
Abstract
Introduction
Although several study protocols reported that vertebral artery hypoplasia can predispose to posterior circulation ischaemia, the role of vertebral artery hypoplasia in the risk of posterior circulation ischaemia still remains controversial. The aim of the present meta-analysis was to investigate the association of vertebral artery hypoplasia and posterior circulation ischaemia.
Patients and methods
We performed a systematic review and random effects meta-analysis of all eligible observational study protocols reporting prevalence rates of vertebral artery hypoplasia in patients with anterior circulation ischaemia and posterior circulation ischaemia.
Results
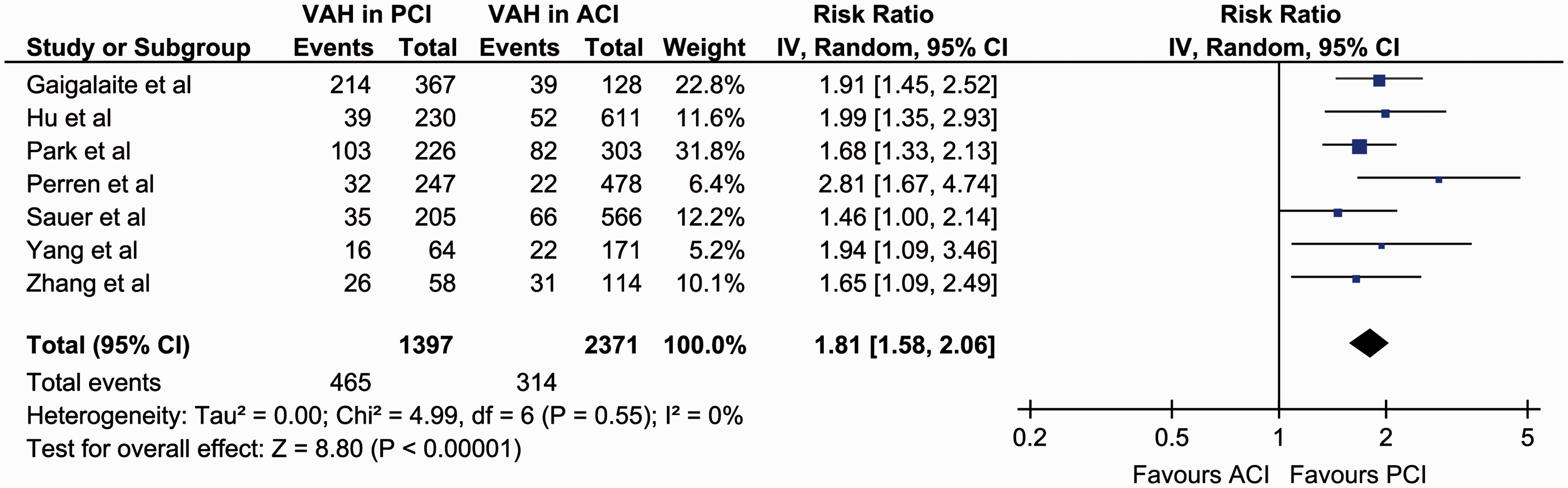
We identified eight study protocols including a total of 3875 acute ischemic stroke patients (mean age: 64.2 years, 61.3% males) and reporting a pooled prevalence of vertebral artery hypoplasia 18.6% (95%CI: 10.8–30.0%). In the overall analysis, a significantly higher probability of vertebral artery hypoplasia presence was found in posterior circulation ischaemia patients compared to patients with anterior circulation ischaemia (risk ratio = 2.12, 95%CI: 1.60–2.82, p < 0.001). In the subsequent sensitivity analysis, vertebral artery hypoplasia was again found to be significantly more prevalent in patients with posterior circulation ischaemia compared to anterior circulation ischaemia (risk ratio = 1.81, 95%CI: 1.58–2.06, p < 0.001), with no evidence of heterogeneity (I2 = 0%, p for Cochran Q = 0.55) between included studies.
