
Abstract
Purpose
A substantial number of patients without a history of atrial fibrillation who undergo surgery develop one or more episodes of atrial fibrillation in the first few days after the operation. We studied whether postoperative transient atrial fibrillation is a risk factor for future atrial fibrillation, stroke and death.
Method
We performed a narrative review of the literature on epidemiology, mechanisms, risk of atrial fibrillation, stroke and death after postoperative atrial fibrillation. We reviewed antithrombotic guidelines on this topic and identified gaps in current management.
Findings
Patients with postoperative atrial fibrillation are at high risk of developing atrial fibrillation in the long term. Mortality is also increased. Most, but not all observational studies report a higher risk of stroke. The optimal antithrombotic regimen for patients with postoperative atrial fibrillation has not been defined. The role of lifestyle changes and of surgical occlusion of the left atrial appendage in preventing adverse outcomes after postoperative atrial fibrillation is not established.
Conclusion
Further studies are warranted to establish the optimal strategy to prevent adverse long-term outcomes after transient, postoperative atrial fibrillation.
A substantial number of patients without a history of atrial fibrillation (AF) who undergo surgery develop one or more episodes of AF in the first few days after the operation. This condition is termed postoperative AF or postoperative atrial fibrillation (POAF). Up to 90% of these episodes resolve spontaneously. A widely held belief is that POAF is benign and has no long-term consequences.1–3 However, recent studies indicate that transient POAF is a risk factor for development of future AF, stroke and death up to several years after the procedure. These are the focus of this review.
Whether the increased stroke and mortality rates are directly related to thromboembolism due to recurrent AF or a higher baseline cardiovascular risk is not established.
Furthermore it is unclear if anticoagulation should be recommended in these patients. The 2016 ESC Guidelines on AF do not provide specific recommendations on type and duration of anticoagulation after POAF, apart from the general weighing of pro-thrombotic and bleeding factors, illustrating the absence of reliable data and evidence. 4
POAF: Epidemiology and pathophysiology
POAF is a common occurrence after cardiac and non-cardiac surgery. The type of surgery is an important determinant with the highest rates reported with combined valve and coronary artery procedures (up to 55%) or isolated coronary bypass surgery (20–40%), intermediate rates after thoracic, non-cardiac surgery (10–20%) and the lowest rates after general, non-thoracic, non-cardiac surgery (0.37–1%).5–8 The incidence of detection of AF is highest on day 2 after surgery. 7 Up to half of the AF episodes recur, usually within days of the first episode. 7 Only 5–10% of patients are discharged with persistent AF.9,10 Symptomatic recurrences prompting medical attention are however infrequent in the first six weeks after discharge.2,11
Multiple risk factors for POAF have been described.12,13 These include type of operation, advanced age, obesity, male gender, prior myocardial infarction (MI) or heart failure, left atrial enlargement, left ventricular hypertrophy or aortic atherosclerosis and intraoperative characteristics including clamp time, pump use and bypass time. In contrast, POAF is reduced by peri- and postoperative medication including betablockers and amiodarone.
The mechanisms involved in POAF development are poorly understood. A multifactorial threshold model is currently favoured where multiple acute and chronic factors synergistically interact to ultimately exceed a POAF ‘threshold’. 14 The acute predisposing factors are directly related to the surgery and include surgical manipulation of the heart itself, intraoperative pharmacological and haemodynamic changes, postoperative inflammation, reperfusion injury with oxidative stress and postoperative increased sympathetic tone promoting ectopic activity and altering atrial refractoriness. Chronic predisposing factors are related to preexistent structural heart changes due to ageing (the most important risk factor for AF) and underlying heart disease, such as atrial fibrosis and atrial enlargement which create a substrate for POAF. Arguments favouring the presence of a preoperative arrythmogenic substrate include the perioperative induction of AF by stimulating the atrium in patients who develop POAF, increased rates of atrial myolysis in the preoperative biopsies of patients, a genetic predisposition to AF and upregulation of specific genes in atrial tissue of patients who developed POAF after coronary artery bypass grafting (CABG).15–18
Early antithrombotic management of AF is heterogeneous with some centres using short-term anticoagulation in case of prolonged (48 or 72 h) or recurrent AF or when cardioversion is needed to stop the arrhythmia, whereas others only treat persistent or permanent AF with anticoagulation. 19 In guidelines POAF is cited as a reversible cause of AF warranting only limited, temporary (4 weeks to 3 months) anticoagulation when sinus rhythm is restored.20–24 Other guidelines do not specify the length of anticoagulation.4,25,26 Cardiac tamponade and pericardial bleeding are often cited as reasons not to use anticoagulation more widely, and may be a specific reason for some not to opt for NOAC or vitamin K antagonists in this setting. 19
POAF has been associated with multiple adverse early outcomes like prolonged admission, early stroke, MI, return to theatre and other adverse events.7,8,27
Long-term consequences of POAF
Summary of outcomes after postoperative atrial fibrillation (POAF).
