
Abstract
Background and Aims:
The purpose of this exploratory study was to expand existing literature on prelinguistic vocalizations by reporting results of the first home-based longitudinal study examining a wide variety of behaviors and characteristics, including early vocalizations, across infants at low and elevated risk of autism spectrum disorder (ASD). The study of vocalizations and vocalization changes across early developmental periods shows promise in reflecting early clinically significant differences across infants at low and elevated risk of ASD. Observations of early vocalizations and their differences during infancy could provide a reliable and essential component of an early developmental profile that would lower the average diagnostic age for ASD. However, studies employing observation of vocalization behaviors have been limited and often conducted in laboratory settings, reducing the external generalization of the findings.
Methods:
The present study was conducted to determine the consistency of previous findings with longitudinal data collected in home environments. Infants in the present study represented elevated risk from two etiological backgrounds, (a) infants born prematurely and with low birth weight and (b) infants who had an older sibling diagnosed with ASD. All data were collected in the infants’ homes and compared with data collected from infants with low likelihood of ASD. The study included 44 participants (31 in the low-risk sample, 13 in the high-risk sample) with vocalization behaviors observed at 6- and 12-months through 20-min semi-structured play interactions with caregivers. Observations were video-recorded and later coded for speech and non-speech vocalizations.
Results:
Differences in the 6-month vocalization behaviors were not statistically significant across risk levels of ASD. By 12 months; however, risk group differences were evident in the total number of vocalizations overall with specific differences across groups representing moderate to large, clinically relevant effects. Infants at low risk of ASD demonstrated significantly greater developmental change between 6- and 12-months than did the infants at high risk. Data were also reviewed for differences across high-risk group etiologies.
Conclusions:
The present study was unique and innovative in a number of ways as the first home-based longitudinal study examining infant vocal behaviors across low and high risk of ASD. Many of the present study findings were consistent with previous cross-sectional investigations of infants at elevated risk for ASD, indicating support for further home-based longitudinal study in this area. Findings also indicated some preliminary subgroup differences between high-risk etiologies of ASD. Vocalization differences across high risk groups had not been previously addressed in the literature.
Implications:
Vocalization differences are notable by 12-months of age between infants at low and elevated risk of ASD and infants at high risk demonstrated reduced developmental changes between 6- and 12-months compared to the infants at low risk. Observation of early infant vocalization behaviors may reasonably occur in the home, providing early childhood professionals and researchers with empirical support for data collection of child-caregiver interactions in this setting. Potential differences across high-risk etiologies warrant further investigation.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder affecting 1 in 54 children in the United States (Maenner et al., 2020) and associated with an overarching economic burden of over $250 billion dollars in the U.S. (Leigh & Du, 2015). At present, an ASD diagnosis is based on behavioral indicators identified using the diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders-5th edition (DSM-5: American Psychiatric Association [APA], 2013) and characterized by deficits in social-emotional reciprocity, nonverbal communicative behaviors, and understanding relationships. Additionally, ASD is characterized by restricted or repetitive patterns of behaviors which can be manifested in stereotypic motor movements or speech, fixated interests, and hypo- or hyper-reactivity to sensory input (APA, 2013). Because of this reliance on behavioral manifestations for diagnosis, it is important to be aware of the observable characteristics consistent with ASD. Although children as young as 18 months of age can be diagnosed with autism, the average age of diagnosis is just over 4 years (Christensen et al., 2018; Maenner et al., 2020).
Early diagnosis
Severity of ASD is dependent on the development of the characteristics noted above and early childhood specialists are encouraged to continuously monitor young children's behavioral symptomatology for diagnostic purposes. Early diagnosis leads to early implementation of interventions that can be tailored to address specific skills and improve function and quality of life for individuals and their caregivers (Hyman et al., 2020).
Having ready and early access to resources and services without experiencing a protracted diagnostic process (see Crane et al., 2016 for further discussion of lengthy diagnostic processes) can be critical in reducing the financial and emotional cost of care over time as early intervention lessens the likelihood of long-term negative effects and is associated with optimal developmental outcomes (Hyman et al., 2020; Orinstein et al., 2014; Whitehouse et al., 2021). Given the high and increasing cost of care (see Leigh and Du, 2015) and the availability and advancement in effective evidence-based early interventions (see Hyman et al., 2020; Orinstein et al., 2014; Whitehouse et al., 2021), the motivation to reduce the diagnostic age of ASD is clear. Recognizing early observable characteristics of ASD, such as those consistent with early communication deficits (Delehanty et al., 2018), play a major role not only in identifying ASD, but also in identifying the broader autism phenotype (BAP: Gerdts and Bernier, 2011; Losh et al., 2008).
Broader autism phenotype
BAP generally consists of deficits in social and communication skills similar to the defining features of ASD including restricted and repetitive behaviors and interests (Gerdts & Bernier, 2011; Losh et al., 2008). Understanding BAP traits and their relation to family members of children with ASD can provide insight regarding severity of ASD symptoms in families (Losh et al., 2008). Gamliel et al. (2009) discovered siblings of individuals with ASD presented with BAP-related behaviors demonstrated by below average performance on linguistic measures. The researchers noted siblings manifested deficits primarily in language, consistent with current knowledge that communication is one of the most severely affected domains in individuals with autism.
High-risk infant populations
Heritability is of importance when considering risk for ASD diagnosis or determining BAP presence. Schwichtenberg et al. (2010) found infants within single-incidence families were more likely to develop ASD than infants within families that have no incidence of ASD. In one of the largest prospective studies of ASD sibling recurrence, Ozonoff et al. (2011) found one of the strongest predictors of ASD diagnosis was the number of affected siblings who were in the family.
Another population considered high risk for later ASD diagnosis are infants born prematurely and with low birth weight (LBW). Many researchers found preterm birth and LBW were critical risk factors of ASD diagnosis (Joseph et al., 2017; Kolevzon et al., 2007; Williams et al., 2008). This infant population is at increased risk for multiple specific neurobiological disorders, including ASD, and research indicates that as gestational age (GA) and birth weight decrease, risk and prevalence for disorder presence increases (Johnson & Marlow, 2011). Preterm infants are born with reduced cerebral volumes, which makes the infants’ brain vulnerable during development after birth (Ment & Vohr, 2008).
Infant vocalization behaviors
Previous research has noted significant connections between infant vocalizations and behavioral characteristics of ASD, including those characteristics consistent with BAP. For example, Paul et al. (2011) found infants at heightened risk of ASD due to heritability produced fewer vocalizations at 12 months of age than same-aged peers at low risk. Findings from their cross-sectional study also indicated that although speech productions increased with age for all participants between 6- and 12-months of age, those infants at heightened risk of ASD produced fewer speech-like vocalizations at all ages observed (Paul et al., 2011). Further, Talbott et al. (2016) found that environmental influences (e.g., maternal vocal responses to infant vocalizations) did not significantly differ in frequency or content for mothers of 9-month-old infants at low and elevated risk of ASD diagnosis, implying that external sources, at most, minimally contribute to very early infant vocal behaviors of infants at risk of ASD.
For older children, including toddlers and preschools already diagnosed with ASD, Warlaumont et al. (2014) found that young children with autism produced significantly fewer speech-like vocalizations than same-aged peers when comparing vocalization samples between 16- to 48-months of age. Plumb and Wetherby (2013) noted similar discrepant findings for children between 18- and 24-months of age. They noted that toddlers later diagnosed with ASD used a significantly lower proportion of speech-like vocalizations and a significantly higher proportion of ‘atypical’ vocalizations (e.g., yelling, squealing, grunting, growling) and distress vocalizations (e.g., crying, whining, screaming) than same-aged peers who were not diagnosed with autism (Plumb & Wetherby, 2013). Warlaumont et al. (2014) also found that, over time, the proportion of speech-like vocalizations for children with autism increased more slower than that of their peers.
