
Abstract
Background & aims
Although the Picture Exchange Communication System (PECS) has been demonstrated to be an effective intervention to teach people diagnosed with autism spectrum disorder a functional communication system, the research indicates variability in PECS outcomes across people and studies. Therefore, the purpose of the current study was to explore child characteristics and treatment variables that may explain the variation in, and potentially predict, PECS outcomes.
Method
A total of 22 children and youth diagnosed with autism or a related developmental disorder, all of whom scored substantially below average on standardized measures of cognitive and adaptive abilities, participated in a PECS intervention.
Results
Participants who achieved high phases of PECS (≥PECS phase IIIb) differed significantly from those who mastered lower PECS phases (≤PECS phase IIIa) in terms of overall, verbal, and nonverbal mental age, matching abilities, and adaptive behavior level. Stimulus generalization was also associated with significant variation in PECS outcome. PECS outcomes could be predicted with good accuracy using a combination of these child characteristics and treatment variables.
Conclusions
The findings from the current study suggest that children with relatively higher cognitive and adaptive skill levels are more likely to achieve higher phases of PECS; further, approaches to generalization training also play a role. Factors such as autism symptom severity and parental ratings of maladaptive behavior were not associated with significant differences in PECS outcomes. However, more research is needed.
Implications
Gaining a better understanding of predictors of PECS outcomes is important to inform intervention, provide more accurate outcome expectations for families, and guide PECS teaching procedures. Although participants were more likely to achieve higher phases of PECS if they had a higher mental age, adaptive skill level, and matching skills, the average scores for these measures were well below those expected for same age peers. These results indicate that PECS is appropriate for use with children with clinically significant deficits in cognitive and/or adaptive abilities. Further, results suggest that even children who demonstrate more severe symptoms of autism and exhibit more challenging behavior can achieve higher phases of PECS.
Keywords
Despite numerous advances in supports and services for people diagnosed with autism spectrum disorder (ASD), many will experience communication deficits that negatively impact social interaction, access to basic needs, and opportunities to foster autonomy. Those who do not develop speech may benefit from the use of augmentative and alternative communication systems. One of the most researched augmentative and alternative communication systems is the Picture Exchange Communication System (PECS; Frost & Bondy, 2002). The research base supporting PECS use has resulted in its categorization as an evidence-based communication approach for people on the autism spectrum (National Autism Center, 2015; Hume et al., 2021).
Although the findings from previous research indicate that PECS can be used to successfully teach a functional communication system, there also appears to be significant variation in communication outcomes, including notable differences in overall level of PECS phase acquired and rate of acquisition. Despite the presence of six phases of PECS, a substantial proportion of studies describe teaching and skill acquisition only within the first four phases and the ability of PECS users to attain the skills outlined in each of these phases is highly variable (e.g., Bock et al., 2005; Ganz & Simpson 2004; Ganz et al., 2008; Sulzer-Azaroff et al., 2009; Tincani et al., 2006; Tincani & Devis, 2010).
This variability in PECS phase acquisition was noted in a research synthesis of single-subject studies (Tincani & Devis, 2010), which showed that, of 41 total research participants, three mastered only phase I, six mastered phase II, 20 mastered phase III, eight mastered phase IV, and phase of mastery was not reported for four participants. The authors hypothesized that the variability may be attributed to three factors: (a) variability in participants’ acquisition rate, (b) experimental time limitations which prevented participants from mastering advanced phases, and (c) varying participant cognitive levels. Sulzer-Azaroff et al. (2009) also noted that many researchers reported teaching only to phase III. The authors hypothesized that, once participants were using PECS as a functional communication system, there may have been a reduction in maladaptive behavior, which may have reduced the incentive to teach more advanced phases.
Similar variability is observed in rate of skill acquisition. For example, Cannella-Malone et al. (2010), Carré et al. (2009), Charlop-Christy et al. (2002), Ganz et al. (2008), Jurgens et al. (2009), and Magiati and Howlin (2003) found that some participants mastered PECS phases in a shorter amount of time than others. Further, there were also differences in rate of skill acquisition across studies; however, variations in data collection and reporting procedures, such as the use of number of sessions, trials, or minutes to record time to mastery, make cross-study comparisons difficult. Regardless, it is evident that acquisition rate is variable both within and across studies. It is feasible that variations in rate of acquisition may impact the level of PECS phase mastered within the time and resource constraints of published research studies.
Analogous variations in outcome are identified in the Intensive Behavioral Intervention (IBI) literature. In fact, following IBI, variations in outcome are often so clinically significant, the terms “responders” and “nonresponders” have been employed as a way of describing the tremendous differences (Sherer & Schreibman, 2005). It is believed that several factors impact outcome following IBI, including a combination of child and treatment variables (Eldevik et al., 2009; Perry et al., 2011). Pretreatment child characteristics found to be correlated with variations in outcome include cognitive level (i.e., IQ), age, presence of nonverbal and verbal imitation, language skills, severity of autism symptoms, social responsiveness, and joint attention. Rapid initial acquisition of new material was also found to be a strong predictor (Sallows & Graupner, 2005). Treatment factors believed to be associated with variations in outcome following IBI include duration of the treatment, intensity (e.g., number of hours of treatment per week), staff skill level (i.e., level of training/experience), and the amount and nature of staff supervision (i.e., supervision vs. consultation; Reichow & Wolery, 2009). Given that both IBI and PECS are applications of applied behavior analysis (ABA), and are both used to support people on the autism spectrum, it is highly plausible that similar child and treatment variables impact PECS outcomes. However, limited systematic research has been conducted to explore these associations. As such, surprisingly little is known about the child characteristics which may impact skill acquisition or the components of PECS training that are essential for achieving success.
