
Abstract
Background and Aims
Individuals with fragile X syndrome (FXS) characteristically struggle with language and communication throughout the life course, but there is limited research on the development of communication before 24 months. The purpose of this study is to describe the early communication of infants and toddlers with FXS using the Communication and Symbolic Behavior Scales-Caregiver Questionnaire (CSBS-CQ), a standardized communication screening measure, as compared to the reported normative data of the CSBS-CQ and identify the percentage of infants and toddlers who scored within the range of concern. Documenting how children with FXS perform on screening measures can provide a quick snapshot of skills to help clinicians determine the need for services.
Methods
Participants were 22 infants and toddlers with FXS between 6 and 29 months. Performance on the CSBS-CQ was compared to the measure's normative data. The CSBS-CQ was completed by mothers, and children were administered the Mullen Scales of Early Learning. Because co-occurring autism is common in FXS, the presence of autism was determined using a clinical best estimate procedure.
Results
Overall and within the domains and subdomains of the CSBS-CQ, infants and toddlers with FXS had significantly lower scores than the normative data. Further, 68.2% of our sample was in the range of concern for their overall communication score. The presence of autism led to consistently lower scores, and more infants and toddlers with FXS + autism scored within the range of concern.
Conclusions
Our findings suggest that delays in early communication are evident in comparison to typically developing norms before 24 months. These findings also emphasize that infants and toddlers with FXS would likely benefit from early language intervention given that 68.2% of our sample was in the range of concern for their overall communication score.
Implications
Early identification and developmental monitoring of children with FXS will help to determine concerns in communication and other domains of development. While early communication broadly may not be an early indicator of autism in FXS, some specific skills, such as eye gaze, may serve as such an indicator. Screening measures, like the CSBS-CQ, may help monitor both early communication impairments and autism symptoms. Infants and toddlers with FXS, regardless of autism status, will benefit from early language interventions.
Keywords
Introduction
Individuals with fragile X syndrome (FXS) characteristically struggle with language and communication throughout the life course (Abbeduto et al., 2007; Finestack et al., 2009; Roberts et al., 2001). The available studies of communication in young children with FXS suggest that delays in communication can be traced to deficits in prelinguistic communication skills (e.g., Flenthrope & Brady, 2010; Roberts et al., 2002), but there is limited research on the development of communication before 24 months. The purpose of the present study was to comprehensively describe the early communication of infants and toddlers with FXS – including social communication, speech communication, and symbolic communication – using the Communication and Symbolic Behavior Scales-Caregiver Questionnaire (CSBS-CQ; Wetherby & Prizant, 2003) as compared to the measure's normative data. Documenting how children with FXS perform on screening measures like the CSBS-CQ can provide a quick snapshot of skills to help clinicians determine the need for services.
Early communication in FXS
FXS is the leading inherited cause of intellectual disability and is caused by a mutation of the FMR1 gene on the X chromosome. This mutation leads to an expansion of CGG trinucleotide repeats to greater than 200 (Santoro et al., 2012), which impacts cognition (Kover et al., 2013; Roberts, McCary, et al., 2016). Because FXS is an X-linked genetic disorder, FXS is more common in males, and males are more severely affected than females. Further, co-occurring autism is present in 25–74% of individuals with FXS (McCary & Roberts, 2013). Together, these factors impact communication development in FXS.
