
Abstract
Background and aims
Basilar artery occlusion is a most devastating form of stroke, and the current practice is to reverse it with revascularization therapies. Pharmacological thrombolysis, intravenous or intraarterial, has been adjuncted or replaced with invasive, endovascular thrombectomy procedures. The preferred approach remains unknown and many recanalizations are futile with no clinical benefit. We sought to determine reasons for futility and weigh the existing reports to find whether endovascular mechanical interventions provide superior outcomes over pharmacological thrombolysis alone.
Methods
After analyzing systematically the reports of outcomes produced by variable basilar artery occlusion recanalization protocols, information was retrieved and reconciled from 15 reports published from year 2005 comprising 803 patients in 17 cohorts. In the largest single-center cohort (162, Helsinki), predictors of futile recanalization (three-month modified Rankin Scale score 4 to 6) were determined.
Results
Good outcome was reported by mechanical approaches either alone or on demand more frequently than by pharmacological, intravenous or intraarterial thrombolysis protocols (35.5% versus 24.4%, p < 0.001), accompanied by higher recanalization rates (84.1% versus 70.9%, p < 0.001). Along with superior recanalization rate at 91%, good outcome was reached by primary thrombectomy in 36% at the cost of substantial futile recanalization rate at 60%, which was lower when using modern stentrievers only (52.8%). In the Helsinki cohort, the single most significant predictor was extensive baseline ischemia, increasing the odds of futility 20-fold (95%CI 4.39–92.29, p < 0.001). Other attributes of futility were ventilation support and history of atrial fibrillation or previous stroke.
Conclusions
Endovascular mechanical approaches have been reported to provide superior outcomes over pharmacological thrombolysis in basilar artery occlusion. Stricter patient selection, most notably to exclude victims of already extended ischemia, would assist in translating excellent recanalization rates into improved clinical outcomes and more acceptable futility rates.
Introduction
Occlusion of the basilar artery is one of the most devastating forms of ischemic stroke. It carries a high mortality of 85–95% if recanalization does not occur, and a substantial part of survivors suffer severe disability, some being in locked in state.1–4 Evidence of the efficacy of different therapy protocols of intravenous (IVT) or intraarterial thrombolysis (IAT) and/or endovascular mechanical treatment is based on retrospective or prospective patient cohorts or registries, since pivotal randomised controlled trials (RCT) do not exist.
Roughly, a third of basilar artery occlusion (BAO) patients reach nondependent outcome (modified Rankin Scale (mRS) 0–3) following thrombolysis. From those with successful recanalization about half will reach nondependent outcome. In noninvasive pharmacological and endovascular mechanical protocols, recanalization of BAO is reached from 60% up to 100% of the patients.3,4 While endovascular mechanical approaches improve recanalization, they have not been proven superior to IVT in increasing good outcomes (GO).
It is widely agreed that meaningful survival after BAO requires rapid access to revascularization, but a considerable proportion of successful recanalizations do not translate into clinical benefit. This defines the term “futile recanalization” (FR). 5 The recanalization rate has been found in a combined analysis of 19 published cohorts to correlate indirectly with mortality, but no correlation with the likelihood of GO was found. 3 Intriguingly, recanalization appears to be a prerequisite for survival but does not at all guarantee meaningful survival. Previous systematic analyses do not advise on how to avoid FR.1,6 This motivated the present systematic analysis to assess the rates of GOs and FR obtained by different therapy protocols in BAO. Since the previously published reports did not fully disclose patient-level data to establish predictors of futility, we analyzed in detail the original data from the largest consecutive cohort of 162 patients treated primarily with IVT in Helsinki.
Materials and methods
Search/inclusion criteria for included studies
We searched PubMed with the terms “basilar occlusion,” “basilar artery occlusion,” and “basilar artery thrombosis.” We also collected relevant published reports and reviews by exploring the reference lists of articles retrieved by our search and from our own files. Reports containing original series data with active recanalization approach and published in English were included. The final study list was generated on the basis of originality and relevance, and the following aspects of recanalization, outcomes, and futility.
Posttreatment recanalization data available as defined in the original publication. Outcome data available from authors for patients with successful recanalization. To retain homogeneity and accessibility to the particular recanalization approach, individual series with more than 10 patients rather than heterogeneous registries were included. To retain contemporary clinical practices in the face of continuously evolving recanalization techniques we collected data from relatively recent series published starting from the year 2005.
Authors of studies were contacted to obtain information not retrievable from the original reports. Information was retrieved from 15 studies which, including the present Helsinki cohort, comprised altogether 803 patients.7–20
Definition of clinical benefit by recanalization therapy is not straightforward. In predominantly carotid territory stroke series, the marker of futility has usually been dependent functional outcome: mRS score 2 or higher. 5 However, BAO patients are at baseline neurologically more severely disabled11,12,21 than patients with carotid territory stroke entering recanalization therapies.5,22 Furthermore, BAO patients are frequently comatose and half require artificial ventilation. 21 It is unfair to judge that the recanalization of BAO in a comatose, tetraplegic patient was futile in a survivor achieving mRS 3. We thus considered mRS 4 or higher to represent the lack of clinical benefit, i.e. FR in BAO.
The Helsinki BAO cohort
The largest cohort was analyzed in detail to identify dominant predictors of recanalization, outcome, and FR in BAO.
