
Abstract
Background
Sex differences in stroke outcomes have been noted, but whether this extends to stroke recurrence is unclear. We examined sex differences in recurrent stroke using data from the Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) trial.
Patients and methods
We assessed the risk of recurrent stroke in women compared to men using data from the POINT trial. Adults
Results
Of 4,881 POINT trial participants with minor stroke or high-risk TIA, 2,195 (45%) were women. During the 90-day follow-up period, 267 ischemic strokes occurred; 121 were in women and 146 in men. The cumulative risk of recurrent ischemic stroke was not significantly different among women (5.76%; 95% CI, 4.84%–6.85%) compared to men (5.67%; 95% CI, 4.83%–6.63%). Women were not at a different risk of recurrent ischemic stroke compared to men (hazard ratio [HR], 1.02; 95% CI, 0.80–1.30) in unadjusted models or after adjusting for covariates. However, there was a significant interaction of age with sex (P=0.04). Among patients
Discussion and Conclusion
Among patients with minor stroke or TIA, the risk of recurrent ischemic stroke and the impact of common stroke risk factors did not differ between men and women.
Introduction
One in four strokes in the US is a recurrent stroke, and approximately 13% of patients with minor stroke/transient ischemic attack (TIA) face recurrent stroke, heart attack, or cardiovascular death within 5 years.1,2 Sex differences in stroke outcomes have been noted, including both post-stroke mortality and patient-reported outcomes.3,4 Further, several sex-specific stroke risk factors have been identified, such as migraine and oral contraceptive use for women and substance use for men.5–9 Some conventional stroke risk factors, including hypertension, diabetes, and metabolic syndrome, may also have a stronger association with incident stroke risk in women than in men.6,9,10 Whether these differences impact stroke recurrence risk has not been definitively assessed. Prior studies, which included a large proportion of stroke mimics 11 or used non-adjudicated administrative claims data,12,13 did not find clear evidence of a sex difference in stroke recurrence.
Several challenges exist in studying sex differences and recurrent stroke risk using observational data. For example, women are less likely to be diagnosed with stroke despite presenting with similar symptoms as men. 11 Additionally, recurrent stroke is often early,2,14 and early recurrent strokes can be misclassified as worsening stroke symptoms rather than new events. To circumvent these challenges, we studied sex differences in stroke recurrence using adjudicated clinical trial data from the Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke (POINT) trial, in which substantial efforts were made to capture early stroke recurrence. 15 First, we examined sex differences in recurrent ischemic stroke rates after minor stroke or TIA. Second, we evaluated sex differences in the strength of the association between common conventional stroke risk factors and recurrence.
Patients and Methods
Design
POINT was a randomized clinical trial that evaluated aspirin and clopidogrel (dual anti-platelet therapy) versus aspirin alone for preventing major ischemic events in patients with minor ischemic stroke or TIA.15,16 In total, 4,881 individuals were enrolled from May 2010 to December 2017, across 269 sites globally. Subsequently, these participants were followed for up to 90 days for the primary composite outcome of cardiovascular events and secondary outcomes including recurrent ischemic stroke. The National Institute of Neurological Disorders and Stroke (NINDS) funded the trial and also made available the deidentified data employed in this analysis. The Weill Cornell Medicine Institutional Review Board granted an exemption for analysis of these data.
Patient population
Adults 18 years and older were randomized into the POINT trial within 12 hours of onset of either minor ischemic stroke (National Institutes of Health Stroke Scale score 0–3) or high-risk TIA (ABCD 2 score ≥4). Brain imaging was obtained before randomization to confirm ischemic stroke and rule out hemorrhage or other symptom etiologies. Patients who were candidates for thrombectomy, thrombolysis, or on anticoagulant therapy were not included in the study. Women who were pregnant or at risk for pregnancy were excluded from POINT because the safety of clopidogrel in pregnant women was not established. 15
Measurements
Our primary exposure variable was self-reported sex. The primary outcome in our analysis was recurrent ischemic stroke that occurred after randomization in POINT. This was defined as (1) the rapid onset of a new focal neurological deficit with evidence of infarction or (2) rapid worsening of an existing deficit attributed to a new infarction. Outcomes of the POINT trial were adjudicated by a blinded endpoint adjudication committee. Covariates included the index event type (minor stroke versus TIA), randomization arm (clopidogrel versus placebo), demographic characteristics, participant site (US versus non-US), and stroke risk factors. Demographics included age, race, and ethnicity. Stroke risk factors included hypertension, diabetes mellitus, coronary heart disease, congestive heart failure, valvular heart disease, atrial fibrillation, carotid atherosclerosis, and history of tobacco use, based on baseline ascertainment. Participants were categorized as having atherosclerosis if they had at least 50% stenosis in either carotid artery at the time of the index event.