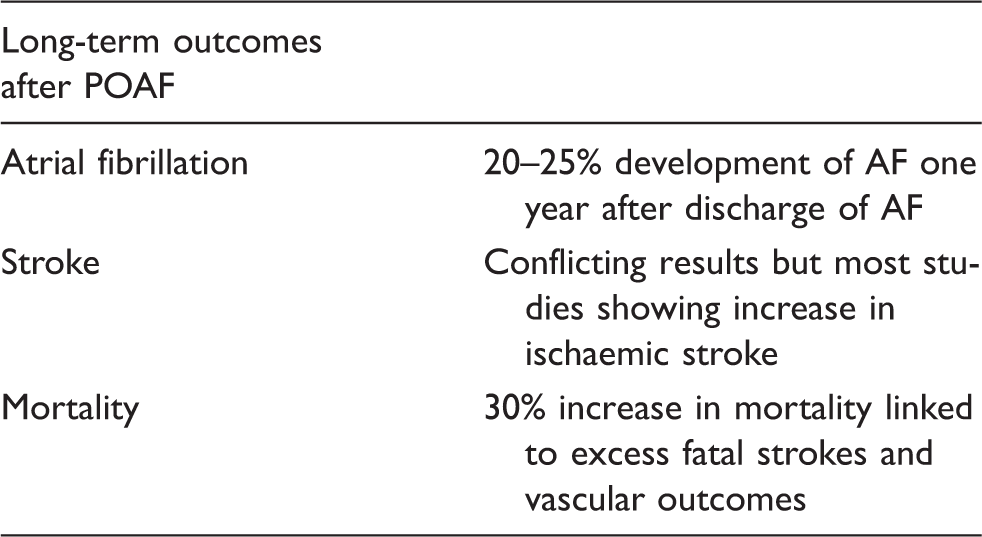
Recurrent AF
Although clinically obvious recurrences are infrequent in the first weeks, POAF portends future AF in the longer term.28–31 In a population based study that analysed AF associated with secondary precipitants (31% had cardio-thoracic surgery), up to 25% of the patients developed recurrent AF within two years. 30 A study from the USA found a cumulative frequency of post-discharge AF for which admission or emergency department presentation was required at one year of 22% in patients with an episode of POAF. 29 POAF was associated with a five- to eight-fold increase in development of future AF, compared to patients without POAF.32,33
Stroke
POAF has been associated with long-term risk of stroke in most studies. In some of these studies no distinction was made between ischaemic and haemorrhagic strokes, and most of the ischaemic strokes were not classified according to etiologic subtypes. The six-month stroke rate was doubled in a multicentre series of POAF after cardiac surgery. 34 In a very large study on POAF after cardiac surgery, the rate of ischaemic stroke was increased with an adjusted hazard ratio of 1.3 after cardiac surgery. Interestingly, ischaemic stroke was even higher with POAF occurring after non-cardiac surgery (hazard ratio of 2.0). 29 A single centre retrospective study of isolated cardiac surgery with extended follow up reported a higher risk of stroke with a hazard ratio of 1.26. 35 Another study reported a doubling of the rate of fatal ischaemic stroke after CABG with POAF. 32 A multicentre study found a fourfold increase in the rate of fatal embolic stroke in patients with POAF after cardiac surgery. 36 In the Framingham study, stroke risks were similar when AF developed in the context of surgery or occurred spontaneously. 30 Four studies, totalling 1766 patients with POAF, however did not show an increased risk of a major adverse cardiac and cerebrovascular events.37–40 A very large Canadian study (n = 18,046) could not identify POAF as an independent risk factor for stroke between discharge and two year follow up (odds ratio (OR) 1.1, 95% confidence interval (CI) 1.0–1.2), although a higher risk of stroke or death was found in patients with POAF and higher CHADS2 scores. 41
Increased mortality
An increased mortality rate, persisting up to 17 years after CABG has been reported by several studies after POAF.8,32,36,42–45 A meta-analysis involving 104,946 found increased mortality in patients with POAF with an OR of 1.28 (95% CI 1.19–1.37). 46 The unadjusted mortality rates at three years were 11.3% with POAF versus 6.1% without POAF. In a multiethnic cohort, blacks had substantially higher mortality with POAF. 43 One study found that treatment with warfarin reduced long-term mortality in POAF by 20%, despite the higher risk profile of patients with POAF. 42 Intriguingly, POAF was not found to be associated with increased mortality in patients with combined CABG and valvular surgery.47,48 It was suggested that the increased surveillance in this population, and stricter adherence to anticoagulation may be responsible for this paradoxical result. 47 Most studies did not identify a reason for the increased mortality, as many studies linked to administrative death registers with little information on causes of death. One study found increased rates of fatal stroke, cardiac arrhythmia, heart disease and heart failure. 45 Another reported excess mortality only related to stroke. 36
