
Abstract
Introduction
Co-occurring conditions like sleep disturbances are prevalent in autism spectrum disorder (ASD) and have been linked to greater variability in clinical presentation, including social communication and behavioral challenges. This study examined the relationship between sleep disturbances and ASD characteristics in school-aged children.
Method
In this descriptive, observational study, 24 children with ASD (ages 6–12) wore actigraphy monitors for up to seven nights to provide objective data on sleep onset latency, total nighttime sleep, and nighttime awakenings. Parents completed sleep diaries and the Autism Spectrum Rating Scale to assess impairments in social and communication, behaviors associated with ASD, and self-regulation.
Results
Of the 24 participants, 23 wore actigraphy monitors. Twenty-two children experienced at least one sleep disturbance, and of these, 21 had usable actigraphy data, with an average of 6.43 nights analyzed. A greater number of sleep disturbances was associated with increased parent-reported social-communication difficulties but lower parent-reported behavioral dysregulation scores.
Conclusions
Findings suggest that sleep disturbances may differentially influence the expression of ASD characteristics across social-communication and behavior. Considering sleep patterns in ASD research and clinical care may enhance understanding of variability in ASD and support the development of targeted interventions.
Autism spectrum disorder (ASD) is a complex neurobiological condition that is characterized by social impairments, restrictive, and repetitive behaviors. Recent surveillance estimates suggest that approximately 1 in 31 children are identified with ASD, although prevalence varies with diagnostic practices, ascertainment methods, and access to services (Fombonne et al., 2021; Shaw et al., 2025; Zeidan et al., 2022). Children with ASD 1 display considerable variability in clinical presentation, language development, cognitive functioning, adaptive skills, and co-occurring conditions—factors that complicate diagnosis, treatment, and research (Al-Beltagi, 2021; American Psychiatric Association, 2013; Bitsika et al., 2018; Casanova et al., 2020; Lai et al., 2014; Wiggins et al., 2022; Zachor & Ben-Itzchak, 2016). Understanding how co-occurring conditions influence this variability is crucial for improving outcomes, particularly because early, targeted intervention can meaningfully support development (Bangerter et al., 2020; Genovese & Butler, 2020; Wiggins et al., 2022).
Among co-occurring conditions, sleep disturbances are among the most common and impactful challenges in ASD, affecting 56% to 80% of children with autism (Abel et al., 2017; Bangerter et al., 2020; Hundley et al., 2016; van der Heijden et al., 2018). These disturbances—such as reduced sleep efficiency, shorter sleep duration, fragmented sleep, and prolonged nighttime awakening—may contribute to behavioral dysregulation, diminished adaptive functioning, and greater caregiver burden. This study examines the relationship between sleep disturbances and distinct ASD characteristics, contributing to the growing body of literature on how sleep influences neurodevelopment and day-to-day functioning in autistic children (Bangerter et al., 2020; Bitsika et al., 2018; Cohen et al., 2018; Zachor & Ben-Itzchak, 2016).
Objective sleep studies in children using actigraphy and polysomnography consistently show more erratic, less efficient sleep in children with ASD compared to neurotypical peers. Autistic children frequently experience increased sleep onset latency (SOL; the interval between bedtime and sleep onset), shorter overall sleep time, earlier morning waking, and prolonged nighttime awakenings, as well as disrupted sleep continuity (Abel et al., 2017; Cohen et al., 2018; Fletcher et al., 2017; Goldman et al., 2009; Kotagal & Broomall, 2012; Sannar et al., 2018; Souders et al., 2009; van der Heijden et al., 2018).
Despite these well-established sleep disruptions, few studies have linked specific types of sleep disturbances (e.g., sleep onset delay, early morning waking, or nighttime awakenings) to distinct ASD symptom domains. Much of the existing literature evaluates sleep globally, reporting broad associations between poor sleep and greater overall ASD severity rather than identifying symptom-specific pathways.
Studies relying on parent report suggest that children with ASD who sleep poorly exhibit heightened sensory sensitivity, hyperactivity, anxiety, and greater ritualistic or compulsive behaviors (Goldman et al., 2011; Hundley et al., 2016; Sikora et al., 2012). Children with increased bedtime rituals may also show greater bedtime resistance and difficulty adapting to environmental or routine changes. However, these findings primarily rely on subjective measures, and few investigations have isolated how particular sleep disturbances relate to specific behavioral, social-communication, or repetitive behavior profiles.