Statistical analysis
The primary statistical analysis entailed use of a Cox proportional hazards model to compare the risk of recurrent stroke in women versus men. We constructed the following stepwise models: (1) unadjusted, (2) adjusted for randomization arm (clopidogrel versus placebo) and event type (stroke versus TIA), (3) additionally adjusted for age, race, ethnicity, and site (US vs non-US), and 4) additionally adjusted for pre-existing stroke risk factors and risk factors ascertained at the time of the index event. Given prior evidence of sex differences in stroke risk factors in younger people with stroke,6,17 we used formal interaction term testing and prespecified subgroup analyses to determine if the association between sex and recurrent stroke differed by age group (
Results
Baseline characteristics of POINT trial participants, stratified by sex.
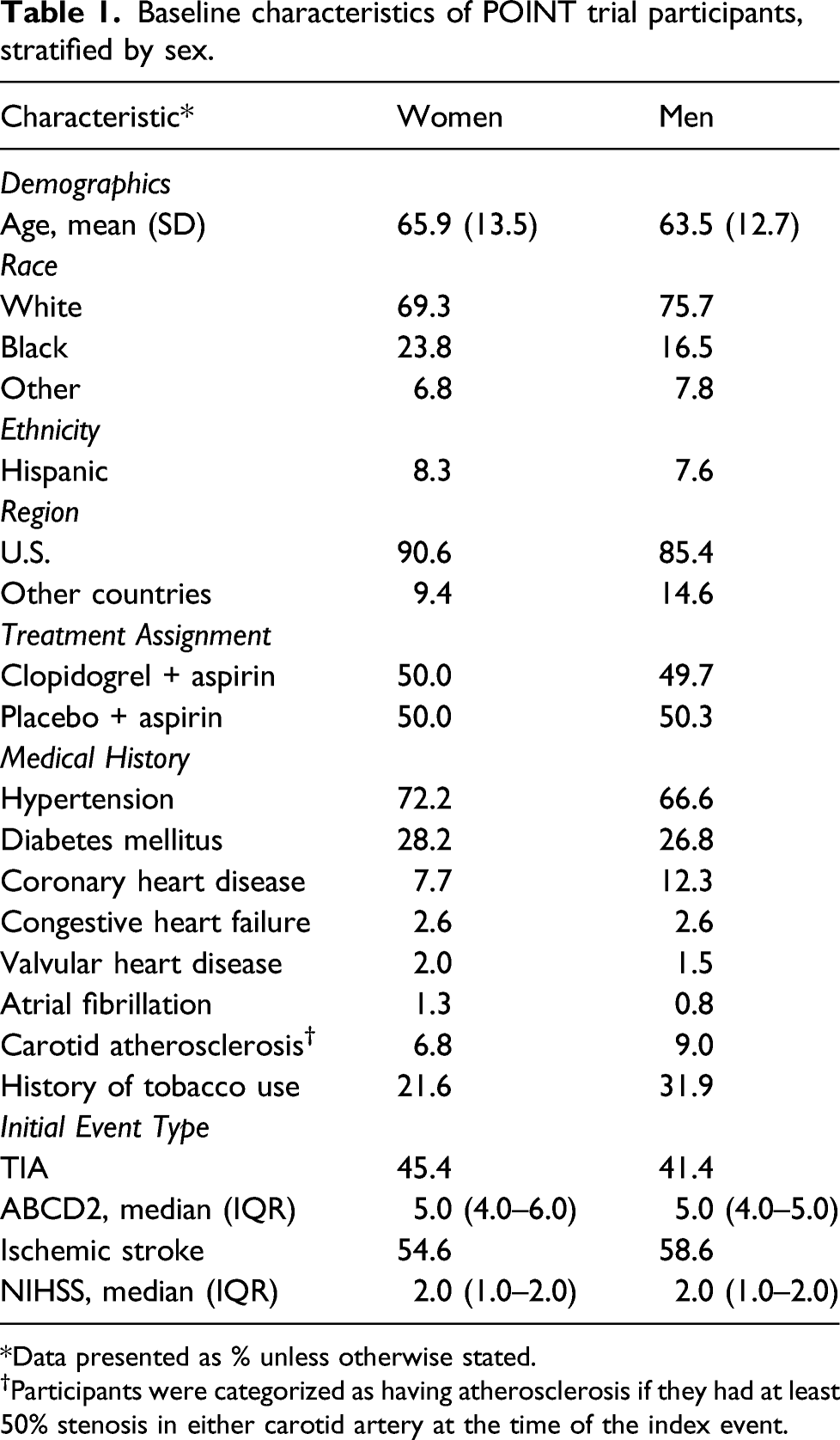
Data presented as % unless otherwise stated.
