
Abstract
Introduction
We aimed to evaluate the preferred treatment strategy for patients with symptomatic cerebral cavernous malformations (CCM).
Methods
In a decision model, we compared neurosurgical, radiosurgical, and conservative management. A literature review yielded the risks and outcomes of interventions, intracerebral hemorrhage (ICH), and seizures. Patients with CCM rated their quality of life to determine utilities. We estimated the expected number of quality-adjusted life years (QALYs) and the ICH recurrence risk over five years, according to mode of presentation and CCM location (brainstem vs. other). We performed analyses with a time horizon of five years.
Results
Using the best available data, the expected number of QALYs for brainstem CCM presenting with ICH or focal neurological deficit was 2.84 (95% confidence interval [CI]: 2.54–3.08) for conservative, 3.01 (95% CI: 2.86–3.16) for neurosurgical, and 3.03 (95% CI: 2.88–3.18) for radiosurgical intervention; those for non-brainstem CCM presenting with ICH or focal neurological deficit were 3.08 (95% CI: 2.85–3.31) for conservative, 3.21 (95% CI: 3.01–3.36) for neurosurgical, and 3.19 (95% CI: 2.98–3.37) for radiosurgical intervention. For CCM presenting with epilepsy, QALYs were 3.09 (95% CI: 3.03–3.16) for conservative, 3.33 (95% CI: 3.31–3.34) for neurosurgical, and 3.27 (95% CI: 3.24–3.30) for radiosurgical intervention.
Discussion and conclusion
For the initial five years after presentation, our study provides Class III evidence that for CCM presenting with ICH or focal neurological deficit conservative management is the first option, and for CCM presenting with epilepsy CCM intervention should be considered. More comparative studies with long-term follow-up are needed.
Keywords
Introduction
Cerebral cavernous malformations (CCM) may present with intracerebral hemorrhage (ICH), seizures, or focal neurological deficit (FND) anatomically related to CCM location or may be incidental findings during cerebral imaging for other reasons. 1 The untreated clinical course of CCM is mainly determined by their location and mode of presentation.2,3
Patients with CCM may be managed conservatively accepting the risk of future ICH, FND, or seizure; alternatively, they may be treated with neurosurgical excision or stereotactic radiosurgery with the chance of reducing the risk of future ICH or FND but also with the risk of treatment complications. This risk of treatment complications is mainly determined by CCM location. 4 Until now, it has not been possible to make strong recommendations about CCM management, 5 because randomized controlled trials have not been performed and observational studies have not reliably identified dramatic effects of CCM intervention. 6 In the absence of such evidence, decision analysis may inform CCM management by modeling the outcome of different management approaches based on the best available data. 7
We developed a Markov decision model to compare quality-adjusted life years (QALY) associated with conservative management, neurosurgical excision, or stereotactic radiosurgery for symptomatic CCM, according to their location and mode of presentation.
Methods
Markov model
The model was designed to simulate three patient cohorts: (1) patients with brainstem CCM presenting with ICH/FND, (2) patients with non-brainstem CCM presenting with ICH/FND, and (3) patients presenting with epilepsy. The cohorts differed in the transition probabilities associated with complications and outcomes after intervention and the occurrence and prognosis of ICH or seizures. We did not study incidental/asymptomatic CCM because their mild clinical course 2 seldom creates a dilemma about their management. 5 We grouped patients with ICH or FND because their clinical impact seems to be equal, 8 and many FND may be undetected ICH. 1 We did not study patients with a solitary seizure separately, because 94% of the people presenting with a solitary seizure develop a second seizure 9 and the International League Against Epilepsy classify people with a CCM and solitary seizure as having epilepsy. 3 The model contained four mutually exclusive health states: well with treated or untreated CCM, disabled (after intervention, epilepsy, ICH, or FND), and death (online Figure e-1).
