
Abstract
Purpose
Parent involvement is crucial for tailored early intervention programs. The Hanen More Than Words (HMTW) program is a parent-implemented language intervention for autistic children. The current study examined the effectiveness of the HMTW program delivered online among Chinese families.
Methods
Using a randomized controlled trial design, 22 Chinese families of autistic children in Hong Kong completed the trial. Baseline and post-intervention assessments were conducted to measure changes in parent-child interaction, parents’ use of linguistic facilitation techniques (LFTs), and children's communication skills. Additionally, the influence of parental self-efficacy and parenting stress on treatment outcomes was explored.
Results
The intervention group demonstrated significant improvements in parent-child attention synchrony. Although the treatment effect on children's spontaneous communication was not significant, the intervention group showed a larger effect size compared to the controls. The treatment outcomes were mainly influenced by the parents’ initial levels of self-efficacy but not by parenting stress.
Conclusion
These findings provide preliminary evidence of the effectiveness of the online-delivered HMTW program for Chinese parents of autistic children. Further research involving a larger sample and focusing on long-term effects is needed.
Over the years, significant progress has been made in understanding the underlying neurobiological mechanisms that contribute to the development of autism, including genetic and environmental factors (Mandy & Lai, 2016; Masi et al., 2017). Advances in screening and diagnosis have allowed the early detection of autism, which can lead to earlier intervention and, as a result, better outcomes (Øien et al., 2021; Zwaigenbaum & Penner, 2018). However, despite these advancements, managing autism remains challenging. The high prevalence of comorbid conditions and the heterogeneous nature of the disorder highlight the need for individualized intervention (National Research Council, 2001). Additionally, the need for long-term specialized services may further exacerbate the fiscal burden faced by families and autistic individuals (Helkkula et al., 2020).
Direct consultation remains the most common service delivery model for language and communication training for autistic children in some regions such as Hong Kong. This traditional model of service delivery has the advantage of controlling various external factors to provide an ideal learning context by professionals. However, given the rapid increase in the prevalence of autism over the past decade (The Government of the Hong Kong Special Administrative Region, 2019), this one-on-one consultation model may not be able to meet the service demand in the community. Without a corresponding growth in the available resources, autistic individuals and their families often face long waiting times. There is, therefore, an urgent need to explore culturally appropriate service delivery models that can provide optimal and evidence-based interventions.
Parent-implemented interventions for autistic children
Constructivist and social interactionist theories of language acquisition suggest that children acquire language through their interactions with their physical and social environment (Piaget, 1971; Vygotsky & Cole, 1978). Parents therefore play a critical role in providing the input, the context, and the scaffolding for children's communication and language development (Hart & Risley, 1995; Roberts et al., 2019). A great deal of evidence shows that children's language development is positively correlated with the amount and quality of language input provided by parents (Haebig et al., 2013; Siller & Sigman, 2002, 2008).
Given the importance of parental involvement in early social and communication development, evidence-based autism treatments involve parents not only as the informants but also as the primary intervention agents (Akemoglu et al., 2020; National Research Council, 2001; Zwaigenbaum et al., 2015). Through working with the child's family system, parents can acquire a broad range of strategies that they can apply to their child's daily life, promoting consistent support and generalization of skills beyond the treatment sessions (Akemoglu et al., 2020; Aldred et al., 2004).
Research has demonstrated the efficacy of parent-implemented language interventions in facilitating receptive and expressive language development in young children with language impairments (Roberts & Kaiser, 2011). Positive effects on parental responsiveness, the rate of communicative acts, and the use of language facilitation strategies have also been noted (Kasari et al., 2014; Roberts & Kaiser, 2011; Siller et al., 2013; Watson et al., 2017). Apart from the evidence obtained in Western countries, recent studies conducted among Chinese populations have provided preliminary evidence supporting the adaptation of parent-implemented intervention for non-Western cultures. Zhou et al. (2018) evaluated a parent-implemented Early Start Denver Model among 58 Chinese autistic toddlers and found significant improvements in language abilities and social communication behaviors in the target group compared to the community control group. Similarly, Liang et al. (2022) reported positive effects on the language and social development among Chinese-speaking autistic children after their participation in a parent-training program. Results of a recent meta-analysis of 21 parent-implemented intervention studies in mainland China, Hong Kong, and Taiwan indicated general large average effect sizes on a variety of child outcome domains (Liu et al., 2020). However, despite these promising results, Liu et al. (2020) also noted that 66.7% of the reviewed studies did not meet the satisfactory quality index. Thus, there is a pressing need to continue to develop and evaluate the efficacy of culturally appropriate, evidence-based parent-implemented interventions for autistic children.
