
Abstract
Background and Aims
Early intervention (EI) for young children with autism spectrum disorder (ASD) must be resource-efficient while remaining effective; thus, clinicians are challenged to create and implement useful methods. Clinical evidence from community-based interventions that include reliable diagnoses, individual EI programs, along with comprehensive descriptions of participants, procedures, and participant outcomes can inform practice, translational research, and local policy. Parent-mediated EI for toddlers with ASD can promote positive developmental outcomes and lifelong well-being, but evidence of successful community uptake of research-based EIs is somewhat limited. The community-based, parent-mediated, evidence-informed QuickStart EI program aims to encourage toddlers’ early social communication, social interactions, and relationship-building, in a community clinic setting.
We aim to (1) describe our adaptations to the evidence-based Parent-Delivered Early Start Denver Model and (2) present promising findings for toddlers with or at risk for ASD and their families who received QuickStart. We also intend to motivate a similar study of EI in real-world situations to advance evidence-based practice and create relevant dialogue and questions for research.
Methods
Complete data were identified and analyzed for up to 89 toddlers diagnosed with, or at risk of, ASD. Pre- and post-intervention parent- or self-report data were analyzed using descriptive statistics and paired-sample t-tests, as appropriate. Pre-intervention measures included demographic information (n = 89) and the Early Screening of Autism and Communication (ESAC; n = 89). Measures taken pre- and post-intervention included the Adaptive Behavior Assessment System-II (n = 60), MacArthur-Bates Communication Development Inventories (n = 58), and the parental sense of competence scale (n = 62). The Measure of Processes of Care (n = 60) was taken post-intervention. On enrollment, parents signed standard clinical agreements that included statements allowing their anonymous data to be analyzed for research.
Results
Using standardized parent/self-report measures, toddler gains were noted for social interaction, language, communication skills, and ASD symptoms, but not for parents’ feelings of competence. Parents identified QuickStart procedures as family centered (Measure of Processes of Care).
Conclusions
The QuickStart EI program, provided to toddlers and their families over 20 weeks in a community clinic, resulted in promising positive behavior and communication changes, as indicated on the parent-response measures, for a moderately large sample of toddlers.
Implications
This study adds to the literature by describing a new EI program with clear procedures by which clinicians can create, provide, and evaluate a readily accessible, community-based EI for toddlers with or at risk of ASD. Methodological limitations inherent to our study design that precluded a control group and necessitated a reliance on available parent-report data are carefully critiqued and discussed.
The toddler years of early development are critical for children to learn important foundational skills that lead to their future productivity and well-being. Effective early intervention (EI) for children with autism spectrum disorder (ASD) is essential to decelerate cascading developmental challenges associated with limited early social interactions and improve developmental trajectories (Piccininni et al., 2017; Wetherby et al., 2018; Zwaigenbaum et al., 2015a). Inaction or delayed action for young children with or at risk for ASD may have lifelong consequences for them as ASD symptoms such as lessened social communication skills and over-selectivity in interests result in fewer opportunities to learn from others (Camarata, 2014). Early detection of ASD and access to EI promote long-term developmental outcomes for children and families, and ultimately for society (Oono et al., 2013; Piccininni et al., 2017; Wetherby et al., 2014; Zwaigenbaum et al., 2015a). To this end, the American Academy of Pediatrics recently updated ASD identification, evaluation, and management guidelines to emphasize swift referral to EI as soon as developmental concerns are identified (Hyman et al., 2020).
Findings of comprehensive research reviews that have informed professional guidelines emphasize the need for readily available efficient, effective, and “community-viable” EI for families (Wetherby et al., 2018, p. 2616). Models of parent-mediated EI that coach parents and other caregivers to serve as interventionists may be effective for short- and long-term learning outcomes for very young children with ASD (Brian et al., 2017, 2022a; Landa, 2018; Nevill et al., 2018; Schertz et al., 2013; Wetherby et al., 2014, 2018; Zwaigenbaum et al., 2015a, 2015b). Moreover, EIs that are developmentally grounded, individualized, focused on comprehensive learning targets, and initiated as soon as concerns are noted, allow the best possible child development to begin (Zwaigenbaum et al., 2015a). Community-based, parent-mediated EI for toddlers at risk for ASD may provide a wider, cost-effective opportunity reach to all toddlers and their families who would benefit from an early launch to enriched learning (Brian et al., 2022a; Cidav et al., 2017; Wetherby et al., 2018; Zwaigenbaum et al., 2015a).
