
Abstract
Background & Aims
Estimates suggest that one in 59 children receive a diagnosis of autism and that early intervention can be effective if applied consistently and intensively. Parent implemented intervention can increase intervention consistency and intensity however, availability of providers, geographical factors, time constraints, and parental stress levels can all act as barriers to service access. Limitations in understanding elements that support family engagement can also impact participation in intervention. Telepractice can increase availability of intervention services and decrease the time and costs associated with face-to-face delivery. Research focused on children with autism has shown that telepractice is acceptable to parents. Despite positive findings for telepractice services with individual clients, limited research has been conducted on telepractice services for parent groups; parent perceptions and preferences regarding intervention; and service delivery methods. This research aimed to investigate parent perceptions of a group intervention programme for autism; the telepractice approach; parent and child outcomes; and parental stress. The purpose of the investigation was to build an understanding of parent's intervention preferences to inform future service offerings, increase choice, and support participation.
Methods
Eleven parents of preschool children with autism participated in a telepractice delivered group training programme called Hanen More Than Words (HMTW). The intervention is traditionally delivered face to face and teaches strategies to facilitate social-communication development in young children.
Quantitative and qualitative measures were used to evaluate parent perceptions of the telepractice HMTW intervention. Data were collected via the Parenting Stress Index, HMTW programme evaluation forms, and online parent survey.
Quantitative data was analysed using descriptive statistics. Pre- and post-intervention comparisons of parenting stress were conducted using paired T-Tests. Open comment field responses were analysed qualitatively using a directed content analysis.
Results
Parents reported high levels of satisfaction with telepractice delivered HMTW across intervention and post programme evaluations. Interactive learning opportunities, group participation, video coaching, individualisation of service, and programme facilitation were identified as key supports to learning.
Parents perceived increased insight into the interaction, learning, and behaviour of themselves and their children. They reported positive changes in strategy implementation and confidence. Parents also perceived improvements in their children's communication, responsiveness, interaction, and play following intervention. Parental stress measurements from pre- to post intervention, were not significantly different.
Conclusions
Telepractice may reduce service barriers and improve access, particularly with the efficiency of a group delivery approach. Utilising technology to deliver group intervention was acceptable to parents and perceived to have positive outcomes for both parent and child. Further investigation into parent perceptions of intervention types and delivery approaches, could facilitate a broader understanding of family needs with respect to service access and engagement.
Implications
Expansion of telepractice offerings can increase efficiencies and service choice for families and providers. Limitations in service availability and barriers to service access and engagement, confirm the importance of pursuing ongoing service improvements and evaluating the preferences of service users. Development of standardised tools to measure and compare parent perceptions across intervention types and service delivery approaches would be beneficial.
Introduction
Autism is a prevalent, lifelong neurodevelopmental condition affecting as many as one in 59 children (Baio et al., 2018). It is characterised by challenges in social communication, restricted, repetitive behaviours and interests, and hyper- or hypo-reactivity to sensory input (APA, 2013). The challenges associated with autism can have a significant ongoing impact on communication, education, employment, social participation, and relationships.
Many young children are diagnosed with autism and research has shown that diagnostic accuracy can be achieved from 18 to 24 months (Barbaro & Dissanayake, 2017; Pierce et al., 2019). Early diagnosis is recommended as it provides opportunities for intervention to commence at a time considered optimal for supporting long term developmental outcomes (Koegel et al., 2014; Landa, 2018). Evidence suggests that early intervention, involving collaboration between clinicians, family, and the child's significant others, can be effective at improving communication and adaptive functioning, and potentially impact cognitive development and autism symptomatology (Bradshaw et al., 2015; Dawson et al., 2010; Landa, 2018; Roberts et al., 2016).
Early Intervention Service Barriers
Despite the potential positive impact of early intervention for children with autism, barriers to service access, knowledge gaps in evidence-based practice, and limited understanding of factors supporting family engagement can all impact service delivery. Engaging families with appropriate services is complex and multi-faceted (Melvin et al., 2021), and evidence remains incomplete regarding intervention preferences and elements that influence engagement with services (Carr et al., 2016; Phoenix et al., 2019). Hackworth et al. (2018) discussed the impact of family socio-demographic characteristics and community social disadvantage on engagement with services, and the importance of individualised support to retention and parental involvement. Romano and Schnurr (2020), identified gaps between research and practice in early intervention service provision impacting family engagement and implementation of intervention strategies. Disparities involved capacity building and coaching skills; inclusion of family priorities, culture and values in intervention planning; ability to target skills across multiple goals and settings; and recognition of caregiver wellbeing and confidence as integral to child development.
Service access barriers faced by families include availability of services and suitably qualified practitioners; limitations in funding, family capacity and support; severity of autism symptomatology; and geographical factors (Braddock & Twyman, 2014; Monz et al., 2019; Smith-Young et al., 2020). Service delivery approaches that may mitigate intervention access barriers have been explored and continue to evolve. Telepractice based services and parent implemented interventions have received significant attention as enablers of service access. Continuing to evaluate the suitability of these early intervention offerings is important for ensuring the availability of a variety of evidence-based services for families.
Telepractice Service Delivery
Telepractice uses technology to connect clients and interventionists to provide services such as health care, assessment, intervention, and education at a distance (Houston et al., 2014; Pierson et al., 2021). It has been used to increase the number and range of people participating in services, and decrease the time and costs associated with face-to-face delivery (Rheuban & Krupinski, 2018). Already, substantial telepractice research has focused specifically on children with autism (Knutsen et al., 2016; Parsons et al., 2017; Sutherland et al., 2018). Evidence has shown that telepractice service delivery is acceptable to parents and that they can be successfully trained to implement intervention strategies with their children (Garnett et al., 2022; Garnett et al., 2019; Little et al., 2018; Pickard et al., 2016; Wainer & Ingersoll, 2013).
Despite positive findings from studies of telepractice services for individual clients, limited research has been conducted on telepractice intervention for groups of parents. A review of group intervention for parents of children with autism (O'Donovan et al., 2019), reported positive trends in parenting behaviour and health, child behaviour, and social support, notwithstanding weaknesses in the quality of some included studies. With growing numbers of families seeking early intervention, potential efficiency gains in time and cost with telepractice group interventions are appealing (Lichtlé et al., 2019; Steiner et al., 2012). Telepractice groups could also potentially provide support and connection for families who may be experiencing a sense of isolation (O'Donovan et al., 2019; Patterson & Smith, 2011). Efficiency and parent support factors create a strong rationale for evaluating a telepractice group intervention approach, adding to current evidence and potentially revealing factors impacting on families seeking services.
Parent-implemented Intervention
Teaching parents to use evidence-based intervention strategies in everyday situations has become accepted practice within early intervention services (Nevill et al., 2018; Tomeny et al., 2019). Parent-implemented intervention potentially increases access to intervention, supports generalization of learned skills, builds capacity and empowerment in parents, and increases hours of intervention for the child (Wainer et al., 2017). Parents can be trained to implement a range of interventions with their children (Edmunds et al., 2019; Gengoux et al., 2019). This can lead to improved child outcomes such as joint attention, communication, and language (Akamoglu & Meadan, 2018; Bradshaw et al., 2015; National Autism Center, 2015; Oono et al., 2013).