In a review of single case design studies, Tincani and Devis (2010) explored the relationship between participant characteristics and participants’ acquisition of PECS. PECS acquisition did not significantly differ based on participants’ gender, diagnosis, or age. Further, in another review, Preston and Carter (2009) found no significant difference in PECS outcomes based on participant age or gender; however, the intervention was found to be less effective for children diagnosed with autistic disorder than participants with other diagnoses, including pervasive developmental disorder–not otherwise specified (PDD-NOS) and other “autistic characteristics.” In another study, three additional child characteristics were identified as variables of interest in PECS outcomes, including joint attention, object exploration, and motor imitation (Flippin et al., 2010). Ganz et al. (2012) conducted a meta-analysis investigating pretreatment characteristics associated with PECS outcomes and found that younger children without additional diagnoses (e.g., intellectual disability), compared to older participants with additional diagnoses, exhibited greater communication skills. Recently, Sievers et al. (2018) conducted a systematic review examining predictors of augmentative and alternative communication outcomes for children diagnosed with ASD. Based on the articles included in the review that implemented a PECS intervention, the findings also indicated that child characteristics may impact outcomes, such as developmental and chronological age (Pasco & Tohill, 2011), expressive language (Gordon et al., 2011), and ASD symptoms (Gordon et al., 2011).
Despite several study authors exploring the relationship between PECS outcomes and child characteristics, the relationship is still unclear. Specifically, some authors suggest younger children may take longer to learn PECS (Ganz & Simpson, 2004). Others suggest that students introduced to PECS at a later age may have a lower likelihood of increasing speech production (Howlin et al., 2007). Further, variables such as cognitive and language functioning have also been posited as factors that may impact rate of skill acquisition and overall communication outcomes (Ganz & Simpson, 2004; Ganz et al., 2008). Additional factors suggested to impact outcomes include the presence or absence of joint attention skills, the level of complexity of children's play, and the number and reinforcing value of the child's preferred activities and materials (i.e., number of reinforcers and how quickly the child satiates on them; Schwartz et al., 1998).
Although these studies provide some understanding of child characteristics that may be associated with PECS outcomes, to date, there have been no systematic attempts to examine the association between PECS treatment variables and communication outcomes. Potentially relevant treatment factors would include treatment intensity, duration, approaches to generalization training, amount of staff training and/or supervision, and treatment fidelity. Given the lack of research exploring treatment variables and PECS outcomes, little is known about the characteristics of treatment essential for improved communication outcomes, or how treatment factors might interact with child factors.
An exploration of the literature reveals significant differences in treatment duration and intensity, with some studies conducting training over a limited number of sessions and a limited number of trials (Anderson et al., 2007; Cannella-Malone et al., 2010; Carré et al., 2009; Ganz & Simpson, 2004; Ganz et al., 2008; Greenberg et al., 2012; Jurgens et al., 2009; Yoder & Stone, 2006a, 2006b), while other studies report on outcomes over longer periods, with unlimited trials spread over the course of the entire day (Koudys et al., 2021; Magiati & Howlin, 2003; Schwartz et al., 1998; Webb, 2000). Teaching practices targeting generalization also vary considerably, with some conducting training in a single, controlled teaching environment, such as a clinic (Greenberg et al., 2012; Yoder & Stone, 2006a), while others conduct teaching in multiple natural settings and/or activities, including the child's home and/or classroom (Carr & Felce, 2006, 2007a, 2007b; Koudys et al., 2021; Kravits et al., 2002; Schwartz et al., 1998). These discrepancies are not surprising when variations in staff training are explored.
Given the large differences in staff training in PECS implementation, it is not surprising that the term “PECS” is often used in applied settings to refer to a variety of approaches involving pictures; even if these approaches often share little more than the use of pictures with the original protocol described by Frost and Bondy (2002). Similar deviations from protocol are found in descriptions of fidelity in published works (e.g., Dooley et al., 2001; Frea et al., 2001; Stoner et al., 2006; Yokoyama et al., 2006). As PECS is a multilevel, manualized system, based on theoretically sound behavioral principles, it is probable that deviations from the protocol may substantially impact outcomes. However, meta-analyses (Preston & Carter, 2009; Sulzer-Azaroff et al., 2009; Tincani & Devis, 2010) have indicated that procedural or treatment fidelity is rarely addressed in a systematic, quantitative fashion in the literature, limiting our ability to assess the association between fidelity and communication outcomes.
Although PECS has been demonstrated to be an effective intervention to help people on the autism spectrum develop a functional communication system, the research indicates variability in PECS outcomes across individuals and across studies. In fact, the results of our initial research that explored the nature of 22 participants’ PECS use in a community setting revealed similar variability. Specifically, although there was significant overall improvement in PECS phase acquisition following PECS training, some participants only mastered one PECS phase while others mastered up to five PECS phases (Koudys et al., 2021). To better understand the outcome variability in the original sample of 22 participants, the present companion study was designed to explore both the child characteristics and treatment factors that may explain the variation in, and potentially predict, PECS outcomes. The results can be used to provide more accurate outcome expectations for families and to guide PECS teaching procedures. The specific research questions included the following:
What are the correlations of PECS outcomes with: child characteristics (i.e., chronological age, cognitive and adaptive skill level, matching abilities, autism symptom severity, and maladaptive behavior ratings) and treatment variables (i.e., treatment fidelity, frequency of PECS trials, duration of training, overall treatment intensity, number of pictures trained, number of situations in which PECS was trained, number of categories of reinforcers trained, stimulus generalization)? Are child characteristics and treatment variables individually and together significant predictors of PECS outcomes using logistic regression?
Based on prior PECS and IBI research, we predicted that a combination of child characteristics and treatment variables would account for some variance in communication outcomes. Further, these characteristics may be used to predict child PECS outcomes. Specifically, we expected that higher cognitive and adaptive skill level and matching abilities would be associated with improved PECS outcomes. In addition, we hypothesized that higher treatment fidelity, frequency of PECS trials, duration of training, number of pictures trained, number of situations in which PECS was trained, and number of categories of reinforcers trained would also be associated with improved PECS outcomes.
Method
Participants
Study participants were the same 22 children/youth who were involved in the companion study (Koudys et al., 2021). Participants included three girls and 19 boys and ranged in age from 2 years, 3 months to 15 years, 0 months (M = 6 years, 6 months; additional participant details are included in Table 1; Reprinted, as modified, from [2021]Koudys et al., 2021).
Descriptive statistics participant characteristics.