Recent research of early communication in FXS focused on examining the different forms of early communication skills—such as eye gaze, gestures, and vocalizations—in FXS before 24 months (Hahn et al., 2017; Hughes et al., 2019; Marschik et al., 2014; Rague et al., 2018). Consistently, these studies have demonstrated impairments in gestures, communicative functions, and spoken language as compared to typically developing infants and infant siblings of children with autism (Hahn et al., 2017; Hinton et al., 2013; Hughes et al., 2019; Kover et al., 2015; Marschik et al., 2014; Rague et al., 2018). These studies have used a variety of behavioral coding approaches (e.g., gestures, potentially communicative behaviors) or parts of caregiver questionnaires (e.g., gesture items on the MacArthur-Bates Communicative Development Inventories-Words and Gestures [Fenson et al., 2006]). To date, no research has characterized early communication profiles comprehensively using the same tool to assess social communication, speech, and symbolic behaviors and report on all aspects of the tool. Documenting how children with FXS perform on comprehensive screening measures, like the CSBS-CQ, can provide a quick snapshot of skills to help clinicians determine the need for services. However, it is important to note that one study of early communication did use the CSBS-CQ longitudinally from 9 to 24 months in 13 infants and toddlers with FXS (Kover et al., 2015), but only provided data on the overall communication abilities of the sample (i.e., Total Communication score). There was no reference group for these CSBS-CQ data in this study despite a comparison group of children with typical development for other measures in the study. Total Communication raw scores for this sample increased from 9 to 24 months, while standard scores decreased, suggesting delays. Although findings from this study are consistent with other studies indicating that early communication in FXS is delayed, especially in relation to age-based standard scores, it is unclear from this study how infants and toddlers with FXS are performing within the more fine-grained domains of communication captured by the CSBS-CQ: social communication, speech communication, and symbolic communication. Below, we review the existing literature on these three primary early communication domains in FXS.
Social communication
The CSBS-CQ captures three aspects of social communication— 1) eye gaze and emotion, 2) gesture use, and 3) communicative functions (i.e., joint attention, behavior regulation; referred to as communication on the CSBS-CQ; Wetherby & Prizant, 2003).
Speech communication
The CSBS-CQ separates speech communication into sounds and words (Wetherby & Prizant, 2003). Therefore, this domain accounts not only for spoken words but also the pre-symbolic forms of spoken communication (e.g., vocalizations and babbling). Research on early vocalizations, including babbling, in FXS is just starting to emerge. This research indicates that although infants and young children with FXS do incorporate vocalizations into their communicative acts (Hahn et al., 2017), they vocalize less (e.g., lower rate of canonical babbling, fewer syllable productions) and engage in fewer conversational turns than typically developing peers (Belardi et al., 2017; Reisinger et al., 2019). However, Hamrick et al. (2019) found no differences in the average amount of vocalizations coded during a standardized communication interaction with an examiner between 22 9-month-olds with FXS and 17 9-month-olds with typical development who were at a low risk for autism. Thus, it is possible that after 9 months, infants and toddlers with FXS do not keep pace with their peers leading to reduced vocalizations, but more research is needed to elucidate the developmental course of vocalizations and babbling in FXS.
Only one study has explored the relationship between early vocalizations and the presence of autism in FXS, despite emerging evidence for this association in children with nonsyndromic autism. Consistent with findings in children with nonsyndromic autism (Fusaroli et al., 2017), infants with FXS who had higher pitch vocalizations (i.e., atypical pitch) at 9-months had more autism symptoms at 24 months (Hamrick et al., 2019). Despite the limited research on vocalizations in infants and toddlers with FXS, vocalizations and babbling support the development of spoken language (i.e., first words) and continue to support communication throughout the life course in typically developing children and children with other neurodevelopmental disorders. Thus, a similar pattern is likely in FXS.
Only one study, to date, has focused on identifying the age of first words in FXS, and indicated that the age of first words in FXS is delayed (mean age 26 months, range of first words 10–45 months; Hinton et al., 2013). This is not surprising given that expressive language skills more broadly are also delayed in FXS (7.5–14.5 months) (Finestack et al., 2013; Roberts et al., 2002, 2007). Similarly, Hahn et al. (2017) noted that no infants with FXS (7.5-14.5 months) in their study produced a spoken word during a 15-to-20 min communication interaction. Beyond this, it is not clear when children with FXS begin to combine words and use phrases. Nonetheless, expressive language skills do increase over time Brady et al., 2020) with many individuals with FXS using spoken language. In a study of boys with FXS between 21 and 77 months (Roberts et al., 2007), performance on verbal and vocal communication domains (e.g., use of vocalizations, different words, and word combinations) were higher than performance on gestural communication, reciprocity (responding to communicative acts, repair strategies), and symbolic communication (e.g., language comprehension, constructive play) during the direct administration of the CSBS-Behavior Sample (Wetherby & Prizant, 2003). Due to the wide age range in this study, there was substantial variability in individual scores and the findings should be interpreted with caution.
