
Abstract
Introduction
Information about the impact of functional outcome after stroke is currently missing on health-related quality of life, survival and costs. This information would be valuable for health economic evaluations and for allocation of resources in stroke health care.
Patients and methods
Data on 297 Swedish patients included in the Third International Stroke Trial were analysed including functional outcome at six months (measured by Oxford Handicap Scale), health-related quality of life up to 18 months (EQ-5D-3L) and survival up to 36 months. We used record linkage to collect data on costs up to 36 months, using national patient registers.
Results
Patients with a better functional outcome level at six months had a significantly better health-related quality of life at 18 months (p < 0.05), better long-term survival (p < 0.05) and lower costs (p < 0.001), for all time points up to 36 months. The difference in costs was mainly due to differences in days spent in hospital (p < 0.005).
Discussion
This study showed an association between functional outcome at six months and health-related quality of life up to 18 months, and costs up to 36 months.
Conclusion
Functional outcome six months after stroke is an important determinant of health-related quality of life, survival and costs over 36 months. Effective interventions aimed at reducing short-term disability levels are therefore also expected to reduce the overall burden of stroke.
Introduction
Each year, stroke affects 16 million people for the first time and causes about 5.7 million deaths worldwide. 1 In Sweden, about 23,000 people have a stroke annually, of whom 20% die within one year, and a high percentage of survivors have long-term residual disabilities, cognitive deficits, emotional problems and reduced health-related quality of life (HRQoL). 2 This places a huge burden on health care and society.3–5 At present, more than 20% of stroke patients are below retirement age, a proportion predicted to increase.6,7 In total, the economic costs are substantial, and the life-time direct costs of a first-time stroke in Sweden have been estimated to 49,000 Euros for men and 60,000 Euros for women (year, 2009 prices). 8
Functional outcome after stroke has been shown to be an important factor for survival, 9 but the impact of functional outcome on HRQoL and costs is less well studied. 10 Having reliable estimates of costs by functional outcome will be valuable for health economic evaluations and for the planning of health care. In this study, we aimed to investigate HRQoL, survival and direct medical costs after ischaemic stroke, for different levels of functional outcome at six months, using data from the Third International Stroke Trial (IST-3) in Sweden.
Patients and methods
IST-3 was a randomised-controlled, open trial of thrombolytic treatment with alteplase within 6 h of onset of ischaemic stroke in 3035 patients. The methods and main results have been reported previously. 11 In short, patients were eligible if they had symptoms and signs of clinically definite acute ischemic stroke; the time of stroke onset was known; treatment could be started within 6 h of onset; computed tomography (CT) or magnetic resonances imaging (MRI) of the brain had reliably excluded both intracranial haemorrhage and structural brain lesions (the latter which could mimic stroke, e.g. cerebral tumour). Of the 3035 patients in the trial, 297 patients were included in Sweden.
The primary outcome in IST-3 was functional outcome at six months, as measured by the Oxford Handicap Scale (OHS). 12 OHS is ordered in seven categories, where OHS 0 signifies no functional deficit, OHS 1: minor symptoms that do not interfere with lifestyle, OHS 2: minor handicap, symptoms that lead to some restriction in lifestyle but do not interfere with the patient’s capacity to look after himself, OHS 3: moderate handicap, symptoms that significantly restricted lifestyle and prevent totally independent existence, OHS 4: moderately severe handicap, symptoms that clearly prevent independent existence though not needing constant attention, OHS 5: severe handicap, totally dependent patient requiring constant attention night and day and OHS 6: death. Secondary outcomes were HRQoL at 6 and 18 months, as measured by the EQ-5D-3L instrument. 13 EQ-5D is a generic HRQoL instrument describing the respondent’s health state in terms of three severity levels in each of five domains (mobility, self-care, usual activities, pain/discomfort and anxiety/depression). A preference-based utility index for each health state can be derived with help from a Swedish tariff where the maximum value 1 represents perfect health and the value 0 represents death. This index is often combined with survival in health economic analysis to estimate quality adjusted life years (QALYs) and therefore often referred to as the QALY weight. 14
