
Abstract
Background
In addition to significant cognitive delays, boys with fragile X syndrome display phenotypic characteristics that include delays in language, inattention, social anxiety, and escape-maintained challenging behaviors. Despite these challenges, families affected by fragile X syndrome often have limited access to center-based intervention programs.
Methods
The present study utilized a multiple baseline design across participants to examine the preliminary effectiveness of a 12-week, parent-implemented spoken language intervention for three 5- to 7-year-old boys with fragile X syndrome. The goal of the intervention was to teach the biological mothers of each boy to use a set of verbally responsive language support strategies while participating in shared book reading activities with her child. All aspects of the intervention, including pre- and post-treatment measures, were delivered into the family’s home via distance video teleconferencing.
Results
Results from this study provide preliminary support for the efficacy of this parent-implemented language intervention approach by demonstrating generalized improvements in both targeted maternal strategy use and measures of child spoken language.
Conclusions
The present study expands upon prior language intervention research utilizing distance delivery of services for families affected by fragile X syndrome. Additionally, the study provides early support for the feasibility of collecting pre- and post-treatment assessments at a distance.
Keywords
Introduction
Fragile X syndrome
Fragile X syndrome (FXS) is caused by a mutation of the FMR1 gene on the X chromosome. The mutation consists of a CGG-repeat expansion, which silences the FMR1 gene, thereby interfering with the production of FMRP, a protein critical for neuronal functioning and experience dependent learning (Greenough et al., 2001; Verkerk et al., 1991). The typical FMR1 allele comprises 5-54 CGG repeats. An individual with 55 to 200 repeats carries the premutation and can have elevated levels of FMR1 mRNA (Hessl et al., 2005). Individuals with the FMR1 full mutation have expansions exceeding 200 repeats and reduced levels of FMRP (Oostra & Willemsen, 2003). Further, FXS is a multigenerational disorder in that a child inherits the disorder from his or her biological mother, who has either the FMR1 premutation or full mutation (Nolin et al., 1996). A recent prevalence study estimated the rate of the FMR1 full mutation to be 1 in 7,143 males and 1 in 11,111 females (Hunter et al., 2014). The prevalence of the FMR1 premutation is higher at an estimated rate of 1 in 430 men and 1 in 209 women (Tassone et al., 2012).
Child characteristics
FXS affects males more severely than females, given the protective presence of an unaffected X chromosome in females (Brown, 2002). In males, the behavioral characteristics of FXS include moderate to severe cognitive impairment, hyperactivity, and inattention (Cornish, Cole, Longhi, Karmiloff-Smith, & Scerif, 2013) escape-maintained challenging behaviors (Machalicek et al., 2014), repetitive and restricted interests (Hessl et al., 2009; Oakes et al., 2016), behaviors consistent with a diagnosis of autism spectrum disorder (ASD; Yu & Berry-Kravis, 2014), and increased levels of anxiety (Cordeiro et al., 2010). Further, language is a core deficit in males with the full mutation, who often exhibit delays in multiple domains of language. Vocabulary, grammar, and pragmatics can all be affected, with delays often exceeding those associated with nonverbal cognition (Abbeduto, Brady, & Kover, 2007). There is, however, much heterogeneity in symptom presentation in this disorder, which can be attributed to influences from background genes and the home environment (Mailick et al., 2014).
Maternal characteristics
Mothers with the FMR1 premutation are at increased risk for mental health concerns, such as depression (Franke et al., 1996) and anxiety disorders (Bailey, Raspa, Olmsted, & Holiday, 2008; Bourgeois et al., 2011). In mothers of children with FXS, there is also evidence for higher levels of expressed emotion, reflected in higher rates of criticism towards, or over-involvement, with the child with FXS, as measured by a procedure termed the Five-Minute Speech Sample (FMSS; Smith, Hong, Greenburg, & Mailick, 2016). High levels of expressed emotion reflect a negative emotional climate within the parent–child relationship (Greenberg et al., 2012). Importantly, there is variability among mothers in symptom presentation, some of which may be attributed to the mother’s genetic makeup as well as to individual differences in child characteristics and in feelings of stress related to raising a child with a disability (Seltzer, Abbeduto, Krauss, Greenberg, & Swe, 2004).
Verbally responsive parenting in FXS
As specified by a transactional model of development (Sameroff & Chandler, 1975), there is evidence that child developmental gains are influenced by environmental factors. For example, Glaser et al. (2003) found that the quality and responsiveness of the home environment was positively associated with adaptive behavioral functioning among children with FXS. A responsive home environment is often mediated through the mother as the primary caregiver. Maternal responsiveness, in general, is defined by how a mother provides for, interacts with, and responds to her child (Brady, Warren, & Sterling, 2009). The general construct of maternal responsivity includes the ways in which the mother talks to and with her child. Such maternal verbal responsiveness has a positive and sustained influence on the development of spoken language skills in children with FXS (Brady, Warren, Fleming, Keller, & Sterling, 2014; Warren, Brady, Sterling, Fleming, & Marquis, 2010). In fact, Brady et al. (2014) found that, when sustained over time, maternal verbal responsiveness was related positively to receptive vocabulary, expressive vocabulary, and the number of different words produced by school-aged children with FXS.
Importantly, the phenotypic characteristics of mothers and children affected by this disorder give rise to the potential for decreased levels of maternal verbal responsivity in families affected by FXS (Sterling, Warren, Brady, & Fleming, 2013). Specifically, barriers to verbally responsive parenting in families affected by FXS include maternal mental health status and/or prolonged developmental delays and challenging behaviors in the child (Abbeduto et al., 2004). These factors provide the impetus for implementing interventions to enhance maternal verbal responsivity in this population. In light of these barriers and evidence for the ongoing facilitative role of maternal verbal responsivity during childhood, we conducted a small pilot study to examine the efficacy of a parent-implemented language intervention that targeted maternal verbal responsivity in three mother–son dyads affected by FXS. We examined treatment-related changes in maternal use of targeted language support strategies and child spoken language outcomes.
Parent-implemented language interventions
Historically, numerous interventions for children with language delays have included a component in which parents are taught to increase their verbal responsiveness (Brady et al., 2009). Teaching parents to use verbally responsive language input was the focus of a play-based early language intervention for toddlers diagnosed with FXS and delivered into the families’ homes by means of distance teleconferencing (McDuffie, Oakes, et al., 2016). This study demonstrated the initial efficacy of using this model of service delivery for young boys with FXS who were pre-verbal or just beginning to make the transition to language production.
In an additional pilot study targeting older school-aged boys with FXS, (McDuffie, Machalicek, et al., 2016) implemented a spoken language intervention based upon teaching mothers to embed the use of three verbally responsive language support strategies into the context of shared, or interactive, book reading (Kaderavek & Justice, 2002; Landry et al., 2012). In the single case design study by (McDuffie, Machalicek, et al., 2016), mothers were taught to use expansions of child utterances, topic-continuing wh-questions, and intonation prompts (i.e., fill-in the blanks) to scaffold the spoken language of boys with FXS as they engaged in a shared book-reading experience. Although the pre- and post-intervention assessments were conducted on-site at a university-based research clinic, all intervention sessions were delivered into each family’s home by means of distance teleconferencing. Results of the study demonstrated that mothers increased their use of the targeted intervention strategies. Additionally, child participants increased the duration of time they remained engaged in telling each story as well as their use of on-topic story-related utterances. All three child participants increased the diversity of vocabulary words used while telling the story and two of three participants increased their mean utterance length, an indicator of syntactic complexity (McDuffie, Machalicek, et al., 2016).