Discussion
The present report is a meta-analysis of retrospective observational study protocols, with all the inherent limitations of included studies. The heterogeneity on the reported rates of vertebral artery hypoplasia could be attributed to differences in population age, sex, race, imaging protocols and vertebral artery hypoplasia definition between included studies.
Conclusion
Our meta-analysis provides further evidence for a possible causal relationship between vertebral artery hypoplasia and cryptogenic posterior circulation ischaemia, an association which undoubtedly deserves further investigation in future prospective study protocols.
Introduction
Cryptogenic embolism has been reported to represent about 10% of the ischemic strokes in posterior circulation. 1 Although several study protocols have reported that vertebral artery hypoplasia (VAH) can predispose to posterior circulation ischaemia (PCI) even in young, the role of VAH in the risk of cerebral ischaemia still remains controversial.2–4
In the present manuscript, we performed a systematic review and random effects meta-analysis of all available cohort studies investigating the association of VAH and cerebral ischaemia.
Methods
Eligible observational study protocols that reported prevalence rates of VAH in patients with anterior circulation ischaemia (ACI) and PCI were identified by searching MEDLINE and SCOPUS databases. The combination of search strings that was used in both database searches included the terms: ‘vertebral artery hypoplasia’, ‘ischemic stroke’ and ‘cerebral ischaemia’. No language or other restrictions were imposed. Last literature search was conducted on 4 July 2016. All retrieved studies were scanned independently by the two authors (AHK and SG), while any disagreement was resolved with consensus. We excluded from the quantitative/qualitative analysis all case series, case reports and studies not reporting VAH prevalence rates on either ACI or PCI.
We calculated the corresponding risk ratios (RRs) in each included study to express the relative risk of VAH presence in both the aforementioned subgroups. A random effects model (DerSimonian–Laird) was used to calculate the pooled RRs. The equivalent z-test was performed for each pooled RR, and if p < 0.05 it was considered statistically significant. We assessed heterogeneity between studies with the Cochran Q and I2 