefly, these results show that at least 30 min of MCAO can evoke selective neuronal death, astrocytic dysfunction and microglial activation in the dorsolateral field of the rat striatum and suggest that a rat model of 30 min.
Conclusion
MCAO can be used to investigate mechanisms of neuronal death and gliosis following brief transient focal cerebral ischemic events for acute transient ischemic attack.
Trial registration number
N/A
AS06-004
FLUCTUATING NEUROLOGY IN ACUTE STROKE DUE TO MULTIPLE EMBOLI – THE IMPORTANCE OF REPEATING THE CT ANGIOGRAM IN AN EVOLVING CLINICAL PICTURE
1Royal Devon and Exeter Hospital, Stroke, Exeter, United Kingdom
Background and Aims
We report a 79 year old man with paroxysmal atrial fibrillation (PAF) treated with aspirin. On arrival he was reviewed immediately by the acute stroke team. He presented with right hemiplegia, dysphasia, and right neglect; NIHSS 16/42. Non-contrast CT excluded haemorrhage and he was thrombolysed. The diagnosis was of left middle cerebral artery (MCA) infarct, with rapid improvement of his hemiplegia. A CT angiogram (CTA) showed left M3 occlusion not amenable to thrombectomy.
During thrombolysis he suddenly became drowsy: repeat CT excluded haemorrhage. He roused to a GCS of 13/15, but with new left hemiplegia, fixed gaze to the right, and mild dysphasia, repeat NIHSS was 24/42. Repeat CTA showed resolution of the left M3 occlusion, but new proximal right MCA occlusion. He was transferred to the regional thrombectomy centre. Thrombectomy was not performed as he had improved significantly on arrival (NIHSS = 7/42).
On discharge, he had mild dysphasia, mild left hemiparesis, left hemianopia and left neglect. Apart from PAF, no alternative cause was identified. He was discharged home on Day 6 with Early Supported Discharge and anticoagulated with Apixaban.
Method
NA
Results
NA
Conclusion
We describe a complex case with fluctuating signs secondary to multiple emboli from untreated PAF. Repeat CTA demonstrated resolution of the initial left MCA occlusion (likely due to thrombolysis) but showed a new right MCA thrombus. This demonstrates the importance of repeating the CTA if a repeat CT head shows no acute findings, as this could reveal early recurrence requiring thrombectomy
Trial registration number
NA
AS06-005
TIME IS LIFE - NOT ONLY BRAIN - FOR ALL STROKE PATIENTS
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine - Nursery, Denia, Spain
4Hospital General de Tomelloso, Neurology, Tomelloso, Spain
Background and Aims
Reducing time delays is essential for patients undergoing reperfusion therapies. However, such a benefit is uncertain when we consider the whole stroke population and, specially, mortality. We investigated the impact of prehospital delay in long term mortality in a series of stroke patients.
Method
382 Patients with acute stroke or TIA were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors in previous studies were collected, as well as data on PD and mortality. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency 12 months after stroke.
Results
Arriving the hospital within the first three hours after stroke onset decreased long term mortality after stroke (OR 0,381; CI 0,169 – 0,860; p = 0,020). Infectious comorbidities during hospitalization (OR 6,407; CI 3,124– 13,138; p < 0,001), a poor nutritional status – serum albumin of less than 3,5mg/dL – (OR 2,274; CI 1, 1,024– 5,052; p = 0,044), and high scores on previous mRS (OR 1,565; CI 1,237 – 1,980; p < 0,001) or NIHSS (OR 1,159; CI 1,096 – 1,226; p < 0,001) favored mortality in the same period.
Conclusion
Arriving the hospital within the first three hours after stroke onset reduces mortality twelve months after hospitalization. New interventions aiming at reducing prehospital delay are needed. This way we would probably increase reperfusion therapy rates. Moreover, by increasing the percentage of patients arriving within the first three hours after stroke, it would be possible to reduce 1-year mortality among stroke patients.
Trial registration number
N/A
AS06-008
PULSE PRESSURE VARIABILITY IS ASSOCIATED WITH FUNCTIONAL OUTCOME DURING THROMBECTOMY IN ACUTE ISCHEMIC STROKE PATIENTS
1Rothschild Foundation, Interventional Neuroradiology, Paris, France
2Sainte-Anne Hospital, Neurology, Paris, France
3Rothschild Foundation, Anesthesiology, Paris, France
4Rothschild Foundation, Neurology, Paris, France
5Hôtel Dieu, Hypertension Unit, Paris, France
6Foch Hospital, Neurology, Suresnes, France
Background and Aims
The impact of blood pressure (BP) variability during mechanical thrombectomy (MT) on prognosis has not been studied. We assessed the association between pulse pressure (PP) variability during MT and 3-month functional outcome in acute ischemic stroke (AIS) patients with large vessel occlusion (LVO).
Method
AIS patients presenting with LVO from January 2012 to June 2016 were included. BP data during MT were prospectively collected in the ETIS registry. Ordinal logistic regression models were used to assess the association of the PP variation coefficient and functional outcome at 3 months.
Results
Among the 343 included patients, PP variability was significantly associated with worse 3-month mRS in univariable (OR = 1.56, 95%CI:1.24-1.96 per 1-unit increase, P = 0.0002) and multivariable shift analysis (adjusted OR = 1.40, 95%CI:1.09-1.79, P = 0.008). PP variability was also associated with unfavorable outcome (mRS 3–6) in univariable (OR = 1.53, 95%CI:1.17-2.01, P = 0.002) and multivariable analysis (adjusted OR = 1.42, 95%CI:1.02-1.98, P = 0.04).
Conclusion
PP variability during MT was independently associated with worse clinical outcome in AIS patients. Whether pharmacological intervention, aiming at reducing BP variability during MT, impacts on functional outcome needs to be determined.
Trial registration number
N/A
AS06-009
DOOR-IN-DOOR-OUT TIMES ACROSS A CANADIAN PROVINCE FOR OPTIMAL ACCESS TO ENDOVASCULAR THERAPY
1University of Calgary, Clinical Neurosciences, Calgary, Canada
2University of Alberta, Neurology, Edmonton, Canada
3Alberta Health Services, Cardiovascular Health & Stroke- Strategic Clinical Network, Calgary, Canada
Background and Aims
Endovascular treatment (EVT) for acute ischemic stroke is highly efficacious but only offered at some tertiary care urban hospitals; therefore, rapid transfer of EVT-eligible patients from non-EVT capable primary stroke centers (PSCs) is critical. This study reviews the door-in-door-out (DIDO) times of ischemic stroke patients from PSCs to EVT Centres in Alberta.
Method
We reviewed data entered into the QuICR (Quality Improvement and Clinical Research) clinical registry from January 2016 to December 2017. The analysis included: the number of patients that were transported, the number of patients that received EVT, the transportation modality, Door-to-Needle times (DNT) at the PSCs, and DIDO times at the PSCs.
Results
There were a total of 51 patients that were transported from a PSC for EVT from 2016-2017 (Figure). The number of transports increased from 13 in 2016 to 38 in 2017. Out of the 38 patients that were transported in 2017, 68% received EVT and 73% arrived via ground ambulance. The median DNT in 2017 for these patients was 46.5 minutes (IQR:31-57.5min), while the median DIDO time was 96.5 minutes (IQR:72-134min). The fastest DIDO times were 40 and 41 minutes. Faster DNT was correlated with faster DIDO times (r = 0.55, p = 0.0012).
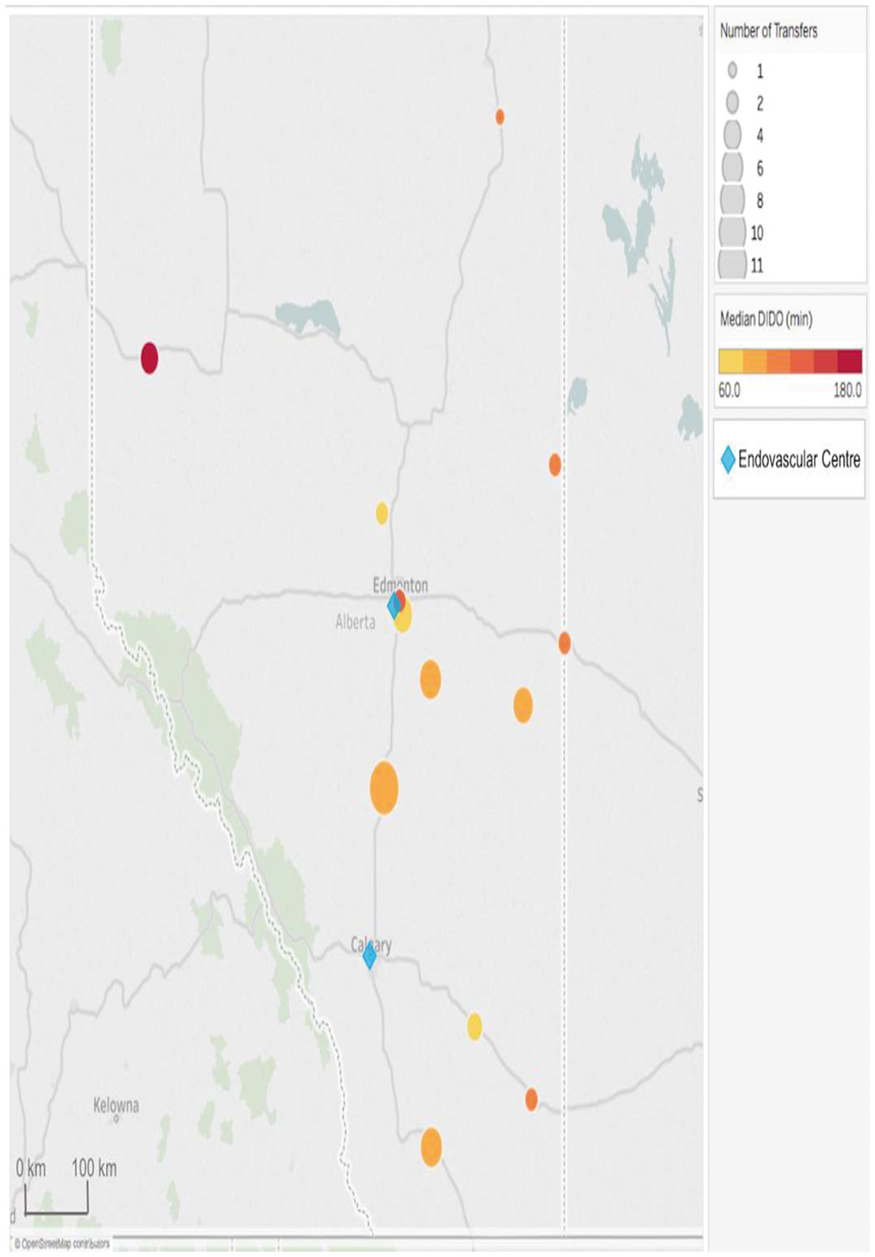
Conclusion
In the Canadian province of Alberta, DIDO times remain high despite quick administration of alteplase; however, fast DIDO times are possible.
Trial registration number
N/A
AS06-010
HOW DO COMMUNITY HOSPITALS PERFORM IN ACUTE ISCHEMIC STROKE TREATMENT IN THE RT-PA ERA?
1faculty of medicine- khon kaen university, Internal Medicine, khon kaen, Thailand
Background and Aims
The Stroke Fast Track Network, which has been development in Thailand to improve stroke care, particularly in community hospitals (CH). This study, aimed to evaluate the quality of acute ischemic stroke care in the various hospital levels.
Method
Data used in this study were randomly selected from the medical records, which are sent to the National Health Security Office for reimbursement purposes between October 2015 and August 2016. Patient demographics, risk factors, stroke subtypes, stroke severity, quality of care indicators and complications were recorded. Pair comparisons between two groups were carried out using Bonferroni correction.
Results
A total of 947 patients, 169 patients from CHs, 629 from regional hospitals (RH) and 149 from tertiary hospital (TH) were included in the final analysis. The CH group had a lower median age and median initial NIHSS than the RH and TH groups (median age = 70, 66 and 67 years, respectively, and initial NIHSS = 6, 8, and 9, respectively). The CH group had shorter onset-to-needle times for rt-PA than the other two groups (147 vs 178.5 and 180 min). The CH group had a lower proportion of asymptomatic intracerebral hemorrhage (0.6%), and lower mortality rate (1.2%) than either the RH or TH group.
Conclusion
Community hospitals have the potential care for acute ischemic stroke patients in the same way as RHs or THs.
Trial registration number
N/A
AS06-011
THE ROLE OF CT PERFUSION IN REAL-WORLD, ACUTE STROKE DECISION-MAKING: A SINGLE CENTER, MIXED METHODS STUDY
1Ottawa Hospital and Research Institute, Neurology, Ottawa, Canada
2King Fahad Medical City, Neurology, Riyadh, Saudi Arabia
3Imam Abdulrahman University, Neurology, Dammam, Saudi Arabia
Background and Aims
In the wake of recent trials, CT Perfusion (CTP) has garnered increasing attention as a means of selecting patients with ischemic stroke for acute reperfusion therapies. We question the logic of using CTP to “extend the window,” and sought to determine: whether CTP is more useful in real-world decision-making to rule patients OUT for reperfusion than rule them IN, and whether neurologists use CTP in this way.
Method
We analyzed a database of images (initial CT and CTP and final CT or MRI) and chart reports obtained from 164 consecutive “stroke code” patients at our tertiary center. We compared initial CTP Cerebral Blood Volume (CBV) ASPECTS score to final CT or MRI ASPECTS score. We searched patient charts for references to CTP in treatment decision-making.
Results
We included 70 patients in the imaging analysis, and 91 in the chart analysis. A low CTP-CBV ASPECTS score (less than 7) reliably ruled out a high final ASPECTS score (100% sensitivity), though a high CTP-CBV ASPECTS score was of limited predictive value. CTP was mentioned rarely in patient charts, and in 5 of 7 cases was used to justify withholding reperfusion therapy.
Conclusion
This study supports our hypothesis that CTP may be of more value to real-world decision-making to rule patients OUT for reperfusion therapies. This work could support a paradigm shift in acute stroke therapy: namely, offering treatment regardless of time, unless exclusionary parameters are met, such as evidence of completed infarction on CT or CTP.
Trial registration number
N/A
AS06-014
FRENCH AGREEMENT STUDY ON THE MANAGEMENT OF ACUTE ISCHEMIC STROKE (FAMOUS): A MULTICENTRIC INTERRATER AND INTRARATER AGREEMENT STUDY
1Fondation Rothschild, Interventional Neuroradiology, Paris, France
2HSHS St. John’s Hospital, HSHS Neuroscience Center, Springfield, USA
3Centre Hospitalier de l’Université de Montréal CHUM- Notre-Dame Hospital, Radiology, Montreal, Canada
4Henri Mondor hospital, Neuroradiology, Creteil, France
5Centre Hospitalier de l’Université de Montréal CHUM- Notre-Dame Hospital, CHUM Library, Montreal, Canada
6University of Alberta Hospital- Mackenzie Health Sciences Centre, Neurosurgery, Edmonton, Canada
Background and Aims
We aimed to assess agreement on intravenous tissue-plasminogen activator (IV tPA) and mechanical thrombectomy (MT) management decisions in acute ischemic stroke (AIS) patients.
Method
Studies assessing agreement of IV tPA and MT were systematically reviewed. An electronic portfolio of 41 AIS patients was sent to randomly selected providers at French stroke centers. Raters were asked 2 questions for each case: (1) Would you perform IV tPA? (2) Would you perform MT? Twenty responders were randomly selected to study intrarater agreement. Agreement was assessed using Fleiss’ Kappa statistics.
Results
The review yielded two single center studies involving 2–5 raters, with various methodologies and diverging results. The electronic survey was answered by 86 physicians (60 vascular neurologists and 26 interventional neuroradiologists). The interrater agreement was moderate for IV tPA treatment decisions (κ=0.565 [0.420–0.680]), but only fair for MT (κ=0.383 [0.289–0.491]) and for combined treatment decisions (κ=0.399 [0.320-0.486]) (Figure 1). The intrarater agreement was at least substantial for the majority of raters.
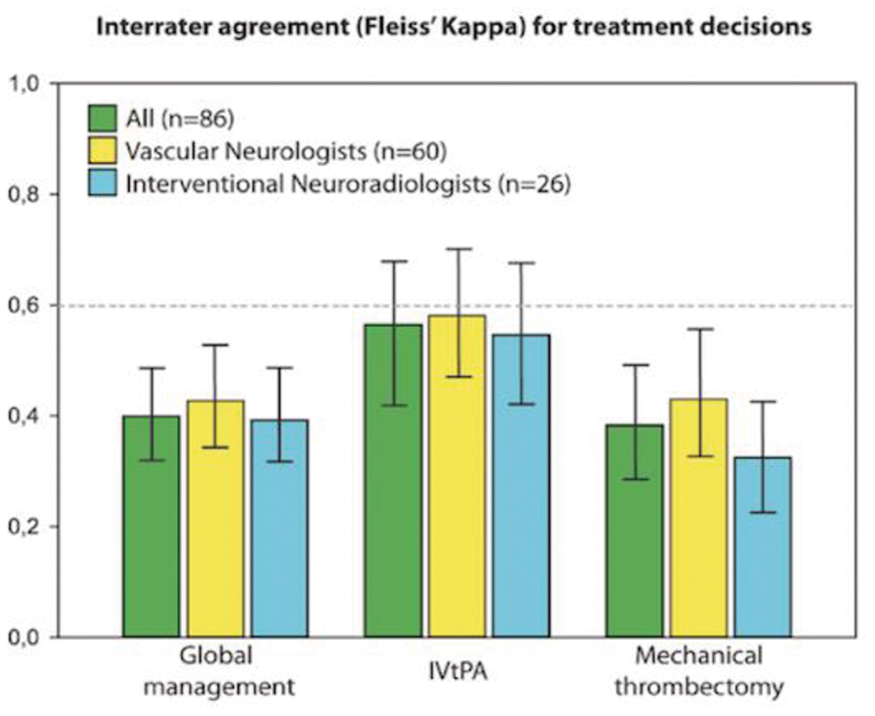
Conclusion
Disagreements regarding the use of IVtPA or MT in the management of AIS patients remain frequent, in spite of available evidence. More inclusive trials may help manage patients for whom uncertainties remain.
Trial registration number
n/a
AS06-015
TIME TO ANTITHROMBOTIC THERAPY AT MONASH HEALTH IN ISCHEMIC STROKE AND TRANSIENT ISCHEMIC ATTACK (TIA)
1Monash Health, Neurosciences, Clayton, Australia
2Monash University, Medicine, Clayton, Australia
Background and Aims
There has been emphasis on timely administration of thrombolysis and clot retrieval but not antithrombotic therapy for ischaemic stroke. The frequency of antithrombotic administration within 48 hours among patients with transient ischemic attack (TIA) was 73% in Australia, while among patients with ischemic stroke this ranged from 21% in New Zealand to 95% in North America. We plan to assess factors associated with time to antithrombotic therapy.
Method
Retrospective study of admissions to the stroke unit at Monash Medical Centre over 12 months in 2015. We collected data on demographic variables, admission diagnoses, time to triage, imaging, and time to administration of antithrombotic. We plot the cumulative event of patients receiving antithrombotic therapy against the time to administration.
Results
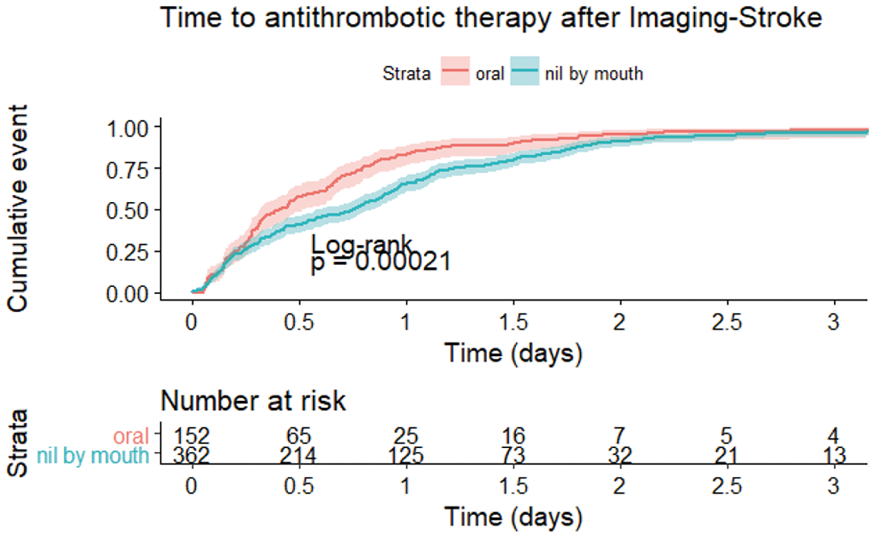
There were 514 patients (age 72.9 ± 14.7) who had an ischemic event, TIA (n = 75) or ischaemic stroke (n = 439). Of those with ischemic stroke, 70.8% of the patients were started on antithrombotic therapy by 24 hours and 92.0% by 48 hours. The use of thrombolytic therapy and nil by mouth status were associated with delay in commencing antithrombotic (p < 0.001). Of those with TIA, 54.7% received antithrombotic therapy within 12 hours, 86.7% within 24 hours and 98.7% at 48 hours. There was no weekend effect (p = 0.9) or after hour effect (p = 0.6) on the time to antithrombotic.
Conclusion
The proportion of patients with ischemic stroke or TIA receiving antithrombotic therapy within 48 hours was higher than previously reported in Australia and New Zealand. Nil by mouth status at presentation was associated with delay in time to therapy.
Trial registration number
NA
AS06-016
OUTCOME OF SUPERFICIAL TEMPORAL ARTERY TO MIDDLE CEREBRAL ARTERY ANASTOMOSIS IN ACUTE PERIOD OF CEREBRAL INFARCTION
1Bucheon St. Mary's Hospital- Catholic University of Korea, Neurosurgery, 부천천, Republic of Korea
Background and Aims
The authors performed urgent superficial temporal artery to middle cerebral artery (STA-MCA)anastomosis in acute period for the patients who was in progressive stroke or failed to fibrinolytic therapy. We investigated the effect of bypass surgery in acute period and good prognostic factors.
Method
The total of 83 patients who presented with major vessel occlusion and underwent emergency STA-MCA anastomosis were enrolled in this study for 9 years. Diffusion/perfusion Magnetic Resonance Image (MRI) and catheter angiography findings are major determinants of decision making of surgery. Only the patient who had small volume of infarction (less than 30cc) and large volume of perfusion defect with MRI study was selected as a surgery candidate.
Results
Initial national institute of health stroke scale (NIHSS) was 2 to 22. Mean volume of infarction was 8.3cc and mean time to peak (TTP) delay area volume was 75cc. NIHSS was higher in perforator infarction group (9.4 vs 3.6). There was no case of post-operation intracerebral hemorrhage or mortality. Post operative perfusion MRI at 1 week revealed full recovery of TTP delay in almost cases. Surgical outcomes according to modified Rankin score (mRS) are as follow ( IV:9, III:11, II:19, I:18.0:27)
Conclusion
Small infarction volume in the watershed area with large perfusion defect can be a good candidate for bypass surgery. It can improve the blood flow in critical area with little risk of reperfusion injury because of low flow characteristics. Bypass surgery in acute period of infarction can be a good option because it has a considerable long time window.
Trial registration number
n/a
AS06-017
IMPACT OF A STROKE PROTOCOL ON THE DOOR-TO-NEEDLE TIME: A FEASIBILITY STUDY
1Ghent University Hospital, Department of Emergency Medicine, Gent, Belgium
2Ghent University Hospital, Department of Neurology, Gent, Belgium
3Ghent University Hospital, Department of Radiology, Gent, Belgium
Background and Aims
Thrombolysis within 4,5 hours of ischemic stroke onset can improve outcome. Guidelines recommend administration of thrombolytics within 60 minutes upon arrival at the hospital, meaning door-to-needle time (DNT) should be less than 60 minutes. The earlier the treatment is started, the greater the benefits. In this study, a stroke protocol was introduced at the emergency department of the Ghent University Hospital with as primary goal to shorten the DNT.
Method
This study was an uncontrolled before-after study. A stroke protocol, consisting of multiple interventions, was implemented and the results from the pre-stroke protocol period (Pre-SP period, from August 15th 2016 until March 5th 2017) were compared to the results of the post-stroke protocol period (Post-SP period, from March 6th 2017 until July 16th 2017).
Results
The median DNT decreased significantly from 57 minutes in the Pre-SP period to 33 minutes in the Post-SP period (P < 0,001). When analyzing all patients included in the study and adjusting the results for other variables that might have an influence on these time intervals, the triage-to-emergency physician time (TET), emergency physician-to-CT time (ECT) and CT-to-needle time (CNT) also decreased significantly. When we analyzed these time intervals for only those who received thrombolysis, the TET and CNT decreased significantly. There was a statistically significant effect of the implementation of the stroke protocol on the number of patients treated with a DNT within 20, 30, 45 and 60 minutes (P = 0.008).
Conclusion
A significant decrease in DNT can be achieved by implementing this stroke protocol.
Trial registration number
N/A
AS06-019
PROGRESSING TOWARD PREHOSPITAL TRIAGE OF ACUTE STROKE USING PREHOSPITAL STROKE SCALES
1Hospital De Cabuenes, Neurology, Gijon, Spain
2Hospital Univeristario Central de Asturias, Neurology, Oviedo, Spain
3Hospital de Jove, Neurology, Gijón, Spain
4Universidad de Chile, Statistic, Chile, Chile
Background and Aims
Early detection of acute stroke (AS)and transfer of the patient to a centre able to provide the appropriate treatment within the therapeutic window continues to be a major challenge in neurological care.NIHSS is the gold-standard diagnostic tool for stroke.The Los Angeles MotorScale (LAMS), in turn, was designed to triage stroke patients before they arrive at the hospital.Our study aims to demonstrate the usefulness of theNIHSS for stroke triage (ST)and to compare its predictive ability to that of theLAMS.Furthermore, we have developed a scale for prehospitalSTin our setting.
Method
We prospectively included all patients transferred to a tertiary hospital as a result of code stroke (CS)activation during a one-year period.They were assessed by prehospital emergency medical services (EMS)using theLAMS andNIHSS.The AUC for both scales were analysed to compare the prediction validities.We also determined whichNIHSS items displayed the most similar scores between theEMS and the neurology department and created a prehospital stroke scale (PSS)specifically designed for our region.
Results
We analysed a total of363patients.Mean age was69years;54%were men.Recanalisation treatment (RT)was applied in147cases (25% increase compared to the previous year).NIHSSscores displayed good inter-rater agreement (prehospital emergency medical services vs neurology department).Likewise, NIHSS andLAMS scores showed a high level of agreement for predicting large-vessel occlusion (LVO).
Conclusion
Recent advances in the treatment forASunderscore the need to adaptCSprotocols to meet each region’s specific requirements.Such modifications may increase the rates of early management and the number of patients receivingRT.PSS are valid, quick-to-administer tools that are used in prehospitalST and helpful for detecting LVO.They constitute a valuable tool for choosing the most appropriate hospital for the patient based on the resources available at each centre.
Trial registration number
N/A
AS06-020
“EPILEPTIC SEIZURE” AS THE FIRST SIGN OF BASILAR ARTERY OCCLUSION
1University Hospital Centre Zagreb, Department of neurology, Zagreb, Croatia
Background and Aims
Stroke due to the acute basilar artery occlusion (BAO) represents a neurological emergency. When suspected following the clinical presentation, prompt neuroimaging and early initiation of recanalisation/reperfusion therapies can lead to the good clinical outcome. The diagnosis is often challenging due to considerable heterogeneity of presenting clinical signs, which graduate from decreased level of consciousness, visual disturbances, cranial nerve abnormalities, quadriplegia.
Method
Seizure as initial presentation of stroke is rare, all about 2% cases, more common with anterior circulation stroke and rare in BAO and posterior circulation stroke. But, involuntary movements at the onset of BAO or brainstem ischemic stroke are not so rare. Movements can range from myoclonus, dystonic movements, rhythmic tonic movements to generalized tonic–clonic “convulsive-like” activities. Such symptoms are sometimes difficult to distinguish from true epileptic seizures, but in emergencies they may help to direct the suspicion and diagnosis of the BAO,
Results
In our paper we present a clinical findings, emergency diagnostic and therapeutic procedures in several patients initially presented with atypical clinical picture and “epileptic attack” i.e. involuntary gestures as the first sign of BAO.
Conclusion
Early diagnosis of BAO is a diagnostic challenge due to heterogeneous clinical symptomatology, including involuntary motion-like epileptic attacks. In emergencies, these unwanted movements may direct the suspicion to BAO. Recognition, confirmation with prompt neurovascular imaging and initiation of early recanalization/reperfusion therapy significantly contributes to a more favorable clinical outcome in this devastating form of stroke.
Trial registration number
N/A
AS06-022
GOOGLING BOUNDARIES FOR OPERATING MOBILE STROKE UNIT FOR STROKE CODES
1Monash Health, Neurosciences, Clayton, Australia
2Monash University, Medicine, Frankston, Australia
3Melbourne Health, Neurology, Melbourne, Australia
4Florey Institute, Stroke, Melbourne, Australia
Background and Aims
It is important to optimize parameters for using mobile stroke unit (MSU) to deliver recombinant tissue plasminogen activator (TPA) at the patient’s location and expedite endovascular clot retrieval (ECR). There are 2 Melbourne hospitals (Royal Melbourne Hospital/RMH, Monash Medical Centre/MMC) designated to provide ECR. We developed a computational model as an app (https://gntem3.shinyapps.io/ambmc/), taking into account traveling time (Google Map API), to explore this issue.
Method
In these spatial simulations, the MSU is based at RMH and delivers TPA at the patient’s location and returns to base for ECR. The app contains widgets for varying the processing time at the patient location (default=20 minutes), performing CT angiography (default=10 minutes). The data were compared against those for usual ambulance metrics (default traveling time =15 minutes, processing time at patient’s location =10 minutes, door to TPA = 30 minutes, door to groin=60 minutes).
Results
In spite of the large area, MSU is superior for delivering TPA to all Melbourne suburbs (76 minutes from RMH) as long as the combined processing and imaging time is < 60 minutes. However, it was superior for providing ECR to only 39.3% of suburbs if the return base is RMH and 63.9% if the return base is both RMH and MMC. If the door to groin is 70 minutes for usual ambulance metrics, then MSU is superior to this in 93.4% of suburbs.
Conclusion
The app can help to define how best to deploy the MSU across Melbourne.
Trial registration number
na
AS06-023
SAMPLE SIZE CALCULATION FOR INTRACEREBRAL HAEMORRHAGE TRIALS BASED ON CT ANGIOGRAPHIC “SPOT SIGN” AND RATE OF GROWTH
1Stroke and Aging Research Group, Department of Medicine- Monash University- and Stroke Unit and Diagnostic Imaging- Monash Medical Centre- Melbourne- Australia, Melbourne, Australia
Background and Aims
To generate sample size calculation for clinical trials based on the predictive value of the “Spot Sign” in predicting spontaneous intracerebral haemorrhage (ICH) expansion.
Method
PubMed, Medline, conference proceedings and manuscript references up to June 2017 were searched for studies reporting “computed tomography angiography” and “spot sign” or “intracerebral haemorrhage” and “spot sign”. The overall rate of ICH growth and ICH growth in presence of positive spot sign is positive are calculated based on random effect assumption (Metafor package in R). Sample size estimates were calculated from data on ICH treated as dichotomous variables.
Results
There were 36 studies describing 6888 patients. The rate of growth with spot sign was 55.4% (95% CI 49.6%-61.1%). A drug which decreases the spot sign ICH growth by 5% would require 1565 patients, 10% decrement requires 391 patients and 20% decrement requires 173 patients in each arm. The rate of growth was 23.1% (95% CI 20.2%-26.0%). A drug which decreases the ICH growth by 5% would require 1026 patients, 10% decrement requires 231 patients and 20% decrement requires 91 patients in each arm (80% power, and 0.05).
Conclusion
The sample size estimates provided here will be useful for planning of clinical trials on intracerebral haemorrhage. Sample size estimates based on ICH growth would require smaller sample size.
Trial registration number
N/A
AS06-024
A CASE OF FAVOURABLE OUTCOME FOLLOWING THROMBECTOMY VIA THROMBOASPIRATION TO POSTERIOR CEREBRAL ARTERY STROKE AND SUPERIOR CEREBELLAR ARTERY STROKE WHEN INTRAVENOUS THROMBOLYSIS IS CONTRAINDICATED
1NHS - Brighton and Sussex University Hospital, Stroke Medicine, London, United Kingdom
Background and Aims
Intra-arterial thrombectomy has demonstrated benefit for patients with acute ischaemic stroke and large vessel occlusions (LVOs). More recently, an equal benefit was shown for both anterior and posterior circulation LVOs.
We are discussing a case of posterior circulation stroke receiving thrombectomy, when intravenous thrombolysis is contraindicated
Method
This 87 year old patient presented with left TACS syndrome (right hemiplegia and dysarthria) and an NIHSS score of 14. His risk factors included HTN, T2DM, IHD and Hypercholesterolaemia.
An unclear onset time meant no intravenous thrombolysis was given.
Based on the CTA findings of left P1 and superior cerebellar artery (SCA) filling defects, the patient received high dose aspirin and a thrombectomy procedure.
The angiogram confirmed the occlusion of the left PCA and SCA. SOFIA distal access catheter was advanced to the interface of the clot and aspiration performed for 2 minutes.
Results
The pre-thrombectomy TICI flow improved from 0 to 3 with thromboaspiration.
His NIHSS score improved to 0 after 24 hours post procedure.
He made a full recovery.
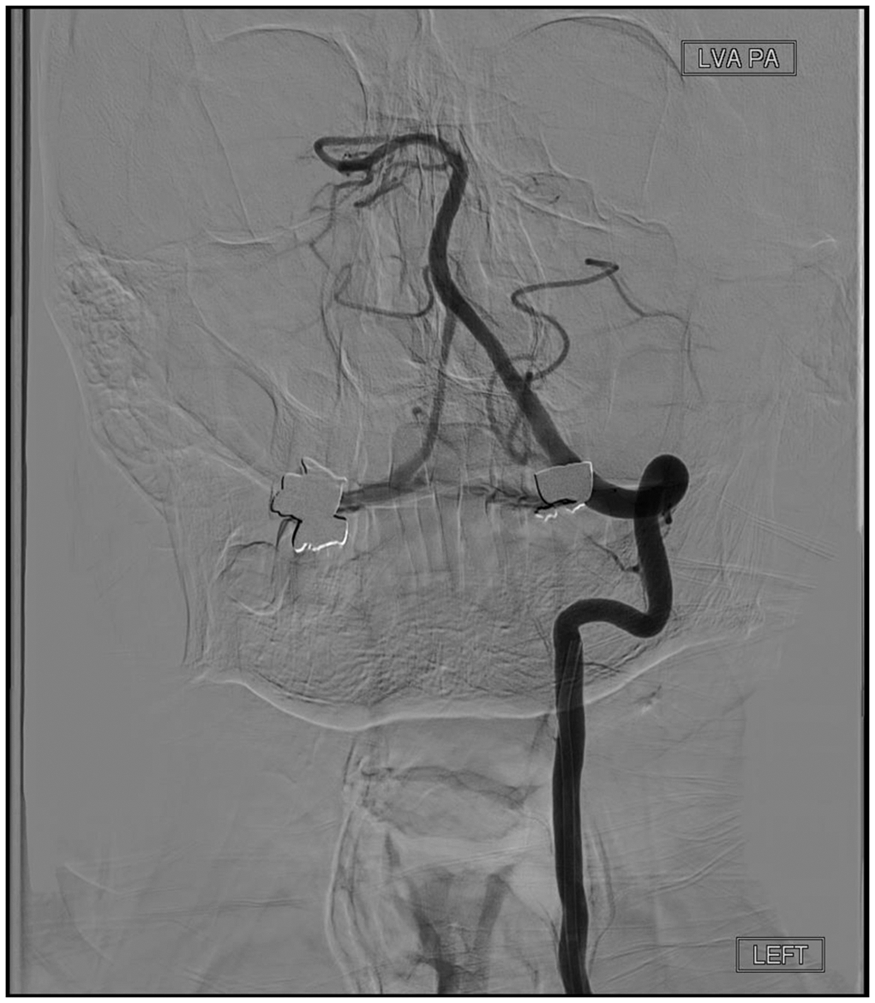
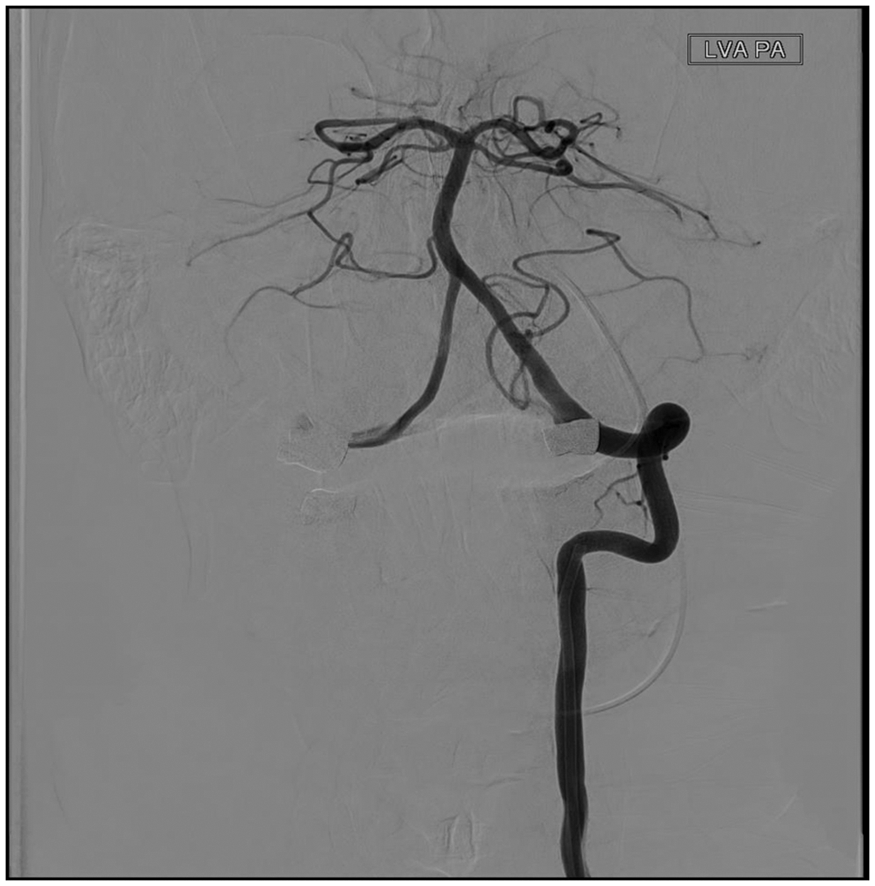
Conclusion
A favourable outcome was achieved with intra-arterial thrombectomy (thromboaspiration) in a posterior circulation stroke when intravenous thrombolysis is contraindicated
Trial registration number
N/A
AS06-025
MECHANICAL THROMBECTOMY IN PATIENTS WITH TANDEM OCCLUSION
1St George's Hospital NHS Trust, Neuroradiology, London, United Kingdom
2St George's Hospital NHS Trust, Neurology, London, United Kingdom
Background and Aims
Randomised trials have proven mechanical thrombectomy (MT) is superior to best medical treatment in patients with acute ischemic stroke. The optimal approach for MT in patients with tandem occlusions (MT + urgent stenting vs. MT + delayed CEA; antegrade stenting vs retrograde stenting) remains controversial. We report the results of our series of MT in patients with a tandem occlusion.
Method
This study was based a prospective observational registry of all consecutive patients treated with MT between May 2016 to July 2017. The treatment decisions (above) were made by the neurointerventionists. For patients that had a carotid stent, 500mg aspirin i.v. was given during the procedure, and a second antiplatelet added after the 24 hour follow-up CT showed no contraindication. Successful recanalisation was defined as modified treatment in cerebral ischaemia (mTICI) 2b/3.
Results
22 had an extracranial carotid occlusion or critical stenosis, 7 of whom went on to have an urgent extracranial carotid stenting. 6 of these 7 patients had successful intracranial recanalisation, 2 of whom died. Of the remaining 15 patients, 5 patients did not have MT, as no access through extracranial occlusion was gained. 10 patients had MT, and 7 of them had successful intracranial recanalisation without urgent carotid stenting with no deaths. The other 3 patients failed recanalisation, 2 of which died. There were no intracranial bleeds in our cohort.
Conclusion
In our case series, successful recanalisation and mortality rates were comparable in both approaches (with or without urgent carotid stenting). Further research is required.
Trial registration number
N/A
AS06-026
GOOD COLLATERALS ASSOCIATED WITH HIGH RECANALIZATION RATE WITH OR WITHOUT THROMBOLYSIS
1St George's Hospital NHS Trust, Neurology, London, United Kingdom
2St George's Hospital NHS Trust, Neuroradiology, London, United Kingdom
Background and Aims
Recent randomised trials have proven mechanical thrombectomy (MT) to be superior to best medical treatment. Small retrospective studies have suggested that good collaterals are associated with better clinical outcome after MT patients with Large Vessel Occlusion (LVO) Stroke. We examined the association between collateral status and clinical outcome after MT.
Method
Our Hyperacute Stroke Unit (HASU) is the first fully operational 24/7 thrombectomy service in the UK, servicing Southwest London and Surrey Trusts.
We collected data on consecutive patients treated with MT from May 2016 to July 2017. Collaterals were retrospectively assessed on baseline CT angiogram (single phase), by two interventional neuroradiologists. Assessors were blinded to clinical outcome. Collaterals were divided into two groups (poor and good).
Successful recanalisation was defined as modified treatment in cerebral ischaemia (mTICI)2b/3. Favorable clinical outcome was set as modified Rankin scale (mRS) <3 at 90 days.
Conclusion
Our data suggests that good collaterals are associated with both recanalization and favourable clinical outcome in stroke patients treated with MT and may not be affected by thrombolysis.
Trial registration number
N/A
AS06-027
“DISTAL ONLY APPROACH” IN ACUTE MCA STROKES WITH TANDEM ICA OCCLUSION
1Hacettepe University, Neurology, Ankara, Turkey
2Hacettepe University, Radiology, Ankara, Turkey
Background and Aims
The current treatment strategy of tandem occlusion, suggesting to recanalize both proximal and distal arteries to provide complete patency, is complex and relatively risky procedure.
Method
Three cases with tandem proximal ICA and MCA occlusion (refers to 9.6% of all MCA strokes thrombectomized in 2017) underwent MCA thrombectomy without any ICA revascularization effort were described.
Results
Case 1: A 60-year-old man with acute left MCA syndrome (NIHSS: 23) received IV tPA. Angiography documented left ICA and MCA occlusion, but patent ACom and PCom. With passing ICA occlusion using modified Dotter method, successful MCA thrombectomy and TICI 3 reperfusion were achieved. Discharge mRS was 4. Case 2: A 70-year-old-man with acute left MCA syndrome (NIHSS 6) was treated with IV tPA. Angiography documented left ICA and MCA occlusions with operative ACom and PCom. MCA thrombectomy through ICA occlusion provided TICI 2b reperfusion. NIHSS decreased to 5. Discharge mRS was 3. MR perfusion showed no extralesional hypoperfusion. Case 3: A 61-year-old-woman was admitted with right MCA syndrome (NIHSS 8). Angiography after IV tPA, showed right ICA and MCA occlusion with patent ACom and PCom. MCA thrombectomy, through ICA occlusion, provided dramatic NIHSS decrease (to 2). mRS was 1. MR perfusion documented minimal perfusion deficit on right hemisphere.
Conclusion
The “distal only approach", described herein, resulted in positive outcomes in 3 acute tandem MCA-ICA occlusion cases with effective Willis’ collaterals. Although this method is seemingly practical, it needs to be compared with combined (either “proximal to distal" or “distal to proximal") approaches.
Trial registration number
N/A
AS06-028
PREDICTORS OF EARLY DRAMATIC RECOVERY AFTER ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE
1Aarhus University Hospital, Department of Neurology, Aarhus C, Denmark
2Aarhus University Hospital, Department of Anesthesiology and Intensive Care-North- Section of Neuroanesthesia, Aarhus C, Denmark
3Texas Stroke Institute, Division of Neurointervention, Dallas- TX, USA
4Aarhus University Hospital, Department of Neuroradiology, Aarhus C, Denmark
Background and Aims
Knowledge of factors associated with immediate response to endovascular treatment (EVT) in ischemic stroke patients may be helpful in the early estimation of prognosis. We sought to identify clinical and imaging factors associated with early dramatic recovery (EDR) in patients after EVT.
Method
We analyzed data from consecutive acute ischemic stroke patients undergoing EVT within 6 hours from symptom onset due to anterior large vessel occlusion between March 2015 to February 2017 at Aarhus University Hospital. EDR was defined as an improvement of more than 7 points on NIHSS at 24 hours. Logistic regression analyses explored the association between key variables and EDR.
Results
Among 128 patients (mean age, 71 years; median NIHSS, 18), EDR was achieved by 69 (53.9%) patients. Demographics, risk factors, and process time variables between patients with and without EDR were similar. Patients with EDR had greater rate of successful (TICI 2b/3) reperfusion (88.4 vs. 45.8%; p = 0.00) and smaller baseline infarcts (median 8.9mL vs, 15.4mL; p = 0.02). The stroke etiology was more often cardioembolic in patients with EDR (60.9 vs. 37.3%; p = 0.01). In multivariable analyses, successful reperfusion (OR, 11.77 (95%CI, 4.20-32.98)), smaller baseline infarct volume (OR, 0.97 (95%CI, 0.95-0.99)), and cardioembolic stroke etiology (OR, 2.65 (95%CI, 1.08-6.46)) were independent predictors of EDR.
Conclusion
EDR was achieved by >50% of ischemic stroke patients after EVT and was associated with baseline infarct size and reperfusion grade. Patients with cardioembolic stroke were more likely to achieve immediate response to EVT. Future studies on the association between ischemic stroke subtype and outcome after EVT are needed.
Trial registration number
N/A
AS06-029
BOTH CT PERFUSION AND NON-CONTRAST CT MAY OVERESTIMATE ISCHAEMIC CORE IN THE EARLY PHASE
1St.Georges University Hospitals NHS foundation Trust, Stroke, London, United Kingdom
Background and Aims
Mechanical thrombectomy (MT) is superior to best medical treatment in patients presenting with acute ischaemic stroke. Most benefit is seen in patients with a small infarct core. Non-Contrast CT (NCCT) is widely used in clinical practice to predict infarct core utilizing The Alberta Stroke Programmed Early CT score (ASPECTS). Although CT perfusion (CTP) is valued for demonstrating ischaemic mis-match, there is controversy as to whether CTP can accurately predict ischaemic core.
Method
We present two patients with ischaemic stroke who presented early following large vessel occlusion. Both patients had NCCT and CTP within 90 minutes from symptom onset to evaluate ischaemic core and mis-match. Both received thrombolysis and MT treatment within 120 minutes from symptom onset. They had neuroimaging (NCCT or MRI) and repeat NIHSS 24 hours post MT treatment.
Results
Both patients had severe stroke syndromes with initial NIHSS of 16 and 20. Both NCCT and CTP demonstrated ischaemic core, with CT angiogram confirmed large vessel occlusion. However follow up imaging at 24 hours showed no acute ischemic changes, with excellent clinical recovery, NIHSS 1 and 0.
Conclusion
Our cases show that both NCCT and CTP may overestimate ischemic core in the early phase from symptom onset. This observation is important to be aware of and could otherwise result in appropriate patients being denied mechanical thrombectomy.
Trial registration number
N/A
AS06-030
A PILOT RANDOMIZED SUB-STUDY OF PATIENTS WITH TANDEM CAROTID OCCLUSION UNDERGOING ENDOVASCULAR THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE IN THE ENDOVASCULAR ACUTE STROKE INTERVENTION (EASI) TRIAL
1Centre Hospitalier de l'Université de Montréal, Neurosciences, Montreal, Canada
2Centre Hospitalier de l'Université de Montréal, Radiologie, Montreal, Canada
Background and Aims
Tandem occlusion refers to stroke due to middle cerebral artery or distal internal carotid artery (ICA) AND a steno-occlusive lesion of the ipsilateral cervical ICA. Optimal acute management of the cervical ICA lesion in patients undergoing endovascular therapy (EVT) for their intracranial occlusion remains uncertain and may include no definitive revascularization or acute stenting.
Method
The EASI (Endovascular Acute Stroke Intervention) trial was a pragmatic, single-centre RCT conducted between 2013 and 2015 comparing EVT versus best medical therapy for patients with stroke due to proximal intracranial occlusion.
Patients assigned to EVT underwent a second randomization when a tandem lesion was identified, allocating them to acute ICA stenting or not. Stenting before or after thrombectomy and antiplatelet regimen were left to the discretion of the treating team. The primary outcome was the proportion of patients with modified Rankin Scale (mRS) score of 0–2 at 90 days.
Results
Of 138 patients, 16 (11.6%) with a tandem lesion were randomized: 9 to acute stenting and 7 to no stenting. Baseline characteristics were similar in both groups. The proportion of patients with a favourable outcome (mRS 0–2) at 90 days was not statistically different (n = 5, 55.6% stenting vs n = 3, 42.9% no stenting, p = 1.0) but very poor outcomes (mRS 5–6) were more frequent in the no stenting group (n = 0, 0% vs n = 4, 57.1%, p = 0.019).
Conclusion
Our pilot trial of patients with tandem occlusion undergoing EVT demonstrates that such a study is feasible. Results are hypothesis-generating and will inform a larger RCT of ICA management in this population.
Trial registration number
NCT02157532
AS06-032
MANAGEMENT OF PATIENTS WITH TANDEM CAROTID OCCLUSION UNDERGOING ENDOVASCULAR THROMBECTOMY FOR ANTERIOR CIRCULATION STROKE: AN INTERNATIONAL SURVEY OF STROKE PHYSICIANS
1Centre Hospitalier de l'Université de Montréal, Medicine, Montreal, Canada
2Université de Montréal, Neurosciences, Montréal, Canada
3Centre de recherche du CHUM, Axe Neurosciences, Montréal, Canada
4Centre Hospitalier de l'Université de Montréal, Radiology, Montreal, Canada
Background and Aims
“Tandem occlusion” refers to an acute occlusion of the middle cerebral artery and/or distal internal carotid artery (ICA) with concurrent steno-occlusive disease of the ipsilateral cervical ICA. In stroke due to tandem occlusion, the benefit of acute stenting of the cervical ICA lesion during the intracranial thrombectomy procedure is uncertain.
Method
We distributed an online survey to stroke physicians and neuro-interventionalists affiliated with the Canadian Stroke Consortium, the Canadian Interventional Neuro Group, the Society of Vascular and Interventional Neurology and international ESCAPE trial collaborators to determine current practice patterns and whether community equipoise existed. Questions were based on clinical scenarios and multiple-choice questions across a Likert-type scale were provided. The survey was sent out in Fall of 2017. After two months, data were extracted and then analyzed using descriptive statistics.
Results
Responses from 162 stroke experts, primarily stroke physicians (40,1%) and interventionalists (45,7%), from Canada (58,6%), the United States (25,9%) and other countries (15,4%) were analyzed. Overall, 31.5% of respondents perform acute stenting of the cervical ICA either occasionally, usually or routinely versus 68.5% who never or almost never stent. The majority of respondents (52% Yes, 23% No, 23% uncertain) agree that there exists equipoise regarding the optimal acute management of the cervical ICA lesion for these patients and 58% would agree to randomize such patients in a trial.
Conclusion
Our international survey suggests variability in practice and the existence of community equipoise which justifies a randomized clinical trial evaluating the use of acute ICA stenting in patients with tandem occlusion undergoing thrombectomy.
Trial registration number
N/A
AS06-033
IMPACT OF THE IMPLEMENTATION OF A MULTIDISCIPLINAR STROKE CODE PROTOCOL FOR PEDIATRIC ISCHEMIC STROKE ON STROKE AWARENESS AND REPERFUSION THERAPIES IN A TERTIARY HOSPITAL
1University Hospital La Paz, Paediatric Intensive Care Unit, Madrid, Spain
2University Hospital La Paz, Neuropaediatry, Madrid, Spain
3University Hospital La Paz, Paediatric Emergency, Madrid, Spain
4University Hospital La Paz, Paediatry, Madrid, Spain
5University Hospital La Paz, Paediatric Haematology, Madrid, Spain
6University Hospital La Paz, Paediatric Anestesiology, Madrid, Spain
7University Hospital La Paz, Neurosurgery, Madrid, Spain
8University Hospital La Paz, Neuroradiology, Madrid, Spain
9University Hospital La Paz, Paediatric Rehabilitation, Madrid, Spain
10University Hospital La Paz, Quality, Madrid, Spain
11University Hospital La Paz, Paediatric Cardiology, Madrid, Spain
12University Hospital La Paz. Madrid Autonoma University. IdiPAZ Health Research Institute, Neurology and Stroke Center, Madrid, Spain
Background and Aims
Our aim is to evaluate the impact of the implementation of a multidisciplinary protocol for the treatment of paediatric acute ischemic stroke (IS) in a tertiary hospital on the awareness of stroke, times to neuroimaging, rates of recanalization therapies and outcomes.
Method
Observational study with retrospective analysis of children who suffered an IS prior (2011-2014) and prospective data collection after the implementation of a paediatric stroke code protocol (2014-2017). We describe time to neuroimaging, final diagnosis, rates of recanalization therapies (intravenous thrombolysis (IVT) or mechanical thrombectomy (MT)), and outcomes at 3 months (modified Rankin Scale, mRS).
Results
Twelve children aged 2–16 years were diagnosed with IS. Prior the paediatric stroke code protocol implementation, stroke were initially suspected only in 2 out of 5 patients with final diagnosis of stroke and both of them were treated with recanalization therapies (one IVT and one MT). After the protocol implementation, 7 children were diagnosed with IS and 3 received recanalization therapies (one IVT and three MT). Median door to neuroimaging time was reduced from 156 (IQR 27-165) to 44 (IQR 43;127) minutes after the protocol implementation. All the children suffering IS in both periods survived and had favorable outcome at three months (mRS 0–2).
Conclusion
After the implementation of the paediatric stroke code protocol in a experienced stroke center, we observed an increase in the awareness of stroke in childhood, with reduction in door to neuroimaging times, albeit the rates of recanalization therapies remained stable at 40% of the children.
Trial registration number
N/A
AS06-034
FIRST RESULTS OF MECHANICAL THROMBECTOMY IN CLINICAL CENTER OF VOJVODINA SERBIA
1Clinical Center of Vojvodina, Emergency Center, Novi Sad, Serbia
2Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia
3Clinical Center of Vojvodina, Radiology, Novi Sad, Serbia
Background and Aims
Mechanical thrombectomy (MT) is now well-established treatment method for selected patients with acute ischemic stroke (AIS) and efforts are being made to incorporate it into the systems of stroke care, reserved for large vessel occlusion anterior circulation. We presented our results in the first year of performing this method.
Method
From November 2016. to December 2017. 17 patients with ischemic stroke in Clinical Centre of Vojvodina, Novi Sad, Serbia were treated with MT, combined with iv - TPA or MT only, using the Penumbra system or Solitaire Stent Retriever. Potential eligibility for MT were evaluated using recommendations from consensus ESO - Karolinska. We compared our results with 3 randomized trials (MR CLEAN, EXTEND-IA and SWIFT PRIME), because of similar study protocol.
Results
10 males (58%) and 7 (42%) females, mean age 62 years, were enrolled in the study, with initial NIHSS 14. Dominant vascular risk factors were hypertension (92%), smoking (50%), atrial fibrillation and dyslipidemia (42%), diabetes (25%). Our Onset To Puncure time (OTP) was 246 minutes while Symptom to Reperfusion time (SOR) was longer than compared to other trials, 312 min. In half of our patients, the target mRS 0–2 was reached in first 90 days. Spontaneous intracerebral haemorrhage was seen in our patients (17%) and mortality (25%) and its significantly higher than in comparative trials.
Conclusion
Our results are not significantly different from the results of comparative trials. Beside better selection of patients and improving operators skills, shortening of time frame for successful thrombectomy is remaining our main goal.
Trial registration number
N/A
AS06-035
IMPACT OF EXTRA-HOSPITALARY STROKE CODE IN PARAGUAY. A PILOT STUDY
1Hospital de Clínicas, Stroke Unit. Neurology Department., San Lorenzo, Paraguay
Background and Aims
Prehospital stroke code (PSC) activation has shown a relevant benefit in stroke patients, reducing pre and in-hospital delays, and directing stroke patients to the adequate centers. In Paraguay, data about reperfusion treatment is not widely known. Recently, a pilot PSC program was implemented in the country. Our aim was to determine the impact of PSC on several outcomes
Method
Observational, single center study. Data collected from a prospective registry, from April 2015 to November 2017. PSC was implemented in November 2016. In reperfusion stroke patients, baseline characteristics, reperfusion timings, and functional outcomes were evaluated between PSC and non-PSC patients.
Results
From 634 stroke patients admitted in the study period, 149 (23.5%) were stroke code. Of them, 32 (21.4%) were PSC, forty received e.v. tPA and one Endovascular Treatment.
The number of stroke code has been increasing through the years (2015: 37, 2016: 50, 2017: 60). From the overall of reperfusion patients treated, the proportion through the years was as follow; 2015:20.5%, 2016:28.2%, 2017:51.2%
No differences in baseline characteristics and functional outcomes between PSC and Non-PSC were found. However, PSC patients had a significant lower mean Door to CT time (mean time 17 Vs. 45min. p = 0.020) and mean door to needle time (mean time 41 vs. 84min. p = 0.006) than non-PSC.
Conclusion
PSC has a positive impact in acute stroke management, reducing delays and increasing the rates of reperfusion treatments. An expanded implementation of PSC in the entire country would lead to spread its benefits nationawide.
Trial registration number
N/A
AS06-036
STROKE SEVERITY VERSUS TIME TO DYSPHAGIA SCREEN AS RISK FACTOR FOR POST-STROKE PNEUMONIA
1Monash Health, Neurosciences, Clayton, Australia
Background and Aims
Aspiration pneumonia is a feared complication of stroke as it is associated with higher mortality and disability. Patients are often kept Nil By Mouth (NBM) until after dysphagia screen and declared safe to resume oral intake. An attractive hypothesis is that pneumonia post stroke is related to immunosuppression and stroke severity. In this study the aim is to assess the proportional contribution of the variables and pneumonia
Method
This is a retrospective study of admissions in 2015. We collected data on demographic variables, admission diagnoses, time to dysphagia screen, and stroke severity. Variables found to be associated with pneumonia (p < 0.1) were entered into hierarchical partition analysis to determine the proportion contribution of each variable. Additionally, this method avoid collinearity (relatedness) among the variables.
Results
Over 12-month period in 2015, there were 795 admissions and 627 patients with ischemic and hemorrhagic stroke (age 71.2 ± 15.4, National of Health Institute Stroke Score/NIHSS 7.6 ± 7.8, male=55.4%). The frequency of pneumonia was 5.4%, week day admission was 43.7% and NBM status was 72.8%. The regression analyses were restricted to 452 patients with reliable time of dysphagia screen. Univariable analyses show stroke severity, time to dysphagia screen, Charlson comorbidity score and age to be significantly associated with pneumonia. Week day versus weekend admission was not associated with pneumonia. The hierarchical partition analysis showed that stroke severity accounted for (76.2%), charlson (11.6%), age (7.9%) and time to dysphagia screen (4.2%)
Conclusion
Stroke severity status play key role in determining risk for post stroke pneumonia in this retrospective study.
Trial registration number
NA
AS06-037
2 YEARS FOLLOW UP OF TANDEM OCCLUSION ACUTE ISCHEMIC STROKES TREATED BY MECHANICAL THROMBECTOMY WITHOUT EXTRA-CRANIAL STENTING
1Besançon University Hospital, Neurology, Besançon, France
2Besançon University Hospital, Neuroradiology, Besançon, France
Background and Aims
Mechanical thrombectomy (MT) is indicated for acute ischemic stroke caused by intracranial occlusion associated with extra-cranial occlusion or sub-occlusion (tandem occlusion). Therefore, very few tandem occlusions were included in the first MT trials and the best type of procedure for these occlusions is not yet known, although widely debated.
Method
All patients who presented with acute ischemic stroke and benefited from an MT in CHRU Besançon between January 1st 2015 and December 31st 2016 were included. They were followed by the Besançon Stroke Registry who collected modified Rankin Scale results at three months. Recurrence and endarterectomy procedures were collected between 15th January and 20th January 2018 by phone call (or medical file when there was no answer).
Results
During the period of inclusion, 27 patients presented with tandem occlusion. Concerning internal carotid artery (ICA) occlusion, the same procedure was performed for every patient: passing through ICA occlusion by guide only or with the help of an angioplasty balloon, then intra-cranial recanalization by aspiration or stent retriever. No ICA stenting was performed. Twenty-six percent had a 0–2 mRS at three months. Three patients had undergone endarterectomy, in a mean time of 286 days after stroke. In January 2018, no patient had had stroke recurrence; median follow-up was 23 months.
Conclusion
Recanalization of intracranial occlusion without ICA stenting at the hyperacute phase seems to be safe at two years. Acute stroke presenting with tandem ICA occlusion must be followed on a long-term basis, since very little evidence-based recommendations exist in hyperacute management.
Trial registration number
N/A
AS06-038
QUALITY OF STROKE CARE IN SLOVAKIA
1Faculty of Medicine- Pavol Jozef Safarik University and University Hospital L. Pasteur- Kosice, Department of Neurology, Kosice, Slovak Republic
2Faculty Hospital Nitra- Slovakia, Department of neurology, Nitra, Slovak Republic
3General Hospital FORLIFE, Department of Neurology, Komarno, Slovak Republic
4Faculty Hospital Skalica, Department of Neurology, Skalica, Slovak Republic
5Hospital Rožňava, Department of Neurology, Rožňava, Slovak Republic
6Faculty Hospital Trnava, Department of Neurology, Trnava, Slovak Republic
7Hospital Galanta - ProCare, Department of Neurology, Galanta, Slovak Republic
8Hospital Brezno, Department of Neurology, Brezno, Slovak Republic
9General Hospital Levoča, Department of Neurology, Levoča, Slovak Republic
10Faculty of Medicine- Comenius University and University Hospital Bratsilava, I. Department of Neurology, Bratislava, Slovak Republic
11Faculty of Medicine- Comenius University and University Hospital Bratsilava, II. Department of Neurology, Bratislava, Slovak Republic
12National Health Information Center Bratislava, National registers, Bratislava, Slovak Republic
13Kepler University Clinic- Linz, Department of Neurology 2- ESO-EAST Steering Committee, Linz, Austria
Background and Aims
Intravenous thrombolysis (IVT) and endovascular treatment (EVT) significantly improve the outcome for ischaemic stroke (IS), but the results also depends on time. Quality control is therefore very important.
Method
We analysed the data from National stroke registry ( which is mandatory for all stroke centers in Slovakia) in March 2017 to evaluate the quality parameters. In the same time data from Registry of Stroke Care Quality in ESO EAST countries were analysed.
Results
In 36 stroke centers 1108 patients were hospitalized, 987 with brain ischaemia (844 stroke, 143 – TIA) and 117 with brain haemorrhage. The rate of acute treatment in IS (IVT, EVT, IVT+EVT) was 16,9% (IVT – 14,8 %, EVT – 3,3%). Door-to-needle time (DNT) £ 20 minutes was in 31,1% of patients, 21-45 min. in 22,2%, 46-60 min. in 14,4% and Ëf60 min. in 32,3% of patients. According SITS registry DNT in 2017 in Slovakia was 37 minutes, what is shorter than in 2016 (47 min.) and 2015 (50 min.). Of 730 patients with IS without AF 641 (88%) were discharged with antiplatelet agents, and of 217 patients with IS and AF 66,7% were discharged with anticoagulant treatment (Warfarin, NOAK), 8,5 % without antithrombotics, and 25,8% on LMWH.
Conclusion
Our goal is to meet even better ESO quality criteria, therefore the Slovak stroke society in collaboration with Ministry of Health at the end of 2017 prepared new guidelines, set up a network of primary and secondary stroke centers and improved collaboration with rescue services.
Trial registration number
N/A
AS06-039
AUDIT ON CT ANGIOGRAM AS INITIAL SCREENING FOR THROMBECTOMY IN PATIETNS PRESENTED WITH ACUTE ISCHEMIC STROKE
1St George's Hospital, Neuroscience Department, London, United Kingdom
Background and Aims
Mechanical thrombectomy (MT) is superior to medical management in stroke patients due to large vessel occlusion (LVO). Emergency screening with CT angiogram (CTA) is required to identify patients with LVO that may be suitable for MT. This audit aimed to assess what proportion of patients admitted to our unit within 6 hours of ictus had CTA, and how many ultimately proceeded for MT.
Method
Using data from Sentinel Stroke National Audit Programme (SSNAP), we identified all local patients admitted to our Hyperacute Stroke Unit (HASU) with an ischemic stroke diagnosis between September and October 2017. For those presenting within 6 hours of ictus, initial stroke imaging modalities and treatment received were reviewed. If CTA was not performed, medical records were reviewed.
Results
120 patients with confirmed ischemic stroke were identified. 87 (72.5%) presented within 6 hours of ictus. 62/87 (71%) had CTA, the remaining 25 did not have CTA as part of their initial stroke imaging as they were deemed unsuitable for MT: 10 patients had MRS>3; 6 had established infarct on initial CT scan; 5 had low National Institute of Health Stroke Scale (NIHSS) scores; 2 had improved significantly (NIHSS 0); 1 had a terminal cancer; 1 patient’s initial presentation was not clearly identified as stroke. 11 had MT. 1 patient presenting at 8 hours from last seen well, proceeded to MT.
Conclusion
This audit demonstrated that all potentially eligible acute stroke patients had CTA screening for MT. Overall, 10% of our acute ischemic stroke admissions proceeded to mechanical thrombectomy.
Trial registration number
N/A
AS06-040
REMOTE ISCHEMIC PERCONDITIONING AMONG ACUTE ISCHEMIC STROKE PATIENTS IN CATALONIA: REMOTE-CAT PROJECT
1Hospital Universitari Arnau de Vilanova de Lleida, Stroke Unit, Lleida, Spain
2Generalitat de Catalunya, Pla Director de les Malalties Cerebrovasculars, Barcelona, Spain
3Institut de Recerca Biomèdica de Lleida IRBLleida, Clinical Neuroscience, Lleida, Spain
4Hospital Universitari de Bellvitge, Stroke Unit, Bellvitge, Spain
5Generalitat de Catalunya, Servei d'Emergències Mèdiques, Barcelona, Spain
6Hospital de la Santa Creu i Sant Pau, Stroke Unit, Barcelona, Spain
7Hospital Universitari Vall d'Hebron, Stroke Unit, Barcelona, Spain
8Institut de Recerca Biomèdica de Lleida IRBLleida, NUTREN–Nutrigenomics Center, Lleida, Spain
9Hospital del Mar, Stroke Unit, Barcelona, Spain
10Hospital Universitari Vall d'Hebron, Radiology department, Barcelona, Spain
11Institut de Recerca Biomèdica de Lleida IRBLleida, Biostatistics Unit, Lleida, Spain
Background and Aims
Remote ischemic conditioning (RIC), consisting of brief episodes of transient limb ischemia, represents a new paradigm in neuroprotection with interesting results in ischemic heart disease patients. We aim to conduct a multicentre study of pre-hospital RIC application in acute ischemic stroke (AIS) patients.
Method
Adults diagnosed of suspected clinical stroke within 8 hours of symptom onset and clinical deficit >0 according to RACE prehospital scale will be randomized 1:1 to RIC or sham. Patients will be stratified by RACE score scale. RIC will be started in the ambulance before hospital admission. RIC will consist of five cycles of electronic tourniquet inflation and deflation (5 min each). To detect a treatment difference of 14% in the outcome, 286 patients will be included for 5% significance and 80% power.
Results
The primary outcome will be the difference in clinical benefit measured by the modified Rankin Scale (mRS) score <3 at 90 days. Secondary outcomes to be monitored will include early neurological improvement rate, treatment related serious adverse event rates, size of the infarct volume, symptomatic intracranial hemorrhage, and metabolomic and lipidomic response to RIC.
Conclusion
Neuroprotective therapies could not only increase the benefits of available reperfusion therapies among AIS patients but also provide an option for patients who are not candidates for these treatments. REMOTE-CAT will investigate the clinical benefit of RIC as a new neuroprotective strategy in AIS.
Trial registration number
ClinicalTrials.gov number: NCT03375762
AS06-042
IS THE “DRIP AND SHIP" THE BEST OPTION FOR PATIENTS ELIGIBLE FOR MECHANICAL THROMBECTOMY IN ALGARVE?
1Centro Hospitalar e Universitário do Algarve, Serviço de Neurologia, Faro, Portugal
2University of Algarve, Biomedical Sciences Department, Faro, Portugal
Background and Aims
Thrombectomy is indicated in acute internal carotid artery occlusion (AICAO). “Drip and ship” or “mothership” are possible strategies to offer thrombectomy in areas without a center capable of thrombectomy (CCoT). The Rapid Arterial oClusion Evaluation (RACE) scale has high specificity for large vessel occlusion. In patients with RACE ≥5,“mothership” to a CCoT is indicated. We aimed to quantify the missed opportunities for mechanical thrombectomy of AICAO in Algarve (280 km apart/3hours by ambulance) from the nearest CCoT.
Method
Retrospective application of the RACE scale in patients with AICAO(June/2015-December/2017) from a region, where “drip and ship” is the implemented strategy. Delay time from patient location at stroke onset to the hospital and to the nearest CCoT was calculated.
Results
We identified 65 patients with AICAO; 45(69,2%) were males; mean age 69 years. Twelve (18,4%) were wake up strokes; 22(33,8%) presented with ≥6 hours of evolution; 30(46,2%) ≤6 hours of onset. All patients (n = 30) who presented ≤ 6 hours of onset had RACE score ≥ 5; a minority of them (4/13,3%) received mechanical thrombectomy. The mean time from patient location to CCoT was 2 hours 38 minutes. The excepted time from patient location to CCoT was ≤6 hours in 27/30(90%) if direct transportation would have been considered, implying additional 23 thrombectomies.
Conclusion
In Algarve, the application of the RACE scale to aid the decision to transport directly to a CCoT would potentially increase the number of patients who undergo thrombectomy. Further studies, taking in consideration the implementation of the scale by first responders as also the costs are needed.
Trial registration number
N/A
AS06-043
DECISION-MAKING COMPETENCE IN PATIENTS WITH ACUTE ISCHEMIC STROKE ELIGIBLE FOR ENDOVASCULAR TREATMENT – IMPLICATIONS FOR FUTURE TRIALS
1Erasmus MC University Medical Centre, Department of Neurology, Rotterdam, The Netherlands
2Erasmus MC University Medical Centre, Department of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
3Erasmus MC University Medical Centre, Department of Public Health, Rotterdam, The Netherlands
4Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
5University Medical Center Utrecht, Neurology and Neurosurgery- Brain Center Rudolf Magnus, Utrecht, The Netherlands
6Maastricht University Medical Center, Department of Radiology, Maastricht, The Netherlands
Background and Aims
Informed consent from acute ischemic stroke patients in person is often required for participation in endovascular treatment (EVT) trials. We aimed to assess decision-making competence in these patients.
Method
We used data from the MR CLEAN Registry (n = 1,628), a Dutch prospective registry of consecutive stroke patients undergoing EVT. We included adult patients with anterior large vessel occlusion treated between March 2014 and June 2016. We predefined which scores on the individual items of the National Institutes of Health Stroke Scale (NIHSS) on admission indicate decision-making incompetence. Primary outcomes were the proportion of patients who were decision-making incompetent and the distribution of individual NIHSS items indicating decision-making incompetence.
Results
Decision-making incompetence was determined in 1,469 of 1,526 (96%) patients. Highest frequencies of predefined scores on the individual NIHSS items indicating decision-making incompetence were ‘Level of Consciousness Questions’ (59%), ‘Best Gaze’ (68%), and ‘Best Language’ (58%) (Figure). Patients who were determined incompetent were older (median 71 vs 66 years, p = 0.043), had higher NIHSS scores (median 16 vs 8, p < 0.001), more often left hemisphere strokes (55% vs 28%, p < 0.001), more proximal arterial occlusions (p = 0.021), lower collateral grade (p = 0.038), and lower ASPECTS (p = 0.001) than patients not scoring any NIHSS items indicating decision-making incompetence.
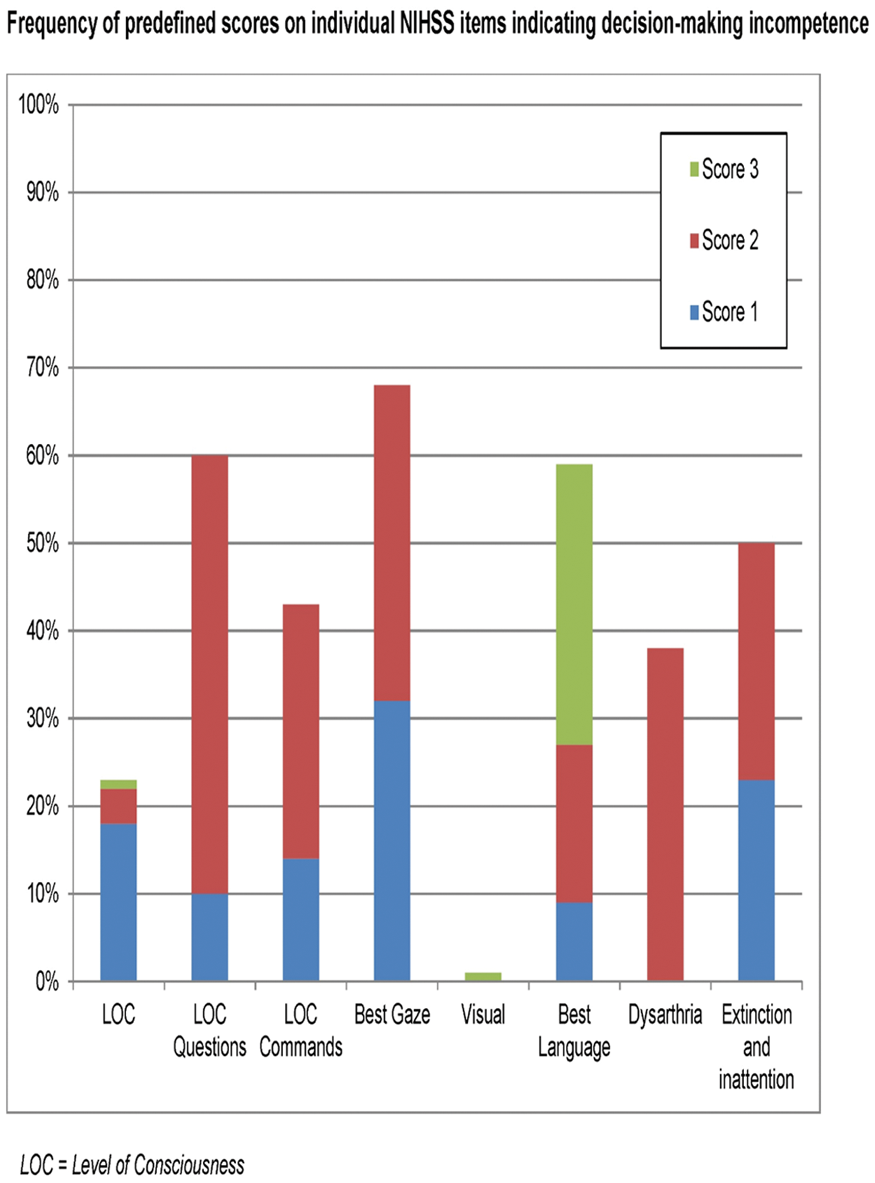
Conclusion
Obtaining personal informed consent for participation in an EVT trial is impossible in 96% of acute stroke patients due to decision-making incompetence.
Trial registration number
N/A
AS06-044
CASE SERIES ON USE OF HYPNOTHERAPY WITH IMAGERY IN PATIENTS PRESENTING WITH FUNCTIONAL STROKE
1University Hospital of North Midland NHS Trust, Stroke Medicine, Stoke on Trent, United Kingdom
2University Hospital of North Midlands NHS Trust, Stroke Medicine, Stoke on Trent, United Kingdom
Background and Aims
5 - 10% of patients presenting with acute stroke are considered to be functional. There are two randomised controlled trial published of use of hypnotherapy in functional neurological disorder, of which one was positive and another negative. This is a case series of patients treated with hypnotherapy for functional stroke symptoms.
Method
Successive patients with a clinical diagnosis of functional stroke supported by normal MRI imaging were offered hypnotherapy. Each treatment session lasted about 60 minutes and was provided by was provided by a single stroke physician trained in the technique.
Results
62 patients were included in the case series. The female: male ratio was 48:14 and the mean (range) NIHSS score was 6 (1- 9). The primary presentation in 53 out of 62 was weakness of the limbs. 33 had a right and 20 a left hemiparesis. The primary presentation in others were severe dysarthria, ataxia, sensory impairment, facial weakness and homonymous hemianopia. 1 out of 62 patients could not be hypnotized. 56 out of 61 patients responded with complete resolution of their symptoms (NIHSS 0). 5 out of 61 responded partially. 47 out of 56 patients who responded to hypnotherapy received one session, rest needed two or more sessions (maximum 5 sessions) for resolution of symptoms. All 55 responding patients were contacted by phone up to 6 months, 50 remained well without recurrence. 5 patients developed new symptoms, which responded to a repeat hypnotherapy treatment.
Conclusion
In this case series, hypnotherapy was successful with rapid and sustained recovery of symptoms.
Trial registration number
N/A
AS06-045
ENDOVASCULAR TREATMENT OF PATIENTS WITH ANEURYSM SUBARACHONOID HEMORRHAGE AND POOR CLINICAL STATUS: EPIDEMIOLOGIC, PROGNOSIS AND COMPLICATIONS ANALYSIS
1Hospital Universitario Central de Asturias, Radiology- Neuroradiology, Oviedo, Spain
2Hospital Universitario Central de Asturias, Radiology, Oviedo, Spain
3Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
4Hospital Universitario Central de Asturias, Intensive Care Unit, Oviedo, Spain
5Hospital Universitario Central de Asturias, Neurosurgery, Oviedo, Spain
Background and Aims
Ruptured aneurysm is the most frequent cause of nontraumatic subarachnoid hemorrhage (SAH). Prognosis depends on clinical status at admission, aneurysm closure success and early solution of complications. There are some papers showing doubts in treating poor clinical status patients, putting forward a bad outcome (mRS>2) rate. In our institution, all these patients are embolized within 24 hours from symptoms onset, supported by a significant clinical benefit outcome percentage.
Method
Patients with aneurysm SAH from 2009 and 2012 admitted at our institution were reviewed. This sums 158 patients, 118 good (group 1) and 40 bad (group 2) clinical status. We analyzed the relationship in both groups with risk factors, aneurysm features, clinical status outcome (mRS), mortality, embolization and postprocedural complications, and mortality.
Results
Group 2 reached higher mortality (17.5%) and worst independence rate (60% mRS>2) respect to group 1 (5.1% of mortality, mRS>2 in 20.3%).
Conclusion
Even though the results described, 40% of patients with poor clinical status were discharged with good independence ranking (mRS<2) in our study. Literature has shown 67%-100% mortality in patients with aneurysm SAH without treatment. This supports our idea to embolize poor clinical status patients. Main factors related to good and poor clinical status are Fisher scale and hydrocephalus at diagnosis CT.
According to our study, a significant percentage of patients with aneurysm SAH and poor clinical status, may obtain prognostic benefit by prompt aneurysm embolization.
Trial registration number
N/A
AS06-046
EARLY SURGICAL MANAGEMENT FOR ACUTE ISCHEMIC STROKE
1Wonkwang University Hospital, Neurosurgery, Iksan, Republic of Korea
Background and Aims
The disappointed results of the Cooperative study further tempered enthusiasm for revasculariztion surgery. There remain a subset of patients who might benefit from surgery but who are not appropriate candidates for medical therapy and endovascular recanalization in ischemic stroke due to intracranial major artery occlusion.
Method
Surgery was given to patients with acute or evolving stroke, or ongoing symptoms despite best medical therapy, and to patients harboring marked hemodynamic impairment. The outcome was evaluated in patients who were treated with early surgery (Group1; microsurgical embolectomy 20, Group 2; STA-MCA bypass 23).
Results
Symptom recurrence occurred during medical treatment in 8 patients and progressive symptoms in the others. Mean time between the onset of symptoms and embolectomy was 6 hours (range 5–10). Bypass was done within 1 week (mean; 2.3 days) after stroke onset. Surgery prevented further stroke recurrence and progression (p < 0.01). Good outcome (mRS ≤3) of Group 1 and 2 were achieved by 15 and 17 patients, respectively. Four patients died (3 brain swelling and 1 cardiac problem).
Conclusion
Surgical revasculariztion, which might be a powerful alternative to mechanical thrombectomy and an ultimate effective therapeutic option in adequately selected cases with interdisciplinary interaction, should be performed rapidly and actively because of narrow time window in patients with recurrent or progressive stroke who are ineligible or failed for mechanical thrombectomy.
Trial registration number
N/A
AS06-048
STREAMLINING INTERDISCIPLINARY COMMUNICATION TO IMPROVE SUSPECTED ACUTE STROKE ASSESSMENT, DIAGNOSIS AND TREATMENT TIMES: PRELIMINARY RESULTS FOR A SMARTPHONE COMMUNICATION APP
1The Florey Institute of Neuroscience and Mental Health, Stroke, Melbourne, Australia
2Monash University, Department of Medicine- School of Clinical Sciences at Monash Health, Monash, Australia
3Ambulance Victoria, Centre for Research and Evaluation, Doncaster, Australia
4Monash University, Epidemiology and Preventive Medicine, Monash, Australia
5Monash University, School of Epidemiology and Preventive Medicine, Monash, Australia
6Bendigo Health Care Group, Bendigo Base Hospital, Bendigo, Australia
7Ballarat Health Services, Ballarat Base Hospital, Ballarat, Australia
8Ambulance Victoria, Loddon Mallee Region, Bendigo, Australia
9The University of Melbourne, Faculty of Medicine- Dentistry and Health Sciences, Melbourne, Australia
10Ambulance Victoria, Grampians Region, Bendigo, Australia
Background and Aims
Rapid assessment, diagnosis and treatment for patients with acute stroke events requires communication between in-field paramedics and multiple hospital clinicians (emergency, medical, neurology, radiology). Treatment delays may occur with information repeated between the interdisciplinary team from different organisations/hospital departments.
Aim
To determine if a smartphone communication app can improve clinical care timelines for patients with suspected acute stroke.
Results
There were 262 patients (no Pulsara™/Pulsara™: n = 81/n=185, both median 75 years, 52%/48% male) with Pulsara™ initiated by paramedics (n = 115) and Emergency Departments (n = 70). Faster paramedic hospital-arrival-to-departure by median 10 minutes (no Pulsara™: 55 minutes [IQR: 43-64]; Pulsara™ 45 minutes [IQR: 35-55]). Faster emergency department door-to-first medical review time by median 18 minutes (no Pulsara™: 23 minutes [IQR: 6–65]; Pulsara™ 5 minutes [IQR: 1–11]) and faster door-to-CT completed by median 51 minutes (no Pulsara™: 81 minutes [IQR: 39-145]; Pulsara™: 27 minutes [IQR: 17-42]). All thrombolysis cases used Pulsara™ (n = 38).
Conclusion
Preliminary evidence supports improved care timelines. Pulsara™ was successfully implemented for the first time outside of America.
Trial registration number
N/A
AS06-049
PREVALENCE OF HIGH ON-TREATMENT PLATELET REACTIVITY AFTER CLOPIDOGREL ADMINISTRATIONM IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Zealand University Hospital- University of Copenhagen, Neurology, Roskilde, Denmark
2Rigshospitalet- University og Copenhagen, Clinical biochemistry, Glostrup, Denmark
Background and Aims
Background
Early anti-platelet therapy is a cornerstone in the prevention of recurrent ischaemic stroke (IS) and transient ischaemic attacks (TIAs) Responsiveness to anti-platelet medications varies among patients. Several studies have reported that patients with ischaemic stroke who exhibit high on-treatment platelet reactivity (HTPR) have an increased risk of vascular events.
Aim
To determine the prevalence of HTPR after the administration of a 300 mg bolus of oral clopidogrel in the acute phase after IS or TIA (<48 h after symptom onset) in a real-world setting.
Methods
In total, 219 clopidogrel naïve patients with IS or TIA received 300 mg of oral clopidogrel on admission. Blood samples from all patients were analysed using the VerifyNow P2Y12 system at 8–24 h after clopidogrel intake. HTPR was defines as Platelet Reaction Units (PRU) >208. Concomitant therapy and the intervals between ictus and blood collection, clopidogrel intake and blood collection, and blood sampling and analysis were recorded for all patients.
Results
HTPR was observed in 28.8% (63/219) samples. After adjustment for age, sex, co-morbidities, and co-medications, none of the tested variables exhibited an association with HTPR or the PRU-value.
Conclusions
The recognition of HTPR to specific anti-platelet agents in the acute phase after stroke may be the first step towards interventions that may further minimize the early recurrent stroke risk. Further large randomized trials including clinical outcome assessments are necessary.
Trial registration number
clinicaltrials.gov number: NCT02607358
AS06-051
DOOR TO GROIN TIME IN PATIENTS WITH ACUTE ISCHEMIC STROKE PRESENTING DURING ON- VS OFF-HOURS, RESULTS FROM THE MR CLEAN REGISTRY
1Maastricht University Medical Center, Neurology, Utrecht, The Netherlands
2Sint Antonius Hospital, Radiology, Nieuwegein, The Netherlands
3Haaglanden Medical Center, Radiology, The Hague, The Netherlands
4Haaglanden Medical Center, Neurology, The Hague, The Netherlands
5Sint Antonius Hospital, Neurology, Nieuwegein, The Netherlands
Background and Aims
A large proportion of patients with acute ischemic stroke receiving endovascular treatment for large vessel occlusion (LVO) present during evenings, nights, weekends or holidays. As team availability might be reduced during off-hours, treatment times might be longer, leading to a lower chance of good functional outcome. The aim of this study is to compare workflow times and functional outcome between patients presenting during on- and off-hours.
Method
We analyzed data from the MR CLEAN Registry, a prospective, multicenter, observational study in the Netherlands and included patients with an anterior circulation LVO between March 2014 and June 2016. Off-hours were defined as Monday to Friday between 17:00 and 08:00, weekends (Friday 17:00 to Monday 8:00) and Dutch National holidays. Primary endpoint was door to groin time (DTGT), secondary outcome was functional outcome (modified Rankin Scale (mRS) at 90 days). We stratified for transfer status and used linear and ordinal regression models.
Results
1488 patients were included of which 959 (64%) presented during off-hours . Corrected DTGT was 14.3 minutes (95% CI: 8.0 – 20.6) longer during off-hours. After stratification only direct referrals had a significant delay of 20.2 minutes (95% CI: 12.0 – 28.5). The delay for transfers was 6.5 minutes (95% CI: -3.3 – 16.3). The off-hour delay did not influence functional outcome (aOR 0.92; 95% CI: 0.74 – 1.14).
Conclusion
Patients treated with EVT during off-hours because of anterior circulation LVO have a longer DTGT which is more pronounced in direct referrals. This delay does not seem to influence functional outcome.
Trial registration number
N/A
AS06-052
CONSENT PROCEDURES AND RELATIONSHIP WITH OUTCOME IN THE RAPID INTERVENTION WITH GLYCERYL TRINITRATE IN HYPERTENSIVE STROKE TRIAL-2 (RIGHT-2)
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Obtaining consent in emergency situations is challenging. Proxy consent allows patients to be recruited when they lack capacity, a common scenario in stroke patients. The rapid intervention with glyceryl trinitrate in hypertensive stroke trial-2 (RIGHT-2) recruits patients in the pre-hospital setting within 4 hours of stroke onset.
Method
In RIGHT-2, informed or proxy consent is taken in the ambulance. A brief assessment of capacity is performed by the paramedic. Patients with capacity provide consent and in patients without capacity, proxy consent is obtained from a relative, carer or friend, or by the paramedic, witnessed by a crew member.
Results
Of 879 participants enrolled into RIGHT-2 as of 15th December 2017, 468 (53.2%) participants gave their own consent; proxy consent was given by a relative/carer/friend for 325 (37%) and by a paramedic for 85 (9.7%). Participants who consented themselves were younger, had less dependency and had less severe strokes than those with proxy consent. Participants who gave their own consent had a lower rate of intracerebral haemorrhage (9% vs 16%) and a higher rate of non-stroke (20% vs 13%) as their final diagnosis than those who gave proxy consent. Consenting patients had better scores for dependency, cognition, disability and quality of life at day 90 than those recruited via proxy consent.
Conclusion
Proxy consent can ensure participants are enrolled rapidly into emergency clinical trials where they may otherwise be excluded due to lack of capacity. These patients have more severe strokes and therefore poorer clinical outcomes.
Trial registration number
The RIGHT-2 trial is registered: ISRCTN26986053
AS06-053
ENDOVASCULAR THROMBECTOMY (EVT) FOR STROKE: EXPERIENCE IN A CANADIAN TEACHING HOSPITAL
1Queen Elizabeth II Health Sciences Centre, Medicine, Halifax, Canada
2Queen Elizabeth II Health Sciences Centre, Diagnostic Imaging, Halifax, Canada
Background and Aims
EVT is now recommended as standard of care in several countries, including Canada. However, implementing EVT in routine practice poses many challenges. We studied the delivery of EVT at our hospital, which serves the province of Nova Scotia (a mixed urban-rural population of about 980,000).
Method
All patients who underwent EVT December 2011 - December 2016 were identified from our prospective registry. Demographics, process measures, imaging characteristics (Alberta Stroke Program Early CT Score [ASPECTS], collateral score, Thrombolysis in Cerebral Infarction [TICI] score), and outcome (modified Rankin score [mRS] approximately 90 days post-EVT) were derived from the registry, and from review of imaging studies and hospital records. Effectiveness was assessed by comparison with patients receiving EVT in the ESCAPE trial.
Results
Ninety-one patients (M:F = 48:43, mean age 64 years; range 39-91) presented to hospital after a mean of 194 min ± 230 min (median=97 min) from last seen normal. In 58%, the ASPECTS was >7, and 80% had good/intermediate collaterals. Alteplase was administered to 72% (75% in ESCAPE, p = 0.97). Retrievable stents only were used. EVT mean duration was 70 min ± 62 min (median = 58 min). Successful recanalization (≥TICI 2b) was achieved in 76% (vs 72.4% in ESCAPE, p = 0.97). Among 54 of 70 patients in whom recanalization was achieved, mRS scores of 0–2, 3–5 and 6 were seen in 57.4, 24.1 and 14.8% respectively; ESCAPE comparators 53, 37 and 10%, p = 0.96, 0.86 and 0.91.
Conclusion
EVT at our hospital yielded results similar to those achieved in the ESCAPE trial.
Trial registration number
N/A
AS06-054
COMPUTER MODELING OF MCA TRUNK AND BRANCH OCCLUSION- IMPORTANCE OF LEPTOMENINGEAL ANASTOMOSES OVER CIRCLE OF WILLIS
1Monash Health, Neurosciences, Clayton, Australia
2Monash University, Medicine- Central Clinical School, Frankston, Australia
3CSIRO, Data61, Melbourne, Australia
Background and Aims
The role of the Circle of Willis (CoW) in salvaging flow in the major vessels (internal carotid [ICA], anterior [Acom] and posterior communicating [Pcom]and basilar artery) has been emphasized over the leptomeningeal anastomoses (LA). We developed a computational model of the cerebral circulation to 1) evaluate the roles of the CoW and LA in restoring flow (>30% of baseline) to the superficial compartment of the middle cerebral artery territory (MCA) under simulated occlusion.
Method
Cerebral vasculature was modelled as a network of pipes with laminar flow along the pipes. The experiments included occlusion of successive distal branches of the MCA while the diameters of LA (0.5-1.5 mm) and circle of Willis (CoW) were varied.
Results
The full results are available at https://gntem3.shinyapps.io/mcasim/. The model showed that the region of reduced flow became progressively smaller as the site of occlusion was moved from the large proximal to the smaller distal arteries. The diameter of the inter-territorial LA needed to be greater than 1.0 mm in order to provide adequate (>30%) flow to selected arteries in the occluded MCA territory. Changing CoW configurations (such as absent proximal ACA (A1), absent proximal PCA (P1) or absent Acom) do not impact flow.
Conclusion
Inter-territorial LA play important supportive roles in simulated occlusion of MCA. Computational modelling provides the ability to experimentally investigate the effect of arterial occlusion on CoW and LA function.
Trial registration number
NA
AS06-055
ENDOVASCULAR THERAPY OF ISCHEMIC STROKE BEYOND THERAPEUTIC TIME WINDOW
1Hospital Clinico San Carlos, Neurology, Madrid, Spain
2Hospital Clinico San Carlos, Radiology, Madrid, Spain
Background and Aims
Endovascular therapy (ET) along with the best medical treatment has been shown as the most effective therapy for ischemic stroke associated with large-vessel occlusion in the first 6 hours since onset. Recently, evidence that supports its effectiveness in image-selected patients between 6 and 24 hours has been published. Our aim is to analyse our series of patients treated with ET beyond the 6-hour therapeutic window
Method
We conducted a retrospective, descriptive study of patients treated with ET in our tertiary referral hospital between January 2010 and December 2017. The inclusion criteria were: occlusion of a large vessel in the anterior circulation, time of clinical evolution (baseline to femoral puncture) greater than 6 hours. We excluded patients whose last baseline situation was beyond 6 hours when the symptoms were objectified. Baseline characteristics, periprocedural complications and functional outcome at 3 months were analyzed
Results
54 patients (55.5% women) with a mean age of 69 years (IQR 56-78) were included. The median time of clinical evolution was 414 minutes (IQR 390-501). Baseline ASPECT median was 8 (IQR 6–8). The median of NIHSS was 18 (IQR 13-22). 22 patients (40,7%) had been previously treated with alteplase (within its therapeutic window). Symptomatic hemorrhage occurred in 7 cases (13%). 6 patients died (11%). 25 patients had a mRS score ≤ 2 at 3 months (48%)
Conclusion
Our study suggests that in selected patients, with favourable basal neuroimaging despite a prolonged evolution time, endovascular therapy could be beneficial even beyond 6 hours from last baseline situation
Trial registration number
N/A
AS06-056
FEASIBILITY OF JUGULAR BULB VENOUS MONITORING IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Ajou university school of medicine, Department of Neurology, Suwon, Republic of Korea
2Ajou university school of medicine, Department of Emergency Medicine, Suwon, Republic of Korea
Background and Aims
Jugular bulb venous monitoring can provide information about cerebral hemodynamics and metabolism. We investigated the feasibility and clinical application of jugular bulb venous monitoring in acute ischemic stroke patients at neurocritical care unit.
Method
From March 2015 to June 2017, we conducted jugular bulb venous monitoring in 33 patients. Five patients were excluded. Venous catheters were placed in internal jugular vein by ultrasound-guided method. Lactate, venous oxygen saturation (SjvO2), and arteriovenous oxygen saturation differnece (AVDO2) were monitored every 4 hours. Metabolic derangement was defined when lactate was more than 2.0 mmol/l. Patients were divided according to presence of clinical deterioration. For long-term prognosis, modified Rankin Scale 5–6 at 3 months were defined as poor outcome.
Results
Twelve patients (42.9%) showed metabolic derangement and experienced more frequent clinical deteriorations than patients without metabolic derangement (n = 9, 64.3% vs. n = 3, 21.4%, p = 0.022). Clinical deterioration was noted in 14 patients, and lactate level was significantly higher (1.44 ± 0.48 vs. 1.04 ± 0.20mmol/l, p = 0.009). Adjusting other potential variables, metabolic derangement was an independent factor associated with clinical deterioration (OR 6.60, 95% CI 1.23-35.44, p = 0.028). Meanwhile, poor outcome group (n = 12) showed no difference on lactate level, but AVDO2 were higher in poor outcome group (29.54 ± 5.51 v. 24.95 ± 5.65, p = 0.041). AVDO2 remained an independent factor for poor outcome after adjusting other factors (OR 3.68, 95% CI 1.08-12.55, p = 0.038).
Conclusion
This study showed that lactate was associated with clinical deterioration, whereas venous desaturation contributed to long-term prognosis. Jugular bulb venous monitoring is a feasible tool in patients with acute ischemic stroke at neurocritical care unit.
Trial registration number
N/A
AS06-058
PREDICTORS OF ENDOVASCULAR TREATMENT AMONG STROKE CODES ACTIVATED WITHIN 6 HOURS FROM SYMPTOM ONSET
1Hospital Universitari Vall d'Hebron, Department of Neurology, Barcelona, Spain
2Hospital Germans Trias i Pujol, Stroke Unit, Barcelona, Spain
3Agència d’Avaluació de Tecnologia i Recerca Mèdiques, Pla Director Malalties Aparell Circulatori/ Malaltia Vascular Cerebral, Barcelona, Spain
4Hospital Universitari Bellvitge, Stroke Unit, Barcelona, Spain
5Hospital Universitari Clinic Barcelona, Stroke Unit, Barcelona, Spain
6Hospital Universitari Vall d'Hebron, Stroke Unit, Barcelona, Spain
Background and Aims
Prehospital stroke code activations reduce wokflow times. We aim to identify predictors of endovascular treatment among activated stroke codes (ASC) within 6 hours from symptom onset.
Method
CICAT is a prospective official mandatory registry of all ASC in Catalunya. We studied all entries from 5 comprehensive stroke centers during 18 months. We recorded demographic, clinical and imaging variables on admission. We explored the relationship between these variables and endovascular treatment (EVT).
Results
From 3944 ASC, 2778 (70.4%) were admitted <6 hours from symptom onset. Mean age was 72 ± 15.3 years, median RACE scale 4 (IQR 2–6), median onset-to-door-time (OTDT) 89 minutes (IQR 54-158), median NIHSS 9 (IQR 4–18), median ASPECTS 10 (IQR 8–10). Final diagnosis was ischemic stroke in 1762 patients (63.4%), with confirmed large vessel occlusion (LVO) in 720 (25.6%); hemorrhagic stroke in 359 (13.0%); TIA in 164 (5.9%), stroke-mimic in 493 (17.7%).
EVT was received by 444 patients (16% of all ACS, 61% of all LVO, 45.4% of ACS with RACE >4). Baseline variables associated with EVT were premorbid mRS <2 (p < 0.01), prehospital RACE >4 (p < 0.01) and admission NIHSS >8 (p < 0.01).
While the rate of ASPECTS =10 progressively decreased over time (p < 0.01), rate of ASPECTS ≥6 did not decrease within 6 hours after the onset (0–3h: 95.1% Vs 3–6h: 94.0%: p = 0.245).
Conclusion
Within 6 hours from onset only 5% of patients showed an ASPECTS <6, and this rate did not significantly increase over time. These data may be useful to generate direct transfer to angio-suite protocols.
Trial registration number
N/A
AS06-059
EVALUATING THE EFFICACY AND SAFETY OF THE CAROTID CASPER-RX STENT IN MECHANICAL THROMBECTOMY FOR ACUTE ISCHEMIC STROKE
1CHUV - Lausanne University Hospital, Diagnostic and Interventional Radiology, Lausanne, Switzerland
2Inselspital - Bern University Hospital, Diagnostic and Interventional Neuroradiology, Bern, Switzerland
3CHUV - Lausanne University Hospital, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
Background and Aims
A new generation of carotid artery stents that uses a dual micromesh layer to reduce embolic events during carotid artery stenting has recently been introduced. We aim to analyze the efficacy and safety of the new CASPER-RX stent in patients experiencing acute ischemic stroke with large vessel intracranial occlusion associated with a tandem lesion (i.e. including a carotid occlusion or severe stenosis).
Method
All consecutive patients treated with carotid CASPER-RX stents were retrospectively analyzed from our stroke registry. Clinical, angiographic and neuroimaging data were analyzed. Endpoints included acute intra-stent thrombus formation, stent occlusion prior to hospital discharge, 3-month modified Rankin score (mRs) and in-hospital symptomatic intracranial hemorrhage.
Results
Twenty-one patients were included of whom ten had tandem and eleven had a haemodynamically significant stenosis. Acute intra-stent thrombus formation occured in 11 patients and required peri-procedural intravenous infusion of anticoagulants and antiplatelets. No stent occlusion occurred prior to hospital discharge. No stroke recurrence was reported at 3 months. Symptomatic intracranial hemorrhage was reported in two patients. MRs at 3 months was 0–2 (favorable) in 15 patients (71%), 3–5 in three patients and 6 in three patients.
Conclusion
In our consecutive series of acute carotid stenting in tandem lesions using the CASPER-RX stent, clot formation during the procedure was frequent. Unless a randomized controlled study demonstrate the non-inferiority of micromesh dual-layer compared to single-layer stents, such devices may not be considered safe in this setting.
Trial registration number
N/A
AS06-060
ENDOVASCULAR TREATMENT IN PATIENTS WITH PREVIOUS DISABILITY
1Hospital Universitari Bellvitge, Neurology, L'Hospitalet de Llobregat, Spain
2Hospital Universitari Bellvitge, Radiology, L'Hospitalet de Llobregat, Spain
Background and Aims
Good functional results after the use of endovascular treatment in ischemic stroke are mainly based on the correct selection of the patient. Criteria such as age > 80 years, onset time unknown or baseline with moderate established core are no longer exclusion criteria for its indication. However, patients with a baseline functional situation of mRS > 1 are not always treated.
Method
We analyzed 766 patients treated in our hospital by thrombectomy between August 2010 and June 2017. We compared the patients treated with baseline mRS 0–1 vs 2–3 before the stroke (65 patients), their epidemiological differences, functional prognosis, hemorrhagic complications and mortality.
Results
There are certain epidemiological differences between the group of Rankin 2–3 regarding Rankin 0–1 (mean age 73+/-8 vs 67+/-7 years, tandem or basilar occlusion 17% vs 25%. Patients with baseline Rankin 2–3 did not present significant differences in TICI 2b-3 recanalization rate than those with Rankin 0–1 (72% vs 75%), with a similar rate of symptomatic hemorrhage (7.5% vs. 6, 4%). In the baseline Rankin 2–3 group the recovery was 33% in the 90days follow-up whereas 32% in those of Rankin 0–1 baseline. Mortality was significantly different in 90 days after stroke, higher in the baseline Rankin group 2–3 (32% vs 16%).
Conclusion
In patients with moderate baseline disability endovascular therapy can be equally effective with a low rate of bleeding complications. The recovery of the baseline functional situation at the third month is similar, however those who do not achieve it have a higher mortality rate.
Trial registration number
N/A
AS06-062
ESTIMATING BODYWEIGHT FOR THROMBOLYSIS IN ACUTE ISCHAEMIC STROKE
1Addenbrooke's hospital, stroke unit, Cambridge, United Kingdom
Background and Aims
Alteplase dosing for patients with acute ischaemic stroke (AIS) is based on bodyweight. In order to facilitate timely thrombolysis at our hospital, bodyweight is estimated. This study aimed to assess whether there is a difference between the actual and estimated weights of patients receiving thrombolysis for AIS.
Method
We reviewed 300 consecutive patient records who underwent thrombolysis for AIS between November 2014 and November 2017. Estimated and actual weight along with admission and post-thrombolysis NIHSS and mRS were collected. Records were excluded where complete data was not obtainable (n = 67).
Results
The mean estimated and actual weights were 74.5kg and 74.3kg respectively (s.d. 14.3; 15.3). There was a good correlation between the estimated and actual weights (r = 0.82) and no statistically significant difference (Wilcoxon signed rank test, p-value = 0.86). The mean difference in weights was -0.21kg (actual - estimated; s.d. 8.95kg). There was no correlation between the difference in weight between methods and the change in NIHSS score at 24 hours (r = −0.04) or change in mRS on discharge (r = −0.13). Bland-Altman analysis demonstrates good agreement between the measurements (Fig.1).
Conclusion
From this data we conclude that estimating bodyweight is sufficient; there is no significant difference between the estimated and actual bodyweight. There are also no meaningful effect on outcome.
Trial registration number
N/A
AS06-066
KAIZEN METHODOLOGY (LEAN HEALTHCARE) APPLIED TO CODE STROKE IN URGENT HOSPITAL CARE
1Hospital Moises Broggi, Neurology Department, Sant Joan Despi, Spain
2Hospital Moises Broggi, Lean Methodology Referent, Sant Joan Despi, Spain
3Hospital Moises Broggi, Intensive Medical Service, Sant Joan Despi, Spain
4Hospital Moises Broggi, Radiology Department, Sant Joan Despi, Spain
5Hospital Moises Broggi, Emergency Department, Sant Joan Despi, Spain
6Hospital Moises Broggi, Planning and Patient Safety Director, Sant Joan Despi, Spain
Background and Aims
Moisès Broggi Hospital is a local reference center for acute stroke patients in Catalonia. Initial door-to-needle (DTN) time was 54 minutes with high variability. We aimed, using Kaizen methodology, to improve DTN time and variability in our center.
Method
Kaizen tool was used as a part of the Lean Healthcare management system. A leader, a methodological reference and a working team gathering representative of different professionals involved in the multidisciplinary approach to code stroke attention were established. A simulation of the attention to a code stroke was recorded and all the process was divided into several small activities. Afterwards, activities were analyzed as to: who should take part, which tools should be applied and minimum necessary time involved. We analyzed which activities could become external and how to optimize the activities that necessarily had to be internal, done from the ‘door' to the ‘needle'. Finally, the procedure was standardized, and presented to the Internal Committee for approval. This was followed by training to all the professionals involved.
Results
The new protocol was implemented in December, 2016. To date, we have reduced the DTN time from 54 to 33 minutes and lowered the variability by 70% (from 63.7 to 19.1 minutes).
Conclusion
Objectifying and quantifying the different components of the circuit from an external methodological perspective made it possible to identify activities that do not add value, that are poorly located or that are not standardized, and agree on a new way of acting that improves the quality of care for patients.
Trial registration number
N/A
AS06-072
CEREBRAL ISCHEMIA IN PATIENTS ON NON-VITAMIN-K-DEPENDENT ORAL ANTICOAGULANTS: THROUGH PLASMA-LEVELS ON ADMISSION ARE ASSOCIATED WITH STROKE SEVERITY
1University Hospital Erlangen, Neurology, Erlangen, Germany
Background and Aims
The severity and clinical course of stroke in patients on Non-Vitamin-K-dependent oral anticoagulants (NOAC) might be affected by the quality of anticoagulation at the time of stroke onset, but clinical data are limited.
Method
Data from our prospective observational registry including all patients admitted with acute cerebral ischemia while taking oral anticoagulants between November 2014 and October 2017 were investigated. Functional through plasma-levels were measured in NOAC-patients using the calibrated Xa-activity (Apixaban, Rivaroxaban, Edoxaban) or the Hemoclot-essay (Dabigatran). The activity of anticoagulation was categorized into low (<50ng/ml), intermediate (50-100ng/ml), or high (>100ng/ml) and its association with clinical and imaging characteristics as well as functional outcome were investigated.
Results
Of 234 patients treated with NOAC on admission, functional through plasma-levels were available in 177 subjects (75.6%). Plasma-levels were found to be low in 49 (27.7%), intermediate in 41 (23.2%), and high in 87 patients (49.2%). Patient groups were similar for relevant demographic parameters. Patients with low plasma-levels had significantly higher scores on the NIHSS on admission (median 8 (IQR 3–15) vs. 4 (1–11) vs. 3 (0–8); p = 0.005) and had a higher risk of persisting neurologic deficits or cerebral infarction on imaging. In addition, occlusion of a large cerebral vessel was more frequent with low plasma-levels (23(46.9%) vs. 9(22.0%) vs. 13(14.9%); p < 0.001). Functional outcome after three month was not different.
Conclusion
Through plasma-levels of NOAC on admission are associated with stroke severity and the risk for large vessel occlusion. Measuring the quality of anticoagulation might be of therapeutic and prognostic relevance.
Trial registration number
N/A
AS06-073
MULTICENTER, RETROSPECTIVE ANALYSIS OF ENDOVASCULAR TREATMENT (EVT) IN NONAGENARIANS WITH ACUTE ISCHEMIC STROKE (AIS): ELIGIBILITY, OUTCOME AND SAFETY
1AZ Sint-Jan Brugge-Oostende av, Neurology, Bruges, Belgium
2Centre Hospitalier Universitaire Vaudois, Neurology, Lausanne, Switzerland
3AZ Groeninge, Radiology, Kortrijk, Belgium
4AZ Sint-Jan Brugge-Oostende av, Radiology, Bruges, Belgium
5Cliniques Universitaires Saint-Luc, Neurology, Brussel, Belgium
6Cliniques Universitaires Saint-Luc, Radiology, Brussel, Belgium
7University Hospital Leuven, Neurology, Leuven, Belgium
8University Hospital Leuven, Radiology, Leuven, Belgium
9Antwerp University Hospital, Neurology, Edegem, Belgium
10Antwerp University Hospital, Radiology, Edegem, Belgium
11University of Leuven campus Kortrijk, Public Health and Primary Care, Kortrijk, Belgium
12AZ Groeninge, Neurology, Kortrijk, Belgium
Background and Aims
With increasing age of AIS patients being admitted to hospitals, more data are needed on indications, complications and outcome of EVT.
Method
Patients with AIS ≥90 years old, treated with EVT alone or bridged with IV thrombolysis, and follow-up data available at 7 and 90 days. Safety assessment: peri-procedural complications, hemorrhagic transformation (SITS-MOST classification), other adverse events. Efficacy and outcome: successful recanalization (TICI 2b-3), 3-months mortality, favorable outcome (Modified Rankin Score (mRS) 0–2).
Results
43 nonagenarians were included (median 92 years; 77% women; median premorbid mRS = 2). Main occlusion sites: carotid-T, M1 and basilar artery in 23, 51 and 7%, correlating with high NIHSS on admission (median=18; IQR 10-24). Bridging with IV thrombolysis was performed in 72% (n = 31). In 76,1% (n = 32) patients, successful recanalization was achieved. In 19% (n = 8) EVT was unsuccessful due to vascular anatomy or clinical evolution. At 3 months, mortality rate was 63 % and favorable outcome 15%.
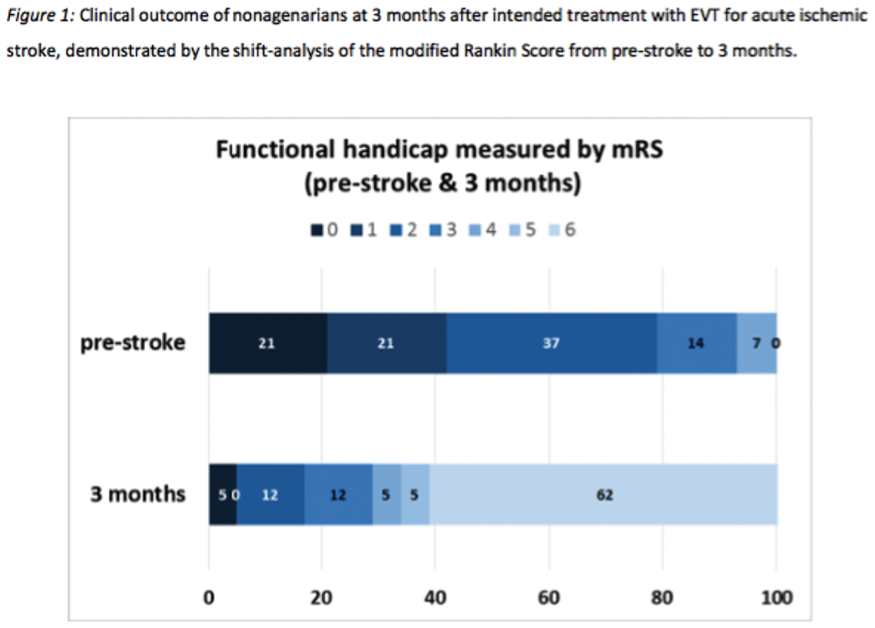
Conclusion
This study shows a substantially poor outcome of AIS in nonagenarians, even when treated with EVT, indicating the need to be strict in patient selection. A high pre-stroke mRS probably contributes to the unfavorable outcome and may be a reason to deter from EVT. More data on potential outcome predictors for EVT in this population are needed, in planned research data will be compared to non-EVT nonagenarians and younger groups.
Trial registration number
N/A
AS06-074
PATIENT VERSUS PROXY CONSENT IN RELATION TO STROKE SEVERITY AND FUNCTIONAL OUTCOME IN THE MR CLEAN TRIAL
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Erasmus MC University Medical Center, Neurology, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Radiology and Nuclear Medicine, Rotterdam, The Netherlands
4Erasmus MC University Medical Center, Public Health, Rotterdam, The Netherlands
5University Medical Center Utrecht, Brain Center Rudolf Magnus- Neurology, Utrecht, The Netherlands
6Erasmus MC University Medical Center, Intensive Care Adults, Rotterdam, The Netherlands
7Academic Medical Center, Radiology, Amsterdam, The Netherlands
8Maastricht University Medical Center, Radiology, Maastricht, The Netherlands
9Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
Background and Aims
The way informed consent is obtained for participation in randomized clinical trials of acute stroke treatment may influence patient selection and therefore the generalizability of trial results. We aimed to determine whether patient versus proxy consent is associated with baseline stroke severity and 90-day functional outcome in stroke patients eligible for endovascular treatment (EVT).
Method
MR CLEAN was a randomized trial of EVT versus no EVT. Written informed consent was obtained from all patients before randomization. We compared characteristics of patients enrolled with patient versus proxy consent. With ordinal logistic regression, we assessed the association of proxy consent with 90-day functional outcome (modified Rankin Scale).
Results
Data on type of consent were available for 395 of 500 enrolled patients (79%), of whom 331 (84%) were enrolled with proxy consent. These patients were older (median 66 versus 62, p = 0.025), had a higher median National Institutes of Health Stroke Scale score (18 versus 14, p < 0.001), more left hemisphere strokes (58% versus 25%, p < 0.001) and lower collateral grade (p = 0.018) than those providing consent themselves. Proxy consent was associated with worse functional outcome (common odds ratio 0.39, 95% confidence interval 0.23-0.62).
Conclusion
Informed consent was provided by proxy for the majority of patients enrolled in the MR CLEAN trial. These patients had more severe strokes and a worse functional outcome. Excluding patients who cannot provide consent themselves will affect the generalizability of trial results.
Trial registration number
Trial registrations: NTR1804 [Netherlands Trial Register] and ISRCTN10888758
AS06-075
SECONDARY TRANSFER FOR THROMBECTOMY: WHICH FACTORS MODIFY THE OUTCOME OF PATIENTS ? RESULTS OF A PROSPECTIVE OBSERVATIONAL STUDY IN A NETWORK OF BELGIAN HOSPITALS
1Centre Hospitalier Chrétien, Neurology- Comprehensive Stroke Center, LIEGE, Belgium
2University of Liège, Psychology & Neuroscience of Cognition – PsyNCogn, Liège, Belgium
3Centre Hospitalier Chrétien, Interventional Neuroradiology, LIEGE, Belgium
4Centre Hospitalier Chrétien, Neuroradiology, LIEGE, Belgium
5Centre Hospitalier de Huy, Neurology, Huy, Belgium
6Klinik St-Josef, Neurology, St Vith, Belgium
7Centre Hospitalier du Bois de l'Abbaye et de Hesbaye, Neurology, Seraing, Belgium
Background and Aims
Thrombectomy is effective in the management of acute stroke. It is not kown if patients benefit more from early thrombolysis at the closest of the nonendovascular capable Primary Stroke Centers (PSC) before transportation to the Comprehensive Stroke Centers (CSC) or if it is better to bypass the PSC.
Method
We reviewed 140 consecutive acute stroke patients treated by thrombectomy . The network is composed of 9 PSC located at a distance from 2.2 to 83 km from the CSC. We considered 10 predictive factors: age, diabetes, hypertension, NIHSS on admission, transfer, delay between stroke onset to emergency admission, iv thrombolysis before thrombectomy, delay between symptoms and device deployment, groin insertion to recanalization time and number of passes to recanalization.
Results
We observed a reduction of 32 minutes between stroke onset and recanalization for patients who bypass the PSC (CSC = 209 min, PSC = 241 min; p = 0.03). The outcomes at discharge or during the follow-up did not significantly differ between groups (p = 0.36 for mRS and p = 0.34 for NIHSS). Multiple linear regression and logistic regression analysis revealed that iv thrombolysis before thrombectomy was the only factors improving the functional prognosis (mRS) of the patients at discharge (p = 0.02) and during the follow-up (p = 0.01).
Conclusion
In a network of PSC far of less than 100 kilometers from the CSC, despite a significant delay of recanalization, we did not observe a significant effect of transfer on the outcomes. The only predictive factor of good prognosis was iv thrombolysis performed before thrombectomy.
Trial registration number
N/A
AS06-077
DIFFUSION-WEIGHTED ASPECTS AS A FUNCTIONAL OUTCOME PREDICTOR IN PATIENTS WITH ACUTE ISCHEMIC STROKE TREATED WITH ENDOVASCULAR THERAPY UP TO 24 HOURS
1ENERI, Buenos Aires, Capital Federal, Argentina
Background and Aims
In acute ischemic stroke patients Diffusion-weighted ASPECTS is correlated with infarct volume and also is an independent factor of functional outcome. Our aim is to assess the impact of pre-treatment Diffusion-weighted ASPECTS on outcomes after endovascular treatment (EVT) within 24 hs.
Method
Patients aged 18-80 years with acute ischemic stroke with large vessel occlusion from anterior circulation eligible for EVT within 24 hours were included in this descriptive, monocentric, ambispective study between 2015 and 2017.
Vascular neurologists and neurorradiologist measured ASPECTS on DWI according to the method by Barber et al. Diffusion-weighted ASPECTS were grouped in ≥ 6 (Group A) or < 6 (Group B).
The primary outcome measured was a modified Rankin scale (mRs) ≤ 2 at 90 days. Secondary outcomes included a successful reperfusion, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) scale 2b/3, mortality rate at 90 days and symptomatic intracranial hemorrhage (SIH).
Results
We included 83 patients, 56 in Group A and 27 in Group B. Demographics data, risk factors, SIH and successful reperfusion did not show significant differences.
The rate of mRS ≤ 2 at 90 days was 69,6% in Group A as compared with 27% in Group B (P = 0.0006 OR = 5.4 IC = 1.9-14.8), the rate of mortality was 3,6% Group A while in Group B was 19% (P = 0,022 OR = 0.16 IC = 0.02-0.90).
Conclusion
Diffusion-weighted ASPECTS ≥ 6 seems to be a good parameter predicting favorable outcome among patients treated by EVT within 24 hs.
Trial registration number
N/A
AS06-078
THE RELIABILITY OF PREHOSPITAL DIAGNOSIS OF STROKE OR TRANSIENT ISCHEMIC ATTACK
1Institute of Psychiatry and Neurology, 2nd Department of Neurology, Warsaw, Poland
2Medical University of Warsaw, 2nd Faculty of Medicine, Warsaw, Poland
3Institute of Psychiatry and Neurology, 1st Department of Neurology, Warsaw, Poland
4Medical University of Warsaw, Department of Experimental and Clinical Pharmacology, Warsaw, Poland
Background and Aims
Early and correct suspicion of acute cerebrovascular accident (CVA) is necessary for shortening time to reperfusion treatment. Our aim was to evaluate the reliability of prehospital diagnosis of stroke or transient ischemic attack made by healthcare professionals referring patients directly to a neurological Emergency Department (ED).
Method
This retrospective analysis included all consecutive patients referred between January 2014 and December 2014 by ambulance physicians, paramedics or outpatient physicians to a neurological ED providing care for the population of 300–350 thousand inhabitants of a highly urbanized area. We calculated sensitivity and positive predictive value (PPV) with 95% confidence intervals (95%CI) for each group of healthcare professionals and compared the proportions of undetected CVAs.
Results
During the study period there were 690 patients with confirmed CVAs, including 639 formally referred by healthcare professionals. The highest sensitivity for detection of any CVA was observed among ambulance physicians (96%, 95%CI: 92-98%), followed by paramedics (85%, 95%CI: 80-90%, p < 0.001) and then outpatient physicians (74%, 95%CI: 70-79%, p < 0.001). PPV for stroke was 83% (95%CI: 77-87%) among ambulance physicians, 73% (95%CI: 65-80%) among paramedics and 56% (95%CI: 47-64%) among outpatient physicians.
Conclusion
Ambulance physicians are highly sensitive in diagnosing any CVA. However, the their prehospital diagnosis of stroke was correct in 8 of 10 cases, and only in 7 of 10 cases if made by paramedics, which indicates the necessity of two-way communication between ambulance and the stroke team before arrival at the ED. Suboptimal sensitivity urges additional training for paramedics and primary care physicians.
Trial registration number
N/A
AS06-080
INFARCTS CORE VOLUME MEASURE BY DIFFUSION-WEIGHTED IN ACUTE ISCHEMIC STROKE AS A PREDICTOR OF FUNCTIONAL OUTCOME AFTER ENDOVASCULAR TREATMENT
1ENERI, Buenos Aires, Capital Federal, Argentina
Background and Aims
Patients who have large cerebral infarctions may not be good candidates for endovascular treatment.
Evaluate the core volume measured on diffusion-weighted as a functional predictor in large vessel occlusion (LVO) strokes of the anterior circulation submitted to endovascular treatment (EVT) within 24 hours.
Method
Patients aged 18-80 years with acute ischemic stroke with LVO of the anterior circulation eligible for EVT within 24 hours were included in this descriptive, monocentric, ambispective study between 2015-2017.
Core volume was manually calculated by vascular neurologist and neurorradiologist separately using Osirix MD 7.5. Core volumes were grouped in ≤50 ml (Group A) or >50 ml (Group B)
The primary outcome measured was a modified Rankin scale (mRs) ≤2 at 90 days. Secondary outcomes included a successful reperfusion, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) scale 2b/3, mortality rate at 90 days and symptomatic intracranial hemorrhage (SIH).
Results
We included 82 patients, 54 in Group A and 28 in Group B. Demographics data and successful reperfusion did not show significant differences.
The rate of mRS ≤2 at 90 days was 68% in Group A as compared with 28.6% in Group B (P = 0.0006 OR = 5.44 IC = 1.99-14.8), SIH in Group A was 1,8% and in Group B was 17,8% (P = 0,016 OR = 0.08 IC = 0.009-0.785), there was no mortality in Group A while in Group B was 25% (P = 0,001 OR = 0).
Conclusion
The core volume measures in diffusion-weighted ≤50 ml in LVO strokes of the anterior circulation treated within 24 hours with EVT had a strong association with better outcomes at 90 days.
Trial registration number
N/A
AS06-081
“USING SMARTPHONES TO DELIVER THE RIGHT CARE AT THE RIGHT TIME AT THE RIGHT PLACE”
1Salford Royal Foundation Trust, Greater Manchester Stroke Operational Delivery Network Coordinator & Paramedic, Salford, United Kingdom
2Salford Royal Foundation Trust & University of Manchester, Clinician Scientist & Honorary Consultant Neurologist, Salford, United Kingdom
Background and Aims
Acute stroke patients benefit from rapid treatment and specialist care at Hyper Acute Stroke Units (HASUs). In areas with a centralised model of care, patients with suspected stroke are taken by ambulance to HASUs, often bypassing their local hospital. Three HASUs serve the population of Greater Manchester (GM) between 06:45-22:45 with one remaining open overnight. The pathway is further complicated by pathway exclusions, intended to divert unstable patients to the nearest hospital. To aid pathway compliance, we developed and piloted a smartphone app to support pathway decision-making.
Method
The “Pre Hospital Pathway Aid” (PHPA) application is designed to support all pre-hospital pathways but initial development and testing has focused on the GM Stroke Pathway. A beta version was provided to 74 paramedics that volunteered to test the app. User feedback was collected within the app and a survey will be undertaken on pilot completion.
Results
Between 17/07/17 and 19/09/17, 44 registered users actively used the live app on 74 separate occasions. 32/74 (43%) diversions to the nearest hospital were prompted. The pathway aid prompted these diversions for reasons such as a negative FAST test, onset >48 hours ago or the presence of a pathway exclusion.
Conclusion
Our pilot data suggest the PHPA app may improve pathway compliance, though the clinical effectiveness of the app cannot yet be determined by our pilot data. We plan to make our app available to all GM pre-hospital clinicians, and will evaluate the clinical effects of this through a ‘before and after study’ using routinely collected HASU data.
Trial registration number
n/a
AS06-082
EFFECT OF MOBILE STROKE UNIT (MSU) CARE IN ACUTE ISCHEMIC STROKE PATIENTS WITH LARGE ARTERY OCCLUSION
1CSB Berlin, University Hospital Charité, Berlin, Germany
2Pineo Medical Ecosystem, Department of Neurology, Tbilisi, Georgia
3Sainte Anne Hospital- Paris Descartes University- INSERM U894, Neurology Department, Paris, France
Background and Aims
Benefits of endovascular therapy in acute ischemic stroke (AIS) patients with large artery occlusion (LAO) are strongly time-dependent. By allowing pre-hospital CT angiography (CTA), prehospital care by Mobile Stroke Units (MSU) have the potential of triaging patients with LAO to stroke centers with endovascular treatment facility providing pre-notification of endovascular teams and therefore reducing time to reperfusion.
Method
We reviewed data of consecutive patients treated by endovascular therapy for AIS with LAO in Charité hospitals, Berlin between February 2013 and May 2017. The primary endpoint was the time of ambulance dispatch-to-groin puncture. Other endpoints included dispatch-to-arterial imaging time and stroke onset-to-groin puncture time.
Results
A total of 354 AIS patients were evaluated, of whom 12 received MSU care with on-board CTA. There was statistically non-significant trend for MSU patients with on-board CTA to have shorter median dispatch-to-groin puncture time compared with other patients (138 [IQR 131-162] min and 160 [132-187] min, respectively, P = 0.19). Median dispatch-to-arterial imaging time and stroke onset-to-groin puncture time were also shorter for MSU compared to standard care (33 [IQR 27-38] min and 57 [48-69] min, P<0.0001; 168 [145-219] min and 180 [150-221] min, P = 0.65; respectively).
Conclusion
Although non-significantly, dispatch-to-groin puncture time in patients delivered by an MSU to comprehensive stroke centers in Berlin was shorter than of those treated with standard prehospital care. Similar trends were observed for secondary endpoints. A larger, prospective study is needed to confirm these findings.
Trial registration number
N/A
AS06-083
IMPACT OF TIME TO RECANALIZATION ON CLINICAL OUTCOME OF ACUTE ISCHEMIC STROKE PATIENTS TREATED WITH MECHANICAL THROMBECTOMY
1Porto Hospital Centre, Neurology, Porto, Portugal
2Porto Hospital Centre, Neuroradiology, Porto, Portugal
3São João Hospital Centre, Neurology, Porto, Portugal
4Trás-os-Montes e Alto Douro Hospital Centre, Neurology, Vila Real, Portugal
Background and Aims
Delays in acute ischemic stroke workflow from symptom onset to successful recanalization may have a negative impact on clinical outcome. The aim was to evaluate the impact of time to recanalization on clinical ouctome.
Method
We analyzed patients treated in our centre in a 2 year-period. Good clinical outcome was defined as 90-day modified Rankin Scale 0–2 or no change in score. Relationship between outcome and time intervals was modeled using logistic regression. Associations between patient, thrombectomy, hospital characteristics and time-intervals was modelled using negative binomial regression.
Results
From 174 patients included, 130 (75%) were recanalized. After adjusting for significant predictors in univariate analysis, qualifying imaging-to-recanalization time (126 vs 166 minutes, p = 0.02) and catheter-to-recanalization time (41 vs 62 minutes, p = 0.04) were significant predictors of good clinical outcome. Symptom-onset-to-qualifying imaging time was not associated with clinical outcome. For every 30 minutes increase in catheter-to-recanalization time the probability of achieving a good clinical outcome dropped 10%. Significant predictors of longer duration were general anesthesia administration (OR 1.22, p = 0.045, 95% CI 1–1.5), occlusion in posterior circulation (OR 1.2, p = 0.007, 95% CI 0.98-1.38) and tandem lesion presence (OR 1.49, p = 0.002, 95% CI 1.16-1.93). A trend was found over stent-retrievers use vs aspiration (OR 1.16, p = 0.08, 95% CI 0.98-1.38) and in patients presenting during work hours versus off hours (OR 0.83, p = 0.06, 95% CI 0.69-1.01).
Conclusion
Qualifying imaging-to-recanalization time was a significant predictor of clinical outcome. General anesthesia use, technical approach and hour of presentation are factors that may contribute to workflow inefficiencies.
Trial registration number
N/A
AS06-084
SHOULD WE DETERMINE PATIENT TRANSFER FROM PRIMARY LOCAL HOSPITALS TO COMPREHENSIVE STROKE CENTERS ACCORDING TO BASELINE ASPECTS?
1Hospital Vall d'Hebron, Stroke Unit, BARCELONA, Spain
2Hospital Germans Trias i Pujol, Stroke Unit, Badalona, Spain
3Hospital Universitari Bellvitge, Stroke Unit, Hospitalet de Llobregat, Spain
4Hospital Clinic, Stroke Unit, Barcelona, Spain
5Agency for Health Quality and Assessment of Catalonia, Stroke Programme, Barcelona, Spain
Background and Aims
Among stroke patients evaluated in local centers (LC), whom should be transferred to comprehensive stroke centers (CSC) for endovascular reperfusion (EVT) is debatable. We aim to analyze the impact of LC-ASPECTS on EVT indication on CSC.
Method
Retrospective analysis of prospective mandatory regional multicenter database of acute strokes. Consecutive patients with intracranial occlusion, LC-ASPECTS and CSC-ASPECTS (evaluated by local investigators) were included.
Results
: 109 patients included, mean age 73 ± 12, median NIHSS 19(12-21). 67(61.5%) received EVT; reasons for exclusion: large infarct and/or absence of mismatch 18(16.5%), recanalization 18(16.5%), clinical improvement 1(0.9%), >1 reason 5(4.6 %).
Median LC-ASPECTS was 10(8–10) after median of 112.5(80-218)min from symptoms onset. Median CSC-ASPECTS was 8(6–10), after median time from LC-CT of 150min (119-173). In 8 patients (7.3%) CSC-ASPECTS was higher than LC-ASPECTS.
Median ASPECTS decrease was 1(0–3). In 17 patients, MRI was performed in CSC and median diference with LC-ASPECTS was 2(0–3.5). Only 13(11.9%) presented CSC-ASPECTS<6.
Patients were clasified by LC-ASPECTS: if 10(n = 64), median CSC-ASPECTS 9(7–10), 6(9.4%) <6. If LC-ASPECTS 8–9(n = 29), median CSC-ASPECTS 7(6–8), 5(17.9%) <6. If LC-ASPECTS 6–7(n = 16), median CSC-ASPECTS 7(6–8), 2(12.5%) <6.
Only baseline NIHSS(p < 0.05) but not LC-ASPECTS(p = 0.3) was associated with clinical improvement (decrease of >4p on 24h-NIHSS). Younger age was the only predictor of final ASPECTS<6(OR 0.95, CI0.91-0.99, p = 0.03) after adjustment for baseline NIHSS, LC-ASPECTS and time between LC- and CSC-ASPECTS.
Conclusion
ASPECTS decrease during transfer of stroke patients from LC to CSC is minimal, with very few patients progressing to CSC-ASPECTS<6 and supporting the strategy of not repeating imaging at CSC for EVT. Only younger age predicted CSC-ASPECTS<6.
Trial registration number
N/A
AS06-085
A TERTIARY STROKE CENTRE SERVING A LARGE RURAL POPULATION – GEOGRAPHY’S IMPACT ON MANAGEMENT
1galway university hospital, Geriatric, galway, Ireland
Background and Aims
Timely access to stroke services is an essential part of hyperacute stroke management. This allows for administration of reperfusion therapy in cases that present within given time windows. Rural populations are at a disadvantage, due to geographical distance from stroke centres. This has become more apparent with the advent of mechanical thrombectomy, as not all tertiary stroke centres provide this treatment. We investigated the impact of door-to-door distance on management in a tertiary stroke centre with a largely rural catchment area.
Method
A single tertiary stroke centre with a catchment area exceeding 300,000 and a large rural component was investigated. A prospective investigation of all acute stroke presentations over three months (October’17-January’18) was performed.
Results
A total of 53 acute ischaemic stroke presentations (<24h symptom onset) were recorded. Of these, 13%(n = 7) were treated with intravenous tissue plasminogen activator (tPA), while 2%(n = 1) received mechanical thrombectomy. A total of 64%(n = 34) had CT angiography performed. The median door-to-door distance was 35.1km (IQR:10.8-57.2), and the median time from symptom onset to presentation was 260mins (IQR:125-541). Of patients who recieved tPA, the median door-to-door distance at symptom onset was 26.4km (IQR:3.75-53.5). The door-to-door distance for the patient who underwent mechanical thrombectomy was 26.4km.
Conclusion
A low rate of mechanical thrombectomy was recorded. Geographical location and a large rural population, some of whom are native Irish speakers, are likely contributory factors. This centre is over 200km from mechanical thrmobectomy services. Rural populations represent a challenge in relation to stroke service organisation, especially with the advent of mechanical thrombectomy.
Trial registration number
N/A
NEUROINTERVENTION – EXCLUDING CLINICAL TRIAL RESULTS
AS07-001
EXPERIENCE OF COVERED CORONARY STENT GRAFTS AS TREATMENT OPTION FOR CAROTID CAVERNOUS FISTULAS WITH FOLLOW-UP RESULTS
1Eulji University Hospital, Neurosurgery, Daejeon, Republic of Korea
Background and Aims
Endovascular detachable balloon occlusion and coil occlusion have been well-established options for the treatment of carotid cavernous fistulas. In recent years, sporadic treatment of CCFs endovascular covered stent grafting is proving an excellent result not only in successful treatment of fistula but also preserving patency of parent artery. We present our experience of CCFs, treated by covered stents, and provide their clinical and angiographic follow-up results.
Method
Four consecutive patients with CCFs underwent the Jostent coronary stent graft (Abbott Vascular, Redwood City, CA) placement alone at our department during 2 years. Two were direct CCFs with a symptom triad and 2 were indirect CCFs with diplopia. These patients had periodic clinical follow-up examinations (at 6–29 months) with all receiving angiographic follow-up examination (at 5–15 months).
Results
Covered stent placement was technically successful in all patients. Immediate post-procedural complete exclusion of the fistula was achieved in 3 and near complete exclusion with small endoleak was observed in 1 after stent placement. ICA patency was preserved in all. Symptoms related to CCFs regressed within 1–14 days in all patients after treatment without thromboembolic events. There was no mortality and no immediate post-procedural morbidity related to the procedure. Final follow-up angiography showed complete exclusion of all CCFs and revealed good stent patency of the ICA without intra-stent stenosis.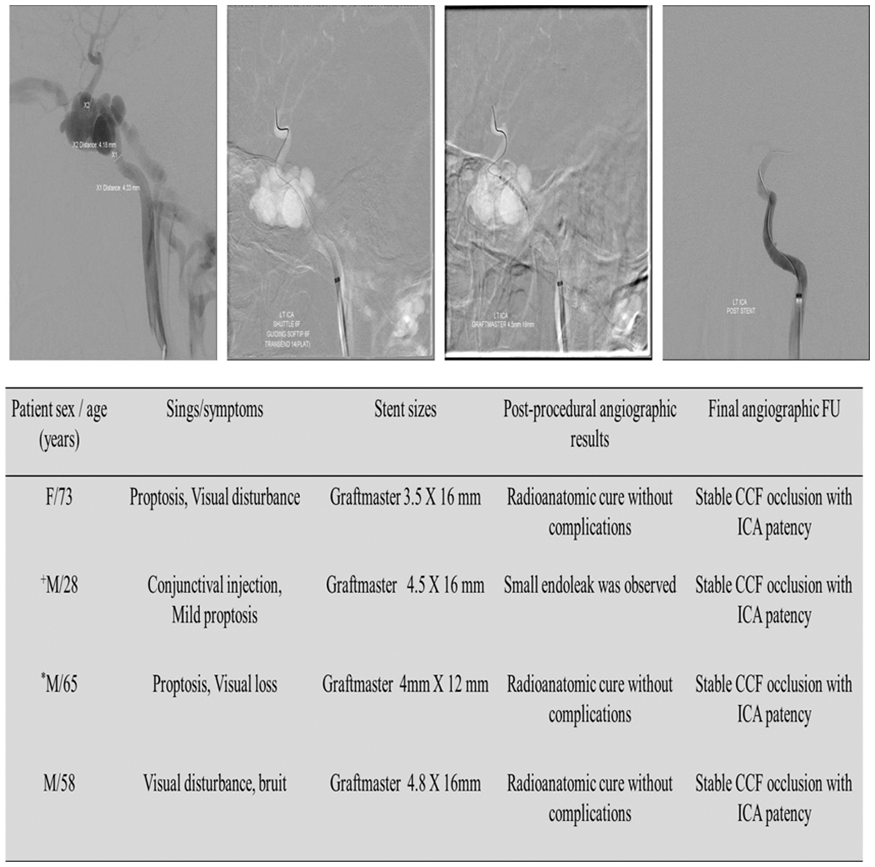
Conclusion
Graft-stents should be considered as an alternative option of treating CCFs and preserving the parent artery by arterial wall reconstruction especially in patients with a fistula that cannot be successfully occluded with detachable balloons or coils.
Trial registration number
N/A
AS07-002
ENDOVASCULAR MECHANICAL THROMBECTOMY VERSUS INTRAVENOUS THROMBOLYSIS FOR ACUTE POSTERIOR CIRCULATION STROKE
1Beijing Tian Tan Hospital - Capital Medical University - China, Interventional Neurology, Beijing, China
2Tangshan Gongren Hospital- Hebei Medical University, Neurology, Tangshan, China
3Neurovascular Imaging Research Core and the UCLA University of California- Los Angeles Stroke Center, Neurology, Los Angeles, China
4Beijing Tian Tan Hospital - Capital Medical University - China, Neurology, Beijing, China
Background and Aims
Endovascular mechanicalthrombectomy (MT) was provensuperior to intravenous thrombolysis (IVT) for patients with acute ischemic stroke (AIS) inanterior circulation due to large vessel occlusion. Whether these positive results are available for patients with acute posterior circulation stroke remains elusive. Our study were to compare clinical outcomes of patients afterMT and IVT alone in acute posterior circulation stroke.
Method
We analyzed consecutive data from two cohorts of patients and matched 1:1 for age, sex, admission NIHSS score, onset-to-treatment time and ischemic stroke subtype from March 2012 to November 2016.The primary outcome was the modified Rankin Scale (mRS, ranging from 0 [no symptoms] to 6[death]) score at 90 days.
Results
Overall, 328 patients were included for analysis, 55 patients were matched in each group, MT group (mean [SD] age, 59[7] years;44 male[80.0%])and IVT group (mean [SD] age,59[11] years;46 male[83.6%]). The baseline NIHSS score showed no differences between the MT and IVT group (23 versus 21, p = 0.853). There were no differences in the duration from symptom onset to treatment time (330 min for MT group versus 277 min for IVT group, p = 0.660). 21(38.2%) patients treated with MT had functional independence (modified Rankin score, 0 to 2) at 3 months compared with 28(50.9%) matching cases (odds ratio [OR],0.596;95% confidence interval [CI],0.279-1.272; p = 0.181). There were no differences in mortality or the occurrence of intracranialhemorrhage between the two groups.
Conclusion
In acute posterior circulation stroke caused by large vessel occlusion, the outcomes after intravenous or endovascular revascularization appear similar.
Trial registration number
N/A
AS07-004
COMPARISON OF TRANSRADIAL AND TRANSFEMORAL APPROACH IN CEREBRAL ANGIOGRAPHY
1The Catholic University of Korea - Incheon St. Mary's Hospital, Neurosurgery, Incheon, Republic of Korea
Background and Aims
Cerebral catheter angiography is gold standard method for cerebrovascular disease. The standard for cerebral angiography is the transfemoral and transradial approaches. The aim of this study is to retrospectively compare the single center results and complications of radial vs. femoral approach.
Method
We reviewed the medical records of 1058 consecutive angiographic studies. Between January 2014 and December 2016, 528 angiographies were conducted via the radial artery while 530 were via femoral artery. The decision of approach whether transradial or transfemoral was on the operator’s discretion. The success rate of examinations, complications, and the time required for angiography were analyzed.
Results
The success rate of angiography was similar (99.3 % in transradial vs 99.5% in trasfemoral). The complication rate is slightly high in transradial group (3.5 % vs 2.7 %). However, the severity of complication was worse in transfemoral group. Most of complications in transradial group were transient arm pain (n = 35) or wound problems (n = 12) which were recovered in a few days. Most of complications of transfemoral were femoral hematoma (n = 27) and cerebral infarct (n = 6) which need bed rest for a few days or permanent sequelae. The time required for angiography were significantly shorter in transradial group (17.22 min) than transfemoral group (28.35) group (p = 0.02).
Conclusion
Transradial approach is useful method for simple cerebral angiography with fewer severe complication and shorter time demand.
Trial registration number
N/A
AS07-005
THE VALUE OF PERFUSION CT AS A PROGNOSTIC FACTOR AFTER MECHANICAL THROMBECTOMY IN ANTERIOR CIRCULATION LARGE VESSEL OCCLUSION PATIENTS
1The Catholic University of Korea - Incheon St. Mary's Hospital, Neurosurgery, Incheon, Republic of Korea
Background and Aims
We conducted a study to determine whether recanalization was faster and whether perfusion CT could be used as a predictor of prognosis.
Method
We retrospectively studied patients who had recanalization therapy with LVO of anterior circulation at our hospital from 2011 to 2015. The CVA CT scan takes a 7 minutes. In these patients, 10 areas such as ASPECT score were designated and scores were given to the lowered areas of CBF, MTT, and CBV compared with the contralateral side, and scoring was performed at 10 points. We checked NIHSS at admission, mRS at discharge, and mRS at 90 days after discharge.
Results
In total, 94 patients met the inclusion criteria of this study. After recanalization, TICI G 2b and 3 were achieved 80 patients (85.10%). Of the total patients, 71 patients (75.53%) had a CBV score of 4points or less and 23 patients (24.47%) had a score of 5points or more. In patients with CBV 4 points or less, good outcome (mRS 0 ∼ 2) was 34 patients (47.88%). In patients with CBV 5 points or more, good outcome (mRS 0 ∼ 2) was 6 patients (26.08%). The mortality rate was 7.04%(5patients) in patient with CBV 4points or less, but there were 30.43%(7patients) in patients with CBV 5points or more.
Conclusion
Mechanical thrombectomy showed better prognosis in LVO patients with CBV score of 4 points or less. There was higher mortality rate in patients with CBV score of 5 points or more. Perfusion CT can be helpful in predicting the prognosis of the patient.
Trial registration number
N/A
AS07-006
ACUTE CERVICAL CAROTID STENTING IN PATIENTS WITH TANDEM OCCLUSIONS: A RETROSPECTIVE SINGLE-CENTRE STUDY
1Hôpital Notre-Dame- Centre hospitalier de l'Université de Montréal, Department of Radiology, Montreal, Canada
2Centre de Recherche du Centre hospitalier de l'Université de Montréal CRCHUM, n/a, Montreal, Canada
3Hôpital Notre-Dame- Centre hospitalier de l'Université de Montréal, Division of Neurology- Department of Medicine, Montreal, Canada
4McGill University, Faculty of Medicine, Montreal, Canada
5Centre hospitalier de l'Université de Montréal, Library, Montreal, Canada
6Hôpital du Sacré-Coeur de Montréal, Division of Neurology- Department of Medicine, Montreal, Canada
Background and Aims
The role of immediate stenting of the cervical internal carotid artery (ICA) is controversial in patients with stroke due to tandem occlusion, defined as ipsilateral severe stenosis or occlusion of the cervical ICA and occlusion of the distal ICA and/or middle cerebral artery. We aimed to compare functional outcomes between patients with and without acute ICA stenting during endovascular therapy (EVT).
Method
We included all patients with tandem occlusions admitted to CHUM Notre-Dame Hospital for EVT between December 2014 and December 2016. Our primary outcome was the proportion of patients with modified Rankin scale (mRS) 0–2 at 90 days. Secondary outcomes were: rate of symptomatic intracranial hemorrhage (sICH), post-EVT intracranial recanalization (TICI score 2b-3) and ICA recanalization.
Results
26 patients underwent acute ICA stenting versus 47 who did not. There was no significant difference (p>0.05) in baseline characteristics between the two groups except for hypertension (77 vs 45%, p = 0.008). The stenting group was associated with a higher rate of ICA recanalization (92 vs 9%, p < 0.0001) but no difference in intracranial recanalization (77 vs 79%, p = 0.86) and sICH (8 vs 4%, p = 0.54). Although a greater proportion of patients undergoing acute ICA stenting had a favourable outcome at 90 days (46 vs 30%), this difference was not statistically significant (p = 0.16).
Conclusion
Patients with tandem occlusion treated with EVT had no significant difference in functional outcome, intracranial recanalization or sICH whether they underwent acute cervical ICA stenting or not. Defining the role of acute ICA stenting in tandem occlusion will require a well-designed randomized controlled trial.
Trial registration number
N/A
AS07-007
ANGIOPLASTY FOR INTRACRANIAL VERTEBROBASILAR STENOSIS: A META-ANALYSIS OF PROCEDURAL RISKS
1University of Illinois at Chicago, Department of Neurosurgery, Chicago, USA
2University of Illinois at Chicago, Center for Clinical and Translational Science, Chicago, USA
3University at Buffalo, Department of Neurosurgery, Buffalo, USA
4Medical University of South Carolina MUSC, Department of Neurology, Charleston, USA
5Northwell Health - North Shore University Hospital, Neurology, Manhasset, USA
6Northwestern University, Department of Neurology, Chicago, USA
Background and Aims
Symptomatic flow-compromised Intracranial vertebrobasilar (VB) stenosis carries a significant risk of stroke. Although flow restoration through endovascular interventions represents the most plausible treatment strategy, the high periprocedural risk of stenting, especially for the basilar artery, has proven prohibitive. Submaximal angioplasty alone may represent a safer strategy. We examined the peri-procedural risks associated with VB submaximal angioplasty.
Method
All English language studies of intracranial angioplasty for atherosclerotic disease were screened. Studies were included in the meta-analysis, based on the following criteria: submaximal angioplasty alone, identifiable peri-procedural outcomes for VB angioplasty, ≥5 patients. Our primary outcome was the 30 day stroke/ death event rate. We used Q statistics to test heterogeneity, and random-effect models using DerSimonian-Laird estimator to summarize effect sizes. Funnel plots and regression tests were performed to detect publication bias.
Results
Six studies, comprising 127 patients, met inclusion criteria. The Q test (p = 0.90) indicated homogeneity across studies. The pooled event rate was 5.9% (95% CI, 2.9%- 8.9%).
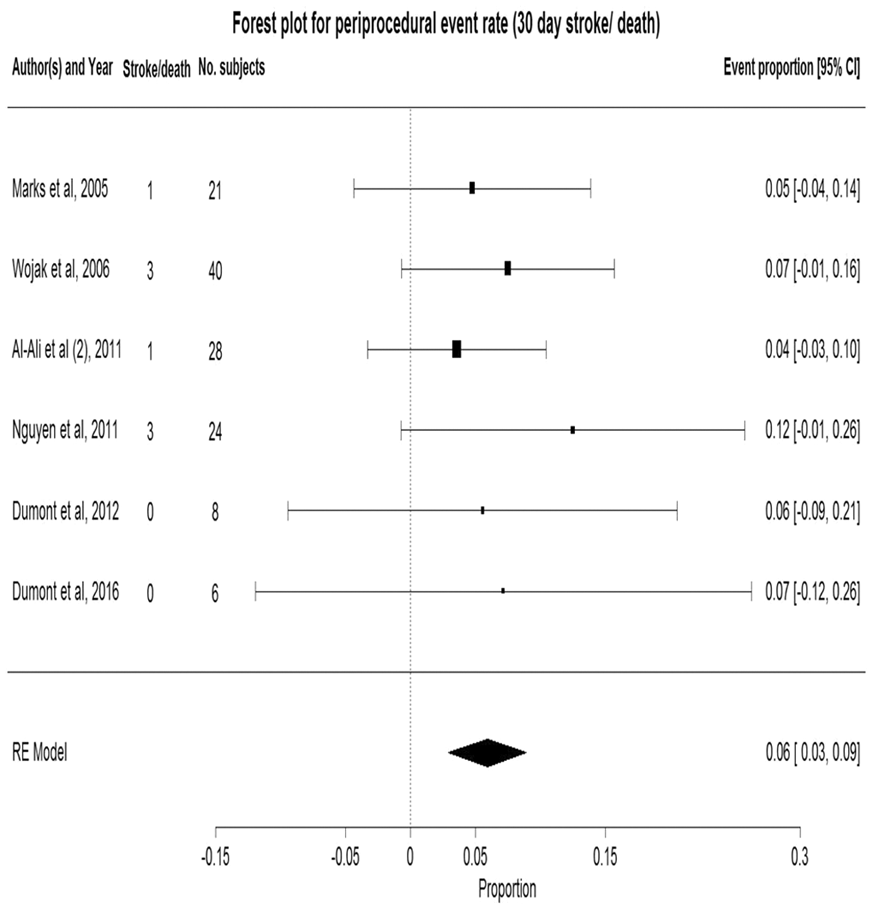
The funnel plot and a non-significant regression test (p = 0.30) indicated no publication bias. Examination for event rate of vertebral vs basilar angioplasty showed no statistically significant risk difference.
Conclusion
Submaximal angioplasty represents a potentially promising intervention for symptomatic intracranial VB stenosis. These results support the need to prospectively examine the safety and feasibility of the intervention in high-risk flow compromised VB patients.
Trial registration number
N/A
AS07-008
ENDOVASCULAR THERAPY WITH OR WITHOUT INTRAVENOUS LOW DOSE ALTEPLASE IN ACUTE STROKE PATIENTS WITH ANTERIOR LARGE VESSEL OCCLUSION
1National Cerebral and Cardiovascular Center, Stroke Care Unit, Suita, Japan
2Hyogo College of Medicine, Neurosurgery, Nishinomiya, Japan
3Hyogo College of Medicine, Clinical epidemiology, Nishinomiya, Japan
4Kobe City Medical Center General Hospital, Neurosurgery, Kobe, Japan
5National Cerebral and Cardiovascular Center, Cerebrovascular Medicine, Suita, Japan
Background and Aims
The impact of prior intravenous thrombolysis using low dose (0.6mg/kg) alteplase on outcomes in large vessel acute stroke patients undergoing endovascular therapy remains unclear.
Method
In a Japanese nationwide registry study, 2420 patients with acute stroke due to LVO were registered between October 2014 and January 2017. Among them, 594 patients with occlusion of the internal carotid artery or the middle cerebral artery M1 portion and who underwent endovascular therapy within 6 hours after onset were analyzed. Prior intravenous thrombolysis (IVT) with low dose alteplase was performed in 368 (62%) patients. Functional outcome was assessed by modified Rankin Scale (mRS) score at 90 days, and symptomatic intracranial hemorrhage (sICH) was evaluate within 72 hours.
Results
In patients with IVT, previous stroke and prior anticoagulant therapy were less common, baseline Alberta Stroke Program Early CT Score was higher, and time from onset to arterial puncture was shorter than in those without IVT. Compared to IVT (-) group, independency (mRS 0–2) and independent ambulation (mRS 0–3) were more frequent in IVT (+) group (49% vs 40%, P = 0.04, and 64% vs 48%, P<0.001, respectively). Prior IVT was associated with independent ambulation (adjusted odds ratio [aOR] 1.64, 95%CI 1.06-2.55) but not with independency (aOR 1.15, 95%CI 0.74-1.79) after adjustment for potential confounders. Also, it did not increase odds of sICH (2.9% vs 2.9%, aOR 1.14, 95%CI 0.36-3.61).
Conclusion
Prior IVT with low dose alteplase before endovascular therapy can modestly improve functional outcome without increasing risk of sICH in acute stroke patients.
Trial registration number
ClinicalTrials.gov Identifier: NCT02419794
AS07-010
CLINICAL EFFECTS OF CONSCIOUS SEDATION VERSUS NON-SEDATION IN ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE
1Busan Paik Hospital - Inje University, Neurology, Busan, Republic of Korea
2Busan Paik Hospital - Inje University, Diagnostic radiology, Busan, Republic of Korea
Background and Aims
Although there is a controversy, several studies have reported that conscious sedation for endovascular treatment (EVT) in acute ischemic stroke (AIS) have better neurological outcome compared with general anesthesia. However, conscious sedation in EVT can be related to complications such as hypotension and respiratory distress. In this single-center study, we investigated the impact of conscious sedation on neurological outcome in AIS patients.
Method
243 patients receiving EVT for AIS in January 2012 to May 2017 were included. All procedures were started without sedation, and the conscious sedation was applied if necessary. Depending on whether sedation was applied, all patients were divided into sedation group and non-sedation group. Age, sex, comorbidities, admission NIHSS score, modified Thrombolysis in Cerebral Ischemia score, time intervals from the puncture to recanalization and three months modified Rankin Scale score were analyzed.
Results
In the non-sedation group 64 of 144 patients (44.4%) and in the sedation group 42 of 99 patients (42.8%) achieved a modified Rankin Scale score ≤2 (P = 0.81) at 3 months. There were no differences in sex, comorbidities, admission NIHSS score, and mTICI≥2b (77.8% versus 70.1%) between two groups. Sedation group were older, more likely to use of IV-tPA, and took more time to recanalization (73 versus 93 minutes).
Conclusion
Because the initiation of conscious sedation after starting EVT, the time interval from the puncture to the recanalization was longer in sedation group. In EVT for AIS, no difference was found between conscious sedation and non-sedation in neurological outcome three months after stroke.
Trial registration number
N/A
AS07-012
FAVORABLE CLINICAL OUTCOME AND SIGNIFICANT REDUCTION IN HOSPITAL WORKFLOW TIMES WITH DIRECT TRANSFER TO ANGIOSUITE: A CASE CONTROL STUDY
1Instituto Nacional de Neurología y Neurocirugía, Vascular Neurology, Ciudad de Mexico, Mexico
2H.E. Centro Médico Nacional SXXI, Department of Neurology, Ciudad de Mexico, Mexico
3Vall d’Hebron University Hospital- Vall d’Hebron Research Institute, Stroke Unit- Department of Neurology, Barcelona, Spain
4São João Hospital Center, Department of Neurology, Porto, Portugal
5Hospital Fernando Fonseca, Department of Internal Medicine-, Amadora, Portugal
6Vall d’Hebron University Hospital- Vall d’Hebron Research Institute, Department of Neuroradiology, Barcelona, Spain
Background and Aims
Demonstrate that direct transfer to angiosuite (DTAS) of patients with suspected large vessel occlusion stroke (LVO) improves workflow times and outcomes.
Method
A case–control matched study of the first 79 DTAS patients with confirmed LVO (cases) and 145 No-DTAS patients (controls). Cases and controls were matched by level of vessel occlusion, age, baseline NHISS and time from symptoms onset to hospital arrival. Dramatic clinical improvement was defined as a decrease in NIHSS greater than 10 points or NHISS >2. Favorable outcome was defined as mRS≤2 at 3 months.
Results
During an 18 months period 95 patients were directly transferred to the angiosuite after admission: 9 (9.7%) showed an ICH on cone beam CT, 13 (14%) did not have a LVO on initial angiogram and 79 (76.3%) had a LVO and received endovascular treatment (EVT, cases). There were no differences in baseline characteristics between groups. The median door-to-groin time (15 Vs 70 minutes; p < 0.01) and onset-to-groin times (229 Vs 289; p < 0.01) were shorter in the DTAS group. At 24 hour the median NHISS was lower in the DTAS group (7 Vs 14; p = 0.01) and the rate of dramatic improvement was higher (50.6% 31.7%; p = 0.04). At 3 months favorable clinical outcome was also higher in the DTAS group (46% Vs 26%; p < 0.01). A logistic regression model pointed age, admission NIHSS and onset-to-groin time as independent predictors of favorable outcome.
Conclusion
DTAS is an effective strategy to reduce workflow time, which may significantly increase the odds favorable outcome.
Trial registration number
N/A
AS07-013
EFFECT OF TIME TO ENDOVASCULAR REPERFUSION IN ANTERIOR CIRCULATION STROKE PATIENTS WITH CLINICAL-DWI MISMATCH BY LARGE ARTERY OCCLUSION
1Dong-A University Hospital, Department of Neurology, Busan, Republic of Korea
Background and Aims
Recent study demonstrated endovascular treatment (EVT) is beneficial in patients with clinical-diffusion mismatch more than 6 hours after the onset of ischemic stroke. The purpose of this study was to assess the influence of onset-to-reperfusion (OTR) time by EVT on clinical outcomes in stroke patients with clinical-diffusion mismatch.
Method
Using a prospective stroke registry database, anterior circulation stroke patients with pretreatment clinical-diffusion mismatch and successful recanalization by EVT were enrolled in this study. The clinical–diffusion mismatch was defined as National Institutes of Health Stroke Scale (NIHSS) score ≥8 and diffusion-weighted imaging (DWI) lesion volume <25 mL. Clinical outcome were compared in patients treated within an early time window and a late time window. Multivariable analysis was performed to predict favorable functional outcomes.
Results
Among 69 patients with clinical-diffusion mismatch, 57 patients (mean age 67.2 years, 52.6% women) were treated with EVT with TICI 2b to 3 reperfusion. The rate of favorable outcome was higher in early reperfusion group (OTR time; 130-24O minutes) compared to in late reperfusion group (OTR time; 241-510 minutes) (71.4% vs. 41.7%, P = 0.03). DWI lesion volume and NIHSS score were not statistically different in two groups. In multiple regression analysis, OTR time (Odds ratio (OR), 0.84 per 15 minutes; 95% confidence interval (CI), 0.73-0.96) was an independent variable associated with favorable outcome along with TICI 3 recanalization (OR, 8.95; 95% CI 2.08-38.6).
Conclusion
In patients with clinical-diffusion mismatch by large artery occlusion, a shorter time from symptom onset to reperfusion by EVT is associated with better clinical outcomes.
Trial registration number
N/A
AS07-017
ANEURYSM ON THE PATH: HOW TO PERFORM THROMBECTOMY IN ACUTE MCA OCCLUSION?
1Hacettepe University, Neurology, Ankara, Turkey
2Hacettepe University, Radiology, Ankara, Turkey
Background and Aims
Presence of a saccular aneurysm on the path to acute cerebral arterial occlusion results not only significant technical challenges, but also serious complications such as rupture.
Method
A saccular aneurysm on the route to occlusive thrombus was found in 8.5% of 35 acute stroke thrombectomies in 2017.
Results
Case-1: A 85-year-old woman presented with acute right MCA syndrome (NIHSS 6) within 2.5 hours. She deteriorated (NIHSS to 10) during tPA infusion. Thrombectomy (direct aspiration followed by 1-pass Catch® retriever) for distal M1 occlusion provided TICI 3 reperfusion. Puncture of intra-thrombus bifurcation aneurysm (3-mm) caused a parietal subarachnoid hemorrhage. Her NIHSS decreased to 2, and mRS was 2. Case-2: A 85-year-old woman presented with left MCA syndrome (NIHSS 22) within 4.5 hours. Left MCA-M2 and ACA-A2 occlusions were found along with a previously-unknown 3-mm anterior communicating artery aneurysm (ACom). Dual thrombectomy (3-pass Catch® retriever then thromboaspiration) procedure resulted in TICI-2b reperfusion in each territory. NIHSS decreased to 19. mRS was 4. Case-3: A 61-year-old woman presented with right MCA syndrome (NIHSS 8) at 3rd hour. Angiography, following IV-tPA, documented right MCA M1 occlusion and a 3-mm unruptured ACom aneurysm. Thrombectomy (direct aspiration followed by 1-pass Catch® retriever) resulted in TICI-3 flow. NIHSS decreased to 2; discharge mRS was 1. In all cases, aneurysms were not secured.
Conclusion
Thrombectomy and IV tPA should not be withheld in stroke patients with saccular aneurysms in the same arterial tree. Trombectomy procedure is standard, and aneurysm repair is not recommended at the same session.
Trial registration number
N/A
AS07-018
EFFECTIVENESS AND SAFETY OF TRANSBRACHIAL COIL EMBOLIZATION FOR UNRAPTURED INTRACRANIAL SACCULAR ANEURYSMS IN ELDERLY PATIENTS
1Shonan Kamakura General Hospital Stroke Center, Stroke Treatment, Kamakura, Japan
Background and Aims
Unraptured intracranial saccular aneurysms are treated usually with not surgical clipping but coil embolization in elderly patients, because coil embolization is less invasive. But some previous studies have reported that in elderly patients it is difficult to cannulate a guiding catheter or complications occur more frequently during procedures.
We aimed to investigate the success rate of transbrachial guide-catheter cannulation and of coil embolization and the incidence of complications in patients aged 80 years or older who underwent coil embolization of unraptured intracranial saccular aneurysms.
Method
We Included in our study unraptured intracranial saccular aneurysm patients 1) who were admitted to our institution from Jan.2011 to Dec.2017, 2) who received transbrachial coil embolization. Patients were divided into two groups; patients aged 80 years or older (group A) and patients aged less than 80 years (group B). We evaluated differences of the effectiveness and safety of coil embolization between group A and B.
Results
One hundred and fourteen patients were analyzed. Fourteen patients were in group A and 100 in group B. Between group A and B, there were no differences in successful embolization (92.9% and 94%, p = 0.86), successful cannulation (100% and 100%, p = 099), and adjunctive technique (71.4% and 70%, p = 0.91). And, there were no difference in thromboembolism (21.4% and 10%, p = 0.20), peripheral vascular complication (14.3% and 6.0%, p = 0.44), and aneurysm perforation (7.1% and 3.0%, p = 0.68).
Conclusion
There were no differences in the effectiveness and safety of transbrachial coil embolization for unraptured intracranial saccular aneurysms between group A and B in our institution.
Trial registration number
N/A
AS07-019
PREDICTORS OF POOR OUTCOME OF THROMBECTOMY IN BASILARY ARTERY OCCLUSION IN CLINICAL PRACTICE: A SINGLE CENTER EXPERIENCE
1University Medical Center Hamburg-Eppendorf, Neurology, Hamburg, Germany
2University Medical Center Hamburg-Eppendorf, Neuroradiology, Hamburg, Germany
Background and Aims
Results from randomized trials of endovascular treatment (ET) of ischemic stroke due to basilar artery occlusion (BAO) are still lacking. We studied predictors of clinical outcome of ET in patients with BAO in clinical practice.
Method
Data of patients with BAO who received ET in our institution between July 2015 and June 2017 were analyzed. Baseline characteristics, procedural and outcome data were evaluated. Outcome was assessed by the modified Rankin Scale (MRS) at 90 days. We performed multivariate logistic regression to identify predictors of clinical outcome.
Results
Thirty-nine patients with BAO (median age: 75 years, 66.7% male) were included. Median NIHSS was 24 (range 1–42). Intravenous thrombolytic therapy was administered in 56.4%. Successful recanalization assessed by a Thrombolysis in Cerebral Infarction (TICI) score ≥2b was achieved in 82%. Independent outcome (MRS 0–2) was observed in 24.3%, while 52.6 % showed poor outcome (MRS 5–6). Higher baseline NIHSS values (p = 0.013) and the absence of successful recanalization (p = 0.004) were associated with higher MRS scores at 90 days, while pretreatment with intravenous thrombolysis, age and sex were not. Failed recanalization was associated with an odds ratio of 13.5 for poor outcome (p = 0.036).
Conclusion
Higher severity of neurological symptoms on admission and unsuccessful recanalization are predictors of poor outcome after thrombectomy in BAO in clinical practice. In our sample, failed recanalization in BAO resulted in a 13fold increase of the risk of death or dependency, which supports the utmost importance of recanalization in the treatment of BAO.
Trial registration number
N/A
AS07-020
FEMORAL COMPLICATIONS DETECTION AT THE STROKE UNIT
1Vall d'Hebrón hospital, Stroke Unit, Barcelona, Spain
Background and Aims
As the number of patients treated with thrombectomy (EVT) has grown exponentially, the frequency of femoral complications increases as well. Our Stroke Unit (SU) has created a protocol for specific nursing care for early detection and prevention of local complications associated with the procedure. It was implemented in February2017 and it adopts a checklist of preventive measures to improve the safety of post-EVT patients. Our aim was to describe the local post-puncture complications detected after the implementation of the nursing care protocol in the SU.
Method
Prospective study of consecutive patients treated with acute endovascular procedures (EVT) or scheduled (angioplasty), admitted to our SU from February-December2017.
Post-cateheterization complications include: groin bleeding (GB), groin hematoma (GH), retroperitoneal hematoma (RH), femoral artery pseudoaneurysm (FAP), and artery dissection (AD). A specific registry was created for data collection during the procedure until patient’s discharge.
Results
In this period, 260patients were treated with EVT, mean age 71+/-12y.o, 67% men. Vascular closure devices were used in 237 cases (91,2%).40patients (15,4%) presented immediate local complications after sheath removal (27GH, 5GB,8other). After 24hours compression, we found 125(49,6%)patients with no signals of groin damage. 57(22,6%) patients presented internal hematoma, 66(26,2%) superficial hematoma, and 4 (1,6%) GB. At discharge, 15(6,1%)patients presented severe procedure related complications: 7DeepGH, 5FAP, 1AD, 2RH. 2 of those patients died because of complications.
Conclusion
In our series, we found a rate of 6,1% of clinically significant groin complications associated the EVT. The registry will contribute to predict the characteristics of patients who present post-EVT complications to prevent more in the future.
Trial registration number
N/A
AS07-021
ACUTE ISCHEMIC STROKE ENDOVASCULAR TREATMENT: PREDICTORS FOR FAVOURABLE FUNCTIONAL OUTCOME
1Hospital Universitario Puerta de Hierro, Neurology Department. Stroke Unit., Madrid, Spain
2Hospital Universitario Puerta de Hierro, Neuroradiology Department., Madrid, Spain
Background and Aims
To analyse factors related to 90 days favourable functional outcome in patients with acute ischemic stroke treated with endovascular treatment.
Method
Observational prospective study. The period studied was from october 2013 to february 2017. Variables related to 90 days functional outcome (Rankin 0–2 vs 3–6) were analysed.
Results
Number of patients 141, Age median (M) ( intercuartil range IQ 1–3) : 68 ( 59-70) Female: 42 %, NIHSS basal M(IQ 1–3): 19 (16-22), time from onset to arterial puncture: M(IQ 1–3): 264 (200-330), favourable arterial recanalization (TICI 3/2b): 70,21%. Rankin0-2 90 days: 46.8%
Differences between groups (Rankin 0–2 vs 3–6 90 days) were analysed. A univariate analysis is performed and a multivariate predictor model is developed : variables selected in the model were : basal glucemia OR (CI 95% ) 0,98 (0.97-0.99) p = 0.038; basal NIHSS OR (CI 95% ) 0,87 ( 0.79-0.95) p = 0.004 , time from onset to arterial recanalization (TR) OR (CI 95% ) 0,996 (0.993- 1.00) p = 0.061 , favourable arterial recanalization (TICI 2B/3) OR (CI 95% ) 14.04 (4.38-44.9) p <0.001 and presence of hemorragic transformation: parenchymatous hemorraghe type (PH) 0.20 (0.04-0.91)
The ROC area under the curve : 0.83 for predicting Rankin 0–2 at 90 days
Conclusion
Predictors for favourable 90 days outcome in patients with acute ischemic stroke treated with endovascular treatment were : in a negative sense basal glucemia, basal NIHSS, TR and PH ; in a positive sense favourable arterial recanalization (TICI 2B/3) being the most relevant factor OR (CI 95%) 14.04 (4.38-44.9) p <0.001.
Trial registration number
N/A
AS07-022
ANGIOPLASTY USING STENT-RETRIEVERS FOR RECURRENT CEREBRAL VASOSPASM IN PATIENTS WITH SUBARACHNOID HEMORRHAGE: A NOVEL APPROACH AND LONG-TERM OUTCOMES
1Chungnam National University Hospital, neurosurgery, Daejeon, Republic of Korea
Background and Aims
Despite existing treatments, cerebral vasospasm in patients with SAH often results in poor outcome. We report our experience using a stent retriever as a mechanical angioplasty device in patients with SAH with recurrent vasospasm.
Method
We performed a retrospective review of patients with SAH (n = 12) treated at our institution between April 2011 to May 2017 who developed delayed vasospasm and recurrence following a single chemical angioplasty. Follow-up treatment included mechanical vasodilation via temporary deployment of a stent retriever in the spastic vessel segments for 3 minutes. An intra-arterial vasodilator was also infused prior to (Group A; n = 5, 14 vessel segments) or after (Group B; n = 7, 39 vessel segments) mechanical vasodilation.
Results
Fifty-three stent retriever-angioplasties were performed within proximal or distal vessel segments. Stent retriever delivery and deployment was feasible in all procedures. Following temporary stent deployment and retrieval, instant vasodilation was obtained in 71% (10/14) and 82% (32/39) in Groups A and B, respectively. Three patients in Group A demonstrated recurrent vasospasm, while no significant recurrence was noted in Group B. Neurological improvement was noted in 60% (n = 3) and 86% (n = 6) of patients post-procedure in Groups A and B, respectively. The absence of an angiographic abnormality at long-term follow-up was found in 7 patients who completed follow-up.
Conclusion
Mechanical angioplasty using stent retrievers for symptomatic recurrent vasospasm in patients with SAH is a feasible and effective treatment option.
Trial registration number
N/A
AS07-024
MULTICENTRIC EXPERIENCE IN DISTAL-TO-PROXIMAL REVASCULARISATION OF TANDEM OCCLUSION STROKE RELATED TO INTERNAL CAROTID ARTERY DISSECTION
1University Hospital Bern, University Institute of Diagnostic and Interventional Neuroradiology, Bern, Switzerland
2Bordeaux University Hospital, Interventional and Diagnostic Neuroradiology Department, Bordeaux, France
3University Hospital Bern, Department of Neurology, Bern, Switzerland
4Montpellier University Hospital, Interventional and Diagnostic Neuroradiology Department, Montpellier, France
Background and Aims
Internal carotid dissection (ICD) is a frequent cause of ischemic stroke in young adults. It may cause tandem occlusions consisting in cervical carotid obstruction is associated with intracranial proximal vessel occlusion. To date, no consensus has emerged concerning endovascular treatment strategy. Our aim was to evaluate our endovascular “distal-to-proximal” strategy in a multicentric cohort.
Method
Prospectively managed stroke databases from two distinct centres were retrospectively studied between 2009 and 2014. We reviewed tandem occlusions related to ICD. Atheromatous tandem occlusions were excluded. The revascularization procedure consisted first of intracranial thrombectomy. Then, cervical carotid stenting was carried out depending on the functionality of the circle of Willis and the persistence of residual cervical ICA occlusion, severe stenosis or thrombus apposition. Efficiency, complications, radiologic and clinical outcome were studied.
Results
34 patients presenting with tandem occlusion stroke secondary to ICD were treated during the study period. Mean age was 52.5 years, mean initial NIHSS was 17.29 (SD = 6.23) and mean delay between onset and puncture was 3.58 hours (SD = 1.1). Recanalization TICIici 2b/3 was obtained in 21 cases (67.65 %). 15 Fifteen patients benefited from cervical carotid stenting. No ipsilateral stroke recurrence occurred in the non-stented subgroup. 21 (67.65 %) presented a favourable clinical outcome after 3 months.
Conclusion
Endovascular treatment of ICD ICD-related tandem occlusion stroke using the “distal-to-proximal” recanalization strategy appears to be feasible, with low complication rates and high rates of successful recanalization.
Trial registration number
N/A
AS07-025
THROMBECTOMY VERSUS MEDICAL TREATMENT IN PATIENTS WITH ACUTE ISCHEMIC STROKE WITH ISOLATED M2 OCCLUSION
1Hospital Universitario Central de Asturias, Neurology, Gijón, Spain
2Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
3Hospital Universitario Central de Asturias, Interventional Neuroradiology, Oviedo, Spain
Background and Aims
Mechanical thrombectomy (MT) is now an available procedure in proximal artery occlusion in the anterior circulation, but its benefits in M2 segment occlusions still remains doubtful.
Method
We studied 61 consecutive patients with an isolated M2 occlusion who were admitted to a stroke unit in a tertiary level hospital, between January 2015 and April 2017. We analyzed clinical outcome (efficacy and safety) in patients with MT and patients with medical treatment alone.
Results
MT was performed in 40 patients (median age 69 ± 11 years, median NIHSS 12.20 ± 4.87). 69% of the cases were proximal M2 occlusions. Median time from symptom onset to recanalization was 249 minutes and successful reperfusion (TICI 2b–3) was achieved in 85.36% of the cases. Medical treatment alone was employed in 21 patients (median NIHSS 9,95 ± 5.99). No significant differences in mortality between both groups during hospitalization were found. Symptomatic intracerebral hemorrhage was the main complication associated with mortality (p = 0.005, OR = 12.5), with no differences between both groups. Modified Rankin Score (mRS) was 1.3 ± 1.59 points in patients treated with MT and 1.6 ± 1.98 in patients with medical treatment alone.
Conclusion
In our study, patients who presented with moderate-severe stroke due to M2 occlusion were safety treated with MT. Moreover, no significant improvement in 90-day functional outcome was observed compared to medical treatment. Differences in age, baseline mRS and severity of the stroke between the two groups may play a role in these results. More studies are needed in order to specify the profile of patients who can obtain maximal benefit from this technique.
Trial registration number
N/A
AS07-026
MANAGEMENT OF ACUTE STROKE DUE TO TANDEM OCCLUSIONS WITH CAROTID STENTING AND INTRACRANEAL THROMBECTOMY
1Hospital Universitario Son Espases, Neurology, Palma de mallorca, Spain
2Hospital Universitario Son Espases, Radiology, Palma de mallorca, Spain
Background and Aims
The management of tandem occlusion represents a major challenge in patients with acute ischemic stroke (AIS), we want to present our results in patients with AIS due to tandem occlusions treated with Mechanical Thrombectomy (TM) and acute carotid stenting.
Method
We performed a retrospective review of our prospective maintained, single-institution database between December 2014 and December 2017. We analyzed demographic, radiological, and clinical outcome data for patients who underwent endovascular treatment for tandem occlusion with acute carotid stenting. A modified Rankin Scale score (mRs) 2 at 90 days was defined as a favorable clinical outcome.
Results
Thirty- four patients were identified for inclusion in the study, the average age of these patients was 61.7 years; the mean National Institutes of Health Stroke Scale score (NIHSS) at presentation was 16.
Twenty three patients received intravenous thrombolysis before undergoing endovascular treatment (68%). The stroke etiology was mainly atherothrombotic (77%). All our endovascular treatments were complete with general anesthesia. The median time from groin to revascularization was 64.5 minutes (IQR 45.25-90). Successful reperfusion rate (modified Thrombolysis In Cerebral Infarction score ≥2b) was obtained in all but one of our patients (97%). The rate of symptomatic intracranial hemorrhage (SICH) was 6%.
The mean NIHSS score were 8 points at 24h postprocedure and 4.5 points at discharge. Good outcome was achieved in 50% of the patients.
Conclusion
In our center the management of tandem occlusions with acute carotid stenting involves good outcome and a low rate of SICH.
Trial registration number
N/A
AS07-027
MECHANICAL THROMBECTOMY FOR BASILAR ARTERY THROMBOSIS, LOCATION AS A DECISIVE FACTOR
1University Hospital Ramón y Cajal, Neurology, Madrid, Spain
2University Hospital La Princesa, Neurology, Madrid, Spain
3University Hospital Ramón y Cajal, Radiology, Madrid, Spain
4University Hospital La Paz, Neurology, Madrid, Spain
Background and Aims
Basilar artery occlusion (BAO) has been excluded from mechanical thrombectomy (MT) clinical trials, although there are studies that support its utility. There are no reports that compare results of MT in BAO according to occlusion location, proximal (PBO) or distal (DBO). Our project evaluates the benefit and risk of MT in PBO and DBO, with data from the Northeast Node of Madrid Stroke Network.
Method
Multicenter prospective registry between 2012-2016 of MT. Patients who underwent BAO were selected and divided into 2 subgroups: PBO and DBO. Data collected included clinical features, procedure times, techniques employed, procedural complications, mortality and independence rates (EmR 0–2) at 3 months.
Results
Fifty three BAO were included: 34 (64%) PBO and 19 (36%) DBO. There were no differences in baseline characteristics or previous intravenous thrombolysis. Average duration of the procedure: PBO 150 min. (42-160) vs 64 (37-73) DBO (p = 0.018), time to recanalization: PBO 411 min. (329-521) vs 417 (297-450) DBO. Twelve (35%) PBO patients required stent implantation compared to non of the DBO group (p = 0.011). Favorable recanalization rates (TICI grades 2b-3) were similar (PBO 88% vs. 89% DBO). Rates of major periprocedural complications (dissection with subarachnoid hemorrhage) were PBO 20% vs. 10% DBO (p 0.349). PBO mortality 38% vs. 15% DBO (p = 0.087) and independence rates at 3 months PBO 32% vs. 47% DBO (p = 0.279).
Conclusion
MT in DBO requires less time, and has a tendency to provide greater benefit and lower risk than in PBO.
Trial registration number
N/A
AS07-029
ENDOVASCULAR TREATMENT OF INTRACRANIAL DURAL ARTERIOVENOUS FISTULAS USING PHIL® (PRECIPITANTING HYDROFOBIC INJECTABLE LIQUID)
1Hospital Universitario Virgen del Rocío, Interventional Neuroradiology, Seville, Spain
Background and Aims
Precipitating Hydrophobic Injectable Liquid (PHIL®) is a new liquid embolic agent. It brings some useful characteristics:homogeneity in radiopacity iodine based without tantalum and no preparation necessary (prefilled), . We report PHIL treatment in one center series of intracraneal DAVFs.
Method
Between February 2015-November 2017, 13 patients with 13 intracraneal DAVFs were treated using PHIL®. We included in the analysis the following variables: clinical presentation, Cognard type, injecting time and microcatheter used, volume of PHIL injected, treatment sessions, target feeders, technical and clinical complications, premorbid and discharge mRS.
Results
Thirteen patients (9 male, 57.8 yo (range:15-77) were treated. Clinical presentation: hemorrhage 7, headache 3, bruit 2, cognitive impairment 1. Location: 5 transverse sinus, 3 tentorium, 2 sigmoid sinus, 2 superior sagittal sinus, 1 anterior fossa. Cognard type: I:1, IIa:1, IIab:2, III:4, IV:5. PHIL volumen mean: 3 cc (range:1-10). Complete angiographic occlusion was achieve in 79% of patients and only one single treatment session was needed in 86% of all of them. Assisted technique using venous coils was employed in two cases and only PHIL for the rest of patients. Two technical complications were recorded, distal MCA embolism and dural sinus perforation, without clinical consequences. After a median follow-up of 15,7 months, only one patient worse in mRS regarding respiratory condition.
Conclusion
In our experience, PHIL embolic agent is safe and effective for DAVFs treatment. The clinical utility of Phil in dural fistulas remain to be verified from ongoing trial.
Trial registration number
N/A
AS07-030
ANATOMICAL FEATURES OF THE VERTEBRAL ARTERY FOR TRANSBRACHIAL APPROACH FOR EMERGENCY THROMBECTOMY IN THE ISCHEMIC POSTERIOR CIRCULATION STROKE
1Shonan kamakura general hospital, stroke treatment, Kamakura, Japan
Background and Aims
In case of the thrombectomy in the posterior circulation for the acute ischemic stroke (AIS) patients, transfemoral approach is common but limited by aortic or peripheral artery conditions and then transbrachial access is an alternative.
Method
We included in our retrospective study patients 1)who were admitted to our institution from October 1st, 2013 to July 13th, 2017, 2)who were diagnosed as acute ischemic stroke due to the basilar artery (BA) occlusion, 3)who underwent cerebral-cervical-thoracic 3D-CT scanning and transbrachial thrombectomy via the dominant sided vertebral artery (dVA) for access to the BA. We evaluated the patient’s baseline features, the dVA, the diameter of the dVA at the level of the fourth cervical vertebral body, the angle formed by the dVA and the subclavian artery (SA), the success rate of the navigation into the BA.
Results
Eleven patients matched our inclusive criteria and were analyzed. Mean age was 77.5years, 6 patients (55%) were men, seven right vertebral arteries (64%) were dominant. The diameter of the dVA ranged from 3.33 to 4.84mm and its average diameter was 4.22mm. The angle formed by two arteries ranged from 47 to 98degree and its average angle was 69degree. Penumbra system was used in 7patients, stent retrievers in 2 patients, both in 2 patients. No transbrachial approach was abandoned.
Conclusion
The diameter of the dVA of 3.33mm or more and the angle formed by the subclavian and vertebral arteries of 47degree or more are anatomical features of the vertebral artery that transbrachial access is more appropriate to navigation of thrombectomy catheters into the BA.
Trial registration number
N/A
AS07-031
CAROTID ENDARTERECTOMY IN ACUTE STROKE: OUR EXPERIENCE
1The Nikiforov Russian Center of Emergency and Radiation Medicine, Cardiovascular surgery, St.Petersburg, Russia
2City hospital No. 26, cardiovascular surgery, St.Petersburg, Russia
Background and Aims
The validity of carotid endarterectomy (CEA) within 6 weeks after carotid-related ischemic events remains debatable. Principal fear are associated with a high hazard of the hemorrhagic transformation. A benefit of early CEA altogether has been established by multiple reports and guidelines. However, a concrete timing and patients’ selection are uncertain at present. There is a plenty of opposite judgement about it. The negative opinion is being based on findings about extremely procedural risks of surgery within the first 2 days after stoke.
Method
Ours clinics have an experience in 329 early CEA within 14 days (from 2 hours) after acute ischemic event in 2010-2017. 22 patients among them (NIHHS<22) underwent an emergency surgery due to thrombosis of internal carotid artery (group 1). CEA within 2–14 days was performed in 307 patients after ischemic stroke with significant carotid stenosis and without CT-signs of hemorrhage (group 2). We used a selective carotid shunt in 8.8% only in cases of critical clamping intolerance. Near infrared spectroscopy (NIRS) level was used as an only criterion for shunting.
Results
The patients after emergency CEA (group 1) had a neurogical deficiency improvement in 72.7%, 9.0% died. The patients in early CEA (group 2) had improvement in 78.5 %. No repeated stroke or recurrent carotid stenosis were revealed in both groups within one-year.
Conclusion
Carotid endarterectomy, performed in acute period of ischemic stroke and under strict indications, is a highly effective method of recurrent ischemic stroke prevention and improves rehabilitation and the quality of life of these patients.
Trial registration number
N/A
AS07-032
ENDOVASCULAR THERAPY (ET) EXPERIENCE IN WAKE-UP STROKES IN A REFERENCE HOSPITAL. COMPARISON WITH ENDOVASCULAR THERAPY IN KNOWN-ONSET STROKES
1Virgen de la Arrixaca Hospital-Murcia., Neurology, Murcia, Spain
2Virgen de la Arrixaca Hospital-Murcia., Neuroloradiology, Murcia, Spain
Background and Aims
Wake-up strokes can be treated with ET by selecting the patients regarding to favorable radiologic findings (ASPECTS>6, good colateral arteries and favorable missmatch). Checking clinical results is important to find out if selection of patients is accurate.
Method
We implemented a descriptive analysis in the wake-up-stroke group that received ET in the period 2010-2018 in Virgen de la Arrixaca hospital. Statistical comparison with known-onset strokes that received ET was made using X2 and t-Student testing .
Results
In a sample of 701 strokes receiving ET, we found 79 wake-up strokes (11.26%).
The medium age was 64 years-old. 51.9% were males, 48.1 women. Cardiovascular risk factors (CVRF) found were: arterial hypertension (66.2%), dyslipemia (40.3%), diabetes mellitus (29.5%), atrial fibrillation (31.2%) and smoking habit (19.5%). Previous to stroke, 28.3% of patients took antiaggregants and 13% anticoagulants. Cerebral media artery was the most affected (48.1%). 10.4% had symptomatic intracranial hemorrhage. Mortality rate was 17.7%. 92.2% achieved good recanalization: Thrombolysis in Cerebral Infarction (TICI) 2b/3 . Rankin scale (mRs) <2 points three months after stroke was found in 35.1%.
Comparing with the known-onset group, we did not find significant statistical differences in CVRF. Neither we found differences in mortality rate, symptomatic hemorrhage, mRs 3 months after stroke, or TICI scales. Stenting the carotid arteries during ET was more frecuent in wake-up strokes (p < 0.05, OR 2.2)
Conclusion
Endovascular treatment in wake-up strokes is as effective as in known-onsets trokes if patients are selected properly. We do not found clinical or outcome differences in our sample.
Trial registration number
N/A
AS07-033
LONGER TIME TO RECANALIZATION OCCURS IN INTERHOSPITAL TRANSFERS FOR MECHANICAL THROMBECTOMY AND IS ASSOCIATED WITH WORSE OUTCOME
1Hospital de Braga, Neurology, Braga, Portugal
2Centro Hospitalar de Vila Nova de Gaia/Espinho, Neuroradiology, Vila Nova de Gaia, Portugal
3Centro Hospitalar de Entre o Douro e Vouga, Neurology, Santa Maria da Feira, Portugal
4Hospital de Cascais Dr. José de Almeida, Neurology, Cascais, Portugal
5Centro Hospitalar de Vila Nova de Gaia/Espinho, Neurology- Stroke Unit, Vila Nova de Gaia, Portugal
Background and Aims
Interhospital transfers (IHT) for mechanical thrombectomy (MT) are essential for stroke patients with large vessel occlusion (LVO) to access the best treatment in high quality centers. IHT is a demanding process which needs to be continuously evaluated, along with its impact on the outcome of patients.
Method
Retrospective study of all ischemic stroke patients treated with MT after direct admission (DA) in a Stroke Center, or admitted in a Stroke Center after IHT from 2 referring hospitals for MT, between Jan/2015 and Jul/2017. DA and IHT groups were compared.
Results
238 patients were included (DA = 101, IHT = 137), median age=74 (IQR = 62-81), 51.7% of female sex, median NIHSS = 17 (IQR = 13-20), median ASPECTS = 9 (IQR = 8-10). The most frequent location of occlusion was isolated M1 (48.7%). Among 137 IHT patients, MT was not performed in 31 (22.6%). Time to recanalization was 251.5min (IQR = 183-302) in DA patients, and 355min in IHT patients (p < 0.001). Binomial logistic regression revealed that IHT was associated with an adjusted odds ratio (aOR) = 0.34 (95%CI = 0.16-0.70, p = 0.004) for the occurrence of 3-month functional independence. However, after inclusion of time to recanalization in the model, IHT was no longer predictive of functional independence (aOR = 0.59, 95%CI = 0.22-1.57, p = 0.289). Each 15-minute delay in time to recanalization was associated with an aOR = 0.92 (95%CI = 0.86-0.98, p = 0.017) for 3-month functional independence.
Conclusion
Longer time to recanalization is associated with a lower likelihood of achieving 3-month functional independence in stroke with LVO. The organization of Stroke Centers/Units and the process of IHT must be optimized to maximize the clinical benefits of MT.
Trial registration number
N/A
AS07-034
ENDOVASCULAR THROMBECTOMY IN 47 PATIENTS WITH ISOLATED M2 OCCLUSIONS: CLINICAL AND REPERFUSION OUTCOMES
1Interventional Neuroradiology, Liverpool Hospital, Sydney, Australia
2Institute of Neurological Sciences, Prince of Wales Hospital, Sydney, Australia
3Neurological Sciences, Ingham Institute for Applied Medical Research, Sydney, Australia
4Prince Of Wales Hospital Clinical School, University of New South Wales, Sydney, Australia
5South Western Sydney Clinical School, University of New South Wales, Sydney, Australia
6Department of Neurology and Neurophysiology, Liverpool Hospital, Sydney, Australia
Background and Aims
Solitary occlusion at the M2 segment of the middle cerebral artery (MCA) occurs in 16-41% of MCA infarctions. Randomized controlled trials provide limited data on whether benefits of endovascular thrombectomy (EVT) in acute ischemic stroke (AIS) extend to occlusions involving the M2 division of the MCA. It was previously thought that since the M2 is smaller, technically more difficult to treat with limited endangered territory that M2 occlusions may not warrant the risks of EVT.
Method
This study is a prospective audit of AIS patients with isolated M2 occlusions undergoing EVT at 2 Australian comprehensive stroke centres between January 2016-October 2017. We evaluated factors associated with functional outcomes, mortality and reperfusion rates. Outcomes were compared to recent studies in EVT with M2 segment occlusions.
Results
Forty-seven patients (age 72.2 ± 12.5 years, 61.7% male) with isolated M2 involvement and median NIHSS 12 (IQR-12) underwent EVT with stent retrievers and/or aspiration. Thirteen (27.6%) patients received thrombolysis. Angiographically, M2 occlusion locations were identified as proximal (68.0%), middle (12.7%) or distal (19.1%). Good recanalization (mTICI 2b/3) was achieved in 100% of the patients. At 90-days, good (mRS 0–2) or excellent (mRS 0–1) functional outcomes were achieved in 33 (70.2%) and 27 (57.4%) respectively, while 7 (14.8%) patients died.
Conclusion
This study shows a high proportion of excellent functional outcomes and relatively low mortality in patients with isolated M2 occlusions treated with EVT. These findings support previous studies demonstrating the benefit and safety of EVT in selected M2 occlusion strokes.
Trial registration number
N/A
AS07-036
SAFE STENTING OF VULNERABLE CAROTID ARTERY LESIONS SHOWING HIGH-SIGNAL IN MR BLACK BLOOD IMAGES
1Shonan Kamakura General Hospital Stroke Center, Stroke Treatment, Kamakura, Japan
Background and Aims
Carotid artery lesions showing high signal in magnet resonance (MR) black-blood (BB) images look at high risk of symptomatic embolic complications following elective carotid artery stenting (CAS). The aim was to investigate if our strategy can safely dilate vulnerable carotid artery lesions showing high-signal in MR black blood images with balloons and stents.
Method
We included in our study patients who underwent elective CAS of MR-BB high-signal lesions between Jan 2015 and Jun 2017. Symptomatic patients underwent CAS 30 days or later after their ischemic events. We performed transbrachial CAS as following; introducing the Spider filter device distal to BB-high lesions through the super-long sheath (6Fr MSK-guide), dilatation of lesions with a 3mm-diameter (low profile) balloon catheter (Shiden) and deployment of CarotidWallstent without post-CAS balloon dilatation. Patients started to take clopidogrel and cilostazol before CAS and continued to do them after CAS. They took Yokukansan (TJ-54) and etizolam during peri-CAS periods. We evaluated symptomatic complications.
Results
Thirty-four patients matched our criteria and were analyzed. Their average age was 77 years. They had stenosis rate of average 70%, which was reduced to 34.5% after CAS. Neither symptomatic ischemic complications nor hyperperfusion syndrome occurred during peri-CAS period.
Conclusion
According to the specific protocol, vulnerable carotid lesions showing high signal in MR-BB images safely were dilated without symptomatic complications.
Trial registration number
N/A
AS07-038
ACUTE ISCHEMIC STROKE ENDOVASCULAR THERAPY PROGRAM: NOVEL EXPERIENCE IN QATAR
1Hamad General Hospital, Neurology, Doha, Qatar
2Hamad General Hospital, Neuroradiology, Doha, Qatar
3Hamad General Hospital, Neurosurgery, Doha, Qatar
4Hamad General Hospital, Neurosciences Institute, Doha, Qatar
Background and Aims
We aim to describe our experience within a newly established Endovascular Therapy Program (EVT) Program in Qatar, and to compare our performance with international standards and recommendations.
Method
Qatar has a population of 2.6 million. Hamad General Hospital (HGH) is the only Tertiary Stroke Center. In this context, a novel EVT Program was created in February 2015 with a 24/7 on call team. Patients selected for EVT were prospectively registered. Demographics and performance measures were summarized and compared with an international interventional society (SVIN) recommendation.
Results
From its inauguration until November 2017, 103 patients received EVT (mean age 49.6 ± 12.44 SD, 88.6% male, median NIHSS 15 (IQR: 11-19), 71 (68.9%) after iv rtPA, median number of passes 2 (IQR: 1–2). Comparison with SVIN recommendation is shown in Table 1. There were 2 (1.9%) patients complicated with embolisms in a non-Target Downstream Territory, 1 dissection and 1 groin hematoma.
Table 1.
Conclusion
Workflow times until the groin puncture were above recommendations, nevertheless radiological and clinical endpoints were within. New strategies are required to solve these deficiencies.
Trial registration number
N/A
AS07-039
MULTI-VESSEL OCCLUSION IN PATIENTS SUBJECTED TO ENDOVASCULAR STROKE TREATMENT: INCIDENCE, ASSOCIATED FACTORS AND CLINICAL IMPLICATIONS IN A PROSPECTIVE REGISTRY OF ENDOVASCULAR CANDIDATES
1Inselspital- University of Bern, Neuroradiology, Bern, Switzerland
2Inselspital- University of Bern, Neurology, Bern, Switzerland
Background and Aims
Patients with embolic large-vessel occlusion may present with additional accompanying occlusions within or distant from the primary occlusion site (=multi-vessel occlusion, MVO). Prevalence of MVO in endovascular candidates was assessed together with an explorative analysis regarding associated factors.
Method
Image data of consecutive endovascular candidates (n = 720) with direct access to angiography were extracted from a prospective registry. Prevalence of MVO was assessed with multimodal MRI/CT and confirmed by intra-arterial angiography. Explorative analysis and clinical relevance was evaluated using multivariate logistic regression.
Results
MVO was present in 10.7% of patients (95%-CI 6.4-13.0%). Two, three and four concomitant occlusions were found in 80.5%, 16.9% and 2.6% of MVO cases, respectively. Detection rate on initial radiological report was 54.5%. Downstream MVO was present in around one-third of MVO (n = 27/77, 35.1%), while all other MVO (n = 50/77, 64.9%) occurred in different territories. Independent factors related to MVO were statin treatment (aOR 0.477, 95%-CI 0.276-0.827), higher systolic blood pressure (aOR per mmHg-increase 1.014, 95%-CI 1.005-1.023) and primary occlusion site M2 (aOR 1.870, 95%-CI 1.103-3.170). MVO was related to lower rates of successful reperfusion (aOR 0.549, 95%-CI 0.316-0.953) and poorer functional outcome (aOR 0.450, 95%-CI 0.222-0.911)
Conclusion
Every tenth patients subjected to angiography for endovascular stroke treatment experiences an MVO. Patients with MVO have higher baseline systolic blood pressure and were less often medicated with statins, an observation which warrants external validation and evaluation regarding its causality. Occurrence of MVO has implication for treatment decisions, affects endovascular treatment success and is predictive of patient outcome.
Trial registration number
N/A
AS07-040
RESCUE THERAPY IN MECHANICAL THROMBECTOMY REFRACTORY OCCLUSIONS WITH DETACHABLE STENT-RETRIEVERS AND GP IIB/IIIA INHIBITORS: A SINGLE CENTER EXPERIENCE
1Hamad General Hospital, Neurology, Doha, Qatar
2Hamad General Hospital, Neuroradiology, Doha, Qatar
3Hamad General Hospital, Neurosurgery, Doha, Qatar
4Hamad General Hospital, Clinical Pharmacy, Doha, Qatar
5Hamad General Hospital, Neuroscience Institute, Doha, Qatar
Background and Aims
Mechanical Thrombectomy (MT) with stent-retrievers is standard of care. Around 25% of the cases do not reach reperfusion, and Rescue Therapies (RTs) are controversial. We aim to present our experience treating refractory occlusions (RO) by means of eptifibatide (GP IIb/IIIa inhibitors) and intracranial stent detachment.
Method
We retrospectively evaluated patients treated with MT in our Center in Doha (Qatar), from April 2015 to November 2017. Those with RO (lack of reperfusion or mTICI ≤ 2a) underwent “off protocol” RT if unstable critical stenosis was detected after 2 passes of stent-retriever. Different approaches were chosen based on expert preference. Thus, a group of patients was treated with eptifibatide alone, whereas another with intracranial stent detachment plus eptifibatide. Radiological and clinical outcome will be described and compared between both groups.
Results
During the study period, 103 patients were selected for MT. 17 (16.5%) underwent RT (5 (29.4%) eftifibatide only and 12 (70.6%) stenting plus eptifibatide). 3 cases did not recanalise (2 from eptifibatide group). 2 experienced re-occlusion on follow up angiography despite initial successful recanalization (one from each group). No patient experienced symptomatic hemorrhagic transformation. However 1 patient died due to malignant infarction. 6 (35.29%) had good outcome (mRS ≤ 2) at 90 days (25% eptifibatide vs 50% stenting; p = 0.58).
Conclusion
Rescue therapy for RO could be a necessary approach to increase the rate of recanalization and functional independence. We have described our experience with different techniques, which requires further discussion and study.
Trial registration number
N/A
AS07-041
TRANSFER SELECTION FOR ENDOVASCULAR THERAPY OF ISCHEMIC STROKE IN A COLLABORATIVE NETWORK: OFF-SITE VERSUS ON-SITE NEUROLOGY SERVICE
1Carl Gustav Carus University Hospital- Technische Universität Dresden, Neurology, Dresden, Germany
2Carl Gustav Carus University Hospital- Technische Universität Dresden, Neuroradiology, Dresden, Germany
Background and Aims
Selection of patients for endovascular therapy (EVT) may depend on the hospital providing first line assessment. We compared clinical characteristics and stroke outcomes between ischemic stroke patients transferred from telestroke hospitals without and non-telestroke hospitals with on-site neurology service.
Method
We analyzed prospective data from our ongoing stroke registry comprising consecutive ischemic stroke patients who underwent emergent EVT for large vessel occlusion in the anterior circulation at our tertiary stroke center between 01/2016 and 12/2017). Patients were transferred within our collaborative stroke network, either from telestroke hospitals following teleconsultation or non-telestroke hospitals following on-site neurological assessment. We compared baseline and clinical variables among these groups as well as stroke outcomes including complete reperfusion (TICI 2b/3), symptomatic intracerebral hemorrhage (sICH), 90-days favorable functional outcome (mRS 0–2) and 90-days survival.
Results
During the 2-years study period, 122 transferred patients underwent EVT: median age 75 years (IQR, 17); 49% men; median NIHSS score 17 (7). Fifty-seven patients (47%) were transferred from telestroke and 65 (53%) from non-telestroke neurological hospitals. No between-group differences were present with regard to demographics, vascular risk factors, tPA rate, onset-to-treatment /-groin-puncture-times, baseline ASPECTS and occlusion site (p>0.05). Rates of complete reperfusion (80% vs. 82%, p = 0.82), post-treatment sICH (0% vs. 6%; p = 0.25), 90-days survival (75% vs. 82%, p = 0.51) and 90-days favorable functional outcome (23% vs. 33%; p = 0.29) were not different between telestroke and non-telestroke patients.
Conclusion
Telemedicine may substitute on-site neurology expertise for selection of ischemic stroke patients potentially amenable to EVT.
Trial registration number
N/A
AS07-042
EVOLUTION OF OUTCOME OF THE TREATMENT WITH MECHANICAL TROMBECTOMY FROM 2010-2016
1Hospital Virgen de la Arrixaca, Neurología, Murcia, Spain
2Hospital Virgen de la Arrixaca, Neurradiología Intervencionista, Murcia, Spain
Background and Aims
Randomized clinical trials have provided data about of optimal characteristics of the candidates patients to mechanical thrombectomy (MT). However, in clinical practice, decisions must establish based on specific clinical cases. Our goal is to analyze whether the patient profile has changed over time in the treatment decision
Method
We described characteristic of patients who were treated with MT in our center from April of 2010 to May of 2016. Seven groups were created to analyze the distribution of clinical-demographic and results variables, using χ2 and Kruskall Wallis test. Good outcome was defined as mRS score of 0–2 at 3 months
Results
630 procedures were performed, with an annual progressive growth. There are no differences in the distribution of clinical characteristics, except that in 2016 fewer patients with auricular fibrillation have been treated. Wake-up strokes have increased significantly, while procedures performed with known time of more than 6 hours of symptoms have decreased. Without trends, significant changes in incidences of carotid tandem occlusion and symptomatic hemorrhage have been evidenced. Procedure times have been reduced significantly progressively. There are no differences in the functional outcome, with a poor prognosis between 46, 9 -55%, or mortality.
Conclusion
In the seven years of experience, a clear increased in the number of patients has benefitted from MT in our center, keeping stable the outcome over time. Each year, procedurés times have been progressively decreased. To improve outcome, more strict inclusion criteria should be established in the selection of patients.
Trial registration number
N/A
AS07-043
PREDICTORS OF THROMBECTOMY REFRACTORY STROKE
1Hospital La Princesa, Neurology, Madrid, Spain
2Hospital La Princesa, Neuroradiology, Madrid, Spain
Background and Aims
Thrombectomy in acute ischemic stroke is not always successful despite multiple attempts (clot aspiration and stent retriever passes). We aim to define the optimal number of attempts for successful recanalization and to describe clinical predictors of thrombectomy refractory ischemic stroke (TRIS) patients, meaning the overshoot of that number, and the clinical outcome of the TRIS patients.
Method
Consecutive patients with acute anterior circulation large artery occlusion treated with mechanical thrombectomy were retrospectively included from December 2011 to March 2017 (n = 219).
Results
The median number of thrombectomy attempts was 2[1-11]. In a receiver operating characteristic (ROC) curve analysis (AUC = 0.8), 4 was the lowest number of attempts with an acceptable rate of satisfactory recanalization (91%). Patients who underwent ≥5 thrombectomy attempts (n = 32, 15%) were defined as TRIS. TRIS patients had higher NIHSS score at admission, no M2-segment occlusion and less acenocumarol intake compared to non-TRIS patients (p < 0.05 in univariate regression; not independent predictors in multivariate regression). TRIS patients had lower rates of functional independence (3 month mRS ≤2; p = 0.002), but no differences in intraprocedural complications, symptomatic bleeding or mortality. Among TRIS patients, final successful recanalization was associated with better outcomes.
Conclusion
Our study suggests a higher risk of unsuccessful recanalization after 4 thrombectomy attempts. TRIS patients were associated with higher NIHSS score at admission, no M2 segment occlusion and no previous acenocumarol intake in univariate analyses. Despite worse functional outcome in TRIS patients, final recanalization still proved beneficial. The role of anticoagulation in TRIS patients would be an interesting avenue for further studies.
Trial registration number
N/A
AS07-045
CLINICAL CHARACTERISTICS, COLLATERAL STATUS AND LONG-TERM OUTCOME IN LATE PRESENTING STROKES UNDERGOING NEUROINTERVENTION
1Shonan Kamakura General Hospital, Stroke Center, 1370-1 Okamoto- Kamakura-city, Japan
Background and Aims
The effect of endovascular treatment performed within 8–24 hours after the onset of acute ischemic stroke (AIS) is uncertain. We investigated clinical characteristics, types of collateral status (CS) and long-term clinical outcome of those patients.
Method
We analysed AIS patients admitted in our Center (Aug. 2014 - Dec. 2017) 1) who underwent CT angiography or MR angiography showing occlusion of the internal carotid artery or M1 segment of the middle cerebral artery 2) who underwent emergent endovascular therapy within 8–24 hours from onset. Based on the time to peak and the peak value of time-intensity curve, we classified collateral status into three types. We searched patient’s baseline characteristics, ASPECTS and NIHSS on admission, types of CS on admission, mRS scores at 90 days.
Results
Totally 20 patients (13 women, mean age 79 y.o.) were included. Their median onset-to-needle time was 14.8 hours, median NIHSS score on admission was 16 and median ASPECTS on admission was 8. In CS type1(poor), type2(moderate) and type3(good), there were 1(5%), 7(30%) and 12 patients (60%). Successful recanalization (TICI = 2b-3) was achieved in 14 patients (70%). Favorable outcome at 90 days after stroke onset (mRS0-2) was reported 5 patients (25%). Sustained disability improvement on mRS by at least 1 level at 90 days was observed in 1 of 1 patient with type1, 4 of 7 patients with type2, 7 of 12 patients with type3 and in total, 12(60%) of 20 patients.
Conclusion
Emergent endovascular therapy within 8–24hours from onset could improve long-term clinical outcome in patients with high ASPECTS and good or moderate CS.
Trial registration number
N/A
AS07-046
STANDARD CT/CTA VERSUS CT PERFUSION RAPID SELECTION OF ACUTE ISCHEMIC STROKE PATIENTS FOR MECHANICAL THROMBECTOMY IN EARLY PRESENTATIONS
1Northwestern university, radiology, chicago, USA
Background and Aims
Although CTP/MRP RAPID selection has been associated with improved clinical outcomes in several randomized controlled trials, variability of imaging selection across multiple trials and methodological concerns of perfusion metrics to define ischemia has resulted in an uncertainty of excluding patients that could benefit from endovascular thrombectomy, especially in the early <6 hour intervention window.2
Method
We compared separate multi-institutional prospective neurointerventional AIS databases (same operators) of consecutive populations that underwent either standard CT/CTA imaging without or with CTP selection for mechanical thrombectomy from November 2015-2017. Statistical analysis for clinical outcomes was performed on both raw mean and percentage of patients achieving functional independence (90 day modified Rankin Score 0–2) using a normal approximation of the Wilcoxon–Mann–Whitney test
Results
In total 127 patients met clinical inclusion criteria, 59 patients underwent standard CT/CTA imaging selection/intervention without exclusion versus 68 patients that underwent CTP selection (31 thrombectomy:37 excluded). Overall 90 day clinical outcomes were insignificant between standard CT/CTA and CTP selection cohorts (mean mRS 2.3 vs 2.3, p = 0.9 and mRS 0–2 54% vs 47%, p = 0.4). On subgroup analysis, CTP selected patients that underwent thrombectomy achieved relatively excellent independent clinical outcomes (mean mRS 1.3, p = 0.02 and mRS 0–2 74.2%, p = 0.03), balancing those excluded from thrombectomy with poorer outcomes (mean mRS 3.2, p = 0.04 and mRS 0–2 24.3%, p = 0.004)
Conclusion
Although CTP selection significantly increases the rate of favorable clinical outcomes in patients treated with mechanical thrombectomy, there may be no overall population benefit or harm in comparison to standard CT/CTA selection alone in the early interventional time window
Trial registration number
N/A
AS07-047
EFFICACY OF ENDOVASCULAR INTERVENTIONAL APPROACHES ON INTRACRANIAL ARTERY DISSECTION
1Neurology & Neuroscience Research Center of Qom University of medical Sciences, Neurology, Qom, Iran
2Neuroscience Research Center of Tabriz University of Medical Sciences, Neurology, Tabriz, Iran
Background and Aims
Intracranial artery dissections are rare and many controversies exist about treatment options. The aim of this study was to evaluate the efficacy and safety of the endovascular approach in patients with an intracranial dissection presenting with different symptoms.
Method
We prospectively evaluated the clinical features and treatment outcomes of 30 patients who had angiographically confirmed nontraumatic intracranial dissections over 4 years. Patients were followed up for 17 months, and their final outcomes were assessed by the modified Rankin Score (mRS) and angiography.
Results
Sixteen (53.3%) patients had a dissection of the anterior circulation, whereas 14 (46.7%) had a posterior circulation dissection. Overall, 83.3% of the patients suffered a subarachnoid hemorrhage (SAH). Grade IV Hunt and Hess score was seen in 32% of the SAH presenting cases. Parent artery occlusion (PAO) with coil embolization was used in 70% of the cases. The prevalence of overall procedural complications was 23.3%, and all were completely resolved at the end of follow-up. No evidence of in-stent occlusion/stenosis or rebleeding was observed in our cases during follow-up. Angiography results improved more frequently in the PAO with coil embolization group (100%) than in the stent-only-treated group (88.9%) (���� = 0.310) and the unruptured dissection group (5/5, 100%) in comparison with the group that presented with SAH (95.8%) (���� = 0.833).
Conclusion
Favorable outcomes were achieved following an endovascular approach for symptomatic ruptured or unruptured dissecting aneurysms. However, the long-term efficacy and durability of these procedures remain to be determined in a larger series.
Trial registration number
N/A
AS07-048
THE “FLYING INTERVENTIONALIST” A NOVEL STROKE CARE CONCEPT FOR RURAL AREAS
1Staedtisches Klinikum München, TEMPiS, Munich, Germany
2Klinikum rechts der Isar- Technical University Munich, Department of diagnostic and interventional Neuroradiology, Munich, Germany
3University of Regenburg, Department of Neurology, Regensburg, Germany
4Kliniken Kreis Mühldorf am Inn, Department of Cardiology, Mühldorf, Germany
5University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom
6Städtisches Klinikum München, Department of Radiology, Munich, Germany
7Charite-Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
Background and Aims
Endovascular treatment (EVT) of stroke patients with large vessel occlusion a) requires high expertise, b) demands rapid treatment, and c) should be available to all eligible stroke patients throughout the country. Rural areas are underserved worldwide.
The aim is to set up an EVT service that meets all three above mentioned requirements.
Method
The comprehensive stroke center sets up a team of neurointerventionalists and assistant staff to perform EVT in rural community hospitals connected to a telestroke network (TEMPiS-Germany). In case of telemedically identified EVT candidates, the team will be flown to the hospital with an exclusive network helicopter. Meanwhile, the patient will be prepared for intervention in local angiography suite. After treatment patient will stay on local stroke unit or intensive care unit for further treatment. Special material (stent-retriever, aspiration catheters, etc.) will be brought by the team for each individual case. Data for concept development were obtained from TEMPiS-EVT-registry.
Results
11 rural hospitals participate. 257 endovascular treatments are expected/year. Median delay (decision-groin puncture) is estimated to be reduced by 100 minutes compared to secondary transfer of patients. EVT team comprises 5 neuroradiologists and 5 assistant staff members from 2 comprehensive stroke centers in Munich. Service will be provided 26 weeks/year starting 01/02/2018. Patients in “non-flying” weeks will be transferred to closest comprehensive stroke center and will serve as control group for evaluation of the concept. First data of the pilot phase will be presented.
Conclusion
Novel health care concepts need to be developed and evaluated for EVT in rural areas.
Trial registration number
N/A
AS07-049
EFFECTS OF HEPARIN DURING ENDOVASCULAR STROKE TREATMENT: A LARGE SINGLE-CENTER ANALYSIS
1Tor Vergata Hospital, Systems Medicine, Roma, Italy
2Royal Melbourne Hospital, Medicine and Neurology, Melbourne, Australia
3Tor Vergata Hospital, Imaging and Interventional Radiology, Roma, Italy
Background and Aims
The effect of heparin during endovascular treatment (ET) has been barely investigated. We evaluated safety and efficacy of heparin use during ET of acute ischemic stroke.
Method
361 patients with large vessel occlusion of anterior circulation were divided into two groups: heparin use (H+:200) and no-heparin use group (H-:161). Baseline and procedural characteristics, successful reperfusion, 3-month good clinical outcome, intracranical haemorrhage (ICH) and mortality were compared between groups.361 patients with large vessel occlusion of anterior circulation were divided into two groups: heparin use (H+:200) and no-heparin use group (H-:161). Baseline and procedural characteristics, successful reperfusion, 3-month good clinical outcome, intracranical haemorrhage (ICH) and mortality were compared between groups.
Results
baseline characteristics differed for age and CT ASPECTS [74 ± 14 vs 68.9 ± 12.2; p = 0.001 and 8(2–10) vs 8(2–10); p = 0.009]. H- patients were more often treated with intravenous thrombolysis (IVT) (69.5% vs 53%; p = 0.001) and thromboaspiration devices (98.6% vs 70.2%, p < 0.001;) and were reperfused earlier (271 ± 57.6 vs 309 ± 102.2 min; p < 0.001). H- patients showed a higher rate of successful reperfusion (82.6% vs 69.5%; p = 0.004) independently of IVT (62.5% vs 54%; p = 0.17). No differences were found in the rate of 3-month good clinical outcome, mortality and any or symptomatic ICH. Multivariate analysis confirmed successful reperfusion to be inversely associated to heparin use (95% CI: 1.1-3.3; OR: 1.9; p = 0.019).
Conclusion
our findings seem to suggest that heparin during ET does not result in different clinical outcome, mortality and rate of hemorrhagic complications but in a lower rate of reperfusion. Further research is needed to explain this finding.
Trial registration number
N/A
AS07-052
DOSE ADJUSTMENT WITH CLOPIDOGREL ORAL SOLUTION IN HYPER-RESPONDERS PATIENTS WITH INTRACRANIAL ANEURYSMS TREATED WITH STENT AND IDENTIFICATION OF CYP2C19 POLYMORPHISMS
1Hospital Universitario Virgen del Rocío, Interventional Neuroradiology, Seville, Spain
2Public Health Unit, Health Management Area South of Seville, Seville, Spain
3Hospital Universitario Virgen del Rocío, Department of Immunology, Seville, Spain
4Hospital Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Describe the individualization of dose adjustments with clopidogrel oral solution in hyper-responders patients with intracranial aneurysm treated with stent.
Method
Prospective study (from 2015 thru June 2017) in patients taking clopidogrel prior to endovascular treatment. Initial values less than 60 PRU (P2Y12 reactivity units) were classified as a hyper-response. Adjustments to the dose with clopidogrel oral solution (1 ml = 5 mg) were made according as needed to reach the target PRU range. The dose of clopidogrel oral solution was gradually reduced (30 mg-20mg-10 mg-5 mg) until 1 ml (5 mg) /day. Characterization of the most common allelic variants of CYP2C19 was carried out in patients.
Results
Fiftteen patients (53 yo, 66% female) with 17 aneurysm treated with 16 stents were classified as hyper-responder. Mean baseline PRU value and the percentage of platelet inhibition were 8.57 ± 11.5 PRU and 92.05 ± 7.5% respectively. Mean time used to decrease the dose of clopidogrel oral solution to 5 mg/day was 13 days in SAH patients and 16 days in the other patients. Modified dosing strategies showed to increase PRU values and decreased the percentage of platelet inhibition (137.42 ± 27.4 and 41.5 ± 14.8%). 123 PRU determinations were performed. No patients suffered thromboembolic events related to the dose adjustment of clopidogrel with 5 mg/day in the follow up. 10 patients were ultrarapid metabolyzers (17 17, 1 17), 3 extensive (1 1) and 2 patients intermediate-poor metabolyzers (1 2 , 2 2).
Conclusion
The individualization of treatment with clopidogrel oral solution using platelet function testing in hyper responder patients may be reasonable.
Trial registration number
N/A
AS07-053
HIGHER ANNUAL OPERATOR VOLUME IS ASSOCIATED WITH BETTER REPERFUSION RATES IN STROKE PATIENTS TREATED BY MECHANICAL THROMBECTOMY IN THE ETIS REGISTRY
1Centre Hospitalier de Versailles, Department of Neurology and Stroke center, Le Chesnay, France
2Gilbert and Rose-Marie Chagoury School of Medicine- Lebanese American University Medical Center, Department of Neurology, Beirut, Lebanon
3Hopital Foch, Department of Neurology and Stroke Center, Suresnes, France
4Université Versailles Saint-Quentin en Yvelines et Paris Saclay, Neurology, Yvelines, France
5Rothschild Foundation, Department of Interventional Neuroradiology, Paris, France
6University Hospital of Nancy, Department of Diagnostic and Interventional Neuroradiology, Nancy, France
7University of Lorraine, Laboratory of Diagnostic and Interventional Adaptative Imaging IADI- INSERM U947, Nancy, France
8Hopital Foch, Department of Diagnostic and Interventional Neuroradiology, Suresnes, France
9Univ. Lille- CHU Lille- EA 2694, Santé publique: épidémiologie et qualité des soins, F-59000 Lille, France
Background and Aims
Mechanical thrombectomy (MT) is a level IA treatment in the acute phase of ischemic stroke (IS). Characteristics of operators have been found to be an independent predictor of the outcome in interventional cardiology for STEMI syndromes.The aim of this study was to analyse if operator characteristics have an impact on reperfusion and complications rates.
Method
ETIS was a prospective, multicentre, observational real world MT registry. We enrolled consecutive IS patients treated by MT in 3 high volume MT centers with 19 operators between January 2012 and March 2017. We determined the following characteristics of operators: number of MT performed per year and total number of years experience since first MT. The rates of mTICI (Thrombolysis In Cerebral Infarction) 2b/3 and procedural complications (acquired new embolic territory infarction, arterial perforation and dissection).
Results
A total of 1541 anterior and posterior stroke patients were enrolled (mean age 67 years; median NIHSS 16). There is a significant operator variation for TICI2b/3 outcome (Intraclass correlation coefficient (ICC) = 0.046, p = 0.027) but not for complications (ICC = 0.005, p = 0.35). There was a dose response relationship between tertiles of annual volume per operator and mTICI2b/3 with an OR of 1.41 (0.91 to 2.20) for the second tertile (27-40 MT/year) and 1.88 (1.17 to 3.01) for the third tertile (> 40 MT/year) in comparison to first tertile (< 27 MT/year) (p = 0.03).
Conclusion
Our data found that favorable reperfusion (mTICI 2b/3) in IS patients treated with MT was associated with higher operator volume of MT per year (i.e.>40 MT peryear).
Trial registration number
N/A
AS07-054
FUNCTIONAL OUTCOMES IN THE VERY OLD FOLLOWING THROMBECTOMY FOR ACUTE STROKE: A MULTI-CENTER ANALYSIS
1Université de Montréal, Faculty of Medicine, Montreal, Canada
2Centre hospitalier de l'Université de Montréal, Division of Neurology, Montréal, Canada
3Centre hospitalier universitaire vaudois, Division of Neurology, Lausanne, Switzerland
Background and Aims
Very old patients were under-represented in recent randomised endovascular trials. We aimed to describe the functional outcome at 3 months after thrombectomy in patients (≥85 years of age).
Method
A cross-sectional analysis of a prospective registry of consecutive patients ≥85 years old treated for acute stroke in 2016-2017 at Hôpital Notre-Dame de Montréal (Canada) and from 2013 to 2017 at Centre hospitalier universitaire vaudois (Switzerland) by intraarterial thrombectomy (with or without intravenous thrombolysis). Eligibility for thrombectomy was determined according to guidelines and a premorbid modified Rankin Score (mRS)≤2. The primary outcome was 3-month mRS and good functional outcomes defined as a mRS≤2.
Results
A total of 141 patients (median (IQR) age 88(4) years, 66% female) were treated for acute stroke (thrombectomy alone (n = 99), thrombectomy ± thrombolysis (n = 42)). Median (IQR) NIHSS was 18 (10) and median ASPECT score 10. Following the intervention, 98 (85%) of these patients had a good TICI score (2B or 3) and 17 (12%) had a symptomatic hemorrhagic transformation. Functional outcome at 3 months was available in 96 patients. 20 (21%) patients had a good functional outcome at 3 months. The mortality rate was 55%.
Conclusion
Three-month functional outcomes are poorer in the very old despite a good premorbid functional status. However, a substantial proportion of patients do have a favorable functional outcome. Larger prospective studies are warranted to evaluate the benefit of thrombectomy in the context of an aging population.
Trial registration number
N/A
AS07-055
USE OF FLOW DIVERTORS BEYOND RECOMMENDATIONS - FOR RUPTURED ANEURYSMS - AN INDIAN EXPERIENCE
1Masterstroke - Stroke and Neurointervention Clinic, Department of Neurology and Neurointervention, NAGPUR, India
2King Edward Memorial Hospital and Research Centre- Pune- India, Department of Interventional Neuroradiology, pune, India
3Apollo Hospital, Departmetn of Interventional Neuroradiology, Ahmedabad, India
4Sterling Hospital, Departmetn of Interventional Neuroradiology, Ahmedabad, India
5King Edward Memorial Hospital and Research Centre- Pune- India, Departmetn of Interventional Neuroradiology, Pune, India
6Apollo Hospital, Departmetn of Interventional Neuroradiology, Nashik, India
Background and Aims
To explore the feasibility of use of flow-divertor (FD) stents for treatment of ruptured intracranial aneurysms; as currently, they are approved only for use in untreatable unruptured ICA aneurysms.
Method
Patients with ruptured intracranial aneurysms, untreatable either by coiling or clipping, were selected for flow divertor stenting with predesigned antiplatelet protocol. Periodic follow-up neurological examination and 6 month follow-up DSA were done.
Results
Flow divertors were deployed for total of 24 ruptured aneurysms, of which 15 were located at ICA, 2 at ACA and 7 in posterior circulation. 6 were saccular, 8 were fusiform whereas 10 were blister aneurysms. 17 were small, 5 were large and 2 were giant aneurysms. 23 Flow divertor stents were used to treat these 24 aneurysms. 2 patients had in-stent thrombus formation during post-deployment checkshoots, which was completely resolved by giving intra-arterial tirofiban and there were no ischemic or hemorrhagic complications in the post-procedure period. 1 had wire related perforation, but it remained clinically silent (as it was controlled by immediate heparin reversal and lowering of blood pressure). 6 monthly follow-up is available for 22 aneurysms of which 20 had total occlusion (91% occlusion rate) and 2 aneurysms had a minor remnant (9%). 2 patients had severe in-stent stenosis (9%) whereas all the branches covered by the FDs remained patent on comparison with baseline DSAs. There was no mortality.
Conclusion
Flow divertor treatment can be a reasonable treatment option for otherwise untreatable ruptured aneurysms; careful case selection remains the key for successful outcome.
Trial registration number
N/A
AS07-056
USE OF FLOW DIVERTORS BEYOND RECOMMENDATIONS - FOR POSTERIOR CIRCULATION ANEURYSMS - AN INDIAN EXPERIENCE
1Masterstroke - Stroke and Neurointervention Clinic, Department of Neurology and Neurointervention, NAGPUR, India
2King Edward Memorial Hospital and Research Centre- Pune- India, Departmetn of Interventional Neuroradiology, Pune, India
3Apollo Hospital, Departmetn of Interventional Neuroradiology, Ahmedabad, India
4Sterling Hospital, Departmetn of Interventional Neuroradiology, Ahmedabad, India
5Apollo Hospital, Departmetn of Interventional Neuroradiology, Nashik, India
Background and Aims
Can flow-divertors, currently approved only for unruptured untreatable ICA aneurysms, be used for posterior circulation aneurysms?
Method
Patients with posterior circulation aneurysms, untreatable either by coiling or clipping, ruptured and unruptured, were selected for flow divertor stenting with predesigned antiplatelet protocol. Follow-up periodic neurological examination and 6 month follow-up DSA were done.
Results
14 posterior circulation aneurysms in 11 patients (8 of vertebral artery, 3 of basilar artery, 1 of superior cerebellar artery and 2 of P1 segment of PCA) were treated with FD, 7 ruptured and 7 unruptured; 8 fusiform and 6 saccular. All 14 aneurysms showed evidence of immediate contrast stasis after deployment of FD. None of the vessels covered by the stents were occluded nor any patient had intra-procedural complication. No patient showed any angiographic evidence of distal thromboembolism or any leak from distal vessel. 2 patients (with 3 aneurysms) developed peri-procedural complications (1 with 2 FDs in-situ developed in-stent thrombosis and 1 had rupture after 5 days) and both expired [Mortality – 2/11 (18%) – both unruptured]. No other patient had any transient or permanent neurological deficits during the 6 month follow-up period. At the 6 month follow-up, all of remaining 11 aneurysms had total occlusion (occlusion rate–100%); none of the them had any in-stent stenosis or covered branch occlusion compared to the baseline DSA.
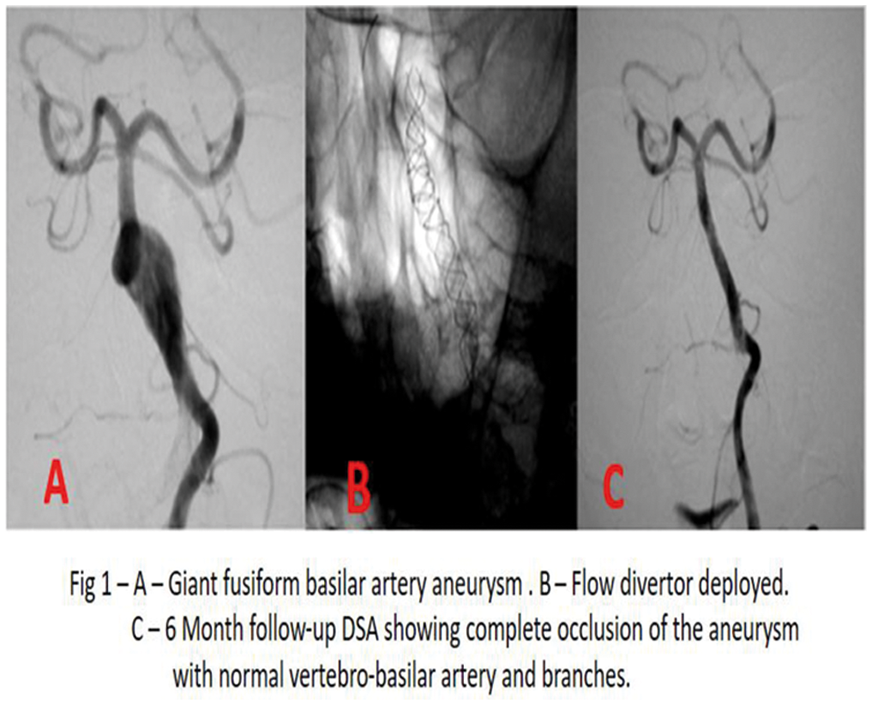
Conclusion
Flow divertor treatment can be a reasonable treatment option in posterior circulation aneurysms including ruptured aneurysms; careful case selection remains the key for successful outcome.
Trial registration number
N/A
AS07-057
“DRIVE THE DOCTOR” - TRANSFERRING THE NEUROINTERVENTIONALIST INSTEAD OF REFERRING THE PATIENT IN ACUTE LVO STROKE: A MATCHED-PAIRS ANALYSIS
1University of Heidelberg, Department of Neuroradiology, Heidelberg, Germany
2University of Heidelberg, Department of Neurology, Heidelberg, Germany
3Klinikum Frakfurt Hoechst, Department of Neurology, Frankfurt, Germany
Background and Aims
Providing ubiquitous interventional service in acute stroke due to large vessel occlusion (LVO) is a major challenge. As an alternative to referring the patient to a comprehensive stroke center (CSC), the neurointerventionalist may be transferred to the patient.
Method
We compared clinical and interventional characteristics of acute stroke patients with LVO either treated in a tertiary care hospital 100km remote by transfer of the neurointerventionalist (“drive the doctor”; DD) or at the CSC site after referral from other hospitals (“drip and ship”; DS) over a comparable distance between 2012 and 2016. To correct heterogeneity in baseline parameters, we matched patients with regard to sex, age, site of occlusion, NIHSS and ASPECTS and compared the clinical outcome and procedural characteristics.
Results
From 60 (DD) and 67 (DS) patients, respectively, 19 pairs were matched. Patients in the DD group were diagnosed after 103 min (vs. 157; p = 0.16) and were treated significantly earlier after diagnosis was made (201 vs. 345 min.; p < 0.001). They had successful recanalization in 94% and good outcome was achieved in 52% while DS patients had successful recanalization in 79% and good outcome in 36% in the DS group (p = 0.34 and 0.33, respectively).
Conclusion
In acute LVO stroke, transferring the neurointerventionalist instead of referring the patient resulted in significantly faster recanalization. Good outcome and successful recanalization were also different, both in favor of the DD group, but this was non-significant due to the small sample size. “Drive the doctor” is a promising concept that should be further evaluated prospectively.
Trial registration number
N/A
AS07-058
IMPACT OF MORE STRICT CORE-BASED SELECTION CRITERIA ON THE FUNCTIONAL OUTCOME OF STROKE PATIENTS OLDER THAN 80 YEARS-OLD TREATED WITH ENDOVASCULAR THERAPY
1Hospital Clínico Universitario de Valladolid, Stroke Unit. Neurology Department, Valladolid, Spain
2Hospital Clínico Universitario de Vallodolid, Stroke Unit. Neurology Deparment, Valladolid, Spain
3Hospital Clínico Universitario de Valladolid, Neuroradolgy Department, Valladolid, Spain
Background and Aims
Previous studies have shown that the impact of baseline core on endovascular therapy (EVT) response increases with age, and recent EVT clinical trials used specific core thresholds for patients >80. We aimed to evaluate the effect of using strict vs. open core-based criteria on the clinical response to EVT in patients >80.
Method
Retrospective analysis of a prospective stroke reperfusion registry from a regional stroke center. We included consecutive patients >80 y.o. with ischemic stroke due to large-vessel-occlusion in the anterior circulation treated by EVT. From May 2015 to December 2016 our selection criteria were based on plain CT-ASPECTS and similar for <80 and >80 age groups. In 2017 we applied more strict criteria for patients >80: ASPECTS 9–10 in plain-CT and core-volume <25cc in CT-perfusion if ASPECTS <9. Primary outcome variable was good functional outcome at third month (mRS≤2). Secondary outcome variables: symptomatic hemorrhagic transformation and mortality. We compared both periods.
Results
We included 71 patients (mean age 84 years; 42% male; median baseline NIHSS 19) of whom 45 (63%) were treated during the first period. Both groups were comparable in baseline NIHSS and ASPECTS. Patients in the second period were more frequently autonomous at day 90 (60% vs 40%; p = 0.022). Being treated after protocol review was independently associated with better functional outcome after a crude logistic regression model (OR:3.3 [1-10,3]; p = 0.035).
Conclusion
Selection of ischemic stroke patients older than 80 for EVT using specific and more strict core-based selection criteria is associated with a better clinical response.
Trial registration number
N/A
AS07-059
IS STROKE ETIOLOGY A PREDICTOR OF SUCCESSFUL RECANALIZATION STATUS IN ACUTE ENDOVASCULAR THERAPY?
1University of Colorado Denver, Department of Neurology, Aurora, USA
2University of Colorado Denver, School of Medicine, Aurora, USA
3University of Colorado Denver, Department of Neurosurgery, Aurora, USA
Background and Aims
Endovascular treatment (EVT) using stent-retriever therapies is considered the gold-standard approach for the treatment of acute ischemic stroke (AIS) in selected patient populations. The Thrombolysis in Cerebral Infarction (TICI) scale measures recanalization. Prior studies have demonstrated that a good neurological outcome depends on procedural success (considered a TICI2b or TICI3 score), collateral status and patient-specific factors. It remains unclear if stroke etiology is a predictor of procedural success. We sought to determine if stroke etiology using the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification was an independent predictor of successful recanalization in acute EVT
Method
We reviewed our retrospectively collected endovascular database at the University of Colorado, Anschutz Medical Center for patients with acute ischemic strokes from January 2014 to June 2017 that underwent EVT. We evaluated baseline characteristics, procedural data, and TOAST classification to determine if there was an association between stroke etiology and TICI grade
Results
A total of 121 patients were analyzed. Our analysis controlled for age, cardiovascular risk factors, previous antithrombotic therapy, baseline National Institutes of Health Stroke Scale score, intravenous thrombolytic therapy (IV tPA), time of onset to IV tPA, and time of onset to reperfusion. There was no association between stroke etiology determined by TOAST classification and successful recanalization status after statistical evaluation using ANOVA test (F (5,117) = 0.48, p = 0.79)
Conclusion
We did not find an association between stroke etiology and successful recanalization in this retrospective case series of over 120 consecutive EVT patients
Trial registration number
N/A
AS07-060
MANAGEMENT OF PATIENTS WITH MINOR CLINICAL DEFICITS DESPITE A LARGE CEREBRAL VESSEL OCCLUSION
1Inselspital Bern- University Hospital- University of Bern, Neurology, Bern, Switzerland
2University Hospital Erlangen, Neurology, Erlangen, Germany
3University Hospital Erlangen, Neuroradiology, Erlangen, Germany
Background and Aims
The optimal management of stroke patients with only minor clinical deficits in spite of an acute large vessel occlusion (LVO) is currently unknown. While pathophysiologic considerations support an early reperfusion therapy of the occluded vessel, those patients were not sufficiently represented in randomized controlled trials and initial medical treatment with rescue-intervention only in case of secondary neurological deterioration is common.
Method
In this monocentric retrospective study all patients who underwent mechanical thrombectomy between 01/2013 and 12/2016 at the University Medical Center Erlangen were investigated. Patients with National Institutes of Health Stroke Scale (NIHSS)<5 on admission were identified and management of these patients was dichotomized according to “acute recanalization” and “initial medical management with rescue-intervention in case of secondary deterioration”. Intra-hospital mortality and functional outcome on day 90 using the Modified Rankin Scale dichotomized according to favorable (mRS 0–2) and poor (mRS 3–6) were assessed.
Results
223 patients (184 (83%) with anterior circulation stroke) were included. Median age was 75 (interquartile range (IQR) 60-80) years, 120 (54%) patients were female. 13 (6%) patients presented with NIHSS<5 on admission. Rescue-intervention (n = 5) was associated with a high rate of poor functional outcome (4 (80%) and a higher intra-hospital mortality compared to immediate thrombectomy (n = 8) (4 (80%) vs. 1 (13%), p = 0.032).
Conclusion
Initial medical management with rescue-intervention in patients with LVO and minor neurological deficits is associated with a high risk of unfavorable outcome. Timely diagnosis and recanalization of LVO should be considered and prospectively examined even in patients with mild symptoms.
Trial registration number
N/A
AS07-062
USE OF PERIPROCEDURAL INTRAVENOUS HEPARIN DURING MECHANICAL THROMBECTOMY FOR ACUTE ISCHEMIC STROKE: RESULTS FROM THE MR CLEAN REGISTRY
1Erasmus MC, Neurology, Rotterdam, The Netherlands
2Erasmus MC, Radiology, Rotterdam, The Netherlands
3Erasmus MC, Public Health, Rotterdam, The Netherlands
4Academic Medical Center, Radiology, Amsterdam, The Netherlands
5Haaglanden Medical Center, Radiology, Den Haag, The Netherlands
6Sint Antonius Hospital, Neurology, Nieuwegein, The Netherlands
Background and Aims
The risks and benefit of periprocedural intravenous (IV) heparin use in patients with ischemic stroke undergoing mechanical thrombectomy (MT) remain uncertain. We evaluated the periprocedural IV heparin use in Dutch stroke intervention centers, and assessed its safety and efficacy.
Method
All patients treated with MT in the Netherlands are registered in the MR CLEAN Registry. Patients registered between March 2014 and June 2016 were analyzed. We used random effects logistic and ordinal regression analysis to compare patients treated with and without periprocedural IV heparin. We adjusted for center-effects and prognostic factors. The primary outcome was symptomatic intracerebral hemorrhage (sICH). Secondary outcomes were successful recanalization (extended thrombolysis in cerebral infarction ≥ 2B), 90-day functional outcome (modified Rankin Scale), and 90-day mortality.
Results
A total of 1488 patients from 16 centers were analyzed, of which 398 (27%) patients received IV heparin (median dose 5000 IU). Between-center variability in heparin use was substantial (range: 0%-94%). There was no excess sICH risk in patients receiving heparin (6% vs. 6%; adjusted odds ratio (aOR) 1.10, 95% confidence interval (CI) 0.63-1.92). Also, no association was found between heparin use and successful recanalization (aOR 1.24, 95%CI 0.89-1.72), functional outcome (adjusted common OR 1.18, 95%CI 0.84-1.65), or mortality (aOR 0.92, 95%CI 0.62-1.38), although all secondary effect parameters point towards benefit.
Conclusion
Among patients treated with MT, substantial between-center variability exists in periprocedural IV heparin use. Its use seems safe, but a randomized trial is needed to confirm this and assess whether this adjunctive therapy is beneficial.
Trial registration number
N/A
AS07-064
THE IMPACT OF A WELL-ORGANIZED STROKE NETWORK ON ACUTE STROKE MANAGEMENT: AN INITIAL DATA OF ACUTE STROKE ENDOVASCULAR THERAPY
1Medicalpark Hospital MLP Care Brain Angiography and Stroke CentreBASC, Neurology Department, Istanbul, Turkey
2Istanbul Aydın University Brain Angiopraphy and Stroke Centre BASC, Istanbul, Turkey
3Istinye University Liv Hospital Brain Angiography and Stroke Centre BASC, Istanbul, Turkey
4GOP MedicalPark Hospital Brain Angiopraphy and Stroke Center BASC, Neurology Department, Istanbul, Turkey
5Istinye University Liv Hospital Brain Angiography and Stroke Centre BASC, Neuroradiology Department, Istanbul, Turkey
Background and Aims
Effective implementation of acute stroke care is strictly related to institutional and geographical limitations. Stroke Network aims to minimize such barriers to secure timely and effective acute treatment. We reviewed the results of the first 3 months experience.
Method
Brain Angiography and Stroke Centre (BASC) Network includes three comprehensive stroke centre (CSC) distributed in
Results
A total of 186 acute stroke patients (Male 57%) were admitted. Median onset-to-door time was 255 minutes. Seventy-four patients received revascularization therapy (27% only IVT, 46% only mechanical thrombectomy (EVT), 27% Bridging therapy). Out of 54 patients that received EVT, 2 patients remained as intention-to-treat and 10 patients (19%) underwent EVT following >6h of onset. The mean NIHSS on admission was 14. The rate of tandem and M1 segment occlusion were 9/54 (17%) and 20/54( 37%) respectively. Median door-to-femoral puncture and femoral puncture-to-recanalization time was 40 and 44 minutes respectively. mTICI ³2b and first-pass recanalization rate was 89% and 54% respectively. At discharge favourable (mRS 0–2) outcome rate was 46%. NIHSS and mRS assessments will be evaluated at 3-months follow-up. In-hospital mortality rate was 4.3%. Only 1 symptomatic haemorrhage occurred (1,9%).
Conclusion
Networking facilitated the access to IVT and/or EVT treatment in eligible patients. Our geographic setting, established interaction between centres and early access to multimodal, automatized, penumbral imaging modalities are major contributing factors in obtaining improved outcomes and benchmark indicators. the resent results.
Trial registration number
N/A
AS07-065
BLOOD-BRAIN BARRIER DISRUPTION AFTER ACUTE ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY: A DYNAMIC CONTRAST-ENHANCED MAGNETIC RESONANCE IMAGING STUDY
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2CIBER de Bioingeniería- Biomateriales y Nanomedicina CIBER-BBN, Biomedical Imaging, Barcelona, Spain
3Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Blood-brain barrier (BBB) disruption may impair the efficacy of mechanical thrombectomy (MT). We aimed to investigate the predictors of diffuse BBB-disruption evaluated through Dynamic Contrast-Enhanced (DCE)-MRI after acute ischemic stroke treated with MT
Method
Thee study included a prospective cohort of 67 patients (median NIHSS = 18) with proximal occlusions in the carotid territory treated with MT and evaluated with a DCE-MRI within 24h after treatment. Patlak-derived K-trans maps were used to obtain the volume of tissue with severely increased BBB permeability within the DWI lesion, defined as regions with K-trans values higher than the 99th percentile of the contralateral non-ischemic tissue.
Results
The volume of infarcted tissue with diffuse BBB-disruption was median (IQR) 0.6 (0.14-2.81) ml. In multivariate models including baseline and treatment-related variables, the variables independently associated with diffuse BBB-disruption were higher pretreatment leukocyte count (adjusted Odds Ratio [aOR]=1.19, 95% confidence interval [95%CI]=1.07-1-32) as well as recanalization beyond 6-hour from stroke onset (aOR = 1.43, 95%CI = 1.09-1-87) or persistent occlusions (aOR = 1.66, 95%CI = 1.22-2.25). In analyses restricted to patients with successful recanalization, longer time to recanalization (aOR = 1.16 per each IQR increase, 95%CI = 1.02-1.31) remained as an independent predictor of diffuse BBB-disruption
Conclusion
Diffuse BBB-disruption was associated with higher pretreatment inflammatory status as well as with longer time of ischemia before recanalization or persistent occlusions. These results highlight the relevance of early recanalization for protecting BBB integrity and give further support to the role of permeability imaging as a promising tool for the evaluation of the effect of adjunctive neuroprotective therapies.
Trial registration number
N/A
AS07-068
ENDOVASCULAR RECANALIZATION IN POSTERIOR CIRCULATION STROKE WITH ASPIRATION DEVICES IS FASTER, EFFECTIVE AND NOT DETRIMENTAL TO OUTCOME COMPARED TO STENT RETRIEVER DEVICES: THE NORDICTUS REGISTRY
1H.U.Donostia, Neurology Department, San Sebastian, Spain
2H. U. Donostia, Radiology, San Sebastian, Spain
3H.U.Donostia, Radiology, San Sebastian, Spain
4Hospital Marqués de Valdecilla., Neurology, Santander, Spain
5H.U. Valladolid, Neurology, Valladolid, Spain
6Hospital U. Central Asturias, Neurology, Oviedo, Spain
7Hospital U Alava, Neurology, Vitoria, Spain
8Hospital Clínico Universitario Santiago, Neurology, Santiago, Spain
9Hospital Galdakao, Neurology, Galdakao, Spain
10H. U. Burgos, Neurology, Burgos, Spain
11Hospital U. Miguel Servet, Neurology, Zaragoza, Spain
12Hospital U. Basurto, Neurology, Bilbao, Spain
13Hospital León, Neurology, León, Spain
14Hospital Vigo, Neurology, Vigo, Spain
15Hospital U. A Coruña, Neurology, A Coruña, Spain
Background and Aims
To describe and compare procedural data and outcome after endovascular therapy (EVT) for posterior circulation acute ischemic stroke (AIS), focusing on the technical device used.
Method
Retrospective analysis of the prospective multicenter reperfusion registry in NORDICTUS, a research network of stroke centers in Northern Spain serving an area of 11.5 M people. Patients with posterior circulation AIS receiving EVT at 13 NORDICTUS stroke centers during 2015-2016 were included. Baseline characteristics, procedural data, and outcomes were evaluated. Patients were divided in three groups according to the device used: stent retriever, aspiration or combination of both.
Results
We included 77 posterior circulation AIS patients (mean age 72, 40% women). The distribution of arterial occlusion was 60 basilar artery, 14 posterior cerebral artery and 3 vertebral artery. Forty patients were treated with stent retriever, 21 with aspiration and 16 used combined therapy. Aspiration, stent retriever and combined therapy groups were comparable regarding main baseline variables. Recanalization TICI 2B/3 was achieved in 19 (91%) patients with aspiration devices, 30 (75%) with stent retriever and 13 (81%) with combination therapy. Groin-to-reperfusion time was shortest in the aspiration group (55 min) as compared to 90 min and 60 min in the stent and combination groups, respectively. Modified Rankin scale 0–2 at three months was achieved in 41 (53%) patients and it was comparable among groups. No differences were seen in terms of safety.
Conclusion
Endovascular recanalization in posterior circulation stroke with modern aspiration devices is faster, effective and no detrimental to outcome compared to stent retriever devices.
Trial registration number
N/A
AS07-069
INTER-HOSPITAL TRANSFER OF PATIENTS WITH ACUTE ISCHEMIC STROKE FOR EVALUATION OF ENDOVASCULAR THROMBECTOMY IS SAFE
1University Hospital/TU-Dresden, Neurology, Dresden, Germany
2University Hospital/TU-Dresden, Neuroradiology, Dresden, Germany
Background and Aims
Telestroke networks may improve the availability of endovascular treatment (EVT) for patients with large vessel occlusion in rural areas. We aimed to determine the safety of inter-hospital transfer in these patients.
Method
We included all patients with acute ischemic stroke who were transferred to our tertiary stroke center for evaluation of EVT between 05/2017 and 11/2017. Data were derived from our prospective EVT registry. We analyzed baseline characteristics including NIHSS scores at the remote hospital prior to transport, NIHSS scores on arrival, acute therapies performed including intravenous thrombolysis and medical interventions associated with inter-hospital transfer. We defined clinical deterioration as an increase of departure to arrival NIHSS score >4 points
Results
In the observed time, 114 patients with acute ischemic stroke were evaluated for EVT at our center. Of these, 75 patients (67%) were transferred from remote hospitals (median age 76 years [IQR 18], 49% male, median baseline NIHSS score 15 [IQR 6]), 49 patients (65%) received intravenous thrombolysis. Median departure-to-arrival time was 36 minutes [IQR 23]. Among transferred patients, 14 (19%) required medical interventions associated with the transfer: 6 patients (8%) were intubated prior to the transport and 8 further patients (11%) required at least 1 medical intervention during the transfer. No patient suffered from a severe complication and 6 (9%) of the non-intubated patients deteriorated clinically during transfer.
Conclusion
Transfer of stroke patients for evaluation of EVT in a telestroke network seems safe. Transfer associated medical interventions are required in a minority of patients
Trial registration number
N/A
AS07-070
ENDOVASCULAR THROMBECTOMY FOR POSTERIOR CIRCULATION TANDEM OCCLUSIONS
1Hospital Universitario Donostia, Neurology, Getxo, Spain
2Hospital Universitario Donostia, Neurology, Donostia, Spain
3Hospital Universitario Donostia, Radiodiagnostic and Interventional Radiology, Donostia, Spain
4Hospital Universitario Marqués de Valdecilla, Neurology, Santander, Spain
5Hospital Clínico Universitario de Valladolid, Neurology, Valladolid, Spain
6Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
7Hospital Universitario de Araba, Neurology, Vitoria, Spain
8Hospital Clínico Universitario de Santiago, Neurology, Santiago de Compostela, Spain
9Hospital de Galdakao, Neurology, Galdakao, Spain
10Hospital Universitario de Burgos, Neurology, Burgos, Spain
11Hospital Universitario Miguel Servet, Neurology, Zaragoza, Spain
12Hospital Universitario Basurto, Neurology, Bilbao, Spain
13Hospital de León, Neurology, León, Spain
14Complejo Hospitalario Universitario de Vigo, Neurology, Vigo, Spain
15Complejo Hospitalario Universitario A Coruña, Neurology, A Coruña, Spain
Background and Aims
Posterior circulation tandem occlusions, particularly those involving basilar artery, have poor prognosis. To date, scarce information has been published regarding endovascular thrombectomy for posterior circulation tandem occlusions.
Method
Descriptive analysis of 14 cases with posterior circulation stroke and tandem arterial occlusion treated with endovascular thrombectomy in six tertiary stroke centers belonging to the research network NORDICTUS (Northern Spain) during 2015-2016.
Results
Median age was 71.5 years-old (range 35-85) and five (36%) were women. Three patients presented a vertebral-basilar artery tandem occlusion, 10 a basilar-posterior cerebral artery tandem occlusion and 1 a vertebral-posterior cerebral artery tandem occlusion. Eight patients received intravenous alteplase previously and 6 patients received direct thrombectomy. Eight patients underwent stent retriever-based thrombectomy, 3 underwent aspiration-based thrombectomy and 3 underwent stent retriever plus aspiration thrombectomy. Mean time onset-to-thrombectomy was 4.32 hours (range 1.03-6.46). Recanalization 2B/3 was achieved in 12 patients (86%) and mean time-to-recanalization was 62.71 minutes (range 10-120). One patient suffered from a local complication during procedure, 2 patients suffered brain oedema and hemorrhagic transformation was not observed. Three patients (21%) were dead at discharge and at 3 months; 9 patients (64%) remained with functionally independent (modified Rankin Scale <3) at 3 months.
Conclusion
Endovascular thrombectomy for posterior circulation tandem occlusions seems to be feasible without major complications and is expected to increase the chances of good outcome in this otherwise dreaded scenario.
Trial registration number
N/A
AS07-071
TREATMENT OF ISCHAEMIC STROKE WITH THROMBECTOMY ALONE AND WITH BRIDGING THERAPY WITH INTRAVENOUS THROMBOLYSIS (TPA) - UK NATIONAL REGISTRY DATA
1Royal College of Physicians, Care Quality Improvement Department, London, United Kingdom
2King's College London, Division of Health and Social Care Research, London, United Kingdom
3University College London, Farr Institute of Health Informatics Research, London, United Kingdom
4Royal Devon and Exeter NHS Foundation Trust, Royal Devon and Exeter NHS Foundation Trust, Exeter, United Kingdom
Background and Aims
We used real-world data from the Sentinel Stroke National Audit Programme (SSNAP), the UK national stroke register (excluding Scotland) to compare the characteristics and early outcomes of patients with acute ischaemic stroke treated with thrombectomy according to use of bridging therapy with tPA.
Method
Patient-level data from 85,122 records in SSNAP were analysed for patients admitted between April 2016 and March 2017. We compared baseline characteristics and early outcomes of patients that had bridging therapy with tPA plus thrombectomy (n = 369) versus thrombectomy alone (n = 211).
Results
Patient characteristics were generally similar between the two groups. Differences include lower prevalence of AF (15% versus 35%, p < 0.001), shorter known onset to arrival time (73 minutes versus 155 minutes, p < 0.001), and more severe stroke (median NIHSS 18 versus 16, p = 0.004) in the tPA group.
Patients receiving bridging tPA had shorter known onset to completion times (300 vs 331 minutes, p = 0.006) but longer arrival to completion times (207 vs 177 minutes, p = 0.016) for thrombectomy. Procedural times were similar in both groups.
There were no differences in reperfusion rates (mTICI) or early outcomes (0–2 NIHSS at 24h, 19% with tPA vs 22%, p = 0.443) between the two groups.
Conclusion
There are some differences in casemix between patients receiving bridging tPA prior to thrombectomy, and those without. Arrival to completion times are longer in the group receiving tPA, presumably reflecting extra time spent on delivering tPA first. Reperfusion rates and early neurological outcomes were similar, which supports ongoing trials to understand the additional efficacy of bridging therapy in patients receiving thrombectomy.
Trial registration number
N/A
AS07-072
DRIP AND SHIP VERSUS MOTHERSHIP AND THEIR INFLUENCE ON THE LIKELIHOOD OF RECEIVING ENDOVASCULAR THERAPY AND ITS OUTCOME
1Hospital Clinico Universitario de Valladolid, Neurology, Valladolid, Spain
2Hospital Clinico Universitario de Valladolid, Radiology, Valladolid, Spain
3Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
Background and Aims
Acute ischemic stroke (AIS) patients who are candidates for endovascular therapy (EVT) may be transferred to the Comprehensive Stroke Center (CSC) via mothership (M) or drip&ship (D&S) systems. We aimed: to (1)evaluate whether M-vs.-D&S influences the probability of receiving EVT,(2)identify variables associated with receiving EVT in the D&Sgroup, and (3)analyze the relationship between the transportation system and EVT-outcome.
Method
Retrospective analysis of our CSC prospective registry (06/2015-12/2016). We included consecutive AIS patients with large-artery occlusion who were eligible for EVT after first CT-scan, performed either at CSC(M) or at referring hospital (RH, D&S). The proportion of candidates receiving EVT per CSC protocol was recorded. D&S patients underwent repeated neuroimaging at CSC. We recorded baseline variables, primary outcome endpoint: 90-day-mRS(0–1, and 0–2), and secondary endpoint: PH-type hemorrhagic transformation.
Results
We analyzed data from 212 patients (median age:72, median NIHSS:18), 115(54%)D&S, and 96(46%)M. No differences in age, NIHSS, or ASPECTS-at-origin were observed. D&S patients showed a longer onset-to-CSC time (336min vs. 194min, p < 0.001) and a worse ASPECTS-at-CSC(p < 0.001). Proportion of candidates qualifying for EVT was lower in D&S(71,62%) vs. M(78, 81%), p = 0.002. Predictors for EVT in the D&Scohort were: ASPECTS-at-origin (OR 1.77[1.3-2.5], p = 0.001) and ASPECTS-decay between RH and CSC(OR 0.55[0.38-0.8], p = 0.002). After EVT, we observed a higher PH-rate (p = 0.02), a lower mRS:0-1rate (p = 0.04), and a trend towards a lower mRS:0-2rate (p = 0.06) in the D&S group in univariate models, associations not resisting multivariable adjustment.
Conclusion
In our CSC network, D&S implied a lower probability of receiving EVT and a trend towards a worse outcome after EVT. Interestingly, ASPECTS-at-origin and ASPECTS-decay between RH and CSC determine the chances of being treated with EVT in D&S system.
Trial registration number
N/A
AS07-073
COMPARISON OF NEW-GENERATION DOUBLE-LAYER MICROMESH CAROTID STENT-SYSTEM VERSUS CAROTID SELF-EXPANDING HYBRID STENT SYSTEM IN SYMPTOMATIC CAROTID ARTERY STENOSIS
1Kantonsspital Aarau, Institut für Neuroradiologie/ Klinik für Neurologie, Aarau, Switzerland
2Kantonsspital Aarau, Klinik für Neurologie, Aarau, Switzerland
3Kantonsspital Aarau, Institut für Neuroradiologie, Aarau, Switzerland
Background and Aims
Carotid artery stenosis is a relevant cause of ischemic stroke. Carotid artery stenting is an emerging alternative treatment option to surgical carotid endarterectomy. Several carotid stent-systems with different stent designs are available. CASPER (MicroVention, Inc., USA) – a double-layer micromesh carotid stent-system designed to prevent peri-procedural embolic release – belongs to the latest generation of carotid stent system. The aim of this study was to assess efficacy and safety of CASPER compared to a carotid self-expending hybrid stent system (Invatec Cristallo Ideal, Medtronic, USA) (Cristallo) in symptomatic carotid artery stenosis (sCS).
Method
A single-center, open-label, retrospective cohort study of 57 consecutive patients with proven sCS between 01/2014–08/2017 executed at a tertiary stroke center in Switzerland. Outcome measures were i) good clinical outcome at 90 days (mRS<2), ii) peri-procedural complications and ischemic events iii) re-occlusion rate and iiii) mortality within 30 days.
Results
22 patients (23% women, median age 75 years (interquartile range (IQR) 71-80) were treated with CASPER, 35 patients (29% women, median age 71 years (IQR 63-76) years) with Cristallo. In both groups, pre-treatment carotid stenosis had similar median NASCET score of 80%. Successful deployment was achieved in all cases without technical failure and similar re-occlusion rates and mortality rate within 30 days. Clinical outcome was similarly beneficial in both groups. In the Cristallo group peri-procedural ischemic event was insignificantly higher (3 vs 0; p = 0.16). Periprocedural complications did not differ significantly between groups.
Conclusion
CASPER and Cristallo demonstrate to be similarly effective and safe in symptomatic carotid artery stenosis.
Trial registration number
N/A
AS07-074
INTRACEREBRAL BLEEDING UNDER DUAL ANTIPLATELETS AFTER EMERGENCY RECANALIZATION OF INTRACRANIAL AND EXTRACRANIAL LARGE ARTERY OCCLUSION
1Otto-von-Guericke University Magdeburg, Neurology, Magdeburg, Germany
2Otto-von-Guericke University Magdeburg, Neuroradiology, Magdeburg, Germany
Background and Aims
To assess bleeding risk of (stent-protected) angioplasty (PTA) of extracranial internal carotid (ICA) occlusion with subsequent dual antiplatelet agents in addition to intracranial endovascular thrombectomy in acute anterior circulation stroke.
Method
Between 01/2009 and 12/2017 515 out of 1801 consecutive patients admitted to our university stroke center with an acute severe anterior circulation stroke underwent endovascular thrombectomy for intracranial large artery occlusion. Admission CT was rated according to ASPECTS and controlled after 24 hours, 4 days, and in case of patients’ clinical worsening.
Results
70 out of 515 patients (13.6%; 48 men; mean age 65.1 years, SD 11.3) underwent additional extracranial PTA for extracranial ICA occlusion/pseudo-occlusion. PTA was stent-protected in 37 patients because of ulcerative or thrombogenic ICA plaque or insufficient dilatation for thrombectomy-catheter passage by sole PTA. 44 patients received dual antiplatelet agents, i.e. ticagrelor in 28 and clopidogrel in 16 in addition to ASA. Chi-square test revealed an association of dual antiplatelet prevention within 24 hours after (stent-protected) PTA and early spontaneous symptomatic intracerebral bleeding (P = 0.028) and a trend for an increased bleeding frequency if ticagrelor has been used instead of clopidogrel (P = 0.075). No bleeding association was found for intravenous thrombolysis (37 patients), intraarterial thrombolysis (19 patients), and ASPECTS at admission (median, 8.5; IQR, 8 to 10).
Conclusion
Clopidogrel/ticagrelor in addition to ASA within 24 hours of intracranial thrombectomy and extracranial (stent-protected) PTA in acute stroke from extra-intracranial tandem occlusion is associated with increased intracerebral bleeding with a trend to higher risk by ticagrelor.
Trial registration number
N/A
AS07-076
FAST PROGRESSORS GET THE MOST BENEFIT FROM THROMBECTOMY DESPITE LARGER PRETREATMENT INFARCT CORES
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Recent trials on mechanical thrombectomy (MT) in late time windows have excluded from treatment patients with large baseline infarct cores (IC). We aimed to compare the quantitative effectiveness of MT in terms of infarct growth (IG) on clinical outcomes in patients with small, medium or large pre-treatment IC.
Method
We studied a prospective cohort of 338 acute stroke patients with proximal occlusions in the carotid territory (256 treated with MT, 82 treated with best medical care (BMC)) who had pre-treatment computed tomographic perfusion (CTP) and 24h follow-up DWI. According to the IC in CTP, patients were classified into 3 subgroups: small (<10cc: n = 81 MT, n = 29 BMC), medium (10-50cc: n = 138 MT, n = 35 BMC) and large (>50cc: n = 37 MT, n = 17 BMC). We compared baseline characteristics, IG between CTP and DWI, and outcome (mRS) at 3 months
Results
Expectedly, increasing pre-treatment IC was associated with greater reduction of IG (IG 5cc with MT versus 35cc with BMC). Yet, the clinical benefit was maximal in patients with IC >50cc (mRS 3 in MT versus mRS 5 in BMC). The clinical benefits were not associated with baseline imbalances between IC groups.
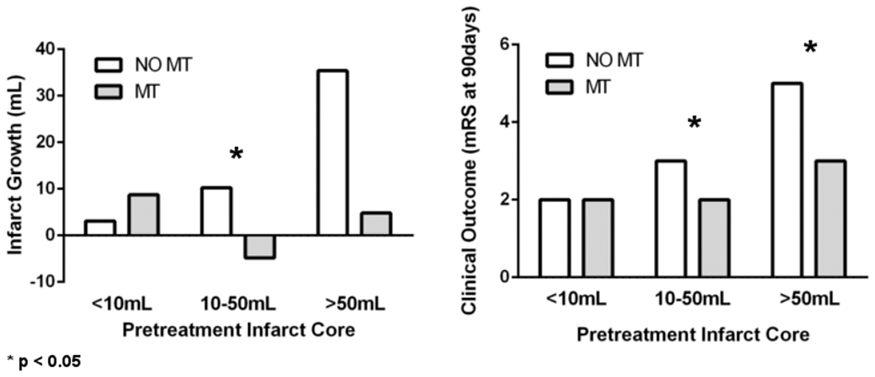
Conclusion
MT may be especially effective in patients presenting with large baseline IC (fast-progressors). These results caution against too restrictive criteria for MT in patients with large vessel occlusions.
Trial registration number
N/A
AS07-078
THROMBECTOMY 6 TO 24 HOURS AFTER STROKE USING THE ALBERTA STROKE PROGRAM EARLY CT SCORE (ASPECTS)
1Centro Hospitalar de Lisboa Central - Hospital Santo António dos Capuchos, Neurology, Lisbon, Portugal
2Centro Hospitalar de Lisboa Central - Hospital de São José, Neuroradiology, Lisbon, Portugal
3Centro Hospitalar de Lisboa Central - Hospital de São José, Unidade Cerebro Vascular, Lisbon, Portugal
Background and Aims
DAWN trial recently established the benefit of mechanical thrombectomy (MT) for patients with occlusion of intracranial internal carotid (ICA) or middle cerebral artery (M1 or M2), last known to be well 6 to 24 hours earlier with deficit-infarct mismatch. We aim to determine outcomes for MT performed at our centre in similar patients with ASPECTS ≥ 7 instead of deficit-infarct mismatch.
Method
Analysis of extracted data, between 2013 and 2017, from local Safe Implementation of Treatment in Stroke (SITS) registry. ASPECTS were calculated by a neuro-radiologist blinded to clinical outcome. Primary endpoint was functional independence (modified Rankin score ≤ 2) at 90 days.
Results
We identified 43 patients with occlusions at the M1-segment (n = 24, 55,8%), M2-segment (n = 12, 27,9%) and intracranial ICA (n = 7, 16,3%). Mean age at stroke onset was 69,7 years (SD ± 12,9). Median admission NIHSS was 14 (IQR 9–19). Stroke onset time was unknown in 20 patients: 14 (32,6%) ‘wake-up strokes’ and 6 (14,0%) ‘daytime unwitnessed-onset strokes’. Median interval between time last known to be well and groin puncture was 575 min (IQR 400-730 min). Rate of functional independence at 90 days was 60,5%. Rate of symptomatic intracranial haemorrhage was 2,3% and 90-day mortality 9,3%.
Conclusion
In our series, patients with ischemic stroke last known to be well 6 to 24 hours earlier and an ASPECTS ≥ 7 treated with MT, functional independence rate at 90 days was similar to DAWN trial result (60,5% vs. 49%). Further research is needed to determine reliability of the ASPECTS in assessing favourable outcome for this time-window.
Trial registration number
N/A
AS07-079
ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE IN DRIP & SHIFT PATIENTS: THE IMPORTANCE OF PERFORMING PERFUSION IMAGING AT THE REFERRING HOSPITAL
1Hospital Clínico Universitario de Valladolid, Neurology, Valladolid, Spain
2Hospital Clínico Universitario de Salamanca, Neurology, Salamanca, Spain
3Hospital Universitario Marqués de Valdecilla, Neurology, Santander, Spain
4Hospital Universitario Donostia, Neurology, Donostia, Spain
5Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
6Hospital Universitario Araba, Neurology, Vitoria, Spain
7Complexo Hospitalario Universitario de Santiago, Neurology, Santiago, Spain
8Hospital de Galdakao, Neurology, Galdakao, Spain
9Hospital Universitario de Burgos, Neurology, Burgos, Spain
10Hospital Universitario Miguel Servet, Neurology, Zaragoza, Spain
11Hospital de Basurto, Neurology, Bilbao, Spain
12Complejo Asistencial Universitario de León, Neurology, León, Spain
13Complexo Hospitalario Universitario de Vigo, Neurology, Vigo, Spain
14Complexo Hospitalario Universitario de A Coruña, Neurology, A Coruña, Spain
Background and Aims
We aimed to evaluate the prognostic impact of the imaging modality performed at referring hospitals in drip and shift (D&S) acute ischemic stroke (AIS) patients receiving endovascular therapy (EVT) within a network of tertiary stroke centers in Northern Spain (NORDICTUS).
Method
We studied consecutive anterior circulation AIS patients treated with EVT in 13 stroke centers after D&S. The use of cerebral perfusion imaging at the first hospital was recorded. Other usual baseline clinical and radiological variables were registered. Primary outcome variable was good long-term outcome (3rd month mRS≤2).
Results
During 2015 and 2016, 245 AIS patients treated with EVT via D&S model in NORDICTUS were included. Of them, 96 (39%) underwent perfusion imaging at the referring hospital. Patients in the perfusion group had a higher use of intravenous thrombolysis (p = 0.001), and showed similar baseline NIHSS and ASPECTS scores, as compared to the non-perfusion group. Most perfusion patients (n = 75, 78%) skipped repeated brain imaging at the stroke center, which meant a significant reduction in door-to-groin time (34 vs. 95 min, p < 0.001). Good outcome rate was higher in the perfusion group (66% vs. 36%, p < 0.001). A multivariable-adjusted logistic regression model showed that perfusion imaging at the referring hospitals predicted good long-term outcome (OR 2.2, [1.07-4.6], p = 0.032).
Conclusion
The use of perfusion imaging at the referring hospitals predicted a better long-term outcome in AIS patients treated with EVT following the D&S model. Perfusion imaging in D&S may help select patients with better collateral capacity and may allow an earlier start of EVT.
Trial registration number
N/A
AS07-081
NEUTROPHIL TO LYMPHOCYTE RATIO ON ADMISSION PREDICTS INTRACRANIAL HEMORRHAGE AFTER ENDOVASCULAR THROMBECTOMY IN ACUTE ISCHEMIC STROKE
1Universitätsklinik Salzburg, Neurology, Salzburg, Austria
2King's College Hospital, Neurology, London, United Kingdom
3Paracelsus Medical University Salzburg, Research Institute for Neurointervention, Salzburg, Austria
4Universitätsklinik Salzburg, Neuroradiology, Salzburg, Austria
Background and Aims
The immune system plays a major role in the development of intracranial hemorrhagic complications in acute ischemic stroke. Higher neutrophil to lymphocyte ratio (NLR) in peripheral blood has been shown to be associated with intracranial hemorrhage (ICH) and poor functional outcome in acute ischemic stroke patients. Here, we studied whether NLR at baseline also predicts hemorrhagic complications and poor functional outcome after endovascular treatment (EVT).
Method
We performed a retrospective analysis of consecutive patients with anterior circulation ischemic stroke who underwent EVT at a tertiary care center from 2012-2016. Follow-up scans from day 2–7 were examined for non-procedure (vessel perforation during catheterization) related ICH. We correlated demographic, clinical and laboratory data with occurrence of non-procedure related ICH.
Results
We identified 187 patients with a median age of 74 years (interquartile range [IQR] 60-81) and a median baseline National Institutes of Health Stroke scale (NIHSS) of 18 (IQR 13-22). One-hundred-thirty-three (71%) patients received intravenous rt-PA. ICH was detected in 31 (16.5%) patients and was associated with higher NLR, larger intracranial thrombus, and prolonged door-to-needle and total intervention times. In multivariate analysis, higher baseline NLR was independently associated with ICH (OR 1.09 per unit increase, 95% CI 1.00-1.20), p = 0.040.
Conclusion
Higher NLR is an independent predictor of ICH after EVT. Further studies should focus on better understanding of the role of the immune system in the development of ICH after attempting mechanical reperfusion.
Trial registration number
N/A
AS07-082
CAROTID STENTING IN THE ACUTE PHASE OF STROKE: ANTIPLATELET THERAPY REGIMEN BASED ON EARLY DUAL-ENERGY CT SCAN
1Hospital Universitario Central de Asturias, Neurology, Gijón, Spain
2Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
3Hospital Universitario Central de Asturias, Interventional Neuroradiology, Oviedo, Spain
4Hospital Universitario Central de Asturias, Neuroradiology, Oviedo, Spain
Background and Aims
Acute tandem occlusions often require carotid stenting. Combination of mechanical and pharmacologic therapies in addition to antiplatelet drugs administered to prevent acute stent thrombosis might increase the risk of intracerebral haemorrhage. We present a protocol of antiplatelet regimen based on early post-procedural Dual-Energy CT (DE-CT).
Method
Consecutive stroke patients with tandem occlusions treated with acute carotid stenting after intracranial thrombectomy in our centre were reviewed. All patients received intravenous lysine acetylsalicylate during the procedure. Dual (aspirin+clopidogrel with or without clopidogrel load) or mono (aspirin) antiplatelet regimen was administered 12-24 hours later according to brain DE-CT findings (figure 1). Carotid ultrasonography was performed at 24h and before discharge. We evaluated the rate of subsequent symptomatic intracranial haemorrhage (SICH) and acute stent thrombosis in each group.
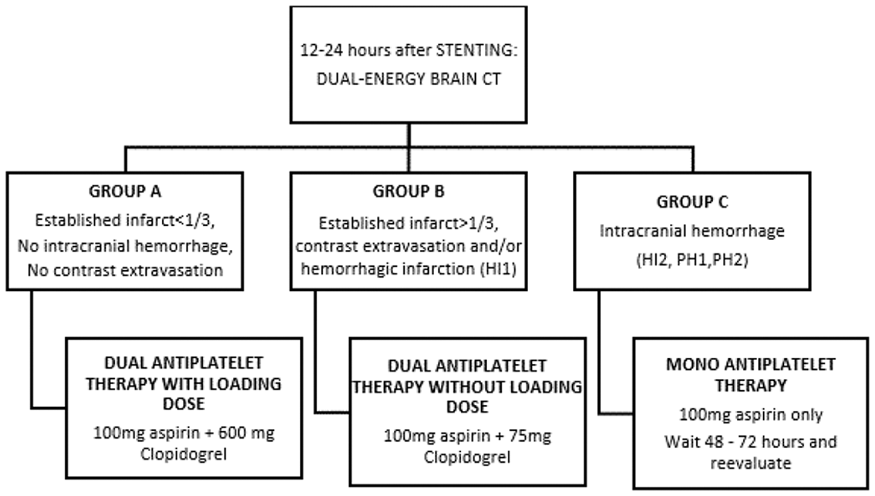
Results
Between June 2014 and December 2016, 50 patients were included (mean age 66 years, 76% men, baseline NIHSS 16, median time from symptom onset to recanalization 266 minutes). According to DE-CT, 24 patients were assigned to GROUP A, 19 to GROUP B and 7 to GROUP C (4 of them had SICH at that time). One patient suffered a subsequent SICH (belonging to GROUP B with a HI1 in first CT). There was only one stent thrombosis without clinical repercussions in GROUP B.
Conclusion
DE-CT may contribute to select antiplatelet regimen after acute carotid stenting in tandem occlusions.
Trial registration number
N/A
AS07-083
ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE DUE TO M2 OCCLUSIONS IN CLINICAL PRACTICE
1Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
2Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
3Haaglanden Medical Center, Neurology, The Hague, The Netherlands
4Academic Medical Center, Radiology, Amsterdam, The Netherlands
5Haaglanden Medical Center, Radiology, The Hague, The Netherlands
6Maastricht University Medical Center, Radiology, Maastricht, The Netherlands
Background and Aims
We aimed to determine functional outcome, technical aspects and complications of EVT in patients with M2 occlusions.
Method
Data was obtained from the MRCLEAN Registry. We included patients with an M2 or M1 occlusion on DSA. We compared functional outcome (mRS 90 days, using ordinal logistic regression) and delta-NIHSS in patients with an M2 occlusion and patients with an M1 occlusion. Recanalization rates (TICI≥2B), symptomatic intracranial hemorrhage (sICH), and complication rate were analyzed. Additionally, anatomical variation in dominance of the M2 branch (difference in trunk thickness) was studied.
Results
In total, 239 (24%) patients with M2 and 742 (76%) patients with M1 occlusions were analyzed. The median delta-NIHSS was -5 (IQR: -10-0) and -4 (IQR:-8-0] (p = 0.22) in M1 and M2 occlusions, respectively. We did not find better functional outcomes in patients with M2 occlusions (acOR 1.23; 95%CI 0.87–1.73). Recanalization (56.4% vs 60.2%; p = 0.34), sICH (6.3% vs 5.9%; p = 0.97), and complication rate (27.7% vs 29.7%; p = 0.65) did not differ between M2- and M1-occlusions. Dominant M2 branch occlusion occurring in 78% of M2 occlusions, versus non-dominant M2 branch occlusion was associated with worse functional outcome (aOR 0.25; 95%CI 0.10-0.64).
Conclusion
Functional outcome, recanalization and complications of EVT in patients with an M2 occlusion do not differ from those with an M1 occlusions. In the majority of M2 occlusions, thrombus was located in a dominant M2 branch, responsible for perfusion of the main part of the MCA territory.
Trial registration number
N/A
AS07-084
STROKE THROMBECTOMY EXPERIENCE IN A NEUROSCIENCES UNIT COVERING A LARGE NON URBAN REGION
1Plymouth Hospitals NHS Trust, Neurology, Plymouth, United Kingdom
Background and Aims
Plymouth Hospital NHS Trust is the Regional Neurosciences Unit in the Southwest of England. Its thrombectomy service covers a large area (6,375sq km) with a sparse population of 2m. It currently runs during weekday working hours and accepts inter-hospital transfers from other areas in the region. These are mostly by land, but due to the rural geography and often poor travel conditions, can be by air ambulance. We performed a retrospective review of our services.
Method
Cases were collated between 2013-2017. Demographics, NIHSS scores and arterial puncture times were extracted from our Radiology & Sentinel Stroke National Audit Program database. Follow up calls were performed to administer a previously validated simplified Modified Rankin Score (smRS) assessment.
Results
Forty cases were treated for proximal anterior circulation clots. Travel distance ranged from 1.3 to 66 miles. 7 deaths occurred in the first 30 days. 17 cases were available to follow up. sMRS was recorded an average 1.5 years after their stroke. Outcomes per smRS category were: 0 (17.6%), 1 (11.7%), 2 (5.9%), 3 (29.4%), 4 (5.9%), 5 (29.4%). The average door to puncture times reduced from 143min to 91 min in line with service changes in 2017. The average outcome smRS reduced 3.2 to 2.3.
Conclusion
A change and streamlining of our thrombectomy services has led to shorter door to puncture times and a reduction in overall smRS. Our review shows the long term functional benefit of this treatment and that is feasible to deliver this service across a large geographical area.
Trial registration number
N/A
AS07-085
PARENCHYMAL HEMATOMA TYPE 1 AS A PREDICTOR OF FUTILE REPERFUSION AFTER ENDOVASCULAR THERAPY FOR ACUTE ISCHEMIC STROKE IN THE NORDICTUS REGISTRY
1Hospital Clinico Universitario de Valladolid, Department of Neurology, Valladolid, Spain
2Hospital Universitario Marques de Valdecilla, Department of Neurology, Santander, Spain
3Hospital Universitario Donostia, Department of Neurology, Donostia, Spain
4Hospital Universitario Central de Asturias, Department of Neurology, Oviedo, Spain
5Hospital Universitario de Álava, Department of Neurology, Vitoria, Spain
6Hospital Clínico Universitario de Santiago, Department of Neurology, Santiago de Compostela, Spain
7Hospital Galdakao-Usansolo, Department of Neurology, Vizcaya, Spain
8Hospital Universitario de Burgos, Department of Neurology, Burgos, Spain
9Hospital Universitario Miguel Servet, Department of Neurology, Zaragoza, Spain
10Hospital Universitario de Basurto, Department of Neurology, Bilbao, Spain
11Complejo Asistencial Universitario de León, Department of Neurology, León, Spain
12Complejo Hospitalario Universitario de Vigo, Department of Neurology, Vigo, Spain
13Complejo Hospitalario Universitario A Cor, Deparment of Neurology, Coruña, Spain
Background and Aims
We aimed to evaluate the relationship between the different patterns of hemorrhagic transformation and futile reperfusion after endovascular therapy (EVT)for acute ischemic stroke (AIS)
Method
Retrospective analysis of the prospective multicenter reperfusion registry in NORDICTUS, a research network of stroke centers in Northern Spain serving an area of11.5 M people. AIS patients who received EVT during2015-2016 in 13NORDICTUS centers were included. Futile reperfusion (FR)was defined as a poor functional outcome (mRS> 2)at day 90 despite complete recanalization after EVT(TICI 2b or 3 grades). Hemorrhagic transformation (HT)on control CT scan was categorized as none, hemorrhagic infarction (HI)1&2, parenchymal hematoma (PH)1&2 and remote hematoma (RH).Multivariable-adjusted logistic regressions were performed to estimate the risk of FR for each HT category, using no-HT as the reference.
Results
From a total of 884 AIS patients treated with EVT, 710(80%),(mean age 72, 51% women, median NIHSS 16)achieved complete recanalization. Of them, 298(42%)experienced FR. Age, baseline NIHSS&ASPECT scores, higher clot burden score, poor collaterals, longer procedure duration, TICI 2b, hypodensity volume and presence of HT on 24-h CT were associated with FR. Multivariable-adjusted regression models showed that PH-2[OR 18, (3–107), p < 0.001]and PH-1[OR 4.4, (1.7-11), p = 0.002], but not HI, predicted FR
Conclusion
Not only PH-2, but also PH-1 emerged as a predictor of futile reperfusion after EVT for AIS. This observation may challenge the current vision of PH-1 as an “asymptomatic” phenomenon after reperfusion therapies.
ion, TICI 2b, hypodensity volume and presence of HT on 24-h CT were associated with FR. Multivariable-adjusted regression models showed that PH-2 [OR 18, (3–107), p < 0.001] and PH-1[OR 4.4, (1.7-11), p = 0.002], but not HI, predicted FR.
Trial registration number
N/A
AS07-086
PREDICTORS OF GOOD RESPONSE TO ENDOVASCULAR TREATMENT OF POSTERIOR CIRCULATION STROKE
1Vall d'Hebron University Hospital, Department of Neuroradiology, Barcelona, Spain
2Vall d'Hebron University Hospital, Department of Neurology, Barcelona, Spain
3Vall d'Hebron University Hospital, Universitat Autònoma de Barcelona, Barcelona, Spain
4Vall d'Hebron University Hospital, MR Unit and Section of Neuroradiology, Barcelona, Spain
Background and Aims
It is not clear which patients benefit from the endovascular treatment of posterior circulation stroke.
Method
We evaluated consecutive patients with acute stroke in the posterior circulation who underwent endovascular treatment from January 2015 to December 2017. Primary outcome was the rate of good outcome as a mRS score 0–3 at three months. Secondary outcome was mortality at one month. We compared clinical, radiological and angiographic parameters with poor and good outcomes. Adjusted logistic regression models established independent predictors of outcomes.
Results
We included 49 consecutive patients (mean age, 70.4 ± 12.5; median NIHSS, 16 IQR 8–30). Good outcome rate was 34% (n = 17). Age (p = 0.006), smoking (p = 0.036), hypertension (p = 0.025), previous mRS (p = 0.01), presence of atherosclerosis lesion (p = 0.026), passes needed to achieve recanalization (p = 0.009) and low procedural cost (p = 0.007) were significantly associated with good outcome. In a multivariate analysis, age (OR 1.106, 95%CI 1.032-1.185, p = 0.005) and atherosclerosis (OR 0.128, 95%CI 0.019-0.853, p = 0.034) were independent predictors of good outcome. Mortality rate was 43% (n = 21). The presence of atherosclerosis lesion (p < 0.0001), the number of passes needed to achieve recanalization (p = 0.025), unsuccessful recanalization (p = 0.013) and high procedural cost (p = 0.007) were significantly associated with poor outcome. The presence of atherosclerosis lesion predicted mortality independently from age, recanalization and previous rtPA (OR 13.7, 95%CI 2.44-77.9, p = 0.003).
Conclusion
The appropriate selection of patients for the endovascular treatment of posterior circulation stroke should take into account the presence of atherosclerosis and age as negative prognostic factors. These selection criteria may improve treatment outcomes and efficiently spent stroke care resources.
Trial registration number
N/A
AS07-088
TANDEM WALKING BETWEEN THE GUIDELINES AND THE TRIALS - REAL LIFE SITUATIONS IN TANDEM OCCLUSION STROKES
1University Emergency Hospital, Neurology Department, Bucharest, Romania
2University Emergency Hospital, Radiology Department, Bucharest, Romania
Background and Aims
Tandem occlusions are an aggravating factor for acute stroke prognosis, as they have a poor response to iv rtPA, and can be particularly difficult to address by endovascular approach.
Method
We present a series of four tandem occlusion acute stroke cases, treated by thrombaspiration in combination with angioplasty, with and without stenting.
Results
3 cases combined a high grade stenosis (two by dissection, one atheromatous) of the cervical segment of the internal carotid artery (ICA) with occlusion of M1 (2 cases) or M2 (1 case) segment of medial cerebral artery (MCA); one case had stenosis of the vertebral artery (V1), combined with a basilar artery occlusion. All cases were treated by a proximal to distal approach, two by baloon angioplasty and two by angioplasty and stenting. Recanalization achieved was TICI 3 in all cases, but despite good recanalization the vertebro-basilar stroke had an unfavorable prognosis. Median door-to-groin time was 227 min. rt-PA was given in one case, the other three being out of the 4.5 hours window (two wake-up strokes). We discuss the treatment combinations in order to avoid acute stent thrombosis, after administration of rt-PA, with a highlight on eptifibatide.
Conclusion
Real life situations find us in the ER caught between the guidelines and the results of new trials proving the efficacy of EVT in an extended time window or raise several problems regarding endovascular treatment following i.v thrombolysis, especially in the particular situation when angioplasty with stenting is necessary in order to perform thrombaspiration.
Trial registration number
N/A
AS07-089
TANDEM OCCLUSIONS AND ENDOVASCULAR TREATMENT
1Hospital Universitari de Bellvitge, Neurology, Barcelona, Spain
2Hospital Universitari de Bellvitge, Radiology, Barcelona, Spain
Background and Aims
The tandem occlusions are associated with strokes of severe clinical impairment and difficulty in their treatment election. The degree of reperfusion of the occluded intracranial vessel may be modest due to the difficulty of carotid access. The treatment of carotid stenosis is not well defined in the guidelines of clinical practice and its results are indeterminate.
Method
We analyzed patients with tandem occlusions treated with interventionism between June 2010 and October 2017. We determined the degree of intracranial recanalization, the use of angioplasty or carotid stent and the functional situation and hemorrhagic complications according to the treatment used.
Results
We reviewed 822 patients treated with thrombectomy, of which 120 presented acute intracranial occlusions associated with critical stenosis or carotid occlusion. 33,3% of the carotids were treated (n = 40), with 55% receiving angioplasty alone (n = 22) and 45% stent (n = 18). The degree of intracranial TICI 2b-3 recanalization was similar to patients with other occluded arteries irrespective of carotid treatment (70% vs 75%). Intracraneal recanalization was reached in 77.5% (n = 31) of treated carotids and 67% of untreated carotids (n = 53). The angioplasty group had slightly better recanalization (stent 71,3%, n = 13 vs. angioplasty 81%, n = 18). The degree of functional independence (mRankin 0–2) in tandem occlusions is lower than other occlusions (41,2% vs 51%) but the treatment of the carotid (stent or angioplasty) did not modify this result or SICH.
Conclusion
Tandem occlusions present an intracranial recanalization similar to the rest of occlusions. The treatment of the carotid does not modify the functional situation in the third month.
Trial registration number
N/A
AS07-090
ACCESS TO ENDOVASCULAR THERAPY FOR ACUTE ISCHEMIC STROKE IN PORTUGAL - EVT-PT STUDY
1Centro Hospitalar Lisboa Norte, Stroke Unit, Lisboa, Portugal
2Centro Hospitalar de São João, Stroke Unit, Porto, Portugal
3Centro Hospitalar Lisboa Central, Stroke Unit, Lisboa, Portugal
4Centro Hospitalar e Universitário de Coimbra, Stroke Unit, Coimbra, Portugal
5Centro Hospitalar do Porto, Stroke Unit, Porto, Portugal
6Centro Hospitalar de Vila Nova de Gaia e Espinho, Stroke Unit, Vila Nova de Gaia, Portugal
7Hospital Garcia de Orta, Stroke Unit, Lisboa, Portugal
8Centro Hospitalar Lisboa Ocidental, Stroke Unit, Lisboa, Portugal
9Hospital de Braga, Stroke Unit, Braga, Portugal
Background and Aims
Endovascular therapy (EVT) for acute ischemic stroke is the state of the art treatment for large artery occlusion and similarly to IV-tpa treatment is highly time-dependent. Due to geographic and population disparities within each country, it is critical to optimize the access of the patients to the centers capable of performing EVT.
We aimed to characterize the frequency and geographic dispersion of EVT access in mainland Portugal.
Method
We included all patients resident in mainland Portugal, that were submitted to EVT between July 2015 and June 2017 in Portuguese hospitals. Geographic dispersion was calculated using the postal code of the patient’s residence and expressed as EVT rate per 100.000 inhabitants. Direct age standardization to 2016 Portuguese population was performed.
Results
1608 EVT procedures were performed during the 24 month period. Gross EVT rate was 8.18/100.000 inhabitants with an increase from the first (6.38/100.000 inhabitants) to the second year (9.99/100.000 inhabitants). Standardized EVT rates per district varied between 1.69/100.000 to 18.0/100.000 inhabitants. A gradient between coast/interior regions and North/South regions was evident on the geographic dispersion maps.
Figure 1. Number of EVTs performed per 100.000 inhabitants, per district (annual average adjusted to age)

Conclusion
This is the first study that characterised the geographic dispersion of EVT in mainland Portugal. A disparity between coast/interior regions and North/South regions was found. EVT access mapping is crucial to evaluate treatment access equity and to develop new health strategies.
Trial registration number
N/A
AS07-091
LARGE-SCALE, CORE-TEAM ASSESSED EVALUATION OF THE SAVE TECHNIQUE
1University Medical Center, Neuroradiology, Göttingen, Germany
2University Hospital Aachen, Neuroradiology, Aachen, Germany
3University Hospital Kiel, Neuroradiology, Kiel, Germany
4University Hospital Cologne, Radiology and Neuroradiology, Cologne, Germany
Background and Aims
The “Stent retriever Assisted Vacuum-locked Extraction” (SAVE) technique has been introduced as an effective embolectomy method in stroke patients suffering from intracranial large vessel occlusion (LVO). We present our multicenter, long-term experience with SAVE.
Method
Retrospective, core-team analysis of 200 patients undergoing embolectomy using the SAVE technique due to intracranial LVO at 4 German centers. Primary endpoints were first-pass and overall complete/near-complete reperfusion, defined as a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2c and 3. Secondary endpoints were number of passes, time from groin puncture to reperfusion, embolization to new territories (ENT), and post-interventional symptomatic intracranial hemorrhage (sICH).
Results
Median age was 78 years (IQR 68-85). Median National Institute of Health Stroke Scale (NIHSS) at admission was 16 (IQR 12-20). Occlusions sites were: ICA-T in 39/200 (19.5%), M1 in 123/200 (61.5%), M2 in 29/200 (14.5%), and others in 9/200 (4.5%) cases. The primary endpoints were documented in 114/200 (57% first-pass mTICI2c or 3) and 154/200 (77% overall mTICI2c or 3) patients, respectively. The overall median time from groin puncture to reperfusion was 35 min (IQR 26-53) with a median of 1 (IQR 1-2) attempts. ENTs were observed in 3 patients (1.5%) and the rate of sICH was 4.6%. The rate of successful reperfusion (mTICI ≥2b) on final angiograms was 95%.
Conclusion
SAVE is an effective, fast and secure embolectomy method. First-line use of SAVE leads to high-rates of complete/near-complete reperfusion.
Trial registration number
N/A
AS07-092
THROMBECTOMY IN BASILAR ARTERY OCCLUSION: A CASE SERIES REVIEW AT A LARGE TERTIARY REFERRAL CENTRE
1Charing Cross Hospital- Imperial College Healthcare Trust, Hyper Acute Stroke Unit, London, United Kingdom
2Charing Cross Hospital- Imperial College Healthcare Trust, Neuroradiology, London, United Kingdom
Background and Aims
Imperial College Healthcare Trust operates London’s largest Hyper-Acute Stroke Unit and the tertiary thrombectomy centre for North West London. We evaluated the outcomes and workload for patients undergoing thrombectomy for basilar artery occlusions (BAO) at our site.
Method
We analysed our prospective patient registry for those undergoing thrombectomy for basilar artery occlusions over a 13-month period from October 2016.
Results
67 patients underwent thrombectomy. 13 (19.4%) were for BAO. 11/13 were male. Median age was 61 (IQR: 46-74). Median pre-morbid MRS was 0 (IQR:0-1).
8/13 were referred from other hospitals, 9/13 were defined as severe at presentation (coma/locked-in/tetraplegic), 7 were intubated pre-procedure. Median time from referral to arrival for the non-local patients was 141 minutes (IQR: 109-169). Median door to groin time was 105 minutes (IQR: 69-156). 6/13 received thrombolysis.
Post thrombectomy 7/13 had TICI 3 recanalization, 2 had 2b, 2 had 2a. Post-procedure 9/13 (69.2%) required admission to ICU, 5/13 required intubation for longer than 24hrs. The median length of intubation was 7 days (IQR:4-14) and 3/13 required a tracheostomy.
The median length of stay was 7.5 days (IQR 4.75-32.25). 9/13 patients had an MRS ≥4 on discharge. 2/13 died, both within 24 hours of procedure.
Conclusion
Our patients had similar outcomes to the BASICS registry which did not show benefit for BAO thrombectomy. The longer than expected transfer times and door to groin may reflect an unwell patient cohort. This review has emphasised the need to improve patient transfer pathways and patient selection to optimise outcomes while awaiting RCT results.
Trial registration number
N/A
AS07-093
SAFETY AND EFFICACY OF DUAL ANTIPLATELET THERAPY IN CAROTID STENTING IN ACUTE ISCHEMIC STROKE PATIENTS WITH TANDEM CAROTID LESIONS WHO UNDERWENT ENDOVASCULAR THROMBECTOMY
1Liverpool Hospital, Department of Interventional Neuroradiology, Sydney, Australia
2Florey Institute of Neuroscience and Mental Health, Stroke Division, Melbourne, Australia
3University of New South Wales UNSW, Prince Of Wales Hospital Clinical School, Sydney, Australia
4Ingham Institute for Applied Medical Research, Stroke & Neurology Research Group, Sydney, Australia
5Prince of Wales Hospital, Institute of Neurological Sciences, Sydney, Australia
6Liverpool Hospital, Department of Neurology & Neurophysiology, Liverpool, Australia
7Hunter Medical Research Institute & John Hunter Hospital- University of Newcastle, Priority Research Centre for Stroke & Brain Injury, Newcastle, Australia
8Western Sydney University, South West Sydney Clinical School- School of Medicine, Sydney, Australia
9University of New South Wales UNSW, South Western Sydney Clinical School, Sydney, Australia
10Prince of Wales Hospital, Department of Neurology, Sydney, Australia
Background and Aims
Tandem carotid lesions in acute ischemic stroke (AIS) pose challenging treatment decisions and have a worse outcome than intracranial large vessel occlusion (LVO) alone. Safety and efficacy data of dual antiplatelet therapy (DAT) in the setting of carotid stenting during endovascular thrombectomy (EVT) are limited. The aim of this study is to assess symptomatic intracranial haemorrhagic (sICH) rates in patients receiving DAT with clopidogrel (DATC) or prasugrel (DATP) whilst undergoing carotid stenting during EVT for LVO.
Method
Consecutive AIS patients with tandem carotid lesions (n = 44) undergoing EVT for LVO who also underwent carotid stenting during the acute neurointervention at two comprehensive stroke centres (January 2016-November 2017) were included. Patients received loading doses of clopidogrel (150-600mg)/aspirin (100-600mg) or prasugrel (15-20mg)/aspirin (300-600mg).
Results
24 patients received DATC (17 males; age = 70.3 ± 11.3y) and 20 patients received DATP (16 males; age = 66.2 ± 9.2y). 6[25%] DATC and 6[30%] DATP patients received prior tissue plasminogen activator (tPA). 10[42%] DATC and all DATP patients also received abciximab (5-20mg) intraoperatively. Symptomatic ICH (parenchymal or subarachnoid) occurred in 4[17%] of DATC and 4[20%] of DATP patients. Stent occlusion/stenosis at 24-hours occurred in 2[8%]/3[12.5%] DATC and in none of the DATP patients. Prior tPA, age and time to reperfusion from stroke onset did not correlate with sICH risk.
Conclusion
DAT with prasugrel during carotid stenting in AIS patients undergoing EVT had similar sICH rates to DAT with clopidogrel and possibly a lower stent occlusion rate. Further studies are warranted to determine the optimal antiplatelet approach for carotid stenting during EVT for LVO.
Trial registration number
N/A
AS07-094
SPONTANEOUS RECANALIZATION OF MAJOR CEREBRAL ARTERIAL OCCLUSION JUST BEFORE EMERGENT CONVENTIONAL ANGIOGRAPHY
1Inha University Hospital, Neurology, Seoul, Republic of Korea
Background and Aims
Mechanical thrombectomy is one of treatment options to the patients with hyperacute ischemic stroke caused by major cerebral artery occlusion. Sometimes, spontaneous recanalization was observed on emergent conventional angiography. However, characteristics of recanalization in hyperacute period remained unknown. Here, we investigated the predictors for recanalization of major cerebral arterial occlusion just before conventional angiography and outcomes of these cases.
Method
We reviewed hyperacute ischemic stroke patients who were admitted from July 2013 to August 2015 and took conventional angiography after identification of major arterial occlusion on MR or CT scans. We analyzed the difference of risk factors, clinical characteristics and outcomes between the spontaneous recanalization group and the others.
Results
A total of 104 subjects were enrolled (70 men, 69.0 ± 10.6 years old). Among them, nine patients had recanalization on conventional angiography before neurointervention(9 men, 66.0 ± 10.2 years old). Spontaneous recanalization group was more frequently associated with men (p = 0.02), embolic stroke etiology (p = 0.05) and the history of diabetes mellitus(p 0.02), compared to non-recanalization group. Duration from stroke onset to MR or CT scan was much shorter in recanalization group than non-recanalization group (63.1 ± 21.2 vs 180.4 ± 276.2 minutes, p < 0.01). Among recanalization group, four subjects (44.4%) had 2 or less modified Rankin Score on 3 months after stroke onset and none had early neurologic deficit or re-occlusion.
Conclusion
Our result suggests spontaneous recanalization might occur within a few hours after stroke onset. This recanalization was associated with men, diabetes mellitus and embolic stroke. Re-occlusion or early neurologic deficit seems to be infrequent in case of the spontaneous recanalization.
Trial registration number
N/A
AS08-001
REHABILITATION AND RECOVERY – EXCLUDING CLINICAL TRIAL RESULTS
STROKE EARLY SUPPORTED DISCHARGE (ESD): THE IMPACT OF PATIENTS’ CHARACTERISTICS AND CLINICAL PROFILE ON REHABILITATION GOAL ATTAINMENT AND CLINICAL OUTCOMES
1Norfolk Community Health and Care NHS Trust, Suffolk Stroke Early Supported Discharge, Bury St Edmunds, United Kingdom
Background and Aims
Stroke Early Supported Discharge (ESD) was introduced to provide a comprehensive stroke specialist therapy input, whilst reducing cost of acute care. ESD resulted in better health-related outcomes (1). A consensus has not yet been established regarding specific ESD patient characteristics and clinical profile (2).
The main aim is to provide clinical data to support the development of an ESD patient profile and eligibility criteria. The paper outlines the relationship between ESD patients’ clinical profile, service provision and clinical outcomes, in terms of disability, goal attainment and institutionalisation rates.
Method
A prospective correlational design was implemented and data was collected for all patients admitted to Suffolk ESD service between August and October 2016, including stroke type and severity, therapy frequency and intensity, as well as clinical outcomes including the Barthel Index (3), Modified Rankin Scale (4) and Goal Attainment Scale (GAS)(5).
Results
Data was collected for 53 patients (Table 1). Data was analysed for all patients in the three groups ({1} goals not achieved, {2} achieved, and {3} achieved to a higher level) according to GAS as shown in Table 2. Results showed significant association between goal attainment and the stroke subtype, severity, disability and length of hospital stay but not age, gender or stroke side (analysis of variance and Chi square tests; p<0.05).
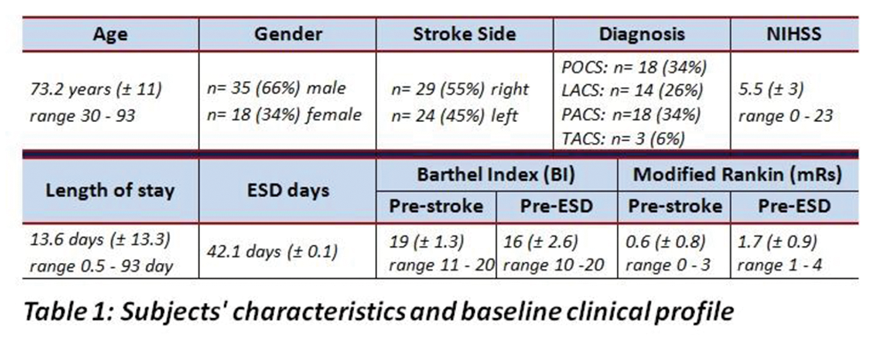
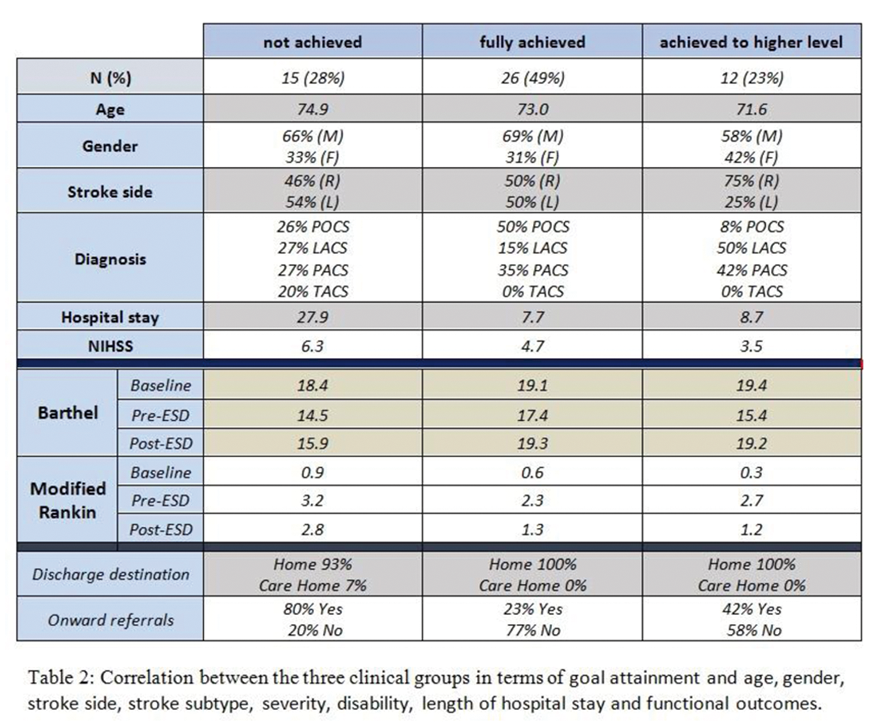
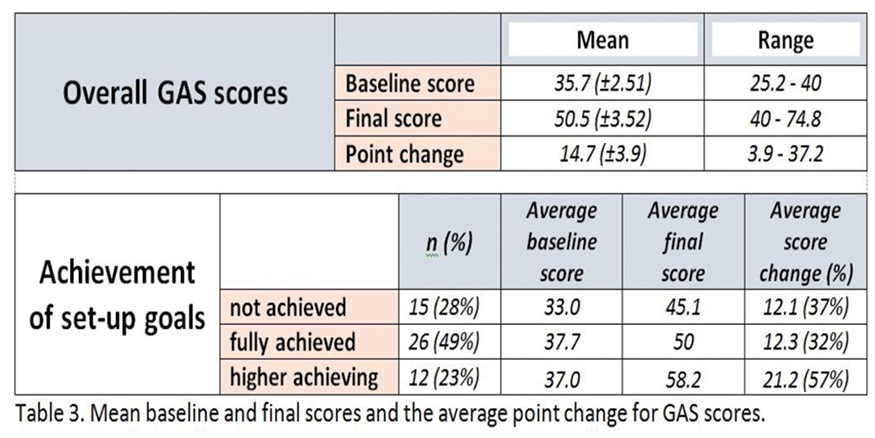
Conclusion
Specific clinical characteristics and disease profile correlate with functional outcomes and could influence goal attainment and functional status. A specific patient cohort seem to benefit the most from ESD services in terms of optimised functional outcomes and recovery.
Trial registration number
N/A
AS08-002
“IN IT TOGETHER”: AN INTERPROFESSIONAL TEAM APPROACH TO REHAB INTENSITY IN INPATIENT STROKE REHAB AT SUNNYBROOK HEALTH SCIENCES CENTRE – ST. JOHN’S REHAB
1Sunnybrook Health Sciences Centre, St.John's Rehab Program, Toronto, Canada
Background and Aims
Guidelines for Quality Based Procedures (QBPs) for Stroke Care have been outlined by Health Quality Ontario. Several QBPs outline specific definitions of a specialized stroke unit, interprofessional rounds and rehabilitation intensity (RI). RI is a key indicator for evaluating efficiency and effectiveness of stroke care. St. John’s Rehab team have developed and implemented several innovative team processes to apply the QBPs requirements.
Method
An interprofessional working group was established with representation from management, professional practice educators and clinicians from the Sunnybrook – St. John’s Rehab team. The team analysed the current state on A3 using gap analysis of i)geographical placement of stroke patients on A3, ii)present team composition and practices, iii)communication efficiencies, and iv) workload measurement data.
Results
Analysis revealed a number of changes to improve RI: innovative modification in locations of stroke patients (cohort), staffing ratios, treatment model, therapeutic space availability, team communication processes and appropriate workload measurement tools. Interprofessional Collaborative team rounds models were developed to provide high-intensity, short-stay rehab and streamline communication and discharge planning. Modifications to workload measurement were implemented to capture the number of daily therapy minutes provided. As a result, stroke patients are receiving on average RI of 123 minutes per active rehab day (a 78% increase from 2010).
Conclusion
As a result of developing multiple quality improvement initiatives and through continuous evaluation, the team has been able to create an innovative model of care that supports and strives towards providing appropriate rehabilitation intensity and individual patient care plans, while ensuring accurate and quality RI reporting.
Trial registration number
NA
AS08-003
ASSOCIATION BETWEEN RETURN TO WORK AND PARTICIPATION IN EVERYDAY LIFE FIVE YEARS AFTER A STROKE IN WORKING AGE PERSONS
1Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
A substantial part of stroke patients are in working age and not everyone return to work (RTW) after a stroke. To not RTW is a risk factor for reduced life satisfaction, and to participate in meaningful activities is of great importance for quality of life. The aim of the study is to investigate if RTW is important for experiencing participation in everyday life after a stroke.
Method
One hundred and nine persons with stroke at age 18-63 years old in 2009-2010 in Gothenburg, participated in a follow up study with mailed questionnaires five years post stroke. RTW was assessed with number of days on sick-leave within five years post stroke at the Social Insurance Agency. Level of participation in four domains (autonomy indoors, family role, autonomy outdoors and social life and relationships) was assessed with the Impact on Participation and Autonomy (IPA-E) in the follow up questionnaires, and was compared between the RTW and no-RTW group.
Results
Ninety four participants did work before the stroke and of those 86 % did RTW within five years post stroke. In all the domains, the majority (55-84 %) reported very good participation, and the RTW group reported a significantly higher participation in all the domains then the no-RTW groups (p < 0.001).
Conclusion
RTW after a stroke seems to not only be important for the person’s life satisfaction or economically for society, but also for the experience of participation in everyday life. This emphasizes the importance of vocational rehabilitation after a stroke.
Trial registration number
N/A
AS08-004
THREE MONTH FOLLOW UP AFTER EARLY INSTITUTIONAL REHABILITATION OF SEVERE STROKE
1Asklepios Kinik Nord- Heidberg, Neurologie und Neurologische Frührehabilitation, Hamburg, Germany
2Asklepios Klinik Harburg, Frührehabilitation, Hamburg, Germany
3Asklepios Klinik St. Georg, Fachübergreifende Frührehabilitation und Physikalische Medizin, Hamburg, Germany
4Asklepios Kliniken Hamburg GmbH, Konzernbereich Qualität, Hamburg, Germany
Background and Aims
There is limited information on long term effects on quality of life after severe stroke followed by early institutional rehabilitation.
Method
Analysis of the Asklepios Hamburg multicenter early stroke rehabilitation registry. All cases fulfilled the criteria of the German coding system for structural characteristic item OPS 8-552. A phone interview three month after discharge was performed to record modified Rankin scale (mRS), 12-Item Short Form Health Survey (SF-12) and further treatment and complications. We used descriptive statistics (median, mean, standard deviation (SD), and proportions, respectively) as well as t-test and Wilcoxon-test for further analysis.
Results
From 10/2015 to 04/2017 complete records of 148 stroke patients (mean age 68.1 years [12.4], 43% female, hemorrhagic [33%] and ischemic [67%] stroke) were analysed. MRS median and proportions at admission, discharge, and at follow up visit 3 month are displayed in table 1.
In 94 patients complete SF-12 could be analysed (table 2).
There was a significant lower value in both scores compared to the german standard sample (p < .001). Compared with the stroke population from the literature, the PHS score was significant lower (p < .01), but the MHS score was not significant different.
Conclusion
We found an increasing improvement in the activity of daily living after discharge from early institutional rehabilitation. Comparing our preliminary results with a stroke population from the literature, MHS was not different despite lower PHS score. Further analysis will focus on the reasons for this result.
Trial registration number
N/A
AS08-005
PROGNOSTIC FACTORS FOR MORTALITY IN STROKE PATIENTS. DOES PREHOSPITAL DELAY PLAY A ROLE?
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine – Nursery, Denia, Spain
4Hospital General de Tomeloso, Neurology, Tomelloso, Spain
Background and Aims
While mortality and dependency are well known consecuences of the delay in the start of reperfusion therapies, prehospital delay has not been stablished as a predictor for mortality in all stroke patients. We conducted a study in stroke patients to investigate the role of prehospital delay in mortality.
Method
382 Patients with acute stroke or TIA were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors in previous studies were collected, as well as data on PD and mortality. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency three months after stroke.
Results
Arriving the hospital within the first three hours after stroke onset decreased mortality three months after stroke (OR 0,136; CI 0,043 – 0,431; p = 0,001). Infectious comorbidities during hospitalization (OR 12,258; CI 4,832 – 31,093; p < 0,001), renal failure (OR 9,053; CI 2,796 – 29,312; p < 0,001), active smoking (OR 4,335; CI 1,045 – 17,992; p = 0,043), systolic blood pressure higher than 185mmHg on admission (OR 5,665; CI 1,690 – 18,985; p = 0,005)., and high scores on previous mRS (OR 1,659; CI 1,209 – 2,277; p = 0,002) or NIHSS (OR 1,251; CI 1,161 – 1,347; p < 0,001) favored mortality in the same period.
Conclusion
A prehospital delay of less than three hours reduces mortality three months after stroke onset. Future interventions should be directed towards increasing the percentage of patients arriving the hospital in the first three hours, which would not only increase thrombolysis and thrombectomy rates, but also decrease mortality.
Trial registration number
N/A
AS08-006
THE EFFECT OF HOME VERSUS REHABILITATION ENVIRONMENT ON ACTIVITY LEVELS OF STROKE SURVIVORS: GO HOME AND SIT LESS
1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia
2Tasmanian Health Service South, Department of Physiotherapy, Hobart, Australia
3Florey Institute of Neurosciences and Mental Health, Stroke Division, Melbourne, Australia
4University of Tasmania, School of Health Sciences, Hobart, Australia
5University of Newcastle, School of Health Sciences, Newcastle, Australia
6University of Newcastle Priority Research Centre for Stroke and Brain Injury, Hunter Medical Research Institute, Newcastle, Australia
Background and Aims
Sedentary time is high and physical activity low in rehabilitation environments after stroke. There is limited understanding of factors which promote activity, and consequently improve function and reduce cardiovascular risk. We aimed to examine whether change in environment (hospital/home) influenced the time spent sitting, upright and walking, as well as factors predicting any change
Method
34 participants with stroke were recruited consecutively from 2 rehabilitation units. An activity monitor (ActivPAL3) was worn for 7 days (24 hours/day) at 2 time points: final week in hospital, and first week home. Other measures included mood (HADS), fatigue (FAS) and physical function (gait speed, 6 min walk). Linear mixed models (adjusted for waking hours) were performed with activity time as the outcome and environment as the exposure
Results
Activity data was available at both time points for 32 (94%) participants (mean age 68 [SD 13] years, 53% male). At home participants spent 45 fewer minutes sitting (95%CI -84,-6 p = 0.023), 45 more minutes upright (95%CI 6,85 p = 0.024), 12 minutes more walking (95%CI 5-19 p = 0.001) and completed 712 additional steps per day (95%CI 188,1236 p = 0.008), compared to the final week in hospital. Depression prior to discharge modified the differences for all activity outcomes (p ≤ 0.05)
Conclusion
Change in environment from hospital to home reduced sitting time and increased time spent in physical activity and daily step count, though depression modified this change. The environment may be a modifiable factor which clinicians can target to reduce sitting time and promote increases in physical activity
Trial registration number
N/A
AS08-007
INCREASING INTENSITY OF PRACTICE AFTER STROKE USING APPS, INTERNET AND SENSORS TO CONNECT PATIENTS AND THERAPISTS REMOTELY: A FEASIBILITY STUDY
1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia
2University of British Colombia, GF Strong Rehabilitation Research Laboratory, Vancouver, Canada
3Southern Cross University, Business development organisational unit, Coffs Harbour, Australia
4University of Tasmania, School of Health Sciences, Hobart, Australia
Background and Aims
Intensity of task practice after stroke is important to improve function, yet adherence to complete exercise programs can be challenging once home. We aimed to determine whether using a chair sensor, tablet application and internet connection could motivate and provide feedback on progress of a sit to stand exercise at home.
Method
Ten participants with stroke completed a 4-week sit-to-stand exercise in the community. Participants learnt how to use the app and chair sensor that a therapist installed in their home. A therapist remotely monitored the exercise program, updated exercise targets, and provided personalised feedback via the app. Feasibility measures included adherence to the prescribed exercise session frequency and number of exercise repetitions (%), and participant satisfaction measures (enjoyment, usability and perceived benefit questionnaires).
Results
Participants (mean age 73.6 years [SD 9.9 years], 50% male, mean gait speed 0.57m/s [SD 0.31m/s] at baseline) performed 125% of the exercise sessions prescribed over the 4 week period. There was a mean exercise repetition adherence of 104% [range 97% to 111%]. Participants rated the system usability as high (78%), enjoyment as high (70%) and rated perceived benefit of the system positively (80%)
Conclusion
It was feasible to prescribe, monitor and progress exercise by connecting participants and therapists remotely using an app and sensor-based system. Exercise session and repetition adherence was high, with positive satisfaction reported by participants. A definitive trial is now required to determine if use of such technology may facilitate greater exercise participation and improve function after stroke
Trial registration number
N/A
AS08-008
TIME IS BRAIN FOR THOSE NOT RECEIVING REPERFUSION THERAPIES, EVEN 1 YEAR AFTER STROKE
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine - Nursery, Denia, Spain
4Hospital General La Mancha Centro, Neurology - Nursery, Alcázar de San Juan, Spain
Background and Aims
Thrombolysis and thrombectomy are therapies with a proven time-dependent benefit on survival and functionality of stroke patients. A benefit in reducing prehospital delay for those who don’t receive such therapies has rarely been studied. We conducted a study to investigate if a sooner hospital arrival (PD < 3 hours) favors functional independency (mRS < 2) 12 months after a stroke.
Method
284 Patients with acute stroke (TIA excluded) who didn’t receive thrombolysis nor thrombectomy were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors were collected, as well as data on PD. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency three months after stroke.
Results
The chance of being functionally independent 1 year after a stroke was higher among those arriving the hospital in the first 3 hours (OR 5,205; CI 95% 2,147-12,619; p < 0,001). Inhospital infectious comorbidities (OR 0,058; CI 95% 0,017-0,204; p < 0,001) and higher scores on previous mRS (OR 0,288; CI 95% 0,209-0,397; p < 0,001) and initial NIHSS (OR 0,809; CI 95% 0,746-0,878; p < 0,001) predicted dependency.
Conclusion
Among patients not receiving reperfusion therapies, the chance of achieving functional independency is clearly higher for those arriving the hospital in the first three hours after stroke onset. Great efforts should be done in the future to increase the number of patients attended in the first three hours after the setting of stroke, in order to minimize the personal, social and economic burden of stroke.
Trial registration number
N/A
AS08-009
PAIN AFTER STROKE: A LONGITUDINAL 5-YEAR FOLLOW UP STUDY
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience- the Sahlgrenska Academy at the University of Gothenburg, Gothenburg, Sweden
Background and Aims
Stroke affects a large global population each year and the number of patients surviving their stroke is steady increasing. Pain is common both in stroke survivors and the general population. Consequences of post-stroke pain can be severe and include reduced quality of life and difficulties in rehabilitation.
The overall aim is to investigate pain 5 years after stroke. Factors potentially related to the experience of pain and unmet needs for pain treatment will be analyzed.
Method
All patients admitted to the Sahlgrenska University Hospital in Gothenburg with first-time stroke during 2009-2010 were eligible for the study. Baseline data was obtained from medical records. Five years post stroke, a set of questionnaires were mailed out to survivors. The questionnaire, which focuses on long-term consequences of stroke, includes two questions of special interest for the present study; “Do you experience pain?” and “Have your needs for treatment of pain been met?”
Results
There were in total 281 respondents (61 %). Pain of varying frequency was reported by 40 % of the patients (n = 108). Unmet needs for pain treatment was reported by 26 % (n = 69). Depression and restricted mobility were both risk factors for more frequent pain, defined as experiencing pain often or always. More frequent pain was significantly associated with poorer quality of life, self-perceived health status and recovery post-stroke.
Conclusion
The results suggest that pain is not uncommon five years after stroke and emphasize the importance of standardized follow up care of stroke survivors in which patients are actively asked about pain.
Trial registration number
N/A
AS08-010
SERUM ALBUMIN AS A PROGNOSTIC FACTOR FOR STROKE PATIENTS THREE MONTHS AFTER STROKE
1Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine - Nursery, Denia, Spain
4Hospital General La Mancha Centro, Neurology - Nursery, Alcázar de San Juan, Spain
Background and Aims
Nutritional status has been described as a potential prognostic factor for stroke prognosis. We conducted a study to investigate the role of serum albumin at admission on the functional prognosis of stroke.
Method
Patients with acute stroke or TIA were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors in previous studies were collected, as well as data on PD. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency three months after stroke. Nutritional deficiency was considered when serum albumin level was below 3,5 mg/dL.
Results
382 patients were included. 224 of them (58,64%) were functionally independent 3 months after stroke, while 158 were dependent. Medium serum albumin was 3,93mg/dL+/−0,44 (4,07 +/− 0,39 vs 3,73 +/− 0,45; p = 0,003). Additionally, 51 patients (14,05%) were considered as suffering nutritional deficiency (8,18% vs 23,08%; p < 0,001). In multivariate analysis for functional independency, nutritional deficiency was an independent predictor of functional dependency 3 months after stroke (OR 0,328; CI 95% 0,117-0,925; p = 0,035).
Conclusion
Nutritional status is a relevant prognostic factor for dependency after stroke, as nutritional deficiency is independently related to functional dependency 3 months after strokes. We propose that serum albumin levels should be determined in all stroke patients to help physicians predict functional status after stroke.
Trial registration number
N/A
AS08-011
LONG TERM FUNCTIONAL PROGNOSIS IS WORSE FOR PATIENTS WITH CHRONIC HYPERGLYCEMIA
1Hospital General La Mancha Centro, Neurology, Alcázar de San Juan, Spain
2Hospital General La Mancha Centro, Endocrinology, Alcázar de San Juan, Spain
3Hospital de Denia, Internal Medicine - Nursery, Denia, Spain
4Hospital Universitario Central de Asturias, Intensive Care Unit - Nursery, Oviedo, Spain
Background and Aims
Diabetes and acute hyperglycemia increase stroke volume and disability in stroke patients, and deliver worse outcomes after reperfusion therapies. Chronic glycemic status has recently been linked to stroke functional outcome, but its impact on long term prognosis has rarely been studied. We conducted a study to investigate the impact of glycosylated hemoglobin (HbA1c) levels on functional outcome 1 year after stroke.
Method
Patients with acute stroke or TIA were prospectively included. Sociodemographic factors, premorbid conditions, and clinical, biochemical and hematological parameters that were considered as possible prognostic factors in previous studies were collected, as well as modified Rankin Scales (mRS) scores at different times. Multivariate logistic regression analyses were conducted to identify factors related to achieving functional independency 12 months after stroke. HbA1c levels higher than 6,4% were considered as pathologic.
Results
382 patients were included. In 217 of them (56,81%) mRS was ≤2 12 months after stroke, while 167 (43,19%) had a mRS≥3. Medium HbA1c on admission was 6,6 +/− 1,55% (6,29+/−1,43% vs 6,76+/−1,70%; p = 0,032). Additionally, 130 patients (34,03%) had HbA1c levels higher than 6,4% (23,08% vs 44,76%; p < 0,001). In multivariate analysis for functional independency, elevated HbA1c level was an independent predictor of functional dependency 1 year after stroke (OR 0,190; CI 95% 0,064-0,568; p = 0,003).
Conclusion
Previous glycemic status is an independent prognostic factor for long term outcome after stroke.Patients with higher HbA1c are more frequently disabled one year after the event. We propose that HbA1c should be determined in all stroke patients to help physicians predict functional outcome after stroke.
Trial registration number
N/A
AS08-012
DETERMINANTS OF ANTIDEPRESSANT TREATMENT AND REHABILITATIVE PARTICIPATION AFTER STROKE
1University of Potsdam, Department of Psychology, Potsdam, Germany
2Ernst von Bergmann Hospital, Clinic of Neurology, Potsdam, Germany
3Humboldt University, Department of Psychology, Berlin, Germany
Background and Aims
Depression is common after stroke, yet substantially undertreated. Additionally, rehabilitative therapies are indicated in most people post-stroke while depressive symptoms may reduce participation. Identifying determinants of antidepressant treatment and predictors of rehabilitative participation enables to improve health care after stroke.
Method
People with ischaemic stroke (N = 294) were consecutively recruited from inpatient rehabilitation. Demographic, psychological, and stroke-related measures were assessed during inpatient stay and one year later. Multiple logistic and linear regression analyses identified determinants of antidepressant treatment and rehabilitative participation in physical, occupational, speech, and neuropsychological therapy.
Results
Use of antidepressants after one year (n = 28/111; 20.1%) was predicted by antidepressant treatment at admission (OR = 48.41), current depressiveness (OR = 3.03), and lower stroke severity (OR = 0.45; all p < .05). Half of the participants (n = 68/136; 50%) used at least one rehabilitative therapy after one year. The number of rehabilitative therapies used was predicted by functional dependency (β = −.43), cognitive impairment (β = −.31), and years of education (β = .25, all p < .001).
Conclusion
As expected, use of antidepressants was predicted by higher depressiveness. Additionally, use of antidepressants was substantially influenced by previous use while patients with severe stroke may be at risk of being undertreated. Rehabilitative participation was predicted by functional and cognitive impairment, and influenced by sociodemographic variables. Patients with lower educational level used these therapies less likely.
Trial registration number
N/A
AS08-013
CAN WE BOOST UPPER EXTREMITY RECOVERY IN CHRONIC STROKE PATIENTS: A RATIONALE FOR THE TRIPLE-COMBINATION OF TDCS PLUS CEREBROLYSIN AND TASK SPECIFIC TRAINING
1Klinik Pirawarth, Neurology, Bad Pirawarth, Austria
Background and Aims
In stroke survivors, motor impairment is a leading cause of disability in activities of daily living. Especially functional recovery of arm and hand function after stroke is still severely limited. Many rehabilitation strategies attempt to enhance motor recovery in stroke patients, however, the effects are mostly limited and outcomes are still poor. Task specific training is still the gold standard for post-stroke rehabilitation, but effect sizes are generally small. Transcranial direct current stimulation (tDCS) is a promsing new technique to optimize the effect of task specific training in the context of UE motor recovery. Cerebrolysin is a neuropeptide preparation with neuroprotective and neurorestorative effects. The combination of these different therapeutic modalities in daily routine might exhibit synergetic effects in improving UE motor recovery.
Method
In this exploratory case studies we investigated subacute and chronic stroke patients with moderate to severe impairment of UE motor function. Patients received a triple-combination-therapy consisting of daily task specific training (minimum 30 minutes 5 days/week), anodal tDCS (20minutes, 5 days/week) and daily administration of the neuropeptid formulation Cerebrolysin 30ml iv.
Results
Effects of the triple therapy on UE motor outcomes (ARAT-Score) compared to patients receiving only task specific training will be reported.
Conclusion
To our knowledge, the effects of the combination of these potentially synergetic acting therapeutic modalities on functional UE recovery has never been studied before.
Trial registration number
N/A
AS08-015
EVALUATION OF MOTOR FUNCTION IMPAIRMENT AFTER STROKE WITH A COMPUTATIONAL ANALYSIS SYSTEM
1Hospital Universitario La Paz, Neurology, Madrid, Spain
2System Friend Inc, System Friend Inc, Hiroshima, Japan
3Universidad Politécnica de Madrid, Bioingeniaría, Madrid, Spain
4Universidad Politécnica de Madrid, Bioingeniería, Madrid, Spain
Background and Aims
Motion capture systems are used in neurological rehabilitation. We aimed to explore the usefulness of MCS to obtain an objective measurement of functional status after stroke.
Method
Prospective observational case-control pilot study.Acute stroke patients and controls performed a battery of exercise in front of the camera Microsoft Kinect® and the movement were analyzed in the three-dimensional space with the software Akira®. The differences in performance before and after each exercise and between both sides of the body were compared between groups. The correlation between the NIHSS score and the mRS score were analyzed. The patients also were evaluated at 3 months.
Results
72 controls and 37 patients were analyzed. The median NIHSS score was 2 (rank 0-12), and the median mRS was 0 (rank 0-4). The measurements that showed better discrimination capacity were those obtained from the abduction of the arm: the shift of the joint angles was different between groups in the frontal plane of the elbow, shoulder, and forearm; all in pronation and supination (p < .001).
Those differences were independent of the NIHSS score, but were moderately correlated to the mRS score at the moment of the evaluation: elbow in supination (Rho = 0.41, P = .01); shoulder in pronation (Rho = 0.45, P = .006) and supination (Rho = 0.64, P<.001).
There were no significant differences in those angles at 3 months.
Conclusion
Computational analysis of movement could be a useful tool for evaluation of upper limb function in stroke patients with slight deficit underestimated using current clinical scales, but correlated with outcome.
Trial registration number
N/A
AS08-016
SEXUAL HEALTH IN STROKE REHABILITATION; UNIT POLICY AND HEALTHCARE PERSONNEL PERSPECTIVE. A MULTICENTER STUDY
1Sunnaas Rehabilitation Hospital, Research department, Nesoddtangen, Norway
2Karolinska Institutet, Department of Neurobiology- Care Science and Society, Stockholm, Sweden
3Karolinska University Hospital, Function area Social work in health, Stocholm, Sweden
4University of Oslo, Institute of clinical medicine, Oslo, Norway
5Stockholm Sjukhem Foundation, n/a, Stockholm, Sweden
Background and Aims
International guidelines on stroke recommend sexual health to be part of standard stroke care. However, sexuality is not addressed with a consistent approach in rehabilitation. Stroke patients and partners have been found to have unmet sexual rehabilitation needs.
The aim was to identify sexual health policies at specialized stroke rehabilitation centers and explore the relationship with healthcare personnel (HCP) perspective on sexual health in stroke rehabilitation.
Method
A prospective cross-sectional study including nine specialized stroke rehabilitation centers in seven countries: Norway, Sweden, United States, Palestine, Israel, China and Russia (i.e. the SIN-stroke network*). Two structured questionnaires were used: 1) each center reported their sexual health policies (a 10 statement audit). 2) HCP (n: 323) answered an anonymous web-questionnaire assessing their knowledge and comfort working with sexual health rehabilitation.
Results
Routines and policies on sexual health varied greatly between the nine centers. A majority of HCP reported lack of knowledge and discomfort providing information about sexuality to stroke patients and spouses. Most HCP expressed a need for more knowledge on the topic. Comfort in giving information to patients and spouses about sexuality was significant associated with HCPs perceived level of knowledge working with sexual issues and with working at centers having implemented routines and policies on sexual health.
Conclusion
Sexual health policies in stroke rehabilitation matters. Education and training for all professions seems necessary for supporting comfort and knowledge among HCP to meet the sexual rehabilitation needs of stroke patients and spouses.
*Langhammer B, et al. Specialized Stroke Rehabilitation Services in Seven Countries. Int J Stroke. 2015;10:236-46
Trial registration number
N/A
AS08-017
GAZE CHARACTERISTICS IN HEMIANOPIA DURING A NATURALISTIC SANDWICH-MAKING TASK AND A TABLE-TOP VISUAL SEARCH TASK
1University of Bristol, Faculty of Health Sciences, Bristol, United Kingdom
2University of Bristol, Experimental Psychology, Bristol, United Kingdom
3Southmead Hospital- North Bristol NHS Trust, Neurolology, Bristol, United Kingdom
Background and Aims
Hemianopia impairs visual search during lab-based tasks (VSTs)1, resulting in longer search times2, increased fixations, and bias towards the hemianopic field3. However, these differences may diminish during real-world tasks4. This study examined visual behaviour during a VST, and a naturalistic sandwich-making task (SWT).
Method
5 participants with homonymous visual field defects, and 10 healthy age-matched controls completed a VST and SWT. Visual behaviour was recorded using an SMI® eye tracker, and analysed using multivariate analysis of variance, controlling for age. Values presented are Mean ± SEM.
6 sandwich-making items (SWT), or 13 recognisable objects (VST) were placed in pre-specified locations on a table. During VST trials (14 total), participants had to locate 2 of 13 objects. During the SWT, participants made 4 different sandwiches (4 trials, each repeated once).
Results
Patients took longer to complete the VST than controls (7.2 ± 1.1 and 3.9 ± 0.52 seconds, p=0.004) and made more fixations (6 ± 2 and 4 ± 1, p = 0.013). Additionally, patients showed a trend of increased number of gaze shifts towards the hemianopic field (3 ± 1 and 2 ± 1, p = 0.064).
During the SWT, patients and controls exhibited similar trial durations (74.9 ± 5.5 and 60.1 ± 5.6 seconds, p = 0.121). Patients made more fixations than controls (30 ± 3 and 23 ± 1, p = 0.023), however there was no directional bias of gaze shifts (10 ± 4 and 10 ± 2, p = 0.307).
Conclusion
Patients exhibited distinct visual behaviour to controls during the VST, but less so during the SWT. During real-world, visuo-motor tasks, patients appear to compensate for visual field defects that limit performance in lab-based VSTs. Further work is needed to elucidate these compensatory mechanisms.
Trial registration number
N/A
AS08-018
EXTERNAL VALIDATION OF PNEUMONIA PREDICTION SCORES AFTER STROKE IN A PROSPECTIVE UK COHORT STUDY
1Sheffield Teaching Hospitals NHS Trust Sheffield UK, Stroke Medicine, Sheffield, United Kingdom
Background and Aims
Stroke associated pneumonia (SAP) affects up to a quarter of stroke survivors. Identifying patients at greatest risk of SAP may help target future preventative interventions. The ISAN, A2DS2, and AIS-APS are scores developed to predict risk of SAP. This study aims to externally validate and compare these clinical scores prospectively among a UK stroke population
Method
Prospective cohort study of 213 stroke patients admitted to a UK hospital over 1 year. SAP prediction scores were calculated. Development of probable or definite SAP was recorded according to CDC criteria. Risk score discrimination was assessed using area under the receiver characteristic curves for each risk prediction model’s published categorization. Sensitivity, specificity, negative predictive (NPV) and positive predictive values (PPV), were compared across scores.
Results
C-Statistics for the ISAN (0.81, 95% CI 0.74 - 0.88), AIS-APS (0.82, 95% CI 0.74 - 0.90) and A2DS2 (0.73, 95% CI .064 - 0.83) indicated good SAP prediction across scores. After categorising each score into 2 discriminators (low/high), A2DS2 exhibited the highest sensitivity (87.5%) while ISAN and AIS-APS displayed higher specificity (both 71.5%). The NPV for each score (ISAN 97.4%, AIS-APS 96.4%, A2DS2 97.5%) indicated accuracy in identifying low risk patients, while the PPV for each score was much lower (range 22.1% to 27.4%).
Conclusion
The ISAN, A2DS2 and AIS-APS all demonstrated validity in predicting SAP in this UK cohort, specifically they identified low risk patients well. Given the ISAN is the most simple, it may have the greatest potential for routine use in clinical practice.
Trial registration number
N/A
AS08-019
ENHANCING STROKE REHABILITATION USING A BALANCE BOARD AND PONG GAME INTERFACE
1The Hillingdon Hospital NHS Foundation Trust, Stroke Medicine, Uxbridge, United Kingdom
2Brunel University London, Clinical Sciences, Uxbridge, United Kingdom
3University of Greenwich, Computing and Information Systems, London, United Kingdom
4The Hillingdon Hospital NHS Foundation Trust, Research and Development, Uxbridge, United Kingdom
Background and Aims
Strokes result in impaired balance and gait, contributing to increased dependence and falls. We explore the use of a novel interface for balance training.
Method
Eight Stroke patients stood on a Nintendo Wii Balance Board and completed a 1-minute trial of:
(1) Physiotherapist-led exercises, in which the physiotherapist instructed the participant to repeatedly lean their bodyweight as far to the left and right as possible.
(2) An exergame (exercise + videogame) task based on the videogame PONG, in which the participant used their balance, moving along the medial-lateral plane, to control a paddle in order to intercept a ball (see Fig. 1).
Medial-lateral limits of stability (a measure of how far an individual can lean to either side without falling) were recorded throughout both conditions. Participants completed a short user-feedback questionnaire.
Results
Medial-lateral limits of stability were significantly greater during Gaming (M = 29.76cm), compared to Therapy alone (M = 25.89cm, p < 0.05). Seven (out of 8) participants swayed significantly greater during Gaming. Seven (out of 8) participants provided positive feedback.
Conclusion
Based on feedback from both patients and physiotherapists this exergame improved engagement and motivation in therapy with objective measures of improved balance. Subsequent to this feasibility trial, we plan to undertake a larger study with a superior board developed by Brunel University as a collaborative project with Hillingdon Hospital.
Trial registration number
N/A
AS08-020
WHAT IS RECOVERY TO STROKE SURVIVORS? A CLINICAL, QUANTITATIVE STUDY USING THE WHO-ICF FRAMEWORK
1Duke-NUS Medical School, Rehabilitation Medicine, Singapore, Singapore
2Singapore General Hospital, Rehabilitation Medicine, Singapore, Singapore
Background and Aims
Current rehabilitation interventions focus on improving activity limitations instead of facilitating participation. Assessment of patient-reported outcomes via a global recovery score (GRS) provides insight into patients’ values which in turn can direct rehabilitation focus on areas associated with self-perceived recovery.
We aim to determine patient-reported levels of post-stroke recovery and identify factors associated with this perception.
Method
This is a cross-sectional study based on the World Health Organization’s International Classification of Functioning, Disability and Health (WHO-ICF) framework. Subjects recruited were at least 1 year post-stroke. GRS was measured using a 0-100 visual analog scale. Domains of impairment, activity limitations and participation restrictions were assessed using National Institutes of Health Stroke Scale (NIHSS), Modified Barthel Index (mBI) and London Handicap Scale (LHS) respectively. The Pearson Correlation was used to evaluate relevant associations.
Results
There were 122 patients. 68% were male with the mean age of 61.0 ± 12.2 years. 66.4% had ischemic stroke and the Charlson Comorbidity Index was 3.80 (IQR 2-5). The self-perceived GRS was 56.8 (IQR 50-80). The mean mBI was 84.5 ± 25.9, NIHSS was 7.63 ± 6.0 and the LHS was 61.5 ± 22.3. The strongest correlation with the GRS was the LHS (r = 0.608, p < 0.01) followed by the mBI (r = 0.526, p < 0.01) and the NIHSS (r = −0.476, p < 0.01).
Conclusion
The ability to participate fully in the community is highly significant to self-perceived recovery post stroke. Deliberate interventions to target participation restrictions need to occur concurrently with the prevailing rehabilitation focus on activity limitations.