Note. n = number; M = mean; SD = standard deviation. Autism severity assessed by the Childhood Autism Rating Scale (CARS; Schopler et al., 1988); mental age assessed by the Stanford-Binet Intelligence Scales, Fifth Edition (Roid, 2003) or Mullen Scales of Early Learning (Mullen, 1995); Adaptive behavior assessed by the Vineland Adaptive Behavior Scales, Second Edition (Sparrow et al., 2005). Matching proficiency derived from nonverbal tasks on the Fluid Reasoning subtest of the Stanford-Binet (5th ed.; SB5). Reprinted, as modified, from Koudys et al. (2021).
These participants were recruited from a community organization serving people on the autism spectrum. All participants were previously diagnosed with autism or a related pervasive developmental disorder (e.g., autistic disorder, PDD-NOS which at the time of the study were the relevant diagnoses under the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision [DSM-IV-TR]; American Psychiatric Association, 2000) prior to the encapsulation of these diagnoses under autism spectrum disorder in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5; American Psychiatric Association, 2013). Diagnostic reports were reviewed for all but one participant. Scores on the Childhood Autism Rating Scale (CARS; see below) indicated that 17 (77.3%) of the children scored in the severe autism range, four (18.2%) in the mild/moderate range, and one (4.5%) in the nonautism range. This one child had a score of 28.5, a value typical of a diagnosis of PDD-NOS under the DSM-IV-TR (Perry et al., 2005). All children met diagnostic criteria for an intellectual disability. Cognitive scores were in the moderate range for five (22.7%), severe range for nine (40.9%) and profound range for eight (36.4%) children. Notably, 13 participants had previously been introduced to PECS. As all child participants had cognitive and language levels substantially below age expectations, including lack of, or limited, speech, parents provided written consent for their children to participate and for publication of their data.
Setting and materials
Research activities and PECS training were conducted in a therapeutic summer camp for children with ASD. Participants attended camp at local churches and participated in regular community outings, including visiting public pools, parks, bowling alleys, libraries, and the science center. During these activities, camp workers provided one-to-one support to children attending the camp. Prior to the start of camp, the camp workers received training on ASD, general behavioral teaching strategies, and safety procedures. Camp workers were encouraged to use behavioral teaching strategies to facilitate child participation in camp activities, to support general skill development, and to manage the occurrence of challenging behavior. Camp sessions ran 5 days a week for 6 h per day. The number of weeks each child attended camp varied from 2 to 7 weeks based on parent choice. Pre-assessments and post-assessments (described below) were also conducted at various locations associated with the camp. All participants were given a PECS binder that included pictures of their preferred items, activities, and locations (e.g., gym, balls, trampolines, scooters, water tables, sand tables, and trains).
Ethical approval for this research was granted through the university Research Ethics Board and the community agency. Ethics procedures and standards governing research involving human participants in Canada were met and the study was conducted in line with the principles of the Declaration of Helsinki.
Measures
Child Characteristics
To obtain standardized information about each participant, a full psychological assessment was conducted at Time 1 (T1) prior to summer camp, measuring cognitive and adaptive levels, as well as autism severity, using the measures listed below. Psychological assessments were conducted by doctoral level clinical psychology graduate students (the first and fourth authors) under the supervision of a doctoral-level licensed clinical psychologist (the second author). Further, information on the child's PECS phase was collected at T1 and T2 (i.e., after summer camp).
Stanford-Binet Intelligence Scales, Fifth Edition
The Stanford-Binet Intelligence Scales, Fifth Edition (SB5; Roid, 2003) is a standardized measure of intelligence designed for use with individuals between the ages of 2 and 85 years, which may be used in the diagnosis of developmental disabilities and exceptionalities (Roid & Pomplun, 2005). A full administration of the SB5 produces a composite score (Full Scale Intelligence Quotient), as well as composite scores for verbal IQ and nonverbal IQ. For this study, we used age equivalent scores of verbal, nonverbal, and overall mental age. We also utilized scores from nonverbal tasks on the Fluid Reasoning subtest to calculate a matching proficiency score. The SB5 has demonstrated excellent reliability and validity and the standardization sample included individuals diagnosed with intellectual and developmental disabilities (Janzen et al., 2004).
Mullen Scales of Early Learning
The Mullen Scales of Early Learning (MSEL; Mullen, 1995) is a measure of developmental functioning for children from birth to 5 years, 8 months. The Mullen assesses development in fine motor skills, visual reception, and receptive and expressive language. The composite score has strong internal and test–retest reliability (Mullen, 1995). Although designed to be appropriate for use with younger children, the Mullen is commonly used in clinical practice with autistic children as it is known that some may meet criteria for an intellectual or developmental disability (Sattler, 2002). Therefore, some children/youth may be unable to complete the items on age-appropriate standardized tests. For this study, we used age equivalent scores of verbal, nonverbal, and overall mental age.
Vineland Adaptive Behavior Scales, Second Edition (Vineland-II)
The Vineland-II (Sparrow et al., 2005) is a questionnaire designed to measure adaptive and maladaptive behavior in individuals between birth and 90 and appears to be a valid measure for use with individuals diagnosed with autism and/or cognitive impairments (Perry et al., 2009). Everyday skills and behaviors are assessed in four domains, including Communication, Daily Living Skills, Socialization, and Motor Skills (only applicable for children 6 years and under); further, it also provides a composite score. Maladaptive behavior is assessed for two areas: internalizing and externalizing and is not included in the Composite Score. For this study we used the Parent/Caregiver Rating Form. We reported the Composite Score, as well as the overall Maladaptive Behavior score.
Childhood Autism Rating Scale
Autism severity was measured using the CARS (Schopler et al., 1988). The CARS is a behavioral observation measure that relies primarily upon direct observation of the child. However, parent report may be used to assist in rating some scales (e.g., fear and nervousness), while semistructured interaction with the child is required to rate other items (e.g., imitation). The CARS is made up of 15 specific categories, which are rated by an observer on a seven-point scale. Scores are summed to obtain a total score (CARS total) with higher scores indicating a greater severity of autism symptoms. A score below 30 is considered to indicate the absence of autism; a score of 30 or greater the presence of autism, with 30 to 36.5 considered mild/moderate autism and 37 or greater, severe autism. Reports indicate excellent reliability and validity (Perry et al., 2005; Schopler et al., 1988). Prior to administering the CARS, the first and fourth authors were required to attend a one-day training on the CARS (based on the Perry et al., 2005 protocol) and achieve research reliability.