A limited number of more detailed investigations provide early evidence of domain-specific relationships. A long-term actigraphy study (20,000 nights of monitoring over 18 months) of 67 children and adolescents with ASD and severe intellectual and social-communication impairments, found that prolonged sleep disruption was associated with increased agitation, meltdowns, externalizing behaviors (e.g., hitting desks and walls and throwing items), and higher scores on a challenging behavior index (Cohen et al., 2018). Other work has linked disturbed sleep more broadly to poorer adaptive functioning and greater ASD symptom severity (Sikora et al., 2012; Zachor & Ben-Itzchak, 2016). Recent research has begun to delineate these associations further, including links between rapid eye movement sleep and social-communication difficulties (Kawai et al., 2023), repetitive behaviors (Passarini et al., 2025), and longitudinal patterns of sleep and symptom severity (Sadikova et al., 2023). These emerging findings underscore the importance of clarifying how specific sleep characteristics may differentially relate to unique ASD characteristics.
Collectively, existing evidence supports a meaningful connection between disturbed sleep and ASD-related behaviors while highlighting a gap in understanding symptom-specific pathways. The present study addresses this gap by examining how discrete actigraphy-derived sleep disturbances relate to specific ASD symptom domains in a sample of children with ASD.
Methods
Design
This descriptive, correlational, cross-sectional study examined sleep characteristics in children with ASD using wrist or shoulder actigraphy and parent-completed sleep diaries.
Setting and Sample
Participants were recruited using a convenience sampling approach from a tertiary hospital database in an urban/suburban area of Cleveland Ohio through a study flyer and targeted email outreach. Email invitations were sent to families of children ages 6 to 12 with an ASD diagnosis identified through University Hospitals Rainbow Babies and Children’s TriNetX electronic medical record database based on ICD diagnostic codes. Emails were distributed in batches of 40 (160 sent in total). Eligibility was confirmed during prescreening, during which caregivers verified the child had received a formal medical diagnosis of ASD by a qualified specialist (e.g., developmental pediatrician, pediatric neurologist, or licensed psychologist) following a comprehensive diagnostic evaluation.
Participants wore a GT3X + Actigraph (ActiGraph LLC, Pensacola, FL) on their wrist or shoulder, for home-based monitoring during the academic year, excluding extended school breaks, to capture typical sleep patterns. Parents completed sleep diaries and agreed not to change medications or therapy during data collection. Exclusion criteria included recent (within 14 days) medication or therapy changes, unstable medical conditions that may require changes in interventional therapy or medication, seizure history, or regressive-onset ASD.
Data Collection
Following IRB approval, parents completed informed consent, provided information about their child's current and historical physical medical conditions, and filled out the Autism Spectrum Rating Scale (ASRS) (Goldstein & Naglieri, 2010). They also received detailed instructions on maintaining sleep diaries and using actigraphy (ActiGraph LLC, Pensacola, FL).
Sleep data were collected over seven consecutive nights, with a minimum of four nights required for inclusion in the analysis. Prior research has demonstrated that at least three nights of actigraphy are sufficient to provide reliable estimates of children's sleep (Adkins et al., 2012). Parents were instructed to place the actigraphy watch on the child's nondominant wrist. If the child was unable to tolerate the device on the wrist, parents were offered a shoulder pocket alternative (Adkins et al., 2012). The actigraph was placed on the child 10 to 30 min before bedtime to capture the full sleep onset period. Compliance and placement were documented by parents in the accompanying sleep diary. Nights were excluded from analysis if the sleep diary reported child illness or sleep occurring in an atypical environment (e.g., sleepovers or time away from home), or if actigraphy data were missing. No device malfunction exclusions were necessary.
Measures
The number of sleep disturbances (increased SOL, wake multiple times, extended wakefulness, early morning wake [EMW]) was collected and quantified, providing a value from 0 to 4 for each participant. A score of 0 indicated no nighttime sleep disturbances, while higher values reflected the number of sleep disturbances. To balance interpretability and reliability in a small sample, disturbances were treated as count-based indicators (0–4), consistent with pediatric sleep assessment frameworks such as the Insomnia Severity Index (Bastien et al., 2001; Morin, 1993), where the presence of multiple disturbance types (e.g., difficulty initiating sleep, maintaining sleep, and early awakening) reflects increasing severity of sleep problems. This approach emphasizes cumulative burden rather than duration or magnitude of individual events, aligning with accepted clinical practice in pediatric sleep assessment.