For the present analysis, we additionally collected data on survival up to 36 months by using data from the Swedish IST-3 follow-up and data on resource utilisation up to 36 months by using data from the Swedish National Patient registry which is held by the National Board on health and welfare. 15 Linkage was conducted via the unique Swedish identification number. For each inpatient stay and outpatient visit, the diagnosis-related group (DRG) and International Classification of Diseases–Tenth revision (ICD-10) codes were retrieved and multiplied with a unit cost. Unit costs were collected from the Cost-per-patient database (KPP) held by the Swedish Associations and Local Authorities, as available by DRG-code and the main ICD code reported at each observation from the National Register. 16 Thus, costs in this investigation are restricted to direct medical costs (i.e. a health care provider perspective). This excludes non-medical costs (e.g. community care costs) and indirect costs associated with productivity losses due to work absence (which anyway are considered low as the strokes occurred in elderly patients). The unit costs represent the average cost at various levels of hospital care (tertiary-, county-, or district level). The DRG-coding system changed in Sweden during 2013, therefore visits before, 2012 used, 2012 year’s costs and visits after, 2012 used, 2013 and, 2014 years’ costs. Inflation in Sweden between, 2012 and, 2014 was close to zero, and no adjustment was therefore performed. Where costs were missing they were imputed with an average cost reported in KPP (7994 Swedish Krona (SEK) = 833 Euro per inpatient day, and, 3126 SEK= 327 Euro per outpatient visit). Costs are presented in Euro (€) and adjusted to 2016 using purchasing power parity with Germany as the target currency (largest Euro market). All calculations were performed using the CCEMG-EPPI-Centre converter using, 2014 as the entry year. 17
Statistical methods and data management
The primary objective was to study the association between OHS score at six months and HRQoL up to 18 months, and survival and costs up to 36 months. Patients were stratified based on their functional outcome, OHS, at 6 months, and were categorized into one of seven OHS groups (OHS 0–6). Only patients with complete data on functional outcome and HRQoL at 6 months and survival up to 36 months were included. Functional outcome was also dichotomised, with OHS 0–2 defined as being independent, and OHS 3–5 as being dependent. 18 For the cost estimates only patients alive at each time point (6, 18 and 36 months, respectively) were included. To compare differences between OHS groups, multiple comparisons of continuous data were performed by analysis of variance, ANOVA. The procedure proposed by Tukey was used to control for multiplicity. Statistical comparisons in order to test differences between two independent groups were made by use of the Student’s t-test for uncorrelated means. Regression modeling methods were used to explore the impact of differences in baseline variables (age, gender, living situation, National Institutes of Health Stroke Scale (NIHSS)) across OHS groups on both costs at 36 months (generalized linear model with log-link and gamma family) and HRQoL at 6 and 18 months (ordinary least-squares model). Baseline variables were excluded (step-wise) from the model unless significant. Association between functional outcome at 6 months and survival up to 36 months was analysed using the Log-rank test. Kaplan–Meier curves, unadjusted and adjusted for age, were computed to assess survival up to 36 months by functional outcome at six months. In addition, descriptive statistics was used to characterize the data. All analyses were carried out by use of the SAS system (SAS 9.4) and the 5% level of significance was considered.
This study was approved by the local Ethical Board, reference number: 02–551, 2014.
Aggregated data from the current study are available from the corresponding author on reasonable request.
Results
Sample characteristics
A total of 297 Swedish patients were included in IST-3. All patients had complete follow-up data on functional outcome, HRQoL at 6 months, and survival at 36 months. Baseline characteristics are summarised in Table 1. The mean age in the population was 81 years and varied between the OHS groups; patients with higher OHS scores were older and had higher NIHSS scores at baseline. In total, 144 of the 297 participants (49%) were females, and this proportion also varied between the OHS groups.
Clinical characteristics at baseline, by level of functional outcome at six months.
