
Abstract
Autism spectrum disorder is a neurodevelopmental condition characterized by significant deficits in social skills that impact youths’ academic, adaptive, and psychological functioning. Social skills deficits are imperative targets for interventions. This pilot study explored the feasibility and preliminary effectiveness of the translated and culturally adapted Arabic version of the UCLA PEERS® among autistic adolescents (ages 11–17) in Saudi Arabia.
The study utilized a quasi-experimental design, collected pre-, post-, and three-month follow-up data, and used focus group discussion and a prospective cohort study with pre- and postintervention assessments. Feasibility was assessed based on subjective methods: recruitment, retention, attendance rate, comprehension of the translated material, and homework completion. Effectiveness was evaluated based on postintervention and three-month follow-up interval changes in scores on three outcome measures: the Social Responsiveness Scale, Second Edition, Child Behavior Checklist, QSQ, and Test of Adolescent Social Skills Knowledge. Written informed consent was obtained from caregivers, and oral assent was obtained from the study participants.
These initial findings support the feasibility and preliminary effectiveness of the PEERS-AA. The outcomes suggested significant improvement in the subjects’ social skills and knowledge of social etiquette, as reported by the adolescents and their parents, with improvements retained at the three-month follow-up. However, there was no reported improvement in the number of get-togethers, which was likely explained by COVID-19 pandemic restrictions and culture-related considerations.
This study represents the first cross-cultural validation trial of an established evidence-based social skills intervention for autistic adolescents in an Arabic-speaking country. The PEERS-AA manual's feasibility and preliminary effectiveness indicate its promising applicability for interventions and research. Further research to evaluate the generalizability and long-term effectiveness of the PEERS-AA program is needed.
Keywords
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by persistent deficits in social communication and interactions across multiple contexts and the presence of restricted, repetitive patterns of behaviors, interests, or activities, according to the Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition - Text Revision (American Psychiatric Association, 2022). The global prevalence of Autism was believed to be less than 1% worldwide, with estimates being higher in high-income nations (Lord et al., 2020b). Recent epidemiological studies indicate a significant global increase in the prevalence of ASD over the past few years (Talantseva et al., 2023). Meimand et al. (2023) systematic review suggested that the prevalence of ASD in the Middle East and North Africa rose by 70% in the period between 1990 and 2019, estimating 7.5% of the new ASD cases globally. In Saudi Arabia, AlBatti et al. (2022) reported a prevalence of ASD was 2.51% (1 in 40 children), consistent with current. Alsulami et al. (2024) reported a prevalence of ASD in children was 0.51% (95% CI: 0.4%–1%), with Saudi Arabia having a significantly higher rate of 1.33%.
Autism significantly impacts children's and adolescents’ academic, adaptive, and psychological functioning (Coie et al., 1995; Elliott et al., 2001; Nelson, 1996) and can increase the risk of other mental health concerns, such as depression and anxiety (Kwan et al., 2020). Additionally, other adverse outcomes have been associated with an Autism diagnosis, including social isolation, rejection, bullying by peers, and low self-esteem (Mitchell et al., 2010).
Social skills deficits become more apparent in the adolescent years, making it a particularly stressful transitional phase and a critical area for intervention. Compared with their neurotypical peers, autistic adolescents often experience greater social isolation, have fewer meaningful friendships and fewer social networks, and are more prone to bullying and victimization. This subsequently increases their risk for depressive symptoms (Lasgaard et al., 2010; Locke et al., 2010; Schroeder et al., 2014). Social skills, mainly conversational skills, significantly correlate with perceived victimization and bullying rates among adolescents on the spectrum (Sterzing et al., 2012).
Group social skills interventions (GSSIs) are programs aimed at improving social performance and social knowledge and are often recommended for children and adolescents on the spectrum (Wolstencroft et al., 2018). A meta-analysis of GSSIs revealed an increase in the effect size of social knowledge in youths’ self-reported measures of social skills, with moderate overall effectiveness attributed to the possible nature of the condition (Gates et al., 2017). Whereas numerous concerns have been articulated toward existing social skills programs, cognitive behavioral therapy-based therapies are recognized as promising treatment methods to alleviate social deficits in autistic adolescents (DaWalt et al., 2018; Laugeson & Park, 2014).
The literature revealed different interventions for Autism, the majority of which were conducted in Western and Asian countries. Dolan et al. showed that autistic youth who completed a social skills intervention focused on friendships had significantly improved vocal expressiveness and an enriched overall quality of rapport (Dolan et al., 2016). A systematic review and meta-analysis revealed significant improvements in social function and cognition among children and adolescents who received any social and behavioral intervention despite their diagnosis and level of deficit in social skills (Darling et al., 2021). The work of Halmelen et al. reflected the importance of helping adolescents successfully transition into adulthood, as friendship support could predict solid functioning in psychosocial domains in the future (Halmelen et al., 2017). There are very few evidence-based interventions for autistic adolescents (Miller et al., 2014), since much of the research addressing social skills interventions in individuals with Autism focuses on children at earlier developmental ages, and as a result, the need for social skills training programs for autistic adolescents is growing (Van Steensel & Heeman, 2017). Among several social skills training programs for individuals with Autism, the Program for the Education and Enrichment of Relational Skills (PEERS®) is one of the few supported by scientific evidence (Laugeson et al., 2012; Laugeson & Frankel, 2011), including a meta-analysis demonstrating significant gains following PEERS® for autistic adolescents (Zheng et al., 2021).