Telepractice and parent-implemented language interventions
Telepractice, which involves the application of telecommunication technologies for health and medical services at a distance, has emerged as a promising means of providing efficient and effective interventions for autistic individuals. This approach offers remote diagnostic options, continuous access to care and the opportunity to involve family members in the child's treatment through effective parent-implemented interventions (American Speech-Language-Hearing Association, n.d.; Solomon & Soares, 2020). Delivery formats of telepractice may include live video conferencing, pre-recorded videos, phone calls, and real-time feedback in a chat room. This approach may offer greater accessibility and convenience for families, particularly in areas where in-person services are limited but in high demand (Snodgrass et al., 2017; Solomon & Soares, 2020).
Single-case studies have demonstrated the efficacy of parent-implemented intervention via telepractice in improving social communication behaviors and language skills in children diagnosed with autism (Vismara et al., 2013; Wainer & Ingersoll, 2015), and decreasing problem behaviors (Lindgren et al., 2016). Additionally, parents have reported high levels of acceptance of the delivery mode (Little et al., 2018; Pickard et al., 2016). However, randomized control trial (RCT) studies examining the efficacy of parent-implemented language and communication interventions via telepractice for autistic children are somewhat limited. The synthesis of results from a recent systematic review supported the potential effectiveness of this delivery model (Akemoglu et al., 2020). However, only 2 of the 12 reviewed studies were RCTs (Ingersoll et al., 2016; Vismara et al., 2018), with most studies using a single-case design.
In Hong Kong, although rehabilitation services have a long history, telepractice is relatively recent with its wide adoption starting in late 2019 due to local social movements and the outbreak of the coronavirus disease in 2019 (COVID-19), which restricted regular inter-personal contact. A 2020 online survey collected the perspectives of 135 speech and language pathologists (SLPs) on telepractice in Hong Kong, with 35% reporting that they had conducted telepractice (Fong et al., 2021), which is significantly lower than the service provision rate (64.1%) in other regions (American Speech-Language-Hearing Association, 2016). Only 25.5% of the SLPs believed that telepractice was as effective as face-to-face services. Reported barriers to the implementation of telepractice included the questionable effectiveness of telepractice as an evidence-based practice; a lack of adequate knowledge about, support for, and training in, telepractice; the inappropriateness of teletpractice for the patient population, and so forth (Fong et al., 2021). Another survey showed high satisfaction and favourable perceptions of telepractice among 41 Hong Kong Chinese students and their parents during the COVID-19 class suspension. However, parents preferred on-site services and considered face-to-face practice more effective (Lam et al., 2021). These local research findings highlight the gap between the accelerating need for telepractice and insufficient evidence-based programs available to the public.
The Hanen More Than Words® Program
The Hanen More Than Words® (HMTW) program is a parent-implemented program developed by Sussman and Lewis (1999), which operates within the social interactionist theoretical framework. It aims to promote reciprocal interaction and social skills in naturalistic contexts for autistic children under the age of six (Weitzman et al., 2017). The HMTW program consists of 8 parent-only group sessions and 3 individualized parent-child sessions at home, facilitated by a Hanen-certified SLP. The program focuses on three key areas: (1) providing parents with the necessary support and knowledge to understand their child's developmental level, (2) increasing parents’ sensitivity and responsiveness to their child's communicative acts, and (3) equipping parents with linguistic facilitation strategies to create opportunities for their child's communicative initiatives and responses.
The effectiveness of the HMTW program has been supported by several outcome studies with varying levels of evidence. Results from a randomized control trial study of 62 young children diagnosed with autism and their parents suggested that HMTW facilitated communication development in children with low baseline object interest (Carter et al., 2011). Although the intervention effect did not reach statistical significance, considerable gains in parental responsiveness was observed both immediately after the intervention and at follow-up assessments, as indicated by large effect sizes. A quasi-experimental study of 51 autistic children with language delay and their families showed significant improvements for the HMTW intervention group in parents’ use of facilitative strategies and children's vocabulary size (McConachie et al., 2005). A recent case-control study conducted in Hong Kong examined the effectiveness of an adapted HMTW program among parents of autistic children and found a main effect of HMTW on increasing children's communication and social skills (Lok et al., 2021). Single-case studies also found positive outcomes in vocabulary and receptive language development, social initiation, and engagement in autistic children after receiving the HMTW program (Girolametto et al., 2007; Noyan Erbaş et al., 2021; Sokmum et al., 2017). In addition, a recent study using a multiple-baseline, single-case experimental design to examine the efficacy of HMTW implementation via telepractice found that both parental responsiveness and child communication behaviors showed significant improvements immediately after the intervention. The effects of the program were maintained over the 3-month follow-up period (Garnett et al., 2022). However, although the effectiveness of the parent-implemented HMTW program in improving language and communication skills in children diagnosed with autism has been demonstrated in several studies, little is known about the effectiveness of HMTW when delivered via telepractice. Moreover, with the exception of Lok et al. (2021), previous studies investigating the parent-implemented HMTW program focused on the Western cultures. It remains unclear whether these interventions would yield comparable effectiveness in different cultural contexts.