We estimated the risks of symptomatic ICH and seizure freedom following conservative management or intervention and also the risks of death, permanent disability, or complete recovery after ICH, seizures, or complications of intervention.
Published estimates of transition probabilities
Using several electronic search strategies, we systematically reviewed published studies of CCM from the inception of Medline and Embase to December 2016 (online Table e-2), to identify the best available studies supplying the relevant probabilities of events and of transition from one health state to another at each node of the decision trees. All event probabilities, transition probabilities, their parameters, distribution, and references to the studies from which these data were derived are described in online Table e-2.
We included studies if they reported outcomes stratified by CCM location (brainstem vs. non-brainstem) and mode of symptomatic presentation (ICH with or without FND vs. epilepsy) for > 95% of participants with CCM. If key studies did not report data in these categories, we contacted corresponding authors for this information. We selected data from the studies with the least biased design according to the Centre for Evidence Based Medicine's Levels of Evidence (www.cebm.net/wp-content/uploads/2014/06/CEBM-Levels-of-Evidence-2.1.pdf). If more than one study fell in the category with the least biased design, we pooled their results to derive an overall transition probability. Results of studies were pooled based on patients' CCM location and mode of presentation. Rates were derived in events per patient-years, based on the number of included patients and median duration of follow-up in each individual study.
Risk of ICH
The risk of ICH from CCM is determined by its location and mode of presentation. 2 We used different ICH recurrence risks according to the type of intervention. We also used different outcomes for ICH from brainstem and non-brainstem CCM. Models allowed for multiple episodes of ICH and for the decrease in risk of the first recurrent ICH over time during conservative management by using the published estimates. 2 For subsequent recurrent ICH, we used the estimate of the ICH recurrence rate in the model's first cycle and the median of the published estimates of ICH recurrence rate in years 2 to 5 for all subsequent cycles of the model.
Risk of seizures
We used different seizure freedom rates, immediately following intervention and for the years thereafter, for the three management strategies. We also estimated the seizure risk of non-brainstem CCM initially presenting with ICH/FND.
Risk of complications
We defined complications as transient disability, permanent disability, and death following intervention and estimated their risks according to CCM location, mode of presentation, and intervention strategy.
Risk of death from other causes
We used age-specific mortality rates for 30-year-old persons from Scottish National health tables to estimate the risk of death from other causes. 10
Model assumptions
Probabilities that were not identified by the literature search were estimated using reasonable assumptions. Data from the retrieved articles did not allow us to estimate ICH rates after SRS stratified by mode of presentation, so we used transition probabilities after SRS based only on CCM location for non-brainstem CCM. 11 We assigned the same risk of seizure freedom after SRS and conservative management, because of the lack of data on seizure freedom after SRS. Due to the paucity of information on disability after ICH and seizure caused by CCM, and the lack of a single measure of disability after these distinct outcomes, we assumed that patients were disabled after ICH if their modified Rankin Scale score was ≥3. We also assumed that the outcome after recurrent ICH was the same as after the first ICH and that people with epilepsy who were not seizure free were disabled until they experienced a year of seizure freedom. Due to the same paucity of information, we modeled that a patient could experience either an ICH or a seizure within the same year.
Survey of QoL among patients with CCM
We identified only two studies of quality of life (QoL) for people with CCM (both after intervention).12,13 Therefore, we designed a survey using SurveyMonkey (www.surveymonkey.co.uk) and asked the Cavernoma Alliance UK (CAUK; www.cavernoma.org.uk) patient support organization to contact patient members on 30 November 2016. The survey contained structured questions to characterize their CCM, clinical history, and QoL using the five-level EQ-5D version of the EuroQol. 14 CAUK contacted non-responders by e-mail once and collected final responses on 16 January 2017.