Hanen More Than Words (HMTW; Sussman et al., 2016) is a parent-implemented, group intervention programme for parents of young children with autism. It is a naturalistic intervention based on social-interactionist theory where the child's learning is scaffolded by the contingent responses of the adult (Abbeduto & Boudreau, 2004; Chapman, 2000; Girolametto et al., 2007). HMTW teaches parents to facilitate their child's social communication development during everyday activities. Group parent training and individual video feedback sessions aim to increase parent understanding and responsiveness to child communication and provide structure within enjoyable activities to support learning (Sussman et al., 2016). Being a group intervention traditionally delivered face to face, HMTW also provides valuable opportunities for parent-to-parent support (Patterson & Smith, 2011).
Parent Perceptions of Telepractice and HMTW
Evaluating parent perceptions of intervention types and delivery methods requires further investigation to determine the feasibility, acceptability and values alignment of interventions for families of children with autism (Vivanti et al., 2018).
Telepractice
Reports of parent satisfaction within current literature are limited with respect to telepractice based services. Early trends indicate that parents express satisfaction with telepractice approaches, particularly when the telepractice intervention involves clinician assistance versus ‘stand-alone’, self-directed online training (Beaudoin et al., 2014; Ingersoll et al., 2016). Existing gaps in understanding parent perceptions of telepractice approaches however, illuminate a need for further investigation.
HMTW
Four published studies have evaluated face-to-face delivery of HMTW to parent groups (Carter et al., 2011; Girolametto et al., 2007; McConachie et al., 2005; Patterson & Smith, 2011). All studies included at least one measure of parent satisfaction. Patterson and Smith (2011) provided a detailed examination of parent experiences using qualitative case study methodology with four participants. Semi-structured interviews and a focus group investigated parent perceptions of HMTW across themes involving information content and quantity, individual participant needs, and factors affecting learning and implementation. Results revealed that parents sought more information about intervention responsibilities, child communication, and expected progress. They wanted less information per session. Working parents and those with recently diagnosed children wanted information about managing intervention in the context of those specific circumstances. Video feedback sessions and parent to parent support were perceived as positive components of the intervention and child factors were perceived to either positively or negatively impact implementation.
Carter et al. (2011) evaluated HMTW in a randomised controlled trial involving 62 families. HMTW participants completed a consumer satisfaction survey developed for the study. Participant satisfaction was high with mean ratings of 5.48 out of 6 for group experience, and 3.46 out of 4 for group leader. McConachie et al. (2005) studied 51 parent–child dyads participating in HMTW. An included measure of parental stress and a questionnaire assessing parent adaptation to having a child with a disability, indicated no significant differences between intervention and control conditions. Girolametto et al. (2007), used multiple case study design to evaluate three parent–child dyads. Following HMTW, parent perceptions were collected via short survey. Parents perceived they were able to apply strategies to support communication, comprehension, interaction, and play. They perceived child improvements in interaction, turn taking, play and verbal communication.
Parental Stress
Parents of young children with autism have generally reported high levels of satisfaction when evaluated within parent intervention studies (Carter et al., 2011; Steiner et al., 2013). Investigation into the experiences of these parents suggests that they often experience higher stress levels than parents of typically developing children, or children with other disabilities (Dabrowska & Pisula, 2010; Davis & Carter, 2008; Estes et al., 2013). Despite the known impact of parent stress on family functioning and managing a child with autism (Bonis, 2016), there has been limited research into the impact of parent-implemented intervention on parent stress levels (Beaudoin et al., 2014; Lichtlé et al., 2019). In the context that parent intervention programmes potentially impact parent stress, inclusion of stress measurement in parent intervention research contributes evidence in this area.
Aims
Barriers have been identified in early intervention service provision, access, and engagement. In response to these barriers, this research aimed to investigate an autism specific, early social-communication intervention, coupled with a contemporary group telepractice service delivery approach. The broader research programme aimed to: (a) establish the feasibility of the group telepractice delivery approach; (b) evaluate the effectiveness of the intervention; and (c) investigate parent perceptions of participating in telepractice HMTW. Outcomes of the feasibility component of the research have been published (Garnett et al., 2019). Results of the effectiveness evaluation have been submitted for publication (Garnett et al., 2022). This paper reports on the investigation into parent perceptions of the HMTW intervention, the telepractice approach, perceived intervention outcomes, and parental stress.
Methods
This study used a convergent mixed methods design involving quantitative and qualitative analysis to evaluate parent perceptions of the telepractice HMTW intervention. The evaluation approach was adopted on the basis that parent participants possessed the specific expertise to report on the intervention experience, and the impact of the intervention on themselves, and their children (Kazdin, 2011). The research programme was approved by the University of Melbourne School of Health Sciences Human Ethics Advisory Group (ID 1238764).
Participants
There were 11 participants in the study, all mothers of children with autism. The children, nine boys and two girls, had a range of abilities and were aged between 2 years, 7 months and 4 years, 7 months prior to commencing telepractice HMTW. Autism symptomatology was measured using the Social Responsiveness Scale, Second Edition (Constantino & Gruber, 2012), with Total Scores ranging from mild to severe. Vineland Adaptive Behaviour Scales, Second Edition (Sparrow et al., 2005), Adaptive Behaviour Composite and Socialization scores were all 70 or below, representing low adaptive functioning. Language was measured using The New Reynell Developmental Language Scales (Edwards et al., 2011). All children received standard scores of 69 (first percentile), indicating severe language impairment.
Parents were aged between 28 and 42 years, lived in an urban location and had two or more children. Ten were living with a partner and one was single. Seven mothers were born in Australia, two in New Zealand, and one each in Portugal and Uruguay. All parents used English as their first language and two parents used an additional language (Vietnamese and Spanish). Education levels varied. Two mothers had completed secondary school, three had a diploma/certificate, three had a degree, and two mothers had postgraduate qualifications. With respect to paid employment, one mother worked full time, two part time, seven were not employed, and one received a government benefit income.
Prior to commencing HMTW, all parents reported reliable internet connection and spent from five to 20 plus hours online per week. Two parents (18%) rated their computer skills as ‘average’ and nine parents (82%) rated themselves as ‘good’ or ‘very good’. Nine parents (82%) had previous video-conferencing experience using either Skype or Face Time, or both. Two parents had accessed a webinar in the past.
Delivery of Intervention
Permission was gained from the Hanen Centre for telepractice delivery of HMTW. The programme was delivered from a clinical setting via Zoom video-conferencing. Parents participated from home using desktop computers, laptops, or tablets.
The HMTW intervention followed the manualized programme format (Sussman et al., 2016). A pre-programme consultation was followed by 11 weeks of intervention comprising eight, 150-min group parent training sessions interspersed with three, 60-min individual video feedback sessions. Parents created home practice plans during group sessions and video-feedback was delivered using evidence based adult coaching methods (Friedman et al., 2012; Trivette et al., 2009). Parents were trained to follow their child's lead and provide motivation and predictability within play, book sharing and daily routines (Sussman, 2012).
Measures and Procedures
Data were collected via the Parenting Stress Index (PSI; Abidin, 2012), HMTW programme evaluation forms, and online parent survey. Data collection tools quantified parent perceptions regarding the intervention. Free comment fields offered a detailed record of parent experiences, providing rationales for perceptions expressed (Creswell & Plano Clark, 2018).