Sleep Diary
The parent sleep diary (CHOC Children's, 2016) recorded the time the child was put down for bed, the observed time sleep was initiated, the number of times the child woke up during the night, the number of minutes the child was awake during the night, the number of hours the child slept, and the time the child got out of bed in the morning. Parents could also document any additional disturbances and note environmental factors that may have affected sleep.
Actigraphy
Actigraphy measures motor activity from which sleep–wake patterns are inferred, providing an objective estimate of sleep duration and fragmentation under naturalistic conditions. Objective sleep onset, total nighttime sleep duration, nighttime awakenings, and wake durations were measured by wrist or shoulder actigraphy (ActiGraph GT3X+, ActiGraph LLC, Pensacola, FL). Sleep efficiency (SE) was calculated as total nighttime sleep divided by time allotted for sleep. Sleep onset and wake times were determined by 10 consecutive minutes of immobility with 60s epochs, per the Sadeh algorithm (Sadeh et al., 1994).
Autism Spectrum Rating Scale
Parents completed the ASRS (Goldstein & Naglieri, 2010), a 70-item standardized measure of ASD symptomatology that takes approximately 20 min to complete. Items are rated on a five-point Likert scale (Never to Very Frequently), with reverse-coded items adjusted prior to analysis. Raw scores were converted to T-scores, providing age- and gender-normed values that facilitate comparisons across individuals and domains. Scores ≥ 60 indicate clinically significant impairment.
The ASRS includes a Diagnostic and Statistical Manual of Mental Disorders (DSM-5)-aligned composite severity score and three subscales—Social-Communication (19 items; capturing pragmatic language, reciprocal interaction, and social use of communication), Unusual Behaviors 2 (24 items; reflecting repetitive behaviors, restricted interests, and sensory sensitivities), and Self-Regulation (27 items; assessing attention, impulsivity, emotional control, and behavioral regulation)—which correspond to core DSM-5 ASD symptom domains. The instrument demonstrates strong psychometric properties, with internal consistency estimates (Cronbach's α) ranging from .74 to .97, test–retest reliability over 2 to 4 weeks ranging from .72 to .93, and discriminant validity studies showing correct classification rates of 92% when distinguishing ASD from the general population (Goldstein & Naglieri, 2010).
Sensory responsiveness was not a primary focus of the study; therefore, a standardized measure was not administered. However, all caregivers reported their child experiences altered sensory responsivity using a yes/no item on the medical history form.
Data Analysis
Descriptive statistics were used to examine sleep diary, actigraphy, and ASRS results. Actigraphy was the primary data source and scored using ActiLife software version 6.13.4 (ActiGraph LLC, Pensacola, FL) with the Sadeh algorithm validated for children. Nights with missing actigraphy were excluded. Sleep diaries were used to record bedtime and contextual factors (e.g., illness and nights away from home) but were not used to replace missing actigraphy data, as parent reports systematically underestimated the frequency and duration of nighttime wakings. Given these discrepancies, the actigraphy data were utilized for primary analyses, while diary data were retained for descriptive and comparative analyses.
One participant who could not tolerate actigraphy was excluded from SOL, wake after sleep onset (WASO), and early morning waking analyses. Among the 23 participants who wore the device, data were collected for 4 to 7 nights (M = 6.43, SD = 0.82) within a 1-week monitoring period. Associations between sleep variables and ASRS T-scores were examined using Pearson correlations, with statistical significance set at α = .05 (two-tailed). Given the exploratory nature and limited sample size, corrections for multiple comparisons were not applied. Findings should therefore be interpreted as hypothesis-generating and preliminary, warranting replication in larger samples.
Correlation analyses included ASRS domain T-scores (Social-Communication, Behaviors, and Self-Regulation) and four actigraphy-derived sleep indices (SOL, number of nighttime awakenings, extended wake episodes, and early morning waking). Scatterplots illustrating these associations are provided in Figure 1 to visualize data distribution and potential outliers. 3

Correlations between sleep disturbances and Autism Spectrum Rating Scale (ASRS) domain scores. Note. Scatterplots illustrate relationships between total number of sleep disturbances (0–4) and ASRS domain scores. Raw (non-T score) values were used to preserve the original distribution for correlational analyses.