The results provided by CAUK were anonymized, without the possibility to trace back individual patients. We summarized responses stratified by respondents' CCM location, presentation and management, and calculated each group's utility value using the EQ-5D-5L Value Set for England. 15 We used the published estimate of population norms for the utility value of the well health state. 16
Health outcomes
We determined the expected number of ICH recurrences, along with differences in QALYs over five years. QALYs were calculated by multiplying the time a person remained in a certain health state by the utility associated with that particular health state and subsequent summing over all health states. Five-year ICH recurrence risk was estimated from the expected number of first ICH recurrences in the different management arms divided by the total number of simulated persons in these arms.
Statistical analysis
In the Markov model, analyses with a life-time horizon proved impossible due to the lack of data. We used cycles of one year and a total time horizon of five years. QALYs were calculated over the five-year time horizon and are presented as the mean outcomes per patient. Effectiveness was discounted at 3.5%, as recommended. 17 We applied half-cycle corrections to all models. Significance was assumed if there was no overlap in the confidence intervals of QALYs between the different strategies. We performed probabilistic sensitivity analysis using Monte Carlo simulations of 10,000 patients per model, to evaluate the effect of varying the input parameters over the ranges given in online Table e-2. We used analysis of covariance methods (ANCOVA) to assess the contribution to the variance of