Parenting Stress Index
The PSI was administered within a broader assessment protocol prior to telepractice HMTW and at one month post intervention. It comprised 101 item, parent self-report form measuring stress within the parent–child system. PSI has been used within autism research with good reported internal reliability (Davis & Carter, 2008; Wainer et al., 2017).
HMTW Programme Evaluation
Participants were provided with six HMTW evaluation forms during the intervention period. They completed evaluations following three group parent training sessions and three video-feedback sessions. Group session evaluations collected open ended information regarding parent likes, dislikes, questions/concerns addressed, and topics of additional interest. Video feedback evaluations collected comments on aspects parents liked/found helpful, that facilitated child progress, support provided by the programme leader, and suggestions for improvement. An overall HMTW programme evaluation gathered parent responses across the following topics: perceived communication and/or interaction changes in both parent and child; helpful/unhelpful aspects of the programme; most helpful programme topics; satisfaction with programme leader; suggestions for change/improvement. Parent satisfaction Likert scale ratings from, 1 - not very helpful, to 5 - very helpful, were included in both video feedback and overall programme evaluations.
Online Parent Survey
The online parent survey was administered to participants at one month, post intervention. It consisted of 61 questions involving Likert scale responses ranging from 1 to 5, yes/no questions, open ended questions, and optional comments (see Appendix). Open ended response options enabled comprehensive reporting of parent perceptions, thus broadening understanding and potentially informing future investigations (Albudaiwi, 2018).
Survey areas targeted for this investigation included parent perceptions of HMTW, the telepractice delivery approach, and perceived outcomes for both parents and children. A lack of pre-existing measures encompassing targeted areas was identified. The online survey was therefore developed, expanding results from parent interviews conducted in an earlier feasibility study (Garnett et al., 2019).
Survey design considered language appropriate to the population being surveyed, sensitivity of included questions, types and consistency of response choices, survey length, and administration method (Langbecker et al., 2017). Pilot testing of the survey to establish face validity was completed by six people familiar with HMTW who had a mix of parenting, allied health, and early intervention experience. Feedback led to the deletion and modification of items that were unclear, ambiguous, redundant, or poorly performing in some other way.
Data Analysis
HMTW programme evaluations and online parent survey responses were analysed using quantitative and qualitative methods. Results were summarised using descriptive statistics including frequency percentages and exemplars.
Quantitative Analyses
Likert rating scales and yes/no questions were quantitively analysed by aggregating and reporting results descriptively.
Pre- and post-intervention comparison of parenting stress, as measured by PSI, was conducted using paired T-Tests with alpha level set at 0.05.
Qualitative Content Analysis
Open comment field responses were analysed qualitatively using a directed content analysis (Hsieh & Shannon, 2005). Data were first sorted into deductively applied categories. Subcategories were identified inductively following subsequent immersion and identification of patterns in wording and theme. A final analysis interpretively collated sub themes within existing subcategories.
Results
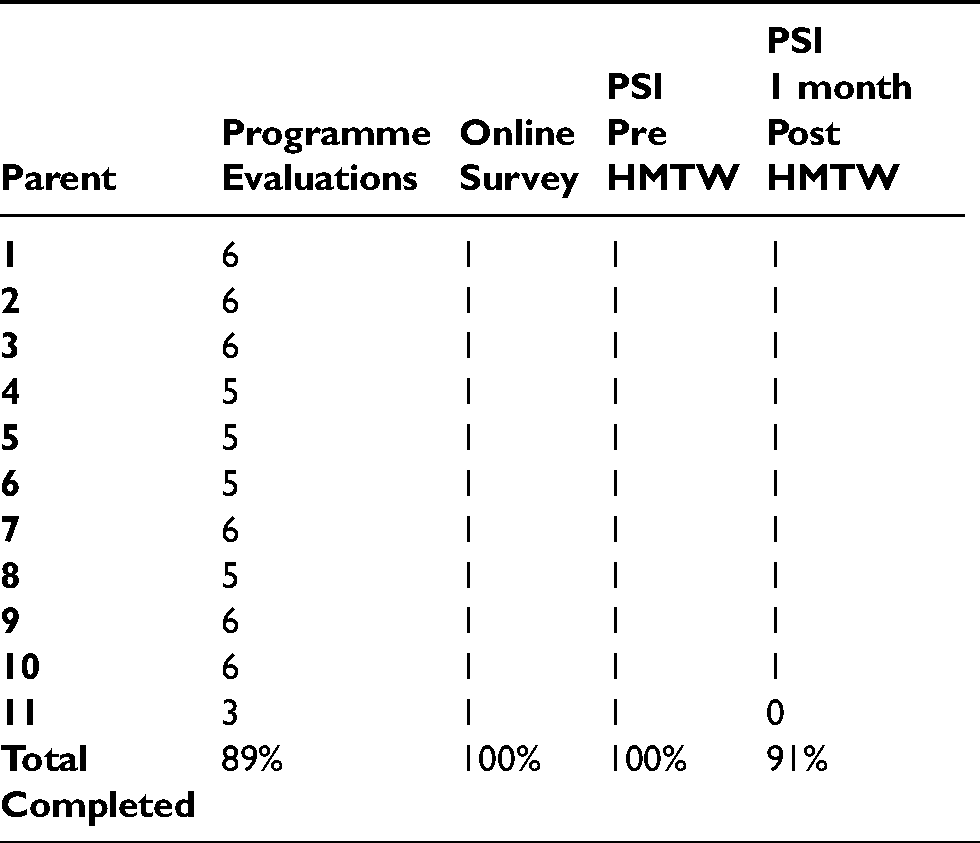
HMTW programme evaluation forms, survey responses, and PSI results measured parent perceptions. See Table 1 for parent outcome measures completed.
Number of parent outcome measures completed.
HMTW evaluation forms and online survey results are reported under content analysis categories, sub-categories, and sub-themes. See Figure 1.

Content analysis categories, subcategories, and sub-themes.
The HMTW Programme
Overall satisfaction with the HMTW programme was rated ‘very high’ by seven participants (64%), and ‘high’ by three participants (27%). One participant (9%) was neither satisfied nor dissatisfied. Eight parents (73%) stated that information provided in the programme was as expected. 10 parents (91%) said it was both easy to understand and implement at home.
Parents were asked whether they would have preferred different speech therapy. Six Parents (55%) said ‘no’, four parents (36%) said ‘don’t know’, and one parent (9%) said ‘yes’. Comments varied; “I found my son and I embraced the principals of the programme really well….”; “[I prefer] more hands on with professionals”; “It's not an either or, situation. I see that my child benefits from more structured speech therapy with ‘homework’, but I’m very pleased to have added plenty of opportunities for extending his language in everyday activities.”
Survey ratings of HMTW components supporting parent participation are presented in Table 2.
Parent ratings of components supporting participation in the HMTW programme (N = 11).

HMTW Programme Components
Group Training Sessions
100% of parents rated group training sessions as ‘helpful’ (36%), or ‘very helpful’ (64%). One parent reported, “all aspects of the programme were great learning tools”, another commented, “loved every bit of it”.
Parents valued information about programme expectations, potential outcomes of intervention, and positioning HMTW in the context of other services. Early in the programme parents desired information about interaction and ideas on engaging in and extending child interests and activities. They wanted, “more about interpreting and interacting”; “greater variety of activities”, and how to “do better activities”. As the programme progressed, parents raised concerns about child behaviour. For example, “How can I keep the child less stressed….?”