Trial registration number
N/A
AS08-021
DYSPHAGIA REHABILITATION FOLLOWING STROKE: MORE THAN JUST FUNCTIONAL RECOVERY
1Trinity College Dublin, Clinical Speech and Language Therapy, Dublin, Ireland
Background and Aims
Emerging research emphasises the significant impact that dysphagia has on the psycho-social health and well-being of persons following stroke. Presently, there is limited information regarding current clinical practice in this area. This study aims to determine the current practices of Speech and Language Therapists (SLTs) internationally when addressing quality of life issues in dysphagia rehabilitation following stroke.
Method
An anonymous cross-sectional, non-experimental survey study was used, consisting of 18 open and closed questions exploring participant’s beliefs, opinions and current clinical practice when managing quality of life issues in dysphagia following stroke. The survey was created and disseminated through international professional bodies and academic institutions, using surveymonkey.com.
Results
223 SLTs responded to the survey, of which 143 currently work with persons with dysphagia following stroke. Respondents report lacking confidence and knowledge when working in this clinical area. Facilitators and barriers to good quality care are identified. Comparisons are made between current practice patterns and known patient care priorities as reported in research to date.
Conclusion
A disparity exists between current clinical practice and patient care priorities when addressing quality of life issues in dysphagia following stroke. Further research and the development of best practice guidelines may contribute to bridging this gap.
Trial registration number
N/A
AS08-022
REHABILITATION AFTER STROKE – ARE THERE URBAN - RURAL DISPARITIES?
1Klinikum Harlaching, Neurologie, München, Germany
Background and Aims
Interdisciplinary stroke rehabilitation delivered in acute and subacute phases has been shown to improve the outcomes of stroke survivors. Several studies have shown an increase of stroke and stroke related mortality and disability in patients living in rural settings compared to patients in urban areas. Little is known about the differences in subacute stroke care in rural and urban areas. We have analysed access to post stroke rehabilitation in patients living in rural areas compared to those living in urban areas in South-East Bavaria.
Method
We conducted a retrospective analysis using Bavarian quality performance data collection (BAQ) 2016 of 20 hospitals participating in the Telestroke network TEMPIS (telemedical stroke network in Bavaria). Hospitals were categorised into rural (12 hospitals), intermediated (6) or urban (2) according to the NUTS-3 (Classification of territorial Units for statistics) urban-rural typology. We compared the frequency of rehabilitation requests in patients having suffered an acute stroke, previously living at home, with a remaining modified Ranking scale of at least 2.
Results
Of 9782 patients with acute stroke, 4925 had been treated in rural, 2659 in intermediate and 2198 in urban hospitals. In urban or intermediate hospitals a rehabilitation was applied for in 74% of patients respectively, in comparison to 68% of patients being treated in rural hospitals (p < 0,05).
Conclusion
A gap remains between post stroke care in patients in rural and urban areas, even in the telemedicine-supported hospitals of the TEMPiS network. More studies are needed to understand this complex phenomenon.
Trial registration number
N/A
AS08-023
A NOVEL APHASIA TRAINING BASED ON BRAIN-COMPUTER INTERFACES
1University Medical Center Freiburg, neurology, Freiburg, Germany
2Brain State Decoding Lab-, Dept. Computer Science- Albert-Ludwig-Universität Freiburg- Germany, Freiburg, Germany
Background and Aims
Effective rehabilitation training approaches for chronic aphasia are scarce.
Method
A novel Brain-Computer Interface (BCI) supported language training was conducted in 8 patients with a left fronto-temporal-parietal infarct and chronic aphasia. In 30 hours of intensive training, word event-related potential (ERP) responses were analyzed using an auditory BCI paradigm, which was previously tested on 20 normally-aged controls. Each trial started with a cueing sentence followed by a rapid stimulus sequence containing 6 bisyllabic words repeated 15 times in pseudo-random order, with only one correctly finishing the sentences. Patients received end-of-trial feedback whether the attended word predicted by the EEG response matched the target word of the trial. The Aachener Aphasie Test (AAT) estimated the training-induced language effects. Pre- and post-training offline EEG sessions assessed training-induced changes of ERP responses.
Results
Per patient, the BCI-supported training realized 26% to 88% of the maximally possible AAT improvement (60% avg.). Figure 1A displays individual (dots) and groupwise changes (bars) of the T-transformed AAT scores showing significant improvements. P300 component showed initially a reduced amplitude and increased latency relative to the controls, and post-training, an increased amplitude and comparable latency (Figure 1B).
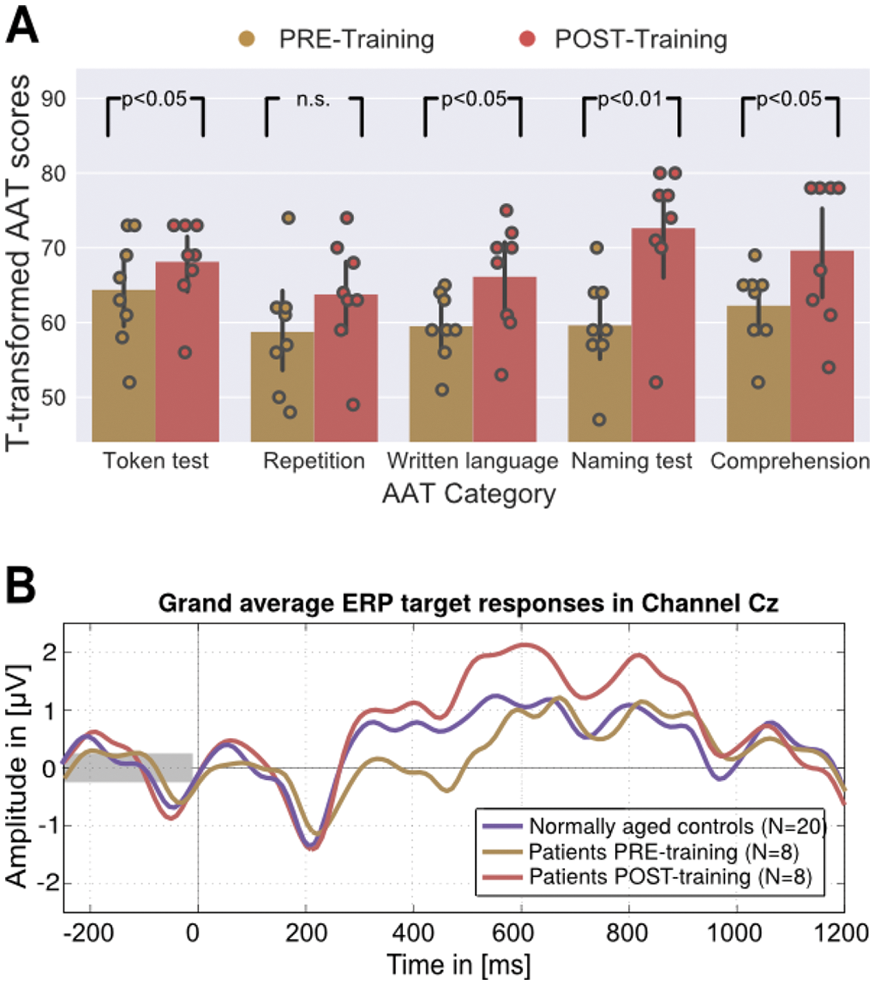
Conclusion
This BCI-supported training is feasible, effective and efficient for chronic stroke patients. ERP changes are thought to reflect increases in neural synchrony as well as strengthened neural connections associated with improved language
Trial registration number
N
AS08-024
SHOULDER PAIN AFTER RECENT STROKE (SPARS): ARE INTERVENTIONS POORLY TARGETTED OR INEFFECTIVE? (NCT 02574000)
1St George's University of London, Dept. Neurology, London, United Kingdom
Background and Aims
Shoulder weakness or subluxation within 72 hours post-stroke significantly increases risk of hemiplegic shoulder pain (HSP) at two months (Nadler 2017). Here we investigated targeted therapy interventions.
Method
Retrospective analysis of consecutive, unselected stroke patients were assessed within 72 hours and followed-up for pain (standardised HSP questionnaire). Muscle power, subluxation and therapy interventions were noted. HSP risk was classified as medium if there was shoulder weakness (Oxford Scale) and high if there was subluxation too. HSP was categorised into “No HSP”, “HSP resolved”, “HSP persisted”, “New HSP”.
Results
121 patients had initial and follow-up data. 50 patients had 140 interventions: shoulder orthosis (10), wheelchair arm support (5), pillow support (31), shoulder taping (4), functional electrical stimulation (2), targeted exercises (43) and general therapy (45). Interventions were targeted at the high (14/121) and medium (47/121) risk HSP patients particularly those with persistent or newly developed HSP. However, even in those with persistent/new HSP, 7/35 high/medium and 17/18 low risk patients had no recorded intervention. Probability of intervention was correlated with risk group (p < 0.0001, ANOVA) and HSP (p < 0.0001, ANOVA) but not associated with recovery.
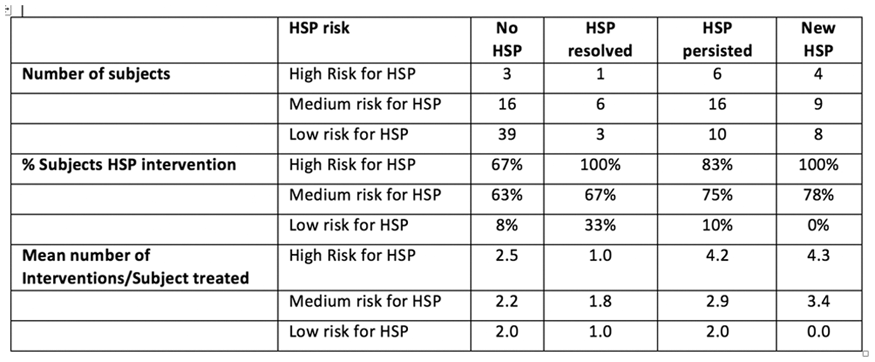
Conclusion
Therapy is targeted towards high/medium risk patients and those with HSP. However, a substantial group are missed. Intervention appears driven by need with little evidence for amelioration or preventative efficacy.
Trial registration number
N/A
AS08-026
CHANGES IN CEREBRAL BLOOD FLOW AND METABOLISM ASSOCIATED WITH NEURITE MORPHOLOGY AFTER MOTOR RECOVERY IN PATIENTS WITH SMALL VESSEL DISEASE
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Osaka, Japan
2National Center for Geriatrics and Gerontology, Department of Psychiatry, Aichi, Japan
3National Cerebral and Cardiovascular Center, Department of Investigative Radiology, Osaka, Japan
4National Cerebral and Cardiovascular Center, Division of Cerebrovascular Rehabilitaion, Osaka, Japan
Background and Aims
Most patients with small vessel disease (SVD) have deficits in executive function as well as processing speed, while stroke severity is mild. We examined changes of cerebral blood flow (CBF) and oxygen metabolism associated with alteration of neurite morphology after motor recovery.
Method
We enrolled 16 ambulant patients (mean 63 y.o., 14 males) with supratentorial SVD who admitted to our hospital within 1 week after stroke onset. All patients underwent conventional rehabilitation until discharge. Neurite orientation dispersion and density imaging (NODDI) model by magnetic resonance imaging and O15-gas positron emission tomography were performed at baseline and 3 months after. Motor recovery was also assessed at these 2-time points.
Results
Nine patients had left lesions and 15 were right handed. They only had disturbance in skilled movement (median NIHSS 1). Increased CBF in insular cortex (p < 0.0001) and precentral gyrus (p < 0.0001) in the left hemisphere, and the right anterior cingulate cortex (p < 0.0001) were observed at 3 months compared with those at baseline. There were no significant changes in cerebral oxygen metabolism between 2 time points. In NODDI model, significant increases of neurite density were demonstrated in the left precentral gyrus (p < 0.0001). Significant motor recovery, assessed by functional independence measure (p = 0.0011), Fugl-Meyer assessment (p = 0.0215), and timed up & go test (p = 0.0073), were also confirmed.
Conclusion
Neurite density and CBF in the left precentral gyrus were significantly increased in patients with mild symptomatic SVD at 3 months after the onset regardless of lesion side.
Trial registration number
N/A
AS08-027
POST-TRAUMATIC STRESS DISORDER AFTER MILD STROKE AND TRANSIENT ISCHAEMIC ATTACK: PSYCHIATRIC CO-MORBIDITY AND SYMPTOM CLUSTER DISTRIBUTION
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Post-traumatic stress disorder (PTSD) is distressing and may be common after stroke and transient ischaemic attack (TIA). A better understanding of the overlap between PTSD with other common post-stroke neuropsychiatric sequelae—depression, anxiety, cognitive impairment can help us develop better psychological support to patients post-stroke/TIA.
Method
We followed up mild stroke and TIA patients at three months using diagnostic psychiatric interview (SCID-DSM-IV) and telephone Montreal Cognitive Assessment (tMOCA).
Results
Of 175 participants (mean age 70; 40% women; 65% stroke; 35% TIA), 11/175, 6% (95%CI 3-11%) met the diagnostic criteria for PTSD. Almost half of all PTSD cases (5/11) were also diagnosed with a depressive episode. All PTSD cases (11/11) were co-morbid with one or more anxiety disorders (phobic disorder or generalized anxiety disorder). Median tMOCA score was 19 and the same in PTSD and non-PTSD cases.
PTSD symptom clusters C) persistent avoidance and numbing of general responsiveness, and D) increased arousal were present in over 10% of our stroke and TIA cohort.
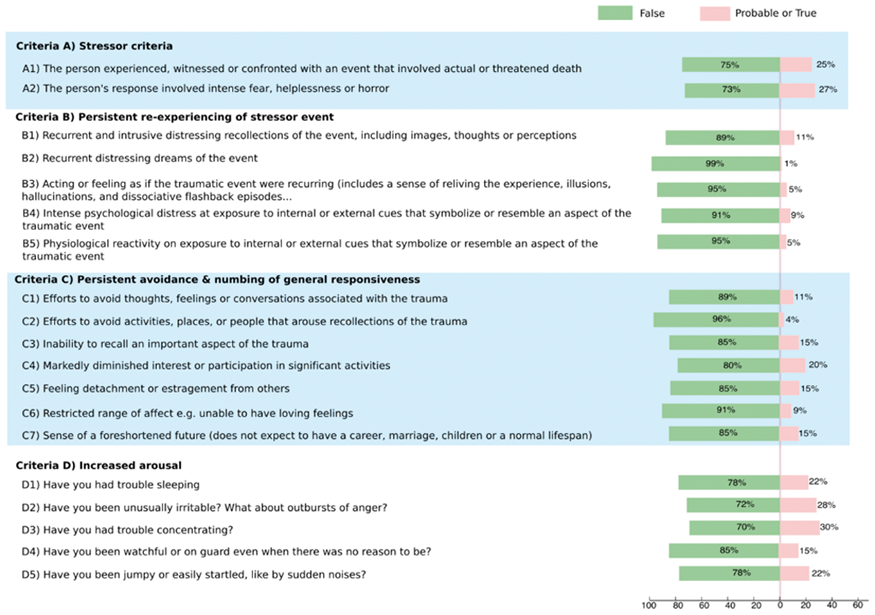
Conclusion
Clinical diagnosis of PTSD is present in around 6% of mild stroke and TIA patients at 3 months. There is considerable overlap between PTSD with depression and anxiety disorders. PTSD symptoms are common even in those without PTSD diagnosis. Psychological support for stroke and TIA should consider targeting these common symptom clusters.
Trial registration number
N/A
AS08-028
UPPER LIMB KINEMATICS IN STROKE AND HEALTHY CONTROLS USING TARGET-TO-TARGET TASK IN VIRTUAL REALITY
1Institute of Neuroscience and Physiology, Clinical Neuroscience and Rehabilitation Medicine, Gothenburg, Sweden
Background and Aims
Virtual reality technique for kinematic assessment has rarely been used in evaluating motor function in stroke despite its availability as a training device in stroke rehabilitation. The aim is to discriminate the upper limb movements between individuals with stroke and healthy controls using kinematic variables from target-to-target task in virtual reality.
Method
Sixty-seven participants (mean age of 65.7) extracted from the Stroke Arm Longitudinal Study at Gothenburg University – SALGOT cohort of non-selected individuals within the first year of stroke, subdivided into moderate (31-57 points) and mild (58-65 points) stroke impairment based on Fugl-Meyer Assessment of Upper Extremity score along with 43 healthy controls performed the target-to-target pointing task. Using a haptic stylus, participants pointed at 32 circular targets that appeared successively in a virtual 3D space to make them disappear. Kinematic parameters captured by the stylus were movement time, velocities and smoothness of movement. Kruskal-Wallis and Mann-Whitney U tests were used to determine if significant differences were present between moderate and mild stroke impairment and healthy controls.
Results
Movement time and mean velocity were discriminative between groups with moderate and mild stroke impairment and healthy controls. The movement time was longer and mean and peak velocity lower for individuals with stroke. The number of velocity peaks, representing smoothness, was higher in stroke groups compared to controls. Movement trajectories in stroke more frequently showed clustering close to the target.
Conclusion
The target-to-target pointing task can provide valuable and specific information about sensorimotor impairment of the upper limb following stroke.
Trial registration number
NCT01115348, NIH National Library of Medicine (May 4, 2010)
AS08-029
FEAR OF FALLING IS INDEPENDENTLY ASSOCIATED WITH AGORAPHOBIA AFTER MILD STROKE AND TRANSIENT ISCHAEMIC ATTACK
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Phobic anxiety is common after mild stroke and TIA patients (Chun et al. 2017). Agoraphobia accounted for the majority of phobic disorders in our recent prospective cohort. Fear of falling (FoF) may contribute to agoraphobia post-stroke/TIA, with or without the presence of mobility problems. FoF can lead to actual falls, muscle deconditioning and impaired functioning. We aim to assess the association between FoF and agoraphobia.
Method
Secondary analysis of a prospective cohort of community-based mild stroke and TIA (n = 175, mean age 70, 40% women). Multivariable logistic regression for outcome: clinical diagnosis of agoraphobia at 3 months. Explanatory variables: i) age, ii) past history of anxiety/depression, iii) ability to walk on discharge, iv) history of actual falls, v) living alone pre-stroke, and vi) Falls Efficacy Scale (FES), a measure of FoF—10 items; each item is scored between 1-10; higher scores indicate greater FoF (Tinetti 1990).
Results
In the fully adjusted model, every 10-point increase on the FES was associated with a 2-fold increase in the likelihood of agoraphobia (adjusted OR 2.47, 95%CI 1.52-3.00). For every decade increase in age, the likelihood of agoraphobia reduced by a third (adjusted OR 0.62, 95%CI 0.39-0.97).
Conclusion
FoF is independently associated with agoraphobia at 3 months after mild stroke and TIA. Older age was associated with decreased likelihood of agoraphobia, consistent with findings that younger people are more at risk of anxiety post-stroke/TIA. Psychological support for stroke/TIA should address FoF even in the absence of mobility issues or history of falls.
Trial registration number
N/A
AS08-030
PHYSICAL ACTIVITY ON PRESCRIPTION AT THE TIME OF STROKE OR TRANSIENT ISCHEMIC ATTACK DIAGNOSIS - A PATIENT PERSPECTIVE
1Sahlgrenska Universitetssjukhuset Östra, Fysioterapienheten, Göteborg, Sweden
2Institute of Neuroscience and Physiology- Sahlgrenska Academy at the University of Gothenburg, Department of clinical Neuroscience, Gothenburg, Sweden
Background and Aims
Physical activity at a moderate or high level is known to reduce the risk of recurrent stroke. Despite this many individuals diagnosed with stroke or transient ischemic attack (TIA) have an insufficient level of physical activity. Physical activity on prescription (PaP) is provided within healthcare to help individuals to change their lifestyle and increase physical activity.
The purpose of this study was to examine how individuals experience receiving physical activity on prescription at the time of stroke or TIA diagnosis and to explore various factors affecting their ability to follow the prescription after discharge from hospital.
Method
Ten in-depth interviews were held with patients who had been admitted to a stroke unit and been diagnosed with stroke or TIA. The results was analysed with qualitative content analysis and are reported with one overall theme and underlying categories and sub categories.
Results
The analysis resulted in the overall theme Participation and individualization is crucial to start and continue with physical activity; containing the categories Experience of support, Barriers and opportunities and Personal motivators.
Conclusion
The study highlights the importance of patient participation and personalization when carrying out activities intended to affect lifestyle regarding physical activity. Important clinical implications are the need to reflect on when and how PaP is prescribed in acute stroke care, as well as the need to ensure proper follow-up; this will create good conditions for long-term effects.
Trial registration number
N/A
AS08-031
EVALUATION OF AN EMBODIED VIRTUAL REALITY DEVICE IN UPPER LIMB REHABILITATION POST-STROKE
1Croydon University Hospital, Stroke and Elderly Care Medicine, Croydon, United Kingdom
Background and Aims
There is increased evidence that intensity in therapy is important in improving outcomes after stroke. Current United Kingdom recommendations state that patients should receive at least 45 minutes of each required therapy, 5 days a week. Virtual reality gaming platforms is an innovative method of improving engagement and intensity of rehabilitation.
This is a small feasibility study to explore the use and efficacy of an immersive virtual reality platform for intensive upper limb rehabilitation on an acute stroke unit.
Method
3 patients were recruited from an acute stroke unit in London. Patients received their normal therapy as well as sessions on the MindMotion Pro; a virtual reality gaming platform. Chedoke McMaster Stroke Assessment scoring was performed at 0 and 4 weeks to assess for changes in upper limb function. Qualitative feedback was collected from patients and their therapists.
Results
All patients saw improvement in their score (Table 1). Patients reported positive effects on mental health and enjoyed the ability to monitor progress easily. Therapists described ease of use of the platform.
Conclusion
The MindMaze Pro shows promise in providing engaging, enjoyable and effective rehabilitation for stroke patients whilst helping to meet therapy targets. It has the potential of improving intensity of therapy especially on weekends. Further work is needed to establish cost-efficacy and to explore long term benefits for various patient cohorts.
Trial registration number
N/A
AS08-034
IMPROVED ACCESS TO INPATIENT STROKE REHABILITATION FOR THOSE WITH COGNITIVE IMPAIRMENT FOLLOWING SUPPORTED IMPLEMENTATION OF A COGNITIVE STRATEGY BASED APPROACH
1Sunnybrook Health Sciences Centre, Regional Stroke Centre, Toronto, Canada
2University of Toronto, Occupational Science & Occupational Therapy, Toronto, Canada
3Sunnybrook Research Institute, St. John's Rehabilitation, Toronto, Canada
4Sunnybrook Health Sciences Centre, Regional Stroke Network, Toronto, Canada
5Holland Bloorview Kids Rehabilitation, Research Institute, Toronto, Canada
6University of Toronto, Physical Therapy, Toronto, Canada
Background and Aims
Patients with cognitive impairment (CI) and stroke do not have consistent access to rehabilitation compared to those without CI, despite evidence of its benefits to them. Lack of rehabilitation team skills and knowledge to treat stroke patients with CI has been identified as a contributing factor. This project aimed to examine inpatient rehabilitation acceptance rates for referred patients with CI before and after the implementation of a knowledge translation (KT) initiative aimed at improving skills in the cognitive-strategy based approach known as Cognitive Orientation to daily Occupational Performance (CO-OP).
Method
Five inpatient rehabilitation teams from a large Canadian city participated in CO-OP KT, which included a workshop, 4-months implementation support, health system support, and a sustainability plan. Referrals and acceptances were extracted from the E-Stroke Rehabilitation Referral System for 14 months pre CO-OP KT and 6 months post. A chi-squared analysis was completed comparing acceptance for patients across CI severity levels and across sites
Results
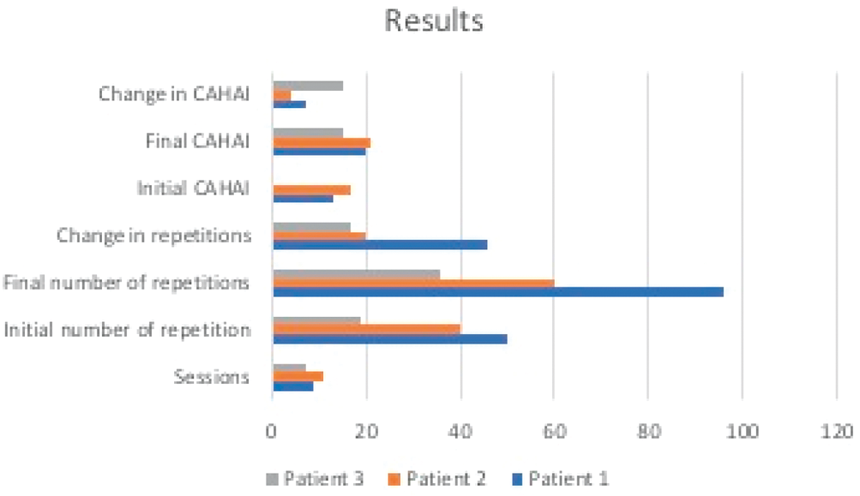
Overall, 4546/5998 (75.8%) patients with CI were accepted pre-intervention compared to 959/1216 (78.9%) post (p = 0.018). Across all sites, significantly more persons with CI were accepted into rehabilitation post intervention (75.3% versus 79.9%; p = 0.002), while there was no significant change among those without CI (77.8% versus 75.5%; p = 0.421). The largest changes were seen in those with moderate CI (74.3% versus 80.8%; p = 0.004). Site-specific differences were also noted.
Conclusion
Access to inpatient stroke rehabilitation improved for persons with stroke and CI after the implementation of a multi-faceted KT intervention to improve skills in a cognitive strategy-based intervention.
Trial registration number
N/A
AS08-035
“STROKE HEALTH”- A DIGITAL TOOL TO SUPPORT SHARED DECISION-MAKING AFTER STROKE
1Institute of Neuroscience and physiology, Dep of Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
Difficulties to understand health-information and describing needs after stroke can lead to a risk of not receiving adequate support. Decision-tools used in preparation for a consultation has been shown to be beneficial, but little is known about users with stroke. The aim was to explore user-needs to enable development of a digital tool to support shared decision-making.
Method
A digital tool, “Stroke health”, including the Post-Stroke Checklist and stroke-related information, was developed according to service-design thinking and practice. First, the “Stroke Health” was tested by persons (n = 7) with prior stroke recruited from the Stroke Association. Second, two focus-group discussions were performed regarding user-needs and possible improvements. Data were analyzed according to Krueger.
Results
The “Stroke health” has the potential to address a range of information needs and serve as preparation for follow-up. Both experienced and inexperienced smartphone/computer users found it easy to use but offered suggestions to improve design and information. The “Stroke health” was expected to enable better communication with clinicians. The risk of not capturing discrete problems were mentioned and possible amendments were discussed. Access to information about that problems are common after stroke was seen as important, in order to normalize their own situation.
Conclusion
The “Stroke Health” could be a resource to lower the threshold to get access to support and be involved in decision-making after stroke. It is of importance to involve the users in the design process to be able to offer a user-friendly tool built on patients’ needs.
Trial registration number
N/A
AS08-038
AN APPRECIATIVE ACTION RESEARCH STUDY TO SUPPORT THE EXPERIENCE OF MULTIDISCIPLINARY PATIENT-CENTRED APPROACHES TO STROKE UNIT CARE AND REHABILITATION.
1Bournemouth University, Faculty of Health and Social Sciences, Bournemouth, United Kingdom
2University of Central Lancashire, Faculty of Health and Wellbeing, Preston, United Kingdom
3University of the West of Scotland, School of Health- Nursing and Midwifery, Glasgow, United Kingdom
Background and Aims
United Kingdom stroke services have a national focus on service improvement through quantitative measures on processes of care. These measures do not account for the context or quality of care, and staff/patient/relative experiences. This study aims to identify and develop approaches to support positive stroke unit care experiences.
Method
CG collaborated with two specialist stroke units in district hospitals in England. Using Appreciative Action Research, participants identified and developed approaches that support meaningful experiences for all participants.
Participants included current stroke in-patients on stroke units (n = 17), their relatives (n = 7) and stroke unit team members (n = 65).
Data were generated over 20 months through 16 semi-structured interviews, observations of usual stroke unit care (213 hours) and 10 discussion groups. Data were co-analysed with participants, and themes developed on their most valued care experiences. Further in-depth analysis was conducted by the authors to confirm themes.
Results
Sharing and reflecting on participants’ narratives of positive caring/rehabilitation experiences increased awareness of the network of human relationships supporting stroke care.
Participants described that ‘pausing’ from physical tasks was essential order to connect with each other.
This enabled staff to:
• Focus on the person (patient, team member or relative) rather than the task
• Understand each other’s’ perspectives, values and roles
• Enable patients and relatives to influence care/rehabilitation focus.
Staff reported improved job satisfaction and well-being as a result of reflecting on positive caring narratives.
Conclusion
Sharing and reflecting positive caring/rehabilitation narratives with patients, relatives and stroke unit team members can support the quality of care experience for all involved.
Trial registration number
N/A
AS08-039
THE IMPACT OF A DEDICATED ORTHOPTIST TO OUR ACUTE STROKE UNIT (ASU) AT ST. GEORGE’S UNIVERSITY HOSPITAL – LONDON
1Moorfields Eye Hospital, Orthoptics, London, United Kingdom
2St. George's University Hospital, Neurology, London, United Kingdom
Background and Aims
The 2016 stroke national clinical guidelines emphasised the importance of orthoptic assessment for patients presenting to ASUs. The orthoptic society recommends orthoptic review within the acute admission. A local audit in 2014 showed 48% of patients with a visual problem saw an orthoptist.
Method
A stroke orthoptist was appointed in January 2017. She accepted all referrals from the multidisciplinary team on the ASU for patients with a visual deficit. From September 18th to December 21st 2017 we re-examined the percentage of patients who received orthoptic input and issued a simplified VFQ-25 questionnaire to patients to examine the difference an orthoptic assessment made to patients’ quality of life.
Results
61 patients were admitted to ASU. 16 (26%) of these had active visual symptoms. The percentage of patients seen by the orthoptist increased from 48% previously to 69%. 24 questionnaires were returned (39% response rate) with 29% reporting poor vision– this aligns with the 26% who had visual symptoms on review of their notes; 44% of the patients with visual concern who returned questionnaires were seen by the orthoptist and 75% of them stated an improved quality of life after orthoptic assessment.
Conclusion
This audit shows that appointing a stroke orthoptist has had a significant positive impact on the visual symptoms of stroke patients – almost three-quarters are now seen and three quarters of those seen feel that their quality of life has been impacted on positively by this encounter. The key limitation of our study is the small sample size.
Trial registration number
N/A
AS08-040
CAN COGNITIVE FUNCTIONS ASSESSED AT VERY EARLY STAGE OF STROKE ONSET PREDICT ADL DEPENDENCE 3 MONTH LATER?
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
2Sahlgrenska University Hospital, Department of Occupational Therapy and Physiotherapy, Göteborg, Sweden
3University of Gothenburg, Centre for Person-Centred Care GPCC, Göteborg, Sweden
Background and Aims
Early prediction of stroke related outcomes have become important due to decreased length of the hospital stay. The aim of the study was to investigate if cognitive functions assessed with the Montreal Cognitive Assessment (MoCA) given 36 hours post stroke can predict dependence in activities of daily living (ADL) 3 month later.
Method
Data were extracted from two databases: the Gothenburg Very Early Supported Discharge Study (GOTVED) and the Swedish Stroke Register - Riksstroke. Neurological functions were assessed with the National institute of Health Stroke Scale (NIHSS) upon admittance to the hospital. Cognitive function and ADL were assessed with the MoCA and the Barthel Index (BI), respectively, within 36 hours of admission. Data about patients' ADL ability 3 month post stroke were extracted from Riksstroke's database - 3 month follow-up module.
Results
Data were available for 369 patients (42% females, mean age 69 years). Three month post stroke 16% of the patients were dependent in ADL. One-half of these patients had very mild neurological deficits (NIHSS ≤2) at the admittance to the hospital and 90% of the patients had cognitive impairments (MoCA ≤25) 36 hours post stroke. The MoCA scores individually predicted ADL dependence at 3 months post stroke (Nagelkerke R2 = 0.12, p < 0.001, AUC = 0.74). The MoCA scores adjusted for age and ADL ability within 36 hours of admission, increased its predictive value for ADL dependence 3 month later (Nagelkerke R2 = 0.26, p < 0.01, AUC=0.80).
Conclusion
The predictive value of the MoCA for ADL dependence 3 month post stroke is limited.
Trial registration number
N/A
AS08-041
EFFECT OF TRAINING EYE HAND COORDINATION USING EMERGING NATURAL USER INTERFACE TECHNOLOGIES TO IMPROVE HAND FUNCTION IN STROKE PATIENTS- A RANDOMIZED CONTROLLED STUDY
1Government Physiotherapy College- Dr. S.N. Medical College - Jodhpur - Rajasthan- India, Physiotherapy, Jodhpur, India
Background and Aims
Eye-hand coordination is essential for humans, as many activities in daily life require precise eye and hand functions. The stroke survivors have poorer eye-hand coordination when using their hemiparetic hand. A significant correlation exists between eye–hand coordination performance and hand function test scores. The aim of this study was to develop a low cost system for testing and training eye and hand coordination using gamification as a tool for improving hand function in chronic stroke patients.
Method
6 subjects (mean age 63.2 ± 4.3 years) with chronic stroke were screened and randomized into experimental and control groups with n = 3 each. Both groups received 1 hour of standard upper limb physical therapy, 6 days a week for total 4 weeks. Experimental group also played a customized eye hand coordination game called “HandEye” using Tobii Eye X® and Leap Motion® for 3 sessions of 2 minutes each. Primary outcome measure was BBT (Box and Block Test).
Results
A significant improvement in scores of BBT was found in both experimental 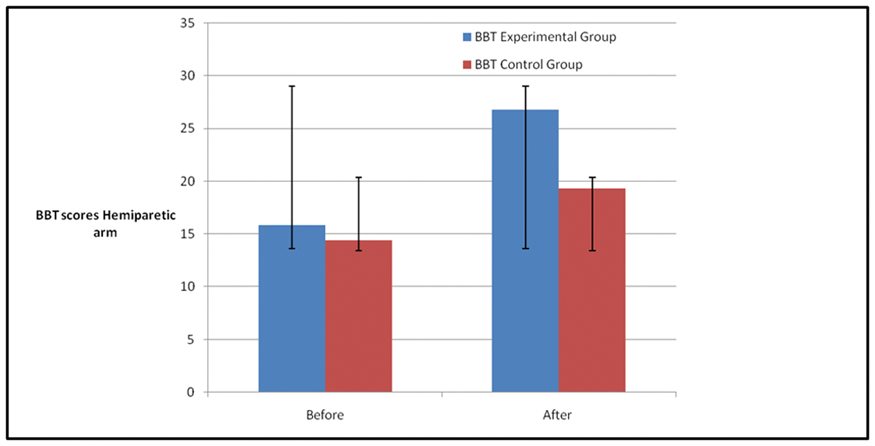
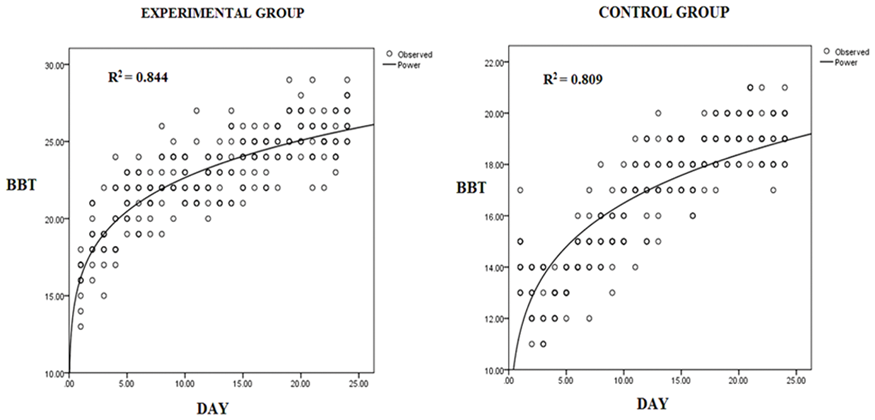
Conclusion
Natural user interface technology and gamification techniques can be useful for hand rehabilitation in stroke survivors.
Trial registration number
N/A.
AS08-043
DOES MOBILITY RESTRICTIONS HAVE AN INFLUENCE ON POST STROKE PAIN?
1Adnan Menderes University, Faculty of Health Sciences / Physiotherapy and Rehabilitation, Aydin, Turkey
2Riga Stradiņš University, Department of Rehabilitation, Riga, Latvia
3University of Gothenburg, Institute of Neuroscience and Physiology- Section for Clinical Neuroscience- The Sahlgrenska Academy, Gothenburg, Sweden
Background and Aims
The aim of this study was to investigate whether the mobility limitations, low vitality, demographic factors and comorbidities can explain Post Stroke Pain (PSP).
Method
Data from 214 community living participants from different parts of Sweden were included in this study. Participants were asked to fill in the Stroke Impact Scale (SIS) to evaluate mobility, Medical Outcomes Study Short Form 36 (SF-36) to evaluate pain, vitality, and The Self-administered Comorbidity Questionnaire (SCQ) for comorbidities. Descriptive statistics were used to show demographic and clinical characteristics of participants. Stepwise multiple linear regression analysis was done to explain the score of pain domain (0-100).
Results
The mean age of all participants in the sample was 66 years (SD=14). 43.4% of the study population were women. The mean pain score of the study population was 68.01 (lower scores indicate more pain). Women had more pain (60.45) than men (73.74). The results also indicated that 12.3% of the participants reported difficulties in sitting without losing balance. The final model with “sitting without losing balance, vitality, female gender’’ explained 22.5% of the variance in the pain score (p < 0.05).
Conclusion
Three factors including sitting balance, vitality and female sex influenced the experience of PSP and its effects on their life. This implies that low motor function (poor sitting balance) as well as low vitality can be factors to address in females having pain after stroke.
Trial registration number
N/A
AS08-044
WORK-RELATED PREDICTORS FOR RETURN TO WORK AFTER STROKE
1Institute of Neuroscience and Physiology, dep of clinical neuroscience- research group rehabilitation medicine, Gothenburg, Sweden
Background and Aims
Disability due to stroke impose a large burden on individuals as well as on society in terms of impaired work ability and sick leave. The reported return to work (RTW) rate after stroke varies globally between 50 to 74 percent.
The aim of this study was to investigate the influence of work-related factors on time to RTW after stroke.
Method
Data from 204 persons with first-time stroke in the years 2009-2010 in Gothenburg, Sweden, who were of working age and had worked prior to their stroke, were analysed. Disease related characteristics were retrieved from medical records, work-related- and socioeconomic data were collected from Statistics Sweden and the Swedish Health Insurance Office up to 6 years post stroke. Cox regression was used to analyse predictors for time to RTW.
Results
The odds of shorter time to RTW were higher among white-collar workers than among blue-collar workers and among workers in larger organizations than among workers in smaller organizations. The odds for shorter time to RTW in this study were also higher when functionally independent at discharge (modified Ranking Scale), of younger age, male sex, and lower educational level.
Men had better odds of shorter time to RTW when being white-collar workers, independent at discharge, and of younger age. For women, being independent at discharge was the only predictor for shorter time to RTW.
Conclusion
Type of work and organizational size are of importance for RTW after stroke. Gender differences indicate the need for further research to improve conditions for women in the RTW process.
Trial registration number
N/A
AS08-045
INCREASED FUNCTIONAL CONNECTIVITY OF CONTRALESIONAL SECONDARY SOMATOSENSORY CORTEX FOLLOWING SOMATOSENSORY REHABILITATION OF STROKE SURVIVORS WITH IMPAIRED TOUCH DISCRIMINATION
1Florey Institute of Neuroscience and Mental Health, Stroke Neurorehabilitation and Recovery, Heidelberg- Melbourne, Australia
2La Trobe University, Occupational Therapy- School of Allied Health, Melbourne, Australia
3Heinrich-Heine-University Düsseldorf, Department of Neurology- Centre for Neurology and Neuropsychiatry- LVR-Klinikum Düsseldorf, Düsseldorf, Germany
Background and Aims
We aimed to identify changes in whole brain functional connectivity (FC) of somatosensory regions following somatosensory rehabilitation designed to help stroke survivors regain a sense of touch.
Method
We investigated resting-state FC of stroke survivors with right (n = 15) or left (n = 17) hemisphere somatosensory lesions pre and post SENSe therapy, and in comparison to age-and-gender matched healthy controls (HCs, n = 15). Whole brain FC was investigated from six regions-of-interest (seeds): primary somatosensory cortex (S1), secondary somatosensory cortex (S2) and thalamus of both hemispheres.
Results
Survivors with right hemisphere lesion showed increased connectivity from contralesional S2 to ipsilesional S1 post- compared to pre-therapy. In addition, prior to SENSe therapy, FC from ipsilesional S1 and thalamus was greater in stroke than HCs in distributed regions; whereas post-therapy FC was greater in stroke than HCs between ipsilesional S1 and ipsilesional thalamus, and with cingulate gyrus. In survivors with left hemisphere lesion, FC was greater from contralesional S2 to contralesional visual area (Brodmann area 19) post- compared to pre-therapy. Pre-therapy, FC from ipsilesional S1 to contralesional fusiform and cingulate regions was greater in HCs compared to stroke; while post-therapy, FC from ipsilesional thalamus to contralesional S1 was greater in stroke.
Conclusion
Changes in functional connectivity of somatosensory network occur following SENSe therapy. Pre-post changes involved increased connectivity from contralesional S2; to ipslesional S1 (following right hemisphere lesion) and to contralesional visual area (following left hemisphere lesion). Changes in connectivity from ipsilesional S1 and thalamus and contralesional S2 were also observed relative to healthy controls.
Trial registration number
ACTRN12613001136796
AS08-046
A LONGITUDINAL PILOT STUDY ON RECOVERY OF MANUAL DEXTERITY IN RELATION TO CORTICOSPINAL EXCITABILITY AND CORTICOSPINAL LESION LOAD AFTER STROKE
1Centre de Psychiatrie et de Neurosciences, Accidents vasculaires cerebraux : determinants du pronostic- recherche translationnelle et medecine personalisee, PARIS, France
2Centre hospitalier Sainte-Anne, Neurology, Paris, France
3Centre de Psychiatrie et de Neurosciences, Biomarqueurs en imagerie : neuro developpement et pathologies cerebrales, Paris, France
4Centre hospitalier Sainte-Anne, Neuroradiology, Paris, France
5FR3636 CNRS- Université Paris Descartes- Sorbonne Paris Cité, Manual Dexterity in health and disease, Paris, France
Background and Aims
Impaired manual dexterity is frequent after stroke and thought to result from corticospinal tract (CST) damage. However, how CST function contributes to functional recovery remains debated. In this prospective longitudinal study we investigated recovery of dexterity and CST injury and excitability in six patients undergoing conventional rehabilitation.
Method
The Finger Force Manipulandum was used to measure force control, finger tapping and independence of finger movements. Structural MRI was used to calculate weighted-CST lesion load, and transcranial magnetic stimulation to measure CST excitability.
Results
Clinical tests showed complete recovery of gross motor hand movements in three patients by six months (maximal Fugl-Meyer Upper Extremity assessment score for hand). At six months, four patients had fully recovered in their ability to accurately control finger force. However, tapping speed and independence of finger movements remained abnormal in all patients at six months when compared to healthy subjects. Recovery in gross motor hand movements and finger force control occurred in those patients with smallest CST lesion load and recovery of CST excitability on TMS, although motor evoked potentials (MEPs) remained of smaller amplitude compared to those evoked from the contralesional side. The two patients with poorest recovery in manual dexterity showed persistent absence of MEPs and greatest structural injury to CST.
Conclusion
Although in a small patient sample, the findings document persistent deficits in manual dexterity after stroke despite good recovery of gross motor hand function and partial recovery of CST excitability, suggesting that CST integrity may be necessary but not sufficient for post-stroke recovery of dexterity.
Trial registration number
N/A
AS08-047
HEALTH CARE AND REHABILITATION CONSUMPTION DURING FIVE YEARS AFTER STROKE
1Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden
Background and Aims
The consequences of stroke often affect a person’s functioning and independence which may lead to a continuous need of rehabilitation and medical attention. The aim of this study was to describe the consumption of health care and rehabilitation during five years after stroke.
Method
Participants with diagnosed stroke were recruited from the stroke units at a hospital in Stockholm, Sweden, during 2006 to 2007. Five years data on in- and out-patient care were collected from the Stockholm County Council’s register.
Results
Of the 121 participants, median age was 65 years and 57% were men. Stroke was classified as mild (Barthel Index 51-100) in 79% of the participants. The number of in-hospital admissions and out-patient visits differed widely in range, table 1. The major part of the total in-patient care, 47% and out-patient care 30%, was used during the first year after stroke. About 80% of the 665 hospital admissions were in medical care and 20% in rehabilitation. Of the 20 639 out-patient visits, rehabilitation represented 27 %. The visits in out-patient rehabilitation were mostly taking place in rehabilitation facilities, 77%, home visits in 11 % and 12 % were non-patients-visits. The most common out-patient rehabilitation visits were to physiotherapists, 39%, physician 23%, occupational therapist 14%, speech and language therapist 10% and psychological-social support 6%.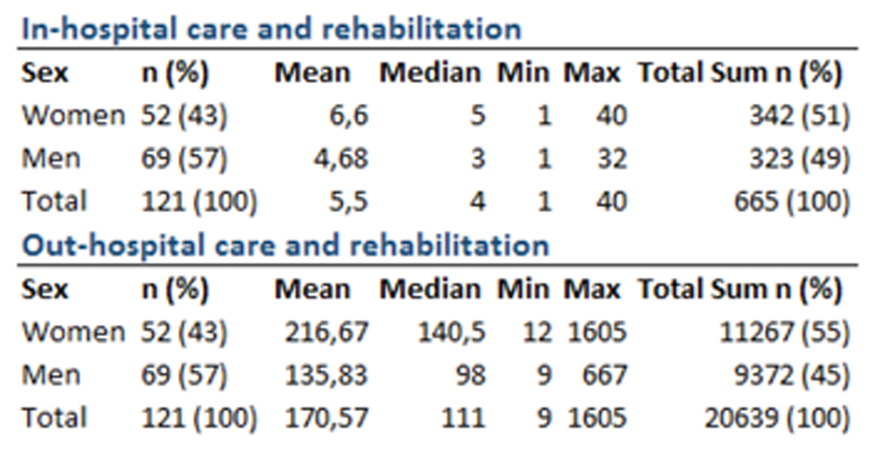
Conclusion
The data show that rehabilitation constituted a smaller part of the total consumption of care and rehabilitation. In further analysis aspects of sex, age and stroke severity will be included.
Trial registration number
N/A
AS08-049
RECOVERY OF KINEMATIC ARM FUNCTION IN WELL-PERFORMING PEOPLE WITH SUBACUTE STROKE: A LONGITUDINAL COHORT STUDY
1UiT The Arctic University of Norway, Department Health and Care Sciences, Tromsø, Norway
2University of Gothenburg, Institute of Neuroscience and Physiology- Rehabilitation Medicine- Sahlgrenska Academy, Gothenburg, Sweden
Background and Aims
Most motor function improvements in people who have experienced strokes occur within the first 3 months. However, individuals showing complete or nearly complete arm function recovery, as assessed using clinical scales, still show certain movement kinematic deficits at 3 months, post-stroke. This study evaluated the changes in upper extremity kinematics, in individuals demonstrating minor clinical motor impairments, 3–12 months post-stroke, and also examined the association between kinematics and the subjects’s self-perceived hand abilities during the chronic stage, 12 months post-stroke.
Method
Forty-two subjects recovering from strokes and having Fugl-Meyer upper extremity motor assessment scores ≥60 were included from the Stroke Arm Longitudinal Study at the University of Gothenburg (SALGOT). Kinematic analyses of a drinking task, performed 3, 6, and 12 months post-stroke, were compared with kinematic analyses performed in 35 healthy controls. The Stroke Impact Scale-Hand domain was evaluated at the 12-month follow-up.
Results
There were no significant changes in kinematic performance between 3 and 12 months, post-stroke. The patients recovering from stroke showed lower peak elbow extension velocities, and increased shoulder abduction and trunk displacement during drinking than did healthy controls, at all time points. At 12 months, post-stroke, better self-perceived arm functions correlated with improved trunk displacements, movement times, movement units, and time to peak velocity percentages.
Conclusion
Kinematic movement deficits, observed at 3 months post-stroke, remained unchanged at 12 months. Movement kinematics were associated with the patient’s self-perceived ability to use their more affected hand.
Trial registration number
ClinicalTrials: NCT01115348
AS08-050
DOG THERAPY IN A STROKE REHABILITATION UNIT
1St. James's Hospital, Stroke, Dublin, Ireland
2St. James's Hospital, Creative Life, Dublin, Ireland
3St. James's Hospital, Stroke- Dept of Medical Gerontology, Dublin, Ireland
Background and Aims
Rehabilitation following Stroke is a complex intervention due to the heterongeneity of clinical presentation. Specialist multi-disciplinary teams are at the core of care of the stroke patient during their recovery and rehabilitation phase.
In our large urban academic hospital, our hospital is founded on four pillars of care, Clinical Care, Research and Development, Education and Training, and Creative Life Centre.
Our Creative Life Coordinator spearheaded the introduction of Dog Therapy as a complimentary aspect of rehabilitation for inpatient stroke patients. The holistic benefit of animals can also additionally benefit staff, families and visitors by creating a happier and more enjoyable environment.

Method
Ruby, our therapy dog, attended our Stroke Unit on a weekly basis, and visited patients who were agreeable to see her. Her owner, and the Institute's Creative Life Coordinator accompanied her on her rounds.
Results
To evaluate the impact of Ruby's interaction, focus groups were conducted with patients and family members, and observations were also documented by the Creative Life Coordinator during the weekly visits.
Patients reported the positive impact that Ruby's visits had on them. Confused and patients who had challenging behaviour were reported by nursing staff as being less upset post visits.
Conclusion
Therapy dogs as a complimentary aspect of care on a rehabilitation unit brings opportunities for patients to interact in a happy and supportive manner. The presence of a therapy dog on a rehabilitation ward has a positive impact on staff members.
Trial registration number
N/A
AS08-051
QUALITY OF LIFE OF STROKE SURVIVORS AND THEIR INFORMAL CAREGIVERS: A PROSPECTIVE STUDY
1Mongolian Stroke Association, Neurology, Ulaanbaatar, Mongolia
Background and Aims
Healthcare improvements have led to increased survival among stroke patients; however, the disability level remains high. These patients require assistance from caregivers, particularly in the first year after stroke. Longitudinal studies of quality of life (QoL) and the factors associated with QoL for both patients and caregivers are limited.
Objectives of the studies are to describe the changes in QoL and determine the factors associated with QoL for stroke patients and their informal caregivers in the first year after stroke.
Method
Multi-centered prospective study was conducted in public hospitals in Mongolia. In this study, 155 first-time stroke patients and their 88 informal caregivers were followed up for 1 year. The WHOQOL-BREF questionnaire was used to assess QoL. The Barthel Index (BI) was administered to the patients at the baseline and after 1 year. A generalized estimating equation analysis was used to determine the factors associated with QoL.
Results
QoL of stroke patients in the domains of physical and environmental aspects improved significantly (p < 0.05) after 1 year; however, social relationship and psychological health declined, but these were not significant. Among caregivers, psychological health and social relationship domains improved significantly. Factors associated with low QoL among stroke patients were advancing age, male patients, being single and less improvements on BI score, and among caregivers were poor physical health and financial difficulties.
Conclusion
Efficient rehabilitation therapy for poststroke patients can improve their QoL. Disability training and financial support for caregivers of poststroke patients might be helpful.
Trial registration number
N/A
AS08-052
LONG-TERM CARE OF STROKE SURVIVORS: IDENTIFYING CIRCUMSTANCES IN WHICH REFERRAL TO SPECIALISTS MAY BE BENEFICIAL USING A MODIFIED RAND APPROPRIATENESS METHOD
1University of Cambridge, Public Health and Primary Care, Cambridge, United Kingdom
Background and Aims
Evidence for long-term care lags behind that for acute stroke care, leading to variations in service provision in primary care across the UK.
Aim
To explore which aspects of long-term stroke care should be managed by primary care and which require referral.
Method
A modified RAND appropriateness method was used. Fictional scenarios were rated for need of referral by an expert 10-person panel. Scenarios were based on long-term post-stroke problem areas identified by published literature.
Round 1:
Online rating of scenarios as follows:
1) Is referral required for this patient?
2) Is specialist stroke referral required?
3) Is this scenario clear?
Round 2:
Face-to-face panel meeting. Aggregate scores from Round 1 were presented along with each panel member’s own scores. Each scenario was discussed and all re-scored as per points 1 & 2 above.
Consensus for referral was defined as a median score of 7-9 on a 9-point scale, without disagreement.
Results
Sixty-nine scenarios were discussed in Round 2. Each was scored for need for referral and then whether this should be to a stroke specialist.
Consensus was achieved for 60 scenarios. 44 were deemed to require referral, of those only 12 for achieved consensus for requiring stroke-specialist referral. There was greater consensus gained in some topic areas (e.g. incontinence, speech) than others (e.g. cognition, employment).
Conclusion
There is broad agreement about when a stroke survivor requires re-referral to specialist care, however there is much less agreement about the destination of referral. These findings will inform a new model of post-stroke primary care.
Trial registration number
n/a
AS08-054
THE EFFECTIVENESS OF EXTRACORPOREAL SHOCK WAVE THERAPY TO REDUCE SPASTICITY OF LOWER LIMB FOR POST–STROKE PATIENTS: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Universitat Internacional de Catalunya, Physioteraphy, Barcelona, Spain
Background and Aims
Recent studies indicate that extracorporeal shock wave therapy (ESWT) is being considered as a new treatment method for spasticity. ESWT is a non–invasive technique where high-energy acoustic impulses produced by different types of generators cause a mechanical stimulus to trigger a chemical reaction (mechanotransduction) in the tissues.
Objective
To establish if ESWT can improve spasticity, range of motion (ROM), balance, pain, gait, activities of daily living in post-stroke patients from a systematic revision of the scientific literature.
Method
CENTRAL, MEDLINE, CINAHL, PEDro, REHABDATA, Scielo, Scopus, Web of Science, Tripdatabase, and Epistemonikos were searched and reference lists screened to identify clinical trials (randomized and nonrandomized) of ESWT, in stroke survivors published until January 2018. Two reviewers independently screened references, selected relevant studies, extracted data, and assessed trial quality. The primary outcome was spasticity; secondary outcomes were ROM, balance, gait and activities of daily living. Due to the heterogeneity of included studies meta-analysis was not possible.
Results
PRELIMINARY: To date a total of 10 studies with 265 participants have been analyzed. The primary targeted muscle was gastrocnemius and secondary was semitendinosus. ESWT showed moderate evidence to reduce spasticity as assessed by the Modified Ashworth Scale and to improve ROM and gait.
Conclusion
PRELIMINARY: ESWT performed with radial or focused modalities could be a good rehabilitation strategy in stroke survivors to reduce spasticity in the lower limb, increase ROM of ankle and improve gait. ESWT does not show adverse events. ESWT is a safe and effective method for reducing spasticity in stroke survivors (subacute and chronic stage).
Trial registration number
PROSPERO 2018 CRD42018083921
AS08-055
SERVICE EVALUATION: DOES ATTENDANCE AT A MULTI-DISCIPLINARY TEAM (MDT) LED LUNCH GROUP AFFECT PATIENTS FUNCTIONAL ACTIVITY LEVELS ON AN ACUTE STROKE WARD?
1Guy's and St Thomas' NHS Foundation Trust, Physiotherapy, London, United Kingdom
2Guy's and St Thomas' NHS Foundation Trust, Speech & Language Therapy, London, United Kingdom
3Guy's and St Thomas' NHS Foundation Trust, Occupational Therapy, London, United Kingdom
4Guy's and St Thomas' NHS Foundation Trust, Dietetics, London, United Kingdom
Background and Aims
Increasing activity through use of an enriched environment is recognised to improve functional outcomes in acute stroke rehabilitation. This service evaluation objective was to identify if attending a MDT lunch group affected patient satisfaction and functional activity across therapy domains.
Method
A descriptive evaluation paired analysis was completed for 18 stroke patients who attended a MDT lunch group (observations for communication and oral intake were carried out on 10 and 14 patients respectively). Patients were aged 46-93 years, with 15 sustaining an ischaemic stroke and 3 a haemorrhagic stroke. Observational data was collected in lunch group and eating at the bedside (usual mealtime) for each patient. This included patients' positioning, mobility (steps taken), communication (number of conversational turns), and oral intake (quantity of food/drink consumed). Qualitative data was collected via a questionnaire to measure patient satisfaction of group attendance.
Results
Mean differences were identified using paired analysis. In lunch group, patients spent 32 minutes longer sitting out when compared to usual mealtimes. Of those able to walk (n = 7), an average of 67 more steps were taken when attending lunch group. 90% of patients took a greater number of conversational turns during lunch group, with an increase of 54 turns on average. In lunch group patients ate 6g and drank 136mls more. 64% of patients preferred attending lunch group.
Conclusion
It is recognised that this is a small sample size, single centre evaluation. However initial findings demonstrate a MDT lunch group increases functional activity and incorporates rehabilitation during mealtimes.
Trial registration number
N/A
AS08-056
IMPACT OF STROKE RESTRICTED TO THE PRIMARY MOTOR CORTEX ON FUNCTIONAL NETWORKS
1University Hospitals Geneva, Clinical Neurosciences, Geneva, Switzerland
2UNIGE, Fundamental Neurosciences, Geneva, Switzerland
Background and Aims
Stroke lesions of primary motor cortex (M1) produce widespread neurophysiological alterations at a distance that underlie clinical deficits. Although structural damage from stroke is focal, loss of function and recovery over time are only partially explained by the size and topography of the lesion. In this study, we take advantage of resting-state (RS) functional connectivity measures to characterize the impact of stroke lesions on the organization and reorganization of brain networks.
Method
We assessed 17 patients with hand paresis due to a first ever stroke restricted to M1. At three time-points (TP) (<10 days, 3 weeks, and 3 months after onset), and together with detailed behavioral motor assessment, we evaluated coupling within nodes of the motor and attentional networks using graph-theory based complex network analysis. Patients were compared to a group of age- and sex- matched healthy volunteers without clinical deficits
Results
Preliminary results indicate a significant decrease in functional connectivity of inter- and intrahemispheric brain motor networks, as well as of dorsal attentional regions in brain damaged-patients compared to controls (p = .048). These changes were selectively observed during the acute stage (TP1). No significant functional differences were present 3 weeks (TP2) and 3 months (TP3) after stroke onset (p > .05). This might be related to the improvement of behavioural motor deficits observed in patients over time.
Conclusion
This study provides new insight into the pathophysiology of motor deficits following stroke and their recovery, and might ultimately contribute to improving prognostic ability and the development of targeted therapeutic interventions.
Trial registration number
N/A
AS08-057
CLINICAL FINDINGS IN EARLY DETECTION OF SWALLOWING DISORDERS IN ACUTE STROKE
1Hospital de Clínicas, Stroke Unit. Neurology Department., San Lorenzo, Paraguay
2Hospital de Clínicas, Neurorehabilitation Department. Hospital de Clínicas, San Lorenzo, Paraguay
Background and Aims
Dysphagia is a major complication, and could be present up to one third of acute strokes. Swallowing disorders can result in aspiration and reduced oral intake. Early detection of swallowing disorders is crucial to avoid potential complications. Our aim was evaluate dysphagia and clinical factors associated through an early dysphagia screen test.
Method
Observational, single center study. Conscious acute stroke patients were evaluated within 48 hours of hospital admission, for trained nurses from the Stroke Unit. An initial screen test was applied to identify dysphagia risk patients and required for full clinical assessment by a professional skilled. We determinate the screen test abnormalities and clinical factors associated.
Results
From 38 acute stroke patients, 26(68.4%) were ICH and 19(50%) female. Median Baseline NIHSS were 7 (IQR 3-11). Initial screen test for dysphagia was referred for full clinical assessment in 6(15.8%) patients as dysphagia risk. Speech impairments occurred in 32%; facial weakness in 36.8 %, reflexes impairments in 15.8%. In univariate analysis, speech impairment due to Fluent and non-fluent aphasia (83.3%Vs.12.5% p = 0.012 and 50%Vs.9.3% p = 0.006 respectively) and baseline NIHSS (median11Vs.5, p = 0.018) were associated with dysphagia risk. Multivariate analysis has shown fluent aphasia as only factor associated to dysphagia risk (OR=32.0 CI= 2.287-41.832p = 0.01).
Conclusion
Dysphagia risk, using an early screen test, was detected in almost 16% of acute stroke patients. Non-fluent aphasia emerge as the only associated factor, even baseline NIHSS including. This clinical finding could help to identify possible swallowing disorder in acute stroke patients.
Trial registration number
N/A
AS08-058
POST-STROKE PARTICIPATION: A QUANTITATIVE INSIGHT USING THE INTERNATIONAL CLASSIFICATION OF FUNCTIONING, DISABILITY AND HEALTH FRAMEWORK
1University of Lyon, University Claude Bernard Lyon 1- HESPER EA 7425, Lyon, France
2University of Lyon, University Lumiere Lyon 2 - GRePS EA 4163, Bron, France
3University of Aix-Marseille, INSERM umr 912 SESSTIM, Marseille, France
4Hospices Civils of Lyon, Public Health Department, Lyon, France
Background and Aims
In 2001, the WHO published the International Classification of Functioning, Disability and Health (ICF) which defined participation restriction as the difficulty to perform activities in daily life and considered contextual factors (personal and environmental) as moderating the association between disabilities and social participation.
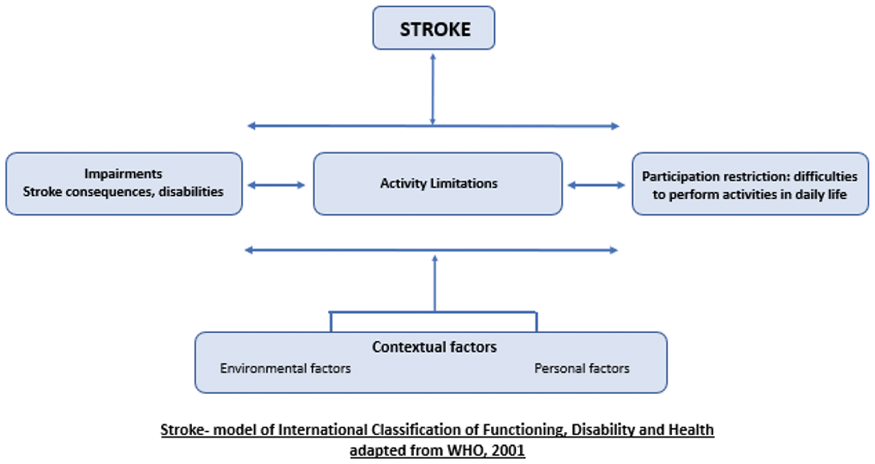
From the patient perspective, participation restriction is a major determinant of life satisfaction. We aimed to better understand the interactions between disabilities, contextual factors and social participation at 6 months post-stroke.
Method
Quantitative self-administered surveys at 6 months post-stroke were sent to a sample of patients recruited from the Stroke 69 cohort, a cohort study of all incident strokes in the Rhône county (France) between November 2015 and December 2016.
Participation was measured with the stroke impact scale ranging from 0 to 100 (maximal participation and no restriction). Firstly, a Focused Principal Component Analysis was conducted, and secondly, a linear multiple regression analysis.
Results
116 patients returned the questionnaire, 63% were men, mean age was 71 years (range [30-95]). The median participation score was 68.8. Increased age (p < 0.05), female gender (p < 0.01), professionally active (p < 0.01), high number of sequelae (p < 0.001), and fatigue (p < 0.05) significantly increased participation restriction at 6 months.
Conclusion
A better understanding of factors associated with participation restriction is important to strengthen existing rehabilitation program, support and management of stroke in clinical practice and daily life.
Trial registration number
N/A
AS08-059
PATIENTS’ PHYSICAL ACTIVITY IN STROKE UNITS: BEHAVIORAL MAPPING IN LATVIA AND SWEDEN
1Riga East University Hospital, Department of Rehabilitation, Riga, Latvia
2The University of Gothenburg- Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
By identification of types and content of care and rehabilitation, which depends on the contextual factors, it would be possible to identify relevant problems as well as to provide foundation for improvement of care and rehabilitation in the Stroke unit.
Objective
To compare levels of patients’ physical activities as well as social interaction within Stroke units in university clinical hospitals in Latvia and Sweden.
Method
Prospective, observational, comparative study using behavioral mapping. Patients admitted at 2 stroke units in Latvia and at 1 stroke unit in Sweden at least 1 day post-stroke were observed over 1 week-day at 10 min intervals between 09.00 and 15.00. At each observation physical activity, location and people present were ascertained. 27 patients from Latvia (51 observation) and 25 patients from Sweden (39 observations) were included.
Results
The physical, social and institutional environment in Stroke units analysed in the study differs. Patients spent alone 55.6%; 64.3% and 44.4% of the observed day-time in Latvian and Swedish study population, respectively. Most of the time patients were inactive lying in bed (83.9%; 90.8% and 63%). Time spent outside the bedroom and interacting with multidisciplinary team (medical and nursing staff, therapists) (35.4%; 26.2% and 27.5%) were different.
Conclusion
In Latvian Stroke units patients spend most of their day-time inactive and alone. Patients in Swedish Stroke unit were more active compared to Latvian population; however they spent most of the time in bed. This emphasizes the opportunity to improve early physical activities after a stroke in both countries.
Trial registration number
N/A
AS08-061
THE ROLE OF ROBOT-ASSISTED GAIT TRAINING IN STROKE PATIENTS
1Polyclinic Glavić, Neurology, Dubrovnik, Croatia
2Polyclinic Glavić- School of Medicine- J.J. Strossmayer University in Osijek, Neurology, Zagreb, Croatia
3University Hospital Center Zagreb- Zagreb School of Medicine, Department of Neurology, Zagreb, Croatia
Background and Aims
Robotic devices are used widely for neurorehabilitation in stroke patients, but due to different devices and inconsistent methods used in published studies, the effect of robotic neurorehabilitation on specific disabilities after stroke remains to be further evaluated. The aim of our study was to investigate the effect of robot-assisted gait training (RAGT) on stroke disability outcome and to detect its correlation to stroke localisation.
Method
33 stroke patients aged 18-60 admitted to our neurorehabilitation center were subjected to RAGT, as well as conventional physical therapy in duration of 12 weeks. Training intensity for both methods was 1 h daily, 5 days a week. We evaluated disability by modified Rankin scale (MRS) at the beginning and end of treatment and observed its relationship to stroke lateralisation (dominant vrs non- dominant hemisphere).
Results
We found statistically significant improvement in the outcome measured by MRS, P<0.001, with effect size of 0.617 . We did not find correlation of improvements with stroke lateralisation.
Conclusion
Our results showed that intensive gait rehabilitation approach blending robotic and conventional physical therapy has significant effects on improving stroke disability. Larger studies are needed to detect influence of stroke lateralisation on neurorehabilitation outcomes.
Trial registration number
N/A
AS08-062
MINDFULNESS BASED STRESS REDUCTION TO SUPPORT SELF-MANAGMENT OF ANXIETY AND DEPRESSION FOLLOWING STROKE: A DEVELOPMENT STUDY
1Glasgow Caledonian University, Nursing and Community Health, Glasgow, United Kingdom
Background and Aims
Anxiety disorders and depression are common after stroke. Anxiety disorders generally are associated with reduced quality of life (QoL) and increased use of healthcare services. Depression is significantly associated with increased mortality, anxiety, and lower QoL amongst stroke survivors. Psychological interventions that promote acquisition of coping skills are recommended.
Mindfulness Based Stress Reduction (MBSR) is a structured, 8-week group-based self-management course, designed to help people cope with physical, psychological or emotional distress. Skills taught are practiced at home. MBSR is effective in people with long-term conditions comorbid with anxiety and depression, which suggests that it could facilitate - self-management of these symptoms for stroke survivors. However, systematic review evidence indicates that attrition is high, with many people not completing the course or finding home practice difficult. We hypothesise that a stroke-specific version of MBSR may help improve adherence, which should improve mastery of skills and subsequent self-management of symptoms, thus reducing burden on individuals and healthcare services.
We aimed to develop a stroke-specific MBSR course.
Method
Thirty stroke survivors and family members/carers took part in MBSR sessions and follow-up focus groups. We analysed the focus group data using a framework approach. Together with stroke survivors and other experts, we then adapted the standard MBSR course.
Results
Findings identified areas for adaption: preparation (accessible information), ‘dose’ (shorter sessions, longer course), approach (slow, repetitive, cognisant of stroke–related impairments), motivation and support (peer/partner support).
Conclusion
Co-creating a stroke-specific MBSR course resulted in meaningful adaptations for testing in future feasibility work.
Trial registration number
N/A
AS08-064
CAN WE PREDICT CLINICAL OUTCOMES AFTER A MODERATE/SEVERE STROKE?
1Nottingham University Hospitals, Stroke Medicine, Nottingham, United Kingdom
2University of Nottingham, Department of Stroke Medicine, Nottingham, United Kingdom
Background and Aims
Predicting outcome of severe stroke allows tailoring the rehab/care needs of the patient. PREP2 has been shown to predict outcome but needs complicated assessments. We hypothesised that Shoulder Abduction and Finger Extension (SAFE) score on day 7 could be used to predict recovery following moderate/severe acute stroke.
Method
Data was from the Efficacy of Nitric Oxide in Stroke (ENOS) trial. ENOS randomised patients with elevated blood pressure, to 7 days of GTN or no GTN, within 48 hours of stroke. Participants had Scandinavian Stroke Scale (SSS) performed at baseline and day 7. The SAFE score was derived from the arm and hand movement components of the SSS. We dichotomised them into mild (SAFE score <=8) and moderate/severe stroke (SAFE score >=9). We analysed day 90 functional outcome using binary logistic or linear regression with adjustment for GTN treatment and baseline severity.
Results
From the ENOS dataset, we identified 2485 patients with moderate/severe stroke at baseline. On day 7, 1715 had a SAFE score of <=8 and 710 had a SAFE score of >= 9 (60 missing data, not analysed). In those with a SAFE score of >=9 on day 7, the 90 day outcome was better in all the outcome measures; modified Rankin Scale (p < 0.001), mortality (p < 0.001), Barthel index (p < 0.001), telephone mini-mental examination score (p < 0.001), Zung depression score (p < 0.001) and quality of life (EQ-5D, p <0.001).
Conclusion
SAFE score alone on day 7 can be used to predict outcome at day 90 in those with a moderate/severe acute stroke.
Trial registration number
ENOS trial ISRCTN99414122
AS08-066
COMPARING ‘REAL WORLD' PATIENTS AND CLINICAL TRIALS ENROLMENT CRITERIA: WHO WOULD BE ELIGIBLE TO PARTICIPATE?
1Bridgepoint Collaboratory for Research and Innovation, Research, Toronto, Canada
2Queens University, Psychology, Kingston, Canada
Background and Aims
The high prevalence of comorbidities in stroke patients poses many challenges for rehabilitation. Yet, many of the Stroke Rehabilitation Best Practice Recommendations lack guidance regarding comorbidities, which may be due to the inability to generalize outcomes from the stroke research literature to ‘real-world’ stroke patients. The applicability of randomized controls trials (RCTs) is partly dependent on the congruency between trial subjects in stroke rehabilitation literature and general patient populations. Our objective was to determine the proportion of stroke patients meeting enrolment criteria of randomized controlled trials in stroke rehabilitation.
Method
Exclusion criteria extracted from a recent systematic scoping review that analyzed 428 RCTs were applied to 110 consecutive patients admitted to a stroke rehabilitation unit from 2012-13 to determine how many patients admitted to a stroke rehab unit would have been eligible to participate in stroke RCTs based on age, cognitive impairment, previous stroke and disease/condition composite exclusion variables.
Results
Approximately 60.1% of the stroke patients admitted to rehabilitation would be excluded from participating in RCTs by one or more exclusion criteria. Notably, 84.5% of patients would have been ineligible for 54% of RCTs based on cognitive impairment.
Conclusion
Results highlight the difference between clinical trials subjects and ‘real world’ stroke patients. Given the high prevalence of comorbidities in ‘real world’ patients, this study emphasizes the importance of including ‘typical stroke patients’ in research studies or supporting the use of alternative methodologies that addresses application of study results to patients with comorbidities.
Trial registration number
N/A
AS08-067
HOW CAN THE ASSISTING HAND ASSESSMENT FOR ADULTS AFTER STROKE (AD-AHA STROKE) INFORM INTERVENTION PLANNING AND MEASURE CHANGE?
1Karolinska Institutet- Stockholm, Department of Women's and Children's Health, Stockolm, Sweden
Background and Aims
Hand skills are vital for the performance of activities in everyday life and using the two hands together is critical to conduct most activities. Still hand function assessments commonly focus on unimanual aspects. The recently developed Ad-AHA Stroke measures how effectively a patient with hemiparesis use his/her affected hand together with the unaffected hand to perform bimanual tasks.
The aim of this presentation is to report the current evidence of the psychometric properties of the Ad-AHA Stroke and to discuss how the results can be used to measure change and guide intervention with the aim to improve the functional us of the affected hand.
Method
Rasch measurement model analysis was based on 144 assessments.
Results
The analysis demonstrated a unidimensional construct and evidence of internal scale validity of the Ad-AHA Stroke scale. The strong reliability and the large person separation ratio indicate that the test will be responsive to change. A strong correlation to outcomes on the Jebsen and Taylor Test of Hand Function and the ABILHAND Stroke indicate external validity. A further useful information generated by the Rasch analysis is the item difficulty calibrations. The patient’s ability measures can be matched to the corresponding item difficulty hierarchy and tells us which the next step would be for improving bimanual performance.
Conclusion
The use of the Ad-AHA Stroke has the potential to broaden the knowledge of how adults following stroke use two hands together. This can guide the development of functional approaches to training that target effective assisting hand use in daily activities.
Trial registration number
N/A
AS08-068
USE OF HYPNOTHERAPY IN CONTROLLING POST STROKE PSYCHOLOGICAL AND EMOTIONAL CHANGES
1University Hospital of North Midland NHS Trust, Stroke Medicine, Stoke on Trent, United Kingdom
Background and Aims
Psychological and emotional changes are common symptoms in stroke survivor. These symptoms could be quite distressing and adversely affects their quality of life. The common symptoms in these patient includes post-stroke anxiety (PSA), post-stroke emotional incontinence (PSEI), post-stroke anger proneness (PSAP), and post-stroke fatigue (PSF) and insomnia. There is clinical evidence for use of hypnotherapy in treating these conditions in non-stroke patients. We reported a case series of patients treated with hypnotherapy with these conditions following stroke.
Method
Patients diagnosed with psychological and emotional changes following stroke were offered hypnotherapy for improvement of the symptoms. Hypnosis with imagery and anchoring technique was used for the treatment. The treatment was provided by single stroke physician trained in the technique and each session lasted for 60 minutes. The audio recording of the sessions given to the patients to practice daily.
Results
Thirty two patients were included for hypnotherapy in this case series. 18 patients had PSA, 5 had insomnia, 4 had PSEI, 3 had PSAP and 2 had PSF. On an average, 6 session were required to control these symptoms. Apart from PSF, all the other group of patients self-reported significant improvement in their symptoms. All the patients who responded also reported increased well-being, motivation. More than 90% of the patient also self-reported satisfactory control of symptoms in 6 months follow-up. None of the patients reported any side effect.
Conclusion
Hypnotherapy can be considered an alternative approach in successfully treating these conditions following stroke and it is very safe.
Trial registration number
N/A
AS08-069
AN AUDIT OF THE DELAY TO CONFIRMATION OF SAFETY OF NASOGASTRIC TUBE PLACEMENT: A QUALITY IMPROVEMENT PROJECT
1William Harvey Hospital, Stroke Medicine, Ashford, United Kingdom
Background and Aims
It was observed that there is often a significant delay from nasogastric tube insertion to confirmation of safe placement by radiography when a satisfactory aspirate can’t be obtained. Local policy mandates confirmation of safe position by a consultant radiologist. This project set out to establish the extent of the problem and to establish where in the service improvements can be made.
Method
All patients with an NG tube requiring imaging confirmation over a two month period were included in this retrospective audit of inpatients on our stroke unit. The delay for each stage in the process was attained, as was the total time for safety clearance.
Results
25 instances of radiographic confirmation were identified. Unavailable documentation of insertion time limited the assessment of total time from insertion to use in 12 patients.

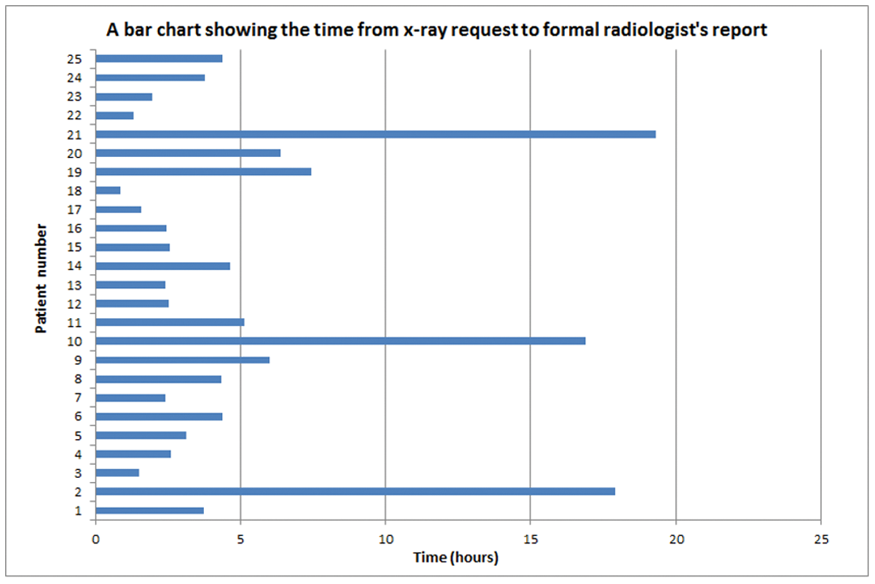
Conclusion
Although confirmation was attained in most cases in an acceptable time frame, there were clearly significant delays in some cases, predominantly in delay to acquisition and reporting. Our radiology department have been informed of the audit findings as have our stroke team. Operational changes will hopefully improve time delays when re-audited in the next two months.
Trial registration number
n/a
AS08-070
EXCITABILITY PROFILE OF THE MOTOR TMS MAP AS A NEW PARAMETER FOR DYNAMICAL INVESTIGATION OF THE HUMAN MOTOR CORTEX
1National Research University Higher School of Economics, Centre for Cognition and Decision making, Moscow, Russia
2Research Center of Neurology, Department of Neurorehabilitation, Moscow, Russia
3Max Planck Institute for Human Cognitive and Brain Sciences, Department of Neurology, Leipzig, Germany
Background and Aims
Cortical mapping with transcranial magnetic stimulation (TMS) is a promising approach for non-invasive tracing of the changes in the motor cortex during rehabilitation after stroke. However, a clear understanding of the test-retest reliability of the different parameters of TMS maps in normal subjects is still missing. Here we propose a new approach which takes into account a complex profile of the cortical excitability over cortical surface potentially allowing a more refined estimation of the neuroplastic changes. We first test its validity in a test-retest TMS mapping study in 16 healthy volunteers.
Method
For standard parameters intra-class correlation coefficient (ICC) was used, while for quantative comparison of the excitability profiles of the muscles’ cortical representations we used earth mover's distance metrics (EMD).
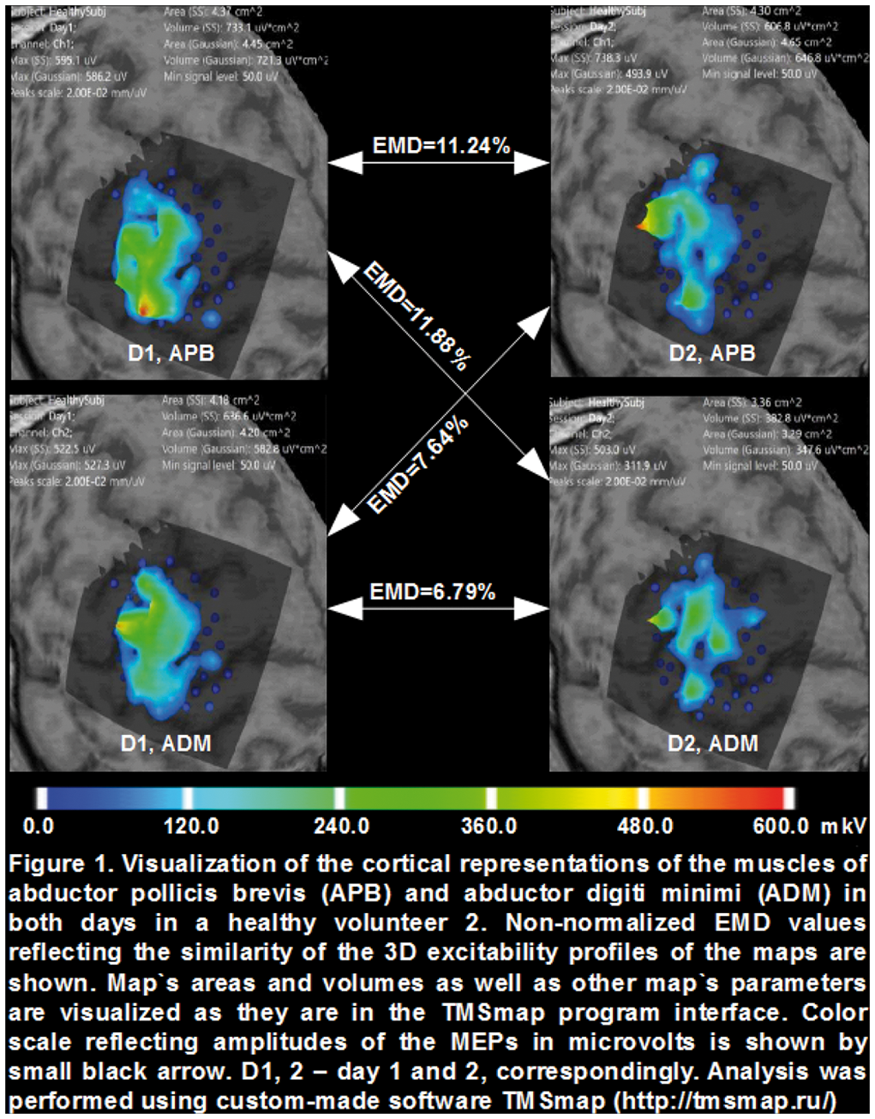
Results
We found that RMT remained the same in all but two subjects. ICC for areas - 0,79 ± 0,11 can be considered as good and for volumes - 0,42 ± 0,06 as poor reproducibility. As for the excitability profile – the reproducibility measurement showed significantly smaller EMD (higher reproducibility) for the same muscle representation than for the different muscles (for same muscles normalized EMD 0,92, for different 1,039, Mann-Whitney criterion p < 0,0001).
Conclusion
Obtained results provide an evidence for the validity of the excitability profile parameter for the test-retest assessment of the motor TMS maps which may be useful for the longitudinal studies in stroke.
Trial registration number
N/A
AS08-072
DOES MYOGRAPHY CONVEY ADDITIONAL INFORMATION BEYOND MOTION SENSORS FOR ARM FUNCTION QUANTIFICATION IN STROKE?
1Imperial College London, Mechanical Engineering, London, United Kingdom
2Imperial College London, Medicine, London, United Kingdom
Background and Aims
Automated systems for quantifying motor function after stroke have been proposed as a higher resolution and more objective alternative to assessment by a clinician. The research proposed in this work investigates the usefulness of information provided by the novel application of myographic sensors in an automated system of post-stroke motor dysfunction.
Method
The motor capture system proposed consisted of two IMUs, placed on the upper and lower segments of the paretic arm of the subject respectively, and a combination of electromyogram and mechanomyogram placed on muscles pertaining to elbow and finger flexion. A total of 28 patients were recruited for this study (FMA motor function score 40.5 ± 4.0) and were instructed to perform tasks from the motor function section of the Fugl Meyer Assessment (FMA). Features were extracted and selected using a combination of domain knowledge and the RELIEF feature selection algorithm.
Results
Out of the 16 motor tasks tested, 12 tasks were found have good classification performance (>60% K-nearest neighbours algorithm). Myographic features were not found to be amongst the most useful features for gross motor tasks involving the entire arm. For motor tasks only involving the wrist and hand which were not measured with IMUs, myographic features alone provided good performance in 57% of the tasks performed.
Conclusion
These results indicate that myography does not provide as accurate information concerning motor dysfunction as IMUs, but could function as a low cost and practical alternative to current automated methods of hand motor function such as an instrumented glove or Kinect sensor.
Trial registration number
N/A
AS08-073
‘CREATE’ COLLABORATIVE REHABILITATION ENVIRONMENTS IN ACUTE STROKE – AN EXPERIENCE-BASED CODESIGN APPROACH (EBCD) TO INCREASING ACTIVITY OF STROKE PATIENTS IN FOUR HOSPITALS IN ENGLAND
1Kingston and St George's Joint Faculty, Health- Social Care and Education, London, United Kingdom
2Alfred Health, Alfred Health, Melbourne, Australia
3School of Population Health & Environmental Sciences, Faculty of Life Sciences and Medicine, London, United Kingdom
4Leeds Institute of Health Sciences, Academic Unit of Elderly Care and Rehabilitation, Leeds, United Kingdom
5King's College London, Florence Nightingale Faculty of Nursing and Midwifery, London, United Kingdom
6Glasgow School of Art, School of Design, Glasgow, United Kingdom
Background and Aims
An Experience-Based Co-Design approach (EBCD) combines participatory research and user experience to redesign healthcare services. Using EBCD for the first time in acute stroke services, CREATE aims to develop and implement service changes to increase opportunities for patients to engage in social, cognitive and physical activities.
Method
Mixed methods include behavioural mapping, non-participant observations of patient activity, semi-structured interviews and patient reported experience and outcome measures. These data were collected pre- and post-introduction of interventions developed using the Experience-Based Co-Design approach.
Results
Pre-implementation behaviour mapping at the first site in London showed that 75% of the time patients were physically inactive, 74% cognitively inactive, and 64% socially inactive. In the Yorkshire site, the figures were 72%, 71% and 55% respectively. 24 staff and 19 patients and carers participated in the co-design groups at both sites prioritising changes to use of space, communication processes and activity opportunities. To date, co-designed interventions across the two sites include provision and increased use of cognitively stimulating board games, puzzles and colouring books; increased participation in singing groups, dog therapy, art groups, breakfast, cookery and lunch supported by volunteers.
Conclusion
There was great enthusiasm for EBCD in the first two stroke units which demonstrated the potential for jointly driven changes to improve opportunities for greater social, cognitive and physical activity in a stroke specific context. The findings of this project aim to provide a template for change to increase activity opportunities that can be used across all inpatient stroke settings.
Trial registration number
N/A
AS08-074
HOW IS LIVING WITH LOCKED-IN SYNDROME? RESULTS FROM THE NORWEGIAN NATIONAL UNIT
1Sunnaas Rehabilitation Hospital, Norwegian National Unit for Rehabilitation of Locked-in Syndrome, Nesoddtangen, Norway
2University of Oslo, Institute of Clinical Medicine, Oslo, Norway
Background and Aims
Locked-in syndrome (LIS) is a rare condition that with regard to function can be defined as the combination of severe tetraparesis and communication impairment leading to complete dependence in activities of daily life, and (close to) normal cognitive function. This study gives an overview of the current Norwegian stroke LIS population.
Method
The Norwegian National Unit for Rehabilitation of Locked-in Syndrome gathers data related to its clinical services in a quality register, possibly the only existing population-based register for LIS. Data from all known patients with LIS are collected during in-patient rehabilitation and yearly follow-up. In addition to demographical and epidemiological data, data regarding all domains of the ICF-model are included.
Results
To date, 21 patients (17 men, 4 women) living in Norway with LIS due to stroke are known to our national service. They are on average 61.0 years old (range 17.0-80.4), and have lived a median of 7.1 years (range 1.8-41.6) with LIS. Ischemia caused LIS in 15 cases, intracerebral hemorrhage in 4 and subarachnoid hemorrhage in 2. Figure 1 shows some of the results that will be presented.
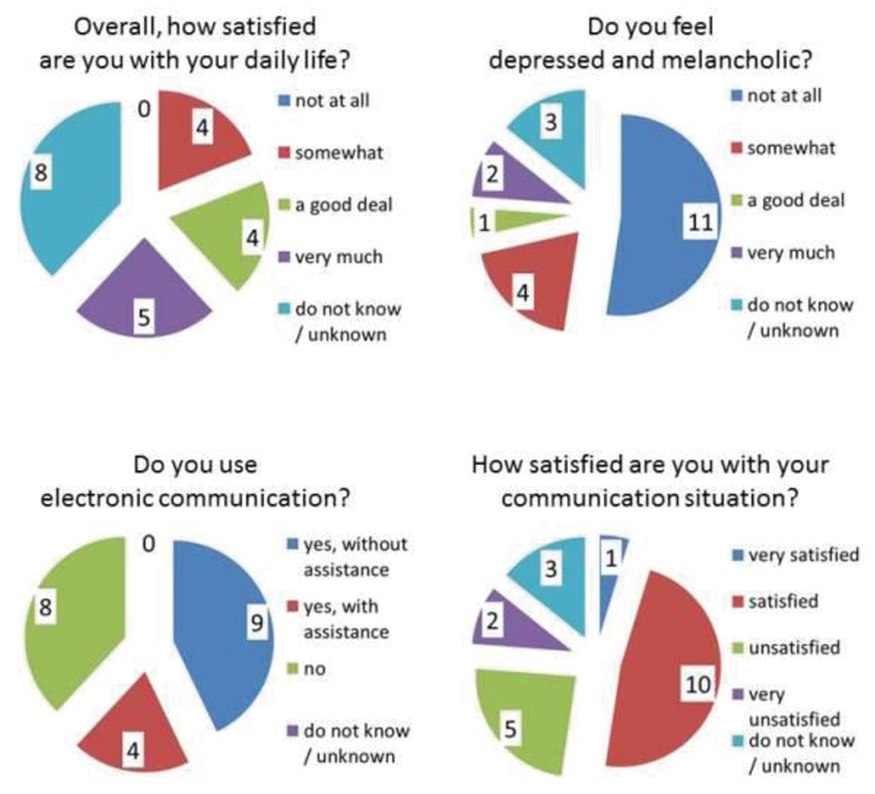
Conclusion
The Norwegian National Unit for Rehabilitation of LIS and its register reveal that a meaningful life with LIS is possible, but also that LIS is a severe condition where more effort is needed to improve patients’ lives and their services.
Trial registration number
N/A
AS08-075
CLINICAL AND PATIENT REPORTED OUTCOMES AT SIX MONTHS IN A LONDON STROKE POPULATION
1University College London Hospital, Hyper Acute Stroke Unit, London, United Kingdom
Background and Aims
Although stroke is a major cause of chronic disability little is known about the pattern and extent of cognitive, functional and patient reported disability at follow up post stroke.
The Stroke Investigation Group in North and central London (SIGNaL) registry captures clinical and patient reported outcomes for all patients presenting with stroke to the University College London Hospitals (UCLH) HASU. The objective of this work is to describe in detail patient performance at follow up for all stroke presentations to a single centre and to identify those factors most associated with determining clinical outcome.
Method
The service admits 1000 patients per year with acute stroke. The SIGNaL registry captures all data relating to baseline assessment, early follow up at 30 days and from a detailed clinical, patient reported and functional assessment at six months. This latter assessment is performed using a locally developed battery of tests that include assessment of cognition, motor function, language and anxiety as well as standard measures of global performance such as MRS.
Results
Since the start of the six months follow up assessment in October 2017 we have collected detailed outcome data on more than 75% of the patient population. Data collection is ongoing and findings from the first 500 patients will be presented, analysed according to stroke sub-type and stroke severity at presentation, baseline treatment received and pre-morbid functional status. An evaluation of the utility of each of the tools in the assessment battery will also be performed.
Conclusion
/
Trial registration number
N/A
AS08-076
ARE PORTUGUESE STROKE UNITS ORGANIZED IN STROKE REHABILITATION?
1Hospital Senhora da Oliveira- Guimaraes, Physical Medicine Rehabilitation, Guimarães, Portugal
2Centro Hospitalar do Médio Ave, Physical Medicine Rehabilitation, Famalicão, Portugal
Background and Aims
Stroke units with multidisciplinary stroke rehabilitation teams (MSRT) are the best place to treat a stroke survivor, not only to reduce mortality rates, shorten hospital lengths and lower the risk of institutionalization, but also to enhance the functional outcome and to decrease the direct and indirect cost of care.
Stroke rehabilitation requires a sustained and coordinated MSRT, highlighting the communication and coordination as essential for achieving the full potential .
Method
All Portuguese stroke units were visited and the caretaking of rehabilitation was assessed. The presence of multidisciplinary teams, time of functional assessment, dysphagia/ neurogenic bladder screnning and discharge planning were evaluated.
Results
All but one of the 27 SU have MSRT coordinated by physiatrist. 96% physiotherapist, 66,7% occupational therapist, 88.9% speech therapist ; 0.4% rehabilitation nurse. Social worker is present in 92.6% of cases, nutritionist in 88.9% and neuropsychologist in 51.9%; only 18,5% have MSRT mettings
Dysphagia is screened in 93,7% of units but neurogenic bladder is only screened in 3,7% .
Discharge planning is performed in 92,6% by physiatrist, but in 59,3% the hospital discharge team has the autonomy for this decision.
Conclusion
In this study, we found a heterogeneous organizational structure of stroke rehabilitation care amongst stroke units. Stroke rehabilitation should be a priority in Portuguese stroke units. Portugal has done a great effort to be effective and efficient in Acute stroke treatment, however, in rehabilitation, there is still a long way to go to achieve excellent organization, which necessarily depends on the efficiency/eficacy of MSRT.
Trial registration number
N/A
AS08-077
CLINICAL AND PATIENT REPORTED OUTCOMES AT 30 DAYS IN A LONDON STROKE POPULATION
1University College London Hospital, Hyper Acute Stroke Unit, London, United Kingdom
Background and Aims
Although stroke is a major cause of chronic disability little is understood about the factors that influence the extent of stroke recovery.
The Stroke Investigation Group in North and central London (SIGNaL) registry captures clinical and patient reported outcomes for all patients presenting with stroke to the University College London Hospitals (UCLH) HASU. The objective of this work is to describe outcomes across the spectrum of stroke presentations to a single centre and to identify factors at presentation that may be associated with clinical outcome and with the patient assessment of the degree of functional recovery.
Method
The service admits 1000 patients per year with acute stroke. Modified Rankin Scale, Stroke Impact Scale and Stroke Recurrence Scale scores are collected for each patient at 30 days using a standardised telephone consultation template. Detailed clinical data, including baseline MRI head imaging in most patients, is also collected at baseline and further follow up is performed at six months.
Results
Since the start of 30 day outcome collection more than 100 outcome data sets have been obtained reflecting successful patient follow up in approximately 70% of the total population of patients presenting to UCLH. Data collection is ongoing and findings from the first 500 patients will be presented. Impact at 30 days on clinical and patient reported outcomes of baseline stroke severity, stroke sub-type, baseline treatment provided, and pre-morbid functional status will be reported.
Conclusion
SIGNaL will create patient centered clinical pathway and may reduce re-admissions at 30 days for patients that are discharged.
Trial registration number
N/A
AS08-079
COLLABORATIVE PHYSIOTHERAPY RELATIVE TO SOLO TRAINING BOOSTS MOTOR PERFORMANCE MORE IN STROKE PATIENTS WITH PARIETAL LESIONS
1Imperial College London, Brain Sciences, London, United Kingdom
2Imperial College London, Human Robotics Group- Bioengineering Dept, London, United Kingdom
Background and Aims
Human interaction is instrumental to supervised physiotherapy, but limited by practical constraints on professionals’ time. We developed a computer game that allows stroke patients to engage in arm exercises with non-specialist partners, e.g. family or other patients, that improves performance and motivation in patients relative to single-player versions. To extend this investigation, we tested whether: 1) lesion location influences performance advantages gained by multiplayer interaction; and 2) performance gains over time are influenced by interactive versus single-player training.
Method
30 hemiparetic stroke patients, without neglect, within 1-week of onset were recruited, and taught an animated visuomotor tracking task with their weak hand, using an adapted tablet-controller (www.gripable.org). Subjects used graduated hand-grip to control the vertical position of one end of a horizontal beam; the other end controlled by either the computer (solo-mode), or a researcher (interactive-mode). Voxel-lesion symptom mapping identified brain regions related to performance gains in interactive relative to single-player modes. Half of patients were tested after 3 x 30-min training blocks over 24 hours.
Results
Performance on visuomotor tracking was inversely proportional to lesions in parieto-occipital and primary motor areas (p < 0.05 corrected). However, only lesions to parietal regions were associated with performance gains during interactive relative to solo-play. This effect persisted after correcting for lesion volume and baseline performance. Subjects who underwent training improved performance by ∼40%, compared to subjects who did not independently of training schedule.
Conclusion
Performance-enhancing effects of collaborative, relative to solo, therapy are experienced more in patients with parietal strokes.
Trial registration number
N/A
AS08-080
EVALUATION OF AN ADVANCED MINDFULNESS PROGRAM LIVE ON INTERNET FOR PARTICIPANTS SUFFERING FROM MENTAL FATIGUE AFTER ACQUIRED BRAIN INJURY
1Institute of Neuroscience and physiology, Clinical Neuroscience, Gothenburg, Sweden
Background and Aims
Mental fatigue is common following an acquired brain injury, having considerable negative impact on work and quality of life. It can take several years of effort, frustration and despair to find the right balance in life. The aim of this feasibility study was to evaluate an advanced mindfulness program delivered live on Internet to individuals who have experienced a traumatic brain injury or stroke and were suffering from long-lasting mental fatigue.
Method
Twenty-one participants who had completed a previous MBSR program (MindfulnessBased StressReduction) attended the advanced mindfulness program, 10 of them live on internet and 11 the same program face-to-face. It was an 8 months program with monthly group meetings (2.5h), and concluded with an all-day retreat. The program included practice of compassion which are central in mindfulness and have significant importance for well-being.
Results
Compared from baseline a decreased mental fatigue (Mental Fatigue Scale) was found (p < 0.001). The assessment after the advanced program showed a sustained positive effect, with no difference between the groups. A significant increased rating for self-compassion was detected (p = 0.003), and improvement was also found after the advanced program. No difference between the groups.
Conclusion
This study showed the possibility to deliver a live, interactive, online advanced mindfulness program to a group of people suffering from mental fatigue after an acquired brain injury and obtain positive effects in the same ranges as for a face-to-face group. This is promising, as the Internet is accessible to many individuals, irrespective of where they live.
Trial registration number
N/A
PREVENTION – EXCLUDING CLINICAL TRIAL RESULTS
AS09-001
THERAPEUTIC REGIMEN OF L-ARGININE FOR PATIENTS WITH MELAS: 9-YEAR, PROSPECTIVE, MULTICENTER, CLINICAL RESEARCH INTEGRATING THE DATA FROM TWO 2-YEAR CLINICAL TRIALS WITH 7-YEAR FOLLOW-UP
1Kurume University, Pediatrics and Child Health, Kurume, Japan
Background and Aims
In order to optimize the therapeutic regimen using oral and intravenous L-arginine for MELAS.
Method
19 patients at 10 medical institutions in Japan were enrolled in two, 2-year, open-label clinical trials of oral and intravenous L-arginine, respectively. The primary endpoint for efficacy in the clinical trial of oral L-arginine was the MELAS stroke scale, while those of intravenous L-arginine were the improvement rates of headache and nausea/vomiting at 2 hours after the completion of the initial intravenous administration. The relationships between the ictuses of stroke-like episodes and plasma arginine concentrations were examined.
Results
Patients, enrolled from December 2008 through June 2011, were followed up until May 2017. 13 patients with interictal MELAS (age: 8 to 47) were assessed for the efficacy and safety of oral L-arginine (0·3-0·5 g/kg/day, tid) for 96 weeks; 10 patients with acute MELAS (age: 9 to 24) were assessed for the symptom-improving effect and safety of intravenous L-arginine (0·5 g/kg/dose). Oral L-arginine extended the interictal phase and decreased the incidence and severity of ictuses. Intravenous L-arginine improved headache, nausea/vomiting, impaired consciousness, and visual disturbance. The maximal plasma arginine concentration was 167 mmol/L when an ictus developed. At the completion of the 2-year clinical trials, the bedriddeness and mortality rates were 0% despite the progressively and eventually life-threatening natures of MELAS, and no treatment-related adverse events occurred. The formulations were well tolerated.
Conclusion
The therapeutic regimen using oral and intravenous L-arginine appropriately may be therapeutically beneficial and clinically useful for patients with MELAS.
Trial registration number
The trials were registered (JMACTR-IIA00023 and JMACTR-IIA00025).
AS09-002
TREATMENT OF NEW ATRIAL FIBRILLATION FOR ACUTE STROKE PATIENTS PRESENTING TO HOSPITAL: TYPE, TIMING, SUITABLILITY AND SUCCESS
1University of Edinburgh, Stroke, Edinburgh, United Kingdom
Background and Aims
For acute stroke admissions with new atrial fibrillation (AF), the time to achieve rate control, the medications used for fast/paroxysmal AF (PAF), and the proportions requiring two agents, are not well-defined. It is unknown how well PAF is managed. The clinical timeline for anticoagulation initiation is variable.
Method
For new admissions (2013-16) with new AF (n = 90), the following were audited: 1] Fast/slow AF. 2] Continuous/paroxysmal AF. 3] Medication(s) selected for either continuous/PAF. 4] Delays/omissions prescribing rate-controlling medication. 5] Timeline of pulse rate control. 6] Delays/type of anticoagulation.
Results
For new AF, 51% presented with rate <90 bpm; 49% fast AF (range 90-160 bpm). 75% were prescribed medication with rate controlling properties - of these: 23% of medications were pre-existing (eg beta-blocker for hypertension); 52% received new medication – digoxin:beta-blocker:other 59%:39%:2%. Treatment commenced after a mean delay of 1.6 days. Fast AF rate control (<90) took 5 days (median). 18% required two rate controlling medications. 13% had PAF: ⅓ received beta-blockers; ⅓ no medication; ⅓ digoxin, respectively. Overall, 68% started anticoagulation: 69% warfarin, 31% NOAC. Stroke-to-prescription of anticoagulation - mean 12.8 days, median 14 days (range 0-78 days).
Conclusion
For new AF: 1/2 presented with fast AF – initial rate control was delayed for 1.6 days; taking 5 days to be effective. 1/5 required two rate-control medications. PAF treatment was sub-optimal: 1/3 received no medication; 1/3 digoxin - despite digoxin being contraindicated for PAF. Delayed anticoagulation varied widely, exposing newly admitted acute stroke inpatients to potential risks of additional embolic events.
Trial registration number
N/A
AS09-003
HOW SUCCESFUL IS ANTI-HYPERTENSIVE AND OTHER SECONDARY PREVENTION MEDICATION AFTER TIA CLINIC ATTENDANCE
1University of Edinburgh, Stroke, Edinburgh, United Kingdom
2NHS Lothian
Background and Aims
The comprehensiveness and adherence to advice for stroke secondary prevention measures are not well-defined. Hypertension is one of the most significant modifiable risk factors for stroke.
Method
Outpatients referred to the TIA / Stroke Clinic following a second event were audited (n = 87) [March 2016 – February 2017]. All had previously attended the Stroke Service when their first TIA / stroke was diagnosed. Secondary prevention advice at the first and advice/implementation at the second appointments, were audited, as follows: anti-hypertensive/-platelet/-coagulant/-cholesterol medications, blood pressure (BP) control, success at stopping smoking.
Results
Comparing first versus second attendances: 60% had a systolic BP > 140 mmHg at the initial attendance (mean 149/81mmHg) versus 56% (mean 144/83mmHg). Mean arterial pressure was: 115mmHg versus 114mmHg (p>0.5). Stroke specialist recommendations for first versus second attendances: i) a target BP: 30% versus 17%, ii) a specific new type of antihypertensive medication: 21% versus 10%. Recommendations (first versus second attendances) to continue/start other secondary prevention showed: anti-platelet/anticoagulant (98% versus 96%); anti-cholesterol medications (87% versus 91%). Patients’ smoking rates were reduced (29% versus 18%).
Conclusion
Although 3/5 patients at first attendance had a systolic BP >140 mmHg, less than 1/3 received a BP target, less than 1/5 received a recommendation for a specific anti-hypertensive medication. By the second attendance, more than 1/2 still had a systolic BP > 140 mmHg. In contrast, for other stroke risk factors, initial delivery of advice and patient compliance were significantly better. Reasons for incomplete anti-hypertensive advice and implementation, and recommendations for improvement are proposed.
Trial registration number
N/A
AS09-004
SAUNA BATHING IS ASSOCIATED WITH A REDUCED RISK OF INCIDENT STROKE: RESULTS FROM THE KUOPIO ISCHEMIC HEART DISEASE STUDY
1Medical University of Innsbruck, Department of Neurology, Innsbruck, Austria
2University of Bristol, Translational Health Sciences, Bristol, United Kingdom
3Emory University, Department of Medicine, Atlanta, USA
4University of Leicester, Diabetes Research Centre, Leicester, United Kingdom
5University of Eastern Finland, Institute of Public Health and Clinical Nutrition, Kuopio, Finland
6Department of Internal Medicine, Central Finland Hospital District, Jyväskylä, Finland
Background and Aims
We aimed to assess the association between frequency of sauna bathing and risk of future stroke.
Method
Baseline habits of sauna bathing were assessed in 1628 adult male and females aged 53 to 74 years (mean age, 62.7 years) without a known history of stroke in the Finnish Kuopio Ischemic Heart Disease prospective cohort study. Three sauna bathing frequency groups were defined: 1, 2-3 and 4-7 sessions per week. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated for incident stroke.
Results
During a median follow-up of 14.9 years, 155 incident stroke events were recorded. Compared with participants who had one sauna bathing session per week, the age and sex-adjusted HRs (95% CIs) for stroke were 0.86 (0.61-1.22) with 2-3 sessions and 0.39 (0.18-0.83) with 4-7 sessions per week (P for trend = 0.025). Upon further adjustment for body mass index, smoking, systolic blood pressure, LDL cholesterol, alcohol consumption, history of type-2 diabetes, socio-economic status, physical activity, and anti-hypertensive, lipid-lowering or aspirin medication, the corresponding HRs (95% CIs) were 0.88 (0.61-1.25) and 0.38 (0.18-0.81) (P for trend = 0.028). The association was not modified by age, sex or other clinical characteristics (P for interaction > 0.10 for all subgroups). It was similar for ischaemic stroke, but modest for haemorrhagic stroke, which could be attributed to the low event rate (34 incident events).
Conclusion
This long-term follow-up study shows that middle-aged to elderly men and women who take frequent sauna baths have a significantly reduced risk of new-onset stroke.
Trial registration number
N/A
AS09-005
HOW EXPERTS DIAGNOSE TIA: A SYSTEMATIC REVIEW
1Ottawa Hospital and Research Institute, Neurology, Ottawa, Canada
Background and Aims
The diagnosis of TIA can be difficult for experts and non-experts alike. Stroke prevention systems are challenged by large volumes of referrals, with many (if not most) patients diagnosed with neither a stroke nor a TIA. We performed a systematic review to describe how experts diagnose TIA.
Method
A systematic literature search was performed according to PRISMA guidelines using MEDLINE, Embase and the Cochrane Library databases. Publications eligible for inclusion were those that included information on the demographic or clinical features experts use to diagnose TIAs or TIA-mimics. Two reviewers independently screened results, selected studies and extracted data. Critical appraisal of included studies was performed using criteria adapted from various quality assessment tools available for qualitative research.
Results
Of 1666 citations, 210 abstracts were selected for full-text screening and 80 publications were ultimately included. Experts were more likely to diagnose TIA based on clinical features including negative symptoms or speech deficits and were less likely to diagnose TIA with positive symptoms, altered level of consciousness, or the presence of non-focal symptoms. Experts commonly included mode of onset (sudden vs. transient), recurrence of attacks, and localizability of symptoms to a distinct vascular territory in the diagnostic decision-making process.
Conclusion
Experts rely on key clinical and demographic features to distinguish TIAs from mimics, which are not currently reflected in widely-used risk scores. Clarifying how experts diagnose TIA may help frontline clinicians to better select patients for referral to stroke prevention clinics.
Trial registration number
N/A
AS09-006
RISK OF RECURRENT ISCHEMIC STROKE IN YOUNG PATIENTS: COMPARISON OF CRYPTOGENIC AND IDENTIFIED CAUSE
1University Hospital Olomouc, Department of Neurology, Olomouc, Czech Republic
2University Hospital Olomouc, Department of Cardiology, Olomouc, Czech Republic
3Palacký University Medical School, Department of Biophysics and Statistics, Olomouc, Czech Republic
Background and Aims
Early and accurate identification of cause of ischemic stroke (IS) is substantial for an effective secondary prevention however in young patients, cause of IS remains often cryptogenic. We aimed to compare the risk of recurrent IS (RIS) between young patients with identified cause (IC) and cryptogenic IS (CIS).
Method
The study set consisted of young acute IS patients < 50 years enrolled in the prospective HISTORY (Heart and Ischemic STrOke Relationship studY) study registered on ClinicalTrials.gov (NCT01541163). In all patients, the brain ischemia was confirmed on CT or MRI. Admission ECG, serum specific cardiac and thrombophilia markers, neurosonology, TEE, 24-hour and 3-week ECG-Holter were performed in all patients to assess cause of IS according to the ASCOD classification.
Results
Of 218 enrolled young IS patients < 50 years (122 males, mean age 40.9 ± 7.5 years), 161 (74%) patients were identified as cryptogenic. During the follow-up (FUP) with a median of 35 months, six (4%) CIS and six (11%) patients with IC suffered RIS (p-0.08). IC patients had RIS significantly earlier after first IS (median 1 vs. 13 months of FUP, p-0.043). No difference was found in the calculated one-year risk of RIS between both groups: 0.021 (95% CI: 0-0.044) for CIS vs. 0.117 (95% CI: 0.028-0.205) for IC patients.
Conclusion
The risk of RIS seems to be similar in young CIS and IC patients, but IC patients suffered RIS significantly earlier. Acknowledgment: Supported by the grant of Ministry of Health of Czech Republic nr. 17-30101A, and by the grant IGA LF UP_018_2018.
Trial registration number
N/A
AS09-007
ASSOCIATION OF POST-STROKE DISABILITY WITH PLASMA CONCENTRATION AND ANTI-XA ACTIVITY OF APIXABAN
1National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita- Osaka, Japan
2National Cerebral and Cardiovascular Center, Divsion of Clinical Chemistry, Suita- Osaka, Japan
3National Cerebral and Cardiovascular Center, Department of Neurology, Suita- Osaka, Japan
Background and Aims
Several studies suggested that physical vulnerability, so-called frailty, affects pharmacokinetics. This study aimed to determine whether post-stroke disability was associated with pharmacokinetics of apixaban in acute ischemic stroke patients.
Method
This single-center, prospective observational study included patients with acute ischemic stroke or transient ischemic attack (TIA) who were admitted to our hospital within 7 days after onset and started apixaban for non-valvular atrial fibrillation from JAN 2012 to DEC 2015. Patients were divided into two groups according to presence of severe disability (mRS 4-5) at discharge (median 18 days of onset). Blood sample was obtained before and 4 hours after taking apixaban. Anti-Xa activity was measured using chromogenic assay, (STA®-Liquid Anti-Xa). Concentration (C) of apixaban was analyzed based on AXA.
Results
We enrolled 167 consecutive patients (78.8 ± 9 years old, 98 men, 152 with ischemic stroke and 15 with TIAs). No significant difference was found between the mRS 0-3 and 4-5 groups in sex (57 vs. 59%), age (79 vs. 78 years), body weight (54 vs. 57 kg), serum creatinine level (0.9 vs. 0.9 mg/dl), creatinine clearance (52 vs. 55 ml/min), apixaban dose (reduced, 48 vs. 43%). Compared with the mRS 0-3 group, C0h, C4h and AXA4h were significantly higher in the mRS4-5 group. After adjusting for age, body weight, serum creatinine, and apixaban dose, plasma concentration and AXA were higher in the mRS 4-5 group than the mRS 0-3 group. (C0h β = 0.16 p = 0.030, C4h β = 0.16 p = 0.019, AXA0h β = 0.15 p = 0.034, AXA4h β = 0.15 p = 0.029)
Conclusion
Post-stroke disability was independently associated with pharmacokinetics of apixaban.
Trial registration number
N/A
AS09-010
PREDICTIVE FACTORS FOR PREOPERATIVE RECURRENCE OF CEREBROVASCULAR SYMPTOMS IN SYMPTOMATIC CAROTID STENOSIS
1HELSINKI UNIVERSITY HOSPITAL, Department of neurology, HELSINKI, Finland
2University of Helsinki, Clinicum- Department of Neurosciences, Helsinki, Finland
3University of Helsinki and Helsinki University Hospital, Department of radiology- Hospital District of Helsinki and Uusimaa Medical Imaging Center, Helsinki, Finland
4University of Helsinki, Molecular Neurology- Research Programs Unit- Biomedicum, Helsinki, Finland
5Helsinki University Hospital, Department of Vascular Surgery, Helsinki, Finland
6University of Helsinki and HUSLAB, Department of pathology, Helsinki, Finland
7Wihuri Research Institute, Wihuri Research Institute, Helsinki, Finland
Background and Aims
Across all stroke subtypes, large artery stroke carries the highest risk for recurrence. Despite initiation of best medical therapy at the onset of cerebrovascular symptoms, some symptomatic carotid stenosis patients suffer recurrent neurological events before undergoing CEA. To help in risk stratification, we searched for factors that predict recurrent events in patients with symptomatic carotid stenosis (50-99%) prior to CEA.
Method
The HeCES2 study is a cross-sectional and longitudinal prospective cohort study, which enrolled 500 carotid stenosis patients scheduled for CEA. Only symptomatic patients were analyzed (median time between index symptom and CEA 11 days (range 0-251)).
Results
Of all 324 symptomatic patients, 39 (12%) had a preoperative recurrent event (median 6, range 0-108 days) after index symptom: 4 ischemic strokes, 16 hemispheric TIAs and 19 AFs. Recurrence rate was 0.4% within 48 hours and 1.4% within 2 weeks. None of the patients with ocular symptoms (AF or RAO) suffered recurrent hemispheric TIA or stroke. In Cox regression analysis, history of hypertension (HR 5.54, 95%CI 1.20-25.55) or CHD (HR 0.34, 95%CI 0.14-0.82), hemispheric TIA as the presenting symptom (HR 3.61, 95%CI 1.51-8.61), LDL-/HDL-cholesterol ratio (HR 1.82, 95%CI 1.29-2. 55) and the number of cerebrovascular attacks prior to index symptom (HR 1.11, 95%CI 1.29-2.55), all were significantly associated with recurrent events.
Conclusion
Overall, the recurrence rate was low and all recurrent strokes occurred in patients presenting initially with hemispheric symptoms. History of cardiovascular disease, LDL-/HDL-cholesterol ratio, presenting symptom and number of cerebrovascular attacks were the strongest predictors for recurrence.
Trial registration number
N/A
AS09-011
HOW EXPERTS DIAGNOSE TIA: IN VIVO CLINICAL DECISION-MAKING MODEL
1Ottawa Hospital and Research Institute, Neurology, Ottawa, Canada
Background and Aims
The diagnosis of TIA can be difficult for frontline practitioners, potentially leading to misdiagnosis and unnecessary referrals. The “gold standard” is diagnosis by an expert physician (usually a neurologist), though little work has been done to characterize how experts arrive at their diagnoses. This project seeks to model how experts diagnose TIA in vivo.
Method
We performed a retrospective chart review of consecutive patients referred to our stroke prevention clinic in a Canadian tertiary care academic centre in 2015. In total, 2077 patient charts met inclusion criteria. We extracted patient demographics, stroke risk factors, elements of the clinical history (pattern of onset, number of events, symptom distribution), imaging findings, and final diagnosis. We performed a multinomial logistic regression model to identify those features predictive of a final diagnosis of definite TIA/stroke and definite non-TIA/stroke.
Results
Factors that were most predictive of definite TIA (all p < 0.001) included: monocular vision loss (OR 34), sudden onset (OR 27.0), homonymous hemianopia (OR 15.6), aphasia (OR 5.0), and unilateral weakness of the arm or leg (OR 3.0). Factors that were least predictive of definite TIA (all p < 0.001) included: loss of consciousness (OR 0.1), amnesia (OR 0.1), jerking movements (OR 0.2), positive visual symptoms (OR 0.2) and stereotyped episodes (OR 0.3).
Conclusion
This model identifies features that are strongly predictive of a diagnosis of TIA or non-TIA and illuminates the expert's decision-making. Once validated, this data may allow for rationalization of referral processes to stroke prevention clinics and better selection of patients for inclusion into clinical trials.
Trial registration number
N/A
AS09-012
OFF-LABEL DOSE REDUCTION OF DIRECT ORAL ANTICOAGULANTS
1University Hospital Rey Juan Carlos, Stroke unit. Neurology, Madrid, Spain
2University Hospital Infanta Sofia, Stroke team. Neurology, Madrid, Spain
3University Hospital Torrejon, Stroke unit. Neurology, Madrid, Spain
Background and Aims
Real-life studies assessing non-vitamin K antagonist oral anticoagulants (NOACs) dose reduction show low doses are being widely prescribed, which may lead to an increase in embolic events. The aim of our study was to analyze NOACs dose reductions.
Method
We retrospectively reviewed NOACs-treated patients between April 2013 and April 2017 from three University Hospital prospective records. Baseline characteristics, doses, reason for reduction and embolic/hemorrhagic events were registered during the follow-up. The primary objective was to evaluate reduced/low dose rate and if the adjustment was based on labeling criteria. Secondary objectives measures were incidence of embolic events and bleeding complications in full dose vs reduced dose during follow-up.
Results
Of 165 patients included, 70 (42.4%) received a reduced dose (mean age 82.4 years SD 7.2, medium CHA2DS2VASc 6 and HASBLED 3). In 22 patients (31.4%) did not meet labeling criteria for a dose adjustment: 9/36 (25%) dabigatran, 5/17 (29.4%) rivaroxaban and 8/17 (47%) apixaban. In 11 cases neurologists adduced an increased bleeding risk and in the remaining 11 there was no apparent clinical justification. During follow-up (mean 14.8 months, SD 10.7), there were 7 embolic events of any severity in patients with full dose, 7 in reduced dose (7.3% vs 10%, p = 0.5); and 6 bleeding events, regardless severity, in both groups (6.3% vs 8.5%, p = 0.3).
Conclusion
In our high risk multicentre series, NOACs dosing was frequently reduced off-label, due to a high bleeding risk a priori assesment. However, no significant differences in the rate of vascular recurrences were observed.
Trial registration number
N/A
AS09-013
PREVENTING STROKE THROUGH SHOPPING CENTRE RISK ASSESSMENTS – AN ACTION DRIVEN APPROACH IN AUSTRALIA’S BIGGEST BLOOD PRESSURE CHECK
1National Stroke Foundation, Office of the CEO, Melbourne, Australia
2National Stroke Foundation, Marketing, Melbourne, Australia
Background and Aims
In 2014, Stroke Foundation launched Australia's Biggest Blood Pressure Check (ABBPC), recognising high blood pressure as a key risk factor for stroke. Initially a one-day event involving free blood pressure checks in capital cities and pharmacy stores nationally, the campaign was extended to one month in 2016, with new partners Priceline Pharmacy and Sisu Wellness. This study sought to evaluate whether consumers took action following the 2017 ABBPC campaign.
Method
A survey was sent to participants found to be at risk of stroke one month after their health check in the shopping centre. The survey asked participants: (1) whether they visited a doctor after their health check; and (2) if they had made any healthy lifestyle changes since having their health check. It also provided additional lifestyle modification advice.
Results
A total of 63,211 free health checks were delivered across Australia from 17 May to 14 June 2017. Thirty-one percent of participants were found to be at high risk of stroke and were referred to their doctor for a comprehensive assessment. Of those high risk participants who agreed to be contacted, 7.5% completed the follow-up survey. Seventy-one percent of survey participants had already visited or planned to visit their doctor to discuss their results, 45% were eating more fruit and vegetables, 42% had increased their exercise levels, and 25% had lost weight.
Conclusion
These results indicate that opportunistic health checks are an effective tool for increasing community awareness of stroke risk factors, identifying those at high risk and prompting them to take action.
Trial registration number
N/A
AS09-014
EVALUATION OF A ‘LIVING WELL AFTER STROKE GROUP' - A NEW AND INNOVATIVE APPROACH TO STROKE SPECIFIC SECONDARY PREVENTION IN A COMMUNITY SETTING
1ST GEORGE's UNIVERSITY OF LONDON, Community Neuro Team, London, United Kingdom
2ST GEORGE's UNIVERSITY OF LONDON, Acute Stroke Unit, London, United Kingdom
Background and Aims
Despite considerable evidence that secondary-prevention group interventions can improve mortality, morbidity and reduce further myocardial infarction no such groups have been evaluated for stroke patients.
This poster will summarise the findings of a project that evaluated the impact and success of the Living Well After Stroke (LWAS) Group in Wandsworth (South West London). The Group was designed as an innovative approach to stroke specific secondary prevention. Using a self-management approach it aims to improve participant’s health, wellbeing and confidence in managing their stroke risk factors.
Method
The Group was evaluated in the following ways:
1) Pre and post group outcome data
2) Post group patient feedback
3) Discovery interviews
4) Cost and attendance analysis of the group
Results
Patients reported improvement in all outcomes with the exception of fatigue.
Outcomes showing the greatest improvement were patients’ understanding of their responsibility for taking care of their own health and their ability to prevent problems with their own health.
Significant improvements were also reported in patient’s understanding and confidence in their knowledge of health problems and their causes and the importance of maintaining a healthy lifestyle.
Conclusion
This project confirmed that the LWAS Group is comparable to other secondary prevention programmes positively addressing similar issues in terms of outcome and attendance rates and is lower in cost than that of a comparable cardiac rehab programme. The group was well evaluated by patients and the outcome data demonstrated improvements in key areas immediately following the group and an increase in confidence in ability to maintain lifestyle changes beyond the group.
Trial registration number
N/A
AS09-018
WHAT PROPORTION OF PATIENTS ADMITTED WITH STROKE OR TIA MAY BE SUITABLE FOR NEWER CHOLESTEROL-LOWERING TREATMENT?
1St George’s Hospital, Department of Neurology, London, United Kingdom
Background and Aims
PCSK9 inhibitors effectively clear low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol (non-HDL-C). Current trials are evaluating efficacy to reduce cardiovascular events. We evaluated stroke admissions potentially eligible for more intensive cholesterol treatment.
Method
Retrospective analysis of consecutive admissions to the stroke unit over 5 months in 2017. Records were hand-searched. Data were collected on diagnosis, risk factors and stroke work-up. The Dutch Lipid Clinic Network Algorithm for Familial Hypercholesterolemia (FH) screening and TOAST classification were used.
Results
We achieved 100% case record ascertainment of 650 patients admitted. 351(54%) had acute ischaemic stroke (AIS) or TIA, 80(12%) haemorrhage and 219(34%) mimic syndromes. Of 351 AIS/TIA patients, 27 had no LDL-C or non-HDL-C testing leaving 324 of whom:
• 6 had possible FH (LDL-C >5.0 mmol/l).
• 23 had LDL-C >4.0mmol/l, or 3.5-3.9mmol/l and concomitant very high vascular risk (>1 vascular bed involved).
• 21 had non-HDL-C >3.4mmol/l and recurrent cardiovascular events. (Evolocumab reduces elevated non-HDL-C which is associated with stroke).
50(15%) patients potentially eligible for PCSK9 inhibitors were identified: mean age 74yrs ( ± 12), 40% hypertension, 34% ischaemic heart disease, 28% atrial fibrillation, 16% diabetes, 8% peripheral vascular disease. 28% had cardioembolic events, 16% lacunar syndrome, 8% symptomatic ICA stenosis >70% and 48% other undetermined aetiology. 50% had history of recurrent cerebrovascular events versus 31% in treatment non-eligible AIS/TIA cohort, p=0.007.
Conclusion
Up to 15% of unselected acute ischaemic stroke or TIA patients were potentially suitable for more intensive cholesterol treatment. Our data may guide sample size selection for stroke trials testing these new drugs.
Trial registration number
N/A
AS09-019
TEMPORAL TRENDS AND ASSOCIATIONS OF PRECEDING ANTITHROMBOTIC TREATMENT AND ACUTE ISCHEMIC STROKE SEVERITY: SOUTH LONDON STROKE REGISTER 2000-2015
1King's College London, 1. School of Population Health and Environmental Sciences, London, United Kingdom
2King's College London, 1. School of Population Health and Environmental Sciences 2. NIHR Biomedical Research Centre- Guy’s and St Thomas’ NHS Foundation Trust and King’s College London- London, London, United Kingdom
Background and Aims
Initial stroke severity is a predictor for disability and mortality. Antithrombotic medication has been used in primary care in patients at risk of ischemic stroke. We evaluated antithrombotic prescriptions prior to first ever stroke, and associations with stroke severity.
Method
A population-based cohort study with data collected from the South London Stroke Register 2000-2015 (n = 3328). The National Institutes of Health Stroke Scale (NIHSS) and Glasgow Coma Scale (GCS) were used to assess stroke severity. Regression models were fitted and adjusted for demographic characteristics, medical history and stroke subtype.
Results
Stroke severity decreased significantly between 2000 to 2015 (p < 0.001). Prior stroke anticoagulant prescriptions among patients with known Atrial Fibrillation (AF) was insignificantly increased by an annual percent change (APC) of 2% (95% CI [-3.1, 8.2]) during the period 2000-2015, whereas prior stroke antiplatelet prescriptions in those without known AF were insignificantly increased between 2000-2005 by an ACP of 9% [-2.6,21.5] and significantly decreased between 2005-2015 by an ACP of -7% [-10.2,-3.0]. Prescriptions of anticoagulant medication among AF patients prior to stroke was associated with reduced stroke severity GCS (p = 0.003) and NIHSS (p = 0.012), while antiplatelet use among non-AF were not statistically significant. No associations were observed between prior-stroke antithrombotics and 7-days mortality. Lower risk of disability, with borderline significant, were observed among AF patients on anticoagulants (Relative-Risk: 0.9 [0.75-1.04]).
Conclusion
Stroke severity reduced in the last two decades and prior to stroke anticoagulant prescribing in AF patients was associated with reduced stroke severity and disability.
Trial registration number
N/A
AS09-020
B- MODE ULTRASOUND- GUIDED SHOCK WAVE- PHOTODYNAMIC COMBINATION THERAPY OF CAROTID ARTERY INTIMAL HYPERPLASIA ACCOMPANIED BY 5- AMINOLEVULINIC ACID- LOADED MICROBUBBLES ADMINISTRATION
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Italian National Research Council, Institute of Translational Pharmacology- IFT, Rome, Italy
3Tabriz University of Medical Sciences- Neurosciences Research Center, Department of Neurosciences, Tabriz, Iran
4Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
Intimal hyperplasia is the major cause of restenosis after percutaneous coronary and carotid interventions such as stenting or angioplasty. Intimal hyperplasia refers to proliferation and migration of vascular smooth muscle cells. In this study, we developed an experimental shock wave- photodynamic combination therapy protocol, and investigated its effectiveness on intimal hyperplasia reduction, wherein diagnostic B- mode ultrasound is combined with shock wave generator, with a goal of increased safety.
Method
The right common carotid arteries endothelial denaturation were performed by ballooning in New Zealand white rabbits. Histopathology results showed the formation of intimal hyperplasia in all of the rabbits’ arteries. Then treatment group underwent combined low- level focused electrohydraulic shock wave (10Kv, 0.2 Hz) therapy and blue laser (417 nm, 10 J/cm2) accompanied by intravenous 5- Aminolevulinic Acid- loaded PESDA (perfluorocarbon- exposed sonicated dextrose albumin) microbubbles administration, photodynamic therapy and simultaneously B- mode ultrasound imaging.
Results
Results from B- mode ultrasound imaging concurrent with shock wave- photodynamic combination therapy, showed the collapsing of microbubbles and feasibility and acute safety of targeting stenotic region in the carotid artery. Also, histopathology results showed a significant reduction in the mean value for smooth muscle cells density, lumen wall mean thickness and percentage of luminal cross- sectional area of stenosis, in the treatment group compared with the other groups (p < 0.05).
Conclusion
Enhanced toxicity effect of 5- Aminolevulinic Acid- loaded PESDA microbubbles, induced by targeted shock wave- photodynamic combination therapy, can cause to reduce intimal layer thickness and significantly dilate the luminal cross- sectional area of stenosis.
Trial registration number
N/A
AS09-022
LONG-TERM (5-20 YEARS) OUTCOME AFTER STA-MCA ANASTOMOSIS AND ULTIMATE INDIRECT BYPASS FOR MOYAMOYA DISEASE
1University of Toyama, Neurosurgery, Toyama, Japan
2Hokkaido University, Neurosurgery, Sapporo, Japan
Background and Aims
There are many reports about short-term (<5 years) outcome after bypass surgery for moyamoya disease. However, recent reports have shown that a certain subgroup of patients may be at risk for subsequent stroke even after 10 years post-surgery. Therefore, this study was aimed to evaluate long-term (5-20 years) outcome after STA-MCA anastomosis and ultimate indirect bypass (encephalo-duro-myo-arterio-pericranial synangiosis; EDMAPS) for moyamoya disease.
Method
This study included 80 patients who were followed up for longer than 5 years after STA-MCA anastomosis and EDMAPS for moyamoya disease between 1997 and 2012. There were 30 pediatric (<18 years) and 50 adult patients. There were 22 males and 58 females. Their mean age was 30.4 ± 19.8 years. Clinical diagnosis included TIA or ischemic stroke in 67 patients, hemorrhagic stroke in 10, and asymptomatic in 3. STA-MCA single or double anastomosis was performed followed by ultimate indirect bypass (EDMAPS) through large front-temporal craniotomy onto 128 hemispheres of 80 patients. All patients were prospectively followed up at outpatient clinic for a mean of 10.8 ± 4.2 years, ranging from 5.1 to 20 years. MRI and MRA were performed once or twice per year.
Results
During follow-up periods, one of 80 patients recurred hemorrhagic stroke (0.12% per patient-year). Radiological examinations demonstrated that the disease progression occurred in the carotid system of non-surgical side in one side and in the PCA in 7 sides (1.1% per side-year).
Conclusion
STA-MCA anastomosis and ultimate indirect bypass (EDMAPS) is the best choice to prevent further cerebrovascular events for longer than 10 years by widely providing surgical collaterals.
Trial registration number
N/A
AS09-025
RAISING STROKE AWARENESS IN GREEK-SPEAKING POPULATION WITH «ΑΠΛΑ» A GREEK EQUIVALENT OF FAST TEST
1251 Helllenic Air Force General Hospital, Neurology, Athens, Greece
2IASO General Hospital, Neurology, Athens, Greece
3National and Kapodistrian University of Athens, Neurology, Athens, Greece
4Athens University of Applied Sciences, Physiotherapy, Athens, Greece
Background and Aims
A structured questionnaire was completed by 97 randomly selected subjects (47.4% women, mean age 41,4), before and after administering an educational leaflet with a clear message about stroke recognition and act. The leaflet described the suggested acronym «ΑΠΛΑ» equivalent to “FAST” as a way of raising awareness for Greek-speaking population in a “single-message” manner.
Method
The meaning of the word «ΑΠΛΑ»(apla) is “simple” and each letter corresponds to one symptom: «Α» for «Άκρο»(ákro) meaning “limb”, «Π» for «Πρόσωπο»(prósopo) meaning “face”, «Λ» for «Λόγος»(lógos) meaning “speech” and «Α» for «Άμεσα»(ámesa) meaning “immediately, right-now”.
Results
Before training 37.1% was able to name correctly 3 signs of stroke, 85.6% recognized the correct action for stroke-patient and 84.5% knew that stroke is curable. After the intervention the percentage of people recognizing the correct symptoms more than doubled (78.4%) and the difference reached considerable statistical significance (p < 0.001), there was an increase in correct answers concerning the action for stroke (88.7%, with a trend to be significant, p = 0.084) and a non-significant raise in the recognition of treatment (98.9%, p = 0.3). The most recognizable sign of stroke pre-training was speech disturbances (83.5%), followed by face drooping (79.3%) and hemiparesis (60.8%).
Conclusion
Overall, the questionnaire showed a very positive impact on recognizing stroke and how and when to react (correct answers after «ΑΠΛΑ» display increased in statistical significant manner p < 0,001). We suggest building an effective public campaign to raise stroke awareness in Greek population with the use of “FAST”-like acronym «ΑΠΛΑ» which both helps symptom recognition and best action in an easy and memorable way.
Trial registration number
N/A
AS09-026
IMPROVING DETECTION OF ATRIAL FIBRILLATION AFTER TRANSIENT ISCHAEMIC ATTACK AND STROKE
1Imperial College Healthcare NHS Trust, Medicine, London, United Kingdom
2St George's University Hospital, Care of the Elderly, London, United Kingdom
3Croydon University Hospital, Care of the Elderly, Croydon, United Kingdom
Background and Aims
Atrial fibrillation (AF) is a known risk factor for embolic stroke. Improved detection of AF reduces the risk of future strokes. Studies have shown that AF detection rates are highest close to the event, underlining the need for prompt diagnosis. Newer Adhesive Ambulatory ECG patch devices (AAECG) may offer alternatives to traditional cardiac telemetry. This pragmatic study aimed to compare AAECG (Zio XT device) against traditional 24 hr ambulatory monitoring.
Method
Patients with minor stroke or TIA were recruited from the TIA Clinic at Croydon University Hospital. Patients had the AAECG applied in clinic and a 24 hour Holter ordered. Patients were subsequently followed up in clinic to review results.
Results
30 patients were recruited. AF was detected in 1 patient using the AAECG and none on the Holter. Patients waited a median of 59 days for the Holter (range 14-102days). Investigations were completed for 29 patients from the AAECG compared to 18 from Holter. All AAECG reports were available in clinic compared to 6 from the Holter.
Cost of the investigation plus follow up was £367 and £440 for a Holter and an AAECG respectively.
Conclusion
Although the Zio system is more expensive in operational costs, it provided a more comprehensive follow up, and allowed timely investigation and management. Nearly half the patients attending the follow up clinic did not have Holter results because of administrative issues. The use of AAECG will allow services to offer “one-stop” TIA clinics leading to improved patient care and experience.
Trial registration number
N/A
AS09-027
COMBINED EFFECT OF INTENSIVE ATORVASTATIN THERAPY AND LOW- LEVEL LASER PHOTOBIOMODULATION THERAPY IMPROVE THE RABBIT CAROTID ARTERY ENDOTHELIAL DYSFUNCTION: MONITORED BY ULTRASONOGRAPHY AND HISTOPATHOLOGY
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Islamic Azad University- Tabriz Branch- Faculty of Medical Sciences, Department of Neurology, Tabriz, Iran
3Iranian Social Security Organization, Alinasab Haspital, Tabriz, Iran
4Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
As is well recognized, the majority of atherosclerosis start with an inflammatory process, resulting in endothelial dysfunction. We developed an experimental intensive atorvastatin therapy combined with photobiomodulation therapy protocol and investigated its effectiveness on inflammation reduction and improvement of endothelial function.
Method
Briefly, New Zealand white rabbits underwent balloon dilatation injury at the right common carotid artery. Then common carotid arteries of the treatment group at lesion region, treated by intensive atorvastatin (6mg/kg/day) administration and low- level laser (635 nm, 100 J/cm2) photobiomodulation irradiation. In order to evaluate endothelial-dependent relaxation, acetylcholine-mediated dilation (AMD) was measured during the infusion of acetylcholine at a rate of 0.5 µg/kg/min and endothelial independent relaxation was evaluated by measuring nitroglycerin mediated dilation (NMD) during the infusion of nitroglycerin at a rate of 5 µg/kg/min.
Results
Results from ultrasonography showed significant differences in AMD between the treated and the non-treated rabbits (p < 0.05), whereas there were no significant differences in NMD between the treatment and normal groups (p>0.05). Also, results from histopathology showed a significant reduction in the mean value for macrophages density within the lesion in the treatment group compared with the non-treatment group (p < 0.05). No microscopic intimal lesions were seen in the normal and treated rabbits, but intimal thickening was observed in the histological studies in the non-treated rabbits.
Conclusion
The pleiotropic, lipophilic and anti-inflammatory effects of atorvastatin therapy, can cause to reduce the lesion macrophages. Also, photobiomodulation therapy cause to macrophage egress from intimal layer and improves endothelial function via increasing endothelial nitric oxide (NO) synthase.
Trial registration number
N/A
AS09-028
B- MODE ULTRASOUND- GUIDED LOW- LEVEL FOCUSED- ELECTROHYDRAULIC SHOCK WAVE THERAPY OF CAROTID ARTERY ADVANCED ATHEROSCLEROTIC PLAQUE ACCOMPANIED BY HDL- LOADED MICROBUBBLES ADMINISTRATION
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Tabriz University of Medical Sciences- Neurosciences Research Center, Department of Neurosciences, Tabriz, Iran
3Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
Atherosclerosis is the leading cause of cerebrovascular disease. The management of atherosclerosis reduces the risk of stroke and its related deaths. In this study, we developed an experimental shock wave therapy protocol, and investigated its effectiveness on advanced atherosclerotic plaque regression, wherein diagnostic B- mode ultrasound is combined with focused- electrohydraulic shock wave generator, with a goal of increased safety.
Method
Briefly, New Zealand white rabbits underwent primary perivascular severe cold injury at the right common carotid artery followed by a 1.5 % cholesterol- rich diet injury for 12 weeks. Histopathology and ultrasonography results showed the formation of advanced atherosclerosis with neovessel - rich plaque and severe stenosis (> 70%) in all of the rabbits’ arteries. The animals treated by low- level focused- electrohydraulic shock wave (8 Kv, 5 Hz) accompanied by HDL- loaded PESDA (Perflurocarbon- Exposed Sonicated Dextrose Albumin) microbubbles administration.
Results
Results from histology, B-mode and color Doppler ultrasonography at the stenotic region showed a significant reduction in the mean value for blood mean velocity, intraplaque neovessels density, wall mean thickness and percentage of luminal cross- sectional area of stenosis and significant increase in the mean value for blood volume flow in the treatment group compared with the other groups (p < 0.05).
Conclusion
Inertial cavitation effect of collapsing microbubbles within neovessels- induced by shock wave therpy accompanied by the reverse cholesterol transport effect of HDL, can cause to destroy the intraplaque neovessels, reduce the lesion lipid content and significantly dilate the luminal cross- sectional area of stenosis.
Trial registration number
N/A
AS09-029
EARLY STAGE ATHEROSCLEROSIS REGRESSION IN THE RABBIT CAROTID ARTERY USING PROTOPORPHYRIN IX– LOADED MICROBUBBLES ADMINISTRATION ACCOMPANIED BY SONO- PHOTODYNAMIC COMBINATION THERAPY PROTOCOL
1Islamic Azad University- Tabriz Branch- Faculty of Basic Sciences, Department of Physics, Tabriz, Iran
2Tabriz University of Medical Sciences, Department of Radiology, Tabriz, Iran
3Islamic Azad University- Tabriz Branch- Faculty of Mechanics, Department of Bioengineering, Tabriz, Iran
Background and Aims
In atherosclerosis, local inflammation and associated macrophage activity can lead to foam cell- rich plaque formation, which results to plaque rupture and thrombosis, making inflammation an important therapeutic target in stroke and cardiovascular disease. Foam cells are generated by uncontrolled uptake of modified LDL, especially oxidized LDL (oxLDL). In this study, we developed an experimental sono- photodynamic combination therapy protocol, and investigated its effectiveness on macrophage foam cells density reduction.
Method
Briefly, New Zealand white rabbits underwent primary balloon dilatation injury at the right common carotid artery followed by a 1.5% cholesterol-rich diet injury for two weeks. Histopathology results showed early stage atherosclerosis or fatty streaks formation in all of the rabbits’ arteries. Then carotid arteries of the treatment group at lesion region, treated using protoporphyrin IX– loaded PESDA (Perflurocarbon- Exposed Sonicated Dextrose Albumin) microbubbles (100 ml/kg, 2-5 ×105 bubbles/ml) administration accompanied by extracorporeal and combined pulsed- low level (P = 3 W, F = 3 MHz, DF = 50% ) focused- ultrasound and low- level red laser (WL = 635 nm, E = 100 J/cm2) system. Foam cells density were evaluated in the treatment group compared with the control group using B-mode ultrasonography and histology.
Results
Results from B-mode ultrasonography and histopathology showed a significant reduction in the mean value for foam cells density within the early atherosclerotic lesion in the treatment group compared with the other groups (p < 0.05).
Conclusion
Enhanced inertial cavitation effect of collapsed microbubbles- induced by focused- ultrasound can cause to enhance anti- inflammatory effect of protoporphyrin IX- mediated photodynamic therapy by laser.
Trial registration number
N/A
AS09-031
ENDOVASCULAR TREATMENT OF SUBCLAVIAN AND INNOMINATE ARTERY OCCLUSIVE DISEASE: A SINGLE CENTER'S EXPERIENCE
1Hospital Clínico Universitario “Lozano Blesa, neurologia, Zaragoza, Spain
2Hospital Clínico Universitario “Lozano Blesa, Cirugia Minimamente Invasiva Guiada por la Imagen, Zaragoza, Spain
Background and Aims
PURPOSE
Subclavian artery stenosis (SAS) is a significant form of peripheral artery disease,. In general, asymptomatic subclavian artery disease is treated with medical therapy and invasive treatment is reserved for the more symptomatic patients.
OBJECTIVE
To review results of primary stenting for innominate and subclavian artery occlusive lesions
Method
Retrospective data were collected from 28 consecutive patients (all men, median age 63 years) having 26 subclavian and 2 innominate artery lesions treated with stenting.
Results
Indication for treatment was transient ischemic attack in 46%, stroke in 14%. 75% stenosis, 25% occluded lesions. Stent were used in 23 lesions and only balloon angioplasty in 5 lesions. The technical success rate of the procedure was 100%, without any cases of death, stroke, and myocardial infarction from the time of stenting to 30 days after the stenting procedure. One puncture site hematoma.
Mean follow-up time was 5.58 years (range 1 to 12). 35% of patients developed in-stent restenosis, only one symptomatic. Mean time to restenosis 29 month (7-61).
Conclusion
Stenting of subclavian and innominate artery lesions is safe, with durable midterm effect and high rate of restenosis, with few longtime complications.
Trial registration number
NA
AS09-033
DOES RANDOM LDL ACCURATELY GUIDE STATIN-BASED MANAGEMENT COMPARED TO FASTING LDL IN PATIENTS WITH ACUTE ISCHEMIC STROKE OR TIA?
1Stony Brook University School of Medicine, Department of Neurology, Stony Brook, USA
Background and Aims
For secondary stroke prevention, American Stroke Association recommends LDL <100 for all adults and <70 for adults with Diabetes. Current practice guidelines include initiation of high intensity Statin for patients with serum LDL above this goal.
The aim of this study is to determine if random lipid profile obtained at arrival at the hospital can reliably guide Statin-based management compared to fasting lipid profile obtained within 72 hours of presentation, in patients with acute ischemic stroke or TIA.
Method
For this retrospective analysis, all patients (776) discharged from Stony Brook University Hospital from 1/1/2016 thru 12/31/2016 with a diagnosis of acute ischemic stroke or TIA were screened. Among them, 394 had both random and fasting LDL levels available and were included. For these cases, the final Statin-based treatment plan is classified as “Same” or “Altered”, comparing management based on random vs fasting levels, with significance calculated using Fisher Exact test.
Results
Among 394 cases, 23 (5.8%) had a change in management based on fasting LDL compared to management predicted by random LDL. 21 of these cases had random LDL between 100-130, implying that 19.6% (21 out of 107) patients with random LDL in this range had a change in management.
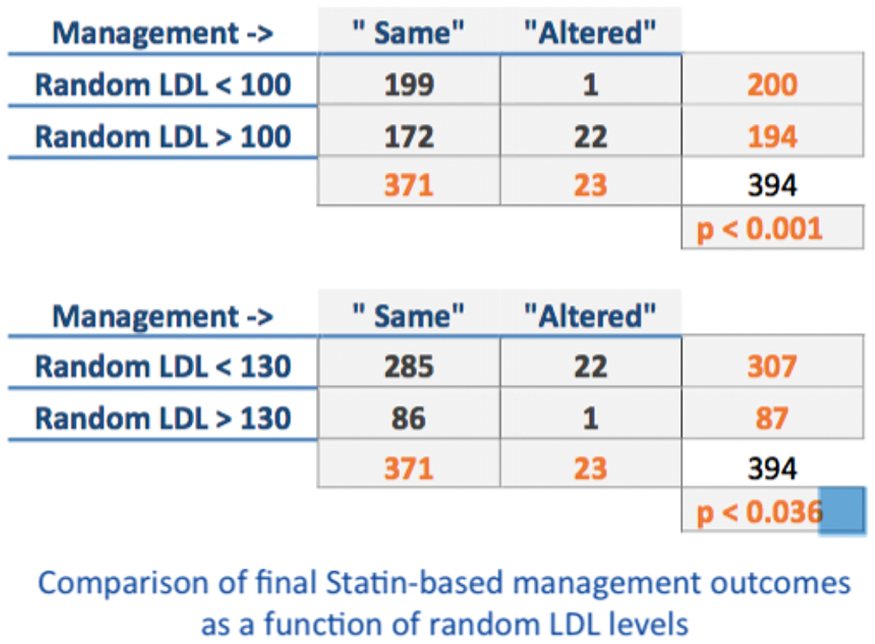
Conclusion
In patients with Acute Stroke or TIA,
Trial registration number
N/A
AS09-036
IS PLASMATIC LP-PLA2 A SURROGATE FOR FDG-PET AS UNSTABLE CAROTID PLAQUE MARKER?
1Hôpitaux universitaire de Genève, Neurology, Genève, Switzerland
2Sainte-Anne Hospital, Neurology, Paris, France
3HEGP, Médecine nucléaire, Paris, France
4Hôpital Sainte-Anne, Laboratoire de Biologie, Paris, France
5HEGP, Chirurgie Cardiovasculaire, Paris, France
6CHU Caen Normandie, Neurologie, Paris, France
7Hôpital Sainte-Anne, Neurologie, Paris, France
8Hôpital Sainte-Anne, Neurology, Paris, France
Background and Aims
Elevated plasma Lp-PLA2, a subtype of the phospholipase A2 superfamily expressed by inflammatory cells within atherosclerotic plaques, has recently been reported as an independent risk factor for stroke. Imaging carotid plaque inflammation using FDG-PET is significantly associated with ipsilateral stroke recurrence, independently of degree of stenosis. In this prospective study, we investigated whether plasma Lp-PLA2 activity is associated with carotid plaque FDG uptake in recently symptomatic stroke patients with >50% ipsilateral stenosis.
Method
Following signed informed consent, consecutive patients >50yrs with a <2-week history of minor diffusion-weighted imaging positive ischemic stroke or proven retinal infarction with 50-99% (NASCET) ipsilateral carotid stenosis, were included. FDG-PET was performed within 7 days of the vascular event using a hybrid PET/CT scanner in conjunction with thin-slice axial neck CT angiography to allow plaque identification, and plaque FDG standardized uptake values (SUV) normalized by jugular vein SUV (target-to-blood ratios, TBR) were determined blind to symptomatic side using ROIs spanning the entire plaque, excluding calcifications. Lp-PLA2 activity was assessed within 5 days of PET.
Results
Thirteen patients (mean age: 70 yrs; 10 men) successfully underwent FDG-PET. Following symptomatic side unblinding, no significant correlation between Lp-PLA2 levels and mean or maximal (average of three highest SUV pixels across 3 slices) symptomatic plaque TBR values was found (Pearson p = 0.643 and 0.994, respectively).
Conclusion
In our cohort with recently symptomatic severe carotid stenosis, no correlation was found between FDG-PET symptomatic plaque uptake and Lp-PLA2 plasma activity, suggesting the latter reflects inflammation not specific to the unstable carotid plaque.
Trial registration number
N/A
AS09-038
ANALYSIS OF ORAL ANTICOAGULANT TREATMENT IN PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION: A NATIONWIDE REGISTRY BASED STUDY 2010-2016
1Tallinn University of Technology, Institte of Cardiovascular Medicine, Tallinn, Estonia
2Tallinn University of Technology, Institute of Cardiovascular Medicine, Tallinn, Estonia
3University of Tartu, Medicine, Tartu, Estonia
Background and Aims
Increase in atrial fibrillation (AF) underlines the importance of treatment with anticoagulants to prevent stroke.
The aim of the study was to evaluate the use and side effects of anticoagulation for AF in Estonia
Method
A nationwide analysis of national health information database (EHIF) (2010 to 2016) and medications use database (Health research database, HRD) (2012 to 2016) was performed.
Results
AF patients comprised 1.13% for men and 1.16% for women in 2010 and 1.95% and 2.16% respectively in 2016. Warfarin was prescribed to 43% of AF patients in 2010, 62% in 2011, 70% in 2012, 67% in 2013, 63% in 2014, 57% in 2015. Purchase rate of first prescription was 96-97%. In 2016 47% were prescribed warfarin and 42% direct oral anticoagulants. The numbers of warfarin users according to EHIF and HRD are depicted (figure 1).
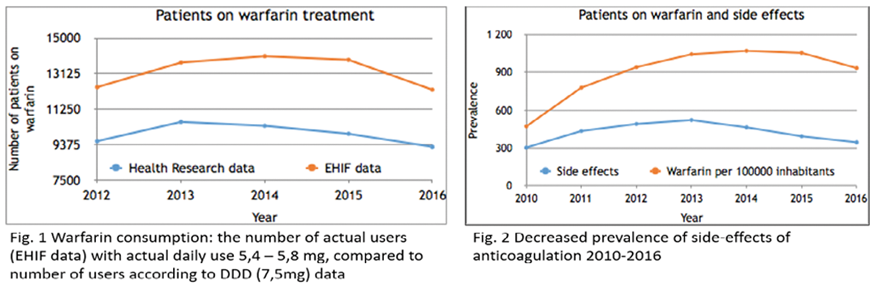
The prevalence of treatment side effects decreased from 4,8% in 2010 to 2,8% in 2015 and 2016 (figure 2). Side effects were most common the age group from 70 to 89. In 2016 anticoagulation was re-started after intracerebral hemorrhage in 14% of patients. Cost of treatment increased significantly after introduction of direct oral anticoagulants.
Conclusion
Increasing prevalence of AF is accompanied by increased used of anticoagulation with no increase in side effects. However, the cost of anticoagulation is increasing significantly.
Trial registration number
N/A
AS09-039
THE IMPACT OF STATIN PRETREATMENT ON ACUTE DWI INFARCT PATTERN IN SYMPTOMATIC INTERNAL CAROTID ARTERY DISEASE
1University Hospital Mannheim, Neurology, Mannheim, Germany
2University Hospital Mannheim, Neuroradiology, Mannheim, Germany
3University Hospital Mannheim, Institute for Clinical Chemistry, Mannheim, Germany
Background and Aims
In addition to lipid lowering and the reduction of stroke incidence, the potential benefit of statin treatment also includes the reduction of clot formation and clot adherence to ruptured plaques.
Method
We compared the initial clinical course and the DW MRI lesion pattern in acute stroke patients with internal carotid artery (ICA) disease (n = 224) who either did (n = 74) or did not (n = 150) receive pre-stroke statin therapy.
Results
In comparison to patients not treated with statins, patients taking lipid-lowering medication exhibited a significantly higher incidence of hypertension (p < 0.001), diabetes (p < 0.05), hyperlipidemia (p < 0.05), stroke (p < 0.01), heart disease (p < 0.001), or peripheral artery disease (p < 0.01). On the other hand, they were also more likely to receive aspirin treatment prior to stroke (p < 0.001). We found no statistical difference between the two groups regarding NIHSS at admission or discharge, or pre- and post-hospital mRS. The level of both total serum cholesterol and LDL was significantly lower in the statin-treated group (p < 0.001). As shown previously, the incidence of a certain stroke pattern was clearly dependent on the degree of stenosis. However, there was also a statistical interaction between statin treatment and stroke pattern, manifested in more DWI-negative and fewer hemodynamic infarctions in the statin-treated group (p < 0.005), as well as between statin treatment and the number of DWI lesions, expressed in fewer lesions in the statin group (p < 0.05).
Conclusion
Our findings suggest an effect of statin therapy on ICA stroke beyond its lipid-lowering property, but the role of confounders (antiplatelet therapy and premorbidity) needs further evaluation.
Trial registration number
N/A
AS09-040
A COMPARISON OF NATIONAL GUIDELINES FOR SECONDARY PREVENTION OF ISCHAEMIC STROKE
1University of Cambridge, Public Health & Primary Care, Cambridge, United Kingdom
2Medicina Familiar y Comunitaria., Centro de salud El Valle, Distrito Sanitario de Jaén, Spain
3Centre for Primary Care and Public Health, Barts and The London School of Medicine and Dentistry, London, United Kingdom
4University of Cambridge, School of Clinical Medicine, Cambridge, United Kingdom
5Northeastern University, Northeastern University, Boston, USA
Background and Aims
National guidelines for secondary prevention of ischaemic stroke are developed independently, and could therefore reach different conclusions or offer different recommendations based on the same body of evidence.
Aim
To compare recommendations on use of antiplatelet, lipid lowering and antihypertensive drugs from a convenience sample of national guidelines on secondary prevention of ischaemic stroke.
Method
Systematic search of grey literature for current guidelines on secondary prevention of ischaemic stroke in adults. Guideline quality was assessed using the AGREE II instrument. Two independent reviewers completed a systematic comparison of indication, choice of drug and outcome targets for antiplatelet, lipid lowering and antihypertensive drugs.
Results
Ten sets of national guidelines (Australia, Canada, France, Germany, Italy, Spain, UK, USA) were compared. All guidelines recommend antiplatelet therapy and statins, but differ with regard to choice of antiplatelet drug and lipid targets. More substantial variation exists within the recommendations for anti-hypertensive therapy, with no agreement on the threshold to initiate treatment, choice of drug or target blood pressure.
Conclusion
Different guidelines not only interpret the same evidence differently, but also apply different research evidence to the same clinical question. It is likely that national guidelines will always differ, due to updates in evidence but especially when they offer highly specific recommendations. This is not an indication that one guideline is wrong and another right, or that more research is necessarily needed. It is however an indication of the challenge in keeping guidelines contemporary and that implementation of a guideline should not be overly dogmatic.
Trial registration number
N/A
AS09-041
AN EFFECTIVE MODEL TO IMPROVE OUTCOME IN TIA CLINIC
1NOTTINGHAM CITY HOSPITAL, Stroke Medicine, Nottingham, United Kingdom
Background and Aims
TIA’s affect over 46,000 new patients every year in the U.K. A one-stop clinic would help to reduce recurrence by prompt diagnosis and secondary prevention. We have attempted to identify the effectiveness of our clinic based on early evaluation, investigations and interventions performed and how this relates to recurrence of TIA/stroke.
Method
Data collected from triage sheets and clinic letters were analysed retrospectively over 7 months. Recurrence rates were calculated from TIA follow-up letters and monitoring re-admission data on the hospital data-base over a 4 week period following discharge.
Results
Out of 333 patients, a majority (69%) of those with ABCD2 ≥ 2 or crescendo TIA were seen within 24 hours. Carotid Doppler were performed within 24 hours for 94% of patients; 11% had clinically significant stenosis. Amongst these 67% were referred for endarterectomy. CT or MRI was performed in 51% of patients, with 85% completion rate in 24 hrs. Initiation of anti-thrombotics (aspirin/clopidogrel) was high (86% ) whilst DOAC’s and warfarin were 7% and 3% respectively. The number of patients on anti-hypertensives and statins were 46% & 73% respectively. Four week recurrence rates of further TIA/stroke were low at 2.3%.
Conclusion
Our recurrence rates are low, likely due to promptness of diagnosis, imaging and secondary prevention within clinic. Although majority of patients were seen within 24 hours of referral, limited resources require continued risk stratification despite new guidance to the contrary. Early initiation of anti-thrombotics and anticoagulants within the clinic is the most effective method of reducing future ischemic events.
Trial registration number
N/A
AS09-042
STAGED CAROTID ANGIOPLASTY TO PREVENT CEREBRAL HYPERPERFUSION SYNDROME
1Hospital San Pedro De Alcantara, Neurología, Cáceres, Spain
2Hospital San Pedro De Alcantara, Neurorradiología intervencionista, Cáceres, Spain
Background and Aims
Cerebral hyperperfusion syndrome (CHS) is one of the most dangerous complications of carotid revascularization treatment. Exhausted cerebral vasoreactivity (CVR) has been associated with an increased risk of CHS. Staged angioplasty could be a therapeutic alternative, with a balloon dilation in a first stage and stent placement in a second time. Our objective is to evaluate the safety of endovascular treatment in two stages in patients at high risk of CHS.
Method
Description of a series of cases.
Results
1.- 53 year-old male with a right-hemisphere ischemic stroke with NIHSS puntuation at discharge (NIHSSd): 15, 95% stenosis of the symptomatic ICA and exhausted CVR. Angioplasty was performed 29 days later, and the stent was placed 60 days after the stroke.
2.- 50 year-old male with a left-hemisphere ischemic stroke with NIHSSd: 6 at discharge, 90% stenosis in the symptomatic ICA and a decreased CRV were detected. Angioplasty was performed on day 15; the stent was placed on day 45.
3.- 73 year-old male with left hemispheric repetitive TIAs. The study showed a subocclusive stenosis (99%) of the symptomatic ICA without intracranial compensation. Angioplasty was performed on day 5; the stent was placed on day 32.
4.- 72 year-old male with a right-hemisphere ischemic stroke with NIHSSd: 4. Angioplasty was performed 46 days later; the stent was placed on day 68.
In all patients, a distal protection filter was used. No patient suffered complications intra or post procedure.
Conclusion
In our experience, staged angioplasty is a safe technique in patients at high risk of CHS.
Trial registration number
N/A
AS09-044
PREVENTION OF STROKE IN INTRACEREBRAL HAEMORRHAGE SURVIVORS WITH ATRIAL FIBRILLATION (PRESTIGE-AF): OBJECTIVES AND DESIGN OF A RANDOMISED CLINICAL TRIAL AND AN OBSERVATIONAL STUDY
1University of Würzburg, Institute for Clinical Epidemiology and Biometry ICE-B, Würzburg, Germany
2Imperial College London, Division of Brain Sciences, London, United Kingdom
3University Hospital Würzburg, Clinical Trial Center, Würzburg, Germany
4Medical University of Graz, Department of Neurology, Graz, Austria
5University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
6Universitat Autònoma de Barcelona, Neurovascular Research Laboratory- Vall d'Hebron Institute of Research VHIR, Barcelona, Spain
7University of Bordeaux, Department of Neurology- Bordeaux University Hospital- and Inserm U1219, Bordeaux, France
8University of Perugia, Stroke Unit and Division of Internal and Cardiovascular Medicine, Perugia, Italy
9Aalborg University, Department of Clinical Medicine- Faculty of Health, Aalborg, Denmark
10University Hospital Heidelberg, Department of Clinical Pharmacology and Pharmacoepidemiology, Heidelberg, Germany
11University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
12SAFE, Stroke Alliance for Europe, Brussels, Belgium
13King’s College London, Department of Primary Care and Public Health Sciences, London, United Kingdom
Background and Aims
Patients with intracerebral haemorrhage (ICH) and concomitant atrial fibrillation (AF) are at high risk of ischaemic stroke (IS) and recurrent ICH. Recent systematic reviews of observational studies suggest that anticoagulation is beneficial, however optimal stroke prevention in ICH patients with AF remains to be established. We present the design of the PRESTIGE-AF trial which aims to identify the best preventive strategy for stroke prevention in ICH survivors with AF.
Method
PRESTIGE-AF is an international, multi-centre study funded by Horizon 2020 aiming to: a) determine whether direct oral anticoagulant (DOACs) are an effective and safe option for stroke prevention in patients with ICH and AF; b) improve personalized risk prediction for recurrent events by multidimensional clinical, biological and imaging data; c) determine public health and economic implications of a potential intervention; d) investigate patient-centered aspects (attitudes/beliefs and psychosocial status) of preventive medicine including the impact of gender.
Results
Central to PRESTIGE-AF is an investigator-led, multi-center, open, parallel-group, prospective, randomised clinical trial being performed in 6 European countries. 654 patients with recent ICH and AF will be randomized to the intervention group receiving DOACs or a control group receiving no anticoagulant. Patients will be followed-up for up to 36 months and will be extensively characterised including clinical characteristics, neuroimaging, blood-based biomarkers, genetics and pharmacological information. Several sub-studies collecting primary data or using existing datasets from different stroke populations will be utilised, in addition to qualitative methodology for patient-centered aspects.
Conclusion
PRESTIGE-AF will provide comprehensive data for guiding preventive decisions in ICH patients with AF.
Trial registration number
N/A
AS09-045
ADHERENCE TO SECONDARY PREVENTION AFTER STROKE – THE NOR-COAST STUDY
1NTNU, Department of Neuromedicine and Movement Science INB, Trondheim, Norway
2NTNU, Department of Public Health and Nursing, Trondheim, Norway
3Haukeland University Hospital, Department of Neurology, Bergen, Norway
4St. Olavs Hospital, Stroke Unit, Trondheim, Norway
Background and Aims
Effectiveness of secondary prevention after stroke is influenced by adherence to treatment and adherence is often suboptimal. We aim to determine the degree of adherence to secondary preventive medication after stroke, identify factors that may impact the adherence and explore associations between adherence and the subsequent risk of post-stroke cognitive impairment (PCI) and new vascular events.
Method
Nor-COAST is an ongoing multicenter, prospective cohort study with focus on PCI. Inclusion criteria are acute stroke hospitalized from May 2015 to March 2017. Follow-ups are performed at 3 and 18 months with assessment of cognitive and physical function, cerebral MRI and blood samples.
Results
817 participants have been included during the recruitment period. Adherence to antihypertensives, statins, antitrombotic and antidiabetic treatment after 3 and 18 months will be evaluated by using medication lists, the 4-item Morisky Medication Adherence Scale and achievement of guideline-defined treatment goals for blood pressure, lipid status and haemoglobin A1c. Information on follow-up routines in primary health care will also be obtained. The Norwegian Cardiovascular Disease Registry will give information about vascular events in the period.
Conclusion
The study will give insight into associations between adherence to preventive measures, achievement of treatment goals and risk of vascular events and PCI, and contribute to valuable knowledge useful for patient care and further research, such as intervention studies to improve adherence and cognitive function after stroke.
Trial registration number
ClinicalTrials.gov Identifier: NCT02650531
AS09-046
TRANSIENT ISCHAEMIC ATTACK DIAGNOSIS AND SUBSEQUENT RISK FACTOR REDUCTION
1Glasgow Caledonian University, Nursing and Community Health, Glasgow, United Kingdom
2Norfolk and Norwich University Hospitals NHS Foundation Trust, Stroke Unit, Norwich, United Kingdom
Background and Aims
Every year 46,000 people in the UK have a first Transient Ischaemic Attack (TIA); 15% will go on to have an ischaemic stroke. Therefore it is important that people receive early diagnosis and medical management, including information about stroke risk and lifestyle changes that might help reduce risk. To design patient-centred self-management interventions as part of TIA treatment, we need to understand patients’ experiences of TIA diagnosis and the factors that motivate them to engage with risk reduction interventions.
We aimed to review the research literature to gain an understanding of patients’ experiences of TIA diagnosis and subsequent engagement with risk reduction interventions.
Method
We used a rigorous method: meta-aggregation. We searched databases including Medline and PsycINFO. We included qualitative studies that focused on the experiences of adults following a TIA diagnosis. We assessed study quality using a CASP checklist and used descriptive statistics and narrative to report the findings. Two reviewers worked independently on all stages; a third reviewer acted as arbiter.
Results
We included 4 studies. The 69 participants (61% male; mean age, 71.6 years) were from the UK and Australia. Three Synthesised Findings emerged from the analysis: Onset (first 24 hours); Impact and effect; Reducing the risk.
Conclusion
Self-management interventions should address individual patient’s awareness and understanding of the potential consequences of a TIA diagnosis. Some patients may require help coming to terms with the impact (social, emotional, financial). Patients should be supported to make changes (prescription medication and lifestyle) to help reduce the risk of stroke.
Trial registration number
N/A
AS09-047
NORWEGIAN STROKE IN THE YOUNG STUDY (NOR-SYS) II, METHODS
1Haukeland University Hospital, Neurology, Bergen, Norway
2Helsinki University Central Hospital, Neurology, Helsinki, Finland
3Haukeland University Hospital, Neuroradiology, Bergen, Norway
4Haukeland University Hospital, Centre for Clinical Research, Bergen, Norway
5Haukeland University Hospital, Heart Disease, Bergen, Norway
6Haukeland University Hospital, Ophthalmology, Bergen, Norway
7Haukeland University Hospital, Ear-Nose-Throat, Bergen, Norway
8Haukeland University Hospital, Physical Medicine and Rehabilitation, Bergen, Norway
9University of Bergen, Neurology, Bergen, Norway
Background and Aims
European long-term follow-up studies have shown that patients with acute ischemic stroke at age <50 years have high mortality rates, new cardiovascular events, cognitive reduction, fatigue, anxiety and depression. «Invisible» consequences are often first discovered after return to previous work. Aims are detecting early arterial disease, cause and consequence finding diagnostics, best prophylaxis and help to regain best possible life-quality.
Method
NOR-SYS II started in March 2016 inclusion of patients at age 15-49 years after acute, arterial, non-traumatic and documented cerebral infarction. Planned inclusion time is 5 years. NOR-SYS II is based on NOR-SYS I.1 A standardized questionnaire is further developed in collaboration with SECRETO, Searching for Explanations for Cryptogenic Stroke in the Young: Revealing the Etiology, Triggers, and Outcome (J. Putaala). NOR-SYS II includes computed tomography and magnetic cerebral imaging, ECG, long-time ECG monitoring, standardized ultrasound of cerebral, pre-cerebral and femoral arteries, echocardiography, sometimes combined with a bubble-test, standardized evaluations by speech and language therapist, occupational therapist, physiotherapist and routine and bio-bank blood samples. After discharge follows standardized testing of vision and hearing, 24-hour blood pressure measurements and measurements of arterial stiffness. Follow-ups are done one week after discharge, after about 3 months and 1 year.
Results
52 patients are included by 22th January 2018
Conclusion
NOR-SYS II is a prospective research program, following young ischemic stroke patients for 1 year. Standardized diagnostics and follow-ups will lead to new knowledge about todayś risk factors, causes and invisible consequences for individualized prophylaxis and improved understanding of the term “fatigue”.
Trial registration number
ClinicalTrials.gov:NCT02762396
AS09-048
EFFICIENCY AND SAFETY OF LEFT ATRIAL APPENDAGE CLOSURE
1Complejo Asistencial Unviersitario de Salamanca, Neurology, Salamanca, Spain
2Complejo Asistencial de Zamora, Comunity Medicine, Zamora, Spain
3Complejo Asistencial Unviersitario de Salamanca, Radiology, Salamanca, Spain
Background and Aims
Left atrial appendage closure is an alternative of stroke prevention for patients with atrial fibrilation and contraindication for anticoagulation. We analyze the characteristics, complications and follow-up of a serie of patients who required the procedure.
Method
We indicated left atrial appendage closure and followed consecutive cases of patients who presented acute ischemic or hemorragic strokes and contraindication for anticoagulation in our centre between July 2009 and December 2017.
Results
The procedure was performed in 97 patients, 49 male and 48 female; all the patients had non valvular arrhytmia, in 66 (68%) it was permanent atrial fibrilation, in 26 (26.8%) paroxistic atrial fibrilation and in 5 (5.2%) it was an atrial flutter. Most of them had concomitant conditions like arterial hypertension in 90% of cases, and mellitus diabetes in 38%. In 57 (58.8%) patients the stroke had been hemorragic and in 40 (41.2%) ischemic. In 4 (4.1%) cases periprocedural complications were reported, with no influence in the final prognosis: 1 case of cardiac tamponade that was treated succesfully, 1 case of transient ischemic attack, 1 case of right coronary artery air embolism and 1 case of device embolism. During our follow-up, with a median of 27 months, one patient had an intracerebral hemorrhage and there were no reports of ischemic strokes. Totally, 10% of patients died and in all cases it was not related to the procedure.
Conclusion
Left atrial appendage closure can be an efficient and safe alternative for secondary stroke prevention in patients with non valvular atrial fibrilation.
Trial registration number
N/A
IMAGING – HYPERACUTE
AS10-002
CAPILLARY TRANSIT TIME HETEROGENEITY USING MR PERFUSION PREDICTS FAVORABLE OUTCOME AND INTRACEREBRAL HAEMORRHAGE IN PATIENTS WITH ISCHEMIC STROKE DUE TO LARGE VESSEL OCCLUSION
1University Hospital Heidelberg, Department of Neurology, Heidelberg, Germany
2University Hospital Heidelberg, Department of Neuroradiology, Heidelberg, Germany
Background and Aims
The DAWN trial showed that endovascular therapy (EVT) is efficient in a prolonged time window for selected patients. However, the rate of favourable outcome declines over time, despite a clinical-imaging mismatch. We aimed at analysing whether microvascular changes depicted by capillary transit time heterogeneity (CTH) on MR perfusion maps might explain this decline.
Method
Retrospective analysis of consecutive patients with acute large vessel occlusion of the anterior circulation who underwent perfusion weighted imaging before EVT. All patients had a relevant PWI-DWI mismatch. Primary endpoints were favourable outcome (mRS<2) and the occurrence of intracerebral haemorrhage (ICH). CTH was calculated using the Perfusion Graphical User Interface. Volume- and voxel-based calculations of CTH were performed. Multivariable analysis were adjusted for age, relevant reperfusion, hypertension, diabetes, atrial fibrillation, NIHSS on admission, use of glycoprotein-IIB/IIIA antagonists, DWI lesion volume and symptom-onset-to-treatment time.
Results
131 patients (median age 73, interquartile range 62-79; median NIHSS 18, IQR 15-21) were included (occlusion site: 51% M1, 21% carotid T, 14% tandem occlusion, 8% M2 and 5% internal carotid artery). Median DWI Volume was 13ml (IQR 5-25). Higher volumes of moderately elevated CTH were positive predictors of favourable outcome (OR 1.18, 95%-CI [1.03-1.35], p = 0.017) and negative predictors of ICH (OR 0.85, 95%-CI: [0.76-0.96], p = 0.007). Moreover, higher absolute voxel-wise CTH values within the area of hypoperfusion (Tmax>6s) were negative independent predictors of ICH (OR 0.85, 95%-CI [0.72-1.00], p = 0.049).
Conclusion
Differences in the microvascular compartment shown by CTH predict outcome in patients with mismatch undergoing endovascular therapy.
Trial registration number
N/A
AS10-003
HOMOGENEOUS APPLICATION OF IMAGING CRITERIA IN A MULTICENTER TRIAL SUPPORTED BY INVESTIGATOR TRAINING: A REPORT FROM THE WAKE-UP STUDY
1Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
2Fraunhofer MEVIS, Institute for Medical Image Computing, Bremen, Germany
3mediri GmbH, mediri GmbH, Heidelberg, Germany
4Girona Biomedial Research Institute, Department of Radiology, Girona, Spain
5University Hospital Schleswig-Holstein, Department of Neuroradiology, Luebeck, Germany
6University-Medical Center Hamburg-Eppendorf, Department of Diagnostic and Interventional Neuroradiology, Hamburg, Germany
7University-Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
Background and Aims
WAKE-UP is a randomized, placebo-controlled trial of thrombolysis in stroke with unknown time of symptom onset using MRI criteria to determine patients’ eligibility for randomization. We describe the investigator image training as well as results of the quality control done by the central image reading board (CIRB).
Method
Investigators at local centers passed a software-based image training prior to being allowed to judge images in the trial. Throughout the trial, the CIRB gave feedback to recruiting centers in cases of disagreement regarding a patient’s randomization. We evaluated the investigators performance in the image training, obtained feedback regarding their experiences with the trial and analyzed results of the CIRB quality control from the first 1069 screened patients.
Results
Four-hundred-and-sixty-one physicians from eight countries took part in the image training, of whom 436 (95%) successfully completed it. In the trial, agreement rates between the local investigators and members of the CIRB were high for the presence of an acute ischemic lesion (94%, κ=0.87) and for the judgment of infarct extent (93%, κ=0.87). Agreement for the criterion of DWI-FLAIR mismatch was 74%, κ=0.60. The majority of investigators reported that the DWI-FLAIR mismatch was the hardest criterion to evaluate but that the image training increased their confidence when assessing it.
Conclusion
Despite its multicenter design, the WAKE-UP study has demonstrated a high level of homogeneity amongst raters in interpreting the imaging criteria for patient randomization, including the novel criterion of DWI-FLAIR mismatch. Systematic image training increased the confidence of investigators in applying imaging criteria.
Trial registration number
EudraCT Number: 2011-005906-32
AS10-004
CTP, ARE YOU TIMING IT RIGHT? A LARGE COHORT STUDY
1University of Basel, Department of Radiology, Basel, Switzerland
Background and Aims
Due to the nature of continuous scanning and calculation methods used in CT Perfusion a complete acquisition of first pass of Iodinated contrast medium through brain tissue is necessary. We present a proposal for optimal scan duration based on evaluation of a large cohort of patients.
Method
Retrospective analysis of attenuation changes arterial input and venous outflow in more than 900 examinations performed using standard CT Perfusion protocol (28 scans for a total of 54 seconds; first 20 scans every 1,5 seconds, last 8 scans every 3 seconds, after intravenous administration of 50 ml of Iodinated contrast medium with a flow of 5 ml/s). Syngo. Via (Siemens) was used for calculations.
Results
Arterial input function: up until the 3rd time point a steady baseline with mean attenuation value of maximally 7 HU (95% CI: −/+ 0,7) was observed; in the last 3 time points levelling of the attenuation curve was noticeable with the last mean attenuation value of 122 HU (95% CI: −/+ 2,7).
Venous output: the last mean attenuation value was 135HU (95% CI: −/+ 3,5) and a levelling of the curve was noticed as well but was pronounced to a lesser extent than in the arterial curve.
Trial registration number
N/A
AS10-005
EVALUATION OF MRI-MODALITIES CONTRIBUTION TO FINAL INFARCT PREDICTION IN ACUTE STROKE
1Charité Universitätsmedizin Berlin, Center for Stroke Research Berlin CSB, Berlin, Germany
2Charité Universitätsmedizin Berlin, Department of Neurosurgery, Berlin, Germany
3Aarhus University, Center of Functionally Integrative Neuroscience CFIN, Aarhus, Denmark
Background and Aims
Stroke-progression based on neuroimaging allows for stratification of acute-ischemic-stroke (AIS) patients to treatment. However, the debate continues which imaging-modalities are most relevant for this purpose. We present a systematic rating of MRI modalities for final-infarct prediction.
Method
In a multi-center retrospective analysis of 195 AIS patients, fluid-attenuated-inversion-recovery (FLAIR), diffusion-weighted-imaging (DWI) and 10 perfusion-parameters were derived from acute MRI scans. They were integrated to predict final-infarct as seen on follow-up T2-FLAIR using the tree-boosting model (XGBoost). We calculated two models for patients with 1) recanalization and 2) persistent-occlusion and ranked the important imaging markers for each case. The contribution of the corresponding imaging-parameter to the model was calculated as the weighted-sum of the modality contribution for each constituent decision-tree in the tree-boosting ensemble-model.
Results
For recanalization we identified the parameters pMTT, oTmax, DWI, TTP, pTmax and for persistent-occlusion TTP, pMTT, pTmax, oTmax, DWI in respective-order as most valuable. The other parameters contributed less than 5% to the prediction in both cases.
Conclusion
Our results emphasize the importance of certain perfusion-imaging parameters for final-infarct prediction. Interestingly, deconvolved-parameters and summary-parameters seem to be most beneficial in different types of stroke patients (recanalized vs persistent-occlusion). This may have important implications for the development of novel prediction tools for acute-stroke patients in the clinical setting.
Trial registration number
N/A
AS10-006
FEASIBILITY AND COSTS OF CT VERSUS MRI-BASED ACUTE STROKE ASSESSMENT – A QUASI-RANDOMIZED CLINICAL TRIAL
1Bispebjerg University Hospital, Department of Neurology, Copenhagen, Denmark
2Bispebjerg University Hospital, Department of Radiology, Copenhagen, Denmark
3Herlev-Gentofte Hospital, Department of Neurology, Herlev, Denmark
Background and Aims
CT-head is feasible in most acute stroke-patients but MRI is more time demanding and infeasible in patients with medical implants or unstable clinical conditions.
The aim of this sub-study was to assess the feasibility, salary-related costs and length-of-hospital-stay of CT versus MRI-based stroke-assessment for acute stroke patients randomized to CT versus MRI prior to intravenous-thrombolytic-treatment (iv-tPA-treatment).
Method
Consecutive acute stroke patients were randomized to CT or MRI prior to potential iv-tPA-treatment. All patients were on admission assessed by a dedicated stroke-team and MR-allocated patients further systematically evaluated for MRI-eligibility.
Results
Four-hundred-forty-four patients were included; of 219 patients randomized to MRI, 107 patients (48.7%) failed the predefined MRI-requirements and had CT instead; 52 (23.7%) patients had inherent MRI-contraindications or failed to deny explicit suspicion of presence of MRI-contraindications, 40 (18.3%) patients were too unrestful or severely ill for MRI of diagnostic quality to be safely conducted and 15 (6.8%) patients did not have MRI due to organizational obstacles. Of 225 patients randomized to CT, 22 (9.8%) patients had MRI due to young age, pregnancy or diagnostic need for MRI.
For the stroke-team, MRI-based assessment obtained 9.6% (p < 0.001) more time and the total gross-salary-costs were 22.9% higher compared to CT-based-assessment.
No deference in length-of-hospital-stay were detected between CT (median 3.5 days (IQR 1-10)) and MRI-allocated patients (median 4 days (IQR 1-8.8)), p = 0.890.
Conclusion
Use of MRI in acute stroke evaluation is more time-demanding, more expensive and offers potential challenges in comparison to CT as first choice of imaging in acute stroke.
Trial registration number
ClinicalTrials.gov Identifier: NCT02780843
AS10-007
TESTING THE CLINICAL-IMAGING MISMATCH SELECTION CRITERIA OF DAWN TRIAL: THERE IS STILL ROOM FOR IMPROVEMENT IN PATIENT SELECTION
1Fondation Rothschild, Interventional Neuroradiology, Paris, France
2HSHS St. John’s Hospital, HSHS Neuroscience Center, Springfield, USA
3Fondation Rothschild, Diagnostic Radiology, Paris, France
4Fondation Rothschild, Research and Biostatistics, Paris, France
Background and Aims
We aimed to conduct an external validation of the selection criteria of the diffusion-weighted-imaging assessment with clinical mismatch in the triage of wake-up and late-presenting strokes undergoing Neurointervention with Trevo (DAWN) trial in a cohort of unknown onset stroke (UOS) patients treated with thrombectomy.
Method
A study cohort of UOS patients was selected from a prospectively collected thrombectomy database. Patients were stratified according to DAWN Groups A/B/C. Group A criteria identified patients≥80 years old with a NIHSS≥10 + DWI volume<21cc; Group B: patients<80 years old with a NIHSS≥10 + DWI volume<31cc; and Group C: patients<80 years old with a NIHSS≥20 + DWI volume ≥31 and <51cc. We compared proportions of patients with a modified Rankin Scale (mRS)≤2 at 3 months follow-up between DAWN-eligible patients and the study cohort and the DAWN trial thrombectomy group.
Results
Out of 102 patients, 60 (59%) were defined as DAWN-eligible. Among these, 26 patients (43%) reached a mRS≤2 at 3 months follow-up (vs. 52/107 patients [49%] in the DAWN trial thrombectomy group;P=0.52) (Figure 1). The proportion of DAWN-ineligible patients for Groups A/B/C with a mRS≤2 were 2/13 patients (15%), 12/22 patients (55%), and 2/7 patients (29%), respectively.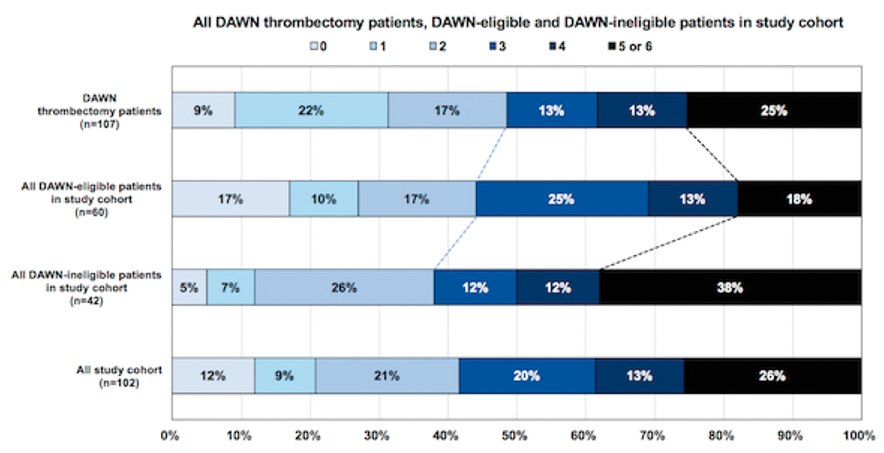
Conclusion
The results of the DAWN trial were externally validated in a UOS cohort. Additional trials are needed to address benefit in patients with larger infarct volumes.
Trial registration number
n/a
AS10-008
SUPERIORITY OF 3D-SWAN COMPARED TO 2D-T2*-WEIGHTED IMAGING IN THE DIAGNOSIS OF HEMORRHAGIC TRANSFORMATION IN THE SETTING OF THROMBOLYSIS
1Bichat Hospital, Neurology, Paris, France
2Bichat Hospital, Radiology, Paris, France
Background and Aims
It has been shown that SWAN is superior to standard T2*-WI for the diagnosis of hemorrhagic lesions. We assessed whether this holds true in the setting of thrombolysis in acute stroke.
Method
We conducted a prospective study on 69 patients who underwent into thrombectomy and/or intra-venous thrombolysis and had a follow up 3T MRI 24-36 hours after. Hemorrhagic transformation (HT) on SWAN and T2*-WI was graded according to the adapted ECASS classification on MRI and hemorrhagic volume was also measured in both sequences. Interpretation of the images was performed by two independent neuro-radiologists blinded to clinical evolution.
Results
HT was detected in 25 patients (36.2%) on SWAN and in 22 patients (31.9%) on T2*-WI with no significant difference. Three HT HI-1 were detected with SWAN but not with T2*-WI, and 2 cases were graded as HI-2 with SWAN and graded HI-1 with T2*-WI. Both parenchymal haemorrhage (PH)-1 and PH-2 were similarly graded by SWAN and T2*-WI. SWAN showed perfect inter-observer agreement for grading HT (Kappa coefficient =1). The volume of the presumed HT measured by SWAN was greater than that measured by T2*-WI (median, 1.78 ml vs 1.20 ml, P=0.04).
Conclusion
After thrombolysis, SWAN detected greater volume of HT compared to T2*-WI. However, this difference had no significant impact on ECASS HT classification.
Trial registration number
N/A
AS10-010
A DIGITAL MAP OF THE ANTERIOR CEREBRAL ARTERY TERRITORY ASSOCIATED WITH ANTERIOR CEREBRAL ARTERY OCCLUSION
1Stroke and Ageing Research STARC, Department of Medicine, Clayton, Australia
2Monash Health, Diagnostic Imaging, Clayton, Australia
Background and Aims
The anterior cerebral artery (ACA) territory has previously been delineated using cadaveric injection studies in subjects without stroke. However, this topography may not be comparable to areas affected after arterial occlusion, due to potential rescue by leptomeningeal anastomoses (LA) between the ACA, posterior cerebral artery (PCA) and middle cerebral artery (MCA). We created a digital atlas of the ACA territory associated with occlusion of the ACA and its branches on CT or MR angiography.
Method
The perfusion deficit (defined by Tmax) on CT perfusion, and infarcts on T2-weighted images were manually segmented and linearly registered onto a standard brain template. Segmented MR images were averaged to yield the probability of infarction at each voxel. We identified sanctuary sites with a low probability of infarction, by comparing perfusion topography with infarct topography at a voxel level.
Results
25 patients (male=11), median age of 74 years (IQR, 62 to 77 years). Regions with the highest probability of infarction were located anteriorly within the anterior cingulate gyrus (0.32) and superiorly within superior frontal gyrus (0.28), likely due to poor collateral blood supply (Figure 1). Sanctuary sites were identified posteriorly and included the paracentral lobule (0.04) superomedially and superolaterally, the precentral gyrus (0.04) and post central gyrus (0.04)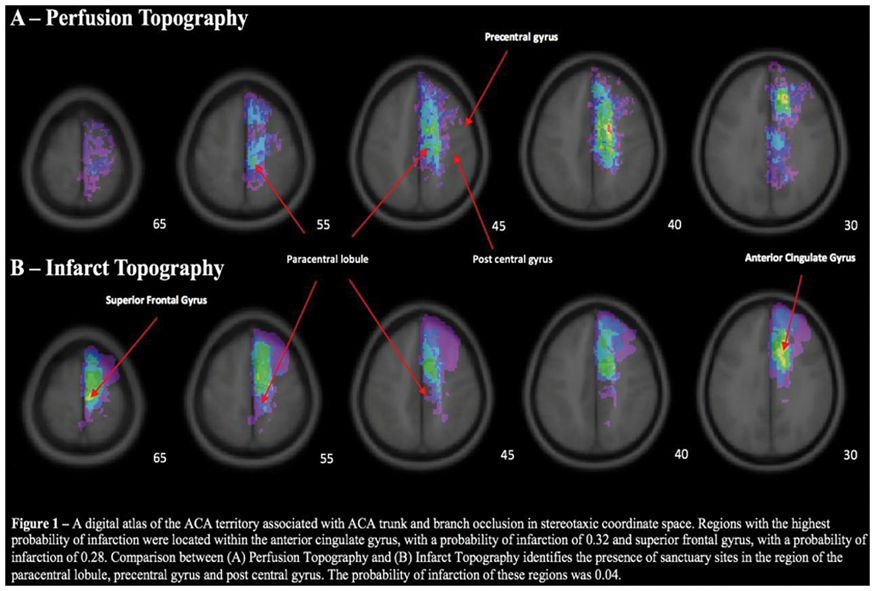
Conclusion
In stroke patients, the compensatory capacity of inter-territorial LA modified risk of infarction of the ACA territory posteriorly, and accounted for the presence of sanctuary sites in important somatosensory and motor areas.
Trial registration number
N/A
AS10-011
EXTERNAL VALIDATION OF BATMAN SCORE FOR BASILAR ARTERY OCCLUSION
1Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Neurology, Seville, Spain
2Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla IBI, Interventional Neurorradiology, Seville, Spain
3Hospital Universitario Virgen Macarena. Instituto de Investigación Biomédica, Neurology, Sevilla, Spain
Background and Aims
The Basilar Artery on Computed Tomography Angiography (CTA) Prognostic Score (BATMAN) is a 10-point image–based novel grading system to predict clinical outcome in basilar artery occlusion (BAO). Our aim was to conduct an external validation of this novel score.
Method
In a prospectively [2012-2017] single-center collected clinical and radiological databases, we retrospectively identified consecutive stroke patients who presented within 24 hours of symptomatic BAO displayed on CTA who underwent endovascular recanalization therapy. Receiver operating characteristic curves and linear regression analyses were used to determine discrimination ability of the score. BATMAN thresholds employed were ≥ 7 (favorable) and < 7 (unfavorable). Good outcome was defined as modified Rankin Scale score (mRs) of ≤3 at 3 months.
Results
Among 47 included patients, unfavorable BATMAN score rate was 59.6%. Unfavorable BATMAN was related to bad clinical outcomes and death (mRs 4-6) at 90 days after discharge (78.3% vs 21.7, p = 0.01). BATMAN showed a sensitivity and specificity of 57.1% and 78.2% respectively for good outcome. The C statistic was 0.72 (95% confidence interval [CI], 0.57-0.87) for the BATMAN score. Unfavorable BATMAN was identified as independent risk predictor of bad outcome and death (mRs 4-6) at 90 days after discharge (Hazard Ratio 4.8 [1.2-17.8], p = 0.019).
Conclusion
In our cohort, the external validation of BATMAN score has demonstrated its accurate ability to predict severe disability and death after BAO. BATMAN is a novel tool to easily identify patients with more likelihood of bad results despite endovascular reperfusion therapies.
Trial registration number
N/A
AS10-013
TEACHING STROKE IMAGING IN THE AGE OF DIGITAL - ONLINE EDUCATION AND ASPECTS TRAINING WEBSITE REVISITED
1University of Calgary, Radiology, Calgary, Canada
Background and Aims
Stroke imaging, reliant on detection of subtle areas of grey/white loss, and vascular imaging necessitating depiction of small structures often in multiple phases requires full image sets in order to adequately visualize the findings, establish the involved areas, and use imaging to guide subsequent decision making. Thus far teaching of stroke imaging has been limited to single images in presentations in order to depict volumetric and often subtle findings and highlight the teaching points. Availability of scrollable stacks of images for the purpose of teaching has been limited by the large size of imaging data, speed of transmission over the web, and specific file format making this only possible on select workstations within the hospital environment but not on personal learning devices or outside.
Method
Using open source web standards and languages such as HTML 5, JavaScript, PHP, and leveraging the organizational power of content management systems, we created a web-based system with fully scrollable images for vascular imaging and acute stroke education.
Results
We successfully created an online web based system using open source tools and technologies.
Conclusion
Emerging web technologies have enabled seamless delivery and processing of large datasets such as medical images, and this improvement in performance and speed could be leveraged in radiology education online. Allowing for richer content delivered right on personal devices available at all times and when convenient for the learner, we hope these additional resources and tools would create a more realistic, enriching and engaging training environment.
Trial registration number
N/A
AS10-015
NO DELAY IN MRI SELECTION OF PATIENTS FOR ENDOVASCULAR THERAPY
1Aarhus University Hospital, Neurology, Aarhus, Denmark
2Texas Stroke Institute, Division of Neurointervention, Dallas-Fort Worth, USA
3Aarhus University Hospital, Anesthesiology and Intensive Care, Aarhus, Denmark
4Aarhus University Hospital, Neuroradiology, Aarhus, Denmark
Background and Aims
Background
GOLIATH was a study designed to study general anesthesia (GA) or conscious sedation (CS) in endovascular therapy (EVT). Magnetic Resonance imaging was used before and after the procedure to study infarct growth.
MRI has been criticized for being too time consuming when evaluation stroke patients. We aimed to study the workflow of patients undergoing MRI as selection before EVT and compare the time measures with CT based studies.
Methods
We randomizing 128 patients with anterior circulation large vessel occlusion stroke within six hours of onset to either GA or CS (1:1 allocation). We studied various time measures to examine if MRI inferred a time delay in treatment and compared it to ESCAPE and SWIFT PRIME, two CT based studies that emphasized on minimizing time delay.
Results
There was no difference in symptom onset to admission (GOLIATH 101 minutes, ESCAPE 107.5 and SWFT-PRIME 109.5 minutes.) In GOLIATH, it only took a median of 9 minutes for the patients to get the scanner, while it took 19 and 16 minutes in ESCAPE and SWIFT-PRIME respectively.
From scan to groin puncture, it took 56.5 minutes in GOLIATH and 51 minutes in ESCAPE (this time interval was not reported in SWIFT-PRIME). The whole period of admission to groin puncture took 68 minutes in GOLIATH and 90 minutes in SWIFT-PRIME (this time interval was not reported in ESCAPE.)
Conclusion
MRI does not result in significant time delay when evaluating stroke patients with large vessel occlusion.
Trial registration number
NCT02317237
AS10-016
FACTORS ASSOCIATED WITH ISCHEMIC CORE AND SALVAGEABLE TISSUE ON CT PERFUSION IN 415 ACUTE MIDDLE CEREBRAL ARTERY OCCLUSIVE STROKE
1Neurocenter of Southern Switzerland, Neurology- Stroke Center, Lugano, Switzerland
2Lausanne University Hopital CHUV, Neurology, Lausanne, Switzerland
3Lausanne University Hospital CHUV, Radiology, Lausanne, Switzerland
4Stanford University and Medical Center, neuroradiology, Stanford, USA
Background and Aims
In acute ischemic stroke (AIS) with large vessel occlusion, the volume of the ischemic core (iC) and the proportion of salvageable tissue [mismatch Ratio, MR = (core+penumbra)/core)] are both predictors of treatment response. We aimed to identify predictors of these two values in AIS with proximal middle cerebral artery (MCA) occlusion undergoing acute CT perfusion (CTP).
Method
We identified all AIS with CTP performed <24hours from stroke onset and M1 (or proximal M2) MCA occlusion in the ASTRAL Registry from 2003 to 2015. We correlated iC volumes and Mismatch Ratio (MR) on CTP with multiple demographic, clinical, metabolic and radiological variables in a multivariate regression analysis (MVA).
Results
415 patients were included, median age was 69 years (IQR 21), admission NIHSS 16 (IQR 11) and 48% were females. Independent factors associated with larger iC volume were: NIHSS, decreased vigilance, neglect, admission creatinine, higher hemoglobin, hyperdense MCA sign, ipsilateral cervical internal carotid stenosis or occlusion, cardiac cause of stroke. Smaller iC volume was predicted by female sex, Clot Borden Score, high ASPECT score and good collaterals. Larger MR was associated with female sex, previous antiplatelets regimen, admission cholesterol level, and good collaterals. Smaller MR was independently associated with NIHSS, higher admission blood pressure, higher hemoglobin.
Conclusion
In acute ischemic stroke with proximal MCA occlusions a potential favourable CTP profile (small ischemic core or large Mismatch Ratio) is strongly predicted by female sex, antiplatelets pretreatment, admission cholesterol level, Clot Burden Score, ASPECT score and good collaterals.
Trial registration number
NA
AS10-017
DIFFUSION WEIGHTED IMAGING NEGATIVE STROKE SYNDROMES
1Hacettepe University Hospitals, Neurology, Ankara, Turkey
Background and Aims
Normal diffusion weighted imaging (DWI) during symptomatic acute phase of ischemic stroke is a rare but well-known phenomenon. The clinical correlates of this condition are not satisfactorily elucidated.
Method
15 patients with DWI-negative stroke, confirmed by repeated MRI, MR perfusion and/or vascular imaging, compiled between 2009 and 2017 in Hacettepe University, along with 77 case reports extracted from germane literature were analyzed in combination. In addition to TIA, stroke mimics such as seizure, migraine, functional disorders and post-stroke-recrudescence were excluded.
Results
Median time (IQR, hours) to initial and confirmatory DWI was 4 (3-6) and 28 (15-71). NIHSS was 4.1 (2-9.5) at the time of first DWI. Major DWI negative syndromes (n = 76) were “brainstem mini-strokes” (49%), “cortical small embolic infarcts” (28%), “pure penumbral stroke” (DWI negative but MR perfusion positive) (6%), “aborted stroke” (early and fully recanalized stroke, only diagnosable in cases with documented acute vessel occlusion) (4%) and “unclassified conditions” (14%). Correlative clinical stroke syndromes (n = 92) include “brainstem/capsular/deep lacunar syndromes” (32%); “ocular syndromes such as INO” (11%), “cortical syndromes such as isolated hand paralysis and elements of Gerstmann syndrome (22%); “Caudal brainstem syndromes” such as lateral medullar syndrome (14%) and “movement disorders” such as hemibalismus (2%). DWI-negative unsubstantiated syndromes such as acute isolated vertigo and major hemispheric syndromes was 19%.
Conclusion
In addition to patients with rapid recovery due to complete reperfusion, acute DWI can be falsely negative in strokes exclusively limited to tract-dense regions such as brainstem and capsula interna. However, the corresponding clinical syndromes are relatively nonspecific.
Trial registration number
N/A
AS10-019
HIGH BLOOD PRESSURE MAY BE ASSOCIATED WITH A BETTER COLLATERALIZATION BUT STILL POOR OUTCOMES IN ACUTE ISCHEMIC STROKE PATIENTS
1Huashan Hospital- Fudan University, Department of Neurology, Shanghai, China
Background and Aims
The relationship among the poststroke blood pressure, collateralization and functional outcome in acute ischemic stroke (AIS) patients is still controversial. The aim of this study is to explore the association of poststroke blood pressure with collateralization and functional outcome in AIS patients with large vessel occlusion.
Method
We enrolled patients with large vessel occlusion who had symptom onset within 6 hours and had complete baseline CT angiography, CT perfusion, clinical profiles and follow-up data. Collateralization was characterized as the volume of delay time (DT) > 3s and DT > 6s lesion on CT perfusion. A poor functional outcome was defined as mRS of 3-6 at 3 months.
Results
A total of 126 patients were enrolled at Huashan Hospital from 2011 to 2017. With every increment of 10mmHg systolic blood pressure (SBP), the odds of poor functional outcome increased by 21% (age and sex adjusted, OR1.21, 95% Confidence interval 1.01 to 1.46, P = 0.04). However, with every increment of 10mmHg diastolic blood pressure (DBP), the volume of DT > 6s lesion downsized by 7.6mL (multivariate adjusted, P = 0.026, Table 1).
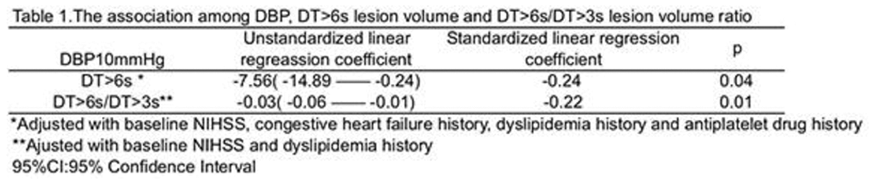
Conclusion
Though higher DBP seems to be associated with a better collateralization, higher SBP may still relate with a poor functional outcome, indicating the other adverse effects resulting from elevated blood pressure. The next step is to enlarge our sample size to further confirm this relationship.
Trial registration number
N/A
AS10-020
INFARCTED CORE VOLUME, ASSESSED BY ACUTE CT-PERFUSION, HOLDS AN INDEPENDENT PREDICTIVE VALUE IN THROMBOLYSED MIDDLE CEREBRAL ARTERY STROKE
1Addenbrooke's hospital, stroke medicine - stroke research group, Cambridge, United Kingdom
Background and Aims
Increasing evidence, reinforced by DAWN trial results, suggests that the amount of infarcted brain tissue is a key predictive factor in acute ischemic stroke.
CT perfusion (CTP) is a validated, cheap, quick, and widely available method to approximate infarcted core and mismatch volumes.
We analysed the prognostic value of CTP in thrombolysed non-lacunar middle cerebral artery (NLMCA) strokes.
Method
All data from thrombolysed NLMCA strokes with available pre-treatment CTP and 3 month modified Rankin Scale (mRS) from our tertiary stroke centre were reviewed. CTP scans were processed with MISTAR® software. Within the perfusion lesion (relative delay time > 3s), two core volume approximations were calculated: Cerebral Blood Flow (CBF) < 30% and Cerebral Blood Volume (CBV) < 60%. Primary outcome was three month mRS ordinal shift. Independent predictors were determined using multivariate ordinal logistic regression models.
Results
We included 237 patients (115 male, median age 76, median NIHSS 12). CBF and CBV-derived core volumes were independently associated with 3 month mRS ordinal shift (adjusted ORs per 1 cc increase: 1.028; 95% (CI 1.014-1.043), p < 0.001; and 1.028, (1.013-1.045), p < 0.001; respectively); as well as age, baseline NIHSS, and arterial occlusion status. Mismatch volumes and collateral status were not independent predictors in multivariate analyses.
Optimally dichotomized core volumes were also independently associated with dichotomized mRS (excellent 0-1; good 0-2; and poor 5-6).
CBF and CBV had similar predictive ability.
Conclusion
CBF and CBV-derived core volumes, calculated with MISTAR® software, were independent outcome predictors, in our cohort of thrombolysed NLMCA strokes, unlike mismatch volumes and collateral status.
Trial registration number
N/A
AS10-021
GHOST INFARCT CORE AND ADMISSION CT PERFUSION - REDEFINING NEUROIMAGING ROLE IN ACUTE ISCHEMIC STROKE
1Centro Hospitalar São João, Department of Neurolgy, Porto, Portugal
2Faculty of Medicine- University of Porto, Department of Clinical Neurosciences and Mental Health., Porto, Portugal
3Hospital Fernando Fonseca, Department of Internal Medicine, Amadora, Portugal
4Instituto Nacional de Neurología y Neurocirugía, Neurology, Mexico City, Mexico
5Vall d’Hebron University Hospital- Vall d’Hebron Research Institute, Stroke Unit- Department of Neurology, Barcelona, Spain
6Universitat Autónoma de Barcelona, Departament de Medicina, Barcelona, Spain
7Vall d’Hebron University Hospital, Department of Neuroradiology, Barcelona, Spain
Background and Aims
Computed tomography (CT) perfusion (CTP) based on cerebral blood volume (CBV) may overestimate infarct core on admission and consequently include ghost infarct core (GIC) in a definitive lesional area. Our goal is to confirm and better characterize GIC phenomenon using CTP- cerebral blood flow (CBF) as the parameter to determine infarct core.
Method
We performed a retrospective analysis of consecutive thrombectomies of middle cerebral or intracranial internal carotid artery occlusions considering noncontrast CT Alberta Stroke Program Early CT Score >6. We used RAPID software to measure admission infarct core based on initial CBF. The final infarct was extracted from follow-up CT. GIC was defined as initial core minus final infarct >10 mL.
Results
123 patients were included. Median National Institutes of Health Stroke Scale score was 18 (13-20), median time from symptoms to CTP was 188 (67 - 288) minutes, and recanalization rate (TICI 2b-3) was 83%. 20 patients presented with GIC. GIC was associated with shorter time to recanalization (150 (105-291) vs 255 (163-367) minutes; p = 0.05) and larger initial CBF-core volume (38 (26-59) vs 6 (0-27) ml; p < 0.001). Time to recanalization < 302 minutes (OR 4.598, 95% CI 1.143 to 18.495, p = 0.032) and initial infarct volume (OR 1.01, 95% CI 1.001 to 1.019, p = 0.032) were identified as independent predictors of GIC.
Conclusion
CTP-CBF < 30% may overestimate infarct core volume, especially in patients imaged in the very early time window and with fast complete reperfusion. CTP-CBF may exclude patients who would benefit from endovascular treatment.
Trial registration number
N/A
AS10-022
SUDDEN COMA FROM ACUTE BILATERAL INTERNAL CAROTID ARTERY OCCLUSION
1Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Bilateral internal carotid artery (ICA) occlusion is an extremely rare cause of sudden coma. We report two clinical cases attended in our hospital.
Method
Two patients, a 93-year-old man and a 87-year-old woman, were transferred to our hospital for a sudden coma. Both patients were receiving long-term oral anticoagulation therapy; case 1: apixaban 2,5mg once daily for an atrial fibrillation; case 2: acenocumarol for a mechanical heart valve. On examination, both patients presented unresponsive coma, quadriplegia and bilaterally positive Babinski signs. However, brainstem reflexes, including the oculocephalic reflex, light reflex and the corneal reflex were preserved (NIHSS:36).
Results
Early computed-tomography (CT) scan signs of infarction, in the territory of both middle cerebral arteries (MCA), and bilateral hyperdense MCA sign, were observed in both cases (ASPECTS<4). CT-angiograms showed a complete occlusion of both ICAs, with sparing of the posterior circulation. CT-perfusion showed an increased mean transit time (MTT) and time to peak (TTP) in the territory of both ICA, with a decreased cerebral blood flow (CBF) and cerebral blood volume (CBV); mismatch was less than 20%. Posterior circulation was prominent as a compensatory mechanism. Aggressive measures were ruled out and both patients died within the first 24h of hospital admission.
Conclusion
Bilateral internal carotid artery occlusion usually presents as a sudden coma with bilateral neurologic deficits, resembling a thrombosis of the basilar artery. This catastrophic stroke syndrome has an extremely poor prognosis.
Trial registration number
N/A
AS10-023
COMPUTER MODEL OF CEREBRAL CIRCULATION- EFFECT OF ANTERIOR CEREBRAL ARTERY TRUNK AND BRANCH OCCLUSION ON FLOW
1Stroke and Ageing Research STARC, Department of Medicine, Clayton, Australia
2Murdoch Childrens Research Institute, Developmental Imaging Group, Parkville, Australia
3Monash Health, Diagnostic Imaging, Clayton, Australia
4CSIRO, Mathematics- Informatics and Statistics, Clayton, Australia
5Monash University, Peninsula Clinical School, Melbourne, Australia
Background and Aims
The circle of Willis (CoW) and leptomeningeal anastomoses (LA) play important supportive roles following intracranial occlusion of the anterior circulation. To evaluate the role of the CoW and LA in maintaining blood flow to the territory of the anterior cerebral artery (ACA) following arterial occlusion.
Method
We developed a computer model of the cerebral vasculature to assess changes in blood flow in the intracranial arteries following vessel occlusion. Arteries were modeled as a network of junctions connected by cylindrical pipes. From a previous study, the diameter of the inter-territorial LA was kept at >1.0mm. Adequate flow was defined as >30% of baseline. A series of experiments based on common occlusion patterns encountered in clinical practice were performed. Variations in the configuration of the CoW was also investigated.
Results
Results of experiments can be found on https://gntem3.shinyapps.io/acasim/. The model showed that the CoW was effective in restoring blood flow to cortical branches (>90%) following proximal ACA (A1) occlusion. But was ineffective (<30%) in A2 occlusion (ACA segment post-Acom). Following occlusion of pericallosal, callosomarginal arteries and their cortical branches, the region of reduced flow (<20%) was downstream from the occlusion, and resulted in neighbouring cortical arteries with known LA demonstrating an increase in flow (>30%). Variations in the CoW (eg. missing Acom) was significant following A1 occlusion.
Conclusion
In ACA stroke, the CoW plays an important but limited role in restoring blood flow following proximal ACA occlusion. In distal occlusions, the compensatory capacity of LA increases flow in selected arteries surrounding the occluded vessel.
Trial registration number
N/A
AS10-024
CORTICOFUGAL FIBRE INVOLVEMENT AND MOTOR OUTCOME IN ANTERIOR CEREBRAL ARTERY STROKE
1Stroke and Ageing Research STARC, Department of Medicine, Clayton, Australia
2Murdoch Childrens Research Institute, Developmental Imaging Group, Parkville, Australia
3Monash Health, Diagnostic Imaging, Clayton, Australia
4Monash University, Peninsula Clinical School, Melbourne, Australia
Background and Aims
A common finding following anterior cerebral artery (ACA) stroke is hemiparesis with a lower limb predominance. Motor outcome appears to be related to loss of integrity of descending corticofugal fibres. To correlate motor outcome with involvement of corticofugal fibres in ACA stroke.
Method
Fibre tracts (from Brodmann area (BA) 4; primary motor (M1) and BA6; supplementary motor (SMA), dorsal and ventral premotor cortices (PMdv)) were defined using diffusion tensor imaging (DTI) on 3T MRI scanner in healthy participants. Infarcts were manually segmented from MRI and co-registered into standard stereotaxic space. We calculate volume of overlap of fibres with segmented infarcts. Relative importance analyses were used (relaimpo package, R) to study the proportional contribution of fibre tracts involvement by infarcts to National Institute of Health Stroke Scale/NIHSS motor subscores.
Results
25 patients (male=11), median age 74 (IQR, 62,77) years. MRI performed at a median interval of 7 (IQR, 2, 56) days after stroke. Median NIHSS of 4 (IQR 2,8) on admission and 0 (IQR 0,4) at 7 days. The R2 for motor deficit on admission was 65.9% (SMA =46.2% [95% CI 27.0%-74.4%], PMdv = 12.5% [95% CI 5.0%-26.5%], M1=5.4% [95% CI 9.1%-16.7%], age=1.8% [95% CI 0.5%-11.3%). The R2 for motor deficit at day 7 was 69.0% and similar to the model on admission. Only 3 patients had motor deficit at 90 days and regression was not performed for this stage.
Conclusion
In ACA stroke, early motor deficit was associated with involvement of corticofugal fibres.
Trial registration number
N/A
AS10-025
ENDOVASCULAR THERAPY IN BASILAR ARTERY OCCLUSION: IMPACT OF RECANALIZATION, THROMBUS BURDEN AND COLLATERALS
1Royal Melbourne Hospital- University of Melbourne, Department of Medicine and Neurology- Melbourne Brain Centre, Parkville, Australia
2University Hospital of Tor Vergata, Stroke Unit- Department of Neuroscience, Rome, Italy
3St. Antonius Hospital, Department of Radiology, Nieuwegein, The Netherlands
4University Hospital of “Tor Vergata”, Department of Biomedicine and Prevention, Rome, Italy
5University of Melbourne, The Florey Institute of Neuroscience and Mental Health, Parkville, Australia
6Careggi University Hospital- University of Florence, Department of Neurology, Florence, Italy
7Royal Adelaide Hospital, Department of Neurology, Adelaide, Australia
8Royal Melbourne Hospital- University of Melbourne, Department of Radiology, Parkville, Australia
9University of Tor Vergata, Department of Interventional Radiology and Neuroradiology, Rome, Italy
10Dresden University of Technology, Department of Neurology and Dresden Neurovascular Center, Dresden, Germany
11St. Antonius Hospital, Department of Neurology, Nieuwegein, The Netherlands
Background and Aims
Whether radiological factors influence the effect of recanalization on outcome in basilar artery occlusion (BAO) is uncertain. We evaluated the associations between recanalization, thrombus burden, collaterals and outcome in endovascular BAO patients.
Method
Clinical and radiological data of consecutive endovascular stroke patients with BAO diagnosed on CT angiography at Royal Melbourne Hospital (Australia), Royal Adelaide Hospital (Australia), University Hospital of Tor Vergata (Italy), Careggi University Hospital (Italy) and from the international BASICS registry were retrospectively analysed. Two investigators assessed the Basilar Artery on Computed Tomography Angiography (BATMAN) score, blinded to clinical outcome. Previously validated dichotomy for favourable BATMAN score (≥7) was used. Good outcome was defined as modified Rankin Scale≤3 within 3 months; successful reperfusion as mTICI 2b-3 (or TIMI 2-3 in BASICS).
Results
We included 170 BAO patients treated with intra-arterial urokinase and/or mechanical thrombectomy (122 with mechanical thrombectomy): mean (SD) age 65(13), median NIHSS 22(IQR 12-30), 36.5% treated beyond 6hours. Recanalization was achieved in 79% patients and was associated with good outcome (p = 0.003). In logistic regression (adjusted for age, NIHSS and time to treatment), recanalization remained associated with good outcome (OR 11, 95%CI 1.2-98, p = 0.03) in the subgroup with favourable BATMAN score but not in patients with unfavourable BATMAN score (OR 3.7, 95%CI 0.7-20, p = 0.1). Treatment beyond 6hours was associated with poor outcome only in patients with unfavourable BATMAN score (adjusted OR 7.2, 95%CI 1.5-35, p = 0.01).
Conclusion
Recanalization is associated with good outcome in BAO patients with good collaterals and less extensive occlusion, independent of clinical severity even in delayed time window.
Trial registration number
N/A
AS10-026
ASPECT SCORE AND TRANSCRANIAL DOPPLER FLOW PARAMETERS IN MIDDLE CEREBRAL ARTERY IN ACUTE BRAIN ISCHAEMIA
1Hospital in Słupsk, Department of Neurology, Słupsk, Poland
2Medical University of Gdańsk, II Department of Radiology, Gdańsk, Poland
3Collegium Medicum in Bydgoszcz- Nicolaus Copernicus University in Toruń, Department of Neurology, Bydgoszcz, Poland
Background and Aims
Transcranial Doppler (TCD) flow parameters assessed with Thrombolysis in Brain Ischaemia (TIBI) score may reflect early brain hypoperfusion. Alberta Stroke Programme early CT score (ASPECT) may also reveal acute brain ischaemia. However, little is known about the relationship between the above parameters. Thus, our goal was to assess the relationship between TCD flow parameters in middle cerebral artery (MCA) and ASPECT score in patients with stroke in MCA territory.
Materials and methods
80 patients with acute MCA ischemia (66 with stroke, mean age 68 yrs and 14 with TIA mean age 68 yrs) were examined. MCA flow was assessed with TCD and scored with TIBI classification on admission and on the 7th day. ASPECT score was established for the CT performed on admission and after 24 h of follow up (with CT or DW-MRI)
Results
A significant correlation was found between ASPECT and the TIBI scores assessed on admission for both, all patients and only those with stroke (r = 0,23; p = 0,04 and r = 0,28; p = 0,02; respectively). In stroke patients, there were also associations between ASPECT score in the follow-up imaging and TIBI score assessed on admission and on the 7th day stroke (r = 0,25; p = 0,04 and r = 0,45; p < 0,01; respectively).
Conclusions
ASPECT score is related to TCD flow parameters in the middle cerebral artery stroke, both in hyper- and subacute phase of stroke.
Trial registration number
N/A
AS10-027
PREDICTORS AND PROGNOSTIC IMPACT OF LEPTOMENINGEAL COLLATERAL FLOW IN PATIENTS WITH PROXIMAL MIDDLE CEREBRAL ARTERY OCCLUSION IN BRAZIL
1USP RP - Neuroscience Department, Neuroscience, Ribeirão Preto, Brazil
2USP - RP - Radiology, Radiology, Ribeirão Preto, Brazil
Background and Aims
Good leptomeningeal collateral flow has been associated with better outcomes in patients with proximal occlusions of the anterior circulation. Few studies have assessed the predictors of good leptomeningeal collateral flow and its impact on clinical outcome in developing countries. We aim to evaluate predictors and prognostic impact of leptomeningeal collateral flow among patients with proximal middle cerebral artery (MCA) occlusion.
Method
We retrospectively analyzed a prospective stroke registry of AIS patients admitted to a tertiary Stroke Center in Brazil, with MCA-M1 occlusion within twelve hours of symptoms onset, admitted from January 2014-June 2017. Leptomeningeal score was evaluated using a previously validated Regional Leptomeningeal (rLMC) score. We evaluated association between rLMC score with clinical variables and outcomes.
Results
From 1559 AIS patients, 121 were analyzed. Demographics: age 67.1 ± 15 years, NIHSS 13 [IQR 11-22]. In linear regression, lower age (B = −0.24; −0.1 to −0.02; p = 0.005), Chagas Disease (B=0,21; 0,51 to 3,74; p = 0,01), smoking (B=0,19; 0,25 to 3,27; p = 0,022) and lower NIHSS (B = −0,26; −0,22 to −0,52; p = 0,002) were associated with better rLMC score. Lower age (B = 0,34; 0,02 to 0,06; p < 0,001), lower NIHSS (B = 0,33; 0,04 to 0,12; p < 0,001), absence of tandem occlusion (B=0,23; 0,33 to 1,62; p = 0,004) and rLMC≥ 17 (B = −0,17; −2 to −0,97; p = 0,03) were associated with better functional outcomes.
Conclusion
Patients with good leptomeningeal collateral flow had lower age, lower NIHSS, Chagas disease and history of smoking. Leptomeningeal collaterals on CT angiography are a reliable marker of good outcome among AIS patients in Brazil.
Trial registration number
N/A
AS10-028
REPERFUSION RESTORES THE OXYGEN METABOLISM OF SEVERELY ISCHEMIC BRAIN TISSUE IN A CLINICALLY RELEVANT ISCHEMIC STROKE MODEL
1Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden
2Karolinska University Hospital, Department of Neuroradiology, Stockholm, Sweden
Background and Aims
The acute treatment of ischemic stroke restores blood flow to the penumbra, regions where an increased Oxygen Extraction Fraction (OEF) sustains viability in the short-term. We employed magnetic resonance imaging (MRI) to examine changes in tissue oxygen metabolism in a M2 occlusion model (M2CAO) that preserves pial collateral flow and allows for controlled reperfusion. The objective was to determine whether reperfusion would result in the restoration of metabolic homeostasis in previously ischemic regions.
Method
OEF and Cerebral Metabolic Rate of Oxygen (CMRO2) were calculated from a Blood Oxygen Level Dependent (BOLD) MRI protocol, examining the R2 and R2* of ischemic tissue, and Dynamic Arterial Spin Labeling perfusion imaging determining cerebral blood flows and volumes. Examinations were performed on Sprague Dawley rats during M2CAO and after reperfusion, with 13 animals included in the analysis. The penumbra was defined as severely hypoperfused brain tissue not recruited into the infarct.
Results
The OEF of the penumbra was significantly increased during M2CAO, but decreased significantly after reperfusion. The OEF of regions recruited to the final infarct were also significantly increased during M2CAO, but did not decrease significantly after reperfusion. No significant difference in regional OEF remained after reperfusion. The CMRO2 of the penumbra was significantly decreased during M2CAO, but increased significantly after reperfusion.
Conclusion
Our results demonstrate the effectiveness of early reperfusion in alleviating metabolic disturbances in ischemic regions, indicating the potential of acute treatment to achieve significant neurological recovery in stroke patients. The results emphasize the potential of metabolic identification of the penumbra through BOLD MRI.
Trial registration number
N/A
AS10-029
RELATIONSHIP BETWEEN THE BURDEN OF CEREBRAL SMALL VESSEL DISEASE AND HEMATOMA VOLUME AND EXPANSION
1West China Hospital of Sichuan University, Neurology, Chengdu, China
Background and Aims
We aimed to investigate the role of individual CSVD markers and total CSVD score in hematoma volume and expansion among primary intracerebral hemorrhage (ICH).
Method
Large hematoma volume was defined as ICH volume >30 ml within 72 hours after ICH onset. Hematoma expansion was defined if the volume on follow-up CT within 72 hours increased >33% or >6 ml when compared with that on baseline CT within 24 hours. CSVD markers, including lacunes, white matter hyperintensities (WMH), cerebral microbleeds (CMBs) and enlarged perivascular spaces (EPVS), and total CSVD score were rated on MRI.
Results
Of the 107 included patients, large hematoma volume was present in 26.2% of (28/107) patients. Sixty patients performed baseline and follow-up CT, among which hematoma expansion was present in 25% (15/60). The prevalence of large hematoma volume was higher in patients with any lacune (OR 6.240, 95% CI 1.146 to 33.989, p = 0.034) and deep lacunes (OR 4.746, 95% CI 1.028 to 21.906, p = 0.046) in deep ICH after correcting vascular risk factors. However, the association of large hematoma volume with WMH, CMBs, EPVS and total CSVD score, separately, was not observed in lobar or deep ICH. We did not find the significant association of hematoma expansion with the four CSVD markers and CSVD score.
Conclusion
In patients with deep ICH, high prevalence of any lacune or deep lacunes was independently associated with large hematoma volume, suggesting that lacunes may have implications for the stratification of hemorrhage treatment. The new finding requires further investigations to validate.
Trial registration number
N/A
AS10-030
MAGNETIC RESONANCE IMAGES SIGNAL CHARACTERISTICS FOR T2-FLAIR AND QUANTITATIVE T2 RELAXATION TIMES AT 3T IN ACUTE STROKE
1University of Bristol, School of Experimental Psychology, Bristol, United Kingdom
2University of Oxford, Acute Vascular Imaging Centre, Oxford, United Kingdom
3University of Glasgow, Queen Elizabeth University Hospital, Glasgow, United Kingdom
Background and Aims
T2 MRI is informative of tissue status and onset time in stroke despite low sensitivity1,2,3 and small changes 2 in early ischaemia. Further complications arise from technical factors including field inhomogeneities and T1 effects.2 We compared T2 signal characteristics at 3T in stroke patients.
Method
ADC, T2-FLAIR and quantitative T2 images (qT2; TSE 3 echoes) were acquired from 12 patients within 9 hours of symptoms. Ischaemic ROIs were manually delineated using ADC images (Figure 1). Signal-to-Noise-Ratio (SNR) and Contrast-to-Noise Ratio (CNR) for T2-FLAIR and qT2 were compared for < 4.5 hours of onset (M = 160mins ± 27, n = 5) and 4.5–9 hours (M = 432mins ± 86, n = 7).
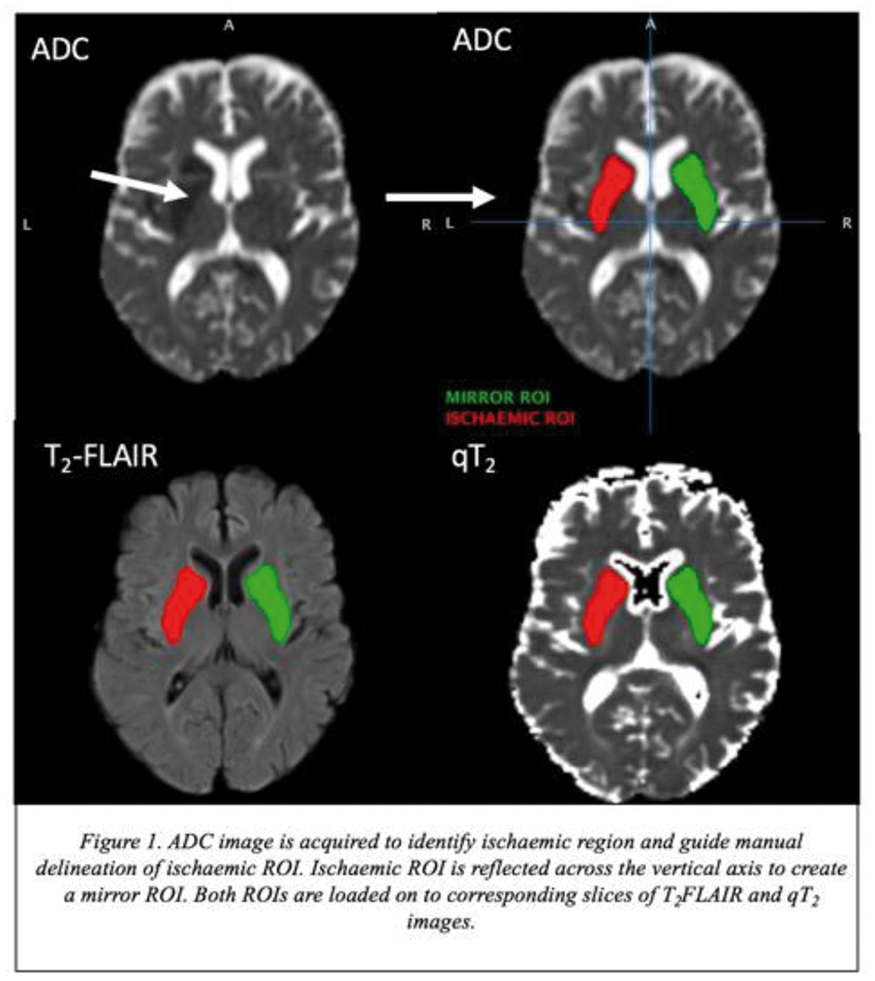
Results
Mean SNR was higher for T2-FLAIR than qT2 within 4.5 hours (92.5 ± 13.9 vs. 38.2 ± 6.6) and after (81.4 ± 17.6 vs. 43.7 ± 22.4). Mean CNR was higher for T2-FLAIR than qT2 within 4.5 hours with greater variability (6.3 ± 4.6 vs. 4.9 ± 0.9). Respective CNRs were comparable after 4.5 hours (6.7 ± 1.7 vs. 7.2 ± 3.8).
Conclusion
qT2 showed less varied contrast than T2-FLAIR in hyperacute stroke patients. qT2 images may be more reliable for tissue state assessment in early ischaemia. All clinical MRI scanners can produce qT2 images at no extra time-cost.
Supported by The Dunhill Medical Trust (R385_1114)
1. Thomalla et al. Lancet Neurol. 2011; 10:978. 2. McGarry et al. Int J Stroke. 2016; 11:677. 3. Cheng et al. JCBFM. 2013; 33:76.
Trial registration number
N/A
AS10-031
MULTIPARAMETRIC APPROACH TO STROKE ONSET TIME ESTIMATION USING QUANTITATIVE MRI AND CLINICAL DATA
1University of Bristol, School of Experimental Psychology, Bristol, United Kingdom
2University of Bristol, School of Clinical Sciences, Bristol, United Kingdom
3University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
Apparent diffusion coefficient (ADC) decreases in ischaemic brain within minutes, but provides no information from onset time in early hours of stroke. Instead, absolute T2 relaxation time changes in a time-dependent manner in ADC lesions, potentially serving as a proxy for onset time to support clinical data in patient management decision making.
Method
MRI were acquired for ADC and T2 relaxation time at 3T from 28 stroke patients (age 31-83Y, 18 thrombolysed) within 9.5h of symptom onset. Ischaemia was delineated as ADC<0.6×10−3 mm2/s, T2 and median absolute deviation m = mad (T2) were determined in ADC lesions.
Results
Neither lesion T2 nor m showed correlation with onset time. Combining the ADC log-volume, λ = ln (V), with m improved the correlation, but including patient age, A, and thrombolysis status ϑ={0,1} made the correlation highly significant (r2=0.817, p = 0.000014, Figure 1):
T = −(3 ± 192) − (98.3 ± 49.4)m + (1145 ± 359)ϑ + (25.0 ± 9.4)λm − (65.8 ± 32.8)mϑ − (12.6 ± 4.4)Aϑ − (7.6 ± 3.6)λ2 − (2.2 ± 1.1)m2 + (0.069 ± 0.030)A2,
where T is the onset time, and the parameter errors are the 95% confidence intervals.
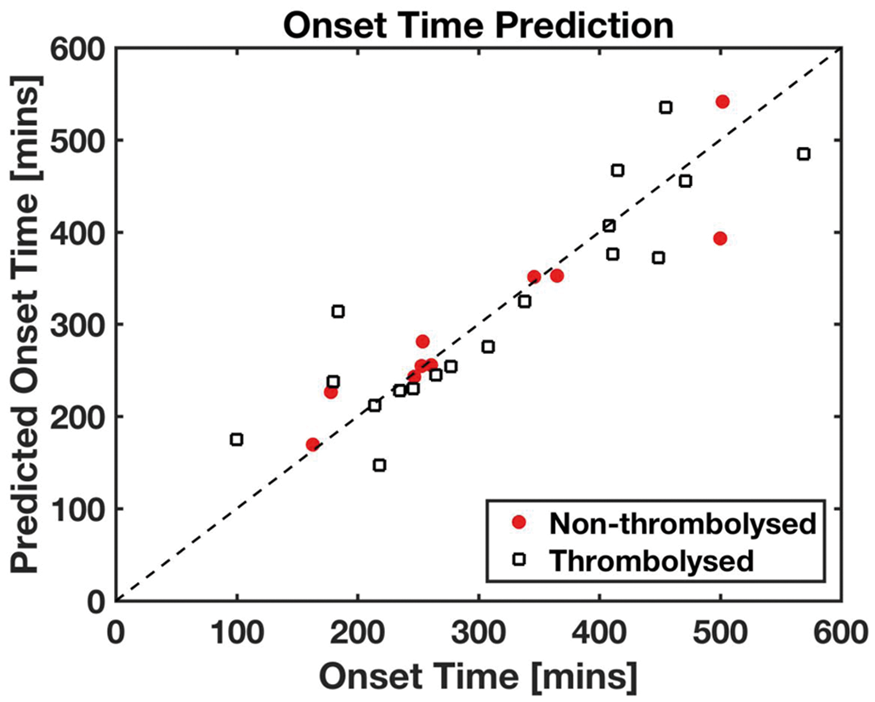
Figure 1. Predicted onset time against known onset time, according to the multiparametric fit.
Conclusion
Quantitative ADC and T2 MRI complemented with patient age and thrombolysis status show remarkably strong correlation with symptom onset. Ongoing MRI projects on stroke aim to address the hypothesis that quantitative MRI combined with clinical data may provide a protocol for stroke timing for patients with unknown onset.
Trial registration number
N/A
AS10-032
PENUMBRA SALVAGE AND INFARCT GROWTH IN ACUTE ISCHEMIC STROKE: MULTIPLE FACTORS EXPLAIN HIGH INTERINDIVIDUAL VARIABILITY
1Lausanne University Hospital, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
2Ospedale Civico di Lugano, Stroke Center- Neurology Service, Lugano, Switzerland
32694-Santé publique : épidémiologie et qualité des soins- Univ. Lille, Department of Biostatistics, Lille, France
4Lausanne University Hospital, Department of Diagnostic and Interventional Radiology, Lausanne, Switzerland
5Stanford University and Medical Center, Department of Diagnostic and Interventional Radiology of Neuroradiology Division, Stanford, USA
Background and Aims
Effective treatment of ischemic stroke requires reperfusion of the penumbral brain tissue. We aimed at investigating predictors of penumbra salvage and infarct growth.
Method
In the Acute STroke Registry and Analysis of Lausanne (ASTRAL) from 2003 to 2016, we selected all middle cerebral artery (MCA) strokes with availability of a good quality CT-angiography <24h and thresholded CT-perfusion. Penumbra salvage (PS) and infarct growth (IG) over 24 hours were correlated in multivariate analyses with clinical, radiological and biochemical variables, and in adjusted analysis with clinical outcome.
Results
In the 551 MCA strokes included, 49.2% were females, median age ( ± IQR) was 68.7 ± 21, admission NIHSS 14 ± 12, and onset-to-imaging time 169.5 ± 283 minutes.
More PS was associated with higher BMI, hemineglect, absence of early ischemic changes, leukoaraiosis, other vascular territory involvement, larger baseline penumbra and a lower clot burden. Less IG was associated with current smoking, lower admission glycemia, larger baseline infarct core, absence of early ischemic changes, chronic vascular brain lesions, other territory involvement, absence of extracranial arterial pathology and hyperdense MCA sign, and lower clot burden.
Adding subacute variables to these analyses, recanalisation were associated with more PS and less IG, and the absence of parenchymal haemorrhage with less IG.
More PS and less IG were independently correlated with better 12 months functional outcome.
Conclusion
Penumbra salvage and infarct growth depend on multiple clinical, metabolic, parenchymal, and arterial variables. These findings may explain variability of treatment response and outcome, and may help select patients for late or more aggressive management.
Trial registration number
N/A
AS10-033
GOOD COLLATERALS ARE A MAJOR DETERMINANT OF THE INFARCT CORE, BUT NOT PENUMBRA VOLUME, IN THE ACUTE PHASE OF STROKE
1Lausanne University Hospital, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
2Neurocenter of Southern Switzerland- Ospedale Civico di Lugano, Stroke Center- Neurology Service, Lugano, Switzerland
3Lausanne University Hospital, Department of Radiodiagnostic and Interventional Radiology, Lausanne, Switzerland
4Department of Radiology- Neuroradiology Division, Stanford University and Medical Center, Stanford, USA
Background and Aims
Determinants of early loss of ischemic tissue (core) or its prolonged survival (penumbra) in acute ischemic stroke are incompletely understood. We aimed to identify radiological variables associated with core and penumbra volumes on CT perfusion (CTP).
Method
In the Acute STroke Registry and Analysis of Lausanne (2003-2015), we identified 415 patients with good quality CTP and proximal middle cerebral artery (MCA) occlusion. Volumes of core, penumbra, and mismatch ratio [MR = (core+penumbra)/core)] were calculated using established thresholds. Collaterals were scored from 0 (absent) to 3 (100% or more) and analysed in an ordinal way. CTP volumes were correlated with multiple radiological variables in multivariate regression analysis.
Results
The median age was 69 years (IQR 21), 49% were female, admission NIHSS was 16 (IQR 11), and delay to imaging 2.2 hours (IQR 1.9). Lower core volumes were associated with higher ASPECTS, absence of hyperdense MCA sign, lower clot burden and good collaterals (see Table). Higher penumbra volumes were correlated with higher clot burden and non-distal intracranial occlusion, but not with collaterals. Higher MR was found in absence of hyperdense MCA sign and of distal intracranial occlusion, and with good collaterals.
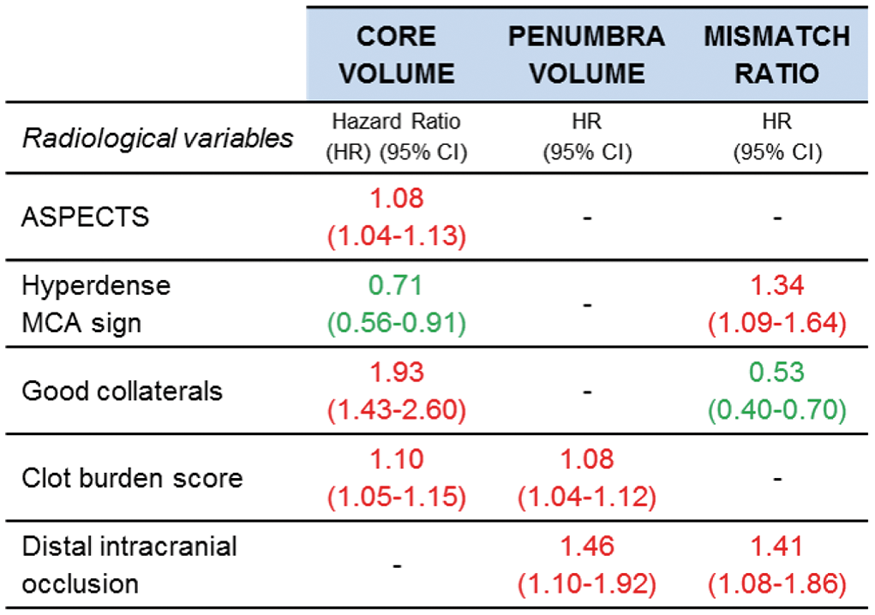
Conclusion
In acute stroke, good collaterals were associated with lower core, but not with higher penumbra volumes. This suggests a major role of collaterals in early tissue loss, but its limited significance as marker of salvageable tissue.
Trial registration number
N/A
AS10-034
HEMODYNAMIC CHARACTERISTICS OF ARTERIAL TRANSIT ARTIFACT ON ARTERIAL SPIN LABELING MAGNETIC RESONANCE IMAGING
1Konkuk University Medical Center- Konkuk University Medical Center, Radiology, Seoul, Republic of Korea
2Daejeon St. Mary’s Hospital- The Catholic University of Korea, Radiology, Daejeon, Republic of Korea
3Daejeon St. Mary’s Hospital The Catholic University of Korea, Neurology, Daejeon, Republic of Korea
4Konkuk University Medical Center- Konkuk University Medical Center, Neurology, Seoul, Republic of Korea
5Daejeon St. Mary’s Hospital The Catholic University of Korea, Neurosurgery, Daejeon, Republic of Korea
6Konkuk University Medical Center- Konkuk University Medical Center, Neurosurgery, Seoul, Republic of Korea
7Siemens Healthcare Ltd., Diagnostic Imaging, Seoul, Republic of Korea
Background and Aims
The presence of arterial transit artifact (ATA) on arterial spin labeling (ASL) is associated with better neurological outcome in acute ischemic stroke patients. However, hemodynamics of ATA has never been explored. In this study, we aimed to evaluate the hemodynamic characteristics of the ATA in patient with acute ischemic stroke caused by a steno-occlusive lesion of the internal carotid artery and/or middle cerebral artery, as compared with multiphase collateral images derived from dynamic susceptibility perfusion MRI (DSC Phase Map).
Method
In a prospectively maintained registry of acute stroke, we identified 99 patients (40 females, mean age: 70.4) with acute ischemic stroke who underwent MRI with pulsed ASL (PASL) and dynamic susceptibility perfusion between November 2015 and August 2017. ATAs on ASL were correlated with contrast-arrival phase of the DSC Phase Map, in which 5 phases (artery, capillary, early venous, late venous, and delayed) were determined by the arterial and venous time-intensity curves.
Results
Among 99 patients, there were 85 patients with positive ATA. The positive ATA group had better clinical outcome than the negative group (3-month modified Rankin scale: 2.3 ± 1.9 vs. 4.1 ± 1.4, P = 0.001). On DSC Phase Map. ATAs appeared in the arterial phase in 76/85 (89.4%) patients and appeared in capillary phase in 9/85 (10.6%) patients.
Conclusion
ATA detected on ASL was well correlated with early collateral flow on DSC Phase Map. This finding may help the understanding of ASL collateral flow and its prognostic value in acute ischemic stroke.
Trial registration number
N/A
AS10-035
ASSESSMENT OF COLLATERAL AND PERFUSION USING ARTERIAL SPIN LABELING MRI IN PATIENTS WITH ACUTE ISCHEMIC STROKE DUE TO LARGE ARTERY STENO-OCCLUSION: CORRELATION WITH NEUROLOGICAL OUTCOME
1Daejeon St. Mary's Hospital- The Catholic University of Korea, Radiology, Daejeon, Republic of Korea
2Konkuk University Medical Center- Konkuk University School of Medicine, Radiology, Seoul, Republic of Korea
3Daejeon St. Mary's Hospital- The Catholic University of Korea, Neurology, Daejeon, Republic of Korea
4Konkuk University Medical Center- Konkuk University School of Medicine, Neurology, Seoul, Republic of Korea
5Daejeon St. Mary's Hospital- The Catholic University of Korea, Neurosurgery, Daejeon, Republic of Korea
6Konkuk University Medical Center- Konkuk University School of Medicine, Neurosurgery, Seoul, Republic of Korea
Background and Aims
Arterial spin labeling (ASL) has been suggested as an imaging method for assessment of cerebral perfusion and collaterals. The aim of this study is to explore association of perfusion and collateral status on ASL with clinical outcome in patients with acute ischemic stroke (AIS).
Method
In a prospectively maintained registry of AIS, 96 cases in 95 patients (38 females, mean age 70.4 ± 11.7) with acute ischemic stroke caused by a steno-occlusion of the unilateral internal carotid artery (ICA) and/or M1 segment middle cerebral artery (MCA) within 8 hours from symptom onset were included in this study. We used 5-point scale scoring system (grade 0 and 1: poor; grade 2: intermediate, grade 3 and 4: good) for assessment of collateral-perfusion on ASL. The association of baseline NIHSS score, stroke risk factors, parameters of EVT, and ASL grade with neurological outcome was analyzed by using logistic regression.
Results
In univariate analysis, younger age, lower initial NIHSS score, absence of hypertension, and better ASL score were associated with a good outcome. In multivariate analysis, better ASL score and lower initial NIHSS score were independent predictors of a good outcome (OR, 3.51; 95% CI, 1.65–7.46; and OR, 0.89; 95% CI, 0.81–0.98). In 53 patients underwent endovascular treatment of 96 cases, only better ASL score was an independent predictor of a good outcome in multivariate analysis (OR, 5.861; 95% CI, 1.11–30.98).
Conclusion
ASL can be used as a non-invasive imaging method for assessment of collateral-perfusion in AIS without exogenous contrast media.
Trial registration number
N/A
AS10-036
INTRACRANIAL CAROTID ARTERY CALCIFICATION AND EFFECT ON ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE PATIENTS
1Erasmus University Medical Center, Radiology & Neurology, Rotterdam, The Netherlands
2Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
3Academic Medical Center, Radiology, Amsterdam, The Netherlands
4Academic Medical Center, Neurology, Amsterdam, The Netherlands
5Maastricht University Medical Center, Neurology, Maastricht, The Netherlands
6Maastricht University Medical Center, Radiology, Maastricht, The Netherlands
7Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
8Erasmus University Medical Center, Radiology & Epidemiology, Rotterdam, The Netherlands
Background and Aims
Intracranial carotid artery calcification (ICAC) may interfere with the safety and efficacy of endovascular treatment (EVT). We assessed the influence of ICAC volume and pattern on the effect of EVT in patients with acute ischemic stroke.
Method
All 500 patients included in the MRCLEAN trial on the effectiveness of EVT were analyzed. The volume (mm3) and pattern (located in tunica intima or tunica media) of ICAC were determined on baseline CT. Functional outcome at 90 days was assessed with the modified Ranking Scale. Next, we investigated the association of ICAC volume and pattern with functional outcome using adjusted ordinal logistic regression models with an interaction term between treatment allocation and ICAC.
Results
We found no association of ICAC volume with functional outcome (acOR per unit increase ICAC volume 0.94 (95%CI 0.84-1.06). Moreover, we found no evidence for effect modification by ICAC volume (p = 0.56). Predominantly medial ICAC pattern was nearly significant associated with poorer functional outcome (acOR 1.63; 95%CI 0.99-2.66). Yet, we found evidence for treatment effect modification by ICAC pattern (p = 0.02): a better functional outcome after EVT in patients with predominantly medial calcification (acOR 2.55; 95%CI 1.38-4.72) and no effect of EVT in patients with predominantly intimal calcifications (acOR 0.76; 95%CI 0.39-1.50).
Conclusion
Predominantly medial calcification pattern of ICAC relates to poorer functional outcome in ischemic stroke patients, but the benefit of EVT in ischemic stroke patients with a medial calcification pattern is larger compared to the treatment effect in patients with a intimal calcification pattern.
Trial registration number
ISRCTN10888758
AS10-038
ASSOCIATIONS OF CLINICAL AND IMAGING CHARACTERISTICS WITH COLLATERAL GRADE ON BASELINE CT ANGIOGRAPHY IN PATIENTS WITHC ACUTE ISCHEMIC STROKE DUE TO LARGE VESSEL OCCLUSION
1Erasmus MC, Dept of Public Health, Rotterdam, The Netherlands
2Erasmus MC, Dept of Neurology- Dept of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
3Academic Medical Center, Dept of Radiology & Nuclear Medicine, Amsterdam, The Netherlands
4Academic Medical Center- Erasmus MC, Dept of Radiology & Nuclear Medicine- Dept of Neurology, Amsterdam- Rotterdam, The Netherlands
5Academic Medical Center, Dept of Radiology & Nuclear Medicine- Dept of Biomedical Engineering & Physics, Amsterdam, The Netherlands
6Erasmus MC, Dept of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
7Academic Medical Center, Dept of Neurology, Amsterdam, The Netherlands
8Maastricht University Medical Center, Dept of Neurology- Cardiovascular Research Institute Maastricht CARIM, Maastricht, The Netherlands
9Maastricht University Medical Center, Dept of Radiology- Cardiovascular Research Institute Maastricht CARIM, Maastricht, The Netherlands
10Erasmus MC, Dept of Neurology, Rotterdam, The Netherlands
Background and Aims
Poor cerebral collateral circulation is associated with poor functional outcome after ischemic stroke and reduces the beneficial effect of endovascular treatment. We aimed to identify clinical and imaging characteristics that are associated with collateral grade on baseline CT angiography (CTA) in patients with acute ischemic stroke due to an anterior circulation large vessel occlusion.
Method
We used data of patients included in the MR CLEAN trial (n = 500) and MR CLEAN Registry (n = 1488). Collateral grade on baseline CTA was scored from 0 (absent) to 3 (good). We used multivariable ordinal logistic regression to assess the association between collateral grade and variables that were previously suggested in the literature.
Results
In total, 1988 patients were analyzed. Distribution of the collateral grades was as follows: grade 0 (7%, n = 123), grade 1 (32%, n = 596), grade 2 (39%, n = 734) and grade 3 (23%, n = 422). Older age (adjusted common odds ratio (acOR) 0.88 per 10 years [95% confidence interval (CI) 0.82 – 0.93]), male sex (acOR 0.65 [95% CI 0.55 – 0.77]) and occlusion of the intracranial segment of the internal carotid artery with or without occlusion of the terminus (ICA(-T)) (acOR 0.64 [95% CI 0.53 – 0.77]) were associated with poorer collateral grades in the multivariable analysis.
Conclusion
Older age, female sex, and occlusion of the ICA-(T) are associated with poorer CTA collateral grades in patients with acute ischemic stroke due to an anterior circulation large vessel occlusion. No independent association was found with cerebrovascular risk factors, such as hypertension, diabetes or extracranial carotid stenosis.
Trial registration number
N/A
AS10-039
CT-RITMO STUDY: RATE OF INFARCTION GROWTH IN ACUTE STROKE CT PERFUSION SEQUENTIAL STUDIES
1La Princesa University Hospital., Stroke Unit. Neurology department., Madrid, Spain
2Ramón y Cajal University Hospital, Stroke Unit. Neurology department, Madrid, Spain
3La Princesa University Hospital., Radiology department., Madrid, Spain
4Ramón y Cajal University Hospital, Radiology department, Madrid, Spain
Background and Aims
Cerebral infarction core can be assessed using CT-Perfusion cerebral blood volume maps (CBV-core). However, no study has evaluated the CBV-core changes during stroke progression yet. The CT-RITMO(
Method
We conducted a retrospective study of consecutive patients with MCA acute stroke transferred between 2 stroke centers and undergoing endovascular treatment, from January 2010 to March 2017. CBV-core was estimated in sequential CT-Perfusion (CTP) studies (first CTP performed in the shipping center and a second one in the treatment center). Clinical and radiological variables were correlated with infarction growth.
Results
N = 50. Mean age: 68,4. Women 54 %. Pretreatment NIHSS 16,1(SD 5,8). Successful recanalization in 86%. Median time (minutes) between CTP: 105[90-121]. Collateral circulation: good 64%, moderate 25%, poor 12%. Mean CBV-Core growth 3,5ml (SD 4,6). CBV-core growth: <5 ml 56%, 5-10 ml 12%, 10-15 ml 24%, > 15 ml 8%. Mean CBV-core velocity of growth: 0,03 ml/minute (SD 0,04). We found direct correlation between CBV-core growth and blood glucose levels (Spearman Rho = 0,33; p = 0,03), creatinine levels (Rho = 0,3;p = 0,05) and pretreatment NIHSS(Rho = 0,28;p = 0,05). Better collateral circulation was associated with lower CBV-core growth. Higher CBV-core growth was associated with worse mRS at 3 months (Rho = 0,35;p = 0,01) and infarction volume at 24h (Rho = 0,44; p = 0,002).
Conclusion
Our study suggests that CBV-core growth tends to be low but with a significant variability. Infarction growth was associated with factors already known as relevant in stroke, but our study points out their importance even for a short period in the hyperacute phase.
Trial registration number
N/A
AS10-040
HYPERGLYCEMIA INCREASES THE RISK OF HEMORRAGIC TRANSFORMATION AFTER MECHANICAL THROBECTOMY IN ACUTE ISCHEMIC STROKE PATIENTS WITH PRE-TREATMENT SEVERE HYPOPERFUSION
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2CIBER de Bioingeniería- Biomateriales y Nanomedicina CIBER-BBN, Biomedical Imaging, Barcelona, Spain
3Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Severe hypoperfusion and hyperglycemia have been associated with the risk of developing a parenchymal hematoma (PH) in acute ischemic stroke treated with reperfusion therapies. Herein, we aimed to evaluate whether hyperglycemia and severe hypoperfusion have synergistic effects in the promotion of PH after mechanical thrombectomy (MT).
Method
We included 258 patients with acute proximal anterior circulation occlusions (median NIHSS=17) treated with MT who had a pre-treatment whole-brain computed tomography perfusion and a post-treatment follow-up MRI. Severe hypoperfusion was defined as the presence of regions with cerebral blood volume (CBV) values lower than 2.5% of normal brain, or very-low CBV (VLCBV)-regions. PH was evaluated in follow-up MRI Gradient-Echo sequences. Glucose levels were recorded at hospital admission. Regression models adjusted for baseline severity and recanalization assessed the association between VLCBV-regions, glucose and the risk of PH.
Results
Baseline glucose levels were median (IQR) 119 (105-141) mg/dl. Thirty-nine (15%) patients had pre-treatment VLCBV-regions, and 42 (16%) developed a PH in follow-up neuroimaging. The presence of VLCBV-regions was associated with an increased risk of PH (adjusted Odds-Ratio (aOR)=3.26, 95%CI=1.42-7.46, p = 0.005)). Pre-treatment glucose levels interacted significantly with VLCBV on the prediction of PH (p = 0.028). In patients with VLCBV-regions, higher pre-treatment glucose levels increased significantly the risk of PH (aOR=3.10 per IQR of glucose increase; 95%CI=1.22-7.87, p = 0.017), whereas this association was not significant in patients without VLCBV-regions.
Conclusion
Pre-treatment hyperglycemia increases the risk of PH after MT in patients with severe hypoperfusion. These two factors should be considered in the evaluation of adjunctive neuroprotective strategies.
Trial registration number
N/A
AS10-041
RETROSPECTIVE ANALYSIS OF CT-PERFUSION PARAMETERS EVOLUTION WITH TIME AND CORRELATION WITH CLINICAL PROGNOSIS, IN A CONSECUTIVE SERIE OF ACUTE ISCHEMIC STROKE ELIGIBLE FOR REVASCULARIZATION THERAPIES
1Geneva University Hospitals, Department of Neurology, Geneva, Switzerland
2Geneva University Hospitals, Department of Neuroradiology, Geneva, Switzerland
Background and Aims
To determine how CT-perfusion parameters (CBF, Tmax) are influenced by time.
Method
We performed a retrospective analysis of patients consecutively admitted in the Emergency Department of Geneva University Hospitals with acute stroke within 6 hours and selected for acute revascularization therapies. Only patients presenting a proximal occlusion of the MCA or of the distal ICA were included. We assessed the correlation between CT-perfusion (with automatic further analysis by the RAPID software) parameters (CBF, Tmax>6sec), recanalization rate (TICI scale), a favorable clinical outcome (defined as a modified Rankin scale of 0-2 at 90 days) and time elapsed from the onset of symptoms.
Results
We included 84 patients. We found a significant inverse correlation between time to imaging and volume of Tmax>6 sec (p = 0.03) and Tmax>8sec (p = 0.006). However, no correlation was found between time to imaging and CBF volume (p = 0.09). Furthermore, in a logistic regression model using clinical outcome as the dependent variable and including the parameters of NIHSS at admission, time to imaging, volumes of Tmax (>6sec and 8sec) and CBF, only CBF resulted to be an independent predictor (p = 0.03).
Conclusion
In our cohort, CBF volume was a significant predictor of clinical outcome, independently of time. Our results, albeit retrospective, might suggest that some CT-perfusion parameters are only partially dependent of time. These data might challenge the rigid timeframe still applied to the selection of ideal candidates to revascularization therapies.
Trial registration number
N/A
AS10-042
INFLUENCE OF PERIVENTRICULAR LEUKOARAIOSIS SEVERITY ON THE PREDICTIVE CAPACITY OF PERFUSION COMPUTED TOMOGRAPHY TO ASSESS FINAL INFARCT VOLUME
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2CIBER de Bioingeniería- Biomateriales y Nanomedicina CIBER-BBN, Biomedical Imaging, Barcelona, Spain
3Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Leukoaraiosis has been shown to affect the accuracy of Computed Tomography Perfusion imaging (CTP) for the prediction of final infarct volume in acute ischemic stroke. We aimed to quantitatively evaluate the impact of leukoaraiosis on the prediction of Non-Viable tissue (NVT) by CTP in acute ischemic stroke treated with thrombectomy.
Method
We retrospectively analyzed 166 patients with acute stroke who had a whole-brain CTP showing a perfusion deficit due to proximal arterial occlusions in the carotid territory and underwent mechanical thrombectomy. Periventricular leukoaraiosis was defined as white matter hyperintensities on a 24-48 hours follow-up MRI according to the Fazekas score (FSPV). Coefficients of determination (R2), intraclass correlation coefficient (ICC) and Bland-Altman plots were used to assess the association between CTP-predicted NVT and final infarct volume measured in the diffusion-weighted image (DWI).
Results
R2 and ICC values differed according to FSPV grade. Patients with absent or mild leukoaraiosis (FSPV 0-1) had significantly higher R2 and ICC values (0.42 and 0.51, respectively) than those with moderate or severe leukoaraiosis (FSPV 2-3; 0.02 and 0.07, respectively). These observations were more apparent in analysis restricted to patients with early recanalization (<4’5 hours from stroke onset) (FSPV 0-1, R2=0.72 and ICC=0.80; FSPV=2-3, R2=0.07 and ICC=0.24). Bland-Altman limits of agreement were narrower in patients with mild or absent leukoaraiosis.
Conclusion
Increased severity of periventricular leukoaraiosis results in a poorer prediction of final infarct by CTP. CTP-derived NVT measures should be interpreted with caution and individualized according to the presence and severity of leukoaraiosis.
Trial registration number
N/A
AS10-043
IMPACT OF RECANALIZATION ON COMPUTED TOMOGRAPHY PERFUSION DEFINITION OF NON-VIABLE TISSUE AFTER ACUTE ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2CIBER de Bioingeniería- Biomateriales y Nanomedicina CIBER-BBN, Biomedical Imaging, Barcelona, Spain
3Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Computed tomography perfusion (CTP) allows the estimation of pretreatment non-viable tissue (NVT) after acute ischemic stroke. However, CTP-predicted NVT obtained after applying validated thresholds (relative Cerebral Blood Flow (rCBF) <30%) may overestimate final infarct volume in the case of early reperfusion. We aimed to evaluate the accuracy of CTP-derived NVT for the prediction of final infarct volume in patients achieving complete recanalization after mechanical thrombectomy (MT) according to time from stroke onset to recanalization.
Method
We included 116 acute stroke patients with intracranial proximal occlusions in the carotid territory successfully reperfused after MT (TICI 3 at the end of the procedure) who had a pretreatment CTP and a 24-hour follow-up DWI. For CTP-predicted NVT calculation, a range of relative thresholds was explored in CBF maps at constant increments. Intraclass correlation coefficient (ICC) and Bland-Altman plots were used to assess the reliability and absolute agreement between CTP-predicted NVT and follow-up coregistered DWI-lesion
Results
The best CTP NVT definition for final DWI-lesion prediction corresponded to the rCBF<30% threshold (ICC=0.751, 95%CI=0.641−0.827). However, time to recanalization modified significantly the association between NVT and final DWI-lesion (p-interaction = 0.04). Patients with recanalization after 4.5 hours had significantly higher ICC values (n = 56; ICC=0.894, 95%CI=0.794−0.942) than those with earlier recanalization (n = 60; ICC=0.378, 95%CI=−0.048−0.630). Bland-Altman showed DWI-lesion overestimation and wider limits of agreement in patients with earlier recanalization.
Conclusion
The reliability of CTP-derived NVT for the prediction of final DWI-lesion is modified according to recanalizacion status. NVT should be interpreted with caution specially when early recanalization is expected.
Trial registration number
N/A
AS10-044
USEFULNESS OF PERFUSION MAPS FROM DIGITAL SUBTRACTION ANGIOGRAPHY IN ACUTE STROKE PATIENTS
1Hospital Clinic, Institut Clinic de Neurociències, Barcelona, Spain
2CIBER de Bioingeniería- Biomateriales y Nanomedicina CIBER-BBN, Biomedical Imaging, Barcelona, Spain
3Hospital Clinic, Radiology Department, Barcelona, Spain
Background and Aims
Perfusion imaging is widely used in Magnetic Resonance Imaging (MRI) and Computed Tomography (CT), but Digital Subtraction Angiography (DSA) is increasingly used for the management of acute ischemic stroke (AIS). We sought to provide a new tool that translates perfusion parameters into procedural DSA images to improve the assessment of perfusion, revascularization and clinical outcomes.
Method
149 angiograms obtained during endovascular treatment (ET) of AIS patients with proximal occlusion in the carotid territory were processed. We implemented a prototype software to compute perfusion-based maps from DSA images: Cerebral Blood Volume (CBV), Cerebral Blood Flow (CBF) and Time To Peak (TTP). We applied a new protocol based on the evaluation of CBV and TTP (CBVTTPp) to assess reperfusion and the scores of this assessment were compared with the performance of TIMI and TICI scales through area under the ROC curves (AUC) as well as through regression analysis with the endpoint of clinical outcome.
Results
The CBVTTPp score showed good inter-rater reliability (weighted Kappa 0.648, 95%CI 0.57−0.73), better classification performance than TIMI and TICI when studied alone and added predictive information when used together with clinical variables and TICI score to predict clinical outcome of AIS patients.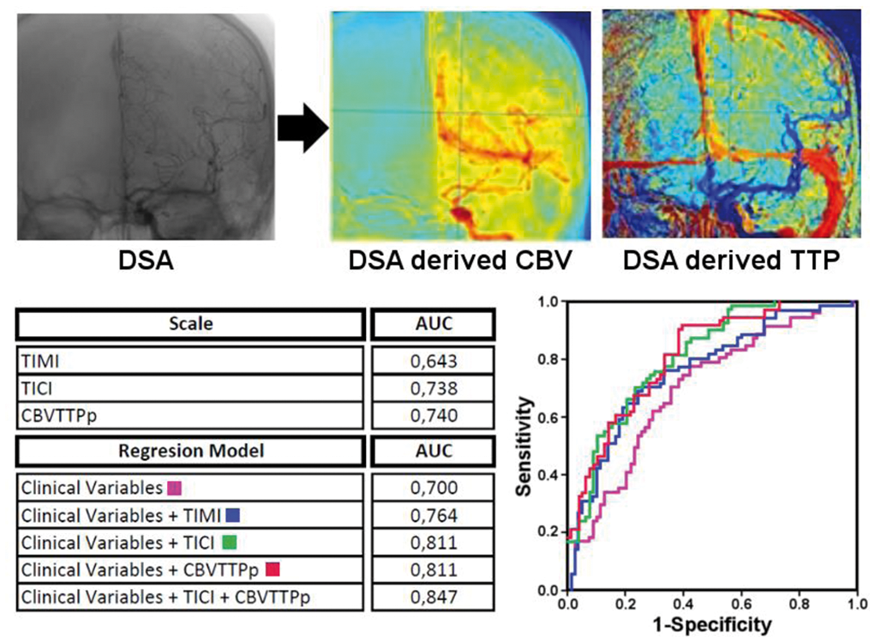
Conclusion
These results make Perfusion-Based DSA maps an attractive tool for the evaluation of reperfusion after EV and the prediction of outcomes in clinical practice.
Trial registration number
N/A
AS10-045
QUALITATIVE ASPECTS: INFARCT LOCATION IN PERFUSION CT AND CT ANGIOGRAPHY SOURCE IMAGES IN ACUTE STROKE AS PREDICTOR OF OUTCOME
1Hospital Universitario La Princesa, Neurology, Madrid, Spain
2Hospital Universitario La Princesa, Neuroradiology, Madrid, Spain
Background and Aims
In addition to infarct volume, infarct location in ASPECTS could have prognostic value. We evaluate the correlation between the involvement of different ASPECTS regions in cerebral blood volume maps of CT perfusion (CBV) and CT angiography source images (CTASI) in patients treated with endovascular therapy (ET) and their outcome.
Method
Retrospective study of consecutive patients with acute ischemic stroke in middle cerebral artery territory treated with ET in our stroke center. ASPECTS was assigned by radiologists and vascular neurologists. Clinical outcome measured using mRS at 3 months (mRS3m).
Results
N=189. 104 women (56.5%). Average age: 67.5(range: 16-100). 92(49.7%) received thrombolysis. 166(89.7%) successful recanalization (TICI≥2b). Average ASPECTS-CT: 8.06, ASPECTS-CBV:7.12, ASPECTS-CTASI:7.91. 23(12.2%) symptomatic hemorrhage. mRS3m ≤ 2: 115(63.9%). More frequently involved deep regions: insula [95(52.5%) in CBV, 101(54.9%) in CTASI] and lentiform nucleus [94(51.9%) in CBV, 88(47.8%) in CTASI]. More frequently involved cortical regions: M1 in CBV [36(19.9%)] and M5 in CTASI [36(19.9%)]. The specific involvement of caudate, lentiform nucleus, insula, M1, M2 or M5 in CBV and/or CTASI was related to worse outcome (p < 0.05). The specific involvement of M1 or M2 in CBV and M2 or M5 in CTASI was related to higher rates of symptomatic hemorrhage (p < 0.05).
Conclusion
In our study the infarct location in caudate, lentiform nucleus, insula, M1, M2 or M5 in CBV and/or CTASI was related to worse outcome. The involvement of M1 or M2 in CBV and M2 or M5 in CTASI was related to higher rates of symptomatic hemorrhage. These results support the importance of early signs of ischemia topography in stroke.
Trial registration number
N/A
AS10-046
TIME DEPENDENCY OF ASPECTS AND E-ASPECTS CORRELATION WITH INFARCT VOLUME
1Hospital Vall d'Hebron, Stroke Unit- Department of Neurology, Barcelona, Spain
2Hospital Prof Doutor Fernando Fonseca, Internal Medicine, Amadora, Portugal
3Hospital Vall d'Hebron, Department of Neuroradiology, Barcelona, Spain
Background and Aims
Alberta Stroke Program Early CT score (ASPECTS) role in predicting patients likely to benefit from endovascular therapy is not well defined. ASPECTS presents a poor interrater reliability, and an automated software (e-ASPECTS) has been created to solve this limitation.
We aim to evaluate correlation between neuroradiologist and software ASPECTS scoring with cerebral blood volume (CBV) infarct core; and correlation of basal imaging with final infarct volume in thrombectomy patients.
Method
We included patients with acute ischemic stroke and large vessel occlusion. We measured ASPECTS and e-ASPECTS on non-contrast CT and CBV infarct core on CT perfusion on admission. Final infarct volume was measured on 24-hour control CT on patients who achieved recanalization (TICI 2b-3) after endovascular thrombectomy.
Results
We included 184 patients (86,9% with MCA occlusion). Median NIHSS was 18 (IQR 13-20), mean time from symptom onset to CT was 191.25( ± 153.10) min. Complete recanalization rate was 82.1%. Median ASPECTS/e-ASPECTS were 9 (IQR 8-10 vs IQR 7.75-10), mean CBV lesion was 57.69( ± 91.70) cc.
Correlation (rs) between ASPECTS and e-ASPECTS was 0.44 (p < 0.01). ASPECTS/e-ASPECTS correlated with CBV after 180 min of symptom onset (rs=−0.26, p < 0.01 vs rs=−0.44, p < 0.05). Both ASPECTS and e-ASPECTS (rs=−0.40 vs −0.43, p < 0.01) correlated with final infarct volume in patients with complete recanalization. In a logistic regression analysis, both ASPECTS (OR 0.56, p < 0.01, CI 0.43−0.72) and e-ASPECTS (OR 0.57, p < 0.01, CI 0.44−0.73) were independent predictors of infarct volume.
Conclusion
ASPECTS and e-ASPECTS correlation with CBV was time-dependent. Both ASPECTS and e-ASPECTS predicted infarct volume after thrombectomy.
Trial registration number
N/A
AS10-049
CLINICAL FEATURES DETERMINING ACCESS TO ADVANCED THROMBECTOMY - A SERVICE IMPROVEMENT INITIATIVE
1Galway university hospital- Ireland, Geriatric and Stroke Medicine, Galway, Ireland
Background and Aims
Mechanical thrombectomy is emerging as a gold standard in acute stroke care and more patients than initially thought may benefit from this therapy. Determining why certain patients do not receive advanced imaging in the acute phase is important in ensuring future access.
Method
Over a 3 month period (October’17-January’18), data was prospectively collected on all acute stroke presentations to a tertiary stroke centre serving a catchment area population of 314,718. All acute ischemic stroke patients presenting within 24 hours of symptom onset were included. We assessed what proportion of patients received advanced imaging, such as CT angiograms (CT-A), in addition to clinical features at presentation.
Results
There were 53 acute ischemic stroke presentations within 24 hours of symptom onset. 55% of patients had clear anterior circulation symptoms, while 23% had clear posterior symptoms. Anatomical location of ischaemia was unclear at presentation in the remainder of cases. 65.4% (n = 34) of patients had CT angiograms (CT-A) performed. 77% of patients with anterior circulation symptoms underwent CT-A imaging, while only 58% of patients with posterior circulation symptoms did. Where anatomical location was unclear at symptom onset or presentation was atypical, 43% of patients underwent CT-A.
Conclusion
Not all patients presenting within 24 hours of symptom onset are receiving advanced imaging. Patients with posterior circulation symptoms and atypical features are less likely to receive advanced imaging. Resource allocation, education and refinements in our stroke pathway are essential to ensure that all potential mechanical thrombectomy candidates are detected. This area is subject to ongoing departmental audit.
Trial registration number
N/A
AS10-050
PROGNOSTIC VALUE OF “ONE STOP SHOP” COMPUTED TOMOGRAPHY (CT), CT-ANGIOGRAPHY (CTA) AND CT-PERFUSION (CTP) PATIENT’S SELECTION FOR STROKE TREATMENT BY MECHANICAL THROMBECTOMY WITH ADAPT TECHNIQUE
1Neuroradiology Unit, Radiology - Maggiore Hospital - UPO University, Novara, Italy
2Interventional Radiology Unit, Radiology - Maggiore Hospital - UPO University, Novara, Italy
3Diagnostic and Interventional Radiology, Radiology - Maggiore Hospital - UPO University, Novara, Italy
Background and Aims
To evaluate CT, CTA and CTP-derived possible predictors of stroke severity, therapeutic success and outcome in mechanical thrombectomy
Method
We treated 30 patients with anterior circulation stroke by mechanical thrombectomy with ADAPT technique. 22 received IV Tpa+endovascular treatment; 8 endovascular treatment only. All Patients underwent to CT, multiphasic CTA and CTP. ASPECTS score, clot length, clot density Ratio, clot burden score, compensatory collateral circulation, mismatch on CTP, ischemic core volume, were measured together with Good clinical outcome at discharge that was defined as an improvement of 8 points on NIHSS score or a modified Rankin Scale (mRS) ≤2, the latter repeatedat at 90 days
Results
Admission NIHSS resulted statistically related to CTP core volume (p 0,015), penumbra volume (p 0,03), clot length (p 0,017) and also premorbid mRS (p 0,001). NIHSS at discharge was predicted by CTP ASPECT (p 0,03), core volume (p 0,04), mismatch (p 0,02) and by CTA CBS (p 0,04) and extent of collaterals (p 0,025).
Good outcome at discharge was obtained in 11 patients (37%) and predicted by ASPECT on NCCT (p 0,049) and TICI (p 0,007), while outcome at 90 days was predicted by ASPECT on NCCT (p 0,048), clot length (p 0,05) and premorbid mRS (p 0,01).
Out of nine patients included by imaging with a premorbid mRS ≥2, two (22%) achieved a good outcome. Mortality at discharge was 23%, increased at 30% at 90 days.
Trial registration number
N/A
AS10-051
RADIOLOGICAL PREDICTORS OF OUTCOME IN BASILAR ARTERY STROKE: THE BASILISK STUDY
1University Hospital of la Princesa, Neurology, Madrid, Spain
2University Hospital of la Princesa, Radiology, Madrid, Spain
Background and Aims
The basilar artery occlusion (BAO) is a medical emergency with a high mortality rate. There are few radiological scores with prognostic capacity in BAO. Our main objective was to study the prognostic capacity of different radiological scales, and to compare them with the BASILISK-score (BASILar Isquemic StroKe-score), a new scale for BAO designed in our centre.
Method
Retrospective study of patients with BAO treated with endovascular therapy in our hospital, excluding non-revascularized patients. Different radiological scores of vertebrobasilar circulation (pc-CTA and BATMAN) and the BASILISK-score were applied in CT-angiography. The BASILISK scale has a score of 10 points. The points are subtracted according to the lack of opacification of different territories of the vertebrobasilar circulation, with higher value for the absence of posterior communicating artery and cerebellar arteries located at middle BAO as main collateral pathways. All scores were correlated with outcome, measured with the mRS at 3 months (3m-mRS).
Results
19 patients. Women 36% (n = 7). Mean age 60,9 years old (SD:15.3). Median NIHSS 6(3-14), median GSC 14(6-15), median mRS3m 3(0-6), three-month death 21.6% (n = 6). Mean time from onset to CT 246.8min (SD:168.4), mean time from CT to recanalization 170.3min (SD:89.8). Primary thrombectomy 63.2% (n = 12). Indeterminate etiology 52.6% (n = 10), cardioembolic etiology 26.3% (n = 5). Association was found between 3m-mRS and the BATMAN-score (Rho Spearman = −0.68, p = 0.004. COR curve: AUC p = 004, Rho Spearman = −0,68) and the BASILISK-score (Rho Spearman = −0.73, p = 0.001. COR curve:AUC p = 001; Rho Spearman = −0,73).
Conclusion
Despite the small number of patients in our study, a good prognostic correlation was found with different radiological scores in patients with BAO. There are more ongoing studies to define the usefulness of BASILISK score in clinical practice.
Trial registration number
N/A
AS10-052
PSEUDOCONTINUOUS ARTERIAL SPIN LABELLING ON MAGNETIC RESONANCE IMAGING IN PATIENTS WITH CAROTID STENOSIS
1University College London, Division of Surgery and Interventional Science, London, United Kingdom
2Sapienza University, Neurosciences- Mental Health and Sensory Organs Department, Rome, Italy
3University College London, Institute of Neurology- Stroke Research Centre, London, United Kingdom
4University College London, Lysholm Department of Neuroradiology, London, United Kingdom
Background and Aims
The presence of a complete circle of Willis and good cerebral collateral circulation is critical in severe carotid stenosis. Arterial Transit Artifact (ATA) in the Arterial Spin Labelling MRI sequence has been correlated with the presence of collaterals. We aim to determine the presence of arterial transit artefacts (ATA) on advanced MR imaging in symptomatic and asymptomatic carotid stenosis patients and to evaluate its significance in these patients.
Method
Patients with internal carotid stenosis who had high resolution MRI perfusion imaging done were retrospectively included. Degree of stenosis was calculated according to NASCET criteria. Patients were divided in two groups: ≥70% and <70% carotid stenosis. Pseudocontinuous arterial spin labelling images were analysed and scored on the presence of ATA’s in both hemispheres.
Results
High resolution perfusion magnetic resonance imaging scanning was done in 54 patients, 30 patients were asymptomatic and 24 symptomatic. ATA’s were present in 6 (20%) and 14 (58%) of the patients, retrospectively (p = 0.005). 20 had <70% stenosis and 34 had >70% stenosis. No patients with >70% stenosis had ATA’s compared to 21 (62%) of the patients with ≥70% stenosis (p < 0.001).
Conclusion
Only patients with ≥70% were shown to have ATA’s. In this group of patients, the presence of ATA’s was more reliable than the degree of stenosis in discriminating symptomatic patients from asymptomatic ones.
Trial registration number
N/A
AS10-054
VITAL PHASE II: VOLUMETRIC IMPEDANCE PHASE-SHIFT SPECTROSCOPY FOR THE NONINVASIVE DETECTION OF HEMISPHERIC BIOIMPEDANCE ASYMMETRY IN A COHORT OF PATIENTS PRESENTING WITH ACUTE ISCHEMIC STROKE
1Icahn School of Medicine at Mount Sinai, Neurosurgery, New York, USA
2Lyerly Baptist Medical Center, Neurosurgery, Jacksonville, USA
3University at Buffalo, Neurosurgery, Buffalo, USA
4Wake Forest Baptist Medical Center, Neurosurgery, Winston-Salem, USA
5University of Tennessee Health Sciences Center, Neurosurgery, Memphis, USA
6Medical University of South Carolina, Neurosurgery, Charleston, USA
7University of Tennessee Health Sciences Center, Neurology, Memphis, USA
Background and Aims
Given the robust evidence supporting thrombectomy in the treatment of acute stroke, accurate triage of patients suffering severe stroke has become an imperative. We previously evaluated the Volumetric Impedance Phase Shift Spectroscopy (VIPS) device (Cerebrotech, Pleasanton, CA) in a derivation study and found that the device was able to detect severe stroke with a sensitivity of 93% and a specificity of 92%. Here we evaluate the use of this portable, easy-to-use non-invasive device for the detection of severe stroke in a population of patients presenting to the hospital as acute stroke codes.
Method
The VIPS device measures bioimpedance on each brain hemisphere separately making it sensitive to asymmetries such as those caused by emergent large vessel occlusion (ELVO). We are currently conducting a multicenter prospective study of adult patients presenting as acute stroke codes who are evaluated with this new technology. The presence or absence of LVO and other severe brain pathology is confirmed on neuroimaging including CT, MR, and/or angiography within 30 minutes of the scan.
Results
The results of this study will be complete by late April and are planned to be presented.
Conclusion
We will present the conclusions of a large scale clinical trial evaluating a new hand-held non-invasive brain scanning device that has the potential to transform stroke triage.
Trial registration number
N/A
AS10-055
PREDICTION OF THE PROGNOSIS OF INTRA-ATRIAL THROMBOLYSIS ACCORDING TO THE APPARENT DIFFUSION COEFFICIENT IN HYPERACUTE CEREBRAL INFARCTION
1Gyeongsang National University Hospital, Department of neurology, Jinju, Republic of Korea
2Jinju Korea hospital, Neurology, Jinju, Republic of Korea
Background and Aims
The apparent diffusion coefficient (ADC) of diffusion-weighted imaging (DWI) is considered to be an index of the ischemic brain damages. The aim of this study was to investigate the prognostic value of ADC of DWI in the prognosis of patients with hyperacute cerebral infarction receiving intraarterial thrombolysis.
Method
From January 2015 to December 2017, 246 patients with hyper-acute cerebral infarction (HCI, <6 h) undergoing intra-aterial thrombolytic therapy were included. DWI was conducted on all the subjects, and ADC maps were generated with Functool software to quantify ADC value. The clinical outcomes (modified Rankin Scale, mRS) of HCI patients were observed for 3 months, and prognostic factors were analyzed.
Results
The ADC values of the poor clinical outcome group (mRS > 3) were significantly higher than those of the good outcome group (mRS ≤ 3) after treatment (90 d) (all P<0.05). The initial National Institutes of Health Stroke Scale (NIHSS) score and baseline ADC value were the independent factors for the prognosis after intra-arterial thrombolysis in multiple logistic regression analysis.
Conclusion
The values of ADC of DWI in patients with hyperacute ischemic stroke may be helpful to predict the prognosis after intra-arterial thrombolysis. Intra-arterial thrombolysis could be considered in hyperacute ischemic stroke patients with radiological rating of stroke MRI.
Trial registration number
N/A
IMAGING – NON ACUTE INCLUDING NEUROSONOLOGY
AS11-002
CAROTID BODY PARAGANGLIOMAS: CONTRIBUTION OF THE VARIOUS IMAGING TECHNIQUES. A REPORT OF NINE CASES
1“Victor Babes” University of Medicine and Pharmacy, Neurology, Timisoara, Romania
2“Dr. Victor Popescu” Emergency Military Hospital, Ophthalmology, Timisoara, Romania
3“Victor Babeş” University of Medicine and Pharmacy, Surgery, Timisoara, Romania
Background and Aims
Carotid body paragangliomas (CBPGLs) are rare neoplasms of the neuroendocrine system that affect the carotid glomus. The aim is to improve their management in our Departments.
Method
This retrospective analysis reports family history, clinical presentation, imaging diagnostics, Shamblin classification, surgical treatment, complications, and the outcome of nine patients with CBPGLs.
Results
All lesions were represented by a painless unilateral cervical mass, with no functional neck tumors. One patient had two different localizations (the second one was a glomus tumor of the right pre lachrymal sac), and a family history for CBPGL. All neck tumors were diagnosed during duplex ultrasound corroborated by magnetic resonance imaging (MRI), and by magnetic resonance angiography. They presented a diameter between 3 and 5 cm (MRI). Complete sub adventitial resection of the tumor was performed in all patients, with no preoperative embolization in any of the cases. The CBPGLs were confirmed on histopathology and immunohistochemistry. Lymph node metastasis was not found in any of the cases. Mortality and perioperative stroke rates were null. Transitory cranial nerve deficit occurred in three cases without permanent palsy. After a follow-up of three years in each patient, there were no signs of tumor recurrence in any of the cases.
Conclusion
Relatively early diagnosis of CBPGL was possible in all patients using multidisciplinary management. Preoperative planning of the surgical procedure by integrated diagnostic imaging was essential in our study to operate only Shamblin group II tumors, minimizing the known risk of complications associated with large CBPGL (group III).
Trial registration number
N/A
AS11-004
PSYCHOSOMATIC SYMPTOMS DURING SOUTH EAST ASIAN HAZE CRISIS ARE RELATED TO CHANGES IN CEREBRAL HEMODYNAMICS
1National University Health System, Division of Neurology- Department of Medicine, Singapore, Singapore
2National University Health System, Department of Medicine, Singapore, Singapore
3National University Health System, Department of Psychological Medicine, Singapore, Singapore
Background and Aims
South Asian forest fires periodically led to widespread haze for a few weeks yearly. The magnitude of health effects of short-term haze exposure remains unknown. However, even some healthy individuals develop psychosomatic symptoms during acute haze crises. We investigated the effects of haze exposure on cerebral hemodynamics, presuming them to be responsible for various psychosomatic symptoms.
Method
74 healthy volunteers participated in this study. Baseline demographics, comorbidities and any new symptoms since the onset of haze were collected. Transcranial Doppler (TCD) ultrasonography was performed to record the blood flow parameters of both middle cerebral arteries (MCA), first in an indoor, air-conditioned environment and later outdoors after 30-minutes of haze exposure. The prevailing level of pollutant standards index (PSI) was recorded. Statistical analyses were performed to compare cerebral hemodynamics between symptomatic and asymptomatic groups of participants.
Results
Median age was 30 years (IQR 26-34) and 45 (60.8%) were female. 35 (47.3%) participants reported new psychosomatic systematic symptoms since haze onset. Significantly lower pulsatility index (PI) in both MCAs were noted in the symptomatic group compared to the asymptomatic group (left MCA: 0.85 vs 0.93, p < 0.001; right MCA: 0.84 vs 0.94, p < 0.001). In symptomatic participants, mean PI decreased from 0.90 to 0.84 (p < 0.008) after haze exposure. There was a moderate negative correlation between PI and number of psychosomatic symptoms experienced by the participants (r = 0.519, p < 0.001).
Conclusion
Haze causes significant alterations in cerebral hemodynamics. Healthy individuals who reported psychosomatic symptoms during the haze period were evaluated to have relatively lower PI on TCD, which represents cerebral vasodilation.
Trial registration number
N/A
AS11-005
TRANSTEMPORAL INVESTIGATION OF BRAIN PARENCHYMA ELASTICITY USING 2-D SHEAR WAVE ELASTOGRAPHY: DEFINITION OF AGE-MATCHED NORMAL VALUES
1Klinikum Augsburg, Neurology, Augsburg, Germany
2Chair and Institute of Environmental Medicine- UNIKA-T- Technical University of Munich and Helmholtz Zentrum München- Germany - German Research Center for Environmental Health- Augsburg- Germany, Center for Environmental Health, Augsburg, Germany
Background and Aims
The goal of our research was to assess the possibility of reliable investigation of brain tissue stiffness using ultrasonographic brain parenchyma elastography with an intact temporal bone.
Method
We enrolled 108 patients after exclusion of intracranial pathology or healthy volunteers. All patients were subdivided by age into groups: 20–40, 40–60 and >60 y. For statistical analysis, the χ2 test and t-test were used.
Results
The mean values, regardless of age and other parameters, were 3.34 kPa (SD = 0.59) on the left side and 3.33 kPa (SD = 0.58) on the right side. We found no correlation between the values, body mass index (r = 0.07, p = 0.48) and sex (t = −0.11, p = 0.91), but we observed a highly significant correlation between the values and age (r = 0.43, p < 0.0001).
Conclusion
We found ultrasonographic brain parenchyma elastography to be a valid, reproducible and investigator-independent method that reliably determines brain parenchyma stiffness. Normal values should serve as a reference for studies on various intracranial lesions.
Trial registration number
N/A
AS11-007
THE VALUE OF NONCONTRAST CRANIAL COMPUTED TOMOGRAPHY IN THE DIAGNOSIS OF CEREBRAL VENOUS THROMBOSIS
1Shahid Beheshty University of Medical Sciences, Student Research Committee- Faculty of Medicine, tehran, Iran
Background and Aims
With its highly variable clinical presentation, the diagnosis of cerebral venous sinus thrombosis (SVT), and especially of deep venous thrombosis (DVT), as rare but important causes of stroke is challenging. Because noncontrast cranial computed tomography is still the imaging technique of choice in most emergency departments, we aimed to investigate its value in the diagnosis of SVT and DVT.
Method
Screening our patient data base in Loghman hakim hospital in 2017, we identified 14 patients with DVT and 27 patients with SVT. We also included a control group of 40 patients who had presented with clinical signs of DVT or SVT but in whom thrombosis was subsequently excluded. MR venography was used as the reference standard. Three independent readers assessed the noncontrast cranial computed tomography for the presence of direct and indirect signs of DVT or SVT. Direct signs included the presence of hyperattenuated sinuses (ie, cord sign) or veins (ie, attenuated vein sign), whereas parenchymal edema and hemorrhage were indirect signs.
Results
The sensitivity and specificity of the attenuated vein sign for the diagnosis of DVT were 100%, and 98.7%, respectively, whereas the sensitivity and specificity of the cord sign for SVT were 59.3% and 92.5%, respectively. The sensitivity and specificity values of noncontrast cranial computed tomography were 94.1% and 96.3% for intracerebral edema and 95.1% and 97.7% for intracerebral hemorrhages, respectively.
Conclusion
Although noncontrast cranial computed tomography is insufficient to exclude a SVT, its value in the emergency diagnosis of DVT seems to be very high.
Trial registration number
N/A
AS11-008
INTRAPLAQUE HEMORRHAGE IN SYMPTOMATIC AND ASYMPTOMATIC PROGRESSIVE CAROTID ARTERY STENOSIS – PILOT STUDY
1University hospital Ostrava, Neurological, Ostrava, Czech Republic
2Charles University and University Hospital Hradec Kralove, Department of Neurology, Hradec Kralove, Czech Republic
3University hospital Ostrava, Radiological, Ostrava, Czech Republic
Background and Aims
Intraplaque hemorrhage (IPH) belongs to potential mechanisms of unstable plaque development. Study aims to compare the IPH occurrence in patients with asymptomatic stable (ASS), asymptomatic progressive (APS) and symptomatic (SS) carotid artery stenosis >50%.
Method
Serial duplex ultrasound (DUS) in a 6-month period and magnetic resonance imaging (MRI) using axial 3DT1w sequence were used for IPH detection in patients with carotid stenosis. Stenoses in patients with ipsilateral stroke/transient ischemic attack within previous 4 weeks or acute ischemic lesion on diffusion-weighted MRI were evaluated as symptomatic. Stenoses with progression of >10% since last DUS examination were evaluated as progressive. Echolucent part of atherosclerotic plaque >8 mm2 on DUS and hyperintensity on 3DT1w-MRI were evaluated as IPH. Differences in IPH occurrence between ASS, APS and SS patients were statistically evaluated.
Results
Totally 32 patients (18 males, mean age 71.3 ± 7.7 years) were enrolled during 18 months; 5 patients with ASS, 18 with APS and 9 with SS. MRI examination was not performed in 3 ASS and 1 SS patient. IPH was detected using DUS/MRI in 1 (20%)/2 (40%) of ASS patients, 9 (50%)/8 (53%) of APS patients, and 5 (56%)/4 (50%) of SS patients (p>0.05 in all cases). IPH on both DUS and MRI were detected in none of ASS patients, 5 (28%) APS patients and 3 (33%) SS patients (p>0.05 in all cases).
Conclusion
No significant difference in IPH occurrence was found between ASS, APS and SS patients. Totally 200 patients will be enrolled to the ongoing study.
Supported by grant MHCR 17-31016A, 16-30965A.
Trial registration number
N/A
AS11-009
CHRONIC DILATATION OF SUPERFICIAL TEMPORAL ARTERY AND MIDDLE MENINGEAL ARTERY ASSOCIATED WITH DEVELOPMENT OF COLLATERAL CIRCULATION AFTER BYPASS SURGERY FOR MOYAMOYA ANGIOPATHY
1Hiroshima University Graduate School of Biomedical & Health Sciences, Neurosurgery, Hiroshima, Japan
Background and Aims
The dilatation of superficial temporal artery (STA) and middle meningeal artery (MMA) were occasionally observed after bypass surgery for moyamoya angiopathy. The purpose of this study was to examine the correlation between angiographic outcomes and MR images, specifically focusing on postoperative dilatation ratio of the STA (rSTA) and MMA (rMMA).
Method
A total of 56 hemispheres in 36 consecutive patients who underwent revascularization for moyamoya angiopathy were evaluated. All patients had angiography and MR images taken before surgery and during the chronic (4.0 ± 1.73 months) phase. Angiographic outcomes were classified into two grades (Good or Poor) according to the extent of the blood supply through direct or indirect bypass, respectively. The rSTA and rMMA was calculated in time-of-flight MR angiography (MRA). The signal changes of ivy signs and flow voids in basal ganglia were also evaluated.
Results
Postoperative collaterals through direct and indirect bypass was good in 30 (53.6%) and 33 (58.9%) cases, respectively. The mean rSTA and rMMA were 36.04 ± 28.79% and 29.15 ± 22.01%, respectively. Ivy signs and flow voids were decreased in 9 (16.1%) and 26 (46.4%) cases, respectively. Univariate analyses demonstrated no significant correlation between the angiographic outcomes and postoperative signal changes on MR images. However, rSTA and rMMA were significantly correlated with good collaterals through direct and indirect bypass, respectively (P = 0.04 and < 0.001).
Conclusion
MRA may be an alternative to angiography. Both rSTA and rMMA estimated the development of collaterals after bypass surgery for moyamoya angiopathy.
Trial registration number
N/A
AS11-010
LESION PATTERNS ON DIFFUSION AND SUSCEPTIBILITY-WEIGHTED MAGNETIC RESONANCE AS A TOOL IN THE ASSESSMENT OF STROKE SUBTYPES
1Complejo Asitencial de León, Stroke Unit. Division of Neurology, LEON, Spain
2Complejo Asistencial de León, Neurology, Leon, Spain
3Complejo Asistencial de León, Stroke Unit. Division of Neurology, León, Spain
4Complejo Asistencial de León, Stroke Unit, León, Spain
5Complejo Asistencial de León, Neurology, León, Spain
6Complejo Asitencial de León, Stroke Unit. Division of Neurology, León, Spain
Background and Aims
The lesion patterns on diffusion (DWI) and susceptibility-weighted (SWI) MRI could be useful to understand the pathogenic mechanisms involved in stroke development. Some topographic patterns have been associated with a specific stroke subtype. In a prospective study, we aimed to assess the characteristics of the different DWI-SWI lesion patterns and its utility in the diagnostic workup of the acute stroke
Method
Consecutive patients with ischemic stroke and a MRI study admitted to a general hospital over a 2-year period were recruited. Lesions on DWI were divided into: 1) Cortical (single/multiple); 2) Cortico-subcortical (single/multiple); 3) Subcortical (</≥15 mm) and small scattered lesions (one/multiple vascular territories). We defined an embolic pattern as (1) multiple lesions in 1 vascular territory (anterior and posterior circulation) (fragmented infarction), (2) acute lesions in > 1 vascular territory and (3) hemorrhagic transformation (SWI). The stroke subtypes were classified by TOAST criteria.
Results
269 patients were enrolled (age 65.4 ± 13.1). 67 were classified as Large-Artery Atherosclerosis (LAA), 68 as Cardioembolic (CE), 22 as small-artery occlusion and 88 as cryptogenic stroke. We found a significant association in these lesion patterns: cortical with CE (OR 3.1; 95% CI: 1.6-5.8); small scattered lesions with LAA (OR 4.7; 95% IC 2.0-10.8). CS and cardiac abnormalities (left atrial enlargement, oval foramen, ventricular and supraventricular arrhythmias) were not associated with a specific pattern.
Conclusion
Specific lesion patterns on DWI/SWI are associated with LAA and CE stroke subtypes. We found no association between CS and a particular topographic pattern
Trial registration number
N/A
AS11-011
QUANTITATIVE ANALYSIS OF BASAL MOYAMOYA VESSELS AND REVASCULARIZATION AREAS AFTER BYPASS SURGERY IN ADULT MOYAMOYA DISEASE
1Seoul National University College of Medicine, Department of Neurosurgery, Seoul, Republic of Korea
2Hallym University College of Medicine, Neurosurgery, Pyeongchon, Republic of Korea
3Hallym University College of Medicine, Neurosurgery, Chuncheon, Republic of Korea
Background and Aims
Quatitative angiographic analysis of basal moyamoya vessels (MMV) and revascularization extent after bypass surgery in adult Moyamoya Disease (MMD) has not been reported. We aimed to quantitatively analyze the extent change of basal MMV and revascularization areas after bypass surgery to evaluate the effectiveness of revascularization surgery in adult MMD.
Method
A total of 168 hemispheres in 135 consecutive patients were retrospectively reviewed. We performed indirect bypass surgery in 81 hemispheres, and combined bypass surgery in 87 hemispheres. The mean interval between surgery and follow-up angiography was 13.2 ± 15.2 months (range, 1-121 months). Image analysis program (M-view: Marotech®) was used for the analysis. We assessed the association between independent variables and the extent of basal MMV, and also investigated the correlation between the decreased extent of basal MMV and the extent of revascularization.
Results
The mean values for the extent of pre- and postoperative basal MMV were 25.7% and 19.9%, respectively. Statistically, a more significant reduction of basal MMV was observed in the combined surgery group compared to the indirect-only group (OR, 2.02; 95% CI, 1.02 to 3.98; P = 0.043). Combined bypass surgery resulted in more favorable extent of revascularization compared with indirect bypass surgery (57.8% vs 44.3%, p < 0.001). The decreased extent of basal MMV had statistically significant relations to the extent of revascularization (p < 0.01).
Conclusion
Favorable revascularization achieved by bypass surgery has a role in reducing the extent of basal MMV in adult moyamoya disease.
Trial registration number
N/A
AS11-012
TMAX AND TMAX-TIME INDEX FROM CT PERFUSION PREDICT THE PROGNOSIS OF PATIENTS WITH ACUTE ANTERIOR ISCHEMIC STROKE AFTER THROMBOLYSIS
1Drum Tower Hospital- Nanjing University Medical School, Department of Neurology, NanJing, China
2GE Healthcare, Medicine, Shanghai, China
3Massachusetts General Hospital- Harvard Medical School, Neurology, Boston, USA
Background and Aims
Time-to-maximum (Tmax) by computed tomography perfusion (CTP) could be used to predict the early reperfusion and brain tissue outcome in patients with acute ischemic stroke. This study aims to show that the clinical prognosis of acute ischemic stroke after rt-PA thrombolysis can be predicted by Tmax and Tmax-time index fromCT perfusion.
Method
We screened patients who underwent CTP imaging scan from March 2014 through September 2017. Patients with acute anterior ischemic stroke who treated with rt-PA thrombolysis and underwent CT perfusion imaging within 48 hours of thrombolysis were enrolled. All of those patients were followed up for 3 months. The association of Tmax, Tmax-time index with 90 day Modified Rankin Scale (mRS)≤1 were examined using receive operating characteristic analysis (ROC) and Cox regression model analysis.
Results
Of 47 patients, 26 were treated with rt-PA thrombolysis and underwent CT perfusion within 48 hours of thrombolysis; of which 7 (26.9%) patients 90 days mRS≤1. ROC revealed that Tmax<1.25s (AUC=0.805, P = 0.019), Tmax/time<1.08 (AUC=0.842, P = 0.009) were the optimal thresholds. Tmax<1.25 s is prediction of 90 days mRS≤1 with sensitivity of 94.7%, specificity of 57.1%. Tmax/time is prediction of 90 days mRS≤1 with sensitivity of 89.5%, specificity of 85.7%. Tmax/time <1.08 is independently predictive of 90 days mRS≤1 in Multivariate analysis with the Cox regression models (P<0.05).
Conclusion
Tmax and Tmax-time index from CT perfusion imaging can predict the clinical prognosis of patients with acute ischemic stroke after thrombolysis, in which Tmax-time performance is better.
Trial registration number
N/A
AS11-013
CALCIFICATIONS OF THE INTRACRANIAL CAROTID ARTERY SELDOM CAUSE STENOSIS: A 4D FLOW MRI STUDY
1Umea University, Pharmacology and Clinical Neuroscience, Umeå, Sweden
2Umea University, Department of Radiation Sciences, Umeå, Sweden
Background and Aims
Up to 75% of strokes have been reported to be independently associated with calcifications in the intracranial internal carotid artery (IICA). This association is unlikely caused by IICA calcifications marking severe stenoses (>50%), such stenoses are rare. However, the mechanism might be marking moderate atherosclerotic IICA stenosis (<50%). Moderate IICA stenoses are hard to assess with existing techniques. The aim of this study was to assess possible associations between IICA calcification, IICA stenosis and clinical features.
Method
Thirty-four patients with recent ischemic stroke/TIA were examined with 4D flow MRI and Computed Tomography Angiography (CTA), and 36 controls were examined with 4D flow MRI. Stenoses were assessed with 4D flow MRI and CTA. Both moderate (<50%) and severe (≥50%) stenoses were considered. Calcifications were assessed with CTA.
Results
Eighteen stenoses were detected, 17% (3/18) were severe and 83% (15/18) were moderate (22-47%). The stenoses were similarly common in IICAs ipsilateral to recent ischemic stroke/TIA (12%), in contralateral IICAs (18%) and in controls (11%), p = 0.64. Among patients with stroke or TIA, a stenosis was seen in 21%, 11% and 1% of IICA segments with severe, moderate and no calcification respectively (p = 0.002).
Conclusion
Stenoses were more common in IICA segments with severe calcifications than in segments with less calcifications. However, it seems that the association between IICA calcifications and stroke is not by marking moderate stenosis as a vast majority of calcified IICA segments did not have a stenosis and the stenoses found were not more common on the ipsilateral side.
Trial registration number
N/A
AS11-015
DISASSOCIATION OF DEFAULT MODE NETWORK SUBSYSTEMS IN HYPERTENSIVE PATIENTS WITHOUT COGNITIVE IMPAIRMENT
1Drum Tower Hospital- Nanjing University Medical School, Department of Neurology, NanJing, China
Background and Aims
Hypertension has a close affinity with brain degeneration and cognitivedecline during the aging process. The default mode network (DMN) plays an important role in the regulation of cognitive function, it is also sensitive to damage in patients with hypertension. The variation of brain’s resting state (RS) functional connectivity (FC) indifferent default mode network subsystems is probably vital to explore neural mechanisms of hypertension on cognitive impairment.
Method
The current research explored abnormalities ofRSFC within the DMN from 30 hypertensive patients with normal cognition (HTN-NC), 25 hypertensive patients with cognitive impairment (HTN-CI) and 19 controls (NT-NC) byseed based analysis.
Results
The FC of HTN-CI was higher than the other two groups despite of the brain regions. However, it showed a DMN subsystems disconnection in the HTN-NC group. Moreimportantly, we found that higher FC activation in dorsal medial subsystems was associated with worsecognitive function. Furthermore, the index related to white matter didn’t correlate with the FC value in our study.
Conclusion
The results demonstrated that the pattern of DMN FC varied in hypertensive patients during different periods of cognitive decline, and the FC alterations in hypertensive patients with normal cognition showed disassociation of DMN subsystems. Those explorations could be predictions for the hypertension induced cognitive impairment and provided us with elicitation about the potential neural mechanism of cognitive decline in hypertensive people.
Trial registration number
N/A
AS11-016
REVERSIBLE DEFICITS OF FUNCTIONAL BRAIN CONNECTIVITY IN PATIENTS WITH CAROTID ARTERY STENOSIS
1University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
2University Medical Center Hamburg-Eppendorf, Department of Diagnostic and Interventional Neuroradiology, Hamburg, Germany
Background and Aims
Carotid artery stenosis is a well-known risk factor for ischemic stroke. Moreover, even in the absence of stroke, asymptomatic carotid stenosis has been associated with cognitive impairment. It has been suggested that disturbed functional brain connectivity might underlie cognitive impairment in asymptomatic carotid stenosis in the absence of structural brain damage. If so, then carotid revascularization should have an effect on the hypothesized brain network disturbances in these patients.
Method
We studied resting-state 64-channel EEG in 12 patients with high grade (≥70%) asymptomatic carotid stenosis before and 30 days after revascularization (carotid endarterectomy or carotid artery stenting). Data were compared with 23 controls of comparable age. We investigated the imaginary EEG coherence in a motor network located within the affected (stenosis side) and unaffected middle cerebral artery territory.
Results
At baseline, we observed decreased connectivity of the alpha (8 – 13 Hz) and beta (14 – 25 Hz) frequency band of EEG oscillations in patients with carotid stenosis compared with healthy controls, particularly on the affected side. After revascularization, a significant increase of functional connectivity was observed. At 6 – 8 weeks after revascularization, patients did not significantly differ from healthy controls anymore.
Conclusion
In summary, we identified oscillatory connectivity changes in asymptomatic patients with impaired brain perfusion resulting from carotid artery stenosis, that normalized after restoration of cerebral blood flow. Hence, electrophysiological changes might be a reversible precursor preceding macroscopic structural damage and behavioral impairment in patients with asymptomatic carotid stenosis.
Trial registration number
N/A
AS11-017
A NEW IMAGING TECHNIQUE TO MONITOR DISEASE ACTIVITY IN SUSAC SYNDROME?
1AZ Sint-Jan Brugge-Oostende AV, Neurology, Brugge, Belgium
2AZ Sint-Jan Brugge-Oostende AV, Internal Medicine, Brugge, Belgium
3AZ Sint-Jan Brugge-Oostende AV, Ophtalmology, Brugge, Belgium
4AZ Sint-Jan Brugge-Oostende AV, Radiology, Brugge, Belgium
Background and Aims
Susac syndrome is a rare auto-immune disorder. It often (though not exclusively) affects young women. Pathophysiologically, it is a non-vasculitic microangiopathy, with involvement of the small vessels of the brain, retina and inner ear, leading to headache, encephalopathy, visual disturbances and sensorineural hearing loss as the key clinical symptoms (1). It can cause significant morbidity if not treated adequately. Aggressive immunosuppressive treatment is therefore justified, but disease course and duration are highly variable. Treatment and disease activity monitoring is through clinical and imaging follow-up.
Method
High resolution black-blood contrast-enhanced T1 images were acquired in a patient with Susac syndrome upon diagnosis and during treatment follow-up.
Results
In our patient, there were several sulcal enhancements visible on this sequence, as demonstrated in Figure 1. Although Susac syndrome is not considered a vasculitis, it appears to show similar findings. Upon follow-up MRI, these black blood sequences were repeated, and each time, sulcal enhancement became less visible. It disappeared completely 6 months after treatment initiation. The patient was also clinically stable at this time. Ten months after diagnosis, the patient had a relapse. At that time, fluo-angiography and black blood imaging demonstrated disease activity, although on DWI no new lesions were detected.
Conclusion
High resolution black-blood contrast-enhanced T1 images might be useful as an imaging marker of disease activity in Susac syndrome and more sensitive than DWI images. Further studies are needed to confirm these results.
Trial registration number
N/A
AS11-018
HIGH INCIDENCE OF MICROBLEEDS ON SWI BRAIN MRI IN QATAR INTRACEREBRAL HEMORRHAGE POPULATION
1Hamad General Hospital, Neurology, Doha, Qatar
Background and Aims
Cerebral microbleed (CMB) on brain MRI is seen in higher frequency in patients with hypertension and may increase risk of intracerebral hemorrhage (ICH)
Our study’s aim was to evaluate the incidence of CMB on brain MRI among ICH patients in Qatar.
Results
584 patients were included in our analysis. Mean age 52+/−12, Sex: M/F: 497/86 (85/15%), GCS:11+/−4, SBP 179+/−35, DBP: 102+/−26. 218 patients underwent brain MRI. CMB were evident in 119/218 cases (55%), mean number of CMBs 9+/−10, median 5 (IQ range: 3-11).
The distribution of CMBs was: superficial (11/119, 9%), deep (52/119, 44%) and diffuse (56/119,47%). Macrobleeds were present in 16/119 cases (13%).
CMBs mainly seen in basal ganglia ICH (45/119, 38%) followed by lobar ICH (41/119,35%). CMBs were related to hypertension (76/119, 64%) and possible hypertension-related (32/119, 27%). Cerebral amyloid angiopathy was suspected in only 6/119, 5% (P < 0.001) of patients.
In the logistic regression analysis, the main risk factors for CMBs were: Hypertension (OR 2.11, CI95%:1.1-4, P = 0.024). In addition, hypertension as an etiology of ICH remained the main predictor of CMBs (adjOR: 3, CI95%:1.3-7, P = 0.013)
Conclusion
CMBs are very common on SWI brain MRI in ICH population. This may be explained by the high prevalence of hypertension in our population
Trial registration number
N/A
AS11-019
HIGH INCIDENCE OF LACUNAR STROKES ON BRAIN MRI IN QATAR INTRACEREBRAL HEMORHAGE POPULATION
1Hamad General Hospital, Neurology, Doha, Qatar
Background and Aims
Our study’s aim is to evaluate the incidence of lacunar strokes and white matter disease and distribution on brain MRI among hemorrhagic stroke patients in Qatar
Method
Our stroke database prospectively collects information on all suspected stroke in our hospital. Patients who suffered from ICH and had brain MRI were included in our study
The following MRI sequences were reviewed:T2 and Flair. The presence of diffuse white matter disease, location and distribution of lacunes were defined in each case.
Results
584 patients were included in our analysis who suffered from ICH.218 patients had brain MRI.
Lacunes were seen in 126/218 cases (58%), mean number of lacunes 9 +/− 6.
The distribution of lacunes: superficial (7/126, 6%), deep (37/126, 29%) and diffuse (84/126, 66%). Diffuse white matter disease were present in 53/216 cases (25%).
Lacunes are mainly seen in the presence of basal ganglia ICH (54/126, 43%) followed by lobar ICH (35/126, 28%) then cerebellar ICH (14/126, 11%) and in the presence of HTN-related ICH (81/126, 64%) and possible-HTN related ICH (33/126, 26%) and only in 4/126, 3% cases with cerebral amyloid angiopathy.(P = 0.003)
In the logistic regression analysis, the main risk factors for lacunes on brain MRI are HTN as risk factor (adjOR 3, CI95%:1.5-6.2, P =0.002) and age (adjOR:1.1, CI95%:1.01-1.09, P<0.001). HTN as an etiology of ICH remains the main predictor of lacunar stroke (adjOR: 3.1, CI95%:1.3-7.3, P = 0.013
Conclusion
Lacunar strokes and White matter disease are very common on brain MRI of patients with ICH. This could be explained by the etiology of HTN.
Trial registration number
N/A
AS11-020
CORONARY ARTERY DISEASE, STROKE AND CAROTID PLAQUE CHARACTERISTICS
1Aristotelian University, A Department of Neurology- AHEPA Hospital, Thessaloniki, Greece
2Gennimatas Hospital, Department of Radiology, Thessaloniki, Greece
Background and Aims
It has been demonstrated that ultrasonic tissue characteristics of carotid plaques and stenosis determine the development of cerebrovascular accident (CVA). The aim of this study was to examine whether the aforementioned indices of plaques constitute associates of myocardial infarction (MI) and CVA.
Method
Analysis involved imaging by duplex of 150 carotid plaques (84 symptomatic, 66 asymptomatic) of more than 50% stenosis on one side and less than 50% stenosis on the other (150 patients, side under study: that of more than 50% stenosis). The images of plaques were analyzed in a computer in a standard way and the Grey Scale Median (GSM) of each was evaluated to distinguish dark (low GSM) from bright (high GSM) plaques. Stenosis was evaluated on duplex. MI was determined on electrocardiographic grounds (n = 42/150, 28%).
Results
Patients with CVA and MI (n = 21) were associated with carotid plaques of tight stenosis (median value: 90%), and hypoechoic nature (median GSM = 0). The corresponding values of stenosis and GSM for the patients in the remaining groups were: with CVA only (n = 63, 80%, 5), MI only (n = 21, 80%, 23) and completely asymptomatic (n = 45, 65%, 29) (p < 0.001).
Conclusion
Our results suggested that stenosis and GSM of carotid plaques constitute associates of MI and CVA. This position might be solidified in natural history studies of asymptomatic individuals (in terms of MI and stroke) with carotid plaques, having as an end point the development of MI and CVA.
Trial registration number
N/A
AS11-021
DEVELOPMENT OF CEREBRAL ANEURYSM CLIPS TO MINIMIZE SUSCEPTIBILITY ARTIFACT BY MAGNETIC RESONANCE IMAGING
1Boramae Medical Center, Neurosurgery, Seoul, Republic of Korea
2Seoul National University Hospital, Neurosurgery, Seoul, Republic of Korea
Background and Aims
Surgical clipping is a major treatment modality in treating cerebral aneurysms. However, in magnetic resonance (MR) imaging, susceptibility artifact due to metal clips impedes postoperative assessments of clipped aneurysms, parent arteries, and adjacent parenchyma. Our goal was to develop an MR-compatible aneurysm clip.
Method
To reconcile mechanical/biologic properties with MR demands, we fabricated a prototypic clip (ZC: straight, 9-mm long), made of zirconia (body) and polyurethane (spring). Mechanical properties, closing forces, open-blade width, and artifact volumes (in vitro and in vivo) by 3T MR imaging of ZC and currently available metal clips (Yasargil [YC: curved, 8.3-mm long] and Sugita [SC: straight, 10-mm long]) were compared, using a canine venous pouch sneurysm model for in vivo study.
Results
Respective closing force (N) values, measured at 1-mm and 8-mm distances from blade tip, were 2.09 and 3.77 in YC, 1.85 and 3.04 in SC, and 2.05 and 4.60 in ZC. Maximum open-blade widths (mm) were 6.8, 9.0, and 3.0 in YC, SC, and ZC, respectively. In vitro artifact volumes of YC and ZC were 26.0- and 1.9-fold greater than corresponding actual volumes. In vivo artifact volumes of YC, SC, and ZC were 21.4-, 29.4-, and 2.6-fold greater than actual volumes.
Conclusion
Compared with two clips in current use, our prototypic clip showed the least susceptibility artifact, with satisfactory closing forces. However, its narrow open-blade width was a weak point. Further experimentation is needed for design refinements and durability testing before human application is feasible.
Trial registration number
N/A
AS11-022
USEFULNESS OF PLAQUE MAGNETIC RESONANCE IMAGING TO DECIDE ON THE TREATMENT MODALITY IN RECURRENT ISCHEMIC STROKE PATIENTS IRRESPECTIVE OF THE DEGREE OF STENOSIS
1Wonkwang University and Hospital, Neurosurgery, Iksan, Republic of Korea
Background and Aims
Measurement of the degree of stenosis is not enough to decide on the treatment strategy for patients with carotid stenosis. Plaque morphology examination is needed for such a decision-making. Thus, we evaluated the usefulness of plaque magnetic resonance imaging (MRI) to decide on the modality of treatment for patients with carotid atherosclerotic plaques.
Method
Fifteen patients presenting with carotid stenosis during recent 2 years were included. They underwent angiography for measurement of the degree of stenosis. Carotid plaques were visualized using MRI.
Results
There were six (40%) stable and nine (60%) unstable plaques. Seven symptomatic patients (77.7%) had unstable lesions and two symptomatic patients (33.3%) had stable lesions ( p = 0.096). There were six (40%) intraplaque hemorrhage (IPH) cases. There were six symptomatic patients (100%) in the IPH group and three symptomatic patients (33.3%) in the non-IPH group ( p = 0.013). The mean stenosis degree was 58.9% in the IPH group and 70.4% in the non-IPH group ( p = 0.094). Symptoms occurred irrespective of the degree of the stenosis in the IPH groups. In the IPH group, the recurrent ischemic cerebrovascular event rate was 33.3%. Particularly, the recurrent ischemic cerebrovascular event rate was 66.7% in the IPH group with mild stenosis treated with medications.
Conclusion
IPH in plaque MRI is significantly associated with ischemic symptoms and has a high risk for subsequent ischemic cerebrovascular events irrespective of the degree of stenosis. Plaque MRI is a useful tool to decide on the modality of treatment in recurrent ischemic stroke patients.
Trial registration number
N/A
AS11-023
PERSISTENTLY ELEVATED MICROVASCULAR RESISTANCE POST-RECANALIZATION ON TRANSCRANIAL DOPPLER: A CLINICAL MARKER OF NO-REFLOW PHENOMENON?
1Austin Health, Department of Neurology, Heidelberg- Melbourne, Australia
Background and Aims
Capillary dysfunction with impaired microvascular reperfusion post-recanalization (no-reflow) is observed in animal models but has not been conclusively demonstrated in humans. This phenomenon could be a potential therapeutic target to improve outcomes after recanalization.
We investigate the utility of Transcranial Doppler (TCD) in detecting acute microvascular changes post-recanalization in stroke patients as a novel biomarker of the no-reflow phenomenon.
Method
Consecutive patients with recanalized acute MCA occlusion by thrombectomy (TICI IIb/III) at a Comprehensive Stroke Centre with high-volume neurovascular laboratory were retrospectively identified (2013-2017). Neurosonographic measures of microvascular resistance (Pulsatility Index [PI] and Resistive Index [RI]) on acute follow-up TCD (within 3-days) were compared between patients and aged-and-gender-matched controls. Radiological outcome was assessed by CT/MRI-ASPECT with ECASS post-treatment hemorrhage classification.
Results
Among 53 patients, the median age and presenting NIHSS was 75 (IQR 66-83) and 15 (IQR 9-19). MCA-PI were frequently asymmetrically-increased (>20%) in the ischemic hemisphere post-recanalization (30.2% vs 7.7%, p = 0.001) regardless of final infarct volume. Absolute values of MCA-PI (47.6% vs 16.0%, p = 0.027) and MCA-RI (19.1% vs 0.0%, p = 0.037) were more frequently elevated beyond normal-ranges compared to controls.
Elevated MCA-PI was associated with less Hemorrhagic Infarction (9.5% vs 45.8%, p = 0.009) and elevated MCA-RI with less peri-infarct hemorrhage of any types (0.0% vs 43.2%, p = 0.037).
Conclusion
Persistently elevated microvascular resistance within the ischemic territory is demonstrable by follow-up TCD and may represent a readily-obtainable clinical biomarker of the no-reflow phenomenon. Larger confirmatory clinical studies evaluating the role of persistent microvascular dysfunction in reperfusion injury are warranted.
Trial registration number
N/A
AS11-024
VALIDATION AND OPTIMIZATION OF BIANCA FOR THE AUTOMATIC SEGMENTATION OF EXTENSIVE WHITE MATTER HYPERINTENSITIES
1Hôpital Lariboisière- APHP, neurologie, PARIS, France
2Huashan Hospital- Fudan University, Neurology, Shanghai, China
Background and Aims
White matter hyperintensities (WMH) are a hallmark of small vessel diseases. Yet, no automated segmentation method is readily and widely used, especially in patients with extensive WMH where lesions are close to the cerebral cortex. BIANCA (Brain Intensity AbNormality Classification Algorithm) is a new fully automated, supervised method for WMH segmentation. In this study, we optimized and compared BIANCA against a reference method with manual editing in a cohort of patients with extensive WMH.
Method
This was achieved in two datasets: a clinical protocol with 90 patients having 2-dimensional FLAIR and an advanced protocol with 66 patients having 3-dimensional FLAIR. We first determined simultaneously which input modalities (FLAIR alone or FLAIR + T1) and which training sets were better compared to the reference. Three strategies for the selection of the threshold that is applied to the probabilistic output of BIANCA were then evaluated. Accuracy of the segmentation was assessed through measures of spatial agreement and volumetric correspondence with respect to reference segmentation.
Results
We identified multimodal inputs (FLAIR + T1), mixed WMH load training set and individual threshold selection as the best conditions to automatically segment WMH in our cohort. A median Dice similarity index of 0.80 (0.80) and an intraclass correlation coefficient of 0.97 (0.98) were obtained for the clinical (advanced) protocol.
Conclusion
Our results suggest that BIANCA is a reliable and fast automatic segmentation method to extract masks of WMH in patients with extensive lesions.
Trial registration number
N/A
AS11-025
HIGH RESOLUTION IMAGING OF REMOTE WHITE MATTER STRUCTURES IN STROKE
1Florey Institute of Neuroscience and Mental Health, Neurorehabilitation, Melbourne, Australia
2Florey Institute of Neuroscience and Mental Health, Imaging, Melbourne, Australia
3LaTrobe University, School of Allied Health, Melbourne, Australia
Background and Aims
Diffusion MRI is key in visualizing white matter (WM) structures. Acquisition resolution is coarse compared to the smaller structures in the brain. This limits spatial resolution of WM structures in fractional anisotropy (FA) maps. Track density imaging (TDI) (Calamante,2010) is designed to achieve super resolution maps with resolutions of a few hundred micrometres. Examples of directionally encoded colour (DEC) maps for both FA and TDI are shown highlighting the superiority of DEC-TDI visualise white matter structures in the somatosensory regions.
Method
Data from one healthy and 1 randomly chosen patient that were a subset of a larger longitudinal stroke study are shown. All patients were >3 months post stroke, and had lesions. MRI was acquired on a 3T Siemens Trio scanner including a T1 and diffusion imaging (b=3000, 60 directions, 2.5mm isotropic). Diffusion data was processed with MRtrix3 (www.mrtrix.org).
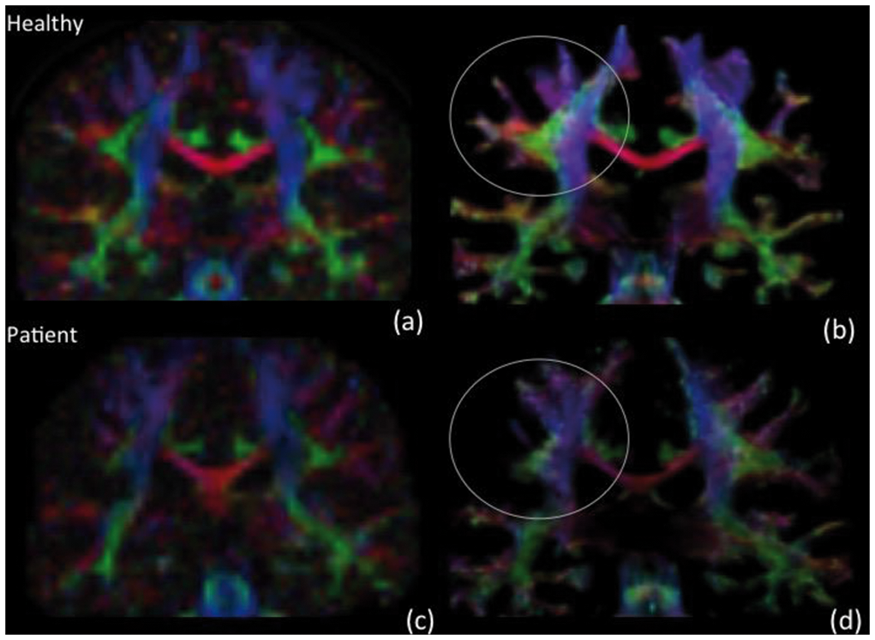
Figure 1 shows a healthy volunteer and 1 stroke patient with sensory deficits on each row. Columns show DEC-FA(a,c) and DEC-TDI(b,d) maps for these subjects. Patient shown had impaired performance in a somatosensory test (tactile discrimination task; a score of 34 compared to a normal score of >50). DEC-TDI allows surviving WM structures close and remote to the damaged sensory regions to be visualised.
Conclusion
TDI is being used in clinical studies (Toselli,2017) due to its ability to provide clearer contrast of WM structures compared to standard DTI techniques. TDI could identify remote WM structures implicated in plasticity associated with recovery due to its improved visualisation of smaller structures.
Trial registration number
n/a
AS11-027
VESSEL WALL IMAGING IN YOUNG ISCHEMIC STROKE PATIENTS
1Donders Institute for Brain Cognition and Behaviour - Radboudumc, Neurology, Nijmegen, The Netherlands
2Radboud University Nijmegen Medical Center, Radiology- Nuclear medicine, Nijmegen, The Netherlands
Background and Aims
high-resolution vessel wall (VW) MRI is a promising technique to directly evaluate the arterial wall. This technique may reveal intra- and extracranial VW abnormalities otherwise not visible on conventional luminography techniques, such as CT-angiography or MR-angiography (MRA). The aim of this study is to evaluate VW abnormalities in young ischemic stroke patients.
Method
in this prospective study, we included 38 consecutive patients with ischemic stroke or TIA aged 18-50 years (mean age 40.6 years [SD 8.2]; 55% male (table 1)), who underwent high-resolution VW-MRI. All MR scans were evaluated by an experienced neuroradiologist.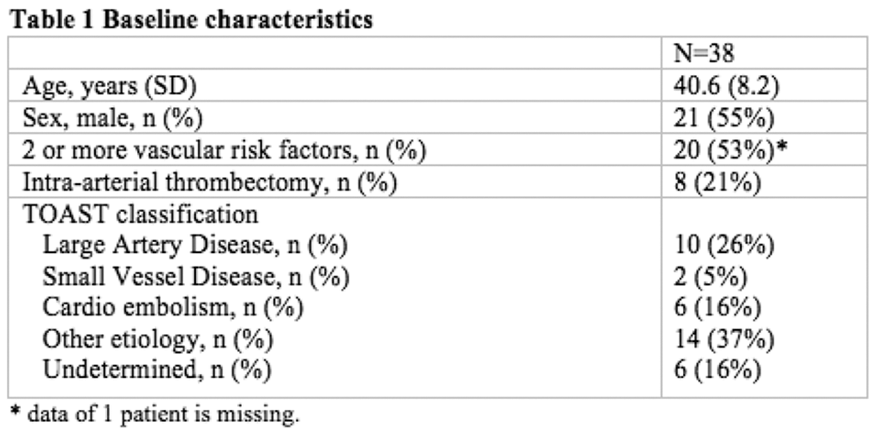
Results
20 patients had MRA abnormalities that were mainly located intracranially (18 patients). These abnormalities included arteriopathies due atherosclerosis (n = 10), vasculitis (n = 1), dissection (n = 3) and post-radiation (n = 1). VW enhancement was detected in 11 patients with MR-angiography abnormalities, 82% located intracranially (table 2). 55% of the enhancement was caused by atherosclerosis. Cerebral vasculitis was diagnosed in 1 patient, who had VW enhancement. None of the patients with carotid dissection had VW enhancement. There were less men with MRA abnormalities with enhancement than without enhancement (73% vs. 27% respectively; p = 0.033).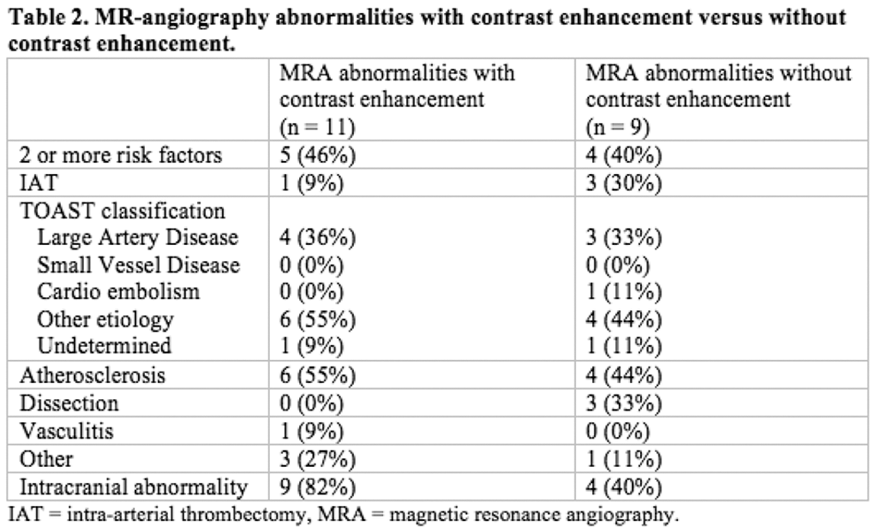
Conclusion
MRA abnormalities, especially located intracranially, are a common finding in young ischemic stroke patients. VW enhancement can be detected in more than 50% of the cases, mainly caused by atherosclerosis. Further research is needed to reliably differentiate the underlying pathologies of the enhancement and the added value of this technique with regard to prognosis.
Trial registration number
N/A
AS11-028
INTERHEMISPHERIC WHITE MATTER INTEGRITY RELATES TO CORTICAL ATROPHY CONTRALESIONAL TO SUBCORTICAL MOTOR STROKE
1University Medical Hospital Hamburg Eppendorf, Neurology, Hamburg, Germany
2University Medical Hospital Hamburg Eppendorf, Neuroloradiology, Hamburg, Germany
Background and Aims
Following acute ischemic stroke, subcortical stroke lesions may induce gray matter atrophy in anatomically connected, yet distant brain regions. Cortical thinning has also been shown on hemispheres contralateral to stroke lesions, most likely due to degeneration of transcallosal, cortico-cortical pathways. In this study, we expand on previous studies by analyzing changes of cortical thickness in contralateral, homologous brain regions indirectly linked to primary stroke lesions via anatomically connected ipsilateral cortical areas.
Method
For this purpose, stroke patients were serially studied by magnetic resonance imaging including diffusion tensor imaging (DTI) and high-resolution anatomical brain imaging. We analyzed changes of gray and white matter integrity from 22 stroke patients (median age 68 years) with upper extremity paresis. Probabilistic fibre tractography was applied to DTI data to identify brain regions connected to stroke lesions and contralesional homologeous areas. Cortical thickness was quantified by semi-automatic measurement (Freesurfer), fractional anisotropy was analyzed to study integrity of white matter pathways.
Results
Primary stroke lesions were mainly connected to cortical motor areas. One year after stroke, significant decreases of cortical thickness were detected in ipsilateral areas connected to ischemic lesions (-5.1%; 95% CI -7.8% to -2.4%, p < 0.001) as well as homologous contralesional brain regions (-3.6%; 95% CI −0.9% to -6.2%; p = 0.012). In addition, we detected specific loss of white matter integrity of both inter- and intrahemispheric white matter measured by fractional anisotropy.
Conclusion
Our results suggest that impact of subcortical lesions extends to contralesional homologous brain areas via degeneration of transcallosal pathways.
Trial registration number
n/a
AS11-029
VALUE OF 99MTC-ECD SINGLE-PHOTON EMISSION CT IN DIAGNOSIS AND RECURRENCE PREDICTION OF POST-STROKE EPILEPSY
1National Cerebral and Cardiovascular Center, Divisions of Neurology- National Cerebral and Cardiovascular Center, Suita, Japan
2National Cerebral and Cardiovascular Center, Divisions of Cerebrovascular Medicine- National Cerebral and Cardiovascular Center, Suita, Japan
Background and Aims
Several studies have shown that 99mTechnetium-Ethyl-Cysteinate-Dimer Single-Photon Emission CT (99mTc-ECD SPECT) is a useful method for identifying the epileptogenic zone localization. However, the association between the hyperperfusion area on SPECT and seizure recurrence remains unclear.
Method
We prospectively enrolled post-stroke epilepsy (PSE) patients who underwent postictal 99mTc-ECD SPECT at our hospital from November 2014 to June 2016. The area of hyperperfusion was determined by visual inspection or subtraction ictal SPECT co-registered to MRI (SISCOM). We determined whether the sides of hyperperfusion was ipsilateral to stroke lesion on CT/MRI or epileptic discharge on EEG, and whether the presence of hyperperfusion area was associated with one-year recurrence of seizure by Pearson’s chi-square test.
Results
We included 41 PSE patients (mean age, 71.6 ± 13.4 years; 61% male); among them, 20 patients (49%) had past history of ischemic stroke, 19 (46%) hemorrhagic stroke, and 2 (5%) both ischemic and hemorrhagic stroke. Hyperperfusion was observed in 22 (54%) patients, of whom 3 were detected only by SISCOM. The hyperperfusion area was ipsilateral to stroke lesion in 18 (82%) of the 22 patients, indicating that the lateralization was significantly concordant (P<0.01). All 6 (27%) patients with the epileptic discharge on EEG had ipsilateral hyperperfusion area (P = 0.01). One-year recurrence of epilepsy was identified in 12 (29%) patients but was not associated with presence of hyperperfusion on 99mTc-ECD SPECT (P = 0.32).
Conclusion
99mTc-ECD SPECT does not predict one-year recurrence of PSE but is as useful as other diagnostic modalities for identifying epileptogenic zone localization.
Trial registration number
N/A
AS11-030
FAT EMBOLISM SYNDROME: A RARE COMPLICATION OF HEMIARTHOPLASTY
1Nottingham University Hospitals NHS Trust, Stroke Medicine, Nottingham, United Kingdom
Background and Aims
A 75-year-old lady sustained a fractured neck of femur and was managed 48 hours later with a left hemi-arthroplasty. Immediately post-operatively, she became agitated with subsequently developed reduced consciousness and obtundation. There were no lateralising signs on neurological examination. Magnetic resonance imaging (Images ADC and DWI) showed very extensive small infarcts and micro-haemorrhages distributed throughout the brain including the cerebral hemispheres, cerebellar hemispheres and the brainstem in a characteristic “starfield” pattern. The appearances were consistent with cerebral fat embolism syndrome (FES) related to the recent fracture and subsequent treatment. She remained in a vegetative state and was palliated over three weeks without recovery.
Method
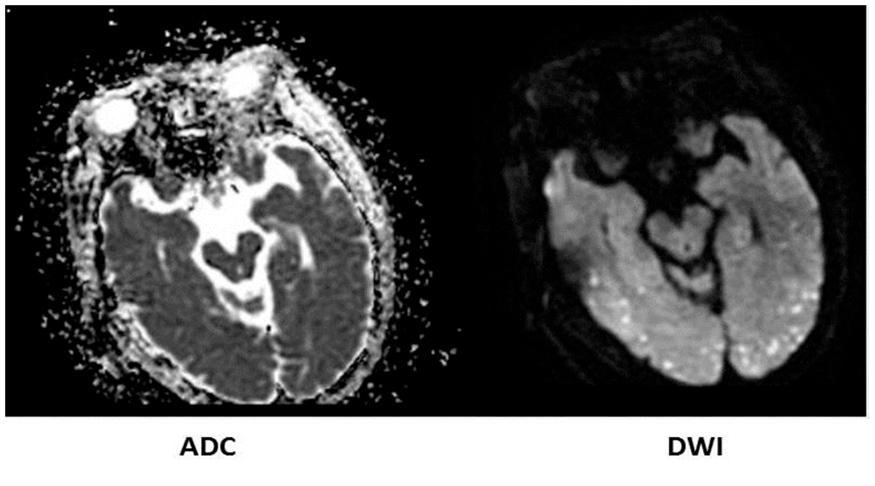
Results
NA
Conclusion
With an incidence of only 0.3% to 2.2%, Fat Embolism Syndrome (FES) is a rare complication reported primarily following long bone fractures.1 It most commonly affects the lungs or brain with the potential to affect any organ or system of the body leading to respiratory failure, neurocognitive deficits, and death in severe cases.2,3 It typically manifests 24-72 hours after the initial insult, however may rarely occur as early as 12 hours, or as late as two weeks.4 FES is a clinical diagnosis as there is no definitive laboratory test that offers confirmation. Out of current imaging modalities available, only MRI of the brain shows obvious perivascular oedema and multiple areas of infarction in a characteristic “starfield pattern”.5
Trial registration number
N/A
AS11-031
BRAIN MRI PROFILE ASSOCIATED WITH ATRIAL FIBRILLATION IN ISCHAEMIC STROKE AND TRANSIENT ISCHAEMIC ATTACK - A PROSPECTIVE COHORT STUDY
1University College Dublin and Mater University Hospital Ireland, Neurovascular Unit For Translational and Therapeutics Research and HRB Stroke Clinical Trials Network Ireland, Dublin, Ireland
2Mater University Hospital- Dublin- Ireland, Radiology Department, Dublin, Ireland
3Beaumont Hospital- Dublin- Ireland, Radiology, Dublin, Ireland
4University College Dublin and Mater University Hospital Ireland, Neurovascular Unit For Translational and Therapeutics Research and HRB Stroke Clinical Trials Network Ireland-, Dublin, Ireland
5Connolly Hospital Blanchardstown- Dublin- Ireland, Stroke, Dublin, Ireland
6Royal College of Surgeons In Ireland- Dublin- Ireland, Department of Geriatric and Stroke Medicine, Dublin, Ireland
7Mater University Hospital Ireland and Royal College of Surgeons In Ireland- Dublin- Ireland, Stroke, Dublin, Ireland
Background and Aims
Long-term ECG monitoring reveals paroxysmal atrial fibrillation (PAF) in up to 30% of patients with cryptogenic ischaemic stroke and transient ischaemic attack (TIA). However, such monitoring is not feasible for all cryptogenic stroke/TIA patients. We hypothesized that a characteristic brain MRI ‘signature’ might be over-represented in patients with atrial fibrillation (AF) and stroke, which may identify patients for targeted prolonged cardiac monitoring.
Method
We investigated clinical and MRI findings associated with AF in a prospective cohort of patients with non-severe (mRS 0-3) ischaemic stroke and TIA. Patients with any AF and those with PAF only were considered separately and compared to those without AF. Forward stepwise logistic regression was used to determine variables associated with AF and PAF.
Results
In 455 stroke (n = 217) and TIA(n = 238) patients, multiple DWI lesions in single or multiple artery territories combined (OR 2.30, CI 1.40-3.76), and multiple DWI lesions in multiple cerebral territories (OR, 3.45 CI 1.70-6.99) were independent predictors of any AF, while single subcortical DWI lesions (OR, 0.43, CI 0.22−0.84) were associated with lower likelihood of AF(model adjusted for age, sex, hypertension, current smoking and leukoaraiosis).
Multiple single-territory or multi-territory DWI lesions (OR 2.12, CI 1.06-4.25) were associated with PAF, while strong trends were observed for multiple lesions in multiple arterial territories (OR 2.44, CI 0.90-6.65) and single subcortical lesions (OR 0.35, CI 0.12-1.02).
Conclusion
Stroke and TIA related to AF is associated with a distinct clinical and MRI profile. Our study provides evidence to support the targeted use of long-term external or implantable rhythm monitoring in selected patients with cryptogenic stroke/TIA and a suggestive MRI profile
Trial registration number
N/A
AS11-032
CROSSED CEREBELLAR DIASCHISIS AFTER STROKE: A VASCULAR PHENOMENON?
1Clinical Neuroscience Center- University Hospital Zurich and University of Zurich, Neurology, Zurich, Switzerland
2Clinical Neuroscience Center- University Hospital Zurich and University of Zurich, Neurosurgery, Zurich, Switzerland
3Clinical Neuroscience Center- University Hospital Zurich, Neuroradiology, Zurich, Switzerland
Background and Aims
Crossed cerebellar diaschisis (CCD) in internal carotid artery (ICA) territory stroke refers to a reduction in blood flow and energy metabolism in the contralateral cerebellar hemisphere. CCD may be due to interruption of cerebro-cerebellar tracts, but a clear clinical correlate of CCD is lacking. We hypothesize that CCD after stroke might indicate severe supratentorial hemodynamic impairment with worse prognosis for recovery.
Method
Duplex sonography and clinical data from stroke patients with unilateral ICAO who underwent blood oxygen level dependent (BOLD)-MRI cerebrovascular reserve (CVR) assessment were analysed. The presence of CCD (either CCD+ or CCD-) was inferred from BOLD-CVR.
Results
Twenty-two patients (11/group) were included. Stroke deficits on admission and at 3 months follow-up were more severe in the CCD+ group. CCD+ patients had similar cerebellar, but lower supratentorial CVR compared to CCD- patients. Flow velocities in the P2 segment of the posterior cerebral artery (PCA) in CCD+ vs. CCD- patients were 66 vs. 47 cm/s ipsi- and 74 vs. 50 cm/s contralaterally (p = 0.02 and 0.04). All other duplex parameters were similar between both groups.
