
Abstract
Introduction
Cervical artery dissections may be preceded by mechanical trigger events, often related to sports.
Methods
Using the MEDLINE database, we identified case reports and case series of sports-related cervical artery dissections. Information of the type of sport, age and gender of the patient, affected vessels, associated infarction, time delay, and neurological sequelae were extracted. Demographic and clinical characteristics were compared between sport groups using analysis of variance and Chi square tests. Differences were further assessed with adjusted post hoc tests and homogenous subsets.
Results
A total of 115 reports describing 190 patients with cervical artery dissections related to 45 different sports were identified. The mean age of all patients was 35 years; 26% of all patients were women. Anterior and posterior circulation, as well as left and right side were affected with similar frequency. Patients belonging to different sport categories differed significantly with regard to age (p < 0.001), gender (p < 0.001), and affected circulation (anterior vs. posterior, p = 0.02). The posterior circulation was most often affected in golf players (88%) and least often in individuals engaging in exercise (23%) and scuba divers (29%). Laterality (left vs. right) and mortality were similar between sport groups.
Discussion
We performed a comprehensive review and analytical evaluation of case reports describing patients with cervical artery dissections after sport. Confirmation of our findings in prospective studies is needed.
Conclusion
Cervical artery dissection has been described in relation to a wide variety of sports. The risk of injury to particular neurovascular structures may depend on the type sport involved. Discipline-specific incidence rates are not known.
Keywords
Introduction
Cervical artery dissection (CAD) is a rare cause of ischemic stroke in the general population. It occurs with an annual incidence of 2.5–3/100.000 1,2 and affects predominantly younger individuals. 3 In patients between 15 and 45 years, it accounts for approximately 20% of all causes of ischemic stroke. 4 CAD can be associated with non-trivial neck trauma such as is seen in motor vehicle accidents, or occur spontaneously. 3 Patients with CAD were found to have sustained neck trauma within one month prior to first symptoms of dissection in 41% of cases. This included sports-related trauma in 6% of cases. 5 Most of those were mild and it is unclear whether or how often the association between mild trauma and CAD is coincidental rather than causal. Thus, in the context of CAD, mild trauma should more precisely be referred to as potential mechanical trigger events. 5 Over the last decades, a growing number of case reports describing patients with CAD that have occurred in relation to sport have been published. Among sports-related CAD, it is unclear whether characteristics of sports matter with regard to site of CAD, or age and gender of affected patients. The degree of, and motivations for, regular participation in sports differs between men and women6–8 and changes with age. 9 Additionally, different sports vary widely in their dynamic and static components and in their risk of impact. 10 We therefore hypothesised that demographic characteristics (age, gender) and clinical manifestations (affected vessels, outcome) of CAD in relation to sport depend on the type of sport involved.
Methods
Study design
Our study consists of two parts. For the first part, we conducted a comprehensive review of the literature. In December 2016, we performed a literature search using the Medline database to identify case reports and case series of patients with CAD that were considered by the authors of the original publication to have occurred in relation to sport. No restriction with regard to publication date was applied. All reports for which at least an English abstract was available online were included in the analysis. Search parameters included the MESH-terms ‘cervical artery dissection’, ‘vertebral artery dissection’ and ‘athletic injuries’ as well as ‘sport’, ‘sports’, and the names of specific sport disciplines (‘soccer, ‘volleyball’, etc.) represented by sportaccord, the umbrella organisation for all Olympic and non-Olympic sport federations. 11 Following the Council of Europe’s definition laid out in the European Sports Charta, 12 we did not include sports primarily involving the mind (such as chess or go), motorised sports, and electronic sports. Bibliographies of identified articles were used to identify further publications. For identified cases, the following parameters were extracted from the reports: age; gender; type of sport preceding CAD; symptoms; location of vascular pathology; presence and anatomic location, or absence, of associated ischemic infarction; time of onset of stroke symptoms; and neurological sequelae.
For the second part, we combined patients described in the identified case reports that had engaged in the same or similar activities into groups of at least 10 patients each and compared demographic and clinical variables between groups.