Parents reported that HMTW comprehensively covered content of interest and answered their questions. They found the information “informative”, “engaging”, and “… easy to follow…”. Programme pace was referred to as, “steady” and “well-paced”. It “provided time for discussion”, and “didn’t drag on”. Videos, interactive activities, small group discussions, power point presentations, and programme resources were all identified as learning supports. Survey results confirmed that interactive activities, practice, and video examples were the highest rated group session components (See Table 2).
Video Feedback Sessions
100% of the parents rated individual video feedback sessions as ‘helpful’ (36%), or ‘very helpful’ (64%). Nine participants (82%) found video feedback sessions to be one of the most helpful components of the HMTW intervention. Evaluations included terms such as “great”, “helpful”, “satisfied”, “really enjoyed”, and “reassuring”.
Parents made positive comments about receiving advice, developing personal insights, and gaining support. Comments (83%), related to personalised ideas and advice about strategies, activities, and child goals. Parents felt that increased insights and understanding were gained by seeing video of their own parent–child interaction, pausing the video frequently, repeatedly, and slowly, then discussing observations with the programme leader. They felt supported by seeing what they did well, (“…positive reinforcement.”), receiving encouragement (“…encouragement around child strengths”), and positive observations (“…pointed out successes”).
Survey results confirmed that ‘live coaching from the speech pathologist’, and ‘using video to review and discuss the interaction’ were the most helpful video feedback components (see Table 2).
Intervention Strategies
Parent comments referenced strategies that facilitated play (31%), extended interaction (23%), and developed social communication goals (19%). Video examples were highly valued to support learning (“… was helpful to see the strategies in action”; “It was great seeing videos of what we were learning.”). Parent's own interaction videos were linked to gaining strategy insights (“I noticed things I did well and could do differently next time.”), and support (“…encouragement around his strengths and further ideas about how to play and keep interactions going well.”).
Highly valued strategies involved interaction and communication (“Gave me good ideas on ways to interact with my child.”; “…able to fine tune skills that were relevant to his communication goals.”), play (“Able to brainstorm ideas – plenty to go on with in playing with him.”), routines (“I found strategies that can be employed in day to day living the most effective.”), language (“Ideas on how to expand language and ways of doing the activity differently”), and book sharing (“Discussed some specific strategies for listening with books, which I will try out.”). Figure 2 details HMTW topics identified by parents as ‘most useful’.
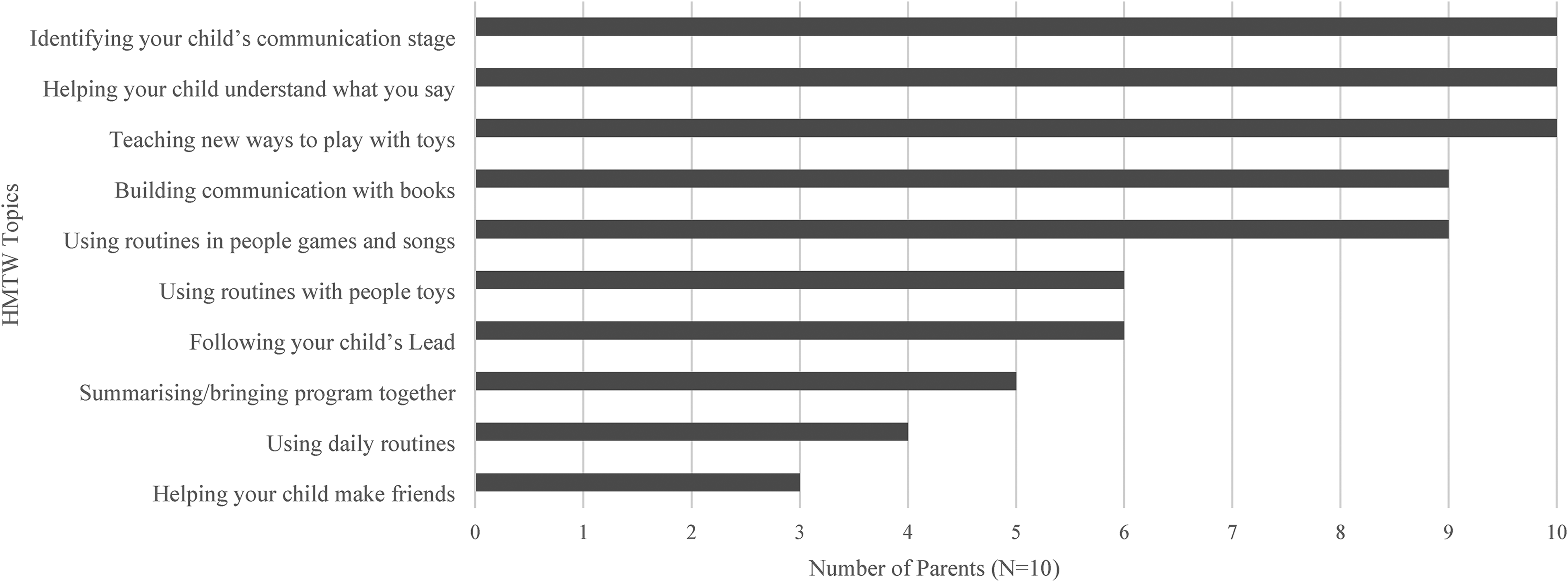
Most useful HMTW topics identified by parents.
Programme Structure and Resources
Parents were asked whether they thought the number and length of HMTW sessions was appropriate. Eight parents (73%) said ‘yes’, one parent preferred an extra 15 min, and two parents suggested slightly shorter sessions. Nine parents (82%) supported their own learning by taking notes, three parents used the parent guidebook, three parents created reminders for themselves, and three parents reviewed emails, handouts, or their own notes.
Programme Leader
Parents commented that learning was facilitated by feedback, guidance, and support from the programme leader. Participation was supported by easy to understand, practical and effective communication; knowledge and ability to answer questions; and provision of relevant information and explanations. Beneficial programme leader attributes were identified as being helpful, engaging, caring about outcomes for families, professional, generous with time, knowledgeable, and patient.
HMTW Programme Benefits and Barriers
Group Support
Positive comments were made by 64% of the participants about support provided by the group. Both personal and learning supports were identified. Personal supports were meeting, interacting with, and getting to know other parents. They included sharing experiences, “hearing other people's stories”, and sharing information. Learning supports were receiving advice, suggestions, and ideas from other parents, planning together, and seeing videos of other parents playing and interacting with their children. 36% of participants reported a desire for more time and opportunity to interact with the other parents in their group.
Programme Structure
Participants communicated potential learning barriers within the HMTW programme structure. They identified, quantity of session content, (“I feel I have enough to digest for this week”; “I thought the session was a bit crammed with information and I was a little confused in the end.”), handouts, (“I would have liked an extra 15 min on top of the 2.5 h for us to fill out forms…”; “Less information on handouts.”), terminology (“…words like, ‘early communicator’ for example, was a bit hard to understand.”), and session length (“Sessions were a bit long and exhausting when I had several appointments on the same day”).
One parent felt better able to work individually, preferring video feedback sessions to group training. Other parents would have liked more opportunities for parent-to-parent interaction within sessions.