Studies of young children with FXS suggest that those with FXS + autism have greater impairments in expressive language than those with FXS only (Philofsky et al., 2004). In contrast, studies of expressive vocabulary and grammar in older children and adolescents have not found significant differences between those with FXS + autism and those with FXS only (Lewis et al., 2006; McDuffie et al., 2010, 2012). It is possible that early in development the differences in expressive language between those with autism and those without are more apparent and as they age these skills become more similar.
Symbolic communication
Symbolic communication involves comprehension and receptive language (Wetherby & Prizant, 2003). These skills are important for word learning and support the use of augmentative and alternative communication to augment spoken language delays for this population (Barker et al., 2019; Dada et al., 2021). In addition to examining language understanding, the CSBS-CQ also examines object use (i.e., how children use, play, and interact with objects in the environment) as part of this domain.
Broadly, research on comprehension indicates that while overall receptive language skills are delayed for children with FXS (Finestack et al., 2013; Roberts, et al., 2007), they do show increases in receptive language abilities over time (Brady et al., 2020). Like expressive language abilities, studies of children and adolescents have not found significant differences between those with FXS + autism and those with FXS only (McDuffie et al., 2010). However, when autism features are measured continuously (i.e., a severity score) instead of categorically (e.g., diagnosis vs. no diagnosis), a negative association has emerged indicating those with more autism features have lower receptive language abilities (McDuffie et al., 2012; Thurman et al., 2017). Despite the difficulties with both receptive and expressive language, limited research has been conducted on word learning in FXS (McDuffie et al., 2013; Benjamin et al., 2015; Thurman et al., 2017).
Object use by infants and toddlers sets the stage for word learning to occur (Pruden et al., 2006). That is, as infants use eye gaze, vocalizations, and gestures to communicate about an object of interest, their communication partners can interpret these communication acts and provide the object label (Brady & Hahn, 2017). For example, if an infant vocalizes and holds up a stuffed bear (i.e., the object) to show it to their communication partner, the communication partner may respond, “Bear! You want the bear?,” linking the word “bear” to the referent (the stuffed bear or object). Delays in object use during play has been noted in children with FXS (Largo & Schinzel, 1985; McDuffie et al., 2015). Consistent with studies on typically developing children (LeBarton & Iverson, 2013; Oakes & Madole, 2000), object interest in preschoolers with FXS was positively related to receptive and expressive language abilities (McDuffie et al., 2015). Research on school-aged children with FXS indicates that they can learn new words and that word learning is more successful when a direct link is made between the label and the object through adult pointing or showing (Benjamin et al., 2015; McDuffie et al., 2013; Thurman et al., 2017).
Explorations of the role of autism features on word learning have yielded non-significant findings about children with FXS in their ability to learn words. This stands in contrast to research indicating negative associations between object interest and autism features in FXS (McDuffie et al., 2015), which mirrors research on individuals with nonsyndromic autism (Ozonoff et al., 2008). It is important to note that the studies of word learning in FXS have focused on school-age children who were able to complete an experimental fast mapping task. As noted in these studies, the samples may not be representative of the broader FXS population, including those with co-occurring autism, due to the inclusion criteria for these studies (i.e., had to use speech as their primary mode of communication, used at least 10 different spontaneous words in the past month, and could respond to simple one-step instructions; Benjamin et al., 2015; McDuffie et al., 2013; Thurman et al., 2017). Therefore, it is unclear how early word learning is related to co-occurring autism in toddlers with FXS.
Present study
The purpose of this study is to describe the early communication of infants and toddlers with FXS using the CSBS-CQ. Specifically, we sought to examine early communication comprehensively and to understand how infants and toddlers compare to normative mean on early communication. The following research question was posed:
What is the pattern of early communication on the CSBS-CQ overall and within each communication domain—Social, Speech, Symbolic—and subdomain—Emotion & Eye Gaze, Gestures, Communication, Words, Sounds, Understanding, Object Use—in infants and toddlers with FXS as compared to the normative mean?
What percentage of infants and toddlers with FXS are in the “range of concern” on the CSBS-CQ overall and within each communication domain—Social, Speech, Symbolic—and subdomain—Emotion & Eye Gaze, Gestures, Communication, Words, Sounds, Understanding, Object Use? When compared to the normative mean, how does a diagnosis of autism impact the pattern of early communication observed on the CSBS-CQ of infants and toddlers with FXS?