Understanding early vocalization patterns can provide insight into a child's ability to compare his/her speech sound productions to those of others (Warlaumont et al., 2014). This contrast between production and reception of speech sounds can impact future communicative development. If infants cannot compare the sounds they make when they engage in vocal play and babble to the sounds that are modeled around them, they may experience a slow transition from pre-speech vocalizations to speech and speech-like vocalizations (Schoen et al., 2011). Infants at risk for ASD and BAP may be less likely to play with speech sounds and practice sounds modeled for them in their own babble, which can then lead to limited use of canonical babbling (Garrido et al., 2017).
One of the most notable studies of vocalization behaviors in infants at elevated risk of ASD was conducted by Paul et al. (2011). The researchers conducted a cross-sectional study of infants at low and high risk of ASD. High-risk infants were those who had an older sibling diagnosed with ASD. Data were collected in a clinical facility and the vocalization samples collected were 5-min in length at 6-, 9-, and 12-months of age. Paul et al. (2011) found no significant differences in observed vocal behaviors of infants across risk groups at 6-months of age, but did not significant differences at 9- and 12-months of age.
Preliminary report findings
A preliminary report (DeVeney & Kyvelidou, 2020) including analysis of a small overlap in the sampling of the present study's 44-participant infant cohort. This report indicated, at the 6-month period, findings for 10 infants at low-risk for a later ASD diagnosis and six at elevated risk (five born prematurely/with LBW and one with an older sibling diagnosed with autism). The preliminary report also included a small 12-month cohort, six participants at low risk and three at high risk (two born prematurely/with LBW and one with an older sibling diagnosed with autism).
In the preliminary report, no significant differences were noted between risk group conditions at 6-months of age. At 12-months, due to the limited sample size, only descriptive statistics were calculated, and inferential statistics were not employed. Differences in vocalizations were noticeable within this small sample across risk groups such that the infants at low risk produced more vocalizations overall, as well as more speech-like and non-speech vocalizations than infants in the high-risk group. Differences over time between 6- and 12-months were calculated for this small sampling and the researchers found that both risk-group conditions exhibited gains in vocal skills, but to a lesser extent for infants in the high-risk group.
Overall, the study of infant vocalization behaviors shows promise in reflecting early clinically significant differences across infants at low and elevated risk of ASD. However, more research is needed before we can determine how early vocalization differences could provide a reliable and essential component of an early developmental profile that would lower the average diagnostic age for ASD.
Study purpose and research questions
The purpose of the present study was to add to the body of available literature regarding vocalization behaviors associated with infants at elevated risk of ASD and/or BAP and expand upon the methodological approaches used for observation of vocal behaviors in naturalistic settings. Although the manner in which vocalizations were coded and analyzed remained consistent with previous studies, several other methodological aspects differed in this work to determine if comparable study outcomes could be reached with changes in methodology. In contrast to the study conducted by Paul et al. (2011), the current study was longitudinal, allowing for both within-subject analyses and between-group comparisons. Also, the current study included preterm infants with LBW in the high-risk sample in addition to infants who had an older sibling with ASD to reflect current research on these two populations of interest for later ASD diagnosis. Additionally, the present study conducted data collection in participant homes to document vocalizations in a naturalistic setting thought to foster parent and child comfort levels that could potentially lead to more robust and representational vocalization samples. Finally, in the current study, researchers collected 20-min vocalization samples with differing conditions in which the infant and caregiver interacted to encourage a variety of infant vocalization opportunities.
In contrast with the preliminary report of infant vocalizations (DeVeney & Kyvelidou, 2020), the present study includes a much larger sample at each time period, 6- and 12-months (44 and 41 in the present study vs. 16 and 6 in the preliminary report). This increase in sample size is particularly notable for the high-risk group with the inclusion of more infants with familial etiology for risk elevation (e.g., 13 vs. 6 participants at high risk in the present study, including five infants with older siblings diagnosed vs. one in the preliminary report). Additionally, the present study includes statistical analyses for the 12-month vocalization data and changes over time across risk conditions. The third research question was not addressed in the preliminary report.
The following research questions were addressed:
Consistent with previous cross-sectional, laboratory-based research, do vocalization behaviors observed in a longitudinal study conducted in the home indicate differences across infants at low and elevated risk of ASD? How do infant vocal behaviors change between 6- and 12-months of age for infants in the low and elevated risk cohorts? Are these noted changes consistent with previous research? Is high-risk etiology (e.g., heritability vs. prematurity/low birth weight) associated with differing vocalization behaviors at 6- or 12-months for infants in the elevated risk cohort?
Based on the previous cross-sectional study in this area conducted by Paul et al. (2011) and the work of Talbott et al. (2016) who found no difference in speech-like productions between 9-month-old infants at low and elevated risk of ASD, the authors hypothesized that for the present study findings, the 6-month vocalization behaviors would not be significantly different across risk groups, nor would these behaviors represent clinically relevant effect sizes. However, by 12-months of age, risk-group differences would be evident in the total number of vocalizations overall, speech-like vocalizations, consonant productions, and non-speech vocalizations such that the infants at low risk would produce significantly more vocalizations overall, more speech-like vocalizations, more varied consonant productions, and more non-speech vocalizations than infants at elevated risk of ASD. Additionally, the authors expected infants in the low-risk group would demonstrate greater change between 6-and 12- months than infants at elevated risk, regardless of etiology for inclusion in the high-risk study condition. For this reason, in the present study, infants in the high-risk group represented combined etiologies such that both heritability and prematurity/low birth weight were considered together when compared with infants at low risk. This hypothesis is consistent with the notion that infant vocalizations will mature and develop over time irrespective of an infant's risk for ASD; however, early acquisition of vocalizations, also known as the “basic vocal ‘tools’” for later speech development (Paul et al., 2011, p. 595), will be a sensitive indicator for ASD-like symptomatology, including BAP. Finally, the authors hypothesized that differences associated with high-risk etiologies may be identifiable in participants’ 6- and 12-month vocalization samples because differences in neurodevelopment between pre-term and full-term infants at the time of birth and after may affect future neurodevelopmental patterns that could impact early vocalization behaviors.
Method
Participants
Infants included in this report were participants in an ongoing longitudinal study, Early Diagnostic Signs of Autism, the aim of which was to identify features of gaze behavior, motor development, and communication skills that could facilitate an early ASD diagnosis. For this longitudinal study, participants needed to be at least 4 months of age at intake with reportedly typical sensory skills (e.g., hearing, vision) and the ability to demonstrate sustained brief periods of independent sitting (e.g., 10 s). The study involved infants born prematurely and with low birth weight (LBW), infants who had an older sibling diagnosed with ASD, and infants at low risk of ASD. Based on inherent attributions, infants were categorized into one of two conditions for the study, high-risk of an ASD diagnosis (HR group) or low-risk of diagnosis (LR group). The HR group included both infants born prematurely and with LBW as well as infants with identified familial risk. The decision to include both high-risk etiologies in one condition for comparisons with the LR group was rendered to test the authors’ hypothesis that infants in the low-risk group would demonstrate greater change in the first year of life than infants at elevated risk, regardless of high-risk etiology.