Results
Demographic Characteristics of the Study Sample
Forty-one families responded to the recruitment materials, and 29 met eligibility criteria. This study was designed to capture typical sleep patterns during the academic year; however, due to COVID-19 school closures, recruitment was discontinued earlier than expected, with 24 participants completing surveys and 23 of these participants completing actigraphy.
Demographic characteristics are presented in Table 1. Of the 24 children with ASD, 75% (n = 18) were male, with a mean age of 9.2 years (SD = 1.72). Four parents reported that their child had a prior sleep disorder diagnosis, however, specific diagnostic categories (e.g., insomnia and sleep apnea) were not collected. The most reported secondary neurological conditions included Attention Deficit Hyperactivity Disorder, anxiety, and delayed speech, while less common diagnoses included obsessive-compulsive disorder, intellectual disability, and depression.
Demographic Characteristics of the Sample (N = 24).

Note. Medical history variables are based on caregiver report.
Actigraph Tolerance
Of the 24 participants, 67% (n = 16) wore wrist actigraphy throughout the study, 29% (n = 7) wore the actigraph in a shirt pocket and one participant could not tolerate either placement.
Regarding data completeness, 58% (n = 14) provided seven full nights of data, 25% (n = 6) provided six nights, 8% (n = 2) provided five nights, and one child provided four nights.
Sleep Patterns
Among the 23 participants with usable actigraphy data, mean sleep efficiency was 85.1% (SD = 5.4%). Participant averages ranged from 80% to 96%, and nightly values ranged from 62% to 99%. The mean total nighttime sleep was 496.2 min (8 h, 16 min; SD = 51.63), with individual nightly values spanning from 5 h and 37 min to 9 h and 22 min.
Several distinct sleep disturbances were observed in participants using actigraphy. Six participants demonstrated prolonged SOL greater than 30 min, with a mean latency of 68.6 min (range = 30–180 min). Nighttime awakenings were common, with 16 participants (70%) experiencing more than 15 awakenings per night (M = 21.6, range = 15–35). Although the average duration of individual wake episodes appeared brief (<30 min), these numerous wake events throughout the night contributed to substantial total WASO and indicated fragmented sleep patterns. Across the sample, the mean total WASO was 69.5 min, with two participants experiencing 30 to 60 min of wake time and seventeen participants (74%) exceeding 60 min per night. Eight participants (35%) experienced extended wake episodes regularly lasting longer than 5 min, with a mean duration of 6.1 min (range = 5–15 min). Additionally, six participants (26%) experienced early morning waking prior to 5:30 a.m., with a mean duration of 17.4 min (range = 5–37.5 min) (Table 2).
Characteristics of Disturbed Sleep Symptoms (Measured With Actigraphy) in Children With ASD (n = 23).

Note. EMW=early morning wake; SOL=sleep onset latency; WASO=wake after sleep onset.
Parent-Report and Actigraphy Comparisons
Across domains, the relationship between the parent diary and actigraphy measures varied (n = 23). Parent-reported and actigraphy total nighttime sleep showed the strongest correspondence (r = .49, p = .017), though parents typically overestimated total nighttime sleep duration. Bland–Altman analysis revealed an average overestimation of 36 min (mean bias = + 36.2 min, SD = 70.4), with wide 95% limits of agreement (−101.8 to +174.3 min), indicating substantial individual variability in estimation accuracy. Agreement for SOL was fair (κ = .26), with about two-thirds of cases matching between methods. EMW demonstrated the strongest association (ρ = .65, p < .001), indicating that parents accurately recognized early awakenings, though this reflects association rather than precise agreement. In contrast, WASO frequency and duration differed substantially between sources (t = –5.17, p < .001; r = .05, p = .82), suggesting that actigraphy detected frequent, brief nighttime awakenings that parents did not perceive. These findings and relationships are described in Table 3.
Associations Between Parent-Reported Sleep Diary Measures and Actigraphy-Derived Sleep Variables (n = 23).