Do infants and toddlers with FXS who are later diagnosed with autism (FXS + autism) differ from those who are not diagnosed with autism (FXS Only) on the CSBS-CQ?
Methods
Participants
Participants were 22 infants and toddlers with FXS (13 males, 9 females; see Table 1 for demographic information) recruited from across the United States as part of a longitudinal study on the emergence and stability of autism in FXS (Roberts, Tonnsen, et al., 2016b; Roberts et al., 2020 for details on the larger study). English was the primary language spoken in the home. As part of the larger study, participants were assessed at standardized intervals—6, 9, 12, 18, 24, and 36 months. However, the CSBS-CQ was added to the battery after some participants had already entered the study, which is why the sample presented in this study is smaller than the larger study. Further, few participants completed the CSBS-CQ multiple times; thus, this study presents data from each participant’s only or first timepoint that the CSBS-CQ was completed.
Participant characteristics for the full study sample (n = 22).

Note. aFor those with multiple time points, the 1st time point was used.
The ADOS-2 was administered at 36, except for two participants had their ADOS-2 at 48 months and one who had their ADOS-2 at 60 months.
Measures
Communication and symbolic behavior scales - caregiver questionnaire (CSBS-CQ)
The CSBS-CQ is a 41-item norm-referenced caregiver report questionnaire that examines communicative competence in children whose functional communication is between 6 and 24 months and whose chronological age is between 6 months and 6 years (Wetherby & Prizant, 2003). The CSBS-CQ has three domains (Social; Speech; Symbolic) and six subdomains, which are combined to create a Total Communication Composite score. For all scores on the CSBS-CQ, higher scores represent greater ability. The Social domain encompasses communication skills like eye gaze, emotions, and gesture use (i.e., social communication). The Speech domain focuses on sounds and words (i.e., spoken/expressive language), and the Symbolic domain focuses on understanding and object use (i.e., comprehension/receptive language). In our study, standard scores were used and compared to the normative mean (Total Communication normative mean = 100, SD = 15; domain and subdomain normative mean = 10, SD = 3). In addition, we examined the range of concern on the CSBS-CQ. For the Total Communication Composite, domain, and subdomain scores, a criterion level for the range of concern has been established based on performance of at least 1.25 standard deviations below the normative mean. Thus, the range of concern for the Total Communication Composite are standard scores of 81 or less and the range of concern for domains and subdomains are standard scores of 6 or less. The CSBS-CQ has well-established reliability and validity (Wetherby & Prizant, 2003).
Mullen scales of early learning
The Mullen Scales of Early Learning (MSEL) is a standardized, observational measure of cognitive abilities and motor skills for children ages birth to 68 months (Mullen, 1995). The MSEL has five domains—Gross Motor, Fine Motor, Visual Reception, Expressive Language, and Receptive Language—that are combined to create an overall composite, the Early Learning Composite. All domains have a mean T-score of 50 with a standard deviation of 10. The MSEL has well-established validity and reliability (Mullen, 1995). An overall nonverbal cognitive ability composite can be created by averaging the Visual Reception and Fine Motor T-scores (Munson et al., 2008). This nonverbal cognitive score was used instead of an overall cognitive score to help control for the influence of language on the Early Learning Composite (Hahn et al., 2017; Munson et al., 2008; Rague et al., 2018).
Clinical best estimate of autism
A clinical best estimate (CBE) procedure was developed from the CBE procedures of Lord and colleagues (Lord et al., 2006; Lord, Petkova, et al., 2012) to determine autism diagnosis based on a review of the Autism Diagnostic Observation Schedule - 2nd edition (ADOS-2; Lord, Rutter, et al., 2012), MSEL, and the Vineland Adaptive Behavior Scales (Sparrow et al., 2005) combined with clinical expertise in autism (see Hogan et al., 2017). The CBE was conducted by a team, including a licensed psychologist, who were all research reliable on the ADOS-2 (Hogan et al., 2017; Roberts et al., 2020). Based on the available data and the team's clinical expertise, diagnoses of (1) no autism, (2) subthreshold autism, and (3) autism were determined (see Roberts et al., 2020 for a full description of CBE procedures). CBE diagnoses were used to identify those with and without autism in our sample. The results of the CBE indicated that 11 children with FXS did not have autism, 10 children with FXS did have autism, and 1 child with FXS had subthreshold autism (who was ultimately included in the co-occurring autism group).