Given the importance of establishing a context for sustained interactions between parent and child, the current study aimed to expand upon these two previously conducted intervention studies. Specifically, we sought to implement a downward extension to a younger age group of the school-age intervention implemented by (McDuffie, Machalicek, et al., 2016). By expanding on this previous line of research, we are able to serve a previously underrepresented age cohort of children with FXS, those in the early school years. This age range is important in that many new skills are being introduced in addition to a number of new demands that may be challenging for the child with FXS to accommodate, suggesting that additional support may be beneficial. Further, stress related to parenting a child with a disability reaches its peak during the early school years and thus the parent–child interaction may be especially impacted at this stage in development (Woodman, 2014). In light of the introduction of new demands in the early school years, such as more structured academic tasks, we felt that delivering the intervention in the context of a structured task, rather than play as used in the toddler intervention of (McDuffie, Oakes, et al., 2016), would be beneficial.
We taught mothers the same language facilitation strategies as had been used by McDuffie, Machalicek, et al., 2016. The intent was to increase the verbally responsive language mothers provided while interacting with their child during shared story-telling using wordless picture books. In addition to examining the preliminary efficacy of this parent-implemented language intervention, the present study sought to examine generalization of treatment gains, as well as whether child gains would be sustained two months after the end of the intervention.
Use of video teleconferencing for intervention delivery
In addition to providing a unique opportunity to observe families in their home environment, utilizing distance technology is of particular importance when conducting research with low incidence populations, such as FXS. Specifically, limited access to services has been identified as a concern for families parenting a child with FXS (Bailey, Skinner, & Sparkman, 2003). Further, when services are available, families who have a child with intellectual disabilities have identified the difficulty of traveling to a clinic as a potential barrier to participation (Statham, Ponder, Richards, Hallowell, & Raymond, 2011). In light of these important factors, the present study aimed to investigate the feasibility of collecting assessment data and implementing the intervention entirely via distance technology (i.e., Skype).
Prior studies have successfully collected both assessment data via distance (Luxton, Pruitt, & Osenbach, 2014) and implemented language interventions via distance (McDuffie et al., 2013; McDuffie, Machalicek, et al., 2016; McDuffie, Oakes, et al., 2016; Oakes, Ma, McDuffie, Machalicek, & Abbeduto, 2015). McDuffie et al. (2013) found that targeted parent behaviors were used as frequently during video-conferencing sessions as they were during face-to-face sessions conducted in the clinic. A study by Grogan-Johnson et al. (2013) found no significant differences between face-to-face and distance delivery of an intervention on the degree of improvement in speech sound production in school-aged children. Further, work by Wainer and Ingersoll (2015) found significant gains in parents’ use of intervention strategies aimed at increasing imitation in children with ASD through a parent-training paradigm administered through online training. Further, these authors were successful in obtaining measures of treatment gains through distance technology (filmed parent–child interactions). These and other studies provide support for the premise that treatment gains can be made in both child and parent behavior through distance delivery of interventions and further, that measures of treatment gains in child skills can be collected via distance technology. Thus, one goal of the present study was to extend the literature by utilizing distance technology to collect pre- and post-treatment language sampling data as a measure of generalized treatment gains in the context of a distance technology-delivered parent-implemented spoken language intervention for young school-aged boys with FXS. The use of such technology to collect outcome data from children with FXS of early school-age has not been attempted previously.
Research questions
The present pilot study was designed to address the following questions in three mother–son dyads affected by FXS who participated in a parent-implemented language intervention:
Does the intervention lead mothers and children to increase their overall frequency of story-related talking? Does the intervention lead mothers to increase their frequency of use of the targeted language support strategies (expansions, open-ended wh-questions, and intonation prompts)? Does the intervention lead children with FXS to increase their lexical diversity, grammatical complexity, and length of engagement in the shared story-telling interaction? Does maternal use of expansions, open-ended wh-questions, and intonation prompts generalize from the shared story-telling interaction to a different language sampling context? Do child gains in lexical diversity and grammatical complexity generalize to a different language sampling context? Do changes in maternal and child behavior persist two months post-intervention?
Methods
Participants
Three boys with a confirmed diagnosis of full mutation FXS, ages 5–7 years, and their biological mothers, ages 36–41 years, participated in this study. These participants were recruited from a database of previous study participants who had agreed to be contacted for future research. Eligibility for the present study stipulated that the child was currently communicating in 1- to 3-word spoken phrases on a daily basis. All mothers gave informed consent to participate in the current study as approved by the institutional review board at the University of California, Davis.
Characteristics of participating dyads at pre-treatment assessment.

ASD: autism spectrum disorder.
Vineland Adaptive Behavior Scales, Second Edition (Vineland-II; Sparrow, Cicchetti, & Balla, 2005).
Childhood Autism Rating Scale (CARS-2; Schopler & Van Bourgondien, 2010).
Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1994), a T score greater than or equal to 63 is considered a positive risk or a case.
Parenting Sense of Competence (Gibaud-Wallston & Wandersman, 1978; Johnston & Mash, 1989), scores between 70 and 96 represent high parental confidence, scores between 51 and 69 represent moderate parental confidence, and scores between 16 and 50 represent low parental confidence.
Parenting Stress Index, Fourth Edition Short Form (PSI-4-SF; Abidin, 2012), scores within the 16th and 84th percentile are considered within the normal range, scores in the 85th to 89th percentile are considered high, and scores in the 90th percentile or higher are considered clinically significant.
Five Minute Speech Sample (FMSS; Magaña et al., 1986), low EE is indicative of a positive parent–child relationship.
Expressive language sampling
In order to assess child spoken language ability at the pre- and post-intervention time points, mother–child dyads were observed in two language sampling contexts that were video-recorded at a distance: (1) a semi-structured parent–child play session; and, (2) an activity-based context that involved making a snack. Parent and child outcome variables were averaged across the two expressive language sampling contexts.
Parent–child play sample
Mother–child dyads were provided with a standard set of developmentally appropriate toys: (1) a train set, (2) a picnic set, (3) magnetic construction blocks, and (4) two puzzles of differing difficulty. These toy sets were mailed to the mother in advance. A graduate student in child development (the first author) initiated a Skype™ call with the mother to observe and record the play session. Mothers were instructed to use the toys to play with their child as they usually would and to play with at least three of the four toy sets. If they remained engaged with a single toy set for more than 5 minutes, they were given a signal to switch to a different toy set. A 10-minute sample, including 3 minutes and 20 seconds of play with the first three toy sets chosen, was transcribed.
Making a snack
Mother–child dyads were asked to make a snack together. The snack could be of the mother’s choice; however, mothers were asked to select a snack that the child would be able to help prepare so that the child would be engaged in the process. A 3-minute sample was transcribed starting from the beginning of snack preparation.
Parent-implemented language intervention
Study design
The study utilized a single-case multiple-probe design across three mother/child dyads (Gast, Lloyd, & Ledford, 2014). In this design, probe data are collected intermittently during baseline in place of the continuous measurement of baseline data. The design requires that baselines for all participants begin at the same point in time and that at least three consecutive baseline sessions be collected prior to the introduction of the intervention for each participant. Following a stable baseline, participants had staggered entry into the intervention phase of the study in which data were collected continuously for 12 weeks. Further, staggered entry into the intervention phase was determined based on a set number of days (Gast et al., 2013), with each dyad entering the intervention phase after the previous dyad completed 3 weeks of intervention. Thus, Dyads 1, 2, and 3 completed 5, 7, and 9 baseline sessions, respectively. At the conclusion of baseline, each mother was individually presented with 2 hours of parent training consisting of a PowerPoint™ presentation, with embedded video clips that provided examples of the targeted intervention strategies. The clinician guided the mother through the PowerPoint™ presentation via Skype™. During these parent education sessions, the clinician and mother discussed each strategy in detail and addressed any questions the mother may have had.
Intervention structure
Average frequency and percent agreement for clinician coaching behaviors and parent response to coaching across dyads.