Patients
The whole cohort includes 208 consecutive patients with angiography-proven BAO treated with the intention of recanalization between January 1995 and May 2013. IVT with 0.9 mg/kg alteplase (recombinant tissue plasminogen activator) was given to 181 (87%) patients, and 97% received concomitant full-dose heparin. Twenty-seven (13%) patients underwent IAT or mechanical endovascular procedure, of whom 18 (67%) also received IVT. Hence, the majority of patients (96%) received IVT as the standard therapy at our institution. Endovascular procedures were performed by the interventional radiologists by individual decision. All patients were prospectively included into the database, and some additional data were retrieved from patients’ charts retrospectively. Our institution approved the study protocol and requires no ethical review for a retrospective analysis of data collected as part of routine clinical care. All patients or their caregivers gave their informed consent regarding the revascularization therapy. All medical conditions and medications refer to the condition prior to the index stroke.
Imaging
Magnetic resonance imaging (MRI) was performed at baseline in 80 (38.5%) patients, whereas computed tomography (CT) was obtained in the rest. Posttreatment MRI or CT was obtained approximately 24 h after thrombolysis and whenever clinical deterioration occurred or intracranial hemorrhage (ICH) was suspected. Pretreatment angiography was CT angiography in 130 (62.5%) patients, time-of-flight MRA in 69 (33.2%) patients, and digital subtraction in nine (4.3%) patients. Posttreatment angiography was available for 76.9% of the patients, which limited the futility analysis to 162 patients. Recanalization in posttreatment angiography was dichotomized as partial to complete (thrombolysis in myocardial infarction/thrombolysis in cerebral infarction (TIMI/TICI) = 2–3) and nil to minimal (TIMI/TICI) = 0–1).23,24
The extent of baseline ischemia was evaluated with the posterior circulation Acute Stroke Prognosis Early CT score (pcASPECTS) for both CT and MRI, as originally reported. 25 Briefly, from a maximum of 10 points (normal), 1 or 2 points were subtracted for ischemic changes as follows: 1 point for left or right thalamus/cerebellum/posterior cerebral artery territory, and 2 points for any part of midbrain or pons. Patients with pcASPECTS < 8 were considered as having extensive ischemic changes. 25 All radiological data were evaluated blinded by two experienced neuroradiologists (HS, OS).
BAO treatment protocol
National Institutes of Health Stroke Scale (NIHSS) is obtained for all patients screened for thrombolysis treatment. According to our written institutional protocol since 199826,27 we distinguish patients with sudden massive onset (phenotype I) and those with progressing symptom presentation (phenotype II).4,27 The protocol advises thrombolysis up to 12 h in case of sudden massive onset. In contrast, for patients with progressing symptom presentation, the cutoff is 48 h from the onset of a monophasic course of progressing symptoms without resolution (i.e., excluding prodromes) characteristic of ischemia in the basilar artery territory, provided that extensive ischemic changes have not yet occurred in the posterior circulation area (particularly in brainstem).
Our protocol for BAO advises full-dose anticoagulation with either intravenous unfractionated heparin or low-molecular-weight heparin continued until the patient is mobilized. We verified the clinical presentation from original medical records to ascertain the individual onset-to-treatment times (OTT).
Outcome measures
We rated poor outcome as mRS = 3–6, GO as mRS = 0–2, and moderate as mRS = 0–3. mRS was assessed by video-trained and certified stroke neurologists either by personal appointment or by telephone interview of patients or caregivers. FR was defined as mRS 4–6 in patients with complete or partial (TIMI/TICI 2–3) recanalization. In the absence of standardized criteria for posterior circulation symptomatic intracranial hemorrhage (sICH), we report sICH according to the European Cooperative Acute Stroke Study II, National Institute of Neurological Disorders and Stroke, and Safe Implementation of Thrombolysis in Stroke criteria.28–30
Statistical analysis
Distributions of the continuous variables were studied and tested for normality. Univariate analyses were performed with t-test, Mann–Whitney U test, or Fisher’s exact test, as appropriate. Based on the univariate analyses, we constructed two models of binary logistic regression (enter method) studying factors associated with (a) recanalization and (b) FR. Variables included in both models were selected based on the univariate analysis with p < 0.1 as cutoff due to a high risk of overfitting. Cross-tabulated data were analyzed using Chi square statistics. Two-sided values of p < 0.05 were considered statistically significant. IBM SPSS 19.0 (SPSS, Inc., an IBM company, New York, USA) was used.
Results
Systematic analysis
The protocols retrieved from the literature that were used to recanalize BAO were quite variable. Most centers used IAT with mechanical thrombus eradication, with or without angioplasty or stenting with a great variety of thrombectomy and stent retriever devices.