Conclusion
In patients with stroke due to ICAO, the presence of CCD indicated 1) more severe stroke deficits, 2) more reduced supratentorial CVR and 3) higher flow in both P2 segments of the PCA. The latter is likely to indicate increased compensatory collateral recruitment through leptomeningeal and PCA collaterals. Our data suggest that CCD may indeed indicate impaired cerebrovascular reserve of the affected ICA territory.
Trial registration number
N/A
AS11-033
DYNAMIC CEREBRAL AUTOREGULATION, AGE AND BLOOD PRESSURE VARIABILITY
1Kantonsspital Lucerne, Neurology and Neurorehabilittion, Lucerne 16, Switzerland
2Kantonsspital Lucerne, Neurology and Neurorehabilitation, Lucerne, Switzerland
3Kantonsspital Lucerne, Department of Radiology, Luzern, Switzerland
4ETH zürich, Automatic Control Laboratory, Zürich, Switzerland
Background and Aims
Whether dynamic cerebral autoregulation (dynCA) is influenced by age and blood pressure variability
Method
In 67 healthy controls (mean age ± SD 45 ± 16 years; 30 females) BP via fingerplethysmography, blood flow velocity (CBFV) in both middle cerebral arteries (MCA) via transcranial Doppler sonography and end-tidal CO2 (ETCO2) via capnography were simultaneously recorded. Using artifact-free recordings over a period of 5 minutes, we assessed coherence and the transfer function parameter gain and phase between BP and CBFV in the frequency ranges of VLF (0.02−0.07 Hz), LF (0.07−0.15), HF range (>0.15). Additionally, the SD of BP was used as an index of BP variability (BPV). For analysis, Pearson correlation and stepwise regression analysis were used.
Results
In the healthy controls (BP, 86 ± 13 mm Hg; ETCO2, 39 ± 4 mm Hg; BPV, 15 ± 6 mm Hg) we found an age dependency only for gain (LF, HF), phase and coherence were age independent in any frequency range. BPV correlated in both MCAs significantly (p≤0.05 – p < 0.001) with gain in the LF and HF range (r = 0.542 – 0.670) and with phase in the VLF and HF range (r = −0.291 – −0.314). ETCO2 did not correlate with gain or phase.
Conclusion
In healthy persons, only gain shows some age dependency leaving phase as an autoregulation parameter useful over all ages. BPV effects are bilaterally present in gain (LF and HF range) and phase (VLF and HF range), and might be more relevant than CO2 for modeling CBFV from BP.
Trial registration number
N/A
AS11-034
QUANTITATIVE SUSCEPTIBILITY MAPPING IN ISCHEMIC STROKE PATIENTS
1Department of Neurology, University Hospital Zurich and University of Zurich, Zurich, Switzerland
2Department of Neuroradiology, University Hospital Zurich, Zurich, Switzerland
3Medical Physics Group- Institute of Diagnostic and Interventional Radiology, Jena University Hospital, Jena, Germany
4Institute for Biomedical Engineering, University and ETH Zurich, Zurich, Switzerland
Background and Aims
Quantitative susceptibility mapping (QSM) is a novel processing method for gradient-echo magnetic resonance imaging (MRI). High signals on susceptibility maps indicate high deoxyhemoglobin content. Prominent vessels have been observed on QSM in patients with ischemic stroke. Their occurrence has been attributed to an increase in oxygen extraction fraction in misery perfused, potentially salvageable brain tissue. We aimed to characterize the susceptibility signal in the infarct and peri-infarct area after successful recanalization.
Method
MRI of patients with MCA-M1 segment occlusion 24-72h after thrombectomy were analyzed. Veins were identified using a signal threshold on susceptibility maps and manually adjusted using ImageJ (NIH). The QSM signal was analyzed within the stroke territory (identified on diffusion weighted images), the boundaries of the ipsilateral MCA territory and on the contralateral MCA territory on six preselected slices.
Results
Data from 14 stroke patients were included. Preliminary results indicate that in successfully recanalized patients, no prominent vessels with high susceptibility signal were found, but veins with reduced susceptibility signal in the infarct compared to the infarct border or contralateral side. We also noted differences in overall venous susceptibility values between patients, which we are currently analyzing further.
Conclusion
Low venous susceptibility within the infarct is caused by low deoxyhemoglobin content. It might indicate normalized oxyhemoglobin levels after recanalization or poor oxygen extraction in the infarct based on cell damage. Further correlation with infarct size and outcome will reveal the potential of QSM to yield new information about the infarcted area and its prognosis for recovery.
Trial registration number
N/A
AS11-035
INCREASED FLOW OF SUPERIOR OPHTHALMIC VEIN IN OCULAR DUPLEX AS SIGN OF ARTERIO-VENOUS FISTULA
1Hospital Universitario La Paz, Neurology, Madrid, Spain
Background and Aims
Arteriovenous fistulas (AVFs) may increase the pressure of the cavernous sinus affecting the flow of orbital vessels. Our aim was to evaluate the utility of ocular Duplex (OD) in the diagnosis and monitoring of AVFs.
Method
Prospective observational study of patients diagnosed of AVF confirmed by angiography. Consecutive OD were performed to evaluate orbital vessels and structures. Peak systolic velocity (PSV) and resistance index (RI) of the ophthalmic artery (OA) and the superior ophthalmic vein (SOV) were recorded. Anatomy of orbital structures was evaluated.
Results
Three cases were identified. Case 1: 58 year old-man presenting with proptosis and conjunctival hyperemia diagnosed of right carotid-cavernous fistula. Case 2: 65 year-old woman presenting with binocular diplopia diagnosed of dural AVF in the anterior cranial fossa dependent on the ethmoidal branches of the right ophthalmic artery. Case 3: 76 year-old woman presenting with aphasia and facial asymmetry secondary to left parietal cerebral heamorrhage due to dural AVF. Ocular Duplex showed an increase in PSV, diameter and RI at SOV in all cases as expression of high cavernous sinus pressure. As especial findings, the case of carotid-cavernous fistula has an inversion of flow at SOV at diagnosis and anterior fossa AVF has a tortuous OA with high PSV. After closure of AVFs, we found that all of OD parameters returned to normal values.
Conclusion
PSV and RI of SOV measured with OD may be useful in the diagnosis and monitoring of hemodynamic repercussion of AVFs to cavernous sinus.
Trial registration number
N/A
AS11-036
RADIATION EXPOSURE OF BRAIN IS WITHIN ACCEPTABLE RANGE EVEN WITH EXTENSIVE AND REPEATED CT-BASED NEUROIMAGING FOR ACUTE ISCHEMIC STROKE
1National University of Singapore, Neurology, Singapore, Singapore
2National University Hospital, Diagnostic Imaging, Singapore, Singapore
Background and Aims
The preferred neuroimaging in acute ischemic stroke continues to remain CT based, largely due to the widespread availability, rapid acquisition, and acceptable image quality. However, whether repeated neuroimaging leads to an increased risk of somatic and genetic effects of ionizing radiation remains debatable. Dose tracking software can automatically monitor the radiation received by patients during computerized tomography (CT) based imaging. We evaluated radiation exposure during standard imaging protocols consisting of non-contrast CT head (NCCT), CT Angiography (CTA) and CT Perfusion (CTP).
Method
Radiation data was retrieved for various CT based imaging studies, performed for ischemic stroke patients during the year 2015. The volume-weighted CT dose index, dose-length product, scan length, effective dose and whole body integral dose were extracted from dose-tracking software. Radiation doses for brain, skin, eye, thyroid and red bone marrow were extracted.
Results
The radiation data for brain imaging for NCCT (n =391), CTA (n = 149) and CTP (n = 61) were retrieved from the institutional dose tracking system attached to a dedicated CT scanners (Phillips iCT256 with iDose4). The calculated effective doses for NCCT, CTA and CTP were 2.56 ± 0.67mSv, 4.45 ± 2.5mSv and 4.47 ± 0.85mSv, respectively. Overall, the effective dose for one complete stroke imaging protocol (NCCT+CTA+CTP) for standard-dose protocol was 11.48mSv. Similarly, radiation exposure to other radiosensitive organs was found to be within the safe range.
Conclusion
Our study demonstrates that radiation exposures of sensitive organs are within acceptable limits when standard neuroimaging protocol is employed for acute ischemic stroke.
Trial registration number
N/A
AS11-037
SILENT ACUTE ISCHEMIC LESIONS IN TRANSIENT GLOBAL AMNESIA
1Charité - Campus Benjamin Franklin, Center for Stroke Research, Berlin, Germany
2Charité - Campus Benjamin Franklin, Department of Neurology, Berlin, Germany
3BIH, Berlin Institute of Health, Berlin, Germany
Background and Aims
Transient Global Amnesia (TGA) is a frequent neurological disorder with sudden onset of symptoms similar to ischemic stroke or transient ischemic attack, but with a specific clinical pattern. Pathophysiological mechanisms underlying TGA are still not completely understood. We performed a study to test the hypothesis that TGA might be of ischemic origin supported by additional ischemic lesions outside CA1.
Method
Consecutive patients clinically presenting with TGA between January 2010 and December 2016 admitted to our hospital were evaluated retrospectively. We analyzed imaging and clinical data in all patients undergoing MRI within 72 h from symptom onset.
Results
140 cases were included into the study. In 49 % of all patients (n = 68/140), MRI showed no acute pathological findings. 51 % (n = 72/140) presented with an acute DWI-lesion in the hippocampal CA1-area. In 9 % (n = 12/140), patients with hippocampal lesions had additional acute DWI-lesions in other cortical regions (nine in MCA-, two in PCA- and two in the vertebrobasilar vascular territory).
Conclusion
The frequency of silent acute ischemic lesions in TGA was 9%. Only patients with hippocampal DWI-lesions had additional lesions. In two thirds of these cases, more than one vascular territory was affected, suggesting a cardiac or cardioembolic cause. Therefore, cardiovascular workup should be considered in patients with TGA.
Trial registration number
clinicaltrials.org NCT02077582
AS11-038
INTEGRITY OF NIGRO-PALLIDAL CONNECTIONS IN STROKE PATIENTS IS ASSOCIATED WITH MOTOR OUTCOME
1University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
Background and Aims
Exofocal postischemic neuronal degeneration describes the delayed death of neurons remote from the primary lesion. This phenomenon is well described for degeneration of the substantia nigra (SN) induced by ischemia in the territory of the middle cerebral artery (MCA). In this context, the role of the integrity of the fibres connecting the SN reciprocally with the Globus Pallidus for the motor outcome remains unclear.
Method
15 patients with ischemic stroke lesions in the territory of the MCA were assessed by means of performance in the Nine-hole-peg (NHP) test and grip force (GF) in the first week after the event and in the chronic phase of recovery. Additionally, diffusion weighted imaging was performed in the sub-acute stage to calculate the tract-specific fractional anisotropy (FA) in nigro-pallidal tracts as a surrogate for microstructural properties. Linear regression models were fitted for the recovery of both NHP and GF.
Results
Of 15 patients with a mean age of 64, 8 had lesions in the dominant hemisphere and the tract-specific FA was 0.51 ± 0.01 for the affected side and 0.52 ± 0.01 for the unaffected side, with a trend in reduction by comparison (paired t-test, p = 0.06). The mean difference between acute and chronic performance was 35.13 ± 10.94s for the NHP and 12.96 ± 2.53kg for the GF. Regression analysis revealed a significant association of the FA with NHP (p = 0.006), but none with GF (p = 0.984).
Conclusion
Integrity of nigro-pallidal tracts appears to be associated with motor function after MCA stroke. This part of the extrapyramidal system might serve as potential target for interventional stimulation strategies.
Trial registration number
N/A
AS11-039
INTER- AND INTRAHEMISPHERIC CORTICAL AND SUBCORTICAL FUNCTIONAL CONNECTIVITY AT REST IS REDUCED IN PATIENTS WITH MORE SEVERE UPPER LIMB SOMATOSENSORY IMPAIRMENTS
1Ku Leuven, Rehabilitation Siences, Leuven, Belgium
2University Medical Center Hamburg-Eppendorf, Department of Neurology, Hamburg, Germany
3Cliniques Universitaires Saint-Luc, Department of Neurology, Brussels, Belgium
4KU Leuven - University of Leuven, Department of Imaging and Pathology, Leuven, Belgium
5Cliniques Universitaires Saint-Luc, Department of Radiology, Brussels, Belgium
6University of Melbourne, Florey Institute of Neuroscience and Mental Health, Victoria, Australia
Background and Aims
Neuroimaging studies examining upper limb somatosensory deficits are scarce.
Aim
To investigate functional connectivity at rest associated with upper limb somatosensory impairments in the early phase post-stroke.
Method
We recruited 20 stroke patients within 4-7 days post stroke with an upper limb somatosensory deficit, and 12 healthy controls. Six network indexes of functional connectivity at rest were created; cortical and subcortical interhemispheric, ipsilesional cortical and subcortical intrahemispheric and contralesional cortical and subcortical intrahemispheric index. General Linear Models were used to investigate group differences; patients with mild to moderate versus severe impaired somatosensory function versus healthy controls, for each somatosensory modality of the Erasmus-modified Nottingham sensory assessment. Covariates age, center and mean framewise displacement were included as nuisance regressors.
Results
Significant lower interhemispheric connectivity was found in severe compared to mild to moderately affected patients and to healthy controls for cortical interhemispheric index for the modalities exteroception, proprioception, and sensory discrimination (p < 0.05), and for subcortical interhemispheric index for exteroception and sensory discrimination (p < 0.05). Additionally, intrahemispheric functional connectivity of severe compared to mild to moderately affected patients and to healthy controls was found to be significantly lower for exteroception for the contralesional subcortical intrahemispheric index (p < 0.05) and for sensory discrimination for the ipsilesional cortical intrahemispheric index (p < 0.05).
Conclusion
Patients with severe somatosensory impairments show significant lower functional connectivity at rest in both cortical and subcortical networks inter- as well as intrahemispherically. Different rehabilitation approaches may be needed for patients with severe compared to patients with mild to moderate somatosensory impairments.
Trial registration number
N/A
AS11-040
NON-INVASIVE ASSESSMENT OF PERFUSION IN ACUTE STROKE - REPRODUCIBILITY OF BOLD DELAY MEASUREMENTS
1Charité – Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
2Humboldt-Universität zu Berlin, Berlin School of Mind & Brain, Berlin, Germany
3Max Planck Institute for Human Cognitive & Brain Sciences, Department of Neurology, Leipzig, Germany
4Charité – Universitätsmedizin Berlin, Department of Biostatistics and Clinical Epidemiology, Berlin, Germany
Background and Aims
Temporal lags in low-frequency oscillations of the blood-oxygenation-level-dependent (BOLD) signal provide a non-invasive measure of blood flow. We investigated the reproducibility of this method, known as BOLD delay, in acute stroke.
Method
Thirty-one patients received resting-state multiband echo planar imaging (TR = 400 ms, TE = 30 ms, FA = 43, multiband factor = 6, voxel size = 3×3×4 mm, 850 volumes) within 24 hours of symptom onset and one day later. None had a visible perfusion deficit. Motion was quantified using framewise displacement for each patient, averaged across timepoints. BOLD delay was calculated using a venous sinus reference, and maps were warped to standard space. The magnitude of the absolute differences in BOLD delay values for each voxel, excluding the ventricles, between the two timepoints was calculated. Statistical analysis was performed using a linear mixed model (to account for the clustering of the data in individuals) and linear regression.
Results
The overall mean absolute BOLD delay difference, including subjects as a random effect and motion as a covariate, was 3.0 s (linear mixed random intercept model, 95% CI = 1.5 s–4.5 s, t = 2.280). Motion was positively associated with absolute differences in BOLD delay (b = 18.8, 95% CI = 8.8–28.8, t = 6.305) and the spread of BOLD delay differences (adjusted R2 = 0.15, b = 10.4, 95% CI = 2.2–18.6, p = 0.0187).
Conclusion
The reproducibility of BOLD delay in acute stroke patients is sufficient for differentiating normally from abnormally perfused tissue but limited by head motion. Variations may additionally be attributed to factors such as delays of neural origin, differences in cardiorespiratory function, or subtle perfusion changes.
Trial registration number
N/A
AS11-041
THE LOCALIZATION OF CEREBRAL INFARCTION IN WERNICKE APHASIA: A RETROSPECTIVE VBM STUDY
1Beijing Tiantan Hospital- affiliated to Capital Medical University, Department of Neurology, Beijing, China
Background and Aims
Since the early works by Broca and Wernicke, the relationship between the localization and size of anatomical cortical damage and aphasia type has been discussed for many years and is one of the most popular concerns of aphasiology.
Method
For this reason, many ‘lesion-defined’ techniques were developed by researchers, of which voxel-based morphometry (VBM) is one of the most commonly used. Wernicke aphasia is believed to be the consequence of the damage at mid-to-posterior portion of the middle temporal gyrus (MTG) of dominant cerebral hemisphere and was classically used to study the relationship between functional impairment and location of brain damage.
Results
Based on prior research, we conducted this study which indicated that Wernicke’s aphasia may be in correlation with infarction at areas associated with the mediating spatial cognition and working memory processing, such as the limbic lobe, frontal lobe, mirrored compensatory region in the right hemisphere and inter-hemispheric area, which is the connection of the left and right hemispheres.
Conclusion
Our findings were consistent with previously published reports: Wernicke’s aphasia may be in correlation with infarction at areas associated with the mediating spatial cognition and working memory processing, such as the limbic lobe, frontal lobe, mirrored compensatory region in the right hemisphere and inter-hemispheric area.
Overall, our results indicate that future research of the brain functional networks of working memory and spatial cognition can better reveal the mechanism of Wernicke’s aphasia.
Trial registration number
N/A
AS11-043
LIPOPROTEIN(A) LEVELS ARE ASSOCIATED WITH STENOSIS IN THE CAROTID ARTERY IN PATIENTS WITH A MILD-TO-MODERATE STENOSIS
1Erasmus University Medical Center Rotterdam, Department of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
2Erasmus University Medical Center Rotterdam, Department of Neurology, Rotterdam, The Netherlands
3Maastricht University Medical Center, Department of Radiology and Nuclear Medicine & CARIM School for Cardiovascular Diseases, Maastricht, The Netherlands
4University Medical Center Utrecht, Department of Radiology, Utrecht, The Netherlands
5Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
6Erasmus University Medical Center Rotterdam, Department of Internal Medicine, Rotterdam, The Netherlands
Background and Aims
Lipoprotein (a) (Lp(a)) is an independent risk factor for cardiovascular disease and recurrent ischemic stroke. Previous studies have shown an association between high Lp(a) levels and stenosis in the coronary arteries. However, the association between Lp(a) levels and atherosclerosis in the carotid artery is yet unknown. The aim of this study was to analyze the association between Lp(a) levels and imaging biomarkers of the atherosclerotic plaque in the carotid artery.
Method
We selected 182 patients of the Plaque At RISK-study (PARISK) in which patients with ischemic symptoms and an ipsilateral carotid artery stenosis of 30-69% were included. Lp(a) concentration was measured in all patients. Imaging biomarkers of carotid atherosclerosis (severity and composition) were determined by MDCTA (n = 162) and MRI (n = 173). We defined elevated Lp(a) as >50 mg/dL. Univariable and multivariable linear and logistic regression analyses were used to investigate the association between Lp(a) levels and markers of atherosclerosis: degree of stenosis, plaque ulceration, presence of calcification, lipid-rich necrotic core (LRNC) and intraplaque hemorrhage, volume of calcifications and LRNC.
Results
Elevated Lp(a) levels were significantly associated with degree of ECST stenosis (beta = 6.71, 95% CI: 1.35-12.07). After adjusting for age, gender, hypertension, hypercholesterolemia, diabetes mellitus and current smoking, the association remained significant (beta = 6.66, 95% CI: 1.28-12.04). Elevated Lp(a) levels were not associated with the other imaging biomarkers.
Conclusion
Lp(a) is significantly associated with degree of stenosis in the carotid artery in patients with a history of ischemic symptoms and a mild-to-moderate carotid artery stenosis.
Trial registration number
N/A
AS11-044
QUANTITATIVE RELAXATION TIME T2 IN CAROTID OCCLUSIVE DISEASE: IMAGING MICROSTRUCTURAL TISSUE DAMAGE ASSOCIATED WITH CHRONIC HEMODYNAMIC FAILURE
1Goethe University, Neurology, Frankfurt a.M., Germany
2Goethe University, Brain Imaging Center, Frankfurt a.M., Germany
3Goethe University, Insitute of Neuroradiology, Frankfurt a.M., Germany
4Goethe University, Institute of Neuroradiology, Frankfurt a.M., Germany
Background and Aims
Chronic hemodynamic impairment in high-grade carotid occlusive disease is suspected to cause microstructural abnormalities that might be subclinical or lead to subtle symptoms including cognitive impairment. Quantitative (q)MRI allows for assessing pathological structural changes beyond macroscopically visible tissue damage. In this study, high-resolution quantitative T2-mapping combined with dynamic susceptibility contrast (DSC)-based perfusion-weighted imaging is used to investigate qT2 changes as a potential marker of microstructural damage in relation to hemodynamic impairment in patients with unilateral high-grade carotid occlusive disease.
Method
18 patients with unilateral high-grade internal carotid or middle cerebral artery stenosis/occlusion were included in the study. After segmentation of normal-appearing hypoperfused white matter and cortical regions, qT2-values and deconvolved perfusion parameters including relative cerebral blood flow (rCBF), relative cerebral blood volume (rCBV) and the rCBF/rCBV ratio as a potential indicator of local cerebral perfusion pressure (CPP) were determined within areas with delayed time-to-peak (TTP) and compared to values from contralateral unaffected areas. Hemispheric asymmetry indices were calculated for all parameters.
Results
qT2 was significantly prolonged (p < 0.01) in hypoperfused tissue and correlated significantly (p < 0.01) with TTP-delay and rCBF/rCBV reduction in white matter. Significant correlations (p = 0.0001) between TTP-delay and rCBF/rCBV ratio were found both in white matter and in cortical areas.
Conclusion
qT2-mapping is suitable to detect hypoperfusion-related microstructural damage in normal-appearing cerebral parenchyma fed by arteries affected by carotid occlusive disease. Analogous to positron emission tomography (PET)-based CBF/CBV, DSC-derived rCBF/rCBV might be an indicator of local CPP. TTP-delay can be considered a reliable surrogate of hemodynamic failure in chronic cerebrovascular disease.
Trial registration number
N/A
AS11-045
MAPPING ELEVATED LACTATE LEVELS AFTER ISCHEMIC STROKE USING PROBE CEST/NOE: A FEASIBILITY PATIENT STUDY AT 3T
1Max Planck Institute for Human Cognitive and Brain Sciences, Nuclear Magnetic Resonance Research and Development Unit, Leipzig, Germany
2Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin CSB, Berlin, Germany
Background and Aims
In ischemic stroke, anaerobic glycolysis leads to a local increase in lactate concentration. Such elevated levels of lactate can be detected using MRI via chemical exchange saturation transfer (CEST) and nuclear Overhauser effect (NOE). In-vivo, resulting Z-spectra exhibit a complex intermingled baseline caused by several broad tissue contributions as well as metabolite signals. Using the recently introduced method Prospective Baseline Enhancement (PROBE) individual metabolite contributions can be detected with the goal to identify ischemic regions around infarcted areas.
Method
The PROBE technique was optimized to achieve a flat baseline for healthy tissue using data from volunteers and applied to three stroke patients (56-80y; 2F/1M). PROBE imaging of a single slice through the center of the stroke lesion was performed on day4 (N = 2) and day2 (N = 1), respectively, after onset. Data processing included normalization, B0 correction, and metabolite detection.
Results
Two subjects showed similar results, while the outcome for one subject was unincisive. Sample results from a thalamic stroke in the right hemisphere: the combined intensity of two lactate peaks (Fig. 1B), where elevated lactate levels coincide with hyperintense regions in the diffusion-weighted image (Fig. 1A).
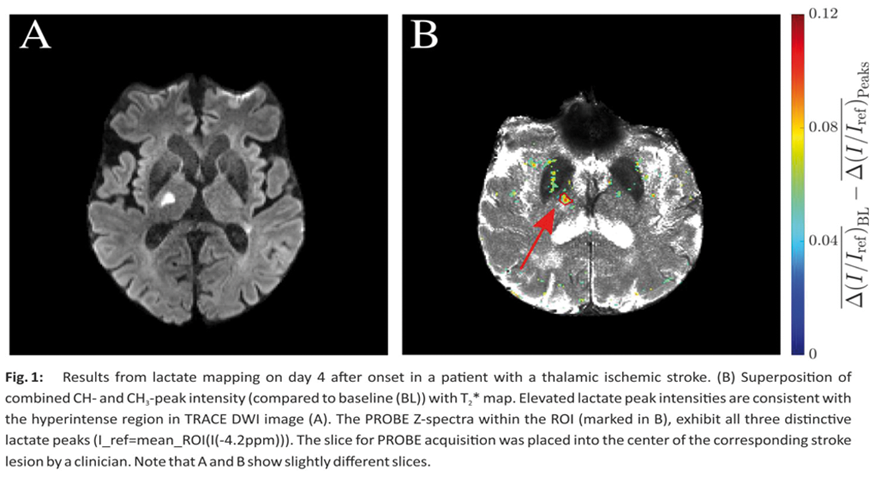
Conclusion
The presumably strong increase in lactate following ischemia leads to detectable changes in PROBE Z-spectra providing a biomarker for affected tissue. The feasibility of PROBE was demonstrated in-vivo for thalamic stroke on a clinical platform at 3T.
Trial registration number
N/A
AS11-046
INVESTIGATION OF LEPTOMENINGEAL ENHANCEMENT IN SUSAC SYNDROME
1Fondation Ophtalmologique Rothschild, Neurology, Paris, France
2Fondation Ophtalmologique Rothschild, Neuroradiology, Paris, France
3Fondation Ophtalmologique Rothschild, Statistics, Paris, France
4Fondation Ophtalmologique Rothschild, Ophtalmology, Paris, France
Background and Aims
To assess the prevalence and the specificity of leptomeningeal enhancement (LME) on 3T postcontrast T2- fluid-attenuated inversion recovery (FLAIR) MRI in susac syndrome (SS).
Method
We compared 1) initial MRI data in SS (n = 10) to pathologic group with multiple sclerosis or isolated optic neuritis patients (n = 73) 2) several MRI (n = 54) for each patient with SS in the follow up (mean: 54 months) to investigate the association between LME and the evolution of the disease. MRIs were examined independently by 2 neuroradiologists 1) who were blinded to the clinical and ophthalmologic angiographic data 2) who assessed LME and parenchymatous abnormalities. An ophthalmologist (blinded to the clinical and radiological data) reviewed all the fluorescein angiographies.
Results
Inter observer agreement in all MRI findings was substantial (Cohen kappa tests >0,5). LME was detected more frequently in SS cases (6/10) than in non SS ((6/73) (p < 0,0004) and differed by 2 characteristics: more frequently supratentorial (6/10 versus 0/73 (p < 0.0001) and multiple foci (>3 foci) involved (5/10 in SS versus 0/73 in non SS; p < 0,0001) (Fisher test). There is a significant association in a mixed-effect logistic model between clinical relapse and increase of LME (OR 6. IC: 1,34-37,7; p = 0,01) and increase of parenchymal lesion (OR = 5. IC: IC: 1.57-59.74). p = 0,02).
Conclusion
LME is frequent in SS and its characteristics are helpful in differential diagnosis. It can be an additional marker of the activity of the disease.
Trial registration number
N/A
AS11-050
HIGH-RESOLUTION MRI (HR-MRI) OF ATHEROSLCEROTIC PLAQUE IN SYMPTOMATIC CAROTID STENOSIS – RELATIONSHIP WITH RISK FACTORS, TREATMENT, AND CT ANGIOGRAPHIC FEATURES
1University College Dublin, Radiography & Diagnostic Imaging, Dublin, Ireland
2St Vincent's University Hospital, Vascular Surgery, Dublin, Ireland
3St Vincent's University Hospital, Stroke service, Dublin, Ireland
4Connolly Hospital, Stroke service, Dublin, Ireland
5St James's Hospital, Stroke service, Dublin, Ireland
6University College Dublin, HRB Stroke Clinical Trials Network Ireland, Dublin, Ireland
7Mater Misericordiae University Hospital, Radiology, Dublin, Ireland
8Mater Misericordiae University Hospital, Neurovascular Unit for Translational and Therapeutics Research, Dublin, Ireland
9Mater Misericordiae University Hospital, Vascular Surgery, Dublin, Ireland
10Royal College Surgeons Ireland, Stroke service, Dublin, Ireland
Background and Aims
Traditional imaging techniques rely on arterial lumen stenosis as an indirect measure of mural plaque. HR-MRI allows direct imaging of mural plaque burden and composition. However, few data exist on the relationship of these parameters to clinical factors in patients with symptomatic carotid stenosis. We investigated the relationship between MR plaque features, clinical characteristics, and plaque morphology on CT angiography.
Method
A sub-group of patients included in the prospective BIOVASC plaque imaging study were included. Inclusion criteria were: (1) Speech/motor TIA or non-severe stroke (Rankin≤3) <72hours (2) Ipsilateral carotid stenosis ≥50% (3) Age≥50 (4) Carotid HR-MRI and CTA performed. Exclusions were pregnancy, malignancy, dementia, renal impairment, cervical irradiation/endarterectomy/stent. Semi-automated analysis of HR-MRI axial plaque images was done using PlaqueView ® and manual analysis of co-registered CTA performed.
Results
27 patients met inclusion criteria (78% men, mean age 66 years, 36% stroke/64%TIA, 39% current smoking). By HR-MRI, maximum plaque wall area was greater in patients with index stroke compared with TIA (p = 0.007). Plaque maximum wall thickness was greater in diabetes (p = 0.016) and statin-untreated patients (p = 0.003). Fibrous cap thickness was greater (p = 0.05) in aspirin-treated patients. When HR-MRI was compared with CTA, high correlations were observed for lumen area (rho = 0.976, p < 0.001), maximum wall thickness (rho = 0.878, p < 0.001), and maximum wall area (Pearson r = 0.981, p < 0.001).
Conclusion
If replicated, our findings may inform the application of plaque HR-MRI and CTA as surrogate markers in future clinical practice and randomised trials for stroke prevention.
Trial registration number
N/A
AS11-053
MCA MEAN BLOOD FLOW VELOCITY INDEX – A PROMISING PREDICTOR OF INTRACRANIAL HEMORRHAGE AFTER STROKE THROMBECTOMY
1Medical University of Graz, Department of Neurology, Graz, Austria
2Medical University of Graz, Department of Radiology- Division of Neuroradiology- Vascular and Interventional Radiology, Graz, Austria
3Medical University of Graz, Institute of Medical Informatics- Statistics and Documentation, Graz, Austria
Background and Aims
In a pilot study, we recently observed that an increased middle cerebral artery (MCA) mean blood flow (MBF) velocity index on transcranial duplex sonography (TCD) was associated with intracranial hemorrhage (ICH) after successful endovascular recanalization of anterior circulation vessel occlusion. This study aimed to further determine the predictive value of the MCA MBF velocity index for postthrombectomy ICH.
Method
Over a seven-year period, we reviewed all ischemic stroke patients with successful endovascular recanalization for anterior circulation vessel occlusion (TICI 2b-3) at our center. Postinterventional TCD sonography served to identify MCA MBF velocity indices ( = MBF velocity of the recanalized divided by the contralateral MCA). Receiver operating characteristic (ROC) curve tested the ability of MCA MBF velocity index values in predicting ICH after thrombectomy.
Results
Of 178 ischemic stroke patients (mean age: 67 ± 12 years, female: 43%) with successful anterior circulation thrombectomy, 35 patients had postinterventional ICH (symptomatic: 10, asymptomatic: 25). MCA MBF velocity index was increased in ICH compared to non-ICH patients (1.32 ± 0.39 versus 1.02 ± 0.32, p < 0.001). The area under the ROC curve for MCA MBF velocity index values in the prediction of ICH after stroke thrombectomy was 0.69 (confidence interval: 0.59−0.79). The cut-off point with the highest sensitivity and specificity was set at 1.25 (sensitivity 69%, specificity 73%) and had a negative predictive value for ICH of 91%.
Conclusion
This study supports a predictive role of TCD sonography detected MCA MBF velocity index for ICH after stroke thrombectomy. In patients with MCA MBF velocity indices below 1.25 postinterventional ICH appears rare.
Trial registration number
N/A
AS11-054
BRAIN MICROBLEEDS ANALYSIS IN PATIENTS WITH LEFT APPENDAGE CLOSURE AND PATIENTS TREATED WITH NEW ORAL ANTICOAGULANTS, PRELIMINARY STUDY
1Universitary Hospital of Salamanca, Neurology Service, Salamanca, Spain
2Universitary Hospital of Salamanca, Cardiology Service, Salamanca, Spain
3Universitary Hospital of Salamanca, Radiology Service, Salamanca, Spain
Background and Aims
Determine the number of microbleeds and appearance speed in patients with non-valvular atrial fibrillation (AF) treated with new oral anticoagulants (NOACs) and left atrial appendage (LLA) closure.
Method
Prospective and Longitudinal study in two groups: patients performed with LLA closure and patients treated with NOACs, paired for embolic and hemorrhagic risk. Basic brain magnetic resonance (1.5 Tesla) with 3D magnetic susceptibility was performed, controlled at 6 and 12 months. The MARS scale was used for microbleeds.
Results
We included 20 patients, 8 with LLA closure and 12 treated with NOACs. The mean age of the group with LLA closuere and NOACs was 82 and 72.3 years respectively; 5 (62.5%) of the group with IC presenting permanent AF, and 9 (75%) in the group of NOACs; 7 (87, 5%) patients with LLA closure presented a stroke, whereas the group with NOACs 10 (83.3%), the median of HASBLED was 4 in patients with LLA closure and 3 in NOACs. 1 (12.5%) patient with LLA closure presented microbleeds in the right subcortical region (MARS 1), in patients with NOACs were 2 (16.7%) (MARS 1). In 6-month control resonance, 1 (12.5%) microbleed was found in NOAC group, in LLA closure group there was no increase in microbleeds. The differences were not statistically significant.
Conclusion
In the preliminary study, there were no statistically significant differences of microbleeds between patients undergoing a LLA closure and treated with NOACs in the control resonance at 6 months. Subsequently, changes will be analyzed again after 12 months.
Trial registration number
N/A
AS11-055
MEASURING CEREBRAL OXYGENATION IN MOYA MOYA USING NEAR-INFRARED SPECTROSCOPY
1St. James's Hospital, Mercer's Institute for Successful Ageing, Dublin, Ireland
2Trinity College Dublin, Department of Medical Gerontology, Dublin, Ireland
3St. James's Hospital, Department of Medical Physics & Bioengineering- Mercer's Institute for Successful Ageing, Dublin, Ireland
4St. James's Hospital, Department of Stroke & Neurovascular Medicine- Mercer's Institute for Successful Ageing, Dublin, Ireland
Background and Aims
Moya moya disease (MD) is associated with a total occlusion of the middle cerebral artery but with maintenance of collateral vessels. Near-infrared spectroscopy (NIRS) derived tissue oxygenation (%TSI) is used as a surrogate for measuring cerebral perfusion to the frontal lobes and anterior circulation.
Method
We collected 10-minute supine measurements on two well and community-dwelling patients with their informed consent. Both had confirmed right-sided MD on magnetic resonance angiography with evidence of collaterals. Beat-to-beat systolic blood pressure (SBP-mmHg) and pulse rate (HR-bpm) was recorded throughout using a calibrated volume clamp method (Finometer NOVA), while near-infra red spectroscopy (NIRS – Artinis Medical) measured regional cerebral tissue oxygen saturation (TSI - %) derived from each hemisphere concurrently.
Results
Patients were aged 58 and 59 respectively and both were male. There was no evidence of frontal cortex infarction on magnetic resonance imaging. In the first patient, baseline TSI was lower by 3% on the occluded side versus the normal side (66.5 +/- 0.68 vs 69.3+/−0.69). In the second patient TSI was lower by 2% (61.3+/−0.48 vs 63.3+/−0.37).
Conclusion
Despite developed collaterals, our two moya moya patients demonstrated identifiably lower cerebral perfusion to the affected hemisphere compared to the non-occluded side. NIRS may have an application in non-invasive identification of large artery occlusion where less extensive collateralisation is present.
Trial registration number
N/A
AS11-059
SENSITIVITY OF MRI SEQUENCES FOR THROMBUS DETECTION IN CEREBRAL VENOUS THROMBOSIS
1Third School of Medicine - Charles University - Hospital Královské Vinohrady, Neurology, Prague 10, Czech Republic
2Third School of Medicine - Charles University - Hospital Královské Vinohrady, Radiology, Prague 10, Czech Republic
Background and Aims
Cerebral venous thrombosis (CVT) is a less frequent cerebrovascular disease. MRI examination plays a pivotal role in the diagnosis assessment; however, findings may be ambiguous since anatomical variability of dural sinuses and evolution of thrombus intensity. Aim of the observation is to assess sensitivity of MRI sequences in different periods of CVT.
Method
We retrospectively evaluated initial MRI findings in 30 patients with CVT established from 2009 to 2017. According to duration of symptoms, MRI was performed in 15 subjects less than 5 days after onset of symptoms (acute phase), in 10 subjects between day 5 and 20 (early subacute phase) and in 5 patients after 20 days (late subacute phase). We searched for presence of intraluminal thrombus on T1WI, T2WI, gradient echo (GE) and post contrast examination.
Results
Hyperintense signal of methemoglobin on T1 WI was seen in 57 % of cases (53 % acute, 80 % early, and 20 % late subacute). Hypointense signal in T2 WI appeared in acute and early subacute period in 62 % and 60 %, respectively. Hypointense signal in GE was found out in 73 % of MRI examinations. Post contrast study revealed thrombus in all acute cases and all but one late subacute case.
Conclusion
In our cohort T1WI and T2WI proved only modest sensitivity for thrombus detection in acute phase of CVT. Post contrast examination followed by GE showed the best results in all phases of CVT assessment. Further research of MRI algorithm in suspected CVT is warranted.
Supported by PROGRES Q32 and Q35.
Trial registration number
N/A
AS11-060
AUTOMATIC MRI QUANTIFICATION OF ISCHEMIC STROKE LESIONS
1Pixyl Medical, Research, Grenoble, France
2Inria Grenoble Rhone-Alpes, Mistis, Montbonnot Saint-Martin, France
3University Grenoble Alpes, Grenoble Institute of Neuroscience, Grenoble, France
4CHU Grenoble Alpes, Research, Grenoble, France
5INSERM, Unit 1216, Grenoble, France
Background and Aims
Manual delineation by an expert is currently the gold standard for lesion quantification, but is resource-intensive, suffers from inter-rater and intra-rater variability, and does not scale well to large population cohorts. We develop an automated lesion quantification method to assess the efficacy of cell therapy in patients after ischemic stroke.
Method
A high-quality sub-acute and chronic stroke dataset was supplied by HERMES (https://clinicaltrials.gov/show/NCT00875654). T1-w and 3D-Flair MRIs were acquired from 20 ischemic stroke patients with MCA infarct at 2 and 6 months post-event. Manual delineation was performed by an expert using the Flair image.
We propose an unsupervised method employing a hidden Markov random field, with innovations to address the challenges posed by stroke MR scans. We introduce a probabilistic vascular territory atlas, adapted to the patient-specific data in a joint segmentation & registration framework, to model the potential progression and delimitation of vascular accidents.
Results
A segmentation example is shown in Fig. 1, and Fig. 2 shows the good correlation observed between manual and automated lesion volume delineation for the two time points.
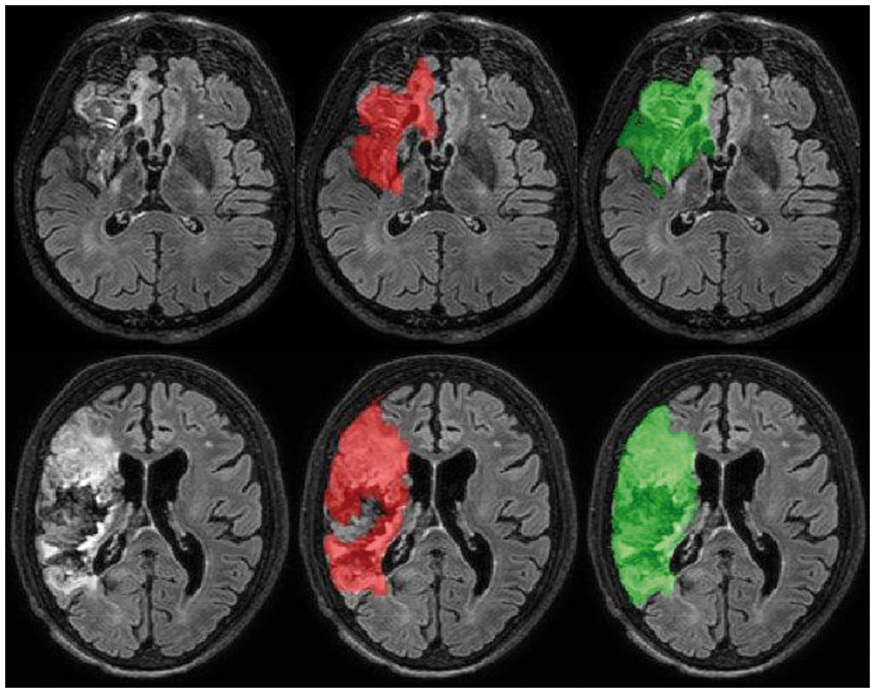
Fig 1: Auto (red) Vs manual (green) segmentation for two difficult cases (top:P04 M2; bottom:P20 M6).
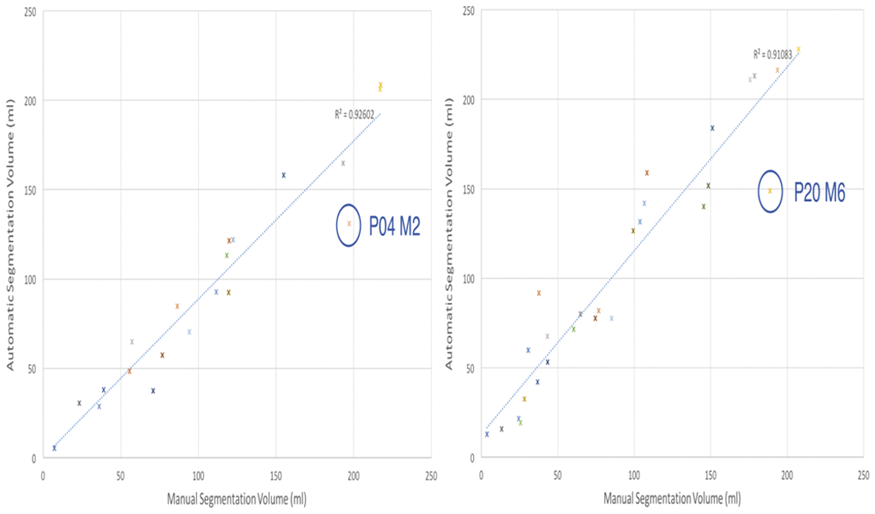
Fig 2: Auto vs manual segmentation for sub-acute (M2, left) and acute (M6, right) ischemic stroke. Circles indicate the cases in Fig.1.
Conclusion
We propose an unsupervised method with the hypothesis that such a class of method is more robust to the diversity of images obtained with different sequence parameters and scanners; a particularly sensitive point for multi-center studies. Interestingly, this approach will be used in the European RESSTORE cohort (http://www.resstore.eu/).
Trial registration number
NCT00875654
AS11-062
EXTENT OF BLOOD-BRAIN BARRIER IMPAIRMENT AND RISK OF HEMORRHAGIC TRANSFORMATION IN ISCHAEMIC STROKE
1Charles University - 2nd Faculty od Medicine, Neurology Department, Prague, Czech Republic
2Institute of Physiology, Czech Academy od Sciences, Prague, Czech Republic
Background and Aims
Impairment of blood-brain barrier (BBB) is an important phenomenon observed in ischaemic stroke. Infarcted tissue is frequently affected by hemorrhagic transformation (HT). The aim of the study is to the regions of ischaemic lesion and ischaemic core with impaired BBB and assess the risk of HT in relation to the extent of BBB impairment in ischaemic stroke.
Method
Prospective study on patients with supratentorial acute ischaemic lesion extending into cortex with negative history of previous stroke. A modified clinical MRI imaging with gadolinium contrast agent was performed 7-12 days after stroke. Automatic algorithms for detection of ischaemic core (hyperintensity on DWI MRI), area of lesion affected by stroke (hyperintensity on FLAIR MRI) and BBB impairment (contrast agent detection) were developed.
Results
The data of 23 patients were analysed (74% men, average age 71 years, median NIHSS 5, 30% received intravenous thrombolysis, in 17% mechanical thrombectomy was performed). HT occurred in 9 (39%) patients. Volume of ischaemic core constituted in average 34% of total volume of region with BBB impairment. Volume of detected ischaemic lesion constituted in average 51% of total volume of region with BBB impairment. Between groups without HT and with HT mean volumes of regions with BBB impairment (18.8 vs. 30.1 ml) did not differ significantly.
Conclusion
Methodology for BBB impairment assessment was adopted. Volume of region with BBB impairment significantly exceeds a region that corresponds to ischaemic lesion detected on MRI (FLAIR, DWI). Patients with HT tend to have larger BBB impairment, although the result was not statistically significant.
Trial registration number
N/A
AS11-063
RE-THINKING SUCCESSFUL REPERFUSION POST ENDOVASCULAR THERAPY IN ISCHEMIC STROKE WITH MR-DCE PERFUSION
1University of Calgary, Department of Clinical Neurosciences, Calgary, Canada
2University of Calgary, Radiology, Calgary, Canada
Background and Aims
The thrombolysis-in-cerebral-infarction (TICI) reperfusion score is highly subjective. We use a novel T1-weighted MR-dynamic-contrast-enhanced (DCE) sequence to objectively measure reperfusion within 5hrs of EVT of ischemic stroke. We hypothesize that MR-perfusion will predict clinical improvement and early DWI growth better than the TICI score.
Method
Reperfusion quality was scored with TICI on the last run of the EVT-DSA (N = 14). At ∼5hrs post EVT, DWI and DCE-perfusion was acquired. DWI was repeated at 24hrs. Relative mean CBF, T0, Tmax and CBV were determined within the 5 hour DWI lesion (initial infarct ROI), the 24 hour subtract 5 hour DWI lesion (final infarct ROI) and non-infarct ROI. Change in NIHSS and infarct growth were used as outcomes. Perfusion parameters were compared between TICI sub-groups. Clinically adjusted linear regression was used to test TICI versus MR-DCE for prediction of clinical and infarct growth respectively.
Results
Figure 1 shows relative perfusion parameters within TICI sub-groups. TICI-2b was not different than TICI<2b (p>0.05). The adjusted linear regression models with the highest R-squared for prediction of change in NIHSS and DWI infarct growth were the MR-perfusion Tmax (p+0.02; R-squared = 0.48) and To (p < 0.01; R-squared = 0.62).
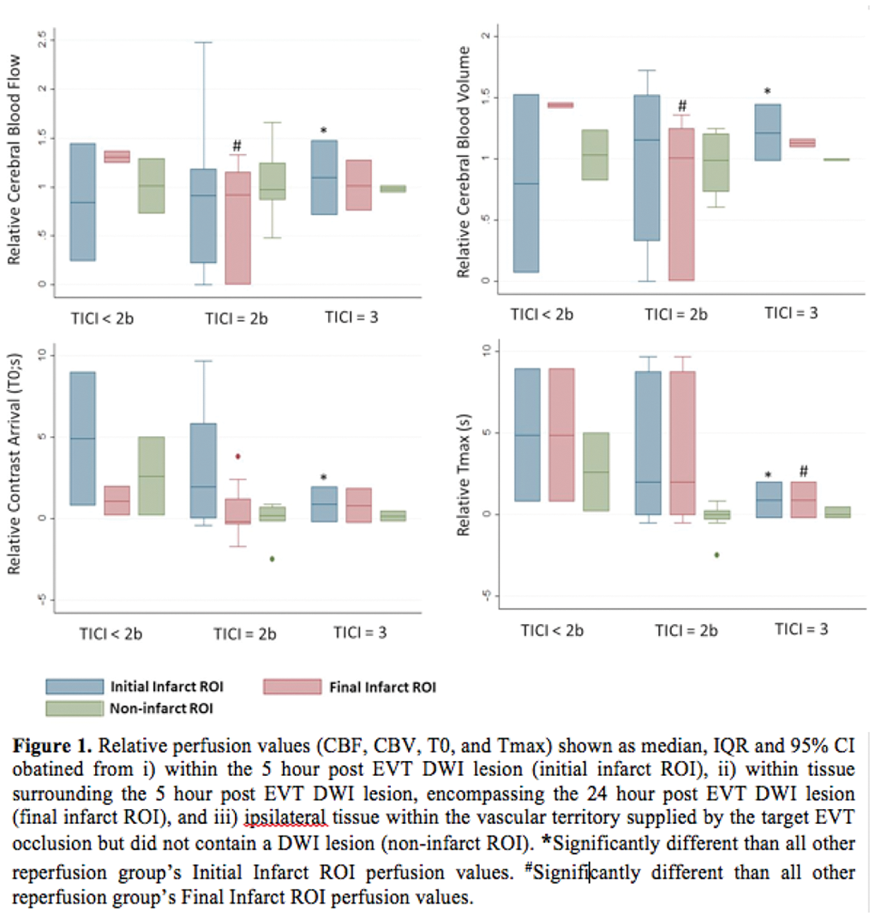
Conclusion
We show that the MR-DCE-perfusion profiles within TICI-2b group are highly variable (Figure 1). Clinical outcome and infarct growth is better predicted with MR-DCE perfusion compared to TICI scoring.
Trial registration number
N/A
SERVICE ORGANISATION
AS12-001
A PERFORMANCE AUDIT OF THE TRANSIENT ISCHAEMIC ATTACK (TIA) SERVICE AT PENNINE ACUTE HOSPITALS NHS TRUST
1Pennine Acute Hospital Foundation Trust, Care Of Elderly, Manchester, United Kingdom
Background and Aims
Approximately 46,000 people in the UK have their first TIA every year (Stroke association, 2012). Timely assessments and appropriate delivery of treatments for TIA patients in the outpatient setting could significantly reduce the risk of developing stroke by 80%. (Johnston SC, 2006)
Method
A retrospective review of all referrals to the Neurovascular Clinics across all four hospital sites (North Manchester, Bury, Oldham and Rochdale) from 1st July 2014 to 1st September 2014 was carried out, with a re-audit in 2017 after changes were implemented. These looked at reasons for referrals and time frame from referral to seeing patients in the clinics.
The changes were of a new community TIA referral proforma and trust online referral proforma to guide non-stroke physicians in making appropriate referrals. Following this, we also designed a simple patient information leaflet to provide adequate information to patients with suspected TIA.
Results
93% of patients were referred using the new TIA referral proforma. The appropriateness of referrals increased from 66.2% to 74.2%. It also showed that the percentage of patients seen within the recommended time frame by the National Institute of Clinical Excellence (NICE) has increased to 78.95% from 68.64%.
Conclusion
This quality improvement project showed significant improvements in the time taken to see patients with suspected TIA in the outpatient setting. Recent changes in the NICE guidelines have significantly increased the number of TIA patients who should be seen within 24 hours, hence an increasing need to maximise the effective use of Neurovascular Clinics.
Trial registration number
N/A
AS12-002
UTILISING TIA AND ACUTE NEUROLOGY SERVICES TO THE MAXIMUM EFFICIENCY
1St George's University Hospitals NHS Trust, Neurology, London, United Kingdom
Background and Aims
TIA clinics are a well-established part of stroke services. About 60% of all patients referred to the TIA service do not have a final diagnosis of TIA. With emergence of acute neurology services, it would be beneficial to combine the strengths of both to improve the percentages of positive TIA diagnosis in the TIA clinic in order to help the most patients. At St George’s we started a “HOT CLINIC” service in August 2016 for acute neurological symptoms (not TIA or seizures).
Objective
To assess the effect of starting this service on the TIA service.
Method
TIA data between March 2016 and March 2017 was analysed. We compared the percentage of TIA/stroke/appropriate patients and percentage of neurological diagnoses before and after the August 2016 start date for acute neurology.
Results
Between March 2016 and August 2016, we saw 317 patients within the TIA service compared to 259 after the acute neurology service started. Of these, 33.4% were diagnosed as TIA/stroke compared to 30.5% after August. The main differential was migraine followed by syncope. Meanwhile, HOT CLINIC referrals went from 5 in August 2016 to 31 in August 2017.
Conclusion
A well thought out model can be used to effectively use both TIA and acute neurology clinics to provide the best care for patients. More education and thought is needed to ensure both services receive the correct types of referrals. GP and acute medical education regarding TIA diagnosis and differentiating this from migraine aura would reduce the burden on the TIA service.
Trial registration number
N/A
AS12-003
THE IMPACT OF THE STROKE EARLY SUPPORTED DISCHARGE SERVICE ON ACUTE STROKE REHABILITATION
1The Hillingdon Hospital NHS Foundation Trust, Stroke Medicine, Uxbridge, United Kingdom
2Central and North West London NHS Foundation Trust, Community Rehabilitation, Uxbridge, United Kingdom
Background and Aims
The Stroke Early Supported discharge service was introduced in Hillingdon, London in October 2016. Once a patient completed their Hyper-acute Stroke investigations and treatment they could be discharged to receive intensive therapy in their own home rather than in a hospital environment. This is potentially beneficial to the patient who prefers the comfort of their home and also the hospital in terms of cost saving from reduced bed days.
We wanted to review the impact of this service on both The Stroke Unit and patients.
Method
A comparison was made of the level of patient dependency (using the Modified Barthel Index) and stroke categorisation (Oxford Stroke Classification) for the 3rd quarter (October-December) in 2015 and 2016 respectively. This represents a snapshot period, before and after the Stroke ESD service was introduced.
Results
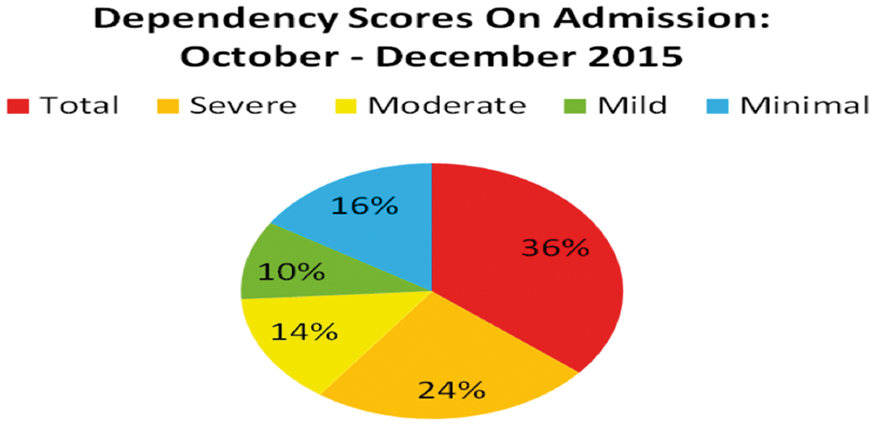
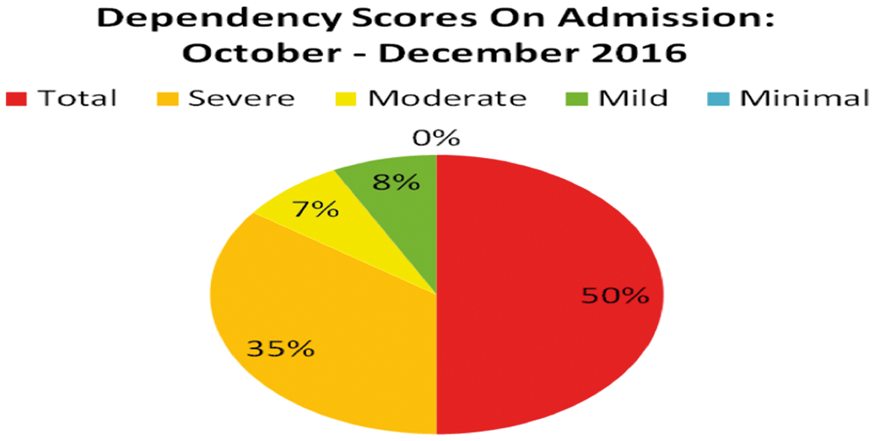
Conclusion
There has been an increase in the level of depedency of Stroke inpatients in The Stroke Unit thereby indicating that a significant number of those less severe Strokes were successfully being treated in the community under the new Stroke ESD service. Patients preferred to be discharged early and the service represented a cost saving in terms of reduced ‘bed-days'.
Trial registration number
N/A
AS12-004
PREHOSPITAL PREDICTION OF THROMBECTOMY ELIGIBILITY: A SYSTEMATIC REVIEW AND 4-ITEM DECISION TREE
1Leiden University Medical Center, Department of Neurology, Leiden, The Netherlands
2Leiden University Medical Center, Department of Medical Statistics, Leiden, The Netherlands
3Leiden University Medical Center, Department of Public Health and Primary Care, Leiden, The Netherlands
4St. Antonius hospital, Department of Neurology, Nieuwegein, The Netherlands
5University Medical Center Utrecht, Department of Radiology, Utrecht, The Netherlands
6Leiden University Medical Center, Department of Radiology, Leiden, The Netherlands
Background and Aims
A prehospital large anterior vessel occlusion (LAVO)-prediction scale could reduce treatment delays in acute stroke by allocating intra-arterial thrombectomy-eligible patients directly to a comprehensive stroke center.
Method
We performed a systematic literature search to identify LAVO-prediction scales. Predictive value was compared in a prospective, multicenter validation cohort of the Dutch acute Stroke study (DUST) by calculating area under the receiver operating curves (ROC-AUC).
Subsequently, with group lasso regression analysis we constructed a prediction model, incorporating patient characteristics in addition to National Institutes of Health Stroke Scale (NIHSS) items. Finally, we developed a decision tree algorithm based on dichotomized NIHSS items.
Results
We identified 7 LAVO-prediction scales. From DUST 1316 patients (35.8% with LAVO) were available for validation. The FAST-ED and RACE scale had a higher ROC-AUC (both >0.81, p <0.01) compared with other scales. Group lasso analysis revealed a LAVO-prediction model containing 7 NIHSS items (ROC-AUC 0.84).
With the GACE (Gaze, facial Asymmetry, level of Consciousness, Extinction/inattention) decision tree, LAVO can be predicted (ROC-AUC 0.76) for 61% of patients with assessment of only 2 dichotomized NIHSS items, and for all patients with only 4 items.
Conclusion
External validation of 7 LAVO-prediction scales showed ROC-AUCs ranging from 0.75−0.83. Most scales, however, are too complex for Emergency Medical Services use and prehospital validation is generally lacking.
GACE is the first LAVO-prediction scale using a simple decision tree as such increasing feasibility while maintaining high accuracy. Further prospective validation in the prehospital setting is needed.
Trial registration number
N/A
AS12-005
SAFETY AND EFFICACY OF TELETHROMBOLYSIS IN NEW STROKE UNIT
1Sverdlovsk Regional Clinical Hospital #1, Stroke Unit, Yekaterinburg, Russia
2Verhnyaya Pyshma Central City Hospital, Stroke Unit, Verhnyaya Pyshma, Russia
3Ural State Medical University, Medical Faculty, Yekaterinburg, Russia
Background and Aims
In new stroke units, we practice telethrombolysis for one year to monitor implementation of the protocol and gain experience. The establishment of a new stroke unit in the territory formerly served by the Regional Stroke Center allowed us to compare bedside thrombolysis with remote thrombolysis in the same territory, population, and ambulance infrastructure.
Method
Twenty-nine consecutive patients who received intravenous thrombolysis via telemedicine in the new stroke unit at Verhnyaya Pyshma Central City Hospital, (Verhnyaya Pyshma, Sverdlovsk region, Russia) from November 2016 to October 2017 were included in the remote thrombolysis group. Retrospectively, 19 patients from the territory served by the new stroke unit underwent thrombolysis at the Regional Stroke Center at Sverdlovsk Regional Clinical Hospital (Yekaterinburg, Sverdlovsk region, Russia) from January 2014 to October 2016 and were included in the bedside group. The primary endpoint was the shift of modified Rankin scale (mRS) score at hospital discharge.
Results
Baseline characteristics of telethrombolysis patients were like those of patients undergoing thrombolysis locally except for more severe disease on admission to the Verhnyaya Pyshma Central City Hospital. In the multivariable model, telethrombolysis did not independently influence functional outcome at hospital discharge (odds ratio for a shift towards a worse outcome on mRS, 0.33; 95% confidence interval, 0.08 – 1.33, p = 0.119). The mortality rate (15.8% vs 20.7%, p = 1.000) and hemorrhagic transformation rate (15.8% vs 21.4%, p = 0.720) at hospital discharge were similar between groups (presented as bedside vs remote).
Conclusion
The implementation of telethrombolysis in the new stroke units appeared to be safe and effective.
Trial registration number
N/A
AS12-006
TELEMEDICINE DIFFUSION IN STROKE NETWORKS: UPDATE OF AN ITALIAN NATIONAL SURVEY
1Neurologic Clinic, Department of Medicine- University of Perugia, Perugia, Italy
2Stroke Unit- l’Unità operativa di Neurologia e di Neurofisiologia, Azienda Ospedaliera Sant’Antonio Abate, Gallarate- Varese, Italy
3Neurologia, Ospedale di Cremona, Cremona, Italy
4Emergency Department, Ospedale San Giovanni Battista- USL Umbria 2, Foligno, Italy
5Urgenze Vascolari Neurologiche, Ospedale Antonio Cardarelli, Napoli, Italy
6Emergency Department, Ospedale di Portoferraio USL 6 Toscana, Portoferraio-Livorno, Italy
7Stroke Unit, Policlinico Umberto I, Rome, Italy
8Stroke Unit, Arcispedale Santa Maria Nuova di Reggio Emilia, Reggio Emilia, Italy
9Stroke Unit, Ospedale di Trento, Trento, Italy
10Stroke Unit, Presidio Ospedaliero dell’Annunziata- Azienda Ospedaliera di Cosenza, Cosenza, Italy
11Emergency Department, Ospedale Santa Maria della Stella- USL Umbria 2, Orvieto, Italy
12Stroke Unit, Ospedale San Giovanni Battista USL Umbria 2, Foligno, Italy
13Stroke Unit, Ospedale San Giovanni Battista- USL Umbria 2, Foligno, Italy
Background and Aims
Prior studies have shown that the use of telemedicine for stroke treatment is not only safe and effective, but it also increases the use of tPA, improving patients outcomes. This study aimed to investigate the diffusion of telemedicine in Italian stroke networks.
Method
We used an online questionnaire to assess: type of setting, volume of activity, access to stroke care between hospitals, the presence of imaging sharing; type of solutions. We have interviewed 26 Italian neurologists, working in main urban areas, from north southward, including rural areas and Italian islands. The sample represented 14 different regions and 18 counties. A majority of neurologists replying to the survey (52 %) worked in large general hospitals, or smaller general hospitals (24%).
Results
The 65% of networks involved in the survey had a low of activity volume while the 35 % had a thrombolysis/year volume above 100 case/y. According to the survey a local stroke network was established in 90% of cases. In the 50% of cases, the hospitals care was not reported as homogeneous within the network. In 30% of interviews was reported an active network for Teleconsult. This was possible in half of cases using personal mobile devices, while only the 30% od them used professional teleconference system, and the last 20% used medical devices.
Conclusion
Our findings demonstrated a relevant diffusion of Teleconsult in Italian stroke networks. The systems adopted are mostly individual solutions not integrated in protocollar pathways. These findings may encourage a systematization of Telemedicine solutions in the country.
Trial registration number
NA
AS12-007
PROCESS EVALUATION OF THE T3 STROKE TRIAL - CLINICIANS VIEWS ON FACTORS FOR SUCCESSFUL IMPLEMENTATION OF EVIDENCE-BASED STROKE PROTOCOLS IN THE EMERGENCY DEPARTMENT
1Nursing Research Institute, Faculty of Health Sciences, Sydney, Australia
2Monash University, Stroke & Ageing Research Centre and Department of Medicine, Melbourne, Australia
3University of Ottowa, Department of Medicine, Ottowa, Canada
4Deakin University, Centre for Quality and Patient Safety Research-, Melbourne, Australia
5National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australia
6University of Sydney, Centre for Diabetes and Endocrinology Research-, Sydney, Australia
7Westmead Hospital, Centre for Diabetes and Endocrinology Research, Sydney, Australia
8University of New South Wales, The Sydney Partnership for Health Education Research & Enterprise, Sydney, Australia
Background
A process evaluation was conducted of a trial to evaluate the effectiveness of nurse-initiated evidence-based protocols to improve the management of the triage, treatment and transfer of patients with stroke in emergency departments (ED). Process evaluations are used in implementation trials to investigate barriers and facilitators to successful implementation.
Aim
To identify the views of emergency department (ED) staff, the conditions needed to successfully introduce a stroke intervention into clinical practice.
Method
Descriptive qualitative study design using face-to-face semi-structured interviews. Purposive sampling was used to select ED clinicians from two high and two low performing intervention sites. Eligible participants were as follows: Medical Directors, Nurse Unit Mangers, bedside nurses and clinical champions. Participants were interviewed about their views on the barriers and facilitators to implementation. Data were analysed thematically and a final set of themes derived.
Results
Twenty-five interviews were completed. Three major themes were the dynamics of change, protocol fidelity and care trajectory. Dynamics of change represents the challenges of achieving implementation in a context of high staff turnover; Fidelity to the protocol represents the impact of organisational factors on intervention fidelity, and Care Trajectory represents the availability of resources along the patient pathway that impacted on whether elements of the protocols were delivered.
Conclusion
Implementing an intervention in the busy and complex setting of the ED can compromise the delivery of evidence-based care protocols. Factors that affect delivery including resources, staff turnover and workplace context require addressing to ensure success implementation.
Trial registration number
Australian New Zealand Clinical Trials Registry: ACTRN12614000939695
AS12-008
PREHOSPITAL CLINICAL TRIAGE MODELLING SUBSTANTIALLY REDUCES TIME TO ENDOVASCULAR THROMBECTOMY IN MELBOURNE, AUSTRALIA
1The Royal Melbourne Hospital, Neurology, Parkville, Australia
2Ambulance Victoria, Research & Evaluation, Melbourne, Australia
3Ambulance Victoria, Clinical Services, Melbourne, Australia
Background and Aims
Clinical triage tools facilitate identification and bypass of patients with suspected large vessel occlusion (LVO) to comprehensive stroke centers (CSC), avoiding lengthy inter-hospital transfers from primary stroke centers (PSC). We estimated the real-world reduction in time to endovascular thrombectomy (EVT) using the Ambulance Clinical Triage-For Acute Stroke Treatment (ACT-FAST) triage algorithm.
Method
All patients in the ongoing ACT-FAST Ambulance Victoria paramedic validation study who were assessed as ACT-FAST-Positive and required metropolitan inter-hospital transfer to the Royal Melbourne Hospital CSC were included. Theoretical time saved by bypass was estimated using Google Maps application-programming-interface calculated scene-to-EVT time for direct transport to the CSC compared to actual inter-hospital transfer times.
Results
A total of n = 13 ACT-FAST-Positive patients were transferred from three PSCs approximately 20min from CSC. The calculated median time difference from scene of ambulance attendance to nearest PSC versus CSC (potential thrombolysis delay) was 12min. Median inter-hospital transfer time was 109min. Bypass to CSC would have reduced median total on-road time by 8min and median time from scene-to-CSC-arrival by 92min (range 52-149min;p < 0.001). At our institution CSC-arrival-to-EVT is 35min longer for direct presentations versus transfers. Bypass would therefore reduce scene-to-EVT by median 57min.
Conclusion
Implementing a paramedic-triaged bypass strategy in Melbourne, Australia is predicted to substantially reduce time to EVT by approximately one hour. Pre-hospital triage would remain beneficial unless transfers times were dramatically reduced, provided CSCs maintain efficient workflow. In this metropolitan region, bypass to CSC would cause minimal delay in intravenous thrombolysis. Full results of ongoing data collection will be available for presentation.
Trial registration number
N/A
AS12-009
EVALUATION OF STROKE CARE QUALITY IN ARMENIA: DATA FROM REGISTRY OF STROKE CARE QUALITY (RES-Q)
1Erebouni Medical Centre, Neurology Department, Yerevan, Armenia
2Medical Centre Surb Grigor Lusavorich, General and Vascular Neurology Department, Yerevan, Armenia
3Yerevan State Medical University, University Neurosurgery Clinic and Comprehensive Stroke Centre, Yerevan, Armenia
4“Armenia” Republican Medical Centre, Neurology Department, Yerevan, Armenia
5Medical Union #2, Neurology Department, Yerevan, Armenia
Background and Aims
Organisation of stroke care remains the backbone of successful stroke management. This study was performed as a part of RES-Q program aiming to monitor stroke care parameters in Armenia.
Method
Data collection was performed prospectively using a standardised forms of the RES-Q study by four leading neurology departments during a predefined period of two month of RES-Q study.
Results
237 stroke patients were recruited during 2 months. 36.7 % were men, median age was 67 years and only 70.9 % of them were with ischemic stroke. 203 patients (86%) were treated in ICU/stroke unit and the median hospital stay was 11 days, mainly due to lack of unavailability of rehabilitation facilities (See Table below). Only 8.1 % of ischemic strokes were screened for atrial fibrillation and prescription of anticoagulant use for AF patients is low. Only minority was treated with thrombolytic agents. Major vascular risk factors were smoking (84.8 %), uncontrolled hypertension. In hospital death rate was 30.8 %.
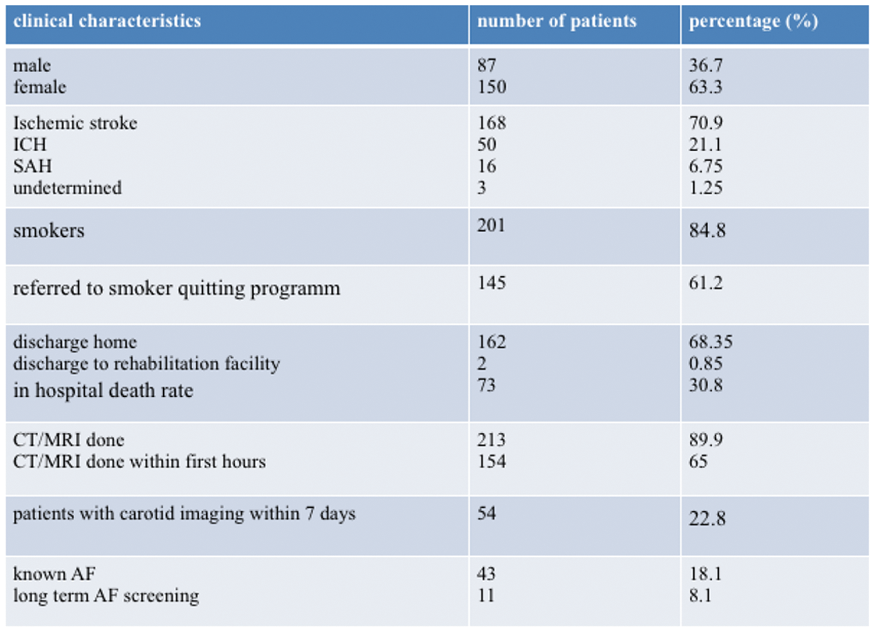
Conclusion
Stroke is a major cause of death and disability in Armenia. Our data show the frequency of specific risk factors and several limitations of stroke care in Armenia. This data may help us to establish a national program to improve the quality of stroke care and management in Armenia.
Trial registration number
N/A
AS12-010
DEVELOPMENT AND EVALUATION OF A TELEMEDICINE CLINIC SERVICE FOR CADASIL
1University of Cambridge, Clinical Neurosciences, Cambridge, United Kingdom
Background and Aims
Genetic forms of stroke such as CADASIL are rare, but have important implications for the family and require specialised care. We run a national CADASIL clinic, where some patients have travel times of up to 10 hours. Following patient feedback, we evaluated alternative methods of providing this care. Funded by the Evelyn Trust, we developed a telemedicine service to carry out follow-up appointments in patient’s own homes using Skype technology.
Method
Telemedicine patients and in-person control patients were asked to fill out the following 3 questionnaires as soon as possible after their follow-up consultation: a satisfaction questionnaire, the Hospital Anxiety and Depression Scale (HADS) and the short form of the State-Trait Anxiety Inventory (STAI-6). Rankin Score and whether patients had a diagnosis of dementia was recorded. Clinicians were also asked to fill in a questionnaire for both appointment types.
Results
57 telemedicine patients and 50 in-person outpatients participated. Mean (SD) age and Rankin score were 53.94(10.82) years and 1.21(1.32). Mean scores on the satisfaction questionnaire were 4.53/5 and 4.69/5 for telemedicine and in-person clinics (p = 0.248). Clinician experience was similar for the telemedicine and in-person appointments (4.55/5 v 4.60/5, p = 0.407). There was a weak but significant negative correlation between Rankin score and patient evaluation score (p = 0.002, Spearman’s rho = −0.314).
Conclusion
A telemedicine follow-up system via Skype achieved similar high levels of patient and clinician satisfaction to that of in-person consultations. This suggests that telemedicine is a viable alternative to in-person appointments for patients with rare stroke disease such as CADASIL.
Trial registration number
N/A
AS12-011
ANALYSIS OF LOCAL PATTERNS OF STROKE PRESENTATION INFORMS SERVICE PLANNING FOR INTRA-ARTERIAL THROMBECTOMY
1Royal Sussex County Hospital, Stroke- Nigel Porter Unit, Brighton, United Kingdom
Background and Aims
The intra-arterial thrombectomy (IAT) service at the Royal Sussex County Hospital, Brighton, UK is currently available in daytime hours with a desire to extend its availability. We investigated the time of day strokes presented to the hospital to ascertain the highest demand for the IAT services
Method
Data were collected on patients with a diagnosis of ischaemic stroke over one year (n = 548). Patients were divided into groups depending on time of day admitted. We estimated the number of patients that may benefit from IAT according to specified criteria. We included patients admitted to hospital within 4.5 hours and 22.5 hours of symptom onset to mirror standard and DAWN trial time frames
Results
For patients admitted within the standard 4.5 hours, 42% presented within weekday working hours and a further 23% up to midnight. 22% presented at weekends up to midnight. In total, 87% of eligible patients presented 8am-midnight 7 days a week and only a further 13% overnight. Within the 22.5 hour time frame, over 7 days, 90% of patients presented between 8am-midnight with 10% presenting overnight
Conclusion
IAT services operating in a resource-limited environment may wish to consider expanding in a step-wise progression that ensures resources are targeted in the most cost efficient way and ensure equity of care provision. Data from Brighton supports previously published evidence regarding the expansion of IAT provision
Trial registration number
N/A
AS12-012
REASONS FOR PREHOSPITAL DELAY IN ACUTE ISCHEMIC STROKE: HINTS ON INCREASING THE RATE OF RECANALIZATION THERAPIES – A PROSPECTIVE COHORT STUDY
1University Hospital Basel, Neurology and Stroke Center, Basel, Switzerland
2University Hospital Basel, Intensive Care Medicine, Basel, Switzerland
Background and Aims
Delays in the prehospital phase jeopardize the chances for stroke patients to be treated with recanalization therapies (RT). Education campaigns targeting potential patients are expensive, and showed contradictory results in terms of increasing the RT rate. We investigated the causes for prehospital delay in stroke patients to identify novel factors to improve.
Method
In this prospective cohort study, we included 337 patients with an MRI-confirmed acute ischemic stroke admitted to the University Hospital Basel Stroke Center between 2015 and 2017. Trained study nurses interviewed all patients along a 28-item questionnaire.
Results
147(44%) patients arrived at the hospital within 4.5h, 190(56%) more than 4.5h after symptom onset. In the first group, 71 patients (48%) received RT compared to 11(6%) in the delayed group. Overall, 96 patients (28%) first alarmed the general practitioner (GP). Among these patients, the delay from symptom-onset to the alarm call exceeded 3h in 53% versus 29% among patients who did not call the GP (p < 0.001). After adjusting for delayed alarming, calling the GP first was associated with a lower rate of RT (aOR 0.39,95%-CI 0.19−0.80, p = 0.01). In patients who first called the GP, delays occurred mostly due to delays in the transportation to the hospital.
Conclusion
Even in a relatively small urban area, prehospital delay occurred in more than half of stroke patients, and was associated with a lower probability of receiving a RT. Calling the GP first, even within 3h of symptom onset, was associated with a reduced RT rate. Information campaigns targeting the GPs may increase RT rates.
Trial registration number
N/A
AS12-013
HIGH CINCINNATI PREHOSPITAL STROKE SCALE SCORE (3/3) AS A TOOL TO DETECT LARGE VESSEL-OCCLUSION STROKE IN THE PREHOSPITAL SETTING
1CHUM-Centre hospitalier de l'Université de Montréal- Axe Neurosciences CRCHUM, Neurosciences, Montreal, Canada
2CHUM-Centre hospitalier de l'Université de Montréal- Axe Neurosciences CRCHUM-, Neurosciences, Montreal, Canada
Background and Aims
Prehospital identification of large vessel occlusion (LVO) stroke may expedite treatment by direct transfer to comprehensive stroke centers (CSC) with endovascular capabilities. The Cincinnati Prehospital Stroke Scale (CPSS) is currently used by Emergency Medical Services (EMS) for prehospital stroke identification. We assessed whether a CPSS score of 3/3 can reliably detect LVO stroke.
Method
We conducted a retrospective analysis of all patients transferred by EMS for suspected stroke to a high-volume CSC over a 12-month period halfway through which EMS diversion of patients with CPSS 3/3 directly to CSC was implemented (6 months pre- /6 months post-implementation). Charts and neuroimaging were reviewed to determine final diagnosis and presence of LVO.
Results
Of 383 patients evaluated during the study period, 224 (58%) had a prehospital CPSS 3/3 score and 159 (42%) had a CPSS<3. Among those with CPSS 3/3, 152 (68%) were diagnosed with acute ischemic stroke, including 62 (28%) LVO stroke. The remainder of CPSS 3/3 were diagnosed with transient ischemic attack 8 (3.6%), intracerebral hemorrhage 35 (15.6%), or mimics 29 (12.9%). Only 12(3%) patients with CPSS<3 had LVO stroke. EMS diversion of CPSS 3/3 to CSC led to a 2.4-fold increase in acute stroke evaluations (n = 124 pre- versus n = 303 post-implementation).
Conclusion
A high (3/3) CPSS score is a simple tool for prehospital LVO detection with easy implementation. Nevertheless, EMS diversion of CPSS 3/3 to CSC substantially increased patient volume. Further studies are warranted to weigh the simplicity of CPSS 3/3 against more specific yet potentially more complex prehospital LVO detection scales.
Trial registration number
n/a
AS12-014
A REVIEW OF THE MECHANICAL THROMBECTOMY SERVICE AT A LARGE UK TEACHING HOSPITAL
1Sheffield Teaching Hospitals, Stroke Department, Sheffield, United Kingdom
Background and Aims
An intra-venous thrombolysis (IVT) service has been established at Sheffield Teaching Hospitals for several years. Mechanical thrombectomy (MT) for acute ischaemic stroke in selected patients has been shown to produce favourable outcomes. Therefore, a new collaborative pathway was created to provide MT for selected patients within working hours.
Method
After several patients have undergone MT we have retrospectively audited against standards taken from The British Association of Stroke Physicians.
Results
12 patients underwent MT between January 2016 and July 2017. 2 patients were excluded as they were clear outliers. 3 of the remaining 10 patients only had MT and did not have IVT due to contraindications.
100% had large vessel occlusions with symptom onset to MT <5hr (mean3hrs19mins, range 1hrs47mins-4hrs35mins). The IVT to groin puncture time was achieved at < 90mins with mean 1hr 4mins (range 57mins-1hr21mins).
Mean groin puncture time to start of revascularisation was 28.9mins (Range 9-65mins). This represents 90% patients meeting the standard of <45mins. Median groin puncture time to end of revascularisation was 66mins (Range 30-163mins). Revascularisation achievement was 70% TICI-grade 2b or above.
One patient suffered haemorrhagic transformation but did not meet the SICH criteria.
Conclusion
We have demonstrated that a MT pathway can be created alongside an established IVT pathway. Our patients were appropriately selected as they had proximal vessel occlusion, received MT within the recommended time and revascularisation rate was high. Areas for ongoing improvement include a customised assessment area within the radiology department, MT flowcharts and a dedicated MT coordinator to improve communication.
Trial registration number
n/a
AS12-016
STROKE AWARENESS AMONG PRIMARY HEALTH CARE ATTENDANTS IN ABHA, SOUTH WESTERN SAUDI ARABIA
1King Khalid University, Neurology Section- department of Medicine - College of Medicine, abha, Saudi Arabia
2King Khalid University, Family and Community Medicine - College of Medicine, Abha, Saudi Arabia
3College of Medicine- Mansoura University, Department of Community Medicine, Mansoura, Egypt
Background and Aims
Awareness about stroke warning signs, risk factors and proper response could improve the outcome and minimize the burden of stroke. This is the first study to examine the awareness of major stroke symptoms, risk factors and response among the population in Abha, Saudi Arabia
Method
A cross sectional study involved 1472 adult subjects. The sample was stratified by the primary healthcare centers (PHCCs) to represent the composition of Abha City’ PHCCs adult attendants. Consecutive persons attending PHCCs on selected days during the study period were invited to participate. A validated questionnaire was used to evaluate the participant’s awareness about stroke. Multivariable logistic regression was used to assess factors associated with awareness of stroke symptoms, major stroke risk factors and response
Results
Only 936 (63.6%) and (43.7%) correctly recognized thrombosis and hemorrhage, respectively, as types of stroke. Commonly identified risk factors were hypertension (55.8%) and dyslipidemia (45.8%).most frequently recognized symptoms were sudden headache (54.1%), dizziness (51.0%) and difficulty in speaking (44.3%). The most frequently reported correct responses were contacting a doctor (73.0%), going to the hospital (67.2%) and calling an ambulance (52.4%). Improper response to stroke (ignoring the condition and/or self-prescribing medications) was mentioned by 18.8%. In binary Females (aOR = 1.70, 95%CI: 1.29-2.25), married and older persons were significantly more prone to have insufficient knowledge of proper response.
Conclusion
Worrying deficit of knowledge about stroke warning symptoms, risk factors and proper response is detected. Health education strategies to improve stroke awareness are urgently required and could potentially prevent and improve outcome of stroke
Trial registration number
N/A
AS12-017
DRIP AND SHIP IN BRUSSELS, “THE WELL-KNOWN WORST TRAFFIC JAMMED CITY IN EUROPE”, A REAL GOOD IDEA?
1Europe Hospitals, Stroke Unit, Brussels, Belgium
2Brussels St-Luc University Hospital, Stroke Unit, Brussels, Belgium
3Brussels St-Luc University Hospital, Interventional Radiology, Brussels, Belgium
4Clinique Saint-Pierre, Stroke Unit, Ottignies, Belgium
5Hôpital de Jolimont, Stroke Unit, Haine Saint-Paul, Belgium
6Clinique Saint-Jean, Stroke Unit, Brussels, Belgium
7AZ Jan Portaels, Stroke Unit, Vilvoorde, Belgium
Background and Aims
We aim to determine if the “drip and ship” paradigm, with first admission in a Primary Stroke Center (PSC), then transfer in a Comprehensive Stroke Center (CSC), could be more hazardous, than “mothership” paradigm (direct admission in CSC) in Brussels.
Method
We conducted a retrospective analysis on stroke patients, admitted in a CSC of Brussels, who benefited a thrombectomy (January 1st, 2016 to September 30st, 2017). The main outcome was the 3-months mRS. Patients were dichotomized in two groups; “drip and ship” (PSC) vs “mothership” (CSC).
Results
106 patients (PSC: 55; CSC: 51) were included in the study. Median 3-months mRS was 2 for PSC patients and 3 for CSC patients (P = 0,46). Details in table 1 and figure 1.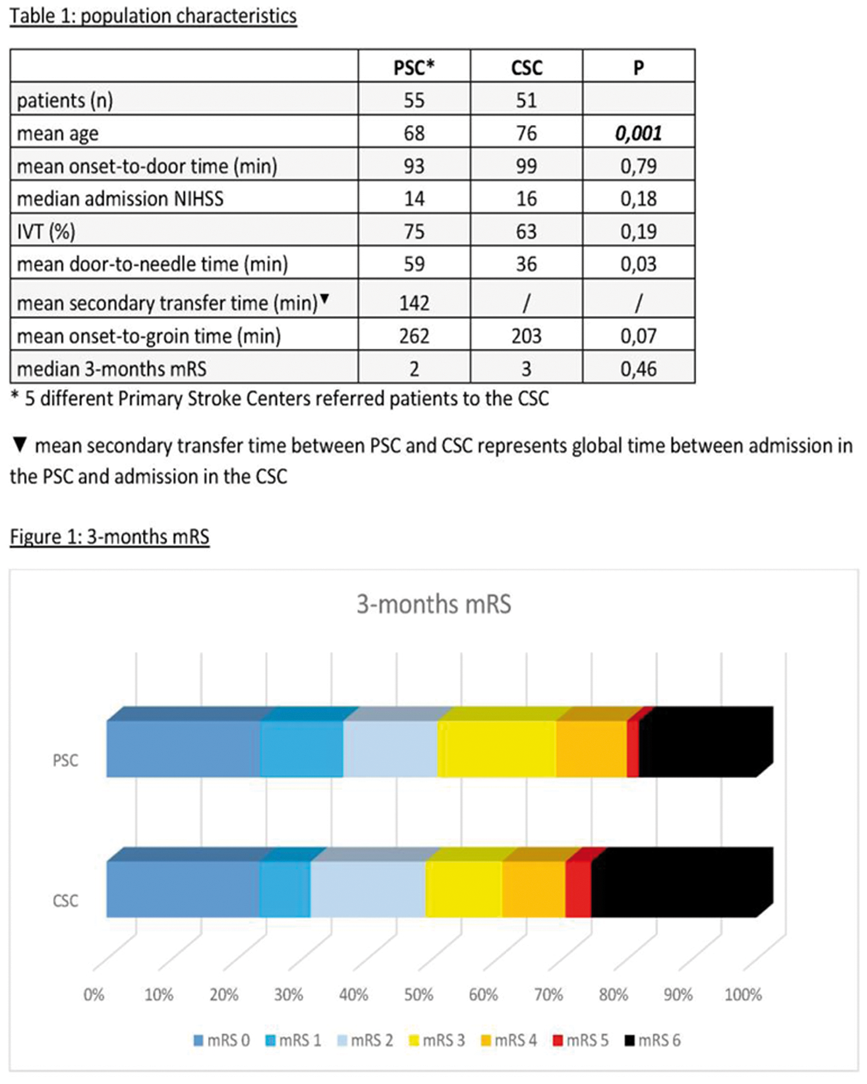
Conclusion
The “Drip and Ship” in Brussels seems not to be hazardous. Despite a longer non-significant delay to groin puncture, there is no significant difference for the 3-months mRS between both groups. This result should be interpreted with caution (retrospective analysis and disparities between groups for age). This study emphasizes also the important problem of secondary transfer from PSC. This is an issue that should be taken into account for all stakeholders.
Trial registration number
N/A
AS12-018
RECOMMENDATIONS OF STROKE COMPETENCE BY THE SWEDISH STROKE COUNCIL
1Institute of Medicine, Department of Medicine, Gothenburg, Sweden
2Sahlgrenska University, Neurology, Gothenburg, Sweden
3Umeå University- and Karolinska Institutet Danderyds hospital- Sweden., Medicine, Umeå, Sweden
4Lunds University, Neurology, Lund, Sweden
Background and Aims
The Swedish Stroke Register (Riksstroke) shows that performance quality indicators of acute stroke care vary substantially, irrespective hospital size. E.g. the proportion thrombolysed patients varied between 2-24%, and door to needle time within 30 minutes between 0-86%. Our aims are to: improve quality, reduce variation and make stroke care more equal, secure competence for rapid reperfusion treatment 24/7, form a basis for education of stroke physicians and nurses and to help organize SU care.
Method
In order to reduce the variations and improve the quality of stroke care the Swedish Stroke Council (SSC) has developed a triangle quality assessment (TQA) method described elsewhere. For the stroke team (non-physicians), specific stroke competence is defined by stroke education according to the Swedish Stroke Association or University studies. However, stroke competence of physicians is not defined. The TQA's show a great variety in stroke competence among Swedish SUs but also in the Emergency departments.
The SSC has defined stroke skills for physicians in all positions from ambulance to regional stroke specialist care. The SSC has also defined competence for doctors and nurses responsible for thrombolysis.
Results
Competence for thrombolysis include: work at SU, competence in performing physical examination and NIHSS, theoretical stroke knowledge, participation and handling several thrombolyses alternatively simulator training, continuous medical education (theoretical and practical). All moments should be approved by the responsible stroke physician. Details will be provided at the presentation.
Conclusion
Definitions of stroke competence are needed to reduce variations in stroke care.
Trial registration number
N/A
AS12-019
AMBULANCE CLINICAL TRIAGE-FOR ACUTE STROKE TREATMENT (ACT-FAST): 3-STEP PARAMEDIC TRIAGE ALGORITHM FOR ENDOVASCULAR THROMBECTOMY
1The Royal Melbourne Hospital, Neurology, Parkville, Australia
2Ambulance Victoria, Research & Evaluation, Melbourne, Australia
3Ambulance Victoria, Clinical Services, Melbourne, Australia
Background and Aims
The Ambulance Clinical Triage-For Acute Stroke Treatment (ACT-FAST) algorithm is a 3-step paramedic triage tool for pre-hospital recognition of endovascular-eligible large vessel occlusion (LVO), designed to improve specificity by recognising only a severe clinical syndrome. ACT-FAST sequentially assesses [1) Unilateral arm fall to stretcher <10sec; 2) Severe language disturbance (right arm weak) or severe gaze deviation/hemi-neglect assessed by shoulder tap (left arm weak)] followed by clinical eligibility questions. We present the results of the ongoing validation study.
Method
The ACT-FAST paramedic validation study commenced in June 2017. Ambulance Victoria paramedics assessed ACT-FAST in all suspected stroke patients pre-hospital in metropolitan Melbourne, Australia, and in the Royal Melbourne Hospital Emergency Department. Algorithm results were validated against a comparator of ICA/M1-occlusion with NIHSS≥6 (Class 1 indication) accepted for endovascular thrombectomy.
Results
A total of n = 87 (ED n = 68, pre-hospital n = 19) assessments were completed in the first 6months. Diagnoses were LVO n = 14(16.1%), non-LVO infarcts n = 33(37.9%), ICH n = 6(6.9%) and no stroke on imaging n = 34(39.1%). ACT-FAST showed 85.7% sensitivity, 90.4% specificity, 63.2% positive predictive value and 97.1% negative predictive value for LVO. Of 7 false-positives, 3 received thrombectomy for non-Class 1 indications (M2 occlusions/dissection), 2 were ICH, and 1 was tumour. Two false-negatives were LVO with mild syndromes.
Conclusion
The 3-step ACT-FAST algorithm is a simple and rapid paramedic-assessed triage tool that shows high accuracy for endovascular-eligible LVO, despite requiring just two examination steps. The streamlined algorithmic approach presents a practical option for implementation in large emergency services. Results at 9months will be available for presentation at ESOC.
Trial registration number
N/A
AS12-020
TRIANGLE QUALITY ASSESSMENT OF STROKE UNITS IN SWEDEN
1Institute of Medicine, Department of Medicine, Gothenburg, Sweden
2Region Västra Götaland, Executive, Gothenburg, Sweden
3Sahlgrenska University Hospital, Neurology, Gothenburg, Sweden
4Umeå University- and Karolinska Institutet Danderyds hospital, Medicine, Umeå, Sweden
5Lund University, Neurology, Lund, Sweden
Background and Aims
The Swedish Stroke Council has developed an instrument for evaluation and improvement of stroke unit (SU) care: the Triangle quality assessment (TQA).
Method
Eight criteria for good stroke care, concerning either availability, competence, procedure or evaluation, were defined using the Swedish National Stroke Guidelines.
A web-based survey with questions regarding each criterion as well data from the National quality register (Riksstroke) was designed. The management of each clinic/SU answered the survey. The results were presented in a combined report and entered into a quality matrix of five degrees from E to A (centre of excellence).
Interdisciplinary assessment teams from all involved SUs were trained. Using the report, a team from SU A evaluated SU B, a team from SU B evaluated SU C, which in turn evaluated SU A. The management was interviewed first and then the team.
Strengths and improvement areas were identified for each criterion and presented to the SU.
Results
Thirty of 72 Swedish SUs have been assessed and around 30 are due 2018. The TQA is performed by the profession and results in learning by assessing and being assessed. The teams take home new working methods, share routines and stimulates improvement work. Unequal medical care is uncovered and hospitals not fulfilling criteria for good stroke care are identified. The TQA leads to both local and regional improvement strategies and new routines.
Conclusion
The TQA is a useful method for knowledge implementation, and management in macro- as well as meso- and micro perspectives.
Trial registration number
N/A
AS12-021
IMPLEMENTATION OF ACUTE STROKE CARE PRACTICE GUIDELINES AND IMPROVEMENT IN STROKE CARE – FOUR YEARS’ EXPERIENCE AT A MIDDLE EASTERN CENTER
1Hamad General Hospital, NEUROSCIENCE, Doha, Qatar
2Hamad Medical Corporation, Emergency medicine, Doha, Qatar
3Hamad Medical Corporation, Neuroscience Institute, Doha, Qatar
Background and Aims
Interdisciplinary guidelines help in improving acute stroke (AS) care. We aim to determine if implementation of AS guidelines improved care of stroke patients in Qatar.
Method
Since the establishment of Neuroscience institute at Hamad Medical Corporation in January 2014, we developed six clinical practice guidelines [AS care in emergency department, inpatient care, rehabilitation, non-surgical intracerebral hemorrhage (ICH), tele-stroke and transient ischemic attack (TIA)] and a stroke database for AS patients care.
Results
5229 patients recorded in database between January 2014-December 2017 (78.1% males). Mean age 53.51 ± 13.8 years, 55.6% (n = 2908) ischemic stroke (IS), 13.3% (n = 697) ICH, 10.9% (n = 568) TIA, 19.3% (n = 1011) with mimics. On admission 68.1% (n = 3561) hypertensives and 48.7% (n = 2547) diabetics. In acute IS, IV thrombolysis increased [8.0% (n = 51) in 2014 to 14.8% (122) in 2017, p < 0.0001], interventional thrombectomies [0.3% (n = 2) in 2014 to 5.0% (n = 41) in 2017, p < 0.0001. Length of stay reduced from 7.8 (95%CI 6.6-8.9) to 5.3 (95% CI 4.9-5.6) days, p < 0.0001) in IS, while 16.4 (95%CI 13.1-19.8) to 10.7 (95%CI 9.2-12.2), p < 0.0001) in ICH. Good prognosis (mRS 0-2) at 90-days improved significantly from 60.4% (n = 545) in 2014 to 70.2% (n = 1189) in 2017, p < 0.0001, while there was a clinically significant reduction in overall mortality (from 6.7% to 5.1%) during the same time.
Conclusion
Introduction of an organized acute stroke service and implementation of guidelines helps in continuous improvement in AS care.
Trial registration number
none
AS12-022
QUALITY OF CARE OF ACUTE STROKE PATIENTS IN LITHUANIA: NATIONAL DATA
1Republican Vilnius University hospital, Department of Neurology, Vilnius, Lithuania
2Vilnius University- Faculty of Medicine, Institute of Clinical Medicine, Vilnius, Lithuania
3Vilnius University Hospital Santaros Klinikos, Department of Neurology, Vilnius, Lithuania
4Lithuanian University of Health Science- Medical Academy, Clinic of Neurology, Kaunas, Lithuania
5Klaipeda Seamen’s Hospital, Department of Neurology, Klaipeda, Lithuania
6Republican Panevezys Hospital, Department of Neurology, Panevezys, Lithuania
7International Clinical Research Center- St. Anne's University Hospital, Department of Clinical Neurology, Brno, Czech Republic
Background and Aims
Quality of care (QOC) of acute stroke patients (ASP) is essential to improve long-term outcomes, decrease mortality and long-term disability. Recent studies have shown that QOC varies across countries and across hospitals in country. The aim of this study was to estimate the QOC of ASP in Lithuania, identify the gaps and suggest ways to improve it.
Method
All ASP (ischemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage) treated in 5 largest stroke centres in Lithuania during October 2017 were included in our study. The RES-Q questionnaire was used. The questions covered imaging, treatment and secondary prevention topics.
Results
330 ASP (ischemic stroke-92.4%, intracerebral hemorrhage-6.4%, and subarachnoid haemorrhage–1.2%) were included. 63.3% (8.6-93.6%) of all patients were treated in a stroke unit. CT or MRI scans were performed in 99.7% (98.9-100.0%) of all patients on admission. 27.9% (7.8-65.0%) of acute ischemic stroke patients received recanalization therapy; the median door-to-needle time was 41 (39 – 57) min. Only 0.92% (0-2.5%) of ASP were screened for dysphagia. AF screening was done in 10.3% (0-68.9%) of ischemic stroke patients, however, none were screened for ≥24 h. On discharge antiplatelet treatment was given to 91.8% (87.5-97.1%) of non-AF patients; anticoagulant treatment – to 83.0% (66.7-95.7%) of AF patients.
Conclusion
We found that the main gaps in QOC of ASP in Lithuania were insufficient screening for dysphagia and cardiac monitoring for AF. Door-to-needle time should be improved as well. Introduction of a dysphagia protocol and education of hospital staff is needed to improve care for ASP.
Trial registration number
N/A
AS12-023
NEURONEGATIVE IMAGING – A FORGOTTEN METRIC?
1Luton & Dunstable Hospital, Stroke medicine, Luton, United Kingdom
Background and Aims
The rate of ischaemic strokes thrombolysed worldwide is increasing – with the current rate being between 20 and 25%. However, it is becoming increasingly clear that a large amount of stroke mimics are also being thrombolysed and, whilst there is no clear data available on the mimic rate, the current London average is approximately 45%.
Secondly, neuronegative imaging has become a forgotten metric and is often excluded from large auditing processes, meaning the importance of accurate clinical assessment is not taken into account.
Method
A literature review was conducted using stroke articles and publicly available data from audit. Evidence was also used from a six-month audit in 2016 at Luton & Dunstable Hospital on patients who received thrombolysis.
Results
Between June and November 2016, 71 patients received thrombolysis at Luton & Dunstable Hospital. Of this cohort, only 9% of patients were found to have no evidence of ischaemia following CT and MRI. Furthermore, of the patients thrombolysed, only 8.5% were diagnosed with a stroke mimic on discharge and only 6% experienced complications.
The low levels of stroke mimic diagnosis and neuronegative imaging indicates that comprehensive clinical assessment is imperative in lowering stroke mimic rates and it is likely that expertise and thorough assessment result in fewer complications secondary to thrombolysis.
Conclusion
We propose the need for large-scale data on stroke mimic rates. Furthermore, the complication rate and neuronegative imaging rate following thrombolysis will need examining in national and international registries in order to promote standards of care in stroke thrombolysis.
Trial registration number
N/A
AS12-024
ACCURACY OF PREHOSPITAL STROKE RECOGNITION BY AMBULANCE MEDICAL STAFF IN SAINT-PETERSBURG, RUSSIA
1Saint Petersburg Research Institute of Emergency Medicine n.a. I.I. Dzhanelidze, Dept. of emergency medical care organisation, Saint-Petersburg, Russia
2Saint Petersburg Research Institute of Emergency Medicine n.a. I.I. Dzhanelidze, Department of acute cerebrovascular pathology and emergency neurology, Saint-Petersburg, Russia
Background and Aims
Stroke mimics are reported at a rate of 9-31% and may overburden the resources of stroke centres. We aimed to study the accuracy of acute stroke recognition by ambulance staff.
Method
Pre-specified neurological signs were systematically recorded in patients with suspected acute stroke consecutively admitted to 9 stroke centers via ambulance. Data were collected prospectively during September 2017. Statistical analysis was performed with Stata 12SE.
Results
We identified 475 patients, 43% men, median age (IQR) 68 (59-80), median admission NIHSS score 4 (0-8). Stroke diagnosis was confirmed in 291 (67%), rejected upon admission in 115 (26.5%), and reconsidered on discharge in 28 (6.5%). Patients with confirmed stroke were older (mean age 70 vs. 65, p < 0.01), with higher NIHSS scores (median admission NIHSS 5 (2-10) vs. 0 (0-2), p < 0.01), had distinct focal neurological deficit (56% vs. 41%, p < 0.01), but less frequent nonspecific (headache, impaired coordination, loss of consciousness) neurological signs (42% vs. 55%, p = 0.011). Speech difficulties (75% vs. 25%, p < 0.01, accuracy 50%), motor deficit (79% vs. 21%, p < 0.01, accuracy 52%), facial asymmetry (81% vs. 19%, p < 0.01, accuracy 43%), hemi-sensory loss (76% vs. 24%, p < 0.01, accuracy 47%), but not visual defect and level of consciousness were associated with final stroke diagnosis. Dizziness was inversely associated with stroke (p < 0.01). None of the stroke signs reported by prehospital staff was predictive of major arterial occlusion.
Conclusion
Accuracy of stroke recognition by prehospital medical professionals is low. Training of emergency medical services should aim to improve stroke recognition in younger patients, minor strokes, atypical clinical presentation.
Trial registration number
N/A
AS12-025
MODELLING THE USE OF A NEW LARGE VESSEL OCCLUSION SCREENING TOOL FOR ISCHEMIC STROKE TRANSPORT DECISION MAKING IN VICTORIA, AUSTRALIA
1University of Calgary, Community Health Sciences and Hotchkiss Brain Institute, Calgary, Canada
2The University of Melbourne, Melbourne Brain Centre at Royal Melbourne Hospital- Department of Medicine, Melbourne, Australia
3University of Calgary, Mechanical and Manufacturing Engineering, Calgary, Canada
4University of Calgary, Electrical and Computer Engineering, Calgary, Canada
5University of Calgary, Community Health Sciences- Hotchkiss Brain Institute- Clinical Neurosciences- Calgary Stroke Program- and Medicine, Calgary, Canada
6University of Calgary, Clinical Neurosciences and Electrical and Computer Engineering, Calgary, Canada
Background and Aims
Clinical triage tools facilitate pre-hospital recognition of large vessel occlusion (LVO) for endovascular thrombectomy (EVT). Tools have variable positive predictive value (PPV), which impacts transport decision-making. We modelled the effects of the Los Angeles Motor Scale (LAMS) and Ambulance Clinical Triage-For Acute Stroke Treatment (ACT-FAST) algorithm, on transport strategies for EVT in Victoria, Australia.
Method
Using conditional probability modelling, the PPV of LAMS≥4 and ACT-FAST from a prospective validation study were combined with the efficacy decay of alteplase and EVT over time to predict the probability of good outcome (mRS 0-1 at 90days) for “drip-and-ship” (alteplase at nearest stroke hospital then transfer for EVT) and “mothership” (bypass to nearest EVT-centre) strategies.
Results
As the PPV of ACT-FAST is higher than LAMS (56% vs 43%) the areas where mothership predicts the best outcome are larger (Figure 1 – Panel A). This is especially pronounced if door to needle times at thrombolysis centres are slow (Figure 1 – Panel B). The absolute probability of good outcome decreases as PPV increases because more LVO strokes, with inherently poorer outcomes than most false positives, are identified.
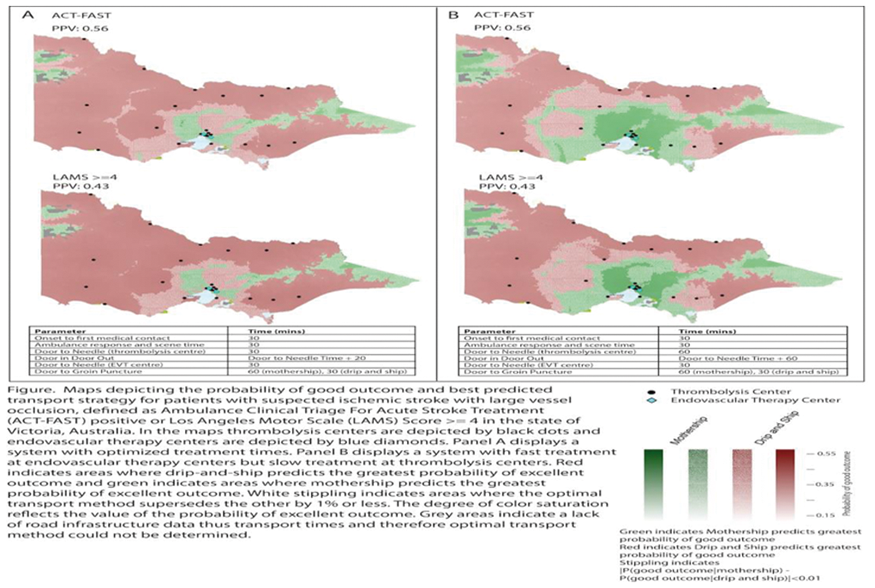
Conclusion
Due to the efficacy of EVT for LVO stroke a LVO triage tool with a higher PPV, such as ACT-FAST, will increase the area where mothership predicts the greatest probability of good outcome for patients with suspected LVO.
Trial registration number
N/A
AS12-026
A NATIONAL STROKE PUBLIC EDUCATION CAMPAIGN IN SINGAPORE INCREASED EARLY ARRIVAL AT HOSPITAL
1National Neuroscience Institute, Department of Neurology, Singapore, Singapore
Background and Aims
Acute reperfusion therapies for ischemic stroke are time-limited. Effectiveness of public education campaigns to improve onset-to-door time have been studied in different countries with varying results. We evaluated the effectiveness of the first national stroke public education campaign in Singapore in increasing the proportion who arrived within reperfusion treatment windows.
Method
A nation-wide ‘FAST’-based stroke public education campaign in Singapore was held in 2016. We prospectively evaluated consecutive patients with acute ischemic stroke admitted to two large tertiary hospitals over two 2-month periods before and after the campaign. Outcome measures were early arrival within 3.5 hours (for intravenous thrombolysis consideration) and within 7 hours (for endovascular therapy consideration), use of the ambulance service and thrombolysis rates.
Results
We recruited 154 patients before the campaign, and 75 patients after, 36.6% of whom of reported having been exposed to the campaign. The proportion of patients who arrived to the hospital early increased from 31.8% to 41.3% (aOR = 1.78 [0.93–3.41]; P = 0.080) for the 3.5-hour window and from 46.1% to 60.0% (aOR = 2.04 [1.08–3.85]; P = 0.027) within the 7-hour window. Neither ambulance use (36.4% vs 42.7%; P = 0.357) nor thrombolysis rates (14.9% vs 16.0%; P = 0.834) improved.
Conclusion
Our inaugural national stroke public awareness campaign was effective in increasing the proportion of patients arriving within acute reperfusion treatment time windows, doubling the proportion reaching hospital within 7 hours of onset. Possible reasons for the campaign’s positive impact include poor rates of early arrival prior to campaign and Singapore’s small geographical area facilitating outreach.
Trial registration number
N/A
AS12-027
ASSESSING ORGANISATIONAL CONTEXT IN EMERGENCY DEPARTMENTS PRIOR TO IMPLEMENTING EVIDENCE-BASED STROKE CARE PROTOCOLS – THE T3 TRIAL CONTEXT ANALYSIS
1Nursing Research Institute, St Vincent’s Health Australia Sydney and Australian Catholic University, Sydney, Australia
2National Centre for Epidemiology and Population Health NCEPH, Australian National University, Canberra, Australia
3School of Medicine and Public Health- Faculty of Health and Medicine, The University of Newcastle, Callaghan, Australia
4Stroke and Ageing Research, School of Clinical Sciences at Monash Health- Monash University, Clayton, Australia
5Florey Institute of Neuroscience and Mental Health, University of Melbourne, Parkville, Australia
6Centre for Diabetes and Endocrinology Research, Westmead Hospital and University of Sydney, Westmead, Australia
7Department of Medicine, University of Ottawa, Ottawa, Canada
8Ottawa Hospital Research Institute, Ottawa Hospital, Ottawa, Canada
9Department of Neurology, John Hunter Hospital, Newcastle, Australia
10Centre for Translational Neuroscience and Mental Health, University of Newcastle, Newcastle, Australia
11Nursing and Midwifery Research Centre, Deakin University, Burwood, Australia
12Department of Medicine, Monash University, Richmond, Australia
13Neurosciences Clinical Institute, Epworth Hospital, Richmord, Australia
14School of Nursing, University of Ottawa, Ottawa, Canada
15Clinical Epidemiology, Ottawa Hospital Research Institute, Ottawa, Canada
Background and Aims
Providing evidence-based care is the gold standard for healthcare delivery. Yet, clinicians often struggle to provide care according to evidence-based recommendations. Clinicians are more likely to adopt evidence-based care in settings with a positive organisational context, such as functioning leadership, teamwork, culture and resources.
We undertook a context analysis of 26 Emergency Departments (EDs) participating in the T3 cluster randomised stroke care implementation trial to examine the associations between contextual factors in ED and processes of stroke care.
Method
Organisational context was assessed using the 10 domains of the Alberta Context Tool by paper-based survey of ED nurses. A mean score was obtained for each hospital, with higher scores indicating a more implementation-friendly context. Evidence-based care was measured via medical record audit of 11 stroke care processes and an overall composite score generated. Associations between context and processes of care were examined using linear regression.
Results
558 ED nurses participated in the survey. Processes of care were obtained from 1591 patient audits. The context domains culture (regression coefficient: 0.64), feedback processes (0.42), staffing (0.21), space (0.36) and resources (0.20) showed weak but significant associations with better processes of stroke care while there were no associations for leadership (0.31), connections (0.43), time (0.38), informal interactions (0.16) and one weak negative association for formal interactions (−0.35).
Conclusion
While context scores mirror previous studies in pediatric and geriatric care facilities, the minimal associations between ED context and evidence-based stroke care may be due to the dynamic and chaotic environment of EDs.
Trial registration number
ACTRN12614000939695
AS12-028
COLLECT ONCE, USE MANY TIMES. DISCHARGING WITH INFORMATION (DWI) -THE BHS SOLUTION
1Ballarat Health Service, Ballarat Base Hospital, Ballarat, Australia
2Florey Institute of Neuroscience and Mental Health, Stroke, Melbourne, Australia
3University of Melbourne, Faculty of Medicine- Dentistry and Health Sciences, Melbourne, Australia
Background and Aims
Prior to the introduction of an individualised discharge care plan, stroke patients received discharge information that did not meet the definition outlined in the Australian Commission on Safety and Quality in Healthcare Acute Stroke Standards, 2015. In response, BHS has produced an individualised discharge care plan using the existing processes to decrease data duplication, minimise time burden of data collection and provide patients with discharge information specific to their stroke. The aim was to develop a person-centred, innovative and time effective individualised discharge care plan for patients, following stroke.
Method
Through the process of data mapping, relevant clinical data fields collected on the existing e-form are automatically shared to the discharge care plan as well as the stroke discharge summary. This process ensures high data integrity, eliminates data duplication and translates clinical information into patient friendly language. As the individualised discharge care plan exists within the BHS electronic medical record, BoSSNET, the document can be completed during the patient’s admission and then provided to the patient upon discharge.
Results
BHS has produced an individualised discharge care plan through existing data collection methods, to provide patients with a discharge care plan following stroke.
Conclusion
The discharge care plan is comprised of data from the existing network of data at BHS. This method will reduce both data duplication and the time burden of data given the absence of a designated resource. Through follow up auditing, it is anticipated the discharge care plan will reveal a positive influence on patient empowerment and outcomes.
Trial registration number
N/A
AS12-029
DRAMATIC IMPROVEMENT OF ACUTE ISCHAEMIC STROKE MANAGEMENT IN THE RHONE AREA BETWEEN 2007 AND 2016: A POPULATION BASED BEFORE AFTER PROSPECTIVE STUDY
1University of Lyon, University Claude Bernard Lyon 1- HESPER EA 7425, Lyon, France
2Hospices Civils of Lyon, Public Health Department, Lyon, France
3Hospices Civils of Lyon, Department of Stroke Medicine, Bron, France
4Hôpital Nord Ouest, Department of Stroke Medicine, Villefranche-sur-Saone, France
5Hôpital Nord Ouest, Emergency Department, Villefranche-sur-Saone, France
6Hospices Civils of Lyon, Emergency department- Centre Hospitalier Lyon Sud, Pierre Benite, France
7Hospices Civils of Lyon, Emergency department- Hôpital Edouard Herriot, Lyon, France
8Hôpital St Joseph St Luc, Emergency department, Lyon, France
9Hospices Civils of Lyon, Emergency department- Hôpital Croix Rousse, Lyon, France
Background and Aims
In 2007 a population-based cohort study (“AVC 69”) on all consecutive patients with an acute ischemic stroke (IS) admitted to any emergency department (ED) or stroke unit of the Rhône area showed that only 9% IS patients were thrombolysed.
Method
In 2016 we conducted a similar study (“STROKE 69”) to assess the effectiveness of all actions implemented in the meantime: Rhône Stroke Units (SU) bed capacities increased from 6 to 18, and a large training program towards emergency physicians and nurses, EMS call center, and firemen, and public campaigns were implemented.
Results
Table 1: Patients characteristics and management modalities
Table 2: Management times (minutes)
Conclusion
Increased access to reperfusion from 9% to 27%, was mostly due to significant in-hospital management times decrease but not from increased public awareness
Trial registration number
NCT02596607
AS12-030
SYSTEMIC FACTORS ASSOCITED WITH STROKE DOOR TO NEEDLE TIME: A COUNTRY WIDE ANALYSIS
1Royal Group of Hospitals, Stroke Unit, Belfast, Ireland
2Altnagelvin hospital, Neurology, Derry, Ireland
3Antrim Area Hospital, Stroke Unit, Antrim, Ireland
4Royal Group of Hospitals, Neurology, Belfast, Ireland
5Craigavon Area hospital, stroke Unit, Portadown, Ireland
6Ulster Hospital, Stroke Unit, Dundonald, Ireland
7Southwest Acute Hospital, Stroke unit, Enniskillen, Ireland
8HSCB, stroke, Belfast, Ireland
9Queens university, statistics, Belfast, Ireland
Background and Aims
Pre-hospital, in-hospital and individual clinical factors are associated with variation in door to needle (DTN) time in acute ischemic stroke (AIS). Published reports are usually from large single centres or multicentre registries. To date, no country-wide analysis of DTN time factors have been presented.
Method
All AIS patients treated with intravenous tissue plasminogen activator (iv-tPA) over 4 years (2013 through 2016) in one European Union country were recorded prospectively, including patient demographics, pre-hospital care, thrombolysis rate and DTN time. Logistic regression was performed to identify factors associated with DTN time
Results
1201 patients from 10556 AIS admissions (11.4%) were treated with iv-tPA in 5 health trusts. Median NIHSS was 10 (IQR 6-17). Median DTN time was 54 minutes (IQR 36-77) with 61% treated < 60 minutes from arrival at Emergency Departments. The arrival method at hospital (ambulance OR 2.3 CI1.4-3.8 ) pre-alert from ambulance (pre-alert OR = 5.3 CI3.5-8.1) and time of day (out of hours, n = 650, OR 0.20 CI 0.22−0.38) all P<0.001, were the most significant factors in determining DTN time. Variation in DTN between centres occurred but was unrelated to volume of stroke admissions.
Conclusion
Ambulance transport with pre-hospital notification and time of day are associated with DTN time on a national level. Most stroke thrombolysis is delivered outside of normal working hours but these patients are more likely to experience treatment delays. Re-organisation of stroke services at a whole system level with emphasis on pre-hospital care and design of stroke teams are required to deliver quality and equitable care in AIS
Trial registration number
n/a
AS12-032
EFFICACY OF A TRAINING PROGRAMME ON “STROKE CODE” AMONG PRIMARY HEALTHCARE PROFESSIONALS: RESULTS IN THE SPANISH STROKE BELT
1Hospital Universitario Virgen Macarena, Neurology, Sevilla, Spain
2Primary Healthcare Service. Seville District., Primary Healthcare Service. Seville District., Seville, Spain
Background and Aims
In the Spanish Stroke Belt, almost 70% of acute stroke cases are initially assessed in Primary Healthcare, so a training programme at this level could be an effective tool to increase “stroke code” activations.
Method
The training session focused on neurological examination and Stroke Code activation criteria. It was applied to 250 nurses and GPs in Primary Healthcare Centers during 2017. A 9-questions survey about stroke diagnosis and management in Primary Care was conducted before and after the training.
Results
Before the training, 32% of surveyed professionals were wrong in questions related to stroke symptoms, like hemianopia, dizziness or instability. 5.7% had difficulties in clinical diagnosis and management of transient ischemic attack. 24.2% of professionals were confused about Stroke Code criteria activation (i.e. wrong contraindications such as age and anticoagulation were assumed). 25% were wrong in management of Stroke Code such as time window for treatment or initial aspirin administration. In the test following the programme, a positive impact was reported by 92%. The number of professionals without any mistakes increased to 48%. The number of professionals with more than one mistake decreased to 45%.
Conclusion
This programme improves knowledge about Stroke Code activation in Primary Healthcare and might be related with the huge increase in the number of thrombolysis plus thrombecthomies performed in the region after the programme implementation.
Trial registration number
N/A
AS12-033
STATE OF NATIONAL AND ESO CERTIFICATIONS FOR STROKE CENTRES/UNITS AMONG ESO MEMBERS
1Haukeland University Hospital, Neurology, Bergen, Norway
Background and Aims
Stroke unit care improves patient outcome. In 2016, the ESO Stroke Unit Committee (SUC) presented, the ESO Stroke Unit and Stroke Centre Certification Process, based on the ESO recommendations.1 Now, we will present the current state of national and ESO certifications for Stroke Units and Stroke Centres by April 2018 among European Stroke Organisations with ESO membership.
Method
ESO Stroke Unit and Stroke Centre Certification processes have successfully started in 2017 and are ongoing. On December 14th 2017, we sent a survey about the existence of regional or national certification programs to all ESO-registered stroke organisations in Europe.
Results
Figure 1 shows the certified ESO Stroke Unit and ESO Stroke Centres and the state of national and regional stroke certification programs by April 2018.
Figure 1: State by April 2018 of national and ESO certifications among European Stroke Organisations with ESO-membership and to organisations from countries with at least a part of their territory in Europe (Figure 1 to be finalized, will be presented on the poster)
Conclusion
ESO certification focusses on own knowledge, skills, and quality to improve stroke patient care. The ESO wants to provide a benchmark for quality of stroke management, to lift stroke care in Europe and to build a network of ESO Stroke units and centres with approved clinical excellence. Some nations in Europe have had national certification programs for years, and a first survey is mandatory in order to build a network.
Trial registration number
N/A
but we are still collecting the results of the survey
AS12-034
COMPARING REAL-WORLD COST-EFFECTIVENESS OF A CENTRALIZED VERSUS DECENTRALIZED STROKE CARE SYSTEM; A NORTHERN NETHERLANDS EXEMPLAR
1University Medical Center Groningen, Epidemiology, Groningen, The Netherlands
2Faculty of Economics & Business- University of Groningen, Economics- Econometrics & Finance, Groningen, The Netherlands
3Health Technology Assessment- University of Groningen- University Medical Center Groningen., Epidemiology, Groningen, The Netherlands
4Faculty of Population Health Sciences- University College London., Applied Health Research, London, United Kingdom
5Faculty of Economics & Business- University of Groningen., Operations, Groningen, The Netherlands
6Faculty of Economics & Business- University of Groningen., Economics- Econometrics & Finance, Groningen, The Netherlands
7University of Groningen- University Medical Center Groningen., Neurology, Groningen, The Netherlands
Background and Aims
Centralization of acute stroke care services increases treatment rates and lowers costs compared to care at community hospitals. The aim of this study was to study the cost-effectiveness of a centralized organizational model in a real-life setting.
Method
Observational data was used from 780 patients in a decentralized system and 267 patients in a centralized system. Datasets from various sources were linked to estimate EuroQol-5D questionnaire (EQ5D) utility values and actual healthcare costs and up to 3 months. Secondary outcomes are lifetime QALYs and healthcare costs, using a probabilistic Markov model.
Results
The mean EQ5D utility value at three months was 0.65 (CI, 0.63 – 0.67) for the decentralized system and 0.69 (CI, 0.65 – 0.73) for the centralized system (P < 0.10). The mean healthcare costs up to 3 months are € 7,096 (CI, 6,285 – 7,908) for the centralized system compared to € 8,131 (CI, 7,647 – 8,614) for the decentralized system (P < 0.05). Results remain stable after correcting for age, gender, stroke severity and distance to hospital (P < 0.05).
Conclusion
A centralized acute stroke care system is cost-effective in a real-world setting. Centralizing acute stroke care significantly improves patient health by optimizing care efficiency, thereby substantially saving healthcare costs.
Trial registration number
N/A
AS12-035
TRANSIENT ISCHAEMIC ATTACK (TIA) SERVICE IMPROVEMENT PROJECT AS PER NATIONAL CLINICAL GUIDELINES FOR STROKE, UK (RCP 2016)
1Sheffield Teaching Hospitals NHS Trust- Sheffield- UK, Stroke Medicine, Sheffield, United Kingdom
Background and Aims
Recently Royal College of Physicians (RCP) updated guidelines for TIA. We created a TIA clinic standardised form in line with these guidelines to ensure provision of timely secondary preventative strategies after TIA. Aim of our project was to ensure TIA service is in compliance with RCP guidelines and is standardised seven days a week.
Method
Patients were identified using our TIA clinic database between October-November 2017. Data collection tool was developed in line with RCP guidelines and notes reviewed. We compared our practice before and after introducing new TIA form.
Results
Medication advice was given in 93.7% and 100% previously during weekday & weekends respectively which improved to 100% using new form all week. Follow up appointments were 100% before & after throughout the week. Life style and driving advice were given in 18.6% and 50% previously, 46.7% and 80% using new form respectively during weekdays while it was 0% & 50% previously, 50% & 75% using new form respectively at weekends. Information leaflets were given to 0% previously throughout the week which improved to 66.6% using new form during the week but remained 0% at weekends. Similarly information given to ring 999 was 6.25% and 0% previously which improved to 66.6% and 25% using new form during weekdays and weekends respectively.
Conclusion
This audit and quality improvement project highlights areas of improvement and certainly showed good results since the introduction of new TIA forms. Given improvement in service with new form, we plan to introduce an electronic form
Trial registration number
N/A
AS12-036
IMPACT OF EVIDENCE-BASED STROKE INTERVENTIONS ON OUTCOMES: HEADPOST TRIAL
1Clínica Alemana de Santiago- Facultad de Medicina Clínica Alemana- Universidad del Desarrollo, Neurology Service- Neurology and Psiquiatry Department, Santiago, Chile
2The George Institute for Global Health, Faculty of Medicine- UNSW, Sydney, Australia
3Facultad de Medicina Clínica Alemana Universidad del Desarrollo, Centro de Estudios Clinicos- Instituto de Ciencias e Innovación en Medicina, Santiago, Chile
4The George Institute China, Peking University Health Sciences Center, Beijing, China
5Nursing Research Institute, St Vincents Health Australia Sydney and Australian Catholic University, Sydney, Australia
6Faculty of Health and Wellbeing, University of Central Lancashire, Preston, United Kingdom
7Facultad de Medicina- Universidad de Chile, Departamento de Ciencias Neurológicas, Santiago, Chile
8Ribeirão Preto School of Medicine- University of São Paulo, Stroke Service- Neurology Division, Ribeirão Preto, Brazil
9Faculty of Medicine- Fukuoka University, Department of Preventive Medicine and Public Health, Fukuoka, Japan
10University of Leicester, Department of Cardiovascular Sciences and NIHR Biomedical Research Unit for Cardiovascular Disease, Leicester, United Kingdom
Background and Aims
Impact of evidence-based stroke care recommendations in relation to hospital organisation is uncertain in many countries.
Aim
Determine associations of evidence-based interventions for acute ischemic stroke (AIS) outcome in a large international multicentre study.
Method
Data are from HeadPoST, a large pragmatic multicenter cluster crossover clinical trial of lying vs. sitting up head positioning after acute stroke conducted across 114 centers in 9 countries. Interventions considered were use of reperfusion treatment (rtPA or EVT) in eligible patients, admission to acute stroke unit, use of antihypertensives, antiplatelets and statins, anticoagulation in atrial fibrillation, swallowing assessment, and physiotherapy in first 7 days of admission. Hierarchical, mixed, logistic regressions, fixed head position and period, random cluster and cluster-period effects, were performed to assess determinants of 90-day poor outcome (mRS 3-6), adjusted for patient and hospital variables.
Results
Among 9,485 included AIS patients, implementation of all interventions in eligible patients was associated with reduced poor outcome (odds ratio [OR] 0.72, 95% confidence interval [CI] 0.60−0.85). After excluding those given rtPA or anticoagulation, implementation of other stroke care interventions was still associated with reduced poor outcome (OR 0.78 95%CI 0.67−0.91). In adjusted analyses, there was no individual hospital characteristic associated to patient outcome. Overall, only 1,445 (15%) of AIS patients received the complete bundle of interventions for which they were eligible, and there was significant regional variation.
Conclusion
Interpretation
As evidence-based stroke care interventions improve outcomes in routine clinical practice, their wider implementation should be encouraged to reduce the burden of stroke, particularly in low resource regions.
Trial registration number
NCT02162017
AS12-037
THE USE OF SIMULATION BASED TRAINING TO IMPROVE DOOR-TO-NEEDLE TIMES IN ACUTE STROKE
1St Vincent's Hospital, Neurosciences, East Melbourne, Australia
2University of Melbourne, Medical Education, Melbourne, Australia
3St Vincent's Hospital, Emergency Medicine, East Melbourne, Australia
4St Vincent's Hospital, Clinical Education and Simulation Centre, East Melbourne, Australia
Background and Aims
Simulation training is increasingly employed in medical education for assessment, learning and, more recently, evaluation of system processes. However, data regarding clinical effectiveness of simulation for acute stroke are lacking. We introduced off-site and in situ simulation to upskill staff and to optimise implementation of a new “code stroke” protocol. We aimed to determine the impact of the simulation program in the clinical setting.
Method
An off-site simulation based training program was developed for members of the stroke team. The simulation scenario was based on a real case (right MCA occlusion) and included use of a simulated patient. We additionally designed an in situ simulation to test and refine the newly developed “code stroke” protocol, prior to implementation. Data were prospectively collected for key clinical performance measures with the primary outcome of interest door-to-needle time (DTN).
Results
Four off-site simulations were run (Jun16-Mar17). The new “code stroke” protocol was tested in the Emergency Department using in situ simulation (Mar17). Immediately post-simulation, the protocol was collaboratively revised to address identified process issues with input from emergency, stroke, radiology, anaesthetic, nursing, clerical and communications team members. “Code stroke” commenced May 2017. We observed a 47 minute reduction in median DTN between the 6 months prior to simulation training (Dec15-May16) and 6 months post (Nov16-Apr17). Reduction in DTN was observed both in-hours and out-of-hours, prior to introducing “code stroke”.
Conclusion
We report the first evidence for simulation training directly translating to improved clinical performance in acute stroke. Further research is required to determine optimal training intervals.
Trial registration number
N/A
AS12-038
TWO-YEAR EXPERIENCE OF IMPLEMENTING A COMPREHENSIVE TELEMEDICAL NETWORK WITHIN A MAINLY RURAL AREA IN GERMANY: THE TRANSREGIONAL NETWORK FOR STROKE INTERVENTION WITH TELEMEDICINE (TRANSIT-STROKE)
1University of Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany
2Clinical Center Main-Spessart, Neurology, Lohr, Germany
3Leopoldina Hospital Schweinfurt, Neurology, Schweinfurt, Germany
4Clinical Center Rhön, Neurology, Bad Neustadt / Saale, Germany
5Clinical Center Aschaffenburg-Alzenau, Neurology, Aschaffenburg, Germany
6Juliusspital, Neurology, Würzburg, Germany
7Clinical Center Helios Frankenwald, Cardiology, Kronach, Germany
8Clinical Center Main, Internal Medicine, Ochsenfurt, Germany
9Clinical Center Helios Erlenbach, Neurology, Erlenbach, Germany
10Clinical Center Capio Franz von Prümmer, Internal Medicine, Bad Brückenau, Germany
11University Hospital Würzburg, Neurology, Würzburg, Germany
Background and Aims
Telemedical stroke networks are an established tool to improve quality of care also in regions without full stroke unit (SU) coverage. We report the experience of the first two years implementing TRANSIT-Stroke in north-western Bavaria (Germany).
Method
Established in October 2014, the TRANSIT network covers a mainly rural region with a catchment area of 1.5 m inhabitants. Hospitals with different expertise in SU care participate in the network: level-III-hospitals (with supra-regional SU, providing teleconsultation), level-II-hospitals (with regional SU), level-I-hospitals (without previous SU care). For a two-year-period (01/2015 to 12/2016), data of eight hospitals were available documented in the stroke register Bavaria for quality assurance and time-trends for a set of 16 evidence-based indicators of process of quality of care (QIs) were evaluated quarterly and compared according to predefined target values.
Results
Overall, 8,327 patients were included (mean age 74.6 years ± 12.8; 48.2% female; I63: 68.6%; I61: 6.5%; G45: 24.6%; I64: 0.4%). In level-I-hospitals, three patterns for development of QIs were observed: a) high adherence ab initio (31%), mainly in secondary stroke prevention; b) improvement over time (44%), predominantly related to stroke specific diagnosis and in-hospital organization; c) no clear time trends (25%). In level-I-hospitals, 11 out of 16 QIs reached predefined target values of quality of care at the end of the observation period. In level-II/III-hospitals, adherence to QI was constantly high over time ab initio.
Conclusion
The implementation of a comprehensive telemedical stroke network resulted in an improvement of quality of care in the whole region.
Trial registration number
N/A
AS12-041
PERCEIVED QUALITY OF CARE TRANSITIONS BETWEEN HOSPITAL AND THE HOME
1Karolinska Institutet, Department of Neurobiology- Care Sciences and Society, Stockholm, Sweden
2Karolinska Institutet, Department of Learning- Informatics- Management and Ethics, Stockholm, Sweden
3Dalarna University, School of Education- Health and Social Studies, Falun, Sweden
4Karolinska Institutet, Department of Clinical Sciences- Danderyd Hospital, Stockholm, Sweden
Background and Aims
There is a lack of knowledge on how patients with stroke in Sweden perceive the current care transitions from stroke unit to the home. Therefore, the aim of this study is to explore the perceived quality of care transitions between hospital and the home for patients with stroke.
Method
A total of 200 patients with stroke referred from stroke unit to home rehabilitation will be included. To date, 190 patients have been included. One week after discharge, the perceived quality of care transitions are assessed with the Care Transitions Measure (CTM). Baseline data on age, sex and stroke severity are collected from medical records.
Results
Preliminary results from 80 participants with a mild stroke (53 men, mean age 70 years), show that a majority perceived a high quality of care transitions. However, 26% did not perceive they had clear health goals or knew how to reach them; 30% did not know what warning signs and symptoms to watch out for; and 20% lacked a written healthcare plan. Further, 24% perceived they had a poor understanding about their health and 29% lacked written understandable information about plans after discharge. In addition, 46% had not clearly understood the possible side-effects of their medications.
Conclusion
The preliminary conclusion shows that there is room for improvement regarding the transition process. Staff at stroke units should acknowledge the importance of informing about subsequent care and rehabilitation after discharge. Specific attention should be drawn towards self-monitoring and increasing patient knowledge about potential side-effects of their medications.
Trial registration number
NCT02925871
AS12-042
IDENTIFYING STROKE CARE PATHWAYS IN THE UK: THE SENTINEL STROKE NATIONAL AUDIT PROGRAMME: INVESTIGATING AND EVALUATING STOKE THERAPY (SSNAPIEST)
1University of Manchester, Centre for Biostatistics, Manchester, United Kingdom
2University of Manchester, Division of Nursing- Midwifery & Social Work, Manchester, United Kingdom
3Royal College of Physicians, Sentinel Stroke National Audit Programme SSNAP, London, United Kingdom
4Kings College London, Division of Health and Social Care Research, London, United Kingdom
5University of Manchester, Manchester Centre for Health Economics, Manchester, United Kingdom
6University of Manchester, Division of Neuroscience & Experimental Psychology, Manchester, United Kingdom
Background and Aims
To further investigate in detail the organisation of post-acute care and multi-disciplinary stroke therapy we first needed to identify the routes (or pathways) that patients experienced through stroke services.
Method
Data from the Stroke Sentinel National Audit Programme (SSNAP), a national stroke register for all strokes occurring in England and Wales, were extracted for July 2013-June 2015. An iterative step-by-step procedure using data driven factors and clinical experience then identified the common pathways patients undertook.
Results
Based on 124,674 stroke patients, 874 possible routes were identified and then consolidated to nine common pathways. Eighty four percent stayed in a single stroke inpatient unit which were split across four pathways; Shorter-stay (<7dys stoke unit average) acute unit > no community rehabilitation (28.3%) or community rehabilitation (19.6%), Longer-stay acute unit > no community rehabilitation (20.6%) or community rehabilitation (16.2%). Fourteen percent transferred to a secondary in-patient rehab unit split into; Shorter-stay acute unit > other in-patient rehabilitation unit > no community rehabilitation (5.3%) or community rehabilitation (6.8%), Longer-stay acute unit > other in-patient rehabilitation unit > no community rehabilitation (0.9%) or community rehabilitation (1.4%). The remaining 1.1% of routes were classed as `other’. Descriptive statistics of baseline demographics, stroke characteristics, and patient stay indicated differences in the patients present in these pathways.
Conclusion
Though variation in the routes through a health care system experienced by stroke patients can seem numerous, common stroke pathways can be observed and help identify patients with similar characteristics and experiences.
Trial registration number
N/A
AS12-043
FACTORS ASSOCIATED WITH THE ONSET-TO-DOOR TIME IN ACUTE STROKE IN GUIPUZCOA (SPAIN)
1Hospital Universitario Donostia, Neurology, Getxo, Spain
2Hospital Universitario Donostia, Neurology, Donostia, Spain
Background and Aims
Acute stroke care in Guipúzcoa is carried out in 3 level II regional hospitals and a single level III hospital with a stroke unit. The objective of this work is to identify factors associated with the onset-to-door time (ODT) in our stroke care model.
Method
Observational study from a prospective registry of patients admitted to the stroke unit of a single hospital within the first 24 hours from the stroke onset. Univariate and multivariate analyses were undertaken to identify factors associated to a prehospital delay (ODT >2 hours).
Results
A total of 197 patients were included: 77% with ischemic stroke, 9% with hemorrhagic stroke and 14% with TIA. Median time to hospital presentation was 160 minutes and 42% presented within 2 hours after symptom onset. To be transported by own means rather than ambulance (OR = 6.7, p = 0.003), previous transfer to a level II hospital (OR = 4.9, p = 0.032), dizziness as clinical presentation (OR = 8.1, p = 0.011) and smoking (OR = 7.0, p = 0.011) were independently associated with prehospital delay. Stroke severity (OR = 1.1, p = 0.003) was associated with lower ODT. Age, sex and distance to the reference hospital, among others, were not associated with prehospital delay.
Conclusion
Smoking, to be transported by own means, previous transfer to a level II hospital, dizziness as first symptom and stroke severity were associated with ODT. Transfer system modifications and community strategies to improve awareness of early symptoms of stroke are expected to help accelerate hospital presentation in acute stroke patients in our region.
Trial registration number
N/A
AS12-044
HUNGARIAN PARTICIPATION IN THE ANGELS, ESO-EAST AND RES-Q PROJECTS
1Semmelweis University, Depatment of Neurology, Budapest, Hungary
2University of Pécs, Department of Neurology, Pécs, Hungary
3IQVIA, Angels Initiative Hungary, Budapest, Hungary
Background and Aims
There is an East-West gap in stroke morbidity and mortality in Europe. Several initiatives have been launched to overcome this disadvantaged situation and to improve stroke care in Central and Eastern Europe. For auditing stroke services, collection of reliable data is essential. The Hungarian Stroke Society aims to promote such activity in the 39 stroke centers throughout the country.
Method
We analyze characteristics of web-based data collection systems in stroke care in Hungary.
Results
Several aspects of acute stroke care have to be reported by stroke centers in Hungary. Financing of intravenous thrombolysis is based on reimbursement from the National Health Insurance Fund for hospitals with the condition that hospitals report online a set of data for each patient. Reimbursement for thrombectomies also requires individual reporting. The Hungarian Stroke Society requests stroke centers to report acute stroke cases, the number of intravenous thrombolyses and mechanical thrombectomies on a monthly basis since 2017. Some stroke centers also report to the SITS-EAST database and to ad hoc international surveys. The most recent of the reporting systems is the RES-Q initiative, supported by the European Stroke Organization and also by the Angels Initiative. In Hungary 23 out of the 39 stroke units already have joined the Angels Initiative and 11 units registered with the RES-Q registry. Until December 2017 six stroke units uploaded data of 460 acute stroke patients to the RES-Q database.
Conclusion
Rationalization of multiple reporting obligations should be solved in order to further improve data entry to the RES-Q registry in Hungary.
Trial registration number
N/A
AS12-045
STROKE NETWORK STRATEGY IN ISTANBUL: A THREE-MONTH PERIOD RESULTS
1MedicalPark Hospitals MLP Care, Neurology Department- Brain Angiography and Stroke Centre BASC, Istanbul, Turkey
2MLP Care Brain Angioprapgy and Stroke Centre BASC, GOP MedicalPark Hospital Neurology Department, Iatanbul, Turkey
3Istinye University Liv Hospital MLP Care Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
4Istanbul Aydın University Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
5Istinye University Liv Hospital MLP Care Brain Angiography and Stroke Centre BASC, Neuroradiology Department, Istanbul, Turkey
Background and Aims
In Istanbul, a city with high population and chaotic traffic, acute stroke patients (ASP) are transferred to the nearest hospital but pre-hospital emergency system is not well organized. We established a Stroke (Brain Angiography and Stroke Centre-BASC) Network including 3 comprehensive stroke centre (CSC) that are strategically located in Istanbul in order to ensure easy-access to the stroke patients.
Method
In BASC Network, the CSCs are a SITS member and Angel Hospital. The patients are treated according to standardized institutional guidelines and evaluated with CT and/or MRI including RAPID software since December 2017. We analysed the preliminary quality performance data of ASP between October - December 2017.
Results
Median onset-to-door (ODT) time of 186 admitted patients (%51 referral) was 255 minutes. Revascularization therapy (27% only IVrTPA, 27% bridging, 46% only endovascular) was performed in 74 patients (39.8%). Within the eligible patients that are admitted within 0-4.5 h period (47.3%) 98% received IVrTPA. Median door-to-needle time (DNT) was 30 minutes. In the 0-6 h period (56.5%) all the eligible patients (44/105), >6 h period 10 patients (10/81) received thrombectomy. Median door-to-femoral puncture time was 40 minutes. The rate of good prognosis (mRS 0-2) at discharge and in-hospital mortality was 49,2% and 3,8% respectively. Follow-up outcome results in 3-months will be announced.
Conclusion
In this newly established stroke network the patients are admitted to the nearest CSC. Although in this kick-off phase the workflow benchmarks are already in line with those recommended well organised CSC, there is still room for improvement.
Trial registration number
N/A
AS12-046
OFF-SITE MULTICENTER IN-AMBULANCE TELESTROKE: A FEASIBILITY STUDY IN TWO BELGIAN ACADEMIC HOSPITALS
1Zealand University Hospital- Roskilde, Department of Neurology- Neurovascular Center, Roskilde, Denmark
2Vrije Universiteit Brussel, Faculty of Medicine and Pharmacy, Brussels, Belgium
3ZorgSaam Hospital, Department of Neurology, Terneuzen, The Netherlands
4Universitair Ziekenhuis Brussel, Department of Rehabilitation Medicine, Brussels, Belgium
5Cliniques Universitaires Saint Luc, Department of Neurology, Woluwe-Saint-Lambert, Belgium
6Universitair Ziekenhuis Brussel, Department of Neurosurgery, Brussels, Belgium
7Universitair Ziekenhuis Brussel, Department of Radiology, Brussels, Belgium
8Vrije Universiteit Brussel, Interuniversity Center for Health Economics Research, Brussels, Belgium
9Vrije Universiteit Brussel, Department of Public Health, Brussels, Belgium
10Universitair Ziekenhuis Brussel, Department of Emergency Medicine, Brussels, Belgium
11Vrije Universiteit Brussel, Research Group on Emergency and Disaster Medicine, Brussels, Belgium
12KU Leuven, Institute for Healthcare Policy, Leuven, Belgium
13Antwerp University Hospital, Department of Emergency Medicine, Antwerp, Belgium
14Antwerp University Hospital, Department of Neurology- Neurovascular Reference Center, Antwerp, Belgium
15University of Antwerp, Research Group on Translational Neurosciences, Dept. of Neurology, Universitair Ziekenhuis Antwerpen
Background and Aims
In-ambulance telemedicine is a promising and scalable approach bringing medical experts virtually to the patients’ location.
Method
The AP19-IATS project has a prospective, multi-center observational design. It aims to implement 24/7 in-ambulance telestroke care in 2 academic hospitals, supported by a group of 6 independent teleconsultants (all senior neurovascular experts) operating from different sites in and outside Belgium. All patients >18 yo, with suspicion of acute stroke and symptom onset <12 hours, transported by ambulance, were eligible for inclusion.
Results
During the trial phase from November 7th until December 22th 2017, 24/7 support via in-ambulance telemedicine was provided by six teleconsultants, resulting in zero missed teleconsultation attempts. Five out of six teleconsultants were not part of the in-hospital stroke team of the participating hospitals. Of 20 attempts, teleconsultation was performed in 14 cases. Unsuccessful attempts were mainly due to technical issues (software update n = 1, teleconsultation device maintenance n = 1, connectivity problems n = 2), in 2 cases additional value of teleconsultation was judged to be lacking by the attending on-site emergency physician (no suspicion of stroke, n = 2). No telemedicine-related adverse events occurred.
Conclusion
This is the first report on 24/7 in-ambulance telestroke in a network of multiple hospitals, supported by a group of six independent teleconsultants. This project has uniquely and successfully demonstrated off-site in-ambulance teleconsultation across hospital and country borders to be feasible and safe, without major organizational issues. Large scale studies are needed to assess long term feasibility and clinical effects of in-ambulance telestroke interventions.
Trial registration number
N/A
AS12-047
QUALITY INDICATORS OF STROKE IN ESTONIA
1University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia
2North Estonia Medical Centre, Neurology Centre, Tallinn, Estonia
Background and Aims
Appropriate management is crucial for reducing the burden of stroke. Measurement of the quality of stroke care as a part of a process of quality improvement is important.
Method
Quality indicators program has been launched in cooperation of the University of Tartu and Estonian National Health Insurance Fund (NHIF) in 2013. The aim of the project is to develop standards for assessment and improvement of health services in Estonia. As a part of the program, 5 stroke indicators were developed. The cases of acute stroke (ICD-10 I63 and I61) were identified retrospectively from the NHIF database. An acute stroke case was defined when the patient had a bill for acute stroke service within 14 days of admission. The cases were linked with the Death Registry and Prescription Database. The results for 2015 and 2016 are presented.
Results
As a total, 77% of patients were managed in Stroke Units in 2015 and 2016 (3699 and 3677 patients, respectively). Of all ischemic strokes 16.4% (95% CI 15.2-17.7%) and 18.2% (95% CI 16.9-19.6) were treated with iv rtPA in 2015 and 2016, respectively. At 12 months after admission with ischemic stroke, 48% (95% CI 45.5-51.1%) of patients with concomitant atrial fibrillation in 2015 and 52% (48.7-54.7%) in 2016 had an active prescription for an oral anticoagulant. The 30-day’s case fatality rate was 21% (95% CI 19.9-22.6%) in 2015 and 20% (18.2 -20.9%) in 2016.
Conclusion
Although the indicators were somewhat behind targets, the management of stroke is comparable or better compared to several Western European countries.
Trial registration number
N/A
AS12-048
EMPOWERING NETWORK COLLABORATION TO IMPROVE THE QUALITY OF CARE FOR ISCHEMIC STROKE PATIENTS: RESULTS OF ANGELS EUROPE EXPERIENCE AT SAN CAMILLO FORLANINI HOSPITAL
1A.O. San Camillo Forlanini, Stroke Unit, Roma, Italy
2A.O. San Camillo Forlanini, Neurology, Roma, Italy
3A.O. S. Camillo Forlanini, Medical Direction, Rome, Italy
4A.O. San Camillo Forlanini, Emergency, Roma, Italy
5Santo Spirito Hospital, Medical Direction, Rome, Italy
6Santo Spirito Hospital, Emergency, Rome, Italy
7Sant'Eugenio Hospital, Neurology - Stroke Unit, Rome, Italy
8Sant'Eugenio Hospital, Medical Direction, Rome, Italy
9G.B. Grassi Hospital, Emergency, Rome, Italy
10S. M. Goretti Hospital, Emergency, Latina, Italy
11S. M. Goretti Hospital, Neurology, Latina, Italy
12S. M. Goretti Hospital, Health Management, Latina, Italy
13A.O. San Camillo Forlanini, Medical Direction, Roma, Italy
Background and Aims
In Italy the percentage of thrombolysed patients has raised in the last years, but there are still differences among and within regions. In Lazio Region (5.8 million citizens), Regional Guidance identifies three complexity levels for stroke care, according to the “Hub and Spoke” Model. The Region is divided in 4 catchment areas (1.8 million citizens per area), each with a II Level Stroke Unit (SU), few I Level SU and several Neurovascular Teams (NVTs). Medical Directors of the Hub Hospitals are responsible for stroke network functioning. The authors’ Area has n.1 Hub, n.2 I level SU and 8 NVTs. In 2015 only the Hub Centre was able to administer thrombolysis to eligible patients. In 2016 San Camillo Forlanini Hospital joined the “Angels Europe” initiative.
Method
The authors used “Angels” support to carry out an organizational assessment of the network, to implement self-assessment tools at multiple level and to organise residential training of health care personnel involved in stroke clinical pathway; on site simulations for training purposes were implemented. Organizational support was provided to reengineer stroke care process in spoke and NVTs centres.
Results
In 2015 thrombolytic procedures were performed only in San Camillo Hub Centre (n.107 treatments). In 2017 the total number of procedures performed within the Area was n.191, thus doubling 2015 result; 41.8% were performed by Hub Centre (n.80) and 58.1% (n.111) by spokes SU and NVTs.
Conclusion
Collaboration with Angels Initiative significantly contributed to improving quality of care and reducing inequalities
Trial registration number
N/A
AS12-049
EXPERIENCE IN THE FUNCTIONING OF THE STROKE UNIT IN THE STRUCTURE OF THE UNIVERSITY CLINIC OF THE ODESSA NATIONAL MEDICAL UNIVERSITY
1University Clinic, Neurology, Odessa, Ukraine
2Odessa National Medical University, Neurology, Odessa, Ukraine
Background and Aims
The stroke unit of the university clinic has been functioning since April 4, 2016. It is organized on the basis of the neurological department of the clinic and includes an intensive monitoring ward and early recovery wards equipped with vital and video monitoring systems and the necessary paraphernalia. This study was aimed to assess the experience of stroke unit work in 2016-2017.
Method
Official reports and medical records for the period of 2016-2017 were analysed.
Results
Patient care is carried out on the principle of a multidisciplinary team, with the participation of a neurologist, cardiologist, therapist, neurosurgeon, vascular surgeion, rehabilitationist, speech therapist, neuropsychologist, ergotherapist. Interaction of the hospital units allows revascularization by mechanical thrombectomy, stenting or carotid endarterectomy. The clinic's stroke unit takes part in international projects such as ESO-EAST, Angels, SITS-EAST, CHRONEX. On the basis of the stroke unit interns from European universities as well as interns and graduate students of ONMedU can improve their skills and competence.
During the stroke center work, 167 patients with acute stroke were treated, including 154 with ischemic stroke, and 13 with hemorrhagic stroke. Post-stroke partial seizures were registered in 7 (4.2%) patients, generalized seizure by type of absence - in one (0.6%) case. Mortality rate was 9.0%. Satisfactory functional results were achieved in 83.2% of patients.
Conclusion
The organization and development of the stroke unit in the structure of the university clinic makes it possible to optimize the provision of emergency medical care to patients with acute disorders of cerebral circulation.
Trial registration number
N/A
AS12-050
THE RESULTS OF THE FIRST TELEPHONE MONITORING WITH THE MEDICAL STUDENTS-LED TELEPHONE SUPPORT IN PATIENTS WITH STROKE ACCORDING TO DATA OF SITS-KYRGYZSTAN
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
Strokes are the major causes of death and disability according to DALY in Kyrgyzstan, where the telephone monitoring was firstly made for the secondary prevention of strokes.
Method
The telephone monitoring was the single possible tool to evaluate the condition of patients, included in stroke registry SITS-Kyrgyzstan, and to collect the information about the outpatient treatment after the discharge. The intervention was made by repeated telephone contact, with counseling on healthy lifestyle, the dosage of antyhypertensives, antiplatelets and anticoagulants to reach target values for blood pressure and blood lipids.
Results
A total of 811 patients included in SITS-Kyrgyzstan and 702 were interviewed. 552 (78.6 %) were included, 78 patients refused to provide an information, relatives of the 32 (4.5%) patients did not know their condition, 40 (5.7%) patients changed their phone number. The median age was 65 years, 64% were female, and 58 % were Kyrgyz. 118 (21.3 %) patients died in 3 months period. Among 434 only 28% were on regular antiplatelets (95%CI 18.2–36.5 and 38% on hypertensive therapy 95% CI 30.8–39.2. Median mRs on the 1st day of the observation was 3 and on 3rd month was 4 (p = 0.001). 31 Participants who monitored weekly after 3 month were more likely than the remainder to have no disability [mRs ≤ 2; relative risk (RR) 2.3; 95% CI 0.86–0.97].
Conclusion
Telephone monitoring in Kyrgyzstan, made for the first time in SITS-registry provided the range of disabilities in 3 months period, was a necessary instrument of gathering the data for medications controlling and corrections.
Trial registration number
N/A
AS12-051
STROKE ACUTE CARE: ACCESSIBILITY FOR MOTHERSHIP PATTERN FROM PATIENT LOCATION
1Université Claude Bernard Lyon 1, EA 7425 HESPER Health Services and Performance Research, Lyon, France
2CH Lucien Hussel, RESCUe Network, Vienne, France
3University Jean Moulin Lyon 3, UMR 5600 CNRS Environnement Ville Société, Lyon, France
4Hospices civils de Lyon, Department of stroke medicine, Bron, France
5INSA, CREATIS- CNRS-UMR5220 Inserm-U1044, Lyon, France
6Hospices civils de Lyon, Public Health Department, Lyon, France
7Hospices Civils de Lyon, Emergency Department, Lyon, France
8CH Lucien Hussel, RESCUe Network and Emergency Department, Vienne, France
Background and Aims
In 2014, there were 140000 hospitalizations for stroke, an increase of 13.7% since 2008. Every minute is crucial for treatment and to reduce the risk of invalidity. This study aims to measure theorical access times from the emergency call to the admission in closest Comprehensive Stroke Center (CSC), regardless of patient area. A better knowledge of travel times allows to improve decision making and inform on patient eligibility according to therapeutic window.
Method
In case of Mothership stroke care pattern, every CSC of Rhône county (France) and border counties were geolocalised using their precise postal addresses. Travel times represent acute stroke care from patient emergency call to admission in nearest CSC. Average times for ambulance (Emergency Medical Service or firemen ambulance) dispatch and times spent on the scene have been calculated from Rhône county prehospital EMS register. Depending on traffic conditions, various scenarios were modeled: difficult weather conditions, traffic jam, emergency, urban/rural traffic.
Results
According to traffic conditions, up to two hours of delays variation under the city are observed. Depending to the ambulance type, this difference is about 45 minutes at maximum. For example, 59 % of the population is eligible in 111 minutes with Prehospital EMS transport in case of regular traffic.
Conclusion
This study could be developed to Drip’n’Ship pattern, to compare and select the more efficient pattern according to patient location. This model could improve decision making process which allows an improvement of care, taking in the same time stroke issues into account that could enhance the treatment delays.
Trial registration number
N/A
AS12-052
CURRENT, FUTURE AND AVOIDABLE COSTS OF STROKE IN THE UNITED KINGDOM: A SOCIETAL COST OF ILLNESS STUDY
1Anita Patel Health Economics Consulting Ltd, NA, London, United Kingdom
2Queen Mary University of London, Centre for Primary Care & Public Health, London, United Kingdom
3London School of Economics & Political Science, Personal Social Services Research Unit, London, United Kingdom
Background and Aims
Despite significant progress in prevention, treatment and rehabilitation, stroke generates significant economic burdens. We estimated its societal costs in the UK to gain a better understanding of current burden (2015), its future trajectory (to 2025 and 2035), and potential for alleviating future costs.
Method
We focused on adults aged ≥45 years. Current average health/social care costs (2015 prices) were estimated using Xu et al.’s (2017) discrete event simulation model which incorporated national stroke audit and regional stroke register data. We estimated informal care and lost employment costs using data from two UK-wide randomised controlled trials. We applied literature estimates of stroke incidence/prevalence for extrapolations to national UK population level. Future cost projections accounted for likely changes in demography, formal care wages, and stroke incidence/prevalence. Incidence/prevalence trajectories and research priorities were elicited from a survey of UK stroke experts.
Results
Current societal costs are £25.6 billion, dominated by informal care costs. Between 2015 and 2035, we estimate increases in: first-time strokes from 117,600 to 187,000 (+59%); stroke survivors from 950,000 to 2,120,000 (+123%); and societal costs from £25.6 billion to £75 billion (+194%). Of experts’ top-five research priorities, improving stroke prevention offered greatest scope for savings (£4 billion).
Conclusion
Numbers of stroke survivors and costs in the UK could more than double in the next 20 years. Investing in priority research areas could alleviate the burden on both formal and informal care sectors.
Xu X-M et al. Eur J Stroke 2017; online first (30 November); 1–10.
Trial registration number
N/A
AS12-053
GLOBAL TELEMEDICINE PLATFORM FOR INTEGRAL CARE TO ACUTE STROKE. BRINGING TREATMENT TO ALL PATIENTS
1hospital virgen del rocio, neurology, seville, Spain
2hospital virgen del rocio, Technological Innovation Group-, seville, Spain
3epes, emergency, seville, Spain
4hospital san juan de dios, critical care, seville, Spain
5hospital san juan de dios, informatics, seville, Spain
Background and Aims
A team of researchers, with experience in telestroke systems, has worked on research and development project founded by “Instituto de Salud Carlos III” whose objective is to design, develop and validate a flexible, reusable, and scalable technology platform capable of supporting the integrated plan for acute stroke care.
Hypothesis: The platform coordinate acute stroke clinical care in all possible scenarios prehospital and hospital care thus creating a network of connected resources. Thereby it is possible to provide an adequate health service offering patient safety, equity in access to the service and optimization of the use of health resources, with a platform easily implementable.
Method
The methodology used is Agile Software Development with modular architecture using free software. The developed system is been piloted in an area of one million inhabitants. It will extend to the Andalusian network of sanitary resources for 8,5 million inhabitants.
Results
Services developed:
Exchange of valuable information, laboratory tests, CT, MRI, and balanced scorecard.
• Communication interfaces based on technical, syntactic and semantic interoperability standards.
• Videoconference allowing the joint exploration.
• Support for clinical decision-making in the field of evidence-based, providing up-to-date clinical, diagnostic and therapeutic recommendations (six automated rules developed).
In addition the system is easy, useful and effective.
Conclusion
This tool has been developed with free software and interoperability standards, thus enabling its use in any healthcare environment. Thereby, the system can be considered portable and easily extended anywhere. This is the most important advantaje over the current situation.
Trial registration number
N/A
AS12-054
IMPLEMENTATION AND THE FIRST RESULTS OF THE STROKE QUALITY REGISTRY RES-Q IN BISHKEK, KYRGYZSTAN
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
RES-Q (REgistry of Stroke Care Quality) is an international multicenter registry developed under the European Stroke Organisation (ESO), to monitor implementation of stroke care best practice. Aim was to implement RES-Q registry in 2 departments in Bishkek, Kyrgyzstan.
Method
The neuro-vascular department of Bishkek City Civil Clinic 1 (BCC1) and the neurological department of the Chui Regional Clinic (ChRC) participated; data were collected for one month, at two different time of the year: November 2016, March 2017. We registered 24 variables, including demographic parameters, types of strokes, median length of stay at hospital, post stroke disability and, treatment at discharge.
Results
We registered 111 cases of strokes, 55% were men; mean age was 61. Ischemic stroke was diagnosed in 71% of cases, parenchymal hemorrhage in 7% and non-traumatic subarachnoid hemorrhage in 7.37%. Median NIHSS score was 4.5 in ChRC and 6 in BCC1. Only 6.82% patients underwent dysphagia screening, and all were in BCC1. Concerning neuroimaging 69,32 % underwent brain MRI or CT scan at BCC1 and 37.5 at ChRC; in terms of timing, only 3.41% of the imaging procedures were performed within 1 hour from hospital admission. Smoking (63.16%), arterial hypertension, atrial fibrillation, ischemic heart disease, non-valvular heart rhythm disturbances, diabetes mellitus were identified as major neurovascular risk-factors. 98% of all patients were admitted in a stroke unit
Conclusion
RES-Q is an effective tool to collect clinical and demographic data in acute stroke patients. It allows clinicians and policy makers realistic planning of health policies and stroke best practice implementation.
Trial registration number
N/A
AS12-055
STROKE MANAGEMENT IN BISHKEK: RESULTS FROM RES-Q STROKE REGISTRY
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
There are few data about the kind of cerebral stroke management practice in use in Kyrgyzstan. RES-Q, an international multicenter registry, allows neurologists to obtain reliable information about everyday practice. Aim: to observe and compare approaches to the acute ischemic stroke management according to RES-Q stroke registry in two departments in Bishkek, Kyrgyzstan.
Method
We analyzed the management of the acute ischemic stroke in Bishkek City Civil Clinic 1 (BCC1) and neurological department of the Chui Regional Clinic (ChRC) in the period of November 2016 and March 2017. Variables included: prescription the antiplatelets, anticoagulants, statins, thrombolytic therapy, endarterectomy, carotid stenting, hemicraniectomy.
Results
We analyzed data from 111 cases of cerebral stroke: 55% men, 71% were diagnosed ischemic stroke; stroke severity was measured with NIHSS, mean score was 5 excluding comatose patients (8% in BCC1, 12,5 % in ChRC). Concerning discharge prescriptions: there were no anticoagulants suggested during the observation; 97.14% of patients at BCC1 and 100% at ChRC were discharged with antiplatelets as secondary prevention strategy; statins were suggested to 45.07% and 80% of patients respectively. None of the patients received recanalization treatment and or hemicraniectomy. All neuroimaging procedures are made outside the hospital in a private regime. As this is time consuming, it represents one of the main barrier to thrombolysis implementation in Kyrgyzstan.
Conclusion
RES-Q is a user-friendly stroke registry and is an important source of clinical, administrative and demographic information. Its implementation in all neurological centers in Kyrgyzstan is critical to stroke management improvement and standardization in the country.
Trial registration number
N/A
AS12-056
LOGISTICS AND EPIDEMIOLOGY OF ENDOVASCULAR TREATMENT IN ACUTE ISCHEMIC STROKE PATIENTS IN THE NETHERLANDS
1University Medical Center Groningen, Epidemiology, Groningen, The Netherlands
2University of Groningen- University Medical Center Groningen., Neurology, Groningen, The Netherlands
3Faculty of Economics & Business- University of Groningen, Operations, Groningen, The Netherlands
4Health Technology Assessment- University of Groningen- University Medical Center Groningen., Epidemiology, Groningen, The Netherlands
Background and Aims
The emergence of Intraarterial Thrombectomy (IAT) has challenged acute stroke care organization both at a national and regional level. Important parameters include distances to primary and comprehensive stroke centers, and effectiveness of interventions as a function of time and availability of ambulance services. Further dissemination of IAT may increase treatment rates, yet, could affect efficient use of scarce resources and effectiveness.
The aim is to study the organizational model and logistics of IAT for ischemic stroke patients in the Netherlands.
Method
Using a simulation modeling approach current performance of hospitals offering IAT in the Netherlands will be quantified. Patient data concerning pathway logistics both pre- and intrahospital will be collected and used to build and validate the simulation models.
Primary outcomes include IAT treatment rates and patient disability according to the modified Rankin Scale. As secondary outcomes the onset-to-treatment time and resource use will be collected.
Results
Results from previous studies will be expanded with results and data of trials performed later in the consortium to represent current patient logistics, time delays and outcomes. Simulation experiments will be performed to assess effectiveness and efficiency of alternative network typologies, i.e. primary and comprehensive stroke services (hybrid system) versus a service delivery based on comprehensive and centralized care. The model will be expanded with cost-data to prepare for elaborate budget impact and cost-effectiveness analyses.
Conclusion
This research fulfills an important clinical and policy need for evaluating the organizational model for IAT treatment in the Netherlands.
Trial registration number
This research is part of the Consortium for new treatments of acute stroke (CONTRAST/MR CLEAN NO IV trial ISRCTN80619088)
AS12-057
LEAN-INSPIRED “DROP-IN” FOR ATRIAL FIBRILLATION-SCREENING WITH THUMB-ECG
1Danderyds Hospital, Strokeunit, Danderyd, Sweden
2Danderyds Hospital, Clinical Physiology, Danderyd, Sweden
Background and Aims
The efforts has increased to find ”silent” atrial fibrillation (AF) in strokeprevention. A diversity of screening-methods are used and the load on the Physiological departments has increased to give access to these investigations.
The resources in hospital care are limited and we must have good logistics to perform and interpret the screening-methods, so that the patient can get a quick diagnosis and treatment. We found out that the time for the Holter-ECG-answers to the clinician could vary greatly between 1 month to > 4 months, at the Stroke open ward clinic at Danderyd Hospital. A great variation in time from referral to signed answers from Phys. lab, gave us an opportunity to create a standardized Lean-inspired process for the patients in need for AF-screening.
Method
We started to use mainly Thumb-ECG:s for 3 weeks screening, already available at the Physiological lab. The patients were welcome to collect it on “drop-in” every afternoon the same day or the day before discharge.
Results
Conclusion
This shows that within an organisation, one can use already available resources to create a more efficient screening procedure in stroke/TIA-patients discharged from the Strokeunit.
Trial registration number
N/A
AS12-058
FRENCH TELESTROKE ORGANISATION “MR WATSON, COME HERE. I WANT YOU.” (ALEXANDER GRAHAM BELL, 10TH MARCH 1876; FIRST PHONE CALL)
1CHU Jean Minjoz- 3- boulevard A. Fleming - 25030 Besançon, Service de Neurologie, Besançon, France
2Haute Autorité de Santé HAS, Paris, France
3Haute Autorité de Santé HAS, Service Indicateurs Pour l'Amélioration et la Qualité et la Sécurité des Soins, Paris, France
Background and Aims
The 4th campaign to collect IPAQSS clinical practice indicators took place in 2017. Clinical practice indicators for “the management of stroke patients” were provided by 549 healthcare institutions in France, each indicating whether it had a neurovascular unit or telestroke.
Method
In 2017, 139 institutions had a neurovascular unit (136 in 2015) and 200 had telestroke (112 in 2015). Amongst these, 134 were spokes (74 in 2015), 48 were hubs (24 in 2015) and 18 acted as both. A random draw of 80 medical files per institution allowed 25.307 files to be analysed, resulting in diagnosis of ischemic or haemorrhagic stroke. The files initially referred by telestroke (1785 in 2017 versus 662 in 2015) were compared with the rest of the files.
Results
The development of telestroke in France between 2015 and 2017 is very clear (+78%). The number of hubs has doubled. The majority of the country has access to a neurovascular unit or telestroke in less than 45 minutes. Patients referred by telestroke (1785) tend to be younger (median age 73 versus 76), male (54.2% versus 53%) and are more likely to undergo thrombolysis (35.9% versus 14.2%).
Conclusion
The purpose of telestroke is not to replace neurovascular units, but in a pragmatic context, its implementation benefits patients, enabling them to receive neurovascular expertise and gain access to thrombolysis.
Trial registration number
N/A
AS12-059
REGISTRY OF STROKE CARE QUALITY (RES-Q): FIRST YEAR RESULTS FROM ESTONIA
1University of Tartu, Department of Neurology and Neurosurgery, Tartu, Estonia
2Tartu University Hospital, Department of Neurology, Tartu, Estonia
3Pärnu Hospital, II Department of Internal Medicine, Pärnu, Estonia
4North Estonia Medical Centre, Neurology Centre, Tallinn, Estonia
Background and Aims
Quality improvement program with the aim to improve the management of stroke in Central and Eastern Europe was launched by ESO-EAST in 2015. The first goal was to measure the current quality of stroke care to define the differences between countries and hospitals in a country level. The first-year results for Estonia (population 1,32 million) are presented.
Method
REgistry of Stroke Care Quality (RES-Q) collecting 24 stroke quality indicators was set up in 2016. In 2017, 3 of 6 hospital with Stroke Units (SU) in Estonia joined RES-Q: 1 central hospital and 2 big regional hospitals.
Results
Totally, 202 stroke cases from 3 centres were registered during the 1 month period (March/April 2017). Most patients (88%) were treated in SUs. The proportion of ischemic strokes was 86%. Fifty-one patients (29%) of ischemic strokes received recanalization therapy, of them 13 (25%) received mechanical thrombectomy (in 2 regional hospitals only). The mean door-to-needle time was shorter in big hospitals (23 min vs 65 min). However, the door-to groin time was 90-100 min. Most patients (63-86%) were screened for atrial fibrillation and received antiplatelets (>92% of patients). Mainly because of contraindications, oral anticoagulants at discharge were prescribed only for 9 (28%) and16 (65%) patients in big hospitals and 2 (100%) in the central hospital.
Conclusion
Half of Estonian SUs participated in the first collection period of the RES-Q project. Although there is enough room for improvement, the management of acute stroke in Estonia is generally good. Two participating stroke centres qualified for the Angels award.
Trial registration number
N/A
AS12-061
CHANGING TIMES - STROKE SYMPTOM ONSET AND SERVICE IMPROVEMENT IN A TERTIARY STROKE CENTRE
1Galway university hospital- Ireland, Geriatric and Stroke Medicine, Galway, Ireland
Background and Aims
Emerging research has demonstrated that the time window for treatment with mechanical thrombectomy may be up to 24 hours in selected patients. To implement this into clinical practice, access to modern imaging techniques to identify those patients who will benefit from treatment is essential.
Method
Over a 3 month period (October’17-January’18), data was prospectively collected on all acute stroke presentations to a tertiary stroke centre serving a catchment area population of 314,718. All acute ischemic stroke patients presenting within 24 hours of symptom onset were included. We assessed what proportion of patients received advanced imaging, such as CT angiograms (CT-A).
Results
There were 53 acute ischemic stroke presentations within 24 hours of symptom onset during the time period. 65.4% (n = 34) of patients had CT angiograms performed. 27 (51%) of patients presented within 6 hours of symptom onset. Patients presenting within 6 hours of symptom onset were more likely to have CT-A performed than those presenting between 6 and 24 hours (74% vs 46%).
Conclusion
Not all patients presenting within 24 hours of symptom onset are receiving advanced imaging. Resource allocation, education and refinements in our stroke pathway are essential to ensure that all cases that may benefit from advanced imaging so potential mechanical thrombectomy candidates are detected. This area is subject to ongoing departmental audit.
Trial registration number
N/A
AS12-062
STROKE MANAGER SERVICE: TWO-YEARS EXPERIENCE WITH POST-ACUTE MANAGEMENT OVER 3-MONTHS AFTER DISCHARGE FROM STROKE UNIT TO IMPROVE MEDICATION, LIFE-QUALITY AND REINTEGRATION
1Clinic of Neurology Bad Neustadt, Stroke Unit/ acute Department, Bad Neustadt, Germany
2Institute of Clinical Epidemiology and Biometry ICE-B, Epidemiology and Biometry, Würzburg, Germany
3Center of telemdicine Bad Kissingen, Telemedicine, Bad Kissingen, Germany
4Rhön Klinikum AG, Medicine Board, Bad Neustadt, Germany
5Clinical Center Main-Spessart, Neurology, Lohr, Germany
6Julius Maximilian University of Würzburg, Neurology, Würzburg, Germany
Background and Aims
In Germany, the inter-institutional post-acute stroke processes suffer from coordination and information discontinuity between the specialized healthcare providers. As stroke hits patients unexpectedly and throws them off track, patients need to organize their way back to daily life after discharge from the hospital. An organized health care network can help patients to recover fast and start with secondary prevention. Therefore, we implemented and evaluated a novel stroke manager service that supports the patients along the post-acute care pathway.
Method
Along admission and discharge from the stroke unit, to rehabilitation center until 3 months after discharge at home, the stroke manager assesses the patients' situation and advises them and their relatives on therapy, medication, risk factors, and reintegration. From June 2015 until March 2017, the stroke unit of the Clinical Center for Neurology Bad Neustadt provided the stroke manager service to 95 patients within an observation study. Inclusion criteria were: no former stroke (I61.*, I63.*,I64), no TIA, informed consent, age between 18 and 75, NIHSS<8, mRS<3.
Results
All patients accepted the stroke manager service and demanded further assistance. 77 patients (81%) filled out the survey after 3 months (65% male, mean nage 62 ± 11 years, 82% BMI > 25, 30% hypertension, mean BI 98,77, mean EQ-5D 0,93 ± 0,0923). 89% need assistance in daily activities, 21% live alone at home, 66% are non-working.
Conclusion
The patients‘ acceptance is high and leads to above average life-quality. It delivers important data for decision-making and valuable information in homecare. Comparison with a control group is in plan.
Trial registration number
N/A
AS12-063
FACTORS FOR DELAYED CALL FOR EMERGENCY MEDICAL SERVICES IN ACUTE STROKE PATIENTS IN COMMUNITY HOSPITALS – DATA FROM POMERANIAN STROKE REGISTRY
1Nicolaus Copernicus University in Torun - Ludwik Rydygier's Collegium Medicum, Department of Neurology- University Hospital No.1, Bydgoszcz, Poland
2Holy Spirit Specialist Hospital, Department of Neurology and Stroke Unit-, Sandomierz, Poland
3Medical University of Gdańsk, Department of Neurology, Gdańsk, Poland
Background and Aims
Delayed call for ambulance reduce the efficacy of acute stroke treatment. We evaluated factors for delayed call for EMS among stroke patients treated at the community-based Polish stroke centers.
Method
Medical records of 8710 patients with stroke (90,25 %) and TIA (9,75 %) consecutively reported to the Pomeranian Stroke Registry from 2010 to 2013 were evaluated.
Results
Delayed call for EMS (>45 min from onset) was reported in 63.33% of patients. Those with delayed call for EMS were characterized by younger age (72 vs 73 yrs; p = 0,03), higher presence of ischemia (82,4 vs 78,3%, p < 0,001), retirement (81,4 vs 78,8%; p = 0,002), living alone (14,7 vs 11,3%; p < 0,001), smokers (21,5 vs 17,5%; p < 0,001), alcohol abusers (2,5 vs 1,8%; p = 0,01) and seizures at stroke onset (17,9 vs 10,7%; p < 0,001). They were also characterized by lower NIHSS on admission (5 vs 8 pts, p < 0,001) and lower presence of regular physician’s care prior stroke (57,7 vs 63,7%; p < 0,001), urban location (34,4 vs 38,1%, p < 0,001), coronary disease (27,4 vs 33,4%; p < 0,001), atrial fibrillation (17,0 vs 24,0%; p < 0,001), pre-stroke anticoagulation (5,7 vs 7,9%; p < 0,001), previous stroke/TIA (27,3 vs 29,9%; p = 0,01), headache (15,3 vs 26,4%; p < 0,001), motor impairment (66,9 vs 73,1%; p < 0,001) and speech disorder (35,3 vs 45,5%; p < 0,001) at stroke onset. Multivariate analysis showed that age, living alone, smoking and tobacco use, seizures, headache, speech deficits, urban location, regular physician’s care prior stroke and atrial fibrillation contributed toward delayed call for EMS.
Conclusion
Delayed call for commonly exists among patients with stroke and transient ischemic attack due to social, clinical and logistic factors. Education should target high risk, living alone and rural patients.
Trial registration number
N/A
AS12-064
THE PRACTICAL APPLICATION OF NEW EU GENERAL DATA PROTECTION REGULATION LEGISLATION TO AN ONGOING INTERNATIONAL STROKE REGISTRY
1St. Anne's University Hospital Brno, Neurology - Stroke, Brno, Czech Republic
Background and Aims
The European Union’s (EU) new General Data Protection Regulation (GDPR) will come into effect on May 25th, 2018. These rules will have a significant impact on registry based research protocols, and will define what and how data can be collected. Registries are an important source of data for measuring the impact of stroke care initiatives, and provide an evidence base for defining clinical best practice. Legislation must balance patient privacy with the need for data collection which facilitates improvements in patient care.
Method
We examined the full GDPR text, as well as current interpretations of the stated rules, in combination with proposed implementations of GDPR for the Czech Republic and EU countries. The GDPR rules were then applied to the Registry for Stroke Care Quality (RES-Q), an ESO-EAST initiative for measuring the quality of stroke in Europe. Relevant sections in GDPR were identified, and compared with RES-Q’s existing data management strategy.
Results
Necessary modifications to RES-Q’s existing policies which were clearly identified were implemented and a new data protection policy was developed. Specific areas where ambiguity was identified included; 1) Informed consent, 2) Anonymization, 3) Pseudonymization, 4) Data preservation and destruction.
Conclusion
GDPR makes significant changes to existing EU and national legislation, and contains many clauses which are intentionally unclear and open to future legal challenges. It is possible to adapt ongoing protocols to comply with GDPR, however the ambiguity currently present has the potential to forestall important research as penalties for non-compliance with GDPR are severe.
Trial registration number
N/A
AS12-065
IMPROVEMENTS TO THE REGISTRY FOR STROKE CARE QUALITY (RES-Q) BASED ON FIRST YEAR USER FEEDBACK
1St. Anne's University Hospital Brno, Neurology - Stroke, Brno, Czech Republic
Background and Aims
The Registry of Stroke Care Quality (RES-Q) was launched by ESO-EAST (Enhancing and Accelerating Stroke Treatment) in November 2016 to provide a tool for monitoring the quality of stroke care in hospitals throughout Europe. RES-Q collects accepted quality of care metrics, based on “Cross-national key performance measures of the quality of acute stroke care in Western Europe” (Norrving et al, 2015). After the first year of operation, feedback was gathered from all participating sites, and an updated version was developed for release in 2018.
Method
RES-Q was initially implemented as a dynamic web form consisting of 25 metrics. Feedback was collected from National Coordinators, Angels Initiative representatives, and directly from sites via RES-Q’s internal contact form. The redesigned form focused on 4 key requirements: 1) Consistency with version 1; 2) Expanded diagnosis and patient transfer monitoring; 3) Definition clarity; 4) Question grouping for dynamic behavior.
Results
The RES-Q committee finalized version 2 of the form in January 2018. Version 2 includes additional metrics for monitoring: 1) Clinically Defined TIA; 2) Cerebral Venous Thrombosis; 3) Transfers between primary and comprehensive stroke centers. The web-enabled form was implemented with dynamic behavior such that additional options do not increase the overall form completion time. Mobile application and paper based questionnaire forms are also being developed.
Conclusion
RES-Q has demonstrated the viability of an accessible, web-based, international registry for monitoring standard stroke care quality metrics. The implementation of the questionnaire is crucial to improving participation while avoiding a selection bias based on adoption criteria.
Trial registration number
N/A
AS12-066
MOBILE STROKE UNIT TREATMENT OF SUSPECTED STROKE IN RURAL ALBERTA
1University of Alberta, Medicine/Neurology, Edmonton, Canada
2Alberta Health Services, Stroke Program Edmonton Zone, Edmonton, Canada
Background and Aims
We hypothesize that rural ischemic stroke patients may potentially benefit even more from Mobile Stroke Units (MSUs) than urban patients based on a greater reduction in stroke onset to treatment time. However most MSUs are urban based. We present our experience with an MSU focused on the treatment of rural patients in Alberta, Canada.
Method
The Northern Alberta Stroke Program’s MSU become operational in February 2017 and serves patients within a radius of 250 KM surrounding the University of Alberta Hospital in Edmonton.
Results
During the initial 10 months of operation, 55 patients were evaluated by the MSU. Thirteen patients (24%) were treated with rt-PA The rendezvous to treatment time was 23 minutes. The remainder of patients were either outside of the treatment window or had alternate etiologies including stroke mimics, TIAs or ICH. Interestingly 19 patients (35%) were evaluated in the MSU and diverted back to the referring hospital. Of 8 patients who received tPA and passed 3 month followup to date the mean presenting NIHSS was 8.6 (range 1, 22); median 5.5 (IQR 3.5, 12.25). The median 3 month NIHSS dropped significantly to 0 (Wilcoxan signed rank test p < 0.05). Of these 8 patients, one patient died, four have a 3 month mRS of 0-1, and seven are mRS 0-2 with all seven survivors returning home.
Conclusion
The MSU offers a novel approach to performing timely evaluation and treatment of suspected stroke patients in rural settings and may help reduce disability and admissions to overcapacity tertiary care facilities.
Trial registration number
N/A
AS12-067
THE QUALITY OF ACUTE STROKE CARE IN POLAND: PRELIMINARY FINDINGS FROM THE RES-Q REGISTRY
1Institute of Psychiatry and Neurology, 2nd Department of Neurology, Warsaw, Poland
2Medical University of Warsaw, Department of Experimental and Clinical Pharmacology, Warsaw, Poland
Background and Aims
The Registry of Stroke Care Quality (RES-Q) incorporated in Angels Initiative was designed to facilitate quality monitoring of acute stroke care. Our aim was to identify major gaps in Polish stroke unit care and approximate the nationwide generalizability of data contributed to RES-Q in year 2017.
Method
We retrospectively analyzed data collected in RES-Q on voluntary basis from January to December 2017. Representativeness of RES-Q data was assessed with reference to the estimated 11.5% national intravenous thrombolysis rate from year 2016.
Results
Of 175 Polish stroke units 44 (25%) declared participation in the registry. At least one case was reported by 36 (21%) units but only 7 (4%) reported >100 cases. Almost 89% of strokes were ischemic, median NIHSS score at admission was 7. Thrombolysis rate was 23% with median door-to-needle time 57 minutes. Early dysphagia screening was performed in 70% of patients. 24-hour ECG monitoring was carried out in 66% of patients. Symptomatic >70% carotid stenosis was diagnosed in 9% of patients and half of them were scheduled for urgent carotid endarterectomy or stenting. Median duration of hospital stay was 10 day with overall 16% hospital mortality. Seventeen percent of patients were discharged to rehabilitation ward and 57% could walk unassisted.
Conclusion
Currently Polish RES-Q data overrepresents better centers and cannot be considered representative for the general population. However, it still provides valuable information for individual centers and allowed to identify dysphagia screening, door-to-needle time and carotid endarterectomy or stenting as the major gaps that need to be addressed.
Trial registration number
N/A
AS12-070
REGISTRY OF STROKE CARE QUALITY (RES-Q) - FIRST REPORT FROM A PORTUGUESE CENTER
1ULS Matosinhos - Hospital Pedro Hispano, Neurology, Matosinhos, Portugal
2ULS Matosinhos - Hospital Pedro Hispano, Neurorradiology, Matosinhos, Portugal
3Centro Hospitalar de São João, Neurology, Porto, Portugal
Background and Aims
The ANGELS initiative aims to optimize acute stroke centers. The prospective registry of 24 variables related to stroke care quality (RES-Q) is a crucial step on that path. Our purpose is to report the baseline results after the RES-Q implementation.
Method
All neurologists from our center were asked to express their idea about the door-to-needle time during the previous year. Then, real data from December 2016 until December 2017 was analyzed.
Results
72 stroke patients were submitted to vascular recanalization treatment. Mean age was 74,5 years-old (SD = 13,5 years), 75% female. 58 were submitted to thrombolysis, 26 were referred to another hospital for thrombectomy, and 8% were submitted to both procedures. The median door-to-needle time was 62,5 (CI 60,5-80,6) minutes. 7 patients (9,5%) had intra-hospital strokes, and median door-needle time was higher in this group but did not reach statistical significance. 76% were evaluated for rehabilitation within the first 72 hours. 8% died before discharge, 44% were discharged home, 5% to a rehabilitation facility and 2% to a long-term care unit. 55,5 % were fully ambulated when discharged. The door-to-needle time subjectively expressed by neurologists on guard underestimated the real time verified by 8 minutes on average.
Conclusion
Implementation of ER protocols and staff education in order to minimize thrombolysis timing, improve intra-hospital stroke protocols and precocious rehabilitation evaluation are the crucial next steps to improve stroke care in our center, reinforcing the relevance of intra-hospital continuous data registry and analysis.
Trial registration number
N/A
AS12-073
STROKE CARE IN GEORGIA – GAPS AND CHALLENGES: PRELIMINARY ANALYSIS OF THE ESO-EAST RES-Q DATA
1Tbilisi State University, Department of Neurology, Tbilisi, Georgia
2Pineo Medical Ecosystem, Department of Neurology, Tbilisi, Georgia
3Kutaisi Referral Hospital, Department of Neurology, Kutaisi, Georgia
4Urgent Neurological Clinic, Stroke Service, Tbilisi, Georgia
5TSMU First University Clinic, Department of Neurology, Tbilisi, Georgia
6N5 Clinical Hospital, Department of Neurology, Tbilisi, Georgia
7St. Ann's University Hospital Brno, Department of Neurology, Brno, Czech Republic
Background and Aims
ESO-EAST is the first comprehensive program implemented in Eastern European countries aiming at improving stroke care and education. An essential part of the program is measuring and then improving stroke care quality in these countries implementing
Method
Data of consecutive stroke patients admitted to centers participating in ESO-EAST program from Georgia have been included in RES-Q. The RES-Q database was open for each center by one-month-per-year basis.
Results
5 centers (4 from Tbilisi, 1 from Kutaisi) participated. In total data of 445 patients (median age 71 years, 55% female) were collected from January 2016 until October 2017. Of those, 415 (93%) were treated in stroke units and 432 (97%) had neuroimaging. 104 patients (24%) underwent dysphagia screening within first 24 hours. Only 2 patients received intravenous thrombolysis. There were no cases of mechanical thrombectomy. Median hospital stay was 8 days. 396 patients (89%) were discharged home. 440 patients (99%) were prescribed antihypertensives at discharge. Of ischemic stroke patients, 94% received antithrombotics and 93% received statins at discharge.
Conclusion
Although non-generalizable for whole country because of few participating centers, the results of our study demonstrate important shortcomings in quality of stroke care in Georgia. This is especially true for acute recanalization therapy (thrombolysis and thrombectomy) in ischemic stroke. A comprehensive causative analysis will allow to tailor the country-specific interventions to fill these quality gaps.
Trial registration number
N/A
AS12-074
DATA ANALYSIS OF RES.Q-REGISTRY FOR 2017 IN UKRAINE
1Kyiv Region Clinical Hospital, Head of Stoke Unit- Department of Neurology, Kyiv, Ukraine
2MC ‘Universal Clinic ‘Oberig’, Head of Stroke Centre, Kyiv, Ukraine
3Institute of Neurology- Psychiatry and Narcology of the National Academy of Medical Sciences of Ukraine, Head of Department of Brain Vascular Pathology, Kharkiv, Ukraine
4Romodanov Neurosurgery Institute- National Academy of Medical Sciences of Ukraine, Director of the Romodanov Neurosurgery Institute, Kyiv, Ukraine
5P. L. Shupyk National Medical Academy of Postgraduate Education NMAPE, Head of Department of Neurosurgery, Kyiv, Ukraine
6Odessa National Medical University, Medical Director of University Clinic- Head of Neurology Depatment, Odessa, Ukraine
7Romodanov Neurosurgery Institute- National Academy of Medical Sciences of Ukraine, Head of Department of Endoscopic and Craniofascial Neurosurgery, Kyiv, Ukraine
8MC ‘Universal Clinic ‘Oberig’, Head of Stroke and Neurorehabilitation Unit, Kyiv, Ukraine
9Volyn Regional Clinical Hospital, Head of Neurology Department, Lutsk, Ukraine
10Institute of Neurology- Psychiatry and Narcology- National Academy of Medical Sciences of Ukraine, Leading Researcher, Kharkiv, Ukraine
11Odessa National Medical University, Head of Stroke Centre- Neurology Department, Odessa, Ukraine
12St. Ann's University Hospital Brno - FNUSA-ICRC, Department of Neurology, Brno, Czech Republic
Background and Aims
Implementation of evidence-based stroke treatments in Ukraine has never been investigated. We present the first results of evaluation of stroke care quality in Ukraine.
Method
Ukraine participates in ESO-EAST to identify gaps in quality of stroke care. Quality metrics are captured on international Registry of Stroke Care Quality (RES-Q). Participation of centers was voluntary and includes collection of all consecutive patients during one month per year period.
Results
74 (69%) neurological and neurosurgical departments (among 107 registered in RES-Q in Ukraine) participated in data analysis, but only 22 (30%) put on more than 30 cases each. 2577 acute stroke cases (SC) were collected from April till November, 2017. Median age was 67 y.o. (52% females). 59% of patients were hospitalized in the specialized stroke units or ICU. Patients undergone neuroimaging in 69% of all SC, 30% was performed within the first hour. Thrombolysis was performed in 3.7% of SC. In-hospital mortality was 7.9% (range 2.27%-50%). The patients had access for rehabilitation in 35%, however only in 6.7% departments rehabilitation facility was available (43% of patients couldn't walk unassisted at discharge). Anticoagulants were given to 42% (33%-100%) of patients with atrial fibrillation.
Conclusion
Fundamental gaps of quality of stroke care were identified in centers participating in ESO-EAST quality improvement program. Based on data from RES-Q, interventions targeting different gaps can be prioritized based especially on their feasibility and cost. Larger number of centers is needed to achieve nation-wide perspective and to collect data from less active and potentially less performing centers.
Trial registration number
N/A
AS12-075
IS POST-ACUTE, COMMUNITY BASED REHABILITATION IN SCOTLAND EVIDENCE BASED?
1University of Nottingham, School of Medicine, Nottingham, United Kingdom
2University of Glasgow, Institute of Health and Wellbeing, Glasgow, United Kingdom
3Scottish Healthcare Audits, Scottish Stroke Care Audit, Edinburgh, United Kingdom
4NHS Lanarkshire, Stroke Managed Clinical Network, Lanarkshire, United Kingdom
5University of Glasgow, Institute of Cardiovascular Medicine, Glasgow, United Kingdom
6Chest Heart and Stroke Scotland, Chest Heart & Stroke Scotland Educational Programmes, Edinburgh, United Kingdom
Background and Aims
Stroke is a clinical priority in Scotland, yet it is unclear whether the recommendations for implementing evidence based post-acute care in national clinical guidelines have been acted upon. The aims of this study were to determine the type of community stroke rehabilitation services that stroke patients are referred to on hospital discharge.
Method
Additional questions were included in the 2017 organisational Scottish Stroke Care Audit (SSCA) asking Managed Clinical Network managers and clinical audit co-ordinators in Scottish health boards to specify whether patients were referred to: a) Early Supported Discharge (ESD) b) Stroke Specific ESD c) Community Rehabilitation (CR) or d) Stroke Specific CR.
Semi-structured interviews with 44 multidisciplinary stakeholders involved in the delivery of ESD or CR were then conducted across three case study sites to further investigate the types of service models.
Results
Seven out of fourteen health boards reported provision of ESD, with one reporting partial stroke-specific ESD. Twelve reported provision of CR with two regarding themselves as stroke-specific.
Framework analysis of qualitative data revealed key themes relating to intervention delivery, monitoring, training and drivers for future service implementation. Strengths and challenges were highlighted. This revealed differences in the adopted models and service fragmentation, together with a variety of factors driving future development. Evidence of stroke education was present across sites.
Conclusion
Findings highlight inequality in the provision of post-acute care in Scotland. This raises questions about the challenges faced in implementing evidence based community stroke care that require further investigation. Opportunities for improving evidence based care were identified.
Trial registration number
N/A
NURSING, ALLIED HEALTH PROFESSIONALS AND CARERS
AS13-001
NARRATIVES AS A TECHNIQUE TO IMPROVE MEDICATION UNDERSTANDING AND USE SELF-EFFICACY IN STROKE: CONTENT DEVELOPMENT USING THE MODIFIED DELPHI METHOD
1Graduate Studies, School of Medicine and Health Sciences- Monash University- Malaysia, Sunway, Malaysia
2Subang Jaya Medical Centre, Neurology and Medical Department, Subang, Malaysia
3Hospital Kuala Lumpur, Neurology Department, Kuala Lumpur, Malaysia
4Monash University, School of Medicine and Health Sciences, Sunway, Malaysia
Background and Aims
The rise of recurrent stroke has urged researchers to explore narrative method in the field of pharmaceutical care. In the past decade, health workers had been vigorously applying the Health Belief Model with various narrative techniques as an adjunct in medication adherence. Recently, narratives via multimedia have gained popularity and displayed a promise of medication adherence. This study aimed to develop a consensus on the contents of learning outcomes and lead questions to improve medication understanding and use self-efficacy among stroke patients.
Method
A modified Delphi method was adapted. First, a few educational experts in stroke proposed a set of learning outcomes and lead questions based on literature reviews, the result of trials and patient education guidelines. Second, three Delphi rounds involving a panel with ten experts representing a mix of experiences in stroke in Malaysia was performed to gain consensus on final content.
Results
Initially, eight learning outcomes and lead questions were proposed for the content objectives. Following Delphi rounds 1 and 2, points were omitted and rephrased. Complete agreement on five learning outcomes and lead questions reached following the final phase; Delphi round 3. Few statistical analysis were applied to each learning outcomes and lead questions to obtain an acceptable mean and SD range which represented 90% consensus.
Conclusion
A consensus on appropriate learning outcomes and lead questions to improve medication understanding and use self-efficacy for stroke patient has been agreed by the expert panel on stroke experiences. It will serve as a base for further development of multimedia narratives.
Trial registration number
N/A
AS13-002
CREATING DIGNIFIED ENCOUNTERS IN UNEXPECTED SUDDEN DEATH BY STROKE – COMMUNICATION AS THE KEY
1Stroke unit, Skaraborg Hospital, Skövde, Sweden
2University West, Department of Health Sciences, Trollhättan, Sweden
3University of Gothenburg, Institute of Health and Care Sciences, Göteborg, Sweden
Background and Aims
Communication is present in all encounters in stroke care and of importance to create a caring relation. A good relation between patients, next of kin and health care staff is crucial, not least in unexpected sudden death by stroke.
The aim of the study was to illuminate communication and its meaning in unexpected sudden death by stroke, as experienced by next of kin and stroke team members.
Method
The design is a secondary analysis of qualitative data from a project on unexpected sudden death by stroke. Material from four interview studies from the project with all in all twelve next of kin of patients who had died due to the acute stroke during hospital stay and twenty-seven stroke team members from stroke units were utilized. Data were analysed with qualitative content analysis.
Results
The analysis reveals communication as the foundation for care and caring in acute stroke care. The overarching theme foundation for dignified encounters in care is built up by six themes illuminating the meaning of communication in unexpected sudden death by stroke.
Conclusion
Communication and its meaning in unexpected sudden death by stroke as experienced by next of kin and stroke team members is one key to create dignified encounters in care when unexpected sudden death by stroke occurs. It gives ground for unanimity about care and possibility to maintain and uphold dignity in care when acknowledging the next of kin familiarity with the patient, giving ground for a person centeredness despite the patients sever illness.
Trial registration number
N/A
AS13-003
“JUST GOT TO LIVE LIFE AS IT COMES”: THE LONGITUDINAL SPOUSAL DYAD EXPERIENCE OF THE TRANSITION TO HOME FOLLOWING A MILD STROKE
1School of Health and Rehabilitation Sciences, Health and Behavioural Sciences Faculty, St Lucia, Australia
2School of Allied Health Sciences, Griffith Health, Mt Gravatt, Australia
Background and Aims
Whilst research into the spousal dyad following mild stroke has started to develop, it has been focussed on the period immediately after the stroke event. Limited knowledge is therefore available in regards to the longitudinal experience of couples following mild stroke. This study aimed to investigate the longitudinal experience of the transition from acute hospital care, to home, in the context of a spousal dyad.
Method
Interpretative Phenomenology explored the experience of one married couple following mild stroke. At the time of the study, the couple was aged in their mid-60s, and the person with stroke (male) was working. Qualitative interviews were conducted separately with the participants at 1-, 3-, 6-, and 9- months post stroke. Coding of data was completed by two members of the research team, and all members were involved in the development and refinement of themes.
Results
Four themes were identified that portrayed the essence of the experience for the couple: (1) The Unexpected, Undesirable and Short-Lived, (2) The Unknown, (3) The New Normal, and (4) Situational Satisfaction.
Conclusion
The findings from the study are consistent with what is known about the initial period following mild stroke for the spousal dyad. Novel findings from this study include: the impact of contextual circumstances on a couple’s transitional experience, and the identification that even in the best of circumstances, people with mild stroke and their partners can experience ongoing questions and life changes. The results indicate there are longitudinal needs regarding information provision and support for the mild stroke population.
Trial registration number
N/A
AS13-004
THE DEVELOPMENT OF STROKE CODE ACTIVATION FOR IN-PATIENTS: PREPARING NURSES IN ACTION!
1National Guard Health Affairs -King Abdulaziz Medical City Riyadh, Stroke Nursing, Reading Berkshire, United Kingdom
Background and Aims
In April 2018, a stroke code activation for in-hospital patients will be introduced at the King Abdulaziz Medical City (KAMC), Saudi Arabia in order to address delays of identifying stroke on inpatient wards. Prior to its launching, developing departmental policies on criteria of stroke code activation and increasing awareness among nurses regarding prompt recognition of stroke symptoms in the ward are therefore imperative.
Method
A stroke code activation pathway protocols for in patients has been developed to envisage a rapid process of assessing patient with a suspected stroke and to provide a timely administration of intravenous thrombolysis and thrombectomy treatments. Also, a Stroke Activation session and Fast SEssion (
Results
More than 1500 nurses are adequately trained, prepared and ready to facilitate the stroke code activation. The stroke code activation pathway protocol has been disseminated to all health allied professionals (nurses, physicians, and therapists) to inform the process. A mock stroke code activation is randomly initiated in the ward to refresh nurses’ and physicians’ integrating the stroke thrombolysis pathway in practice.
Conclusion
Education remains the cornerstone of preparing nurses in action for a stroke code activation project. It is an exciting learning opportunity for all nurses to get involved in hyperacute management of stroke care. It is an excellent example of empowering nurses into an advanced level of expertise.
Trial registration number
N/A
AS13-005
COPING STRATEGIES, QUALITY OF LIFE AND LIFESTYLES: NEW APPROACHES IN ACUTE ISCHEMIC STROKE
1Universitat Rovira i Virgili, Nursing Department. Hospital Verge de la Cinta, Tortosa, Spain
2Hospital Universitari Vall d'Hebron, Stroke Unit, Barcelona, Spain
3Universitat de Girona, Nursing Department, Girona, Spain
4Universitat de Girona, Psychology Department, Girona, Spain
5Hospital Universitari Germans Trias i Pujol, Neuroscience Department, Badalona, Spain
6Universitat Rovira i Virgili, Nursing Department, Tortosa, Spain
7Institut Català de la Salut Terres de l'Ebre, Universitat Rovira i Virgili, Tortosa, Spain
Background and Aims
To study coping strategies, health behaviors, neurological-functional outcome, and quality of life (QoL) inpatients with acute ischemic stroke (AIS), previously randomized in the clinical trial (REVASCAT®), either tomechanical thrombectomy (MT) or control medical treatment (C).
Method
Demographic variables and neurological (NIHSS), functional (mRS), stroke impact (SIS-16), copingstrategies (COPE-28), therapeutic adherence (structured interview) and related QoL (EQ-5D) scales were evaluatedat 3 and 12 months after randomization in 82 AIS patients (MT, n = 42; C, n = 40) admitted in two REVASCAT strokecenters between 2012 and 2016. Between groups comparisons were made by using T-test, Mann-Whitney, and chi-square test. Also multiple linear regression models were performed to establish the relationship between QoL andvariables related to the patient outcomes.
Results
Conclusion
Patients treated with MT show greater neurological and functional recovery, improvements in healthbehaviors and lifestyles and perception of QoL. This group showed better strategies to afford health troubles at longterm.
Trial registration number
N/A
AS13-006
ENDOVASCULAR THERAPY AFTER ACUTE ISCHAEMIC STROKE - EXPERIENCES AND NEEDS OF PATIENTS
1Aarhus University Hospital, Neurology, Aarhus, Denmark
2Aarhus University Hospital, Intensive Care, Aarhus, Denmark
Background and Aims
The most recently approved treatment for major stroke is EVT. Ischaemic stroke is a serious diagnosis and demands urgent action in order to mitigate the extent of brain damage. Unfamiliar symptoms like paralysis, aphasia or cognitive impairment are for the most a violent and chocking experience. No previous studies have explored experiences and needs of patients going through the EVT pathway. The aim of this study was to explore the experiences and needs of patients going through the endovascular therapy (EVT) pathway.
Method
Semi-structured interviews and participant observations were carried out. Data were collected from April 2016 to January 2017. Data were analysed using Ricoeur's theory of interpretation, capturing meaning and ensuring comprehensive understanding.
Results
The acute phase of the stroke pathway was nearly erased of patients' memories, however concrete recollections of feeling anxious, powerless and uncertain were clear. Patients took a passive part and put themselves in charge of the staff. The receiving nurse being present during the entire pathway seemed to prompt calmness and reassurance. Long termly the patients suffered from various difficulties and felt like running against a wall when seeking actual information and advice according to their specific challenges and wishes.
Conclusion
The findings highlights the importance of health professionals acknowledging that also patients with positive recovery may have various needs long termly. The impact of a stroke goes far beyond physical disability and this knowledge might be fundamental to the successful delivery of clinical and social services to people with stroke.
Trial registration number
N/A
AS13-007
IS ONLINE STROKE-SPECIFC EDUCATION SUITABLE, ACCEPTABLE, AND EFFECTIVE FOR THE CONTINUED PROFESSIONAL DEVELOPMENT OF STROKE UNIT STAFF? AN EVALUATION OF THE STROKE-FACTS ONLINE EDUCATIONAL RESOURCE
1University of Central Lancashire, The Stroke Research Unit- Faculty of Health & Wellbeing, PRESTON, United Kingdom
Background and Aims
People affected by stroke require care from staff with appropriate knowledge. The Stroke-Specific Education Framework (SSEF) details the knowledge healthcare professionals (HCPs) require to deliver safe and effective care. Research shows undergraduate programmes may not equip staff with SSEF levels of required knowledge. We developed Stroke-FACTS, an educational resource aligned to the SSEF, to supplement multidisciplinary undergraduate curriculum. This research aimed to evaluate the suitability, acceptability, and effectiveness of Stroke-FACTS for the education of practicing HCPs.
Method
All HCPs (N = 26) delivering care in a stroke unit in north-west England were invited to participate. A mixed-methods design included pre/post testing of participant knowledge against the SSEF, completion of Stroke-FACTS, and a survey of HCPs perceptions.
Results
Eighteen HCPs were recruited. Of the ten HCPs (Nurses (N = 6); Healthcare Assistants (N = 4)) completing the study, 90% had unmet learning needs according to the SSEF. A Wilcoxon signed-rank test revealed a statistically significant increase in HCP knowledge following completion of Stroke-FACTS, Z = −2.023, p < .043, with a medium effect size (r = .45). HCPs felt the resource was suitable for practicing staff (90%), and an acceptable addition to continued professional development (100%).
Conclusion
The findings support previous research suggesting that practicing HCPs have unmet stroke-specific learning needs. Access to educational resources, like Stroke-FACTS, can potentially increase knowledge. Utilising frameworks to identify learning needs, and develop educational resources, can contribute to the provision of clinically relevant teaching. Further evaluation is required to understand impact on not only knowledge, but on patient outcomes when rolled out more widely.
Trial registration number
N/A
AS13-008
IMPROVING CLINICAL KNOWLEDGE: OUR EXPERIENCE OF DELIVERING A SUBARACHNOID HAEMORRHAGE (SAH) EDUCATION PROGRAMME
1Salford Royal NHS Foundation NHS, Department of Neurosurgery, Manchester, United Kingdom
2Salford Royal NHS Foundation Trust, Department of Learning and Development, Manchester, United Kingdom
3Salford Royal NHS Foundation Trust, Department of Neurosurgery, Manchester, United Kingdom
Background and Aims
High quality nursing care is integral in optimising patient outcome following SAH. Neurosurgical practice has become more subspecialised during the last decade, both for medical staff and with the advent of disease specific specialist nurses. However ward based nurses are required to maintain a broad knowledge base. In order to increase and maintain knowledge relating to SAH, we developed a disease specific educational programme. We present the methods used to deliver this programme and the change in level of knowledge.
Method
This specialist nurse led 2 day educational workshop is attended by nursing staff and allied health professionals involved in the care of patients with subarachnoid haemorrhage. The workshop is designed to cover the entire patient-journey and is delivered by members of the neurovascular team. All attendees complete a pre-workshop assessment to ascertain baseline understanding of SAH; this is repeated at the end of the programm.
Results
177 nurses and allied health professionals have attended the programme over 10 years. Subjectively the programme is well evaluated by all candidates, who report improved knowledge and understanding, confidence and awareness of the patient journey from admission to discharge and beyond. There was a significant improvement in pre vs post test scores (pre mean 32% (SD = 15) post mean 71% (SD = 14) paired t-test p < 0.0001). All participants have demonstrated improvements in their test scores with a mean improvement of 38% (SD = 14)
Conclusion
Our data suggest that this programme is well received by nursing staff and improves participants knowledge of SAH.
Trial registration number
N/A
AS13-009
THE EFFECTS OF PHYSIOTHERAPY AND REHABILITATION ON MOTOR RECOVERY, ACTIVITIES OF DAILY LIVING, QUALITY OF LIFE AND DEPRESSION IN ISCHEMIC STROKE PATIENTS
1Baskent University Faculty of Health Sciences, Physiotherapy and Rehabilitation, Ankara, Turkey
Background and Aims
The aim of our study was to determine the effects of the patient-specific physiotherapy rehabilitation program based on the neurodevelopmental treatment approach on motor recovery, activities of daily living, quality of life, anxiety and depression in patients with ischemic stroke.
Method
The 47 ischemic stroke patients were enrolled to the study between August 2010-May 2012. The patients had a physiotherapy rehabilitation program (included exercises such as strengthening for weak tonic muscles in inner range, elongation, functional activities) for 20 sessions. Motor Assessment Scale (MAS), Functional Independence Measure (FIM), Stroke Specific Quality of Life (SSQOL), and Hospital Anxiety Depression Scale (HADS) were assessed before and after treatment. The satisfaction of the patients was questioned with a 5-question Likert-type scale.
Results
There was a statistically significant difference in MAS and FIM between pre- and post-treatment (p < 0.05). No statistically significant change was found in SSQOL and HADS (p>0.05). In patient satisfaction scale, 1(2.1%) patient reported ‘complete improvement’, 11(23.4%) patients reported ‘improvement’, 31(66%) patients reported ‘partially improvement’, 3(6.4%) of the patients reported ‘no change’ and 1(2.1%) patient reported ‘symptoms worsened’.
Conclusion
In our study, we found that the physiotherapy program based on neurodevelopmental therapy, was effective on motor recovery and activities of daily living, but not on quality of life, anxiety and depression in the short term. The effects of improvements in motor and functional activities on the quality of life, and psychological status will occur for a longer time. The absence of the control group and the follow-up period is a significant limitation of our study.
Trial registration number
The study was started at August 2010. Therefore, the clinical registration number was not required for the study at that time. The study was approved by the Clinical Ethics Committee of the Baskent University (KA10/72) and all patients gave their informed consent.
AS13-010
A MULTIDISCIPLINARY SIMULATION TRAINING PROGRAMME IN THE HYPERACUTE STROKE UNIT
1St Helens & Knowsley Teaching Hospitals NHS Trust, Stroke Medicine, Prescot, United Kingdom
2St Helens & Knowsley Teaching Hospitals NHS Trust, Education Training & Development, Prescot, United Kingdom
Background and Aims
High-quality care of stroke patients delivered on Hyperacute Stroke Units (HASUs) has been one of the primary contributors to reductions in stroke mortality and institutionalisation. Effective multidisciplinary management of the unwell stroke patient is an essential skill unique to this environment. Simulation training is a well-recognised means of training for improving confidence and competence in high-pressure acute situations. A small evidence base exists on simulation training specifically for stroke medicine.
Method
We established a simulation programme focusing on unwell patients and acute deterioration on the high-dependency Hyperacute Stroke Unit. The monthly sessions were performed in the HASU itself, attended by nursing and therapy staff. The aim was to improve confidence in identifying and managing acutely unwell patients in clinical team members who may not have formal clinical assessment training.
Dedicated simulation trainers facilitated sessions, using a Laerdal SimMan 3G system with Laerdal LLEAP software. A clinical area was used for realism and to identify latent errors arising from the clinical environment itself. Video recording allowed immediate debriefing with objective feedback for the group.
Results
Formal staff feedback showed increased confidence in basic assessment of unwell stroke patients and improved team-working.
Conclusion
A high-quality stroke-orientated simulation programme can be established with standard simulation equipment and techniques. All members of the stroke multidisciplinary team can benefit, showing subjective improvements in team-working and confidence. Further work is needed on objective measures but we would encourage other HASUs to develop their own simulation programmes.
Trial registration number
N/A
AS13-011
THE IMPORTANCE OF EARLY AUDIOLOGICAL ASSESSMENT AND AURAL REHABILITATION IN STROKE PATIENTS
1NHS Lothian, Audiology Department, Edinburgh, United Kingdom
Background and Aims
Hearing loss can accelerate atrophy in the auditory areas of the brain, especially if left untreated. Hearing aids can help preserve a person's perception, cognition and how the brain processes sounds, including speech. Given how the peripheral and higher auditory centres are structured, both ischaemic and haemorrhagic strokes may disturb any level of the auditory pathway and lead to hearing deficits and central auditory processing problems. A pilot of an Audiology Stroke pathway offering priority aural assessment and rehabilitation was designed and implemented. The results showed that 69% of patients referred had been misdiagnosed as having central problems such as aphasia and global impairment. Their performance at assessments post stroke had been exacerbated by hearing loss and/or central auditory problems.
Method
The pathway has since been used as an official clinical protocol; we look at audiological manifestations from 136 stroke survivors with 27 different types of strokes and haemorrhages.
Results
Clinical findings indicate a higher prevalence of central auditory problems and more marked or asymmetrical hearing losses contralaterally to the site of lesion. The vast majority of patients and family members reported hearing deficits following stroke. 95.5% of stroke survivors referred were found to require aiding. Hearing aid uptake was higher in stroke survivors than in regular patients. Data analysis indicates it takes significantly longer for this patient group to acclimatise to wearing hearing aids.
Conclusion
Early aural intervention following stroke appears to be crucial not only for optimal aural rehabilitation but also for the stroke survivor’s optimal rehabilitation in general.
Trial registration number
N/A
AS13-012
CONVENIENT AND SAFE PATIENT IMMOBILIZATION SYSTEM FOR HYPERACUTE THROMBECTOMY UNDER CONSCIOUS SEDATION
1Chungnam National University Hospital, neurosurgery, Daejeon, Republic of Korea
Background and Aims
Recently, Intra-arterial thrombectomy using Stentriever or suction catheter is very popular for the hyperacute stroke. And There’s an ongoing debate about the better method between conscious sedation and general anesthesia. For the thrombectomy under conscious sedation state, adequate patient immobilization is one of the most important prerequisites for the safer and efficient procedure. Here we present our own patient immobilization system for daily use.
Method
We have designed and revised our own patient immobilization accessories for some intra-cranial interventional procedures such as thrombectomy using Stentriever and chemical angioplasty for vasospasm under conscious sedation. In this presentation, we will show you the developmental processes for the most updated version with descriptive pictures and explanations
Results
We have done more than 135 cases of intra-cranial thrombectomy under conscious sedation with this system without any unintended events. It takes less than a minute for set up before start of procedures and keeps the patient under minimal movement. To use this system was helpful for the safer and efficient procedures. The operator felt comfortable and no disturbance to the maneuver by these devices.
Conclusion
This our own patient immobilization system for interventional intracranial procedure on angiomachine under conscious sedation is a helpful and safe tool for the better Results
Trial registration number
N/A
AS13-013
BEHAVIOURAL CHANGES TO AVOID INCONTINENCE ARE LEADING TO ILL HEALTH, POORER HEALTH OUTCOMES AND INCREASED EXPENDITURE
1cambridge university foundation trust, stroke unit, cambridge, United Kingdom
Background and Aims
Dehydration is common in older people: free living, in care and in hospital. Dehydration is the cause and effect of ill health. Many common hydration assessments are inaccurate in the elderly due to physiological changes, hence dehydration maybe undetected, leading to increased mortality, poorer health outcomes, longer length of hospital stay and increase resource use. Dehydration is strongly associated with risk of stroke and poorer stroke outcomes. To better understand this issue, we investigated patient behaviour and beliefs through a service evaluation during 2015-17.
Method
We conducted three focus groups with older people (>65years): 1. Post stroke group n = 11. 2. Free living community group n = 10. 3. Hospitalised patients n = 7. We undertook brief questionnaires in emergency department n = 40, and on the stroke unit n = 7. We used a phenomenological approach to data collection and analysis. All questionnaires and field notes were analysed, themed and cross checked between interviews. Key themes were rechecked with interviewees for accuracy.
Results
The majority of older people restrict their fluid intake to manage continence, and avoid ‘accidents’. By controlling their intake they are able to continue to engage with social life outside the home, and avoid frequent nocturnal visits to the toilet, this was especially prevalent in hospital setting. 52% of respondence drank less 800mls a day. The data demonstrated low awareness of dehydration and impact on health.
Conclusion
Patient behaviour is contributing to increase morbidity, mortality and use of resources. Education, information around importance of hydration alongside continence support is required to address these important issues.
Trial registration number
n/a
AS13-014
A COMPARATIVE STUDY OF COGNITIVE STATUS IN STROKE SURVIVORS WITH AND WITHOUT TYPE 2 DIABETES MELLITUS
1veterinary organization, veterinary, Mashhad, Iran
2Birjand university of medical scienses, nursing, birjand, Iran
3Farabi hospital, out patient, Mashhad, Iran
4Farabi hospital, neurosurgery, Mashhad, Iran
5Farabi hospital, surgery, Mashhad, Iran
Background and Aims
Stroke is one of the leading causes of disability in the world. A high proportion of stroke survivors as well as type 2 diabetic patients had met the cognitive impairment. This study compared cognitive status in stroke survivors with and without diabetes.
Method
This comparative study was conducted on 30 consecutive stroke survivors from a neurology and stroke clinic. They were divided into two groups: stroke survivors with diabetes (n = 15) and without diabetes (n = 15). The inclusion criteria were the age of over 50 years old, a history of stroke more than one year, history of diabetes more three years and also more than 5 years schooling. Data on the patients’ demographic information gathered using a questionnaire, and Mini mental Status Exam (MMSE) were applied to assess cognitive status. Two groups according to sex, age, education, blood pressure and systemic diseases were group matched.
Results
The mean score of MMSE in stroke survivors without diabetes was significantly higher than with diabetes group (P = 0.03). A significant negative correlation was noted between MMSE scores and duration of diabetes in the diabetic group (r = −0.2, P = 0.03). A significant difference was noted in the mean score of MMSE according to sex (P = 0.03) in diabetic group.
Conclusion
Stroke with diabetes may worsen cognitive function in survivors. Caregivers should pay special attention to these patients according their sex and duration of diabetes.
Trial registration number
N/A
AS13-015
IMPACT OF FAMILY SUPPORT ON MEDICATION ADHERENCE AND COGNITION IN STROKE PATIENTS
1Birjand university of medical sciences, nursing, Birjand, Iran
2Farabi hospital, outpatient clinic, Mashhad, Iran
3Farabi hospital, neurosurgery, Mashhad, Iran
4Farabi hospital, surgery, Mashhad, Iran
5veterriology organization, veterriology, mashhad, Iran
Background and Aims
The prevalence of post-stroke cognition impairment is high and varies. Family support is believed to affect the quality of patient care and illness outcome. The purpose of this study was to determine Impact of family support on medication adherence and cognition in stroke patients.
Method
The randomized control trial study was conducted on 50 patients from a neurology and stroke clinic. They were randomly divided to intervention (n = 25) and control (n = 25) groups. The inclusion criteria were the age of over 50 years old, a history of stroke more than one year and also more than 5 years schooling. Data on the patients’ demographic information and their family gathered using a questionnaire, for two groups Morisky Medication Adherence Scale (MMAS), social support questionnaire – family version (SSQ) and Mini mental Status Exam (MMSE) were applied. The key family members of the intervention group were taught according to their educational needs in small groups.
Results
In intervention group mean of MMSE score was significantly increased after intervention (P = 0.03) however in the control group there was no significant difference. In intervention group a significant correlation was noted between SSQ scores and MMAS scores after intervention (r = 0.62, P = 0.01) but, there was no significant correlation in the control group.
Conclusion
Family support instruction based on the educational needs of family members, may improve medication adherence and cognitive status with indirect effect.
Trial registration number
N/A
AS13-016
COGNITIVE IMPAIRMENT IN STROKE PATIENTS FIVE YEARS POST-STROKE IS ASSOCIATED WITH ANXIOUS AND DEPRESSIVE SYMPTOMS IN FAMILY MEMBERS
1Royal College of Surgeons in Ireland, Psychology, Dublin, Ireland
2Royal College of Surgeons in Ireland, Medicine, Dublin, Ireland
3Royal College of Surgeons in Ireland, Clinical Research Centre- Beaumont Hospital, Dublin, Ireland
4Royal College of Surgeons in Ireland, Population Health Sciences, Dublin, Ireland
5Mater Misericordiae University Hospital, Geriatric Medicine, Dublin, Ireland
6Connolly Hospital Blanchardstown, Geriatric Medicine, Dublin, Ireland
Background and Aims
Cognitive impairment is common post-stroke, and is associated with increased levels of disability and dependency, leading to a greater burden on family members. The aim of this study was to explore associations between cognitive impairment in stroke survivors and anxious or depressive symptoms in family members five years post-stroke.
Method
As part of a five-year follow-up of the Action on Rehabilitation and Secondary Prevention Interventions in Stroke (ASPIRE-S) cohort of stroke patients, family members completed a self-report questionnaire. Symptoms of anxiety and depression were assessed using the HADS-A and CES-D. Cognitive impairment in stroke survivors was assessed using the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE score >3.3).
Results
77 family members participated, of whom 71 completed the HADS-A, and 51 the CES-D. Family members were spouses/partners of stroke patients (n = 49, 63.6%), adult children (n = 22, 38.6%) or siblings (n = 6, 7.8%). The majority was female (n = 62, 80.5%). Depressive symptoms were evident in 25.5% of family members, with 19.7% reporting symptoms of anxiety. Twenty-two stroke patients (29.0%) were identified as having evidence of cognitive impairment. Family members of stroke patients with cognitive impairment were significantly more likely to report depressive [OR (95% CI): 8.00 (1.99, 32.14)] or anxious symptoms [OR (95% CI): 7.00 (2.05, 23.87)].
Conclusion
Cognitive impairment in stroke patients is significantly associated with depressive and anxious symptoms in family members. Family members play a key role in the care and rehabilitation of stroke patients. Enhancing their psychological wellbeing and identifying possible ways to decrease burden is thus essential.
Trial registration number
N/A
AS13-017
UTILISATION AND PERCEIVED EFFECTIVENESS OF TREATMENT FOR CHRONIC PAIN FOLLOWING STROKE
1University of Melbourne, Florey Institute of Neuroscience and Mental Health, Melbourne, Australia
2La Trobe University, Occupational Therapy- School of Allied Health, Melbourne, Australia
3University of South Australia, School of Physiotherapy, Adelaide, Australia
Background and Aims
Chronic pain is common following stroke, yet current evidence for effective treatments targeting chronic pain for this problem is limited.
We aimed to identify current utilisation of treatments for chronic pain for people with stroke, and the perceived effectiveness of interventions utilised.
Method
An online survey for people with chronic pain following stroke was developed. Data was sought about current usage of medication and non-medication therapies and participants' beliefs regarding effectiveness for their chronic pain.
Results
A total of 136 participants with chronic pain following stroke completed the study. 127 (93.4%) reported that they were currently receiving treatment for their chronic pain condition. 116 (85.3%) reported taking medication, either prescribed or non-prescribed, while 98 (72.1%) were receiving non-medication based therapy. Of those receiving treatment, physiotherapy and anti-inflammatory medications were the most commonly reported interventions. Use of multimodal approaches was common, with combination medication therapy reported by 54 (46.6%) of participants receiving treatment, and 2 or more non-medication therapies by 43 (43.8%). Despite good access to, and utilisation of treatments for chronic pain (62 (53.4%) of participants reported poor effect with medications and 46 (46.9%) reported poor effect with non-medication therapies.
Conclusion
Despite often reporting that treatment is ineffective, people with chronic pain following stroke continue to seek and utilise many treatments for this disabling condition. Further research is indicated to greater understand pain following stroke to enable development of effective treatments.
Trial registration number
N/A
AS13-019
PAIN MANAGEMENT IN STROKE PATIENTS AFTER IMPLEMENTATION OF THE PAIN MAP IN THE STROKE UNIT
1Institute Health Science Research Germans Trias i Pujol, Neuroscience, Barcelona, Spain
2Germans Trias i Pujol Hospital, neuroscience, barcelona, Spain
Background and Aims
Pain prevalence among inpatients requires continuous evaluation. New communication technologies open up new opportunities for pain monitoring. The Pain Map is a tool that reports pain values and recurrence in real time, allowing early treatment of pain. Our aim is to evaluate the level of pain in patients admitted to the stroke Unit of the Germans Trias Hospital under the standard of <15% of patients with EVA >3 pre-and post-implementation of the Pain Map 2016-2017.
Method
Pain Map was implemented in January 2016; the specialist nurse receives a daily up-to-date report of the patient's pain situation. If moderate pain is detected, the clinical nurse is contacted. Population: 1.078 stroke patients (2016:537;2017:541). Variables: number of pain evaluations, Visual Analogue Scale (VAS) values and number of re-evaluations.
Results
Assessed sample of 22.222 pain forms in 1.078 patients. The average maximum pain was 0.22 points in 2016 and 0.28 in 2017 (0-10). The 88.8% (958) of patients had a pain record. The prevalence of higher pain >3 VAS was 1.94% (11) in 2016 versus 2.3% (12) in 2017; and severe pain (VAS>7) was 0.18% (1) versus 0.27% (2). The re-evaluation of pain in an hour was 6.10% (2016) versus 9.3% (2017); after two hours descended from 35.21% to 32.17% (p < 0.001)
Conclusion
Significant pain was not observed in stroke patients in our sample. There is moderate compliance in the registration of pain but the implementation of the Pain Map has allowed an early multidisciplinary approach. Systematic re-evaluation of pain is superior after the implementation of the instrument
Trial registration number
N/A
AS13-020
HOSPITAL-BASED SOFTWARE FOR OPTIMIZATION OF TRIAGE, WORK-UP AND TREATMENT OF ACUTE ISCHEMIC STROKE PATIENTS
1Rambam Health Care Campus, Neurology, Haifa, Israel
Background and Aims
The acute ischemic stroke is a medical emergency which may cause neurological and functional disability, deterioration in quality of life, and death. Modern treatments have a relatively narrow time window, calling thus for prompt identification of eligible patients.
Method
In order to optimize the process of triage, work-up and treatment of acute ischemic stroke patients Department of Neurology, in cooperation with the Computing Department, developed software for quick and comprehensive data extraction from hospital computerized database “Prometheus”. This database contains all possible details about patients hospitalized in the Rambam Health Care Campus, Haifa, Israel from the end of 1999. The software enables immediate access and processing of any relevant information in acute ischemic stroke patients from the entrance to the hospital till the treatment initiation and further until discharge.
Results
A special “Stroke Forum” was formed to discuss efficacy of acute stroke patients triage, work-up and treatment based on software data and make recommendations to optimize the whole process of management of acute ischemic stroke patients. The Forum includes neurologists and neurology nurses, emergency medicine staff, neuroradiology and interventional team and representatives of the hospital administration.
Conclusion
The forum discussions are focusing mainly on patients who eligible for IV TPA or interventional treatment. Results of discussions are transformed into hospital protocols and guidelines leading to optimization of work-up and treatment algorithm in acute ischemic stroke patients.
Trial registration number
N/A
AS13-021
IMPACT OF A TRAINING PROGRAMME ON PAIN MONITORING IN A STROKE UNIT
1Germans Trias i Pujol Research Institute, Neuroscience, Barcelona, Spain
2Germans Trias i Pujol Hospital, Neuroscience, Barcelona, Spain
Background and Aims
Pain management is an indicator of the quality of healthcare systems, being <15% of patients with Visual Analogue Scale (VAS) >3 recommended in clinical practice guidelines. Our aim is to evaluate the level of pain in patients admitted to the stroke in our centre after a training program
Method
Pre-test and post-test study was performed. 30 nurses from the stroke unit did a theoretical-practical course on VAS and Pain Assessment in Advanced Dementia (PAINAD) scale during 4 hours. A sample of 1.078 patients admitted in the stroke unit during two years (2016:537;2017:541). Number of pain evaluations, VAS values, number of re-evaluations and drugs consumption were recorded
Results
Assessed sample of 22.222 pain forms in 1.078 patients. The average maximum pain was 0.22 points in 2016 and 0.28 in 2017 (0-10). The 88.8% (958) of patients had a pain record. The prevalence of higher pain >3 VAS was 1.94% (11) in 2016 versus 2.3% (12) in 2017 and severe pain (VAS>7) was 0.18% (1) versus 0.27% (2). The re-evaluation of pain in an hour was 6.10% (2016) versus 9.3% (2017); after two hours descended from 35.21% to 32.17% (p < 0.001). Patients with communicational disorders or End-of-life situation (assessed by PAINAD), showed a significant decrease in analgesics 55.2% (2016) versus 19.5% (2017) (p < 0,001) and increase for hypnotics and sedatives 6.89% to 34.74% (p < 0,002)
Conclusion
Significant pain was not observed in stroke patients in our sample. There is moderate compliance in the registration and evaluation of pain; nevertheless, the training program increases the systematic re-evaluation of pain
Trial registration number
N/A
AS13-022
ALLIED HEALTH PROFESSIONALS COMPLETING A MASTER’S DEGREE IN NEUROREHABILITATION BOOST THEIR ACADEMIC CAREER AND PARTICIPATE IN CLINICAL RESEARCH PROGRAMMES
1Danube University Krems, Department For Clinical Neurosciences and Preventive Medicine, Krems, Austria
Background and Aims
Since 2002 the Department for Clinical Neurosciences at Danube University Krems runs an interdisciplinary Master’s courses in Neurorehabilitation designed specifically for allied health professionals, thereby supporting the academisation of physiotherapists, occupational therapists and speech therapists. The aim of this study was to investigate students’ career choices and career development after graduation and how this affects their professional career.
Method
An online survey was sent to 326 alumni of the Master’s courses Neurorehabilitation and Neurorehabilitation Research with 37 open- and closed-ended questions on study experience and career development.
Results
The total response and completion rates were 38% (n = 124) and 94.3% (n = 117), respectively. 82% (n = 102) of the participants were females, 18% (n = 22) were males with a mean age of 43.4 years ( ± 9.1 SD). Allied health professions represented in the survey were medical doctors (6%) speech and language therapists (13%), occupational therapists (21%) and physiotherapists (54%). Academic and personal expectations were mostly met, with a reported satisfaction rate of 73% on average. Regarding career choices and development, 16% (n = 19) of survey participants reported a pay rise since graduation, 14% (n = 17) now held a managing position at work, 35% (n = 42) were active in teaching at universities and colleges and 12% (n = 14) reported that they had become involved in part-time or fulltime research.
Conclusion
Beyond a better understanding of evidence-based medicine and scientific methodology, the Master’s courses at Danube University Krems support students’ professional development and encourage career opportunities. The academisation of allied health professionals is important and could promote new career models for this professional group.
Trial registration number
N/A
AS13-025
USING QUALITY IMPROVEMENT METHODOLOGY TO IMPROVE INTERMITTENT PNEUMATIC COMPRESSION DEVICE USE AFTER ACUTE STROKE
1Royal Infirmary of Edinburgh, Stroke Medicine, Edinburgh, United Kingdom
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Venous Thromboembolism (VTE) is a common complication of acute stroke. Evidence supports the use of Intermittent Pneumatic Compression (IPC) to reduce the risk of VTE and improve survival when used for immobile patients up to 30-days following stroke. IPC is recommended in UK and European Stroke Guidelines yet use in clinical practice has been inconsistent. In 2016 <50% of eligible patients in Scotland were offered IPC and so this remains a focus for Quality Improvement (QI) activity. We used QI methodology to identify interventions with the overall aim of improving use of IPC for immobile patients after acute stroke.
Method
We constructed process maps, used the Pareto principle to identify interventions and iterative Plan Do Study Act (PDSA) cycles. Data were collected prospectively, monthly from a randomly sampled population of in-patients within our 44-bed Stroke Unit. We introduced checklists to improve patient identification, improved IPC prescribing and introduced patient information /leaflets to improve patient engagement.
Results
Between September 2017 and January 2018 the proportion of sampled patients who met the criteria for IPC use remained stable (50-70%). The use of checklists improved the identification of patients, and IPC sleeve sizing, from zero to 43% but this was not maintained. A pre-prepared prescription improved our prescribing of IPC from 14% to >90% for 3 consecutive months.
Conclusion
Quality Improvement interventions can be helpful in ensuring the successful implementation of evidenced based medicine. Further work is required to ensure that improvements are maintained so that patients receive effective interventions in clinical practice.
Trial registration number
N/A
AS13-026
REALIZATION OF A MODEL FOR THE ANALYSIS OF THE “DYSPHAGIA” PHENOMENON IN THE NURSING HANDOVER OF A NEUROLOGY WARD
1Ospedale Forlanini-San camillo, RN- MSN- Phd Nursing Science-Nursing Research Unit- Sapienza University of Rome, Rome, Italy
2San Camillo Forlanini Hospital, RN Head Nurse - ICU Neurosurgery, Rome, Italy
3San Camillo Forlanini Hospital, MD- PhD Stroke Unit, Rome, Italy
4San Camillo Forlanini Hospital, RN MSN Director of Health Professions Department, Rome, Italy
5San Camillo Forlanini Hospital, Clinical Pathway Area, Rome, Italy
6San Camillo Forlanini Hospital, RN- MSN- Phd Nursing Science, Rome, Italy
7San Camillo Forlanini Hospital, Director General, Rome, Italy
8San Camillo Forlanini Hospital, Medical Director, Rome, Italy
9San Camillo Forlanini Hospital, Administrative Director, Rome, Italy
10University of L’Aquila- Italy, Associate Prof. Nursing Science Department of Health- Life and Environmental Sciences, L'Aquila, Italy
11Sapienza University of Rome, Associate Prof. Nursing Science- Director of Nursing Research Unit- Department of Public health and Infectious Diseases, Rome, Italy
Background and Aims
The Automatic Analysis of the text (AAT) uses a multidimensional statistic algorithm to recognise quantitative information and data in descriptive and not structured materials.
The aim of this work is to identify wording patterns within nursing handovers of the Neurology Ward of a Community Based Hospital, serving 1,6 million people catchment area.
Method
A retrospective survey has been carried out over 1445 nursing reports. The resulting database has been processed with the TalTac2 software, to test consistency between a theoretical model of care of dysphagia and its practice implementation through the analysis of text of handovers.
Results
The database of handovers referred to 63 patients, 21 were diagnosed with dysphagia (nursing diagnosis) on admission. According with the AAT consistency between the theoretical model of care and its practice implementation was low (less than 25%) .
Conclusion
We may interpret the lack of correspondence of the dysphagia model and its implementation in two ways: 1) the model of care is not fulfilled; 2) the text of handovers does not fully reflect the actual nursing practice. As a preliminary it should be recalled that all nursing notes were in paper format, which means that there is a lack of awarness of the key importance of nursing notes to improve health care delivery.
Trial registration number
N/A
AS13-028
IMPACT OF A MULTIDISCIPLINARY DYSPHAGIA PROTOCOL IN THE STROKE UNIT
1Universitary Hospital Rey Juan Carlos, Stroke unit. Neurology, MADRID, Spain
2Universitary Hospital Rey Juan Carlos, Swallow rehabilitation, Madrid, Spain
3Universitary Hospital Rey Juan Carlos, Dysphagia Unit Nursing. Otorhinolaryngology, Madrid, Spain
4Universitary Hospital Rey Juan Carlos, Dysphagia Unit. Otorhinolaryngology, Madrid, Spain
5Universitary Hospital Rey Juan Carlos, Endocrinology and nutrition, Madrid, Spain
6Universitary Hospital Rey Juan Carlos, Dietetic, Madrid, Spain
7Universitary Hospital Rey Juan Carlos, Speech therapy. Rehabilitation., Madrid, Spain
8Universitary Hospital Rey Juan Carlos, Rehabilitation, Madrid, Spain
9Universitary Hospital Rey Juan Carlos, Stroke unit Nursing, Madrid, Spain
Background and Aims
Acute stroke is the most common cause of oropharyngeal dysphagia. It affects 37-78% of stroke patients and increases the risk of aspiration pneumonia (AP), the most frequent infectious complication in stroke. Our objective was to measure the impact of a dysphagia protocol in our stroke unit (SU).
Method
We prospectively include all patients with stroke/TIA from September-2013 to March-2017 (protocol implemented in February-2014). Analysis periods: historic (HP 9/2013-1/2014), initiation (IP :2/2014-6/2014), consolidation (CP:7/2014-3/2017). The stroke neurologist decides depending on a priori risk of dysphagia if the first assessment is made by SU-nurse (low risk) or by and specialised dysphagia-nurse (high risk). Adjusted odds ratios and 95%CI were obtained for AP diagnosis; in-hospital and 90-day mortality and 90-day independence rate (mRS 0–2).
Results
839 patients were included: 80 HP/100 IP/659 CP. Baseline characteristics between groups were fairly comparable. Dysphagia diagnosis was 40%HP vs 43%IP vs 51.7%CP. The incidence of AP was 28.8%HP vs 10%IP vs 7.7%CP(p = 0.0001). In-hospital mortality rate was 16.3%HP vs 10%IP vs 7.9%CP(p = 0.01). Adjusted regression analysis revealed that, compared to the HP: AP was 9.5 and 12.2 times lower in IP and CP respectively; independence rate was 5.7 and 4.8 times higher in IP and CP respectively; in-hospital mortality risk was reduced by 54% and 68% in IP and CP and 90-day mortality was 3 times lower in CP.
Conclusion
Our dysphagia protocol was associated with a lower risk of AP, lower hospital and 90-day mortality and a higher probability of independence at 90-days. The reduction in mortality was largely associated with lower AP occurrence.
Trial registration number
N/A
AS13-029
SIX MONTH REVIEWS FOR STROKE SURVIVORS RESIDENT IN CARE HOMES: USE OF THE MODIFIED GREATER MANCHESTER STROKE ASSESSMENT TOOL (MGM-SAT)
1University of Manchester, Division of Neuroscience and Experimental Psychology, Manchester, United Kingdom
2Salford Royal NHS Foundation Trust, NIHR CLAHRC Greater Manchester, Salford, United Kingdom
3University of Manchester, Alliance Manchester Business School, Manchester, United Kingdom
4University of Manchester, Stroke Research, Manchester, United Kingdom
Background and Aims
The Greater Manchester Stroke Assessment Tool (GM-SAT) is a structured evidence-based needs assessment, developed to support longer term, post-stroke reviews in the community. Following UK-wide implementation of GM-SAT, expert consultation helped revise the tool and its relevance for reviews of care home residents. We aimed to explore the feasibility, usefulness and acceptability of the modified GM-SAT (mGM-SAT) in care homes.
Method
1) Observational study of unmet needs and actions identified during reviews in care homes;
2) Qualitative interviews of reviewers’ and reviewees’ experiences using mGM-SAT.
Results
Twelve professionals reviewed 74 stroke survivors (mean 83 years) in eight care homes. A wide range of unmet needs and actions for follow up were identified e.g. medicines-related; cognition/communication; extended activities of daily living. Reviewers found mGM-SAT was a useful, comprehensive tool for this population; helping legitimise and normalise needs that may not have been elicited without this structured tool. Layout and formatting improvements were suggested. Reviewers identified organisational barriers to implementation including: locating reviewees and booking reviews; communicating planned actions to GP and other agencies. Limited data were available from 13 reviewees who valued the review but had poor detailed recall of the process or outcomes.
Conclusion
The mGM-SAT proved feasible and useful in reviewing the needs of care home residents with stroke. Post-stroke reviews are an important ‘safety-net’ for this vulnerable population of care home residents. To ensure implementation into practice we are merging the original and modified GM-SAT into a single tool and updating guidance for reviewers before shortly making it freely available online.
Trial registration number
N/A
AS13-030
BALANCE IMPAIRMENT AFTER MILD STROKE
1Oslo University hospital and University og Oslo, Department of Physiotherapy and Department of Geriatric Medicine- and Faculty of Medicine, Oslo, Norway
2Norwegian Institute of Public Health, The Norwegian Knowledge Centre for the Health Services, Oslo, Norway
3Norwegian University of Science and Technology, Department of Neuroscience, Trondheim, Norway
4Oslo University hospital, Department of Geriatric Medicine, Oslo, Norway
5Bærum Hospital- Vestre Viken, Department of physiotherapy, Bærum, Norway
6Oslo University hospital and University of Oslo, Department of Geriatric Medicine and Facilty of Medicine, Oslo, Norway
7Vestfold Hospital Trust- Oslo University hospital and University og Oslo, Norwegian National Advisory Unit on Aging and Health and Department of Geriatric Medicine- and Department of Health Sciences, Oslo, Norway
Background and Aims
Due to new treatments, the number of patients without overt impairments after stroke is increasing. The study “Hidden impairments after stroke" aims to characterize mild impairments, and the sub-study aims to explore balance impairments in patients with mild stroke.
Method
Patients in working age suffering a first-ever mild stroke (NIHSS ≤ 3) were included. We used the Balance Evaluation Systems Test (BESTest), which gives a total score (0-108) and subsectional scores for different types of balance (0-15/18/21 depending on section), and the Mini-BESTest (0-28) to assess balance. There is no established cut off scores on the BESTest for the present population, so we used cut off for the lowest quartile to identify patients with balance impairments.
Results
In total 127 patients (age 55.6 11.3)) had a mean BESTest score 91.1 (19.4), and the lowest quartile 27 patients (age 58.7 (10.8)) had a BESTest score 64.7 (21.5). In the BESTest subsections the largest differences between total group and lower quartile were measured in Dynamic balance (0-21) 15.8 vs 9.0 and in Reactive balance (0-18) 14.6 vs. 7.6. The Mini-BESTest for total group was 21.4 (6.5), and for the lowest quartile 12.2 (5.9).
Conclusion
There was a wide range of balance impairments in this sample of patients with mild stroke. Using the BESTest, we identified Dynamic Balance and Reactive Balance to have the lowest scores and the largest difference between the total and the lower quartile. Clinicians should be aware of these balance impairments.
Trial registration number
N/A
AS13-031
ORGANISING SUPPORT FOR CARERS OF STROKE SURVIVORS (OSCARSS): A PROGRESS UPDATE FROM THIS ONGOING CLUSTER RANDOMISED CONTROLLED TRIAL
1University of Manchester, DNEP- Room G800, Manchester, United Kingdom
2University of Manchester, Division of Neuroscience and Experimental Psychology, Manchester, United Kingdom
3Salford Royal NHS Foundation Trust, NIHR CLAHRC Greater Manchester, Salford, United Kingdom
4University of Manchester, Clinical Biostatistics, Manchester, United Kingdom
5University of Manchester, School of Healthcare Sciences, Manchester, United Kingdom
Background and Aims
Informal carers provide invaluable support for stroke survivors but this can affect their own health and well-being. We co-developed an approach to identify and support carers’ needs and aim to explore the implementation of this approach into practice, and its clinical and cost-effectiveness compared to usual care.
Method
Mixed-methodology, longitudinal, multi-site cluster randomised controlled trial (cRCT) with embedded qualitative study, health economic analysis and process evaluation.
Clusters are Stroke Association services randomised to the new approach (intervention) or usual care (control). Staff in intervention clusters are trained in the intervention. Adult carers referred to participating services are invited to participate.
cRCT carer participants provide demographic data at study entry and outcome data at three and six months, through self-reported postal questionnaires. Outcomes are: caregiver strain and burden, mood, experience of caring, satisfaction with services, and economic burden (care provision and service utilisation). A sub-sample of carers are invited to a qualitative telephone interview to enrich quantitative findings.
The process evaluation collects quantitative and qualitative data from staff to explore: training acceptability; practice changes over time; intervention fidelity; and staff experiences of intervention and control.
Results
This trial is currently open to recruitment. Research ethics approval was granted and 35 clusters across the UK have been randomised (18 intervention; 17 control). To date, 300 carers have been recruited to the cRCT, a 64% consent rate with low attrition (7%) at the three month primary outcome point. The qualitative, process evaluation and health economics sub-studies are progressing well.
Conclusion
Recruitment closes July 2018.
Trial registration number
AS13-032
DEVELOPMENT AND VALIDATION OF A NEW MEALTIME ASSESSMENT TOOL FOR PATIENTS WITH DYSPHAGIA
1S Camillo Forlanini Hospital, Nursing and Health Allied, Rome, Italy
2S Camillo Forlanini Hospital, Neuroscience, Rome, Italy
3S Camillo Forlanini, Nursing and Health Allied, Rome, Italy
4S Camillo Forlanini Hospital, Nursing and Healt Allied, rome, Italy
5S Camillo Forlanini Hospital, Hospital Management, Rome, Italy
Background
Meal observation describes and analyze patient behavoiur while taking their meal minimizing influences of the observer; it is a component of the dysphagic patient evaluation process during and after the rehabilitation phase. Tools for meal observation and in particular the MAT, for the ease of administration contemplate the possibility of involvement of the care giver, thus expanding the opportunities for use of the tool.
Aim
to develop and validate a questionnaire that could be administered by both health personel and caregivers to explore patients’ mealtime behavior: the meal time assessment tool.
Method
The development and validation process was divided into three phases. The first phase included the identification of items for the questionnaire. The second phase involved pilot testing of the first version of the tool. In the final phase caregivers and the treating speech therapist administered the MAT to adult inpatients with diagnosed or undiagnosed oropharyngeal dysphagia. Correlation and internal consistency were evaluated with De Pippo and Cronbach alpha test (> 0,70).
Results
we enrolled 140 adult caregivers, MAT Cronbach Alpha was 0.710; we used the test of De Pippo (ROC curve) to verify the sensitivity and the specificity of the scale: results demonstated 97% sensitivity and 90% specificity. Hence it was possible to establish a patology-score cut off.
Conclusion
The validation process led to the conclusion that the MAT is a valid, reliable and stable scale. It is designed as a user-friendly tool for non-professionals to work with.
Trial registration number
N/A
DIAGNOSIS/INVESTIGATION OF STROKE ETIOLOGY
AS14-001
PERFUSION ABNORMALITY IN POSTERIOR INFERIOR CEREBELLAR ARTERY TERMINATION OF VERTEBRAL ARTERY ON ARTERIAL SPIN LABELING AND DYNAMIC SUSCEPTIBILITY CONTRAST PERFUSION MRI
1Hanyang University Guri Hospital, Radiology, Guri, Republic of Korea
Background and Aims
A posterior inferior cerebellar artery (PICA) termination of vertebral artery has been regarded as a normal variation of vertebrobasilar circulation. However, the perfusion condition of PICA territory in the cerebellum has not been evaluated. This study aims to present the perfusion abnormality in PICA termination of vertebral artery (PICA-VA) on arterial spin labeling (ASL) and dynamic susceptibility contrast (DSC) perfusion MRI.
Method
Sixteen patients (M:F = 8:8, 49-90 years old) who conducted brain MRI including MR angiography, and ASL and DSC perfusion MR studies and are found to have PICA-VA, are evaluated in this study. PICA-VA are associated with ipsilateral hypoplastic vertebral artery in 14 patients, and bilateral fetal type posterior cerebral artery in 2 patients.
Results
Hypoperfusion in PICA territory is detected on both ASL and time to peak (TTP) map of DSC perfusion MRI in 11 patients (68.7%), on only TTP perfusion MRI in 2 patients (12.5%), on only ASL perfusion MRI in 1 patient (6.3%) and not on both perfusion MRI in 2 patients (12.5%). Any clinical manifestations of vertebrobasilar insufficiency are not accompanied in 2 patients (12.5%).
Conclusion
PICA-VA that is regarded as normal variation, considerably have hypoperfusion in PICA territory of cerebellum. PICA-VA could have the clinical significance, especially in vertebrobasilar insufficiency, so perfusion study such as ASL or DSC perfusion MRI may help to evaluate the clinical status of vertebrobasilar insufficiency.
Trial registration number
N/A
AS14-002
ATTITUDES TOWARDS THE MANAGEMENT OF DWI-NEGATIVE STROKE AMONGST UK STROKE PHYSICIANS
1The University of Manchester, Faculty of Biology- Medicine and Health, Manchester, United Kingdom
2The University of Manchester, Division of Neuroscience and Experimental Psychology, Manchester, United Kingdom
3The University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
4The University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
Background and Aims
Diffusion-weighted magnetic resonance imaging (DW-MRI) is the gold-standard imaging technique used in diagnosis of acute ischaemic stroke. While the sensitivity has been variably reported in literature, many physicians argue that these represent stroke mimics. We sought to analyse opinion and current clinical practice of “DWI-negative stroke” among UK stroke physicians.
Method
An online survey (Survey Monkey) consisting of 10 questions, designed to evaluate attitudes and opinions of DWI-negative stroke amongst UK stroke clinicians was circulated via the British Association of Stroke Physicians (BASP) and analysed descriptively.
Results
79 BASP members working across 49 acute NHS trusts in the UK took part in the survey. The majority of the respondents were consultant stroke physicians (78%). 70% perceived the proportion of DW-MRI negative strokes to be between 1% and 10%. The majority (76%) felt mild strokes (National Institute of Health Stroke Scale ≤ 5) was associated with MR-DWI negativity; lacunar (68%) or posterior circulation strokes (53%) were most commonly representative of DW-MRI negative strokes. 65% would treat on a high clinical suspicion of stroke despite DW-MRI negativity, with 10% recommending a repeat MR scan and 25% suggesting alternative diagnoses. If DW-MRI stroke was diagnosed, the majority (78%) would offer life-long antiplatelet therapy with 8% not offering any anti-platelet treatment.
Conclusion
This survey suggests that there is wide variation in the diagnosis, interpretation and approach to management of DW-MRI negative strokes suggesting the need for further research to evaluate long term outcomes.
Trial registration number
N/A
AS14-003
CEREBRAL VEINS AND DURAL SINUS THROMBOSIS: A REVIEW OF 73 CASES
1“Victor Babeş” University of Medicine and Pharmacy, Neurology, Timisoara, Romania
2“Dr. Victor Popescu” Military Emergency Hospital, Ophthalmology, Timisoara, Romania
3“Victor Babeş” University of Medicine and Pharmacy, Internal Medicine-Nephrology, Timisoara, Romania
Background and Aims
Cerebral veins and dural sinus thrombosis (CVT) generally manifest in various non-specific clinical forms. The aim is to identify CVT risk factors, to describe the demographic, clinical, laboratory, and neuroimaging data, and to evaluate the treatment and outcome.
Method
We analyzed 73 CVT consecutive patients, that were examined at admission, at 30 days, at 90 days, and after twelve months, using the mRS scores.
Results
Mean age was 37.3 years (SD 7.5); 48 were women, 79.2% of them being fertile. The most frequent neurological syndrome was intracranial hypertension. CT showed direct signs of dural sinuses thrombosis in 12 cases, and venous cerebral infarcts in 28 patients. MRI/MRA/CTA identified thrombosis of SSS in 47 patients, lateral sinus in 30 cases, cavernous sinus in five patients, etc. Emissary vein thrombosis was identified in five cases; 19 out of 73 MRI had a normal prior CT. DSA revealed isolated cortical vein occlusion in 5 cases. Risk factors were identified in 50 patients (68.5%); hereditary thrombophilia being the most common (25 cases). All patients received anticoagulant therapy. After 12 months from admission, functional outcome was good, with a mRS score ≤2 in 43 patients (58.9%), moderate/severe disability in 22 cases (30.1%), the death rate being 11% (8 patients). Severity of CVST was found to be associated with presence of rapidly worsening symptoms (p = 0.001), and occlusion of 4 or more sinuses (p = 0.005).
Conclusion
CVT was common in women of fertile age. The outcome was favorable if the patients were promptly diagnosed and adequately treated.
Trial registration number
N/A
AS14-004
TRANSIENT GLOBAL AMNESIA: AN EMOTIONAL TRIGGER FOR A VASCULAR EVENT?
1Hospital Espírito Santo de Évora EPE, Stroke Unit, Évora, Portugal
2Hospital Espírito Santo de Évora EPE, Internal Medicine, Évora, Portugal
3Hospital Espírito Santo de Évora EPE, Neuroradiology, Évora, Portugal
Background and Aims
Transient global amnesia (TGA) is described has a benign neurological condition, defined by a presence of an amnestic period, with duration of no longer then 24h. The purpose of the presence study is to characterize the patients with TGA.
Method
From January 2004 to November 2017, 50 patients were admitted with TGA diagnosis, 39 were eligible for this study. A comprehensive analysis of the clinical data (including neuropsychological evaluation and follow up period) was performed.
Results
30 patients were female. Mean age was 63 ± 15y. Prevalent vascular risk factors were dyslipidemia and HBP. In 15 patients, the episode occurred in the afternoon, with duration of <8 hours. An emotional stressful life event was present in 35 patients. At admission, more than half presented a systolic >140mmHg. In the MRI hyperintensive signal in hippocampus was observed in 12 patients (either bilateral or unilateral). During follow up period, new MRI showed no abnormalities, 2 patients had a cerebrovascular event, and in neuropsychological evaluation was observed slow processing speed, impairment in verbal fluency and severe anxiety symptoms.
Conclusion
TGA was prevalence in women, with dyslipidemia and HBP as the most common vascular risk factors. From the follow up: no abnormalities on control MRI, the neuropsychological profile showed slow processing speed, impairment in verbal fluency and anxiety symptomatology. Vascular risk factors were present, although an ischemic etiology seems to be a faraway possible explanation due to the nonexistent atherosclerotic factor. Can it be a vascular response to stress?
Trial registration number
N/A
AS14-005
ECONOMIC EVALUATION OF INSERTABLE CARDIAC MONITORS IN THE DIAGNOSIS OF OCCULT AF FOLLOWING CRYPTOGENIC STROKE: RESULTS FROM THE DUTCH HEALTHCARE SETTING USING INPUTS FROM CRYSTAL-AF
1The Leeds Teaching Hospital NHS Trust, Cardiology, Leeds, United Kingdom
2University of Birmingham, Centre for Cardiovascular Sciences, Birmingham, United Kingdom
3Harvard Clinical Research Institute, Economics and Quality of Life Research, Boston- MA, USA
4Symmetron Ltd., Health Economics and Outcomes Research, London, United Kingdom
5Medtronic International, CRHF Health Economics and Outcomes Research, Tolochenaz, Switzerland
6Medtronic Trading NL BV, Reimbursement and Health Economics, Eindhoven, The Netherlands
7Medtronic Inc., CRHF Health Economics and Outcomes Research, Mounds View- MN, USA
8The University of Melbourne, Florey Department of Neuroscience and Mental Health, Melbourne, Australia
Background and Aims
Secondary prevention in patients with cryptogenic stroke (CS) remains challenging. Although anticoagulation effectively prevents stroke in atrial fibrillation (AF) patients, intermittent AF can be difficult to detect with conventional cardiac monitoring. CRYSTAL-AF (a 441-patient RCT) showed that, over 36 months, Insertable Cardiac Monitors (ICMs) diagnose AF in up to 10 times more CS patients than standard diagnostics. This study evaluated the cost-effectiveness of using ICMs in the Netherlands to identify CS patients with asymptomatic intermittent AF.
Method
A lifetime Markov model was developed, assigning patients to health states according to the presence and detection of AF, assuming use of anticoagulation in those with a positive diagnosis, whilst modeling the occurrence of Stroke/TIA, bleeds and death. Frequency and volume of standard tests were based on the control arm of CRYSTAL-AF. Costs were based on the Netherlands healthcare setting. Discounting was applied at 4% per annum for costs and 1.5% per annum for QALYs.
Results
In the base-case, the model predicted an incremental cost-effectiveness ratio (ICER) of €24,715/QALY gained in the scenario under which novel anticoagulants are initiated after an AF diagnosis. The scenario employing warfarin did not result in substantial differences, with an ICER of €24,657/QALY gained. In Monte Carlo simulation, 91% of times ICMs were cost-effective (below €80,000/QALY).
Conclusion
Results suggest that ICMs are cost-effective for patients in the Netherlands presenting with CS, with ICERs being well within the threshold used in the Netherlands, and probabilistic analysis and sensitivity analyses showing a high probability of cost-effectiveness across a range of scenarios.
Trial registration number
NCT00924638
AS14-006
DISRUPTION OF BLOOD-BRAIN BARRIER ATTRIBUTES TO TRANSIENT NEUROLOGIC SYMPTOM AFTER DIRECT BYPASS SURGERY FOR MOYAMOYA ANGIOPATHY – A PRELIMINARY STUDY -
1Hiroshima University Graduate School of Biomedical & Health Sciences, Neurosurgery, Hiroshima, Japan
Background and Aims
The instability of blood-brain barrier (BBB) was recognized for moyamoya angiopathy (MMA); however, the instability of BBB function after bypass surgery for MMA has never been investigated. The purpose of this study was to evaluate the perioperative serum levels of BBB-related proteins in MMA patients based on the hypothesis that postoperative hemodynamic change may cause the disruption of BBB, which may attribute to transient neurological symptom (TNS).
Method
A total of 13 hemispheres in 12 patients with MMA were prospectively investigated. A direct bypass surgery was performed in all cases. The serum levels of occludin (OCLN), claudin 5 (CLDN5) and vascular endothelial (VE)-cadherin were quantitated using enzyme linked immunosorbent assay before and postoperative day (POD) 1, 4 and 7, respectively. TNS was evaluated as reversible neurologic dysfunction without any postoperative infarction or hemorrhage.
Results
Successful patency of the direct bypass was obtained in all cases. The serum levels of OCLN were increased on POD 1, and the following changes of OCLN were decreased on POD 4 and 7, respectively. On the other hand, there was no remarkable fluctuation on those of CLDN5 and VE-Cadherin. TNS was observed in 6 (46.2%) cases. In 2 cases with severe TNS lasting 6 and 13 days after the surgery, the serum levels of OCLN on POD 1 were markedly elevated over 10 folds higher than baseline.
Conclusion
The OCLN could be associated with the disruption of BBB and be a biomarker to predict the TNS after bypass surgery for MMA.
Trial registration number
N/A
AS14-007
PATHOGENESIS AND PROGNOSIS OF NONFISTULOUS CEREBRAL VARICES
1Seoul National University College of Medicine, Department of Neurosurgery, Seoul, Republic of Korea
2GangNeung Asan Hospital, Department of Neurosurgery, Gangeung, Republic of Korea
Background and Aims
Pathogenesis of nonfistulous cerebral varices is not well known. Lasjaunias suggested venous obstruction as a hypothetical cause. The aim of this study is to identify the origin of nonfistulous cerebral varices by the analysis of 25 cases and the review of literature.
Method
25 patients with cerebral varices (> 5 mm) without arteriovenous shunts were found by the search of medical and radiologic records of Seoul National University Hospital. Clinical data and radiologic data about numbers, sizes, locations, associated anomalies, and vascular anatomic relationships among CVs and anomalies were collected.
Results
Mean number of CVs per patient were 1.72 ± 1.2. Mean diameter of the largest CVs were 6.99 ± 2.61 mm. 8 patients had compromise of vein of Galen and straight sinus. 4 of these 8 patients had sinus pericranii. 5 CVs were draining veins of giant developmental venous anomalies. 3 patients were associated with migration anomalies. 3 patients had Sturge-Weber syndromes. 6 isolated cerebral varix cases were found. CVs were not usually directly proximal to the venous obstruction. Instead, CVs developed as alternative collateral drainage routes of venous obstructions.
Conclusion
Nonfistulous CVs greater than 5 mm are possibly pathogenetically heterogeneous group. A subgroup of CVs is probably developmentally caused by venous obstructions. CVs are closely related to congenital anomalies and the other anomalies including developmental venous anomaly and sinus pericranii in the origin.
Trial registration number
N/A
AS14-008
TRANSESOPHAGEAL ECHOCARDIOGRAPHY IN ACUTE STROKE – REASONABLE IN YOUNG PATIENTS OR ONLY IN THE ELDERLY?
1University Medical Center Freiburg, Neurology and Clinical Neurophysiology, Freiburg, Germany
2Mediclin Staufenburg Klinik Durbach, Medicine, Durbach, Germany
Background and Aims
Indication of transesophageal echocardiography (TEE) for the diagnostic work-up in cryptogenic stroke is unclear.
Method
From 2010 to 2011we prospectivelyincluded 485 consecutive stroke patients who underwent routine diagnostics including TEE. Stroke etiology was classified according to the TOAST classification. The rate of high- and potential-risk sources in TEE (TOAST criteria) in cryptogenic stroke was evaluated in <55, 55-74, and ≥75year-old patients. Plaques ≥4 mm thickness or with superimposed thrombi ( = complex plaques) of the proximal descending aorta (DAo) were considered a high-risk source.
Results
Without TEE, etiology of stroke was cryptogenic in 329 (67.8%) patients and TEE determined etiology in 158 (48.4%) of those. In patients aged <55, 55-74, ≥75 years TEE detected the following embolic sources: complex plaques including DAo ≥4 mm thickness = 6 (7.1%), 79 (49.1%) and 52 (63.4%) or with superimposed thrombi = 0 (0.0%), 5 (3.1%) and 7 (8.5%); left atrial flow velocity ≤30 cm/s = 0 (0.0%), 1 (0.6%) and 2 (2.4%); spontaneous echo contrast = 0 (0.0%), 1 (0.6%) and 6 (7.3%); PFO plus ASA = 18 (20.9%), 32 (19.9%) and 14 (17.1%), respectively. TEE led to oral anticoagulation in 57 (17.3%) patients and to PFO-closure in one patient.
Conclusion
TEE was valuable for determining exact stroke etiology and led to oral anticoagulation in 17% of patients with cryptogenic stroke. Impact of TEE in patients ≤55 years was limited to the detection of septal anomalies. In older patients, however, it was highly valuable to identify complex atheroma and indicators of intermittent atrial fibrillation.
Trial registration number
N/A
AS14-010
EMBOLIC STROKES OF UNDETERMINED SOURCE IN THE RENISEN STROKE REGISTRY: COMPARISON OF PATIENT FEATURES AND EVOLUTION DURING ADMISSION
1Hospital Universitari Mutua Terrassa, Neurology service, Terrassa, Spain
2Biomedical Research Institute IRB Lleida, Clinical Neuroscience group, Lleida, Spain
3Hospital Universitari Arnau de Vilanova, neurology, Lleida, Spain
4Hospital Universitari Josep Trueta, Neurology, Girona, Spain
5Hospital Donostia-Donostia Ospitalea, Neurology, San Sebastian., Spain
6Hospital Universitari Germans Trias i Pujol, Neurology, Badalona, Spain
7Hospital Universitario La Paz, Neurology, Madrid, Spain
8Hospital Universitario de Valladolid, Neurology, Valladolid, Spain
9Hospital Moisés Broggi, Neurology, Sant Joan Despí, Spain
10Hospital de Mataró, Neurology, Mataró, Spain
11Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
12Hospital Joan XXIII, Neurology, Tarragona, Spain
13Hospital de León, Neurology, León, Spain
14Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
15Hospital Verge de la Cinta, Neurology, Tortosa, Spain
Background and Aims
Information about clinical characteristics and evolution among embolic stroke of undetermined source (ESUS) patients from large registries is limited. We have compared the evolution during admission and the characteristics of ESUS subjects with other etiological subtypes.
Method
We prospectively studied 13280 ischaemic strokes from 19 university hospitals. Previously, 4163 patients were classified as undetermined due to two causes or incomplete evaluation (TOAST criteria) and 2463 patients with transient symptoms without neuroimaging lesion were excluded. Subjects were classified after the diagnostic work-up as large-artery atherosclerosis (LAA, n = 2489), cardioembolism (CE, n = 5974), small-vessel disease (SV, n = 2499), other causes (OC, n = 498), and ESUS (n = 1820). In all ESUS subjects vascular imaging, ECG monitoring and echocardiography were performed.
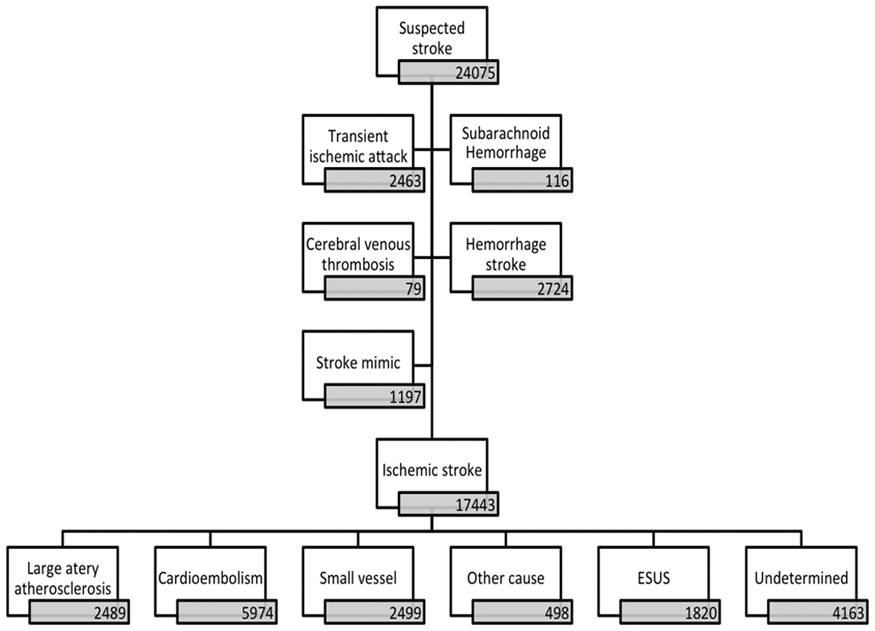
Results
ESUS subjects were younger than LAA, CE and SV (66.7 [14.4] vs. 71,5 [11,6], 75.5 [15.3] and 71.4 [12.6] p < 0.001) and had less proportion of traditional risk factors. Stroke severity, measured by NIHSS, was higher in LAA and CE than in ESUS (5.0 [2.0-12.0] and 8.0 [3.0-17.0] vs. 4.0 [2.0-9.0] p < 0.001). Evolution during admission was significantly better in ESUS. Only 14 (0,8%) ESUS died versus 119 (4.8%) LAA, 514 (8.6%) CE, 52 (2.1%) SV and 20 (84.0%) OC, p < 0.001.
Conclusion
ESUS patients have specific clinical characteristics and evolution during admission. They are younger, with less severe stroke and lowere mortality rate than other etiologic subtypes.
Trial registration number
N/A
AS14-011
NEUTROPHIL-TO-LYMPHOCYTE RATIO AND PLATELET-TO-LYMPHOCYTE RATIO AS FACTORS TO PREDICT IN HOSPITAL MORTALITY IN ACUTE ISCHEMIC STROKE
1Korea University Anam Hospital, Neurology, Seoul, Republic of Korea
Background and Aims
The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) have emerged as independent prognostic markers in stroke. The aim of this study was to investigate the predictive role of the NLR and PLR at admission in patients with acute ischemic stroke.
Method
This study included 3,107 consecutive patients who were admitted to Korea University Anam Hospital for acute ischemic stroke. NLR and PLR were calculated from the differential counts of leukocytes and platelet counts drawn at admission. Primary endpoint was mortality during hospitalization.
Results
The mean age of 3,107 patients was 67.9 years and 59.1% were male. A total of 66 (2.1%) patients died during hospitalization. The NLR of the deceased were higher than the survivors (6.19 vs 3.56 p = 0.001). PLR showed similar pattern without statistical significance (166.79 vs 139.21, p = 0.135). Receiver operating characteristics (ROC) curve analysis revealed that the NLR 3.82 (AUC: 0.662) and PLR 216.67 (AUC: 0.534) were the most powerful predictor of in-hospital mortality, respectively. The mortality rate of patients with both NLR and PLR values above cut-off value was significantly higher (4.8% vs 1.8%, p = 0.001). Binary logistic regression analysis also support this finding with statistical significance (p = 0.019).
Conclusion
Higher values of both NLR and PLR were independently associated with in-hospital mortality with the advantage of being inexpensive and readily available.
Trial registration number
N/A
AS14-012
DIAGNOSING FUNCTIONAL STROKE MIMIC VERSUS TRANSIENT ISCHEMIC ATTACK IN AN MRI NEGATIVE MULTIETHNIC COHORT
1Hamad Medical Corporation, Neurology, Doha, Qatar
Background and Aims
It is important to correctly diagnosis Transient ischemic attacks (TIA) and differentiate them from functional stroke mimics (FSM) as they have very different treatment strategies. We review our experience with the two entities in MRI negative patients.
Method
We retrospective reviewed the Stroke database over a 21 month period identifying all MRI negative cases with a diagnosis of TIA or FSM . The diagnosis was by general or stroke neurologist.
Results
We identified 327 cases including 175 FSM and 152 TIAs. Mean age of FSM was 41 Vs 47 for TIAs (p < 0.001). Males comprised 71.9% of the cohort. There with 3 ethnic groups, Arabs 44%, South Asians 37% and others 19%.
FSM was more frequent in females (67.4% vs Vs 48.1% males as FSM). TIAs were more common in males (51.9% Vs 32.6% females) (p = 0.002). Arrival to emergency was by ambulance in 61.1% of FSM Vs 45.4% in TIAs (p = 0.04).
64.8% of Arab patients where FSM whereas 61.5% of the south Asians were labeled as TIAs (p < 0.001).
Clinical symptoms of facial weakness and dysphasia was associated with the diagnosis of TIA (p < 0.05). The mean ABCD2 scores for TIAs were 2.5 + 1.8 Vs 0.6 + 1.3 for FSM (p < 0.001). Thrombolysis was given in 10.9% FSM Vs 0.7% in TIAs (p < 0.001)
Conclusion
In this mixed ethnic population, we noted that patients with TIAs were more likely to be South Asian and had higher ABCD2 scores. FSM was more frequently seen in Arabs and in female patients. The high rates of thrombolysis in FSM patients is of concern.
Trial registration number
N/A
AS14-013
RESTENOSIS AFTER CAROTID ENDARTERECTOMY: COMPARISON OF THREE SURGICAL TECHNIQUES AND USAGE OF INTRAOPERATIVE SHUNT
1UCL, Division of Surgery and Interventional Science, London, United Kingdom
2UCL, Institute of Neurology- Stroke Research Centre, London, United Kingdom
3University Hospital Basel- Basel University, Department of Neurology and Stroke Unit, Basel, Switzerland
Background and Aims
Closure of the carotid artery during carotid endarterectomy is conventionally done with or without patch, or closure with eversion technique. We report data on carotid restenosis from the International Carotid Stenting Study comparing these techniques, and the association of intraoperative shunt usage.
Method
Patients who underwent carotid endarterectomy in the study were divided into closure with patch angioplasty, primary closure, and eversion endarterectomy. Patch angioplasty was used as the reference technique. Intraoperative shunt usage was reported. Primary outcomes were restenosis of ≥50% and ≥70% to the end of follow-up.
Results
790 patients had carotid endarterectomy with restenosis data at 1- and 5-years after surgery. 511 (64.7%) had patch angioplasty, 232 (29.4%) primary closure, and 47 (5.9%) eversion endarterectomy. The cumulative incidence of ≥50% restenosis at 5-years was respectively 25.9%, 37.2%, and 30.0% per group. There was no difference in risk between the eversion group compared to patch angioplasty (hazard ratio [HR] 0.90, 95% CI 0.45-1.81, p = 0.77). Primary closure had significantly higher risk of restenosis (HR 1.45, 95% CI 1.06- 1.98, p = 0.02). The cumulative incidence of ≥70% restenosis seems greater in the primary closure group, however this was not significant (12.1% vs. 7.1%, HR 1.59, 95% CI 0.88-2.89, p = 0.124). There was no difference in shunt usage on the cumulative incidence of restenosis at either 1- or 5-years.
Conclusion
Shunt usage had no impact on restenosis. Restenosis was more common in carotid endarterectomy with primary closure than conventionally with a patch closure.
Trial registration number
N/A
AS14-014
CIRCADIAN VARIATION OF EFFICACY OF INTRAVENOUS RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Chungbuk National University Hospital, Neurology, Cheongju, Republic of Korea
2Dankook university hospital, Neurology, Cheon-an, Republic of Korea
Background and Aims
A few studies reported that time of stroke, especially ischemic stroke, was influenced by circadian rhythm. The serum concentration of plasminogen activator inhibitor-1 was shown to have clear circadian variation, which could influence platelet aggregation, blood viscosity, and endogenous/exogenous fibrinolytic activity. The aim of our study is to investigate whether the effect of IV rtPA could be influenced by circadian time.
Method
1,923 patients were finally enrolled for the analysis. The patients were stratified according to stroke onset time by every 4 hours. NIHSS at emergency room, NIHSS at 24 hours after IV rtPA administration, NIHSS at discharge, and a change of follow-up NIHSS from iNIHSS were analyzed. Three stroke subgroups according to TOAST classification were separately reviewed. 3month modified Rankin Scale was used to compare a long term outcome between groups.
Results
The whole group analysis showed that the 23-3h group had the highest cNIHSS1 and followed by 3-7h group although statistically insignificant. LAA, CE group showed the same pattern as the whole groups, and cNIHSS1 of the 3-7h group was higher than that of 23-3h in patients with SVO group. No statistical significance was found. The prevalence of patients with favorable outcome defined by 3month mRS 0 or 1 was not different according to LNT. However, in LAA group, 23-3h group showed a tendency of higher prevalence than other groups.
Conclusion
This analysis did not show a definite circadian difference of the efficacy of IV rtPA, measured by the changes of NIHSS and 3mon mRS in acute ischemic stroke patients.
Trial registration number
n/a
AS14-015
ASSOCIATION OF CANCER CELL TYPE AND EXTRACELLULAR VESICLES WITH COAGULOPATHY IN PATIENTS WITH LUNG CANCER AND STROKE
1Samsung Medical Center, Neurology, Seoul, Republic of Korea
2Samsung Biomedical Research Institute, Clinical Research Center, Seoul, Republic of Korea
3Samsung Medical Center, Hemato-oncology, Seoul, Republic of Korea
Background and Aims
Coagulopathy is an important cause of stroke in cancer patients. However, underlying mechanisms and clinical factors related to coagulopathy remain unclear. Cancer cells secrete extracellular vesicles (EVs), and circulating EVs in cancer patients are reportedly associated with clinical outcomes. We hypothesized that certain characteristics of cancer affect coagulopathy in patients with lung cancer and ischemic stroke.
Method
Consecutive patients with active lung cancer and acute ischemic stroke were prospectively studied. Volume and pattern of acute brain infarcts and plasma levels of circulating tumor EVs (CD326, CD133, and CD144) were measured using flow cytometry. In vitro experiments investigated the pathophysiological mechanisms underlying cancer-associated coagulopathy
Results
Of 114 patients, 95 (83.3%) had an adenocarcinoma cell type and 95 (83.3%) had distant metastasis. Acute brain infarct volumes were larger (P = 0.009) and circulating EV levels were higher (P<0.01 for all EVs) in patients with an adenocarcinoma cell type than in those with other cell types. The presence of metastasis was not associated with infarct volume or circulating EV levels. Coagulation assays demonstrated dose-dependent shorter clotting times after treatment with EVs from adenocarcinoma cell lines than with use of EVs from squamous cell carcinoma. These findings were confirmed by coagulation assays using circulating EVs from patients with adenocarcinoma and stroke and from those with conventional stroke mechanisms.
Conclusion
Our findings indicate that cancer cell type is associated with circulating EV levels and coagulopathy in patients with lung cancer and stroke.
Trial registration number
ClinicalTrials.gov: NCT02743052
AS14-016
THE INFLUENCE OF CAROTID ARTERY OCCLUSION ON THE OCCURRENCE OF NONFOCAL CEREBRAL SYMPTOMS
1UMC Utrecht, Department of Neurology and Neurosurgery- Brain Centre Rudolf Magnus, Utrecht, The Netherlands
2UMC Utrecht, Julius Centre for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Patients with symptomatic carotid artery stenosis more often experience nonfocal cerebral symptoms than patients without carotid stenosis. This association has not been examined in patients with occlusion of the carotid artery. We therefore studied the relationship between carotid artery occlusion and the occurrence of nonfocal cerebral symptoms.
Method
We included 67 patients with carotid artery occlusion and 62 patients without carotid stenosis (<50%). All patients had a history of ischaemic stroke or transient ischaemic attack (TIA) in the anterior circulation that had occurred >6 months before inclusion. Both groups were interviewed with a standardized questionnaire on the occurrence of the following nonfocal cerebral symptoms: blurred vision, bilateral weakness, unsteadiness, isolated vertigo, nonrotatory dizziness, paresthaesia, unconsciousness, confusion, and amnesia in the preceding six months. We calculated risk ratios (RRs) with 95% confidence intervals (CIs) for the occurrence of at least one and at least two different nonfocal cerebral symptoms after adjustment for age, sex, systolic blood pressure, and time interval between most recent ischaemic stroke or TIA and interview.
Results
In the total of 129 patients, unsteadiness (46; 36%) and nonrotatory dizziness (31; 24%) were reported most often. Patients with carotid artery occlusion more often experienced at least one (61% vs. 44%; aRR 1.46; 95%CI 1.00-2.14) and more often at least two (28% vs. 11%; aRR 3.32; 95%CI 1.56-7.10) different nonfocal cerebral symptoms as compared with patients without carotid occlusion.
Conclusion
Nonfocal cerebral symptoms occurred more often in patients with carotid artery occlusion than in those without carotid artery occlusion.
Trial registration number
N/A
AS14-017
E-MEDICINE HELPS DIAGNOSING AND CLASSIFYING UNDERLYING CAUSES OF STROKE
1Instituto Nacional de Neurologia Y Neurocirugia- Mexico City and Paris-Diderot- Sorbonne University, Neurology and Stroke Center Bichat Hospital- Paris, Mexico City, Mexico
2Paris-Diderot- Sorbonne University, Neurology and Stroke Center- Bichat hospital, Paris, France
3Lille University, Biostatistics, Lille, France
Background and Aims
After an ischemic stroke or a TIA, the presence of underlying potential causes drives the preventive treatment, based on guidelines. ASCOD phenotyping has been designed to determine the most likely potential cause, without neglecting the concomitant presence of other underlying causes less likely or not directly related to the stroke.
Method
we developed an algorithm to automatically phenotype stroke patients in all main causal diseases (
Results
ASCOD App is a free application now available online and can be downloaded from specific e-stores (Apple Sore and Google Play Store) in English, French, German, Spanish, Portuguese, Mandarin, Cantonese, Japanese, and Korean languages. After entering patient data, the application generates a report on potential, possible or unrelated underlying causes that helps preventive treatment decision making.
Conclusion
ASCOD app is the first application available at bedside to find out potential causes of stroke and guides preventive treatment.
Trial registration number
N/A
AS14-018
GENE EXPRESSION AND ISCHEMIC STROKE ETIOLOGY: CARDIOEMBOLIC FEATURES. A SYSTEMATIC REVIEW AND VERIFICATION ANALYSIS
1Vall d'Hebron Institute of Research, Neurovascular Research Laboratory, Barcelona, Spain
2University of Florence, Neuroscience Section- Department of Neurofarba, Florence, Italy
3Charité University Hospital Berlin, Department of Neurology and Center for Stroke Research Berlin, Berlin, Germany
4University of California at Davis Medical Center, Lawrence J. Ellison Ambulatory Care Center- Department of Neurology, Sacramento, USA
5Vall d’Hebron University Hospital, Stroke Unit- Department of Neurology, Barcelona, Spain
Background and Aims
Optimization of secondary prevention treatment after ischemic stroke falls upon correct and rapid etiological classification, but etiology remains undetermined in one-third of patients. Diagnostic improvement has been suggested by the use of molecular biomarkers, including gene expression markers. We planned a compilation of the transcriptomics available data, a verification analysis of relevant candidates and their validation in several stroke cohorts.
Method
Published studies analyzing high-throughput gene expression in blood samples to discriminate cardioembolic (CE) strokes were found in PubMed until November 2016 and were complemented with similar in-house microarrays data. Significant regulated genes present in at least 2 studies were considered as candidates and validated by RT-qPCR in 50 CE and 50 atherothrombotic (LAA) strokes (<6h from onset) and in 20 cryptogenic strokes (<48h from onset) with long-term Holter monitoring.
Results
After microarrays data screening, 67 genes appeared to be regulated in CE strokes. Up-regulation of CREM, PELI1 and ZAK was verified at transcript level in CE vs. LAA (p = 0.010, p = 0.003, p < 0.001, respectively), with a combination of at least two markers showing 82% specificity and 56% sensitivity to discriminate CE (p < 0.001). In cryptogenic strokes with subsequent AF detection, only PELI1 revealed significance (p = 0.033).
Conclusion
The proved discriminatory capacity of these markers even in cryptogenic strokes might bring their use as early biomarkers up, while the relationship between transcript and protein levels should be further assessed.
Trial registration number
N/A
AS14-019
RECURRENT EMBOLIC STROKE IN YOUNG ADULT PATIENT WITH HEART AMYLOIDOSES
1Mother Theresa University Hospital, Departement of neurovascular disease, Tirana, Albania
2Mother Theresa University Hospital, Departement of neuroradiology, Tirana, Albania
3Mother Theresa University Hospital, Head Departement of neurovascular disease, Tirana, Albania
Background and Aims
Ischemic stroke incidence in young adults has been increasing over the past years. Identifying the cause of ischemic stroke in young adults is very important to prevent stroke recurrence. Etiologic work up in these patients is of major importance, given the potential numerous underlying causes. This is the case of a young adult female patient, with recurrent stroke in different vascular territories. The purpose of this study was to explore different etiologic approaches and work up needed to identify the underlying cause of ischemic stroke in young adult patients.
Method
Multiple etiologic work up for this patient was performed. It included: transesophageal echocardiography, cardiac markers, autoimune assays, biochemical check, coagulation control, viral control, cardiac mri, doppler ultrasound of carotid arteries.
Results
Autoimmune assays, viral control, doppler ultrasound of carotid arteries was normal. Inflammatory markers were elevated with a slightly high homocysteine level and very high c reactive protein. Transesophageal echocardiography revealed asymmetrical septal thickening, granular and sparkling myocardial appearance suggesting of cardiac amyloidosis. This was later confirmed by cardiac magnetic resonance imaging, which revealed infiltration in the myocardium.
Conclusion
Multiple etiologies must be investigated in recurrent ischemic stroke in young adult patients. These data support the need for a more in depth investigation of the causes of stroke in the young.
Trial registration number
N/A
AS14-020
RELATION BETWEEN ISCHEMIC STROKE AND LEGNTH OF INTERNAL CAROTID STENOSIS
1University Hospital Wuerzburg, Neurology, Würzburg, Germany
2University Hospital Wuerzburg, Neuroradiology, Würzburg, Germany
Background and Aims
High-grade carotid stenosis (CS) >70% is a leading cause of ischemic stroke. However, a considerable percentage of stroke survivors with a symptomatic CS have <70% stenosis. Different characteristics such as fibrous plaques or thin ruptured cap have been identified as markers for unstable plaques resulting in cerebral embolism. Whether the length of the CS is also associated with a high risk of ischemic stroke has never been investigated.
Method
In a retrospective observational study, 204 CS in 167 stroke patients were identified. The degree of CS was measured by ultrasound, the length by ultrasound, MR-angiography and/or DSA. Plaque echogenicity was classified into predominantly hypoechogenic, mixed or predominately echogenic category.
Results
A statistically significant inverse relation between the length and degree of CS was found among symptomatic CS (ρ = − 0.29, p = 0.002) but not among asymptomatic CS (ρ = 0.05, p = 0.71). Symptomatic CS <70% were slightly longer (median: 18mm) than asymptomatic CS <70% (median 15.5mm) (p = 0.18). In a multivariate analysis, ipsilateral ischemic stroke was significantly associated with the degree of CS (≥70% vs. <70%; OR 11.04, 95%CI 2.99-40.71, p < 0.001). A borderline significance was found when plaque echogenicity was put into the model (echolucent vs echogenic; OR 3.14, 95%CI 1.0-9.89, p = 0.051), but not with stenosis length (OR 0.97, 95%CI 0.89-1.07, p = 0.56).
Conclusion
Stroke occurrence in patients with <70% CS might be – to some extent - related to plaque length. Whether stroke patients with a long but <70% CS might profit from a carotid revascularization remains to be confirmed in a large study.
Trial registration number
N/A
AS14-021
PHOSPHOLIPASE A2 AND ETIOLOGICAL MECHANISMS OF ISCHEMIC STROKE
1Centro Hospitalar da Universidade de Coimbra, Neurology, Coimbra, Portugal
2Centro Hospitalar de Coimbra, Internal Medicine, Coimbra, Portugal
Background and Aims
Lipoprotein-associated phospholipase A2 (Lp-PLA2) is secreted by hematopoietic and inflammatory cells, and it is considered a biomarker for atherosclerotic plaque. In population-based studies, Lp-PLA2 emerged as an independent risk factor for atheromatous vascular events in coronary and cerebrovascular diseases. Its impact in coronary disease has already been demonstrated; however its influence in cerebrovascular etiology is still unknown.
Method
Observational, prospective study of acute ischemic stroke patients with cardioembolic, atherothrombotic or lacunar etiology (TOAST Etiological Classification), and ESUS patients. For all patients, Lp-PLA2 was dosed in peripheral blood between day 3 and 14 post-event with “Lp-PLA2 - SNIBE" kit. Non-parametric statistical analyses and ANOVA were performed.
Results
A total of 96 patients were enrolled, mean age of 75.31 ( ± 11.88) years, 41 males (42.7%); 12.5% with lacunar stroke, 16.7% atherothrombotic, 46.9% cardioembolic and 24% ESUS. The distribution of Lp-PLA2 levels was not homogeneous between etiologies (ANOVA test, F = 2.982, p = 0.035), being lower in ESUS: 143.3 ( ± 42.8) ng/mL. The mean level was 160.5 ( ± 50.8) ng/mL for lacunar events, 156.2 ( ± 55.3) ng/mL in atherothrombotics and 175.3 ( ± 54.6) ng/mL in cardioembolics. There was no statistical significance for previous vascular risk factors, history of coronary disease or ischemic stroke (Mann-Whitney test). There was also no statistical difference between Lp-PLA2 and mRS score 3 months post-event.
Conclusion
Lp-PLA2 levels are not homogeneous among the etiologic mechanisms of ischemic stroke, being reduced in ESUS patients and similar between lacunar, cardioembolic and atherothrombotic, which reinforces the existence of distinct pathophysiological mechanisms in ESUS patients.
Trial registration number
N/A
AS14-022
ATRAUMATIC CONVEXAL SUBARACHNOID HEMORRHAGES IN PATIENTS WITH HEMODYNAMICALLY SIGNIFICANT CERVICAL OR INTRACRANIAL ATHEROSCLEROTIC DISEASE
1Hospital de Braga, Neurology, Braga, Portugal
2Centro Hospitalar e Universitário de Coimbra, Stroke Unit, Coimbra, Portugal
3Centro Hospitalar de Vila Nova de Gaia / Espinho, Stroke Unit and Neurology Department, Vila Nova de Gaia, Portugal
Background and Aims
Atraumatic convexal subarachnoid hemorrhage (cSAH) is a rare entity, comprising less than 10% of all SAH. The etiological differential diagnosis of cSAH include cervical or intracranial atherosclerotic disease. Our aim was to characterize a population of patients with cSHA with hemodynamically significant cervical or intracranial atherosclerotic disease.
Method
Retrospective multicenter study, describing patients with cSAH associated with cervical or intracranial atherosclerotic disease. Patients with any cerebral vascular malformation were excluded.
Results
Of the 12 patients included, 9 were male, mean age was 60 years (47-83). Four patients were previously under antiplatelet therapy and no patient was anticoagulated. The most frequent initial clinical manifestation was permanent focal neurological signs (50%). During the course of illness, the most prevalent clinical manifestations were permanent or transitory focal neurological signs (11/12) and headaches (7/12). Atheromatous lesion location was cervical internal carotid artery (n = 6), middle cerebral artery (n = 4) and intracranial internal carotid artery (n = 2). Eleven patients showed a high-grade stenosis (>70%) or occlusion ipsilateral to cSAH. cSAH was ipsilateral to the atheromatous lesion in all cases, one patient had bilateral cSAH and two patients showed disseminated cHSA (>4 sulci). Regarding secondary prevention, 6 patients were medicated with dual antiplatelet therapy, 5 with single antiplatelet therapy and 1 was anticoagulated. One patient was submitted to angioplasty and another to endarterectomy.
Conclusion
Atherosclerotic large vessel disease is a rare cause of cSAH but this etiological diagnosis has clinical and therapeutic implications.
Trial registration number
N/A
AS14-023
FRANK’S SIGN AND STROKE SUBTYPES: RELEVANCE IN REFINING THE CLINICAL PROFILE OF CRYPTOGENIC STROKE (ESUS)
1Hospital Universitari Dr. Josep Trueta, Neurology-Stroke Unit, Girona, Spain
2Hospital Universitari Dr. Josep Trueta, Neurology, Girona, Spain
Background and Aims
Frank’s sign (FS) has been described as a predictor of coronary, cerebrovascular and peripheral arterial disease. Few studies have analysed its prevalence and relevance in stroke patients, and no studies have focused on the prevalence and usefulness by stroke subtypes (SSS-TOAST).
Our objective was to analyse the prevalence of FS in stroke patients as a whole and by stroke subtype and to evaluate its potential usefulness in embolic stroke of unknown source (ESUS).
Method
Prospective study, consecutive patients admitted to our Stroke Unit. Presence of FS and correlation with age, sex, pathological history, cardiovascular risk factors, previous treatment, stroke subtype, NIHSS-Rankin, sonographic findings and neuroimaging were analysed.
Results
We included 100 consecutive patients. The prevalence of FS was 63.6% as a whole and 57.1%, 68.8%, 62.1% and 70.8% in small-vessel disease, atherothrombotic, cardioembolic and ESUS strokes, respectively. FS was significantly associated with older age (74.9 ± 12.6 vs. 63.6 ± 12.2, p < 0.01), arterial hypertension (70.0 vs. 46.4, p = 0.02), diabetes (80.0 vs. 55.9, p = 0.01), ischaemic heart disease (76.7 vs. 57.4, p = 0.05), ultrasonographic markers of atheromatosis (76.5 vs. 47.5%; p <0.05), especially carotid stenosis >50%, and stroke severity at admission (NIHSS 7.8 vs. 4.4). Absence correlates with haemorrhagic stroke, smoking habit (43.8 vs. 73.2, p = 0.01) and moderate alcohol intake (50% vs. 71, p = 0.05).
There was a differential pattern in ESUS patients according to the presence or absence of SF.
Conclusion
FS has a similar prevalence in the different stroke subtypes and is associated with an atherothrombotic profile. In ESUS the FS may be useful in guiding aetiological study.
Trial registration number
N/A
AS14-024
DIAGNOSTIC VALUE OF MAGNETIC RESONANCE BLACK-BLOOD THROMBUS IMAGING ON ISOLATED CORTICAL VEIN THROMBOSIS
1Xuanwu Hospital-Capital Medical University, Neurology, B, China
Background and Aims
Precise diagnosis of isolated cortical vein thrombosis (ICoVT) has been difficult and challenging. We explored a novel MR black-blood thrombus imaging technique (MRBTI) for precise detection of ICoVT.
Method
Between June 2014 and December 2017, 32 consecutive patients with clinical presentations suspected of ICoVT were prospectively recruited. All the patients and 18 cortical venous segments of each patient were respectively evaluated both by conventional imaging and MRBTI techniques. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), areas under curves (AUC) and Youden index were used to evaluate the diagnostic value of MRBTI in detecting ICoVT.
Results
Among 37 suspected ICoVT patients, 18 patients were diagnosed as proven ICoVT by conventional imaging and 23 isolated and thrombosed cortical venous segments were detected in the proven ICoVT patients by conventional imaging as well. 17 of 18 (93.5%) proven ICoVT patients were definitely confirmed by MRBTI and another one was detected to have concurrent venous sinus thrombus. 23 of 23 (100%) segments with isolated thrombi were correctly identified by MRBTI. The sensitivity, specificity, PPV, NPV, AUC and Youden index for MRBTI were 94.4%, 100%, 100%, 95%, 97.2% (95% confidence interval 90.9-100%, P<0.001) and 0.944 based on patients. The sensitivity, specificity, PPV, NPV, AUC and Youden index for MRBT based on segments were 100%, 100%, 100%, 100%, 100 (95% confidence interval 100-100, P<0.001) and 1.
Conclusion
MRBTI allows selective visualization of isolated cortical vein thrombus and accurately excludes venous sinus thrombi and can be used as a promising first-line diagnostic imaging tool in detecting ICoVT.
Trial registration number
N/A
AS14-025
THE ROLE OF A NEWLY DEVELOPED CLINICAL PROBABILITY SCORE AND D-DIMERS FOR THE PREDICTION OF CEREBRAL VENOUS THROMBOSIS
1Inselspital- University Hospital of Bern, Department of Neurology, Bern, Switzerland
2Academic Medical Center- University of Amsterdam, Department of Neurology, Amsterdam, The Netherlands
3Department of Experimental Vascular Medicine- Academic Medical Center- University of Amsterdam, Department of Plasma Proteins- Sanquin Research- Amsterdam, Amsterdam, The Netherlands
4Inselspital- University Hospital of Bern, Diagnostic and Interventional Neuroradiology, Bern, Switzerland
5Experimental Haemostasis Group- Department for BioMedical Research- University of Bern, Department of Medicine- Inselgruppe- Tiefenauspital, Bern, Switzerland
6University of Bern, Experimental Haemostasis Group- Department for BioMedical Research, Bern, Switzerland
Background and Aims
The diagnostic value of D-dimers in cerebral venous thrombosis (CVT) has not yet been fully established. A clinical score to stratify patients with possible CVT into groups with high/intermediate/low CVT probability would be helpful to increase the diagnostic value of D-dimers.
Method
This prospective study, included 359 consecutive adult patients (09/2009-02/2016) with clinical possibility of CVT presenting at the University Hospitals of Bern/Amsterdam (n = 196/163). On admission, patients underwent neurological examination, MR- and/or CT-venography and measuring of D-dimers (ELISA-test).
Results
In 94/25.8% patients CVT was confirmed by imaging. For all patients, predictive value of D-dimers for CVT was as follows ≥650mcg/l vs. ≥500mcg/l (Sens:76.6%/Spec:77.3%/NPV:90.3%/ACC: 77.2% vs. Sens:89.4%/Spec:66.4%/NPV:94.6%/ACC:72.4%). The optimal estimate of clinical probability was based on 7 variables (1 point each) identified by multivariate analysis: duration of symptoms (subacute/chronic i.e. >48hours/>7days), focal deficits, seizures, disturbed consciousness, vomiting, drugs with potential procoagulant side effect, known coagulopathy. A cut-off of ≤2 best identified patients with low CVT probability (NPV 93.4%). 183/51.0% patients had a low probability score, of whom 12/6.5% had CVT. The CVT frequency was 28.6% (34/119)/84.2% (48/57) in patients with an intermediate/high probability score (score 3-4/≥5). ROC curves of the clinical score/D-dimers to predict CVT showed an AUC of 0.853/0.83. All patients in the low probability CVT group had D-dimers ≥500 mcg/l.
Conclusion
If D-dimers were measured alone, best cut-off for CVT prediction was ≥650mcg/l. The presented new clinical risk score for CVT prediction may be helpful as a pre-test as none of our CVT patients showed low clinical probability for CVT and D-dimers <500mcg/l.
Trial registration number
N/A
AS14-026
IMPLEMENTATION OF ENDOVASCULAR THERAPIES FOR STROKE IS BOOSTING CERVICAL ARTERY DISSECTION DIAGNOSIS
1Hospital Universitario Virgen Macarena, Neurology, Sevilla, Spain
2Hospital Universitario Virgen del Rocío, Neurology, Sevilla, Spain
3Hospital Universitario Virgen del Rocío, Interventional Neuroradiology, Sevilla, Spain
Background and Aims
Cervical arterial dissection (CAD) is involved in 1 to 2% of all strokes in the general population. Its diagnosis is often a challenge and it might be underestimated. We present the evolution of CAD rate diagnosis following the implementation of endovascular treatment for ischemic stroke in a European region.
Method
All patients with CAD diagnosed in two University Hospitals of Seville were included from January, 2015 to December, 2017. We collected demographic data, clinical variables, diagnosis time and imaging techniques used for the diagnosis. Implantation of 24h-365d mechanical thrombectomy in the city started on August 15th, 2016. We compared CAD diagnosis rates performed before this date and afterwards.
Results
We identified 42 CAD patients with a mean age of 47.5 ± 11.45 years. Carotid artery was involved in 28 patients (66.7%) and vertebral artery in 14 (33.3%). We found 14 cases diagnosed before (1.18% of all ischemic stroke) and 28 (2.19%) after implantation of neurointerventional therapy (p < 0.001). Of these 28 cases, in 18 diagnosis was done in acute phase and angiography was performed in 16 of them. CAD was not suspected by CT-angiography in 11 cases due to small dissections (2) or total occlusion (9). Endovascular treatment was performed in 14 patients.
Conclusion
CAD diagnosis is rising in recent years, essentially due to a constant improving of imaging techniques. CT-angiography might underestimate many CAD patients and the rapid access to arteriography for thrombectomy in boosting CAD diagnosis in few hours, even in patients with low level of CAD suspicion.
Trial registration number
N/A
AS14-028
TARGETS FOR IMPROVING DISPATCHER IDENTIFICATION OF ACUTE STROKE
1University of Helsinki and Helsinki University Hospital, Neurology and Clinical Neurosciences, Helsinki, Finland
2University of Helsinki, Molecular Neurology at the Research Programs Unit, Helsinki, Finland
3University of Helsinki and Helsinki University Hospital, Emergency Medicine and Services at the Department of Emergency Care, Helsinki, Finland
4Hätäkeskuslaitos, Emergency Response Center Administration, Kerava, Finland
5Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
6Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience/Neurology at the Institute of Neuroscience and Physiology, Gothenburg, Sweden
Background and Aims
Accurate identification of acute stroke by Emergency Medical Dispatchers (EMD) is essential for timely and purposeful deployment of Emergency Medical Services (EMS), and a prerequisite for operating mobile stroke units. However, precision of EMD stroke recognition is currently modest. We sought to identify targets for improving dispatcher stroke identification.
Method
Dispatch codes and EMS patient records were cross-linked to investigate factors associated with an incorrect dispatch code in a prospective observational cohort of 625 patients with acute stroke or transient ischemic attack (TIA), transported to our stroke center as candidates for recanalization therapy. Call recordings were analysed in a subgroup that received an incorrect low-priority dispatch code indicating a fall or unknown acute illness (n = 46).
Results
Out of 625 acute stroke/TIA patients, 450 received a high-priority stroke dispatch code (sensitivity 72.0%; 95% CI, 68.5-75.5). Clinical factors independently associated with dispatcher missed acute stroke included fall at onset (aOR, 1.86; 1.24-2.78), altered mental state (aOR, 2.62; 1.59-4.31), older age (aOR [per year], 1.02; 1.01-1.04) and a bystander caller (aOR, 3.72; 1.48-9.34). Of the analysed call recordings, 71.7% revealed targets for improvement, including failure to recognize a FAST-symptom (21/46 cases, missed speech disturbance in 18/21 cases), or failure to thoroughly evaluate patient symptoms (12/46 cases).
Conclusion
Based on our findings, efforts to improve dispatcher stroke identification should primarily focus on improving recognition of acute speech disturbance, and implementing systematic screening of FAST-symptoms in emergency calls revealing an acute fall or altered mental state.
Trial registration number
N/A
AS14-029
THE ROLE OF VWF, FVIII, ADAMTS13 AND INFLAMMATORY RESPONSE IN THE OUTCOME OF ACUTE ISCHEMIC STROKE MECHANICAL THROMBECTOMY PROCEDURE
1University hospital Ostrava, Radiology department, Ostrava, Czech Republic
2University hospital Ostrava, Neurology department, Ostrava, Czech Republic
3University hospital Ostrava, Pathology department, Ostrava, Czech Republic
4University hospital Ostrava, Blood centre, Ostrava, Czech Republic
5Spadia Lab, Immunology department, Ostrava, Czech Republic
6Department of Applied Mathematics, VŠB-Technical University of Ostrava, Ostrava, Czech Republic
7University hospital Ostrava, Hematooncology department, Ostrava, Czech Republic
Background and Aims
• Mechanical thrombectomy (MT) is the method of choice for acute ischemic stroke therapy after failure of intravenous thrombolysis (IVT)
• The aim of this study was to determine the significance of elevated vWF and/or low ADAMTS13 for the prognosis of patients with stroke
• The second goal was to describe the cellular response to inflammation accompanying cerebral ischemia in the acute and reparative stages
• The final goal was to describe the histological structure of extracted emboli with high level of vWF
Method
• At the time of procedure and later on day 5 ± 2 days from the stroke onset the blood samples was collected to examine blood clotting abnormalities (among others vWF and ADAMTS13) and the immune response
• Formalin-fixed specimens were embedded in paraffin and stained with hematoxylin and eosin, antibodies against vWF, anti-CD31 (to identify platelets, neutrophils, and monocytes) and Carstairs’ method (to identify fibrin and platelets)
Results
• Patients with NIHSS>15 had significantly higher vWF levels (P = 0.003) at admission (median: 216; IDR: 137–374), while those with NIHSS≤15 had lower vWF levels (median: 175; IDR: 132–276)
• Patients with worse 3M-mRS (3–6) had significantly higher vWF levels (P<0.001; median: 225; IDR: 160–379) than those with 3M-mRS of 0–2 (vWF levels, median: 174; IDR: 118–298)
Conclusion
• In our group of patients with LVO, MT led to high TICI 2–3 recanalization outcome in 89% of patients and good clinical outcome 3M-mRS of 0–2 in 49 (47%) cases
• Patients with worse clinical outcome had significantly higher vWF levels in plasma and also vWF/ADAMTS13 ratio was significantly higher
Trial registration number
N/A
AS14-030
CHALLENGES IN CLASSIFYING ISCHEMIC STROKE
1Clinical stroke research unit, Neurological department- Rigshospitalet- Glostrup, Copenhagen, Denmark
2Radiologic department, Radiologic department- Herlev and Gentofte hospital, Copenhagen, Denmark
3Danish center for sleep medicine, Department of neurophysiology- Rigshopitalet- Glostrup, Copenhagen, Denmark
Background and Aims
The TOAST classification is the most frequently used to categorize etiology of index ischemic stroke, but does not necessarily reflect the often heterogeneous vascular pathophysiology in the individual. The association between TOAST and measures for small and large vessel disease was assessed.
Method
Consecutive admitted acute ischemic stroke patients had a standard stroke work-up and were classified according to TOAST (large artery atherosclerosis (LAA), cardioembolism (CE), small-vessel occlusion (SVO), other determined etiology and undetermined etiology (including two or more etiologies)). The total small vessel disease (SVD) score (0-4) was calculated based on cerebral MRI. The assessment was supplemented with ankle brachial index (ABI), estimated glomerular filtration rate (eGFR) and peripheral reactive hyperemia index (RHI)(EndoPAT®).
Association between the tests and the TOAST groups was tested with fisher’s exact test, anova or Kruscal-Wallis when appropriate.
Results
99 ischemic stroke patients were included, median age 68 years (range 36-88), 44% women.
As expected, LAA and CE etiology were associated to carotid stenosis (P = 0.037) and atrial fibrillation (AF) (p < 0.001), respectively. We found no association between the TOAST groups and the SVD score (p = 0.59), ABI (p = 0.47), eGFR (p = 0.79) or RHI (p = 0.40).
Conclusion
AF and carotid stenosis were associated to relevant TOAST groups, as their presence define their group, however total SVD score was not associated to the TOAST SVO group. ABI, eGFR and estimates of endothelial function (RHI) were not associated with TOAST.
Especially for research purposes, we need an operational classification system including the range of stroke pathophysiologies in the individual patient.
Trial registration number
clinicaltrials.gov: NCT02111408
AS14-031
V1 SEGMENT DISSECTION OF VERTEBRAL ARTERY
1Ankara Univesity Medical School, Neurology, Ankara, Turkey
2Ankara Univesity Medical School, Radiology, Ankara, Turkey
Background and Aims
Vertebral artery dissection (VAD) is a well recognized cause of ischemic stroke in young adults. The most common location is the V3 segment of the vertebral artery. V1 segment dissection has also been reported in previous studies. The aim of this study was to investigate risk factors, the frequency of symptoms, etiology, prognosis and outcomes in patients with V1 segment dissection of vertebral artery.
Method
The medical records of 8 consecutive patients who were admitted with V1 segment dissection of vertebral artery from January 2014 to April 2017 were evaluated, retrospectively. The demographic data, clinical presentation, the National Institutes of Health Stroke Scale (NIHSS) scores at admission, etiology and outcome of the patients were recorded.
Results
A total of 8 patients with V1 segment of VAD (6 males [75%] and 2 females [25 %]; mean age 56.1 ± 16.8 years) were reviewed, retrospectively. The diagnosis was confirmed with cranial and cervical CT angiopraphy. The past medical history of hypertension (62.5%), diabetes mellitus (37.5%), hyperlipidemia (50%), coronary artery disease (25%) were observed. One patient had neuro-Behcet’s disease in past medical history. The most common clinical presentation was focal neurologic sign followed by acute headache and dizziness. The median NIHSS score was 2 at admission. Seven patients received oral anticoagulant therapy. Only one patient was treated by prednisolone due to neuro-Behcet’s disease The outcome was favourable in all patients.
Conclusion
VAD is associated with nonspecific symptoms such as dizziness, vertigo, headache, or neck pain. V1 dissection should be considered in etiology of posterior system ischemic stroke.
Trial registration number
N/A
AS14-032
GETTING ON YOUR NERVES: OVER-INVESTIGATION, REFERRAL AND TREATMENT OF BELL’S PALSY
1Cambridge University Hospitals NHS Foundation Trust, Department of Stroke Medicine, Cambridge, United Kingdom
Background and Aims
Bell’s Palsy (BP), an idiopathic paralysis of CN VII, results in facial weakness and dysarthria. Pathologically it is distinct from acute stroke, and must be discerned through careful history and neurological examination.
Method
We retrospectively studied electronic medical records of all patients with a discharge diagnosis of BP over 3years (10/2014-10/2017) at Cambridge University Hospital, UK.
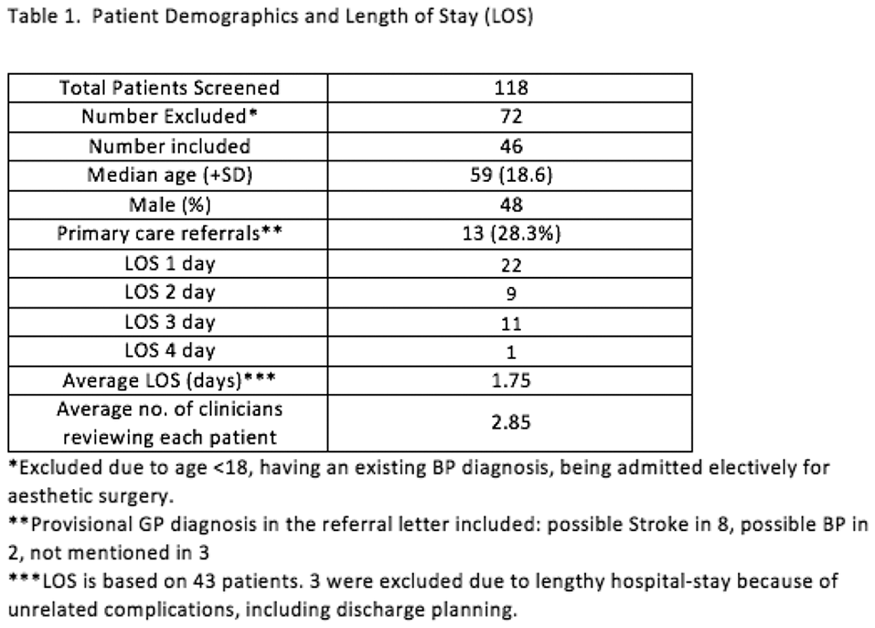
Results
From 46 patients included, 13 presented to the emergency department (ED) after initial assessment by general practitioner, 8 of whom were referred as a possible stroke. Only 1 patient was discharged directly from ED and the average hospital stay was nearly 2 days, during which each patient was assessed by 2-3 clinicians. Uncertainty in diagnosing BP was evident in both ED and medical teams, many failing to notice or consider ‘progression of symptoms’ in the history, vital to differentiate BP from stroke. 83% of patients underwent CT and/or MRI head (many where BP was provisional diagnosis) and 59% were referred to stroke/neurology for specialist opinion. 6 patients received antiplatelets, 2 were even thrombolysed and TIA-clinic follow-up was arranged for 4 patients.
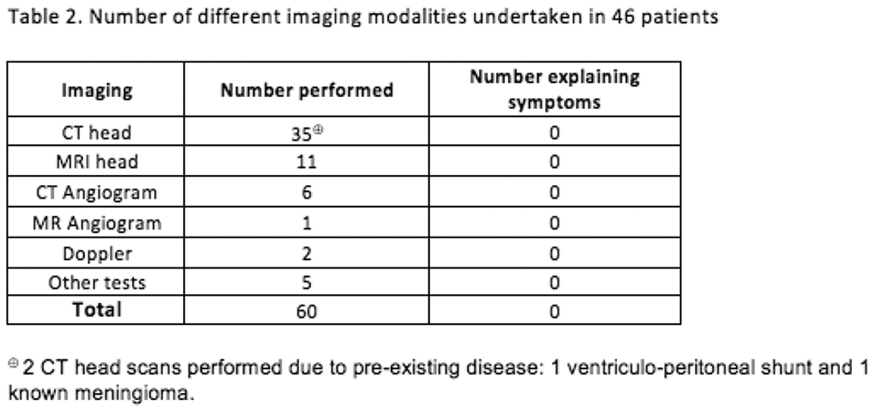
Conclusion
BP should ideally be managed in primary care and self-referring patients should be discharged from ED. Our study shows a lack of confidence (and possibly awareness) amongst clinicians, including GPs and senior medical staff, in diagnosing BP. Continuous education amongst non-specialists is required to avoid inappropriate referrals in both primary and secondary care which can lead to considerable patient stress and waste of medical resources through bed occupancy, over-investigation and inappropriate treatment.
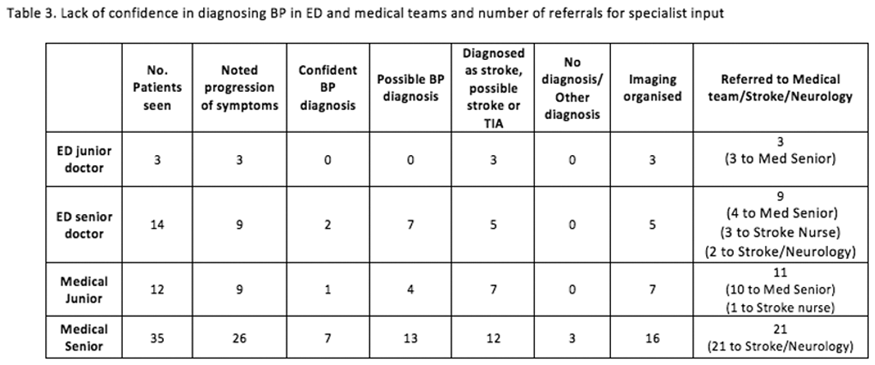
Trial registration number
N/A
AS14-033
EVALUATION OF EPICARDIAL FAT THICKNESS IN YOUNG PATIENTS WITH CRYPTOGENIC STROKE
1Şişli Hamidiye Etfal Training and Research Hospital, Department of Cardiology, Istanbul, Turkey
2Şişli Hamidiye Etfal Training and Research Hospital, Department of Neurology, Istanbul, Turkey
Background and Aims
Epicardial adipose tissue (EAT) is metabolically active and an important predictor of metabolic and cardiovascular diseases. The aim of this study was to investigate the epicardial adipose tissue measurement with echocardiography in young patients with cryptogenic stroke (CS).
Method
We studied 77 volunteers: 40 patients with CS (mean age 43 ± 8 years,16 females) and other 37 healthy subjects (mean age 38 ± 7 years, 20 females). All basic biochemical parameters were analyzed and echocardiographic epicardial fat thickness (EFT) were measured in all subjects. All imaging and examinations were done in terms of etiology in the patients. The categorical and numerical variables were compared using the chi-square test and independent t-test, respectively. Correlations were analyzed using the Spearman and Pearson correlation tests. ROC curve analysis was performed to determine cutoff high risk value of EFT.
Results
In comparison with the control group, the patients with CS had significantly higher EFT (5.51 ± 0.82, 3.96 ± 0.51, p < 0.01). Furthermore, there were positive correlations between EFT and C-reaktive protein (r = 0.284; p < 0.05). A cutoff high risk EFT value of 4.6 mm showed a sensitivity and specificity of 87.5% and 81.1%, respectively.
Conclusion
We found that echocardiographic EFT was significantly higher in young patients with CS. Increased EFT might be a novel risk factor in these patients.
Trial registration number
N/A
AS14-034
FALL IN THE PROPORTION OF ATHEROTHROMBOTIC STROKE IN THE LAST DECADE. SUCCESS OF CURRENT MEDICAL TREATMENT?
1FLENI, Vascular neurology division, Buenos Aires, Argentina
Background and Aims
Etiologic subtypes of ischemic strokes (IS) are mostly influenced by vascular risk factors (VRF). In recent years, several population strategies have been implemented in order to better control VRF. We evaluated the evolution of the proportion of large artery (LAD) and small vessel disease (SVD) in the last 20 years and the concomitant use of statins and antihypertensive drugs.
Method
Medical records of consecutive patients with acute IS were evaluated in our center. Demographic features, VRF, previous treatment and etiologic subtype of IS classified by TOAST criteria were evaluated. These variables were compared in 2 periods: 1997-2006 (P1) and 2007-2017 (P2). Comparisons between groups were calculated using the Fisher's exact test.
Results
We included 2416 patients. A substantial decline in the proportion of LAD and SVD strokes in the last decade was founded. Despite persistence or increase in the prevalence of VRF, there was an increase in the use of therapeutic strategies for control of them.
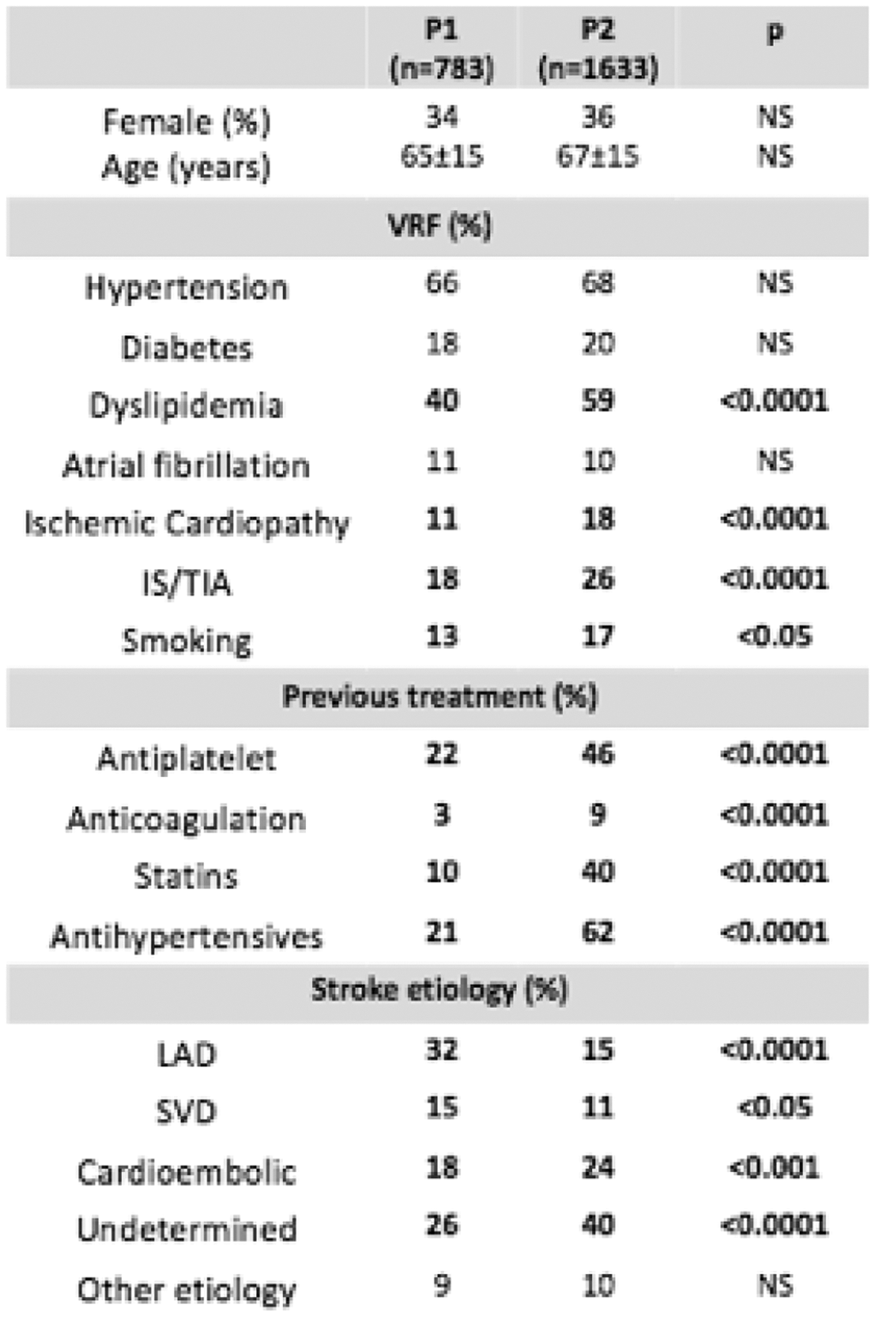
Conclusion
In the last decade, a substantial drop in the proportion of IS of atherothrombotic etiology was observed for both large and small strokes. The higher rate of use of preventive pharmacological strategies could explain, at least in part, these findings.
Trial registration number
N/A
AS14-035
HOW OFTEN ARE DETECTED PFOS CAUSALLY-RELATED IN PATIENTS WITH CRYPTOGENIC ISCHEMIC STROKE?: PUBLICATION BIAS-ADJUSTED ESTIMATES
1University of California Los Angeles, Stroke, Los Angeles, USA
2University of California Los Angeles, Comprehensive Stroke Center and Neurology, Los Angeles, USA
Background and Aims
Management of cryptogenic ischemic stroke (CIS) patients would be aided by estimates of the frequency with which detected PFOs are pathogenic (causally-involved) or incidental (present but unrelated), adjusted for potential publication bias in reported case-control studies.
Method
We analyzed case-control studies of the frequency of echocardiographic detection of PFO among patients with cryptogenic vs known cause strokes. When present, publication bias was corrected using the trim and fill method, and frequency of pathogenic relatedness derived via Bayes’ theorem (Ali 2009).
Results
Systematic search identified 23 case-control studies enrolling of 3364 patients, including 11 studies in younger (age 18-55 years old), and 5 studies or sub studies in older patients. Funnel plot analysis indicated publication bias was moderate for studies of younger (Figure), minimal for studies of older, and absent for studies of age-inclusive patients. In younger patient studies, relative risk of PFO in unadjusted analysis of 2.57 (95CI 1.90-3.47) was lowered in bias-adjusted analysis to 2.32 (95CI 1.74-3.11). Bayes’ theorem derivations showed that, among CIS patients, detected PFOs are causally related in 73% of younger, 55% of older, and 67% of age-unrestricted patients.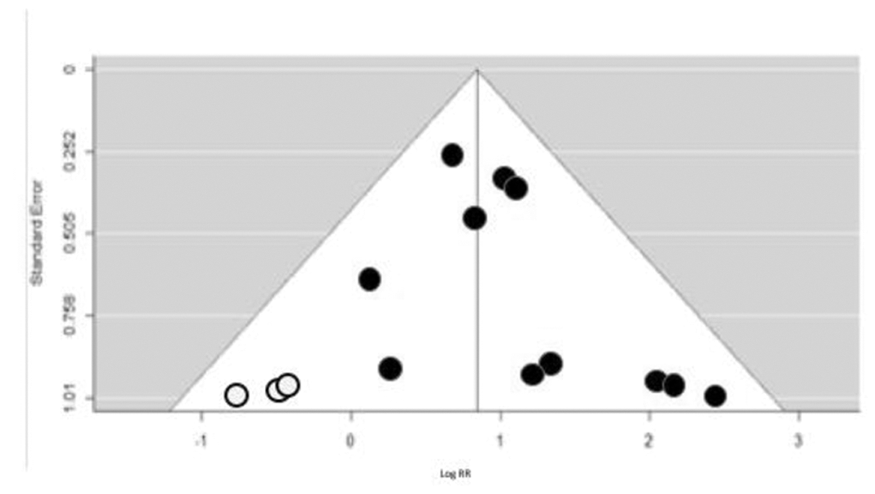
Conclusion
There is evidence of modest publication bias in the stroke-PFO case-control literature. But after correction for bias, rates of PFO pathogenic involvement remain substantial among patients with otherwise cryptogenic ischemic stroke: detected PFOs are likely causally-related in three-quarters of younger and half of older patients.
Trial registration number
N/A
AS14-036
FIESTA: A NOVEL SCORE TO DIFFERENTIATE ACUTE ISCHEMIC STROKE FROM STROKE MIMICS
1University of Helsinki, Molecular Neurology at the Research Programs Unit, Helsinki, Finland
2University of Helsinki and Helsinki University Hospital, Neurology and Clinical Neurosciences, Helsinki, Finland
3University of Helsinki and Helsinki University Hospital, Emergency Medicine and Services at the Department of Emergency Care, Helsinki, Finland
4Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience/Neurology at the Institute of Neuroscience and Physiology, Gothenburg, Sweden
5Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
Background and Aims
Stroke mimics (SM) complicate admission evaluation of stroke code patients, especially when head computed tomography (CT) is negative. We sought to design a novel score to help identify SMs and select patients for additional magnetic resonance imaging.
Method
Acute stroke code patients (n = 471) without findings on admission native CT and NIHSS>0 were randomized into derivation (n = 326, 27% SMs) and internal validation (n = 145, 26% SMs) cohorts. Multivariate analysis was used to evaluate predictive value of parameters associated with a SM diagnosis, and a clinical score was developed based on logistic regression coefficients. Performance was compared to existing scores using area under the receiver-operating characteristic curve (AUC-ROC) analysis.
Results
The
Conclusion
We propose a novel SM score with more elaborate weighting of score components compared to the FABS score, and easier application than the TM-score. Prehospital patient selection and the proportion of SMs differ widely between emergency medical service systems. Thus, existing scores should be compared locally to find the most accurate and practical score to apply.
Trial registration number
N/A
AS14-037
MULTIPLE ACUTE CEREBRAL INFARCTS IN MORE THAN ONE ARTERIAL TERRITORY ARE ASSOCIATED WITH CANCER: THE BERGEN NORSTROKE STUDY
1Haukeland University Hospital, Department of Neurology, Bergen, Norway
2University of Bergen, Department of Clinical Medicine, Bergen, Norway
3Stavanger University Hospital, Centre for Age-related Medicine, Stavanger, Norway
4Haukeland University Hospital, Department of Neurosurgery, Bergen, Norway
Background and Aims
The etiology of multiple acute cerebral infarcts in more than one arterial territory (MACI) is in most cases associated with cardioembolism. However, the presence of cancer should always be considered as a possible underlying mechanism due to its procoagulant activity. We sought to investigate if MACI are more frequent in patients with active cancer and whether patients with MACI have more severe strokes compared to patients with single acute cerebral infarct (SACI).
Method
1884 patients with acute cerebral infarcts on DWI were retrospectively reviewed by medical records. We identified all patients who were diagnosed with cancer during a period from 6 months before to 6 months after the stroke. MACI was defined as DWI lesions in either anterior circulation bilaterally or left or right anterior circulation or posterior circulation. Stroke severity was measured by NIHSS. Data were analyzed using Mann-Whitney U test and multivariate logistic regression.
Results
MACI were present in 141 patients (7.5%) and active cancer was identified in 49 patients (2.6%). Active cancer was more frequent in patients with MACI as compared to patients with SACI (17/141; [12.1%] vs. 32/1711 [1.8%]; p < 0.001). After adjustment for several potential confounders, MACI was associated with active cancer (OR 5.33; 95%; CI 2.1 -13.5). Median NIHSS score at discharge was significantly worse in MACI patients compared to SACI patients (2 [IQR: 1–6] vs. IQR: 1[0-4]).
Conclusion
Cancer should be always considered when identifying the etiology of MACI. The presence of MACI significantly contributes to increased stroke severity at discharge.
Trial registration number
N/A
AS14-038
EMBOLIC STROKE OF UNDETERMINED SOURCE IN JUVENILE STROKE PATIENTS: MULTINATIONAL DATA FROM THREE TERTIARY CARE CENTERS
1University Hospital Dresden, Neurology, Dresden, Germany
2University of Lausanne- Switzerland, Stroke Center- Neurology Service- Department of Clinical Neurosciences-, Lausanne, Switzerland
3University of Thessaly- Larissa- Greece, Department of Medicine, Larissa, Greece
4Hellenic Cardiovascular Research Society, Neurology, Athens, Greece
5San Raffaele Scientific Institute, Stroke Unit- Department of Neurology and Neurophysiology, Milan, Italy
Background and Aims
Embolic stroke of undetermined source (ESUS) may be less common in juvenile than in elderly patients. We sought to determine the frequency of ESUS in patients with juvenile stroke and its predictive role on stroke outcomes.
Method
We retrospectively abstracted data on all stroke patients aged 18-45 seen at three tertiary hospitals between 1992 and 2015. Stroke etiology was determined using TOAST criteria, whereas unknown etiology was further classified according to recently introduced ESUS criteria. Predictors of stroke outcomes including favorable functional recovery at discharge (mRS≤2) and in-hospital death were assessed using logistic regression models.
Results
We identified 702 juvenile acute ischemic stroke patients: median age 40 (IQR, 10), 53% men, baseline NIHSS score 4 (IQR, 10). Of 249 (35.5%) patients with non-identifiable causes, 122 (17.4%) were classified as ESUS. Except for arterial hypertension (12.3% vs. 20.9%, p = 0.03), no differences regarding sex, age, vascular risk factors and baseline stroke severity (p>0.05) were present between ESUS and non-ESUS patients. The rates of in-hospital mortality (1.6% vs. 4.7%) and favorable functional recovery at discharge (77.9% vs. 67.6%) differed between the two groups. After adjustment for age, stroke severity and tPA treatment, ESUS emerged as positive predictor of favorable functional outcome at discharge (OR: 2.94; 95%CI, 1.36-6.38, p = 0.006).
Conclusion
Our data suggest that ESUS is relatively frequent in a large multinational cohort of juvenile stroke patients. Its predictive role on clinical outcomes may differ from those with identifiable stroke causes in this patient population, and needs to be explored in future investigations.
Trial registration number
N/A
AS14-039
CLASSIFICATION OF ISCHAEMIC STROKE AETIOLOGY: RELIABILITY AND ITS EFFECT ON TRIAL ‘POWER’
1University of Glasgow, Institute of Neuroscience and Psychology, Glasgow, United Kingdom
2University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
3Queen Elizabeth University Hospital, Department of Neurology- Institute of Neurological Sciences, Glasgow, United Kingdom
Background and Aims
Increasingly, stroke research is concerned with interventions for particular aetiological subtypes. Inter-observer variability in aetiological classification has an impact on trial ‘power’. We modelled the potential effect of misclassification on a hypothetical trial of anticoagulant in Embolic Stroke of Undetermined Source (ESUS).
Method
We used systematic-review to quantify the reliability (inter-observer variability) of stroke classification systems. We modelled the effect of this misclassification in a hypothetical trial of anticoagulant in cardioembolic stroke (CE) contaminated by patients with non-cardioembolic (non-CE) stroke aetiology. We randomly sampled data from previous acute trials that included anticoagulant in CE and non-CE, stored within the Virtual International Stroke Trials Archive (VISTA). We described outcomes in terms of survival censored at 90 days, and used boot strapping to describe the effect of varying misclassification rates on sample size required to detect a between group difference from intervention across 5000 permutations.
Results
From 4553 titles, we found 14 articles describing the common stroke classification systems. The inter-observer reliability of the classification systems varied from ‘fair’ to ‘very-good’ and suggested misclassification rates of 5% and 20% for our modelling. The hypothetical trial was able to show difference in survival between anticoagulant and antiplatelet in CE with N = 198 both arms. Contamination of treatment and control arms with 5% misclassified participants increased N to 237 and with 20% misclassification increased N to 352.
Conclusion
Aetiological classification are associated with inter-observer variability and the resulting misclassification may reduce trial power. This may explain the neutral result in a recent trial of anticoagulant in patients with ESUS.
Trial registration number
N/A
AS14-040
STROKE RECURRENCE RELATED TO COMPLEX ATHEROMATOUS AORTIC PLAQUES EMBOLISM, IT IS THE TIME TO DECIDE TREATMENT
1Hospital Vall d'Hebron - Barcelona, Stroke Unit, Barcelona, Spain
2Hospital Vall d'Hebron - Barcelona, Neuroradiology, Barcelona, Spain
3Hospital Vall d'Hebron - Barcelona, Cardiology, Barcelona, Spain
Background and Aims
Complex atheromatous aortic plaques (CAAP) are a source of stroke embolism but previous studies didn't find the best secondary prevention treatment.
Method
From January 2012 to July 2017, CAAP screening in acute phase of stroke in ESUS patients were realized by Angio CT
We performed a transesophageal echocardiography (TTE) in subacute phase we assessed the size of plaques, presence of ulcerated plaques and mobile components. All patients with CAAP were treated with high dose statins plus double antiplatelet treatment or oral anticoagulation (OAC) based on the presence of mobile components. Follow up with analysis of recurrence in this cohort was done.
Results
157 patients were screened. CAAP detection by CTA was 57% (88/157).
TEE was performed in 73 patients: recurrence of stroke (n = 9) (12%) was associated with bigger endoluminal plaques (6.7 ± 3.5 vs. 4.8 ± 2.6 mm, p < 0.001), ulcerated plaques (26.9% vs 4.3%, p = 0.005), and with presence of thrombus or mobile components (26.3 % vs. 5.7 %, p = 0.014). All patients with presence of mobile thrombus (n = 19) received oral anticoagulation (OAC) ; In 16 patients ( 85%), OAC were withdrawn after 3 months with control TEE that confirmed the disappearance of mobile parts. We confirmed stroke recurrence with neuroimaging in 5/ 16 patients (31%) and association with active smoking (60.0% vs. 7.1%, p = 0.013 ).
Conclusion
Complex atheromatous aortic plaques are relevant stroke sources of embolism. A subgroup of patients may benefit of chronic oral anticoagulation in order to avoid stroke recurrence. New trials with new oral anticoagulants (NOAC) are expected.
Trial registration number
N/A
AS14-041
DISTAL VERSUS PROXIMAL MIDDLE CEREBRAL ARTERY OCCLUSION: DIFFERENT MECHANISM AND PROGNOSIS
1Kyung Hee University, Neurology, SEOUL, Republic of Korea
Background and Aims
Middle cerebral artery (MCA) supplies the largest area of cerebral hemisphere, and MCA occlusion may cause major infarction. However, not much is known of the location of the MCA occlusion and the difference according to the location of MCA occlusion.
Method
We have enrolled patients with MCA occlusion. The location of MCA occlusion was presented the length of remnant MCA in the ipsilesional MCA over the length of contralateral M1 were measured. The patients were dichotomized to proximal and distal MCA occlusion. Clinical and radiological characteristics were compared between the two groups. Factors associated with the neurological change during admission were investigated.
Results
181 patients were enrolled. The location of MCA occlusion showed a bimodal peak [at the proximal (n = 99) and distal MCA (n = 82)]. Patients with proximal MCA occlusion patients had more hyperlipidemia and were more associated with large artery atherosclerosis (73% vs. 56%) In the other hand, distal MCA occlusion was more associated with hypertension, atrial fibrillation and cardioembolic stroke (35% vs. 10%). Cardioembolic stroke (OR = 4.339, p < 0.001) was independently associated with distal MCA occlusion. Basal ganglia involvement was similar between the two groups (48% vs. 39%; p = 0.21), whereas hemorrhagic transformation was more frequent in distal MCA occlusion (10% vs 23%; p = 0.02). Patients with distal MCA occlusion showed more improvement in NIHSS during admission. Presence of FLAIR vessel sign and distal MCA occlusion was independently associated with improvement of neurological deficit during admission.
Conclusion
The mechanism of stroke differs according to the location of MCA occlusion.
Trial registration number
N/A
AS14-042
ESTIMATED EJECTION FRACTION IN PATIENTS WITH ACUTE ISCHEMIC STROKE AND LEFT VENTRICULAR THROMBI
1Campbell University, School of Osteopathic Medicine, Buies Creek, USA
2Duke University, Dept. of Neurology, Durham, USA
Background and Aims
Echocardiography is often performed on patients with acute ischemic stroke in order to identify cardiac sources in suspected embolic events. This study aimed to delineate ejection fraction (EF) estimates on initial echocardiography in patients with acute stroke and left ventricular (LV) thrombi.
Method
This was a retrospective cohort study, utilizing an academic institutional database to identify patients with diagnosis codes for acute ischemic stroke. Patient records were then filtered by CPT codes in order to select patients who underwent transthoracic, transesophageal echocardiography, cardiac CT, and/or cardiac MRI. Further filters were applied to identify the subset of patients on therapeutic anticoagulation. Patients lacking LV thrombi on cardiac imaging were further excluded, as well as patients whose cardiac thrombus was identified >14 days before or after presenting with acute ischemic stroke. EF ranges and modality for first identifying LV thrombi were analyzed.
Results
A total of 39 patients were identified for the described cohort. Patient EF ranges are detailed in Figure 1. The most common range into which patients fell was 20-29%, but two patients did have normal EF of 55% or greater. The overwhelming majority (n = 37) of LV thrombi were identified on non-invasive transthoracic echocardiography (94.7%).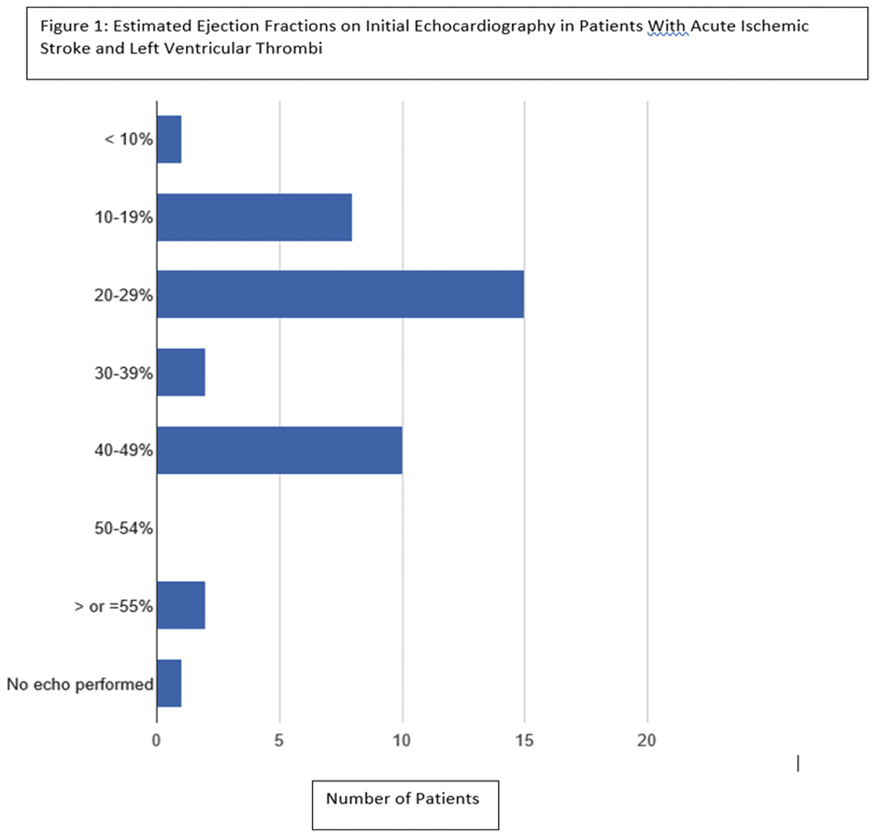
Conclusion
The large majority of patients with acute ischemic stroke and LV thrombi have reduced EF on echocardiography, but LV thrombi are still possible when EF is estimated as normal.
Trial registration number
N/A
AS14-043
EMBOLIC STROKES OF UNDETERMINED SOURCE: PREVALENCE AND PATIENT CHARACTERISTICS FROM A SINGLE TERTIARY CARE CENTER FROM EASTERN INDIA
1Director and Head, Neurology, Kolkata, India
2AMRI Hospitals- Mukundapur, Neurology, Kolkata, India
Background and Aims
Cryptogenic strokes comprise about 25% of all ischemic strokes. Recent evidence suggests that majority of non-lacunar cryptogenic stroke are embolic. Rightly, these strokes have been reclassified as embolic strokes of undetermined source (ESUS). We aimed to look at frequency and clinical features of ESUS patients from our stroke unit database.
Method
We analysed consecutive patients admitted in our stroke center over the last 5 yrs and identified the patients fulfilling the criteria for ESUS. Baseline and discharge NIHSS, vascular risk factors, medical & imaging records and patient demographics were recorded.