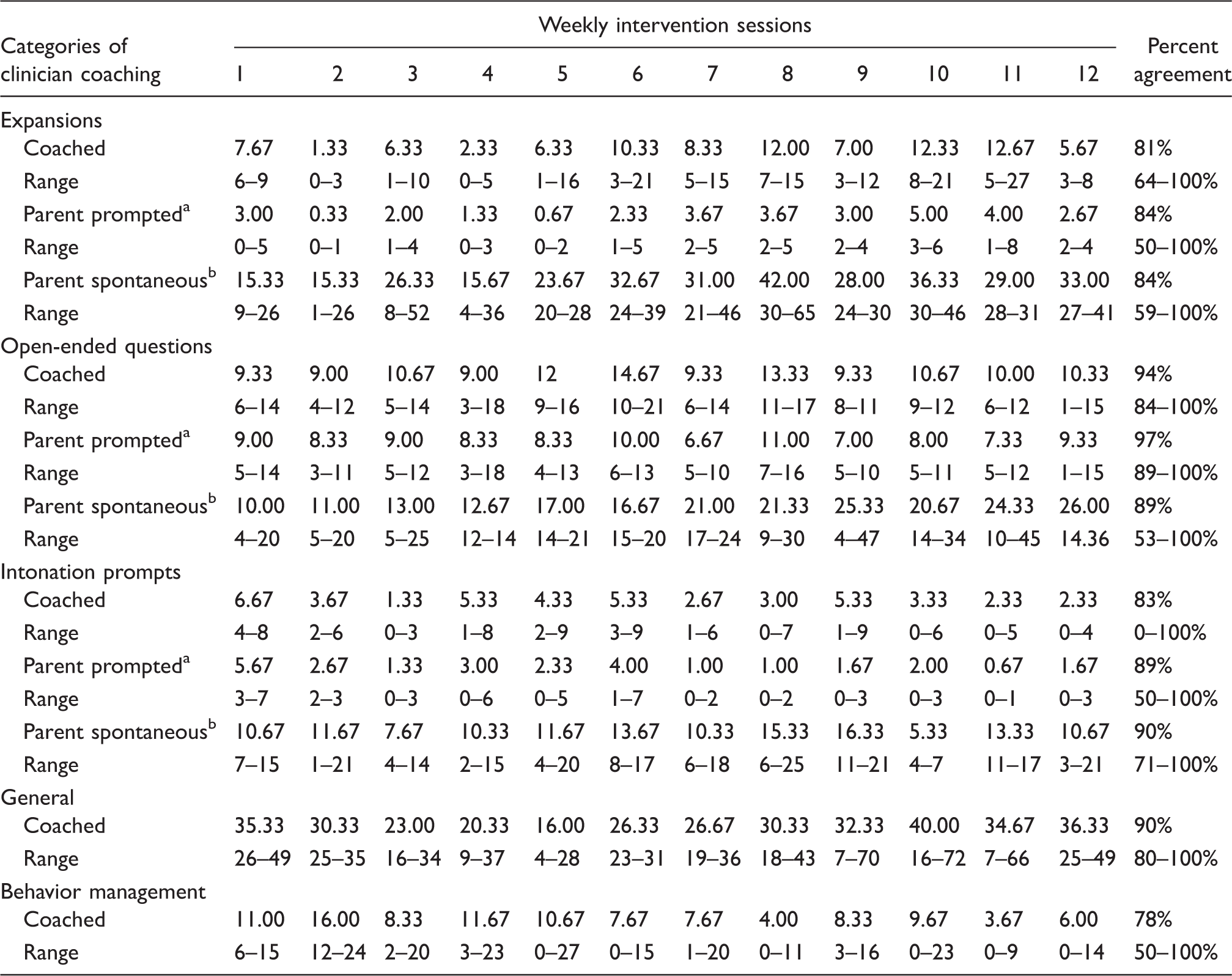
Parent response to clinician prompt for strategy use.
Parent spontaneous use of targeted strategy.
Following each coaching session, dyads were asked to independently engage in the story-telling activity once again using the strategies practiced during coaching. This session was called the homework session and lasted approximately 15 minutes. The homework session was independently recorded by the mother on the laptop using Photo Booth™ software and transmitted to study staff via cloud-based data sharing software (Dropbox™). The mothers were not given instructions regarding the duration of the homework interaction, only that they should repeat the same book used during coaching and practice using strategies that were coached by the clinician. Upon receipt of the homework session, the clinician reviewed the video and then provided additional guidance to each parent during a distance-based feedback session. During this feedback session, the clinician would review video clips from the homework with the mother, highlighting aspects of the session that showed proficiency in strategy use and also highlighting areas for improvement. This session lasted for approximately one hour and did not involve the child.
The final weekly session was a data collection session during which the parent and child again completed the shared story-telling activity. Data collection sessions lasted for approximately 15 minutes. The clinician observed and recorded this session, but did not provide feedback.
The four session types (coaching, homework, feedback, and data collection) were repeated weekly for 12 weeks and a new book was used each week.
The expressive language sampling procedures were again administered after the completion of the intervention to provide post-intervention measures of generalization. At two months’ post-intervention, dyads completed three follow-up data collection sessions as a measure of intervention maintenance. These sessions consisted of a shared book-reading interaction between the mother and child using a previously unseen set of wordless books. Parent and child outcome variables were averaged across the three novel wordless books.
Intervention context
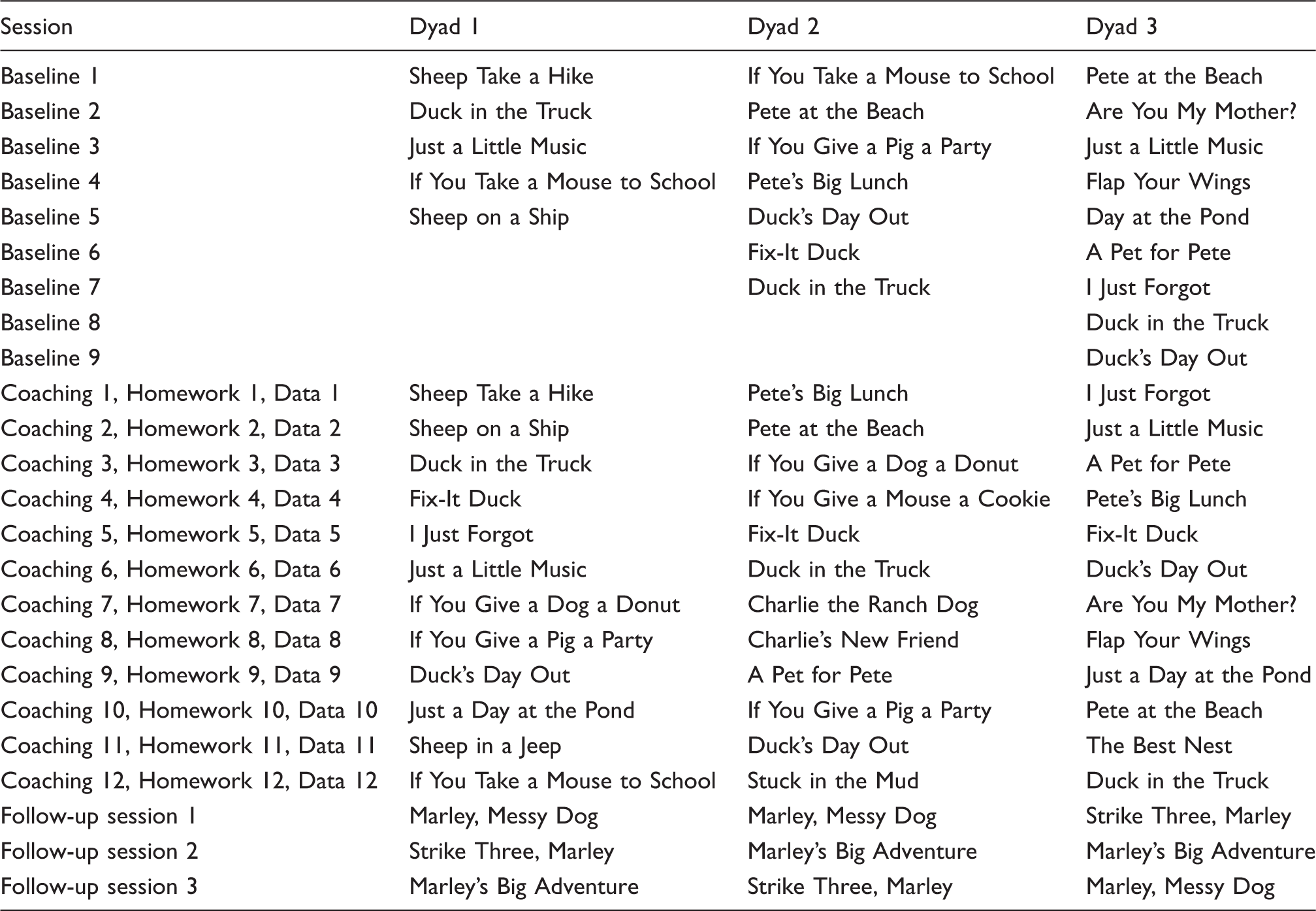
Wordless picture books used for shared story-telling.