PEERS® was initially developed in the United States and evaluated in several randomized controlled trials (RCTs), which have shown efficacy (Hill et al., 2017; Laugeson et al., 2009). The program demonstrated immediate gains in various social skills for autistic adolescents without intellectual disabilities (Dolan et al., 2016; Laugeson et al., 2009; Laugeson et al., 2012). The program has also shown long-term treatment effects, even 1–5 years after the intervention (Mandelberg et al., 2014). Additionally, substantial decreases in social anxiety symptoms in autistic adolescents were revealed in comparison with a control group (Hill et al., 2017). Furthermore, an increase in parent-reported get-togethers in a group of adolescents with brain injury was reported, with gains maintained at 26 weeks following treatment (Gilmore et al., 2022). A study examining the neural function of adolescents after completing the PEERS® program revealed that autistic adolescents no longer differed from typically developing adolescents in terms of EEG asymmetry (Van Hecke et al., 2015). A modified 16-week version has been developed for young adults, with efficacy established through multiple RCTs with delayed treatment groups (Gantman et al., 2012; Laugeson et al., 2015), with results replicated cross-culturally (Oh et al., 2021; Płatos et al., 2022).
Although social skills group interventions are often thought to be more effective in their countries of origin, they have also been verified in different countries, revealing the potential for generalizability, even in different cultural contexts (Miller et al., 2014). The PEERS® program has been successfully translated and adapted to several other non-English-speaking European and Asian countries (e.g., Boon-yasidhi, 2021; Lao et al., 2023; Płatos et al., 2022; Rabin et al., 2018; Shum et al., 2019; Yamada et al., 2020; Yoo et al., 2014). Most recently, Sittanomai et al. (2021) published the results of the PEERS® program adapted to fit Thai culture, which showed high feasibility and effectiveness in 12 adolescents and their families. This was evident from the high parent satisfaction rate and improvement in multiple social skill domains and adaptive functioning, while also decreasing the rate of maladaptive behaviors.
Cross-cultural replication studies have been conducted with Asian and European samples; however, that is not the case in the Middle East and North Africa, as there are no similar programs in Arabic-speaking communities. Furthermore, Arabic evidence-based interventions are scarce; hence, programs that focus on improving the social competence of adolescents with Autism are invaluable, making the present study unique and significant. This study explored the feasibility and effectiveness of applying the translated and culturally adapted version of the PEERS® in a clinical setting among autistic adolescents in Saudi Arabian society. We anticipated overall feasibility as predicted by weekly attendance, the intervention completion rate, assignment compliance, and comprehension of the materials delivered. We hypothesized that the Arabic-translated and culturally adapted version of the PEERS® (PEERS-AA) would improve the social skills of autistic adolescents despite the modification of cultural differences and lack of formal social skills training programs for neurotypical children and adolescents.
Methods
The present study used a quasi-experimental design, collecting pre-, post-, and three-month follow-up data. This design is appropriate for examining the feasibility of a novel intervention. The study was conducted in two main phases: translation and cultural adaptation, followed by adapted manual piloting.
Translation and Cultural Adaptation of the PEERS®
For this Arabic Social Skills Project Initiative, the original manual was translated via a multistage approach (forward translation, focus groups, and feedback sessions). The first four authors initially underwent official PEERS® Certified Training from the UCLA PEERS® Clinic and were qualified as PEERS® certified providers. The original version of the PEERS® Treatment Manual (Laugeson & Frankel, 2011) was then translated into a formal Arabic version and reviewed extensively. In the second stage, focus groups were held by the research team to better adapt wording to simple formal Arabic and culturally adapted examples. The main principles of each training session and instructions were expressed in formal Arabic. At the same time, the conversational scripts in role-play were further modified into a generic Saudi dialect to facilitate the delivery of the lessons. The process of translation, validation, and shaping of the manual into a culturally appropriate version was supervised by the program developer. Three main areas requiring cultural adaptation were identified before the translation. This included choosing appropriate friends, specifically adolescent friend groups (parent session number 3/adolescent session number 4), get-togethers (session number 8), and teasing and handling embarrassing feedback (session 10).
Finally, the translated version was further reviewed and modified by Autism-specialized experts in the Kingdom of Saudi Arabia before they attended a series of focus group discussions. After this, they were asked to evaluate the translated manual independently. To further adapt the treatment manual to the local context, weekly feedback from caregivers and the intervention team during the program's implementation was recorded for further adaptation of the program on an ongoing basis.
Recruitment and Screening
The intervention occurred at two child and adolescent psychiatry departments attached to a military hospital and a university hospital in Riyadh, Saudi Arabia. Convenience sampling was employed, where 25 participants were recruited through advertisements in Autism support groups or clinician referrals from the involved centers. Electronic medical charts and telephone screening data were reviewed to explain the research plan to parents, who were candidates for an initial interview. Three families declined the intervention, and 22 were screened through a phone interview utilizing the UCLA PEERS® manual phone script (Laugeson & Frankel, 2010); they were then invited to an in-person intake interview with both parents and adolescents via a preintake assessment form (Table 1 and Table 2) translated from the original manual (Laugeson & Frankel, 2010). Separate interviewers met individually with adolescents and their parents to assess the adolescents’ cognitive and overall social functioning and ensure that the adolescents were motivated to participate in the program and learn the skills being offered, free of coercion from parents.
Characteristics of the Pilot Sample.