Inclusion criteria for the HR group included (a) the infant had an older biological sibling diagnosed with ASD (familial) or (b) the infant was born less than 37-weeks’ gestation and with a birth weight lower than 2500g (prematurity and LBW). Infants who were (a) born after 37-weeks’ gestation with a birth weight of 2500g or more and (b) did not have an older biological sibling diagnosed with ASD met the criteria to be in the LR group. Namely, infant participants who were not known to have high-risk attributes composed the LR condition of the study.
Participant exclusion criteria for the study, regardless of risk categorization, included the presence of any neuromuscular conditions affecting balance, head injury, genetic disorder(s) that may be linked to increased risk of ASD, and any orthopedic diagnoses. Infants exposed to prenatal illicit drug use or excessive alcohol use were also excluded. When asked what their child's primary language was and if any other languages were spoken in the home, all caregivers indicated that participants were acquiring General American English (GAE) as a dialect in monolingual environments. GAE is the predominant dialect of the English language spoken in the United States and is also commonly referred to as Standard American English or Mainstream American English (Oetting, 2020).
Age adjustments were made for participants born prematurely by subtracting the number of weeks the child was born prematurely from his/her chronological age. This full correction for prematurity was completed according to guidelines noted in the Mullen Scales of Early Learning (MSEL: Mullen, 1995) for all participants born prematurely through 12 months chronological age. Also using MSEL guidelines (Mullen, 1995), when participants who were born prematurely were 12–17 months chronological age, the investigators incorporated a half correction for chronological age and no correction for chronological age was calculated after participants were 18 months of age.
Participants were recruited from an urban area in the Midwest of the United States through word of mouth advertisements that included social media postings and employee announcements sent to local universities. Participants for the HR group were also recruited from clinical partners working with children diagnosed with ASD and their families (e.g., community resource providers, neonatal/perinatal service providers). The participant sample included 23 males and 21 female infants. Parents identified their infant's ethnicity as Caucasian (n = 32), Black, not of Hispanic origin (n = 5), Hispanic (n = 1), Asian/Pacific Islander (n = 2), and Other (n = 4). Parent participants identified their own ethnicity as Caucasian (n = 36), Black, not of Hispanic origin (n = 4), Hispanic (n = 2), and Asian/Pacific Islander (n = 2).
General study procedures
All of the study procedures, including the recruitment strategy and process for obtaining caregiver consent, were reviewed and approved by the local institutional review boards affiliated with the researchers’ universities to provide a safeguard for the ethical consideration of each participant's rights.
In accordance with these approved procedures, the data collections completed for the study were homebased. Initial data collections were individualized for participants based on their age and ability to independently sit, though most infants were 4–5 months of age at intake. Throughout data collections, standardized assessments and caregiver-response questionnaires were administered in addition to the collection of vocalization, eye tracking, and postural data (see Table 1 for an outline of data collection procedures).
Data collection measurement tools from the early diagnostic signs of autism project utilized in the present study.

Data collections included administration of standardized assessments and caregiver-response questionnaires. These assessment tools (see Table 1 for time and description of use) included the Communication and Symbolic Behavior Scales - Developmental Profile (CSBS-DP: Wetherby and Prizant, 2002); the MacArthur-Bates Communicative Development Inventories: Words and Gestures (CDI: Fenson et al., 2007); the Mullen Scales of Early Learning (MSEL: Mullen, 1995); Social Communication Questionnaire (SCQ: Rutter et al., 2003); and the Social Responsiveness Scale (SRS: Constantino, 2002). Table 2 includes a description of participant performance on assessments administered alongside vocalization sampling. The following tasks and measures were also routinely included in data collection procedures: head circumference measurements, eye gaze tracking with presented social and nonsocial visual stimuli, and postural sway during independent sitting. For a more comprehensive description of the overall longitudinal study procedures see DeVeney and Kyvelidou (2020).
Mean (and standard deviation) for assessment tools administered at the initial and second vocalization samplings.
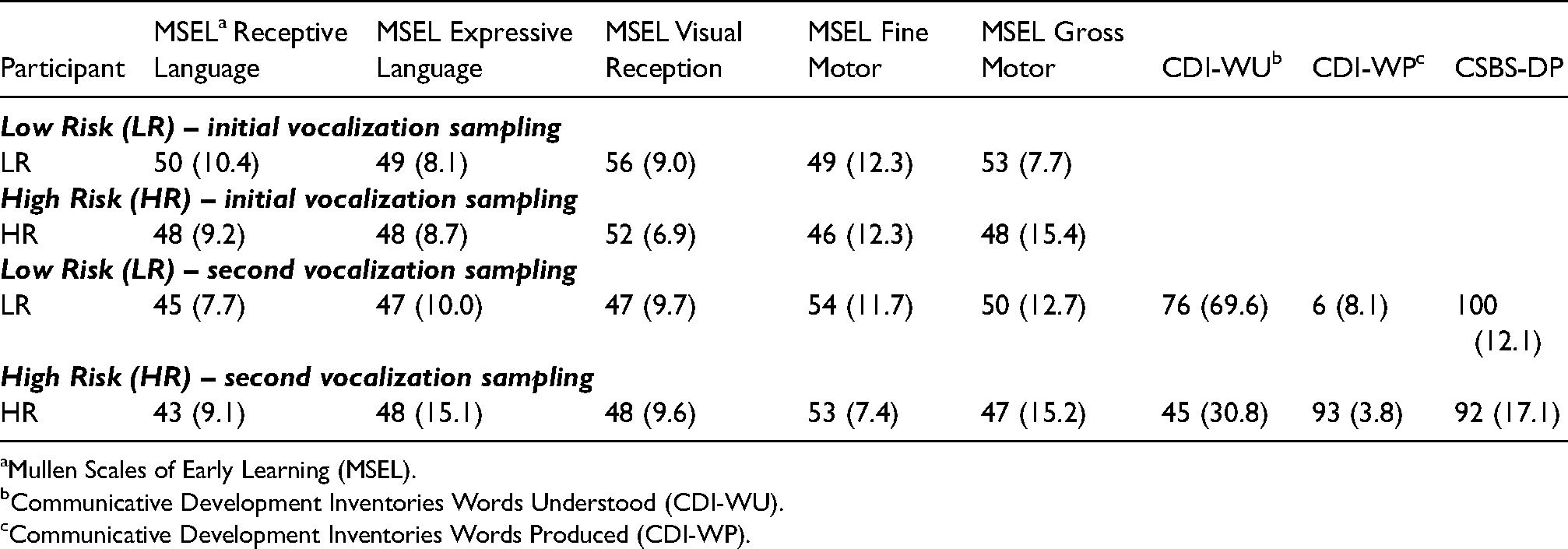
Mullen Scales of Early Learning (MSEL).
Communicative Development Inventories Words Understood (CDI-WU).
Communicative Development Inventories Words Produced (CDI-WP).
Vocalization sample procedures
For each participant, vocalization data was collected at 6-months of age during the 3rd home visit and at 12-months of age during the 6th home visit. The decision was made to focus on these two distinct time points (6- and 12-months) in the present study to elucidate differences in vocal productions within the first year of life and to provide data comparable to the distal time points used by Paul et al. (2011). Initial vocalization samples, those collected at the 6-month data collection visit, included 31 participants in the LR group (14 male, 17 female) and 13 participants in the HR group (9 male, 4 female). Of those in the HR group, 8 were born prematurely and with LBW (5 male, 3 female) and 5 were younger siblings of children diagnosed with ASD (4 male, 1 female).
