
Abstract
Purpose
The purpose of this paper is to review and synthesize data from different countries in the Middle East on stroke and its potential risk factors.
Method
A systematic review of all published stroke articles in the Middle East between 1980 and May 2015 was conducted.
Findings
Sixty-four papers were included in the review. The incidence rate for all strokes ranged between 22.7 and 250 per 100,000 population per year. The prevalence rate for stroke ranged between 508 and 777 per 100,000 population. Among studies reporting gender differences, 75% reported a high male-to-female ratio among stroke patients. The mean age of stroke was within the sixth and the seventh decade. Ischemic stroke was the most reported type followed by intracerebral hemorrhage and subarachnoid hemorrhage. Hypertension was the most reported risk factor followed by diabetes. The overall case-fatality rate within one month was 12–32%.
Discussion
During the last decades, there was an increase in stroke incidence and mortality rates in the Middle East. The Middle East faces low rates of self-awareness and control of noncommunicable diseases and also lacks knowledge for stroke risk factors, awareness, causes, and symptoms.
Conclusion
There is an urgent need to develop more efficient and accurate methods to measure stroke in the Middle East. There is also a significant call to increase public awareness and implement interventions on stroke and its risk factors and symptoms to help people understand the negative impact of stroke on quality of life and potentially prevent this disease.
Background
The epidemiology of stroke is changing rapidly all over the globe. Over the 1990–2013 period, there was a significant increase in stroke incident events, survivors, and deaths for both ischemic and hemorrhagic stroke and a substantial increase in the absolute number of disability-adjusted life years (DALYs) due to ischemic stroke. 1 In 2013 alone, there were 10.3 million new strokes with 67% ischemic strokes, 6.5 million stroke deaths with 51% ischemic stroke deaths, 25.7 million stroke survivors and among those 71% had ischemic stroke, and 113 million DALYs due to stroke with 58% due to ischemic stroke. 1 The proportional contribution of stroke deaths and stroke-related DALYs compared to all diseases varies meaningfully between developed and developing countries, with the majority of stroke burden borne by low- and middle-income countries. 2 The global stroke burden continues to increase where it is expected that stroke will move to the fourth place as a commonest cause of an ongoing disease burden by 2020. 3