Targeted intervention strategies
Mothers received training on four language facilitation strategies that were designed to (a) increase the amount of verbally responsive language they provided to their children during the shared story-telling interactions and (b) prompt the child to verbally or gesturally participate in the story-telling interaction. The four language facilitation strategies were
Story-related talking: Mothers were encouraged to use verbal language to describe the important details and sequence of the story. The goal of story-related talking was to provide models of nouns, verbs, adjectives, adverbs, and function words to the child in addition to models of more advanced grammatical constructions. Mothers were given a written script for each story to provide them with some ideas about the kinds of language they could use while telling the story. Mothers were encouraged to go beyond the script and use their own ideas while interacting with their child. Expansions of child utterances: Mothers were encouraged to add new semantic or grammatical information to the story-telling interaction in a way that was contingent upon child comments about the story; for example, if the child said “castle,” the mom could expand this utterance by saying “Pete built a sand castle.” The goal of expansions was to provide models of vocabulary and grammar that related to the core meaning of the child’s immediately preceding utterance. Open-ended questions: Mothers were encouraged to ask their child open-ended questions that related to the content/topic of story, for example, “What are duck and sheep doing?” This strategy was important for prompting the child to use on-topic utterances that related to the story content and to assess comprehension of important story details. Intonation prompts: The mothers were taught to provide the beginning of an utterance and use expectant waiting to prompt the child to complete the utterance by using a word or words they might not be able to use independently, for example, “Charlie’s new friend is a ——.”
Video-teleconferencing equipment
All pre-treatment assessments, baseline and intervention sessions, and post-treatment and maintenance assessments were collected using video-teleconferencing technology. Each family was provided with a MacBook Pro™ laptop computer equipped with Skype™, Dropbox™, and Photo Booth™ software, and a web browser (i.e., Safari™). Unique, nonidentifying accounts were created for the families to utilize Skype™ and Dropbox™. Mothers elected to use their personal tablets (i.e., iPad™) and earpieces (i.e., Bluetooth or headphones) for all sessions. Sessions were recorded using Ecamm Call Recorder™ for Skype™. The video-teleconferencing equipment was mailed to each family. To orient mothers to the technology, the first author scheduled an individual Skype™ call with each mother to review the various applications and to identify a location in their home for the calls to take place.
Transcription and coding
All parent–child baseline, coaching, and data-collection sessions, as well as the expressive language samples and post-intervention follow-up sessions, were video-recorded using Ecamm Call Recorder™ for Skype™. Homework sessions were video-recorded via Photo Booth™ and sent to the clinician via Dropbox™. All video-recorded samples were transcribed using Systematic Analysis of Language Transcripts (SALT; Miller & Iglesias, 2008), a software program that enables the systematic transcription of samples of spoken language. Transcription was completed by highly trained research assistants following the procedures described by Abbeduto, Benson, Short, and Dolish (1995). Transcription involved a first draft by a primary transcriber, feedback from a second transcriber, and final editing by the primary transcriber. Use of this process averages >90% inter-observer agreement (Kover, McDuffie, Abbeduto, & Brown, 2012). Finalized SALT transcripts were used to generate the child outcome measures for (a) lexical diversity (i.e., number of different words used by the child) and (b) grammatical complexity (i.e., child’s mean length of utterance (MLU) in morphemes).
In addition to the variables generated by SALT, a trained observer coded maternal and child utterances from the transcripts. Maternal utterances were coded for expansions of child utterances, use of open-ended questions, and intonation prompts, as well as utterances in which the mother provided models of language related to the events of the story. A composite score including the frequency of expansions, open-ended questions, intonation prompts, and models of story-related events was computed and termed maternal story-related talking. Child utterances were coded for non-story-related talking (i.e., “What is for dinner?”) and utterances that were self-repetitions (i.e., if a child said “Duck drives car. Duck drives car.” the second utterance would be coded as a self-repetition). The frequency of non-story and self-repetition utterances was subtracted from the total number of child complete and intelligible utterances as calculated by SALT to derive the frequency of child story-related talking. Child engagement was coded using Procoder for Digital Video using 5-second partial interval coding. For each 5-second interval, a trained observer decided whether the child was engaged, not engaged, or if the child interval was uncodable (i.e., video and/or audio stopped working). A child was considered engaged if they were talking about the book and/or jointly attending during the shared story-telling activity for at least 3 of the 5 seconds in each interval. The metric for child engagement was the number of engaged intervals during a shared story-telling session, converted to minutes and seconds. Twenty percent of the coded transcripts and coded engagement files were randomly selected from each phase (i.e., baseline, intervention, and post) and independently recoded to determine inter-coder agreement. Total percent agreement was calculated using the gross method in which the smaller number is divided by the larger number and multiplied by 100 (Gast & Ledford, 2009). Inter-coder agreement for coded variables of interest was 92% for open-ended questions, 91% for expansions, 98% for intonation prompts, 95% and 93% for maternal and child story-related talking, respectively, and 94% for child engagement.
Data analysis
Visual analysis of the data was used to evaluate gains in maternal strategy use and child spoken language. Further, for research questions 1 through 3, intervention effect sizes were calculated using nonoverlap of all pairs (NAP) which assesses the degree of overlap between baseline and intervention phases as well as baseline and follow-up phases (Parker & Vannest, 2009; Parker, Vannest, & Davis, 2011). NAP values between .93 and 1.00 represent strong treatment effects, values between .66 and .92 represent moderate effects, values between .50 and .65 represent weak effects, and NAP values below .5 represent deteriorating performance (Parker & Vannest, 2009). Importantly, when compared to other nonoverlap-based indices commonly used for measuring effect sizes in single-case research, NAP is reported to yield superior results in accurately quantifying the effectiveness of an intervention (Parker & Vannest, 2009).
Results
Maternal and child story-related talking
All mother–child dyads increased their average use of story-related talking during the intervention (see Figure 1 and Table 4). The mother in Dyad 1 showed an immediate increase in her level of story-related talking from baseline to intervention. The child in Dyad 1 also showed an immediate increase in his level of story-related talking from baseline to intervention. There were no overlapping data points between baseline and intervention phases for either the mother or child in Dyad 1. The effect size, as represented by NAP, was 1.00 for both mother and child, indicating a strong effect of treatment for story-related talking.