The second vocalization sample, collected at the 12-month data collection visit, included 29 participants in the LR group (12 male, 17 female) as 2 samples were not usable due to recording errors during data collection that compromised the sample's quality and length. For the HR group, 12 (9 male, 3 female) participant samples were included in analysis. Of these, 7 were samples from participants born prematurely and with LBW (5 male, 2 female) and 5 were younger siblings (4 male, 1 female). One participant's 12-month sample was not usable due to poor audio quality.
Vocalizations were video and audio recorded for later transcription during a 20-min play observation with a primary caregiver. The play observations involved semi-structured play interactions with caregivers using methodology based on that of Iverson and Wozniak (2007) with 5-min segments of (a) face-to-face interaction with the caregiver, (b) play with soft-crinkle books, (c) play with rattles, and (d) play in a jump seat. These varied play contexts reflected the investigators’ efforts to obtain a representative sample of each infants’ vocalization behaviors. The researchers controlled for time such that each sample was 20 min in length with 5-min segments of each of the four types of play contexts targeted. The following instructions were provided to caregivers participating in the play observations, “The communication observation is geared toward getting a sense of [your child's] communication skills when s/he has toys and you to interact with. This will take 20 min and we’ll video record it so we can go back later to describe and categorize [your child's] communications. Every five minutes, I’ll hand you a different toy or give you an instruction on what to do next. Overall, I want to see what kinds of activities [your child] enjoys. I’d like to see how [your child] communicates when s/he enjoys what s/he is doing. So, play and have fun. Help [your child] enjoy what s/he's doing.” Caregivers were provided with examples for the face-to-face interaction segment to remind them of ways they could play with their child in this manner. Games or routines such as peek-a-boo, patty cake, rocking, or bouncing were suggested prior to the start of the observation recording. For ease of transition and to maintain consistency across participants, each observation began with face-to-face play. Following 5 min of interaction, parents were handed some books and encouraged to continue play. After 5 additional minutes, the researcher exchanged the books for rattles, and finally, after 5 more minutes, the parents were instructed to put their infant in the jump seat and continue play. If infants did not want to part with the books or rattles at the specified time, they were allowed to keep these items in addition to the new items introduced.
Caregivers participating in play for the vocalization samples were primarily mothers. The initial vocalization sample data included 29 mothers and 2 fathers interacting with their infants in the LR group and 12 mothers and 1 father interacting with their infants in the HR group. The second vocalization sample included 23 mothers and 6 fathers for the LR group and 11 mothers and 1 father for the HR group.
After the vocalization samples were collected, caregivers were asked to characterize their infant's overall rate of communication during the sample as ‘more communicative than usual,’ ‘typical,’ or ‘less communicative than usual.’ During the initial vocalization sample, 11 participant caregivers from the LR group reported their child was ‘less communicative than usual’ and 1 caregiver reported the child was ‘more communicative than usual.’ All others reported communication as ‘typical.’ For the HR group, 3 caregivers reported their child was ‘less communicative.’ All others reported communication as typical. For the second vocalization sample, 9 participant caregivers from the LR group and 6 from the HR group reported their child was ‘less communicative’, 1 caregiver reported their child was ‘more communicative’, and all others characterized their child's rate of communication as ‘typical.’
After the vocalization samples were video-recorded, they were converted to audio files and transcribed from the audio files by coders blind to participant condition and age. Coding procedures were consistent with procedures reported by previous researchers (Garrido et al., 2017; Paul et al., 2011). Audio files were analyzed according to Paul and colleagues’ coding criteria (2011). For a detailed description of the vocalization coding criteria used in the present study, see Figure 1.

Vocalization coding scheme flow chart. 1Coders noted the presence of vegetative sounds and raspberries but did not include in this report as they were not reported in the original coding schemes used by Paul et al. (2011) and Sheinkopf et al. (2000). 2See text for further description and discussion of the ‘atypical’ categorization.
Distinctive vocalizations were noted as those marked by an audible breath in between utterances/babble which indicated a stoppage of phonation. Vocalizations were further coded as speech-like or non-speech. To be considered speech-like, vocalizations included recognizable consonants and/or vowels that could be represented by phonetic symbols of the international phonetic alphabet (IPA). Vocalizations that could not be confidently transcribed or attributed to the infant participant were not included for further analysis. The samples were transcribed using broad phonemic transcription with IPA symbols for speech-like vocalizations, which were then further coded for presence of linguistic content and canonical babble. A consonant inventory was produced from the speech-like samples.
The nature of non-speech vocalizations were coded as those indicating “delight,” “distress,” or “atypical” non-speech sounds. It should be noted that there is not a consensus amongst researchers regarding the categorization of “atypical” non-speech vocalizations. Some researchers (e.g., Paul et al., 2011; Sheinkopf et al., 2000) categorized squeals, grunts, growls, and yells as ‘atypical’ non-speech productions. However, others consider these kinds of vocalizations to be typical, commonly-accepted protophones with a functional developmental purpose in language acquisition (see Nathani et al., 2006; Oller et al., 1999; Oller et al., 2013). In an effort to maintain consistency with the coding scheme used by Paul et al. (2011) and facilitate comparison of study outcomes, the present study included ‘atypical’ as a categorical distinction inclusive of squeals, grunts, growls, and yells. Non-speech vocalizations categorized as “raspberries” were noted during the coding process, but not included in the present coding scheme, to maintain consistency with procedures used by Paul et al. (2011).
IPA transcriptions were completed by three graduate students studying speech-language pathology who completed previous coursework in phonetic transcription of English speech sounds and were trained on the present study coding scheme by the first author, a licensed and trained speech-language pathologist. Each student was trained separately on the vocalization coding scheme and then coded at least two audio files to 90% agreement with the first author.
Following training, interrater reliability was determined with a 10% sample of audio files. Reliability between each student coder and the first author ranged from 90–95% for identification of vocalizations, 90–95% for identification of speech-like productions, 90–97% for prelinguistic speech productions, 90–100% for canonical syllables and subtypes of non-speech vocalizations. There was a range of 90–100% agreement on the total number and type of consonants produced.
Coders separately transcribed audio files after training. Ambiguous vocalizations were resolved through joint listening and discussion with the first author.
Analysis strategy
For the vocalization data collected at 6- and 12-months, descriptive statistics, nonparametric inferential analyses, and estimates of effect size were used to examine risk-group vocalization behaviors observed. Nonparametric inferential analyses were used because the sample size was small and there were differential group sizes at 6- and 12-months.
To determine vocalization differences across the two groups, statistical tests were calculated with use of the Statistical Package for Social Sciences (SPSS) version 24.0 (IBM, 2016). Due to the exploratory nature of the present study and its limited sample size, experiment wise-adjusted alpha procedures to account for multiplicity were not conducted. As with all inferential statistics, sample size strongly influences the p-value of a statistical analysis such that small samples make small p-values less probable. The present study represents an exploratory study with a small sample size; therefore, adjustments for multiple testing were not conducted as statisticians have critiqued the use of multiple test corrections in these instances and found them problematic (see Cohen, 1990; Wilkinson, 1999). Thus, for the present study results, the acceptable significance value was ≤0.05 for all comparisons. Because the relative clinical magnitude of the group mean differences could be calculated regardless of sample size, effect sizes were estimated using Cohen's d (Cohen, 1988) by dividing pooled standard deviations of each risk groups’ mean differences (Hojat & Xu, 2004). However, for non-significant findings, effect sizes must be interpreted with caution as the confidence interval around them includes zero. Differences across the participants in the HR group based on high-risk etiology and differences across risk group performance over time were determined through descriptive statistics. Vocalization variables were examined using either frequency or proportion to maintain consistency and facilitate comparison with findings from Paul and colleagues’ study (2011). Mann-Whitney U tests were conducted to determine differences in vocalizations between infant groups. Cohen's d was calculated to determine the clinical importance of between-group differences and allowed for between-group analysis unaffected by sample size (Hojat & Xu, 2004).