Systematic reviews in the recent past identify methodological limitations to EI studies including small sample sizes, a paucity of randomized controlled trials (RCTs), and inconsistent outcome measures (French & Kennedy, 2018; Karst & Van Hecke, 2012). Recently, there is emerging a body of RCT evidence (Brian et al., 2017, 2022a; Stadnick et al., 2015; Wetherby et al., 2014) finding positive effects on social communication, language, and play skills development (Sandbank et al., 2020). However, there remains a continuing concern for better study quality (Sandbank et al., 2020). Given the current appreciation for the dynamic and complex nature of EI for ASD, rigorous attention from investigators is needed, including in community-partnered participatory research (Brookman-Frazee et al., 2016; Sandbank et al., 2020; Vivanti et al., 2018; Wetherby et al., 2014).
Benefits of parent-mediated EI for ASD
Evidence indicates that parents can learn to use intervention strategies in daily activities and interactions with their toddlers to augment learning (Estes et al., 2014; Hampton & Kaiser, 2016; Landa, 2018; Oono et al., 2013; Schreibman et al., 2015; Wetherby et al., 2018). As parents become competent in helping their child learn at home, they also generalize these skills to other environments, which is vitally important but often challenging to achieve in traditional intervention models (Rogers et al., 2019a, 2019b). Additionally, parent-mediated EI can result in decreased family stress, positive feelings about intervention, and valuable knowledge of child development (Estes et al., 2014; Karst & Van Hecke, 2012; Weitlauf et al., 2022). Parent-mediated, family focused EIs are effective in promoting the achievement of family identified goals (Hwang et al., 2013), parent–child relationships (Carter et al., 2011), and notably, improving parents’ satisfaction with care (Oono et al., 2013).
Additional benefits for parents and their very young children with ASD are supported by evidence (Bentenuto et al., 2020; Bradshaw et al., 2015; Hampton & Kaiser, 2016; Karst & Van Hecke, 2012; Landa, 2018; Oono et al., 2013; Vivanti et al., 2018; Wetherby et al., 2018; Zhou et al., 2018). For instance, precursors of important foundational social and communication development are boosted because gains occur during a time of rapid overall development and also during the window of time when the symptoms of ASD tend to unfold (Landa, 2018, p. 7); this is also a time when cognitive and adaptive skills might improve significantly (Bentenuto et al., 2020). Benefits for parents and children include improved interaction skills for better relationships and learning, while the family waits for other services, or when access to professional intervention is not feasible (Franz & Dawson, 2019; Zhou et al., 2018).
High-dose EI, though most effective for child outcomes (Landa, 2018), is cost-prohibitive for most community clinical programs. Low-dose EI is cost-friendly and results in significant main effects on parent behaviors, but changes for children on measures of verbal and nonverbal performance, or on ASD symptoms, have not been as reliably reported, depending on the program (Rogers et al., 2019a, 2020; Sandbank et al., 2020; Wetherby et al., 2018). However, evidence is evolving of child gains following brief parent-mediated interventions, particularly in naturalistic developmental behavioral interventions (Brian et al., 2022a; Sandbank et al., 2020). Specifically, early development in infants and toddlers at high risk for ASD is augmented in lower-dose EI when parents learn to use child-responsive strategies (Landa, 2018; Wetherby et al., 2018). In one example, enhancements to a low dose/intensity treatment, where a developmentally grounded (Camarata, 2014; Schreibman et al., 2015), social curriculum was taught to parents, resulted in significant child changes at the 6-month follow-up (Landa, 2018). Landa showed that a hybrid model that combined parent-mediated intervention with direct, clinician-implemented intervention, resulted in significant child developmental gains (Landa, 2018).