Maternal and child story-related talking across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review. Mother and child shared story-telling: average performance across baseline, intervention, and follow-up phases. MLU: mean length of utterance; NDW: number of different words.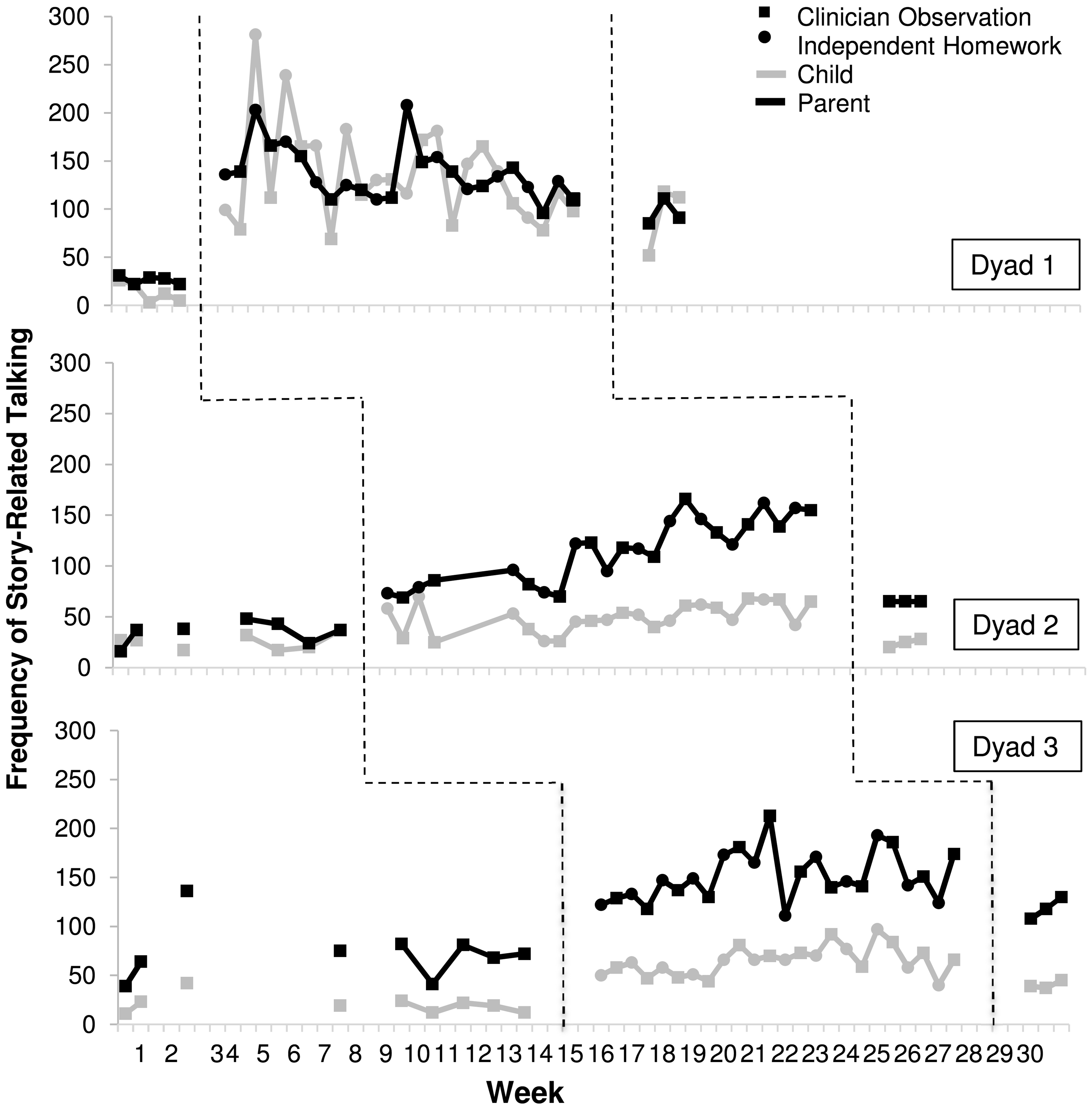

The mother in Dyad 2 had a small, immediate increase in her level of story-related talking, which continued to increase slightly throughout the intervention phase. She showed no overlapping data points between baseline and intervention. The child in Dyad 2 showed a slight increase in story-related talking from baseline to intervention. For this child, four out of the seven baseline sessions overlapped with data points early in the intervention phase. The effect size, as represented by NAP, was 1.00 for maternal story-related talking and .92 for child story-related talking, both indicating a strong effect of treatment.
Although the mother in Dyad 3 had high rates of story-related talking during baseline, she still showed an immediate increase in her level of story-related talking from baseline to intervention. Overall, for this mother, level of story-related talking increased but was variable throughout the 12 weeks of intervention sessions. One of nine baseline data points overlapped with intervention data points. The child in Dyad 3 also showed a slight, immediate increase in story-related talking from baseline to intervention, and had one baseline data point that overlapped with the intervention phase. The effect sizes, as represented by NAP, were .97 and .99 for maternal and child story-related talking, respectively, indicating a strong effect of treatment.
Maternal use of targeted intervention strategies
Mothers showed varying levels of performance as they learned to use the targeted intervention strategies (see Table 4).
Expansions
The mother in Dyad 1 had an immediate increase in her use of expansions from baseline to intervention. Her use of this strategy was variable across the intervention phase, but did not overlap with baseline. The mother in Dyad 2 had a slight but immediate increase in her use of expansions from baseline to intervention and there were no overlapping data points between baseline and intervention, and this mother had a gradual increase in frequency of use of expansions over the 12 weeks of intervention sessions. The mother in Dyad 3 had an immediate increase in her use of expansions from baseline to intervention. Her use of this strategy was variable across the intervention phase, but did not overlap with baseline performance levels. The effect size, as represented by NAP, for all three of the mothers’ use of expansions was 1.00, indicating strong effects of treatment for each mother (see Figure 2).
Maternal use of expansions across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.
Open-ended questions
For Dyad 1, maternal use of open-ended questions immediately increased from baseline to intervention. Use of this strategy was variable throughout the intervention, but did not overlap with baseline data. For Dyad 2, the mother had an immediate increase in her use of open-ended questions and showed a steady overall increase in use of this strategy over the course of the 12 intervention sessions. The mother in Dyad 2 had no overlapping data between baseline and intervention phases and increased her use of open-ended questions from baseline to intervention. The effect size, as represented by NAP, for the mothers in both Dyads 1 and 2 was 1.00, indicating strong effects of treatment. The mother in Dyad 3 also increased her use of open-ended questions from baseline to intervention. Her use of this strategy was variable during the intervention sessions and data from three baseline sessions overlapped with intervention sessions. The effect size, as represented by NAP, was .98, indicating a strong effect of treatment (see Figure 3).
Maternal use of open-ended questions across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.
Intonation prompts
Although intonation prompts were used at a lower frequency relative to the other targeted strategies, all mothers showed an increase in their use of this strategy during the intervention phase. The mother in Dyad 1 had an immediate increase from baseline to intervention, and although her strategy use was variable across intervention sessions, there was no overlap between baseline and intervention sessions. The effect size, as represented by NAP, was 1.00, indicating a strong effect of treatment. The mother in Dyad 2 had a slower uptake of this intervention strategy and her use of this strategy remained variable throughout the intervention phase. Although Dyad 2 mother’s overall use of intonation prompts increased from baseline to intervention, five intervention sessions overlapped with performance during baseline. The effect size, as represented by NAP, was .92, indicating a moderate effect of treatment. The mother in Dyad 3 had an overall increase in her use of intonation prompts from baseline to intervention, but her use of this strategy was variable across the intervention phase and three baseline data points overlapped with intervention. The effect size for the mother in Dyad 3, as represented by NAP, was .93, indicating a strong effect of treatment (see Figure 4).
Maternal use of intonation prompts across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.