Information retrieved from 15 reports with the inclusion of the Helsinki cohort comprised altogether 803 patients. In six cohorts, 406 patients were treated pharmacologically with IVT or IAT with or without glycoprotein IIb/IIIa antagonists as a “bridging” agent (Figure 1). Three cohorts (185) had mixed techniques, with patients treated primarily or adjunctively with IVT or IAT with on-demand mechanical endovascular approach such as stenting or first-generation thrombectomy devices (such as MERCI®, AngioJet®, Penumbra®). In eight cohorts (212) patients received primary thrombectomy with similar devices but lately also modern stentrievers (such as Solitaire®, Trevo®, Revive®). Five of these cohorts used solely these stentrievers (N = 103). Four studies (70/212, 33.0%) had a proportion of patients treated with bridging IVT. Two studies consisted of two cohorts that we analyzed separately due to their difference in the recanalization techniques.16,20
The results of systematic analysis of 15 studies reporting 17 cohorts of BAO recanalization included in the systematic analysis. The cohorts7–20 are grouped according to the primary treatment modality starting from the left: (1) pharmacological treatments, including intravenous, intraarterial thrombolysis with and without bridging with intravenous thrombolysis or antiplatelet agents, (2) mixed techniques as patients were treated primarily or adjunctively with systemic or intraarterial thrombolysis with on-demand mechanical endovascular approach such as stenting or earlier thrombectomy devices (such as MERCI®, AngioJet®, Penumbra®), (3) primary thrombectomy and/or stenting with a continuum of variable devices (such as AngioJet®, Penumbra®, MERCI®, Wingspan®, Solitaire®, Trevo®), (4) only stentrievers (such as Solitaire®, Trevo®, Revive®). In all mechanical protocols, it was possible to use small intraarterial doses of thrombolytics or stenting when deemed necessary to perfect recanalization. In the stentriever study by Mourand, 19 out of 31 patients received intravenous tPA as a bridging therapy before Solitaire® stentriever procedure to all patients.
19
In the cohorts of Nagel et al.,
16
patients treated solely with intravenous tPA (15 of 147) were excluded for this analysis. Note that recanalization is calculated as percentage from the whole treated cohort and futile recanalization is calculated as the percentage from the recanalized patients only.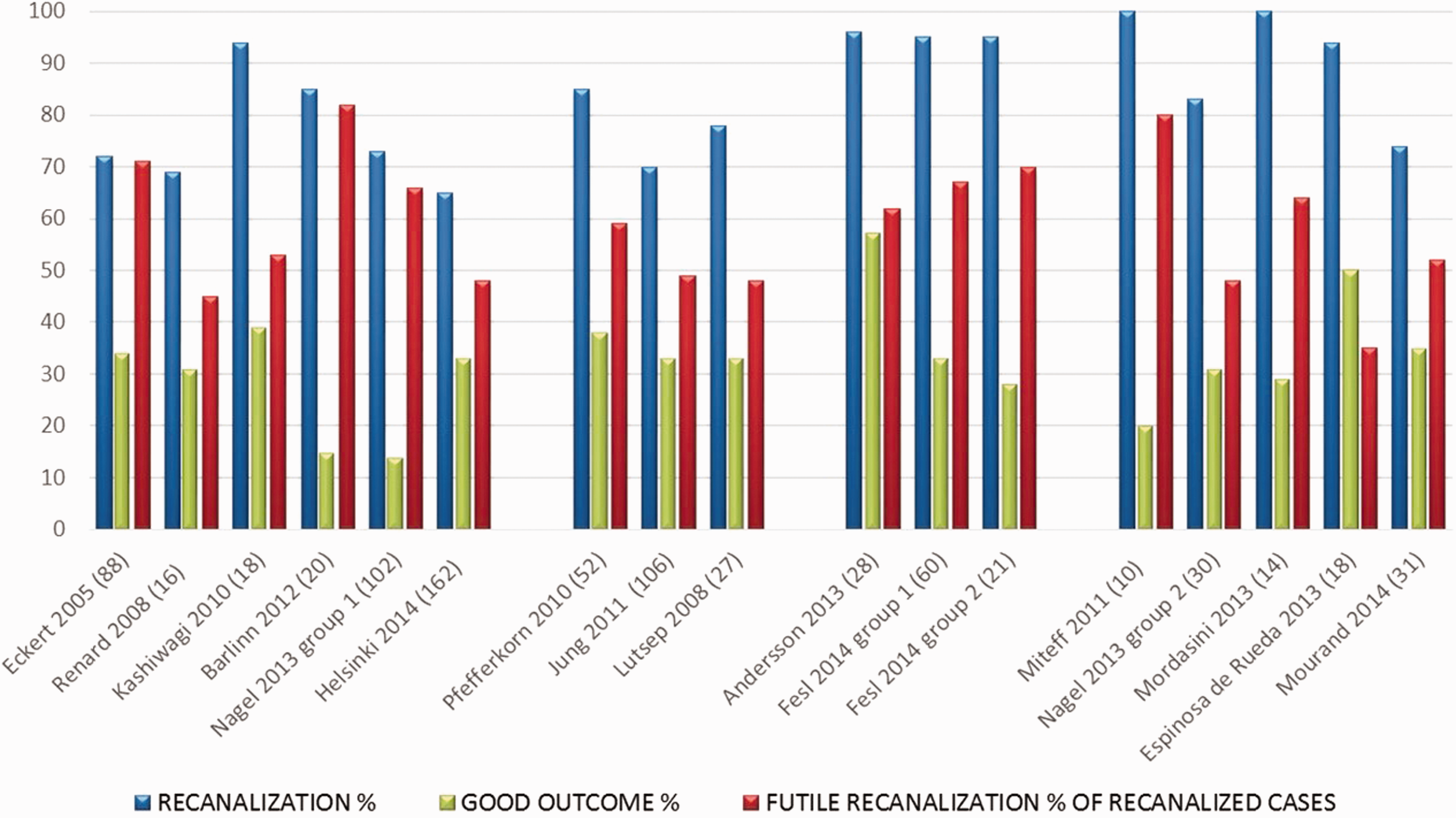
For the total of 803 included patients, recanalization was reported mostly as TIMI/TICI 2a-3, and for uniformity, we rearranged the data to reflect this definition in the reports that had originally used TIMI/TICI 2b-3 definition. The overall recanalization percentage was 77.5% (622/803). GO score predominantly at three months was reached in 29.9% (240/803) and ranged from 14 to 57% of patients in the individual series. FR was present in 57.1% (355/622) ranging from 35 to 82% of the patients in different cohorts (Figure 1).