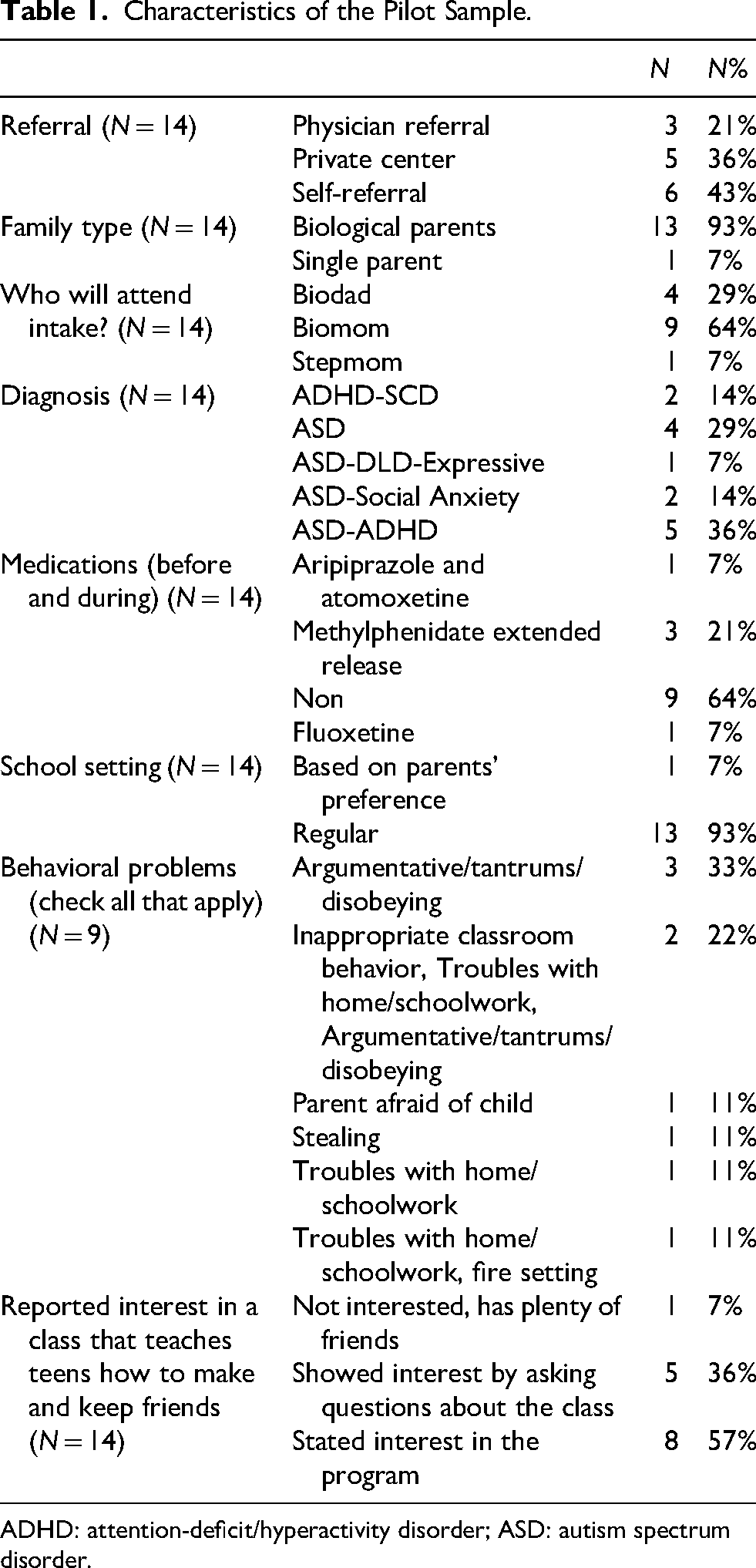
ADHD: attention-deficit/hyperactivity disorder; ASD: autism spectrum disorder.
Questions About Social Behavior and Friendships of the Participants.

Participants
The inclusion criteria of the study included the following: (1) individuals aged 11–17 years, (2) who were motivated to attend the program; (3) who met the clinical criteria for the diagnosis of Autism or social-pragmatic (communication) disorder (SCD), confirmed by child and adolescent psychiatrists; (3) who demonstrated adequate verbal fluency confirmed by full-scale IQ scores of 70 or above on the basis of standardized testing performed at the intervention centers; (4) who were experiencing marked social difficulties as reported by parents/youth in a structured intake interview outlined in the PEERS® treatment manual (Laugeson & Frankel, 2010); and (5) who had a parent willing and able to attend the intervention and serve as a social coach. The exclusion criteria included adolescents with any mental illness or behavioral challenge that would impede participation or require alternative treatment (e.g., IQ below 70, uncontrolled attention-deficit/hyperactivity disorder [ADHD], schizophrenia, bipolar disorder, or self-injurious behavior).
Procedures
Four clinical psychology interns were recruited as cotherapists and research assistants. Their primary duties included conducting intake assessments, supervising pre–post survey completion, and serving as cotherapists in the adolescent group. The PEERS® certified providers then conducted a one-week training workshop on the program and research protocol with the clinical psychology interns. Weekly training sessions were conducted over 12 weeks. Training included didactic lessons covering each session's guiding principles and format of the PEERS-AA manual, with a focus on role plays.
Participants who met the inclusion criteria were invited to a pre-engagement group. The group utilized a format similar to the program, with parallel adolescent and parent groups. The aim was to allow the adolescents to get to know each other and the therapists before the intervention group started, explain the group's structure, and discuss the end-of-group graduation. The formats of the sessions were reviewed with the parent group, and additional concerns regarding the group, intervention, and privacy were discussed. Written informed consent from the caregivers and oral assent from the adolescent study participants were obtained during the intake appointment. All the interviews and assessments were conducted in formal Arabic by child and adolescent psychiatrists and psychologists on the research team and were translated into English for documentation.