The Telepractice Approach
Participants were either ‘satisfied’ (55%) or ‘very satisfied’ (45%) with the telepractice delivery approach. All parents (100%) indicated that telepractice met their expectations, that they could participate as desired, and felt supported by the group. Ten parents (91%) said they would like to participate in telepractice based services in future and would recommend telepractice to other parents. One parent commented, “Wonderful course. The telepractice method was an extremely beneficial method.” One parent did not want future telepractice services and was unsure whether to recommend telepractice to others.
Parents all rated telepractice as ‘effective’ or ‘very effective’ in supporting all but two HMTW activities. ‘Participating in break out group discussions’ and ‘Planning and practicing home plans’ were considered ‘neither effective nor ineffective’ by one parent. A different parent said, “Going into break off rooms and getting ideas off other mums was helpful.” Survey results are presented in Table 3.
Parent ratings of telepractice effectiveness in supporting participation in the HMTW programme (N = 11).

Telepractice Participation
Technology
Parent experience using technology to access HMTW was ‘very positive’ for six parents (55%), ‘positive’ for four parents (36%) and, ‘neither positive nor negative’ for one parent (9%). Most parents participated with laptop computers, followed by desktop computers and tablets. Computers were considered beneficial to participation with respect to audio and visual quality however, ‘ease of use’ was rated as a limitation by two participants. All parents using a tablet or smart phone rated ‘ease of use’ as a benefit and screen size was identified as a limitation (See Table 4 for detail).
Devices used to participate in HMTW with identified benefits and limitations (N = 11).

*Many parents used more than one device. Data represents the number of parents who used each device and number/percentage identifying benefits and limitations.
Supports and Resources
Parents were asked about learning and resource requirements prior to commencing telepractice. One parent commented, “I just needed a bit of coaching on how to set up for video conferencing.” One parent needed to obtain a laptop (borrowed), and one parent purchased a webcam. One parent said, “I didn't need to buy anything, but a set of headphones is very handy.”
Information about video conferencing software, links for accessing sessions, and online coaching supported technology use (“Set up email initially that explained the ZOOM software…”; “Relevant links…., verbal coaching from our course leader during sessions.”). Information about transferring files, determining suitable internet speeds, completing editable forms, and updating relevant software were also valued.
Participants were asked what could improve the telepractice experience. Four parents suggested increased informal group discussion time and one parent commented on the importance of screen breaks, “Me taking sufficient breaks from the screen (personally), which I did take after the first session.” Six parents (55%) said they would have liked an online chat group to enable discussions outside sessions. Two parents suggested a parent workbook would have been helpful.
Potential Barriers
Seven parents (64%) identified telepractice barriers. Two parents (18%) reported difficulty setting up devices, “My laptop needed repairs part way through the course, so I needed to work out how to install zoom to other devices. It wasn't very tricky though.” Three parents (27%) reported difficulty joining sessions, “Sometimes it would not log on properly and audio wasn’t working well.” Four parents (36%) experienced some difficulty during participation (“My internet dropped out unexpectedly in the first session and I was unable to reconnect with the group for 5 min.”; “Bad internet connection can mean that the video/visual and audio are not in sync.”).
Technical challenges could be rated from 1 (major negative impact) to 100 (no negative impact). Ratings ranged from 50 to100 and averaged 90. Parents who experienced technical challenges were able to solve them and responses indicated minimal impact to participation. One parent commented,
Comparison with Face-to-Face Delivery
Telepractice Benefits
Identified benefits included travel, convenience, comfort, time, flexibility, and caring for children. Comments summarised perceived benefits. “It was all done in the comfort of my own home.”; “I can't travel, it would be too much for me.”; “I am very time poor and don't have much support so it was good to be able to participate from home.”; “Flexibility, could still participate with sick children.” One parent summarised, “I really liked the online aspect of the course, meaning it was easy to participate in the training. No logistics with needing to be offsite etc. I would highly recommend undertaking the course in this format.”
Learning and Group Cohesion
Six parents (55%) thought telepractice would make no difference to learning and implementing HMTW content. Five parents (45%) were unsure. When asked whether there were components of telepractice HMTW they would have preferred to do face to face, seven parents (64%) said ‘no’, three parents (27%) were unsure, and one parent said ‘yes’, “Break times!”
Eight parents (73%) felt there was group cohesion during telepractice sessions, one (9%) did not, and two (18%) were unsure. When comparing telepractice group cohesion with face-to-face groups, three parents (27%) thought it would be the same and seven (64%) were not sure. Comments supported both opinions, “There may have been more opportunity for general discussions if in the same physical space together.”; “…hard to replicate the informal cup of tea-time chats in an online format.”; “I think we all got along well and if we were face to face, it would be no different because we'd still be able to communicate and get along.”
Cost and Travel
Six (55%) parents said they would willingly pay for a HMTW programme and five (45%) were not sure. Eight parents (78%) felt their experience would be no different whether they paid for it or not. Cost was identified as a common barrier, “…I found the programme to be excellent. The only problem would be the cost for us”; “It is quite an expensive programme. Cost would be the deciding point”.
Nine parents (82%) said telepractice delivery would not affect their willingness to pay for HMTW however, six parents (55%) expected telepractice to be cheaper. (“I think it should be cheaper than a face-to-face programme although it is such a valuable tool, I would have no hesitation in paying for the telepractice delivery method.”; “Whether face to face or a programme run via telepractice, we still were getting all the information of the programme.”)
Parents quantified the travel time they would willingly undertake to access face to face HMTW instead of telepractice. Responses ranged from, “I can’t travel”, to “30 min – 1 h travel time”. See Figure 3 for results.