incremental QALYs of individual input parameters for all variables. This allowed us to determine which input parameters contributed most to the variance of incremental QALYs in each model. Determining whether variables for which assumptions had been made had a considerable contribution to the variance in QALYs allowed us to establish the robustness of the model to these assumptions. We used SPSS Statistics (version 22.0.0.1, IBM) to estimate and compare variable frequencies and distributions, TreeAge (Pro 2017, R1.0. TreeAge Software, Williamstown, MA) to model outcomes for each decision tree and perform the sensitivity analyses and R (version 3.3.0, package earth) to perform the ANCOVA.
Patient consent and ethical approval
Before designing the survey, we used a decision tool from the UK Health Research Authority (HRA, https://www.hra.nhs.uk/approvals-amendments/what-approvals-do-i-need/) to check whether HRA or ethical approval would be needed. The UK HRA standards deemed there was no need for HRA or ethical approval. The survey was approved and conducted by the Executive Committee of CAUK. The results provided by CAUK were anonymized, without the possibility to trace back individual patients. Patients provided informed consent for their anonymized information to be published in this article when responding to the survey.
Results
Survey
From the 761 CCM patients invited to complete the survey, 207 (27%) responded. We excluded eight incomplete responses and another 59 because they had a spinal cavernous malformation or asymptomatic CCM. We estimated utility values for each model (Figure 1) according to CCM location and mode of presentation from subgroups of the included 140 adults with CCM (characteristics described in online Table e-3) who provided responses.