The interventions were delivered over 12 weeks between October 2021 and March 2022 by four PEERS®-certified providers and four clinical psychology interns as coleaders. The parent group leaders were two child and adolescent psychiatrists. In contrast, the adolescent group leaders included one child and adolescent psychiatrist and one child and adolescent clinical psychologist. Four coleaders assisted the group leaders throughout the treatment sessions. Two coleaders, one for each center, were trained on the program by the research team prior to implementation; in addition, they were supervised by the group leaders weekly in all content and intervention processes. All treatment team members met for one hour after each group for feedback and fidelity testing. The flowchart for the recruitment process and selection of study participants is presented in Figure 1.

Flowchart for the Recruitment Process and Selection of Study Participants.
Outcome Measures
The outcome measures for this pilot study were chosen based on their availability in Arabic, the clinical context in which the study was conducted, and the literature review.
Feasibility Assessment
The feasibility of the study was assessed by the adolescents’ and their parents’ weekly attendance rates, homework completion rates, and overall treatment completion rates. Phone interviews were conducted with participants who failed to attend a session to record reasons for noncompliance and offer assistance for future attendance if possible.
Assessment of Effectiveness
Owing to the small sample size and the nature of the study, effectiveness was measured by assessing adolescent social skills knowledge (Test of Adolescent Social Skills Knowledge [TASSK]), and parental-reported changes in adolescent behavior were measured by validated measures (Social Responsiveness Scale, Second Edition [SRS-2], Child Behavior Checklist [CBCL], and QSQ).
Primary Outcomes
Parent-Reported Measures
Parents were asked to complete a set of measures before the intervention (Time 1), immediately after the intervention (Time 2), and three months following treatment (Time 3) to evaluate the effectiveness and durability of the intervention.
Social Responsiveness Scale, Second Edition
The SRS-2 was used to assess social functioning before the intervention, immediately after the intervention, and three months after treatment (Constantino, 2012). The scale is a standardized 65-item rating scale used to measure the severity of Autism symptoms as they occur in natural social settings. It has two forms: a parent-completed form and a teacher-completed form. The SRS-2 is appropriate for children and adolescents aged 4–18 years. It generates scores for five subscales: social awareness, social cognition, social communication, social motivation, restricted interests, and repetitive behavior. Aldosari and others (2019) translated the Arabic version of the SRS-2 for the Social Communication Questionnaire validation project. The research team obtained a license to use the translated version from the original publisher.
Quality of Socialization Questionnaire-Parent
The Quality of Socialization Questionnaire-Parent (QSQ-P; Laugeson & Frankel, 2010) is a self-report measure adapted from the Quality of Play Questionnaire (QPQ; Frankel & Mintz, 2011) to better capture adolescent social engagement. The QSQ-P includes 12 items assessing the frequency of hosted and invited get-togethers with peers in the past month and conflict during get-togethers. The QPQ number of playdates in children successfully discriminates clinical populations from community controls (Frankel & Mintz, 2011). The QSQ-P has been used as an outcome measure in previous studies of the PEERS® for adolescent social skills intervention (Laugeson et al., 2009, 2012) and represents an ecologically valid, real-world outcome of social engagement. The QSQ-P was administered to parents before the intervention, immediately after the intervention, and three months following treatment to assess changes in adolescent social engagement.
Adolescents-Reported Measures
Test of Adolescent Social Skills Knowledge
The Test of Adolescent Social Skills Knowledge (Laugeson & Frankel, 2010) is a 26-item criterion-based assessment of adolescents’ knowledge of the skills taught in the PEERS® for adolescent intervention. The items include sentence stems and two response options. There are two items for each of the 13 skills-based lessons, excluding the graduation session. Higher scores on this measure suggest increased adolescent social skill knowledge. The TASSK was administered to the adolescents before the intervention, immediately after the intervention, and three months after the intervention to evaluate the effectiveness of the intervention. The English version of the TASSK was translated by four research team members involved in translating the PEERS® manual. A multistage process was utilized, including translation and then back translation, followed by conducting focus group discussions on culturally adaptive wording and ensuring that the layout was consistent with the manual's content.
Quality of Socialization Questionnaire-Adolescent
The Quality of Socialization Questionnaire-Adolescent (QSQ-A; Laugeson & Frankel, 2010) is similar to the parent-completed QSQ-P measure described above. However, the QSQ-A assesses the frequency and quality of most get-togethers from the adolescent's perspective.
Secondary Outcomes
Child Behavior Checklist 2–3
The CBCL was used to investigate parent-reported changes in adolescents’ behavioral and emotional problems. The CBCL is a parent-reported questionnaire in which parents rate the adolescent on various domains of psychopathology (Achenbach & Edelbrock, 1991) (Achenbach, 2001). It assesses internalizing and externalizing behaviors across 16 domain subscales. The 2001 revision of the CBCL, CBCL/6–18, comprises eight syndrome domains: anxious, depressed, somatic complaints, social problems, thought problems, attention problems, delinquent behavior, and aggressive behavior. Parents were asked to complete the questionnaire before the intervention, immediately after the intervention, and three months after the end of the intervention (Achenbach, 2001).
The psychometric properties of the Arabic translation were previously studied in a sample of 694 three-year-old children as part of a community-based epidemiological study in the United Arab Emirates (Yunis et al., 2007). All the data are presented as T scores, with higher T scores indicating more problems. For this study, internalizing, externalizing, and total CBCL scores were evaluated.