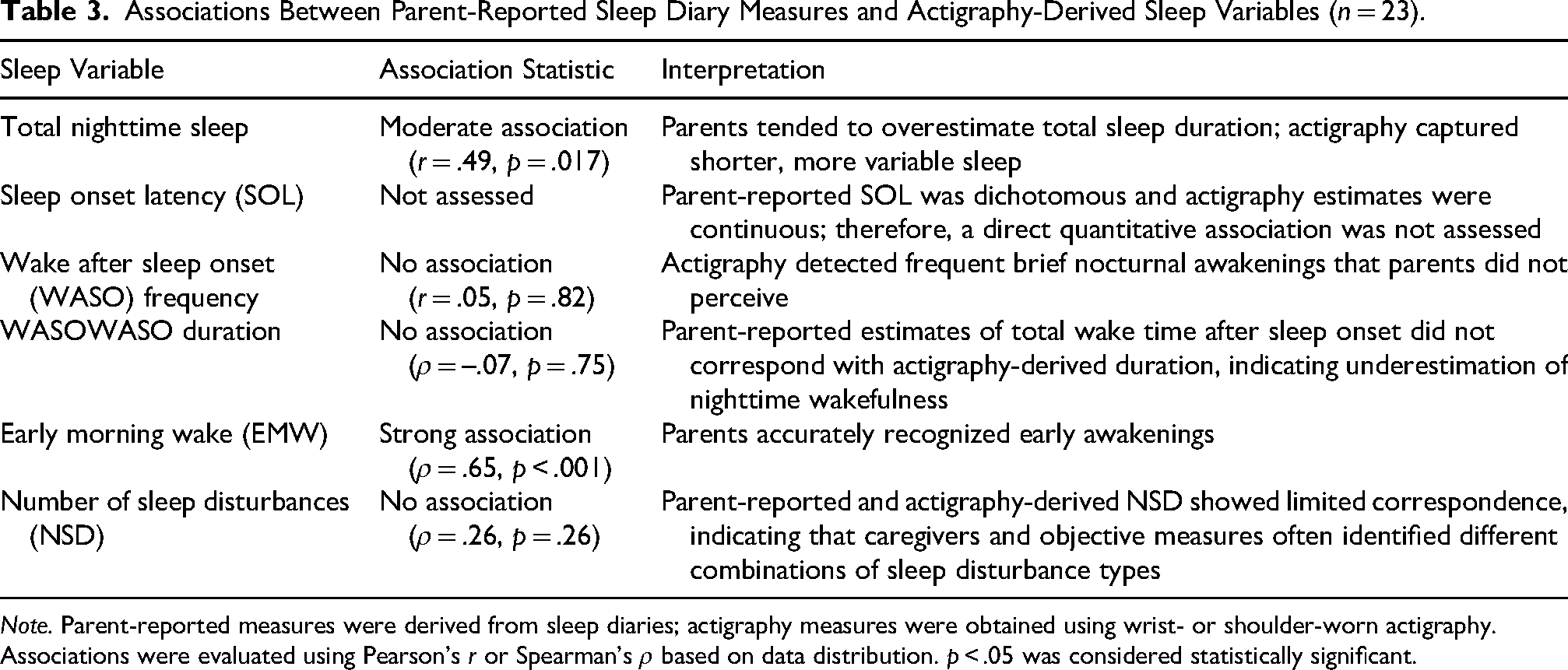
Note. Parent-reported measures were derived from sleep diaries; actigraphy measures were obtained using wrist- or shoulder-worn actigraphy. Associations were evaluated using Pearson's r or Spearman's ρ based on data distribution. p < .05 was considered statistically significant.
Taken together, these findings highlight that actigraphy captured more fine-grained variability in sleep continuity and arousals, whereas parent reports better reflected perceived restfulness and overall adequacy of sleep. EMW was a shared point of recognition, whereas wake after sleep onset duration and the number of subtle disturbances were less consistently observed. These results support the continued use of actigraphy as the primary objective tool for pediatric sleep assessment, while recognizing the contextual insight parents contribute about sleep quality and daily functioning.