Quality of life (utility values derived from the EQ-5D-5L index score) completed by 140 patients who responded to the survey, stratified by CCM location, mode of presentation, and receipt of any CCM intervention. The thick horizontal bars indicate the median. The height of the box corresponds to the difference between the 75th and 25th percentiles (i.e., the interquartile range [IQR]). Circular outliers are values between 1.5 and 3 IQRs from the end of a box. Asterisked outliers are values >3 IQRs from the end of a box. There was no statistically significant difference in median utility values between groups (Kruskal–Wallis test p = 0.264). ICH: intracerebral hemorrhage.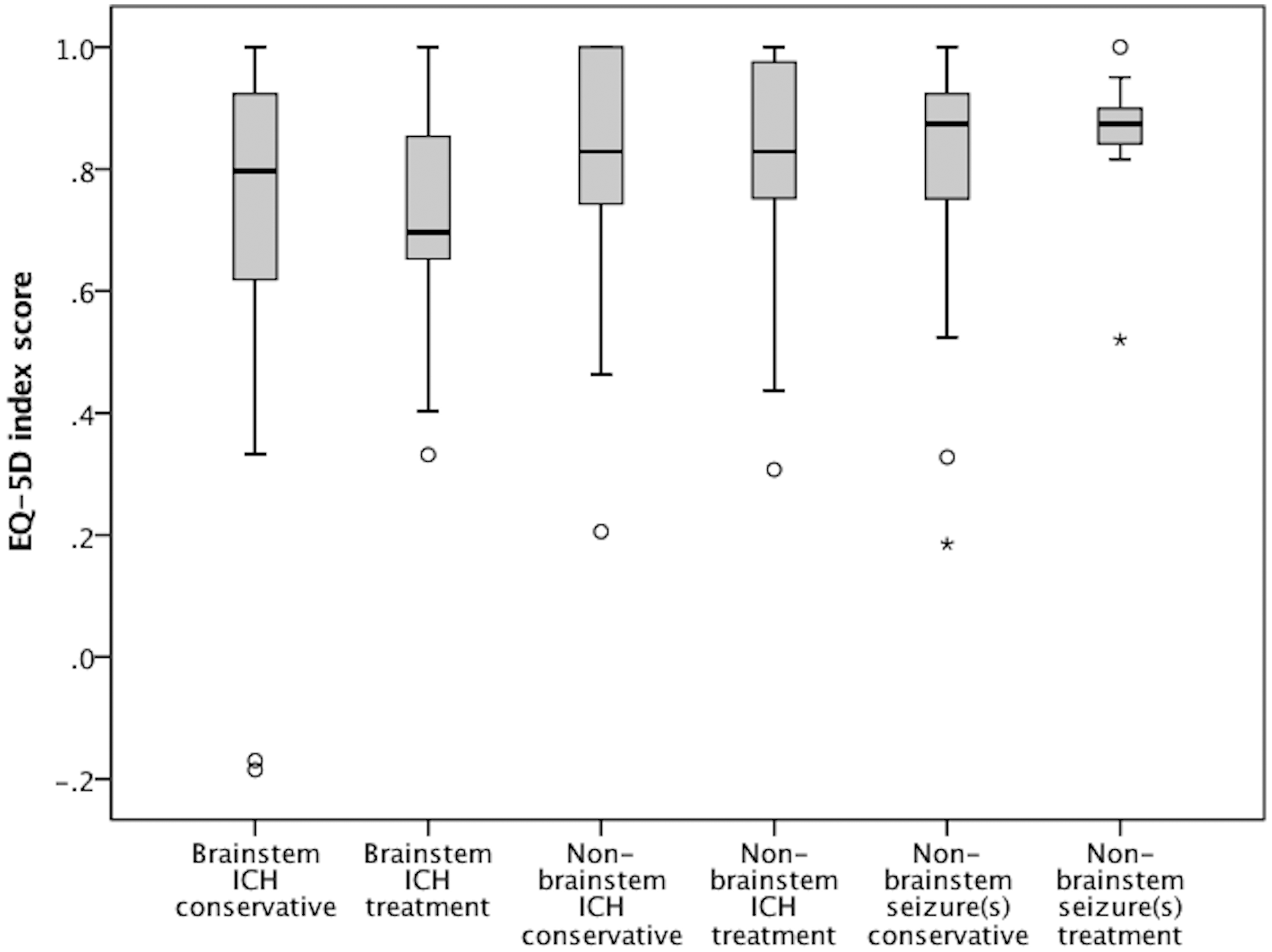
New episodes of ICH
Five-year outcomes (mean of 2000 iterations in simulated cohorts of 10,000 adults with symptomatic CCM) stratified by CCM location, mode of presentation, and type of management
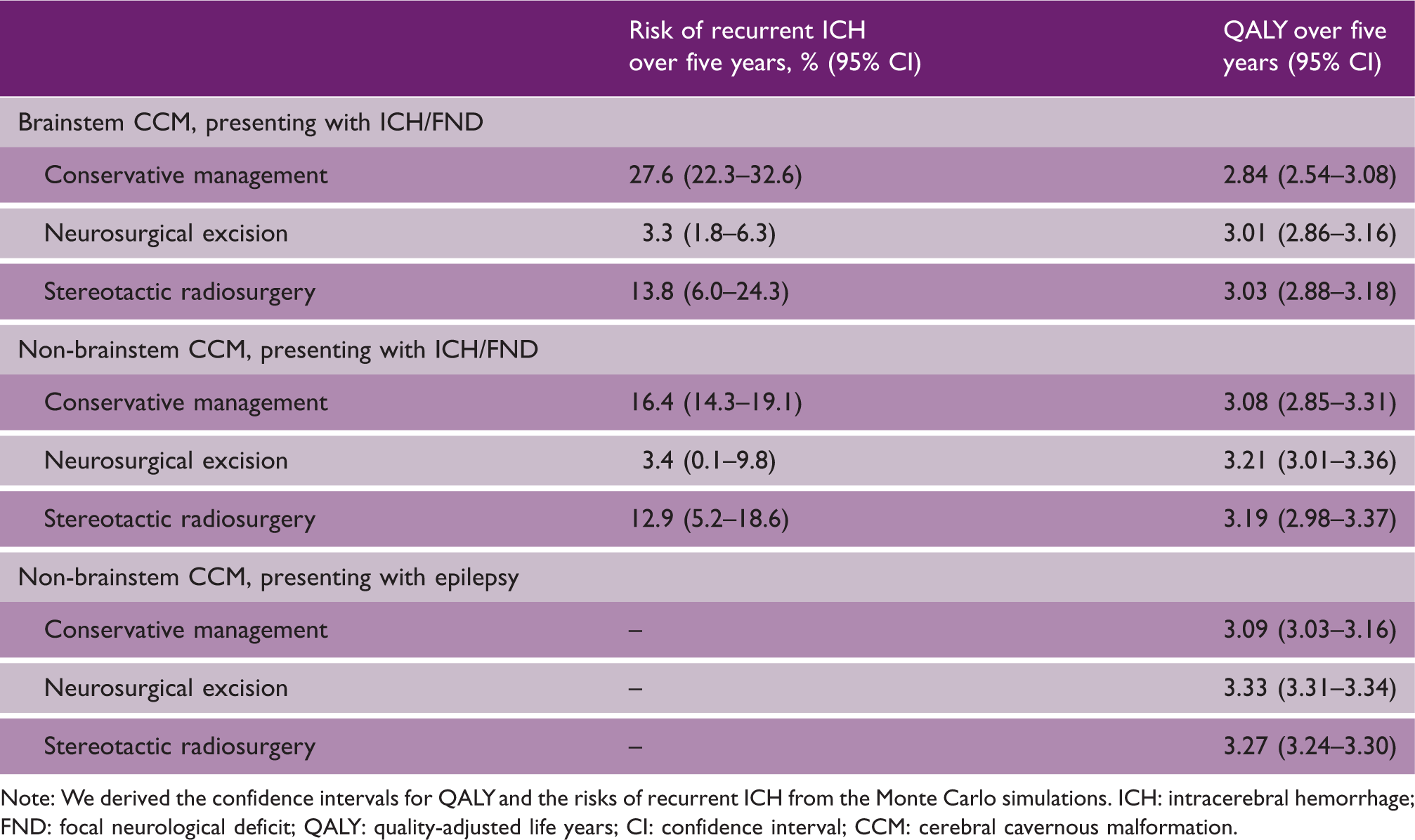
Note: We derived the confidence intervals for QALY and the risks of recurrent ICH from the Monte Carlo simulations. ICH: intracerebral hemorrhage; FND: focal neurological deficit; QALY: quality-adjusted life years; CI: confidence interval; CCM: cerebral cavernous malformation.
QALYs
For persons presenting with ICH/FND, despite differences in the risk of recurrent ICH over five years, there were no statistically significant differences between management strategies in QALYs over five years, regardless of CCM location (Table 1). For persons presenting with epilepsy, intervention was superior to conservative management and neurosurgical excision was superior to radiosurgery.