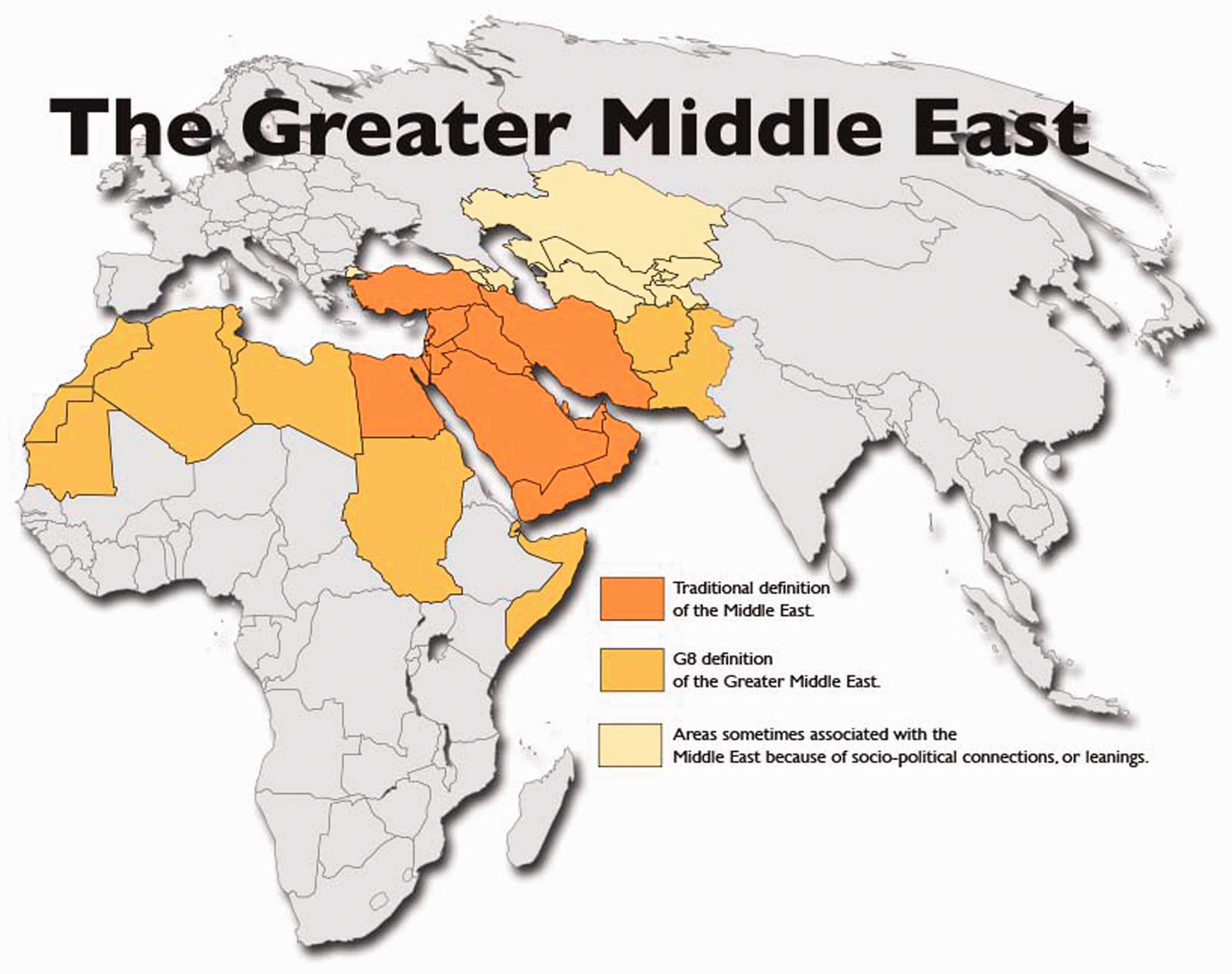
There is a scarcity of reliable information on stroke and its epidemiology in the Middle East (ME). There is also no unique and clear definition of the ME. Three reviews have been published on the epidemiology of stroke in this region but included or excluded countries from North Africa or South Asia.4–6 Therefore, the purpose of this paper is to review and synthesize data on stroke and its potential risk factors from the countries stated by the World Atlas traditional definition of the ME and by the National Geographic Atlas of the ME (2003)—ME: The Focus.7,8
Methods
Search and acquisition
The ME countries include Egypt, Iran, Turkey, Iraq, Saudi Arabia, Yemen, Syria, United Arab Emirates, Israel, Jordan, Lebanon, Oman, Kuwait, Qatar, Bahrain, Cyprus, and the State of Palestine (Figure 1).7–9
Map of the Middle East. The traditional definition of the Middle East. Reproduced with permission from World Atlas.
7
A systematic review of all published stroke articles in the ME was conducted. Different key words were used to identify publications on stroke in the ME, including “Stroke,” OR “Cerebrovascular Accidents,” OR “Ischemic Stroke,” OR “Cerebral H(a)emorrhage,” OR “Subarachnoid H(a)emorrhage,” AND “Middle East,” OR “Arabian Gulf,” OR “Arab Countries,” OR “North Africa,” OR “Egypt,” OR “Iran,” OR “Turkey,” OR “Iraq,” OR “Saudi Arabia,” OR “Yemen,” OR “Syria,” OR “United Arab Emirates,” OR “Israel,” OR “Jordan,” OR “Palestine,” OR “Lebanon,” OR “Oman,” OR “Kuwait,” OR “Qatar,” OR “Bahrain,” OR “Cyprus.”
A broad search was first initiated on computer-based search engines including Medline/PubMed and Scopus/ScienceDirect. The World Health Organization website and specific countries journals were consulted. The search was limited to publications between 1980 and May 2015 and to papers published in English, French, or Arabic languages. The reference sections of all relevant papers were manually searched for additional papers inclusions. The new citations were also acquired, assessed, and if accepted, were subject for additional reference searches (Figure 2).