Results
Out of 685 ischemic stroke patients admitted over last 5 yrs, 153 (22.33%) had large vessel disease, 91 (13.28%) had small vessel disease, 169 (24.67%) had cardio-embolic stroke, 251 (36.64%) had undetermined etiology while 21(3.06%) had stroke with other determined etiology. Out of 251 patients with undetermined etiology, 45(17.92%) fulfilled the ESUS criteria. The mean age of ESUS and non ESUS patients was 62 and 68 years respectively. Among ESUS patients hypertension, Diabetes, dyslipidemia and smoking were present in 72%, 47%, 15% and 11% compared to 87%, 59%, 29% and 22% respectively in non ESUS patients respectively. Median NIHSS scores of ESUS and non ESUS patients at admission were 6 (25-1) and 9 (34-1) respectively. Only 3 patients (7%) among ESUS received oral anticoagulation on discharge.
Conclusion
In our study ESUS comprised about 7% of total ischemic stroke. They were younger with mild stroke and had less vascular risk factors. Antiplatelets remained the standard antithrombotic regime in them.
Trial registration number
N/A
AS14-044
CEREBRAL CONVEXITY SUBARACHNOID HAEMORRHAGE AS A TRANSIENT ISCHAEMIC ATTACK MIMIC: A RETROSPECTIVE CROSS SECTIONAL STUDY
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2Institute of Neurology, Department of statistical science, London, United Kingdom
Background and Aims
Spontaneous (non-traumatic) cerebral convexity subarachnoid haemorrhage (cSAH) can present with focal neurological symptoms that resemble those of transient ischaemic attack (TIA). Misdiagnosis of cSAH as TIA might result in inappropriate antithrombotic therapy and an increased risk of further intracranial haemorrhage. We investigate differences in clinical features and risk factors between patients with cSAH and suspected TIA.
Method
We did a single-centre, retrospective cross-sectional case-control study, including 19 patients with cSAH (identified from radiological and clinical databases of patients assessed in the National Hospital for Neurology and Neurosurgery and UCLH Comprehensive Stroke Service) and 76 (i.e. 4 per case) age and gender matched controls (from a database of consecutive UCLH TIA clinic attendances). We reviewed presenting symptoms and vascular risk factors. Chi squared analysis was used to compare clinical features and risk factors between patients with and without cSAH.
Results
Migratory symptoms (32% vs 3% p < 0.001), sensory disturbance (47% vs. 14% p = 0.02) and recurrent stereotyped events (47% vs. 20% p = 0.013) occurred more frequently in those with cSAH compared with the suspected TIA control group who had other final diagnoses. Hypercholesterolaemia was less common in cSAH (16% vs 53% p = 0.004).
Conclusion
Simple clinical features could help identify individuals with transient neurological events at higher risk of having had cSAH, and guide investigation pathways and clinical treatment, especially regarding the use of antithrombotic drugs. Further research in a second larger population might allow development of a clinical scoring tool.
Trial registration number
N/A
AS14-047
CONTRIBUTION OF BLOOD BIOMARKERS TO THE DIAGNOSIS OF CARDIOEMBOLIC STROKE
1Medical University of Graz, Department of Neurology, Graz, Austria
2Medical University of Graz, Department of Internal Medicine- Division of Cardiology, Graz, Austria
3Medical University of Graz, Department of Internal Medicine- Division of Angiology, Graz, Austria
4Medical University of Graz, Department of Radiology- Division of Neuroradiology- Vascular and Interventional Radiology, Graz, Austria
5Medical University of Graz, Clinical Institute of Medical and Chemical Laboratory Diagnostics, Graz, Austria
Background and Aims
Cardioembolic strokes might be effectively prevented by anticoagulation. Blood biomarkers helping to suggest cardioembolic etiology and to steer the complex diagnostic work-up would therefore be of great advantage. This study addresses the possible contribution of biomarkers associated with thromboembolism (NT-proBNP and D-dimer) to the diagnosis of cardioembolic stroke.
Method
Over a seven months period, we prospectively investigated all ischemic stroke patients admitted to our Stroke Unit for this study. All patients underwent a complete stroke work-up including cerebral imaging (CT and/or MRI), neurosonography, electrocardiography, cardiac rhythm monitoring (for at least 24 hours) and echocardiography. Blood to determine NT-proBNP and D-dimer levels was drawn immediately after admission.
Results
Of 188 ischemic stroke patients (age: 69 ± 14 years, female: 38%), 67 had cardioembolic (36%), 73 non-cardioembolic (49%) and 48 cryptogenic strokes (25%), based on extensive work-up. NT-proBNP and D-dimer levels were significantly higher in cardioembolic vs. non-cardioembolic strokes (2543 vs. 707 pg/ml, p < 0.001; 2.4 vs. 1.4 µg/ml, p < 0.001). The area under the curve (AUC) of NT-proBNP obtained for the diagnosis of cardioembolic stroke was 0.81. The cut-off point with the highest sensitivity and specificity was set at 525 pg/ml (sensitivity: 82%, specificity: 77%). The AUC of D-dimer in cardioembolic stroke was 0.69, with a cut-off set at 0.75 µg/ml (sensitivity: 67%, specificity: 69%).
Conclusion
In concordance with previous studies, NT-proBNP has reasonable diagnostic accuracy for stroke related to cardiac embolism. Nevertheless, sensitivity and specificity are too low to essentially improve the diagnostic work-up. The contribution of D-dimer levels is even more limited.
Trial registration number
N/A
AS14-048
UTILITY OF TRANSTHORACIC ECHOCARDIOGRAPHY IN DIAGNOSTIC EVALUATION OF ISCHEMIC STROKE
1Beth Israel Deaconess Medical Center, Neurology, Boston, USA
Background and Aims
Identification of etiology of acute ischemic stroke (AIS) is crucial for optimizing secondary preventive strategy. Transthoracic echocardiography (TTE) is routinely performed as part of standard workup. However, the overall yield of TTE is unclear and many patients may undergo unnecessary investigations. We sought to investigate the utility of TTE as part of AIS workup.
Method
We reviewed consecutive AIS cases admitted to a tertiary stroke center over a 15 month period. Data was gathered on demographics, medical history, suspected etiology using TOAST classification, relevant TTE findings, including elongated left atrium, low ejection fraction, PFO or valve/ventricular thrombus, and whether TTE led to further workup and/or treatment change
Results
Among 548 AIS patients (median age 71[59-81] years, 50% female), 482 (87%) underwent TTE. Clinically relevant findings were observed in 183 (38%) patients, leading to additional workup in 41(8.5%). Further workup was associated with younger median age (58[50-65] vs 72[62-81], p < 0.0001, and was less likely in suspected large vessel etiology (p = 0.02). Abnormal TTE lead to treatment change in 24(5%) patients; 22/24 were started on anticoagulation. TTE results were less likely to influence treatment changes in older patients (71[60-80] vs 58[49-69] years, p = 0.02) with known atrial fibrillation (p = 0.01).
Conclusion
Despite relevant clinical findings on TTE in 38% patients, it ultimately resulted in treatment change in 5%. The lowest treatment yield was observed in older patients with established atrial fibrillation. Our findings suggest that TTE might be overused in routine stroke care and highlight the need for more refined patient selection to optimize resource utilization.
Trial registration number
N/A
AS14-049
ENDOVASCULAR TREATMENT EXPERIENCE OF ACUTE POSTERIOR CIRCULATION STROKE
1MedicalPark Hospital MLP Care Brain Angiopraphy and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
2Istinye University Liv Hospital Brain Angiography and Stroke Centre BASC, Neurology department, Istanbul, Turkey
3Istinye University Liv Hospita Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
4Istanbul Aydın University Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
5GOP MedicalPark Hospital Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
6Istanbul Aydın University Medicalpark Hospital Brain Angiography and Stroke Centre BASC, Neurology Department, Istanbul, Turkey
7Istinye University Liv Hospital Brain Angiography and Stroke Centre BASC, Neuroradiology department, Istanbul, Turkey
Background and Aims
Identifying the etiology of posterior circulation stroke (PCS) may be challenging. The vascular pathologies should be well analysed by appropriate imaging techniques. In selected patients stenting may be necessary to obtain stroke prevention. We reviewed acute PSC patients’ data of a newly formed high-volume comprehensive stroke centre network.
Method
Between October - December 2017, all the patients who were consecutively admitted to the Brain Angiography and Stroke Centre (BASC) network are evaluated with CTA, MRA and/or DSA. The BASC data is prospectively collected. The results of PCS patients were reviewed.
Results
Of 186 acute stroke patients 41(%21) patients (mean age 65) were PCS. Median NIHSS score and onset-to-door time was 4 and 746 respectively. These patients were admitted later than anterior circulation stroke (ACS) patients (p:0.002). Four patients (9.8%) received IV r-TPA. As intention-to-treat 6 patients were evaluated with emergent DSA, only 3 of them received endovascular revascularization therapy. During hospitalisation period diagnostic DSA was performed in 7 more patients. Atrial fibrillation (AF) rate was 25%. Vertebrobasilar atherosclerotic disease detected in 18(43%), 3 of whom also had AF. Seven patients underwent angioplasty/stenting therapy. Vertebral artery dissection was detected in 2 patients one of them treated with acute stenting.
Conclusion
In this cohort, PCS patients arrived to the hospital later than ACS patients. Even though the AF frequency was similar, the percent of proximal vessel disease was higher compared to literature and accordingly the rate of proximal vessel stenting was also high.
Trial registration number
N/A
AS14-050
AGE AND VESSEL-SPECIFIC PREVALENCE OF INTRACRANIAL AND EXTRACRANIAL ARTERIAL STENOSIS IN CAUCASIAN PATIENTS WITH TIA AND STROKE: A POPULATION-BASED STUDY
1Centre for the Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
There are few published data on the prevalence of intracranial stenosis in older Caucasian TIA/ stroke patients and imaging in many centres is restricted to carotid ultrasound, potentially missing disease in the intracranial vessels, vertebral arteries and distal carotids.
Method
From 2011 to 2017, a population-based sample of consecutive patients with TIA and minor ischaemic stroke (NIHSS≤3), irrespective of age, underwent 3.0T MR angiography for assessment of the intracranial and cervicocranial arteries, including the aortic arch. We determined the age and vessel-specific prevalence of ≥50% stenosis.
Results
Of 758 eligible patients (mean/SD age = 70.0/13.7 years; 96% Caucasian), 304 patients (40.1%) had 425 ≥50% vessel stenosis; 113 (26.6%) at the carotid bifurcation and 312 (73.4%) at other sites. 124 (16.4%) patients had ≥50% intracranial stenosis. Prevalence of ≥50% stenosis increased from 30/173 (17.3%) at <60 years to 94/170 (55.3%) at ≥80 years (ptrend<0.0001), particularly for intracranial disease (OR, 95%CI, for >80 years: carotid bifurcation -1.75, 0.87-3.54, p = 0.11; other extracranial -1.74, 0.94-3.24, p = 0.07; intracranial -3.14, 1.65-5.96, p = 0.0003), with prevalence of intracranial stenosis reaching 60% at ≥90 years. Overall, 175 (41.2%) of all 425 ≥50% vessel stenoses were potentially symptomatic, of which only 42 (24.0%) were at the carotid bifurcation.
Conclusion
The majority of arterial stenosis in Caucasian patients with TIA and minor stroke is at sites other than the carotid bifurcation. Rates of intracranial stenosis are particularly high in older patients, and although intervention will only rarely be indicated, the type and intensity of medical treatment may need to be modified.
Trial registration number
N/A
AS14-051
STROKE IN PATIENTS WITH ONCOLOGICAL COMORBIDITY
1Tyumen regional hospital №2, Regional neurovascular center, Tyumen, Russia
2Tyumen state medical university, Department of Hospital Therapy, Tyumen, Russia
Background and Aims
Vascular and oncological diseases take one of the leading places in the structure of adult mortality.
Assess the relationship between risk factors, clinical course and outcome in patients with stroke and oncological comorbidity.
Method
The study enrolled 2158 case histories of patients with acute cerebrovascular accident treated in our hospital in 2016. The combination of stroke and oncological comorbidity was observed in 61 cases (2.8 %).
Results
The medium age of patients was 69 ± 5.2 years (54% men). Ischemic stroke was observed in 88%, TIA in 3.3%, hemorrhagic stroke in 8.2%. Recurrent stroke was in 37% cases. Vascular risk factors were: arterial hypertension in 95%, carotid stenosis in 34%, coronary heart disease in 29%, peripheral artery disease in 15%, atrial fibrillation in 23.7%, diabetes mellitus in 25.4%. 49% of patients had an oncological anamnesis <1 year, 27% of patients from 1 to 5 years, >5 years - 24%. In 12% of cases oncology was detected fir the first time. Oncology was located in gastrointestinal tract (31%), lungs (11%), gynecological organs (13%). High frequency of cryptogenic stroke was noted (31.5%). Severe anemia was in 17%. Increased coagulation in the blood test was noted in 72.4%. Mortality in the analyzed group was twice higher than in the general group.
Conclusion
The combination of stroke and oncology is a relatively rare variant of comorbidity. Hypercoagulation is important in the pathogenesis of ischemic stroke in combination with oncology. Oncopatology is a factor that worsens the course and prognosis of patients with stroke.
Trial registration number
N|A
AS14-052
FOLLOW UP IN EMBOLIC STROKE OF UNDETERMINED SOURCE: NEW CLINICAL TREATMENT ALGORITHM INCLUDING LONG-TERM CARDIAL MONITORING AND PFO CLOSURE IN A PROSPECTIVE OPEN-LABEL OBSERVATIONAL STUDY
1Ludwig Maximilians University, Department of Neurology, Munich, Germany
2Ludwig Maximilians University, German Center for Vertigo and Balance Disorders, Munich, Germany
3Ludwig Maximilians University, Institute for Stroke and Dementia Research, Munich, Germany
4Ludwig Maximilians University, Department of Medicine 1, Munich, Germany
5University of Heidelberg, Department of Neurology, Heidelberg, Germany
*These authors contributed equally
Background and Aims
Recent trials of patent foramen ovale (PFO) closure to prevent recurrent stroke found overall stroke reduction in the PFO closure group compared with antiplatelet therapy alone. However several aspects in the management of patients with embolic stroke of undetermined source (ESUS) with/without PFO remain unclear.
Method
An interdisciplinary cardio-neurological treatment algorithm was developed to standardize the management of patients with ESUS (see figure). All patients received long-term cardiac monitoring (e.g. implantable cardiac monitor, ICM). Depending on the age of the patient (cut off ≥ 60 years) and the transesophageal detection of a relevant PFO there will be an assignment to different treatment regimens including antiplatelet therapy, oral anticoagulation (OAC) and PFO closure. Follow-up period will be at least 36 months. The study was approved by local authorities and patients gave informed consent.
Results
The algorithm has been implemented in January 1, 2018. Since then, 15 patients (age 65y, 48-87y) have been included. Mean CHA2DS2VASC-score was 5 (3-7). Four patients were found to have a PFO. 7 patients were implanted with ICM. 10 patients received antiplatelet therapy and 5 OAC.
Conclusion
This open-label prospective observational study will help to resolve various unanswered questions regarding the treatment regimen of ESUS patients with and without PFO. We will demonstrate patients included in the study up to 05/2018. The results will have implications for future management of patients with ESUS and might help identifying patients best suited for PFO closure.
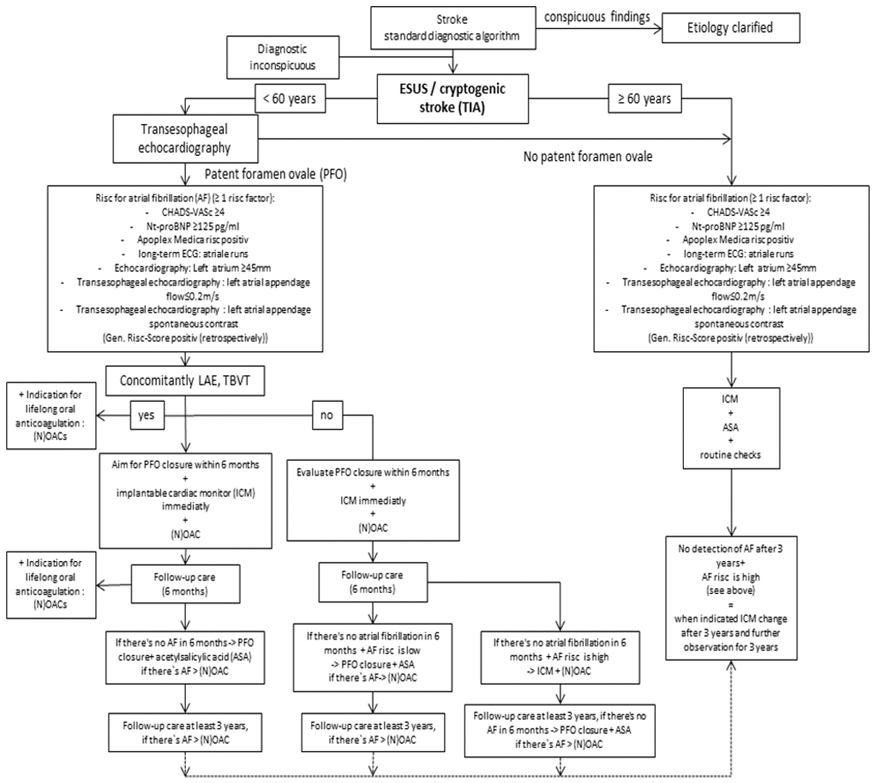
Figure 1: Flow chart of treatment algorithm in patients with embolic stroke of undetermined source (ESUS)
Trial registration number
N/A
AS14-054
ARTERIAL VASOSPASM CAUSING STROKE IN A CASE OF PNEUMOCOCCAL MENINGITIS
1East Kent Hospitals NHS Foundation Trust, Neurology, Canterbury, United Kingdom
2King's College London, Neurology, London, United Kingdom
Background and Aims
Stroke is a potentially devastating complication seen in approximately 15% of patients with community-acquired bacterial meningitis (CABM). We present a case with radiological demonstration of transient large vessel constriction, suggesting vasospasm as the underlying aetiology.
Method
N/A
Results
56 year old woman, who is a current smoker, presented with neck stiffness and confusion and was started on empirical antimicrobials for potential CNS infection. The next day she was noted to have right hemiparesis, non-fluent aphasia and gaze preference to the left side. MRI brain revealed left parietal diffusion restriction suggestive of acute infarction. MR-angiogram demonstrated a short segment of narrowing in the M2 segment of the left middle cerebral artery (MCA). CSF examination revealed a neutrophilia, low glucose and raised protein and subsequently pneumococcal PCR was positive. 10 mg of dexamethasone every six hours was commenced for four days. Clinically she rapidly improved and made a full recovery. Repeat MR-angiogram after 9 days showed resolution of the left MCA narrowing and no evidence of atherosclerotic disease elsewhere.
Conclusion
This case helps to demonstrate how stroke should be considered in a deteriorating patient with CABM, even if the patient has few conventional stroke risk factors. Both vasculitis and vasospasm have previously been proposed as the underlying mechanism of stroke in CABM. Arterial vasospasm was suggested by the imaging findings in the presented case. Treatment with dexamethasone has been shown to reduce mortality and morbidity in pneumococcal meningitis, although its role in reducing vasospasm is uncertain.
Trial registration number
N/A
AS14-055
CARDIAC DIVERTICULUM: A RARE CAUSE OF CARDIOEMBOLIC STROKE
1Neurologist - Department Of Neurology, Complejo Hospitalario de Toledo, Toledo, Spain
Background and Aims
Cardioembolic stroke is between 25-40% of the cases of stroke. When we think about this type of stroke, atrial fibrillation is the main cause found. However, there are other less frequent but no less important in the origin of ischemic stroke
Method
Women 48 years. Migraine in treatment with propranolol. She is in hospital by right hemispheric TIA. Duration 30 minutes. Clinical presentation: Central facial paralysis and dysarthria
Results
Cranial CT - two chronic ischemic lesions: left cerebellar and right temporoinsular.
Blood Studies - no findings.
IRM - chronic ischemic lesions in different vascular territories:right insular region, left cerebellar hemisphere and left occipital lobe.
Transthoracic echocardiogram - Saccular aneurysm that disrupts thel inferobasal myocardia miocardial. Neck 13 mm
Cardiac MRI - left ventricular diverticulum
Conclusion
Ventricular wall defects are classified in diverticulum, aneurysms, and hernias. The diverticulum retain normal cardiac structure, with its three histological layers, are connected with the main chamber through a narrow hole. In retrospective studies, a prevalence of 0,76% has been estimated. After echocardiography, cardiac MRI study is often necessary to characterize these defects and for differential diagnosis. In most of the cases have an asymptomatic course, but in some patients can be associated with high rates of morbidity-mortality associated with heart failure or thromboembolism. The treatment are not fully defined:if the diverticulum is small in size and the patient is asymptomatic, it is likely that a wait-and-see attitude is as indicated. The indefinite anticoagulation is indicated in cases of systemic embolism documented, as our patient.
Trial registration number
N/A
AS14-056
FAST (PFO-RELATED STROKE PROBABILITY): A NEW-INDEX TO PREDICT PATHOGENICITY OF PFO IN CRYPTOGENIC ISCHEMIC STROKE
1University of Florence, NEUROFARBA, Florence, Italy
2Azienda Ospedaliero Universitaria Careggi, Cardiotoracovascolare, Florence, Italy
3University of Bologna, Pediatric, Bologna, Italy
Background and Aims
Role of patent foramen ovale (PFO) in cryptogenic ischemic stroke (CS) remains matter of debate. Rope score index (Kent et al, 2013) estimating probability of PFO related stroke, is mainly based on vascular risk factors particularly age and does not completely satisfy clinical needs.
Aim
to create a new index (
Method
index was created joining Rope score variables with clinical/neuroradiological/echocardiographic characteristics suggested from literature. Index was applied to CS (n = 91) and NCS (n = 23) to evaluate its capability to discriminate between the twos
Results
Figure shows FAST index. Higher score is associated with higher probability of PFO pathogenicity. Compared to NCS, CS patients had significantly higher FAST (12,31 ± 2,39 vs 10,56 ± 3,01; p = 0,004) but not Rope-index score (7,14 ± 1,51 vs 6,83 ± 1,72; p = 0,384). ROC curve analysis showed moderate affidability of the index (area under the curve 70%; p = 0.003 with 68.9% sensibility, 73.9% specificity, 26.1% false positive, 69.3% diagnostic accuracy). ROC curve analysis allowed to set at 12 the cut-off over which the pathogenicity of PFO was higher.
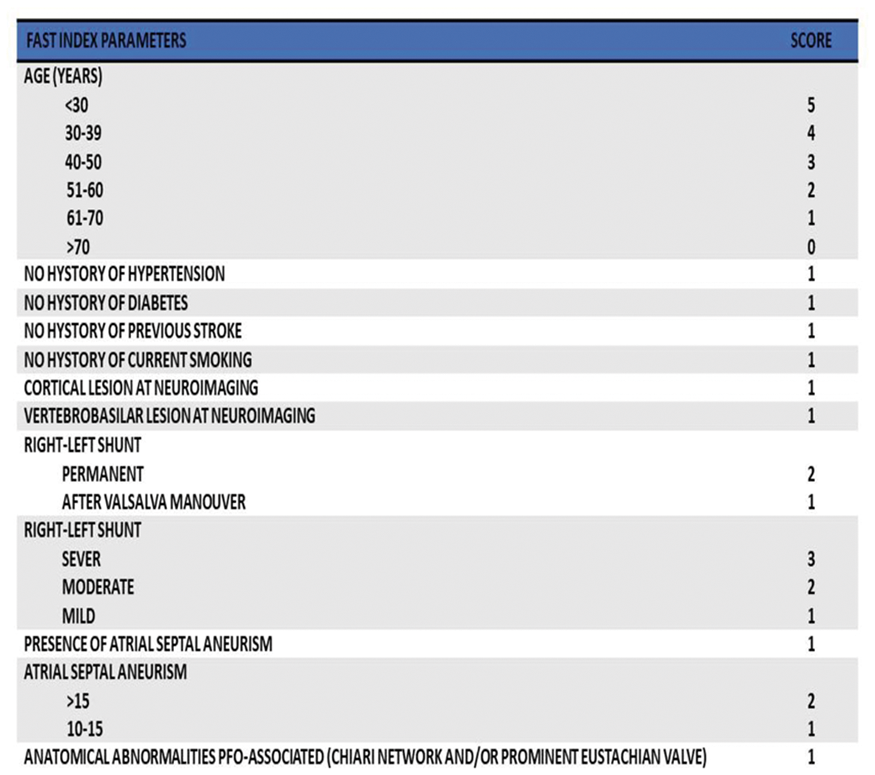
Conclusion
from these preliminary data FAST index seem to be a promising score to discriminate between pathogenic and incidental PFO. These results and the comparison with other indexes deserve to be confirmed and explored in larger studies.
Trial registration number
N/A
AS14-057
STROKE IN NEWBORNS, INFANTS AND SMALL CHILDREN: CLINICAL ASPECTS
1State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Department of Pediatrics- Clinic of Child Neurology, Chisinau, Moldova
2State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Department of Pediatrics, Chisinau, Moldova
3State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Department of Genetics, Chisinau, Moldova
4Territorial Medical Association Botanica- Center of family doctors number 2, Neurology, Chisinau, Moldova
Background and Aims
Stroke in children is much less prevalent than in adults and is manifested with nonspecific clinical symptoms. The aim of this study was to analyze the clinical symptoms of stroke in children depending on age, using the method of logistic regression.
Method
The analysis was carried out on a group of 216 children with stroke, admitted in the pediatric neurology departments. The clinical symptoms were evaluated through logistic regression method.
Results
Statistical analysis allows modeling of suggestive symptoms of stroke in children depending on their age. In newborn these are: seizures (p = 0,000), non-focal neurological signs (p = 0,002), altered state of consciousness (p = 0,006), generalized motor abnormalities (p = 0,004). In children from 28 days to one year of life these are: seizures (p = 0,006), hemiparesis (p = 0,000), decreased ability to squeeze the fist (p = 0,004), consciousness disorders (p = 0,003). In children from 1 to 3 years, these are: hemiparesis (p = 0,003), seizures (p = 0,000), sensory disorders (p = 0,004), focal movement disorders (p = 0,002). Brain magnetic resonance imaging data in newborn demonstrated that the most affected sites are the left hemisphere (67,8%), anterior and middle cerebral arteries (63,9%); multifocal lesions are in 33,2% of cases. In children from 1 to 3 years the middle cerebral artery is affected in 55,6% and the left hemisphere in 78% of cases.
Conclusion
Diagnosis of stroke in children can often be delayed since the clinical symptoms are subtle and nonspecific, often being misdiagnosed. Logistic regression method allows establishing suggestive stroke symptoms, attributed to the category of age, which can help substantially improving the diagnosis.
Trial registration number
N/A
AS14-058
PATENT FORAMEN OVALE IN CRYPTOGENIC AND NOT CRYPTOGENIC ISCHEMIC STROKE YOUNG PATIENTS
1University of Florence, NEUROFARBA, Florence, Italy
2Azienda Ospedaliero Universitaria Careggi, Cardiotoracovascolare, Florence, Italy
Background and Aims
patent foramen ovale (PFO) is found in about 25% of healthy subjects. In ischemic stroke (IS) patients its frequency reaches 50-60%. The pathogenetic role of PFO in cryptogenic ischemic stroke (CS) remains matter of debate.
Aim
to compare CS with not CS (NCS) both having PFO to define whether distinctive characteristics exist to state PFO causality in stroke pathogenesis, assuming that it can be considered incidental in NCS and potentially pathogenetic in CS.
Method
retrospective analysis of clinical, neuroradiological, and ecocardiographic characteristiscs of IS patients with PFO under 50 yrs of age admitted to the Stroke Unit or visited in the Heart-Brain team outpatient service of Careggi Hospital, Florence. Pathogenesis of stroke according to TOAST classification. Cryptogenic stroke defined according to Saver et al (NEJM 2016)
Results
Compared to NCS patients (n = 23) with PFO, CS patients (n = 91) with PFO had significantly higher frequency of history of Valsalva like manoeuvres pre-stroke (19,6% vs 0%; p = 0,06), milder neurological deficits on discharge (mean NIHSS 1,13 ± 3,43 vs 3,47 ± 5,88; p = 0,041) and higher frequency of vertebro-basilar IS (47,3% vs 21,7%; p = 0,027). CS had higher frequency of permanent PFO, severe right-left shunt, severe atrial septal aneurism, and prominent Eustachian valve (p = 0,005).
Conclusion
Several clinical, radiological and echocardiographic characteristics seem to distinguish CS from NCS patients with PFO and may be of help to estimate its pathogenicity and to decide between closure and medical therapy. Our results are in line with clues coming from recently published positive clinical trials on PFO closure.
Trial registration number
N/A
AS14-059
VERTEBRAL ARTERY OCCLUSIVE DISEASE: DATA FROM THE ANGIOGRAPHICALLY CONFIRMED VERTEBRAL ARTERY (ACVAD) DISEASE REGISTRY
1Zeenat Qureshi Stroke Institute- St. Cloud- Minnesota USA, Neurology, St. Cloud, USA
Background and Aims
We performed this study to identify basic demographic and clinical characteristics of adult patients with angiographically confirmed vertebral artery occlusive disease (VAOD).
Method
All patients aged 18 years or older who had angiographically confirmed (using catheter-based cerebral angiograms to ensure diagnostic accuracy) VAOD, defined as stenosis of ³50%, were included. The demographic and clinical characteristics (including associated clinical symptoms), and angiographic features including severity and location of stenosis, and collateral pathways were ascertained using pre-defined criteria.
Results
Of 56 patients with VAOD, (mean age ± SD; 65.4 ± 11.7 years, 44.6% women), 37.5% were classified as suffering from moderate stenosis (50-69%), 16.1% from severe stenosis (70-99%) and 46.4% from occlusion of at least one vertebral artery. The stenosis was unilateral and bilateral in 42 and 14 patients, respectively. Collateral flow was seen in 23 patients either through anastomoses of distal vertebral artery with ascending cervical artery or occipital artery (n = 5) or retrograde filling from contralateral vertebral artery (n = 18). Twenty patients had concurrent diagnosed coronary artery disease and nineteen had stenosis ≥50% or occlusion in the internal carotid artery. Of the 56 patients, 9 patients had acute infarction on neuroimaging in vertebral or basilar artery distribution within preceding 3 months. Of the total of 20 patients who had recurrent symptoms of vertebrobasilar insufficiency, 8 underwent angioplasty and/or stent placement.
Conclusion
Registries such as ACVAD are of unique importance in order to provide a better understanding of asymptomatic and symptomatic vertebral artery occlusive disease and assist in designing future clinical trials.
Trial registration number
N/A
AS14-060
THYROID FUNCTION AND STROKE ETIOLOGY
1Special Hospital for Cerebrovascular Diseases Sveti Sava, Neurology, Belgrade, Serbia
2Clinic for Neurology- Clinical Center of Serbia, Emergency Neurology, Belgrade, Serbia
3Faculty of Medicine- University of Belgrade, Neurology, Belgrade, Serbia
Background and Aims
Thyroid disorders (TD) are often verified in patients with stroke. There is a growing pool of clinical and experimental data suggesting potential influence of thyroid function on causes and prognosis of ischemic events. Purpose of this single-center retrospective study was to assess a role of pre-existing untreated TD in etiology of acute ischemic stroke (AIS).
Method
We have obtained medical records for all adult patients with first-ever AIS treated in one-year period. Patients with radiological confirmation of stroke and thyroid function test performed in first 72 hours after stroke onset were eligible. Patients with previous central nervous system damage of any type, modified Rankin score of 2 and more, malignancy, previously treated TD, or thyroid function altering medications were excluded from analysis.
Results
A total of 331 patients with AIS and thyroid function assessment were analyzed, based on which they were divided in three groups: euthyroid, hyperthyroid and hypothyroid. We found high prevalence of TD in this cohort (25,1%) and analyzed baseline data. Regarding etiology of stroke, there was no statistically significant difference between the three groups. Nevertheless, we observed an inclination for both cardioembolism and atrial fibrillation in hyperthyroid patients, where lack of statistical significance could be explained by relatively small sample size.
Conclusion
We found no verification of TD influence on stroke etiology. However, given the study limitations, more investigation is needed to confirm these findings.
Trial registration number
N/A
AS14-061
DETECTION OF ATRIAL FIBRILLATION USING 7-DAY HOLTER MONITOR IN PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE
1Kyushu Medical Center, Department of Neuroendovascular surgery, Fukuoka, Japan
2Hirosaki Stroke and Rehabilitation Center, Department of Internal Medicine, Hirosaki, Japan
3Jikei University School of Medicine, Department of Neurology, Tokyo, Japan
4Kyorin University, Department of Stroke and Cerebrovascular Medicine, Mitaka, Japan
5Kyushu Medical Center, Department of Cerebrovascular Medicine and Neurology, Fukuoka, Japan
6National Cerebral and Cardiovascular Center, Department of Neurology, Suita, Japan
7National Cerebral and Cardiovascular Center, Department of Cerebrovascular Medicine, Suita, Japan
Background and Aims
Detecting covert atrial fibrillation (AF) in patients with Embolic Stroke of Undetermined Source (ESUS) is highly relevant in antithrombotic therapy for secondary prevention. However, routine short duration ECG monitoring (e.g. 24-hour Holter) may not detect AF. We conduct a study to evaluate the effectiveness of a novel wireless belt-like 7-day Holter monitor (EV-201, Parama-Tech inc., Japan) for detecting AF in patients with recent ESUS after completion of a standard clinical work-up.
Method
This is a multi-center prospective observational study (clinicaltrials.gov identifier : NCT02801708) involving 5 centers. The inclusion criteria is patients with recently diagnosed ESUS and no history of AF. All the patients receive the 7-day Holter monitoring. The primary outcome is detection of any AF on the monitoring.
Results
Between September 2014 and December 2017, a total of 206 patients (78 women ; mean age 68.9 years) were enrolled. During a median device-wearing time of 167.9 hours, the 7-day Holter monitor detected AF in 15 patients (7.3%, 95% confidential interval 4.1 – 11.7%). The interval from start of the examination to first detection of AF was over 24 hours in 11 of the 15 patients, and even 72 hours in 7. After the examination, 14 of the 15 patients with newly identified AF were switched from an antiplatelet agent or warfarin to a non-vitamin K oral anticoagulant, whereas none of the patients without AF was.
Conclusion
The 7-day Holter monitoring in patients with ESUS may increase the detection rate of AF, leading to a relevant change of antithrombotic therapy.
Trial registration number
N/A
AS14-062
RECURRENT STROKES IN A YOUNG MAN: WHEN ANTI-PLATELET THERAPY ISN'T ENOUGH
1Luton & Dunstable University Hospital, Stroke Unit, Luton, United Kingdom
2Buckinghamshire Healthcare NHS Trust, Neurology, Amersham, United Kingdom
Background and Aims
A 39-year old man with no significant comorbidities or family history presented with an ischaemic infarct. Despite thorough investigation and secondary prevention management he proceeded to have 4 further symptomatic strokes over the following 2 years.
Method
Case report.
Results
This patient had normal carotid doppler studies, bubble contrast echo, thrombophilia and autoimmune screen, 7 day ECG monitoring, MR imaging of vasculature from the aortic arch to the brain, CT imaging of the chest, abdomen and pelvis, CSF analysis, cerebral angiography and brain biopsy. The persistent recurrence of strokes and presence of mild vessel wall enhancement on vasculitis protocol MRI brain led to the initiation of a trial of immunosuppression resulting in cessation of further ischaemic events.
Conclusion
Primary CNS vasculitis is a rare but important cause of stroke in young people associated with significant morbidity and mortality when untreated. Its diagnosis requires the presence of an acquired neurological deficit of unknown origin associated with evidence of CNS vasculitis and absence of systemic vasculitis. It presents a diagnostic challenge due to the low sensitivity and specificity of its investigations. It is therefore important to maintain a high level of suspicion for this condition in young patients with recurrent strokes even with negative results.
Trial registration number
N/A
AS14-063
INTRACRANIAL STENOSIS IN THE NORTH OF SPAIN: AN OBSERVATIONAL STUDY
1Centro Medico de Asturias, Neurology, Oviedo, Spain
Background and Aims
Intracranial stenosis (IS) are commonly reported in asiatic countries, being considered infrequent in western countries, even anecdotic in some countries like Spain.
Method
Patients followed in our Ultrasound laboratory from May 2010 to December 2017. All the stenosis were confirmed by other neruoimaging technique.
Results
155 patients had intra other extracranial stenosis/occlusion, 34% (n = 52): IC stenosis. 69% men. Mean age at diagnosis: 70.13 +/-14.8 years old. Previous diagnosis: 52% arterial Hypertension, 29% diabetes, 44% hyperlipidemia. 24% smokers. 15% concomitantly extracranial pathology and 6% multiple IS. 60% symptomatic IS. 53% MCA affected. Etiology: 77% artherosclerosis, 15% Evanescent thrombosis. 92% medical treatment. Follow up: 10% death. 15% cerebrovascular events. Symtomatic IS: more frequently younger patient (65.97+/-16.2 yo vs 76.29 +/-9.9, P = 0.006), male (81% vs 52%, P = 0.030), tobacco use (45% vs 7%, P = 0.025) and less prior antiplatelets use (29% vs 62%, P = 0.019). We found no significant differencies between symptomatic and asymptomatic IS regarding prior other vascular risk factors, previos drugs (statins, ARB, ACE inhibitors and latter complications.
Conclusion
IS in our media is not so uncommon, reaching up to 30% of the patients attended in our hospital. More studies should elucidate its real frequence in European contries, and possible differences among diferent regions of the same country.
Trial registration number
N/A
AS14-064
RISK FACTORS FOR VERTEBRAL ARTERY STENO-OCCLUSIVE DISEASE
1Zeenat Qureshi Stroke Institute- St. Cloud- Minnesota USA, Neurology, St. Cloud, USA
2Zeenat Qureshi Stroke Institute- St. Cloud- Minnesota- USA, Neurology, St. Cloud, USA
Background and Aims
Diabetes, hypertension and smoking have been described as risk factors for carotid artery disease and cerebrovasculature disease in general. We performed a case control study to examine the effect of hypertension, smoking, and diabetes including other factors which may increase the risk of vertebral artery disease (VAD).
Method
Medical records of all aged 18 years or older who had angiographically confirmed vertebral artery stenosis ≥50% were reviewed. Demographic and associated risk factors were ascertained. Controls were selected from the National Health and Nutrition Examination Surveys matched according to age, sex, and ethnicity. A step wise logistic regression was performed to identify the effects of risk factors on occurrence of vertebral artery disease.
Results
There were 56 patients with cerebral angiography confirmed VAD with mean age 66.0 ± SD 12.5 years; 55.4% were men. There were 747 exact controls matched from the NHANES database. In the multivariate analysis hypertension (odds ratio [OR], 5.9; 95% CI, 2.7 – 12.8), Diabetes (OR, 3.5; 95% CI, 2.0 – 6.0), Hyperlipidemia (OR, 4.9; 95% CI, 2.3 – 10.7), Coronary artery disease (OR, 5.7; 95% CI, 3.0 - 10.7) and past cigarette smoking (OR, 3.7; 95% CI, 2.1-6.7) were associated with increased risk of vertebral artery disease even after adjusted for age.
Conclusion
Hypertension, diabetes, hyperlipidemia, coronary artery disease and past cigarette smoking increase the risk for development of vertebral artery disease. The increased risk persists even after cessation of cigarette smoking, which suggests the importance of early abstinence from smoking and controlling all mentioned risk factors.
Trial registration number
N/A
EPIDEMIOLOGY OF STROKE
AS15-001
IN-HOSPITAL MANAGEMENT OF ACUTE STROKE IN THE REPUBLIC OF MOLDOVA – ANALYSIS OF FIRST DATA OF THE RES-Q AS A PART OF ESO-EAST PROJECT
1NicolaeTestemitanu State University of Medicine and Pharmacy, Neurology nr.1, Chisinau, Moldova
2NicolaeTestemitanu State University of Medicine and Pharmacy, Neurology nr.2, Chisinau, Moldova
3Institute of Neurology and Neurosurgery, Admission unit, Chisinau, Moldova
4Institute of Neurology and Neurosurgery, Neuroemergencies, Chisinau, Moldova
5“Holy Trinity” Municipal Clinical Hospital, Neurology, Chisinau, Moldova
6Municipal Clinical Hospital, Neurology, Balti, Moldova
7Shaare Zedek Medical Center, Brain Division, Jerusalem, Israel
Background and Aims
Currently no national database exists in the Republic of Moldova that provides information on the overall approach of management of acute stroke patients.
The purpose of the study was to identify the gaps existing at the in-hospital acute stroke management in the Republic of Moldova based on RES-Q (Registry of Stroke Care Quality) data.
Method
We collected data of all consecutive acute ischemic and haemorrhagic stroke patients in 4 hospitals in the Republic of Moldova for one month. The information was entered in the on-line RES-Q. The statistical analysis of data was performed centrally.
Results
251 acute stroke patients from 4 hospitals were included. 83% presented with ischemic stroke and 17% - with hemorrhagic stroke. The mean age was 66.8 years (52.5% male). The in- hospital mortality rate was 23.6%. Only 37.8% of patients were admitted to Intensive Care Stroke Units. The diagnosis of stroke was confirmed by brain CT / MRI in 95.1% of cases. Thrombolytic treatment with rtPA was applied to 1.2% of patients. Patients diagnosed with atrial fibrillation were given anticoagulants in 62% of cases. Antiplatelet are most commonly prescribed at discharge for secondary stroke prevention (99%), followed by antihypertensive (80%) and statins (66.7%). 17.3% of patients were discharged to a neurorehabilitation unit.
Conclusion
RES-Q registry data revealed that the acute stroke treatment and the access to the neurorehabilitation units are the weakest segments of the in-hospital stroke management in the Republic of Moldova.
Trial registration number
N/A
AS15-002
FREQUENCY OF CLASSICAL CROSSED MEDULLARY SYNDROMES IN THE MRI ERA
1National Institute of Neurology and Neurosurgery, Division of Neurology, Mexico City, Mexico
2National Institute of Neurology and Neurosurgery, Stroke Clinic, Mexico City, Mexico
3University of Maryland School of Medicine, Department of Neurology, Baltimore, USA
Background and Aims
Classical crossed medullary syndromes (CCMS), initially described in the previous two centuries, are taught to neurological trainees around the world but it is not known how often they are the presenting semiology in patients with MRI-confirmed medullary infarction (McMI). The objective of our study was to determine the frequency of CCMS in patients with McMI.
Method
Medical records of patients with McMI seen at our center (1998-2017) were reviewed to determine their initial clinical findings and to ascertain if they presented with one CCMS.
Results
102 patients had an McMI. All of these patients had clinical and imaging features of a medullary infarction but 64 (63%) did not have a CCMS: most of these patients had a non-classical crossed syndrome (83%). The rest had an uncrossed syndrome. Only 38 patients (37%) had a CCMS at presentation: in 14 (6 with concomitant cerebellar infarction), the clinical presentation matched Wallenberg's description (1895). An additional 14 patients (3 with concomitant cerebellar infarction) had a similar presentation but their thermoalgesic examination was not adequately described. In 7 patients, the presenting clinical features matched Opalski's description from 1946 (one of these patients had a cerebellar infarction), in two it matched that of Babinski-Nageotte (1902) and in one it matched Reinhold's (1894).
Conclusion
Most patients with McMI do not have a CCMS but among the third of patients who have a classical presentation, the most common was Wallenberg's syndrome.
Trial registration number
N/A
AS15-003
FREQUENCY OF ANATOMICAL LESIONS OF ISCHEMIC STROKE IN POSTERIOR CIRCULATION
1UHC Mother Teresa, Neurosciences, tirana, Albania
Background and Aims
A posterior circulation (PC) stroke is classically defined by infarction occurring within the vascular territory supplied by the vertebrobasilar (VB) arterial system. The vertebral arteries (VAs) arise from the right and left subclavian arteries and travel cranially through the transverse foramina of the cervical vertebrae. When reaching the foramen magnum, they pierce the dura mater to start their intracranial course. Both VAs join at the pontomedullary junction forming the basilar artery (BA).
Posterior circulation strokes represent approximately 20% of all ischemic strokes.
To study the frequency of anatomical lesions of ischemic stroke in posterior circulation.
Method
We include in this study 91 patients (52M +39F, who was admitted at the Service of Cerebrovascular Disorders in UHC “Mother Teresa”, Tirana, Albania. They was admitted in this service, for the first time ischemic stroke, with different etiologies, during Feb 2017 to Oct 2017.
MRI of brain was made for all of them during the hospitalization.
Results
From this study resulted that 30 patients (32,9%) presented ischemic lesion in PICA territory, 24 patients (26,4%), presented ischemic lesion in PCA territory, 9 patients (9,9%), presented ischemic lesion in AICA territory, 6 patients (6.6%) presented ischemic lesion in TOB territory, 10 patients (11% ) in ICVA ( Intracerebral Vertebral artery) and 12 patients (13.2%) non localization.
Conclusion
As in the other studies, ischemic stroke in PICA territory, is the most frequent, and ICVA stroke is less. Other studies needed to verify this findings, with more patient included.
Trial registration number
n/a
AS15-004
FACTORS INFLUENCING SURVIVAL FROM HAEMORRHAGIC STROKE IN AN URBAN UK CENTRE
1Queen Elizabeth Hospital Birmingham, Stroke Medicine, Birmingham, United Kingdom
2Heartlands Hospital, Stroke Medicine, Birmingham, United Kingdom
3Queen Elizabeth Hospital Birmingham, Statistics, Birmingham, United Kingdom
4Sandwell General Hospital, Stroke Medicine, Birmingham, United Kingdom
Background and Aims
Haemorrhagic stroke (HS) has a high case fatality. Serving an ethnically diverse, low-income population, we retrospectively reviewed registry data to determine how certain parameters influenced 30-day survival.
Method
By reviewing registry data and excluding SAH and haemorrhagic transformation of infarcts, we identified 404 HS cases admitted between 2010-2015. We examined how age, sex, ethnicity, hypertension, diabetes, atrial fibrillation, anticoagulation, HbA1c and haematoma location related to 30-day survival. Fisher’s exact test was used for univariable analysis and binary logistic regression for multivariable analysis.
Results
In univariable analysis, the 30-day survival for males and females was 69% and 54% respectively (p = 0.002). 67% of patients with history of hypertension were alive at 30 days compared to 50% of patients without (p = 0.001). 71% of patients with deep, and 48% with lobar haematoma were alive at 30 days (p < 0.001). Ethnicity and diabetes mellitus did not significantly influence this.
In multivariable analysis, age (p < 0.001), hypertension (p = 0.001) and haematoma location (p = 0.002) were significantly associated with 30-day survival.
In the 169 patients that HbA1c was available, there was no association with survival (p = 0.36).
Conclusion
In this cohort, history of hypertension favourably influenced the 30-day survival, possibly via premorbid antihypertensive treatment. Where available, HbA1c was not associated with survival. However, recognising bias due to incomplete data, retrospective analysis and no pre-specified hypothesis, we propose that a prospective study is done to determine the effect of history of hypertension and HbA1c on clinical outcomes from HS in the UK.
Trial registration number
N/A
AS15-005
EVALUATION OF RISK FACTORS FOR STROKES IN PATIENTS UNDER 45 YEARS OLD ADMITTED AT LOGHMAN HAKIN HOSPITAL, IRAN DURING 2015-2017
1Shahid Beheshty University of Medical Sciences, department of neurology, tehran, Iran
Background and Aims
Strokes in young adults are reported as being uncommon, comprising 10%–15% of all stroke patients. However, compared with stroke in older adults, stroke in the young has a disproportionately large economic impact by leaving victims disabled before their most productive years. The present study aims to evaluate causes of ischemic stroke in young adult patients admitted to a Loghman hakim hospital over a period of 3 years.
Method
We retrospectively reviewed the records of patients with a first-ever stroke in the age range of 15–45 years who were admitted to the Loghman hakim hospital between 2015 and 2017.
Results
Sixty three young adults with ischemic stroke were identified. The etiological diagnoses were: undetermined in 36% of patients, large-artery atherosclerosis in 21%, cardioembolism in 17%, non-atherosclerotic vasculopathy in 17%, and other specific etiologies in 9%. The prevalence of hypertension, cigarette smoking and habitual alcohol consumption was significantly higher in men than in women.
Conclusion
strokes in young adults are a major public health problem and further research, with standardized methodology, is needed in order to give us more precise epidemiologic data. Given the increasing incidence of stroke in the young, there is an objective need for more research in order to reduce this burden. specific causes (non-atherosclerotic vasculopathy, large-artery atherosclerosis, cardioembolism and hematological disorder) are identified in the majority of patients.
Trial registration number
N/A
AS15-006
EVALUATION OF BARRIERS TO DELIVERY OF TISSUE PLASMINOGEN ACTIVATOR FOR PATIENTS WITH ISCHEMIC STROKE AT LOGHMAN HAKIN HOSPITAL, IRAN IN 2017
1Shahid Beheshty University of Medical Sciences, department of neurology, tehran, Iran
Background and Aims
Intravenous thrombolysis is an approved treatment method for patients with acute ischemic stroke and is recommended by multiple guidelines. However, it seems that it is less frequently used in the developing countries compared to the developed countries. The purpose of this study was to estimate the percentage of patients with acute ischemic stroke, eligible for intravenous thrombolytic therapy, at Loghman hakim hospital, Iran, and to determine the main barriers for implementation of this method.
Method
Over one year, 586 patients who were admitted to the emergency department were enrolled into the study. Factors recorded were demographic information,, past medical history, time between onset of symptoms and hospital arrival, stroke type, frequency of patient missed thrombolytic therapy and causes.
Results
A total of 586 patients referred to loghman hakim hospital during 2017. 142 (24.2%) patients arrived at hospital within 3 hours of the onset of symptoms (early enough for intravenous thrombolytic therapy). However, 97.4% (571/586) of these patients missed thrombolytic therapy due contraindications. The remaining 15 patients (10% of those who arrived within 3 hours and 2.6% of all cases) were eligible for thrombolytic therapy.
Conclusion
The major barriers for thrombolytic therapy for patients with acute ischemic stroke in this setting were delays in hospital arrival.
Trial registration number
N/A
AS15-007
FACTORS DELAYING HOSPITAL ARRIVAL OF PATIENTS WITH ACUTE STROKE
1Shahid Beheshty University of Medical Sciences, department of neurology, tehran, Iran
Background and Aims
Optimal time of referral after stroke and the use of new therapies, such as recombinant tissue plasminogen activator, could accelerate symptoms recovery after stroke. The aim of this study was to investigate factors contributing to the delay in referral to hospitals after the occurrence of acute stroke.
Method
This descriptive study included 927 patients, who had referred to the Loghman hospital during years 2015-2016. Time of referring to medical center, the time of occurrence of stroke, risk factors, clinical symptoms of stroke, way of referring, distance from medical center and type of stroke by using a questionnaire were recorded.
Results
The mean age of patients in this study was 68.35 years old. Overall, 593 patients (63.9%) were male and 82.9% had ischemic stroke. Mean time of referral to first treatment center and Loghman hospital was 2.32 and 5.42 hours, respectively. A total of 31.7% patients arrived to Loghman hospital, within less than 2 hours. Factors that prolonged time to presentation were male gender, ischemic stroke, low education, being at a location far from the medical center, referral from other medical centers, being single, having no witness during stroke, and having a stroke at home, and during night.
Conclusion
Time elapsed from onset of symptoms to hospital arrival is influenced by low education, being at a location far from the medical center, referral from other medical centers, being single, having no witness during stroke, and having a stroke at home, and during night.
Trial registration number
N/A
AS15-011
CEREBRAL VENOUS THROMBOSIS: CLINICAL PROFILE, TREATMENT AND FOLLOW-UP
1Évorás Hospital, Stroke Unit and Internal Medicine2, Évora, Portugal
2Évorás Hospital, Internal Medicine2, Évora, Portugal
3Évorás Hospital, Neuropsychology Unit, Évora, Portugal
4Évorás Hospital, Stroke Unit and Neurology Unit, Évora, Portugal
5Évorás Hospital, Stroke Unit and Neuroradiology Unit, Évora, Portugal
6Évorás Hospital, Stroke Unit and Cardiology, Évora, Portugal
7Évorás Hospital, Stroke Unit, Évora, Portugal
Background and Aims
cerebral venous thrombosis (CVT) is a rare condition. It affects younger patients and has different clinical presentations. The aim of study was to evaluate clinical profile, management and outcome of patients (pts) admitted with CVT in a stroke unit located in a rural Portuguese community.
Method
during 14 years (2004-2017), 3961 pts were admitted with stroke. We evaluated clinical and outcome data of 39 consecutive pts (mean age 49.3 ± 17.8; 64.1% female) with CVT. The diagnosis was suspected by clinical presentation and confirmed radiologically. Follow-up (mean 23.3 ± 21.8; median 16 months) included clinical, functional (NIHSS scale) and imaging data evaluation.
Results
the incidence of CVT was 1.0%. Clinical presentation was headache in 24 pts (61.5%) and encephalopathy in 11 pts (28.2%). Eight pts had isolated intracranial hypertension syndrome. Vascular risk factors were present in 27pts (69.2%): 1.6 ± 0.9. Ten women (40.0%) used oral contraceptives. Prothrombotic conditions were found in 7 pts (17.9%). Neoplasm was diagnosed in 5 pts (12.8%). Two or more sinus were involved in 23pts (59.0%). Parenchymal brain lesions were present in 21 pts (53.8%). The treatment was anticoagulation in 36pts (92.3%) and endovascular in 3 (7.7%). There was one recurrence and one acute hydrocephalus (2.6%). Three inpatients died (7.7%) and 6 (15.4%) died during follow-up. An improved functional outcome occurred (NIHSS in admission 3.32 ± 5.79; last evaluation 2.38 ± 5.21 p < 0.05).
Conclusion
CVT is a rare cause of stroke. Mean age was higher than in literature. We found different associated conditions. Clinical presentation was variable. The functional prognosis was good.
Trial registration number
N/A
AS15-012
GOOGLING MAPS OF TRANSIENT ISCHEMIC ATTACK ACROSS LOCAL GOVERNMENT AREAS IN VICTORIA
1Monash Health, Stroke Unit, Melbourne, Australia
2Monash University, School of Clinical Sciences- Department of Medicine, Melbourne, Australia
3Frankston Hospital, Department of Medicine, Melbourne, Australia
4Monash University, Central Clinical School, Melbourne, Australia
5University of Melbourne, Health Outcomes Research Group- Centre for Palliative Care, Melbourne, Australia
Background and Aims
Understanding of the prevalence and regional risk of transient ischemic attack (TIA) is important to planning health service. To our knowledge there are no previous attempts to map regional variation in TIA rate across Victoria, Australia or in other countries. We aimed to compare and map the incidence and Standardised Morbidity Ratio (SMR) of TIA between Victorian Local Government Areas (LGAs).
Method
Victorian hospital administrative data between 2001-2011 were used to define TIA cases and patients’ LGA of residence. Population data by LGA and geocodes of the shapefiles (boundary of LGA) for each LGA were obtained from the Australian Bureau of Statistics for the purpose of mapping TIA cases by location. Spatial regression accounting for age and hypertension was conducted using SpatialEpi package in R (version 3.2.0).
Results
43,088 cases of TIA were identified across 2001-2011. SMR across LGAs ranged between 0 to 9.98. Our choropleth map demonstrates the highest SMRs in the rural North-Western LGAs of Victoria. The lowest SMRs were observed in Melbourne and the Yarra Valley region. Spatial regression shows similar effect of higher rate (coefficient 2.27-2.54) in the North-Western LGA over 10 years.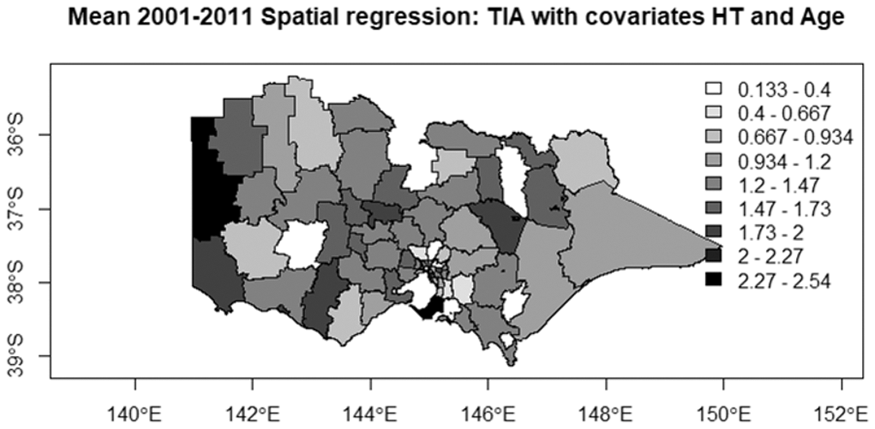
Conclusion
SMR for TIA based on LGA population is higher in North-Western Victoria compared to other regions. The lowest observed SMR is concentrated in Metropolitan Melbourne and surrounds.
Trial registration number
N/A
AS15-013
TRENDS IN TREATMENT AND OUTCOMES AFTER ISCHEMIC STROKE OVER A DECADE IN CHINA: INSIGHTS FROM CHENGDU STROKE REGISTRY DATABASE
1Department of Neurology - West China Hospital, Neurology, Chengdu, China
Background and Aims
We sought to assess whether the treatment during hospitalization, and outcomes at discharge and 3 months after stroke onset had been improved during last decades in China.
Method
We analyzed data regarding ischemic stroke patients within 7 days after stroke between 2002–2005 and 2012–2015 from a prospective and consecutive database, Chengdu Stroke Registry Database, to identify the improvement in stroke management and prognosis between the two time periods. Poisson regression analysis was employed to identify the significant difference of in-hospital mortality, and 3-month disability, disability/mortality between 2002-2005 and 2012-2015.
Results
Of 3003 ischemic stroke patients included (2002–2005: n = 1314; 2012–2015: n = 1689) in the final study, there was a statistically significant increase in using antiplatelet agents (92.1% vs 83.0%), statins (80.8% vs 10.1%), and thrombolysis (3.7% vs 1.4%) during 2012-2015, and an increase trend for anticoagulation application, though not significant (7.5% vs 6.2%). In-hospital mortality declined significantly from 48/1314 patients (3.7%) in 2002-2005 to 19/1689 (1.1%) in 2012-2015 (adjusted RR 0.55 [95% CI 0.31–0.97]). Compared to 2002-2005, patients in 2012-2015 showed a higher 3-month cumulative survival rate (94.7% vs 91.8%; P = 0.002, log rank test) and a lower risk of 3-month mortality (5.3% vs 8.2%; unadjusted RR 0.31 [95% CI 0.18–0.52]), though the adjusted analysis showed no significant difference in 3-month mortality (adjusted RR 0.98 [95% CI 0.71–1.34]). In contrast, 3-month mortality/disability in 2012-2015 decreased significantly, and the adjusted RR was 0.78 (95% CI 0.68–0.88).
Conclusion
Acute ischemic stroke management and outcomes have been improved during the last decade in China.
Trial registration number
N/A
AS15-014
CURRENT STATE OF STROKE ISSUE IN UZBEKISTAN – IMPROVING STROKE MANAGEMENT QUALITY
1Tashkent institute of postgraduate medical education, Neurology, Tashkent, Uzbekistan
2Kepler University Clinic, Department of Neurology 2, Linz, Austria
Background and Aims
A dedicated study on the quality of care for patients with stroke in Uzbekistan has not previously been conducted. The goal of the project is to analyze the current situation and establish regular stroke quality measurement of stroke care in Uzbekistan.
Method
A study of the status of stroke care (head center and 12 branches) was carried out. Uzbekistan is participating in ESO-EAST Project. First results of the International Registry of Stroke Care Quality RES-Q were analyzed.
Results
For the last 3 years (2015-2017) 31,272 patients with acute stroke (75% ischemic, 25% hemorrhagic) were hospitalized in the emergency medicine system. Hospital letality was 12.7% (6.0% ischemic, 19.4% hemorrhagic). The mortality rate over 3 years from hemorrhagic stroke decreased by 4%. The average annual rate of recurrent stroke decreased by 10%. The RES-Q study was conducted in 2 centers (in 401 patients). 99% of them were admitted to the stroke unit. 78% of patients received neuroimaging during the first 4h. NIHSS was estimated in 11%. The length of stay in the stroke department was 11.8 days. 42% of patients were transferred for rehabilitation to neurological wards. Thrombolysis rate was 2% (8 Pts).
Conclusion
Serious problems in providing of emergency care for stroke patients have been identified. These can be improved by training of specialists working in stroke centers. Further strengthening of the technical equipment of stroke centers and creation of stroke country-network are required. The RES-Q data will provide the basis for identifying lacks of the stroke service and future performance progress.
Trial registration number
N/A
AS15-017
INTERLEUKIN 6 TRANS-SIGNALLING AND RISK OF FUTURE ISCHEMIC STROKE
1Karolinska Institutet, Department of Medicine and Department of Clinical Science- Danderyd Hospital, Stockholm, Sweden
2Karolinska Institutet, Unit of Cardiovascular Epidemiology at the Institute of Environmental Medicine, Stockholm, Sweden
3Karolinska Institutet, Unit of Biostatistics at the Institute of Environmental Medicine, Stockholm, Sweden
Background and Aims
Interleukin 6 (IL6) trans-signalling, driven by the binary complex of IL6 and the soluble IL6 receptor (sIL6R), exerts pro-inflammatory effects in the vascular wall. The binary IL6:sIL6R complex is inactivated by sgp130 through the formation of the ternary IL6:sIL6R:sgp130 complex. Studies on IL6 signalling and ischemic stroke are scarce and with diverging results.
Aim of the study was to investigate if IL6 trans-signalling, estimated by a ratio between the active binary and inactive ternary complex, is associated with ischemic stroke risk.
Method
Serum levels of IL6, sIL6R and sgp130 were measured at baseline in a prospective cohort of 60 year old men and women living in Stockholm 1997-1998 (n = 3263) and used to derive the nanomol/liter concentration of the binary and ternary complex. Incidence of ischemic stroke was ascertained through linkage to the national patient registry. Prevalent cardiovascular disease and incident coronary events were excluded. Cox regression models were used to estimate the risk of ischemic stroke (n = 164), expressed as hazard ratio (HR) with 95% confidence interval (CI), associated with the binary/ternary complex ratio. Estimates were adjusted for the common cardiovascular risk factors.
Results
A binary/ternary IL6 complex ratio higher than the median, representing a relative excess of the active binary complex was associated with increased risk of ischemic stroke (adjusted HR 1.61; 95% CI 1.17-2.22).
Conclusion
IL6 trans-signalling, estimated by the binary/ternary IL6 complex ratio, is associated with the risk of future ischemic stroke, indicating that it could be a marker of inflammatory risk and possibly used to identify candidates for anti-inflammatory treatment.
Trial registration number
N/A
AS15-018
STUDY OF STROKE INCIDENCE IN ASEER REGION, SOUTHWESTERN SAUDI ARABIA
1King Khalid University, Neurology Section- Department of Medicine- College of Medicine, abha, Saudi Arabia
2College of Medcine- King Khalid University, Department of Family and Community Medicine, Abha, Saudi Arabia
3College of Medicine- Mansoura University, Department of Community Medicine-, Mansoura, Egypt
Background and Aims
Recent data regarding first stroke incidence in Saudi Arabia, in general and in Aseer region in particular, are scarce and even lacking. The aim was to study first time stroke incidence in Aseer region, southwestern Saudi Arabia
Method
All first stroke patients admitted to all hospitals in Asser region over one-year period (January through December 2016) were included. Stroke patients outside Aseer region were excluded from the study. Incidence per 100,000 and concomitant 95% CI were computed
Results
study included 1249 first-time stroke patients giving an overall minimal incidence rate of hospitalized first-time stroke of 57.64 per 100,000 person-years (95% CI: 57.57 - 57.70). A steady increase was noticed by age to reach a figure of 851.81 (95% CI: 849.2 - 854.5) among those aged 70 years and more. Overall, the incidence rate among females (48.14; 95% CI: 48.04 - 48.24) was lower compared to males (65.52; 95% CI: 65.1 - 66.0)
Conclusion
Taking into consideration the expected rise of elderly due to the prominent medical services provided by the Saudi government leading to subsequent change in the horizontal and vertical age distribution structure of the population an increase in number of stroke patents is expected. It is suggested to establish a national wide stroke surveillance system in the Kingdom. The objective is to report, analyze and maintain an updated overview for stroke status in Saudi Arabia.
Trial registration number
N/A
AS15-019
TREND IN THE INCIDENCE OF STROKE IN PEOPLE UNDER 65 YEARS OF AGE FROM 2002 TO 2015: ANALYSIS OF 57,713 CASES
1University of Queensland, Centre for Sensorimotor Performance, Brisbane, Australia
Background and Aims
Data from UK and USA’ studies show that the average age of stroke patients is falling. Give that stroke is the main cause of adult disability, we want to understand if the same is true in Australia.
Method
Our retrospective study included 244,276 admissions to Hospitals in Queensland between 2002 and 2015 for stroke and related issues (ICD = I60-I69). 151,733 admissions had stroke (I60-I64) as a principal diagnosis, of which 57,713 were defined as first ever episode. We analyzed the patient data on the basis of age range (under or equal 65 and over 65 years of age) and year of admission.
Results
Data from 57,713 patients reveals that the crude incidence rate of stroke patients age 25-64 x 100,000 inhabitants increased from 44 to 62 (p < 0.0001). It represents a jump of + 18/100,000 from 2002 to 2015.
Moreover preliminary data shows that younger people seem to get to the hospital later than older ones, missing the chance for acute therapy and facing a worse outcome with chronic disability.
Conclusion
As a word of caution, the results have yet to be adjusted for catchment area changes, new stroke units opening, and changes in population statistics. Nonetheless, our study suggests that stroke is becoming more frequent in younger Australians. Primary and secondary prevention techniques are effective, as results from older shows, but that they need to be carried over to younger at-risk groups too, together with an awareness campaign.
Trial registration number
N/A
AS15-020
SEX DIFFERENCE IN SPECIFIC-CAUSE MORTALITY AFTER STROKE: THE AUSTRALIAN STROKE CLINICAL REGISTRY
1University of Tasmania, Menzies Institute for Medical Research, Hobart, Australia
2Pham Ngoc Thach University of Medicine, Department of Public Health Management, Ho Chi Minh, Vietnam
3La Trobe University, College of Science- Health and Engineering- School of Allied Health, Bundoora- Victoria, Australia
4Monash University, Department of Medicine- School of Clinical Sciences at Monash Health, Victoria, Australia
5University of Sydney, The George Institute for Global Health, Sydney, Australia
6University of Queensland, School of Medicine- Sunshine Coast Clnical School, Brisbane, Australia
7Royal Hobart Hospital, Neurology Department, Hobart- Tasmania, Australia
8University of Melbourne, Florey Institute Neuroscience and Mental Health, Heidelberg, Australia
Background and Aims
All-cause mortality after stroke is greater in women than men. Our aim was to examine whether there are sex differences in the causes of death (COD) or the potential contributing factors.
Method
1-year COD were obtained by linking first-ever strokes (2010-2013) admitted to 35 hospitals participating in the Australian Stroke Clinical Registry to national death registrations. COD were categorised as stroke, ischemic heart disease (IHD), other cardiovascular disease (CVD, e.g. hypertension), cancer, and other causes. Competing risk models were used to estimate female:male specific hazard ratios (sHRs) of death with adjustment for factors that differed between men and women (sociodemographics, stroke severity assessed by ability to walk on admission).
Results
Among 9,441 events (46% women), women were 7 years older (median age 78 vs 72, p < 0.001) than men, had more severe stroke (32% vs 41% able to walk on admission, p < 0.001), received similar acute care therapies, and had greater all-cause mortality (25.4% vs 19.1% p < 0.001). Women had greater risk of death due to stroke (sHRunadjusted 1.65, 95% CI 1.42-1.91) and other CVD (sHRunadjusted 1.65, 95% CI 1.29-2.12), but these differences were substantially attenuated after adjusting for age, stroke severity (stroke: sHRadjusted 1.19, 95% CI 1.02-1.40; other CVD: sHRadjusted 1.12, 95% CI 0.85-1.48). In contrast, women less often died from IHD (sHRadjusted 0.58, 95% CI 0.43−0.77), or from cancer (sHRadjusted 0.67, 95% CI 0.49−0.91).
Conclusion
COD after first stroke differ between genders with women having more deaths attributed to stroke or other CVD, reinforcing the need to manage cardiovascular risk factors.
Trial registration number
N/A
AS15-021
STROKE RECURRENCE AND MORTALITY IN NORTHEASTERN GREECE: THE EVROS STROKE REGISTRY
1School of Medicine - Democritus University of Thrace, Department of Neurology, Alexandroupolis, Greece
2“Attikon University Hospital”- National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece
3AHEPA University Hospital- Aristotle University of Thessaloniki, Hypertension Excellence Center- 1st Department of Internal Medicine, Thessaloniki, Greece
4School of Medicine - Democritus University of Thrace, Department of Neurosurgery, Alexandroupolis, Greece
5University of Ioannina School of Medicine, Department of Neurology, Ioannina, Greece
6School of Medicine - Democritus University of Thrace, Department of Radiology, Alexandroupolis, Greece
7AHEPA University Hospital- Aristotle University of Thessaloniki, Division of Endocrinology and Metabolism, Thessaloniki, Greece
8School of Medicine - Democritus University of Thrace, Second Department of Internal Medicine, Alexandroupolis, Greece
9School of Medicine - Democritus University of Thrace, First Department of Internal Medicine, Alexandroupolis, Greece
Background and Aims
Data are scarce on both stroke recurrence and mortality in Greece, in rural areas particularly. We analyzed data from a prospective population-based study evaluating first-ever stroke patients in the Evros Prefecture, a region of a total 147,947 residents located in North Eastern Greece.
Method
Adult patients with first ever stroke were registered during a 24-month period (2010-2012) and followed up for 12 months. We calculated cumulative incidences of stroke mortality and recurrence, with corresponding 95% confidence intervals (95%CI). Cox proportional hazards and logistic regression models were used to identify independent determinants of 1-year mortality and 1-year functional dependence (mRS-scores of 3-6) respectively.
Results
We prospectively documented 703 first ever stroke cases [mean age: 75 ± 12 years; 52.8% males; ischemic stroke: 80.8%, intracerebral hemorrhage: 11.8%, subarachnoid hemorrhage: 4.4%, undefined: 3.0%) with a total follow-up time of 119,805 person-years. We estimated the cumulative incidence of recurrent stroke at 30 days (2.0%, 95%CI: 1.2-3.6%), 90 days (4.2%, 95%CI: 2.8-6.2%) and 1-year (9.4%, 95%CI: 7.2-12.4%). We additionally estimated the cumulative incidence of mortality at 30 days (22.1%, 95%CI: 18.3-24.5%), 90 days (26.1%, 95%CI: 23.0-29.6%) and 1-year (36.2%, 95%CI: 32.7-40.0%). The risk of 1-year mortality was independently (p < 0.05) associated with advancing age, history of hypertension, lower GCS-score and increasing admission NIHSS-score. The likelihood of 1-year functional dependence was independently (p < 0.05) associated with age, gender, smoking, lower GCS-score and increasing admission NIHSS-score.
Conclusion
This is the largest to date population-based study in Greece providing novel data on 1-year stroke outcomes (recurrence, mortality and disability) in South-Eastern Europe.
Trial registration number
N/A
AS15-022
HEADACHE OR CERVICAL PAIN AS THE ONLY SYMPTOM OF INTRACRANIAL ARTERY DISSECTION
1National Cerebral and Cardiovascular Center, Department of Crerebrovascular medicine, Suita- Osaka, Japan
2National Cerebral and Cardiovascular Center, Division of Stroke Care Unit, Suita- Osaka, Japan
3National Cerebral and Cardiovascular Center, Department of Neurology, Suita- Osaka, Japan
Background and Aims
Intracranial artery dissection (IAD) often accompanies headache or cervical pain, but little is known about details of IAD patients with pain as the only symptom.
Method
We enrolled patients with pain as the only symptom on visit from all IAD patients who were admitted to our hospital between March 2011 and November 2016 and reviewed backgrounds, clinical courses, sites of dissected artery, pain semiology, and neurological outcomes.
Results
In total of 64 patients with IAD, 25 (39%) had pain as the only symptom. Of these, 19 were male and median age was 51 years old (IQR 44-52). Previous headache history was identified in seven patients (37%). Fifteen (60%) had acute onset pain and 22 (88%) complained of occipital or posterior cervical pain. Median interval between symptom onset to visit was 6 days (IQR 3-13.5). Twenty-four (96%) were referred to our hospital with MRA abnormal findings. Identified vascular risk factors were as follows: hypertension in 11 patients (44%), dyslipidemia in 8 (32%) and current smoking in 9 (36%). None had diabetes mellitus. The vertebral artery was the most frequently affected site (23, 92%) and bilateral vertebral arteries were affected in two. Two (8%) developed minor ischemic stroke (NIHSS 1 and 6) after admission and all were independently discharged home.
Conclusion
The vertebral artery was commonly affected in IAD patients with pain as the only symptom. Most of them had acute occipital or neck pain. Although ischemic stroke occurred in 8% after admission, clinical outcome at discharge was generally preferable.
Trial registration number
N/A
AS15-023
STROKE IN HIV INFECTED PATIENTS. IS IT MORE FREQUENT AND ARE THEY ATTENDED WORSE?
1OSI Donostialdea Hospital Universitario Donostia., Neurología, Donostia, Spain
2OSI Donostialdea Hospital Universitario Donostia., Enfermedades infecciosas, Donostia, Spain
Background and Aims
It is believed that HIV-infected patients have a higher risk of stroke and that they receive a different acute phase attention. The aim of this study is to determine if this is true in our environment.
Method
Retrospective analysis of a series of cases of stroke in a HIV population in Gipuzkoa since 2009. The attention in the emergency room and the reason for not been admitted in the stroke unit (SU) are analized when this occurs.
Results
30 patients were included (mean age 56 years, range 45-80), 80% male. Incidence of 3.04 cases per 1000 patient-year. Baseline characteristics: Parenteral drug use (67%), HBP (46%), smoke (63%), mean CD4 of 665 cells with undetectable viral load in 83%. 67% were ischemic stroke (IS) and 33% hemorrhagic stroke (HS). 50% of IS and 20% of HS were admitted to the SU. No thrombolysis or thrombectomy was performed and mortality at discharge was 25% in IS and 60% in HS. The reason for not entering the stroke unit were: >24h from the beginning of symptoms (39%) and need of orotracheal intubation (28%). In 22%, no neurological care was requested despite fullfilling criteria for admission to the stroke unit.
Conclusion
HIV-infected patients have an increased incidence of stroke at younger ages, in spite of good immunologic control and no HTB. In our enviroment, the main reason for not entering stroke units is a delay in the search of care. It would be advisable to implement health education on early detection of stroke in this population.
Trial registration number
N/A
AS15-024
CEREBRAL VENOUS THROMBOSIS: CLINICAL FEATURES AND RISK FACTORS, DATA FROM A MONOCENTRIC COHORT STUDY OVER 5 YEARS
1Besancon University Hospital, Neurology, Besancon, France
Background and Aims
Cerebral venous thrombosis (CVT) is a rare cause of stroke. In large cohorts, multiple risk factors are identified and CVT patients often present with more than one of them. We aim to analyse if these risk factors are consistent in a real-life practice.
Method
We conducted an observational study of retrospective data from a prospective cohort, the Besançon Stroke Registry, the prospective registry of the Department of Neurology at Besançon University Hospital (France), from January 2013 to December 2017. The diagnosis of CVT was confirmed in all patients using magnetic resonance imaging or angiographic computed tomography. The demographic, clinical, radiological and outcome data were recorded.
Results
Forty-five adult patients were diagnosed for cerebral venous thrombosis in our centre, including 26 women, with a mean age of 48 years (ranging from 18 to 88). Clinical manifestations leading to diagnosis were headache, seizures and altered level of consciousness. The main risk factors were cancer (8 patients), meningitis (4), hematologic malignancy (4), thrombophilia (3), autoimmune disease (2), oral contraceptives (6) and smoking (3). Eleven cases remained cryptogenic.
Conclusion
The supposed multifactorial physiopathology of CVT should lead us to consider systematic assessment and follow-up.
Trial registration number
N/A
AS15-025
NEUROVASCULAR MIMICS: AN UPDATE FROM THE TIA CLINIC
1Bradford Royal Infirmary, Dept of Neurology/Stroke Medicine, Bradford, United Kingdom
Background and Aims
Conditions mimicking neurological disease are well recognised and are common presentations to the neurovascular clinic. Where symptoms are transient, distinction between pathologies may be challenging. We aimed to quantify presentations to the TIA clinic addressing demographics and features of neurovascular mimics.
Method
All patients presenting to the Bradford TIA clinic between 1st Jan 2017 – 31st Dec 2017 were studied. Investigations, Demographics and final diagnosis were recorded. Trends were recorded and patients were grouped by final diagnosis.
Results
426 (186, 43.7% Male) were seen over the 12 month period. Average age was 68 years with no difference for gender. Average time from referral to appointment was 2.74 days. The majority of patients were diagnosed as having suffered a stroke (26 patients, 6.1%) or TIA (182 patients, 42.72%). 188 patients (44.1%) were identified as having a mimicking diagnosis. For the TIA mimics, where a final diagnosis was attributable, the one fifth were felt to have migraine (37 patients), one tenth felt to have symptoms attributable to hypotension (19 patients) and 5% felt to have symptoms that were either psychological (9 patients) or due to peripheral nerve lesions (9 patients). Patients with TIA were more likely to be older than migraneurs (72.39yrs vs 53.38 yrs, p <0.0001). Females were more likely to be represented in the migraneurs (73.0% vs 51.6%, p = 0.02).
Conclusion
Neurovascular mimics make up a significant proportion of presentations to the TIA clinic. An awareness of common presentations and their frequencies may help in attributing a final diagnosis.
Trial registration number
N/A
AS15-026
GENDER STROKE DIFFERENCES IN A PORTUGUESE COMMUNITY-BASED INCIDENCE STUDY
1Faculdade de Medicina da Universidade do Porto, Departamento de Neurociências Clínicas e Saúde Mental, Porto, Portugal
2Centro Hospitalar São João- Porto, Serviço de Neurologia, Porto, Portugal
3Universidade do Porto, Instituto de Ciências Biomédicas Abel Salazar, Porto, Portugal
4Hospital de Santo António-Centro Hospitalar do Porto, Serviço de Neurologia, Porto, Portugal
Background and Aims
Stroke is a major health problem and several studies reported gender stroke differences. Our aim is to further enhance the current knowledge about this issue.
Method
Information was retrieved from a community-based prospective register of patients that had a stroke between October 2009-2011. We studied gender differences regarding demographic data, vascular risk factors, stroke type, stroke severity (NIHSS), 28-days modified Rankin scale (mRS) and case fatality (at 30 and 90 days).
Results
From 721 stroke patients, 45.4% were men. Women were older (75.0 ± 13.6 vs. 67.3 ± 14.8 years), had a worse pre-morbid mRS (39.3% vs. 25.4%, p < 0.001), a higher prevalence of hypertension (p < 0.004) and atrial fibrillation (p < 0.001); previous myocardial infarction was more frequent in men (p < 0.001) as well as smoking habits (p < 0.001). Ischemic stroke was more common in women than men (87.6% vs. 81.0%, p < 0.04). Twenty-eight days’ outcome was worse in women (mRS>1, 77.2% vs. 70.6%, p < 0.05). No differences were found in stroke severity (median NIHSS = 4) and case fatality at 30 and 90 days, after adjusting for age and pre-morbid mRS.
Conclusion
Gender stroke severity and mortality were not different in spite of sex differences pertaining stroke profile - age, vascular risk factors, stroke type and outcome. Our results are somewhat discrepant from those described in literature; more research is needed to understand if this may be due to changes in stroke standard of care.
Trial registration number
N/A
AS15-027
EPIDEMIOLOGY STUDY AND CHANGING TRENDS IN MANAGEMENT OF CEREBRAL SINUS THROMBOSIS IN TWO MAJOR LONDON HYPER-ACUTE STROKE UNITS
1Northwick Park Hospital, Stroke, London, United Kingdom
2Charing Cross Hospital, Stroke, London, United Kingdom
Background and Aims
Cerebral sinus thrombosis (CST) is a rare but important cause of Stroke with incidence of 3-4 per million patients. We have done a retrospective study into causes and treatment outcomes for cases of cerebral sinus thrombosis in two major London hyper-acute stroke units over three consecutive years
Method
We observed data from patient notes, imaging results and clinic letters.
Results
There were 24 confirmed cases of CST for total of 7200 admissions in two units. 20 were female and 4 male patients. Median age was 41.5 years.
Majority of patients had good functional baseline.
Headache was the commonest presentation, followed by seizures and motor-sensory symptoms.
Multiple aetiologies including localized and systemic causes were identified in 84% patients. The rest had no cause identified at followup.
Majority of patients recovered back to good functional baseline.
Mortality rate was 12.5% and all those patients had diagnosis of malignancy.
All the patients except two (who had malignancy) were switched to oral anticoagulants, with a growing preference for DOACs (Direct oral anticoagulants) observed, after initial therapy with lower molecular weight heparin (LMWH). One patient was lost to follow up.
Complications such as chronic headaches due to raised intracranial pressure and subarachnoid haemorrhage were noted in two cases each.
Conclusion
The majority of patients recovered well with timely anticoagulation however Endovascular thrombectomy (ET) and decompression hemicraniectomy which are rare treatment options were performed in two cases. Evidence for ET in CST is not yet proven from randomised controlled trials, but both of our patients showed good recanalization and functional recovery.
Trial registration number
n/a
AS15-028
EARLY LIFE FACTORS AND RISK OF ADVERSE OUTCOMES 3 YEARS POST-MINOR ISCHAEMIC STROKE
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Disadvantages in early life (EL) including lower education, premorbid intelligence (IQ) and childhood socioeconomic status (SES) are associated with an increased stroke risk in adulthood. However it is unclear whether EL factors effect long-term post-stroke outcomes. We aimed to examine the association between childhood SES, education and premorbid IQ and outcomes post-minor ischaemic stroke.
Method
Lacunar or minor cortical ischaemic stroke (NIHSS<8) patients were followed-up 3-4 years post-stroke. We collected information on childhood SES at age 11 (rooms per person, parent’s occupation and indoor/outdoor toilet location), education and premorbid IQ (National Adult Reading Test [NART]). We assessed recurrent vascular events (stroke or myocardial infarction [MI]), cognition (Addenbrooke’s Cognitive Examination–Revised [ACE-R]) and physical functioning (Timed Get Up and Go [TUG], 9-Hole Peg Test [9HPT]).
Results
At 3-4 years, 223/264 participants (84.47%) were followed-up (mean age = 66, SD = 12, range 34-96 at index stroke). Multiple vascular events were reported by 87 patients (61 strokes, 18 MI’s, 8 both). When adjusting for other early life factors, intermediate (vs high) Father’s occupation was associated with an increased risk of multiple strokes (OR = 8.58, 95% CI = 1.21-93.24). Having an outside toilet was associated with poorer mobility (TUG; B = 1.34, 95% CI = 1.05-1.72). Lower premorbid IQ was associated with poorer cognition (ACE-R; B = 1.01, 95% CI = 1.00-1.01). No other significant associations, including with education, were found.
Conclusion
The results add to the growing evidence that EL SES factors are independently associated with worse post-stroke outcomes. These results should be replicated in larger samples to determine their true effect.
Trial registration number
NA
AS15-029
COMORBIDITY OF CEREBRAL INFARCTS AND MALIGNANCIES: A 12-YEAR NATIONWIDE ANALYSIS IN HUNGARY
1Semmelweis University, Depatment of Neurology, Budapest, Hungary
2Hungarian Academy of Sciences, Institute of Experimental Medicine, Budapest, Hungary
Background and Aims
Both short- and long-term outcome after stroke are affected by comorbidities. We set forth to identify malignant diseases associated with cerebral infarction in the Hungarian population diagnosed with cerebral infarction.
Method
In the framework of the National Brain Research Program we analyzed the anonymized database of the National Health Insurance Fund that covers the total population of Hungary, for the period of 2004-2015. Those inhabitants were considered to have cerebral infarctions who had an ICD-10 diagnosis of I63 or I64 reported by health care providers. Of these subjects we used record linkage to find those with diagnosed malignancy (ICD-10 C00-C97). The temporal pattern of malignancies were categorized as a./ diagnosed in any year before, b./ in the same year or c./ in any subsequent year relative to the first diagnosis of cerebral infarction.
Results
In the 12-year period 835,937 persons had a diagnosis of cerebral infarction among the inhabitants of Hungary. Of them, 40,515 had diagnosed malignancy in any preceding year, 56,158 in the same year and 135,846 patients in any subsequent year relative to the first diagnosis of cerebral infarction. Of the malignancies metastatic and ill-defined tumors (C76-C80), gastrointestinal tumors (C15-C26), melanoma (C43-C44) and tumors of the respiratory system (C31-C39) were the most prevalent. Malignant comorbidity was more frequent in those with cerebral infarction compared to those without it (p < 0.001).
Conclusion
One out of 9 patients has a malignancy identified before or in the year of cerebral infarction. Patients hospitalized for stroke should be screened for malignant comorbidity.
Trial registration number
N/A
AS15-030
DOES EDUCATION MODIFY THE RELATIONSHIP BETWEEN PREMORBID IQ AND COGNITION FOLLOWING MILD ISCHAEMIC STROKE?
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
It has been established that lower premorbid intelligence (IQ) and education are associated with increased stroke risk and subsequent cognitive impairment and dementia. Education is often used as a proxy for premorbid IQ, however this relationship has been widely debated. Few studies examine the independent relationship of these factors on stroke risk and post-stroke outcomes, so the associations are unclear. We aimed to examine the effect of education on the relationship between premorbid IQ and cognition post-mild ischaemic stroke.
Method
Patients diagnosed with lacunar or minor cortical ischaemic stroke (NIHSS<8) were followed-up at 3-4 years. We assessed premorbid IQ (National Adult Reading Test [NART]), cognition (Addenbrooke’s Cognitive Examination - Revised [ACE-R]) and collected demographic information including years of education.
Results
At 3-4 years, 223/264 (84.7%) participants were followed-up (mean age = 66, SD = 12, range 34-96 at index stroke). Scores ranged from 54-100 (mean = 88.32, SD = 8.92) on the ACE-R (n = 151) and 92.31-128 (mean = 112.50, SD = 8.44) on the NART. Years of education ranged from 8-23 (mean = 11.72, SD = 2.98) with 30 reporting high education (>13 years). Visual inspection of the data suggests a weaker relationship between NART and ACE-R scores for high vs low education. Although we found no significant interaction when controlling for age, mean years of education and the frequency of high education are small.
Conclusion
The results from this exploratory analysis suggest that education may modify the relationship between premorbid IQ and cognition. Although tentative, these findings suggest that further exploration of this relationship in larger samples with varying degrees of education is needed.
Trial registration number
NA
AS15-031
PRE-STROKE PSYCHOSIS AND ITS ASSOCIATION WITH LEVELS OF HEALTH, RESOURCE UTILIZATION AND CARE PROCESS AFTER ISCHEMIC STROKE: A REGISTER-BASED STUDY
1Karolinska Institutet, Department of Clinical Science and Education- KI-SÖS, Stockholm, Sweden
2Karolinska Institutet, Karolinska Institutet Stroke research Network at Södersjukhuset, Stockholm, Sweden
3Karolinska Institutet, Medical Management Centre, Stockholm, Sweden
4University of Gothenburg, Institute of Neuroscience and Physiology- Rehabilitation medicine, Gothenburg, Sweden
Background and Aims
Approximately 1% of the global population is diagnosed with psychosis or schizophrenia. These patients generally consume higher amounts of healthcare resources whilst their somatic health is worse. The objective with the present study was to analyze potential differences (health, resources, care process), comparing stroke patients with and without previous psychosis/schizophrenia.
Method
Ischemic stroke patients from 7 regions in Sweden were identified via ICD-10 codes (I63) in regional administrative systems and the Swedish Stroke Register; approximately 70% of Sweden’s stroke cases during 2008-2011 were included (n = 46,350). Relevant patient-level data from national registries were linked to enable multivariate regression analysis; data on socioeconomics, mortality, municipality services, social insurance, and filled prescriptions. History of psychosis/schizophrenia was defined via ICD-10 codes F20-29 (n = 389).
Results
The psychosis patients were younger (mean 5 years). Patient-reported general health and functional outcome (3 and 12 months after stroke) were significantly lower in the psychosis subgroup. Stroke recurrence risk was higher. Pre-stroke psychosis patients had a lower frequency of reperfusion treatment than the non-psychosis group, and showed significantly higher proportion moving to special housing. Time at stroke unit were the same as were first-year levels of somatic care. Dispensation of antihypertensives were less common.
Conclusion
Our findings emphasize the importance of taking not only somatic comorbidity but also mental comorbidity into account during stroke treatment, and for evaluation or comparisons, as mental comorbidity (e.g. psychosis) may have a significant impact the year preceding and the two years succeeding the stroke event.
Trial registration number
N/A
AS15-033
AN ASSOCIATION STUDY OF THE MATRIX METALLOPROTEINASE-7, -26 GENETIC POLYMORPHISMS ON THE RISK OF ISCHEMIC STROKE
1Shin Kong WHS Memorial Hospital, Department of Neurology, taipei, Taiwan R.O.C
2Taipei Medical University, School of Public Health- College of Public Health, Taipei, Taiwan R.O.C
Background and Aims
Previous studies indicated that matrix metalloproteinase-7 (MMP-7) and MMP-26 were associated with plaque stability. Therefore, we aimed to study the association of genetic polymorphisms of MMP-7, -26 with ischemic stroke.
Method
A total of 1000 study subjects (500 ischemic stroke patients and 500 age-, sex- matched healthy controls) were recruited in our study. Information of demographic data, lifestyle, and disease history were collected from the study subjects using a structured questionnaire. The genotypes of selected SNPs from MMP-7 (rs10502001, rs11568818) and MMP-26 (rs2499953, rs2499966) were determined by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). Multivariate logistic regression models were used to analyze the relationship between genetic polymorphisms and risk of ischemic stroke.
Results
After adjusting age, gender, education, obesity, smoke, alcohol, hypertension, diabetes and heart diseases, a protective effect for ischemic stroke was found in study subjects with MMP-26 rs2499966 A allele (OR = 0.633, 95%C.I. = 0.461−0.868). There was a 23.7% decreased risk of developing ischemic stroke for each additional A allele (p for trend = 0.039). In study subjects with obesity, a 3.5-fold (95%C.I. = 1.840-6.596) increased odds for ischemic stroke were observed in MMP-7 rs10502001 T allele carriers. However, this was not seen in the subjects without obesity.
Conclusion
MMP-26 rs2499966 A allele was protective against ischemic stroke. However, a higher risk for ischemic stroke was seen in MMP-7 rs10502001 T allele carriers in obesity subgroup. Therefore, subjects who carry MMP-7 rs10502001 T allele have to avoid becoming obesity.
Trial registration number
N/A
AS15-034
ASSOCIATION OF WEIGHT CHANGE FOLLOWING SMOKING CESSATION WITH RISK OF STROKE IN YOUNG MEN
1Seoul National University, Department of Biomedical Sciences, Seoul, Republic of Korea
2Seoul National University Hospital, Department of Family Medicine, Seoul, Republic of Korea
3National Health Insurance Service, Big Data Steering Department, Wonju, Republic of Korea
Background and Aims
Smoking cessation is associated with reduced risk of stroke, but weight gain attributable to smoking cessation may negatively affect cardiovascular benefits from quitting cigarette smoking. In the present study, we aimed to investigate the association of smoking cessation and weight change with risk of stroke using a nationwide, population-based cohort of young men.
Method
Male enrollees without history of stroke between age of 20 and 39 (n = 1,308,031) were recruited from the two consecutive health examinations between 2002 and 2005 from the National Health Insurance Service database. The subjects were followed from January, 2006 through December, 2015. Incident events of stroke were identified with hospitalization records. We used Cox proportional hazard models adjusted for cardiovascular risk factors and weight change to calculate hazard ratio (HR) and 95% confidence interval (95% CI).
Results
Compared to continual smokers, recent quitters (<4 years) and long-term quitters (≥4 years) had reduced risk of stroke (HR 0.84: 95% CI: 0.78−0.91 for recent quitters, and HR 0.58; 95% CI: 0.53−0.64 for long-term quitters, respectively) after adjusting for cardiovascular risk factors. Additional adjustment for weight change did not significantly alter the protective association of smoking cessation with stroke among quitters.
Conclusion
The findings of our study suggest that quitting cigarette smoking is associated with reduced risk of smoking despite the subsequent weight change from smoking cessation.
Trial registration number
N/A
AS15-036
FACTORS PREDICTING RISK OF 30-DAY RECURRENCE AFTER ISCHEMIC STROKE OR TIA: THE BERGEN NORSTROKE STUDY
1Haukeland University Hospital, Neurology, Bergen, Norway
2University of Bergen, Department of Clinical Medicine, Bergen, Norway
3Norwegian Health Association, Research, Oslo, Norway
4Stavanger University Hospital, Centre of age-related medicine, Stavanger, Norway
Background and Aims
Incidence of recurrent stroke is highest the first 30 days after the initial ischemic stroke (IS) or TIA, but there is scarce knowledge about causes behind early recurrence. We aimed to determine etiologies behind 30-day recurrence of IS or TIA. We hypothesized that there might be some patients who are especially prone to early recurrence.
Method
Medical records of 1874 patients in the NORSTROKE-registry, discharged alive from our stroke unit in the study period, were reviewed retrospectively. Recurrence was defined as admittance with a new IS or TIA after being discharged alive after the index event. Stroke etiology was determined by review of electronical medical journals and imaging data. We classified etiology by the TOAST classification, but considered also more specific causes. Cox multiple regression was used to calculate hazard ratios (HR).
Results
33 patients (1.76%) were readmitted within 30 days after the index stroke. Recurrence was caused by large-artery atherosclerosis (LAA) in 21 patients, by active malignancy in 6 patients and by cardioembolism in 3 patients. Small vessel occlusion, aneurysm and postoperative complication was cause for recurrence in 1 patient each. LAA had a HR of 13.63 for 30-day recurrence (p < 0.001). Patients with active cancer had a HR of 12.65 for 30-day recurrence (p < 0.001).
Conclusion
Patients with LAA are at highest risk of recurrent IS or TIA. Active cancer was a important cause of 30-day recurrence. It may therefore be reasonable to screen early recurring patients without LAA for cancer.
Trial registration number
N/A
AS15-037
POST-STROKE COGNITIVE IMPAIRMENT: A SYSTEMATIC REVIEW OF DISEASE PROGRESSION MODELS
1Royal College of Surgeons in Ireland, Psychology, Dublin, Ireland
2Economic and Social Research Institute, Social Research, Dublin, Ireland
Background and Aims
The aim was to review existing models of post-stroke cognitive impairment (CI) disease progression, to inform development of the StrokeCog epidemiological model of post-stroke CI.
Method
Pubmed, EMBASE and the NHS Economic Evaluations Database were searched for relevant articles published in English since 2000. Included articles described an epidemiological or economic model tracking disease progression of CI and/or stroke over time, e.g., Markov or microsimulation models. Titles and abstracts were screened by one reviewer, followed by full text of potentially relevant articles. Data was abstracted from eligible articles using a standard form. Models were evaluated against pre-specified criteria for the StrokeCog model, agreed by expert consensus.
Results
5,723 abstracts were screened, followed by full text review of 398 articles. There were 72 eligible articles for CI and 54 for stroke (two articles modelled stroke and CI). The dominant model type in both reviews was a Markov cohort-level state transition model. Models of CI assume continuous disease progression, whereas models of stroke assume stability in the absence of stroke recurrence.
Conclusion
To date, epidemiological modelling of post-stroke cognitive impairment has been extremely limited. It requires a synthesis of two existing approaches - modelling the ongoing risk of transition to a worse cognitive state, and the increased risk of deterioration associated with a recurrent stroke.
Trial registration number
N/A
AS15-038
COMPARISON OF IMPUTATION METHODS FOR MISSING VALUES IN CLINICAL STROKE DATABASES
1Charité - Universitätsmedizin Berlin, Center for Stroke Research, Berlin, Germany
2Charité - Universitätsmedizin Berlin, Department of Neurosurgery, Berlin, Germany
Background and Aims
Missing-values are a prevalent challenge in analysis of clinical data of stroke patients. Deletion of patient entries with missing-values is common, but is a discouraged practice. Methods that estimate missing-values are recommended. Here, we explore the difference between simple imputation of the mean vs. hot-deck imputation (“sampling”) and multiple-imputation-by-chained-equations (“MICE”).
Method
We used a clinical database based on the 1000+ stroke study with 380 completed-entries patients. We selected 13 common clinical parameters including numerical and categorical values: gender, treatment, occlusion, hyperlipidemia, diabetes, hypertonia, hours-to-MRI, age, mRS-pre-stroke, acute-NIHSS, discharge-NIHSS, discharge-mRS and discharge-TOAST. We simulated missing-values from 5% to 30% and then imputed them using the mean, random-sampling and MICE method. The error was calculated as the mean-squared-error (MSE) of the normalized data for numerical parameters and as the error-rate (percentage of misclassified values) for categorical data. The analysis was repeated 50 times and the methodologies were compared using the Wilcoxon signed-rank test.
Results
Simple imputation of the mean led to a significantly lower error-rate within numerical and categorical parameters (average error-rate 0.04 and 0.32 respectively) compared to the random sampling (p < 0.00000004 and p < 0.02 respectively) as well as the MICE method (p < 0.00000003 and p < 0.009 respectively) over the range of simulated missing values. No significant difference was found between the random-sampling and the MICE.
Conclusion
Simple imputation by mean is simple to apply and our results suggest that it might perform better than more sophisticated and time-consuming methods for clinical stroke data.
Trial registration number
N/A
AS15-039
ISCHEMIC STROKE AS AN EARLY MANIFESTATION OF NEOPLASIA
1HCU Lozano Blesa, Neurología, Zaragoza, Spain
Background and Aims
Patients with cancer frequently associate cerebrovascular complications. In some occasions the ischemic stroke is the first manifestation of a hidden neoplasia.
Our aim was to study the appearance of ischemic stroke as a possible first manifestation of a hidden neoplasia
Method
Retrospective unicentric longitudinal study of patients diagnosed with ischemic stroke followed by diagnosis of neoplasia between the years 2012 - 2016
Results
Of the 2036 patients diagnosed with ischemic stroke between the years 2012-2016, 1.5% had been diagnosed with neoplasia in the period studied, with an average from the diagnosis of stroke of 478 days.
In our sample, 23 were male (74%) and 8 female (26%), with an average age of 80 years. As cardiovascular risk factors, 30% had a history of smoking, 66% had high blood pressure, 38% had dyslipidemia and 29% had diabetes mellitus.
Of the neoplasms detected, 40% are divided between lung carcinoma and glioblastoma multiforme, followed by colorectal carcinoma.
Conclusion
Both ischemic stroke and neoplasms are frequent pathologies in the general population that share risk factors for their developmentIschemic stroke can be an early manifestation of the existence of a hidden neoplasia
Trial registration number
No
AS15-040
ANALYTICAL PARAMETERS IN ACUTE ISCHEMIC ICTUS AND ASSOCIATION OF HIDDEN NEOPLASM
1HCU Lozano Blesa, Neurología, Zaragoza, Spain
Background and Aims
Patients with cancer frequently associate cerebrovascular complications. In some occasions the ischemic stroke is the first manifestation of a hidden neoplasia.
Our aim was to analyse the different analytical parameters determined in acute ischemic stroke and assess their ability to predict the presence of a hidden neoplasia
Method
Retrospective study of cases and controls in patients diagnosed with ischemic stroke between 2012-2016 with subsequent diagnosis of neoplasia in the following 6 months.
The determinations of sodium, potassium, chloride, calcium, bilirubin, albumin, cholesterol, speed of globular sedimentation, C-reactive protein, lactate dehydrogenase, alkaline phosphatase, uric acid, homocysteine, lipoprotein A, hemoglobin and lupus anticoagulant were analyzed.
The results obtained were compared with those of a control group extracted from a sample of patients who had presented a diagnosis of ischemic stroke between 2012-2016 without subsequent diagnosis of neoplasia.
Results
Of the 2036 patients diagnosed with ischemic stroke between the years 2012-2016, 31 patients (1.5%) had been diagnosed with neoplasia in the period studied, and of these 11 (35%) had been diagnosed with neoplasia in a period maximum of 6 months after the vascular event. Significant differences were obtained between both groups in Calcium (p = 0.001), Ac. Uric (p = 0.007) and VSG (p = 0.019).
Conclusion
In our series, 35% of the patients diagnosed with neoplasia after ischemic stroke were diagnosed in the following 6 months. In relation to patients who did not develop neoplasia, our group presents higher values of speed of globular sedimentation and lower values of calcium and uric acid
Trial registration number
No
AS15-041
EPIDEMIOLOGY OF RURAL/URBAN STROKE DISPARITIES IN THE GREATER CINCINNATI / NORTHERN KENTUCKY STROKE STUDY
1University of Cincinnati, Neurology and Rehabilitation Medicine, Cincinnati, USA
2Cincinnati Children's Hospital Medical Center, Biostatistics & Epidemiology, Cincinnati, USA
3University of Cincinnati, Emergency Medicine, Cincinnati, USA
4Indiana University, Neurology, Bloomington, USA
5Michael E. DeBakey VA Medical Center, Neurology, Houston, USA
6Baptist Health Neuroscience Center, Neurology, Miami, USA
Background and Aims
Stroke mortality is higher in rural areas than urban, in the U.S. and internationally. Limited data exist as to why. We sought to evaluate whether the Greater Cincinnati/Northern Kentucky Stroke Study (GCNKSS) could be used to evaluate these disparities.
The GCNKSS is a population-based epidemiologic study capturing all ischemic stroke cases in a five-county region surrounding Cincinnati, Ohio, USA, with a total population of 1.3 million. Census areas within the region contain a wide variety of population densities, but due to proximity to Cincinnati, few meet commonly-used rurality criteria.
Method
Among residents of the GCNKSS region, we identified all hospitalized adult ischemic stroke cases in 2010 by screening ICD-9 codes 430–436, with cases verified by study physicians. We geocoded cases to census tracts based on home address and evaluated the tract-level correlation between stroke rate and tract characteristics including population density, rural fraction, and percent impervious development. We analyzed both unadjusted and after unconfounding for age, race, and a composite socioeconomic deprivation index.
Results
We identified 1633 individuals suffering strokes during the study period (54.1% female, 20.1% black). After adjustment for confounders, population density was significantly associated with stroke rate. An interquartile (∼17,000 people/km2) decrease of population density was associated with an increase of 0.15 strokes/1000 people/year.
Conclusion
Rural/urban disparities in stroke persist even in areas like the GCNKSS considered by some metrics to be non-rural. This suggests the GCNKSS can be used to study rural/urban stroke disparities and supports an understanding of rurality as a continuum, rather than a binary variable.
Trial registration number
n/a
AS15-044
BASELINE CHARACTERISTICS AND LONG TERM OUTCOME OF ESUS IN A HOSPITAL-BASED POPULATION
1Università degli Studi di Palermo, Department of Experimental Biomedicine and Clinical Neurosciences- University of Palermo- Italy, Palermo, Italy
Background and Aims
The construct of Embolic Stroke of Undetermined Source (ESUS) was created in order to distinguish, among the cryptogenic strokes, those who might have an embolic origin. We evaluate the percentage of ESUS in a hospital-based cohort, describing characteristics at baseline and follow-up.
Method
A retrospective analysis was performed on consecutive patients admitted to our Neurology Department (from January 2010 to December 2015) with an ischemic stroke (IS), selecting those who fulfilled ESUS criteria. Patients were evaluated at baseline and at follow-up (2017) with a telephonic interview and an outpatient visit. The primary end-point was mortality; the secondary outcomes were TIA/stroke recurrence and functional outcome (mRS). Dead was assessed both by telephone interview and death certificate, while the last were used for the recording of causes of death.
Results
Of 750 patients admitted to our ward with IS, 177 met ESUS criteria. The mean age of ESUS patients (69,01; SD:13.2) was lower than IS group (72,3 SD 13,6). Despite frequency of death in ESUS patients was lower (18%vs30%), mean survival was significantly lower (400 vs 990 days, p = 0.001). Cox regression showed that NIH-SS was the most relevant risk for death independently from stroke subtypes (IS vs ESUS). Stroke/TIA recurred in 21 % of patients. The modified Rankin Scale (mRS) evaluation suggested that ESUS patients presented an improvement of disability.
Conclusion
In our cohort, nearly 25% of patients met ESUS criteria. ESUS patients were younger than IS patients, but had less severe strokes with a lower mortality rate and better functional outcome on follow-up.
Trial registration number
N/A
AS15-045
CLINICAL CHARACTERISTICS OF STROKE IN YOUNG PEOPLE
1Azerbaijan State Advanced Training Institute for Doctors named after A. Aliyev, Neurology and clinical neurophysiology, Baku, Azerbaijan
2Republican Clinical Hospital named after acad. M. Mirgasimov, Neurology, Baku, Azerbaijan
Background and Aims
In the past decade, strokes at young age is more common. The aim of our research was to study the clinical features of stroke in young people.
Method
The study was conducted in neurology departments of the Republican Clinical Hospital named after M. Mirgasimov (Baku, Azerbaijan). Within 3 years (2014-2016), 145 patients aged from 18 to 45 were examined [men 74 (51%), women 71 (49%)]. Patients were performed by a complete neurological, somatic, laboratory, ultrasonography, neuroimaging examination.
Results
The average age of patients was 35, for men - 36, for women - 34 years. 39 (27%) of patients, were in the younger age group (18-30 years), and 106 (73%) in older age group (31-45 years). In 116 (81%) patients, stroke was noted as a primary, in 29 (19%) recurrent. 82 (56%) patients had ischemic stroke (IS), 41 (28%) an intraparenchymal hemorrhage, 13 (9%) subarachnoid hemorrhage (SAH) and 9 (7%) venous sinus thrombosis (VST). It was found that in the older age group, IS and SAH occurs more often (Table 1).
Table 1. Percentage of stroke types in young people.

In 6 (21%) patients from 29, who had recurrent stroke, the cerebrovascular accident repeated at the age of 18-30 and in 23 (79%) in 31-45. The distribution of stroke by sex showed that young women predominate among patients with VST (Table 2).
Table 2. Percentage of stroke types in young people be sex.

Conclusion
At young age, IS prevails. In the older age group, ischemic stroke and SAH are more common. VST is more common in women.
Trial registration number
N/A
AS15-046
PREVALENCE, DEMOGRAPHICS AND RISK FACTORS OF INTRACRANIAL ATHEROSCLEROTIC STENOSIS IN ISCHEMIC STROKE PATIENTS AT A TERTIARY CARE NEUROLOGICAL HOSPITAL IN WESTERN INDIA
1Vadodara Stroke Center, Stroke Research, Vadodara, India
Background and Aims
Intracranial Atherosclerotic Stenosis (ICAS) is a common cause of Ischemic Stroke (IS) in Asia, associated with a high risk of stroke recurrence. No data is available to our knowledge, on the prevalence of ICAS in Western India. Aim was to study prevalence, demographics and risk factors of ICAS in IS patients at a tertiary care Neurological Hospital in Western India.
Method
We retrospectively collected data on all IS patients admitted at Vadodara Institute of Neurological Sciences between January 2014 and May 2017. We excluded patients on whom MRA and/or CTA imaging of intracranial vessels was not done. ICAS was defined as stenosis or occlusion > 50%. We excluded normal variants (hypoplastic Vertebral artery and hypoplastic A1 segment of Anterior Cerebral Artery and P1 segment of Posterior Cerebral Artery) of intracranial vasculature.
Results
Data was collected on 687 patients of whom 267 (38%) had ICAS and of those 267, 209 (78%) were symptomatic ICAS, 58 (22%) had asymptomatic ICAS while 33 patients had both symptomatic as well as asymptomatic ICAS. Mean age was 59 years with male preponderance. Hypertension was present in 54%, while DM (33%), Hyperlipidemia (44%), Smoking (24%) and CAD (7%), NIHSS ≥ 5 (68%), hyperhomocysteinemia (≥ 15 micromole/L) (42%) of ICAS patients. No significant difference in vascular risk factors, NIHSS or hyperhomocysteinemia between ICAS IS patients and non ICAS IS patients.
Conclusion
We report a prevalence of 31% of symptomatic ICAS in our IS patients. Aggressive secondary stroke prevention needs to be considered in our IS population with ICAS.
Trial registration number
n/a
AS15-047
PREVALANCE AND CLINICO-RADIOLOGICAL CHARACTERISTICS OF ACUTE HEMORRHAGIC STROKE PATIENTS FROM A SINGLE TERTIARY CARE CENTRE FROM EASTERN INDIA
1AMRI HOSPITAL-MUKUNDUPUR, NEUROLOGY, KOLKATA, India
2Amri Hospital Mukundapur, Neurology, Kolkata, India
Background and Aims
Incidence of intracerebral hemorrhage (ICH) in Asia is twice as high as in Western countries. Location of stroke apart from clinical severity play important role in determining the treatment outcome. We aim to look for frequency and clinico-radiological feature of ICH patients from our centre.
Method
We retrospectively surveyed consecutive patients admitted over the last 5 yrs with spontaneous non traumatic ICH. Baseline and discharge NIHSS, vascular risk factors, medical & imaging records and patient demographics were recorded. Hemorrhage caused by trauma, anticoagulant or thrombolytic drugs, brain tumor, aneurysm or vascular malformation were excluded
Results
Out of 1122 total stroke patients admitted, 437(38.94%) had ICH. Among hemorrhagic strokes, 300 (68.64%) were male while 137 (31.35%) were female. Of 437 patients, 192 (43.93%) had basal ganglia, 95 (21.73%) had thalamus, 76 (17.39%) had lobar, 32 (7.32%) had cerebellar, 28(6.40%) had brain stem and 14 (3.20%) had primary intraventricular hemorrhage (IVH). Out of 437 patients, 167(38.21%) had intraventricular extension most commonly associated with thalamic (72.63%), followed by brain stem (64.28%), cerebellar (50.00%), basal ganglia (19.27%) and lobar bleed (17.10%). Among the vascular risk factors hypertension (79%) was commonest followed by diabetes (46%), smoking (18%) and dyslipidemia (12 %). Mean age at admission was 56 yrs [19-89]. Median NIHSS at admission was 11(1-40). Mortality was highest with brain stem bleed (22%), and least with basal ganglia (3%).
Conclusion
In our study, commonest location of hemorrhage was basal ganglia with male preponderance. Patients with Brain stem and IVH had worst outcome with hypertension being the commonest association.
Trial registration number
N/A
AS15-048
DECREASING STROKE INCIDENCE AND LONG-TERM CASE FATALITY IN ITALY
1University of L’Aquila- 67100- L’Aquila- Italy, Department of Neurology and Stroke Unit- AZH, L'Aquila, Italy
2University of L’Aquila- 67100- L’Aquila- Italy, Department of Neurology, L'Aquila, Italy
Background and Aims
We assessed first-ever strokes (FESs) incidence and case-fatality rates (CFRs) in a defined population, reflecting national trends.
Method
Prospective population-based registry including all the residents with a FES in 2011-2013 followed up to 3 years to ascertain CFRs. Present data were compared with those obtained in 1994-1998.
Results
Data from 1,238 patients with a FES in 2011-2013 were compared to those of 4,353 patients in 1994-1998. Mean age ± SD at stroke onset was higher in 2011-2013 than in 1994-1998 (76.1 ± 12.6 vs 74.8 ± 11.4 years; P = 0.001). FES incidence in 2011-2013, standardized by the 2011 European population, was 107 per 100,000 person-years and lower than that observed in 1994-1998 [275 per 100,000 person-years; incidence rate ratio 0.39, 95% confidence interval (CI) 0.36−0.43]. In 2011-2013, there were 71.4% ischemic strokes (ISs), 21.1% intracerebral hemorrhages (ICHs), 4.4% subarachnoid hemorrhages (SAHs), and 3.1% ill-defined events; the corresponding proportions in 1994-1998 were 82.6%, 13.5%, 2.7%, and 1.2% (P<0.001).
The 2011-2013 CFR was 43.5%, lower than the 54.1% of 1994-1998 (SMR 0.72, 95% CI 0.69−0.76). CFRs were lower for IS (37.0% vs 51.3%, SMR 0.66, 95% CI 0.61−0.70) and ICH (57.5% vs 69.2%, SMR 0.77, 95% CI 0.70−0.83) and stable for SAH (43.6% vs 44.9%, SMR 1.25, 95% CI 0.84-1.86).
Trial registration number
N/A
AS15-050
SPATIAL STROKE INEQUALITIES REVEALED THANKS TO GEOGRAPHIC INFORMATION SYSTEM: DATA FROM STROKE 69 COHORT
1University of Lyon - Université Claude Bernard Lyon 1, EA 7425 HESPER Health Services and Performance Research, Lyon, France
2CH Lucien Hussel, RESCUe network, Vienne, France
3University Jean Moulin Lyon 3, UMR 5600 CNRS Environnement Ville Société, Lyon, France
4Hospices Civils de Lyon, Emergency Department - Edouard Herriot Hospital, Lyon, France
5Hospices Civils de Lyon, Public Health Department, Lyon, France
6Hôpital Nord Ouest, Department of Stroke Medicine, Villefranche-sur-Saone, France
7Hôpital St Joseph St Luc, Emergency Department, Lyon, France
8Hôpital Nord Ouest, Emergency Department, Villefranche-sur-Saone, France
9Hospices Civils de Lyon, Emergency Department - Centre Hospitalier Lyon Sud, Pierre Benite, France
10Hospices Civils de Lyon, Emergency Department - Hopital Croix Rousse, Lyon, France
11CH Lucien Hussel, RESCUe network and Emergency Department, Vienne, France
12Hospices Civils de Lyon, Department of Stroke Medicine, Bron, France
Background and Aims
This study aimed to analyze the spatial repartition of stroke patients thanks to Geographic Information System (GIS).
Method
This is an analysis on 2518 patients included in a population-based cohort study (STROKE 69) on all consecutive patients with an acute stroke admitted to any emergency department (ED) or Stroke Unit of Rhône county from November 2015 to June 2016. Every patient was geolocalised using their precise residential postal addresses (80% of strokes arised at home). Stroke repartition was calculated for 1000 inhabitants at city scale and a global indicator of spatial autocorrelation, Moran’s Index, was applied. Furthermore, the Local indicator of Spatial Autocorrelation (LISA) indicates the local pattern of spatial clusters.
Results
As the p-value was significant and Moran’s I was positive, the repartition of strokes may be considered as clustered. High stroke density clusters (HH and HL clusters) have significantly gather more strokes than other places. The cities of Low-low (LL) clusters in the south of Rhône may be explained by border effects, due to the existence of close EDs in the adjacent county.
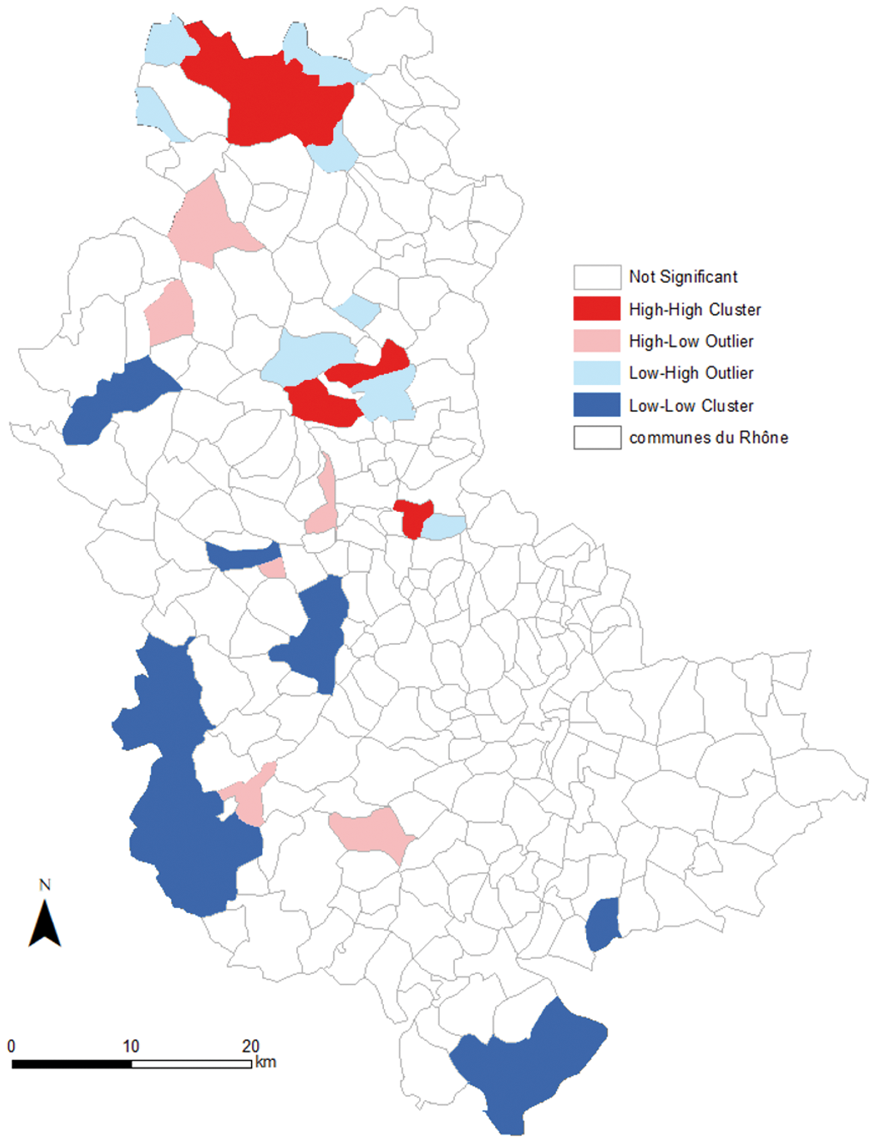
Conclusion
This kind of analysis allows to estimate more precisely the spatial repartition and to raise hypotheses regarding environmental and socio-economic factors that could explain this repartition.
Trial registration number
N/A
AS15-052
CLINICAL FEATURES OF CEREBROVASCULAR DISEASES IN A SPANISH CITY IN NORTH AFRICA. “STROKE IN THE FRONTIER OF EUROPE”
1Regional Hospital of Melilla- Spain, Internal Medicine - Neurology Service, MELILLA, Spain
Background and Aims
Perform a descriptive and inferential study of patients with cerebrovascular disease in a regional hospital in the frontier of Europe and Africa.
Method
We realized a descriptive analysis of inpatients with cerebrovascular disease from January to December 2015. The patients were divided in two groups (ischemic and hemorrhagic). We describe the clinic presentation, etiologies, injury area and a bivariate analysis using Chi squared test and Mann Whitney U Test.
Results
There were 106 patients, 52.8% of them were women. The median age was 71,08 years ( ± 13,53), 40.6% of Patients were from Bere ber ethnic. 83 patients (79%) had ischemic stroke and 22 (21%) had hemorrhagic stroke. The average lenght of stay was 9,99 ± 10,53 days. The mortality was 16% (17 patients). The most common etiology of ischemic stroke were atheroembolic disease (42.6%), cardioembolic (25.2%) and lipohyalinosis (15%). The most common etiology of hemorrhagic stroke were hypertensive (40.9%) and spontaneous (36.4%). The affected areas in of ischemic stroke were middle cerebral artery (48,1,5%), two or more areas (16%) and vertebrobasilar territory (15.1%) and only 7.8% were treated with IV rt-PA.
Conclusion
The mean age is lower than all rest of Spain. Ischemic stroke was due atherothrombotic disease and the main factor for hemorrhagic stroke was high blood pressure, very probably due poor control. Does not exist yet a easy access to a adequate treatment for hyperacute stroke. It was fundamental to realize this study in our region, because according to the characteristics of cerebrovascular disease, we can propose preventive measures.
Trial registration number
N/A
AS15-054
SOCIODEMOGRAPHIC CHARACTERISTICS OF PATIENS WITH CEREROVASCULAR DISEASES IN ONE CITY ON THE EUROPE-AFRICA BORDER
1Regional Hospital of Melilla, Internal Medicine - Neurology Service, Melilla, Spain
Background and Aims
Perform a study of patients with cerebrovascular disease in a regional hospital of Melilla, Spain; analyzing demographic characteristics with cerebrovascular disease type and comorbidities.
Method
We realized a retrospective descriptive transversal analysis of inpatients with cerebrovascular disease from January to December 2015. The patients were divided in two groups (ischemic and hemorrhagic). We described the characteristics comparing their median values between ethnic groups, using Chi squared test and Mann Whitney U Test.
Results
There were 106 patients, 52.8% of them were women. The mean age was 71,08 years ( ± 13,53). Only 71.7% had social security, 40.6% were from Bere ber ethnic and 29 % were of them were non-EU. 83 patients (79%) had ischemic stroke and 22 (21%) had hemorrhagic stroke. The average lenght of stay was 9,99 ± 10,53 days. The mortality was 16% (17 patients). 68.9% of patients had HBP; 37.7% had DM, 22.6% dyslipidemia, 17% AF, 15.1% coronary artery disease, 11.3% neoplasia, 10.4% heart failure and 8.5% dementia, all these features without significant statistical differences between ethnic groups. After hospital discharge up to 40% of the patients had dependence for basic activities of daily living.
Conclusion
There is a high frequency of patients with cerebrovascular diseases without social security and non-EU citizens that been have seen in our hospital. Patients with ischemic cerebrovascular disease are older and have more disability and associated comorbidities. We did not find significant statistical differences in the comparison of the demographic and clinic characteristics of the ethnics groups.
Trial registration number
N/A
AS15-055
THE EPIDEMIOLOGY OF SYMPTOMATIC CAROTID STENOSIS IN ACUTE ISCHEMIC STROKE PATIENTS IN TWO LARGE HOSPITALS IN THE NETHERLANDS
1Academic Medical Centre, Neurology, amsterdam, The Netherlands
2St. Antonius Ziekenhuis, Neurology, Nieuwegein, The Netherlands
3Erasmusmc Rotterdam, Neurology, Rotterdam, The Netherlands
4Erasmusmc Rotterdam, Radiology, Rotterdam, The Netherlands
Background and Aims
Current prevalence estimates of carotid stenosis are between 12 to 25%. However, based on clinical observation this percentage seems an overestimation. The aim of this study was to estimate the prevalence and predictor effects of symptomatic internal carotid artery (ICA) stenosis in patients with transient ischemic attack (TIA) or acute ischemic stroke.
Method
We included all consecutive adult patients admitted to two hospitals in the Netherlands in 2014, who suffered from amaurosis fugax, retinal infarction, cerebral TIA or cerebral infarction in a distribution area of the ICA. Primary outcome was the presence of ipsilateral ICA stenosis. Multivariable logistic regression was performed to estimate the effect of predictors for the presence of 50-100% ICA stenosis.
Results
We analyzed 883 patients of whom 110 (12.5%) had a symptomatic ipsilateral carotid stenosis. Ninety-nine patients (11.2%) were men with 50-99% ICA stenosis or women with 70-99% stenosis. White patients have an increased risk of ICA stenosis and occlusion compared to non-white patients (21.8% vs 11.7%). Increasing age (OR 1.0; 95%CI 1.0-1.1), male sex (OR 2.7; 95%CI 1.7-4.4), retinal ischemia (OR 2.2; 95%CI 1.0-4.7) and peripheral vascular disease (OR 3.3; 95%CI 1.8-6.2) are important predictors for 50-100% ICA stenosis.
Conclusion
The prevalence of patients with an indication for carotid intervention in this study is lower than preceding literature. Possible explanations for a decline in carotid stenosis prevalence are improvement of secondary prevention and increasing awareness of risk factors for atherosclerosis. This more current prevalence can be used in power analysis for future research.
Trial registration number
N/A
AS15-056
STROKE IN THE MIDDLE-EAST AND NORTH AFRICA: A 2-YEAR PROSPECTIVE OBSERVATIONAL STUDY OF STROKE CHARACTERISTICS IN THE REGION. RESULTS FROM THE SITS-MENA REGISTRY
1Rashid University Hospital, Department of Neurology, Dubai, United Arab Emirates
2Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
3Karolinska Institutet, Department of Clinical Neuroscience, Stockholm, Sweden
4Mongi Ben Hamida National Institute of Neurology, Department of Neurology, Tunis, Tunisia
5Hassan II University Hospital, Department of Neurology, Fez, Morocco
6Cairo University, Department of Neurology, Cairo, Egypt
7Imam Husain Hospital- Shahid Beheshti University of Medical Sciences, Department of Neurology, Tehran, Iran
8Blida University Hospital- Franz Fanon Hospital, Department of Neurology, Blida, Algeria
9Faculty of Medical Sciences- Lebanese University, Neurology Division, Hadath, Lebanon
10King Abdulaziz Medical City, Department of Neurology, Riyadh, Saudi Arabia
11Hamad General Hospital, Department of Neurology, Doha, Qatar
12Ain Shams University Hospital, Stroke Unit, Cairo, Egypt
13King Abdulaziz University, Department of Neurology, Jeddah, Saudi Arabia
Background and Aims
Stroke incidence and mortality is reported to have increased in the Middle-East and North African (MENA) countries during the last decade.
Method
This was a prospective observational study to examine baseline characteristics of stroke patients in the MENA region and to compare the MENA vs. non-MENA stroke cohort in the SITS International Registry.
Results
Of 13822 patients with ischemic and hemorrhagic stroke registered using the SITS All Patients Protocol between June 2014 and May 2016, 5897 (43%) were recruited in MENA. The median onset-to-door time (OTD) was 5 hours (2:20-13:00), median NIH Stroke Scale (NIHSS) score was 8 (4-13), and age 65 years (56-76). Hypertension (66%) and diabetes (38%) were the prevailing risk factors. Large artery stenosis > 50% (25.3%) and lacunar strokes (24.1%) were the most common ischemic stroke etiologies. In comparison, non-MENA countries had OTD 5h50min (2:00-18:45), median NIHSS 6 (3-14), and age 66 years (56-76), with other large artery disease and cardiac embolism as the main ischemic stroke etiologies, Hemorrhagic strokes (10.0%) were less common than in non-MENA countries (13.9%). In MENA, a low proportion of patients (21%) were admitted to stroke units.
Conclusion
Stroke patients in MENA countries are slightly younger, have more often diabetes and slightly more severe ischemic strokes, commonly of atherosclerotic or microvascular etiology and less often hemorrhagic strokes. Admission to stroke units and long-term follow-up needs to be improved and it is suspected that cardiac embolism and atrial fibrillation are currently underdiagnosed in MENA countries.
Trial registration number
N/A
AS15-057
ETIOLOGIC AND PROGNOSTIC STUDY OF YOUNG ISCHEMIC STROKE IN ALGERIA
1Faculté De Médecine de Constantine, Medicine, Constantine, Algeria
Background and Aims
ischemic strokes in young adults are rare. They etiologic and prognostic have some particularities. Cervical artery dissection is the most frequently etiology; however 25 at 40% of ischemic stroke in young remain without definite causes. This study investigated the etiologic and prognostic aspects of ischemic stroke young in the region of Constantine in the east of Algeria.
Method
This is a retrospective and prospective observational study conducted at the neurology department of the University Hospital in Constantine. The criterion for inclusion was confirmed ischemic stroke by an neuroimaging and age> 15 years old and ≤ 50 years. an exhaustive exploration etiologque was achieve We study the risk factors and the etiologies according to TOAST classification. Mortality was noted at one month and NIHSS was used in our study.
Results
228 wemens and 163 men with an average age 41, 25 years. cardiac causes are the main etiologies found with 23.53%, cervical artery dissection in 12.80%,. lacunar stroke in 12.27%, atherosclerosis in 7.16% and 34.78% are undetermined cause. The main risk factor found are tobacco (17.62%), hypertension (15.06), migraine ( 7.77% ) and diabetes in 7.51%.
average NIHSS at admission was 6.6, mortality was 8.44%. 33 patients (8.44%) had one seizure during hospitalization.
Conclusion
Our study found that the main etiology of ischemic stroke in our young Algerian population remains the embolic heart disease, cervical artery dissection and ischemic lacuna. While over a third remains without a known cause hence the necessity to push the explorations to understand the mechanism and identify the etiology.
Trial registration number
N/A
AS15-058
EMBOLIC STROKES OF UNDETERMINED SOURCE IN POLISH STROKE REGISTRY
1Institute of Psychiatry and Neurology, 2nd Department of Neurology, Warsaw, Poland
2Medical University of Warsaw, Department of Experimental and Clinical Pharmacology, Warsawa, Poland
Background and Aims
We aimed to provide a descriptive analysis of embolic stroke of undetermined etiology (ESUS) population based on a long-term prospective Polish patients stroke registry.
Method
We retrospectively analyzed data collected in a detailed registry regarding consecutive patients admitted for first-ever ischemic stroke (IS) between January 2001 and December 2015. We used Org 10172 in Acute Stroke Treatment classification supplemented with ESUS criteria proposed by the Cryptogenic Stroke/ESUS International Working Group. We additionally compared patients ≤60 years and >60 years of age within the ESUS group.
Results
During the study period there were 3008 (1615 females and 1393 males) patients admitted for first-ever stroke. The most frequent cause of IS was undetermined (38.7%), followed by cardioembolic (27.7%), large artery atherosclerosis (18.2%), small vessel disease (11.9%) and other determined (3.6%). We identified 326 patients as ESUS, which accounted for 10.8% of all strokes and 28% of strokes of undetermined etiology. ESUS patients were the youngest and in 30% had ≤60 years of age. Compared to all types of stroke but for those with small vessel disease, ESUS patients were most often independent before stroke. They had the least severe neurological deficit at admission and the best outcome at discharge. ESUS patients ≤60 years were more frequently independent at discharge than ESUS patients >60 years.
Conclusion
Approximately 11% of patients from our registry met ESUS criteria. ESUS patients were the youngest, suffered the least severe strokes and had more favorable outcome at discharge than other groups except for those with small vessel disease.
Trial registration number
N/A
AS15-060
SHORT-TERM EXPOSURE TO AMBIENT FINE PARTICULATE MATTER AND THE RISK OF SPONTANEOUS INTRACEREBRAL HEMORRHAGE IN ALGARVE, PORTUGAL
1University of Algarve, Biomedical Sciences and Medicine, Faro, Portugal
2Centro Hospitalar Univeristário do Algarve, Neurology, Faro, Portugal
3University of Bergen, Department of Clinical Medicine, Bergen, Norway
4Neurosciences and Mental Health Neurology- Hospital de Santa Maria- CHLN-, EEG/Sleep Laboratory, Lisbon, Portugal
Background and Aims
The association between short-term ambient particulate matter ≤ 2.5 μm diameter (PM2.5) and spontaneous intracerebral hemorrhage (SICH) occurrence is unclear. We aimed to study the association of ambient PM2.5 with occurrence of SICH in Algarve, Portugal.
Results
308 patients were included (2010-2015); mean age 70.8 years. The mean values (μg / l) of PM2.5 were higher on the case days (Lag1: 7.76, Lag2: 7.64, Lag3: 7.74) compared to control period (Lag14-17: 6.77). For each 10 μg/ l, the likelihood of SICH increased 5.7 % (OR = 1,057. 95%CI = 1,020-1,095. P = .002). Considering the average PM2.5 from Lag1,23, the odds of SICH (P <0.05) was higher in patients > 70 years (OR = 1,064, 95% CI = 1,009-1,122); patients with pre-SICH mRS ≤ 2 (OR = 1,061, 95% CI 1,022-1,101); non lobar (OR = 1,054, 95% CI = 1,012-1,099); in the morning (OR = 1,067, 95% CI = 1,012-1,125), in the fall (OR = 1,118, 95% CI = 1,031-1,213) and winter (OR = 1,064, 95% CI = 1,002-1,129); and at low values of minimum and maximum temperature.
Conclusion
Short-term increases of PM2.5 are associated with occurrence of SICH in Algarve, a region of low ambient pollution.
Trial registration number
N/A
PROGNOSIS AND OUTCOME AFTER STROKE
AS16-001
PREVALENCE AND PREDICTORS OF 3-MONTH FATIGUE IN PATIENTS WITH TIA AND MINOR STROKE: A CASE-CONTROL STUDY
1Extremadura University Medical School, Biomedical Sciences, Badajoz, Spain
2Hospital Universitario Infanta Cristina., Stroke Center. Neurology Department, Badajoz, Spain
3Hospital de Neurorehabilitación Casaverde, Neurology Area, Mérida, Spain
4Extremadura University Medical School, Psychology and Social Anthropology Department, Badajoz, Spain
Background and Aims
The persistent and significant fatigue affects the daily life of major-stroke survivors, but the evidence suggests that transient ischemic attack (TIA) and minor stroke patients also experience significant fatigue. There are some population-based studies examining the prevalence of fatigue in patients with minor stroke and TIA and very few studies of predictors of fatigue in these ones. This study aimed to determine if fatigue prevalence in patients is different to population controls, and to explore predictors of fatigue.
Method
Ninety-two consecutive patients with minor stroke or TIA were compared with 89 controls of the same age. The Fatigue Assessment Scale (FAS) was administered to both groups to compare prevalence. Multivariate logistic regression analysis was used to determine predictors of fatigue.
Results
The prevalence of substantial fatigue was 72.8% (23.5% in controls) and extreme fatigue was 20,7% (0.0% in controls) in patients. There are not was a clear association between fatigue and age (OR 1.00; IC95%: 0.96-1.04). The only baseline variables independently associated with an increased risk of fatigue at 3 months after stroke were dyslipidemia (OR 2.10; IC95%: 103-4.30; p = 0.038), tobacco use (OR 1.86; IC95%: 0.94-3.71; p = 0.075), physical inactivity (OR 3.49; IC95%: 1.48-8.20; p = 0.01), and gender male (OR 2.10; IC95%: 1.05-4.15; p = 0.036).
Conclusion
Minor stroke and TIA patients had higher prevalence of fatigue three months after stroke than the general population sample, which may be partly explained by the stroke population being in poorer health overall. Dyslipidemia, tobacco use, physical inactivity, and gender male were independent clinical predictors of fatigue.
Trial registration number
N/A
AS16-002
PROGNOSTIC VALUE AND CAUSE OF HEADACHE AS A SYMPTOM AT ISCHEMIC STROKE ONSET
1Kharkiv Medical Academy of Postgraduate Education, Department of Neurology, Kharkov, Ukraine
2Kharkiv Stroke Center, Neurology, Kharkiv, Ukraine
Background and Aims
The aim of this study was to identify the endothelial dysfunction in patients, which is related to the development of headache in acute ischemic stroke and access predictive value of headache.
Method
We collected headache characteristics using a semi-structured questionnaire in 84 participants from the Kharkiv Acute Stroke Study within 24 hours after ischemic stroke onset and formed 2 groups: 1st – with headache (44 patients) and 2nd – without headache (40 patients). We compared impact on stroke outcomes using clinical features, including in-hospital stroke in evolution, and changes in National Institutes of Health Stroke Scale on discharge. Endothelial dysfunction was assessed by evaluating presence of desquamated endotheliocytes, estimating vasoregulation endothelial factors (nitric oxide and endothelin-1) in the blood.
Results
Compared with patients without onset headache, those with onset headache had a higher level of nitrite (3,97 ± 0,19 umol/l versus 3,13 ± 0,18 umol/l, p < 0,05), a lower level of endothelin-1 (0,57 ± 0,01 pmol/l versus 0,69 ± 0,01 pmol/l, p < 0,05), a lower level of the number of desquamated endotheliocytes in the blood (5,15 ± 0,23 versus 8,34 ± 0,26, p < 0,01), a lower frequency of stroke in evolution (3,8% versus 6,2%, p < 0,05), greater improvement in National Institutes of Health Stroke Scale score on discharge (0,10 versus - 0,22, p < 0,05).
Conclusion
Patients who experienced headache in association with ischemic stroke have a less endothelial dysfunction and a better vascular prognosis than those without concomitant headache. This may, at least partly, reflect changes in the vascular endothelium system with a high role of NO to perform headache and protective collateral circulation.
Trial registration number
N/A
AS16-003
CHARACTERISTICS ASSOCIATED WITH OUTCOME IN FIRST-EVER POSTERIOR FOSSA STROKE PATIENTS
1Charité-Universitätsmedizin, Department of Biostatistics and Clinical Epidemiology, Berlin, Germany
2Institute of Psychiatry and Neurology, Department of Radiology, Warsaw, Poland
3Charité-Universitätsmedizin, Center for Stroke Research, Berlin, Germany
Background and Aims
Factors like infarct volume, infarct location and symptom severity can considerably influence long-term outcome in posterior fossa strokes. Therapy decision can sometimes be complicated by discrepancies between infarct volume and clinical severity. We aimed to evaluate imaging and clinical parameters possibly influencing long-term outcome in first-ever posterior fossa stroke patients.
Method
Imaging was performed on a 3 T MRI scanner. Sixty-one out of 1795 patients from the observational 1000Plus and LOBI studies (clinicaltrials.org NCT00715533, NCT02077582) were enrolled meeting the inclusion criteria of first-ever posterior fossa stroke and MRI examination within 24 hours after symptom onset. Infarcts were classified as belonging to proximal, middle, or distal territory location in the posterior fossa. Good outcome was defined as modified Rankin Scale Score ≤ 1 at 3 months.
Results
The largest lesion volumes on DWI day 0 and FLAIR day 6 were found in the middle territory location with a median volume of 0.4 mL on DWI, 1.0 mL on FLAIR day 6 versus 0.1/0.3 mL in the proximal, and 0.1/0.1 mL in the distal territory location of the posterior fossa respectively. Parameters associated with poor outcome were older age (p = 0.005), higher NIHSS on admission/discharge (p = 0.016, p = 0.001), larger FLAIR day 6 lesion volumes (p = 0.013), and dysphagia (p = 0.02). There was no significant association between infarct location and mRS at day 90.
Conclusion
Infarct volume and clinical severity, but not infarct location were the main contributors to poor long-term outcome in first-ever posterior fossa strokes.
Trial registration number
N/A
AS16-004
LIPID PARADOX IN STATIN-NAIVE ACUTE ISCHEMIC STROKE
1Kaohsiung Medical University Hospital, Division of Cardiology- Department of Internal Medicine, Kaohsiung, Taiwan R.O.C
2Chang Gung University, Clinical Informatics and Medical Statistics Research Center, Keishan, Taiwan R.O.C
3University of Sydney, The George Institute for Global Health, Sydney, Australia
4Linkou Chang Gung Memorial Hospital, Department of Neurology, Kweishan, Taiwan R.O.C
Background and Aims
Lipid level is recommended the lower the better in cardiovascular disease. Lipid paradox can be seen under stressful condition in some diseases. This study wished to clarify the prognostic significance of admission lipids on mortality in acute ischemic (IS) and hemorrhagic stroke (HS).
Method
The data was collected from Stroke Registry In Chang-Gung Healthcare System (SRICHS) between 2009 and 2012. Stroke was classified into IS and hypertension-related HS. Primary outcomes were 30-day and 1-year mortality by linkage to national death registry.
Results
Among 18,268 patients, 3,746 IS and 465 HS were eligible for analysis. In IS, lower admission total cholesterol (TC<163.5 mg/dL) and lower non-high-density lipoprotein cholesterol concentrations (Non-HDL-C<130.5 mg/dL) were associated with higher 30-day (TC: HR = 1.78, p = 0.002; Non-HDL-C: HR = 1.53, p = 0.027) and 1-year mortality (TC: HR = 1.33, p = 0.006; Non-HDL-C: HR = 1.33, p = 0.008). Lower low-density lipoprotein (LDL<100 mg/dL, HR = 1.30, p = 0.01) and lower TC/HDL ratio (<4.06, HR = 1.28, p = 0.016) were associated with higher 1-year mortality. In HS, lipid profiles were not associated with mortality, but higher uric acid concentrations (UA≥8.0 mg/dL) showed significance at 30-day (HR = 4.61, p = 0.002) and 1-year mortality (HR = 3.18, p = 0.012). Higher admission fasting glucose was associated with 30-day and 1-year mortality in both IS and HS (p≤0.001) and lower admission blood pressure (BP) with 30-day and/or 1-year mortality in IS (p < 0.05). Synergic effects were found when lower lipid incorporated with higher NIHSS, lower BP and higher fasting glucose (p < 0.05).
Conclusion
Lipid paradox can be seen in statin-naïve acute IS but not HS with lower admission lipid levels being associated with higher mortality.
Trial registration number
N/A
AS16-005
HISTORY OF ASPIRIN USE DOES NOT AFFECT PROGNOSIS IN PATIENTS WITH NON-CARDIOEMBOLIC ISCHEMIC STROKE
1Queen Elizabeth Hospital, Division of Neurology- Department of Medicine, Hong Kong, Hong Kong S.A.R
Background and Aims
Aspirin treatment failure is proposed to be a risk factor for recurrent ischemic stroke. This study would like to determine the risk of ischaemic stroke recurrence, cardiovascular events and death in patients suffered from acute non-cardioembolic ischaemic stroke, with or without previous aspirin use.
Method
This study is an observational retrospective cohort study. Consecutive acute ischaemic stroke patients were recruited. The primary outcome is recurrent acute ischaemic stroke within 24 months. The secondary outcomes are any cardiovascular events as well as all causes mortality occurred within 24 months.
Results
A total of 264 acute ischaemic stroke patients were admitted during the study period. 98 were excluded because of cardioembolic cause of stroke, while 3 were excluded because they were younger than 40. Among these patients, 43 has history of aspirin use. Aspirin users are significantly older, are more likely to have history of hypertension, diabetes mellitus, hyperlipidaemia and history of cerebrovascular of ischaemic heart diseases compare to aspirin naïve patients. The recurrent stroke rate of aspirin users and aspirin naïve patients were 9.3% and 9.2% respectively. The rate of recurrent cardiovascular events of aspirin users and aspirin naïve patients were 16.3% and 15.8% respectively. Previous aspirin users have a higher mortality (20.9%) comparing to those aspirin naïve patients (10.8%) but the difference did not reach statistical significance.
Conclusion
The prognosis of acute non-cardioembolic ischaemic stroke patients with clinical aspirin failure is comparable to that of aspirin naïve patients in the current study.
Trial registration number
N/A
AS16-006
DIVERSE ISCHEMIC POSTCONDITIONING PROTOCOLS AFFECT THE INFARCTION SIZE IN FOCAL ISCHEMIC STROKE
1Chonnam National University Hospital, Neurosurgery, Gwangju, Republic of Korea
Background and Aims
Ischemic postconditioning (IPostC), induced by cycles of transient brain ischemia and reperfusion, is well known to be neuroprotective. However, no optimal single protocol for IPostC has been established because the effectiveness of the IPostC may depend on various parameters, including the species tested and the tissue characteristics. Therefore, we investigated whether different algorithms of IPostC have similar neuroprotective effects in experimental animal models
Method
We induced stroke through middle cerebral artery (MCA) suture occlusion in a focal ischemia model in mice. IPostC was conducted through repeated, brief MCA occlusion 2 min after reperfusion, followed by different ischemia/reperfusion protocols. The infarction size and functional neurological scores were measured after surgery.
Results
IPostC was conducted with different protocols, resulting in diverse effects. IPostC performed 2 minutes after reperfusion, followed by 3 cycles, significantly reduced the infarction size 3 days after stroke.
Conclusion
IPostC was confirmed to reduce infarction size as a function of the numbers of cycles of brief MCA occlusion that were performed.
Trial registration number
N/A
AS16-007
ESTIMATED GLOMERULAR FILTRATION RATE, ANEMIA AND OUTCOMES IN PATIENTS WITH ISCHEMIC STROKE
1the second affiliated hospital of Soochow University, Neurology, Suzhou, China
2Beijing Tiantan Hospital- Capital Medical University, Department of Neurology, Beijing, China
3Illinois Neurological Institute Stroke Network- Sisters of the Third Order of St. Francis Healthcare System- University of Illinois College of Medicine, Neurology, Peoria, USA
Background and Aims
Anemia is highly prevalent in patients with low estimated glomerular filtration rate (eGFR), the combined effect of anemia and low eGFR on the prognosis of outcome after stroke has not been well studied.
Method
Data of ischemicstroke patients in the prospective cohort study of China National Stroke Registry was reviewed. According to the levels of eGFR and hemoglobin, patients were categorized into four groups: low eGFR (< 60 mL/min per 1.73 m2) or normal eGFR (≥ 60 mL/min per 1.73 m2) with or without anemia. Multivariable logistic regression method was used to analyze the association between low eGFR with or without anemia and the poor functional outcome, dependence, mortality and stroke reoccurrence at 3 months and 1 year after stroke
Results
This study included 8,303 stroke patients. After adjustment for the confounding factors, low eGFR alone increased risk of mortality (Odds ratio [OR] = 1.50, 95% confidence interval [95% CI]1.14-1.97), but anemia alone was not associated with any of poor outcome at 1-year of follow up. In patients with both low eGFR and anemia, there was an increased risk of poor functional outcome (OR 1.73, 95% CI 1.30-2.29), mortality (OR 2.64, 95% CI 1.94-3.59) and stroke reoccurrence (OR 1.42, 95% CI 1.06-1.91) during 1-year of follow up, except that the dependence (OR 1.17, 95% CI 0.83-1.64).
Conclusion
Ischemic strokepatients with concurrent low eGFR and anemia had increased risks of poor functional outcome, mortality and stroke reoccurrence, but not dependence during 1-year follow up.
Trial registration number
N/A
AS16-008
EARLY PROGNOSIS AND FUNCTIONAL OUTCOME OF SPONTANEOUS INTRACEREBRAL HEMORRHAGE. A MONOCENTER STUDY
1University of Lübeck, Neurology, Luebeck, Germany
Background and Aims
Spontaneous intracerebral hemorrhage is a serious disease with poor outcome. The aims of the present study were to determine the frequency of in-hospital mortality and good functional outcome (mRS£2) as well as to investigate the associated factors in patients suffering from intracerebral hemorrhage and treated conservatively.
Method
During an 8-year period (2007–2015), 613 consecutive patients (mean age, 72 ± 13 years; female sex, 51%, median NIHSS score 10) with sICH who were admitted to the Department of Neurology at the University of Lübeck, Germany were enrolled and prospectively evaluated. Univeriate and logistic regression analyses were used to estimate the associated factors in a mono-center study.
Results
During a mean hospitalization of 12 ± 8 days, 148 patients (24%) died and 192 patients (31%) survived the sICH with good functional outcome at discharged.
The in-hospital mortality was significantly increased by a female sex (OR, 2.0; 95%-CI, 1.2-3.4; p = 0.009), NIHSS score >10 (OR, 10.5; 95%-CI, 5.6-19.5; p>0.001), previous anticoagulation (OR, 2; 95%-CI, 1.0-3.8; P = 0.032) and hemorrhage with intraventricular extension (OR, 2.8; 95%-CI, 1.7-4.7; P<0.001). Contrariwise a previous hypertension was associated with decreased in-hospital mortality (OR, 0.35; 95%-CI, 0.19−0.64; P = 0.001).
Among survivors, the good functional outcome (mRS£ 2) at discharge from hospital was significantly decreased by an age >70 (OR, 0.56; 95%-CI, 0.35−0.9; p = 0.017), NIHSS >10 at admission (OR, 0.07; 95%-CI, 0.04−0.13; P<0.001) and development of pneumonia (OR, 0.35; 95%-CI, 0.2−0.6; P<0.001).
Conclusion
Our findings may help clinicians estimating the risk of mortality and survive in patients suffering from sICH. Further studies are needed to confirm our study.
Trial registration number
N/A
AS16-009
EFFECTIVE RESTORATIVE ACTION OF NEW NOOTROPIC PREPARATIONS AFTER ISCHEMIC STROKE
1Taras Shevchenko National University of Kyiv, ESC “Institute of biology and medicine”, Kyiv, Ukraine
Background and Aims
Inflammation plays an important role in pathogenesis of ischemic stroke and other forms of ischemic brain injury. Violations of cerebral blood supply as a result of stroke lead to significant side effects that are associated with a reduction in functional activity of immune cells. Recovery of immune response is important component of ischemic disease treating. The aim of our work was to study effect of new nootropic preparations (mitocorrectin, cerebral) on immunocompetent and endothelial cells.
Method
MT-4 (T- cell line), Raji (B-cell line) and pig aortic endothelial cells (PAE) were used. Cells were incubated in the medium RPMI under standard conditions. Cytotoxic/ proliferative effect on cultured cells was determined using cytofluorymetric analysis and MTT-test.
Results
According to the study, cerebral is pro-proliferative factor for MT-4 and Raji cells, as evidenced by its ability to increase the number of cell proliferative pool (G2 / M + S) in 1.2 and 1,8 times respectively and decrease the level of apoptosis in 2 times compared with control. In addition, cerebral showed pro-angiogenic properties on endothelial cells in 1.5-fold increase of cell proliferation compared with the control.
It has been found that the effect of mitocorrectin on cultured endothelial cells for 24 h resulted in an increase 1.8-fold in the population of proliferative cells pool under the influence of mitocorrectin. While mitocorrectin showed little immunomodulating action in relation to immunocompetent cells.
Conclusion
Cerebral showed expressed immunomodulating and pro-angiogenic effects and can be effective to recovery of immune response, which is important in post-stroke period at ischemic complication.
Trial registration number
N/A
AS16-010
PNEUMONIA INCREASES MORTALITY RISK IN PATIENTS ADMITTED WITH ACUTE ISCHEMIC STROKE INDEPENDENTLY OF STROKE SEVERITY
1AHEPA University Hospital, First Propedeutic Department of Internal Medicine, Thessaloniki, Greece
Background and Aims
Patients admitted with acute ischemic stroke have increased risk for pneumonia bit it is unclear whether pneumonia simply reflects the severity of stroke or independently affects the outcome. The aim of the present study was to evaluate this association.
Method
We prospectively studied 922 consecutive patients admitted with acute ischemic stroke (42.2% males, age 79.6 ± 6.9 years). The severity of stroke was assessed at admission with the National Institutes of Health Stroke Scale (NIHSS). The outcome was assessed with dependency rates at discharge (modified Rankin scale 2-5) and in-hospital mortality.
Results
During hospitalization, 113 patients developed pneumonia (12.3% of the total study population). Patients who developed pneumonia had higher rates of dependency at discharge than patients who did not develop pneumonia (89.7% vs. 58.4%, respectively; p < 0.001). Independent risk factors for dependency at discharge were age (relative risk (RR) 1.08, 95% confidence interval (CI) 1.04-1.12, p < 0.001), history of prior ischemic stroke (RR 1.89, 95% CI 1.22-2.94, p < 0.005) and NIHSS at admission (RR 1.49, 95% CI 1.39-1.62, p < 0.001). Patients who developed pneumonia had higher in-hospital mortality rates than patients who did not develop pneumonia (43.4% vs. 4.7%, respectively; p < 0.001). Independent risk factors for in-hospital mortality were diastolic blood pressure at admission (RR 1.05, 95% RR 1.03-1.08, p < 0.001), NIHSS at admission (RR 1.18, 95% CI 1.14-1.23, p < 0.001) and pneumonia (RR 5.44, 95% CI 2.54-11.65, p < 0.001).
Conclusion
In patients admitted with acute ischemic stroke, the development of pneumonia during hospitalization increases the risk of in-hospital mortality independently of stroke severity.
Trial registration number
N/A
AS16-011
IS FUNCTIONAL OUTCOME DIFFERENT IN POSTERIOR AND ANTERIOR CIRCULATION STROKE?
1Krankenanstalt Rudolfstiftung, Neurology, Vienna, Austria
2Danube University Krems, Clinical Neuroscience, Krems, Austria
3Medical University VIenna, Neurology, Vienna, Austria
4Krankenhaus Barmherzige Brüder Vienna, Neurology, Vienna, Austria
5Kepleruniversitätsklinikum Linz, Neurology 2, Linz, Austria
6Medical University Innsbruck, Neurology, Innsbruck, Austria
Background and Aims
Background
There is limited evidence whether functional outcome of posterior circulation stroke (PCS) is comparable to that of anterior circulation stroke (ACS).
Methods
We analyzed the 3-month functional outcome measured by the modified Rankin Scale (mRS) of patients with acute ischemic stroke/TIA enrolled into the Austrian Stroke Unit Registry. Infarct localization was stratified according to the Oxfordshire Community Stroke Project Classification. Propensity score matching was used to control for covariate imbalances and to match patients with PCS/ACS. Based on matched patients proportional odds models for different patient populations were calculated.
Results
9208 patients (4604 PCS/4604 ACS) were analyzed, 954 of those (477 in each group) were treated with intravenous thrombolysis (IVT). Overall, PCS was associated with worse functional outcome compared to ACS (OR 1.19, 95%CI 1.1-1.28, p < 0.0001). In particular, functional outcome was worse in PCS with ODT>270 minutes (OR 1.34, 95%CI 1.17-1.54, p < 0.0001) or in PCS with unknown ODT (OR 1.26, 95%CI 1.13-1.42, p < 0.0001), however, we did not detect any difference in functional outcome between ACS and PCS in patients with an ODT≤270 minutes (1-180 minutes: OR 0.92, 95%CI 0.78-1.09, p = 0.3554; 181-270 minutes: OR 1.04, 95%CI: 0.79-1.37, p = 0.7689). In patients treated with IVT, functional outcome was not significantly different between PCS and ACS.
Conclusion
In our study, PCS was associated with worse outcome compared to the anterior circulation if patients arrived later than 4.5 hours or if the symptom onset is unknown. Therefore, patients triage needs to implement symptoms found in patients with PCS.
Trial registration number
N/A
AS16-012
INSULIN RESISTANCE AND CLINICAL OUTCOMES AFTER ACUTE ISCHEMIC STROKE
1Kyushu University, Department of Health Care Administration and Management, Fukuoka, Japan
2Kyushu University, Department of Medicine and Clinical Science, Fukuoka, Japan
3Kyushu University, Department of Epidemiology and Public Healt, Fukuoka, Japan
4Kyushu University, Center for Cohort Studies, Fukuoka, Japan
Background and Aims
This study aimed to determine whether insulin resistance is associated with clinical outcomes after acute ischemic stroke.
Method
We enrolled 4655 patients with acute ischemic stroke (age 70.3 ± 12.5 years [mean ± standard deviation]; 63.5 % men) who had been independent before admission, were hospitalized in 7 stroke centers in Fukuoka, Japan from April 2009 to March 2015, and did not receive insulin therapy during hospitalization. Homeostasis model assessment of insulin resistance (HOMA-IR) score was calculated by using fasting blood glucose. Study outcomes were neurological improvement (≥4-point decrease in National Institutes of Health Stroke Scale score or score 0 at discharge), poor functional outcome (modified Rankin scale ≥3 at 3 months), and 3-month prognosis (stroke recurrence and all-cause mortality). Logistic regression analysis was used to evaluate the association of HOMA-IR score and the clinical outcomes.
Results
HOMA-IR score was negatively associated with neurological improvement (odds ratio [95% confidence interval], 0.68 [0.56–0.83], top quintile vs. bottom quintile) and positively with poor functional outcome (2.02 [1.52–2.68], top quintile vs. bottom quintile) after adjusting for potentially confounding factors, including diabetes and body mass index. HOMA-IR was not associated with stroke recurrence or mortality within 3 months of onset. The associations were maintained in non-diabetic or non-obese patients.
Conclusion
These findings suggest that insulin resistance was independently associated with poor neurological recovery and subsequently poor functional outcome without increasing the risk of short-term stroke recurrence or mortality in patients with acute ischemic stroke.
Trial registration number
N/A
AS16-013
MORTALITY AND DISABILITY IN STROKE PATIENTS IN ROMANIA : QUALITY ASSESSMENT OF STROKE CARE INSIDE RES-Q REGISTRY AND ESO- EAST PROJECT
1University Hospital Buharest, Neurology, Bucharest, Romania
2Institute of Cerebrovascular Diseases, Neurology, Bucharest, Romania
3Cluj Napoca Emergency County Hospital, Neurology, Cluj Napoca, Romania
4Clinical Hospital of Emergency Oradea, Neurology, Oradea, Romania
5Elias University Emergency Hospital, Neurology, Bucharest, Romania
6Emergency Clinical Hospital “Prof Dr Nicolae Oblu”, Neurology, Iasi, Romania
7Clinical County Emergency Hospital Timisoara, Neurology, Timisoara, Romania
8Colentina Clinical Hospital, Neurology, Bucharest, Romania
9Emergency County Hospital Suceava, Neurology, Suceava, Romania
10Mures County Clinical Emergency Hospital, Neurology, Targu Mures, Romania
Background and Aims
To perform the first assessment of the quality of stroke care in Romania based on the 21 quality indicators. We analyzed the data from RES-Q Registry as a part of ESO – EAST project.
Method
Romania participated with 10 centers, collecting data from 1060 stroke patients discharged from the hospitals between 1-31 March 2017.
Results
Romania occupied the fourth place, after Czech Republic (26 centers, 2100 patients), Poland (28 centers, 1465 patients) and Ukraine (100 centers, 1300 patients). The large number of patients reflects the high incidence of stroke in Romania. Ischemic stroke represented 88,27%; the rate of recanalization treatment (pharmacologic or endovascular) was low, only 2.26%. Intrahospital mortality was 15,9%, with large differences between centers. Among the identified causes were the high severity of stroke upon admittance, the insufficient number of beds in the stroke units and the lack of a proper dysphagia screening in the first 24 hours (2,08% ), the later leading to a large number of deaths due to bronchopneumonia. The destination at discharge was ”home” for 73,02% of survivors, with only 6.04% reffered for neuro-rehabilitation, although more than 50% of the patient could not walk independently. For this item we identified two determinants: lack of a specialized team or insufficient human resource inside the hospitals, and more important, lack of specialized units for neuro- rehabilitation in our country.
Conclusion
The data will be registered again in March 2018 and will be reffered to the Ministry of Health in order to improve quality of stroke care in Romania
Trial registration number
N/A
AS16-014
ANEMIA AT ADMISSION IS ASSOCIATED WITH POOR CLINICAL OUTCOME IN CEREBRAL VENOUS THROMBOSIS
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Helsinki University Central Hospital, Neurology, Helsinki, Finland
3Institute of Neuroscience and Physiology- Sahlgrenska Academy at University of Gothenburg, Neurology, Gothenburg, Sweden
Background and Aims
Anemia is a predictor of poor outcome in ischemic and hemorrhagic stroke. We examined this relationship in patients with cerebral venous thrombosis (CVT).
Method
Consecutive adult patients with CVT were included from three academic hospitals between 1987 and 2016. Anemia at admission was scored according to World Health Organization definitions (men <8.1 mmol/L, non-pregnant women <7.5 mmol/L, pregnant women <6.9 mmol/L). Patients were excluded if they had missing baseline hemoglobin. Poor outcome was defined as a modified Rankin Scale (mRS) score ≥3 at last follow-up. Mortality was also analyzed separately. We adjusted for age, sex, cancer, oral contraceptive use, and center of recruitment.
Results
Out of 546 patients, 483 were eligible. Median age was 42 (IQR 28-54) and 67% were women. Anemia at admission was present in 118 patients (24%). Patients with anemia more often had a history of cancer (20% vs. 7%). Median duration of follow-up was 6 months (IQR 5-7). Overall, 76 patients (16%) had a poor outcome. Patients with anemia had a higher risk of mRS ≥3 at follow-up (aOR 2.4, 95% CI 1.4-4.2). We found no association with mortality (aOR 1.7, 95% CI 0.8-3.8).
Conclusion
Anemia at admission is frequent and associated with poor clinical outcome in patients with CVT.
Trial registration number
N/A
AS16-015
PREMORBID MALNUTRITION IDENTIFIED BY THE NUTRITIONAL RISK INDEX IS ASSOCIATED WITH THE RISK OF INFECTION IN PATIENTS WITH ISCHEMIC STROKE
1Seoul National University Hospital, Neurology, Seoul, Republic of Korea
Background and Aims
Infection is a common complication after stroke. Furthermore, malnutrition is associated with unfavorable outcome in patients with stroke. Therefore, we investigated that premorbid undernutrition identified by objective method, Nutritional Risk Index (NRI) was related to the risk of infection after ischemic stroke.
Method
A consecutive 852 patients who were admitted within 7 days after ischemic stroke onset between October 2010 and October 2015 were included. We assessed initial nutritional status using NRI, and NRI formula as follows: NRI = (1.519×serum albumin, g/dL) + {41.7×present weight/ideal body weight (kg)}. The patients were categorized into three groups on the basis of NRI [No risk (NRI >97.5), Moderate risk (NRI 83.5–97.5), and Severe risk (NRI <83.5)]. We compared the clinical characteristics and NRI according to the presence of infection.
Results
Among the included patients (mean age, 67.7 years, male, 60.6%), 85 (10.0%) patients experienced infection during hospitalization. The proportion of lower NRI patients (Moderate and Severe risk) was significantly greater in the infection group (45.9% vs. 17.9% and 10.6% vs. 2.7%, P <0.001). Moreover, higher NRI patients were less likely to be admitted to the intensive care unit (P = 0.004). A multivariate analysis revealed that lower NRI groups had a higher risk of infection [Odds ratio (95% confidence interval); Moderate risk 3.98 (1.95–8.13); Severe risk 4.21 (1.10– 6.14), P for trend = 0.001].
Conclusion
Our study demonstrated that lower NRIs predicted infection complications and severe infection after ischemic stroke. This suggests that assessment of malnutrition could be a useful predictor for infection following stroke.
Trial registration number
N/A
AS16-016
HIGH NEUTROPHIL TO LYMPHOCYTE RATIO IS ASSOCIATED WITH STROKE-ASSOCIATED PNEUMONIA
1Seoul National University Hospital, Neurology, Seoul, Republic of Korea
2Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Neurology, Seoul, Republic of Korea
Background and Aims
Although there are a variety of risk factors and predictive models of stroke-associated pneumonia (SAP), more objective and easily accessible markers are still needed. In this study, we evaluated the relationship between the neutrophil to lymphocyte ratio (NLR) and SAP in acute ischemic stroke patients.
Method
We assessed 1,317 consecutive acute ischemic stroke patients. SAP was defined according to the modified Centers for Disease Control and Prevention criteria. The severity of pneumonia was rated using scores from the Pneumonia Severity Index (PSI), the quick Sequential Organ Failure Assessment (qSOFA), and the Acute Physiology and Chronic Health Evaluation (APACHE) II. The NLR was calculated after dividing absolute neutrophil counts over absolute lymphocyte counts.
Results
Among the total patients, SAP occurred in 112 (9.0%) patients. Using a multivariate analysis, NLR [adjusted OR = 1.55; 95% confidence interval, 1.14-2.10, P = 0.005] remained significant after adjusting confounders. In addition, age, atrial fibrillation, previous stroke history, initial National Institutes of Health Stroke Scale score, and high-sensitivity C-reactive protein were also significant, independent of NLR. NLR was higher in severe pneumonia groups when we assessed it by all PSI (P < 0.001), qSOFA (P < 0.001), and APACHE II scores (P = 0.004). Furthermore, patients who had SAP showed worse clinical outcomes both during hospitalization and after discharge.
Conclusion
We demonstrated that a higher NLR predicted SAP in acute ischemic stroke patients. The NLR would help to select high-risk patients in time and provide clues for further studies about preventive antibiotic therapy.
Trial registration number
N/A
AS16-017
USEFULNESS OF COMBINED WHITE BLOOD BELL COUNT AND BLOOD GLUCOSE FOR PREDICTING IN-HOSPITAL OUTCOMES IN ACUTE ISCHEMIC STROKE
1The Second Affiliated Hospital of Soochow University, Department of Neurology, Suzhou, China
2School of Public Health- Medical College of Soochow University, Department of Epidemiology, Suzhou, China
3The Affiliated Wujiang Hospital of Nantong University, Department of Neurology, Suzhou, China
4University of New South Wales, The George Institute for Global Health, Sydney, Australia
5Suzhou Hospital Affiliated to Nanjing Medical University, Department of Neurology, Suzhou, China
Background and Aims
We investigated the association between combination effect of white blood cell (WBC) count and blood glucose upon hospital admission and in-hospital mortality and pneumonia in acute ischemic stroke (AIS) patients.
Method
A total of 3,124 AIS patients enrolled from December 2013 to May 2014 across 22 hospitals in Suzhou city were included. We divided patients into 4 groups: NWNG (normal WBC count and normal glucose), NWHG (normal WBC count and higher glucose), HWNG (higher WBC count and normal glucose) and HWHG (higher WBC count and higher glucose). Cox proportional hazard and logistic model was used to estimate the effect of combination effect of WBC count and blood glucose on all-cause in-hospital mortality and pneumonia in AIS patients.
Results
Patients with HWHG were associated with a 2.89-fold increase in the risk of in-hospital mortality in comparison to NWNG (adjusted HR 2.89; 95% CI, 1.59–5.23; P-trend <0.001) after adjusting for potential covariates. The risk of pneumonia is significant higher in patients with HWHG comparison to those with NWNG (adjusted OR 2.62; 95% CI, 1.67–4.10; P-trend <0.001). The C-statistic of the combination of WBC count and blood glucose was significantly larger than WBC count or blood glucose alone for in-hospital mortality and pneumonia (all p < 0.01).
Conclusion
High WBC count with high blood glucose levels at admission was independently associated with in-hospital mortality and pneumonia in AIS patients. Moreover, the combination of WBC count and blood glucose appeared to be a better predictor than WBC count or blood glucose alone.
Trial registration number
N/A
AS16-018
THE CHANGE IN CIRCULATING INSULIN-LIKE GROWTH FACTOR I (IGF-I) AFTER ISCHEMIC STROKE IS INDEPENDENTLY ASSOCIATED WITH OUTCOME
1Institute of Medicine, Department of Internal Medicine, Gothenburg, Sweden
2Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
3Hunter Medical Research Institute- University of Newcastle, x, Newcastle, Australia
4Institute of Biomedicine, Department of Clinical Genetics, Gothenburg, Sweden
Background and Aims
Insulin-like growth factor I (IGF-I) has neuroprotective and regenerative effects in experimental ischemic stroke (IS). However, observational studies in IS patients have shown varying associations for IGF-I with outcome, which may be due to that changing serum IGF-I (s-IGF-I) are more important than absolute s-IGF-I. We investigated whether decreases in s-IGF-I between the acute time point (median 4 days) and three months (ΔIGF-I, further transformed into ΔIGF-I-quintiles, ΔIGF-I-q) were associated with IS severity and outcome.
Method
In the Sahlgrenska Academy Study on Ischemic Stroke (SAHLSIS), Gothenburg, Sweden, IS patients with s-IGF-I measurements available were included (n = 354; 65% males, mean age 55 years). Baseline stroke severity was evaluated by the National Institutes of Health stroke scale (NIHSS) and converted into NIHSS-quintiles (NIHSS-q). Outcome was assessed using the modified Rankin Scale (mRS) at 3 and 24 months.
Results
Generally s-IGF-I decreased (positive ΔIGF-I), but in the most severe NIHSS-q, s-IGF-I did not change. After correction for sex and age the 3rd ΔIGF-I-q showed the greatest association to mRS 0-2 [Odds ratio, (OR) 5.11, 95% confidence interval (CI) 2.19-12.0], and after 24 months the 5th ΔIGF-I-q (OR 3.63, 95% CI 1.40-9.38). The associations remained significant after multivariate correction for diabetes, smoking, hypertension and hyperlipidemia after 3 months, but were reduced to trends (p = 0.057) after 24 months.
Conclusion
This establishes that a post-stroke s-IGF-I decrease from day 4 after IS until three months, is independently associated with favorable IS outcome after 3 months. The causality is however uncertain and discussed.
Trial registration number
N/A
AS16-019
PREVALENCE AND PREDICTORS OF POSTTRAUMATIC STRESS FOLLOWING TRANSIENT ISCHEMIC ATTACK
1University of Heidelberg, Department of Neurology, Heidelberg, Germany
2University of Heidelberg, Department of General Internal Medicine and Psychosomatics, Heidelberg, Germany
Background and Aims
Transient ischemic attack (TIA) increases the risk for posttraumatic stress disorder (PTSD), but predictors of posttraumatic stress following TIA are largely unknown. We investigated prevalence and predictors of posttraumatic stress during the hyperacute phase and after three months in TIA patients with special emphasis on psychosocial resilience factors.
Method
Consecutive hospitalized TIA patients were prospectively included into this longitudinal investigation (05/2016-06/2017). Sociodemographic variables, clinical characteristics and common cerebrovascular risk factors were assessed during hospitalization (T1). Posttraumatic stress, anxiety and depression were assessed at T1 and after three months (T2). Potential psychosocial predictors of PTSD (peritraumatic dissociation, social support, sense of coherence, mindfulness and attachment style) were estimated via self-rating questionnaire at T1.
Results
Overall 73 patients were enrolled at T1 (median age 69.0 years (IQR: 58-77); 63% male; median ABCD2 score 4 (IQR 3-5)). Median posttraumatic stress score at T1 was 4.0 (IQR 2.0-7.0), indicating mild symptoms. Follow up data (T2) were available in 61 patients (83.6%); 15 of these (24.6%) were classified as having PTSD. These patients were younger (p < 0.001), suffered less often from arterial hypertension (p = 0.023) and atrial fibrillation (p = 0.036), had lower ABCD2 scores (p = 0.012) and were more often active smokers (p = 0.011). Based on hierarchical regression, age, psychiatric history, peritraumatic dissociation and social support at T1 predicted posttraumatic stress severity at T2. Sense of coherence and mindfulness improved the model, attachment style did not.
Conclusion
Posttraumatic stress is common after TIA. Factors characterizing patients at risk and pointing towards supportive interventions should be further explored.
Trial registration number
N/A
AS16-020
POST-STROKE HYPERGLYCEMIA AND GLUCOSE VARIABILITY: THE KEY FACTORS UNDERLYING POOR OUTCOMES IN PATIENTS WITH DIABETES MELLITUS
1La Paz University Hospital, Neurology, Cáceres, Spain
2La Paz University Hospital, Neurology, Madrid, Spain
3Sant Pau y Santa Creu, Neurology, Barcelona, Spain
4La Paz University Hospital, Endocrinology, Madrid, Spain
5Navarra General Hospital, Neurology, Navarra, Spain
6Donostia Hospital, Neurology, Donostia, Spain
7Basurto Hospital, Neurology, Bilbao, Spain
8San Pedro de Alcántara Hospital, Neurology, Cáceres, Spain
9Gregorio Marañón University Hospital, Neurology, Madrid, Spain
10La Paz University Hospital, Biostatistic, Madrid, Spain
Background and Aims
Diabetes Mellitus (DM) has been identified as a prognosis factor of poor outcome after ischemic stroke (IS) but the mechanism underlying it has not been elucidated yet. We analysed the influence of DM, post-stroke hyperglycaemia, glucose variability (GV) and HbA1c in the prognosis of IS.
Method
Secondary analysis of the GLIAS II study. Acute stroke patients were classified into two study groups: DM group (patients with previous history of DM) and a non-DM group. Capillary finger-prick glucose levels were measured every 4 hours the first 48 hours after a IS. Glycaemia >155mg/dL was the cut-off point of post-stroke hyperglycemia. GV was measured by the standard deviation (SD) of the mean glucose values. HbA1c was tested in all patients. The outcomes were death or dependency and mortality at 90 days.
Results
213 patients were included. 64 (30%) had a previous history of DM. No differences in death or dependency (mRS score >2: 31.7% DM vs. 26.4% non-DM; P = .500) at three months were found. The DM group showed a trend to higher mortality (12.7 % vs. 5.7%, P = .096). The logistic regression analysis adjusted by the stroke severity showed that GV and post-stroke hyperglycaemia were independently associated with mortality at three months. Post-stroke hyperglycemia was also associated with higher risk of death or dependency. DM and HbA1c were not related with the outcome.
Conclusion
The presence of post-stroke hyperglycaemia and GV were associated with poor prognosis after IS independently of the diagnosis of DM and HbA1c values.
Trial registration number
N/A
AS16-021
PREDICTORS OF RECOGNISING, EARLY AND RIGHT THERAPY OF ISCHEMIC STROKE AND FOLLOW UP
1Evangelical Hospital Unna, Neurology, Unna, Germany
2University of Duisburg-Essen, Medicin, Essen, Germany
3St. Marienhospital, Neurology, Luenen, Germany
Background
Even though effekt of rekanalisation therapies for acute stroke has been proved to be highly effektive, most of stroke patients still reaches hospitals outside the time window
Aims
We aimed at identifying factors decisive for timely arrival at the hospital of patients with acute stroke within the therapeutic time window.
Method
In two regional stroke units in North-Rhine-Westfalia, Germany 895 consecutive patients with ischaemic stroke or TIA were surveyed after admission to hospital and 3 months later.
Results
Only 44.9 % of subjects reached the hospital within 4 hours and 54% within 6 hours, respectively. 12.3% received rTPA, 3.1% thrombectomy. Patients who notified emergency service were more likely to arrive in due time (OR 2.3 95% CI [1.1-4.9]). Knowledge of stroke symptoms (OR = 1.2 95% CI [1.1-1.4]) and private health insurance (OR = 3.9 95% CI [1.1-13.9]) were associated with a timely arrival.
At discharge 46.8 % of timely arrived patients were symptom free compared to 30.9% of those who arrived late the (Chi-Quadrat = 27.8, df = 6, p = 0.001). Three months later, clinical outcome of timely arrived patients still was better (Chi-Quadrat = 3.66, df = 6, p = 0.72).
Conclusion
Despite free access to medical care the acute treatment of stroke in Germany is still insufficient. More than a half of stroke victims arrive too late and do not receive adequate treatment. The results call for public awareness campaign in order to increase the number of timely arriving stroke patients.
Trial registration number
N/A
AS16-022
EARLY IDENTIFICATION OF HIGH-RISK TIA OR MINOR STROKE USING ARTIFICIAL NEURAL NETWORK
1Prince of Wales Hospital- The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Sha Tin, Hong Kong S.A.R
2The Chinese University of Hong Kong, Shenzhen Research Institute, Shenzhen, China
3Chinese Academy of Sciences, Shenzhen Institutes of Advanced Technology, Shenzhen, China
4The Second Affiliated Hospital of Guangzhou Medical University, Department of Neurology, Guangzhou, China
Background and Aims
The risk of recurrent stroke following a transient ischemic attack (TIA) or minor stroke is high. The accuracies of commonly used scoring systems to predict stroke recurrence in such patients are limited. In this study, we investigated the efficacy of artificial neural network (ANN) in identifying patients at high risk of stroke after an acute TIA or minor stroke.
Method
Consecutive patients with acute TIA or minor stroke presenting at a tertiary hospital during a two-year period were recruited. We collected the demographics, and clinical and imaging data at baseline. The primary outcome was recurrent ischemic stroke within 1 year. We applied an ANN model to predict recurrent stroke based on 19 independent variables obtained at baseline, with a learning algorithm based on back-propagation. A 5-fold cross-validation approach was employed to testing the model.
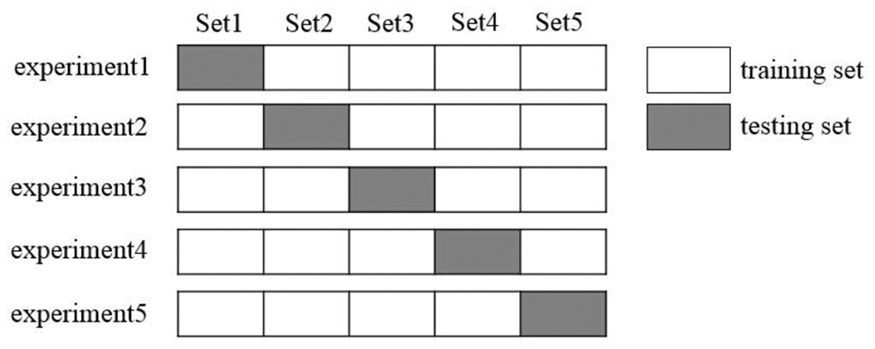
Results
A total of 451 acute TIA or minor stroke patients were enrolled. Forty (8.9%) patients had a recurrent ischemic stroke within 1 year. Another 40 patients were randomly selected from the remaining 411 patients with no recurrent stroke, for training and testing of the ANN model. The median sensitivity, specificity and accuracy of the ANN model to predict recurrent stroke at 1 year, among the 5 attempts of cross-validation, was 75%, 85.7% and 76.3%, respectively.
Conclusion
This pilot study indicated that an ANN could be an effective method in early risk stratification of acute TIA or minor stroke patients. Further studies are warranted for verification and improvement of the current ANN model.
Trial registration number
N/A
AS16-023
ALTERED BARORECEPTOR SENSITIVITY AND HEART RATE VARIABILITY AFTER STROKE PREDICT INCREASED BLOOD PRESSURE VARIABILITY
1University of East Anglia, Ageing and Stroke Medicine, Norwich, United Kingdom
2University of Aberdeen, Ageing Clinical & Experimental Research Team, Aberdeen, United Kingdom
Background and Aims
Increased beat-to-beat blood pressure variability (BPV) is associated with a poor prognosis post-stroke. Cardiac baroreceptor sensitivity (BRS) and heart rate variability (HRV) are reduced after stroke and beat-to-beat BPV increased. As baroreceptors regulate short-term blood pressure (BP) stability, impaired BRS may be a causative mechanism for increased beat-to-beat BPV after stroke.
Method
Patients with TIA or mild stroke (N = 158), of recent onset, underwent 10 minutes of beat-to-beat BP recording with measurement of BRS and HRV. Systolic, diastolic, and mean arterial BPV were derived as the standard deviation, coefficient of variation, and average real variability (ARV). Pearson’s rho was used to assess correlations between BRS, HRV, and BPV indices. Stepwise multiple regression was performed to investigate if BPV was predicted by BRS or HRV after accounting for other factors known to influence BPV.
Results
Mean low frequency HRV was 591.3 ± 998.0ms2, high frequency HRV 704.9 ± 1322.3ms2, and BRS 11.7 ± 8.8ms/mmHg. There were moderate correlations between high frequency HRV and diastolic ARV (r = 0.53, p < 0.001) and mean arterial ARV (r = 0.43, p < 0.001), and between BRS and diastolic ARV (r = 0.36, p < 0.001). Other correlations were weak or non-significant. After stepwise regression increased systolic, diastolic and mean arterial ARV were predicted by high frequency HRV and stroke diagnosis, with systolic BP ARV also related to changes in BRS.
Conclusion
HRV and BRS were correlated with beat-to-beat ARV and both were predictors of increased BPV in some models. Strategies to improve cardiac BRS and reduce BPV early post-stroke may prove important therapeutically.
Trial registration number
N/A
AS16-025
IMPACT OF ANTI – NMDAR GLUN1 ANTIBODIES ON LONG-TERM CARDIOVASCULAR RISK AFTER STROKE – THE PROSPECTIVE COHORT WITH INCIDENT STROKE BERLIN (PROSCIS-B)
1Center for Stroke Research Berlin CSB, Neurologie, Berlin, Germany
2Deutsches Zentrum für Neurodegenerative Erkrankungen, Klinik für Neurologie mit Experimenteller Neurologie, Berlin, Germany
Background and Aims
Anti-N-Methyl-D-Aspartat-Receptor (NMDAR) antibodies have been repeatedly measured in serum of healthy subjects without a neuropsychiatric disease. A previous study demonstrated smaller delta MRI lesions in anti-NMDAR antibody seropositive compared to seronegative stroke patients. In the present work, we aimed to evaluate the association between anti-NMDAR GluN1 antibodies and long–term cardiovascular risk in ischaemic stroke patients.
Method
Data from the PROSpective Cohort with Incident Stroke Berlin (PROSCISB; NCT01363856) was used. We included patients with mild to moderate stroke events (NIHSS ≤ 15). Anti-NMDAR GluN1 antibodies were measured with cell-based assays. The primary outcome was a combined vascular endpoint defined as either recurrent stroke, myocardial infarction, or all-cause mortality up to 3 years after stroke. A Kaplan Meier survival curve was used to show the time-to-event for patients with and without such antibodies. Cox regression analysis adjusted for potential confounders (age, sex, cardiovascular-risk factors, stroke severity and stroke aetiology) was used to obtain Hazard ratios for cardiovascular risk in seropositive patients.
Results
We included 583 first-ever ischaemic stroke patients with antibody measurement (Mean age: 67, 39% female). Of those 13% (76) were anti-NMDAR GluN1 antibody seropositive (IgM: n = 49, IgA: n = 43, IgG: n = 2, Titer ≥ 1:10). We recorded 95 cardiovascular events (recurrent stroke: n = 43, MI: n = 5, all-cause mortality: n = 47). In an adjusted Cox regression model, 3-year cardiovascular risk was increased in anti-NMDAR GluN1 seropositive patients (HR:1.8 95%CI:1.1-3.0).
Conclusion
Our study showed that the presence of anti-NMDAR GluN1 antibodies in the acute phase of ischaemic stroke is independently associated with increased long-term cardiovascular risk.
Trial registration number
NCT01363856
AS16-026
IS THE BRUSH SIGN A RADIOLOGICAL PREDICTOR OF POORER CLINICAL OUTCOME IN ISCHEMIC STROKE?
1Hôpital Saint Joseph, Neurology, Paris, France
2Hopital Henri Mondor, Radiology, Creteil, France
3Hôpital Saint Joseph, Centre de recherche clinique, Paris, France
Background and Aims
The brush sign (BS) refers to hypointense lines along the course of subependymal and medullary veins in the deep hemispheric white matter on MRI susceptibility weighted sequences (SWS). It was described in patients with MCA ischemic stroke, but its clinical relevance remains uncertain.
Method
Patients admitted to the Stroke Unit at Saint Joseph Hospital, Paris, between May 2014 and December 2015 for a MCA ischemic stroke and with early (< 24h of stroke onset) high-quality MRI-SWS were included. We assessed whether the BS could predict an unfavorable outcome at 3 months according to the modified Rankin Scale (mRS). NIHSS at admission and MCA occlusion on MRI were also considered. In this paper, only results of patients not eligible for hyperacute revascularization are presented.
Results
A total of 122 patients were included, 58 of which had mRS notified at 3 months. Proportion of patients with a good outcome (mRS 0–2) was significantly lower in the BS group compared to the Non Brush sign (NBS) group (13.8% vs 65.5%, OR: 4.75 p = 0.019). Subsequent analyses concerned the 122 patients. Mean NIHSS at admission was significantly higher in the BS group (12.4 [1-25] vs. 4.9 [0-21], p < 0.001) and M1 or M2 occlusions were significantly more frequent (28.7% vs 3.2%, OR: 41.12 p < 0.001 and 10.7 % vs 3.2%, OR: 11.75 p < 0.001, respectively).
Conclusion
BS seems to be a powerful radiological predictor of poorer clinical outcome for MCA ischemic stroke patients, at least for those who cannot benefit from hyperacute revascularization procedures.
Trial registration number
N/A
AS16-027
RECURRENT RATE OF STROKE AFTER RT-PA TREATMENT
1faculty of medicine- khon kaen university, medicine, khon kaen, Thailand
2Faculty of Medicine- Khon Kaen University- Khon Kaen- Thailand, Department of Medicine, khon kaen, Thailand
Background and Aims
Thrombolytic therapy is a standard treatment of acute ischemic stroke and there is limited data of recurrent stroke rate after thrombolytic treatment. To study prevalence, duration and risk factor of recurrent stroke compared between patients treated with thrombolytic therapy (recombinant tissue plasminogen activator; rt-PA) and patients without thrombolytic therapy.
Method
Retrospective analytical study by retrieving data from the National Health Security Office database, Thailand between 1st October 2011 and 30th September 2014.
Results
The total 120,545 acute ischemic stroke patients; 4,610 (3.82%) patients were treated with rt-PA and 115,935 (96.18%) were not treated with rt-PA. The difference of recurrent stroke rate between rt-PA group versus non-rt-PA group is not significant (7.0% (323/4,610) versus 7.33% (8,502/115,935); p value = 0.33). Recurrent stroke patients in rt-PA group were ischemic stroke 88.54% (286/323) and hemorrhagic stroke 11.46% (37/323). Recurrent stroke patients in non-rt-PA group were ischemic stroke 86.38% (7,344/8,502) and hemorrhagic stroke 13.62% (1,158/8,502) during 1-year follow up period. Mean duration of recurrent ischemic stroke and hemorrhagic stroke in non-rt-PA group were 8.4 month (95%CI: 7.1-10.6) and 8.9 month (95%CI: 8.6-9.3) respectively.
Conclusion
Mean duration of recurrent stroke in both groups were around 8 months except in rt-PA treated group with hemorrhagic stroke recurrence was 5.5 months.
Trial registration number
N/A
AS16-028
EFFECTS OF CILOSTAZOL ON SEVERITY AND FUNCTIONAL OUTCOME IN ISCHEMIC STROKE: A PRELIMINARY REPORT
1Fukuoka Kieikai Hospital, Stroke Center, Fukuoka, Japan
2Steel Memorial Yawata Hospital, Stroke Center, Kitakyushu, Japan
3Kyushu Central Hospital, Department of Neurosurgery, Fukuoka, Japan
4Jichi Medical University, Division of Neurology- Department of Medicine, Shimotsuke, Japan
Background and Aims
Antiplatelet therapy is the global standard for secondary prevention of non-cardioembolic ischemic stroke.
Method
From 2008 to 2013, 1287 patients were admitted within 7 days after the onset of stroke. A total of 666 patients with a modified Rankin Scale (mRS) score of 0 prior to ischemic events were included in this study.
Results
Prior to ischemic events, 119, 28, 25, and 8 patients were prescribed aspirin, cilostazol, clopidogrel, and ticlopidine, respectively. The National Institutes of Health Stroke Scale score on admission (aNIHSS) and at discharge (dNIHSS), mRS at discharge (dmRS), and Barthel Index at discharge (dBI) were compared among the groups with or without predetermined antiplatelet agents. All four parameters were significantly better in the cilostazol group compared with the non-cilostazol group (p = 0.024, p = 0.019, and p = 0.010, respectively). However, no significant differences were found among other antiplatelet agents. The prevalence of atrial fibrillation and chronic heart failure was similar between the groups, but CE was significantly less frequent in the cilostazol group than in the non-cilostazol group (p = 0.027). Therefore, we re-analyzed 538 patients after excluding patients with CE. Both dNIHSS and dmRS remained significantly better in the cilostazol group than in the non-cilostazol group. In multivariate adjusted analysis, prescription of cilostazol prior to ischemic events (p = 0.022) was a factor that affected a favorable outcome (dmRS ≤2).
Conclusion
In ischemic stroke, severity and functional outcome are improved if cilostazol is prescribed prior to events. Reduction of cardiogenic embolism may partly explain this effect, although other neuroprotective effects of cilostazol may be contributory.
Trial registration number
N/A
AS16-029
SERUM ANTIOXIDANT AND OXIDATIVE MARKERS ARE ASSOCIATED WITH CLINICAL NEUROLOGICAL OUTCOMES IN ACUTE STROKE PATIENTS
1Loghman Hakim Hospital-Shahid Beheshti University of Medical science, Skull Base Research Center, Tehran, Iran
2The Research Institute of the McGill University Health Center, Centre for Research in Neuroscience, Montreal, Canada
3Loghman Hakim Hospital-Shahid Beheshti University of Medical science, Brain Mapping Research Center, Tehran, Iran
4School of Pharmacy- Shahid Beheshti University of Medical Sciences, Department of ClinicalPharmacy, Tehran, Iran
5Loghman Hakim Hospital-Shahid Beheshti University of Medical science, Anesthesiology Research Center, Tehran, Iran
Background and Aims
Disruption of oxidant-antioxidant balance may lead to oxidative stress which is known as a mechanism contributing to ischemic stroke. However, the early changes in serum levels of oxidative stress markers and clinical neurological outcomes have not clearly established. This study aims at measuring serum concentration of major indicators of antioxidant and oxidant among patients within 24 h after onset of the stroke symptoms, and investigating their relation with the clinical status of patients.
Method
Serum levels of Q10 (CoQ10), superoxide dismutase (SOD) and malondialdehyde (MDA), as oxidative markers, were measured in 76 patients and 34 healthy individuals. Severity of the neurological deficit, functional disability and cognitive status in ischemic subjects were respectively studied with national institute of health stroke scale (NIHSS), modified ranking scale (MRS) and mini-mental state examination (MMSE).
Results
Stroke patients had significantly lower serum level of CoQ10 and SOD as compared to controls (27.34 ± 35.40 ng/ml, 18.58 ± 0.76 u/ml p < 0.05) respectively, whereas serum MDA level was significantly higher (38.02 ± 2.61 µm p < 0.05). The significant negative correlation was detected between the serum CoQ10 level and scores of NIHSS and MRS. Similar association was discerned between the SOD level and the neurological deficit score. Serum MDA level was also found to be strongly correlated with all three neurological scales.
Conclusion
These findings revealed that serum level of CoQ10, SOD and MDAcan significantly change early after ischemic stroke and they are substantially associated with clinical neurological outcomes.
Trial registration number
N/A
AS16-030
CAUSES AND PREDICTORS OF HOSPITAL READMISSIONS AFTER SPONTANEOUS INTRACEREBRAL HEMORRHAGE IN ALGARVE, PORTUGAL
1University of Algarve, Biomedical Sciences and Medicine, Faro, Portugal
2Univeristy Hospital Center of Algarve, Neurology, Faro, Portugal
3University of Bergen, Department of Clinical Medicine- Center for Neurovascular Diseases- Haukeland University Hospital, Bergen, Norway
Background and Aims
After the acute phase, spontaneous intracerebral hemorrhage (SICH) survivors face the risk of complications and hospital readmissions. Despite its relevance, the number of studies on the topic is scarce. We aimed to identify the causes and predictors of hospital readmissions after SICH in Algarve, Portugal.
Method
Retrospective analysis of a single-center community representative cohort (2009-2015) of SICH survivors. The outcome was the first unplanned readmissions within the first 365 days after discharge. Hospital readmissions were characterized as early (< 90 days) and late (91-365 days). Logistic regression was used for predictive analysis.
Results
Of the 360 SICH survivors, 357 (99.2%) had available one-year follow-up data. Approximately one-third (116 /32.5%) were readmitted in the first-year; the majority 67 (57.8%) were early readmitted. A non-statistically significant trend towards earlier readmission of severely impaired survivors at index discharge (log-rank, P = 0.457) was observed. Pneumonia, endocrine/nutritional/metabolic disturbances and cardiovascular complications were the most common causes of readmissions. The likelihood of being readmitted within one year was increased by: prior to index SICH history of one to three (OR, 3.8; 95% CI 1.76-8.20) and multiple/≥ 4 (OR, 9.68; 95% CI 3.82-24.56) emergency department visits; pneumonia during index SICH hospitalization (OR, 3.46; CI 1.76-6.80) and discharge to nursing or convalescence units (OR, 1.43; 95% CI 0.93-2.11).
Conclusion
The rate of hospital readmissions after SICH is high in Algarve and most causes are potentially preventable. Risk factors are identifiable during the index hospitalization. Readmissions can potentially be reduced by improvement of both acute care including transitional phase and post-acute SICH care.
Trial registration number
N/A
AS16-033
EARLY INFECTION AND SINGLE WORD REPETITION PREDICT POST-STROKE APHASIA LONG TERM OUTCOME
1Centro Hospitalar e Universitário de Coimbra, Neurology, Coimbra, Portugal
2Centro Hospitalar e Universitário de Coimbra, Internal Medicine, Coimbra, Portugal
3Centro Hospitalar e Universitário de Coimbra, Neuroradiology, Coimbra, Portugal
Background and Aims
Better understanding of clinical predictors of aphasia outcome is of the most utmost importance, in patients’ rehabilitation planning, expectation management and further physiopathology understanding.
Aim
To identify clinical predictors of long term post-stroke aphasia outcome.
Method
We conducted a longitudinal observation study of patients with left-MCA stroke with aphasia. Patients were evaluated at baseline, day 7 and 6 months with NIHSS and Aphasia Rapid Test (ART). Other demographic variables and vascular risk factors were collected. A linear regression was performed to identify best predictors of ART at 6 months.
Results
We included 113 patients, with 81 reaching the final evaluation. ART at 6 months was predicted by the occurrence of infection during hospitalization (β = 11.992, 95%CI = [7.148, 16.836], p = 0.002) and by the single word repetition task at baseline (β = 1.621, 95%CI = [0.917, 2.325], p = 0.003).
Conclusion
We report the association of aphasia outcome with infection during hospitalization and with the score in a single word repetition task at baseline. Infection has been previously reported to impact negatively the outcome in stroke patients. We extended this finding to aphasia recovery. Repetition is associated with left arcuate fasciculus, which has been found to predict aphasia outcome. We report the first clinical marker of aphasia prognosis, which may be of great interest in a clinical setting.
Trial registration number
N/A
AS16-034
‘NON-OFFICE HOUR EFFECT’ ON ACUTE IN-HOSPITAL STROKE PATIENTS: AN OUTCOME ANALYSIS IN MULTI-CENTER STROKE REGISTRIES IN TAIWAN
1National Central University, Department of Biomedical Science and Engineering, Taoyaun, Taiwan R.O.C
2Landseed Hospital, Department of Neurology, Taoyaun, Taiwan R.O.C
3Division of Neurology, Department of Internal Medicine, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan R.O.C
4Department of Neurology, Chi-Mei Medical Center, Tainan, Taiwan R.O.C
Background and Aims
In-hospital stroke (IHS) patients, 2.2-17% of all acute stroke patients, have been reported to have delay in the definite diagnosis and worse outcome than patients with community-onset stroke (COS). This study postulated that IHS patients who are onset during non-office hours may be at increased stroke severity, time to evaluation and treatment, and prognosis.
Method
We retrieved IHS patients in the databases of prespecified stroke registries from three teaching hospitals in Taiwan from July 2010 to December 2015. The patients were grouped according to their onset of acute stroke on office hours (Monday to Friday, 8 am to 6 pm) or non-office hours (weekend or Monday to Friday nighttime). The diagnosis was confirmed by appropriate neuroimaging studies, in-charge neurologists and the medical records were reviewed.
Results
Among total 408 IHS patients included in the study, 221 (54.2%) were with their stoke onset on non-office hours. Initial stroke severity as median NIHSS scores of IHS patients on non-office hours were similar to those on office hours (15 vs 16, p = 0.97). Patients with IHS on non-office hours had insignificantly higher use of thrombolysis (4.6% vs 1.2%, p = 0.05), but with longer alert-to-neurologists (1.3 vs 0.6 hours, p < 0.002) than those on office hours. However, the in-hospital mortality (22.2% vs 21.4%, p = 0.47) was no significant compared with that on office hours
Conclusion
Our study demonstrated more than half IHS were identified on non-office hours. IHS patients on non-office hours had increased use of thrombolysis and non-office effect didn’t exist in most quality of care of IHS.
Trial registration number
N/A
AS16-035
EVALUATION OF FACTORS ASSOCIATED WITH MORTALITY DURING 7 YEARS AFTER STROKE
1Riga Stradins University, Department of Rehabilitation, Riga, Latvia
2Riga East University Hospital, Rehabilitation Clinic, Riga, Latvia
Background and Aims
The objective of this study was to evaluate how prestroke risk factors, neurological symptoms and the level of disability shortly after stroke are associated with post stroke mortality during 7 years after stroke for persons that have been treated in the stoke unit.
Method
The data of 231 patients who were treated in the Stroke unit at the Riga East University Hospital between February 1 and July 20, 2009 were included in the study. Prestroke risk factors (type of stroke, arterial hypertension, diabetes mellitus, atrial fibrillation, smoking, alcohol abuse, obesity, recurrent stroke, age, gender), neurological symptoms (motor deficit, sensory disturbance, aphasia, post-stroke urinary incontinence (PSUI), mental status) and limitations of activities (feeding, bathing, grooming, dressing, toilet use, transfers, mobility, stairs) early after stroke were used as independent variables in the stepwise Cox proportional hazard analysis to analyse the mortality during 7 years following stroke.
Results
145 patients had died during the study period. The final model for each group of factors included only one of the factors used for the analysis. Patients who had alcohol abuse were 40% more prone to die earlier. The hazard for those with PSUI is 1.72 times higher than those without PSUI. The independence in grooming showed for 39% lower chance to die earlier.
Conclusion
Alcohol abuse as a prestroke risk factor, post stroke urinary incontinence as a neurological symptom and dependence in grooming as a factor of disability were associated with earlier mortality during seven years after stroke.
Trial registration number
N/A
AS16-036
PARAMEDIAN THALAMIC ISCHEMIC INFARCTION:A RETROSPECTIVE CLINICAL OBSERVATION
1The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Neurology, Wenzhou, China
Background and Aims
The study aimed to evaluate the clinical features in patients with bilateral and unilateral paramedian thalamic infarcts.
Method
Twenty-one patients with paramedian thalamic infarcts were included, and their case records were reviewed. We focused on the patients’ neuroimaging and neurological symptoms including the duration of coma, vertical gaze palsy, and memory impairment. The causes of bilateral and unilateral paramedian thalamic infarcts were also investigated.
Results
Nine patients had bilateral paramedian thalamic infarcts and 12 patients had unilateral lesions. As an initial symptom, coma had occurred in 5 patients with bilateral lesions and 4 patients with unilateral lesions. Bilateral vertical gaze palsy and memory impairment were found in both groups. Most of them recovered well, except 1 patient who died due to bilateral thalamic paramedian infarction.
Conclusion
Our results show that both bilateral and unilateral paramedian thalamic infarcts can cause coma, vertical gaze palsy, and memory impairment. This may promote our understanding of paramedian thalamic infarction.
Trial registration number
N/A
AS16-037
DECOMPRESSIVE SURGERY IN AGED PATIENTS WITH SPACE-OCCUPYING MCA INFARCTION (DECAP): A PROSPECTIVE OBSERVATIONAL STUDY
1University Hospital- Technische Universität Dresden, Neurology, Dresden, Germany
2University Hospital- University of Heidelberg, Neurology, Heidelberg, Germany
3Ostalb-Klinikum, Neurology, Aalen, Germany
4University Hospital- University of Ulfm, Neurology, Ulm, Germany
5Institute of Medical Biometry and Informatics- University of Heidelberg, Medical Biometry, Heidelberg, Germany
6University Hospital- Technische Universität Dresden, Neurosurgery, Dresden, Germany
7Klinikum Augsburg, Neurology, Augsburg, Germany
Background and Aims
Decompressive surgery (DS) improves survival rates and functional outcome in patients with space-occupying middle cerebral artery (MCA) infarction. We sought to determine clinical outcome measures in a cohort of elderly patients with MCA infarction treated with DS.
Method
We performed a prospective, single-center observational study including patients aged 61 years and older with MCA infarction treated with DS. Functional outcome was evaluated at 3, 6 and 12 months. Primary endpoint was the functional outcome defined as modified Rankin Scale (mRS) score at 6 months after hemicraniectomy. Secondary endpoints included outcome measures at 12 months.
Results
We included 40 elderly patients with MCA stroke and DS treated between 2012 and 2017 at our university hospital (median[IQR] patient age 64[62-67] years, median[IQR] NIHSS 17[16-21], dominant hemisphere n = 22). DS was performed within 31(23-53) hours (median[IQR]) after symptom onset. At 6 months after DS, 6 of 40 patients (15%) were moderately or moderate-severely disabled (mRS score 3 or 4), 19(47.5%) were severely disabled (mRS score 5), and 15(37.5%) had died. Compared to a cohort of elderly MCA stroke patients treated with hemicraniectomy within the DESTINY-II trial, patients of the single-center cohort had a lower probability for favourable functional outcome at 6 months (mRS scores of 0-4 ; OR 0.239[95%CI:0.082−0.696]. Case-fatality rate at 12 months was 43%.
Conclusion
In our single-center cohort of elderly patients with space-occupying MCA infarction and decompressive surgery, lethality at 6 months was comparable to previously reported data. Probability for survival without severe disability in our cohort was relatively low.
Trial registration number
NA
AS16-039
ASSOCIATION BETWEEN PREMORBID COGNITIVE STATUS AND POST-STROKE CASE-FATALITY: THE DIJON STROKE REGISTRY
1Dijon Stroke Registry - EA7460 - University Hospital and Medical School of Dijon, Neurology, Dijon, France
Background and Aims
Although it is has been suggested that dementia may confer a greater risk of early death in patients suffering a stroke, whether mild cognitive impairment (MCI) could influence post-stroke prognosis is not clearly elucidated. We aimed to assess the association between premorbid cognitive status and 90-day case-fatality of stroke patients in a population-based setting.
Method
All patients with either ischemic stroke (IS) or spontaneous intracerebral haemorrhage (ICH) were prospectively identified among residents of Dijon, France (155,000 inhabitants), using a population-based registry, between January 2013 and December 2015. Baseline characteristics including demographics, vascular risk factors, premorbid treatments, prior mRS score, and NIHSS score at onset were collected. Prestroke cognitive status was assessed based on a review of medical files, and interview of patients and their relatives. Association between cognitive status and case-fatality at 90 days was evaluated using Cox regression analysis.
Results
773 patients were recorded (Mean age 75.3 ± 16.3 years; 53.8% women; 84.5% IS). Information about prestroke cognitive status was obtained in 716 patients (92.6%), among whom 99 (13.8%) had MCI and 98 (13.7%) had dementia. Case-fatality at 90 days was 8.6% in patients without cognitive impairment, 22.7% in patients with MCI, and 39.4% in demented patients (log-rank test p < 0.001). In multivariable analysis, prestroke MCI (HR = 2.24; CI 95%: 1.23-4.10, p = 0.008) and dementia (HR = 4.41; CI 95%: 2.52-7.71, p < 0.001) were both associated with 90-day case-fatality.
Conclusion
This population-based study demonstrates that post-stroke vital prognosis is influenced by premorbid cognitive status. Both prior dementia and MCI increases the risk of death in stroke patients.
Trial registration number
N/A
AS16-040
PREDICTORS OF 30-DAY MORTALITY IN PATIENTS WITH INTERNAL CAROTID ARTERY OCCLUSION RELATED ACUTE CEREBROVASCULAR SYNDROME IN ALGARVE, PORTUGAL
1Algarve's University Hospital Centre, Neurology, Faro, Portugal
2University of Algarve, Biomedical Sciences and Medicine, Faro, Portugal
Background and Aims
The prognosis of internal carotid artery occlusion (ICAO) related acute cerebrovascular syndrome (ACS) is poor. However, the mortality rates found in the literature vary. Identification of predictors of 30-day mortality is fundamental for adequate prognosis stratification. We aim to evaluate the 30-day mortality, including its predictors of ICAO related ACS in Algarve, Portugal.
Method
Retrospective study of a community representative case-series (2012-2016) with acute ischemic stroke (AIS) or transient ischemic attack (TIA) associated to ICAO documented on carotid Doppler ultrasound. The primary outcome was 30-day mortality.
Results
One-hundred-thirty-five cases occurred; 68.9% were mal; the mean age was 69.25 years. 93.3% has AIS; 36.3% presented with total anterior circulation infarct (TACI); 37.8% had atrial fibrillation (AF). Contralateral significant carotid stenosis was identified in 31.9% cases and 68.9% had cerebral compensatory mechanisms as assessed by transcranial Doppler. The 30-day mortality rate was 8.9%. Older age (78 vs 68 years, p = 0.016), AF (66.7% vs 35.0%, p = 0.031), absence of cerebral compensatory mechanisms (50.0% vs 17.8%, p = 0.016) and TACI syndrome (75.0% vs 32.5%, p = 0.003) were associated with higher mortality. In a logistic regression model, older age (p = 0.04), TACI syndrome (OR 18.35, IC95% 2.079-162.024, p = 0.009) and previous ACS (OR 6.53, IC95% 1.032-41.368, p = 0.04) emerged as independent predictors of 30-day mortality.
Conclusion
Older age, TACI syndrome and a previous history ACS were associated with higher 30-day mortality after adjusting for covariates. Although this cohort is small, this data suggests that special attention should be paid to this subgroup of very high-risk patients.
Trial registration number
N/A
AS16-041
IMPACT OF BLOOD PRESSURE LEVELS WITHIN FIRST 24 HOURS AFTER MECHANICAL THROMBECTOMY ON CLINICAL OUTCOME IN ACUTE ISCHEMIC STROKE PATIENTS
1KZ a.s.- Masaryk Hospital, Neurology, Ústí nad Labem, Czech Republic
2Palacký University Medical School and Hospital, Department of Neurology, olomouc, Czech Republic
3KZ a.s.- Masaryk Hospital, Department of Radiology, Ústí nad Labem, Czech Republic
Background and Aims
Despite technical success and early management of mechanical thrombectomy (MT) for acute ischemic stroke (AIS), not all treated patients reach a good clinical outcome. Different factors may have impact on outcome. We aimed to assess the influence of blood pressure in first 24 hrs after MT on clinical outcome.
Method
All consecutive AIS patients treated with MT using stent-retrievers were enrolled in the retrospective bi-center study. Neurological deficit was assessed with National Institutes of Health Stroke Scale (NIHSS) and clinical outcome after 3 months with modified Rankin scale (mRS) with a score 0-2 for good outcome. Recanalisation was rated using the Thrombolysis in Cerebral Infarction (TICI) scale. Blood pressure (BP) levels within first 24 hours after MT were collected and statistically analyzed.
Results
Of 709 treated patients, completed BP levels were collected in 690 patients (350 males, mean age 71 ± 12 years). Patients with mRS 0-2 had significantly lower median of systolic BP (SBP) compared to patients with poor outcome (130.5 vs. 140.0 mm Hg, p < 0.0001). Logistic regression analysis showed median of SBP (p < 0.0001; 95% CI: 0.965 - 0.987) maximal measured SBP (p < 0.0001; 95% CI: 0.972 - 0.987) and median of diastolic BP (p−0.006; 95% CI: 0.972 - 0.995) within first 24 hours after MT as predictors of good clinical outcome after MT.
Conclusion
Strict correction of blood pressure within first 24 hrs after MT seems to may have a positive impact on clinical outcome in treated patients.
Trial registration number
N/A
AS16-042
LONG-TERM OUTCOMES OF YOUNG ISCHAEMIC STROKE BY TOAST SUBTYPE: THE SOUTH LONDON STROKE REGISTER
1King's College London, School of Population Health and Environmental Sciences, London, United Kingdom
Background and Aims
To investigate the changes in a range of outcomes up to 10 years after stroke in young ischemic patients aged 15-54 years as compared to those over 55 years.
Method
Data from the South London Stroke Register (SLSR) were studied. Ischaemic stroke subtypes were classified based on Trial of Org 10172 in Acute Stroke Treatment (TOAST). Outcomes included death, disability, activity, depression, anxiety and quality of life. T-test, Chi-square test, and Fisher exact test were performed when appropriate. A best-fit curve for each long-time outcome up to 10 years was produced using the locally-weighted scatter plot smoothing (LOWESS) regression method.
Results
2,864 patients experienced a first-ever ischaemic stroke between 1999 and 2016, of which 421 (14.7%) were young patients aged 15-54 years as compared to 2,443 (85.3%) patients aged 55 years and over. Young patients were more likely to be male, black, smokers, drinkers, and have lower prevalence of most vascular risk factors, as compared to older patients. Young large-artery atherosclerosis (LAA) and cardioembolism (CE) patients with poor functional outcomes were more likely to be male, to have hypertension. Generally, young patients had better functional outcomes but worse mental consequences than older patients. Among young patients, those with small-vessel occlusion (SVO) had a better functional outcome and a worse mental consequence than those with LAA and CE.
Conclusion
Long-term outcomes appear to be influenced by aetiological stroke subtypes and onset age. Long-term treatment strategies tailored to the needs of different subtypes are needed for young ischemic stroke patients.
Trial registration number
N/A
AS16-044
LONG-TERM PROGNOSIS FOR DEATH AND DISABILITY IN THE SWEDISH STROKE REGISTRY
1Lund University, Department of Neurology, Lund, Sweden
Background and Aims
Longitudinal long-term prognostic data after stroke based on recent large cohorts are sparse. We therefore collected and analyzed data on survival and functioning based on the Swedish Stroke Register (RiksStroke).
Method
Beyond the Swedish Stroke Register’s routine follow-up surveys at 3 months and 1 year, additional surveys were conducted in 2016 on two half year cohorts with stroke 3 and 5 years earlier. Dependence in activities of daily living (ADL) was defined as Modified Rankin Scale of 3 or higher. Mortality data of the original cohorts, analyzed by Kaplan-Meier, were obtained from the Swedish population register.
Results
The study included 23 488 patients (87.3 % with ischemic stroke (IS); 12.7 % with intracerebral hemorrhage (ICH)). Proportion lost to follow-up in surveys was 12.7 - 22.4 %.
Early mortality was higher for ICH than for IS, whereas beyond 1 year, survival declined at about the same rate for both groups.
In the pre-stroke ADL independent group (69.1 % of cohort) the proportions of poor outcome (ADL dependent or dead) at 3 months were 40.8% for IS and 64.3 % for ICH, and at 5 years, 65.9 % for IS and 77.7 % for ICH. For patients dependent in ADL pre-stroke (30.9 % of cohort), survival at 5 years was 15.8 % for IS and 12 % for ICH.
Conclusion
Despite advances in stroke care long-term prognosis remains a cause for concern. Only 1 in 3 patients with ischemic stroke and 1 in 5 patients with intracerebral hemorrhage had a favorable outcome at five years.
Trial registration number
N/A
AS16-045
MRI PREDICTORS OF HEMORRHAGIC TRANSFORMATION IN 474 CONSECUTIVE STROKE PATIENTS TREATED BY IV THROMBOLYSIS
1Centre Hospitalier de Versailles, Department of Neurology and Stroke Center, Le Chesnay, France
2Gilbert and Rose-Marie Chagoury School of Medicine- Lebanese American University Medical Center, Neurology Department, Beirut, Lebanon
3Univ. Lille- CHU Lille- EA 2694, Santé publique: épidémiologie et qualité des soins, F-59000 Lille, France
4Centre Hospitalier de Versailles, Department of Radiology, Le Chesnay, France
5Hopital Prive de Parly 2, Radiology Department, Le Chesnay, France
6Hopital FOCH, Department of Neurology and Stroke Center, Suresnes, France
7Université Versailles Saint-Quentin en Yvelines et Paris Saclay, Neurologie, Yvelines, France
Background and Aims
Clinical and biological risk factors of hemorrhagic transformation (HT) after IV thrombolysis (IVT) have been well established in several registries such as SISTMOTS. The added value of MRI parameters have been studied in small samples and are controversial. We aim to evaluate the added value of MRI variables in HT in the above clinical and biological factors.
Method
We enrolled between January 2011 and August 2017, a total of 474 consecutive patients with brain infarction (BI) treated by IVT alone at our primary stroke center. Baseline demographic, clinical, biological and imaging characteristics were collected. MRI parameters were: volume of brain infarction in cm3 (B1000 diffusions, ADC< 500.10-6 mm2/s), parenchymal Flair hyperintensity, hyperintense vessel sign, number of microbleeds, subcortical white matter hyperintensity (Fazekas scale) and thrombus length.
Results
301 patients out of 474 were included (64%). Main causes of exclusion were combined thrombectomy (n = 88) and no MRI before IVT (n = 44). In bivariate analyses, HT was significantly associated with the presence of more hyperintense vessel sign, thrombus length (> 8mm), higher BI volume (B1000 and ADC < 500). In multivariate analysis only BI volumes were significantly associated with HT. The discrimination value of the multivariable model including both DWI volume and clinical model (AUC, 0.80; 95%CI, 0.74 to 0.86) was significantly improved compared to the model based only on clinical variables (p = 0.012).
Conclusion
Brain infarction volume on DWI appears to be the only predictive MRI parameter adding value to clinico-biological parameters in HT.
Trial registration number
N/A
AS16-046
INCREASED BLOOD PRESSURE VARIABILITY PREDICTS POOR SHORT-TERM FUNCTIONAL OUTCOME
1University of Leicester, Cardiovascular Sciences, Leicester, United Kingdom
2University of East Anglia, Faculty of Medicine and Health Sciences- Norwich Medical School, Norwich, United Kingdom
3University of Oxford, Nuffield Department of Clinical Neurosciences- John Radcliffe Hospital, Oxford, United Kingdom
Background and Aims
Blood pressure variability (BPV) following acute ischaemic stroke (AIS) may be of prognostic significance. We investigated the effects of increasing BPV on short-term functional outcome.
Method
240 AIS patients from three centres (152 male (63.33%), median age 70.5 (64-78)) were prospectively studied. Enhanced casual blood pressure (BP) was measured within 48 hours of symptom onset using OMRON 705‐IT. BPV was defined using standard deviation (SD) and coefficient of variation (CoV); functional outcome at one month was assessed as death or major disability (modified Rankin scale (mRS) ≥3). Regression analyses reporting odds ratios and confidence intervals (CI) performed used variability indices of systolic BP, diastolic BP, mean arterial pressure (MAP), pulse pressure (PP) and heart rate (HR) to predict outcome.
Results
BPV estimated as SD of diastolic BP (1.23; 95% CI, 1.07 to 1.41, p 0.003) and MAP (1.17; 95% CI 1.03 to 1.34, p 0.018), and CoV of MAP (1.16; 95% CI 1 to 1.33, p 0.048) emerged as predictors of death or major disability at 1 month post-AIS. Though models were adjusted for age, sex and baseline mRS (≥3), such observations could not be made for any variability parameters of systolic BP, PP and HR. Additionally, increasing mean diastolic BP (1.05; 95% CI 1 to 1.09, p 0.028) and MAP (1.03; 95% CI 1 to 1.06, p 0.038) were also predictors of 1 month functional outcome.
Conclusion
Increasing BPV, particularly mean and SD of diastolic BP, and mean, SD and CoV of MAP are independent predictors of 1 month functional outcome post-AIS.
Trial registration number
N/A
AS16-047
ACCEPTABILITY OF BLOOD PRESSURE VARIABILITY MEASUREMENT TECHNIQUES FOLLOWING ACUTE ISCHAEMIC STROKE
1University of Leicester, Cardiovascular Sciences, LEICESTER, United Kingdom
2University of East Anglia, Faculty of Medicine and Health Sciences- Norwich Medical School, Norwich, United Kingdom
3University of Oxford, Nuffield Department of Clinical Neurosciences- John Radcliffe Hospital, Oxford, United Kingdom
Background and Aims
Blood pressure variability (BPV) following acute ischaemic stroke (AIS) is associated with neurological, functional and cognitive outcome. We compared the completeness of BP device readings, and their patient acceptability for BPV measurement and definition.
Method
240 AIS patients from three centres were enrolled (152 male (63.33%), median age 70.5 (64-78)). BP data were collected within 48 hours of symptom onset. Enhanced casual BPs were monitored using OMRON 705‐IT; Spacelabs 90207 ambulatory BP monitor (ABPM) assessed 24 hour BP; non-invasive beat-to-beat BP was monitored using the Finometer, and Vicorder® for pulse wave activity. Patients were subsequently invited to complete a questionnaire exploring the acceptability and tolerability of the Finometer and ABPM.
Results
Device readings were achieved using: OMRON 705‐IT (n = 240, 100%); Finometer (n = 235, 97.92%); Vicorder (n = 227, 94.58%); ABPM (n = 204, 85%). Questionnaire feedback was provided by 129 (53.75%) participants; experiences of pain (n = 3, 2.4%), skin irritation (n = 3, 2.4%) and bruising (n = 2, 1.61%) were reported in using the Finometer, and also ABPM (pain n = 20, 16.81%; skin irritation n = 16, 13.33%; bruising n = 9, 7.5%). Moreover, 116 (89.9%) subjects stated a preferred BP device: OMRON 705‐IT (n = 54, 46.55%), Finometer (n = 43, 37.07%) and ABPM (n = 19, 16.38%).
Conclusion
Completeness of device readings is important for BPV measurement and definition; however this may be influenced by individual patient preferences, including specific experiences of comfort, pain, skin irritation and bruising. These may influence patient acceptability and completeness of recordings in device selection for BPV measurement and prognosis prediction in AIS patients.
Trial registration number
N/A
AS16-048
DOES STATIN USE IMPROVE LONG TERM OUTCOMES AFTER STROKE?
1King's College London, HSCR, London, United Kingdom
2King's College London, School of Population Health and Environmental Sciences, London, United Kingdom
Background and Aims
15 million people worldwide have a stroke every year. Stroke survivors have a one in six chance of recurrence in the five years following stroke. The benefit of statins on stroke incidence is well known. However, the relationship between statin use, and recurrence and survival outcomes remains controversial. We investigate the relationship between statin prescription and ischaemic stroke, stroke recurrence and survival in patients with first-ever ischemic stroke in a cohort with up to 20 years of follow-up.
Method
We used the population-based South London Stroke Register for the years 1995-2015. Patients were assessed at time of first ever stroke, three months and annually thereafter. Cox proportional hazards analysis was used to assess the effect of statin prescriptions pre- and post-stroke on stroke severity, recurrence and survival.
Results
Pre-stroke statin prescription was not associated with a reduction in severity of the initial stroke. Patients prescribed statins both pre- and post-stroke showed a 24% reduction in mortality (aHR = 0.76, 0.60−0.97) when compared to patients that were not prescribed statins. Patients who were prescribed statins pre-stroke and stopped post-stroke showed greater risk of mortality (aHR = 1.85, 1.10-3.12) and stroke recurrence (aHR = 3.25, 1.35-7.84) compared to those not prescribed statins at any time. No association was found between statin use and recurrence.
Conclusion
This observational study provides evidence that statins play a significant role in improving survival rates after a stroke and discontinuation immediately after stroke may be detrimental. Adherence to the National Guidelines that promote statin treatment in primary and secondary prevention should, therefore be monitored.
Trial registration number
N/A
AS16-049
IMPACT OF THE SOCIOECONOMIC STATUS ON SURVIVAL AFTER ACUTE ISCHEMIC STROKE: A POPULATION-BASED STUDY IN A REGION WITH UNIVERSAL HEALTHCARE COVERAGE
1Stroke Programe. Agency for Health Quality and Assessment of Catalonia, Stroke Programe, BARCELONA, Spain
Background and Aims
Differences in stroke mortality by socioeconomic status (SES) exist but are heterogeneous in high-income countries. Objective: to assess the impact of SES on 30-day and longer-term mortality in patients with an acute ischemic stroke (AIS) living in a region with universal healthcare coverage.
Method
We used healthcare administrative data to identify AIS hospitalizations (index cases, ICD-9: 433.x1, 434.x1, 436) occurred among Catalonia’s residents between Jan15-Dec16. Data included age, gender, reperfusion therapies (99.10, 39.74), and the basic healthcare area of residence (BHCAR). Patients were followed up until Sep17 by linkage to the Central Registry of Insured Persons. The SES index consists of 9 components and reflects socioeconomic differences between BHCAR. Adjusted logistic and Cox regression models using the Huber-White cluster sandwich estimator of variance were used to analyze the effect of SES (per quartiles) on survival.
Results
We analyzed 16,815 AIS patients. Those living in BHCAR with high SES were older (mean 76 years, SD 13 vs 73 years, SD 13; p-value: <0.001), and received higher treatment rates (17% vs 15.6%; p-value: 0.28) than those living in BHCAR with lower SES. During follow-up 5,174 died (31%). Patients living in low SES areas had a higher adjusted 30-day mortality compared to those living in higher SES areas (OR: 1.22 [1.08-1.38], p < 0.01). No differences between SES quartiles were observed in longer-term mortality (HR: 1.01 [0.91-1.13]; p: 0.81).
Conclusion
In our study population, SES plaid a role in 30-day mortality only. More studies are needed to explain the mechanism of these associations.
Trial registration number
N/A
AS16-050
PROGNOSTIC MODEL OF OUTCOMES OF NON-TRAUMATIC INTRACEREBRAL HEMORRHAGE
1Grodno State Medical University, Neurology and neurosurgery, Grodno, Belarus
2Grodno State Medical University, Clinical laboratory diagnostics and immunology, Grodno, Belarus
Background and Aims
Intracerebral hemorrhage (ICH) is the most fatal and disabling stroke type. The purpose of this study was to develop a model for outcome prognosis of ICH more precise than the existing ones.
Method
This study includes 150 cases with spontaneous ICH treated by Regional Rehabilitation Clinical Hospital, Grodno during 2009-2011 years. We included in our research patients with primary ICH, defined as not associated with subarachnoid or traumatic hemorrhage, arteriovenous malformation, brain tumor or other structural lesion. A multivariate regression analysis was performed to determine informative variables.
Results
The multivariable model for outcome prognosis was elaborated by analysis of 150 patients using 23 clinical, amnestic, laboratory and neuroradiological parameters. There were age, Rankin scale before ICH, history of any stroke, history of diabetes mellitus, atrial fibrillation, level of consciousness on admission (Glasgow Coma Scale), glucose level, activated partial thromboplastin time, prothrombin time, platelets, white cell count, absolute monocytes count, ratio of neutrophils/ lymphocytes (the Krebs index), ESR, blood cells in the CSF, ALT, AST, ICH location, ICH volume, intraventricular hemorrhage, hydrocephalus, midline shift, compressed ambient cisterns, NIHSS on admission.
The lethal outcome during 1 month was chosen as the grouping variable. The structure of classification matrix, Wilks' Lambda level equal to 0.28, F level equal to 2.48, p < 0.0185 indicate the correctness of this classification. The sensitivity of proposed model is 100%, the specificity – 95.7%.
Conclusion
It was found that the referred model excels previously created predictive instrument and may be used in clinical practice.
Trial registration number
N/A
AS16-051
STROKE RECOVERY AT ONE YEAR IN PATIENTS WITH COGNITIVE IMPAIRMENT: A POPULATION BASED STUDY
1King's College London, HSCR, London, United Kingdom
2King's College London, School of Population Health and Environmental Sciences, London, United Kingdom
Background and Aims
Cognitive impairment is prevalent after stroke, affecting approximately a third of survivors and impacting quality of life and care needs of the patient. We sought to evaluate associations between cognitive impairment within three months and mortality and functional recovery up to one year.
Method
The South London Stroke Register is a population cohort register of individuals with a first stroke in the South London area. Cognitive function was measured using Mini-Mental State Examination (impaired<24) or Abbreviated Mental Test (impaired<8), activities by the Barthel index (disabled< = 14). Cox and logistic regression models were fitted to study associations between cognitive impairment at seven days, three months and change between these on one-year mortality and physical disability adjusting for demographic, socio-economic and clinical covariates.
Results
1,155 individuals recorded with a stroke between January 1995 and June 2016 had cognitive impairment measured at both seven days and three months (27% of 4,296 who survived to three months). Cognitive impairment was associated with an increased risk of mortality and disability. Any deterioration on the cognitive impairment scale between seven days and three months was associated with an increased risk of death at one year (adjusted hazard ratios 1.8, 95% CI 1.04-3.24) and an increased risk of physical disability at one year (adjusted odds ratio = 2.1, 1.32-3.38) compared to maintaining the same level.
Conclusion
Both progression and improvement of cognitive impairment are frequent after stroke. Deterioration in cognition over the first few weeks after a stroke may indicate the need for early referral to specialist treatment.
Trial registration number
N/A
AS16-052
CONTINUED NATIONWIDE DECLINE IN STROKE RELATED IN-HOSPITAL MORTALITY IN UNITED STATES
1Texas Tech University Health Sciences Center, neurology, El Paso, USA
Background and Aims
Previously a downward trend in stroke related in-hospital mortality was noted from 1996 to 2006 reflecting advancements in acute stroke care. Given ongoing improvement in acute stroke care models and therapies, our study assessed nationwide patterns in in-hospital mortality related to acute stroke for next decade
Method
Patients with acute stroke were identified from the nationwide in-patient sample database for the years 2007 to 2014 using International Classification of Diseases, Ninth Revision procedure codes. Time trends in the proportion of stroke hospitalizations that resulted in death were assessed.
Results
Between 2007 and 2014, overall stroke hospitalizations increased from 1017 414 in 2007 to 2008 to 1114 960 in 2013 to 2014, whereas percentage stroke hospitalizations that resulted in death decreased from 8.98% in 2007-2008 to 7.34% in 2013-2014 (P<0.0001). Unadjusted Odds of mortality decreased regardless of stroke type: ischemic stroke (IS) (OR 0.798, 95% CI 0.762 to 0.835), subarachnoid hemorrhage (SAH) (OR 0.885, 95% CI 0.810 to 0.968), and intracerebral hemorrhage (ICH) (OR 0.865, 95% CI 0.824 to 0.908). In multivariate analysis these odds remained significant (IS: OR 0.813, 95% CI 0.770 to 0.859), SAH: OR 0.680, 95% CI 0.611 to 0.757, ICH: OR 0.707, 95% CI 0.664to 0.754) after adjusting with age, gender, race, medical comorbidities, in-hospital complications, insurance status and APRDRG Severity scale).
Conclusion
There is continued decline in Nationwide In-Hospital Mortality among hospitalized acute stroke patients. This reflects ongoing improvement in stroke care models and advancement in therapies.
Trial registration number
N/A
AS16-053
GENETIC POLYMORPHISMS INFLUENCE VASCULAR COGNITIVE IMPAIRMENT AFTER STROKE
1Taipei Medical University, School of Public Health, Taipei, Taiwan R.O.C
2Taipei Medical University, Graduate Institute of Neural Regenerative Medicine, Taipei, Taiwan R.O.C
3Taipei Medical University, Department of Neurology, Taipei, Taiwan R.O.C
4National Taiwan University, Stroke Center and Department of Neurology, Taipei, Taiwan R.O.C
Background and Aims
Stroke considerably increases the likelihood of dementia. Post-stroke vascular cognitive impairment (VCI) is classified as vascular mild cognitive impairment (VaMCI) and vascular dementia (VaD). Little is known about the inflammatory variants on the risk of VCI after stroke. To identify the genetic variations of individual susceptibility on inflammation might decrease the risk of VCI and provide promising avenues for strategies of prevention.
Method
40 VCI ischemic stroke patients and 40 frequency-matched age and sex non-VCI ischemic stroke patients were enrolled to identify inflammation related variants associated with VCI and confirmed. Additional 110 ischemic patients were recruited as external validation group. All ischemic stroke patients were assessed by Montreal Cognitive Assessment (MOCA) Taiwan Version. Blood samples were collected within 7 days, 3 months and 1 year after stroke.
Results
The MOCA scores of GG genotype was higher than that of AA + AG genotype in the recessive model of PANX1 (rs12793348). The MoCA scores of CT + TT genotype was significantly lower than that of CC genotype in the dominant model of LTN1 (rs61735768). Furthermore, amyloid beta 42 (AB42), amyloid beta 40 (AB40) and soluble receptor for advanced glycation end products (sRAGE) in patients with ischemic stroke. The results showed that rs2305458 of HS1BP3 was correlated with the expression of tau, AB42 and AB40 protein in ischemic stroke patients. Besides, rs10407035 of PLEKHG2 was associated with the protein expression of sRAGE.
Conclusion
The association of genetic polymorphisms of amyloid beta, TLR4, RAGE and immune mechanism-related genes with MoCA scores were observed.
Trial registration number
N/A
AS16-055
ASSOCIATION BETWEEN LDL-C/HDL-C RATIO AND HEMORRHAGIC TRANSFORMATION IN ACUTE ISCHEMIC STROKE PATIENTS
1West China Hospital of Sichuan University, Stroke Clinical Research Unit and Department of Neurology, Chengdu, China
Background and Aims
Low-density lipoprotein cholesterol (LDL-C) levels were negatively associated with hemorrhagic transformation (HT), but high-density lipoprotein cholesterol (HDL-C) levels were positively associated with HT. The association between LDL-C/HDL-C ratio and HT in acute ischemic stroke (AIS) patients remains unclear.
Method
Data from the Chengdu Stroke Registry on consecutive AIS patients admitted to West China Hospital within 7 days of stroke onset from January 2016 to June 2017 were included. Clinico-demographic characteristics including lipid profiles tests were collected. Patients were divided into three categories based on LDL-C/HDL-C ratio tertiles. HT was defined by the magnetic resonance imaging or computed tomography.
Results
We enrolled 968 patients (612 males; mean age, 63.89 ± 14.60years), of whom 116 patients (11.98%) presented with HT. According to LDL-C/HDL-C ratio tertiles (tertile 1<1.70; tertile2 = 1.70-2.48; and tertile3>2.48), all patients were divided into three categories including tertile 1(n = 320, 190 males, mean age, 66.72 ± 15.32years), tertile 2(n = 330, 204 males, mean age, 63.39 ± 14.34years) and tertile 3(n = 318, 218 males, mean age, 61.56 ± 13.65years). The number of HT was 55(17.2%), 31(9.1%) and 30(9,7%) from tertile 1 to tertile 3. After adjustment for age, male gender, atrial fibrillation, SBP and National Institutes of Health Stroke Scale score on admission, a low LDL-C/HDL-C ratio was significantly associated with HT (OR 0.517, 95%CI 0.308 to 0.866, P = 0.012).
Conclusion
Our research founded that a low LDL-C/HDL-C ratio was independently associated with HT in AIS patients within 7 days. Future work should be aimed to elucidate how lipid levels contribute to HT and explore comprehensive factors of predicting HT.
Trial registration number
N/A
AS16-056
PREDICTIVE ACCURACY OF THE POST-STROKE DEPRESSION PREDICTION SCALE (DEPRES)
1Martin-Luther-University Halle-Wittenberg, Institute for Health and Nursing Science, Halle, Germany
2University Medical Center Utrecht, Nursing Science- program in Clinical Health Science, Utrecht, The Netherlands
3University Medical Center Utrecht, Julius Center for Health Science and Primary Care, Utrecht, The Netherlands
Background and Aims
To identify patients at risk for depression after stroke in the second month after stroke, the Post-Stroke Depression Prediction Scale (DePreS) had been developed.
Initial evaluation of the DePreS demonstrates good predictive performance with an area under the curve of 0.78 (95% CI 0.72−0.85). This study provides an evaluation of the predictive performance of the DePreS in a new sample of patients with stroke, able to communicate adequately.
Method
In a prospective multicenter observational in three stroke units in the Netherlands and Germany, 93 consecutive patients were included. The risk for depression was measured in the first week post stroke using the DePreS. In the second month post stroke, the presence of major depressive disorder was established with the Composite International Diagnostic Interview.
Results
Of the 93 included patients, 17 (18,3%) were diagnosed with major depressive disorder. With a cut-off value of ≥ 0 the DePreS performed best with a sensitivity of 0.65 (95% CI 0.42−0.87, a specificity of 0.74 (95% CI 0.64−0.84), a positive predictive value of 0.35 (95% CI 0.19−0.52), and a negative predictive value of 0.90 (95% CI 0.80-1.00). The AUC was 0.71 (95% CI 0.56−0.86).
Conclusion
The DePreS shows a good ability to eliminate patients with a low risk for depression after stroke. This limits the burden of structural diagnostic follow-up only to patients with a high risk. The instruments enable clinicians to estimate the risk of PSD in the first week after stroke by means of routine data.
Trial registration number
This study was registered prospectively (DRKS00011546)
AS16-057
RISK OF EARLY STROKE AFTER TRANSIENT ISCHEMIC ATTACK TREATED IN A SPECIALIZED TIA UNIT – A BEFORE-AFTER ANALYSIS AT A TERTIARY STROKE CENTER
1Klinikum Kassel, Department of Neurology, Kassel, Germany
2Klinikum Kassel, Department of Emergency Medicine, Kassel, Germany
Background and Aims
Transient ischemic attacks (TIA) play an important role in the work-flow of stroke centers. Guidelines recommend treatment of TIA patients in stroke units. Risk of recurrent TIA/stroke after TIA has decreased over past years to 5% (day 90). It is unclear whether TIA patients can be sufficiently treated outside stroke Units. Aim is to analyse treatment of TIA patients in a dedicated TIA unit to safety, feasibility and impact on recurrence rates.
Method
Single-center observational study from our German tertiary stroke center. Until 04/2016 patients suspected of stroke/TIA were treated in the certified stroke unit. In 05/2016, a specialized/dedicated TIA unit was setup adjacent to the emergency dept. to improve work-flow and allow stroke unit focus on the more severely afflicted patients. Patients have been prospectively registered with regard to baseline, demographic and clinical data (NIHSS, pmRS, vascular risk factors, comorbidities, ABCD2-score etc.). TIA/stroke recurrence rates for patients treated between 05/2016 and 04/2017 and controls 05/2015-04/2016 (stroke unit)) were compared. Likewise, secondary outcomes of safety and feasibility were compared as was the predictability of TIA/stroke recurrence by ABCD2-score.
Results
515 patients were admitted to the TIA unit. 231 (44.9%) had a TIA, 97 (18,8%) an acute ischemic stroke, 187 (36,3%) other diagnosis. This TIA-cohort was compared to 230 TIA-patients treated in the stroke unit. Detailed results will be presented.
Conclusion
We assume that treating TIA patients in a dedicated TIA unit incorporated in the emergency room is equally safe and feasible as in a stroke unit and may improve work flow.
Trial registration number
N/A
AS16-058
IS ADDITIONAL THROMBOLYSIS WORTHWHILE IN TANDEM OCCLUSIONS TREATED WITH THROMBECTOMY?
1Christian Doppler Medical Center, Neurology, Salzburg, Austria
2University Medical Center Maribor, Neurology, Maribor, Slovenia
3King's College Hospital, Neurology, London, United Kingdom
4General Hospital Varazdin, Anesthesiology, Varazdin, Croatia
5Christian Doppler Medical Center, Neuroradiology, Salzburg, Austria
Background and Aims
Ischemic stroke related to Tandem Internal carotid and Middle cerebral artery (TIM) occlusion is a challenging condition where endovascular treatment (EVT) is an emerging revascularization option. This study aimed to evaluate prognostic factors in the context of EVT for TIM occlusion.
Method
It was performed a retrospective study of consecutive patients with TIM occlusion admitted within 6 hours from symptom onset. We recorded etiology of stroke, clinical deficits at stroke onset and discharge, details of EVT, final infarct volume (FIV), in-hospital mortality, and outcome at 3 months.
Results
Among 73 patients with TIM occlusion, 53 were treated with EVT. Intravenous thrombolysis with tissue-plasminogen activator (t-PA) was performed in the majority (69.8%) of cases. EVT achieved successful recanalization with a thrombolysis in cerebral infarction (TICI) grade of 2b or 3 in 67.9%. Good outcome (modified Rankins scale score 0-2) was observed in 37.7%. The rate of in-hospital mortality was 28.3%. Univariate analyses indicated the association of good outcome with younger age (p = 0.011), higher cholesterol and low-density lipoprotein levels (p = 0.026 and p = 0.011, respectively), higher erythrocyte count (p = 0.017), t-PA treatment (p = 0.015), successful recanalization with EVT (p = 0.014) and smaller FIV (p < 0.001). We found a trend for better outcome in patients with non-cardioembolic cause of stroke (p = 0.058).
Conclusion
Additional administration of t-PA, successful recanalisation, and smaller FIV are associated with good outcomes in the setting of TIM occlusion receiving EVT. The prognostic relevance of blood lipids and erythrocyte count deserves further studies.
Trial registration number
N/A
AS16-059
FACTORS, TRENDS AND LONG-TERM OUTCOMES FOR STROKE PATIENTS RETURNING TO WORK: THE SOUTH LONDON STROKE REGISTER (SLSR)
1Guy’s and St Thomas’ NHS Foundation Trust, Department of Ageing and Health, London, United Kingdom
2King’s College London, Primary Care and Public Health Sciences, London, United Kingdom
Background and Aims
There is limited information on factors, trends and outcomes in return to work (RTW) at different time-points post-stroke. This study aims to identify these in a multi-ethnic urban population.
Method
Patterns of RTW were identified in individuals in paid work prior to first-ever stroke in the population-based SLSR between 1995-2014. Outcomes including the Barthel Index (BI), Hospital Anxiety and Depression Scale and 12-Item Short-Form survey were assessed at 1 year (1y), 5 years (5y) and 10 years (10y) post-stroke. Multivariable logistic regression examined associations between patient characteristics and RTW.
Results
Among 5609 patients, 940 (17%) were working prior to their stroke (mean age 53 years), of which 319 (34%) were working 3 months post-stroke, declining to 250 (27%) at 1y, 230 (25%) at 5y and 93 (10%) at 10y. Factors associated with RTW, after logistic regression, included receiving thrombolysis (p < 0.01) and occupational therapy (p < 0.01) at 1y and increasing age (p < 0.05) at all three time-points. RTW within 1y increased the likelihood of working at 5y (OR: 7.6; 95% CI: 3.5-16.2) and 10y (3.8; 1.0-14.5). Of those who were independent at follow-up (BI≥19), 39% were working at 1y, 47% at 5y and 69% at 10y. Anxiety, depression and lower self-rated health were all associated with RTW at 1y (p < 0.01) and 5y (p < 0.05).
Conclusion
A large proportion of stroke survivors remain unemployed despite functional independence, however this proportion reduces with time. Individuals returning to work after stroke can experience anxiety, depression and lower self-perceived quality of life in the long-term.
Trial registration number
N/A
AS16-061
A SYSTEMATIC REVIEW OF STROKE, DELIRIUM AND ALLIED HEALTH INTERVENTIONS; AN EXERCISE IN FUTILITY
1Ballarat Health Services, Ballarat Base Hospital, Ballarat, Australia
2Florey Institute of Neuroscience and Mental Health, Neuroscience and Mental Health, Melbourne, Australia
3University of Melbourne, Faculty of Medicine- Dentistry and Health Sciences, Melbourne, Australia
Background and Aims
Delirium is a neglected complication of stroke and characterised by fluctuating disturbance of consciousness, inattention and deficits in cognition. It is generally associated with poor functional outcome, increased morbidity and mortality, and greater incidence of institutionalisation.
Method
We planned a systematic review to study the impact of delirium on post- stroke rehabilitation. However, there is a surprising lack of published research. We then expanded our search to include all acute medical and surgical admissions.
Results
A number of studies were identified that showed correlation between delirium and poor functional outcome, and greater rates of institutionalisation and mortality. This impact was greater in patients with significant pre-existing co-morbidity and poorer functional status prior to admission. We found a single case study that attempted to address the issue of the negative impact of delirium on participation in rehabilitation. No research specifically addresses the impact of delirium on post-stroke rehabilitation, or factors that might influence short-term outcomes in these patients.
Conclusion
This literature search has identified an important gap in current research. We need to understand the impact of delirium on participation in post-stroke rehabilitation and outcome. If a discrepancy in participation is identified, it will allow for improvements in directed interventions in those at risk, including the use of non-pharmacological and pharmacological therapy. This will ultimately result in reduced burden of disease for patients, carers and the healthcare system. The promise of ever-improving acute stroke care will come to naught, if patients are unable to benefit from unhindered participation in rehabilitation.
Trial registration number
N/A
AS16-062
CHANGE IN NIHSS IS A USEFUL PREDITOR FOR EFFECTIVENESS OF ENDOVASCULAR THROMBECTOMY AFTER THROMBOLYSIS IN ELDERLY PATIENTS
1Tokai University Hachioji Hospital, Department of Neurology, Tokyo, Japan
2Tokai University Hachioji Hospital, Department of Neurosurgery, Tokyo, Japan
Background and Aims
Recently, it has been demonstrated that mechanical endovascular thrombectomy (EVT) after thrombolysis improves final outcome in patients with emergent large vessel occlusion. However, modified Rankin scale (mRS) at 3 months may not be a very good marker for its effectiveness, because initial mRS is frequently more than 3 in elderly patients. The aim of the present study is to elucidate usefulness of change in NIHSS as a predictor for effectiveness of EVT.
Method
Sequential 32 patients (68.4 ± 12.6 year old) who underwent the bridging therapy were enrolled retrospectively. According to the change in NIHSS by EVT, we dichotomized these subjects into good responsive (GR) group (>4, n = 12) and poor responsive (PR) group (<3, n = 20), and compared these two groups in various measures.
Results
1) At infusion of t-PA, NIHSS in the GR group (13.8 + 6.2) was significantly (p < 0.05) lower than that in the PR group (19.7 + 7.6). 2) DWI-ASPECTS in the GR group (9.1 + 1.5) was significantly (p < 0.05) higher compared with that in the PR group (5.8 + 2.8). 3) The recanalization rate (>TICI 2b) in the GR group was 100%, while that in the PR group was 50%. 4) The mRS at 3 months in the GR group (1.8 + 2.1) was significantly lower (p < 0.01) than that in the PR group (4.4 + 0.9). 5) Good recovery ratio (mRS at 3 months; 0-2) in the GR group was 9/12 (75%), while that in the PR group was 0%.
Conclusion
The change in NIHSS >4 could be a more useful marker for successful recanalization with EVT after thrombolysis especially in the elderly patients.
Trial registration number
32
AS16-063
PREDICTORS OF IN HOSPITAL AND ONE YEAR MORTALITY AFTER STROKE
1Faculties of Pharmacy and of Public Health- Lebanese University, Laboratory of Clinical and Epidemiology Research, Beirut, Lebanon
2Henri Mondor Hospital AP-HP, Department of Neurology, Creteil, France
3Lebanese University, Faculty of Medicine, Beirut, Lebanon
4Hotel Dieu de France- Saint Joseph University, Faculty of Medicine, Beirut, Lebanon
Background and Aims
We examined mortality rates during the first year after an acute stroke and major predictors of short-term (in-hospital) and long-term (1 year) mortality.
Method
Data were collected on hospitalized stroke patients during a 1-year period. Mortality rates for stroke were assessed in-hospital and 1-year post stroke and predictors of death were evaluated using Cox regression analysis.
Results
A total of 203 Lebanese stroke patients were included. Cumulative mortality rates were 13.3% at in-hospital discharge and 20.7% at 1-year.
Stroke severity, decreased level of consciousness and presence of infectious complications were independent prognostic factors for increased mortality.
The hazard ratio for in-hospital death patients increased with an Intensive Care Unit admission (HR 12.7, 95% CI 3.0–53.7, p = 0.001), hypertension (HR 4.2, 95% CI 1.0–17.8, p = 0.051) and when a surgery was needed (HR 2.3, 95% CI 1.0–5.5, p = 0.053).
The hazard ratio (HR) for patients surviving the acute stroke phase significantly increased with a higher level of dependency in daily living activities (DLA) at hospital discharge (modified Rankin Scale: HR 3.2, 95% CI 1.4–7.3, p = 0.005; Barthel Index: HR 0.2, 95% CI 0.06–0.6, p = 0.006) and with Atrial Fibrillation (HR 3.2, 95% CI 1.1–9.5, p = 0.032).
In multivariate survival analyses, death predictors in-hospital (stroke severity and infectious complication) also predicted death at 1-year; however, dependency in DLA, hypertension and recurrent stroke were additional predictors of long-term mortality.
Conclusion
While markers of severe stroke and infectious complications were major predictors of in-hospital death, comorbidities were added for long-term mortality predictors. Improved control of these factors can potentially reduce long-term mortality in stroke victims.
Trial registration number
N/A
AS16-064
PREDICTORS OF READMISSION AFTER ACUTE ISCHEMIC STROKE IN A TERTIARY CARE CENTER OF PAKISTAN
1Aga Khan University Hospital, Medicine, Karachi, Pakistan
Background and Aims
Stroke is one of the leading causes of disability both in developing as well as developed nations. Among those who survive the acute period, there remains a risk of recurrent vascular events or other stroke related non vascular complications leading to re-hospitalizations and increasing economic and health care related burden, especially in a country with limited availability of health insurance schemes.
Method
We performed the study to evaluate the frequency and factors affecting readmission within one month of discharge among patients with acute ischemic stroke who were admitted to the stroke unit of the Aga Khan University Hospital, Pakistan, during January to December 2016. Retrospective review of data was performed on 1109 patients who fulfilled the inclusion criteria. Logistic regression was performed to evaluate for factors associated with readmission.
Results
Of the 1109 patients discharged after acute stroke, 115 (10.3%) were readmitted within one month. The most frequent causes for readmission were found to be recurrent strokes, infections particularly chest and urinary tract, seizures, electrolyte imbalances and cardiovascular events. Older age, higher MRS score at discharge and multiple underlying stroke risk factors were independent predictors of readmission.
Conclusion
Survivors of acute stroke are a vulnerable population with a higher likelihood of requiring readmission from certain stroke or non stroke related complications. Recognition of these factors and cautious monitoring may help develop strategies for quality of care improvement in these patients.
Trial registration number
N/A
AS16-065
DECISION CURVE ANALYSIS OF CLINICAL PREDICTION MODELS FOR 30 DAY MORTALITY FOLLOWING STROKE USING SOUTH LONDON STROKE REGISTER
1King's College London, School of Population Health & Environmental Sciences, London, United Kingdom
2NIHR Biomedical Research Centre, Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, London, United Kingdom
Background and Aims
Numerous prediction models for stroke mortality exist but none of them are widely used in clinical practice. We compared the accuracy and clinical utility of three existing prediction models for stroke mortality within the first 30 days after stroke, in the population of South London. Models evaluated were iScore, PLAN and Six simple variable scores.
Method
5846 patients with first-ever stroke from the South London Stroke Register from 1995 to 2016 were included in the study. Comparative analyses of the performance of prediction models were based on discrimination (Area under the receiving operating curve), calibration (Hosmer-Lemeshow test) and clinical utility through the decision curve analysis (DCA).
Results
The rate of mortality within 30 days post stroke was 24% in the study population. All three models demonstrated diminished performance in the study population, compared with that reported in their development cohorts. The accuracy for predicting 30-day mortality after stroke for iScore, Six Simple Variable model and PLAN score were 0.63 (95% CI, 0.61−0.64), 0.61 (95% CI, 0.59−0.62) and 0.60 (95% CI, 0.58−0.61) respectively. The decision curve analysis for the three models indicated a greater benefit over the range of threshold values of iScore predictive model.
Conclusion
Assessment of impact is an important aspect in the evaluation of clinical prediction models. The IScore model demonstrates greater clinical utility across a range of threshold probabilities and in different subgroups.
Trial registration number
N/A
AS16-066
SYMPTOMATIC AND ASYMPTOMATIC INTRACRANIAL STENOSIS STUDY (SAISS): A PROSPECTIVE STUDY OVER 3 YEARS
1Inselspital- University Hospital of Bern, Department of Neurology, Bern, Switzerland
2Inselspital- University Hospital of Bern, Diagnostic and Interventional Neuroradiology, Bern, Switzerland
Background and Aims
Intracranial stenoses are an important cause of TIA/ischaemic stroke, especially in Non-Caucasians. Data on vascular risk factors, clinical and imaging findings and outcome in Caucasian patients with intracranial stenoses are scarce.
Method
In this prospective observational study (05/2012-06/2017) at the Bernese Stroke Center, we compared vascular risk factors, MR-imaging and long-term outcome in patients with symptomatic versus asymptomatic intracranial stenoses on current standard treatment.
Results
Among 73 patients (40% women, median age 64y) 45/62% had symptomatic intracranial stenoses. Symptomatic disease patients did not have more vascular risk factors (p = 0.139) and had a similar degree of stenoses (≥50%: 84.4% vs. 71.4%; p = 0.181) as asymptomatic patients, but more frequently anterior circulation stenoses (75.6% vs. 46.4%; p = 0.012) and a trend towards more perfusion deficits in the territory of the stenoses (75.6% vs. 53.6%; p = 0.053). Outcome of symptomatic and asymptomatic patients did not differ at last follow-up (mRS 0-1: 66.7% vs. 81.5%; p = 0.179, survival: 100% vs. 96.3%; p = 0.380). During 69’515 patient-days, frequencies of ischaemic strokes in the intracranial stenosis territory (11.4% vs. 0%; p = 0.083) and endovascular interventions (6.8% vs. 0%; p = 0.232) did not differ significantly between symptomatic and asymptomatic patients. Symptomatic disease was strongly associated with TNA (36.4% vs. 10.7%; p = 0.016; HR 4.76, 95%CI 1.24-18.29) and TIA (29.5% vs. 7.4%; p = 0.027; HR 5.24, 95%CI 1.08-25.43), showing higher risk of TNA (log-rank-p = 0.029) and TIA (log-rank-p = 0.038) during 3-years-follow-up-time than asymptomatic disease.
Conclusion
One in ten patients with intracranial stenosis had an ischaemic stroke in the intracranial stenosis territory during follow-up. There is an unmet need for more effective prevention of recurrent events in symptomatic disease patients.
Trial registration number
N/A
AS16-067
CONVULSIVE STATUS EPILEPTICUS AFTER STROKE
1Karadeniz Technical University, Department of Neurology, Trabzon, Turkey
Background and Aims
The main objective of our study was to determine the risk factors associated with convulsive status epilepticus (CS) after stroke.
Method
We retrospectively reviewed 2350 stroke patients admitted to our hospital between January 1999 and December 2015. A total of 218 (9.8%) patients who had post-stroke first time seizures were included in the study. Medical records concerning stroke type, etiology, functional disability, time of onset of CS following the stroke, type of seizure, electroencephalography (EEG), and neuroimaging findings were compared between the patients with or without CS after stroke.
Results
A total of 17 (7.8%) of the 218 patients had CS. 14 (82.4%) patients had CS manifested by generalized in onset and 3 (17.6%) patients had seizures that were partial in onset. Univariate analysis revealed that CS after stroke occured more frequently among female patients (p = 0.041), patients with severe (mRS>3) initial (p = 0.005) and discharge (p = 0.003) mRS scores. Patients with CS after stroke had higher mortality rates at one month (p = 0.017).
Conclusion
CS is a serious complication after stroke with higher mortality rates at one month and severe functional disability is associated with a higher risk of CS after stroke.
Trial registration number
N/A
AS16-068
EEG: DIAGNOSTIC UTILITY IN THE HASU & ASU
1St Georges Hospital, Neurosciences Dept, London, United Kingdom
Background and Aims
To establish how EEG informs the management of patients in a comprehensive UK stroke service.
Method
Retrospective identification of patients who underwent EEG over a two-year period (June 2015 to June 2017). Review of imaging, EEG reports and clinical notes to identify rationale for the investigation and extent clinical management was influenced.
Results
Out of approximately 4000 admissions to the stroke unit, 53 patients (1.3%) had an EEG during stroke unit admission. 35 were in stroke patients and 18 in subjects with stroke mimics (e.g. encephalitis).
In the stroke patients, 33 EEGs were done for a suspected seizure diagnosis and 2 (6%) for other reasons (i.e. encephalopathy). 13 EEGs (37%) were to investigate suspected non-convulsive status epilepticus (NCSE). 20 EEGs (57%) were for other suspected seizure diagnoses. 10 EEGs in total (28.5%) were epileptiform and of these, 3 EEGs (8.5%) specifically identified “NCSE” or “epilepsy partialis continua (EPC)”. EEG findings in these patients altered management. Of the remaining 25 EEGs (71.5%), 14 EEGs (40%) indicated cerebrovascular disease, 8 (23%) were encephalopathic and 3 (8.5 %) were normal.
Documentation review showed that epileptiform activity did not necessarily result in initiation of AEDs or treatment modification. Conversely, a non-epileptiform EEG did not exclude a clinical diagnosis of epilepsy subsequently being made.
Conclusion
EEGs are requested very sparingly. The most useful indication was NCSE. Other indications for seizures in stroke patients did not necessarily result in a change in diagnosis or management.
Trial registration number
N/A
AS16-069
COGNITIVE IMPAIRMENT AFTER MINOR STROKE AND TRANSIENT ISCHEMIC ATTACK AND ITS RELATION TO THE FUNCTIONAL OUTCOME
1Universitätsklinikum Leipzig, Department of Neurology, Leipzig, Germany
2Universitätsklinikum Leipzig, Department of Neuroradiology, Leipzig, Germany
3Carl-von-Basedow Klinikum, Department of Neurology, Merseburg, Germany
Background and Aims
Post-stroke cognitive impairment (PSCI) is a common finding that may critically impact on patient’s outcome even in the setting of transient or minor ischemic affection. However, the course of PSCI and its association with neurological deficits, functional dependency and stroke volume are scarcely studied.
Method
In this prospective single-centre study, cognitive status was assessed with Mini Mental Status Examination (MMSE), neurological deficits with NIHSS and functional dependency with Barthel index (BI) at multiple time points (days 1, 7, 30, 90 and 180) in patients with first ever minor stroke (n = 73, 64.7 ± 12.8 years, baseline NIHSS 2.3 ± 2.1) and transient ischaemic attack (TIA; n = 24, 62.8 ± 16.3 years). Infarct volume was assessed at day 7 by magnetic resonance imaging.
Results
In patients with minor stroke, MMSE was significantly affected at day 1 (26.9 ± 5.0), improved significantly towards day 7 (28.0 ± 3.3) and recovered until day 30 (day 30: 28.8 ± 2.1, day 90: 28.9 ± 1.6, day 180: 29.0 ± 1.7). An equal course of recovery was found for BI, while NIHSS had fully recovered not until day 90. Multiple linear regression analyses yielded best prediction of functional dependency at day 180 by the NIHSS (beta −0.58), followed by infarct volume (beta −0.28) and MMSE (beta 0.22), but not by age or sex. Patients with TIA exhibited identical MMSE and BI at every time point investigated.
Conclusion
Cognitive impairment is temporarily affected in patients with minor stroke, but their mid-term functional dependency is primarily related to neurological sequelae caused by the ischaemic event and to a quite lesser extent to PSCI.
Trial registration number
N/A
AS16-072
INCIDENCE MORTALITY AND FUNCTIONAL OUTCOME AFTER INTRACEREBRAL HEMORRHAGE ACCORDING TO SEX, AGE AND ETHNIC GROUP IN QATAR
1Hamad General Hospital, Neurology, Doha, Qatar
2University Of Alberta Hospital, Neurology, Edmonton, Canada
Background and Aims
To investigate incidence of short-term case fatality and clinical outcome after intracerebral hemorrhage (ICH) using stroke database from the main tertiary hospital in Qatar
Method
Our stroke database is based on prospective data collection of patients with TIA, ischemic stroke or ICH.
Ninety-day case fatality was stratified by age and sex after ICH and ischemic stroke using logistic regression
Results
90 days Case fatality rate after ICH was 92/401 cases (23%), compared with 79/1663 (5%) with Stroke
Case fatality rate stratified by sex in ICH: Male 22% versus female 29% (P = 0.2) and in Ischemic stroke: male 4% versus 9% female (P< 0.001)
90 days case fatality rate stratified by age in ICH revealed high rate in younger age and elderly: (26% for 18-45 years, 19% for 45-65 years, 31% for >65 years old)
90 days case fatality rate stratified by age in IS revealed high rate in elderly: (1.2% for 18-45 years, 4% for 45-65 years, 10% for >65 years old)
In the multiple logistic regression analysis for ICH: Age >65 (adjOR: 1.9, CI95%:0.8-4.4, P = 0.12) and baseline NIHSS (adjOR: 1.2, CI95%:1.2-1.3, P< 0.001) are correlative with mortality at 90 days.
In the multiple logistic regression analysis for IS: Age>65 (adjOR: 2.9, CI95%:1.7-5, P<0.001) and baseline NIHSS (adjOR: 1.2, CI 95%:1.2-1.3, P<0.001) are correlative with mortality at 90 days.
Conclusion
More than one-quarter of individuals die in the first 90 days after hemorrhagic stroke, and patients younger than 45 years are more likely to die after ICH than ischemic stroke in our patient’s population
Trial registration number
N/A
AS16-073
COMPUTED TOMOGRAPHY ANGIOGRAPHY COLLATERAL SCORES AND OUTCOMES AFTER ACUTE REPERFUSION THERAPIES FOR BASILAR ARTERY OCCLUSION
1Ribeirão Preto Medical School - University of São Paulo, Department of Neurosciences and Behavioral Sciences, Ribeirão Preto, Brazil
2Ribeirão Preto Medical School - University of São Paulo, Department of Internal Medicine - Radiology Division, Ribeirão Preto, Brazil
Background and Aims
Introduction
Collateral status is strongly recognized as one of the most important prognostic factors in anterior circulation large vessel occlusion strokes. Recently, posterior circulation CTA collateral scores have been also linked to outcomes in acute basilar artery occlusion (BAO). Objectives: We aim to analyze which previous published CTA collateral score better predicts outcomes in BAO.
Methods
Retrospective analysis of consecutive BAO patients from a prospective stroke registry, treated with acute reperfusion therapies (intravenous thrombolysis or endovascular therapy). BAO was confirmed through CTAs, which were also used to evaluate the Posterior Circulation Collateral Score (PC-CS) and the Basilar Artery on Computed Tomography Angiography (BATMAN) score. Favorable outcome was defined as mRS ≤3 at 90 days.
Results
between January/2011 and July/2017, 30 BAO patients were identified. Nine (30%) patients were treated with IVT only and 21 (70%) with endovascular therapy. Favorable outcomes were achieved in 11 (37%) patients and mortality was 30%. In univariate analysis, NIHSS, Glasgow coma scale, mild-to-moderate symptoms on admission, successful recanalization and PC-CS were predictors of favorable outcomes. In multivariate analysis, PC-CS remained as an independent predictor of favorable outcomes. The AUC for PC-CS was 0.68 (95%CI 0.47−0.89; p = 0.04). BATMAN score and the presence of both posterior communicating arteries were not related to favorable outcomes.
Conclusion
Collateral flow assessment using PC-CS is an independent predictor of favorable outcomes among acute BAO patients treated with acute reperfusion therapies.
Trial registration number
N/A
AS16-074
CEREBRAL SMALL VESSEL DISEASE, FASTING GLUCOSE, LDL CHOLESTEROL LEVELS AND 3-MONTH OUTCOME AFTER SPONTANEOUS HYPERTENSIVE INTRACEREBRALHEMORRHAGE
1Beijing Tiantan Hospital - Capital Medical University, Neurology Department, Beijing, China
Background and Aims
Cerebral small vessel disease (SVD), abnormal fasting glucose and low density lipoprotein cholesterol (LDL-C) levels are well-known risk factors for spontaneous intracerebral hemorrhage (ICH). MRI-visible perivascular spaces (PVS) are a sensitive neuroimaging marker of SVD. We aimed to explore the association between PVS levels, serum glucose levels, cholesterol levels and the 3-month outcome after spontaneous hypertensive intracerebral hemorrhage (HICH).
Method
We included 250 consecutive patients from a prospective HICH cohort. The PVS in the BG and CS regions were assessed on a validated 4-point visual rating scale (0 = no PVS, 1 = <10, 2 = 11–20, 3 = 21–40, and 4 = >40) by two observers independently and predefined severe PVS as score >2. Clinical information was obtained using standardized forms and hospital routine blood sample tests. Outcome was assessed at 90 days using the modified Rankin Scale (Good outcome: mRS: 0-2 vs. Bad outcome: mRS 3-6).
Results
In univariate analyse, severe PVS was associated with bad 3-month outcome (p = 0.025). In the multivariable logistic regression, high fasting glucose levels (odds ratio [OR] 5.29, 95% confidence interval [CI] 1.55–18.11, p = 0.008) and low LDL-C levels (0.27, 0.01–0.75, p = 0.012) were independently associated with bad HICH outcome in 3 months.
Conclusion
High fasting glucose levels and low LDL-C levels are independently associated with bad outcome in 3 month after HICH. Both the glucose and cholesterol controls are essential for HICH patients.
Trial registration number
N/A
AS16-075
PLATELET MARKERS PREDICT EARLY OUTCOME IN ISCHEMIC STROKE: THE SICFAIL (STROKE INDUCED CARDIAC FAILURE IN MICE AND MEN) COHORT STUDY
1University of Wuerzburg, Institute for Clinical Epidemiology and Biometry, Wuerzburg, Germany
2University Hospital of Wuerzburg, Department of Neurology, Wuerzburg, Germany
3University of Wuerzburg, Rudolf Virchow Center for Experimental Biomedicine, Wuerzburg, Germany
4University Hospital of Wuerzburg, Institute of Experimental Biomedicine, Wuerzburg, Germany
5University Hospital of Tuebingen, Department of Cardiology, Tuebingen, Germany
6Klinikum Main Spessart, Department of Neurology, Lohr, Germany
7University Hospital of Essen, Department of Neurology, Essen, Germany
8University of Wuerzburg, Comprehensive Heart Failure Center Wuerzburg, Wuerzburg, Germany
Background and Aims
Platelets play a critical role in vascular disease pathogenesis, e.g. by mediation of thrombosis, inflammation and tissue-repair. Data from patients with coronary heart disease (CHD) suggest that expression levels of specific platelet receptors predict patient outcome but their prognostic role in ischemic stroke (IS) remains unclear.
Method
Data collection was embedded in the prospective hospital-based SICFAIL-cohort-study assessing the natural course of cardiac function after IS. Blood samples at day 3 ± 1 were analyzed using flow-cytometry for mean fluorescence intensity (MFI) of following platelet-markers: CXCR4, CXCR7, HMGB1, CD84, CD42b, CD61, CD62 ± ADP-stimulation, CD40, CD41, CD42d, GPVI. Definition of early outcome was change of NIHSS from day 1 to 3 and poor outcome at day 3 (NIHSS≥5). In an exploratory approach linear and logistic analysis, adjusted for age and baseline-NIHSS, were performed to assess the distinct associations between MFI-levels and early outcome.
Results
101 patients with acute IS were recruited (65% male; 66 ± 14y; baseline-NIHSS 4.6 ± 4.3). Linear regression showed a statistically significant association of CXCR7-MFI (β = −0.97, p = 0.01) and stimulated-CD62p-MFI (β = −0.07, p = 0.01) with reduced NIHSS-recovery. Logistic regression yielded a statistically significant association of CXCR7-MFI (OR = 3.5; 95%-CI 1.4-9.1; p = 0.01), HMGB1-MFI (OR = 2.1; 95%-CI 1.0-4.1; p = 0.04) and CD84-MFI (OR = 1.3; 95%-CI 1.0-1.6; p = 0.02) with poor outcome.
Conclusion
High MFI of CXCR7, HMGB1, CD84 and elevated sensitivity of platelets to stimulation were linked to early unfavorable outcome. Results are partly contradictory to CHD-data where e.g. high CXCR7-levels were protective for early-outcome. Observed associations might be caused by chance, differences in methodology or organ-specific variations. Therefore, replicating the data of this pilot study is required.
Trial registration number
N/A
AS16-076
PREDICTIVE FACTORS OF DISABILITY AND MORTALITY: A COMPARISON OF ISCHEMIC STROKE AND HEMORRHAGIC STROKE
1Faculty of Medicine Duta Wacana Christian University, Neurology, Semarang, Indonesia
2Faculty of Medicine Duta Wacana Christian University, Neurology, Yogyakarta, Indonesia
Background and Aims
Stroke is one of the leading cause of morbidity and mortality in Indonesia. Various factors increasing disability or death on stroke is not yet clearly described in Indonesia. This study aimed to compare the predictive factors of disability and mortality on ischemic stroke (IS) and hemorrhagic stroke (HS).
Method
This study was a retrospective cohort study, conducted at Bethesda Hospital, Yogyakarta, Indonesia. The data were obtained from 6350 subjects, consists of 4892 IS and 1458 HS patients from 2009 to 2017. Stroke outcome measured by using modified Rankin Scale, clustered into 3 groups. Group 1 was subjects with moderate and moderately severe disability, group 2 was subjects who dead, and group 3 was subjects without no significant disability or with slight disability. Each group analized by various variable: age, gender, stroke history, symptoms, comorbidities, and complications.
Results
Subjects were dominated by male age >60 year. Limb weakness was the main symptom. Both in IS and HS, hypertension was the most common comorbidity and gastrointestinal bleeding was the most common complication. Decubitus ulcer was the most significant factor of disability in IS (OR:7.704, 95%CI: 3.659-16.219, p:0.000), followed by gastrointestinal bleeding, and pnemonia. Gastrointestinal bleeding was the most significant factors of disability in HS (OR:9.520, 95%CI: 3.726-24.324, p:0.000), followed by pnemonia and aphasia. Gastrointestinal bleeding was also significant to mortality in IS (OR:94.075, 95%CI: 39.954-221.507, p:0.003) and HS (OR:53.665, 95%CI: 19.626-146.744, p:0.000).
Conclusion
Complications are the main factor contributing to disability and mortality in IS and HS patients, especially decubitus ulcer and gastrointestinal bleeding.
Trial registration number
N/A
AS16-077
THE ASSOCIATION OF NEUTROPHIL-LYMPHOCYTE RATIO AND LYMPHOCYTE-MONOCYTE RATIO WITH THREE-MONTH CLINICAL OUTCOME AFTER MECHANICAL THROMBECTOMY FOLLOWING STROKE
1St George’s University Hospitals NHS Foundation Trust, Neurology, London, United Kingdom
Background and Aims
Neutrophil-Lymphocyte ratio (NLR) and Lymphocyte-Monocyte ratio (LMR) are associated with clinical outcomes in malignancy, cardiovascular disease and stroke. Here we investigate their relationship following mechanical thrombectomy (MT) for middle cerebral artery (MCA) stroke.
Method
Data were analysed from a prospective database of consecutive patients who underwent MT at a UK centre from May 2016-July 2017. Data included demographics, treatment parameters (e.g. recanalization using the TICI score), infarct size (in relation to MCA territory, table) and haemorrhagic conversion (using ECASS classification, table). The clinical outcome was modified Rankin score (mRS) at three months. NLR and LMR were calculated from the first full blood count taken within 24 hours of thrombectomy. Statistical analyses used ANOVA for comparison and Spearman Rho for correlation.
Results
121 patients (mean age 66.4 ± 16.7, 63 female) underwent thrombectomy. With worsening mRS, NLR increased and LMR decreased (both significantly, figure).
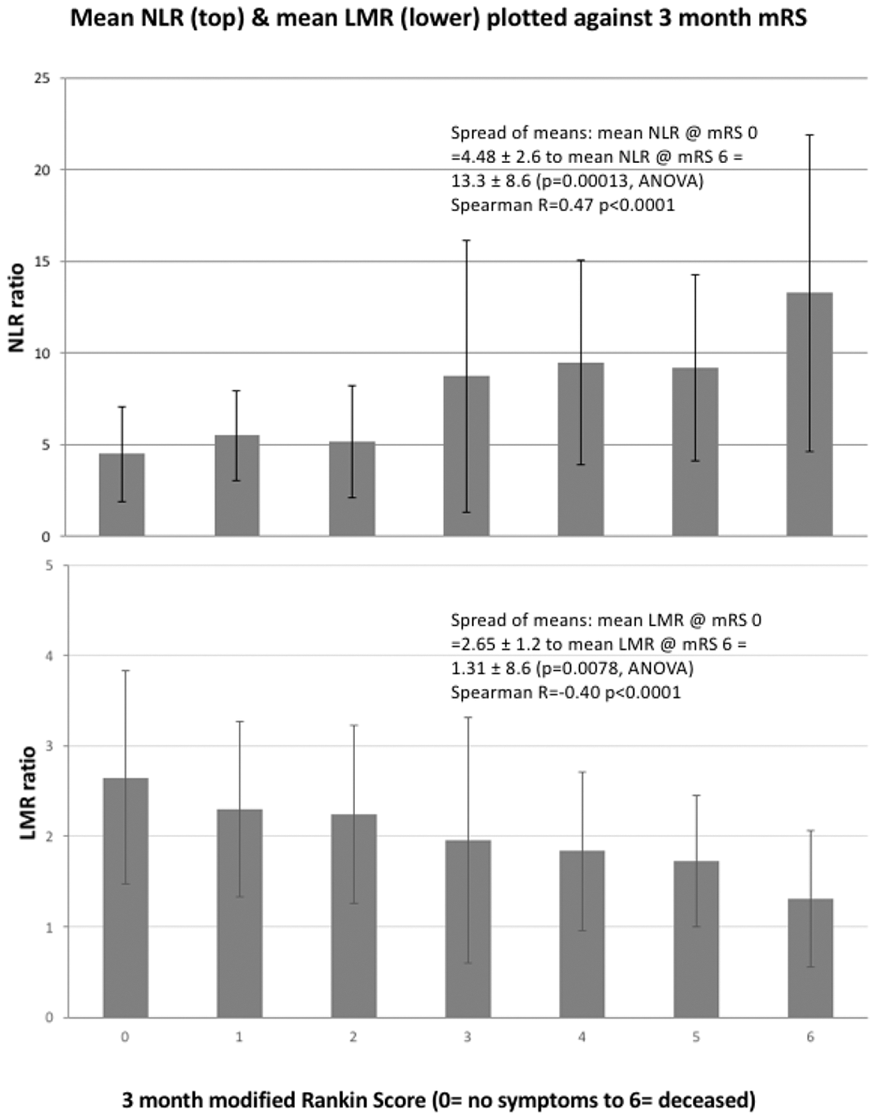
NLR and LMR were related neither to recanalisation nor haemorrhagic conversion but varied significantly with infarct size.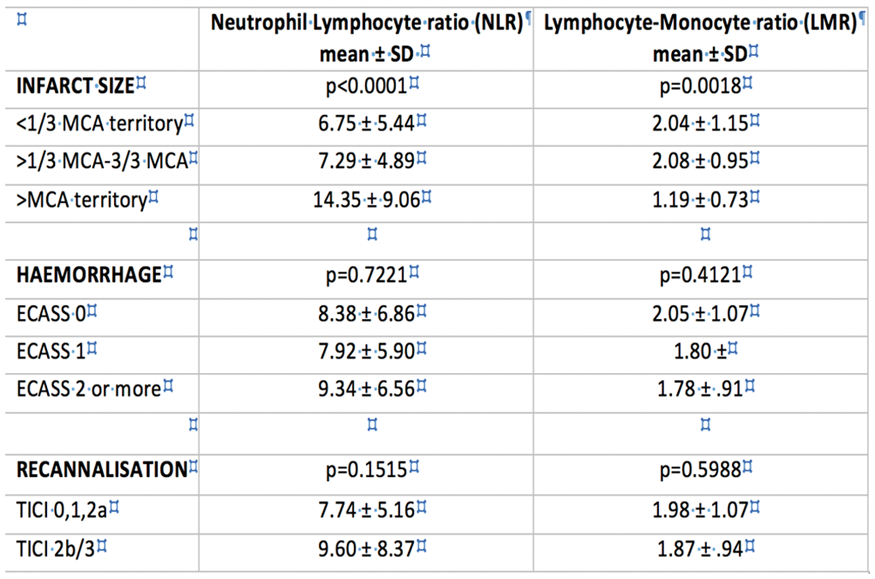
Conclusion
NLR and LMR, calculated early post MT, are related to three-month clinical outcome. These ratios may be attributable to infarct size and warrant further exploration as potential prognostic markers.
Trial registration number
N/A
AS16-078
OBESITY PARADOX IN ACUTE ISCHEMIC STROKE: POOR PROGNOSIS IS NOT FOUND IN OBESE PATIENTS, PROBABLY DUE TO AN ANTI-INFLAMMATORY RESPONSE
1Hospital Clínico Universitario de Santiago, Neurology, Santiago de Compostela, Spain
2Instituto de Investigación Sanitaria de Santiago de Compostela, Laboratorio de Investigación en Neurociencias Clínicas, Santiago de Compostela, Spain
Background and Aims
The concept of “obesity paradox” describes the unexpected improved prognosis found in several diseases in patients with excessive body weight. Contradictory findings have been reported regarding stroke, and the possible role of inflammation in this phenomenon has not been evaluated.
Method
We performed a prospective case-control study with ischemic stroke patients admitted to our Stroke Unit to study the obesity paradox in ischemic stroke. Cases were defined as obese patients (body mass index -BMI- ≥ 30 kg/m222), and controls were non-obese patients (BMI < 30 kg/m22). Patients were evaluated during hospitalization and at 3 months after stroke for clinical, inflammatory and neuroimaging variables.
Results
Over a period of 33 months, 98 patients were included (48 controls and 50 cases). Obese patients exhibited more cardioembolic strokes (46% vs. 31.2%, p = 0.249), more hemorrhagic transformations (30% vs. 12.5%, p = 0.035), and more infections during hospitalization (28% vs. 16.7%, p = 0.179) than controls. In obese patients we found a decrease of pro-inflammatory markers (IL-6 levels) and an increase in anti-inflammatory markers (IL-10 levels) during the first week after ischemic stroke. On the other side, in non-obese patients we found and increase of IL-6 in the same period, whereas IL-10 remains stable. No differences in functional outcome at 3 months were found between obese and non-obese patients.
Conclusion
Despite having several factors strongly associated with bad outcome, obese patients do not show a worse outcome after ischemic stroke. We postulate that obesity can counterbalance the inflammatory reaction through an anti-inflammatory stream enhanced in acute phase of stroke.
Trial registration number
N/A
AS16-080
HEALTH QUALITY PROGNOSTIC FACTORS IN PATIENTS WITH ATHEROTHROMBOTIC STROKE
1Saint-Petersburg City Hospital N 26, Department of neurology, Saint-Petersburg, Russia
2First Saint-Petersburg I.P. Pavlov State Medical University, Department of physical methods of treatment and sports medicine, Saint-Petersburg, Russia
3First Saint-Petersburg I.P. Pavlov State Medical University, Department of neurology, Saint-Petersburg, Russia
4Almazov National Medical Research Centre, Department of neurology, Saint-Petersburg, Russia
5First Saint-Petersburg I.P. Pavlov State Medical University, Department of anesthesiology and resuscitation, Saint-Petersburg, Russia
Background and Aims
Our study’s purpose was to investigate health quality prognostic factors in elderly patients with atherothrombotic stroke due to atherosclerotic carotid stenosis (ACAS).
Method
Insulin-like growth factor (IGF) family and non-lipid atherosclerosis biomarkers serum levels, clinical and social markers were evaluated in 124 patients with 50-99% ACAS and 24 healthy volunteers. Age range was 50-80 years. Health quality was accessed at not less than 90 days from enrollment.
Results
In patients with ACAS modified Rankin scale (mRs) (τ = 0,635, p < 0,001) and National Institutes of Health Stroke Scale (NIHSS) (τ = 0,377, p < 0,001) levels increase and Mini-mental state examination (MMSE) (τ = –0,323, p = 0,001) levels decrease were associated with total European Quality of Life Questionnaire score (EQ-5D) increase. IGFBP-1 (τ = –0,245, p = 0,040) and asymmetric dimethylarginine (ADMA) (τ = –0,272, p = 0,034) serum levels decrease and IGF-2 (τ = 0,263, p = 0,034) level increase correlated with EQ-5D visual analogue scale (VAS) increase. Medical observation (p = 0,015), presence of work (p = 0,005), and higher education (p = 0,012) were associated with lower EQ-5D total score.
Conclusion
IGF-activity suppression and ADMA activation in patients with ACAS predict their poor health quality. Lower disability degree, stroke severity and cognitive impairment, presence of medical observation and work and higher education are positive health quality prognostic factors in these patients.
Trial registration number
N/A
AS16-081
POST STROKE DEPRESSION AND STROKE ETIOLOGY – ACUTE AND AFTER SIX MONTHS
1Clinical stroke research unit, Neurological department- Rigshospitalet- Glostrup, Copenhagen, Denmark
2Radiological department, Radiological department- Herlev and Gentofte hospital, Copenhagen, Denmark
3Danish center for sleep medicine, Department of neurophysiology- Rigshospitalet- Glostrup, Copenhagen, Denmark
Background and Aims
Post stroke depression (PSD) is frequent and related to poor functional outcome and increased mortality. Data regarding association to stroke etiology and particular small vessel disease (SVD) are sparse.
Method
We designed an observational study in acute stroke patients followed for six months. PSD was assessed with Hamilton 6-item depression scale (Ham-D6), Hospital anxiety and depression scale (HADS), Global depression scale administered by patient (GDS-patient) and examiner (GDS-examiner) and WHO-5 well-being questionnaire. Ischemic stroke etiology was classified by the TOAST criteria and a total SVD score, based on MRI, was calculated in all TOAST groups. Stroke severity and history of depression were included as confounders.
Results
110 patients were included, 92 completed follow-up. Median age: 68 years (range 36–88), men: 56%, ischemic strokes: 90%. Over time the prevalence of depression decreased from 38% to 10% (p < 0.0001) according to Ham-D6 and from 13% to 4% (p = 0.03) according to HADS. The other questionnaires also indicated improvement, but didn’t reach significance.
Patients with large artery atherosclerosis (LAA) etiology were most severely affected by PSD according to Ham-D6 (p = 0.01) and GDS-patient (p = 0.04). Improvement in PSD was independent of TOAST.
Self-rated symptoms (GDS-patient) improved with increasing SVD score (p = 0.034), but well-being (WHO-5) improved with decreasing SVD score (p = 0.031). Depression rated by the other questionnaires were independent of the SVD score.
Conclusion
Patients with LAA etiology were most severely affected by PSD. The PSD improved over time independent of TOAST groups. Association to the total SVD score was inconclusive and needs further investigation.
Trial registration number
clinicaltrials.gov: NCT02111408
AS16-083
SLEEP DISORDERED BREATHING AND SMALL VESSEL DISEASE IN STROKE: ACUTE AND SIX MONTHS FOLLOW-UP
1Clinical stroke research unit, Neurological department- Rigshospitalet- Glostrup, Copenhagen, Denmark
2Radiological department, Radiological department- Herlev and Gentofte hospital, Copenhagen, Denmark
3Danish center for sleep medicine, Department of neurophysiology- Rigshospitalet- Glostrup, Copenhagen, Denmark
Background and Aims
Sleep disordered breathing (SDB) is frequent after stroke and associated to poor outcome and increased mortality. The association between stroke etiology, especially small vessel disease (SVD), and SDB and SDB over time is uncertain.
Method
This observational study included stroke patients within seven days from onset, and re-tested after six months. Polysomnography was performed and the apnea hypopnea index (AHI) calculated. Sleepiness was scored by Epworth sleepiness scale (ESS) and sleep quality by Pittsburgh sleep quality index. The ischemic strokes were classified according to the TOAST classification and a total SVD score was calculated based on MRI. Age, sex and stroke severity were included as confounders.
Results
We included 101 patients and 58 patients had follow-up. Median age 68 years (range 36-88), 57% men and 90% ischemic strokes. AHI decreased over time, median -3.9, range -8.3 – −0.7 (p = 0.01). Sleepiness decreased over time (p = 0.01), but sleep quality was unchanged (p = 0.6).
We found no association between AHI and the TOAST classification groups.
The total SVD score was associated to AHI at follow-up (ANOVA: p = 0.033), but not in the acute phase (p = 0.08). The number of patients with indication for treatment for SDB (AHI>15) at both the acute state and follow-up increased with increased SVD score (Fishers’ exact test: p < 0.001).
Conclusion
SDB and sleepiness improved during the first six month after stroke. AHI and treatment-requiring SDB in both the acute state and follow-up was associated to increased SVD score, but not the TOAST classification groups. Stroke patients should be tested for SDB.
Trial registration number
clinicaltrials.gov: NCT02111408
AS16-084
THE EFFECT OF TRANSDERMAL GLYCERYL TRINITRATE IN ACUTE STROKE PATIENTS WITH CAROTID STENOSIS: DATA FROM THE EFFICACY OF NITRIC OXIDE IN STROKE TRIAL
1University of Nottingham, Stroke- Division of Clinical Neurosciences, Nottingham, United Kingdom
Background and Aims
There is concern that blood pressure lowering in acute stroke may compromise cerebral perfusion and worsen outcome in the context of carotid stenosis. The effect of glyceryl trinitrate (GTN) on outcome in acute stroke patients with carotid stenosis is unclear. We sought to assess GTN’s effect in this context using data from the Efficacy of Nitric Oxide in Stroke (ENOS) trial.
Method
ENOS randomised 4011 patients with acute stroke and raised systolic blood pressure to transdermal GTN or no GTN within 48 hours of onset. The primary outcome was the modified Rankin Scale (mRS) at day 90. Ipsilateral carotid stenosis was split: <30%; 30-50%; 50-70%; >70%. Bilateral carotid stenosis was split: <30%; 30-50%; >50%. Data are odds ratios (OR) with 95% confidence intervals (CI) adjusted for baseline prognostic factors.
Results
2023 (60.5%) ischaemic stroke participants had carotid imaging. Compared with participants with <30%, >70% ipsilateral stenosis was associated with an unfavourable shift in mRS at 90 days (OR 1.88, 95% CI 1.44-2.44, p < 0.001). Those with >70% stenosis who received GTN had a favourable shift in mRS (OR 0.56, 95% CI 0.34−0.93, p = 0.024) compared to those who received no GTN. Tendencies towards less dependency, albeit non-significant, were seen in 30-50% and 50-70% groups. No differences in mRS were seen across groups of bilateral stenosis or between those who received GTN or not.
Conclusion
Severe ipsilateral carotid stenosis is associated with poorer functional outcome at 90 days following ischaemic stroke. GTN appears safe in acute stroke patients with ipsilateral or bilateral carotid stenosis.
Trial registration number
N/A
AS16-085
FACTORS ASSOCIATED WITH FAVORABLE OUTCOME OF BASILAR ARTERY OCCLUSION PATIENTS INTUBATED ON HOSPITAL ADMISSION
1University of Helsinki, Molecular Neurology Research Program, Helsinki, Finland
2Helsinki University Hospital - University of Helsinki, Department of Neurology, Helsinki, Finland
3Helsinki University Hospital - University of Helsinki, Helsinki Medical Imaging Center, Helsinki, Finland
Background and Aims
Roughly a third of basilar artery occlusion (BAO) patients present comatose on admission. Frequently coma on admission is regarded to be associated with poor outcome. However, there is a group of comatose BAO patients who might still achieve fair outcome after recanalization therapy. We set out to study which factors are associated with better outcome in BAO patients presenting intubated on admission.
Method
We analyzed 261 consecutive BAO patients treated in Helsinki University Hospital between June 1995 and January 2017 in whom 117 presented intubated on admission. Favorable outcome was defined as a modified Rankin Scale (mRS) 0-3 at 3 months.
Results
Favorable outcome was achieved in 22.4% of comatose patients. Patients with favorable outcome were younger (mean age 54 years vs. 66 years; p = 0.001) and had less often atrial fibrillation 7.7% vs. 28.9%; p = 0.026). Successful recanalization was essential for favorable outcome with 100% of patients in mRS 0-3 group vs. 50.8% of mRS 4-6 group achieving recanalization (p < 0.0001). Extensive baseline ischemia, evaluated with the posterior circulation Acute Stroke Prognosis Early CT Score (pc-ASPECTS) < 8 (43.3% vs. 19.2%; p = 0.026), and development of symptomatic intracranial hemorrhage (sICH) (20.2% vs. 0.0%; p = 0.011) were associated with poor outcome.
Conclusion
Despite coma on presentation, more than 2 out of 10 patients survive BAO favorably and the number rises to 4 out of 10 if recanalized. This likelihood is higher if the patients are younger and lack atrial fibrillation and extensive ischemic signs at baseline
Trial registration number
N/A
AS16-086
PINK PUFFER PROFILE IN CEREBROVASCULAR DISEASES
1Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Neurology, Ariano Irpino AV, Italy
2Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Internal Medicine, Ariano Irpino AV, Italy
3Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Cardiology, Ariano Irpino AV, Italy
4Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Intensive Care, Ariano Irpino AV, Italy
5Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Radiology, Ariano Irpino AV, Italy
6Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Laboratory, Ariano Irpino AV, Italy
7Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Infantile Neuropsychiatry, Ariano Irpino AV, Italy
Background and Aims
Cardiac biomarkers are increased in cerebrovascular conditions, especially in class III/IV, C/D New York Heart Association (NYHA) and American Cardiology Association (ACA) scales. Delta criterium allows differential diagnosis between acute and chronic conditions before the appearance of ischaemic signs at electrocardiogram (ECG) / echography (Fiori P. et al, 2017). The aim of our current study is to assess the impact of pulmonary emphysema.
Method
So far, we recruited 63 acute strokes (AS), 32 chronic cerebrovascular conditions (CCVD), 25 other neuropsychiatric diseases (OND). They underwent ECG and chest ray and/or CT at emergency department, blood withdrawal within 24 hours, echocardiography within one week.
Results
Preliminary results show significant higher levels of troponin ths (tro ths) and N-terminal-pro-Brain Natriuretic Peptide (NT-pro-BNP) levels in class III/IV, C/D NYHA and ACA AS and CCVD affected with emphysema (group A) compared to those without it (group B). Glasgow Coma Scale, Glasgow Outcome Scale were lower and Modified Rankin Scale was higher in the former compared to the latter. Central hyperventilation decreases pCO2 levels without compensating pO2 deficit.
Conclusion
In “pink puffers” a mismatch between ventilation and perfusion is present. Low pCO2 may impair cerebral vasodilatation. Low pO2 reduces penumbra and enlarges necrotic ischaemic core. Structural pulmonary damage may account for concomitant chronic cerebrovascular sufferance, apoptotic neuronal death, lack of response to Non-Invasive Positive Pressure Ventilation.
Trial registration number
N/A
AS16-087
GENDER-BASED DIFFERENCE OF CARDIOEMBOLIC STROKE LONG-TERM MORTALITY IN LATVIA FROM 2014 TO 2016
1Pauls Stradins Clinical University Hospital, Neurology, Riga, Latvia
2Pauls Stradins Clinical University Hospital, Cardiology, Riga, Latvia
Background and Aims
In this study tried to evaluate a gender based the long-term mortality of cardioembolic stroke in Latvian population.
Method
In a prospective study were included all patients cardioembolic stroke patients admitted to P. Stradins Clinical University Hospital, Riga, Latvia from 2014 to 2016. Patients were divided in two groups based of gender. We evaluated the in-hospital mortality in these patients and performed 30d-90-180d-365d follow-up by phone. Only contacted stroke survivors were included in further study. The mortality rates in both gender groups were compared accordingly.
Results
A total of 1479 patients were included in this study- 65,18% (964) women and 34,82% (515) men. The average age was 78,46 (SD-8,033) in women and 73,43 (SD- 9,599) in men. A total in-hospital mortality was 13,18% (195) with 11,26% (58) in men and 14,21% (137) in women. Of 1209 patients discharged 81,74% (1014) were contacted for follow-up. The mortality rates are shown in table below.
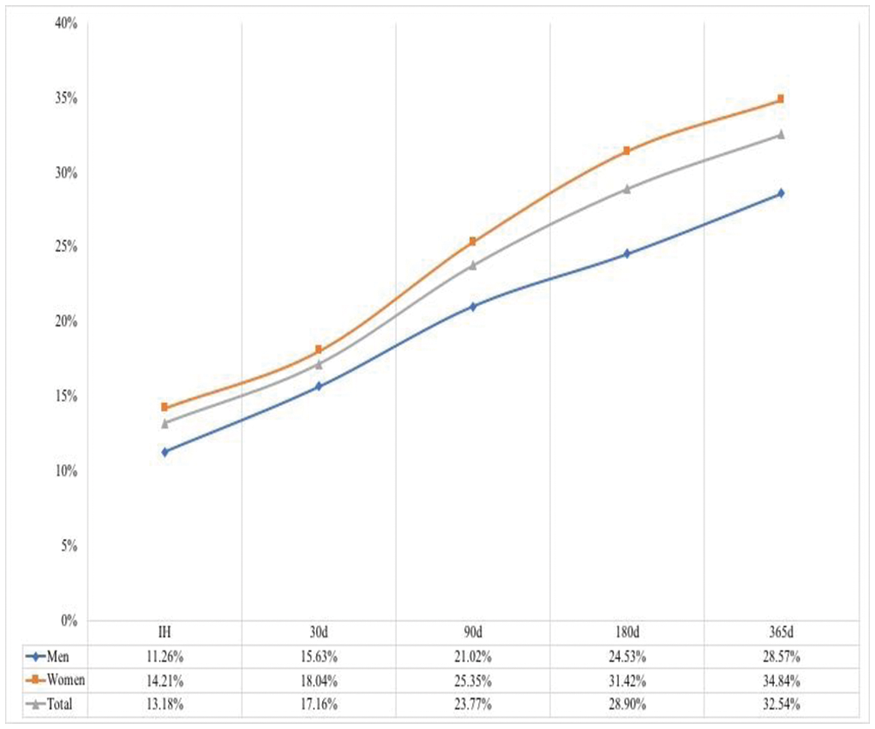
Conclusion
Our study shows that cardioembolic stroke mortality rates are higher in women then in men.
Trial registration number
N/A
AS16-088
BLUE BLOATER PROFILE IN CEREBROVASCULAR DISEASES
1Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Neurology, Ariano Irpino AV, Italy
2Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Internal Medicine, Ariano Irpino AV, Italy
3Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Cardiology, Ariano Irpino AV, Italy
4Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Intensive Care, Ariano Irpino AV, Italy
5Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Radiology, Ariano Irpino AV, Italy
6Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Laboratory, Ariano Irpino AV, Italy
7Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Infantile Neuropsychiatry, Ariano Irpino AV, Italy
Background and Aims
Cardiac biomarkers are increased in cerebrovascular conditions, especially in class III/IV, C/D New York Heart Association (NYHA) and American Cardiology Association (ACA) scales. Delta criterium allows differential diagnosis between acute and chronic conditions before the appearance of ischaemic signs at electrocardiogram (ECG) / echography (Fiori P. et al, 2017). The aim of our current study is to assess the impact of chronic pulmonary disease with decompensated congestive heart failure and pleural effusion.
Method
So far, we recruited 368 acute strokes (AS), 89 chronic cerebrovascular conditions (CCVD), 25 other neuropsychiatric diseases (OND). They underwent ECG and chest ray and/or CT at emergency department, blood withdrawal within 24 hours, echocardiography within one week.
Results
Preliminary results show significant higher levels of troponin ths (tro ths) and N-terminal-pro-Brain Natriuretic Peptide (NT-pro-BNP) levels in class III/IV, C/D NYHA and ACA AS and CCVD affected with chronic pulmonary heart disease with decompensated congestive heart failure and pleural effusion (group A) compared to those without pleural effusion (group B). PO2 levels, Glasgow Coma Scale, Glasgow Outcome Scale were lower, pCO2 and Modified Rankin Scale were higher in the former compared to the latter.
Conclusion
A malignant circulatory profile, characterized by increased mismatch between ejection fraction and pulmonary arterial pressure, may account for resistance to treatment and negative prognosis. Non-Invasive Positive Pressure Ventilation may help in increasing oxygenation and reducing hypercapnia and risk of haemorrhagic complicances.
Trial registration number
N/A
AS16-089
PINK PUFFER AND BLUE BLOATER PROFILE IN ACUTE STROKE
1Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Neurology, Ariano Irpino AV, Italy
2Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Internal Medicine, Ariano Irpino AV, Italy
3Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Cardiology, Ariano Irpino AV, Italy
4Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Intensive Care, Ariano Irpino AV, Italy
5Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Radiology, Ariano Irpino AV, Italy
6Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Laboratory, Ariano Irpino AV, Italy
7Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Infantile Neuropsychiatry, Ariano Irpino AV, Italy
Background and Aims
Cardiac biomarkers are increased in cerebrovascular conditions, especially in class III/IV, C/D New York Heart Association (NYHA) and American Cardiology Association (ACA) scales. The aim of our current study is to evaluate the impact of respiratory failure and the differences between pink puffers and blue bloaters.
Method
So far, we recruited 431 acute strokes (AS), 121 chronic cerebrovascular conditions (CCVD), 25 other neuropsychiatric diseases (OND). They underwent ECG and chest ray and/or CT at emergency department, blood withdrawal within 24 hours, echocardiography within one week.
Results
Preliminary results show significant lower O2 saturation and higher levels of pCO2, heart rate, troponin ths (tro ths) and N-terminal-pro-Brain Natriuretic Peptide (NT-pro-BNP) levels in class III/IV, C/D NYHA and ACA blue bloater AS (group A) compared to pink puffer AS (group B). A greater improvement at Glasgow Coma Scale, Glasgow Outcome Scale and Modified Rankin Scale was observed in the latter compared to the former.
Conclusion
Respiratory failure worsens ischaemic sufferance and negatively interferes with recovery. High pressure and volume overload in blue bloaters increase the risk of cardiac ischaemic damage with subsequent poor neurological outcomes. Diuretics and novel therapeutical agents, as recombinant brain natriuretic peptide and sacubitril, may be pivotal in restoring circulatory function in these patients. Bridge therapy with low molecular weight eparins may be useful for preventing hromboembolism. Non-Invasive Positive Pressure Ventilation may be helpful in increasing perfusion and limiting diffusion-restricted volume in both pink puffers and blue bloaters, particularly in the latter.
Trial registration number
N/A
AS16-090
ASSOCIATION BETWEEN LEUKOCYTE AND HEMORRHAGIC TRANSFORMATION AFTER ISCHEMIC STROKE
1West China Hospital of Sichuan University- Stroke Clinical Research Unit, Department of Neurology, Chengdu, China
Background and Aims
Leukocyte infiltrated into the ischemic tissue after ischemic stroke is associated with blood-brain-barrier damage and may cause hemorrhagic transformation (HT). Whether leukocyte is associated with HT after ischemic stroke and whether the association depends on stroke etiology remains an open question.
Method
Acute ischemic stroke patients within 7 days from stroke onset were included. Blood samples were obtained within 24 hours after admission. HT was defined as hemorrhage presented on follow-up MRI or CT but not on baseline CT. Stroke was divided into five categories according to the criteria of the Trial of Org 10172 in Acute Stroke Treatment (TOAST).
Results
We included 973 patients (mean age 63.94 ± 14.60 years; 63% male). HT occurred in 115 patients (11.82%). Leukocyte was grouped into quartiles(Quartile 1: < 6.22, Quartile 2 : 6.22-7.66, Quartile 3: 7.67-9.31, Quartile 4: > 9.31), and Quartile 1 was set as reference. Univariate analysis identified risk of HT was higher in Quartile 3 ( OR 2.205, 95% CI 1.217-3.994 ) and Quartile 4 (OR 2.075, 95% CI 1.140- 3.778). In multiple regression analysis, leukocyte were independently associated with HT in all ischemic stroke patients (OR 2.104, 95% CI 1.080-4.099), and in the subgroup of cardio-embolic stroke (OR 4.411, 95% CI 1.372- 4.179), but not in the subgroup of the other three types of stroke.
Conclusion
Leukocyte counts were significantly associated with the risk of HT in all ischemic stroke patients, especially in cardio-embolic stroke patients.
Trial registration number
N/A
AS16-091
USING A NOVEL AND NONINVASIVE CEREBRAL AUGMENTATION INDEX AS EVALUATED BY EXTERNAL COUNTERPULSATION TO PREDICT LONG-TERM CLINICAL OUTCOME AFTER ACUTE ISCHEMIC STROKE
1The Chinese University of Hong Kong, Medicine & Therapeutics, Shatin- N.T., Hong Kong S.A.R
2The 3rd Affiliated Hospital of Zhong Shan University, Rehablitation, Guang Zhou, China
Background and Aims
External counterpulsation (ECP) is a non-invasive method used to augment cerebral blood flow of patients with ischaemic stroke via induced hypertension. We aimed to whether the cerebral augmentation index (CAI) evaluated by ECP can predict clinical outcomes after acute ischemic stroke.
Method
We enrolled acute ischemic stroke patients within 7 days after stroke onset. Bilateral middle cerebral arteries of patients were monitored using transcranial Doppler (TCD). Flow velocity changes before, during and after ECP were, respectively, recorded for 3 min. The cerebral augmentation index (CAI) was the increase in percentage of the middle cerebral artery mean flow velocity during ECP compared with baseline. TCD data were analysed based on the side ipsilateral or contralateral to the infarct. The modified Rankin Scale (mRS) (good outcome: mRS 0∼2; poor outcome: mRS 3∼6) was evaluated 3 months after the index stroke.
Results
106 patients were included (mean age, 63.8 ± 10.9 years; 88.7% males). At month 3 after stroke onset, univariate analysis showed that the National Institutes of Health Stroke Scale at recruitment was significantly higher in the poor outcome group, while the ipsilateral CAI was significantly lower in the good outcome group than that in the poor outcome group (3.82 ± 3.04 vs 6.82 ± 6.66, p = 0.048). Multivariate logistic regression showed that ipsilateral CAI was independently correlated with an unfavourable functional outcome after adjusting for confounding factors.
Conclusion
The higher degree of cerebral blood flow velocity augmentation on the side ipsilateral to the infarct induced by ECP is independently correlated with an unfavourable functional outcome after acute ischemic stroke.
Trial registration number
N/A
AS16-092
HIGH LEVELS OF COAGULATION FACTORS FVIII AND FXI ARE ASSOCIATED WITH OUTCOMES AFTER FIRST STROKE
1Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin, Berlin, Germany
2Charité - Universitätsmedizin Berlin, Insitute for Biometry and Clinical Epidemiology, Berlin, Germany
3Leiden University Medical Center, Department of Clinical Epidemiology, Leiden, The Netherlands
Background and Aims
Though recurrence risk is high following ischemic stroke, little is known about risk factors for secondary events. The coagulation factors VIII, XI, and XII (FVIII, FXI, and FXII) have been implicated in first thrombotic events; our aim was to elucidate their role in outcomes after first stroke.
Method
The PROSpective Cohort with Incident Stroke Berlin (PROSCIS-B) study followed participants aged 18 and older after first mild to moderate ischemic stroke event for a median of three years until occurrence of recurrent stroke, myocardial infarction or all-cause mortality. High coagulation factor activity levels (p75) were compared to low/normal levels, and quartiles were used to assess dose response. We used Cox proportional hazards models adjusted for age, sex, and cardiovascular risk factors to estimate hazard ratios (HRs).
Results
In total, 92 events occurred in 570 included participants, resulting in an absolute risk of 6.5/100 person-years. High FVIII showed the strongest relationship with the combined endpoint (HR = 2.05, 95%CI 1.28-3.29). High FXI levels were also associated with an increase in relative risk (HR = 1.80, 95%CI 1.09-2.98) and quartile analyses indicated this relationship is dose-responsive. Contrarily, high FXII levels were not significantly associated with the combined endpoint (HR = 0.86, 95%CI 0.49-1.51).
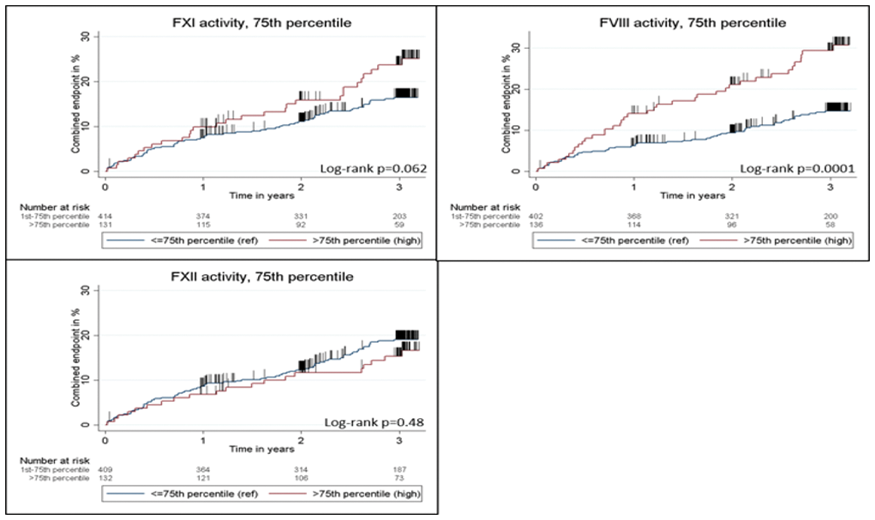
Conclusion
High levels of coagulation proteins FVIII and FXI are associated with an increased risk of combined cardiovascular/all-cause mortality endpoint in the three-year period after first ischemic stroke.
Trial registration number
N/A
AS16-093
PREDICTORS OF EARLY DEATH IN CEREBRAL VENOUS THROMBOSIS
1Academic Medical Center University of Amsterdam, Neurology, Amsterdam, The Netherlands
2Helsinki University Central Hospital, Neurology, Helsinki, Finland
3University hospital Inselspital, Neurology, Berne, Switzerland
4Sahlgrenska University Hospital, Neurology, Gothenburg, Sweden
5Royal Adelaide Hospital, Neurology, Adelaide, Australia
6National Institute of Neurology and Neurosurgery Manuel Velasco Suarez, Neurology, Mexico City, Mexico
Background and Aims
Contemporary studies have shown a steady decline in mortality of cerebral venous thrombosis (CVT). We examined current causes and predictors of early death in CVT.
Method
We used data from the International CVT Consortium, which contains information of consecutive adult CVT patients of 6 centers from 6 countries admitted between 2000 and 2017. We used logistic regression analysis to determine baseline predictors of death within 30 days of diagnosis.
Results
Data from 923 patients with CVT were included. Median age was 43 years (IQR 30-55) and 65.6% were female. Forty-eight patients (5.2%) died within 30 days (31 within 7 days). Predictors of death were coma at admission (OR 6.42, 95% CI 3.20-12.90), pre-existing cancer (OR 3.61, 95% CI 1.58-8.23), intracerebral hemorrhage (OR 4.72, 95% CI 2.36-9.42), thrombosis of the superior sagittal sinus (OR 2.18, 95% CI 1.10-4.33), and thrombosis of the deep cerebral venous system (OR 2.08, 95% CI 1.03-4.21). Patients who died within 30 days were less often treated with anticoagulation (77.1% versus 93.5%, p < 0.001), and more often underwent endovascular treatment (27.1% versus 5.7%, p < 0.001) and decompressive hemicraniectomy (21.3% versus 4.2%, p < 0.001). A new intracerebral hemorrhage occured in 21 out of 48 patients (43.8%) who died within 30 days. The main cause of death was cerebral herniation (83.3%).
Conclusion
In this large international study, early death occurred in 5% of CVT patients. Coma and baseline intracerebral hemorrhage were the strongest predictors of early death. A new intracerebral hemorrhage occured in >40% of patients who died within 30 days.
Trial registration number
N/A
AS16-094
INFLAMMATORY CYTOKINES IN ACUTE ISCHEMIC STROKE
1Institute of Emergency Medicine, Neurology nr. 2, Chisinau, Moldova
Background and Aims
Stroke is a frequent cause of death and long-term disability worldwide. Proinflammatory cytokines play a key role in the progression of the irreversible ischemic lesions. The presence of anti-inflammatory mediators may prevent secondary ischemic injury. Objectives: 1) To assess the relationship between stroke severity and the serum levels of IL-1b, IL-6, IL-10, and TNF-a; and 2) To analyze the neurological outcome after 7 days of ischemic stroke onset and expression of interleukins.
Method
We measured the serum levels of IL-1b, IL-6, IL-10, and TNF-a in 75 patients with acute stroke. The blood level of IL-1b, IL-6, IL-10, and TNF-α was determined by ELISA Neurological impairment was scored using the National Institute of Health Stroke Scale (NIHSS) within the first 24 hours and the 7th day after stroke onset. Eleven healthy subjects were analyzed as controls.
Results
The IL-1b, IL-6, IL-10, and TNF-a levels in the 1st and 7th day of patients hospitalization was higher significantly in comparison with the control group (fig.1). There has been established the correlation between the inflammatory cytokines values and NIHSS score. It can be stated that the most powerful relationship was with IL-1b (r = 0,73) (fig.2, fig.3, fig.4, fig.5).
Conclusion
Increased IL-1b, IL-6, IL-10 and TNF-a concentrations are present in early stroke period and are associated with the degree of neurological deficit. Measurement of IL-1 b, IL-6, IL-10 and TNF-a may be useful for the follow-up of clinical outcome after ischemic stroke.
Trial registration number
N/A
AS16-095
VERBAL MEMORY EFFECTS IN ISCHAEMIC STROKE PATIENTS WITH THE APOLIPOPROTEIN EPSILON-4 ALLELE
1The Florey Institute of Neuroscience and Mental Health, Behavioural Neuroscience, Heidelberg, Australia
2Austin Health, Neurology, Heidelberg, Australia
Background and Aims
Cognitive impairment is common after ischaemic stroke. Our aim was to examine the effect of a known genetic risk factor for cognitive impairment and dementia – the apolipoprotein E (APOE) epsilon-4 (ε4) allele – on cognition in ischaemic stroke patients three months after stroke.
Method
We recruited ischaemic stroke patients of all types from three hospitals in Melbourne. Patients completed detailed cognitive assessments three months after stroke. Six domains were assessed: attention, processing speed, executive function, language, visuospatial function, and memory (verbal, visual). Z-scores were calculated using age-appropriate norms. APOE gene single nucleotide polymorphisms (SNPs)(rs7412, rs429358) were genotyped on venous blood using TaqMan® SNP Genotyping assays (Thermofisher, Australia) on a ViiA™ 7 (Applied Biosystems).
Results
We compared 21 carriers of the APOE ε4 allele with 21 non-carriers from our larger cohort. Groups did not differ on any demographic or clinical variable (Table 1). Stroke locations were also comparable between groups (Oxfordshire Criteria, p = 0.27). Days elapsed between stroke onset and assessment did not differ in the carrier (median (IQR) = 99 (84,135)) and non-carrier (median (IQR) = 89 (82,102)) groups (p = 0.26). Carriers and non-carriers performed similarly in all cognitive domains (p>0.05) except verbal memory: carriers performed worse than non-carriers on measures of immediate recall (p = 0.009) and retention (p = 0.047), but not on a measure of delayed recall (p = 0.06).
Conclusion
The APOE ε4 allele may be a risk factor for verbal memory dysfunction after ischaemic stroke.
Trial registration number
N/A
AS16-096
RELATION OF B-TYPE NATRIURETIC PEPTIDE AND SEVERE STROKE IN ACUTE ISCHEMIC STROKE WITH ATRIAL FIBRILLATION
1Hallym University Sacred Heart Hospital, Neurology, Anyang- Gyeonggi-do, Republic of Korea
Background and Aims
The aim of this study is to investigate whether the B-type natriuretic peptide (BNP) is associated with initial stroke severity and infarct volume in acute ischemic stroke (AIS) patients with atrial fibrillation (AF).
Method
We studied a total of 242 AIS patients with AF who were admitted within 72 h of the onset of symptoms. The BNP levels were measured with a standardized method when patients were admitted to hospital. Initial stroke severity was assessed using the NIH Stroke Scale (NIHSS) scores. Infarct volume was measured using DWI. We performed bivariate and multivariable median regression analyses to examine the association between the BNP and NIHSS scores and DWI infarct volumes.
Results
Mean age 73 years, and 54.1% women. The median NIHSS score at presentation was 7 points (interquartile range [IQR] 2-16) and the median DWI infarct volume was 21.3 cc (IQR 3.4-73.2). Spearman’s rank correlation analysis showed that the raw BNP levels were significantly positively correlated with both initial NIHSS scores (r = 0.33; P < 0.001) and DWI infarct volumes (r = 0.45; P<0.001). Multivariate median regression analyses demonstrated that the BNP was independently associated with an increase of 2.7 points in the NIHSS in the NIHSS (95% confidence interval [CI] 1.3-3.5; P<0.001) and an increase of 16.7 cc in DWI infarct volume (95% CI 12.6-20.8; P < 0.001).
Conclusion
The BNP may be a useful marker of severe stroke and large infarct, which is related to severe atrial dysfunction and the large atrial thrombus in patients with AF.
Trial registration number
N/A
AS16-097
A COMPARISON OF TRENDS IN PROCESSES OF STROKE CARE AND OUTCOMES BETWEEN PATIENTS WITH IN-HOSPITAL AND COMMUNITY-ONSET STROKE USING THE SOUTH LONDON STROKE REGISTER
1King's College London, School of Population Health & Environmental Sciences, London, United Kingdom
2Guy's and St Thomas' NHS Foundation- Trust and King's College London, NIHR Comprehensive Biomedical Research Centre, London, United Kingdom
3Guy's and St Thomas' NHS Foundation Trust, Department of Ageing and Health, London, United Kingdom
Background and Aims
Acute care and outcomes for stroke have improved over the past decade. We aimed to determine whether patients who had their stroke in hospital (in-hospital stroke, IHS) experienced similar improvements in care and outcomes as those who were admitted with stroke (community-onset stroke, COS).
Method
Data from an inner-city stroke register were used to evaluate trends in processes of care and outcomes across three cohorts (1995–2001, 2002–2008, 2009–2015). Kaplan-Meier survival curves and predictors of survival (Cox proportional hazards models) were calculated.
Results
Out of 5,119 admitted stroke patients registered between 1995 and 2015, 552(10.8%) were IHS. Over the study period, brain imaging rates increased to 100% for both groups. Rates of stroke unit care rose in both groups, but remained lower for IHS (1995-2001: 12.4% (IHS) vs. 32.2% (COS), 2009-2015: 65.4% (IHS) vs. 86.3% (COS), P<0.001). In 2009–2015, thrombolysis rates were lower for ischaemic IHS (13.8% (IHS) vs. 17.8% (COS), P = 0.290) and median hospital-stay was longer after IHS (17 days (IHS) vs. 7 days (COS), P<0.001).
In 2009-2015, rates of in-hospital death were 26.7% (IHS) vs. 13.7% (COS, P<0.001). 5-year mortality rates declined for IHS from 80.8% (1995-2001) to 51.1% (2009-2015) and for COS from 58.9% (1995-2001) to 35.2% (2009-2015). After adjusting for socio-demographic factors, pre-stroke disability, vascular risk factors, stroke severity/subtype, and hospital care processes, IHS remained associated with 24% higher mortality compared to COS (HR 1.24; 1.08–1.42).
Conclusion
Despite improvements, processes of care and outcomes for IHS remain poorer than for COS. IHS patients need to enter evidence-based hospital pathways more effectively to experience their well-established benefits.
Trial registration number
N/A
AS16-098
INTERLEUKIN-6 INDEPENDENTLY PREDICTS LATE FATALITY AND POOR FUNCTIONAL OUTCOME AFTER TRANSIENT ISCHAEMIC ATTACK (TIA) AND NON SEVERE STROKE
1University College Dublin, Stroke Clinical Trials Network Ireland, Dublin, Ireland
2Mater Misercordiae University Hospital, Stroke Service, Dublin, Ireland
3University College Dublin, Conway Institute, Dublin, Ireland
4St Vincent's University Hospital, Medicine for the Older Person, Dublin, Ireland
5James Connolly Memorial Hospital- Blanchardstown, Medicine for the Older Person, Dublin, Ireland
6Mater Misercordiae University Hospital, Clinical Biochemistry, Dublin, Ireland
7St James University Hospital, Stroke Department, Dublin, Ireland
8Mater Misercordiae University Hospital, Stroke Clinical Trials Network Ireland, Dublin, Ireland
9Beaumont University Hospital, Neurology, Dublin, Ireland
10St Vincent's University Hospital, Stroke, Dublin, Ireland
11Royal College of Surgeons in Ireland, Stoke, Dublin, Ireland
12Mater Misercordiae University Hospital / University College Dublin, Stroke Clinical Trials Network Ireland, Dublin, Ireland
Background and Aims
Atherosclerotic plaque inflammation is associated with major vascular events (MVEs), including stroke. The CANTOS trial recently demonstrated that canukinumab, an interleukin-1 antagonists, reduced risk of MVEs. Interleukin 6 (IL6) is an ‘upstream' central inflammatory pathway cytokine, which stimulates ‘downstream' acute phase response proteins (eg C-reactive protein [CRP]). We investigated the relationship between IL-6, CRP, other inflammatory cytokines and outcome after TIA and non-severe stroke.
Method
The BIO-STROKE and BIO-TIA studies included patients with TIA and non-severe stroke (Rankin ≤3) <72 hours after symptom onset. Exclusion criteria included malignancy, infection, recent trauma / surgery, TIA mimics or recurrent stroke before phlebotomy/MRI. Plasma high-sensitivity CRP and IL-6 were measured by mass spectrometry and IL1, IL8, IL10, IL12, interferon-alpha and tumour necrosis factor by ELISA. Follow up occurred at 7, 28, 90&365 days.
Results
Of 726 patients included (483 strokes, 243 TIA), median age was 70. Carotid stenosis >50% was present in 23.6%.
Median IL-6 was 5.86pg/ml (stroke), 4.25pg/ml (TIA),3.06pg/ml (control)(p < 0.001). Median hsCRP was 3.75mg/L, 2.36mg/l and 1.87mg/L in the stroke, TIA and control groups respectively (p < 0.001).
On mutivariate logistic regression, after adjustment for age, prior stroke, carotid stenosis and diabetes mellitus, IL6 independently predicted all-cause mortality at 1 year (OR 1.68, p = 0.02) and functional outcome (Rankin ≤ 2) at 1 year (p = 0.04), with a trend for recurrent stroke at 1 year (OR 1.26, p = 0.06).
CRP independently predicted 1 year all cause mortality (OR 1.71 p = 0.013) but not other outcomes. Other inflammatory cytokines did not predict outcomes.
Conclusion
In patients with TIA/non-severe stroke, IL-6 may have utility as a prognostic marker and may guide selection of patients for anti-inflammatory preventive therapy.
Trial registration number
NA
AS16-099
STROKE/TIA IN ASIAN AND NON-ASIAN POPULATIONS: SUBGROUP ANALYSIS OF THE RANDOMIZED PERFORM STUDY
1Tokyo Women's Medical University, Department of Neurology, Tokyo, Japan
2Hôpital Bichat, Department of Neurology and Stroke Center, Paris, France
3Université de Lille, CHU Lille- EA 2694 - Santé publique : épidémiologie et qualité des soins, Lille, France
4Hôpital Lariboisière, Department of Neurology, Paris, France
5University of Barcelona, Hospital Clinic de Barcelona, Barcelona, Spain
6Beth Israel Deaconess Medical Center, Harvard Medical School, Massachusetts, USA
7University of Glasgow, Robertson Centre for Biostatistics, Glasgow, United Kingdom
8Royal Brompton Hospital, NHLI Imperial College, London, United Kingdom
9University of Heidelberg, Department of Neurology, Mannheim, Germany
10Universität Bern, Neurologische Klinik und Poliklinik, Bern, Switzerland
11University of Oxford, Department of Clinical Neurosciences, Oxford, United Kingdom
12Hôpital Bichat, Department of Cardiolog, Paris, France
13Hôpital Fernand Widal, Department of Biostatistic, Paris, France
Background and Aims
We aimed to compare the nature and prognosis of non-cardioembolic stroke/TIA between Asian and non-Asian populations on antiplatelet monotherapy.
Method
We analyzed data from the PERFORM study, in which 19,100 patients (2,178 Asian; 16,922 non-Asian) with non-cardioembolic ischemic stroke/TIA were randomized to aspirin or terutroban and followed for 2 years. The primary outcome was a composite of major adverse cardiovascular events (MACE; nonfatal myocardial infarction, nonfatal stroke, and cardiovascular death).
Results
There was no difference in MACE risk between patients from Asian and non-Asian countries (11.1% vs 10.5%; p = 0.39). However, those from Asian countries were at significantly higher risk of intracranial hemorrhage (2.4% vs 1.3%; hazard ratio [HR] 1.87; 95% CI 1.34-2.60; p < 0.001) and major bleeding (5.4% vs 4.1%; HR 1.30; 95% CI 1.04-1.61; p = 0.02). Stroke risk was significantly higher in Asian than non-Asian populations among patients with lacunar stroke (7.4% vs 4.5%; p = 0.02). Multivariable analysis identified population-specific predictors for MACE; diastolic blood pressure (HR per 5 mm Hg 1.08; 95% CI 1.01–1.16; p = 0.03) and diabetes mellitus (HR 1.36; 95% CI 1.22–1.52; p < 0.001) were independent predictors for patients from Asian and non-Asian countries, respectively.
Conclusion
Compared with patients from non-Asian countries, those from Asian countries had a 1.9-fold higher risk of hemorrhagic stroke when given antiplatelet therapy for secondary prevention after non-cardioembolic stroke/TIA. The knowledge of population disparities in vascular risk and the factors that contribute to them will help develop targeted prevention strategies.
Trial registration number
ISRCTN66157730
AS16-100
ASSESSMENT TOOLS FOR FUNCTIONAL INDEPENDENCE AND RESIDUAL DISABILITY AFTER STROKE: ARE THEY COMPARABLE?
1Samsung Medical Center, Physical and Rehabilitation Medicine, Seoul, Republic of Korea
2School of Medicine- Chungnam National University, Department of Rehabilitation Medicine, Daejeon, Republic of Korea
3Konkuk University School of Medicine, Department of Rehabilitation Medicine, Seoul, Republic of Korea
4Yonsei University College of Medicine, Department and Research Institute of Rehabilitation Medicine, Seoul, Republic of Korea
5Chonnam National University Medical School, Department of Physical and Rehabilitation Medicine, Gwangju, Republic of Korea
6Pusan National University Yangsan Hospital, Department of Rehabilitation Medicine, Yangsan, Republic of Korea
7Wonkwang University School of Medicine, Department of Preventive Medicine, Iksan, Republic of Korea
8Kyungpook National University Hospital, Department of Rehabilitation Medicine, Daegu, Republic of Korea
9Jeju National University Hospital- University of Jeju College of Medicine, Department of Rehabilitation Medicine, Jeju, Republic of Korea
10Hallym University, Department of Statistics, Chuncheon, Republic of Korea
11Ewha Womans University, Department of Health Convergence, Seoul, Republic of Korea
12Korea Center for Disease Control, Division of Chronic Disease Control, Osong, Republic of Korea
Background and Aims
To investigate the correlations between the modified Rankin Scale (mRS) grades and Korean version of modified Barthel Index (K-MBI) scores in assessing the residual functional status of stroke survivors.
Method
K-MBI and mRS were administered to 5,759 ischemic stroke patients at 3 months after onset of stroke. The sensitivity and specificity were calculated at all possible K-MBI score cutoffs for each mRS grade in order to obtain the optimally corresponding K-MBI scores and mRS grades. The area under the curve (AUC) for receiver operator characteristic curves and was calculated.
Results
The K-MBI cutoff points with the highest sum of sensitivity and specificity were 100 (sensitivity 0.940; specificity 0.612), 98 (sensitivity 0.904; specificity 0.838), 94 (sensitivity 0.885; specificity 0.937), 78 (sensitivity 0.946; specificity, 0.973), and 55 (sensitivity 937; specificity 0.986) for mRS grades 0, 1, 2, 3, and 4, respectively. The AUC was 0.791 for mRS grade 0, 0.919 for mRS grade 1, 0.970 for mRS grade 2, 0.994 for mRS grade 3, and 0.991 for mRS grade 4.
Conclusion
The K-MBI ranges for representing mRS grades were variable. mRS grades 0, 1, and 2 had narrow K-MBI score ranges, while mRS grades 3, 4, and 5 showed broad K-MBI score ranges. mRS grade seemed to sensitively differentiate mild residual disability of stroke survivors, whereas K-MBI can provide more specific information of the functional status of stroke survivors with moderate to severe residual impairment. (This work was supported by the Research Program funded by the Korea Centers for Disease Control and Prevention (2016E3300302)).
Trial registration number
NCT03402451
AS16-101
THE PATTERN OF PENETRATION AND ASPIRATION IN ACUTE STROKE SURVIVORS
1University of Nottingham, Stroke Trials Unit- Division of Clinical Neurosciences, Nottingham, United Kingdom
2University of Nottingham, Division of Medical Sciences & GEM, Nottingham, United Kingdom
3University of Manchester, Division of Diabetes- Endocrinology and Gastroenterology, Manchester, United Kingdom
Background and Aims
Aspiration is common in acute stroke survivors with dysphagia, is associated with increased pneumonia rates, and is an independent predictor of mortality. However, studies evaluating the nature and pattern of penetration and aspiration post-stroke are lacking.
Method
The Penetration-Aspiration Scale (PAS) was used to rate baseline videofluoroscopic swallowing studies of 17 dysphagic stroke survivors from the STEPS trial of pharyngeal electrical stimulation (onset <14 days, mean 74 years). Analysis was performed on 6 x 5ml boli and 1 x 50ml bolus (thin fluids with contrast agent at 40% wt/vol), recorded at 25 f/s. Every swallow to clear each 5ml or 50ml bolus was counted, given a PAS score and labelled a primary or secondary (clearing) swallow.
Results
In total, 285 swallows were viewed. Due to poor image quality, 7% of swallows were excluded. At a bolus level, for 5ml/50ml swallows, results showed 68%/42% normal swallows, 14%/27% penetration and 18%/31% aspiration respectively. At a subject level, 5ml: only 3 patients scored within normal limits for all boli; 50ml: no subject swallowed without showing penetration or aspiration at some point. Higher penetration and aspiration scores occurred on 50ml. Aspirated material was rarely fully cleared, even in those subjects who demonstrated a cough response (5ml: 2%, 50 ml: 0%).
Conclusion
Aspiration in post-stroke dysphagia appears to fluctuate in presentation within and between boli. Bedside assessments should take into account variability and sample enough swallows. In addition, clinicians should not assume coughing clears aspirated material. Quality of image capture must be optimised for future studies.
Trial registration number
N/A
AS16-102
LONG-TERM OUTCOME OF STROKE PATIENTS: DATA FROM A MULTICENTER COHORT OF LEBANESE STROKE PATIENTS
1Lebanese University, Laboratory of Clinical and Epidemiology Research, Beirut, Lebanon
2Henri Mondor Hospital AP-HP, Department of Neurology, Creteil, France
3Lebanese University, Faculty of Medicine, Beirut, Lebanon
4Saint Joseph University- Hotel Dieu de France, Faculty of Medicine, Beirut, Lebanon
Background and Aims
Stroke is one of the leading causes of death and disability worldwide. The objective of this study was to determine the long-term outcome of stroke patients in terms of impairment, disability, handicap, and quality of life.
Method
The survivors and/or their caregivers were interviewed in hospital, at 3-, 6-, and 12-months post stroke. The questionnaire included the Barthel Index, the modified Rankin Scale, the NIHSS and the Stroke Specific Quality Of Life (SSQOL). The paired samples T-test was used to compare repeated measures.
Results
Thirty-one percent of the survivors were severely or moderately disabled, 27.1% were mildly disabled, and 42.1% were functionally independent 1-year post stroke vs. 53.9%, 18.2% and 27.8% at hospital discharge respectively. The mean SSQOL 1-year post stroke was 175 ± 54 vs. 152 ± 54 at hospital discharge (P<0.001).
Conclusion
More than half of our stroke patients had improvement at one year. These findings can help inform future health policy and service planning regarding the longer term management of patients with stroke.
Trial registration number
N/A
AS16-104
FACTORS INFLUENCING ADHERENCE TO SECONDARY PREVENTION MEDICATION AFTER ISCHEMIC STROKE: A PROSPECTIVE POPULATION-BASED COHORT STUDY IN RHONE AREA OF FRANCE
1Hospices Civils of Lyon, Public Health Department, Lyon, France
2University of Lyon, University Claude Bernard Lyon 1- HESPER EA 7425, Lyon, France
3Hospices Civils of Lyon, Emergency Department- Hôpital Edouard Herriot, Lyon, France
4Hospices Civils of Lyon, Department of Stroke Medicine, Bron, France
5Hôpital Nord Ouest, Department of Stroke Medicine, Villefranche-sur-Saone, France
6Hôpital St Joseph St Luc, Emergency Department, Lyon, France
7Hôpital Nord Ouest, Emergency Department, Villefranche-sur-Saone, France
8Hospices Civils of Lyon, Emergency Department- Centre Hospitalier Lyon Sud, Pierre Benite, France
9Hospices Civils of Lyon, Emergency Department- Hôpital Croix Rousse, Lyon, France
Background and Aims
Identifying factors associated with medication adherence to secondary prevention medication is important among ischemic stroke (IS) patients to reduce the risk of recurrence.
Method
We conducted a prospective population-based cohort study (“STROKE 69”) on all patients with an acute IS admitted to any emergency department or stroke unit of the Rhône area (november 2015 to june 2016). Medication adherence was evaluated with the 8-items Morisky scale 3 months after the IS. Characteristics of patients and acute IS management were investigated.
Results
Conclusion
Aging and calling EMS were associated with a higher adherence. Surprisingly, having a history of stroke/TIA and being professionally active tended to be associated with a decreased adherence. These results need to be further investigated in a larger cohort with multivariate analyses.
Trial registration number
NCT03153020
AS16-105
AGE AND SEX SPECIFIC RISK PROFILES AND IN-HOSPITAL OUTCOME IN 2,476 SUBJECTS FROM A MULTICENTRE COHORT
1Hospital Arnau de Vilanova, Stroke Unit, Lleida, Spain
2Hospital Dr. Josep Trueta., Stroke Unit, Girona, Spain
3Hospital de Donostia, Stroke Unit, San Sebastián, Spain
4Hospital de la Paz, Stroke Unit, Madrid, Spain
5Hospital Trias i Pujol, Stroke Unit, Badalona, Spain
6Hospital Clínico, Stroke Unit, Valladolid, Spain
7Hospital Moisés Broggi, Stroke Unit, Esplugues de Llobregat, Spain
8Hospital de Mataró, Neurology Department, Mataró, Spain
9Hospital de la Santa Creu i Sant Pau, Stroke Unit, Barcelona, Spain
10Hospital Universitario de Santiago de Compostela, Stroke Unit, Santiago de Compostela, Spain
11Hospital Joan XXIII, Neurology, Tarragona, Spain
12Hospital de León, Neurology, Leon, Spain
13Hospital Ramón y Cajal, Stroke Unit, Madrid, Spain
14Hospital de Tortosa, Stroke Unit, Tortosa, Spain
Background and Aims
We aimed to determine the age and sex related patterns and predictors of the clinical course in a large multi-centre registry (from Spain’s nationwide hospital-based stroke registry, RENISEN) of admitted haemorrhagic stroke (HS) patients.
Method
We prospectively studied 2,573 HS from 19 university hospitals. Post traumatic intracranial hemorrhage, post-fybrinlosis HS and subarachnoid hemorrhage were excluded. data were analysed by age groups: 18 to 39, 40 to 49, 50 to 59, 60 to 69, 70 to 79, 80 to 89 and ≥ 90 years). Significant disability was defined as a modified Rankin score (mRS) at discharge>2.
Results
The mean (SD) age was 71.2 (13.2) years. 964 (39.1%) subjects were women and 772 (31.3%) were >80 years old. 1690 (68.5%) had mRs >2 at discharge. Older patients were more likely to be female and exhibit primary aetiologies. Previous treatment with anticoagulants was more frequent in women than in men. Older subjects and women were less likely to be admitted to a stroke unit or have a stroke code activated. Age (OR 1.56, 1.41-172), female sex (OR 1.32, 1.04-1.67), diabetes mellitus (1OR.37,1.04-1.81), NIHSS (OR 1.30, 1.24-1,92) at admission and febrile syndrome (OR 2.90, 2.06-4.08) were predictors of poor outcome.
Conclusion
Clinical characteristics, aetiology and management differed with respect to age group and sex. The poorest outcome was in elderly patients. Strategies need to be implemented to ensure equal care was given to all age groups and sex.
Trial registration number
NA
AS16-106
IMPACT OF PREMORBID FRAILTY ON STROKE OUTCOMES
1Colchester General Hospital, Stroke unit, Colchester, United Kingdom
Background and Aims
Frailty amongst stroke patients is increasing and is associated with poorer outcomes. We sought to evaluate the impact of frailty on stroke outcomes in our population which has higher frailty rates than the national average.
Method
Design
Prospective cohort analysis. Stroke subjects admitted over a 4 year period in a district general hospital in UK were included. Data collected prospectively of all patients with stroke was used for analysis.
Frailty was defined as prestroke modified Rankin score of 3 and above (3-5)
Results
Frail patients present with slightly higher severity of stroke, and are slightly less likely to receive thrombolysis. They have a much higher incidence of stroke related complications such as pneumonia, and Urinary tract infections. They are more likely to be placed on palliative care. There is a higher likelihood of death and new institutionalisation.
Key results are presented in Table 1.
Premorbid Rankin score of 3-5 association with increased mortality was retained (Odds ratio: 1.5934(1.1978 to 2.1196) when corrected for other covariates such as stroke type, NIHSS, age, gender, history of Atrial Fibrillation, heart failure, Diabetes. So was the association for UTI, palliative care on discharge and new institutionalisation.
Conclusion
Frail patients present with slightly higher severity of stroke, slightly less likely to receive thrombolysis, have a much higher incidence of stroke related complications including death and higher likelihood of new institutionalisation. By being aware of the association with prestroke frailty and poor outcomes, clinicians can improve outcomes by augmenting evidence based care provision for frail patients.
Trial registration number
N/A
AS16-107
SELECTION OF ACUTE STROKE PATIENTS FOR MECHANICAL THROMBECTOMY: THE MAGNIFICENT SEVEN SCORE
1Comprehensive Stroke Center, Department of Systems Medicine- University of Tor Vergata, Rome, Italy
2Santa Lucia Foundation, Neurorehabilitation Unit, Rome, Italy
3Royal Melbourne Hospital- University of Melbourne, Department of Medicine and Neurology, Parkville, Australia
4University of Tor Vergata, Department of Diagnostic and Molecular Imaging- Interventional Radiology and Radiotherapy- Neuroradiology, Rome, Italy
Background and Aims
Mechanical thrombectomy (MT) is the recommended treatment for acute ischemic stroke patients with large vessel occlusion (LVO). However, use of MT is increasing in recent years and this is burdened by high procedural costs. We tested whether a new prognostic score may be useful to select LVO patients for MT and exclude those who are unlikely to benefit from endovascular therapy.
Method
Prospective patients collected from our endovascular stroke registry were assessed for imaging and clinical outcome measurements. Good outcome at 3 months was defined as modified Rankin Scale (mRS) ≤ 2. We derived a new prognostic score called the MAGNIFICENT SEVEN score (MSS) including clinical and radiological prognostic factors of poor outcome in LVO patients treated with MT. Receiver Operating Characteristics curve analysis and the area under the curve (AUC) were used to assess the discrimination ability of the score.
Results
Among 312 patients suitable for analysis 114; 198 (63.5%) had a poor outcome at 3 months. After multivariate logistic regression analysis, pre-stroke mRS, age, admission glycemia, NIHSS, collateral Flow, Clot Burden Score, Alberta Stroke Program Early CT score were used to create MSS. MSS had a good prognostic accuracy with an AUC of 0.834 [95% CI: 0.79−0.88]. The risk of poor outcome was 93.9% and mortality was 55.6% in the subgroup of patients with higher risk score, regardless successful reperfusion and time to arterial puncture.
Conclusion
The MSS seems to be a useful tool to select patients for MT, but external validation is needed.
Trial registration number
N/A
AS16-108
SPASTICITY SEVERITY AFTER STROKE AND RELATION TO HAND MOTOR RECOVERY AND CORTICO-SPINAL TRACT INTEGRITY
1Karolinska Institutet, Department of Clinical Sciences- Division of Rehabilitation Medicine- Danderyd Hospital, Stockholm, Sweden
2Centre de Psychiatrie et Neurosciences, Inserm U894, Paris, France
Background and Aims
Spasticity of muscles controlling the hand is common after stroke, however, its impact on hand motor recovery and neural correlates are poorly understood. This longitudinal observational study investigated hand spasticity after stroke in relation to motor recovery, secondary complications and lesion location.
Method
Sixty-one patients were assessed at three weeks (T1), three (T2) and six months (T3) after stroke. Neural (NC) and viscoelastic (EC and VC) stretch-resistance in wrist and finger flexors were quantified with the NeuroFlexor method. Clinical evaluation included Fugl-Meyer (FMA-HAND), Box and Block Test (BBT), passive range of movement (ROM) and pain (FMA-subscale). Magnetic Resonance Imaging data were analyzed for weighted corticospinal tract lesion load (wCST-LL) and voxel-based lesion symptom mapping (VLSM).
Results
Four spasticity subgroups were defined: early severe (SS, n = 10), early moderate (MS, n = 10), late developing (LS, n = 17) and no spasticity (NS, n = 24). All groups except SS improved in FMA-HAND to T3. SS and LS had no recovery in BBT. SS showed a larger loss of ROM and more frequent arm pain at T3. wCST-LL predicted NC at T3, also when including FMA-HAND and lesion volume as covariates. VLSM showed that lesioned white matter below the cortical hand knob correlated positively with spasticity.