PECS Phase
To determine each participant's PECS skill level at T1 and T2, a PECS Phase Assessment was conducted. Prior to conducting the assessment, participants were offered a variety of items or activities believed to be preferred by the child (based on parent and/or camp worker report). Offered items/activities generally included toys (e.g., trains and puzzles), sensory activities (e.g., water play and light up toys), playground activities (e.g., swings and slides), interactive activities (e.g., chase and tickles), and drinks or snacks (e.g., crackers and juice). Items or activities reliably selected by the participant were used during the assessment. These items were made visible, but not accessible to participants. Each participant's pictures and/or PECS communication binder were easily accessible. PECS performance was systematically tested, without the use of prompts. The assessment continued until the participant demonstrated proficiency at one phase but not the next, or until all phases were assessed. Child PECS performance was recorded using a PECS Phase Checklist which was based on the checklists included in the Second Edition PECS Training Manual (Frost & Bondy, 2002). The first and fourth authors used a consensus approach to determine the specific PECS phase(s)––if any––that each participant performed independently. The accuracy of each participant's assessed PECS level was later confirmed by video review.
The result of this assessment, referred to as PECS outcome, was treated as a dichotomous variable (i.e., all participants who demonstrated mastery of PECS phases ≥ IIIb were categorized as high phase outcome and all participants who demonstrated mastery of PECS phases ≤ IIIa were categorized as low phase outcome). The PECS phases were categorized in this manner due to the particular skills required for each phase. Specifically, phases I and II do not require visual discrimination skills, and phase IIIa requires simple visual discrimination (i.e., between pictures of a preferred and nonpreferred item). Phase IIIb and above require complex visual discrimination (i.e., discrimination between pictures of two or more preferred items), and phases IV and above require complex visual discrimination within a sequential task (i.e., sentence construction).
Treatment Variables
The treatment period in this study refers to the time (M = 28.7 days, range: 14–34) children attended camp and were taught to use PECS. Several sources of data were collected during this time. Descriptive statistics for treatment variables are shown in Table 2.
Descriptive statistics treatment variables.
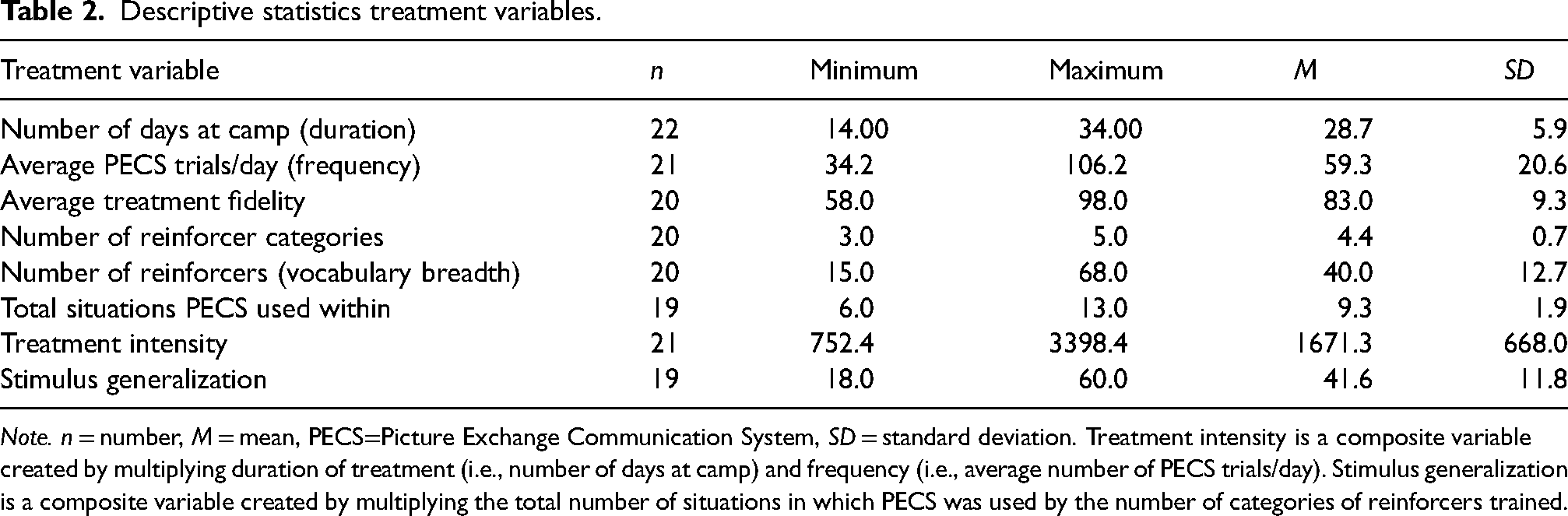
Note. n = number, M = mean, PECS=Picture Exchange Communication System, SD = standard deviation. Treatment intensity is a composite variable created by multiplying duration of treatment (i.e., number of days at camp) and frequency (i.e., average number of PECS trials/day). Stimulus generalization is a composite variable created by multiplying the total number of situations in which PECS was used by the number of categories of reinforcers trained.
PECS Treatment Fidelity
During the first and last weeks of camp, each camp worker's PECS treatment fidelity was assessed. Five PECS teaching trials were conducted for each camp worker–child dyad during regular camp activities. These trials were video recorded. Two graduate students collected data on the camp workers’ accuracy of PECS teaching from video using a PECS phase checklist developed for this study based on checklists created by Pyramid Educational Consultants (used with permission). To determine the percent accuracy of treatment fidelity, the number of teaching steps implemented correctly by the camp worker was divided by the total number of items on the checklist and multiplied by 100. Interobserver agreement (IOA) was calculated for a random selection of 25% of videos. An agreement was scored if both observers scored the step as correct or both as incorrect. IOA was calculated as the number of steps with agreement, divided by the total number of steps, multiplied by 100. IOA was 97% (range: 92%–100%). Given that many camp workers were asked to work with a different participant during camp, due to logistical and support purposes, fidelity was assessed with the worker who was most frequently working with the client during each timepoint. Therefore, the fidelity assessment associated with a particular child may have been conducted with a different camp worker at T1 and T2.