Selection of articles.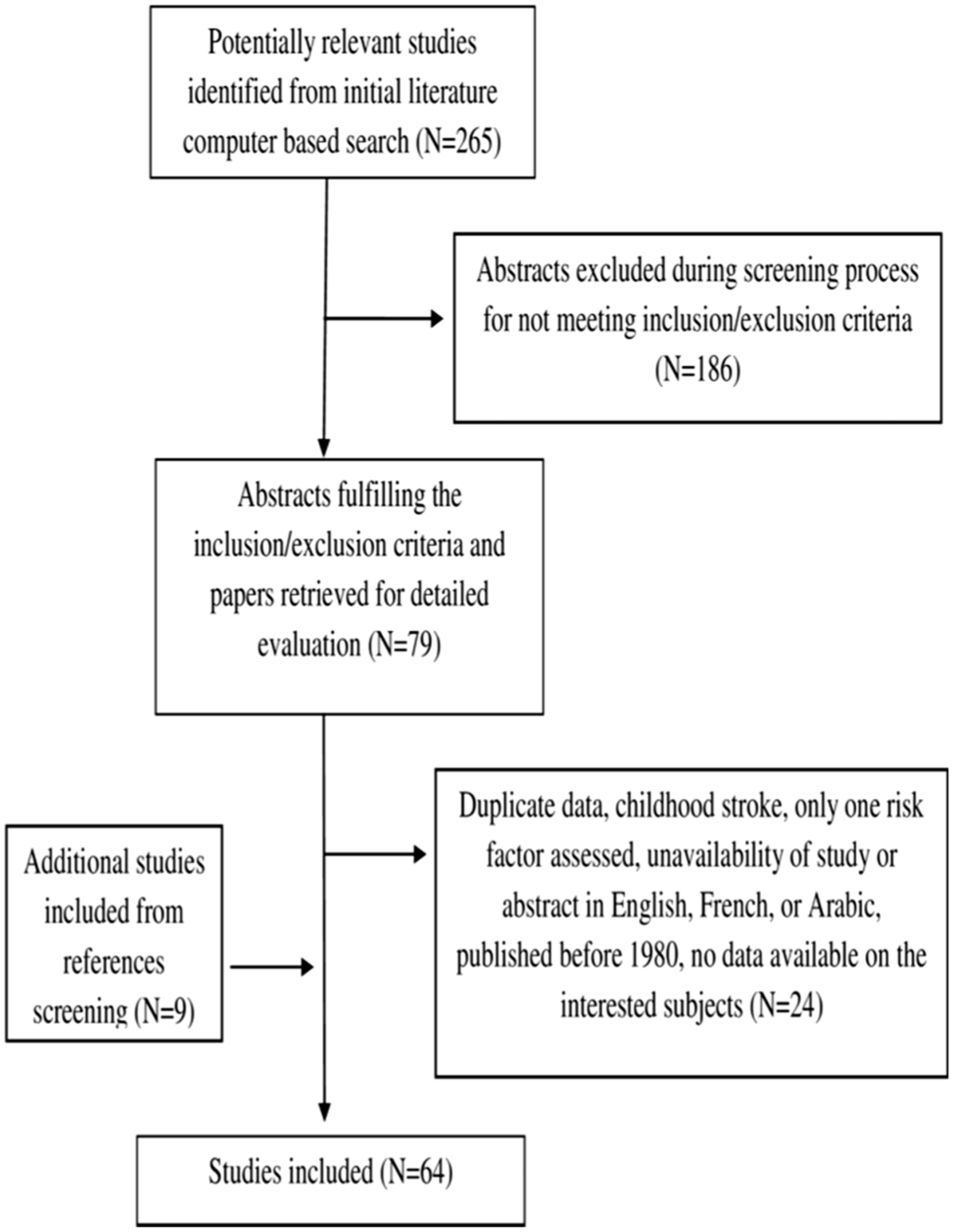
Outcomes
Due to the divergence of outcomes in existing studies and in an effort to synthesize the results from studies, a subset of seven variables was selected for the purposes of this review, including, incidence, prevalence, gender differences, mean age, types, risk factors, and outcome of stroke.
Inclusion and exclusion criteria
To be eligible, the study has to be conducted in any of the ME countries listed previously, contain data about the interested outcomes and be available in English, French, or Arabic, should have more than one risk factor assessed and be published in a peer-reviewed journal, and should not consider childhood stroke (age < 15) or be a duplicate of another study.
Data extraction and analysis
Data regarding outcomes were extracted from all relevant articles and analyzed descriptively. No meta-analysis was conducted due to the divergence in studies methodologies and data sources.
Results
Incidence of stroke in the Middle East.