Procedure
As part of a larger assessment battery (see Roberts, Tonnsen et al., 2016; Roberts et al., 2020 for details), mothers completed the CSBS-CQ (Wetherby & Prizant, 2003), and trained research assistants administered the MSEL to children at each assessment. The ADOS-2 was also administered to children at 36-months. However, three children did not complete a 36-month assessment but completed assessments after 36 months: two children completed a 48-month assessment, and one child completed a 60-month assessment. The data from these assessments were used for determining autism status using the CBE procedure. Assessments occurred at either the child's home or in a family-friendly laboratory at the University of South Carolina.
Analytic plan
To answer our research question, we present the mean CSBS-CQ standard scores along with the normative mean scores of the CSBS-CQ to describe patterns of early communication in FXS. Also, we present the percentage of infants and toddlers with FXS who fall within the range of concern based on the CSBS-CQ publisher's established criterion. To explore the impact of autism on early communication in FXS, we present data for the full sample, FXS Only, and FXS + autism.
Results
Descriptive pattern of early communication on the CSBS-CQ
Overall and within the domains and subdomains of the CSBS-CQ, none of the infants and toddlers with FXS had CSBS-CQ standard scores at or above the normative mean (i.e., no participants scored above normative mean of 100 on Total Communication or scored above the normative mean of 10 on the domains and subdomains; Figures 1 to 4). One-sample t-tests indicated that the differences between CSBS-CQ scores (overall and within each domain) were significantly different from the normative mean (see Table 2). Further, 68.2% of infants and toddlers were in the range of concern for their overall communication score (see Table 2). Within the domains and subdomains of the CSBS-CQ around 50% of the sample fell into the range of concern.

CSBS-CQ total communication score. Note. Solid line represents the normative mean of a standard score of 100. Dashed lined represents the range of concern of a standard score of 81 or less.

CSBS-CQ social domain and subdomains. Note. Solid line represents the normative mean of a standard score of 10. Dashed lined represents the range of concern of a standard score of 6 or less.
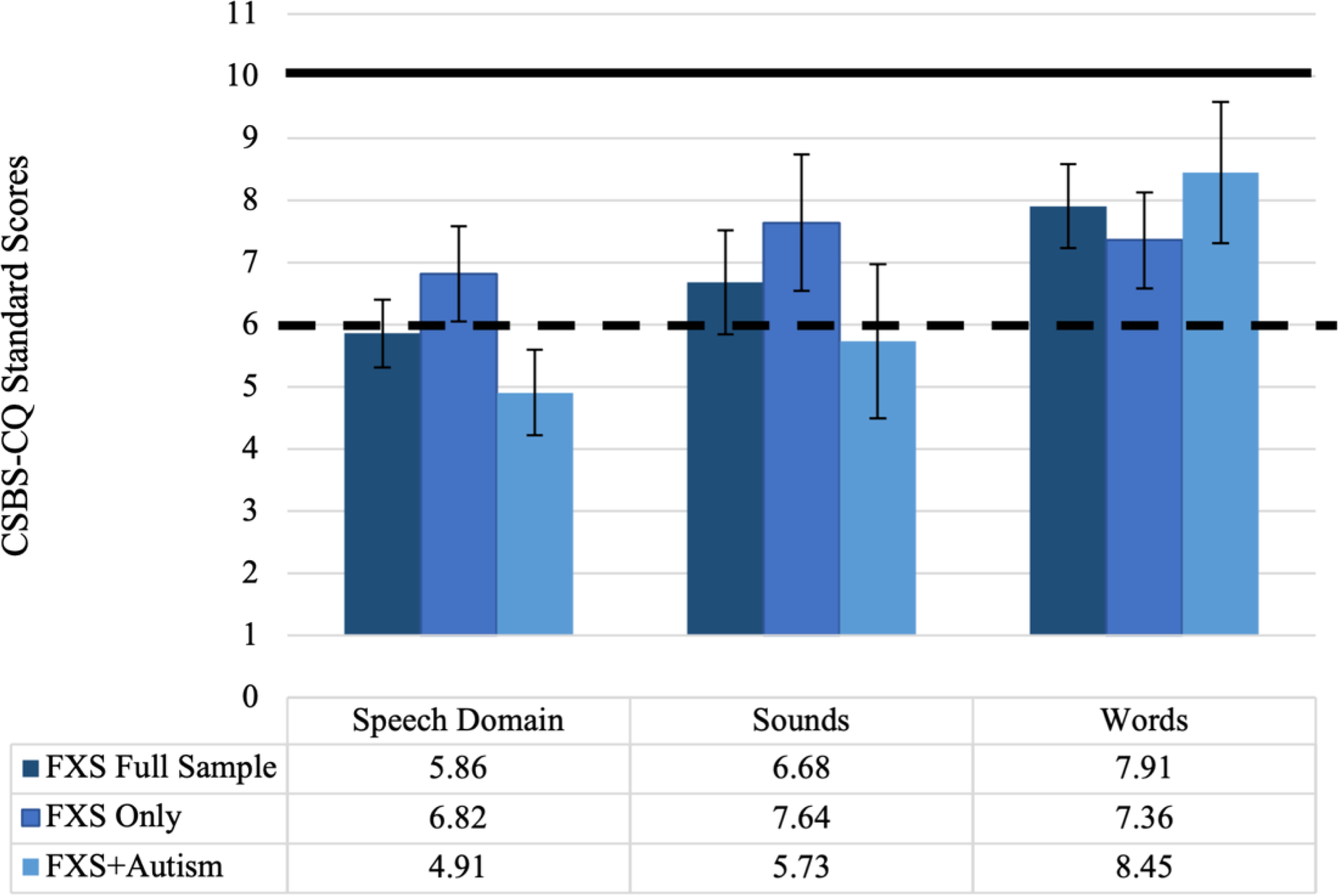
CSBS-CQ speech domain and subdomains. Note. Solid line represents the normative mean of a standard score of 10. Dashed lined represents the range of concern of a standard score of 6 or less.