Statistical analysis
Nominal data are presented as proportion and continuous data as mean with 95% confidence interval (calculated using Wilsons’s method for proportions 13 ). Proportions were compared to the hypothesised proportion of 0.5 using an asymptotic one-sample binomial test. If multiple one-sample tests were performed, the significance level was adjusted using the Bonferroni method. Between-group differences of continuous variables were assessed using univariable analysis of variance with Tukey’s Honestly Significant Difference (HSD) post hoc test and analysis of covariance, as appropriate. The normality assumption was confirmed by one sample Shapiro-Wilk test. Equality of variances was assessed using Levene’s test. Nominal data were compared using Fisher’s exact Chi square test with Bonferroni-corrected post hoc pairwise comparisons. A two-sided p value of less than 0.05 was considered statistically significant. Data were analysed with IBM SPSS Statistics version 21 (IBM Corp.; Armonk, NY, USA) and MATLAB (Mathworks, Inc.).
Results
Types of sport described to have preceded CAD (n = 190).

Indicates which types of sports are included in between-group analyses (all groups with at least 10 cases). ‘Yes’: forming a main group, ‘(+)’: part of main group, ‘−’: not included in further analysis, ‘/’: some of its constituents are included in between-group analyses.
CAD: cervical artery dissections.
Demographic and clinical characteristics of all sport-related CAD cases (n = 190).
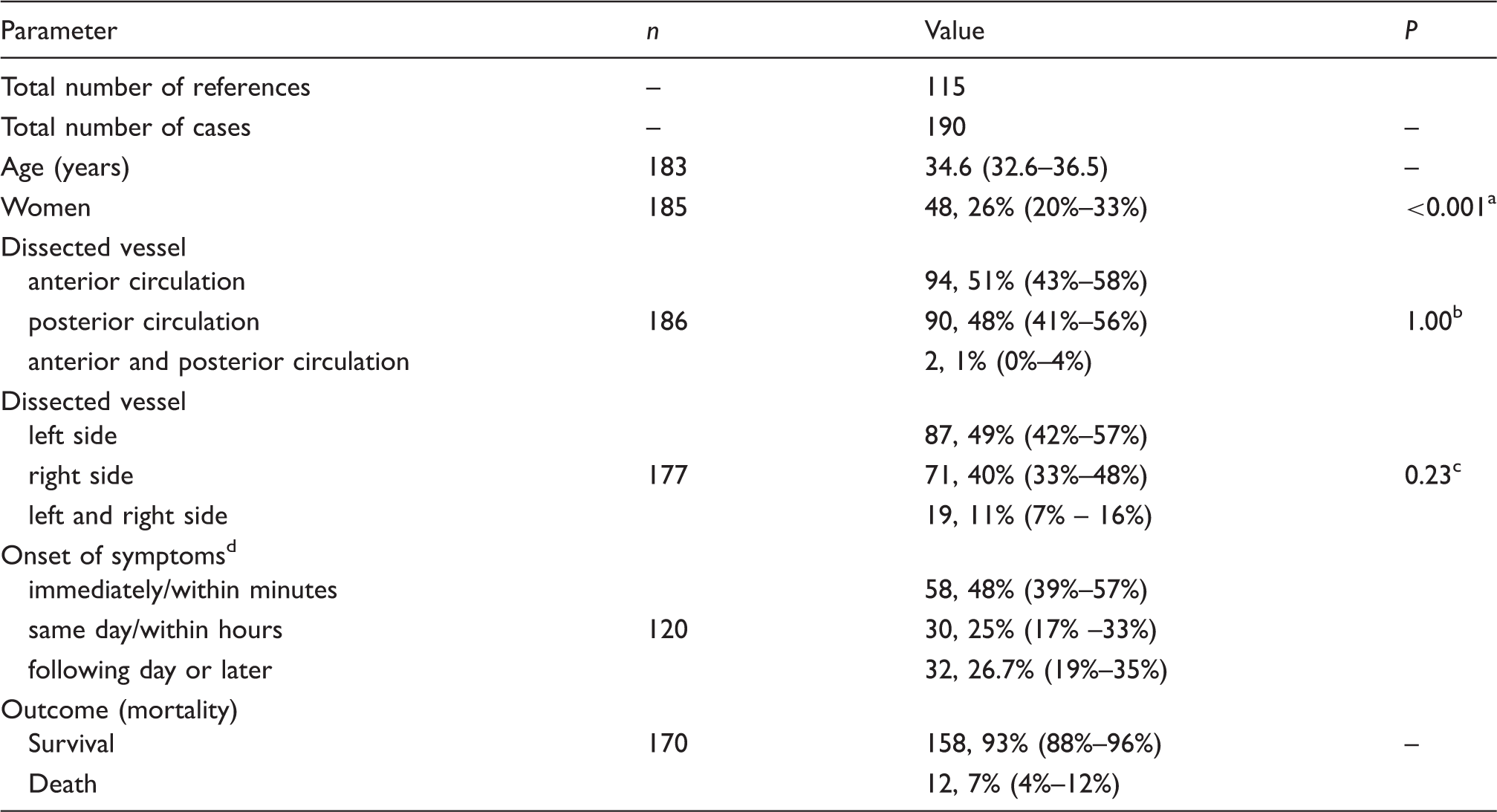
Note: Continuous data are displayed as mean (95% confidence interval). Categorical data are displayed as absolute number and proportion (95% confidence interval).