Parental characteristics and intervention outcomes
Parent-implemented interventions heavily rely on effective parental engagement and implementation of strategies (Brown & Woods, 2015; Roberts & Kaiser, 2011). To maximize desirable outcomes, it is crucial to examine parental characteristics that may impact their engagement and ability to implement strategy. Parenting stress, arising from challenges parents face in meeting their child's needs, has been found to influence the intervention outcomes for autistic children (Stadnick et al., 2015; Strauss et al., 2012). Research reported that higher levels of parenting stress can hinder a child's progress in early learning (Robbins et al., 1991), social communication (Stadnick et al., 2015), and behavioral functioning (Osborne et al., 2008), while others found that it can facilitate children's cognitive (Rickards et al., 2007) and language ability (Strauss et al., 2012). Another critical factor in the success of parent-implemented interventions is parental self-efficacy, which refers to parents’ beliefs about their ability to be effective and successful in parenting (Jones & Prinz, 2005). Research has indicated that high self-efficacy leads to more active treatment involvement (Solish & Perry, 2008; Trunzo, 2006) and effective strategies implementation (Hastings & Brown, 2002), resulting in better child intervention outcomes (Hoza et al., 2000; Jones & Prinz, 2005; Warren et al., 2011). In contrast, lower self-competence leads to inconsistent strategy implementation (Coleman & Karraker, 2000). Interestingly, a recent HMTW intervention study found that children whose parents had lower self-efficacy achieved better outcomes than those whose parents had higher levels of self-efficacy (Lok et al., 2021). Therefore, examining these parental factors can lead to broader and more holistic evaluation of the intervention effectiveness, beyond intrinsic factors associated with the child.
The purpose of the present study was twofold: (1) to investigate the efficacy of a telepractice-delivered HMTW program in improving parents’ verbal and nonverbal responsiveness and children's communication initiations and responses; and (2) to explore the potential effects of baseline levels of parental self-efficacy and parenting stress on the treatment outcomes. The findings of this study may contribute to a greater understanding of the effectiveness of telepractice-delivered HMTW and highlight the importance of considering cultural context and individual differences in intervention process.
Method
Ethical approval for this study was obtained from the Human Research Ethics Committee (HREC) of The University of Hong Kong. All procedures and protocols adhered to the ethical guidelines set forth by the HREC and were conducted in accordance with the principles of research practice.
Participants
Participants were recruited from a Non-Governmental Organization (NGO) in Hong Kong that supports families with children with specific needs. Children were included if they: (a) were from Cantonese-speaking Chinese families living in Hong Kong; (b) had a diagnosis of autism; (c) were between 36 and 72 months old; (d) had no other diagnosis of neurodevelopmental disorders; and (e) had verbal language abilities ranging from single words to emerging two-word combinations.
The NGO staff provided the research team with a list of eligible families who expressed interest in participating in research studies. Subsequently, the research team contacted these families to provide detailed information about the study, its purpose, and the requirements for participation. A total of 46 parent-child dyads were recruited. Upon receiving parents’ written consent, the Autism Diagnostic Interview-Revised (ADI-R; Rutter et al., 2003) was administered by qualified examiners to confirm the autism diagnosis of the participating children. One child did not meet the ADI-R diagnostic cut-off and was excluded. The remaining 45 parent-child dyads were assigned to one of two groups through computer-generated random assignment. The treatment group (n = 25, 17 boys and 8 girls) received the HMTW program in addition to their regular therapy if there was any, while the control group (n = 20, 18 boys and 2 girls) continued with or without their regular therapy as status quo during the intervention phase and were enrolled to the HMTW program after the study period. However, only 12 out of 25 participants in the treatment group and 10 out of 20 participants in the control group successfully submitted valid videos for analysis (see below).
Procedure
All participating parents were asked to complete an online demographic questionnaire, along with the Chinese version of the Parenting Sense of Competence Scale (Chinese version) (PSOCC; Ngai et al., 2007) and the Parental Stress Scale (PSS-C; Cheung, 2000). The raw scores of the Action and Gesture sections of the Cantonese version of the MacArthur-Bates Communicative Development Inventories (CDI; Tardif & Fletcher, 2008) were administrated to assess the non-verbal communication ability of the children. The mean score was 40.17 (SD = 11.74) out of a total score of 65. Prior to the intervention phase, parents were asked to submit a 3-min video of their typical daily interactions with their child at home. During the intervention phase, parents in the treatment group received the online HMTW training. They attended eight 2.5-h parent-only online group training sessions conducted by licensed SLPs over a period of three months. Three individual video-conferencing feedback sessions were carried out between the group sessions, with the same SLP providing feedback to each parent. Post-intervention videos were collected from both groups within one month after the program. The baseline and post-training videos of parent-child interaction were analysed to assess the parents’ effective use of the taught intervention strategies and the children's verbal communication ability.