Conclusion
Severe hand spasticity impairs motor recovery, ROM and may increase risk for development of arm pain. This study provides the first data showing that spasticity is related to lesion load of the CST. The significance of early quantification of spasticity for prediction of motor outcome and rehabilitation planning will be discussed.
Trial registration number
N/A
AS16-109
PRE-STROKE PHYSICAL ACTIVITY COULD INFLUENCE COGNITION IN PATIENTS WITH SUBACUTE STROKE
1Institute of Neuroscience and Physiology, Dep of Clinical Neuroscience, Göteborg, Sweden
Background and Aims
Physical activity pre-stroke has been proven to be effective as prevention. No previous study has described how pre-stroke physical activity influence cognitive function after stroke. The aim was to investigate the influence of pre-stroke physical activity in patients with subacute stroke.
Method
Data from 820 patients in Swedish stroke registers was used and analyses with logistic regression was performed with Montreal Cognitive Assessment (MoCA) as dependent variable. Pre-stroke age, sex, smoking, diabetes, physical activity measured with Saltin-Grimby Physical Activity Level Scale (SGPALS) and protective treatments (statin and hypertension treatment) were independent variables.
Results
Mean age of 73 years, 44.4% were women, 93.9 % with had ischemic stroke. Most patients had mild stroke (80.4%). Half (51.1%) of the patients reported pre-stroke physical inactivity.
In total 481 (58.7%) patients were assessed with MoCA out of whom 215 patients (44.6 %) had normal cognition. The most common cause to not assess with MoCA was dementia or severe cognitive deficit in 62 patients (7.6%).
Patients who reported light or moderate physical activity levels were more likely to present normal cognitive function in a model also including age as a predictor (physical activity OR = 1.86, CI = 1.29-2.70, age OR = 1.04, CI = 1.03-11.06). The model predicted 13.5% of the cognition outcome.
Conclusion
This study suggests that pre-stroke physical activity and younger age can result in better cognitive function during subacute phase after stroke. Increased levels of exercise and physical activity can decrease cognitive dysfunction for adults after stroke, even though the effects are limited.
Trial registration number
N/A
AS16-110
MYASTHENIA AN UNUSUAL CAUSE OF POST STROKE FATIGABILITY- STUDY FROM A TERTIARY CARE HOSPITAL IN INDIA
1Amrita Institute of Medical Sciences, Stroke Medicine, Kochi, India
2Amrita Institute of Medical Sciences, Centre for Neurosciences, Kochi, India
3Amrita Institute of Medical Sciences, Neuroimmunology, Kochi, India
Background and Aims
30-70% of stroke survivors experience fatigue following the stroke. It is often misinterpreted as tiredness, a part of post stroke depression or other cognitive issues after a stroke. It is a major obstacle in the rehabilitation and has a negative impact on the overall recovery from stroke and ultimately deteriorates the quality of life of the patient.
We describe the patients presented with fatigue in the post stroke period
Method
We incidentally identified five follow up patients presenting to the stroke outpatient clinic with variable degree of recovery from stroke with serologically positive myasthenia gravis. Relevant information of the patient including the follow up data was collected from the hospital electronic database as well as patient medical records. Clinical examination video of patients available before and after treatment was assessed by a blinded assessor to analyse the treatment outcome.
Results
Total of 5 patients was identified to have post stroke fatigability and sero positive myasthenia gravis. Out of this, 3 were females and the mean age was 62 ± 8.51. Of this, 3 patients had large ischemic hemispheric strokes and 2 patients had intra cerebral haemorrhage. All of the patients had documented proximal as well as neck muscle fatigability. Median time from stroke onset to symptoms was 13 months. All patients responded to cholinergic therapy and had significant improvement in motor function. 2 patients had adverse events of the cholinergic drugs but resolved upon dosage modification.
Conclusion
Myasthenia gravis can also be a cause of post stroke fatigue and if identified promptly can be treated well
Trial registration number
N/A
AS16-111
PREDICTION OF OUTCOME AFTER ISCHAEMIC STROKE USING BIOMARKERS
1Institute of Neuroscience & Physiology, Department of Psychiatry & Neurochemistry- University of Gothenburg, Mölndal, Sweden
2Sahlgrenska University Hospital, Clinical Neurochemistry Laboratory, Mölndal, Sweden
3UK Dementia Research Institute, at UCL, London, United Kingdom
4UCL Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
5Institute of Neuroscience & Physiology, Department of Clinical Neuroscience- University of Gothenburg, Gothenburg, Sweden
6Institute of Clinical Sciences, Department of Anaesthesiology and Intensive Care- University of Gothenburg, Gothenburg, Sweden
7Institute of Clinical Sciences, Department of Radiology- University of Gothenburg, Gothenburg, Sweden
Background and Aims
Stroke is a major public health problem that can cause long-term disability, lasting brain damage or death. In this study, we investigated the use of Tau and NFL to understand the progression of neuronal damage and their relationship to outcome in acute ischemic stroke.
Method
Blood samples were taken from 90 patients at arrival to hospital and 2h, 24h, 48h, 72h and 3 months after endovascular treatment of large vessel occlusions. The concentrations of Tau and NFL were measured in serum using simoa assays. Early neurological changes from arrival to hospital were assessed by NIHSS at 24h, 3days and at discharge. Volume of infarction was calculated at day 1 with CT and day 3 with MR. Outcome was estimated using mRS at 3 months.
Results
Tau and NFL increased and NIHSS decreased over time. At 3 months, Tau levels were back to normal whereas NFL was still significantly high. Both biomarkers correlated to outcome at all time points except Tau at 3 months. Tau and NFL correlated to outcome and to CT and MR volumes, and could differentiate between good and poor outcome. Individually, the best time for prediction of poor outcome was 2h for Tau, 72h for NFL and 24h for NIHSS.
Conclusion
The combination of Tau at 48h and NIHSS at 24h gave the best prediction of outcome with a sensitivity of 86.5% and specificity of 85.7%. This combination could, at an early time point, help to reduce the time needed for neurological examinations.
Trial registration number
N/A
AS16-113
EXTERNAL VALIDATION OF THE ASTRAL STROKE RECURRENCE SCORE
1CHUV, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
2San Raffaele Scientific Institute- Milan- Italy, Department of Neurology and Neurophysiology, Milan, Italy
3Helsinki University Hospital, Department of Neurology, Helsinki, Finland
4University of Helsinki, Clinical Neurosciences, Helsinki, Finland
5Larissa University Hospital, Department of Medicine, Larissa, Greece
6Hellenic Cardiovascular Research Society, Stroke Division, Athens, Greece
Background and Aims
Patients surviving an ischemic stroke have an increased probability of further cardiovascular events, with the highest risk during the first year. We aimed at developing and validating a score predicting stroke recurrence over 12 months after an acute ischemic stroke.
Method
Study outcome was an ischemic or hemorrhagic stroke during the first 12 months after the index ischemic stroke. An integer score was built from the results of the multivariable Cox regression analysis performed on the derivation cohort (from ASTRAL registry, Lausanne). External validation was performed on three independent cohorts (from Athens Stroke Registry, Helsinki Young Stroke Registry and San Raffaele Hospital, Milan), assessing calibration, predictive performance (Brier score, Kullback-Leibler score) and discriminative ability (c-index).
Results
Features of the study cohorts are displayed in Table-1a. Figure-1 shows the final Cox regression model with variables best predicting 1-year stroke recurrence, corresponding Hazard Ratios and integer points composing the score. Score calibration, predictive performance and discriminative ability on the three validation cohorts are shown in Table-1b.
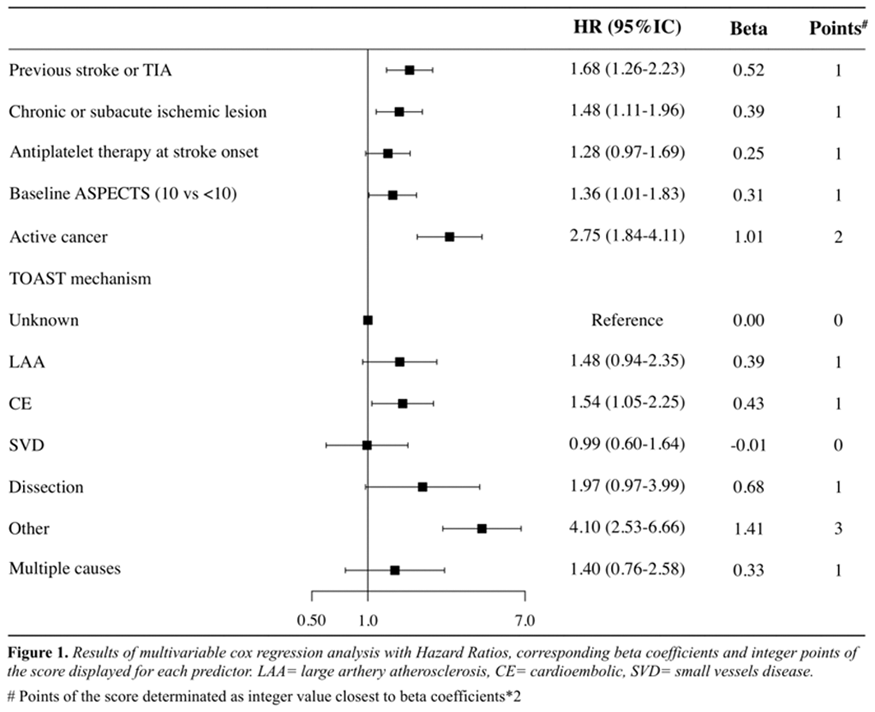
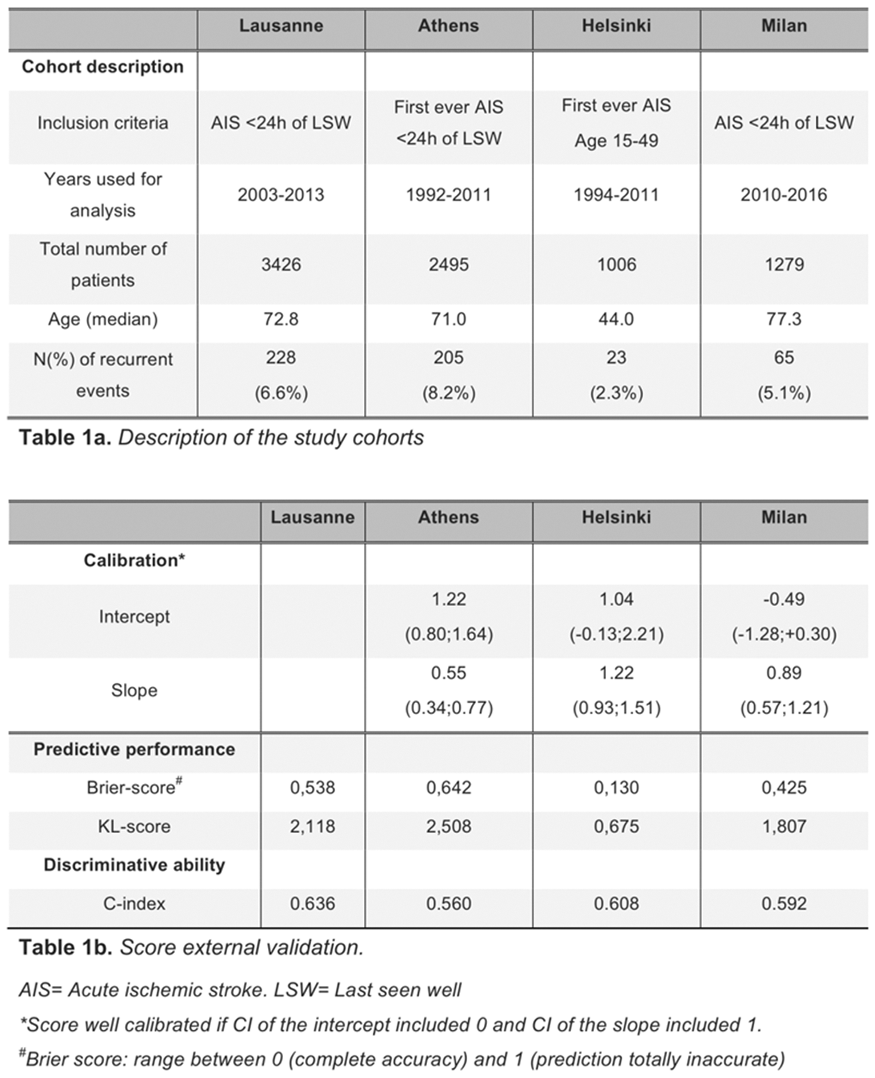
Conclusion
Our recurrence score performed well in two external validation cohorts of ischemic stroke patients. It seemed less applicable in another cohort of first-ever strokes.
Trial registration number
NA
AS16-115
DYSPHAGIA IN HEMISPHERIC POST-STROKE: BIOMECHANICAL AND NEUROPHYSIOLOGICAL SWALLOWING EVALUATION
1Hospital de Mataró, Gastrointestinal Physiology Laboratory, Mataró, Spain
2Instituto de Salud Carlos III, Centro de Investigación Biomedica en Red de enfermedades hepáticas y digestivas CIBERehd., Barcelona, Spain
Background and Aims
Post-stroke oropharyngeal dysphagia (OD) is a common disorder associated with negative outcomes such as malnutrition and dehydration, respiratory infections and aspiration pneumonia. The aim of the study was to describe the pathophysiology of post-stroke OD by assessing changes in swallowing (biomechanical analysis) and in afferent and efferent swallowing pathways (neurophysiological analysis).
Method
We studied 20 patients with hemispheric stroke (>3 months from onset) and chronic OD (Penetration-Aspiration Scale -PAS- >2). We evaluated the kinematics of the swallow response with videofluoroscopy (PAS and laryngeal vestibule closure time [LVCT]); we obtained the sensory evoked potentials with pharyngeal electrical stimulation (pSEP; 200µs, 75%-tolerance threshold, 0.2Hz) at CP3/CP4 and, pharyngeal motor evoked-potentials (pMEP) with transcranial magnetic stimulation bilaterally.
Results
Participants presented good functional capacity, high prevalence of malnutrition (50%) and mild stroke severity (Table 1). The highest PAS score was 5.10 ± 2.31, and 35% of patients presented aspiration associated with delayed LVCT (322.22 ± 87.28ms). In the affected hemisphere, we found delayed pSEPs in P1 (p = 0.09) and N2 (p = 0.005) peaks and reduced amplitude in P1-N2 (p = 0.024) and N2-P2 (p = 0.011) peaks, and only generally reduced pMEPs amplitude bilaterally and slightly reduced duration (ns) (Table 2).
Conclusion
We found severely impaired biomechanics of oropharyngeal swallow response with high mean PAS scores, high prevalence of aspiration and delayed LVCT in a mild stroke severity population. Neurophysiological evaluation showed preserved motor pathways and impaired conduction and integration of pharyngeal sensory inputs at stroke site as a key feature of chronic mild post-stroke OD patients.
Trial registration number
N/A
AS16-116
THE RELATIONSHIP BETWEEN DYNAMIC BALANCE TESTS APPLIED IN CLINICAL SETTINGS AND LABORATORY IN PATIENTS WITH STROKE
1Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Izmir, Turkey
2IZMIR KATIP CELEBI UNIVERSITY, Physiotherapy and Rehabilitation, IZMIR, Turkey
3Dokuz Eylul University, Institute of Health Sciences, Izmir, Turkey
4Dokuz Eylul University Faculty of Medicine, Neurology, Izmir, Turkey
Background and Aims
To evaluate the relationship between dynamic balance tests performed in clinical settings and laboratory in stroke population
Method
Timed Up and Go Test (TUG) was used as clinical test. The results compared with sit-to-stand (STS), step-quick-turn (SQT), and walk across (WA) tests data from Neurocom Balance Master System. Statistical analyses were performed using SPSS software version 22.
Results
21 males and 19 female participants were included. The mean age was 64,87(SD = 10,63) across participants. There was a moderate positive correlation between TUG and weight transfer (r = 0.368; p = 0.025), and moderate negative correlation between TUG and body weight rising index percentage (r = −0.432; p = 0.008) during STS. There was a moderate positive correlation between TUG and SQT left and a strong positive correlation between TUG and SQT right (r = 0.434; p = 0.007; r = 0.717; p < 0.001, respectively). Additionally, we found strong negative correlation between TUG and step length (r = −0.652; p < 0.001).
Conclusion
There were a moderate to strong relationship between TUG and Balance Master System data. Our study confirms that TUG test is a useful and reliable tool to use in clinical settings. When the time and cost effectiveness of TUG is considered we strongly recommend the use of it to assess the dynamic balance of patients with chronic stroke.
Trial registration number
N/A
AS16-117
HEART FAILURE IS NOT ASSOCIATED WITH A POOR OUTCOME AFTER MECHANICAL THROMBECTOMY IN LARGE VESSEL OCCLUSION
1University Medical Center, Neurology, Göttingen, Germany
2University Medical Center, Neuroradiology, Göttingen, Germany
3University Medical Center, Cardiology, Göttingen, Germany
Background and Aims
Heart failure is associated with a poor outcome in stroke with an increased mortality and morbidity. But it remains uncertain, if thrombectomy in patients with large vessel occlusion (LVO) in the anterior circulation is less effective in patients with heart failure compared to patients without.
Method
Here we retrospectively analyzed echocardiographic data of all patients in our stroke database (n = 314) for the presence of heart failure and other cardiac conditions associated with heart failure. Furthermore we collected the baseline characteristics, neurological and neuroradiological parameters.
Results
In the analysis 59 (27.2 %) patients suffered from heart failure, measured by the ejection fraction in the echocardiography according to the current guidelines. We corrected our data for age, ASPECTS and time from onset to recanalization.
The analysis revealed that heart failure in patients with LVO and mechanical thrombectomy is not associated with a poor outcome measured by the modified Rankin Scale after 90 days (3.0 vs. 2.69; p = 0.424). Moreover they did not show any difference in mortality than the patients without heart failure (26.15 % vs. 26.16 %; p = 0.999).
Conclusion
Heart failure is not associated with a poor outcome after mechanical thrombectomy in LVO.
Trial registration number
N/A
AS16-118
PREDICTING OUTCOME OF INTRAARTERIAL TREATMENT FOR ACUTE ISCHEMIC STROKE WITH MACHINE LEARNING ALGORITHMS
1Leiden University Medical Center, Neurology department, Leiden, The Netherlands
2Academic Medical Center, Bioengineering department, Amsterdam, The Netherlands
3Leiden Institute of Advanced Computer Sciences, Exploratory Data Analysis Group, Leiden, The Netherlands
4University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
5Erasmus Medical Center, Neurology department, Rotterdam, The Netherlands
6Leiden University Medical Center, Department of biostatistics, Leiden, The Netherlands
7University Medical Center Utrecht, Radiology department, Utrecht, The Netherlands
8Erasmus Medical Center, Department of public health, Rotterdam, The Netherlands
9Antoniusziekenhuis, Neurology department, Nieuwegein, The Netherlands
10Academic Medical Center, Radiology department, Amsterdam, The Netherlands
11Academic Medical Center, Department of Clinical Epidemiology- Biostatistics and Bioinformatics, Amsterdam, The Netherlands
12Leiden University Medical Center, Radiology department, Leiden, The Netherlands
Background and Aims
Intraarterial treatment (IAT) is an effective therapy for ischemic stroke patients with a proximal arterial occlusion. To further improve stroke care, it is essential to identify patients who will benefit from IAT and those who will not. Machine learning seems a promising tool for pursuing such personalized treatment as it is highly capable of assessing complex interactions and non-linear relations between variables.
Method
We used clinical data of patients from the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MRCLEAN) Registry. We used the following machine learning algorithms: RandomForest, SupportVectorMachine, NeuralNetwork, and Superlearner and compared these to classic logistic regression models using various variable selection methods. We performed nested cross-validation to correct for model optimism. Our outcome was functional independence, defined as modified Rankin Scale (mRS) of ≤2 three months after stroke. Model performance was assessed through area under the ROC-curve (AUC).
Results
In our study, 1526 patients were included, of whom 564 (37%) were functionally independent at three months. Machine learning and logistic regression models showed equally high performance. Best performing machine learning algorithms were RandomForests (AUC:0.86;95%CI:0.82−0.91) and SuperLearner (AUC:0.86;95%CI:0.81−0.91). Using LASSO for variable selection resulted in the best performing logistic regression model (AUC:0.86;95%CI:0.81−0.90).
Conclusion
Machine learning algorithms were equal to logistic regression in predicting three-month mRS. Their equal performance may be explained by the relatively large population compared to number of variables, and potentially few important interactions or non-linear relations between variables in our clinical dataset, tempering the added value of machine learning.
Trial registration number
N/A
AS16-121
THE RELATIONSHIP BETWEEN CENTER OF GRAVITY AND CLINICAL BALANCE TESTS AND FALLS EFFICACY IN CHRONIC STROKE POPULATION
1Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Izmir, Turkey
2IZMIR KATIP CELEBI UNIVERSITY, Physiotherapy and Rehabilitation, IZMIR, Turkey
3Dokuz Eylul University, Institute of Health Sciences, Izmir, Turkey
4Dokuz Eylul University Faculty of Medicine, Neurology, Izmir, Turkey
Background and Aims
This study aimed to investigate the relationship between centre of gravity (COG) and Berg Balance Scale (BBS) and falls efficacy in patients with chronic stroke.
Method
We compared the results of BBS, COG and Falls Efficacy Scale (FES-I). Data regarding with COG gathered from Neurocom Balance Master System as sway velocity. Trial of Org 10172 in Acute Stroke Treatment (TOAST) was used to classify ischemic stroke subtypes. Statistical analyses were performed using SPSS software version 22.
Results
The study included 33 participants (16 Female, 17 Male). The mean age was 65.42(SD = 9,4) and the mean of time stroke onset was 5,6(SD = 4.1) years. According to TOAST classification 40% of patients had large-artery atherosclerosis and 20% had small-vessel occlusion. We found a moderate negative correlation between BBS and sway velocity when eyes open and closed (r = −0.331; p = 0,069, r = −0.389; p = 0.030, respectively) and a strong negative correlation between BBS and FES-I (r = −0.557; p = 0.001). Additionally there was a moderate positive correlation between FES-I and sway velocity when eyes open and closed (r = 0.444; p = 0,012, r = −0.382; p = 0.034, respectively).
Conclusion
The study has shown that there are some changes in COG in chronic stroke population and these changes correlated with balance parameters. We believe that improvement in balance functions will help to decrease sway velocity and also risk of falls in this patient group.
Trial registration number
N/A
AS16-122
ACTIVITY LIMITATIONS IN MIDLIFE STROKE SURVIVORS
1University of Michigan, Epidemiology, Ann Arbor, USA
2Boston University School of Medicine, Vascular Neurology- Department of Neurology, Boston, USA
3Boston University School of Public Health, Biostatistics, Boston, USA
4Boston University School of Medicine, Neurology, Boston, USA
Background and Aims
Little is known about post-stroke activity limitations in midlife. Our objective was to describe and compare activity limitations in stroke survivors and stroke-free controls by age group (45-64, 65-84, ≥85), and to compare age groups with respect to differences between cases and controls.
Method
Incident strokes were identified from the Framingham Study (1981-2014). Activity limitations were ascertained at post-stroke follow-up visits (median 228.5 days [IQR = 191-495]). For each stroke case, three age, sex, and cohort-matched stroke-free controls were selected. Conditional logistic regression was used to compare activity limitations in cases and controls within age group; differences by age group assessed with interaction terms.
Results
Twenty-six midlife strokes were identified (mean age 57 (sd = 5), 35% women). The majority did not report activity limitations; 2 (7.7%) reported limitations with all activities. Midlife stroke cases reported greater odds of activity limitations than controls but results were not significant. Post-stroke activity limitations were prevalent in older ages and significant differences between cases and controls were evident in those 65-84 and ≥85 years. Age significantly modified these associations with the largest differences in those 65-84 (Table).
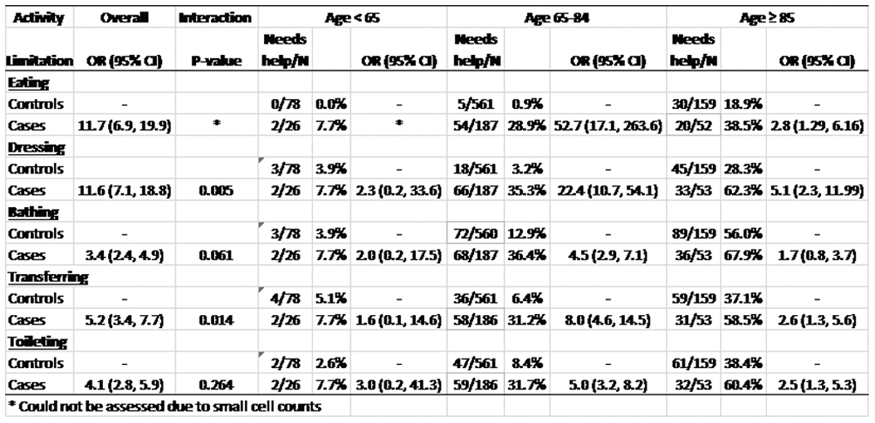
Conclusion
Post-stroke activity limitations were uncommon in midlife but prevalent in elderly, with the largest impact of stroke in those 65-84 years. Research is needed to understand the unique outcomes midlife stroke survivors face due to their younger age.
Trial registration number
N/A
AS16-123
POST STROKE FATIGUE IMPACTS EXECUTIVE FUNCTIONS, ANXIETY, DEPRESSION AND QUALITY OF LIFE
1Sahlgrenska University Hospital, Dept. of Rehabilitation Medicine, Gothenburg, Sweden
2Institute of Neuroscience and Physiology, Department of Clinical Neuroscience and Physiology- University of Gothenburg, Gothenburg, Sweden
Background and Aims
Fatigue, emotional distress and reduced working memory are often the subjectivley most common disabling experience after stroke.
Aims to further understand the multifactorial nature of fatigue, its casual effects and implications on executive functioning, emotional status and quality of life.
Method
Outpatients at the rehabilitation clinic were neuropsychologically assessed with the WAIS-III NI working memory, and the self-rating scales: Fatigue Impact Scale (FIS), Dysexecutive Questionnaire (DEX), Hospital Anxiety and Depression Scale (HADS) and EQ-5D the dimension of health-related quality of life (QoL). Results were analysed through correlations and linear regressions with QoL as the dependent variable.
Results
31 patients, 14 men / 17 women, ages Md = 52 years, weeks since stroke Md = 28, with a reduced working memory. Fatigue and executive problems respectively was reported by 87%, anxiety 42%, depression 19%, while 58% perceived a lower QoL than average.
Correlations was seen between fatigue and respectively executive functions, anxiety, depression and QoL, between executive functions and anxiety, between depression and anxiety. Depressive patients reported a lower QoL. Regression analysis showed impact of fatigue on executive functions, anxiety and depression with remaining effect on QoL.
Conclusion
Post stroke fatigue showed an impact on executive functions, anxiety, depression an QoL.
Fatigue seems to hinder the capacity in executive functioning, like mentally planning, keeping track and organizing. The more dysexecutive difficulties the lower emotional well-being and increasing feelings of not being capable of handling the everyday life was connected to a lower quality of life.
Trial registration number
N/A
AS16-124
COGNITIVE FUNCTION AND RETURN TO WORK 7 YEARS POST-STROKE. OUTCOMES REGARDING STROKE LOCALIZATION WITH FOCUS ON BRAINSTEM OR CEREBELLUM STROKE. RESULTS FROM THE SAHLSIS STUDY
1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
2Institute of Biomedicine-, Department of Clinical Pathology and Genetics, Gothenburg, Sweden
3Institute of Biomedicine, Department of Clinical Pathology and Genetics, Gothenburg, Sweden
Background and Aims
Background
Little is known about the effect of stroke in brainstem or cerebellum concerning cognition, stroke outcomes and return to work.
Aims
To investigate and describe stroke outcome, cognitive function and work situation for persons with stroke in the brainstem or cerebellum initially and at follow-up 7 years post-stroke as compared with stroke localization in the right or left hemisphere.
Method
Patients were examined initially and after 7 years post stroke with the National Institute of Health Stroke Scale (NIHSS), the modified Rankin Scale (mRS) and at 7 years post-stroke also with the Barrow Neurological Institute Screen (BNIS) concerning cognitive function.
Results
Data from 139 persons < age 65 were present at the 7 year follow-up (82 men, 57 women). Mean age at stroke was 47 years, 54 had right (RH), 59 left hemisphere (LH) stroke and 26 had stroke in the brainstem or cerebellum (B/C).
At 7 years the RH, LH and B/C groups all had a NIHSS median of 0 and between 85 – 89% had a mRS score of 0-2 (functional independence). Mean BNIS total score was RH: 42.1 LH: 38.6 and C/B: 40.0 (max total score 50, cut off 47).
Initial proportion of actively working was 83% (RH) and 85% (LH and B/C). At 7 years fewer persons were working: RH: 35%, LH: 68% and C/B: 50%.
Conclusion
Patients with a stroke localization in brainstem or cerebellum have the same level of cognitive deficits as patients with other stroke localizations and did not return to work to a higher extent.
Trial registration number
N/A
AS16-125
NEUTROPHIL-TO-LYMPHOCYTE RATIO PREDICTS POST-STROKE PNEUMONIA IN ACUTE ISCHEMIC STROKE
1Uz brussel, Neurology, jette, Belgium
2Clinique Saint-Jean, Department of Neurology, Brussels, Belgium
Background and Aims
High Neutrophil-to-Lymphocyte ratio (NLR) on admission has been associated with poor prognosis in acute ischemic stroke (AIS). Our goal was to investigate the predictive value of NLR and other clinical variables for post-stroke pneumonia (PSP).
Method
We retrospectively retrieved clinical and laboratory measures (absolute neutrophil count (ANC) and absolute lymphocyte count (ALC)) from the electronic record system of 192 patients with AIS who had routine blood sampling within 24h from onset. The NLR was defined as ANC/ALC. Patients were divided into 2 groups: those who developed pneumonia within the first week after admission (n = 30) and those who didn’t (n = 162). Logistic regression analysis and receiver operating characteristics (ROC) curves were used to identify predictors of PSP.
Results
At logistic regression analysis, male gender, severe dysarthria (NIHSS score 2), dysphagia and NLR were independent risk factors for PSP, with odds ratios (OR) of 3.4 (p = 0.025, 95% CI = 1.2–10.2), 8.5 (p = 0.005, 95% CI = 1.9–38.2), 7.8 (p = 0.001, 95% CI = 2.2–26.9) and 1.4 (p = 0.000, 95% CI = 1.2–1.7) respectively. A cut-off of 4.3 for NLR was determined on ROC curve (sensitivity = 70%, specificity = 79%). Area under the curve was 0.78 ± 0.05. Patients having an NLR above 4.3 are 11.9 times more at risk for PSP than patients with an NLR below 4.3 (OR = 11.9, p = 0.000, 95% CI = 3.8–36.9). Cross-validation (67/33% validation training set) showed misclassification probability of 12.6%-21.8%.
Conclusion
Our results suggest that NLR, dysphagia, dysarthria and male gender are independent predictors of PSP within the first week after stroke onset.
Trial registration number
N/A
AS16-126
DOES NIHSS SCORE PREDICT ACUTE IN-HOSPITAL COMPLICATIONS IN PATIENTS WITH POSTERIOR CIRCULATION STROKES?
1Masterstroke - Stroke and Neurointervention Clinic, Department of Neurology and Neurointervention, NAGPUR, India
2Bangur Institute of Neurosciences- IPGMER- Kolkata, Department of Neurology, Kolkata, India
Background and Aims
The National Institutes of Health Stroke Scale (NIHSS) is widely used to evaluate stroke severity and final outcome after a stroke. It is unclear whether baseline NIHSS score at admission can also predict in-hospital neurological and medical complications (NMC), especially in patients with posterior circulation (PC) strokes.
Aim
To determine whether NIHSS score was associated with in-hospital NMC in patients with PC strokes.
Method
This prospective study included patients of PC strokes admitted in a tertiary care centre in India over one year period (n = 100). NMC included neurological deterioration (worsening by ≥4 points of the NIHSS score) and all other medical complications that the patients developed during their hospital stay prior to their discharge/in-hospital mortality.
Results
30.3% of patients with ischemic and 54.2% of patients with hemorrhagic stroke developed NMC. Patients who experienced NMC had higher mean baseline NIHSS score for ischemic (6.4 versus 4.2, P <0.01) as well as for hemorrhagic stroke (17.1 versus 12.1. P <0.01). Using receiver-operating characteristic curve analysis, it was found that NIHSS > 4 for ischemic strokewas associated with NMC, however, a cut-off value for hemorrhagic stroke could not be established. Also, patients having diabetes (p = 0.02) and cardioembolism (p = 0.04) as the stroke mechanism had significantly higher risk of NMC.
Conclusion
In posterior circulation stroke patients, increased baseline NIHSS score at admission was associated with increased risk of in-hospital neurological and medical complications. This association applied to ischemic as well as hemorrhagic strokes. The clinical significance of these findings requires further evaluation in larger prospective studies.
Trial registration number
N/A
AS16-127
SEX DIFFERENCES IN THE RISK OF RECURRENT VASCULAR EVENTS AFTER STROKE AT YOUNG AGE IN A 12-YEAR TIME PERIOD
1Radboud University Medical Center- Donders Institute for Brain- Cognition and Behaviour, Neurology, Nijmegen, The Netherlands
2Brain Center Rudolf Magnus- University Medical Center Utrecht, Neurology and Neurosurgery, Utrecht, The Netherlands
3Julius Center for Health Sciences and Primary Care- University Medical Center Utrecht, Neurology, Utrecht, The Netherlands
Background and Aims
Young stroke patients are often at crossroads in their lives and need accurate information regarding their prognosis. There is little data on stroke recurrence or other vascular events following stroke in young adults, especially not in the era of secondary prevention. We investigated recurrent stroke and other vascular events in young stroke patients in the Netherlands.
Method
We constructed a cohort by linking national registries (Hospital Discharge-, Cause of Death- and Population Register) using ICD-9/-10 codes for ischemic-, undefined stroke and intracerebral hemorrhage. The cohort consisted of patients aged 18-49 years who experienced first-ever stroke between 1998 and 2010. Outcomes were ischemic-, undefined stroke, intracerebral hemorrhage, ischemic heart disease, and other vascular events.
Results
We identified 15257 patients (mean age 41.8 ± 6.8 years; 53.3% women), 8444 (55.3%) ischemic-, 3736 (24.5%) undefined stroke and 3077 (20.2%) intracerebral hemorrhage. During 12-year follow-up period, 125 (1.5%) patients developed recurrent ischemic stroke, 62 (1.7%) recurrent undefined stroke and 37 (1.2%) recurrent intracerebral hemorrhage. Following any stroke, 559 (3.7%) developed ischemic heart disease, and 189 (1.2%) another vascular event. Women more often experienced recurrent ischemic stroke (2.6% of women, 2.2% of men; p = 0.01) than men, whereas men were more likely to experience ischemic heart disease (5.1% of men, 2.4% of women; p < 0.001).
Conclusion
In young stroke patients recurrence-rate of ischemic stroke is higher in women than men, whereas the occurrence of ischemic heart disease is higher in men than women. These differences suggest varying etiological mechanisms among young adults according to sex, which warrant further clarification.
Trial registration number
N/A
AS16-128
“IT HITS US OVER THE HEAD YOU DON’T KNOW, YOU DON’T UNDERSTAND”: THE ROLE OF PATIENTS’ ILLNESS REPRESENTATIONS IN IMPROVING HEALTH POST-STROKE OUTCOMES
1University of Lyon, University Claude Bernard Lyon 1- HESPER EA 7425, Lyon, France
2University of Lyon, University Lumiere Lyon 2 - GRePS EA 4163, Bron, France
3University of Aix-Marseille, INSERM umr 912 SESSTIM, Marseille, France
4Hospices Civils of Lyon, Public Health Department, Lyon, France
Background and Aims
Appropriate stroke self-management constitutes a major component of health outcomes optimization, especially in patients with low or moderate stroke disability. According to the common-sense model theory (CSM) of self-management, how persons engage with treatment and effective behaviors depends on 1) their representations about which symptoms are part of the illness, 2) their beliefs about causes, 3) how long their illness might last, 4) what consequences it has on their life, and 5) whether they think the condition can be controlled with medication or actions. To investigate the role of patients’ illness representations in guiding their behavior about the management of their health conditions we used the CSM.
Method
Semi-structured interviews were conducted to investigate the 5 components of CSM in 24 patients with a mRS ≤1 and mostly hidden stroke consequences, 6 months after stroke.
Results
Patients struggled remembering acute phase and notably information they received. They did not make any association between their behaviors and stroke occurrence but believed in external causes (stress, burn-out, heredity…).
They considered returning to pre-stroke level was not attainable and did not recognize their symptoms as hidden stroke consequences. Even if they were adherent to their medications and improved their health habits, their sense of control regarding recurrence and recovery remained low.
All patients experienced difficulties to develop clear representations of their post-stroke condition which caused important negative emotional impact.
Conclusion
Providing more targeted support for understanding beliefs related to condition, based on the CSM, may increase medication adherence, recovery and hence post-stroke quality of life.
Trial registration number
N/A
AS16-129
OUTCOME PREDICTORS FOR PATIENTS WITH MECHANICALLY RECANALIZED BASILAR ARTERY OCCLUSIONS
1Klinikum rechts der Isar, Neuroradiology, München, Germany
2Klinikum rechts der Isar, Neurology, München, Germany
3Inselspital Bern- University of Bern, Neurology, Bern, Switzerland
Background and Aims
While mechanical thrombectomy has evolved as an evidence-based approach for treating large-vessel occlusion in the anterior circulation, its efficacy remains debated in posterior circulation strokes, especially basilar artery occlusions. Aim of this study was to identify variables predicting outcome for this severe stroke subtype.
Method
A retrospective single-center analysis of 115 basilar artery occlusion treated with 2nd generation thrombectomy devices was carried out. Uni- and multivariate analyses were performed to identify clinical, anatomical, occlusion related and interventional variables predicting favorable (mRS ≤ 3) patient outcome.
Results
Univariate analysis showed an association of good patient outcome with: Age (p = 0.033), no diabetes mellitus (p = 0.001), lower admission NIHSS and mRS (p = 0.000 and 0.000), incomplete occlusion (p = 0.001) and shorter thrombus (p = 0.000), non stenotic occlusion type (p = 0.003), good pcomA-collateralization (p = 0.000), complete recanalization (p = 0.000). In the multivariate regression analyses, highest impact on patient outcome could be shown for stenotic occlusion type (OR = 5,706, p = 0.046), diabetes (OR = 17.472, p = 0.033) and complete recanalization (OR = 0.102, p = 0.009). Time to recanalization showed no clear association.
Conclusion
Complete recanalization is strongly associated to good patient outcome in basilar artery occlusions, while underlying stenosis and diabetes are negatively associated. Time to recanalization showed no clear impact on patient outcome.
Trial registration number
N/A
AS16-130
ANATOMICAL VARIATIONS INFLUENCE STROKE PROGNOSIS AFTER THROMBECTOMY
1Hospital Universitario La Princesa, Neurología, Madrid, Spain
2Hospital Universitario La Princesa, Radiología, Madrid, Spain
Background and Aims
Changes in the normal anatomy of the circle of Willis may favour cerebrovascular disorders but how these conditions may influence stroke prognosis has not yet been studied. We aimed to analyse the influence of vessel anatomy on recanalization results and functional recovery in patients with stroke due to large vessel occlusion.
Method
We performed a retrospective study of consecutive patients with middle cerebral artery (MCA) stroke undergoing endovascular treatment at our center. Anatomical variations of the circle of Willis were identified on baseline computed tomographic angiography. We assessed the dominance of either superior or inferior main divisions of the MCA and the M1/M2 angle (angle between distal M1 segment and proximal M2 segment) by digital subtraction angiography. We correlated these variables with radiological and clinical outcomes.
Results
N = 190. Posterior communicating artery hypoplasia was the most common anomaly (50.5%) followed by the fetal origin of the posterior cerebral artery (fPCA) (23.2%). In a logistic regression model, patients with hypoplastic P1 segments were more likely to have a better collateral circulation (p < 0.05), a lower 24-hour infarct volume (p < 0.05) and better functional outcomes evaluated at 3-month mRS (p < 0.01). In those patients with M1/M2 angles greater than 130º there was a trend towards fewer number of stent-retriever passes needed to complete recanalization (p = 0.09).
Conclusion
In our study, fPCA was found to be an independent predictor of better radiological and functional outcomes in patients with acute stroke. Other anatomical variations did not significantly influence the results of thrombectomy. We have not found any similar references in literature.
Trial registration number
N/A
AS16-131
THE NEUROPSYCHOLOGICAL ASSESSMENT AND PROGNOSIS IN PATIENTS WITH CEREBRAL VENOUS THROMBOSIS
1Istanbul Faculty of Medicine- Istanbul University, Department of Neurology, İstanbul, Turkey
Background and Aims
Cerebral venous thrombosis (CVT) is a rare disease with various clinical presentations generally with a favorable prognosis. Our aim was to assess the neuropsychological profile after the acute phase of CVT and its association with neuroimaging characteristics.
Method
Twenty-four patients (16 females, mean age:33.2 ± 9.3 years) with a follow-up period of 6.4 ± 3.1 years diagnosed with CVT were included. The Addenbrook Cognitive Assessment (ACE-R) was used for neuropsychological evaluation and the results were compared with the age and sex matched healthy Turkish controls. The participants also completed the Beck Depression and Anxiety Inventory. The clinical, radiological findings and long-term follow-up data were collected from patient files.
Results
The ACE-R total score was significantly lower in patients with CVT with left hemispheric cortical infarcts compared to healthy controls (78.5 versus 83.1, p = 0.004). Memory and language skills are impaired in patients with left hemispheric cortical infarcts compared to the control group (19.3 ± 4.1 versus 22.2 ± 2.2 p = 0.021, 21.8 ± 2.5 versus 23.1 ± 1.6 p = 0.007 respectively).
Anxiety scores were significantly higher in the whole CVT group than the control group (24.6 ± 7.2 versus 13.7 ± 4.4, p < 0.001). Depression scores were also higher in CVT patients without reaching statistical significance.
Conclusion
Compared to healthy controls, CVT patients with left hemispheric venous infarcts had mild cognitive impairment but moderate anxiety and depression emerged as a common finding affecting all CVT patients.
Trial registration number
N/A
AS16-133
OUTCOME AFTER INTRAVENOUS THROMBOLYSIS IN PATIENTS WITH ACUTE LACUNAR STROKE, AN OBSERVATIONAL STUDY BASED ON THE SITS INTERNATIONAL REGISTRY
1Karolinska Institute, Department of Clinical Neuroscience, Stockholm, Sweden
2University of Perugia, Division of Cardiovascular Medicine, Perugia, Italy
3Karolinska Institute, Institute of Environmental Medicine, Stockholm, Sweden
4Postgraduate Institute of Medical Education and Research, Department of Neurology, Chandigarh, India
5Hospital Universitario de Caracas, Neurology Department, Caracas, Venezuela
6Hospital de Clínicas de Porto Alegre, Neurology Service, Porto Alegre, Brazil
7Istinye University, Stroke Rehabilitation and Research Unit, Istanbul, Turkey
8Sapienza University, Emergency Department Stroke Unit, Rome, Italy
9Karolinska University Hospital, Department of Neurology, Stockholm, Sweden
Background and Aims
Intravenous thrombolysis (IVT) for lacunar stroke (LS) is debated, as the underlying pathophysiological mechanism may not be thrombogenic. Our aim was to investigate outcomes after IVT in LS in the SITS International Stroke Registry.
Method
We identified clinically suspected LS by both NIHSS subscores at baseline and ICD-10 codes at discharge. IVT patients were collected from SITS-IVT dataset which predominantly were from Europe and non-IVT patients from SITS-All-patient dataset were predominantly from South America and Asia. We compared LS patients treated with IVT to LS not treated with IVT. Outcome measures were functional independence (modified Rankin Scale [mRS] score ≤2), excellent outcome (mRS ≤1), and mortality at 3 months. We also performed a matched-control comparison of symptomatic Intracerebral Hemorrhage (SICH) between IVT treated LS patients and IVT treated non-LS patients.
Results
Median age for LS patients (n = 5831) receiving IVT was 65y vs. 64y and NIHSS score was 6 vs. 3 compared to non-IVT treated LS patients (n = 1221). IVT-treated LS patients had higher adjusted odds of functional independence (adjusted odds ratio [aOR] = 1.65, 95% CI = 1.28-2.13) and of an excellent outcome (aOR = 1.49, 1.22-1.82). Mortality at 3 months was similar in the two groups (aOR = 0.57, 0.29-1.13). LS patients treated with IVT had lower odds for SICH (aOR = 0.33, 0.19−0.58 per SITS, aOR = 0.40, 0.27−0.57 per ECASS-2) than matched controls.
Conclusion
Our results suggest that clinically suspected LS patients should not be denied IVT treatment as their bleeding risk is lower and IVT treatment does not lead to worse functional outcome.
Trial registration number
N/A
AS16-134
NEUROLOGICAL DEFICIT ITEMS ASSOCIATED TO 3-MONTHS POOR FUNCTIONAL OUTCOMES AFTER MINOR STROKE
1Hospital Basurto, Neurology, Bilbao, Spain
Background and Aims
A variable percentage of patients with minor stroke (MS) have significant disability (mRankin >2) after 3 months. It is unclear which variables are associated with a poor outcome in this population.
Objective
To analyze the variables associated with a poor functional outcome (mRankin >2) in independent patients (mRankin 0-1) at three months after a minor stroke (MS) as defined by a NIHSS ≤4.
Method
All patients with acute ischemic MS and no baseline disability (mRankin <2) consecutively admitted to the Neurology Department of a general hospital during a 4-year period were included.
Variables collected included initial NIHSS, and Rankin at three months; neurological deficit (ND), recorded as moderate-severe involvement in Moto function, Sensitivity, Language, Visual and Ataxia. Any other ND was registered as minor symptoms. The association between the registered variables and functional outcomes was assessed by logistic regression.
Results
298 patients were included (table 1)
Logistic regression analysis showed a significant association with: Motor OR 4,33(IC 95% 2,23-8,41), Ataxia OR 2,95(IC 95% 1,51-5,77) and Minor Symptoms OR 2,55(IC 95% 1,47-4,4)
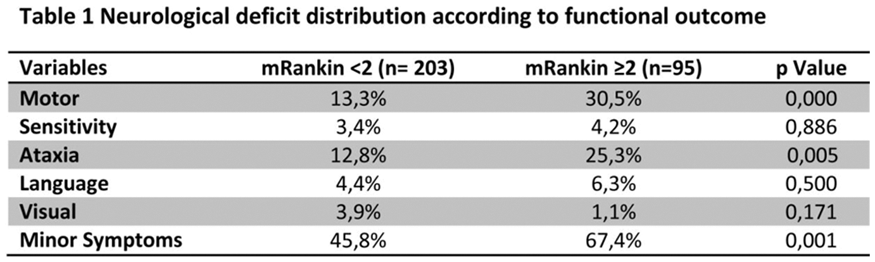
Conclusion
A 31,8% of MS patients had an unfavorable functional outcome. Moderate to severe involvement in motor function, ataxia, and the presence of minor symptoms were significantly associated with a poorer prognosis.
Trial registration number
N/A
AS16-135
NIHSS AS A PRIMARY ENDPOINT IN TRIALS ON ENDOVASCULAR TREATMENT FOR ACUTE ISCHEMIC STROKE: A SURROGATE ENDPOINT ANALYSIS OF TWO RANDOMIZED CONTROLLED TRIALS
1Erasmus MC University Medical Center, Department of Neurology, Rotterdam, The Netherlands
2Erasmus MC University Medical Center, Department of Radiology & Nuclear Medicine, Rotterdam, The Netherlands
3Erasmus MC University Medical Center, Department of Public Health, Rotterdam, The Netherlands
4Academic Medical Center, Department of Radiology, Amsterdam, The Netherlands
5University of Cincinnati Gardner Neuroscience Institute, Department of Neurology and Rehabilitation Medicine, Cincinnati- OH-, USA
6Medical University of South Carolina, Department of Public Health Sciences, Charleston- SC, USA
7Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
8Maastricht University Medical Center, Department of Neurology, Maastricht, The Netherlands
9Maastricht University Medical Center, Department of Radiology, Maastricht, The Netherlands
Background and Aims
The 90-day modified Rankin Scale (mRS) is the most commonly used primary endpoint in stroke trials, but it has limitations. The National Institutes of Health Stroke Scale (NIHSS) is frequently used as a secondary outcome measure at an earlier time point. The aim of this study was to evaluate the NIHSS as a primary endpoint in trials on endovascular treatment (EVT) for acute ischemic stroke.
Method
We applied the ‘Prentice criteria’ to evaluate NIHSS 1 day and 5-7 days after EVT as potential primary endpoints in the positive MR CLEAN and neutral IMS III. The four Prentice criteria evaluate a surrogate endpoint against a true endpoint (Figure). We adjusted for age, baseline NIHSS, collateral score, and time of symptom onset to randomization.
Results
The Prentice criteria were met for NIHSS at 1 day and 5-7 days in both trials. In MR CLEAN (n = 500), the effect of EVT on ordinal mRS decreased from common odds ratio 1.70 (p < 0.01) to 1.34 (p = 0.11) and 1.21 (p = 0.30) after adjustment for NIHSS at 1 day and 5-7 days respectively; in IMS III (n = 643), no effect of EVT on mRS (p = 0.07) or NIHSS (p = 0.56 and p = 0.28) was found.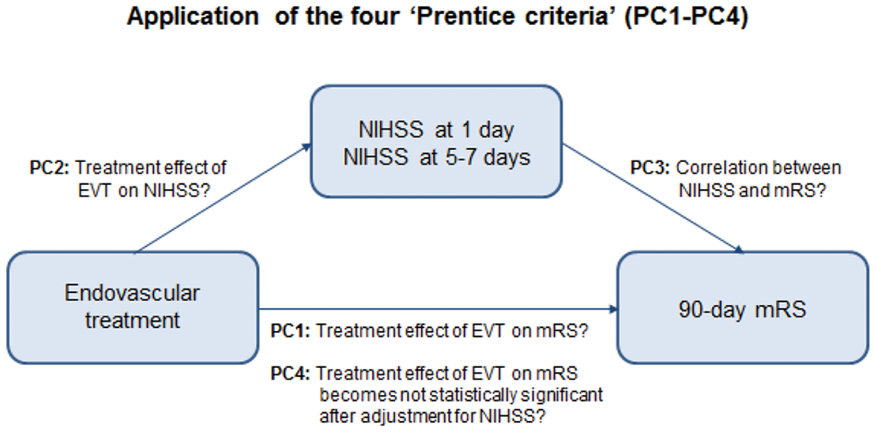
Conclusion
NIHSS within one week may be used as a primary endpoint in phase II(b) trials. This could minimize loss to follow-up, provide early trial results, and reduce trial costs.
Trial registration number
N/A
AS16-136
HIGH LIPOPROTEIN(A) LEVELS INCREASE LONG-TERM RISK OF CARDIOVASCULAR EVENTS AND DEATH IN ISCHEMIC STROKE PATIENTS: RESULTS OF THE PROSPECTIVE COHORT WITH INCIDENT STROKE (PROSCIS) STUDY
1Center for Stroke Research Berlin CSB, Neurology, Berlin, Germany
Background and Aims
Lipoprotein (a) [Lp(a)] levels are an independent risk factor for myocardial infarction and ischemic stroke. The long-term risk of recurrent events in stroke patients with elevated Lp(a) levels is unknown.
Method
Patients who participated in the PROSCIS study and had a follow-up visit three years after first-ever stroke were eligible for inclusion. Lp(a) levels were measured by an isoform-insensitive nephelometry assay. High Lp(a) levels were defined as ≥50mg/dl. We assessed the risk of the composite endpoint of recurrent stroke, myocardial infarction, and death using Cox regression analyses.
Results
590 patients were included in the analyses (median age 68[59-76], 62% male, median NIHSS 2[1-5]). 153 patients (26%) had elevated Lp(a) levels. After three years of follow-up 98 patients (17%) reached the predefined composite endpoint (43 strokes, 5 myocardial infarctions, and 50 deaths). 32 out of 153 patients (21%) of patients with elevated Lp(a) reached a composite endpoint, compared to 66 out of 437 patients (15%) with low Lp(a) levels (p = 0.09). The risk for a composite endpoint after three years was significantly higher in patients with elevated Lp(a) levels after adjustment for potential confounders (hazard ratio, 1.60; 95% confidence interval, 1.02–2.39; P = 0.04).
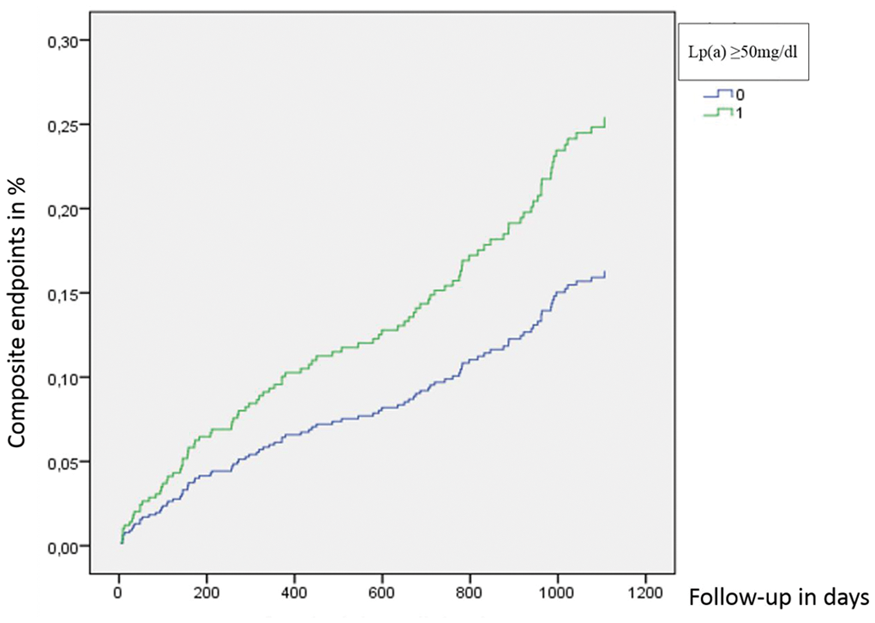
Conclusion
This study is the first to demonstrate that Lp(a) levels greater than 50mg/dl independently increase long-term risk of cardiovascular events and death. Clinical trials should investigate causality using new Lp(a)-lowering treatment options.
Trial registration number
N/A
AS16-137
THROMBOPHILIC GENES’ POLYMORPHISMS: THE POSSIBILITY TO FORECAST THE ONSET AND THE OUTCOME OF THE ARTERIAL ISCHEMIC STROKE IN YOUNG
1Ural Federal University named after the first President of Russia B.N. Yeltsin, Laboratory of Brain and NeuroCognitive Development, Yekaterinburg, Russia
2Clinic City Hospital 23, Stroke Unit, Yekaterinburg, Russia
3Ural State Medical University, Psychiatry Department, Yekaterinburg, Russia
4City Clinic Pediatric Hospital 9, Pediatric Neurological Department, Yekaterinburg, Russia
Background and Aims
Ischemic Stroke (AIS) leads to palsies, epilepsy, mental retardation, etc. Thrombophilia is described as a risk factor for the first AIS in young, but its role for disability outcome hasn’t been investigated thoroughly.
Method
The forecast cohort study. Inclusion criteria: age 18-45 y.o.; AIS confirmed by brain CT/MRI scan, informed consent. 12 single nucleotide polymorphisms (SNPs): FGB:-455G>A, F2:20210G>A, F5:1691G>A, F7:10976G>A, F13:103G>T, ITGA2:807C>T, ITGB3:1565T>C, PAI-1:-675 5G>4G, MTHFR:677С>Т, MTHFR:1298А>С, МТRR:66А>G, MTR:2756А>G) in 131 blood samples were identified by polymerase chain reaction. After 5 years follow-up 80 patients were recognized as disabled (Dis, Rankin Scale 3-5), 51 - nondisabled (NotDis).
Results
Quantitative analysis showed that only the carriers of some certain combinations as well as 5-6 SNPs in total number of polymorphisms raised the risk of the disable outcome (table).
Table.
Forecast value of thrombophilic SNPs in young patients with AIS
*- calculation took into account both hetero- and homozygous (not wild) alleles.
Conclusion
There are no clear SNPs which inevitably lead to disability after young AIS, however 5 and more SNPs i.q. carriage of combination including fibrinogen, platelets receptors, fibrinolytic system, and folic acid enzymes SNPs have the most diagnostic value and seem to be the good applicants to become such genes-candidates combinations.
Trial registration number
N/A
AS16-138
TROPONIN T ELEVATION IN ACUTE INTRACRANIAL HEMORRHAGE
1CHU Poitiers, Department of Neurology, Poitiers, France
2CH Saint-Louis, Department of Neurology, La Rochelle, France
3CHU Poitiers, Clinical Investigation Center INSERM CIC-P 802, Poitiers, France
Background and Aims
Troponin T elevation is associated with increased stroke severity and mortality, and with worsened clinical outcomes. However, most studies have involved acute ischemic stroke patients.
We aimed to evaluate high-sensitivity troponin T elevation frequency in our cohort of acute intracerebral hemorrhage (ICH) patients, to identify clinical, radiological and biological factors associated with troponin increase, and to study its prognostic impact.
Method
Consecutive patients admitted to our tertiary care academic stroke center from January 2012 to December 2016 for radiologically-confirmed ICH within 24 hours of symptom onset were included. Clinical, radiological, EKG and biological variables were collected, including high-sensitivity troponin T levels. Patients with secondary ICH, severe renal insufficiency, or recent ( <14 days) acute coronary syndrome, ischemic stroke or cerebral catheter angiography were excluded.
Results
Of the 232 included patients (mean age 74.9 ± 12 years, 58.6% men), 50% had high (>14ng/L) troponin T levels. Older age, male sex, higher admission glycaemia, previous ischemic stroke or TIA, mild-to-moderate renal insufficiency and EKG anomalies were independently associated with troponin elevation at multivariate analysis. Six-month mortality rate was 32%. Acute phase troponin T increase was not associated with poor clinical outcome (mRS >2).
Conclusion
Troponin T elevation occurred in half our acute ICH patients. Older age, male sex, higher admission glycaemia, previous ischemic stroke or TIA, mild-to-moderate renal insufficiency and EKG anomalies were independently associated with troponin elevation, which was not associated with poor clinical outcome during follow-up.
Trial registration number
N/A
AS16-139
CIRCULATING VASCULAR ENDOTHELIAL GROWTH FACTOR INDEPENDENTLY ASSOCIATES WITH WORSE POST-STROKE OUTCOME
1Institute of Medicine- The Sahlgrenska Academy at University of Gothenburg, Department of Internal Medicine, Gothenburg, Sweden
2Institute of Neuroscience and Physiology- The Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience, Gothenburg, Sweden
3Institute of Neuroscience and Physiology- The Sahlgrenska Academy at University of Gothenburg, Department of Psychiatry and Neurochemistry, Gothenburg, Sweden
4Institute of Biomedicine- the Sahlgrenska Academy at University of Gothenburg, Department of Pathology and Genetics, Gothenburg, Sweden
Background and Aims
Vascular endothelial growth factor (VEGF) promotes angiogenesis, lymphogenesis, neuroprotection and increases plasticity. Local brain VEGF is thought to play a role in the repair process following ischemic stroke (IS) whereas high serum VEGF (S-VEGF) appears to correlate with worse stroke severity. Most studies looking at the association between S-VEGF and outcome have shown variable results, lack long term follow-up and are limited by small study populations. Our aim was to investigate whether S-VEGF in the acute phase and after three months was associated with IS severity and long-term outcome for up to two years. Binary regression models were used to assess the associations.
Method
S-VEGF was analyzed in patients (n = 492, 36% females, mean age 57 years) included in the Sahlgrenska Academy Study on Ischemic Stroke (SAHLSIS). Stroke severity was classified according to the National Institutes of Health Stroke Scale (NIHSS) and outcome at three and twenty-four months was evaluated using the modified Rankin Scale (mRS), further transformed into favorable (mRS 0-2) or unfavorable (mRS 3-6) outcome.
Results
Neither acute nor three-month S-VEGF correlated (significantly) with worse NIHSS at baseline or three months after IS. S-VEGF in the acute phase correlated with unfavorable outcome after two years (r = 0.126 p = 0.005 n = 485), and similarly, S-VEGF after three months correlated with unfavorable outcome after two years (r = 0.145 p = 0.002 n = 465). The worse outcome by acute S-VEGF was not attenuated when adjusting for initial stroke severity and cardiovascular confounders.
Conclusion
Although S-VEGF is not associated with worse stroke severity it is clearly associated with worse unfavorable long-term outcome.
Trial registration number
n/a
AS16-140
WORK AFTER A SUBARACHNOID HAEMORRHAGE, WHO AND WHY?
1Fundación Instituto de Investigación Sanitaria de Aragón IIS, Neurology, ZARAGOZA, Spain
2Clinical University Hospital “Lozano Blesa”, Neurology, Zaragoza, Spain
3Social Security Institute, Neurology, Zaragoza, Spain
4Clinical University Hospital “Lozano Blesa”, Rehabilitation Medicine, Zaragoza, Spain
Background and Aims
Determining the return to work rate, the associated factors and the work disability degree after a subarachnoid haemorrhage (SAH)
Method
Retrospective study of labor-active patients (18-65 years) admitted to our center suffering from SAH between 2005 and 2015. Socio-demographic, clinical and radiological variables were collected. Patients with traumatic SAH were excluded.
Results
53 patients, 33 (62.3%) returned to work and 20 (37.7%) had a permanent work disability (PWD). Table I shows the demographic and clinical characteristics. The main factors significantly associated with PWD were: a higher score on the NIHSS scale at admission (p = 0.001) and at discharge (p = 0.000), a higher score at the Rankin scale at 3 months (p = 0.000), epileptic seizures (p = 0.022), dysarthria (p = 0.022) and motor symptoms (p = 0.017), aneurysmal SAH (p = 0.004), vasospasm (p = 0.047), hydrocephalus (p = 0.004) and a Hunt score and Hess> IV score (p = 0.000).
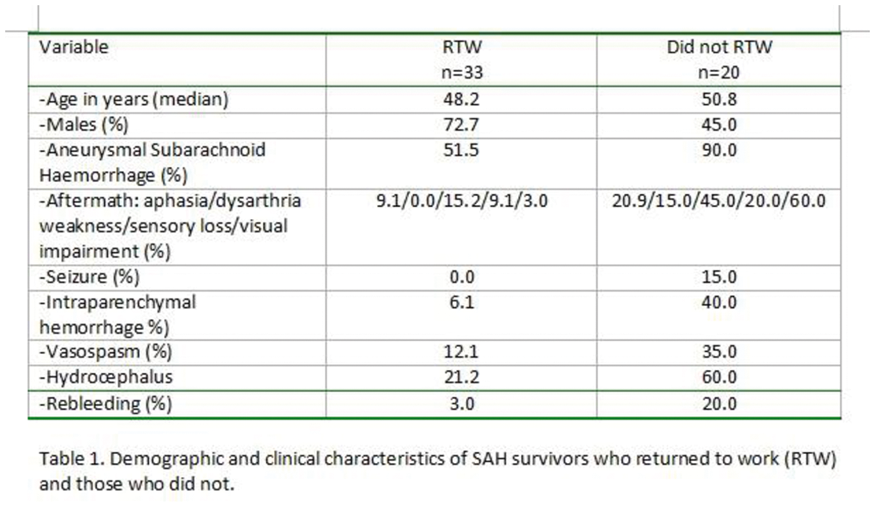
Conclusion
SAH has got a great socio-economic impact due to its generation of dependence, because most cases occur in young, healthy and completely independent people. In our study, 37.7% had an PWD after a SAH, which was related to motor conditions, vasospasm, hydrocephalus, epilepsy and aneurysmal aetiology.
Trial registration number
N/A
AS16-141
HEMISPHERIC LATERALITY AND CLINICAL OUTCOME IN REVASCAT POPULATION
1Hospital Germans Trias i Pujol, Stroke Unit- Department of Neuroscience, Barcelona, Spain
2Hospital Clínic de Barcelona, Unitat Funcional de Patologia Vascular Cerebral-, Barcelona, Spain
3Universitat Politécnica de Catalunya, Department of Biostadistics, Barcelona, Spain
4Hospital de la Vall d'Hebron, Stroke Unit, Barcelona, Spain
5Hospital de Bellvitge, Stroke Unit, Hospitalet del Llobregat- Barcelona, Spain
6University of Pittsburgh Medical Center, Stroke Institute- Department of Neurology-, Pittsburgh, USA
Background and Aims
A metaanalysis of recent endovascular trials have confirmed the benefit of mechanical thrombectomy (MT) in all ASPECT score strata (0-5, 6-8, 9-10) but the effect was marginal in the lowest scores. Since hemispheric laterality may have distinct influence on clinical outcome, we aimed to study whether ASPECT scores had different prognostic effects according to the affected hemisphere in acute stroke patients receiving MT.
Method
This is a secondary post hoc study of REVASCAT clinical trial. Favourable outcome (modified Rankin score, mRS, ≤ 2 at 3 months) was compared between treatment groups adjusted for age, initial stroke severity, occlusion site, ASPECT score and laterality. We analysed ASPECT strata and laterality by treatment interaction.
Results
Out of 206 REVASCAT patients, 113 had infarcts on the right (RH) and 93 on the left hemisphere (LH). Treatment effect was higher in RH patients (adjusted OR, 3.20; 95%CI 1.21 to 8.62) than in LH patients (aOR, 1.20; 0.30 to 4.22) without significant interaction (p = 0.26). Treatment by ASPECT strata interaction was significant in the RH infarcts (p = 0.010) but not in the LH ones (figure).
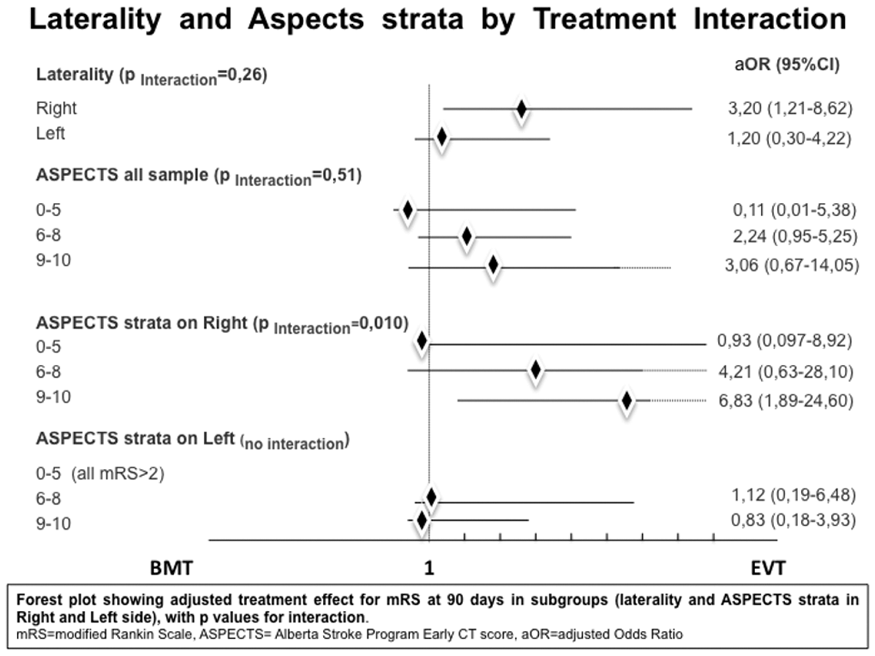
Conclusion
Treatment effect in REVASCAT was shown in both hemispheric infarcts. Right side lesions had higher odds of functional independence at 3 months and treatment effect significantly differed according to the ASPECT score.
Trial registration number
N/A
AS16-143
INCIDENCE AND LONG-TERM PROGNOSIS OF LACUNAR STROKE
1Department of Neurology and Stroke Unit- AZH, University of L’Aquila- 67100- L’Aquila- Italy, L'Aquila, Italy
Background and Aims
Our study provides updated information on incidence and long-term prognosis of lacunar stroke.
Method
Cases of first-ever ischemic stroke (FEIS) were ascertained in a three-year population-based prospective registry. Patients were followed up to 3 years after the event.
Results
Out of 884 FEIS, 110 (12.4%) were lacunar (68 men; 61.8%) and 774 (87.6%) were non-lacunar (354 men; 45.7%). Crude annual incidence rate for lacunar strokes was 12.3/100,000 (95% confidence interval [CI] 10.0-14.6): 15.6/100,000 (95% CI 10.1-21.0) in men and 9.1/100,000 (95% CI 6.26-11.9) in women (p = 0.012). The corresponding rate standardized to the 2011 European population was 9.6/100,000 (95% CI 7.8-11.4): 12.7/100,000 (95% CI 9.6-15.8) in men and 7.0/100,000 (95% CI 4.8-9.2) in women (p = 0.034). Patients with lacunar strokes were younger (mean age 70.9 ± 11.8 vs 76.8 ± 13.2 years; P<0.0001) and had higher proportions of arterial hypertension (76.4 vs 63.0%; p = 0.006) and cigarette smoking (27.3 vs 19.3%; p = 0.0002) than patients with non-lacunar stroke. Atrial fibrillation was more frequent in non-lacunar than in lacunar stroke (27.0 vs 10.9%; p = 0.0002). At the Kaplan-Meier analysis, the30-day, 1-year, and 3-year survival was higher in lacunar than in non-lacunar stroke (98.2% vs 79.8%; p < 0.0001; 94.6% vs 68.3%; p < 0.0001, and 90.1% vs 59.4%; p < 0.0001, respectively), whereas the 30-day, 1-year and 3-year survival free from any vascular event, was similar (99.0% vs 99.1%, p = 0.486, 93.5% vs 94.5%, p = 0.230 and 88.1% vs 89.1%, p = 0.157, respectively).
Conclusion
Despite a relatively favorable long-term prognosis of lacunar stroke, strategies for early tailored preventive measures should be adopted, mostly in men.
Trial registration number
N/A
AS16-144
EARLY NEUROLOGIC DETERIORATION AFTER MECHANICAL THROMBECTOMY IN ANTERIOR CIRCULATION ACUTE ISCHEMIC STROKE PATIENTS WITH UNFAVOURABLE COMBINATION OF CIRCLE OF WILLIS CONFIGURATION AND OCCLUSION LOCALIZATION
1Republican Vilnius University Hospital, Department of Interventional Radiology, Vilnius, Lithuania
2Vilnius University, Faculty of Medicine, Vilnius, Lithuania
3Vilnius University, Faculty of Medicine- Institute of Clinical Medicine, Vilnius, Lithuania
4Republican Vilnius University Hospital, Department of Neurology, Vilnius, Lithuania
Background and Aims
In acute ischemic stroke (AIS) patients, infarct growth rate depends on collateral circulation. We propose that configuration of circle of Willis (CoW) and intracranial occlusion localization may largely influence the overall collateral flow and early neurological deterioration, whether one or more arterial territories are affected.
Method
Anterior circulation AIS (AC-AIS) patients who were treated in Republican Vilnius University hospital during 2014–2017 and underwent mechanical thrombectomy (MTE) were included. Target group was defined as having >1 arterial territory affected and control group as having single territory affected. Each patient from target group was matched with 2 control group patients regarding age and IVT status. Early neurologic deterioration was defined as NIHSS score ≥4-point increase or death at 7 days.
Results
From 142 patients 48 cases (16 patients in target group and 32 patients in control group) were included in the final analysis. Target group patients had lower ASPECTS compared to control group (6,5 [IQR 6-7] vs. 8 [IQR 8-9], p < 0.01, respectively) and lower percentage of good ASPECTS collateral circulation score (33 vs. 97%, p < 0.01, respectively). Successful recanalization (TICI 2b/3) has been achieved in a lower proportion of target group patients (73 vs. 91%, p = 0.134). Early neurologic deterioration was associated with multiple territories affected (OR 12.69; 95% CI 2.19-73.42; p = 0.005), results remained significant after TICI score was added to the regression model.
Conclusion
Our results suggest that the unfavourable combination of CoW configuration and occlusion localization leading to >1 arterial territories being affected is associated with early neurologic deterioration of AC-AIS patients after MTE.
Trial registration number
N/A
AS16-145
RECENT TRANSIENT ISCHEMIA BEFORE ISCHEMIC STROKE INDUCES ISCHEMIC TOLERANCE IN CLINICAL PRACTICE. DATA FROM THE MULTICENTRE STUDY ESTOICA
1Hospital Universitari Arnau de Vilanova, Stroke Unit, Lleida, Spain
2Hospital Universitario de Pamplona, Stroke Unit, Pamplona, Spain
3Hospital del Mar, Stroke Unit, Barcelona, Spain
4Hospital de Son Espases, Stroke Unit, Palma de Mallorca, Spain
5Hospital Parc Taulí, Stroke Unit, Sabadell, Spain
6Hospital de la Santa Creu i Sant Pau, Stroke Unit, Barcelona, Spain
7Hospital Gregorio Marañón, Stroke Unit, Madrid, Spain
8Hospital Ramón y Cajal, Stroke Unit, Madrid, Spain
9Hospital la Paz, Stroke Unit, Madrid, Spain
10Hospital General de Albacete, Stroke unit, Albacete, Spain
Background and Aims
Ischemic precondioning (IPC) consist in brief periods of ischemia that activates different endogenous neuroprotective pathways that confers tolerance to later episodes of permanent cerebral ischemia (ischemic tolerance [IT]). We wanted to determine if clinical practice ischemic stroke (IS) patients with a recent transient ischemic attack (TIA) have better outcome than patients without.
Method
We prospectively recruited 541 consecutive IS patients who were attended to by a neurologist during the first 24 h after the onset of symptoms from ten University Hospitals of Spain. Diffusion weighted imaging MRI was performed in 365 (67.5%). According to previous evidence, patients were classified and analyzed in two groups according to the time interval between prior TIA and stroke: TIA < = 7 days (TIA group) and non TIA or TIA> 7 days (non-TIA group). Primary outcome was the proportion of patients with modified Rankin score <3 at 90 days.
Results
40 (7.4%) had had previous 7-day TIA. Compared to non-TIA group, patient from TIA-group were significantly more likely to have large artery atherosclerosis (30.0% vs 15.4%; p = 0.005) and had significantly lower NIHSS score at admission (4.0 [1.0-6.0] vs. 6.0 [3.0-13.0] p < 0.001). TIA-group had also significantly better outcome at 90 days than non-TIA group (proportion of mRS<3: 72.5% vs. 56.8%, p = 0.037) and lower infarction volume (0.7 [0.1-8.3] mL vs. 2.8 [0.6-16.0] p = 0.009)
Conclusion
Recent previous TIA is related to better clinical and neuroimaging outcomes suggesting a neuroprotective effect. It would be interesting to identify pathways associated with this effect in order to guide biomarker discovery and neuroprotective drug synthesis.
Trial registration number
N/A
AS16-146
STATIN TREATMENT FOR SECONDARY PREVENTION IN PATIENTS WITH CARDIOEMBOLIC STROKE: SYSTEMATIC REVIEW AND META-ANALYSIS
1University of Thessaly, Department of Medicine, Larissa, Greece
2General hospital of Thessaloniki “Agios Pavlos" -Greece, Department of Medicine, Thessaloniki, Greece
3Eginitio Hospital- National and Kapodistrian University of Athens-, First Department of Neurology, Athens, Greece
4Imperial College, Division of Brain Sciences- Department of Stroke Medicine, London, United Kingdom
5Leeds Teaching Hospitals NHS Trust and Medical School- University of Leeds, Stroke Service- Department of Neurosciences, Leeds, United Kingdom
6University of Ioannina, Department of Internal Medicine, Ioannina, Greece
7Hellenic Cardiovascular Research Society, Hellenic Cardiovascular Research Society, Athens, Greece
Background and Aims
It is unclear whether statin treatment should be offered to patients with cardioembolic stroke for secondary prevention. We aimed to investigate the association between statin treatment and outcomes in patients with cardioembolic stroke through a systematic review and meta-analysis of all available evidence.
Method
We searched PubMed and Web of Science until 08/01/2018 for eligible observational or interventional studies. The outcomes assessed were stroke recurrence, myocardial infarction, major cardiovascular events and mortality.
Results
Among 174 studies identified in the search, 4 were eligible (n = 5730; 13224 patient-years of follow-up). There was no significant difference between patients treated with statin and those not in the rate of stroke recurrence [odds-ratio (OR): 0.92, 95% confidence intervals (95%CI): 0.68-1.24], myocardial infarction (OR: 1.28, 95 %CI: 0.85- 1.92) and major cardiovascular events (OR: 0.53, 95%CI: 0.11- 2.53). There was lower rate of mortality (11% vs. 14% respectively, OR: 0.45, 95%CI: 0.26−0.79, RRR: 21%, ARR: 3%, NNT: 33) in patients treated with statin compared to those who were not.
Conclusion
Patients with cardioembolic stroke treated with statin have lower mortality compared to those without, despite similar rates of stroke recurrence and myocardial infarction. This study provides level B evidence to justify the use of statin also in patients with cardioembolic stroke.
Trial registration number
N/A
AS16-147
LONG-TERM RISK OF RECURRENT STROKE AND CORONARY EVENTS AFTER ISCHEMIC STROKE: RESULTS FROM THE SAHLGRENSKA ACADEMY STUDY ON ISCHEMIC STROKE
1Institute of Biomedicine, Department of Pathology and Genetics, Gothenburg, Sweden
2Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Gothenburg, Sweden
3Statistiska Konsultgruppen, Statistiska Konsultgruppen, Gothenburg, Sweden
4Institute of Medicine, Department of Molecular and Clinical Medicine, Gothenburg, Sweden
Background and Aims
Studies of coronary events after stroke in the long term are scarce. We sought to investigate the long-term risk of stroke recurrence and coronary events, and their predictors in young and middle-aged ischemic stroke patients.
Method
This is a longitudinal study of 1,086 consecutive adult cases with ischemic stroke before 70 years of age, and 600 community controls without cardiovascular disease at baseline. Participants were followed through national registers and medical records. Cox regression models were developed to identify predictors of vascular events.
Results
One-hundred-seventy-six cases experienced recurrent stroke (median follow-up 7 years) and 84 a coronary event (median follow-up 8 years), whereas the corresponding numbers were 12 and 32 for controls (median follow-up 10 years). The event rate (ER) for stroke was 10 times greater for cases than controls, whereas the coronary event rate was twice as high (ER per 1,000 person years 23.8 (95% confidence interval (CI) 20.4-27.6) versus 1.9 (95% CI 1.0-3.3) and 10.6 (95% CI 8.4-13.1) versus 5.2 (95% CI 3.5-7.3), respectively). Independent associations were detected for living alone and recurrent stroke (adjusted hazard ratio (HR) 1.67 (95% CI 1.23 - 2.27), p = 0.001) and for pre-stroke sedentary leisure time and coronary events (adjusted HR 2.16 (95% CI 1.33 - 3.52), p = 0.002). In addition, age and previous cardiovascular disease were independently associated to both outcomes.
Conclusion
Ischemic stroke patients remain at elevated risk for recurrent vascular events for many years after stroke. We identified living alone and sedentary leisure time as novel predictors of recurrent stroke and coronary events.
Trial registration number
N/A
AS16-148
RECURRENT VASCULAR EVENTS AFTER EMBOLIC STROKE OF UNDETERMINED SOURCE IN YOUNG ADULTS
1Hospital Egas Moniz - Centro Hospitalar Lisboa Ocidental, Neurology, Lisbon, Portugal
2CEDOC - Nova Medical School - Universidade Nova de Lisboa, Neurology, Lisbon, Portugal
3Hospital Fernando Fonseca, Internal Medicine, Lisbon, Portugal
Background and Aims
The existing knowledge about baseline characteristics and recurrent vascular events in young patients with embolic stroke of undetermined source (ESUS) is scarce. We compared baseline characteristics and risk of recurrent vascular events and vascular death between ESUS and non-ESUS young patients.
Method
We included consecutive patients aged 18 to 55 years with first-ever ischemic stroke admitted between January 1, 2009, and November 30, 2017. ESUS patients were identified and recurrent cerebrovascular events, composite vascular events and vascular death were compared between ESUS and non-ESUS patients. Survival analysis using incidence-rate (IR) ratios was performed. Adjusted risks were calculated using Cox proportional hazard analyses.
Results
294 patients were included, 88 (30%) classified as ESUS. This subgroup was younger (mean age 45.0 ± 7.5 years versus 47.1 ± 7.8 years), less often diabetic (10.2% versus 20.0%) and had more frequently migraine (18.2% versus 7.3%). Mean follow-up time was 3.8 ± 2.7 years. IR ratios for recurrent cerebrovascular events, composite vascular events and vascular death were respectively 0.64 (IR: 2.6 person/year vs 4.1 person/year; 95% CI 0.25–1.46), 0.47 (IR: 3.3 person/year vs 7.1 person/year; 95% CI 0.21–0.94) and 0.50 (IR: 0.9 person/year vs 1.8 person/year 95% CI 0.09–1.79). After adjusting for baseline characteristics there were no differences in the risk of composite vascular events (hazard ratio 0.57, 95% CI 0.29–1.15).
Conclusion
In our cohort, ESUS patients were younger, less often diabetic and had more frequently migraine. There were no differences in recurrent vascular events and vascular death between ESUS and non-ESUS young patients.
Trial registration number
N/A
AS16-149
PREDICTION OF SUB-ACUTE POST-STROKE INFECTIONS WITH MARKERS OF HEART RATE VARIABILITY
1University of Jena, Center for Sepsis Control and Care CSCC, Jena, Germany
2University of Jena, Department of Neurology, Jena, Germany
Background and Aims
Infections following acute stroke pose severe complications and stroke-induced immunodepression is a main risk factor for severe infections. Notably, the activity of the autonomous nervous system (ANS) affects stroke-induced immunodepression. The study Predictors of Sepsis (PRED-SEP) investigated the predictive value of markers of heart rate variability (HRV) for post-stroke infection, SIRS or severe sepsis.
Method
PRED-SEP is a prospective, observational, monocentric cohort study. German Clinical Trials Register Number: DRKS00003392. Included are 287 patients with ischemic infarction in the territory of the middle cerebral artery without an ongoing infection at admission. Recruitment is completed. HRV indices were processed by standardized algorithms from 24-h-Holter-ECG. ECG-recordings started within the first 24h after admission. Patients were screened daily for signs of infection. Primary endpoint is development of infection up to day 5, secondary endpoints are development of SIRS and severe sepsis. Predictive value of HRV adjusted for clinical data are analyzed by logistic regression models.
Results
Preliminary analyses indicate that HRV-indices, especially very low frequency band power (VLF), are associated with development of sub-acute (day 3 to 5) post-stroke infections. Adjustments for clinical parameters (preconditions, stroke-severity and -localization) are ongoing.
Conclusion
HRV-indices seem to predict the development of post-stroke infections. Continuous monitoring of autonomic function using HRV-indices in addition to clinical parameters could provide valuable information regarding, for example, the timely initiation of antibiotic therapy.
Trial registration number
German Clinical Trials Register Number: DRKS00003392
AS16-150
EARLY CLINICAL OUTCOME OF PATIENTS WITH POSTERIOR CIRCULATION STROKE AND INTRACRANIAL STENO-OCCLUSIVE ARTERIAL DISEASE
1Neurology Clinic - Clinical Centre of Serbia, Emergency Department, Belgrade, Serbia
Background and Aims
There is limited data in literature about outcome of patients with posterior circulation stroke due to intracranial steno-occlusive arterial disease. The aim of our study was to present demographic and clinical data, early outcome and predictors of outcome in group of patients with stroke and vertebrobasilar steno-occlusive disease.
Method
This is a retrospective study conducted from June 2013. to June 2017. on 34 patients diagnosed with posterior circulation stroke caused by intracranial steno-occlusive arterial disease. Patients with stroke of cardioembolic origin were excluded from study. We analyzed the associations of demographic factors, risk factors, and the clinical and radiological characteristics of posterior circulation stroke with poor outcome at discharge, which was defined as death or dependency (mRS ≥ 3).
Results
In our cohort (27 males and 7 females patients, mean age of 55 years), 18 patients (53%) had a poor outcome at discharge. The univariate analysis identified factors related to poor outcome: NIHSS on admission (p−0.000), altered consciousness on admission (p = 0.003), acute course of disease (p = 0.038), atherosclerotic etiology of intracranial steno-occlusive disease (p = 0.016), steno-occlusive basilar artery disease (p = 0.006) and somatic complications during hospitalization (p = 0.019). None of these analysed variables were significant predictors of poor outcome based on multivariate analysis.
Conclusion
In our group of patients with posterior circulation stroke half of them had a poor outcome, but we didn’t identify independent predictors of death or disability. Probably, the larger sample size is needed.
Trial registration number
N/A
AS16-151
ASSESSING THE IMPACT OF CARE IN A TELEMEDICINE-BASED STROKE NETWORK USING PATIENT-CENTERED HEALTH-RELATED QUALITY-OF-LIFE OUTCOMES
1Thomas Jefferson University, Department of Neurological Surgery, Philadelphia, USA
2Thomas Jefferson University, Department of Neurology, Philadelphia, USA
3Shore Medical Center, Performance Improvement Regulatory and Safety, Somers Point, USA
4Pocono Medical Center, Quality and Safety, East Stroudsburg, USA
5Chestnut Hill Hospital, Nursing Administration, Philadelphia, USA
6Roborough Memorial Hospital, Performance Improvement, Roxborough, USA
7Roborough Memorial Hospital, Therapy Services, Roxborough, USA
8Pottstown Memorial Medical Center, Stroke Program, Pottstown, USA
9Mercy Health, Neurology, Philadelphia, USA
10Atlanticare, Neurosciences Program, Philadelphia, USA
11Roborough Memorial Hospital, Physical Therapy, Roxborough, USA
Background and Aims
Robotic-Telepresence-based Telemedicine Networks (RTPTN) deliver acute ischemic stroke (AIS) assessments at higher rates – and with greater accuracy – than other models of telemedicine-based care. Clinical trials do not clearly demonstrate the impact of RTPTN on patients’ functional outcomes. The present research examines the feasibility of using health-related-quality-of-life (HR-QoL) measures (NIH/NINDS PROMIS/Neuro-QoL) as alternatives to a standard measure of neurologic disability (modified Rankin scale [mRS]).
Method
From January 2015-December 2017, AIS patients were prospectively identified during RTPTN evaluations across 10 hospitals. MRS and HRQoL responses were captured at 3-month intervals, post-discharge, for up to 6 months. We performed a correlational analysis of mRS and HR-QoL responses and modeled the effect of patients’ characteristics on: a) probability of good functional outcome (mRS = 0-1); and b) HR-QoL T-scores (centered on demographics of U.S. population, 50 ± 10 [SD]).
Results
Overall, 304 patients were consented (52 expired; 57 were excluded). Participants (n = 247) were assessed at 3 and 6 months post-discharge. Mean age was 68 ± 15 years, median NIHSS was 9 (IQR = 4), and rate of IV-tPA was 49%. NeuroQoL (AdjR2 = 0.8, p < .001) and PROMIS (AdjR2 = 0.7, p < .001) scores were correlated with mRS scores. Positive outcomes at 6 months were associated with NIHSS scores <5 (p < .0001) and IV-tPA administration (p = .04). IV-tPA was associated with higher T-scores in NeuroQoL (OR, 1.5; 95%CI 1.01-2.2, p = 0.04) and PROMIS (OR, 1.3; 95%CI 1.1-1.6, p < 0.01) at 6 months.
Conclusion
This study demonstrates HR-QoL assessments are complimentary to standard measures of neurologic disability. Furthermore, it shows IV-tPA administration is positively associated with good functional outcome and quality-of-life after stroke.
Trial registration number
N/A
AS16-152
TRAJECTORY OF DEPRESSIVE SYMPTOMS AFTER FIRST STROKE: EXPLORING RACE/ETHNIC DIFFERENCES
1University of Michigan School of Public Health, Epidemiology, Ann Arbor, USA
2University of Michigan Institute for Social Research, Survey Research Center, Ann Arbor, USA
Background and Aims
Race/ethnic minorities experience worse stroke outcomes compared with Whites. Race/ethnic differences in post-stroke depression (PSD) may be one contributor but data are lacking. This study aimed to investigate race/ethnic differences in long-term changes in depressive symptoms among survivors of first-ever stroke from a nationally representative sample of US middle-aged and older adults.
Method
A total of 16,807 stroke-free respondents from the Health and Retirement Study (HRS) aged ≥50 were followed from 1998 to 2014 for first-ever stroke. Depressive symptoms were assessed using the 8-item Center for Epidemiologic Studies Depression Scale (CESD), with higher scores indicating more depressive symptoms. Linear mixed-effects models accounting for the complex design of the HRS were used to examine the influence of incident stroke on rate of change in depressive symptoms and race/ethnic differences in trajectories of PSD. Multiple imputation by chained equations was used to impute missing values of CESD due to proxy interviews.
Results
During follow-up, 1,678 respondents reported first-ever stroke. Stroke onset was associated with higher CESD scores after adjustment for sociodemographic characteristics (0.62 points, 95% Confidence Interval = 0.40−0.83). The rate of decline in depressive symptoms was steeper post- compared with pre-stroke (P = 0.040). Although Blacks and Hispanics had higher CESD scores after stroke onset, there were no statistically significant differences in rate of change in depressive symptoms pre- and post-stroke compared to Whites.
Conclusion
Stroke onset was associated with elevated depressive symptoms and a greater decline afterwards. Post-acute stroke care should consider prevention and treatment of worsening depressive symptoms to aid in recovery.
Trial registration number
N/A
AS16-153
FACTORS THAT INFLUENCE THE OUTCOME AND THE EMERGENCY CALL AMONG NON-THROMBOLYSED STROKE PATIENTS IN HUNGARY
1Nyírő Gyula Hospital-OPAI, Neurology, Budapest, Hungary
2Eötvös Loránd University, Department of Probability Theory and Statistics, Budapest, Hungary
3University of Debrecen, Department of Health Management and Quality Assurance, Debrecen, Hungary
4Semmelweis University, Department of Neurology, Budapest, Hungary
Background
There is a lack of literature about what was the immediate action of patients ineligible for thrombolysis when the stroke symptoms were observed and its effect on their prognosis. We examined such stroke patients on admission and also performed a follow-up study.
Aim
Our aim was to explore the relationship between ambulance call and prognosis.
Method
We examined 253 patients between 2013 and 2014 in Neurology of Nyírő Gyula Hospital–OPAI in Hungary with a follow up period of maximum 12 months. We analyzed the relationship between the National Ambulance Service notification, NIHSS, mRankin and survival. We used descriptive statistics, linear and logistic regressions and Cox proportional hazards model.
Results
NIHSS (OR = 1.19, CI95%:[1.19-1.27], p < 0.001) and atrial fibrillation (OR = 2.25, CI95%:[1.15-4.41], p = 0.019) significantly increased the odds of ambulance call.
The analysis of mRankin and survival concluded that higher NIHSS leads to worse prognosis, whereas ambulance call had no significant effect. Higher NIHSS significantly increased the odds of death (OR = 1.18, CI95%:[1.13-1.24], p < 0.001 and the mRankin score both on leaving the hospital (coefficient = 0.252, CI95%:[0.217−0.287], p < 0.001) and follow-up (coefficient = 0.22, CI95%:[0.149−0.251], p < 0.001). The Cox model gave similar results.
Conclusion
According to the results, patients who had more severe symptoms were more likely to call ambulance and also had worse prognosis. Calling the ambulance itself had no significant effect on the prognosis. Not calling ambulance lowers the chance for systemic thrombolysis or thrombectomy in centers where these interventions are available, thus patients should call ambulance even if the symptoms are mild.
Trial registration number
N/A
AS16-154
THE EUROPEAN-AUSTRALIAN COOPERATIVE ACUTE STROKE STUDY (ECASS) CLASSIFICATION OF HAEMORRHAGIC INFARCTION APPLIED TO THE BRAIN CT 24 HOURS POST MECHANICAL THROMBECTOMY
1St George’s University Hospitals NHS Foundation Trust, Neurology, London, United Kingdom
Background and Aims
Currently, there is no standardised method for categorising haemorrhagic infarction (HI) post mechanical thrombectomy (MT). The situation post MT is complicated by contrast leakage intermingling with haemorrhage on the routine 24-hour CT brain. We investigated the utility of the European-Australian Cooperative Acute Stroke Study (ECASS) method categorising HI (already used post thrombolysis) in a series of MT patients.
Method
Data were analysed using a database of consecutive patients who underwent MT at a UK centre (May 2016-July 2017. Data included demographics, treatment parameters (e.g. recanalization using the TICI score) and infarct size (in relation to MCA territory). Hyperdense changes (a combination of blood and contrast staining) were categorised as HI from 0 to 4 using the ECASS system (figure). Clinical outcome was modified Rankin score (mRS) at three months.
Results
120 patients (mean age 66.4 ± 16.7, 63 female) underwent MT and had a 24 hour CT brain for analysis. There was no association between HI and thrombolysis, unsuccessful recanalisation or reperfusion times. ECASS groups 3 and 4 were amalgamated for statistical comparison. More extensive HI was present in larger infarcts. HI was associated with worse outcome for medium sized infarcts (p = 0.034, Kruskall-Wallis).
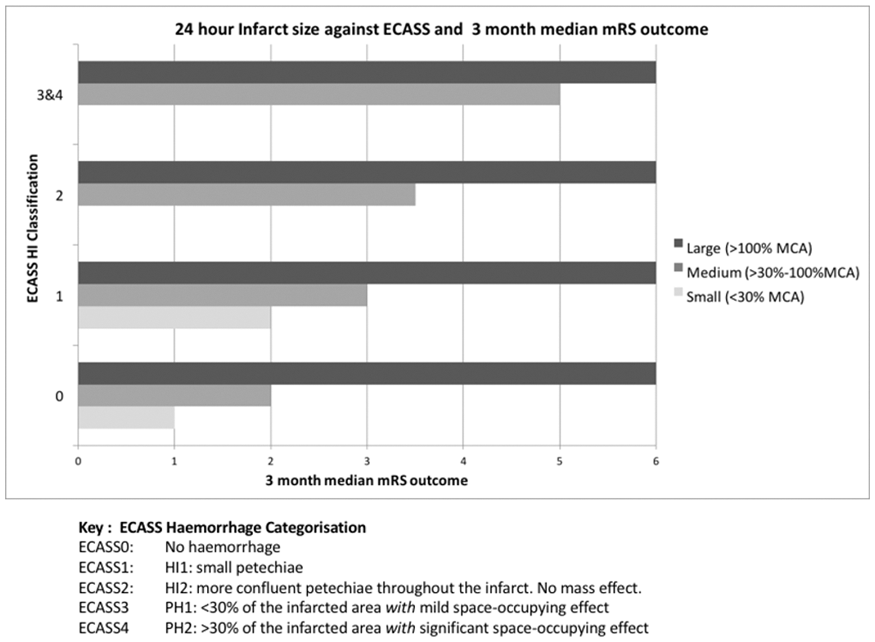
Conclusion
The ECASS Classification has additional clinical utility in describing haemorrhage after MT. The extent of HI is associated with 3-month outcome in patients with medium sized infarcts.
Trial registration number
N/A
AS16-156
ASSOCIATION OF SOCIOECONOMIC STATUS WITH MEDICATION PERSISTENCE AND ADHERENCE AFTER AN ACUTE ISCHEMIC STROKE
1Duke University, Sanford School of Public Policy, Durham-NC, USA
2Duke University School of Medicine, Duke University, Durham-NC, USA
3Duke University, Duke-Margolis Center for Health Policy, Durham-NC, USA
4Duke University, Duke Global Health Institute, Durham-NC, USA
5Beijing Tiantan Hospital, Department of Neurology, Beijing, China
6China National Clinical Research Center for Neurological Diseases, Capital Medical University, Beijing, China
Background and Aims
Stroke is the leading cause of disease burden in China. Although several medications can modify risk for stroke recurrence, few studies have examined barriers to continuing prescribed medications. This study aimed to examine the association of family income, health insurance and educational attainment with the continuation of prevention medications for three months following stroke hospital discharge.
Method
Patients with ischemic stroke discharged from 219 hospitals participating in the Chinese National Stroke Registry II were contacted by phone to determine their use of antiplatelets, anticoagulants, antihypertensives, statins and diabetes medications three months from hospital discharge. Persistence was defined for each patient as continuation of all medications prescribed at hospital discharge, and adherence considered continuation with the number of total prescribed medications per patient compared with the study population median adherence (67%).
Results
Among 11,868 patients, 46.8% continued taking all medications prescribed and 57.1% were adherent at three months. Having health insurance (versus self-pay) was not associated with medication adherence, overall persistence or persistence of any medication class. Patients with family income ≤1000 RMB/mo versus higher income had lower adherence and were less persistent overall (44.3% versus 47.8%). Elementary and middle school education versus high school or higher had lower adherence and were less persistent overall (45.9% versus 49.3%). Table 1 presents unadjusted and adjusted odds of persistence and adherence.
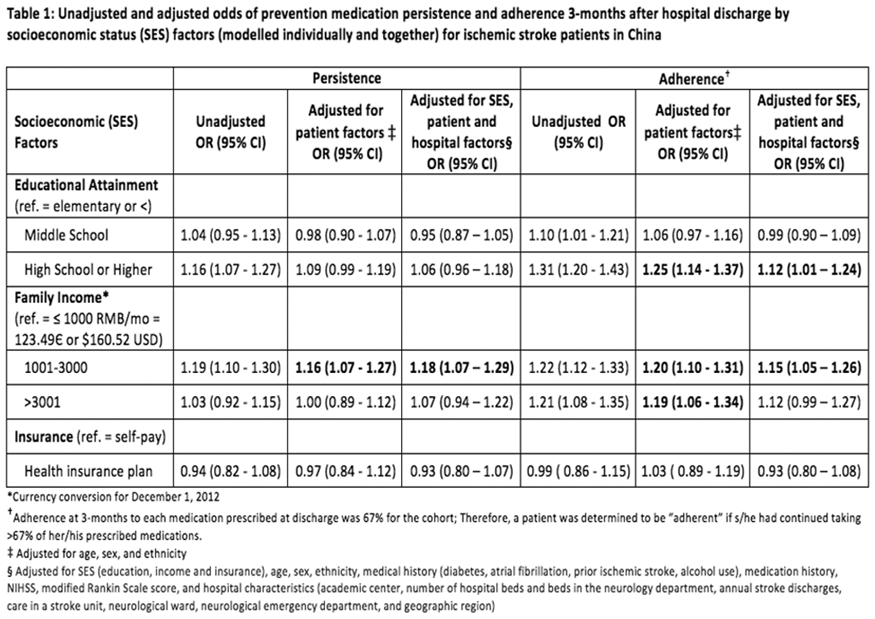
Conclusion
In this cohort of stroke survivors in China, socioeconomic status was associated with medication persistence and adherence three-months post-stroke. Findings may have implications for public health and health services secondary prevention interventions.
Trial registration number
N/A
AS16-157
PREDICTORS OF POOR OUTCOME DESPITE SUCCESSFUL RECANALIZATION IN PATIENTS WITH LARGE VESSEL OCCLUSION STROKE TREATED WITH ENDOVASCULAR THERAPY
1Rothschild Foundation hospital, Department of Interventional Neuroradiology, Paris, France
Background and Aims
Previous clinical studies revealed that despite successful recanalization nearly one in two patients with treated with EVT experienced an unfavourable clinical outcome after AIS. The aim of our study was to identify baseline prognostic factors of poor clinical outcome in EVT-treated patients with successful recanalization.
Method
We reviewed our monocentric prospectively collected endovascular database for patients with anterior circulation AIS from December 2011 to May 2017 who had successful recanalization (TICI score of 2b or 3). A poor outcome was defined as a 3-months mRS of 3 or more.
Results
A total of 594 patients were included. Among them, 302 (51%) patients experienced a poor outcome. Multivariate logistic regression indicated that age (OR = 5,64(3,28-9,68)), high baseline NIHSS score (>20, OR = 5,74(3,29-10,0)), low DWI-ASPECT score (<7, OR = 2,24(1,39-3,61)), onset to recanalization delay (> 360 minutes, OR = 1,63(1,03-2,59)), no IV t-PA infusion (OR = 1,59(1,02-2,47)), diabetes mellitus history (OR = 2,00(1,15-3,47)), high blood glucose level (>1,26 g/L, OR = 1,85(1,14-3,00)) and high blood neutrophils count (>8000, OR = 1,56(1,02-2,39)) were associated with poor clinical outcome.
Conclusion
In this retrospective series, baseline severe stroke criteria and delayed EVT-induced reperfusion were associated with poor outcome in accordance with previous studies. Interestingly, no IV t-PA infusion, both high neutrophil count and hyperglycemia, known from experimental studies to be associated with downstream microvascular thrombosis (DMT) were independently associated with poor outcome. Our data support efforts to develop DMT targeting therapy in association with EVT in AIS.
Trial registration number
N/A
AS16-159
ASSOCIATION BETWEEN ONSET-TO-ARRIVAL TIME AND FUNCTIONAL OUTCOME AT DISCHARGE IN ACUTE ISCHAEMIC STROKE
1King's College London, School of Population Health & Environmental Sciences, London, United Kingdom
2Royal College of Physicians London, Stroke Programme, London, United Kingdom
3Stroke Unit, London, United Kingdom
Background and Aims
Few studies have examined the association between onset-to-arrival time and functional outcomes in acute ischaemic stroke, particularly in patients not receiving reperfusion therapy. Our study aims to investigate if early arrival to a hospital is associated with good functional outcome (mRS ≤ 1) at discharge.
Method
Data were collected from the nationwide, registry-based Sentinel Stroke National Audit Programme. We included all adult patients aged >16 admitted to hospital with acute Ischaemic Stroke in England and Wales between the 1st of April 2013 and the 31st of March 2017. We used a multilevel logistic regression analysis to adjust for potential demographic (age, sex, ethnicity) and clinical (pre-stroke functional status, comorbidities, stroke severity, arrival by ambulance and reperfusion therapy) confounders at the patient level, as well as potential differences between centres.
Results
165,301 patients with ischaemic stroke from 224 different hospitals were included in the analysis. 85,427 (52%) were male, 146,179 (88%) were white, median NIHSS was on arrival was 4 (IQR: 2-10), and median onset-to-arrival time was 156 minutes (IQR: 82-474), with 49,021 patients arriving within 1.5 hours of stroke onset. After adjustment, patients arriving within 1.5 hours and between 1.5 and 3 hours after stroke onset had slightly increased odds of having a good functional outcome at discharge (OR 1.21 [95%CI 1.15-1.27] and 1.08 [95%CI 1.03-1.13]) compared to those arriving after 24 hours.
Conclusion
Early hospital arrival within 3.0 hours after ischaemic stroke onset is associated with good functional outcome at discharge even after adjusting for stroke severity and reperfusion therapy.
Trial registration number
N/A
AS16-161
LONG-TERM OUTCOME OF STROKES RELATED TO PATENT FORAMEN OVALE. ANALYSIS OF LOCAL POPULATION FROM CODOCIA STUDY
1Complejo Hospitalario Universitario Albacete, Neurology, Albacete, Spain
2Hospital Universitari de Girona Doctor Josep Trueta, Neurology, Girona, Spain
Background and Aims
CODICIA study analysed in 2004 the outcome of patients recruited in 17 Spanish hospitals, suffering an ischemic stroke of undetermined origin in terms of functional outcome and probability of relapse, according to the presence of patent foramen ovale (PFO).
The present study revaluate these outcome in the sample recruited in our centre after more than 15 years.
Method
The study included patients age >18 years, with recent cryptogenic ischemic stroke or TIA (to TOAST criteria). A transcranial Doppler was done for determining the presence of right-to-left shunt, following the standardised guidelines. The present study followed up all patients recruited in our centre and recorded the presence of relapses and good functional status (0-1 points in mRankin scale).
Results
The 30 patients included in CODICIA study in our hospital were contacted 15’7 years after the first stroke. The basal date were 44% women, mean age 57 years, 33% smokers, 33% hypertension, 11% diabetes, 44% PFO. There were 1’59%/year relapses in PFO group, whereas 2’55% in nonPFO group (p 0’15). The proportion independent patients was 66’7% in PFO group and 14’3% in nonPFO patients (p <0’01). The multivariate analysis confirmed the presence of PFO as a predictor of good outcome. Among patients with PFO, the mRankin do not differed in case of relapse.
Conclusion
This substudy reinforces the idea that patients with FOP have a very favorable prognosis, even the few cases with recurrences. This should redefine the benefit of closing the oval of the foramen, which is expensive and is not free from risks
Trial registration number
N/A
AS16-162
MISJUDGMENT OF PRE-MORBID FUNCTIONAL STATUS ADVERSELY AFFECTS OUTCOMES IN STROKE PATIENTS UNDERGOING ENDOVASCULAR THERAPY FOR LARGE VESSEL OCCLUSION
1University Hospital Dresden, Neurology, Dresden, Germany
2University Hospital Dresden, Neuroradiology, Dresden, Germany
Background and Aims
Endovascular therapy (EVT) trials enrolled ischemic stroke patients inter alia according to pre-morbid functional status; however, this information is commonly lacking in real-world setting. We hypothesized that misjudgment of pre-morbid functional status adversely affects outcomes in these patients.
Method
Data derived from our prospective registry of ischemic stroke patients undergoing EVT for large vessel occlusion in anterior circulation (01/2016-12/2017). Considering all information accumulated during hospital course, pre-morbid modified Rankin scale (mRS) was independently re-assessed and compared with pre-treatment assessments. Misjudgment was defined as any difference in the mRS categories between first- and second-look assessments. Multivariable model was built to adjust for confounding variables of unfavorable outcome (mRS 3-6) and death at 90-days.
Results
We studied 209 patients: median age 75 years (IQR, 17); 46% men; median NIHSS 16 (7). Second-look assessment of pre-morbid mRS revealed 79 (38%) cases initially being misjudged by ≥ 1 category and 15 (7%) by ≥ 2 categories. None of the first-look mRS categories were retrospectively adjusted to a lower category. Patients whose mRS were misjudged were older (79 [14] vs. 74 [17], p < .001), more severely affected (NIHSS 17 [7] vs. 16 [7], p = .01) and suffered more frequently from diabetes (44% vs. 24%, p = .005) and atrial fibrillation (73% vs. 48%, p = .001) than those with consistent mRS assessments. Any misjudgment of pre-morbid mRS emerged as predictor of 90-days unfavorable outcome (OR = 3.11; 95%CI 1.31-7.38, p = .01) and death (OR = 2.21; 95%CI 1.09-4.52, p = .029).
Conclusion
Thorough pre-treatment assessment of pre-morbid functional status appears decisive for proper selection of EVT candidates.
Trial registration number
N/A
AS16-163
FACTORS ASSOCIATED WITH POOR FUNCTIONAL PROGNOSIS IN PATIENTS WITH MINOR STROKE
1FIB Hospital Gregorio Marañón CIF: G83195305, neurology, MADRID, Spain
Background and Aims
Previous studies alert about the possibility of ending-up with a poor outcome in patients suffering “minor stroke.” The objective of this study is to identify factors related to poor functional outcome or death within this subgroup.
Method
Retrospective study of a prospective cohort of patients with ischemic “minor stroke” admitted in an acute stroke unit during 2015. “Minor stroke” was defined as a baseline National Institute of Health Stroke Scale (NIHSS) score between 1 and 4[AA1]. Factors related with poor functional outcome or death at 3 months (defined as a Modified Rankin Scale score of 3-6) were identified using an univariate and multivariate logistic regression analysis.
Results
207 patients were included, 123 (58.9%) males. Mean age 68.07 (SD 14.54). Baseline NIHSS: median (IQR) 2 (1-3). 29 patients (14%) were functionally dependent or died [AA2] at 3 months. Age ≥80 years, baseline NIHSS score, “unknown onset” stroke, leukoaraiosis, large artery occlusion (LAO) and clinical fluctuation, were related with poor outcome/death in the univariate analysis. After the multivariate analysis, Age ≥80 years (OR: 2,59 [CI 95%: 1.06-6.32; p < 0.001]), baseline NIHSS (OR: 2.22 [CI 95%: 1.47-3.35; p < 0,001]), clinic fluctuation (OR: 5.01 [CI 95%: 1.44-17.49; p = 0,011]) and LAO (OR: 3.26 [IC 95%: 0,96 – 10,9; p = 0.057]). ) were identified as independent predictors of poor outcome.
Conclusion
A proportion of “minor strokes” may have a poor outcome. Identifying factors associated with poor outcome may be useful for selecting patients who may benefit from more aggressive treatments.
Trial registration number
N/A
AS16-166
QUANTIFYING PARTICIPATION IN THE FIRST YEAR POST-STROKE: COMPARISON OF THE ACTIVITY CARD SORT AND THE UTRECHT SCALE FOR EVALUATION OF REHABILITATION-PARTICIPATION ACROSS INTERNATIONAL COHORTS
1Florey Institute of Neuroscience and Mental Health, Stroke Neurorehabilitation and Recovery, Heidelberg- Melbourne, Australia
2La Trobe University, Occupational Therapy- School of Allied Health, Melbourne, Australia
3Maastricht University Medical Center, Department of Psychiatry and Neuropsychology, Uterecht, The Netherlands
4Washington University in St Louis, Occupational Therapy, St Louis, USA
Background and Aims
The World Health Organisation identifies participation as a valued outcome; yet relatively little is known about the trajectory of participation outcomes post-stroke. We aimed to quantify participation in the first year post stroke across international stroke cohorts from Australia and the Netherlands. We asked: What are the actual activities that survivors re-engage in during the first year post-stroke relative to their pre-morbid level of activity?
Method
A subset of patients were identified for whom participation data were available over the first year post-stroke, i.e. at 2-3 and 12-months post-stroke. Participation measures employed were the Activity Card Sort-Australia (ACS-Aus), (Australian stroke cohort START-PrePARE; n = 100) and the Utrecht Scale for Evaluation of Rehabilitation-Participation (USER-Participation) (Netherlands cohort Restore4Stroke; n = 395). Data from the two measures was recoded to identify common patterns in activities which were retained, gained or discarded due to the stroke. Data were analysed to describe the course of participation in the first year post-stroke.
Results
In total 217 patients from the Restore4stroke cohort and 92 patients from the START cohort were included. Patient groups were comparable in terms of demographic and stroke characteristics. The frequency of vocational activities increased up to one year post-stroke in the Restore4stroke cohort but remained stable for START patients. Household and leisure activities remained stable.
Conclusion
Actual activities that stroke survivors re-engage in during the first year post-stroke were characterised and compared across two international stroke cohorts. Clinicians can use this information in identifying persons at risk of long-term unfavourable outcome and target rehabilitation programs accordingly.
Trial registration number
START - NCT00887328 and ACTRN12610000987066
Restore4stroke -Dutch Trial Register NTR3051
AS16-167
SELF-ASSESSMENT AND QUANTIFICATION OF THE S.A.F.E. PROGNOSTIC TEST FOR ARM WEAKNESS AFTER STROKE
1Imperial College London, Bioengineering, London, United Kingdom
2Imperial College London, Brain Sciences, London, United Kingdom
3Imperial College, Brain Sciences, London, United Kingdom
4Imperial College Healthcare NHS trust, Brain Sciences, London, United Kingdom
Background and Aims
Assessment of arm function is complex and expert-dependent, but critical for prognostication and treatment stratification after stroke. A simple, two-stage functional test – Shoulder Abduction + Finger Extension (S.A.F.E.) – can reliably distinguish patients who will recover arm function at 6 months, and thus explains a large degree of the variance of arm function post-stroke. However the test is observer dependent and relatively imprecise. We developed a method to quantify the functional components of the S.A.F.E score, and to allow for easy self-assessment of S.A.F.E by patients with a view to home monitoring.
Method
We utilised a pair of commercial sensors that can detect finger-flexion and extension (gripAble™ ) and shoulder abduction (‘Myo™’ inertial motion unit armband sensors). A bespoke software was developed that illustrated to patients on an avatar the arm movements to be tested, with realtime sensor feedback. We tested 20 hemiplegic stroke patients and 5 healthy controls; and compared software measures with goniometer-measured joint angles, and clinician-judged MRC power (both blinded to software measures). A 1-3 minute calibration step was required prior to use.
Results
Arm joint angles were reliably recorded by the gripAble-Myo system. Finger extension and shoulder abduction estimated by a clinician using the Medical Research Council motor score correlated closely with sensor measures of force and range of motion (r = 0.80 – 0.86; p < 0.01). All subjects were able to complete the study without prompting or guidance.
Conclusion
A relatively simple system of commercially-available sensors allows for accurate self- S.A.F.E. quantification.
Trial registration number
N/A
PATHOPHYSIOLOGY OF STROKE
AS17-001
POTENTIAL ROLE OF OXIDATIVE STRESS AND ANTIOXIDANT SERUM STATUS IN PATIENTS WITH FOCAL CEREBRAL ISCHEMIA IN ANTERIOR CIRCULATION
1Clinical Center of Nis, Clinic of Neurology, Nis, Serbia
2Special psychiatric hospital “Gornja Toponica”- Nis- Serbia, psychiatry, Nis, Serbia
Background and Aims
Oxidative stress is a disorder that appears as a result of a disturbance between prooxidant and antioxidant balance. This disturbance takes place in a number of neurological diseases (e.g. multiple sclerosis), and is also an important predisposing factor for a stroke (e.g. diabetes mellitus). Aim was to compare antioxidant status of serum total and direct bilirubin, albumin and creatinine in stroke patients with healthy controls, and patients with multiple sclerosis.
Method
Subjects were divided into three groups (97 stroke, 78 healthy and 81 multple sclerosis patients). Only patients with well defined clinical symptoms and correlation on MSCT/MRI of the brain were included (signs of cerebral ischemia in anterior circulation). All patients were divided into groups regarding onset (<50 years, ≥50 years) and sex. Severity of the disease was assessed with National Institutes of Health Stroke Scale at admission, and outcome was assessed with Modified Rankin Scale at hospital discharge.
Results
Serum antioxidant status was significantly lower in stroke and MS group compared with healthy controls (p < 0,05). There was no significant difference in serum antioxidant status between patients with stroke and those with MS. Regarding clinical presentation on admission and outcome on discharge, we found correlation with serum levels of measured parameters (p < 0.05) which indicates lower antioxidant status in patients with severe disease and worse outcome.
Conclusion
Our findings suggest that there is a potential role of oxidative process in stroke pathology, which can be helpful for patients that could receive supporting therapy providing better clinical outcome.
Trial registration number
N/A
AS17-002
FLUCTUATING LEVELS OF CONSCIOUSNESS WITH VASCULAR ORIGIN: A CASE SERIES
1Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
Background and Aims
We present a series of clinical cases with four patients with coma, fluctuating levels of consciousness and vertical ophthalmoplegia which revealed synchronous bilateral paramedian thalamic infarcts.
An adequate differential diagnosis is essential in patients with an acutely decreased level of consciousness.
Method
The study included three men, aged 83, 63 and 62 years, with a previous Rankin score of 0, and an 88-year-old woman with Rankin score 3. Three of them showed different factors of vascular risk. In all cases, the clinical presentation included a sharp decrease of the level of consciousness. The neurological examination revealed coma and fluctuating level of consciousness with vertical ophthalmoplegia in all patients. Apart from these symptoms, they presented other neurologic signs, and one of the patients also showed cognitive and behavioral alterations. In only one of the patients, reperfusion therapy with intravenous fibrinolysis was performed.
Results
The emergency neuroimaging tests were normal, and later studies revealed bilateral thalamic infarcts in all cases. On discharge, all the patients still presented altered oculomotor responses. In two cases, the fluctuations in the levels of consciousness disappeared, and there was a partial improvement in the other two.
Conclusion
Percheron artery syndrome requires a high degree of diagnostic suspicion, because it can very easily be confused with other pathologies that show an acute decrease in the level of consciousness, and which are managed differently. It is essential to pay attention to specific aspects of the physical examination, rather than to the neuroimaging tests available in hospital emergencies.
Trial registration number
N/A
AS17-003
HLA AND KILLER CELL IMMUNOGLOBULIN-LIKE RECEPTOR (KIRS) GENOTYPING IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Policlinico Palermo, Medicina Interna, Palermo, Italy
2Giuseppe Giglio Hospital- Cefalù, Pronto Soccorso Unit, Cefalù, Italy
3Policlinico Palermo, Dipartimento di Scienze per la Promozione della Salute e Materno Infantile “G. D'Alessandro"- Universita' degli Studi di Palermo Italy., Palermo, Italy
4University of Bari, School and Chair of Allergology- Dipartimento delle Emergenze e Trapianti d'Organo, Bari, Italy
5Policlinico Palermo, Dipartimento di Biopatologia e Biotecnologie Mediche-, Palermo, Italy
6Policlinico Palermo, Dipartimento di Biopatologia e Biotecnologie Mediche, Palermo, Italy
7Policlinico Palermo, Dipartimento di BioMedicina Sperimentale e Neuroscienze Cliniche, Palermo, Italy
Background and Aims
In humans, a major component of NK and T cell target recognition depends on the surveillance of human leukocyte antigen (HLA) class I molecules by killer immunoglobulin-like receptors (KIRs). The aim of our study was to implement the knowledge about the immunological genetic background of acute ischemic stroke susceptibility in relation to the frequency of the KIR genes and HLA alleles
Method
Between November 2013 and February 2016, consecutive patients with acute ischemic stroke were recruited. As healthy controls we enrolled subjects without acute ischemic stroke. KIR aplotype and HLA allele phenotyping has been performed
Results
Subjects with acute ischemic stroke in comparison to controls showed a higher frequency of 2DL3, 2DL5B, 2DS2 and 2DS4 KIR genes and a lower frequency of HLA-B-Bw4I alleles. Subjects without acute ischemic stroke showed a higher frequency of interaction between KIR 2DS2 and HLAC2. We also observed an higher frequency of 2DL3 and 2 DL4 KIR genes in subjects with LAAS subtype. Multiple logistic regression analysis showed a protective effect towards stroke of HLA-B-Bw4I and of interaction between KIR 2DL2 and HLAC1 whereas a detrimental effect was observed with regard of interaction between KIR 2DS2 and HLAC2 and between KIR 2DL2 and HLA-C1_A.
Conclusion
Our findings of a higher frequency of activating KIR genes seem to be consistent with findings previously reported patients with coronary syndrome. This higher frequency of “proinflammatory" genes in subjects with ischemic stroke could also explain the immunoinflammatory activation of the acute phase of stroke.
Trial registration number
N/A
AS17-004
PYRAMIDAL SIGNS IN LATERAL MEDULLARY INFARCTION WITH IPSILATERAL WEAKNESS
1National Institute of Neurology and Neurosurgery, Division of Neurology, Mexico City, Mexico
2National Institute of Neurology and Neurosurgery, Stroke Clinic, Mexico City, Mexico
3University of Maryland School of Medicine, Department of Neurology, Baltimore, USA
Background and Aims
The etiology of ipsilateral weakness (IW) in lateral medullary infarction is still an ongoing discussion. Pyramidal, cerebellar, and sensitive causes have been proposed. The objective of our study was to describe the clinical findings in patients with MRI-confirmed lateral medullary infarction (McLMI) and IW.
Method
Medical records of patients with McLMI and IW seen at our center (1996-2017) were reviewed to describe their clinical findings (especially pyramidal signs). Patients with concomitant cerebellar infarction were excluded. Muscle strength was graded using the Medical Research Council (MRC) Scale.
Results
12 patients had an McLMI with IW. 11 (91%) patients had ipsilateral hemiataxia. 10 (83%) patients performed at least active movement against gravity and slight resistance (MRC ≥4–). The rest (n = 2) performed active movement against gravity. Of the total patients with available information (n = 9), in 6 this weakness was cleared in less than 35 days (median: 4 days; range: 1-34 days). Hyperreflexia (3+) was found in only three patients. Babinski sign was found in only one patient. Of the total with available information (n = 9), Trömner sign was found in only one patient. The patient without hemiataxia neither had hyperreflexia nor Babinski sign. Ipsilateral hemisensory loss was found in 4 patients.
Conclusion
Pyramidal signs are uncommon in patients with McLMI and IW, even in those without hemiataxia. Weakness in these patients is usually transient.
Trial registration number
N/A
AS17-006
IS THERE ANY RELATIONSHIP BETWEEN STROKE SIZE AND ACUTE ELEVATION OF BLOOD PRESSURE IN YOUNG PATIENTS?
1Hospital Britanico de Buenos Aires, Neurology, Ciudad Auronoma de Buenos Aire, Argentina
2Hospital Britanico de Buenos Aires, Neuroradiology, Buenos Aires, Argentina
Background and Aims
Many studies showed that blood pressure (BP) rises during acute ischemic stroke (IS). Different mechanisms have been proposed to explain this phenomenon, being stroke volume (SV) among them. Young patients should be a useful model for understanding the natural course of BP during the first hours of an IS because they have less vascular risk factors (VRF) and other medical conditions that could alter the autonomic system function and therefore modify BP.
Method
All patients between 18 and 55 years-old admitted within the first 24hours of an IS and studied with MRI were evaluated. An observer blinded to BP values assessed SV. Data analyzed: socio-demographic variables, VRF, systolic BP (SBP) and diastolic BP (DBP) on admission. Statistical analysis: Mean and SEM for quantitative variables, percentages for qualitative, Spearman method for correlations.
Conclusion
Increase BP during acute IS did not depend on stroke size in young patients.
Trial registration number
N/A
AS17-007
VITAMIN D DEFICIENCY AND STROKE RISK IN AN IRISH POPULATION
1St James's Hospital, Mercer's Institute for Successful Ageing, Dublin, Ireland
2St James's Hospital, Department of Stroke and Neuromuscular Medicine- Mercer's Institute for Successful Ageing, Dublin, Ireland
Background and Aims
Vitamin D deficiency is associated with higher stroke incidence and worse stroke outcome. Stroke incidence increases by >25% during Irish winters. Vitamin D deficiency is common in Irish people because of low levels of sunlight, especially during the winter. We determined the prevalence of Vitamin D deficiency in Irish stroke patients.
Method
We measured vitamin D levels in subjects admitted with stroke (over 4 consecutive summers and winters) to a University Hospital Stroke Service to determine the prevalence of deficiency (25-hydroxyvitamin D <30nmol/l). We also compared our results with bone, hypertensive and cognitively impaired cohorts from the nationally representative Trinity, Ulster, Department of Agriculture (TUDA) study.
Results
Data on 158 subjects (Mean age 73.5, 64 (40.5%) Female) were identified (53: June-September vs. 103: December-March). Of these 34 (21.5%) were receiving vitamin D supplementation. Median unsupplemented levels were 30nmol/l (range <10-86 nmol/l) and 60 (48.4%) subjects were vitamin D deficient (36.8% summer, 53.5% winter, p=0.15 chi sq). Vitamin D level did not correlate significantly with age or length of stay. Vitamin D deficiency was substantially more prevalent than in the TUDA Bone (13.8%) and Hypertensive (27.3%) cohorts despite similar ages (mean respective ages 70, 71). It was also greater than in the much older Cognitive cohort (43.6%, mean age 80) (all p < 0.001 chi sq).
Conclusion
Vitamin D deficiency is very common in the Irish stroke population and more common than in comparable high-risk cohorts.
Trial registration number
N/A
AS17-009
THE EFFECT OF MECHANICAL REPERFUSION OUTCOME FOLLOWING AN OCCLUSIVE STROKE ON THE REGIONAL EXPRESSION OF MATRIX METALLOPROTEINASE-9 IN RAT BRAIN
1National University of Ireland Galway, Physiology, Galway, Ireland
2National University of Ireland Galway, Curam, Galway, Ireland
Background and Aims
This study investigated the effect of different mechanical reperfusion outcomes following occlusive stroke on a marker of blood brain barrier dysfunction – matrix metalloproteinase-9 (MMP-9).
Method
Male Sprague Dawley rats underwent 2 hour middle cerebral artery occlusion (MCAO) (n = 6-14 per group). Following occlusion, different reperfusion strategies were employed for a further 2 hours; either full, partial or no reperfusion, simulating cerebral blood flow (CBF) restoration that may occur during thrombectomy. In sham-operated animals, filament insertion was omitted.
Results
Physiological parameters, including temperature, haemodynamics, blood glucose and gases were within normal parameters with no difference between groups throughout. MCAO caused a drop in CBF to 50% of pre-occlusion level (F(3,37)=10.57; p < 0.001). Reperfusion approach had a significant effect on CBF (F(2,27)=5.12; p < 0.05); 78%, 53% and 43% of sham levels for full, partial and no reperfusion groups respectively. Occlusion resulted in significant infarction (F(3,26)=3.03; p < 0.05), most prominent in non-reperfused animals, and also significant oedema (F(3,26)=5.49; p < 0.01). Occlusion resulted in increased MMP-9 expression in the lesioned hemisphere in the frontal cortex (F(1,52)=15.51; p < 0.001), striatum (F(1,52)=39.98; p < 0.001), anterior temporal cortex (F(1,52)=63.85; p < 0.001) and posterior temporal cortex (F(1,52)=13.34; p < 0.001), but not the hippocampus (F(1,52)=2.00; ns). MMP-9 expression was higher in animals not reperfused than those fully or partially reperfused, particularly in the striatum (F(3,52)=11.53; p < 0.001) and anterior temporal cortex (F(3,52)=10.35; p < 0.001).
Conclusion
Permanent occlusion resulted in greater infarct, oedema and MMP-9 expression than full or partial reperfusion, supporting the clinical benefits of early thrombectomy and indicating the benefit of even partial reperfusion.
Funding: Enterprise Ireland and Industrial partners Neuravi
Trial registration number
N/A
AS17-010
FASL DEFICIENCY ATTENUATES CYTOTOXICITY OF CD8+ TCELLS AFTER ISCHEMIC STROKE
1Drum Tower Hospital- Nanjing University Medical School, Department of Neurology, NanJing, China
Background and Aims
After the onset of stroke, infiltrated CD8+ T cellsaggravate brain injurythrough FasL orcytotoxic granules. We previously reported that FasL mutation could attenuate brain inflammation in experimental stroke, however, the exact mechanisms were undefined. Thus, this study tested the hypothesis whether FasL could modulate the cytotoxicity of CD8+ T cells or not.
Method
In vivo, flow cytometry was used to detected the numbers and functions of brain-invading CD8+ T cells in the mice brain after middle cerebral artery occlusion (MCAO).CD8+ T cells from WT and FasL mutant (gld) mice wereinjected into Rag1-/- mice and then induced MCAO. After 3 days of reperfusion, infarct volumes, functional outcomes and gila cells activation were evaluated. In vitro, CD8+ T cells were co-cultured with neurons or microglia for 24hours. The cytotoxicity of CD8+ T cells, neuronal death and polarization of microglia were measured.
Results
FasL deficiency reduces CD8+ T cells cytotoxicity after MCAO in the brain. And FasL deficiency in CD8+ T cells confers brain protection after MCAO in Rag1-/- mice. Neuronal death and M1 microglia polarization were weakened after FasL on CD8+ T cells was blocked or dysfunctional. Besides, FasL deficiency attenuates CD8+ T cells activation induced by microglia.
Conclusion
FasL deficiency attenuates cytotoxicity of CD8+ T cells after ischemic stroke.
Trial registration number
N/A
AS17-011
DISRUPTION OF ASTROCYTES/OLIGODENDROCYTES GAP JUNCTIONS CONTRIBUTES TO IMPAIRED OLIGODENDROGENESIS IN ISCHEMIC WHITE MATTER INJURY
1Drum Tower Hospital- Nanjing University Medical School, Department of Neurology, NanJing, China
Background and Aims
Gap junctions are the molecular basis for the panglial syncytium and are vital for oligodendrocyte survival as well as white matter integrity. Disruption of astrocyte-oligodendrocyte (A/O) gap junctions has been shown in several demyelinating central nervous system disorders. However, their involvement in cerebral ischemia remains largely unknown.
Method
Ischemic white matter injury in mice was induced by long-term bilateral carotid artery sclerosis (BCAS). White matter injury was examined by MBP staining. Cognitive impairment of BCAS mice was assessed by Novel object recognition and Morris water maze test. Expression of connexin30 and connexin32 in astrocytes and oligodendrocytes, respectively, was measured by real-time PCR and immunofluorescence. Brdu was used to label pre-oligodendrocytes and newly generated oligodenrocytes. Oligodendrogenesis was calculated by the ratio of newly generated oligodendrocytes among total oligodendrocytes.
Results
White matter injury was induced in BCAS mice at 30 days post ischemic injury. BCAS mice show reduced novel object recognition ability. Compared to the control group, the learning and memory ability was impaired in BCAS mice. Both the expression of Cx30 and Cx32 in astrocytes and oligodendrocytes was decreased in BCAS. Moreover, co-localization of Cx30 and CX32 was damaged in BCAS mice, indicating that A/O gap junction was damaged in ischemic white matter injury. In addition, oligodendrogenesis was inhibited in BCAS mice as demonstrated by decreased Brdu-labeled newly generated oligodendrocytes.
Conclusion
Disrupted A/O gap junction contributes to the impaired oligodendrogenesis in ischemic white matter injury, and eventually leads to cognitive impairment.
Trial registration number
N/A
AS17-012
DOUBLE NEGATIVE T CELLS PROMOTE NUEROINFLAMMATION IN ACUTE ISCHEMIC STROKE BY INDUCING ACTIVATION OF PROINFLAMMATORY MICROGLIA
1Drum Tower Hospital- Nanjing University Medical School, Department of Neurology, NanJing, China
Background and Aims
CD3+CD4-CD8-T cells (double-negative T cells, DNTs) have diverse functions in immuno-related diseases. We have demonstrated FasL mutant (gld) mice attenuated brain inflammation after ischemic injury, with a dramatic accumulation of DNTs in brain. We hypothesized that DNTs modulate neuroinflmmation by promoting microglial activation post-stroke.
Method
Middle cerebral artery occlusion (MCAO) was induced in FasL mutant (gld) and C57BL/6J mice. Splenic DNTs post-stroke were cocultured with microglia, followed by quantification of inflammatory cytokines in the supernatant measured by Cytometric Bead Array (CBA). Specificity of detrimental DNTs effects was confirmed by adoptive transfer experiments in Rag1-/- mice lacking functional lymphocytes. Subtypes of T lymphocytes and microglia were measured by flow cytometry and immunofluorescence.
Results
DNTs accumulated significantly in the ischemic cerebral hemisphere in B6 mice 1d and 3d after MCAO, and contributed to pro-inflammatory activation of microglia via releasing more tumor necrosis factor (TNF)-α. Rag1-/- mice reconstituted with DNTs developed significantly increased brain infractions and more activation of pro-inflammatory microglia. Mechanistically, proteomic analysis revealed that the inflammatory function of DNTs was correlated with FasL/PTPN2/TNF-α pathway, inhibition of PTPN2 abolished the decreased expression of TNF-α in DNTs from gld mice, and simultaneously improved activation of pro-inflammatry microglia. Finally, ablation of FasL in DNTs using anti-FasL antibodies or Rag1-/- mice reconstituted with gld DNTs improved the anti-inflammatory microglial activation and reduced the brain injury.
Conclusion
Infiltrated DNTs contribute to neuroinflammation, promote pro-inflammatory microglial activation and aggravate brain injury after ischemic stroke, the possible mechanism may involve the FasL/PTPN2/ TNF-α pathway in DNTs.
Trial registration number
N/A
AS17-013
SERUM CLAUDIN-5, A POTENTIAL BIOMARKER REFLECTING BLOOD-BRAIN BARRIER DYSFUNCTION IN ACUTE/SUBACUTE CEREBRAL VENOUS THROMBOSIS WITH VENOUS INFARCT
1Xuanwu Hospital-Capital Medical University, Neurology, B, China
2Xuanwu Hospital-Capital Medical University, Neurology, Beijing, China
Background and Aims
Cerebral venous thrombosis (CVT) with venous infarct often develops into severe CVT. Blood-brain barrier (BBB) dysfunction plays a crucial role in the development of venous infarct. Currently, there are no valuable biomarkers to reflect BBB dysfunction associated with venous infarct. Herein, we analyzed whether claudin-5, occludin and matrix metalloproteinases-9 (MMP-9) could serve as biomarkers reflecting BBB dysfunction in acute/subacute CVT patients.
Method
Blood and cerebrospinal fluid were prospectively obtained from acute/subacute CVT patients, chronic CVT patients and healthy control group. Claudin-5, occludin and MMP-9 were measured using ELISA kits. The roles of the biomarkers reflecting BBB dysfunction were analyzed using one way ANOVA, generalized linear models and diagnostic tests.
Results
A total of 52 CVT patients were enrolled, including 43 patients (30 with venous infarct and 13 without) with acute/subacute stage and 9 patients with chronic stage. Compared with patients without venous infarct, serum claudin-5 was significantly increased (p=0.025) in acute/subacute CVT patients with venous infarct and still significantly associated with venous infarct in acute/subacute CVT patients (b=849.61, P=0.020) after adjustment for age, sex, systolic blood pressure and high-sensitivity C-reactive protein. Areas under the curves (AUC) indicated moderate discriminatory capabilities of serum claudin-5 on venous infarct in acute/subacute CVT (AUC=0.700, 95%CI: 0.541-0.859, P=0.039).
Conclusion
These findings suggest that serum claudin-5 maybe a clinically valuable biomarker for reflecting BBB disruption in acute/subacute CVT patients with venous infarct. Larger cohorts to precisely evaluate early predictive value of serum claudin-5 for BBB dysfunction in CVT patients are warranted.
Trial registration number
N/A
AS17-016
NETWORK LESION MAPPING IN PURE MOTOR CHRONIC ISCHAEMIC STROKE PATIENTS IDENTIFIES DISRUPTIONS IN GLOBAL AND LOCAL NETWORK ARCHITECTURE
1Universitätsklinikum Hamburg-Eppendorf, Neurology, Hamburg, Germany
2École polytechnique fédérale de Lausanne, Centre of Neuroprosthetics, Lausanne, Switzerland
Background and Aims
Many neurological functions are distributed across cerebral networks and are contingent on the interplay between cortical and subcortical areas. Part of the pathophysiology of stroke is the disruption of these networks as a result of neuronal death. We study the structural connectome of stroke patients and quantify how the their network architecture differs from healthy controls.
Method
17 patients with subcortical ischaemic stroke and motor symptoms as well as 21 age-matched healthy controls underwent T1-weighted MRI and DTI imaging. Their anatomical brain networks were approximated by probabilistic tractography. In a hierarchical analysis, multilinear mixed-models were first used to assess alterations of the global network architecture of stroke hemispheres. In a second step, network lesion mapping identified the cortical and subcortical regions most strongly affected by the lesion-induced white matter disruptions.
Results
Compared to healthy controls, stroke hemispheres showed reduced connectivity strength, decreased global efficiency, and increased clustering. The largest local connectivity deficits were observed in the pre-/postcentral and inferior/superior parietal cortices as well as the basal ganglia and the thalamus. Affected white matter tracts were predominantly connecting cortical and subcortical areas.
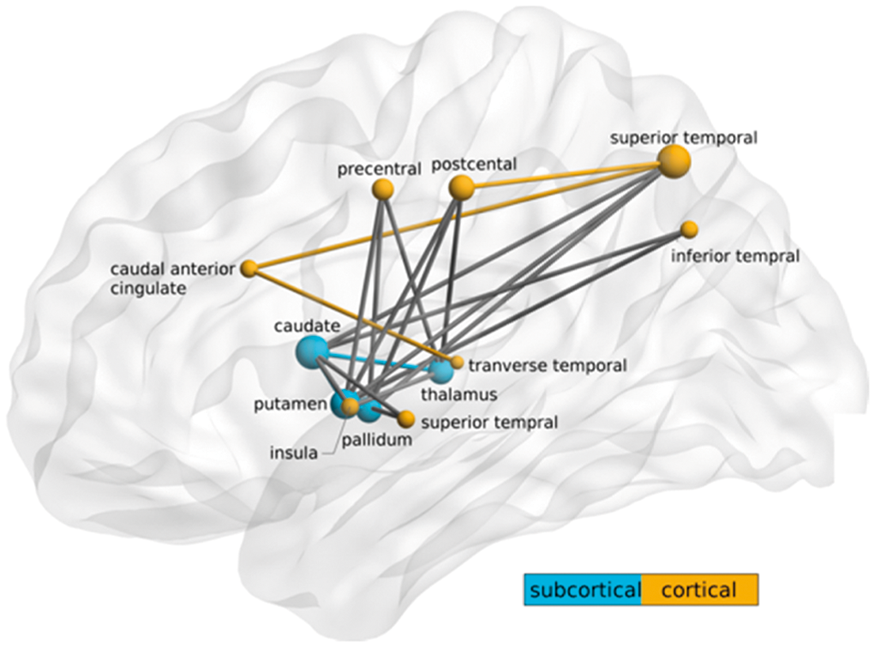
Conclusion
Pure motor stroke patients displayed significant alterations in the global network architecture of the ipsilesional hemisphere. These changes localized to a cortico-subcortical subnetwork consisting of regions associated with planning, execution and control of motor functions.
Trial registration number
N/A
AS17-017
NEUROLOGICAL SYMPTOMS AND RISK FACTORS IN REPERFUSION SYNDROME AFTER CAROTID REVASCULARIZATION: BEYOND THE HYPERPERFUSION SYNDROME
1Hospital Universitario Central de Asturias, Neurology Service, Oviedo, Spain
2Hospital Universitario Central de Asturias, Bone and Mineral Research Unit, Oviedo, Spain
3Hospital Universitario Central de Asturias, Radiology Service, Oviedo, Spain
4Hospital Universitario Central de Asturias, Vascular Service, Oviedo, Spain
5Lausanne University Hospital, Stroke Center- Neurology Service, Lausanne, Switzerland
Background and Aims
The cerebral hyperperfusion syndrome is a well-known syndrome after carotid- endarterectomy (CEA) and carotid artery stenting (CAS), decreasing the potential benefit of these interventions
Method
We studied consecutive patients with internal carotid artery (ICA) stenosis who underwent a CEA and CAS (February 2005-May 2016) in a tertiary level University Hospital. We investigated all patients with new neurological symptomatology after carotid revascularization (NSACR) not attributable to recurrent ischemia.
Results
Of 1’029 consecutive patients 83 patients (median age 72.2 years, 30.1% female) fulfilled the inclusion criteria. 59% underwent CEA and 41% CAS. NSACR included the following symptoms, alone or in combination: 38.5% new headaches, 31.3% confusional episodes and 31.3% focal neurological deficit, 13.2% seizures, and 13.2% visual hallucinations. Intracranial hemorrhage and cerebral edema were seen each in 10.8% of the cases. Transcranial Doppler studies were normal in the majority of the patients. The comparison with a matched control group showed that intermittent (OR 8.5 1,05-69,94) and persistent (OR 4.4 0.78-25.23) high blood pressure (HBP) during the procedure presented a greater risk for CHS syndrome, whereas treatment with statins seemed protective.
Conclusion
CHS definition should be enlarged to include visual hallucinations and confusional states. The main risk factor for CHS was periprocedural high blood pressure, and statin pretreatment seemed protective. This knowledge may help to prevent CHS in elective carotid revascularization.
Trial registration number
N/A
AS17-019
SECONDARY BRAIN DAMAGE AND OUTCOME IN ISCHAEMIC STROKE PATIENTS WITH A HISTORY OF MIGRAINE
1Leiden University Medical Center, Neurology, Leiden, The Netherlands
2Leiden University Medical Center, Radiology, Leiden, The Netherlands
3University Medical Center Utrecht, Radiology, Utrecht, The Netherlands
4University Medical Center Utrecht, Neurology, Utrecht, The Netherlands
5St. Antonius Hospital, Neurology, Utrecht, The Netherlands
6VU Medical Center, Neurology, Amsterdam, The Netherlands
Background and Aims
Patients with a history of migraine might be susceptible for spreading depolarisations which are known to affect vascular and neuronal function and penumbra recovery after stroke. We investigated whether these patients have more secondary brain damage after stroke and less favourable outcomes compared with patients without migraine.
Method
We included patients from a prospective multicentre ischemic stroke cohort. Lifetime migraine history was based on International Classification of Headache Disorders-II criteria. Patients underwent non-contrast CT, CT angiography and CT perfusion and follow-up CT after 3-5 days. On admission, presence of perfusion deficit, infarct core, penumbra and blood brain barrier permeability (BBBP) were assessed. Markers of brain damage at follow-up included presence of malignant oedema, haemorrhagic transformation and final infarct volume. Clinical outcome was evaluated using the modified Rankin scale (mRS) after 3 months. We calculated adjusted relative risks (aRR) or difference of means (aB) with regression analyses.
Results
We included 600 patients of whom 43 had migraine. Patients with migraine had as often as patients without migraine perfusion deficits on admission (aRR:0.98,95%CI 0.77-1.25), similar infarct core area (ASPECTS<8 aRR:0.95, 95%CI:0.45-2.00), penumbra area (ASPECTS<8 aRR:0.90, 95%CI:0.60-1.34), mean BBBP (aB:-0.08, 95%CI:-3.11–2.96), malignant oedema (0% in migraine, 5% in no migraine), haemorrhagic transformation (aRR:0.26, 95%CI:0.04–1.73), final infarct volume (aB:-14.8, 95%CI:29.9-0.2) and poor clinical outcome after 3 months (mRS>2 aRR:0.50, 95%CI:0.21–1.22).
Conclusion
Our results suggest that patients with migraine do not have significantly more secondary brain damage or poor outcome after ischemic stroke compared with patients without migraine.
Trial registration number
ClinicalTrials.gov Identifier: NCT00880113
AS17-020
MACAQUE MODEL OF IN SITU THROMBOEMBOLIC STROKE
1CYNBIOSE, Cynbiose, Marcy l'Etoile, France
2CYCERON, UMR-S U1237 PhIND, Caen, France
3CarMeN Laboratory, INSERM u1060, Lyon, France
Background and Aims
Novel insights into the pathophysiology of the neurovascular unit after stroke call for the use of new strategies to improve stroke treatment. Unfortunately, despite the plethora of drugs that display clear beneficial effects in animal models of experimental ischemia, their subsequent use in clinical trials has proven disappointing. As such, one is forced to consider that new animal models of focal cerebral ischemia may be required before translation to clinical trials.
Method
In situ microinjection of thrombin is used to trigger a local clot formation in the middle cerebral artery of adult male rhesus monkeys. Animals are submitted to MRI (3T) analyses including angiography, T2, FLAIR, diffusion, perfusion and T1 procedures at 2, 24 hours, 7, 15 and 90 days after stroke onset. Motor function assessment, particularly manual dexterity and digit strength, is performed over the 3-months period post-stroke by using an adaptation of the hand dexterity task (Moore et al, 2010).
Results
In situ thrombin injection leads to immediate clot formation that leads to both cortical and subcortical ischemic injuries which display all the characteristics of the clinical situation. The major clinical deficits, consistent with cerebrovascular damage, include contralateral motor and sensory dysfunctions and, visuospatial neglect.
Conclusion
We describe an original model of in situ clot formation in which imaging, physiological and functional analyses mimic human stroke evolution. In order to improve on a similar model developed in mice (Orset et al., 2007), we provide here a non-human primate model of stroke which we consider to be more relevant to pre-clinical studies
Trial registration number
N/A
AS17-021
ANTI-INFLAMMATORY EFFECT OF DHA IN MICE SUBMITTED TO ISCHEMIC STROKE
1the Third Affiliated hospital, Sun Yat-sen University, Guangzhou, China
Background and Aims
The study aimed to investigate the anti-inflammatory effect of DHA in mice suffering from a cerebral ischemia/ reperfusion injury.
Method
In this study, the focal cerebral ischemia in mice was induced by middle cerebral artery occlusion (MCAO) for 1 h, and the mice were treated with DHA just before reperfusion. The ischemic infarct volume was recorded 24 h after the MCAO. In addition, numbers of inflammatory cells in the blood, spleen, ipsilateral brain were determined by flow cytometry, while cytokines and chemokines levels were determined by RT-PCR and protein array.
Results
Our results showed that DHA treatment decreased infarct volume significantly compared with control group, it downregulated inflammatory cells, such as macrophage, B cells, T cells, and reduced expression levels of cytokines and chemokines, especially the levels of IL-1rα, G-CSF, CXCL1.
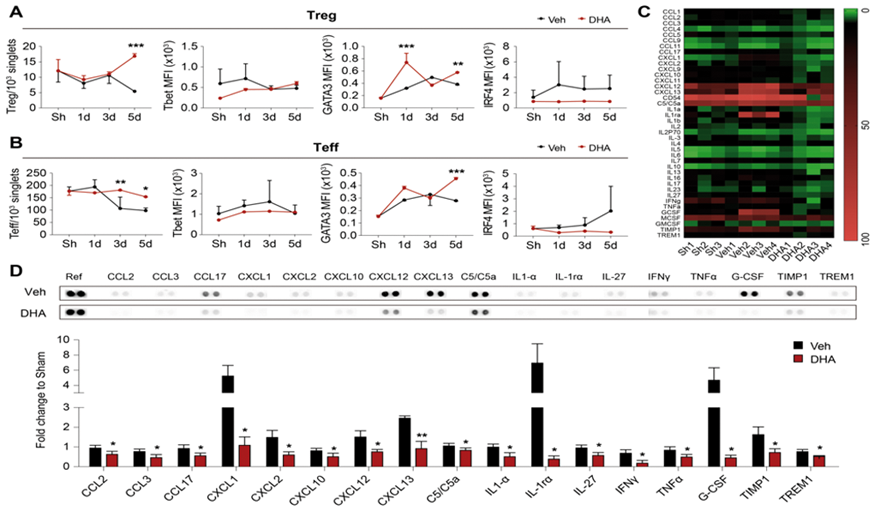
Conclusion
Our results suggest that DHA protects against cerebral ischemia/reperfusion injury.and displays anti-inflammatory actions.
Trial registration number
N/A
AS17-022
CEREBRAL INFARCT VOLUME AND COLLATERAL CIRCULATION IN YOUNG VERSUS OLDER ADULTS WITH ACUTE ISCHEMIC STROKE
1Beth Israel Deaconess Medical Center, Division of Stroke and Cerebrovascular Diseases, Boston, USA
Background and Aims
After acute ischemic stroke (AIS), older adults tend to have worse outcomes compared to young adults. One potential explanation is differences in cerebral collateral circulation (CCC). Multiple studies have shown that a robust CCC is associated with smaller infarcts, improved clinical outcomes, and lower rates of hemorrhagic transformation. We undertook this study to examine CCC status and the role it plays in determining infarct size and outcome in young and older adults with AIS.
Method
We studied 142 consecutive patients presenting with AIS secondary to occlusion of the proximal MCA. We measured final infarct volumes on DWI MRI and graded the CCC on CTA. Patients were divided into 2 groups based on age; >55 and ≤55 years. Univariate and multivariate logistic regressions were performed to test the relationship between age, CCC, and various clinical outcome measures.
Results
Younger age (≤55 years) was associated with better CCC (p = 0.0281) and mRS (p = 0.0003). Infarct volumes did not vary significantly with age. There was no significant interaction between age and collateral status on infarct volume.
Conclusion
In this cohort, younger adults had better CCC and clinical outcomes, but there was no interaction between age and collateral status on infarct volume. This suggests that the beneficial effect of good CCC is not blunted by age, and that older adults with AIS can derive similar benefits from good CCC. This takes on new significance as the time windows for reperfusion therapy become individualized, and novel strategies to augment CCC are developed.
Trial registration number
N/A
AS17-023
EXPRESSION OF M2-RELATED CYTOKINES AND GENES IN ISCHEMIC STROKE PATIENTS
1University of Antwerp, Cell biology and Histology, Antwerp, Belgium
2Universitair Ziekenhuis Antwerpen, Neurology, Antwerp, Belgium
3University of Antwerp, Translational Neuroscience, Antwerp, Belgium
Background and Aims
Post-stroke development of immunesuppression underlies increased susceptibility towards infectious complications, affecting mortality and patient outcome. Inducing cellular preference towards the anti-inflammatory M2 phenotype in innate immune cells can impair innate bactericidal defense. In this study, we examined the anti-inflammatory cytokine profile and the expression of M2-related genes in the blood of ischemic stroke patients.
Method
Thirty adult patients with ischemic stroke and 20 age-matched control subjects were included. Patients had no incidence of infection prior to hospital admission. Blood and serum samples were collected in the stroke-unit of the Antwerp University Hospital at admission and one, two and three days after symptom onset. Cytokine concentrations were measured in serum and transcript analysis of M2-related genes was performed in whole blood samples. As development of infection is an important complication of stroke, we also studied and identified 10 patients in our cohort that developed early infectious complications (within seven days after ischemic stroke), comprising pneumonia (80%) and UTI (20%) infections.
Results
Stroke patients showed significantly increased levels of anti-inflammatory cytokines IL-4, IL-10 and IL-33 alongside pro-inflammatory cytokines IL-6 and TNFa but no change in IL-5 and IL-13 levels. Upregulation of serum cytokine levels of IL-4, IL-10 and IL-6 correlated with development of early infections. Furthermore, IL-33 and IL-1b could only be measured in serum samples from patients that later developed infectious complications.
Conclusion
To conclude, we show here that ischemic stroke leads to upregulation of anti-inflammatory cytokines, which is correlated with an increased risk for developing infectious complications.
Trial registration number
N/A
AS17-024
STUDY OF CAVEOLIN-1 PROTEIN LEVELS IN EXPERIMENTAL MODELS OF CEREBRAL ISCHEMIA AND TREATMENT WITH RT-PA
1University of Girona, Biology, Girona, Spain
2Girona Biomedical Research Institute IdIBGi, Neurology, Girona, Spain
3University of Girona, Chemistry, Girona, Spain
4Universidad Complutense de Madrid, Neurovascular Research Unit, Madrid, Spain
5University Hospital Complex of A Coruña, Neurology Service, A Coruña, Spain
Background and Aims
The recombinant tissue plasminogen activator (rt-PA) has been associated with increased blood-brain barrier (BBB) permeability during stroke insult. Caveolin-1 (cav-1) is a key protein in the regulation of endothelial cell permeability. Our aim was to study the cav-1 protein levels under ischemic conditions and treatment with rt-PA.
Method
Cav-1 protein levels were analyzed by Western Blot at 0, 3, 6, 24 and 72h post-reperfusion of oxygen and glucose deprivation (OGD) and rt-PA administration in bEnd3 murine endothelial cell line. In an in vivo thromboembolic model +/- rt-PA, cerebral tissue cav-1 levels were analyzed at 24h post-occlusion of the middle cerebral artery (MCAO) by immunofluorescence and serum cav-1 levels at 3, 6 and 24h post-MCAO by ELISA.
Results
Cav-1 increased significantly in the bEnd3 cell line from 0 to 72 h post-reperfusion in OGD condition. However, when rt-PA is administered, cav-1 protein levels significantly decreased versus OGD condition at all analyzed times and versus CTRL rt-PA condition at 6 and 24 hours post-reperfusion. In vivo, serum levels of cav-1 tended to increase at 6h post-MCAO only in the rt-PA treated MCAO group. In cerebral tissue, significant cav-1 increased levels in the ischemic area were only observed in the rt-PA treated MCAO group. Cav-1 tissue levels correlated positively with edema, infarct volume and hemorrhagic area at 24h post-MCAO. Cav-1 serum levels at 3h post-MCAO correlated negatively with the hemorrhagic area at 24h post-MCAO.
Conclusion
rt-PA modifies cav-1 expression in response to ischemic conditions in both analyzed experimental models.
Trial registration number
N/
AS17-025
CEREBRAL ISCHEMIC PRECONDITIONING PLAYS A PROTECTIVE ROLE BY REDUCING THE EXCITATORY AMINO ACIDS TOXICITY
1Jilin University, Neurology, changchun, China
Background and Aims
Cerebral ischemia-reperfusion injury is a multi-target and multi-process cascde reaction. The mechanism of endogenous protection by ischemic preconditioning arises at the historic moment. The purpose of this study is to explore the protective effects of cerebral ischemic preconditioning on cerebral ischemia-reperfusion injury, as well as the mechanism of Connextion 43 (Cx43) and excitatory amino acid transporter 2 (EAAT2 ) in ischemic preconditioning.
Method
In vitro, primary astrocytes cultures were pepared from cerebral cortex of Wistar neonatal rats. OGD group was given glucose oxygen deprivation (OGD) 12h /reintroduction 6h. Preconditioning (IPreC) group received OGD 30min treatment 24h before OGD12h. The activity of astrocytes was detected by CCK-8 and flow cytometry. The concentration of glutamate in the supernatant was detected. The hemichannels opening state was detected by small nucleic acid permeability test. The expression level of Cx43 and EAAT2 was observed by Wetern Blotting and co-focal microscope.
Results
CCK-8 and flow cytometry results showed that preconditioning could significantly increase the activity of astrocytes, while the concentration of extracellular glutamic acid was decreased, and the opening of hemichannels were decreased, and the contents of Cx43 and EAAT2 decreased significantly.
Conclusion
Cerebral ischemic preconditioning can reduce the expression of Cx43 and EAAT2 protein, and promote the closure of hemichannels, thereby reducing extracellular glutamate concentration, reducing excitatory amino acid toxicity, and playing a protective role in brain.
Trial registration number
N/A
AS17-026
TRANSTHORACIC ECHOCARDIOGRAPHY IN LACUNAR STROKES: IMPLICATIONS IN SECONDARY ISCHEMIC STROKEPREVENTION
1Vadodara Stroke Center, Stroke Research, Vadodara, India
Background and Aims
Lacunar Strokes(LS) are caused by thickening of arterial media and obstruction of the origin of small size penetrating arteries and arterioles by intimal plaques. LS are clinically characterized by classic lacunar syndromes (pure motor, pure sensory, sensorimotor, ataxic-hemiparesis and dysarthria-clumsy hand) with radiological lesion less than 1.5 cm in with no obvious large vessel disease or cardioembolic source (CE). Transthoracic echocardiography (TTE) is extensively used for etiological evaluation of ischemic stroke (IS) for detection of CE source but its utility in LS is debated. The aim of this study was to evaluate potential use of TTE in LS.
Method
We performed retrospective chart review of IS patients admitted at Vadodara Institute of Neurological Sciences between January 2015 and December 2017. Data was collected on demographics, risk factors and TTE findings. Potentially CE TTE findings were enlarged LA diameter, Akinetic and hypokinetic left ventricular wall motion (LVWM), Left Ventricular thrombus and EF less than 40%.
Results
Out of 624 patients, 156(25%) were LS patients having mean age 63 years and male preponderance. Hypertension was risk factor in 60% of LS patients while DM(28%), CAD(6%), Smoking (27%) and hyperlipidemia (52%). There was no difference in mean age/sex/risk factors between LS and non-LS IS patients. TTE revealed abnormalities in 33 patients: 3 with enlarged left atrial diameter, 15 with akinetic LVWM, 10 with hypokinetic LVWM and 5 with EF less than 40%.
Conclusion
TTE findings revealed potential CE source in 21% of our LS patients and should be considered in evaluation of LS patients for management of secondary prevention of IS.
Trial registration number
n/a
AS17-027
STORAGE OF BLOOD CLOTS FOR HISTOLOGICAL ANALYSIS: HOW LONG IS TOO LONG IN SALINE AND FORMALIN?
1National University of Ireland Galway, Physiology, Galway, Ireland
2National University of Ireland Galway, Curam, Galway, Ireland
Background and Aims
To investigate the histological composition of blood clots following mechanical thrombectomy, it is key to ensure optimum storage for highest quality histology and immunofluorescence. We investigated how long is too long for storage of clots in saline and formalin.
Method
Human blood was obtained from the Irish Blood Transfusion service. Whole blood and fibrin rich clot analogues were made under dynamic flow conditions. Clots were stored in saline, or 10% buffered formalin for 1 hour (h), 24h, 48h, 1 week (w), 2w, 4w. Additionally, clots were stored in formalin for the extended periods of 2 and 6 months. 5 micrometre slices were cut, stained with Massons Trichrome to visualise RBCs, white blood cells (WBCs) and fibrin. Preliminary analysis of the integrity of clot components used a scoring system (0: low; 1: sub-par; 2: high). Autofluoresence was also assessed using a relative scale.
Results
The clots in saline for longer than 1 week showed evidence of degradation of RBCs and WBCs, but fibrin remained intact (median score: 1, 1, 2 respectively). Clots stored in formalin for up to 2 months were qualitatively similar to those stored for all shorter periods (median score: 2 per component). However, 6 month samples showed considerably reduced integrity of all components (0, 1, 0 respectively). Autofluorescence increased time dependently, being most pronounced at 6 months.
Conclusion
For optimum histology and immunofluorescence, blood clots should be left in saline and formalin for no longer than 1 week and 2 months respectively.
Acknowledgements: Science Foundation Ireland (Grant Number 13/RC/2073) and Cerenovus.
Trial registration number
N/A
AS17-028
REMOTE PERCONDITIONING ENHANCES NEURO PROTECTION AND COLLATERAL BLOOD FLOW DURING ISCHEMIA IN DISTAL CEREBRAL ISCHEMIC RAT MODEL (MCAO) THROUGH AMPK-ENOS PATHWAYS
1Hamad Medical Corporation, Neurosciences Institute, Doah, Qatar
2University of Alberta, Department of Medicine, Edmonton, Canada
Background
The technique of Remote Ischemic preconditioning (RIPerC) has been studied in experimental ischemic and clinical trials in patients with cardiac and cerebral ischemia. However, the mechanisms for protection behind Remote Ischemic preconditioning (RIPerC) are still not fully understood. Here we investigated the neuroprotective efficacy and the role of AMPK-eNOS pathways in limb RIPerC using a distal middle cerebral artery occlusion (MCAO) rat model.
Methods
Here the adult male rats were subjected to (MCAO) followed by perconditioning (3*15 minutes) treatment after 2h. Laser speckle contrast imaging (LSCI) was used to measure the collateral flow augmentation due to RIPerC during distal (MCAO). Western Blotting, and RT-PCR techniques were used to measure p-AMPK, eNOS 24 h, post MCAo.
Results
LSCI revealed that RIPerC Augmented collateral flow into distal segments. Notably, while control rats exhibited an initial dilation followed by a progressive narrowing of pial arterioles 60 to 150 –min post-MCAo, this constriction was prevented or reversed by RIPerC. RIPerC significantly reduced early ischemic damage measured 6h after stroke onset. We also found by Western Blotting, that compared to control rats RIPerC significantly increased the activation of p-AMPK post MCAO. RT-PCR further showed that increased p-AMPK activity translated into up regulation of e-NOS in RIPerC treated animals suggesting that perconditioning mediated collateral enhancement may be mediated through AMPk-eNOS pathway.
Conclusion
Our results suggest that RIPerC Augmented collateral flow into distal segments and the subsequent prevention of collateral collapse via RIPerC is neuroprotective and potentially due to the activation of AMPK- eNOS pathway.
Trial registration number
N/A
AS17-029
DELAYED CEREBRAL ISCHAEMIA AFTER SUBARACHNOID HAEMORRHAGE IN PATIENTS WITH A HISTORY OF MIGRAINE
1Leiden University Medical Center, Neurology department, Leiden, The Netherlands
2University Medical Center Utrecht, Neurology department, Utrecht, The Netherlands
3Academic Medical Center, Neurosurgery department, Amsterdam, The Netherlands
4The Hague Medical Center, Intensive Care department, The Hague, The Netherlands
5University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Spreading depolarizations are thought to play a role in the pathophysiology of delayed cerebral ischaemia (DCI) after aneurysmal subarachnoid haemorrhage (SAH). Since migraine patients are probably more susceptible to spreading depolarizations, we investigated whether they are at increased risk for DCI.
Method
We included SAH patients from three hospitals in the Netherlands. We assessed migraine history with a validated migraine screener. We calculated adjusted hazard ratios (aHR) with 95% confidence intervals (CI) with multivariable Cox regression to adjust for possible confounders and assessed interaction by age and sex.
Results
We included 542 SAH patients with complete data on migraine and DCI, of whom 103 (19%) had a history of migraine (61 with aura). Mean age of all patients was 57 years and 391 (72%) were women. Patients with a history of migraine did not more frequently develop DCI than patients without (22% versus 28%, aHR:0.78;95%CI:0.49–1.25). Additionally, no increased risk for DCI was found in migraine patients with aura or in women. We found a statistically significant interaction between migraine and age with an increased risk of DCI among young migraine patients (Pinteraction=0.011, Table).
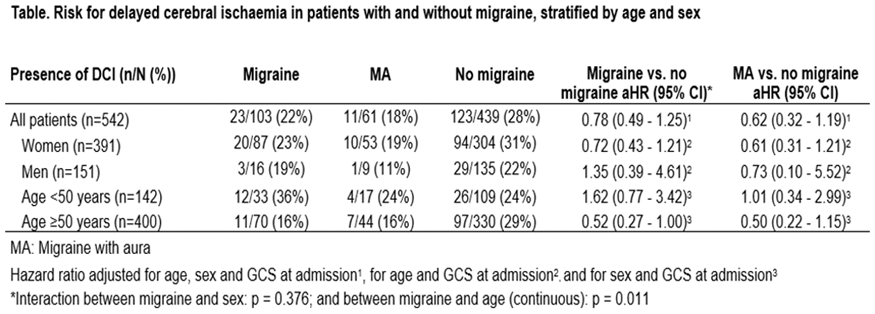
Conclusion
Our results suggest that young migraine patients may have an increased risk of DCI. Future studies with a larger number of young patients are needed to further investigate this subgroup of SAH patients.
Trial registration number
N/A
AS17-030
LYMPHOCYTE TO MONOCYTE RATIO AND MONOCYTE SUBTYPES ARE PREDICTORS OF SEVERITY AND OUTCOME IN ACUTE ISCHEMIC STROKE
1Stroke Unit. Hospital Universitario Fundación Jiménez Díaz- IIS-FJD, Neurology, Madrid, Spain
2Neurovascular Research Unit- Faculty of Medicine- Universidad Complutense de Madrid, Pharmacology Department, Madrid, Spain
3Hospital Universitario Fundación Jiménez Díaz- IIS-FJD, Haematology Department. Hospital Universitario Fundación Jiménez Díaz- Madrid- Spain., Madrid, Spain
4Stroke Unit. Hospital Universitario 12 de Octubre, Neurology Department., Madrid, Spain
Background and Aims
Monocytes are heterogeneous cells that play a key role in the pathophysiology of acute ischemic stroke. Depending on the mechanism by which they are activated, they adopt proinflammatory or anti-inflammatory phenotypes according to their expression of lipopolysaccharide receptor (CD14) and Fcg receptor III (CD16). Low lymphocyte to monocyte ratio (LMR) has recently been associated with stroke severity and poor long-term outcome. In this prospective case-control study, we assessed whether LMR, the different monocytes subsets and related cytokines can predict clinical course and outcome of acute ischemic stroke (AIS) and transient ischemic attack (TIA) patients.
Method
We established a group of AIS and TIA patients and a control group from two stroke units. We registered demographic factors, previous medical history of cardiovascular risk factors and diseases. Blood and plasma samples were collected at acute stage (baseline within first 12 hours). Flow cytometry studies and quantitative analysis of different plasma cytokines using a customised cytometric bead array were performed. Neurological evaluation of severity was done daily during hospitalization and at day 90 using NIHSS scale, and functional outcome using the modified Rankin Scale (mRS).
Results
Our results show an increased number of total blood monocytes in AIS and TIA patients, and also an increased number of classical monocytes (CM; CD14+ CD16-) but not of intermediate (IM; CD14+CD16+) and non-classical (NCM; CD14-CD16++). Total CM were associated with stroke severity (higher NIHSS) and classical LMR (LMRc) with better outcome (lower mRS).
Conclusion
CM and LMRc may be a predictor of clinical outcome of AIS and TIA patients.
Trial registration number
N/A
AS17-032
INTERLEUKIN-6 (IL-6) IS A POTENTIAL BIOMARKER OF PLAQUE-DERIVED SYSTEMIC INFLAMMATION IN PATIENTS WITH TRANSIENT ISCHAEMIC ATTACK AND CAROTID STENOSIS
1University College Dublin, Stroke Clinical Trials Network Ireland, Dublin, Ireland
2Mater Misercordiae University Hospital/Royal College of Physicians Ireland, Stroke, Dublin, Ireland
3University College Dublin, Conway Institute, Dublin, Ireland
4St Vincent's University Hospital, Medicine for the Older Person, Dublin, Ireland
5James Connolly Memorial Hospital- Blanchardstown, Medicine for the Older Person, Dublin, Ireland
6University College Dubline, Conway Institute, Dublin, Ireland
7Mater Misercordiae University Hospital, Clinical Biochemistry, Dublin, Ireland
8St James University Hospital, Stroke, Dublin, Ireland
9Mater Misercordiae University Hospital, Stroke Clinical Trials Network Ireland, Dublin, Ireland
10Mater Misercordiae University Hospital, Stroke, Dublin, Ireland
11Beaumont University Hospital, Department of Neurology, Dublin, Ireland
12Royal College of Surgeons Ireland, Stroke, Dublin, Ireland
13Mater Misercordiae University Hospital/University College Dublin, Stroke Clinical Trials Network Ireland, Dublin, Ireland
Background and Aims
Blood inflammatory biomarkers may aid patient selection for prevention therapies targeting plaque inflammation. However, the contribution of recently-symptomatic carotid plaque to the systemic inflammatory biomarker profile is typically confounded by acute brain infarction. To investigate the plaque-derived component of systemic inflammation in acute cerebrovascular disease, we studied inflammatory biomarkers in TIA patients with carotid stenosis, in whom the confounding effects of brain infarction should be minimal.
Method
The BIO-TIA study was a prospective cohort study of blood/imaging biomarkers in stroke physician-confirmed TIA presenting within 72 hours of symptoms. Exclusion criteria were malignancy, infection, recent trauma/surgery, recurrent stroke prior to phlebotomy/MRI. Plasma hsCRP and IL-6 were measured by mass spectrometry and IL1, IL8, IL10, IL12, interferon-α (INF) and tumour-necrosis factor (TNF) by ELISA. MRI was performed within 72 hours of symptom-onset.
Results
Overall, 237 TIA patients were included (59 [24.9%]with carotid stenosis ≥50% [TIA-CS]). In TIA-CS patients, median age was 73, 62.7% were male. 37.2% had DWI positive findings on MRI.
Compared with non-TIA controls, pro-inflammatory cytokines were elevated in TIA-CS patients (IL-6 p < 0.001; IL-8 p = 0.005; INF-α p = 0.009; TNF p =0.004). Compared to TIA patients without stenosis, only IL-6 (5.3pg/mL versus 3.94pg/mL, p <0.001) was greater in TIA-CS patients. Similar results were found after exclusion of TIA-CS patients with DWI hyperintensity (IL-6 p < 0.001; CRP p = 0.01; IL-8 p = 0.006; INF-α p = 0.002, compared with controls).
Conclusion
Our findings suggest that in patients with TIA, serum IL-6 may reflect inflammatory atherosclerotic plaque and may aid future selection of patients for anti-inflammatory stroke preventive therapies.
Trial registration number
NA
AS17-033
RANDOMIZED DOUBLE-BLIND CROSSOVER STUDY ON THE EFFECTS OF VENLAFAXINE ON NEUROVASCULAR AND SUDOMOTOR FUNCTION
1Dresden International University, Health Sciences, Dresden, Germany
2Bavaria Hospital Kreischa, Department of Neurology, Kreischa, Germany
3Universitätsklinikum Carl Gustav Carus Dresden, Department of Neurology, Dresden, Germany
4Rhön-Klinikum, Department of Psychosomatic Medicine, Bad Neustadt, Germany
Background and Aims
Research has indicated that selective serotonine and noradrenaline reuptake inhibitors (SNRIs) such as venlafaxine but not purely serotonergic SSRIs are associated with an increased risk of ischemic stroke but the underlying pathophysiology is poorly understood. We aimed to assess whether venlafaxine treatment is associated with sympathetic noradrenergic disturbances that might indicate a predominantly noradrenergic mechanism whereby SNRI increase neurovascular risk.
Method
Twelve healthy male subjects were enrolled to orally receive 37.5 mg of venlafaxine per day for 7 days and subsequently 75 mg for another 7 days. Placebo was administered to the subjects for 14 days under randomized double-blind crossover conditions. Sympathetic cutaneous neurovascular function was assessed using laser Doppler flowmetry and sympathetic sudomotor function via sympathetic skin response on the upper extremities before start of medication as well as at 0.5, 3, 5 and 7 hours after the last dose. Assessment was undertaken under resting conditions and following sympathetic stimulation.
(Figure)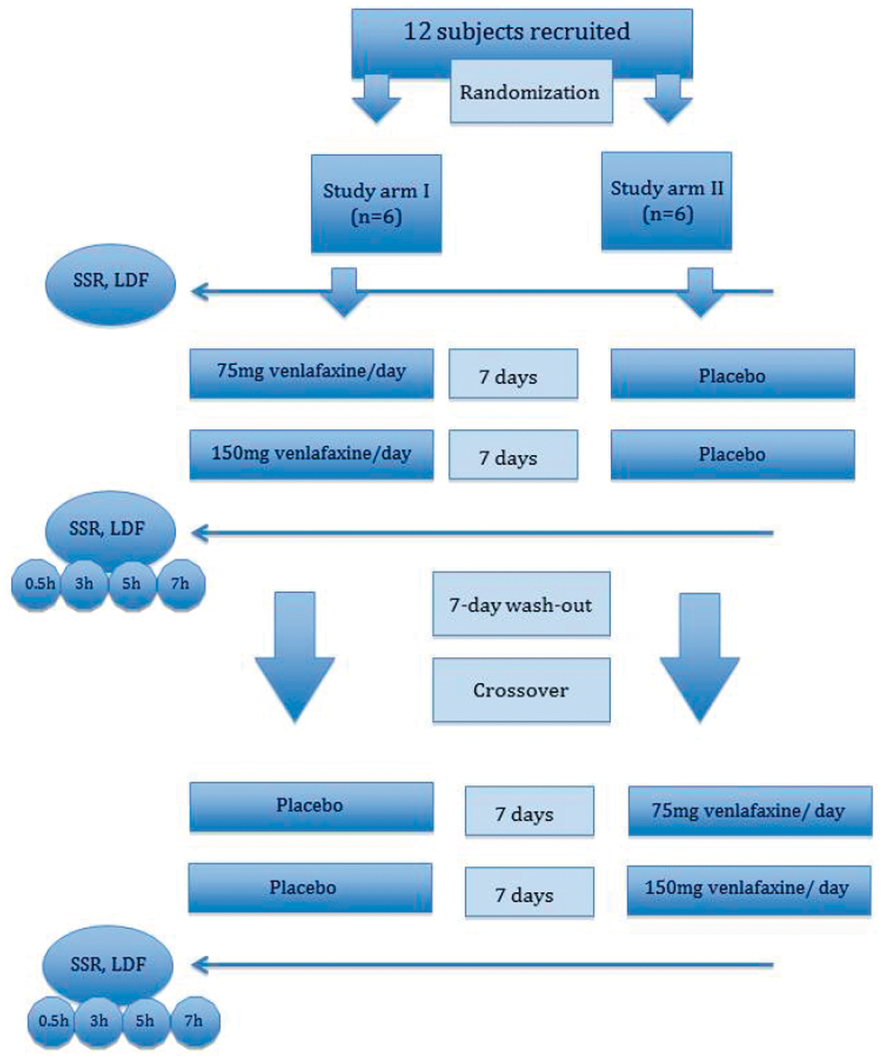
Results
Neither venlafaxine nor placebo has altered integrity of sympathetic neurovascular and sudomotor function when post treatment values were compared to baseline (p = ns). Moreover there was no difference in sudomotor or neurovascular function between groups at any time point of measurement (p = ns). These findings were independent of whether testing was undertaken under resting conditions or upon sympathetic activation.
Conclusion
In our study, venlafaxine has displayed no effect on sympathetic small vessel and sudomotor function in healthy subjects. However, the external validity of this observation warrants confirmation in a larger cohort.
Trial registration number
N/A
AS17-034
PHENOTYPIC AND FUNCTIONAL CHARACTERIZATION OF HUMAN CIRCULATING NEUTROPHILS IN ACUTE PHASE OF ISCHEMIC STROKE
1Saint Antoine Hospital, Neurology and Stroke Unit, Paris, France
2INSERM, UMRS 938- CdR Saint- Antoine- team “Immune System- Neuroinflammation and Neurodegenerative Diseases”- Hôpital St-Antoine, Paris, France
3Sorbonne Université, Faculté de Médecine, Paris, France
4Sorbonne Université, UPMC Univ Paris 06- UMRS 938- CdR Saint-Antoine- Hôpital Saint-Antoine, Paris, France
5Pitié Salpêtrière Hospital, Stroke Unit, Paris, France
6Foch Hospital, Neurology and stroke unit, Suresnes, France
Background and Aims
Ischemic stroke (IS) is a leading cause of death and disability. Emerging data suggest that neutrophils (PMNs) play a key role after IS and constitute a promising target in stroke therapy. However, clinical trials that had targeted PMNs failed to improve recovery in acute IS patients underlining the need for better understand the involvement of PMNs during IS. The aim of our study was thus to characterize phenotypes and functions of human circulating PMNs at the acute phase of IS. This study was performed in whole-blood conditions in order to minimize activation due to isolation procedures.
Method
We analyzed circulating PMNs phenotypes and functions in 27 patients over 18 years, with cerebral infarction less than 6 hours and without evidence of infection, and compared them with 17 age-matched healthy subjects.
Results
During the acute phase of IS, PMNs exhibit an activation state characterized by increased CD11b expression and increased reactive oxygen species (ROS) production and an altered homeostasis which could partially explain increased PMNs oxidative burst. In addition, we observed a lower level of circulating neutrophils extracellular traps (NETs).
Conclusion
PMNs alterations observed in our study, i.e. increased ROS production may be involved in brain injury and clinical outcome. Furthermore, decreased level of circulating NETs within days of focal stroke might play a key role in the increased susceptibility to bacterial infections observed in IS patients. Additional studies are needed to further clarify PMNs functions and determine their involvement in the functional prognosis of patients.
Trial registration number
N/A
AS17-035
EPILEPTIC DISCHARGES IN THE ACUTE PHASE OF STROKE
1Ghent University Hospital, Neurology, Gent, Belgium
Background and Aims
Stroke is a common cause of seizures, especially in the elderly population. However, the incidence, associated factors and influence on outcome of interictal epileptic discharges and subclinical electrographic seizures following acute stroke are unknown.
Method
In this ongoing prospective study, 31 patients with an ischemic stroke (n = 29) or intracerebral hemorrhage (n = 2) underwent long-term video-EEG monitoring within 3 days of stroke. Epileptic discharges (spikes, spike-waves, PLEDs or electrographic seizures) were analysed on the EEG and correlated with clinical and neuroradiological patient characteristics, the occurrence of clinical seizures and functional outcome at day 7 (NIHSS).
Results
In 7/31 (23%) of patients epileptic activity was recorded on the EEG. Two patients (6%) had electrographic seizures. Two patients (6%) had clinical seizures at stroke onset, of which one had interictal spikes and electrographic seizures on the EEG. The occurrence of epileptic discharges was not associated with functional outcome or any of the studied patient characteristics.
Conclusion
Despite the small study population, epileptic discharges were frequently found. Their significance in the acute phase of stroke needs to be elucidated. Identification of associated factors and the influence on outcome need to be addressed in a larger study population.
Trial registration number
NCT01862952
AS17-037
REDUCING THE NUMBER OF MICROGLIA DOES NOT AFFECT STROKE OUTCOME
1San Raffaele Scientific Institute, Institute of Experimental Neurology INSPE, Milano, Italy
2University of Zürich, Institute of Experimental Immunology, Zurich, Switzerland
Background and Aims
Microglial cells are the parenchymal mononuclear phagocytes of the central nervous system (CNS). Although during development and in the adult, microglial cells have been described to maintain neuronal functions, their role in acute pathological conditions such as cerebral ischemia remains elusive. Aim of this work was to unravel the role of microglia in acute experimental ischemic stroke.
Method
Mice lacking more than 50% of reduction of microglia, Il34Lacz/LacZ mice, and mice treated with the CSF-1R inhibitor, PLX3397, causing more than 90% loss of microglial, were subjected to transient proximal 45 minutes middle cerebral artery occlusion.
Results
Il34Lacz/LacZ and control animals, subjected to ischemic stroke were in terms of disability and ischemic lesion volume comparable, despite a better survival rate of Il34Lacz/LacZ mice. Interestingly Il-34 deficiency did not affect microglia proliferation: at 7 days post ischemia (dpi) microglia cell numbers in the ischemic hemisphere were similar between Il-34 deficient and control animals. Indeed microglia proliferation during acute stroke does not rely on IL-34 but rather on CSF-1. Treatment with the CSF-1R inhibitor PLX3397 before stroke led to more than 90% microglia ablation, this severe ablation persisting even at 7dpi. Nevertheless even persistent severe microglia cell reduction did not affect stroke outcome.
Conclusion
We here conclude that reducing the total number of microglia per se does not impact acute stroke outcome. Affecting subtypes of microglia may rather have an impact in stroke.
Trial registration number
N/A
RISK FACTORS FOR STROKE
AS18-001
BRAIN TRAUMA AN IMPORTANT RISK FACTOR FOR STROKE
1Sir ganga ram hospital, Neurosurgery, Lahore, Pakistan
Background and Aims
Over the last century, stroke due to head trauma has become a leading cause of death particularly among young individuals.
We aim to analyse the huge proportion of ischemic stroke as a result of head injuries occurring in lower middle income countries like Pakistan. The study also targets to provide surgeons, health planners, nurses and hospital managers with the useful information which may help for the further workup of stroke. The main aim is to investigate and prevent the burden of stroke caused by head injuries.
Method
A prospective study was done in Sir Ganga Ram Hospital from May 2015 to May 2016. Informed consent was obtained. Epidemiological, clinical and management data were collected for the study.
Results
Out of 100 patients, 76 were males. The median age was 20.0 years (SD=13.3). Fights (n = 20, 38.5%) and road traffic accidents (n = 19, 52.4%) were the most common causes of head injury leading to stroke. The initial GCS had a significant correlation with the outcome. The mortality rate was 31.1%. Of all patients 81.3% were managed conservatively.
Conclusion
We concluded that prevention of road traffic accidents and improvement of conservative care were identified as major methods in order to lessen the burden of stroke. Further studies on stroke patients in low-income countries should be done so that new interventions can be made.
Trial registration number
N/A
AS18-006
CEREBROVASCULAR COMPLICATIONS IN PROLONGED ANTIHYPERTENSIVE THERAPY IN MEN WITH ESSENTIAL HYPERTENSION
1Azerbaijan State Advanced Training Institute for Doctors named after A. Aliyev, Neurology and clinical neurophysiology, Baku, Azerbaijan
2Azerbaijan State Advanced Training Institute for Doctors named after A. Aliyev, Theraphy, Baku, Azerbaijan
3Azerbaijan State Advanced Training Institute for Doctors named after A. Aliyev, Therapy, Baku, Azerbaijan
Background and Aims
Arterial hypertension (AH) ranks first in the structure of mortality from cardiovascular diseases and is a risk factor for cerebrovascular diseases, including stroke. Obviously, the role of antihypertensive therapy (AHT) in prevention of cerebrovascular complications of hypertension is beyond doubt. The aim of this study was to observe the rate of cerebrovascular complications with long-term AHT in patients with essential hypertension.
Method
225 men aged 30-59 years with AH were examined. All patients took various antihypertensive drugs, both in the form of monotherapy, and their various combinations. All patients were examined by a neurologist. Before entering to the study, it was not found any disorders of nervous system associated with AH.
Results
With prolonged AHT, complications of hypertension were observed in 29 patients (21.1%) at different treatment times, 3 of which (2.2%) died from other causes. In 12 patients (8.7%) equally fatal and nonfatal cerebrovascular complications were detected. Against the background of continuous treatment, the complication of hypertension arose on average 8.6 ± 4.5 years. In 75% of cases, betablockers were used in 9 of 12 patients with cerebrovascular complications with AHT, 5 of them developed a fatal stroke (55.6%), and 4 had nonfatal (44.4%).
Conclusion
It was found that fatal and nonfatal cerebrovascular complications appeared mainly in patients taking betablockers, both in the form of monotherapy, and their combination. Long-term AHT allows not only to adequately control of blood pressure, but also to reduce the frequency of its complications, in particular, ischemic strokes, while long-term treatment with betablockers does not prevent their development.
Trial registration number
N/A
AS18-007
PROGNOSTIC SIGNIFICANCE OF CLINICAL-ANTHROPOMETRIC, BIOCHEMICAL, METABOLIC, VASCULAR-INFLAMMATORY AND MOLECULAR-GENETIC MARKERS IN THE DEVELOPMENT OF THE FIRST ISCHEMIC STROKE
1Moscow centre of speech patology and neurorehabilitation, healh, Moscow, Russia
Background and Aims
The study of the prognostic model for the fist ishemic stroke
Method
196 patients who underwent the first ischemic stroke and 119 people who did not suffer a stroke, corresponding to age, place of residence and nationality to a group of patients, were examined. The main anthropometric, clinical, biochemical and metabolic parameters were assessed; markers of vascular inflammation and endothelial dysfunction. Genotyping of single nucleotide polymorphisms of genes: IL8, ADIPOQ, ADIROR, APOB, APOC-IV, BDNF, GRM3.
Results
The following parameters were statistically significant with the first ischemic stroke: weight, BMI, OT, homocysteine, insulin, adiponectin, cystatin C, ApoA1, Apo B, OHL, XC-HDL, LDL, TG, CRB-sh , glucose, uric acid, IL-1b, IL-4, IL-6, IL-8, TNF-a, VEGF-A. The binary logistic regression method was used to construct the forecast model. The final independent model includes the following independent variables: weight, SD-2, adiponectin, Apo A1, IL-1b, IL-4, ADIPOQ (rs17366743), GRM3 (rs2228595), R2 value of Nagelkerk was 0.839. The percentage of agreement between the model and the “training sample” was 90.7%. The percentage of consent of the model with the “independent sample” was 87.1%, the overall percentage of the model's agreement for all patients was 89.8%. In accordance with the received data, the ROC-curve (Receiver Operating Characteristic) was constructed, the area under the ROC-curve was 0.92.
Conclusion
Of all the parameters studied in the study, the largest contribution to the probability of development of the first IS, according to the model obtained, is made by the parameters: diabetes, adiponectin, Apo A1, IL-4.
Trial registration number
N/A
AS18-008
HERPES SIMPLEX INFECTION AND STROKE
1Tbilisi State Medical University HTMC Clinic, Neurology/Neurosurgery, Tbilisi, Georgia
2The First University Clinic of Tbilisi State Medical University, Neurology, tbilisi, Georgia
3Petre Sarajishvili Institute of Neurology, Neurology, tbilisi, Georgia
Background and Aims
Infective vasculities can cause the inflammation of cerebral vessels and high coagulation state that can become the risk for ischemic stroke
Method
75 ischemic stroke patients, 40 male/35 female, aged 50-75 with anamnesis of herpes simplex infection during 3 months previously of stroke have been investigated. All major risk factors of stroke (Atherosclerosis, diabetes mellitus, hypertension, atrial fibrillation, cardiac diseases smoking, alcohol abuse) were researched. Stroke severity assessed by NIHSS scale. Brain MRI (1.5 Tesla) was done. Blood investigated for antinuclear antibodies (ANA) and Antineutrophil cytoplasmic antibody (ANCA) by Enzyme- linkedimmunosorbent Assay (ELISA) method, C reactive protein and coagulation, serology for herpes simplex virus (HSV ½). Statistics were done by SPSS -14.0. Pearson correlation and Multivariate logistic regression (entered stepwise model) were performed.
Results
All patients showed positive serology for herpes infection, 48 positive for HSV1, 27 patients –for HSV2. Blood C reactive protein was elevated in all patients (18 ± 5.1), blood ANA was elevated in 75 % of patients (11.0 U ± 4.2) and Anti PR 3 (c-ANCA) in 50% of patients (0.97U ± 0.05). Positive correlation was found between blood ANA and ANCA levels with Blood INR levels in stroke patients (R=+0.45 and R=+0.27 respectively, P<0.05). Multivariate logistic regression revealed the significance of blood high ANA and ANCA levels in conjunction with diabetes for severity of stroke measured by NIHSS (p < 0.05). There was not significant correlation between ANA and ANCA and ischemic lesion size on MRI scans
Conclusion
Herpes simplex virus can cause the infectious vasculitis in several immunocompromised patients and by increasing the inflammatory reactions might help to the ischemic stroke development.
Trial registration number
N/A
AS18-009
A COMPARISON OF BLOOD PRESSURE VARIABILITY ASSESSED OVER VARYING TIME PERIODS USING DIFFERENT METHODS OF MEASUREMENT IN PATIENTS WITH CEREBROVASCULAR DISEASE
1University of East Anglia, Ageing and Stroke Medicine, Norwich, United Kingdom
2University of Aberdeen, Ageing Clinical & Experimental Research Team, Aberdeen, United Kingdom
Background and Aims
Blood pressure variability (BPV) is an independent cardiovascular risk factor and can be measured as short, medium or long-term variations. However, whether variability over different timescales is a singular phenomenon is unclear.
Method
Patients with a recent TIA or mild stroke (N=154), underwent 10 minutes beat-to-beat BP recording, daytime ambulatory BP monitoring (ABPM), and seven days self-BP monitoring (SBPM). BPV of systolic BP (SBP) and diastolic BP (DBP) for each method was derived as standard deviation (SD), coefficient of variation (CV), average real variability, maximum, and maximum-minimum difference. Beat-to-beat data shows variability over minutes, ABPM variability over hours, and SBPM variability over days. Each measurement method was compared against the others for every BPV index using Pearson’s correlation coefficient and their agreement for categorising participants by quartile of BPV was assessed using the kappa statistic.
Results
There were moderate correlations between beat-to-beat and between-hour maximum DBP (r=0.35, P<0.01), beat-to-beat and SBPM maximum SBP (r=0.47, p < 0.01) and DBP (r=0.32, p < 0.01), and ABPM and SBPM maximum SBP (r=0.45, p < 0.01), SD (r=0.32, p < 0.01), and CV (r=0.35, p < 0.01). All other correlations between measurement methods were either weak or non-significant. Agreement for categorising participants by quartile of BPV was either weak or non-significant for all comparisons.
Conclusion
Short-term BPV (either over minutes or hours) and medium-term BPV (over days) are not strongly correlated regardless of the method used to derive variability. It is likely that BPV over different timescales relates to different underlying physiology and pathophysiology and may have different prognostic values.
Trial registration number
N/A
AS18-010
A COMPARISON OF DIFFERENT METHODS OF ASSESSING AND CALCULATING BLOOD PRESSURE VARIABILITY POST-STROKE OR TIA
1University of East Anglia, Ageing and Stroke Medicine, Norwich, United Kingdom
2University of Aberdeen, Ageing Clinical & Experimental Research Team, Aberdeen, United Kingdom
Background and Aims
Blood pressure variability (BPV) is an independent cardiovascular risk factor. It can be calculated using various indices yet whether they provide different information has not been investigated for shorter-term blood pressure (BP) measurements.
Method
Recent TIA or mild stroke patients (N=154) underwent daytime ambulatory BP monitoring (ABPM), 10 minutes beat-to-beat BP recording, and seven days self-BP monitoring (SBPM). BPV of systolic and diastolic BP for each method was derived as standard deviation (SD), coefficient of variation (CV), average real variability (ARV), maximum, and maximum-minimum difference (MMD). For each method indices were compared using Pearson’s correlation coefficient and their agreement for categorising participants by quartile of BPV was assessed using the kappa statistic.
Results
SD strongly correlated with CV (all r>0.9, p < 0.01) and MMD for all methods (all r>0.8, p < 0.01) except diastolic BP from ABPM. CV strongly correlated with MMD (all r>0.7, p < 0.01) except for diastolic BP from ABPM. ARV strongly correlated with SD, CV, and MMD from SBPM (all r>0.7, p < 0.01), but less so from ABPM (r=0.4-0.5, p < 0.01) and beat-to-beat BP (r=0.3-0.5, p < 0.01). Agreement by quartile of BPV was good (K>0.5) for all methods between SD/CV and SD/MMD, and for SD/ARV from SBPM (all p < 0.01).
Conclusion
There is overlap between different indices of BPV calculation. ARV, which accounts for the time series of measurements, correlated more strongly with other indices when there were fewer BP measurements with longer between them. Further data regarding the prognostic value of different parameters is needed to reach a consensus about their use.
Trial registration number
N/A
AS18-011
RISK OF AN ARTERIAL HYPERTENSION AND STROKE IN POPULATION WITH VITAL EXHAUSTION IN RUSSIA/SIBERIA: GENDER FEATURES. WHO PROGRAM MONICA-PSYCHOSOCIAL EPIDEMIOLOGICAL STUDY
1Institute of Internal and Preventive Medicine - branch of Institute of Cytology, Collaborative laboratory of cardiovascular diseases epidemiology, Novosibirsk, Russia
Background and Aims
To determine the gender differences in influence of vital of exhaustion (VE) on risk of arterial hypertension (AH) and stroke in population of 25-64y in Russia/Siberia.
Method
Under the third screening of the WHO epidemiological program MONICA-psychosocial random representative sample including both genders aged 25–64y was surveyed in Novosibirsk in 1994 (n = 1386, mean age 44.9 ± 0.4y; 49.7% women). VE was estimated at baseline.
Results
Prevalence of VE was as follows: 66.8% in men (14.6% - high level), 75.7% was in women (44.4% - high level). Over the first 5 years the risk of AH was higher in men HR=3.2 than women HR= 1.9 with VE (p for all <0.05). AH risk in men was 1.6 and 1.4-fold higher over 10 years and 16 years of follow-up, respectively. AH risk increased in divorced men HR = 3.3 (p <0.05) and in older age group HR = 5.7. As for women AH risk was higher in individuals with lower education HR = 1.8 with VE. Stroke risk was higher in female HR=3.34 compared with male HR=3.1 with VE. But risk of stroke was higher in those men with primary education HR= 4.8; in divorced HR= 3.8 and widowed men HR=3.6.
Conclusion
There is higher prevalence of VE in female compared to male. Risk AH is higher in men but stroke in women with VE.
Trial registration number
N/A
AS18-012
ISCHEMIC CEREBROVASCULAR DISEASE RISK CHARTS FOR SPANISH POPULATION
1Hospital Clínico Universitario “Lozano Blesa, Neurology, Zaragoza, Spain
2San José Primary Care Centre, Family Medicine, Zaragoza, Spain
Background and Aims
Atherothrombotic ischemic stroke is one of the mean causes of morbidity and mortality in Spain, leading to an important socio-sanitary cost. Although risk factors are well established, there are no specific risk charts for daily use in our work environment for primary prevention.
To elaborate a predictive algorithm and a risk chart based on the major cardiovascular risk factors.
Method
A 5-year follow-up, prospective and analytic cohort study was done, including a primary care population (1924 men, 2498 women >40 years) who accomplished the inclusion criteria. By logistic regression, a predictive equation and a risk chart were designed.
Results
The main risk factors within the studied population were age, smoking and atherogenic index. The likelihood of ischemic atherothromotic stroke was explained with 98,3% of probability by the following equation: P= 1/1 + 2,7182818284 ^ [11,1+ (0,087 x AGE) + (0,83 IF SMOKER) + ((0,331 x (LDL/HDL))].
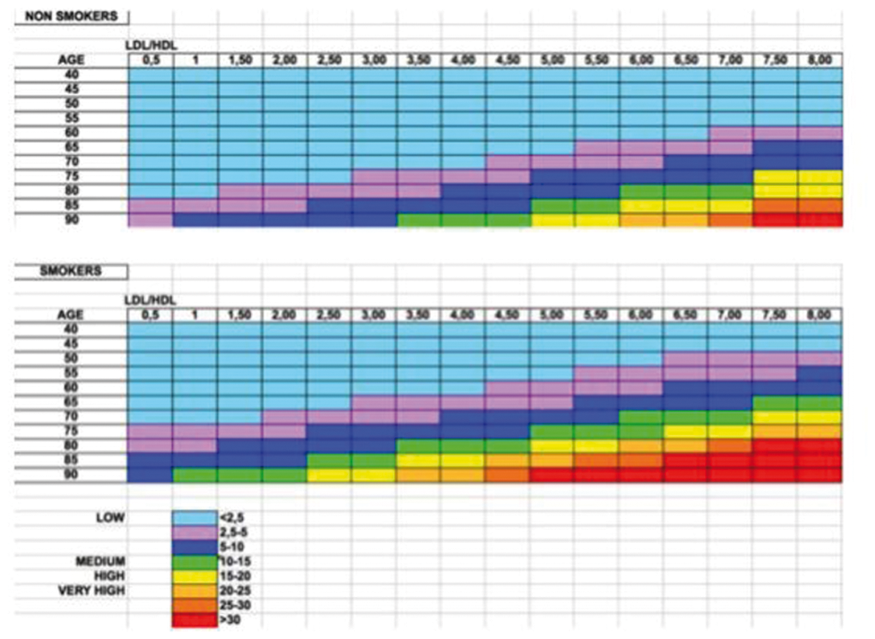
Conclusion
A tool for decision-making is presented, preferably by means of cholesterol management, once the rest of the factors are under control, in order to ameliorate the incidence of stroke. It is required to carry on with this line of research so as to achieve more predictive variables.
Trial registration number
N/A
AS18-013
EARLY EXTENDED CARDIAC MONITORING IN ISCHAEMIC STROKE INCREASES RATE OF PAROXYSMAL ATRIAL FIBRILLATION DETECTION: A TWO YEAR RETROSPECTIVE STUDY
1North Middlesex University Hospital, Stroke Medicine, London, United Kingdom
Background and Aims
Paroxysmal atrial fibrillation (PAF) is a common cause of cardioembolic stroke and detection is important to guide post-stroke management. Cardiac monitoring is advised in clinical guidelines but the modality, timing and length of such monitoring is often poorly defined.
We hypothesized that early, extended cardiac monitoring improves PAF detection and have explored this through retrospective study of acute stroke unit patients over a two year period.
Results
Fifty-eight of 193 patients (30.0%) were found to have PAF with a mean time of 10.8 days between stroke onset and testing. Patients with PAF were significantly older than patients with no PAF defected (77.3 vs 71.5 years, p < 0.05). There was no significant difference between timing of monitoring after stroke (11.4 days vs 10.5 days, p>0.5) or sex (61.4% vs. 60.0% male, χ2 p>0.05). 86.0% of PAF patient were anti-coagulated prior to discharge. The rate of PAF detection within the inpatient cohort was significantly higher than outpatients (30% vs. 0.6%, p < 0.05) who often had monitoring performed several weeks after stroke onset.
Conclusion
Our findings suggest early, extended cardiac monitoring in ischaemic stroke is effective in identifying PAF and has cost-benefit implications for using three-lead holter monitoring
Trial registration number
-
AS18-014
PREVALENCE OF PATENT FORAMEN OVALE IN CRYPTOGENIC STROKE AT OLDER AGES: A POPULATION-BASED TRANSCRANIAL DOPPLER STUDY
1University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Percutaneous closure of large patent foramen ovale (PFO) has recently been shown to be superior to medical treatment alone for prevention of recurrent stroke after cryptogenic TIA/non-disabling stroke at age ≤60 years. The justification for trials in older TIA/stroke patients depends on the association between PFO and cryptogenic events at older ages, where previous studies have been conflicting, and on the population-burden of PFO-associated events. We therefore performed a large population-based screening study of contrast-enhanced transcranial Doppler (bubble-TCD).
Method
We determined the prevalence of any PFO, and of “large” PFO (> 20 microbubbles), in consecutive patients with cryptogenic (TOAST criteria) vs other TIA/non-disabling ischaemic stroke subtypes in a population-based study (Oxford Vascular Study; 2014-2017), stratified by age, and extrapolated to the UK population.
Results
Among 572 patients (mean/SD age = 70.0/13.7; 439/76.7% aged >60 years), bubble-TCD was done in 523 (91.4%) cases in which it was technically possible. PFO was associated with cryptogenic events (97/264 vs 60/259, OR=1.93, 95%CI 1.32-2.82, p = 0.001) overall, and in those aged >60 years (68/190 vs 44/207, 2.07, 1.32-3.23, p = 0.001). Of 41 patients with large PFOs and cryptogenic events, 25 (61%) were aged >60-years, which extrapolates to 5951 patients per year in the UK.
Conclusion
Bubble-TCD is feasible in the majority of older patients with TIA/non-disabling stroke, and the association of PFO with cryptogenic events remains, with a substantial burden of large PFOs at the population-level.
Trial registration number
N/A
AS18-015
TWENTY-FOUR HOUR AMBULATORY CENTRAL HAEMODYNAMICS AND ARTERIAL STIFNESS IN PATIENTS WITH LACUNAR STROKE
1Hospital de Sant Joan Despí Moisés Broggi, Neurology, Sant Joan Despí BARCELONA, Spain
2Hospital de Sant Joan Despí Moisés Broggi, Cardiology, Sant Joan Despí BARCELONA, Spain
3Hospital de Sant Joan Despí Moisés Broggi, Medicine, Sant Joan Despí BARCELONA, Spain
4Hospital de Sant Joan Despí Moisés Broggi, Epidemiology, Sant Joan Despí BARCELONA, Spain
Background and Aims
We aimed to evaluate the role of 24h- brachial and central blood pressure (BP) and arterial stiffness in the physiopathology of lacunar stroke (LS).
Method
Patients > 18 years old admitted to our institution between July 2015 and July 2017 were included after a first episode of ischemic stroke. Subjects with mRS> 2 and history of heart failure were excluded. The aortic pulse wave velocity (aPWV), augmentation index (AiX), 24h ambulatory brachial and central BP were measured by means of Mobil-O-Graph device between 7 and 30 days after stroke.
Results
We evaluated 71 subjects, mean age: 64.7 ± 13.9 years, 62% men. Twenty-two patients had a LS and 49 cases a non-LS. Office BP in the emergency department were higher in LC as compared as non-LS(mean (SD) mm Hg: 173(37)/153(28) respectively; p < 0.004). After adjusting for age, daytime systolic and diastolic brachial BP were significantly higher in LS patients; Systolic BP: 133(12) vs 123(13), p = 0.005, and diastolic BP: 81(9) vs 75(9) mm Hg (p = 0.047). The differences in daytime central BP (cBP) were also statistically significant: daytime systolic cBP: 122(14) vs 114(12); p = 0.040; daytime diastolic cBP: 84(10) vs 77(10), p = 0.053. After adjusting for age, daytime pulse pressure (PP) was significantly higher in LS patients as well: 52.4(12.2) vs 48.7(11.3) mm Hg ; p = 0.045). No differences were found for aPWV or Aix.
Conclusion
Daytime CBP and PP were significantly higher in LS. This might suggest a role for central haemodynamics and arterial pulsatility in the development of LS.
Trial registration number
N/A
AS18-016
PREVALENCE AND PROGNOSIS OF HYPERTRIGLYCERIDEMIA AND HYPOTRIGLYCERIDEMIA IN ACUTE ISCHEMIC STROKE
1Ankara Univesity Medical School, Neurology, Ankara, Turkey
Background and Aims
Hypertriglyceridemia (hyperTG) has been demonstrated to be an important, independent risk factor for cardiovascular diseases in experimental, genetic, and epidemiological studies. Regarding data have been not enough for such a relationship for stroke since less attention on triglycerides. This study aimed to determine the prevalence and risk assessment of hyperTG and hypotriglyceridemia (hypoTG) in our stroke registry.
Method
We reviewed the charts of 619 patients with acute ischemic stroke. HyperTG was defined as being over than 149 mg/dl and hypoTG was defined as being less than 50 mg/dl based on the guidelines of the National Cholesterol Education Program (NCEP) III categorization. The demographic data, risk factors, the National Institutes of Health Stroke Scale (NIHSS) scores, hemoglobin level, thrombocyte count and C reactive protein level at admission, mortality in hospital, recurrent stroke and the modified Rankin Scale (mRS) scores in follow-up period were recorded.
Results
A total of 182 (32.3%) patients [104 males (57.1%) and 78 females (42.9%); mean age 64.5 ± 12.01 years] had hyperTG. Otherwise, there were 25 (4.4%) patients (12 males (48%) and 13 females (52%); mean age 70.9 ± 17.4 years) with hypoTG. On logistic regression analysis, only diabetes mellitus (DM) was significantly associated with hyperTG in acute ischemic stroke patients (P<0.05).
Conclusion
HyperTG was seen in 32.3% of acute ischemic stroke in our registry. Otherwise, hypoTG was seen in 4.4% of acute ischemic stroke in our registry. DM appears to be the major risk factor for acute ischemic stroke patients with hyperTG.
Trial registration number
-
AS18-017
SERUM FATTY ACIDS’ LEVEL AND STROKE SUBTYPES IN MIDDLE- OR OLD-AGED ACUTE STROKE PATIENTS
1Shonan Kamakura General Hospital Stroke Center, Stroke Treatment, Kamakura, Japan
Background and Aims
Middle-aged patients may have higher serum saturated fatty acids (SFA), whereas old-aged patients may have higher serum n-3 polyunsaturated fatty acids (PUSFA) . The aim of our retrospective study was to investigate serum fatty acids (FA)’ level and stroke subtypes in Japanese middle- and old-aged stroke patients.
Method
We included stroke patients between September 2015 and March 2017 who took examination for palmitic acid (PA) and stearic acid (SA) as saturated fatty acids (SFA), oleic acid (OA) as monounsaturated fatty acid (MUSFA), linoleic acid (LA) and arachidonic acid (AA) as n-6 PUSFA, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) as n-3 PUSFA. We compared FA and stroke subtypes in patients aged between 50 and 74 years (Middle age) with those in patients aged 75 years or older (Old age).
Results
One hundred ninety-one patients met our inclusive criteria. Ninety-one patients belonged to Middle age and hundred to Old age. In Middle and Old age, PA was 763 and 663 (μg/ml) (p < 0.001), SA was 224 and 193 (p < 0.0001), OA was 702 and 586 (p < 0.0001), LA was 882 and 746 (p < 0.0001), AA was 158 and 140 (p < 0.005), EPA was 64 and 79 (p < 0.05) and DHA was 131 and 142 (p = 0.09). In Middle and Old age, the incidence of lacunar or atherosclerotic stroke was 66 and 42% and cardioembolic stroke was 16 and 36% (p < 0.01).
Conclusion
Patients who had higher SFA, MUSFA and n-6 PUSFA suffered from atherosclerotic stroke at Middle age, whereas patients who had higher EPA suffered from cardioembolic stroke at Old age.
Trial registration number
N/A
AS18-018
SKIING RELATED STROKE: CAUSES, TREATMENT AND OUTCOME
1CHUV, Stroke Center- Neurology Service- Department of Clinical Neurosciences, Lausanne, Switzerland
2Hospital Beatriz Angelo, Neurology, Lisbon, Portugal
Background and Aims
Previous studies described ischemic stroke temporally related to specific triggers, but only one series collected patients with ischemic stroke (AIS) following downhill skiing, all caused by cervical arteries dissection. Here we aimed at describing our series of AIS temporally related to ski practice focusing on their frequency, pathogenesis, clinical presentation and prognosis.
Method
We maintained a prospective list of Skiing-Related Strokes (SRS) since 2003 and till 27.2.2017. A comparison group of non-SRS patients, matched for age and gender, was identified from all AIS patients included in our stroke registry (ASTRAL) during the same time period.
Results
In the 12-year observation period were identified 17 SRS (4 females, median age 51 years) and 51 matched non-SRS . Vascular risk factors, stroke features and outcome were similar in the two groups. Stroke mechanism was arterial dissection in 11/17 SRS (65%) and in 7/51 control patients (14%, p < 0.05). Among the 11 patients with SRS caused by dissection, 8 reported minor falls during skiing, 1 had a major head trauma without loss of consciousness, and 2 no traumatism. Ski-related dissections were not different by all other dissections in term of age, vascular risk factors, number of arteries involved, stroke initial severity and three months outcome (median baseline NIHSS 13.5 vs 10, 3-months mRS ≤2 72% vs. 58% for ski-related vs. non ski-related respectively).
Conclusion
Arterial dissection was a significantly more frequent stroke mechanism if compared to matched controls, but other mechanisms occurred as well. . Minor or moderate skiing-related traumatisms preceded most SRS with dissections.
Trial registration number
NA
AS18-019
THE ASSOCIATION OF VASCULAR RISK FACTORS AND SEVERITY OF WHITE MATTER HYPERINTENSITIES IN DIFFERENT STROKE SUBTYPES
1Yeungnam University Medical Center, Neurology, Daegu, Republic of Korea
Background and Aims
Although mechanisms underlying progression of white matter hyperintensities (WMH) are still poorly understood. We aim to investigate the association between common vascular risk factors and the severity of WMH in each stroke subtype of large artery atherosclerosis (LAD) and small vessel occlusion (SVO).
Method
Consecutive patients admitted due to ischemic stroke or TIA were included (n = 841). LAD and SVO were defined according to the SSS-TOAST classification. WMH were categorized into two groups: no/mild and moderate/severe using Fazekas scale. Demographics, vascular risk factors and laboratory results were compared between the two groups (LAD vs SVO) in total and separately.
Results
A total of 228 patients who underwent brain MRI within seven days after onset were eligible (n = 170 in LAD, n = 58 in SVO). Older age and hypertension were independent risk factors of moderate/severe WMH (OR = 3.94 [2.46-6.30] with an increased age of 10 years; OR = 5.14 [1.70-15.56], P=0.004 for hypertension) after adjustment of common cardiovascular risk factors. In patients with LAD, independent risk factors of moderate/severe WMH were age (OR = 3.86 [1.83-8.12] for every ten-year increase, P<0.001) and hypertension (OR = 5.64 [1.51-21.1], P=0.01). On the other hand, age was the only independent risk factor in patients with SVO (OR = 3.03 [1.28-7.19] for every ten-year increase, P=0.012).
Conclusion
This study showed that there is a different association between hypertension and severity of WMH in each stroke subtype. Other potential mechanisms of WMH, those not associated with traditional vascular risk factors, may be associated with progression of WMH.
Trial registration number
N/A
AS18-020
INCIDENCE AND RISK FACTORS OF PERIOPERATIVE STROKE IN THORACIC ENDOVASCULAR AORTIC REPAIR (TEVAR) AND ENDOVASCULAR ANEURYSM REPAIR (EVAR) IN SONGKLANAGARIND HOSPITAL
1Prince of Songkla University, Internal medicine, Songkhla, Thailand
2Prince of Songkla University, Community medicine, Songkhla, Thailand
3Prince of Songkla University, Surgery, Songkhla, Thailand
4Prince of Songkla University, Anesthesiology, Songkhla, Thailand
5Prince of Songkla University, Epidemiology Unit, Songkhla, Thailand
Background and Aims
Stroke has emerged as a complication of thoracic endovascular aortic repair (TEVAR) and endovascular aortic repair (EVAR). Identifying risk factors for TEVAR and EVAR–related stroke is important to minimize the periprocedural stroke.
Method
This retrospective 1:4 case-control study enrolled all patients underwent TEVAR and EVAR operations from January 2008 to June 2015. Patients’ demographic data and clinical characteristics during pre-, intra-, and post- operative periods were analyzed by descriptive statistics to identify factors associated with perioperative stroke. Independent risks for were further determined by multivariate analysis.
Results
There were 774 patients included. Perioperative stroke occurred in 17 cases (2.2%). Nine patients (53%) had strokes within 24 hours post operation. The overall in-hospital mortality rate was 29%. Independent risk factors of perioperative stroke were previous stroke or TIA (OR 9.19; 95%CI 1.56-54.19, p = 0.014), abnormal radiological findings of aorta (OR 15.05; 95%CI 2.54-89.22, p = 0.003), prolong operation time more than 390 minutes (OR 13.9; 95%CI 2.67-72.28, p < 0.001), occurrence of intraoperative hypotension more than 4 times (OR 11.98; 95%CI 2.69-53.31, p = 0.001), average duration of hypotension more than 10 minutes (OR 26.09; 95%CI 5.07-134.14, p < 0.001), blood loss more than 600 mL (OR 13.9; 95%CI (2.67-72.28), p = 0.002), and post-operative hyperglycemia (OR 9.6; 95%CI (1.8-51.19), p = 0.008).
Conclusion
Though stroke complicated with TEVAR and EVAR is uncommon, it is associated with a high mortality. The recognition of the perioperative stroke risks will facilitate early prevention of the risks properly.
Trial registration number
N/A
AS18-021
DAYLIGHT SAVING TIME (DST). RISK FACTOR FOR ACUTE ISCHEMIC STROKE?
1St John's Hospital, Neurology and Stroke Center, Budapest, Hungary
2DRK Hospital, Cardiology, Neuwied, Germany
3Semmelweis University, First Department of Obstetrics and Gynecology, Budapest, Hungary
Background and Aims
Daylight Saving Time (DST) means, that the clocks are turned forward 1 hour from spring to autumn. DST interferes with the biorhythm twice a year, which influences the circulation, thereby the risk of stroke. Thrombolysis performed due to acute ischemic stroke (associated with a narrow time window) allows a precise assessment of the effect of DST on stroke development.
Method
The number of thrombolysis performed within the period between 2006 and 2015 was analyzed. Anonymized nationwide data on the dates and daily numbers of it was provided by the National Health Insurance Fund. DST start and end dates are internationally known. We compared the mean number of thrombolysis on the day of transitions with that the day before and after, and during the preceding and following one week and month. The corresponding periods were compared to the annual mean. Statistical analysis was performed by Student t- or Mann-Whitney U-tests.
Results
The day of the DST start date was associated with an increased, whereas that of the DST end date with a surprisingly decreased risk; however, this short-term analysis did not show significance (p DST start = 0.1419, p DST end = 0.8904). The analysis of the one-week incidence demonstrated a significant increase in the thrombolysis number (pDSTstart= 0.0046, pDSTend=0.0004), whereas the long-term analysis likewise failed to reveal significant difference (pDSTstart=0.5567, pDSTend=0.5916).
Conclusion
Our results evidence the negative impact of DST transitions on the human body. The incidence of acute ischemic stroke increase in relation to both the DST start and end dates.
Trial registration number
N
AS18-022
HYPERHOMOCYSTEINEMIA IS NOT ASSOCIATED WITH SYSTEMIC ARTERIAL STIFFNESS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Chung-Ang University College of Medicine, Neurology, Seoul, Republic of Korea
Background and Aims
Hyperhomocysteinemia is reported to be a risk factor for vascular calcification, atherosclerosis, and cerebrovascular disease. The aim of this study was to determine the association between hyperhomocysteinemia and brachial-ankle pulse wave velocity (baPWV) in patients with stroke.
Method
We identified consecutive patients with acute ischemic stroke who visited a tertiary university hospital within seven days of symptom onset between January 1, 2011 and April 30, 2017. The hyperhomocysteinemia was defined as serum level of homocysteine > 11 umol/L. The average of baPWV measured on both sides was categorized into quartiles. The association between homocysteine and baPWV was tested using chi-square test and logistic regression analysis.
Results
A total of 1624 patient were enrolled in this study. Mean age was 68.5 +/- 12.5 years and male was 882 (54.3%). Hyperhomocysteinemia was found in 1074 (66.1%). On bivariate analysis, baPWV was significantly associated with age, sex, hypertension, diabetes mellitus, smoking, systolic blood pressure, highly sensitive C reactive protein, estimated GFR, and hyperhomocysteinemia. However, the association between hyperhomocysteinemia and baPWV was not significant on multivariable logistic regression. Age, hypertension, diabetes mellitus, and systolic blood pressure remained significant on multivariable analysis.
Conclusion
Despite previous studies showed the association between homocysteine and arterial stiffness in general population, our study did not show significant association between them in stroke population. We presumed that potent vascular risk factors such as hypertension and diabetes rather than homocysteine play a more important role in damaging vessel wall in stroke patients.
Trial registration number
N/A
AS18-024
RISK FACTORS FOR INFARCT GROWTH IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Academic Medical Center, Biomedical Engineering and Physics, Amsterdam, The Netherlands
2Academic Medical Center, Department of Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3VU University Medical Center, Department of Radiology, Amsterdam, The Netherlands
4Texas Stroke Institute, Department of Radiology, Dallas, USA
5Maastricht Univeristy Medical Center, Department of Radiology, Maastricht, The Netherlands
6Maastricht Univeristy Medical Center, Department of Neurology, Maastricht, The Netherlands
7Erasmus Medical Center, Department of Radiology and Nuclear Medicine, Rotterdam, The Netherlands
8Erasmus Medical Center, Department of Public Health, Rotterdam, The Netherlands
9Academic Medical Center, Department of Neurology, Amsterdam, The Netherlands
Background and Aims
An increase in infarct lesion growth after treatment is associated with decreased functional outcome in patients with acute ischemic stroke (AIS). This study aims to identify predictors of infarct growth after 24 hours of stroke onset.
Method
One-hunderd-fourty-seven AIS patients with anterior proximal occlusions and with 24 hour and 1-week follow up NCCT scans were retrospectively selected from the MRCLEAN trial database. Lesion volumes were used to determine relative and absolute infarct growth. In univariate analysis, variables associated with relative and absolute infarct growth larger than 30% and 20mL, respectively, with p < 0.20 were selected for multivariate analysis. Odds ratios were calculated from the multivariate logistic regression model to identify independent associations with relative and absolute infarct growth.
Results
The mean age was 66(range:26–85)years and median admission NIHSS score was 17(range:4-29). Median infarct volumes of 35(IQR:19-88) mL and 56(IQR:30-120) mL were observed after 24 hours and 1-week, respectively. Seventy (48%) patients had a relative infarct growth and 53(36%) patients had an absolute infarct growth. In multivariate linear regression, a left sided large vessel occlusion and higher collateral grade were independently associated with relative infarct growth with an adjusted OR of 2.7(p = 0.006, 95% CI:1.3-5.3) and 1.7(p = 0.012, 95% CI:1.1-2.7), respectively. No variable was significantly associated with absolute infarct growth in multivariate linear regression.
Conclusion
In our population, left-sided large vessel occlusion and higher collateral grades are associated with relative infarct growth after 24 hours of stroke onset. Patients with lower collateral grade had larger lesion at 24 hours and hence, a lower potential of infarct growth.
Trial registration number
ISRCTN10888758
AS18-025
ASSESSMENT OF URIC ACID CONCENTRATION IN PATIENTS WITH ALZHEIMER DISEASE, PARKINSON DISEASE AND ACUTE STROKE
1Medical University of Warsaw- Faculty of Health Science, Department of Neurology, Warsaw, Poland
2Medical Center Neuroprotect, Medical Center Neuroprotect, Warsaw, Poland
Background and Aims
Literature data indicate uric acid as a risk factor of stroke and neuroprotective agent in neurodegenerative disease, especially Parkinson Disease (PD). There are some controversial data concerning Alzheimer Disease (AD) due to coexistence of vascular hypothesis in this disease. Objective of the work was the analysis of uric acid concentration in patient with AD, PD and stroke and analysis of other vascular risk factor in individual groups.
Method
60 patients were examined:20 patients with stroke, AD and PD. The level of uric acid, BMI and vascular risk factors were determined in each group of patients. Average concentration value of uric acid in individual groups was compared with laboratory standard (6 mg/dl).
Results
The results obtained indicate statistically significant differences in uric acid concentration between the groups of patients with stroke and PD (p = 0.015). No statistically significant differences were observed between groups PD and AD, and between AD and stroke. Statistically significant difference in the concentration of uric acid in women was found in stroke and PD groups (p = 0.001) and in AD and PD groups (p = 0.009). There was also the presence of the influence of hypertension on the uric acid level and the lack of influence of dyslipidemia on the level of uric acid.
Conclusion
The results of our study confirm the hypothesis about the effect of high uric acid values on stroke and low uric acid values on PD. The lack of differences between stroke and AD groups is confirmed by the vascular hypothesis of both diseases, which is particularly important for women. .
Trial registration number
N/A
AS18-026
PREDICTIVE FACTORS OF CEREBROVASCULAR EVENTS FOLLOWING CAROTID ARTERY STENTING
1HUV Macarena. IBIS., Neurology, Sevilla, Spain
2HUV Rocío. IBIS., Neurology, Seville, Spain
3H. Vall d'Hebron, Interventional Neuroradiology, Barcelona, Spain
4H. Vall d'Hebron, Neurology, Barcelona, Spain
5H. Reina Sofía, Interventional Neuroradiology, Córdoba, Spain
6H. Reina Sofía, Neurology, Córdoba, Spain
7HU Salamanca, Interventional Neuroradiology, Salamanca, Spain
8HU Salamanca, Neurology, Salamanca, Spain
9HV de la Arrixaca, Interventional Neuroradiology, Murcia, Spain
10HV de la Arrixaca, Neurology, Murcia, Spain
11HUC Asturias, Neurology, Oviedo, Spain
12HUC Asturias, interventional Neuroradiology, Oviedo, Spain
13H Clínico de Valencia, Interventional Neuroradiology, Valencia, Spain
14H Clínico de Valencia, Neurology, Valencia, Spain
15HU Cruces, Neurology, Bilbao, Spain
16HU Cruces, Interventional Neuroradiology, Bilbao, Spain
17HUV Rocío. IBIS., Interventional Neuroradiology, Seville, Spain
Background and Aims
Carotid artery stenting (CAS) is an effective and minimally invasive method for the treatment of extracranial carotid artery stenosis. The aim of the present study was to search for independent risk factors to predict cerebrovascular events following CAS in order to identify high risk patients and make CAS even safer among those.
Method
HISPANIAS, a national prospective multicenter study with 14 recruiting hospitals, collected data from 757 patients who underwent CAS. We analyzed morbidity and mortality within 30 days after CAS looking for factors that might be associated with cerebrovascular events (stroke and TIA).
Results
The HISPANIAS cohort included 80.3% males with mean age of 70.7 years, 38.6% were diabetics, 76.6% hypertensives, 61.6% had dyslipidemia, 29.5% heart disease, 28.1% were smokers and 10.4% had atrial fibrillation. Cerebrovascular complications occurred in 42 patients (5.6%), including TIA in 24 patients (70.8% ipsilateral; mean 2.79 days after CAS) and stroke in 28 patients (72.2% ipsilateral; mean 6.72 days after CAS). Main independent clinical predictors of stroke/TIA identified by logistic regression were: females OR 3.8 (1.05-14.2, p = 0.041) and diabetes OR 7.4 (1.7-31.7, p = 0.007). For stroke alone the main independent predictors in the logistic regression (age, diabetes, systolic blood pressure, post-CAS systolic peak MCA velocity) allowed to build a predictive model with an AUC=0.89.
Conclusion
Elderly, females and diabetic patients are more vulnerable to perioperative cerebrovascular complications after CAS. Moreover, some hemodynamic measurements might help to define the stroke risk in this population in order to improve cerebrovascular events prevention.
Trial registration number
N/A
AS18-027
GENDER DIFFERENCES IN PATIENTS WITH STROKE AND ATRIAL FIBRILLATION
1Peoples' Friendship University of Russia /RUDN University, Neurology department, Moscow, Russia
2Research Center of Neurology, 2nd neurology department, Moscow, Russia
Background and Aims
Atrial fibrillation (AF) in stroke patient is often accompanied by other gender-specific stroke risk factors, which can change strategies for the stroke management
Method
We examined main stroke risk factors and medical compliance in 140 patients with stroke and AF , 69 (49%) men, 71 (51%) women (data were examined separately). Neurological deficit severity was evaluated using NIHSS and mRS. CHA2DS2VASc were used to estimate thromboembolism risk.
Results
Arterial hypertension was detected in 133 (95%)patients, rheumatism - 5 (4%), diabetes mellitus (DM) – 32 (23%), coronary artery disease (CAD) - 42 (30%), congestive heart failure - 91 (65%), carotid atherosclerosis (CA)- 86 (61%), chronic kidney disease (CKD) –117 (84%) patients. 50(36%) were taking antihypertensive drugs before their stroke, 25(17%) – anticoagulants, 8(6%) – statins. Men were younger (mean age: 67(63;76) vs 74(66;79), (p = 0,006). Men more often had severe CA: 14% vs 7% (p = 0,058), CAD 41% vs 20% (p = 0,005) and more higher plasma creatinine levels: 100(88;118) vs 86,5(73,5;107) mcmol/L (p = 0,0005). Men more often were taking statins: 13% vs 3% (p = 0,025), and had lower low density lipoprotein cholesterol: 1,7(1,3;2,3) vs 2,3(1,6;2,8) mcmol/L (p = 0,003) and lower blood glucose: 5,6(4,9;5,9) vs 5,9(5,1;7,2) mcmol/L (p = 0,013). CHA2DS2VASc was lower in men: 6(5;6) vs 7(6;8) ,р=0,0001. There were no other significant differences between men and women.
Conclusion
Patients with AF had wide range of cardiovasular risk factors and poor medication adherence. Gender-specific stroke prevention must include not only improvement of adherence to anticoagulation therapy, but also consider higher risk of atherosclerosis complications and CKD in men, and DM in women.
Trial registration number
N/A
AS18-028
IMPACT OF SHORT-TERM EXPOSURE TO TRAFFIC-RELATED AIR POLLUTION ON ISCHEMIC STROKE SEVERITY AND MORTALITY
1IMIM - Hospital del Mar Research Institute, Neurovascular Research Group, Barcelona, Spain
2ISGlobal, Environmental Epidemiology, Barcelona, Spain
3IADEA-CSIC, Institute of Environmental Assessment and Water Research, Barcelona, Spain
Background and Aims
Air pollution has been related to a pro-thrombotic state. This effect could influence the initial severity of an acute ischemic stroke (AIS) and ultimately, short-term prognosis.
Method
2252 AIS patients were recorded in a hospital-based prospective stroke register (BASICMAR 2005-2014) in Barcelona (Catalonia, Spain) and followed up for 3 months. Daily and hourly concentrations of PM2.5 and black carbon (BC) and meteorological data were obtained from monitoring stations in the city. Time-lags (from previous 72h to acute stroke onset) were analyzed. Primary outcomes were severity (measured as initial NIHSS) and mortality at 3 months. Adjusted linear (for NIHSS) and logistic (for 3-month mortality) regression models were used.
Results
No association was found between PM 2.5 and BC exposure and initial severity. Previous 72 hours stroke onset exposure to BC was associated with a higher mortality at 3 months (OR = 1.22, p = 0.059). Sensitivity analysis showed that those exposed to BC 72 hours previous to stroke onset and that did not receive rtPA had higher mortality (OR = 1.26, p = 0.040). This effect was not observed in those that received rtPA.
Conclusion
No association was observed between short-term exposure to PM2.5 and BC and initial AIS severity. Patients exposed to BC 72 hours prior to stroke onset showed higher 3-month mortality and this effect was mainly observed in those that did not received rtPA.
Trial registration number
N/A
AS18-029
CLINICAL MANIFESTATION OF STROKE PATIENTS WITH PRIMARY THROMBOCYTHEMIA ACCORDING TO JAK2 MUTATION
1Inha University Hospital, Neurology, Seoul, Republic of Korea
Background and Aims
primary thrombocythemia is a rare disease and usually presents with headache, bleeding, and splenomegaly. JAK2 mutation is one of common gene mutation, which caused primary thrombocythemia. However, the clinical manifestation of ischemic stroke patients with essential thrombocytosis, especially related to JAK2 mutation, remains uncertain.
Method
We selected the patients with primary thrombocythemia from our stroke registry from 2005 to 2016 and analyzed the demographic and laboratory findings according to JAK2 mutation.
Results
Among 9358 patients in stroke registry, only 44 (0.4%) patients had the primary thrombocythemia (mean age 66.1 ± 10.2, male 22). Mean platelet count was 672 ± 258 *103/μL and 20(45%) had the JAK2 mutation. Twenty five patients (56%) had the cryptogenic stroke etiology and cardioembolism and transient ischemic attack were also frequently observed (18% and 14%, respectively). Three (6.8%) patients died within 3 months of stroke onset. There was no difference in the demographic profile and the frequency of hypertension, diabetes mellitus, dyslipidemia and current smoking between the patients with JAK2 mutation and those without. The platelet counts were not different between two groups, either. The patients without JAK2 mutation had more frequent accompanying cancer than those with JAK2 mutation (42% vs. 11%, P = 0.03).
Conclusion
Our data suggest that the primary thrombocythemia is rare disorder in stroke population and that this platelet disorders is most associated with the cryptogenic stroke among stroke etiology. If a stroke patient with primary thrombocythemia had no JAK2 mutation, the possibility of hidden malignancy should be considered.
Trial registration number
N/A
AS18-030
DIETARY AND LIFESTYLE PRACTICES OF STROKE PATIENTS IN THE YEAR FOLLOWING STROKE
1Florey Institute of Neuroscience and Mental Health, Stroke Neurorehabilitation and Recovery, Heidelberg- Melbourne, Australia
2La Trobe University, Occupational Therapy- School of Allied Health, Melbourne, Australia
3The Royal Melbourne Hospital, Department of Medicine- Melbourne Brain Centre, Melbourne, Australia
Background and Aims
Guidelines for stroke management recommend that stroke patients improve their dietary and lifestyle risk factors to prevent recurrent stroke. The extent to which this occurs has not been reported.
Method
Participants included 219 stroke patients (64% male), aged 27-95 years receiving usual care. We observed dietary and lifestyle risk factors of adult stroke patients in the year following stroke in a longitudinal stroke cohort study. We report the percentage who met national guidelines prior to stroke (baseline) and at 3 months and 12 months post-stroke. Risk factors included smoking, diet, fruit and vegetable consumption, salt intake, physical activity, alcohol consumption, body mass index (BMI) and waist circumference.
Results
Risk factors remained generally stable throughout the study. After 12 months, significantly more patients met recommendations for alcohol consumption (86%) and episodic drinking (76.6%). Other changes during 12 months were not significantly different from baseline. The proportion of patients meeting dietary recommendations remained low after 12 months, including whole diet (68.7%) and fruit and vegetable intake (58.3%). Fewer patients met physical activity recommendations (29.2%) and smoking rates decreased (11.9%). Patients with BMI and waist circumference within the healthy range increased (32.3% and 21.7% respectively). Compared with females, males were younger, had experienced less severe stroke, and met dietary and lifestyle guidelines less frequently.
Conclusion
There is little improvement in the diet and lifestyle risk factors of patients in the first 12-months post-stoke. Greater emphasis on diet and lifestyle modification strategies is needed to reduce the risk of recurrent stroke.
Trial registration number
NCT00887328 and ACTRN12610000987066
AS18-032
THE ADVERSE EFFECT OF MULTIPLE COMORBIDITY ON FUNCTIONAL OUTCOME IN PATIENTS WITH ISCHEMIC STROKE OR TRANSIENT ISCHEMIC ATTACK
1Seoul National University Hospital, Department of Neurology, Seoul, Republic of Korea
2Kangdong Sacred Heart Hospital, Department of Neurology, Seoul, Republic of Korea
Background and Aims
Multiple comorbidities have negative impact on functional outcomes in cardiovascular diseases including ischemic stroke. However, their individual association with acute ischemic stroke (AIS) or transient ischemic attack (TIA) remains to be elucidated. This study aims to evaluate the impact of comorbidity on functional outcome in patients with AIS or TIA.
Method
A total of 2,449 AIS and 248 TIA patients were included for the analysis. Functional outcome was dichotomized into excellent outcome (modified Rankin scale[mRS] at 3 months 0, 1) and non-excellent outcome (mRS≥2). Logistic regression analysis between comorbidity conditions and outcomes was performed.
Results
The mean age was 67.1, and 60.3% were male. Among the patients, 44.0% in AIS patients and 12.9% in TIA patients had non-excellent outcome. In patients with AIS, diabetes mellitus (adjusted odds ratio[aOR] 1.23, p = 0.025), previous history of stroke (aOR 1.52, p < 0.001), dementia (aOR 3.39, p < 0.001), moderate to severe kidney disease (aOR 2.52, p < 0.001), solid (aOR 1.85, p < 0.001) and metastatic tumor (aOR 6.45, p < 0.001) were predictors of non-excellent outcome after adjustment. In patients with TIA, congestive heart failure (OR 14.33, p = 0.032) were associated with non-excellent outcome in the univariate analysis, but not in the multivariate analysis. The Charlson Comorbidity Index score was significantly associated with non-excellent outcome in AIS group (aOR 1.29, p < 0.001), but not in TIA group (aOR 0.93, p = 0.692).
Conclusion
This study demonstrated that multiple comorbidity has a significant impact on functional outcome in patient with AIS, but not in TIA. This suggests that treatment of comorbid conditions is important as well as the index stroke itself.
Trial registration number
N/A
AS18-034
ASTROCYTE-DERIVED VEGF DRIVES BLOOD-BRAIN BARRIER DISRUPTION UNDER HIGH SALT CIRCUMSTANCE
1The Third Affiliated Hospital of Sun Yat-sen University, Department of Neurology, Guangzhou, China
Background and Aims
Increasing salt intake in the human diet is associated with cerebrovascular diseases and inflammatory disease in central nervous system, which show a core feature of the blood-brain barrier (BBB) disruption. However, the direct impact of high salt (HS) environment on BBB is unclear. In the current study, we aimed to investigate the relationship between high salt and the blood-brain barrier.
Method
From October 2016 to April 2017, 36 patients were enrolled within 6 hours after acute ischemic stroke at the time of their first attack. Excluding cerebrovascular diseases, 23 healthy controls were selected from the medical Examination Center from the same time. We conducted an observational study in which sodium intake was estimated from sodium excretion in urine samples. Then we set up high salt diet (HSD) model by male Sprague-Dawley rats aged 8 weeks to 2 groups who received a sodium-rich chow containing 8% NaCl and 1% saline for 30 days and 60 days to explore the specific mechanism of high salt on BBB.
Results
We found significant differences in urinary sodium levels between first-onset acute stroke patients and healthy individuals. We observed that HSD signifcantly promoted BBB disruption with increased VEGF release from reactive astrogliosis and loss of tight junction (TJ) proteins expression without apparently altering blood pressure.
Conclusion
Our study demonstrates that a higher sodium intake is linked to acute stroke, which may be due to the increased release of VEGF from reactive astrogliosis.
Trial registration number
N/A
AS18-036
LENGTH-OF-STAY AND DEMOGRAPHICS IN ACUTE ISCHEMIC STROKE WITH LEFT ATRIAL OR LEFT VENTRICULAR THROMBUS
1Campbell University, School of Osteopathic Medicine, Buies Creek, USA
2Duke University, Dept. of Neurology, Durham, USA
Background and Aims
Cardiac imaging is often performed on patients with acute ischemic stroke, particularly when stroke etiology is unknown. However, little has been published on the demographics of patients with acute ischemic stroke who are identified as having left atrial or ventricular thrombi during their diagnostic evaluations.
Method
This was a retrospective cohort study, utilizing an academic institutional database to identify patients with diagnosis codes for acute ischemic stroke. Patient records were then filtered by CPT codes in order to select patients who underwent transthoracic, transesophageal echocardiography, cardiac CT, and/or cardiac MRI. Further filters were applied to identify the subset of patients on therapeutic anticoagulation. Patients lacking left atrial or ventricular thrombi on cardiac imaging were further excluded, as well as patients whose cardiac thrombus was identified >14 days before or after presenting with acute ischemic stroke.
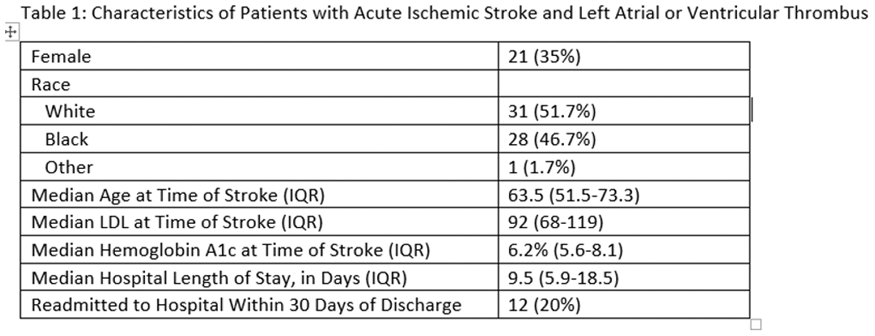
A total of 60 patients were identified for the described cohort. Data pertaining to sex, race, age, and baseline LDL and hemoglobin A1c at presentation are detailed in Table 1. Median length-of-stay was 9.5 days (IQR 5.9-18.5), and 20% of patients were readmitted within 30 days of discharge.
Conclusion
Among this cohort of patients, men and those of black race were disproportionately represented. These patients demonstrate somewhat prolonged lengths-of-stay, with relatively high readmission rates.
Trial registration number
N/A
AS18-037
DOES THE PRESENCE OF SYMPTOMS RELATED TO CAROTID STENOSIS SEVERITY CORRELATE WITH SERUM LIPOPROTEIN LEVELS?
1Hospital Universitario La Princesa, Neurología, Madrid, Spain
Background and Aims
Relationship between serum lipoprotein levels (SLL), higher levels of low-density lipoprotein cholesterol (LDL-C) and/or lower levels of high-density lipoprotein cholesterol (HDL-C), and carotid stenosis is well established. However, the association between carotid stenosis severity with HDL-C is not so consistent. We examined the relationship between SLL, the grade of carotid stenosis and whether the stenosis was symptomatic or not.
Method
Retrospective study of patients with >50% carotid stenosis attended at our stroke unit, from january 2011 to january 2017. Symptomatic carotid stenosis (SCS) or asymptomatic carotid stenosis (ACS) were defined according to the presence of acute ischemic stroke. We measured SLL (HDL-C, LDL-C, total cholesterol and atherogenic risk) at the moment of the diagnosis, as well as other clinical features and previous treatment.
Results
N = 92. Mean age: 73,1 (SD 10’8), women 28,3%, SCS 60%, previous statin therapy 60%. Mean LDL levels in SCS: 98,64 mg/dl, and in ACS: 86,56 mg/dl. Mean HDL levels in SCS: 44,71 mg/dl, and in ACS: 44,16 mg/dl. No association was found between SLL neither with grade of carotid stenosis severity nor with the presence of symptoms or not (p>0’05). The proportion of patients with ACS was significantly higher in patients on previous statin therapy (p < 0’05).
Conclusion
We didn’t found significant association between SLL, carotid stenosis severity and the presence of symptoms, probably due to the fact of being a high selected sample of patients with severe stenosis. The relationship between ACS and patients on statin therapy may support a protective effect of this drug against stroke.
Trial registration number
N/A
AS18-038
ABNORMAL BRAIN VASOMOTOR REACTIVITY IN PATIENTS WITH LOW ANKLE BRACHIAL INDEX
1Médica Sur, Neurología, Ciudad de México, Mexico
2Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Neurología y Psiquiatría, Mexico, Mexico
Background and Aims
Diseases related to ischemic vascular events (cerebral (CVD), coronary and peripheral arterial disease (PAD)) are the leading cause of death and disability worldwide and are due to atherothrombosis. PAD is a marker of generalized atherosclerosis and is susceptible to be studied in a noninvasive way, measuring the ankle brachial index (ABI). Studies have shown that the incidence of ischemic CVD increases gradually as ABI decreases. Transcranial Doppler (TCD) evaluation of cerebral circulation (CC) estimates the degree of involvement of cerebral hemodynamics when occlusive disease exists and identifies patients at increased risk for cerebral ischemia. Therefore, the detection of alterations of CC represents an additional tool for the evaluation of cardiovascular risk in patients with abnormal ABI.
To determine the frequency of CC abnormalities associated with abnormal ABI in patients with high cardiovascular risk
Method
Patients older than 50 years with previous cardiovascular disease or with high vascular risk were included, ABI was measured and a DTC with apnea test was performed. The flow velocities of both middle cerebral arteries (MCA) were measured and the breath holding index (BHI) was calculated in each case.
Results
A total of 79 patients were evaluated, 41.8% of the patients had abnormal ABI, of which 52.2% presented BHI ≤ 0.5%/sec and 27.3%> 0.5%/sec, p = 0.027, IRR, with a correlation coefficient r = 0.335, p = 0.003.
Conclusion
In patients with high cardiovascular risk, the presence of an abnormal ABI is associated with alterations of cerebral vasoreactivity, which is considered a determinant of cerebral ischemia.
Trial registration number
N/A
AS18-040
THE PROGNOSTIC MODEL FOR DETERMINING THE RECURRENT STROKE
1Moscow centre of speech patology and neurorehabilitation, healh, Moscow, Russia
Background and Aims
The study of the relationship between various parameters: clinical-anthropometric, biochemical, metabolic, vascular-inflammatory, molecular-genetic and the development of the recurrent ischemic stroke, and the development of a prognostic model for determining the probability of its occurrence.
Method
196 patients who underwent the first ischemic stroke were examined. The observation was 3 years and 58 patients had a second ischemic stroke. The groups were compared by main parameters: biochemical, metabolic, markers of vascular inflammation and endothelial dysfunction. Genotyping of single nucleotide polymorphisms of genes: IL8, ADIPOQ, ADIROR, APOB, APOC-IV, BDNF, GRM3 using ready-made TaqMan probes was carried out.
Results
Based on the results of the correlation analysis, the following parameters were statistically significant with the recurren ischemic stroke: gender, weight, insulin, adiponectin, HDL, TG, CRP-sh , glucose, uric acid, IL-4, VEGF-A. The binary logistic regression method was used to construct the forecast model.
Conclusion
Based on the data obtained in this study, a probability model for the development of the recurrent ischemic stroke was obtained. Of all the parameters studied in the study, the largest contribution to the probability of development of the recurrent ischemic stroke, according to the model obtained, is made by the parameters: adiponectin adn gender.
Trial registration number
N/A
AS18-041
PREDICTORS OF SEVERE ACUTE ISCHEMIC STROKE IN THROMBOLYSED PATIENTS
1Faculty of Medicine, University of Belgrade, Belgrade, Serbia
2Department of Emergency neurology, Neurology Clinic- Clinical centre of Serbia, Belgrade, Serbia
Background and Aims
The National Institutes of Health Stroke Scale (NIHSS) baseline score strongly predicts outcome in patients with acute ischemic stroke (AIS). The aim of our study was to determine predictors for severe AIS in thrombolysed patients.
Method
A total of 514 thrombolysed patients were classified according to the baseline NIHSS score into two groups- patients with baseline NIHSS score ≤ 15 (n = 346) and patients with baseline NIHSS score > 15 (n = 168).
Results
The presence of atrial fibrillation was higher in patients with severe AIS (24% vs. 34.5%, p = 0.012), but a smaller number of smokers were recorded in this group (36.1% vs. 26.8%, p = 0.035). Initial glycaemia also was higher in patients with severe AIS (median: 6.4 vs. 6.8, p = 0.021). In this group, there was a greater involvement of the carotid vascular area (76.9% vs. 92.9%, p < 0.001) and left hemisphere (39.9% vs. 57.7%, p < 0.001). Also, there was determined significant influence of the etiology on the stroke severity (p < 0.001). Multivariate analysis showed that incorporating the carotid vascular area increases the risk for the development of severe AIS (OR, 3.345; 95% CI,1.614–6.931; p < 0.001). Large arteries atherosclerosis (OR, 7.736; 95% CI,2.527–23.679; p < 0.001), cardioembolism (OR, 7.986; 95% CI,2.526–25.244; p < 0.001), other determined (OR, 4.657; 95% CI,1.311–16.547; p = 0.017) and undetermined (OR, 6.786; 95% CI,2.297–20.042; p = 0.001) etiologies, also increase the risk of its development, compared to small-vessel disease as a referent category.
Conclusion
Predictors for the development of severe AIS in thrombolysed patients are- involvement of the carotid vascular area, large arteries atherosclerosis, cardioembolism, other determined and undetermined etiologies.
Trial registration number
N/A
AS18-042
VASCULAR RISK FACTORS IN DIABETICS WITH ISCHEMIC STROKE: HAVE THEY CHANGED IN THE LAST 15 YEARS?
1SAS/ Hospital Universitario Virgen Macarena, Vascular Risk Unit. Internal Medicine, Seville, Spain
2Hospital de Valme, Neurology, Seville, Spain
3Hospital Macarena, Internal Medicine, Seville, Spain
4Hospital Virgen Macarena, Internal Medicine, Seville, Spain
5Hospital Virgen Macarena., Internal Medicina, Seville, Spain
6Hospital Virgen Macarena., Internal Medicine, Seville, Spain
Background and Aims
The epidemic incidence of ischemic stroke (IS) in diabetic patients is closely associated with the action of different vascular risk factors (VRF). We aimed to evaluate whether these VRF have changed in the last 15 years.
Method
Retrospective study on diabetic patients with IS discharged from the Hospital Macarena, Hospital de la Merced and Hospital de Valme, Seville, Spain, between 1999–2001 and 2013–2016.
Results
We included 764 patients (40.9% of the IS population), 394 men and 370 women, with an average age of 71 ( ± 9) years. Comparing the two periods we observed that patients were now older 73.7 ( ± 9) vs 69.5 ( ± 8) years (p = 0.0001), with a similar percentage of males (51% vs. 52%, p = Not significant-NS). The main VRF were hypertension (85.5 % vs 75.6%, p = 0.001), dyslipidemia (60.6 % vs 36%; p = 0.0001), smoking (12.9% vs 16.8% p = 0.027), AF (24% vs 19.4%; p = NS), and previous stroke (26.7% vs 25.7%, p NS). At discharge, less VRF control recommendations (19.4% vs 41.5%; p = 0.0001) and diet recommendations (56.2% vs 77.5%; p = 0.0001) were given, being aspirin the main antiplatelet used in both periods (45.7% vs. 41.9%; p = NS).
Conclusion
Now diabetic patients with IS are older, present a higher prevalence of hypertension and dyslipidemia and a lesser prevalence of smoking, which is possibly related to population aging, but also to a better control of VRF. Recommendations on VRF control at hospital discharge are clearly deficient
Trial registration number
N/A
AS18-043
CLINICAL AND EPIDEMIOLOGICAL ASPECTS OF THE ISCHEMIC STROKE IN PATIENTS WITH DIABETES MELLITUS TYPE 2
1Tyumen regional hospital №2, Regional neurovascular center, Tyumen, Russia
2Tyumen state medical university, Department of Hospital Therapy, Tyumen, Russia
Background and Aims
To study the clinical and epidemiological characteristics of patients with acute ischemic stroke and type 2 diabetes.
Method
From 656 case histories of patients with ischemic stroke treated in our clinic during 2015 year we evaluated 105 case histories (16%) of patients with type 2 diabetes. We evaluated the duration and effectiveness of control over the course of diabetes, risk factors, baseline blood glucose level, glycosuria, a vascular region, type of stroke (TOAST), the degree of carotid stenosis, the severity of the stroke (NIHSS), mortality and degree of disability (mRS).
Results
The medium age of patients was 68 ± 5.2 years. Recurrent stroke was in 25% cases. In 10% cases the diabetes was diagnosed for the first time. In 53% patients with certain diagnosis of diabetes the duration of the desease was more than 5 years. Hypoglycemic took 75% of stroke patients, 40% patients controlled their blood glucose level and only 18% took the diet. The prevalence of vascular risk factors was: overweight or obesity in 89% of patients, hypertension in 95%, coronary heart disease in 84%, myocardial infarction in 19%, atrial fibrillation in 25% of cases. Medium baseline glycemic index was 10.35 ± 2.7 mmol/l. Glycosuria was in 49% of cases (n = 52), ketonuria was in 24% (n = 25). The mortality rate in patients with ischemic stroke and diabetes was 14.3% vs 10.9% in all stroke patients (n = 656). At discharge from the hospital 45.5% of patients had mRS score ≤ 2.
Conclusion
Type 2 diabetes is associated with ischemic stroke and increases the risk of adverse outcome.
Trial registration number
N/A
AS18-044
IMPACT OF DIABETES MELLITUS ON FIRST-EVER ISCHEMIC STROKE
1University of L’Aquila- 67100- L’Aquila- Italy, Department of Neurology and Stroke Unit- AZH, L'Aquila, Italy
Background and Aims
We evaluated the impact of diabetes mellitus (DM) on first-ever ischemic stroke (FEIS) severity and long-term prognosis.
Method
Cases of FEIS were ascertained in a three-year period and followed up to 3 years.
Results
Out of 884 FEIS patients, 849 (445 women, 52.4%) were categorized as diabetics or non-diabetics; 211 (24.9%) were diabetics (125 women, 59.2%) and 638 non-diabetics. DM prevalence <64 years of age was similar in men and women (21.4% vs 15.8%; p = 0.470), and increased in women >65 years (29.8% vs 21.3%; p = 0.012). With respect to non-diabetics, diabetics had more frequently peripheral arterial disease (12.8% vs 3.0%, p < 0.0001), higher NIHSS score at stroke onset (median score 8, interquartile range (IQR) 4–16 vs median score 6, IQR 3–12; p = 0.0007) and higher mRS score at discharge (median score 4, IQR 2-5 vs median score 3, IQR 2-5; p < 0.0001). At the multivariate Cox regression analysis, the NIHSS score at stroke onset was a predictor of 30-day mortality (HR=1.07, 95% CI 1.05–1.09; p < 0.001). DM and NIHSS score at stroke onset were predictors of 1-year mortality (HR=1.38, 95% CI 1.01–1.88; p = 0.044 and HR=1.06, 95% CI 1.05–1.08; p < 0.001 respectively). The NIHSS at stroke onset was an independent predictor of 3-year mortality. At the Kaplan-Meier analysis, 30-day, 1-year and 3-year survivals were higher in non-diabetics than in diabetics (85.9% vs 72.3%; p < 0.0001; 76.2% vs 59.6%; p < 0.0001, and 66.7% vs 54.0%; p < 0.0001 respectively).
Conclusion
The contribution of DM to FEIS severity and long-term prognosis is relevant. New preventive strategies are needed, mostly in elderly women.
Trial registration number
N/A
AS18-045
THE ROLE OF ANDROGEN DEFICIENCY IN THE DEVELOPMENT OF ISCHEMIC STROKE IN MIDDLE-AGED AND ELDERLY MEN
1Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
Background and Aims
The occurrence of a cerebral stroke, results in the simultaneous exposure of several risk factors. Consequently, the prediction of cerebral stroke should be multifactorial and change in testosterone levels may lead to stroke.
Method
A total of 142 males of middle and old age were examined. 40 of them are middle-aged men (mean age 48.6 ± 1.8) and 102 elderly patients (s=67.5 ± 1.5) with ischemic stroke. Neurological status, lipid spectrum, testosterone level, MRI of the brain were studied in all patients. To assess daily activity, was used Barthel Scale
Results
In the men of middle age of 45–52 year olds (n = 16), the serum testosterone level is 10 nmol/l, and in 53–60 years old patients (n = 24) is 9.2 nm/l, and for men elderly the age of 60–70 year-old patients (n = 45) serum testosterone level is 8.3 nm/l, and> 70 years old patients (n = 57) is equal to 6.8 nmol/l. (test rate 12–33 nmol/l, 345–950 ng/dL). According to the results of the Barthel scale, in middle-aged patients was mild degree of disability (Bi> 70 points) was observed in 25.6% of patients, severe (Bi < 30 points) - in 6.4%. And elderly patients revealed that a mild degree of disability (Bi> 70 points) in 31.2% of patients, severe (Bi <30 points) - in 56.4%.
Conclusion
Based on the studies conducted, with age testosterone levels decrease in men, which directly increases the risk of ischemic stroke and increases the degree of disability.
Trial registration number
101227
AS18-046
PAST HISTORY HEADACHE (PHH) IN PATIENTS WITH CERVICAL ARTERY DISSECTION (CEAD)
1Research Center of Neurology, Department of Early Rehabilitation for Patients with Stroke and Other Neurological Diseases, Moscow, Russia
2Research Center of Neurology, Department of Clinical Neurophysiology, Moscow, Russia
Background and Aims
To analyze the frequency, clinical and electrophysiological characteristics of PHH in CeAD patients.
Method
227 patients with CeAD were studied. The comparison group included 35 patients with migraine. 35 CeAD patients who had PHH and all migraine patients underwent EEG and visual evoked potentials (VEP).
Results
101 out of 227 patients had PHH
The visual EEG analysis less often found rhythmic disorganization in PHH patients than in migraine. The hyperventilation caused a slight increase in the spectral power of Teta, Delta waves in PHH patients and significant enhancement in migraine. Pattern reversal VEP had a greater latency and smaller amplitude of cortical responsesin PHH patients than in migraine (p =0,028 and =0,037, respectively). The flash VEP amplitude was lower in PHH patients than in migraine (p = 0.01).
Conclusion
PHH in CeAD patients meets migraine criteria in 15.4 %, while in 29.1% patients- not meet (non-migraine PHH). Central mechanisms, namely, the hypersensitivity of the cerebral cortex playing the main role in migraine pathogenesis, are not significant in PHH genesis. The great importance appears to have dysplastic changes in the wallof extra-intracranial arteries that predispose both to headache and dissection.
Trial registration number
N/A
AS18-047
KNOWLEDGE OF POPULATION OF KYRGYZSTAN ABOUT THE MEDITERRANEAN DIET AS A PREVENTIVE FACTOR AGAINST STROKE AND HEART DISEASES
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
Food in Kyrgyzstan is presented mostly by carbohydrates as a cultural aspect. Mediterranean diet (MD), despite its efficacy, is not known for the majority of population in Kyrgyzstan. We conducted a cross-sectional study to evaluate the style of nutrition and healthy profile of patients with IS in Kyrgyzstan.
Method
280 (180 patients underwent ischemic stroke (IS) and 100 controls) people were interviewed with our special questionnaire, including the questions about the food preference, amount, the proportion of carbohydrates and components of the MD (olives, greenery, nuts) in diet.
Results
Age range was 42 to 86 years; median age was 60,16. 47% were women. According TOAST ischemic strokes there was a prevalence of large artery atherosclerosis (LAA) (56,9%). In the group large artery atherosclerosis we found significantly higher consumption of animal fats and carbohydrates (OR = 2.8 and 4.1 respectively (95% 3.1–4.6, 3.8–6.4), low consumption of vegetables (p = 000.1), fruits and water less than 2 l in daily intake. 87,5% (p = 0.001) do not prefer olives and olive oil. 85,7% of patients do not live a healthy lifestyle, are physically inactive (OR 5.1 (95% 2.1–11.1), 40,6% were smokers. Only 6.3% of all found time for exercises. BMI in all TOAST subtypes was not significantly different and was 25 (p = 0.01), but lower in control group (24).
Conclusion
Because of traditional food intake (high consumption of animal fat and carbohydrates), Kyrgyz people tend to be overweight, have higher BMI and do not adhere MD. Kyrgyz inhabitants need to change food preferences in order to change rates for IS.
Trial registration number
N/A
AS18-048
PATHOLOGICAL MORNING BLOOD PRESSURE SURGE IN PATIENTS WITH RECENT ISCHEMIC STROKE
1SAS/Hospital Universitario Virgen Macarena, Vascular Risk Unit. Internal Medicine, Seville, Spain
2SAS/Hospital Virgen de Valme, Neurology, Seville, Spain
3SAS/Hospital Virgen del Rocio, Risk Factors. Internal Medicine, Seville, Spain
Background and Aims
An exaggerated morning blood pressure surge (MBPS) has been associated with stroke. We aimed to analyze the frequency of pathological MBPS in patients with recent ischemic stroke (IS).
Method
We included 86 patients with IS. A 24-hour ambulatory blood pressure monitoring (ABPM) was performed 6 months after stroke. MBPS was defined as the difference between the mean systolic BP during the 2 hours after waking and arising minus the mean systolic BP during the hour that included the lowest BP during sleep. MBPS values> 25 mmHg were considered pathological.
Results
We included 45 lacunar (52%), and 41 non-lacunar IS (48%), mean age 68 +/− 11, years; males 56 (65%); with a previous history of hypertension in 58 (67%), Diabetes in 29 (34%), dyslipidemia in 40 (46.5%) and smoking in 26 (30%) patients. 67(78%) patients received antihypertensive treatment. In 33 (38%) cases, the patients received a evening dose of antihypertensive. In the ABPM, the mean MBPS was 24 +/− 14 mmHg. Pathological MBPS was detected in 40 patients (46.5%), with a mean of 36 +/− 9 mmHg. A pathological MBPS was associated with an older age (66 +/− 11 vs 71 +/− 10 years, p = 0.041) and a higher frequency of altered office BP values (19.5% vs 47,5%, p = 0.01), on the contrary it was not associated with gender, previous risk factors, antihypertensive treatment nor chronotherapy.
Conclusion
A pathological MBPS is frequent in patients with recent IS. Further studies are necessary to assess the prognostic importance of these findings.
Trial registration number
N/A
AS18-049
CARDIOVASCULAR DISEASES REGISTRY (RECVASA): FOCUS ON RISK FACTORS FOR STROKE IN PATIENTS WITH CARDIOVASCULAR COMORBIDITIES
1National Medical Research Center for Preventive Medicine, Department of Clinical Cardiology and Molecular Genetics, Moscow, Russia
2National Medical Research Center for Preventive Medicine, Department of Preventive Pharmacotherapy, Moscow, Russia
3I.P. Pavlov State Medical University, Department of Hospital Therapy, Ryazan, Russia
4National Medical Research Center for Preventive Medicine, Laboratory of Biostatistics, Moscow, Russia
5National Medical Research Center for Preventive Medicine, Department of Integrated Prevention Programs, Moscow, Russia
6National Medical Research Center of Cardiology, Directorate, Moscow, Russia
Background and Aims
To evaluate the risk for stroke in comorbid patients with arterial hypertension (AH), ischemic heart disease (IHD), chronic heart failure (CHF) and atrial fibrillation (AF) enrolled in the outpatient registry RECVASA.
Method
RECVASA registry included 3690 patients with cardiovascular diseases (CVD) from 3 outpatient clinics in Ryazan region of Russia. For this analysis, we took patients with the combination of 2–4 CVD (3.0 ± 0.9). Incidence of non-fatal stroke was estimated during 4-year follow-up period.
Results
2934 patients were included in our analysis (27.7% men, age 68.5 ± 12.9 years). 11.1% patients had history of stroke (HSTR). Mean follow-up was 3.7 ± 0.9 years. Lost to follow-up was 4.5%. 504 (17.2%) patients died from all causes and 154 (5.2%) had non-fatal stroke. Risk ratio (RR) of non-fatal stroke and 95% confidential interval (CI) were analyzed in multifactor Cox model. The next factors had an effect on risk of stroke: age - 1.06 (1.05–1.08); HSTR - 3.21 (2.27–4.55); AF 1.94 (1.27–2.96); blood pressure (BP)<110/75 mmHg - 2.72 (1.02–7.31); heart rate (HR)>=90/min - 2.10 (1.23–3.56); administration of ACE inhibitor (ACEI) - 0.54 (0.36–0.80). The next factors had no significant effect on risk of stroke: sex; BP>=140/90 mmHg; AH; CHF (NYHA 1–2 and 3–4); IHD; history of myocardial infarction; administration of angiotensine receptor blockers, antithrombotic drugs, beta-blockers; calcium channel blockers, diuretics, statins (p>0.05).
Conclusion
The RECVASA study revealed during 4-year follow-up period higher risk for stroke in comorbid cardiovascular patients with HSTR, AF, BP<110/75 mmHg, HR>=90/min. In patients with ACEI administration risk for stroke was 1.9 times less.
Trial registration number
N/A
AS18-051
THE RISK FACTOR OF SURVIVAL BETWEEN ELDERS SUFFERING STROKES IN UZBEKISTAN: OBSERVATION FROM A NATIONALLY REPRESENTATIVE SAMPLE
1Tashkent Medical Academy, Neurology, Tashkent, Uzbekistan
Background and Aims
Stroke was the leading cause of death in Uzb from 2008 to 2016. Deaths due to stroke now rank second only to cancer, with more deaths resulting from strokes than from any other single pathology. It is important to understand stroke prognosis among elderly, because aged population is growing rapidly. The aim of the present study was to discern factors affecting survival in stroke patients from a nationally representative elderly sample.
Method
A total of 99 stroke survivors, from a representative national sample of elders aged >/=65 years on December 31, 2016, whose strokes occurred in the period 2010–2016, were followed for mortality until July 1, 2017. Personal data were gathered through home interviews conducted by well-trained community nurses, and mortality data were obtained from the national census office by using identification card numbers.
Results
Women experienced a higher mortality rate (139.8 per 1000 person-years) than men (126.4 per 1000 person-years), as age-adjusted for WHO world-population figures. Stroke patients who received continuous treatment for diabetes experienced mortality risks similar to those of patients without diabetes and much lower risks than those with discontinuous diabetes treatment. Cognitive impairment was also an independent predictor of survival (relative risk 2.69, P<0.05).
Conclusion
This first report on the various prognostic factors related to survival of elderly stroke patients in Uzbekistan Kazakh population emphasized the benefit of continuous diabetes treatment in improving survival chances. These stroke patients should also be monitored for cognitive and mobility impairments and undergo rehabilitation.
Trial registration number
920628
AS18-054
EVALUATION OF SLEEP APNOEA SHOULD BE PART OF ROUTINE RISK ASSESSMENT IN STROKE PATIENTS
1Nottingham University Hospitals NHS Trust, Stroke Medicine, Nottingham, United Kingdom
Background and Aims
Obstructive sleep apnoea (OSA) is a potentially modifiable risk factor for vascular diseases including stroke. Early diagnosis and treatment of sleep apnoea should potentially reduce the risk of stroke. Atrial fibrillation (AF), hypertension, diabetes, vascular dementia, cardiac arrhythmias, dyslipidaemia and arrhythmias are associated with OSA.
Method
In a cohort of 252 consecutive patients admitted to the stroke unit, we assessed pre-stroke symptoms to look for OSA. Out of these, 92 were excluded as mimics or with a non-stroke diagnosis. We used two apnoea assessment scales: Epworth (ES) and STOP-BANG (SB) scores.
Results
Out of a total 150 consecutive patients with a diagnosis of stroke, the risk of clinical OSA as measured by ES and SB was reported as ‘mild’ in 56% (85/150) and ‘moderate-severe’ in 38% (57/150). The prevalence of AF was 8.23% (7/85) in mild OSA and 17.5% (10/57) in moderate-severe OSA; hypertension 37% (32/85) in mild OSA and 66% (38/57) in moderate-severe OSA; diabetes was 11% (10/85) mild OSA and 31% (18/57) with moderate-severe OSA; and ischaemic heart disease was 8% (7/85) in mild OSA and 21% (12/57) in moderate-severe OSA.
Conclusion
OSA is a commonly recognised risk factor for stroke and it should receive high priority when assessing stroke patients. We therefore recommend that evaluation for OSA should be included routinely through the use of Epworth and STOP-BANG scores in the initial assessment of stroke patients so that appropriate measures can be taken. A greater awareness is required among public, general practitioners and stroke teams.
Trial registration number
N/A
AS18-055
STROKE RISK FACTORS IN THE POPULATION OF REPUBLIC OF MOLDOVA AND STRATEGIES OF PRIMARY PREVENTION
1Institute of Emergency Medicine, Department of Neurology, Chisinau, Moldova
2State University of Medicine and Pharmacy “Nicolae TestemiÉ>anu”, Laboratory of Neurobiology and Medical Genetics, Chisinau, Moldova
Background and Aims
Stroke is one of the leading causes of morbidity and mortality worldwide. A good management of risk factors can lead to significant improvements in the incidence of stroke. Herein, we aimed to investigate stroke risk factors in the population of Republic of Moldova.
Method
In November 2015, we initiated an epidemiological study in 2 villages located in the northern and central regions of the Republic of Moldova. Our study protocol included: questionnaire, physical and neurological examinations, ECG, Doppler/Duplex ultrasound of carotid arteries and laboratory tests. Informed consent was obtained from all subjects.
Results
In this study were included 812 subjects, 487 (60%) women and 325 (40%) men with a mean age 48.1 ± 14.1 years. Obesity was one of the most common risk factors, idenfied in 600 (74%) subjects; 346 (43%) had a body mass index (BMI) >30, while 257 (32%) were overwighted and 197 (32%) were normal weighted. Hypertension was identified in 290 (36%), 37 (5%) had atrial fibrillation and 58 (7%) - diabetes mellitus. Increased total cholesterol (C) was found in 450 (55%), increased LDL-C in 232 (29%) and decreased HDL-C in 110 (14%) subjects. Abdominal circumference significantly correlated with systolic blood pressure (BP) (r=0.43, p < 0.0001), diastolic BP (r=0.40, p < 0.0001), BMI (r=0.85, p < 0.0001) and uric acid levels (r=0.35, p < 0.0001).
Conclusion
Abdominal as well as general obesity, dyslipidemia and arterial hypertension were the most common identified risk factors. Our preliminary results indicate that in the studied population the modifiable risk factors predominate and their prevention, and control requires an interdisciplinary strategic approach.
Trial registration number
N/A
AS18-057
PROGNOSIS AFTER ISCHEMIC STROKE IN DIABETIC PATIENS
1SAS/Hospital Virgen de Valme, Neurology, seville, Spain
2SAS/Hospital San Juan de Dios, Internal Medicine, Seville, Spain
3SAS/Hospital Universitario Virgen Macarena, Vascular Risk Unit. Internal Medicine, Seville, Spain
Background and Aims
Diabetes increases the risk of cardiovascular events and stroke. We aimed to assess the prognosis after ischemic stroke (IS) in diabetic patients.
Method
Retrospective study on patients with IS discharged from the Hospital de Valme and San Juan de Dios, Seville, Spain, during the first 6 month of 2016. Patients were followed up for one year. We compared diabetic and non-diabetic patients.
Results
We included 152 patients, mean age 70 (+/− 12) years, 60 (39.4%) were diabetics. Diabetic patients had more frequently hypertension 93.3% vs 70.7% vs (p = 0,003) and dyslipidemia (81.7% vs 46.7%, p = 0.001). After one year 6 diabetic patients and 5 non-diabetics had died (10% vs 5,4%, p non significant), though vascular events and death were more frequent among diabetics (31.7% vs 16.3% p = 0.03). The main events were new IS 13 cases, followed by TIA 11 cases.
Conclusion
Diabetic patients with IS have worse prognosis than non-diabetic patients. A better control of risk factors is essential in these patients.
Trial registration number
N/A
AS18-058
IS CAROTID STIFFNESS A POSSIBLE SURROGATE FOR STROKE IN LONG-TERM SURVIVORS AFTER NECK RADIOTHERAPY?
1University Clinical Center, Department of Vascular Neurology, Ljubljana, Slovenia
2Institute of Oncology, Radiotherapy Department, Ljubljana, Slovenia
Background and Aims
The risk for cerebrovascular late effects among childhood cancer survivors is considerable. According to recent studies it is not clear which marker could be reliable for the screening of cerebrovascular diseases among the long-term survivors of childhood cancer. The purpose of this study is to analyse arterial stiffness and intima media thickness as possible early markers of later occurring stroke
Method
Twenty-three patients, treated for HD in childhood, were included. They had received radiation therapy to the neck with 20- 65 (med.30) Gy. Twenty-six healthy controls, matched in age, sex, BMI, arterial hypertension, smoking history and total cholesterol levels were compared. High-resolution colour-coded duplex sonography and power Doppler sonography of the carotid arteries were performed and intima –media thickness, number and quality of plaques were measured. Arterial stiffness indices were calculated.
Results
Plaque deposits and/or arterial wall calcinations were found in 24 out of 43 (55.8 %) vessels in cancer survivors group and 0 out of 52 vessels in the group of healthy controls (p < 0.01). We found significant group differences for all the stiffness parameters we used (P < 0.05), but there was no difference in intima–media thickness between cases and controls (p = 0.92). In a multivariate model, carotid pulse wave velocity was positively associated with smoking.
Conclusion
The arterial stiffness has appeared as a possible surrogate marker for stroke in long-term survivors of childhood cancer. Smoking habit might have an additional negative influence on vascular aging in the group of patients after neck radiotherapy.
Trial registration number
N7A
Motivation
The detection of an appropriate surrogate marker for stroke is necessary in order to introduce it into follow-up guidelines. This could enable us to detect LTSCC who are at risk of developing cerebrovascular events. Many studies in adults and some in LTSCC found IMT as possible surrogates. Anyway the results are not consistent. Arterial stiffness was proposed as a possible surrogate cardiovascular morbidity in LTSCC. However, the stiffness indices were not systematically studied. Therefore, we analysed indices of arterial stiffness besides intima media thickness as possible early markers of later occurring stroke.
RARE CAUSES, STROKE IN THE YOUNG
AS19-001
VALIDATION OF A NOVEL QUESTIONNAIRE TO SCREEN MIGRAINE IN YOUNG PATIENTS WITH ISCHEMIC STROKE AND STROKE-FREE CONTROLS
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
Background and Aims
Migraine is a well-known risk factor for ischemic stroke (IS). We designed a structured and concise questionnaire for screening both migraine with (MA) and without aura (MO) for a research setting, and conducted a validation study including both young patients with IS and stroke-free control subjects.
Method
We enrolled patients aged 18–49 years with a first-ever cryptogenic IS and age- and sex-matched stroke-free controls in an ongoing case-control SECRETO study (NCT01934725). We performed screening of migraine using the questionnaire including 13 screening questions. A clinical diagnosis of migraine was done by an independent senior headache-neurologist based on International Headache Society criteria, blinded to participant status and clinical data. For inter-rater agreement, we considered kappa-value over 0.75 as an excellent agreement.
Results
We included 50 patients (median age 41 years; 23 women) and 50 control subjects (42 years; 24 women). Based on both the migraine-specific questionnaire and clinical evaluation, 22 (44%) patients had MA, inter-rater agreement (Cohen’s kappa) of 0.84. 4 (8%) vs. 6 (12%) patients had MO, kappa 0.78. Kappa value for any type of migraine was 0.84. Corresponding values for controls based on the questionnaire vs. clinical evaluation were for MA 5 (10%) vs. 7 (14%), kappa 0.81, and for MO 9 (18%) vs 10 (20%), kappa 0.81, respectively. For any type of migraine in control subjects, kappa was 0.77.
Conclusion
Our migraine-screening questionnaire is valid to identify persons with MA and MO with an excellent agreement between the screening questionnaire and experienced clinician in both patients and healthy controls.
Trial registration number
N/A
AS19-002
THE NOVEL ORAL ANTICOAGULANTS (NOACS) FOR THE TREATMENT OF CEREBRAL VENOUS THROMBOSIS: A SERIES OF 32 PATIENTS
1University of Medicine and Pharmacy, Neurology, Ho Chi Minh, Vietnam
2People 115, Cerebrovascular Disease, Ho Chi Minh, Vietnam
Background and Aims
Cerebral venous thrombosis (CVT) are less frequent than other types of strokes and have a quite different clinical presentation. Recent availability of NOACs provides an alternative option of systemic anticoagulation in various thromboembolism conditions.
The aim of this study was to present a series of 32 cerebral venous thrombosis patients treated with NOACs (including dabigatran and rivaroxaban).
Method
We recorded clinical, imaging, and follow-up characterization (outcome, recanalization, complications) of all patients admitted with cerebral venous thrombosis and treated with NOACs (including dabigatran and rivaroxaban) between May 2016 and July 2017. Modified Rankin Scale was used to assess clinical severity; excellent outcome was defined as modified Rankin Scale at three-months of 0 to 1. Recanalization was assessed with MR angiography.
Results
Thirty two patiens were included, 15 were treated with rivaroxaban and 17 with dabigatran. Overall outcome was excellent in 94%, and all patients showed at least partial recanalization, complete recanalization is 50%. No complications occurred.
Conclusion
NOACs maybe have clinical benefit in the treatment of cerebral venous thrombosis. Further prospective assessment with randomized controlled studies is warranted.
Trial registration number
N/A
AS19-003
A PEDIATRIC ACUTE STROKE PROTOCOL DECREASES THE TIME TO DIAGNOSIS OF ACUTE-ONSET FOCAL NEUROLOGIC DEFICITS IN A CHILDREN'S HOSPITAL EMERGENCY DEPARTMENT
1Boston Children's Hospital, Neurology, Boston, USA
2Boston Children's Hospital, Stroke and Cerebrovascular Center, Boston, USA
3Children's National Medical Center, Neurology, Washington, USA
4Boston Children's Hospital, Radiology, Boston, USA
5Boston Children's Hospital, Psychiatry, Boston, USA
Background and Aims
Treatment of children with acute ischemic stroke with tissue plasminogen activator (tPA) or endovascular thrombectomy requires timely diagnosis. Widespread diagnostic delay prompted pediatric centers in the United States to develop multidisciplinary teams to respond emergently to children with acute-onset focal neurologic deficits. We describe here a decrease in the time to diagnosis of children presenting to the emergency department (ED) with acute-onset focal neurologic deficits after the establishment of a pediatric stroke alert system.
Method
Clinical and demographic information were reviewed for children who presented to the Boston Children's Hospital ED with acute-onset focal neurologic deficits for 2.5 years before and after the implementation of a stroke alert system.
Results
Sixty-eight children presented with acute-onset focal neurologic deficits after implementation of a stroke alert system. Thirteen children presented with such symptoms before establishment of a stroke alert system. Time from ED arrival to the start of neuroimaging decreased significantly after implementation of a stroke alert system (median 196 v. 82 minutes before and after stroke alert system implementation, respectively; p < 0.01). Children considered potential tPA candidates experienced the shortest time to neuroimaging after ED arrival (median 54 v. 89.5 minutes for potential tPA candidates v. non-tPA candidates, respectively; p < 0.01).
Conclusion
Establishment of a stroke alert system at a children's hospital decreased the time to diagnosis of children presenting to the ED with acute-onset focal neurologic deficits. Timely diagnosis of stroke in children is essential to enabling treatment with tPA or thrombectomy.
Trial registration number
N/A
AS19-004
STROKE AFTER CARDIAC CATHETERIZATION IN CHILDREN
1Boston Children's Hospital, Neurology, Boston, USA
2Boston Children's Hospital, Stroke and Cerebrovascular Center, Boston, USA
3Children's National Medical Center, Neurology, Washington, USA
4Boston Medical Center, Pediatrics, Boston, USA
5Boston Children's Hospital, Radiology, Boston, USA
6Boston Children's Hospital, Psychiatry, Boston, USA
Background and Aims
Children with congenital and acquired heart disease are at high risk for stroke. Post-catheterization strokes account for 15–37% of strokes in children with cardiac disease. Risk factors, clinical presentation, and safety of treatment in these children have not been well-defined. We describe here post-catheterization strokes at a tertiary children's hospital in the United States.
Method
Clinical and demographic information were reviewed for children who had an acute stroke within 20 days of cardiac catheterization at Boston Children's Hospital between December 2006 and July 2016. We excluded children who also had a cardiac arrest, cardiac surgery, extracorporeal membrane oxygenation, a ventricular assist device, or an arrhythmia proximate to their stroke.
Results
We identified 23 post-catheterization strokes. The most common types of catheterization were balloon dilation for pulmonary vein stenosis (n = 7) and systemic pulmonary collateral closure (n = 6). The most common presenting symptoms were arm weakness (n = 10) and seizure (n = 8). The median time from the end of catheterization to the onset of symptoms was 31 hours (range 105 minutes to 19.8 days); all but 1 child presented within 4 days of catheterization. Three children were treated with intravenous thrombolysis or mechanical thrombectomy.
Conclusion
While stroke after cardiac catheterization is rare, improved understanding of this entity is important since children with cardiac disease and stroke have high morbidity and mortality. Reducing this morbidity and mortality requires interventions aimed at prevention and more rapid identification of post-catheterization strokes. Better understanding stroke after cardiac catheterization will enable development of targeted preventive and therapeutic measures.
Trial registration number
N/A
AS19-007
THE CARDIOPATHY IS LEAKING. WHEN EPIDEMIOLOGY CONFOUNDS US
1Complejo Asistencial Universitario de Salamanca, Neurology, Salamanca, Spain
2Complejo Asistencial Universitario de Salamanca, Radiology, Salamanca, Spain
Background and Aims
To expose a case report about an infrequent cause of stroke, in a cocaine ex- consumer young patient.
Method
A 29-years-old-man, cocaine ex-consumer, convicted to jail, that is found in the flour, without left hemibody mobility, labial commissure deviation and poor articulation when speaking. Stroke code was activated.
In the neurologic exploration, we detected complete right hemispheric deficit, NIHSS 19.
In neuroimage we found an occlusion in the proximal segment of the right middle cerebral artery, and mismatch in right hemisphere. Thrombolysis and rescue thrombectomy were performed, without significant changes.
In control CT we found an ischemic infarct with hemorrhagic transformation.

In ecocardiogram, we found dilatation of the left ventricle with moderated asymmetric hypertropia at multiple locations, abundant lateral trabeculation and akinesia at multiple locations. Left ventricular ejection fraction was 45%.
Results
In cardiac MRI, we found a left ventricular non-compaction cardiomyopathy.
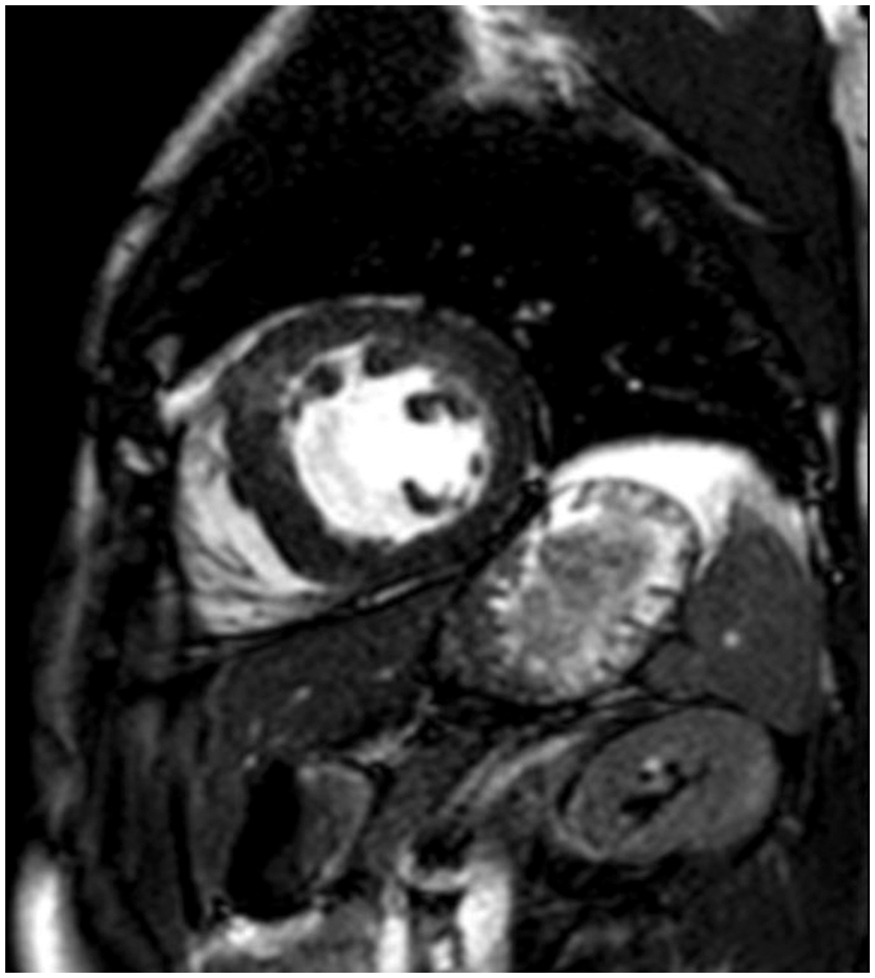
Conclusion
In spite of our patient past of consumption of cocaine, and his epidemiology environment, we diagnosed a stroke with an infrequent etiology: cardioembolic cardiopathy. We should always consider them.
Trial registration number
N/A
AS19-008
LONG TERM OUTCOME OF LOCAL SYMPTOMS IN SPONTANEOUS CERVICAL ARTERY DISSECTION
1Medizinische Universitaet Innsbruck, Neurology, Innsbruck, Austria
2BKH Kufstein, Neurology, Kufstein, Austria
Background and Aims
Spontaneous cervical artery dissection (sCAD) is a frequent cause of stroke in the young. Local symptoms such as headache, Horner’s syndrome, cranial nerve palsy and pulsatile tinnitus are common in sCAD. Data on long term outcome of these symptoms are scarce.
Method
In the ReSect-study all patients with a sCAD treated at the Innsbruck University Hospital since 1996 (n = 259) were invited to attend a standardized follow-up examination. Those who did not want to take part in the study were analysed through retrospective chart review. We analysed long term follow up of local symptoms and additionally of Horner’s syndrome and cranial nerve palsies caused by brain stem ischaemia.
Results
Local symptoms were evident in 212 (81.9%) of all sCAD patients with head-/neck pain being the most frequent one (n = 205,79.2%), followed by Horner’s syndrome (n = 42,16.2%), tinnitus (n = 19,7.3%) and lower cranial nerve palsy (n = 13,5.0%). Head-/neck pain relieved within a median of 13.5 days and all patients with cranial nerve palsy or tinnitus had full remission under conservative management. None of the patients received endovascular treatment of the underlying dissection. Horner’s syndrome was resolved in three quarters of cases (n = 9,24.3%). Additional 16 and 12 subjects with sCAD had Horner’s syndrome or lower cranial nerve palsy caused by brainstem ischaemia. Prognosis was less favourable in these patients as none showed full remission during follow up period.
Conclusion
Local symptoms in sCAD have an excellent prognosis. Their favourable natural course in our cohort argues against interventional treatment of underlying vessel pathologies in sCAD with local symptoms.
Trial registration number
N/A
AS19-010
ENDOTHELIAL FUNCTION IN YOUNG-ONSET CRYPTOGENIC ISCHEMIC STROKE: A PROSPECTIVE PILOT STUDY
1Helsinki University Hospital, Department of Neurology, Helsinki, Finland
2University of Helsinki, Clinical Neurosciences, Helsinki, Finland
3University of Helsinki and Helsinki University Central Hospital, Abdominal Center Nephrology, Helsinki, Finland
4University of Helsinki, Research Programs Unit- Diabetes and Obesity, Helsinki, Finland
5Folkhälsan Research Center, Folkhälsan Institute of Genetics, Helsinki, Finland
6HUS Medical Imaging Center- Helsinki University Central Hospital and University of Helsinki, Department of Clinical Physiology and Nuclear Medicine, Helsinki, Finland
7Heart and Lung Center- Helsinki University Hospital and University of Helsinki, Department of Cardiology, Helsinki, Finland
8Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
9The Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience- Institute of Neuroscience and Physiology, Gothenburg, Sweden
Background and Aims
Approximately one third of young-onset ischemic strokes (IS) remain cryptogenic after an extensive diagnostic work-up. We hypothesized that factors leading to endothelial dysfunction may be part of the cryptogenic IS pathogenesis.
Method
We prospectively enrolled 115 patients aged 18–49 with a recent imaging-positive cryptogenic IS in this single-center pilot study within a larger consortium (NCT01934725). Endothelial function was measured non-invasively with a peripheral arterial tonometry (Endo-PAT®) both at baseline and at a 3-month control visit. Natural log transformation of Reactive Hyperemia Index (lnRHI) was used to estimate endothelial function. Variables associated with lnRHI (P<0.2) in bivariate comparison (preexisting hypertension, diabetes, lipid components, renal function [eGFR], waist-to-hip ratio) were entered into a linear regression analysis using the backward-stepwise approach adjusted for age and sex.
Results
Mean lnRHI was 0.76 (SD +/−0.25) at baseline and 0.73 (SD +/−0.26) at 3-month visit (p = 0.275). Median delay from stroke-onset to lnRHI measurement was 9 days. At baseline, adjusted linear regression showed waist-to-hip ratio (beta -0.411; p < 0.001) and diabetes (beta -0.187; p = 0.033) to associate with a lower lnRHI (endothelial dysfunction). At 3-months, hypertension (beta -0.214; p = 0.029) and a high low-density lipoprotein cholesterol level (beta -0.230; p = 0.020) were associated with low lnRHI.
Conclusion
Endothelial dysfunction is associated with abdominal obesity, diabetes, hypertension, and hypercholesterolemia in young patients with new onset cryptogenic IS. Notably, factors associated with endothelial function were different immediately after an incident IS and 3 months after, suggesting this vascular event and its treatment may affect the patient risk profile related to endothelial function.
Trial registration number
N/A
AS19-011
CEREBROVASCULAR DISEASE IN ANTIPHOSPHOLIPID SYNDROME: 20 YEAR EXPERIENCE IN A UNIVERSITY HOSPITAL
1Ramón y Cajal University Hospital, Neurology, Madrid, Spain
Background and Aims
Antiphospholipid syndrome (APS) is an autoimmune disorder for which optimal clinical management remains controversial. Specific immunologic profiles may have prognostic relevance.
Method
We conducted a retrospective analysis of the electronic database of our stroke centre university hospital Neurology Department and included patients admitted due to APS related cerebrovascular disease from 1997 to 2017. Clinical, immunological and therapeutic variables were registered.
Results
Seventeen patients (82% female, mean age of 48 ± 17 years) were included. Seven patients (41%) were receiving antithrombotic therapy because of previous thrombosis; 3 antiplatelets (AP), 2 oral anticoagulants (OAC), 1 AP+OAC and 1 subcutaneous heparin (SH). Twelve patients presented with ischemic stroke, 4 patients with transient ischemic attack (TIA) and 1 patient with cerebral venous thrombosis (CVT). Triple antiphospholipid antibodies (aPL) positivity was detected in 5(29%) and lupic anticoagulant (LA) in 12(71%). On discharge most patients (9, 53%) were prescribed vitamin K antagonists (VKA), 1 dabigatran 110mg bid plus AP, 2 VKA+AP and 4 AP. After 4.9 ± 4.5 year’s follow-up, 3 recurrences (1 stroke and 1 retinal artery occlusion in 1 patient and 2 TIA) and 5 deaths (4 related to APS or antithrombotic therapy complications) were registered. Nine patients were functionally independent (mRS 0–2) and 3 were functionally dependent (mRS 3–4) at the end of follow-up. Neither triple aPL nor LA positivity were significantly associated with stroke/TIA recurrence or death.
Conclusion
In our experience, APS related cerebrovascular disease had significant morbidity and mortality. Clinical management was heterogeneous. No predictors of poor prognosis were detected, although small sample size may be responsible.
Trial registration number
N/A
AS19-013
DISSECTION OF ARTERIA OPHTHALMICA PRESENTING AS SUBACUTE MONOCULAR BLINDNESS
1Bispebjerg Hospital- Copenhagen University, Neurological, Copenhagen, Denmark
2Bispebjerg Hospital- Copenhagen University, Neuroradiology, Copenhagen, Denmark
Background and Aims
Intracranial artery dissections, once considered a rare disease, have become increasingly recognized as a cause of stroke in young and middle-aged individuals. Early diagnosis is essential because anticoagulation or antithrombotic therapy can help prevent primary or secondary ischemic events and possibly increase rates of recanalization.
Method
Case report
A 37-year old previously healthy man with subacute onset of blurred unilateral vision in the evening with symptom progression to monocular blindness during the night. There were no headaches or ocular pain
Results
Ophtalmoscopic fundus findings showed red cherry spot and maculae pallor. CTC showed a hyperdense a. ophthalmica. CTA showed irregularity of the a. ophthalmic lumen, but no occlusion or mural thrombus. TOF MRA showed hyperintensity of the vessel wall suggesting intramural hematoma. To further characterize these findings we supplemented with 3D fat-saturated/suppressed and high resolution MRI T1 imaging, which showed intima hematoma/intramural hematoma and pseudoaneurism. Medical treatment with dual antiplatelet (clopidogrel 75mg and aspirin 75mg daily) was prescribed for 3 months followed by mono-therapy with aspirin 75mg daily. Vision on the left eye was not regained
Conclusion
Monocular loss of vision can result from dissection of the ophthalmic artery, to our knowledge not reported previously. MRI with 3D fat-saturated T1 and high resolution MRI ensured the diagnosis and follow-up in our case of intracranial artery dissection complicated by pseudoaneurism. However, the diagnosis is a challenge for radiologists and neurologist
Trial registration number
N/A
AS19-015
PULMONARY ARTERIOVENOUS FISTULA: UNCOMMON CAUSE OF STROKE IN YOUNG PATIENTS
1Fundación Jimenez Diaz, Neurology, Madrid, Spain
Background and Aims
To describe an infrequent etiology of stroke in a 22-year-old male patient.
Method
Clinical case description.
Results
A 22-year-old male who has a personal story of viral myopericarditis and familial adenomatous polyposis that was colectomized. He presented a sudden transient episode of 15 minutes of coordination deficit in the right limbs. Three hours later he suffered an episode of dysarthria, holocranial headache and gait instability for the next two hours. There was no signs of neurological deficit in the examination. Cerebral MRI showed multiple acute ischemic lesions in both cerebellar hemispheres. The transesophageal echocardiogram showed patent oval foramen without interatrial septal aneurysm. The patient was heterozygous for the C677T mutation of the MTHFR gene. A thoraco-abdominopelvic CT showed a 13mm arteriovenous fistula in the lower lobe of the right lung. The rest of the complementary tests were normal. The patient was managed with embolization of the fistula without any complication and he remained asymptomatic.
Conclusion
Pulmonary arteriovenous fistulas are a rare cause of stroke in young patients. They must be taken into account in order to establish the etiology of stroke in young patients in which no other cause has been found. They are treatable lesions, so the stroke risk recurrence may be reduced in diagnosed and treated patients.
Trial registration number
N/A
AS19-016
ATRIOESOPHAGEAL FISTULA - A RARE CAUSE OF BRAIN EMBOLIZATION
1Faculty of Medicine in Pilsen- Charles University and Faculty Hospital Pilsen, Department of Neurology, Pilsen, Czech Republic
2Faculty of Health Studies- Pardubice University and Pardubice Hospital, Department of Neurology, Pardubice, Czech Republic
3Faculty of Medicine in Pilsen- Charles University and Faculty Hospital Pilsen, Department of Medical Imaging, Pilsen, Czech Republic
Background and Aims
Catheter ablation is a highly effective treatment of atrial fibrillation leading in a large number of patients to removal of symptoms or complete suppression of the arrhythmia. Rare, but serious complication of this treatment is the formation of atrioesophageal fistula. At present, only a few dozens of cases have been documented worldwide.
Method
In this paper we describe the case of air embolism in the brain caused by atrioesophageal fistula in a 62-year-old patient, which occured 4 weeks after radiofrequency isolation of the pulmonary veins with a sudden guadriparesis and a transient quantitative disturbance of consciousness. At the same time, there were signs of sepsis. Several days later, other symptoms developed - dysphagia, haematemesis, progression of sepsis and diffuse brain and spinal cord involvement by air and septic emboli. Chest CT has confirmed clinical suspicion of atrioesophageal fistula.
Results
In spite of intense treatment, artificial pulmonary ventilation, catecholamine support and combined broad-spectrum antibiotic therapy the condition deteriorated and the patient died on the 14th day of hospitalization.
Conclusion
The main purpose of this report is to highlight this very rare complication of catheter ablation, which often occurs 2–4 weeks after the interventional procedure, among other things, by a sudden neurological deficit.
Supported by the project Ministry of Health, Czech Republic for Conceptual Development of Research Organization 00669806 Faculty Hospital in Pilsen, Czech Republic
Trial registration number
N/A
AS19-018
VITAMIN D LEVELS IN YOUNG ACUTE ISCHEMIC STROKE PATIENTS UNDER 55 YEARS OLD
1Recep Tayyip Erdogan University Faculty of Medicine, Neurology, Rize, Turkey
Background and Aims
Observational studies indicate that low concentrations of plasma 25-hydroxy Vitamin D (25(OH)D) are associated with hypertension and ischemic stroke. Management of hypertension and treatment of Vitamin D deficiency could help in effective prevention of stroke. Vitamin D levels have been shown to be low in all stroke patients, but studies evaluating the relationship with young patients are limited. In this study, we aimed to investigate the association of vitamin D deficiency with acute ischemic stroke in young patients under 55 years old.
Method
Patients under 55 years old who were diagnosed with acute ischemic stroke between November 2013 and January 2017 retrospectively screened. This study include 74 patients in study group and 191 individuals in the control group. The research findings were obtained as using the SPSS v23.0 program.
Results
Vitamin D levels; 54.1% of the study group was inadequate, 17.6% was lack of Vitamin D and 28.4% was normal, 99% of the control group was normal and 1% was inadequate. There was a statistically significant difference between the two groups (p < 0.05).
Conclusion
Recent studies indicate that providing optimal Vitamin D levels under 50 years old can reduce stroke risk. The etiology of young stroke differs from older cases. Studies evaluating the association with young stroke and Vitamin D deficiency are limited. Although the relationship of genetic variants of Vitamin D receptors with cardiovascular diseases has been detected, the relation with ischemic stroke has not been shown yet. There is a need for studies in this area.
Trial registration number
Not needed
AS19-019
DIAGNOSTIC AND PROGNOSTIC CRITERIA OF CONNECTIVE TISSUE DYSPLASIA FOR CERVICAL ARTERY DISSECTION
1Research Center of Neurology, Department of Early Rehabilitation for Patients with Stroke and Other Neurological Diseases, Moscow, Russia
Background and Aims
Arterial wall weakness due to dysplastic changes one of the cause of spontaneous cervical artery dissection (sCeAD).
The aim of study was to assess clinical signs of connective tissue dysplasia (CTD) in CeAD patients and assess their predictive value for dissection development.
Method
We examined 82 patients (mean age 38,3 ± 13,5; 63%females,) with sCeAD, verified by MRI/MRA and 40 healthy volunteers matched for age and sex (control group). 48 signs of CTD included in diagnostic criteria for the vascular type of Ehlers–Danlos syndrome, Marfan syndrome, joint hypermobility and some others were studied. Headache in the past history (HPH) was also evaluated. Each sign was counted as positive or negative, resulting in an individual score.
Results
Mean CTD score was higher in patients than in control (7,9 ± 3,6 vs 4,6 ± 2,5; p < 0.0039). 8 out of 48 CTD signs and HPH which were more frequent in patients with sCeAD than in control (p < 0.05) were divided into main (HPH, arterial hypotension, extensive bruising widened atrophic scars, p = 0.022–0.011) and additional (translucentskin, hight palate, nasal bleeding, blue sclera, predisposition to constipation, p = 0.05–0.034). Logistic regression model showed that the presence of 4 main and 2 additional signs predict CeAD in 75–77%(ROC analysis: AUC 0.90, 95% CI, 0.84–0.96).
Conclusion
Clinical CTD signs are prevalent in patients with sCeAD. The presence of the 4 main and 2 additional CTD signs has a high predictive value of sCeAD and can be used as its diagnostic and prognostic criteria.
Trial registration number
N/A
AS19-021
TESTING FOR ANTIPHOSPHOLIPID SYNDROME IN THE YOUNG STROKE POPULATION
1University College London Hospital, Rheumatology, London, United Kingdom
2University College London Hospital, Stroke, London, United Kingdom
3University College London Hospital, Haematology, London, United Kingdom
Background and Aims
The 2016 UK National Clinical Guideline for Stroke recommend testing for antiphospholipid syndrome (APS) in people with ischaemic stroke or transient ischaemic attack (TIA) where other causes have been excluded, especially in patients under 50 years1. We aimed to determine how many patients were not tested and their characteristics.
Method
Setting
Regional stroke referral centre for North Central London. Review of consecutive records, ischaemic stroke/TIA patients <50 years presenting between January 2015-July 2016. Diagnosis, aetiology (TOAST criteria), risk factors and history of miscarriage were reviewed.
Results
Of 236 patients <50years, 62(26%) were not tested for APS at time of event, 32(52%) male, mean age 41yrs (SD 7.60). 26(42%) were ischaemic stroke, 36(58%) TIA (22% definite, 78% possible). In the majority 48(77%) aetiology was unknown but 4(6%) cardioembolism, 1(2%) small vessel occlusion, 9(15%) other. 23(37%) had no stroke risk factors, 15(24%) 1 risk factor, 16(26%) 2 risk factors, 6(10%) 3 risk factors and 2(3%) 5 risk factors. History of miscarriage was often not documented (29/30, 97%). History of venous thromboembolism was not documented in 57(92%). 11(21%) were tested for APS at another time, 7 after the event (range 1–19 months) and 4 before the event (range 7–20 months).
Conclusion
26% of patients under 50 with ischaemic stroke/TIA were not tested for APS. Amongst those 61% had ≤1 risk factor. History of miscarriage and venous thromboembolism were poorly documented. Those aged under 50 who lack classical stroke risk factors or clear aetiology represent a potentially high risk group in whom antiphospholipid testing is appropriate.
Trial registration number
N/A
AS19-022
MITOCHONDRIAL DISEASE - AN IMPORTANT CAUSE OF STROKE-LIKE EPISODES IN YOUNG ADULTS
1Brighton & Sussex University Hospitals NHS Trust, Neurology, Brighton, United Kingdom
2Brighton & Sussex University Hospitals NHS Trust, Stroke Medicine, Brighton, United Kingdom
Background and Aims
A 29-year-old man presented with two generalised tonic-clonic seizures followed by headache and visual disturbance. Past history included migraine and longstanding hearing loss attributed to childhood ear infections. Examination revealed right homonymous hemianopia and semantic language difficulties. CT brain was normal. Brain MRI showed subtle cortical signal change in left occipital and temporal lobes.
His visual and cognitive deficits persisted, and repeat MRI one week later showed dramatic increase in signal change in the left posterior cerebral artery territory with associated restricted diffusion. Differential diagnosis included ischaemic stroke, autoimmune encephalitis or a mitotic lesion. Echocardiogram, 24-hour ECG and blood tests including viral and inflammatory screen were normal. Genetic testing for mitochondrial disorder was sent due to his young age.
Three weeks later he was re-admitted with seizures and right-hand apraxia. Repeat MRI showed further spread of the signal change to involve parietal and anterior temporal lobes. Lactate was raised in the serum (5.5mmol/L) and CSF (6.2mmol/L).
Genetic blood tests eventually revealed a heteroplasmic m.3243A>G pathogenic mutation of MT-TL1. This is the most common mutation causing MELAS (mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes), which can present in young adults with headache, seizures, muscle weakness, sensorineural hearing loss and stroke-like episodes.
This case is a reminder to consider mitochondrial disease in young patients with stroke-like presentations. Raised CSF or blood lactate should increase suspicion, as should ischaemia-like changes which do not respect vascular territory. Management includes careful patient counselling and practical advice including avoiding infections, dehydration and exhaustion.
Method
–
Results
–
Conclusion
–
Trial registration number
–
AS19-023
CLINICAL FINDINGS IN YOUNG STROKE PATIENTS IN PARAGUAY. A DESCRIPTIVE STUDY
1Hospital de Clínicas, Stroke Unit. Neurology Department., San Lorenzo, Paraguay
Background and Aims
Stroke rates have been increasing in young people in the last decades around the world, being a relevant cause of mortality and severe disability in this group. Data about young stroke patients in Paraguay is not widely known. Our aim was determinate baseline characteristic, and etiology in young stroke patients in our population.
Method
This a descriptive, observational, single center study. Young stroke was defined by age between 18–50 year-old. Data collected from a prospective registry of patients admitted in our Stroke unit, from April 2015 to December 2017.
Results
From 651 patients, 129 were young stroke (19.8%). Mean age was 40.4 (SD ± 9.7) yo. Sixty one percent were ischemic and 40.2% were female.
Intracerebral Hemorrhage (ICH) was significant more frequent in young than ≥51 years-old group (38.7 % Vs. 22.7% p <0.001). Hypertension was the most frequent risk factor in both; ICH and ischaemic, showing higher rates in ICH (60% Vs. 38.1% p = 0.06).
In ICH group, hypertensive microangiophaty (48%), undetermined (30%), and Arteriovenous Malformation (14%) were the most common cause. In ischemic group, undetermined (50.6%) and cardioembolic (21.5%) cause were the most frequent etiology.
Conclusion
Higher rates in young stroke patients were seen than other series. ICH rates is remarkably higher in young stroke comparing with those ≥ 51 years-old group, being hypertensive microangiophaty the most frequent etiology. Hypertension would have an important impact in these findings. Forward multicenter studies are needed to confirm these findings.
Trial registration number
N/A
AS19-025
ASSOCIATION BETWEEN FACTOR V GENE POLYMORPHISM AND RISK OF ISCHEMIC STROKE: A META-ANALYSIS
1King Khalid University, Neurology - College of Medicine, abha, Saudi Arabia
2All India Institute of Medical Sciences, Department of Neurology-, New Delhi, India
3Beth Israel Deaconess Medical Center- Harvard Medical School, Department of Neurology- Stroke Division-, Boston, USA
Background and Aims
Ischemic stroke (IS) is a complex, multifactorial and polygenic disease. Reports on relationship between Factor V G1691A single nucleotide genepolymorphism and ischemic stroke have revealed inconsistent results. Weconducted an updated meta-analysis to determine the role of Factor Vsingle nucleotide gene polymorphism in ischemic stroke
Method
we did literature using academic electronic databases i.e PubMed, Trip Data Base, EBSCO and Google Scholar, last search up to September2017. Pooled odds ratios (ORs) and 95% confidence intervals (CIs) werecalculated from fixed or random effects models whichever applicable using software STATA version 13
Results
Forty case-control studies met the inclusion criteria, which included6860 cases and 18025 controls. Altogether, 19 studies in young adults (age < or = 40 years) and 17 studies were conducted in old stroke (age>40). Four studies did not report the mean age at recruitment. Significant association between Factor V G1691A gene polymorphism and risk of ischemic stroke were observed under dominant model (OR 1.40; 95% CI: 1.22 to 1.62, P-value <0.001). Stratified analysis suggested substantial association of Factor V gene polymorphism and risk of Ischemic stroke in cases with onset at young age (OR 1.84; 95% CI: 1.47 to 2.30,) but was not statistical significant in cases at old age (>40 years).
Conclusion
Factor V G1691A single nucleotide gene polymorphism was associatedwith risk of ischemic stroke mainly in young adults. Further researchwith adequately powered prospective studies in homogenous subjects arerequired to determine the nature of association in young stroke
Trial registration number
N/A
AS19-026
THE INFRECUENT CEREBRAL ANTERIOR ARTERY STROKES, SPECIAL CHARACTERISTICS TO TAKE INTO ACCOUNT. ANALYSIS OF A SAMPLE
1Virgen de la Arrixaca Hospital-Murcia., Neurology, Murcia, Spain
Background and Aims
Cerebral anterior artery strokes (CAA) are very infrecuent and there are few samples published. They have special clinical, etiological and prognostic characteristics which are important to be known.
Method
We put forward a descriptive analysis of a sample of CAA strokes from Virgen de la Arrixaca hospital collected since 2009. We evaluate thrombolytic therapy and the main causes that exclude this treatment. We consider good functional outcome Rankin scale (mRs) ≤2. We turn into dichotomous the National Institute of Health Stroke Scale (NIHSS: ≤8,>8) in order to analyse with X2 test the possible relation between mRs and NIHSS.
Results
In a sample of 2764 strokes, only 17 strokes involved CAA isolated (0.62%). This percentage is similar to the samples published (0.4–3%)
Thrombolitic treatment with alteplase was given in 27.8%. The main cause of exclusion was to reach the hospital out of time (>4.5 hours).
Cardioembolic etiology was the most frecuent (27.8%) followed by atherothrombotic.
We did not found statistical relation between low NIHSS score and mRs≤2 (p≥0.05).
Conclusion
CAA strokes are quite unusual.
Low NIHSS scores have no relation with better outcome. It may be due to the lower limb paresis predominantly, which restrain the gait. Neurocognitive impairment may also influence.
Initially, some patients do not give importance to an isolated leg paresis. That may delay the first medical attention and make not posible thrombolitic treatment.
Trial registration number
N/A
AS19-027
COCAINE USE AND STROKE
1Hospital Universitario Fundacion Alcorcon, Neurology, Madrid, Spain
Background and Aims
Cocaine is an independent cerebrovascular risk factor for ischemic and hemorrhagic stroke, especially among people under 55 years of age. Cocaine is associated with cerebrovascular disease through a number of different mechanisms.
Our objective is to describe the epidemiological characteristics, symptoms, prognosis and recurrence of patients with acute stroke and cocaine use.
Method
Retrospective analysis of patients with acute ischemic stroke and positive cocaine urine screen on admission from January 2015 to December 2017.
Results
We analyze 10 patients with acute stroke (9 ischemic, 1 subarachnoid hemorrhage) and positive cocaine. 100% were male, and median age was 38.5. 90% were smokers and 30% cannabis users. 40% of them had comorbid psychiatric history. Only 30% had other vascular risk factors. Median NIHSS on admission was low (2,1) with low rate of neurological complications. 100% had good outcome at 3 months.80% were anterior circulation strokes, and 50% were lacunar syndromes. Only 20% had an established infarction on magnetic resonance imaging and 100% had a complete normal etiological study. 2 patients had a new stroke in the follow up and both were lacunar. Only 30% admitted cocaine use before the results of the toxic analysis were reported.
Conclusion
Cocaine abuse is a growing epidemic that will probably result in an increased prevalence of ischemic strokes. In our work, when compared to previous studies, a low morbidity and mortality were observed. Cocaine should always be considered as a possible cause of stroke in young patients, even if the patient denies its use.
Trial registration number
N/A
AS19-029
GLIOBLASTOMA PRESENTED AS STROKE MIMIC
1Complejo Asistencial Universitario Salamanca, Neurology, Salamanca, Spain
Background and Aims
OBJECTIVE
Brain tumors are not usually considered in the etiology of cerebral infarcts in clinical practice. The objective is report a case of Glioblastoma whose initial manifestation was a stroke mimic.
Method
A clinical case
Results
We present the clinical case of a 70-year-old woman with a personal record of hypercholesterolemia. She doesn’t have any relevant family history; and she was ex-smoker for 10 years. The patient was first admitted in the Department of Neurology in October 2017 with symptoms of a sudden fluctuating aphasia of motor predominance. The initial neuroimaging (brain CT without contrast) showed a hypodense subcortical left lesion that was initially oriented as subacute ischemic infarction, adding to that clinical-radiological suspicion the existence of a moderate stenosis (50–70%) of the left internal carotid artery. Over the following weeks the patient presented a clinical worsening with the appearance of focal epileptic seizures with normal EEG and good response to carboxamide, as well as progressive right hemiparesis. Given this evolution, radiological control with contrast CT was requested, where progression of the described lesion was observed, with marked vasogenic edema and hyper-uptake that suggested malignant intracerebral neoplasia. The treatment performed was surgical excision where the finding of Glioblastoma was confirmed
Conclusion
Glioblastoma should be considered in the etiology of acute ischemic stroke, where neuroimaging plays an important diagnostic role, enabling a more immediate therapeutic approach, with a consequent impact on survival
Trial registration number
N/A
AS19-030
BIOINFORMATIC AND MOLECULAR ANALYSES IN SKIN BIOPSIES OF CADASIL PATIENTS TO EVALUATE CHANGES IN THE AFFINITY OF ITS LIGANDS
1Fundació Docència i Recerca MútuaTerrassa- Hospital Mútua de Terrassa, Stroke Pharmacogenomics and Genetics, Terrassa, Spain
2Vall d’Hebron Institute of Research- Hospital Vall d’Hebron, Neurovascular Research Laboratory, Barcelona, Spain
3The Manchester Metropolitan University of All Saints, Healthcare Science, Manchester, United Kingdom
4IMIM-Hospital del Mar, Dermatology Department, Barcelona, Spain
5IMIM-Hospital del Mar, Neurology Department, Barcelona, Spain
6Hospital MutuaTerrasa, Neurology Department, Terrassa, Spain
7Biomedicine Institute of Seville- IBiS/Hospital Universitario Virgen del Rocío/CSIC/University of Seville, Neurology Department, Sevilla, Spain
8Hospital Universitario Virgen Macarena, Neurology Department, Sevilla, Spain
9Universitat Pompeu Fabra/IMIM- Barcelona Research Park of Biomedicine PRBB, Structural Bioinformatics Laboratory GRIB, Barcelona, Spain
10Sant Pau Institute of Research- Hospital de la Santa Creu i Sant Pau, Stroke Pharmacogenomics and Genetics, Barcelona, Spain
Background and Aims
CADASIL is caused by mutations in the NOTCH3 gene. These mutations affect the number of cysteines causing protein misfolding and receptor aggregation. The recent discovery of cysteine-sparing NOTCH3 mutations in CADASIL has called this mechanism into question. The aim of this study is to find other possible pathogenic mechanisms that could be involved in CADASIL, through bioinformatic studies.
Method
A bioinformatic study was performed through DisGeNET and GUILD software with five NOTCH3 mutations: R607C, R182C, Y220C, V1183M and P496L, to find ligands that lose its binding to Notch3. To evaluate the findings observed, an immunohistochemistry study was performed in 7 confirmed CADASIL patients and 5 healthy controls. Skin biopsies were obtained to conduct a quantitative analysis of immunohistochemistry expression of H2A Histone Family Member X (H2AX) to evaluate DNA damage. To compare H2AX expression, a Mann-Whitney test was performed.
Results
Regardless of having cysteine or cysteine-sparing NOTCH3 mutations, bioinformatic studies showed changes in the affinity of several proteins to Notch3. One of them was Ku70, a DNA-repair protein. The quantitative analysis of H2AX (a marker of DNA damage) has not found a significant difference (p < 0.05) between CADASIL patients and controls.
Conclusion
Bioinformatic studies showed changes in the affinity of Ku70 to Notch3, independently of cysteine or cysteine-sparing NOTCH3 mutations. However, significant differences in DNA damage were not observed in the skin biopsies of CADASIL patients and controls. Further studies should be performed to confirm these results.
Trial registration number
N/A
AS19-031
FAMILIAL CLUSTERING OF ISCHEMIC STROKE AND MENDELIAN STROKE ASSOCIATED GENES. RESULTS FROM WHOLE EXOME SEQUENCING
1Skåne University Hospital, Department of Clinical Sciences Lund- Neurology- Lund University and Department of Neurology and Rehabilitation Medicine- Neurology- Skåne University Hospital-, Lund, Sweden
2Region Skane and Lund University, Department of Clinical Genetics and Pathology- Laboratory Medicine, Lund, Sweden
Background and Aims
Familial clustering is found in 13% of young-onset stroke probands in the Lund Stroke Register. Among 4,467 young probands with stroke, we selected 20 subjects with suggestive monogenic heredity for stroke but no previously known genetic cause for whole exome sequencing (WES) evaluation.
The aim was to detect monogenic causes of stroke by using a comprehensive stroke gene panel in patients with familial stroke clustering.
Method
WES of the 20 probands was performed on Ion Proton (Life Technologies), using base and variant calling by Torrent Suite. Ion Reporter Libraries were generated with Ion AmpliSeq Exome RDY kit. The data were filtered against a structured, comprehensive panel including genes associated with stroke and stroke related subtypes. Conventional filtering methods were used and only variants with MAF<1% were considered.
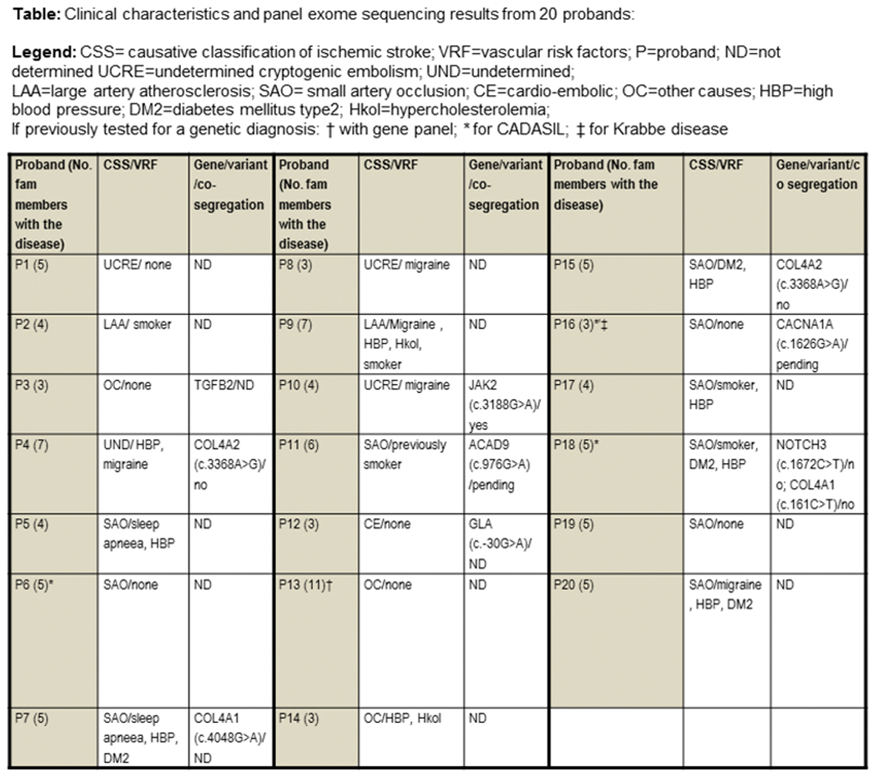
Results
Nine of 20 investigated probands carried possible pathogenic mutations in known genes relevant for stroke (table). Sanger sequencing confirmed this in 6, did not confirm in 1 and could not be performed in 2 cases. In the 6 families, additional affected and/or unaffected family members were also genotyped. Only one suspected mutations in JAK2 co-segregated with stroke in these families.
Conclusion
Our results suggest that there are additional monogenic causes for familial stroke. Alternatively, familial clustering of stroke may result from oligogenic mechanisms.
Trial registration number
N/A
AS19-033
PEDIATRIC ISCHEMIC STROKE, A CASE REVIEW
1Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
2Hospital Universitario Ramón y Cajal, Pediatric Intensive Care Unit, Madrid, Spain
Background and Aims
Pediatric ischemic stroke (IS) is uncommon, and diagnosis is usually difficult. Children have been excluded from randomized clinical trials that support reperfusion therapies for IS treatment. Therefore, management of this patients is controversial.
Method
Retrospective review of pediatric IS admitted to the hospital from 2007 to 2017.
Results
Twelve cases were recorded (7 female). Mean age was 10 +/− 3.7 years old. Most frequent TOAST subtype was IS of other determined etiology (6 cases: 3 focal arteriopathies, 1 moya moya disease, 1 sickle cell disease and 1 cervical artery disección), followed by cryptogenic stroke (5 cases). Carotid territory was the most frequent (77%). Definitive diagnostic imaging test was cranial CT in 7 cases and MRI in 6 cases. Prehospital stroke code activation was efficient in 2 cases. Median time from initial symptoms to admission was 2 hours (0.5 hours - 4 days), and median time from admission to diagnosis was 12 hours (40 min – 4 days), with most cases (77%) diagnossed beyond time window for reperfusion therapies. One patient received intravenous tPA and thrombectomy was succesfully perfomed in 2 patients. Good clinical outcome at 90 days (mRS 0–2) was achieved in 85%. No mortality was registered.
Conclusion
Pediatric IS etiology may differ from adult subtypes. Improving pediatric stroke code activation could help reducing delays in diagnosis and may provide reperfusion therapies for these patients.
Trial registration number
N/A
AS19-034
TYPE A AORTIC DISSECTION AND STROKE: CLINICAL PROFILE. A RARE AND SEVERE CAUSE OF STROKE
1Hospital de la Princesa, Neurología, Madrid, Spain
2Hospital de la Princesa, Unidad de cuidados intensivos, Madrid, Spain
Background and Aims
Aortic dissection is an infrequent cause of acute ischemic stroke and there are few case series reported in caucasic population. Our aim is to describe clinical-radiologic features of type A acute aortic dissection (typeA-AAD) with acute neurological symptoms as clinical presentation.
Method
We describe a series of patients with typeA-AAD (ascending aorta affected) admitted to our center with suspected stroke between 2010–2016.
Results
N=4. Mean age 62(SD:4,5). Women 25%. Hypertension 3(75%), dyslipidemia 2(50%) smoker 2(50%). Time from presentation of symptoms to CT: mean 97,5 minutes (SD:20,6). Clinical presentation: 2 patients had left hemisphere syndrome (NIHSS:3 and NIHSS:28), another one sudden coma (GSC:4) and the last one showed right hemisphere syndrome (NIHSS17). 3(75%) showed hypotension (<100/50) and one patient normotension (126/55). None of the patients reported chest pain. Braquiocephalic artery and right common carotid were involved in 2 patients. The other patients had left common carotid and left subcavia affected, one of them with braquiocephalic artery also involved. Early infarct signs in plane CT appeared in one patient but Perfusion-CT imaging was remarkably abnormal in all patients. AngioCT was not perfomed in one case and thrombolytic therapy was administered. Two patients underwent surgery. One of them survived.
Conclusion
Stroke is an infrequent presentation form of AAD and clinical presentation was heterogeneous in our serie, with patients tending to have neurological deficit with hypotension. Perfusion-CT must be carefully evaluated as the decreased blood flow could be related to the affection of supraaortic vessels. Routinary angio-CT in stroke evaluation should be considered in order to avoid thrombolysis in these patients.
Trial registration number
N/A
AS19-035
INCREASED RISK OF SIMULTANEOUS ACUTE ISCHEMIC STROKE AND DEEP VEIN THROMBOSIS IN PATIENTS WITH ACTIVE CANCER
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
2Hospital de la Santa Creu i Sant Pau, Hematology, Barcelona, Spain
3Hospital de la Santa Creu i Sant Pau, Oncology, Barcelona, Spain
Background and Aims
Patients with cancer have an increased risk of thrombosis mainly due to hypercoagulability. We investigated the frequency and risk factors of deep vein thrombosis (DVT) of patients with active cancer and simultaneous acute ischemic stroke (AIS) and the outcome implications.
Method
Prospective and descriptive study of consecutive patients with AIS and active cancer (2015–2017). We excluded patients under palliative care and those with an incomplete stroke evaluation. To screen for DVT, we performed a bedside ultrasonography of lower limbs. In a subgroup, we evaluated the presence of right-to-left shunt (transcranial ultrasound or transesophageal echocardiography). We collected demographic data, vascular risk factors, previous venous thrombosis (>6 months), treatments, cancer features (type, localization, histology, stage, chemotherapy), laboratory data (including D-Dimer), stroke etiology (TOAST), and 3-month outcome (modified Rankin Scale).
Results
We included 52 patients (mean age 74.6 ± 11.1y, 61.5% were men) and 65.4% had a solid cancer. We found DVT in 8/52(15.3%) patients. Right-to-left shunt was significantly more frequent in patients with DVT (40% vs 0%, p = 0.022). DVT patients showed significantly higher frequency of previous vein thrombosis (50% vs 4.5%, p = 0.003), cryptogenic stroke (75.0% vs 34.1%, p = 0.016) and higher concentrations of D-Dimer (median:12392 vs 1325µg/L, p = 0.009), compared with those without DVT. The outcome was not different between both groups. D-Dimer and previous vein thrombosis were independent predictors of DVT.
Conclusion
We observed that 15.3% of patients with AIS and active cancer had DVT. Considering the diagnostic and management implications, routine test in this group of patients should include an ultrasonography of lower limbs.
Trial registration number
N/A
AS19-036
A RARE CAUSE OF STROKE MIMIC IN A YOUNG PATIENT
1Plymouth Hospitals NHS Trust, Neurology Level 10, Plymouth, United Kingdom
Background and Aims
We report a rare cause of a stroke mimic due to intravascular large B cell lymphoma (IBCL). IBCL is a very rare and aggressive form of non–Hodgkin lymphoma with a predilection for blood vessel walls and skin. Diagnosis is extremely challenging and often made post-mortem.
Method
Case report
Results
A 45 year-old Jehovah’s witness with a background of depression was referred with a 3 day history of speech decline and altered behaviour. Initial CT head showed an established cerebellar infarct however subsequent MRI revealed multiple areas of restricted diffusion in keeping with multi-territory infarcts. Extensive tests failed to reveal a cause for her stroke (e.g. transthoracic and bubble contrast echocardiography, blood screens for Fabry, thrombophilia and vasculitis; CSF was acellular including cytology with only slight elevation of protein; CT scan of thorax/abdomen/pelvis showed mild splenomegaly; CT angiography of cerebral vessel was unremarkable).
She received pulsed steroids for presumed cerebral vasculitis with limited clinical improvement. 34 days following her admission she deteriorated with reduction in conscious level, pyrexia and haemolytic anaemia confirmed on Direct Coomb’s test. A repeat CT head revealed acute intraparenchymal haemorrhage. She died shortly afterwards. On post-mortem examination IBCL was present throughout the sampled brain tissues with secondary infarction and haemorrhage.
Conclusion
IBCL is a rare cause of stroke. In this case the diagnosis remained elusive due to the relative absence of disease outside the brain. A diagnosis of IBCL should be considered in patients with multi-territory infarcts without a clear cause (e.g. vasculitis, atrial fibrillation).
Trial registration number
N/A
AS19-037
SPONTANEOUS SUBDURAL HEMATOMA IN A CASE OF ANTIPHOSPHOLIPID SYNDROME EVOLVING INTO SYSTEMIC LUPUS ERYTHEMATOSUS: DIAGNOSTIC CHALLENGE AND TIMING FOR RESUMING ANTICOAGULANTS
1Hospital Enche' Besar Hajjah Khalsom- Kluang, Medicine, Kluang, Malaysia
2Hospital Enche' Besar Hajjah Khalsom- Kluang, Radiology, Kluang, Malaysia
3Hospital Kuala Lumpur, Medicine, Kuala Lumpur, Malaysia
Background and Aims
Bleeding in antiphospholipid syndrome (APS) is facilitated by thrombocytopenia, anticoagulants, uncontrolled hypertension and hypoprothrombinemia. Spontaneous intracranial bleed (ICB) is less frequent than ischemia but more debilitating. Its management can be challenging.
Method
We reported a 43-year-old woman who first presented with fever and anemia. She was a known primary APS, on warfarin for 5 years. At day 3, she developed dense right hemiplegia and expressive aphasia. She was normotensive.
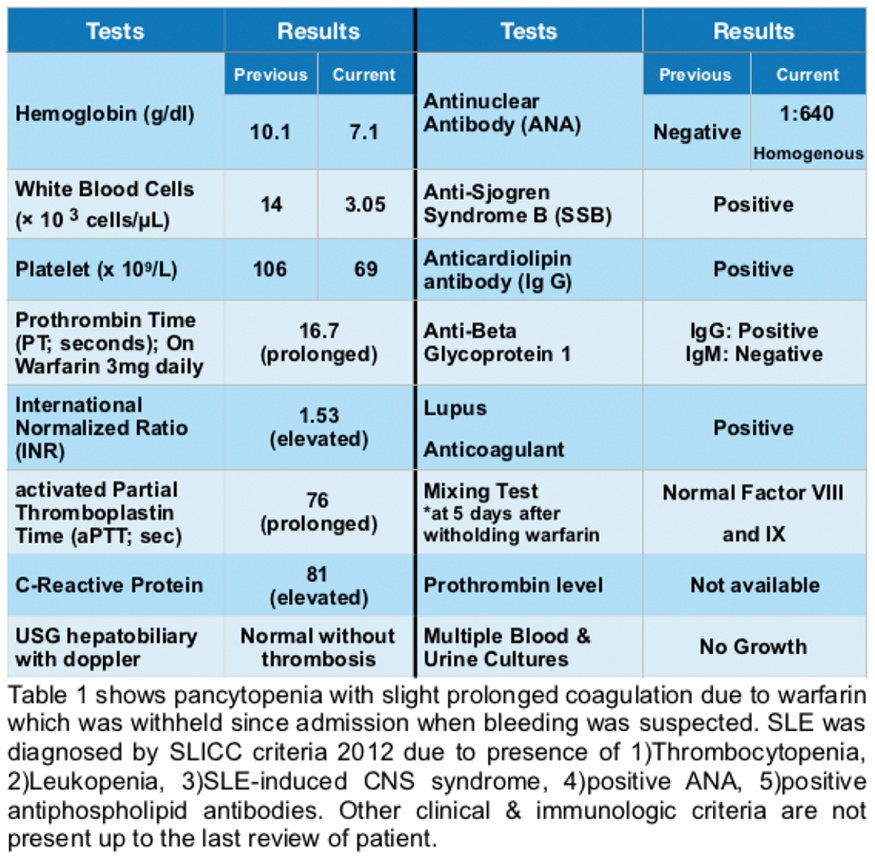
Results
CT head showed an epidural hematoma (EDH) without evidence of trauma. However, craniotomy confirmed a large encapsulated subdural hematoma (SDH) without aneurysm or AV malformation, evacuation was done. Hence, an acute-on-chronic SDH mimicked EDH on CT. MRI brain done after craniotomy showed no significant abnormality. Post-operatively, her platelet count reduced to < 50x109/L. Antinuclear antibody was positive, hence diagnosis of active SLE with secondary APS was made. We started oral prednisolone 1mg/kg/day and platelet normalised within a week. She was given prophylactic-dosed anticoagulant followed by therapeutic dose when platelet count >100x109/L two weeks post craniotomy. She was discharged at week 4 without neurological deficit.
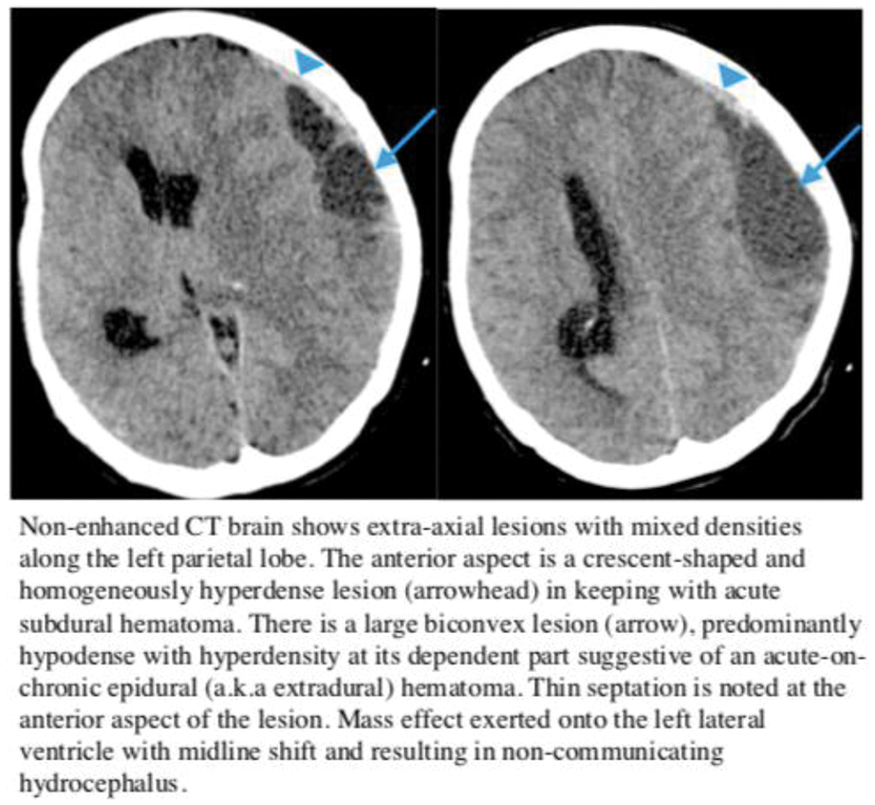
Conclusion
ICB should be anticipated in APS especially with risk factor (thrombocytopenia in this case). The underlying disease - active SLE should be diagnosed promptly and treat with immunosuppressants. Recurrent ICB in APS is high with use of anticoagulant. The timing to start anticoagulant for high risk of thromboembolism is recommended at 7–10 days after the onset of ICB. However, bleeding risk (thrombocytopenia in our patient) should be considered.
Trial registration number
N/A
AS19-038
A RARE CASE OF TRAUMATIC MIDDLE CEREBRAL ARTERY THROMBOSIS WITHOUT INTERNAL CAROTID ARTERY DISSECTION
1Royal Victoria Hospital Belfast, Stroke Unit, Belfast, United Kingdom
Background and Aims
Trauma is a well-recognised cause of middle cerebral artery (MCA) infarction. Most cases are attributable to arterial dissection, particularly of the internal carotid artery. Here we describe a rare case of localised M1/M2 thrombosis following blunt head trauma.
Method
A 59 year old male presented with facial injuries resulting from blunt head trauma on a building site. Emergency imaging of his head and neck demonstrated skull fractures and extensive soft tissue swelling.
His Glasgow Coma Scale (GCS) was 12. He was intubated and ventilated and managed in the intensive care unit (ICU).
On day 2 of his admission sedation was weaned. He was noted to be agitated with a dense right hemiparesis. Magnetic resonance (MR) imaging revealed an extensive area of acute infarction in the left MCA territory with associated mass effect. MR Angiography demonstrated partial occlusion of the left MCA at the M1-M2 junction, but no arterial dissection. He underwent emergency decompressive hemi craniotomy. After a prolonged period of rehabilitation residual deficits include severe articulatory and functional dyspraxia, right inattention and reduced upper limb function.
Results
Literature review finds similar cases describing localised rupture of the intima and elastic lamina of the vessel at post mortem examination. Other suggested mechanisms include arterial vasospasm.
Conclusion
This case demonstrates the importance of monitoring for stroke syndromes after blunt head trauma.
Trial registration number
N/A
AS19-040
ANATOMICAL VENOUS VARIANTS AND PHYSIOLOGICAL ADAPTIVE CHANGES IN CHILDREN WITH CEREBRAL SINOVENOUS THROMBOSIS
1LHSC, Paediatrics, London, Canada
2Sick Kids Hospital, Pediatrics, Toronto, Canada
3SickKids Hospital, Diagnostic Imagiung, Toronto, Canada
4SickKids Hospital, Diagnostic Imaging, Toronto, Canada
5SickKids Hospital, Pediatrics, Toronto, Canada
Background and Aims
There is no data regarding anatomical variants of the intracranial venous system and their influence in pediatric cerebral sinovenous thrombosis (CSVT) . We aim to describe the frequency of anatomical venous variants and how it affects the course in children with CSVT.
Method
Retrospective reviewed of children (term neonates – 18 years), with CSVT over 6 years (Jan 2008 – Jan 2014). Clinical features, risk factors for thrombosis and anticoagulant therapy. Radiological features (MR/MR venography and/or CT/CT venography) included location of the thrombus, presence/type of venous anatomical variation, hemorrhagic venous infarction and venous collateralization. Clinical outcomes were measured by the paediatric stroke outcome measure (PSOM) and radiological outcome was measured by early versus late thrombus recanalization at follow-up. The frequency of variations was compared to age and sex matched controls.
Results
Fifty-one children were identified. Twenty-two (43%) had anatomical variants at presentation compared to 29 (57%) with typical anatomy. These included 19 (86%) children with abnormal morphology (hypoplasia/absence of a major dural sinus) and 5 (23%) children with persistent fetal structures. Seven (14%) had prominent venous collaterals on follow-up imaging of which 3 (6%) were not associated with other venous variants. There were no significant clinical/radiological differences between children with variants vs typical anatomy. Controls without CSVT had a slightly higher prevalence of anatomical venous variants 26/51 (51%).
Conclusion
Anatomical variants are seen in the majority of children with and without CSVT. Its influence on the brain’s ability to tolerate venous congestion due to thrombosis merits further study.
Trial registration number
N/A
AS19-043
CLINICAL DIFFERENCES OF CRYPTOGENIC ISCHEMIC STROKE IN YOUNG PATIENTS WITH AND WITHOUT PATENT FORAMEN OVALE
1Kuopio University Hospital, Neurology, Kuopio, Finland
2Helsinki University Hospital, Neurology, Helsinki, Finland
3Haukeland University Hospital, Cardiology, Bergen, Norway
4Tampere University Hospital, Neurology, Tampere, Finland
5Turku University Hospital, Division of Clinical Neurosciences, Turku, Finland
6Oulu University Hospital, Neurology, Oulu, Finland
7Istanbul University, Faculty of Medicine, Istanbul, Turkey
8Azienda Unità Sanitaria Locale - IRCCS, Neuromotor Physiology, Reggio Emilia, Italy
9Hospital de Santa Maria, Neurology, Lisboa, Portugal
10Haukeland University Hospital, Neurology, Bergen, Norway
11Sahlgrenska University Hospital, Neurology, Gothenburg, Sweden
12University Medicine Greifswald, Neurology, Greifswald, Germany
13Helsinki University Hospital, Cardiology, Helsinki, Finland
Background and Aims
Patent foramen ovale (PFO) is a frequent finding in young patients with cryptogenic ischemic stroke (IS). However, little is known about clinical characteristics of PFO-related stroke. We compared acute circumstances and symptomatology between cryptogenic IS with and without PFO.
Method
We included patients with cryptogenic IS at age 18–49 enrolled in the multicenter SECRETO study (NCT01934725) who underwent standardized transesophageal echocardiography with Valsalva maneuver and contrast to examine presence of PFO (any degree of shunt). We compared demographics, premonitory symptoms, mode of symptom onset, neurological and cardiac symptoms (chest pain/palpitation), and occurrence of Valsalva inducing activity or heavy physical exertion within 2 hours prior to stroke in patients with and without PFO.
Results
Of the 201 patients (mean age 38.6+/−8.0 years; 57.1% men; median admission NIH Stroke Scale [NIHSS] score 2, range 0–20; 21.7% treated with iv-thrombolysis, 6.9% with thrombectomy), 109 (54.2%) had PFO. PFO patientś symptom onset was more often abrupt than gradual compared to non-PFO patients (79.4% vs. 64.1%; P = 0.002), aphasia more common (36.7% vs. 19.6%; P = 0.008), but nausea/vomiting (16.5% vs. 29.3%; P = 0.030) and headache less frequent (31.2% vs. 46.7%; P = 0.024). PFO patients had lower NIHSS score (median 1 vs. 3; P<0.001). In logistic regression adjusted for age and sex, mode of stroke onset, aphasia, and lower NIHSS score were independently associated with PFO-related IS.
Conclusion
Cryptogenic IS patients with PFO had more often sudden symptom onset suggestive of embolic etiology than non-PFO-patients, albeit they had milder symptoms on admission.
Trial registration number
NCT01934725
AS19-045
A RARE CASE OF STROKE IN THE YOUNG
1Salford Royal NHS Foundation Trust, Stroke Medicine, Salford, United Kingdom
Background and Aims
Recent data suggest an increasing incidence of stroke in young adults, accounting for around 10–15% of all strokes.
Vasculitis is a rare cause of strokes in young, with incidence in rates in Europe between 0.4 to 1.5 per million.
Takayasu vasculitis affects young females between 5 to 40 years of age.
It is common in patients originating from Far East, Japan and India.
Environmental factors and genetic susceptibility are thought to play a role in etiology.
Method
We report a case of young female who presented with disabling ischemic strokes as a first manifestation of Takayasu vasculitis. We also highlight salient features of the disease.
Results
A 28 year old lady presented with acute left sided facial droop and hemiparesis. MR brain showed multiple infarcts in different vascular territories. An angiogram showed widespread narrowing and stenosis affecting the brachiocephalic trunks, right subclavian artery, pulmonary artery and common carotid arteries. She fulfilled the diagnostic criteria for Takayasu vasculitis and was commenced on immunosuppressive therapy. The disease course was stable initially, but she then went on to have disabling bilateral MCA territory strokes despite being on multiple agents including cyclophosphamide. She was then commenced on Tocilizumab, and has not had any further events in the short follow-up period since.
Conclusion
Takayasu vasculitis may lead to disabling strokes but is a potentially controllable condition.