Despite superior recanalization at 91.0%, GO was reached by primary thrombectomy in 36.3% at the cost of a substantial FR rate of 60.1% (Figure 2). From these eight cohorts, those five using solely modern stentrievers had more favorable FR rates of 52.8%, while the rates of recanalization and GO were 86.4 and 34.0%, respectively. Pharmacological recanalization methods (IVT or IAT) alone yielded mediocre efficiency: 70.9% rate of recanalization, GO in 24.4%, and FR in 57.6% of the patients. Protocols combining thrombolysis and variable on-demand endovascular mechanical therapies had most favorable outcome profiles; GO and FR rates being 34.6 and 51.8%, respectively (Figure 2).
The averaged results of the systematic analysis per treatment modality. Note that recanalization is calculated as percentage from the whole treated cohort and futile recanalization is calculated as the percentage from the recanalized patients only. Note also that the bars labeled stentrievers represent a subgroup of the thrombectomy group. The pharmacologically treated cohorts had statistically significantly inferior results in recanalization and good outcome in comparison to those treated with primary or adjuncted mechanical endovascular treatments (see Table 1).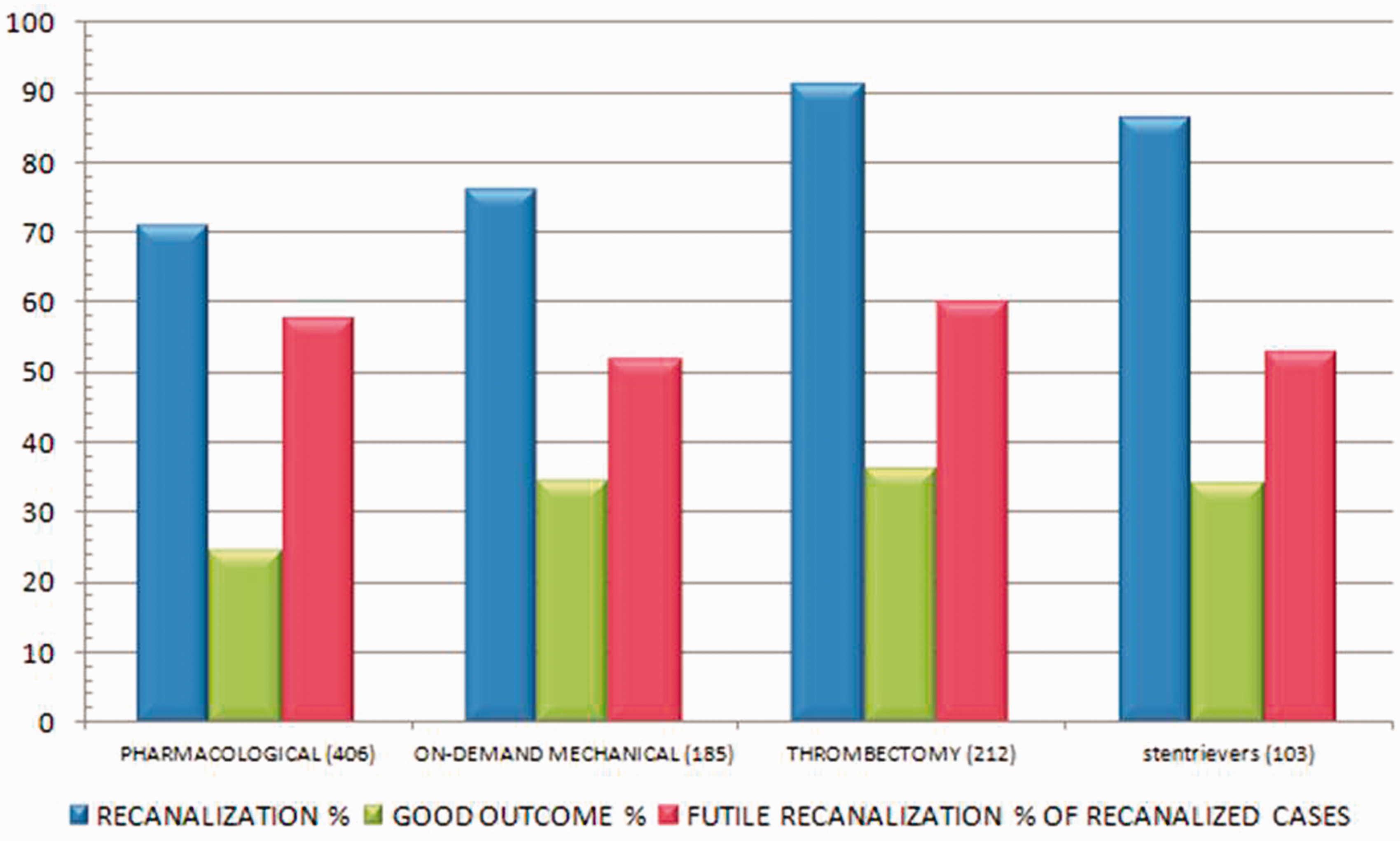
Cross-tabulation of the data retrieved by the systematic analysis.