Results
Six-month vocalization sampling
Speech-like and non-speech vocalizations were summarized for each participant group (see Tables 3–5) for the six-month (initial) vocalization sample. Overall, distributions of the prelinguistic vocalization behaviors for each group were similar. Statistical analyses, as indicated below, revealed no significant differences in the prelinguistic vocalization behaviors across risk groups for the initial vocalization sample. Effect sizes, reported in Tables 3 and 5, did not indicate clinically important differences across groups and were generally considered to be of small, negligible importance based on the effect size categorization provided by Cohen (1988).
Mean (and standard deviations) for vocalizations across the low- and high-risk groups with significance (p-value) and estimates effect size for the initial vocalization sample.

Mean (and standard deviations) for vocalizations across the low- and high-risk groups with significance (p-value) and estimates effect size for the second vocalization sample.

*statistically significant finding (p ≥ 0.05).
** not a statistically significant findings as p = 0.052.
Mean (and standard deviations) for differences in vocalization behaviors between the initial and second vocalization samples for each risk group.
*statistically significant finding (p ≥ 0.05).
Total frequency of vocalizations
Differences in the total number of vocalizations including those coded as speech-like as well as those coded as non-speech for infant participants across low- and high-risk groups were determined. Distributions of vocalization frequency across risk groups were similar. Vocalization frequency from samples collected at six-months of age was not significantly different between LR (mean rank = 22.05) and HR participants (mean rank = 23.58), U = 216, z = 0.360, p = 0.718, using an exact sampling distribution for U (Dineen & Blakesley, 1973). The average number of total vocalizations was also similar for both groups (see Table 3), although there was more variability surrounding the point of central tendency for those representing the HR group (M = 56.08, SD = 32.39) than for those in the LR group (M = 49.71, SD = 22.58). Only small, negligible clinical importance (d = 0.25) was identified regarding differences in frequency of total vocalizations across risk groups at this sampling time.
Frequency of speech-like vocalizations
Differences across risk groups for the frequency of speech-like vocalizations at six months were determined. The statistical analysis indicated nonsignificant findings for differences between the LR (mean rank = 22.53) and HR participants (mean rank = 22.42), U = 201, z = -0.026, p = 0.979. Measures of central tendency and variability around the mean for both groups were similar, LR (M = 29.68, SD = 18.69) and HR (M = 31.69, SD = 20.34). An effect size of d = 0.11 indicated only small, negligible clinical importance for the frequency of speech-like vocalizations for the initial vocalization sample.
Consonant inventories
The consonants included in each participants’ inventory were categorized as early-, middle-, and late-developing according to the developmental acquisition order described by Shriberg (1993) to maintain consistency with the reporting format for findings in this area used by Paul et al. (2011). At 6-months, central tendency and the distribution of variability around it for the total number of consonants were similar for the LR (M = 4.13, SD = 2.28) and HR groups (M = 4.46, SD = 2.40). Statistical analyses were conducted to determine differences in consonant use between risk groups and supported descriptive data. Risk groups were not significantly different for total consonant use (U = 223, z = 0.540, p = 0.585), early-developing consonant use (U = 214, z = 0.313, p = 0.754), middle-developing consonant use (U = 222, z = 0.604, p = 0.546), or late-developing consonant (U = 198, z = -0.207, p = 0.836). More information regarding consonant inventories can be found in the article's supplemental materials.
The effect size for the difference in total number of consonants between risk groups was small (d = 0.15). When considering each developmental category of acquisition separately (early, middle, late) findings for risk-group means, variability distribution around the mean, and effect size were consistent with findings for the total number of consonants (see Table 3). Means and standard deviations were similar across risk group categorization and small, negligible effect sizes, ranging from d = 0.07–0.20, were noted.
For all infant participants regardless of risk group condition, the consonant inventories reflected higher use of early-developing consonants, those considered less motorically-complex, than middle- and late-developing consonants. Late-developing consonant production was nearly absent from the initial vocalization samples and represented by sparse use of /l/ in 4% of participants from the LR group and in 8% of participants from the HR group (see Table 3).
Percent canonical syllables
Use of canonical syllables in babbling was also not significantly different across the two risk groups in the initial vocalization sample. LR (mean rank = 22.15) and HR groups (mean rank = 23.35) did not demonstrate statistical differences in percent canonical syllable use, U = 213, z = 0.297, p = 0.766. This finding supported descriptive data for the two risk-groups, LR (M = 9.28, SD = 0.12) and HR (M = 9.01, SD = 0.12). The effect size was small (d = 0.02).
Non-speech vocalizations
Descriptive analysis indicated similarities in the data as both LR (M = 20.03, SD = 17.51) and HR groups (M = 24.40, SD = 17.94) showed similar distributions of non-speech vocalizations in general from the initial vocalization sample. The groups were not significantly different in their overall use of non-speech vocalizations, U = 241, z = 1.017, p = 0.309. The effect size was small (d = 0.12).
When the types of non-speech vocalizations (i.e., delight, distress, atypical) were analyzed between risk groups, both groups showed similar production averages for non-speech vocalizations across the sub-categorical distinctions. All effect sizes representative of these discrete non-speech vocalization categories, ranging from d = 0.13 to d = 0.26, reflected little practical importance. More information regarding subcategories of non-speech vocalizations can be found in the article's supplemental materials.
Twelve-month vocalization sampling
Speech-like and non-speech vocalizations were summarized for each participant group (see Tables 6–7). Significant differences were noted for the total number of vocalizations and differences for speech-like productions were notable but did not achieve significance. Effect sizes varied overall (see Tables 6 and 8). However, moderate to large effect sizes (i.e., ≤ 0.5) indicated clinical importance for the number of total vocalizations, number of speech-like vocalizations, consonant use (e.g., total number of consonants, early-developing and middle-developing consonants), and production of non-speech distress vocalizations between groups.
Mean (and standard deviations) for vocalizations across the high-risk groups with significance (p-value) and estimates of effect size for both vocalization samples.

High Risk Siblings (HR-SB).
High Risk Premature and Low Birth Weight (HR-PR).
Mean (and standard deviations) for non-speech vocalization categories across high-risk groups with estimates of effect size for both vocalization samples.

Total frequency of vocalizations
The descriptive analyses (Table 4) indicated dissimilar means and standard deviations between the LR (M = 76.10, SD = 33.15) and HR groups (M = 53.30, SD = 28.50) for total vocalizations. Statistical differences in the total number of vocalizations of infant participants across risk groups were determined. Total vocalizations were significantly higher in the LR group (mean rank = 23.59) than in the HR group (mean rank = 14.75), U = 99, z = -2.149, p = 0.031, using an exact sampling distribution for U. Based on the effect size categorization provided by Cohen (1988), these differences in total vocalizations were representative of moderate to large clinical importance, d = 0.69.