Sensitivity analyses
The results of the ANCOVA showed that for brainstem CCM, the case fatality following ICH is the most important for explaining uncertainty of incremental QALYs gained with neurosurgical or radiosurgical intervention compared to conservative management. The ICH rate in the first two years following radiosurgery is the most important for explaining uncertainty of incremental QALYs gained between radiosurgical and neurosurgical intervention.
For non-brainstem CCM, the case fatality after ICH and the utility after intervention are for CCM the most important for explaining uncertainty of incremental QALYs gained with neurosurgical or radiosurgical intervention compared to conservative management. Utility after intervention is the most important for explaining uncertainty of incremental QALYs gained between radiosurgical and neurosurgical intervention.
For CCM presenting with epilepsy, utility after conservative management and after intervention for CCM are the most important for explaining uncertainty of incremental QALYs gained with neurosurgical or radiosurgical intervention compared to conservative management. The utility after CCM intervention is most important for explaining uncertainty of incremental QALYs gained between radiosurgical and neurosurgical intervention.
Discussion
This decision analysis showed that outcomes over five years were similar for all strategies for brainstem and non-brainstem CCM presenting with ICH or FND, despite the decrease in ICH rates after intervention. Outcomes were better after neurosurgical or radiosurgical intervention compared to no intervention for CCM presenting with seizures. Variance in these models' estimates was most affected by estimates of case fatality after ICH and the utility value for disability.
This is the first decision analysis for the management of CCM. Our findings are consistent with the few previous comparative studies of outcome after CCM intervention or conservative management, some of which have found benefits associated with CCM intervention, and others have found harms. 4 The better outcomes associated with intervention in CCM presenting with seizures we found, concurs with emerging comparative observational studies. Our data show that the gain in QoL is not only statistically significant but also clinical relevant, with an additional three months of good QoL gained within the initial five years after intervention.
Study summary
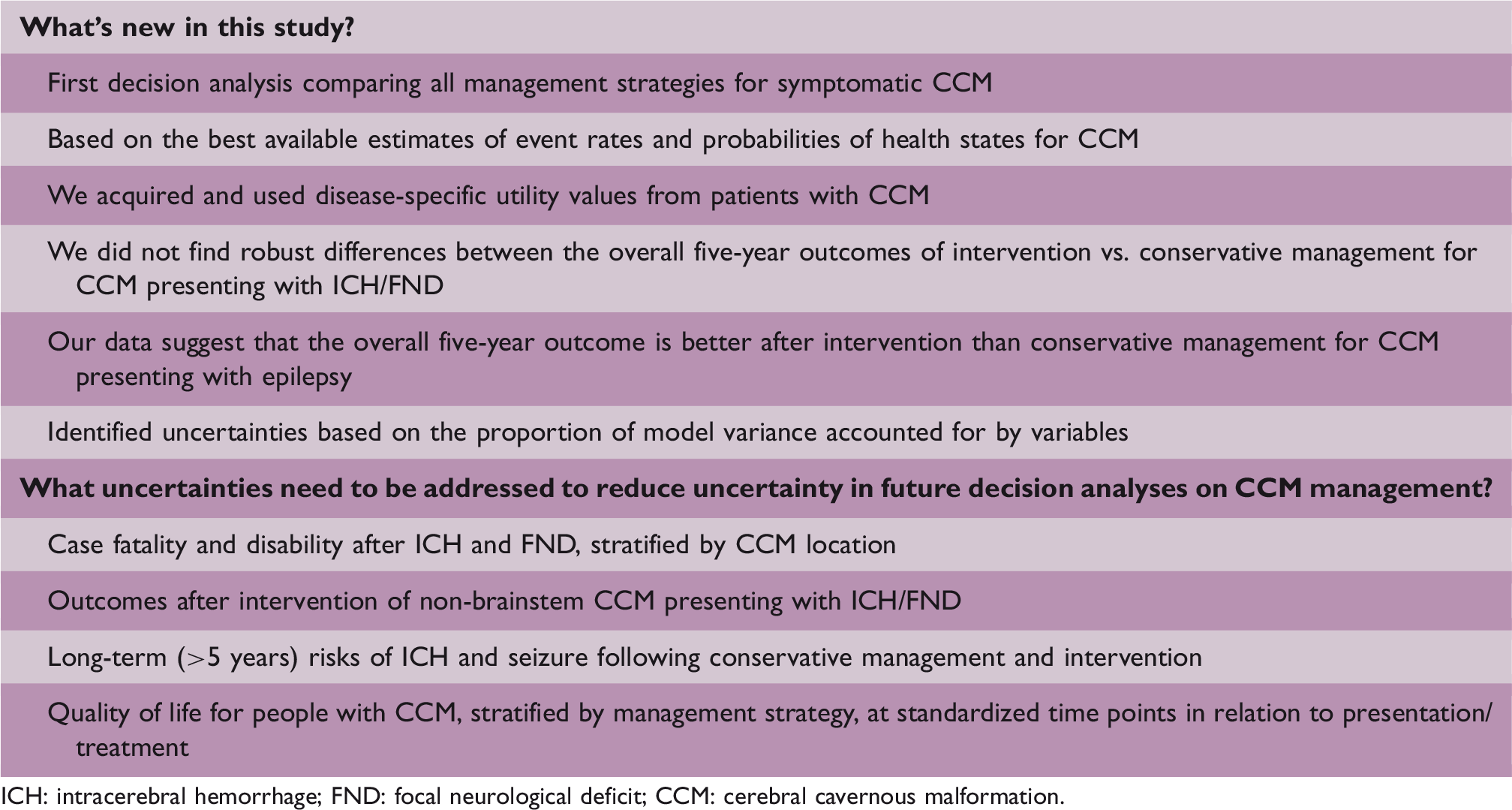
ICH: intracerebral hemorrhage; FND: focal neurological deficit; CCM: cerebral cavernous malformation.