Child measures of spoken language and engagement
Child measures of lexical diversity, grammatical complexity, and duration of engagement in the shared story-telling activities are presented Table 4.
Child lexical diversity
Relative to baseline sessions, all three children showed an increase in lexical diversity as measured by the number of different words used while engaging in the shared story-telling interactions with their mothers during the intervention (see Figure 5). The child in Dyad 1 increased the number of different words used from baseline to intervention. The child in Dyad 2 increased the number of different words used from baseline to intervention. Lastly, the child in Dyad 3 increased the number of different words used from baseline. For Dyads 1 and 3, there was a strong effect of treatment on lexical diversity (NAP =1.00 and .99, respectively), and a moderate effect of treatment for Dyad 2 (NAP = .87).
Child number of different words used across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.
Grammatical complexity
There was variable performance in grammatical complexity across the three dyads, with two of the children showing an overall increase in MLU in morphemes while engaging in the shared story-telling interactions with their mothers during the intervention (see Figure 6). For the child in Dyad 1, MLU increased from baseline to intervention. For the child in Dyad 3, there was a slight increase in MLU from baseline to intervention. In contrast, MLU for the child in Dyad 2 decreased slightly from baseline to intervention. Effect sizes for child grammatical complexity varied across the three dyads; showing a strong effect of treatment for Dyad 1 (NAP = .98), a moderate effect of treatment for Dyad 3 (NAP = .81), and a deteriorating effect of treatment for Dyad 2 (NAP = .42).
Child mean length of utterance in morphemes across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.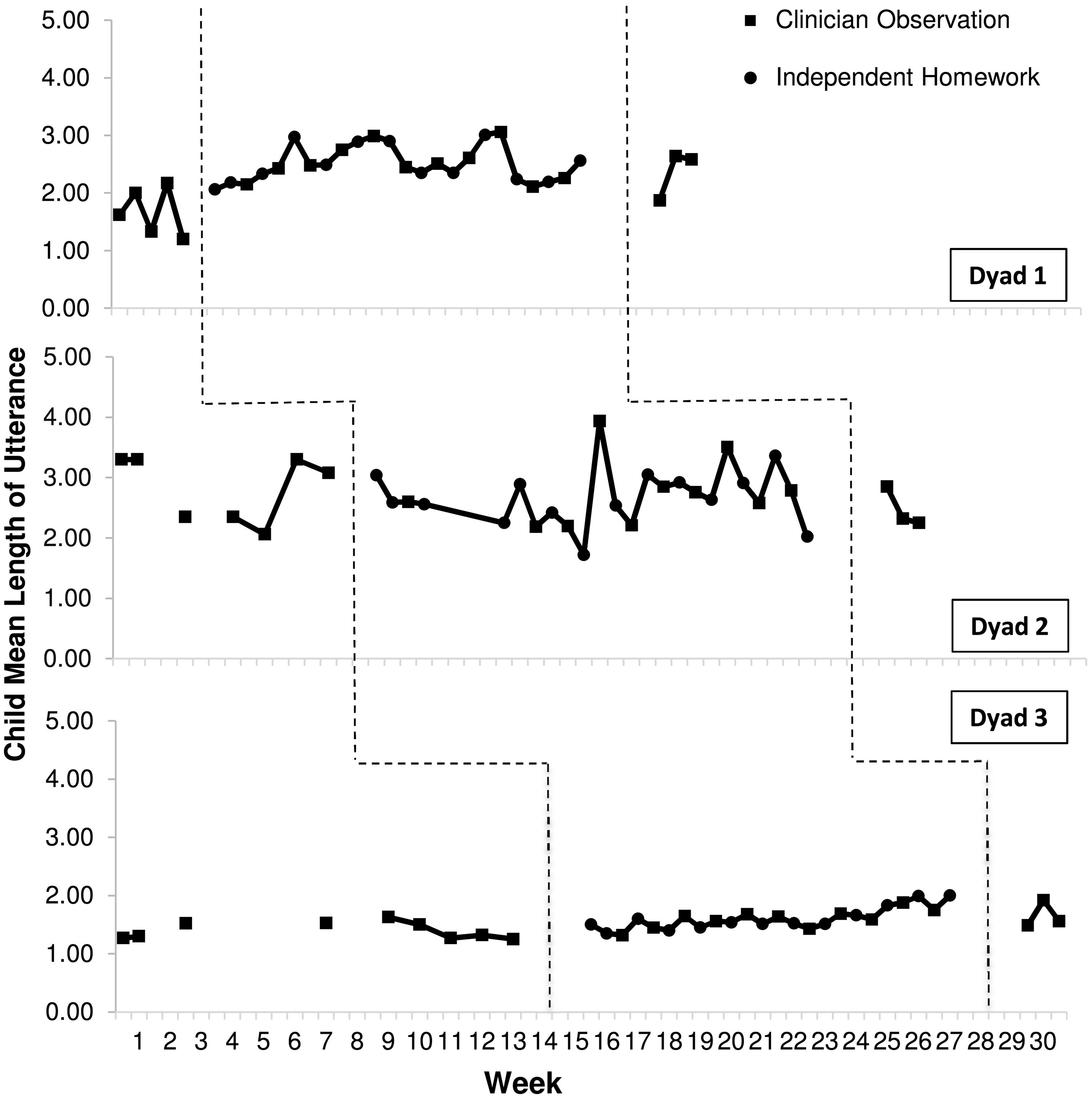
Engagement
All three children increased the time they spent engaged in the shared story-telling activities (see Figure 7). The child in Dyad 1 increased from an average of 2 minutes and 12 seconds during baseline to 14 minutes and 30 seconds during intervention. The child in Dyad 2 increased his length of engagement from an average of 3 minutes and 10 seconds during baseline to 12 minutes during intervention. The child in Dyad 3 increased from an average of 8 minutes and 39 seconds during baseline to 14 minutes and 58 seconds during intervention, with three data points overlapping between phases. Overall, there was a strong effect of treatment on engagement for the children in Dyads 1 and 2 (NAP = 1.00) and a moderate effect of treatment on engagement for the child in Dyad 3 (NAP = .87).