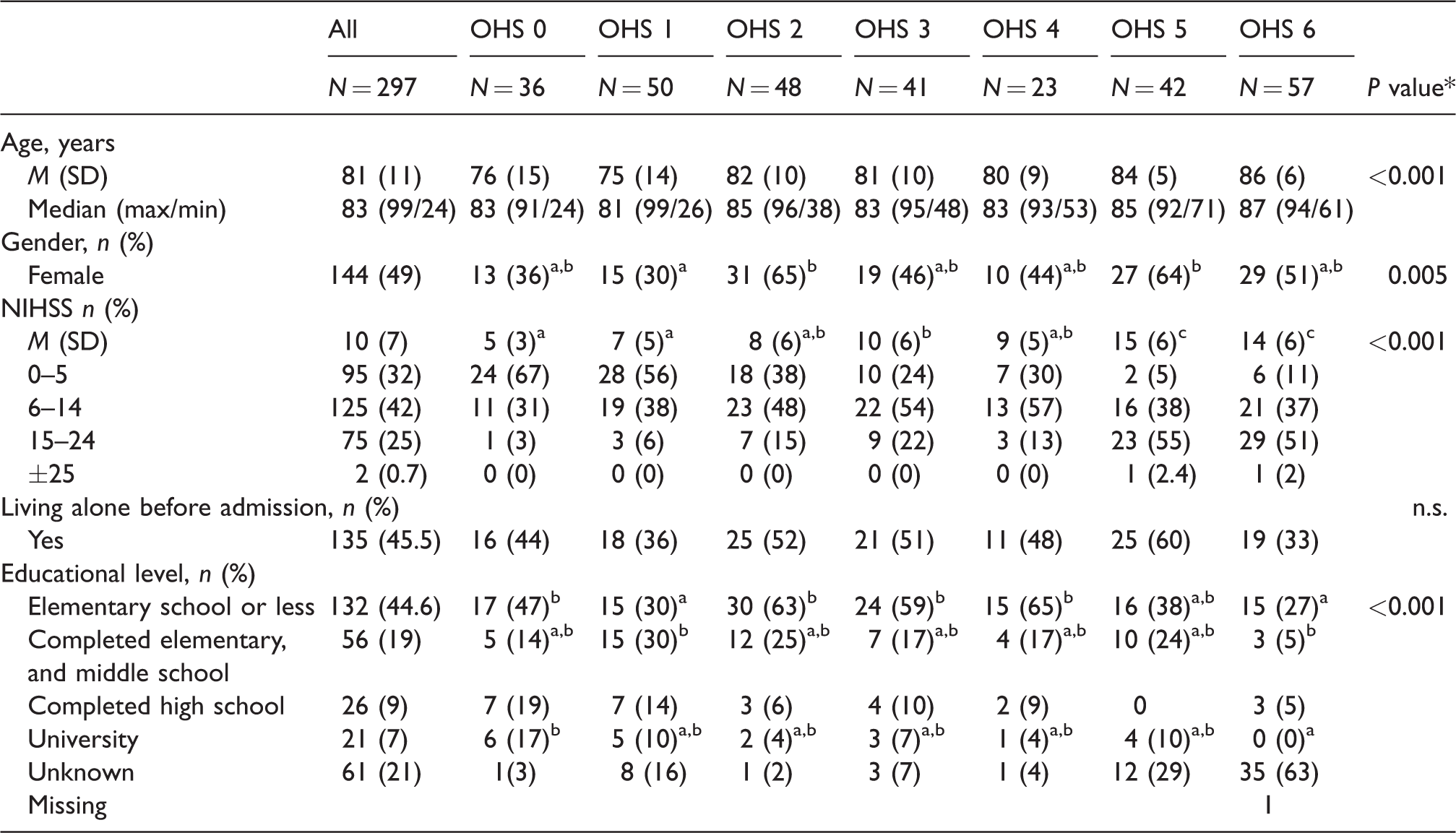
Note: *P value for one-way analysis of varaince (ANOVA) analysis with Tukey correction.
Showing significant differences between groups, a = lowest, c = highest.
OHS: Oxford Handicap Scale; NIHSS: National Institutes of Health Stroke Scale; n.s, not significant.
HRQoL and survival
Patients with a better functional level had a higher HRQoL value at 6 and 18 months (p < 0.05, Table 2). The findings remained stable when controlling for baseline differences across OHS groups, and the only significant predictor was age and only for the 18 months outcome. Controlling for age changed the mean HRQoL scores at 18 months by up to 3 per cent with the highest impact in OHS group 5 increasing the mean score from 0.57 to 0.59 (Supplementary material, Figure S1).
Health utility index (QALY-weights) measured with EQ-5D-3L at 6 and 18 months by functional outcome, OHS, at six months.