Data Analysis
The data were analyzed via JMP version 15.0. Descriptive analysis was used for the study variables; categorical variables are represented by frequencies and percentages, whereas continuous variables are represented by means or medians and standard deviations. Inferential statistics in the form of paired t-tests or Wilcoxon-ranked tests were used to estimate the difference between the measurements at each time point and the baseline. Paired t-tests were used for normally distributed continuous variables, whereas Wilcoxon-ranked tests were applied for non-normally distributed data or small sample sizes. Analysis of variance was conducted to assess the effect of the PEERS-AA program and the mean difference between baseline, one-month, and three months postintervention. To further explore the effect of the PEERS intervention over time, a post hoc pairwise analysis using the Wilcoxon rank test was conducted to compare the preintervention (Time 1) with postintervention (Time 2) and preintervention (Time 1) with three months postintervention (Time 3) on the outcome. The total T score and changes in severity were used to reflect overall social responsiveness. McNemar's test or Kendal's tau test was used to estimate significant associations for paired categorical or ordinal data, respectively, for nonparametric paired comparisons. A p value less than 0.05 was considered statistically significant.
Ethical Consideration
Ethical approval was obtained from Prince Sultan Military Medical City (Approval Number: [1488]) and King Abdullah bin Abdulaziz University Hospital (Approval Number: [21–0224]). Informed written consent was secured from the parents or legal guardians of all participants, and verbal assent was provided by the participating adolescents.
Results
Participants
This pilot sample consisted of 12 participants who were diagnosed with Autism and two with SCD. Among those participants, 43% were self-referred to our clinic, whereas 36% were referred from private centers. Most families in the sample had biological parents, with mothers attending the intake session for 64% of the participants. Three of the 14 participants had a sibling with Autism. Most of them (93%) were enrolled in mainstream school classes. Nine participants had behavioral problems (four with tantrums and argumentative, disobedient behaviors, two with inappropriate classroom behavior, two with homework difficulties, and one with stealing issues). When asked about other treatments, more than half of the participants were not on any medications (64%), while three of them (21%) were taking methylphenidate extended release, one was taking fluoxetine, and the other was taking both aripiprazole and atomoxetine. Most participants with Autism were diagnosed with another comorbid condition, with five diagnosed with comorbid ADHD and two diagnosed with social anxiety disorder (36% and 14%, respectively). In contrast, 29% of the participants were diagnosed with Autism only, and 14% were diagnosed with both SCD and ADHD. The detailed characteristics and demographic information of the participants in the pilot sample are presented in Table 1.
The participants’ responses to questions about social behavior and friendships are shown in Table 2 (Supplement). All but one participant expressed interest in taking a class on making and keeping friends. However, the one who was not interested agreed to try it when the option of leaving at any point was explained to him. Most participants (62%) did not socialize with their schoolmates; among those who did, only 20% named four or more of their friends. Furthermore, 70% of the participants spent their free time alone, 93% had access to electronic devices and video games at home, and 57% did not spend time with friends regularly. Among the 43% who socialized with friends, approximately 67% had yet to do so over the previous month. Most participants spent their free time playing with electronics and participating in other activities (see Table S2 in the supplements).
Treatment Outcome
Analysis of variance and post hoc pairwise analysis via the Wilcoxon rank test revealed a statistically significant increase in the average self-reported knowledge of social skills (TASSK) score across the three time points (F (1.5,13.4) = 18.9, p = .001). There was a significant increase in the TASSK score at postintervention T2 (16 ± 3.9) compared with preintervention T1 (10.7 s.d 2.6) with p = .002 and at three months postintervention T3 (17 ± 3.1) compared with preintervention T1 with p = .001 (Table 3 and Figure 2).
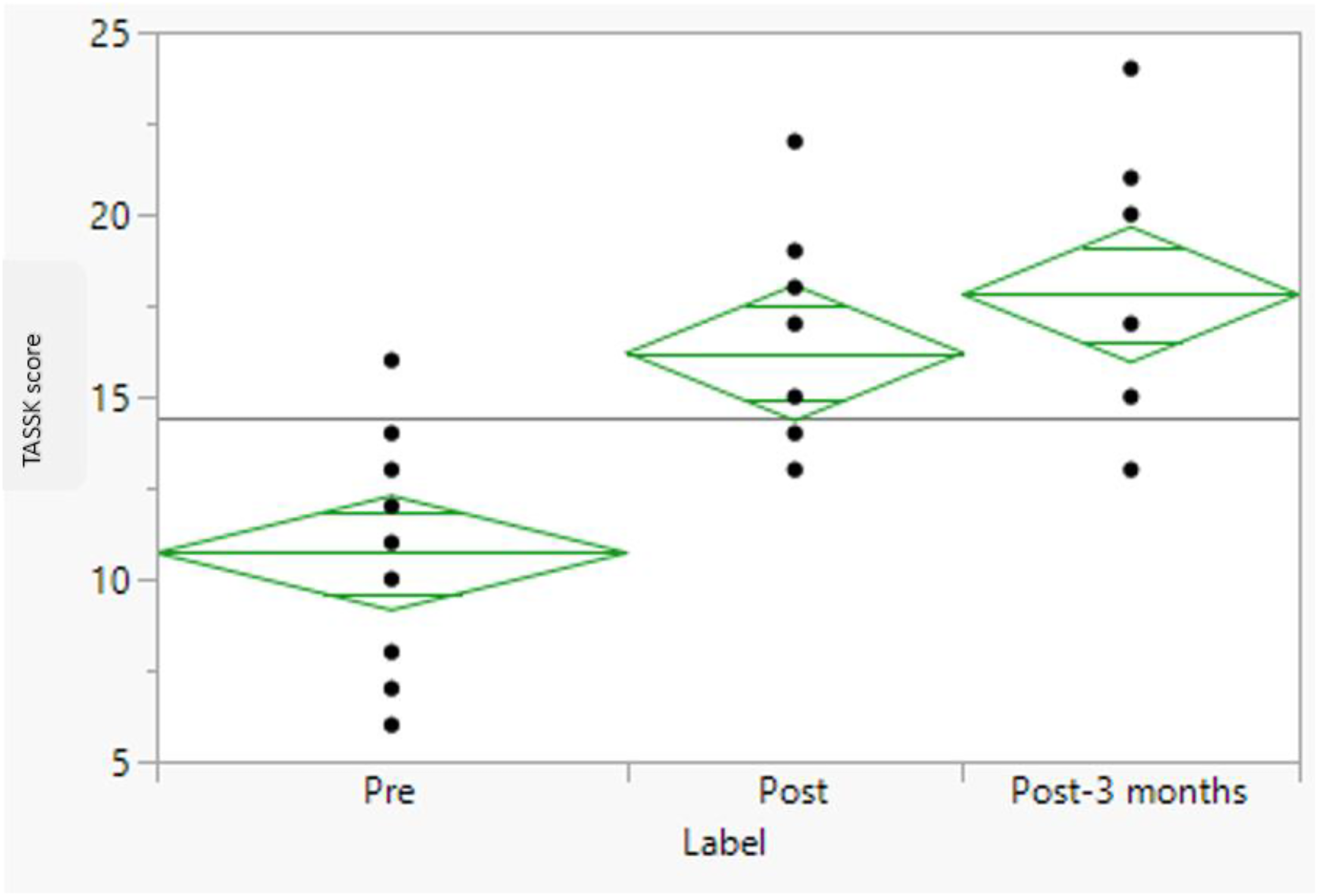
Boxplot of the Test of Adolescent Social Skills Knowledge (TASSK) Scores Across the Three Follow-up Time Points (p = .001).