Attrition and the final sample
Within the treatment group, three participants did not submit baseline videos and withdrew just after Time 1 (pre-intervention phase). Additionally, three participants dropped out before Time 2 (post-intervention phase). Among the 19 participants who successfully completed the intervention, five submitted invalid videos that the baseline and post-intervention videos did not capture the same participating parent, and another two post-intervention videos were significantly shorter than the required duration of 3 minutes. In the treatment group, parents who failed to submit valid post-intervention videos had attended less than 2 sessions, while those who submitted valid post-intervention videos had attended over 80% of the sessions. Regarding the control group, four participants withdrew just after Time 1 due to their inability to submit baseline videos. Another four participants dropped out after Time 1 and before Time 2. Among the 12 participants who remained after the intervention, one participant did not submit the post-intervention video, and one's post-intervention video was significantly too short (see Figure 1). The mean age of the children at the enrolment was 37.8 months (SD = 11.6), comprising 16 boys and 6 girls. The primary caregiver participants consisted of 18 mothers and 4 fathers. Based on the parents’ reports, nine children in the treatment group and eight in the control group also received concurrent individual speech and language therapy during the intervention phase.

Flow of the participants throughout the study.
Pre-intervention group comparison
The baseline characteristics of the two groups were compared using a one-way ANOVA based on the pre-intervention continuous variables (i.e., parent and child outcome variables, parental self-efficacy and stress levels) and Fisher's exact test was employed for categorical variables (i.e., child's age and sex, mother's education level, household income). Other than the control group obtaining higher baseline levels of parent-child attention synchronization than the HMTW group [F(1,20) = 8.71, p < .01], there were no between-group differences in sociodemographic characteristics, predictors, or other outcome variables (see Table 1).
Comparison of Participants’ Pre-intervention Characteristics

Note.
One-way ANCOVA and Fisher's exact test were applied for continuous and categorical variables, respectively;
Education level: 1-Primary or below, 2-Secondary, 3-Senior Secondary, 4-Diploma/ Tertiary education, 5-University or above;
Household income: (HKD/per month) 1-Below 6,000, 2-6,000–9999, 3-10,000–19,999, 4-20,000–29,000, 5-30,000–59,999, 6-50,000–79,999, 7-80,000–99,999, 8-Above 100,000
PSOCC = Parenting Sense of Competence Scale (Chinese version);
PSOCC-E = Parenting Sense of Competence Scale (Chinese version) - Efficacy;
PSOCC-S = Parenting Sense of Competence Scale (Chinese version) - Satisfaction;
PSSC = Chinese Parental Stress Scale.
The online Hanen More Than Words® Program
Modifications were made to adapt the online HMTW program for Chinese participants. The teaching materials, including the HMTW demonstration video clips, PowerPoint slides, and handouts, were translated into Chinese by qualified MTW trainers using the forward-backward translation method, with official permission obtained from the Hanen Centre. The original demonstration video clips were used with Chinese subtitles added. Detailed technical instructions were provided to parents on how to use the electronic program materials. Some practice activities were modified for online viewing, such as replacing flip charts with fillable charts on PowerPoint slides.
The HMTW program consisted of 8 group sessions and 3 individual sessions. All sessions were conducted online via the Zoom video-conferencing platform and the medium of instruction was Cantonese, which was the native language of all the participants, the SLP instructor and a research support staff. The research support staff, who was familiar with the MTW program, coordinated and oversaw each online section as well as provided technical support to the group.
The content of each group session included a combination of instructor presentation, video analysis, group discussion, and role-play activities. The focus of the group sessions was to provide parents with information about early language and communication development stages and to teach parents strategies that facilitate positive social interaction with their child. During the individual videoconferencing sessions, parents engaged directly with the HMTW instructor and demonstrated the strategies acquired during group workshops while interacting with their child. With the immediate feedback and personalized coaching from the HMTW instructor, these one-on-one sessions aimed to create an interactive learning environment where parents could refine and apply their skills effectively.
Treatment fidelity
To ensure that the implementation of the program was consistent with the recommended content and delivery quality and style, the modified online Chinese HMTW program was implemented by SLPs who were certified by the Hanen Centre and had completed a 3-day More Than Words® Certification workshop. The instructors were required to follow a specific protocol outlining how to deliver the content for each session and document the topics, activities, and goals set for parents in each session. Checklists outlining the required tasks for each session were prepared. The instructor and the research support staff made use of the checklist to ensure all were completed in the session. The research support staff would also remind the instructor during the session in case there were any missing tasks. The completed checklists for each session were submitted to the project coordinator, and the accuracy of the checklist was verified by checking against each recorded session.
Measures
Parental self-efficacy
PSOCC (Ngai et al., 2007) was used to assess the parents’ belief in their capability to manage the demands of parenting. The PSOCC has good internal consistency, construct validity, and test-retest reliability (Ngai et al., 2007). It consists of 16 items forming two subscales: Efficacy (PSOCC-E) and Satisfaction (PSOCC-S). The Efficacy subscale measures parents’ self-perception of their ability to be effective and successful in parenthood, while the Satisfaction subscale measures the extent to which parents are satisfied with their parenting role. Higher scores indicate higher levels of parental self-efficacy and satisfaction.