Frequency of speech-like vocalizations
The descriptive data showed variability in distributions across risk groups regarding the number of speech-like vocalizations coded during the second vocalization sampling (Table 4). Significance testing indicated differences in mean rank (LR mean rank = 23.34; HR mean rank = 15.33), U = 106, z = -1.950, p = 0.052, but these differences did not meet the conventional level of significance common to social sciences (p ≤ 0.05). An effect size of d = 0.68 reflected moderate to large clinical importance.
Consonant inventories
Consistent with the initial vocalization sample analysis, consonants were categorized as early-, middle-, and late-developing according to Shriberg; (1993) classic ordered system. At 12-months, central tendency and variability distribution measures were calculated for total consonant use in both the LR (M = 6.83, SD = 2.35) and HR groups (M = 5.50, SD = 1.68). Risk groups were not significantly different for total consonant use (U = 118, z = -1.628, p = 0.113), early-developing consonant use (U = 129, z = -1.333, p = 0.195), middle-developing consonant use (U = 120, z = -1.649, p = 0.127), or late-developing consonant (U = 168, z = -0.223, p = 0.877). The effect sizes for differences in total number of consonants, early-developing, and middle consonants ranged from d = 0.59 to d = 0.48, indicating moderate clinical importance. Later-developing consonant use represented a small, negligible effect, d = 0.12.
Infants across risk groups produced more early-developing consonants than middle and late during the second vocalization sample. However, individual consonant representation within developmental categories was variable. For example, production of early-developing consonants ranged from sample representation of 86% (/m/ and /h/ productions) to 3% (/p/) for the LR group and 100% (/h/) to 8% (/p/) for the HR group. Later-developing consonants were not used by the majority of infant participants at 12-months of age. For example, production of individual consonants representing this category ranged from 17% (/l/) to 0% use (/θ/, /z/, /ð/, and /ɹ/) for the LR group and 8% (/ɹ/ and /ʃ/) to 0% (all other sounds in the category) for the HR group.
Percent canonical syllables
Use of canonical syllables was also not significantly different across the two risk groups in the second vocalization sample. LR (mean rank = 21.60) and HR groups (mean rank = 19.54) did not demonstrate statistical differences in percent canonical syllable use, U = 157, z = -0.503, p = 0.621. This finding supported descriptive data for the two risk-groups, LR (M = 23.24, SD = 0.26) and HR (M = 18.54, SD = 0.19) and the effect size was small (d = 0.20).
Non-speech vocalizations
Descriptive analysis indicated similarities in the data as both LR (M = 20.14, SD = 16.49) and HR groups (M = 25.20, SD = 13.84) showed similar distributions of non-speech vocalizations. The groups were not significantly different in their overall use of non-speech vocalizations, U = 183, z = 0.244, p = 0.810. The effect size was negligible (d = 0.00).
When the types of non-speech vocalizations (i.e., delight, distress, atypical) were analyzed, both groups showed similar production averages for non-speech vocalizations categorized as “delight” and “atypical.” However, differences were noted for non-speech “distress” vocalizations between the LR (M = 11.76, SD = 13.66) and HR groups (M = 5.50, SD = 6.87). Although effect size estimates for “delight” and “atypical” were negligible, the effect size estimate for “distress” was of moderate clinical importance, d = 0.51).
Comparison of 6- and 12-month prelinguistic vocalization samples
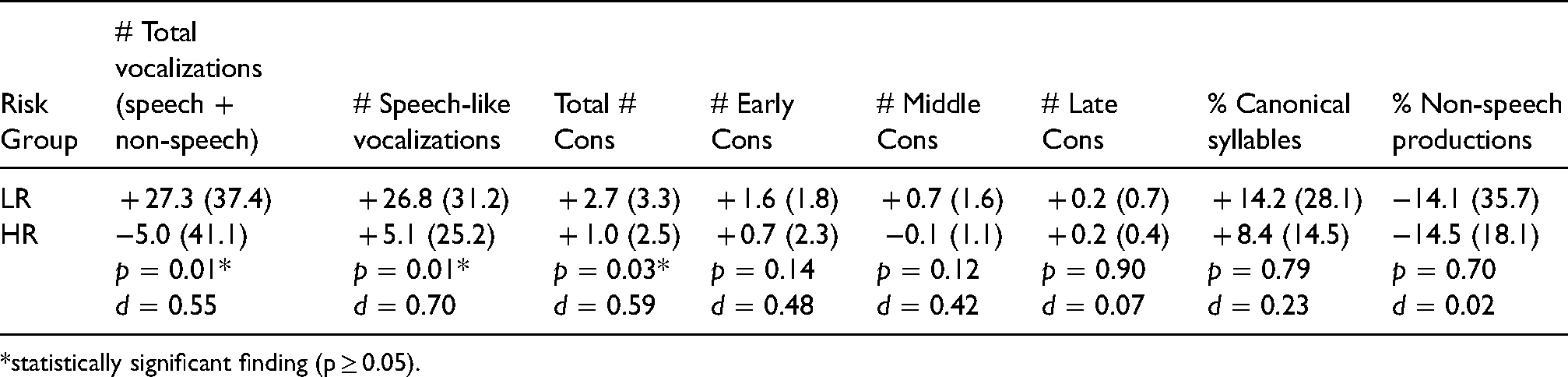
As shown in Table 5, a comparison of findings from the two samples indicated change over time in vocalization acquisition such that infants with low-risk status generally followed a trajectory of increasing vocal skill between the initial and second vocalization samples. For instance, means for total vocalizations increased over time as did speech-like vocalizations, and consonant and canonical syllable use, while non-speech productions decreased.
The trend toward vocal skill gains demonstrated by infants in the LR group was also demonstrated by participants from the HR group, but to a lesser extent with variation noted. Although the total number of vocalizations indicated a slight decrease, speech-like vocalizations increased, as did most consonant production measures and canonical syllable use. Non-speech productions decreased from the initial to second sample.
Similar to initial vocalization sample findings, infants from both risk groups produced more early-developing consonants than middle and late. Although production of later-developing consonants increased compared to the initial vocalization sample, this category continued to represent the least used across risk groups.
Statistically significant differences were noted over time between the low- and high-risk groups for total vocalizations. Risk groups were significantly different across the two time samples for total vocalization use (U = 86.5, z = -2.508, p = 0.012), number of speech-like vocalizations (U = 89.5, z = -2.423, p = 0.015), and total consonants used (U = 99.5, z = -2.153, p = 0.031). Additionally, effect sizes for these differences over time ranged from d = 0.55 to d = 0.70, indicating effects of moderate practical importance (Cohen, 1988). Effect sizes for other variables compared for change over time indicated medium to negligible effects, d = 0.48 (change in the number of early consonants used) to d = 0.02 (change in the percentage of non-speech productions over time).
Differences in vocalization behaviors across high-risk etiologies
To examine differences in vocalization behaviors within the HR group, descriptive statistics (e.g., mean and standard deviation), nonparametric inferential analyses, and estimates of effect size were employed.
ptAs indicated in Table 6, analysis of the two vocalization samples revealed no significant differences between subgroups in the high-risk category of the present study, younger siblings of children diagnosed with ASD (HR-SB) and infants born prematurely and with low birth weight (HR-PR). Although all findings were non-significant, the HR-SB subgroup, on average, produced more speech-like vocalizations, total consonants, middle consonants, late consonants, and percentage of canonical syllables than did the HR-PR subgroup. The HR-PR subgroup produced, on average, more total vocalizations and a larger percentage of non-speech productions than the HR-SB subgroup. In the 12-month sample, the HR-SB subgroup produced, on average, more total vocalizations, speech-like vocalizations, total consonant use, early consonant use, middle consonant use, late consonant use, and percentage of canonical syllables than the HR-PR subgroup. The HR-PR subgroup produced, on average, a larger percentage of non-speech productions than the HR-SB subgroup.