Child duration of engagement across baseline, intervention, and follow-up phases. Clinician observation data points are sessions in which the clinician observed the mother and child in real time via Skype. Independent homework data points are sessions in which the mother and child completed the book sharing activity independently via Photo Booth and then sent to the clinician for review.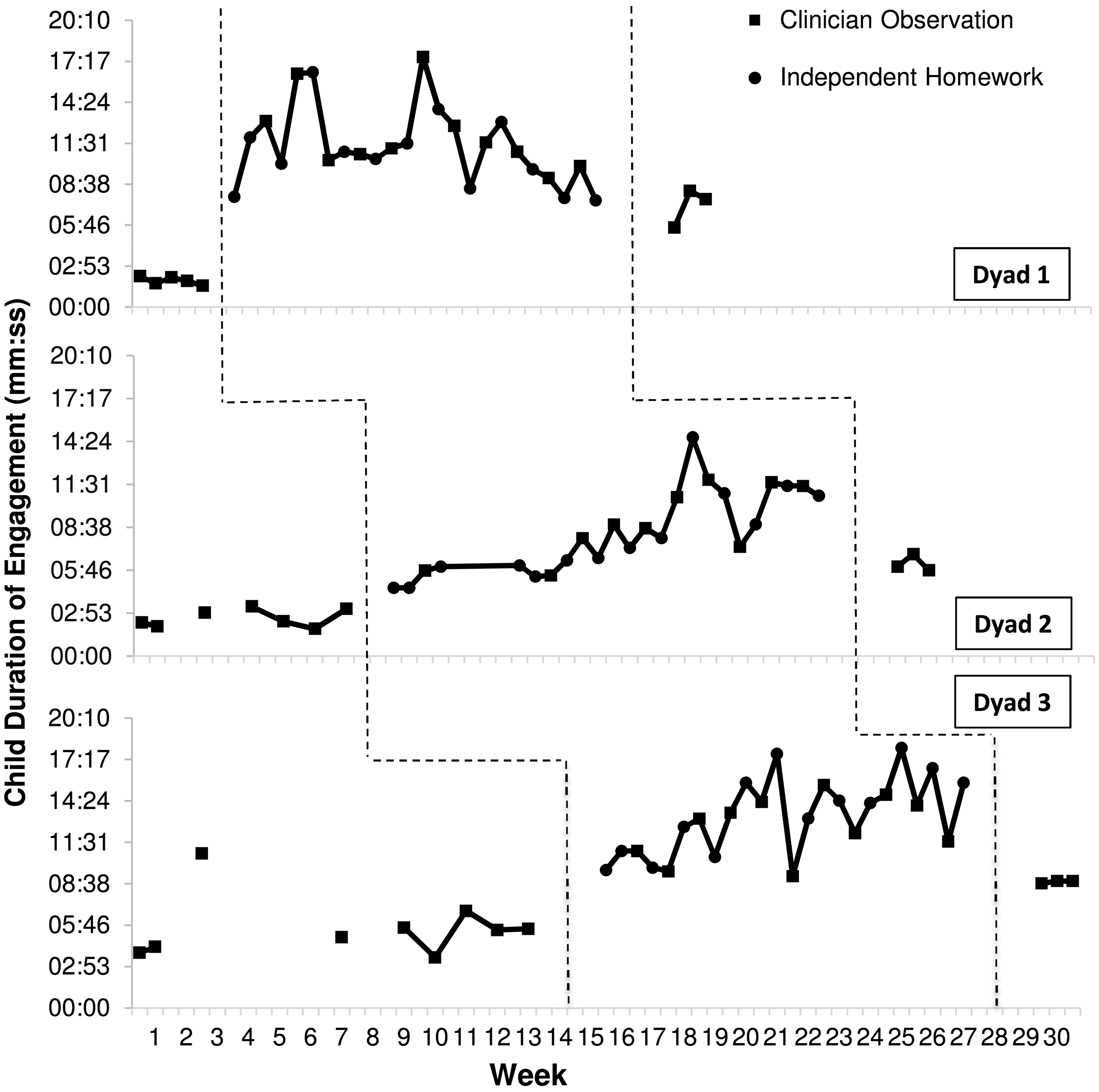
Generalization of treatment gains: Expressive language sampling
Expressive language sampling: generalization of intervention effects.

MLU: mean length of utterance; NDW: number of different words.
Intervention effects at the two-month follow-up
Mother and child performance at the two-month follow-up was averaged across the three shared story-telling interactions using novel books (see Table 4). For story-related talking, all three of the mothers used less story-related talking relative to intervention; however, performance remained higher than during baseline. When comparing baseline and follow-up phases, there was a strong effect of treatment on story-related talking for the mothers in Dyads 1 and 2 (NAP = 1.00) and a moderate effect of treatment for the mother in Dyad 3 (NAP = .89). For child story-related talking, the children in Dyads 1 and 3 used less story-related talking relative to the intervention phase; however, story-related talking remained higher than their performance during baseline. The child in Dyad 2 returned to baseline performance at the two-month follow-up. There was a strong effect of treatment on story-related talking for the children in Dyads 1 and 3 (NAP = 1.00 and .93, respectively) and a weak effect for the child in Dyad 2 (NAP = .50).
The mothers varied in their maintenance of intervention strategies, with all three mothers showing a decrease in strategy use compared to their performance during intervention sessions. The mothers in Dyads 1 and 3 maintained a higher level of performance at the two-month follow-up relative to their performance during baseline. The exception to this pattern was the use of intonation prompts by the mother in Dyad 3 who approached baseline performance in the use of this strategy. The mother in Dyad 2 returned to baseline performance in her use of open-ended questions and intonation prompts; however, her use of expansions was slightly improved compared to baseline. Effects of treatment varied across maternal strategy use when examining overlap between baseline and follow-up phases of the intervention. There was a strong effect of treatment for all three mothers in the use of expansions (NAP = 1.00). For maternal open-ended questions, there was a strong effect of treatment for the mothers in Dyads 1 and 3 (NAP = 1.00 and .98, respectively) and a moderate effect of treatment for the mother in Dyad 2 (NAP = .67). Lastly, for intonation prompts, there was a strong effect of treatment for the mother in Dyad 1 (NAP = 1.00); a moderate effect of treatment for the mother in Dyad 3 (NAP = .72) and a deteriorating effect of treatment for the mother in Dyad 2 (NAP = .36).
For number of different words, the children in Dyads 1 and 3 had lower performance at the follow-up compared to intervention sessions; however, their numbers of different words remained higher than used during baseline sessions. There was a strong effect of treatment for Dyads 1 and 3 (NAP = 1.00 and .96, respectively). Number of different words for the child in Dyad 2 returned to baseline levels of performance at the two-month follow-up, indicating a weak effect of treatment (NAP = .55). For grammatical complexity, the child in Dyad 1 had a lower MLU at the two-month follow-up when compared to the average for intervention sessions, but higher than his MLU at baseline. The child in Dyad 2 had a lower MLU when compared to both baseline and intervention performance. The child in Dyad 3 had a slightly higher MLU at the follow-up when compared to the averages from baseline and intervention sessions. There was a moderate effect of treatment on MLU for the children in Dyads 1 and 3 (NAP = .87 and .81, respectively) and a deteriorating effect of treatment for the child in Dyad 2 (NAP = .24). For length of engagement, the children in Dyads 1 and 2 had shorter engagement at follow-up than during the intervention phase; however, both were higher than in baseline, indicating a strong effect of treatment (NAP = 1.00). The child in Dyad 3 returned to baseline performance for length of engagement, indicating a weak effect of treatment (NAP = .55).
Discussion
The present study was designed as a downward extension of a shared story-telling intervention focused on improving the spoken language of young school-aged boys with FXS. The study is unique in that all aspects of the intervention, including the pre- and post-treatment assessments, were delivered by means of distance video-teleconferencing technology, allowing families to access the intervention regardless of geographic location and making enrollment in the intervention possible without a trip to the clinic. Importantly, during an informal debriefing with the families upon completing the intervention, no families reported issues with technology as being a hindrance to their involvement or enjoyment of the intervention. Additionally, generalization of intervention effects was evaluated using expressive language sampling, which provides a standardized, yet naturalistic, procedure for evaluating spoken language performance.
The majority of boys with FXS can use spoken language to communicate their basic needs and wants, but their ability to sustain communication within the context of a back-and-forth interaction with a conversational partner is severely limited. Impulsivity, a short attention span, repetitive and stereotyped utterances, and escape-maintained challenging behaviors are all likely to interfere with the ability to engage in reciprocal interactions about a shared topic of conversation. However, few interventions have been designed specifically for children with FXS, and fewer still with a focus on language. We previously developed a spoken language intervention based upon establishing shared story-telling interactions with a caregiver using wordless picture books. We tested this intervention with older school-aged and adolescent boys with FXS and observed positive changes in engagement, lexical diversity and grammatical complexity. In the present study, we sought to evaluate the effects of such an intervention with younger boys with FXS whose spoken language consisted of one- to three-word phrases. In this intervention, we taught mothers to provide enriched language input to their children such that the children would have the opportunity to hear and practice using developmentally advanced vocabulary and grammar in a meaningful and highly scaffolded context.