Parenting stress
PSSC (Cheung, 2000) was administered prior to the intervention to measure parents’ subjective feelings of strain and stress levels before the program. This scale includes 17 items assessing two aspects, Parental Strain and Parental Satisfaction, in relations to stressors within the parent-child relationship. The PSSC has good internal consistency, test-retest reliability, and construct and content validity, as reported in previous research (Cheung, 2000). A higher PSSC score indicates a higher stress level experienced by the respondents.
Outcome measures
Parents’ and children's communicative behaviors were coded using the baseline and post-intervention parent-child interaction recordings. A coding scheme was developed by the first author who coded all the data using the INTERACT, an observational computer system (Mangold, 2022). Parent outcomes were measured within the 3 min video recordings on three communication variables: (1) parent-child attention synchronization, (2) parental responsiveness (verbal and nonverbal), and (3) the use of linguistic facilitation strategies (LFTs). Coding for parent-child attention synchronization and parental responsiveness were adapted from Siller and Sigman (2002) and Yoder et al. (2015) respectively. Parent-child attention synchrony and responsiveness refer to how well parents demonstrate sensitivity to the child's current focus of attention and whether they follow the child's lead and promptly provide quality language input or positive affection (Mahoney et al., 1986; Mahoney & Perales, 2003, 2005). The outcome variables included the proportion of parent-child attention synchronization, which was the percentage of total child-directed attention intervals in which a parent shared the same attentional focus, and the proportion of parental responsiveness, which was the percentage of total child-directed attention intervals in which an undemanding parental response occurred. LFTs were coded based on Qi et al. (2023) including the techniques of expansion, linguistic mapping, imitation, and modelling and prompting. The definition of each LFTs can be found in the Supplementary Information online.
Using partial interval coding, on the first pass, we identified the codability for each 5-s interval (i.e., both parent and child were presented on screen). The second pass determined whether there was at least one child-directed attention episode (i.e., the child looked at object, played with a toy, engaged in activities, or made communicative acts) in each codable interval. On the third pass, intervals in which the parent and child shared the same attentional focus were marked as parent-child attention synchronization. On the next pass, parental responsiveness (i.e., parent provided either verbal or nonverbal responses that were relevant to the child-directed attention without redirecting, controlling or demanding the child's behaviors) was identified. On the final pass, parents’ use of LFTs were coded.
Children's communicative acts were coded for: (a) vocalizations (i.e., babbling, word approximations) and verbalizations (i.e., actual words, meaningful speech) directed towards the parent, and (b) nonverbal behaviors, including eye gaze and positive affect, directed towards the parent, as well as use of gesture. Target child outcome variables were the total number of child communicative acts and the spontaneous verbal communication. Spontaneous verbal communication is defined as the child communicating spontaneously or initiating a conversation using words or vocalization without prompting or speaking from an adult (Wetherby et al., 1988).
Coding reliability
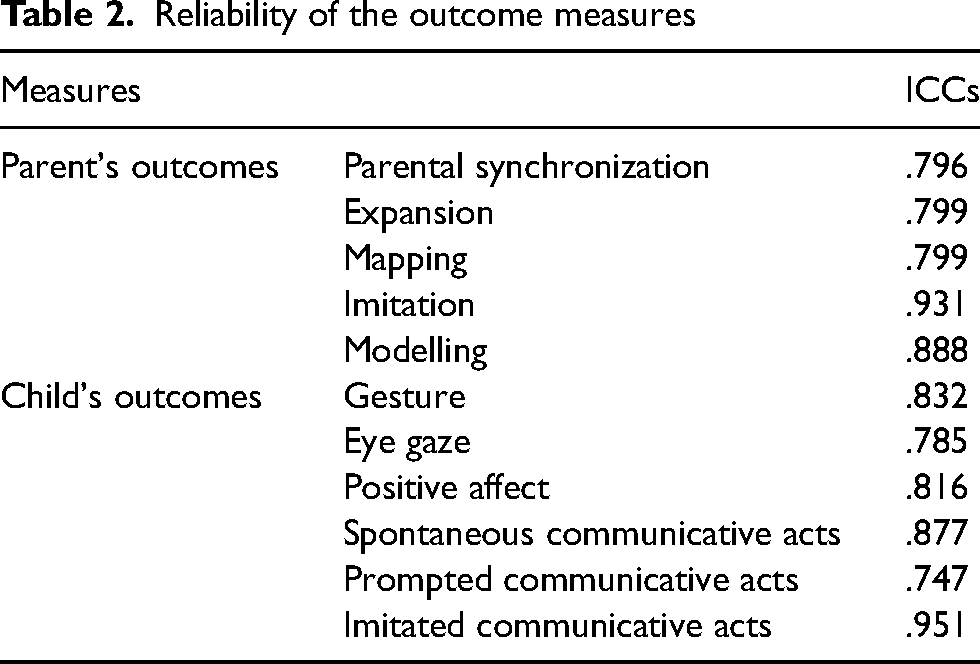
A second coder who was experienced in transcribing child-directed speech practiced the coding with the INTERACT software by referring to the coding scheme and five coded videos without the group membership or the pre- and post- intervention state. Mismatches were resolved through discussion with the first coder and elaborations were added to the coding scheme to enhance consistency. To evaluate inter-rater coding reliability, eight sets of videos (i.e., 20%) were coded by the second coder independently. Intraclass correlation coefficients (ICCs) were calculated for parent and child outcome measures (Shrout, 1998). ICCs of all the measures ranged from 0.747 to 0.951, indicating a satisfactory reliability (see Table 2).