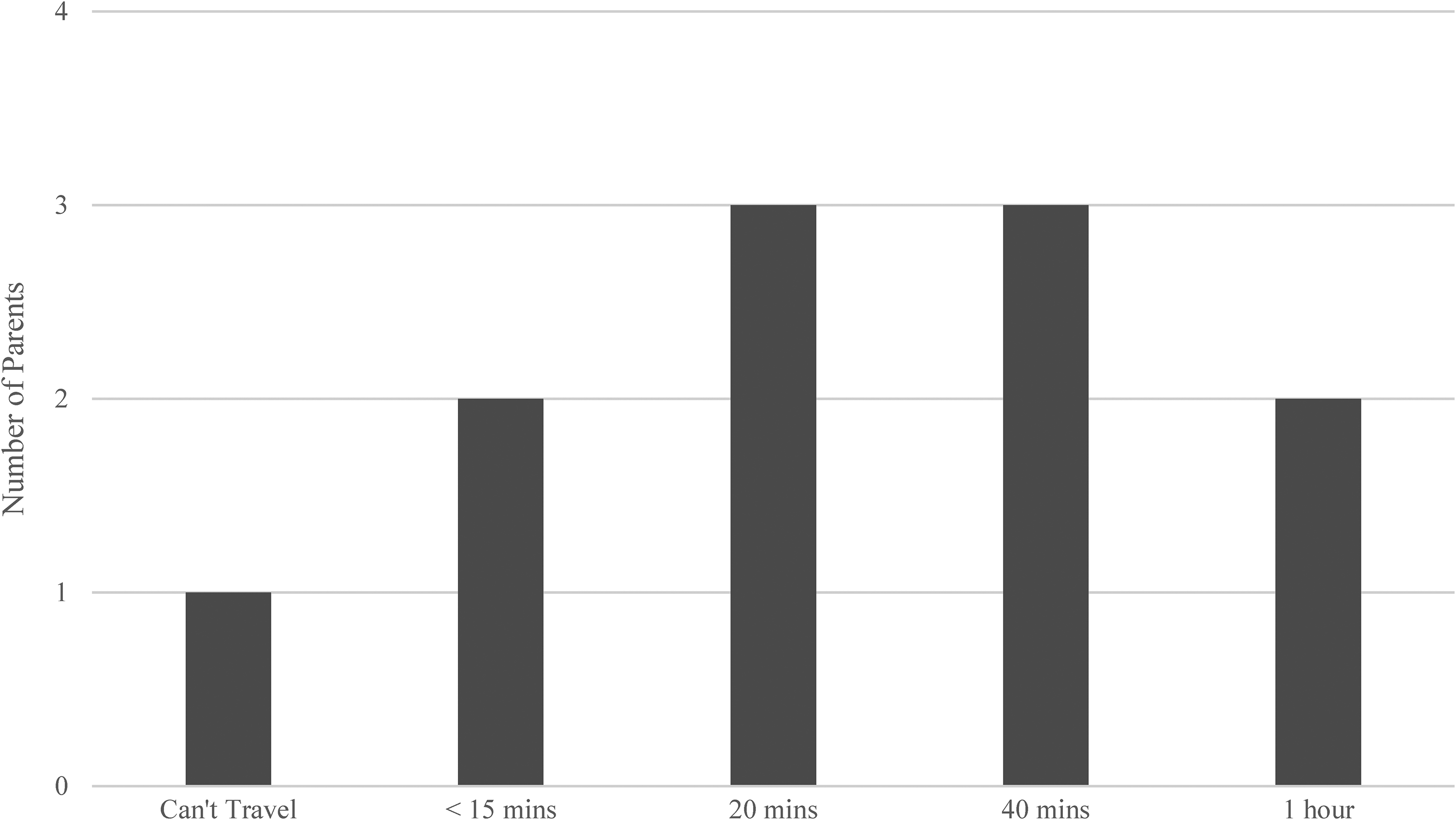
Time parents would be willing to travel to access HMTW face to face (N = 11).
Perceived Intervention Outcomes
Parent Outcomes
Insight and Understanding
Parents reported increased understanding of their own interactive behaviours. For example, “I gained a better understanding of turn taking in conversations and how to balance asking questions with social comments.”; “I don't think I ever gave him enough opportunities to speak. I would just play a game or interact with him and I did all the talking.” Insights about children's interests and behaviours were reported, “I understand more now what he needs from me based on his behaviours and sensory preferences”; “I have put myself in my child's shoes.” There were also insights about motivation and learning, “These are really great sessions and help to complement and reinforce the learning during the weeks.”; “I am able to enjoy playing with my son more as I see the difference these techniques have made.” and, about goal planning, “Yes, it helped to establish his current strengths and weaknesses and direct what we can next focus on.”
Strategy Implementation
Following HMTW, parents rated changes in communication with their child as, ‘significant change for the better’ (73%), or ‘small change for the better’ (27%). All parents reported they were ‘very likely’ (73%), or ‘somewhat likely’ (27%), to continue using HMTW strategies post intervention.
Parents reported applying a range of strategies to achieve social communication goals. 67% of parent comments related to interaction and following the child's lead. “I feel I can interpret his needs more.”; “I am waiting a lot more and giving him time to send a message.”; “I can interpret his nonverbal communication more easily.”; “I wait for my son to show an interest in things first, instead of initiating all the time.” Comments also mentioned play and/or routine related strategies, “I think once I knew how to [use the strategies], it made interaction through play and so much easier.”; “I still use the MTW strategies everyday with routines and play with my child.” Some comments referred to strategies supporting language, “Because I am able to keep him engaged longer, I am able to work more on his language and joint attention.”; “I know the importance of expanding his play and how to encourage language during it.” Further comments implied generalisation of skills, “I have learned how to incorporate the strategies into everyday tasks.”; “I have even shared this information with his grandparents who also spend quite a bit of time with him …”.
Confidence
All parents reported they were a
Parent confidence ratings following telepractice delivered HMTW (N = 11).

Child Outcomes
Ten parents (91%) perceived their child had changed following participation in telepractice HMTW. Changes were described, “He is more verbal…”; “more interactive and interested in playing…”; “she wants to be with me a lot more”; “…approaches me more to play with him, without prompting…”; “…able to communicate more effectively.”; “keener on playing with people, more confident with pretend play…”; “…seems to be repeating and saying a lot more.” One parent said: “Definitely a huge improvement in my child. He has come so far since the programme. Every day he progresses and it's all thanks to knowledge I acquired …If I look at when I first submitted a 10 min video prior to doing the programme and then my 10 min video at end of the programme, the difference is amazing. It's just made play between us so much easier and it doesn't feel like a chore.”
Seven parents (64%) reported improvements with play and books, “….is initiating play more.”; “He is now doing so much pointing while reading books and giving me great joint attention.” Other comments referred to improvements in child responsiveness, “things that I thought he wasn’t taking notice of, he brings it up in other play sessions that make me realise he was really listening and understanding.”
One parent facing significant challenges with her child, still perceived progress. “My child is a reluctant communicator at the best of times but the programme has definitely made a difference to her. Would I say her communication has improved “a lot"? - probably not. But there has been definite improvement all the same.”
Parental Stress
Eleven parents completed the PSI at pre-intervention and 10 at post intervention. Paired T-Test results (alpha 0.05; n = 10) indicated no significant differences from pre- to post-intervention for total stress domain (p = 0.460), child domain (p = 0.449), and parent domain (p = 0.705). See Table 6 for results.
Parenting stress Index scores pre intervention and 1 month post HMTW intervention.