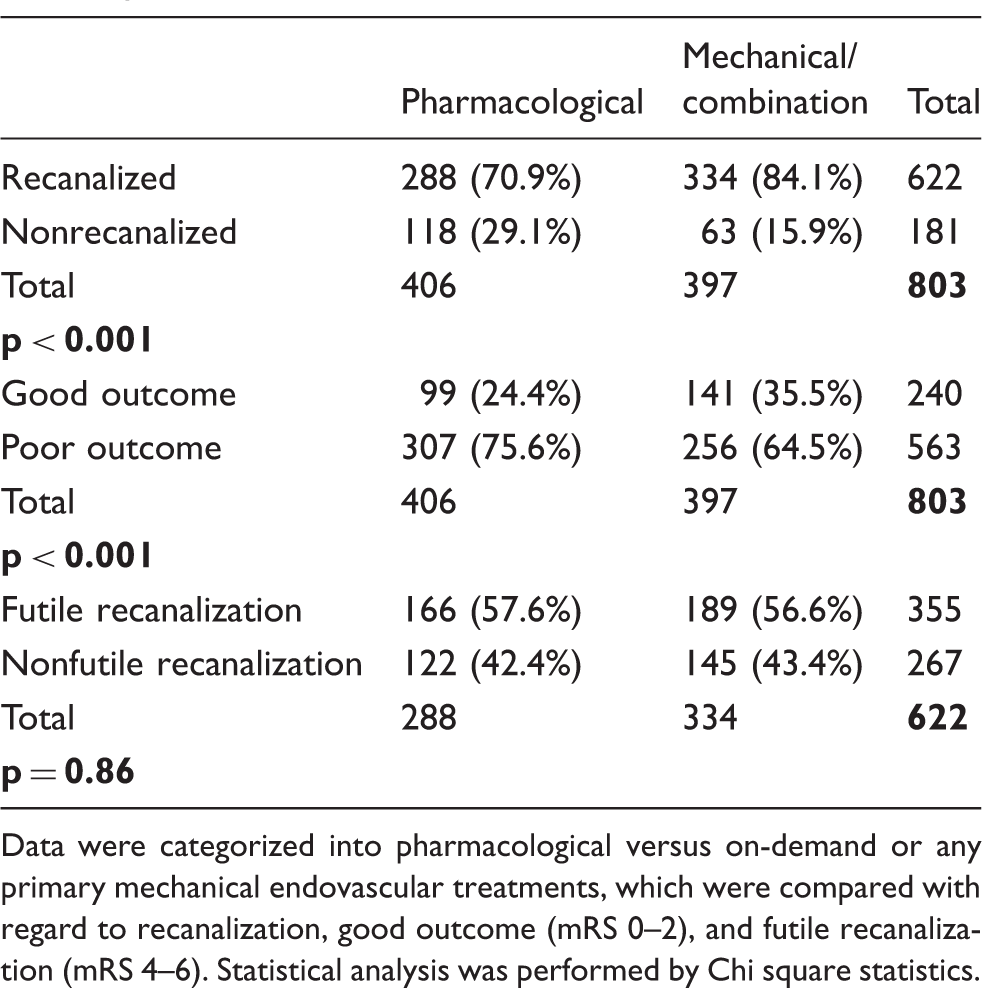
Data were categorized into pharmacological versus on-demand or any primary mechanical endovascular treatments, which were compared with regard to recanalization, good outcome (mRS 0–2), and futile recanalization (mRS 4–6). Statistical analysis was performed by Chi square statistics.
Predictors of recanalization and futility
In the largest BAO cohort of 162 patients from Helsinki, the recanalization rate was 66%, GO at 33%, and FR rate 42% (Figure 3, Supplemental Table 1). In addition to the profound effects of age and baseline NIHSS, ventilation support and pcASPECTS < 8 were associated with worse chances of recanalization as well as FR in the univariate analysis. Interestingly, history of atrial fibrillation or prior stroke was associated more likely with FR but not with recanalization. Atrial fibrillation favored recanalization but also FR (Table 2). The development of any ICH or sICH by variable definitions28–30 associated with nonrecanalization as well as with FR (Supplemental Table 1).