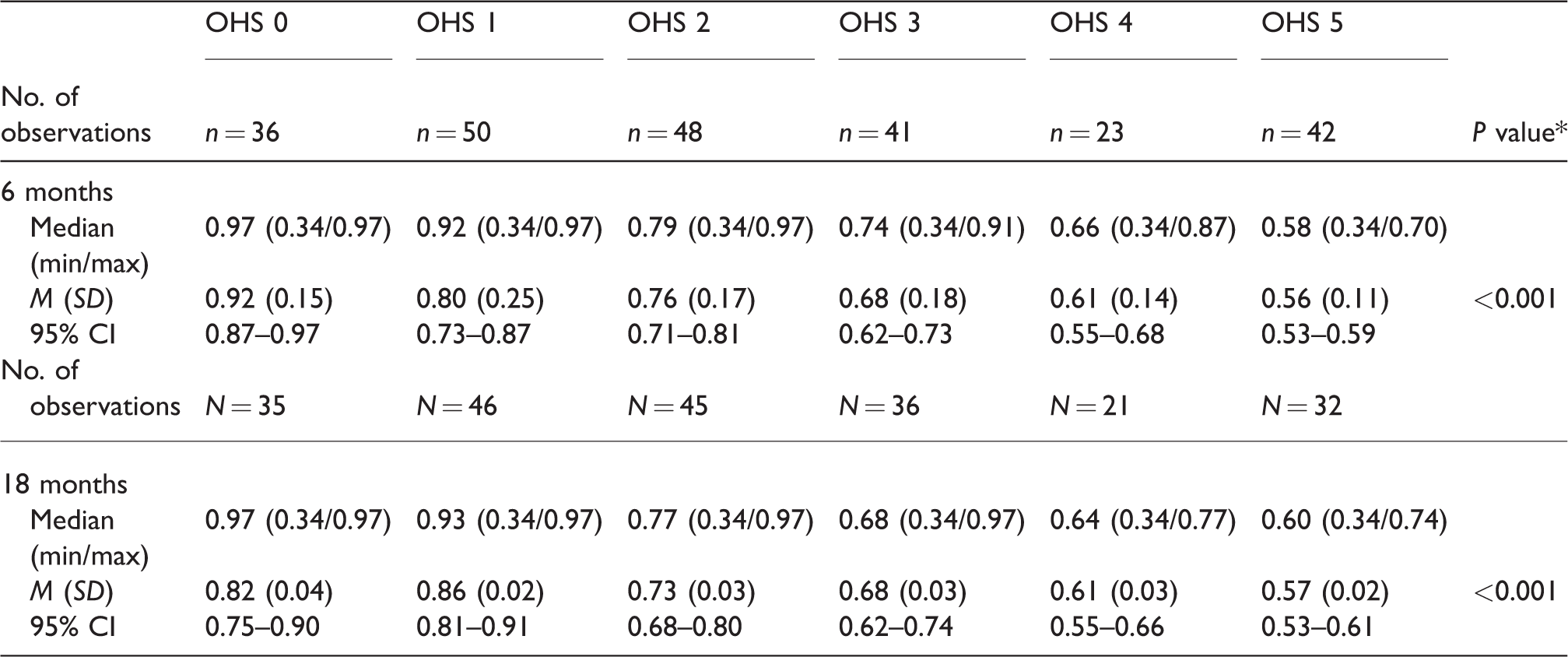
Note: CI: Confidence interval; SD: standard deviation; QALY: quality-adjusted life year; OHS: Oxford Handicap Scale.
P value represents the mean difference in QALY-weight between all groups of functional outcome OHS 0–5 using one-way ANOVA with Tukeys correction.
There was a statistically significant difference in survival up to 36 months between independent (OHS 0–2) and dependent (OHS 3–5) patients at six months (p < 0.05, Figure 1), and this difference sustained when adjusting for age (p < 0.01). In the period between 6 and 36 months post baseline, 25 patients (19%) had died in the independent group, and 31 patients (29%) in the dependent group (p = 0.054).