Behavioral Characteristics
All 24 participants scored in the clinically elevated range for ASD characteristics (≥ 60) on the ASRS. The ASRS mean DSM-5 composite score was 70.33 (SD = 5.85; range: 59–84). Domain-specific scores indicated a wide distribution of severity: social-communication impairment (M = 67.79, SD = 7.28), behaviors (M = 67.21, SD = 5.59; range: 56–77), and self-regulation (M = 63.12, SD = 6.39; range: 50–76). Some participants demonstrated minimal impairment in at least one domain; specifically, 8% (n = 2) scored in the average range for social communication, 13% (n = 3) for behaviors, and 25% (n = 6) for self-regulation. Social-communication severity was not significantly correlated with behavioral dysregulation (r = –.31, p = .15), with the two domains sharing less than 10% of variance. Cronbach's alpha values for ASRS subscales ranged from .83 to .86, which was acceptable though slightly lower than previously reported (.86–.95) (Goldstein & Naglieri, 2010).
Correlations Between Sleep and ASD Characteristics
Pearson correlation 4 analyses revealed significant associations between sleep disturbances and ASD clinical characteristics. An increased number of sleep disturbances positively correlated with social-communication impairment (r = .51, p = .014) and inversely correlated with behavioral dysregulation (r = –.55, p = .007). No significant associations were found between overall sleep disturbances and self-regulation impairment (r = –.32, p = .13) or the DSM composite score, which reflects overall ASD characteristics (r = –.11, p = .61).
Examination of specific sleep disturbances yielded additional findings. Among the 23 participants with usable actigraphy data, total WASO duration (average total nightly wake time) was not significantly associated with social-communication scores (r = .15, p = .49). However, longer total WASO durations were significantly associated with lower behavioral dysregulation scores (r = –.42, p = .047). When examining the average duration of individual awakenings, participants whose mean awakening length exceeded five minutes significantly correlated with greater social-communication impairment (r = .55, p = .007) and lower behavioral dysregulation (r = –.42, p = .047). EMW was also associated with increased social-communication impairment (r = .44, p = .037). In contrast, delayed SOL, and frequent nighttime awakenings (>15 per night) were not significantly associated with ASD characteristics (Table 4).
Correlations Between Actigraphy-Derived Sleep Disturbances and Impaired Social-Communication and Behavioral Regulation Scores in Children With ASD (n = 23).
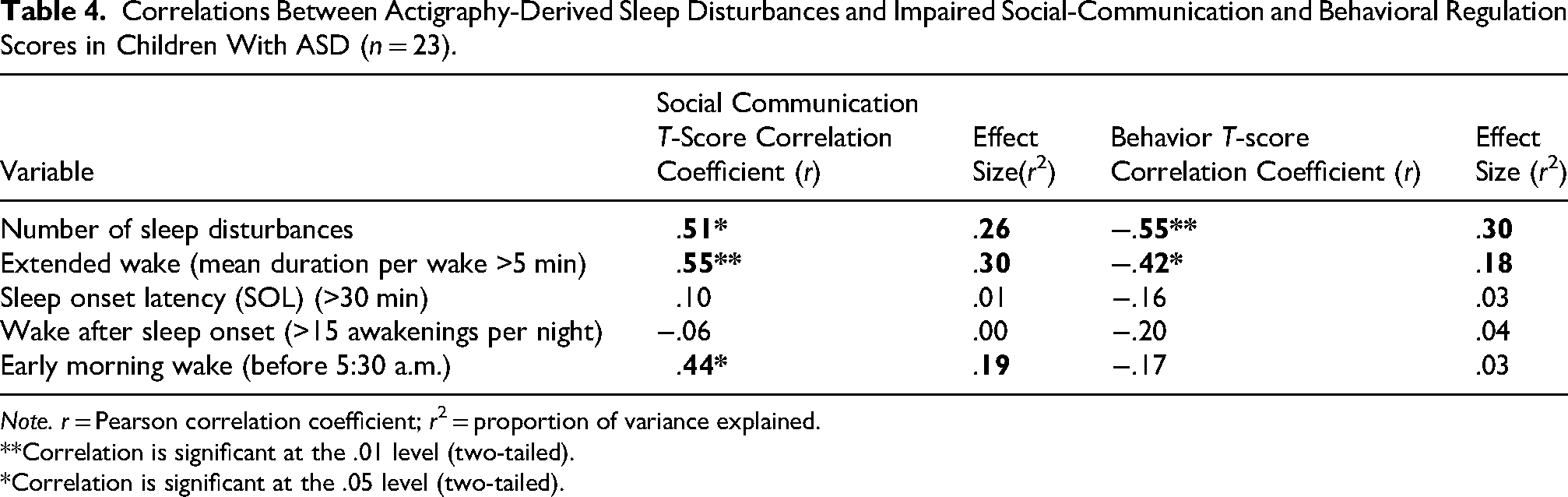
Note. r = Pearson correlation coefficient; r2 = proportion of variance explained.