Effect of baseline infarct and recanalization on clinical outcome and futility. Outcome results of the Helsinki cohort arranged to reflect the effect of recanalization and extensive baseline infarction (pcASPECTS score <8). Note that recanalization is calculated as percentage from the whole treated cohort and futile recanalization is calculated as the percentage from the recanalized patients only. Data are arranged according to the three-month mRS score expressed with different colors. R+ = recanalization and R− = nonrecanalization. Logistic regression of parameters associated with recanalization and futile recanalization (mRS 4–6). Results from the Helsinki cohort. Variables included in both models were selected based on the univariate analysis with p < 0.1 as cutoff due to a high risk of overfitting (45 cases of FR, 107 total cases). OTT was not independently associated with outcome even when tested as categorical variable. NIHSS on admission and ventilation support were tested separately due to strong interaction between these two factors.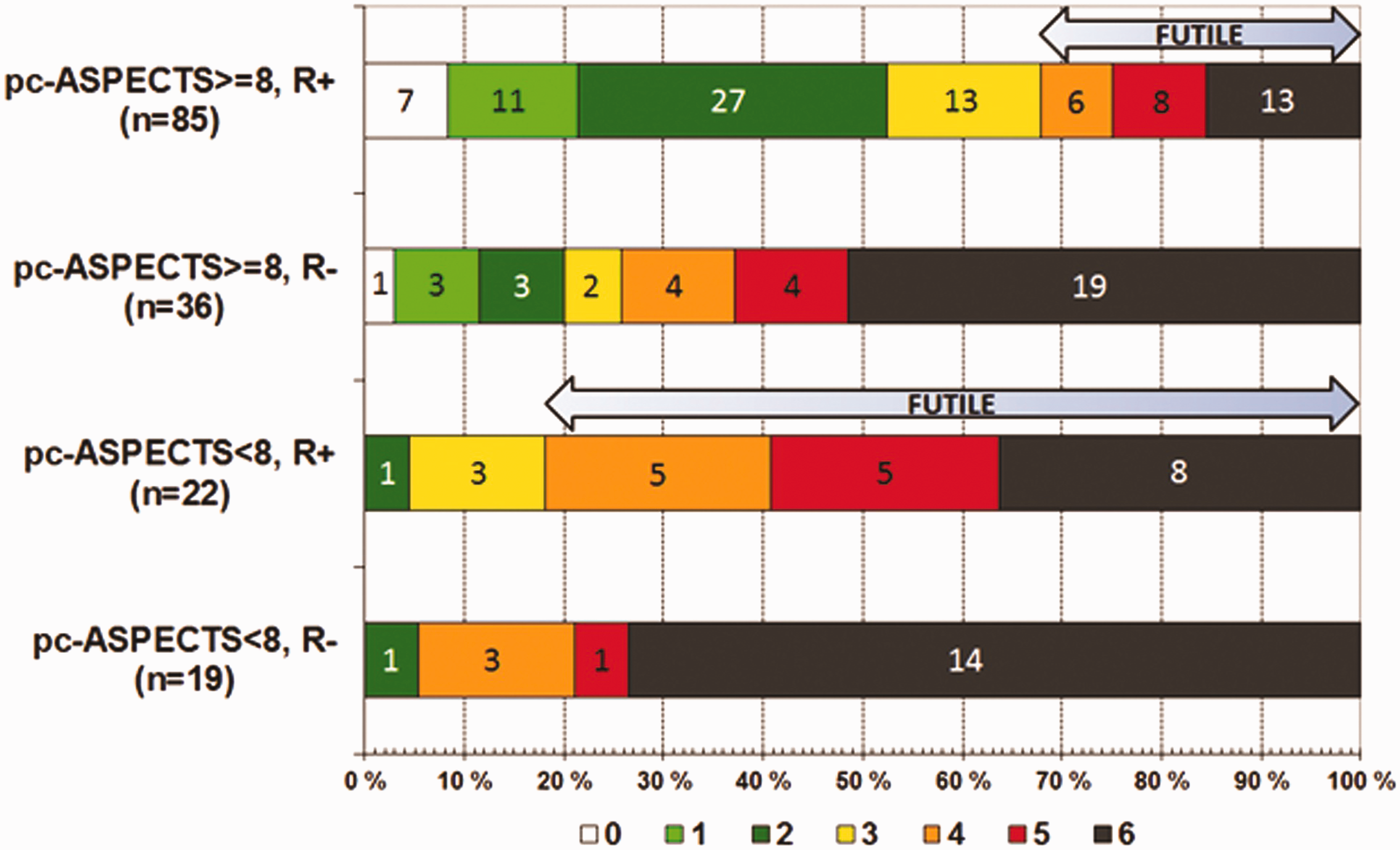
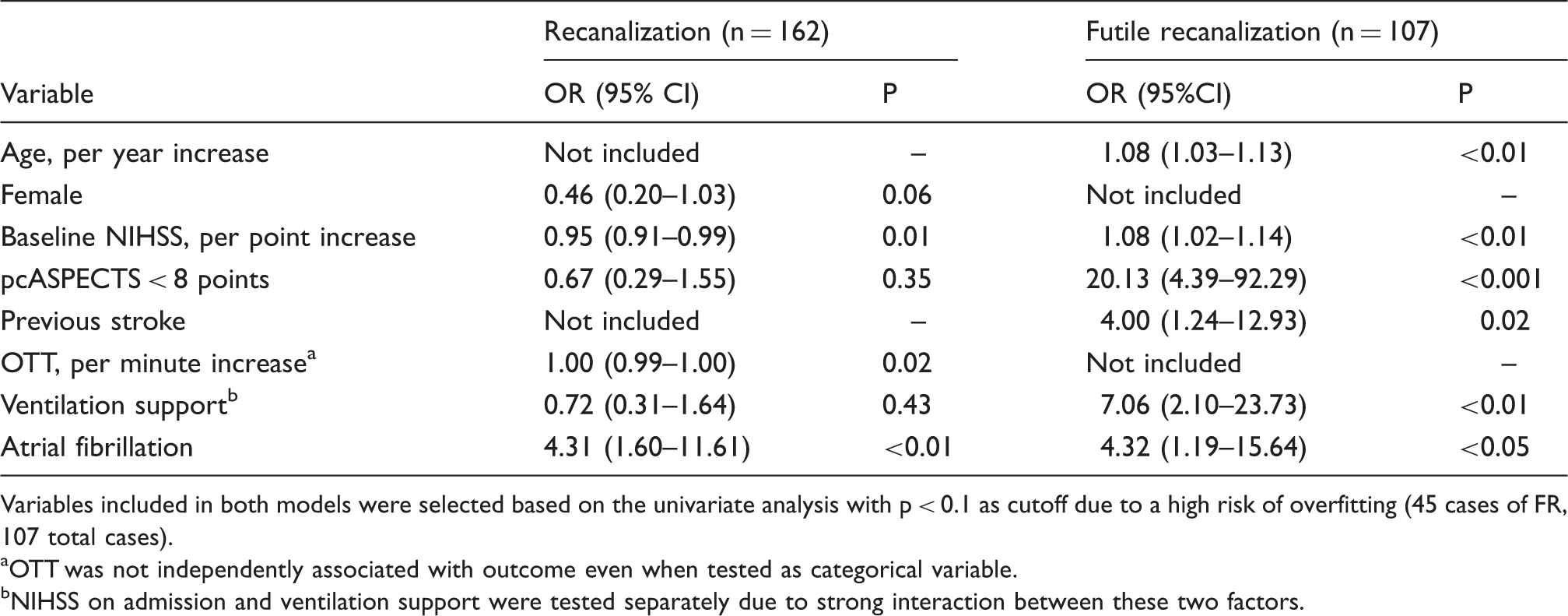
In the multivariable analysis of futility, the most striking predicting variable was the extent of baseline ischemia (pcASPECTS < 8), increasing the odds of FR 20-fold (95%CI 4.39–92.29, p < 0.001) (Table 2). There was a 2.5-fold increase in the fraction of FR from 32% in patients recanalized with baseline pcASPECTS ≥ 8 to 82% in patients recanalized with pcASPECTS < 8. Simultaneously, the odds of GO shrinked from 53% to only 5% (Figure 3).