Null hypothesis: category ‘woman’ occurs with probability of 0.5.
Null hypothesis: equal probability for ‘anterior circulation’ and ‘posterior circulation’.
Null hypothesis: equal probability for ‘left side’ and ‘right side’.
Onset of symptoms attributable to cerebral ischemia relative to sportive activity.
CAD: cervical artery dissections.
We identified eight categories of sports with at least 10 cases reported. Thereby, a
total of 116 patients were included in further analyses (Table 1). Mean age was significantly
different between sport categories
(p < 0.001). Age was lowest in the group of
patients that suffered a dissection while playing football (21.4 years
[13.1–29.7 years]) and highest in the group of golfers (48.3 years
[41.4–55.2 years]). Post hoc tests identified four
homogenous subsets with regard to age: golf players were significantly older than
participants of football, basketball, and combat sports; football players were also
significantly younger than runners, tennis players, and people engaging in
exercise/weight lifting and scuba diving (Figure 1(a)). The proportion of female
patients also differed significantly between groups
(p < 0.001). It was higher than 50%
in only two groups (exercise/weight lifting and running); no female patients
suffering a CAD were reported for football, golf, and combat sports.
Post hoc analysis of homogenous subsets yielded two subsets that showed no
overlap for, and thereby separated, exercise/weight lifting/running on one hand and
golf/combat sports on the other hand (Figure 1(b)). The distribution of anterior
circulation vs. posterior circulation CAD was significantly different between groups
(p = 0.02). This difference remained
significant after adjustment for age
(p = 0.02). Bonferroni corrected post hoc
analyses indicated a significant higher proportion of posterior circulation