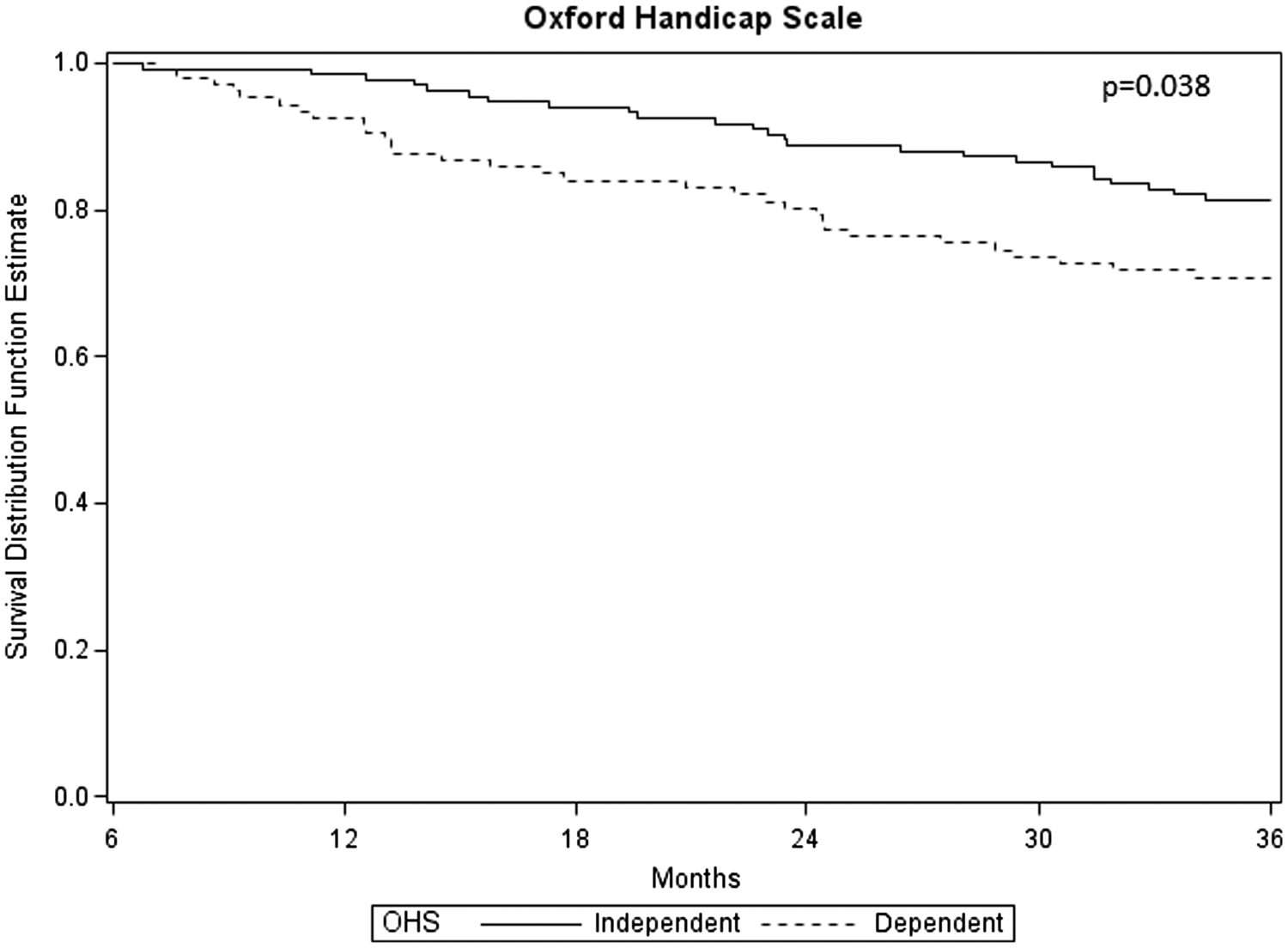
Kaplan–Meier curves of survival up to 36 months by functional outcome, independent (OHS 0–2) versus dependent (OHS 3–5), at 6 months.
Costs
Cumulative costs up to 36 months are shown in Table 3, for both in-hospital stays and outpatient visits. The difference in costs related to hospital stays, was mainly due to differences in mean number of days spent in hospital, ranging from 8 to 42 days at six months, across OHS groups (Supplementary material, Table S3). The differences in total costs between patients who were independent (OHS 0–2) and those who were dependent (OHS 3–5) at six months were significant, at all time points (p < 0.005). However, Figure 2 shows that the total cumulative costs at end of follow-up were lower among patients with the highest OHS score, OHS 5. For out-patient care patients with OHS 5 utilized the least resources of all groups. The analyses also showed that males had a higher cost at OHS 0, and females had a higher cost at OHS 1–5. In the regression model, NIHSS at baseline was (together with OHS group) a significant predictor of 36 months total costs. Controlling for NIHSS changed the mean costs up to 16% (Supplementary material, Figure S2).