Trial registration number
N/A
AS19-046
EPILEPSY IN CHILDREN WITH PERINATAL STROKE
1State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Medical Genetics, Chisinau, Moldova
2State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Pediatrics, Chisinau, Moldova
3Institute of Mother and Child, Pediatrics, Chisinau, Moldova
4Institute of Mother and Child, Medical Genetics, Chisinau, Moldova
Background and Aims
According to some studies epilepsy after perinatal stroke occurs in 67% of the children. It was reported numbers that vary from 15% to 54%.
To assess the risk in children that suffered perinatal stroke for developing epilepsy after their first year of life. To find association between risk factors and the time of developing seizures.
Method
We collected data on 140 children with perinatal stroke (period defined between 20th week of pregnancy and first 28 days of life) between 2009–2016 and established the risk factors for developing seizures. We determined the period of developing seizures and the association between the type of stroke and the type of epilepsy.
Results
At a mean follow-up of 36 months, from 140 children about 37,86% (53 children) were found to have epilepsy, classified as folows: 16,42% - generalized; 20% - focal; 1,43% - unknown onset. According to the type of stroke, we found that 66,42% of patients have ischemic stroke; 18,57% - hemorrhagic and 9,28% - mixt. Patients underwent investigations like MRI, CT, EEG (electroencephalography). Stroke size on MRI was significantly associated with development of epilepsy, with a risk of remote seizures 8,3 times higher in those with larger stroke size.
Conclusion
Children with perinatal stroke had a high risk for developing epilepsy. Seizures occurred in 37,86 % of patients during the follow-up period. Larger stroke size was associated with higher risk of seizure. These data suggest that prolonged treatment with anticonvulsant agents may not be indicated for seizure prophylaxis after perinatal AIS.
Trial registration number
N/A
AS19-047
BILATERAL MALIGNANT MCA-INFARCTION DUE TO VASOSPASM AFTER CONSUMPTION OF CANNABIS AND ALCOHOL
1Jena University Hospital, Hans Berger Department of Neurology, Jena, Germany
2Jena University Hospital, Institute of Pathology, Jena, Germany
3Jena University Hospital, Department of Neuroradiology, Jena, Germany
Background and Aims
The association between cannabis abuse and the occurrence of ischemic stroke is controversial. Although several cases have been reported, a correlation could not be proved in a cohort study.
Method
We report the tragic and fatal course of a 27-year-old man without pre-existing medical conditions who developed acute hemiplegia left following consumption of alcohol (5 drinks) and cannabis with friends. The emergency team intubated him due to a severe agitation.
Results
Initial native computer tomography (CT) imaging and CT-angiography in an external hospital revealed no occlusion of major cerebral arteries. Systemic thrombolysis with rt-PA was administered 2h20 after symptom onset. Subsequently, the patient was transferred to our hospital. In the reperformed CT with angiography and perfusion-imaging, media discontinuation on both sides with extensive bilateral perfusion reductions in the MCA- and ACA-territory were detectable without relevant mismatch. Imaging most likely corresponded to vasospasm. Without a mismatch, no neuro-intervention could be performed and the patient was admitted to our intensive care unit.
Already the next morning, the CT showed a nearly complete bilateral infarction of the cerebral hemispheres with incipient entrapment. Subsequently, the patient developed a progressive brainstem areflexia. After 111h, irreversible brain function failure was detected. The family gave consent to organ donation. Heart, lung, both kidneys, liver and pancreas could be transplanted. Autopsy of brain and brain vasculature is ongoing.
Conclusion
In the toxicological analyses, no other drugs besides cannabis could be detected. No other cause for bilateral vasospasm could be found.
Trial registration number
N/A
AS19-048
CAROTID DIAPHRAGM. A RARE OR AN UNRECOGNIZED ENTITY?
1ASST Papa Giovanni XXIII, Neurology, Bergamo, Italy
2ASST Papa Giovanni XXIII, Neuroradiology, Bergamo, Italy
Background and Aims
Carotid diaphragm (CD) is considered a focal form of fibromuscular dysplasia, and a rare causes of ischemic stroke. We have collected three cases of CD over a 2-year period, suggesting that its frequency may be higher than previously thought.
Method
We have prospectively collected all cases of CD among patients with ischemic stroke or TIA admitted to our Stroke Unit during the last two years. A CD was diagnosed when CT- or MR-angiography showed an image of a spur arising from the posterior wall of the carotid and a thin septum in axial images at this level, without signs of atherosclerosis of the ipsilateral bifurcation.
Results
Out of 671 patients, 3 cases showed a CD (0.45%). They were 3 women aged 34, 59, and 64 years. One patient had had a previous ipsilateral territorial stroke 7 years before the index event. The 64-year-old case had a symptomatic contralateral atherosclerotic carotid occlusion, while the CD was asymptomatic. The CD was bilateral in 1 case. Only one case had positive findings at Duplex ultrasound. Two patients underwent stenting of the symptomatic diaphragm.
Conclusion
Although infrequent, a carotid diaphragm seems to be not so exceptional among patients with ischemic stroke or TIA. Since slightly less than 50% of our patients had a CT- or MR-angiography, the frequency of CD may well be higher than the one we found, especially among women. Differentiation from mural thrombus or atherosclerotic lesions may not be straightforward in all cases.
Trial registration number
N/A
AS19-049
THE PLACE OF ENCEPHALO-DURO-ARTERIO-MYO-SYNANGIOSIS IN ADULT MOYAMOYA DISEASE
1National Institute of Clinical Neurosciences, Neurology, Budapest, Hungary
2Kenessey Albert Hospital, Neurology, Balassagyarmat, Hungary
3National Institute of Clinical Neurosciences, Neurosurgery, Budapest, Hungary
Background and Aims
Moyamoya disease is a progressive, occlusive disease of the cerebral vessels with specific involvement of the circle of Willis and its feeding arteries. The name moyamoya (Japanese for "puff of smoke") refers to abnormal vascular collateral networks developing around the stenotic vessels, usually on both sides. Pathologically, it is characterized by fibrocellular intimal thickening in the walls of the terminal part of the internal carotid arteries. The proliferating intima may contain lipid deposits. It may have a genetic background; a specific gene locus and susceptibility loci have been identified.
Its prevalence of mixed population is below 1/1000000, higher in Japanese, with a mortality rate of 10% in adults and 4% in children. Half of those affected suffer a gradual cognitive loss, probably due to recurrent strokes.
Method
We present the case of a young female patient with Moyamoya disease, and work up the moyamoya cases in our institution, as well as the literature on surgical procedures, especially encephalo-duro-arterio-myo-synangiosis. We elaboration of the history, comorbidities, treatment and outcome of the moyamoya cases in our institution is in process.
Results
Our patient underwent an apparently successful (2 year follow up, with control imaging revealing the strengthening and growth of one peripheral artery) encephalo-duro-arterio-myo-synangiosis. Our literature research confirms the usefulness of this technic.
Conclusion
Moyamoya disease is a mysterious entity with probable genetic origin. The relatively high case number in our institution - around 50 - suggests a higher incidence than expected. The revascularisation method of encephalo-duro-arterio-myo-synangiosis is a useful treatment option also in adults.
Trial registration number
N/A
AS19-050
DIAGNOSTIC ASPECTS OF EPILEPSY IN CHILDREN WITH PERINATAL BRAIN INJURIES
1State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Pediatrics, Chisinau, Moldova
2SPRI Mother and Child Institute, Pediatrics, Chisinau, Moldova
3State Medical and Pharmaceutical University - -Nicolae Testemitanu - -, Medical Genetics, Chisinau, Moldova
4SPRI Mother and Child Institute, Medical Genetics, Chisinau, Moldova
Background and Aims
The diagnosis of EP (epilepsy) is opportune and important, especially knowing consequences for the child.
Determining of some peculiarities of the diagnosis of EP in the child suffered from CPL (cerebral perinatal lesions).
Method
As parts of a prospective longitudinal case-control study were observed 259 children who developed EP following the CPL. They were followed in 1 – 3 months until the age of 48 ± 12 months. Control group - 334 “practically healthy” children. EEG (electroencephalography), cerebral MRI, testing of serum levels of NF (neurotrophic factors) using enzyme-linked ELISA assay were performed. The data were treated by software Statistica 7.0, MS EXCEL.
Results
We diagnosed the following types of epilepsies: generalized (81,5%), focal (18,5%). In 1/3 of cases (34,4%) were positive history of neonatal seizures. The majority of the EP manifested in infancy (90,3%), most often between 3 and 6 months (34,4%). We established strong correlations between imaging data and resistant EP (rxy=-0,72) and medium correlations (rxy=-0,53) with controlled EP. EEG changes were correlated with the type of seizures (rxy=-0,72). We found nonspecific patterns of EEG activity: isolated or diffuse slow activity and clustered peaks with periodic generalizing, followed by epileptiform activity. Low serum levels of NF are correlated with EEG changes, i. e., BDNF (rxy=-0,72) and CNTF (rxy=-0,74), which suggested severe course of EP.
Conclusion
EP are part of basic CPL complications, with prevailing of generalized forms. Association of structural anomalies and changes in cerebral bioelectric activity, in conjunction with the NF deficit, allow to predict the course of EP.
Trial registration number
N/A
AS19-051
AN UNUSUAL INFECTIVE CAUSE FOR STROKES
1Luton & Dunstable University Hospital, Stroke Unit, Luton, United Kingdom
2Luton & Dunstable University Hospital, Radiology Department, Luton, United Kingdom
Background and Aims
A 25-year-old Romanian male presented in shock then developed seizures and a left hemiparesis. Early imaging confirmed cerebral infarcts and further investigations showed an unusual infective aetiology.
Method
Case report
Results
This patient attended the emergency department in shock following a collapse. His ECG showed inferolateral ischaemia and troponin was raised. CT aorta showed normal vasculature and an incidental liver cyst. Initial cerebral imaging was normal but after he developed a left hemiparesis, repeat imaging showed a right fronto-temporal infarct with small contralateral infarcts Echocardiography demonstrated a patent foramen ovale but no evidence of endocarditis. Further imaging characterised the liver cyst as suggestive of hydatid disease and contrast-enhanced MRI brain demonstrated bilateral enhancing lesions consistent with hydatid cysts. Anti-hydatid treatment resulted in regression of these lesions.
Liver ultrasound scan:
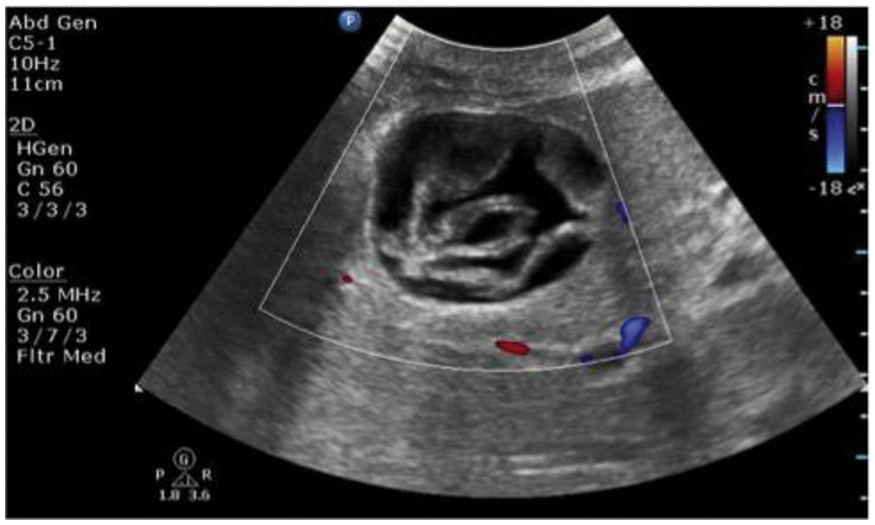
Conclusion
This case demonstrates how a ruptured hydatid cyst can cause strokes and subsequent cerebral hydatidosis via a patent foramen ovale without detectable colonisation of the endocardium. Cerebral hydatid disease occurs in just 1–2% of all cystic echinococcoses but resultant strokes have only been recognised previously when cardiac colonisation has occurred. Although rare this cause should be considered in patients from endemic areas as treatment with anti-helminthics and anti-platelets has provided good clinical and radiological outcomes.
Trial registration number
N/A
AS19-052
ISCHEMIC STROKE IN THE YOUNG: THE EXPERIENCE OF THE STROKE UNIT OF CAREGGI HOSPITAL (FLORENCE)
1University of Florence, NEUROFARBA, Florence, Italy
Background and Aims
Ischemic stroke (IS) under 50 years of age represents around 10% of all IS. Frequency of cryptogenic stroke (CS) in this class of age is elevated.
Aim
to describe a series of patients under 50 years of age admitted for IS and to compare the characteristics of CS vs not CS (NCS).
Method
retrospective analysis of patients < 50 years of age consecutively admitted to the Stroke Unit of Careggi Hospital between 1st January 2000 and 30 April 2017.
Results
337 young patients admitted for vascular events, 273 (81%) IS, mean age 40,07 ± 7,81 yrs, 42.5% females. Systemic thrombolisis performed in 19%, endovascular treatment in 16.5%. Classic cardiovascular risk factors mainly smoking highly represented, alcool consumption in 16.9%, illicit drug abuse in 16.2%. Patent foramen ovale (PFO) found in 45.9%. Artery dissection was found in 20% of cases, CS in 46.9%. Fabry disease not found.
Compared to NCS (n = 145), CS (n = 128) had milder clinical presentation (mean NIHSS 5,55 ± 6,74 CS vs 7,88 ± 8,12 NCS; p = 0,014), higher frequency of cortical lesions (p = 0,029), of patent foramen ovale (PFO) (p = 0,001), of prominent Eustachian Valve (p = 0,047), of migraine (p = 0.030), and were less hypertensive (p < 0.001).
Conclusion
Our study confirms that IS in the young is not a rare entity, the clinical presentation is mild/moderate, artery dissection remains the most frequent pathogenetic subtype. CS seem to be mainly of the ESUS type; the pathogenetic role of PFO in this subgroup has to be carefully evaluated.
Trial registration number
N/A
AS19-053
POSTVARICELLA VASCULOPATHY PRESENTING WITH ACUTE ISCHEMIC STROKE AND PROXIMAL INTRACRANIAL VESSEL DISSECTION
1Geneva University Hospitals, Neurology, Genève, Switzerland
Background and Aims
Post Varicella Zoster Virus (VZV) vasculopathy is a rare cause of stroke most frequent in children than in adults. Immunosuppression is a risk factor to develop postvaricella arteriopathy which typically affects the distal internal carotid artery and the proximal M1 segments.
Method
Here, we present a HIV-positive adult patient presenting with acute stroke and proximal middle cerebral artery (MCA) dissection related to VZV vasculopathy.
Results
A 36-year-old HIV positive female was admitted to the Emergency Room for acute middle cerebral artery stroke due to proximal M1 occlusion. A bridging therapy was started with intravenous rtPA followed by an endovascular procedure which revealed a dissection of the proximal (M1) segment of the left MCA requiring stenting placement. Because of the unusual pattern combining intracranial M1 dissection and history of HIV, CSF examination was performed, revealing mild pleiocytosis (22/mm3) and a positive VZV PCR. A low CD4 count (144) and a high number of HIV copies (>1.000.000) were identified in blood. A treatment with intravenous aciclovir and oral anti-retroviral therapy was immediately started. Evolution was favourable with a NIHSS at discharge of 1.
Conclusion
In our patient, HIV infection with low CD4 count due to poor compliance may have caused of reactivation of latent VZV infection. In patients with proximal vessel occlusion and a history of HIV infection, CSF examination should be considered.
Trial registration number
N/A
AS19-054
CEREBRAL VENOUS THROMBOSIS AT OSLO UNIVERSITY HOSPITAL 2008–2017
1Oslo University Hospital, Neurology, Oslo, Norway
2Oslo University Hospital, Geriatrics, Oslo, Norway
3Oslo University Hospital, Radiology, Oslo, Norway
4Oslo University Hospital, Neurosurgery, Oslo, Norway
Background and Aims
Cerebral venous thrombosis (CVT) is an uncommon cause of stroke. Baseline symptoms can vary considerably resulting in delayed diagnostics. The purpose of this study was to assess risk factors and management in patients treated at Oslo University Hospital.
Method
Patients admitted to Department of Neurology, Neurosurgery or Geriatrics from January 2008 to November 2017 with CVT were retrospectively selected from the patient administrative system using ICD-codes I67.6 and I63.6. Information on symptoms, risk factors, etiology, diagnostics and management was then collected from the medical records.
Results
130 patients with CVT were identified, 104 (80.0 %) with non-traumatic CVT (nCVT) and 26 (20.0 %) with traumatic (tCVT). In the nCVT group the average age was 45.3 ( ± 18.4) and 71.2 % were females. Headache was the most common symptom reported by 83.7%, followed by nausea (49.0%), weakness (29.8%), seizure (24.0%) and sensory deficits (20.2 %). Among female patients <50 years (n = 42), 14.3 % occurred during pregnancy/puerperium and 38.1% on estrogen-containing contraceptives. Etiological investigations showed that hereditary thrombophilia was the main cause in 15 %, a combination of different causes in 1/3 whereas no pro-thrombotic condition was identified in 1/3. All acute patients with nCVT were treated with anticoagulation, 6.7 % with endovascular treatment and 6.7 % with neurosurgical interventions. 18 patients (69.2 %) with tCVT had skull fracture.
Conclusion
CVT should be considered in women presenting with new onset of headache while treated with oral contraceptive pills and in patients with skull fracture.
Trial registration number
N/A
AS19-055
REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME: A CASE SERIES OF 7 PATIENTS
1Hospital de Braga, Neurology, BRAGA, Portugal
Background and Aims
Reversible cerebral vasoconstriction syndrome (RCVS) is characterized by recurrent ‘thunderclap’ headaches with reversible multifocal narrowing of the cerebral arteries, with or without focal neurological deficits. Dynamic arterial changes can be seen on angiography, but clinical deficits resulting from infarction or haemorrhage may be persistent. We analysed clinical, neuroimaging and outcome data of patients with angiographically confirmed RCVS.
Method
Retrospective study of patients admitted with the diagnosis of RCVS between August/2015-September/2017 in our institution.
Results
Seven patients with RCVS were included. Mean age was 41 years (23–67), 4 were male. RCVS was spontaneous in 3 patients and triggered in 4: vasoactive substances – selective serotonin reuptake inhibitors (n = 1), cannabinoids (n = 1) –, postpartum (n = 1) and autonomic dysfunction in Guillain-Barré syndrome (n = 1). Recurrent ‘thunderclap’ headache was the main presenting symptom (n = 6). Several complications were observed: subarachnoid haemorrhage (n = 2), focal intracerebral haemorrhage (n = 1), cerebral infarction (n = 1) and seizures (n = 1). Persistent focal neurological deficits occurred in 3 patients. The first angiographic study was normal in 2 patients, with mean time from symptom onset to diagnosis of 8 days and mean time from diagnosis to normalisation of arteries of 107 days (12–254).
Conclusion
RCVS diagnosis may be cumbersome, particularly when headaches are the sole clinical presentation or when the first angiographic study is normal. Differentiating RCVS from primary headaches may be difficult, and this syndrome should always be included in the differential diagnosis of thunderclap headaches, even if the initial investigation is negative.
Trial registration number
N/A
AS19-056
ACUTE ISCHEMIC STROKE AS THE INITIAL PRESENTATION OF TAKAYASU ARTERITIS IN A 16-YEAR-OLD GIRL
1ENERI - CLINICA LA SAGRADA FAMILIA, NEURORADIOLOGY, Capital Federal, Argentina
2Eneri-Clinica La Sagrada Familia, Neuroradiology, Capital Federal, Argentina
Background and Aims
Takayasu arteritis is a rare chronic disease of unknown etiology that affects the aorta and large vessels. Affects mainly women and is more prevalent in Asia and Latino-American countries. The clinical symptoms are variable and range from asymptomatic cases to arterial claudication and end-organ ischemia depending on location and severity of the lesions. The involved arteries usually developed wall thickening, stenosis and occlusion with aneurysmal dilatation and arterial dissections as uncommon findings. Neurological manifestations without systemic symptoms are rare.
Method
We present a case of a 16-year-old female with an unremarkable past medical history that was admitted to our emergency department with a history of a 48-hour severe right-sided hemiparesis and aphasia.
Results
Magnetic resonance and angiography (MRA) of the neck and the brain was performed revealing an acute left median cerebral artery (MCA) territory ischemic stroke and total occlusion of the left common carotid artery (CCA) and its branches. The MRA also showed proximal severe stenosis of the right CCA, left subclavian and both vertebral arteries. The patient received corticoid and endovascular treatment with a carotid wall stent and was discharged a week later with minimal right-sided hemiparesis.
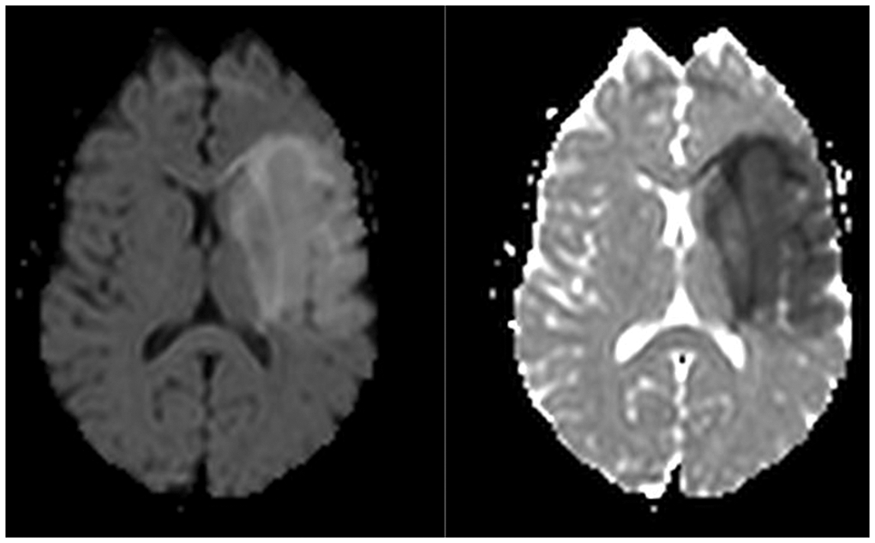
Conclusion
Although ischemic stroke as the initial manifestation of Takayasu arteritis is uncommon, it should be considered as a differential diagnosis in young patients with acute stroke. Early detection and treatment is essential in order to prevent progression of the disease and neurological disabilities.
Trial registration number
N/A
AS19-058
HYPERTENSIVE ENCEPHALOPATHY AND MULTIPLE ISCHEMIC STROKE AS INITIAL PRESENTATION OF FABRY DISEASE
1MacKay Memorial Hospital, Neurology, Taipei, Taiwan R.O.C
2MacKay Medical College, Medicine, New-taipei, Taiwan R.O.C
Background and Aims
Fabry disease is an X-linked inborn error of glycosphingolipid catabolism resulting from deficient α-galactosidase A activity. Fabry-specific manifestations, such as early stroke, progressive renal and cardiac failure, due to systemic cellular accumulation of globotriaosylceramide, may be partly avoided or delayed by early enzyme replacement therapy (ERT). However, correct diagnosis was often delayed up to 20 years.
Method
We reported a case of young male presenting hypertensive encephalopathy following by multiple stroke as initial manifestation of Fabry disease.
Results
This 38-year-old male patient, a heavy smoker and hypertension without treatment for 2 years, was admitted firstly on Dec 31 2012 due to hematuria. Malignant hypertension (BP: 267/155 mmHg), azotemia (BUN/Cr:58/5.5 mg/dL), type B aortic dissection were found. Sudden conscious change happened 24 hours later with stupor consciousness, fixed mid-dilated pupils, irregular breathing and quadriplegia. MRI showed multiple scattered infarcts in bilateral cerebrum and right cerebellum and abnormal T2 FLAIR high signals involving brainstem, bilateral middle cerebellar peduncle & bilateral thalami, suspicious for posterior reversible encephalopathy syndrome or osmotic demyelination. His consciousness regained and weaned from ventilator after aggressive BP management but became paraparesis since first discharge. He was admitted again on Sep 2016 due to infection induced acute decompensated heart failure and acute on chronic renal failure. Heart echo showed hypertrophic cardiac myopathy. Screening for Fabry disease showed positive result and confirmed as classical form. Though ERT was given, he underwent regular dialysis later.
Conclusion
In young patients with unexplained stroke, left ventricular hypertrophy and renal insufficiency, screening for Fabry disease is warranted.
Trial registration number
N/A
INTRACEREBRAL HEMORRHAGE
AS20-001
CEREBRAL VENOUS OUTFLOW PARTICIPATES IN PERIHEMATOMAL EDEMA AFTER SPONTANEOUS INTRACEREBRAL HEMORRHAGE: A CROSS-SECTIONAL STUDY
1Beijing Tian Tan Hospital - Capital Medical University - China, Neurology, Beijing, China
2Beijing Tian Tan Hospital - Capital Medical University - China, Ultrasound, Beijing, China
Background and Aims
To detect whether perihematomal edema (PHE) after spontaneous intracerebral hemorrhage (sICH) is associated with cerebral venous outflow volume (CVFV) in the internal jugular veins (IJVs) and vertebral veins (VVs).
Method
Newly diagnosed cases of sICH between April 2016 and March 2017 were enrolled. On computed tomography (CT), absolute PHE volume was calculated as the difference between total lesion volume and ICH volume. Relative PHE volume was defined as absolute PHE volume divided by ICH volume. CVFV was determined by Doppler ultrasound. Patients were divided according to mean values of absolute PHE at 3 and 12 days, and relative PHE (rPHE) at 3 and 12 days.
Results
Significant differences were observed in smoking, alcohol consumption, glycosylated hemoglobin (GHb), sIVH, and CVFV in PHE at 72 h. Only sIVH and CVFV were significantly different at 12 d in PHE. In rPHE, GHb and sIVH were significantly differed at 72 h. No significant difference was observed at 12 d in rPHE. The multivariate analyses showed that CVFV was independently associated with late PHE (PHE at 12 ± 3 d) but not with early PHE (PHE at 72 h) and rPHE.
Conclusion
These results suggest that cerebral venous outflow may take part in the process of the formation of PHE after sICH.
Trial registration number
N/A
AS20-002
ANNUAL TRENDS OF THE CLINICAL FEATURES OF INTRACEREBRAL HEMORRHAGE FOR 6 YEARS
1Research Institute for Brain and Blood Vessels -Akita, Department of Stroke Science, Akita, Japan
Background and Aims
Direct oral anticoagulants (DOACs) are recently introduced in the clinical use for stroke prevention, and they are reported to show lower risk of intracerebral hemorrhage (ICH) compared with warfarin. It might be interesting whether the number of ICH patients is decreasing or not, and whether there is any change of clinical backgrounds in ICH patients. This study aimed to reveal the annual change of clinical features in recent ICH patients with antithrombotic medication including DOACs.
Method
Between 2010 and 2015, acute ICH patients were consecutively screened (n = 658). Hematoma size was assessed by brain CT images on admission. Outcome was measured by modified Rankin Scale (mRS). Favorable outcome was defined as mRS 0–2. Annual trends were compared in three periods, 1P:2010–2011, 2P: 2012–2013 and 3P:2014–2015.
Results
Percentage of ICH patients with antithrombotics was slightly decreased for 6 years (p = 0.245: 32.9% in 1P, 27.4% in 2P and 26.0% in 3P). Frequency of antiplatelets and DOACs was inversed (p = 0.001: 56.3% and 1.4% in 1P, 52.5% and 4.9% in 2P, 40.4% and 22.8% in 3P, respectively). Mortality was not changed among the observation period (6.9% in 1P, 24.6% in 2P and 17.5% in 3P). Frequency of favorable outcome was slightly increased (p = 0.176: 28.5% in 1P, 34.6% in 2P and 38.5% in 3P). Hematoma size was not changed (29.9 ± 41.7ml in 1P, 41.2 ± 59.1ml in 2P and 25.7 ± 33.8ml in 3P).
Conclusion
Number of ICH patients with antithrombotics was decreasing for 6 years. Among them, percentage of DOACs was increasing and the outcome became better in 6 years.
Trial registration number
N/A
AS20-003
INTRACRANIAL HEMORRHAGE IN PATIENTS WITH ATRIAL FIBRILLATION RECEIVING ORAL ANTICOAGULATION WITH WARFARIN OR EDOXABAN
1Johns Hopkins University, Neurology and Anesthesiology/Critical Care Medicine, Baltimore, USA
2Brigham and Women’s Hospital- Harvard Medical School, TIMI Study Group- Department of Cardiovascular Medicine, Boston, USA
3Dana-Farber/Brigham and Women’s Cancer Center, Center for Neuro-Oncology, Boston, USA
4Massachusetts General Hospital, Department of Neurology, Boston, USA
5Daiichi Sankyo, Europe GmbH, Munich, Germany
6Daiichi Sankyo, Pharma Development, Basking Ridge, USA
Background and Aims
Anticoagulants prevent thromboembolism in atrial fibrillation (AF) patients but increase intracranial hemorrhage (ICH). In ENGAGE AF-TIMI 48, 2 edoxaban (oral FXa inhibitor) regimens were noninferior to warfarin in preventing stroke or systemic embolism, while both significantly reduced ICH.
Method
We reviewed demographics, ICH characteristics, and outcomes in patients with ICH in the trial.
Results
Of 21,105 patients in ENGAGE AF-TIMI 48, 322 (1.53%) had ≥1 ICH, totaling 341 ICH events; 166 patients (2.36%) with warfarin (W), 88 (1.25%) with higher-dose edoxaban regimen (HDER), and 68 (0.97%) with lower-dose edoxaban regimen (LDER) (p < 0.001). Intraparenchymal hemorrhage (IPH) (HR 0.55 [95% CI 0.38–0.78]) and subdural hematoma (SDH) (HR 0.36 [0.22–0.58]) were reduced with HDER versus W, while subarachnoid hemorrhage (SAH) and ischemic stroke with hemorrhagic transformation (ISHT) were similar (both p>0.05). LDER reduced IPH (HR 0.33 [0.21–0.50]), SAH (HR 0.31 [0.12–0.78]), and SDH (HR 0.26 [0.15–0.45]), while ISHT was increased (HR 2.48 [1.09–5.63]) versus W, due to more ischemic strokes with LDER (333/7034=4.7% versus 235/7036=3.3%). 185 subjects had spontaneous ICH, 97 traumatic, and 48 unknown etiology. Compared to W, edoxaban reduced spontaneous ICH (HDER: HR 0.58 [0.41–0.81], LDER: HR 0.52 [0.36–0.74]) and traumatic ICH (HDER: HR 0.38 [0.23–0.63], LDER: HR 0.31 [0.18–0.53]). Fatality rates post-ICH were similar in the 3 arms (W: 48%, HDER: 50%, LDER: 47%; p = 0.92).
Conclusion
Edoxaban reduced all ICH compared to warfarin, including both spontaneous and traumatic. Both edoxaban regimens reduced IPH and SDH while LDER also had lower rates of SAH but higher rates of ISHT.
Trial registration number
Subgroup analysis of NCT00781391.
AS20-004
PREDICTORS OF SEVERITY OF HYPERTENSIVE RESPONSE IN ACUTE INTRACEREBRAL HAEMORRHAGE
1The George Institute for Global Health, Neurological and Mental Health, Sydney, Australia
2Oslo University Hospita, Department of Neurology, Oslo, Norway
3The George Institute for Global Health, Professional Unit, Sydney, Australia
Background and Aims
Early elevation in blood pressure (BP) known as acute hypertensive response is common in patients with spontaneous intracerebral hemorrhage (ICH), and a known predictor of a poor outcome. We aimed to identify the independent predictors.
Method
We pooled INTERACT1 (n = 404) and INTERACT2 (n = 2839) of acute ICH patients (<6 hrs of onset) with elevated systolic BP (SBP, 150–220 mmHg) who were randomized to intensive (target SBP < 140 mmHg) or guideline-recommended (target SBP <180 mmHg) management. BP at randomisation was measured at least twice and at least two minutes apart using the non-paretic arm (or right arm in situations of coma or tetraparesis) with the patient supine. Multivariable linear regression was used to determine associations.
Results
Among 3233 patients, the mean age was 63.4 (12.8) years, mean SBP 179.3 (17.1) mmHg and 36.8% were female. History of hypertension (estimate 2.295, SE 0.691), admission glycemia > 6.5 mmol/lt (3.132, 0.618), elevated heart rate (1.238, 0.222 per 10-bmp increase), and higher NIHSS (0.154, 0.047 per 1-point increase) were significantly associated with hypertensive response at baseline. The use of antithrombotics (-3.742, 0.954) and time from onset to randomization (-0.992, 0.255 per 1-hour increase) were inversely associated with hypertensive response.
Conclusion
For patients with acute ICH, if they are with history of hypertension, elevated blood glucose and heart rate, severe neurological deficit, not on antithrombotics, and presented earlier, more frequent BP measurement is required and more intensive BP treatment may be needed.
Trial registration number
INTERACT studies are registered with ClinicalTrials.gov, numbers NCT00226096 and NCT00716079
AS20-005
EFFECTIVENESS OF INTRAVENTRICULAR FIBRINOLYSIS IN COMBINATION WITH EXTERNAL VENTRICULAR DRAINAGE FOR TREATMENT OF INTRAVENTRICULAR HEMORRHAGE WITH ACUTE OBSTRUCTIVE HYDROCEPHALUS
1Bach Mai hospital, Emergency Department, Hanoi, Vietnam
2Hanoi Medical University, Department of Emergency and Critical Care Medicine, Hanoi, Vietnam
3Thai Binh University of Medicine and Pharmacy, Department of Science Management, Thai Binh, Vietnam
4Bach Mai hospital, Poison Control Center, Hanoi, Vietnam
5Hanoi Medical University, Department of Neurology, Hanoi, Vietnam
Background and Aims
Intraventricular hemorrhage (IVH) is a negative prognostic factor in intracerebral hemorrhage (ICH). In Vietnam, the mortality among IVH patients with acute hydrocephalus requiring external ventricular drainage (EVD) was 57.7%. The aim of our study was to evaluate effectiveness of combined IVF by low-dose rtPA with EVD in IVH patients with acute hydrocephalus.
Method
In this non-randomized controlled study, participants with a routinely placed EVD, in emergency department with stable, ICH volume < 30 ml, and IVH obstructing the 3rd or 4th ventricles were assigned to combined IVF by low-dose rtPA (1mg every 8 hours, maximum: 9mg) with EVD (intervention) or EVD alone (control).
Results
Between Nov 30, 2011, and Dec 30, 2014, 80 patients were selected: 35 to the interventional and 45 to the control group. Primary outcomes: mortality rates in the control were higher than that in the interventional group at 30 days (42% vs. 11.4%, respectively; p < 0.01) and at 90 days (62.2% vs. 20%; respectively, p < 0.01). Secondary outcomes: mRS0–3 at 30 days in the control (6.7%) was lower than that in the interventional group (28.6%) (p < 0.05); and GOS3–5 also improved in the interventional group at 30 days (control: 24.4%; interventional: 74.3%; p < 0.01) and at 90 days (control: 42.3%; interventional: 90.3%; p < 0.01). There were no significant differences in complications between the two groups.
Conclusion
In our study, combined IVF by low-dose rtPA with EVD in IVH patients with acute hydrocephalus improved significantly mortality rates and good functional outcomes comparing with EVD alone.
Trial registration number
N/A
AS20-008
EARLY EVALUATION OF THE CORTICOSPINAL TRACT USING FRACTIONAL ANISOTROPY PREDICTS MOTOR AND FUNCTIONAL OUTCOME IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE
1Dr Josep Trueta Hospital, Neurology, Girona, Spain
2Germans Trias i Pujol Hospital, Neurology, Badalona, Spain
Background and Aims
Intracerebral hemorrhage (IH) is a frequent cause of disability and death in general population. From 30 to 50% of patients die in the first 30 days and only 20% live independently at 6 months.
Intensive therapies and do not resuscitate orders during the first 24 hours of stroke, are independent predictors of worse outcome.
We aimed to determine whether the evaluation of corticospinal tract (CT) through fractional anisotropy (FA), is able to predict motor and functional outcomes at 3 months.
Method
A prospective study was performed in which a cerebral magnetic resonance with diffusion tensor imaging (DTI) sequences were obtained in the first 12 hours from IH onset. Clinical severity, IH volume, location of corticospinal tract damage on DTI, and ratios of fractional anisotropy (rFA) between affected and unaffected sides of the CT were evaluated. The rFA was determined in 3 different levels: internal capsule, pons and the mean of hundreds of measurements along the CT (named total CT).
Results
A total of 54 consecutive patients (33.3% women; 70 years) were enrolled.
5 patients died during follow-up. Of the remaining 49, 24 (48.97%) were functional dependent (mRS=3–5) at 3 months.
rFA of the total CT was the only independent predictor of long-term motor outcome (odds ratio, 27.4; 95% confidence interval, 1.717–438.28; P<0.019) and of functional dependency (odds ratio, 5.9; 95% confidence interval, 1.014–34.85; P<0.048).
Conclusion
rFA in the first 12 hours is a independent predictor of long-term motor and functional outcomes in patients with IH. CT evaluation with FA should be considered in these patients.
Trial registration number
N/A
AS20-009
PEAK TROPONIN I LEVELS ARE ASSOCIATED WITH FUNCTIONAL OUTCOME IN INTRACEREBRAL HEMORRHAGE
1University Hospital Erlangen, Neurology, Erlangen, Germany
2University Hospital Erlangen, Neuroradiology, Erlangen, Germany
Background and Aims
To investigate the associations of troponin I levels during hospital stay with functional outcome in patients with atraumatic intracerebral hemorrhage (ICH).
Method
Observational single-center study including conservatively treated ICH patients over a 9-year period. Patients were categorized according to peak troponin I level during hospital stay (≤0.040ng/ml; 0.041–0.500ng/ml; >0.500ng/ml) and compared regarding baseline and hematoma characteristics. Multivariable analyses were performed to investigate independent associations of troponin levels during hospital stay with functional outcome – assessed using the modified Rankin scale (favorable 0–3/unfavorable 4–6) – and mortality after 3 and 12 months. To account for possible confounding propensity-score (PS)-matching (1:1;caliper 0.1) was performed accounting for imbalances in baseline characteristics to investigate the impact of troponin I values on outcome.
Results
Troponin elevations (>0.040ng/ml) during hospital stay were observed in 308/745 (41.3%) patients and associated with poorer status on admission (GCS/NIHSS) and more frequent intraventricular involvement (>0.040ng/ml: 204/308 (66.2%) versus ≤0.040ng/ml: 182/437 (41.6%); p < 0.001). Multivariable analysis revealed troponin I levels during hospital stay to be independently associated with unfavorable outcome after 12 months (Risk-ratio (95%CI): 1.030 (1.009–1.051) per increment of 1.0ng/ml; p = 0.005), but not with mortality. After PS-matching, patients with troponin I elevation (≥0.040ng/ml) versus those without had a significant higher rate of unfavorable outcome after 12 months (mRS 4–6 at 12 months: ≥0.040ng/ml: 179/266 (71.3%) versus <0.040ng/ml: 141/248 (56.9%); p = 0.001).
Conclusion
Troponin I elevations during hospital stay occur frequently in ICH patients and are independently associated with functional outcome after 3 and 12 months, but not with mortality.
Trial registration number
N/A
AS20-010
HIGHER NIHSS SCORE AT PRESENTATION IS ASSOCIATED WITH MORE SEVERE BBB DISRUPTION DURING THE FIRST 24 HOURS AFTER PRIMARY ICH
1National Institute of Neurological Disorders and Stroke, Stroke Branch, Bethesda, USA
2NIH, Stroke Branch, Bethesda, USA
Background and Aims
Primary intracerebral hemorrhage (ICH) is thought to be associated with a diffuse inflammatory response that is likely detrimental and results in opening of the blood-brain barrier (BBB). The time course of this process is not well understood.
Method
Patients with acute primary ICH who had a perfusion weighted MRI scan within the first 24 hours were identified from the NIH Natural History of Stroke study. BBB permeability images where generated from those who had adequate quality perfusion weighted source images. A whole brain permeability measure was calculated as the mean value of voxels demonstrating increased permeability due to gadolinium accumulation in the parenchymal space. Permeability, which is expressed as a percent leakage, was compared with the admission NIHSS score and discharge mRS using linear regression. Poor functional outcome on discharge was defined as discharge mRS>3.
Results
A total of 20 patients were included in the analysis. The mean age was 63 years. The median NIHSS score and mean hematoma size was 5 and 9.6 mL, respectively. Higher NIHSS score on admission was significantly associated with the severity of BBB disruption (p = 0.008). For the 17 patients who had mRS recorded on discharge, there was a trend to worse outcome with higher BBB disruption (p = 0.058) with twice the likelihood of a poor functional status at discharge[OR;(95%Cl): 2.33;(-0.47–5.15)] for every 1 percent increase in whole brain BBB disruption.
Conclusion
BBB disruption is higher in ICH patients with a poor clinical status within hours of presentation. These findings suggest a rapid inflammatory response plays a role in ICH-induced brain injury.
Trial registration number
N/A
AS20-011
POTENTIAL COST-EFFECTIVENESS OF MINIMALLY-INVASIVE ENDOSCOPIC-GUIDED NEUROSURGERY VERSUS MEDICAL TREATMENT IN SPONTANEOUS SUPRATENTORIAL INTRACEREBRAL HEMORRHAGE
1Radboudumc, Neurology, Nijmegen, The Netherlands
2Radboudumc, Health Evidence & Operating Rooms, Nijmegen, The Netherlands
3Erasmus Medical Center, Neurosurgery, Rotterdam, The Netherlands
Background and Aims
Open craniotomy to reduce hematoma volume has failed to improve functional outcome in patients with spontaneous supratentorial intracerebral haemorrhage (ICH). Innovative minimally-invasive surgical techniques with limited secondary tissue damage may improve health outcome and reduce healthcare costs.
We aim to assess the potential cost-effectiveness of minimally-invasive endoscopic-guided neurosurgery (MIEGS) in addition to usual care versus usual care alone in spontaneous supratentorial ICH, prior to a phase-III randomized clinical trial.
Method
We constructed a decision-analytic state transition (Markov) model, which assumed a 12% relative improvement in good functional outcome (defined as a modified Rankin Scale score of 0–3) to determine the effect of MIEGS versus usual care on quality-adjusted life-years (QALYs) and direct healthcare costs. Model parameters were derived from literature supplemented with retrospective data. Primary outcome was incremental cost-effectiveness ratio at a lifetime horizon. We performed probabilistic sensitivity and threshold analysis to address uncertainty.
Results
If MIEGS improves functional outcome by 12%, incremental costs were €9,913 (95%-CI, €7,886 to €11,569)/ per patient, whereas average health gain was 0.24 (95%-CI, -0.18 to 0.29) QALY per patient. The incremental cost-effectiveness ratio was €40,509 per QALY. Sensitivity analysis determined that MIEGS was always more effective but also more expensive, yet in all simulations well below a threshold of €80,000 per QALY. MIEGS had to improve good functional outcome by at least 6.4% (95%-CI, 5.1% to 8.2%) to stay below this threshold.
Conclusion
In patients with spontaneous supratentorial ICH, minimally-invasive endoscopy-guided neurosurgery has the potential to be cost-effective, which warrants a phase-III randomized clinical trial.
Trial registration number
N/A
AS20-012
EARLY IN-HOSPITAL EXPOSURE TO STATINS AND OUTCOME AFTER INTRACEREBRAL HEMORRHAGE - RESULTS FORM THE VIRTUAL INTERNATIONAL STROKE TRIALS ARCHIVE
1Charité Universitätsmedizin Berlin, Klinik für Neurologie mit Experimenteller Neurologie & Center for Stroke Research Berlin, Berlin, Germany
2University of Glasgow, Institute of Cardiovascular and Medical Sciences & Institute of Neuroscience and Psychology, Glasgow, United Kingdom
3University of Pennsylvania, Department of Neurology, Philadelphia, USA
Background and Aims
We aimed to assess whether prevalent statin users who continued to use statins during the acute phase after primary intracerebral hemorrhage (ICH) have improved functional outcome at 90 days.
Method
Data were obtained from the Virtual International Stroke Trials Archive (VISTA). Patients were categorized into four groups according to early in-hospital statin exposure. Statin continuation was defined as treatment given within 2 days after the event among prevalent statin users. Multiple logistic regression analyses were conducted to explore the association between statin exposure and favorable functional outcome (mRS≤3 at 90 days).
Results
We included 921 patients (mean age 66 ± 12, 64% male, median baseline GCS 15 [IQR 13–15], median ICH volume 15ml [IQR 7–30ml], none on oral anticoagulant). Compared with patients without exposure to statins before and early after the event (n = 790, favorable outcome 48%, reference), continued statin use was associated with favorable outcome (n = 57, favorable outcome 72%, unadjusted odds ratio 2.8, 95% confidence interval [CI] 1.6–5.1, adjusted OR [adjOR] 2.7, 95%CI 1.4–5.3). Discontinued statin use (n = 40, adjOR 0.8, 95%CI 0.3–1.7) and new early statin use (n = 32, adjOR 1.4, 95%CI 0.6–3.3) were not. The association between continued statin use and outcome remained robust in sensitivity analyses restricted to patients able to take oral medication within 72 hours (n = 606, adjOR 2.9, 95%CI 1.3–6.9) or one-week-survivors (n = 833, adjOR 2.6, 95%CI 1.3–5.1).
Conclusion
Prevalent statin users who continued statin treatment during the initial phase after primary ICH had improved functional outcome at 90 days compared to patients without statin exposure before and early after ICH.
Trial registration number
N/A
AS20-013
SIGNIFICANCE OF BLEND SIGN IN INTRACEREBRAL HEMORRHAGE: INTERACT2 STUDY
1the Second Affiliated Hospital of Soochow University, Neurology, Suzhou, China
2The george institute of global health, Mental and neurological group, Sydney, Australia
Background and Aims
To determine whether blend sign at baseline on noncontrast CT is associated with hematoma expansion, edema expansion and clinical outcomes after intracerebral hemorrhage (ICH) in the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT2) dataset.
Method
INTERACT2 was a randomized controlled trial of early intensive vs. guideline-recommended blood pressure (BP) lowering in ‘hypertensive’ ICH (<6 hrs) patients. The blend sign was defined as hematoma with two well-defined components, a relatively hypoattenuating area and adjacent hyperattenuating region. Multivariable logistic regression models were used to detect the association between blend sign and hematoma expansion, edema expansion and clinical outcomes.
Results
Of 2207 participants, 318 (14.4%) had blend sign. In multivariable analysis, the hematoma expansion volume from baseline to 24 hours in patients with blend sign was significant large than those without blend sign (9.1ml; 95% confidence interval [CI], 5.7–12.5 vs. 5.9 ml; 95%CI, 4.1–7.6; P = 0.049). The edema expansion volume from baseline to 24 hours in patients with blend sign was also significant large than those without blend sign (3.7 ml; 95%CI 2.5–4.9 vs. 2.6 ml; 95%CI, 2.0–3.2; P = 0.048). However, no significant association between blend sign and death (odds ratio [OR] 1.19; 95%CI, 0.80–1.77; P =0.397), death or major disability (0.75; 95%CI, 0.55–1.02; P = 0.064) at 90 days were found after adjusting for confounders.
Conclusion
The presence of blend sign on noncontract CT at baseline independently predicts hematoma expansion and edema expansion, but not 90 days clinical outcomes among ICH patients.
Trial registration number
N/A
AS20-014
MANAGEMENT OF ANTICOAGULATION IN PATIENTS WITH INTRACRANIAL HEMORRHAGE AND PROSTHETIC HEART VALVE
1Städtisches Klinikum München GmbH, Neurology, München, Germany
Background and Aims
For patients with prosthetic heart valves anticoagulation is recommended. Management of anticoagulation in patients with mechanical heart valves and intracranial hemorrhage (ICH) is uncertain. Aim was to identify risk of adverse effects in case of converting oral anticoagulation to heparin versus total discontinuation of anticoagulation in patients with ICH and prosthetic heart valves.
Method
The registry of the Tele Stroke Unit network TEMPiS includes all consecutive patients receiving teleconsultation in 21 participating hospitals. Data from 07/2003 to 09/2017 were searched for patients with ICH and mechanical heart valve. We compared outcome of patients with immediate conversion from oral anticoagulation to heparin versus temporary discontinuation of anticoagulation. Outcomes include intrahospital hematoma expansion, occurrence of new ICH, ischemic stroke and death.
Results
31 patients with acute ICH with prosthetic heart valve were identified. 19 of these were immediately converted to heparin. In this group 7 patients (37%) suffered from intracranial bleeding complications, 2 (11%) from ischemic stroke. Two patients (11%) died. In 10 patients (53%) none of the predefined complications occurred. In 12 patients anticoagulation was completely discontinued. In those 2 (17%) intracranial bleeding complications were seen, and 4 patients (33%) died. In 7 patients (58%) none of the predefined complications occurred.
Conclusion
Both treatment groups are at high risk for complications. Differences between discontinuation versus conversion of anticoagulation warrants further studies.
Trial registration number
N/A
AS20-015
FACTORS ASSOCIATED WITH CORTICAL SUPERFICIAL SIDEROSIS AND HEMORRHAGIC RISK IN A PROSPECTIVE OBSERVATIONAL COHORT STUDY
1University Hospitals of Strasbourg, Neurology, Strasbourg, France
2Lille University Hospital, Neurology, Lille, France
3Lille University Hospital, Neuroradiology, Lille, France
4Saint-Anne Hospital, Neuroradiology, Paris, France
Background and Aims
Unselected prospective studies on cortical superficial siderosis (cSS) are scarce. We aimed to determine the prevalence of cSS, its clinical and neuroimaging associated markers and its influence on the risk of recurrent intracerebral hemorrhage (ICH) in a prospective observational ICH cohort.
Method
We investigated clinical and radiological markers associated with cSS using multivariable analysis. In survival analyses, we used Cox models to identify predictors of recurrent ICH after adjusting for potential confounders.
Results
Of the 258 patients included in the study, 49 (19%; 95%CI 14–24) had cSS at baseline. Clinical factors independently associated with the presence of cSS were: increasing age (OR 1.03 per one year increase; 95%CI 1.001–1.06; p = 0.044), pre-existing dementia (OR 2.62; 95%CI 1.05–6.51; p = 0.039), history of previous ICH (OR 4.02; 95%CI 1.24–12.95; p = 0.02). Among radiological biomarkers, factors independently associated with the presence of cSS were: ICH lobar location (OR 24.841; 95%CI 3.2–14.47; p < 0.001), severe white matter hyperintensities score (OR 5.51; 95%CI 1.17–5.78; p = 0.019) and absence of lacune (OR 4.46; 95%CI 1.06–5.22; p = 0.035). During a median follow-up of 6.7 years (IQR 2.9–8.4), recurrent ICH occurred in 19 patients. Disseminated cSS (HR 4.69; 95%CI 1.49–14.71; p = 0.008) on baseline MRI was the only independent predictor of recurrent symptomatic ICH.
Conclusion
In a prospective observational cohort of spontaneous ICH, clinical and radiological markers associated with cSS suggest the implication of underlying cerebral amyloid angiopathy. Disseminated cSS may become a key prognostic neuroimaging marker of recurrent ICH that could be monitored in future clinical trials dedicated to ICH patients.
Trial registration number
N/A
AS20-016
ICHO SCORE: A NEW SCORE TO PREDICT FUNCTIONAL OUTCOME IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE
1Hospital Universitari Dr. Josep Trueta, Neurology. Stroke Unit, Girona, Spain
2Girona Biomedical Research Institute, Radiology, Girona, Spain
3University of Girona, Department of computer science, Girona, Spain
Background and Aims
Intracerebral hemorrhage (ICH) is a leading cause of stroke-related morbidity and mortality. We propose a model based on clinical and imaging parameters to predict functional outcome: the ICHO score.
Method
We evaluated 280 consecutive patients with acute ICH, recording demographics, vascular risk factors, stroke severity, location, and volumes of hematoma and of perihematomal edema (PHE) at baseline, 24 h, and 72 h (Olea Sphere 3.0, La Ciotat, France). Functional outcome was assessed at 3 months with the modified Rankin scale (mRS). Independent predictors of poor outcome were identified by multiple regression analysis. The best model was selected by Bayesian information criterion.
Results
Patients with poor outcome (66%) were older [72(61–78) vs. 64(54–74), p < 0.001], had higher NIHSS scores at admission [17(12–19) vs. 5(3–9), p < 0.001]; higher systolic pressure [148(134–164) vs. 143(128–152.5), p = 0.02]; higher glucose [114(101–139) vs. 105(95–116.5), p = 0.011]; larger hematoma volume at baseline [24.28(10.1–43.3) vs. 6.81(2.46–12.02), p < 0.001], 24h [28.95(14.85–52.34) vs. 7.22(2.82–13.16), p < 0.001], and 72h [28.75(12.35–56.17) vs. 7.13(3.4–12.66), p < 0.001]; greater PHE volume at baseline [11.39(5.1–24.7) vs. 4.6(1.38–8.92), p < 0.001], 24 h [19.72(9.01–40.15) vs. 6.76(3.08–12.43), p < 0.001], and 72h [29.97(14.48–53.27) vs. 10.29(4.95–17.42), p < 0.001]; greater involvement of basal ganglia (p = 0.001); and more frequent midline shift (p < 0.001). The best predictors were age, 24h-NIHSS, and hematoma volume at 72h. The ICHO score was determined as: mRS at 3 months = -0.837 + (0.032 x age) + (0.152 x 24h-NIHSS) + 0.011 x 72h-hematoma volume).
Conclusion
The ICHO score might be a valid clinical grading scale for 3-monh functional outcome after ICH; further validation in different populations is needed.
Trial registration number
N/A
AS20-017
INDEPENDENT VALIDATION OF THE HEMATOMA EXPANSION (HEP) SCORE: A NON-CONTRAST PREDICTION TOOL
1Ottawa Hospital Research Institute, Medicine- Division of Neurology, Ottawa, Canada
2Calgary Stroke Program, Clinical Neurosciences, Calgary, Canada
3Sunnybrook Health Sciences, Division of Neuroradiology and Department of Medical Imaging, Toronto, Canada
4Hospital Universitari Vall d'Hebron, Neurology, Barcelona, Spain
5Dr. Josep Trueta University Hospital, Neurology, Girona, Spain
6Elblandklinikum Meissen Academic Teaching Hospital of the Technische University, Neurology, Dresden, Germany
7Institute of Psychiatry and Neurology, Neurology, Warsaw, Poland
8Charles LeMoyne Hospital, Medicine, Longueuil, Canada
9Ottawa Hospital Research Institute, Diagnostic Imaging: Neuroradiology Section, Ottawa, Canada
10Dalhousie University, Neurology, Halifax, Canada
11All India Institute of Medical Sciences, Neurology, New Delhi, India
12Apollo Gleneagles Hospitals, Neurology, Kolkata, India
13Boston Medical Center, Neurology, Boston, USA
14Beth Israel Deaconess Medical Centre, Neurology, Boston, USA
Background and Aims
In 2015, Yao et al. (Neurocrit Care,23:179–187) developed the Hematoma Expansion Prediction (HEP) Score, an 18-point nomogram-derived non-contrast prediction scale with six variables: 1) time to CT, 2) dementia history, 3) smoking status, 4) antiplatelet use, 5) Glasgow coma scale, and 6) presence of subarachnoid hemorrhage. Using data from the prospectively collected PREDICT-ICH cohort, we aimed to independently validate this prediction tool.
Method
We generated a receiver operating characteristic (ROC) curve assessing the discriminative value of the HEP score in predicting significant hematoma expansion (defined as: ≥6mL or ≥33%). Sensitivity, specificity, positive and negative predictive values (PPV/NPV) were calculated for each score point. Independent predictors of expansion, including HEP score, were determined using multivariable logistic regression modelling. Covariates were selected through exploratory analysis. Spot sign was included as a covariate in post-hoc analysis.
Results
292 patients were included in primary analysis with HEP scores ranging from 0–10. Hematoma expansion occurred in 94 patients (32%). ROC curves comparing HEP score to expansion had an area under the curve of 0.639 (95% CI: 0.57–0.70). Youden’s method showed an optimum score of 3. HEP Scores ≥ 3 (Sens 85%, Spec 30%, PPV 46%, NPV 75%, aOR 2.42 [CI:1.20–4.90], p < 0.014) accurately predicted significant expansion. PPV increased with higher scores, but at the cost of lower sensitivities. When spot sign was included in regression analysis, the HEP score was not significantly associated with expansion.
Conclusion
The HEP score is predictive of hematoma expansion and has use in scenarios where technological access is limited and contrast is not available.
Trial registration number
N/A
AS20-019
USING ZEBRAFISH TO MODEL HAEMORRHAGIC STROKE
1University of Manchester, School of Biological Sciences, Manchester, United Kingdom
Background and Aims
Our understanding of the disease mechanisms underlying intracerebral haemorrhage (ICH) is incomplete and as such, our ability to prevent ICH or improve outcomes once bleeding has occurred is limited. It is essential, therefore, that we continue to interrogate ICH pathophysiology using new pre-clinical approaches. The aim of this work was to investigate the use of zebrafish as an alternative model system for studying the causes and pathological consequences of ICH.
Method
Zebrafish larvae are transparent, allowing for easy visualisation of brain tissue in intact animals. Spontaneous brain haemorrhage was induced using genetic and chemical manipulation. Live imaging of larvae derived from transgenic zebrafish reporter lines (expressing fluorescent proteins in a range of cell types) was performed to record cellular responses in the brain immediately after ICH. Locomotor function following ICH was also analysed.
Results
We show that spontaneous brain haemorrhage in zebrafish larvae is associated with 1) significant cell death within the brain, 2) increased activation of macrophages within brain injury sites, 3) a significant reduction in locomotor function and 4) increased expression of the inflammatory cytokine interleukin-1β (il-1β). Furthermore, we show that inhibition of il-1β is protective against brain cell death in this model.
Conclusion
Zebrafish larvae are a powerful system for studying ICH biology in real-time, allowing for observations which are not possible using rodents. These data indicate that the pathological consequences of brain bleeding are conserved between zebrafish and humans, thereby validating the use of this model as an important new tool for studying ICH pre-clinically.
Trial registration number
N/A
AS20-020
THE FUNCTIONAL OUTCOME OF PRIMARY INTRACEREBRAL HEMORRHAGE IN PATIENTS WITH ORAL ANTICOAGULANT OR ANTIPLATELET THERAPY
1Faculty of Medicine, neurology, Novi Sad, Serbia
2Clinical Center of Vojvodina, Emergency Center, Novi Sad, Serbia
3Faculty of Medicine, Faculty of Medicine, Novi Sad, Serbia
Background and Aims
An escalation in the use of oral anticoagulants (OAC) and antiplatelet therapy (AT) has led to a surge in the incidences of primary intracerebral hemorrhage (pICH). The presented study aims at determing the effect of this therapy aproach on the functional outcomes following pICH.
Method
Retrospective study included 246 adult patients with first time diagnosed pICH, hospitalized at the Clinic for Neurology and the Emergency Centre in Novi Sad, from January 2014 to December 2015. Patients were divided into three groups: OAC, AT and without OAC/AT.
Results
157 males (63.8%) and 89 (36.2%) females with mean age of 67.9 were enrolled in the study. 50 (20.3%) patients were on OAC, and 20 (8.2%) on AT, while the other 176 (71.5%) didn't take OAC/AT in the premorbid period. In 40% patients of OAC group initial NIHSS was 14–20, while the other two groups had NIHSS 0–6. The mRS was calculated for 154 (62.6%) survivors. For about 2/3 patients in all three groups, pICH had a poor functional outcome (mRS ≥3), but without statistically significant difference in initial NIHSS score or mRS at discharge among groups. OAC users had the highest mortality rate in the first 24 hours (OR = 2.5). Patients in the other two groups (50%/71%) recorded a significant tendency for survival (p < 0.000) (OR = 1.5).
Conclusion
Early mortality (in first 24h) was specific for AC users. AT users and those without OAC/AT didn't have significant effect on the incidence of mortality of pICH.
Trial registration number
N/A
AS20-021
PREDICTORS OF HEMORRHAGE AFTER ENDOVASCULAR THERAPY: FINDINGS FROM THE INTERRSECT STUDY
1University of Ottawa- Ottawa Hospital Research Institute, Medicine Neurology, Ottawa, Canada
2Calgary Stroke Program, Clinical Neurosciences, Calgary, Canada
3Girona Biomedical Rsch Institute IDIBGI- Hosp Universitari Dr Josep Trueta, Diagnostic per la Imatge, Girona, Spain
4Hospital Clínico Universitario de Valladolid, Neurology, Valladolid, Spain
5Keimyung University, Neurology, Daegu, Republic of Korea
6Miller School of Medicine, Neurology, Miami, USA
7Chosun Univ Sch of Medicine and Hosp, Neurology, Daegu, Republic of Korea
8St. Anne’s Hospital and Masaryk University, Neurology, Brno, Czech Republic
9University of British Columbia, Neurology, Vancouver, Canada
10Queens University, Neurology, Kingston, Canada
11Bezmialem Vakif Üniversitesi Nöroloji, Neurology, Istanbul, Turkey
12University of Sherbrooke, Medicine, Sherbrooke, Canada
Background and Aims
While recent endovascular therapy trials have had a minimal number of adverse events, intracerebral hemorrhage (ICH) still occurs. The predictors of ICH with endovascular therapy remain unclear. We assessed predictors of hemorrhage following endovascular thrombectomy using data from the prospectively collected, multicenter INTERRSeCT study.
Method
Patients undergoing endovascular therapy +/− intravenous alteplase (tPA) were enrolled and received baseline CT/CTA, follow-up CTA/Angiogram and 24-hr CT/MRI images. Primary outcome was any ICH as per the ECASS classification of hemorrhage. Secondary outcome was significant ICH (PH1/PH2). We assessed the relations between ICH and baseline ASPECTS scoring, thrombus location, residual flow, collateralization, tPA use, and final recanalization state. Multivariable regression with stepwise selection was used to adjust for relevant covariates.
Results
Of 242 patients who met inclusion criteria, 58 (24%) had an ICH at 24 hours (HI1 53%, HI2 19%, PH1 7%, PH2 21%). Post-procedure hemorrhage was associated with lower ASPECTS scores (p < 0.001), ICA (p = 0.004), proximal M1 (p = 0.008), and mid-M1 (p = 0.002) thrombus locations, and serum glucose (7.6 vs. 6.7; p = 0.027). When adjusted for covariates, lower ASPECTS score (OR: 1.41 per point lost; 95% CI: 0.57–0.88; p < 0.002), mid-M1 thrombus location (OR: 2.03; 95% CI: 1.03–4.01; p < 0.041), and serum glucose (OR:1.15, 95% CI: 1.01–1.35, p < 0.033) independently predicted the presence of post-procedure ICH. Significant ICH was associated with ICA thrombus (OR:2.96, 95% CI:1.05–8.33, p < 0.04) after adjusting for relevant covariates.
Conclusion
Early ischemia defined by imaging, mid-M1 thrombus location, and increased serum glucose are associated with increased risk of hemorrhage in patients undergoing combination tPA and endovascular therapy.
Trial registration number
N/A
AS20-022
ASSOCIATION BETWEEN THE EDINBURGH CT AND GENETIC DIAGNOSTIC CRITERIA FOR LOBAR INTRACEREBRAL HAEMORRHAGE ASSOCIATED WITH CEREBRAL AMYLOID ANGIOPATHY AND RISK OF RECURRENT INTRACEREBRAL HAEMORRHAGE
1The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Melbourne, Melbourne Brain Centre at The Royal Melbourne Hospital, Melbourne, Australia
3Newcastle University, Institute of Neuroscience and Institute for Ageing, Newcastle, United Kingdom
4Newcastle upon Tyne Hospitals National Health Services Foundation Trust, Department of Neuroradiology, Newcastle, United Kingdom
5The University of Edinburgh, Row Fogo Centre for Research into Ageing and the Brain, Edinburgh, United Kingdom
6The University of Edinburgh, UK Dementia Research Institute at The University of Edinburgh, Edinburgh, United Kingdom
Background and Aims
The Edinburgh diagnostic criteria based on CT ± APOE genotype are accurate for diagnosing pathologically-proven CAA-associated lobar intracerebral haemorrhage (ICH), but whether they are associated with a higher risk of recurrent ICH is unknown.
Method
We conducted a 3-year, population-based, prospective inception cohort study using multiple overlapping sources of case ascertainment and follow-up of ICH in 2010 to 2013 in Lothian, Scotland; during this study, and until 2016, we recruited adults who consented to APOE genotyping. A radiologist rated brain CT appearances using Edinburgh criteria masked to clinical, genetic and histopathological features. We determined APOE genotype using peripheral blood and/or brain tissue. A neurologist validated recurrent ICH diagnoses using clinical and imaging records.
Results
Among 196 adults with lobar ICH in the population-based study, using CT-only Edinburgh criteria, the recurrent ICH rate was significantly lower in adults with low CAA probability over four year follow-up (n = 54, 2.6 [95%CI 0.6–6.7] per 100 patient-years) versus adults with intermediate/high CAA probability (n = 142, 9.4 [95%CI 5.6–14.5] per 100 patient-years; HR 0.29 [95%CI 0.08–0.98], p = 0.03).
Among 133 adults with lobar ICH, using CT and APOE Edinburgh criteria, the recurrent ICH rate was non-significantly lower in adults with low CAA probability over four years follow-up (n = 32, 3.6 [95%CI 0.6–11.2] per 100 patient-years) versus adults with intermediate/high CAA probability (n = 101, 9.5 [95%CI 5.3–15.3] per 100 patient-years; HR 0.40 [95%CI 0.09–1.76], p = 0.21).
Conclusion
After lobar ICH, recurrent ICH risk appears higher among patients with intermediate/high probability of CAA according to the Edinburgh criteria. We encourage external validation of these findings.
Trial registration number
N/A
AS20-023
DIAGNOSIS OF CEREBRAL AMYLOID ANGIOPATHY-ASSOCIATED LOBAR INTRACEREBRAL HAEMORRHAGE: DIAGNOSTIC TEST ACCURACY SIMULATION STUDY
1The University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2The University of Edinburgh, Row Fogo Centre for Research into Ageing and the Brain, Edinburgh, United Kingdom
3The University of Edinburgh, UK Dementia Research Institute at The University of Edinburgh, Edinburgh, United Kingdom
Background and Aims
Cerebral amyloid angiopathy (CAA) is a diffuse small vessel disease. Cortical biopsy is the pathological reference standard in life, but it potentially results in false negatives (CAA missed by biopsy) and false positives (CAA in the biopsy but sparse in the whole brain). We aimed to compare simulations of cortical biopsy against autopsy for CAA diagnosis.
Method
We identified adults with first-ever symptomatic intracerebral haemorrhage (ICH), who died and underwent research autopsy as part of a prospective, population-based, inception cohort. We compared two published pathological approaches to rating the tissue block obtained from the lobe affected by ICH (simulated cortical biopsy) against the whole-brain reference standard at autopsy. A neuropathologist staged and graded CAA using a standardised consensus rating scale, and we categorised lobar ICH as CAA-associated if global cerebral summed parenchymal CAA score was ≥9.
Results
Among 69 adults with lobar ICH (median age 83 years [IQR 78–86], 26 [38%] men), 42 (61%) were CAA-associated at research autopsy. The presence of any CAA in simulated cortical biopsy (Vonsattel grade ≥1) was 100% (95%CI 90–100) sensitive for CAA-associated ICH, but 70% (95%CI 50–86) specific due to 8/27 false positives. The presence of complete replacement of a vessel wall with amyloid in simulated cortical biopsy (Vonsattel grade ≥2) was 95% (95%CI 83–99) sensitive and 78% (95%CI 57–91) specific due to 6/27 false positives.
Conclusion
Cortical biopsy appears sensitive enough to rule out CAA-associated lobar ICH, but its specificity is moderate in comparison to whole-brain assessments.
Trial registration number
N/A
AS20-024
CT IMAGING MARKERS OF CAA, APOE GENOTYPE AND RECURRENT ICH RISK
1UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Stroke Research Center- Department of Brain Repair and Rehabilitation, London, United Kingdom
2University Hospital and University of Basel, Stroke Center and Neurology, Basel, Switzerland
3UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Neurogenetics Laboratory, London, United Kingdom
4UCL Institute of Neurology, Department of Statistical Science, London, United Kingdom
5University College London Hospitals NHS Foundation Trust, Departement of Haematology, London, United Kingdom
6National Hospital for Neurology and Neurosurgery, Lysholm Department of Neuroradiology-, London, United Kingdom
7UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Department of Brain Repair and Rehabilitation, London, United Kingdom
8School of Clinical Sciences- University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
9University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
10University of Glasgow- Queen Elizabeth University Hospital, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
11UCL Institute of Neurology and The National Hospital for Neurology and Neurosurgery- Queen Square, Neuroradiological Academic Unit- Department of Brain Repair and Rehabilitation, London, United Kingdom
Background and Aims
We analysed the risk of recurrent intracerebral haemorrhage (ICH) using APOE e4 genotype and CT imaging markers that are hypothesised to be associated with CAA.
Method
In a prospective ICH cohort study (CROMIS-2 ICH), we analysed CT scans for presence of subarachnoid haemorrhage (SAH) and “finger-like projections” (FLP). We used blood samples to determine APOE genotype. Patients were followed up for at least 6 month for recurrent ICH. We calculated annualized rate of recurrent ICH (=total of observed ICH/patient-years of follow-up) and compared groups using the log-rank test.
Results
The final cohort contained 336 patients with lobar ICH (median age 76 years, IQR 70–83; median ICH volume 17.4mL IQR 6.8–35.1mL). SAH was present in 135 patients (40.2%), FLP in 80 (23.8%) and 104 (30.5%) patients had at least one APOE e4 allele.
During a total follow-up period of 487.5 patient years, 22 patients had recurrent ICH (4.5%/year). The rate of recurrent ICH increased with the number of positive markers: 2.4%/year in patients without any marker, 5.0%/year in patients with 1 or 2 markers, and 11.2%/year in patients having all 3 markers (p = .034). Patients having both CT markers (SAH+FLP) and those having all 3 markers had a significantly higher rate of recurrent ICH compared to patients without these markers (12.2%/year vs. 3.3%/year for both CT markers, p = .003 and 11.2%/year vs. 3.9%/year for all 3 variables, p = .026).
Conclusion
APOE e4 and CT markers associated with CAA can identify patients with increased risk of recurrent ICH.
Trial registration number
n/a
AS20-025
ANTITHROMBOTIC DRUGS RESUMPTION AFTER INTRACEREBRAL HAEMORRHAGE AND SUBSEQUENT RISK OF MAJOR VASCULAR EVENTS
1Université Lille- Inserm U1171- Degenerative and Vascular Cognitive Disorders- CHU Lille, Department of Neurology, Lille, France
2Groupement des Hôpitaus de L'Institut Catholique de Lille, Department of Neurology, Lomme, France
3Rudolf Magnus Institute of Neuroscience- University Medical Centre, Department of Neurology and Neurosurgery, Utrecht, The Netherlands
4Academic Medical Center- University of Amsterdam, Department of Neurology, Amsterdam, The Netherlands
5School of Clinical Sciences- University of Edinburgh, Division of Clinical Neurosciences, Edinburgh, United Kingdom
6Université Lille- EA 2694- CHU Lille, Department of Biostatics and Public Health, Lille, France
7Donders Institute for Brain- Cognition and Behavior- Radboud University Medical Center, Department of Neurology, Nijmegen, The Netherlands
Background and Aims
The optimal treatment strategy concerning restarting or not antithrombotic drugs in intracerebral haemorrhage (ICH) survivors is unknown, because of the competing risk of ischemic and haemorrhagic events. We assessed the association between restarting antithrombotic drugs and the risk of major vascular events in a multinational cohort of ICH.
Method
We gathered data from three hospital-based cohorts (Lille, n = 545; Utrecht, n = 389; Amsterdam, The Netherlands, n = 403) and one community-based study (Lothian, n = 295) of ICH. We included 272 patients (median age 75 years, interquartile range 65–82; 56% males) who took antithrombotic drugs for secondary prevention of thromboembolic events or atrial fibrillation, and survived at least 30 days after ICH. We assessed the association between restarting antithrombotic drugs and the occurrence of major vascular events (ischaemic or haemorrhagic) by Cox regression modelling.
Results
Restarting antithrombotic drugs was not associated with major vascular events (HR 1.24; 95% confidence interval (CI) 0.78–1.98) nor with haemorrhagic events (HR 0.99; 95%CI 0.41–2.41) during a follow up of 4.7 years (IQR 2.2–6.1). Compared to avoiding antithrombotic drugs, restarting antiplatelet agents (HR 1.94; 95%CI 1.02–3.71), but not anticoagulation (HR 1.31; 95%CI 0.60–2.82), was associated with thromboembolic events. In patients with non-lobar ICH, restarting antithrombotic drugs was associated with major vascular events (HR 2.07; 95%CI 1.13–3.78), and thromboembolic events (HR 2.30; 95% CI 1.12–4.69). No significant association was observed in patients with lobar ICH.
Conclusion
Antithrombotic drugs seem safe after ICH and not associated with an increase in haemorrhagic events. Randomised controlled trials are needed to confirm their benefit.
Trial registration number
N/A
AS20-026
INFLUENCE OF HAPTOGLOBIN ON OEDEMA EXTENSION DISTANCE AFTER INTRACEREBRAL HAEMORRHAGE
1Stroke Research Centre, Institute of Neurology- University College London, London, United Kingdom
2Clinical Neurosciences, Clinical and Experimental Sciences- Faculty of Medicine- University of Southampton, Southampton, United Kingdom
3Department of Statistical Science, University College London, London, United Kingdom
4Neuroradiological Academic Unit, Department of Brain Repair & Rehabilitation- University College London, London, United Kingdom
5Neurogenetics Laboratory, The National Hospital of Neurology and Neurosurgery, London, United Kingdom
6Haemostasis Research Unit, Department of Haematology- University College London, London, United Kingdom
7Centre for Clinical Brain Sciences, School of Clinical Sciences- University of Edinburgh, Edinburgh, United Kingdom
8Institute of Cardiovascular Sciences, University of Birmingham, Birmingham, United Kingdom
9Institute of Neuroscience & Psychology, University of Glasgow- Queen Elizabeth University Hospital, Glasgow, United Kingdom
Background and Aims
After intracerebral haemorrhage (ICH) the brain is exposed to extracellular haemoglobin and its toxic breakdown products haem and iron. Haptoglobin (Hp) is an acute-phase protein involved in neutralizing haemoglobin. Hp expression level is influenced by the Hp copy number variant (CNV) (Hp1 versus Hp2), and the rs2000999 single nucleotide polymorphism (SNP). Hp1-1 has previously been associated with better outcomes after ICH. We investigated the effect of these genetic variations on perihaematomal oedema (PHO), a potential mediator of effects on outcome, measured by oedema expansion distance (OED; potential marker of inflammation and haemoglobin toxicity).
Method
Patients were enrolled from the ICH arm of CROMIS-2, a prospective observational study. Hp CNV was determined by two methods: quantitative polymerase chain reaction (PCR) and conventional PCR. Hp SNP was determined using Kompetitive Allele-Specific PCR. Measurement of PHO volume on acute CT scan (within three days) was performed via a semi-automated, threshold-based approach.
Results
Among 738 included patients Hp CNV genotype was 122 Hp1-1 (16.55%), 364 Hp2-1 (49.39%) and 244 Hp2-2 (34.06%). Distribution of the Hp SNP genotype was: 23 A:A (3.22%), 235 A:G (32.87%) and 457 G:G (63.92%). Neither Hp CNV nor SNP genotype was associated with OED in either univariable or multivariable linear regression analysis that included systolic blood pressure, antihypertensive medication, anticoagulation, time to CT, ICH volume and location.
Conclusion
We found no association of either Hp CNV or SNP with acute PHO. If haptoglobin genetic variants influence outcome, it is likely mediated by mechanisms other than through reducing acute PHO.
Trial registration number
N/A
AS20-027
AMYLOID SPELLS AND CORTICAL SUPERFICIAL SIDEROSIS: A COMBINATION WITH AN INCREASED RISK OF INTRACRANIAL HEMORRHAGE
1Hospital General Universitario Gregorio Marañón, Stroke Unit - Vascular Neurology Section- Neurology Department, Madrid, Spain
Background and Aims
Transient focal neurological symptoms are a recently recognized clinical presentation of cerebral amyloid angiopathy (CAA), often called “amyloid spells” (AS). Our aim is to describe the clinical-radiological features of a series of patients with AS.
Method
We included 9 patients presenting with recurrent transient focal neurological symptoms and radiological features related to CAA.
Results
Mean age was 74 and 3 patients were women. All patients described transient, stereotyped and recurrent episodes (5 patients had >10 episodes). A gradual spread of the symptoms was present in 7 patients. Electroencephalography did not show epileptiform features in any patient. Initially, 2 patients were misdiagnosed as recurrent transient ischemic attack (TIA), 5 as seizures and 2 were diagnosed as both. 2 patients were prescribed antiplatelet therapy. A cerebral MRI with T2* gradient-recalled echo sequence showed cortical superficial siderosis (cSS) in 4 patients, cortical microbleeds (CMB) in 1 patient and both features in 4 cases. After a median follow-up of 24 months, 4 patients developed an intracranial hemorrhage (ICH), all of which had cSS in the previous cerebral MRI and 1 was on antiplatelet therapy.
Conclusion
AS represent an underdiagnosed entity often mimicking TIA, seizures or migraine aura. This misdiagnose can lead to the prescription of antiplatelet or anticoagulant therapy, which increases the risk of ICH. Our results suggest that cSS might be a radiological marker especially related to an increased risk of bleeding. A T2* gradient-recalled echo MRI should be performed in elderly patients with transient focal neurological symptoms with atypical characteristics.
Trial registration number
N/A
AS20-028
RISK OF RECURRENT INTRACEREBRAL HAEMORRHAGE AND ISCHAEMIC STROKE AFTER INTRACEREBRAL HAEMORRHAGE: MULTICENTRE PROSPECTIVE COHORT STUDY
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3University College London, Haemostasis Research Unit- Department of Haematology, London, United Kingdom
4University College London, Lysholm Department of Neuroradiology and the Neuroradiological Academic Unit, London, United Kingdom
5University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
6University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
7Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
8Institute of Neuroscience & Psychology, Neuroscience, Glasgow, United Kingdom
Background and Aims
Survivors of intracerebral haemorrhage (ICH) are at risk of both recurrent ICH and new ischaemic stroke, leading to uncertainty concerning the benefits and risks of treatment with antithrombotic drugs (antiplatelet agents and anticoagulants). ICH location (lobar vs deep) might influence the balance of risk for recurrent ICH and ischaemic stroke, but data are limited.
Method
We included data from participants with ICH in a prospective multicentre observational study and investigated the incidence of ischaemic stroke and recurrent ICH, according to index ICH location (lobar vs. deep) and other baseline clinical and imaging factors.
Results
We included 1074 patients, mean age 73 years (SD 12 years); 436 (41%) ICH were lobar, and 638 (59%) were non lobar. After a median follow up period of 213 days (IQR 187 to 410), there were 62 outcome events: 27 ischaemic strokes and 35 ICH. Lobar ICH location was independently associated with higher risk of recurrent ICH than non-lobar ICH: rate 39.5 per 1000 patient years vs. 11.7 per 1000 patient years; adjusted HR 2.95; 95% CI 1.41 to 6.17, p = 0.004, whilst there is a suggestion of a lower risk of incident ischaemic stroke in patients with lobar-ICH: rate 9.6 events per 1000 patient years vs. 20.9 per 1000 patient years; adjusted HR 0.46; 95% CI 0.18 to 1.15, p = 0.095
Conclusion
In ICH survivors, those with lobar ICH have a higher risk of future ICH. Further studies are needed to define whether treatment effects differ according to ICH location.
Trial registration number
N/A
AS20-029
FATAL ORAL ANTICOAGULANT RELATED INTRACRANIAL HEMORRHAGE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1“Attikon University Hospital”- National and Kapodistrian University of Athens, Second Department of Neurology, Athens, Greece
2University of Ioannina School of Medicine, Department of Neurology, Ioannina, Greece
3Johannes Wesling Medical Center- Ruhr University Bochum, Departments of Neurology and Neurogeriatry, Minden, Germany
4Universitätsklinikum Essen, Department of Neurology, Essen, Germany
5Massachusetts General Hospital, J. P. Kistler Stroke Research Center, Boston, USA
6University of Perugia, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
7University Hospital of Genève, Department of Neurology, Geneva, Switzerland
8University of Tennessee Health Science Center, Department of Neurology, Memphis, USA
Background and Aims
Intracranial hemorrhage (ICH) is the most feared complication in patients treated with oral anticoagulants due to non-valvular atrial fibrillation (NVAF). Non-vitamin K oral anticoagulants (NOACs) reduce the risk of ICH compared to vitamin K antagonists (VKAs). We performed a systematic review and meta-analysis to evaluate the risk of fatal NOAC-related ICH compared to VKA-related ICH.
Method
We calculated the corresponding risk ratios (RRs) in each included study to express the relative risk of fatal ICH among all patients receiving oral anticoagulation with either NOACs or VKAs. We additionally evaluated the mortality rates in NOAC-related ICH in patients treated with and without NOAC-specific reversal agents (idarucizumab or andexanet alpha). Case fatality was evaluated at 30–90 days following symptom onset.
Results
Our literature search identified 6 eligible studies (4 RCTs and 2 open-label trials of NOAC-specific reversal agents). In pairwise analyses NOACs were found to have lower risk of fatal ICH compared to VKAs (RR=0.46, 95%CI: 0.36–0.58) with no heterogeneity (I2=0%) across included RCTs. However, the case fatality rate was similar in NOAC-related and VKA-related ICH (RR=1.00, 95%CI: 0.84–1.19) with no evidence of heterogeneity (I2=0%). In the indirect analysis case fatality rate of NOAC-related ICH in patients treated with specific reversal agents was lower compared to the rest (17%, 95%CI: 11%-24% vs. 41%, 95%CI: 34–49%; p < 0.001; Figure).
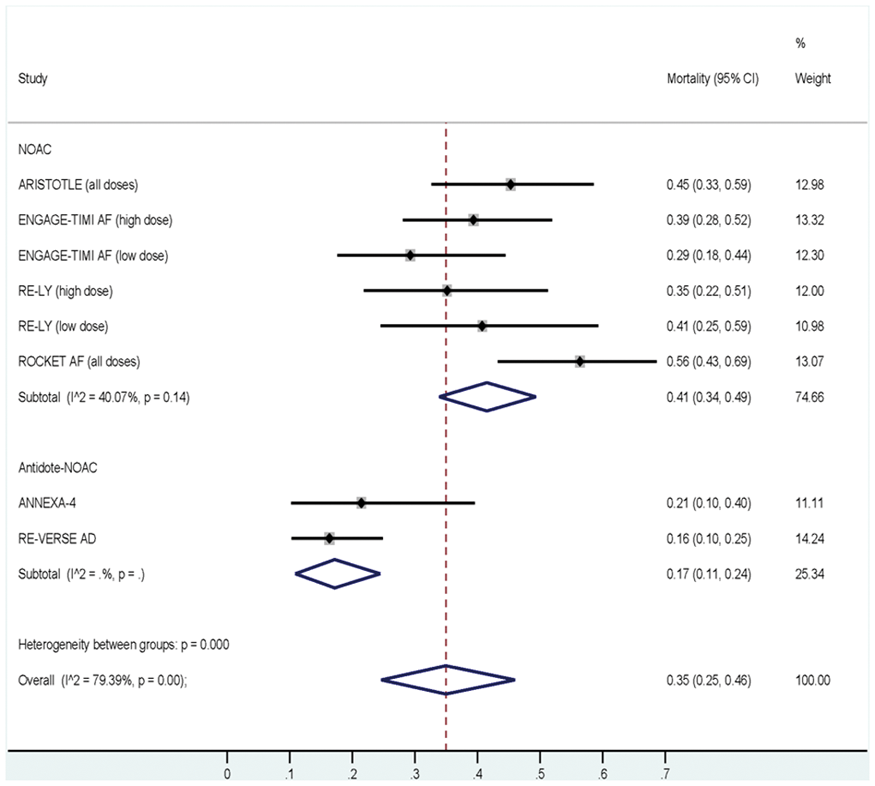
Conclusion
NOACs halve the risk of fatal ICH in NVAF patients compared to VKAs, while indirect comparisons indicate that NOAC-specific reversal agents may be associated with lower case fatality rate in NOAC-related ICH.
Trial registration number
N/A
AS20-030
VALIDATING CHA2DS2-VASC IN PATIENTS WITH INTRACEREBRAL HAEMORRHAGE AND ATRIAL FIBRILLATION
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3University College London Hospital, Haemostasis Research Unit- Department of Haematology, London, United Kingdom
4Institute of Neurology, Department of Brain Repair and Rehabilitation, London, United Kingdom
5University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
6University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
7Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
8University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
The CHA2DS2-VASc score has been validated in a number of different atrial fibrillation (AF) patient populations. However, it has not been validated in patients with intracerebral haemorrhage (ICH) and AF.
Method
We included data from a prospective multicentre study of patients with imaging confirmed ICH (CROMIS-2 ICH) and concurrent AF. CHA2DS2-VASc scores were generated for each patient. ROC curves, Hosmer-Lemeshow tests and corresponding risk estimates comparing subsequent ischaemic stroke events against the CHA2DS2-VASc risk estimates were then derived. The observed and predicted risks were then plotted against each other for a visual approximation of fit. We tested the calibration of the CHA2DS2-VASc score by fitting a logistic regression model with ischaemic stroke as the outcome and the predicted log-odds of ischaemic stroke (from CHA2DS2-VASc) as the only predictor.
Results
322 patients were included in the final analysis. There were 17 ischaemic stroke events, 7 major bleeding events (all recurrent ICH) within a median follow up period of 228 days (IQR 186 to 420). The median CHA2DS2-VASc score was 4 (IQR 3 to 5). Compared to the risk predictions adapted from Lip et al our findings showed excellent agreement (Hosmer-Lemeshow goodness of fit: p = 0.85). Calibration satisfactory (slope 1.02 and intercept 0.21, p = 0.80), with no evidence of difference. The C statistic was 0.64
Conclusion
The CHA2DS2-VASc scoring system has similar predictive value in ICH survivors with AF compared to other populations, so might be useful in estimating the risk of ischaemic stroke in this population.
Trial registration number
N/A
AS20-032
NEUROIMAGING CHARACTERISTICS AND CLINICAL OUTCOMES IN FUNCTIONALLY INDEPENDENT PATIENTS PRESENTING WITH ORAL ANTICOAGULANT RELATED NON-TRAUMATIC INTRACEREBRAL HEMORRHAGE
1Beth Israel Deaconess Medical Center- Harvard Medical School, Neurology, Boston- MA, USA
2University of Tennessee Health Science Center, Department of Neurology, Memphis, USA
3School of Medicine- University of Athens, Second Department of Neurology- “Attikon” Hospital, Athens, Greece
4University of Ioannina School of Medicine, Neurology, Ioannina, Greece
5St. Josef-Hospital- Ruhr University of Bochum, Neurology, Bochum, Germany
6Geisinger Medical Center, Neurology, Danville, USA
7Yong Loo Lin School of Medicine- National University of Singapore, Neurology, Singapore, Singapore
8Henry Ford Hospital, Neurology, Detroit, USA
9West Virginia University Charleston Division, Neurology, Charleston, USA
10University of Perugia, Stroke Unit and Division of Cardiovascular Medicine, Perugia, Italy
11Essentia Health-Duluth Clinic, Neurology, Duluth, USA
12Medstar Washington Hospital Center, Neurology, Washington DC, USA
13AHEPA University Hospital- Aristotelian University of Thessaloniki, Second Department of Neurlogy, Thessaloniki, Greece
14Metropolitan Hospital, Acute Stroke Unit, Piraeus, Greece
15University of Thessaly, Neurology, Larissa, Greece
16"Attikon" Hospital- School of Medicine- National and Kapodistrian University of Athens, Laboratory of Haematology and Blood Bank Unit, Athens, Greece
Background and Aims
We have previously reported smaller hematoma volume and lesser presenting neurologic deficits in patients with intracerebral hemorrhage (ICH) due to direct oral anticoagulants (DOACs) as compared to vitamin K antagonists (VKA). We sought to prospectively validate our findings in functionally independent patients prior to index event.
Method
We prospectively evaluated clinical, laboratory and imaging data from consecutive patients with non-traumatic, anticoagulation-related ICH admitted at 15 tertiary stroke care centers over a 12-month period.
Results
Our cohort comprised 196 ICH patients: 62 DOAC-related (mean age 75.0 ± 11.4 years, 54.8% men) and 134 VKA-related (mean age 72.3 ± 10.5 years, 73.1% men). There were no differences in vascular comorbidities, HAS-BLED, CHA2DS2-VASc scores, antiplatelet and statin use; VKA-related ICH were more likely to be lobar (60.4% vs 32.2%, p < 0.001). DOAC-related ICH patients had lower median baseline hematoma volume (13.8 [2.5–37.6] vs 19.5 [6.6–52.0] ml, p = 0.026) and were less likely to have severe neurologic deficits on admission (NIHSS>10) (37% vs 55.3%, p = 0.025). VKA-ICH had higher median 24-hr hematoma volume (20.0 [6.8–59] vs 15.9 [2.5–32.7] ml, p = 0.02) and were more likely to have significant hematoma expansion (37.4% vs 17%, p = 0.008) and midline shift (47 vs 36%, p = 0.03) at 24hrs. Pretreatment with DOACs was independently associated with smaller baseline hematoma volume and lower likelihood of severe neurological deficits in multivariable models adjusting for potential confounders.
Conclusion
We confirmed our previous findings in a prospective, multi-center cohort of functionally independent ICH patients. Patients with DOAC-related ICH have smaller baseline hematoma volume and lower odds of severe neurological deficits compared to VKA-related ICH.
Trial registration number
N/A
AS20-033
FREQUENCY OF BRAIN DEATH IN ACUTE CEREBROVASCULAR DISEASE RELATED MORTALITY
1Texas Tech University Health Sciences Center, neurology, El Paso, USA
Background and Aims
Despite the frequent occurrence of brain death in intensive care unit, the prevalence rate of brain death in ischemic stroke (IS), intracranial hemorrhage (ICH) and subarachnoid hemorrhage (SAH) is not known at national level. In addition the prevalence of cardiac arrest in these patients is not established.
Method
From 2012, ICD-9-CM includes a specific code for brain death (348.82). Brain death patients were identified from the nationwide in-patient sample database for the years 2012 to 2014. Associated in-hospital cardiac arrest patients were also identified under each category. Demographics, medical comorbidities, in-hospital complications, procedures, length of stay and hospital charges were compared.
Results
Rate of brain death was highest in SAH related mortality (22%, 1840 brain deaths/ 62285 in-hospital mortality), followed by ICH, (12.5%, 5760 brain deaths/ 45945 in-hospital mortality) and ischemic stroke (3%, 1840 brain death/62285 in-hospital mortality). Majority of the patients had brain death secondary to neurological insult (ICH n = 5260, 91.3%; SAH 2625 (80.6%) and IS n = 1640, 89.1%) without any secondary diagnosis of in-hospital cardiac arrest. Length of stay was shorter in patients with SAH and ICH (mean 2.92 ± 4.13 days and 2.53 ± 3.56 days respectively) compared to IS patients (mean 4.93 ± 10.2 days, p < 0.001) suggesting brain death is an early event in hemorrhagic stroke.
Conclusion
: Brain death in the majority of cerebrovascular patients occurs as a result of primary neurological insult without associated cardiac arrest. It occurs much earlier in hemorrhagic stroke compared to ischemic stroke.
Trial registration number
N/A
AS20-034
CLINICAL CHARACTERISTICS OF INTRACRANIAL HEMORRHAGES IN PATIENTS TREATED WITH DIRECT ORAL ANTICOAGULANTS IN SECONDARY STROKE PREVENTION
1Hospital Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Risk of hemorrhagic complications in patients anticoagulated after acardioembolic stroke is double than in primary prevention. Direct oral anticoagulants (DOACs) reduce the risk of intracranial hemorrhage (ICH) by 50% compared to warfarin. We present our clinical experience of ICH secondary to DOACs in secondary prevention.
Method
We performed an observational, retrospective study of anticoagulated patients with DOACs in secondary prevention of stroke from October 2010 to June 2015 at our centre. Clinical, radiological and ICH variables were collected.
Results
We included 425 patients (57.7% dabigatran, 24.7% rivaroxaban and 17.6%apixaban). 53.4% were women, mean age 77.1 ± 10.2 years. The mean follow-up was 20 ± 18.1 months. Median CHA2DS2-VASc was 5 (2–8) and HAS-BLED was 2 (1–4). During follow-up there were 10 (2.3%) ICH, median of 36 months (7–78) from the beginning of treatment, incidence rate: 0.015 cases/person-year. Patients were receiving treatment with Dabigatran (8), Apixaban (1) andRivaroxaban (1). There were 5 spontaneous intraparenchymal hematomas, 3 post-traumatic subarachnoid hemorrhage, an intraventricular hemorrhage and a subdural hematoma. Anticoagulation was reversed in 3 cases. There were 2 deaths related to ICH. At 3 months 70% presented mRS≤2. Anticoagulation was discontinued in 4 patients (intraparenchymal hemorrhages). Same DOAC was reinitiated in 3 patients, in one DOAC was changed, and one percutaneous leftatrial appendage closure was performed.
Conclusion
The rate of ICH in patients with DOACs in secondary stroke prevention was similar to that of the pivotal studies and patients presented low disability.
Trial registration number
n/a
AS20-035
ACUTE ISCHEMIC LESIONS 8 WEEKS AFTER ACUTE INTRACRANIAL HEMORRHAGE: PRELIMINARY RESULTS OF A COHORT STUDY
1Bispebjerg Hospital, Neurology, Copenhagen, Denmark
2Bispebjerg Hospital, Radiology, Copenhagen, Denmark
3Klinikum Frankfurt-Höchst, Neurology, Heidelberg, Germany
Background and Aims
Ischemic events may be common after intracerebral hemorrhage (ICH), especially if anti-thrombotica have been discontinued. The aim of this analysis is to determine the rate of silent infarctions at 8 weeks after ICH and its associations to stroke risk factors.
Method
Patients in an inclusion cohort with ICH underwent repeated MRI-scans after the initial diagnosis was made based on CT-scan. MRI was performed on a 3-tesla scanner. The initial MRI-scan (at 72 hours) included T1, T2-flair, diffusion weighted imaging (DWI) and susceptibility weighted imaging (SWI), post-contrast sequences and multivoxel MRI spectroscopy. The follow up scan (at 8 weeks) included T1, T2-FLAIR, DWI and SWI. An acute ischemic lesion was defined as DWI/ADC- lesions separated from the hematoma cavity. The lesions had to be present on the follow up MRI, but not on the initial scan.
Results
61 patients with ICH were included into the protocol. The median (IQR) age was 65.5 (54.5–74.8) years. Patients underwent the initial MRI with a median (IQR) delay of 2.0 (1.0–4.0) days from symptom onset. On follow-up MRI, 5 patients (10.4%) had acute ischemic lesions. Of the patients with ischemia, four were asymptomatic and one had TIA symptoms that could have been related to the lesion location but had not led the patient to contact a physician. In one patient, a non-vitamin-K oral anticoagulant (indication atrial fibrillation) was stopped on admission for ICH. None of the patients were on anti-platelet drugs.
Conclusion
Silent ischemic lesions occurring during follow up after ICH may be common and of clinical relevance.
Trial registration number
N/A
AS20-037
CORTICAL SUPERFICIAL SIDEROSIS IN PATIENTS WITH CARDIOEMBOLIC STROKE AND LONG-TERM ORAL ANTICOAGULATION: FREQUENCY, ASSOCIATED VARIABLES AND RISK OF INTRACRANIAL HEMORRHAGE DURING FOLLOW-UP
1HOSPITAL SANTA CREU I SANT PAU, Neurology, BARCELONA, Spain
2Hospital de la Santa Creu i Sant Pau- IIB Sant Pau Biomedical Research, Neurology, Barcelona, Spain
3Hospital del Mar, Radiology, Barcelona, Spain
4Hospital Germans Trias i Pujol, Unitat RM IDI, Badalona, Spain
5Hospital Arnau de Vilanova, Neurology, Lleida, Spain
6Hospital de Granollers, Neurology, Granollers, Spain
7Hospital La Fe, Neurology, Valencia, Spain
8Mutua de Terrassa, Neurology, Terrassa, Spain
9Hospital Ramón y Cajal, Neurology, Madrid, Spain
10Hospital Universitario La Paz- Instituto de Investigación IdiPaz, Neurology, Madrid, Spain
11Hospital Verge de la Cinta, Neurology, Tortosa, Spain
12Hospital del Mar, Neurology, Barcelona, Spain
13Hospital de Mataró, Neurology, Mataró, Spain
14Hospital Virgen del Rocío, Neurology, Sevilla, Spain
15Hospital La Rioja, Neurology, Logroño, Spain
16Hospital de Albacete, Neurology, Albacete, Spain
17Hospital Santiago de Compostela, Neurology, Santiago de Compostela, Spain
Background and Aims
Cortical superficial siderosis (cSS) is associated with a high risk of intracerebral hemorrhage (ICH) and treatment with oral anticoagulants (OA) may enhance this risk. We investigated the frequency, associated variables and risk of subsequent ICH in patients with cardioembolic stroke and cSS.
Method
Patients were participants of a multicenter observational study (HERO study, NCT02238470). Participants were older than 65y, had ischemic stroke (IS) attributed to cardiac embolism, and were new users of OA. A baseline magnetic resonance was performed within 1 month after the index IS. Two neuroradiologists, blinded to clinical data, evaluated the presence and extension of cSS (focal or disseminated) on T2*-GRE and/or SWI sequences. We collected vascular risk factors, CHAâ,,DSâ,,-VASc and HASBLED scores, prior treatment with antiplatelets, type of OA, presence of microbleeds and white matter lesions, and ICH during follow-up. Statistics: Bivariate analyses, logistic regression analysis, Kaplan-Meier survival curves.
Results
We studied 870 patients (age 77.6 ± 6.6 y, 48% men). cSS was detected in 27 (3.1%, 24 focal/3 disseminated) patients. Presence of cSS was associated with previous ICH (OR 14.7, 95%CI 14.5–14.89, p = 0.002) and advanced liver disease (OR 6.6, 95%CI 6.6–6.7, p = 0.017). After a mean follow-up of 23 ± 6.7 months, 18(2%) patients suffered an ICH. Only 1(3.7%) patient with cSS suffered an ICH. Presence of cSS was not associated to ICH (log rank test, p = 0.52)
Conclusion
In patients with cardioembolic stroke, cSS is an uncommon finding and is associated with previous ICH and liver disease. In our study cSS was not associated with an increased risk of ICH in patient receiving OA.
Trial registration number
N/A
AS20-039
WHICH FACTORS ARE ASSOCIATED WITH THE NATURAL RATE OF HAEMATOMA RESOLUTION AFTER ICH? A POOLED ANALYSIS OF MEDICAL PATIENTS FROM THE MISTIE AND CLEAR TRIALS
1Salford Royal NHS Foundation Trust, Manchester Academic Health Science Centre, Salford, United Kingdom
2Division of Cardiovascular Sciences- School of Medical Sciences- Faculty of Biology-, Medicine and Health- University of Manchester- Manchester Academic Health Science Centre, Manchester, United Kingdom
3Johns Hopkins Medical Institutions, Division of Brain Injury Outcomes, Baltimore- MD, USA
Background and Aims
Experimental evidence suggests that the immune system facilitates haematoma resolution after intracerebral haemorrhage (ICH) and prompt clearance may improve outcomes by limiting injury to the perihaematomal brain. We sought to determine factors associated with the rate of haematoma resolution in clinical ICH, including markers of the peripheral and central inflammatory response.
Method
Patients randomised to standard care in MISTIE II, MISTIE III and CLEAR III were included in this retrospective analysis. Perihaematomal oedema (PHO) at day 3 and haematoma volume on all CT scans from the diagnosis to day 30 were measured by threshold-based, semi-automated segmentation. Haematoma surface area at baseline was calculated by the sum of [region-of-interest perimeter x slice thickness] for each haematoma. To remove early haematoma expansion, volumes prior to day 3 were excluded. A linear regression line was then fitted to volume cube roots to determine each patient’s resolution rate. A multifactorial linear regression model was then used to determine factors associated with resolution.
Results
Of 416 patients, we excluded 61 due to missing data and 89 without haematoma volumes after day 20 post-onset, leaving 266 in the final analysis. The mean rate of clearance was 0.89 cm/day (SD: 0.58 cm/day). Surface area:volume ratio was associated with haematoma resolution rate (p = 0.014) but no other factors were significantly associated, including age, baseline white blood cell count, platelet count, baseline haematoma volume and PHO volume.
Conclusion
Our study demonstrates that only the shape of the haematoma (as described by surface area:volume ratio) significantly influences resolution rate.
Trial registration number
N/A
AS20-040
NEUROINFLAMMATORY PATHWAYS IN INTRACEREBRAL HEMORRHAGE, A SYSTEMATIC LITERATURE ANALYSIS
1Beijing Tiantan Hospital - Capital Medical University, Neurology Department, Beijing, China
Background and Aims
Neuroinflammatory responses are key factors leading to secondary brain injury after intracerebral hemorrhage (ICH). However, the role of neuroinflammation after ICH remain poorly defined. We aimed to summarize current knowledge on inflammatory cells and cytokines involved in the neuroinflammatory pathway after ICH.
Method
We systematically searched Medline and EMBASE using terms 'neuroinflammatory' or 'neuroinflammation' and 'intracerebral hemorrhage' for human or animal data. We found 123 relevant papers and extracted data on species, experimental method, inflammatory cells, cytokines and catalogued these to summarize the neuroinflammatory pathway and potential therapeutic targets after ICH .
Results
We included 64 studies, on inflammatory cells and cytokines involved in the neuroinflammatory pathway after ICH. Cerebral microglia and macrophages are mostly studied inflammatory cells in ICH models, 23 observations are related to microglia activation, immune response and microgliosis; and 10 are about recruitment and activation of macrophages. A variety of inflammatory mediators such as MMP-9, TNF-α, NF-κB, IL (1, 3, 6, 10, 13, 14, 17, 18), prostaglandin E2 are invovled in TLR4/NF-κB, JAK2-STAT3, p38MAPK/PKC, Nrf2/ARE, cAMP-Epac pathways contribute to neuroinflammatory injury after ICH and cAMP-PKA pathway for neuroprotection.
Conclusion
Neuroinflammatory pathways contributes to secondary brain damage and poor outcomes after ICH. Better understanding of ICH neuroinflammatory pathway is essential to identify potential therapeutic targets in ICH treatment.
Trial registration number
N/A
AS20-041
VALIDITY OF INTRACEREBRAL HAEMORRHAGE DIAGNOSIS IN THE DANISH STROKE REGISTRY AND THE DANISH NATIONAL PATIENT REGISTRY
1Odense University Hospital, Department of Neurology, Odense, Denmark
2University of Southern Denmark, Department of Clinical Research- Faculty of Health Sciences, Odense, Denmark
3Odense University Hospital, Department of Radiology, Odense, Denmark
4Centro Español Investigación Farmacoepidemiológica CEIFE, Centro Español Investigación Farmacoepidemiológica CEIFE, Madrid, Spain
5University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
6Odense University Hospital, Department of Neurosurgery, Odense, Denmark
7University of Southern Denmark, Clinical Pharmacology and Pharmacy- Department of Public Health, Odense, Denmark
Background and Aims
The Danish Stroke Registry (DSR) and the Danish National Patient Registry (DNPR) are frequently used as resources for stroke research. The validity of intracerebral haemorrhage (ICH) diagnoses in these registries is uncertain.
Method
We estimated the positive predictive value (PPV) of ICH diagnosis for a sample of 500 patients from the DSR (patients recorded under ICH diagnosis) and DNPR (ICD-10, code I61) during 2010–2015, using discharge summaries and brain imaging reports. We estimated PPVs for any ICH (a-ICH) and spontaneous ICH (s-ICH) alone. Further, we assessed the specificity of ICH diagnosis in DSR by evaluating a sample of 200 patients recorded in the registry under diagnoses of ischemic stroke (n = 100), or unspecified stroke (n = 100).
Results
In the DSR, the PPVs were 94% (95% CI, 91%-96%) for a-ICH and 85% (95% CI, 81%-88%) for s-ICH. The PPVs in DNPR were 88% (95% CI, 84%-91%) for a-ICH and 75% (95% CI, 70%-79%) for s-ICH. Among the 54 cases that were not verified as a-ICH the majority were due to other types of intracranial haemorrhage, e.g., subdural haematoma (48%), or ischemic stroke with or without haemorrhagic transformation (37%). In DSR, we identified no cases of s-ICH among patients recorded with ischemic or unspecified stroke diagnoses.
Conclusion
The validity of ICH diagnoses in both DSR and DNPR is sufficiently high to support their use in epidemiologic studies. The percentage of ICH cases that represented spontaneous haemorrhages was similar in the 2 registries.
Trial registration number
N/A
AS20-042
INTRACEREBRAL HAEMORRHAGE LOCATION CLASSIFIED USING DISCHARGE SUMMARIES AND BRAIN IMAGING REPORTS: FEASIBILITY STUDY
1Odense University Hospital, Department of Neurology, Odense, Denmark
2University of Southern Denmark, Department of Clinical Research- Faculty of Health Sciences, Odense, Denmark
3Odense University Hospital, Department of Radiology, Odense, Denmark
4Centro Español Investigación Farmacoepidemiológica CEIFE, Centro Español Investigación Farmacoepidemiológica CEIFE, Madrid, Spain
5University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
6Odense University Hospital, Department of Neurosurgery, Odense, Denmark
7University of Southern Denmark, Clinical Pharmacology and Pharmacy- Department of Public Health, Odense, Denmark
Background and Aims
Intracerebral haemorrhage (ICH) location has received increasing attention in recent years, as it is associated with underlying cause and prognosis. It is unclear whether ICH location can be classified accurately by using routinely-available clinical data.
Method
We identified a sample of 500 patients in the Danish Stroke Registry (recorded under ICH diagnosis) and the Danish National Patient Registry (recorded under code I61, ICD-10) during 2010–2015. We retrieved discharge summaries and brain imaging reports (referred to as minimal data) that were assessed by 4 physicians to confirm the diagnosis. Further, spontaneous ICH (s-ICH) was subdivided by location into lobar, deep, infratentorial, ‘unclassifiable’ (i.e., due to large ICH), or insufficient information. In a subsample (n = 100), we also used extensive data, i.e., we validated ICH diagnosis and location by assessing full medical records and by visual inspection of original brain imaging studies.
Results
Minimal data identified a diagnosis of any ICH type in 446 (89%) of patients, of whom 387 (87%) had suffered s-ICH. s-ICH was located as follows: 35% lobar, 37% deep, 16% infratentorial, 9% unclassifiable, and 3% insufficient information. Evaluation of extensive data in the subsample of 100 patients led to re-classification of 1 out of 81 cases originally classified as s-ICH. A single case, classified as non s-ICH based on minimal data, was reclassified as s-ICH based on extensive data. Further, visual inspection of brain imaging studies verified location in 94% cases of s-ICH.
Conclusion
Discharge summaries and brain imaging reports were feasible and valid for identifying ICH location.
Trial registration number
N/A
AS20-043
CHARACTERIZATION OF CEREBRAL MICROBLEEDS AND MICROINFARCTS IN PATIENTS WITH SPONTANEOUS INTRACEREBRAL HEMORRHAGE; A 7T MRI AND HISTOPATHOLOGY STUDY
1University Medical Center Utrecht, Department of Neurology and Neurosurgery, Utrecht, The Netherlands
2Massachusetts General Hospital and Harvard Medical School, J. Philip Kistler Stroke Research Center, Boston, USA
3University Medical Center Utrecht, Department of Radiology, Utrecht, The Netherlands
4University Medical Center Utrecht, Department of Pathology, Utrecht, The Netherlands
5VU Medical Center, Department of Pathology, Amsterdam, The Netherlands
6Massachusetts General Hospital and Harvard Medical School, Neuropathology Service- C.S. Kubik Laboratory for Neuropathology, Boston, USA
7Massachusetts General Hospital and Harvard Medical School, Alzheimer Research Unit- Department of Neurology, Boston, USA
8Radboud university medical center, Department of Neurology- Donders Institute for Brain- Cognition and Behaviour- Centre for Neuroscience, Nijmegen, The Netherlands
Background and Aims
Spontaneous intracerebral hemorrhage (ICH) is caused by hypertensive vasculopathy (deep ICH) and cerebral amyloid angiopathy (lobar ICH in elderly patients). Aim of the current study was to gain insight in the underlying small vessel disease in patients with spontaneous ICH with post-mortem 7 tesla (7T) MRI and histopathology of focal microvascular lesions.
Method
From the biobank of the UMC Utrecht and the Netherlands Brain Bank we selected 20 patients (12 women, 8 men) who died as a consequence of ICH (8 deep, 9 lobar, 3 infratentorial). From each case, we scanned three formalin-fixed coronal slabs with 7T MRI using high resolution T2 and T2*-weighted sequences. Acquired images were screened for cerebral microbleeds (CMBs) and cortical microinfarcts (CMIs). From each case we sampled at least one CMB and one CMI and processed the samples for histopathological analysis.
Results
We found 132 cortical CMIs and 204 CMBs on the MR images. In lobar ICH we found more CMIs and CMBs (115 CMIs, 155 CMBs) than in deep (17 CMIs, 46 CMBs) and infratentorial ICH (0 CMIs, 3 CMBs). Of 88 lesions selected for histopathological analysis, we could retrieve 47 lesions (53%) on corresponding sections (47% CMIs; 53% CMBs). We found 52 additional lesions upon microscopy, of which 40 could be identified on MRI in retrospect. CMIs on MRI were confirmed to be acute or old CMIs at histopathology. The pathologic substrates of CMBs included acute and older microhemorrhages and hemorrhagic CMIs.
Conclusion
CMBs and CMIs are more prevalent in lobar ICH compared to non-lobar ICH.
Trial registration number
N/A
AS20-044
INFLUENCE OF TIME TO ADMISSION ON THE OUTCOME IN PATIENTS WITH ACUTE INTRACEREBRAL HEMORRHAGE
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
2Hospital del Mar, Neurology, Barcelona, Spain
3Hospital San Bernardo, Neurology, Salta, Argentina
Background and Aims
Guidelines about spontaneous intracerebral hemorrhage (ICH) recommend a rapid diagnosis and management to reduce the likelihood of unfavourable long-term outcome. Nevertheless, the impact of the time-sensitive diagnostic and therapeutic measures on the outcome is not well known. Our aim was to determine the influence of the time to admission to a tertiary stroke center on the 3-month functional outcome.
Method
We retrospectively studied a prospective database of consecutive patients with ICH attended at two tertiary stroke centers within the first 24 hours from symptoms onset from 2013 to 2017. We excluded patients with an unknown or wake-up onset, a previous modified Rankin scale (mRS)>3 and those in whom withdrawal of life-sustaining interventions were decided <24 hours from admission. We collected the time from the ICH onset to admission, demographic, clinical, radiological data and the 3-month outcome (favourable when mRS ≤3). We performed bivariate and multivariable logistic regression analyses.
Results
From a total of 959 patients, 412 met the inclusion criteria (mean age 72 ± 13y, and 53.9% were men). Patients were admitted after a median of 120 minutes (interquartile range 60–360). Time to admission was inversely associated to favorable outcome with an OR (per 60 minutes) of 1.10 (95%CI:1.06–1.19; p = 0.002) after adjustment for age, baseline blood glucose, international normalized ratio, use of antiplatelet agents, Glasgow Coma Scale score, ICH volume, and intraventricular hemorrhage.
Conclusion
Our results suggest that in patients with an acute ICH, a shorter time to admission to a tertiary stroke center is associated with a better functional outcome.
Trial registration number
N/A
AS20-046
ACUTE INFLAMMATORY RESPONSE IS CORRELATED WITH HEMATOMA VOLUME BUT DOES NOT AFFECT ITS EXPANSION RATE
1Centro Hospitalar de São João, Neurology, Porto, Portugal
2Faculty of Medicine of Porto University, Clinical Neurosciences and Mental Health, Porto, Portugal
3Centro Hospitalar de São João, Neuroradiology, Porto, Portugal
4Hospital Beatriz Angelo, Internal Medicine, Lisboa, Portugal
Background and Aims
Hematoma volume and its expansion are major predictors of outcome in spontaneous intracerebral haemorrhage (sICH). Also, a systemic inflammatory and stress response, translated by hyperglycaemia and increased neutrophil to lymphocyte ratio (NLR) was related to sICH. We aimed to study if NLR and hyperglycaemia are related to hematoma volume or growth.
Method
From January to December 2014 we evaluated all the sICH patients admitted to our centre. Small (<30 ml) and large hematomas (>=30 ml) were measured at baseline and in at 24–72 hours follow-up CT scan. Hematoma growth was considered if enlargement was >33%. Clinical and laboratorial parameters were analysed.
Results
We included 177 patients. Large hematomas (25%) were associated with higher NIHSS scores (28 ± 13 vs 10 ± 11 pts, p < 0.001), lower Glasgow coma scale (8 ± 4 vs 13 ± 3 pts, p < 0.001), higher glucose level (175 ± 71 vs 141 ± 48, p = 0.002) and NLR (9.7 ± 11 vs 6.7 ± 5.7, p = 0.008). Hematoma growth, however, did not show relationship with NLR or hyperglycaemia.
Conclusion
The presence of high glucose level at admission, as well as increased NLR, a probable manifestation of stress response, were associated with large hematomas and to clinical neurological severity, but they did not affect hematoma expansion rate. This could be new area for therapeutic intervention.
Trial registration number
N/A
AS20-047
MORTALITY RATES FOR NOAC VERSUS VKA ASSOCIATED INTRACEREBRAL HEMORRHAGE: A SWEDISH STROKE REGISTER STUDY
1Lund University, Neurology, Malmö, Sweden
2Lund University, Neurology, Lund, Sweden
Background and Aims
Intracerebral hemorrhage (ICH) is the most devastating adverse effect of treatment with oral anticoagulants. Data on prognosis after ICH associated with novel oral anticoagulants (NOAC) compared to vitamin-K antagonists (VKA) are sparse. We compared prognosis for survival following NOAC-ICH versus VKA-ICH based on data in the Swedish Stroke Register (Riksstroke).
Method
Using data from Riksstroke and the Swedish Cause of Death Register between 2012–2016, we compared all-cause 90-day mortality for patients with NOAC-ICH vs VKA-ICH using a univariate Kaplan-Meir survival analysis. Log-rank test was used to compare mortality estimates between groups.
Results
We included a total of 2483 patients, 300 with NOAC-ICH and 2183 with VKA-ICH. In both groups, mean age was 79 years, and 58% were male. Atrial fibrillation was present in 84.7% in the NOAC group, and 82.4% in the VKA group. Level of consciousness on admission was drowsy in 26.8% and comatose in 19.1% in the NOAC-ICH group, versus 21.6% and 18.3%, respectively, in the VKA-ICH group. No significant difference between NOAC-ICH and VKA-ICH was found for all-cause 90-day mortality (44.3% NOAC-ICH vs 42.6% VKA-ICH; p = 0.53) (Figure 1). Findings are unadjusted for confounding factors.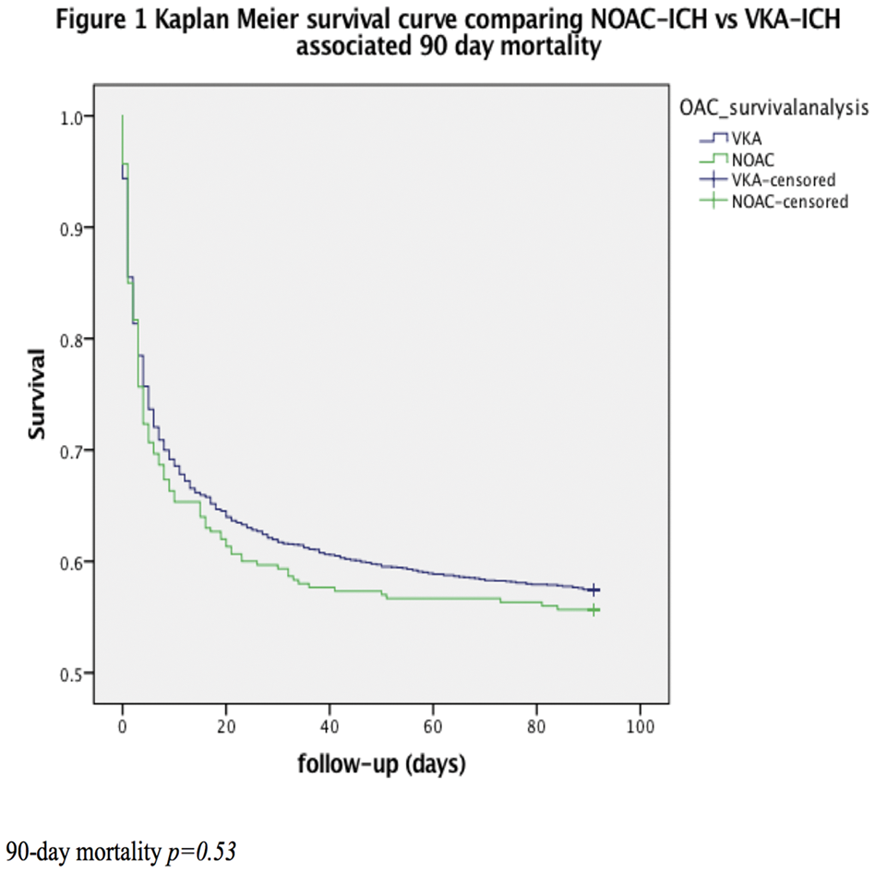
Conclusion
In the largest study to date on anticoagulant related ICH, we found no significant difference in mortality at 90 days between NOAC-ICH vs VKA-ICH. Further analyses will be presented.
Trial registration number
N/A
AS20-048
NIHSS IS A BETTER PREDICTOR OF OUTCOMES IN ICH COMPARED TO GCS AND HEMATOMA VOLUME. INFORMATION THEORY APPROACHES APPLIED TO DATABASES FROM INDIA AND US
1Kasturba Medical College- Manipal University, Neurosurgery, Manipal, India
2Yale School of Medicine- Yale University, Neurology, New Haven, USA
3Michael E. DeBakey VA Medical Center, Neurology, Houston, USA
4Manipal Institute of Technology, Electrical Engineering and Electronics, Manipal, India
Background and Aims
While baseline NIH Stroke Scale (NIHSS) is a strong predictor of outcomes in ischemic stroke, its predictive value in spontaneous intracerebral hemorrhages (ICH) has not been well studied. The Glasgow Coma Scale (GCS) or/and NIHSS along with age, hematoma volume, and location have been routinely reported in clinical trials of ICH. We applied information theory precepts to understand which baseline variable alone or combination best predicts 90-day modified Rankin Score (mRS) outcomes.
Method
Two ongoing prospective studies of ICH (KMC Manipal University, India, n = 510; Yale University, n = 243) were utilized. Analysis was restricted to subjects with all baseline (NIHSS, GCS, age, hematoma volume, laterality) and 90-day mRS variables available. 90-day mRS was modeled by proportional odds logistic regression in terms of baseline variables alone or in combinations. Akaike Information Criterion (AIC), an information theory construct was calculated for each model. The model with smallest AIC is considered the best predictor.
Results
141 subjects satisfied inclusion/exclusion criteria (median NIHSS:17, range:0–39; median GCS:13, range:3–15; mean age:61.8; median hematoma volume:14, range:0–110). Considering one variable at a time, the model with NIHSS had the smallest AIC:436.39 (GCS:438.52, hematoma Volume:477.29, Age:510.84). The model with combination of NIHSS, age, and hematoma volume had the lowest AIC (418.23) of all combinations and thus the best predictor of 12 models considered.
Conclusion
NIHSS is a better predictor of outcomes vis-à-vis GCS and the combination of NIHSS, age and hematoma volume better than GCS, age, and hematoma volume even considering laterality. We suggest that ICH trials report NIHSS in preference to GCS.
Trial registration number
N/A
AS20-049
PATIENT AND PHYSICIAN COMMUNICATION PRIORITIES IN SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1Queen's University- Kingston Health Sciences Centre, Medicine- Division of Neurology, Kingston, Canada
2Kingston Health Sciences Centre, Stroke Network of Southeastern Ontario, Kingston, Canada
3Queen's University- Kingston Health Sciences Centre, Critical Care & Medicine- Division of Neurology, Kingston, Canada
4Kingston Health Sciences Centre, Surgery- Division of Neurosurgery, Kingston, Canada
5Kingston Health Sciences Centre, Patient Experience Advisor, Kingston, Canada
Background and Aims
Spontaneous intracerebral hemorrhage (sICH) is a neurologic emergency presenting numerous communication challenges and prognostic uncertainty. Qualitative studies of communication in critical care suggest there may be unaddressed priorities for patients/patient representatives (PPR) in challenging acute care contexts such as sICH.
Method
We surveyed physicians who regularly manage sICH as well as PPRs with diagnoses compatible with sICH at our centre. 15 physicians and 4 PPRs enrolled.
Results
Physicians encountered a mean 20.08 ( ± 12.69) patients with sICH in the past year. SICH hematoma volume on CT was the leading variable used estimate risk of death, with 80.6% ( ± 4.8%) reporting it was likely/very likely to influence their estimate. 83.3% ( ± 8.3%) responded that the patient’s baseline functioning/comorbid status was likely/very likely to influence their estimate of post-sICH quality-of-life. Comparison of physician and PPR responses to our survey suggest areas of concordance and discordance between the groups in terms of recalled experiences with communication (Figure 1). Word clouds display emerging themes related to communication priorities (Figure 2).
Conclusion
Together, these results present a model for rapid uptake of patient, alongside physician input, to inform prospective studies of communication in stroke and neurocritical care.
Trial registration number
N/A
AS20-050
RECRUITMENT CHALLENGES IN MRI STUDIES OF ACUTE INTRACEREBRAL HAEMORRHAGE: EXPERIENCE FROM THE TICH-2 MRI SUBSTUDY
1University of Nottingham, Stroke Trials Unit, Nottingham, United Kingdom
2University of Nottingham, Radiological Sciences, Nottingham, United Kingdom
3University of Nottingham, Sir Peter Mansfield Imaging Centre, Nottingham, United Kingdom
Background and Aims
Magnetic Resonance Imaging (MRI) is widely used in clinical practice and in trials for ischaemic stroke; however, relatively few large multicentre trials for intracerebral haemorrhage have used MRI. We describe the main recruitment challenges faced in the TICH-2 MRI substudy, which is nested within TICH-2, a multi-centre randomised placebo-controlled trial of tranexamic acid in intracerebral haemorrhage (ISRCTN93732214).
Method
TICH-2 participants at recruiting centres were eligible for the substudy. Centres were asked to record, if applicable, the reason for non-recruitment. The recruitment window was day 2 to day 14 post-randomisation.
Results
Figure 1 shows the distribution of reasons for non-recruitment (N=169). Clinical instability was the main reason for non-recruitment, accounting for 34.3% of the cases. The mean NIHSS scores (as per TICH-2 protocol) for unrecruited patients classified as clinically unstable were 19 (range 5–32, N=57), 21 (range 0–40, N=51) and 20 (range 1–38, N=37) for baseline, day 2 and day 7 post-randomisation, respectively. In contrast, for recruited patients (N=142) the mean scores were 10 (range 0–28, N=141), 8 (range 0–26, N=139) and 8 (range 0–31, N=132). Other important factors for non-recruitment include difficulty obtaining consent, patient refusal, claustrophobia and transfer to other hospitals.
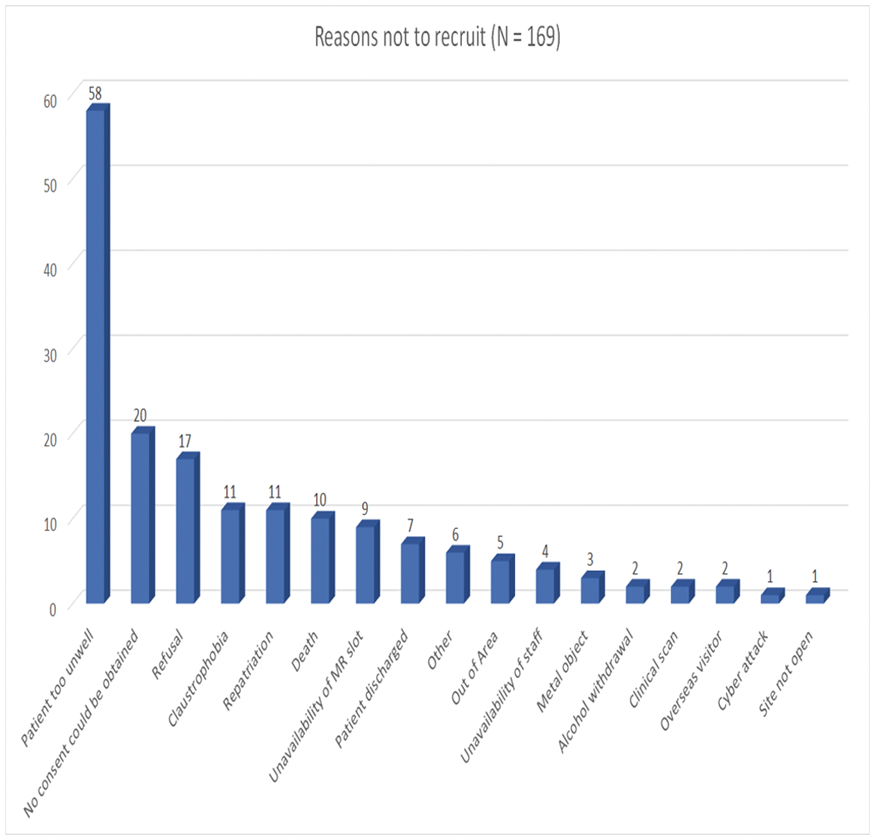
Conclusion
Clinical instability in intracerebral haemorrhage poses a challenge for recruitment into MRI studies. This, and other factors, should be taken into consideration when designing clinical trials of intracerebral haemorrhage involving MRI.
Trial registration number
N/A
AS20-053
DOES SPONTANEOUS INTRACEREBRAL HAEMORRHAGE WARRANT DECOMPRESSIVE HEMICRANIECTOMY?
1Kasturba Medical College, Neurosurgery, Manipal, India
Background and Aims
Role of Decmpressive Hemicraniectomy (DC) with clot evacuation in Spontaneous Intracerebral Hemorrhage (SICH) is controversial. We conducted a retrospective analysis to assess the outcomes of DC vs mini craniotomy (MC) with hematoma evacuation in patients with SICH.
Method
A review of Hospital SICH registry was performed to search for patients who underwent surgical evacuation of hematoma at Kasturba Medical College, India from January 2015 to December 2017. We compared MC with DC, with regard to GCS, shift from midline, time from ictus to surgery, post-surgical hematoma volume, hospitalization period and mRS at 90 days.
Results
A total of 94 patients underwent surgical evacuation of hematoma in the study period. Sixty-One patients underwent MC while 33 patients underwent DC. Preoperative hematoma volume, midline shift, time from the ictus to surgery and hospital stay were similar between both groups. The incidence of residual hematoma in immediate post-operative scan was higher in patients who underwent MC (P = 0.02) and resolution of midline shift was higher in patients offered DC (P = 0.05) There was no statistical significance difference in the outcome mRS at 90 days (P = 0.426) and GCS on discharge (P = 0.317) among the two groups. Mortality was also similar in the two cohorts (P = 0.903). Nine patients underwent a second surgery to replace the bone flap.
Conclusion
Decompressive Hemicraniectomy had better rates of clot evacuation and resolution of midline shift which however failed to translate to better outcomes and survival. Its adds to the social and economic burden of SICH by warranting a second surgery for replacing the bone flap.
Trial registration number
N/A
AS20-054
MODERATE SIZED HYPERTENSIVE INTRACEREBRAL HEMATOMAS – WHY DO THEY DIE?
1Kasturba Medical College, Neurosurgery, Manipal, India
Background and Aims
Spontaneous Intracranial Hemorrhage (SICH) with Volume >30ml is associated with poor outcome. The reasons are multifactorial, with mass effect, midline shift and herniation being the major factors in large clots. However, the reasons for poor outcome in moderate sized SICH are not well studied.
Method
Patients with supratentorial hematoma volume 20–29ml calculated on Plain CT from our SICH register at Kasturba Medical College Hospital, INDIA, were included in this study. Basic clinical characteristics, GCS, radiological characteristics, and 90-day outcomes of these patients were recorded using the mRS Scale.
Results
A total of 88 patients fulfilled the above criteria and were included in this study. Mean age of the patient was 57.19 years with 66 males and 22 females. Mean hematoma volume was 22.62ml and GCS on presentation was 11. Twenty-six patients succumbed to the illness at the end of 90 days. Hematoma growth (P = 0.007), Black Hole sign (P = 0.002), Left sided Hematomas’ (P = 0.013), poor GCS on admission (P = 0.020), and External Ventricular Drainage (P = 0.037) were significant factors predicting mortality. Age, intraventricular extension (IVE) of hematoma, hydrocephalus, blood glucose on presentation were not predictors of mortality in smaller hematomas.
Conclusion
Hematoma expansion, black hole sign and GCS on presentation are the most important predictors of mortality in moderate sized hematomas. Left sided hematoma’s also have greater mortality compared to their right sided counterparts. Size of hematoma, age, IVE and location are not significant predictors like in larger sized bleeds.
Trial registration number
N/A
AS20-055
ASSOCIATION BETWEEN NEW ARTERIAL THROMBOTIC EVENTS AND MORTALITY AMONG SURVIVORS OF INTRACEREBRAL HEMORRHAGE
1Weill Cornell Medicine, Clinical and Translational Neuroscience Unit- Department of Neurology, New York, USA
Background and Aims
To determine the association between arterial thrombotic events including acute ischemic stroke and myocardial infarction (MI) and mortality in survivors of intracerebral hemorrhage (ICH).
Method
We performed a retrospective cohort study using emergency department visits and hospitalizations in New York, California, and Florida from 2005–2013. Patients with ICH were identified using previously validated ICD-9-CM diagnosis codes. Patients with ischemic stroke or MI prior to or within the index hospitalization for ICH were excluded. Our exposure variable was an arterial thrombotic event, defined as the composite of ischemic stroke and MI. The primary outcome was mortality. Cox proportional hazards analysis was used to determine the association between a thrombotic event and mortality, while adjusting for demographics, stroke risk factors, and Elixhauser comorbidities. ICH was modeled as a time-varying covariate to minimize immortal-time bias.
Results
We identified 122,605 patients with ICH, of whom 6,821 (5.6%) had a subsequent arterial thrombotic event. Patients with an thrombotic event were older (mean age, 70.0 versus 68.6 years), and had more medical comorbidities. The 5-year cumulative mortality rates for patients with and without arterial thrombotic events were 26.2% and 12.9%, respectively. After adjustment for demographics, Elixhauser comorbidities, and vascular risk factors including atrial fibrillation and valvular heart disease, patients with an arterial thrombotic event had an increased risk of mortality compared to those without (hazard ratio, 2.4; 95% CI, 2.2–2.5).
Conclusion
Arterial thrombotic events are associated with a heightened risk of mortality in patients with prior ICH.
Trial registration number
N/A
AS20-056
DOES BASELINE BLOOD PRESSURE PREDICT THE TYPE OF STROKE:OUR EXPERIENCE IN QATAR
1Hamad General Hospital, Neurology, Doha, Qatar
Background and Aims
Hypertension on initial presentation in stroke patients has been associated with high significant risk of primary intracranial haemorrhage (ICH).
Our study is to evaluate wither baseline SBP and DBP can predict type of stoke in an acute setting. We hypothesize the high SBP and DBP does predict ICH.
Method
Our stroke database prospectively collects information on all suspected stroke at Hamad General Hospital.
We included all patients with ischemic stroke, ICH, TIA, CVST and mimics in our analysis.
Results
4133 patients from May 2014 to May 2017 were included in our analysis. Median age 55 years (IQR45–64), Sex:M 3263 (79%)/F 870(21%) and NIHSS 3 (IQR 1–7).
There are 2386 (57.7%),606(14.7%), 458 (11.1%), 34(0.8%) and 648 (15.7%) patients with ischemic stroke, ICH, TIA, CVST and mimics respectively.
Mean baseline SBP in the presence of ischemic stroke were 156mmHG ± 30, TIA 149mmHG ± 25, ICH 178mmHG ± 36, CVST 125mmHG ± 19 and stroke mimics 142mmHG ± 25 (P< 0.001) respectively. Mean DBP in the presence of ischemic stroke were 89 mmHG ± 19, TIA 86mmHG ± 15, ICH 102mmHG ± 24, CVST 77mmHg ± 14 and stroke mimics 81mmHG ± 16 (P < 0.001) respectively.
In the logistic regression analysis with adjustment to common risk factors, acute stroke patient with baseline SBP>200 is 6 times likelihood of having ICH than other type of stroke (adj OR:6.2,95 % CI,4.6–8.4, P = 0.001) and patient with SBP 150 to 200 range is 3 times likelihood of having ICH(adj OR:2.7, 95 %CI,2.1–3.4, P = 0.001).
Conclusion
Baseline SBP and DBP can predict the likelihood of stroke ‘typé. SBP>200 is highly correlated with presence of ICH.
Trial registration number
N/A
AS20-057
FEASIBILITY OF EARLY INTENSIVE BLOOD PRESSURE LOWERING IN PATIENTS WITH INTRACEREBRAL HEMORRHAGE (ICH) - THE USE OF A SIMPLE SYSTEMATIC TREATMENT ALGORITHM
1Aarhus University Hospital, Department of Neurology, Aarhus C, Denmark
2Aarhus University Hospital, Department of Clinical Genetics, Aarhus, Denmark
3Aalborg University, Department of Clinical Medicine, Aalborg, Denmark
4Aalborg University Hospital, Department of Clinical Medicine, Aalborg, Denmark
Background and Aims
In the acute phase of ICH more than 75% have elevated blood pressure (BP). In a recent randomized clinical ICH trial (INTERACT2) intensive BP lowering (systolic level <140 mmHg) within 6 hours from symptom onset, was associated with decreased hematoma expansion and borderline reduction of disability or death after 3 months.
We aim to investigate whether a rapid BP reduction can be obtained in everyday clinical practice using a simple treatment algorithm.
Method
This is a prospective single-center cohort study of spontaneous ICH patients admitted to the Stroke Unit, Aarhus University Hospital, Denmark. Patients with a systolic BP >140 mmHg were treated according to the algorithm. The pharmacological agents used were glyceryl trinitrate patch, intravenous labetalol and oral nimodipine.
Results
157 patients were included during one year. Results were stratified by duration of symptoms until imaging <6 hours (n = 101) and >6 hours (n = 56). In the two groups 87% and 82% were treated with the algorithm, respectively. Systolic BPs are summarized in figure 1. Within 1 hour, from admission, 28% of patients with a symptom duration <6 hours reached target systolic BP and 76% within 6 hours. For the patients with a symptom duration >6 hours 40% and 68% reached target BP after 1 and 6 hours, respectively.
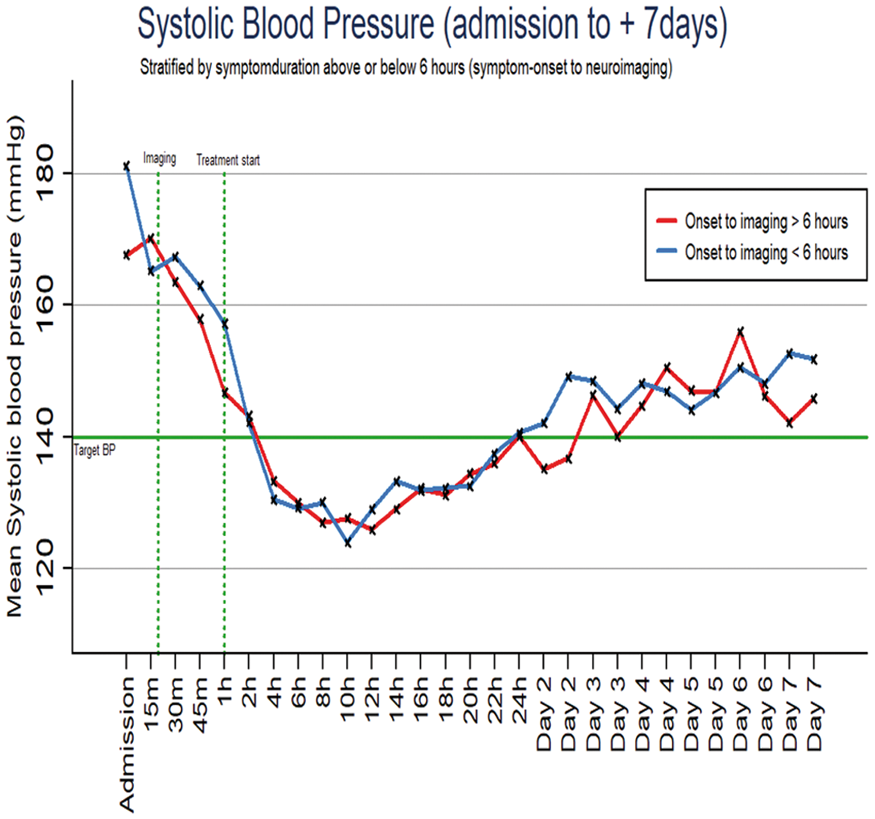
Conclusion
Rapid BP reduction can be obtained in everyday clinical practice using a simple algorithm.
Trial registration number
N/A
AS20-059
CT BRAIN IMAGE CLUSTERING FOR DIFFERENTIATION OF INTRACEREBRAL HAEMORRHAGE; A NOVEL ALGORITHM
1Universiti Kebangsaan Malaysia, Faculty of Engineering & Built Environment, Bangi, Malaysia
2Universiti Kebangsaan Malaysia, Neurology and Radiology- Faculty of Medicine, Cheras, Malaysia
3Ballarat Health Services, Ballarat Base Hospital, Ballarat, Australia
4University of Melbourne, Faculty of Medicine- Dentistry and Health Sciences, Melbourne, Australia
Background and Aims
Hypertensive haemorrhage (HH) and cerebral amyloid angiopathy haemorrhage (CAAH) are difficult to differentiate on clinical grounds, although there are distinguishing imaging features. The gold-standard, MRI, can differentiate between more obvious cases but CT remains the preferred modality due to accessibility and cost, especially in developing economies.
Method
In this study, CT brain images (n = 40) of primary ICH were acquired from the UKM Medical Centre, Imaging Centre Patient Database. The DICOM images were anonymized to remove the metadata and resized into 256 x 256 pixels to standardize image resolution. Skull removal and normalization were required in further processing of the images to improve identification of the ICH bleed location through the k-means clustering algorithm.
Results
K- means clustering identified 7 clusters, namely; grey matter (2 clusters), white matter, cerebrospinal fluid (2 clusters) and hematoma (2 clusters), as visualized in Figure 1. The significance of the extracted clusters will be analysed using texture feature extraction. Further, the Support Vector Machine (SVM) classifier algorithm will be used to classify the different type of ICH bleed using the significant features.
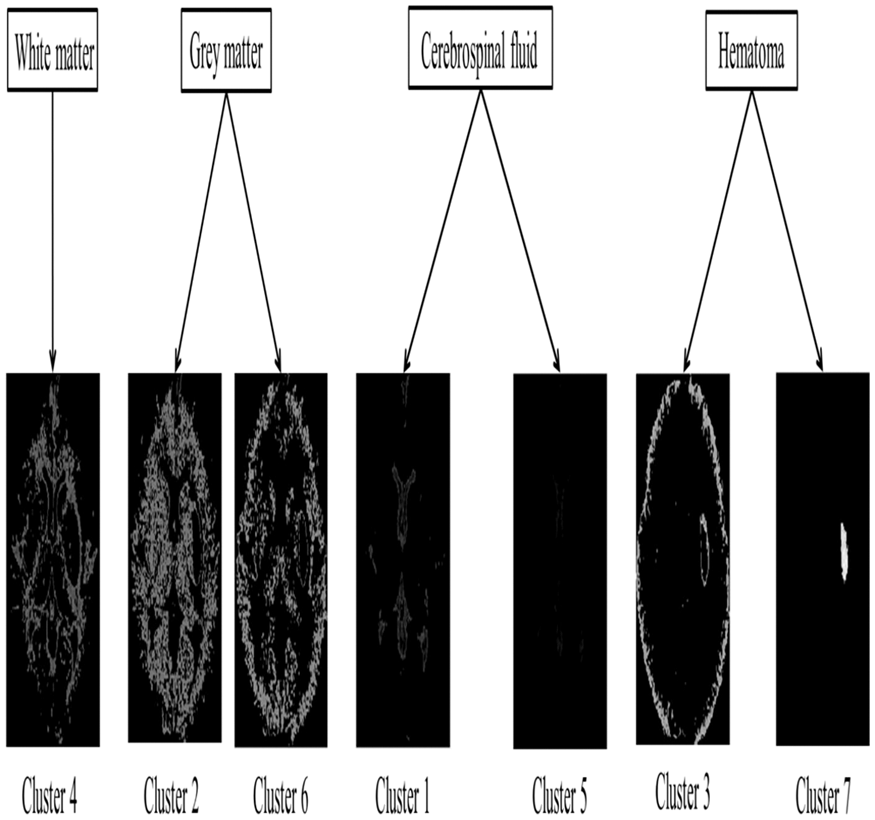
Conclusion
The proposed segmentation technique is expected to help differentiate between HH and CAAH on CT.
Trial registration number
N/A
AS20-060
PATIENTS WITH INTRACEREBRAL HEMORRHAGE AND NEED FOR RED BLOOD CELL TRANSFUSION MAY BENEFIT FROM A RESTRICTIVE TRANSFUSION PRACTICE
1University Hospital Erlangen, Neurology, Erlangen, Germany
2University Hospital Erlangen, Transfusion Medicine and Haemostaseology, Erlangen, Germany
3University Hospital Erlangen, Neuroradiology, Erlangen, Germany
Background and Aims
Data regarding the influence of anemia and its treatment – using red blood cell transfusions (RBCT) – on functional outcome in intracerebral hemorrhage (ICH) do barley exist. Large randomized trials investigating RBCT excluded neurocritical-care patients, therefore evidence on transfusion thresholds remain highly debated. The aim of the present study was to delineate the impact of RBCT on functional outcome and to identify an optimal transfusion threshold.
Method
Prospective institutional cohort study investigating as primary outcome the dichotomized functional status (modified Rankin-Scale (mRS)=0–3 versus 4–6) at 3 and 12 months according to treatment exposure (RBCT versus non-RBCT) in consecutive (n = 610) ICH patients. Sub-analyses comprised patients that received RBCT to analyze transfusion thresholds. Confounding was addressed by propensity-score (ps)-matching and adjusted regression analyses.
Results
We identified 610 eligible ICH patients, of which 82(13.4%) received RBCT with a median of 2(2–4) units transfused at 9(4–13) days after admission. Confounders associated with RBCT consisted of younger age (p < 0.01), poorer neurological status (p < 0.01), larger ICH-volume (p < 0.01), and increased intraventricular hemorrhage (p < 0.01). After balancing for confounding by ps-matching, patients that received RBCT showed a significantly decreased rate of favorable functional outcome at 3(RBCT:6/80(7.5%)-versus-non-RBCT:39/144(27.1%);p < 0.01) and 12-months (RBCT:14/80(17.5%)-versus-non-RBCT:48/144(33.3%);p = 0.01). Sub-analyses showed that a restrictive transfusion regime (at hemoglobin levels <4.65mmol/l) was independently associated with favorable functional outcome (risk-ratio:3.01(1.03–8.77);p = 0.04).
Conclusion
RBCT in patients with spontaneous ICH was associated with poorer functional outcome even after rigorous correction for confounders. RBCT delivered at restrictive transfusion thresholds were independently associated with improved outcome at one year. The findings presented here strongly warrant randomized controlled investigations.
Trial registration number
n/A
AS20-061
IS HIGH ADMISSION BLOOD GLUCOSE A PREDICTOR OF OUTCOME IN SPONTANEOUS INTRACEREBRAL HAEMORRHAGE?
1Kasturba Medical College, Neurosurgery, Manipal, India
Background and Aims
High Blood glucose levels on admission have been associated with poor outcome in patients with Spontaneous Intracerebral Hemorrhage (SICH). However high blood glucose values are often associated with other poor prognosticators like large hematoma volume (vol>30ml), Intraventricular Extension (IVE) of hematoma and poor GCS (GCS<8).
Method
A Retrospective study from our hospital based SICH register at Kasturba Medical College, India between February 2015 to June 2017, to validate the prognostic value of elevated blood glucose on admission. Outcome mRS and mortality were recorded at 90 days.
Results
A total of 510 patients were included in our study. Mean blood glucose values were 158.34mg/dl (42mg/dl-407mg/dl). High Blood Glucose values on admission was a predictor of mortality in our entire cohort (P = <.001, 95%CI = 1.004–1.011). We dichotomised our cohort into two groups, based on blood glucose levels of 160mg/dl defined by the mid point of ROC Curve (0.718, 0.544). Mean blood glucose levels in these two groups were 124.45mg/dl and 220.61mg/dl and mortality at 3 months were 74 and 84 patients respectively. When we excluded patients with hematoma volumes >30ml, IVE and GCS<8; blood glucose values on admission failed to show any statistical significance (P = 0.06, 95% CI = 0.999–1.029) with respect to mRS at discharge (P = 0.111), mRS at 3 months (P = 0.212) and mortality at 90days (P = 0.163).
Conclusion
High blood glucose value is not an independent predictor of mortality in SICH. It is a result of catastrophic ICH, explained by the stress theory and cannot be used as a reliable independent predictor of outcome in SICH.
Trial registration number
N/A
AS20-062
RISKS FOR INTRACRANIAL HEMORRHAGE IN PATIENTS WITH GLIOBLASTOMA OR BRAIN METASTASES AND ATRIAL FIBRILLATION WITH AND WITHOUT ANTICOAGULATION
1University of Heidelberg, Neurology, Heidelberg, Germany
2University of Heidelberg, Medical Biometry, Heidelberg, Germany
Background and Aims
Patients with glioblastoma (GBM) or brain metastases (BM) and atrial fibrillation (AF) might be under increased risk of intracranial hemorrhage (ICH) during anticoagulation (AC). Our aim was to assess this risk.
Method
Our institution’s database (from 2006 to 2016) was screened for patients with GBM or BM and AF with an indication for prophylactic anticoagulation according to their CHA2DS2-VASc-Score (>/=2). AC was either performed with heparins, phenprocoumon or novel oral anticoagulants. Applying the propensity score method, patient cohorts (matched according to primary tumor, age, sex, therapy) were generated (GBM [or BM] with AF +/− AC, GBM [or BM] without AF/AC, no GBM [or BM] but AF on AC). ICH was defined as any new blood on imaging. A logistic mixed effects model was calculated to compare the risk for ICH between the three groups.
Results
In total 174 patients were identified of which 48 with GBM (31% on AC) and 38 with BM (45% on AC) were matched. In both GBM groups 12% of patients suffered from ICH, whereas 6% of patients with AF only suffered ICH (follow-up median 8 months). 16% of patients with BM and AF had ICHs, whereas 5% of patients with BM only and 8% with AF only had ICHs (follow-up median 5,5 months). The logistic mixed effects model revealed no significant difference between the groups.
Conclusion
ICHs occurred most in patients with BM and AF although the cohorts might be too small to detect significance in logistic regression. There was no difference in GBM patients.
Trial registration number
N/A
AS20-063
DECOMPRESSIVE HEMICRANIECTOMY IN SUBCORTICAL SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1Ochsner Clinical Foundation/Louisiana State University Health Science Center, Neurocritical Care/Neurosciences, new orleans, USA
2University of Queensland, School of Medicine, New Orleans, USA
3Ochsner Clinic Foundation, Neurocritical Care, New Orleans, USA
4Ochsner Clinic Foundation, Neurosurgery, New Orleans, USA
Background and Aims
Decompressive hemicraniectomy (DHC) is beneficial in patients with acute ischemic stroke. However, the knowledge and benefit in hemorrhagic strokes continues to evolve. Previous studies have included cortical and subcortical intracerebral hemorrhage (SCICH) in their analysis. We report outcomes of a matched series of DHC in subcortical ICH.
Method
We reviewed out Get-with-the-stroke guideline database and identified all patients with SCICH. Cases with SCICH with hemicraniectomy were matched conservatively managed patients by Age (+/− 10 years), gender, and ICH hematoma volume category 0–30, 30–60, >60 ml. Outcome was measured at hospital length of stay (LOS), disposition at inpatient discharge, 90-day Glasgow outcome score (GOS).
Results
Seven SCICH cases with DC were matched with 22 patients managed conservatively without DHC. There was no difference in clinical characteristics between groups. Discharge disposition did not differ between groups. Despite a higher GOS ≥3 at 90 days amongst DC cases, there was no significant different between groups (71.3% vs 54.5% p = 0.665). However, hospital LOS was significantly different (26.5 vs 12.5 days p = 0.006).
Conclusion
DC for subcortical intracerebral hemorrhage was associated with a prolonged hospital stay. Despite a higher survival rate, the difference was not significant between groups. DC may not be effective alone in improving outcomes. Further studies in the benefit of DC in SCICH are needed.
Trial registration number
N/A
AS20-065
PATIENTS WITH NON-HYPERTENSIVE SPONTANEOUS INTRACEREBRAL HEMORRHAGE ARE MORE LIKELY TO EXPERIENCE HEMATOMA GROWTH COMPARED TO PATIENTS WITH HYPERTENSIVE SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1University Hospital/TU-Dresden, Neurology, Dresden, Germany
2University Hospital/TU-Dresden, Neuroradiology, Dresden, Germany
Background and Aims
Arterial hypertension is a major cause of spontaneous intracerebral hemorrhage (ICH). We sought to determine the rates of hematoma growth in patients with hypertensive ICH compared to non-hypertensive ICH etiology.
Method
We performed a retrospective, single-center, observational cohort study. We included all consecutive patients with spontaneous ICH who were admitted to our tertiary stroke center between 2010 and 2013. Data acquisition was performed via electronic chart review including demographic characteristics, baseline NIHSS scores and neuroradiological findings. We extracted all patients with baseline and follow-up CT images available for review and semiautomatically assessed hematoma volumes. We defined hematoma growth according to PREDICT criteria (i.e., absolute growth >6cc or relative growth >33%) and compared rates of hematoma enlargement in patients with hypertensive ICH and non-hypertensive ICH etiology.
Results
Of 392 patients, complete imaging data were available in 122 patients (55% male, median age 73 years [IQR 15], baseline NIHSS score 11 [IQR 14]). Of these, 100 patients (82%) had a hypertensive ICH. Median time between baseline and follow-up CT was 21 hours (IQR 14). Overall, hematoma growth was present in 16 patients (12.2%). Patients with hypertensive ICH were less likely to have hematoma growth compared to patients with non-hypertensive ICH etiology (5/100 patients (5%) compared with 11/22 patients (50%), respectively; Fisheŕs exact test, p = 0.0001).
Conclusion
Our data suggest that patients with non-hypertensive ICH may be more likely to suffer hematoma enlargement compared with patients who have a hypertensive ICH.
Trial registration number
N/A
AS20-066
DOES SURGERY REDUCE MORTALITY IN PATIENTS WITH A CEREBELLAR ICH? OBSERVATIONS FROM AN INTERNATIONAL, MULTICENTRE, POOLED DATA SET
1University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
2Salford Royal NHS Foundation Trust, Greater Manchester Neurosciences Centre, Manchester, United Kingdom
3Royal Melbourne Hospital, Department of Medicine and Neurology, Melbourne, Australia
4Department of Neurology, Christchurch Hospital, Christchurch, New Zealand
5Department of Radiology, Christchurch Hospital, Christchurch, New Zealand
6Helsinki University Hospital and Clinical Neurosciences, Department of Neurosurgery, Helsinki, Finland
7Helsinki University Hospital and Clinical Neurosciences, Department of Neurology, Helsinki, Finland
8Prince of Wales Hospital, Department of Imaging and Interventional Radiology, Hong Kong, Hong Kong S.A.R
9Prince of Wales Hospital, Department of Medicine and Therapeutics, Hong Kong, Hong Kong S.A.R
Background and Aims
Haematoma evacuation and/or external ventricular drainage (EVD) are often performed for cerebellar intracerebral haemorrhage (ICH), but there is no clear consensus between neurosurgeons regarding when to operate, which operation to perform and whom to operate on. We pooled registry data from five international centres to determine the association between surgery and risk of death and whether this differs by type and timing of surgery.
Method
Data describing baseline, clinical, and radiological characteristics, surgical management and 30-day mortality for spontaneous cerebellar ICH were pooled. Using multiple logistic regression, we determined factors associated with the decision to operate and then tested for associations between 30-day mortality and surgery, adjusting for key prognostic factors. Finally, we tested if type of surgery (EVD alone vs. haematoma evacuation +/− EVD) and timing of haematoma evacuation (≤24h vs. >24h post-onset) were associated with 30-day mortality.
Results
30-day mortality was 34.3% (n = 113/329 patients), 47 (14.3%) had haematoma evacuation +/− EVD, and 22 (6.7%) had an EVD alone. Younger age (OR:0.96, 95%CI:0.94–0.98;p < 0.001) and larger ICH volume (OR:11.74, 95%CI:4.37–31.49;p < 0.001) were associated with surgery. Surgery was independently associated with lower 30-day mortality (OR:0.35, 95%CI:0.16–0.79; p = 0.012). There was no association between 30-day mortality and type of surgery (OR:0.70, 95%CI:0.22–2.25; p = 0.699) but we found a reduced odds of death with early surgery (OR:0.28, 95%CI:0.078–0.97; p = 0.045)
Conclusion
Surgical treatment of cerebellar ICH is independently associated with reduced 30-day mortality. Surgery within 24h of onset (vs. >24h) is associated with reduced mortality but we found no effect for type of surgery
Trial registration number
N/A
AS20-067
TEMPORAL EVOLUTION OF INTRACRANIAL HEMORRHAGE ASSOCIATED WITH VITAMIN K ANTAGONISTS IN SPAIN: FROM TAC RESGISTRY 1 TO TAC REGISTRY 2
1Hospital Universitario La Princesa, Neurology, Madrid, Spain
2Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
3Hospital Universitario Central de Asturias, Neurology, Oviedo, Spain
4Hospital Clínico Universitario San Carlos, Neurology, Madrid, Spain
5Hospital de Basurto, Neurology, Bilbao, Spain
6Hospital Universitario de Bellvitge, Neurology, Bellvitge, Spain
7Complejo Hospitalario Universitario de Navarra, Neurology, Pamplona, Spain
8Complejo Hospitalario Universitario A Coruña, Neurology, A Coruña, Spain
9Hospital Universitario Gregorio Marañón, Neurology, Madrid, Spain
10Hospital Universitario Salamanca, Neurology, Salamanca, Spain
11Complejo Hospitalario Universitario Vigo, Neurology, Vigo, Spain
Background and Aims
To assess possible changes in epidemiology, characteristics and outcome of intracranial hemorrhage associated with vitamin K antagonists (ICH-VKA).
Method
We evaluate patients with ICH-VKA included in TAC-Registry1(TR1) and TAC-Registry2(TR2) studies. Country-wide, retrospective, observational multicentric studies that included all adult patients with ICH associated with anticoagulation admitted to Neurology Departments. TR1: September 2012-August 2013, TR 2: year 2015.
Results
TR1: 21 hospitals, population area: 8,155,628 inhabitants, N = 235, annual incidence ICH-VKA: 2.88/100,000. TR2: 29 hospitals, population area: 11,864,971 inhabitants, N = 331, annual incidence ICH-VKA: 2.79/100,000. Both groups had similar baseline characteristics. ICH-VKA represented in TR1 1.14% of Neurology admitted patients, 1.94% of all strokes and 13.62% of ICH; in TR2 1.22%, 2.04% and 16.42% respectively. Average INR at admission: 2.84 (SD: 1.4) in TR1 and 2.75(DS 1.1) in TR2 (p = NS). Only 37.6% in TR1 and 39.8% in TR2 presented INR in range at admission. Most frequent location: deep regions: 37.4% TR1, 46.2% TR2(p <0.05). In TR1 there were more hemispheric hemorrhages (17% vs 5.4% p 0.001), in TR2 more intraventricular hemorrhages (17.4% vs24.5%, p <0.05). The average mRS3m was similar (p = NS): TR1 4.12 (SD: 2.07), TR2 4.04 (DS 2.12), 24% were independent at 3 months in both groups and 3 months mortality represented 42.6% and 38.7 % respectively (p = NS).
Conclusion
ICH-VKA incidence remains stable in recent years. Nevertheless, its relative frequency among ICHs has increased. Its poor outcome and association with variable INR ranges remains constant, representing a problem still unsolved.
Trial registration number
N/A
AS20-068
PREVIOUS TREATMENT WITH NOAC IS ASSOCIATED WITH SLOWER ULTRA-EARLY INTRACRANIAL HEMATOMA GROWTH COMPARED WITH VITAMIN K ANTAGONISTS
1Centro Hospitalar e Universitário de Coimbra, Neurology, Coimbra, Portugal
2Centro Hospitalar de São João, Neurology, Porto, Portugal
3Faculdade de Medicina da Universidade do Porto, Department of Clinical Neurosciences and Mental Health, Porto, Portugal
4Hospital de Braga, Neurology, Braga, Portugal
5Hospital Egas Moniz- Centro Hospitalar de Lisboa Ocidental, Neurology, Lisboa, Portugal
6Nova Medical School- Universidade Nova de Lisboa, Cedoc, Lisboa, Portugal
7Hospital São Francisco Xavier- Centro Hospitalar Lisboa Ocidental, Medicine, Lisboa, Portugal
8Universidade de Coimbra, Faculdade de Medicina, Coimbra, Portugal
Background
Ultra-early hematoma growth (UHG) estimates the initial hematoma expansion rate in acute non-traumatic intracranial hemorrhage (ICH), representing a marker of its hemostatic properties. Patients with ICH and oral anticoagulation are at particular risk of hematoma expansion, however the impact of different anticoagulants has not yet been fully ascertained.
Aims
To compare UHG in patients on NOAC and vitamin K antagonists (VKA).
Method
Multicentre and retrospective cohort study, which included consecutive patients with acute non-traumatic ICH on oral anticoagulation admitted during 30-months period, with baseline ICH volume and time from symptom-onset to first CT-scan available for analysis. Medical records were analysed for clinical and demographic data. UHG was defined as the relation between baseline ICH volume (mL)/time of symptom-onset to first CT-scan (hours), with volume obtained by planimetry. Univariate analysis was performed and propensity score matching (PSM) analysis was used to evaluate UHG differences in VKA- and NOAC-treated patients.
Results
Among 131 patients included, 18 (13.7%) were anticoagulated with a NOAC and 113 (86.3%) with a VKA. On univariate analysis, NOAC-treated patients were older (p = 0.003), presented higher CHA2DS2VASc score (p = 0.033) and higher admission systolic-BP (p = 0.005). Median UHG on univariate analysis did not show significant differences (2.42 mL/h vs. 1.93 mL/h, p = 0.470). On PSM analysis, with a match in 18 NOAC- and 18 VKA-treated patients, median UHG was higher in VKA-treated patients (VKA 5.73 mL/h vs. NOAC 1.93 mL/h, p = 0.026).
Conclusion
Our study showed a higher UHG in VKA- when compared to NOAC-treated patients using matching statistics.
Trial registration number
N/A
AS20-069
PHYSICIAN CONCORDANCE WITH EEG GUIDELINES AND PROGNOSTIC FACTORS FOR OBTAINING EEG IN INTRACRANIAL HEMORRHAGE PATIENTS ADMITTED TO INTENSIVE CARE UNIT
1University of Massachusetts Medical School, Neurology, Worcester, USA
Background and Aims
Electroencephalography (EEG) aids seizure detection in intracerebral hemorrhage (ICH). However, physician adherence to EEG guidelines for assessing electrographic seizure activity in ICH patients is uncertain. We sought to determine physician adherence to EEG guidelines and assess potential clinical confounders that impact guideline adherence.
Method
Retrospective analysis of 330 patients with ICH (49% women, 42% lobar hemorrhage) admitted to a neurological intensive care unit at a single tertiary care academic center between 01/2013–12/2015. Multivariable logistic regression models were constructed to determine clinical confounders for physician adherence to guidelines for obtaining EEG. Model fit was compared using C-statistics (area under the curve [AUC]).
Results
Overall, 83 (25.2%) underwent EEG. 190 (57.6%) of included patients fulfilled criteria for obtaining EEG per existing guidelines, 78 (41.1%) of whom underwent EEG (sensitivity 94.0%). Of 140 patients not fulfilling criteria, 135 (96.4%) did not have an EEG (specificity 54.7%). The C-statistics of guideline adherence to predict EEG in unadjusted analyses was 0.74 (95%-CI 0.69–0.80). After adjustment for age, admission Glasgow coma scale score, and presence of a clinical seizure during hospitalization the C-statistics of guideline adherence to predict EEG was 0.85 (95%-CI 0.81–0.90). Model performance was similar when forcing withdrawal of care/in-hospital death into the model.
Conclusion
Our data suggest that physicians based their decision to obtain EEG in patients with ICH on clinical criteria beyond those recommended for the routine EEG criteria. Ongoing analyses are aimed at understanding the impact of physician non-adherence to EEG guidelines on patient care.
Trial registration number
N/A
AS20-070
NON-CONTRAST COMPUTED TOMOGRAPHY MARKERS OF INTRACEREBRAL HEMORRHAGE GROWTH TO PREDICT FUNCTIONAL OUTCOME
1Hospital de la Santa Creu i Sant Pau, Neurology, Barcelona, Spain
2Hospital de la Santa Creu i Sant Pau, Radiology, Barcelona, Spain
Background and Aims
Several markers in baseline non-contrast computed tomography (NCCT) of intracerebral hemorrhage (ICH) predict hematoma growth (HG). We aimed to study whether NCCT markers of HG predict functional outcome after ICH.
Method
We retrospectively evaluated a prospective database of consecutive patients with spontaneous ICH. We included patients who underwent baseline NCCT within 6 hours of ICH onset. We collected clinical and radiological data, including ICH volume and HG (increase in hematoma volume of ≥33% or >6 mL within 72 hours), and functional outcome (poor when modified Rankin scale >3 at 90 days). Two independent raters evaluated in baseline NCCT the presence of the following markers: irregular shape, heterogeneous density, hypodensities, swirl sign, blend sign, and black hole. Statistics: inter-rater agreement (κ statistic), bivariate and multivariable logistic regression analyses.
Results
A total of 103 patients were included with a mean age of 74 ± 12years, and 46%were women. HG was detected in 39%. Irregular shape, heterogeneous density, hypodensities, swirl sign, blend sign, and black hole were observed in 59.2%, 32%, 55.3%, 41.7%, 7.8% and 33% of patients, respectively. All signs showed a good inter-rater agreement (κ>0.6). After adjustment by age, irregular shape (OR:5.3; 95%CI:1.1–25.6) and heterogeneous density (OR:5.2; 95%CI:1.2–22.7) were independent predictors of HG. Irregular shape, hypodensities and swirl sign were associated with poor functional outcome in the bivariate analysis, but not after adjusting for age, ICH volume and Glasgow coma scale score.
Conclusion
In our study, irregular shape and heterogeneous density were independent markers of HG. These NCCT markers were not associated to functional outcome.
Trial registration number
N/A
AS20-071
ADVANCE STUDY: AUTOMATED DETECTION AND VOLUMETRIC ASSESSMENT OF INTRACEREBRAL HEMORRHAGE
1Grady Memorial Hospital- Emory University School of Medicine, Marcus Stroke Center- Department of Neurology, Atlanta, USA
Background and Aims
Acute intracerebral hemorrhages (ICHs) often bring severe neurological consequences and often require neurocritical care. Reliable ICH volume measurements are of great importance for patient prognostication and management. Existing semi-automated detection systems experience some pitfalls. We present a fully automated artificial intelligence algorithm for ICH detection.
Method
We performed single center retrospective analysis of non-contrast CTs (NCCTs), randomly picked from prospective cohort of acute stroke patients, with and without parenchymal ICHs, admitted at a stroke center, from 2014–2017. Experienced stroke neurologists graded NCCTs with a semi-automated tool (OsiriX MD v.9.0.1) for presence and volume of ICH, and also presence of intraventricular hemorrhage (IVH). Viz-ICH® v2.0 – a Convolutional Neural Network programmed to fully automatically detect ICH (presence and volume) analyzed same studies.
Results
Interim analysis of 284 subjects: 132 with ICH and 152 controls. For the ICH group, mean age of 58.3 ± 11.7, bNIHSS 10[3–19], ICH volume of 13[5–24] mL, males 51.5%, hypertension 75.8% and presence of IVH 47.8%. Intra-class Correlation Coefficient (uncontrolled for IVH): a=0.983 (IC95%=0.979–0.987; p = <0.001). For presence of ICH, AUC of 0.951(CI95% 0.921–0.981, p < 0.001), sensitivity 90.2%, specificity 99.99%, PPV 100%, NPV 92.2%, accuracy 95.5%. Maximal running time of the algorithm was under 15 seconds.
Conclusion
Viz-ICH Algorithm can precisely predict the presence and volume of ICHs, on an independent fashion, and also differentiates parenchymal bleeding from IVHs, with a good reliability.
Trial registration number
N/A
AS20-072
HYPERACUTE TREATMENT OF ANTICOAGULANT ASSOCIATED INTRACEREBRAL HAEMORRHAGE - 'TIME IS BRAIN' - REDUCING TIME TO TREATMENT
1Mater Misericordiae University Hospital, Stroke, Dublin, Ireland
Background and Aims
Intracerebral haemorrhage (ICH) associated with anticoagulation is increasing. Prothrombin Complex Concentrate (PCC) is part of management of vitamin K antagonist (VKA) and direct oral anticoagulant (DOAC) associated ICH. We sought to reduce time from diagnosis to treatment with PCC in these patients.
Method
From April 2016 to January 2018 we prospectively analysed patients presenting to ED of the Mater Misercordiae University Hospital with ICH on anticoagulation – VKA or DOAC. Following literature review and based upon the pathway used in The Greater Manchester Comprehensive Stroke Centre a new protocol was devised and implemented. Key changes included 1. Availability of PCC (Octaplex ®) in a blood products fridge in ED. 2. Using Point of Care INR testing in ED and 3. Prescription of PCC, by strict protocol, without need for prior approval by the on-call Haematologist. These new changes were implemented in April 2017.
Results
A total of 41 patients with anticoagulant associated ICH were admitted to ED: 19 patients prior and 22 patients post protocol implementation. Median age pre- and post-protocol implementation was 80 (IQR: 72–84) vs. 79 years (IQR 69–87), respectively. Median scan to needle time pre protocol was 150 minutes (IQR 85–226min) and post protocol was 50.5min (IQR 31–115min) p = 0.019. Median door to needle time pre protocol was 382min (IQR 205–562min) and post protocol was 147.5 min (IQR 65–291min) p = 0.008
Conclusion
A protocol to reduce door to needle time and scan to needle time in treatment of anticoagulant associated ICH was highly successful. Faster treatment, we hope, will improve outcomes.
Trial registration number
n/a
AS20-073
LONG-TERM PROGNOSIS IN INTRACEREBRAL HEMORRHAGE
1İstanbul Faculty of Medicine: İstanbul University, Neurology, İstanbul, Turkey
2İstanbul Faculty of Medicine: İstanbul University, Neurosurgery, İstanbul, Turkey
Background and Aims
Our aim was to define long-term prognosis and prognostic effect of demographic features, risk factors, hematoma characteristics and treatment in ICH.
Method
Patients (571) admitted to the Department of Neurology, Istanbul Faculty of Medicine in 1994–2016 and to the Department of Neurosurgery in 2000–2014, ≥18 years, diagnosed with non-traumatic ICH were included. Modified Rankin Score (mRS) (mRS 0–2 good, mRS≥3 poor prognosis), Barthel Index (BI), 3-month mortality, employment status, recurrent bleeding, presence of post-ICH epilepsy and cumulative survival were evaluated.
Results
Three hundred twenty-six of the patients (57.1% male, mean age:60.6 ± 15.2 years) were followed-up for 40 ± 50.11 (0,03 – 226) months. Two hundred twenty-one patients had died at the end of follow-up. Age (p = 0,001), whether ICH is the first or recurrent stroke (p = 0,007) and NIHSS score at onset (p < 0,0001) were independent factors determining prognosis. Whether ICH is the first or recurrent stroke (p = 0,008), neurological status at 48 hours (p = 0,018), NIHSS score (p < 0,0001) and consciousness level (p = 0,01) at onset were independent factors predicting 3 months mortality. Surgically treated patients had worse prognosis in univariate logistic regression analyses (p <0.0001). Only 17.6% of the previously employed (43% ) patients were able to return to work in the long term. Nine patients (5.4%) had recurrent ICH, 8 patients (7%) had post-ICH epilepsy and cumulative survival was 37%.
Conclusion
Age, and ICH severity at onset are important factors for long-term prognosis, deferred surgical treatment as a last measure to prevent mortality does not seem to impact overall prognosis.
Trial registration number
N/A
AS20-074
MICRORNA AND MRNA EXPRESSION IN HIGH AND LOW VOLUME INTRACEREBRAL HEMORRHAGE
1Ochsner Medical Centre, Institute of Translational Research, New Orleans, USA
Background and Aims
Intracerebral hemorrhages (ICH) occur with extravastion of blood unto brain parenchyma, leading to upregulation of inflammatory processes. MicroRNA (miRNA) and mRNA expression profile may serve as biomarkers in ICH. We profile miRNA and mRNA in high volume (HV) (>30mL) vs low volume (LV) (<30 mL) ICH.
Method
HV (n = 6) and LV (n = 6) ICH were used for paired miRNA microarray and digital gene expression (DE-Seq) analysis. Results were analyzed using Bioconductor/R. Top 500 upregulated/downregulated mRNA and miRNA (p < 0.05) were used for Gene Set Enrichment Analysis (GSEA) using the Benjamini-Hochberg (BH) cut-off (pValue<0.05) in miRWalk.
Results
We identified 13 upregulated and 31 downregulated miRNA. Functional analysis of downregulated miRNA showed a predominance of pathways involved in proliferation, apoptosis, and oxidative stress resistance. Conversely, no KEGG pathway enrichment was found for upregulated miRNA. GO terms enrichment for upregulated miRNA included NF-kappaB transcription factor activity, protein ubiquination, and ion channel activity; downregulated miRNA are associated with apoptosis and sphingolipid biosynthetic processes. Upregulated mRNA exhibited enrichment for osteoclast differentiation, RAP1, FOXO, AMPK, and TNF signaling pathways. Downregulated mRNA KEGG pathways associated with regulation of cell proliferation, apoptosis, and stem cell renewal. GO terms enriched for upregulated mRNA consists of inflammatory and cell migratory pathways. Downregulated mRNA associated with decreasing cell proliferation and upregulating apoptotic processes.
Conclusion
Apoptosis and decreased cell proliferation processes are predominant in LV ICH patients whereas HV ICH favored inflammatory and cell migratory pathways. Evidence of these pathways demonstrate miRNA and mRNA profiling has potential for utilization as biomarkers in ICH.
Trial registration number
N/A
AS20-075
SERUM MAGNESIUM LEVELS AND OUTCOMES IN PATIENTS WITH ACUTE SPONTANEOUS INTRACEREBRAL HEMORRHAGE
1University of Tennessee Health Science Center, Neurology, Memphis, USA
2West Virginia University Charleston Division- Charleston- West Virginia- USA, Neurology, Charleston, USA
3University of Tennessee Health Science Center, Neurosurgery, Memphis, USA
Background and Aims
Magnesium (Mg) has potential hemostatic properties. We sought to investigate the potential association of serum Mg levels (at baseline and at 48 hours) with outcomes in patients with acute spontaneous intracerebral-hemorrhage (ICH).
Method
We reviewed data on all spontaneous ICH patients with available Mg levels at baseline, over a 5-year period. Clinical and radiological outcome measures included initial hematoma volume, admission NIHSS and ICH scores, in-hospital mortality, favorable functional outcome (FFO: modified Rankin Scale (mRS) scores: 0–1] and functional independence (FI: mRS scores of 0–2) at discharge.
Results
Our study population consisted of 299 ICH patients (mean age: 61 ± 13 years, mean admission serum Mg: 1.8 ± 0.3 mg/dL) Increasing admission Mg levels strongly correlated with lower admission NIHSS (Spearman’s r: -0.141; p = 0.015), lower ICH score (Spearman’s r: -0.153; p = 0.009), and lower initial hematoma volume (Spearman’s r: -0.153; p = 0.012). Higher admission Mg levels were documented in patients with FFO (1.9 ± 0.3mg/dL vs. 1.8 ± 0.3mg/dL; p = 0.025) and FI (1.9 ± 0.3 mg/dL vs. 1.8 ± 0.3 mg/dL, p = 0.022) at discharge. No association between serum Mg levels at 48 hours and any of the outcome variables was detected. In multiple linear regression analyses, a 0.1mg/dL increase in admission serum Mg was independently and negatively associated with the cubed root of hematoma volume at admission (regression coefficient: -0.020, 95%CI: -0.040, -0.000; p = 0.049), and admission ICH score (regression coefficient: -0.053, 95%CI: -0.102, -0.005; p = 0.032).
Conclusion
Higher admission Mg levels were independently related to lower admission hematoma volume and lower admission ICH score in patients with acute spontaneous ICH.
Trial registration number
N/A
AS20-076
OUTCOME OF INTRACEREBRAL HEMORRHAGE ON DIFFERENT ORAL ANTICOAGULANTS
1University Medical Centre, Department of Neurology, Ljubljana, Slovenia
2University Medical Centre, Clinical Institute of Radiology, Ljubljana, Slovenia
3University of Ljubljana, Institute of Pathophysiology, Ljubljana, Slovenia
4University of Ljubljana, Institute of Physiology, Ljubljana, Slovenia
Background and Aims
We compared outcomes of patients with intracerebral hemorrhage (ICH) on direct oral anticoagulants (DOAC) to those on vitamin K antagonist (VKA).
Method
We conducted a retrospective study of 135 consecutive patients on oral anticoagulants, admitted to our tertiary stroke center with acute non-traumatic ICH between 1st January 2013 and 23rd November 2016. Outcome measures were mortality and hematoma volume (HV). Functional outcomes were estimated using National Institutes of Health Stroke Scale (NIHSS).
Results
108 patients had VKA-related ICH and 27 had DOAC-related ICH. Mean HV was 20.6 mL (interquartile range [IQR] 7.5–57.8 mL) for VKA-related ICH vs. 22.3 mL (IQR 8.6 – 78.4 mL) for DOAC-related ICH (p = 0.8081). Mean NIHSS score on admission was 12.0 (IQR 6.0 – 21.0) for VKA-related ICH vs. 18.0 (IQR 3.8 – 21.8) for DOAC-related ICH (p = 0.5321). Mortality was 56% in the VKA group vs. 50% in the DOAC group (p = 0.6711). In the survival subgroup, mean HV was 8.4 mL (IQR 3.2 – 31.4 mL) for VKA-related ICH vs. 16.4 mL (IQR 7.1 – 29.2 mL) for DOAC-related ICH (p = 0.3231). Admission NIHSS score was 8.0 (IQR 4.0 – 11.0) for VKA-related ICH vs. 4.0 (IQR 1.0 – 20.0) for DOAC-related ICH (p = 0.9871). Additionally, advanced age was predictive of higher mortality in both groups.
Conclusion
Our analysis did not find statistically significant differences in mortality, HV or functional outcome between the two groups. Anticoagulant-related ICH has high mortality and unfavorable outcome irrespective of anticoagulant type.
Trial registration number
N/A
AS20-077
EFFECT OF ADMISSION BLOOD PRESSURE ON INTRACEREBRAL HEMORRHAGE VOLUME AND ITS EARLY GROWTH
12nd Faculty of Medicine- Charles University and Motol University Hospital, Neurology, Prague, Czech Republic
Background and Aims
Acute intracerebral hemorrhage (ICH) is typically associated with increase of blood pressure (BP). High level of pretreatment BP seems to be a predictor of poorer outcome in ICH patients. The underlying mechanism is still unclear and controversial; however, the association with hematoma volume and its enlargement is mostly suspected. The aim of our study was to assess the impact of admission BP on initial hematoma volume size and its 24 hours progression.
Method
110 patients with acute nontraumatic ICH were included in the study. The first in hospital measured BP value was evaluated. Hematoma volume was measured on the baseline CT scan using 3D Slicer. Control CT scan was performed within 24 hours of admission. Primary outcome was the admission ICH volume, secondary outcome the presence of hematoma enlargement on the control CT scan.
Results
We did not find any correlation between admission BP and hematoma volume (p = 0,259, r=0,12). High BP (cut off levels of 140, 160, 180, 200, 220mmHg systolic BP) did not increase the risk of hematoma enlargement (p>0,05).
Conclusion
Our results do not indicate any cause-effect relationship between admission BP and hematoma size or its growth. Therefore, we hypothesize that the poor outcome of ICH patients with high elevation of pretreatment BP might be caused by other mechanism (e.g. cerebral edema, need of more rapid and aggressive BP lowering, presence of cardiac or autonomic dysfunction).
Trial registration number
N/A
AS20-079
INTRACOMPARTMENTAL PRESSURE GRADIENTS IN THE VENTRICULAR SYSTEM IN SPONTANEOUS INTRAVENTRICULAR HEMORRHAGE: RESULTS FROM THE CLEAR III TRIAL
1Johns Hopkins Medical Institutions, Neurology, Baltimore, USA
2Johns Hopkins University School of Medicine, Neurology, Baltimore, USA
3Johns Hopkins Bloomberg School of Public Health, Biostatistics, Baltimore, USA
4University of Chicago, Neurosurgery, Chicago, USA
Background and Aims
Intracranial hypertension is a prognostic factor for poor outcome of spontaneous intracerebral with intraventricular hemorrhage (ICH/IVH). Intracompartmental pressure gradients may exist around focal ICH/IVH and may adversely affect tissue perfusion. External ventricular drain (EVD) position is an important determinant of IVH removal efficiency with thrombolytics which may impact accuracy of intracranial pressure (ICP) measures.
Method
We report time course of ICP in 108 subjects from the CLEAR III trial, with pragmatic placement of ≥2 simultaneous EVDs with ICP recordings every 4 hours for up to 10 days. We performed linear regression analysis of ICP differences by EVD side ipsilateral vs. contralateral to dominant IVH volume and included interactions with variables affecting compartmental pressures.
Results
Mean (SD) age was 60(10) years, with mean ICH and IVH volume 9.1(8.1) and 39(25.5) mL respectively. For EVDs placed on opposite ventricle sides, mean ICP was significantly higher in EVDs placed ipsilateral to dominant IVH volume vs. contralateral: 11.9 vs. 10.9 mmHg; p = 0.004. Contralateral placed EVDs were significantly less likely to report ICP>30mmHg than ipsilateral EVDs (Odds ratio=0.41; 95%CI:0.20–0.84; p = 0.02). Differences in ICP between opposite side EVDs were significant for ICH volume>10mL, modified Graeb score>18, age<60, %IVH removal and third ventricle obstruction at end of intraventricular treatment (saline vs. alteplase), and intraventricular saline assignment.
Conclusion
Intermittent pressure gradients exist within the intraventricular cavity in spontaneous IVH and may affect ICP interpretation. Due to importance of EVD position to optimize IVH clearance and minimize intracranial hypertension, consideration should be given to EVD location in relationship to these clinical goals.
Trial registration number
NCT00784134
ATRIAL FIBRILLATION, CARDIOEMBOLISM & HEART-BRAIN INTERACTIONS
AS21-001
SYSTEMIC INTRAVENOUS THROMBOLYTIC THERAPY OF CONCOMITANT ACUTE ISCHEMIC STROKE AND ACUTE MYOCARDIAL INFARCTION – A CASE REPORT
1University Hospital- Masaryk University, Department of Neurology, Brno, Czech Republic
2University Hospital- Masaryk University, Department of Cardiology, Brno, Czech Republic
3University Hospital- Masaryk University, Department of Radiology, Brno, Czech Republic
Background and Aims
The simultaneous occurence of acute ischemic stroke and acute myocardial infarction is rare but serious condition in clinical practice. We report a case of successful treatment with intravenous thrombolysis, followed by elective percutaneous coronary intervention (PCI)
Method
Results
A 56-year-old female was admitted to the stroke unit with a history of dysarthria, hemineglect and severe left-sided hemiparesis. CT head scan identified the old lacunar infarct in the left basal ganglia, CT angiography revealed right posterior cerebral artery occlusion. Electrocardiogram and emergency echocardiography were performed due to chest pain and revealed ST segment elevation due to myocardial infarction (STEMI). The patient was treated with intravenous thrombolysis and immediately referred to a comprehensive cardiovascular centre. During thrombolysis, chest pain and ST segment elevation subsided and neurological symptoms partially improved. After six days dual antiplatelet therapy was initiated and coronary angiography revealed 70% stenosis on the left anterior descending artery. The condition was treated by PCI with a stent implantation. The adopted strategy turned out to be the fastest and the most successful treatment methods of two vulnerable atherosclerotic plaques of different locations causing thrombotic occlusion in cerebral and coronary circulation. Neurological and cardiological status including left ventricular systolic dysfunction were fully recovered within one year.
Conclusion
Currently there are no evidence-based guidelines for management of patients with concomitant stroke and acute myocardial infarction. Treatment decisions in these cases are empirical and individualized. Our case report shows that intravenous thrombolysis might be the effective method for the treatment of ischemic stroke complicated by parallel STEMI.
Trial registration number
N/A
AS21-002
MIGRAINE WITH VISUAL AURA A RISK FACTOR FOR INCIDENT ATRIAL FIBRILLATION
1Palmetto Health University of South Carolina, Neurology, Columbia, USA
2Emory University, Epidemiology and Internal Medicine, Atlanta, USA
3University of Minnesota, Medicine, Minneapolis, USA
4Wake Forest School of Medicine, Epidemiology and Internal Medicine, Winston Salem, USA
5Heart and Vascular Institute- University of Pittsburgh, Medicine, Pittsburgh, USA
6Arnold School of Public Health- University of South Carolina, Epidemiology, Columbia, USA
7Johns Hopkins University School of Medicine, Neurology, Baltimore, USA
8Gilling’s School of Public Health- University of North Carolina, Epidemiology, Chapel Hill, USA
Background and Aims
Migraine with visual aura is associated with cardioembolic stroke risk. The aim of this study was to test association between migraine with visual aura and atrial fibrillation (AF).
Method
Participants in the Atherosclerosis Risk in Communities cohort were interviewed for migraine history in 1993–1995, and were followed for incident AF through 2013. AF was adjudicated using electrocardiograms, discharge codes, and death certificates. Multivariable Cox proportional hazards models were used to study the relation between migraine and its subtypes with incident AF, compared with a control group without headaches. Mediation analysis was conducted to test if atrial fibrillation was a mediator of migraine with visual aura associated cardioembolic stroke risk.
Results
Of 11,939 participants assessed for headache and without prior AF or stroke, 426 reported migraines with visual aura, 1,090 migraine without visual aura, 1,018 non-migraine headache and 9,405 no headache. Over a 20-year follow-up period incident AF was noted in 232 (15%) out of 1,516 with migraine, 142 (14%) out of 1,018 with non-migraine headache and 1,623 (17%) of 9,405 without headache. After adjustment for multiple potential confounders, migraine with visual aura was associated with increased risk of AF compared to no headache (HR 1.30, 95% CI 1.03–1.62) and to migraine without visual aura (HR 1.39, 95% CI 1.05–1.83). Mediation analysis (Baron and Kenny’s causal-steps approach) suggests AF as a mediator of migraine with visual aura - cardioembolic stroke association.
Conclusion
Migraine with aura was associated with increased risk of AF. The migraine with aura associated AF, may lead to ischemic strokes.
Trial registration number
N/A
AS21-003
CORTEX-INVOLVED ISCHEMIC STROKE AND SUBTYPES OF ATRIAL FIBRILLATION
1Beijing Tiantan Hospital- Capital Medical University, Tiantan Clinical Trial and Research Center for Stroke- Department of Neurology, Beijing, China
2Beijing Tiantan Hospital- Capital Medical University, Vascular Neurology- Department of Neurology, Beijing, China
3Beijing Tiantan Hospital- Capital Medical University, Neuro-intensive Care Unit- Department of Neurology, Beijing, China
Background and Aims
Cortex-involved (Both cortical and cortical-subcortical) lesions are typically caused by embolic stroke, of which Atrial fibrillation (AF) is the common cause. The aim of this study was to investigate the associations between cortex-involved stroke, vascular risk factors and the subtypes (discovery time and duration) of AF.
Method
Between October 2013 and June 2015, 1511 acute ischemic stroke or TIA patients within 7 days after stroke onset were enrolled in the prospective, multicenter cohort study at 20 Chinese hospitals. The primary aim of this trial is to define the true frequency of AF-associated stroke. The final analysis of this substudy included 243 AF patients with required MRI sequences. AF was diagnosed by 6-day Holter monitoring and ECG and classified by duration of 24 hours. Two stroke specialists blinded to the clinical information reviewed MRI(DWI, FLAIR, T1WI, T2WI). The third stroke specialists assessed the conflicts. Adjusted large artery atherosclerosis, the associations between Cortex-involved lesions, vascular risk factors and the subtype of AF were evaluated by multivariate regression analysis.
Results
Of 243 acute ischemic stroke patients with AF, 190 were known AF and 53 were new-detected AF. there were 28 with AF persistent more than 24 hours and 25 persistent less than 24hours in newly detected AF. Cortex-involved lesions were significantly related to newly detected AF persistent more than 24 hours (OR = 4.517, 95%CI 1.490–13.696, P = 0.0077), Proteinuria (OR = 3.431, 95%CI 1.530–7.692, P = 0.0213) and glycosylated hemoglobin (OR = 0.632, 95%CI 0.464–0.861, P = 0.0036).
Conclusion
Compared to previously known AF, Newly detected AF persistent more than 24 hours was robustly associated with cortex-involved ischemic stroke.
Trial registration number
N/A
AS21-004
COMPARISON OF ATRIAL FIBRILLATION DIAGNOSIS AND ORAL ANTICOAGULATION UTILIZATION AMONG ISCHEMIC STROKE PATIENTS WITH VS. WITHOUT INSERTABLE CARDIAC MONITORS
1Weill Cornell Medicine, Neurology, New York, USA
2Brown University, Neurology, Providence, USA
3Northwestern University, Cardiology, Chicago, USA
4Cone Health Medical, Cardiology, Greensboro, USA
5Medtronic, Diagnostics and Monitoring Research, Mounds View, USA
Background and Aims
Oral anticoagulation is highly effective for preventing recurrent stroke in patients with atrial fibrillation (AF). However, real-world data comparing rates of AF diagnosis and OAC utilization between ischemic stroke patients with vs. without insertable cardiac monitors (ICM) are limited.
Method
Using de-identified Optum EHR data from 2011–2016, we included cardiovascular disease patients with ischemic stroke (ICD-9 codes 434.11/434.91, ICD-10 codes I63.4/I63.5/I63.8/I63.9) and ≥180 days of follow-up, no pacemaker or defibrillator, and no prior AF diagnosis or anticoagulant prescription. Within this cohort, we identified patients receiving an ICM within 90 days of stroke and another group (matched for age, gender, CHADS2 score, year and length of hospitalization) without ICM but with index ischemic stroke over a similar period. Kaplan-Meier estimates for AF diagnosis and oral anticoagulant initiation rates between the two groups are reported.
Results
A total of 886 ICM and 886 non-ICM patients (65.3 ± 12.2 years, 52% male) with stroke were included. At 2 years, the rates of AF diagnosis (29.7% vs. 8.3%, p < 0.001, Panel A) and anticoagulant prescription (26.5% vs. 8.3%, p < 0.001, Panel B) were significantly higher among ICM vs. non-ICM patients.
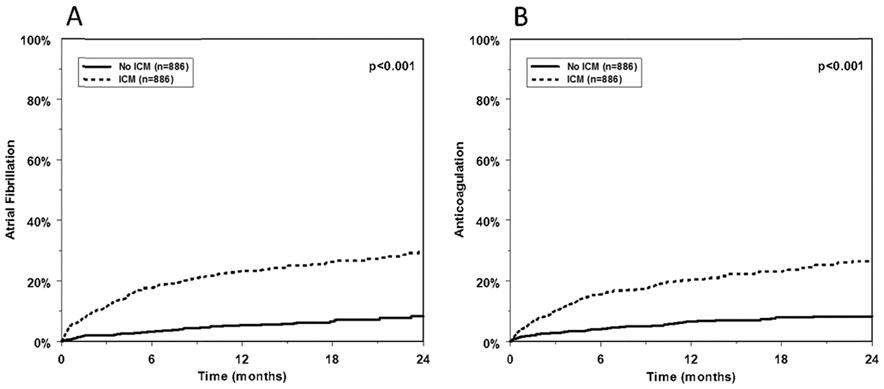
Conclusion
In a large real-world ischemic stroke population, monitoring with an ICM was associated with significant increases in AF diagnosis and anticoagulant prescription, which would be expected, based on the balance of available data, to decrease rates of recurrent stroke.
Trial registration number
N/A
AS21-005
DIRECT ORAL ANTICOAGULANTS AFTER STROKE: ARE OUR PATIENTS CORRECTLY TREATED?
1Hospital Universitario Marques De Valdecilla, Neurology, Santander, Spain
Background and Aims
Direct oral anticoagulants (DOACs) are effective drugs in the prevention of stroke in patients with non-valvular atrial fibrillation (NVAF). To assess the percentage of patients receiving the correct dose of DOACs after an ischemic stroke or TIA. To detect factors involved in an incorrect dosage of these drugs.
Method
Retrospective analysis of consecutive patients admitted to our stroke unit during a period of 5 years with a diagnosis of NVAF, and for whom treatment with DOACs was prescribed. Demographic and vascular risk factors, previous treatments, clinical parameters and hemorrhagic risk, type of DOACs and dose at discharge were evaluated. Statistical analysis: t-Student, Mann-Whitney U, chi-square and logistic regression analysis.
Results
341 patients were included in the study (mean age 74.96 ± 9.13 years, 60.4% males). 62 patients (18.2%) received doses of DOACs lower than those indicated and 8 patients (2.3%) were treated with doses higher than those indicated. The factors related to the underdosing of the DOACs were the high age (OR 1.257; 95% CI 1.018–1.551; p = 0.034), the concomitant treatment with antiplatelet agents (OR 4.997; 95% CI 2.171–11.502; p <0.001) and presenting a filtrate glomerular <50 ml/min/1,73 m2 and/or creatinine> 1.5 mg/dl (OR 0.111; 95% CI 0.014–0.895; p = 0.039).
Conclusion
Approximately 20% of our patients received an incorrect dose of DOACs. This could contribute to an increase in the recurrence of acute cerebrovascular disease and increase the risk of hemorrhagic complications.
Trial registration number
N/A
AS21-008
ENDOVASCULAR TREATMENT OF ACUTE ISCHEMIC STROKE IN PATIENTS DURING AND BEFORE CARDIAC SURGICAL PROCEDURE
1The National center for Neurosurgery- Astana- Kazakhstan, Department of Neurovascular disorders, Astana, Kazakhstan
Background and Aims
Endovascular treatment results assessment in patients during and before cardiac surgical procedure and acute ischemic stroke.
Method
10 patients’ treatment outcomes was analyzed. CT and angiography revealed occlusions of the internal carotid, middle cerebral and basilar arteries. Following parameters were evaluated: time from the onset of ischemic stroke prior to endovascular treatment, TICI scale degree of recanalization, ICH within 24 hours from the onset of ischemic stroke and functional independence of patients (modified Rankin Scale) 1 and 3 months after surgery.
Results
Acute ischemic stroke developed during 1–4 days after cardiosurgery in four patients, prior to cardiosurgery in two patients, and in four cardiac patients. Selective thrombolysis was performed in three cases with the occlusion of M2-M3 (TICI 2B, 3); five patients underwent thromboextraction with occlusion of ICA and M1 (TICI 3), M1-M2 (TICI 2A, 2B, 3); two patients were performed with thromboextraction with thrombolysis for occlusion of the basilar artery and M1-M2 of the MCA (TICI 3). Symptomatic intracranial hemorrhage was detected in one patient after 11 hours of selective thrombolysis with M2 occlusion (TICI 3). The mRS after 1 month: mRS 0 (40%), mRS 1 (20%), mRS 2 (20%), mRS 4 (20%); 3 months after surgery: mRS 0 (60%), mRS 1 (20%), mRS 2 (10%), mRS 4 (10%). In the postoperative period, there were no mortality.
Conclusion
Endovascular treatment in the first 6 hours after the onset of acute ischemic stroke once again demonstrates the efficacy and good functional outcome according to the mRS after 3 months of surgery.
Trial registration number
N/A
AS21-009
EFFECTIVENESS AND SAFETY OF RIVAROXABAN VERSUS WARFARIN IN PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION AND A NON-SEX-RELATED CHA2DS2-VASC SCORE OF 1
1University of Connecticut School of Pharmacy, Pharmacy Practice, Storrs, USA
2McMaster University, Department of Medicine, Hamilton, Canada
3New England Health Analytics, Department of Pharmacoepidemiology, Granby, USA
4Bayer AG, Real-World Evidence Generation, Berlin, Germany
5Southcoast Health System, Department of Cardiac Electrophysiology, Fall River, USA
Background and Aims
The pivotal rivaroxaban clinical trial focused on enrolling high-risk patients with nonvalvular atrial fibrillation (NVAF). We sought to assess the effectiveness and safety of standard dose rivaroxaban vs. warfarin in NVAF patients with 1 low-risk, nonsex-related stroke risk factor.
Method
Using US MarketScan claims data from 11/2011–12/2016, we identified oral anticoagulant (OAC)-naïve NVAF patients with a single nonsex-related stroke risk factor assigned 1-point in the CHA2DS2-VASc score and ≥12-months of continuous insurance coverage prior to the qualifying OAC dispensing. Standard dose rivaroxaban users (20 mg once daily) were 1:1 matched to warfarin users using propensity scores calculated based on demographics, comorbidities, stroke and bleeding risk factors and concomitant medications (with residual standardized differences <0.1 achieved for all covariates after matching). Patients were followed until an event, OAC discontinuation/switch (30-day permissible gap), insurance disenrollment or end of follow-up. Rates of stroke/systemic embolism (SSE) and major bleeding were compared.
Results
Upon Cox regression, 6,626 rivaroxaban users were matched to 6,626 warfarin users. Mean ± standard deviation (SD) follow-up was 0.7 ± 0.8 years and mean HASBLED score was 2.0 ± 1.0. Rivaroxaban was associated with a significant 40% reduction in the hazard of SSE; without impacting major bleeding risk (Figure).
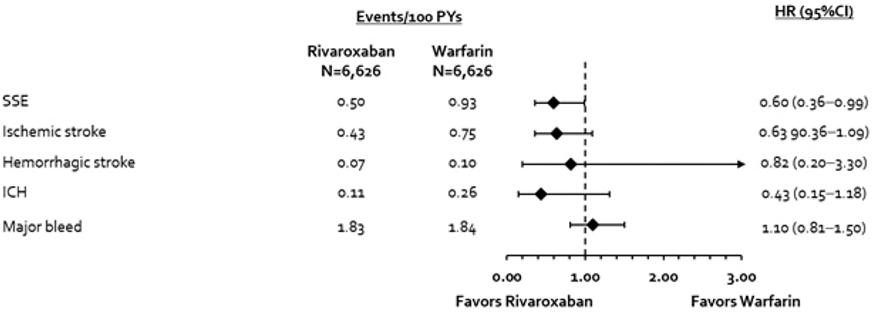
Conclusion
This real-world study suggests rivaroxaban’s is effective and safe compared to warfarin in NVAF patients with 1 low-risk, nonsex-related stroke risk factor.
Trial registration number
N/A
AS21-010
CLINICAL CHARACTERISTICS OF ISCHEMIC STROKE IN PATIENTS TREATED PREVIOUSLY WITH DIRECT ORAL ANTICOAGULANTS
1Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Clinical guidelines recommend direct oral anticoagulants (DOACs) for secondary prevention of ischemic stroke (IS) in atrial fibrillation (AF). Optimal management of recurrent IS on DOAC therapy is controversial.
Method
Prospective registry (2010–2015) of patients with AF treated with DOACs in secondary prevention of IS. Demographic, clinical variables, IS recurrence and its management were analyzed.
Results
We included 425 patients, 53.4% women, with a mean age of 77.1 ± 10.2 years, mean CHA2DS2VASc 5 ± and HASBLED 2 ± , treated with dabigatran (57.7%), rivaroxaban (24.7%), and apixaban (17.6%), with a mean follow-up of 20 ± 18.1 months. Thirty-four incidental IS (7.95%) were registered in a median time of 7 months from treatment onset (1–52);14 (41.2%) were transient ischemic attacks. Annual rate of IS was 0.05 cases/person-years. All recurrent IS patients were receiving the correct dose of DOACs according to the label, and mean glomerular filtration rate in the event was similar to baseline (61.8 ± 31ml/min). Reperfusion therapies were performed in 5 patients (4 intravenous thrombolysis and 1 mechanical thrombectomy). Twenty patients (58.8%) were independent (mRS ≤2) at three months, while one patient died (2.9%). For further IS prevention, 21 patients retained the same DOAC, 7 were switched to a different DOAC, and 1 to acenocoumarol. Two patients underwent left appendage closure in addition to DOAC therapy.
Conclusion
In our experience with patients treated with DOACs in secondary IS prevention, incidence and clinical features of recurrent IS was similar to the pivotal trials. Clinical decisions following recurrent IS were individualized, in the absence of formal guidelines.
Trial registration number
N/A
AS21-011
ATRIAL FIBRILLATION IMPACT ON MILD COGNITIVE IMPAIRMENT PREVALENCE IN ELDERLY: CASE-CONTROL STUDY
1Sechenov First Moscow State Medical University, Neurology Clinic, Moscow, Russia
2Sechenov First Moscow State Medical University, Chair of Internal Diseases, Moscow, Russia
Background and Aims
Atrial fibrillation (AF) shares several risk factors for cognitive disorders, especially with cerebrovascular impairment. This study was aimed to investigate cognitive performances in patients with and without AF but having comparable cardiovascular risks.
Method
We enrolled 49 patients with AF (AF+) and 45 patients without AF (AF-). After exclusion patients with signs of major cognitive decline according to DSM-V criteria and those who showed low Sensitivity of cueing (<0.66) in Free and Cued Selective Reminding Test (FCSRT), we performed analysis of 37 and 40 patients in AF+ and AF- groups respectively according to Montreal Cognitive Assessment test (MoCA) and Geriatric Depression Scale (GDS). Groups were comparable for middle age and MoCA results. The cut-off value for MoCA was 23 points to provide better sensitivity to Mild Cognitive Impairment (MCI).
Results
14 patients (37.8%) in AF+ group and 25 patients (62.5%) in AF- group were marked as having MCI based on MoCA result. No difference was found in the MoCA results between groups (p = 0.28). Subgroup analysis showed no influence of blood pressure control (Fisher exact test, AF+ p = 0.74, AF- p = 0.3), antihypertensive treatment (AF+ p = 1, AF- p = 0.65), anticoagulant treatment (p = 0.68) on cognitive performances. There were no correlations in AF group between MoCA result and GDS (Spearman coefficient s = 0.02), Glomerular filtration rate (GFR) (s = 0.01), CHA2DS2-VASc score (s = 0.03). AH group showed no correlation with GDS (s = 0.06), GFR (s = −0.19).
Conclusion
Our study did not reproduce previous literature data of AF negative impact on cognitive functions in comparison with the control group with shared cardiovascular risks.
Trial registration number
N/A
AS21-012
OUTCOME OF ATRIAL FIBRILLATION-RELATED STROKE IN A MULTIETHNIC COHORT
1Hamad Medical Corporation, Neurology, Doha, Qatar
2Hamad Medical Corporation, Cardiac Research Center, Doha, Qatar
Background and Aims
Atrial fibrillation (AF) is an important risk factor for stroke; it is associated with increased morbidity and mortality, with limited data being available on AF-related stroke from the Middle East.
Method
A retrospective analysis of Stroke database at Hamad General Hospital, Doha, Qatar, from 1st January 2014 thru 18 October 2017 was performed. All cases admitted with stroke and established AF or new onset AF during admission were included in the analysis.
Results
AF was present in 260 (6.4%) of the total database patients population.
The mean age was 65.4 + 16 years for the AF Stroke cohort, with females representing 33.8%.
Arabs from the Middle East and North Africa region (including Qataris) comprised 66.2% of the AF cohort whereas South Asians the biggest ethnic group in the database (51.6% of the total cases) contributed 23.8% and other ethnicities 10%.
In the multivariate model age odds ratios (OR) 1.11 (1.02 – 1.2, 95% CI) (p = 0.015), female gender OR 8.86(1.07–73.36,95% CI) p = 0.043) and stroke severity on the National Institute of Health Stroke Scale (NIHSS) OR 1.37(1.12 – 1.68, 95% CI) (p = 0.003) predicted a poor outcome on Modified Rankin Score (mRs = 3–6) at 90 days irrespective of other risk factors in this cohort. Whereas ethnicity, presence of non-lacunar stroke and diabetes mellitus were not (p>0.05)
Conclusion
Age, female gender and severe stroke are associated with poor outcomes in AF-related stroke in a younger, multiethnic, low AF-related stroke incidence population
Trial registration number
N/A
AS21-013
DDIMER LEVELS FOR SUBSEQUENT OCCULT ATRIAL FIBRILLATION PREDICTION IN STROKE PATIENTS
1IMIM-Hospital del Mar, Neurology, Barcelona, Spain
Background and Aims
The aim of the present study was to evaluate whether elevated D-dimer levels can predict subsequent occult atrial fibrillation (oAF) in patients with an acute ischemic stroke (IS) or transient ischemic attack (TIA).
Method
From 2007 to 2016 consecutive patients with a final diagnosis of IS/TIA, were registered. Inclusion criteria were: Stroke Unit admission, blood sample drawn at arrival to test D-dimer levels, sinus rhythm on ECG at admission, no history of AF or other cardioembolic disease, complete vascular study, and 3-months follow-up.
Results
Of 1042 patients included, oAF was detected in 108 (10.4%). These patients were older (p < 0.001), more often women (p < 0.001), chronic heart failure as well as chronic kidney disease were more prevalent (p < 0.001 and p = 0.042, respectively), were more often IS than TIA (p = 0.015), and stroke severity was higher at admission (p < 0.001). D-dimer levels were positively associated to oAF diagnosis (p < 0.001). Multivariate analysis including these 7 variables revealed that increased D-dimer levels remained an independent predictor for oAF diagnosis (p = 0.007). For every 200 ng/ml increase of D-dimer levels, the risk of oAF detection increased a 12%. Age (OR 1.04 [CI 95% 1.02–1.06], p < 0.001), initial stroke severity (OR 1.08 [CI 95% 1.04–1.11], p < 0.001), and CHD (OR 2.54 [CI 95% 1.25–5.13], p = 0.01) were the remaining independent predictors. D-Dimer levels were negatively associated with the time of oAF diagnosis (r=-0.229; p = 0.017).
Conclusion
Higher plasma D-dimer concentration in acute IS/TIA patients is a risk marker for new-oAF diagnosis. D-dimer levels are higher as closer to the oAF diagnosis.
Trial registration number
N/A
AS21-014
LONG-TERM IMPACT OF RESIDUAL SHUNT AFTER PATENT FORAMEN OVAL CLOSURE ON STROKE RECURRENCE
1Department of Neurosciences and Mental Health- Hospital de Santa Maria - CHLN, Stroke Unit, Lisboa, Portugal
2Hospital de Santa Marta - CHLC, Cardiology, Lisboa, Portugal
3Department of Neurosciences and Mental Health- Hospital de Santa Maria - CHLN, Neurosonology, Lisboa, Portugal
Background and Aims
Patent Foramen Oval (PFO) closure may be recommended in some cryptogenic stroke patients. Residual shunt after PFO closure identified by transesophageal echocardiography or transcranial Doppler (TCD) has been reported. However the long-term impact of residual shunt on stroke recurrence is not established.
We aimed to identify and quantify the residual shunt at long-term (at least one year) by TCD and to evaluate its association with stroke recurrence.
Method
Observational retrospective study of patients with cryptogenic transient ischemic attack (TIA) or ischemic stroke (IS) observed on the stroke unit or outpatient clinic submitted to percutaneous closure of the PFO from 2000 to 2016. Patients without TCD post procedure or clinical follow-up were excluded. The following data was retrieved from clinical files and complemented by information from the Cardiology department: Demographic, TIA/IS date and characteristics, procedural-related, long-term TCD results regarding residual shunt (absence, mild, moderate or severe), and stroke recurrence after PFO closure.
Results
Forty nine patients were included (mean 45 years-old, 55% men), 78% (n = 38) with IS and 22% (n = 11) with TIA. PFO was associated to atrial septal aneurysm in 55% (n = 27). Mean time of TCD evaluation was 5.3 years after PFO closure. Residual shunt was detected in 65% (n = 32) and it was mild in most of them (n = 25). One patient had a stroke recurrence not related to the PFO (vasculitis).
Conclusion
Although long-term residual shunt was identified in 65% of the patients submitted to PFO closure, it was mild in most of them and not associated with stroke recurrence.
Trial registration number
N/A
AS21-015
INCIDENCE AND DETERMINANTS OF CEREBROVASCULAR EVENTS IN OUTPATIENTS WITH STABLE CORONARY ARTERY DISEASE
1Lille University Hospital, Department of neurology & stroke centre, Lille, France
2Lille University Hospital, Department of Cardiology, Lille, France
3Lens Hospital, Department of Cardiology, Lens, France
Background and Aims
There are limited data on cerebrovascular events (CVE) in patients with stable coronary artery disease (CAD). To study the risk of CVE, the relative proportion of ischaemic stroke (IS) and intracranial haemorrhage (ICrH), and their prognostic factors in stable CAD.
Method
The CORONOR registry prospectively recruited, between February 2010 and April 2011, 4184 unselected stable CAD outpatients. All events occurring during a 5-year follow-up were adjudicated
Results
Ninety-six patients had an IS and 34 had an ICrH, reaching a cumulative incidence after 5 years of 3.2[2.7–3.8]% . During the same period, 677 deaths and 170 MIs (ST-elevation MI, n = 55; non-ST-elevation MI, n = 115) occurred. In elderly individuals, the number of CVEs was higher than that of MIs and largely exceeded that of ST-elevation MIs. Predictors of IS were: previous history of stroke (subhazard ratio [SHR]=3.16[1.95–5.14]), absence of statin therapy at inclusion (SHR=2.45[1.47–4.10], increasing age (SHR=1.45[1.16–1.82] per 10-year increase), and diabetes mellitus (SHR=1.65[1.10–2.49]). Predictors of ICrH were: combination of vitamin K antagonists with an antiplatelet agent at inclusion (SHR=5.41[2.49–11.75], single antiplatelet therapy as reference), and increasing age (SHR=1.47[1.12–1.93] per 10-year increase)
Conclusion
In stable CAD patients, the brain deserves attention. In patients at high risk of IS, secondary prevention could be intensified. Our results raise awareness of the hazard of the association of antiplatelet drugs with oral anticoagulants in stable CAD patients. While improving the prevention of future vaso-occlusive events should be our ultimate goal in CAD patients, the net clinical benefit of our treatments should carefully be studied.
Trial registration number
N/A
AS21-016
PREDICTION OF ATRIAL FIBRILLATION IN A MULTIETHNIC STROKE COHORT
1Hamad Medical Corporation, Neurology, Doha, Qatar
2Hamad Medical Corporation, Cardiac Research Center, Doha, Qatar
Background and Aims
Atrial fibrillation (AF) is an important risk factor for stroke, particularly in the elderly. There is limited data on AF-related stroke from the Middle East.
Method
A retrospective review of the Stroke database at Hamad General Hospital, Doha, Qatar, from 1st January 2014 thru 18 October 2017 was performed.
Results
The data of 4082 patients (81.4% male, mean age 55.4+ 13.3 years) were reviewed.
AF was present in 260 (6.4%) patients and of these 106 (2.6%) had new-onset AF.
Arabs from the Middle East and North Africa region (MENA)(including Qataris) comprised 66.2% the AF cohort, whereas South Asians the biggest ethnic group in the Database (51.6% of total cases) contributed 23.8% of AF cases and other ethnicities 10%. The mean age of non-AF stroke was 54.7 + 12.8 vs. 65.4 + 16 years for AF Stroke (p < 0.001).
While females represented (17.6%) of the non-AF cohort, they represented (33.8%) of the AF cohort (p < 0.001).
In multivariate model both Age odd ratios (OR) of 1.03(1.02 – 1.05, 95% CI) (p < 0.001) and gender OR 1.96 (1.25–2.98, 95% CI) (p = 0.001) predicted the presence of AF in this cohort. Similarly, NIHSS, presence of cardiac disease, presence of non-lacunar strokes and posterior circulation strokes were also independent predictors for the presence of AF (OR (1.05, 2.2, 2.49 and 2.06 respectively) (p < 0.05).
Conclusion
Age, female gender, stroke severity , presence of cardiac disease, non-lacunar and posterior circulation strokes were associated with AF-related stroke in a younger, multiethnic, gender skewed low AF prevalence population. AF-stroke occurs a decade younger than in the Western populations.
Trial registration number
N/A
AS21-017
EARLY VERSUS LATE ANTICOAGULATION ADMINISTRATION FOR ISCHAEMIC STROKE ASSOCIATED WITH ATRIAL FIBRILLATION: OBSERVATIONAL PROSPECTIVE MULTICENTRE INCEPTION COHORT STUDY
1Institute of Neurology, Brain repair and rehabilitation, London, United Kingdom
2University College London, Department of Statistical Science, London, United Kingdom
3University College London Hospital, Haemostasis Research Unit- Department of Haematology, London, United Kingdom
4University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
5University of Birmingham, Institute of Cardiovascular Sciences, Birmingham, United Kingdom
6Institute of Neurology, Department of Molecular Neuroscience, London, United Kingdom
7University of Glasgow, Institute of Neuroscience & Psychology, Glasgow, United Kingdom
Background and Aims
The optimal time to start oral anticoagulation (OAC) in patients with ischaemic stroke due to non-valvular atrial fibrillation (AF) is unclear. We reviewed OAC timing in relation to 90 day clinical outcomes as a post-hoc analysis from the CROMIS-2 observational study.
Method
Patients were included in this sub study if information on time to OAC initiation was available. The primary outcome was the composite of ischaemic stroke, TIA, intracerebral haemorrhage (ICH) or death within 90 days of the qualifying stroke or TIA. We performed adjusted Cox regression analyses to compare early (0 to 4 days) and later (5 to 90 days) OAC initiation.
Results
We included 1,272 patients, mean age 76 (SD 10) years of which 543 (43%) were female. OAC was started between early in 358 (28%) patients and later in 916 (72%) patients. Patients started on early OAC were younger, less likely to have been thrombolysed, had less severe strokes, and a lower pre-stroke mRS. There were 45 outcome events in 42 individual patients: 7 (2%) in the early (0 ICH, 5 ischaemic strokes, 2 deaths) and 38 (4%) in the late OAC group (2 ICHs, 16 ischaemic strokes and 20 deaths). There was no significant difference in the risk of the composite outcome in adjusted analysis (HR 0.78, 95% CI 0.33 to 1.89, p = 0.588)
Conclusion
Our data support starting OAC early after stroke in selected patients, but the benefits and risks need to be tested in randomised trials over a range of stroke severities.
Trial registration number
N/A
AS21-018
RISK FACTORS ASSOCIATED WITH STROKE AFTER TRANSCATHETER AORTIC-VALVE REPLACEMENT: ON THE WAY TO PREVENT IT
1Hospital Universitario Virgen Macarena, Neurología, Sevilla, Spain
2Hospital Universitario Virgen Macarena, Cardiovascular Surgery, Sevilla, Spain
3Hospital Universitario Virgen Macarena, Endovascular, Sevilla, Spain
Background and Aims
Transcatheter aortic-valve replacement (TAVR) is a safe and effective option for severe aortic stenosis treatment. Stroke is one of its most important complications. We aimed to explore stroke incidence after TAVR in a real-life population and compare it with TAVR trials and also tried to identify predictive factors for stroke
Method
179 TAVR patients from 2010–2016 performed by endovascular and cardiovascular surgeons were followed for one year. Baseline characteristics, stroke incidence and possible associated factors were recorded and compared to those in SURTAVI and PARTNER2 trials.
Results
Baseline variables: 62% females, mean age 80years, 83% hypertensives, 47.5% diabetics, 51% had dyslipidemias. 40.8% had coronary disease and 35.8% atrial fibrillation (AF) before TAVR. At follow-up new-onset AF was detected shortly following TAVR in 8.4% and 2.8% in the first year. Total incidence of stroke was 6.7% (12); 8 were ischemic, 3 hemorrhagic and 1 TIA. 75% of them occurred in late period, while only 25% in the first 30 days. No factors were associated with stroke appearance, except for a trend to among those being more hypertensive (82% vs 100%, p = 0.1).
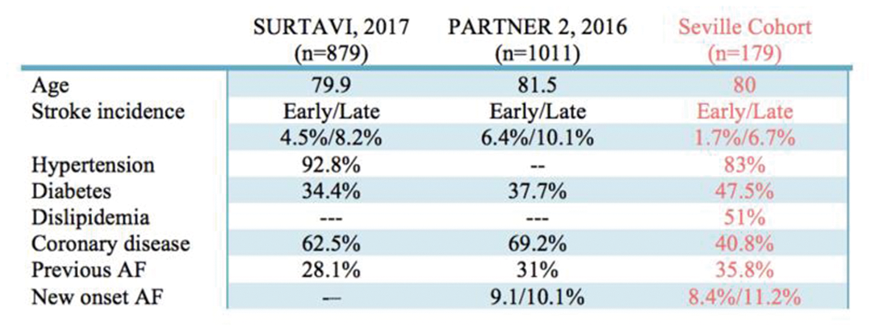
Conclusion
In our sample, stroke incidence following TAVR is similar than in large clinical trials, despite the fact that real-life patients use to have higher vascular risk factors burden. Assessment by a Vascular Neurologist prior to procedure to control risk factors and optimize prevention could be the key to reduce post-TAVR stroke incidence. Biomarkers identification to predict high-stroke-risk profile would be desirable since there is a lack of stroke predictors in this population.
Trial registration number
N/A
AS21-019
RISK FACTORS FOR ATRIAL FIBRILLATION IN PATIENTS WITH EMBOLIC STROKE OF UNDETERMINED SOURCE (ESUS)
1University Medicine Greifswald, Department of Neurology, Greifswald, Germany
2University Medicine Greifswald, Department of Cardiology- Deutsches Zentrum für Herz-Kreislauf-Forschung German Center for Cardiovascular Disease- DZHK, Greifswald, Germany
3University Medicine Greifswald, Department of Cardiology, Greifswald, Germany
Background and Aims
Since the publication of embolic stroke of undetermined source (ESUS) criteria, it has not been possible to determine at admission which patients suffer from yet undetermined atrial fibrillation (AF). We searched criteria that identify patients who will benefit most from invasive ECG-recording for AF detection.
Method
We enrolled 100 consecutive patients admitted for ESUS to our Department in 2016 who underwent insertion of insertable loop recorders (ILR, Medtronic Reveal LINQ). Cardiovascular risk factors and diseases, and AF detection were retrieved. We calculated CHA2DS2VASc-Score and arrhythmia score consistent of characteristics enhancing the chance of AF (diabetes, left atrial fibrillation, arterial hypertension, and current alcohol abuse).
Results
Within a mean observation time of 362 days, AF was detected in 17 of 100 patients (n = 9, 52.9% male). Patients with AF more often were ≥75 years old (52.9% vs. 27.7% for those without AF, p = 0.0088), had left atrial dilatation (58.8% vs. 25.3%, 0.0065), and more often had current alcohol abuse (23.5% vs. 9.6%, n.s.) than patients without AF (n = 58, 70.9% male).
In multiple logistic regression models controlling for age and sex, AF was significantly associated with left atrial dilatation (OR 3.12 (95%CI 1.002–9.708) and alcohol abuse (OR 7.96, 1.51–41.85). Odds ratios relating AF with a 1-point increase on the arrhythmia score or the CHA2DS2VASc score were 2.42 (1.229–4.778) and 1.529 (1.085–2.154).
Conclusion
Higher age, atrial dilatation, and current alcohol abuse are associated with AF detection in patients with ESUS. This may help to better choose patients who benefit from AF detection by ILR.
Trial registration number
N/A
AS21-020
PREDICTING ATRIAL FIBRILLATION IN ISCHAEMIC STROKE: A SYSTEMATIC REVIEW
1Ballarat Health Services, Ballarat Base Hospital, Ballarat, Australia
2Calvary Public Hospital, Stroke Service, Canberra, Australia
3Australian National University, ANU Medical School, Canberra, Australia
4Florey Institute of Neuroscience and Mental Health, Neuroscience and Mental Health, Melbourne, Australia
5University of Melbourne, Faculty of Medicine, Melbourne, Australia
Background and Aims
There has been renewed research interest in atrial fibrillation (AF) and increased stroke risk in the last decade. The occurrence of embolic stroke in the absence of AF has given rise to the new description of embolic stroke of undetermined source (ESUS). Current data suggests that AF is detected in approximately 30% of ESUS patients. Traditional methods, like 24-hour telemetry, detect AF in a small proportion of ESUS, while using prolonged Holter monitor or implantable loop recorders improves detection further. The latter, while being a more sensitive tool, is invasive and costly. Should we continue focusing on detection or expand to include accurate prediction of AF? In addition, do clinical predictors of AF exist?
Method
We conducted a systematic review of the literature to identify clinical predictors of AF.
Results
There is a body of research on predicting risk of AF. Identified variables include age, sex, cardiovascular risk factors, and ECG and echocardiogram abnormalities. We identified several tools ranging from moderate to strong predictive models for AF. However, none included recent biochemical tests and novel ECG changes.
Conclusion
We suggest that a mix of established and new variables and parameters be used to create a composite tool, enabling clinicians to accurately predict risk of AF in patients with ESUS, and informing decision-making regarding use of oral anticoagulants in preventing embolic events. Once developed, the tool will be tested in a suitable population. Generalizability should be a key feature of the tool to ensure equitability of use, in developed and developing economies.
Trial registration number
N/A
AS21-021
EARLY DABIGATRAN TREATMENT AFTER ISCHEMIC STROKE DOES NOT RESULT IN HEMORRHAGIC TRANSFORMATION
1University of Alberta, Medicine, Edmonton, Canada
2Population Health Research Institute- McMaster University, Medicine, Hamilton, Canada
3University of Ottawa, Medicine, Ottawa, Canada
Background and Aims
Early anticoagulation after stroke in atrial fibrillation (AF) patients remains controversial, due to potential hemorrhagic transformation (HT). The safety of initiating dabigatran within 14 days of stroke is unknown, as these patients were excluded from phase III trials.
Method
We enrolled participants with AF and acute ischemic stroke/TIA (<14 days, NIHSS≤3) treated with dabigatran in a prospective, multi-centre open label cohort. CT scans prior to and 7 days after dabigatran initiation were assessed centrally for HT and graded using ECASS criteria (hemorrhagic infarct (HI) 1/2, parenchymal hemorrhage (PH) 1/2).
Results
We enrolled 100 participants, 65 male, mean age 71.9 ± 13.6 years and infarct volume 7.3 ± 15.1 ml. Median (IQR) time from onset to first dabigatran dose was 2 (1–5) days, median NIHSS 1 (0–2). Pre-treatment HT was present in 4 patients (all HI1). Time to dabigatran initiation was correlated with infarct volume (r=0.61, P<0.0001). No patients developed symptomatic HT. Asymptomatic progression from HI1 to HI2 occurred in 1 patient on the day 7 scan. Asymptomatic HI1 developed in 6 patients. The only predictor of HT was infarct volume (OR = 1.075 [1.023–1.130], P<0.004). Six of 7 (86%) patients with new HT/progression were functionally independent (mRS=0–2) at 30 days, which was similar to those without HT (87%, p = 0.644). Recurrent ischemic events occurred within 7 days of treatment in 4 patients (3 strokes, 1 systemic embolus), and 50% of these patients were disabled at 30 days.
Conclusion
Early dabigatran treatment did not precipitate symptomatic HT after minor stroke. Early recurrent ischemic events may be clinically more important.
Trial registration number
NCT02415855 (CLINICALTRIALS.GOV).
AS21-022
SERUM LIGHT-CHAIN NEUROFILAMENT, A BRAIN LESION MARKER, IS ASSOCIATED WITH THE CHA2DS2-VASC SCORE AMONG PATIENTS WITH ATRIAL FIBRILLATION: A CROSS-SECTIONAL STUDY
1University of Basel Hospital, Department of Neurology, Basel, Switzerland
2University of Basel Hospital, Clinical Trial Unit- Department of Clinical Research, Basel, Switzerland
3Bern University Hospital, Institute of Primary health Care- Department of Internal Medicine, Berne, Switzerland
4Cantonal Hospital of Baden, Department of General Internal Medicine, Baden, Switzerland
5Hôpital Cantonal Fribourg, Department of Internal Medicine, Fribourg, Switzerland
6Luzerner Kantonsspital, Department of Cardiology, Lucerne, Switzerland
7Ospedale Regionale di Lugano, Department of Cardiology, Lugano, Switzerland
8Bürgerspital Solothurn, Department of Cardiology, Solothurn, Switzerland
9Centre Hospitalier Universitaire Vaudois, Departemnt of Cardiology, Lausanne, Switzerland
10University of Basel Hospital, Cardiology Division- Department of Medicine, Basel, Switzerland
11Bern University Hospital, Department of Neurology, Berne, Switzerland
12Felix Platter Hospital, Memory Clinic, Basel, Switzerland
13University of Basel Hospital, Department of Radiology, Basel, Switzerland
14University of Basel Hospital, Medical Image Analysis Center, Basel, Switzerland
15University of Zürich, Biostatistics and Prevention Institute, Zürich, Switzerland
16McMaster University, Population Health research Institute, Hamilton, Canada
Background and Aims
Serum light-chain neurofilament (sNfL) is an emerging biomarker for neuroaxonal injury in inflammatory, neurodegenerative and vascular brain disease. Its role as a potential neurological outcome marker in heart disease has not been investigated. Our aim was to study if sNfL is associated with the CHA2DS2-VASc score, a validated score predicting stroke risk in patients with atrial fibrillation (AF).
Method
sNfL was measured at baseline in 278 patients with AF included in the SWISS-AF cohort study (mean age 73, 75% male) 90% of whom were under oral anticoagulation. Linear regression was used to investigate associations between log-transformed sNfL and (1) CHA2DS2-VASc alone, (2) CHA2DS2-VASc adjusted for age, and (3) all components of the score (congestive heart failure, hypertension, age, diabetes, stroke and TIA history, vascular disease, sex) in a multivariable analysis.
Results
sNfL was significantly associated with the CHA2DS2-VASc score (figure), also after correction for age (p < 0.001). On average, sNfL levels increased by 22.3 % per unit increase in CHA2DS2-VASc score. In the multivariable model including the score components, age (4.7% increase per year) and diabetes (62.5% increase) were independently associated with sNfL (p < 0.001 each), as was stroke history by trend (29.4% increase; p = 0.06).
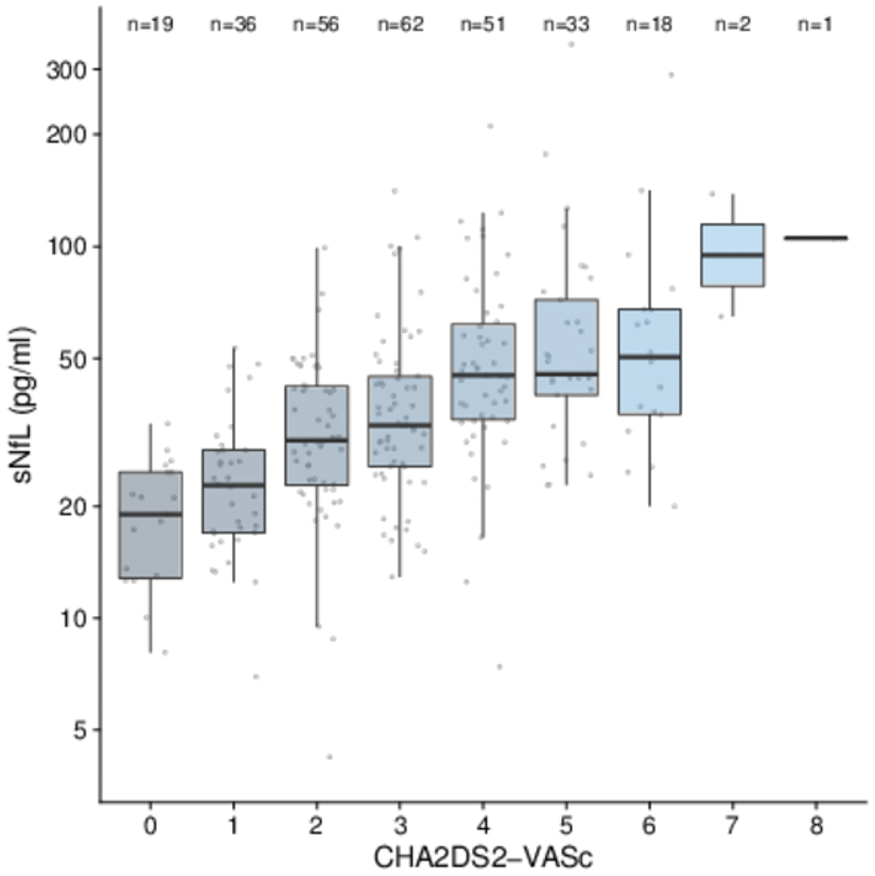
Conclusion
Our findings indicate increasing subclinical neuroaxonal injury with increasing CHA2DS2-VASc score among patients with AF. The mechanisms underlying this association remain to be elucidated.
Trial registration number
N/A
AS21-023
NEWLY DISCOVERED VERSUS KNOWN ATRIAL FIBRILATION IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1University clinic for neurology, Urgent Neurology, Skopje, FYR Macedonia
Background and Aims
To investigate the frequency of newly discovered versus known atrial fibrillation (AF) in patients who developеd acute ischemic stroke, associated risk factors, course and outcome of the disease.
Method
We analyzed the medical records of acute ischemic stroke patients hospitalized between 2014 and 2017 at our department. We assessed physical and neurological examination, modified Ranking Scale (mRS) score on admission and at discharge, laboratory tests, CT and/or MRI of the brain, electrocardiogram (ECG) monitoring for a period of 2 weeks and consultation with cardiologist. Vascular risk factors (hypertension, diabetes mellitus, dyslipidemia, heart diseases, smoking, peripheral arterial diseases) and previous stroke were evaluated. Statistical analysis was performed with the programme Statistica for Windows 12.
Results
Of the 960 patients in the study, 268 (27,9%) had atrial fibrillation. Newly discovered AF was registered in 65 (6,8%), while 203 (21,1%) patients had known AF. There was no statistical difference in terms of age, gender, clinical presentation, associated risk factors and outcome between the two groups (p>0.05). Compared to the rest, patients with AF (newly discovered or known) had higher mRS score on admission and at discharge from the hospital and had lethal outcome in higher percentage (p < 0.05).
Conclusion
AF, whether newly discovered or known, significantly increases the risk of stroke and affects its prognosis and outcome.
Trial registration number
N/A
AS21-024
“NEURO-HOLTER”: A NEW TECHNOLOGY FOR THE STROKE ETIOLOGY DIAGNOSIS. PILOT STUDY
1University Hospital of La Princesa, Stroke Unit, Madrid, Spain
Background and Aims
The search for the etiology of cryptogenic strokes is a diagnostic challenge. Currently, conventional 24-hour Holter-ECG records have a diagnostic rate for the detection of atrial fibrillation (AF) of only 4.6%. We evaluate the benefit and feasibility of a new technology based on biomedical textiles (Nuubo ®) that allow the prolonged recording of ECG without affecting the quality of life of the patient.
Method
It is a prospective study of patients with cryptogenic stroke or TIA discharged from the Stroke Unit or seen in a Vascular Consultation. A 2-week ECG recording was performed in all patients. The interpretation of the obtained signal was made through a patented software evaluated by the Neurology Service with the supervision of the Cardiology Service. The clinical variables and the results obtained were collected to proceed with their descriptive analysis.
Results
N = 44. Mean age: 72 years, 41% women. Subtype: 84% stroke, 16% TIA. The mean score on the CHA2DS2-VASc scale was 4.6. The indexed left atrium volume was available in 66% patients with a mean value of 32.06 ml/m2. A new detection of AF was achieved in 11.36% (5/44).
Conclusion
This new device based on non-implantable biomedical textiles has increased the detection of AF more than doubled over conventional devices in this group of patients. Future studies with a larger number of patients are necessary to confirm these findings and identify possible risk factors.
Trial registration number
N/A
AS21-026
LOW INCIDENCE OF ATRIAL FIBRILLATION IN RECURRENT STROKES IN A COHORT OF CRYPTOGENIC STROKE PATIENTS ON LONG TERM CARDIAC MONITORING
1Cone health, stroke center, Greensboro, USA
2cone health, CHMG Heartcare, Greensboro, USA
Background and Aims
Long term monitoring studies have detected atrial fibrillation in upto 30% of cryptogenic stroke patients but incidence of atrial fibrillation amongst recurrent strokes in this population is not well described.
Method
Review of electronic medical charts of our prospective cohort of cryptogenic strokes who underwent implantable loop recorder (ILR ) from February 2014 to September 2017. All patient’s met ESUS criteria and were enrolled in atrial fibrillation clinic with structured remote follow-up. All recurrent strokes were confirmed by vascular neurologist.
Results
442 patients underwent ILR placement. 32 had recurrent strokes at upto 3.5 years follow up. Age range (48–85) mean 65.71.56.25% (18/32 ) were males.- Mean time to recurrent stroke was 218.65 days (8–1285). Only 5 of these (15.5% ) had atrial fibrillation detected. 27/32 (84.5%) strokes yet remained of cryptogenic etiology. Atrial fibrillation was detected after 13,117,34,251 and 167 days after ILR implantation. All patients were started on anticoagulation (3 on apixaban and 2 on rivaroxaban). Imaging pattern of these recurrent stroke patients suggested cortical infarcts in 16 with 4 patients having multiple infarcts while 16 patients had subcortical infarcts with 5 showing multiple infarcts. There were no significant differences in imaging patterns of recurrent strokes patients with atrial fibrillation with 3 /5 patients having cortical and 2/5 having subcortical small infarcts.
Conclusion
In our prospective cohort of cryptogenic stroke patients atrial fibrillation was found in only 15.5% of recurrent strokes. Imaging charecteristics did not differ in recurrent stroke patients with or without atrial fibrillation.
Trial registration number
no
AS21-027
ATRIAL FIBRILLATION DETECTION AND STROKE RECURRENCE IN PATIENTS WITH EARLY INSERTABLE CARDIAC MONITOR. A CASE-CONTROL STUDY
1Hospital Del Mar, Stroke Unit. Neurology, Barcelona, Spain
2Hospital del Mar, Cardiology, Barcelona, Spain
Background and Aims
Paroxysmal atrial fibrillation (pxAF) is the underlying cause of most patients with cryptogenic strokes (CrS). Several methods for AF detection have been used, but current guidelines are not specific about the best strategy. AF detection rate varied between 5–20% with external ECG-monitoring and up to 25–35% with insertable cardiac monitor (ICM). The aim of our study was to assess the AF-detection rate in CrS admitted in stroke unit (SU) with early ICM, in comparison to a standard non-invasive outpatient strategy.
Method
Case-control study, including prospective first acute ischemic cryptogenic stroke/TIA patients with ICM before discharge compared with retrospective patients without ICM. A 24–36h ECG-monitoring in SU and 3D-transthoracic echocardiography were performed before ICM implantation (5–7 day after stroke). The primary outcome was newly detected AF lasting more than 30 seconds. Early anticoagulation was started in patients with AF detection. Secondary outcome included stroke recurrence.
Results
65 cases/81 controls with CrS between 50–89 years. There were no differences in age, sex or vascular risk factors. AF was detected in 35(53.8%) cases and 21(25.9%) controls, p < 0.001. Detection in cases was earlier than in controls: 36(15–169) vs94(54–303);p = 0.099 days. Stroke recurrence was found in 2(3.1%) cases vs. 9(11.1%) controls;p = 0.058. Time to recurrence was 10 ± 9.1 months without differences between groups.
Conclusion
In our study the rate of AF detection was as high as 53.8% in cases with ICM, more than twice than in controls with conventional external monitoring. Time to AF detection was very short and recurrence lower, outlaying the importance of early implantation of ICM and anticoagulation therapy.
Trial registration number
N/A
AS21-029
CARDIOGENIC CEREBRAL EMBOLISM IN NON-VALVULAR ATRIAL FIBRILLATION
1The National Pirogov Medical Surgical Center- National Center of Cerebrovascular, Neurology, Moscow, Russia
2Scientific research Institute of emergency care named N.V. Skliphosovskiy- Moscow- Russia, Neurology, Moscow, Russia
Background and Aims
The embolic stroke in AF suggests a high diagnostic significance for the detection of microembolic particles in the cerebral blood. Previous studies have shown an extremely low frequency of detection of MES in patients with AF, which does not correspond to the quantity of cerebral vascular complications.
Determine the frequency of registration of microemboli and prognostic significance of MES as an independent marker for the development of cardiogenic cerebral embolism in non-valvular AF.
Method
42 patients with and without the transferred cardioembolic vascular events were divided into two groups respectively (n1=22, n2=20). MES registration was performed by the method of bilateral Doppler monitoring of the MCA on the SOMOMED-300M device at the beginning of the study, 10 days later, 6 and 12 months.
Results
During the observation period, cerebral microemboli were detected in 3(7.1%) patients of cases (1(4%) patient from the first and 2(11%) patients from the second group). There was no significant relationship between the presence of MES in the cerebral arteries and embolic complications (vascular death, repeated AIS and/or TIA in the ipsilateral hemisphere) in patients with AF(p>0.05).
Conclusion
During the period of observation, 7 MES were detected in both groups. The revealed material microembolic signals in patients with AF are not associated with the transferred cardioembolic event (stroke or TIA) and may have a platelet valvular nature. Cardiogenic cerebral embolism in patients with non-valvular AF is realized by the formation of large, fibrin-erythrocyte thrombi in the left heart, not available for Doppler detection in the distal sections of the cerebral arteries.
Trial registration number
N/A
AS21-030
CARDIAC BIOMARKERS AND CEREBRAL ISCHAEMIA
1Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Neurology, Ariano Irpino AV, Italy
2Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Internal Medicine, Ariano Irpino AV, Italy
3Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Cardiology, Ariano Irpino AV, Italy
4Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Infantile Neuropsychiatry, Ariano Irpino AV, Italy
5Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Radiology, Ariano Irpino AV, Italy
6Ospedale S. Ottone Frangipane - ASLAV - II University of Naples, Laboratory, Ariano Irpino AV, Italy
Background and Aims
Troponin ths (Tro ths) and N-Terminal-pro-Brain Natriuretic peptide (NT-pro-BNP) are increased in cerebrovascular conditions, especially in class III/IV, C/D New York Heart Association and American Cardiology Association scales. The aim of our study was to assess the relation with the involved cerebral region.
Method
So far, we recruited 552 acute ischaemic stroke (AS). They underwent blood withdrawals at day 1, 3 and 7. Computerized Tomography and/or Magnetic Resonance Imaging were performed at admission, after 24 hours and, if necessary, repeated later.
Results
No significant differences of cardiac biomarkers were related to the region of the AS (Internal Carotid Artery, Middle Cerebral Artery, Anterior Cerebral Artery AS: Tro ths 73,4 sd 430,2 pg/ml, NT-pro-BNP 3898,6 sd 6648,4 pg/ml; Vertebro-Basilar AS: Tro ths 60 sd 153,5 pg/ml; NT-pro-BNP: 3607,9 sd 6143,7 pg/ml, p ns). These results were confirmed in subgroup analysis among cardiac biomarkers in fronto-parietal (Tro ths 24,93 sd 19,37 pg/ml; NT-pro-BNP 1717,1 sd 1996,4 pg/ml), temporo-insular (Tro ths 23,9 sd 15,1 pg/ml; NT-pro-BNP 2581 sd 4166,1 pg/ml), capsulo-nuclear (Tro ths 27,73 sd 27,27 pg/ml; NT-pro-BNP 2022,4 sd 2435,5 pg/ml), occipital (Tro ths 41,68 sd 42,57 pg/ml; NT-pro-BNP 2398,8 sd 2198,4 pg/ml), cerebellar-brainstem (Tro ths 30,6 sd 26,4 pg/ml; NT-pro-BNP 2080,8 sd 2771,9 pg/ml) AS. Levels of cardiac biomarkers, as the extension of cerebral ischaemia, were related to the severity of cardiac dysfunction, responsible of diffuse hypoxic encephalopathy in severe cases.
Conclusion
Our data highlight the importance of cardiological evaluation for assessing the risk of reduced perfusion and increased diffusion-restricted cerebral tissue in AS.
Trial registration number
N/A
AS21-031
PAROXYSMAL ATRIAL FIBRILLATION DETECTION AFTER CRYPTOGENIC STROKE: A SINGLE CENTER EXPERIENCE
1Hospital Clínico Universitario Lozano Blesa, Neurology, Zaragoza, Spain
2Hospital Clínico Universitario Lozano Blesa, Cardiology, Zaragoza, Spain
Background and Aims
Long-term implantable cardiac monitoring following early post stroke resulted in a high rate (12 – 38%) of paroxysmal atrial fibrillation and flutter (PAF) detection in cryptogenic stroke (CS) patients according to previous studies. Our institution protocol involves a late insertable cardiac monitoring (ICM) placement compared with previous data. Our aim was to asses the PAF detection rate achieved with our protocol.
Method
We retrospectively reviewed CS patients admitted to our institution who underwent ICM implantation during outpatient follow-up from June 2015 to December 2017. We analysed the PAF rate detection, time from stroke to IMC placement, and time between ICM placement and PAF detection.
Results
37 CS patients underwent ICM placement (56.8% males, mean age 74.38 years). The median time between stroke and IMC placement was 226.6 days [range 18 – 642]. PAF was detected in 10 (27%) CIS patients during the study period (18.9% atrial fibrillation; 8.1% atrial flutter). The median time from device insertion to PAF detection was 82.5 days [range 3–295] and 336.6 days [37 – 729] between stroke and PAF detection. The median follow-up time was 337.95 days [range 115–853]. All the patients with PAF detection were anticoagulated (12.5% with warfarin, 87.5% with direct oral anticoagulants).
Conclusion
ICM insertion in the subacute phase of stroke resulted in a substantial rate of PAF detection in our institution. When ICM cannot be placed early after stroke, placement during the outpatient evaluation should be also considered.
Trial registration number
N/A
AS21-032
EMBOLIC STROKE OF UNDETERMINED SOURCE WITH ABNORMAL TRANSESOPHAGEAL ECHOCARDIOGRAPHY: HOW FAR ARE THESE PATIENTS FROM ATRIAL FIBRILLATION STROKE PATIENTS?
1Hospital de Clínicas - Federal University of Parana, Neurology Division, Curitiba, Brazil
Background and Aims
Although not necessary for the diagnosis of Embolic Stroke of Undetermined Source (ESUS), transesophageal echocardiography (TEE) may help stratify its recurrence risk, by the identification of potential sources of emboli.
Aim
to compare the occurrence of an endpoint composed by recurrent stroke, cardiovascular death and myocardial infarction (MI) in ESUS patients with normal TEE, ESUS patients with abnormal TEE and atrial fibrillation (AF) stroke patients.
Method
A retrospective analysis of a prospective data bank was conducted, including all consecutive patients with first-ever ischemic stroke (IS) admitted between October 2012 and January 2017. The ischemic stroke was considered secondary to atrial fibrillation based in the TOAST criteria and ESUS according to Cryptogenic Stroke/ESUS International-Working-Group criteria. Based on the findings observed in the TEE, ESUS patients were classified in to normal TTE and to abnormal TEE.
Results
The primary endpoint occurred in all the three groups at the same rate (p = 0,429). The time to the occurrence of the primary endpoint did not differ significantly among ESUS patients with or without TEE abnormalities (p = 0,319). Overall, the use of oral anticoagulants (OA) had a significant protective effect on the primary endpoint (p = 0,002).
Conclusion
With or without TEE abnormalities, ESUS patients presented similar rates of recurrent stroke, cardiovascular death and MI, when compared to AF patients. ESUS patients might benefit from OA’s prescription, irrespective of the presence of embolic sources on TEE.
Trial registration number
N/A
AS21-033
IS 24 HOUR ECG MONITORING THE INVESTIGATION OF CHOICE TO DIAGNOSE PAROXYSMAL ATRIAL FIBRILLATION?
1Worcester Royal Hospital, Stroke Department, Worcester, United Kingdom
Background and Aims
Atrial fibrillation (AF) is the most common sustained adult cardiac arrhythmia causing ischaemic strokes. Paroxysmal AF (PAF) is undetected and untreated if sufficient ECG monitoring is not performed adequately. Adequate diagnosis of AF following an ischaemic stroke is vital in preventing further strokes. Current guidelines recommend a minimum of 24 hours ECG monitoring after a stroke to exclude PAF. We want to study if this recommendation is reliable in diagnosing PAF.
Method
In this retrospective study, we investigated the detection rate of PAF with prolonged ECG monitoring in 100 stroke patients admitted over 6 months to Worcester Royal Hospital. Data was collected using patient notes and standards were set against the Royal College of Physicians Stroke Guidelines UK.
Results
This study included ninety-seven 24-hour tapes, two 72-hour tapes and one 7-day tape. Among 100 eligible stroke patients, 9 (9%) patients were found to have PAF from 24-hour ECG monitoring. 3 out of 5 known AF patients showed AF in 24 hour monitoring which were excluded from the total of 9 identified AFs. 6 AFs were newly diagnosed which gives a pick up rate of 6.52%. The two 72-hour and the 7-day tape in the study did not pick up AF in the presenting stroke patients.
Conclusion
Prolonged ECG monitoring for more than 24-hours duration is required in order to maximise the diagnosis of PAF. Optimal duration of ECG monitoring should be further investigated.
Trial registration number
N/A
AS21-034
STRATIFYNG THE RISK OF ATRIAL FIBRILLATION WITH MULTIMODAL LEFT ATRIA BIOMARKERS IN CRYPTOGENIC STROKE
1Vall d'Hebrón hospital, Stroke Unit, Barcelona, Spain
2Vall d'Hebrón hospital, Research Lab, Barcelona, Spain
3University Hospitals Virgen Macaren-Virgen del Rocio, Stroke Unit, Sevilla, Spain
4University Hospital of Valladolid, Stroke Unit, Valladolid, Spain
Background and Aims
Traditional predictors of AF are unsuitable in elderly stroke patients. We tested the hypothesis that the combination of two correlated atrial dysfunction markers (NT-ProBNP and Left atria Strain) may improve the selection of patients at risk of AF.
Method
We performed a prospective multicentric study of cryptogenic stroke patients (CRYPTO AF Registry) during 3 years. Subjects underwent 30 days Holter monitoring and complete diagnosis evaluation (CT/MRI, Doppler CT, Echocardiography, 24h CEM.) NT-ProBNP level was obtained and Left atrial strain (LAS) was assessed by speckle tracking echocardiography. We calculated the validity (sensitivity (S) and E (specificity) of both markers by ROC curves analysis.
Results
Two hundred and eighty-one patients were included. Median age was 75 years (69–83). Comparing patients with AF detection, we did not find any difference in age (a trend), sex, hypertension, diabetes, CHA2DS2VASC score, NIHSSS, left atria volume and left ventricle ejection fraction. NT-ProBNP level was higher in patients with AF detection 346.9 pg/ml Vs. 203.5 pg/ml (p = 0.028) and Left Atrial Strain was lower 18.66% Vs. 27.43% (p = 0.003). The AUC of NT-ProBNP was 0.65, NT-ProBNP >102 pg/ml (S 96%, E 33%) and Left Atrial Strain was 0.73, LAS<19.28% (S 50%, E 80.4%). The combination of both showed an AUC of 0.76, 0.23 (S 94%, E 50%). The rate of AF in High-risk group (NT-ProBNP >102 & LAS<19.28%) was 10-fold the rate in Low risk group (NT-ProBNP <102 & LAS>19.28%).
Conclusion
The use of multimodal atrial dysfunction markers (NT-ProBNP &LAS) improved their validity for AF detection in elderly cryptogenic stroke patients.
Trial registration number
N/A
AS21-035
STROKE RISK PREDICTION WITH CORTICAL MICROINFARCTS IN PATIENTS WITH ATRIAL FIBRILLATION
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, Hong Kong, Hong Kong S.A.R
2The Chinese University of Hong Kong, Department of Imaging and Interventional Radiology, Hong Kong, Hong Kong S.A.R
3Queen Elizabeth Hospital, Department of Medicine, Hong Kong, Hong Kong S.A.R
4Northern District Hospital, Department of Medicine, Hong Kong, Hong Kong S.A.R
5Pamela Youde Nethersole Eastern Hospital, Department of Medicine, Hong Kong, Hong Kong S.A.R
6United Christian Hospital, Department of Medicine, Hong Kong, Hong Kong S.A.R
7Yan Chai Hospital, Department of Medicine, Hong Kong, Hong Kong S.A.R
Background and Aims
Cortical microinfarcts (CMI) detected by MRI brain, is a recently emerged radiological marker, representing microscopic regions of ischaemic-related cell death at brain cortex. They are most commonly observed in patients with small vessel disease, vascular dementia, Alzheimer’s disease, lacunar strokes and cerebral amyloid angiopathy. Recent studies have also demonstrated their association with subclinical cardiac diseases. However, it remains uncertain if CMI can help predict stroke risk in patients with AF. The purpose of this study is to evaluate if CMI is associated with clinical ischaemic stroke or transient ischaemic attack (IS/TIA) in patients with AF.
Method
In this prospective multicenter study, we recruited AF patients on oral anticoagulants for 3T MRI brain. Presence of CMI was correlated with other small vessel disease markers and IS/TIA.
Results
A total of 517 patients were included in this study. CMIs were observed in 58 (11.2%) of patients. Patients with CMIs were more likely to have IS/TIA (82.8% vs 65.8%, p = 0.001) and higher mean CHA2DS-VASc score (5.26 ± 1.86 vs 4.64 ± 1.81, p = 0.020) compared to patient without CMI. From multiple logistic regression, CMI, white matter score, hyperlipidaemia, hypertension and CHA2DS2-VASc scores were independent predictors for IS/TIA. Comparing to CHA2DS2-VASc scores alone, combining CMI with CHA2DS2-VASc scores improves risk prediction modestly for IS/TIA.
Conclusion
This proof-of-concept study suggests that CMI may help predict stroke risk in patients with AF. CMI may serve as an adjunctive risk-stratification tool when decision for anticoagulation is difficult base on clinical risk factors alone.
Trial registration number
NA
AS21-036
WHEN DOACS AFTER CARDIOEMBOLIC STROKE?
1Aomori Prefectural Central Hosptal, Neurology, Aomori, Japan
Background and Aims
Because of their high efficacy and safety, the use of direct oral anticoagulants (DOACs), instead of warfarin (WF), has recently increased to prevent the recurrence of cardioembolic stroke (CES). Due to their rapid onset of action, DOACs are expected to be introduced during the acute phase of CES; however, such an approach is not actively recommended due to the lack of conclusive evidence..
Method
This study aimed to investigate the actual anticoagulation therapy administered to our patients in the acute phase of CES to our department between April 2015 and March 2016, we retrospectively reviewed the medication used for anticoagulation, timing of therapy initiation, and the presence or absence of complications such as hemorrhage.
Results
Ninety seven patients were diagnosed CES (60 men and 37 women) during the study period. Anticoagulation therapy was administered to 80 patients; WF was used in 29 patients and DOAC in 51. The therapy was initiated by the second day of admission in 44 patients (WF in 11 and DOAC in 33), indicating that 65% of patients given DOAC had started therapy by the second day of admission. Hemorrhagic complications were noted in 13 patients (1 treated with WF and 12 with DOAC), but none were severe enough to require treatment.
Conclusion
DOACs can actually be used in the acute phase of CES without causing any major problems. We anticipate the establishment of further clinical evidence that can clarify details, such as the timing for optimal initiation of DOACs according to severity levels.
Trial registration number
N/A
AS21-037
HEMORRHAGIC TRANSFORMATION IN PATIENTS WITH ACUTE ISCHEMIC STROKE AND ATRIAL FIBRILLATION: TIMING OF THE INITIATION OF ORAL ANTICOAGULANT THERAPY AND OUTCOMES
1University of Perugia, Stroke Unit, Perugia, Italy
Background and Aims
In patients with acute ischemic stroke and atrial fibrillation (AF), early anticoagulation prevents ischemic recurrence, but associated hemorrhagic transformation (HT) remains a major concern. The aims of this study in consecutive patients with acute stroke and AF were: 1) to evaluate the incidence of early HT; 2) to evaluate the time to initiation of oral anticoagulant therapy in patients with HT; 3) to correlate the presence of HT with ischemic recurrence; and 4) to assess the influence of HT on clinical outcome at 90 days.
Method
HT was diagnosed by brain CT performed 24–72 h after stroke onset. Three-month ischemic recurrence were defined as the composite of ischemic stroke, TIA or systemic embolism. Three-month mortality or disability (mRS>2) were also evaluated.
Results
Among the 2,183 patients enrolled, 241 (11.0%) had HT. Patients with and without HT initiated oral anticoagulant therapy after a mean 23.3 days and 11.6 days, respectively from index stroke (p = 0.0001): 11/241 patients (4.6%) with HT had an ischemic recurrence compared to 96/1942 patients (4.9%) without HT. On multivariate analysis, HT was associated with mortality or disability at 90 days (OR 1.71, 95% CI 1.24–2.35, p = 0.001).
Conclusion
Early HT was observed in 11% of patients with acute stroke and AF. In patients with HT, the time to initiation of anticoagulants was about 12 days later than patients without HT. This delay was not correlated with ischemic recurrence at 90 days. HT was significantly associated with mortality or disability at this follow-up time.
Trial registration number
N/A
AS21-038
CLINICAL CHARACTERISTICS OF CARDIOEMBOLIC STROKE WITH OR WITHOUT ATRIAL FIBRILLATION
1Ajou University Hospital, neurology, Suwon-si, Republic of Korea
Background and Aims
Devastating cardioembolic (CE) stroke is responsible for approximately 20% of all ischemic strokes. Nonvalvular atrial fibrillation is the most frequent cause of CE strokes and is potentially preventable cardiac dysfunction. To reduce the stroke recurrence besides this ordinary embolic source from atrial fibrillation, stroke neurologists have taken into account other causative embolic abnormalities. Therefore, we are to investigate clinical and radiological characteristics in CE stroke patients with or without atrial fibrillation.
Method
We analyzed the consecutive 1,529 patients from a prospective stroke registry over 4 years. We selected the patients who were assigned as CE mechanism according to well-defined TOAST classification in weekly adjudication meeting. We also divided atrial fibrillation into permanent or persistent, paroxysmal, and non-atrial fibrillation groups with at least 72-hour monitoring at stroke unit care. Stroke patterns were categorized to territorial, non-territorial or scattered, borderzone, and subcortical subtypes.
Results
We analyzed a total of 364 stroke patients with CE. As compared with atrial fibrillation-positive group (n = 307), atrial fibrillation-negative group (n = 57) was younger (73.0 ± 11.2 vs. 64.3 ± 15.1; p < 0.001) and more severe on baseline NIH stroke scale (11.2 ± 7.7 vs. 6.8 ± 7.2; p < 0.001). Territorial pattern were more prevalent toward permanent or persistent type of atrial fibrillation; and borderzone pattern more prevalent toward paroxysmal and non-atrial fibrillation group. There was no difference of future stroke recurrence score between the groups.
Conclusion
This study suggests that CE stroke without atrial fibrillation appear to be associated with mild initial presentations and more common borderzone and non-territorial patterns, which can be representing less clot burden in such cases.
Trial registration number
N/A
AS21-039
PROSPECTIVE STUDY OF DETECTION OF PAROXYSMAL ATRIAL FIBRILLATION WITH VERY EARLY PROLONGED HOLTER MONITORING IN CRYPTOGENIC AND NON-CRYPTOGENIC STROKE
1Groupe Hospitalier Paris Saint Joseph, Neurology and Neurovascular Department, Paris, France
2Centre Médico-Chirurgical Ambroise Paré, Département of Electrophysiology and Pacing, Neuilly-sur-Seine, France
3Groupe Hospitalier Paris Saint Joseph, Cardiology, Paris, France
4Groupe Hospitalier Paris Saint Joseph, Neurology and Neurovascular Department- Université Paris Descartes-Sorbonne, Paris, France
Background and Aims
Prolonged Holter monitoring for the detection of paroxysmal atrial fibrillation (PAF) is usually performed after cryptogenic stroke and initiated late after injury. We aimed to monitor patients very early following stroke and to compare the rate of PAF in those with cryptogenic and non-cryptogenic stroke.
Method
This prospective, monocentric study was conducted over a 2-year period among patients > 65 y-o admitted for ischemic stroke. Monitoring with the LivaNova SpiderFlash® device began as soon as possible after the stroke. Recordings were assessed by a pacing cardiologist, who was unaware of patient characteristics. We looked for PAF (episodes longer than 30 seconds) and assessed anticoagulation consecutively.
Results
A total of 405 patients was screened and 102 were prospectively recruited (mean age 70 ± 4, 58% men, 57% with cryptogenic stroke). Holter monitoring began 5 ± 1 days after stroke and lasted 19 ± 2 days. PAF was diagnosed in 14 (14%) patients (mean age 75 ± 7). The first PAF episode was recorded 9 ± 6 days after the beginning of record. PAF episodes were observed in 13.7% and 13.6% of patients with cryptogenic and non cryptogenic stroke, respectively, and the same rate was observed in those with atherosclerotic or lacunar stroke. In all 14 PAF+ patients, prolonged anticoagulation was prescribed.
Conclusion
In this prospective series of patients > 65 y-o, early recording did found PAF in both groups with cryptogenic and non cryptogenic stroke in the same proportion, and anticoagulation was proposed to PAF patients. The clinical significance of PAF episodes within the first weeks after stroke remains to be precised.
Trial registration number
ClinicalTrials.gov NCT02778321
AS21-040
PROPORTION OF EHRA/ESC LEFT ATRIAL APPENDAGE CLOSURE (LAAC) CANDIDATES BEFORE AN ACUTE STROKE ASSOCIATED WITH ATRIAL FIBRILLATION (AF): 12-MONTH OUTCOME IN THE WATCH-AF REGISTRY
1Bichat Hospital, Neurology, Paris, France
2Hospices Civils de Lyon, Neurology, Lyon, France
Background and Aims
Because of contra-indications, frailty, cognitive impairment, co-morbidities or patient refusal, or perceived low risk of stroke or high bleeding risk, many patients with AF are not treated with long-term oral anticoagulant (LTOAC). Among them, the proportion of candidates for LAAC before stroke and their 12 months outcome after stroke is not well known.
Method
Consecutive patients admitted within 24 hours of symptom onset of an acute stroke associated with AF in two stroke centers had systematic data collection (e.g., CHADSVASC, HASBLED) at 6 and 1 months before stroke, at admission, discharge, 2 and 8 days, 3, 12 months post stroke. The primary endpoint was death or dependency (mRS>3). Potential candidates for LAAC were based on ERHA/ESC recommendations.
Results
Among 400 enrolled patients, 237 patients had a known AF before baseline. In these patients CHADSVASC was 0 in 5.1%, 1 in 11.5%, ≥2 in 83.3% and HASBLED ≥3 in 33.8% of them before stroke. LTOAC was given in none of patients with CHADSVASC 0, in 15.4% of patients with CHADSVASC 1, and in 61.7% in patients with CHADSVASC ≥2. Among 225 patients with CHADSVASC ≥ 1, 51 (22.6%) had EHRA/ESC LAAC indication. Their 12-month rate of death or dependency was 61.2% [95% CI, 48.0–74.7] as compared to 34.5% [95% CI, 27.7–42.4] in remaining patients (P<0.0001).
Conclusion
Among patients with AF before stroke and CHADSVASC≥ 1, 22.6% were ERHA/ESC candidates for LAAC. The 12-month post stroke outcome of patients who were EHRA/ESC candidates for LAAC before stroke was much severe than other patients.
Trial registration number
N/A
AS21-041
ASSOCIATION BETWEEN HIGH-SENSITIVITY CARDIAC TROPONIN LEVEL AND SEVERITY OF CEREBRAL WHITE MATTER LESIONS IN PATIENTS WITH ACUTE ISCHEMIC STROKE
1Charité - Campus Benjamin Franklin, Klinik für Neurologie, Berlin, Germany
2Charité-Universitätsmedizin Berlin, Center for Stroke Research, Berlin, Germany
3Charité-Universitätsmedizin Berlin, Berlin Institute of Health, Berlin, Germany
4Charité-Universitätsmedizin Berlin, DZNE German Center for Neurodegenerative Diseases, Berlin, Germany
5Charité-Universitätsmedizin Berlin, DZHK German Center for Cardiovascular Research, Berlin, Germany
Background and Aims
Previous studies suggested an association between cognitive impairment, dementia and cardiac diseases. Our aim was to assess whether there is a link between cardiac troponin levels (hs-cTnT) as a marker of subclinical myocardial injury and severity of white matter lesions (WML) as a marker of subclinical brain injury in stroke patients.
Method
We retrospectively analyzed consecutive acute ischemic stroke patients admitted to Charité-University Hospital, Berlin from 2011–2013. All participants included in our analysis underwent 3T-cMRI and serial hs-cTnT measurements. We graded severity of WML using the age-related white matter severity score (ARWMS). We excluded patients with hs-cTnT >52 ng/l or dynamic change of hs-cTnT >50% to account for possible acute hs-cTnT elevation. We performed quantile regression analysis to determine whether the association between hs-cTnT (dichotomized at the 99th percentile, 14ng/l) and WML depends on WML severity. Adjustment was made for age, sex and vascular risk factors.
Results
A total of 860 patients were analyzed (median age 73 years, 44.8% female, median ARWMS 6). Patients with elevated hs-cTnT had more extensive WML than those without (median ARWMS 8 vs. 5, adjusted coefficient 1.09, 95% CI 0.63–1.55). In addition, quantile regression analysis showed that the association between WML and hs-cTnT elevation was stronger in patients with severe WML (coefficient 1.77, 95% CI 1.06–2.48 at 75% WML-percentile; coefficient 2.86, 95% CI 0.48–5.24 at 90% WML-percentile).
Conclusion
Our data indicate an association between subclinical myocardial injury and severity of white matter lesions with an effect that is potentially dependent on the WML load.
Trial registration number
N/A
AS21-042
AORTIC DISSECTION MASQUERADING AS A “CODE STROKE”: A PROSPECTIVE CASE SERIES
1Academic Medical Center AMC, Neurology, Amsterdam, The Netherlands
Background and Aims
Acute aortic dissection is an uncommon disease (incidence in the general population is 2.6–3.5 per 100 000 person-years) with a high morbidity and mortality. Approximately 17–40% of these patients present with neurological symptoms, but the incidence of acute aortic dissection in a “code stroke” population is unknown. We report incidence, clinical manifestations, radiological findings and outcomes of patients with an acute aortic dissection in a code stroke population.
Method
We used data from a single-center prospective registry of consecutive adult patients who presented to the emergency department in 2017 with neurological deficits suggestive of an acute stroke (“code stroke”). All such patients routinely undergo non-contrast CT of the brain and CT-angiography of the aortic arch, cervical and intracranial arteries.
Results
Of 996 “code strokes”, 496 (50%) had an acute ischemic stroke. Four patients (0.4%) had a type A Stanford classification acute aortic dissection (see table). The incidence of an acute aortic dissection was 402 per 100 000 person-years (0.4%) in the “code stroke” population and 806 per 100 000 person-years (0.8%) in the acute ischemic stroke population. Pain was a distinguishing feature in all four, neurological symptoms varied. Three survived.
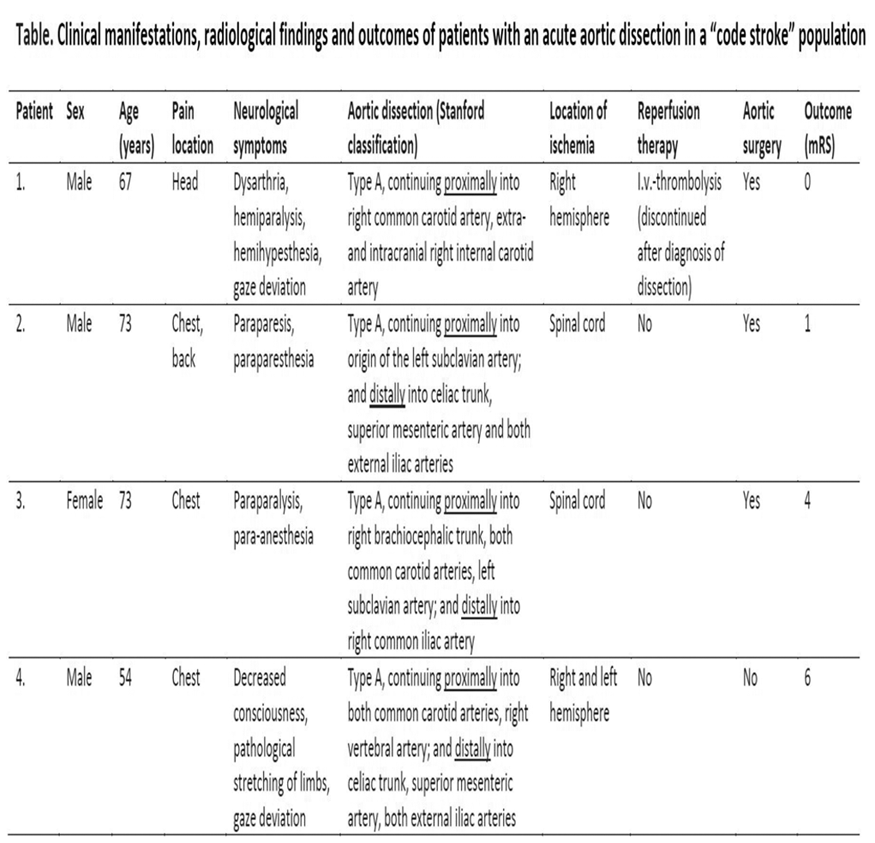
Conclusion
About 1/200 “code stroke” patients have an acute aortic dissection. Given the potential ramifications of missing this diagnosis, imaging of the entire aortic arch is important in “code stroke” patients.
Trial registration number
N/A
AS21-044
TROPONIN ELEVATION AND AUTONOMIC DYSFUNCTION AFTER ISCHEMIC STROKE: INSIGHTS FROM THE SICFAIL (STROKE INDUCED CARDIAC FAILURE IN MICE AND MEN) PROSPECTIVE COHORT STUDY
1University of Würzburg, Institute of Clinical Epidemiology and Biometry, Würzburg, Germany
2University of Würzburg, Interdisciplinary Center for Clinical Research, Würzburg, Germany
3University Hospital Würzburg, Department of Neurology, Würzburg, Germany
4University Hospital Würzburg, Department of Internal Medicine, Würzburg, Germany
5University of Würzburg, Comprehensive Heart Failure Center, Würzburg, Germany
6University of Zürich, Psychiatric Hospital, Zürich, Switzerland
7University Hospital Essen, Department of Neurology, Essen, Germany
8University Hospital Würzburg, Clinical Trial Center, Würzburg, Germany
Background and Aims
Troponin elevation can be observed in ischemic stroke (IS) patients in the acute phase, the majority of them without cardiac symptoms. This phenomenon might be caused by autonomic dysfunction due to sympathovagal imbalance with sympathetic overweight. We investigated whether high troponin values are associated with reduced heart rate variability (HRV), an established marker of autonomic dysfunction.
Method
Data were collected within the hospital-based SICFAIL study assessing the natural course of cardiac function after IS. Baseline investigation included cardiac history, physical examination, and echocardiography. Four HRV time domain variables were calculated for a subset of patients undergoing routine 24-hour Holter monitoring. Blood samples were collected 2–4 days after stroke. Multivariable logistic regression was used to determine the association of HRV time domain variables and elevated troponin, adjusted for age, gender, stroke severity, systolic dysfunction (ejection fraction ≤ 55%), impaired kidney function (glomerular filtration rate <60 ml/min/1.73m2), insular lesion, previous beta-blocker use, history of myocardial infarction, angina, and hypercholesterolemia.
Results
Complete baseline information was available from 154 IS patients who underwent 24-hour Holter monitoring between January 2014 and April 2015. Troponin was elevated (>14ng/L) in 42 patients (27%). In multivariable analysis, systolic dysfunction (OR 6.00 95% CI 2.06–17.47), impaired kidney function (OR 3.59 95% CI 1.17–10.97) and age (OR per year 1.07 95% CI 1.03–1.11) were associated with increased troponin values.
Conclusion
In this analysis, troponin elevation was associated with concomitant disease conditions. The role of autonomic dysfunction in troponin elevation, as assessed by HRV, has to be elucidated further.
Trial registration number
N/A
AS21-045
STROKE SEVERITY AND MORTALITY IN PATIENTS WITH NEWLY DIAGNOSED ATRIAL FIBRILLATION
1University of L'Aquila, Department of Neurology and Stroke Unit, L'Aquila, Italy
2University of L’Aquila, Department of Neurology and Stroke Unit, L'Aquila, Italy
Background and Aims
Atrial fibrillation (AF) is a major risk factor for stroke. We investigated the burden of newly diagnosed AF (NDAF) among first-ever ischemic stroke (FEIS) patients.
Method
Prospective population-based registry including all the residents with a FEIS in 2011–2013.
Results
Out of 884 patients with FEIS, 285 had documented AF and 64 (22.5%) NDAF. At the multivariate analysis, age ≥80 years and arterial hypertension were independently associated with AF. NDAF patients with respect to those previously diagnosed AF (PDAF) had similar risk factors and thromboembolic risk (median premorbid CHA2DS2VASc score [IQR]; 4 [3–5] vs 4 [3–5]; P = 0.469), lower proportion of premorbid antithrombotic therapy (75.0% vs 41.5%; P<0.001), higher stroke severity at onset (median NIHSS score[IQR] 12.5 [5–19] vs 8 [4–16]; P = 0.016), and higher 30-day (32.3% vs 25.9%) and 1-year (53.8% vs 38.6%) case-fatality rates. Cox regression analysis including age, sex, NDAF, NIHSS score at onset, and premorbid antithrombotic therapy showed that among AF patients, premorbid antithrombotic therapy at 30 days (HR 1.89; P = 0.021), and NIHSS score at 30 days (HR 1.06; P<0.001) and at 1 year (HR 1.07; P<0.001) were independent predictors of mortality.
Conclusion
In nearly one-fifth of AF-related FEIS the arrhythmia is diagnosed at the time of the event. The worse prognosis in NDAF patients is mainly driven by higher stroke severity and lower proportion of patients on antithrombotics than in PDAF. Screening for AF among individuals aged ≥80 years with arterial hypertension, and treating them with the most appropriate drugs may reduce stroke severity and mortality.
Trial registration number
N/A
AS21-046
12-MONTH OUTCOME IN PATIENTS WITH STROKE AND ATRIAL FIBRILLATION NOT DISCHARGED ON ANTICOAGULANT: THE WATCH-AF REGISTRY
1GH Bichat Claude Bernard, Neurology and Stroke center, Paris, France
2Hopital Neurologique Pierre Wertheimer, Neurology and Stroke Center, Bron, France
Background and Aims
In patients with acute stroke associated with atrial fibrillation (AF) many cannot be discharged on oral anticoagulant. Outcome of these patients compared to those on long-term oral anticoagulant (LTOAC) is not well known.
Method
Consecutive patients admitted within 24 hours of symptom onset of an acute stroke associated with AF in two stroke centers had systematic CHADSVASC, HASBLED, ATRIA, NIHSS, mRS, Barthel, IADL, MMS, STRATIFY scores as well as INR, TTR, GFR collected 6 and 1 months before stroke, at admission, discharge, 2 and 8 days, 3, 12 months post stroke. The primary endpoint was death or dependency (mRS≥4) and secondary endpoint recurrent brain infarction or hemorrhage.
Results
Among 400 patients (369 brain infarction, 29 brain hemorrhage, 2 both), mean age was 79 years. Baseline NIHSS was ≥5 in 32.1% of patients. 157 patients were not discharged on LTOAC (died before discharge, too frail-bedridden or demented, patient refusal, temporary or definitive contra-indication to LTOAC). At 12 months, the primary and secondary endpoints occurred in 25.5% [95% CI, 20.4–31.7] and 17.9% [95% CI, 13.5–23.4] respectively in 243 patients discharged on LTOAC, and 55.0% [95% CI, 47.4–63.0] and 49.4% [95% CI, 41.8–57.5] in those not on anticoagulant (p < 0.001 for both). After multivariable analysis, patients not on LTOAC at discharge were almost twice more likely to be dead or dependent at 12 months (HR = 1.77 [95%CI, 1.25–2.50], p < 0.001).
Conclusion
Patients not discharged on LTOAC have a high risk of death or dependency at 12 months. Treatment such as left atrial appendage closure should be trialed.
Trial registration number
N/A
AS21-047
ELECTROCARDIOGRAPHIC PREDICTORS OF ATRIAL FIBRILLATION IN CRYPTOGENIC STROKE
1Azienda Ospedaliera Universitaria Senese, Stroke Unit- Department of Neurological and Neurosensorial Sciences, Siena, Italy
2University of Siena, Department of Medical Sciences- Surgery and Neurosciences, Siena, Italy
3University of Siena, Department of Economics and Statistics, Siena, Italy
Background and Aims
Prolonged screening for the presence of atrial fibrillation (AF) is recommended after cryptogenic stroke (CS) and different electrocardiographic markers have been proposed as tools to identify patients at high-risk for AF. The aim of this study was to evaluate the relationship among different electrocardiographic parameters and in-hospital AF occurrence after acute CS.
Method
222 patients with CS underwent 12-lead resting ECG at admission and 7-day inhospital ECG monitoring. The following indices were evaluated: P-wave dispersion (PWD)(that is the difference between the maximum P wave duration and the minimum P wave duration), P-wave index (that is the standard deviation of P wave duration across all 12 leads), P-wave axis, PR interval, atrial size.
Results
AF was detected in 44 patients. AF-group had significantly higher PWD, P-wave index, PR interval and greater frequency of abnormal P-wave axis in comparison with no-AF group. The following variables were found to be predictors for AF: age (OR:1.41 for 5 years, 95% CI:1.15–1.72), PWD (OR:1.92 for 10 ms, 95% CI:1.45–2.55), abnormal P-wave axis (OR:3.31, 95% CI:1.49–7.35).
Conclusion
In CS, high PWD and abnormal P-wave axis are independent predictors of AF, representing useful tools to identify patients at high-risk of AF.
Trial registration number
N/A
AS21-048
PREVIOUSLY KNOWN VERSUS NEWLY DIAGNOSED ATRIAL FIBRILLATION AND CARDIOEMBOLIC ISCHEMIC STROKE OUTCOME: THE NORDICTUS REGISTRY
1Hospital Clínico Universitario de Valladolid, Stroke Department, Valladolid, Spain
2Hospital Clínico Universitario de Valladolid, Stroke Unit. Neurology Deparment, Valladolid, Spain
3Hospital de Basurto, Stroke Unit. Neurology Department, Bilbao, Spain
4Hospital Marqués de Valdecilla, Stroke Unit. Neurology Department, Santander, Spain
5Hospita Universitario Santiago de Compostela, Stroke Unit. Neurology Department, Santiago de Compostela, Spain
6Hospital Universitario Lozano Blesa, Stroke Unit. Neurology Department, Zaragoza, Spain
7Complejo Hospitalario Universitario A Coruña, Stroke Unit. Neurology Department, A Coruña, Spain
Background and Aims
We tested the hypothesis that stroke outcome may differ in acute ischemic stroke (AIS) patients with previously known atrial fibrillation (AFib) vs. in patients in whom AIS is the first manifestation of a newly diagnosed AFib.
Method
Retrospective analysis of the prospective registry in NORDICTUS, a research network of stroke centers in Northern Spain serving an area of 11.5 M people. We included consecutive patients with an AIS caused by AFib admitted to five NORDICTUS stroke centers from January 2015 to December 2017. Common demographic, clinical, radiological and prognostic variables were recorded during admission. AFib was categorized in previously known vs. new diagnosis, and AIS outcome in both groups was compared. Brain infarct volume was considered the primary outcome variable, whereas secondary outcome variables were NIHSS and mRS at discharge.
Results
We included 905 patients with AFib-related AIS (mean age 78 years, 52% men, median previous CHA2DS2-VASC = 4), of whom 640 (71%) had a previous AFib diagnosis. Compared to the new-AFib group, patients in the previous AFib group were older, had significantly higher CHA2DS2-VASC and HAS-BLED scores and similar NIHSS on admission. Previous AFib was associated with a larger mean infarct volume (223 cc. vs 17cc.; p = 0.005), and higher NIHSS (p = 0.007) and mRS (p = 0.001) scores at discharge. A multivariable-adjusted linear regression model showed that prior AFib was independently associated with a larger infarct volume (beta 254, p = 0.03).
Conclusion
Cardioembolic AIS patients with previously known AFib have worse outcomes than those with newly diagnosed AFib.
Trial registration number
N/A
AS21-049
SNAPSHOT OF ANTICOAGULATION PRACTICE IN AN INNER LONDON BOROUGH IN PATIENTS WITH KNOWN DIAGNOSIS OF ATRIAL FIBRILLATION: TIME FOR CHANGE
1North Middlesex University Hospital, Stroke Medicine, London, United Kingdom
Background and Aims
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia. It is a strong risk factor for embolic stroke, such that anticoagulation is recommended for the majority of patients. However, many patients for whom anticoagulation is indicated do not receive appropriate therapy
To assess anticoagulation usage in patients with known AF prior to hospital admission.
Method
A standardized proforma was designed to collect data from inpatient notes and electronic letters for inpatients over four months in a district general hospital
Results
One hundred seven patients were included, of whom 36% were not anticoagulated. Of these, only 37% had a documented reason for withholding therapy despite a mean CHA2DS2-VASc of 5. Common reasons included bleeding risk and risk of falls. Warfarin was the agent of choice in 48% of patients and Direct Oral Anticoagulants (DOACs) in 52%. Concerningly, 76% of patients on warfarin were admitted with an INR not in range; 56% of which were subtherapeutic. Of those on DOACs, only 75% were on the appropriate dose. Notably 37% of patients not anticoagulated prior to admission were initiated on therapy on discharge
Conclusion
Many patients in whom anticoagulation is indicated are receiving inappropriate dosage, or are not receiving treatment at all, thus increasing their risk of embolic stroke. Many are identified and anticoagulated during acute admissions, indicating inadequate anticoagulation in the community. There is pressing need for changes in anticoagulation practices in community urgently
Trial registration number
-
AS21-050
12-MONTH BLEEDING RISK IN PATIENTS WITH STROKE AND ATRIAL FIBRILLATION(AF) NOT DISCHARGED ON ANTICOAGULANT: THE WATCH-AF REGISTRY
1GH Bichat Claude Bernard, Neurology, Paris, France
2Hospices Civils de Lyon, Neurology, Lyon, France
Background and Aims
In patients with acute stroke associated with AF many cannot be discharged on long-term oral anticoagulant (LTOAC). Their bleeding risk compared to those on LTOAC is not well known.
Method
Consecutive patients admitted within 24 hours of symptom onset of an acute stroke associated with AF in two stroke centers had systematic CHADSVASC, HASBLED, NIHSS, mRS, Barthel, IADL, MMS, STRATIFY scores collected at admission, discharge, 2 and 8 days, 3, 12 months post stroke. We evaluated the hemorrhagic stroke and major bleeding (MB, according to ISTH) incidence.
Results
Among 400 patients (369 brain infarction, 29 brain hemorrhage, 2 both), 157 patients were not discharged on LTOAC. Among them 42.7% had CHADS VASC2 ≥5 and 22.3% HASBLED ≥3, 10.8% STRATIFY ≥2 (high risk of fall), 7.0% low IADL≤2, 14.0% MMS ≤24 as compared to 32.5%, 18.1%, 6.2%, 4.1% and 22.6% in patients discharged on LTOAC. At 12 months, brain hemorrhages and MB occurred in 3.5% and 0.8%, respectively in 243 patients discharged on LTOAC, and 15.9% and 7.0%, respectively in those not on LTOAC (p < 0.001 for both). After multivariable analysis, patients not anticoagulated had a 5-fold and 10-fold increase in the risk of brain hemorrhage and MB, respectively (HR = 4.67 [95%CI, 1.94–11.27], p < 0.001 and HR = 10.63[95% CI, 2.11–53.53]] p = 0.005).
Conclusion
Patients not discharged on LTOAC had an unexpectedly high increase risk in brain hemorrhage and major bleeding at 12 months as compared to that of patients discharged on LTOAC. Alternative preventive treatments in patients not discharged on anticoagulant are needed.
Trial registration number
N/A
AS21-051
AFFECTED VASCULAR TERRITORIES IN PRESUMED CARDIOEMBOLIC STROKE IN PATIENTS WITH LEFT ATRIAL OR VENTRICULAR THROMBI
1Duke University, Dept. of Neurology, Durham, USA
2Campbell University, School of Osteopathic Medicine, Buies Creek, USA
Background and Aims
Left atrial and ventricular thrombi are identified in a subset of patients with acute ischemic stroke. Cerebrovascular territories affected by stroke (i.e. to which thrombi embolize) has not previously been published. The aim of this analysis was to identify vascular distributions of infarctions in high-probability cardioembolic strokes.
Method
This was a retrospective cohort study, utilizing an academic institutional database to identify patients with diagnosis codes for acute ischemic stroke. Records were then filtered by CPT codes to select patients who underwent transthoracic or transesophageal echocardiography, cardiac CT, and/or cardiac MRI. Further filters were applied to identify the subset of patients on therapeutic anticoagulation. Patients lacking left atrial or ventricular thrombi on cardiac imaging were further excluded, as well as patients whose cardiac thrombus was identified >14 days before or after presenting with stroke. A vascular neurologist reviewed the brain magnetic resonance images (or head CT images for patients who did not undergo MRI) and classified the vascular territories for each acute infarction.
Results
Sixty patients were identified for the cohort described above, and a total of 84 acute ischemic infarctions were found on neuroimaging. Ten patients had multifocal infarctions affecting multiple vascular territories. Table 1 details vascular territories affected. The left middle cerebral artery territory was most frequently involved (n = 28, 46.7%), followed by the right middle cerebral artery territory (n = 21, 35%). Anterior circulation territories were disproportionately affected (72 of the 84 infactions, or 85.7%).
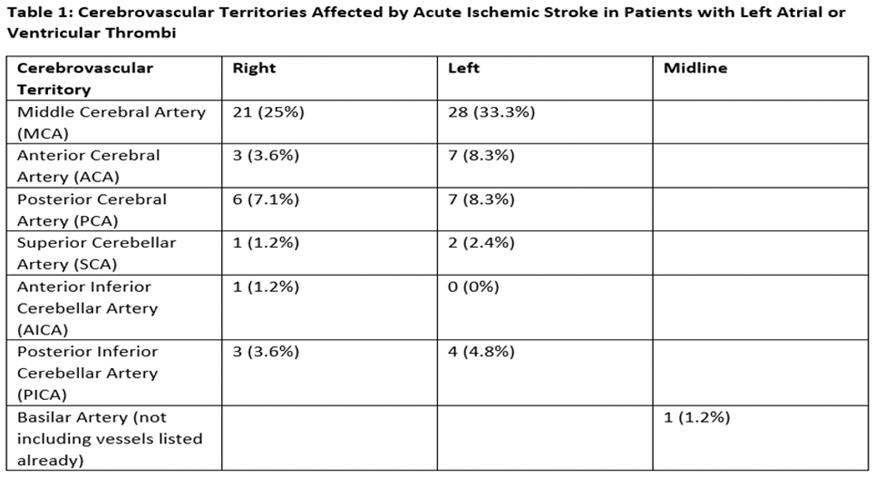
Conclusion
Anterior circulation territory acute infarctions of unclear etiology warrant cardiac imaging to identify a potential cardioembolic source.
Trial registration number
N/A
AS21-052
CARDIOEMBOLIC VS ATHEROSCLEROTIC STROKE ETIOLOGY AND COLLATERAL STATUS IN THE MR CLEAN REGISTRY
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Onze Lieve Vrouwe Gasthuis, Neurology, Amsterdam, The Netherlands
3Erasmus University Medical Center, Radiology, Rotterdam, The Netherlands
4Academic Medical Center, Radiology & Nuclear Medicine, Amsterdam, The Netherlands
5University Medical Center Utrecht, Neurology and neurosurgery- Brain Center Rudolf Magnus, Utrecht, The Netherlands
6Maastricht University Medical Center, Neurology- Cardiovascular Research Institute Maastricht CARIM, Maastricht, The Netherlands
7Erasmus University Medical Center, Neurology, Rotterdam, The Netherlands
Background and Aims
Cardioembolic stroke develops relatively quickly, whereas large-artery atherosclerosis develops over years. Theoretically, chronic brain hypoperfusion might promote formation of intracranial collateral arteries. We assessed the association between stroke etiology and collateral status.
Method
We report consecutive patients who underwent endovascular treatment for anterior circulation large vessel occlusion, included between March 2014 and June 2016 in the MR CLEAN Registry, a prospective, observational study in The Netherlands. Stroke etiology was determined using TOAST criteria. We compared patients with cardioembolic stroke to those with large-artery atherosclerosis. Collateral score (Tan, 2009) was categorized into poor (grade 0–1) vs good (2–3). Clinical outcome measures were ΔNIHSS (baseline NIHSS–NIHSS at 24–48 hours), mRS score at 90 days and symptomatic intracranial hemorrhage (sICH) rate.
Results
Of 1526 included patients, 459 (30%) had cardioembolism and 197 (13%) had large-artery atherosclerosis. Patients with cardioembolism were older (median 75 vs 70 years, P<0.001), more often female (54% vs 36%, P<0.001), more often had a middle cerebral artery occlusion (79% vs 51%, P<0.001), and higher pre-stroke mRS scores (mRS≥3: 15% vs 4%, P<0.001) than patients with large-artery atherosclerosis. Cardioembolic stroke patients more often had poor collaterals (40% vs 29%, P = 0.009). ΔNIHSS (adjusted β -0.656, 95% CI -2.245–0.943), mRS at 90 days (aOR 0.965, 95%CI 0.645–1.441) and sICH (aOR 0.457, 95%CI 0.192–1.084) did not differ significantly between groups.
Conclusion
Patients with cardioembolic stroke had poorer collaterals than patients with atherosclerotic stroke. This difference did not translate into a worse clinical outcome after endovascular treatment.
Trial registration number
N/A
AS21-053
PREVALENCE AND IMPLICATIONS OF CEREBRAL MICROBLEEDS IN PATIENTS WITH ATIRAL FIBRILLATION: ASSOCIATED RISK FACTORS AND PREDICTIVE MODEL
1Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla, Neurology, Seville, Spain
2Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla, Radiology, Seville, Spain
3Hospital Clínic, Radiology, Barcelona, Spain
4Instituto de Biomedicina de Sevilla, Neurovascular Research Laboratory, Sevilla, Spain
5Hospital Universitario Virgen del Rocío, Radiology, Seville, Spain
6Senior Project Manager, Andalusian Healthcare Ministry, Sevilla, Spain
7Universidad de Loyola, Neuropsychology Department, Sevilla, Spain
8Hospital Universitario Virgen Macarena/Instituto de Biomedicina de Sevilla, Neurology Department/Neurovascular Research Laboratory, Sevilla, Spain
Background and Aims
Cerebral Microbleeds (CMBs) are defined as small (usually < 10 mm) areas of signal void with associated blooming seen on T2*-weighted MRI sequence. The number of CMBs (≥ 5) and its location are associated with an increased risk of ICH in AF patients, in whom OAC is indicated. The aim of this study is to determine the prevalence of and risk factors for CMBs in patients with AF.
Method
Patients with a history of AF who scored 0–1 in the CHADS2 score were selected from Seville urban area using the Andalusian electronic healthcare database (DIRAYA). A 3T-brain MRI was performed. Demographic and clinical data were collected.
Results
443 patients were included from May 2015 to June 2016. 74 patients (16.7%) presented CMB’s on the MRI. 46 patients (62.1%) presented 1 CMB, 22(29.8%) presented 2–4 CMBs and 6(8.1%) presented ≥ 5 CMBs. The most frequent localization was cortical-subcortical (53.2%). Univariate analysis showed that an older age, renal impairment and a higher punctuation on HASBLED score were associated with CMBs. After logistic regression analysis, an older age (OR 1.05,95% CI 1.01–1-09, p = 0.02) and renal impairment (OR 10.14,95% CI 1.7- 60.5, p = 0.011) were independent risk factors for CMBs.
Conclusion
An older age and renal impairment were associated with CMBs in patients with AF. Although further investigations are needed to evaluate the benefit/risk profile of OAC in these patients, this group of patients might benefit from a neuroimaging screening to be offered the best anticoagulation therapy in order to improve stroke prevention minimizing ICH risk.
Trial registration number
N/A
AS21-054
SPONTANEOUS INTRACEREBRAL HEMORRHAGE IN ANTICOAGULATED PATIENTS: DIFFERENCES BETWEEN NON-VITAMIN ANTAGONIST ORAL ANTICOAGULANTS (NOACS) AND VITAMIN K ANTAGONISTS (AVK)
for the NORDICTUS Investigators
1Hospital Clínico Universitario de Santiago, Neurology, Santiago de Compostela, Spain
2Hospital Universitario de Donostia, Neurology, Bizkaia, Spain
3Complejo Hospitalario Universitario A Coruña, Neurology, A Coruña, Spain
4Hospital Marqués de Valdecilla, Neurology, Santander, Spain
5Hospital de Basurto, Neurology, Bilbao, Spain
6Hospital Universitario Miguel Servet, Neurology Department, Zaragoza, Spain
7Hospital Clínico Lozano Blesa, Neurology Department, Zaragoza, Spain
Background and Aims
Our objective is to know if there are differences in the neuroimaging characteristics and the short-term evolution of patients with spontaneous cerebral hemorrhage who are undergoing non-vitamin antagonist oral anticoagulants (NOACs) or vitamin K antagonists (VKA).
Method
We prospectively included all patients admitted with spontaneous cerebral hemorrhage who were under treatment with oral anticoagulants from January 2015 to December 2016 in 6 Hospitals in Spain. We analyzed baseline characteristics (age, sex, previous history, baseline NIHSS, CHAD2S2-Vasc, HASBLED) neuroimaging (location, volume and ventricular or subarachnoid contamination) and outcome variables (NIHSS and mRS at discharge, in-hospital mortality and days of hospitalization).
Results
174 patients were included (78.8 ± 7.89 years, 53% males). 156 (89.7%) received VKA and 18 (10.3%) NOACs. Patients under treatment with NOACs had a higher score on the CHAD2S2-Vasc scale before hemorrhage (4 [3-5] versus 5 [4–6], p = 0.016), less history of diabetes (16.7% vs to 37.8%, p = 0.042), lower levels of INR (1.23 vs. 2.59, p <0.001) and lower volume of initial hemorrhage (8.64 [2.0–43-20] vs. 16.0 [5.94–61.90], p = 0.031). There were no differences in both groups regarding baseline NIHSS, hemorrhage location, mortality, days of hospitalization or the functional outcome at discharge.
Conclusion
Patients with ACODs have smaller initial volumes of cerebral hemorrhage compared to VKA, however there are no differences in short-term outcome between both groups of patients.
Trial registration number
N/A
AS21-055
EVALUATION OF SERUM BIOMARKERS RELATED TO ATRIAL REMODELING IN PATIENTS WITH UNDETERMINED STROKE ETIOLOGY
1Hospital de Santa Maria- Centro Hospitalar Lisboa Norte, Neurology, Lisboa, Portugal
2Instituto de Medicina Molecular, JMFerro Lab, Lisboa, Portugal
3Hospital Egas Moniz, Neurology, Lisboa, Portugal
4Hospital Beatriz Ângelo, Neurology, Loures, Portugal
5Hospital de Santa Maria- Centro Hospitalar Lisboa Norte, Cardiology, Lisboa, Portugal
Background and Aims
Patients with undetermined ischemic stroke etiology may have cardiac structural changes that are not currently considered associated with cardioembolism. In a previous study using cardiac MRI we found that patients with undetermined stroke had a particular left atrium (LA) phenotype with higher levels of fibrosis and reduced LA ejection fraction than patients with specific stroke causes, suggesting an atrial disease associated with stroke. We aimed to determine if this LA phenotype could be translated in different levels of serum biomarkers related to atrial remodeling.
Method
Consecutive sample of patients, admitted from 2014–2017 for ischemic stroke, aged >50 years. Patients with structural changes on echocardiography currently considered causal for stroke in TOAST were excluded. Patients underwent a 3Tesla cardiac MRI. We measured serum levels of P-Selectin (endothelial dysfunction), matrix metalloproteinase-2 (MMP-2, remodeling), tenascinC (remodeling), galectin-3(fibrosis), and N-terminal of brain natriuretic peptide (NT-proBNP;myocyte stress). Non-parametric statistic tests with Bonferroni corrections were used.
Results
We included 122 patients with a mean age (standard deviation) of 68.8(9.2) years. Six patients were excluded due to cardiomyopathies. Eighteen patients with cardioembolism (atrial fibrillation), 56 undetermined etiology and 42 other causes were included. Patients with cardioembolic and undetermined stroke had statistically significant higher serum levels of MMP-2 and NT-proBNP than patients with other stroke causes. Levels of MMP-2 and NT-proBNP in patients with undetermined stroke were intermediate between the ones obtained in patients with cardioembolic stroke and other specific causes.
Conclusion
Serum levels of MMP-2 and NT-proBNP that were found in patients with undetermined stroke support the hypothesis of an atrial disease.
Trial registration number
NA
AS21-056
ISCHEMIC STROKE IN PATIENTS TREATED WITH ANTICOAGULANTS: RETROSPECTIVE ANALYSIS FROM HOSPITAL-BASED REGISTER
1Careggi University Hospital, Stroke Unit, Florence, Italy
2Institute of Neuroscience, Italian National Research Council, Florence, Italy
3Universisty of Florence, Department of Neurosciences- Psychology- Drug Research and Child Health, Florence, Italy
Background and Aims
Oral anticoagulation lowers the risk of stroke in patients with Atrial Fibrillation (AF), the most important cause of cardioembolic stroke. Effective anticoagulation is relevant to avoid major adverse events and treatment compliance is the main aim to achieve good anticoagulation control. We describe patients with acute ischemic stroke (AIS) occurred under anticoagulant treatment.
Method
Retrospective analysis of AIS patients admitted to our Stroke Unit between September 2015 and December 2017. Data were collected using hospital based register.
Results
Out of 682 AIS patients, 76 (11.1%; mean age 79 ± 8 years) were on anticoagulants before stroke: 42 (55.3%) on warfarin, 21 (27.6%) on direct oral anticoagulants (DOACs), and 13 (17.1%) on low molecular weight heparin (LWMH). At admission, 52 (68.4%) patients presented suboptimal anticoagulant treatment. 34/42 (80.9%) warfarin patients had subtherapeutic international normalized ratio (INR). Among DOACs patients, 11/21 (52.4%) received suboptimal treatment (6 inappropriate dosage, 2 poor adherence, 3 both causes). LWMH was underdosed in 9/13 (69.2%) patients. No difference in stroke severity and risk factors distribution was found comparing suboptimal anticoagulation regimen versus in-label treatment, while cardioembolic stroke was significantly more frequent in the first group (85.2 vs 50%; p = 0.0013).
Conclusion
In our sample, a large portion of patients had suboptimal anticoagulant treatment; in particular, DAOCs and LWMH were used at inappropriate doses and/or in poor compliant patients in more than half of the cases. Therefore, a greater emphasis should be given to prescribe the recommended dose for the specified patients according to age, glomerular filtrate, body weight.
Trial registration number
N/A
AS21-057
SAFETY AND EFFICACY OF DABIGATRAN FOR SECONDARY STROKE PREVENTION IN PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION-MULTICENTER PROSPECTIVE REGISTRY BY TAIWAN STROKE SOCIETY
1MacKay Memorial Hospital, Neurology, Taipei, Taiwan R.O.C
2Taipei Medical University Hospital, Neurology, Taipei, Taiwan R.O.C
Background and Aims
Stroke in nonvalvular atrial fibrillation (NVAF) patients is usually devastating if not adequately prevented. AF patients with stroke are at higher risk of recurrence. Dabigatran, a direct thrombin inhibitor has had been approved as an appropriate preventive option. This multicenter observational prospective cohort study tried to investigate the safety and efficacy of Dabigatran prescribed under routine clinical practice for secondary stroke prevention in NVAF patients.
Method
Patients with history of stroke or TIA, started Dabigatran within 3-months of study initiation or after new index-stroke were enrolled. After patients’ consent, we recorded data on their demographics, AF disease information/medical history, laboratory tests and concomitant medications during baseline and follow-up visits. The rate of stroke recurrence, bleeding, gastrointestinal events as well as the drug adherence were evaluated.
Results
From Dec 2013 till Apr 2017, 653 patients (M/F:399/254) participated, mean age 71.4 ± 10.4, mean follow-up 205 days. The median CHA2DS2VASc score was 5; HAS-BLED scale was 3. Low dose Dabigatran (110 mg BID) were prescribed in 85% patients. Recurrent ischemic stroke was diagnosed in 18 patients/TIA in 2; MI in 5; death in 17 (3%; 0.77 %; 2.6%). Hemorrhagic complications were recorded in 46 patients, 56 events (8.6%), of which 13 were major bleeding (1.99%): intracerebral (3), gastrointestinal (7), genitourinary (2), retroperitoneum (1). Male, age≧75 y/o were risks of bleeding but no difference between low dose and standard dose.
Conclusion
The use of low dose Dabigatran in real-world clinical setting among high risk NVAF patients in Taiwan was still associated with comparable efficacy and acceptable safety outcomes.
Trial registration number
N/A
AS21-058
CLINICAL PRACTICE DATA IN THE TREATMENT WITH DIRECT ORAL ANTICOAGULANTS IN PATIENTS WITH ISCHEMIC STROKE
1Fundación Instituto de Investigación Sanitaria de Aragón IIS, Neurology, ZARAGOZA, Spain
2Clinical University Hospital "Lozano Blesa", Neurology, Zaragoza, Spain
Background and Aims
Analysing the frequency of renal function monitoring in patients with direct oral anticoagulants (DOAC), and the rate of ischemic or hemorrhagic events
Method
Retrospective review of patients admitted to our center within January 2014-December 2016 in which they started treatment with DOAC after a cardioembolic ischemic stroke due to non-valvular atrial fibrillation (NVAF).
Results
138 patients, of which 71 were men (51.4%). The average age was 78.94 ( ± 8.63). The DOAC used were: 74 (53.6%) apixaban, 33 (23.9%) rivaroxaban, 30 (21.7%) dabigratran, 1 (7%) edoxaban. 37 patients previously had anticoagulant treatment, 73% were with VKA and 27% with DOAC. During the follow-up, 73 patients (52.9%) underwent renal function monitoring at 3 months, 74 (53.6%) at 6 months, and 85 (61.6%) at 12 months. The complications are detailed in Table 1: 6 patients (4.3%) had an intracranial haemorrhage, 4 (2.9%) gastrointestinal and 8 external haemorrhages (5.8%). 6 (4.3%) of the patients had an ischemic stroke or a transient ischemic attack.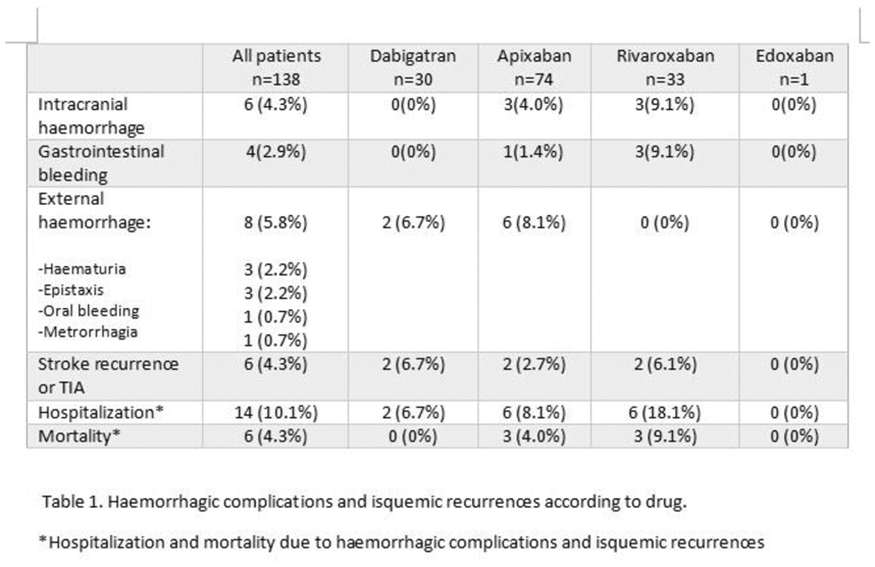
Conclusion
Due to their favorable pharmacokinetic properties, DOAC are effective drugs with a good safety profile, however, we believe that a more strict monitoring of renal function is necessary due to their high rate of elimination via this route and the risk of complications derived from the lack of monitoring.
Trial registration number
N/A
AS21-059
FACTORS INFLUENCING THE CHOICE OF ORAL ANTICOAGULANTS FOR PREVENTION OF CARDIO-EMBOLIC STROKE IN PATIENTS WITH ATRIAL FIBRILLATION
1Şişli Hamidiye Etfal Education and Research Hospital, Neurology, Istanbul, Turkey
2Şişli Hamidiye Etfal Education and Research Hospital, Radiology, Istanbul, Turkey
3İstanbul Bilim University, Neurology, Istanbul, Turkey
Background and Aims
Atrial fibrillation (AF) is associated with increased risk of ischemic stroke. Anticoagulant therapy either with warfarin or with non-vitamin K oral anticoagulants (NOACs) has been proven to be efficacious in lowering this risk. The aim of our study is to determine factors that influence agent selection for anticoagulation in acute cardio-embolic stroke patients with AF.
Method
We prospectively evaluated two hundred seventy-one consecutive patients with acute cardio-embolic stroke with AF treated with warfarin or NOACs who were admitted to our center between June 2015 and July 2017. Warfarin and NOACs groups were compared in terms of demographic features, risk factors, CHA2DS2VASc scores, NIH Stroke Scale (NIHSS) score on admission and discharge, modified Rankin scores (mRS), infarct size, leukoaraiosis, cerebral micro-bleeds (CMBs), stroke recurrence and complications.
Results
The study population consisted of 271 patients that 125 of them were on warfarin treatment. None of the risk factors were significantly different between two groups except ischemic heart disease and previous stroke. There were no significant differences between two groups in terms of CHA2DS2VASc, leukoaraisosis and CMBs.İnfarct size, both NIHSS scores and mRS of NOACs group were significantly higher than warfarin group (p < 0.002, 0.001, 0.02 and 0.001 respectively). Recurrent ischemic stroke occurred in 3 patients in warfarin group versus 2 in NOACs group. Intracerebral hemorrhage was seen in 2 patients in warfarin group and 1 patient in NOACs group.
Conclusion
In this study, the most important factor that influence the preference between warfarin and NOACs was the infarct size, the severity of the disease at the beginning and the clinical status at hospital discharge. Although the follow-up period is not long enough we couldn’t comment on stroke recurrence.
Trial registration number
N/A
AS21-060
USEFULNESS OF N-TERMINAL PRO B-TYPE NATRIURETIC PEPTIDE FOR ATRIAL FIBRILLATION SCREENING IN PRIMARY STROKE PREVENTION
1Institut de Recerca- Hospital Universitari Vall d'Hebron- Universitat Auntónoma, Neurovascular Research Laboratory, Barcelona, Spain
2Institut d'Investigació en Atenció Primària "Jordi Gol" IDIAP, CAP el Temple, Tortosa, Spain
3Hospital Universitario Virgen del Rocío, Cardiology, Seville, Spain
4Institut d'Investigació en Atenció Primària "Jordi Gol" IDIAP, Unitat de Suport a la Recerca de Barcelona, Barcelona, Spain
5Hospital Universitari Vall d'Hebron, Biochemistry Unit, Barcelona, Spain
6Hospital Universitari Vall d'Hebron, Stroke Unit, Barcelona, Spain
Background and Aims
Atrial fibrillation (AF) screening programs have not shown a clear usefulness in stroke prevention. In this study we aimed to test whether N-terminal pro B-type natriuretic peptide (NT-proBNP) differentiates between different patterns of AF in a high risk population.
Method
The AFRICAT is an observational, multicenter, population-based study which aims to develop a multimodal screening program for AF in primary care centers combining clinical, biological and electrocardiographic information. In the pilot phase of the study, we randomly selected 100 patients aged 65–75, with previous diagnosis of hypertension and diabetes. Atrial fibrillation was assessed by conventional electrocardiogram (ECG), and patients without AF in ECG received four weeks monitoring with a wearable Holter device (Nuubo™). Depending on past medical history (PMH) for AF, ECG findings and Holter, five groups were compared: no AF, PMH+ECG-, PMH-ECG+, PMH+ECG+ and PMH-ECG-Holter+. NT-proBNP was measured in serum by immunoassay (Roche Laboratories) and was compared between these groups.
Results
From the included 100 patients, total incidence of AF was 20%. Distribution across the different groups was: No AF: 80%; PMH+ECG-: 1%; PMH-ECG+:6%; PMH+ECG+: 6%; PHM-ECG-Holter+: 7%. NT-proBNP levels were different across the different subgroups (p < 0.0001), being higher in patients with AF present at the time of ECG (Figure 1A). When just patients without AF diagnosis by PMH or ECG were included, patients with AF diagnosis in Holter had higher levels of NT-proBNP (p = 0.031, Figure 1B).
Conclusion
Measurement of NT-proBNP is a useful tool to be included in AF screening programs in primary care.
Trial registration number
N/A
AS21-061
EHRA/ESC LEFT ATRIAL APPENDAGE CLOSURE (LAAC) CANDIDATES AT DISCHARGE AFTER A STROKE ASSOCIATED WITH ATRIAL FIBRILLATION (AF): 12 MONTHS OUTCOME. THE WATCH-AF REGISTRY
1HCL Hopital Wetheimer, Stroke Unit, BRON, France
2Bichat Hospital, Stroke Unit, Paris, France
3Bichat Hospital, Statistic, Paris, France
Background and Aims
Because of frailty, cognitive impairment, co-morbidities, patient refusal, or perceived low risk of stroke or high bleeding risk, many patients with stroke and AF cannot be discharged on long-term oral anticoagulant (LTOAC). Among them, the proportion of candidate for LAAC and their 12-month outcome is not well known.
Method
Consecutive patients admitted within 24 hours of symptom onset of an acute stroke associated with AF in two stroke centers had systematic data collection (e.g., CHADSVASC, HASBLED, mRS, Barthel, IADL, MMS, STRATIFY scores) at admission, discharge, 2 and 8 days, 3, 12 months post stroke. The primary endpoint was death or dependency (mRS≥4) and secondary endpoint recurrent brain infarction or hemorrhage (BIBH). Potential candidates for LAAC were based on ERHA/ESC recommendations.
Results
Among 400 enrolled patients (369 with brain infarction, 29 with brain hemorrhage, 2 with both). Among 157 patients not discharge on LTOAC, 42/400 (10%) were EHRA/ESC LAAC indication. At 12 months, death or dependency occurred in 10.4% and BIBH in 12.3% in 243 patients discharged on LTOAC, as compared to 71.6% and 46.8% respectively in patients not discharged on LTOAC and not candidate for LAAC, and to 17.2% and 27.3% in patients with temporary contra-indication to LAAC (atrial thrombus or still too frail), and to 7.6% and 21%, respectively, in patients with LAAC indicated (adjusted p < 0.001 for all comparisons).
Conclusion
10% of patients with stroke associated with atrial fibrillation were EHRA/ESC candidate for LAAC. Their 12-month risk was twice the risk of patients discharged on LTOAC.
Trial registration number
N/A
AS21-062
PREVALENCE OF AND FACTORS ASSOCIATED WITH SYSTOLIC DYSFUNCTION IN ISCHEMIC STROKE PATIENTS: THE SICFAIL (STROKE INDUCED CARDIAC FAILURE IN MICE AND MEN) COHORT STUDY
1University of Wuerzburg, Institute for Clinical Epidemiology and Biometry, Wuerzburg, Germany
2University Hospital Wuerzburg, Department of Neurology, Wuerzburg, Germany
3University of Wuerzburg, Comprehensive Heart Failure Center, Wuerzburg, Germany
4University of Wuerzburg, Interdisciplinary Center for Clinical Research, Wuerzburg, Germany
5Klinikum Main-Spessart, Department of Neurology, Lohr am Main, Germany
6University Hospital Wuerzburg, Department of Internal Medicine I, Wuerzburg, Germany
7University Hospital Essen, Department of Neurology, Essen, Germany
8Universtiy Hospital Wuerzburg, Clinical Trial Center, Wuerzburg, Germany
Background and Aims
Systolic dysfunction (SD) is an established risk factor for ischemic stroke (IS). Conversely evidence from animal studies suggests that IS itself might cause SD. However, reliable data on the frequency of SD in IS and factors associated with its occurrence are lacking.
Method
Data were collected within the ongoing prospective hospital-based SICFAIL cohort study assessing the natural course of cardiac function after IS. In consecutive patients, cardiac function was assessed at baseline (median 4 days after IS) including clinical examination, echocardiography performed by an expert sonographer and detailed cardiac medical history. SD was defined as left ventricular ejection fraction (LVEF) ≤ 55%. Logistic regression was performed to identify factors associated with SD prevalence.
Results
Between January 2014 and February 2017 696 subjects met inclusion criteria; baseline echocardiography was possible in 634 (91.1%). 13.8% (95%CI 11.3–16.6%) showed evidence for SD (range LVEF 22–55%). Men had a higher probability of SD (OR 2.77, 95%CI 1.58–4.86). Further, NT-ProBNP above 125 pg/ml (OR 7.73, 95%CI 3.13–19.04), pre-stroke myocardial infarction (OR 2.54, 95%CI 1.32–4.88) and heart rate day 3 after IS (OR 1.02, 95%CI 1.00–1.04) increased probability of SD. No other statistical significant association was found, e.g. for stroke severity or TOAST classification. Restricting analysis to assessment of cardiac function within 5 days after IS did not change results substantially.
Conclusion
This is the first study providing reliable data on the prevalence of SD in subjects with IS and identifying factors associated with its prevalence. Ongoing Follow-up will show the prognostic value.
Trial registration number
German Clinical Trials Register (DRKS): DRKS00011615
AS21-063
ROLE OF TCD EMBOLI-MONITORING IN EVALUATION OF EFFICACY OF ANTICOAGULANT THERAPY IN PATIENTS WITH NONVALVULAR ATRIAL FIBRILLATION
1Jessenius Faculty of Medicine in Martin Commenius University in Bratislava, Neurology Clinic, Martin, Slovak Republic
2Jessenius Faculty of Medicine in Martin Commenius University in Bratislava, Ist Internal Clinic, Martin, Slovak Republic
Background and Aims
Atrial fibrillation (AF) is a risk factor for stroke but, despite anticoagulation therapy, the risk of stroke is not completely eliminated. We evaluated the presence of microembolic signals (MES) by TCD emboli-monitoring in AF patients receiving various anticoagulation therapies.
Method
In total, 103 patients were divided into four therapeutic groups (receiving warfarin, dabigatran, rivaroxaban, or apixaban; 22 patients in each group) and a control group (15 patients). Common stroke risk factors were evaluated, such arterial hypertension, ischemic heart disease, history of TIA/stroke, diabetes mellitus, and hyperlipidemia. TCD emboli-monitoring was performed on bilateral middle cerebral arteries for 45–60 minutes.
Results
No statistically significant differences were determined regarding the presence of risk factors between all groups. We found 2 MES in the warfarin group, 1 in the rivaroxaban group, 4 in the dabigatran group, and 0 in the apixaban group. One patient had positive MES in the control group. No statistical differences were seen when the groups were compared with the control group or with each other.
Conclusion
TCD emboli-monitoring can be used for MES detection in patients with AF receiving anticoagulation therapy and thus for the identification of patients at high risk of stroke occurrence/reoccurence.
Trial registration number
N/A
AS21-064
3 AND 12 MONTHS FOLLOW-UP AFTER LEFT ATRIAL APPENDAGE CLOSURE IN STROKE PATIENTS
1GH Bichat Claude Bernard, Neurology and Stroke center, Paris, France
2GH Bichat Claude Bernard, Radiology, Paris, France
3GH Bichat Claude Bernard, Cardiology, Paris, France
4GH Pitie-Salpetriere, Cardiology, Paris, France
Background and Aims
ERHA/ESC guidelines recommend left atrial appendage closure (LAAC) in stroke patients with non-valvular atrial fibrillation and contra-indications to long-term oral anticoagulant (LTOAC). The aim of this study was to evaluate the 3- and 12-month clinical and imaging outcome after the LAAC in stroke patients.
Method
Clinical, biological, cardiac work-up (TTE/TEE, Cardiac-gated CT angiography (CCTA)) and neuroimaging data were systematically collected before LAAC, 3 and 12 months after LAAC in consecutive stroke patients with ERHA/ESC LAAC indication.
Results
27 stroke patients (19 brain infarction, 6 brain hemorrhage, 2 both), with mean age of 78 years had LAAC performed because of contra-indication to LTOAC (n = 23, 85%) or for recurrent stroke under adequate anticoagulant therapy (n = 4, 15%). 26 (96%) had CCTA before LAAC (to exclude thrombus and evaluate LAA shape). At 3 months, 2 patients were dead because of recurrent hemorrhagic stroke and 22/25 patients (88%) had CCTA. 4 patients (18%) had thrombus on the LAAC device and one of them had a symptomatic ischemic stroke. None of the other patients had asymptomatic lesion on brain MRI. At 12 months, 22/25 patients (88%) had CCTA, 1 patient had persistent thrombus on LAAC device (despite anticoagulant therapy) and 1 patient had asymptomatic ischemic stroke on MRI (without thrombus on CCTA) and none of the other (24) patients had symptomatic recurrent stroke.
Conclusion
Systematic follow-up imaging leads to a better understanding of natural evolution of LAAC procedure in stroke patients.
Trial registration number
N/A
AS21-065
CONTINUOUS NON-INVASIVE 4-WEEK ECG MONITORING REVEALS ATRIAL FIBRILLATION IN PATIENTS WITH RECENT EMBOLIC STROKE OF UNDETERMINED SOURCE
1Helsinki University Central Hospital HUCH, Neurology, Helsinki, Finland
2Hospital District of Helsinki and Uusimaa HUS, Internal medicine, Lahti, Finland
3Helsinki University Central Hospital HUCH, Clinical Physiology, Helsinki, Finland
4Helsinki University Central Hospital HUCH, Cardiology, Helsinki, Finland
5South Karelia Central Hospital, Internal medicine, Lappeenranta, Finland
Background and Aims
Atrial fibrillation (AF) frequently escapes routine stroke workup due to its unpredictable and often asymptomatic nature, leaving a significant portion of patients at high risk of recurrent stroke. Recent trials emphasized continuous ECG monitoring in the detection of occult AF. We screened AF in patients meeting the embolic stroke of unknown source (ESUS) criteria using an external miniaturized recorder attached to an electrode plaster.
Method
Patients aged ≥50 with recent ESUS (e.g., no AF in 24–48h Holter) were prospectively screened and assigned to wear a 1-lead ECG-device capable to record continuous ECG for up to 4 weeks. Electrodes were replaced every 3–4 days. Primary outcome was proportion of patients completing at least 80% of monitoring. Secondary outcome measures included incidence of AF and number of patients with oral anticoagulation therapy initiated after AF detection.
Results
57 patients were monitored (mean age 64.5+/−8.2 years, delay from stroke to the start of monitoring 23.8+/−29.9 days). 51 patients (89.5%) completed at least 80% of the desired monitoring period. We detected AF >=30 seconds in 7 patients (12.3%), all of whom initiated anticoagulation therapy. AF was revealed in 6 patients (85.7%) within the first week of monitoring. Compared to patients without AF, patients with AF were older (70.6+/−5.1 vs 63.6+/−8.3 years, P<0.011) and more obese (Body Mass Index 30.0+/−3.4 vs 26.6+/−4.6, P<0.039.)
Conclusion
Prolonged ECG monitoring with an external device using plaster electrodes is feasible in ESUS patients. A relatively large proportion of underlying AF was detected in ESUS patients.
Trial registration number
N/A
AS21-066
PRESENTING DATA ON PRIMARY PREVENTION OF STROKE IN THE PACEMAKER POPULATION, ARE WE MISSING AN OPPORTUNITY?
1Royal United Hospitals Bath NHS Foundation Trust, Cardiology, Bath, United Kingdom
2Royal United Hospitals Bath NHS Foundation Trust, Stroke, Bath, United Kingdom
Background and Aims
Current guidelines suggest monitoring for atrial fibrillation (AF) in cases of apparent cryptogenic stroke. Previous studies have shown a high prevalence of AF on prolonged implantable loop recorder (ILR) monitoring (CRYSTAL AF). In patients with stroke and prior pacemaker implantation, there is the opportunity to demonstrate the prevalence of AF, and investigate whether these patients are appropriately treated.
Method
We audited patients with pre-existing pacemakers who subsequently suffered a stroke during the follow-up period. We interrogated pacemaker data from 2006–2016 for evidence of subclinical atrial fibrillation prior to stroke, and analysed medical records to obtain anticoagulation status.
Results
80 from 2,558 (3.1%) patients with pacemakers suffered a stroke/TIA in the study period. All patients had a CHA2DS2VASc score >1. Only one patient suffered a haemorrhagic stroke. Interrogation of pacemaker notes showed that 36/80 (45%) patients had documentation of AF prior to stroke presentation. Records for 8 could not be obtained. 20 of the remaining 28 (71%) were not anticoagulated. Whilst some patients may have had established contra-indications, or adverse reactions, to anticoagulation, it was apparent that information communicated to Primary Care regarding the detection of AF on device follow-up was unclear, and ambiguous. This has been addressed to improve patient care.
Conclusion
The prevalence of subclinical AF in patients prior to stroke may be higher than previously reported. This supports the use of extended monitoring with implantable devices such as pacemakers. A streamlined system for identification of AF and initiation of anticoagulation is crucial to minimise occurrence of stroke.
Trial registration number
N/A
AS21-067
ACCURACY OF THE ROPE SCORE TO EVALUATE THE SIZE OF A FORAMEN OVAL PATENT AS EVALUATED BY TRANCRANIAL DOPPLER WITH BUBBLE STUDY
1Hospital Santa Maria, Neurology, Alhos Vedros, Portugal
Background and Aims
Recent clinical trials showed that patients with a large Patent foramen ovale (PFO) are the ones who benefit the most from PFO closure. The RoPE score was created to determine the probability of a cryptogenic stroke being attributable to a PFO. However some center have been using it to select patients for PFO closure.
We aimed to evaluate the accuracy of the Rope score to predict a large right-to-left shunt as evaluated by transcranial Doppler with bubble study
Method
Observational retrospective study. All patients with cryptogenic stroke that underwent transcranial Doppler with bubble study at an university hospital between 2015–2017 were included inn this study. Data was colected regarding demographics, ROPE score components and shunt size by as quantified by transcranial Doppler. A large shunt was defined as the presence of either a curtain pattern or shower pattern. ROC curve and C-statistics were obtained. Statistical significance was set at p < 0.05
Results
Of the 292 patients with cryptogenic stroke, 99 (34%) had shower/curtain pattern on Doppler examination. The area under the ROC curve was 0.51 (confidence interval 95%[CI],0.45–0.58). A cutoff point of ≥6 had a 50% (95%[CI], 44.3%-55.7%) sensitivity and a 52% (95%[CI], 46.3%-57%) specificity. A cutoff point of ≥7 had a 32% (95%[CI], 27%-37.4%) sensitivity and a 69% (95%[CI], 63.7%-74.3%) specificity
Conclusion
RoPE Score had a low acuity for the detection of an hemodynamically significant PFO on transcranial Doppler examination. Our results suggest that caution should be taken when using the RoPE scale as a tool of selection for PFOs closure.
Trial registration number
N/A
AS21-068
EARLY PRESCRIPTION OF NOACS AFTER STROKE - RETROSPECTIVE DATA
1V.N. Karazin Kharkiv National University, Department of Clinical Neurology- Psychiatry and Narcology, Kharkiv, Ukraine
2Kharkiv Raiway Clinical Hospital #1, Neurology Department #1, Kharkiv, Ukraine
Background and Aims
There is no data from clinical trials about initiation of anticoagulants treatment after Ischemic Stroke. Most commonly used tool is Diener's Law - 1-3-6-12 days after stroke onset based on severity and risk of hemorrhage.
But before Day 12 in severe stroke patient with Atrial Fibrillation we can find Deep Vein Thrombosis in him during this period.
We prescribed NOACs from day 1 after stroke despite the severity and checked all cases of bleeding during first 10 days (hospital stay)
Method
87 patient with ischemic stroke (average NIHSS 8,7) were prescribed with NOACs within 48 hours after the stroke onset based on creatinine clearance (dabigatran 110 mg BID or 150 mg BID, rivaroxaban 15 mg QD or 20 mg). CT or MRI scan was done before prescribing NOACs to rule out any hemorrhages. In case of clinical deterioration follow-up neuroimaging was done. And in case of DVT symptoms venous ultrasound was performed.
Results
7 patients died during first days (2 of them had PH2 hemorrhages). 3 of survived patients developed brain hemorrhage - 1 PH2, 2 PH1. 1 patient developed DVT with further anticoagulant treatment. 76 patients didn't have any hemorrhagic or thrombotic complications.
Conclusion
Early NOAC prescription even in severe embolic stroke didn't show increase of brain bleeding (3,5% of PH2, 2,3% of PH1 hemorrhages) even in severe stroke and helped to prevent early thrombotic complications (only 1,15%). Further prospective studies are needed to confirm our findings.
Trial registration number
N/A
COGNITION AND VASCULAR COGNITIVE IMPAIRMENT
AS22-001
SCREENING FOR COGNITIVE IMPAIRMENT WITH THE MONTREAL COGNITIVE ASSESSMENT IN SPANISH PATIENTS WITH MINOR STROKE OR TRANSIENT ISCHAEMIC ATTACK: A VALIDATION STUDY
1Extremadura University Medical School, Biomedical Sciences, Badajoz, Spain
2Centro de Neurorehabilitacion Casaverde, Neurology area, Mérida, Spain
3Hospital Universitario Infanta Cristina, Neurology, Badajoz, Spain
4Extremadura University, Psychology and Social Anthropology Department, Badajoz, Spain
Background and Aims
Non-disabling cerebrovascular events, which include mild ischaemic stroke and transient ischaemic attack (TIA), generally result in either short-lasting or mild neurological symptoms, but these patients are at an increased risk of a recurrent cerebrovascular event. The patients therefore receive considerable medical attention and treatment for physical symptoms and risk factors. However, their cognitive function is often neglected. We aimed to establish the cut-off point of the Montreal Cognitive Assessment (MoCA) in screening for mild cognitive impairment (MCI) within 90 days of TIA.
Method
A total of 50 patients were recruited. They received the MoCA test. MCI was defined clinically by a formal neuropsychological test battery (NEURONORMA).
Results
The average age of recruited patients was 57.7 ± 8.0 years, the majority of patients being men (70.0%) and all patients with greater equal or than primary school level of education. Thirty-seven (74.0%) subjects were classified into MCI group; 29 (58%). The number of domain affected was: one, 14(28%); two, 9(18%); three, 8(16%) and four, 6(12%). The optimal cut-off point for MoCA in discriminating patients with MCI from those with no MCI was 25 (sensitivity 76.9%, specificity 77.8%, positive predictive value 55.6%, negative predictive value 90.3%) and the Receiver operating characteristic curve analysis, 0.831 (95%CI 0.715–0.947).
Conclusion
More than half of the sample had cognitive impairment as determined by the formal battery of neuropsychological tests. A MoCA cut-off score of 25 is optimally sensitive and specific for detecting MCI after mild stroke or TIA in the subacute stroke phase. Therefore, it should be implemented in routine clinical practice.
Trial registration number
N/A
AS22-002
CORRELATION HIGH SENSITIVITY C REACTIVE PROTEIN WITH COGNITIVE IMPAIRMENT IN ACUTE ISCHEMIC STROKE
1Sardjito General Hospital/ Gajah Mada University School of Medicine, Departement of Neurology, Yogyakarta, Indonesia
Background and Aims
The incidence of acute cognitive impairment in stroke patients occurred in about 80% of patients and 38–73% of them became impaired permanently. The Increased inflammatory markers as a response to stroke inflamation are associated with poor outcomes in stroke patients. HsCRP level is one of the vascular cognitive impairment predictor in infarction stroke patients.
This study aims to determine the correlation of hsCRP levels in determining the occurrence of cognitive function disorder in patients with acute ischemic stroke at RSUP Sardjito Yogyakarta
Method
The design was prospective cohort observational study, with the subject of the first acute ischemic stroke patients. Cognitive impairment was assessed using the MoCA Ina score at discharge. The hsCRP level was examined in the Pramita laboratory at onset <72 h. All data was processed with computerized statistical analysis.
Results
A total of 30 subjects followed the study with mean age 61.93 ± 11.916 years and hsCRP levels of 3.35 ± 2.23 g/dL. The result of bivariate analysis showed that one factor significantly influence cognitive impairment of ischemic stroke patients, that is hsCRP levels (r = -0,538, p = 0,002)). Multivariate analysis showed that hsCRP levels (β = -0.5, p = 0.003) were independent factors affecting cognitive impairment of acute ischemic stroke
Conclusion
Based on this study, there is a correlation between hsCRP levels with acute ischemic stroke cognitive impairment, that is, the higher hsCRP levels, the lower MoCA Ina values
Trial registration number
N/A
AS22-003
THE NEUROAID II (MLC901) IN VASCULAR COGNITIVE IMPAIRMENT STUDY (NEURITES): BASELINE RESULTS
1National University of Singapore, Department of Pharmacology, Singapore, Singapore
2National Geriatric Hospital, Neurology, Hanoi, Vietnam
3University of Santo Tomas Hospital, Neurology and Psychiatry, Manila, Philippines
4School of Public health- University of Hong Kong, Statistics, Hong Kong, Hong Kong S.A.R
5National Neurological Institute, Neurology, Singapore, Singapore
6Singapore General Hospital, Neurology, Singapore, Singapore
7Raffles Neuroscience Centre, Neurology, Singapore, Singapore
Background and Aims
A substantial number of patients are cognitively impaired after a non-disabling stroke, Vascular cognitive impairment no dementia (VCIND) of moderate severity has a higher risk of incident dementia as well as dependency and death. MLC901 has its origins from Traditional Chinese Medication (TCM) and has been shown to be effective in cellular and animal models of stroke, as well as having neuroprotective and neuroregenerative properties in global ischemia models with prevention of necrosis and apoptosis of hippocampal CA1 neurons after global ischemia, and improved functional recovery in spatial memory. NEURITES tests the hypothesis that NeuroAiD II is safe and effective in the treatment of post-stroke cognitive impairment.
Method
NEURITES is a 24-week, multi-center, double-blind, randomized, placebo-controlled phase II study of NeuroAiD II in patients with VCIND. The primary outcome is executive function as measured by Verbal Fluency and Color Trails Test 1 & 2. Secondary outcomes include cognitive function, behavior, depression, and activities of daily living. Safety will be assessed using adverse events, laboratory tests and vital signs.
Results
NEURITES has recruited a total of 103 patients by November 2017 from sites in Singapore, Philippines and Vietnam. Baseline data on demographics and clinical characteristics will be reported.
Conclusion
NEURITES is investigating the efficacy of a TCM on VCIND. It is performed in compliance with international guidelines and using Western clinical trial standards.
Trial registration number
Clinical trials.gov-NCT01847924.
AS22-004
ANTI-PLATELET AGENT AND POST-STROKE COGNITIVE CHANGE IN TAIWANESE
1Kaohsiung Municipal Ta-Tung Hospital, Neurology, Kaohsiung, Taiwan R.O.C
Background and Aims
Patients with ischemic stroke would have heterogeneous cognitive outcomes. It is important if the anti-platelet agent can benefit cognition beyond stroke prevention. Cilostazol, one of the anti-platelet agents, has benefits in cognitive function for it can inhibit the aggregation and production of beta-amyloid. The study will report the post stroke cognitive change in relation to anti-platelet agents.
Method
A prospective study has conducted to observe the cognitive change of stroke patient treated with cilostazol or aspirin. For each recruited individual, the baseline periventricular (PWMH) and deep white matter hyperintensities (DWMH). medical history, and demographic characteristics were analyzed in relation to the baseline and following up psychometrics, cognitive ability screen instrument (CASI) and mini-mental status examination (MMSE), after 6 months.
Results
In total, 150 patients, 85 treated with cilostazole, initial MMSE 18.2 ± 7.4 and CASE 63.1 ± 23.4, and 65 with aspirin, MMSE 20.4 ± 7.3 and CASE 70.0 ± 24.0, have recruited into the study. The severity of PWMH and DWMH was significantly associated with MMSE (p < 0.001) and CASI (p < 0.001). After following up, 65.4% patients have improved in CASI and 73.1% in MMSE score. In improved in CASI group, 52.9% of patients were treated with cilostazol and aspirin 47.1% (p = 0.573). In MMSE group, 55.3% patients were treated with cilostazole and aspirin 44.7% (p = 0.904).
Conclusion
WMH would have poor cognition function. Cilostazole or aspirin would not differ cognitive outcome. Given to the limited sample size and low baseline psychometric of cilostazole group, a large sample size with randomized sampling study is needed to examine these issues.
Trial registration number
N/A
AS22-005
COGNITIVE TRAJECTORY IN RECOVERY PERIOD OF ISCHEMIC STROKE: THE ROLE OF NEUROINFLAMMATION, MICRO-, AND MACROSTRUCTURAL BRAIN PATHOLOGY
1Perm State Medical University, Neurology, Perm, Russia
2Perm State Medical University, Radiology, Perm, Russia
3Institute of Ecology and Genetics of Microorganisms, Immumology, Perm, Russia
Background and Aims
Post-stroke cognitive impairment is clinically heterogeneous condition with variable prognosis. Aim of study is to evaluate the role of neuroinflammation and cerebral structural factors in the development of cognitive impairment in the recovery period of ischemic stroke.
Method
In 55 patients we assessed cognitive status in acute and recovery period of ischemic stroke. In acute period we determined the concentration of interleukin 1β, 4, 6, 10 and TNFα in liquor and serum, as well as a number of MRI morphometric parameters, fractional anisotropy of the main regions of interest and other instrumental data.
Results
Predictors of cognitive trajectory are listed in tab.1.
Table 1. Predictors of cognitive trajectory in recovery period of ischemic stroke.
Conclusion
The cognitive trajectory in recovery period of ischemic stroke is determined by the profile of neuroinflammation and microstructural integrity of the ipsilateral superior longitudinal fasciculus, as well as the severity of atherosclerosis of the ipsilateral carotid artery, the level of high density lipoproteins and lateral ventricular dilation in the acute period of the disease.
Trial registration number
N/A
AS22-006
THE UTILITY OF CEREBRAL HEMODYNAMIC, MEASURED WITH TRANSCRANIAL DOPPLER, TO PREDICT CONVERSION OF MILD COGNITIVE IMPAIRMENT TO ALZHEIMEŔS DISEASE
1Ciudad Real University Hospital, Neurology, Ciudad Real, Spain
2Albacete Hospital, Neurology, Albacete, Spain
Background and Aims
There is a vascular hypothesis to explain the etipathogenesis of Alzheimeŕs disease (AD). It is based on epidemiological, clinical, pharmacological and anatomopathological studies. Stronger evidences are:
1. Changes in brain perfusion are a risk factor for AD
2. Hypertensive microangiopathy and atherosclerosis in elderly people can trigger and exacerbate AD.
We aimed to elucidate if disturbances in cerebral hemodynamic are able to predict the development of the AD. It will support its use as a biomarker.
Method
A cohort of patients with mild cognitive impairment (MCI) was recruited. We assessed their cerebrovascular function by a Transcranial Doppler Examination (TDE) measuring the pulsatility index (PI) and the apnea index (AI).
Results
These where the results:
- Conversion from MCI to AD is more frequent in patients with disturbances in the cerebral hemodynamic at the time of the diagnosis.
-The presence of a basal AI of 1.44 predicts with 76% sensitibity and 52% especificity the progress in the next year from MCI to AD.
-Patients who develop AD a year after the diagnosis of MCI suffer more damage in their cerebral hemodynamic than the patients who maintain MCI.
-Elevated PI in MCI patients is related with progression to AD in the next year.
Conclusion
Cerebral blood flow may reveal useful information for identifying candidates for future AD treatment trials, especially in the preclinical phases of the disease.
Trial registration number
N/A
AS22-007
EXECUTIVE FUNCTION IN SYMPTOMATIC CAROTID STENOSIS
1Hospital Espírito Santo de Évora EPE, Stroke Unit, Évora, Portugal
2Salamanca University, Depto. Psicología Básica- Psicobiología y Metodología, Salamanca, Spain
3Hospital Espírito Santo de Évora EPE, Luscan, Évora, Portugal
Background and Aims
Executive impairment is one of the main cognitive complications following stroke. The aim of this study is to characterize the executive function among stroke patients with symptomatic carotid stenosis.
Method
thirty ischemic stroke patients with symptomatic internal carotid stenosis and 30 ischemic stroke without stenosis were eligible for inclusion, matched by gender, age and scholar grade. A comprehensive clinical and neuropsychological assessment was conducted during the first two weeks after the vascular event, before being subjected to carotid revascularization treatment.
Results
Most of the participants were male, with a mean age 65.3 ± 13.9 and 34% had between 4-6 years of scholar education. More than half had a right side lesion and 46% were classified has PACI. In the stenosis group, 50% had a moderate to severe stenosis and 57% had no collateral circulation mechanism. Stroke patients with stenosis performed worst in screening tests, like MMSE (p < .002) and Clock Drawing Test (p < .001), when compared to stroke patients without stenosis. Significant statistical differences were observed in most of the tests applied, however only two: TMT B and Similarities seem to discriminate results between the stroke group (p < .05).
Conclusion
Both groups showed impairment in executive function. However patients with symptomatic stenosis seem to have difficulties in most of the executive domains studied, nevertheless shifting, reasoning and abstraction domains seem to discriminate from stroke patients with and without stenosis. These findings may have an important role while applying screening tests, therapeutic decision and adherence, and on developing more tailored rehabilitation programs.