For clinical practice, our data can be used to inform patients about the effects of the different management strategies for the initial five years after the CCM has become symptomatic and to inform patients on the lack of data for effects after these initial five years. Because we were unable to determine a consistently superior management strategy for CCM presenting with ICH or FND, we interpret the results of our study as Class III evidence that for these CCM conservative management in general is the first option. For CCM presenting with epilepsy, our data provide Class III evidence that both CCM interventions are superior to conservative management which concurs with emerging comparative observational studies. 19 It should be kept in mind, however, that this conclusion is based on results from analyses with a five-year time horizon, and not with a remaining life-time horizon.
For future research, implications are that several estimates of outcome – especially QoL – remain to be determined. More robust data are required for estimates that were shown to be most important in explaining the variance in QALYs between the different management strategies. More studies comparing management strategies for CCM are required to test the hypothesis that intervention is superior to conservative management in certain sub-groups of patients. Because of the lack of convincing effects in existing observational studies and this decision analysis, a randomized controlled trial would be the ideal study design to determine the most effective management strategy for CCM by mode of presentation and location. More data on long-term seizure risk after conservative management or intervention are needed for CCM presenting with seizure(s). More comparative studies for CCM presenting with ICH/FND are needed to estimate treatment effects on QoL, which would be useful as input for future randomized controlled trials.
Supplemental Material
Supplemental material for Radiosurgical, neurosurgical, or no intervention for cerebral cavernous malformations: A decision analysis
Supplemental Material for Radiosurgical, neurosurgical, or no intervention for cerebral cavernous malformations: A decision analysis by Leon A Rinkel, Rustam Al-Shahi Salman, Gabriel JE Rinkel and Jacoba P Greving in International Journal of Stroke
Footnotes
Acknowledgments
The authors are grateful to the members of Cavernoma Alliance UK for assisting with the survey of QoL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.