†Participants were categorized as having atherosclerosis if they had at least 50% stenosis in either carotid artery at the time of the index event.
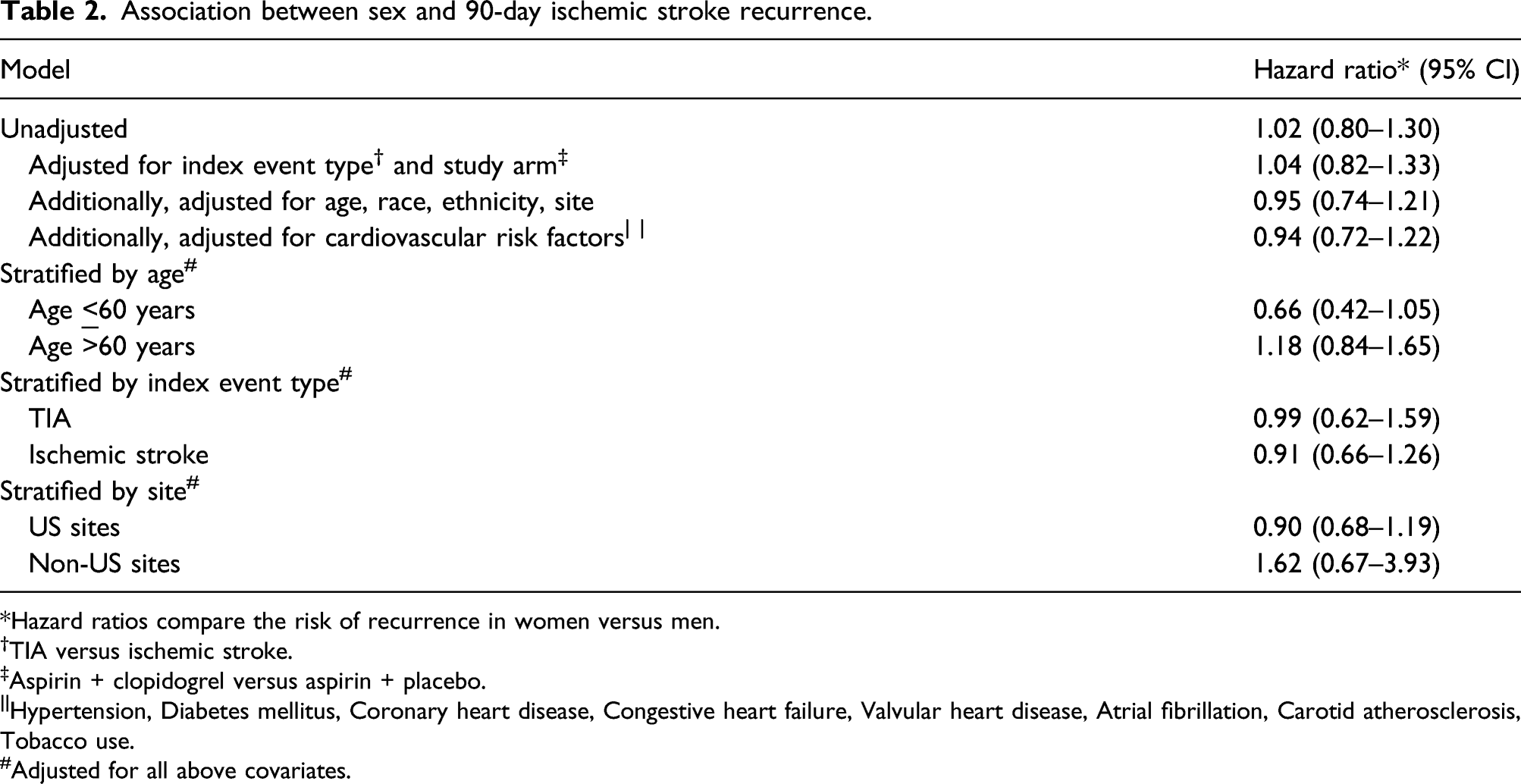
During the 90-day follow-up period, 267 (5%) ischemic strokes occurred; 121 were in women and 146 in men. The cumulative risk of recurrent ischemic stroke was not significantly different among women (5.76%; 95% CI, 4.84%–6.85%) compared to men (5.67%; 95% CI, 4.83%–6.63%) (Figure 1). In an unadjusted Cox proportional hazards model, women were not at a different risk of recurrent stroke as compared to men (hazard ratio [HR] 1.02, 95% CI 0.80–1.30). After stepwise adjustment for covariates, there was no association between sex and 90-day recurrent ischemic stroke risk, including in the final model, which was adjusted for index event type, study treatment assignment, demographics, and vascular risk factors (HR 0.94; 95% CI 0.72–1.22) (Table 2). Title: Kaplan–Meier curves demonstrating risk of recurrence stroke by sex in the Platelet-Oriented Inhibition in New Transient Ischemic Attack or Minor Ischemic Stroke Trial. Caption: The rate of recurrent stroke was similar in men and women enrolled in the Platelet-Oriented Inhibition in New Transient Ischemic Attack or Minor Ischemic Stroke Trial over 90 days. Association between sex and 90-day ischemic stroke