**Correlation is significant at the .01 level (two-tailed).
*Correlation is significant at the .05 level (two-tailed).
Discussion
Children with ASD exhibit diverse combinations of behavioral, social, and communication impairments, yet the underlying reasons for these varied presentations remain an active area of research (Bertelsen et al., 2021; Bitsika et al., 2018). Identifying factors that contribute to these differences remains an important area of investigation. In this sample, social-communication and behavioral dysregulation were not significantly correlated, suggesting relatively limited shared variance between these domains. This pattern is consistent with heterogeneity in ASD clinical profiles and supports examining domains separately (Bertelsen et al., 2021; Bitsika et al., 2018).
While sleep disturbances are well-documented in ASD and known to impact daily functioning in both autistic and non-autistic individuals (Abel et al., 2017; Bangerter et al., 2020; Cohen et al., 2018), this study did not identify significant associations between the number of sleep disturbances and overall ASD characteristics in this sample. However, a greater number of sleep disturbances was associated with more severe social and communication delays, aligning with previous research (Bangerter et al., 2020; Johnson et al., 2018). In contrast, sleep disturbances showed an unexpected inverse association with behavioral dysregulation (Cohen et al., 2018; Kawai et al., 2023), while no relationship was detected between sleep and self-regulation difficulties.
Together, these results suggest that sleep disruption may relate differently to specific ASD symptom domains. The absence of significant associations between sleep disturbances and behavioral or self-regulation impairment severity may reflect clinical heterogeneity (e.g., medications, co-occurring conditions, and individualized supports) and statistical factors such as small sample size and intercorrelated ASRS domains, which can yield suppression or instability in bivariate estimates. Measurement issues may also contribute, as the composite “number of disturbances” may be less sensitive than specific sleep indices (e.g., WASO duration or early morning waking), which showed stronger associations in this sample. It is also possible that differences in expressed ASD characteristics have distinct relationships with specific aspects of sleep disruption, highlighting the need for future studies to examine more specific dimensions of behavior and regulation.
These exploratory findings are consistent with prior work suggesting that ASD phenotypes may reflect multiple underlying neurobiological pathways. These pathways may contribute to domain-specific profiles (Bertelsen et al., 2021; Lombardo et al., 2019). The observed negative correlation between sleep disturbances and behavioral dysregulation implies that factors beyond sleep disruption alone—such as neurodevelopmental differences or adaptive coping mechanisms-may contribute to the variability in behavior in ASD. Importantly, current DSM-5-TR diagnostic criteria conceptualize autism as a single spectrum condition and do not differentiate subtypes based on whether social-communication difficulties or restricted and repetitive behaviors are more prominent (American Psychiatric Association, 2022). It remains unclear how specific ASD symptom expression independently and interactively contributes to overall functioning and developmental trajectories across childhood (Bertelsen et al., 2021; Lombardo et al., 2019; Wiggins et al., 2022).
Emerging work has begun to explore these domain-specific relationships between sleep and ASD characteristics, and the present findings lend preliminary support to the idea that different sleep characteristics may relate differently to social versus behavioral features (Bertelsen et al., 2021; Bitsika et al., 2018). Further research with larger, more diverse samples is needed to explore the interplay between sleep, ASD symptom expression, and potential ASD subtypes as well as how these relationships change over time. A clearer understanding of these patterns may lead to more personalized intervention strategies, particularly sleep-focused behavioral supports (e.g., bedtime-routine modification and behavioral sleep hygiene training) and individualized care approaches that consider each child's unique sensory and behavioral profile.
Strengths and Limitations of the Study
This study, focused on families from a Midwestern U.S. city and its suburbs, contributes to the growing literature on sleep and ASD by integrating both objective and subjective sleep measures. A key strength was using actigraphy to measure sleep disturbances, quantifying aspects of sleep that were not consistently captured in parent reports, particularly in the number of WASO events and the duration of nighttime awakenings (Table 3). These differences underscore the importance of objective sleep measures in ASD research.