dissections in golf players (88% [64%–97%]) than in
exercisers (23% [8%–50%]) and scuba divers
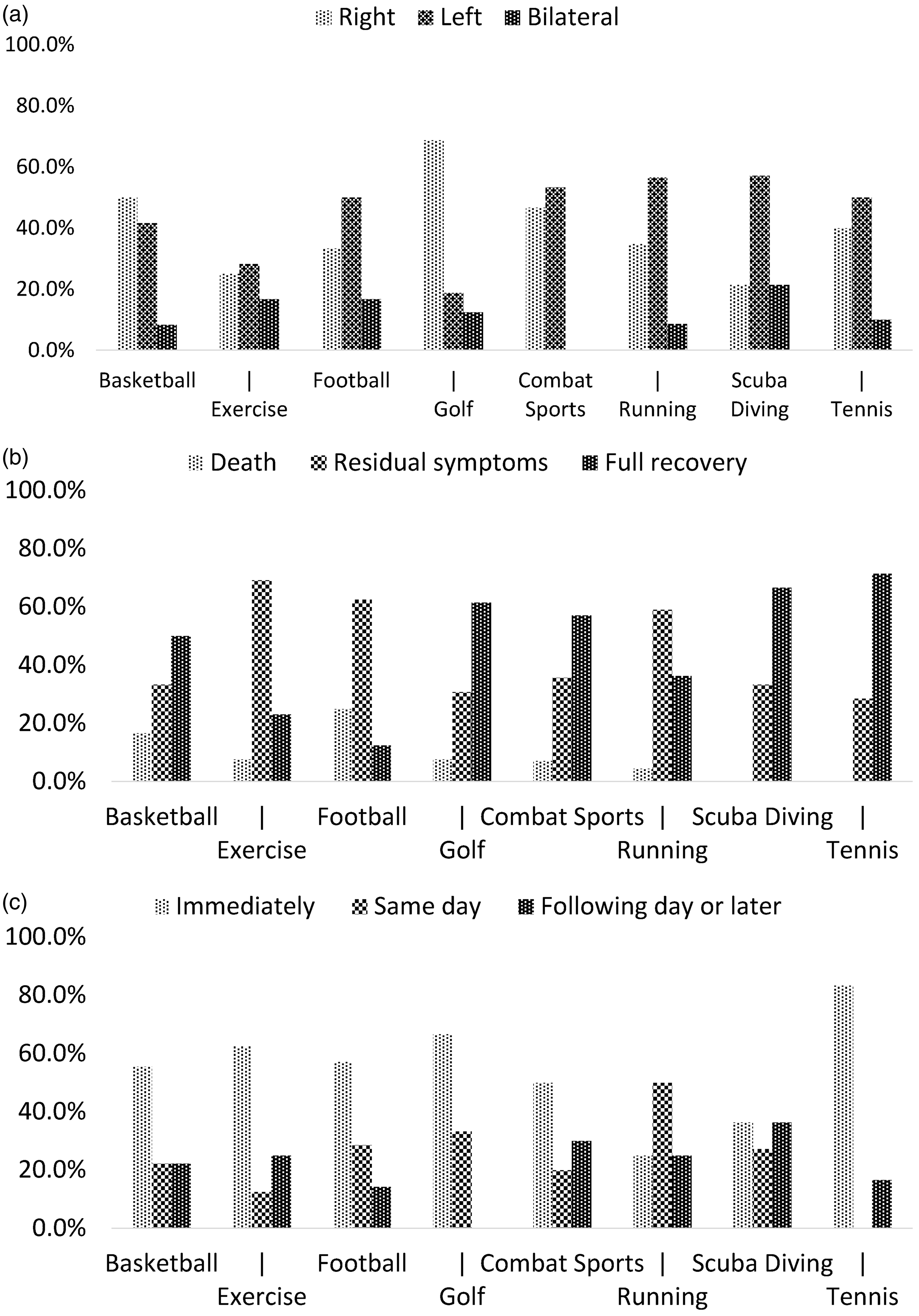
(29% [12%–55%], Figure 1(c)). The left and the right side of
the cervicocephalic vasculature was affected similarly in different sports
(p = 0.29). The outcome after CAD in
relation to sport across the categories ‘death’, ‘residual
symptoms’, and ‘full recovery’ did not depend on the type of
sport preceding the injury (p = 0.51). No
differences between groups were observed with regard to the time interval between
the sportive activity and the onset of stroke symptoms
(p = 0.71). Detailed results of group
specific analyses are presented in Figure 2. Demographic and clinical characteristics of patients
with cervical artery dissection according to type of sport. Side of affected vessels, outcome, and time delay
before stroke symptoms of CAD patients according to type of sport. The
distributions of the side of affected vessels (Panel A), of outcome
(Panel B), and of the time interval between sportive activity and onset
of stroke symptoms (Panel C) were not significantly different between
groups (p > 0.05). CAD stands
for cervical artery dissection.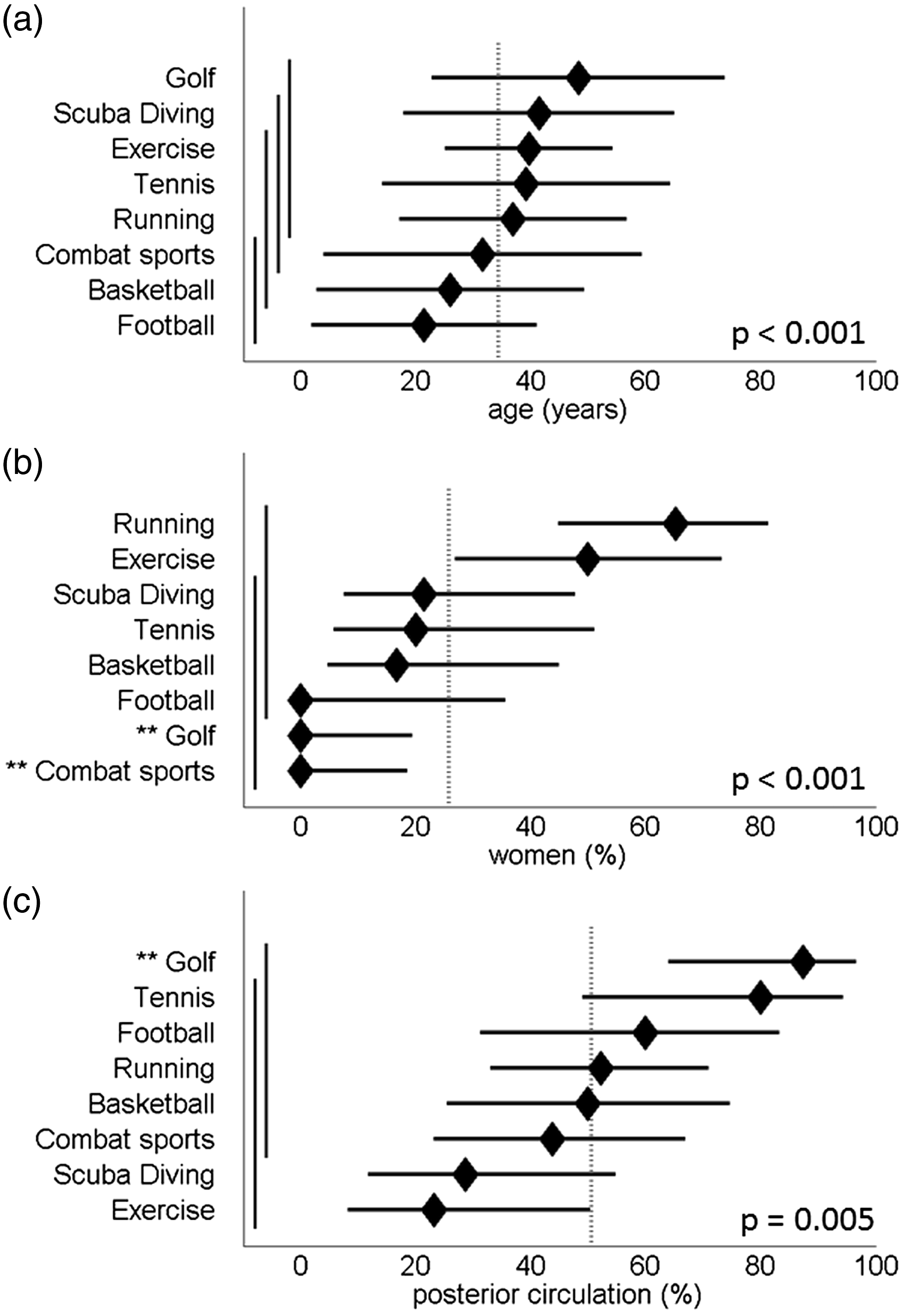
Discussion
Main findings
We provide the most comprehensive collection so far and a systematic analysis of case reports describing patients with CAD in relation to sport. Our main finding was significantly different distributions of posterior vs. anterior circulation CAD in different sports with the highest proportion of posterior circulation CAD in golf and the lowest in exercise/weight lifting and scuba diving. The number of patients being described in the scientific literature varies widely for different types of sport from only 1 (e.g. paddle ball, wrestling) to 23 (running/jogging).
Gender