Reliability of the outcome measures
Results
Attrition rates
Thirty-one out of the 45 participants (69%) remained at Time 2. Those in the treatment group had attended over 80% of the sessions. The attrition rate was calculated by dividing the number of dropouts (lost to contact) at Time 2 by the number of initial participants. Specifically, the attrition rate was 24% (6/25) for the intervention group and 40% (8/20) for the control group at Time 2.
Statistical analyses
The data analyses were performed using SPSS version 29. A significance level of 0.05 was used throughout the analysis. The Levene's Test for Equality of Variances was conducted to assess the assumption of homogeneity between the HMTW and control groups. Results indicated that there was no significant difference between the variances.
Primary analyses
A mixed effect repeated measures ANOVA were conducted to examine the main effects of time (i.e., baseline and post-intervention) and and intervention assignment (i.e., HMTW vs. control groups), as well as the interaction of time and intervention assignment for all parent and child outcomes (Table 3). Effect sizes (ηp2) were reported for the significant tests and interpreted as small (0.01–0.059), medium (0.06–0.139), or large (0.14 or greater) (Cohen, 1992). Parents in the intervention group showed more robust growth in parent-child attention synchronization, F(1, 20) = 8.22, p = .010, with a large effect size (ηp2 = 0.291), but not in other outcomes. The differences in child verbal communication between the intervention and the control groups did not reach statistical significance, but a large effect size of ηp² = 0.126 was observed.
Effect of condition on parent and child outcomes

To examine the contribution of baseline levels of parental self-efficacy and parenting stress to the changes in the parent and child outcomes (parent-child attention synchronization, parental responsiveness, child total communication acts and child spontaneous communication), a series of hierarchical linear regression were conducted. The corresponding baseline measure of the dependent variable was entered into the model in step 1, followed by PSOCC-E and PSSC and, finally, the parent's education level. Table 4 summarizes the results. Parental self-efficacy (i.e., PSOCC-E) and parental education level, but not parental stress, significantly predicted the parental responsiveness during post-intervention after controlling for the baseline performance. The predictors, parent's efficacy (i.e., PSOCC-E) and parental education level, accounted for 27% and 17% of the total variance respectively.
Results of hierarchical linear regression analyses.

p < .05.
Discussion
The current research made use of a randomized controlled trial design to investigate the efficacy of the HMTW program delivered via telepractice among Cantonese-speaking Chinese families aiming to examine the feasibility and the preliminary effectiveness of this online parent-implemented intervention. Results indicated a significant main intervention effect on improving parent–child attention synchronization. Treatment effect of other parental measures was statistically not significant. However, small effect sizes of the parental responsiveness, the use of linguistic mapping, imitation, modelling, and prompting as LFTs were observed. Despite the non-significant treatment effects on the child communication outcomes, child spontaneous verbal communication was found to show a large effect size of the intervention. In general, the findings of the current research provide preliminary evidence of the effectiveness of a telepractice-delivered HMTW program in Chinese families affected by autism.
Parent outcomes
The HMTW program grounded in social-interactionist theory, focuses on improving parents’ sensitivity, contingent responsiveness, and scaffolding strategies to support their child's communication improvement (Garnett et al., 2022; Girolametto et al., 2007). As expected, the intervention effects on the changes in the parental behaviors were the most immediate and noticable. The observation was consistent with those of previous research examining the effectiveness of parent-implemented language interventions in improving parent-child synchrony (Green et al., 2010; Siller et al., 2013). The current findings revealed that parents were able to master this skill even via an online mode of training.
Regarding parental responsiveness, a non-significant main effect with a small effect size was found. In the literature, the effects of parent training programs on parental responsiveness are mixed. Several randomized control trial studies on parent-implemented interventions for autistic children reported significant effects on parental responsiveness (Kasari et al., 2014; Siller et al., 2013; Solomon et al., 2014; Watson et al., 2017), while others reported no significant changes (Carter et al., 2011; Rogers et al., 2012). The robustness of the effect may depend on the treatment intensity. For example, Rogers et al. (2012) studied the effectiveness of the parent-implemented Brief Early Start Denver Model over a period of 12 weeks and reported null results in parental responsiveness. Studies reporting significant results involved more frequent hands-on practice and a higher treatment dosage (Kasari et al., 2014), which is likely to support parents in developing better responsiveness. Compared to the previous studies, the treatment intensity of the program in the current study was relatively low which may therefore lead to non-significant intervention effects.