Detecting recurrent AF after a diagnosis of POAF
The true rate of recurrent AF after discharge is largely unknown. Many episodes of AF likely remain undetected because of short in-hospital monitoring and early discharge. AF was identified on post-discharge wearable recorders in 41/302 (13.6%). 49 Using a transtelephonic loop recorder between day 6 and day 30 after surgery, AF was found in 8.8% of patients. 50 Another study in the immediate post-discharge period found AF in 42% within 30 days of surgery using 4x daily 30 s monitoring strips for 30 days obtained on a smartphone. Another study using self screening with a handheld device found recurrent AF in 58% of POAF patients. Surprisingly, AF was also detected in patients who did not have POAF. 51 The majority of episodes were asymptomatic. 49 52 51 Longer term studies (>30 days) using implantable cardiac monitors have not been performed. It is well established that screening techniques like pulse measurement, serial ECG or Holters may miss relevant episodes of AF because of the often intermittent nature of the arrhythmia. 49 The studies which identified a high rate of AF after POAF used routinely obtained ECG or clinical examination to diagnose AF and likely underestimate the true frequency of AF in this population. POAF may be analogous to intermittent AF after cryptogenic stroke, a situation in which intermittent monitoring techniques have been shown to be poorly sensitive compared to continuous monitoring techniques. 53
Prevention of thromboembolism with POAF
Lifestyle changes
Weight reduction and exercise have been shown to reduce AF symptoms and AF burden in patients with intermittent AF who are candidates for cardiac ablation.54,55 Specific studies in POAF have to our knowledge not been performed and it is unclear whether this strategy reduces thromboembolism.
Antithrombotic regimens after cardiac and non-cardiac surgery
Aspirin is generally recommended after CABG, but has not been tested specifically in patients with POAF.56–58 By nature, atherosclerotic vascular disease is universal in patients undergoing CABG. 58 In addition, aspirin has been shown to substantially reduce the rate of venous graft occlusion in patients who receive a saphenous venous graft. 57 The role of other antiplatelet agents like clopidogrel or other P2Y12 receptor antagonists or dual antiplatelet therapy is less well defined. 56 Anticoagulant-based strategies after CABG have been less well studied than antiplatelets. In a meta-analysis of randomised trials, anticoagulation reduced the rate of venous graft occlusion compared to placebo, but not compared to aspirin. 59 In two small trials, the combination of aspirin and anticoagulants had higher venous graft patency rates than anticoagulants alone.56,59 Given the absence of benefit over aspirin and the higher bleeding risk, anticoagulants are currently not recommended for secondary prevention after CABG. Antithrombotic agents are not recommended after non-cardiac surgery.