Trial registration number
N/A
AS22-009
PREDICTORS OF LONG-TERM IMPAIRED PROCESSING SPEED AFTER STROKE
1School of Public Health & Psychosocial Studies Faculty of Health & Environmental, National Institute for Stroke and Applied Neurosciences, Auckland, New Zealand
2School of Public Health & Psychosocial Studies Faculty of Health & Environmental, Biostastistics Department, Auckland, New Zealand
Background and Aims
Impaired Processing Speed (IPS) affects up to 50 to 70 % of stroke survivors and has a major influence on post-stroke cognitive dysfunction, affecting quality of life and increased dependence on others. Few studies have examined predictors of IPS after stroke, and there is a paucity of data in terms of long-term prevalence. This study examined baseline predictors associated with long-term impaired processing performance in an existing population-based cohort, four years after stroke.
Method
IPS was assessed using the Symbol Digit Modalities Test (SDMT), at four years after stroke in a sample drawn from an existing population-based study (n = 133, mean age =67.0 ± 13.4). Baseline predictors were obtained at time of stroke and/or within two weeks of the acute event. Multivariate linear and logistic models were used to identify baseline predictors (reported as OR with 95%CI) and prevalence of long-term IPS.
Results
Four years after stroke 62% of survivors had IPS indicated by a mean score < 40 on the SDMT (m = 36.9 ± 11.2). There were significant associations between long-term IPS and the following baseline factors: older age (OR 3.03, 95% CI 0.9–9.3, p = 0.05), previous stroke (OR 2.74, 95% CI 1.0–7.4, p = 0.05), cholesterol (OR 2.72, 95% CI 1.3–5.4, p = 0.01), hypertension (OR 1.82, 95% CI 0.9–3.6, p = 0.05), coronary artery disease (OR 3.35, 95% CI 1.6–9.6, p = 0.01), and arrhythmia (OR 4.40, 95% CI 1.5–12.4, p = 0.01).
Conclusion
IPS remains highly prevalent long after stroke. Early identification of those who are at higher risk of IPS is vital to target rehabilitation interventions, improving overall outcomes.
Trial registration number
N/A
AS22-011
DYNAMIC CHANGES OF COGNITIVE CONDITIONS IN PATIENTS AFTER DIFFERENT TYPES OF CARDIAC SURGERY
1"Institute of Neurology- Psychiatry and Narcology of the NAMS of Ukraine" SI, Department of Brain Vascular Pathology, Kharkiv, Ukraine
Background and Aims
To prevent development of severe cognitive impairments, it is necessary to determine a profile of dynamic changes of cognitive conditions in patients after different types of cardiac surgery (CS).
Method
The prospective study included 27 patients (mean age 58.6 ± 5.3 years old) with ischemic heart disease after various types of CS (coronary artery stenting (CAS) (48.1%), aortocoronary bypass (AcB) with artificial blood circulation (ABC) (18.5%) and AcB without ABC (33.3%)). All the patients were assessed for their cognitions with Mini Mental State Examination (MMSE), the Frontal Assessment Battery (FAB), and the Montreal Cognitive Assessment (MoCA). A baseline examination of the patients was performed after 6–12 months after CS and a repeated examination was performed after 12 months after the baseline one. Between 1st and 2nd assessments, the patients received standard hypolipidemia, hypotensive, and disaggregation therapies.
Results
In all patients, regardless of the CS type, mean MMSE scores were changed insignificantly on the 2nd assessment as compared with the 1st one. MoCA scores were decreased by 1 point at average in patients with CAS and patients with AcB with ABC: (26.0 vs. 24.9) and (23.8 vs 22.9) respectively. In patients with AcB without ABC, the MoCA score was slightly increased (23.6 vs. 24.4). All the patients had a tendency to increasing their FAB scores.
Conclusion
The MoCA was more sensitive to cognitive changes in patients after CS, as compared with MMSE. According to the MoCA results, a direction of cognitive changes after 18–24 months after CS was depended on the CS type.
Trial registration number
N/A
AS22-012
CLINICAL RISK FACTORS PREDISPOSING TO VASCULAR COGNITIVE DECLINE IN ATHEROSCLEROTIC PATIENTS
1University of Wisconsin - School of Medicine and Publich Health, Neurological Surgery, Madison, USA
2University of Wisconsin - School of Medicine and Publich Health, Medicine - Cardiovascular Division, Madison, USA
3University of Wisconsin-Madison, Medical Physics, Madison, USA
4University of Wisconsin - School of Medicine and Publich Health, Neurology, Madison, USA
Background and Aims
We have previously shown that in patients with significant large vessel atherosclerosis, the degree of vascular cognitive decline could be predicted by the instability of that atherosclerotic plaque, as measured by strain in the pulsating carotid artery plaque. We here study those clinical risk factors which strengthen that relationship.
Method
We studied 89 patients with significant (Ëf60%) atherosclerosis, 45 symptomatic and 44 asymptomatic. All were studied for vascular cognitive decline (NINDS battery) and vascular wall strain by ultrasound, as well as their major clinical risk factors and serum levels of inflammatory markers. Analysis was done with non-parametric testing.
Results
A statistically significant relationship enhancing the plaque instability/cognitive decline relationship was seen with positive family history (p = 0.02). This relationship is enhanced by hyperlipidemia (p = 0.009), hypertension (p = 0.019) or carotid bruit (p = 0.005) which also works in a synergistic fashion (p = 0.002). In a subset of 40 patients, proteomic antibody array showed significant increases in serum levels of the inflammatory markers IL1B (p = < 0.01), fibrinogen (p = <0.05), and TIMP1 (p = <0.05) were present in the symptomatic as compared to asymptomatic or control patients.
Conclusion
These markers suggest a significant process of pro-inflammatory cytokines affecting adhesion molecules, viscosity, and tissue remodeling may play a systemic role in vascular cognitive decline for which instability of the carotid plaque may be a mechanical biomarker. This relationship is enhanced by the genetic and biochemical factors which determine family history, hyperlipidemia, and hypertension which could be modifiable factors in the process of vascular cognitive decline.
Trial registration number
N/A
AS22-016
THE QUEEN SQUARE COGNITIVE ASSESSMENT FOR STROKE (QS-CAS): IMPROVING ON THE MONTREAL COGNITIVE ASSESSMENT (MOCA)
1National Hospital for Neurology and Neurosurgery, Neuropsychology, London, United Kingdom
2UCL Institute of Neurology, Stroke Research Group, London, United Kingdom
Background and Aims
The MoCA is a popular cognitive screening tool. However, studies comparing MoCA performance with neuropsychological assessments have shown that it lacks sensitivity to stroke-relevant domains (e.g. visual memory and speed of processing) and insufficiently assesses key domains (e.g. attention/working memory and executive functions). The aim of the study was to examine whether the test accuracy of the MoCA can be improved with additional tailored screening items.
Method
142 patients with sub-acute stroke were administered the QS-CAS which is an assessment tool that consists of the MoCA and additional newly developed tailored screening items assessing visual memory and speed of processing, as well as attention/working memory and executive functions. Performance on the QS-CAS was compared with performance on neuropsychological assessment.
Results
20% of patients were classified as “cognitively intact” on the traditional MoCA alone (>25). Of those patients, 72% failed on the additional attention/working memory screening items, 52% on the speed of processing items, 35% on the visual memory items and 32% on the executive screening items. In addition, 54% of patients who scored full marks on the visuospatial/executive items of the MoCA (5/5) failed on at least one of the additional executive screening items. Poor performance on the tailored screening items was strongly correlated with poor performance on neuropsychological assessment in the corresponding domain.
Conclusion
Our findings show that the QS-CAS improves the test accuracy of the MoCA. Supplementing the MoCA with our additional tailored screening items may be a time- and cost-efficient way of improving detection of post-stroke cognitive deficits.
Trial registration number
n/a
AS22-018
ASSOCIATIONS BETWEEN COGNITIVE IMPAIRMENT, VULNERABILITY AND MORTALITY POST-STROKE: FINDINGS FROM A FIVE-YEAR FOLLOW-UP OF THE ASPIRE-S COHORT
1Royal College of Surgeons in Ireland, Psychology, Dublin, Ireland
2Royal College of Surgeons in Ireland, Medicine, Dublin, Ireland
3Royal College of Surgeons in Ireland, Clinical Research Centre- Beaumont Hospital, Dublin, Ireland
4Royal College of Surgeons in Ireland, Geriatric and Stroke Medicine- Beaumont Hospital, Dublin, Ireland
5Royal College of Surgeons in Ireland, Population Health Sciences, Dublin, Ireland
6Connolly Hospital Blanchardstown, Geriatric Medicine, Dublin, Ireland
7Mater Misericordiae University Hospital, Geriatric Medicine, Dublin, Ireland
Background and Aims
While previous research has examined vulnerability as a predictor of mortality in general older population samples, no study to date has explored vulnerability as a predictor of mortality in a post-stroke cohort. The aim of this study was to examine predictors of mortality in patients five years post-stroke, focusing on cognitive impairment and vulnerability in addition to cardiovascular risk factors.
Method
Patients from the ASPIRE-S (Action on Secondary Prevention Interventions and Rehabilitation in Stroke) cohort were followed 5 years post-ischaemic stroke. Cardiovascular risk factors were assessed at 6 months post-stroke. Cognitive impairment was assessed using a cut-off of <26 on the Montreal Cognitive Assessment. Vulnerability was defined as a score of ≥3 on the Vulnerable Elders Scale. Mortality and date of death were ascertained using hospital records, death notifications and contact with general practitioners. Predictors of mortality were explored using multivariate Cox proportional hazard models. Adjusted hazard ratios (HR) and 95% confidence intervals (CI) are presented.
Results
Sixty-three of 256 patients (24.6%) assessed at six months post-stroke had died within 5 years. Cognitive impairment [HR (95% CI): 2.19 (1.42, 3.39)], vulnerability [HR (95% CI): 5.23 (2.92, 9.36)], atrial fibrillation [HR (95% CI): 2.31 (1.80, 2.96)] and dyslipidaemia [HR (95% CI): 1.90 (1.10, 3.27)] were associated with increased risk of 5-year mortality.
Conclusion
Vulnerability, cognitive impairment, atrial fibrillation and dyslipidaemia at six months were associated with increased risks of mortality five years post-ischaemic stroke. Identification and management of these risk factors should be emphasised in post-stroke care.
Trial registration number
N/A
AS22-019
IMPACT OF COPD AND HB ON COGNITIVE FUNCTION IN THE ELDERLY
1Center for Stroke Research Berlin CSB, Charité - Universitätsmedizin Berlin, Berlin, Germany
2Institut für Biometrie und Klinische Epidemiologie, Charité - Universitätsmedizin Berlin, Berlin, Germany
3Therapist, Zentrum für ambulante Neuropsychologie und Verhaltenstherapie, Berlin, Germany
Background and Aims
Both chronic obstructive pulmonary disease (COPD) and haemoglobin (HB) level have been suggested to influence cognition possibly through long-term reduced oxygen availability in the brain. Thus far, no studies have examined the contributions of HB and COPD in a combined analysis.
Method
We investigated the association of COPD and HB with cognition through delayed words recall as well as with cognitive motor function through time to complete five char-rises in the well-established English Longitudinal Study of Ageing (ELSA). Coefficients were estimated in a mixed linear-regression model and adjusted for age, test-repetitions, sex, depression, diabetes, cholesterol, hypertension, prior stroke, prior myocardial-infarction, heart-failure, smoking and alcohol. COPD was defined using lung-function parameters and clinical symptoms in five categories. HB was coded as a continuous variable.
Results
COPD as well as HB were associated with cognition in a model adjusted for sex, number of test-repetitions and age. Coefficients for the effect of COPD on cognition showed a decrease by one-fourth of a standard deviation for the comparison of COPD-category 3 vs. 0 (-0.23,95%CI:-0.3 to -0.15) while for the effect of HB on cognition an increase with HB-levels was seen (0.03,95%CI:0.01 to 0.05). For cognitive motor function, effects were even more pronounced (0.27,95%CI:0.18–0.36, in COPD category 3 vs.0 and -0.04,95%CI:-0.05 to -0.02, for HB). Effects were attenuated to different degrees after additional adjustment for confounders in both models and the impact of specific confounders differed between the two outcomes.
Conclusion
HB and COPD show discrete contributions on different cognitive functions with varying impact of confounding factors.
Trial registration number
NA
AS22-020
CEREBRAL SMALL VESSEL DISEASE CHANGES OVER TIME: DEVELOPMENT OF A PROGRESSION SCORE AND ITS RELATION TO COGNITION
1Vall d’Hebron Research Institute- Universitat Autònoma de Barcelona, Neurovascular Research Laboratory, Barcelona, Spain
Background and Aims
Accumulation of cerebral small vessel disease (cSVD) markers over time may affect cognition. We aimed to explore whether a score combining the appearance of several markers relates to cognition in a longitudinal study.
Method
Data from the ISSYS cohort, a prospective study of hypertensive patients aged 50–70, dementia and stroke-free at baseline. Subjects underwent brain MRIs, cognitive screening tests (Dementia Rating Scale 2nd version –DRS-2–) and cognitive diagnosis (mild cognitive impairment –MCI– or normal aging) at baseline and follow-up.
Presence of incident lacunar infarcts (LI); deep cerebral microbleeds (dCMB); marked progression of white matter hyperintensities (WMH) and basal ganglia enlarged perivascular spaces (BG-EPVS) was summed (one point each) to obtain a cSVD progression score.
Relationship between cSVD progression score, follow-up DRS-2 scores (total, attention, executive function, memory) and incident MCI was studied in multivariate models adjusting by age, sex, education, follow-up time and baseline cognition and vascular risk factors.
Results
345 participants, 55.4% male, median age 65, were followed-up for 4.1 years.
3.8% showed incident LI, 2.9% dCMB, 23.7% marked increment of WMH and 18.8% BG-EPVS. Regarding cSVD score, 64.3% scored 0, 24.6% scored 1 and 11% scored ≥2. Patients showing ≥2 markers experienced a significant decrease in executive function (adjusted mean = -0.290; standard error = 0.108) compared to subjects with 1 or 0 markers (0.031; 0.071 and 0.039; 0.043, respectively; p = 0.019). 9.2% of the sample showed incident MCI and no association was found with cSVD progression score.
Conclusion
Executive function decline relates to progression in ≥2 points in cSVD progression score.
Trial registration number
N/A
AS22-021
ALZHEIMER'S DISEASE-LIKE AΒ DEPOSITION IN REMOTE REGIONS AFTER CEREBRAL INFARCTION MAY ASSOCIATE WITH POST-STROKE COGNITIVE IMPAIRMENT IN NONHUMAN PRIMATES
1The First Affiliated Hospital- Sun Yat-Sen University, Department of Neurology and Stroke Center, Guangzhou, China
Background and Aims
Stroke-induced amyloid-beta (Aβ) deposition in remote brain areas is a consistent phenomenon in rodents. However, there is some inconsistency between rodent, nonhuman primates and human findings. Here we investigate the dynamic Aβ accumulation in remote regions and its relationship with cognitive impairment after cerebral infarction in cynomolgus monkeys.
Method
Animals were subjected to left middle cerebral artery occlusion (MCAO) (n = 12) or sham operation (n = 4), and the MCAO monkeys were further divided into three subgroups: 45 day (n = 2), 3 month (n = 6) and 1 year (n = 4). Cognitive assessment was evaluated 1 year after operation. Thalamus and hippocampus were harvested to detect dynamic Aβ expression using immunohistochemistry assay. Pearson correlation analyses were used to determine the association between Aβ deposition and cognitive impairment.
Results
Intraneuronal Aβ deposition were detected in the thalamus and hippocampus 45 days after stroke, which were more evident 3 months following operation. Interestingly, extracellular plaque-like Aβ aggregation were found in the thalamus and hippocampus 1 year post ischemic stroke and their intensities were stronger than those 3 months after stroke. Moreover, neurons in the thalamus and hippocampus were declined 1 year compared with those 3 months following stroke. The corresponding cognitive evaluation suggested cognitive impairment of these monkeys, which was correlated with Aβ deposition in the hippocampus 1 year after stroke.
Conclusion
Our findings suggest that Aβ deposits can be induced in remote cognitive regions after cerebral infarction in nonhuman primates, which may correlate with cognitive impairment after stroke.
Trial registration number
N/A
AS22-023
ABNORMAL INTRINSIC BRAIN ACTIVITY PATTERNS IN LEUKOARAIOSIS PATIENTS WITH COGNITIVE IMPAIRMENT: A RESTING STATE FMRI STUDY
1Beijing Tiantan Hospital- Capital Medical University- China National Clinical Re, Neurology, Beijing, China
Background and Aims
Leukoaraiosis (LA), also called cerebral white matter lesions (WMLs), are present in over 50% of elderly people. Most studies showed an association with increased risk of cognitive decline, especially in attention, executive function, and information processing speed domains. However, the underlying neural mechanism of how LA affect the cognition is still incompletely elucidated. Modern laboratory techniques may help to identify this issue.
Method
To explore the amplitude of the low-frequency fluctuations (ALFF) of whole brain in leukoaraiosis patients with cognitive impairment. Here we utilized resting-state functional magnetic resonance imaging (R-fMRI) to measure the amplitude of low-frequency fluctuations (ALFF) in 28 LA patients with vascular mild cognitive impairment (LA-VaMCI), 18 LA with vascular dementia (LA-VaD) and 28 age- and sex-matched healthy controls.
Results
We showed that there were widespread differences in ALFF in many brain regions, predominantly including the right inferior temporal gyrus (ITG) and posterior cingulate cortex/precuneus (PCC/PCu). Compared to controls, the LA-VaD patients had decreased ALFF values in the PCC/PCu and increased ALFF values mainly in temporal regions. The LA-VaD patients had increased ALFF values mainly in ITG. Finally, Close correlations were found between the ALFF values of Pcu and the memory test scores of LA-VAD patients.
Conclusion
Our study suggests that in leukoaraiosis patients have widespread abnormalities in intrinsic brain activity, which might further affect cognitive performance.
Trial registration number
N/A
AS22-024
INTIMA-MEDIA THICKNESS IN PATIENTS WITH NEUROCOGNITIVE IMPAIRMENT
1Univeristy Emergency Hospital, Neurology, Bucharest, Romania
Background and Aims
Measurement of intima-media thickness (IMT) represents a non-invasive method to evaluate subclinical atherosclerosis. The aim of our study was to determine the association between IMT and neurocognitive impairment (NCI).
Method
We included 86 patients with arterial hypertension divided into two groups one with NCI ranging from mild to severe aged between 47 and 90 years (70.2 ± 11.4) and the second group without NCI aged between 44 and 86 years (61.8 ± 11.1). Patients with other comorbidities beside hypertension and dyslipidemia that could alter the neuropsychological exam were excluded. Due to significant differences of age between the groups we performed multivariate analysis with adjustment for age.
Results
When we evaluated the association between IMT and NCI we found that IMT values do not associate with NCI (p = 0.1). Also, IMT is not an independent predictor for NCI when adjusting for age and dyslipidemia. When analyzing the association between the presence of atherosclerosis and NCI we observed that there is no statistical significant difference between the prevalence of atherosclerosis in the two groups (12.5% in the group without NCI versus 19.5% in the group with NCI).
Conclusion
Although there are a lot of contradictory results in the literature regarding the association between IMT and NCI, our study shows that there is no association between them, subclinical and clinical atherosclerosis are not indicative for the presence of NCI, although as some longitudinal studies suggests may be a predictor of future NCI and of its progression.
Trial registration number
N/A
AS22-025
POST STROKE COGNITIVE IMPAIREMENT AND STROKE ETIOLOGY – ACUTE AND AFTER SIX MONTHS
1Clinical stroke research unit, Neurological department- Rigshospitalet- Glostrup, Copenhagen, Denmark
2Radiological department, Radiological department- Herlev and Gentofte hospital, Copenhagen, Denmark
3Danish center for sleep medicine, Department of neurophysiology- Rigshospitalet- Glostrup, Copenhagen, Denmark
Background and Aims
Cognitive impairment (CI) is common after stroke and is related to poor functional outcome and increased mortality. Data regarding association to stroke etiology and particular small vessel disease (SVD) are sparse.
Method
An observational study in acute stroke patients followed for six months. CI was assessed with Montreal Cognitive Assessment (MoCA) and Trial Marking Test part A and B (TMT-A, TMT-B). Etiology was classified according to TOAST; large artery atherosclerosis (LAA), cardioembolism (CE), small vessel occlusion (SVO), other determined etiology (OD) and undetermined etiology (UD). A newly defined total SVD score was calculated in all TOAST groups based on MRI. Age and stroke severity were included as confounders.
Results
We included 110 patients and 73 completed follow-up. Median age: 68 years (range 36 – 88), men: 56%, ischemic strokes: 90%. The cognitive function improved over time, MoCA: mean difference 1.5 (95% confidence interval 1.0–2.0, p < 0.001), TMT-A: mean difference 5.5 (95% confidence interval 2.5–8.5, p < 0.001) and TMT-B: mean difference 19.5 (95% confidence interval 7.0–37.5, p < 0.01).
CI at follow-up, assessed with MoCA, was more frequent in patients with LAA, CE and UD etiology compared to SVO etiology (logistic regression: p = 0.02 for each comparison).
CI increased with increasing SVD score both in the acute state (TMT-B p>0.01) and at follow-up (TMT-A p = 0.01).
Conclusion
CI improved during the first six months after a stroke. Patients with SVO (TOAST) etiology were least affected by CI. Independent of the TOAST criteria, CI increased with increasing SVD score.
Trial registration number
clinicaltrials.gov: NCT02111408
AS22-026
CEREBRAL MICROBLEEDS MAY CONTRIBUTE TO COGNITIVE DECLINE AFTER ISCHEMIC STROKE
1University Hospital Wuerzburg, Neurology, Wuerzburg, Germany
2Institute of Psychology- University of Würzburg, Cognitive Psychology, Würzburg, Germany
Background and Aims
About one-third of stroke patients will subsequently develop vascular cognitive decline (VCD) or vascular dementia. Whereas white matter hyperintensities were shown to predict cognitive decline following stroke, little is known about the significance of cerebral microbleeds (CMB) in the development of VCD. The present study aimed to investigate whether CMB contribute to VCD already in the early course after ischemic stroke, and - if so – whether distinct cognitive domains are affected more preferentially by CMB.
Method
In a prospective cohort study, cognitive performance was examined in 33 stroke patients showing ≥1 CMB on MRI. Matched for age, gender, clinical and radiological characteristics, 22 stroke survivors without CMB served as a control group. Neuropsychological testing was performed in both groups using the Consortium to Establish a Registry for Alzheimer's Disease (CERAD)-plus test battery. This assessment was conducted in CMB-positive stroke patients (mean ± standard deviation (SD)) 196 ± 5 days and in control patients 208 ± 4 days after the index event.
Results
Patients with CMB scored significantly lower on both the 15-item Boston Naming Test (p = 0.027) and the word-list learning test (p = 0.026). Moreover, they showed a significantly impaired phonematic fluency (p = 0.037) as compared to the control group. No significant differences were found between the groups regarding word-list recall, constructional praxia, Trail-Making-Test and Mini-Mental State Examination.
Conclusion
Six months after stroke, cognitive abilities are more severely affected if patients are CMB-positive. Stroke survivors with CMB might more often experience impaired executive functions and verbal memory. However, further studies are needed to confirm these findings.
Trial registration number
226/16
AS22-028
NEURONAL DEPOPULATION, NOT SILENT CEREBROVASCULAR DISEASE, MEDIATE COGNITIVE DYSFUNCTION IN CHAGAS DISEASE
1Universidade Federal da Bahia, Biomorfologia, Salvador, Brazil
2Hospital Universitário Professor Edgard Santos, Fonoaudiologia, Salvador, Brazil
3Universidade Federal de Minas Gerais, Cardiologia, Belo Horizonte, Brazil
4Brown University, Neurology, Providence, USA
Background and Aims
Chagas disease is associated with cognitive dysfunction, but its mechanism in not well known, especially in stroke-free individuals. We aimed to investigate brain imaging biomarkers as potential mediators of cognitive dysfunction.
Method
Cross-sectional study of stroke-free individuals from a university-based heart failure clinic. Chagas exposure was defined by ELISA serologic test. Stroke was excluded based on the Questionnaire for Verifying Stroke-Free Status. Individuals underwent cognitive testing (cognitive tests categorized into memory, visuospatial and executive function domains) and 1.5-Tesla brain MRI with semi-automated (MRIcro software) volume measurements (brain, cerebellum and white matter hyperintensity normalized for intracranial volume), silent infarct count and metabolite measurements (N-acetyl aspartate - NAA, choline, myoinositol; all relative to creatine). Cognitive tests and MRI analyses were performed by investigators blinded to Chagas status. Linear regression was performed for each cognitive domain Z-score. We then tested for potential mediation by each of the MRI meausurements.
Results
We studied 398 individuals, age 55 +/− 13 years, 194 (49%) Chagas. Linear regression adjusted for age, sex, left ventricle ejection fraction and educational level confirmed the association between Chagas and visuospatial dysfunction (Beta=-0.245, p = 0.012), but not other cognitive domains. Only NAA/creatine levels differed comparing Chagas and non-Chagas individuals (1.75 vs 1.81, p = 0.028). Mediation analysis estimated that NAA levels explained 49% of the effect of Chagas on visuospatial Z-score.
Conclusion
The neuronal biomarker NAA mediates a significant proportion of cognitive dysfunction found in Chagas disease. In stroke-free individuals, silent cerebrovascular disease does not seem to play a significant role.
Trial registration number
N/A
AS22-030
COGNITIVE DECLINE, PRIMARY HEALTHCARE SERVICE USE AND RECEIPT OF INFORMAL CARE WITHIN 5 YEARS POST-STROKE
1Royal College of Surgeons in Ireland, Psychology, Dublin, Ireland
2Royal College of Surgeons in Ireland, Medicine, Dublin, Ireland
3Royal College of Surgeons in Ireland, Clinical Research Centre- Beaumont Hospital, Dublin, Ireland
4Royal College of Surgeons in Ireland, Dublin, Ireland
5Royal College of Surgeons in Ireland, Population Health Sciences, Dublin, Ireland
6Geriatric Medicine, Dublin, Ireland
7Connolly Hospital Blanchardstown, Geriatric Medicine, Dublin, Ireland
Background and Aims
The aim of this study was to profile cognitive decline 5 years post-stroke, and to explore associations with primary healthcare service use and informal care.
Method
Patients from the Action on Secondary Prevention Interventions and Rehabilitation in Stroke (ASPIRE-S) cohort were followed up at 6 months and 5 years post-stroke. Cognitive impairment was assessed using the Montreal Cognitive Assessment (MoCA), with cognitive decline defined as a decrease of at least 2 points. Primary healthcare service use was defined as the number of general practitioner visits in the previous 12 months (0 to 4 or 5 or more visits). Informal care was defined as any unpaid care received by stroke patients from family members, neighbours or friends.
Results
One hundred patients had cognitive assessment at both 6 months and five years post-stroke. Cognitive decline was evident in 66 (66.0%) patients at 5 years. Increasing age was significantly associated with cognitive decline [OR (95% CI): 1.05 (1.01, 1.09)]. Controlling for age, cognitive decline was associated with a greater number of GP visits in the previous 12 months [OR (95% CI)): 4.73 (1.27, 17.61)], but not with likelihood of receiving informal care [OR (95% CI): 1.20 (0.35, 4.07)].
Conclusion
Cognitive decline is evident in a significant number of patients five years post-stroke, and is associated with increased use of primary healthcare services. Further research is required to explore predictors and outcomes of cognitive decline post-stroke.
Trial registration number
N/A
AS22-031
DEFECTIVE HIPPOCAMPAL NEUROGENESIS INDUCES DEFICITS IN SPATIAL MEMORY IN A MOUSE MODEL OF CEREBRAL HYPOPERFUSION
1University Complutense, Pharmacology, Madrid, Spain
Background and Aims
Vascular cognitive impairment (VCI) is defined by alterations in cognition attributable to cerebrovascular causes that can range from subtle deficits to complete vascular dementia. One of the most important causes of VCI is chronic cerebral hypoperfusion (CCH), which produces white matter lesions triggered by oxidative stress, inflammation and blood-brain barrier damage (Iadecola, 2013). Several studies have linked a faulty neurogenesis with poor outcome after CCH in rats (Silvilia et al., 2008; Choi et al., 2016). However, the spatial memory deficits that underlie CCH and are developed by a defective hippocampal neurogenesis have not been studied so far.
Method
Ten-week-old male C57Bl/6 mice were subjected to bilateral common carotid artery stenosis (BCCAS) or sham operation. Hippocampus-dependent spatial memory deficits were evaluated 3 months after surgery using the Novel Object Location (NOL) and Y-maze tests. Neurogenesis was quantified at 1, 3, 7, 14, 28 days and 3 months by immunohistochemical studies.
Results
BCCAS-animals showed spatial memory deficits demonstrated by a lower time in the closed arm of the Y-maze and lower exploration time of the novel object than their sham-operated counterparts (recognition index: sham 1.13 ± 0.05 vs. BCCAS 3 months 0.85 ± 0.13). Doublecortin positive cells showed a significant decrease (sham 117.7 ± 3.13 vs. BCCAS 3 months 93.04 ± 6.2 cells) in mice subjected to BCCAS with no differences in progenitors proliferation measured as Ki67+ cells.
Conclusion
CCH in rodents produces deficits in hippocampus-dependent spatial memory in the short and long term which are associated to a decrease in the number of neuroblasts.
Trial registration number
N/A
AS22-032
PERFORMANCE IN THE BRIEF MEMORY AND EXECUTIVE TEST, BUT NOT MONTREAL COGNITIVE ASSESSMENT, IS ASSOCIATED WITH STRUCTURAL BRAIN CHANGES IN CHRONIC OBSTRUCTIVE PULMONARY DISEASE PATIENTS
1ST GEORGE's UNIVERSITY OF LONDON, Clinical Pharmacology, LONDON, United Kingdom
2Southmead Hospital, Academic Respiratory Unit, London, United Kingdom
3ST GEORGE's UNIVERSITY OF LONDON, Neurosciences, London, United Kingdom
4ST GEORGE's UNIVERSITY OF LONDON, Respiratory, London, United Kingdom
Background and Aims
COPD is associated with cognitive dysfunction, which may be related to structural brain changes as a result of cerebral small vessel disease. The aim of this study was to identify if cognitive dysfunction was related to structural brain changes in a cohort of COPD patients.
Method
This was a prospective cohort study of COPD patients with no history of stroke or dementia. Participants underwent assessment of COPD severity, cardiovascular risk, and completed cognitive assessment including Test of Premorbid Function (TOPF[UK]), Montreal Cognitive Assessment (MoCA) and Brief Memory and Executive Test (BMET). Participants went on to complete structural brain 3T MRI to evaluate white matter hyperintensities, and whole brain, grey and white matter and CSF volumes. Bivariate and partial correlation analyses were performed to determine the association of cognitive performance with structural brain changes.
Results
56 patients were recruited (mean ± SD age 69 ± 8). 28 participants (50%) had cognitive impairment according to published BMET cut-offs (age-adjusted cut off score ≤13/16). 34 participants (61%) had cognitive impairment according MoCA score (cut off score <26/30). 53 patients completed structural brain 3T MRI. After adjusting for premorbid function (TOPF[UK]) using partial correlation, BMET score was positively correlated with normalised whole brain volume (r=0.373, p = 0.01) and normalised grey matter volume (r=0.365, p = 0.012). MoCA score was not associated with any brain volume parameter.
Conclusion
Impaired cognitive performance on the BMET, but not MoCA, was associated with reduced whole brain and grey matter volume in a cohort patients with COPD.
Trial registration number
N/A
AS22-034
NEUROPROTECTIVE EFFECT OF LITHIUM ON A RAT MODEL OF GLOBAL CEREBRAL ISCHEMIA
1Adnan Menderes University Faculty of Medicine, Neurology Department, Aydin, Turkey
2Adnan Menderes University Faculty of Medicine, Pathology Department, Aydin, Turkey
3Adnan Menderes University Faculty of Medicine, Biochemistry Department, Aydin, Turkey
4Adnan Menderes University Faculty of Medicine, pharmacology Department, Aydin, Turkey
Background and Aims
Lithium (Li) has neuroprotective effects by inhibiting lipid peroxidation and protein oxidation. However there is still insufficient data about its effects in chronic ischemic conditions such as global cerebral ischemia.
Method
We analyze the oxidative stress parameters including nitric oxide (NO), malondialdehyde (MDA), glutathione (GSH), glutathione reductase (GSH-R), catalase (CAT), myeloperoxidase (MPO) and superoxide dismutase (SOD) levels in ischemic prefrontal cortex (PFC) and hippocampal tissue of rats (sham operated, Li treated with low dosage (40mg/kg) and high dosage (80mg/kg), global cerebral ischemia without treatment). The spatial learning disability was also assessed at the end of 28 days of treatment by Morris water maze (MWM) test and brain tissues were collected for biochemical and pathological analyses.
Results
In prefrontal cortex tissue there was a decrease in the elevation of NO, MPO and MDA levels in rats having Li. We also found a significant increase in GSH, GSH-R, CAT and SOD levels in treated groups independent of dosage. MWG test data showed that learning ability in Li taking groups was better in comparison to dementia group. In pathological investigation Li treated rats had significantly less apopitosis in hippocampus CA1 neurons than untreated control group. We also found less apopitosis in rats having higher dosage of Li (80mg/kg) treatment when compared with rats having lower dosage of Li (40mg/kg).
Conclusion
These findings support that Li has antioxidant and neuroprotective property in global cerebral ischemia with less apopitosis in hippocampal CA1 neurons. Our data support that Li has antioxidant and neuroprotective effects in global cerebral ischemia.
Trial registration number
N/A
AS22-036
ADJUSTMENTS MODELS AND BEHAVIORAL CHANGES IN PATIENTS WITH ISCHEMIC AND HEMORRHAGIC STROKE IN EARLY REHABILITATION PERIOD IN KYRGYZSTAN
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
Cognitive impairment (CI) in stroke patients are poorly investigated in Kyrgyzstan. Aim:to determine the neuropsychological profile and the degree of CI in patients in the acute period of ischemic (IS) and hemorrhagic stroke (HS) in the sample of Bishkek City Civil Clinic 1.
Method
The case-control study included 100 patients in the acute period of Is and HS. A group included patients with cardioembolic (CES) and lacunar stroke (LS), was compared with patients with atherothrombotic stroke (ATS). All patients were evaluated on the NIHSS scale; MoCA test, FAB test, clock drawing test, “Schulte Table” technique; Spielberger's Test Anxiety, the Bartell index.
Results
The mean age of patients was 50.5 ± 9.8 years, women were 45.2%. We found severe CI in patients with a duration of hypertension more than 10 years 14.6 ± 6.8 points (p = 0.2). In the HS group, severe neurological impairment according to NIHSS 9.5 ± 2.6 points (p = 0.012) was combined with moderate CI according to MOCA test: 14.7 ± 3.8 (p = 0.03). The most pronounced CI with moderate frontal FAB dysfunction was found in the CES, with a direct correlation with the severity of stroke according to NIHSS (11,1 ± 3,5) and high personal and moderate situational anxiety (p = 0.006). Patients with CES showed a high dependence on others on the Bartell scale (74.4 ± 3.7).
Conclusion
A relationship was found between the duration of hypertension, the large size of the stroke and the severity of CI, cardioembolic strokes demonstrated the worse cognitive deficit.
Trial registration number
N/A
AS22-037
WHITE MATTER INTEGRITY USING DIFFUSION TENSOR IMAGING FOLLOWING TRANSIENT ISCHEMIC ATTACK
1University of Calgary, Neuroscience, Calgary, Canada
2Seaman Family MR Center, Foothills Medical Center, Calgary, Canada
3Hotchkiss Brain Institute, Foothills Medical Center, Calgary, Canada
4University of Calgary, Radiology, Calgary, Canada
5University of Calgary, Community Health Sciences, Calgary, Canada
6Calgary Stroke Program, Clinical Neurosciences, Calgary, Canada
7University of Calgary, Medicine, Calgary, Canada
8University of Calgary, Psychology, Calgary, Canada
9Neuropsychology Service, Foothills Medical Center, Calgary, Canada
Background and Aims
Transient ischemic attack (TIA) increases the risk of developing dementia later in life. Measurement of microstructural changes in white matter (WM) using diffusion tensor imaging (DTI) tractography has potential for identifying individuals at greatest risk of cognitive decline. We hypothesized that patients with TIA have abnormal DTI parameters in WM tracts compared to controls.
Method
Patients presenting with high risk TIA but free of dementia, and healthy volunteer controls were recruited acutely and underwent structural MRI, inclusive of DTI sequences (31 directions b1000). Axial diffusivity (AD), fractional anisotropy (FA), mean diffusivity (MD) and radial diffusivity (RD) values were measured from the cingulum, superior longitudinal fasciculus, uncinate fasciculus, fornix and genu. A mixed effect regression was used assess the effects of TIA on DTI parameters controlling for age, vascular risk factors, intracranial volume, WM hyperintensities volume and premorbid intelligence.
Results
Of the 148 patients included in this analysis, 96 were TIA patients, 79 (53.4%) were females. The average age of the patients in TIA and control groups was 68.1(SD=9.5) and 64.5 (SD=10.2), respectively. A mixed-effects regression revealed that TIA patients exhibited an increase in MD (P<.0001) only in the fornix and an overall decrease in FA (P<.0001) when compared to healthy controls, after controlling for all covariates.
Conclusion
There are significant differences in DTI parameters for TIA patients and healthy controls, supporting the presence of incipient microstructural disease in the fornix. Future work aims to identify deterioration of DTI measures over time and their relation to potential vascular and neurodegenerative etiologies.
Trial registration number
N/A
AS22-038
CEREBRAL AMYLOID ANGIOPATHY-RELATED INFLAMMATION (CAA-RI) PRESENTING AS ACUTE CONFUSION IN AN OLDER PERSON
1Nottingham University Hospitals NHS Trust, Stroke Medicine, Nottingham, United Kingdom
Background and Aims
A 77-year-old female presented to our hyper-acute Stroke Unit with sudden onset agitation and dysarthria. A similar presentation had occurred in the past. On MRI (Figure 1) there was swelling and hyperintensity of the left parietal lobe extending to the occipital lobe, with the signal change extending to the cortical boundary. Numerous micro-haemorrhages were throughout the cerebrum in a lobar distribution particularly around the left parietal swelling. Normal flow voids are seen in the major intracranial vessels.
A year ago she was diagnosed with Inflammatory Cerebral Amyloid Angiopathy (CAA) and treated with IV methylprednisolone. On this occasion the symptom of delirium recurred and a diagnosis of reversible encephalopathy was made. She was again treated with steroid successfully.
Method
Figure 1
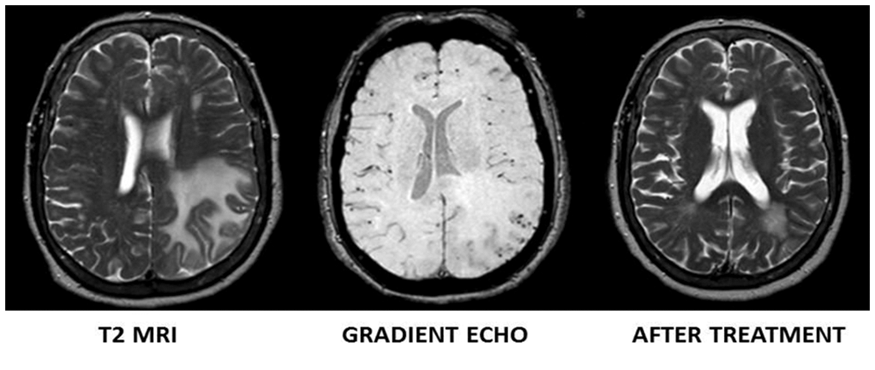
Results
N/A
Conclusion
CAA-related inflammation (CAA-ri) is a distinct subset of CAA1, 2 with a presentation of acute or sub-acute cognitive decline rather than haemorrhage. Diagnostic tests include neuroimaging, CSF studies and brain biopsy. CSF may show higher level of autologous anti-Amyloid β antibodies than non-inflammatory form of CAA according to a small study3. MRI features include potentially reversible leukoencephalopathy with patchy or confluent white matter hyper-intensities and multiple micro-haemorrhages seen on gradient echo on T2 weighted MRI sequences. Treatment for CAA-ri is not standardized, however glucocorticoid or cytotoxic agent e.g. cyclophosphamide is often used as an initial agent. Clinical and radiological improvement is often seen after immunosuppression. Duration of treatment is not well-established and needs to be individualized. Patients can be categorized in 3 different patterns of response: improvement, relapsing or progressive2.
Trial registration number
N/A
AS22-039
DIFFUSION TENSOR IMAGING TRACTOGRAPHY AND COGNITION OF TRANSIENT ISCHEMIC ATTACK PATIENTS
1University of Calgary, Neuroscience, Calgary, Canada
2Seaman Family MR Center, Foothills Medical Center, Calgary, Canada
3Hotchkiss Brain Institute, Foothills Medical Center, Calgary, Canada
4University of Calgary, Radiology, Calgary, Canada
5University of Calgary, Community Health Sciences, Calgary, Canada
6Calgary Stroke Program, Clinical Neurosciences, Calgary, Canada
7University of Calgary, Medicine, Calgary, Canada
8University of Calgary, Psychology, Calgary, Canada
9Neuropsychology Service, Foothills Medical Center, Calgary, Canada
Background and Aims
Transient ischemic attack (TIA) patients experience an increased dementia risk. Assessment of white matter (WM) microstructural changes using diffusion tensor imaging (DTI) tractography and cognitive testing has the potential to identify individuals at the greatest risk. We hypothesized that TIA patient’s poor cognitive performance can be predicted by DTI parameters.
Method
Data were collected from 96 dementia-free TIA patients and 52 healthy volunteer controls, who were recruited acutely and underwent structural MRI, DTI (31 directions b1000), and cognitive testing. Fractional anisotropy (FA) and mean diffusivity (MD) were measured in the cingulum, superior longitudinal fasciculus, uncinate fasciculus, fornix and genu. Study participants’ demographic, clinical, and imaging data characteristics were compared across TIA and control groups. Mixed-effects regression analysis was used to assess the association between DTI parameters and cognition in the executive function, memory, and processing speed domain, adjusting for age, vascular risk factors, intracranial volume, WM hyperintensities volume and premorbid intelligence.
Results
TIA patients exhibited lower scores on visual memory (P<0.01), verbal memory (P<0.003), and processing speed (P<.0001) domains than healthy controls. DTI parameters within the fornix (lower FA and higher MD) and cingulum (lower FA) were predictive of lower test scores in TIA patients, compared to healthy controls.
Conclusion
This study confirms the prognostic utility of DTI parameters in predicting cognitive scores. These findings suggest that imaging biomarker should be incorporated into prognostic tools, in addition to demographic and clinical markers, for predicting dementia in patients at greater risk of cognitive decline.
Trial registration number
N/A
AS22-040
ASYMPTOMATIC CAROTID STENOSIS, WHITE MATTER DISEASE AND COGNITION: CONTRIBUTIONS TO A CLINICAL PROFILE
1University of Sao Paulo, Department of Neurosciences and Behavioral Science, Ribeirao Preto, Brazil
2University of Sao Paulo, Department of Physics, Ribeirao Preto, Brazil
Background and Aims
Patients with carotid stenosis, without history of stroke or transient ischemic attack are considered to be asymptomatic. However, many of those patients might have high burden of white matter hyperintensities (WMH) and cognitive decline that may precede clinical events, suggesting a high risk for stroke. In the present study, we aimed to assess the association between ACAS, WMH and cognitive decline.
Method
Eleven patients (69,72 ± 8,29 years, 6 women) with ≥70% ACAS unilateral were compared with 11 healthy elderly controls (62 ± 7,36 years, 6 women) using a comprehensive neuropsychological battery and T2-weighted FLAIR MRI. Lesion segmentation was performed by the SPM-12 using an automatic algorithm. Mann-Whitney U Test, Spearman correlation coefficients were used to explore associations among scores of neuropsychological tests and burden of WMH between groups.
Results
Compared controls, patients showed higher WMH lesion burden in the studied tracts (p <0.05) and lower performances on information processing speed, memory, attention and executive functions (p < 0.05) tests. 65% of patients fulfill criteria for vascular cognitive impairment. The cerebral hemisphere ipsilateral to ACAS showed a higher burden of WMH compared to the contralateral one (p = 0.03). Correlations between lesion burden and cognitive impairment were found for both groups (p < 0.05). The reduced number of associations between lesion burden on WM tracts and cognitive domains may suggests different risk profiles among patients with severe ACAS.
Conclusion
Vascular cognitive impairments and high burden of WMH are common in patients with ACAS and should be explored as markers of high risk of stroke and dementia in those patients.
Trial registration number
N/A.
SMALL VESSEL DISEASE
AS23-002
RISK FACTORS FOR MRI-VISIBLE PERIVASCULAR SPACES IN SPONTANEOUS HYPERTENSIVE INTRACEREBRAL HEMORRHAGE PATIENTS: A COHORT STUDY
1Beijing Tiantan Hospital - Capital Medical University, Neurology Department, Beijing, China
Background and Aims
Cerebral small vessel disease (SVD) is associated with cognitive decline, depression, increased mortality and disability in stroke patients. MRI-visible perivascular spaces (PVS) are a sensitive neuroimaging marker of SVD. We aimed to explore the risk factors of MRI-visible PVS burden in two topographical regions (in the basal ganglia [BG] and centrum semiovale [CS]) in a cohort of spontaneous hypertensive intracerebral hemorrhage (HICH) patients.
Method
We included 250 consecutive patients from a prospective HICH cohort. The PVS in the BG and CS regions were assessed on a validated 4-point visual rating scale (0=no EPVS, 1=<10, 2 =11–20, 3=21–40, and 4=>40) by two observers independently. Clinical information was obtained using standardized forms and hospital routine blood sample tests. We predefined severe PVS as score >2 and tested their associations with demographic characteristics as well as blood sample by multivariable logistic regression.
Results
In the multivariable logistic regression, severe CS PVS (odds ratio [OR] 5.56, 95% confidence interval [CI] 2.23–13.87, p < 0.001) and age (1.08,1.04–1.12, p < 0.001) were independently associated with increased BG PVS severity. Male gender (0.28, 0.95–13.90, p = 0.024) and patients with high serum creatinine levels (4.55, 1.05–19.71, p = 0.043) were independently associated with severe CS PVS.
Conclusion
MRI-visible PVS in different regions are inter-related and have different risk factors in patients with spontaneous HICH, which may accelerate discovery of effective treatments for PVS, SVD and HICH.
Trial registration number
N/A
AS23-004
EEG PECULIARITIES IN PATIENTS WITH A DIFFERENT BURDEN OF THE BRAIN SMALL VESSEL DISEASE
1“Institute of Neurology- Psychiatry and Narcology of the NAMS of Ukraine” SI, Department of Brain Vascular Pathology, Kharkiv, Ukraine
Background and Aims
The investigation of the cerebral electrogenesis peculiarities in patients with different MRI markers of the brain small vessel disease (bSVD) might determine strength/quality of the association between EEG parameters and the burden of the disease, as well as establish EEG-correlates of the bSVD course.
Method
In the prospective study, 40 patients (mean age 62.51 ± 1.38 years old) with different bSVD burden and without history of stroke were assessed for a number of EEG parameters (rhythm indices, power ratios (alpha/delta, (delta+theta)/(alpha+beta)), brain symmetry index (BSI)). A total score on the scale of bSVD burden (0-4 points) was determined according to MRI results.
Results
With an elevation of the bSVD burden from 1 to 4, a significant increasing of delta-index (from 19.23% to 35.78%, respectively; p <0.01), and a significant decreasing of alpha-index (from 42.75% to 19.02%, respectively; p < 0.001) were recorded. The alpha-ratio also was linearly decreased (from 2.74 to 0.55, respectively; p < 0.001) and (delta+theta)/(alpha+beta)-ratio was increased (from 0.41 to 1.15, respectively; p < 0.01). Correlation analysis have confirmed the existence of strong associations between bSVD burden and the delta-index (r=0.76), the alpha-index (r=-0.83), (delta+theta)/(alpha+beta)-ratio (r=0.64), and alpha/delta-ratio (r=-0.80). The BSI was also increased with scores of bSVD burden: 0.06–0.10 for bSVD burden of 1–2, and 0.12–0.15 for bSVD burden of 3–4.
Conclusion
Values of EEG-correlates of cerebrovascular impairments in patients with bSVD were related with the score of bSVD burden. The indices of delta- and alpha-activity, as well as alpha/delta- and (delta+theta)/(alpha+beta)-ratio can be considered as EEG-correlates of bSVD burden.
Trial registration number
N/A
AS23-005
TOTAL SMALL VESSEL DISEASE SCORE AND SUBSEQUENT CEREBROCARDIVASUCULAR EVENTS IN NEUROLOGICALLY HEALTHY ADULTS: 6.5 YEARS FOLLOW-UP IN THE KASHIMA SCAN STUDY
1Saga University, Internal medicine, Saga, Japan
2Saga University, Radiology, Saga, Japan
3National Center for Global Health and Medicine, Radiology, Tokyo, Japan
4Yuai-Kai Oda Hospital, Radiology, Kashima, Japan
Background and Aims
We prospectively explored the association between the total small vessel disease (SVD) score obtained with MRI and cerebro-cardiovascular events in neurologically healthy Japanese adults.
Method
The presence of SVD features, including lacune (s), cerebral microbleed (s), moderate or severe white matter changes, and moderate or severe basal ganglia perivascular spaces on MRI (1point if present, respectively), was summed to obtain a “total SVD score” (range 0-4). A total of 1,411 subjects (mean age, 59.1 years; 47% male) were classified into 3 group: those with a total SVD score of 0 (n = 1000), 1 (n = 292), and ≥2 points (n = 102). Non-fetal or fetal cerebro-cardiovascular events were defined as our primary end point. The hazard ratio [HR] of the events during the follow-up period were calculated using the Cox proportional hazards model with adjustments for age, sex, hypertension and diabetes mellitus. Cumulative events-free rates were estimated by the Kaplan-Meier method.
Results
During a mean follow-up of 6.5 ± 3.0 years, 43 cerebro-cardiovascular events (including cerebral infarction [n = 15], intracerebral hemorrhage [n = 3], subarachnoid hemorrhage [n = 1], ischemic heart disease [n = 21], acute heart failure [n = 2], aortic dissection [n = 1] occurred in 42 subjects. A higher SVD score was associated with an increased risk of cerebro-cardiovascular events (HR per unit increase: 1.74, 95%CI, 1.19–2.71, p = 0.006). The events were significantly more common among subjects with higher total SVD score (p < 0.000.1, log rank test).
Conclusion
This study offered an additional evidence of the total SVD score, suggesting this scoring system may be a promising tool to predict subsequent stroke or cardiovascular diseases.
Trial registration number
N/A
AS23-006
FATAL CASE OF CEREBRAL AMYLOID ANGIOPATHY DECADES AFTER A DURAL GRAFT
1Hopital Lariboisiere/universite Paris Diderot/INSERM U 1161, Service de neurologie/Centre de référence des maladies vasculaires rares du cerveau et de l'oeil CERVCO, Paris, France
2Hopital Lariboisiere, Service de neurologie, Paris, France
3Hôpital Bichat, Service de Neurologie, Paris, France
4Hopital Lariboisiere/universite Paris Diderot/INSERM U 1161, Laboratoire de génétique, Paris, France
5CHU de Rouen, Service de génétique, Paris, France
6Hôpital Lariboisière, Laboratoire d'anatamo-pathologie, Paris, France
7Hopital Lariboisiere/universite Paris Diderot/INSERM U 1161, Service de neurologie, Paris, France
8Hôpital Pitié-Salpetriere, Laboratoire de neuropathologie, Paris, France
Background and Aims
Injection of brain homogenates from APP transgenic mice can seed Abeta deposition in the host brain of primates. More recently, cerebral parenchymal and vascular amyloid deposits were observed in iatrogenic Creutzfeldt-Jakob disease (iCJD) caused by injection of cadaver derived growth hormone (cGH). The presence of aggregated abeta was confirmed in cGH batches. This raised the hypothesis that hormone preparations contained Abeta aggregates able to seed amyloid formation two decades after their injection. Dural grafts with or without iCJD have also been suspected to seed Abeta misfolding. Seeded Abeta aggregation, however, was not previously associated with clinical manifestations.
Method
We report a clinical autopsy case of a 46-year-old woman who died of intracerebral hemorrhages caused by cerebral amyloid angiopathy (CAA), presumably related to contaminated cadaveric dura, grafted 44 years before death.
Results
The patient had a severe cerebral contusion at the age of two. A dural defect was filled by a graft of human cadaveric dura mater. At the age of 46, she died of repeated lobar hematomas. Microscopical examination revealed a severe CAA, parenchymatous Aβ deposits, and a tauopathy limited to exceptional tangles. Genetic testing excluded known mutations and deletions involved in hereditary Abeta CAA (APP, PSEN1, PSEN2). The APOE genotype was ε2/ε3.
Conclusion
The probability that the dural graft was causal in our case is high: the young age, the absence of mutation and the severe CAA in the near absence of tauopathy are in favor of that mechanism. The incubation period would be particularly long, explaining why CAA was symptomatic.
Trial registration number
N/A
AS23-010
APATHY IS ASSOCIATED WITH DISRUPTION TO DISTINCT, LARGE-SCALE WHITE MATTER NETWORKS
1University of Cambridge, Department of Clinical Neurosciences, Cambridge, United Kingdom
2Donders Institute for Brain- Cognition and Behaviour- Radboud University Nijmegen Medical Centre, Department of Neurology, Nijmegen, The Netherlands
3St. George's University of London, Neuroscience Research Centre- Molecular and Clinical Sciences Research Institute, London, United Kingdom
4University of Oxford, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Apathy is a common and debilitating syndrome in many neurological conditions, but its underlying neurobiology remains poorly understood. This complicated by depression, an overlapping but distinct neuropsychiatric syndrome. Research has shown that apathy, but not depression, is associated with widespread white matter damage. We test the hypothesis that apathy is a disconnection syndrome using network analysis to study the relationships between apathy and white matter networks in patients with cerebral small vessel disease (SVD), a vascular pathology characterised by white matter damage.
Method
331 SVD patients completed measures of apathy and depression and underwent MRI. White matter networks were constructed using DTI and tractography. First, path analysis was used to test the mediating effect of network integrity on the relationship between radiological markers of SVD and apathy. Second, we examined differences in whole brain measures of network integrity between participants with only apathy, only depression, comorbid apathy and depression, and a control SVD group free of neuropsychiatric symptoms. Finally, we examined regional network correlations with apathy while controlling for depression.
Results
Path analysis results indicated that the relationship between SVD markers and apathy was fully mediated by network integrity. Between-group comparisons revealed that SVD patients with apathy, when compared to other SVD patients, were impaired on whole brain measures of network density and efficiency. Regression analyses revealed that apathy was primarily associated with connectivity in medial premotor and frontostriatal regions.
Conclusion
These results suggest that apathy is caused by the disconnection of white matter tracts underlying action initiation and effort-based decision-making for reward.
Trial registration number
N/A
AS23-011
PREDICTORS OF INTRACEREBRAL HEMORRHAGE AMONG LACUNAR STROKE PATIENTS TREATED WITH ASPIRIN: PORCELAIN STUDY SUB-ANALYSIS
1Nippon Medical school Tamanagayma Hospital, Neurology, Tokyo, Japan
Background and Aims
We are investigating the utility of low-dose aspirin for secondary stroke prevention in patients with non-cardioembolic stroke. Recently we had reported that the lacunar stroke as an index stroke was the significant and only predictor of intracerebral, not intracranial, hemorrhage (ISTH2017). So that we further analyzed the risk factor of “intracerebral” hemorrhage (ICeH) only among lacunar stroke patients.
Method
PORCELAIN study includes three randomized, double-blinded, prospective, aspirin-comparator study conducted in Japan, i.e. S-ACESS study (2008; aspirin vs sarpogrelate), CSPS 2 study (2010; aspirin vs cilostazol) and JASAP study (2011; aspirin vs Aggrenox). All three studies enrolled only patients with non-cardioembolic stroke. We combined and reanalyzed the patients randomized to aspirin-arm from each studies. In this sub-analysis, we limited the patients who were diagnosed lacunar stroke as an index stroke and compared between patients with ICeH and those without according to background patient profiles.
Results
From total 2726 aspirin treated cases, 1789 patients with lacunar stroke as an index stroke were included in this sub-analysis (female 28.3%, mean age 64 y/o). All cases were administrated 81mg aspirin per day. During 715 days mean observation period, 129 ICeHs were documented. The history of diabetes was the only significant negative predictor of ICeH (HR=0.36; 014–0.94: p = 0.037) after multivariate logistic regression analysis, whereas the history of hypertension and the blood pressure (both systolic and diastolic) on registration were not significant.
Conclusion
The history of hypertension was not a significant predictor of ICeH among lacunar stroke patients treated with low-dose aspirin.
Trial registration number
N/A
AS23-012
CLINICAL PREDICTORS OF PARKINSONISM AND DEMENTIA IN PATIENTS WITH CEREBRAL SMALL VESSEL DISEASE; A DISTINCTIVE PATTERN
1Radboudumc, Neurology, Nijmegen, The Netherlands
2Jeroen Bosch Ziekenhuis, Neurology, 's Hertogenbosch, The Netherlands
3Radboud University, Donders Institute for Brain- Cognition and Behaviour- Centre for Cognitive Neuroimaging, Nijmegen, The Netherlands
Background and Aims
Patients with cerebral small vessel disease (SVD) have a heterogenous clinical course, while some remain without symptoms, others develop parkinsonism, dementia or both. Our aim was to identify cognitive and motor symptoms that predict parkinsonism or dementia in SVD patients.
Method
Participants were from the RUN DMC study, a prospective cohort of 503 SVD patients with nine year follow-up. Parkinsonism and Dementia were diagnosed according to respectively the UKPDS brain bank and DSM IV criteria. Hazard ratios were calculated for incident parkinsonism and dementia separately using Fine and Gray method with death as a competing risk.
Results
After a median follow-up of 8.6 years, 32 of 501 participants developed parkinsonism (6.4%) and 65 developed dementia (13.0%). While motor symptoms (presence of hypokinesia HR1.32 95%CI [1.08–1.62]) and rigidity HR1.24 95%CI [1.02–1.51]) were significantly associated with developing parkinsonism, they were not associated with dementia when adjusted for age, education and presence of depressive symptoms. However cognitive tasks demanding attention and psychomotor speed such as the paper-pencil test were significantly associated with both parkinsonism (HR2.19 95%CI [1.26–3.79] per SD) and dementia (HR2.11 95%CI [1.29–3.45] per SD). Memory tasks (MMSE<26 HR2.51 95%CI [1.33–4.73], 15 word learning test HR1.29 95%CI [1.12–1.48] per word below average) were only associated with a higher risk of dementia.
Conclusion
Using simple clinical tests, a distinct clinical pattern is visible years before diagnosis of parkinsonism and/or dementia in SVD patients. Taking these differences in account might improve personalized preventive management for dementia and/or parkinsonism in these patients.
Trial registration number
N/A
AS23-013
EFFECT OF CILOSTAZOL ON PREVENTION OF RETINAL ARTERY STENOSIS AND CEREBRAL SMALL VESSEL DISEASE IN ACUTE LACUNAR INFARCTION PATIENTS
1Hong-Ik hospital, Neurology, Seoul, Republic of Korea
Background and Aims
Cilostazol, phosphodiesterase inhibitor, has antiplatelet and vasodilating effect. We aimed to investigate the effect of cilostazol on retinal artery stenosis and in line with cerebral small vessel disease.
Method
A total of 48 consecutive acute lacunar infarction patients for the first time in life were enrolled. We evaluated initial arteriole-to-venule ratio (AVR) and Fazekas grade. We arbitrarily separated patients into two groups. Cilostazol group was treated with cilostazol 200mg/day and control group with either aspirin 100mg/day or clopidogrel 75mg/day or triflusal 600mg/day for 2 years. Primary endpoint was AVR and Fazekas grade change and secondary endpoint was incident ischemic stroke recur.
Results
Initial demographic, medical and laboratory characteristics of the two groups showed no statistically significant difference. In cilostazol group, AVR increased after treatment (p = 0.010) and Fazekas grade showed no significant change (p = 0.596). In control group, on the other hand, there was no AVR change (p = 0.925) but increase of Fazekas grade (p = 0.045). There was no difference in ischemic stroke recurrence between two groups (p = 0.293). Although the overall frequency of recurrent cerebral ischemic event did not differ, hemorrhagic stroke incidence was higher in control group without statistical significance (p = 0.091).
Conclusion
This study identified cilostazol treatment potently increases retinal microvascular dilatation, prevents cerebral small vessel disease progression and reduce hemorrhagic stroke incidence at the same time compared to other antiplatelet treatment.
Trial registration number
N/A
AS23-014
A NOVEL MUTATION OF COL4A1 RESPONSIBLE OF FAMILIAL PORENCEPHALY AND SEVERE HYPERMETROPIA
1Hôpital Erasme - ULB, Neurology, Bruxelles, Belgium
2Hôpital Erasme - ULB, Neuropediatrics, Bruxelles, Belgium
3CHU Angers, Pediatric, Angers, France
Background and Aims
COL4A1 is a gene responsible for a broad spectrum of syndromes characterized by small vessel involvement of variable severity, including neurological manifestations (porencephaly, aneurysms), ophthalmologic (retinal artery tortuosity and Axenfeld-Rieger anomaly), renal (renal cysts, microscopic hematuria) and systemic (cramps, Raynaud's phenomenon, arrhythmias).
Method
We studied a non-consanguineous family (fig.1) with 3 cases of porecencephaly. IV-2 and IV-5 developed left and right hemiplegia respectively, had hypermetropia (8.50 and 15 dioptres (D)). IV-2 has epilepsy under valproic acid. IV-5 had mild psychomotor retardation and slight elevation of CK. IV-4 is hyperopic, microcephalic, with light mental retardation and the MRI shows a porencephalic cyst. The father has severe hypermetropia (7 D), bilateral cataract and nonspecific abnormalities of brain white matter. His mother suffers from lameness attributed to a forceps delivery: this has allowed suspecting an unknown hereditary pathology and a dominant inheritance. A genetic analysis reveals for father and three out five children a COL4A1 mutation of the type (c.2228G> T [p. Gly743Val]), not reported previously.
Fig.1
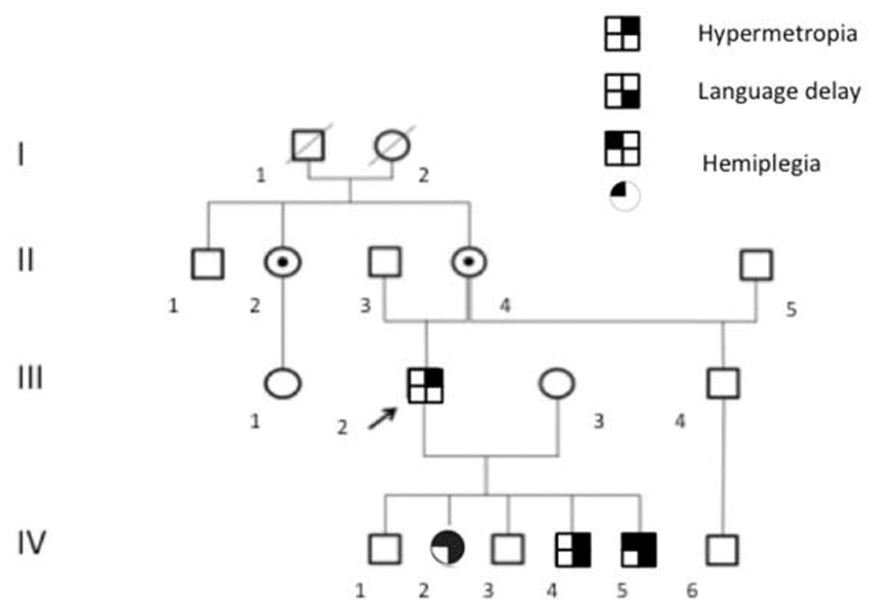
Fig.2
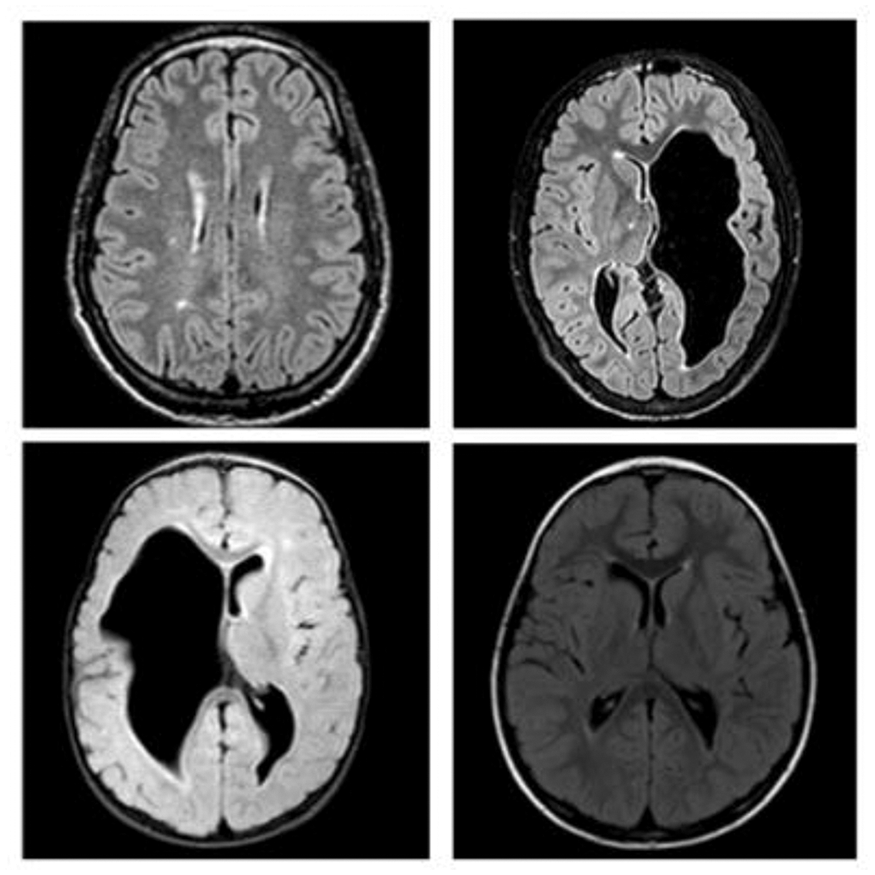
Results
We discover a new autosomal dominant mutation of COL4A1. Glycine is chemically different, highly conserved and crucial for the formation of α1α1α2 heterotrimers of collagen IV. The systemic balance shows cerebral and ocular involvement.
Conclusion
A mutation of the COL4A1 gene must be suspected in case of congenital porencephaly, early white matter abnormalities, ocular and renal abnormalities with familial history suggesting autosomal dominant inheritance with incomplete penetrance. For asymptomatic patients biannual monitoring of renal function, with cerebral and vessel imaging and ophthalmologic follow-up are indicated.
Trial registration number
N/A
AS23-015
CORTICAL SUPERFICIAL SIDEROSIS PROGRESSION AS A NOVEL DISEASE BIOMARKER IN CEREBRAL AMYLOID ANGIOPATHY: IMPLICATIONS FOR FIRST-EVER INTRACEREBRAL HAEMORRHAGE RISK IN AN MRI-CLINICAL COHORT STUDY
1Massachusetts General Hospital, JPK Stroke Research Center, Boston, USA
Background and Aims
Cortical superficial siderosis (cSS) is an emerging hemorrhagic signature of cerebral amyloid angiopathy (CAA). cSS progression might represent new CAA-bleeding events and is an attractive biomarker, but has not yet studied. We investigated cSS progression and its clinical relevance for incident lobar intracerebral hemorrhage (ICH) risk, in probable CAA presenting without ICH.
Method
Consecutive symptomatic patients with probable CAA who underwent MRI at baseline and during follow-up were analyzed. cSS progression was assessed by comparison of the baseline and follow-up images. Patients were followed prospectively for incident symptomatic ICH. Cox proportional hazard models were used to investigate cSS progression and first-ever ICH risk.
Results
The cohort included 118 probable CAA patients: 72 (61%) presented with transient focal neurological episodes and 46 (39%) with cognitive complaints. Fifth-two patients (44.1%) had cSS at baseline. During a median scan-interval of 2.2 years, cSS progression was detected in 33 (28%) patients. In multivariable logistic regression, cSS presence at baseline (OR: 4.04; 95%CI: 1.53–10.70, p = 0.005) and appearance of new lobar microbleeds (OR: 4.24; 95%CI: 1.29–13.9, p = 0.017) were independent predictors of cSS progression. In clinical follow-up (median post-final MRI: 1.34, IQR: 0.3–3 years), cSS progression predicted increased symptomatic ICH risk (HR: 3.76; 95%CI: 1.37–10.35, p = 0.010) in multivariable Cox regression.
Conclusion
cSS progression is common among CAA patients and a reasonably strong predictor of subsequent lobar ICH risk. These findings are useful clinically and have implications about the mechanistic link between superficial bleeding and ICH in CAA. cSS progression could be a candidate biomarker for trials in the field.
Trial registration number
n/a
AS23-016
IMPACT OF WHITE MATTER HYPERINTENSITIES ON ONE-YEAR STROKE RECURRENCE
1Dongguk University, Neurology, Goyang-si, Republic of Korea
2Seoul National University Bundang Hospital, Neurology, Seongnam, Republic of Korea
Background and Aims
Using a large sample-sized patients and quantitative measurement of WMH, we investigated the impact of WMH on stroke recurrence, type of recurrence (ischemic vs. hemorrhagic).
Method
A total of 7101 ischemic stroke patients were enrolled. Type of stroke recurrence were prospectively captured. WMH were stratified into quartiles. To examine the independent impact of WMH on the type of stroke recurrence, we used cox regression and competing risk analysis as appropriate.
Results
Mean age was 67.8 (standard deviation 12.7) and 4170 (58.7%) were men. During 1-year, 345 (4.9%) patients had recurrent stroke – 286 ischemic strokes, 28 hemorrhagic strokes, 25 unclassified strokes, and 6 transient ischemic attacks. Cox regression analysis showed that WMH quartiles were independently associated with recurrent all strokes. Compared with the first quartile, adjusted hazard ratio (HR) for fourth quartile was 1.84 (95% confidence interval 1.27 – 2.68, Table). Competing risk analysis demonstrated that only the fourth quartile of WMH was associated with recurrent ischemic stroke after adjusting for covariates (adjusted HR 1.54, 95% confidence interval 1.07 – 2.29). With respect to hemorrhagic stroke, WMH quartiles strongly associated with recurrent hemorrhagic stroke (p for trend = 0.003). Compared to the first quartile, adjusted subdistribuion HR for third and fourth quartiles were 12.1 (95% confidence interval 1.5 – 99.0) and 29.5 (3.6 – 242.1), respectively.
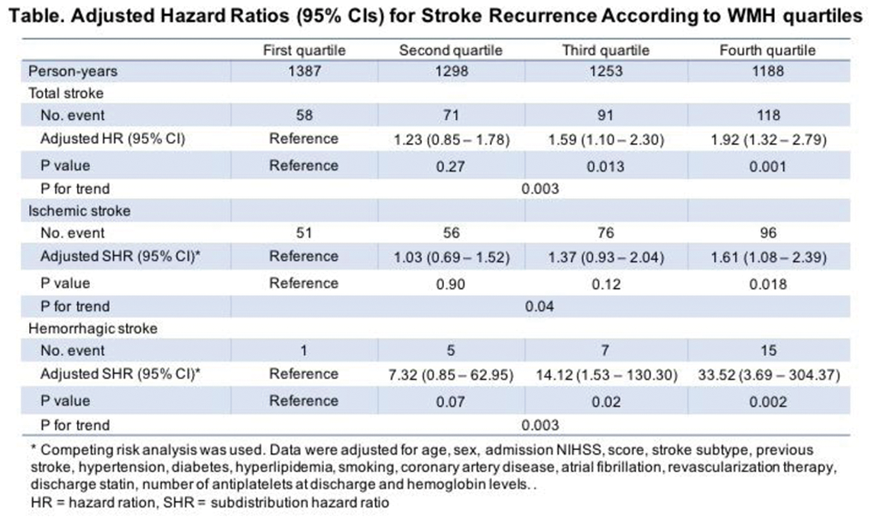
Conclusion
WMHs are more strongly associated with recurrent hemorrhagic stroke than ischemic stroke. Our data implicate that WMHs might be used as a risk marker of recurrent hemorrhagic stroke in patients with ischemic stroke.
Trial registration number
N/A
AS23-017
EXTRACRANIAL ARTERY STENOSIS IS CORRELATED WITH TOTAL MRI BURDEN OF CEREBRAL SMALL VESSEL DISEASE IN ISCHAEMIC STROKE PATIENTS
1The First Affiliated Hospital- Sun Yat-Sen University, Department of Neurology and Stroke Center, Guangzhou, China
Background and Aims
Extracranial artery stenosis (ECAS) is related to individual markers of cerebral small vessel disease (cSVD). However, little has been reported on the association between ECAS and the total burden of cSVD as assessed by magnetic resonance imaging (MRI). We aimed to investigate the relationship between ECAS and total cSVD burden in patients with acute ischaemic stroke.
Method
We included consecutive patients who underwent colour Doppler ultrasonography and brain MRI for evaluation of acute stroke. The presence and total MRI burden of cSVD, including lacunar infarctions (LIs), white matter hyperintensities (WMHs), cerebral microbleeds (CMBs) and enlarged perivascular spaces (EPVS), were investigated. ECAS was classified by severity: absent or mild stenosis, moderate stenosis, severe stenosis, or occlusion. The relationships among ECAS and total MRI burden of cSVD were examined.
Results
Two hundred and thirty-eight patients were included in this study. The mean age of the participants was 61 ± 12 years, and 73.2% of them were male. Hypertension, current smoking, hyperlipidaemia and diabetic mellitus were frequent among the patients (66.9%, 45.6%, 43.9% and 35.1%, respectively). Kruskal-Wallis test and the post-hoc analysis showed that the severity of ECAS was higher in severe burden group than moderate burden group and absent to mild burden group respectively (Corrected P = 0.003 and 0.001, respectively). Ordinal regression indicated that ECAS was significantly and independently associated with total cSVD burden after adjustment for the other vascular risk factors.
Conclusion
In this study, high levels of ECAS were associated with coexisting advanced cerebral cSVD in acute ischaemic stroke and TIA patients.
Trial registration number
N/A
AS23-018
COMBINATION OF RETINAL ABNORMALITIES AND THE MRI MARKERS FOR ASSESSING THE TOTAL CEREBRAL SMALL VESSEL DISEASE BURDEN IN TIA/ISCHAEMIC STROKE PATIENTS
1The First Affiliated Hospital of Sun Yat-sen University, Department of Neurology and Stroke Center, Guangzhou, China
Background and Aims
Retinal vessels is a distribution of intracranial vessels outside the brain, and accumulating evidence shows the association among cerebral small vessel disease (cSVD) and retinal microvascular abnormalities. The purpose of this study was to investigate whether combining the retinal and MRI features captures overall characteristics of cSVD by testing the associated with the risk factors of the individual magnetic resonance imaging (MRI) features.
Method
We included consecutive patients who underwent retinal photography and brain MRI. The scores combining retinal and MRI features of cSVD were investigated. Ordinal regression was used to assess the association between vascular risk factors and the combined cSVD scores.
Results
Two hundred and sixty-three patients were included in the study. In all included patients, the median age was 61y (interquartile, 51∼70 y), and 72.2% of the patients were male. Hypertension, current smoking, hyperlipidaemia and diabetic mellitus, were frequent among the included patients (65.8%, 44.9%, 42.2% and 33.8%, respectively). The proportions of the patients with the combined cSVD score ranging from 0 to 5 were 14.0%, 17.5%, 17.5%, 17.0%, 20.9% and 13.3%, respectively. Age (OR 1.09, 95% CI 1.06–1.11), hypertension (OR 2.39, 95% CI 1.46–3.91) and previous stroke/TIA (OR 1.83, 95%CI 1.01–3.31) were significantly and independently associated with the combined cSVD score.
Conclusion
Hypertension, age and previous stroke/TIA, are significantly associated with the combined cSVD score in TIA/ischaemic stroke patients. The combined cSVD score captures the overall features of cSVD, and it may therefore be an effective method for evaluating the total cSVD burden.
Trial registration number
N/A
AS23-019
AUTOMATED RETINAL IMAGE ANALYSIS TO DETECT WHITE MATTER HYPERINTENSITIES IN STROKE- AND DEMENTIA-FREE HEALTHY SUBJECTS - A CROSS-VALIDATION STUDY
1The Chinese University of Hong Kong, Department of Medicine and Therapeutics, New Territories, Hong Kong S.A.R
2The Chinese University of Hong Kong, Therese Pei Fong Chow Research Centre for Prevention of Dementia, New Territories, Hong Kong S.A.R
3The Chinese University of Hong Kong, Division of Biostatistics- Jockey Club School of Public Health and Primary Care, New Territories, Hong Kong S.A.R
Background and Aims
Retinal imaging with artificial-intelligence assisted analysis has the potential to become a simple and reliable tool for screening population-at-risk of cerebrovascular disease and dementia. We aimed to develop an algorithm with automatic retinal imaging in identifying asymptomatic subjects with high burden of white matter hyperintensities (WMH).
Method
We performed automated retinal image analysis (ARIA) in 180 community dwelling, stroke and dementia-free healthy subjects. ARIA is fully automatic and validated in separate disease cohorts. WMH on MRI brain was graded using ARWMC scale by an independent accessor. 126(70%) subjects were randomly selected for model building, 27(15%) for model cross-validation, and remaining 27(15%) for testing; all 180 subjects were used for evaluation of model accuracy to predict WMH burden.
Results
All 180 subjects completed ARIA with successful analysis. The mean age was 70.3 +/− 4.5 years, 70(39%) were male. Risk factor profiles were: 106(59%) hypertension, 31(17%) diabetes, and 47(26%) hyperlipidemia. Severe WMH (defined as global ARWMC grading >=2) was found in 56(31%) subjects. The performance for detecting severe WMH (sensitivity, SN; and specificity, SP) for model building (SN 96.7%, SP 80.6%), model validation (SN 100%, SP 87.5%), and testing (SN 100%, SP 83.3%) was excellent. The overall performance was SN 97.6% and SP 82.1%, with PPV 94% and NPV 92%. Moreover, there was good correlation with WMH volume (log-transformed) in the building (R=0.92), validation (R=0.81), testing (R=0.88) and overall (R=0.90) models, respectively.
Conclusion
We developed a robust algorithm to automatically evaluate retinal fundus image that can identify community subjects with high WMH burden.
Trial registration number
N/A
AS23-022
PLATELET AND HAEMOGLOBIN LEVELS IN PATIENTS ON ISOSORBIDE MONONITRATE AND/OR CILOSTAZOL WITH LACUNAR ISCHAEMIC STROKE: DATA FROM THE LACI-1 TRIAL
1University of Nottingham, Stroke- Division of Clinical Neurosciences, Nottingham, United Kingdom
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Cilostazol and isosorbide mononitrate (ISMN) have properties that may be of benefit in the context of cerebral small vessel disease and lacunar ischaemic stroke. As both drugs may influence platelet and haemoglobin levels, we sought to assess their effects using data from the lacunar intervention trial-1 (LACI-1).
Method
LACI-1 recruited 57 patients with lacunar ischaemic stroke and randomised them to ISMN or cilostazol in isolation, or combined for 9 weeks. One group received both drugs but with a delayed start. Full blood counts were taken at baseline, and weeks 3 and 8. Platelet function was assessed with remote measurement of surface expression of P-selectin (CD62P) using kits sensitive to aspirin or clopidogrel at the same timepoints. Differences in haemoglobin and platelet levels and platelet function were assessed by multiple linear regression with adjustment for baseline value.
Results
Haemoglobin levels did not differ between the treatment groups at week 8 (Table), whilst platelet levels were slightly higher in those who received cilostazol compared with no cilostazol. No differences were noted in platelet function in unstimulated, aspirin or clopidogrel testing between groups.
Conclusion
Cilostazol and isosorbide mononitrate have no clinically concerning effects on haemoglobin and platelet levels and function in the short to medium term. Further assessment of the safety and efficacy of these medications following lacunar ischaemic stroke is warranted.
Trial registration number
N/A
AS23-023
PERIPHERAL AND CENTRAL HAEMODYNAMICS IN PATIENTS ON ISOSORBIDE MONONITRATE AND/OR CILOSTAZOL WITH LACUNAR ISCHAEMIC STROKE: DATA FROM THE LACI-1 TRIAL
1University of Nottingham, Stroke- Division of Clinical Neurosciences, Nottingham, United Kingdom
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Cilostazol and isosorbide mononitrate (ISMN) have effects that may be beneficial in patients with cerebral small vessel disease and lacunar ischaemic stroke. We assessed their haemodynamic effects in the lacunar intervention-1 (LACI-1) trial.
Method
Patients with lacunar ischaemic stroke were randomised to immediate ISMN, cilostazol, or their combination for 9 weeks. A fourth group received both drugs but with a delayed start. Peripheral blood pressure (BP) and heart rate (HR), and central haemodynamics (central BP, Augmentation index [AI] unadjusted and normalised to HR 75bpm, Buckberg index [BI], pulse wave velocity [PWV] were measured using the Sphygmacor) at baseline, and weeks 3 and 8. Haemodynamic differences were assessed by multiple linear regression adjusted for baseline. Data are mean difference (MD) with 95% confidence intervals (CI).
Results
We recruited 57 patients; those allocated cilostazol alone were older but otherwise the groups were well-balanced at baseline. At week 8, BP did not differ between the treatment groups, whilst HR was significantly higher in those taking cilostazol vs. no cilostazol (MD 6.42, 95% CI 1.17–11.68, p = 0.017). BI (subendocardial perfusion) was significantly lower in those randomised to cilostazol vs. no cilostazol and in those randomised to both drugs vs. either drug. There was a tendency towards reduced AI (arterial stiffness) adjusted for HR in those taking cilostazol vs. no cilostazol and ISMN vs. no ISMN.
Conclusion
In patients with lacunar ischaemic stroke, cilostazol increased HR (a recognised effect) which may account for the reduced BI; both agents may reduce arterial stiffness. Larger trials are warranted.
Trial registration number
N/A
AS23-025
PREVALENCE AND PREDICTORS OF CEREBRAL MICROANGIOPATHY DETERMINED BY PULSATILITY INDEX IN ASYMPTOMATIC POPULATION. DATA FROM THE ILERVAS PROJECT
1Hospital Universitari Arnau de Vilanova, Stroke Unit, Lleida, Spain
2Hospital Universitari Arnau de Vilanova, Servei d'Endocrinologia i Nutrició, Lleida, Spain
3Hospital Universitari Arnau de Vilanova, Respiratory Medicine, Lleida, Spain
4IRBLleida, Vascular and Renal Translational Research Group, Lleida, Spain
5IRBLleida, Clinical Neurosciences Group, Lleida, Spain
6IRBLleida, NUTREN–Nutrigenomics Center, Lleida, Spain
Background and Aims
Little is known about the prevalence of cerebral microangiopathy (CM), which is related to cognitive impairment, in asymptomatic population. Pulsatility index (PI) is an easily measurable parameter of cerebral vascular resistance in Transcranial dúplex (TCD) of the middle cerebral artery (MCA) study. It is a surrogated marker of CM. We aimed to determined the prevalence of CM in low to moderate vascular risk subjects
Method
We included 3,721 subjects aged between 45 and 70 years without previous history of vascular disease or diabetes mellitus and with at least one other vascular risk factor from the ILERVAS project (Lleida, Catalonia). Patients underwent TCD to determine MCA-PI. Possible CM was defined by MCA-PI>1.0. Carotid and femoral arteries ultrasound study, body mass index (BMI), pulse pressure (PP) and laboratory data were also recorded
Results
439 (11.8%) subjects were excluded due to low quality of TCD images. Median age was 57 [52–62] years and BMI 28.6 [25.8–31.8] kg/m2. Possible CM was found in 424 (12.9%) subjects. CM patients had higher prevalence of plaques (77.4% vs. 66.4%. p < 0.001) than non-CM. PI had a positive linear correlation with the number of territories with plaques (r = 0.130, p < 0.001), the total plaque area (r = 0.082, p < 0.001), the glycosylated haemoglobin levels (r = 0.065, p < 0.001); and a negative correlation with the glomerular filtration rate (r = −0.120, p < 0.001). Age, male gender and PP were predictors of possible CM (Beta coefficients: 0.172, 0.089 and 0.406 respectively, all p-value<0.001).
Conclusion
The proportion of hidden possible CM is not negligible. The planned 10-year follow-up will describe the clinical relevance of abnormal IP
Trial registration number
ClinicalTrials.gov Identifier: NCT03228459
AS23-027
NOVEL DTI MARKER IS ASSOCIATED WITH PROCESSING SPEED DEFICITS IN SMALL VESSEL DISEASE WITHOUT APPARENT CLINICAL SYMPTOMS
1The Chinese University of Hong Kong, Medicine and Therapeutics, Hong Kong, Hong Kong S.A.R
2The Chinese University of Hong Kong, Imaging and Interventional Radiology, Hong Kong, Hong Kong S.A.R
Background and Aims
Peak width of skeletonized mean diffusivity (PSMD) is a novel and robust marker for cerebral small vessel disease (SVD). PSMD was associated with processing speed in CADASIL and sporadic SVD patients and outperformed conventional imaging markers. However, whether PSMD is a sensitive imaging marker such that the association is demonstrated in SVD subjects without apparent clinical symptoms is less studied.
Method
Community elderlies recruited had clinical, neuropsychological assessments performed at baseline and 3rd-year follow-up. PSMD and conventional SVD imaging markers were measured at baseline: i) white matter hyperintensity, ii) lacune count, iii) microbleed count, and iv) brain atrophy. SVD was defined as having moderate WMH volume load (median cutoff: ≥ 4mL) or with lacune or microbleed. The association between imaging variables and processing speed were analysed using linear regression model, with adjustment to age and education.
Results
Overall, the addition of √PSMD improved the regression model explaining processing speed deficits (F = 11.25; p = 0.001). Comparing SVD (n = 506) and controls (n = 325), √PSMD was significantly associated with processing speed deficits in the SVD group (β=−0.206; p = 0.011). The √PSMD contribution outperformed conventional imaging markers (WMH volume β=0.181; p = 0.015, other markers were N.S.). At 3rd year follow-up, baseline √PSMD also outperformed other markers and was the only significant marker associated with processing speed deficits in the SVD group (β=−0.252; p = 0.011).
Conclusion
PSMD has added value to the overall imaging contribution to processing speed in SVD without apparent clinical symptoms. Further, PSMD outperformed conventional SVD imaging markers in contributing to processing speed deficits, both at baseline and follow-up.
Trial registration number
N/A
AS23-028
THE CORRELATION BETWEEN ENDOTHELIAL DYSFUNCTION AND DEPRESSIVE DISORDER IN MIDDLE-AGED PATIENTS WITH HYPERTENSION-ASSOCIATED MICROANGIOPATHY
1I.M. Sechenov First Moscow State Medical University, Department of Nervous Diseases, Moscow, Russia
Background
Endothelial dysfunction (ED) is the one of the causes of depressive disorders development in middle-aged patients with hypertension-associated microangiopathy.
Aim
To evaluate the correlation between the specter of endothelial dysfunction biomarkers and depressive disorders in middle-aged patients with hypertension-associated microangiopathy.
Method
In the population-based cohort clinical study that was conducted in out-patient clinics we enrolled 262 patients (42,1% men, 57,9% women, mean age 54,2 ± 7). Depressive symptoms were evaluated for HADS scale. Enzyme Linked Immunosorbent Assays methodology and ELISA Multiscan EX reagents (Biomedica Inc.;Fujirebio Diagnostics Inc.) were used for evaluation of endothelial inflammation-associated plasma ED biomarkers (CRB and monocytic chemoattractant protein-1 (МСР-1), vasoconstriction-associated (endothelin-1 and NO-synthase activity), endothelial damage-associated (S100 and the number of desquamated endotheliocytes (DE)), blood rheology biomarkers (fibrinogen, vWF).
Results
We calculated the Integral Parameter of ED (IPED) that is the sum of CRB, МСР-1, endothelin-1, fibrinogen, DE concentration levels. The contribution of these parameters in the resulting factor was about the same (Factor Score Coefficients –0,36; –0,34; 0,25; 0,23 и –0,47 respectively).
Enrolled patients were randomized in 2 groups: patients with (1 group, n = 139) and without (2 group, n = 123) depressive disorder. The mean IPED score in 1 group was 0,12 ± 0,04, in 2 group –– 1,14 ± 0,3; р<0,05.
Strong correlation between IPED and depression was found in correlation analysis (r = –0,83; р<0,05).
Conclusion
Our results indicate that there is correlation between increased level of endothelial dysfunction biomarkers (CRB, МСР-1, endothelin-1, fibrinogen, DE) and depressive disorders in middle-aged patients with hypertension-associated microangiopathy.
Trial registration number
N/A
AS23-029
EVALUATING SEVERITY OF WHITE MATTER CHANGES FROM CT WITH CONVOLUTIONAL NEURAL NETWORK
1Clinical Neuroscience- University of Helsinki, Department of Neurology, Helsinki, Finland
2Combinostics Ltd., Combinostics Ltd., Tampere, Finland
Background and Aims
The severity of white matter changes (WMC), a surrogate for cerebral small vessel disease (CSVD) is evaluated in magnetic resonance imaging (MRI) with Fazekas scale (Fazekas 1-3). There are several studies aiming to specify the MRI findings in CSVD. Still the commonest imaging globally is computed tomography (CT). The possibility to quantify the WMCs volume in CT would give a tool for WMC research and also in case of stroke.
Method
CT- and MRI-images of 91 patients in the Helsinki University Hospital, Finland, which were conducted within time interval from 1 day to 6 weeks, were included in the analyses. Exclusion criteria were tumors, cortical infarcts, bleedings (except microbleedings in Fazekas 2–3 could be included) and multiple sclerosis and obvious contusions.
WMSs were segmented from CT images using convolutional neural network (CNN). The ground truth for the training of CNN was generated using cNeuro® (Combinostics Oy, Tampere, Finland) image quantification tool, that utilizes expectation-maximization algorithm to segment WMCs from MRI FLAIR images. The training and testing of CNN was performed using 2-fold cross-validation.
Results
High correlation of 0.89 was obtained between the WMC volumes of MRI and CT segmentations. The correlation between the CT WMC volume and Fazekas score was 0.74. When estimating the Fazekas score from WMC volumes, the CT segmentation classified correctly 75.8% of patients.
Conclusion
CNN-based segmentation of CT images can evaluate the severity of CSVD in order to support clinicians in treatment decisions.
Trial registration number
N/A
AS23-030
DYNAMIC CEREBRAL AUTOREGULATION IS DISTURBED IN CONTROLLED HIGH BLOOD PRESSURE
1Kantonsspital Lucerne, Neurology and Neurorehabilittion, Lucerne 16, Switzerland
2Kantonsspital Lucerne, Department of Radiology, Lucerne 16, Switzerland
3ETH zürich, Automatic Control Laboratory, Zürich, Switzerland
Background and Aims
Whether dynamical cerebrovascular regulation is different in patients with controlled high blood pressure (HBP) and different stages of small vessel disease (SVD) compared to healthy persons.
Method
In 25 healthy controls (mean age ± SD, 64 ± 15 years; 7 females, BP, 91 ± 15 mm Hg; ETCO2, 39 ± 4 mm Hg) and in 40 patients (mean age 64 ± 13 years; 14 females, BP 90 ± 16, ETCO2, 39 ± 4 mmHg ) with HBP and different stages of SVD (Fazekas classification) BP via fingerplethysmography, blood flow velocity (CBFV) in both middle cerebral arteries (MCA) via transcranial Doppler sonography and end-tidal CO2 (ETCO2) via capnography were simultaneously recorded. Using artifact-free recordings over periods of 5 minutes, we assessed coherence and the transfer function parameter gain and phase between BP and CBFV in the frequency ranges of VLF (0.02–0.07 Hz), LF (0.07–0.15), HF range (>0.15). Analysis was performed with comparison of means (ANOVA or t-test), with correlation and stepwise regression analysis.
Results
Neither gain nor phase in any frequency range was different in the HBP patients with or without SVD. Compared to controls of similar age and sex distribution, significant differences (p < 0.05 – <0.005) were found for coherence (controls 0.46 ± 0.12 vs patients 0.54 ± 0.12, right MCA), gain (left: 0.18 ± 0.20 vs 0.35 ± 0.30; right: 0.19 ± 0.22 vs 0.36 ± 0.33) and phase (left: 1.07 ± 0.37 vs 0.84 ± 0.35; right: 1.04 ± 0.42 vs 0.76 ± 0.28) in the VLF range and for phase (left: 0.74 ± 0.23 vs 0.60 ± 0.23; right: 0.74 ± 0.26 vs 0.63 ± 0.27) in the LF range.
Conclusion
In controlled HBP, the CBF regulation is disturbed at longlasting CBF changes of 20–50 seconds.
Trial registration number
N/A
AS23-032
STRUCTURAL BRAIN CHANGES AND DEPRESSIVE SYMPTOMS IN OLDER ADULTS: FINDINGS FROM 4 COHORT STUDIES
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Edinburgh, Geriatric Medicine- Department of Clinical and Surgical Sciences, Edinburgh, United Kingdom
3University of Edinburgh, Centre for Cognitive Ageing and Cognitive Epidemiology, Edinburgh, United Kingdom
4University of Aberdeen, Institute of Medical Sciences, Aberdeen, United Kingdom
5University of Amsterdam, Clinical Epidemiology- Biostatistics and Bioinformatics, Amsterdam, The Netherlands
Background and Aims
Depressive symptoms are common in older people and are a major cause of morbidity and mortality. In older adults they are associated with brain atrophy and cerebral small vessel disease (cSVD), particularly white matter hyperintensities (WMH). The impact of total cSVD burden on symptoms of depression has not been studied.
Method
We analysed data from community dwelling participants from 4 cohort studies: STRADL (N=280), The Dutch famine cohort (n = 118), the Lothian Birth Cohort 1936 (n = 617) and the Simpson cohort (n = 110). The presence of each cSVD feature was analysed individually and summed to form a total “cSVD score” (range 1–4). WMH volume and brain volumes were measured in the LBC 1936 and Simpson cohort. The Hospital Anxiety and Depression Scale (HADS) assessed depressive symptoms. Data were adjusted for risk factors, analysed separately for each cohort and then meta-analysed.
Results
Across all cohorts (n = 1125) presence of one or more cortical infarct (B = 0.08, p = 0.01) and more cerebral atrophy (B=0.09, p = 0.002) were associated with higher depressive symptoms. Higher WMH volume was associated with higher depressive symptoms (Simpson cohort, B = 0.24, p = 0.01). Higher total brain volume (B = −0.22, p = 0.001), intracranial volume (B = −0.11, p = 0.03) and global white (-0.13, p = 0.004) and grey matter volume (B = −0.12, p = 0.01) were associated with lower depressive symptoms (LBC 1936).
Conclusion
These findings support an association between WMH, brain atrophy and depressive symptoms in older adults. It is unclear whether total cSVD burden is associated with depressive symptoms in these relatively healthy cohorts. Associations should be examined in those with more vascular disease and more depressive symptoms.
Trial registration number
n/a
AS23-034
CADASIL SCALE CALIBRATION
1AOU Careggi, Emergency Department - Stroke Unit, Florence, Italy
2University of Florence, Department of Statistics “G. Parenti”, Florence, Italy
3University of Florence, NEUROFARBA Department- Neurosciences Section, Florence, Italy
4University of Siena, Department of Medicine- Surgery and Neurosciences- Medical School, Siena, Italy
5San Jacopo Hospital, Neurology Unit, Pistoia, Italy
6Madonna del Soccorso Hospital- San Benedetto del Tronto, Division of Neurology, Ascoli Piceno, Italy
7University of Milan, "L Sacco” Department of Biomedical and Clinical Sciences, Milan, Italy
Background and Aims
CADASIL is a small vessel disease caused by NOTCH3 gene mutations. The genetic test is the diagnostic gold standard. A CADASIL scale was proposed as a screening tool to select patients in the clinical setting for genetic analysis.1 Here we calibrated the proposed scale in a larger sample of patients who underwent the genetic test.
Method
We applied the scale to 77 CADASIL (probands) and 132 NOTCH3–negative patients. An ad-hoc optimization algorithm was then applied weighing each variable of the scale with integer values (1-5). For each combination of weights, a cutoff score was chosen by maximizing the total number of correct cases classifications. This produced an efficiency frontier of scales evaluated on the basis of sensitivity and specificity. A bootstrap method was finally used to make inference about the scales obtained on efficiency frontier.
Results
Post-optimization, the CADASIL scale belonged to the efficiency frontier. Sensitivity and specificity were 96.1% and 50%, maintaining the original cutoff (14). Specificity raised to 59% and 70% for cutoff values of 15 and 16, with simultaneous reduction of sensitivity (76.6% and 68.8%).
Conclusion
The CADASIL scale remained accurate in selecting patients for NOTCH3 analysis. The lower the cutoff used, the lower the probability to miss affected patients, but more false positive cases might be included. Specificity was reduced in comparison with the previously published data, probably for the inclusion of high number of NOTCH3-negative patients with a phenotype very similar to CADASIL (CADASIL-like patients).
1Pescini et al., Stroke 2012;43:2871–2876
Trial registration number
N/A
AS23-035
SERUM NEUROFILAMENT LIGHT CHAIN PREDICTS PROGRESSIVE MICROSTRUCTURAL DAMAGE AND PSYCHOMOTOR SPEED DECLINE IN CEREBRAL SMALL VESSEL DISEASE
1University Hospital Basel, Neurology and Stroke Center, Basel, Switzerland
2Radboud University Medical Center, Donders Institute for Brain- Cognition and Behaviour, Nijmegen, The Netherlands
3University Hospital Basel, Neurologic Clinic and Policlinic- Departments of Medicine- Biomedicine and Clinical Research, Basel, Switzerland
4University Hospital- LMU Munich, Institute for Stroke and Dementia Research, Munich, Germany
Background and Aims
Serum neurofilament light-chain (sNfL) is a circulating marker for neuroaxonal injury and was shown to be associated with disease burden in cerebral small vessel disease (SVD). Here we explored the predictive value of sNfL for disease progression in SVD.
Method
We studied 258 (mean age 62.4 ± 7.7 years, 59.3% male) patients with sporadic SVD from the RUN DMC study longitudinally with a follow-up period of 8.7 ± 0.2 years. At baseline, sNfL was measured by an ultrasensitive single-molecule array assay. We assessed both baseline presence/severity and progression over time of white matter hyperintensity (WMH) volume, presence of lacunes, microbleed count, brain atrophy and mean diffusivity (MD) values. Subjects underwent cognitive testing including memory, psychomotor speed and executive function to assess cognitive decline over time.
Results
At baseline, sNfL-levels were associated with MD values, WMH volume, as well as presence of lacunes and mircobleeds after correction for age. The strongest association was observed for MD (β0.142; 95%CI [0.160–1.012]; p = 0.007). sNfL-levels were associated with psychomotor speed cross-sectionally (β-0.161; 95%CI [-0.946; -0.134]; p = 0.009), as well as with decline in psychomotor speed over time (β0.141; 95%CI 0.033; 0.634]; p = 0.030). Serum NfL-levels at baseline were associated with progression of SVD markers and cognitive decline over the follow-up period. After correction for age, sNfL was independently related to incident lacunes as well as changes in mean diffusivity.
Conclusion
In SVD, serum NfL is strongly related to microstructural tissue damage and its progression over time. Serum NfL may thus potentially serve as a marker for disease monitoring and outcome in SVD.
Trial registration number
N/A
AS23-036
TWO NEW GENETIC MUTATIONS OF CADASIL DISEASE
1University Hospital of Salamanca, Neurology, Salamanca, Spain
Background and Aims
CADASIL disease is a genetic disease that causes microvascular dysfunction. More than 200 mutations have been described, especially involving cysteine residues.
We present two cases of patients with CADASIL disease due to two new different mutations in NOTCH 3 gene.
Method
Case 1: 73-year-old female admitted for an acute lacunar stroke in 2016. The personal history included lacunar infarcts in 1997, 2013 and 2015. Her mother had stroke and dementia and her daughter had migraine. Later on, she developed subcortical cognitive impairment. Cranial MRI showed multiple chronic ischemic lesions in deep white matter, chronic lacunar infarcts, an acute lacunar infarction and thalamic-mesencephalic microbleeds.
Case 2: 61-year-old female consulted for a prolonged episode of migraine. She has a family history of migraine. Cranial MRI showed extensive leukoencephalopathy due to small vessel disease. She had no cardiovascular risk factors nor history of stroke
Results
Case 1: The molecular NOTCH 3 study showed an heterozygosity mutation 19th exon [c.3748T> C (p. Cys1250Arg)].
Case 2: The molecular NOTCH 3 study showed an heterozygosity mutation 19th exon [c.3875> G (p. Ser1292Cys)].
Conclusion
These mutations have not been described in molecular databases but the analysis with prediction programs indicates that they are probably pathogenic. Since the clinical and radiological data are highly suggestive of CASADIL disease, we have requested a cutaneous biopsy to confirm the diagnosis and to give genetic counseling. These new pathogenic mutations would enrich the mutation spectrum of NOTCH3 gene.
Trial registration number
N/A
AS23-037
HETEROGENEOUS ORIGIN AND EVOLUTION OF MICROBLEEDS IN CEREBRAL SMALL VESSEL DISEASE
1Radboud university medical centre- Donders Institute for Brain- Cognition and Behaviour- Centre for Cognitive Neuroscience, Department of Neurology, Nijmegen, The Netherlands
2Image Sciences Institute, University Medical Center Utrecht, Utrecht, The Netherlands
3Medical University of Graz, Department of Neurology, Graz, Austria
4Radboud university- Donders Institute for Brain- Cognition and Behaviour, Centre for Cognitive Neuroimaging, Nijmegen, The Netherlands
5Institute for Stroke and Dementia Research ISD, University Hospital LMU, Munich, Germany
Background and Aims
Cerebral microbleeds are assumed to be chronic lesions with a primary hemorrhagic origin. These assumptions have both been challenged by recent imaging and histopathological studies. Therefore we aimed to investigate the origin and evolution of microbleeds with our high frequency serial imaging RUN DMC – InTENse study.
Method
Participants were 54 individuals from the RUN DMC study (mean age 70.2 years [SD 6.5]; 63% male) with mild to severe cerebral small vessel disease (CSVD) on previous MRIs (2006, 2011, 2015). Exclusion criteria were large-artery disease, atrial fibrillation, dementia and Parkinson’s disease. Participants received monthly 3T MRIs for 10 consecutive months, including susceptibility-weighted imaging for detection of microbleeds.
Results
At baseline, 20 participants had a total of 39 microbleeds (84.6% lobar, 12.8 % deep, 2.6 % infratentorial). During the time course of the study period one microbleed disappeared. Additionally, we identified 8 new microbleeds in 5 individuals, of which 75% (n = 6) were indicative of primary microbleeds, while 25% (n = 2) co-located with an acute infarct and a FLAIR lesion, suggesting that these microbleeds were hemorrhagic infarcts (Figure 1).
Conclusion
In participants with CSVD, microbleeds of similar appearance as detected on MRI can originate both from hemorrhage and from an infarct. Over time, new microbleeds may appear but they also can vanish. Therefore the origin as well as the evolution of microbleeds in CSVD is heterogeneous.
Trial registration number
NA
AS23-038
CEREBROVASCULAR REACTIVITY IMPAIRMENT IN ISCHAEMIC STROKE AND CEREBRAL SMALL VESSEL DISEASE PATIENTS IS ASSOCIATED WITH INCREASED INTRACRANIAL VENOUS PULSATILITY BUT NOT DECREASED CEREBRAL BLOOD FLOW
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
Cerebral small vessel disease (SVD) is increasingly associated with altered cerebral haemodynamics, while associations with reduced cerebral blood flow are becoming less clear. We utilised hypercapnic cerebrovascular reactivity (CVR) and phase contrast blood flow MRI to investigate cerebral haemodynamic changes in SVD.
Method
We used BOLD MRI while breathing 6% CO2 to quantify CVR and phase contrast MRI to quantify arterial blood flow and pulsatility index (PI) in the cerebral arteries, veins and CSF in patients with minor ischaemic stroke and SVD. We quantified CVR in seven subcortical regions which we averaged to produce mean grey matter and white matter CVR values.
Results
52 patients (mean age 67.6 ± 8.4, 14 females, median WMH volume 11.3ml) completed CVR and pulsatility scans. White matter CVR decreased with increasing venous PI in the straight sinus, superior sagittal sinus (SSS), transverse sinus and internal jugular vein (IJV) (all p < 0.05), but was not associated with cerebral blood flow or arterial PI. SSS and IJV PI remained statistically significant (p < 0.05) after correcting for age and systolic blood pressure, which remained a strong trend after correcting for white matter hyperintensity (WMH) volume.
Conclusion
CVR falls as intracranial venous pulsatility increases, but is not related to lower cerebral arterial blood flow suggesting a disassociation between resting CBF and the ability of the small vessels to vasodilate in response to CO2 as they become stiffer. Larger studies will determine if the association between CVR and intracranial pulsatility is independent of a co-association with WMH.
Trial registration number
N/A
AS23-039
LUNG DISEASE SEVERITY IS ASSOCIATED WITH WHITE MATTER HYPERINTENSITIES IN PATIENTS WITH CHRONIC OBSTRUCTIVE PULMONARY DISEASE
1ST GEORGE's UNIVERSITY OF LONDON, Clinical Pharmacology, LONDON, United Kingdom
2Southmead Hospital, Academic Respiratory Unit, Bristol, United Kingdom
3ST GEORGE's UNIVERSITY OF LONDON, Respiratory, London, United Kingdom
Background and Aims
Previous studies exploring the association of chronic obstructive pulmonary disease (COPD) with structural brain changes on MRI have found inconclusive results. The aim of this study was to identify if severity of lung disease and cardiovascular risk were associated with structural brain changes in a cohort of COPD patients.
Method
This was a prospective cohort study of COPD patients with no history of stroke or dementia. Structural brain 3T MRI was performed to evaluate the number and volume of white hyperintensities as well as whole brain, grey and white matter and CSF volumes. Bivariate and partial correlation analyses were performed to determine the association of COPD severity (lung function, COPD assessment test score, exacerbation frequency, pulse oximetry) and cardiovascular risk (smoking pack years, blood pressure, pulse wave velocity, lipid and glycaemic profiles, body mass index, brain natriuretic peptide) with structural brain disease.
Results
56 patients were recruited (mean ± SD age 69 ± 8). 53 patients completed structural brain 3T MRI. White matter lesion number was strongly correlated with age (r = 0.525, p < 0.001), brain natriuretic peptide (r = 0.435, p = 0.001) and QRISK®2 score (r = 0.55, p < 0.001), with weaker associations with markers of lung health, COPD assessment test score (r = 0.284, p = 0.04) and hypoxaemia (r = −0.346, p = 0.014). After adjusting for age, COPD assessment test score (r = 0.519, p = 0.001) and hypoxaemia (r = −0.374, p = 0.019) remained significantly correlated with white matter lesion number.
Conclusion
This study demonstrated that in addition to age, underlying COPD health status and hypoxaemia may predict white matter lesions in COPD patients.
Trial registration number
N/A
AS23-040
WHAT ARE THE HISTOLOGICAL SUBSTRATES OF SMALL VESSEL DISEASE AS SEEN ON IMAGING? A SYSTEMATIC REVIEW OF POST-MORTEM IMAGING-HISTOLOGY CORRELATIONS
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
Background and Aims
The imaging features of small vessel disease (SVD) have been described with agreed definitions and grading systems. However, the underlying pathophysiology is not fully understood.
Method
We assessed papers comparing post-mortem imaging with histology to determine to what extent our knowledge of SVD pathology is based on neuroimaging features, the population characteristics this knowledge is based on, the methods and histological terminology used and the quality of these studies.
Results
44 papers compared post-mortem magnetic resonance imaging to histological appearances with a mean quality score of 14.45/27 ( ± SD 2.94); many neglect critical features of study design, general and specific methods and clinical characteristics of their cohorts, particularly those associated with SVD such as vascular risk factors.
Of these, white matter lesions identified on neuroimaging have been studied most extensively: 27 papers with about 1182 subjects. Commonly identified pathological substrates are described but not found consistently. The extent to which imaging represents the histological burden is unclear although histological abnormalities are found in normal-appearing white matter in lesional brains, confirming in vivo functional imaging findings.
Methods for making comparisons vary, most are dependent on subjective comparisons of gross anatomical features and many do not account for imaging artefact. Histological definitions also vary but are often not defined at all.
Conclusion
Common histological substrates of SVD can be identified in the literature, but a lack of consensus regarding their definitions and of high quality studies comparing imaging-histological appearances limit our ability to fully understand their associations and SVD pathophysiology.
Trial registration number
N/A
AS23-041
BIOCHEMICAL ASSESSMENT OF SEVERITY AND MECHANISMS OF WHITE MATTER INJURY IN HUMAN POST-MORTEM WHITE MATTER IN NEURORADIOLOGICALLY DOCUMENTED SMALL VESSEL DISEASE
1University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
2University of Bristol Medical School, Learning & Research level 2- Southmead Hospital, Bristol, United Kingdom
Background and Aims
Specific neuroimaging abnormalities of cerebral white matter (WM) have been attributed to small vessel disease, implicated in many cases of dementia. However, the pathogenesis is poorly understood. Biochemical methods have been developed which measure specific vessel wall constituents, proteins altered by tissue hypoxia, and others extravasated through leaky vessels, in post-mortem brain tissue. We have used these to analyse WM in intracerebral haemorrhage (ICH), Alzheimer's disease (AD) and age-matched controls.
Method
Cerebral WM samples were obtained from 18 cases of AD (mean age 78.8 ± SD 12.5), 26 mostly deep ICH (79.0 ± 10.2) and 35 controls (64.6 ± 9.8). Hypoxia was estimated by the myelin associated glycoprotein: proteolipid protein-1 ratio (MAG:PLP1), reduced in hypoxia, and vascular endothelial growth factor (VEGF) level, which rises. von Willebrand factor (vWF) level indicates microvessel density, and platelet derived growth factor receptor-b (PDGFRB) and fibrinogen estimate pericyte content and blood-brain-barrier integrity. Endothelin-I and angiotensin-II mediate vasoconstriction.
Results
VEGF was higher in ICH than control WM and MAG:PLP1 reduced. vWF tended to be raised in ICH, but not significantly. There was strong correlation between VEGF and vWF. PDGFRB and fibrinogen were increased in AD but not ICH. Endothelin-I reduced in AD and ICH. There was no change in angiotensin-II.
Conclusion
There is evidence of cerebral WM hypoxia in ICH, associated with a physiological endothelin-1 response and increased microvessel density. In AD, WM vessels leak fibrinogen although pericyte protein is increased. We are analyzing further structural and biochemical variables for correlation with in vivo neuroimaging findings.
Trial registration number
N/A
AS23-043
SYSTEMIC VASCULAR CHARACTERISTICS IN PATIENTS WITH CEREBRAL WHITE MATTER HYPERINTENSITIES
1Royal Devon & Exeter Hospital, Stroke Medicine, Exeter, United Kingdom
2University of Exeter Medical School, Diabetes and Vascular Research Centre, Exeter, United Kingdom
Background and Aims
Cerebral small vessel disease (SVD) is associated with increased risk of dementia, stroke and disability. Cerebral white matter hyperintensities (WMH) are found in patients with and without history of cerebrovascular disease (CVD) and are recognised surrogate markers for cerebral SVD. Currently there are no clear targets or strategies for the treatment of cerebral SVD. We studied the systemic vascular function and its relationship with cerebral WMH to inform potential modifiable vascular treatment target.
Method
112 participants with and without a history of CVD underwent macrovascular and microvascular function tests and an MRI head scan. WMH volume was calculated from MRI images using Freesurfer software.
Results
Increased carotid intima media thickness and carotid-femoral pulse wave velocity were associated with cerebral WMH (β=1·1 p = 0·001 and β=1·66, p < 0·0001 respectively). Adjusted cerebral resistance index (p = 0·03) and brachial flow mediated dilation time to peak (p = 0·001) were associated with the severity of cerebral WMH independent of age and sex. Post occlusive reactive hyperaemia time as a measure of microvascular reactivity was associated with WMH after adjustment for age and sex (p = 0·03). Ankle Brachial Pressure Index and urinary albumin excretion rate predicted the severity of cerebral WMH (p = 0·02 and 0·01 respectively). Age and hypertension were the most important risk factors for WMH severity (p < 0·0001).
Conclusion
Cerebral WMH are associated with hypertension, microalbuminuria, increased arterial stiffness, impaired vascular reactivity and increased cerebrovascular resistance. Treatments that target these vascular markers may prove beneficial in halting the development or progression of cerebral WMH.
Trial registration number
N/A
AS23-044
ASSOCIATION OF WHITE MATTER HYPERINTENSITIES AND LATE-LIFE DEPRESSION – INSIGHTS FROM LARGE-SCALE COHORT STUDIES
1University Medical Center Hamburg-Eppendorf UKE, Department of Neurology, Hamburg, Germany
Background and Aims
The vascular depression hypothesis postulates that white matter hyperintensities of presumed vascular origin (WMH) may induce late-life depression via disruption of frontal-subcortical circuits involved in emotion regulation. Initially only adressed by cross-sectional studies, in the recent years more longitudinal cohort studies started investigating in this issue. We aim to provide an overview of insights on vascular depression derived from recent prospective studies.
Method
We performed a selective review. Articles were included if they met the following inclusion criteria: (1) investigation of the association of WMH and late-life depression, (2) data from a prospective cohort study. Data extraction was performed by full-text reading articles and standardized extraction of pre-specified information.
Results
We reviewed 15 studies. 13 studies utilized fully-quantitative WMH measurement and 5 different questionnaires were applied for depression assessment. 11 studies delivered significant results for the association of WMH and late-life depression. Studies not showing significant results had lower mean sample size, their participants had lower baseline WMH volume and were younger. Studies that differentiated between WMH localizations suggest that deep WMH are more strongly associated with depressive symptom development than periventricular WMH.
Conclusion
To summarize, the majority of available studies report an association of white matter hyperintensities with depression in elderly subjects and by this support the vascular depression hypothesis. Studies with contradictory findings showed methodological limitations.
Trial registration number
N/A
AS23-045
INVESTIGATING THE RELATIONSHIP BETWEEN SUBCORTICAL HYPERINTENSITIES ON 3T MRI BRAIN AND ORTHOSTATIC HYPOTENSION ON ACTIVE STAND TESTING IN AN AGEING POPULATION
1St. James's Hospital, Gerontology, Dublin, Ireland
Background and Aims
To investigate whether there is a relationship between burden of subcortical hyperintensities on MRI brain and failure of stabilisation of blood pressure on active stand test, and so test the hypothesis that repeated episodes of transient hypoperfusion contribute to development of such hyperintensities.
Method
440 community-dwelling participants ≥65 were randomly chosen from a nationwide dataset of >8,000 individuals and underwent 3T MR brain. Scans were scored for subcortical hyperintensities according to Scheltens’ scale. Cohen’s kappa coefficient determined inter-rater agreement.
Lying-to-standing orthostatic test (active stand) was performed on same individuals during same wave of data collection. Beat-to-beat blood pressure was measured non-invasively using digital photoplethysmography (Finometer®) for 2 minutes post-stand.
Orthostatic hypotension (OH) at a given timepoint defined as ≥20mm Hg systolic (or ≥10mm Hg diastolic) drop in blood pressure from baseline recordings.
Scheltens’ score was analysed with respect to OH at 3 timepoints (10s, 40s, 110s). Potential confounders were incorporated into statistical model.
Results
A statistically significant relationship between Scheltens’ score and OH at 110s was established (p = 0.003), i.e. those individuals with hypotension at 110s had significantly more subcortical hyperintensities than those whose blood pressure had recovered.
There was no significant relationship between Scheltens’ score and OH at 10s or 40s timepoints.
Well-established relationships between subcortical hyperintensities and both hypertension and age were maintained throughout model buildup, as was downstream association with stroke.
Conclusion
In this population of community-dwelling participants, there is a statistically significant relationship between burden of subcortical hyperintensities and (previously uninvestigated) failure of stabilisation on active stand test at 110s.
Trial registration number
N/A
AS23-046
MIRNA-27A-3P AND MIRNA-222-3P AS NOVEL REGULATORS OF PHOSPHODIESTERASE 3A (PDE3A) IN ENDOTHELIAL FUNCTION?
1Copenhagen University Hospital Herlev, Department of Neurology- Stroke unit- Neurovascular laboratorium, Herlev, Denmark
2Steno Diabetes Center Copenhagen, Type 1 Diabetes biology, Gentofte, Denmark
3Copenhagen University Hospital Herlev, Department of Peadiatrics, Herlev, Denmark
4University of Copenhagen, Department of Pharmacy, Copenhagen, Denmark
Background and Aims
Cerebral Small Vessel Disease stroke (CSVD) accounts for 25% of cerebral ischemic strokes. CSVD is a leading cause of cognitive decline and functional loss. microRNAs (miRNA) modulate gene function/expression, widely used as disease biomarkers in many diseases. cAMP degrading enzyme phosphodiesterase 3a (PDE3a) is present in endothelial cells and relevant to cerebrovascular and endothelial function. PDE3 inhibitor, Cilostazol®, is currently used for secondary prevention of stroke. Modulation of PDE3a by miRNAs may highlight possible targets to amend endothelial dysfunction and treat CSVD.
Method
In silico analysis predicted 67 PDE3a miRNAs (Targetscan, context score < −0.01). miRNAs were ranked based on expression values (Kalari et al. 2016) and context scores. Co-expression meta-analysis of miRNA targets was performed using Co-Meta to create miRNA clusters. KEGG pathway were used to create miRNA regulatory networks. Transfection of hcmec/D3 cell line with miRNA mimics miR-27a-3p and miR-222-3pe, followed by western blot to validate PDE3a as target of the miRNAs.
Results
Target prediction resulted in 67 PDE3a miRNAs. 49 miRNAs found expressed in hcmec/D3 cell line (Kalari et al.). miRNAs were ranked based on expression values and context scores. mirCo analysis of two top clusters miR-221/miR-222 and miR-27a/miR-27b/miR-128 supported their role in cerebral vascular functions. Validation experiments with miRNA mimics confirmed PDE3a as target of miR-27a-3p and miR-222-3p.
Conclusion
miR-221/miR-222 and miR-27a/miR-27b/miR-128 are predicted miRNAs of PDE3a. miRNAs are involved in pathways essential to cerebral and vascular integrity, suggesting their role in neurogenesis, angiogenesis after cerebral injury and endothelial function. PDE3a is validated as target of miR-27a-3p and miR-222-3p.
Trial registration number
N/A
SAH, ANEURYSMS AND VASCULAR MALFORMATIONS
AS24-001
HYPOFRACTIONATED READIOSURGERY FOR LARGE CEREBRAL ARTERIOVENOUS MALFORMATION: A CASE SERIES AND FOLLOW UP RESULTS
1The Chinese University of Hong Kong, Surgery, Hong Kong, Hong Kong S.A.R
2The Chinese University of Hong Kong, Clinical Oncology, Hong Kong, Hong Kong S.A.R
Background and Aims
Treatment of large cerebral arteriovenous malformation (AVM) is of increased risk and can be challenging. Radiosurgery is commonly employed for treatment of AVM that are deep seated or located in eloquent area. However, efficacy of single dose RS is limited by AVM size. We have previously adopted a hypofractionated RS for large AVM radiosurgery and we aimed to assess their efficacy as compared to single dose radiosurgery in our institute.
Method
We retrospectively reviewed the radiosurgery record in an university-affiliated regional neurosurgical referral centre in Hong Kong from January 1998 to September 2017. We retrieved patient records of AVM undergoing RS with imaging and clinical follow up assessments at 4 or more years afterwards.
Results
Thirty-five patients were recruited into the current study. Age was 32+/−14 years and 18(51%) were male. Thirteen (37%) presented with hemorrhage related to AVM and 17(49%) had prior AVM treatment. The AVM volume was 25+/−21cm3. AVM obliteration without new or increased deficit was achieved in 18(51%). Thirteen (37%) underwent hypofractionated RS and 22 (63%) underwent single dose RS. The AVM volume was higher in hypofractionated RS (37+/−30cm3 versus 18+/−7cm3, p = 0.045). There was a trend towards higher AVM obliteration without new or increased deficit in hypofractionated RS (62% versus 41%, OR 2.3 95%CI: 0.6–3.4, p = 0.238).
Conclusion
In selective large AVM patients, hypofractionated RS resulted in higher AVM obliteration without new or increased deficit as compared to single dose RS.
N/A
AS24-002
GROWTH AND RUPTURE OF UNRUPTURED INTRACRANIAL ANEURYSMS
1University of Helsinki, Clinical Neurosciences, Espoo, Finland
Background and Aims
To investigate risk factors for growth and rupture of unruptured intracranial aneurysms (UIAs) in a long-term prospective follow-up study.
Method
The series consists of 87 patients with 111 UIAs diagnosed before 1979, when UIAs were not treated. Risk factors for UIA growth were analyzed in relation to subsequent rupture.
Results
The median follow-up time between aneurysm measurements was 21.7 years (mean 19.2, range 1.2–51.0 years). In 40 of the 87 patients (46%), the UIAs increased in size >1 mm and in 31 patients (36%) >3 mm. During 1669 person-years, 27 patients suffered from an aneurysm rupture (1.6% per year). All 27 ruptured aneurysms grew during the follow-up of 324 person-years (mean growth rates 6.1 mm, 0.92 mm/year, and 37%/year) while growth without rupture occurred in 13 patients during 302 follow-up years (3.9 mm, 0.18 mm/year, and 4%/year) and no growth in 47 patients during 1043 follow-up years. Independent risk factors for UIA growth (> 1 mm) in all patients were female sex (adjusted odds ratio 3.08, 95% confidence interval 1.04–9.13) and smoking throughout the follow-up time (3.16, 1.10–9.10), while only smoking (4.36, 1.27–14.99) was associated with growth resulting in aneurysm rupture. Cigarette smoking at baseline predicted subsequent UIA growth, while smoking at the end of the follow-up was associated with growth resulting in aneurysm rupture.
Conclusion
Cigarette smoking is an important risk factor for UIA growth, particularly for growth resulting in rupture. Cessation of smoking may reduce the risk of devastating aneurysm growth.
Trial registration number
N/A
AS24-007
SURGICAL TREATMENT OF TRAUMATIC INTRACRANIAL ANEURYSMS: EXPERIENCES AT A SINGLE CENTER OVER 30 YEARS
1Chonnam National University Hospital, Neurosurgery, Gwangju, Republic of Korea
Background and Aims
Traumatic intracranial aneurysms (TIAs) are rare and associated with high rates of morbidity and mortality. We describe our experiences with TIAs at our institution.
Method
We retrospectively reviewed records from patients who underwent treatment for TIAs between January 1986 and December 2015. For each patient, clinical data, including age, sex, type of trauma, location of aneurysms, clinical presentation, time elapsed between trauma and operation, treatment, and outcome were reviewed.
Results
Data from 5,532 patients diagnosed with cerebral aneurysms were reviewed from January 1986 to December 2015 in our hospital. Of these, 13 cases (0.23%) were TIAs. Most occurred after blunt brain trauma (12/13, 92%). The most common locations were the distal anterior cerebral artery (7/13, 53%) followed by the internal carotid artery (ICA) (5/13, 38%). Delayed intracerebral hemorrhage (ICH) was the major presentation at the time of aneurysmal rupture (70%). Most patients underwent surgical treatment (10/12, 83.3 %), which included clipping (5/10), trapping (3/10), aneurysmal excision and bypass (1/10), and aneurysmal excision and coagulation (1/10). Two TIA cases that were located in the ICA were treated with coil embolization and detachable balloon occlusion, respectively. Most cases had good recovery (5/12, 41.7 %); three and one had moderate and severe disability, respectively; one was in a vegetative state; and two patients died.
Conclusion
TIAs are an uncommon complication of head trauma. TIAs should be considered when unexpected new symptoms develop in patients with head trauma. Early diagnosis and prompt treatment could help to improve final clinical outcomes.
Trial registration number
N/A
AS24-008
POSTERIOR CIRCULATION PEDIATRIC ANEURYSMS MANAGEMENT OUR EXPERIENCE
1ALL INDIA INSTITUTE OF MEDICAL SCIENCES - NEW DELHI, NEUROSURGERY, NEW DELHI, India
2All India institute of medical sciences, Neuroradiology, New Delhi, India
3All India institute of medical sciences, Neurosurgery, New Delhi, India
Background and Aims
Pediatric posterior circulation aneurysms are rare, complex poorly understood lesions on which only limited literature is currently available. We share our experience of managing this condition, hoping to enhance our knowledge of this rare entity.
Method
Pediatric patients (< 18 years of age) with posterior circulation aneurysm managed at our institute from January 2005 and April 2017 were included in this retrospective study. Demographic, clinical, radiological and management details were retrieved from hospital records and detailed analysis of the characteristics of the aneurysms and methods of treatment provided was undertaken.
Results
Total 20 patients (M:F- 15:6, mean age 13.1yrs) were treated during this period. Majority of the patients (75%) had presented with subarachnoid hemorrhage. Most common location of aneurysm was in the vertebra-basilar and vertebral artery 31.81% followed by basilar artery and PCA 27.72% each. Dissecting aneurysms (77.27%) and large size ones (63.63%) were the most common type noted. Of the 15/22 aneurysms treated 13 underwent endovascular management (parent vessel sacrifice in 8 and parent vessel preservation in 5 aneurysms), one patient underwent surgery and one patient underwent medical management for CNS tuberculosis. At follow up one patient had recurrence of aneurysm and one patient expired after discharge from. Overall good outcome was present in 18 (90%) patients (GOC - 4/5)
Conclusion
Vertebro-basilar and vertebral artery are the most common location for posterior circulation aneurysm in pediatric population and most are of dissecting variety. Endovascular treatment is the main stay of management. Overall good outcome was observed.
Trial registration number
NA
AS24-009
RADIOSURGICAL, NEUROSURGICAL OR NO INTERVENTION FOR THE TREATMENT OF CEREBRAL CAVERNOUS MALFORMATIONS: A DECISION ANALYSIS
1University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands
2University of Edinburgh, Centre for Clinical Brain Sciences, Edinburgh, United Kingdom
3University Medical Center Utrecht, Department of Neurology and Neurosurgery- Brain Centre Rudolf Magnus, Utrecht, The Netherlands
4University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Patients with cerebral cavernous malformations (CCM) may be managed conservatively, or with neurosurgical or radiosurgical intervention. Randomised trials have not been performed and observational studies have not reliably identified dramatic effects of treatment. Using decision analysis, we aimed to evaluate the preferred treatment strategy for patients with symptomatic CCM.
Method
In a decision model, we compared three strategies: 1) neurosurgical, 2) radiosurgical, and 3) conservative treatment. A literature review yielded the risks and outcomes of interventions, intracerebral haemorrhage (ICH) and seizures. Patients with CCM rated their quality of life to determine utilities. We estimated the expected number of quality-adjusted life years (QALYs) and the ICH recurrence risk over five years, according to mode of presentation (ICH or focal neurological deficit [FND] vs. other) and CCM location (brainstem vs. other).
Results
The expected number of QALYs for brainstem CCM presenting with ICH or FND was 2.84 (95% confidence interval [CI]: 2.54–3.08) for conservative, 3.01 (95%CI: 2.86–3.16) for neurosurgical, and 3.03 (95%CI: 2.88–3.18) for radiosurgical treatment; those for non-brainstem CCM presenting with ICH or FND were 3.08 (95%CI: 2.85–3.31) for conservative, 3.21 (95%CI: 3.01–3.36) for neurosurgical, and 3.19 (95%CI: 2.98–3.37) for radiosurgical treatment. For CCM presenting with epilepsy, QALYs were 3.09 (95%CI: 3.03–3.16) for conservative, 3.33 (95%CI: 3.31–3.34) for neurosurgical, and 3.27 (95%CI: 3.24–3.30) for radiosurgical treatment.
Conclusion
This study provides Class III evidence that conservative management and intervention for CCM presenting with ICH or FND are associated with similar QALYs over five years; for CCM presenting with epilepsy, intervention seems the preferred strategy.
Trial registration number
N/A
AS24-010
DURAL ARTERIOVENOUS FISTULA AFTER CEREBRAL VENOUS THROMBOSIS: A SYSTEMATIC REVIEW OF CLINICAL FEATURES, TREATMENT AND OUTCOMES
1University of Manchester, Manchester Medical School, Manchester, United Kingdom
2Salford Royal NHS Foundation Trust, Greater Manchester Neurosciences Centre, Salford, United Kingdom
3University of Manchester, Cardiovascular Domain, Manchester, United Kingdom
4Salford Royal NHS Foundation Trust, Department of Neuroradiology, Salford, United Kingdom
5University of Manchester, Centre for Biostatistics, Manchester, United Kingdom
6University of Manchester, Institute of Brain- Behaviour and Mental Health, Manchester, United Kingdom
Background and Aims
Dural arteriovenous fistulae (DAVF) are an uncommon complication of cerebral venous thrombosis (CVT). It is unclear why some patients develop dAVF after CVT, the timeframe for development nor the optimal treatment or outcome. We reviewed existing literature to identify demographics, complications and management of DAVF.
Method
A systematic review was performed using multiple electronic databases with PRISMA guidance. Published studies reporting DAVF at, or after CVT diagnosis and unpublished local service data were included. Manuscripts were independently screened for inclusion by two reviewers and data analysis undertaken descriptively, using summary statistics.
Results
45 patients were included from 37 manuscripts and local service data. 62.5% cases were male. The median age of CVT diagnosis was 54, being higher for male than female (56.5 vs 47.0 years, p = 0.032). Median time of onset of DAVF after CVT was 12 months (range 1 – 132 months, excluding 23 cases with concomitant DAVF and CVT diagnoses). Treatment was endovascular in 55.1% cases, surgical in 18.4%, and conservative in 22.4% with radiological resolution reported in 38.8% cases and improvement in clinical features in 51%. No radiological or clinical outcomes were reported in 44.9% and 38.8% cases respectively.
Conclusion
In contrast to the female preponderance both for CVT and dAVF the male preponderance for dAVF after CVT was striking, as was the relatively older ages reported. Reporting of outcomes was poor, highlighting a need for disease registries with standardised reporting to better understand risk factors for developing an uncommon complication of an uncommon disease, and its treatment.
Trial registration number
N/A
AS24-011
INTRAOPERATIVE USE OF TRANSCRANIAL MOTOR/SENSORY EVOKED POTENTIAL MONITORING IN THE CLIPPING OF INTRACRANIAL ANEURYSMS: EVALUATION OF FALSE POSITIVE AND FALSE NEGATIVE CASES
1Asan Medical Center, Department of Neurosurgery, Seoul, Republic of Korea
Background and Aims
Somatosensory and motor evoked potentials (SEP and MEP) are often used to prevent ischemic complications during aneurysm surgeries. However, surgeons often encounter cases with suspicious false positive and false negative results from intraoperative evoked potential (EP) monitoring, but the incidence and possible causes for these results are not well established
Method
From January 2012 to April 2016, 1514 patients underwent surgery for unruptured intracranial aneurysms (UIA) with EP monitoring. An EP amplitude decrease of 50% or greater compared with the baseline amplitude was defined as a significant EP change. Correlations between immediate postoperative motor weakness and EP monitoring results were retrospectively reviewed. The sensitivity, specificity, positive and negative predictive values, and incidence of false positives and false negatives of intraoperative MEP monitoring were calculated.
Results
There were 18 patients with a symptomatic infarction (1.18%) and 4 cases of with a symptomatic hemorrhage (0.26%). A total of 15 patients showed motor weakness, with 10 detected by an immediate postoperative motor function test. Fifteen false positive cases (1.25%), and eight false negative cases (0.53%) were reported. Therefore, MEP results during UIA surgery resulted in a sensitivity of 0.10, a specificity of 0.94, positive predictive value of 0.01, and negative predictive value of 0.99.
Conclusion
Intraoperative EP monitoring has high specificity and negative predictive value. Both false positive and false negative findings were present. However, it is thought that a more meticulously designed protocol will make EP monitoring a better surrogate indicator of possible ischemic neurologic deficits.
Trial registration number
N/A
AS24-012
PSEUDOANEURYSM FORMATION AFTER REPETITIVE SUCTION THROMBECTOMY USING A SUCTION CATHETER -CASE REPORT
1Chungnam National University Hospital, Department of Neurosurgery, Daejeon, Republic of Korea
Background and Aims
As the recent advance of suction catheters in endovascular field, the use of manual aspiration thrombectomy for patients with hyperacute ischemic stroke with large vessel occlusion has increased. Although contrast leakage and subarachnoid hemorrhage have been reported during this kind of procedures, there was no report of pseudoaneurysm formation due to vessel injury by suction catheters.
Method
We present a case of 60-year-old woman who presented to our emergency room with dysarthria and left-sided weakness. She underwent suction thrombectomy 5 times using Penumbra suction catheter for acute middle cerebral artery (MCA) occlusion and significant contrast leakage occurred during the procedure. On follow-up angiogram on post-operative day 15, we found a pseudoaneurysm and we treated with detachable coil embolization.
Results
We experienced contrast leakage during repetitive suction thrombectomy for a patient with acute MCA occlusion that later became a significant pseudoaneurysm.
Conclusion
Neurosurgeons who perform suction thrombectomy should keep in mind the possibility of vessel injury that results in the formation of a pseudoaneurysm, especially at the branching site or tortuous segments.
Trial registration number
N/A
AS24-017
PERI-OPERATIVE DUAL ANTIPLATELET THERAPY FOR THE COIL EMBOLIZATION OF UNRUPTURED BRAIN ANEURYSMS: THE EFFICACY AND THE SIDE EFFECT
1The Jikei University Kashiwa Hospital, Neurology, Kashiwa-shi, Japan
2The Jikei University School of Medicine, Neurosurgery, Tokyo, Japan
Background and Aims
The dual antiplatelet therapy (DAPT) using aspirin and clopidogrel before coil embolization has been a commonly used antiplatelet protocol in unruptured aneurysm. However, few studies have done to evaluate the relationship between the duration of the DAPT and its efficacy. In the present study, the different durations of the pre-operative DAPT and their related efficacy was retrospectively analyzed.
Method
A total of 380 unruptured brain aneurysm patients (male, n = 97; median age, 61 y) who underwent coil embolization were retrospectively evaluated. The patients were categorized into 3 different groups depending on the duration of the DAPT: Group A (within 3days), Group B (4–6 days) and Group C (7 days or longer). The platelet aggregation profiles are evaluated on the day of procedure. Post-operative MRI and neurological findings between the 3 groups were compared and the statistical analyses was performed.
Results
Diffusion weighted image performed the day after the operation showed that 272 (72%) patients had any high intensity lesion in the affected area of the treated artery, and 13 (3.4%) presented symptomatic infarction. The both adenosine diphosphate (ADP) and collagen aggregation were significantly decreased with longer DAPT period (ADP aggregation of Group A, B, C; 54%, 52%, 47% (P<0001), collagen aggregation ; 51%, 45%, 41% (P<0001)). The symptomatic infarction tended to decrease with longer DAPT period without statistical significance (Group A, B, C; 5.6%, 3.6%, 2.6%).
Conclusion
Longer DAPT period significantly reduced both the ADP and collagen aggregation. The rate of symptomatic thromboembolic event tended to decrease with longer DAPT period without statistical significance.
Trial registration number
N/A
AS24-018
CAN DISCHARGE DESTINATION BE USED AS A SURROGATE FOR GLASGOW OUTCOME SCALE (GOS) DEFINED OUTCOMES AT 3 MONTHS IN SUBARACHNOID HAEMORRHAGE (SAH)?
1University Hospital of Wales, Neurosurgery, Cardiff, United Kingdom
2Salford Royal NHS Trust, Neurosurgery, Manchester, United Kingdom
3University of Manchester, School of Medical sciences, Manchester, United Kingdom
Background and Aims
The best time to assess outcome after an acute neurological insult to the brain is debated. Timing needs to balance the practicalities of recording a robust measure and ensuring that recovery has reached a plateau at a group level. The aim of this study was to determine if discharge home can be used as surrogate of outcome at 3 months in SAH patients.
Method
This is a retrospective analysis of outcomes of SAH patients identified from a prospective database (March 2016-September 2017). Positive and negative predictive values and accuracy of discharge home for favourable outcome (GOS 1–3) at 3 months post SAH were calculated.
Results
Most patients were female, n = 139 (70%), and n = 45 (23%) presented in poor grade. 142 (71%) patients were discharged home directly from hospital, and 152 (76%) of patients had achieved a favourable outcome at 3 months. The probability of a favourable outcome at 3 months when a patient was discharged home was 98% (CI 85.0–95). The probability of an unfavourable outcome when a patient was not discharged home was 76% (CI 66–84). The overall probability that a patient will be correctly classified was 92% (87–95).
Conclusion
This data suggests that discharge home is a good surrogate marker for outcome at 3 months. This observation needs confirming in a larger dataset that includes multiple centres and more patients in poor grade.
Trial registration number
N/A
AS24-019
RECANALIZATION OF THE ANEURYSM ORIGINATING FROM THE POSTERIOR COMMUNICATING ARTERY AFTER COIL EMBOLIZATION: INCIDENCE AND RISK FACTORS
1Korea University Ansan Hospital, Neurosurgery, Ansan-si, Republic of Korea
Background and Aims
Recanalization is a major problem in the embolization of cerebral aneurysms. We aimed to analyze the recanalization of the aneurysm originating from the posterior communicating artery and its risk factors after coil embolization.
Method
This retrospective study included 37 aneurysms originating from the posterior communicating artery treated with coil embolization. We analyzed the association of various factors (the shape and size of aneurysm, presence of subarachnoid hemorrhage, presence of fetal origin posterior communicating artery, use of stents, coil packing density, and modified Raymond-Roy classification) with recanalization. Recanalization was defined as flow filling at the neck of aneurysm or aneurysm sac on magnetic resonance angiography or conventional angiography compared to the image at the time of treatment. To calculate the coil packing density, volume of aneurysms, and volume of coils, we used an on-line system available at www.angiocalc.com.
Results
Recanalization developed in 13 (35.1%) out of 37 patients. Multiple logistic regression analysis indicated that recanalization of coiled aneurysm was associated with fetal origin posterior communicating artery presentation (P = 0.045) and coil packing density ≥ 18% (P = 0.037).
Conclusion
Our data suggest that presenting with fetal origin posterior communicating artery and low coil packing density (<18 %) are predisposed recanalization of aneurysms originating from the posterior communicating artery after coil embolization.
Trial registration number
N/A
AS24-020
THE SELF-REPORTED NEEDS OF PATIENTS FOLLOWING SUBARACHNOID HAEMORRHAGE
1Salford Royal NHS Foundation Trust, Department of Neurosurgery, Manchester, United Kingdom
2University of Manchetser, Division of Cardiovascular Sciences, Manchester, United Kingdom
3University of Manchester, Centre for Biostatistics, Manchester, United Kingdom
4University of Manchester, Department of Neurosurgery, Manchester, United Kingdom
Background and Aims
Despite advances in the acute care of patients who suffer subarachnoid haemorrhage, post discharge services remain under-developed. Clinical measures are commonly used to assess outcome and quality of life, but patient-reported needs and the extent to which they are met have not been measured.
The aim of this study is to describe the frequency and type of self-reported met and unmet needs of subarachnoid haemorrhage survivors, and explore whether these differ early and late in recovery.
Method
A cross sectional postal survey of 400 SAH survivors to measure needs and the extent to which they were met in two groups of survivors; those 1–2 years and 3–5 years following subarachnoid haemorrhage.
Results
Two hundred and three (51%) participants responded, 63% were female and the mean age was 55 years. Eighty-six percent of survivors reported one or more need following subarachnoid haemorrhage, of whom 78% described one or more to be unmet (median 6 range 1–19) The most commonly reported need related to fatigue (66%). The most commonly reported unmet need related to temper and irritability (85%). There was no statistical difference in the number of needs or unmet needs between the two groups, a greater need in relation to memory was reported by those early in recovery (n = 73 v 48, p = 0.01).
Conclusion
Most subarachnoid haemorrhage survivors have unmet needs both early and late in recovery. Future research should explore factors associated with unmet needs and aim to inform the development of rehabilitation service models to address the long-term needs identified.
Trial registration number
N/A
AS24-021
THE RELATIONSHIP BETWEEN BLOOD GLUCOSE VARIABILITY AND IN-HOSPITAL MORTALITY OF ANEURYSMAL SUBARACHNOID HEMORRHAGE
1Beijing TianTan Hospital-Capital Medical University, Department of Neurology, Beijing, China
Background and Aims
It is well known that increased fasting blood glucose in stroke is associated with poor prognosis in stroke. But a cross-sectional study of a single time point does not fully demonstrate the multidimensional relationship between blood sugar and stroke mortality. Our study aimed to study the relationship between the dynamic changes of fasting blood glucose and the mortality during hospitalization in patients with aneurysmal subarachnoid hemorrhage.
Method
We retrospectively analyzed 351 patients with aneurysmal subarachnoid hemorrhage who were treated in neurological intensive care department of Tiantan hospital in September 2014 -2017 September. During the patient's hospitalization, we monitored the patient's fasting blood glucose for at least 14 days. According to the fasting blood glucose monitoring results:early admission within the first 24 hours of fasting blood glucose is greater than 7mmol/L and after 13 days of fasting blood glucose is higher than 10mmol/L, the patients were divided into four groups:
Results
Univariate analysis showed that admission temperature, creatinine, glycosylated hemoglobin, Hunt-Hess, CT-fisher and GCS score and aneurysm treatment were associated with the death during hospitalization. Multivariate logistic regression analysis showed that the poor glycemic control group and blood glucose elevated later group were associated with death.(OR = 16.327; 95%CI=2.956–89.194; OR = 13.360; 95%CI=1.458 to 122.417).
Conclusion
In the high volume treatment capacity center of cerebrovascular disease, if the fasting blood glucose is elevated, continuous dynamic monitoring should be carried out.
Trial registration number
N/A
AS24-022
ANEURYSMS OF CEREBRAL ARTERIES, MANIFESTED WITH EPILEPTIC SEISURES
1Republican Research and Clinical Center of Neurology and Neurosurgery, neurosurgical department, Minsk, Belarus
2Republican Research and Clinical Center of Neurology and Neurosurgery, laboratory of pathophysiology of nervous system, Minsk, Belarus
3Republican Research and Clinical Center of Neurology and Neurosurgery, director, Minsk, Belarus
Background and Aims
To establish size, localization of cerebral aneurysms, types and time of epileptic seizures occurrence in patients with epilepsy on the background of unruptured aneurysms of cerebral arteries.
Method
The study included 225 patients with unruptured aneurysms of cerebral arteries. Epileptic seizures prior to identification of the cerebral aneurysms were observed in 17 people. All patients were performed computed tomography angiography and electroencephalography.
Results
Frequency of seizures occurrence was 7,6 %. The time of their occurrence before the aneurysms identification ranged from 1 day to 30 years. 2 patients (11,8%) had focal seizures, 13 patients (76,4%) - generalized tonic-clonic seizures, 2 patients (11,8%) – combination of focal and generalized tonic-clonic seizures. The analysis of cerebral aneurysms sizes revealed the following data: in 3 cases there were giant aneurysms (greater than 25 mm in diameter), in 14 cases seizures occurred in patients with aneurysms of normal size (4–15 mm). Aneurysm localization distribution was as follows: 8 patients (47%) had aneurysm of the middle cerebral artery (MCA), 6 (35%) - aneurysm of the internal carotid artery (ICA), 3 patients (18%) - aneurysm of the anterior cerebral artery (ACA).
Conclusion
So it is necessary to think of aneurysms in patients with epileptic seizures for prevention hemorrhagic stroke. According to our data, epileptic seizures occurred in patients with aneurysms of giant and normal sizes. They met more often in the localization of aneurysms in the CMA, but they also took place in the localization of aneurysms on the ICA and ACA.
Trial registration number
N/A
AS24-024
IMPROVED PREDICTION OF DELAYED CEREBRAL ISCHEMIA IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HEMORRHAGE WITH MACHINE LEARNING
1Academic Medical Center, Biomedical Engineering & Physics, Amsterdam, The Netherlands
2Academic Medical Center, Neurology, Amsterdam, The Netherlands
3Academic Medical Center, Radiology, Amsterdam, The Netherlands
4Academic Medical Center, Neurosurgical Center Amsterdam, Amsterdam, The Netherlands
5Academic Medical Center, Clinical Epidemiology- Biostatistics and Bioinformatics, Amsterdam, The Netherlands
Background and Aims
Delayed Cerebral Ischemia (DCI) is a severe complication in patients with aneurysmal subarachnoid hemorrhage. Several predictors associated to DCI have been identified based on logistic regression. However, their accuracy is generally low. We hypothesize that Machine Learning (ML) algorithms for the prediction of DCI using a combination of clinical and image data might lead to higher predictive accuracy.
Method
Clinical and CT image data from 366 patients with aneurysmal subarachnoid hemorrhage were included. Three types of analysis were performed to predict DCI. First, logistic regression models were used with known clinical DCI predictors. Second, all clinical data were used with ML algorithms. Third, image features were extracted from the CT-images using an auto-encoder, combined with clinical data and used with ML algorithms. Accuracy evaluation was based on the Area Under the Curve (AUC) with the 95% Confidence Interval (CI).
Results
The AUC of the logistic regressions ranged between 0.54 and 0.63. For the ML algorithms with clinical data there was a small, but significant, improvement in accuracy (AUC=0.68, 95%CI (0.65 - 0.69)). Notably, size of the aneurysm was used in many of the models. The accuracy was highest for ML models that also include image features (AUC=0.74, 95% CI (0.72 - 0.75)).
Conclusion
Machine Learning algorithms significantly improve the prediction of DCI in patients with a SAH, particularly when image features are also included. Our experiments suggest that aneurysm characteristics are also associated to the development of DCI.
Trial registration number
N/A
AS24-025
SYSTEMATIC REVIEW AND META-ANALYSIS OF THE ANGIOGRAPHIC EVOLUTION OF NECK RESIDUAL (CLASS II) ANEURYSMS
1Texas Tech University Health Sciences Center, Neurology, El Paso, USA
Background and Aims
Coiled intracranial aneurysms are more likely than clipped aneurysms to recur and the degree to which neck residuals can be considered a favorable outcome after initial treatment is questionable. Our systematic review aimed to evaluate the existing data on the natural history of neck residuals with regards to recanalization rate (Class II worsening to Class III) versus rate of progressive occlusion or obliteration (Class II to Class I).
Method
The Raymond–Roy Occlusion Classification (RROC) was used in order to define neck residuals in this study. Based on PRISMA methodology, we reviewed 1105 studies and selected 22 studies, to characterize the angiographic evolution of class II neck residuals to recanalization (Class III) or obliteration (Class I).
Results
A total of 1002 class II aneurysms were included in the analysis. The average angiographic follow-up after initial treatment was 13.8 ± 9.0 months. Upon angiographic follow-up a total of 150 (14.9%) aneurysms recanalized, 429 (42.8%) evolved to progressive occlusion, and 423 (42.2%) remained stable (no change in classification). Additionally, out of 696 class II aneurysms with available data, 156 (22.4%) had stand-alone coiling, 508 (73.0%) underwent stent-assisted coiling, and 32 (4.6%) had balloon-assisted coiling.
Conclusion
There is a greater tendency of neck residual (Class II) aneurysms to remain stable or evolve to progressive occlusion versus worsening to Class III.
Trial registration number
N/A
AS24-026
ASPIRIN AND ANTICOAGULANT USAGE ON OUTCOMES AFTER RUPTURED ARTERIOVENOUS MALFORMATION (AVM): A NATIONWIDE INPATIENT SAMPLE ANALYSIS
1Texas Tech University Health Sciences Center, neurology, El Paso, USA
Background and Aims
In nationwide study, use of aspirin (ASA) or anticoagulant were associated with differential mortality rates after aneurysmal subarachnoid hemorrhage however their impact on outcomes of ruptured AVM is unclear.
Method
Data from the Nationwide Inpatient Sample (NIS; 2006–2014) were analyzed with a primary diagnosis of SAH with a diagnosis of AVM. Patients were divided in two groups: ASA/anticoagulant use versus none. Multivariable logistic regression was performed to calculate the adjusted odds of in-hospital mortality, a non-routine discharge (except home), or poor outcome (death, discharge to institutional care. Multivariable linear regression was used to evaluate length of hospital stay. Covariates included patient demographics, comorbidities, APDRG severity scale, and treatment method of AVM.
Results
11066 patients with ruptured AVM were included. Patients taking either ASA (2.5 %, n =273) or anticoagulation (1.7 %, n =185) were significantly older and had a greater burden of comorbid disease (hypertension, hyperlipidemia, atrial fibrillation & renal disease, p < 0.001). Inpatient mortality (10.9 % either aspirin/anticoagulation vs 9.2 % neither, p = 0.63) Length of stay (9.3 ± 8.7 days vs 11.0 ± 13.5 days p = 0.11) were not significant. In multivariable logistic regression models for outcome, discharge disposition was better in ASA/Anticoagulation group (home discharge OR 2.36, CI 1.40–3.98, p = 0.001) but inpatient mortality was not different (OR 0.79, CI 0.34–1.82, p = 0.58).
Conclusion
In this study, neither long-term ASA nor anticoagulant use was associated with differential mortality after ruptured AVM. ASA/Anticoagulant use was associated with favorable discharge to home.
Trial registration number
N/A
AS24-027
DEFINING HYDROCEPHALUS AFTER ANEURYSMAL SUBARACHNOID HAEMORRHAGE
1Salford Royal NHS Foundation Trust, Neurosurgery, Manchester, United Kingdom
2Salford Royal NHS Foundation Trust, Neurology, Manchester, United Kingdom
Background and Aims
Ventriculomegaly is invariably seen at presentation in aneurysmal subarachnoid haemorrhage (aSAH) and practice for cerebrospinal fluid (CSF) diversion varies. A simple imaging measure to predict the need for CSF diversion at presentation may be of benefit. Our aim was to derive and test a threshold bicaudate index (BCI) above which CSF diversion should be considered.
Method
Derivation and test cohorts were extracted from our single-centre prospective registry (2009-present). The derivation cohort (2009–2015) included WFNS grade 1–2 aSAH patients who deteriorated clinically, had a repeat CT brain and were treated with CSF diversion. BCI was measured on post-deterioration CTs and the lower limit of the 95% confidence interval (95%CI) was taken as the hydrocephalus threshold. The test cohort included aSAH patients from 2016. For WFNS≥2 patients, we compared BCI on diagnostic CTs with use of CSF diversion within 48 hours of admission.
Results
The derivation cohort (n = 62) received an external ventricular (n = 57, 92%) or lumbar drain (n = 5, 8%). Mean post-deterioration BCI was 0.21 (95%CI:0.19–0.22) for age <65 years and 0.24 (95%CI:0.22–0.27) for age ≥65 years. In the test cohort (n = 105), there was no significant difference in BCI on diagnostic CT between good (WFNS 1-3) and poor (WFNS 4-5) grade patients (mean[95%CI]: 0.15[95%CI:0.14–0.16] vs. 0.17[95%CI:0.15–0.19], p = 0.159). 20/66 (30%) WFNS≥2 patients exceeded our BCI thresholds (0.19, 0.22) and 16/20 (80%) had CSF diversion. An additional 13/66 (20%) patients underwent CSF diversion without exceeding BCI thresholds.
Conclusion
Our threshold values require further testing but may provide an objective measure to aid clinical decision making in aSAH.
Trial registration number
N/A
AS24-030
RELATIONSHIP OF HEADACHE AND COIL EMBOLIZATION IN PATIENTS WITH UNRUPTURED INTRACRANIAL ANEURYSMS: A PROSPECTIVE ANALYSIS
1Hallym University, Neurosurgery, HwaSeong-Si, Republic of Korea
Background and Aims
To investigate the association between headache outcomes and coil embolization and to identify potential factors associated with different headache outcomes in patients with unruptured intracranial aneurysms (UIAs) after treatment with coil embolization.
Method
A prospective study of patients with planned coil embolization for UIAs was conducted. The changes in headache patterns, headache-related disability, and depression were assessed before coil embolization and at 3 days and 2 and 6 weeks after coil embolization. All variables were analyzed to identify factors associated with different headache outcomes
Results
Fifty-nine (72%) of 82 patients reported headaches prior to coil embolization. Of these, improvements in the severity of headaches were reported by 42 patients (71%). In addition to a significant reduction in headache severity, significant reductions in headache-related disability and depression scores were also observed. Demographic factors, aneurysmal characteristics, or procedural factors were not found to be significantly associated with improvement in the severity of headaches after coil embolization. In addition, the number of microemboli on diffusion weighted imaging (DWI) was not significantly associated with improvement of headaches after coil embolization.
Twenty-three patients reported no headaches before coil embolization, and 3 (13%) patients reported new onset headaches after coil embolization. All new onset headaches were mild and dull in nature without combined symptoms in the temporal area.
Conclusion
Our study suggested that regardless of headache characteristics, the aneurysm size (even those < 5 mm in diameter), technique used (stent-assisted or not stent-assisted), and coil embolization of UIAs resulted in headache improvement in most patients with pretreatment headaches.
Trial registration number
HC13OISI0070
AS24-034
PREVENTABLE POOR OUTCOME FROM REBLEEDING BY EMERGENCY ANEURYSM OCCLUSION IN PATIENTS WITH ANEURYSMAL SUBARACHNOID HEMORRHAGE
1Brain Center Rudolf Magnus - UMC Utrecht, Department of Neurology and Neurosurgery, Utrecht, The Netherlands
2Neurosurgery of NeuroCenter- Kuopio University Hospital- Kuopio- Finland, Department of Neurosurgery, Kuopio, Finland
3University Medical Center Utrecht, Radiology, Utrecht, The Netherlands
Background and Aims
The risk of rebleeding is highest during the initial hours after aneurysmal subarachnoid hemorrhage (aSAH), but the aneurysm is not occluded in all patients immediately after admission. We studied the proportion of patients with poor outcome from early in-hospital rebleeding that can be prevented by three emergency aneurysm occlusion regimes.
Method
From our prospectively collected database we retrieved from all aSAH patients admitted between July 2007 and July 2017 data on clinical condition on admission, time of rebleeding, and outcome at three months.
Results
Of 1391 consecutive aSAH patients, 923 were in good clinical condition and had an aneurysm on initial imaging that was amenable for treatment. Poor outcome from rebleeding could have been avoided by treatment <4 hours after admission during day time shifts in 4 (0.4% [95% CI 0.2 – 1.1]) patients (number needed to treat [NNT] 250), by treatment <1 hour during daytime shift in 9 (1.0% [95% CI 0.5 – 1.8]; NNT 111), and treatment <1 hour at 24/7 basis in 16 (1.7% [95% CI 1.1 – 2.8%]; NNT 59).
Conclusion
Emergency aneurysm occlusion can reduce poor outcome due to rebleeding, but only in small proportions of patients. Whether such strategies lead to improved outcome for all patients and are cost-effective is highly uncertain.
Trial registration number
N/A
AS24-036
SAFETY AND FEASIBILITY OF TOLIVAPTAN FOR THE TREATMENT OF EUVOLEMIC HYPONATREMIA AFTER ANEURYSMAL SUBARACHNOID HEMORRHAGE (ASAH)
1Thomas Jefferson University, Neurosurgery, Philadelphia, USA
Background and Aims
Euvolemic hyponatremia is prevalent in aSAH patients and associated with poor outcome, gait imbalance, cognitive impairment, and prolonged length of stay. We sought to determine the efficacy and safety profile of the aquaporin inhibitor tolivaptan in a cohort of aSAH patients.
Method
Inception cohort of consecutive aSAH patients at a high volume academic center from 2011–2016. We collected the patient’s volume status at the time of tolivaptan administration and the change in sodium (Na) was analyzed using the double-sided matched pairs Wilcoxon-Rank-Test. Measured outcomes were in-hospital mortality, cerebral vasospasm (cVSP), cerebral infarction, and the modified Ranking Scale at 3 months.
Results
In total, 40 patients were included. Mean age was 56 ± 11 years, 52% (n = 21) were woman, median (Md)-H&H was 3 (IQR=2) and Md-Modified-Fisher was 3 (IQR=2). Median volume balance at time of tolivaptan administration was 3.5L (IQR=5L). The lowest Md-Na was 128mEq/L (IQR=3) and highest Md-Na post tolivaptan was 137mEq/L (IQR=5), mean-difference 9.7mEq/L. p < .001. In-hospital mortality was 0.2%, cVSP was 20% (n = 8), cerebral infarction was 0.7% (n = 3), and Md-mRS at 3-months was 0 (IQR=2).
Conclusion
Our data suggest that tolivaptan administration in euvolemic hyponatremic aSAH patients was associated with significant correction of Na levels. Though a higher rate of cVSP was observed, the incidence of cerebral infarct and in-hospital mortality were low. Our findings require further study.
Trial registration number
N/A
AS24-038
SAFETY AND EFFICIENCY OF TREATMENT PROTOCOLS OF PATIENTS WITH SAH AHA/ASA 2009 AND 2012
1Ural State Medical University- Yekaterinburg- Russia., Medical Faculty-, Yekaterinburg, Russia
2Сlinical Institute of Brain., intensive care unit, Yekaterinburg-, Russia
3Ural State Medical University- Yekaterinburg- Russia., MD- PhD-Professor, Yekaterinburg, Russia
4Сlinical Institute of Brain., General Director, Yekaterinburg-, Russia
5Sverdlovsk Regional Clinical Hospital#1, Stroke Unit, Yekaterinburg, Russia
Background and Aims
In the treatment of vasospasm with SAH from 2011, we abandoned 3-H therapy, adopted the concept of maintaining euvolemia. To assess the treatment introduced a scale of aggressiveness of therapy.
Method
A total of 380 patients were included in the study; of them 193 patients, whose treatment corresponded to the AHA/ASA 2012 (Group A) protocol and 187 patients to the recommendations of the AHA/ASA 2009 (Group B). Evaluated the aggressiveness of therapy, complications, the results of treatment.
Results
Groups are comparable in age and severity. Aggressiveness of therapy in group B was 5.0 (4.5, 5.4) and was higher than group A 3.4 (3.1, 3.7) (p <0.0001). Acute pulmonary injury in group B occurred in 24.1%, and in group A in 14.0% (P = 0.0014). In group B, PE was recorded, 9.6%, and in group A 2.1% (P = 0.0032). Intracranial hypertension in group A developed 19.7%, and in group B, 34.2% (P <0.0001). An analysis based on the Glasgow outcome scale showed differences between groups (p = 0.0009). The outcome in group A was 0.7 points better with 95% CI (0.2, 1.2). Mortality in group A is 14.5%, in group B - 23% (p = 0.034).
Conclusion
3-H therapy did not justify the expected effect in the prevention of DCI, but led to an increase in complications. Activities aimed at providing physiological indicators reduced medical complications and mortality. The 2012 AHA/ASA recommendations are considered to be the most effective and safe approach in the prevention and treatment of angiospasm in SAH.
Trial registration number
N/A
AS24-039
HIGHER RISK OF INTRACRANIAL ANEURYSMS AND ANEURYSMAL SUBARACHNOID HAEMORRHAGE IN SIBLINGS THAN IN CHILDREN OF PATIENTS WITH ANEURYSMAL SUBARACHNOID HAEMORRHAGE
1University Medical Center Utrecht, Neurology, Utrecht, The Netherlands
2University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
First-degree relatives (FDR’s) of patients with aneurysmal subarachnoid haemorrhage (aSAH) have an increased risk of both unruptured intracranial aneurysms (UIA) and aSAH. We assessed whether the type of kinship (parents, siblings, or children) of the FDR’s of aSAH patients influences this risk.
Method
We used all available data from the prospectively collected database of families with familial aSAH seen in our outpatient clinic between 1994–2016. We constructed pedigrees for all families with ≥2 FDR’s with aSAH, probable aSAH or UIA. The proband was defined as the affected family member who was first brought under medical attention. We compared both the proportion of aSAH and UIA in subgroups of FDR’s in relation to the proband by calculating risk ratios (RR) with children as a reference.
Results
A total of 154 families were identified, with 1259 FDR’s of whom 146 had aSAH and 63 of the 326 screened FDR’s UIA. Siblings had a higher risk of aSAH (RR 1.6, 95% CI: 1.1–2.4) and parents a lower risk (RR 0.4, 95% CI: 0.2–0.8; RR 0.6,95% CI: 0.4–0.97 when analyzing aSAH and probable aSAH together). Siblings also had a higher risk of UIA (RR 2.3, 95% CI: 1.2–4.1, age adjusted RR 2.0,95% CI: 1.1–3.9) than children.
Conclusion
Siblings of patients with familial aSAH have a significant higher risk of both UIA and aSAH and parents have a lower risk of aSAH compared to children. The type of kinship is a relevant factor to consider in the risk prediction and screening advice in families with familial aSAH.
Trial registration number
N/A
AS24-040
TREATMENT OF INTRACRANIAL ANEURYSMS:COMPARISON OF ENDOVASCULAR AND SURGICAL TREATMENT
1Hospital Universitario de La Princesa, Unidad de Ictus. Servicio de Neurología., Madrid, Spain
Background and Aims
Management of intracranial aneurysms could be conditioned by aneurysm rupture. We analyze periprocedural complications and outcomes in intracranial aneurysm treatment.
Method
Retrospective observational study of patients treated for intracranial aneurysms, both ruptured (with subarachnoid hemorrhage) and unruptured, from 2011 to 2017 at our center. Demographic, anatomical and clinical variables were measured. Endovascular and surgical techniques were compared in terms of safety and outcomes.
Results
N=249. 146(58,6)% were treated for unruptured aneurysms (UA),103(41,4%) were treated for ruptured aneurysms (RA). Treatment options for both groups were: simple coil embolization (61[25,2%]), balloon-assisted embolization (73[30%]), stent-assisted embolization (21[8,6%]), flow diversion stent (42[17,3%]), surgical clipping (42[17,3%]) and clipping+hematoma evacuation (4[1,6%]).
Periprocedural complications were: aneurysm rupture/hemorrhage (11[4,4%]), ischemic stroke (8[3,2%]), bleeding (6[2,4%]), infection (2[0,8%]), arterial dissection (1[0,4%]), others (9[3,6%]).
RA treated in the subacute phase (24–72h from onset of hemorrhage) were associated to a higher rate of periprocedural complications (24,3%) than those treated in the first 24 hours (8,7%) and after 72h (19,2%)(p = 0,05). No correlations were observed between the complication rate and the time of intervention for each technique separately.
Surgical clipping was associated to more periprocedural complications in RA(75%) than in UA(25%)(p = 0.006). No such differences were observed for endovascular techniques.
We found no correlation between the technique type and the periprocedural complications, mRS and mortality at 3 months, and neck remnant in both RA and UA groups. Patients with RA that required surgery had a higher rate of remaining neurological deficit (p < 0,007).
Conclusion
In our study periprocedural complications in ruptured aneurysms were more frequent in aneurysms treated between 24 and 72h. Aneurysm rupture could increase periprocedural complications with surgery, therefore endovascular management could be a safer alternative for ruptured aneurysms.
Trial registration number
N/A
AS24-041
ATRAUMATIC CONVEXITY SUBARACHNOID HEMORRHAGE, A DIAGNOSTIC CHALLENGE
1Hospital La Princesa, Neurología, MADRID, Spain
Background and Aims
Atraumatic convexity subarachnoid hemorrhage (acSAH) is an uncommon form of subarachnoid hemorrhage. We present a case serie of patients with acSAH.
Method
All patients with diagnosis of acSAH identified from hospital records (2008–2017) were included. We retrospectively reviewed clinical and radiological characteristics, etiology of the hemorrhage and outcome.
Results
N=17. Age average: 73,1 years (range: 40–88), 64,7% female, 58,8% arterial hypertension, 17,6% diabetes mellitus, 35,3% dyslipidemia. One patient had previous intracranial haemorrhage. 41,2% antiplatelet treatment, 17,6% anticoagulant treatment. Clinical presentation: One had thunderclap headache, 10 TIA/crisis-like, 2 generalized seizures, 1 thunderclap headache+generalized seizures, 2 thunderclap headache+TIA/crisis-like, 1 asymptomatic. 58,8% received antiepileptic drugs, only one patient didn’t improve clinically. MRI of the brain was performed in 53%, finding hemosiderosis and microbleedings in 62,5%. acSAH involved >5 sulci in 23,3%, and was bihemisferic in 23,5%. The most frequent location was left fronto-parietal (29,4%). Etiology: 5 (29,4%) probable cerebral amyloid angiopathy (CAA), 3 (17,6%) attributable to anticoagulation treatment, 1 reversible cerebral vasoconstriction syndrome, 1 post-thrombectomy cerebral hyperperfusion syndrome, 1 cerebral sinus thrombosis, 1 atypical hemorrhagic transformation after cerebral infarction, 1 arterio-venous fistula, 4 (23,5%) unknown. In the follow-up, 12,5% had another intracranial hemorrhage (intraparenchymal hemorrhages). Median 3-months mRS: 2.
Conclusion
In our serie acSAH had a heterogeneous clinical presentation, being the most frequent TIA/crisis like. acSAH could have many underlying etiologies that will condition the outcome, CAA was the most frequent, maybe even underrepresented in elderly patients due to the lack of MRI studies.
Trial registration number
N/A
AS24-042
CHARACTERISTICS OF PATIENTS WITH DELAYED CEREBRAL ISCHEMIA AFTER SUBARACHNOID ANEURYSMATIC HEMORRHAGE
1Hospital São Paulo, Neurology, São Paulo, Brazil
Background and Aims
Delayed cerebral ischemia (DCI) is defined as the occurrence of focal neurology impairment or a decrease in the level of consciousness (2 points in Glasgow coma scale) for at least one hour, in the context of a subarachnoid aneurysm hemorrhage (SAH). The symptoms should not be explained by other causes such as fever, seizure or hydrocephalus. If these neurologic symptoms are attributed to sonographic or angiographic arterial spasm, it is characterized as symptomatic vasospasm.
Method
We present the clinic characteristics of patients from Hospital São Paulo (São Paulo- Brazil) with DCI after subarachnoid aneurysmatic hemorrhage who also had a sonographic arterial spasm. These patients were submitted to either hypertension induction or endovenous vasodilator (milrinone) treatment.
Results
During one year, 11 patients of our service had documented DCI after SAH. The majority of our sample was female (59%) and an average age of 46 years old. The average Hunt-Hess scale was 2,6; the World Federation of Neurosurgical Societies SAH grading scale was 2; the modified Fisher scale was 2,3. Ninety percent of our patients were submitted to surgical clipping in a mean time of 8 days after the hemorrhage. The preferred therapy to treat DCI was endovenous Milrinone, according to Montreal's Protocol.
Conclusion
Aneurysmatic SAH is a devastating condition and the exact pathophysiology of DCI remains uncertain. Our sample describes our experience in treating DCI and the most prominent characteristics of the patients with this complication. A greater knowledge of this entity is essential to improve SAH's morbidity rates.
Trial registration number
N/A
AS24-043
A SERIE OF 322 RUPTURED AND UNRUPTURED CEREBRAL ANEURYSMS: BEYOND THE SIZE
1Dr Josep Trueta Hospital, Stroke Unit- Neurology, Girona, Spain
2Germans Trias i Pujol Hospital, Interventional Neuroradiology Unit- Neuroscience, Badalona, Spain
3Germans Trias i Pujol Hospital, Neurosurgery- Neuroscience, Badalona, Spain
Background and Aims
Prevalence of cerebral aneurysms is around 3% in general population. Nowadays remains unclear some features related to the aneurysm rupture mechanism.
We aimed to determine if previous vascular risk factors, treatments, or anatomy and aneurysm location were different in patients with ruptured aneurysms compared to those with unruptured aneurysms.
Method
A prospective study was performed between 2000 and 2017 in our hospital. A total of 322 aneurysms in 283 patients (65.2% women; 55.8 years) were enrolled. Of them, 41.4% were smokers, 6% were alcohol abusers, 45.7% had high blood pressure and 31.3% had dyslipidemia.
According to the status at the moment of the diagnosis, the aneurysms were divided in ruptured (53.7%) and unruptured (46.3%). No statiscally significance differences were observed in terms of gender, age and vascular risk factors.
Results
Patients from unruptured group were more frequently under treatment with statins (30.2% vs 17.8%, p = 0.012), had less lobulated aneurysms (57.5% vs 76.1%, p = 0.001) and were less frequently located in the anterior communicating artery (14.8% vs 26.6%, p < 0.001) and posterior communicating artery (9.4% vs 25.4%, p < 0.001). Patients from ruptured aneurysms group had lower sac diameters compared to unruptured aneurysms (6.52 mm vs 7.5 mm, p < 0.000).
In the logistic regression, non statin use, lobulated aneurysms and both anterior and posterior communicating arteries location, were independently associated with ruptured aneurysms.
Conclusion
Aspects other than classical risk factors and aneurysm size, are involved in the rupture process of cerebral aneurysms.
Trial registration number
N/A
AS24-044
SUBARACHNOID HEMORRHAGE, BEYOND THE ANEURYSM
1Hospital La Princesa, Neurología, MADRID, Spain
Background and Aims
non-traumatic subarachnoid hemorrhage (SAH) is classified as: aneurysmal SAH (aSAH), perimesencephalic SAH (pSAH) and non-aneurysmal non-perimesencephalic SAH (npSAH). We evaluated the clinical and prognostic differences between these groups.
Method
Retrospective observational study based on data collected prospectively from patients admitted to our hospital with SAH (2008–2017). Demographic, clinical, radiologic and prognostic variables were recorded.
Results
N=165. aSAH n = 122 (73,9%), npSAH n = 28 (17%), pSAH n = 15 (9,1%). We found significant differences for demographic variables: mean age (npSAH 60,1 ± 14,8, aSAH 57 ± 14,4, pSAH 47,9 ± 7) (p < 0,01) and sex ratio (women aSAH 77,9%, npSAH 53,6%, pSAH 46,7%) (p < 0,01). No significant differences for vascular risk factors were found. Regarding clinical variables we found significant differences for: initial Hunt&Hess grade (median = 1 for pSAH, median = 2 for aSAH and npSAH) (p < 0,01), Glasgow Coma Scale (GCS) (median = 15 for pSAH, median = 14 for aSAH and npSAH) (p < 0,01), patients requiring ventricular drainage (39,3% npSAH, 35,2% aSAH, 0% pSAH) (p < 0,05), development of delayed cerebral ischemia (DCI) (27% aSAH, 14,3% npSAH, 0% pSAH) (p < 0,05). We also found significant differences for prognostic variables: median mRS at discharge 0 for pSAH, 1 for aSAH and npSAH (p < 0,01). The hospital stay in days was longer in aSAH, followed by npSAH and pSAH (median: 17, 12, 9 respectively) (p < 0,001).
Conclusion
Significant differences between these three groups were found for: mean age, sex ratio, initial Hunt&Hess and GCS, ventricular drainage, DCI, mRS and hospital stay. pSAH had an excellent clinical situation and prognosis. Special interest deserves the group of HSAnp, with clinical characteristics and prognosis resembled HSAa.
Trial registration number
N/A
AS24-045
HYPERTONIC SALINE SOLUTION (HTS3%) AFTER ANEURYSMAL SUBARACHNOID HEMORRHAGE (ASAH) DOES NOT AFFECT SODIUM (NA) BALANCE
1Thomas Jefferson University, Neurosurgery, Philadelphia, USA
2Thomas Jefferson University, Neurology and Neurosurgery, Philadelphia, USA
Background and Aims
Euvolemic hyponatremia is prevalent in aSAH patients and is associated with poor outcome, gait imbalance, cognitive impairment and prolonged length of hospital stay. We sought to determine the effect of HTS3% on sodium trends in an interim analysis of the ongoing HTS3% clinical trial.
Method
The “Safety and Feasibility of HTS3% After aSAH Hemorrhage (HS3)” is a randomized, single-center, single-blinded clinical trial designed to evaluate if a protocol of volume expansion with HTS3% is safe and effective in patients with aSAH for the prevention of cerebral vasospasm and hyponatremia. Within 72 hours of index hemorrhage, aSAH patients were randomized to receive prophylactic intravenous (i.v) HTS3% bolus injections of 250ml per 6hrs for 7 days via central line vs. routine fluid management with isotonic fluids as per our local management protocol based on multi-professional guidelines for the management of aSAH. Na levels from admission (D0) and up to 10 days (D10) were compared using Mann-U-Whitney test for non-parametric data.
Results
In total, 19 patients participated in the interim analysis of Na balance. Mean age was 50 ± 12 years, 63% (n = 12) were females, 52% (n = 10) were white, Median (Md) Hunt and Hess was 3 (IQR=0), Md-modified-Fisher was 3 (IQR=1). No significant differences observed in Md-Na levels from D0-D10 (Fig 1).
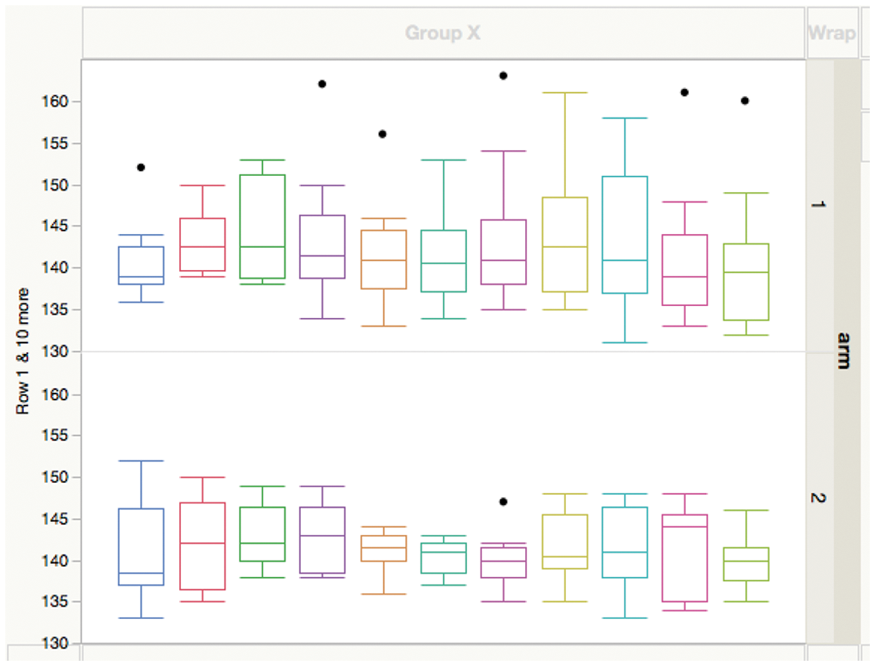
Fig 1: Na (mEq/L) trends. Arm 1 = HTS3%, Arm 2 = Standard fluid management. (Mann-U-Whitney)
Trial registration number
NCT02432157
APHASIA, NEGLECT AND OTHER CORTICAL DEFICITS
AS25-001
METHODS OF MONITORING FIDELITY IN TRIALS OF COMPLEX BEHAVIOURAL INTERVENTIONS: THE COMPARE FIDELITY PROTOCOL
1La Trobe University, Allied Health, Bundoora, Australia
2Macquarie University, Cognitive Science, Sydney, Australia
3University of Sydney, Health Sciences, Sydney, Australia
4University of Queensland, UQ Centre of Clinical Research, Brisbane, Australia
5University of Technology Sydney, Mathematical and Physical Sciences, Sydney, Australia
6Edith Cowan University, Psychology and Social Sciences, Joondalup, Australia
7Monash University, Clinical Sciences, Melbourne, Australia
8Monash Health, Speech Pathology, Melbourne, Australia
Background and Aims
Treatment fidelity is a complex evaluative process critical for achieving quality in intervention studies. Its objective is to determine whether an intervention was delivered as intended. Despite its benefits, treatment fidelity has been inconsistently reported in behavioural intervention studies with only 14% of aphasia treatment studies explicitly reporting on treatment fidelity. Complex interventions, such as those for post-stroke aphasia, pose particular challenges to fidelity monitoring.
Method
The COMPARE study is an Australian-based 3-arm randomised controlled trial (planned sample size n = 216) which aims to determine whether two intensive and contrasting treatments (constraint induced aphasia therapy; multi-modality aphasia therapy) for chronic post-stroke aphasia are superior to usual care. Based on the theoretical models underlying the trial interventions, we developed a fidelity protocol to monitor and enhance treatment delivered by multiple clinicians across Australia. The fidelity protocol adheres to the recommended standards outlined in the TiDIER statement (a template for reporting interventions stemming from the CONSORT 2010 and SPIRIT 2013 statements).
Results
An overview of the protocol will be presented, including the theoretical rationale, methods, challenges and results to date. Data will be presented on the assessment measures, which include (a) standardised clinician training, (b) video recording all assessment and treatment sessions, (c) providing feedback in real-time to clinicians, and (d) monitoring for therapist drift.
Conclusion
The COMPARE fidelity protocol offers one solution to the challenges of monitoring and enhancing treatment fidelity within behavioural change interventions. Our solution may be of utility to a wide range of trials of complex interventions.
Trial registration number
N/A
AS25-002
WHERE DOES THALAMIC APHASIA STEM FROM? ASSOCIATION WITH LEFT ANTERIOR ISCHEMIC LESION
1Charité Universitätsmedizin Berlin Campus Benjamin Franklin, Department of Neurology, Berlin, Germany
2Charité Universitätsmedizin Berlin Campus Benjamin Franklin, Centre for Stroke Research CSB, Berlin, Germany
Background and Aims
Aphasia is typically associated with left cortical lesions but can also occur following thalamic ischemic lesions. The thalamus is thought to be involved in thalamo-cortical language networks. Case reports have shown aphasia after anterior and left thalamic lesions. However, to this date, no study could connect aphasia to a specific anatomical region of the thalamus. We hypothesized, that aphasia is associated with left anterior thalamic lesions.
Method
Retrospective analysis of 1064 patients (criterion: MRI within 48h upon admission showed ischemic stroke). Aphasia was assessed by the admitting physician and follow-up was performed by speech therapists. On MRI scans thalamic lesions were categorized into 4 anatomic regions according to Carrera/Bogousslavsky 20061.
Results
Of 1064 patients 52 presented with an isolated lesion in the thalamus ("ILT"=isolated lesion thalamus, 4.9%). Aphasia was less frequent in “ILT” than in all other, cortical and subcortical, infarctions (11.5% vs. 26.7%, p = 0.014). In patients with “ILT”, aphasia was only seen after left anterior thalamic lesion (n = 6, 100%, p < 0.001).
Conclusion
We were able to demonstrate an association of aphasia with lesions of the left anterior thalamus. While a lateralization of speech in the thalamus has been discussed, no specific region could be identified to this date. Lesion of the anterior nuclei could lead to functional or metabolic disconnection within the language network (diachisis) causing disruption in lexical-semantic properties. Further prospective investigation is needed to determine the role of the thalamus in aphasia.
1. Carrera E, Bogousslavsky J. The thalamus and behavior: effects of anatomically distinct strokes. Neurology. 2006;66(12):1817–1823.
Trial registration number
N/A
AS25-003
APHASIA DETECTION WITH NIH STROKE SCALE ITEM 9 “BEST LANGUAGE”
1Lund University, Department of Clinical Sciences- Neurology, Lund, Sweden
2University of Gothenburg, Division of Speech and Language Pathology, Gothenburg, Sweden
Background and Aims
It is unclear how well the National Institutes of Health Stroke Scale (NIHSS) sub-item 9 detects aphasia in stroke patients. We therefore studied if NIHSS sub-item 9 is reliable for diagnosing aphasia in the acute phase of ischemic stroke compared to a more detailed language screening tool; the Language Screening Test (LAST). We also assessed the incidence of aphasia in patients with first-ever ischemic stroke using NIHSS sub-item 9.
Method
119 patients with first-ever ischemic stroke were prospectively and consecutively included in Lund Stroke Register Study. Exclusion criteria: non-native Swedish language; altered consciousness; diagnosed dementia or psychiatric diagnosis. Patients were evaluated with NIHSS sub-item 9 by a nurse (up to 7 days post stroke onset) followed by a more detailed language screening with LAST (range 0–15, ≤14 indicate aphasia) by a speech therapist. Assessments were made within 24 hours. Data were analysed using LAST as ‘gold standard.’
Results
26 patients (22%) had aphasia according to NIHSS sub-item 9 (distribution of scores 1–3 were n = 16, n = 5, n = 5, respectively) in comparison to 34 patients (29%) according to LAST, with a median score of 11. Assuming LAST as gold standard, NIHSS sub-item 9 gave 15 false negatives for aphasia (LAST scores ranging from 8 to 14) and 7 false positives for aphasia, corresponding to a sensitivity of 56% and specificity of 92%.
Conclusion
Sub-item 9 = “best language” of the NIHSS has a rather low sensitivity and sometimes miss-classifies patients with mild to moderate aphasia, when compared with a diagnostic tool more dedicated towards aphasia.
Trial registration number
N/A
AS25-004
RECOVERY OF LANGUAGE FUNCTION AND PROGNOSTIC FACTORS DURING THE FIRST YEAR AFTER ISCHEMIC STROKE
1Samsung Medical Center, Physical and Rehabilitation Medicine, Seoul, Republic of Korea
2Yonsei University College of Medicine, Department and Research Institute of Rehabilitation Medicine, Seoul, Republic of Korea
3Pusan National University Yangsan Hospital, Department of Rehabilitation Medicine, Yangsan, Republic of Korea
4Korea Center for Disease Control, Division of Chronic Disease Control, Osong, Republic of Korea
Background and Aims
We examined the recovery pattern of language function and influencing factors until 1 year after onset of ischemic stroke.
Method
We analyzed data of 235 patients with first-ever ischemic stroke who completed Korean Frenchay Aphasia Screening Test (K-FAST) at 7 days, 3 months, 6 months, and 1 year after stroke onset. Repeated measures ANOVA was used to investigate changes of language function among each time points and subgroup analysis was done according to K-FAST score at 7 days. Multiple logistic regression analysis were performed to investigate influencing factor for K-FAST score at 1 year. Broca's, Heschl's, and Wernicke's area were selected for lesion involvement.
Results
In the improvement of K-FAST score, significant differences were noticed between each assessment points. In the subgroup analysis, only severe group demonstrated significant differences of mean K-FAST scores among all assessment time points (p < 0.05). Negative factors for K-FAST category shift were involvement of Wernicke's area and old age, whereas positive factors were female, alcohol consumption, and involvement of Heschl's gyrus. Obesity and stroke lesion volume were positively related to K-FAST score improvement.
Conclusion
The results show that recovery of language function differently occurred according to the initial severity of aphasia. Patients who initially presented larger stroke lesion volume or patients who had involvement of Heschl's gyrus paradoxically demonstrated more recovery in delta K-FAST at 1 year after onset. (This work was supported by grants from the Korea Centers for Disease Control and Prevention (2016E-33003-02) and the National Research Foundation of Korea by the Korean government (MSIP) (NRF-2017R1A2A1A05000730).
Trial registration number
NCT03402451
AS25-005
EFFECTS OF TDCS IN MODULATING THE AFTER-EFFECT OF PRISMATIC LENSES TRAINING IN SUBACUTE STROKE PATIENTS WITH NEGLECT
1San Raffaele Hospital, INSPE- Neurorehabilitation Dept., Milan, Italy
Background and Aims
neglect treatment with prismatic lenses (PL) has been demonstrated to be effective in improving hemispatial neglect. This study aimed to compare the effect of cathodal transcranial direct current stimulation (c-tDCS), anodal tDCS (a-tDCS) or sham stimulation in modulating the PL effect in stroke patients.
Method
fifteen subacute stoke patients with pathological performance on the Behavioral Inattention Test (BIT) battery, indicative of neglect, were included in this study. Patients underwent to a-tDCS over the right posterior parietal cortex (PPC), c-tDCS over the left PPC and sham stimulation during three PL training sessions (with PL of 10◦ rightward shift), in random sequence and separated by at least 1 day. Thirty “invisible” pointing (visual target not visible) were performed before and after each session to evaluate the after-effect of the PL training.
Results
leftward shift after PL training was significantly reduced by a-tDCS over the ipsilasional PPC in comparison with c-tDCS over the contralesional PPC (p = 0.019) and sham stimulation (p = 0.047). No difference in the after-effect was obtained comparing the c-tDCS and sham stimulation. Error correction during the PL training do not significantly differed among the three sessions.
Conclusion
a-tDCS over the ipsilesional PPC reduced the leftward deviation possibly interfering with the network involved in visuo-motor adaptation to PL training.
Trial registration number
N/A
AS25-006
THEMIS-SV: AUTOMATIC CLASSIFICATION OF LANGUAGE DISORDERS FROM SPEECH SIGNALS
1Institutionen för svenska språket, Department of Swedish, Göteborg, Sweden
Background and Aims
Brain injuries resulting from stroke can affect the production of speech resulting in different types of language impairments, such as aphasia (Brookshire and McNeil, 2014; Plowman et al., 2012). Studying these productions manually is an extremely cumbersome and time consuming process. The aim of this paper is to present THEMIS-SV: a system that enables the automatic transcription of speech signals and the segmentation of vowels and consonants in Swedish.
Method
The input of the system are recordings of speech. The system processes the recordings and returns an output with three tiers: the utterance tier, the word tier, and the vowels/consonants tier (see Figure 1).
Results
The output of the system is a fast and reliable transcription and segmentation of speech, which is very close to transcriptions and segmentations performed manually. The automatic segmentation of speech enables targeted acoustic measurements, such as measurements of consonant spectra, formant frequencies of vowels, fundamental frequency, pauses, speech rate, etc. and other acoustic measurements that have been known to differentiate between the different types of language disorders (see Figure 2).
Conclusion
The method proposed here can be employed for the analysis of speech of individuals with post-stroke aphasia and other language disorders and constitutes a promising step towards a fully automated differential diagnostic tool for language disorders.
References
R. Brookshire, M. McNeil, Introduction to Neurogenic Communication Disorders-E-Book, Elsevier Health Sciences, 2014.
E. Plowman, B. Hentz, C. Ellis, Post-stroke aphasia prognosis: A review of patient-related and stroke-related factors, Journal of evaluation in clinical practice 18 (2012) 689–694.
Trial registration number
N/A
AS25-007
THE TYPE OF POST-STROKE APHASIA AND RELATIVE FACTORS: A RETROSPECTIVE OBSERVATIONAL STUDY ON 882 CHINESE PATIENTS
1Beijing Tiantan Hospital - Capital Medical university, Department of Neurology, Beijing, China
Background and Aims
The incidence of post-stroke aphasia ranges from 21% to 38%. Several factors can influence the type of post-stroke aphasia. To investigate the correlation between these factors and the type/serverity of post-stroke aphasia, a retrospective observational study was conducted.
Method
This study recruited 882 post-stroke aphasiacs who met the inclusion criteria and were admitted to the Department of Neurology of Beijing Tiantan Hospital, Capital Medical University from January 2004 to December 2014. The criteria of handedness instituted by Peking University First Hospital was used to judge patients’ handedness. Western battery aphasia was used to assess aphasic types. Patients were divided into youth, middle-aged and elderly groups.
Results
It was found post-stroke aphasia was not solely determined by the location of the lesion. Age and the type of stroke were closely related to the type of aphasia. Male patients showed a significantly higher incidence of aphasia after a stroke and a younger average age of onset than their female counterparts. Two forms of aphasia - global and Broca’s were the most common ones observed in both genders.
Conclusion
Age and types of stroke influence the type of aphasia, while sex does not. Males have a significantly higher level of morbidity due to aphasia, and a younger age of stroke onset than females. Broca’s and global aphasia are the most common types of aphasia in both males and females, followed by anomic and trans-cortical motor aphasia. The type of aphasia is not correlated with the location of the lesion, and it changes as the disease progresses.
Trial registration number
N/A
AS25-008
ACUTE SYMPTOMS OF NEGLECT PREDICT LONG-TERM FUNCTIONAL OUTCOME AFTER LEFT HEMISPHERIC STROKE ESPECIALLY FOR PATIENTS WITH LANGUAGE IMPAIRMENT
1Faculty of Social Sciences, Department of Psychology, Gothenburg, Sweden
2the Skaraborg Institute for Research and Development, the Skaraborg Institute for Research and Development, Skövde, Sweden
3Institute of Bioscience, Department of Cognitive Neuroscience and Philosophy, Skövde, Sweden
4Institute of Neuroscience and Physiology, Sahlgrenska Academy, Gothenburg, Sweden
5Institute of Biomedicine, Sahlgrenska Academy, Gothenburg, Sweden
Background and Aims
Visuospatial inattention (VSI) and language impairment (LI) post-stroke have often been associated with unfavorable short-term functional outcome. This study aimed at investigating the presence of VSI and LI following a hemispheric stroke and to investigate if these early symptoms predict long-term functional outcomes. Results from the left hemispheric group are presented.
Method
A consecutive cohort of 163 left hemispheric ischemic stroke patients was assessed for VSI, using Star Cancellation Test, in median 7 days after admission (interquartile range 1–5 days). LI was assessed with the language item in the Scandinavian Stroke Scale (within the first 7 days). Seven years later, 105 survivors without recurrent stroke were assessed for functional outcomes by the modified Rankin Scale (mRS) and the Frenchay Activities Index (FAI).
Results
VSI was frequent (20.9%) early after a left hemispheric stroke. The regression model significantly identified VSI and neurological deficits as significant independent predictors of mRS (R2 = .49, p < .001) and for FAI the significant predictors were VSI and LI (R2 = .37, p < .001). Presence of LI was significantly related with unfavorable long-term outcomes but only in combination with the presence of VSI (p < .001).
Conclusion
The study emphasizes the importance of identifying early symptoms of VSI after left hemisphere stroke and particularly so for individuals with severe symptoms of LI, since this combination in the acute phase indicated an increased risk of unfavorable outcomes.
Trial registration number
N/A
AS25-009
ASSESSING APRAXIA OF SPEECH AFTER STROKE USING THE APRAXIA OF SPEECH RATING SCALE: REPORT FROM A RELIABILITY TRIAL
1Karolinska Institute, CLINTEC- Division of Speech and Language Pathology, Stockholm, Sweden
Background and Aims
Speech and language impairments are common sequele after stroke, resulting in aphasia or motor speech disorders such as dysarthria or apraxia of speech. Apraxia of speech (AOS) is recognized as a diagnosis, but few attempts have been done to specify criteria into a standardized assessment-battery. In 2014, Strand and colleagues at the Mayo clinic presented a new assessment tool for AOS diagnosis; The Apraxia of Speech Rating Scale (ASRS). The ASRS showed excellent intra- and inter-rater reliability for assessing neurodegenerative speech and language disorders.
The purpose of this study was to examine the reliability across clinicians when applying the ASRS in patients with speech and language impairments after stroke. An additional aim was to examine the sensitivity of the instrument in assessing patients with severe AOS.
Method
A Swedish version of the ASRS was administered to patients 2 - 6 weeks' post stroke onset. Video-recordings of the patients' speech were generated. Five speech and language pathologists viewed each video and independently rated the presence and severity of AOS by using the ASRS.
Results
The overall inter-rater reliability was fair for the total score. There was high variation in item-level agreement, for several items the disagreement was high.
Conclusion
The results indicate that for clinicians without the expertise knowledge of AOS as the original raters, the ASRS may not be optimally suited. They also imply that the ASRS in its present version is not designed for assessing severe AOS and raises questions as to how assessment of patients with AOS following stroke could be improved.
Trial registration number
N/A
AS25-010
SYSTEMATIC ANALYSIS OF AGRAMMATIC ERRORS AND CHARACTERIZATION OF THE LANGUAGE PROFILE IN TURKISH SPEAKING PATIENTS WITH BROCA’S APHASIA
1Istanbul University, Aziz Sancar Institute of Experimental Medicine- Department of Neuroscience, Istanbul, Turkey
2Istanbul Faculty of Medicine, Department of Neurology- Behavioral Neurology and Movement Disorders Unit, Istanbul, Turkey
3Istanbul Faculty of Medicine, Department of Neurology- Edip Aktin Stroke Unit, Istanbul, Turkey
4Istanbul University, Hulusi Behçet Life Sciences Center- Neuroimaging Lab, Istanbul, Turkey
Background and Aims
Cerebrovascular damage to dorsal perisylvian areas of left hemisphere may cause agrammatic aphasia (a.k.a. Broca’saphasia).
The goal of this study is to characterize the language profile in agrammatic aphasia in Turkish.
Method
Five patients with Broca’s aphasia and 9 controls were given a novel picture description task and language samples were recorded using a digital voice recorder. All language samples were analyzed using Systematic Analysis of Language Transcripts (SALT) Software.
Results
Patients produced 28.1 words per minute, 37.4% of their speech output consisted of efforts and their speech was interrupted by an average of 4.6 pauses. Controls were more fluent with 95,7 words per minute, efforts were recorded only in 4.9% of their total speech output and almost no pauses were noted. Although patients made frequent phonemic paraphasias, no semantic paraphasias were recorded in both groups. Number of complex sentences were significantly lower for the patients, as well. Patients with Broca’s aphasia had almost no errors while using bound morphemes as verb inflections and verb stems were never used without inflections. Moreover, in a subsequent single-word comprehension test, patients performed comparable to controls.
Conclusion
Although Broca’s aphasia in Turkish has similar characteristics compared to aphasia seen in Indo-European languages as shown by decreased fluency with effortful speech, frequent phonemic errors and intact single-word comprehension, the use of bound morphemes can be preserved in Turkish aphasics even in the cases with severe agrammatism. As an inflectional language, preservation of the use of morphemes is a distinguishing feature in agrammatic aphasia in Turkish speaking patients.
Trial registration number
N/A
AS25-011
A CASE OF MIMICKING STROKE SEIZURE, CAUSED BY GANGLIOGLIOMA
1A. Vorokchobov City Clinical Hospital № 67, Stroke Unite, Krasnogorsk, Russia
2A.I. Burnazyan Federal Medical and Biophysical Center, neurology, Moscow, Russia
Background and Aims
Many disorders may mimic stroke and seizures are probably one of the most challenging disorders, which may mislead a doctor, resulting in a bad outcome.
Method
An 60-year-old male was admitted as an emergency with a short episode of abrupt onset of aphasia. Aphasia lasted approximately 3–5 minutes, no other symptoms including loss of consciousness were present. The examination in Stroke Unite revealed no abnormalities in neurological status. Computed tomography (CT) brain scan showed changes in keeping with cerebral small vessel disease. He was first managed as TIA, but further questioning lead to hypothesis that it might have been a seizure. His wife recalled that aphasia was preceded with bizarre left arm posture, which was interpreted by doctors as dystonic posturing. A routine scalp EEG captured a clinical seizure with epileptiform changes arising from the left temporal region. Electroencephalography changes comprised continuing rhythmic 4 to 5 Hz theta activity throughout the left hemisphere, maximal in the temporal region. Brain MRI was performed, with showed left temporal ganglioglioma.
Results
The patient was transferred to a neurosurgery department.
Conclusion
More precise evaluation is needed in some cases of common symptoms, which at first sight may seem due to some vascular disorder.
Trial registration number
n|a
WOMEN AND STROKE
AS26-003
SPECIFIC RISK FACTORS, CLINICAL FEATURES AND OUTCOME IN YOUNG WOMEN WITH ISCHEMIC STROKE
1University clinic for neurology, Urgent Neurology, Skopje, FYR Macedonia
Background and Aims
Aim of this study was to investigate risk factors of young adult female patients (< 45 years) with first ever ischemic stroke and to obtain information on outcome and follow-up.
Method
This study was conducted at the Department for Urgent Neurology, University Clinic of Neurology in Skopje, Macedonia. Young adult female patients admitted due to first episode of ischemic stroke were prospectively studied. Follow-up period was 3 years after discharge from hospital. Specific risk factors, clinical features and investigations, stroke reccurence and residual disability with Modified Rankin Scale (mRS) score were evaluated. The residual functional disability was assessed by the modified Rankin scale at discharge, 3 months and 3 years after the stroke, respectively.
Results
We analyzed 449 female patients with ischemic stroke, out of which, 15 (3,3%) were young females aged 30+-5 years. Specific risk factors included hypercoagulable state during puerperium, migraine with aura, patent foramen ovale, use of oral contraceptives and smoking (p < 0.05). No significant difference was seen in the clinical or imaging features (p>0.05). Moderately severe or severe disability with mRS score >3 was seen in 4 patients (26,6%), moderate disability with mRS score ranging 1–3 was registered in 5 (33,3%) and 6 patients (40%) were without significant disability with mRS=0. The 3-year survival rate was 100% and residual disability improved in 82%. No reccurent stroke was registered.
Conclusion
Identification of specific risk factors might help to identify young women who have increased risk for ischemic stroke. In general, with appropriate diagnosis and treatment, outcome is favourable.
Trial registration number
N/A
AS26-004
CEREBRAL VENOUS AND SINUS THROMBOSIS: WOMEN VERSUS MEN
1University clinic for neurology, Urgent Neurology, Skopje, FYR Macedonia
Background and Aims
To explore the gender differences between women and men with cerebral venous and sinus thrombosis (CVST) in terms of risk factors, neurologic characteristics, outcomes and prognosis.
Method
The medical records of patients with CVST admitted to our hospital during a 5 years period were assessed. We analyzed gender specific differences, thrombophilic risk factors, clinical presentations and imaging examination results. Modified Rankin scale (mRS) was used to measure clinical severity at the time of onset, discharge and follow up visits.
Results
A total of 35 patients with CVST was analyzed. Female to male ratio was 1,9:1. Median age was 34,5 years and women were significantly younger (p < 0.05). Gender specific differences included presence of acquired hypercoagulable state (pregnancy, puerperium, use of oral contraceptives, hormonal replacement therapy) in 75 % of women. No significant differences in terms of neurologic characteristics or imaging results were observed (p>0.05). Women had a better prognosis than men (complete recovery 92% vs 75%, p <0.05), especially the ones with gender specific risk factors.
Conclusion
There are important differences between women and men with CVST, women with gender-specific risk factors have a better outcome.
Trial registration number
N/A
AS26-005
SEX DIFFERENCES IN CONSECUTIVE ACUTE ISCHEMIC STROKES: CAUSES, CLINICAL PRESENTATION AND OUTCOMES
1HFR - Hopital Cantonal Fribourg, Neurology, Fribourg, Switzerland
2Institute of Social and Preventive Medicine- University of Lausanne, Institute of Social and Preventive Medicine, Lausanne, Switzerland
3CHUV, Stroke Center- Neurology Service- Department of Clinical Neurosciences- CHUV, Lausanne, Switzerland
Background and Aims
We aimed to investigate sex differences of causes, clinical presentation and outcomes in a large consecutive cohort of acute ischemic strokes (AIS).
Method
Patients from the Acute STroke Registry and Analysis of Lausanne were included from 03/2003–04/2016. Multivariate analysis regarding clinical, pathophysiological and biological variables was conducted. 12 months functional outcome applying mRS shift analysis and 12 months mortality were compared after adjustment for potential confounders.
Results
The 1761/3993 female patients (44%) were older and had more preexisting handicap than male patients. Other than well-known comorbidities and risk factors that are more frequent in women (migraine, hypothyroidism, depression) or men (past cancer, coronary artery disease, low ejection fraction and alcohol abuse), we found women to have lower BMI, more pretreatment with antihypertensives, and less with antidiabetic/lipid lowering drugs. Clinically, NIHSS was similar, but men more often had cerebellar findings. Stroke due to large-artery atherosclerosis, small vessel disease or multiple/coexisting causes was found less often in women who had less previous cerebrovascular events than men. In the adjusted 12 months mRS shift analysis, female sex was associated with less favorable outcome (OR:0.85;p = 0.018), but 12 months mortality was not statistically increased (OR:1.21;p = 0.159).
Conclusion
In this retrospective analysis of 3993 consecutive AIS patients, female patients more often had preexisting handicap, higher age and less frequent stroke of large-artery atherosclerotic, lacunar or multiple/coexisting etiology. Also, female sex was associated with more handicap at 12 months, whereas there was no significant association in terms of mortality compared to men.
Trial registration number
N/A
AS26-006
AGE-SPECIFIC STROKE PROFILES AND OUTCOMES IN WOMEN
1University of Glasgow, Institutes of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
2Medical University of South Carolina, Department of Neurology, South Carolina, USA
3Cedars Sinai Medical Centre, Department of Neurology, Los Angeles, USA
4University of Gothenburg, Department of Clinical Neuroscience at Institute of Neuroscience and Physiology, Gothenburg, Sweden
5University of Duisburg, Department of Neurology and Stroke Unit, Essen, Germany
Background and Aims
We aimed to explore sex differences in index stroke severity and functional outcomes, and the factors associated with poor functional outcomes in women.
Method
We analysed anonymised data from registry-based populations within the Virtual International Stroke Trials Archive (VISTA). Generalised linear modelling described relationships among demography, clinical factors, and functional outcome by modified Rankin Scale (mRS) at 1 year, by sex and age at onset (18–45, 46–55, 56–75, and >75 years). For women, we described whether baseline variables were specific-effect-modifiers of age, and the factors that were associated with mRS within each age stratum.
Results
In 6,632 patients (median age=70, IQR [60,78]; n = 3,001 [45.3%] female), after adjusting for age, presence of atrial fibrillation (AF), hypertension, diabetes, prior stroke, pre-stroke independence, hemisphere affected, and type of stroke we observed no sex differences in initial stroke severity by National Institutes of Health Stroke Scale (NIHSS; p = 0.27). Women aged between 56–75 years had poorer mRS scores at 1 year than men aged 56–75 years (p = 0.009; OR [95% CI]=1.3 [1.1,1.5]) after adjusting for covariates. In women, AF in those aged>75years (p = 0.009, OR [95% CI]=1.6 [1.1, 2.3]; hypertension in those aged 46–55 years (p = 0.0002, OR [95% CI] = 5.1 [2.2,12] and diabetes in those aged 56–75 years (p = 0.014, OR [95% CI]=1.5 [1.1,2.2] were each associated with increased odds of poor mRS at 1 year, but were not significant in any other age stratum.
Conclusion
We observed no sex differences in index stroke severity, however sex differences in functional outcomes at 1 year were present in those aged 56–75years.
Trial registration number
n/a
AS26-007
WOMEN PARTICIPATE IN UNPAID WORK MORE THAN MEN IN THE FIRST YEAR AFTER STROKE: THE PSYCHOSOCIAL OUTCOMES IN STROKE (POISE) COHORT STUDY
1George Institute for Global Health, Neurological and Mental Health, Sydney, Australia
2University of New South Wales, Faculty of Medicine, Sydney, Australia
3The University of Sydney, Sydney Medical School, Sydney, Australia
4Brain and Mind Centre, Psychiarty, Sydney, Australia
5The University of Central Lancashire, Faculty of Health and Wellbeing, Preston, United Kingdom
Background and Aims
While returning to paid work is a crucial marker of stroke recovery, little is known about whether levels of unpaid work differ by sex following stroke.
Method
POISE (Psychosocial Outcomes In StrokE) was a prospective, multicentre observational study that recruited individuals, 18–64 years, within 28 days of stroke from New South Wales, Australia. Unpaid work was classified as: unpaid domestic work for the household; unpaid care of others; looking after own child (ren) without pay or looking after someone else’s child (ren) without pay. This was graded as <5, 5–14; 15–29 and 30 hours or more per week. Data were collected on pre-stroke, 28 day, 6 and 12 month follow-up. The primary outcomes were the gender differences and factors associated with participation in unpaid work after stroke.
Results
Eighty percent of women and 52% of men engaged in >5 hours per week of unpaid work prior to stroke, by 12 months after stroke this became 69% and 53%, respectively. For women, there were significant associations in participation in unpaid work at 12 months with having financially dependent children (OR, 3.54; 95% CI, 1.23–10.18) and with the absence of depression at 28 days post stroke (OR, 13.82; 95% CI, 1.01–188.42). In men, having financially dependent children (OR, 1.46; 95% CI, 1.06–1.99) was significant.
Conclusion
More women engaged in unpaid work pre-stroke and at 12 months after stroke but this gap narrows somewhat following stroke due to a fall in the level of unpaid work carried out by women.
Trial registration number
N/A
AS26-008
SAFETY OF SURGERY IN PREGNANCY-RELATED HEMORRHAGIC STROKES : A SINGLE-CENTER EXPERIENCE OF 20 YEARS
1Catholic Kwandong University International St. Mary's Hospital, Neurosurgery, Incheon, Republic of Korea
2Yonsei University Severance Hospital, Neurosurgery, Seoul, Republic of Korea
Background and Aims
Hemorrhagic stroke during pregnancy can cause serious problems to mother and fetus, but its cerebrovascular causes have not been understood.
Method
Medical records between January 1994 and June 2016 who had pregnancy-related hemorrhagic strokes were retrospectively reviewed in our institution. Reasons of hemorrhage, gestational age, methods of delivery, maternal modified Rankin Scale (mRS) at discharge were investigated for analysis.
Results
There were 11 hemorrhagic strokes related to pregnancy treated surgically. The mean age of these patients was 28.5 years old with the range of 23∼37. Cerebrovascular diseases (CVDs) were found in 8 patients (72.7%), comprised of arteriovenous malformation (AVM, 37.5% of CVD-associated hemorrhage), aneurysm, cavernous malformation and moyamoya disease (25%, 25%, 12.5%, respectively). Most CVD-related hemorrhage occurred in 2nd trimesters, whereas most hemorrhage without CVDs occurred in 3rd trimesters. Seven patients who had AVM, aneurysm and cavernous malformation underwent craniotomy and surgical removal of lesions, and 1 patient with moyamoya disease had extraventricular drainage (EVD) only. The other 3 patients who had eclampsia or unknown cause of hemorrhage received EVD or catheterization for intracerebral hematoma. Although there were one maternal death and 1 therapeutic abortion, mean maternal mRS scores on discharge was 1.3, and condition of babies after delivery was all good.
Conclusion
Preexisting CVDs are main causes of pregnancy-related hemorrhagic stokes, but their surgical results are excellent like non-pregnant patients. Therefore, active investigation and aggressive management of cerebrovascular lesion is necessary for pregnant patients with intracranial hemorrhage.
Trial registration number
N/A
AS26-009
THE ROLE OF OXIDATIVE STRESS IN MENSTRUAL RELATED MIGRAINE: A VASCULAR TYPE HEADACHE
1Adnan Menderes University Faculty of Medicine, Neurology Department, Aydin, Turkey
2Adnan Menderes University Faculty of Medicine, Biochemistry, Aydin, Turkey
Background and Aims
Menstrually related migraine (MRM) is a headache disorder occurring in reproductive-aged women relevant to menstrual cycles. Attacks occur with decreases in estrogen and may be relevant to oxidative stress which hasn't been clear yet. Our aim was to investigate oxidative stress markers during menstrual cycle which may be important in pathophysiology of MRM as a vascular type headache.
Method
20 patients with MRM (32.65 ± 8.75 age) and 20 healthy volunteers (30.25 ± 8.6 age) were included in our study. All subjects were examined during an attack-free interval and blood samples were taken in order to study estrogen, progesteron, LH, FSH, nitric oxide (NO), malondialdehyde (MDA), superoxide dismutase (SOD) , glutathione (GSH) and glutathione reductase (GSH-Rd) in midfollicular and midluteal phases of the menstrual cycle.
Results
There was no statistical significant difference between the control and the patient groups in according to age, menstrual cycle duration and hormones. GSH-Rd (62.96 ± 17.22 vs 84.69 ± 38.64, p = 0.04) and SOD (3834.44 ± 1423.8 vs 4562.41 ± 1825.3, p = 0.003) of MRM group were found elevated in the luteal phase when compared with follicular phase but this couldn't be detected in the control group.
Conclusion
Our results suggested that the antioxidant system in the follicular phase is inadequate relative to healthy subjects in MRM. The antioxidant defence system have to be taken into account to understand the pathophysiology of MRM and therefore need further studies.
Trial registration number
N/A
AS26-010
DIFFERENCES BETWEEN WOMEN AND MEN IN USE OF ANTITHROMBOTIC DRUGS IN PATIENTS WITH STROKE AND ATRIAL FIBRILLATION
1Oslo Universitetssykehus HF, Department of Medicine, 0424 Oslo, Norway
2Oslo Universitetssykehus HF, Department of Neurology, 0424 Oslo, Norway
3Norwegian University of Science and Technology, Norwegian Stroke Registry, Trondheim, Norway
Background and Aims
Women who suffer stroke are older than men, have more cardioembolic aetiology including atrial fibrillation (AF) and suffer from more severe strokes. We aimed to investigate whether the use of antithrombotic drugs is different in women and men with stroke and AF.
Method
We used data from the Norwegian Stroke Registry 2016 and extracted people with detected AF, both known and detected during the hospital stay. Using the Chi-square test we compared the use of different antithrombotic drugs prior to stroke and upon discharge.
Results
Out of 8650 patients, 2290 (26.5%) had AF. There were significantly more AF among women than men (27.7 vs 25.5%, p = 0.02). On admission, there were no differences between women and men in the use of aspirin (31.2 vs 32.1%, p = 0.495), clopidorgrel (1.9 vs 2.5%, p = 0.327) or warfarin (21.8 vs 23.6, p = 0.30). Women were less likely to be on treatment with other anticoagulants (19.4 vs 23.4%, p = 0.017). At discharge, there were no differences in the use of either warfarin or other anticoagulants, however, men were more often on treatment with aspirin (17.1 vs 21.8%, <0.001) and clopidogrel (1.8 vs 4.1%, p = 0.002).
Conclusion
The proportion of AF is higher among women than among men. Women were less likely than men to be treated with other anticoagulants prior to the stroke, but not on discharge. Men with AF received more antiplatelet drugs on discharge than women with AF, and this could reflect differences in age or other comorbidities.
Trial registration number
N/A
AS26-012
SEX DIFFERENCES IN ACUTE SPONTANEOUS INTRACEREBRAL HEMORRHAGE – A DANISH HOSPITAL BASED STUDY
1Bispebjerg Hospital, Department of Neurology, Copenhagen, Denmark
2Klinikum Frankfurt-Höchst, Klinikum Frankfurt-Höchst, Frankfurt. Germany, Germany
Background and Aims
Data on gender differences in Intracerebral Hemorrhage (ICH) remains scarce. The purpose of this study was to explore a cohort of patients with ICH from a Danish hospital for sex differences in risk factors, clinical presentation and outcome.
Method
This study was a retrospectively planned analysis based on a prospectively collected cohort of patients with first ever ICH. Major known risk factors, admission and radiological characteristics, clinical course, outcome and mortality were compared between genders.
Results
127 women (F) and 173 men (M) with ICH were included into the analysis. Women were older than men (74 years (F) vs 67 (M), p < 0.001), more men had diabetes (4% (F) vs 13% (M), p = 0.008), alcohol abuse (4% (F) vs 19% (M), p < 0.001), or received lipid lowering therapy (14% (F) vs 28% (M), p = 0.003). Co morbidity (Charlson Score) was higher in men (0 (F) vs 1 (M), p = 0.006). There were no significant differences in admission characteristics (NIHSS, GCS, onset to scan), radiological characteristics (ICH volume, IVH, SAH, spot sign, midline shift, hydrocephalus), clinical course (early neurological deterioration, surgery, do not resuscitate orders). There was no significant difference in outcome (day 90 outcome, mRS 0–3 (good outcome) vs 4–6 (poor outcome), p = 0.279) or 1-year mortality (29% (F) vs 25% (M), p = 0.512) or 1-year mortality (Kaplan-Meyer curves, p = 0.407).
Conclusion
Women were significantly older but in spite of this men had more co-morbidities as well as alcohol abuse. No differences were observed in clinical presentations or outcome.
Trial registration number
N/A
AS26-013
OUTCOME OF PATIENTS TREATED WITH INTRAVENOUS THROMBOLYSIS BY SEX
1Hospital San Pedro De Alcantara, Neurología, Cáceres, Spain
Background and Aims
Being a woman could lead to a worse prognosis in the response to rtPA. We aimed to evaluated differences between rtPA response by sex.
Method
Consecutive cohort of stroke patients treated with rTPA. Two groups: GA, women and GB, men. Early evolution was defined as hemorrhagic transformation (HT), difference of NIHSS in first 24 hours and mortality at 7days. Medium-term evolution (90days) such as mRS score, mortality and Independence (mRS≤2). Long-term evolution (1year) such as mRS score, mortality and independence in that period. Chi-square test were used to compare categorical variables and T-student to quantitative ones. We used multivariable regression with prognostic factors.
Results
293 patients (GA 137, GB 156). We found differences in age (70,6 +/− 12,7 vs 65,4 +/−12,6; p < 0,001), AF (21,2% vs 12,2%, p = 0.04), cognitive impairment (6,6% vs 1,9%, p = 0,045), smoking (10,2% vs 30,1%, p < 0,0001), alcohol use (2,9% vs 24%, p < 0,001), and door-to-needle time (84,3 +/−54,9 vs 99,8 +/−64,3, p = 0,03).
In early evolution, we did not observe differences between the variables. The univariate analysis at 90days showed a trend towards lower mortality in women (10.8% vs 18%, p = 0.08), without differences in the others. Differences after the adjusted analysis by demographic variables and by characteristic in the acute phase were not found. In long-term evolution, a trend to worse mRS score in women was found (2.4 ± 1.9 vs 2.1 ± 1.7, p = 0.08), without differences in the rest of univariate analysis neither the adjusted analysis.
Conclusion
In our cohort, there were no differences in the response to rtPA depending on the sex of the patient.
Trial registration number
N/A
AS26-015
EXPLORING THE SEX DIFFERENCES IN ATRIAL FIBRILLATION AND STROKE IN A COHORT OF 1178 PATIENTS WITH 10 YEAR FOLLOW UP
1Bispebjerg University Hospital, Neurology, Copenhagen, Denmark
Background and Aims
Clinical practice suggests a difference between men and women, we wanted to explore the differences in our stroke cohort.
Method
A well-described stroke cohort was included between 1998–2001. Discharge diagnose of either ischaemic stroke or Transitory Ischaemic Attack (TIA) was selected for the analysis (n = 1178). Known and found risk factors as well as results of the examinations were registered. A 10-year follow up was performed focusing on vital status, atrial fibrillation (AF) and reoccurrence of ischemic stroke or TIA.
Results
The distribution of men and women was equal as well as the ratio of TIA and ischaemic stroke (75.2% vs 75.7% ischaemic stroke women vs men).
The women were significantly older (75 vs 69) p < 0.001)
AF was known or found in 21.1% of the women vs 15.1% (P<0.001),
At 10 years follow-up, AF was reported in 36.7% of women and 26.5% of men (P<0.001)
Diabetes was present in 10.6% of the women vs 17.1% of the men (P<0.001) Hypertension and vital status at follow-up was not significantly different in the two groups.
Conclusion
Atrial fibrillation is far more prevalent in women with ischaemic stroke/TIA than men; women with AF are older than men and differ in risk factor profile. Rates of AF increases further during long term follow up reaching the highest frequency in women. Personalised medicine in secondary stroke prevention could be an answer to the increasing evidence of gender differences in stroke and should be explored.
Trial registration number
N/A
AS26-017
EVALUATION THE RISK OF DEVELOPMENT OF STROKE IN REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME
1Tashkent Medical Academy, Nenrology, Tashkent, Uzbekistan
Introduction
Reversible cerebral vasoconstriction syndrome (RCVS) characterized by acute-onset, severe thunderclap headaches, reversible segmental, multifocal vasoconstriction of cerebral arteries, with or without focal neurological signs. RCVS may caused in 16% cases of TIA, in 4-56% cases of ischemic stroke, in 34% subarachnoid hemorrhage.
Purpose
evaluation the risk of development of stroke in patients with RCVS
Methods
We analyzed 30 patients with thunderclap headache. The average age of patients was 54.7 ± 1.8 (40 to 66) years, of them 12 men (40%) and 18 women (60%). All patients examined neurological status, biochemical blood analysis, radiological methods MRI, MRA.
Results
The average duration of the pain was 50,25 ± 5.7 minutes (15–180). this pain attack was observed in 5 patients -10 times, in 7 patients- 6 times, in 8 patients-3, in 5 – 2 times. In 18 patients (60%) occured local neurologic signs which all of them had mild hemiparesis , in 2 patients observed abnormal speech, The patients’ average systolic blood pressure was 146.25 ± 9.8 mm Hg (110–170 mm Hg), the average diastolic blood pressure of 92 ± 5.8 mm Hg (70–110 mm Hg). 16 patients examined by MRI and 3 patients found picture of ischemic stroke. Also, 4 patients examined by MRA, found multifocal vasoconstriction in brain`s arteries. In 19 patients all symptoms completely were disappeared after 10–12 weeks, in 1 patient remained mild hemiparesis
Conclusion
The results of study shows, reversible cerebral vasoconstriction syndrome is most common in women; Also, RCVS may be the risk factor of the development of stroke in 18.75% cases.
Trial registration number
N/A
AS26-019
POSTPARTUM REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME: AN ENTITY TO CONSIDER IN PUERPERIUM HEADACHE
1Hospital Universitario Fundación Alcorcón, Neurology, Alcorcón, Spain
Background and Aims
Postpartum reversible cerebral vasoconstriction syndrome (PRCVS) is characterised by severe headaches, with or without acute neurological symptoms, during the puerperium. We describe two patients with complicated PRCVS.
Method
Description of two clinical cases
Results
A 33 year-old woman with a history of migraine, multiple sclerosis and a recent delivery with acute thunderclap occipital headache that had lasted for three days. MRI showed left frontal non-aneurysmal subarachnoid hemorrhage and multiple milimetric acute ischemic injuries. Angiography detected vessel wall narrowing in both middle cerebral arteries. Lumbar puncture was anodyne. She was first diagnosed of isolated Central Nervous System vasculitis and clophosphamide was started. After clinical improvement weeks after, a new angiography was realized with a complete resolution of observed abnormalities.
A healthy 37 year-old woman presents with a two hour history of hypoesthesia on right upper limb, severe headache and hypertension. She had given birth three weeks before. MRI showed left postrolandic infarction and angiography detected mild left vertebral artery stenosis and severe left internal carotid artery stenosis with possible associated dissection that was treated with angioplasty. During hospitalization she had two self-limited episodes of aphasia, so anticoagulation was started. She completely recovered and an angioMRI three months after showed a complete resolution of intracranial abnormalities.
Conclusion
PRCVS is an entity to consider in woman with recent delivery and severe headache that can associate neurological deficits. Patients can develop several neurological complications as ischaemic and haemorrahagic stroke. Differential diagnosis is wide and has to include CNS vasculitis. An early intra and extracraneal study is recommended.
Trial registration number
N/A
AS26-020
GENDER DIFFERENCES IN EFFECT ON PATIENTS WITH ACUTE ISCHEMIC STROKE FOLLOWING THROMBOLYSIS: A 11-YEAR COHORT STUDY IN NORTHERN TAIWAN
1MacKay Memorial Hospital, Neurology, Taipei, Taiwan R.O.C
Background and Aims
Intravenous (IV) recombinant tissue plasminogen activator (rt-PA) has become the standard care in selected patients with acute ischemic stroke (AIS). Stroke women without treatment of thrombolysis have a worse clinical outcome than men, but given thrombolysis, their outcome is similar or better compared with men. The main objective is to determine whether there is a gender difference in clinical outcomes among Asian AIS patients following thrombolysis.
Method
We conducted a retrospective cohort analysis of 345 AIS patients treated with IV rt-PA within 3 hours from stroke onset in a medical center in Northern Taiwan. The baseline characteristics, clinical features, baseline National Institute of Health Stroke Scale score , radiological and laboratory data, onset to needle time, stroke mechanism and outcomes were compared between the sexes.
Results
From July 2005 to December 2016, 63 men (31.0%) and 36 women (25.3%) had an excellent functional outcome, defined as modified Rankin Scale score of 0–1 at 90-days after thrombolysis. There are no gender differences in both crude (p = 0.252) and adjusted odds ratio (p = 0.965) of the excellent functional outcome after adjusting for age, glucose, hypertension, atrial fibrillation, stroke subtypes, dyslipidemia, baseline NIHSS score, and time from symptom onset to thrombolysis. Noticeably, women waited significantly longer than men from hospital arrival to thrombolysis (p = 0.01).
Conclusion
The usual “poorer” outcome of untreated stroke women is nullified after thrombolysis resulting in the similar outcome between treated men and women. This finding may suggest that the greater benefit for stroke women from thrombolysis than men
Trial registration number
N/A
AS26-021
DO WOMEN SUFFER MORE FROM STROKE?
1Clinical Center of Serbia, Emergency Neurology, Belgrade, Serbia
2Medical Faculty, University of Belgrade, Belgrade, Serbia
Background and Aims
Previous research suggests that sex differences exist in the epidemiology, etiology and outcome from acute ischaemic stroke (AIS). We tried to determine the association of gender on stroke severity, risk factors, in hospital mortality and early outcome after AIS.
Method
We retrospectively analyzed patients with AIS who were hospitalized at the Department of Emergency Neurology, in the period from January 1, 2016, to Decembar 31,2016. Comparison was made according to gender and age, stroke severity, measured by National Institutes of Health Stroke Scale (NIHSS) scores, etiology of disease according to TOAST classification and functional outcome at discharge, measured by the modified Rankin Scale (mRS). Good and poor outcomes were defined as mRS ≦2 and mRS>2.
Results
A total of 226 patients (139 men and 87 women) were included in the analysis. Women were older (mean age 67,5 vs 59,5, p < 0,001), had more offten atrial fibrilation (40% vs 23%, p < 0,001) and more comorbidites (p = 0,041) than man. Women had greater stroke severity (mean NIHSS 7,65 vs 5,23 p = 0,026), and poorer functional outcomes (mRS>2) at discharge (p < 0,001). Multiple regression analysis revealed that female sex and stroke severity were associated with the poorer outcome after stroke. The in-hospital mortality rate was not significantly different between women and men.
Conclusion
Women were on average older, had more comorbidity than men, and more often had cardioembolic stroke, which could explain a worse outcome. However, after adjustment for age, comorbidities, and stroke severity femaile sex still remain indipendent risk factor for poor outcome after stroke.
Trial registration number
N/A
AS26-025
FREQUENCY OF DIFFERENT TYPES OF STROKE IN PREGNANCY AND PUERPERIUM: CASE STUDIES FROM MOSCOW HOSPITALS IN 2017
1Pirogov Russian National Research Medical University, Neurology- Neurosurgery and Medical Genetics, Moscow, Russia
2Pirogov Russian National Research Medical University, Research Institute of Cerebrovascular Pathology and Stroke, Moscow, Russia
3Perinatal Medical Center, Department of miscarriage, Moscow, Russia
4Perinatal Medical Center, Radiology, Moscow, Russia
5Yudina Moscow city hospital, Neurology, Moscow, Russia
6Vorohobov city hospital 67, Regional Vascular Center, Moscow, Russia
Background and Aims
Pregnancy and puerperium period are associated with an increased risk of stroke. Due to the various possible causes of cerebrovascular complications in women during pregnancy their diagnostic become challenging problem for neurologists and obstetricians. In this study we evaluated frequency, risk factors and causes of pregnancy-related strokes in 3 obstetric hospitals in Moscow in 2017.
Method
Prospective analysis (etiology, risk factors, treatment and outcome) of ischemic and hemorrhagic stroke, TIA, cerebral venous thrombosis (CVT) cases in women during pregnancy and postpartum period in 3 Moscow obstetric hospitals in 2017 was conducted.
Results
The frequency of ischemic stroke was 2 per 16177 deliveries: 1 case in patient with sever preeclampsia with PRES and 1 due to amniotic fluid embolism. For hemorrhagic stroke – 1 patient with AVM per 16177. For CVT – 2 per 16177 (both had hereditary thrombophilia and onset in first trimester of pregnancy). Evaluation of TIA was carried out only in one hospital and observed in 3 patients with different risk factors for young stroke per 2715. More detailed data is shown in the picture below.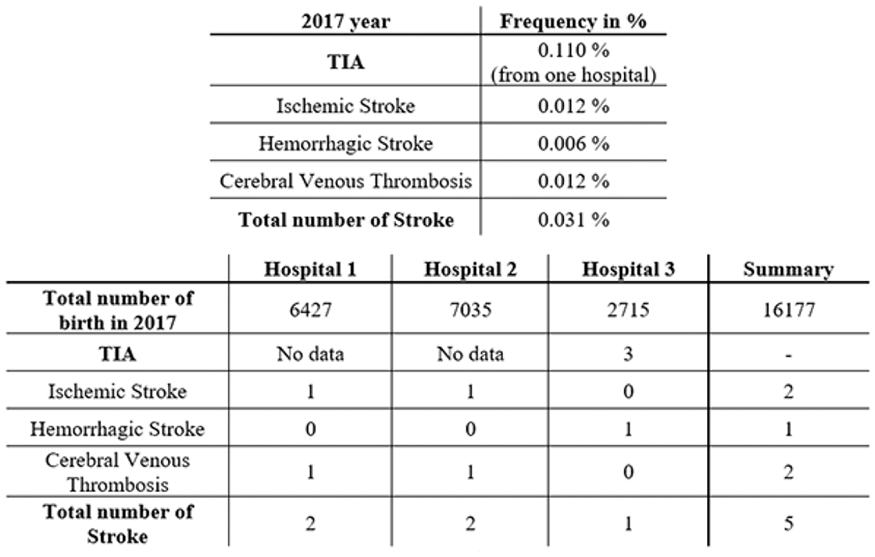
Conclusion
Observed cases of ischemic stroke were associated with pregnancy related complications, while TIA, hemorrhage and CVT were associated hematological disorders and vascular abnormalities.
Trial registration number
N/A
YOUNG STROKE PHYSICIANS AND RESEARCHERS: RESEARCH DESIGN WORKSHOP FOR STUDIES IN DEVELOPMENT
AS27-001
A MIXED METHODS STUDY TO IMPROVE JOINT DECISION-MAKING WITH PATIENTS AND FAMILIES ON TREATMENTS AFTER SEVERE STROKE
1University of Edinburgh, Centre for Clinical Brain Sciences, EDINBURGH, United Kingdom
2University of Edinburgh, Usher Institute of Health and Population Sciences, Edinburgh, United Kingdom
Background and Aims
Many people who are well think survival with severe disability is unacceptable. However, many stroke treatments increase the chance of surviving with severe disability. Therefore, informed decisions about the use of these treatments is necessary.
We aim to develop a tool to facilitate the process of joint decision-making with patients and families.
Method
A mixed methods study:
(1) To validate prediction models in severe stroke: prospective cohort study of around 400 consecutive admissions with severe stroke with follow up to specific complications and treatments at 1 week and outcomes (disability or death) at 6months
(2) To elicit goals and expectations from treatment, and stability of decisions over time: qualitative study of around 50 participants with follow up at a week and 6 months. Feedback is also obtained on potential tools to aid decision-making.
Results
(1) Recruitment into the longitudinal cohort is ongoing.
(2) Family interviews (n = 24) have identified that decision-making about treatments after stroke requires a period of observation, support from friends and relatives, discussion regarding preferences and wishes and information from clinicians. Majority report that the patient would find survival with severe disability unacceptable. Different individuals wished information in different formats; either verbal, written, audio or visual aids. Most relatives found that viewing brain scans helped their understanding of the situation.
Conclusion
Relatives felt that patients would not value survival with severe disability. Decision-making happened over several days. Information needs to be available in different formats. Ongoing interviews with patients, rather than families, will provide insight into their views and goals.
Trial registration number
N/A
AS27-002
FACTORS ASSOCIATED WITH THE DEVELOPMENT OF POST-STROKE FATIGUE, ANXIETY, DEPRESSION AND SLEEP DISORDERS IN THE PERIODS OF ACUTE STROKE AND SIX MONTHS POST-STROKE
1Clinical Hospital Dubrava, Department of Neurology, Zagreb, Croatia
Background and Aims
Neuropsychological and mood disorders including fatigue, anxiety, depression and sleep disturbances are frequent symptoms encountered after stroke. Despite their affect on recovery and outcome, they often overlooked and not properly assessed. The aim of this study is to evaluate the association between the type of stroke, etiology, neuroradiological characteristics, localization of the stroke and patient comorbidity, with the prevalence of fatigue, anxiety, depression and sleep disorders during the acute stroke period (at the time of hospital discharge) and at the six-month follow-up period.
Method
Patients aged 18 years and older, who have suffered an acute stroke, will be included in the study. Exclusion criteria will be severe aphasia (assessed using an aphasia screening test), severe cognitive impairment (MMSE<20), subarachnoid hemorrhage (SAH), transient ischemic attack (TIA), a prior history of anxiety and depression, psychosis, terminal illness and thyroid disorders. All patients will have a CT or MRI. In order to assess stroke severity, the National Institute of Health Stroke Scale (NIHSS) will be used upon admission and a Modified Rankin Scale (mRS) upon hospital discharge. Each enrolled participant will be assessed using the following rating scales upon discharge and at the six month follow-up period:Fatigue Severitiy Scale-9 (FSS-9), Modified Fatigue Severity Scale (MFIS), Montgomery and Asberg Depression Rating Scale (MADRS), Hamilton Depression Scale HAM-D), Hospital Anxiety and Depression Scale (HADS), Beck Depression Inventory (BDI) and the Epworth Sleepiness Scale (ESS). Rating scales will also be obtained from age-matched healthy control subjects.
Results
Results are expected to identify the prevalence and risk factors for neuropsychological disorders post-stroke.
Conclusion
Identifying predictive factors for neuropsychological and mood disturbances after a stroke could lead to early intervention in patients at high risk.
Trial registration number
N/A
AS27-003
SERUM BIOMARKERS OF BLOOD BRAIN BARRIER INTEGRITY TO PREDICT HEMORRHAGIC TRANSFORMATION OF ISCHEMIC STROKE: A PROSPECTIVE STUDY
1Nicolae Testemitanu State University of Medicine and Pharmacy, Neurology Department nr.1, Chisinau, Moldova
Background and Aims
Hemorrhagic transformation (HT) of ischemic stroke is associated with low outcome and higher disability/mortality rate. Actual predictive tools are mostly based on clinical and imaging data. Serum biomarkers are an attractive, still underused domain in cerebro-vascular diseases management.
The aim of our research is to determine the correlation between the serum level of blood brain barrier (BBB) integrity biomarkers and the risk for hemorrhagic transformation in acute ischemic stroke.
Method
The planned trial will be a prospective cohort study with 2 research groups, each including 55 patients with acute ischemic stroke (adult patients admitted within 24h from firsts symptoms): L1 – working group – with hemorrhagic transformation, L0 – control group, without hemorrhagic complication.
Results
The eligible patients, according inclusion criteria, will be clinically assessed by NIHSS scale and perform a native cerebral CT scan at admission. For identification of L1 group patients, a repeated scan will be done at 72h from admission and/or in case of clinical worsening and at discharge. Matrix metallo-proteinases 2 and 9 (MMP-2, MMP-9) serum levels will be established in all patients selected in the trial within 24h from admission as biomarkers of BBB integrity and predictive markers of HT. Disability and mortality rates will be calculated at discharge and 3 months’ follow-up.
Conclusion
We expect to confirm the correlation between the serum levels of MMP-2 and MMP-9 and the risk for HT, the disability and mortality rate in acute ischemic stroke patients. Our results could improve acute stroke management in our country, regarding selection of patients for thrombolysis.
Trial registration number
N/A
AS27-004
CARDIAC ARRHYTHMIAS AND IN-HOSPITAL MORTALITY IN 63 CASES OF ISCHEMIC STROKE INVOLVING THE INSULA
1National Institute of Neurology and Neurovascular Diseases, Stroke Unit Department, Bucharest, Romania
2Faculty of General Medicine- “Carol Davila” University of Medicine and Pharmacy, Neurology Department, Bucharest, Romania
3Faculty of General Medicine- “Carol Davila” University of Medicine and Pharmacy, Medical Semiology Department, Bucharest, Romania
4University Emergency Hospital, Nephrology Clinic, Bucharest, Romania
5National Institute of Neurology and Neurovascular Diseases, Neurology Department, Bucharest, Romania
Background and Aims
There is not universal agreement in the published studies whether insular involvement in acute ischemic stroke is associated with higher mortality mediated by severe arrhythmias. We explored the putative association between insular involvement in ischemic stroke and electrocardiographic (ECG) abnormalities and in-hospital mortality.
Method
Prospective study on 110 patients admitted to stroke unit with acute (<24 hours from onset) ischemic stroke with no history of arrhythmias, including atrial fibrillation (AF), or severe heart failure. We analyzed the data provided by up to 5 days continuous ECG monitoring. TOAST criteria were used for the etiologic classification of ischemic stroke.
Results
Insular lesions were detected in 63 (57.27%) patients. New AF was present in 35 (31.81%) patients. Significantly more ventricular premature contractions (VPC) in couplets (P 0.045) and bigeminism (p 0.049) were detected in patients with cardioembolic stroke. AF detection was not statistically significantly associated with insular infarction. ST depression was correlated with insular lateralization, being greater for patients with left insular injury (p 0.02). There was no relationship between insular lesion and other types of significant arrhythmias. The 12.72% in-hospital mortality had a tendency to be correlated with the number of VPC runs, but this association failed to reach statistical significance (p = 0.08).
Conclusion
These findings support only the relationship between ST depresion and insular lesion. Insular involvement was not a risk factor for death, nor were insula lateralization or AF. AF was most probably the cause of cardioembolic stroke and not the consequence of stroke-induced insular lesions.
Trial registration number
83
AS27-007
EFFECT OF REMOTE ISCHEMIC POSTCONDITIONING AFTER MIDDLE CEREBRAL ARTERY OCLUSION ON PROTEIN EXPRESSION
1Institut de Recerca Biomèdica de Lleida, Clinical Neurosciences Group, Lleida, Spain
2Hospital Arnau de Vilanova de Lleida: Stroke Unit, Institut de Recerca Biomèdica de Lleida: Clinical Neurosciences Group, Lleida, Spain
Background and Aims
Remote Ischemic PostConditioning (RIPostC) emerges as a possible estrategy to mitigate post-reperfusion damage in cerebral ischemia. We developed a mouse model of RIPostC after cerebral ischemia and we identify changes in protein expression related to infarction reduction.
Method
CD1 mice between 2–3 months old were divided into two groups. Group 1 (n = 4) underwent 60’ occlusion of the middle cerebral artery. Group 2 (n = 4) underwent the same procedure of cerebral ischemia followed by RIPostC (3 cycles of 10’ of femoral artery ischemia and 5' of reperfusion). All the animals were sacrificed at 48h. The brain was stained with 2% triphenyltetrazoliumchloride (TTC) to calculate the infarcted area using the Image J software. The volume was calculated by adding the 1mm sections and was expresed as the percentage of corrected infarct volume. We performed an array of antibodies using plasma samples obtained at 6 hours postischemia to identify biomarkers related to the RIPostC phenomenon.
Results
A significant decrease in the corrected infarct volume was observed in those animals submitted to the RIPostC compared to those animals only submited to cerebral ischemia (8.47% vs. 17.98%, p = 0.0047). In addition, the expression of two proteins was significantly different between the two groups (p <0.05).
Conclusion
The proposed RIPostC model after occlusion of the middle cerebral artery is valid to study the RIPostC phenomenon. Two proteic biomarkers that measure the response to RIPostC have been identified. This model opens a new field to investigate new therapies focused in IS acute phase.
Trial registration number
N/A
AS27-008
DESIGNED TO SENSE AND MOVE. PRODUCT DESIGN AS A GAME-CHANGER IN THE DEVELOPMENT OF SYSTEMS FOR SENSORIMOTOR REHABILITATION AFTER STROKE
1Università Iuav di Venezia, Design and Planning in Complex Environments - Design Sciences, Venezia, Italy
Background and Aims
Design affects the way we experience the world every day: from the handle of a door to the interface of a smartphone, we experience a designed world in all our actions. The application of design thinking to rehabilitation aims to investigate the possibilities of development of an user-friendly environment, in which the users are both the patient and the therapists, to create a system that enhances the rehabilitative experience through the use of gamification strategies, driving the patient into a state of flow and engagement that results into an optimization of the rehabilitative experience.
Method
The research has been conducted as part of a doctorate in Design Sciences, optimized with the interdisciplinary investigation through robotics and neurosciences, with the support of tools from the Design Research Methodology (DRM) for the literature studies and from ethnographic approaches (e.g. on-field observation in a Stroke Unit and interviews). Quick-sketching and rapid prototyping have been instruments for the design and the investigation of the concept development.
Results
The result is the design of a concept for a system to be used for sensorimotor rehabilitation of the lower limbs in bedridden patients, integrating teachings on rehabilitative procedures, haptic stimulation and physical interaction with virtual gaming dynamics to improve the patient’s involvement with the rehabilitation.
Conclusion
As external figures with technical and humanistic background, designers can become a connector between the physician, the patient and the engineers in order to develop systems that integrates advanced technologies into the rehabilitative therapy to make it a more effective and pleasant experience.
Trial registration number
N/A
AS27-009
ANTICIPATING INTRACRANIAL HYPERTENSION BEFORE IT CAN HARM: OPTIC NERVE SONOGRAPHY TO MONITOR INTRACRANIAL PRESSURE AFTER STROKE
1University Hospital Zurich and University of Zurich- Switzerland, Neurology, Zurich, Switzerland
Background and Aims
Intracranial hypertension (IH) is a dangerous complication of large vessel ischemic or hemorrhagic stroke. Since invasive intracranial pressure (ICP) monitoring devices are not always feasible, patients are usually followed based on clinical symptoms. However, medications or comorbidities of stroke complicate clinical IH assessment.
Method
The goal of this study is to implement optic nerve sonography (ONS) as an easy, non-invasive method to monitor ICP after stroke. We will derive ICP from sonographic measurement of the optic nerve sheath diameter (ONSD). ONS has been used for ICP estimations in neurological conditions such as head trauma and benign intracranial hypertension. Own preliminary data show that ONSD is indeed increased ipsilateral to stroke.
Results
We are planning a single-center, prospective study, where ONSD will be repeatedly assessed in patients with large vessel ischemic or hemorrhagic stroke up to 120 hours after stroke onset. GCS and NIHSS are obtained every 6 hours in clinical routine, and will be used along with neuroimaging (CT/MRI) to confirm IH. The presence of IH will be defined as midline shift ≥ 3mm or GCS decrease > 2 points without any other cause based on clinical judgement. Cut-off values for ONSD that best predict the presence of IH will then be determined by a receiver operating characteristic (ROC) curve. Sensitivity, specificity and positive predictive value of this threshold to predict IH will be calculated.
Conclusion
In future studies, ONSD could be tested as a parameter to aid in decisions for surgical interventions aimed to release ICP in stroke patients.
Trial registration number
N/A
AS27-010
CHANGE IN INCIDENS OF VENOUS SINUS THROMBOSIS FROM YOUNG WOMEN TO ELDERLY MEN
1Aarhus University- Denmark, Neurological department, Aarhus C, Denmark
Background and Aims
Cerebral venous thrombosis (CVT) is an uncommon form of stroke with a variable presentation. We examined trends in the diagnosis from 2005–07 and 2016 at our center.
Method
Patient data from Department of Neurology, Aarhus University Hospital, Aarhus, Denmark, was extracted from the electronic patient file. The two time periods were compared.
Results
Eight patients from 2005–07 and 15 from 2016 were found. Median age increased from 31 to 61 years, respectively (p = 0.02). In the early years all were women, and 7/8 were caused by oral contraceptive therapy (OCT). In 2016, 10/15 had unknown etiology, 8/15 were women (p = 0.06 for difference in sex). Seizures were more frequent among younger patients. Time from symptoms onset to admission decreased significantly from 27 to 3 days (p = 0.02). Times from admission to diagnose were decreased from 1.5 to 1 day, which was non-significant.
Discussion
An increased number of patients were hospitalized in 2016 compared to 2005–07. Patients from 2016 were averagely 30 years older than in 2005–07. Significantly fewer patients had oral OCT and significantly more had unknown etiology in 2016. Days from symptomes until admission were significantly decreased in 2016 compared to 2005–07, but the change in time from admission to diagnose was non-significant. In general, younger patients had more frequent seizures than older patients
Conclusion
More elderly men with unknown etiology were diagnosed with CVT in the later time period. In general, younger patients had more frequent seizures than older patients.
Trial registration number
N/A
AS27-011
MEETING THE NEEDS OF THE MILD STROKE POPULATION THROUGH TARGETED INTERVENTIONS – A PILOT STUDY
1School of Health and Rehabilitation Sciences, Health and Behavioural Sciences Faculty, St Lucia, Australia
2Griffith University, School of Allied Health Sciences, Mt Gravatt, Australia
3University of Queensland, School of Health and Rehabilitation Sciences, St Lucia, Australia
Background and Aims
People with mild stroke are frequently able to mobilise, communicate, and complete activities of daily living independently, leading to a quick discharge from hospital. A large proportion of this population, however, experience difficulties when re-engaging with more complex activities. As mild stroke occurrences increase, and the age continuum at which they occur broadens, meeting the needs of this population in the least resource intensive manner becomes difficult. It is suggested that two different styles of self-management services be trialled: (1) a health application that targets younger populations (<65) and (2) a telehealth service that targets older populations (>65). This project will aim to trial these services and determine their feasibility and acceptability for the suggested age categories, with a primary focus on return to occupations. Secondary objectives will look at the impact on community reintegration and quality of life.
Method
Mixed-methods pilot study involving 50 participants with mild stroke. Participants will be split into 5 groups of 10 participants: (1) <65 years receiving health application, (2) <65 years receiving telehealth services, (3) >65 years receiving health application, (4) >65 years receiving telehealth, and (5) standard care group. Quantitative measures will be used over the initial 6-months post-discharge to measure occupational gaps, quality of life, service satisfaction, and community reintegration. Qualitative interviews will aim to gain insight into patient experiences of the services and return to community living.
Results
The results of this study will contribute to the refinement of interventions, which will then be tested in a large Randomised Controlled Trial.
Conclusion
N/A
Trial registration number
N/A
AS27-012
THE EFFECTS OF SLEEP ON WALKING AND BALANCE IN PATIENTS WITH STROKE
1IZMIR KATIP CELEBI UNIVERSITY, Physiotherapy and Rehabilitation, IZMIR, Turkey
2Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Izmir, Turkey
Background and Aims
Learning during sleep is a complex procedure which is not completely understood. There is extensive evidence for positive effects of sleep on motor learning in young people; however, the effect of sleep on motor learning and neural plasticity is not well understood in patients with stroke. Previously, a number of studies have investigated the effects of sleep on motor learning and declared improvements. These studies mostly used tasks related to upper extremity functions and memory. To our best knowledge, neither research has studied the effects of sleep on lower extremity activities and balance. Therefore, we aim to investigate the effects of sleep on motor learning in lower extremity activities and balance performances.
Method
We plan to include patients with chronic stroke based on MRI scan. Participants will be able to walk 10 meters independently. After the selection of participants, they will be divided into two groups randomly. Both groups will receive game-based rehabilitation by use of Wii Fit. Control group will perform exercises early in the morning and will instruct to not sleep at least following 12 hours. Experimental group will do exercises late in the night and will be advised to sleep after they finish the exercises as soon as possible. Actigraphy will be used to monitor the participants. All participants will perform the exercises 3 times in a week for 8 weeks. Before and after the programme Berg Balance Scale (BBS) score, Timed Up and Go Test (TUG) scores, and fMRI scans of patients will be compared.
Results
N/A
Conclusion
N/A
Trial registration number
N/A
AS27-013
ATRIAL CARDIOPATHY MARKERS IN CRYPTOGENIC STROKE PATIENTS: A PROSPECTIVE STUDY
1University Hospital of Padua, Stroke Unit and Neurovascular Ultrasound Lab - Department of Neurosciences, Padova, Italy
Background
Patients with cryptogenic stroke (CS) still receive an untargeted secondary prevention treatment. There is increasing evidence that most CS are embolic and related to an atrial cardiopathy (AC), which might determine stroke through a disrythmic mechanism or less frequent mechanisms (myocyte/endothelial dysfunction, dilatation…). AC is still defined only through surrogate markers (ECG/echographic and biomarkers). Presently, the only opportunity to give the patient a targeted anticoagulant therapy is detecting atrial fibrillation (AF). The presence of microembolic signals (MES) at transcranial Doppler (TCD) is a reliable surrogate marker of higher risk of stroke recurrence.
Method
We will enroll all consecutive patients admitted to the Stroke Unit in a six-months period and diagnosed with CS. We will analyze biomarkers (NT-proBNP at admission), ECG markers (p-wave terminal force, paroxysmal supraventricular tachycardias, premature atrial contractions), echographic markers (left atrial size/volume). All patients will undergo a 60-minutes TCD monitoring for MES detection with bilateral insonation of middle cerebral artery within the first 24 hours from stroke onset, at 7 and 30 days. During a 3-years follow-up we will check for recurrent stroke, atrial fibrillation and death.
Results
N/A
Conclusion
N/A
Trial registration number
N/A
AS27-018
IMPROVED DETECTION OF ACUTE LACUNAR INFARCTS ON NON-CONTRAST CT USING A FREQUENCY-SELECTIVE NON-LINEAR BLENDING
1University Hospital- TU Dresden, Institute for Diagnostic and Interventional Neuroradiology, Dresden, Germany
2University Hospital- TU Dresden, Clinic and Polyclinic for Neurology, Dresden, Germany
Background and Aims
Acute lacunar infarcts (LI) are difficult to detect by computed tomography (CT) within the first hours of stroke onset. We hypothesize that non-contrast CT (NCCT) post-processing with frequency-selective non-linear blending (best contrast/BC) increases the accuracy in detecting acute LI.
Method
We retrospectively analysed NCCT scans and baseline data of 34 consecutive patients with acute thalamic LI which were not detected on initial NCCT but confirmed with subsequent diffusion-weighted magnetic resonance imaging (DW-MRI). We collected CT densities of LI using a coregistration algorithm to perform post-processing.
Unprocessed, window-optimized and BC-optimized NCCT of patients with LI and age-matched controls will be reviewed by three expert neuroradiologists in a blinded fashion. Accuracy, sensitivity, specificity and predictive values for detection of LI will be calculated using follow-up MRI serving as reference standard.
Results
On NCCT, Hounsfield Units (HU) of acute thalamic LI were significantly reduced compared to corresponding contralateral tissue (29.6 ± 3.1 HU vs. 33.3 ± 2.6 HU; p = 7.7E-09). Compared with acute infarcts, old LI had significantly reduced HU (16.6 ± 4,1 HU; p = 1.2E-09). Based on these results, optimized window level/width to detect acute LI on NCCT are 30/9 HU. Optimized BC parameters are a center/delta of 30/9 HU at a slope of 5. Blinded evaluation with these settings is planned.
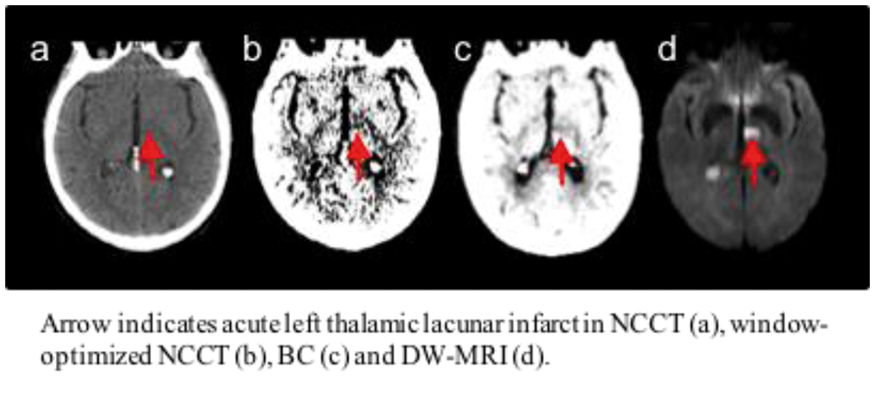
Conclusion
Our analysis will determine whether NCCT post-processing with frequency-selective non-linear blending (BC) can improve the accuracy in detecting acute LI.
Trial registration number
N/A
AS27-019
THROMBOLYSIS AND ENDOVASCULAR WORKFLOW NETWORK (TEFLON) TRIAL - A NOVEL SYSTEMS-BASED APPROACH TOWARDS REDUCING REPERFUSION TREATMENT DELAYS ACROSS TWO MAJOR COMPREHENSIVE STROKE CENTRES IN SYDNEY
1Liverpool Hospital, Department of Neurology & Neurophysiology, Sydney, Australia
2Hunter Medical Research Institute- John Hunter Hospital and School of Medicine & Public Health- The University of Newcastle, Priority Research Centre for Stroke & Brain Injury, Newcastle, Australia
3The Sydney Partnership for Health- Education- Research and Enterprise SPHERE, Mindgardens, Sydney, Australia
4Ingham Institute for Applied Medical Research, Stroke & Neurology Research Group, Sydney, Australia
5Western Sydney University WSU, South Western Sydney Clinical School- School of Medicine, Sydney, Australia
6University of New South Wales UNSW, South Western Sydney Clinical School, Sydney, Australia
7Liverpool Hospital, Department of Interventional Neuroradiology, Sydney, Australia
8University of New South Wales UNSW, Prince Of Wales Hospital Clinical School, Sydney, Australia
9Prince of Wales Hospital, Institute of Neurological Sciences, Sydney, Australia
10The Florey Institute of Neuroscience and Mental Health, Stroke Division, Melbourne, Australia
11St Vincent's Health, Nursing Research Institute, Sydney, Australia
12Australian Catholic University, School of Nursing, Sydney, Australia
13Liverpool Hospital, Department of Emergency Medicine, Sydney, Australia
14University of Sydney, Emergency Medicine- Central Clinical School, Sydney, Australia
15University of New South Wales UNSW, The Sydney Partnership for Health- Education- Research and Enterprise SPHERE, Sydney, Australia
16John Hunter Hospital, Department of Neurology, Newcastle, Australia
17Hunter Medical Research Institute HMRI and School of Medicine & Public Health- The University of Newcastle, Priority Research Centre for Stroke & Brain Injury PRCSBI, Newcastle, Australia
Background and Aims
Speedy delivery is a crucial factor in ensuring reperfusion therapy approaches deliver most benefit per unit cost. Systems based approaches in reducing the time to reperfusion are important in delivery of best patient outcomes and best value care. Using a combination of adaptive collaborative workflow embedded within a knowledge translation framework,
Method
We propose to conduct an implementation and knowledge transfer trial of a package intervention aiming to identify and address system of care gaps in acute stroke reperfusion treatment delivery across two Comprehensive Stroke Centres (CSCs) in Sydney, Liverpool and Prince of Wales Hospitals. Following a baseline phase, processes of care will be mapped and measured, clinicians and management stakeholders will be consulted and a new workflow model of care developed - the TEFLON system-based model. We will then conduct a preliminary pre- versus post- implementation controlled trial of the TEFLON model (Fig 1).
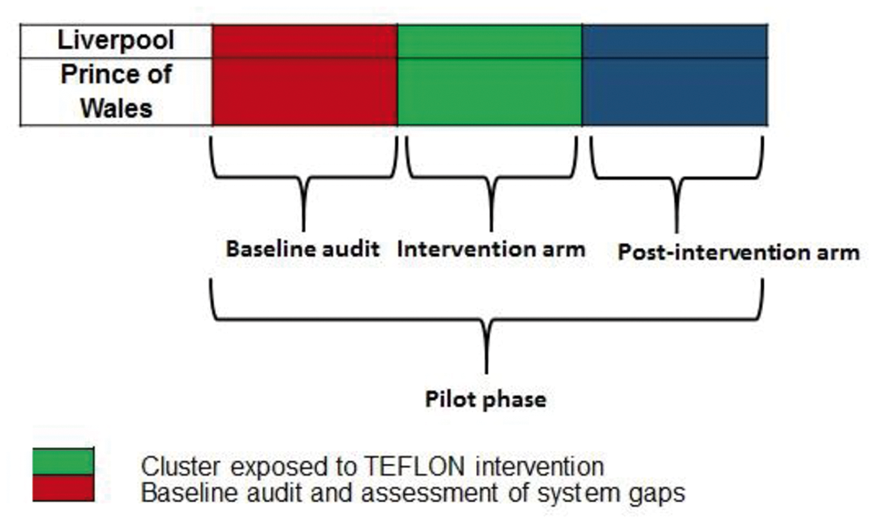
Results
The primary outcomes of this initial phase of TEFLON will be improvements in the process of care and in reducing treatment delays – specifically clinically meaningful reductions in door to needle or groin time (DNT/DGT) of 20 minutes.
Conclusion
If successful, this model will provide improved efficiency in the delivery of reperfusion therapy across two major hospitals in Sydney. This will provide a strong platform for city-wide (Sydney), state-wide (NSW), and potentially national rollout of a system-based reperfusion implementation plan (Fig 2).
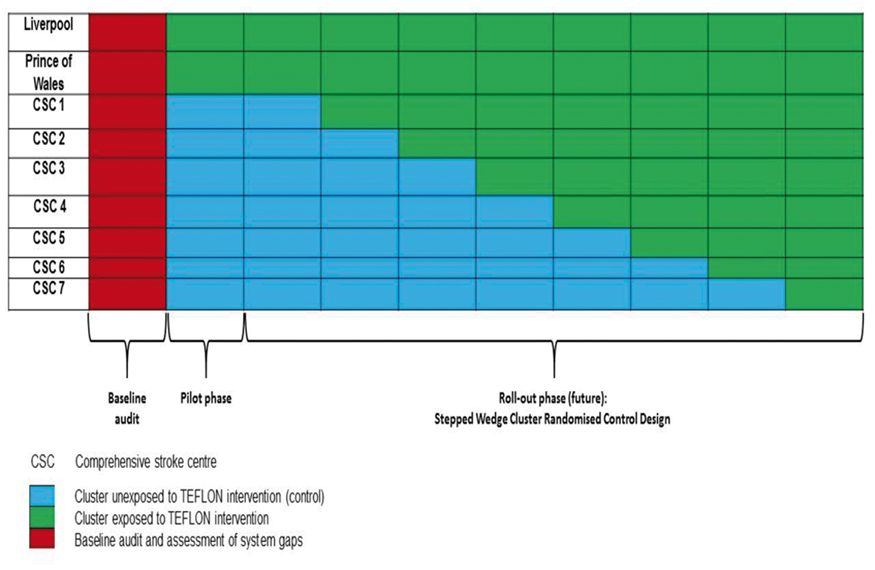
Trial registration number
N/A
AS27-020
LONG-TERM OBSERVATIONS AFTER TRANSIENT MIDDLE CEREBRAL ARTERY OCCLUSION (TMCAO) IN MICE
1University Hospital Frankfurt, Neurology, Frankfurt am Main, Germany
2Goethe University Frankfurt, Medicine, Frankfurt, Germany
3Institute for Stroke and Dementia Research Munich, Stroke Research, Munich, Germany
Background and Aims
The challenge of translating preclinical into clinical advances in stroke research is partly due to limitations of the established in-vivo models. TMCAO in mice models closely the I/R injury of patients with acute vessel stem occlusion and recanalization. Due to high mortality of this model long-term observations were hitherto impossible. A new care protocol comprising close clinical monitoring and individual care increases the survival rate > 70% and was used to get first representative insights into the dynamics of post-reperfusion inflammation and regeneration. Special focus was on the contribution of S1P as it is known to be a crucial regulator of barrier integrity and immune cell migration.
Method
C57Bl/6 mice underwent tMCAO vs. sham operation and were supported according to a recently established protocol. Brains were removed after 24 hours or 7 days respectively, separated into the ipsilateral and contralateral hemisphere and processed for microvessel and subsequent mRNA isolation for whole transcriptome mRNA-sequencing.
Results
After 24 hours, intracellular S1P production by SphK1 and secretion by Spns2 is highly upregulated while expression of S1P-Lyases is decreased, which normalizes during tissue remodeling. The overall dynamic changes from an inflammatory condition, dominated by IL1-beta and IL6 to a highly proliferating condition determined by massive increase of KI paralleled by upregulation of microglial and ECM markers.
Conclusion
Intense post-stroke care allows first representative insights into the long-term dynamics of cerebral I/R injury and indicative testing of future therapeutic strategies. In analogy to stroke-unit monitoring and support of patients, this approach contributes to successful translational stroke research.
Trial registration number
N/A
AS27-021
LATIN AMERICAN STROKE REGISTRY
1Instituto Nacional de Neurologia y Neurocirugia, Subdireccion de Neurologia, Mexico, Mexico
2Universidad de Costa Rica, Subdireccion de Neurologia, San Jose, Costa Rica
3Hospital de Clínicas. Facultad de Ciencias Médicas., Subdireccion de Neurologia, Asuncion, Paraguay
4Instituto Nacional de Ciencias Neurológicas, Subdireccion de Neurologia, Lima, Peru
5Hospital Juarez de Mexico, Subdireccion de Neurologia, Mexico, Mexico
6Hospital Universitario Fundación Santa Fe de Bogotá, Departamento de Neurología, Bogota, Colombia
7Hospital General de Mexico, Departamento de Neurologia, Mexico, Mexico
8Hospital General 450, Departamento de Neurologia, Durango, Mexico
9Hospital Fundación Valle del Lili, Subdireccion de Neurologia, Cali, Colombia
10Hospital Pablo Arturo Suarez, Dirección de Neurologia, Quito, Ecuador
11Hospital Civil del Guadalajara, Subdireccion de Neurologia, Guadalajara, Mexico
12Institute for Neurological Research- FLENI, Dirección de Neurologia, Buenos Aires, Argentina
13Hospital Regional del ISSSTE, Subdireccion de Neurologia, Morelia, Mexico
14Hospital Nacional Guillermo Almenara Irigoyen, Departamento de Neurologia, Lima, Peru
Background and Aims
Few centers in Latin America (LA) have established stroke registries. Our study collects data obtained from patients admitted with stroke in differents centers of LA. Using this data, we attempted to define the profile of risk factors and outcomes.
Method
The demographic data, stroke description, ancillary tests, vascular risk factors, and modified Rankin scale (mRs) were registered. Cerebral Infarction (CI) subtyping was based on the ASCOD phenotyping. Primary outcomes included mRs, recurrence and death at 3 months of follow-up.
Results
We included 2239 patients with a follow-up of 3 months. The mean age was 61 ± 17.5 years. There were 1210 males (53.4%) included in the study. CI was present in 81%, Transient ischemic attack (TIA) 3%, intracerebral hemorrhage (ICH) in 15.3% and cerebral venous thrombosis (CVT) in 0.7%. Hypertension was the major risk factor (64.7%) followed by diabetes (28.1%) When ASCOD phenotyping was applied, atherosclerosis was present in 25.2%, small-vessel disease in 6.5%, cardiac pathology in 21.5%, other causes in 8.3% and dissection in 0.9% as the main etiology. However, in 37.7% the etiology is unknow due to insufficient workup to rule out the disease. Overall, the mortality rate was 24.2%. The recurrence rate was 20%. Poor outcome (mRs>3) was found in 33.3% of patients.
Conclusion
The Latin American Stroke Registry is an effort to show the differences and similarities with other populations. Hypertension is the major risk factor. We found that the etiology in 37.7% of the IC is uncertain. The implementation of a systematized registry significantly improved our clinical practice.
Trial registration number
N/A
AS27-022
MANAGEMENT OF SYMPTOMATIC INTRALUMINAL THROMBUS OF THE INTERNAL CAROTID ARTERY
1University of Colorado, Neurology, Aurora, USA
2University of Colorado, Vascular Surgery, Aurora, USA
Background and Aims
Intraluminal thrombus of the internal carotid artery (IT-ICA) is an infrequent finding in acute ischemic stroke (AIS). Nonocclusive thrombi are often found incidentally on angiographic studies increasing the risk of recurrent AIS and Large Vessel Occlusion (LVO). We aimed to describe the variation in the treatment of IT-ICA and evaluate for differences in recurrent AIS and intracerebral hemorrhage (ICH)
Method
A database of 1485 consecutive computed tomography angiography, magnetic resonance angiogram, and digital subtraction angiography was created retrospectively between September 1, 2011, and December 1, 2016. Radiology reports were queried for keywords including intraluminal, floating, clot, or thrombus. We identified cases of intraluminal thrombus of the extracranial ICA in patients over the age of 18.
Results
Of 84 radiology reports with intraluminal thrombus, 37 patients (44%) had IT-ICA and AIS (mean age 59 years; interquartile range (IQR) 50–71). Median NIH Stroke Scale was 8 (IQR 3–14), 8 (21.6%) patients received IV-tPA alone, 10 (27%) had LVO and underwent mechanical thrombectomy. Severe ICA stenosis was observed in 17 (46%) patients, 11 (29.7%) had CEA and 3 (8%) ICA stenting. Medical management included single antiplatelet (31, 83.7%), dual antiplatelet (8, 21.6%) and anticoagulation (34, 92%). There was no statistically significant difference in the rate of ICH or recurrent AIS between the treatment groups.
Conclusion
Most patients with IT-ICA and AIS were treated with anticoagulation and antiplatelet therapy. More than 10% of patients had recurrent AIS, and 16% had complications of ICH. The best treatment strategy to prevent recurrent AIS and minimize hemorrhagic transformation remains unclear.
Trial registration number
N/A
EXPERIMENTAL/TRANSLATIONAL MEDICINE
AS28-001
IMPACT OF METABOLIC DISORDERS ON THE MICROHEMORRHAGE BURDEN IN THE MOUSE BRAIN
1University of Lille 2, U1171 Laborory of Pharmacology, Lille, France
Background and Aims
Diet-induced metabolic disorders represent a set of vascular risk factors, which are suspected to contribute to the progressive appearance of cognitive decline in humans. This link seems of particular importance when the disorders are present from middle age. We suggest that the weakened cerebral vasculature may be prone to rupture, thus leading to microbleeds that may have functional consequences.
Method
To challenge this hypothesis in a non-confounding context, mice free from brain disease were fed with normal diet (ND) or high-fat diet (HFD) for 12 months, and then injected with nanoparticles to induce a disseminated pattern of microbleeds, and challenged for motor and cognitive functions through a series of behavorial tests.
Results
Compared to ND mice, HFD mice presented an increased brain microhemorrhagic score (+45%). While the whole motor activity of ND mice was unchanged by the presence of microbleeds, the spontaneous activity of HFD mice with microbleeds was significantly reduced (-72%), when compared to non-lesioned mice. Among the lesioned mice, the HFD mice exhibited a 70% reduced spontaneous activity, and were unable to realize the cognitive tests. The visual recognition memory of ND mice was decreased by 74% compared to those without lesions.
Conclusion
We suggest that microbleeds are no more silent lesions for the normal brain function at middle age, and that diet-induced metabolic disorders may increase the severity of this microbleed-induced cognitive impairment.
Trial registration number
N/A
AS28-002
2-CL-MGV-1 REDUCES NEURONAL APOPTOSIS IN THE THALAMUS AND HIPPOCAMPUS AND AMELIORATES COGNITIVE DEFICITS AFTER CORTICAL INFARCT IN HYPERTENSIVE RATS
1The First Affiliated Hospital- Sun Yet-sen University, Department of Stroke and Neurology Center, Guangzhou, China
2Israel Institute of Technology, Department of Neuroscience, Haifa, Israel
Background and Aims
Cortical infarction causes neuronal apoptosis in the ipsilateral non-ischemic thalamus and hippocampus, which is potentially associated with post-stroke cognitive deficits (PSCD). We examined the effects of the novel TSPO ligand 2-Cl-MGV-1 on PSCD, mitochondrial apoptosis, and secondary damage in the thalamus and hippocampus after cortical infarction.
Method
114 hypertensive rats underwent successful distal middle cerebral artery occlusion (dMCAO, n = 76) or sham procedures (n = 38). 2-Cl-MGV-1 or DMSO as vehicle was administrated 2 hours after dMCAO and then for 6 or 13 days (n =19 per group). Cognition was tested using the Morris water maze. Secondary degeneration and mitochondrial apoptosis in the thalamus and hippocampus were assessed using Nissl staining, immunohistochemistry, terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL), JC-1 staining, and immunoblotting 7 and 14 days after dMCAO.
Results
Infarct volumes did not significantly differ between the vehicle and 2-Cl-MGV-1 groups. There were more neurons and fewer glia in the thalamus and hippocampus in the vehicle groups than in the sham-operated group 7 and 14 days post-dMCAO. 2-Cl-MGV-1 significantly ameliorated cognitive impairment, and decreased neuronal death and glial activation when compared to vehicle treatment (P<0.05). The collapse of mitochondrial transmembrane potential and cytoplasmic release of apoptosis-inducing factors and cytochrome c was prevented within the thalamus. Caspase cleavage and the numbers of TUNEL+ or Nissl atrophic cells were reduced. This was accompanied by upregualtion of Bcl-2 and downregualtion of Bax (P<0.05).
Conclusion
2-Cl-MGV-1 reduces neuronal apoptosis via mitochondrial-dependent pathways and attenuates secondary damage in the non-ischemic thalamus and hippocampus, potentially contributing to ameliorated PSCD.
Trial registration number
N/A
AS28-003
EFFECTS AND MECHANISM OF SDF-1Α/CXCR4 PATHWAY ON CEREBRAL NEUROGENESIS AND ANGIOGENESIS IN RECOVERY PHASE AFTER INTRACEREBRAL HEMORRHAGE IN RATS
1Sichuan University, the Stroke Clinical Research Unit- Department of Neurology- West China Hospital, Chengdu, China
Background and Aims
Central nervous system constitutively express SDF-1/CXCR4 which promotes the migration of neural precursor cells, proliferation, differentiation of neurons, and regulates neuronal loop formation. Following intracerebral hemorrhage (ICH), whether SDF-1α/CXCR4 regulates or participates in neurovascular regeneration is unclear, as are the pattern recognition receptors and signaling pathways involved.
Method
ICH was induced by injection of collagenase in Sprague-Dawley rats. Then the SDF-α/CXCR4 axis inhibitor AMD3100 were injected intraperitoneally every day in the following 14 days. Injection of saline were set as a control group. A sham group was treated with saline instead of collagenase and then with saline in the following 14 days. Observe all animal’s modified neurological severity scores (mNSS) at 1, 3, 7, 10, and 14 day after ICH. Expression of the following proteins was measured by western blot: SDF-1α, CXCR4, BDNF, VEGF, and p-ERK. The number of cells positive for 5-bromo-2-deoxyuridine or doublecortin was determined by immunohistochemistry.
Results
Levels of SDF-1α, CXCR4, BDNF, VEGF, and p-ERK were significantly higher 14 days after ICH than at baseline, as were the numbers of 5-bromo-2-deoxyuridine- or doublecortin-positive cells. Daily administration of AMD3100, which inhibited SDF-α/CXCR4 axis, reduced the recovery of neurological function. Administration of AMD3100 significantly reduced all ICH-induced increases of Brdu+/DCX+/CD31+ cells increases.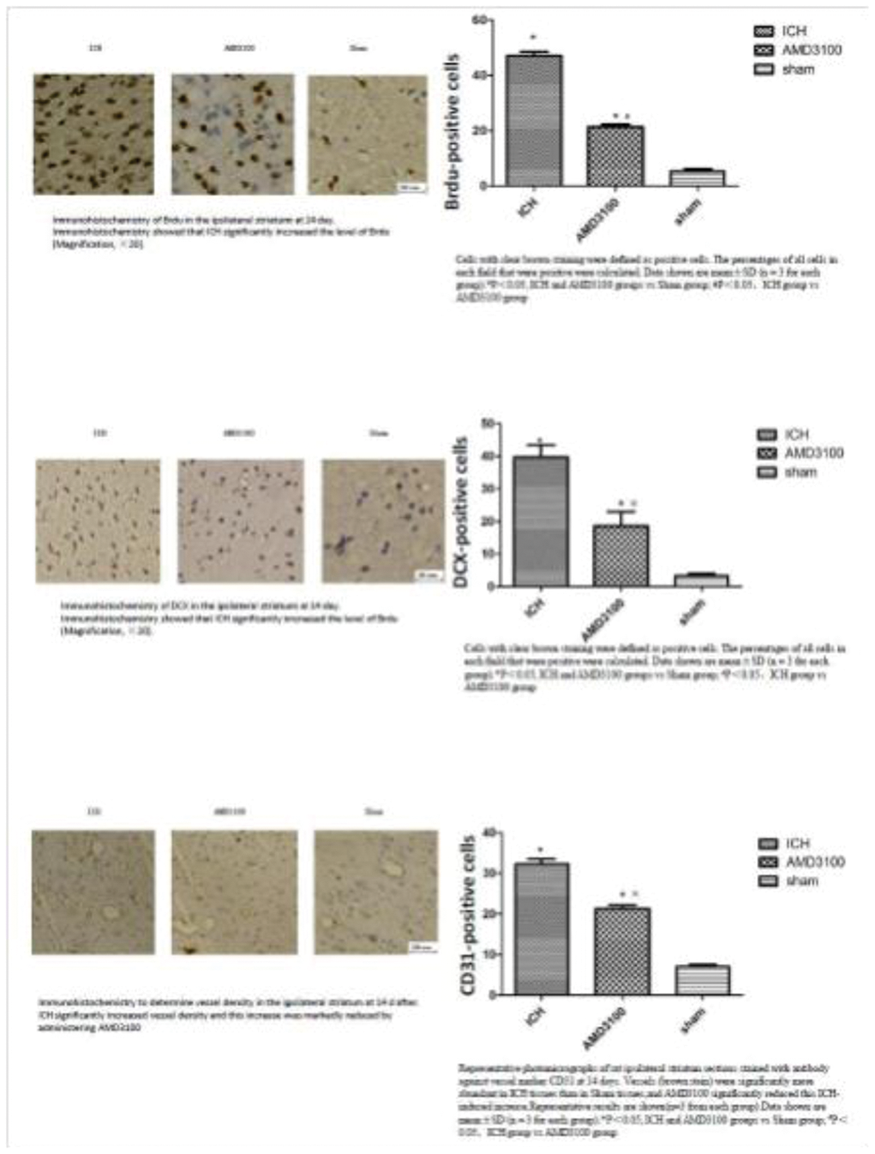
Conclusion
SDF-1α/CXCR4 upregulation accompanied VEGF, p-ERK, and BDNF increases around ICH lesions. Inhibition of the binding of SDF-1α and CXCR4 impede neurovascular regeneration, suggesting that SDF-1α /CXCR4 involved in neurovascular unit repair.
Trial registration number
N/A
AS28-004
LONG-TERM IMPAIRED PERFORMANCE ON THE OBJECT RETRIEVAL-DETOUR TASK OF EXECUTIVE FUNCTION IN A NONHUMAN PRIMATE MODEL OF STROKE
1the First Affiliated Hospital of Sun Yat–Sen University, Department of Neurology and Stroke Center, Guangzhou, China
Background and Aims
Post-stroke cognitive impairment occurs frequently in the patients with stroke, but the underlying mechanisms are not known. We aim to evaluate the executive function twelve months post stroke in a nonhuman primate model of stroke, whose brain is structurally and functionally similar to human.
Method
Eight adult male cynomologous monkeys (4-5 years old, 4.5–5.5 kg) were used in the study. Four of them received unilateral permanent middle cerebral artery occlusion distal to the M1 branch to induce focal cerebral ischemia, and the other four received sham operation. Cognitive function was evaluated using the object retrieval task with barrier-detour twelve months after the experimental stroke.
Results
In trials classified cognitively as easy, performance of the task was similar between the two groups. In trials classified cognitively as hard, when a reaching detour around the transparent barrier was necessary to retrieve the reward, the stroke group significantly increased barrier reaches, making 2.5 times as many barrier reaches as the control group (0.28 VS 0.11, P = 0.027). The stroke group also increased the reach number per trial (1.28 VS 1.11, P = 0.027), and made less successful responses per trial (0.76 VS 0.90, P = 0.033) compared with controls. No difference between the two groups was found in terms of perseverative responses and initiation time.
Conclusion
The performance on the object retrieval-detour task of executive function twelve months after unilateral permanent middle cerebral artery occlusion was impaired in nonhuman primate stroke model, which can serve as a translational model to study the underlying mechanisms of post-stroke cognitive impairment.
Trial registration number
N/A
AS28-005
A DOSE- RESPONSE STUDY TO IDENTIFY THE MINIMAL EFFECTIVE DOSE OF EXOSOMES THAT PROMOTE RECOVERY AFTER STROKE
1La Paz University Hospital- Neuroscience Area of IdiPAZ Health Research Institute- Autonomous University of Madrid, Neuroscience and Cerebrovascular Research Laboratory- Department of Neurology and Stroke Center, MADRID, Spain
Background and Aims
Exosomes have shown efficacy in functional recovery in stroke animal models.
To identify the minimal effective dose of exosomes to enhance brain repair and recovery after stroke in rats.
Method
Sprague-Dawley rats were subjected to subcortical stroke. 24hours after stroke, exosomes were administrated. Groups:Sham; Control:stroke+saline; stroke+low dose (50µg exosomes); stroke+intermediate dose (100µg exosomes); stroke+high dose (200µg exosomes). We evaluated: motor function at 24hours, 7 and 28days, lesion volume and tract connectivity by MRI at 24hours and 28days, cell death by TUNEL and brain repair markers:GFAP(Glial Fibrillary Acidic Protein), MOG(Myelin Oligodendrocyte Glycoprotein), MBP(Myelin Basic Protein), BDNF(Brain Derived Neurotrophic Factor), Syp (Synaptophysin), Olig-2(Oligodendrocyte) by immunofluorescence at 28days.
Results
All exosomes doses showed an improvement in functional evaluation compared to control (p < 0.05). Between treatments, high doses of exosomes demonstrates better recovery than low and intermediate doses at early times, but not at 28 days. We did not observe reduction of lesion size in treated compared to control groups, however, all doses showed the same significant increase in tract connectivity compared to control group at 28 days (p < 0.01). Cell death was decreased in all doses compared to control group (p < 0.01). All doses decreased GFAP expression and increased MOG, MBP and Syp expression compared to control group (p < 0.05).BDNF and Olig-2 expression was higher in low doses compare to intermediate and high doses (p < 0.05).
Conclusion
50µg,100µg and 200µg of exosomes improves the functional recovery, tract connectivity and expression of brain repair markers. Low dose is as effective as intermediate and high doses.50µg of exosomes is the minimal effective dose to enhance brain repair and recovery in stroke.
Trial registration number
N/A
AS28-006
MODULATION OF GUT MICROBIOTA IMPROVES OUTCOMES AFTER STROKE BY REDUCING LIPOPOLYSACCHARIDE-INCUCED INFLAMMATION IN THE ISCHEMIC BRAIN IN DIABETIC MICE
1Juntendo University School of Medicine, Neurology, 2-1-1 Hongo Bunkyo-ku, Japan
2Juntendo University Urayasu Hospital, Neurology, Chiba, Japan
3Juntendo University Graduate School of Medicine, Probiotics Research Laboratory, Tokyo, Japan
Background and Aims
Gut dysbiosis, an imbalance of gut microbiota, is associated with host inflammation due to the translocation of Gram-negative bacteria-derived lipopolysaccharide (LPS) molecules resulting from an increased gut permeability. Inflammation plays a key role in the pathophysiology of ischemic stroke. Here we investigated the effect of gut dysbiosis on acute ischemic brain injury.
Method
Fecal bacteria was analyzed via 16S and 23S rRNA-targeted quantitative reverse transcription-polymerase chain reaction in type 2 diabetic mice (db/db) following focal cerebral ischemia in the presence or absence of oral antibiotic pre-treatment.
Results
Oral administration of the non-absorbable antibiotic polymyxin B selectively attenuated fecal bacterial count of the Gram-negative bacteria Enterobacteriaceae, and reduced plasma LPS levels and gut permeability without changing plasma glucose levels in db/db mice. In addition, antibiotic pre-treatment significantly reduced infarct size, blood-brain barrier leakage, and inflammatory reactions in the brain, and improved neurological function, and survival rates following cerebral ischemia. These results were associated with a reduction in LPS, Toll-like receptor 4 (an LPS receptor), and inflammatory cytokine levels in the ischemic brain.
Conclusion
The findings suggest that LPS-induced inflammation may be a mechanism that links gut dysbiosis to ischemic cerebral injury, and that modulation of gut microbiota may be a potential therapeutic strategy to improve stroke outcome.
Trial registration number
N/A
AS28-007
APOA1-MILANO REDUCES THE INFARCT VOLUME IN A RAT MODEL OF ISCHEMIC STROKE
1INSERM U698, Neurology, PARIS, France
2Inserm U1148, Neurology, Paris, France
3Bichat hospital, Department of neurology and stroke center, Paris, France
Background and Aims
Previous animal experiments have shown that the injection of human high-density lipoprotein (HDL) in a rat model of acute ischemic stroke reduced the final infarct volume as well as hemorrhagic transformations (HTs). However, several liters of human blood would be necessary in order to obtain a sufficient dose of purified HDLs for a single patient. Using a similar methodology, we aimed at testing whether ApoA1-Milano, a recombinant mutant human apoA1, easy to produce in large quantities, would lead to similar effects.
Method
The first experiment evaluated the effects of ApoA1-Milano on the infarct volume, when injected immediately or 4 hours after monofilament occlusion of the middle cerebral artery (MCAO). A second experiment evaluated the volume of HT after co-administration of tissue plasminogen activator (tPA) and ApoA1-Milano. The final infarct and HT volumes were assessed.
Results
The injection of ApoA1-Milano performed immediately or 4 hours after MCAO significantly reduced the infarct volume compared with control saline solution (33.9[25.7–40.1] versus 43.6[37.4–48.7] [p = 0.03] [Figure 1A] and 37.5[29.3–45.9] versus 48.5[44.0–55.1] [p = 0.03] [Figure 1B], respectively). Compared with tPA, simultaneous injection of ApoA1-Milano and tPA showed similar HT volume (20.1[8.8–25.7] versus 14.3[7.9–23.5];p = 0.61).
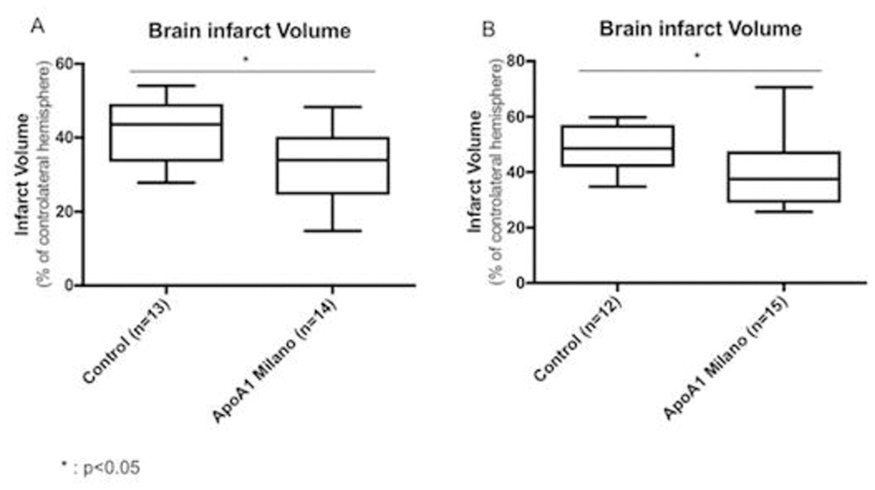
Conclusion
Administration of ApoA1-Milano was associated with a reduced infarct volume, suggesting a possible neuroprotective effect of ApoA1-Milano similar to that observed with human HDL in previous experiments.
Trial registration number
n/a
AS28-008
VASCULAR COGNITIVE IMPAIRMENT IN EXPERIMENTAL HYPERTENSION: THE MICROGLIAL CULPRIT
1Maastricht University, CARIM - School for cardiovascular diseases, Maastricht, The Netherlands
2Maastricht University, MH&NS – School for Mental Health and Neuroscience, Maastricht, The Netherlands
Background and Aims
Hypertension is a major risk factor for cerebral small vessel disease, which is the most prevalent cause of vascular cognitive impairment. Microglial activation, myelin loss, and short-term memory impairment have shown to be present in Angiotensin II (AngII) induced hypertensive mice. In this study, we aim to decipher the contribution of microglia to vascular cognitive impairment in AngII induced hypertensive mice via depletion of microglia.
Method
Cx3Cr1GFP/WTxThy1YFP/0 reporter mice were generated to visualize microglia and neurons. Mice were infused for 12 weeks with AngII or saline and treated with a highly selective CSF-1R inhibitor (PLX5622) to deplete microglia or vehicle. Systolic blood pressure (SBP) was measured via tail-cuff and carotid pulsatility by velocity doppler. Short- and long-term spatial memory was assessed during an Object Location and Morris Water Maze task
Results
SBP, heart weight and carotid pulsatility index were increased by AngII and were not affected by PLX5622. Short-term memory was significantly impaired in AngII infused mice treated with a vehicle. In contrary, the AngII infused mice with PLX5622 treatment showed no significant impairment in short-term memory. Histological analyses revealed a major decrease in density of Cx3Cr1+ cells after PLX5622 treatment (-99% in Saline groups; -92% in AngII groups; pPLX5622<0.0001). This was confirmed by flow cytometry showing a decreased count of CD45intCx3Cr1hiCD11bhi cells (-94% in Saline groups; -83% in AngII groups; pPLX5622<0.0001).
Conclusion
In AngII induced hypertensive mice, short-term memory impairment is absent when microglia are depleted. This supports the hypothesis that microglia are involved in the pathophysiology of hypertension related cognitive impairment.
Trial registration number
N/A
AS28-009
THE EFFECT OF GLIPTINS TO IMPROVE FUNCTIONAL OUTCOME AFTER STROKE IN MICE IS MEDIATED BY THE CXCR4/SDF-1ALPHA PATHWAY
1Karolinska Institut, Clinical Science and Education, Stockholm, Sweden
2PXBioVision GmbH, PXBioVision GmbH, Hannover, Germany
3University of Turin, Department of Drug Science and Technology, Turin, Italy
4Boehringer Ingelheim Pharma GmbH & Co. KG, 2Department of CardioMetabolic Diseases Research, Biberach, Germany
Background and Aims
Dipeptidyl peptidase-4 (DPP-4) inhibitors (gliptins) decrease hyperglycemia by inhibiting glucagon-like peptide-1 (GLP-1) cleavage. Gliptins can also improve stroke outcome in rodents independently of GLP1R. However, the underlying mechanisms are unknown. Stromal cell-derived factor-1a (SDF-1α) is a DPP-4 substrate and CXCR4 agonist that promotes beneficial effects in injured brains. However, SDF-1α involvement in gliptin-mediated neuroprotection is unproven. We aimed to determine whether gliptins improve stroke outcome via SDF-1α/CXCR4 and identify additional targets behind the efficacy.
Method
Adult, male C57bl6/j mice (n = 101) underwent transient focal cerebral ischemia. Linagliptin was administered for 3 days or 3 weeks. The CXCR4-antagonist AMD3100 was administered starting a day before ischemia. Stroke outcome was assessed by measuring upper-limb function and brain tissue damage. Active GLP-1, gastric inhibitory polypeptide (GIP) and SDF-1α were quantified by ELISA in serum and brain. Mass spectrometry was used to identify additional gliptin-mediated effectors in brain tissue samples.
Results
Sustained, post-ischemic treatment with linagliptin reduced motor impairment (p < 0.01) and tissue damage (p < 0.05). Linagliptin increased serum levels of GLP-1 (p < 0.0001), GIP (p < 0.05) and SDF-1α (p < 0.05). However, only SDF-1α levels were increased in the brain (p < 0.001). Linagliptin also decreased the presence of neurogranin-derived peptides and peptides from an isoform of myelin basic protein (MBG, p < 0.05). The inhibition of SDF-1α/CXCR4 pathway diminished the positive effects of linagliptin on stroke outcome (not different from vehicle).
Conclusion
We propose a gliptin-mediated neuroprotective mechanism via SDF-1α, which could affect Ca2+ homeostasis, altering neurogranin and MBG processing and potentially decreasing calpain activity. These results provide new insights into restorative gliptin-mediated effects against stroke.
Trial registration number
N/A
AS28-010
GROWTH HORMONE DEFICIENCY IS FREQUENT AFTER RECENT STROKE
1University of Newcastle, Medicine, Newcastle, Australia
2John Hunter Hospital, Neurology, Newcastle, Australia
3University of Newcastle, Hunter Medical Research Institute, Newcastle, Australia
4University of Gothenburg, Internal Medicine, Gothenburg, Sweden
5University of Melbourne, Medicine, Newcastle, Australia
Background and Aims
It has recently been recognised that traumatic brain injury can result in significant pituitary dysfunction. It is not yet known, however, whether a similar form of dysfunction occurs after stroke. Pituitary dysfunction after stroke would represent a novel area of research and available experimental evidence suggests that growth hormone has positive effects on neuronal regeneration and motor recovery.
Method
We performed an arginine human growth hormone (GH) stimulation challenge and a pituitary assay which included TSH, T3, T4, cortisol, luteinising hormone and testosterone on clinically and radiologically diagnosed ischemic stroke patients within a week of symptom inset. GH peak level/BMI was used to assess presence of deficiency.
Results
Thirteen stroke patients were successfully tested and included in this study. The median baseline NIHSS was 10 (range 7–16), median age 71 (range 54–78) and the median time since stroke was 7 days (range 4–10). Of the 13 patients, 7 (54%) had GH deficiency when the and two had a borderline response (mean abnormal GH peak 4.4). Six of eight men had low serum testosterone (mean low testosterone result 3.2nmol/L, normal rage 9–38nmol/L) and 1 of 5 females had low luteinising hormone (<0.2IU/L, normal range 5.2–62IU/L). Two patients had low IGF-1 concomitant with GH deficiency. Lastly, TSH, T3, T4 and cortisol were within normal reference ranges for all patients.
Conclusion
After major ischemic stroke, low GH levels are common. This has potentially important implications considering the experimental data suggesting benefits of GH for neuronal regeneration and functional recovery after stroke
Trial registration number
N/A
AS28-012
A NEW MODEL OF THROMBOEMBOLIC STROKE IN AWAKE MICE
1University of CAEN, UMR-S U1237 “Physiopathology and Imaging of Neurological Disorders” - PhIND - INSERM/EFS/Univ. Caen-Normandie Team “tPA and neurovascular disorders” Centre CYCERON, CAEN, France
Background and Aims
Stroke is a neurovascular disease killing 6 million people a year. The therapeutic care include pharmacological treatment with tissue plasminogen activator (rtPA) injection within the 4.5 hours after symptom onset possibly associated to thrombectomy. However, 90% of the patients are not eligible to those therapies. Despite research efforts, all new molecules validated in animal models have failed in clinical trials. The reason for this conundrum is unclear, but we postulate that the anaesthetics used for preclinical studies influence the formation and evolution of lesions, and hinder pharmacological strategies effects. It is well admitted that anaesthetics have many effects on the cerebral vasculature, metabolism, blood flow and pressure. Therefore, we developed a new stroke model in awake mice to avoid any interferences with the stroke physiopathology.
Method
Under general anaesthesia, a 3D-printed prosthesis was bond to mice skull allowing immobilization of the head of awaken animals, and the middle cerebral artery was exposed for the future occlusion step. Twenty-four hours after, clot formation was induced by microinjection of thrombin in the artery lumen, either in awake or anaesthetized (control) animals.
Results
Preliminary results showed a reduction of the infarct volumes in awake compared to anaesthetized mice. Functional recovery assessed using the strength test, showed different patterns in awake and anesthetized groups.
Conclusion
This work demonstrates the feasibility to perform awake thromboembolic stroke in mouse, avoiding potential interaction between anaesthesia and lesion evolution or treatments. Thus, it would provide an increased success rate for subsequent clinical trials.
Trial registration number
N/A
AS28-013
STIMULATION OF THE MESENCEPHALIC LOCOMOTOR REGION ATTENUATES NEURONAL LOSS AND CYTOKINE EXPRESSION IN THE PERILESIONAL AREA OF PHOTOTHROMBOTIC STROKE IN RATS
1University Hospital Wuerzburg, Neurology, Würzburg, Germany
Background and Aims
Inflammation plays an important role in the pathophysiology of stroke. To a certain extent, the brain is able to regulate immune response via the cholinergic anti-inflammatory pathway (CHAIP). Vagal nerve stimulation has been shown to attenuate neuroinflammation after experimental stroke via CHAIP. The mesencephalic locomotor region (MLR) encompasses cholinergic cells and is connected indirectly to the sensorimotor cortex. Whether high-frequency stimulation (HFS) of the MLR reduces perilesional inflammation after stroke of the sensorimotor cortex has not been addressed so far.
Method
Male Wistar rats underwent photothrombotic stroke of the right sensorimotor cortex and implantation of a stimulating microelectrode into the ipsilesional MLR. Three hours after intervention, either HFS or sham stimulation of the MLR was applied for 24 hours; thereafter, rats were sacrificed. Infarct volumes were calculated from consecutive hematoxylin and eosin-stained brain sections. Perilesional inflammatory response was determined by flow cytometry and immunohistochemistry. Neuronal apoptosis was analyzed by TUNEL staining.
Results
Neuronal apoptosis was significantly reduced in the ischemic penumbra of rats after MLR-HFS, whereas infarct volumes did not differ between both groups. Importantly, MLR-HFS reduced significantly the release of cytokines and chemokines (TNFα, IL-6, CXCL1, CCL2) within the ischemic penumbra. Infiltration of immune cells at the sides of ischemic injury remained unaltered when both, stimulated and unstimulated animals were compared.
Conclusion
MLR-HFS can improve neuronal survival in the perilesional area of photothrombotic stroke, most likely by modulating the inflammatory response. Whether this perilesional humoral immune activity is mediated via CHAIP has to be confirmed in further studies.
Trial registration number
N/A
AS28-014
INTENSIVE BLOOD PRESSURE LOWERING REDUCES HEMATOMA VOLUME IN EXPERIMENTAL INTRACEREBRAL HEMORRHAGE
1University Hospital, Department of Neurology, Frankfurt am Main, Germany
2Georg-Speyer-Haus, Institute for Tumor Biology and Experimental Therapy, Frankfurt am Main, Germany
3Institute of Neurology Edinger-Institute, Goethe-University, Frankfurt am Main, Germany
Background and Aims
Blood pressure is often elevated in the acute phase of intracerebral hemorrhage (ICH) and linked with a poor outcome. Recent clinical trials provided mixed results on whether intensive blood pressure lowering after ICH is safe and effective in terms of reducing mortality and improving functional deficits. The aims of this translational study were to evaluate the influence of intensive blood pressure lowering in acute ICH on hematoma volume and to explore the pathophysiological background.
Method
In total, 84 spontaneously hypertensive rats (SHR) were used. ICH was induced by intrastriatal collagenase injection. We established a model of rapid blood pressure lowering after ICH by oral administration of nifedipine to achieve systolic blood pressure values of approximately 130 mmHg (vs. 185 mmHg for controls). We assessed functional outcome and hematoma growth 24h after ICH. Histopathological analysis and post-mortem MRI were performed to evaluate ICH characteristics, edema formation and inflammatory response.
Results
Rapid blood-pressure lowering significantly reduced hematoma volume as compared to the control group (88.6 µl vs. 146.3 µl, n = 9, p = 0.023). Neurological deficit (mNSS) was significantly improved in the intensively treated group (7 vs. 13 points, p = 0,011). Histopathological analysis revealed no differences for edema formation, blood-brain barrier disruption and inflammatory processes between both groups at 24h and 72h after ICH, confirmed by explorative MRI analysis.
Conclusion
The results of our experimental study suggest that intensive blood pressure lowering in the acute phase of ICH improves functional outcome. The reduction in ICH volume seems to be the main mediator whereas other pathophysiological processes remain unchanged.
Trial registration number
N/A
AS28-015
ASTROCYTE-DERIVED EXOSOMES ENHANCE STROKE RECOVERY VIA PROSTAGLANDIN D2 SYNTHASE EXPRESSION
1Juntendo University School of Medicine, Neurology, Bunkyo-ku, Japan
2Juntendo University Urayasu Hospital, Neurology, Urayasu, Japan
3Keio University, Physiology, Shinjuku-ku, Japan
Background and Aims
In the peri-infarct area after stroke, axons were regenerated but were inhibited by astrocyte scar formation. The direct effect and underlying molecular mechanisms of astrocyte-derived exosomes on axonal outgrowth after ischemia are not known.
Method
Using Semaphorin 3A (Sema3A) inhibitor, we explored neuronal signaling of axonal outgrowth after ischemia in middle cerebral artery occlusion (MCAO) model rats and in cultured cortical neurons challenged with oxygen-glucose deprivation (OGD). We assessed whether this inhibitor suppressed astrocyte activation and regulated astrocyte-derived exosomes to enhance axonal outgrowth after ischemia.
Results
In MCAO rats, we administered Sema3A inhibitor into the peri-infarct area from 7 to 21 days, and we found that phosphorylated high-molecular weight neurofilament (pNFH)+ axons were increased together with suppression of glial fibrillary acidic protein+ astrocytes, and thereby functional recovery were promoted at 28 days. In cultured neurons, we observed that Rho family GTPase 1 (Rnd1)/R-Ras/Akt/Glycogen Synthase Kinase 3beta (GSK-3β) signaling, and selective expression of phosphorylated GSK-3β in axons enhanced pNFH+ axons after OGD. In cultured astrocytes, Sema3A inhibitor suppressed activation of astrocytes induced by OGD. Exosomes secreted from ischemic astrocytes treated with Sema3A inhibitor further promoted axonal elongation with prostaglandin D2 synthase (ptgds) expression on microarray analysis. GSK-3β+ and PTGDS+ neurons were robustly increased after treatment with Sema3A inhibitor in the peri-infarct area.
Conclusion
Not only neuronal Rnd1/R-Ras/Akt/GSK-3β signaling and axonal GSK-3β expression, but also the function of astrocyte-derived exosomes with ptgds contribute to axonal outgrowth and functional recovery after stroke.
Trial registration number
N/A
AS28-017
PROTEOMIC PROFILING AND BIOINFORMATICS ANALYSES OF LOW LEVEL LASER-TREATED HYPOXIC ASTROCYTES
1Kaohsiung Medical University Hospital, Department of Physical Medicine and Rehabilitation, Kaohsiung, Taiwan R.O.C
2Kaohsiung Medical University- College of Medicine, Graduate Institute of Clinical Medicine, Kaohsiung, Taiwan R.O.C
3Kaohsiung Medical University- College of Medicine- School of Medicine, Department of Physical Medicine and Rehabilitation, Kaohsiung, Taiwan R.O.C
4Kaohsiung Medical University, Department of Medical Imaging and Radiological Sciences, Kaohsiung, Taiwan R.O.C
5Kaohsiung Medical University- College of Medicine, Graduate Institute of Medicine, Kaohsiung, Taiwan R.O.C
Background and Aims
The application of low-level laser therapy (LLLT) in brain ischemia provides clinical significance in stroke management. The aim of this study was to explore the neuroprotective effect of LLLT in hypoxic astrocytes.
Method
Mouse brain astrocytes were subjected to normoxic (20% O2) or hypoxic environment (0.05% O2) for 24 hours at 37°C incubator and confirmed its hypoxic induction by hypoxia-inducible factors (HIFs) expression. The MTT assay was performed to assess cell viability of astrocytes after hypoxic induction. Normoxic and hypoxic-treated astrocytes were subjected to LLLT at total fluence of 4J/cm² for 2 days, and cell lysates were collected for proteomic profiling using LC-MS/MS analyses. The differentially expressed proteins between normoxic, hypoxic and LLLT-treated astrocytes were identified and analyzed.
Results
The increased expression of HIF-2α was observed in hypoxic-treated astrocytes by western blot analysis. There was no significant difference in cell viability between normoxic and hypoxic-treated astrocytes by MTT assay. Through LC-MS/MS analyses, 25 differentially expressed proteins were identified in hypoxic astrocytes. Based on bioinformatics analyses, these proteins were involved in glucose metabolism, with ERK1/2 being the central connecting hub. In addition, increased HS90B, LDHA and THIO were involved in HIF signaling and NRF2-mediated oxidative stress response. Moreover, 6 differentially expressed proteins identified in LLLT-treated hypoxic astrocytes were involved in post-transcriptional protein regulation through acetylation. Filamin (FLNA) was identified to interact with HS90B, which potentially facilitated LLLT-treated hypoxic astrocyte migration.
Conclusion
The current findings suggested novel proteins involved in the potential mechanisms of neuroprotective effects exerted by LLLT in brain ischemia.
Trial registration number
N/A
AS28-019
SELECTIVE INHIBITION OF THE TRANSENDOTHELIAL LEUKOCYTE MIGRATION BY KNOCK-IN MUTATION OF VE-CADHERIN RESULTS IN SMALLER INFARCTS IN A MOUSE MODEL OF MIDDLE CEREBRAL ARTERY OCCLUSION
1Münster University Hospital, Department of Neurology, Münster, Germany
2Max-Planck-Institute of molecular biomedicine, Vascular cell biology, Münster, Germany
Background and Aims
Transendothelial leukocyte migration and vascular permeability are both regulated by tyrosine phosphorylation of the adhesion molecule VE-cadherin. Dephosphorylation of Y731 of VE-Cadherin induces selective leukocyte diapedesis, whereas the phosphorylation of Y685 of VE-Cadherin is required for inflammation-induced, unspecific vascular permeability (plasma leaks). In the current project, we use knock-in mice expressing either a Y731F mutant or a Y685F mutant of VE-Cadherin to investigate the effects of a selective inhibition of the transendothelial leukocyte migration on endothelial integrity, brain edema, infarct volumes, postischemic inflammation and neurological outcomes in a mouse model of middle cerebral artery occlusion (MCAO).
Method
Mice expressing either the Y731F mutant or the Y685F mutant of VE-Cadherin and their littermates (n = 10–11 per group) were subjected to 45 minutes of MCAO. A neuroscore, the rotarod test and the foot fault-test were employed to assess functional outcomes. Infarct volumes were determined three days after MCAO.
Results
Infarct volumes were significantly smaller after selective inhibition of the transendothelial leukocyte migration (52.33 mm3 ± 4.72 mm3 vs. 70.43 mm3 ± 6.48 mm3, p < 0.05, t-test). Restricting the inflammation-induced, unspecific vascular permeability did not influence infarct volumes and functional outcomes. Flow cytometry and immunohistochemical analyses to investigate endothelial integrity, brain edema and postischemic inflammation are ongoing.
Conclusion
Selective inhibition of the transendothelial leukocyte migration by knock-in mutation of VE-Cadherin results in smaller infarct volumes and may improve outcomes after ischemic stroke.
Trial registration number
N/A
AS28-020
TP53 ARG72PRO POLYMORPHISM CONTROLS PRECONDITIONING-PROMOTED NEUROPROTECTION AND MODULATES TIA-INDUCED ISCHEMIC TOLERANCE
1Institute of Biomedical Research of Salamanca- University Hospital of Salamanca. Institute of Functional Biology and Genomics. University of Salamanca-CSIC, Molecular Neurobiology, Salamanca, Spain
2Stroke Unit- University Hospital of Valladolid- University of Valladolid, Department of Neurology, Valladolid, Spain
3Institute of Biomedical Research of Salamanca- University Hospital of Salamanca- University of Salamanca, Department of Statistics, Salamanca, Spain
4IRB Lleida. UdL, Clinical Neurociences Group, Lleida, Spain
5Stroke Unit. University Hospital Arnau de Vilanova.IRBLleida. UdL, Clinical Neurociences Group, Lleida, Spain
Background and Aims
Cerebral preconditioning (PC) is one of the most important endogenous mechanisms responsible for the increased resistance to damage after stroke. Patients with transient ischemic attacks (TIA) prior ischemic stroke may potentially be in a preconditioned state. Recently, we have described that PC-mediated neuroprotection against ischemic insult is promoted by p53 destabilization, which is mediated by its main regulator MDM2 (murine double minute 2 gene). Moreover, we have previously described that Arg72Pro SNP controls susceptibility to ischemia-induced neuronal apoptosis and governs the differential functional outcome of individuals after stroke. Here, we studied the role of human Tp53 Arg72Pro polymorphism SNP on PC-induced ischemic tolerance.
Method
Primary cortical neurons were obtained from p53 knock-in mice expressing human polymorphic variants Arg72-p53 and Pro72-p53. To induce PC, neurons were exposed to 20 mM NMDA for 2 hours prior to a subsequent lethal ischemia induced by oxygen and glucose deprivation (OGD; 90 min). Apoptosis, mitochondrial membrane potential (DiIC-staining), Caspase-3 activity and protein levels were analysed.
Results
Our results showed that neurons expressing Pro72-p53 variant exhibited higher PC-mediated neuroprotection as compared with Arg72-p53 neurons. PC prevented ischemia-induced nuclear and cytosolic p53 stabilization only in Pro72-p53 neurons. However, PC failed to prevent ischemia-induced mitochondrial p53 stabilization, which occurs in Arg72-p53 neurons. Finally, we found that the good prognosis is associated to TIA within one-month prior to ischemic stroke was restricted to patient harbouring the Pro72 allele.
Conclusion
Tp53 Arg72Pro SNP modulates the PC-induced neuroprotection against a subsequent ischemic insult.
FEDER, ISCIII(CP0014/00010;PI15/00473;RD12/0014/0007; RD16/0019/0018;CM14/00096) and Junta de Castilla y Leon BIO/SA35/15.
Trial registration number
N/A
AS28-021
NOSE-TO-BRAIN DRUG DELIVERY FOR THE TREATMENT OF STROKE: NEUROPROTECTIVE EFFECTS OF THE ANGIOTENSIN AT2-RECEPTOR AGONIST C21 IN EXPERIMENTAL STROKE IN RATS
1University of Southern Denmark, Cardiovascular & Renal Research, Odense, Denmark
2University of Florida, College of Medicine, Gainesville, USA
3University of Florida, Dept. of Physiology and Functional Genomics, Gainesville, USA
4RISE Research Institute of Sweden, none, Gothenburg, Sweden
5Barrow Neurological Institute, Dept. of Neurology, Phoenix, USA
6Attoquant Diagnostics GmbH, none, Vienna, Austria
Background and Aims
Recent preclinical studies by 7 independent groups have highlighted the neuroprotective potential of post-stroke stimulation of the angiotensin AT2-receptor (AT2R) using Compound 21 (C21), a selective small-molecule AT2R agonist. However, C21 only poorly penetrates the BBB. Therefore, we tested the neuroprotective effects of C21 delivered by intranasal trans-olfactory, or nose-to-brain (N2B) application.
Method
Male Sprague-Dawley rats underwent endothelin 1-induced MCAO in three experiments: (i) Rats received 0.9% saline or C21 (1.5ug/kg) at 1.5, 4, 24 and 48h post-stroke, using an intranasal catheter for N2B application, along with daily neurologic assessments (Bederson and Garcia score) and 72h infarct size analysis. (ii) Blood pressure and heart rate were measured by telemetry transducer recording. (iii) C21 levels in plasma and target brain regions were measured in naïve and stroke animals.
Results
(i) Post-stroke N2B delivery of C21 elicited a signifcant reduction of cerebral infarct size (44.23 ± 4.12, n = 9) compared with saline-treated controls (25.39 ± 4.71, n = 13) [p < 0.0075]. C21-treated rats also displayed highly significant improvements in neurological function (p < 0.01). (ii) N2B delivery of C21 did not significantly alter baseline or post-stroke blood pressure or heart rate. (iii) C21 was detected in therapeutically relevant concentrations in the target brain tissue in both naïve (0.82 nM; n = 8) and stroke (0.82 nM; n = 8) animals after N2B administration.
Conclusion
Our results demonstrate that N2B delivery of the AT2R agonist C21 exerts protective effects after ischemic stroke without affecting blood pressure or heart rate. These studies suggest N2B administration as potential future route of application of C21 to stroke patients.
Trial registration number
N/A
AS28-022
MDM2 309T>G POLYMORPHISM, A FUNCTIONAL SNP IN THE MDM2 PROMOTER THAT REGULATES PROTEIN LEVELS AND FUNCTIONAL OUTCOME AFTER STROKE
1Institute of Biomedical Research of Salamanca, University Hospital of Salamanca - University of Salamanca, Salamanca, Spain
2Institute of Functional Biology and Genomics, University of Salamanca-CSIC, Salamanca, Spain
3Health Research Institute of Santiago de Compostela, University Clinical Hospital, Santiago de Compostela, Spain
Background and Aims
MDM2 is the main negative regulator of p53, which plays a key role in neuronal apoptosis after ischemia. A functional polymorphism in the MDM2 promoter, known as SNP309T>G, modulates MDM2 protein expression, which may affect p53 apoptotic activity. Here we studied the role of MDM2 on neuronal apoptosis and the impact of the MDM2 SNP309T>G on stroke prognosis.
Method
Primary cortical neurons were subjected to oxygen and glucose deprivation (OGD), then MDM2 and p53 mRNA and protein levels were measured. The MDM2-p53 interaction was disrupted by neuronal treatment with nutlin-3a. Small interfering RNA (siRNA) was used to knockdown MDM2 expression. The link between the MDM2 SNP309T>G and functional outcome based on the modified Rankin scale (mRS) was analysed in a cohort of 408 patients with ischemic stroke (IS) and 128 patients with non-traumatic intracerebral hemorrhage (ICH).
Results
OGD induced MDM2 expression in neurons. Disruption of the MDM2-p53 interaction with nutlin-3a and MDM2 knockdown by siRNA promoted p53 accumulation and increased neuronal susceptibility to OGD-induced apoptosis. We showed that patients harbouring the G allele had higher levels of MDM2 expression and better functional outcome after stroke than those with the T/T genotype. The T/T genotype was also associated with increased infarct volume in IS and increased residual cavity volume in ICH patients.
Conclusion
The MDM2-p53 interaction modulates neuronal susceptibility to apoptosis after ischemia. The MDM2 SNP309 regulates MDM2 expression, which determines the functional outcome of patients after stroke.
Funded by FEDER, ISCIII (PI15/00473;RD16/0019/0001;RD16/0019/0018) and Junta de Castilla y León (IES007P17).
Trial registration number
N/A
AS28-023
12/15 LOX INHIBITION AMELIORATES HIPPOCAMPUS ASSOCIATED NEURONAL DAMAGE AND MITOCHONDRIAL DYSFUNCTION IN MICE SUBJECTED TO HYPOBARIC HYPOXIA
1University of Delhi, Dr B.R Ambedkar Center for Biomedical Research-, Delhi, India
2Dr B.R Ambedkar Center for Biomedical Research-, Delhi, India
Background and Aims
Oxidative stress is thought to be the critical effectors in hypobaric hypoxia induced cognitive dysfunctions. 12/15 Lipoxygenase has recently been described as potent mediator of oxidative stress and is closely associated with cognitive decline. The present study was designed to decipher the underlying role of 12/15LOX on hypobaric hypoxia induced memory impairment and neuronal damage.
Method
Balb/c mice were subjected to hypobaric hypoxia, simulating condition at 7620m altitude. Baicalein, a specific inhibitor of 12/15 LOX was administered to mice. Behavioral paradigm, histopathological assessment and mitochondrial integrity was assessed to establish the involvement of 12/15 Lipoxygenase in the hypobaric hypoxia neuro-pathology.
Results
Hypobaric hypoxia episode was accompanied by an increased level of 12/15 LOX and its metabolite 12(S) HETE. The hippocampus CA3 region was found to be mostly affected and showed sign of cellular apoptosis as characterized by elevated activity of caspase-3, 9 & 8. Working memory impairment seen in mice after hypobaric hypoxia was attenuated following baicalein treatment along with reduced level of caspase activation and HIF-1α. Further, impediment of 12/15 LOX decreased NO level by down-regulating the expression of iNOS, nNOS but not eNOS. A significantly elevated level of cytochrome C was associated with increased 12/15 LOX colocalisation with mitochondria that got reversed following 12/15 LOX inhibition.
Conclusion
12/15 LOX influences the hypobaric hypoxia pathology and its inhibition using baiclein was found to be neuroprotective. Its co-localization with mitochondria and subsequent increased level of cytochrome c further highlighted importance of its interplay with the mitochondrial associated machinery.
Trial registration number
N/A
AS28-024
APTOLL, A NEW THERAPEUTIC APPROACH TO ISCHEMIC STROKE
1AptaTargets S.L., Scientific Department, Madrid, Spain
2Aptus Biotech S.L., Scientific Department, Madrid, Spain
3Hospital Ramón y Cajal, Biochemistry Research, Madrid, Spain
4University Complutense, Pharmacology, Madrid, Spain
Background and Aims
The devastating consequences of ischemic stroke are induced -at least in part- by the inflammatory response triggered in the first hours after stroke onset. In this arena, TLR4 receptor plays a key role activating resident cells, promoting inflammatory cell infiltration and, therefore, inducing the release of proinflammatory molecules that exacerbates brain damage after ischemia (Caso et al., Circulation 2007). ApTOLL is an aptamer that has been selected and optimized to block TLR4 activation in the acute phase, showing an outstanding profile reducing brain damage after ischemic stroke. Specifically, ApTOLL has been tested in rat and mouse models of permanent and transient experimental ischemia (31.35% ± 16.7% mid protection) (Fernández et al. Under 2nd editorial review). ApTOLL’s development program is currently ongoing, to demonstrate the protective effect could be reproduced in stroke patients. To this aim, regulatory preclinical studies have been conducted before the first administration in humans.
Method
Pharmacokinetic and toxicity studies were performed in rats and monkeys both in vitro and in vivo.
Results
ApTOLL shown neither drug-to-drug interactions nor off-target reactions in vitro. Moreover, Cmax showed linear kinetics over the dose range studied in rats. Administration of ApTOLL to rats did not induce remarkable toxicological alterations. Maximum tolerated dose study in monkeys did not show alterations in biochemistry, coagulation parameters or pathological findings.
Conclusion
Regulatory preclinical studies with ApTOLL have shown adequate pharmacokinetic properties and absence of toxic side effects. Therefore, clinical trial with healthy volunteers will be ready to start in 2018.
Trial registration number
N/A
AS28-025
FUNCTIONAL DEFICITS FOLLOWING INTRACEREBRAL HEMORRHAGE IN RATS
1Ghent University Hospital, Department of Neurology- Laboratory for Clinical and Experimental Neurophysiology Neurobiology and Neuropsychology- LCEN3, Ghent, Belgium
Background and Aims
The rat collagenase model is a frequently used animal model to study intracerebral hemorrhage (ICH), in which bacterial collagenase is injected, usually in the striatum, resulting in motor deficits. The ventral striatum appears to play a role in anhedonia, a symptom of depression, and anxiety. In this pilot study we evaluated deficits in motor function and emotion regulation in a rat model for striatal hemorrhage.
Method
Six male Sprague-Dawley rats were injected with collagenase (0.20U in 0.7µl saline, n = 3) or saline (0.7µl, n = 3) in the left ventral striatum (0.5AP 3.5ML 6DV relative to bregma). The rats were tested for motor deficits at day -1, 3, 5 and 7, by means of the cylinder test, a neurological test battery and the forelimb placing test. The saccharine preference test and forced swim test were performed to test for depressive-like behavior. Anxiety was tested using the elevated plus maze and light-dark box. After 2 weeks, the rats were euthanized to evaluate the extend of the hemorrhage using histology.
Results
Collagenase induced a bleeding in the ventrolateral striatum in all three animals. Significant motor deficits were present in the forelimb placing test on day 3 (p < 0.05). Tests for depressive-like behavior and anxiety did not show significant changes compared to control animals.
Conclusion
The hemorrhage was more ventrally located compared to previous research and caused a measurable motor deficit. A larger trial is warranted to evaluate changes in emotion regulation.
Trial registration number
N/A
AS28-028
INHALED NITRIC OXIDE REDUCES VASCULAR INFLAMMATION AFTER EXPERIMENTAL STROKE
1Institute for stroke and dementia ISD, Experimental Stroke Research, Munich, Germany
Background and Aims
Inhaled nitric oxide (iNO) protects the brain from ischemic injury following cerebral ischemia (Terpolilli et al., Circ Res 2012). So far, selective vasodilatation of penumbral collaterals was suggested to be the main mechanism. The aim of the current study was to investigate whether NO, which is also known to inhibit leukocyte adhesion, affects neuroinflammation after experimental ischemic stroke.
Method
Middle cerebral artery occlusion (MCAo) was induced in C57BL/6 mice for 60 min. iNO (50 ppm) was initiated at the beginning of reperfusion. Three hours later leukocytes were stained with Rodamine 6G and imaged in the ischemic penumbra by in vivo two-photon microscopy. Rolling and adhesion of leukocytes on the vascular endothelium were recorded and analyzed by using IMARIS 3D imaging software.
Results
No adherent leukocytes were observed in sham operated mice. Cerebral ischemia resulted in significant rolling (11 +/− 7 cells/ROI) and sticking (12 +/− 9 cells/ROI) of leukocytes to venular and capillary endothelium three hours after MCAo. In animals receiving iNO the amount of adherent and rolling leukocytes was reduced by 75% (p < 0.05) and 98% (p < 0.00001) respectively.
Conclusion
Rolling and sticking of leukocytes to the endothelium of venules and capillaries after cerebral ischemia was almost completely blunted (-75 and -98%, respectively) upon treatment with iNO. In addition to its vasodilatatory activity, this effect of iNO may represent a novel mechanism on how inhaled NO mediates neuroprotection. These findings further support the clinical evaluation of iNO as an acute therapeutic for ischemic stroke.
Trial registration number
N/A
AS28-029
EFFECTS OF PREGABALIN ON BRAIN EDEMA, NEUROLOGIC AND HISTOLOGIC OUTCOMES IN EXPERIMENTAL TRAUMATIC BRAIN INJURY
1Endocrinology and Metabolism Research Center- Institute of Basic and Clinical Ph, Physiology, Kerman, Iran
2Neuroscience Research Center- Neuropharmacology Institute- Kerman University of Medical Sciences- Kerman- Iran-, Pharmacology, Kerman, Iran
Background and Aims
Brain edema and increased intracranial pressure (ICP) are among the main causes of neurological disturbance and mortality following traumatic brain injury (TBI). Since pregabalin neuroprotective effects has been shown, this study was performed to evaluate the possible neuroprotective effects of pregabalin in experimental TBI of male rats.
Method
Adult male Wistar rats were divided into 4 groups: sham, vehicle, pregabalin 30 mg/kg and pregabalin 60 mg/kg. TBI was induced in vehicle and pregabalin groups by Marmarou method. Pregabalin was administered 30 min after TBI. Sham and vehicle groups received saline. Brain water and Evans blue content, and histopathological changes were evaluated 24 h after TBI. The ICP and neurological outcomes (veterinary coma scale, VCS) were recorded before, 1h and 24 h post TBI.
Results
The results showed a significant reduction in brain water content and ICP, and a significant increase in VCS of pregabalin group (60 mg/kg) as compared to vehicle group (P<0.05). Also, pregabalin reduced brain edema and apoptosis score as compared to vehicle group.
Conclusion
Post TBI pregabalin administration revealed a delayed but significant improvement in ICP and neurological outcomes in experimental TBI. The underlying mechanism (s) was not determined and needs further investigation.
Trial registration number
N/A
AS28-030
INTERACTION OF LEUKOCYTES WITH THE CEREBROVASCULAR ENDOTHELIUM IS SUFFICIENT TO DAMAGE NEURONS FOLLOWING EXPERIMENTAL ISCHEMIC STROKE
1Institute for stroke and dementia ISD, Experimental Stroke Research, Munich, Germany
2Department of Neurosurgery- National Cerebral and Cardiovascular Center, Department of Neurosurgery, Suita Osaka, Japan
3Universitätsklinukum Gießen, Neurochirurgie, Gießen, Germany
Background and Aims
Cerebral ischemia causes activation of inflammatory processes, including recruitment of leukocytes to cerebral vessels. Even to date, however, it is still unclear how this process mediates post-ischemic brain damage. The aim of the current study was therefore to investigate the impact of leukocyte-endothelium interaction (LEI) on neuronal cell death following cerebral ischemia.
Method
C57BL/6 mice were subjected to 60 min of middle cerebral artery occlusion (MCAo). LEI, leukocyte transmigration, and neuronal cell death were investigated within the first hour and 2, 5, 9, and 15 hours after MCAo by 2-PM and epifluorescence in vivo microscopy and ex vivo by light sheet and confocal microscopy.
Results
Five hours after reperfusion neuronal cell death starts rising while the interaction of leukocytes with the endothelium already reached its peak. By inhibiting the leukocyte adhesion molecule CD18 LEI was reduced by 60% (P<0.01) and the number of viable neurons increased by 5-fold (P<0.01). Migration of leukocytes into the brain was not affected by inhibition of LEI.
Conclusion
Our results suggest that infiltration of leukocytes into the post-ischemic brain may not be related to neuronal cell death. Rather these findings suggest that the interaction of leukocytes with the cerebro-vascular endothelium is sufficient to induce neuronal cell death after cerebral ischemia. The mechanisms underlying this process warrant further investigation.
Trial registration number
N/A
AS28-031
THE ROLE OF CAVEOLIN-1 IN A MOUSE MCAO STROKE MODEL: TOWARDS A PROTECTIVE STRATEGY FOR THE NEUROVASCULAR UNIT
1CHUV, Department of clinical neurosciences, Lausanne, Switzerland
2Cnrs Umr 5287, Incia, Bordeaux, France
Background and Aims
A complex matrix of events occurs within the first days after stroke with disruption of the Blood Brain Barrier (BBB) contributing to neuronal death, neurological deterioration and mortality. Nitric Oxide (NO) modulates Cerebral Blood Flow, inflammation, BBB disruption and oxidative stress. Caveolin-1 (Cav-1) proteins assemble to form caveolae involved in endocytosis, transcytosis and exocytosis. Cav-1 is also involved in modulating NO synthesis and stabilization of the tight-junction proteins between endothelial cells. Thus, Cav-1 seems to be a critical protein underlying several roles in the neurovascular unit
The main goal of this project is to characterize Cav-1 changes in a mouse cerebral ischaemia-reperfusion model to improve our knowledge on the pathophysiology of the BBB disruption after stroke and to develop novel therapeutic approaches to restore its function.
Method
We investigated the role of Cav-1 by comparing Wild Type (WT) and genetically modified Cav-1−/− mice in a transient Middle Cerebral Artery Occlusion (MCAO) model. Standardized outcome measures: lesion volume, behavioural tests (Neuroscore, Rotarod, Adhesive Removal and Open Field), and immunofluorescence staining have been collected at different time-points and up to 7 days after brain injury.
Results
Larger lesion volumes and greater motor deficits in the Cav-1 KO mice were highlighted. All together, these results point towards a potential protective role of endogenous Cav-1 in the first days after stroke.
Conclusion
Characterization of the Cav-1 KO mice helps understanding the role of caveolins in brain injuries. As endogenous Cav-1 appears to have a beneficial effect, mimicking caveolin functions could then be considered as a neuroprotective strategy.
Trial registration number
does not apply
AS28-032
INHIBITION OF STROKE-ELEVATED ENDOTHELIAL Α5Β1 INTEGRIN WITH THE SMALL PEPTIDE ATN-161 STABILIZIES THE BLOOD-BRAIN BARRIER AND IS NEUROPROTECTIVE
1University of Kentucky, Neuroscience, Lexington, USA
2University of Kentucky, Neurosurgery, Lexington, USA
3University of Kentucky, Neurology, Lexington, USA
Background and Aims
Stroke is a leading cause of death and disability with limited therapeutic options. We have demonstrated that endothelial cell-selective α5β1 integrin (a fibronectin receptor expressed in development, but not adult cerebrovasculature under physiologic conditions) knockout mice are profoundly resistant to changes in blood-brain barrier (BBB) integrity and brain injury after ischemic stroke. Therefore, we hypothesize that therapeutic inhibition of α5β1 would result in a more intact BBB, thus reducing infarct volume and improving functional recovery.
Method
Wild-type mice underwent transient middle cerebral artery occlusion, and were treated with the α5β1 inhibitor, ATN-161 (1mg/kg IP), immediately after reperfusion, PSD1, and PSD2. Immunohistochemistry determined α5β1 expression through post-stroke day (PSD) 4. Stroke volume (TTC and MRI at PSD3), functional behavior (Neuroscore through PSD14), and BBB permeability (MRI and qPCR of claudin-5 and MMP9 at PSD3) was analyzed. In vitro, brain endothelial cells underwent oxygen-glucose deprivation (OGD). Permeability was determined by FITC-dextran migration measurements. α5β1 and claudin-5 expression was determined by immunocytochemistry.
Results
Luminal, peri-infarct α5β1 cerebrovascular expression was noted by PSD2 and increased exponentially by PSD4. ATN-161 treatment resulted in significantly smaller infarcts, improved functional recovery, and a stabilized BBB. Finally, in vitro studies demonstrated that OGD increased permeability, increased α5β1 expression, and decreased cell-surface expression of the tight junction protein claudin-5, changes that could be prevented by ATN-161.
Conclusion
Collectively, our results show that inhibition of α5β1 with ATN-161 results in smaller infarct volumes through reduction of BBB permeability, and thus could represent a novel therapeutic target for ischemic stroke.
Trial registration number
N/A
AS28-033
COCKTAIL OF FLAVONOIDS AND ANTHOCYANINS PROTECT AGAINST BEHAVIORAL AND BIOCHEMICAL CHANGES IN AN ISCHEMIA STROKE MODEL OF DROSOPHILA
1PBMMEC, BC, MYSURU, India
2PBMMEC, Bt Bc Mb, Mysuru, India
Background and Aims
Ischemia/referfusion has been implicated in most of the stroke pathophysiology. Marked redox markers and mitochondrial dysfunction has also been associated with etiology of the stroke-after effects. Here the tested hypothesis is that Selaginella flavonoids (SF) and selected anthocyanins (AC) abrogate ischemia/ reperfusion (I/R, 20h)-induced biochemical and behavioral changes in drosophila.
Method
Drosophila treated with SF/AC were challenged with I/R (1%) for 20h. Phenotypic manifestations were assessed by employing a battery of behavioral assays for stroke (climbing, Y-maze, passive avoidance). Drosophila exposed to I/R were treated with SF/AC and were tested for behavior index using fly T-maze and OFT. Terminally, the hippocampi were biochemically assessed for mitochondrial dysfunction, oxidative stress and ache activity.
Results
I/R exposure induced significant behavioral aberrations among drosophila evident from the mazes. The passive avoidance score was also found reduced among the I/R drosophila indicating severe dementia traits. SF/AC supplements attenuated the I/R-induced behavioral anomalies. Additionally SF/AC treatment reduced ache activity, oxidative stress (reduced malondialdehyde), and nitric oxide among I/R-group. Further, mitochondrial membrane permeability was improved among SF/AC groups exposed to I/R. Among drosophila, I/R-induced general aggressive behavior, ache and oxidative markers were also abrogated by SF/AC supplements.
Conclusion
We report the potent neuro-attenuatory propensity of Selaginella flavonoids and other Anthocyanins against I/R-induced oxidative stress, however studies are warranted for long term implications.
Trial registration number
N/A
AS28-034
HIGH-SALT DIET RESULTS IN EXACERBATED INFLAMMATORY RESPONSE AND MIGRATING VESICLE FORMATION FOLLOWING EXPERIMENTAL STROKE
1Universtity of Münster, Department of Neurology, Muenster, Germany
2University of Münster, Department of Anesthesiology and Intensive Care Medicine, Münster, Germany
Background and Aims
High-sodium chloride promotes pro-inflammatory immune cell polarization shift, astrocyte loss and osmotic demyelination, all of which influence the outcome following stroke. Despite its translational relevance, the functional importance of NaCl in stroke pathophysiology is still unclear. We analyzed the effects of high-salt diet in a mouse model of middle cerebral artery occlusion.
Results
NaCl-diet resulted in worsened functional outcome (p < 0.05), increased infarct volume (p < 0.05), loss of astrocytes (p < 0.001) and cortical neurons (p < 0.05). Most importantly, we firstly describe the massive induction of migrating vesicle formation after NaCl-diet and ischemic stroke. Immunohistochemistry, electron microscopy and proteomics were carried out for the characterization of migrating vesicles. Plain formation of apoptotic blebs or exosomes could be excluded. Furthermore, we show that vesicles incorporate cytosol of surrounding neurons, potentially inducing neuronal cell damage and augmenting brain injury following stroke. Highlighting the clinical importance of these findings, we provide evidence of migrating vesicle formation in infarcted parenchyma of human stroke patients.
Conclusion
In summary, our current study introduces the migrating vesicles as novel mechanism in stroke pathophysiology and identifies dietary salt as a potential setting screw to attenuate migrating vesicle formation and neuronal damage after stroke.
Trial registration number
N/A
AS28-035
PROGNOSTIC VALUE OF EARLY ENDOTHELIAL PROGENITOR CELLS MOBILIZATION AFTER AN ACUTE ATHEROTHROMBOTIC STROKE
1Hospital De La Santa Creu I Sant Pau, Neurology, Barcelona, Spain
2Hospital De La Santa Creu I Sant Pau, Cytometry, Barcelona, Spain
Background and Aims
Circulating Endothelial Progenitor Cells (cEPC) are bone marrow-derived cells with capacity of forming and repairing blood vessels. Their prognostic role after an ischemic stroke is controversial. We aimed to demonstrate the prognostic value of early EPC mobilization after an acute atherothrombotic stroke.
Method
We conducted a prospective study of consecutive patients with an acute atherothrombotic stroke from 2015 to 2017 (NCT03218527). We excluded patients with a modified Rankin Scale (mRS) score>3 after the stroke. A blood sample was obtained at day 7 ± 1 from the stroke. EPC were identified by flow cytometry using a triple-staining method (CD133+/CD309+/CD34+). We recorded demographic data and neuroimaging findings during hospitalization. At three months of follow-up we collected stroke recurrences and mRS score.
Results
We included 48 patients with a mean age of 75 ± 10y, 34 (70%) were men. EPC were detectable in 30 (63%) patients and the median count was 0.02% (IQR 0–0.05) of the mononuclear cells. 33 patients presented an acute infarction on the neuroimaging and 15 were considered transient ischemic attacks. There were 12 stroke recurrences during the follow-up (25%). Mobilization of EPC (any count) was independently associated with the risk of presenting an infarction on the neuroimaging (OR 7.37 95%CI 1.61–30.74). However, cEPC were not associated with the risk of stroke recurrence nor with the functional outcome at three months of follow-up.
Conclusion
In patients with an acute atherothrombotic stroke, early EPC mobilization predicted the presence of an acute infarction on the neuroimaging. EPC levels were not associated with vascular recurrences nor with functional outcome.
Trial registration number
N/A
AS28-036
A NOVEL BIOPHYSICAL MODEL BASED ON THE VASCULAR TREE FOR THE SIMULATION OF ARTERIAL FLOW AND PERFUSION PRESSURE IN CEREBROVASCULAR DISEASE
1Charité - Universitätsmedizin Berlin, Department of Neurosurgery, Berlin, Germany
2Charité - Universitätsmedizin Berlin, Center for Stroke Research Berlin CSB, Berlin, Germany
Background and Aims
Personalized medicine is a challenge in stroke management. It calls for individual patient biomarkers enabling stratification to treatment. Neuroimaging biomarkers, e.g. perfusion imaging, are promising candidates, but often necessitate the application of non-standardized, potentially harmful or time-consuming methods. To overcome this limitation, we present a biophysical model simulating flow in arteries and brain perfusion pressure based on routine structural vessel imaging.
Method
The simulation is based on the Hagen-Poiseuille equation and exploits the analogy of a vascular tree to an electric circuit. Autoregulation of brain vessels is considered. Blood pressure is a boundary condition. The simulation depicts the vascular tree as a network of branches and nodes and finally perfusion supply areas. For each branch the flow and for each supply area perfusion pressure can be simulated.
Results
We implemented the following pipeline as a software prototype: 1) Segmentation of the vascular tree from routine Time-of-Flight (TOF)-images, 2) Annotation of brain vessels, 3) Simulation. We can simulate individual critical clinical information about tissue-at-risk due to stenosis/occlusion under different blood pressure conditions (Figure 1). A laptop with the simulation will be available at the conference for testing.
Conclusion
We present a personalized medicine approach allowing simulation of critical perfusion information without the need for additional perfusion imaging. Clinical validation will be performed next.
Trial registration number
N/A
AS28-037
MONOMETHYL FUMARATE MITIGATES ISCHEMIA REPERFUSION INJURY BY ACTIVATING NRF2/HO1 PATHWAY IN EXPERIMENTAL MODEL OF ISCHEMIC STROKE IN RAT
1All India Institute of Medical Sciences- AIIMS- New Delhi, Department of Pharmacology, New Delhi, India
2All India Institute of Medical Sciences- AIIMS- New Delhi, Department of NMR and MRI facility, New Delhi, India
3All India Institute of Medical Sciences- AIIMS- New Delhi, Department of Pathology, New Delhi, India
Background and Aims
Despite advances in understanding the pathophysiology of cerebral ischemia, tPA remains to be the only treatment option, leaving stroke a major cause of mortality and long term disability. Increasing number of evidences suggest that activating endogenous antioxidant pathway by stimulation of nuclear factor erythroid-2-related factor 2 (Nrf2) can play a key role in cellular defense against oxidative stress in ischemic penumbra. The study was planned to test the hypothesis that monomethy fumarate (MMF) exerts neuro-protective role via activation of Nrf2/HO1 pathway.
Method
Middle cerebral artery occluded using a 3.0 monofilament in Male Sprague Dawley rats (270 ± 20g) for 90 min was confirmed by Laser Doppler flow meter. MMF (10 mg/kg) was administered at two time points, 30 min post ischemia and 5 min post reperfusion. Twenty four hours later, neurobehavioral parameters were assessed followed by T2 imaging using 7.0T animals MRI to assess effect on infarct. After MRI, rats were euthanized, perfused with paraformaldehyde, cryosections were stained with Nrf2, HO1 and NeuN followed by counterstaining with DAPI.
Results
Post occlusion, cerebral blood flow reduced by 80.2 ± 2.9% of baseline and post reperfusion 70.4 ± 4.1% of blood flow was restored. MMF treatment significantly (p < 0.05) improved neurobehavioral parameters and cerebral infarct when compared to MCAo group. Immunofluorescence study revealed increase in expression of Nrf2 in neurons, HO1 in neuron and non-neuronal cells in peri-infarct region of MMF group when compared with MCAo group.
Conclusion
Our results indicate the neuro-protective effect of MMF in ischemia reperfusion injury by activating Nrf2/HO1 pathway.
Trial registration number
N/A
AS28-038
INVESTIGATING THE EFFECT OF RAPAMYCIN ON BRAIN PERICYTE CONSTRICTION AND CELL DEATH FOLLOWING OXYGEN GLUCOSE DEPRIVATION
1University of Oxford, Radcliffe Department of Medicine, Headington, United Kingdom
2Kuwait University, Department of Physiology- Faculty of Medicine, Kuwait City, Kuwait
3University of Oxford, Department of Oncology, Headington, United Kingdom
Background and Aims
Evidence suggests brain pericyte “death in rigour” plays a role in no-reflow phenomenon following reperfusion in stroke (Hall, 2014). Our previous work identified mammalian target of rapamycin (mTOR) inhibition as an endogenous neuroprotectant (Papadakis, 2013). Our aim was to determine if mTOR inhibition with rapamycin reduces pericyte constriction and cell death following oxygen glucose deprivation (OGD) in vitro.
Method
Cultures of rat pericytes were prepared as described previously (Abbott, 2010). We used an electrical impedance system (icellegence) to measure changes in pericyte contractility. Pericytes were exposed to 24 hours of OGD. Treatment groups: vehicle (ethanol), 10nM rapamycin and 100nM Rapamycin, administered at the beginning of OGD (n = 3, per group). Pericytes were exposed to OGD or normoxia for 2, 8 or 12 hours. Treatment groups were the same as above (n = 6, per group). Cell viability and apoptosis were assessed by Propidium Iodide/Annexin V staining.