Changes in parents’ use of LFTs were not significant. The general positive trends observed in the treatment group results suggested that the parents showed an increased use of imitation strategy when interacting with their children. The small effect size of the imitation strategy was consistent with the findings of a recent single-case intervention study using the online HMTW program (Garnett et al., 2022). Similarly, minimal intervention effects were observed in parents’ use of expansion, linguistic mapping strategies, modelling and prompting. Expansion involves a parent elaborating on the child's utterances by adding phonetic, semantic, and/or syntactic details. Linguistic mapping is when parents describe the child's actions, focus of interests, and unintelligible vocalization with one or a few words (McDuffie & Yoder, 2010). Modelling and prompting strategies refer to the use of verbal modelling, gestural or physical prompting to encourage appropriate communication skills in children. These strategies aim to provide a child with exposure to appropriate language models and facilitate spontaneous communication (Liao et al., 2022; Venker et al., 2012). Children in the current study experienced difficulties in not only speech and language development but also social communication, including decreased social motivation, communication initiation and shared engagement (Zwaigenbaum et al., 2013). These difficulties imposed additional challenges on parents in immediately interpreting their child's ambiguous communicative signals. The child's limited verbal communication intent in addition to delayed language development may further hinder parents’ ability to expand their vocalizations. This may potentially explain the minimal changes in parents’ use of various LFTs after a relatively short-term intervention in the present study. However, significant improvements in parents’ use of LFTs, including imitation and expansion, after attending an in-person HMTW program had been reported in McConachie et al. (2005). The discrepant results may suggest that linguistic facilitation may not be easy for parents to master and apply flexibly after the online training alone. A higher dosage of intervention targeting linguistic facilitation strategies, and more explicit direct coaching from the SLPs would be necessary to support parents’ learning (Carter et al., 2011; Kasari et al., 2014; Rogers et al., 2019).
Child outcomes
Child's general communication outcomes in the treatment group did not show significant change. However, a large effect size of the HMTW intervention with respect to child’s spontaneous communication indicated that the online program may be effective in supporting the child in producing communication initiatives. Kasari et al. (2014) pointed out that the effect of intervention models that target increasing parental sensitivity and responsiveness may not be sustainable and powerful enough to support children's language development, and quality input and interaction are essential. However, as discussed above, the online program had not yet induced significant growth in parents’ responsiveness and use of LFTs. Lack of significant improvement in children's communication ability was expected. It might be possible that if the parent-child dyads were followed for a longer period and training in higher dose, parents’ facilitation may become more skilful, and improvement in children's communication may be observed.
Parental factors associated with treatment outcome
Only parental self-efficacy and parental education level were found to predict the post-intervention parental responsiveness. Parents with high levels of parental self-efficacy were found to be more likely to make changes to their responsiveness after training and the observations were consistent with previous findings. High self-efficacy parents are more actively engaged in the treatment process with their children (Trunzo, 2006) and show more effective parenting strategy implementation (Hastings & Brown, 2002), thus leading to better child intervention outcomes (Hoza et al., 2000; Jones & Prinz, 2005; Warren et al., 2011).
Concerning parental education, our findings found that parents with relatively lower education levels seemed more responsive than those with high education levels. It may be possible that the former were more receptive to the instructors’ training as they considered the instructors as the role model to learn. Despite parental education level having been shown to be a powerful predictor of children's development outcomes (DiPietro, 2000), the mechanism of its influence on the treatment effect for autistic children is still not clear. Mixed results have been observed across various studies. For example, a number of studies reported that higher maternal education levels correlated with higher treatment gains in therapist-implemented interventions (Ben Itzchak & Zachor, 2011; de Veld et al., 2017). In contrast, Gulsrud et al. (2016) reported that parental education levels did not predict the joint attention treatment outcomes for autistic children after participating in a parent-implemented intervention. Given the mixed findings, parental education may not be a reliable measure to determine the suitability of a parent-training program to be prescribed. At least, parents with low education level should not be deprived from the opportunities of receiving this type of parent training programs in practice.
Baseline levels of parenting stress did not significantly predict any treatment outcomes. This finding has added a piece of evidence to the mixed results indicated by the previous research (Osborne et al., 2008; Stadnick et al., 2015; Strauss et al., 2012). Several studies suggested that children whose parents with higher levels of parenting stress tend to make less improvements in the treatment outcomes (Robbins et al., 1991; Stadnick et al., 2015), while others indicated that greater parenting stress has been found to predict better gains (Rickards et al., 2007; Strauss et al., 2012). Moreover, a recent study has demonstrated the moderating effect of parenting stress on the relationship between the intervention assignment and children's treatment outcomes, suggesting differential treatment effects for parents with high, medium, or low levels of baseline stress (Watson et al., 2017). Given the limited available findings regarding the influence of parenting stress on intervention delivered through telepractice, further investigation is warranted.