Comparisons of the Means of the PEERS-AA Assessment Tools at the Three-Time Follow-Up Points.

ANOVA: analysis of variance; CBCL: Child Behavior Checklist; QPQ: Quality of Play Questionnaire; TASSK: Test of Adolescent Social Skills Knowledge.
* p values and F values were calculated via a general linear model, repeated measures analysis of variance.
^ Mean differences, SE, and p values were calculated via paired t-tests or Wilcoxon rank tests on the basis of normality assumptions.
The Percentage Differences of the Nominal Scores of the PEERS-AA Over the Three Points of Follow-Up for the Pilot Sample.

The parent-reported SRS-2 also revealed a statistically significant decrease in the average score over time (F (1.7, 13.7) = 19.03, p = .001), indicating improvement. This difference was also observed at the pairwise level, both postintervention T2 (65.5 ± 6.8) compared with preintervention T1 (76 ± 8.1) with p = .001, and three months postintervention T3 (64 ± 10.7) compared with preintervention T1 with p = .001 (Figure 3 illustrates the means, medians, and quartiles of SRS-2 scores). However, the number of gatherings and friends and the total score of the QSQ did not significantly change postintervention T2 or three months postintervention T3 compared with preintervention T1, neither in the parents nor in the children's scales. Differences in the mean scores of the CBCL were examined individually (i.e., per behavior) and in total. A difference in scores was found in the domains of aggressive behaviors (F (1.4, 12.6) = 10.4, p = .001), internalization (F (1.4, 12.4) = 5.6, p = .013), and externalization (F (1.8, 17.6) = 11.7, p = .001) at the three months postintervention. Although the total CBCL scores tended to decrease over time (time 1 = 65 ± 8.7, time 2 = 64 ± 2.3, time 3 = 62 ± 5.5), the difference was not statistically significant. For details, see Table 3.
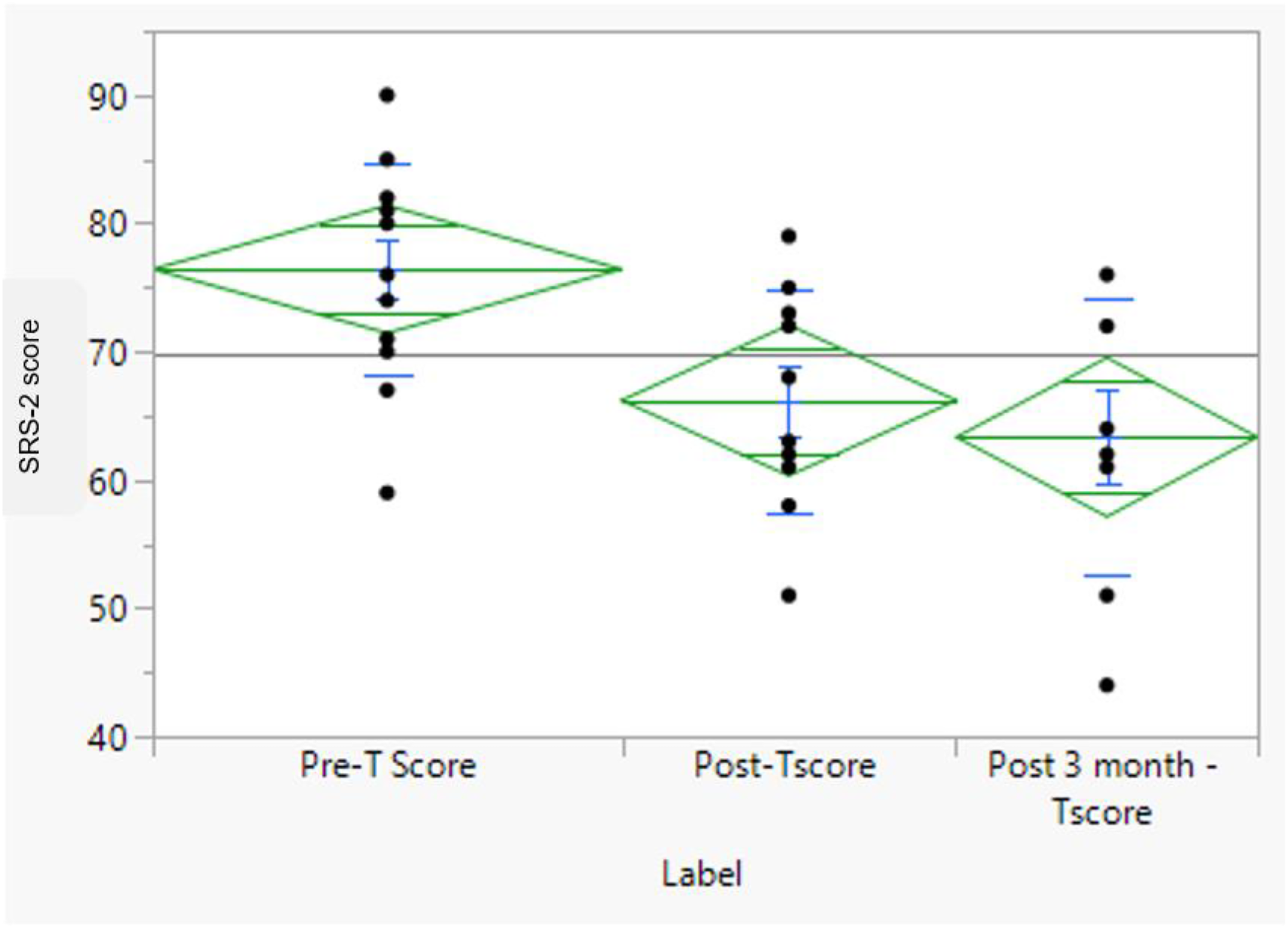
Boxplot of the Social Responsiveness Scale, Second Edition (SRS-2) Scores Across the Three Follow-up Time Points (p = .001).
To further evaluate the effect of the PEERS-AA program, another analysis using the nominal classification of most variables was performed (Table 4). The SRS-2 scores were regarded as normal (≤59), mild (60–65), moderate (66–75), or severe (≥76), whereas the CBCL scores were regarded as normal (≤59), borderline (60–64), or significant (≥65). McNemar's and Kendall's tau tests revealed a decreasing trend in the SRS-2 percentages of moderate (11% vs. 36%) and severe (22% vs. 57%) cases at three months postintervention follow-up (Time 3) compared with preintervention (Time 1) (p = .001). When the CBCL domains were examined, there were fewer significant internalizing behaviors at the three-month postintervention follow-up than at the preintervention follow-up (64% vs. 86%) and fewer borderline externalizing behaviors after the third month (27% vs. 50%). The total CBCL score appeared to be lower in patients with significant scores during the Time 3 follow-up than in those with significant scores during the Time 1 assessment (46% vs. 79%); however, this difference was not statistically significant in the pairwise analysis (see Table S4 in Supplementary Material).