CT: computerized tomography; ICD-10: International Classification of Diseases 10; MRI: magnetic resonance imaging; 95% CI: 95% confidence intervals stated when available; PIC: practical Iranian criteria classification for etiologic and topographic diagnosis of brain infarction; WHO: World Health Organization.
Clinical definition: stroke was defined as an ischemic focal neurological deficit that persisted at least for 24 h.
Data reported on age-adjusted incidence rate.
Data reported in 2007.
Data reported in 1992.
Study included ischemic stroke patients only.
Data reported in 2000.
Data reported in 2001.
Data reported in 2002.
Data reported in 2003.
Data reported in 2004.
Data reported in 2005.
Data reported in 2006.
Study included young ischemic stroke patients only.
Data reported in 1988.
Data reported in 1996.
Study included subarachnoid hemorrhagic patients only.
Incidence
For studies including all age ranges, the incidence rate for all strokes in the ME ranged between 22.7 per 100,000 population per year in Iran and 250 per 100,000 population per year in Egypt.12,17 It ranged between 22.7 and 180 per 100,000 population per year for first ever and recurrent stroke,13,17 and between 29.8 and 250 per 100,000 population per year for first ever stroke.12,61
For studies including only patients above 18 years old,10,11,14,67 the incidence rate ranged between 15.9 and 181 per 100,000 population per year.14,67 The incidence rate for patients above 45 or 50 years old ranged between 275 and 354 per 100,000 population per year.23,24
The incidence rate for ischemic stroke was reported between 43.17 and 164 per 100,000 population per year.18,37
Two studies from Iran reported a rising incidence from 84.16 to 103.23 per 100,000 population per year over four years and from 48.6 to 103.4 per 100,000 population per year over six years.19,20 Table 1 summarizes the reported incidence rates of stroke in the ME.
Overall, during the last decades, there was an increase in stroke incidence rate in the ME (please see Supplementary Material Figure I).
Prevalence
Only Egypt reported an overall prevalence of nonfatal stroke. The prevalence rate for first ever and recurrent stroke ranged between 508 and 777 per 100,000 population in 1992 and 2001–2013, respectively.13,15 The prevalence of stroke was found to increase steeply with advancing age and to be higher in males than females.12–15
Gender differences
Among studies reporting gender differences, 75% reported a high male-to-female ratio. A great predominance of males to females was found in certain studies from Qatar, Saudi Arabia, and one from Iraq which may be explained by the demographic characteristics of these countries. 48
Three studies from Iran, Lebanon, and Saudi Arabia indicated a 1:1 ratio of male to female.25,43,60 Eleven studies (six studies in Iran, one in Kuwait, two in Palestine, one in Iraq, and one in Saudi Arabia) found that females predominate males in number of stroke cases.18–20,24,26,31,35,41,44,45,60
In Iran, six out of the 15 studies included in the current review indicated a high female-to-male ratio.18–20,24,26,31 In Palestine, females showed more stroke cases than males in both studies included where women represented 51.07% in the study including all stroke patients and 54.25% in the ischemic study.44,45 The female predominance was referred to the presence of undiagnosed stroke among men or to the poor control of stroke risk factors among women in Palestine, 44 and in Iraq, to the unpleasant situation in this country during the last 30 years. 35 In Saudi Arabia, females represented the highest percentage of 64% of all ischemic stroke patients included in Qutub descriptive study. 62
Mean age
The mean age of stroke was within the sixth and the seventh decade, ranging from 59 to 71.38,59 Four studies from Qatar and one study from Saudi Arabia reported a mean age of stroke lower than other ME countries, ranging between 56.9 and 58 years old.46–48,50,65
Three studies from Iran reported a mean age of stroke for women to be lower than for men, ranging between 59 and 63 years old, compared to men, which ranged between 61 and 66 years old.21,22,30 One study from Egypt reported that while the thrombotic and hemorrhagic stroke were rapidly increasing after the age of 40 years, the peak period for embolic stroke was between the age of 20 and 40 years. 13
In regards to stroke survivors, three studies showed that the risk of nonsurviving a stroke increases with age.28,43,45 In Lebanon, the mean age for nonsurvivors was 71.1 ± 13 years; in Palestine, it was 73.11 ± 11.19 years; and in Iran, the mean age of deceased was 67.3 ± 14.6 years.