Daily PECS Use at Camp
Camp workers collected data during each camp activity, across the entire 6h day. To determine the number of PECS trials conducted per day, camp workers used tally counters to collect data on the frequency of independent exchanges (i.e., participant exchanged a picture without any assistance) and prompted exchanges (i.e., participant required assistance to exchange a picture). Data that could not be sensitively captured using tally counters were collected using phase-specific data sheets (e.g., accuracy of picture selection [phase IIIa/b], accuracy of sentence construction [phase IV]). To determine the total frequency of PECS trials conducted each day, the data from these two sources were totaled. These data sheets were also used to determine the number of days each participant attended camp (i.e., duration) and the number of days it took participants to master PECS phases (i.e., rate). To determine the nature and number of items/activities requested, and the number of reinforcer categories these were derived from (e.g., toys, food/drink, activities, places, and other), data were also collected on the number of different reinforcers requested daily. To determine the environments and activities PECS was used in, or the total situations in which PECS was used, data on these details were also captured on daily data logs. It was not feasible to conduct IOA for the daily data collected by camp workers. However, to enhance the reliability of the data, camp workers (a) participated in a data collection training that involved collecting data from video, (b) received individual coaching on data collection with a requirement to achieve acceptable levels of reliability (i.e., ≥ 80%), and (c) received regular supervision on their data collection accuracy from camp directors.
Using the data collected through direct observation, two composite variables, treatment intensity, and stimulus generalization, were calculated. Treatment intensity involved collapsing the variables frequency and duration, multiplying them to get one composite variable. Stimulus generalization was created by multiplying two critical facets of generalized behavior change (i.e., setting/situation generalization and response generalization; Cooper et al., 2019); specifically, the total number of situations in which PECS was used was multiplied by the number of categories of reinforcers trained (see Table 2).
Procedure
Psychological and Baseline (T1) Assessments
Assessments were completed for each child approximately 1 week prior to the start of camp. During the initial assessment, PECS Phase Assessment, cognitive testing (i.e., SB5 and MSEL) and measures of autism severity (i.e., CARS) were completed. In addition, several other tasks that assess children's understanding of pictures and objects were conducted as part of a companion study (McFee, 2011). While the child was participating in the assessment, parents completed the Vineland-II.
Camp Worker Training and PECS Intervention
After the T1 PECS Phase Assessment was complete, an individualized, phase-specific PECS program was developed for each participant (Supplemental Appendix A). The individualized program followed the prescribed teaching strategies designed by Frost and Bondy (2002). Each program included phase-specific PECS information and a copy of this program was given to each participant's assigned camp worker, the program director, and the participant's parents. Most camp workers were university or college students specializing in areas such as early education, psychology, kinesiology, and social work. They had limited experience working with children or youth on the autism spectrum. Some camp workers were professionals, including a speech language pathologist, occupational therapist, teacher, and an early interventionist. Prior to the start of camp, each camp worker attended a 1-week training on ASD, behavioral teaching strategies, and safety procedures, as well as a one-day PECS overview training and a 2h training on data collection for each phase of PECS. Each participant's assigned camp worker received one session of individualized coaching on their assigned participant's PECS program and was required to achieve ≥80% accuracy in teaching prior to working with their assigned participant.
PECS training took place across all camp activities using the protocol designed by Frost and Bondy (2002). Camp workers were encouraged to ensure children's PECS binders were readily available and to create communication opportunities using different reinforcers, within different settings and activities. Consistent with the established practices of the summer camp, the mastery criterion for each phase of PECS was 80% independent PECS exchanges over 3 days. To support fidelity in PECS training, accuracy in data collection, and to monitor child progress, camp workers and child participants were regularly observed by camp directors.
Outcome (T2) Assessments
At T2, the PECS Phase Assessment was readministered. Camp workers were observed implementing PECS with their assigned participant and teaching fidelity was reassessed. All postassessments were conducted on-site at the summer camp within regular camp activities.
Results
Research Question 1: What are the Correlations of PECS Outcomes With Child Characteristics and Treatment Variables?
Correlations among child characteristics are presented in Table 3 and among treatment variables in Table 4.
Correlations among child characteristics.

Note. CARS=Childhood Autism Rating Scale; MA = mental age; PECS=Picture Exchange Communication System; SB5 = Stanford-Binet (5th ed.).
*p < 0.05, **p < 0.01.
Correlations among treatment variables.
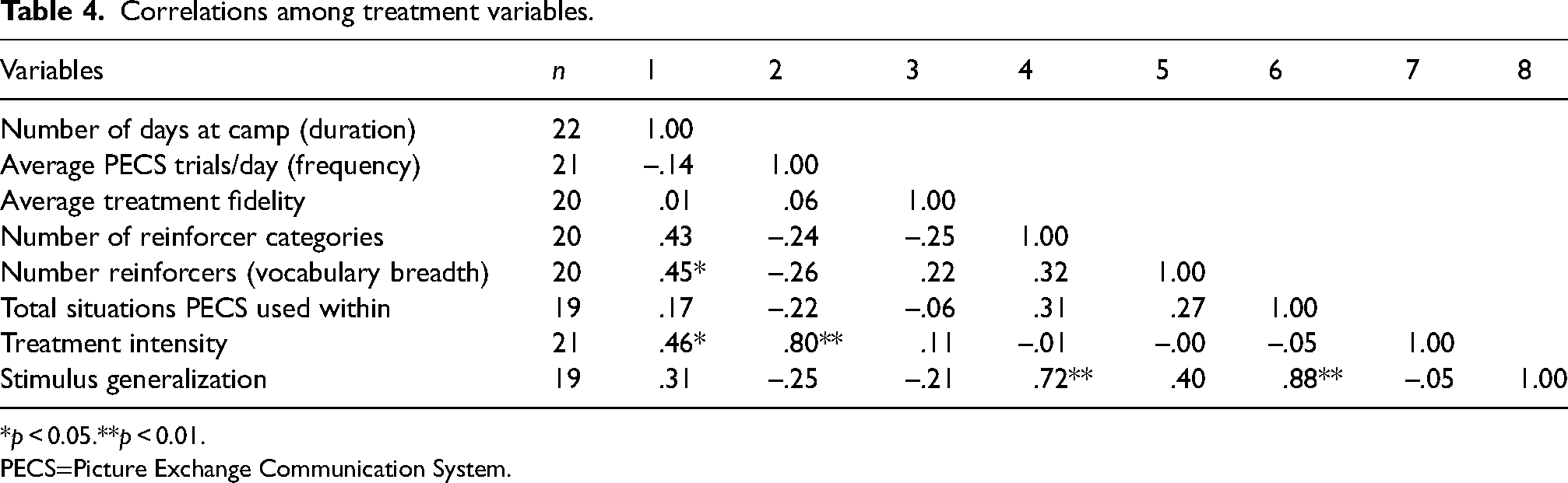
*p < 0.05.**p < 0.01.