Feasibility
Among the 14 participants who joined the program from the beginning, 10 completed the program until graduation, resulting in a 28.6% attrition rate. Those who withdrew from the program cited scheduling issues, lack of motivation, and severe social anxiety as reasons for dropping out. Among the participants who continued the program, 100% attended 11 sessions out of 13, and 50% completed all 13 sessions, with a 100% completion rate at the three-month postintervention follow-up point. The overall assignment completion rate was 60%. Anecdotally, parents reported observing benefits since the program's initiation. The participants and their caregivers reported improved social skills, communication, self-esteem, and relationships with their parents and siblings at home. Repeating the assignment weekly was considered positive, as the participants became less stressed and more confident with time.
Discussion
This pilot study explored the feasibility and preliminary effectiveness of the Arabic adaptation of PEERS® for Adolescents (PEERS-AA). The findings revealed significant improvement in adolescent social skills and knowledge of social etiquette, as evidenced by self-reports and parent reports; however, the frequency of get-togethers did not significantly increase following treatment. Despite running amid the COVID-19 pandemic, the treatment responded positively despite running during uncertain times and social distancing restrictions. The maintenance of treatment gains months after the intervention highlights the role of parental involvement in social coaching, promoting parental assistance in generalizing and maintaining social skills.
This study demonstrates the efficacy of treatment for an Arab and underserved population, namely, autistic adolescents with low support needs who exhibit social challenges related to making and keeping friends. In contrast to the majority of existing social skills training interventions, the study employed a parent-assisted manualized intervention designed to improve the friendship skills of autistic adolescents, thereby promoting the continued generalization of newly acquired skills. In addition, it assessed the change in social competence at a 14-week follow-up assessment to determine the success of treatment maintenance.
The results of this study support the feasibility of the PEERS-AA program for autistic adolescents in Saudi Arabia. Despite the relatively small sample size, the attrition rate in this study was 28.6%, which was slightly higher than that reported in previous studies, ranging from 8% to 24% (Rabin et al., 2018; Schohl et al., 2014; Veytsman et al., 2022; Yoo et al., 2014). In addition, those who continued the intervention completed most of the sessions, and 100% completed the follow-up at three months, indicating satisfactory adherence.