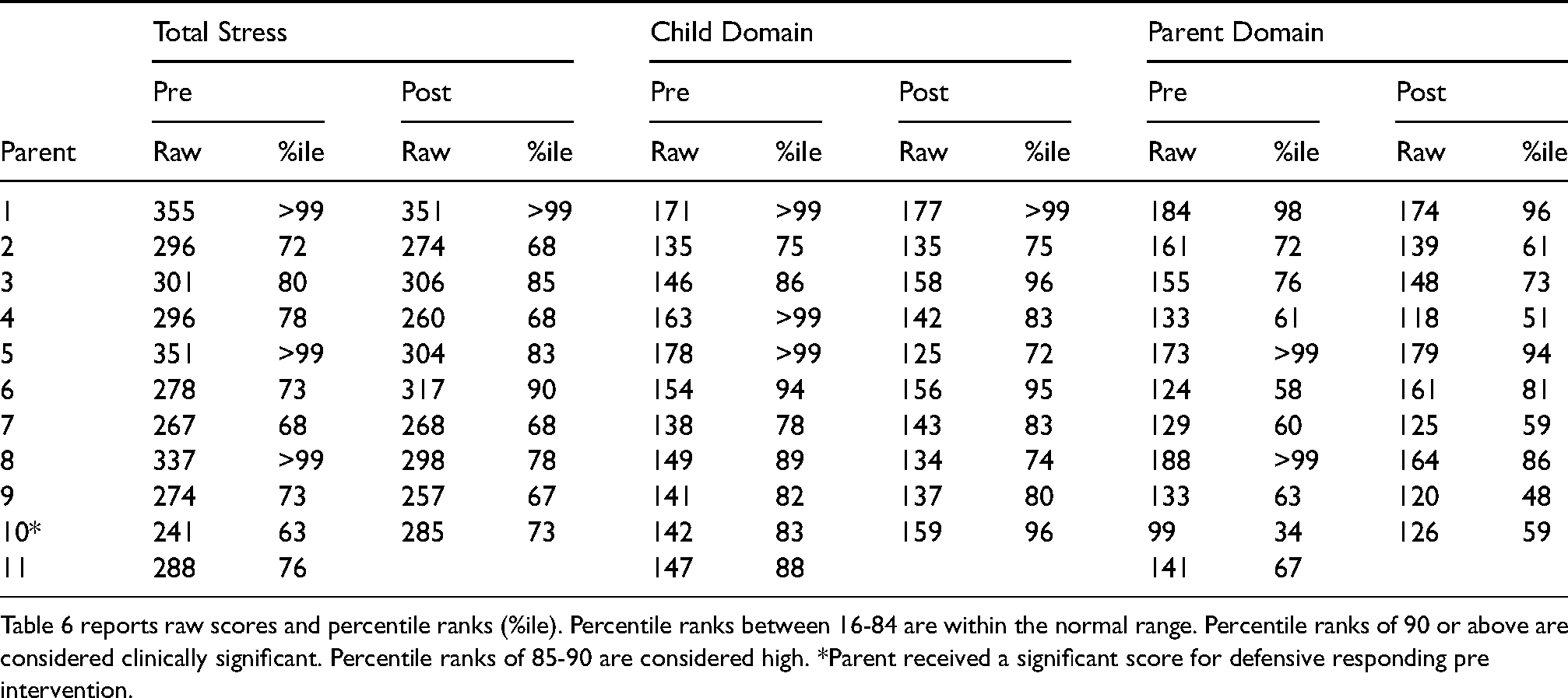
Table 6 reports raw scores and percentile ranks (%ile). Percentile ranks between 16-84 are within the normal range. Percentile ranks of 90 or above are considered clinically significant. Percentile ranks of 85-90 are considered high. *Parent received a significant score for defensive responding pre intervention.
Total stress scores were generally consistent from pre to post intervention. Two parents with clinically significant pre intervention scores moved to normal range post intervention. Two parents with normal range pre-intervention scores increased at post intervention to high and clinical range scores.
Survey ratings of parent stress following telepractice HMTW saw seven parents (64%) rate themselves as ‘a little less stressed’, two parents (18%) as ‘significantly less stressed’, and two parents (18%) as ‘no change’.
Discussion
Evaluating the acceptability of intervention approaches for families of children with autism has been identified as a gap in current research literature (Vivanti et al., 2018). Consequently, this research investigated parent perceptions following participation in group telepractice HMTW. Parent satisfaction with telepractice HMTW was consistent across repeated evaluations collected during the programme and in response to a post programme survey. Factors impacting parent learning, perceived intervention outcomes, and implications for service delivery are discussed.
Factors Impacting Parent Learning
Interactive Learning Opportunities
Learning required active engagement. Results confirmed the importance of active participation and reflection opportunities in the intervention, with practice activities and parent–child interaction video discussions considered most helpful by parents. Findings support previous research identifying practice, evaluation, and reflection as essential components of effective adult learning, important for skill acquisition (Trivette et al., 2009). Caregivers have previously reported that opportunities to problem solve and reflect have been beneficial to their learning (Salisbury et al., 2017).
Group Participation
Two thirds of participants gained support through group participation and expressed a desire for increased opportunities for group interaction. A systematic review of mental health interventions for parents of children with autism (Catalano et al., 2018), recognised the importance of parent-to-parent engagement as potentially one of the most effective factors in supporting parental wellbeing. Perceived group benefits in this study included personal supports gained through meeting and sharing experiences with other parents, and learning supports obtained through ideas and suggestions of others. This finding was consistent with previous work by Patterson and Smith (2011) who found participants valued group support during HMTW, particularly with respect to strategy learning and implementation. Group experience was also rated highly in the HMTW study by Carter et al. (2011).
Video feedback and Coaching
Individual video recording, coaching, and reviewing parent–child interactions with the programme leader were highly rated components of the HMTW programme. This reflects findings by Wainer and Ingersoll (2013), where parents expressed a desire for more video examples, coaching, and feedback when learning intervention strategies. In Stahmer et al. (2017), parents identified that working with a therapist was one of the most useful aspects of the intervention, and a recent systematic review by Camden et al. (2019), found interventions focusing on parent behaviours using a coaching approach, potentially resulted in greater improvements in parent skill development and child behavioural change.
Programme Facilitation
Parents valued a skilled and experienced programme leader. Beneficial facilitation skills included effective communication, professionalism, organization, flexibility, knowledge, ability to answer questions, and provide guidance. Literature has linked clinician communication skills and knowledge translation to increased parent satisfaction and involvement (King et al., 2017; Øien et al., 2010; Phoenix et al., 2019). In this study, participants required a programme leader who could support strategy implementation in the context of complex developmental presentations and child behaviour challenges. Being helpful, caring, and generous with time were also perceived as positive leader attributes. A lack of these specialist skills and attributes in a programme leader could represent a risk to successful parent engagement.
Individualisation of Service
Individual coaching and collaborative review of parent–child interaction videos by the parent and programme leader were the most highly rated of all HMTW programme components. The need to individualise services to meet the differing needs of families has been recognized in previous research (Carr et al., 2016; Phoenix et al., 2019). Parents valued personalised discussion regarding application of strategies and expressed greater understanding of themselves and their children following individual video feedback sessions. Parents also confirmed the importance of individualisation with regards to intervention delivery components. They expressed different preferences for use of written materials, group versus individual learning, session length and frequency, content load, preparation time, and opportunities for group interaction.
Varying parent preferences highlight the need for caution in applying a ‘one size fits all’ approach to service delivery. The findings support the importance of service choice and individualisation to enable engagement with a broad range of families. Individualising services aligns with early intervention recommendations, highlighting the need to consider family characteristics such as parent capacity and preferences, when providing early intervention supports (Roberts et al., 2016).
Learning Outcomes
Parent Strategy Implementation and Understanding
Following telepractice HMTW, parents reported improvements in communicating with their children and considered themselves likely to continue using learned strategies. Consistent with results reported by Girolametto et al. (2007), participants perceived they could implement strategies to support interaction, play, language development, and child social communication goals. Parents also described increased insight and understanding about their own interactive behaviours, motivations and learning, and their child's interests and behaviours. These insights affirm the naturalistic, social-interactionist philosophy underlying the intervention. It is possible that the child's learning was scaffolded by adult responses (Abbeduto & Boudreau, 2004; Chapman, 2000; Girolametto et al., 2007), but also that adult insights and understanding, were facilitated by observing child responses within cycles of social interaction.
Confidence
Following HMTW, all parents expressed greater confidence in playing with their children and setting communication goals for them. They reported confidence in understanding and engaging with their children and working with other service providers. Increased confidence in planning and implementing intervention indicates a capacity building component to HMTW which could potentially expand to other caregivers (Salisbury et al., 2017). It may also relate to increased self-advocacy, which has been linked to success for parents in acquiring services for their children (Smith-Young et al., 2020).