Ventilation support increased FR sevenfold (2.10–23.73, p < 0.01) and previous stroke fourfold (1.24–12.93, p = 0.02) (Table 2). The paradoxical univariate associations of atrial fibrillation to both recanalization and FR were maintained fourfold in the multivariable analysis. OTT was not independently associated with GO. The attributes of futility have been broken out according to the etiologic group in Supplemental Figure 1.
Evolution of futility, GO, and secular trends
During the whole period of BAO recanalization therapy in Helsinki, on average 11 patients have been treated annually. To allow scrutiny of the outcome and futility results as a function of secular trends we have broken out the essential results into roughly 20 treated patients’ batches within 1995–2013 (Supplemental Figure 2). Since the publication of our initial institutional management guidelines of BAO recanalization in 1998,26,27 very few clear protocol changes have been implemented during this time. The definitions of time delays have not changed. The major evolutions during this time were following.
Between years 2005 and 2010 the computed tomography angiography (CTA) has more or less replaced MRA as the primary diagnostic imaging modality. The average OTT of BAO thrombolysis has gradually more than halved from roughly 23 h during 1998–2005 to 9 h during 2006–2013 (Supplemental Figure 3). During corresponding years the door-to-needle time (DNT) has dropped significantly almost fivefold from roughly 14 to 3 h, while the onset-to-door time has fluctuated from roughly 9 to 6.5 h (supplemental Figure 3). Only in the last three years on-demand endovascular mechanical treatments (11 out of 23) have been performed actively.
The rates of GO and FR appear not to have changed in the face of these “secular trends” in general BAO diagnostics and streamlining of management.
Discussion
This is the first systematic analysis comparing the clinical benefit and utility of successful recanalizations of BAO treated with multimodal recanalization therapies. An endovascular mechanical approach with or without an adjuncted pharmacological protocol was associated with improved treatment results in comparison to pharmacological thrombolysis (IVT or IAT) protocols (Table 1). While the rates of GO have reached 36% with primary thrombectomy, it appears that up to 60%, of BAO recanalizations ended up futile. Using solely stentrievers had a more favorable FR of 53%, while 34% reached GO (Figure 2). The detailed analysis of the largest series in Helsinki suggests that the single most important adjustable patient selection characteristic to associate with futility is baseline ischemic changes as defined by pcASPECTS score below 8.
Previous systematic analyses and registry data have demonstrated that a significant difference in the outcomes cannot be found following IVT and IAT of BAO.1,2,6 This, as well as communications with contacted source study authors led us to an analysis with regard to endovascular mechanical treatments and pharmacological thrombolysis (IVT or IAT) only (Table 1, Figures 1 and 2). Technical advances in the newer stentrievers are close to perfection, with recanalization rates around 90% (Figures 1 and 2). Nevertheless, even complete recanalizations by primary thrombectomies have not translated into GO, 20 supported here also by FR rate of 53–60%. While pharmacological approaches have an apparent ceiling effect, a strong incentive for adopting mechanical devices was found. Cost–benefit calculation would perhaps favor their rapid deployment as an on-demand procedure, which had the lowest FR rate of 52%. Improved patient selection based on parenchymal imaging with plain noncontrast CT, CTA source images and pcASPECTS score to start with, can probably improve the FR rates of thrombectomy protocols. 25 Similar predictive value of pcASPECTS scoring based on MR DWI has been reported, 31 suggesting that either technique is useful.