Cumulative mean costs of hospital stays, out-patient visits and total cost by functional level at six months, including 95% confidence intervals.
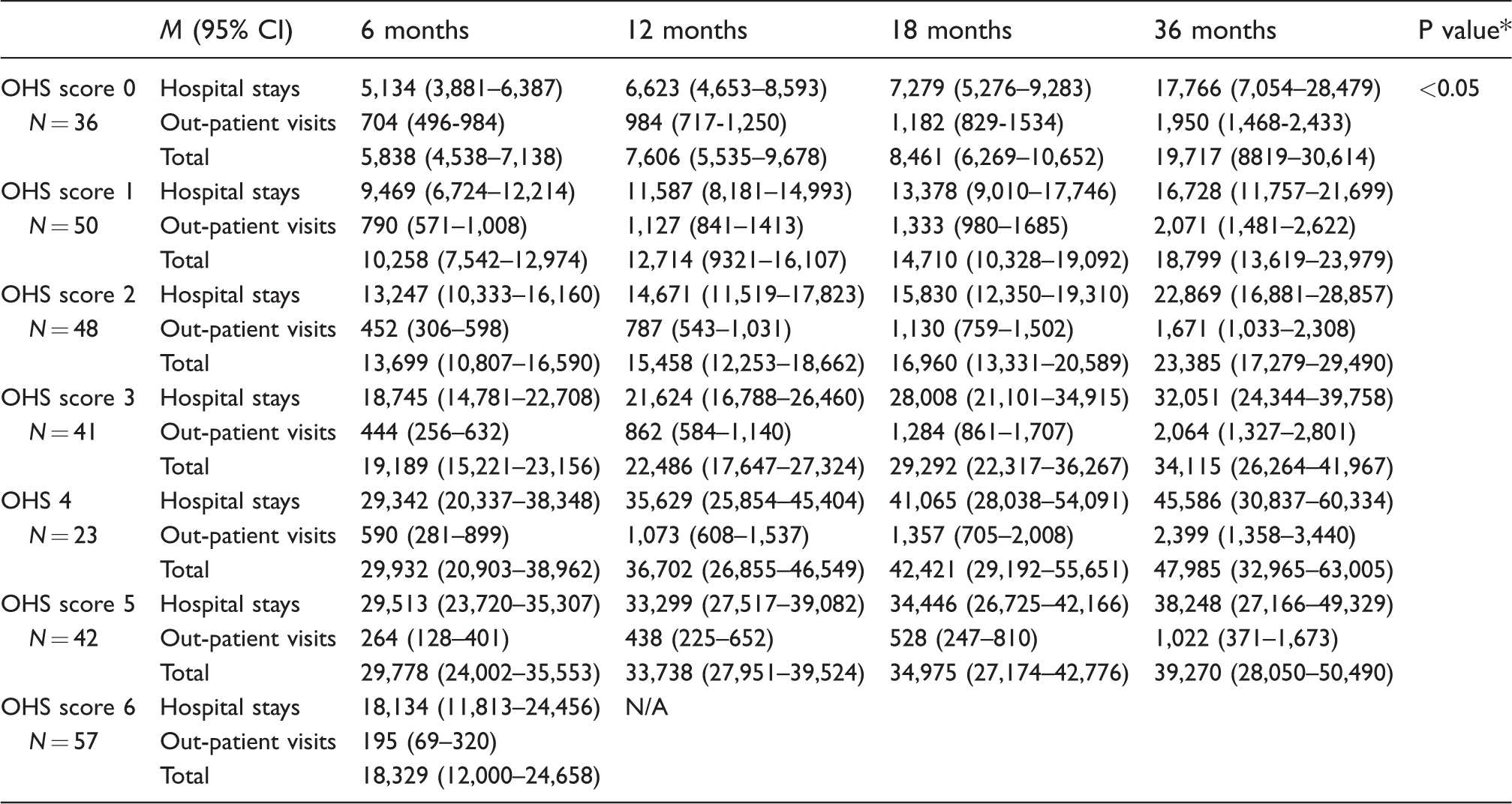
Note: Costs displayed are in Euro adjusted to 2016 using purchasing power parity with Germany as the target currency (largest Euro market). All calculations are done using CCEMG-EPPI-Centre Cost Converter. https://eppi.ioe.ac.uk/costconversion/default.aspx.