statistics. For the qualitative interpretation of heterogeneity, I2 values of at least 50% were considered to represent substantial heterogeneity, while values of at least 75% indicated considerable heterogeneity, as per the Cochrane Handbook. 5 All statistical analyses were conducted using Review Manager (RevMan) Version 5.3 software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and Comprehensive Meta-analysis Version 2 software (Borenstein M, Hedges L, Higgins J, et al. Englewood, NJ: Biostat, 2005).
Results
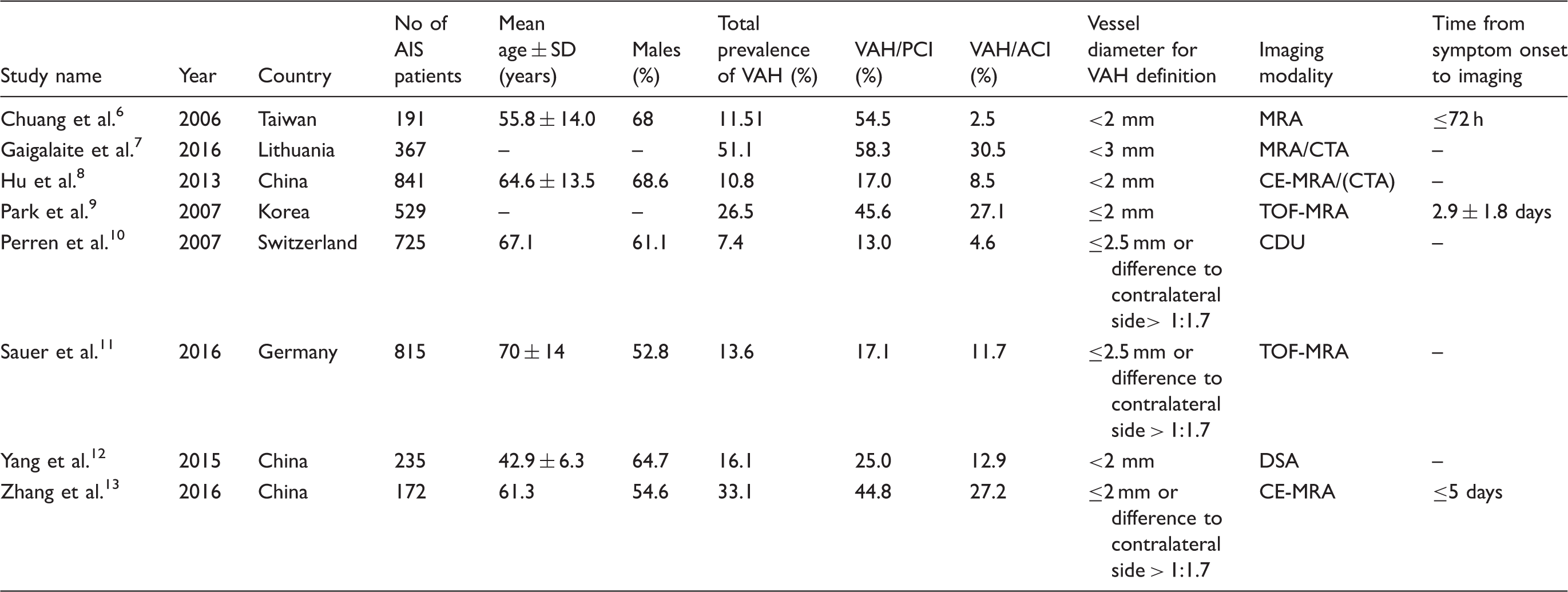
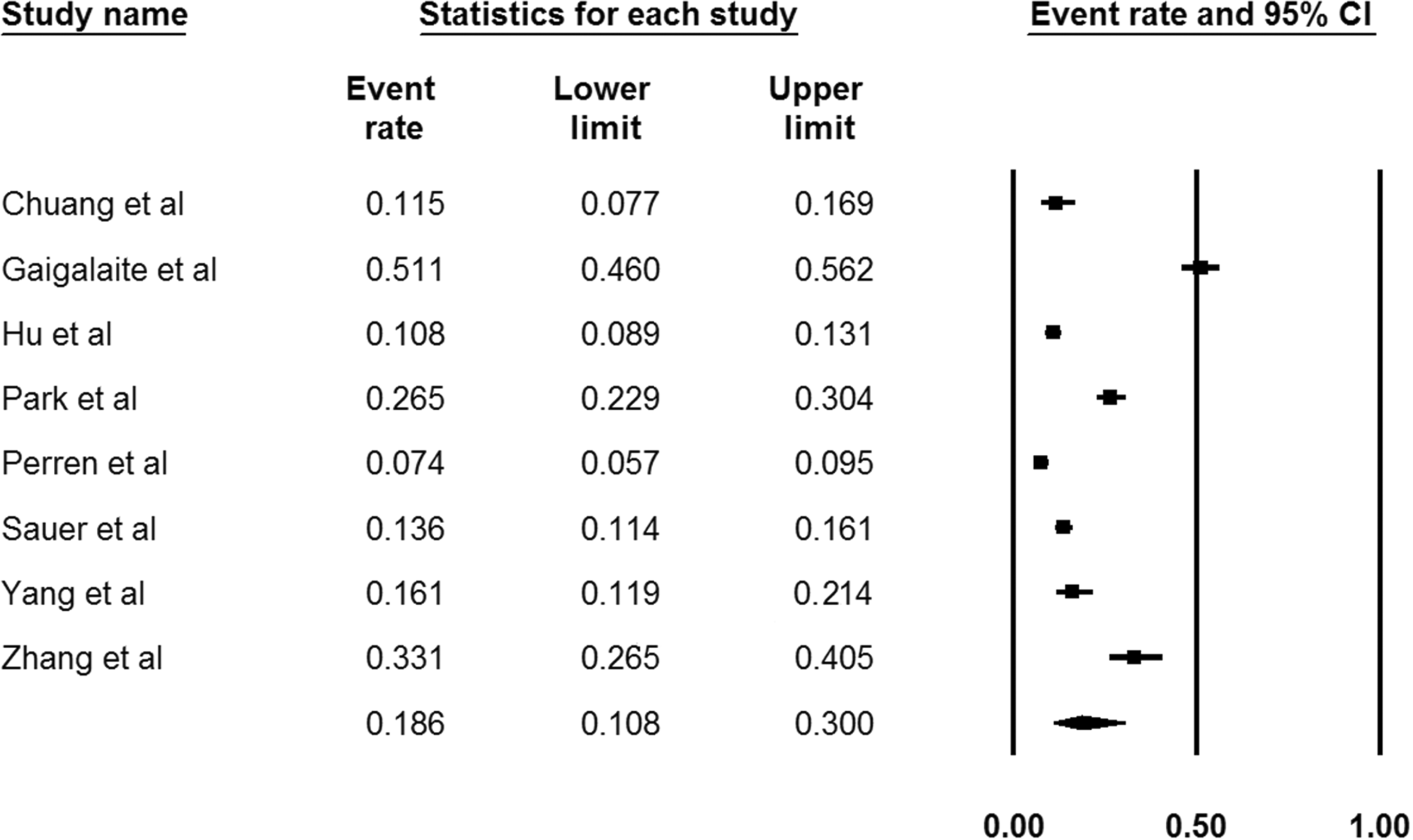
Our systematic literature search on MEDLINE and SCOPUS databases highlighted eight potential studies,6–13 reporting VAH prevalence rates in both patients with ACI and PCI (Figure 1). Included study protocols recruited a total of 3875 acute ischemic stroke patients (mean age: 64.2 years, 61.3% males; Table 1) and reported a pooled prevalence of VAH in 18.6% (95%CI: 10.8–30.0%; I2 = 98%, p for Cochran Q < 0.001; Figure 2).