The limited imaging data available from individual study centers were not sufficient to analyze the predictors of futility across all analyzed data (803). Therefore, we performed a detailed analysis of our large cohort (162). Age, baseline NIHSS, ischemic CT changes, and ventilation support associated significantly with FR. Rather paradoxically, OTT and DNT reduction did not evolve in correlation with the rate of FR (Supplemental Figures 2 and 3). Halving of OTT and even fivefold reduction in the DNT delays in Helsinki after 2005 were not followed by noticeable therapeutic improvement (Table 2, Supplemental Figures 2 and 3, Supplemental Table 2). Also our previous data suggest that symptom duration does not predict prognosis in thrombolyzed BAO. 32 The issue of long time window in BAO recanalization therapies has recently been discussed. 33 During the perilous time period from symptom onset to treatment, recanalization at any point of time can potentially salvage the brain stem from eventual necrosis caused by imminent reinforcement and further building up of the clot. 33
In the Helsinki cohort, previous stroke appeared as a robust predictor of futility, even after patients with extensive baseline ischemia had been excluded (Supplemental Table 3, Supplemental Figure 1). Half of the patients with FR lacking extensive baseline ischemia had a history of previous stroke. Interestingly, while embolic origin and atrial fibrillation favored recanalization, they also predicted FR, which may reflect poorly developed collaterals in contrast to arteriosclerotic origin. BAO caused by dissections seems to fare well when treated with recanalization therapy.
How many favorable outcomes would be lost should patients with pcASPECTS < 8 be denied revascularization? Considering the whole period of revascularization therapy in Helsinki since 1998, only four patients (mRS 3 in three and mRS 2 in one) would have been denied a non-FR from 41 patients with pcASPECTS < 8 within the 107 consecutive patients examined for recanalization (Supplemental Figure 2). The serious antithesis for administering IVT and on-demand thrombectomy for patients with extensive baseline ischemia are the 18 patients with FR, 10 of whom remained severely debilitated with mRS 4 or 5. However, the timing of BAO recanalization by IVT has not been monitored and based on this IVT series it cannot be assumed that prompt and complete recanalization by thrombectomy would necessarily produce identical outcome distribution.
It is often stated that multimodal imaging should be used to select patients who could still have clinical benefit from recanalization. However, as reported previously, 32 even the plain noncontrast CT and determination of the pcASPECTS score will assist tremendously in selecting the patients with potentially meaningful recovery. If the pcASPECTS score is below 8 there is probably no additional imaging to gain more accurate prognostic information in this desperate situation where hardly anyone will recover meaningfully following recanalization.
How do the recently published RCTs proving the efficacy of anterior circulation thrombectomy relate to BAO?34–36 Since these trials did not include posterior circulation occlusions, they did not add to the database necessary for revising therapy guidelines concerning BAO. However, since the on-demand mechanical approach after pharmacological recanalization attempts was superior to thrombolysis alone in the current systematic analysis, there is absolutely no disagreement. In aggressive management of imminent devastating infarctions, it seems of paramount importance for therapeutic efficacy to exclude patients with extensive baseline infarctions in both vascular territories. Also the effect of the need of mechanical ventilation, multiplying sevenfold the likelihood of futility (Table 2), resembles the blunted therapeutic effect of thrombectomy in patients requiring general anesthesia in the MR CLEAN trial. 37 All but one of the eight cohorts using primary thrombectomy approach in BAO reported using general anesthesia.
Study limitations
We realize that the systematically analyzed material consists of only ad hoc reports of consecutive series rather than clinical trials, and a considerable publication bias may exist. Besides additional data heterogeneity, some centers reported their recanalization results based on periprocedural angiographic imaging and others with repeat CT angiography approximately at one day after recanalization therapy. Furthermore, we could not retrieve data on the timing of recanalizations, which may be different in the compared therapeutic approaches. Furthermore, there may also be variability in reporting the start and duration of BAO based on clinical symptoms, which we are unable to eliminate in a systematic literature analysis.
In conclusion, these data suggest that endovascular mechanical treatments do assist in achieving superior recanalization rates and improved outcomes than pharmacological thrombolysis protocols (IVT or IAT) alone. Among intracranial major trunk occlusions, BAO is the most amenable to recanalization by thrombolytic therapy (71%, Figure 2), but stentrievers can reach even higher recanalization rates and presumably faster. Still, FR rates remain high and should be monitored in benchmarking stroke management protocols. In the advent of ever perfecting recanalization devices, we may have been too enthusiastic just to rush BAO patients into the hands of expert interventionalists. It should be considered based on baseline imaging whether the vascular territory to be recanalized still benefits from revascularization. However, more systematic data, e.g. in a RCT or a prospective registry, are necessary to determine the optimal strategy for BAO recanalization of viable brain stem to avoid therapeutic futility. The present data are by no means a substitute for a RCT, and centers treating BAO actively with recanalization therapy are encouraged to participate in RCTs to acquire prospective data on the efficacy of variable BAO recanalization protocols.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lindsberg, Silvennoinen, Salonen list no disclosures. Sairanen and Nagel received travel expenses to a scientific conference with the support of from Boehringer Ingelheim Pharmaceuticals Inc. Nagel has received counseling fees from Brainomix Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Academic stroke research in Helsinki is supported by financial resources from governmental and nonprofit foundations, the Helsinki University Central Hospital governmental subsidiary funds for clinical research (DS, PJL), the Finnish Medical Foundation (DS), the Finnish Academy (PJL), the Sigrid Jusélius Foundation (PJL), the Maire Taponen Foundation (TS, PJL), and the Paavo Nurmi Foundation (PJL).
Informed consent
In the Helsinki University Hospital, all patients or their caregivers gave their informed consent regarding the revascularization therapy.
Ethical approval
Our institution approved the study protocol, and requires no ethical review for a retrospective analysis of data collected as part of routine clinical care.
Guarantor
PJL
Contributorship
PJL researched literature and conceived the study. DS, SN, HS, OS and TS were involved in protocol development, patient recruitment and analysis of clinical and radiological data. PJL wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.