recurrence. *Hazard ratios compare the risk of recurrence in women versus men. †TIA versus ischemic stroke. ‡Aspirin + clopidogrel versus aspirin + placebo. ||Hypertension, Diabetes mellitus, Coronary heart disease, Congestive heart failure, Valvular heart disease, Atrial fibrillation, Carotid atherosclerosis, Tobacco use. #Adjusted for all above covariates.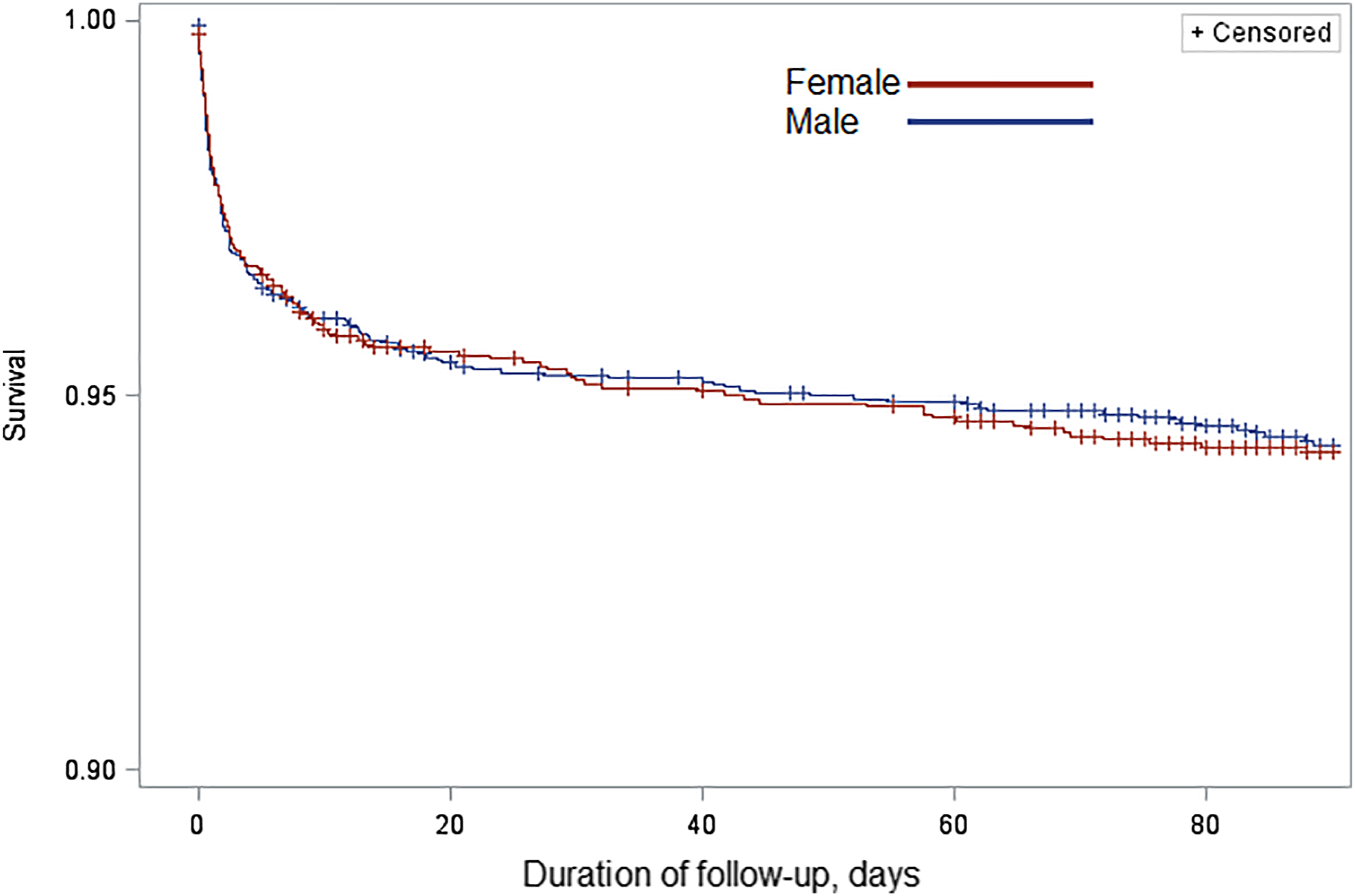
Formal interaction testing revealed a significant interaction between age group (
Last, we assessed sex differences in the relationship between conventional stroke risk factors and recurrent ischemic stroke. Overall, in adjusted models, the associations between conventional risk factors and recurrent ischemic stroke were as follows: diabetes (HR, 1.52; 95% CI, 1.15–2.00), hypertension (HR, 1.29; 95% CI, 0.93–1.79), carotid atherosclerosis (HR, 2.8; 95% CI, 2.01–3.90), and tobacco use (0.76; 95% CI, 0.56–1.03). Significant interactions with sex for diabetes (P=0.11), hypertension (P=0.70), carotid atherosclerosis (P=0.17), and tobacco use (P=0.88) were not seen.
Discussion
Among participants in the POINT randomized controlled trial with minor ischemic stroke or high-risk transient ischemic attack, we did not find an association between sex and 90-day risk of ischemic stroke recurrence. Additionally, sex did not modify the association between common conventional stroke risk factors and recurrent ischemic stroke.
Our findings build on prior work on sex differences in stroke recurrence. A prior analysis of data from a prospective cohort study based in Canada found men and women had a similar risk of 90-day ischemic stroke after presenting with stroke-like symptoms. 11 In this study, 452 of the 1,648 patients enrolled were diagnosed with a stroke mimic. In contrast, our use of data from the POINT trial ensured that all patients in our analysis had an adjudicated ischemic stroke or transient ischemic attack as their index event. Further, the POINT trial carefully included and adjudicated early recurrent events, which may have been missed otherwise in an observational study design. These methodological differences may explain the higher 90-day recurrence rate in the POINT trial (∼5% vs ∼2%). An alternate explanation is that the mean age in POINT was relatively young, with a relatively low prevalence of high-risk conditions such as atrial fibrillation.19–21 Additional prior studies on the association between sex and stroke recurrence include analyses of administrative claims data from a rural region of the United States 12 and for diabetic patients in Ontario, Canada. 13 Though these data were from narrowly defined populations and lacked granular clinical data, their findings were similar to ours.