Types of stroke
Ischemic stroke was the most reported type in studies including all types of stroke (60–90.1%),10,11,40 followed by intracerebral hemorrhage (6.5–30.7%),57,67 and subarachnoid hemorrhage (0.4–10.4%).30,34
Nonlacunar infarction was reported in 40–76.5% of stroke,20,71 while lacunar infarction in 8.9–59.7%.20,41 The majority of studies reported a rate of lacunar infarction less than 35%. Two studies reported high occurrence of lacunar infarction: Jordan reported to have 51% of ischemic patients with lacunar infarction, 39 and Kuwait, reported 59.7% lacunar patients of the 62 ischemic patients included. 41
Stroke subtypes in the Middle East.

ICH: intracerebral hemorrhage; non-L/L: non-lacunar/lacunar; SAH: subarachnoid hemorrhage.
Risk factors
Frequency of risk factors in stroke cases admitted to hospitals in the Middle East.

AF: atrial fibrillation; DM: diabetes mellitus; FH: family history of stroke; HBP: hypertension; IHD: ischemic heart disease; MI: myocardial infarction; RHD: rheumatic heart disease; TIA: previous history of transient ischemic stroke.
Other important risk factors reported include migraine, anticoagulant drugs, alcohol intake, blood disorders, sickle cell disease, cervical bruit, oral contraceptive, and depression.
Reported data on “M” men and “W” women separately.
Previous history of stroke.
Data reported in 2006.
Reported data on “S” survivors and “NS” nonsurvivors separately.
Reported data on “H” hemorrhagic and “I” ischemic patients separately.
Data only for hemorrhagic patients.
Outcome of stroke
The average in hospital length of stay (LOS) varied between eight and 63 days for all types of stroke,11,25,46,53 and between seven and 12 days for ischemic stroke.24,38 In Iran, women had significantly longer LOS compared with men, and patients with a history of ischemic heart disease had a higher LOS compared to patients without ischemic heart disease. 24 Thrombotic subtypes had the lowest LOS and the subarachnoid hemorrhage had the highest LOS in a cross-sectional study conducted in Iran. 25
The overall case-fatality rate within one month of all types of stroke was 12–32%.19,25,34,47,54,61,63 In-hospital case-fatality rate of stroke was 8–28%.13,20,36,38,43–46,57,60,67
During the last decades, there was an increase in stroke case-fatality rate in the ME (please see Supplementary Material Figures IIA and IIB).
In regards to stroke type, the ischemic stroke-fatality rate was low, ranging from 2.8% to 36%,13,18–20,24,28,30,37–39,41,47,61,62,67,73 in comparison to hemorrhagic stroke fatality, ranging from 5.5 to 46.7%.13,19,20,28,30,38,46,47,54,61,65,67,73
Different studies reported that most death occurred during the first week after the events, especially for hemorrhagic strokes.12,19,28 There was a significant correlation between age and the mortality rate.20,41,42,45,63 However, other factors were also found to be related to mortality, including brain herniation, 18 hypertension, ischemic heart disease,24,64 coma, complete paralysis, medical complications during hospitalization, 36 and lack of antiplatelet therapy. 41
Stroke survivors face the burden of poor to severe outcome at hospital discharge. A study conducted in Israel reported that 34% of patients with acute stroke faced severe handicap at discharge and an additional 29% had moderate handicap. 38 In Kuwait, 77.7% of stroke patients were discharged with neurologic deficit, 46 and in Turkey, severe disability was significantly more frequent among females at the time of discharge. 70
Young stroke
The definition of young stroke varied: < 45, 64 and between 15 and 45 years of age.29,49,66 The mean age was 28.6–37.1 years.49,64 The incidence rate was eight per 100,000 population per year in Iran, 18 and the subarachnoid hemorrhage was reported at 2.69 per 100,000 population per year in Qatar. 51
For stroke subtypes, Khan reported in a prospective study that 42.5% of his ischemic patients had lacunar infarction, 49 compared to only 2.42% and 7.5% reported by Ghandehari and Moud and Awada, respectively.29,66 Awada also reported intracerebral hemorrhage at 32.5% compared to 9% of subarachnoid haemorrhage. 66
The common causes of stroke in young ischemic strokes included cardioembolic (19.5–54% of cases), atherosclerosis (6.45–28% of cases), and undetermined causes (28.2–34.5% of cases).29,66 The most likely causes of young hemorrhage were hypertension (39% of patients aged 40–45 years), arteriovenous malformations (32% of patients aged 20–29 years), aneurysm (13% of patients 30–39 years old), and blood dyscrasias (58% of 1–9 years old patients). 64