Furthermore, despite the novelty of such interventions in a cultural context, this adaptation of the PEERS® for Adolescents program is generally acceptable to adolescents and their families, with few modifications. Areas that need cultural adaptation include choosing appropriate friends, obtaining them, and handling teasing, bullying, and feedback. The homework completion rate was above 60%, providing further support for the feasibility of this study. However, multiple difficulties were encountered, most notably with the “get-together” and “finding friends” assignments. This was similar to the findings of other studies from Eastern Asian countries (Shum et al., 2019; Yamada et al., 2020; Yoo et al., 2014) compared with North American studies. Culturally, it is not uncommon for extended families to meet at the grandparents’ houses and for cousins to be considered friends. To integrate the “get-together” and “finding friends” assignments into the cultural context, the research team added the option to host get-togethers at the grandparents’ house. With this modification, the number of get-togethers increased to an average of two during the program; however, this number was still lower than that reported by North American and European studies (Płatos et al., 2022; Zheng et al., 2021). Pandemic-related restrictions were also reported as limiting the ability to attend the program and the activities and venues available to carry out homework assignments. The older adolescent group was noted to have a lower assignment completion rate during that time. Despite these difficulties, the positive responses and outcomes of the intervention support the feasibility of the PEERS-AA program. In order to maintain fidelity, all members of the treatment team met for one hour following each group session for feedback and to informally evaluate adherence to the PEERS-AA curriculum. This practice was to ensure consistent implementation and allow for prompt adjustments based on the team's observations.
Knowledge of social skills increased after the program was completed, as measured by the self-reported TASSK. Moreover, there was a significant improvement in Autism-related social difficulties, as indicated by lower scores on the parent-reported SRS-2. These findings are in line with those of the original study and its replication in the United States and other countries (21–20; Laugeson & Park, 2014; Schohl et al., 2014; Shum et al., 2019; Van Hecke et al., 2015; Yoo et al., 2014). The involvement of parents in the implementation of social skills is a unique part of the PEERS® program that is usually absent from most social skills interventions (Darling et al., 2021). A meta-analysis by Wolstencroft et al. (2018) revealed that GSSIs that included concurrent parent groups were more effective than those that did not (Wolstencroft et al., 2018). Furthermore, the treatment gains were mainly sustained for at least three months after the program's completion, corroborating previous studies’ findings supporting its durability (Laugeson et al., 2012; Shum et al., 2019; Yoo et al., 2014). The prolongation of the treatment effect could be partly attributed to improved parental abilities and increased participation in carrying out the supervision and coaching of their adolescents, which continued even after the treatment was completed.
Although the CBCL scale was used, our results did not replicate previous findings indicating a significant decrease in specific problem behaviors among autistic adolescents after PEERS® treatment (Mandelberg et al., 2014; Schohl et al., 2014). At the three-month postintervention follow-up, the total CBCL score was noticeably lower in the significant patients than at the baseline assessment. Although emotional and behavioral changes following PEERS® have been studied less in North America, the current Korean studies (Yoo et al., 2014) reported improvements among adolescents.
In this sample, social gatherings were the function of the extended family, and teenagers met the same group of relatives every time. This led to the success of get-togethers, especially with adolescents who have good relationships with their relatives. Contrary to initial expectations, most adolescents did not form new relationships, which could be understood in light of the COVID-19-related pandemic restrictions that limited the willingness and ability to participate in in-person social gatherings. Another contributing factor could be understood from a cultural lens; first, parents would be expected to plan get-togethers for their youth among each other, rather than the youth planning their get-togethers. Hence, parental openness and means to plan such events might be limited, as parents might find it foreign to plan get-togethers with new parents for their teens to socialize. Second, parents’ perceived need to plan for their children with relatively similar socioeconomic status, level of education, and cultural background can complicate the process of planning these events.
Limitations and Future Directions
The Arabic translation and cultural adaptation of the PEERS® for adolescent social skills intervention showed promising results for Autistic adolescents in Saudi Arabia despite cultural and linguistic differences. However, it is not without limitations that should be taken into consideration. First, when the pilot was developed, the infrastructure of Autism services in Saudi Arabia and the limited validated measures in Arabic were among the most significant challenges. Moreover, the region's need for more evidence-based intervention programs to compare results was considered a significant challenge. Despite the feasibility and preliminary effectiveness of the PEERS-AA for the adolescent program, the small sample size and the lack of a control group and observational methods limit the generalizability of results. Parent-reported measures could be subjected to parents’ metacognition, awareness of their teens’ limitations, expectations of teens and programs, and cultural expectations.
Further studies are needed to test the efficacy and sustainability of the PEERS-AA program, utilizing observational measures obtained from teachers and peers, such as focus groups conducted with teachers and students, and a checklist built to measure the direct behavioral changes to compensate for the need for evidence-based interventions in Arabic.
In conclusion, this study offers preliminary insights into the feasibility and preliminary effectiveness of the PEERS-AA for the Adolescents program, with encouraging results indicating its potential applicability and use for future research. Additionally, it sheds light on the need to invest in developing culturally adapted intervention programs and assessment tools to support those with neurodevelopmental disabilities. However, the results should be interpreted with caution, given the study's exploratory design and limited sample size. Furthermore, this study highlights the need for community-centered social outlets that allow autistic adolescents to socialize with their peers.
Supplemental Material
sj-docx-1-dli-10.1177_23969415251371547 - Supplemental material for Feasibility and Preliminary Effectiveness of the Arabic Version of the Program for the Education and Enrichment of Relational Skills (Peers-AA) for Autistic Adolescents in Saudi Arabia
Supplemental material, sj-docx-1-dli-10.1177_23969415251371547 for Feasibility and Preliminary Effectiveness of the Arabic Version of the Program for the Education and Enrichment of Relational Skills (Peers-AA) for Autistic Adolescents in Saudi Arabia by Afnan A. AlMarshedi, Marwah Ahmad Behisi, Hussain Mohammed Al-Taweel, Tamer Mohammed Albasuony, Saad Mohammed Almuqrin, Samah Hazem Alkhawashki, Aqeel Talal Alkhiri, Saleh Mohammed Alsalehi, Fatimah Abdulrahman Alhaidar, Yasser Ad-Dab’bagh and Elizabeth Ann Laugeson in Autism & Developmental Language Impairments
Footnotes
ORCID iDs
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.