Results
OGD caused constriction of pericytes before cell death (1 hour vs. 12 hours post-OGD, respectively). Rapamycin showed a dose depended trend to reduced constriction between 3 and 6 hours after OGD (p = 0.053 100nM vs. Vehicle, One-way ANOVA with post-hoc Dunnett’s test). 12 hours OGD caused a significant reduction in pericyte viability (p < 0.0001, two-way ANOVA). Rapamycin did not have a significant effect on pericyte viability after 12 hours of OGD.
Conclusion
Rapamycin appears to reduce pericyte constriction without changing pericyte viability. Future work will seek to determine the mechanism of reduced constriction and if rapamycin can reduce pericyte constriction and improve capillary perfusion post-stroke in vivo.
Trial registration number
n/a
AS28-039
EFFECTS OF INTRA-ARTERIAL AND INTRAVENOUS TRANSPLANTATION OF INDUCED PLURIPOTENT STEM CELL-DERIVED NEURAL PROGENITOR CELLS ON ISCHEMIC STROKE RECOVERY IN RATS
1Pirogov Russian National Research Medical University, Department of Neurology- Neurosurgery and Medical Genetics, Moscow, Russia
2Pirogov Russian National Research Medical University, Research Institute of Cerebrovascular Pathology and Stroke, Moscow, Russia
3Research Centre of Medical Genetics, Stem cells genetics, Moscow, Russia
4Koltzov Institute of Developmental Biology, Problems of regeneration, Moscow, Russia
5Sklifosovsky Research Institute for Emergency Medicine, Radiology, Moscow, Russia
6Vavilov Institute of General Genetics RAS, Laboratory of Epigenetics, Moscow, Russia
7Institute of Biomedical Chemistry, Cell Biology, Moscow, Russia
Background and Aims
Induced pluripotent stem cell-derived progenitor cells (iNPCs) can be genetically reprogrammed from a patient’s own somatic cells and according to the recent pioneering research may be a promising therapeutic strategy for an autologous and multifunctional cell therapy for stroke. The aim of this study was to evaluate the therapeutic effects of iNPCs after their intra-arterial and intravenous transplantation in rats after MCAO.
Method
Male Wistar rats 24h after 90 minutes MCAO were randomly attributed to the following groups: intra-arterial (IA) (n = 10) and intravenous (IV) (n = 15) infusion of iNPCs (5x105), control group (n = 12). For evaluation of therapeutic effects and infarct volume behavioral test and 7T-MRI and were performd at 1d, 7d, 14d after MCAO (before histology).
Results
IV administration of iNPCs significantly reduces neurological deficit only 14d after MCAO, while IA administration of iNPCs improves survival, stroke volume and functional recovery already after 7d from stroke onset (fig.1).
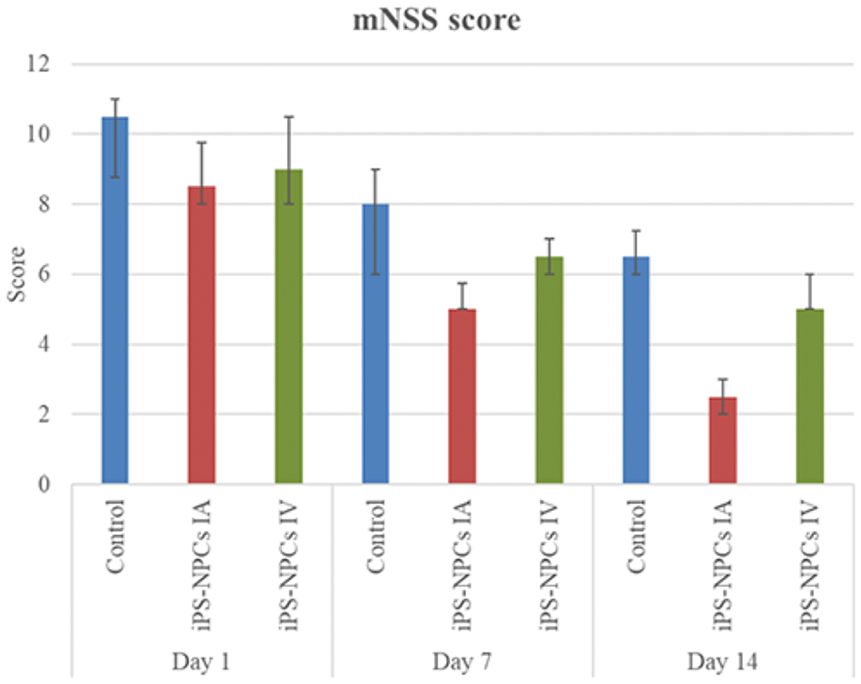
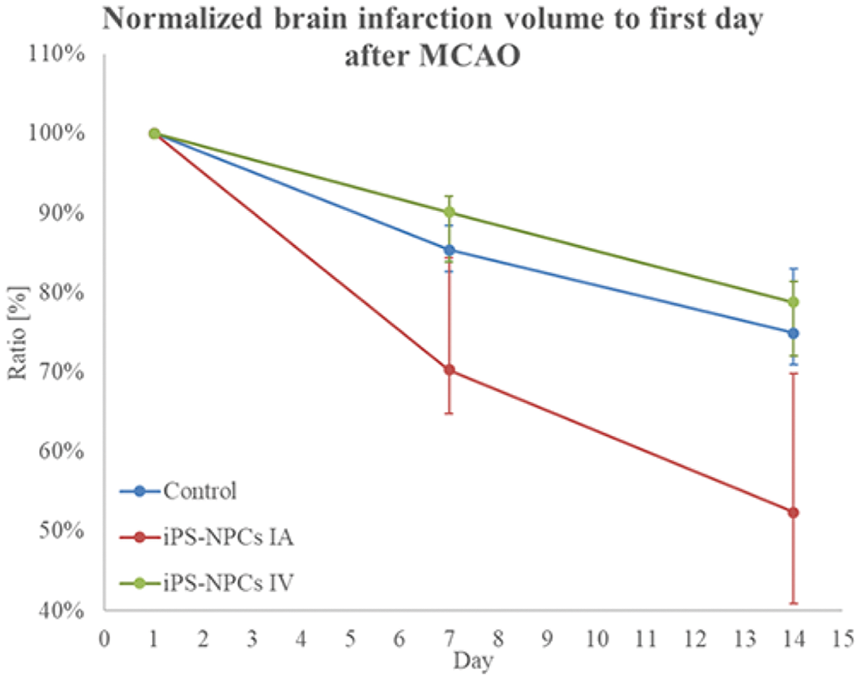
iNPCs are capable to migrate through the blood–brain barrier (fig.2).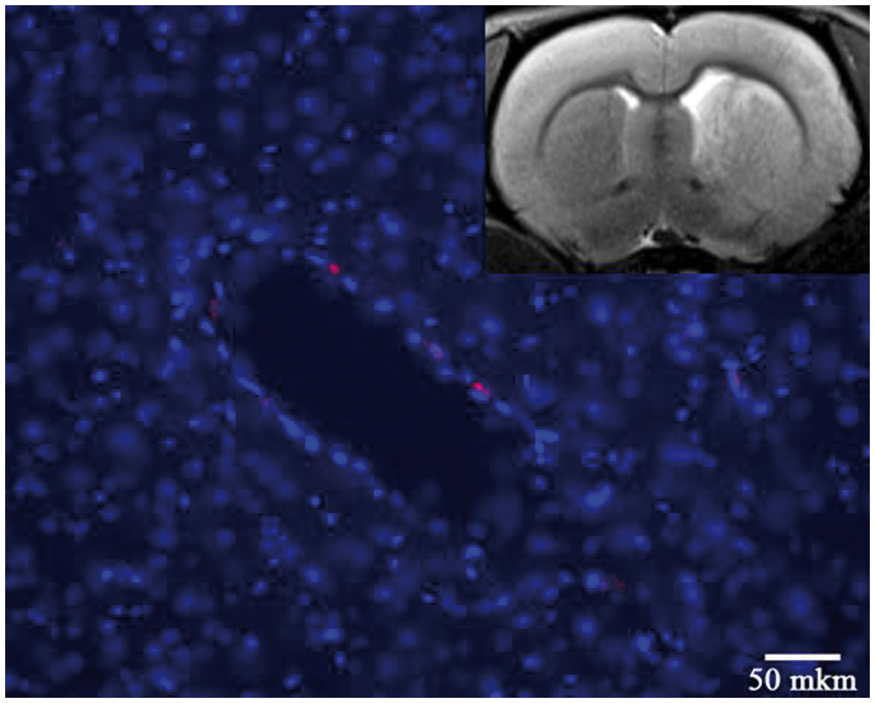
Conclusion
We have shown that IV and IA iNPCs transplantation improved recovery after stroke. However, intra-arterial transplantation has more prominent therapeutic effects. This work was supported by Ministry of Education and Science of the Russian Federation (RFMEFI60417X0184)
Trial registration number
N/A
AS28-040
QUANTITATIVE EVALUATION OF BLOOD ON MRI
1Pirogov Russian National Research Medical University, Research Institute of Cerebrovascular Pathology and Stroke, Moscow, Russia
2Pirogov Russian National Research Medical University, Department of Neurology- Neurosurgery and Medical Genetics, Moscow, Russia
3Pirogov Russian National Research Medical University, Department of Medical Biophysics, Moscow, Russia
Background and Aims
Detection of blood on MRI is an important and relevant task for emergency radiology. Many factors can influence on visualization of blood, such as hemoglobin form, time after hemorrhage, presence of clot, pulse sequences and etc. The aim of this study was to create semi-automatically algorithm to define hemoglobin species on MRI.
Method
Special phantom with fixed temperature at magnetic field with 7T strength was used. Conventional MRI images and T1, T2, T2* maps and apparent diffusion coefficient map was measured. Spectrophotometry was used to control of hemoglobin form and erythrocytes membrane status (figure 1). Additionally, hemorrhage stroke was modeled in rat with dynamic MRI examination (figure 2).
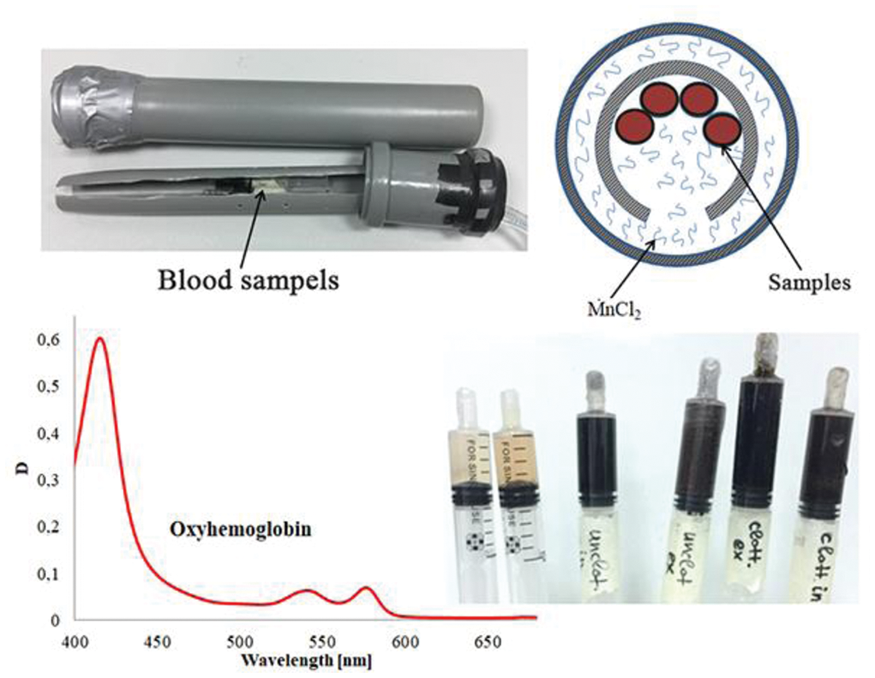
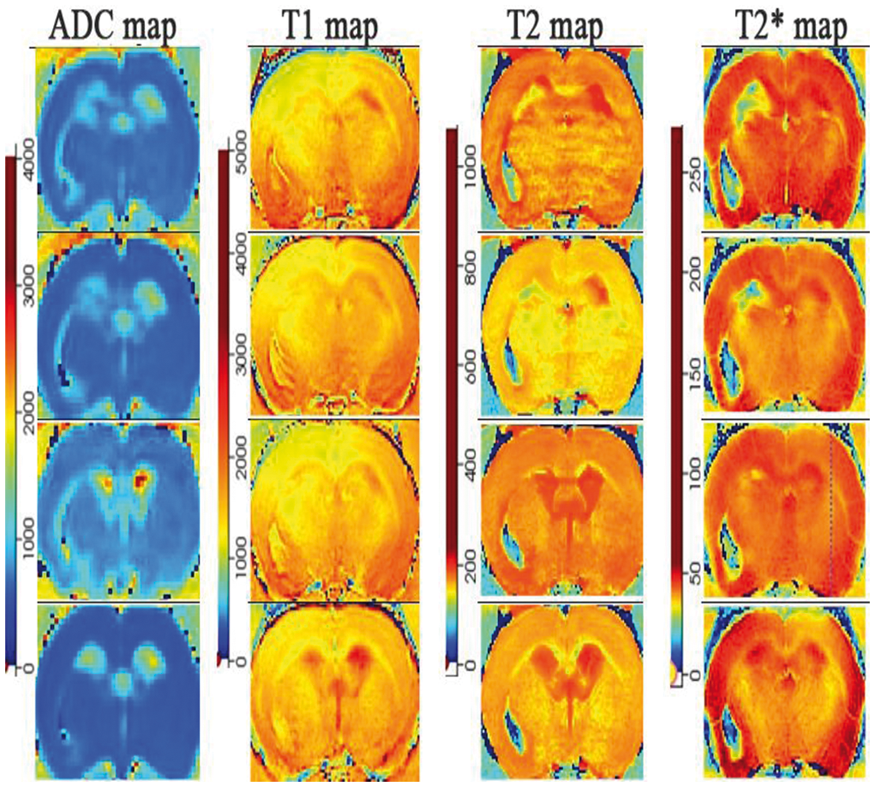
Results
Qualitative and quantitative MRI data of different determinations of blood (clot, free, plasma) total number of 15 was evaluated. In vivo MR in dynamics of rat with intracerebral hemorrhagic were obtained (from injection up to 21 day).
Conclusion
We have shown that semi-automatically algorithm trained on our data can detect different hemoglobin form in hemorrhagic stroke in rat. This method makes possible quantitative evaluation of blood on MRI, but still needs more improvements.
Trial registration number
N/A
AS28-041
COMPARISON OF HUMAN THROMBUS COMPOSITION RETRIEVED IN SEPARATE PASSES DURING THROMBECTOMY IN ACUTE ISCHEMIC STROKE
1Cerenovus- Galway Neuro Technology Centre, Neuravi Thromboembolic Initiative, Galway, Ireland
2Galway-Mayo Institute of Technology, Galway Medical Technology Centre, Galway, Ireland
3Beaumont Hospital, Department of Neuroradiology, Dublin, Ireland
Background and Aims
Mechanical thrombectomy may involve several attempts/passes to remove the occluding thrombus in acute ischemic stroke. To date, the histologic analysis of human thrombi has involved the combined analysis of all thrombus fragments from multiple passes without distinction between fragments retrieved in individual passes. Our novel study compares the composition of thrombi retrieved in each pass.
Method
Thrombi from 60 consecutive stroke patients were collected following thrombectomy at Beaumont Hospital, Dublin, Ireland. Thrombus fragments retrieved in separate passes were fixed separately and processed histologically. Initial characterisation through semi-quantitative rating using Martius Scarlet Blue stained slides was performed. Thrombi retrieved in separate passes were classified as red blood cell (RBC) rich, fibrin rich or mixed.
Results
From the 60 cases (136 passes in total), thrombus fragments were retrieved in 79% of passes. Semi-quantitative analysis showed that fewer passes were required to retrieve RBC-rich thrombi compared to fibrin-rich thrombi (mean 1.2 versus 3 passes respectively). The number of passes required to retrieve RBC-rich and mixed thrombi was not statistically different (Figure 1).
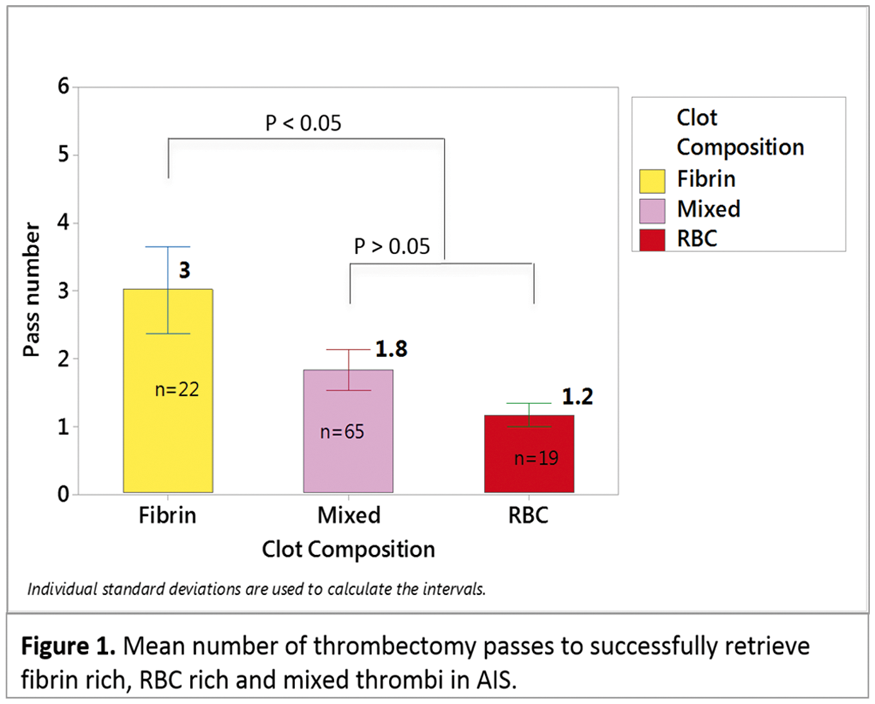
Conclusion
This research provides the first histological comparison of AIS thrombi retrieved in separate thrombectomy passes. Initial analysis suggests that fibrin-rich thrombi require multiple attempts at retrieval. An understanding of the thrombus composition is important for device selection and particularly for developing technologies that can be used to successfully retrieve difficult thrombi.
Trial registration number
N/A
GENETICS, ‘OMICS AND BIOMARKERS
AS29-001
RELATIONSHIP BETWEEN TUMOR NECROSIS FACTOR-ALPHA (-308G/A, +488G/A, -857C/T AND -1031T/C) GENE POLYMORPHISMS AND RISK OF ICH IN NORTH INDIAN POPULATION: A HOSPITAL BASED CASE-CONTROL STUDY
1All Indian Institute of Medical Sciences AIIMS, Neurology, New Delhi, India
Background and Aims
Genetic factors may play a role in the susceptibility of Intracerebral hemorrhage (ICH). The present case-control study hypothesized that genetic polymorphisms in Tumor Necrosis Factor- α (TNF-α) gene may affect the risk of ICH. We investigated the association of four single nucleotide polymorphisms (-308G/A, +488G/A, -857C/T and -1031T/C) within TNF-α gene promoter and their haplotypes with the risk of ICH in North Indian population.
Method
Genotyping was determined by using SNaPshot method for 100 ICH patients and 100 age-sex-matched ICH free controls. Conditional logistic regression analysis with adjusting multiple demographic and risk factor variables was used to calculate the strength of association between TNF-α gene polymorphisms and risk of ICH. Haplotypes were reconstructed using PHASE 2.0 and patterns of Linkage disequilibrium (LD) analysis were done by using Haploview version 4.2.
Results
TNF-α +488G/A gene polymorphism was found to be independently associated with the risk of ICH under dominant [GG +GA vs. AA] (OR = 3.1; 95%CI 1.2 to 8.2; p = 0.001) and allelic [G vs. A] (OR = 2.2; 95%CI 1.2 to 4.2; p = 0.007) models. However, no significant association between -308G/A, -857C/T and -1031T/C gene polymorphisms and risk of ICH was observed. Haplotype analysis showed that 308A-488G-857C-1031T and 308G-488A-857T-1031T haplotypes were significantly associated with the increased risk of ICH. Strong LD was observed for +488G/A and -857C/T TNF-α polymorphisms (D’=0.72, r2 = 0.01).
Conclusion
Our findings suggest that TNF-α +488G/A polymorphism may be an important risk factor for ICH, whereas -308G/A, -857C/T and -1031T/C gene polymorphisms may not be associated with risk of ICH in North Indian population.
Trial registration number
N/A
AS29-002
BODY TEMPERATURE AND INFLAMMATORY MARKERS THE FIRST WEEK AFTER STROKE – SEARCHING FOR BRAIN FEVER
1Örebro University Hospital, Neurology, Örebro, Sweden
Introduction
Fever after stroke is strongly associated with a poor outcome, and may be caused by a number of complications such as bacterial infections or deep vein thrombosis. Complicating the clinical decision making, the stroke itself is thought to be able to cause endogenous fever (from here on referred to as brain fever). However, the knowledge regarding brain fever is limited.
Aim
The aim of this exploratory study was to assess patterns of body temperature and inflammatory biomarkers in stroke patients, in search of a common non-infectious temperature peak that could reflect brain fever. We stipulated that brain fever would have a predictable temporal pattern and that it would correlate to stroke severity.
Methods
Fifteen patients underwent daily clinical examination and collection of blood samples for analysis of C-reactive protein (CRP) and white blood cells count, during one week after stroke.
Results
The majority of patients (10/15) presented at least one occasion of elevated body temperature (≥37.5°C), and these occurred at seemingly random time points in respect to the stroke. Body temperature was during most of the days unrelated to stroke severity. An exception was the first day, during which stroke severity correlated to body temperature enough to approach significance (r = 0.51, p-value=0.089).
Conclusion
The fact that the hyperthermic episodes after stroke appeared at random time points make them unlikely reflections of brain fever. A possible exception is the first 24 hours, during which temperature seemed associated to stroke severity, which could be in line with brain fever.
Trial registration number
N/A
AS29-003
ASSESSMENT OF THE POLYMORPHIC GENES VARIANTS OF THE LIPID AND CARBOHYDRATE METABOLISM, VASCULAR INFLAMMATION AND NEUROTRANSMITTER SYSTEM IN THE FIRST ISCHEMIC STROKE
1Moscow centre of speech patology and neurorehabilitation, healh, Moscow, Russia
Background and Aims
Aim
To study the relations of polymorphic variants of the genes: АРОЕ, MTHFR, IL8, IL6, TNF-а, VEGFA, ADIPOQ, ADIROR, APOB, APOА-V, APOC-IV, LPL, LP(a), BDNF, GRM1, GRM3 and development of the first ischemic stroke (IS).
Material and methods
The alleles frequencies and genotypesassessed for 20 mono-nucleotide polymorphic gene variants in 435patients, who had first IS, and 229 persons with no stroke, comparablewith age, gender, place of living and ethnicity. Genotyping ofpolymorphisms was done with the prepared TaqMan probes.
Results
For polymorphisms АРОВ (rs676210) and IL8 (rs1803205) there was significant difference between groups in the variety of minoralleles and genotypes. Conclusion. There is significant relation of mononucleotidepolymorphisms of the genes АРОВ (rs676210) and IL8 (rs1803205) withthe development of first IS in the studied groups.
Conclusion
There is significant relation of mononucleotidepolymorphisms of the genes АРОВ (rs676210) and IL8 (rs1803205) withthe development of first IS in the studied groups.
Trial registration number
N/A
AS29-005
MULTI-OMICS ANALYSIS TO CHARACTERIZE HUMAN BRAIN ISCHEMIA: AN INTEGROMIC APPROACH TO DISCOVER NEW BIOMARKERS AND POTENTIAL TARGETS FOR NEUROPROTECTION
1Vall d'Hebron Institute of Research, Neurovascular Research Laboratory, Barcelona, Spain
2Vall d'Hebron Institute of Research, Statistics and Bioinformatics Unit, Barcelona, Spain
3University Medical Center of Geneva, Translational biomarker group- Speciality Internal Medicine department, Geneva, Switzerland
Background and Aims
Neuroprotective drugs have not succeeded in their translation to stroke treatment and new biomarkers are sought to help in stroke management. The use of proteomics and transcriptomics to characterize the human brain after stroke and to understand stroke pathophysiology might help develop new therapeutic strategies, including biomarkers’ monitoring.
Method
Flash-frozen post-mortem brain samples from infarct core (IC) and healthy contralateral (CL) areas of 6 stroke patients were analyzed through quantitative label-free mass-spectrometry proteomics and gene expression microarrays. Selected candidates were replicated in 5 new brain samples by Western Blot or RT-qPCR. Verified candidates were qualified by ELISA in blood temporal profiles of 11 ischemic strokes (<4.5h, 24h, 7d). Integrative analysis of both omics was performed by regularized canonical correlations and was combined with biological annotations (miXomics & mogsa R packages).
Results
From the 90 proteins and 192 genes altered in IC areas (FDR<0.1, fold-change>|3|), 14 candidates were replicated in brain and 8 were detected in blood with different temporal profiles, mostly showing higher levels in the hyperacute phase. When both omics datasets were merged, a network of the best correlations highlighted new gene-protein connections and underlined sets of molecules involved in immune system and inflammation, cell metabolism and synaptic transmission, with different contribution of genes and proteins in those pathways.
Conclusion
We have integrated and validated changes due to ischemia at protein and transcript levels in human brain samples. Some of the discovered candidates showed potential as stroke biomarkers and some flagship molecules might be interesting therapeutic candidates.
Trial registration number
N/A
AS29-008
ISCHEMIC TOLERANCE BIOMARKERS: FROM DISCOVERY TO VALIDATION
1Institut de Recerca Biomèdica de Lleida, Clinical Neurosciences Group, Lleida, Spain
2Hospital Arnau de Vilanova de Lleida: Stroke Unit, Institut de Recerca Biomèdica de Lleida: Clinical Neurosciences Group, Lleida, Spain
3Hospital de la Santa Creu i Sant Pau, Department of Neurology, Barcelona, Spain
4Complejo Hospitalario de Navarra, Department of Neurology, Pamplona, Spain
5Hospital Universitario Ramón y Cajal, Deparment of Neurology, Madrid, Spain
6Hospital Universitari Son Espases, Department of Neurology, Mallorca, Spain
7Hospital del Mar, Department of Neurology, Barcelona, Spain
8Hospital Universitario La Paz, Department of Neurology, Madrid, Spain
9Hospital General Universitario Gregorio Marañón, Department of Neurology, Madrid, Spain
10Hospital de Sabadell- Corporació Sanitària i Universitària Parc Taulí, Department of Neurology, Sabadell, Spain
11Hospital Universitario de Albacete, Department of Neurology, Albacete, Spain
Background and Aims
Although Transient Ischemic Attacks is related to high risk of stroke recurrence if correct management is not guaranteed, transient ischemia could contribute to the development of ischemic tolerance (IT). The study of biomarkers related to IT in humans is gaining a great deal of interest in seeing the changes in gene expression that could lead to endogenous neuroprotection and the release of neuroprotective pathway substances.
Method
60 patients who had suffered an ischemic stroke (IS) were selected for this study. 15 of them had suffered a TIA 24 hours prior to IS(Group 1) and 15 more between 24 hours and 7 days prior to IS(Group 2). The remaining 30 patients, did not suffer any TIA prior to IS(Group 3). Patients of each group were divided in three more groups compensated by sex, age and etiology. 9 arrays of antibodies (1,000 proteins in duplicate) were performed in all groups using basal plasma samples. Array’s lectures were normalized respect a reference array. T-Student test was carried out and the correction of BonFerroni (p < 0.000016) was applied in order to identify potential biomarkers.
Results
The mean age was 68.9(SD 9.9) years and the proportion of sexes 4:1 (male:female). The distribution of etiologies was 2: 1: 1: 1 (large artery atherosclerosis:cardioembolism:small vessel:ESUS). Four proteins showed significant differences expression in their relative expression between Group 1 and Group 3.
Conclusion
The technology of antibody arrays had allowed the identification of 4 proteins involved with the IT phenomenon. We will validate our results in a larger cohort of subjects using ELISA’s technology.
Trial registration number
N/A
AS29-009
SERUM AMYLOID PROTEIN IS ASSOCIATED WITH OUTCOME FOLLOWING ACUTE ISCHAEMIC STROKE: DATA FROM THE REMOTE ISCHAEMIC CONDITIONING AFTER STROKE TRIAL (RECAST)
1University of Nottingham, Stroke- Division of Clinical Neurosciences, Nottingham, United Kingdom
2University of Nottingham, Vascular Medicine- Division of Medical Sciences and GEM- School of Medicine, Derby, United Kingdom
Background and Aims
Remote ischaemic per-conditioning (RIC) in experimental ischaemic stroke is neuroprotective. Several neurohumoral, vascular and inflammatory mediators are implicated.
Method
The REmote ischaemic Conditioning After Stroke Trial (RECAST) was a pilot blinded sham-controlled trial in patients with ischaemic stroke, randomised to receive four 5-minute cycles of RIC within 24 hours of ictus. Plasma taken pre-intervention, immediately post-intervention and on day 4 was analysed for nitric oxide (nitrate/nitrite) levels using chemiluminescence and other biomarkers were analysed by enzyme-linked immunosorbent assay (ELISA): alpha-2-macroglobulin (A2M), serum amyloid protein (SAP), e-selectin, vascular endothelial growth factor (VEGF). Biomarkers were correlated with outcome (Day 90 National Institutes of Health Stroke Scale [NIHSS], modified Rankin scale [mRS], Barthel index [BI]) using Pearson’s correlation coefficient.
Results
In all 26 patients, an increase in SAP (pre- to post-intervention) positively correlated with worse day 90 mRS (r = 0.429, p = 0.029) and negatively with worse BI (r = −0.392, p = 0.048), whilst an increase in SAP from day 0 to 4 positively correlated with worse day 90 NIHSS (r = 0.400, p = 0.043), mRS (r = 0.505, p = 0.008) and negatively with worse BI (r = −0.439, p = 0.025). RIC reduced SAP levels from pre- to post-intervention (n = 13, 2-way ANOVA, p < 0.05), whilst sham did not. No significant changes over time or by treatment, or correlations with outcome were seen for A2M, e-selectin, nitric oxide or VEGF.
Conclusion
Increased plasma levels of SAP are associated with worse clinical outcomes after ischaemic stroke. RIC reduced SAP levels from pre- to post-intervention. Larger studies assessing biomarkers and efficacy of RIC in acute ischaemic stroke are warranted.
Trial registration number
N/A
AS29-010
PREDICTORS OF CLINICALLY RELEVANT BLEEDING AND OVERDOSE IN PROSPECTIVELY FOLLOWED COHORT OF DABIGATRAN TREATED STROKE PATIENTS
12nd Medical Faculty- Charles University, Neurology, Prague, Czech Republic
2Na Homolce Hospital, Molecular genetics, Prague, Czech Republic
3Pharmakl- spol. s.r.o., Clinical pharmacology, Prague, Czech Republic
Background and Aims
Dabigatran is direct thrombin inhibitor used in secondary prevention of stroke in patients with atrial fibrillation. RELY trial showed that genetic variants could contribute to interindividual variability in concentrations of dabigatran. Minor allele of the CES1 (rs2244613) was associated with lower exposure to active metabolite and with a lower bleeding risk compared to wild-type allele. Aim was to determine the influence of CES1 genotype on occurrence of clinically relevant bleeding (CRB) or plasmatic levels above the therapeutic range in dabigatran treated stroke patients.
Method
Prospective observational monocentric study in consenting stroke patients initiated on dabigatran. Outcome was any CRB or through plasmatic concentration (cmin) over 300 ng/ml. DNA analysis of CES1 polymorphism rs2244613 was done with RFLP analysis. Through concentration of dabigatran was measured with liquid chromatography-tandem mass spectrometry after initiation and repeated every 12 months.
Results
110 patients after cardioembolic stroke, mean age 70,2 (SD 12.7), 56 (50.9%) women, were enrolled. Mean follow-up time was 19.9 months. 68 (61.8%) patients were wild-type, 37 (33.6%) were minor allele heterozygotes and 5 (4.5%) were homozygous minor allele carriers. There were 8 episodes of CRB and 4 patients with cmin above 300 ng/ml. Carriers of minor allele were less likely to have the outcome, HR 0.124 (95% CI 0.02 – 0.96, p = 0.046).
Conclusion
Patients with minor allele had significantly lower risk of CRB or increased level of dabigatran. Dabigatran dosing based on pharmacogenetics should be studied in future trials with aim to increase the safety of treatment.
Trial registration number
N/A
AS29-011
PLASMA CELLULAR FIBRONECTIN AND THE SEDAN SCORE FOR PREDICTION OF PARENCHYMAL HEMATOMA AFTER STROKE THROMBOLYSIS
1University of Helsinki and Helsinki University Hospital, Neurology and Clinical Neurosciences, Helsinki, Finland
2University of Helsinki, Molecular Neurology at the Research Programs Unit, Helsinki, Finland
3University of Helsinki and Helsinki University Hospital, Emergency Medicine and Services at the Department of Emergency Care, Helsinki, Finland
4Sahlgrenska Academy at University of Gothenburg, Department of Clinical Neuroscience/Neurology at the Institute of Neuroscience and Physiology, Gothenburg, Sweden
5Sahlgrenska University Hospital, Department of Neurology, Gothenburg, Sweden
Background and Aims
Cellular fibronectin (c-Fn) is a promising biomarker for predicting post-thrombolytic intracranial hemorrhage in acute ischemic stroke. We sought to perform external validation of c-Fn, and evaluate benefits of combining c-Fn and the SEDAN score (range 0-6), originally validated for assessing post-thrombolytic risk of symptomatic intracranial hemorrhage (sICH).
Method
Our cohort included 274 thrombolyzed ischemic stroke patients. Pre-treatment plasma c-Fn was measured with ELISA. Hemorrhage identified within 36 hours post-treatment was stratified according to the Heidelberg Bleeding Classification. The European-Australasian Acute Stroke Study II (ECASS-II) definition of sICH was used.
Results
A parenchymal hematoma (PH) occurred in 28 (10.2%) and sICH in 10 (3.6%) cases. The SEDAN score predicted risk of both PH (AUC-ROC 0.73 [0.64–0.82]) and sICH (AUC-ROC 0.79 [0.64–0.94]). In the whole cohort, c-Fn was elevated almost significantly in PH but not in sICH (p = 0.061 and p = 0.502). However, utility was evident within the SEDAN 1–3 subgroup, where c-Fn was significantly higher in PH patients (p = 0.029, AUC-ROC 0.64 [0.52–0.76] for PH prediction). A predictive rule (SEDAN 1-3 with c-Fn≥5.8 µg/mL or SEDAN 4-6) provided a sensitivity of 89%, specificity of 50%, positive predictive value of 17% and negative predictive value of 98% for predicting PH.
Conclusion
Plasma c-Fn improved PH prediction in the SEDAN 1-3 subgroup, in which the risk of intracranial hemorrhagic complications is relatively low. Combining c-Fn and SEDAN allows stratification of patients into groups of very low and high PH risk, which could improve patient selection into future clinical trials aiming to reduce hazardous post-thrombolytic hemorrhagic complications.
Trial registration number
N/A
AS29-013
A GENOME WIDE ASSOCIATION STUDY IN PATIENTS WITH INTRACRANIAL AND EXTRACRANIAL ATHEROSCLEROSIS
1Fundació Docència i Recerca Mútua Terrassa, Stroke Pharmacogenomics and Genetics, Terrassa, Spain
2Vall d'Hebron Institute of Research VHIR, Neurovascular Research Laboratory, Barcelona, Spain
3The Manchester Metropolitan University of All Saints, HealthCare Science Department, Manchester, United Kingdom
4Hospital Universitario Virgen del Rocío, Radiology Department, Sevilla, Spain
5Institute de Biomedicine of Seville- IBiS/Hospital Universitario Virgen del Rocío/CSIC/University of Seville, Department of Neurology, Sevilla, Spain
6Institut de Recerca Hospital de la Santa Creu i Sant Pau, Stroke Pharmacogenomics and Genetics, Barcelona, Spain
7Hospital Clínico Universitario de Valladolid, Department of Neurology, Valladolid, Spain
Background and Aims
Large-artery intracranial/extracranial atherosclerosis (ICAs/ECAs, respectively) are a major cause of stroke worldwide. Genome-Wide Association studies (GWAs) identified genes associated with Aterothrombotic stroke, such as HDAC9 or TSPAN2. However, ICAs and ECAs have not been directly analyzed by GWAs using risk scores.
Method
We studied 509 Caucasian subjects: 195 patients with ICAs and/or ECAs (94.6% symptomatic), and 315 population-based controls. For each patient we calculated two scores depending on the number of ICAs (Score1) and the combination of ICAS/ECAs severity (Score2). Stenosis severity was scored as one (stenosis <50%) or two (stenosis >50%), measured using arteriography (ICAs) and Doppler (ECAs).
Genetic analysis was performed using Human Core Exome (Illumina). For quality controls, 1000G imputation and association analysis we used PLINK, R, IMPUTE2 and SNPTEST following previous recommendations. We used as covariates sex, age and principal components.
Results
After quality controls 8,047,349 SNPs, 173 patients and 315 controls were analyzed. None SNP in HDAC9 nor TSPAN2 was significantly associated with our Scores.
One locus at 11q14 was genome-wide associated (P<10E-08) with Score 1. Two loci were genome-wide associated with Score 2, one at 1p13, the nearest gene has been associated with heart arrhythmias and the other at 18q21, the nearest gene has been associated with calcified aortic stenosis in mi-RNA expression studies.
Conclusion
A GWAs in ICAs and ECAs patients has revealed potential genes associated with ICAs presence and with combination of ICAs and ECAs severity. These findings need to be replicated in other independent cohorts to confirm these results.
Trial registration number
N/A
AS29-014
GENETIC ASSOCIATION OF LEUKOCYTES LEVELS DURING THE ACUTE PHASE OF STROKE
1Fundació Docència i Recerca Mútua Terrassa, Neuroscience Department- Stroke Pharmacogenomics and Genetics, Terrassa, Spain
2Vall d'Hebron Institute of Research VHIR, Neurovascular Research Laboratory, Barcelona, Spain
3Massachusetts General Hospital, Departmet of Neurology, Boston, USA
4Hospital Universitario Central de Asturias HUCA, Neurology Department- Stroke Unit, Oviedo, Spain
5Hospital Germans Tries i Pujol, Department of Neurology, Badalona, Spain
6Institut Hospital del Mar d'Investigacions Mèdiques IMIM, Neurovascular Department, Barcelona, Spain
7The Manchester Metropolitan University of All Saints, Healthcare Science, Manchester, United Kingdom
8Fundació d'Investigació Sanitaria Illes Balears, Neuroscience Laboratory, Palma de Mallorca, Spain
9Hospital Universitari Mútua Terrassa, Department of Neurology, Terrassa, Spain
10Washington University School of Medicine, Emergency Medicine, Saint Louis, USA
11Washington University School of Medicine, Department of Psychiatry, Saint Louis, USA
12Institute de Biomedicine of Seville- IBiS/Hospital Universitario Virgen del Rocío/CSIC/University of Seville & Hospital Universitario Virgen Macarena, Department of Neurology, Seville, Spain
13Washington University School of Medicine, Department of Neurology, Saint Louis, USA
14Sant Pau Insitute of Research, Stroke Pharmacogenomic and Genetics, Barcelona, Spain
Background and Aims
Several genes are associated with stroke risk, however, little is known about stroke outcome. Neutrophils and other immune cells have a key role in inflammation during the acute phase of stroke and have been associated with poor functional and neurological outcome.
We aim find genetic risk factors associated with neutrophils levels (NL) and white blood cell counts (WBCc) during the acute phase of ischemic stroke.
Method
Ischemi stroke patients from 6 Spanish cohorts with data of NL and WBCc during the acute phase (<24h stroke onset) were included in this study. Genotyping was performed with Axiom-Biobank (Affymetrix) and Omniquad-2.5M Core-Exome (Illumina). We performed a SNP association analysis using as covariates age, sex, NIHSS at baseline and principal components (SNPTEST software) for each cohort, and a metanalysis (METAL software). Quality controls of imputation, association analysis and metanalysis were performed following previous recommendations.
Results
1,575 and 963 patients were analyzed for WBCc and NL respectively. We found a correlation with stroke outcome measured at third month with mRS score (p-value = 2.98 × 10−4 WBCc; p-value = 1.0 × 10−6 NL). We found Genome-Wide significant associations for NL and WBC, on Chromosome 6 (Top-SNP, p-value = 2.6 × 10−8) and on Chromosome 11 (Top-SNP: p-value = 2.6 × 10−8) respectively. Those SNPs were not previously associated with NL or WBCc on other GWAS performed on healthy population.
Conclusion
We have found new genetic associations with NL and WBCc during the acute phase of stroke. These SNPs were not previously associated with leukocytes levels in healthy population, suggesting a different modulation of immune cells during the acute phase of stroke.
Trial registration number
N/A
AS29-016
PREVALENCE OF PROTHROMBOTIC GENE MUTATIONS IN PATIENTS WITH CEREBRAL VENOUS SINUS THROMBOSIS
1Neuroscience Research Center NSRC, Neurology Department, Tabriz, Iran
2Connective Tissue Research Center, Department of Medical Genetics, Tabriz, Iran
3Liver and Gastrointestinal Disease Research Center, Internal Medicine, Tabriz, Iran
Background and Aims
Cerebral venous thrombosis (CVT) is not an uncommon neurovascular disorder with higher prevalence in Iranian population. The reason for this higher rate in not known. Thrombophilia caused by gene mutation is a common cause of CVT. The aim of this study was to assess the prevalence of thrombophilic gene mutations in Iranian CVT patients.
Method
In a case-control study from October 2014 to December 2015, all patients (n = 70) with a definite diagnosis of CVT, who were referred to Imam-Reza and Razi hospitals, had been enrolled. As for the control group, 82 healthy controls (with the same ethnicity and origin) with no family history of venous or arterial thrombosis were selected and matched for age and gender. Common gene mutations involved in thrombophilia were assessed in all the participants.
Results
The median age in CVT group was 37 (29–42) years and 56 (80%) were female. Headache was the most common presenting symptom (57%) and super sagittal sinus was the most common involved sinus (52%). the frequency of Factor-V-Leiden, Factor-V-Leiden HR2, Factor prothrombin II, MTHFR (667C/T), and MTHFR (1298A/C) mutations were significantly higher in the CVT group in comparison with control group.
Conclusion
The results of this study suggest that some of the prothrombotic gene mutations are more common in CVT patients and detection of these mutations by clinicians may help them to decide on the duration of treatment and refer the patients and their family members to valuable genetic consultation.
Trial registration number
N/A
AS29-017
PROGNOSTIC VALUE OF COPEPTIN DYNAMICS OVER 5 DAYS AFTER ONSET OF ISCHEMIC STROKE
1University Hospital Zurich, Neurology, Zurich, Switzerland
2University Hospital Basel, Endocrinology, Basel, Switzerland
Background and Aims
The release-kinetics of copeptin after acute ischemic stroke (aIS) are unknown. We hypothesize that copeptin-change (CC) over time may be an even more accurate predictor of outcome as compared to mere copeptin baseline (BC) levels.
Method
Copeptin was serially measured in 348 aIS patients. Outcome measures were unfavorable functional outcome (modified Rankin-Scale (mRS) >2 points) and mortality at 90 days. CC was evaluated by calculating the beta-coefficients for copeptin-change over time (admission, day 1, 3, 5). We fitted multivariate logistic regression models to estimate adjusted odds-ratios (OR, 95%CI) for the association of CC with functional outcome, and adjusted hazard-ratios (HR, 95% CI) for the association with mortality. The discriminatory accuracy was determined by the area under the receiver-operating-characteristic (AUC) curve.
Results
Out of 348 patients 140 had a mRS >2 and 33 died. CC was not significantly associated with functional outcome in contrast to BC. However, CC was an independent predictor for mortality (adjusted HR 1.83; 95%CI 1.27–2.65) comparable to BC levels (HR 3.94; 95%CI 1.63–9.53). Both CC (AUC 0.92, p = 0.022) as well as BC (AUC 0.91, p = 0.036) significantly added incremental value to known vascular risk factors and demographics (AUC 0.88, model without biomarkers) for mortality. The comparison of the model including CC as compared to the model including BC showed no incremental prognostic value (p = 0.7).
Conclusion
CC over the first 5 days showed a strong association with 90-day mortality, but CC compared to BC provided no significant additional information; therefore, no repeated measures are need for an accurate prognosis.
Trial registration number
ClinicalTrials.gov: NCT00390962
AS29-019
USE OF HUMAN ANTIBODY MICROARRAYS TO IDENTIFY POTENTIAL BIOMARKERS RELATED TO STROKE ETIOLOGIES
1Institut de Recerca Biomèdica de Lleida, Clinical Neurosciences Group, Lleida, Spain
2Hospital Arnau de Vilanova de Lleida: Stroke Unit, Institut de Recerca Biomèdica de Lleida: Clinical Neurosciences Group, Lleida, Spain
3Hospital Arnau de Vilanova de Lleida, Department of Vascular Surgery, Lleida, Spain
Background and Aims
The main goal was to identify proteins for etiology recognition in ischemic stroke (IS) patients. For this purpose, we used arrays containing 1000 antibodies against human blood circulating antigens.
Method
200 IS patients were included in the study. They were divided regarding their stroke etiology: 97 patients with IS due to non valvular atrial fibrillation (NVAF), 49 patients with atherothrombotic (ATM) IS and 57 with Small Vessel (SV) IS. For each group, three pools of samples were compensated by sex and age, with which 9 human antibody arrays (Raybiotech) were performed using basal plasma samples, and therefore obtaining the relative expression of 1000 proteins in duplicate. T-student statistical test and Bonferroni correction were applied in all comparisons (p-value<0.00005).
Results
The mean age of AF IS was 81,7 years (SD 7.6), of ATM IS was 75’9 (SD 11.1) and SV IS was 68,4 (SD 12.2) years. Three proteins showed a significant increase in their expression when we compared SV IS with NVAF and ATM IS: LRP-1, that has been linked with various factors related to IS risk; BMP-2, that is an anti-fibrotic biomarker and was considered a potential plasma indicator of inflammatory status; and GDF-9.
Conclusion
All in all, we identified possible biomarkers specifically related to SV IS. We conclude that antibody arrays are a good tool for pre-screening on biomarker discovering, but the obtained results must be validated with more precise techniques and with individual samples in order to determine the role of this proposed biomarkers in SV IS.
Trial registration number
N/A
AS29-020
RELATIONSHIP BETWEEN SERUM C-REACTIVE PROTEIN (CRP) AND SEVERITY OUTCOME IN PATIENT WITH INTRACEREBRAL HEMORRHAGE FROM NORTH INDIAN POPULATION: A HOSPITAL BASED STUDY
1All India Institute of Medical Sciences, Department of Neurology, New Delhi, India
2All India Institute of Medical Sciences, Department of Biochemistry, New Delhi, India
3All India Institute of Medical Sciences, Department of Neurobiochemistry, New Delhi, India
Background and Aims
Intracerebral hemorrhage (ICH) having high morbidity and mortality rates worldwide. CRP has been emerged as important prognostic biomarker for determining functional outcome in patient with ICH.
Aim
To determine the relationship between the serum CRP level in patients with ICH and outcome measured by modified Rankin Scale (mRS) at three months.
Method
In this study, 250 patients with ICH recruited within 72 hours of onset from Neurology ward, Department of Neurology at All India Institute of Medical Sciences, New Delhi. After obtaining written informed consent from patients/proxy, 4ml of blood sample collected and analysed for CRP level by ELISA method. All subjects were telephonically followed by using mRS scale at three months after the recruitment.
Results
The data has been analysed for 244 patients. Mean CRP was 40.6 mg/L (SD ± 33.6). The mean age of the patient was 54.9 years (SD ± 12.89). 35.2% participant was female. A total of 108 (43.2%) deaths were observed. The mean values of CRP at 0,1,2,3,4,5,6 category of mRS were 1.7, 36.7(30.4), 31.9 (22.7), 35 (29.7), 42.9(32.5), 42.7 (41.7), 42.9 (33.8) respectively. Cases were categorised into two groups; good outcome (mRS: 0–3) and bad outcome (mRS: 4–6). ICH cases with bad outcome had significantly higher mean CRP value than patients with good outcome (42.9 vs 33.9; p value =0.04 ttest with unequal variance).
Conclusion
The findings of present study suggested that the high CRP level at baseline may be a significant predictor of functional outcome at three months in patients with ICH.
Trial registration number
N/A
AS29-021
MIRNA REGULATORY NETWORKS AS BIOMARKERS FOR SEIZURES IN SPONTANEOUS ICH
1Ochsner Clinic Foundation, Institute of Translational Research, New Orleans, USA
2Ochsner Clinic Foundation/Louisiana State University Health Science Center, Neurocritical Care/Neurology/Neurosurgery/Neurosciences, New Orleans, USA
Background and Aims
Approximately 10% of patients experience seizures post spontaneous intracerebral hemorrhage (SICH). Etiology of seizures in SICH is unknown, although cerebral injury and iron deposition may be contributory factors. MicroRNA(miRNA) are regulators of gene expression and may serve as biomarkers for pathological processes associated with cerebral injury. We profiled known miRNA to identify regulatory networks as biomarkers for seizures following SICH.
Method
SICH with (n = 3) and without (n = 9) seizures and health (n = 3) patients were consented. Blood (5mL) was collected in Paxgene Blood RNA tubes. Total RNA (1ug) was used for profiling of 2,515 miRNA using µParaflo Microfluidic Biochip. Differential miRNA expression and hierarchical clustering was determined using the t-test (p < 0.05 and 2-fold change). Gene targets of significant miRNA and gene set enrichment analysis (GSEA) were identified using TarBase and miRWalk and the adjusted Benjamini-Hochberg p-value (p < 0.05) cut-off.
Results
We found 13 highly expressed miRNA: 2 up-regulated and 11 down-regulated. 41 additional significant miRNA were found and expressed at low levels: 18 up-regulated and 24 down-regulated. GSEA of up-regulated miRNA for KEGG pathways identified enrichment for cell-cycle, FoxO, and neutrophin signaling pathways. Biological processes that are enriched are associated with protein modifications and cell cycle. Conversely, no significant enrichment was found for down-regulated miRNA. Molecular functions GO terms enriched for up-regulated miRNA are numerous and diverse; whereas, down-regulated miRNA are mainly associated with ion channel activity.
Conclusion
MiRNAs differentiated ICH complicated with seizures and functional network analysis demonstrated involved signaling pathways and bio-processes. This suggests that miRNA regulatory network are potential biomarkers of seizures following spontaneous ICH patients.
Trial registration number
N/A
AS29-025
THE ROLE OF C-TERMINAL-PRO-ENDOTHELIN-1 IN PREDICTING ISCHEMIC STROKE OUTCOME
1University Hospital Zurich, Department of Neurology, Zurich, Switzerland
2University Hospital Wuerzburg, Neurology, Wuerzburg, Germany
3University Hospital Basel, Department of Endocrinology- Diabetes & Metabolism, Basel, Switzerland
Background and Aims
Endothelins have shown to play a role in ischemic stroke pathophysiology. However, only controversial data in mainly small studies exist. We aimed at evaluating the incremental prognostic value of endothelin-1 in a well-described cohort of acute stroke patients.
Method
In this prospective cohort-study we measured endothelin-1 levels of 362 ischemic stroke patients within 72h of symptoms onset. Outcome measures were functional outcome (defined as a modified Rankin Scale of ≤2 for good and ≥3 for unfavourable outcome) and mortality after 90 days. We calculated logistic regression and cox proportional hazards models, respectively, to estimate the association of endothelin-1 with our outcome measures after adjusting for demographic and medical risk factors. To assess the discriminatory accuracy and the incremental value of endothelin-1 beyond known risk factors, we calculated and compared the area under the receiver operating characteristics (AUC) curve.
Results
In the univariate analysis endothelin-1 was associated with unfavourable outcome with an OR of 1.32 [95% CI, 1.16 – 1.51] and with mortality with a HR of 1.45 [95% CI, 1.29 – 1.63]. After adjusting, endothelin-1 remained an independent predictor for mortality with an adjusted HR of 1.58 [95% CI, 1.34 – 1.85] but not for functional outcome. Adding endothelin-1 to the cox-regression model for mortality, the discriminatory accuracy improved from 0.89 [95% CI, 0.84 – 0.94] to 0.92 [95% CI, 0.88 – 0.96] p < 0.001.
Conclusion
Endothelin-1 was an independent predictor of mortality adding incremental prognostic value beyond traditional demographic and vascular risk factors. These results need further validation in independent larger cohorts.
Trial registration number
N/A
AS29-027
ASSOCIATION BETWEEN CIRCULATING PLASMA CONCENTRATIONS OF MESENCEPHALIC ASTROCYTE-DERIVED NEUROTROPHIC FACTOR (MANF) AND LONG-TERM OUTCOMES AFTER ISCHEMIC STROKE
1Institute of Biomedicine, Department of Clinical Pathology and Genetics, Gothenburg, Sweden
Background and Aims
Mesencephalic astrocyte-derived neurotrophic factor (MANF) is expressed in brain and secretory tissues. Data from experimental stroke models show that MANF is neuroprotective. We hypothesized that MANF predicts post-stroke outcomes.
Method
We included cases from the Sahlgrenska Academy Study on Ischemic Stroke, evaluated at 3-month and 7-year follow-ups (n = 220), and age- and sex-matched controls. Plasma was collected at baseline (median 4 days post stroke) and at follow-ups in cases, and once in controls. We quantified relative MANF concentrations by proximity extension assay (Olink® NEUROLOGY panel). We scored cases by NIH stroke scale (NIHSS) at baseline, and NIHSS and modified Rankin Scale (mRS) at follow-ups. We developed regression models to identify associations between MANF and poor outcomes (increasing NIHSS/mRS >2).
Results
Median MANF in arbitrary units was 6.7 (interquartile range 5.6–7.5) at baseline, 6.1 (5.2–7.2) at 3 months, 5.4 (4.7–6.1) at 7 years, and 3.6 (3.0–5.1) in controls. There was no association between MANF and traditional vascular risk factors or NIHSS at baseline. When adjusting for age, previous stroke and baseline NIHSS, independent associations between 3-month MANF and 7-year outcomes were detected (odds ratio 1.52 (95% confidence interval (CI) 1.07–2.14) for mRS>2 and NIHSS beta=0.28 (95% CI 0.02–0.55) per one unit increase in MANF). These associations were retained when adjusting also for 3-month hsCRP and IL-6 levels.
Conclusion
This is the first study reporting an association between plasma MANF and post-stroke outcomes. The mechanisms involved need to be investigated and the source for circulating MANF remains to be established.
Trial registration number
N/A
SYSTEMATIC REVIEW AND META-ANALYSIS
AS30-002
MICROBIOLOGICAL ETIOLOGIES OF PNEUMONIA COMPLICATING STROKE: A SYSTEMATIC REVIEW
1Salford Royal Foundation Trust, Stroke Medicine, Salford, United Kingdom
Background and Aims
Identifying the causal pathogens of pneumonia complicating stroke is challenging and antibiotics used are often broad spectrum, without recourse to the microbiological etiology. We aimed to review existing literature to identify organisms responsible for pneumonia complicating stroke, prior to developing a consensus based approach to antibiotic treatment.
Method
A systematic literature review of multiple electronic databases was undertaken, in accordance with Cochrane and PRISMA guidance. Published studies of hospitalized stroke patients, which identified microbiological etiologies for pneumonia complicating stroke up to 1stJanuary 2017, were considered. Analysis included summary statistics and random-effects meta-analysis where appropriate.
Results
15 studies (40% IS, 60% IS and ICH) involving 7968 patients were included. Where reported (60%), the majority of pneumonia occurred within 1 week of stroke (78%). Reported frequency of positive culture data (15% to 88%) varied widely. When isolated, aerobic Gram negative bacilli (AGNB, 38%) and Gram positive cocci (GPC, 16%) were most frequently cultured; commonly isolated organisms included Enterobacteriaceae (21.8%: Klebsiella pneumoniae, 12.8% and Escherichia coli, 9%), Staphylococcus aureus (10.1%), Pseudomonas aeruginosa (6%), Acinetobater baumanii (4.6%) and Streptococcus pneumoniae (3.5%). Sputum was most commonly used to identify pathogens, in isolation (40%) or in conjunction with tracheal aspirate (15%) or blood culture (20%).
Conclusion
Whilst analysis was limited by small and heterogeneous study populations, limiting determination of microbiological causality, this review suggests AGNB and GPC are frequently associated with pneumonia complicating stroke. This supports the need for a consensus based approach in antibiotic usage and further targeted antibiotic treatment trials for enhanced antibiotic stewardship.
Trial registration number
NA
AS30-003
GLUCAGON-LIKE PEPTIDE 1 RECEPTOR AGONISTS AND PROTECTION AGAINST STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1School of Medicine - University of Ioannina, Internal Medicine, Ioannina, Greece
Background and Aims
Glucagon-like peptide 1 receptor (GLP-1R) agonists, a novel class of antidiabetic agents, have been reported to exert neuroprotective effects in experimental stroke models, especially if treatment starts before stroke. We aimed to assess available data regarding the risk of stroke in diabetic individuals treated with GLP-1R agonists.
Method
We conducted a meta-analysis of randomized, placebo-controlled trials (RCTs) involving GLP-1R agonists with cardiovascular outcomes and/or safety as primary endpoints.
Results
Four eligible multicenter (n = 32,895) prospective double-blinded RCTs (ELIXA, LEADER, SUSTAIN, EXSCEL) were published up to November 2017. The analysis showed a non-significant trend towards a reduction of the risk of stroke in patients taking GLP-1R agonists compared with placebo (odds ratio, OR 0.88, 95%CI: 0.76–1.03, p = 0.109; Q-value = 3.57, p = 0.31; I2 = 15.95%). After excluding ELIXA trial, which included patients at high cardiovascular risk with a recent myocardial infarction, the net benefit was significant (OR 0.85, 95%CI: 0.74–0.99, p = 0.04; Q-value = 2.145, p = 0.342; I2 = 6.76%).
Conclusion
Available data from RCTs dedicated to cardiovascular safety at least partially support the promising findings from previous experimental studies indicating protective effects of treatment with GLP-1R agonists against stroke. Nonetheless, the issue of neuroprotection of these agents needs to be investigated in future clinical studies focusing on stroke.
Trial registration number
ELIXA: NCT01147250
LEADER: NCT01179048
SUSTAIN: NCT01720446
EXSCEL: NCT01144338
AS30-005
THROMBECTOMY 6-24 HOURS AFTER STROKE IN DAWN TRIAL INELIGIBLE PATIENTS
1University of Pittsburgh, Neurology, Pittsburgh, USA
2University of Pittsburgh, Neurosurgery, Pittsburgh, USA
Background and Aims
The DAWN trial demonstrated benefit of endovascular thrombectomy (ET) in patients presenting 6–24 hours after acute ischemic stroke due to anterior circulation large vessel occlusions (LVO). Strict criteria were employed for patient selection. We sought to evaluate the characteristics and outcomes of patients treated outside the DAWN trial.
Method
A retrospective review of acute ischemic stroke admissions to a single DAWN trial-participating comprehensive stroke center was performed during the trial enrollment period (November 2014-February 2017) to identify all patients presenting in the 6–24-hour time window. These patients were further investigated for trial eligibility, baseline characteristics, treatment and outcomes.
Results
About half (204) of the 15% (407) patients presenting to our CSC within 6–24 hours since last seen well (LKW) and NIHSS Score ≥6 (total-2667), harbored a proximal or distal anterior circulation LVO. All DAWN criteria were met by 22% (45) of patients. Of the 159 patients not meeting DAWN criteria, ET was performed outside of clinical trial participation in 29% of patients. In patients with good baseline (mRS 0–1) receiving ET, functional independence rates (mRS 0–2) at 3 months in 26 patients meeting DAWN criteria and 29 patients not meeting DAWN criteria were comparable (54% vs 41%, p value=0.35).
Conclusion
29% of patients not meeting DAWN criteria but with an anterior circulation LVO received ET with safety and efficacy outcomes comparable to patients meeting DAWN criteria. These data indicate a larger population of patients who can potentially benefit from ET in the 6–24-hour time window if more permissible criteria are applied.
Trial registration number
N/A
AS30-006
SHORTER DOOR-IN TO DOOR-OUT TIME IS ASSOCIATED WITH HIGHER LIKELIHOOD OF ENDOVASCULAR THERAPY
1University of Pittsburgh, Neurology, Pittsburgh, USA
2University of Pittsburgh, Emergency Medicine, Pittsburgh, USA
Background and Aims
Endovascular thrombectomy (ET) leads to improved clinical outcomes in patients presenting with large vessel occlusions (LVO); however outcomes are typically worse in patients triaged to a inter-facility transfer. A further understanding of the sources and impact of transfer delays is essential to improve outcomes in this population.
Method
Data were analyzed from consecutive acute ischemic stroke patients with proximal LVO transferred to our comprehensive stroke center for consideration of ET. The following variables were studied: door-in-door-out time (DIDO), baseline NIHSS/mRS, initial CT ASPECT, site of LVO, treatment and clinical outcome.
Results
309 patients were transferred from 14 referral hospitals to our CSC (January-December 2016). 61 patients (20%) had a LVO in the anterior circulation (n = 53) or basilar artery (n = 8). 40 (66%) underwent ET and 21 (34%) did not undergo ET – due to clinical improvement (33%), large core or poor ASPECTS (48%), premorbid disability (5%), hemorrhagic transformation (5%) and time from symptom onset >24 hours (9%). Median DIDO time in the ET group was significantly better than in patients who did not get ET (98.5 minutes vs 185 minutes, p value=0.001). After 90 minutes of DIDO time, the likelihood of undergoing ET decreases by 7% with every additional 10 minutes of DIDO time. In multivariable regression analysis, younger age and lower baseline NIHSS scores predicted good outcome in the ET group.
Conclusion
Shorter DIDO time is associated with higher likelihood of receiving ET. DIDO time should be used as a clinical performance metric for stroke referring hospitals.
Trial registration number
N/A
AS30-007
DWI-NEGATIVE STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS OF FREQUENCY AND OUTCOMES
1The University of Manchester, Faculty of Biology- Medicine and Health, Manchester, United Kingdom
2The University of Manchester, Division of Neuroscience and Experimental Psychology, Manchester, United Kingdom
3The University of Glasgow, Institute of Cardiovascular and Medical Sciences, Glasgow, United Kingdom
4The University of Manchester, Division of Population Health- Health Services Research and Primar, Manchester, United Kingdom
5The University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
Background and Aims
Diffusion-weighted magnetic resonance imaging (DW-MRI) is often used in the diagnosis of acute ischaemic stroke. However, its sensitivity has been variably reported and DW-MRI negative strokes are sometimes postulated to represent stroke mimics. We sought to determine the frequency and reported outcomes of DW-MRI negative strokes.
Method
A systematic literature review of multiple electronic databases using pre-defined search criteria was undertaken, in accordance with PRISMA guidance. Published studies of adults with ischaemic stroke who underwent DW-MRI were included and a meta-analysis was undertaken.
Results
15 studies involving 4602 patients were considered suitable for meta-analyses. The overall reported frequency of DW-MRI negative strokes was 9% (95% CI = 6.8%-11.7%, I2 = 80.2%). The frequency of DW-MRI negative minor stroke (NIHSS≤5, or as defined in the study) was 17% (N=1666, 95% CI = 8.7%-26.7%, I2 = 93.4%). Only 1 study reported 1-year outcome with comparable stroke recurrence rate. While baseline characteristics were poorly reported (26%), DW-MRI negative stroke patients had a higher proportion of ischaemic heart disease (27%) and previous strokes (18%), in comparison to DW-MRI positive strokes. Lacunar strokes (43%) or posterior circulation strokes (24%) were most commonly associated with negative DW-MRI.
Conclusion
The review was limited by small sample sizes and substantial heterogeneity. Our study suggests the need for continuing stroke prevention treatment if the clinical suspicion of stroke remains high, despite negative DW-MR imaging. Larger well designed studies are needed to evaluate long term outcomes including recurrent stroke risk, cognitive and functional outcomes.
Trial registration number
N/A
AS30-008
EFFECTS OF DIABETES MELLITUS AND ADMISSION GLUCOSE ON OUTCOMES IN PATIENTS TREATED WITH MECHANICAL THROMBECTOMY: A META-ANALYSIS
1The First Affiliated Hosipital of Nanjing Medical University, The Department of Interventional Radiology, Nanjing, China
2Nanjing Medical University, School of Nursing, Nanjing, China
Background and Aims
The influence of diabetes mellitus (DM) and admission glucose level (AGL) on outcomes in acute ischemic stroke (AIS) patients receiving mechanical thrombectomy is unclear. We performed a meta-analysis to evaluate outcomes of patients treated with mechanical thrombectomy, according to DM and AGL.
Method
We systematically reviewed studies in PubMed reporting outcomes of mechanical thrombectomy and their relationship with DM or AGL. We took functional independence (modified Rankin score ≤2 at 3 months) as the primary outcome.
Results
Data from 13870 patients in 52 articles were included. Patients with history of DM had significant lower odds of functional independence both in unadjusted (Figure 1) and multivariable analysis (OR, 0.48; 95% CI, 0.33–0.71). Similarly, higher AGL was associated with unfavorable functional outcome in unadjusted meta-analysis (Figure 2) and the combined adjusted OR (95% CI) per 1 mmol/L increase in AGL was 0.87 (0.83–0.92) for functional independence. Recanalization rates and symptomatic intracranial hemorrhage were not related to AGL, and they also had no differences in patients with or without DM.
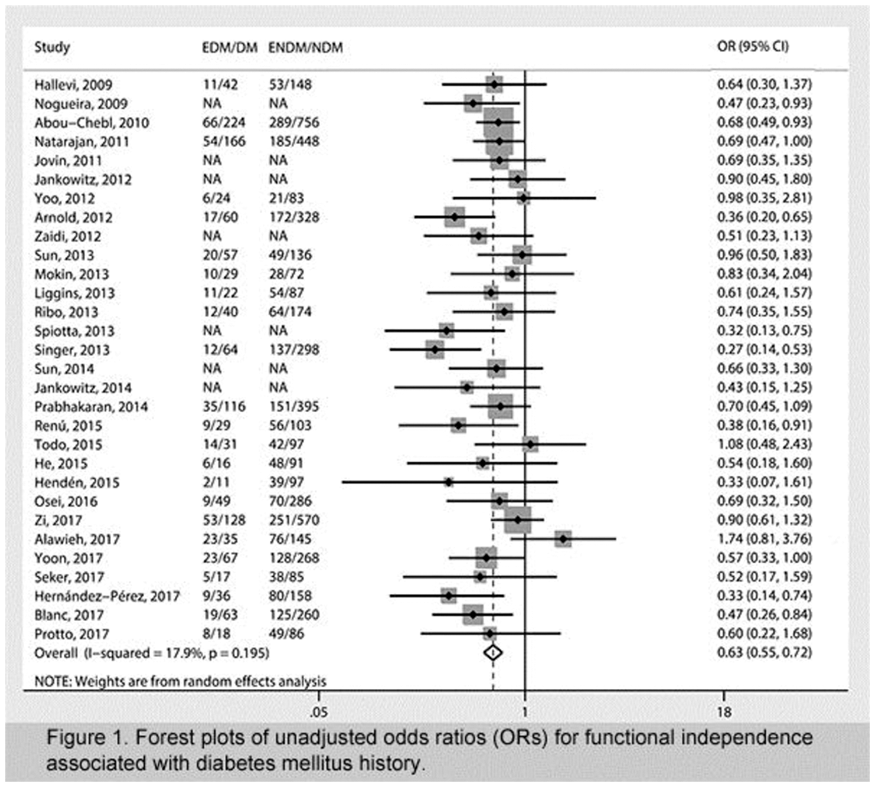
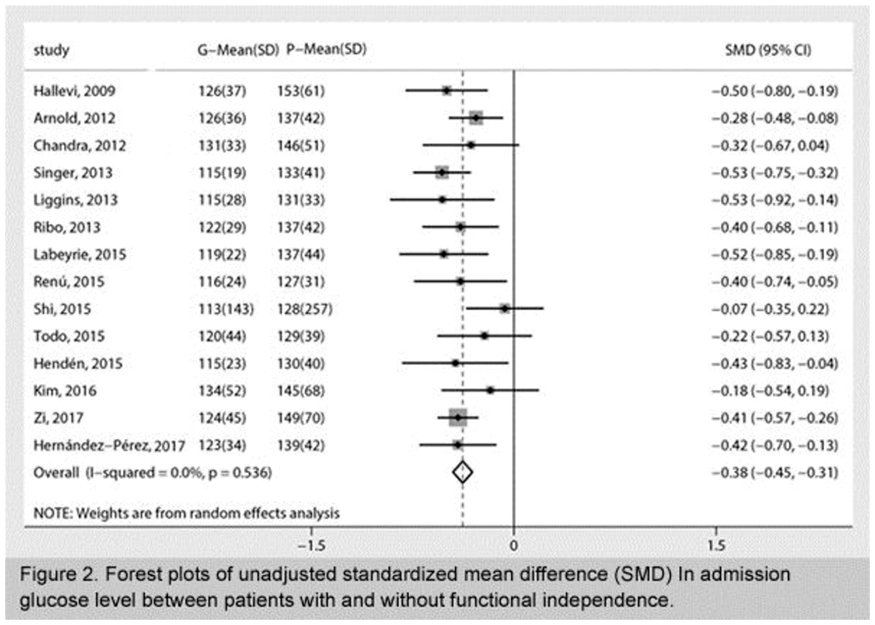
Conclusion
Our results indicate that history of DM and AGL are associated with unfavorable functional outcome at 3 months after mechanical thrombectomy in AIS patients.
Trial registration number
N/A
AS30-009
EENCEPHALODUROARTERIOSYNANGIOSIS FOR HEMORRHAGIC MOYAMOYA DISEASE: LONG-TERM OUTCOME OF A CONSECUTIVE SERIES OF 95 ADULT PATIENTS FROM A SINGLE CENTER
1The people's Liberation Army 307 Hospital, neurosurgery, Beijing, China
Background and Aims
To investigate long term outcomes after encephaloduroarteriosynangiosis (EDAS) for the treatment of hemorrhagic moyamoya disease (MMD) and identify the risk factors for recurrent hemorrhages.
Method
We retrospectively reviewed 95 patients with haemorrhagic MMD who were treated with EDAS at 307 Hospital PLA. Clinical features, angiographic findings, and clinical outcomes were investigated. Rebleeding incidences were compared between anterior or posterior hemorrhagic sites. Kaplan–Meier survival analysis and Cox proportional hazard regression models were used to estimate rebleeding risks post EDAS.
Results
The average age at symptom onset was 37.1 years for adult patients. The ratio of female to male patients was 1.16:1. In 61 of 95 hemorrhagic hemispheres (64.2%), the anterior choroidal artery or posterior communicating artery (AChA-PCoA) was extremely dilated, with extensive branches beyond the choroidal fissure, which only occurred in 28 of 86 nonhemorrhagic hemispheres (32.6%). 57 incidences were classifed as anterior hemorrhages and 38 as posterior. Sixteen of 95 patients (16.8%) suffered cerebral rebleeding after a median follow-up time of 8.5 years. The annual rebleeding rate was 2.2%/person/year. The incidence rate was higher for the posterior group than for the anterior group, however, this difference was not statistically significant (p>0.05). Cox regression analysis revealed that the age of symptom onset (P = 0.028) was a predictor of rebleeding strokes.
Conclusion
EDAS proves beneficial for patients with hemorrhagic MMD. Dilation of the AChA-PCoA is associated with the initial hemorrhage of MMD, and rebleeding is age-related. Patients with hemorrhagic MMD should undergo follow-up over the course of their lives, even when neurological status is excellent.
Trial registration number
N/A
AS30-012
HIGH OPERATOR AND HOSPITAL VOLUME ARE ASSOCIATED WITH A DECREASED RISK OF DEATH AND STROKE FOLLOWING CAROTID REVASCULARISATION. A SYSTEMATIC REVIEW AND META-ANALYSIS
1University Medical Center Utrecht, Department of Vascular Surgery, Utrecht, The Netherlands
2University of Oxford, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
3University of Oxford, MRC Population Health Research Unit- Clinical Trial Service Unit, Oxford, United Kingdom
4University Medical Center Utrecht, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Operator and hospital volume have been proposed as a proxy for outcomes following carotid endarterectomy (CEA) or carotid artery stenting (CAS). The magnitude and clinical relevance of this relationship is debated.
Method
We searched PubMed and EMBASE for studies reporting on the association between operator or hospital volume and procedural outcome following CEA or CAS. Obtained or estimated relative risks (RRs) and odds ratios (ORs) with 95%-confidence intervals (CI) were pooled with a generic inverse variance random-effects model.
Results
For CEA, a decreased risk of death or stroke for high operator volume was found with a pooled adjusted OR of 0.50 (95%CI 0.28–0.87), and a pooled unadjusted RR of 0.59 (95%CI 0.42–0.83); for high hospital volume with a pooled adjusted OR of 0.62 (95%CI 0.42–0.90), and a pooled unadjusted RR of 0.68 (95%CI 0.51–0.92). For CAS, a decreased risk of death or stroke for high operator volume was found with an adjusted OR of 0.43 (95%CI 0.20–0.95), and an unadjusted RR of 0.50 (95%CI 0.32–0.79); for high hospital volume with an adjusted OR of 0.46 (95%CI 0.26–0.80), and no significant decreased risk in a pooled unadjusted RR of 0.72 (95%CI 0.49–1.06).
Conclusion
We found associations between high operator and high hospital volume and a decreased risk of procedural death and stroke after CEA and CAS, indicating that aiming for a high volume might help to reduce procedural complications. Further research is needed to establish the optimum volume thresholds balancing a minimum adverse event rate and practical feasibility.
Trial registration number
N/A
AS30-013
THE ASSOCIATION BETWEEN OPERATOR SPECIALIZATION AND PROCEDURAL OUTCOMES FOLLOWING CAROTID REVASCULARISATION: A SYSTEMATIC REVIEW AND META-ANALYSIS
1University Medical Center, Vascular Surgery, Amsterdam, The Netherlands
2University Medical Center, Vascular Surgery, Utrecht, The Netherlands
3University of Oxford, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
4University of Oxford, MRC Population Health Research Unit- Clinical Trial Service Unit- Nuffield Department of Population Health, Oxford, United Kingdom
5University Medical Center, Julius Center for Health Sciences and Primary Care, Utrecht, The Netherlands
Background and Aims
Different competences and skills are required and obtained during medical specialization that might be associated with the procedural outcomes of CEA or CAS. The magnitude and clinical relevance of the association between operator specialization and procedural outcomes is debated.
Method
We systematically searched PubMed and EMBASE until August 21, 2017 for randomized clinical trials and observational studies. The primary outcome was death and stroke combined. The secondary outcomes were death, stroke, myocardial infarction, death, stroke, and myocardial infarction combined, and cranial nerve injury (in case of CEA). Obtained or estimated risk estimates were pooled with a generic inverse variance random effects model.
Results
A total of 35 studies (data on CEA: 27, data on CAS: 9) were included. For CEA, pooled risk estimates showed a lower unadjusted risk for vascular surgeons compared to neurosurgeons, and compared to general surgeons for death and stroke, death, and stroke. For vascular surgeons compared to cardiac surgeons for stroke. For neurosurgeons compared to general surgeons, compared to cardiovascular surgeons and compared to thoracic surgeons for death. In a limited number of studies on CAS, no statistically significant increased or decreased risks on outcomes following CAS were found comparing operator specializations. The number of studies that adjusted for (potential) case-mix differences between specialties was limited.
Conclusion
Operator specialization is found to be associated with the risk on procedural outcomes for CEA, but only limited data for CAS is available. Future research is needed to elucidate which factors explain the observed differences in procedural outcomes.
Trial registration number
N/A
AS30-014
DIAGNOSTIC ACCURACY OF THE CT ANGIOGRAPHIC “SPOT SIGN” FOR PREDICTING INTRACEREBRAL HAEMATOMA GROWTH
1Stroke and Aging Research Group, Department of Medicine- Monash University- and Stroke Unit and Diagnostic Imaging- Monash Medical Centre- Melbourne- Australia, Melbourne, Australia
Background and Aims
To study the predictive value of the “Spot Sign” in predicting spontaneous intracerebral haemorrhage (ICH) expansion.
Method
PubMed, Medline, conference proceedings and manuscript references up to June 2017 were searched for studies reporting “computed tomography angiography” and “spot sign” or “intracerebral haemorrhage” and “spot sign”. The positive (PLR) and negative (NLR) likelihood ratios were calculated using MetaDisc. The PLR needs to be ≥5 and NLR ≤0.1 for a test to be clinically useful.
Results
There were 36 studies describing 6888 patients. This current analysis includes 23 studies that were not used in previous meta-analyses. The frequency of haematoma growth was 21%. The PLR and NLR for the CTA spot sign indicating haematoma growth were 4.25 (95% CI 3.52–5.13) and 0.48 (95% CI 0.41–0.56) respectively. The sensitivity analyses show a plateau in PLR and NLR of 4.3 and 0.48. The heterogeneity chi square was 214.36–250.24 (p < 0.001) and inconsistency I2 was 83.7–86%.
Conclusion
The PLR for the CTA spot sign did not reach the desired threshold of 5 to be clinically useful. The heterogeneity around this estimate adds to uncertainty. The high NLR suggest that the absence of the CTA spot sign does not guarantee a lack of ICH growth.
Trial registration number
N/A
AS30-015
SYSTEMATIC REVIEW OF CT ANGIOGRAPHIC “SPOT SIGN” FOR PREDICTING MORTALITY
1Stroke and Aging Research Group, Department of Medicine- Monash University- and Stroke Unit and Diagnostic Imaging- Monash Medical Centre- Melbourne- Australia, Melbourne, Australia
Background and Aims
To study whether presence of the CT angiographic “Spot Sign” for spontaneous intracerebral haemorrhage (ICH) expansion is predictive of mortality.
Method
PubMed, Medline, conference proceedings and manuscript references up to June 2017 were searched for studies reporting “computed tomography angiography” and “spot sign” or “intracerebral haemorrhage” and “spot sign”. Positive (PLR) and negative (NLR) likelihood ratios were calculated using MetaDisc. The PLR needs to be ≥5 and NLR ≤0.1 for a test to be clinically useful.
Results
There have not been previous systematic reviews correlating the spot sign to clinical outcome. There were 36 studies describing 6888 patients and 32 clinical outcome measures. However, there were only 3 outcome measures with sufficient comparability across the studies. PLR, and NLR for in-hospital mortality by spot sign were 2.47 (95% CI 1.59–3.82) and 0.62 (95% CI 0.46–0.82) with a plateau of 2.7 and 0.6 respectively across 10 studies. PLR and NLR for 3 month mortality by haematoma expansion were 0.41 (95% CI 0.35–0.47) and 0.8 (95% CI 0.78–0.83) with a plateau of 2.0 and 0.8 respectively across 8 studies.
Conclusion
Overall, there is limited data available on clinical outcomes stratified by the “spot sign”. Based on the available information, the PLR and NLR did not meet respective thresholds of 5 and 0.1 required to have clinical utility.
Trial registration number
N/A
AS30-016
CEREBROVASCULAR EVENTS AFTER SURGERY VERSUS CONSERVATIVE THERAPY FOR MOYAMOYA DISEASE: A META-ANALYSIS
1KU Leuven, Department of Neurosciences- Experimental Neurology- VIB – Center for Brain & Disease Research, Leuven, Belgium
2KU Leuven, Department of Neurosciences, Leuven, Belgium
Background and Aims
To determine the effect of a neurosurgical intervention in patients with moyamoya disease on the risk of cerebrovascular events.
Method
We included studies with at least 10 moyamoya disease patients in either intervention or control group which investigated cerebrovascular events during a minimal follow-up period of 1 year after a neurosurgical intervention vs. conservative therapy. The primary outcome was any stroke and we prespecified three subgroups: adult, ischemic moyamoya and hemorrhagic moyamoya patients. Secondary outcome events were ischemic stroke, hemorrhagic stroke and mortality. We performed a random effects meta-analysis to calculate odds ratios (OR).
Results
We included 2486 patients from 10 studies. The rate of any stroke was 14% in surgical treated compared to 30% in non-surgical treated patients (OR 2.6, 95%CI 1.6–4.5). In subgroup analyses we identified this association in patients presenting with hemorrhagic moyamoya, but not ischemic moyamoya disease. The secondary endpoint of hemorrhagic stroke was 5% in patients who underwent a surgical intervention compared to 19% in conservatively treated patients (OR 3.7, 95%CI 1.9–7.3). In addition we observed a reduction in mortality, 1% vs. 3% (OR 3.1, 95%CI 1.3–7.5), but did not identify an association between surgical treatment and the outcome of ischemic stroke (10% vs. 14%; OR 1.4, 95%CI 0.9–2.2).
Conclusion
Surgical intervention in moyamoya disease is associated with a decreased risk of stroke most striking in patients presenting with hemorrhagic moyamoya disease. The relationship was present between surgical treatment and the outcome of hemorrhagic, but not ischemic stroke.
Trial registration number
N/A
AS30-017
EFFECT OF ACUPUNCTURE FOR URINARY RETENTION AFTER STROKE: A SYSTEMATIC REVIEW
1King's College London, School of Population Health and Environmental Sciences, London, United Kingdom
2Beijing University of Chinese Medicine, School of Basic Medicine, Beijing, China
3Korea Institute of Oriental Medicine, Korean Medicine, Daejeon, Republic of Korea
Background and Aims
To assess the effects and safety of acupuncture for post-stroke urinary retention (UR).
Method
18 mainstream databases and 16 clinical trials registries in four different languages (English, Chinese, Korean, and Japanese) were searched to identify published RCTs worldwide. RCTs comparing any conventional treatment plus acupuncture versus the conventional treatment alone were eligible for inclusion. The likelihood of bias was assessed by using the Cochrane risk of bias tool. Two outcome measures, the cure rate and response rate, were used to assess the effect of acupuncture plus mainstream therapy over mainstream therapy alone. Meta-analysis was performed using RevMan 5.3 software.
Results
20 randomized clinical trials were included with 1322 participants. Catheterization and urination training with acupuncture has a favorable effect on UR than without acupuncture (cure rate: relative risk (RR) from 1.61 [1.20, 2.18] to 1.76 [1.24, 2.50] by two different assessment criteria, and response rate: RR from 1.18 [1.03, 1.35] to 1.34 [1.16, 1.56] by two different assessment criteria). Acupuncture also has a favorable effect on UR with comparison to medicine alone (cure rate: RR: 1.71 [1.19, 2.46] and response rate: RR: 1.33 [1.12, 1.58]). Catheterization with acupuncture is better than catheterization with urination training (cure rate: RR: 1.86 [1.31, 2.65] and response rate: RR: 5.20 [2.51, 10.79]).
Conclusion
Acupuncture appears to increase cure rates for patients who develop UR after stroke, but the trials included are small and some with quality problems. There is a need to confirm the effect of acupuncture on treating UR with further high-quality and standardized RCTs.
Trial registration number
N/A
AS30-018
PREVALENCE OF ANXIETY WITHIN THE FIRST YEAR AFTER STROKE: A SYSTEMATIC REVIEW AND METAANALYSIS
1University of Gothenburg, Neuroscience and Physiology- Rehabilitation medicine, Göteborg, Sweden
2University of Gothenburg, Neuroscience and Physiology- Health and Rehabilitation, Göteborg, Sweden
3Sahlgrenska university hospital, Occupational therapy and Physiotherapy, Göteborg, Sweden
Background and Aims
Anxiety is associated with decreased quality of life and depression, but gets less attention than other psychological consequences after stroke. The aim was to estimate prevalence of anxiety in the first year after stroke.
Method
Searches in EMBASE, MEDLINE, PsycINFO, Cochrane Library, Amed and CINAHL were conducted in May 2015 and April 2017. Included were studies of populations with a hemorrhagic or ischemic stroke or transient ischemic attack, anxiety categorized on a rating scale during the first year after stroke. Two reviewers independently screened and included studies and assessed quality using a checklist. Studies using the Hospital Anxiety and Depression Scale – Anxiety (n 31) were included in a meta- analysis using the random effects model. Heterogeneity was assessed using the Q-test and I² was used to estimate heterogeneity.
Results
Of 4453 titles screened, 37 studies were included comprising 13756 participants with mean ages from 52 to 79 years, assessed within 2 weeks to 1 year after stroke. Most studies were of medium quality. The pooled prevalence of anxiety within the first year was 29.3% [(95% CI 24.8 – 33.8), (I² = 97%, p < 0.00001)] which is higher than previously shown. Frequency 0-2 weeks post stroke was 34.8% (95% CI 24.9 – 44.6%), 2 weeks -3 months 23.2 (95% CI 16.3–30.1%) and 3 -12 months 35.6% (95% CI 17.7–54.3.
Conclusion
One third of the stroke population may have an anxiety disorder and the prevalence seems to increase, why routine screening may be worth considering in order to provide appropriate interventions.
Trial registration number
N/A
AS30-019
RADIOLOGICAL GRADING SCALES FOR PREDICTING DELAYED CEREBRAL ISCHEMIA IN ANEURYSMAL SUBARACHNOID HEMORRHAGE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Academic Medical Center, Biomedical Engineering & Physics, Amsterdam, The Netherlands
3Academic Medical Center, Radiology, Amsterdam, The Netherlands
4Academic Medical Center, Neurosurgical Center Amsterdam, Amsterdam, The Netherlands
Background and Aims
Delayed cerebral ischemia (DCI) is a severe complication of aneurysmal subarachnoid hemorrhage (aSAH). The extent of subarachnoid blood on admission CT-scan is a strong predictor of DCI. However, it is unclear which radiological scale has the most prognostic value. The purpose of this review was to assess the associations of the Fisher scale, modified Fisher scale, and Hijdra sum score with clinical DCI.
Method
We performed a MEDLINE and EMBASE search from 1980 until 20th of June 2017. Radiological grade and occurrence of clinical DCI were extracted along with Odds Ratio’s (OR) for occurrence of DCI. When possible, pooled ORs with 95% confidence intervals were calculated per grade increase on the radiological scale.
Results
Fifty-three studies were included. Fourty-two studies included the Fisher scale, 11 the modified Fisher Scale, and 5 the Hijdra sum score. The Fisher scale was associated with DCI in 62% of the studies compared to 88 – 100% for the other scales. The pooled OR (95% CI) for DCI was 1.53 (1.01 – 2.32) for Fisher 2, 3.21 (1.87 – 5.49) for Fisher 3, and 2.21 (1.49 – 3.28) for Fisher 4, respectively. DCI occurred most frequently (42%) in modified Fisher 4.
Conclusion
The Fisher scale, modified Fisher scale, and Hijdra sum score are all associated with clinical DCI. In contrast to the Fisher scale, the risk of DCI increases per grade increase on modified Fisher scale. As a grading scale should be linear with prognosis, the modified Fisher scale may be preferred for future SAH related studies.
Trial registration number
N/A
AS30-020
RES-Q REGISTER IN BULGARIA
1University Hospital, Second clinic of Neurology with ICU and Stroke unit, Varna, Bulgaria
Background and Aims
Currently in Bulgaria there is no an official national registry of acute ischemic stroke patients who underwent thrombolytic treatment. Therefore, there is no possibility to perform a national analysis of the impact of different treatments on the outcome of the disease. The aim of our study is to make evaluating characteristic from the Res-Q database, related with the quality parameters incuded in the Res-Q register from all centers in Bulgaria until 2018.
Method
Since there is no a national registry of AIS patients, and for the aim of analyzing the results from our research data related to treatment optimization, we have to compare the generalized analysis of the data at the clinic to the database of the remaining centers included in the RES-Q.
Results
Based on the results from the Res-Q register for the period 2016–2018, In 2017 the number of registered patients with ischemic stroke was 127 as 3 (2,36%) of them had thrombolysis, as there were no registered patients with door-to-needle time under 60 minutes. In 2018 from 495 patients, 58 (11,72%) are treated with thrombolysis, as the door-to-needle time was under 60 minutes in 44 (75%) of them and under 45 minutes in 25(43%).
Conclusion
There is, significant improvement with regard to the results of intravenous thrombolysis. Inclusion of more centers for treatment of strokes into the Res-Q registry and the good cooperation between them, results in an improvement in stroke treatment results in Bulgaria, indicating the importance of complete and regular data entry.
Trial registration number
N/A
AS30-021
WEARABLE SENSORS FOR CLINICAL APPLICATIONS IN STROKE, PARKINSON’S DISEASE AND EPILEPSY: A MIXED-METHODS SYSTEMATIC REVIEW
1Neuroscience and physiology, Clinical neuroscience- Rehabilitation Medicine, Gothenburg, Sweden
2Neuroscience and physiology, Clinical neuroscience, Gothenburg, Sweden
Background and Aims
Wearable technology is increasingly used to monitor neurological disorders. The purpose of this systematic review was to synthesize knowledge from quantitative and qualitative clinical research using wearable sensors in stroke, Parkinson’s disease (PD) and epilepsy.
Method
A systematic literature search was conducted in PubMed and Scopus spanning from 1995 to January 2017. A synthesis of the main findings, reported adherence and missing data from quantitative studies is provided. Clinimetric properties of measures derived from wearables in laboratory, free-activities in hospital and free-living environment were summarized. Qualitative thematic synthesis was conducted to explore user experiences and acceptance of wearables.
Results
Out of 104 eligible studies 50 quantitative and 6 qualitative studies had sufficient reporting quality and were included for data extraction and synthesis. In stroke upper extremity activity, walking and physical activity have been studied in laboratory and during free activities. In PD the focus was on quantification of cardinal motor symptoms and medication evoked adverse symptoms in both laboratory and free-living environment. In epilepsy, wearables were used to detect and differentiate seizures in hospital settings. Adherence varied between 63% and 97%, technical errors accounted 3–14% and human error for 4–24% of missing data. Three analytic themes emerged from the thematic synthesis: acceptable integration in daily life, lack of confidence in technology and the need to consider individualization.
Conclusion
Wearables may provide information of clinical features of interest in stroke, PD and epilepsy but knowledge regarding the clinical utility and usability for supporting clinical decision making remains to be established.
Trial registration number
N/A
AS30-023
CONTROL COMPARISONS AND RISK OF BIAS IN RANDOMISED CONTROLLED TRIALS (RCT) OF REHABILITATION AFTER STROKE: AN ANALYSIS OF APHASIA REHABILITATION SYSTEMATIC REVIEW DATA
1Glasgow Caledonian University, Nursing- Midwifery and Allied Health Professions Research Unit, Glasgow, United Kingdom
2Glasgow Caledonian University, Institute for Applied Health, Glasgow, United Kingdom
3University College Cork, Speech and Hearing Sciences, Cork, Ireland
4University of Sheffield, School of Health And Related Research ScHARR, Sheffield, United Kingdom
Background and Aims
Choice of a control comparator in RCTs of rehabilitation may increase the risk of bias. Pharmacological trials employ inert placebo-control comparisons whereas attention-control interventions aim to control for the benefits derived from the notice and involvement that rehabilitation RCTs participation entails. We reviewed the delivery and content of attention-control comparisons in RCTs of speech and language therapy (SLT) for people with aphasia after stroke.
Method
Data Sources: Data from a Cochrane review of SLT for aphasia after stroke following a search of electronic databases (including CENTRAL, MEDLINE, EMBASE, CINAHL, AMED and SpeechBITE) (inception to September 2015).
Methods: We conducted direct and indirect comparisons between SLT, attention-controls and no-therapy controls. We extracted intervention details using the template for intervention description and replication checklist. Language ability, drop-outs and non-adherence was independently double data extracted. Standardized mean differences and risk ratios (95% confidence intervals) were calculated.
Results
Seven RCTs (n = 447) compared SLT with attention-control interventions. Targeted rehabilitation of specific language structures was only described in SLT interventions. Control and SLT interventions however shared several active intervention components; social support, language stimulation, functional language practice and materials. Interventions’ format, location, frequency, intensity, duration and dose were matched. Distinctions between interventions were diminished.
Conclusion
Social support interventions are unsuitable attention-control placebos in RCTs of aphasia rehabilitation. SLT utilises social interactions for therapeutic purposes to support the delivery of targeted language rehabilitation. The distinction between the interventions’ content and delivery was eroded to such an extent that the trials may have lacked sensitivity to detect differences.
Trial registration number
NA
AS30-025
CAN WE IMPROVE THE STATISTICAL ANALYSIS OF VASCULAR PREVENTION TRIALS?: RESULTS FROM THE OPTIMISING THE ANALYSIS OF VASCULAR PREVENTION TRIALS (OA-PREVENTION) COLLABORATION
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom
Background and Aims
Vascular prevention trials typically use binary event outcomes, although this is inefficient statistically and gives no indication of severity; outcomes could therefore be polychotomised, with ordering determined by severity. OA-Prevention aims to identify the most efficient type of outcome and analysis technique for vascular prevention data in randomised controlled trials (RCTs).
Method
Chief investigators of vascular prevention RCTs were asked to share individual patient data from their trials. The most commonly shared outcome was stroke. Extensions of this outcome were analysed using various statistical techniques (e.g. Mann-Whitney U test [MWU], t-test) and results of these analyses were then ordered within each trial set and given a rank; the most significant result (smallest p-value) was given the lowest rank. The Freidman and Duncan’s multiple range tests were then performed to assess significant differences between tests.
Results
Data from 35 trials (257,749 patients) were shared with the collaboration. Thirteen trials had multiple comparator arms, resulting in 59 datasets. Using the severity data provided, a 4-level stroke outcome was derived (Fatal/Non-fatal/TIA/None) for 35 datasets. In a direct comparison, analyses performed on this extended outcome (e.g. MWU, ordinal logistic regression) were more efficient than those performed on a binary stroke/no-stroke outcome (p < 0.001); the most efficient was the MWU test with a mean rank of 4.69.
Conclusion
Methods that are used when analysing polychotomised outcomes appear to be more efficient than those used for binary outcomes. This finding is to be further tested using data from the OA-Prevention collaboration.
Trial registration number
N/A
AS30-026
OPTIMAL ANTIPLATELET THERAPY IN MODERATE TO SEVERE ASYMPTOMATIC AND SYMPTOMATIC ATHEROSCLEROTIC CAROTID STENOSIS: A SYSTEMATIC REVIEW OF THE LITERATURE
1The Adelaide and Meath Hospital, Neurology, Dublin, Ireland
2Glenfield Hospital, Department of Vascular Surgery, Leicester, United Kingdom
3University of Strasbourg, Department of Vascular Surgery, Strasbourg, France
4Rigshospitalet University of Copenhagen, Dept. of Vascular Surgery, Copenhagen, Denmark
5University of Patras Medical School, Department of Vascular Surgery, Patras, Greece
6University of Oxford, Nuffield Department of Surgical Sciences, Oxford, United Kingdom
7University Medical Center Utrecht, Department of Vascular Surgery, Utrecht, The Netherlands
8Hospital de Galdakao-Usansolo, Department of Angiology and Vascular Surgery, Bizkaia, Spain
9University College London Medical School, Department of Vascular Surgery, London, United Kingdom
10School of Medicine- Trinity College Dublin, Irish Centre for Vascular Biology, Dublin, Ireland
Background and Aims
Carotid stenosis patients are at risk of cerebrovascular events despite antiplatelet therapy. Data on prescribed antiplatelet regimens have not been comprehensively-collated from trials to guide optimal therapy in this population.
Method
We searched Medline, Ovid, Embase, Web of Science and Google Scholar from 01/1988 to 03/2016 for randomised trials in patients with symptomatic or asymptomatic extracranial moderate-severe carotid stenosis on any form of antiplatelet therapy in which cerebrovascular outcome events were reported.
Results
Twenty-two studies were deemed eligible for inclusion. Data from one RCT showed a non-significant benefit from aspirin vs. placebo in asymptomatic carotid stenosis, but it is still reasonable to recommend aspirin (81–325mg daily) for prevention of vascular events in these patients. Low-medium dose aspirin (81–325mg daily) is superior to higher doses (>650mg daily) at preventing recurrent vascular events in patients undergoing endarterectomy. Data from endovascular treatment (EVT) trials support peri-procedural treatment of asymptomatic and symptomatic patients with 81–325mg of aspirin daily. The use of peri-procedural aspirin-clopidogrel in patients undergoing EVT is based on one pilot trial, but appears safe. Short-term treatment with aspirin-dipyridamole or aspirin-clopidogrel are equally effective at reducing micro-embolic signals on transcranial Doppler ultrasound in patients with ≥50% symptomatic carotid stenosis. There is insufficient evidence to recommend routine aspirin-clopidogrel combination therapy to reduce the risk of ‘recurrent clinical ischaemic events’ in patients with symptomatic moderate-severe carotid stenosis.
Conclusion
This systematic review facilitates an evidence-based approach to ‘optimal antiplatelet therapy’ in carotid stenosis patients. Future trials should randomise such patients to receive different antiplatelet regimens.
Trial registration number
N/A
AS30-027
STATIN PRE-TREATMENT AND MICRO-EMBOLIC SIGNALS IN LARGE ARTERY ATHEROSCLEROSIS: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Attikon University Hospital, Second Department of Neurology, Athens, Greece
2Metropolitan Hospital, Stroke Unit, Pireus, Greece
3Ruhr University Bochum- St. Josef-Hospital, Neurology, Bochum, Germany
4University of Ioannina- School of Medicine, Neurology, Ioannina, Greece
5St Vincent’s University Hospital- University College Dublin, Neurology, Dublin, Ireland
6Vascular Neurology Research Foundation- The Adelaide and Meath Hospital- Dublin- incorporating the National Children’s Hospital, Neurology and Stroke Service, Dublin, Ireland
7School of Medicine- Trinity College Dublin, Academic Unit of Neurology, Dublin, Ireland
8Royal Free Campus- UCL Institute of Neurology, Clinical Neurosciences, London, United Kingdom
9University Hospital Geneva and Medical School, Neurology, Geneva, Switzerland
10Attikon University Hospital- National and Kapodistrian University of Athens, Second Department of Internal Medicine, Athens, Greece
11Yong Loo Lin School of Medicine- National University of Singapore, Neurology, Singapore, Singapore
12University of Alberta, Neurology, Edmonton, Canada
13University of Calgary, Clinical Neurosciences, Calgary, Canada
Background and Aims
Observational data from a recent study indicate that statin pretreatment (SP) in patients with acute cerebral ischaemia (ACI) due to large artery atherosclerosis (LAA) is associated with both a lower incidence of micro-embolic signals (MES) and reduced MES burden during transcranial Doppler ultrasound (TCD) monitoring.
Method
We performed a systematic review and meta-analysis of available observational studies reporting MES presence/absence and/or MES burden, categorized according to SP status, in patients with ACI due to symptomatic LAA (≥50% ipsilateral carotid stenosis). In studies with partially-published data, authors were contacted for previously-unpublished information. We also performed sensitivity analysis of studies with data on MES burden categorized according to SP status, and an additional subgroup analysis in patients receiving higher-dose SP (atorvastatin 80mg or rosuvastatin 40mg daily).
Results
Seven eligible study protocols were identified (568 patients, 55% with SP). SP was associated with a reduced risk of MES detection during TCD-monitoring (RR=0.60, 95% CI: 0.38–0.95), with substantial heterogeneity between studies (I2=57%, Figure A). In studies reporting MES burden, a significantly lower number of MES were identified in patients with compared with those without SP (mean difference = −0.97, 95%CI: -1.70 to -0.24; Figure B), with no evidence of heterogeneity between studies (I2=47%). Subgroup analysis revealed that higher-dose SP reduced the risk of detecting MES (RR=0.23, 95%CI: 0.06–0.88), with no evidence of heterogeneity between studies (I2=0%, Figure C).

Conclusion
SP appears to be associated with a lower MES incidence and burden in patients with ACI due to LAA, possibly with a more pronounced benefit from higher-dose SP.
Trial registration number
N/A
AS30-028
IMPACT OF DYSPHAGIA ASSESSMENT AND MANAGEMENT ON RISK OF STROKE-ASSOCIATED PNEUMONIA IN ACUTE STROKE: A SYSTEMATIC REVIEW
1Sheffield Teaching Hospitals Foundation NHS Trust, Speech and Language Therapy, Sheffield, United Kingdom
2Sheffield Hallam University, Faculty of Health and Wellbeing, Sheffield, United Kingdom
3Royal College of Physicians, Sentinel Stroke National Audit Programme, London, United Kingdom
4Salford Royal Foundation Trust, Greater Manchester Comprehensive Stroke Centre, Salford, United Kingdom
5University of Manchester, Division of Cardiovascular Sciences, Manchester, United Kingdom
Background and Aims
Patients with dysphagia are at increased risk of stroke-associated pneumonia (SAP). There is wide variation in the way patients are screened and assessed. This systematic review addressed “How do methods of dysphagia assessment and management during the first 72 hours of admission affect the risk of SAP?” The objective was to identify which methods influence the risk of SAP in acute stroke.
Method
Electronic databases (CINAHL, COCHRANE, EMBASE, MEDLINE and SCOPUS) were systematically searched for studies reporting dysphagia screening, or assessment, or management in acute stroke. The primary outcome was SAP. Eligible studies were critically appraised, data extracted and summarised. Heterogeneity was evaluated using random effects models.
Results
Twelve studies including data on 87824 patients were included. There was marked heterogeneity in study design between the included studies, which precluded meta-analysis. Nine studies were prospective observational studies. Two used a quasi-experimental design and 1 was a retrospective review. Type of dysphagia screening protocol varied widely. There was limited information on what comprised a specialist swallow assessment and alternative feeding was the only management strategy where data were analysed in relation to SAP. Use of a formal screening protocol, early dysphagia screening and assessment by a speech and language pathologist (SLP) was associated with a reduced risk of SAP.
Conclusion
There is variation in assessment and management of dysphagia in acute stroke. There is moderate evidence from observational studies only that early screening and specialist swallow assessment by a SLP may reduce the odds of SAP.
Trial registration number
N/A
AS30-029
STEM CELL THERAPY IN PATIENTS WITH ISCHEMIC STROKE: A META-ANALYSIS
1All India Institute of Medical Sciences- New Delhi, Neurology, New Delhi, India
Background and Aims
Stem cell therapy has emerged as a potential therapy for the treatment of stroke. We performed a meta-analysis of published studies using stem cell therapy in patients with ischemic stroke (IS).
Method
Literature was searched using Sciencedirect.com, Google Scholar, MEDLINE, PubMed, EMBASE, Trip Database, Cochrane library and clinicaltrial.gov to identify studies on stem cell therapy in IS till December, 2017. STATA version 13 was used for carrying out meta-analysis. Selection Criteria: We included comparative non-randomized trial, or randomized controlled trials (RCT) if stem cell were infused to treat patients with IS in any phase after the index stroke. Fixed effect model was used if heterogeneity was less than 50%, otherwise random effects model to compute the standardized mean difference in stroke outcome between intervention and control group.
Results
Four randomized trials and four non-randomized comparative trials were included in the present meta-analysis. Significant improvement in term of standardized mean difference in stroke outcome was observed in the stem cell therapy group as compared to controls (SMD 0.43, 95% CI 0.25 to 0.59, P<0.001). The pooled difference in the safety outcomes was not significant between both the groups.
Conclusion
Our meta-analysis suggests that stem cell therapy is safe, feasible and may have potential to improve outcome in patients with stroke. Well designed randomized controlled trials are required to provide more information on the efficacy of stem cell transplantation in patients with IS.
Trial registration number
None
AS30-033
IS CEREBRAL ISCHAEMIA ON DIFFUSION-WEIGHTED IMAGING AFTER REVASCULARISATION OF CAROTID STENOSIS A SURROGATE OUTCOME MEASURE FOR PROCEDURAL STROKE? A SYSTEMATIC REVIEW AND META-ANALYSIS
1University Hospital Basel, Neurology and Stroke Center, Basel, Switzerland
2UCL Institute of Neurology, Brain Repair and Rehabilitation, London, United Kingdom
3London School of Hygiene and Tropical Medicine, Medical Statistics- Faculty of Epidemiology and Population Health, London, United Kingdom
Background and Aims
Aim
To investigate if DWI lesions after carotid artery stenting (CAS) or endarterectomy (CEA) provide a surrogate outcome measure for peri-procedural stroke.
Methods
We selected all studies where DWI scans were obtained before and within 7 days after CAS or CEA for symptomatic or asymptomatic carotid stenosis. The clinical outcome was ischaemic hemispheric stroke up to 30 days after treatment. The surrogate outcome was the presence of ≥1 new DWI lesion after treatment (DWI+). The correlation between the log odds of stroke and DWI+ was estimated in a bivariate random effects logistic regression model across studies and subgroups for CAS and CEA separately. Relative risks of DWI+ and stroke in studies comparing CAS vs. CEA were estimated using fixed-effect Mantel-Haenszel models.
Results
71 studies, reporting 75 separate CAS subgroups (4455 procedures) and 29 separate CEA subgroups (1708 procedures) were included. The average risks of DWI+ and stroke were 36% and 2.8% in CAS patients and 10.2% and 1.5% in CEA patients, respectively. Across CAS subgroups, the log odds of DWI+ correlated significantly with the log odds of stroke (correlation coefficient 0.68, p = 0.032). Correlation was not significant across CEA subgroups. In 17 studies comparing CAS vs. CEA, the relative risks (95% confidence intervals) of DWI+ and stroke were 4.25 (3.44–5.24) and 2.45 (1.47–4.10), respectively.
Conclusion
These findings support the use of DWI as a surrogate outcome measure for peri-procedural stroke in CAS. Randomized studies comparing treatment effects on DWI lesions and clinical stroke are needed to further validate surrogacy.
Trial registration number
N/A
AS30-034
ALCOHOL INTAKE AND RISK OF ISCHEMIC STROKE : A DOSE-RESPONSE META-ANALYSIS
1Nowon Eulji Medical Center- Eulji University, Neurology, Seoul, Republic of Korea
2Ilsan Paik Hospital- Inje University, Neurology, Goyang, Republic of Korea
3Seoul Medical Center, Neurology, Seoul, Republic of Korea
Background and Aims
The correlation between alcohol intake and stroke risk has been controversial. These controversies may be attributed to heterogeneity of stroke subtypes, potential differential effects across sex and race/ethnic groups, and different beverage types and amounts of alcohol consumed. The aim of this study was to evaluate the effects of alcohol intake on the incidence and mortality of ischemic stroke using a dose-response meta-analysis considering various subgroup.
Method
We searched the PubMed, EMBASE, the Cochrane Library databases, PsycINFO, Wprim, and domestic databases including RISS, KoreaMed, Kmbase, NDSL for relevant articles published up to December 2016. From 21 observational studies (17 cohorts), the different dose categories of alcohol intake were compared with the non-drinkers between sexes for the incidence and mortality of stroke.
Results
Compared with non-drinker, alcohol intake of light (-10 g/d) and light-to-moderate (10–20 g/d) amount reduced Ischemic stroke incidence (RR 0.60, 95% CI 0.42–0.88; 0.61, 0.40–0.93, respectively), which was observed only in female population, not in male. Very high intake (> 120 g/d) resulted in increased incidence of ischemic stroke (5.05, 1.53–16.67). Compared with non-drinker, alcohol intake of moderate-to-high (40–60 g/d) amount increased Ischemic stroke mortality (5.05, 1.53–16.67) in male population, while light intake (-10 g/d) resulted in reduced ischemic stroke mortality in female (0.60, 0.50–0.72).
Conclusion
Moderate-to-high and very high alcohol intake increased the risk of stroke incidence and mortality in men, but light and light-to-moderate alcohol intake decreased the risk in women compared with non-drinkers.
Trial registration number
N/A
AS30-036
SYSTEMATIC REVIEW OF PUBLISHED AND UNPUBLISHED DATA ON PREVALENCE OF PATENT FORAMEN OVALE IN CRYPTOGENIC STROKE AT OLDER AGES
1Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, Oxford, United Kingdom
Background and Aims
Percutaneous closure of large patent foramen ovale (PFO) has recently been shown to be superior to medical treatment alone for prevention of recurrent stroke after cryptogenic TIA/non-disabling stroke at age ≤60 years. However, the associations of PFO and cryptogenic events at older ages are conflicting.
Method
We compared the age-specific prevalence of PFO in consecutive patients with cryptogenic vs. other TIA/non-disabling ischaemic stroke (TOAST criteria) in a population-based study (Oxford Vascular Study; 2014–2017) using contrast-enhanced transcranial Doppler (bubble-TCD) and pooled our results in a systematic review of published studies of PFO prevalence (transoesophageal echo-TOE or bubble-TCD) by stroke subtype at older ages.
Results
Of 523 patients (190 aged >60 years), 157 (30.0%) were found to have a PFO. Compared to patients of known aetiology, cryptogenic cases were associated with a higher prevalence of PFO overall (97/264 versus 60/259, OR = 1.93, 95%CI 1.32–2.82, p = 0.001) and in those aged >60 years (68/190 versus 44/207, OR = 2.07, 1.32–3.23, p = 0.001). On pooling with data from two previous smaller studies of bubble-TCD, the association remained highly significant at age >60 years (n = 741; OR = 2.35, 1.42–3.90, p = 0.0009; phet = 0.15) and was also consistent with the equivalent estimate from five TOE studies (n = 1280; OR = 2.20, 1.15–4.22, p = 0.02; phet=0.03), particularly across the four larger (recruitment >100 patients) studies (2.82, 1.76–4.52, p < 0.0001; phet=0.21).
Conclusion
Given the relatively consistent association of PFO and cryptogenic stroke in patients aged >60 years, trials to compare closure vs. best medical treatment in patients with large PFO and otherwise cryptogenic stroke are justified at older ages.
Trial registration number
N/A
AS30-037
THE EFFECTIVENESS OF VIRTUAL REALITY INTERVENTIONS IN THE TREATMENT OF BALANCE IMPAIRMENT IN PATIENTS WITH CHRONIC STROKE: A SYSTEMATIC REVIEW
1IZMIR KATIP CELEBI UNIVERSITY, Physiotherapy and Rehabilitation, IZMIR, Turkey
2Dumlupinar University, Division of Physiotherapy and Rehabilitation, Kutahya, Turkey
3Dokuz Eylul University, School of Physical Therapy and Rehabilitation, Izmir, Turkey
Background and Aims
To evaluate the effectiveness of virtual reality interventions for improving balance in patients with chronic stroke
Method
Studies were identified from electronic databases (CINAHL, EMBASE, MEDLINE, AMED, JBI, COCHRANE, and PEDro) searched to June 2015. Two review authors assessed studies for inclusion, extracted data and evaluated trial quality. PRISMA Checklist has been used as primary guideline.
Results
A total of 397 studies were screened. After inclusion and exclusion criteria applied three randomised controlled trials were included. These studies presented the results of 72 participants. All of the included studies reported improvement in intervention and control groups after treatments. Only one study showed a significant difference in favour of intervention group.
Conclusion
Virtual reality interventions improve the static and dynamic balance and develop the skills of functional independence as much as conventional rehabilitation does. Neither virtual reality interventions nor conventional therapy approaches are superior to one another in this patient population. Further studies with large sample sizes and good methodological quality are needed to establish strong evidence.
Trial registration number
N/A
AS30-038
LONGITUDINAL EVALUATION OF COGNITION AFTER STROKE - A SYSTEMATIC REVIEW
1Florey Institute of Neuroscience and La Trobe University, Neurorehabilitation, Melbourne, Australia
2La Trobe University, Occupational Therapy- School of Allied Health, Melbourne, Australia
3Washington University in St. Louis, Occupational Therapy, St. Louis, USA
4Florey Institute of Neuroscience, Stroke division, Melbourne, Australia
5University of Haifa, Occupational Therapy, Haifa, Israel
6La Trobe University, School of Allied Health, Melbourne, Australia
Background and Aims
Cognition is one of the areas more commonly affected by stroke, however the trajectory of recovery of cognitive function is relatively unexplored. The aim of this review was to identify studies that have investigated cognition longitudinally post-stroke and to identify the instruments used.
Method
A targeted search was conducted to identify longitudinal studies and clinical trials reporting cognitive outcomes on adults (18+) who sustained a hemorrhagic or ischemic stroke. Seven databases were examined: PsycINFO, Embase, MEDLINE, Pubmed, Web of Science, and CINAHL. Studies on pediatric, adolescents, animal studies, and investigations on SAH, and TIA were excluded.
Results
A total of 1,072 papers were identified, sixty-two papers met our inclusion criteria. In a preliminary analysis, we identified 172 instruments evaluating 82 different cognitive functions longitudinally. Memory, attention, and executive function were the cognitive domains more commonly assessed. The MMSE was the most frequently used instrument, with 33 studies (53%) using this assessment serially. Other findings indicate that most longitudinal and follow-up studies (76%) do not assess cognition beyond 12-months post-stroke; and that 73% of these papers used more than one assessment to evaluate cognition at multiple time points. There were no studies using performance-based assessments longitudinally.
Conclusion
Our results show that there is large variability in both the cognitive assessments used and the domains they target. Studies looking at post-stroke cognitive function beyond the one-year mark are scarce. These issues, combined with non-representative samples, dropouts, and practice effects, make identifying the true trajectory of post-stroke cognition from the current literature extremely difficult.
Trial registration number
N/A
AS30-039
HAS THE INCREASE IN THE RATE OF ANTICOAGULATION HAD AN IMPACT ON THE RATE OF STROKE ? ANALYSIS OF NATIONAL PRESCRIBING DATA
1St Vincent’s University Hospital and St Columcille’s Hospital, Medicine for the Elderly, Dublin, Ireland
2Health Service Executive, department of Public Health, Dublin, Ireland
3University College Dublin, Health Research Board Stroke Clinical Networks Ireland., Dublin, Ireland
4Royal College of Physicians of Ireland, National Clinical-Programme for Stroke, Dublin, Ireland
5St James's Hospital and University of Dublin- Trinity College., National Centre for Pharmacoeconomics, Dublin, Ireland
6Mercer's Institute for Successful Ageing- St. James's Hospital, St. Jame's Hospital-, Dublin, Ireland
Background and Aims
The availability of Direct Oral Anti Coagulants (DOACs) and increased attention towards detecting atrial fibrillation have resulted in an increase in the number of people anticoagulated.
We examined whether the increase in rate of anticoagulation was associated with changes in the incidence of intra cerebral haemorrhages and infarcts
Method
We compared the annual haemorrhagic stroke (ICD I60 and I61) and cerebral infarcts (I63) data admitted to public hospitals from 2009 to 2016 and compared them with national medicines prescribing data for anticoagulants (Warfarin and DOACs). Data was compared with baseline incidence period 2004–2008.
Results
The number anticoagulated increased by 84% over the period January 2010 to January 2017 (33073 – 60800). Numbers receiving Warfarin dropped by 30.7% in that time. Proportion of patients on DOACs increased from 0.9% to 62.9% over this seven years.
Baseline average rate of ischaemic stroke increased by 3.6% per annum (4174- 4781 (14.5%)) in the baseline period but only 0.5% from 2009–2016 (4781- 4994 (3.4%)). Rate of haemorrhagic stroke fell by 2.1% per annum on average in the baseline period (1374-1256 (8.6%)) but increased by 1.2% on average from 2009–2016 (1256-1358 (8.1%)). There was no correlation between annual change in bleed incidence and change in anticoagulation prescriptions (r-0.07. p = 1.0)
Conclusion
An 84% increase in rate of anticoagulation was associated with slowing in the rate of increase in ischaemic stroke and a non-correlated, marginal increase in haemorrhagic stroke incidence. The increase in anticoagulation with DOACs is one possible explanation for the less than expected increase in stroke incidence.
Trial registration number
N/A
AS30-040
RANDOMISED TRIAL OF DIFFERENT METHODS OF AUTHOR CONTACT IN ORDER TO RECEIVE DATA FOR A SYSTEMATIC REVIEW OF RANDOMISED STROKE TRIALS
1University of Nottingham, Nottingham Clinical Trials Unit, Nottingham, United Kingdom
2University of Nottingham, Division of Clinical Neuroscience, Nottingham, United Kingdom
Background and Aims
Systematic reviews often rely on the acquisition of data in order to carry out analysis. But such data sharing may never happen. We carried out a randomised trial investigating two approaches for contacting authors identified in a systematic review attempting to acquire central adjudication data from stroke trials, with the aim of seeing which method elicits the most complete response.
Method
A primary and secondary research active author were selected as contacts for each stroke trial. Authors were randomised to either a short email with a protocol attached, or a longer email which contained detailed information. A maximum of two emails were sent to each author to obtain a response. The primary outcome was whether a response was received.
Results
88 trials were identified in the systematic review. 76 authors were randomised (36 to Short [trials = 45], 40 to Long [trials = 43]). There were 69 responses, with 19 non-responders. There was no evidence of a difference in response rate between trial arms (Short vs Long, O.R 0.83, 95% C.I: [0.30, 2.28]). More authors responded to the first email if allocated to the Short group (21 vs 15). However, there was no difference in time to response between trial arms (Short vs Long, H.R 0.86, 95% C.I: [0.54, 1.39]). Overall, 27% of authors responded within a day and 22% of authors never responded.
Conclusion
Email length did not have an impact on the number of responses received when acquiring data for a systematic review involving stroke trials, or the time taken to receive these responses.
Trial registration number
N/A
AS30-042
META-ANALYSIS OF REAL-WORLD EVIDENCE ON DIRECT-ACTING ORAL ANTICOAGULANTS VERSUS VITAMIN K ANTAGONIST AMONG PATIENTS WITH NON-VALVULAR ATRIAL FIBRILLATION
1University of Connecticut, School of Pharmacy, Storrs, USA
2Bayer AG, Health Economics and Outcomes Research, Berlin, Germany
3Bayer AG, Health Economics and Outcomes Research, London, United Kingdom
4University of Glasgow, HEHTA- Institute of Health & Wellbeing, Glasgow, United Kingdom
5Université Paris-Dauphine, PSL Research University- LEDa-LEGOS, Paris, France
6Aix Marseille Université, Faculté de Médecine, Marseille, France
7Creativ-Ceutical, Health Economics and Outcomes Research, London, United Kingdom
8Creativ-Ceutical, Health Economics and Outcomes Research, Paris, France
9Centre Hospitalier Universitaire Trousseau et Université François Rabelais, Cardiologie, Tours, France
Background and Aims
Numerous real-world studies comparing direct-acting oral anticoagulants (DOACs) to vitamin K antagonists (VKAs) in non-valvular atrial fibrillation (NVAF) have been published. This meta-analysis provides a synthesis of the available evidence.
Method
Searches on Medline, Embase, Cochrane databases and grey literature sources were performed up to 12/2016. Non-randomized NVAF studies with >50 patients comparing DOAC to VKA, and reporting ischemic stroke (IS), intracranial hemorrhage (ICH) or persistence were identified. When patient overlap between or within studies were detected, the result with the most statistically precise confidence interval was used. Studies were pooled using fixed and random-effect models (fixed-effect results were used when I2<50%) and reported as hazard rations (HRs) and 95% confidence intervals (CIs).
Results
562 citations were reviewed, 49, 79 and 18 compared rivaroxaban, dabigatran and apixaban to VKA and were included. Compared to VKA, rivaroxaban was associated with less IS (HR=0.83; 95%CI=0.75–0.93), ICH (HR=0.68; 95%CI=0.52–0.90) and non-persistence (HR=0.62; 95%CI=0.60–0.65). Dabigatran was associated with less IS (HR=0.79; 95%CI=0.65–0.97) and ICH (HR=0.45; 95%CI=0.36–0.58) but no difference on non-persistence (HR=0.91; 95%CI=0.53–1.55) compared to VKA. Apixaban demonstrated no difference in IS (HR=1.01; 95%CI=0.87–1.17), was associated with less ICH (HR=0.41; 95%CI=0.28–0.60) and no difference on non-persistence (HR=1.08; 95%CI=0.81–1.45) compared to VKA.
Conclusion
This meta-analysis suggests rivaroxaban and dabigatran but not apixaban are associated with a decreased hazard of IS and that rivaroxaban is associated with a decreased hazard of non-persistence versus VKA. All DOACs were associated with less ICH. DOACs appear to be at least as effective and safe as VKA for stroke prevention in NVAF.
Trial registration number
N/A
AS30-043
PERIPROCEDURAL ANTI-THROMBOTIC TREATMENT DURING ACUTE MECHANICAL THROMBECTOMY FOR ISCHEMIC STROKE: A SYSTEMATIC REVIEW
1Erasmus MC, Neurology, Rotterdam, The Netherlands
2Erasmus MC, Radiology, Rotterdam, The Netherlands
3Erasmus MC, Public Health, Rotterdam, The Netherlands
4University of Washington School of Medicine, Medicine Division of Hematology, Seattle, USA
5University of Washington School of Medicine, Neurology, Seattle, USA
Background and Aims
More than one-third of patients undergoing acute mechanical thrombectomy (MT) for ischemic stroke do not recover. This may be partially explained by incomplete microvascular reperfusion (IMR). IMR might be attenuated by anti-thrombotics (i.e. anti-platelet agents and heparin). The aim of this review was to assess the potential safety and functional outcome of periprocedural anti-platelet or heparin use during acute MT for ischemic stroke.
Method
Pubmed, Embase, Medline, Web-of-science, Cohrane and Google Scholar were searched systematically for studies investigating the safety and functional outcome of periprocedural anti-platelet or heparin treatment during acute MT for ischemic stroke. The primary outcome was symptomatic intracerebral hemorrhage (sICH). Secondary outcomes were good functional outcome after 3–6 months (modified Rankin Scale 0–2) and mortality within 6 months.
Results
807 Studies were identified through the search, of which 18 studies were included. The sICH risks for periprocedural anti-platelet use ranged from 6% to 17% and for heparin from 5% to 12%. Three out of five studies reporting relative effects of anti-thrombotics on sICH risk showed that the use of anti-thrombotics increased this risk. One out of two studies presenting relative effects for anti-platelet agents showed favorable results on good functional outcome. The two studies reporting relative effects of heparin found it to improve functional outcome.
Conclusion
Periprocedural use of anti-platelet agents or heparin increases sICH risk. However, several studies show promising results regarding functional outcome. Randomized trials are warranted to address the question whether sICH risk could be outweighed by improved functional outcome.
Trial registration number
N/A
AS30-044
DELIRIUM SCREENING IN ACUTE STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS OF INCIDENCE, SCREENING TOOLS AND SCREENING FREQUENCIES
1Nordsjællands Hospital - Hillerød, Dept. of Neurology, Hillerød, Denmark
2Zealand University Hospital- Roskilde, Dept. of Neurology- Center for Neurophysiology, Roskilde, Denmark
Background and Aims
Delirium in acute stroke patients is a serious complication with adverse effects on functional outcome. The precise incidence of delirium during the hospitalization for acute stroke is unknown.
We performed a systematic literature review to address whether the choice of delirium screening tool, frequency of use and the type of health professional carrying out the screening influence the number of delirious patients detected in a population of acute stroke patients.
Method
A systematic review protocol was registered at the PROSPERO register. We searched MEDLINE, EMBASE and PsycINFO and included pro- and retrospective cohort studies which tested for delirium in any way during hospitalization of adult patients with acute stroke. Article screening, selection and data extraction were carried out independently by two reviewers.
Results
24 unique populations were included in the review. Delirium incidence ranged from 1.4% to 75.6% in total and narrowed down to approx. 10% to 30% for studies using the screening tools Confusion Assessment Method (CAM) and Delirium Rating Scale (DRS(-R-98)). There was no clear correlation between delirium incidence and the frequency of delirium screening or the type of health professional using a given tool.
Conclusion
The broad range in delirium incidence reported may to some extent be explained by the choice of screening tool, but the different tools may also under- or over-diagnose some delirium subtypes. Delirium is a common complication with a heterogeneous symptom expression that can be difficult to recognize in some patients and may be wrongly diagnosed in others.
Trial registration number
N/A
AS30-045
SAFETY OF THROMBOLYSIS IN SMALL VESSEL DISEASE ACUTE ISCHEMIC STROKE - SYSTEMATIC REVIEW AND METAANALYSIS
1Medical University of Gdansk, Department of Neurology, Gdansk, Poland
Background and Aims
Symptomatic intracerebral hemorrhage (sICH) is the most frequent severe complication related to intravenous thrombolysis (iv-rtPA) of ischemic strokes. However, although basically considered to be safe, the multi-study based ratio of rtPA-related sICHs in a subgroup of patients with small vessel disease stroke (SVDS) remains unknown.
Method
We systematically reviewed PubMed and Scopus bases towards original comparative (vs placebo) and observational studies investigating the risk of rtPA-related sICHs in SVDS (OCSP or TOAST classifications). The metaanalysis was performed using fixed effect model with Peto odds ratio (Peto OR), and random effects model with Freeman-Tukey transformation.
Results
We found 3 comparative and 13 observational studies showing the ratios of rtPA-related ICHs in SVDS. One comparative trial found no complications, whereas the metaanalysis of the two remaining showed no difference between iv-rtPA and placebo (Peto OR = 4.08, 95% CI:0.92–18.04, I^2:0%; Figure 1). The combined (16 studies summing up to 3052 patients) pooled rate of rtPA-related ICH in this group was 0.23% (95% CI, 0%-0.96%), I^2:46%; Figure 2.
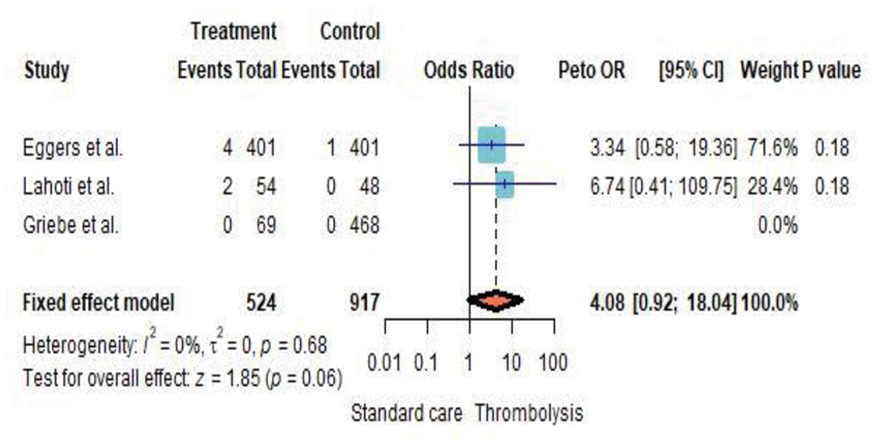
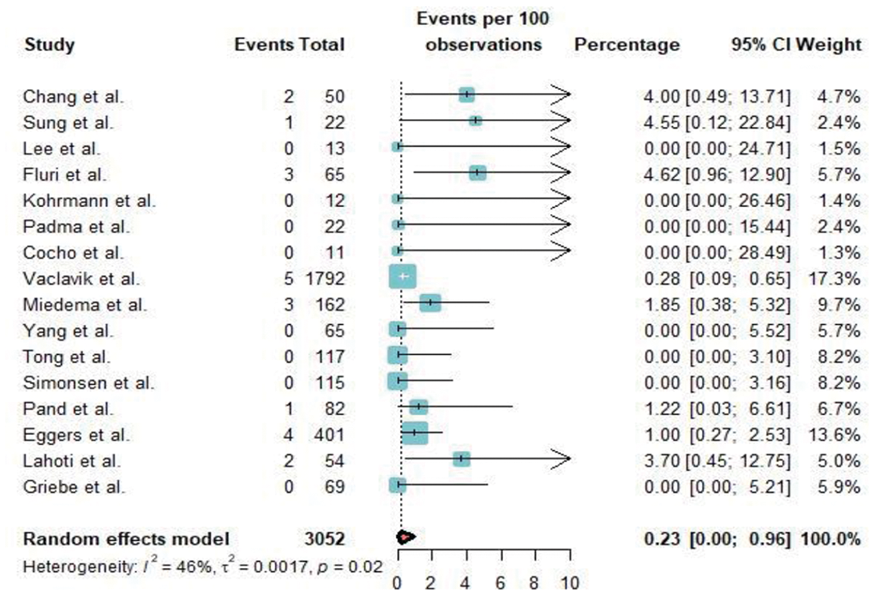
Conclusion
There is a very low risk of rtPA-related ICH in SVDs. Management of SVDS demands separate analyses towards potential different therapeutic approaches.
Trial registration number
N/A
AS30-046
EFFECT OF WORKFLOW IMPROVEMENTS ON TIME TO TREATMENT IN ENDOVASCULAR STROKE THERAPY: A SYSTEMATIC REVIEW
1Erasmus MC University Medical Centre, Department of Neurology, Rotterdam, The Netherlands
2Erasmus MC University Medical Centre, Department of Public Health, Rotterdam, The Netherlands
Background and Aims
Rapid initiation of endovascular stroke therapy (EVT) is associated with better clinical outcome. Time to treatment is influenced by pre-hospital and in-hospital processes. We performed a systematic review on the effectiveness of specific workflow improvements.
Method
Medline, EMBASE, Cochrane Central, Web of Science, Google Scholar, and Google were searched until November 2017 for studies evaluating the effect of one or more workflow improvements. Selection of relevant studies and data extraction was performed by two independent reviewers. Primary outcome was difference in time from stroke onset to treatment between intervention group and control group.
Results
Fifty studies (2 randomized controlled trials, 13 pre-post studies, and 35 studies reporting observational data) were selected for analysis (n = 8,234), including 17 multicenter studies. Most frequently reported were no general anesthesia (26 studies), early activation of the neuro-interventional team (7 studies), and continuous education and feedback of involved hospital staff on workflow metrics (6 studies). Mean or median time to treatment was reduced in 47 intervention groups (90%). This reduction was statistically significant in 25 interventions (median time-difference of 11 of 25 interventions was 36 minutes, range 10–73), including 9 studies reporting multiple simultaneously implemented workflow improvements. One study (2%) reported a significantly longer time to treatment.
Conclusion
Workflow improvements have a positive effect on time from stroke onset to EVT. Now we need well-designed controlled implementation studies to find out if these workflow improvements increase safety and good functional outcome after thrombectomy.
Trial registration number
N/A
AS30-047
DIRECT ENDOVASCULAR TREATMENT VERSUS INTRAVENOUS RTPA FOLLOWED BY ENDOVASCULAR TREATMENT IN PATIENTS WITH ACUTE ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Academic Medical Center, Neurology, Amsterdam, The Netherlands
2Academic Medical Center, Radiology and Nuclear Medicine, Amsterdam, The Netherlands
3Academic Medical Center, Radiology and Nuclear Medicine- Biomedical Engineering and Physics, Amsterdam, The Netherlands
Background and Aims
Endovascular treatment (EVT) has become standard-of-care for acute ischaemic stroke caused by proximal anterior circulation occlusions. The additional benefit of intravenous thrombolysis (IVT) in patients undergoing EVT is being debated.
Method
We conducted a systematic review and meta-analysis comparing IVT+EVT to direct EVT. We included studies with ≥10 patients, that used 2nd generation devices, and performed multivariable analyses. Our primary outcome was functional independence (modified Rankin Scale score [mRS] 0–2) at 90 days. Safety outcomes included symptomatic intracranial haemorrhage (sICH). We applied a fixed effects model.
Results
Out of 4.007 search results, we included 14 studies with data of 4693 patients (1855 direct EVT). All studies had an observational design (10 retrospective). Four studies reported on direct EVT in patients without contraindications for IVT. In the unadjusted analysis, IVT+EVT was associated with a higher likelihood of functional independence than direct EVT (summary OR [sOR] 1.31,95%CI 1.15–1.48). In the analysis with adjusted ORs, the effect estimate lost statistical significance (sOR 1.14, 95%CI 0.94–1.39). In the analysis of studies including only patients without IVT contraindications, the point estimate reversed and indicated better outcomes in the direct EVT group (sOR 0.86, 95%CI 0.62–1.19). There was a trend of increased sICH risk in the IVT+EVT group in both the unadjusted analysis (sOR 1.26, 95%CI 0.92–1.71) and subgroup without IVT contraindications (sOR 1.52, 95%CI 0.90–2.57).
Conclusion
Better outcomes after IVT+EVT compared to direct EVT observed in non-randomized studies may be explained by residual confounding. Randomized trials are needed.
Trial registration number
N/A
AS30-048
COGNITIVE DECLINE AND PROGRESSION TO DEMENTIA FOLLOWING HEMORRHAGIC OR ISCHEMIC STROKE: A SYSTEMATIC REVIEW AND META-ANALYSIS
1Harvard T.H. Chan School of Public Health, Epidemiology, Boston, USA
Background and Aims
We aimed to: 1) Assess the risk of cognitive decline and progression to dementia following hemorrhagic or ischemic stroke; and 2) assess role of stroke-related factors on cognitive decline among stroke survivors.
Method
A search was conducted on MEDLINE and EMBASE for reports published between 2009 and January 15 2018. Prior to 2009, studies were extracted from published meta-analyses. Studies were included if: 1) Reported on stroke subtype; 2) assessed dementia and cognition outcomes, and; 3) followed up patients for at least three months after stroke. Risk of bias in included studies was assessed using Newcastle-Ottawa scale.
Results
The database search yielded 2,769 studies (EMBASE=1,953 and MEDLINE=816). 2,029 studies, after removing duplicates, were screened in the title and abstract phase and 217 eligible studies were included for full-text screening. Meta-analyses of: 1) Combined incidence rates of dementia by stroke subtype, and; 2) pooled odds ratios of stroke-related factors and cognitive decline will be conducted in eligible studies.
Conclusion
IMPLICATIONS: Delineating risk of cognitive decline and progression to dementia among stroke survivors is crucial to guide monitoring and screening in these patients. Given the limited power in individual cohorts, previous studies were unable to assess risk by stroke subtype and other stroke-related factors. This systematic review will synthesize the findings of included studies and provide combined incidence rates and pooled odds ratios.
Trial registration number
N/A
AS30-049
DOES PREVIOUS TRANSIENT ISCHEMIC ATTACK INFLUENCE ISCHEMIC STROKE PROGNOSIS? – SYSTEMATIC REVIEW AND META-ANALYSIS
1Hospital Egas Moniz - Centro Hospitalar Lisboa Ocidental, Neurology, Lisboa, Portugal
2CEDOC - Nova Medical School - Universidade Nova de Lisboa, Neurology, Lisbon, Portugal
3Hospital de Santa Cruz - Centro Hospitalar Lisboa Ocidental, Cardiology, Lisbon, Portugal
Background and Aims
Observational studies have shown conflicting results about the impact of previous transient ischemic attack (prev-TIA) on ischemic stroke (IS) prognosis. Although ischemic preconditioning has been suggested as a potential neuroprotective mechanism, secondary prevention treatment after a first TIA could explain better outcomes in future events. We aimed to conduct a systematic review and meta-analysis of observational studies designed to study the influence of prev-TIA on IS prognosis.
Method
We analysed studies indexed to MEDLINE, Embase and Scopus (up to October 2017), reporting IS outcome according to the occurrence of prev-TIA. Studies were grouped according to their definition of good outcome. We used a random-effects model to pool effect on outcome according to prev-TIA. Meta-regression model was used to explore the potential effect of preadmission antithrombotics on outcome.
Results
15 studies were selected including 22335 patients, 2350 (10.5%) with prev-TIA. Two subgroups were defined: 1) good outcome at discharge (modified Rankin Scale ≤ 1), 3 studies, 12358 patients, 795 (6.4%) with prev-TIA; 2) good outcome at 3 months (modified Rankin Scale ≤ 1), 4 studies, 813 patients, 238 (29.3%) with prev-TIA. Both at discharge and at 3 months, prev-TIA was associated with better outcomes (OR: 1.37; CI 95% 1.12–1.68 and OR: 2.29; CI 95% 1.59–3.29). Meta-regression analyses did not revealed a significant effect of preadmission antithrombotics on 3-month outcome (CI 95% -0.007–0.006; p = 0.912).
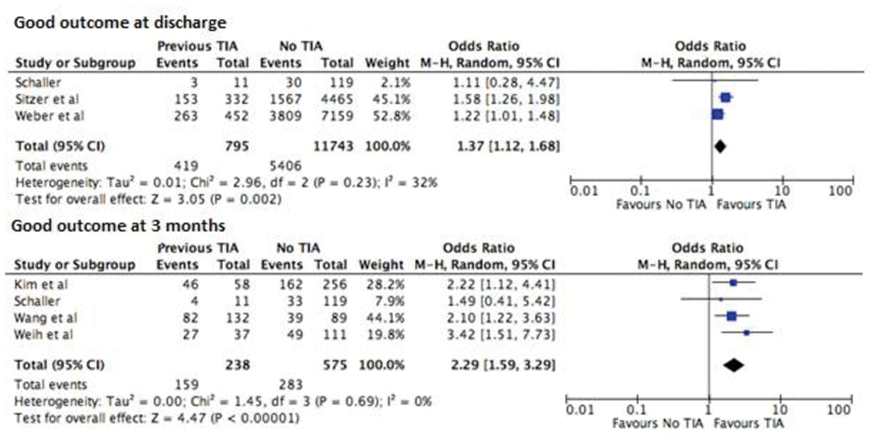
Conclusion
Previous TIA may have an impact on ischemic stroke prognosis independently of preadmission antithrombotics. The high heterogeneity between studies on outcome assessment precluded more comprehensive results.
Trial registration number
N/A
AS30-050
METHODOLOGICAL QUALITY OF CEREBROVASCULAR DISEASES RESEARCH ARTICLES PUBLISHED IN THE KEY UKRAINIAN NEUROLOGICAL JOURNAL
1Ukrainian Anti-Stroke Association, Education- research and publishing projects, Kiev, Ukraine
2Ukrainian Anti-Stroke Association, Directorate, Kyiv, Ukraine
Background and Aims
Our former review (2012) of methodological quality of Ukrainian research articles on cerebrovascular diseases has revealed severe shortcomings.
Method
We have reviewed all research articles on cerebrovascular diseases, published during the years 2016–17 in the key Ukrainian neurological journal, which is supervised by the leading Ukrainian neurological research institute and professional society. Totally, 10 articles were reviewed: 6 clinical trials of pharmacotherapeutic interventions and 4 researches on mechanisms of disease. The quality issues were assessed in 3 domains: planning and management of investigation, ethical items, and statistical items.
Results
Quality of all publications was poor in all domains. None of studies had clear aim and protocol. Although all pharmacological trials were declared as prospective and randomized, none of the articles contained any description of randomization procedure, and none was blinded. The groups in the trials were initially either not compared, or poorly comparable. None of the articles has mentioned approval by ethical committee and regulatory institution. The informed consent was received from participants only in one of 7 prospective studies. None of the studies has declared any conflict of interest, despite in 5 of them it was obvious, as the used pharmacological agents were mentioned by their trade names. Serious mistakes in statistical analysis were revealed in all reviewed articles.
Conclusion
Quality of Ukrainian research articles on cerebrovascular diseases is extremely poor. The problem requires further deeper investigation to reveal the ways for its solution.
Trial registration number
N/A
AS30-51
STROKE DIAGNOSIS USING HINTS IN PATIENTS PRESENTING WITH ACUTE VESTIBULAR SYNDROME: A SYSTEMATIC REVIEW
1University of Nottingham, Stroke- Division of Clinical Neuroscience, Nottingham, United Kingdom
2Nottingham University Hospitals NHS Trust, Stroke, Nottingham, United Kingdom
3Oslo University Hospital, Dept. of Neurology, Oslo, Norway
4Oslo University Hospital, Dept. of Geriatrics, Oslo, Norway
Background and Aims
Patients with posterior circulation stroke presenting with acute vestibular syndrome (AVS- vertigo, nausea/vomiting and gait unsteadiness) often have minimal clinical signs at the time of presentation. NIHSS is not reliable and CT scans cannot exclude acute posterior circulation ischaemia. A positive HINTS test with any of three signs: normal horizontal head impulse, direction changing nystagmus, and skew deviation of the eyes is suggestive of central cause including acute stroke. This systematic review examined the effectiveness of abnormal HINTS in posterior circulation stroke in patients presenting with AVS.
Method
We searched MEDLINE (1966 to 21 December 2017), EMBASE (1980 to December 2017), Web of Science and scanned bibliographies of relevant articles to identify studies on clinical features and diagnostic evaluation. We included studies in which HINTS was done primarily to identify posterior circulation stroke with diagnosis (infarct or haemorrhage) confirmed using magnetic resonance imaging (MRI).
Results
Six studies (644 patients) with AVS were identified. Two studies had patients with ABCD2 score of 4 and one study examined the relationship between truncal ataxia and posterior circulation stroke. Acute stroke was confirmed in 218 patients (29.8%). There was a 11-fold increased risk in posterior circulation stroke in those patients with a positive HINTS test compared to those with no abnormality (O.R. 11.50, 95% CI 3.50–38.32).
Conclusion
HINTS test appears to differentiate posterior circulation stroke from peripheral causes in AVS. Since posterior circulation stroke has the same risk of poor outcome as those of anterior circulation, methods to use HINTS in emergency settings need further investigation.
N/A
CASE REPORTS
AS31-001
NON-BACTERIAL THROMBOTIC ENDOCARDITIS WITH TROUSSEAU'S SYNDROME IN A PATIENT WITH OCCULT LUNG CANCER AND RECURRENT ISCHAEMIC STROKE
1ST GEORGE's UNIVERSITY OF LONDON, Stroke Medicine, LONDON, United Kingdom
Background and Aims
We present the case of a 73 year old gentleman, previously independent with a background of hypertension and non-insulin dependent diabetes mellitus, who presented with recurrent ischaemic strokes.
Method
He was investigated extensively, including extra and intracranial CT, repeat MRI, serological tests including a normal vasculitic screen, and a normal transthoracic echo. A likely primary lung malignancy was identified radiologically on both CT and PET scan. After recurrent events as an inpatient, a transoesophageal echo confirmed non-bacterial vegetations on his mitral valve, in keeping with non-bacterial thrombotic (marantic) endocarditis. Of note, prior to admission, he had presented with two isolated episodes of migratory thrombophlebitis. This was diagnosed in retrospect as Trousseau’s syndrome.
Results
Literature review identified that very few cases of non-bacterial or marantic endocarditis have been diagnosed prior to post mortem, and indeed majority of cases reported were in advanced or terminal malignancy rather than a presenting factor. Of note, cutaneous manifestations of non-bacterial thrombotic endocarditis are reported, including Trousseau syndrome.
Conclusion
We present this as a reminder to clinicians of the association between skin presentations indicative of underlying thrombotic state and concealed malignancy. Non-bacterial thrombotic endocarditis should be considered in patients with unexplained recurrent cerebral ischaemic events.
We will provide a review of the medical literature regarding non-bacterial thrombotic endocarditis and a clinical reminder of Trousseau’s syndrome.
Trial registration number
N/A
AS31-002
THE IMPORTANCE OF SWIFT VASCULAR SURGICAL AORTIC DISSECTION REPAIR DURING HYPERACUTE STROKE: TWO CASE STUDIES ILLUSTRATE POTENTIAL FOR EXCELLENT NEUROLOGICAL OUTCOMES
1University of Edinburgh, Stroke, Edinburgh, United Kingdom
Background and Aims
Aortic dissection (AD) is an established cause of ischaemic stroke. Surgical repair of AD can successfully reverse neurological deficits due to acute ischaemic stroke. Delays initiating vascular surgical repair are common due to delays in diagnosis, imaging, vascular referral and hesitation or disinclination to operate due to perception of poor outcome by some vascular surgeons.
Method
n/a
Results
Case 1: A 64 year-old man presented to A&E with chest pain radiating to the back. In hospital the following day marked hypotension developed with differing blood pressures in each arm. There was rapid progression to reduced conscious level, dense left hemiparesis and hemi-neglect. CT imaging confirmed extensive type A AD and excluded brain haemorrhage. Surgical AD repair commenced within 2.5 hours of stroke onset. This patient left hospital 5 days later without residual neurological deficit. Case 2: A 59 year-old man presented with chest pain and left hemiparesis during an acute stroke due to AD. After urgent transfer from a peripheral hospital to our tertiary vascular surgical centre, a Type A AD was repaired, approximately 5 hours after stroke onset. Post-operatively, left sided hemiplegia and dysphagia were associated with right hemispheric infarction. Following rehabilitation, this patient required sheltered housing with a degree of residual deficit.
Conclusion
These cases are an important reminder to Stroke Physicians working with Vascular Surgeons that surgical AD repair should be considered urgently, within a critical time window after onset of acute ischaemic stroke. The literature and potential for complete/near complete resolution of ischaemic neurological injury is also reviewed.
Trial registration number
N/A
AS31-003
THE VIRAL MASQUERADE: TWO CASES OF VIRAL ENCEPHALITIS MIMIKING STROKE
1University of Edinburgh, Stroke, Edinburgh, United Kingdom
Background and Aims
Mimics of stroke present on-going diagnostic challenges for Stroke Specialists. Infectious encephalitis constitutes a medical emergency; viral herpes simplex encephalitis (HSE) is the commonest UK cause. Morbidity and mortality can be high, necessitating prompt diagnosis and treatment.
Method
n/a
Results
Case 1: 33 year male presentation: sudden-onset right facial and limb weakness, right paraesthesia, dyspraxia, ataxia and dysphasia. Thrombolysis for suspected ischaemic stroke followed normal CT head/ CT angiogram. Following thrombolysis neurological findings improved. Subsequent MRI: right frontal cortical T2 high signal - in a left-handed patient, however persistent headache, uncharacteristic aggression, agitation, subsequent photophobia, pyrexia and dysphasia, later triggered treatment for CNS infection. CSF: lymphocytosis, moderately increased protein - consistent with viral encephalitis. Acyclovir improved most symptoms; but headaches and decreased concentration persist.
Case 2: 70 year male presentation: fall with head injury and pyrexia, after several weeks of confusion. CT head: reportedly evolving strokes in left frontal, temporal and possibly right parietal lobes. After Stroke Unit admission, antibiotics commenced for unknown sepsis. The patient deteriorated - reduced consciousness and tonic-clonic seizures. CSF: inconclusive results; viral PCR negative. EEG: periodic focal sharp waves over left temporal area, characteristic of HSE. Complete recovery followed acyclovir.
Conclusion
In both cases, experienced Stroke Physicians initially diagnosed ischaemic stroke in the acute setting. Viral PCR was negative in both cases. We will discuss these cases, characteristic imaging and the literature, as an important reminder to Stroke Physicians that viral encephalitis, often causing acute focal neurological deficit, is a rare but important mimic of acute stroke.
Trial registration number
N/A
AS31-005
EIGHT-AND-A-HALF SYNDROME WITH HEMIPARESIS: A POSSIBLE NINE SYNDROME
1Hospital Enche' Besar Hajjah Khalsom- Kluang, Medicine, Johor, Malaysia
2Hospital Enche' Besar Hajjah Khalsom- Kluang, Radiology, Johor, Malaysia
Background and Aims
“Eight-and-a-half” syndrome consists of “one-and-a-half” syndrome (OHS) and ipsilateral lower motor neuron (LMN) facial nerve palsy (1½+CN7=8½). This disorder is seen in an unilateral dorsal pons lesion which involves close proximity of 1) paramedian pontine reticular formation (PPRF) or abducen nerve, 2) ipsilateral medial longitudinal fasciculus, and 3) facial nerve fascicle. 1&2 are responsible for horizontal gaze and OHS. Additional involvement of pontine corticospinal tract results in contralateral hemiparesis and configuring a "nine" syndrome (8½+½ = 9). Various etiologies have been described and mostly infarcts. Recognition of this rare condition is important for precise lesion localisation.
Method
We report a middle-aged man with hypertension presented with sudden onset of double vision, left facial and right sided body weakness.
Results
Horizontal ocular movement showed left OHS with presence of left conjugate gaze palsy and left internuclear ophthalmoplegia. Vertical eyes movement and convergence were preserved. He had left peripheral facial palsy with right hemiparesis. No cerebellar sign. MRI at day 14 demonstrated an infarct in facial colliculus of the left dorsal pons. He was given aspirin and statins. Three weeks later, hemiparesis resolved completely and ocular palsy improved significantly.
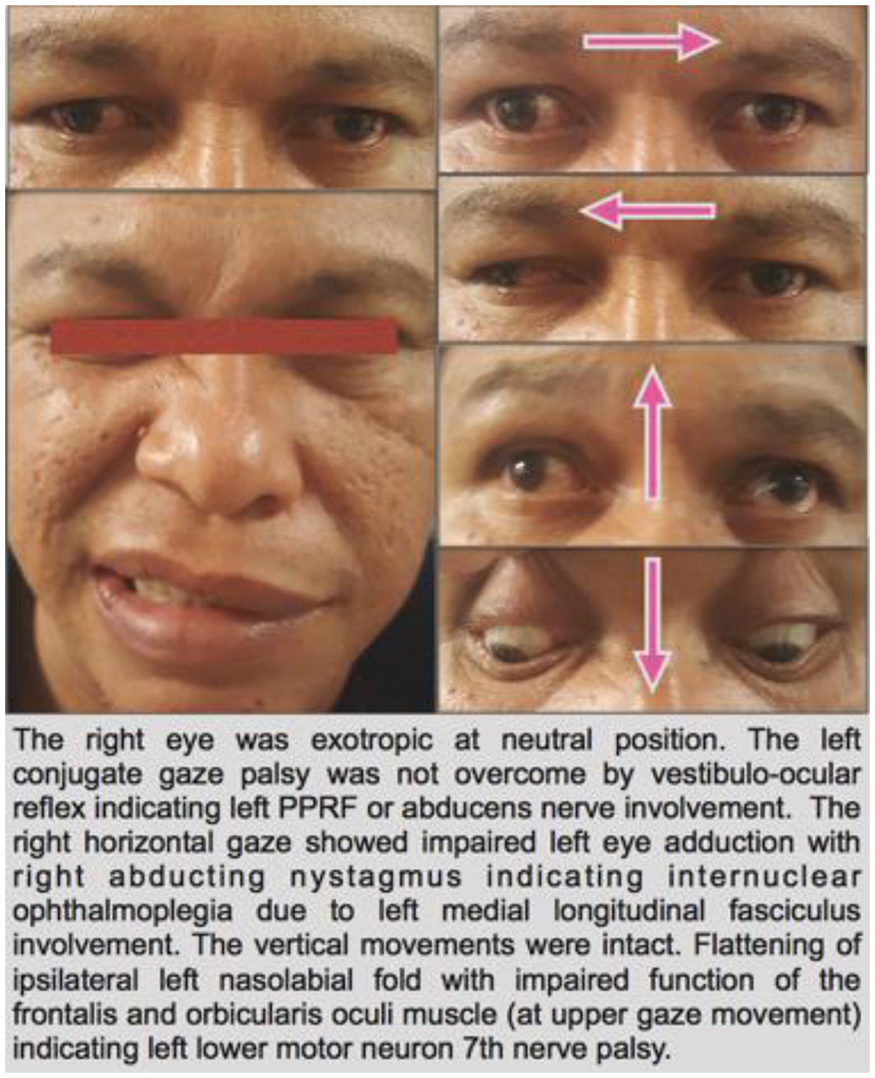
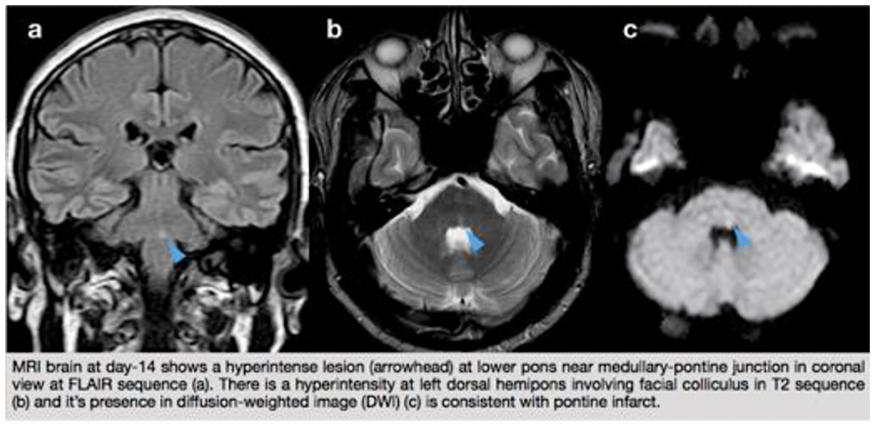
Conclusion
This is an eight-and-a-half syndrome in a setting of stroke. OHS is rarely an isolated finding and the accompanying signs are frequent. OHS with LMN facial nerve palsy and hemiparesis configures "nine" syndrome, a widened spectrum of 8½ syndrome. Recognition of this rare condition allows precise localisation of the lesion to ipsilateral lower pons and thus choice of imaging.
Trial registration number
N/A
AS31-006
SUCCESSFUL INTRAVENOUS ALTEPLASE USE IN FOUR PATIENTS WITH ACUTE ISCHEMIC STROKE AFTER DABIGATRAN REVERSAL WITH IDARUCIZUMAB
1Klinikum Darmstadt, Neurology, Darmstadt, Germany
2Klinikum Darmstadt, Radiology, Darmstadt, Germany
Background and Aims
Idarucizumab has been recently approved as an antagonist for the direct oral anticoagulant (DOAC) dabigatran. As there is a lack of data available on the safe use of idarucizumab in everyday clinical practice for dabigatran reversal before intravenous thrombolysis, we are presenting four patients with ischemic strokes under dabigatran treatment who were treated with idarucizumab before intravenous alteplase use.
Method
The four patients were treated at the Department of Neurology in the period of November 2016 to March 2017. All data were collected retrospectively. The mean patient age was 84 years (76–91).
Results
All patients included in this case series were successfully treated with alteplase after dabigatran reversal, without a secondary hemorrhagic transformation of the ischemic infarct, or intracranial hemorrhage being provoked. To evaluate the severity of the ischemic stroke, we used the universally employed National Institutes of Health Stroke Scale (NIHSS). On arrival in the Department of Neurology the average NIHSS was 6.75; upon transfer from the stroke unit it was 3.25. Two patients went into neurorehabilitation after their hospital stay, and two patients were directly discharged from the hospital because of their improved condition.
Conclusion
According to our clinical experience and the case reports to date, we assume that the dabigatran reversal with idarucizumab with subsequent intravenous thrombolysis in acute ischemic stroke does not entail an increased bleeding risk. We therefore suggest the effect to be studied in wider clinical multicenter trials to investigate the safety of the method.
Trial registration number
N/A
AS31-007
EMBOLIC SULCAL ARTERY STROKE : REPORT OF TWO CASES
1Changi general Hospital, Neurology, singapore, Singapore
Background and Aims
Sulcal arteries are branches of the anterior spinal artery (ASA). Unilateral sulcal artery infarcts are rare, and have been previously described secondary to vertebral dissection.
Method
Two patients with unilateral sulcal artery infarcts, secondary to unique embolic aetiology, are described.
Results
A 64 year male, was admitted with recurrent hemoptysis and underwent bronchial artery embolization (BAE). Immediately post procedure, progressive (over 6 hours) right lower limb numbness, weakness (MRC grade 2–3) and urinary retention was reported. Brown-Sequard syndrome (BSS; sensory level T6) was noted on exam. Magnetic resonance imaging (MRI) of the thoracic spine showed focal T2 hyperintensity at T3/4 (Figure 1a). Sulcal artery stroke (SAS), as a complication of BAE was diagnosed. Complete motor recovery was noted over 8 weeks.
A 74 year male, with known cervical myelopathy and chronic aortic dissection (abdominal) presented with acute onset abdominal pain, right lower limb numbness and weakness (MRC grade 0–1). BSS was diagnosed, (sensory level T 7–8); MRI spine showed short segment T2 hyperintense lesion at T4/5 right hemicord (Figure 1b). Aortic imaging showed dissection flap at mid-descending aorta. SAS, secondary to embolic complication of aortic dissection was diagnosed. Slow improvement to ambulation (50 ms) with aid was noted.
Both patients were managed conservatively; anti-platelets (previously given for ischemic heart disease) were continued, and rehabilitative measures initiated.
Conclusion
Clinical outcomes of sulcal artery infarcts are better in comparison with ASA infarcts.
Trial registration number
N/A
AS31-010
HYPERTHYROIDISM: A RARE CAUSE OF A RARE TYPE OF STROKE
1Alfred Health, Department of Neurology, Melbourne, Australia
Background and Aims
We present two cases of cerebral venous sinus thrombosis (CVST) due to hyperthyroidism.
Method
A 27 years old female developed severe headache and then arm clumsiness prior to a generalised seizure. Magnetic Resonance Venography (MRV) showed extensive thrombus of the superior saggital sinus but no parenchymal haemorrhage. No obvious cause was found and she was discharge on warfarin based anticoagulation. She re-presented with worsening headache 8 months later, despite therapeutic anticoagulation. MRV now demonstrated thrombosis of right transverse, sigmoid, superior petrosal sinuses and jugular bulb. A smooth goitre was also apparent and antibody associated thyrotoxicosis was confirmed. Her thyrotoxicosis was pharmacological treated and her symptoms and CVST resolved.
A 63 years old male crashed his car with a generalised seizure but no head injury. Thrombosis of the left transverse and sigmoid dural venous sinuses and a left sided superficial cortical vein was seen on MRV. He was noted to be tachycardic and was biochemically hyperthyroid and found to have a toxic nodule on further thyroid imaging. This was subsequently treated with radioactive iodine. He has been well since with no symptoms or radiological signs of recurrent CVST.
Results
Thyrotoxicosis can cause hypercoagulability by a number of mechanisms including: increased plasma von Willebrand factor levels, improved platelet function, increased factor II, VII, VIII, and X factors and increased plasminogen activator protein (PAI-1).
Conclusion
Hyperthyroidism has been previously described in small case reports of venous thrombosis and should be considered in patients presenting with unprovoked CVST or progression of thrombosis despite adequate anticoagulation.
Trial registration number
N/A
AS31-012
FAHR’S DISEASE IN A 26 YEAR OLD FEMALE. A CASE REPORT
1Corazon Locsin Montelibano Memorial Regional Hospital, Internal Medicine, Bacolod City, Philippines
Background and Aims
Fahr’s disease is a rare, degenerative neurological disorder characterized by idiopathic symmetrical and bilateral intracranial calcification. Prevalence of <1:1,000,000, usually presents at middle age group (40–50) rarely in the young. Diagnosis requires certain clinical criteria: absence of biochemical abnormalities and somatic features; absence of infection, trauma, toxic cause; presence of progressive neuropsychiatric dysfunction with onset of symptoms at 4th – 5th decade of life, presence of bilateral basal ganglia calcification visualized on neuroimaging and family history with autosomal dominant inheritance or sporadic.
Method
We report the case of a 26 year-old female who presented with stiffening of upper and lower extremities with no loss of consciousness. Her symptoms started thirteen years prior when she had sudden onset of tetanic contraction of extremities, she had consult and managed as seizure disorder with poor compliance to Phenobarbital.
Results
Blood test were done; complete blood count, creatinine, magnesium, sodium, calcium, urinalysis, arterial blood gas, fasting blood sugar, erythrocyte sedimentation rate, complement, thyroid hormones, intact parathyroid hormones are within normal range. Chest xray, electrocardiogram and electroencephalogram were unremarkable. Computed Tomography scan brain plain demonstrated bilateral cerebellar, basal ganglia and frontal gray-white matter calcification. Magnetic Resonance Imaging had abnormal hyper-intense signals area seen in both basal ganglia, corona radiata white matter areas, cerebellar hemispheres
Conclusion
Fahr’s disease is a rare neuropsychiatric degenerative disorder. Patient with classical clinical manifestation should be consistent with the neuroimaging findings moreover our patient presented with more rare entity with early onset of symptoms.
Trial registration number
n/a
AS31-013
ISOLATED CENTRAL AND BRANCH RETINAL ARTERY OCCLUSION WITHOUT OTHER THROMBOEMBOLIC EVENT AFTER CAROTID ARTERY STENTING
1Konyang University Hospital- College of Medicine- Konyang University, Neurosurgery, Daejeon, Republic of Korea
Background and Aims
The complications associated with carotid artery stenting (CAS) may occur during or after the procedure and generally present as neurological symptoms due to embolism or thrombus. Embolisms from the carotid bifurcation may be cause of central retinal artery occlusion (CRAO) and branch retinal artery occlusion (BRAO). We report two cases of CRAO and BRAO after CAS in the carotid stenosis.
Method
<Case I>
53 year-old man was admitted to the hospital with right hand clumsiness. Diffusion weighted magnetic resonance imaging (DW-MRI) showed a high signal lesion on Lt hemisphere, and a neck magnetic resonance angiogram (MRA) and cerebral angiogram showed severe stenosis with decreased distal blood flow in proximal part of internal carotid artery.
<Case II>
64 year-old man was admitted due to cerebral infarction in right hemisphere. MRA and cerebral angiogram showed severe stenosis in proximal part of internal carotid artery.
Results
<Case I>
During and after CAS, there was no significant abnormal findings and events. However, the patient complained of decreased visual acuity in his left eye in next day after the CAS. Left eye fundus photography revealed a cherry-red spot on the macula, the retina's multiple edema and CRAO. The patient visual acuity was not improved.
<Case II>
After few hours after CAS, the patient complained of blurred vision in his right eye. Ophthalmologic evaluation was revealed BRAO, inferior temporal artery occlusion. The symptom was gradually much improved after few weeks
Conclusion
Endovascular surgeons should keep in mind the risk of permanent or partial vision loss after CAS.
Trial registration number
N/A
AS31-014
BILATERAL INTERNAL CAROTID ARTERY DISSECTIONS FOLLOWING CHIROPRACTIC NECK MANIPULATIONS
1Imperial College NHS Trust, Stroke, London, United Kingdom
Background and Aims
A case report on the suspected cause of bilateral internal carotid dissection in an otherwise fit and healthy young man.
Method
Case report and subsequent literature search.
Results
Internal carotid artery dissection (ICAD) is a common cause of strokes in young adults with numerous causes including varying degrees of neck trauma. We describe a case of a previously fit and well 40 year old gentleman presenting with acute left upper limb weakness. His computed tomography angiography (CTA) showed an acute dissection of the right extracranial internal carotid artery (ICA) with associated mural haematoma as well as a chronic dissection of left ICA. Upon detailed history taking, he revealed he has regular chiropractic neck manipulations and has done so for many years.
Conclusion
A search of the literature has shown conflicting evidence on the relationship between ICA dissection and chiropractic manipulations. This is confounded by the small number of case reports and also that many patients sought out a chiropractor in the first place due to existing neck pain.
However, given the two dissections in this case are of different ages and that he had no other risk factors, it is felt the chiropractic neck manipulations are most likely the cause of the bilateral ICA dissections.
Trial registration number
N/A
AS31-015
HEMIBALLISM OF VASCULAR ORIGIN: A CASE SERIES
1Hospital Universitario de Salamanca, Neurology, Salamanca, Spain
Background and Aims
Hyperkinetic disorders may have several causes, and the vascular origin is one of the less common.
We present a series of four clinical cases of patients with hemichorea or hemiballism with an acute onset, secondary to ischemic or hemorrhagic brain lesions.
Method
Our series includes elderly patients, with multiple cardiovascular risk factors in all cases and a rather good prior quality of life. The start of the clinical picture was similar in all cases: involuntary movements on one side of the body with a sudden onset, unaccompanied by any other focal neurologic signs. Ischemic or hemorrhagic brain lesions were observed in all four cases (in two of them on the basal ganglia and in the other two on the cortico-subcortical areas). The origin of the stroke was varied.
Results
In three of the cases, there was a clear improvement of the movements after the administration of neuroleptics, mainly tetrabenazine. In one of the cases, control of the symptoms was more complex, and it required the combination of several drugs from different pharmacological groups.
Conclusion
It is important to establish a correct differential diagnosis, because these neurological manifestations may be associated to other disorders which have an effective etiological treatment, such as hyperglycemia.
Trial registration number
N/A
AS31-016
SUBARACHNOID HAEMORRHAGE DUE TO BERRY ANEURYSM PERFORATION DURING MECHANICAL THROMBECTOMY FOR ACUTE ISCHAEMIC STROKE: A CAUTIONARY TALE
1Salford Royal Foundation Trust, Greater Manchester Neurosciences Centre, Salford, United Kingdom
2Salford Royal Foundation Trust, Department of Neuroradiology, Salford, United Kingdom
3Salford Royal Foundation Trust, Department of Neuropathology, Salford, United Kingdom
Background and Aims
Mechanical thrombectomy has become an established treatment option for patients with ischaemic stroke due to intracranial artery occlusion. The technique improves outcomes for patients but is not without potential complication. We present a case of sub arachnoid haemorrhage due to perforation of a middle cerebral artery bifurcation aneurysm.
Method
A 78 year old female with no antecedent history suffered a severe left sided stroke an hour prior to initial assessment. Computed tomography (CT) head showed changes of early ischaemia in the right hemisphere and CT angiography showed occlusion of the terminal internal carotid artery (ICA)/proximal middle cerebral artery (MCA). Her blood pressure of 238/110, precluded intravenous thrombolysis so she was taken to the angiography suite for mechanical thrombectomy. It proved impossible to open the MCA and during the procedure contrast extravasation was noted from the right MCA and the procedure was abandoned.
Results
Repeat brain imaging demonstrated subarachnoid haemorrhage and a total anterior circulation stroke, the patient died on day 4. Post mortem examination demonstrated right hemisphere cerebral infarction and extensive subarachnoid haemorrhage from a ruptured MCA bifurcation berry aneurysm.
Conclusion
The aneurysm wasn’t detected on non-invasive angiography nor initial digital subtraction angiography as contrast wasn’t demonstrated distal to the ICA/MCA occlusion. This case illustrates a rare complication. A late phase CTA may better delineate post occlusion anatomy and identifying an aneurysm in such a position may inform the thrombectomy technique.
Trial registration number
N/A
AS31-017
A WOLF IN SHEEP’S CLOTHING: PAINLESS TYPE A THORACIC AORTIC DISSECTION PRESENTING AS TIA
1Royal United Hospitals Bath NHS Foundation Trust, Acute Stroke Unit, Bath, United Kingdom
2Royal United Hospitals Bath NHS Foundation Trust, Radiology, Bath, United Kingdom
Background and Aims
We present the case of a 70 year old retired carpenter who had been referred by his general practitioner to the weekend rapid access Transient Ischaemic Attack (TIA) clinic as a high risk TIA. The day before he had experienced an half hour episode of numbness and weakness in his L leg whilst sawing in his workshop along with feeling faint and lightheaded. He did not notice any other neurology nor reported any other symptoms apart from having felt tired and lacking energy for two weeks previously.
Method
On assessment in the TIA clinic on Saturday no focal neurology was noted. He was asked about neck or chest pain and did not report experiencing either. Clinical protocol at weekends constitute CT/CT angiography to assess carotids (carotid duplex scan is not available at weekends).
Results
CTA from aortic root to the Circle of Willis revealed an incidental Type A thoracic aortic dissection. An extended CTA of the complete aorta was performed. This demonstrated an extensive type A aortic dissection from aortic root (dilated to 6.5 cm) to the aortic bifurcation, with the R renal artery arising from the false lumen. He was transferred to the tertiary cardio-thoracic centre and underwent thoracic aortic dissection repair the next day.
Conclusion
Aortic dissection is painless in 5 – 15% of cases. Focal neurological deficit is particularly common in this group (19%) and can mimic cerebral ischaemic events. Care needs to be taken to differentiate between these two conditions.
Trial registration number
n/a
AS31-018
INTRAVENOUS THROMBOLYSIS FOR EARLY RECURRENT ISCHEMIC STROKE ASSOCIATED WITH AORTIC ARCH THROMBUS
1Aristotle University Of Thessaloniki, 2nd Department of Neurology, Thessaloniki, Greece
2Aristotle University Of Thessaloniki, Department of Radiology, Thessaloniki, Greece
3National & Kapodistrian University of Athens, 2nd Department of Neurology, Athens, Greece
Background and Aims
Aortic arch atheromatosis and thrombus is a risk factor for recurrent stroke.
Method
-
Results
A 51-year-old woman presented with a transient episode of aphasia. Clinical examination, neurosonologic examination and transthoracic echocardiography were all normal. MRI showed minor cortical infarcts in the left MCA territory. She was started on aspirin and five days later, she developed aphasia, right hemianopsia and right hemiplegia. Trancranial Doppler confirmed occlusion of the left MCA and urgent CT showed only the known minor infarction. Since mechanical thrombectomy (MT) was not available, we proceeded to off-label intravenous thrombolysis (IVT), resulting within 24h to near-complete reversal of the deficit. CT angiography revealed an aortic arch floating thrombus (AAT-image). The patient was discharged on acenocoumarol and 40 days later the thrombus had completely dissolved.

Conclusion
This is the second case of IVT in a setting of stroke attributed to AAT, and the first case of early recurrent stroke treated safely and effectively with IVT, in presence of AAT. If imaging of the aortic arch is not performed, infarctions associated with aortic arch atheromatosis may be mischaracterized as ESUS. Safety of MT and IVT in presence of AAT is unknown but both treatments may be considered in disabling strokes. Patients with small infarcts and mild/no deficits after an initial stroke might be considered for IVT in case of early recurrence.
Trial registration number
N/A
AS31-021
CHRONIC SUBDURAL HEMATOMA, ATRIAL FIBRILLATION AND ISHEMIC STROKE, CONSIDERATIONS ABOUT TREATMENT OPTIONS, A CASEREPPORT
1Østfold Hospital, Department of Neurology, Kalnes, Norway
2Akershus University Hospital, Department of Neurology, Oslo, Norway
3Østfold Hospital, Department of Radiology, Kalnes, Norway
4Oslo University Hospital, Department of Cardiology, Oslo, Norway
Background and Aims
A 84-year-old man presented with acute left sided hemiparesis, central facial palsy and dysarthria (NIHSS 11). In March 2014 the patient had a right sided frontal infarction. A paroxysmal atrial fibrillation (PAF) was found and anticoagulation (dabigatran) was initiated. Six months later, the patient acquired bilateral traumatic subdural hematomas (SDHs). Dabigatran was discontinued and the right sided SDH was drained twice. Owing to persistent bilateral SDH, anticoagulation use was not recommended. On admission the patient underwent rapid assessment and neuroimaging.
Method
Figure
CTP: Decreased perfusion to the right MCA territory.
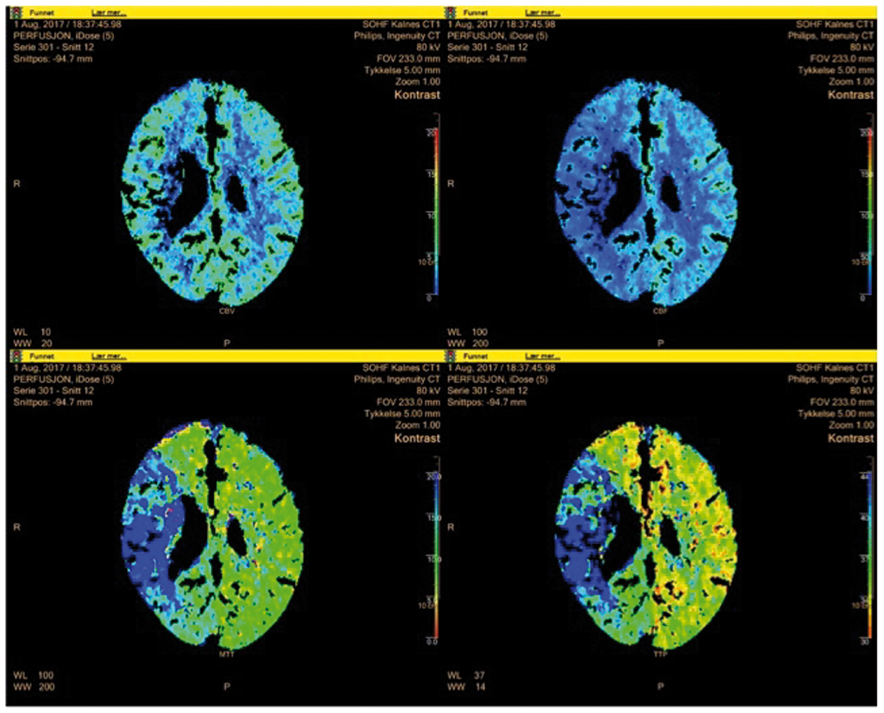
Results
Neuroimaging showed a proximal MCA occlusion with a large salvageable penumbra. Due to a left sided SDH causing midline shift, intravenous thrombolysis (IVT) was contraindicated. The patient underwent endovascular thrombectomy (EVT).MRI Scanning 24 hours post EVT only showed the old frontal infarction. NIHSS 48 hours after EVT was 3. Low dose anticoagulation (Apixaban) was initiated. His 3-month post stroke mRS was 0
Conclusion
Patients with persistent SDH and significant risk of ischemic stroke present a challenge to treating physicians. We present a case of excellent outcome (mRS 0) owing to rapid EVT where IVT was contraindicated. The complexity of prophylactic anticoagulant therapy in patients where persistent SDH and stroke risk coexist is a clinical and radiological challenge.
Trial registration number
N/A
AS31-022
MOYAMOYA DISEASE IN THE DIFFERENTIAL DIAGNOSIS OF MULTIPLE SCLEROSIS: A CASE REPORT
1National and Kapodistrian University of Athens, 1st Department of Neurology- Eginition Hospital, Athens, Greece
2University of Athens Medical School, Research Unit of Radiology and Medical Imaging, Athens, Greece
3National and Kapodistrian University of Athens, Department of Radiology- Aretaion Hospital, Athens, Greece
Background and Aims
Moyamoya disease (MMD) manifestation may be insidious in young female patients presenting with unspecific neurological symptoms and atypical white matter lesions in brain Magnetic Resonance Imaging (MRI), mimicking Multiple Sclerosis (MS).
Method
Herein we present a case of a young female patient with MMD.
Results
A 44-year old woman experiencing transient numbness of her right-sided face and arm was referred to our Unit due to small brain lesions in MRI, with a possible diagnosis of MS or of a systemic autoimmune disease. For years, she had been complaining of intermittent weakness of her left arm, but it had been attributed to psychosomatic problems. Neurological examination was unremarkable except from plantar and jerky deep tendon reflexes. Diagnostic work up with brain Magnetic Resonance Angiography revealed findings typically seen in MMD, confirmed with Digital Subtraction Angiography. Antiplatelet therapy was initiated, however few days later, she developed suddenly global aphasia and right hemiparesis (National Institutes of Health Stroke Scale/NIHSS 6). Brain MRI revealed an acute infarct in the distribution of the left Middle Cerebral Artery. Although thrombolysis was not performed due to the increased risk of hemorrhage in MMD patients, significant improvement of the patient’s health status was noted at discharge (NIHSS 3).
Conclusion
In young patients with transient neurological symptoms suggestive of Multiple Sclerosis and atypical white matter lesions in MRI, MMD should be considered in the differential diagnosis.
Trial registration number
N/A
AS31-023
SELECTIVE EC-IC BYPASS FOR REVASCULARIZATION OF ACUTE OR CHRONIC CEREBRAL HYPOPERFUSION REGION
1Scientific research institute of emergency medicine n.a. N. V. Sklifosovskiy, Neurosurgery, Moscow, Russia
Background and Aims
New method of EC-IC bypass for revascularization of cerebral hypoperfusion areas by merging neuronavigation (NN), perfusion (SPECT) and angiographic (CT-AG) data. The routine method of EC-IC bypass means the suturing of the superficial temporal artery (STA) to one of the cortical branches (M4 segment) of the middle cerebral artery (MCA). We perform the bypass without respect to the location of hypoperfused region. We offer new method of selective EC-IC bypass in patients with acute or chronic cerebral ischemia in attempt to optimize results of our intervention.
Method
We perform the perfusion study (SPECT in our cases) and angiographic study (we use CT-AG). Then merge perfusion maps with angiographic studies, outline the region of hypoperfusion, search and mark the recipient intracranial artery (RA) that supply our region of interest. Then we search and mark donor extracranial artery (DA) that run near our RA, outline the extend of boneflap. Thereafter we upload planned data into the frameless NN, mark all extracranial (DA projection, bone flap borders) and use contact probe before opening dura to plan the dura incision with respect to the planned RA projection. Finally we perform the EC-IC bypass in classic fashion.
Results
Three patients were operated, there was no complications. Postoperatively we use SPECT to dynamically asses cerebral perfusion (all patients have better values) and CT-AG and ultrasound to control latency of bypasses on first and thirtieth post days (all bypasses were working)
Conclusion
New method could be used for treatment of patients with ischemia of different origin
Trial registration number
N/A
AS31-025
FEATURES OF DIFFERENTIAL DIAGNOSIS OF STROKE AND PML IN YOUNG PATIENTS
1medicine, neurology, Moscow, Russia
Background and Aims
Features of differential diagnosis of stroke and PML in young patients
Progressive multifocal leukoencephalopathy (PML) is a rapidly progressing demyelinating disease of the central nervous system caused by activation of the JC-virus (John Cunningham-virus), capable of mimicking various CNS-diseases, including acute stroke.
We give an observation from our own clinical practice.
Method
We give an observation from our own clinical practice.
Results
The 35-year-old patient was hospitalized with a preliminary diagnosis «stroke» with complaints of disorientation, emotional lability, decreased memory for current events, dizziness, fluctuations in blood pressure from 90/60 to 140/90 mm Нg. Two years ago, after traveling to Thailand, he abruptly lost weight, which was associated with a "healthy lifestyle": balanced nutrition, enhanced training. Became more likely to get colds; did not visit doctors. Six months ago he suffered a right-sided bronchus pneumonia (diagnosed by computed tomography of the lungs).
A clinical blood test revealed lymphopenia up to 1.9–3.2*109. Anti-HCV - was detected; immunobloting (+); JC-virus was detected by PCR of CSF.
Neuroimaging (MRI brain in Flair, T2, DVI) revealed progressive multifocal leukoencephalopathy of the brain, as well as signs of intracranial hypertension. The most indicative were the tomograms in the Flair mode (Figure 1.).
Conclusion
Due to the doctors' lack of knowledge of PML, such patients are very often hospitalized in stroke departments, which complicate timely treatment, contribute to a worsening of the prognosis and makes biased statistics of outcomes of strokes.
Trial registration number
N/A
AS31-026
REPEATED MECHANICAL THROMBECTOMY FOR RECURRENT PROXIMAL MIDDLE CEREBRAL ARTERY OCCLUSION
1Medical University of Graz, Department of Neurology, Graz, Austria
2Medical University of Graz, Department of Radiology- Division of Neuroradiology- Vascular and Interventional Radiology, Graz, Austria
Background and Aims
Mechanical thrombectomy (MT) is the gold standard treatment for ischaemic stroke due to large vessel occlusion (LVO) of the anterior circulation. Whether MT can also be effectively and safely performed in recurrent LVO is largely unclear. We present the case of a patient with recurrent LVO who was successfully treated by MT twice within nine days.
Method
Case report.
Results
A 66-year old female patient was admitted with right total anterior circulation stroke (TACS) syndrome (NIHSS: 13). Brain CT was unremarkable and CT-angiography revealed right MCA-M1 occlusion. IV thrombolysis was contraindicated because of recent major surgery. MT was successfully performed (symptom-to-recanalization time 130 minutes). The patient recovered well (NIHSS: 0, mRS: 1 at discharge after one week). Aetiological work-up was unremarkable aside from exulcerated plaques with <50% stenosis in the right carotid artery bifurcation.
One day after discharge, the patient was readmitted with wake-up stroke and again had right TACS (NIHSS: 16). MRI showed severe diffusion-perfusion mismatch and once more right MCA-M1 occlusion. The patient again underwent successful MT and once more showed remarkable neurological improvement (NIHSS 0, mRS 1). Extensive cardiac workup did again not reveal evidence for cardioembolic sources. Therefore, the ipsilateral exulcerated carotid plaque formation was considered the most likely cause for the recurrent strokes and carotid thromboendarterectomy was performed. In an 18-months follow-up period the patient had no further events.
Conclusion
Repeated MT for recurrent LVO stroke within a short time frame appears feasible in carefully selected patients. The collection of such cases via registries is desirable.
Trial registration number
N/A
AS31-028
CEREBRAL VENOUS THROMBOSIS IN A YOUNG FEMALE PATIENT IN POSTPARTUM PERIOD
1The National center for Neurosurgery- Astana- Kazakhstan, Department of Neurovascular disorders, Astana, Kazakhstan
Background and Aims
Cerebral venous thrombosis is a rare pathology with an incidence of less than 1% in the structure of all strokes.
CASE
22-year-old woman gravida 2, parity 2, both pregnancies ended with neonatal death. Patient presented to the hospital on postpartum day 3 with first ever-manifested seizures, GCS – 15, NIHSS – 3, blood pressure 160/80.
CT showed thrombosis of the upper sagittal sinus, hemorrhage in the parietal lobe of the left hemisphere and acute ischemia site in the right parietal lobe.
Immunological examination revealed high levels of homocysteine-15.55, antiphospholipid screening IgG - 20.529 (norm <10) and IgM - 0.0996 (norm <10).
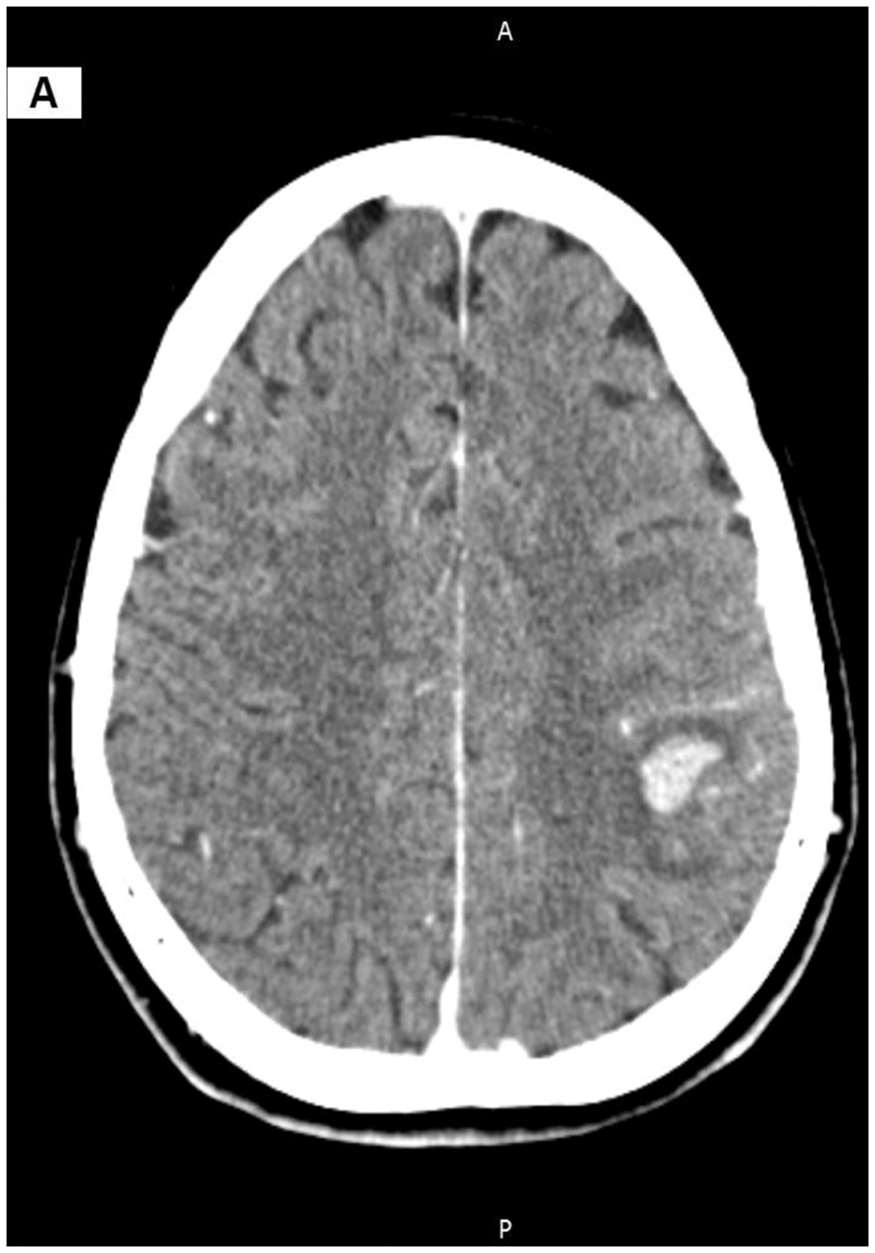
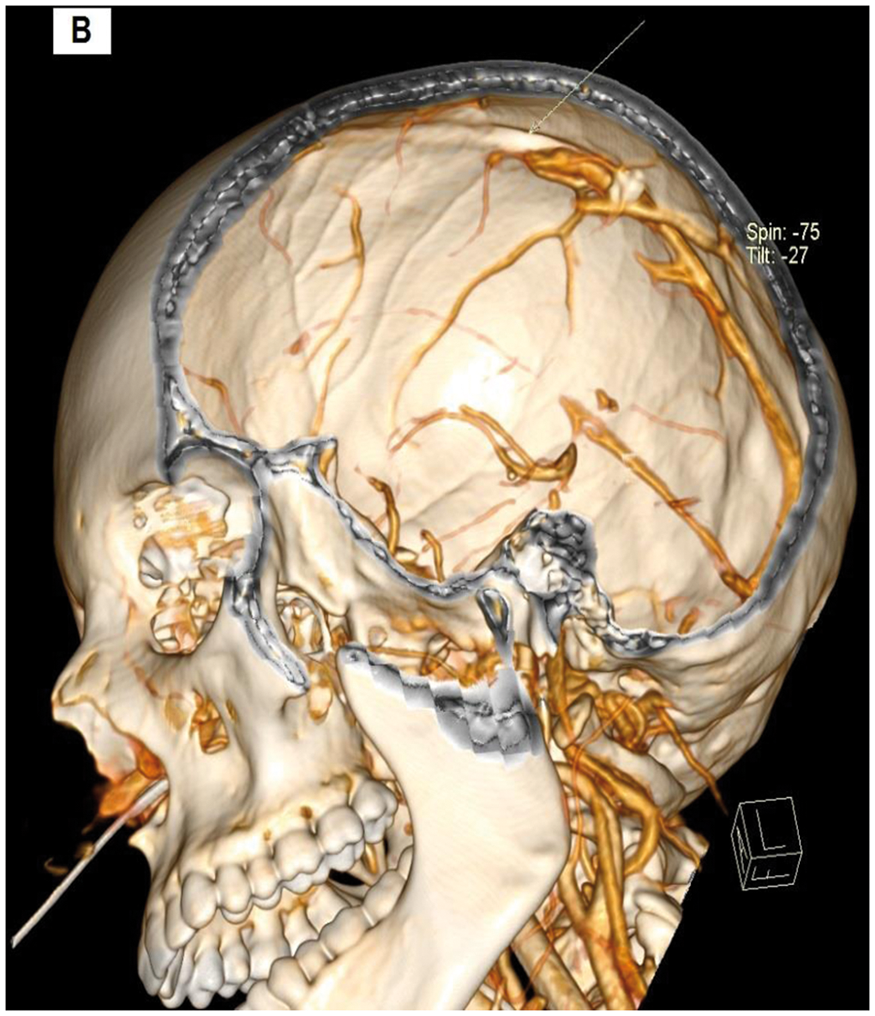
Fig.1. CT image displaying hemorrhage in the parietal lobe of the left hemisphere and acute ischemia
site in the right parietal lobe (A) and thrombosis of the upper sagittal sinus (B).
Results
On 10th day, repeated CT revealed positive dynamics with apparent recanalization of the upper sagittal sinus, resorption of hemorrhage in the left parietal lobe.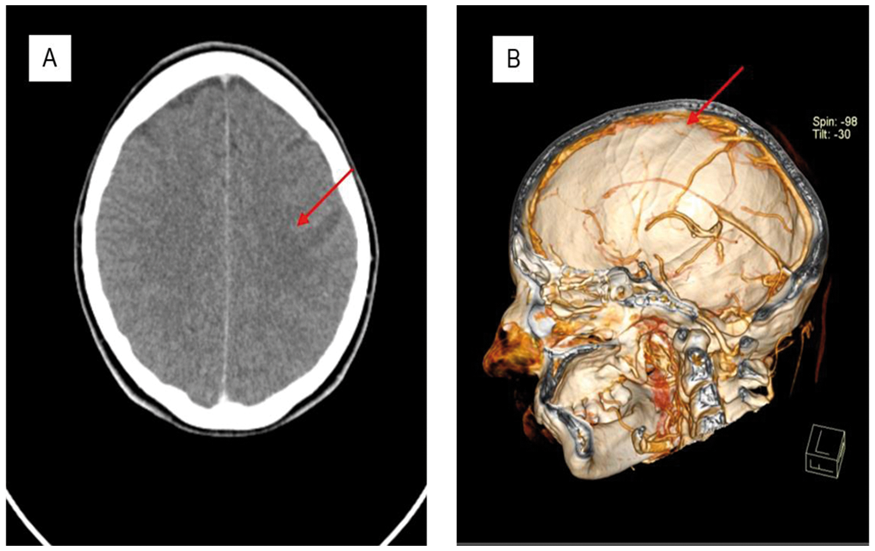
Discussion
Based on full workup patient was diagnosed with ischemic stroke associated with antiphospholipid syndrome, thrombosis of the upper sagittal sinuses (middle third of the sagittal sinus). Given the positive dynamics the early administration of direct anticoagulants in the acute period with further prolongation of indirect anticoagulants with the achievement of INR within 2-3 highly suggested. Administration of anticoagulants can last up to 6 months until recanalization of the sinuses and veins of the brain.
Trial registration number
N/A
AS31-029
AN UNUSUAL STROKE MIMIC: SPONTANEUS SPINAL EPIDURAL HEMATOMA. CASE REPORT AND REVIEW OF THE LITERATURE
1Hospital De Cabuenes, Neurology, Gijon, Spain
2Hospital Univeristario Central de Asturias, Neurology, Oviedo, Spain
Background and Aims
The proportion of stroke mimics in hospital-based intravenous thrombolyses registers varies between 1–16%. Some studies mention cervical or spinal lesions among the conditions that could simulate stroke, including spontaneous spinal epidural hematoma (SSEH), which is rare (tenemos algun dato de prevalencia?). Most patients with spontaneous spinal epidural hematoma (SSEH) present with paraplegia or tetraplegia but, although uncommon, acute hemiparesis may be the initial manifestation. In this context physicians may be inclined to consider first a cerebral stroke.
Method
An 82-year-old women with a history of atrial fibrillation treated with warfarin was admitted to the hospital for sudden right hemiparesis. She reported suffering of severe sharp cervical pain since the day before.
Results
On neurological examination she presented right hemiparesis with a muscle strength score of 2/5 without facial palsy, INR value was 2,7 and CT angiography of the brain was normal. Acute lacunar stroke was suspected at first and the patient was admitted to the Neurology Department[MR1]. During the next few hours she complained of severe persistent cervicalgia and developed left-sided hypoaesthesia, also withouth involving the face, so a spinal insult was suspected instead. Cervical spine MRI demonstrated the presence of an C3-C5 epidural haematoma compressing the spinal cord and urgent evacuation of the blood clot was performed. The patient was able to walk at discharge.
Conclusion
SSEH is a rare condition, and its presentation as hemiparesis infrequent, which often leads to misdiagnosis with stroke. Complaints of back pain and the absence of involvement of the face should arise suspicion.
Trial registration number
N/A
AS31-031
ACUTE GENERALISED EXANTHEMATOUS PUSTULOSIS (AGEP) SECONDARY TO APIXABAN
1The Hillingdon Hospital NHS Foundation Trust, Stroke Medicine, Uxbridge, United Kingdom
2London North West Healthcare NHS Trust, Geriatric Medicine, London, United Kingdom
3London North West Healthcare NHS Trust, Dermatology, London, United Kingdom
4Royal Berkshire NHS foundation Trust, Trauma and Orthopaedics, Thatcham, United Kingdom
Background and Aims
Acute generalized exanthematous pustulosis (AGEP) is a severe generalized pustular rash of acute onset, with serious cutaneous adverse reaction and systemic inflammation. It is known to be caused by drugs and the treatment involves stopping the offending drug and applying topical steroids. On reviewing the literature, we did not find this condition described to occur secondary to Apixaban. We found one case, however of AGEP occurring secondary to another Factor Xa inhibitor, Rivaroxaban.
Method
We describe a 78 year old lady who had a fall and sustained a fractured left neck of femur. She had a left hemiarthroplasty then developed fast AF post-operatively. She was started on Apixaban. 24 hours later she developed a pustular rash that started on the chest and spread rapidly to affect her arms, legs and back.
Results
She was seen by our Dermatologist who started the patient on steroids. A skin biopsy confirmed AGEP on histology. There were no other new medications implicated.

Conclusion
We believe this is the first described case of AGEP secondary to Apixaban.
Trial registration number
N/A
AS31-032
CEREBRAL AIR EMBOLISM AS A COMPLICATION OF IDIOPATHIC PULMONARY FIBROSIS. A CASE REPORT
1Campus Bio-Medico di Roma, Neurology Unit, Roma, Italy
2San Filippo Neri Hospital, Neurology Unit, Rome, Italy
3San Filippo Neri Hospital, Neuroradiology Unit, Rome, Italy
Background and Aims
Cerebral air embolism (CAE) is a cerebral infarction caused by the air intake in the vascular structures. Most cerebral air emboli are caused by iatrogenic factors, such as invasive cardiac and pulmonary procedures. There are few reports on CAE occurring in non-iatrogenic situations.
We report an unusual case of CAE not related to any medical intervention.
Method
A 79-year-old man was admitted to our hospital sent to the emergency room, for acute onset of oral rhyme deviation followed by non-responsiveness. At the first evaluation, the patient was alert, didn’t perform simple orders, had hypotonia at the 4 limbs in the absence of active motility.
Results
A computed tomography (CT) scan of the head revealed bilateral parietal-occipital air emboli, mainly on the right. We also performed a chest CT and found a small pneumothorax flap on the right with associated pneumomediastinum, which gradually improved over the clinical course. We also found honeycomb lung compatible with a framework of idiopathic pulmonary fibrosis with associated obstructive chronic bronchopneumopathy (BPCO). On day 2, Head CT scan showed that the size and number of the air emboli disappeared. Diffusion-weighted magnetic resonance imaging, performed a week later, revealed altered signal intensity in cortical-subcortical parietal-occipital area bilaterally. In the following days, the patient showed a left brachial-crural plegia with improvement of clinical conditions. Subsequently, he was sent to the neuro-rehabilitation structure.
Conclusion
This clinical report confirms that CAE can occur in a non-iatrogenic situation, especially in a patient with pulmonary vulnerability as idiopathic pulmonary fibrosis.
Trial registration number
N/A
AS31-034
INTERNAL CAROTID ARTERY FENESTRATION: CASE PRESENTATION
1Complejo Asistencial Universitario de León, Neurology, León, Spain
2Complejo Asistencial Universitario de León, Radiology, León, Spain
Background and Aims
Fenestration of the internal carotid artery is an extremely rare congenital cerebrovascular condition. It results from fusion failure or persistence of the primitive arterial network during the early embryonic stages.
Method
A case report of internal carotid artery fenestration associated with ischemic stroke, originally misdiagnosed as carotid artery dissection.
Results
A 56-year-old right-handed male was admitted to our department for a one-day case history of right hand clumsiness. He was a smoker and hypertensive.
Clinical examination revealed a mild weakness in the intrinsic musculature of the right hand.
Magnetic resonance imaging and angiography of the brain arteries revealed ischemic acute lesions in the left middle cerebral artery territory. Brain arteries were normal.
Carotid duplex showed an image suggesting unstable plaque versus thrombus in the posterior wall of the internal carotid artery, with a turbulent flow which estimated a probable stenosis of about 50–70%.
Posterior computed tomographic angiography revealed double-lumen development on the left distal internal carotid artery, suggesting artery dissection.
With the aim of reaching a final diagnosis, we requested a carotid vascular MRA which revealed a fenestration of the extracranial internal carotid artery, causing a dilatation and parcial thrombosis of one of its lumen.
The patient was prescribed aspirin and atorvastatin and his symptoms dissapeared after rehabilitation.
Conclusion
There are some false-positive neuroimaging findings for the diagnosis of craniocervical arterial dissection, among them is the artery fenestration. Although this diagnosis is usually incidental, the possibility of a trombus or embolus formation is much higher in a fenestrated artery than in a normal one.
Trial registration number
N/A
AS31-036
THE CHALLENGES OF DIAGNOSING AND TREATING CHARLES BONNET SYNDROME
1University Hospital Wuerzburg, Neurology, Wuerzburg, Germany
Background and Aims
Charles Bonnet syndrome (CBS) is characterized by complex visual hallucinations in visually impaired but otherwise psychologically normal individuals. CBS is primarily diagnosed in patients with an ophthalmic disease but is also seen in stroke patients with hemianopsia. Treatment of these hallucinations is challenging and there is no standardized treatment so far. Here, we present a stroke patient suffering from CBS who was treated successfully with melperone.
Method
A 82-year-old female patient with a history of arterial hypertension and diabetes mellitus presented with an acute right-sided loss of vision. A cerebral MRI revealed an acute ischemic stroke within the left and an old infarction involving the right occipital lobe. A few days after infarction, she noticed simple geometric shapes in form of ornaments exclusively in her right visual field followed by complex shapes in terms of faces and human bodies moving in a bizarre manner. An electroencephalogram did not show epileptic activity. When she was examined by a psychiatrist, she was fully oriented and without signs of mental illness. These findings allowed diagnosing a CBS according to the criteria ofGold & Rabins. To treat the hallucinations, a therapy witharipiprazole (5mg daily) was initiated.
Results
The two-month intake of aripiprazole did not reduce the frequency of hallucinations. Therefore a therapy with melperone (25mg daily) was administered resulting in a disappearance of the visual hallucinations.
Conclusion
Melperone might offer a potent treatment in patients with persistent hallucinations. However, its effectiveness has to be proved in a larger cohort of CBS-patients.
Trial registration number
N/A
AS31-038
AN UNWELCOME SURPRISE: THE PERSISTENCE OF THE HYPOGLOSSAL ARTERY - A VERTEBROBASILAR STROKE CASE REPORT
1Ospedale “G. Brotzu”, Radiology, Cagliari, Italy
Background and Aims
Vertebrobasilar stroke is one of the most serious and inauspicious cerebro-vascular accidents burdened with high mortality and severe disability. When this condition occurs in an abnormal anatomical picture, the knowledge of the different variants is fundamental for the planning of the endovascular treatment. Among the vascular anomalies occurring in development of supraortic trunks, we can recognize the persistent carotid-vertebrobasilar anastomoses (persistent trigeminal artery, persistent otic artery, persistent hypoglossal artery and proatlantal artery).
Method
This case presents a wake-up stroke in a 44-year-old woman with rapid worsening of neurological symptoms and hyperintensity signal in both cerebellar hemispheres, both occipital lobes and posterior ponto-mesencephalic area on DWI sequence at MR examination. MR Angiography demonstrated a basilar artery occlusion, in its distal tract, with left vertebral artery hypoplasia and absence of the right vertebral artery. The preliminary Angiographic examination highlighted the presence of a persistent hypoglossal artery arising from the left internal carotid artery as the main feeder of the basilar artery. Furthermore, abundant thrombotic material was found in the left common carotid artery and in the proximal tract of the internal carotid artery, slightly below the origin of the persistent hypoglossal artery.
Results
We proceeded to direct mechanical thrombectomy with thrombaspiration of the basilar artery thrombus and, subsequently, to a carotid artery stenting.
Conclusion
Considering the rarity of these anatomical abnormalities, the preoperative description of these variants is crucial for the success of interventional procedures.
Trial registration number
N/A
AS31-039
ACUTE POSTERIOR MULTIFOCAL PLACOID PIGMENT EPITHELIOPATHY(APMPPE), AN UNUSUAL CAUSE OF RECURRENT STROKE
1Basurto University Hospital, Neurology, Bilbao, Spain
2Basurto University Hospital, Internal Medicine, Bilbao, Spain
3Basurto University Hospital, Ophtalmology, Bilbao, Spain
Background and Aims
APMPPE is an uncommon immunologic disease of unknown etiology. It is characterized by chorioretinal disease and its typical findings in the dilated fundus examination (DFE). Systemic and neurological manifestations can occur. We present a case of recurrent vertebrobasilar strokes associated with APMPEE.
Method
A 58-year-old female was admitted to our Stroke Unit with right hemiparesis and fluctuating mild dysarthria due to a paramedian pontine stroke. She had a previous diagnosis of psoriasic arthritis and no vascular risk factors. Unfractionated heparin (UFH) was administrated with clinical stabilization, switched to antiaggregation 72 hours later. Patient showed acute left weakness 48 hours later secondary to a new pontomedullary stroke and returned to previous treatment with UFH. She developed a locked-in syndrome in admission with partial recovery. Prior to hospital admission, the patient had been suffering from blurred vision and fever. At hospital, she was evaluated by Ophtalmologist and Reumathologist because of worsening ocular symptoms.
Results
Laboratory studies included ESR 107, CRP 10.5 and positive ANAS(anti-DFS70). CSF revealed lymphocytic pleocytosis and raised proteins. DFE, OCT and laboratory tests supported diagnosis. Normal Holter monitor (1 week), transthoracic echocardiography, supra-aortic trunk echodoppler, arteriography and body-scanner ruled out systemic, cardiologic and atherotrombotic etiologies. Patient received corticosteroids and azathioprine with a good clinical outcome. After discharge, she was transferred to a rehabilitation center.
Conclusion
Neurological involvement in APMPEE is rarely reported. The most common neurologic complication is cerebral vasculitis and subsequent strokes. Clinical findings, laboratory tests and DFE support diagnosis. Early identification and treatment can improve the outcome of patients.
Trial registration number
N/A
AS31-040
CONTRAST INDUCED ENCEPAHLOPATHY - A RARE STROKE MIMIC
1Southend University Hospital NHS Foundation Trust, Stroke Medicine, Southend on Sea, United Kingdom
Background and Aims
Neurotoxicity from iodinated contrast agents is a known but rare complication of angiography and cardiovascular digital subtraction angiography. As contrast penetrates the blood-brain barrier cerebral oedema results with altered neuronal excitability. Clinical symptoms can include focal neurological deficits. We describe a rare case of contrast induced encephalopathy.
Method
A 67 year old lady presented with dysarthria and agitation following iodinated contrast media administered 4 hours previously for a coronary angiogram. There was no haemorrhage or infarct on CT. NIHSS score was 7 and the patient was thrombolysed.
Results
The following morning an MRI was conducted. There was no restricted diffusion or infarct, despite persistent clinical symptoms. At this time contrast induced encephalopathy was suspected. There was a slow progressive clinical improvement with complete resolution of presenting symptoms at 48h.
Conclusion
Neurotoxicity from iodinated contrast agents is a rare complication of angiography. The infrequency with which it is encountered makes it a diagnostic challenge. Contrast encephalopathy can be suspected in a symptomatic patient after exclusion of thromboembolic and haemorrhagic complications. Our report demonstrates this rare stroke mimic which should be recognised by doctors performing DSA angiography.
Trial registration number
N/A
AS31-041
CARDIAC FINDINGS IN A COMPREHENSIVE CEREBRO-VASCULAR-CARDIAC MRI (CVC-MRI) PROTOCOL FOR ONE-STOP ETIOLOGIC IMAGING IN ACUTE STROKE
1Neurology, Neurology, Homburg, Germany
Background and Aims
Current state-of-the-art for etiologic workup in stroke is a combination of cerebral and vascular imaging in combination with duplex sonography and cardiac diagnostics including echocardiography and ECG. We established a comprehensive MRI protocol, combining cerebral, vascular and cardiac examinations in one session (CVC-MRI) in order to provide a one-stop etiologic imaging. As most stroke specialists are not familiar with cardiac MR-images, we intend to present four cases with cardiac imaging findings obtained with CVC-MRI.
Method
Presentation of four cases with instructive findings in cardiac MR-imaging and acute stroke.
Results
Case 1: Embolic Stroke in 42 yr old patient. The patient had no history of cardiac disease but CVC-MRI revealed cardiac scarring after transmural infarktion with adjacent Thrombus that was overlooked in initial TTE but then confirmed in second.
Case 2: CVC-MRI revealed high grade Aortic stenosis in a patient with acute embolic stroke.
Case 3: Impaired cardiac function with ejection fraction of 25% in a patient with acute embolic stroke.
Case 4: Endocarditis with vegetation on the mitral valve in a patient with acute embolic stroke.
Conclusion
CVC-MRI may help to identify cardiac etiologies of stroke that may be overlooked with standard care. It may also be an alternative in patients who refuse to undergo more invasive methods such as TEE.
Trial registration number
N/A
AS31-043
CAPSULAR GENU SYNDROME. AN UNDERDIAGNOSED DISORDER
1Hospital Universitario de Canarias, Neurology, La Laguna, Spain
Background and Aims
Capsular Genu Syndrome is a forgotten entity, described by Tatemichi in 1992, which is found in patients with internal capsular genu infaction, disconnecting the thalamus from the orbito-frontal cortex. The clinical presentation varies, although patients usually show behavioral problems, abulia, amnesia, confabulations and lack of insight. Post-stroke cognitive impairment can be found in up to 1/3 of stroke survivors.
Method
A report of two cases assisted in our reference area in 2017.
Results
We present two males, A and B, both previously independent and with vascular risk factors. A: 72 years-old man with a previous frontal ictus in 2016, independent after discharge. He developed sudden behaviour changes, with irritability, mood oscillations, apathy and hyporexia. He didn't show any other neurologic deficits, so at first he was labelled as a confusional syndrome. In a brain CT-scan we found a new stroke in the anterior limb of the left internal capsular genu and thalamus. B: 77 years-old man who after a fall started being abstracted, having episodic memory failures, sleeping disorders and spatial disorientation. In the brain CT-scan was found a lacunar lesion in the right capsular genu.
Conclusion
Strategic strokes can induce acute cognitive impairment or behaviour changes, in some occasions can be misunderstood as a confusional syndrome. These results emphasize the importance of lesion location and the necessity of an assessment of cognition in these cases.
Trial registration number
No clinical trial
AS31-044
SPONTANEOUS SPLENIC RUPTURE SECONDARY TO DABIGATRAN: THE LAST IN A SERIES OF UNFORTUNATE EVENTS
1Royal Berkshire Hospital, Acute Stroke Unit, Oxford, United Kingdom
2Royal Berkshire Hospital, Acute Stroke Unit, Reading, United Kingdom
Background and Aims
N/A
Method
N/A
Results
We present the case of a previously well 77 year old lady who had an accidental fall in her garden, resulting in a fracture of her left ankle. After manipulation of the fracture, she developed sudden onset shortness of breath. An echo led to the diagnosis of Takotsubo cardiomyopathy, along with a massive elevation in cardiac troponin. She underwent an angiogram which showed normal coronary arteries; however, shortly after the procedure, she developed receptive and expressive dysphasia. An MRI head confirmed a left parietal infarct. She was recovering well on the acute stroke unit, and was eventually started on dabigatran on the basis that her cardiomyopathy was the likely source of her embolic infarcts. The following day, she developed severe abdominal pain and her oxygen saturations began to fall. No obvious cause was found on chest or abdominal radiographs and she was treated with simple analgesia and antibiotics in view of raised inflammatory markers. Three days later, she had on-going abdominal pain and her haemoglobin began to drop. Eventually a CT chest, abdomen and pelvis revealed spontaneous splenic rupture, and she was successfully treated with praxbind and blood transfusions.
Conclusion
This was an unusual case of multiple complications following a simple fall, culminating in a rare complication of DOAC therapy. This case highlights the importance of considering this diagnosis in patients with unexplained abdominal pain who have been started on anticoagulation, as well as the importance of continuing to pursue a diagnosis in patients with unexplained symptoms.
Trial registration number
N/A
AS31-045
A SYNDROME OF ACUTE CEREBELLAR AND HIPPOCAMPAL RESTRICTED DIFFUSION: A POTENTIALLY FATAL STROKE MIMIC
1University of Cincinnati, Neurology and Rehabilitation Medicine, Cincinnati, USA
2University of Tennessee Health Science Center, Neurology, Memphis, USA
Background and Aims
Abnormally restricted diffusion on MRI is often associated with ischemic stroke, but other conditions can present similarly. We present six cases of an unusual pattern of restricted diffusion in the bilateral hippocampi and cerebellar cortices. This pattern of injury is distinct from findings typical for ischemic, anoxic, or toxic injury, suggesting it may represent a novel syndrome.
Method
We identified an ad hoc series of patients at our two institutions between years 2014–2017 who presented to the neurosurgical ICU with severe, otherwise-unexplained cerebellar edema and retrospectively identified several commonalities in history, presentation, and imaging.
Results
Between two institutions, we identified six patients – ages 35 to 59 years, four male – with similar presentations. Most patients presented with opiate overdose and some degree of hypoxia. All patients demonstrated similar imaging findings of restricted diffusion in the bilateral hippocampi and cerebellar cortices, as well as patchy restricted diffusion in the basal ganglia (figure). Due to cerebellar edema causing obstructive hydrocephalus, patients required either osmotic therapy or surgical decompression. The five patients who survived to discharge demonstrated variable degrees of physical and memory impairment on discharge and followup.
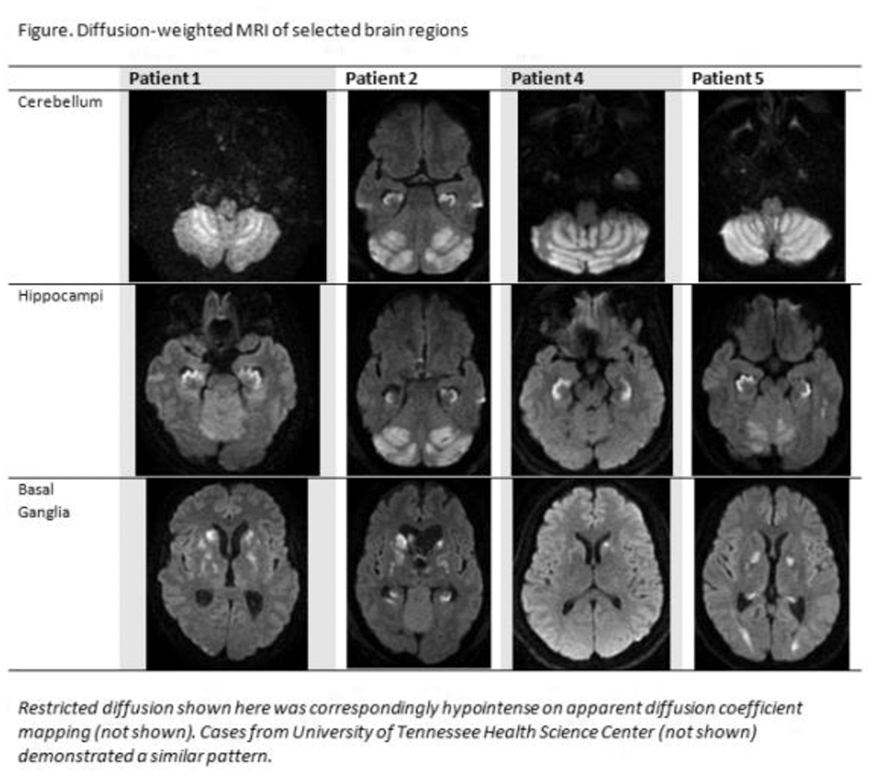
Conclusion
We present findings of a potentially novel syndrome involving a particular pattern of cerebellar and hippocampal restricted diffusion, with imaging and clinical characteristics distinct from ischemic stroke. Given a potential risk of obstructive hydrocephalus, early identification and intervention of this syndrome may be critical.
Trial registration number
n/a
AS31-046
THROMBOLYSIS IN NON-APPARENT BRAIN TUMOURS ON NON-CONTRAST CT – TWO CASES
1Colchester General Hospital, Stroke Unit, Colchester, United Kingdom
Background and Aims
Non-contrast CT (NCCT) is the pre-thrombolysis modality of choice in acute stroke assessment.
We present two cases of normal NCCT and subsequent MRI revealing undiagnosed brain tumour. There were no adverse outcomes following thrombolysis.
Method
Case 1: 67 years old male with hypertension was admitted with acute expressive and receptive aphasis and NIHSS of 6
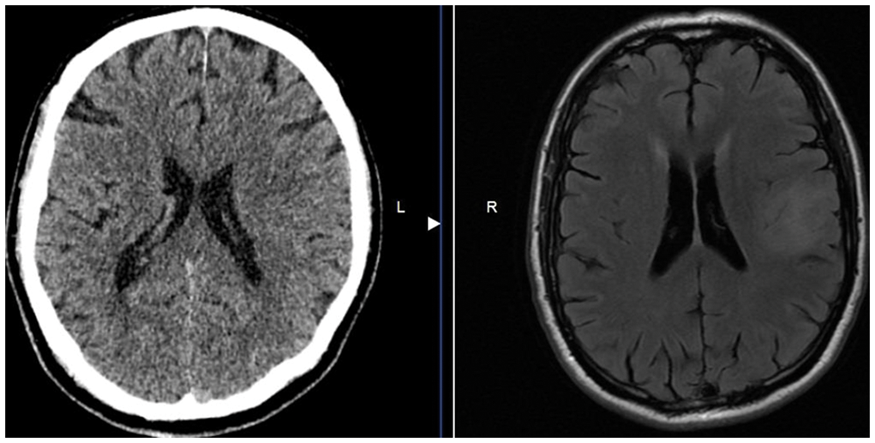
Case 2: 79 years old female with hypertension was admitted with acute expressive and receptive aphasia with NIHSS of 6
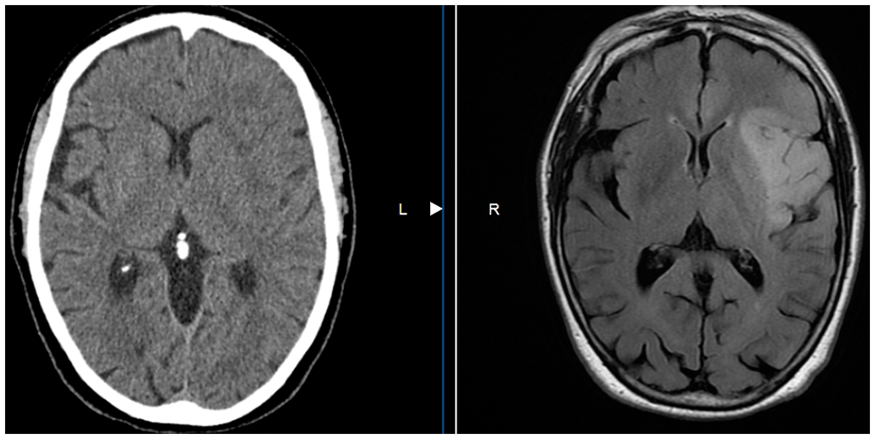
Results
Relatively normal appearing NCCTs but subsequent abnormal MRI revealed slow growing glioma.
Conclusion
These cases add further unintentional data to support the data that thrombolytic therapy for acute stroke appears to be safe in patients with primary brain tumors, with similar rates of ICH.(1)
Ref:
1. J Clin Neurosci. 2015 Mar;22(3):474–8
Trial registration number
N/A
AS31-048
ISHEMIC INTERNUCLEAR OPHTHALMOPLEGIA: ETIOLOGICAL SPECTRUM
1Hacettepe University Hospitals, Neurology, Ankara, Turkey
Background and Aims
Ischemic INO (internuclear ophthalmoplegia) is rare but an important clinical stroke syndrome surely due to its localizing value. Etiological spectrum of ischemic INO has not been studied satisfactorily with modern methods.
Method
Demographic, etiologic, risk factor and imaging profiles of 16 patients with isolated INO, referring to 0.6% of acute ischemic stroke admissions during the last 9 years, were documented.
Results
Acute ischemic INO lesions had two characteristic localizations on diffusion-weighted images (DWI) merging with MLF determined by DTI. In 9 cases (57%), lesions were located in the anterior part of mesencephalon at the level of inferior colliculus, conforming to occlusion of the distal segment of interpedincular fossa arteries. All lesions were flame-shaped with their base contacting the anterior border of midbrain aqueduct. In 7 (43%) cases, acute infarcts were located in the dorsomedial tegmental areas of the midpons – the territory of paramedian tegmental long anteromedial arteries, and were in contact with the anterior margin of the 4th ventricle. The lesion size was quite small, with an average volume of 0.26 (0.1 to 1) cc. The cause of stroke was embolism, except for a 50% basilar artery stenosis in one case. Presumed origin of embolism was cardiac in 3, procedural in 3, artery-to-artery in 2 and cryptogenic in 7. Vascular imaging documented mild-to-moderate basilar artery (BA) tortuosity in 6 cases, and BA irregularity in 2 cases.
Conclusion
The major cause of ischemic INO is embolism, not small vessel disease (lacune) or basilar artery branch atheroma.
Trial registration number
N/A
AS31-049
INTRAVENOUS THROMBOLYSIS IN STROKE AFTER DABIGATRAN REVERSAL BY IDARUCIZUMAB: OUR EXPERIENCE AND REVIEW OF LITERATURE
1Gubbio-Gualdo Hospital- USL Umbria 1, U.O. Neurologia, Gubbio, Italy
2Città di Castello Hospital - USL Umbria 1, U.O. Neurologia, Gubbio, Italy
3Gubbio-Gualdo Hospital- USL Umbria 1, U.O. Medicina, Gubbio, Italy
4Università degli Studi di Perugia - Azienda Ospedaliera di Perugia, Cardiologia e Fisiopatologia Cardiovascolare, Perugia, Italy
5Gubbio-Gualdo and Città di Castello Hospitals - USL Umbria 1, U.O. Neurologia, Gubbio, Italy
Background and Aims
The preventive approach in cardio-embolic stroke due to non-valvular atrial fibrillation was radically changed after the marketing of the non-vitamin K antagonist oral anticoagulants (NOACs). The favourable benefit-risk profile of these “new” drugs makes them preferable to warfarin. Until now dabigatran is the only one with a specific antidote approved for clinical use: idarucizumab. This drug is capable of reversing the anticoagulant activity of dabigatran very quickly without procoagulant effect. However idarucizumab is not extensively studied in the acute phase of ischaemic stroke. In this paper we describe our experience in this topic and review the available information in literature.
Method
We analysed our stroke registry in order to identify the patients who were eligible to thrombolysis during treatment with dabigatran in the last two years. We also performed a literature review to identify all the available
Results
We only found cases series and case reports; we did not find other types of studies.
In addition to our patients, the cases described in literature confirmed the safety and the efficacy of idarucizumab in emergencies setting and its usefulness in ensuring the applicability of i.v. thrombolysis.
Conclusion
We think that the available registries on the use of NOACs, their reversal and eventual thrombolytic treatment, may provide the necessary amount of evidence on this topic; since the implementation of a clinical trial on this subject is rather improbable.
Trial registration number
N/A
AS31-050
CNS VASCULOPATHY SECONDARY TO LEPTOMENINGEAL CARCINOMATOSIS FROM PROSTATE CANCER
1Addenbrooke's Hospital, Department of Stroke Medicine, Cambridge, United Kingdom
2Addenbrooke's Hospital, Department of Clinical Neurosciences, Cambridge, United Kingdom
Background and Aims
Leptomeningeal metastases associated with prostate cancer are extremely rare, and occur in the context of previously metastatic, and castration-resistant, disease. Specific treatment options are largely unknown, and its clinical course is rapidly progressive. Central nervous system (CNS) vasculopathies are well described as causes of neurological symptoms, and can be associated with metastatic meningeal disease.
Method
We present the case of a 69 year old gentleman presenting with progressive confusion, dysarthria and right-sided weakness. Initial neuroimaging was suggestive of ischaemic strokes affecting the thalamus and cerebellum. Computed tomography (CT) angiography (CTA) demonstrated multiple intracranial foci of stenosis in the anterior and posterior circulation. Subsequent cerebrospinal fluid (CSF) cytology and immunochemistry demonstrated prostate adenocarcinoma cells. He was therefore diagnosed with leptomeningeal spread of prostate cancer, with a secondary CNS vasculopathy.
Results
He was referred to the prostate oncology team and commenced on degarelix as maximal androgen blockade. His performance status precluded further chemotherapy or radiotherapy. He had been noted to have a history of prostate cancer treated with radical prostatectomy, with no evidence of biochemical recurrence or metastatic disease at previous follow up visits. His symptoms progressively worsened despite treatment, and he died approximately five weeks after admission.
Conclusion
This is a novel case of meningeal spread of previously non-metastatic prostate cancer with an associated vasculopathy and stroke-like syndrome. We review the literature surrounding risk factors, diagnostic challenges and prognosis of meningeal spread in prostate cancer and CNS vasculopathy.
Trial registration number
N/A
AS31-051
PEDUNCULAR HALLUCINOSIS AS THE PRESENTING FEATURE OF MIDBRAIN/PONTINE INFARCT
1Cambridge University Hospitals NHS Trust, Department of Stroke Medicine, Cambridge, United Kingdom
Background and Aims
Visual hallucinations, a common presentation in acute medical patients with infection and psychosis, is a relatively rare presentation of hyperacute stroke. We describe a case of visual hallucinations as the presenting feature of pontine/midbrain infarct.
Method
Case Report
An 84-year old female presented with 3-day history of horizontal diplopia and unsteadiness. Past medical history included hypertension, old lacunar infarct and surgically-corrected bilateral cataract. Onset of symptoms was preceded by short-lived episodes of vivid visual hallucinations whenever she closed her eyes of people with “weird” faces and animals on either side of visual field approaching her. The hallucinations resolved upon falling asleep and she was able to distinguish them from reality. Sleep was unimpaired.
On examination, right internuclear opthalmoplegia, mild left-sided ataxia, truncal ataxia was found. Visual fields, visual acuity and cognition were normal.
Results
MRI showed an acute infarct at the junction of pons/lower midbrain. She was found to have polycythemia vera, being treated with intermittent venesection. On discharge at day 12, diplopia had resolved.
Conclusion
Peduncular hallucinosis (PH), a rare form of visual hallucinations, is characterised by acute onset of transient vivid, colourful hallucinations involving moving characters or animals, which are distinguishable from reality. PH has been reported in midbrain, pontine and thalamic lesions of inflammatory, malignant or most commonly, vascular origin. The likely mechanism is disruption of visual cortex connectivity via damage to thalamocortical pathways. This case serves as a reminder to consider mesencephalic infarct/haemorrhage in cases of acute onset vivid hallucinations, and to carefully examine for occulomotor disturbances and ataxia.
Trial registration number
N/A
AS31-052
SIMULTANEOUS THROMBECTOMY AND COILING OF AN UNRUPTURED ANEURYSM IN A PATIENT WITH A CARDIOEMBOLIC STROKE
1Hospital Ramón y Cajal, Neurology, Madrid, Spain
2Hospital Ramón y Cajal, Radiology, Madrid, Spain
Background and Aims
Mechanical thrombectomy in acute stroke for large-vessel occlusion in anterior circulation is effective. The experience in the realization of simultaneous thrombectomy and packing with coils of an unruptured aneurysm is limited. We report the first case of succesful mechanical thrombectomy and simultaneous coiling in a patient with a cardioembolic stroke and a previous unruptured aneurysm in the middle cerebral artery (MCA).
Method
A 54-year-old man with history of hypertension, non-valvular atrial fibrilation (NVAF) CHA2DS2VASc-1 (before ischemic stroke), a non-clipped MCA aneurysm and subarachnoid hemorrhage, presented with mutism and right hemiplegia in the anesthetic awaking after a pulmonary vein ablation for NVAF. rtPA was contraindicated in this patient so endovascular therapy was directly performed.
Results
The patient presented with complete left MCA symptoms (NIHSS-25). The vital signs and laboratory tests were normal. Multimodal CT imaging revealed an unruptured aneurysm (13,2x12,7 mm), ASPECTS 9, with ischemic penumbra and complete occlusion of M1 segment. Mechanical thrombectomy was performed (door-needle time 145 minutes, general anesthesia). The thrombus was removed with an aspiration-catheter (ACE-68), with an inferior MCA division remaining occluded (TICI-2a). Thereafter, aneurysm was treated successfully with coiling. A cranial CT performed 24 hours post-thrombectomy showed a small infarction on M3-M5-M6 territory. Patient was discharged with dabigatran 150mg/12h started after 10 days. He had sensory aphasia (NIHSS-7, mRS-3) and no hemorrhagic events were recorded during follow up (6 months).
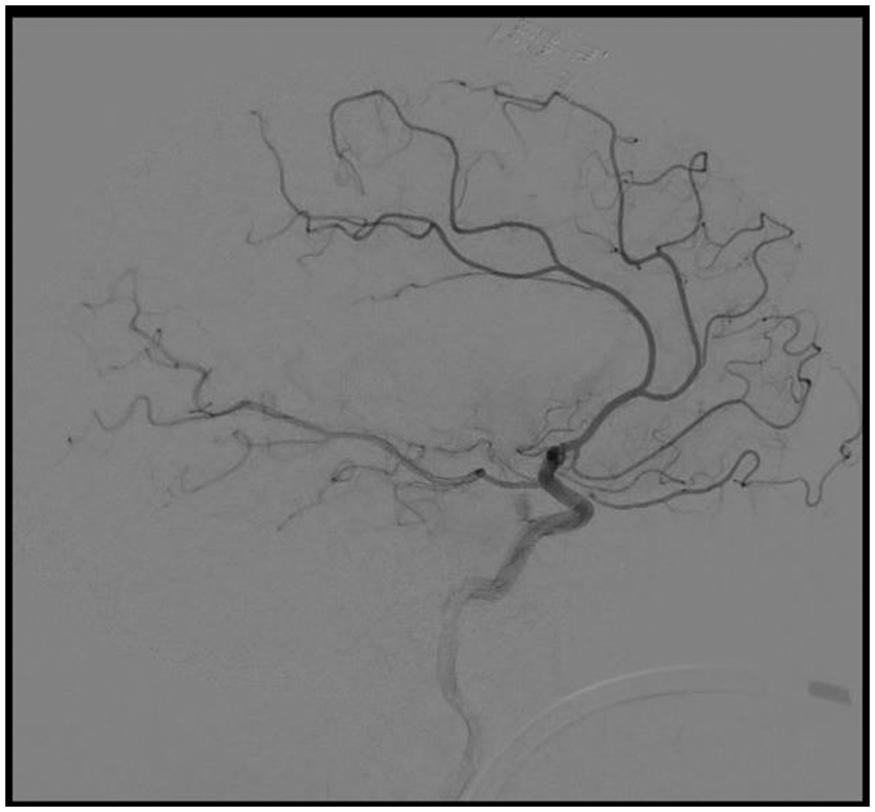
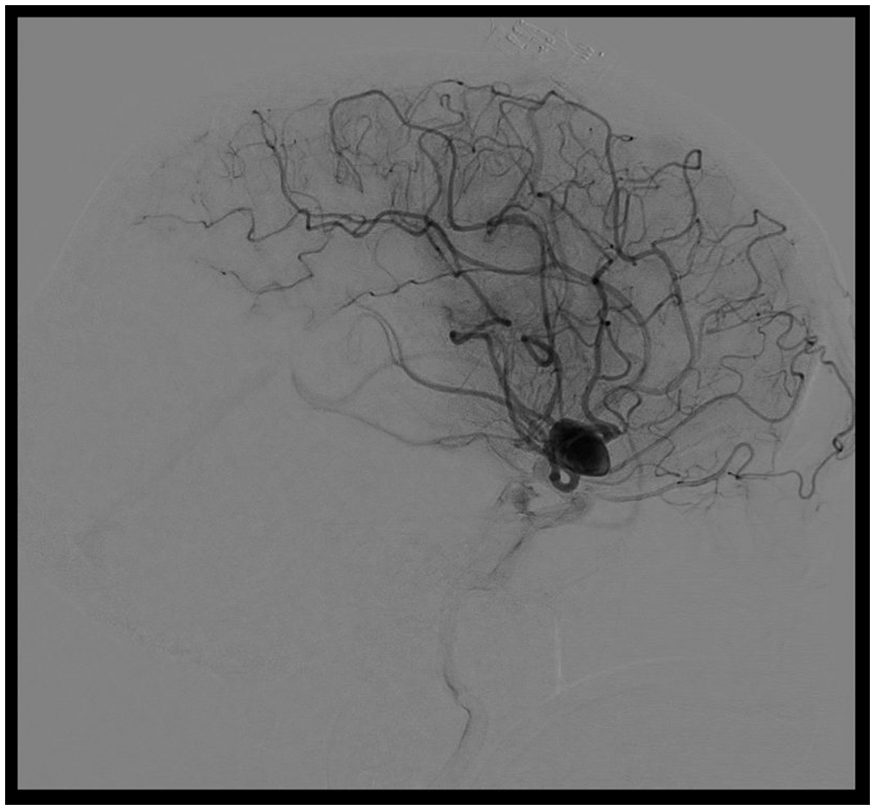
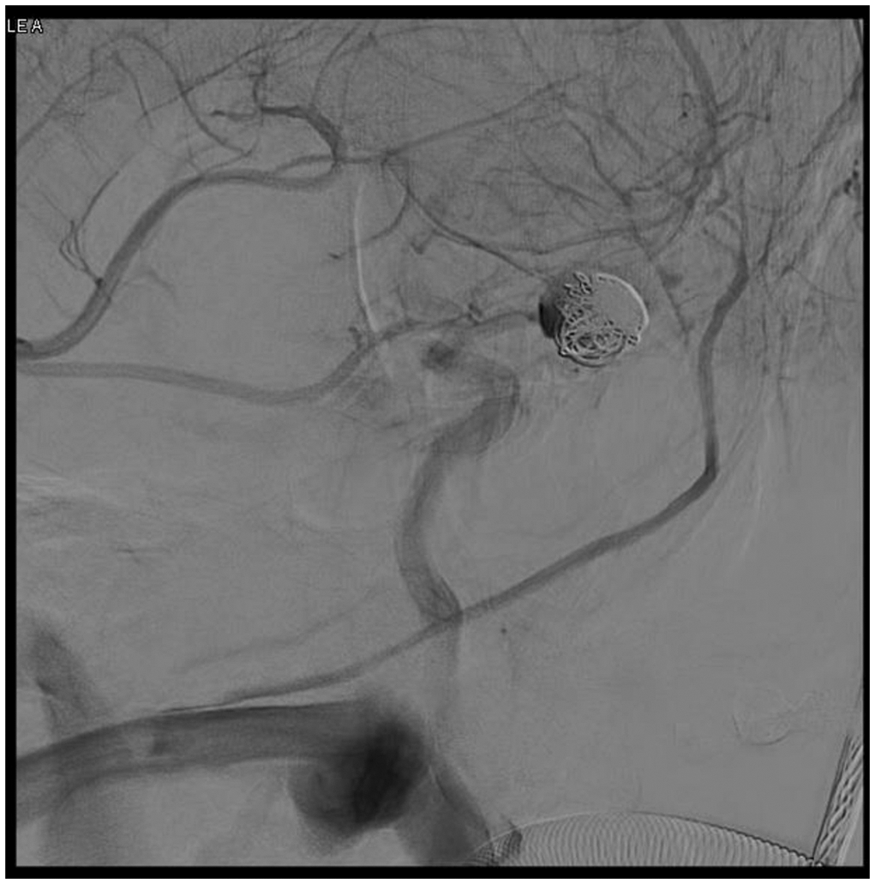
Conclusion
Our case shows that simultaneous mechanical thrombectomy and coiling of unruptured aneurysms is feasible with an excellent clinical result and allows to prevent further ischemia.
Trial registration number
N/A
AS31-053
MES MONITORING IN PATIENTS WITH LARGE ARTERY OCCLUSIONS OF THE ANTERIOR CIRCULATION TREATED WITH MECHANICAL THROMBECTOMY: A CLINICAL CASE
1University of Padova, Department of Neurological Sciences, Padova, Italy
Background and Aims
Mechanical thrombectomy (MT), in addition to intravenous thrombolysis (IVT), is currently recommended to treat ischemic stroke patients with large artery occlusions of the anterior circulation. Yet, not all patients experience clinical improvement after a successful recanalization and to determine the cause of occlusion could be a diagnostic challenge.
Method
A 79 years old man referred to our hospital with sudden onset of left hemiparesis, dysarthria and hemineglect. He reported an history of hypertension, dyslipidemia and smoking habit. A cerebral CT scan was negative for hemorrhage while an AngioCT scan of cerebral vessels showed a right proximal middle cerebral artery (MCA) occlusion. He was treated with IVT and MT with successful artery recanalization. During periprocedural Transcranial Doppler (TCD) monitoring, numerous bilateral microembolic signals (MES) suddendly appeared, followed by the disappearance of the flow signal in the left MCA. The patient presented a generalized seizure and then underwent to a second MT procedure which was partially successful.
Results
Control CT scan showed a large ischemic lesion in the left MCA territory. During stroke unit monitoring atrial fibrillation was never recorded and echocardiography was negative for ventricular thrombi. An aortic AngioCT scan showed an extended irregular plaque in the descending arch. Patient died after a week due to pulmonary complications in status epilepticus.
Conclusion
Atheroembolism from aortic arch is an unrecognized cause of multiembolic stroke to be kept into account. TCD is an helpful tool to real time monitor hemodynamics changes in EVT-treated stroke patients and may give important diagnostic clues.
Trial registration number
N/A
AS31-054
GIRL WITH CONSECUTIVE CRYPTOGENIC STROKE AND PATENT FORAMEN OVALE
1Ramón y Cajal Hospital, Neurology, Madrid Spain, Spain
2Ramón y Cajal Hospital, Pediatric Intensive Care, Madrid Spain, Spain
3Ramón y Cajal Hospital, Pediatric Cardiology, Madrid Spain, Spain
Background and Aims
The role of patent foramen ovale (PFO) closure to prevent ischemic stroke recurrence remains controversial. Its efficacy for the prevention of recurrence after cryptogenic stroke has been proven in recently published clinical trials, especially in young patients when large shunts are observed. Children have been excluded from these trials.
Method
Case report
Results
A nine years old girl had a cryptogenic ischemic stroke in the left thalamus. Cardioembolic sources, carotid stenosis or thrombophilia were not found. She was discharged without sequelae and started treatment with aspirin. Four years later, she was admitted to hospital with sudden onset dizziness, vomiting and right limb and gait ataxia. Magnetic resonance showed an acute right cerebellar infarction. She had favourable clinical outcome in few days with complete remission of symptoms. Transcranial doppler and transesophageal echocardiography showed presence of PFO with large interatrial shunt (>30 microbubbles). PFO closure was performed during admission. She was discharged on dual antiplatelet therapy and she was switched to clopidogrel alone after two months. No further recurrence have been recorded during follow up.
Conclusion
In selected cases, children with cryptogenic stroke may be considered to perform PFO closure to prevent ischemic stroke recurrence.
Trial registration number
N/A
AS31-055
OCULAR ISCHEMIC SYNDROME: THE FIRST MANIFESTATION OF BILATERAL COMMON AND INTERNAL CAROTID ARTERIES OCCLUSION
1Hospital de Braga, Neurology, Braga, Portugal
Background and Aims
Ocular Ischemic Syndrome (OIS) is a rare form of ischemia of both segments of the eye. It’s caused by ocular hypoperfusion due to stenosis or occlusion of the carotid arteries mainly due to atherosclerosis. OIS as the first manifestation of bilateral carotid occlusion is rare.
Method
Case-report
Results
A 63-year-old man with history of smoking, excessive alcohol intake, dyslipidemia and polyglobulia, had progressive loss of vision for one month and bilateral periorbital pain in decubitus associated with conjunctival hyperemia for ten days. On the admission day, there was a short-lasting episode of altered state of consciousness associated with involuntary movements of the upper limbs, which had also occurred two days earlier. Neurological examination revealed a bilateral hypovision. Ophthalmologic examination showed a greatly reduced visual acuity in both eyes, medium mydriasis, rubeosis iridis, retinal microaneurysms and cotton-wool spots. CT showed two watershed infarcts in the right frontal and left parieto-occipital location. CTA revealed occlusion of both common and internal carotid arteries. Doppler ultrassound confirmed severe atheromatous disease and showed normal flow in external carotid arteries and inverted flow in ophthalmic arteries. At discharge, the patient maintained hypovision with no other focal deficits. Patient was treated with dual antiplatelet therapy, high-dose statin and general recommendations for vascular risk factor control and hypotension prevention were made.
Conclusion
Our patient presented an OIS as the first manifestation of bilateral occlusion of the carotid arteries. It’s important to alert that ocular manifestations may precede those of the cerebrovascular system, and thus, potentially life-threatening events can be prevented.
Trial registration number
N/A
AS31-059
CEREBRAL AIR EMBOLISM: A NON-THROMBOTIC CAUSE OF STROKE
1University of Florence, NEUROFARBA Department- Neuroscience Section, Florence, Italy
2Azienda Ospedaliero Universitaria Careggi, Stroke Unit, Florence, Italy
3University of Milan, “L. Sacco” Department of Biomedical and Clinical Sciences, Milan, Italy
Background and Aims
The majority of ischemic strokes are of an embolic nature and are commonly due to occlusion of the brain arteries by clots. Less frequently, emboli may consist of non-thrombotic material. Cerebral air embolism (CAE) is a rare cause of non-thrombotic stroke. It may occur as complication of medical procedures, although non-iatrogenic sources have been also reported.
Method
We report three patients with CAE admitted to hospital for the treatment of different heart diseases.
Results
In two patients, neurological disturbances developed soon after central venous catheter (CVC) manipulation, while in the third one symptoms occurred after persistent cough. All of them experienced seizures, loss of consciousness and bilateral neurological signs. Acute brain computed tomography (CT) revealed intracranial air bubbles while multiple ischemic lesions were shown on neuroimaging repeated in the following days.
Conclusion
CAE may occur during CVC placement, removal or manipulation and also consequent to non-iatrogenic conditions such as pulmonary diseases, even if this latter is rare. Clinical manifestations are similar to those of thrombotic ischemic strokes, although some features such as decreased consciousness and seizures are more frequent in CAE. CAE is characterized by multiple ischemic lesions and is associated with high mortality rate.
Stroke secondary to CAE is rare but should be suspected especially in the case of in-hospital strokes. Brain CT is useful to detect cerebral air bubbles when performed in the hyperacute phase. Hyperbaric oxygen therapy is the gold standard treatment for CAE within the first four to six hours after onset of neurologic symptoms.
Trial registration number
N/A
AS31-060
CEREBRAL VENOUS THROMBOSIS TREATED WITH DIRECT ORAL ANTICOAGULANTS: A CASE SERIES
1Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Cerebral venous thrombosis (CVT) is an uncommon cause of stroke. Standard treatment is based on anticoagulation with heparin followed by an oral vitamin K antagonist (VKA). Direct oral anticoagulants (DOACs) are the best option for stroke prevention in patients with non-valvular atrial fibrillation but there is no clinical evidence to support their use for CVT.
Method
We report three cases of patients with CVT treated with DOACs in our Comprehensive Stroke Center from January 2014 to December 2017.
Results
All patients (2 women aged 31 and 35 years-old and a 69-year- old male) received initial anticoagulant therapy with subcutaneous low molecular weighted heparin (LMWH). Two patients were discharged on VKAs, but due to the impossibility for reaching therapeutic levels after dose modifications, they were switched on ACOD (Rivaroxaban 20mg and Dabigatran 150mg). The other patient was discharged on Dabigatran 110mg due to previous intracranial hemorrhage secondary to a cavernoma. During follow up visits along 2 ± 1 years, magnetic resonance imaging (MRI) demonstrated complete venous repermeabilization in one patient and partial recanalization in two patients. No bleeding or thromboembolic complications were recorded during follow up.
Conclusion
In selected cases, DOACs may be safe and an effective for the treatment of CVT.
Trial registration number
N/A
AS31-061
THE USE OF DIFFUSION WEIGHTED T2 SPINAL MRI AS AN AID TO DIAGNOSING ANTERIOR SPINAL ARTERY SYNDROME
1Mater Dei Hospital, Department of Neuroscience, MOSTA, Malta
2Mater Dei Hospital, Department of Neuroscience, Msida, Malta
3Mater Dei Hospital, Department of Radiology, Msida, Malta
Background and Aims
Anterior Spinal Artery Syndrome remains in most cases a clinical diagnosis and a diagnosis of exclusion. Whereas Diffusion Weighted Magnetic Resonance Imaging (DW MRI) has long been used in the brain, its use in the spine is still an expanding field in neuroradiology. Its use in this case is the only example available in literature of a spinal cord infarct secondary to Anterior Spinal Artery Syndrome evident on MRI. Its use early on in the presentation will confirm the diagnosis and enable management decisions to be made not just on clinical acumen.
Method
A case of a 40 y/o lady previously healthy who presents with acute flaccid diplegia, areflexia and dissociated sensory loss with sole preservation of fine touch, vibration and joint position sense is described.
Results
In this case, the use of DW MRI confirmed the diagnosis with evident diffusion restriction starting at the level of T2, thereby confirming spinal cord infarction starting at the level of T2 and progressing distally along the whole length of the spinal cord.
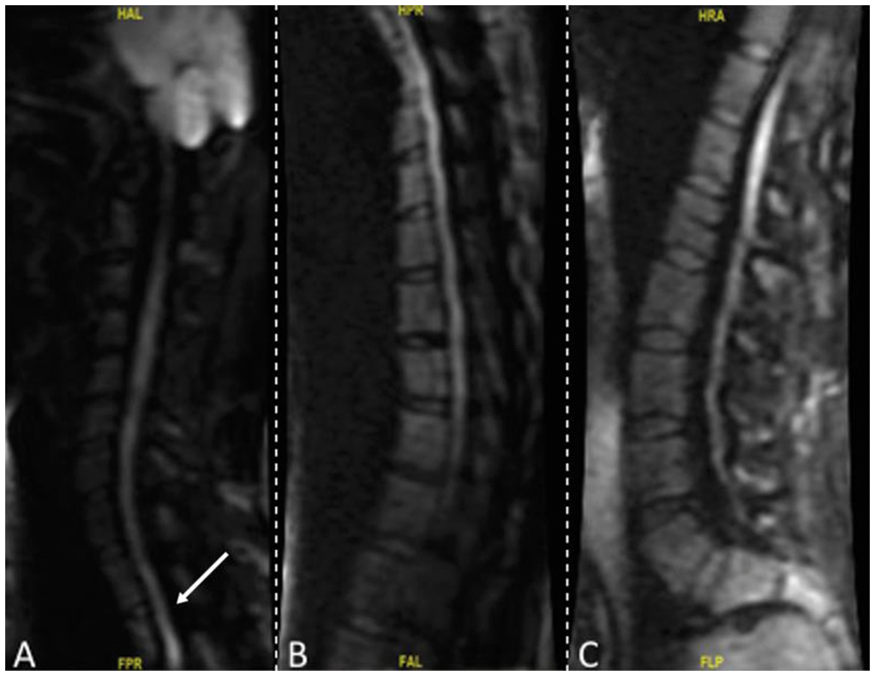
Conclusion
The use of Diffusion-Weighted T2 MRIs of the spinal cord has enabled the diagnosis of Anterior Spinal Artery Syndrome via investigative means. This in turn also provides the clinician more time for intervention.
Trial registration number
N/A
AS31-062
TIME IS BRAIN: ULTRAFAST RECANALIZATION AFTER ACUTE ISCHAEMIC STROKE WITH LARGE VESSEL OCCLUSION. REPORT OF 3 CASES
1St. Johns Hospital Vienna, Department of Neurology, Vienna, Austria
2St. Johns Hospital Vienna, Department of Radiology, Vienna, Austria
Background and Aims
Acute ischaemic stroke with large vessel occlusion (LVO) has a poor outcome without fast treatment. Fast-as-possible reperfusion of the occluded artery is the primary therapeutical goal.
Method
We present three cases with very fast extra- and intramural processes and reperfusion after less than 90 minutes after onset. All three patients suffered from a MCA-syndrome with an observed onset and high NIHSS at admission.
Fig. 1: Intramural times in minutes
Conclusion
The personal and logistical effort of LVO treatment (IV thrombolysis and MT) is high and time-consuming. These cases show that it is possible to keep the intrahospital delay clearly below 40 minutes. Our intrahospital processes offer to the most of the patients with LVO in the anterior circulation recanalization within 50 minutes after hospital admission. The details of our intrahospital flows will be presented at the ESOC 2018.
Trial registration number
N/A
AS31-064
MECHANICAL THROMBECTOMY IN A YOUNG STROKE PATIENT WITH DUCHENNE MUSCULAR DYSTROPHY
1Ruhr University Bochum, Neurology- St. Josef-Hospital, Bochum, Germany
2Ruhr University Bochum, Radiology- St. Josef-Hospital, Bochum, Germany
3Ruhr University Bochum, Anaesthesiology- St. Josef-Hospital, Bochum, Germany
Background and Aims
Duchenne muscular dystrophy (DMD) is an X-linked recessive skeletal muscle myopathy which is caused by mutations in the dystrophin gene. Lack of dystrophin also results to cardiomyopathy, which raises significantly the stroke risk in DMD-patients. However, data about therapeutic opportunities in the acute setting are scarce in literature. So far, only two cases receiving IV thrombolysis are described, one of them with fatal outcome.
Method
Case report of a case of successful mechanical thrombectomy (MTE) in an acute ischemic stroke (AIS) patient with DMD and associated dilatative cardiomyopathy.
Results
A 20-year old DMD-patient was transferred at 08:56 h to our department due to wake up stroke with severe right-sided hemiparesis and aphasia (NIHSS=20). Last-seen-normal was at 03:00 h. Cerebral CT-scan revealed only slight early ischemic changes (ASPECT-Score=8). CT-angiography detected occlusion of left middle cerebral artery (LMCA). MTE started rapidly at 9:23 h and using direct thrombus aspiration (Penumbra System®) complete recanalization was achieved 20 min later (TICI-grade 3). Considering the specific risks of general anesthesia in DMD, the procedure was performed with propofol, remifentanil and rocuronium. The patient recovered quickly from the acute symptoms, due to preexisting hypotonic tetraparesis his NIHSS-score at discharge was 12 points.
Conclusion
To the best of our knowledge, this is the first report on MTE in a patient with DMD related cardioembolic stroke. In contrast to the few reports with IV thrombolysis, MTE seems to represent an optimal treatment option. Specific characteristics of DMD-patients like anesthetic regimen should be taken into account.
Trial registration number
N/A
AS31-065
A CASE REPORT OF A CADASIL PATIENT WITH SUSPECTED PARKINSON DISEASE
1Fundació Docència i Recerca MútuaTerrassa- Hospital Mútua de Terrassa, Stroke Pharmacogenomics and Genetics, Terrassa, Spain
2CHUAC, Neurology Department, A Coruña, Spain
3IMIM-Hospital del Mar, Neurology Department, Barcelona, Spain
4Biodonostia Health Research Institute, Neurodegenerative Disorders Area, San Sebastián, Spain
5Donostia University Hospital, Neurology Department, San Sebastian, Spain
62CIBERNED- Network Center for Biomedical Research in Neurodegenerative Diseases, Neurodegenerative Diseases, Madrid, Spain
7Univ. de Bordeaux, Institut des Maladies Neurodégénératives, Bordeux, France
8CNRS- Institut des Maladies Neurodégénératives, Neurology Department, Bordeaux, France
9Vall d’Hebron Institute of Research- Hospital Vall d’Hebron, Neurovascular Research Laboratory., Barcelona, Spain
10Vall d’Hebron Institute of Research- Hospital Vall d’Hebron, Neurovascular Research Laboratory, Barcelona, Spain
11The Manchester Metropolitan University of All Saints, Healthcare Science, Manchester, United Kingdom
12Hospital Mútua de Terrassa, Neurology Department, Terrassa, Spain
13Biomedicine Institute of Seville- IBiS/Hospital Universitario Virgen del Rocío/CSIC/University of Seville, Neurology Department, Sevilla, Spain
14Hospital Universitario Virgen Macarena, Neurology Department, Sevilla, Spain
15Sant Pau Institute of Research- Hospital de la Santa Creu i Sant Pau, Stroke Pharmacogenomics and Genetics, Barcelona, Spain
Background and Aims
CADASIL is caused by mutations in NOTCH3. Migraine, psychiatric disturbance, small subcortical infarctions, and dementia are the main symptoms, with an MRI with confluent white matter hyperintensities (WMH). Extrapiramidal features have not been frequently reported but vascular parkinsonism could appear. Usually, vascular parkinsonisms are characterized by symmetric symptomatology, not tremoring, normal DaT-scan and poor response to levodopa treatment.
Method
We report a case of CADASIL with suspected Parkinson Disease instead of vascular parkinsonism.
Results
A 65 year-old female with CADASIL disease and a p.R607C mutation in NOTCH3 gene presented an asymmetric parkinsonism: right rest tremor, bradykinesia, loss of weight, fatigue and hypomimia among other symptoms. The MRI showed diffuse WMH without strategic infarcts. The DaT-scan evidenced an asymmetric presynaptic dopaminergic degeneration with left predominance. A myocardial MIBG scintigraphy was not performed. Levodopa and dopaminergic agonist treatments were established with a successful response.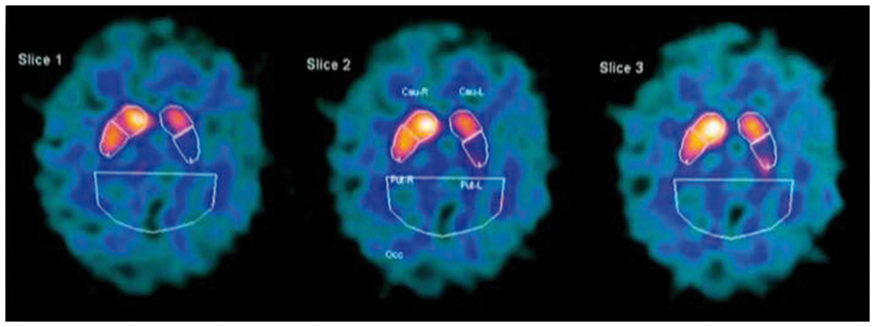
Conclusion
This is the first case of a CADASIL patient with suspected Parkinson Disease instead of vascular parkinsonism. She presented asymmetric parkinsonism, asymmetric DAT-scan alteration and good response to levodopa and dopaminergic agonists, suggesting Parkinson Disease. A myocardial MIBG scintigraphy would help to differentiate between vascular parkinsonism and Parkinson Disease.
Therefore, it is mandatory to evaluate whether a CADASIL patient with extrapyramidal symptoms could present Parkinson Disease, as an appropriate treatment could improve the quality of life of the patient.
Trial registration number
N/A
AS31-066
A RARE ANASTOMOTIC VESSEL IN ASSOCIATON WITH UNILATERAL AGENESIS OF INTERNAL CAROTID ARTERY AND BRAIN ANEURYSM
1Eneri - Clínica La Sagrada Familia, Neuroradiology, Buenos Aires, Argentina
Background and Aims
Variations in the normal anatomy of the brain arteries may influence the development of arterial disease, such as aneurysms, dolichoectasia and atherosclerosis due to arterial remodeling that can occur in the presence of shear stress in the arterial walls. The most frequent anatomical variants include remnants and anomalies of the normal embryological development like fenestration, duplications, hypoplasia, agenesis and persistent primitive arteries. Occasionally these anatomical variations can entail risks for morbidity and mortality when associated with stroke and aneurysms.
Method
We present a case of a 46-year-old female with a rare anatomical variation of the brain vasculature where unilateral agenesis of internal carotid artery (ICA) was found.
Results
The patient had a family history of subarachnoid hemorrhage (SAH) and presented with intense sudden headache and nausea. Clinical examination and laboratories were unremarkable. Computed tomography (CT) brain scan brain showed signs of SAH and magnetic resonance angiography (MRA) identified absence of the right ICA and the presence of an unusual intercavernous anastomotic vessel originated from the left ICA continuing as the right median cerebral artery. The MRA, also shown the presence of an anterior communicating aneurysm that measured 10 x 8 mm where both anterior cerebral arteries originated.
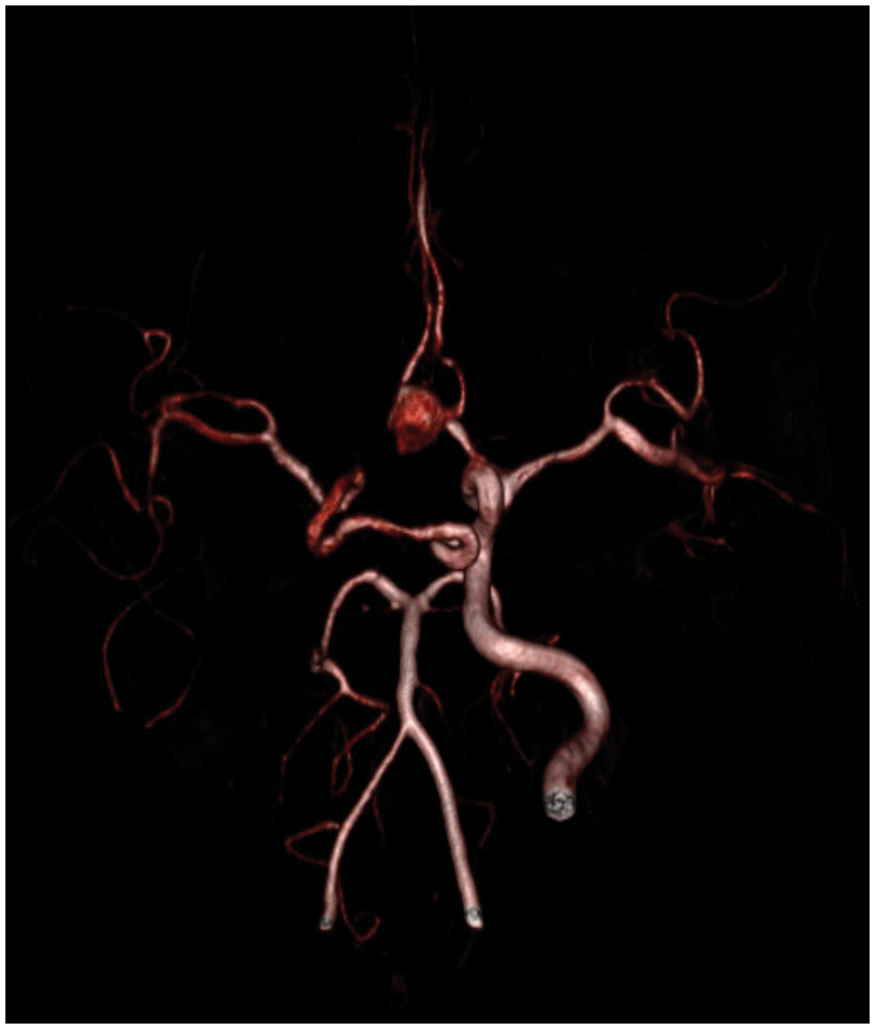
Conclusion
Although some of these anatomical variations are common and discovered as incidental findings, there are others that have low incidence rates as the one we present here with 0,01% of cases. Knowledge of these anatomical variants is important as some of these might turn pathological, symptomatic or could be associated with vascular disease.
Trial registration number
N/A
AS31-067
SPONTANEOUS NON-TRAUMATIC DISSECTION MIMICKING HYPERDENSE MIDDLE CEREBRAL ARTERY SIGN
1L.A. Vorokchobov City Clinical Hospital № 67, Stroke Unite, Moscow, Russia
2A.I. Burnazyan Federal Medical and Biophysical Center, neurology, Moscow, Russia
Background and Aims
Clinical case
Method
The patient K., 40 y.o., female, was admitted to Stroke Unit with speech impairment (motor aphasia). She was hospitalized 8 hours after acute onset of right-sided weakness and aphasia preceded by hot bath. Motor deficit resolved before the admission. Systemic thrombolytic therapy was not performed due to the exceeding time of the therapeutic window and modest neurological deficit (NIHSS 3). There was no history of trauma, arterial hypertension, arrhythmia, oral contraceptive use, alcohol, drugs consumption. The patient also had no history of any chronic disease associated with coagulation abnormalities, no habitual miscarriage, no visible symptoms of connective tissue disorders. Native CT performed at admission showed hyperdense middle cerebral artery (MCA) sign and no signs of acute ischemic and hemorrhagic changes. CT-angiography (CTA) of intracranial arteries was performed in order to estimate the risk of malignant cerebral infarction. CTA scans showed local subcortical ischemia with involvement of the Broca’s area. Left middle cerebral artery was not occluded but thinned and distal branches were visible. Transcranial Doppler showed asymmetric blood flow velocity in the MCAs with 50% difference D>S, left MCA dilatation and defect of contrast enhancement. Duplex ultrasound of precerebral arteries showed left internal carotid artery occlusion due to the dissection (local dissection of intima-media complex).
Results
n/a
Conclusion
The particular interest of this clinical case resides in neurovisualisation data which may have led to the wrong diagnosis. Hyperdense MCA sign was caused by the blood clot formation in the false lumen of the dissected MCA, which mimicked MCA occlusion.
Trial registration number
n/a
AS31-068
CENTRAL HYPOVENTILATION SYNDROME FOLLOWING POSTERIOR CIRCULATION STROKE
1Broomfield Hospital, Stroke Medicine, Chelmsford, United Kingdom
Background and Aims
Posterior circulation Strokes constitutes around one fifth of all ischaemic strokes. Despite the unforeseeable nature and rarity of acquired hypoventilation syndrome in brain-stem stroke, it should be managed with mechanical ventilation over a prolonged period. Effective monitoring and vigilance for a prolonged period is essential in patients exhibiting signs of apnoea after a brain stem event to prevent cardiorespiratory arrest in brainstem stroke.
Method
N/A
Results
N/A
A 51-year-old gentleman was admitted to the acute stroke unit with right-sided weakness and dizziness. MRI imaging confirmed a pontine infarct. Two days later the patient suffered a cardiac arrest. He returned to spontaneous circulation but required intubation and ventilation. Over the next 2 days his presenting symptoms of weakness and dizziness improved but two extubation attempts failed within hours due to apnoeic episodes. A tracheostomy was performed and he was maintained on ventillatory support. A central hypoventilation syndrome secondary to brainstem stroke was suggested as the cause for his apnoeic episodes. After successfully weaning off the ventillator, which was complicated by one further episode of apnoea, patient was decannulated and transferred back to the stroke ward after 26 days. 48 hours following transfer from intensive care the patient suffered a respiratory arrest followed by a second cardiac arrest and died. Central hypoventilation syndrome is a relatively rare complication of posterior circulation stroke. Apnoeic episodes can happen even after a period of quiescence warranting extra vigilance over a prolonged period in the intensive care unit
Trial registration number
N/A
AS31-069
AUDITORY HALLUCINATIONS AS A RARE PRESENTATION OF STROKE
1Brighton & Sussex Universities Hospital NHS Trust, Stroke Unit, Brighton, United Kingdom
Background and Aims
A 74 year old woman presented to the Royal Sussex County Hospital with speech and language problems. She had noticed, and recorded in her diary, periods of auditory hallucinations which she described as ‘a full choir’. She commented that she was hearing ‘different tunes, notes and tones’ which came on suddenly and were now happening many times each day. She had not been troubled by these symptoms, but was prompted to seek medical advice due to difficulties completing her usual crosswords and puzzles, and she had noticed difficulty expressing her thoughts to a friend. She had no other significant past medical history.
Method
-
Results
On examination she was hypertensive, and had an expressive dysphasia. No other focal neurological signs were elicited. Whilst a computed topography scan of her head did not reveal any clear abnormality, magnetic resonance imaging showed acute and sub-acute changes in the left middle cerebral artery territory suggestive of embolic events. Her initial electrocardiogram showed normal sinus rhythm, however 24 hour outpatient monitoring demonstrated atrial flutter and she was later anti-coagulated with apixaban.
Conclusion
Auditory hallucinations are uncommon phenomena which can be caused by an acute stroke. Whilst they have been reported in some small case series in lesions of the brainstem, they are rarely seen after cortical strokes. We present this case as a reminder of one of the rarer presentations of stroke, and the necessity to consider a central cardio-embolic cause.
Trial registration number
-
AS31-070
HEMORRHAGIC TRANSFORMATION FROM ISCHEMIC PERFORATING ARTERIES AROUND MICROBLEED FOLLOWING WINNING RT-PA THROMBOLYSIS IN THE BASILAR BRANCH ATHEROMATOUS DISEASE
1Kindai University Hospital, Stroke Centre, Osaka-Sayama, Japan
Background and Aims
Asymptomatic cerebral microbleed is never contraindication for rt-PA thrombolysis of ischemic stroke.
Method
A case of successful thrombolysis for minor stoke within 3 hour after onset succumbed to 6-hour-delayed massive hemorrhagic transformation from a microbleed in the ischemic brain.
Results
A 62-year-old male was transfer to our center 2 hours after sudden attacks of gait disturbance and slurred speech. Neurological examination showed dysarthria, left ataxic hemiparesis, and disturbance of consciousness accompanied by gaze suppression to the right, that reached NIHSS score 7. His medical history consisted of diabetes, hypertension with no antithrombotic medication and stroke. CT showed no early ischemic signs. Thrombolysis with intravenous rt-PA started from 50 minutes of door-to-needle duration enough to achieve complete shrinking neurological deficits for initial 30 minutes during the injection, when DWI detected a ventral-to-dorsal wedge signal in the mid-pons with neither detectable FLAIR high signal or the adjacent constricted/occluded vertebra-basilar arteries. We also noted a 1-mm diameter of T2*-positive microbleed that were overlapped by the DWI positive infarcts. While his blood pressure had been kept in 160–170/70–90 mmHg after rt-PA. He suddenly complained of thunderclap headache with recurred left hemiparesis with right ophthalmoplegia 3 hours after thrombolyis execution. CT demonstrated the 2-cm-diameter pontine hemorrhage centering around the microbleed. The hematoma expanded to midbrain and the forth ventricle with coma and tetraplegia subsequently.
Conclusion
Because cerebral microbleed represents hemorrhage-prone microangiopathy, fibrinolytic and effective rt-PA jeopardized hemorrhagic ruptures for ischemic perforating arteries vulnerable to reperfusion injury even in the minor stoke with branch atheromatous disease.
Trial registration number
N/A
AS31-071
TWO UNUSUAL CASES OF ISCHAEMIC STROKE CAUSED BY INTERNAL CAROTID SHEATH INFLAMMATION SECONDARY TO INFECTION
1Hull Royal Infirmary, Stroke Medicine, Hull, United Kingdom
Background and Aims
Patient A – an 86 year old gentleman presenting with right arm weakness and dysarthria and a four month history of periauricular pain. CT head revealed a soft tissue mass involving the left carotid canal and jugular foramen, with bony destruction and extension into the middle ear and mastoid air cells. An MRI revealed multiple areas of acute infarction in this territory and was consistent with malignant otitis externa and skull base osteomyelitis causing left internal carotid compression, carotid sheath inflammation and subsequent stroke. Despite Intravenous broad-spectrum antibiotic he had progressive occlusion of his ICA and further embolization.
Patient B – a 68 year old gentleman presented with sudden onset left sided weakness. MRI head revealed multiple acute infracts in the right MCA watershed zone. The right internal carotid artery showed extrinsic compression secondary to an inflammatory soft tissue mass involving the carotid sheath, extending from the right skull base to C4. Staphylococcus aureus was isolated. Despite timely antibiotic therapy further infective lesions were detected at C3-C6 and L2-L4.
Method:
Both these cases illustrate that infective skull base lesions are frequently fulminant and can cause progressive compression of the affected artery and arterial sheath inflammation (arteritis), despite broad-spectrum antibiotics (which need to be continued for 6–8 weeks). They have high risk of recurrence and usual warrant follow up with surveillance imaging (CT recommended).
Trial registration number
AS31-072
A CASE OF CEREBRAL VENOUS SINUS THROMBOSIS IN A PATIENT WITH LARGE B-CELL LYMPHOMA AND RECENT DURAL PUNCTURE
1North Tees and Hartlepool Foundation trust, Care of the Elderly, Stockton-on-Tees, United Kingdom
Background and Aims
Cerebral venous sinus thrombosis (CVST) is a known stroke mimic and present in 1% of stroke cases. The incidence rate of CVST is rare of despite the high risk of thrombosis in lymphoma patients. It also can be associated with intrathecal (IT) chemotherapy.
Method
56 year old man presented with an acute onset right sided hemiparesis and speech disturbance. He had been diagnosed with stage 4 diffuse B cell lymphoma and had finished 3 cycles of IT methotrexate 2 weeks prior. An urgent CT head showed a large intraparechymal acute haematoma in the left parietal lobe and an Magnetic resonance (MR) imaging showed a venous infarct with haemorrhage secondary to a dural venous anamoly with thrombosis. No other causative factors were identified. The patient was managed with subcutaneous low molecular weight heparin therapy (LMWH) and made slow recovery.
Results
Cases of CVST are commonly linked to acute leukaemias but rare in lymphomas. Lumbar punctures and intrathecal therapy is one of the rare reported causes of CVST and they usually occur within a day to 14 days. MR with T2-weighted imaging and MR venography are preferred diagnostic tests. Our case illustrates that one should have high index of suspicion of CVST in patients with lymphoma and recent dural puncture to aid further appropriate imaging and management.
Conclusion
Acute treatment is with weight based (LMWH) followed by vitamin K antagonist irrespective of the presence of haemorrhage and carries a good prognosis. Fibinolytic or surgical treatment are restricted to cases refractory to medical treatment.
Trial registration number
N/A
AS31-073
ASPERGILLUS ASSOCIATED MCA INFARCTION :A CASE REPORT
1St. Vincent's hospital- school of medicine- The catholic university of Korea, Neurology, Suwon, Republic of Korea
Background and Aims
Aspergillus is common in environment and usually it has low pathogenicity. The incidences of CNS fungal infection have increased as according to extensive use of immunosuppressive agent and the number of AIDS patients. CNS infection of aspergillus had high mortality and morbidity because of the disease and the tolerability of antifungal agents including amphotericin B and fluconazole. We experienced a case of direct CNS invasion of aspergillus.
Method
A 86-year-old woman admitted to internal medicine due to urinary tract infection. She was consulted to the department of neurology because of her chronic headache. She experienced intermittent headache since 3 years ago. Her headache was recently aggravated after fever developed. Left side weakness and sudden onset confusion were developed on 4th admission day. Neurologic examination showed proptosis on her right eye and positive sign for neck stiffness. Cerebrospinal fluid was clear with lymphocyte dominant leukocytosis (WBC 80/mm3). Diffusion weighted MRI and Orbit MRI showed acute MCA territory infarction and enhanced lesion in right orbital apex and right cavernous sinus. The lesion extended to right pterygopalatine fossa and nasopharynx. Occlusion of right ICA was revealed on brain CT angiography. The result of biopsy from nasal cavity was consistent with aspergillus species.
Results
Her neurological status and medical condition was gradually worsen despite antifungal agents and at 14 days of hospitalization, she transferred to day care center.
Conclusion
Aspergillus more often spread by hematogenous than direct invasion, but our patient is rare case of MCA infarction resulting from ICA occlusion by direct invasion of aspergillus.
Trial registration number
N/A
AS31-074
ANCA-NEGATIVE GRANULOMATOSIS WITH POLYANGIITIS PRESENTING AS AN INTRACRANIAL TUMOR SPREADING FROM THE NASAL CAVITY, AND MULTIPLE BRAIN INFARCTIONS
1University of Helsinki, Clinical Neurosciences, Helsinki, Finland
2Helsinki University Hospital, Department of Neurology, Helsinki, Finland
3Helsinki University Hospital, Department of Medicine, Helsinki, Finland
4University of Helsinki, Clinicum, Helsinki, Finland
5Meilahti Hospital, HUS Medical Imaging Center, Helsinki, Finland
6Helsinki University Hospital, Department of Radiology, Helsinki, Finland
7HUSLAB, Department of Pathology, Helsinki, Finland
8Helsinki University Hospital, Department of Pathology, Helsinki, Finland
Background and Aims
Central nervous system (CNS) involvement in granulomatosis with polyangiitis (GPA) has been considered rare.
Method
A 76-year-old Caucasian woman was referred to neurological emergency unit with a history of four transient aphasia attacks. A saddle nose appearance and severe hypertension (230/95 mmHg) were noted.
Results
Brain computer tomography revealed a white matter hypodensity in the base of the left frontal brain lobe. Magnetic resonance imaging showed chronic paranasal sinus inflammation, which had spread through the skull base into the anterior cranial fossa. Later on the patient developed severe headache, slight dysarthria, episodic vertigo with diplopia, intermediate cognitive impairment, and a resting tremor. Vast serum and cerebrospinal fluid examinations taken at 1 and 4 months were unremarkable, including negative ANCA-antibodies. A stereotactic brain biopsy was performed at four months revealed small vessel vasculitis with no necrotizing or granulomatous features. A control brain MR-angiography (MRA) and MRI showed arterial caliber variation compatible with intracranial arteritis and multiple acute brain infarctions. High-dose intravenous methylprednisolone (1.5 g x 1) treatment was immediately commenced followed by oral prednisolone (60 mg daily) and three intravenous cyclophosphamide cycles (1000 mg every two weeks). Cyclophosphamide was continued orally at a dose of 2 mg/kg daily for two months. Three months later a clear radiological and clinical improvement was noted.
Conclusion
The clinical picture combined with the radiological findings and histology of small vessel vasculitis in CNS, was found to be best compatible with “moderately certain” ANCA-negative GPA. To diagnose a limited ANCA-negative GPA, several differential diagnoses need to be excluded.
Trial registration number
N/A
AS31-075
CASE REPORT: INTRACRANIAL DISSECTION MISSED BY 1.5T MRI AND CT-A. NEW OPPORTUNITIES WITH 3.0T MRI WITH HIGH RESOLUTION T1-FATSUPPRESSION
1Bispebjerg University Hospital, Department of Stroke, Copenhagen, Denmark
2Bispebjerg University Hospital, Department of Neuroradiology, Copenhagen, Denmark
Background and Aims
Intracranial dissections are a well-known cause of subarachnoid hemorrhage (SAH) and some dissections only consist of an intramural hematoma, without intravascular bulging. Angiography is therefore of little use in diagnosing these cases. Our case compares different imaging methods.
Method
A 36 year old woman was admitted with thunderclap headache. Prior to admission she had suffered from two weeks of neck pain.
Results
Computed tomography angiography (CTA) of neck and brain showed an extracranial vertebral artery dissection in the V2 segment. Due to worsening of headache and new on-set photophobia and nausea she was readmitted two days later at a stroke department. CT revealed a SAH around the brainstem. No changes were seen regarding the extracranial vertebral dissection on CTA. Seven days after onset of thunderclap headache a 1.5T MRI with T1-fatsupression only confirmed previous findings. A 3T MRI with high resolution T1-fatsuppression (HR-T1FS) performed next day showed an intramural hematoma in the intracranial part of the vertebral artery (V4 segment), however, not connected to the extracranial vertebral dissection at V2.
Conclusion
Retrospectively the extracranial dissection may explain the two weeks of neck pain, while the thunderclap headache was caused by the intracranial dissection with secondary SAH.
Our case indicates that 3T HR-T1FS is more sensitive than regular T1FS at 1.5T and can detect dissections with intramural hematoma which can be missed on CTA. This case underlines the need of further investigations when clinical and imaging findings are contradictory.
Trial registration number
N/A
AS31-077
A CASE OF MULTIPLE MYELOMA PRESENTING WITH TIA-MIMIC
1Kosin University College of Medicine, Neurology, Busan, Republic of Korea
Background and Aims
Suspected transient ischemic attack (TIA) is a common diagnostic challenge for physicians. It is important to identify TIAs promptly because of the high early risk of ischemic stroke, requiring urgent investigation and preventive treatment. On the other hand, it is also important to identify TIA ‘mimics’, to avoid unnecessary investigations and inappropriate long-term prevention treatment. Now we report a case of multiple myeloma of spine in misdiagnosis for TIA.
Method
Case report
Results
A 72-year-old man was presented with sudden onset of left leg weakness during walking. He could not stand up or even no more walk. When he visited emergency room, his leg weakness had disappeared. Diffusion weighted imaging demonstrated no acute lesion in the brain. Full blood count showed anemia (Hb 7.8 g/dL) and mild thrombocytopenia (platelet count 118,000/uL). Clopidogrel was administered following the diagnosis of TIA and transfused to him with packed red cell. Two hours after admission to the stroke unit, he complained back pain and left leg weakness. On neurological examination, the motor power in left lower limb was grade 3/5 in MRC scale. Increased muscle tone and deep tendon reflex were observed in his lower limb. The whole spine MRI revealed pathologic fracture of T10 with cord compression. He was underwent an emergency surgical decompression. The next day, laboratory findings and skull X-ray compatible with multiple myeloma.
Conclusion
The transience and sudden attack of symptoms makes historical features paramount in establishing the diagnosis of TIA. The clinicians should consider possibility of TIA-mimics.
Trial registration number
N/A
AS31-078
TO COME HOME AFTER A STROKE: PATIENTS’ EARLY EXPERIENCES OF HEALTH AND RECOVERY IN THEIR HOME SETTINGS
1Chalmers University of Technology, Architecture- Dep. Building Design, Gothenburg, Sweden
2Dalarna University, School of Education- Health and Social Studies, Falun, Sweden
3Karolinska Institutet, Neurobiology- care sciences and society, Stockholm, Sweden
4Lund University, Neurology, Lund, Sweden
Background and Aims
Healthcare systems and services for stroke patients are increasingly performed within home settings where both, people with moderate and severe disability can receive care. However, at present little knowledge is available in regard to early stroke phases and how the interaction with the physical environment of home settings might affect rehabilitation outcomes. The aim of this work was thus, to increase our understanding in regard to the interplay between home settings and people’s rehabilitation process, a month after stroke onset.
Method
A cross-sectional interdisciplinary investigation was conducted using validated measures in face-to-face interviews and by observing the participants’ interactions with their home settings. People with stroke (N = 16) that had a mild disability, and cognitive and communicative abilities to participate in an interview of approximately 2 hours, were recruited in the study and their data was collected within 4 to 7 weeks after stroke onset. Information was collected in regard to their experience of the physical and social home environment, their attachment to place, self-efficacy and the quality of continuity of care from the hospital to the home. Moreover, data about their recovery and overall health were collected with, Stroke Impact Scale and the EQ-5D.
Results
Preliminary results suggests the existence of a relation between recovery levels, self-efficacy and the perceived quality of the physical environment of home settings.
Conclusion
More detailed results and their implication for early rehabilitation phases of stroke patients within home settings will be discussed.
Trial registration number
N/A
AS31-080
AN ALTERNATIVE CAUSE OF STROKE IN A YOUNG PATIENT WITH BETA-THALASSEMIA
1Croydon University Hospital, Stroke, LONDON, United Kingdom
Background and Aims
Beta Thalassemia confers a stroke risk due to the hypercoagulable state of the patient. We present an interesting case which highlights other important causes of stroke in patients with beta-thalassemia.
Method
A 35-year-old man was admitted with a 4-day history of headache, intermittent left sided weakness and reduced vision in the left eye. He had a background of beta-thalassemia major and splenectomy. Medications included folic acid, penicillin V, and hydroxycarbamide. Examination demonstrated a soft systolic murmur, and mild left sided weakness. Visual acuity was markedly reduced in the left eye and fundoscopy revealed evidence of a left inferior branch retinal artery occlusion. Haematology investigations were in keeping with thalassemia and iron studies showed evidence of iron overload.
Results
MRI brain demonstrated foci of infarctions in the left corona radiata and corpus collosum, as well as tiny foci of restricted diffusion in the left parietal and right frontal lobes. He went on to have an echocardiogram showing diffuse extensive calcification in keeping with thalassemia-induced cardiomyopathy, and a mobile mass in the left ventricular outflow tract. He was commenced on anticoagulation and had no further events.
Conclusion
Thalassaemia does not in itself predispose to stroke, but a hypercoagulable state due to iron overload is known to increase the risk of thromboembolism. There have been case reports of cardiogenic embolism in the presence of siderotoxic cardiomyopathy in beta-thalassemia. It is vital that patients with known thalassaemia have urgent cardiac investigations to rule out cardiac emboli as a cause of an ischaemic stoke.
Trial registration number
N/A
AS31-081
MYOCARDIAL INFARCTION AND STROKE SECONDARY TO CHEST SEPSIS AND REACTIVE THROMBOCYTOSIS
1St Vincent's Hospital, Neurosciences, East Melbourne, Australia
2St Vincent's Hospital, Medicine, East Melbourne, Australia
3University of Melbourne, Medical Education, Melbourne, Australia
4St Vincent's Hospital, Haematology, East Melbourne, Australia
5St Vincent's Hospital, Cardiology, East Melbourne, Australia
Background and Aims
Reactive thrombocytosis is common in acute hospital settings but not generally considered prothrombotic. We present an unusual case of multiple vascular bed thromboses occurring without traditional vascular risk factors.
Method
A 48-year-old female presented with acute inferior ST-elevation 1 day post discharge for treatment of antigen-positive pneumococcal pneumonia. Comorbidities included menorrhagia associated iron deficiency anaemia. On arrival she developed left hemiplegia (NIHSS 10). Imaging demonstrated a right MCA occlusion with large ischaemic penumbra.
Intravenous alteplase was commenced. Endovascular clot retrieval extracted a platelet-fibrin rich thrombus with cerebral reperfusion achieved 137mins post onset. Following ECR, ST-elevation persisted and coronary angiogram was performed. No angiographic evidence of epicardial coronary artery disease was demonstrated. Upon sheath removal, a large clot was noted. Given the procoagulant state, dual antiplatelet therapy and unfractionated heparin were commenced.
Results
Mild weakness (NIHSS 3) and a small subcortical infarct were apparent on day 8. Bloods revealed microcytic anaemia and pro-inflammatory state (Hb 88g/L, platelet 1148x109/L, C-reactive-protein 105mg/L). Thrombophilia screen, transoesophageal echocardiogram and bronchoscopy were normal. Haematological parameters normalised within 3 weeks. She was discharged day 10 and returned to work (mRS 1).
Conclusion
Reversible thrombocytosis causing cerebral and cardiovascular thrombosis occurred post community acquired pneumonia with coexisting iron deficiency. Population studies demonstrate increased stroke risk following pneumococcal pneumonia. Sepsis-associated inflammation may promote hypercoagulability through alterations in endothelial function and microstructural changes to clot characteristics. Increased stroke risk in iron deficiency anaemia is potentially driven by reactive thrombocytosis with concurrent haemodynamic changes. Non-traditional risk factors are important considerations in ischaemic stroke aetiology.
Trial registration number
N/A
AS31-082
ACUTE CARBON MONOXID INTOXICATION MIMICKING AN ACUTE COMPLETE MCA SYNDROME PRESENTED FOR I.V. THROMBOLYSIS AND THROMBECTOMY
1Johannes Wesling Klinikum, Department of Neurology, Minden, Germany
Background and Aims
We report a 53 year old female patient presenting to our neurological emergency room with an acute complete left sided MCA syndrome in an unclear time window.
Method
CT and CTA showed no specific findings, therefore the already initiated IV thrombolysis and thrombectomy procedures were stopped before bolus and puncture. Duplex sonography of the cervical extra- and intracranial vasculature had no evidence of arteriosclerosis or dissection. MRI, however, revealed bihemispheric, small, left-sided lesions on diffusion weighted imaging. We performed lumbar puncture due to febrile temperatures (38.7 ° Celsius) without any pathological results.
Results
During this emergency workup we received additional information regarding a potential carbon monoxide (CO) intoxication confirmed with a CO value of 18.7%. The patient experienced rapid improvement of symptoms with normobaric hyperoxygenation (FI O2 >90%) via a demand-mask. The only remaining symptoms at hospital discharge were mild cognitive impairments. Six weeks later after rehabilitation, minor gliotic scars were seen where the former DWI lesions were located. There were no cognitive impairments clinically and in neuropsychological testing.
Conclusion
The presentation of non-lethal CO-intoxication as a stroke mimic nearly undergoing (non-indicated) IV thrombolysis and endovascular therapy to our knowledge has not been published in the literature.
Trial registration number
N/A
AS31-083
CEREBRAL VENOUS AIR EMBOLISM AFTER GASTROINTESTINAL ENDOSCOPY
1Basurto University Hospital, Neurology, Bilbao, Spain
Background and Aims
Cerebral air embolism (CAE) is an uncommon entity associated with high morbidity and mortality rates. We describe a case of CAE following a colonoscopy.
Method
A 70-year-old male with vascular risk factors and Crohńs disease developes acute right hemispheric symptoms after colonoscopy. On physical examination, the patient showed left hemiplegia, homonymous hemianopsia, dysarthria and central facial palsy with a NIHSS score of 16. Right MCA stroke was suspected.
Results
Blood test and electrocardiogram were normal. Multimodal CT did not show ischemic changes and presence of gas bubbles in right posterior parietal cerebral parenchyma and superior sagital sinus were detected. CT angiography and perfusion-CT were normal. Revascularization techniques were dismissed as no vascular oclussions were found and CAE diagnosis was established. Transthoracic echocardiogram did not found atrial septal defect. Patient was transferred to another hospital to perform hiperbaric oxygen therapy with no clinical changes. Two potential physiopathological mechanisms were considered in this patient: a paradoxical air embolism in to the cerebral arterial circulation versus retrograde cerebral venous air embolism. Absence of artery oclussion and gas bubbles in venous sinus support the second mechanism.
Conclusion
CAE in an infrequent condition with poor prognosis despite intensive treatment. It is a rare adverse event in endoscopic procedures. Detection of gas bubbles in the CT scan supports the diagnosis. Among other treatments, hiperbaric oxygen treatment can be considered in these patients.
Trial registration number
N/A
AS31-084
CANCER AS A POTENTIAL CAUSE OF CRYPTOGENIC STROKE: A CASE REPORT
1Society of Serbian neurologists- EFNS, Department of cerebrovascular disease- Clinic of neurology, Novi Sad, Serbia
Background and Aims
Background
Ischemic strokes of undetermined etiology can be non-embolic and embolic, which include paroxysmal atrial fibrillation, minor cardiac causes, atheroembolism, paradoxical embolism through patent foramen ovale (PFO) and cancer associated stroke. Hypercoagulability accounts as the most important mechanism of malignancy caused stroke. Once the traditional risk factors are excluded as the cause of stroke, we can refer to d-dimer levels as the surrogate marker for hypercoagulability.
Method
Case Report
A 69-year old woman was admitted to Neurology Clinic for sudden onset of right-sided weakness and difficulties of speech. She had a history of hypertension and diabetes.
Results
Physical examination confirmed neurological deficit. Duplex ultrasonography scan of carotid arteries was normal. Computed tomography (CT) of the brain showed infarction of the right cerebellum as well as frontoparietal infarction on the left side. Since vaginal bleeding and ascites were observed, the patient underwent CT of the abdomen that revealed tumor mass located in the pelvis. Tumor markers for ovarian cancer (CA 125, HE4) were elevated. During hospitalization she developed signs for deep vein thrombosis that was confirmed by ultrasound examination. The patient was treated with low molecular weight heparin and refered to gynecologist for further investigation.
Conclusion
LMWH has been widely used for treating stroke patients with cancer, but its efficacy has not been well studied. Direct oral anticoagulants (DOAC) are being considered for treatment of malignancy related cryptogenic stroke. The use of DOAC can certainly lead to better compliance but further studies are needed to determine its safety and efficacy.
Trial registration number
N/A
AS31-085
RECURRENT ISCHEMIC STROKE TREATED WITH MECHANICAL THROMBECTOMY DURING A PREGNANCY: A CASE REPORT
1St. Anne's University Hospital Brno, Department of Neurology, Brno, Czech Republic
2St. Anne's University Hospital Brno, Department of Radiology, Brno, Czech Republic
Background and Aims
Although the evidence from large randomized controlled trials confirmed that mechanical thrombectomy is effective in selected patients with an intracranial proximal artery occlusion, pregnancy was excluded from the study protocols. The described case depicts an endovascular treatment of recurrent acute ischemic stroke in pregnancy.
Method
Case report
A 19-year-old woman during her 12th gestational week was admitted to our comprehensive stroke center suffering from acute ischemic stroke within the territory of left internal carotid artery. The National Institute of Health Stroke Scale (NIHSS) during admission was 17. She had a history of aneurysmal subarachnoid hemorrhage, endocarditis 4 years ago and ischemic stroke with occlusion of M2 segment of left middle cerebral artery (MCA) successfully treated with mechanical thrombectomy (at discharge NIHSS 0) seventeen days before recent stroke.
Results
The urgent MRI at our hospital showed an acute and subacute ischemic lesion involving the left basal ganglia and the occlusion of M1 segment of left MCA. Due to her above mentioned history, she was treated with mechanical thrombectomy alone using stent retriever. Complete recanalization was achieved with no evidence of hemorrhagic transformation on control MRI. Transesophageal echocardiography identified thrombus in left ventricular outflow tract. The patient was discharged with NIHSS 0 and received anticoagulation therapy.
Conclusion
Mechanical thrombectomy (even doubled within the 17 days apart) was, in this case, feasible and successful and might be considered as option for treatment of sever ischemic stroke with M1 or M2 occlusion in pregnancy.
Trial registration number
N/A
AS31-086
IPSILATERAL VOCAL CORD PARALYSIS AFTER ACUTE ANTERIOR ISCHEMIC STROKE
1The Ohio State University Wexner Medical Center, Neurology, Columbus- OH, USA
Background and Aims
Vocal cords are innervated by the recurrent laryngeal nerve and superior laryngeal nerve which are branches of the vagus nerve. The nucleus ambiguous is the motor nucleus of the vagus nerve and it is located in the medulla. It receives stimuli from the bilateral hemispheres through the corticobulbar tracts. A previous study of 54 patients with stroke and vocal cord paralysis reported 11 patients with contralateral vocal cord paralysis following one hemispheric acute ischemic stroke. The finding questioned the bilateral hemispheric innervation of the nucleus ambiguous. We present the first case of transient ipsilateral vocal cord paralysis after acute anterior ischemic stroke.
Method
We present a sixty-two-year-old female patient with past history significant for hypertension who presented with acute right-sided weakness and aphasia. she was outside the window for thrombolytic-therapy.
Results
CT-head was unremarkable. MRI-brain diffusion scan showed partial middle cerebral artery ischemic stroke while CT-angiogram of the head and neck showed complete extracranial and intracranial left internal carotid artery occlusion. CT-perfusion showed large penumbra. She partially improved after induced hypertensive therapy. She was able to pronounce few words; however, her voice was hypophonic. The otolaryngology team was consulted for vocal-cords evaluation.
She underwent Flexible fiberoptic laryngoscopy which showed a paralyzed left vocal cord. The right cord was fully mobile. Chest x-ray showed no pathology. Few months later, a repeat laryngoscopy exam revealed resolution of the paralysis.
Conclusion
Higher cortical injury, like in stroke, can cause ipsilateral vocal cord paralysis although commonly seen with bilateral injury and to lesser extent contralateral injury.
Trial registration number
N/A
AS31-087
THE PREVALENCE OF DELIRIUM ON NEUROLOGICAL INTENSIVE CARE UNIT AND STROKE UNIT: AN EMPIRIC STUDY
1Universitätsklinikum des Saarlandes, Neurologie, Homburg, Germany
Background and Aims
To determine the prevalence of delirium on neurological intensive care Units.
Method
The study was a project over 3 months, collecting patient data of the neurological intensive care unit such as the stroke unit. Altogether there were 220 patients admitted to the study. The main goal of the study was to determine how many patients developed a delirium while their inpatient stays. Which factors such as age and length of the hospital stays favor a delirium? The data was collected by choosing different types of instruments. On the one side there was the CAM-ICU and the RASS. On the other side the medication such as benzodiazepine, neuroleptic or opiate usage as well as the observation of heart rate, blood pressure and body temperature. Also documented were the fixation and the ventilation of the patient. These information were collected three times a day; the first test in the morning between 8 and 10 o’clock, the second one between 17 and 19o’clock and the last one between 23 and 1 o’clock. Those specific times were chosen as these were the times where most of the problems, such as patients developing a delirium, starting to scream or were just not able to handle anymore without sedation, had occurred beforehand on these specific units.
Results
Preliminary results show a tendency towards a high delirium rate.
Conclusion
Exact research about delirant behaviour of patients in different age groups and disease patterns.
Trial registration number
N/A
AS31-088
ISOLATED INTERNUCLEAR OPHTHALMOPLEGIA (INO) CAUSED BY A LACUNAR INFARCTION: A CASE REPORT AND REVIEW OF THE LITERATURE
1Alcorcón Hospital, Neurology, Madrid, Spain
Background and Aims
Midbrain and pontine strokes are well defined in literature as etiologies of internuclear ophthalmoplegia (38%), multiple sclerosis (34%) or unusual cases (28%). Only 30–52% of these ischemic lesions could be identified by MRI. Our objetive is taking into consideration that lacunar brainstem infarctions with positive MRI can be also a cause of isolated INO.
Method
We present a 72 year-old male with mRS=0 and history of hypertension for which he was taking amlodipine and a previous left ischemic oculomotor palsy totally recovered for which he was on clopidogrel and pantoprazole daily. He was presented at the emergency room with sudden binocular diplopia 3 hours after onset.
Results
On examination, he showed normal gaze in primary position, restriction of the right eye adduction and left eye abduction showed tortional nystagmus. Convergence was impaired. The rest of the neurological examination was unremarkable. CTA showed no hemorrhage, great vessel oclussion nor intracraneal stenosis. He was admitted to the stroke unit where no arrhythmias were detected on the monitorization during one day. Hypertensive cardiopathy was seen on the transthoracic echocardiogram but no embolic sources were found. Finally, MRI showed a right midbrain lacunar acute ischemic stroke. He was discharged home 2 days later on clopidogrel. At 90 days, the patient was totally recovered (mRS=0).
Conclusion
Isolated INO can be the sole manifestation of lacunar pontine stroke targeting longitudinal medial fasciculus, but it is ocassionally located in midbrain. It generally carries good prognosis.
Trial registration number
N/A
AS31-089
EXCESSIVE HIGH PLASMA CONCENTRATIONS OF APIXABAN IN A PATIENT SUSPECTED TO SUFFER ACUTE STROKE
1Heidelberg University, Department of Clinical Pharmacology and Pharmacoepidemiology, Heidelberg, Germany
2Heidelberg University, Department of Neurology, Heidelberg, Germany
3Imperial College London- Faculty of Medicine, Department of Medicine, London, United Kingdom
Background and Aims
The value of quantifying direct oral anticoagulants (DOAC) concentrations in neurological emergency situations is largely unknown.
Method
We implemented routine DOAC concentration measurements in patients with suspected acute stroke and in consenting patients single nucleotide polymorphisms of the relevant pharmacokinetic DOAC target structures P-glycoprotein (ABCB1), breast cancer resistance protein (ABCG2), and cytochrome P450 (CYP) 3A5 were determined using real-time PCR.
Results
A 75-year-old woman on apixaban (2x5 mg/d) due to atrial fibrillation experienced a sudden weakness of her left leg, fell, and remained undetected 12 h on the floor. On admission, brain imaging was normal but electrophysiological examination revealed a sciatic nerve lesion. Laboratory results showed rhabdomyolysis, renal and liver impairment (creatine kinase 31,269U/l, eGFR 38.1 ml/min/1.73m2, ASAT 863U/l, and ALAT 186U/l). Apixaban concentration/dose ratio was 9900 (ng/ml)/(mg/kg/d) three hours after drug intake and 8100 at trough (expected range: 249− 463). The half-life was substantially prolonged to ∼ 31.5 h (normal: 12 h), which cannot be explained by moderate renal or liver impairment. Known drug-drug interactions were excluded. Simvastatin (10 mg/d) might have contributed to rhabdomyolysis, but the dose was rather low. Genomic testing revealed a CYP3A5*3/*3 genotype, which is associated with low or absent expression of functional CYP3A5.
Conclusion
Measuring DOAC concentrations in neurological emergency situations can reveal unexpectedly high drug concentrations, which cannot be predicted by using routine clinical and laboratory criteria and require genetic work-up. To prevent severely elevated DOAC levels and associated bleeding risks, selection criteria to monitor patients on DOACs should be developed.
Trial registration number
N/A
AS31-091
BLOOMING OF CEREBRAL MICRO-BLEED POST IV THROMBOLYSIS IN ACUTE ISCHAEMIC STROKE
1St. James's Hospital, Medicine for the Elderly, Dublin 8, Ireland
2Trinity College Dublin, Centre for Medical Gerontology, Dublin 2, Ireland
Background and Aims
Cerebral Micro-Bleeds (CMBs) increase the risk of haemorrhagic transformation following IV thrombolysis and controversy exists over whether they are a contraindication for thrombolysis.
Method
An 81 year old female presented with a 5-hour history of left hemiplegia (NIHSS 5). CT/CTA showed a right occipital infarct and bilateral vertebral arteries stenosis with no large vessel occlusion (LVO). Her ECG showed rate-controlled Atrial Fibrillation. She was admitted, given Aspirin 300mg and managed in the Hyper-Acute Stroke Unit. MRI Brain day 3 showed acute infarction of the right temporo-occipital region and thalamus, Gradient Echo sequence (GRE) showed multiple CMBs throughout the parenchyma including a small lesion in the pons. She developed new onset left hemiparesis on day 9 of admission. NIHSS was 12 and CT/CTA showed the established infarct and no LVO. The decision was made to administer lose-dose IV rTPA 0.6 mg/kg given her recent infarct, antiplatelet therapy and CMBs on MRI. Repeat NIHSS was 6 at 24 hours and MRI Brain was performed.
Results
Repeat MRI showed interval increase in extent of the known acute right temporo-occipital infarct and blooming of a previous micro-bleed in the left paracentral pons on GRE as shown in the image below.
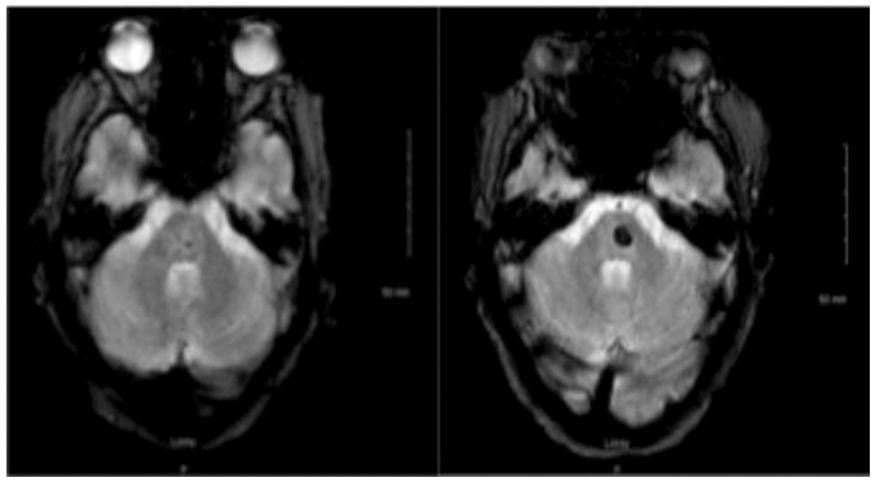
Conclusion
Low-dose rTPA can cause enlargement of CMBs. Age of CMBs cannot be determined accurately on MRI.
Trial registration number
N/A
AS31-092
BILATERAL MIDDLE CEREBRAL ARTERY STROKE TREATED WITH DOUBLE THROMBECTOMY. REPORT OF TWO CASES
1Hospital Universitario La Princesa, Neurología, Madrid, Spain
2Hospital Universitario La Princesa, Radiología, Madrid, Spain
Background and Aims
Bilateral middle cerebral artery (MCA) occlusion in patients with acute ischemic stroke is an extremely rare entity whose treatment has not been established.
Method
We report two cases of acute bilateral MCA occlusion treated with endovascular therapy at our center.
Results
Case1: A 68 year-old female with history of atrial fibrillation treated with antiplatelets presented with impaired consciousness, speech disorder and right-sided hemiparesis (NIHSS:12) with unknown onset time. A multiparametric CT showed a total occlusion of the proximal M1 segment of the left MCA and another occlusion in the proximal right M2 segment. Early recanalization of the left MCA was achieved but the right MCA remained occluded despite multiple stent-retriever passes. A CT performed 24 hours after the procedure demonstrated a bilateral cerebral infarction with hemorrhagic transformation (IH2). Three months after the stroke she was dependent in daily life activities (mRs4).
Case2: A 82 year-old female with history of hypertension, hypercholesterolemia and diabetes under antiplatelet therapy presented with acute onset of aphasia and left-sided hemiparesis (NIHSS:16). A baseline CT was normal and intravenous thrombolysis was started without neurological improvement. A CT-angiography showed a double artery occlusion (left M1 segment and right carotid T). Both arteries were recanalized within six hours of stroke onset but a MRI showed an extensive infarction and the patient finally died of respiratory complications.
Conclusion
Stroke due to acute bilateral MCA occlusion is a rare entity difficult to diagnose with unknown prognostic factors and high morbimortality despite successful treatment. We have not found any similar references in literature.
Trial registration number
N/A
AS31-093
18 YEAR OLD FEMALE WITH FOCAL CEREBRAL ARTERIOPATHY RELATED TO CHRONIC METHYLPHENIDATE TREATMENT
1Son Espases Hospital, Neurology, Palma de Mallorca, Spain
2Son Espases Hospital, Pharmacy, Palma de Mallorca, Spain
3Son Espases Hospital, Radiology, Palma de Mallorca, Spain
Background and Aims
Focal cerebral arteriopathy defines an angiographic pattern of unilateral stenosis or irregularity of distal internal carotid artery (ICA) and its branches. This condition accounts for 20% of pediatric arterial ischemic stroke, and could be triggered by different insults: inflammmatory, infectious, toxic or adjuvant thrombotic factors may take part in a multifactorial process.
Method
We present clinical and complementary findings in a patient with an ischemic stroke secondary to focal cerebral arteriopathy.
Results
A 18 year old female was admitted to our emergency department with a left M1 acute occlusion. She underwent endovascular treatment achieving complete recanalization despite a difficult procedure due to middle cerebral artery (MCA) irregularity.
The angiographic study revealed marked stenosis of the distal ICA and proximal MCA and anterior cerebral artery ACA arteries, with contrast enhancement of the blood vessel on the Magnetic Resonance Angiography (MRA).
After a thorough examination that ruled out other causes, the focal vasculitic process was attributed to chronic metilphenidate treatment combined with paliperidone and hormonal contraceptive therapy.
The patient received combined antithrombotic and corticosteroid treatment with oral prednisone.
Follow-up MRA 6 months later showed partial improvement of the arterial narrowing without contrast enhancement of the blood vessel.
Conclusion
Vasculitis related to metilphenidate intake is a rare condition that should be taken into account in the etiological study of pediatric and young adults stroke.
Trial registration number
N/A
AS31-094
ANTICOAGULATION IN PATIENTS WITH ATRIAL FIBRILATION AND CEREBRAL MICROBLEEDS, A NOT UNCOMMON DILEMMA IN DAILY CLINICAL PRACTICE
1Hospital Universitario Fundación Alcorcón, Neurology, Alcorcón, Spain
Background and Aims
Cerebral amyloid angiopathy (CAA) is a common finding in elderly patients which can cause cerebral microbleeds (CMBs). Atrial Fibrillation (AF) is also frequent in this age. The coexistence of both patologies is not uncommon in daily clinical practice. We present a patient with that condition.
Method
Description of a clinical case.
Results
91 years old man, with history of hypertension, ex-smoker, AF treated with acenocoumarol and cardioembolic right Middle Cerebral Artery infarct, admitted in our emergency department because of general discomfort. In neurological examination he puctuated four points in NIHSS, due to motor aphasia. Basal and vascular CT were normal and INR was in anticoagulant range. We discontinued acenocoumarol, started Low Molecular Weight Heparin (LMWH) and he was hospitalized in our neurology department becoming asymptomatic the day after admission. In MRI he had multiple CMBs (more than five), suggesting CAA, and leukoaraisois. He had a score of 5 in CHA2DS2VASc and 3-4 in HASBLED so we decided to keep low dose of LMWH (40mg/12h). He was dischargued asymptomatic. Control MRI didńt show new bleeds despite anticoagulation.
Conclusion
CMBs are asocciated with ischaemic stroke and intracraneal haemorrhage (ICH). CMBs number was associated with recurrente ICH, specially when they are more than five, and anticoagulation increase this risk. Previos studies suggest that, when this patients need to be anticoagulated, as AF patientes, they should receive non-vitamina K antagonists or left atrial appendage oclusion, but there isńt randomizad trials published to guide this decision. In our concrete case we decide to start treatment with LMWH.
Trial registration number
N/A
AS31-095
HEMORRHAGIC REVERSIBLE CEREBRAL VASOCONSTRICTION SYNDROME: A REPORT ON 2 CASES
1Son Espases Hospital, Neurology, Palma de Mallorca, Spain
2Son Espases Hospital, Radiology, Palma de Mallorca, Spain
Background and Aims
Reversible Cerebral Vasoconstriction Syndrome (RCVCS) is clinically characterized by severe and often recurrent headaches, sometimes accompanied by focal neurological deficits. Intraparenchimal hemorrhages appear in 10 to 20% of the patients and tend to occur within the first week while cerebral vasoconstriction is maximum on angiography between 2 to 3 weeks after onset. This dynamic nature can hamper the diagnosis.
Method
We present clinical and radiological findings in two patients with hemorrhagic RCVCS and normal neuroimaging at onset.
Results
A 51 year old woman presented with severe headache and visual loss. A right parietal hemorrhage was diagnosed on the CT scan, but initial cerebral angiography was normal. A magnetic resonance performed one week later revealed segmental vasospasm of cerebral arteries that resolved over a few weeks.
A 48 year-old woman with thunderclap headache presented normal examination and neuroimaging on admission. A second CT scan performed 10 days later showed a right frontal hemorrhage. Direct cerebral angiography showed diffused cerebral vasoconstriction.
Conclusion
RCVCS is caused by a dynamic disfunction of the cerebrovascular tone, with a distal-to-proximal progression. The main angiographic abnormalities can appear days to weeks after onset of symptoms, so, in the presence of a high degree of clinical suspicion, normal neuroimaging does not exclude RCVCS and a follow-up study may be justified.
Trial registration number
N/A
AS31-096
WATCH YOUR CATCH: TWO CASES OF EFFECTIVE MECHANICAL THROMBECTOMY IN LARGE CEREBRAL VESSEL OCCLUSION BY TUMOR FRAGMENTS
1Klinikum Osnabrück, Neurology, Osnabrück, Germany
2Klinikum Osnabrück, Radiology, Osnabrück, Germany
3Klinikum Osnabrück, Pathology, Osnabrück, Germany
Background and Aims
Cerebral vessel occlusion by tumor fragments is a rare cause of ischemic stroke.
Method
We report two cases of effective mechanical thrombectomy in which large cerebral vessel occlusion by tumor fragments was the initial manifestation of neoplastic disease.
Results
In the first case, a 73 year old man presented to our emergency department with right-side hemiparesis and aphasia due to left middle cerebral artery occlusion. Mechanical thrombectomy was performed immediately and the patient recovered completely. Histological examination of the embolus revealed tissue consistent with cardiac papillary fibroelastoma. In the second case, a 45 year old woman with acute onset right-side hemiparesis and aphasia was diagnosed with left middle cerebral artery occlusion. Mechanical thrombectomy retrieved an embolus that appeared atypical macroscopically. Immunhistochemical analysis confirmed tissue of an angioinvasive lung carcinoma of the left upper lobe as the origin of cerebral embolism.
Conclusion
These two cases show that histopathologic analysis of mechanical thrombectomy specimens may help to identify rare causes of stroke.
Trial registration number
N/A
AS31-097
RARE CASE OF RECCURENT BASILAR ARTERY THROMBOSIS - CASE REPORT
1Faculty Hospital Trnava, Dpt. of Neurology, Trnava, Slovak Republic
2Faculty Hospital Trnava, Dpt. of Radiology, Trnava, Slovak Republic
Background and Aims
Trombosis of basilar artery presents approximately 1% of all strokes, however it’s very serious form of ischemic stroke and without adequate treatment. The outcome of most patients is associated with severe disability or death.
Method
Thanks to advances in diagnostics and therapy, outcome of many patients have improved. Current options of treatment the basilar artery occlusion is intraarterial or intravenous thrombolytic therapy. Other option is endovascular recanalization by using mechanical thrombectomy.
Results
We present rare clinical case of patient with symptoms of infratentorial stroke, initial NIHSS score 19 points. CT angiography verified occlusion of basilar artery. Patient was treated with systemic rt-PA and with aspiration mechanical thrombectomy, full recanalization was achieved, TICI 3. Patient’s state has improved, NIHSS decrease to 1 point.
Conclusion
Four days later sudden onset of somnolence occurred, again with symptoms of infratentorial stroke, NIHSS 15 points. CT angiography verified top of basilar artery occlusion. Full recanalization was achieved again by using the aspiration thrombectomy. Patient was later discharged home with NIHSS 3 points and mRs 3 points. On 3 months follow-up patient’s mRs was 1 point.
Trial registration number
N/A
AS31-098
POOR PROGNOSIS DESPITE SUCCESSFUL THROMBEKTOMY: TWO CASE REPORT
1Sisli Hamidiye Etfal Education and Research Hospital, Neurology, Istanbul, Turkey
2Sisli Hamidiye Etfal Education and Research Hospital, Radiology, Istanbul, Turkey
3Istanbul Bilim University, Neurology, Istanbul, Turkey
Background and Aims
Stroke is a major health problem worldwide. Revascularization therapies are the hallmarks of acute stroke treatment. The aim of this presentation is to evaluate the the causes of poor prognosis despite the successful revascularization.
Results
Large MCA infarction was reveled and decompressive craniectomy was performed in both cases despite successful revascularisation procedures. Furthermore, extracranial carotid artery stenting simultaneously with the thrombolytic theraphies was controversial. First patient had reocclusion of the stent.
Conclusion
Improvement after revascularization does not imply complete normalization of perfusion. Optimal stroke therapy should result in both recanalization and reperfusion.
Trial registration number
N/A
AS31-099
SPINAL CORD INFARCTION AFTER LEFT LOBECTOMY AND CONTINUOUS THORACIC PARAVERTEBRAL BLOCK
1Hospital Universitario Ramón y Cajal, Neurology, Madrid, Spain
Background and Aims
Continuous thoracic paravertebral block (PVB) is commonly used and has a low incidence of complications. Despite negative aspiration of cerebrospinal fluid (CSF), the catheter may be inserted in the intrathecal space. We report a spinal cord infarction after left lobectomy with video-assisted thoracoscopic surgery (VATS) and PVB following surgery
(a)
Conclusion
If neurological symptoms appear after PVB placement, complications at the spinal cord should be suspected, and spinal cord infarction should considered in differential diagnosis.
Trial registration number
N/A
AS31-100
A CASE OF NEUROMYELITIS OPTICA MISTAKEN AS A SPINAL STROKE
1Kyrgyz State Medical Academy, Neurology, Bishkek, Kyrgyzstan
Background and Aims
It’s necessary to differentiate the Neuromyelitis Optica (NO) from brainstem and thoracic location spinal strokes due to possible similar course at the onset of the disease.
Method
We described the case of a 33-year-old woman suffering from NMO in which a spinal cord lesion was mistaken for a spinal stroke. The patient was directed to the study of antibodies to aquaporin 4. The lesions of the spinal cord imaged with T2-weighted MRI were longitudinally extensive and were confused with spinal stroke.
Results
Lower paraparesis developed first, then a Lhermitte’s symptom and stiffness in the trunk joined, followed by a deterioration of vision on the right eye. The incomplete atrophy of the optic nerve on the right eye was diagnosed. Initially, the patient as treated for a spinal stroke due to the findings on the spinal MRI: in the DWI mode, a focus of small sizes was noticed in the brainstem and upper thoracic region as well as the swollen right optic nerve with the use of contrast. But later because of the undular course, an autoimmune disease was suspected. The positive titres of the aquaporin 4 antibodies confirmed NMO.
Conclusion
Ischemic strokes in brainstem appear often due to the dissection of vertebral artery and following the trauma, having the acute course, what differs them from the autoimmune disease. Focal lesions in thoracic spine can be provoked by occlusion in anterior spinal arteries, what is very rare but mostly are typical for the transverse myelitis and multiple sclerosis as well as autoimmune neuromyelitis.
Trial registration number
N/A
AS31-101
CHALLENGES IN ANTICOAGULATION THERAPY FOLLOWING ISCHEMIC STROKE IN PATIENTS WITH ATRIAL FIBRILLATION
1Keele University, Medical School 3rd Year, Stoke on Trent, United Kingdom
2University Hospital of North Midland NHS Trust, Stroke Medicine, Stoke on Trent, United Kingdom
Background and Aims
Patients with ischemic stroke and atrial fibrillation, determining optimal timing of anticoagulation for secondary prevention is of challenge. Current ESC guidelines recommend initiation of anticoagulation in AF patients 1–12 days post stroke, depending on stroke severity.
Method
We report a case, whereby a 62 years old patient presented with a left TACI
Results
She had a thrombus in M1of left MCA with NIHSS and ASPECT score of 19 and 9. Thrombolysis followed by Mechanical Thrombectomy (MT) achieved a TICI3 score and improvement in NIHSS to 1. Twenty-four hours post thrombolysis, CT head revealed a left basal ganglia infarct (2.5cm) with Hemorrhagic Transformation (HT1). Decision to anticoagulate on day 6 post stroke was taken.
Five days later, the patient suffered a right TACI, with an NIHSS of 17 and thrombus in M1 segment of right MCA. As thrombolysis was contraindicated, MT was repeated and TICI3 flow achieved. NIHSS reduced to 5 with repeat CT confirming a 1.5cm infarct within the right lentiform nucleus. With high risk of further embolic episodes, split dose low molecular weight heparin was initiated to reduce the risk of further embolic stroke. Three days later, NIHSS deteriorated to 19 and CT head confirmed Parenchymal Hemorrhage (PH1). Anticoagulation was stopped and six weeks rehabilitation followed, reducing NIHSS to 4 and MRS to 2. With resolution of the Haemorrhage, oral anticoagulation with Apixaban was resumed. Three months follow up showed NIHSS and MRS of 1.
Conclusion
In conclusion, timing of anticoagulation following stroke is always a challenge, as this case highlights.
Trial registration number
N/A
AS31-102
RECCURENT THROMBECTOMY IN PACIENT WITH PARADOXICAL EMBOLISM - CASE REPORT
1Faculty Hospital Trnava, Dpt. of Neurology, Trnava, Slovak Republic
2Faculty Hospital Trnava, Dpt. of Radiology, Trnava, Slovak Republic
Background and Aims
We present a case report of 52-years-old male patient with inherited hypercoagulability and reactive thrombocytosis, pulmonary hypertension, hospitalized at the coronary unit due to reccurent pulmonary artery embolization despite anticoagulation. ECHOKG revealed atrial septum aneurysm bulging to left atrium.
Method
Due to acute onset of dysarthria and left side weakness /NIHSS 11 pts/ patient underwent brain CT and no acute ischemic lesions were present. CT angiography revealed occlusion of top-of-basilaris and V4 segment of right vertebral artery. Systemic thrombolysis was administered without any improvement. Persistent occlusion was seen on DSA, with aspiration thrombectomy was full recanalization achieved and patient´s neurological status improved to NIHSS 7 pts.
Results
On next day new side hemiparesis appeared again, NIHSS was 14 pts. Brain CT revealed subacute ischemic lesion in right cerebellar hemisphere. CTAG demonstrated occlusion of M2 segment of right arteria cerebri media. Again with use of aspiration thrombectomy was full recanalization achieved and NIHSS decreased to 4 pts.
Conclusion
Thrombosis of bilateral arteria femoralis superficialis was visualised with ultrasound examination. TCD emboldetection revealed right-to-left shunt. TEECHOKG confirmed foramen ovale apertum with left-to-right shunt and large right-to-left shunt. Foramen ovale apertum was closed with Amplatz occluder. Caval filter was implanted as prevention of next embolization. According to hematologist and cardiologist treatment with warfarin was started.
Trial registration number
N/A
AS31-103
SMALL VESSEL DISEASE AND INTRACEREBRAL HEMORRHAGES ASSOCIATED WITH NOVEL PATHOGENIC VARIANTS OF COL4A1
1Neurology Resident, Neurology Department, Braga, Portugal
2Hospital de Braga, Neurology Department, Braga, Portugal
3Centro Hospitalar do Porto, Neuropathology Unit- Neurosciences Department, Porto, Portugal
4Universidade do Porto- Instituto de Biologia Molecular e Celular- Instituto de Investigação e Inovação em Saúde, Centro de Genética Preditiva e Preventiva, Porto, Portugal
Neurological manifestations associated with COL4A1 gene mutations include porencephaly, infantile hemiparesis, HANAC syndrome (hereditary angiopathy with nephropathy, aneurysm and muscle cramps) and also cerebral small vessel disease with hemorrhages without other additional manifestations.
Method
N/A
Family A: Three members affected: index case, his mother and daughter. Index case: male without previous diseases, was admitted at the age of 53 with hemispheric cerebellar hemorrhage. MRI revealed leucoencephalopathy (Fazekas II). Mother: history of arterial hypertension, diabetes, chronic renal disease and kidney cysts. Between the age of 54 and 77 she experienced recurrent, spontaneous, deep and cortical cerebral hemorrhages, currently presents vascular cognitive impairment (VCI). MRI revealed leucoencephalopathy (Fazekas III). Daughter: 31 years old, with symptoms of recurrent vertigo. MRI revealed leucoencephalopathy (Fazekas I). Genetic study of COL4A1 identified a novel variant in exon 32 [c.2563G>C; p.(Gly855Arg)] in these members.
Family B: One member affected. Female, without previous diseases, admitted at age of 38 with deep spontaneous haemorrhage. During hospitalization, she experienced successive and recurrent cortico-subcortical hemorrhages. At the age of 48 she had simultaneous basal ganglia hemorrhages. She currently presents VCI. MRI revealed leucoencephalopathy (Fazekas I). Genetic study of COL4A1 identified a novel variant in exon 47 [c.4232G>C; p.(Gly1411Ala)].
Conclusion
Discussion
There are less than 80 families described in the literature with COL4A1 mutations, which are more often associated with early onset CNS manifestations. Our work describes clinical features of the first two Portuguese families with small vessel disease and cerebral hemorrhages associated with novel pathogenic variants of COL4A1.
Trial registration number
N/A
AS31-104
AMYLOID BLEED IMMEDIATELY FOLLOWING NORMAL GRADIENT ECHO MR SCAN
1St. James' Hospital, Stroke medicine, Dublin, Ireland
2St James' Hospital, Stroke medicine, Dublin, Ireland
Background and Aims
Amyloid Angiopathy can present radiologically in a number of ways including with cortical or subcortical microhaemorrhages or large intracerebral haemorrhages which may be multiple.
Method
We present the case of a woman who suffered a large amyloid bleed within 20 minutes of completion of a Gradient Echo MR to determine extent of Amyloid Angiopathy.
Results
A 74 year old woman presented to hospital with an episode of transient worsening confusion and disorientation lasting <30 minutes on a background of similar episodes over the previous 4 months. CT brain at the time of a previous episode had been reported normal but urgent CT on presentation suggested the presence of a very small area of subarachnoid haemorrhage over the left parietal lobe. A diagnosis of possible amyloid spells was made and an MR scan of Brain with Gradient Echo (T2*) sequences was performed. This showed three small areas of superficial siderosis consistent with a diagnosis of Amyloid Angiopathy. On being transferred back to the Stroke Unit the patient suffered a sudden onset of dense right hemiplegia and receptive aphasia. She was resuscitated and transferred back to the CT for rescan. This showed a large left fronto-parietal haemorrhage, discrete from the areas of siderosis. She was transferred back to the stroke unit but died 4 weeks later after suffering a further intraparenchymal haemorrhage in the right cerebral hemisphere.
Conclusion
Large intra-parenchymal amyloid bleeds can occur suddenly and catastrophically without radiological evidence of prior microhaemorrhage or siderosis in the vicinity of the bleeding.
Trial registration number
N/A
AS31-105
SPINAL INFARCT RELATED TO CEREBRAL AMYLOID ANGIOPATHY
1University Hospital of Salamanca, Neurology, Salamanca, Spain
Background and Aims
Cerebral amyloid angiopathy (CAA) is a cortical and leptomeningeal vessels arteriopathy. CAA spectrum includes intracranial, intraventricular, subarachnoid or subdural hemorrhages. The spinal hemorrhage is a rare manifestation only described in some case reports.
Method
85-year-old man with a personal history of moderately differentiated prostate carcinoma with bone metastasis in T9 treated with hormonotherapy. He was admitted to the hospital due to lumbar pain, paresis of the lower left limb and loss of sphincter control. The next day he was paraplegic and the lumbar pain disappeared. There was no history of fever nor infectious symptoms. The exploration revealed a flaccid paraplegia with muscular stretch reflexes abolished in the lower limbs, the cutaneous-abdominal reflexes were present, the cutaneous-plantar reflexes were indifferent, the sensitivity was preserved and there was loss of sphincter control.
Results
The urgent spinal magnetic resonance (MRI) showed an acute myelopathy from D1 to spinal cone suggestive of ischemic origin. Cranial computed tomography showed parietal bilateral subarachnoid hemorrhage with secondary intraventricular component. Cranial angiography MRI as well as medullar and vertebral arteriography ruled out vascular malformations. The lumbar puncture revealed a hemorrhagic cerebrospinal fluid without other alterations.
Conclusion
The spinal infarct in CAA has not been described before. CAA has been documented in a minority of meningeal spinal vessels and has not been observed in the parenchymal spinal cord vessels. We believe that the spinal infarct was due to the vasospasm of the anterior spinal artery induced by the blood in the subarachnoid space in the context of CAA.
Trial registration number
N/A
AS31-106
RECURRENT BLEEDING, A RARE CAUSE
1Jena University Hospital, Neurology/Neurocritical Care, Jena, Germany
Background and Aims
Anticoagulant therapy reduces the risk of cerebral and systemic embolization in patient with atrial fibrillation, but increases the risk of bleeding, especially in patients with unrecognized coagulation disorders.
Method
We would like to present the case of a patient with atrial fibrillation and oral anticoagulation with rivaroxaban who suffered from a cerebral hemorrhage. Subsequently the anticoagulation was stopped, the bleeding was treated conservatively.
Results
After interventional occlusion of the LAA and DAPT a cardiac tamponade occurred, resulting in a surgical resection of the left atrial appendage.
A few months later the patient was presented with an acute rightsided hemiparesis and consecutive thrombolysis resulting in multilocular cerebral hemorrhages.
Reviewing the laboratory results we found a persistent prolongation of prothrombin time, which was caused by an isolated factor VII-deficiency.
Conclusion
We would like to discuss diagnostic investigations (malabsorption, inhibitors of coagulation factor VII, hereditary factor VII deficiency) and management of patients which rare coagulation disorders.
Trial registration number
N/A
AS31-107
SPONTANEOUS RUPTURE OF CEREBRAL ANEURYSM AFTER THROMBECTOMY IN A CASE OF ACUTE ISCHEMIC STROKE WITH PROXIMAL OCCLUSION
1Centre Hospitalier Chrétien, Neurology- Comprehensive Stroke Center, LIEGE, Belgium
2Centre Hospitalier Chrétien, Interventional Neuroradiology, LIEGE, Belgium
3Centre Hospitalier Chrétien, Neuroradiology, LIEGE, Belgium
Background and Aims
Unruptured cerebral aneurysm may be hidden by a proximal occlusion in some cases of acute ischemic stroke. The consequence of the recanalization of the occluded vessel by thrombectomy and the revascularisation of the aneursym is not well known.
Method
A 78 year-old woman was transferred from a primary stroke care center to our comprehensive stroke center, after iv thrombolysis, because of acute ischemic stroke due to a right proximal (M1) mean cerebral artery occlusion. After 2 passes, partial recanalization was achieved (TICI 2a) and revealed an aneurysm of 5 mm expanding from the parietal branch, which ruptured soon after the recanalization during the procedure, leading to the death of the patient.
Results
In the literature, we identified 12 reported cases of intracranial aneurysms that were visualized after recanalization of the occluded vessel. Aneurysms were visualized after acute endovascular thrombolysis in 5 cases, after thrombectomy in 3 cases, after IV tPA in 1 case, and after spontaneous recanalization in 3 cases. Aneurysms ruptured during endovascular therapy in only 2 cases, one of which after thrombecotmy. Mechanism of rupture is not well kown but in absence of direct perforation by the device of thrombectomy, abrupt reperfusion due to recanalization may be one explanation.
Conclusion
The presence of an aneurysm hidden by the proximal occlusion should be carefully assessed during the procedure of recanalization. At the light of this case and others reported in the literature, the recanalization may lead to an immediate rupture of the aneurysm.
Trial registration number
N/A
AS31-108
A STROKE-LIKE PRESENTATION DUE TO BALO CONCENTRIC SCLEROSIS
1Shrewsbury and Telford NHS Trust, Stroke department, Telford, United Kingdom
Background and Aims
A young woman presented with a ‘stroke like’ episode subsequently found to be due to a rare form of multiple sclerosis, Balò concentric sclerosis (BCS).
Method
A literature search was conducted (5/1/2018) using the key words: ‘Baló concentric sclerosis ‘ and ‘Stroke ‘ finding only 30 PUbMed and 5 Medline references respectively. Few case reports exist of such a presentation.
Results
The Hungarian neuropathologist Josef Baló published a case report in 1928 of a young man with a new hemiparesis who was found at autopsy to have lesions described as encephalitis periaxialis concerntrica. With the advent of MRI, imaging characteristically shows an onion ring or whorled appearance. Recently it has been classified to lie within the spectrum of atypical idiopathic inflammatory demyelinating disorders, and practically is considered as a form of relapsing-remitting MS. It is more common in Chinese and Filipino populations with an estimated 2:1 female predilection with on-going uncertainty as to the relative role of genetic or environmental predespositions.
We describe a 33 year old lady presenting acutely with left arm heaviness, incoordination and paraesthesia. She had no vascular risk factors and no relevant past medical or family history. MRI confirmed a classical BCS ringed lesion within the white matter of the right frontal gyrus, Lumbar puncture showed raised lymphocytes and oligoclonal bands.
Conclusion
Stroke-like presentations are not uncommonly found to be due to MS but rarely of the atypical BCS type. BCS shows a characteristic onion ring appearance on MRI.
Trial registration number
N/A
AS31-109
INFECTIVE ENDOCARDITIS AS A RISK FACTOR FOR MULTIFOCAL STROKE
1V. N. Karazin Kharkiv National University, Department of Clinical Neurology- Psychiatry and Narcology, Kharkiv, Ukraine
2Kharkiv Railway Clinical Hospital #1, Neurology Department #1, Kharkiv, Ukraine
Background and Aims
A 54 year old male presented with headache, left-side hemiparesis, loss of consciousness, left-side hemihypesthesia (NIHSS 5, GSC 13). He had a history of hypertension, prosthetic aortic valve, atrial fibrillation and was on warfarin (INR=2.6).
Method
NCCT scan showed right-side ischemia 65x44x60 mm. Reperfusion was not done as he was on warfarin with high INR.
Results
In 7 day he developed a fever (38 C), dyspnea along with bulbar syndrome and worsening of his left-side hemiparesis (NIHSS 15, GCS 11) TTE and 2nd CT were done - no new brain lesions but vegetation on aortic valve. He was prescribed with vancomycin and gentamicin. Follow-up blood culture test was positive for S. aureus and CT in 5 day after deterioration showed brainstem stroke. Treatment was continued with antibiotics and warfarin (under INR control) In 10 days patient was discharge from the hospital (NIHSS 10, mRS 3)
Conclusion
Infective endocarditis with emboli from vegetations is one of the causes of embolic stroke (and very often with multifocal lesions). So all patient with prosthetic heart valves and stroke even if they are on anticoagulants should be investigated with TEE or TTE for vegetations development and treated properly with antibiotics if those are found.
Trial registration number
N/A
AS31-110
NOTHING IS AS CLEAR AS IT SEEMS: A TRICKY CASE OF STROKE
1Department of Neurological Disorders- Neurology, Santa Chiara Hospital, Trento, Italy
2Department of Cardiovascular Diseases- Santa Chiara Hospital, Department of Cardiosurgery, Trento, Italy
3Department of Cardiovascular Diseases- Santa Chiara Hospital, Department of Vascular Surgery, Trento, Italy
4Department of Cardiovascular Diseases- Santa Chiara Hospital, Department of Cardiology, Trento, Italy
Background and Aims
Many studies focused on stroke etiology, given its great importance in correctly setting secondary prevention. Nevertheless, a relevant percentage of strokes still remains cryptogenic. To better stratify cryptogenic strokes, a neuroradiological classification has been proposed, based on infarct morphology and topography, introducing the concept of embolic stroke of undetermined sources (ESUS). However, the diagnostic reliability of such classification may not reflect patient’s clinical situation.
Method
.
Results
A 64-years old woman referred to our hospital for fuzzy vision and dizziness, with evidence of bilateral upward gaze palsy and no convergence on neurological examination. She reported a history of smoking-habit, hypertension, dyslipidaemia and autoimmune setting with tiroiditis, rheumatoid arthritis and systemic scleroderma. Acute CT scan excluded hemorrhages and AngioCT did not reveal relevant extra and intracranial stenosis. No alteration in cardiac rhythm were detected on ECG-monitoring. An MRI scan showed a minute (0.5 mm) recent thalamo-mesecephalic infarct, suggeting a lacunar stroke, and she was put on antiplatelet treatment. Transthoracic echocardiogram showed extensive atherosclerosis of aortic arch, which was further investigated throught trasesophageal echo, revealing two pedunculated and mobile thrombi protruding into brachiocephalic artery. Anticoagulation with LMWE was promptly started, but during hospitalization, patient experienced acute arm ischemia of right radial artery that required embolectomy. Patient was ultimately referred to cardiosurgical substitution of aortic arch.
Conclusion
Despite misleading anamnesis and infarct MRI-findings, a comprehensive diagnostic work-up identified microembolization from aortic plaques as the cause of patient’s symptoms. This enabled to correctly classify the observed lesion as embolic, with remarkable consequences on therapeutic strategy.
Trial registration number
.
AS31-111
RED FLAGS IN A PROTOTYPICAL CASE OF VZV-VASCULOPATHY
1APSS - Ospedale Santa Chiara, Department of Neurological Disorders- U.O. Neurologia, Trento, Italy
2APSS - Ospedale Santa Chiara, Department of Radiology- Neruoradiology, Trento, Italy
Background and Aims
Zoster is a well-known risk factor for stroke. Varicella zoster virus (VZV) can infect cerebral arteries after re-activation. VZV-vasculopathy is challenging because of heterogeneous and evolving phenotype and possible unfavourable course without prompt treatment. We report a prototypical case.
Method
Case report
Results
A 84-year-old healthy and immunocompetent woman referred to emergency department because of confusional state during fever. Under supervision she presented a tonic-clonic seizure of left limbs followed by persistent vigilance impairment, left side hemiparesis with anesthesia and right-forced gaze version. During previous months she suffered right ear pain and deafness without local rash and progressive cognitive impairment. Head CT scan showed a right medial frontal hypo-density and EEG showed background slow activity with right sharp waves. Otoscopy showed a recent right middle ear acute otitis. Carotid and heart ultrasound, ECG, blood exams were unremarkable. Cerebrospinal fluid (CSF) exam showed 3 lymphocytes and normal protein and glucose concentrations, whereas PCR revealed the presence of VZV-DNA. Acyclovir, prednisone and levetiracetam were introduced, associated to aspirin. Brain MRI and angiography studies showed an ischemic stroke in the territory of an irregular right anterior cerebral artery and diffuse post-gadolinium leptomeningeal enhancement. After three-months follow-up, patient was well oriented with mild gaze impairment and left side hemiparesis.
Conclusion
VZV-vasculopathy should be suspected not only in stroke patients with history of Zoster but also in atypical stroke presentations associated with a recent evolving cranial neuralgia or encephalopathy; immunosuppression is not a prerequisite especially in older patients. VZV-DNA search on CSF should be performed.
Trial registration number
N/A
AS31-112
ARTERIAL INVASION – COMPLICATION OF A COMMON VIRUS
1Hospital de Braga, Neurology, BRAGA, Portugal
Background and Aims
Varicella zoster virus (VZV) is the only virus that has been shown to replicate in arteries and produce vasculopathy. Many cases of HIV-associated vasculopathy most probably indicate an undiagnosed VZV vasculopathy.
Method
Case-report
Results
A 37-year old Mozambican woman presented with a 3-week history of headaches and fever, followed by horizontal diplopia one week before hospital admission. Neurological examination revealed isolated left eye abduction limitation. Admission brain CT and CT angiogram were unremarkable. Brain MRI revealed pontomedullary junction meningeal thickening and enhancement. Lumbar puncture disclosed 105 leukocytes (87% lymphocytes) and positive VZV DNA. Blood tests showed positive anti-HIV 1 with plasma viral load of >1 million copies/μL. Intravenous acyclovir and antiretroviral therapy were started, but deterioration occurred, with depressed level of consciousness, complex ophthalmoparesis, dysphagia, dysarthria, right motor deficit and ataxia. High dose steroid therapy was instituted. A second brain MRI with angiogram revealed multiple recent, bilateral, supra and infratentorial ischemic lesions and multifocal stenosis in the anterior and posterior circulation. She completed treatment with 21 days of acyclovir and slow tapering steroids, besides antiretroviral therapy, with good clinical response.
Conclusion
A negative angiogram does not exclude the diagnosis of VZV vasculopathy, most likely because disease in small arteries is not detected as readily as in large arteries. In HIV-infected patients, the natural course of VZV vasculopathy is modified by immunosuppression, and progression of vascular changes is more frequent despite treatment with intravenous acyclovir.
Trial registration number
N/A
AS31-113
EARLY LEFT ATRIAL APPENDAGE CLOSURE AFTER SUBARACNOID HEMORRHAGE
1Complejo Asistencial Unviersitario de Salamanca, Neurology, Salamanca, Spain
2Complejo Asistencial Unviersitario de Salamanca, Radiology, Salamanca, Spain
Background and Aims
Oral anticoagulants are the treatment of choice for ischemic stroke prevention in patients with non-valvular atrial fibrillation but there is an increased risk of bleeding associated to the use of these drugs. In patients with previous intracranial hemorrhage, oral anticoagulation therapy triples this risk of bleeding and left atrial appendage closure has been shown as a good alternative.
Method
We report a case of early left appendage closure after acute subaracnoid hemorrhage due to oral anticoagulation.
Results
An eighty-year-old woman presented to the emergency room complaning of intense cephalea that started three days before with associated dizziness and nausea; it was persistent despite analgesic therapy. In physical examination only postural tremor was seen and CT images showed an hyperdense material taking up left frontal convexity sulcus, suggesting subaracnoid hemorrhage. Given the high atherothrombotic and cardioembolic risks (history of bilateral carotid stenosis with repeated ischemic strokes, ischemic hearat disease with coronary revascularization and permanent atrial fibrillation), left atrial appendage closure was performed in 24 hours, and antithrombotic therapy was prescribed.
Conclusion
Patients with acute bleeding and atrial fibrilation suppose a clinical setting of controversial treatment, without conclusive data in randomized studies about the optimum time for reintroduction of anticoagulation. Left atrial apprendage closure could reduce the embolic risk during the early post-hemorrhage period, and would allow a safer use of antithrombotic therapy in patients with both cardioembolic and atherothrombotic risk.
Trial registration number
N/A