In agreement with previous findings,130,131 almost 75% of patients in our sample were male. Additionally, our results indicate that gender of CAD patients is distributed unevenly between different types of sports. Questionnaire-based surveys have shown that women and men prefer different types of sport.6,132 Thus, gender differences in the type of sports among patients with sport-related CAD are likely to reflect different degrees of participation in particular types of sports rather than gender-specific vulnerabilities to suffer sport-related dissections of the cervical arteries, although we cannot exclude this possibility.
Age
The mean age of patients analysed in our study was 35 years which is approximately 10 years younger than the mean age reported previously for CAD patients.2,3,133 Higher percentages of younger people as compared to the elderly 132 participating in sport or exercise may be responsible for this difference. Similarly to gender, age of CAD patients was significantly different between types of sport. Participants of basketball and football were approximately half the age of golf players and also significantly younger than scuba divers. In our opinion, these imbalances most likely reflect different age structures associated with different types of sport. Indeed, golf and scuba diving require substantial financial resources for training, certification, purchase of equipment, green fees (for golfing), and associated travel. As financial means tend to accumulate with age, 134 these types of sport may be less popular among younger people and may be preferentially performed by older people. 135 Younger individuals, on the other hand, may more often engage in sports like basketball, football, and exercise which are often taught in school, are associated with less costs, and form an integral part of college life in many countries.