Hypertension was the most reported risk factor (32–40%) followed by diabetes (16–32.5%) and smoking (26–27.5%), respectively.49,66
The average hospital stay for ischemic young stroke patients was estimated at 18 days. 49 The case-fatality rate for young ischemic patients was reported at 2.5 and 7%,49,66 and for young hemorrhagic stroke at 21 and 27%.64,70 In Saudi Arabia, only one-third of young cerebral hemorrhagic stroke patients returned to independent living after stroke incidence. 64
Stroke diagnosis in included studies, role of stroke unit and management of acute stroke
No studies included in the present systematic review reported on the time between the arrival to the hospital and neurology evaluation and no studies reported on the time between the arrival and the transfer to an in-patient setting. However, in a prospective observational hospital-based study conducted in Qatar, only 17.5% of ischemic stroke patients arrived at the hospital within 3 h from stroke onset. 46 A prospective study in Isfahan, Iran, stated that 66.2% of stroke patients were hospitalized during the same day of onset, 28.7% were hospitalized 1–2 days after stroke, and 4.5% of stroke patients were admitted to the hospital between three and seven days after stroke. 19 In Turkey, the admission of stroke patients depended on the availability of beds, and therefore, minor strokes might get managed on an ambulatory basis due to the shortage of beds as stated in a prospective study conducted in the Neurology Department of Istanbul Medical School (one of the three state university neurology clinics in Istanbul). 70
Computed tomography (CT) was the most emergency brain imaging performed for stroke patients in the ME. Thirty-one clinical series stated the percentage of stroke patients undergoing brain CT scan or magnetic resonance imaging (MRI).10–16,18–22,24,28,29,36,38,42,44,46,47,50,51,53,54,57,59,60,61,67,69,70 The percentage of patients undergoing brain CT varied between 7653 and 100%.12–16,18,20–22,24,28,29,42,44,47,50,51,54,67,69,70 Only five studies reported on times from arrival at the emergency department to undergoing head CT22,38,47,57,67; the average time varied between 2.1 h 46 and three days of admission. 55 In a census conducted in Iran, 3.94% of stroke patients had a brain imaging from eight to 28 days of stroke onset. 22 In Turkey, the lower rate of performing MRI and magnetic resonance angiography in females was thought of as being the result of higher incidence of severe hemispheric strokes and atrial fibrillation with lower incidence of posterior circulation symptoms. 70 In Israel, 32 and 28% of stroke patients had a carotid duplex in two studies conducted by Bentur and Resnizky and Tanne et al., respectively, and 5% of patients had transcranial Doppler in both studies.36,38
In Israel, thrombolysis (intravenous or intraarterial) was used for 0.5% of patients with acute ischemic stroke and for 1% of those presenting within 6 h of symptom onset. 38 Moreover, antithrombotic and warfarin were prescribed for 94 and 44% for patients with ischemic stroke or TIA, respectively. 38 Seventy-seven percent of stroke patients were treated with aspirin and 2.8% with ticlopidine in a hospital-based study in Saudi Arabia. 53 In Palestine and Bahrain, 92.5 and 79% of stroke patients with hypertension were discharged with antihypertensive medications and 98 and 83% were discharged with antiplatelets, respectively,11,45 and 82.3% of patients in Bahrain commenced on aspirin within 48 h of admission. 11
Quality features of included studies
Twenty-seven included studies have a retrospective design10,11,17,20,23,27,37,39–41,45,47,51–55,57,63–69,72,73 compared to 16 having a prospective study design.13,19,21,22,26,30,34,35,38,42,44,46,49,50,60,70 Two studies have both, a retrospective and a prospective design.43,59
Many included studies miss clear definition of stroke,13,15,17,23,27,30–34,36,38,39,43–45,51,54,56,58,59,62–68,70,72,73 have a small sample size14–16,21,23,26,32,40,41,43,49,51,53,56,62,66,71 and lack age-adjusted incidence rate,10,11,13–15,17–23,29,30,47,51,54,61,67 and/or 95% confidence intervals for this rate.10–15,17,18,20,21,29,31,42,44,51,54,67 The majority of studies are hospital-based (52 studies out of 64 included),10,11,17,19,20,23–28,30–37,39–60,62–70,72,73 and eight studies are community or population based.12–16,18,21,22 None of the studies included was designed to represent national population for data accuracy except in Israel. 38
Discussion
Sixty-four clinical series were included in this review with the majority of studies from Iran and Saudi Arabia.