CSBS-CQ symbolic Domain and Subdomains. Note. Solid line represents the normative mean of a standard score of 10. Dashed lined represents the range of concern of a standard score of 6 or less.
Comparison of the CSBS-CQ to the normative mean.

Note. The normative mean standard score for CSBS-CQ Total Communication is 100 and the normative mean standard score for CSBS-CQ domains and subdomains is 10.
Impact of autism
When the sample was divided by later diagnosis of autism, both groups had significantly lower CSBS-CQ Total Communication scores when compared to the CSBS-CQ normative mean of 100 (see Table 3). The percentage of infants and toddlers in the range of concern who were later diagnosed with autism was much higher, 81.8%, than those who did not receive an autism diagnosis, 54.5% (see Table 2). Generally, there was a lower percentage of infants and toddlers with FXS Only (vs. those with FXS + autism) in the range of concern across all domains and subdomains.
Comparison of the CSBS-CQ between those with FXS only and those with FXS + Autism.

However, within the different domains and subdomains, each group performed differently. Infants and toddlers with FXS Only had significantly lower scores on the three domain scores when compared to the normative mean of 10 but did not have significantly lower scores on five of the subdomains (Emotion & Eye Gaze, Communication, Gestures, Sounds, and Understanding) when compared to the normative mean of 10. In contrast, infants and toddlers with FXS + autism had significantly lower scores on all domains and subdomains, except for the Words subdomain, when compared to the CSBS-CQ normative mean of 10.
Given the different patterns observed between the two groups in comparison to the normative mean, we also examined differences between the two groups of interest on the CSBS-CQ. Infants and toddlers with FXS Only scored higher than those with FXS + autism on all CSBS-CQ domains and subdomains, except for the Words subdomain (see Figures 1 to 4). However, statistically significant differences between the two groups were only observed for the CSBS-CQ Total Communication score and the Symbolic domain, such that those with FXS + autism had lower scores than those with FXS Only (see Table 3). Also, while they did not reach a p-value below .05, the scores for Communication, Understanding, and the Speech domain were trending (p < .10), indicating higher scores for those with FXS Only.