P value for differences in total costs related to functional outcome (independent vs. dependent) using one-way analysis of variance (ANOVA) with a post hoc Tukey correction.
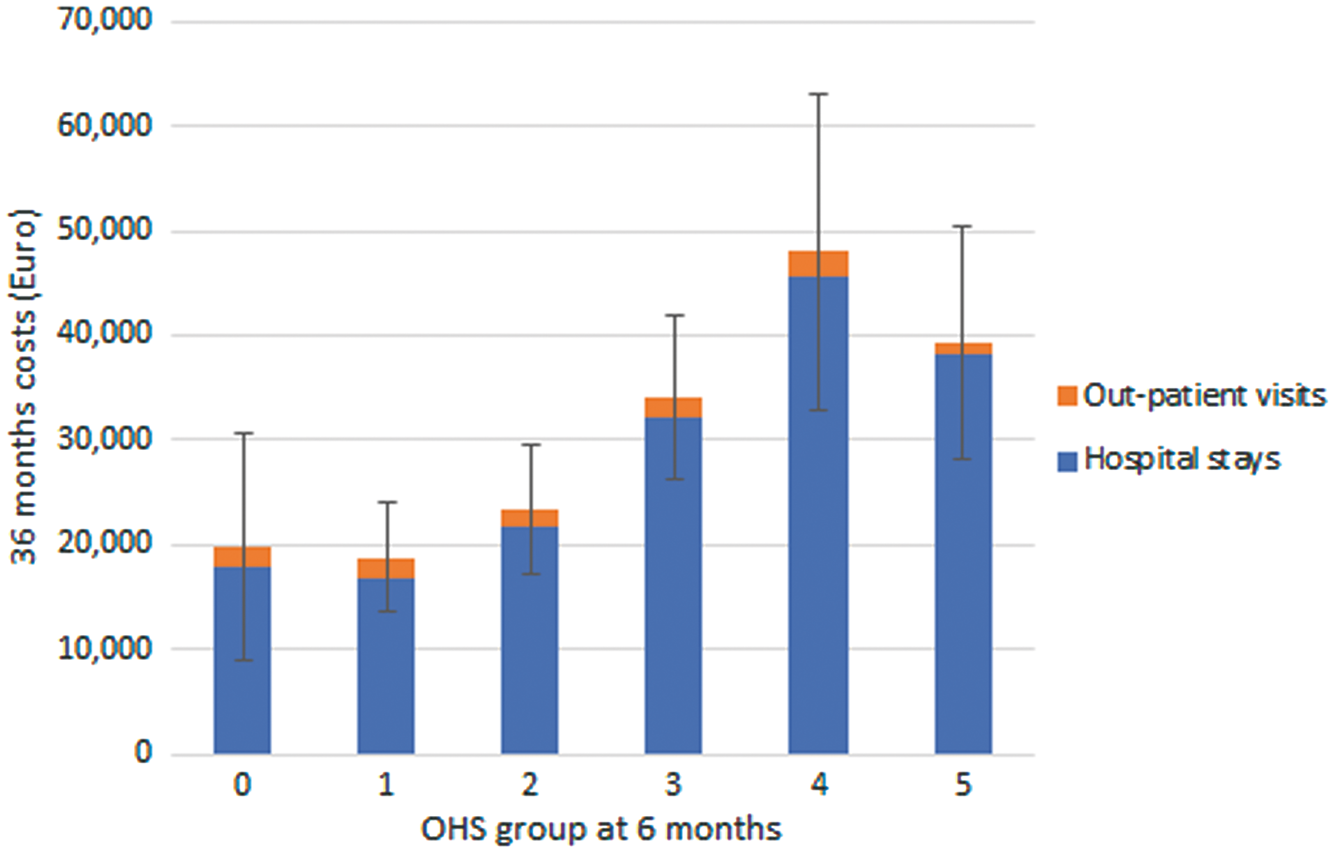
Cumulative 36 months mean total costs by functional level at six months, including 95% confidence intervals.
Discussion
In this study, we have found an association between functional outcome at 6 months and HRQoL up to 18 months and survival and costs up to 36 months. The impact of functional status on survival has also been shown by Slot el al. 9 However, the impact on quality of life and costs has not been shown before. We found a clear association between functional status and QALY weights both at 6 months and at 18 months as measured by EQ5D. We also found an increase in health care cost among patients with a poorer functional outcome. If a treatment can shift a patient’s functional outcome from OHS 4–5 to OHS 0–2, the potential benefit could be substantial also in monetary values. This is of importance for the planning of health care and for decision making by clinicians.