Flow chart presenting the selection of eligible studies. Baseline characteristics of included studies. ACI: anterior circulation ischaemia; AIS: acute ischemic stroke; CDU: colour duplex ultrasound; CE: contrast enhanced; CTA: computed tomography angiography; DSA: digital subtraction angiography; MRA: magnetic resonance angiography; PCI: posterior circulation ischaemia; SD: standard deviation; TOF: time of flight; VAH: vertebral artery hypoplasia. Pooled prevalence of vertebral artery hypoplasia reported in the included study protocols.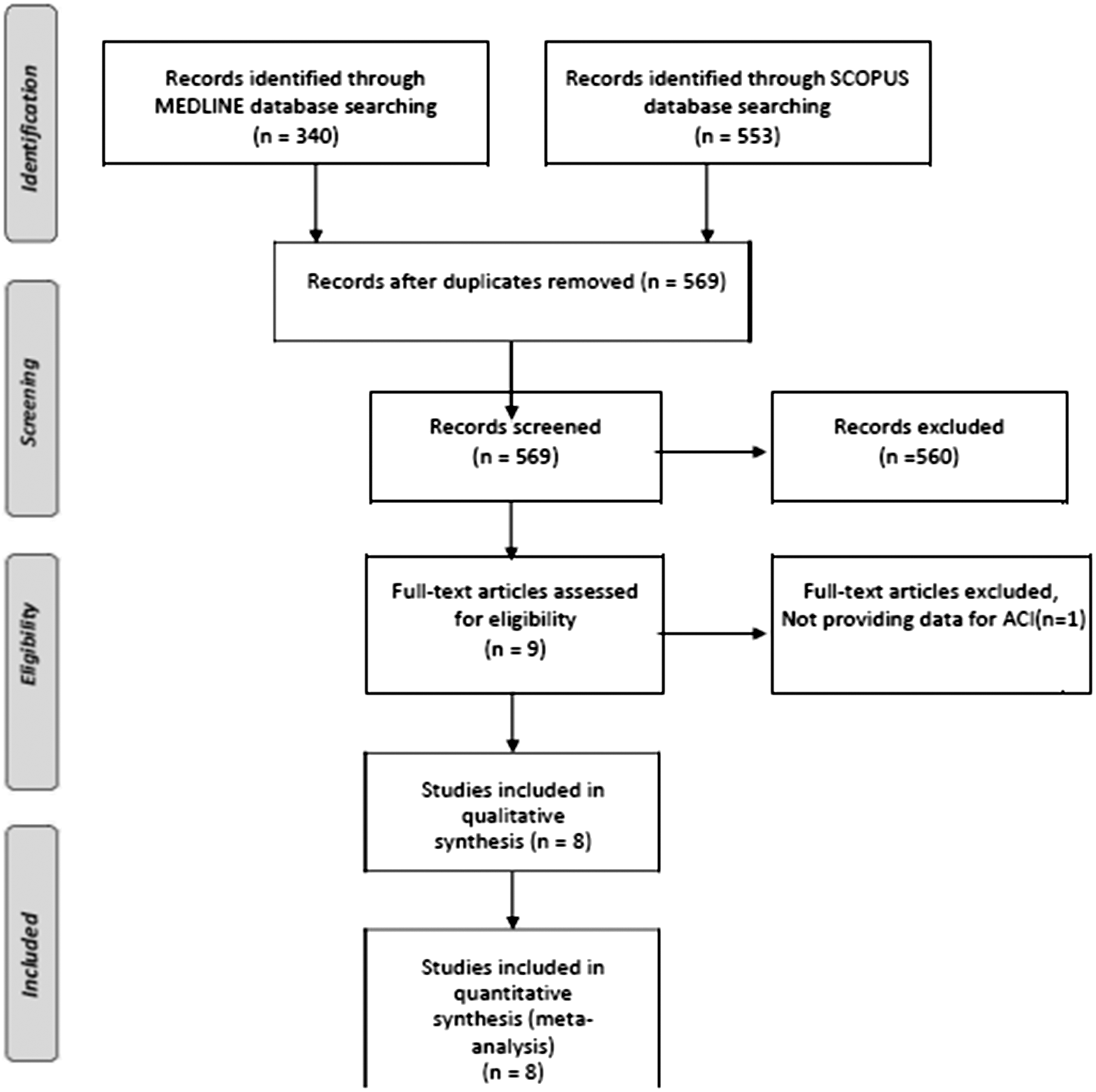
In the overall analysis of all included studies, significantly higher rates of VAH presence were found in patients with PCI (31.8% (95%CI: 19.2–48.0%)) compared to patients with ACI (12.8% (95%CI: 7.6–20.7%)) (RR = 2.12, 95%CI: 1.60–2.82, p < 0.001; Figure 3), with considerable heterogeneity among included studies (I2 = 75%, p for Cochran Q < 0.001). In the subsequent sensitivity analysis, after excluding a small-sized study reporting a considerably higher effect size compared to the other studies,
6
VAH was found to be significantly more prevalent in patients with PCI (29.2% (95%CI: 16.6–46.2%)) compared to ACI (15.0% (95%CI: 9.0–24.0%)) (RR = 1.81, 95%CI: 1.58–2.06, p < 0.001; Figure 4), with no evidence of heterogeneity in remaining studies (I2 = 0%, p for Cochran Q = 0.55).