Discussion
The purpose of this study was to comprehensively describe the early communication of infants and toddlers with FXS using the CSBS-CQ, a standardized communication screening measure. To achieve this aim, we compared the pattern of early communication of infants and toddlers with FXS to the normative data of the CSBS-CQ and identified the percentage of infants and toddlers who scored within the range of concern.
Descriptive pattern of early communication
Our results indicate that overall and within the domains and subdomains of the CSBS-CQ, infants and toddlers with FXS had significantly lower scores than the normative sample. These findings are not surprising given that communication and language impairments are common in FXS (Abbeduto et al., 2007; Finestack et al., 2009). These results are also consistent with the only other study in FXS that has used the CSBS-CQ (Kover et al., 2015), which noted that CSBS-CQ Total Communication scores for most infants and toddlers were below the normative mean of 100 between 9 and 24 months, though there were a few infants and toddlers that did score above the normative mean of 100 at 9 and 12 months. Importantly, Kover et al. (2015) did not compare performance on the CSBS-CQ between infants and toddlers with FXS to infants with typical development that were used as a comparison for other measures in the study. Thus, our study expands our understanding of the emergence of communication delays in FXS as compared to normative data across early communication skills. Together, our findings and the prior findings of Kover et al. (2015) suggest that communication delays emerge as early as 9 months.
Our findings further highlight the broad impact of autism on early communication abilities in FXS. Once we divided the full sample by autism status, both groups continued to have significantly lower scores overall and within the domains CSBS-CQ than the normative mean. However, differences emerged within the subdomains for the CSBS-CQ for both groups in comparison to the normative mean. Infants and toddlers with FXS + autism had significantly lower scores on all but one subdomain (i.e., Words) of the CSBS-CQ. In contrast, those with FXS Only had significantly lower scores on the subdomains of Words and Object Use, but they also had scores that were not significantly different from the normative mean on the other five subdomains (Emotion & Eye Gaze, Communication, Gestures, Sounds, and Understanding). In addition, comparisons between infants and toddlers with FXS with and without autism indicated that those with FXS Only scored significantly higher than those with FXS + autism on the Total Communication score and the Symbolic domain. Further, infants and toddlers with FXS Only outperformed those with FXS + autism in all CSBS-CQ domains and subdomains, except for the Words subdomain. These findings are consistent with other studies of early communication in FXS that have noted greater delays in early communication/language are related to increased likelihood of autism or the later diagnosis of autism (Hahn et al., 2017; Hamrick et al., 2019; McDuffie et al., 2012; Philofsky et al., 2004; Rague et al., 2018; Thurman et al., 2017).
Percentage in the range of concern
Of critical clinical importance is the identification of those who are within the range of concern for early communication impairments and would likely benefit from early language intervention. The utility of using a screening measure, like the CSBS-CQ, is that clinicians can obtain information about if children are at risk of communication delays and may benefit from further evaluation and, potentially, intervention. It appears that most infants and toddlers with FXS would likely benefit from early language intervention given that 68.2% of our sample was in the range of concern for their overall communication score, and approximately 50% of the sample fell in this range on most domains and subdomains. However, it is somewhat surprising that more infants and toddlers were not scoring within the range of concern, given the well-established communication and language impairments reported in those with FXS (Abbeduto et al., 2007; Finestack et al., 2009).
Early identification for communication intervention is especially important for those who are later diagnosed with autism with 81.8% of our sample scoring within the range of concern for Total Communication on the with over 60% of the sample with FXS + autism scoring the range of concern on the domains of the CSBS-CQ. Further, more infants and toddlers with FXS + autism were within the range of concern for all subdomains of the CSBS-CQ, except for the Words subdomain. In contrast, 54.5% of infants and toddlers with FXS Only were in the range of concern for Total Communication with 50% or less scoring within the range of concern on all domains or subdomains. Taken together, and like previous research examining the impact of autism on early communication in FXS, our results indicate that the presence of co-occurring autism is associated with greater communication impairments in FXS (Flenthrope & Brady, 2010; Hahn et al., 2016, 2017; Rague et al., 2018).