Parental Stress
Children with autism commonly present with behavioural and sensory challenges that impact parent stress levels (Bonis, 2016; Dabrowska & Pisula, 2010; Davis & Carter, 2008; Estes et al., 2013). Reflecting this, PSI results in this study represented high or clinically significant scores for several parents, particularly in the child domain which assesses behaviours that parents frequently find challenging. Overall, from pre- to post intervention, PSI results were not significantly different. This was unsurprising in the context of a short-term communication intervention and was consistent with McConachie et al. (2005), who found no significant differences between HMTW intervention and control conditions on a measure of parenting stress.
PSI results provide confirmation that parenting stress levels did not increase significantly following HMTW; nor did they decrease. Standardised measures of parenting stress following intervention in other parent training studies, have also demonstrated non significant reductions in parenting stress (Lichtlé et al., 2019). Parent's perceived stress levels following intervention however, differed from standardized results with nine parents (82%) perceiving less stress following intervention. This is consistent with a study by Ingersoll et al. (2016), who also reported reductions in perceived parent stress following a time limited autism intervention. Although short term communication interventions cannot change family living circumstances and are unlikely to change many child behaviours, it is possible that feelings of competency developed by parents through intervention, could positively influence their perceptions of stress.
Child Communication
All parents perceived improvements in their children following participation in telepractice HMTW. Parent feedback described changes in verbal and non-verbal communication, responsiveness, interaction, play, and ability to communicate effectively. Perceived child outcomes were consistent with quantitative communication outcome findings from the telepractice HMTW effectiveness evaluation by Garnett et al (2022), and with improvements in interaction, turn taking, play, and verbal communication, perceived by parents in Girolametto et al. (2007).
Implications for Service Delivery
Telepractice Delivery Method
All parents were satisfied with group telepractice intervention, reporting that telepractice met their expectations, enabled participation, and provided group support. Findings reinforced previous studies evaluating parent satisfaction with telepractice, particularly approaches involving individualised clinician assistance (Beaudoin et al., 2014; Ingersoll et al., 2016; Little et al., 2018; Pickard et al., 2016).
The research confirmed that the expansion of a traditional face to face group intervention programme to telepractice, was not only feasible and potentially effective (Garnett et al., 2019; Garnett et al., 2022), it was also highly acceptable to participating families. Although parents did not have an opportunity to experience and compare telepractice HMTW with face-to-face delivery directly, more than half the parents speculated that the learning experience would be the same.
With telepractice being increasingly used to provide services to families of children with autism, there has already been substantial relevant research (Knutsen et al., 2016; Parsons et al., 2017; Sutherland et al., 2018). In the current COVID-19 pandemic environment however, personal protective measures are necessary and regulatory changes are enabling broader application of telepractice services (Commonwealth of Australia, 2021; Havens, 2020). Ongoing research evidence to guide this burgeoning area of service delivery is therefore essential.
Despite the promise of telepractice services in increasing service access, it is recognised that technology and computer literacy remain obstacles to its adoption by some people (Kruse et al., 2018). Telepractice design utilising commonly available devices will ensure parents require fewer technology and informational resources to enable participation. Development of relevant technological expertise by clinicians will also need to evolve. Capacity to support increased access to telepractice services could be at risk if service providers are not suitably trained and resourced.
Cost
When seeking to understand and support parent engagement with services, cost and service availability have been identified as significant barriers to access and ongoing engagement (Shepherd et al., 2018). Cost was perceived as a potential barrier to HMTW participation in this study. Parents that felt able to pay, were equally willing to pay for telepractice or face-to-face delivery however, more than half the parents expected telepractice to be cheaper than face-to-face service. This expectation is consistent with research identifying cost savings in terms of travel time and expenses, for families and providers using telepractice (Little et al., 2018). Savings may also be gained by service providers in terms of facility costs (Lindgren et al., 2016).
Utilising a group telepractice approach could ameliorate cost barriers, as well as addressing geographical constraints, and provide additional service choice. Parental expectations of a cheaper service may increase participation, but could also become a barrier if actual costs were not acceptably cheaper, thereby misaligning with expectations and/or being financially inaccessible.
Limitations
The small number of participants in this study limits generalisability of results and raises concerns regarding the representativeness of the sample. All parents were already engaged with early intervention services, volunteered to participate, and the programme was delivered by an experienced leader. Participants therefore, potentially experienced different perspectives regarding the intervention than less engaged families, those from more diverse backgrounds, or those receiving intervention from a less experienced practitioner. Despite this, the qualitative information presented provides a rich source of data to inform future delivery of group telepractice interventions.
The parent perceptions investigation did not use standardised outcome measurement which has been identified as a limitation in previous group-based parent intervention studies (O'Donovan et al., 2019). The directed content analysis approach involved informed bias by the researcher based on knowledge of previous evidence and participants could get cues from the questions, potentially influencing responses (Hsieh & Shannon, 2005).
Future Directions
Factors that are considered important for effective early intervention include understanding and developing children's abilities, advocating for their needs, providing parent support, and facilitating access to services (Wainer et al., 2017). This investigation identified factors supporting parents to remain engaged in a specific intervention programme and factors enhancing their experience, but did not address engagement of families in early intervention services more broadly. Development and application of standardised tools to measure and compare parent perceptions across interventions and service delivery approaches in the early intervention domain would be advantageous. Assessing individual parent and family factors within such tools could also enable evaluation of the influence of elements such as socio-economic status, family culture, and wellbeing on family engagement, parent strategy implementation, and child and family outcomes. Standardised measurement of parent perceptions could facilitate a broader understanding of family needs with respect to service access and engagement (O'Donovan et al., 2019), thus informing ongoing early intervention service development.
Evidence of skill maintenance and long-term outcomes following parent-implemented intervention remains limited (Hong et al., 2018). Learnings from this study could be enhanced through future HMTW research including larger participant numbers and longer-term measurement of both parent strategy use and parental stress levels. More detailed investigation into the role of social support in parent group intervention and consideration of potential adverse effects would also be beneficial (O'Donovan et al., 2019).
A review of telepractice intervention characteristics by Camden et a,l. (2019) recommended that, “Future trials should compare telerehabilitation interventions to well-described evidence-based face-to-face interventions and document their cost-effectiveness.” This recommendation would be appropriately applied to future HMTW research.
Summary and Conclusions
This research built an understanding of parent experiences and preferences within group telepractice HMTW, its components, and service delivery method. A measure of parenting stress confirmed information regarding the social validity of the approach. Results contribute information to inform future service offerings that could increase intervention choice, and support access and engagement for families of children with autism.
Continuing to develop, expand and evaluate telepractice services can increase efficiencies and choice for families and providers. Limitations in service availability and barriers to service access and engagement, confirm the importance of pursuing and evaluating ongoing service improvements.
The quote below highlights the experience of one family who participated in telepractice HMTW. With continued learning about effective and engaging service provision, it is hoped this could be the experience of many.
“I found the leader's information like opening a present that I had kept in a drawer and didn’t even realise it was there. She helped me gain more confidence in myself as a parent in not being afraid to try new things. I was scared about playing with my child because I always expected he would have a tantrum and not want me to join in his play, but since doing this programme, it has been the exact opposite. I learned more about my child in this time that I never thought I would learn. He actually loves playing with me.”
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.