PECS=Picture Exchange Communication System.
Correlations between child characteristics and treatment variables are presented in Table 5. Results reveal moderate and significant correlations between adaptive behavior; overall, nonverbal, and verbal mental age; and the number of reinforcer categories, as well as the composite variable of stimulus generalization. These correlations suggest that participants with higher adaptive and cognitive skill levels received training in the use of PECS across a broader range of reinforcer categories, while participants with lower adaptive and cognitive skill levels received training across a narrower range of reinforcer categories. Age, autism severity, matching skills, and PECS phase mastery at T1 were not significantly associated with either variable. Interestingly, a moderate significant negative correlation was found between ratings of maladaptive behavior on the Vineland-II and the frequency of PECS trials per day. These results suggest that children who demonstrated more maladaptive behavior received fewer PECS training trials per day or vice versa.
Correlations among child characteristics and treatment variables.

Note. MA = mental age; PECS=Picture Exchange Communication System.
*p < 0.05. **p < 0.01.
Child Characteristics Associated With Outcome Variation
The relationships of PECS outcomes to child characteristics and treatment variables were further explored using independent t-tests comparing two subgroups of children, those with low- and high-phase outcomes.
Results are shown in Table 6 and reveal that participants who achieved high or low phases of PECS did not differ significantly in chronological age, autism severity, or parental ratings of maladaptive behavior. However, participants with higher cognitive and adaptive skill level, and matching abilities, were more likely to achieve higher PECS phases. Large effect sizes, ranging from 1.04 to 1.51, were found for these comparisons. Not surprisingly, significant differences were also found between high- and low-phase groups in terms of initial PECS phase, suggesting that participants who began the study at a higher PECS phase were more likely to achieve a higher PECS phase by the end of camp, t(19) = −3.04, p = .007, d = 1.42.
Comparison of child characteristics associated with high and low phase PECS outcomes.

Note. ≤ Phase IIIa n = 9, ≥Phase IIIb n = 12. MA = mental age. CARS=Childhood Autism Rating Scale; PECS=Picture Exchange Communication System; SB5 = Stanford-Binet (5th ed.).
Treatment Variables Associated With Outcome Variation
Similar comparisons were conducted for high versus low PECS phase outcome in relation to treatment variables, as displayed in Table 7. No significant differences were found in terms of treatment fidelity, frequency of PECS trials, duration of training, number of pictures trained, or overall treatment intensity. However, significant differences between the two groups were found for the number of situations in which PECS was trained, t(16) = −3.27, p = .005, d = 1.56. A difference approaching significance (but with a large effect size) was also found in terms of the number of categories of reinforcers trained, t(17) = −2.01, p = .060, d = 0.89. As expected, significant differences were also found between the two outcome groups for the composite variable stimulus generalization, t(16) = −3.35, p = .005, d = 1.61. Together, these results suggest that participants who achieved higher phases of PECS were more likely to have been trained to use PECS in a broader number of training environments and to request reinforcers from different categories.
Comparison of treatment variables associated with high and low phase PECS outcomes.

Note. ≤ Phase IIIa n = 9, ≥Phase IIIb n = 12; PECS=Picture Exchange Communication System.
Research Question 2: Are Child Characteristics and Treatment Variables Significant Predictors of PECS Outcomes?
Sequential logistic regressions were run to determine the combination of variables that would lead to the best prediction of PECS outcome. It was necessary to limit the number of variables entered into the model due to the small number of participants. For this reason, we separately explored how child characteristics contributed to PECS outcomes and how treatment variables contributed to PECS outcomes—while controlling for initial PECS phase.
Child Characteristics as Outcome Predictors
The variables included in the model were based on the results of the previous analyses (i.e., mental age and initial PECS phase) and literature (i.e., CARS). We entered initial PECS phase at step 1, mental age at step 2, and CARS at step 3 (Table 8).
Prediction of PECS phase outcome from selected child characteristics while controlling for initial PECS phase.

Note. CARS=Childhood Autism Rating Scale; MA = mental age; PECS=Picture Exchange Communication System; SB5 = Stanford-Binet (5th ed.).
The most accurate prediction resulted from the model that included initial PECS phase and mental age. This model predicted low PECS phase achievement with 88.9% accuracy and high PECS phase achievement with 91.7% accuracy. Overall prediction was 90.5%, reflecting a 20% improvement in classification over a model with only the constant and initial PECS phase. The odds ratio for the model with the best classification (i.e., initial PECS phase plus mental age) indicates that with each additional PECS phase mastered at T1 children were approximately ten times more likely to be within the high PECS phase group at T2, Exp(B) = 9.70. Further, if mental age increases by 1 month, the odds of achieving a higher PECS phase increases by a factor of 1.71. Although the R2 should be interpreted with caution for logistical regressions, the model accounts for approximately 60% of the total variance in outcomes. However, the addition of the CARS at step 3 did not improve the predictive power of the model and, in fact, decreased the accuracy of predicting the children in the high PECS phase group at T2.