As noted, research on early communication in FXS has often focused on specific skills—eye gaze, vocalizations, gestures—that are also examined within the CSBS-CQ. Available research suggests that young children with FXS use eye gaze effectively to establish and maintain social interactions (Hahn et al., 2017; Marschik et al., 2014; Roberts et al., 2002). When examining our full sample, this appears to be consistent with extant research. However, once the sample was divided by autism status, we observed that 63.6% of young children with FXS + autism were in the range of concern for Emotion & Eye Gaze, while only 18.2% of young children with FXS Only were in the range of concern for this subdomain. Further, for those with FXS Only Emotion & Eye Gaze was the subdomain with the lowest percentage of children in the range of concern. This suggests early impairments in eye gaze that mirror research on early identification and risk markers of autism (Ozonoff et al., 2010; Zwaigenbaum et al., 2013) and supports recent research indicating that reduced eye gaze in infancy is predictive of later autism features (Roberts et al., 2019). Another subdomain with a high percentage of young children with FXS + autism within the range of concern was Sounds (81.8%). This finding provides additional support to recent research indicating that the properties of early vocalizations in infants with FXS may serve as an early indicator of autism (Hamrick et al., 2019).
Previous research has also suggested an early impairment in gesture use in FXS (Flenthrope & Brady, 2010; Hahn et al., 2017; Hughes et al., 2019; Marschik et al., 2014; Rague et al., 2018; Roberts et al., 2002). Interestingly, across the whole sample, regardless of autism status, 45.5% of infants and toddlers with FXS were in the range of concern for gesture use. Many of the prior studies used behavioral coding of gestures during a communication interaction (i.e., Flenthrope & Brady, 2010; Hahn et al., 2017; Hughes et al., 2019; Marschik et al., 2014; Roberts et al., 2002), which likely provided a more comprehensive description of the type and frequency of gesture use in young children with FXS. Rague et al. (2018), however, did use a caregiver report measure (MacArthur-Bates Communicative Development Inventories-Words and Gestures) to capture gesture use in infants and toddlers with FXS. Unlike the CSBS-CQ, this measure asks respondents if their child uses 13 communicative gestures along with 51 actions and imitations rated as present or absent. In contrast the CSBS-CQ, asks respondents if they’ve seen their child use “gestures that are easily understood by others” (e.g., giving objects, showing objects, pointing, and waving) rated as never, sometimes, or often and then asks if they have seen their child perform 10 different gestures. Thus, using a comprehensive early communication measure may provide insight into overall areas in need of intervention, early markers of autism, and phenotypic features within early communication associated with FXS.
Limitations
Although this study is one of the first to examine the early communication abilities in comparison to normative data in FXS, there are several limitations. Our sample size was small, especially once the sample was separated by later diagnosis of autism. Therefore, our findings should be interpreted with caution and warrant replication with a larger sample. We did not have a direct comprehensive behavioral examination of early communication, such as the CSBS Behavior Sample, to provide additional insight into the skills reported by mothers on the CSBS-CQ. Nevertheless, although parents may be inaccurate reporters, their perspectives are also crucial as they are likely to be more attuned to their child's communication and able to interpret behaviors and skills that other communication partners would not recognize. Further, the use of screening measures can provide clinicians with additional information prior to a direct evaluation.
Conclusion
The present study adds to the growing literature that is identifying profiles of early communication in FXS. These findings suggest that delays in early communication are evident in comparisons to typically developing norms before 24 months. Also, differences in early communication were observed between children with FXS who were later diagnosed with autism. While early communication broadly may not be an early indicator of autism in FXS, some specific skills, such as eye gaze, may serve as such an indicator. More research is needed to examine the relationship between different early communication skills and autism outcomes in this population.
Taken together, early identification and developmental monitoring of children with FXS will help to determine increasing concerns in communication, and other domains of development. Screening measures, like the CSBS-CQ, may help monitor early signs of autism. Caregiver-report measures may be particularly useful when it comes to developmental monitoring because they are cost-effective and require minimal time from the family. Understanding the developmental course of early communication skills has implications for language interventions, including the potential timing of interventions and potential intervention targets.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. This research was supported by grants from the National Institute of Mental Health (L40 MH108014, R01 MH090194) and the National Institute of Child Health and Human Development (F31 DC018219). No other conflicting interests are present for the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Mental Health, (grant number F31 DC018219, L40 MH108014 , R01 MH090194).