Overall analysis on the reported prevalence of vertebral artery hypoplasia in patients with anterior cerebral ischaemia compared to patients with posterior cerebral ischaemia. Sensitivity analysis on the reported prevalence of vertebral artery hypoplasia in patients with anterior cerebral ischaemia compared to patients with posterior cerebral ischaemia.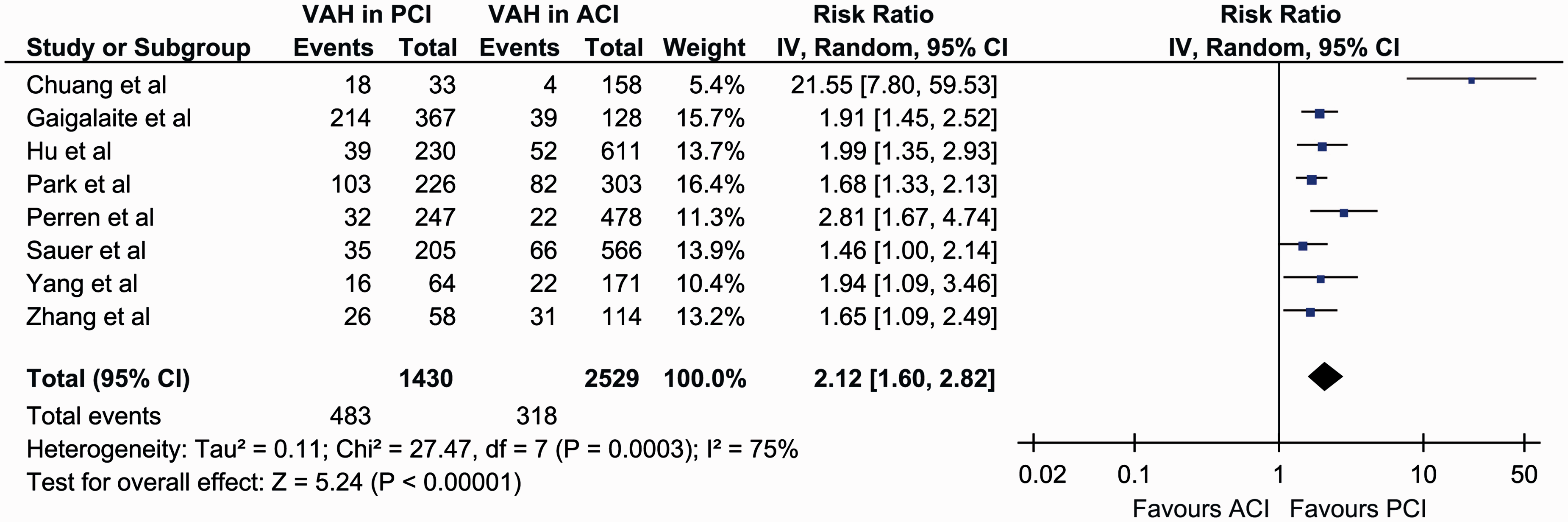
Discussion
In our meta-analysis of available cohort studies, we found that VAH is present in approximately one out of five patients with ischemic stroke, while is almost twice more prevalent in patients with PCI compared to patients with ACI.
We found that the total prevalence of VAH varied significantly among the included studies. This heterogeneity could be attributed to the differences in mean population age across the included studies,6–13 as a higher prevalence of reported VAH-related PCI is anticipated in younger patients with cryptogenic stroke due to the increase of all other stroke aetiologies (large vessel disease, lacunar, cardioembolic) and stroke risk factors with age.14,15 Apart from age differences, racial (Asian versus Caucasian) and gender (female versus males) disparities across included studies could reflect imbalances in stroke subtypes and stroke mechanisms,16–18 and thus be partially responsible for the observed differences in the reported VAH prevalence rates.