A review of effect sizes calculated across vocalizations findings indicated primarily minimal to moderate effects for most findings derived from the 6-month sample except for the number of middle and late-developing consonants produced and presence of canonical syllables. The effect sizes for these consonant productions and canonical syllable use, ranged from d = 0.51 (canonical syllables) to d = 0.81 (middle consonants) and were considered to be large, suggesting the potential for crucial practical importance across these differences (Cohen, 1988). For the 12-month sample, effect sizes again indicated small to moderate effect sizes with the exception of total number of consonants, late-developing consonants, canonical syllable use, and non-speech productions. The effect sizes associated with these findings indicated large, clinically-relevant effects ranging from d = 0.53 (non-speech productions) to d = 0.70 (canonical syllables).
Table 7 depicts subgroup differences in non-speech vocalization categories of delight, distress, and atypical productions across the two vocalization samples. For the 6-month sample, non-speech vocalizations expressing distress and atypical productions both suggested large, clinically-relevant effect sizes (d = 0.87 for distress and d = 0.85 for atypical). However, by the 12-month sample, all non-speech differences were minimal.
Discussion
The aim of the present study was to address three research questions. First, did the observed vocalization behaviors indicate differences across infant risk for ASD? Second, how do vocalization behaviors change between 6- and 12-months of age for infants in low and elevated risk cohorts? Finally, third, is high-risk etiology associated with differing vocalization behaviors at 6- or 12-months for infants in the elevated risk cohort? We found that at 6- months of age, there were no significant differences in vocalizations across risk group cohorts, but by 12-months, significant differences were noted. We also found that, over time, vocalization behaviors changed between 6- and 12-months such that both risk groups indicated increasingly complex skill acquisition, but the HR group exhibited this to a lesser extent than the LR group. In terms of differences in infant vocal behavior across high-risk etiologies, some differences were noted in the present study sample including vocalization frequency overall, speech-like vocalizations, use of consonants and canonical syllables, and non-speech productions.
Vocalization behavior differences across risk groups at 6 months of age
Prior to the study, based on the findings from Paul et al. (2011) study, the researchers hypothesized that the targeted 6-month vocalization behaviors would not be significantly different across risk groups nor would these behaviors represent clinically relevant effect sizes. The study findings indicated this hypothesis should be retained. We did not observe vocalization behaviors that indicated differences across risk groups such that infants at high risk produce fewer vocalizations overall, fewer speech-like vocalizations, more non-speech vocalizations, fewer consonant types, and fewer canonical syllable shapes.
These findings support those of Paul et al. (2011) who also found no significant differences in observed vocal behaviors of infants across risk groups at 6-months of age. Thus, the 6-month vocalization findings indicated convergence regardless of methodological differences between the present study and the study conducted by Paul et al. (2011) that included differences in the data collection environment (home vs. clinic, respectively), sample size (20-min samples vs. 5-min), HR-group composite (younger siblings and infants born prematurely and with low birth weight vs. only younger siblings of children diagnosed with ASD), and research design (longitudinal vs. cross-sectional). Additionally, these non-significant findings associated with small, negligible effect sizes collected using direct analysis of infant vocal behaviors were congruent with findings derived from retrospective home video analysis (e.g., Chericoni et al., 2016).
Because differences in vocal behaviors for infants at high risk of an ASD diagnosis may represent inactive alignment of sound productions to match those present in the infant's linguistic environment, Schoen et al. (2008, 2011) theorized that differences in vocal behaviors may not be observable until the time when the infant transitions to the use of sounds for speech. At that time, close to a child's first birthday, the expectation would be for the child to successfully convey messages using real-word productions composed of speech sounds present in the ambient language environment. Until that time, differences in prelinguistic vocal behavior may be difficult to observe and code, as evidenced by the present research literature in this area. However, early vocalization patterns remain an important area of study to facilitate comparison of change over time by providing much-needed baseline data points by which to measure further developmental progress, or lack thereof.
Vocalization behavior differences across risk groups at 12 months of age
By 12-months of age, the researchers originally hypothesized that risk-group differences would be evident such that the infants at low risk would produce significantly more vocalizations behaviors than the elevated-risk cohort. Present study findings offered partial support for this hypothesis. Statistically significant risk-group differences associated with moderate-to-large effect sizes were noted for overall vocalizations such that the LR group produced more total vocalizations than the HR group. Similarly, although the finding for speech-like vocalizations was not significant (p = 0.052), it did represent a large, clinically-relevant effect size.
These findings are aligned with those of Paul et al. (2011) in that speech-like vocalizations differed between the risk groups and more were produced by infants at low risk. However, Paul et al. (2011) did not find significant differences in total vocalizations, as were indicated by this study and they found significantly low frequency of non-speech vocalizations at 12-months for their low-risk group. They noted, “pre-speech sound development is a sensitive indicator of the rate and degree to which infants at risk for ASD are following the developmental path to language acquisition” (Paul et al., 2011, p. 594). More research is needed to determine the vocalization indicators truly of early developmental interest. However, in broader terms, this study indicated support for differences noted between major measures of early vocal behavior in which infants at low risk produce “more” and infants at high risk produce overall “less.” This broad finding is consistent with the findings of other researchers (Gamliel et al., 2009; Sheinkopf et al., 2000) although the precise language measures at which these observations were recorded varied. Additionally, researchers studying gestural output noted the same phenomena (see Manwaring et al., 2018; West et al., 2020).
Notably, the present study findings as well as those of previous research efforts (e.g., Chericoni et al., 2016; Iverson & Wozniak, 2007; Paul et al., 2011; Talbott et al., 2016; West et al., 2020), differed from those indicated by Swanson et al. (2018); Swanson et al. (2018) found an opposing effect in which the high-risk group produced more vocalizations than the low-risk group of infants at 9 months of age. They identified a subgroup of “hypervocal” infants (p. 64) who produced significantly more vocalizations than expected by the researchers and raised the condition group average in this area. To date, other researchers have not replicated the findings associated with their study. It is possible that differences in vocal observation and coding methodology, risk-group inclusionary criteria, and infant age may explain differences in study findings. For example, Swanson and colleagues used continuous, yet variable digital recording with wearable devices and coded vocalizations by count, length, and duration rather than for speech-like/non-speech content. In addition, the HR group in Swanson and colleagues’ study were comprised solely of infants whose older siblings were diagnosed with autism. Also, Swanson and colleagues collected data at 9-months of age only. Or, in fact, true differences may exist within subgroups of infants at high risk of ASD, as some were noted within the present study as well. Determining factors related to high-risk etiology are a logical next step for research efforts in this area. Swanson et al. (2018) as well as others (see Warlaumont et al., 2014) have noted deficits in the “social feedback loop” (Warlaumont et al., 2014, p. 1314) may contribute to hypervocal infant behavior involving more non-speech vocalizations when increased vocalizations do not educe timely and contingent adult responses.