Treatment Variables as Outcome Predictors
The variables included in the model were based on the results of the previous analyses (i.e., initial PECS phase and generalization factors) and literature (i.e., treatment intensity). Initial PECS phase was entered at step 1, treatment intensity at step 2, and stimulus generalization at step 3 (see Table 9).
Prediction of PECS phase outcome from selected treatment variables while controlling for initial PECS phase.

Note. PECS=Picture Exchange Communication System.
The model with initial PECS phase and treatment intensity was found to have good model fit, χ2 (2, n = 18) = 8.55, p = .014. The addition of stimulus generalization improved fit, χ2 (3, n = 18) = 17.81, p < .001. Prediction for the model which included both treatment variables was strongest, approaching 90% accuracy overall (87.5% for low PECS phase achievement, 90.0% for high PECS phase achievement).
An examination of odds ratios for the model with the best classification (i.e., initial PECS phase plus treatment intensity plus stimulus generalization) indicates that, with each additional PECS phase mastered at T1, children were approximately eight times more likely to achieve higher PECS phase outcomes at T2, Exp(B) = 7.74. Further, for each point increase in stimulus generalization, the odds of achieving a higher PECS phase increases by a factor of 1.49. Interestingly, the odds ratio for treatment intensity, that is, Exp(B) = 1.00, suggests that changes in treatment intensity have minimal impact on PECS phase outcome. Again, although the R2 should be interpreted with caution for logistical regressions, the model accounts for approximately 63% of the total variance in outcomes.
Child Characteristics and Treatment Variables as Outcome Predictors
Although it would have been ideal to explore both child characteristics and treatment variables as predictors, while controlling for initial PECS phase, power limitations precluded this investigation. Instead, we included child characteristics and treatment variables based on the findings of the previous analyses, without controlling for initial PECS phase. Mental age was entered at step 1, treatment intensity at step 2, and stimulus generalization at step 3 (Table 10).
Prediction of PECS phase outcome from selected child characteristics and treatment variables without controlling for initial pecs phase.

Note. PECS=Picture Exchange Communication System; MA = mental age.
The most accurate prediction occurred in the model with all three variables (i.e., mental age, treatment intensity, and stimulus generalization) and the overall prediction was 88.9%. Low and high PECS phase outcome were predicted with 87.5% and 90.0% accuracy, respectively. An examination of odds ratios for the model including all three variables indicates that, with each one month increase in mental age, the odds of children achieving a higher phase of PECS increases by a factor of 1.39. Similarly, a one-unit increase in stimulus generalization increases the odds of achieving a higher PECS phase by a factor of 1.22. Again, the odds ratio for treatment intensity, that is, Exp(B) = 1.00, suggests that changes in treatment intensity have minimal impact on PECS phase outcome. R2 indicates that, taken together, the variables of mental age, treatment intensity, and stimulus generalization account for approximately 58% of variation in PECS outcomes.
Discussion
The present study explored the associations between child characteristics, treatment variables, and PECS outcomes. Further, the use of child and treatment variables to predict PECS outcomes was also explored. Participants who achieved higher phases of PECS (phase IIIb or above) differed significantly from those who mastered lower PECS phases (phase IIIa or below) in terms of mental age (overall, verbal, and nonverbal), matching abilities, and adaptive behavior level. These results are consistent with earlier research in behavioral interventions with children with ASD (Eldevik et al., 2009; Perry et al., 2011; Sallows & Graupner, 2005). It is important to note, however, that although participants were more likely to achieve higher phases of PECS if they had a higher mental age, adaptive skill level, and matching skills, the average scores for these measures (even in the high PECS phase group) were well below those expected for same age peers. These results indicate that PECS is appropriate for use with children with clinically significant deficits in cognitive and/or adaptive abilities.
Perhaps more surprisingly, no significant differences were found between the two PECS outcome groups on factors such as autism severity and parental ratings of maladaptive behavior. In terms of autism ratings, both groups’ mean scores were within the severe range. These results suggest that even children who demonstrate more severe symptoms of autism and those who exhibit more challenging behavior can achieve higher phases of PECS. This is an important finding given the established connection between the acquisition of a functional communication system and the prevention or reduction in maladaptive behavior (Koudys et al., 2021; Tiger et al., 2008).
Finally, some children in the study had some previous experience with PECS and initial PECS phase (i.e., PECS phase at T1) was significantly associated with differences in PECS outcomes at T2. This means that participants who started camp at a higher phase were more likely to be using PECS at a higher phase at the end of camp. Although these results are unremarkable on their own, they are important in guiding our interpretation of other findings. Specifically, when exploring the impact of treatment variables on PECS outcomes, duration of treatment (i.e., number of days at camp) was found not to be related to differences in outcome. Although it is not possible to separate the possible child characteristics associated with prior PECS gains, it could be reasoned that those children starting camp as experienced PECS users were exposed to PECS training for a longer duration, and they may have differed in other unknown ways (e.g., parent motivation). Given the possible overlap between these factors, caution should be taken when interpreting results that suggest minimal impact of treatment duration on PECS outcomes. Indeed, it is possible that increased intervention duration and opportunity may lead to increased PECS phase acquisition.
In the current study, only one treatment factor was found to be associated with significant differences in PECS outcome: total situations in which PECS was trained. However, it is important to note that another treatment factor, number of categories of reinforcers trained, was approaching significance. When these two variables were combined to create a composite variable termed “stimulus generalization”, a very large effect size was found, suggesting that the combination of these treatment factors may be associated with significant variations in outcome. There was also an association approaching significance between variations in PECS outcomes and the number of categories of reinforcers trained (e.g., food, toys, and activities), but not between PECS outcomes and the overall number of reinforcers trained. This suggests that diversity of reinforcers trained may contribute uniquely to PECS outcomes. However, more information is required on the impact of these variables, as multiple child and intervention factors may affect the relationship, such as the child's interest in a variety of toys, activities, and other putative reinforcers. Surprisingly, frequency of trials, a factor associated with treatment intensity or quantity, was not found to be associated with significant variation in outcome. However, it is important to note that the average frequency of PECS trials was 60, which is above the recommended number of trials per day (i.e., 40; Frost & Bondy, 2002). Therefore, these results should be interpreted cautiously as a minimum number of PECS teaching trials may be necessary to effect positive outcomes. Overall, results of the present study suggest that PECS training should incorporate facets of generalization training such as teaching across multiple environments and reinforcers to promote generalized PECS use (Frost & Bondy, 2002).