Even though it has been reported that VAH can be reliably diagnosed and categorised on cervical MRI scans, 19 the differentiation of VAH from both stenosis20,21 and occlusion 22 still remains challenging. Moreover, taking also into account that contrast-enhanced magnetic resonance angiography has been associated with an increased rate of false positive results in the detection of VA stenosis 23 and that CTA has been reported to have a higher sensitivity and positive predictive value than time-of-flight MRA for the detection of intracranial vessel stenosis and occlusion, 24 the use of different imaging modalities in included studies and the lack of information on the time interval from stroke onset to vessel imaging for most study protocols (Table 1) should be regarded as significant limitations of the present meta-analysis and another potential source of heterogeneity on the reported prevalence rates of VAH. It is therefore evident that as all flow-dependent imaging studies bare a high risk of false positive results, the imaging has to be evaluated by a specialist to confirm the diagnosis of VAH. Although cerebrovascular ultrasound was used for the definition of VAH in only one of the included studies, 10 the ultrasound’s flow profile could be used as an initial screening tool to differentiate between stenosis and hypoplasia, 25 with other imaging modalities (CTA, MRA, DSA) confirming the final diagnosis at a later stage.
Finally, even though VAH is one of the most common congenital vascular variations there is still no standard definition. 2 In the included studies, the threshold of VA diameter for the definition of VAH ranged from 2 to 3 mm (Table 1) and an additional criterion of VA asymmetry diameter ratio of more than 1:1.7 was applied in three out of eight studies.10,11,13 The disparities in VAH definition could therefore be at least partially responsible for the heterogeneity across included studies and for the strikingly high prevalence of VAH reported in one of the study protocols. 7
The association between VAH and PCI has also been consistently highlighted in all included studies, except from one, 11 suggesting thus a potentially increased risk of PCI in patients with VAH. Even though Sauer et al. 11 reported that they found no clear evidence of a causal relationship between VAH and cerebral ischaemia, they reported that in their cohort VAH was associated with younger age (p = 0.037), stroke localisation in posterior circulation (p = 0.009) and with cerebrovascular ischemic events of ‘undetermined’ aetiology (p = 0.042, although non-significant after Bonferroni correction). 11 Therefore, the only negative study so far on the association of VAH and PCI if interpreted from a different point of view might further enhance the possibility of a causal association, rather than reject it.
Apart from the included cohort studies, several imaging study protocols have also independently reported that VAH can predispose to posterior circulation regional hypoperfusion,26,27 and that when combined other risk factors can result in the clinical manifestation of PCI. 28 This theory suggests that normally when blood flow on the one vertebral artery is temporarily reduced, the flow on the opposite vertebral artery is compensatory augmented to provide sufficient flow in the basilar artery, but in severe VAH the blood flow is reduced to a greater degree than the contralateral vertebral artery can reverse resulting thus in unbalanced haemodynamics and in inadequate blood supply to the brain. 29
Small diameter arteries have also been reported to be more vulnerable to stenosis or occlusion, as its low flow velocity predisposes to prothrombotic or atherosclerotic processes in the presence of conventional vascular risk factors, 30 and therefore PCI may occur as a result of artery-to-artery embolism from the low-flowed stenotic VA. 31 VAH has also been associated with an increased risk of ipsilateral VA dissection compared to the normal counterpart, providing thus another possible stroke pathomechanism of artery-to-artery embolism from the hypoplastic vessel, 32 while the increased vessel diameter of the contralateral to the hypoplastic VA could provide a route prone to the transfer of cardiac emboli due to its low resistance and increased blood flow. 33
According to the aforementioned data, we consider that all patients with PCI and VAH should undergo a comprehensive diagnostic stroke workup to exclude both other VA abnormalities (dissection, stenosis or occlusion) and occult cardioembolism.34–36 Since no data are available to date on either the primary or secondary stroke prevention of patients with VAH, VAH patients with PCI and no other evident stroke aetiology should be treated according to the current guidelines for cryptogenic stroke.37,38
In conclusion, we considered that our meta-analysis of available retrospective cohort studies indicates a possible association between VAH and cryptogenic PCI. As only retrospective data are available to date, this association undoubtedly deserves further investigation in future prospective study protocols not only to elucidate further the potential causality but also to provide invaluable data on the underlying stroke mechanisms and potential therapeutic approaches.
Footnotes
Acknowledgements
None declared.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable (the present report is a review of already published studies).
Guarantor
AHK.
Contributorship
AHK and SG researched literature and conceived the study. AHK and SG wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.