Site of vascular injury
The site of vascular injury may vary according to the type of sport. For example, as noted previously by Choi et al, 57 golfers tend to have CAD in the posterior rather than in the anterior circulation and predominantly on the right side. The authors suggest that rotational forces on the vertebral arteries that occur during the swing may be responsible for this observation. Our analysis adds further evidence to the presumption that sport-specific mechanisms of injury translate into an unbalanced distribution of damage to cervical vessels. Data by Metso et al. 136 suggest that the proportion of vertebral artery dissection as opposed to internal carotid artery dissection may increase with age. In our study, however, there was no association between CAD location and age, and adjustment for age did not account for the variation of CAD location (anterior vs. posterior) between types of sport. If it is true that participation in specific sports is associated with an increased risk of injury of particular neurovascular structures, this could serve as guidance for the development of better protective gear, the introduction of safer techniques, and adaptions to the rules of the sport with the ultimate goal to minimise long-term morbidity and mortality. From a clinical point of view, it may also be relevant to include this information when counseling patients diagnosed with spontaneous CAD about possible trigger factors.
Parameters not included in the analytical evaluation
We included the presence and location of ischemic infarctions associated with sport-related CAD in our individual case descriptions. However, because of large heterogeneity in the methodological ascertainment of ischemic infarction (clinical, CT, MRI, craniotomy, autopsy) no descriptive analyses and between-group comparisons were possible. Similarly, we found that the occurrence of cardiovascular risk factors such as arterial hypertension, atherosclerosis, dyslipidemia, atrial fibrillation, and diabetes mellitus as well as the results of investigations for rarer connective tissue disorders such as Ehlers-Danlos syndrome, Marfan syndrome, or Osteogenesis imperfecta were reported inconsistently in the literature. Only one case report described a patient with a proven connective tissue disorder: a 35-year-old women who suffered bilateral vertebral artery dissections in relation to scuba diving and was diagnosed with a mild phenotypic variant of osteogenesis imperfecta. 17 Recent studies have shown that patients with CAD often have clinical features of connective tissue abnormalities 137 but rarely meet criteria for established hereditary connective tissue diseases.137,138 Furthermore, most publications included in our study did not contain specific information about the presence or absence of migraine, which was recently suggested to be a synergistic factor in the pathogenesis of CAD in young stroke patients. 139
With regard to anatomical parameters, it has been noted that arterial tortuosity is more prevalent among CAD patients than among matched controls.140–142 Whether the degree of arterial tortuosity reflects underlying risk factors such as (undiagnosed) connective tissue disease or represents an additional independent risk factor, e.g. by negatively affecting blood flow hemodynamics and wall shear stress, is uncertain. Similar to the clinical parameters mentioned earlier, case reports used for this study did not systematically report the degree of vascular tortuosity of their patients. None withstanding, it can be hypothesised that this risk factor also increases the likelihood of suffering a CAD after sport-related mechanical trigger events.
Limitations
We are aware of the following limitations: First, the design of our study does not allow to make inferences about incidence rates. Indeed, such a calculation would require detailed information about the number of individuals participating in each sport, stratified by country (popularity of each sport may differ from region to region) and time period. There may have been additional sources of distortion stemming from publication bias, recall bias, and geographic variation in the availability of diagnostic modalities needed to identify CAD. Second, we do not have data on the risk of recurrent dissection after a sports-related CAD. Third, the comparative analysis with regard to the site of vascular injury has limited topographical resolution with regard to the segments of the vertebral and internal carotid arteries involved (V1–V4 and C1–C7, respectively). Last, the case reports we included in our analytical evaluation described patients who suffered a CAD in temporal association with engagement in sports; inherent to the methodology of case reports, a causal relationship could not be established.
Conclusion
We used an analytical approach to systematically evaluate the currently existing evidence regarding sports-related CAD in the form of case reports. We found that age, gender, and the site of vascular injury differ between types of sports. Well-designed prospective studies are needed to gain a better understanding of the incidence and the clinical characteristics of CAD that occur in relation to individual sports.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ludwig Schlemm is participant in the BIH-Charité Clinical Scientist Program funded by the Charité – Universitätsmedizin Berlin and the Berlin Institute of Health.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
LS.
Contributorship
LS conceived the study, researched the literature, performed the data analysis, interpreted the data, and wrote the first draft of the manuscript. MEn and MEb were involved in conceiving the study, searching the literature, and interpretation of the data. CHN and STE were involved in searching the literature. Additionally, all authors critically reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.