Anticoagulation after POAF
A limited number of studies assessed anticoagulation in patients with POAF. Most studies were retrospective, were performed in the immediate postoperative phase and had short-term follow up. In two studies after CABG no clear benefit of anticoagulation emerged in terms of ischaemic stroke prevention and there was no unequivocal temporal relationship between POAF and ischaemic stroke occurrence.60,61 By contrast, a Japanese study found a significant ischaemic stroke reduction with early anticoagulation (in combination with an antiplatelet agent) after POAF and a temporal relationship between POAF and ischaemic stroke occurrence. 62 One observational study found no benefit of anticoagulation with warfarin in patients who had POAF after general thoracic surgery, but most patients had low CHADS2 scores in this population and consequently event rates were low. 63 One large observational study found a significantly reduced long-term mortality risk in patients who were discharged on warfarin after CABG, despite the fact that these patients had a higher rate of congestive heart failure, hypertension, diabetes and hyperlipidemia. 42 Direct oral anticoagulants (DOAC) have not been specifically tested in patients with POAF, as patients with recent cardiac surgery or so called transient causes of AF were excluded in the large randomised trials of DOAC versus warfarin or aspirin.
Mechanical approaches to left atrial appendage closure
Surgical ligation, excision and oversewing or stapling of the left atrial appendage (LAA) are commonly performed to reduce thromboembolism originating in the LAA after CABG or mitral valve surgery. Satisfactory long-term anatomical results are not always achieved. These strategies do not revert the hypercoagulable state associated with AF and do not reduce the risk of emboli originating in the left atrium. Although appealing, it remains unclear if surgical ligation actually reduces stroke risk. A meta-analysis of observational studies suggested a reduction in stroke with LAA closure, but noted that high quality data were lacking. 64 A randomised trial is currently underway to assess whether closure reduces stroke risk on top of usual treatment in patients who undergo cardiac surgery and have a history of AF. 65 Patients with POAF without a history of AF are not eligible for this trial. Endovascular closure of the LAA for POAF has not been studied yet as most of the literature has focused on surgical closure and would expose the patient to an additional procedure.
Remaining questions and conclusions
Further studies are needed to understand the natural history of POAF using modern AF detection techniques. Future studies will also need to identify risk factors that increase the risk of stroke amongst patients with POAF. We also need to better understand the role of lifestyle changes in patients with POAF as prevention of permanent AF may in theory be achieved by intervening on the underlying pathophysiological pathways at its earliest stages. Given the high rate of AF after POAF and the difficulties in detecting AF through reported symptoms or intermittent screening techniques, the role of modern anticoagulants with a safety profile comparable to aspirin needs to be established. The type, timing and duration of early postoperative anticoagulation also deserves study given the postoperative bleeding risk that leaves many physicians hesitant to start anticoagulation. Similarly, the role of surgical intervention to reduce thromboembolic risk in POAF needs to be determined. Addressing these issues may have a significant population health impact as POAF is a common postsurgical event with potentially preventable adverse long-term outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: VT has received honoraria and speaker fees and participated in consultancy boards from Bayer, Daiichi-Sankyo, Medtronic, Pfizer, Boehringer-Ingelheim and Astra Zeneca. OF, RL and GD report no conflicts of interest. HH received consulting and speaker fees from Boehringer-Ingelheim, Bayer, BMS-Pfizer, Daiichi-Sankyo, Cardiome, Merck and Biotronik.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable
Informed consent
Not applicable
Guarantor
VT.
Contributorship
VT researched literature and conceived the study. VT wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Authors’ note
RL is a senior clinical investigator of FWO Flanders.