In the present study and unlike the study conducted by Paul et al. (2011), at 12-months, the LR and HR groups produced, on average, nearly the same percentage of non-speech vocalizations. Further examination of non-speech vocalizations showed that both groups produced typical and atypical vocalizations with nearly the same frequency, but the LR group produced more distress-related vocalizations than the HR group. At this time, we cannot determine if this finding is consistent with additional existing literature (e.g., Plumb and Wetherby, 2013; Schoen et al., 2011) that young children with ASD, or those later diagnosed with ASD, were more likely to produce atypical vocalizations than peers at low risk. However, it is important to consider early vocalization patterns in conjunction with other developmental skills and observable behaviors not in an isolated context to make decisions regarding early ASD diagnosis (Garrido et al., 2017).
Vocalization behavior differences over time
The second research question associated with the present study related to changes in infant vocal behaviors between the 6- and 12-month vocalization samples. In the present study, infants in the LR group largely followed a developmental pattern of increasing vocalization, as indicated by increases across factors such as total vocalizations, speech-like vocalizations, and consonant and canonical syllable use. This finding was expected and consistent with previous research findings (Gamliel et al., 2009; Paul et al., 2011). Also consistent with previous reports (Gamliel et al., 2009; Paul et al., 2011; Warlaumont et al., 2014) was the finding that participants in the HR group also followed an overall pattern of increasingly complex skill acquisition, but to a lesser extent and at a somewhat slower pace than the LR cohort by 12 months of age for most metrics observed. Infants in the HR group showed statistically significant less change over time in the total number of vocalizations, speech-like vocalizations, and total consonant use compared with infants in the LR group. Schoen et al. (2008; 2011) proposed that slowed transitions between developmental stages of pre-speech could be an early symptomatic feature of ASD behavioral characteristics. These findings may also reflect a delay in early speech-language skills that could resolve or lessen in severity over time, consistent with findings related to toddlers with late language emergence (for further discussion on this topic, see Camarata, 2014; Rescorla & Dale, 2013). Without knowing ASD diagnostic status, it is difficult to infer predictive meaning from the present study findings regarding later speech-language abilities; however, this information provides insight into the potential influence of BAP on the trajectory of early vocalization development, particularly speech-like vocalizations, as well as early indication of ASD-like behavioral symptomology in the communication domain (APA, 2013).
The present study finding for non-speech productions, that they decreased over time, was also consistent with the findings from Paul et al. (2011). These findings imply a gradual transition from infant reliance on non-speech vocalizations to more effective and complex speech-like vocalizations that eventually convey linguistic content for communicative messages, demonstrated by infants across risk group categorization.
Vocalization behavior differences as a function of high-risk etiology
The third research question addressed the notion that high-risk etiology (e.g., familial heritability vs. prematurity/low birth weight) may be associated with differing vocalization behaviors at 6- or 12-months for infants in the high-risk cohort. The present study findings indicated some preliminary subgroup differences that could be of moderate-to-large clinical importance including vocalization frequency overall, speech-like vocalizations, use of consonants and canonical syllables, and non-speech productions. For many of these metrics, the presence of clinically-significant differences tended to increase with age up to 12-months indicating that, over time, these etiologically specificities may be more observable. Unfortunately, at this time, there is a dearth of available literature to which comparisons of the present study findings can be made. Perhaps issues related to etiology offer some explanatory power to inconsistent findings across infant risk studies as most notable studies within this area of research focus primarily or solely on infant siblings of children already diagnosed. However, more meaningful comparative studies may be conducted now that the research community has a better understanding of additional infant risk conditions of ASD, namely infants born prematurely and with low birth weight. More research is needed to address the lack of information regarding the role of etiology in the manifestation of early vocalization behaviors.
Study limitations
As with any study, the present research has several limitations for generalization beyond the participants involved. First, it represents a small sample, particularly for the high-risk group representation. This limited sample size is indicative of the exploratory nature of the present study which was innovative in its home-based nature of data collection and inclusion of multiple etiological conditions for the high-risk group, offering an opportunity for preliminary comparisons. To that end, use of Cohen's d effect size to denote high clinical relevance may be misleading given the small sample size and the subtle and modest observable group differences that may not rise to the level of detection by parents or clinicians. Given the limited sample size of the HR group, it is possible that these effects do not truly represent clinically meaningful differences. Replication of the study with a larger and more diverse cohort of infant participants would be advantageous. Additionally, aligned with the exploratory nature of the study, the data collection points were limited to 6- and 12-month samples. Additional data collection across multiple months would lead to a more nuanced perspective of early vocalization behaviors and a better sense of when early important differences in vocalization behaviors can be detected.
For future directions, with the present study, review of the vocalization data in context with eye gaze and postural data to compile differentiated diagnostic profiles would be intriguing. Also, incorporating “quality” vocalization coding such as those used by McDaniel et al. (2020) coupled with “quantity” coding would allow for more robust and nuanced study findings in this area. Finally, use of a structured measurement tool like the Stark Assessment of Early Vocal Development-Revised (SAEVD-R) as utilized by Nathani et al. (2006), may provide increased measurement reliability for assessing discrete vocal development behaviors across infant risk groups.
Clinical implications
When the findings of the present exploratory study are viewed in the context of previous research findings, clinical implications can be gleaned for practical application. Early childhood professionals need to be aware of risk group status as well as the developmental differences that may accompany ASD and ASD-like symptomology (i.e., BAP). Early childhood professionals need to also be aware that an ASD diagnosis is behaviorally based and precursors of the behaviors noted may differ in important ways much sooner than current diagnostic evidence indicates. For example, although the average age of an ASD diagnosis is 50–52 months of age (just over 4 years of age), as noted by the present study, differences in vocalization behaviors evident by 12-months of age are observable between infants at low and elevated risk of ASD. Observable and clinically-relevant vocalization behaviors may be an important component of an early developmental profile that could eventually lead to a reduced diagnostic age for ASD and these observations, whether completed in the home or laboratory setting, seem to converge in agreement.
Conclusion
The present study is unique and innovative in a number of ways as the first home-based longitudinal study examining infant vocal behaviors across low- and high-risk groups for ASD and the first direct-observation vocalization study to include high-risk infants from two etiological backgrounds. The study included infants born prematurely and with low birth weight as well as infants who had an older sibling diagnosed with ASD and compared their early vocalization behaviors at 6- and 12-months to infants at low risk as well as with each other. Consistent with previous cross-sectional research conducted in a clinical laboratory setting, differences at 6-month were not significantly different across risk groups. By 12-months of age, statistically significant group differences were noted in the total number of vocalizations and moderate to large clinically relevant effects were found for a number of the behaviors noted at this age. Whereas both risk groups demonstrated developmental changes in vocalization behavior between 6- and 12-months of age, those observed by infants at low-risk were greater and significantly differed from infants at high-risk for total vocalizations, speech-like vocalizations, and total consonants used. Preliminary differences across high-risk group from different etiologies indicated potentially clinically relevant findings for some vocalization behaviors studied including total number of consonants, late-developing consonants, canonical syllable use, and non-speech productions; however, replication of these findings are needed to further determine areas of interest between high-risk infants.
Supplemental Material
sj-docx-1-dli-10.1177_23969415211057658 - Supplemental material for A home-based longitudinal study of vocalization behaviors across infants at low and elevated risk of autism
Supplemental material, sj-docx-1-dli-10.1177_23969415211057658 for A home-based longitudinal study of vocalization behaviors across infants at low and elevated risk of autism by Shari L. DeVeney, Anastasia Kyvelidou and Paris Mather in Autism & Developmental Language Impairments
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nebraska University System Science. Collaborative Grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.