The analyses also showed a decrease of costs for functional level OHS 5 compared to functional level OHS 4. This can presumably be explained by the fact that more patients with OHS score 5 live in nursing homes, whereas more patients with OHS score 4 are still in hospital. Nursing homes in Sweden are municipality financed and the cost is therefore not captured in this investigation. We also discovered a difference in costs between men and women within separate functional levels, and this was especially evident in OHS 0, where the costs for men were almost twice as much compared to women. The reason for this might be that males are more often dependent on their spouses with daily chores such as washing, cooking and cleaning etc, and therefore evaluated differently in functional level.19,20 For OHS scores 1–5, on the other hand, we saw a decreased cost for males compared to women. This is possibly explained partly by the fact that we did not include costs for unpaid informal care, which have been estimated to 6 per cent of the total societal cost of stroke. 3 This may have bearings on total costs for men, as more male stroke patients are discharged earlier with a spouse assisting in the daily activities than vice versa. This finding also indicates that stroke care may differ for women and men, both as caretakers of spouses with stroke and as stroke patients. Future studies should be aiming at increasing the understanding of this difference. Interestingly, it has been described by Jonsson et al. 21 that the quality of life of the patient is the most important determinant of the quality of life of the informal carer, thus would interventions aiming at increasing the quality of life for the patient also lower the burden for the informal carer. 21
The regression models showed that despite differences between OHS groups at baseline, this did not have large impact on the differences across groups in costs or HRQoL. Different baseline variables were significant predictors depending on outcome and time period. It seems that OHS group at six months explains most of the variation in costs and HRQoL.
Previous studies on cost of stroke by functional category (mRS) are heterogeneous, and show divergent results.22–25 We found a cumulative cost for OHS 1 of 18,799 Euros at 36 months, and for the OHS 4 level, we show a total cost of 47,985 Euros at 36 months. At 18 months, we found that OHS 3 corresponded to a mean total cost of 29,292 Euros, which is somewhat higher than the 21,324 Euros found in two other studies.26,27 The difference may be explained by the fact that we have used registry-based observations for all health care provided to the patients during the follow-up, and not only costs from institutional care.
The strengths of this study include the long follow-up time (three years) and complete outcome data retrieved from national registers of high quality. In accordance with European stroke Organisation’s guideline, we present functional outcome as a complete ordinal scale including those for patient that died. We also present cost data for individual groups of patients, allowing for future meta-analysis of aggregated data of similarly grouped patients. However, although national registers in Sweden are of high quality there are always limitations in registries such as missing data, incomplete data and incorrect registration. Costs were based on functional level at six months, except in the case of death, although, patients may be at a worse or better state over time. Our method of censoring costs by excluding patients dying in between two visits may have resulted in over- or underestimated mean costs. However, comparing our reported estimates to the mean observed costs of all irrespective of time of death did not change the results by much (less than 13%, details available upon request). Finally, our study does not include all relevant costs from a societal perspective, including primary care, community care, rehabilitation and indirect costs. 5
Conclusion
In conclusion, functional outcome at six months is an important driver for HRQoL, survival and long-term costs after stroke. Effective interventions aimed at reducing short-term disability levels are therefore also expected to reduce the overall burden of stroke. These data can be used in health economic evaluations of treatments for stroke patients.
Footnotes
Acknowledgements
Veronica Murray (deceased in 2014) initiated, planned and obtained funding for this study. We would like to thank Professor Peter Sandercock who participated in the early planning of this study. We also thank Leif Lundstedt and Åke Karlsson at Swedish Associations and Local Authorities for help with the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from AFA Försäkring, Hjärt- och Lungfonden, and STROKE-Riksförbundet.
Informed consent
Written informed consent was obtained from all subjects before the study.
Ethical approval
This study was approved by the local Ethical Board, reference number: 02–551, 2014.
Guarantor
EL.
Contributorship
ASR, EB and EL researched literature, applied for ethical approval, and contributed to the development of the data. All authors contributed to the methodology of the project, and the statistical analysis plan. ASR, AG and PN carried out the statistical analysis, and all authors interpreted the data. ASR wrote the first draft of the manuscript. All authors reviewed, and edited the manuscript and approved the final version of the manuscript.