The ME countries are on the list of developing countries by the World Bank where the mean age of stroke is slightly younger that the one reported by developed countries. 74 The lower mean age of stroke is due to differences in population age structure including high prevalence of young people 48 and limited life expectancy 75 that is caused by higher rates of noncommunicable diseases compared to developed countries. 76
The incidence rate available from the ME before the year of 2000 indicates a low unadjusted incidence rate of stroke compared to most developed countries. 77 The ME incidence rates ranged from 29.8 to 180 per 100,000 population per year in 1993–97,13,61 compared to crude stroke incidence rates of 112–223 per 100,000 population per year in 1990–99 among high-income countries. 77 However, the stroke incidence rates in the ME have increased dramatically over the past decade, exceeding by then the level seen in some high-income countries; incidence rates for ME countries ranged from 22.7 to 250 per 100,000 population per year in 2000–2014,12,17 compared to crude stroke incidence rates of 112–223 per 100,000 population per year in 2000–8 among high-income countries. 77 The ME unadjusted incidence rate of stroke is also higher than the sub-Saharan Africa's, ranging 31–223 per 100,000 population per year in 1986–2004, 78 but within Asia incidence rate of first ever stroke (116–219 per 100,000 population per year in China). 79
Only five included studies provided an age-adjusted incidence rate, 89.9–250 per 100,000 population per year in 2007–8,12,44 which is still higher than the age-adjusted annual incidence rate in high-income countries reported at 85 per 100,000 population per year in 2000–8. 77
Ischemic stroke was the most reported subtype of stroke, followed by intracerebral hemorrhage and subarachnoid hemorrhage. Our proportion frequencies of stroke subtypes are within the range of high-income countries. 77 However, the high rate of lacunar infarction found in two studies is somehow similar to the Japanese data,39,41,80 which may be related to the elevated blood pressure, diabetes, and/or obesity and the poor control of those diseases as well as to the advanced age among cases. 81
Hypertension was the most prevalent risk factor for stroke, followed by diabetes, dyslipidemia, and cardiac diseases, respectively. The ME suffers from high rates of noncommunicable diseases where the prevalence of hypertension in the ME is unacceptably high among adults aged 25 years and older, reaching 30% of this population, 82 and diabetes rates attaining 11% of the population. 5 Moreover, the highly prevalent risk factors pattern is similar among the majority of the ME countries as well as the low rate of self-awareness and control of noncommunicable diseases.83–86 Additionally, the ME lacks knowledge for cerebrovascular risk factors, awareness, causes, and symptoms as seen in many studies,87,88 which is a concern, especially in increasing the chances of patients of benefiting from acute intervention including thrombectomy,89,90 thrombolysis,91,92 and stroke unit treatment.
Stroke patients in the ME have an average hospital stay longer than other low- and middle-income countries, such as China, which has the longer hospital stay compared to other countries with an average of 20 days. 93 The average LOS for patients with ischemic stroke is similar to the United States average, which ranges from six to 12 days,94,95 and shorter than the average LOS found in Canada (17–47 days), 96 and some countries in Europe (18–105 days) and Asia.97,98
While the early stroke case fatality in high-income countries decreased during the last four decades, the early stroke case fatality in the ME has increased. The mean total stroke case fatalities within one month in the ME was 14.3% in 1990–99,47,54,61 which is lower than the one reported by high-income countries, 22.2%, during the same period. 77 However, in 2000–8, the mean total stroke case fatalities within one month in the ME was 26.4%,19,25,34 indicating a higher mean than the one reported by high-income countries (19.8%) during the same period. 77 One study from Iran reported an early stroke case fatality at 32%, comparable to sub-Saharan Africa figures (33%). 78
The percentage of stroke patients undergoing CT scan in the ME is close to the United States percentage (92–95%), 99 and Europe (79–87%), 100 in many studies included. The availability of information in regard to time to neurology evaluation and transfer to in-patient setting as well as to the role of the stroke unit in the care and management of acute stroke are very limited in the studies included in this review, thus, we cannot drive conclusions about the variations in treatments between the ME and other countries without supplementary information.