With the demonstrated importance of fidelity on treatment gains in the IBI literature (e.g., Långh et al., 2017), it was surprising that treatment fidelity was not associated with significant differences in PECS outcome. However, given the high degree of fidelity demonstrated by nearly all direct staff, results may reflect a lack of variation in teaching fidelity. Therefore, it is unknown how more significant deviations from the intervention protocol may have impacted PECS outcomes. Alternatively, as the psychometric properties of the checklists are unknown, it is possible that they do not sensitively capture the teaching components with the most significant impact on PECS outcomes. More research should be conducted to explore the nature and number of deviations from protocol that can occur without negatively impacting PECS outcomes.
Results of logistic regression models that controlled for initial PECS phase while separately exploring child characteristics and treatment variables as predictors of outcome suggest that PECS outcomes can be predicted with good accuracy. Specifically, a model that controlled for initial PECS phase, and then explored the addition of mental age as a predictor accurately classified 90.5% of cases. Another model that controlled for initial PECS phase, and then explored the addition of treatment intensity and stimulus generalization, classified outcomes with approximately 89% accuracy. Both models provide impressive classification, and account for a considerable amount of outcome variance, providing support for the original hypothesis that child characteristics and treatment variables together impact outcome. As such, a third model was explored, which included both child and treatment factors. This final model, containing mental age, treatment intensity, and stimulus generalization provides comparable classification (89%). Although this final model does not control for initial PECS phase (because of statistical limitations), and as such must be interpreted with caution, it provides a preliminary model for predicting PECS outcomes. Results suggests that a small number of child characteristics and treatment variables, together, may account for a considerable amount of variation in outcome and can be used to predict outcome with substantial accuracy. It is important to note that there are significant correlations between child characteristics and treatment variables (i.e., mental age and stimulus generalization). Further, neither variable is an independent predictor. Therefore, in the current research it is not possible to isolate the individual contributions of each of these variables. However, it does appear that these variables, together, may contribute in important ways to PECS outcomes. Of course, independent replication of these findings is needed.
Limitations and Future Directions
As is expected in any clinical study, there are several limitations which must be considered when interpreting the findings. As thoroughly discussed in Koudys et al. (2021), the study did include a small sample that may not be representative despite best efforts during the recruitment process. The sample size limits the statistical power for analysis, meaning we may not have been able to detect some differences or effects that would have emerged in a larger sample (possible for treatment intensity, for example). Although attempts were made to monitor treatment fidelity to evaluate its impact on child outcomes, data were only collected at two time points and these assessments were conducted with the assigned camp worker at the time; results should be interpreted in the context of this limitation.
The results of a preliminary analysis of the child characteristics and treatment variables associated with outcome variation in a relatively homogenous sample of children and adolescents are presented in this study. However, PECS is currently used with a diverse array of individuals, across age ranges and diagnostic categories. Future studies should explore the use of PECS with diverse populations, including those with varying cognitive, adaptive and language abilities, those with various co-occurring diagnoses, and those with physical limitations. Studies that explicitly explore the impact of PECS training within these different populations may help identify whether, and to what extent, similar child characteristics and treatment variables account for outcome variations. In addition, studies exploring PECS use within diverse populations and settings should examine the possible interactions, or transactional relationships, between child characteristics and treatment variables.
Finally, more research needs to be conducted to accurately identify the treatment variables associated with best outcomes. This study suggests that generalization factors are highly associated with improved outcomes, while intensity appeared to have negligible influence. Yet higher initial PECS phase, which is ostensibly linked to length of treatment, was associated with improved PECS outcomes. Further, research from other behavioral and educational interventions suggests that number of teaching trials and duration of treatment are important treatment variables (e.g., Granpeesheh et al., 2009; Luiselli et al., 2000). Future studies should explore these characteristics in greater detail, including the impact of broader ranges of treatment intensity, such as short or long periods of intervention and few or many trials per day, on both rate of acquisition and overall communication gains.
Conclusion and Clinical Implications
An important goal of this research was to understand factors associated with variations in PECS outcomes, to provide more accurate outcome expectations for families, and to guide PECS teaching procedures. Although more research needs to be conducted with a larger sample, results from the current study suggest that children with relatively higher cognitive and adaptive skill levels are more likely to achieve higher phases of PECS. However, it is important to emphasize that even children with substantial impairments in cognitive and adaptive skills were able to learn to use PECS effectively, suggesting that even those with significant limitations in these domains benefitted from the intervention. Importantly, autism severity and parent ratings of maladaptive behavior were not associated with variations in outcome, suggesting that even children demonstrating more severe symptoms of autism and maladaptive behavior can acquire communication skills through PECS. The clinical implications of these results should not be underestimated.
Very large effect sizes were found for the impact of stimulus generalization factors on PECS outcome; specifically, children who mastered higher phases of PECS were more likely to have received training in the use of PECS across a variety of situations, using reinforcers from different categories. These results suggest that PECS training should focus on generalization factors from the beginning, emphasizing the use of PECS across reinforcer categories and across environments/activities.
Supplemental Material
sj-docx-1-dli-10.1177_23969415231221516 - Supplemental material for Predictors of Picture Exchange Communication System (PECS) outcomes
Supplemental material, sj-docx-1-dli-10.1177_23969415231221516 for Predictors of Picture Exchange Communication System (PECS) outcomes by Julie Koudys, Adrienne Perry, Carly Magnacca and Kristen McFee in Autism & Developmental Language Impairments
Footnotes
Declaration of Conflicting Interests
Authors 2, 3 and 4 have no conflicting/competing interests. Author 1 was a consultant to Pyramid Educational Consultants of Canada, Inc., a company that may be affected by the research reported in the enclosed paper, at the time this study was conducted. No compensation for this research was provided by Pyramid Educational Consultants of Canada, Inc. Rigorous protocols were put in place to manage any potential conflicts arising from this arrangement.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.