Interventions based on shared story-telling are known to improve many foundational aspects of language and pre-academic skills for young children (Landry et al., 2012). Additionally, shared story-telling is frequently used by speech/language pathologists as a context for embedding language intervention activities (Kaderavek & Justice, 2002). We reasoned that the visual structure of an illustrated book would provide a joint topic of conversation and help to maintain a shared focus of attention during the parent/child interaction. We also reasoned that the sequence of actions depicted in the book would scaffold the progression of story-related talking. In addition to encouraging mothers to use story-related talking, we taught mothers to use three additional language facilitation strategies: expansions, open-ended questions, and intonation prompts. Topic-continuing expansions used contingent upon child communication acts were hypothesized to provide additional semantic and grammatical information to children as they engaged in the shared story-telling interaction. Both open-ended questions and intonation prompts were hypothesized to encourage children to take a turn in the story-telling interaction, which also enables the mother to respond to such prompted child utterances with a contingent expansion of her own.
We found that all three mothers increased the amount of story-related talking that they provided to their children during shared story-telling. Although the amount of story-related talking used by mothers decreased from treatment to follow-up, the level of story-related talking remained considerably higher than baseline levels. This finding is important because talking about the story is one primary way in which mothers can provide follow-in language input to children. An increase in story-related talking was paralleled by an increase in the amount of time children and their mothers were able to stay engaged in each shared story-telling interaction. Increased engagement in the context of more story-related talking can be expected to foster a continuing cascade of positive effects on language learning.
Maintaining engagement in a learning activity is especially challenging for children with FXS who may, over time, miss out on many opportunities for learning due to their short attention spans and their escape-maintained challenging behaviors. These child characteristics make the potential for participating in ongoing shared story-telling activities even more important. All three child participants in the intervention also increased the amount of story-related talking they produced during intervention sessions relative to baseline. Two of the three children maintained some increases in story-related talking at the follow-up but not at as high a level as during intervention sessions. Given the challenges of participating in sustained social interactions, it is plausible that the children had difficulty maintaining the effects of treatment at the follow-up session. However, one difference between intervention sessions and follow-up sessions was that, during weekly intervention activities, the child was exposed to each book for the first time during coaching and, thus, was essentially seeing the book for the second time during homework sessions and for the third time during data collection sessions. During follow-up sessions, data were collected only during the child’s first exposure to each book. This lack of repeated experience with the stories may help to explain why the amount of story-related talking for child participants was slightly lower during follow-up sessions than during intervention sessions.
Mothers were able to learn to use the three targeted language support strategies during intervention sessions. As was the case for story-related talking, two mothers did maintain some of their gains at the follow-up assessment, whereas the mother in Dyad 2 reverted to her level of baseline performance. Because this was a relatively brief intervention, it might have been unreasonable to expect that mothers would maintain their use of the targeted strategies at the follow-up. Additionally, mothers may not have continued to practice shared story-telling with their children once the intervention sessions were concluded. Perhaps the limited time frame of the intervention and the lack of opportunities for continued practice with the shared story-telling format made it difficult for the mothers to consolidate their intervention gains and maintain these gains at the two-month follow-up. Future studies should examine the effect of extending the intervention for a longer time frame or providing mothers with booster sessions and additional storybook materials to help them maintain strategy use after the conclusion of the intervention.
The children in Dyads 1 and 3 increased both the number of different words they used as well as their grammatical complexity at the two-month follow-up when compared to their performance during baseline. Even though the child in Dyad 3 had only a small increase in utterance length, this increase seemed stable from intervention to follow-up. This child had other developmental concerns in addition to FXS (e.g., he had low muscle tone and cleft) which may also have negatively impacted his ability demonstrate gains in spoken language. For this child, we did feel that the noted increase was clinically significant given his developmental level. Alternatively, the child in Dyad 2 did not show sustained improvement at the two-month follow-up when compared to his baseline performance. This is potentially reflective of his mother’s decrease in strategy use at the follow-up time point as well.
All three children increased their overall level of engagement in the shared story-telling activity and this effect persisted until the two-month follow-up for the children in Dyads 1 and 2. This finding is important in that time spent engaged in such tasks could be an important precursor to language gains in the future. By increasing the amount of time a child spends engaged in an interactive context with a verbally responsive parent, the amount of language input that can be experienced by the child increases cumulatively, which is an important starting point for continuing language development.
One aspect of this study that should be highlighted was the use of expressive language samples, collected at a distance, as an outcome measure. Expressive language sampling using conversation and narrative language contexts has been frequently used as an outcome measure in descriptive studies of older children with FXS (Finestack & Abbeduto, 2010; Kover & Abbeduto, 2010; Kover et al., 2012) and has many benefits for use in treatment studies (Berry-Kravis et al., 2013). Further, the collection of these samples via distance in the home allowed for a more representative sample of the child’s language in relation to the intervention and eliminated the burden of travel on the family.
In this study, we used two activity-based language samples, play and making a snack, to remotely collect descriptive data on spoken language use by both the mother and the child. Mothers used more expansions, open-ended questions, and intonation prompts during the language samples at the post-intervention compared with the pre-intervention. It is important to note that, in these language samples, mothers were generalizing use of these intervention strategies to two new contexts (play and snack) that differed substantially from the shared story-telling interaction. Even the mother in Dyad 2, who did not maintain her use of the targeted strategies during shared story-telling at the two-month follow-up, did show generalized improvement in the use of all three strategies in the language sampling context. These findings are important in that they demonstrate that mothers continued to use the intervention strategies to provide their children with enhanced verbal language input during everyday activities in the home following the conclusion of the intervention. This generalization is critical given the importance of children being exposed to a variety of language-rich environments throughout development. Additionally, relative to the pre-intervention, the children all used a larger variety of different words during the language sampling activities at the post-treatment and also showed an increase in grammatical complexity although this was marginal for the child in Dyad 2.
Not surprisingly, there was variation within the three dyads in both maternal uptake of the intervention strategies and magnitude of child language growth. As seen in the literature, maternal mental health status could be a contributor to the use of verbally responsive language for mothers who are affected by the FXS premutation (Sterling et al., 2013). However, there were no self-reports of mental health challenges for the three mothers who participated in the current study. This could be due to a procedural limitation in how mental health was assessed and should be considered in future projects. Another possible explanation for the differences in performance could be variability across the three children. One potential contributor could be the presence of challenging behaviors. Although all three children exhibited challenging behaviors consistent with that of the FXS phenotype, escape- and attention-maintained challenging behaviors were observed more frequently for the child in Dyad 2. Further, these behaviors persisted longer into the intervention when compared to the other children. Therefore, the shift of focus towards behavior management and lower demand strategies, such as having the child point to the page, as opposed to the use of language support strategies could be one possible explanation for the slower maternal uptake of language intervention strategies and limited child changes observed for Dyad 2.
Limitations and future directions
The present study is limited by the small sample size and thus, the results should be interpreted with caution. Although it appears promising that this intervention was successful in teaching mother’s useful strategies which to promote their child’s spoken language, these methods should be examined with a larger sample size and should be compared to strategy use by a nontreatment group. Further, this intervention could have been improved by either a longer period of treatment or by booster sessions following the end of the 12-week intervention. Although the generalization of treatment gains seen during the expressive language samples provides early evidence that these samples were a valid measure, next steps will expand upon this study to further explore the reliability and validity of these approaches to measuring developmental gains via distance technology.
Footnotes
Acknowledgment
First and foremost, we would like to thank the families who participated in this project. We would also like to thank Melissa Mello for her suggestions regarding challenging behavior, as well as Amy Banasik, Sarah Nelson, Robyn Tempero-Feigles, and Vivian Nguyen for their assistance with coding. This work was done as part of a thesis submitted in partial satisfaction for an M.S. in Child Development at the University of California, Davis. The author would like to thank her thesis committee members Leonard Abbeduto, Andrea McDuffie, Peter Mundy, and Siwei Liu for their guidance.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported in part by the National Institute of Child Health and Human Development [grant number U54 HD079125].
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.