Intervention attrition rates
The attrition rates of 24% for the intervention group and 40% for the control group are relatively higher than our expectation, and the typically observed dropout rates reported in other telehealth caregiver training programs (Akemoglu et al., 2020; Vaagan et al., 2023). Telepractice has the advantages of saving commute time and hence supporting more flexible training schedule. However, there may be other constraining factors such as accessibility to stable internet connectivity, technology-related challenges, and participant expectations of the programs (Law et al., 2021; Kruse et al., 2018). As a relatively novel training approach, parents may require an adjustment period to align their expectations and adapt to this mode of learning. The high attrition rates observed in this study may, in part, reflect the learning curve associated with this new and evolving method of intervention delivery in Hong Kong. It may in fact highlight the importance of considering the local context and the unique challenges associated with the adoption of telehealth practices in different regions.
Telepractice as a service delivery mode
Telepractice may be a promising solution in bridging the gap between services requirement for autistic children and the availability of service providers (Baharav & Reiser, 2010). Yet, it is important to acknowledge that the dynamics of communication in online sessions may differ from those in face-to-face services (Akamoglu et al., 2018). For instance, building rapport is crucial in programs likes the HMTW program, but developing rapport remotely may be challenging due to the reduced communication openness. Aggarwal et al. (2015) found that some parents expressed discomfort in sharing personal experiences openly during telepractice. Parents may also find it difficult to manage their child while communicating with the SLP via video. Similarly, SLP instructors also reported difficulties in observing parent-child interaction when the camera angle was blocked or limited (Aggarwal et al., 2015). These challenges may lead some parents to perceive telepractice as less effective than face-to-face practice, resulting in reduced participation and responsiveness. Technical difficulties can cause further frustration (Ashburner et al., 2016). Therefore, for parents who struggle with multi-tasking or lack of adequate knowledge of information technology, extra support has to be given. Thus, intervention provided via telepractice without consideration of individual needs may not adequately support every parent of autistic child in effective learning and implementing the taught skills. To enhance the effectiveness of an online HMTW program in general, the following modifications are suggested. Firstly, face-to-face sessions can be organized to build rapport and trust between parents and the SLPs prior to and in between the online sessions. Secondly, booster coaching sessions or extended HMTW programs can be offered towards the end of the treatment program, as intervention strategies become more complex. Thirdly, when offering such a service, parent (e.g., parental self-efficacy, knowledge and skills of information technology) and child's (e.g., developmental level, and problematic behaviours) baseline characteristics that may influence skill acquisition should be taken into account to maximize the treatment efficacy (Vismara et al., 2013). Future research directions can focus on investigating who will benefit the most from the treatment and under what circumstances. The information can support clinicians when selecting the most suitable treatment options based on clients’ individual characteristics.
Clinical significance
This study provides empirical evidence supporting the effectiveness of online HMTW in improving parental sensitivity and responsiveness, substantiating the potential feasibility of the adaptation of the program for the Chinese population. With positive trends obtained in children's spontaneous communication outcomes, it is possible that, by increasing the treatment dosage and following up for a longer duration, more significant positive results can be obtained.
Limitations and future directions
The current study has several limitations that warrant consideration. First, the retention rate in the current study appeared to be not satisfactory. It may limit the generalizability of the study's findings to a broader population. Moreover, the dropout has implications for the statistical power of the study, given that the dataset was obtained from a relatively small sample size. Second, the quality and content variability in the self-recorded videos may pose challenges to the accuracy and reliability of the study results. The delivery of the HMTW program via telepractice required parents to self-record the baseline and post-training videos, which may result in significant variations in the quality of the recordings. In addition, the lack of standardization in the content and activities of the parent-child interaction videos could affect the evaluation of the intervention's actual impact on the outcomes. Third, post-intervention potential generalization effects were not addressed; only immediate outcomes were examined.
To address these limitations, future research should implement targeted strategies to minimize dropout rates, such as addressing technological barriers or participants’ expectations. Implementing standardized procedures for video recording, including guidelines for content and activities, can improve the accuracy and reliability of the collected data. Future investigations could also explore the long-term impact of the intervention in a larger sample size by including a maintenance phase to assess post-intervention generalization effects. Furthermore, future studies should take into account parent and child characteristics, such as parental mental health status, parents’ broader autism phenotype, child's autism symptom severity and cognitive ability, as well as external factors like social support and family resources, to comprehensively evaluate the program's efficacy which may assist in intervention selection for different clients (Binns & Oram Cardy, 2019; Oono et al., 2013).
Supplemental Material
sj-docx-1-dli-10.1177_23969415241245096 - Supplemental material for Empowering Hong Kong Chinese families with autism: A preliminary study of the online Hanen More Than Words Program
Supplemental material, sj-docx-1-dli-10.1177_23969415241245096 for Empowering Hong Kong Chinese families with autism: A preliminary study of the online Hanen More Than Words Program by Xin Qi, Qiwei Zhao and Carol K. S. To in Autism & Developmental Language Impairments
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health and Medical Research Fund (grant number 16172071).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.