Taken together, our findings suggest that the overall rate of recurrent ischemic stroke is similar in women and men, despite the influence of sex-specific risk factors unique to men and women.8,17,22,23 This has several possible explanations. First, it is possible that the effects of sex-specific risk factors unique to women and men are similar in magnitude, resulting in similar overall recurrence rates at the group level. Second, the effects of sex-specific risk factors may be too modest, relative to the large effect of conventional stroke risk factors, 24 to result in an appreciable difference in recurrence rates. Third, trial participation may obscure sex differences in stroke recurrence due to potential healthy participant selection bias and the controlled environment of the trial. Fourth, it is possible that sex differences in recurrence do exist, but among age groups (such as octogenarians and nonagenarians) not well represented in this analysis. Notwithstanding, our findings do not suggest that there exists an unidentified and influential sex-specific risk factor for ischemic stroke recurrence. Additionally, while prior research has suggested that the strength of the relationship between conventional stroke risk factors and incident stroke risk varies by sex, 10 this does not appear to be the case for recurrent ischemic stroke.
We identified a possible interaction between age and sex, with women having a non-significantly lower rate of recurrence than men under age 60. This may be due to a higher burden or greater severity of conventional stroke risk factors in young men than in young women. 25 Alternatively, differences in care may also account for our findings. Specifically, some young women with recurrent stroke may have been misdiagnosed with a stroke mimic and not reported to the trial,7,26 although this is unlikely given the rigorous nature of follow-up in POINT. Third, this finding may be due to chance in this post-hoc analysis. Yet, given the increasing incidence of stroke in younger adults,27–29 surveillance for sex differences in outcomes including recurrent stroke in this population may be warranted.
The strengths of our analysis include the use of a multicenter clinical trial dataset with adjudicated 90-day ischemic stroke outcomes. Our findings should be interpreted considering several limitations. First, the POINT trial was not designed to address sex differences in stroke recurrence; therefore, sex-specific risk factors were not tabulated in the trial. Additionally, we analyzed data for a clinical trial population, which excluded pregnant women. Pregnancy-related stroke is a unique clinical scenario that is not accounted for by these data, thus highlighting the potential lack of generalizability to the greater public. However, pregnancy-related stroke is rare and including it would have unlikely changed our results.17,30 Generalizability may be further limited for the additional reason that the POINT trial population does not fully represent stroke across the lifespan; sex differences in high-risk conditions, such as atrial fibrillation,19,20 among older individuals may not be reflected in our findings. Second, the trial had a 90-day follow-up period; so, it is unclear if our results hold true for long-term recurrence. Third, the POINT trial excluded participants with moderate and severe ischemic stroke, so these results may not be generalizable to all people with ischemic stroke. However, there was no interaction by event type (ischemic stroke versus TIA), so it is unlikely that our results are specific to minor ischemic stroke alone.
Conclusions
Among people with minor ischemic stroke and high-risk transient ischemic attack, men and women had a similar short-term ischemic stroke recurrence risk, and sex did not modify the impact of conventional stroke risk factors on recurrent ischemic stroke risk.
Footnotes
Acknowledgments
This research is based on the National Institute of Neurologic Disease and Stroke’s Archived Clinical Research data (Trial name: Platelet-Oriented Inhibition in New TIA and Minor Ischemic Stroke; Principal Investigator: S. Clairborne Johnston, MD, PhD; grant number: 1U01S062835-01A1) received from the Archived Clinical Research Dataset web site.
Declaration of conflicting interests
EB and SSO declare that there is no conflict of interest. HK serves as a principal investigator for the NIH-funded ARCADIA trial (National Institute of Neurological Disorders and Stroke U01NS095869) which receives in-kind study drug from the BMS-Pfizer Alliance for Eliquis® and ancillary study support from Roche Diagnostics, serves as Deputy Editor for JAMA Neurology, serves as a steering committee member of Medtronic’s Stroke AF trial (uncompensated), and serves on an endpoint adjudication committee for a trial of empagliflozin for Boehringer-Ingelheim. NP has received grants from the Leon Levy Foundation and the New York State Empire Clinical Research Investigator Program unrelated to this work and personal compensation for medicolegal consulting.
Funding
NP was supported by the Florence Gould Endowment for Discovery in Stroke for this work and receives funding from the NIH/NIA (K23AG073524).
Informed consent
Informed consent was not sought for this article because this was a retrospective analysis of existing, deidentified data.
Ethical approval
The Weill Cornell Medicine Institutional Review Board granted an exemption for analysis of these data because this was a retrospective analysis of deidentified data.
Trial registration
Guarantor
NP.
Contributorship
EB and NP researched literature and conceived the study. EB wrote the first draft of the manuscript. NP performed statistical analyses. All authors reviewed and edited the manuscript and approved the final version of the manuscript.