According to Benamer, there is no available data from Arab countries about the use of different treatments of stroke. 101 However, certain high-income and upper middle-income countries in the ME such as Qatar, 102 United Arab Emirates,103,104 Israel, 105 and Iran 106 are improving stroke care including thrombolysis treatment, radiology teams, and rehabilitation services. Saudi Arabia is still struggling with stroke care where there are only 10 trained stroke neurologists in the country mainly in the capital, nine endovascular interventionalists and less than 20 qualified and trained physiatrists. 107 Moreover, two-thirds of Saudi Arabia neurologists never used thrombolysis on a stroke patient, one-third were against using thrombolysis, and another third lacked knowledge about thrombolysis. 101 Therefore, it is very important to conduct studies on the role of the stroke unit in the management of acute stroke in the ME in order to evaluate where the ME stands in stroke management and treatment. However, until the establishment of the proper infrastructure for the use of thrombolytic therapy or thrombectomy in the ME, it is significantly important to focus on effective strategies for a primary and secondary prevention for stroke.
A large number of studies emphasize the importance of economic factors as predictors of stroke mortality and burden. 108 The availability of adequate resources has a great impact on case fatality and long-term morbidity, and the access to prevention, treatment, and follow-up has a direct effect on stroke mortality and ongoing disability from stroke. According to Kim and Johnston, the incremental cost-effectiveness ratio of aspirin for acute stroke is $100–$700 per DALY averted. 108 Therefore, in certain environments, where resources are limited, a given expenditure on a certain therapy for secondary prevention, such as aspirin, may have some impact on the stroke burden. However, according to the World Bank data, around 15.4, 21.2, and 37.3% of the population of the ME lower middle-income countries, Egypt, Iraq, and Yemen, respectively, live below the poverty line with less than $2 a day. 109 Hence, the question is whether the unfortunate people in the ME with such a low daily income would be able to afford any treatment or follow-up to prevent stroke. As a result, stroke may increase suffering for patients and families and be a burden to society.
The limitations of this review include scarcity in epidemiological studies with similar methodology and epidemiologic measures of stroke in the ME. Sudlow and Warlow suggested different criteria to compare stroke incidence worldwide, later updated by Feigin and Vander Hoorn.110,111 None of the studies included in our comparison of stroke incidence rate fulfill the proposed criteria for comparison as well as the updated version due to methodological weaknesses, mainly through missing clear definition of stroke in certain studies, lack of community-based case ascertainment, absence of age-adjusted incidence, absence of 95% confidence intervals, and having a retrospective design. This may have played a significant role on the great variability of the reported epidemiological parameters in the studies. However, it is important to keep in mind that the ME may have improved in stroke case ascertainment over the last two decades which may be the reason for increased stroke incidence and fatality rates compared to the past.
The ME has a comparable younger population, with more than 40% of the population less than 15 years old and only 4% over the age of 65. 112 This may have an impact on the stroke incidence rates reported as the majority is not age adjusted. Moreover, the number of patients presented to hospitals may not represent the real number of stroke patients since a large number of patients tend to consult doctors before seeking hospitals, which may have a significant impact on data collection and reported incidence rates. Furthermore, the absence of the severity of stroke in the majority of studies, the unreported number of patients who were not admitted to hospitals, and the retrospective design of a great number of the studies may have had a significant impact on the case-fatality rate reported in the ME.
Conclusion
The epidemiology of stroke is changing rapidly and the global stroke burden continues to increase worldwide. The younger population of the ME indicates that the stroke will increasingly become a burden in the coming years. There is an urgent need to develop more efficient and accurate methods to measure stroke in the ME. There is also a significant call to increase public awareness and implement interventions on stroke and its risk factors and symptoms to help people understand the negative impact of stroke on quality of life and potentially prevent this disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable
Informed consent
Not applicable
Guarantor
Maya El-Hajj, Clinical and Epidemiological Research Laboratory, Faculty of Pharmacy, Lebanese University, Hadath, Lebanon
Contributorship
Not applicable
Acknowledgements
None