A primary limitation was the absence of a neurotypical comparison group, limiting generalizability. Recruitment relied on voluntary response through local support networks and a children's hospital and was discontinued earlier than planned due to COVID-19-related closures. Although all participants scored in the clinically elevated range on the ASRS (consistent with confirmed ASD diagnoses), limited within-group variability may have constrained observed associations. The study was exploratory, and the small number of participants within each sleep disturbance subtype (including categories with as few as two participants) limited the ability to examine symptom variability across sleep profiles. The high prevalence of sleep disturbances may also reflect self-selection bias. To improve feasibility and reduce clinical confounding, the sample was restricted to a narrow age range and excluded children with seizure disorders or regressive-onset ASD. These criteria limit generalizability and may underrepresent children with more severe neurodevelopmental presentations and associated behavioral challenges, potentially influencing observed associations between sleep and behavioral dysregulation (Cano-Villagrasa et al., 2023).
Actigraphy data reflected nighttime actigraphy only, with devices typically placed 10 to 30 min before bedtime. Standard protocols often recommend 30 to 60 min before bed. Information on daytime naps was not collected, which may have influenced nighttime sleep parameters. Another limitation of the study was that medical information was limited to a general parent-report history form rather than detailed documentation of specific medical or psychiatric diagnoses, including sleep disorders. Standardized sensory assessments, school placement, current therapies, and caregiver characteristics were not obtained. Future studies should incorporate these contextual variables to characterize sample heterogeneity and clinical correlates more fully.
Behavioral dysregulation was assessed using the ASRS, which captures DSM-5-aligned autism-related behavioral symptoms across multiple domains; future studies may incorporate measures of externalizing behavior (e.g., the Aberrant Behavior Checklist) to further clarify sleep-behavior relationships. In parallel, research identifying distinct social-communication and behavioral subtypes within ASD (Bertelsen et al., 2021) demonstrates the value of examining clinical domains separately when evaluating relationships between sleep and ASD in clinical research.
Conclusions
This study assessed sleep patterns in 24 children with varying ASD clinical profiles. Notable differences emerged between children with more severe social-communication impairments and those with more pronounced behavioral challenges. Actigraphy provided a more objective measure of sleep continuity and nighttime awakenings than parent reports, reinforcing the importance of objective sleep measurement in ASD research. Among the 23 participants with usable actigraphy data, increased sleep disturbances were associated with more social-communication delays and higher frequency and duration of WASO. Contrary to expectations, no positive correlation was found between sleep disturbances and behavioral dysregulation; instead, an inverse relationship emerged. These findings provide preliminary evidence to support the concept of potential ASD sleep-related phenotypes and underscore the importance of domain-specific research focused on ASD clinical profiles in larger, more diverse samples.
Understanding the interplay between co-occurring health conditions and ASD clinical profiles could offer deeper insight into its complexity. Differentiating children with pronounced behavioral dysregulation from those with significant social-communication delays may refine ASD classification and guide more personalized intervention strategies. Such an approach has the potential to enhance the effectiveness of behavioral and therapeutic interventions and improve individualized treatment plans, ultimately leading to better outcomes for children with ASD.
Footnotes
Acknowledgments
This study was implemented for SM's dissertation work with support of Case Western Reserve University, Frances Payne Bolton School of Nursing and University Hospitals Cleveland Medical Center Nursing and Clinical Research Center. Dr. Mary Anthony and Denise Karshner of the Kent State University College of Nursing provided professional writing support.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional standards.
Consent to Participate
Informed consent was obtained from parents of all individual participants included in the study. Participants over the age of 7 were required to sign an assent (if developmentally appropriate).
Consent for Publication
Not applicable. This article is not submitted or under review by any journal. An earlier version of this article is available as a preprint on Research Square but this article is available for publication. Doi: 10.21203/rs.3.rs-2674526/v1
Author Contributions
SM collected, analyzed, and interpreted patient data. SM and MM were major contributors to writing the article. Both authors read and approved the final submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the National Institute for Nursing Research Pre-Doctoral Ruth L. Kirschstein National Research Service Award (NRSA) (T32) NIH T32 NR015433 2018-2020 and Sigma Theta Tau Nursing Research Grant (Alpha Mu Chapter). Neither entity participated in study design nor data collection.
Availability of Data and Materials
Data that support the findings of this study are available from University Hospitals Cleveland Medical Center (UHCMC), but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of UHCMC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.