Interaction strategies such as promoting sensitive parental responsiveness, turn-taking, following the child's lead, imitation, and progressive matching are all skills necessary for toddler learning (Camarata, 2014; Sandbank et al., 2020; Schreibman et al., 2015; Wetherby et al., 2018). Moreover, reducing core deficits and associated features of ASD that interfere with infants’ and toddlers’ active participation in early interactions is considered imperative to improve their outcomes (American Speech-Language-Hearing Association (n.d.). When parents’ capacity to use responsive engagement strategies is developed through coaching, a collaborative process (Movahedazarhouligh, 2021), transactional benefits within the dyad occur resulting in improved child social communication and language outcomes (Hampton & Kaiser, 2016; Landa, 2018; Wetherby et al., 2018).
Purpose
EI for young children with or at risk for ASD must be resource-efficient while remaining effective; thus, clinicians need to determine which methods are most useful. Clinical evidence from community-based interventions that include reliable diagnoses, individual EI programs, along with comprehensive descriptions of participants, procedures, and participant outcomes can inform practice, translational research, and local policy. Parent-mediated EI for toddlers with ASD can promote positive developmental outcomes and lifelong well-being, but evidence of successful community uptake of research-based EIs is somewhat limited (Stadnick et al., 2015). The community-based, parent-mediated, evidence-informed QuickStart EI Program was developed to stimulate toddlers’ early social communication, social interactions, and relationship-building in a community clinic setting.
We aim to (1) describe our adaptations to a current, evidence-based EI that resulted in a parent- and therapist-delivered hybrid model of the parent-delivered ESDM (P-ESDM; Rogers et al., 2012) and (2) present promising findings for children with or at risk for ASD and their families receiving services in a community clinic. We also intend to encourage a similar study of EI in real-world situations to advance evidence-based practice and create relevant dialogue and questions for research.
Methods
Ethical considerations
All procedures involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics approval to analyze the data and publish the findings was obtained from the research department of the Children's Hospital of Eastern Ontario. Data were analyzed post-hoc, following completed participation in the QuickStart program.
Setting
QuickStart was delivered in an established community clinic for the treatment of ASD between 2013 and 2018 in Ottawa Canada. During that time there was a two-year or more waitlist for government-funded EI services and no publicly funded parent-mediated programs. Based on a local pilot study (Gaines et al., 2021), QuickStart was provided to families by the QuickStart registered charity (QuickStart Early Intervention for Autism, 2022) to fill the EI need.
Participants
Any family in Ottawa with concerns about their toddler having ASD was offered the QuickStart EI, fully funded by the charity (QuickStart Early Intervention for Autism, 2022). As parents and professionals learned about QuickStart referrals came via a registered psychologist, the Children's Hospital of Eastern Ontario, other intervention projects, social workers, and speech-language pathologists (SLP). The clinical dataset held data on parent report measures for 132 QuickStart families and thus was explored for complete data that could be analyzed for evidence of child and parent outcomes. Complete baseline data for 89 families were available from the clinical dataset; up to 62 families had pre–post-data, depending on the measure. Different families had complete data per measure. All the toddlers were diagnosed with, or at high risk for, ASD.
Families
Pre-intervention measures included demographic information (n = 89) and the Early Screening of Autism and Communication (ESAC; n = 89). Measures taken pre- and post-intervention included the Adaptive Behavior Assessment System-II (ABAS-II, n = 60), MacArthur-Bates Communication Development Inventories (MB-CDIs, n = 58), and the parental sense of competence (PSOC) scale (n = 62). The measure of processes of care (MPOC; n = 60) was taken post-intervention. For reasons not recorded, 43 families left QuickStart without completing all measures. On enrollment, parents signed standard clinical agreements that included statements allowing their anonymous data to be analyzed for research. Figure 1 presents the numbers of participants with complete data for each measure, used in analyses.
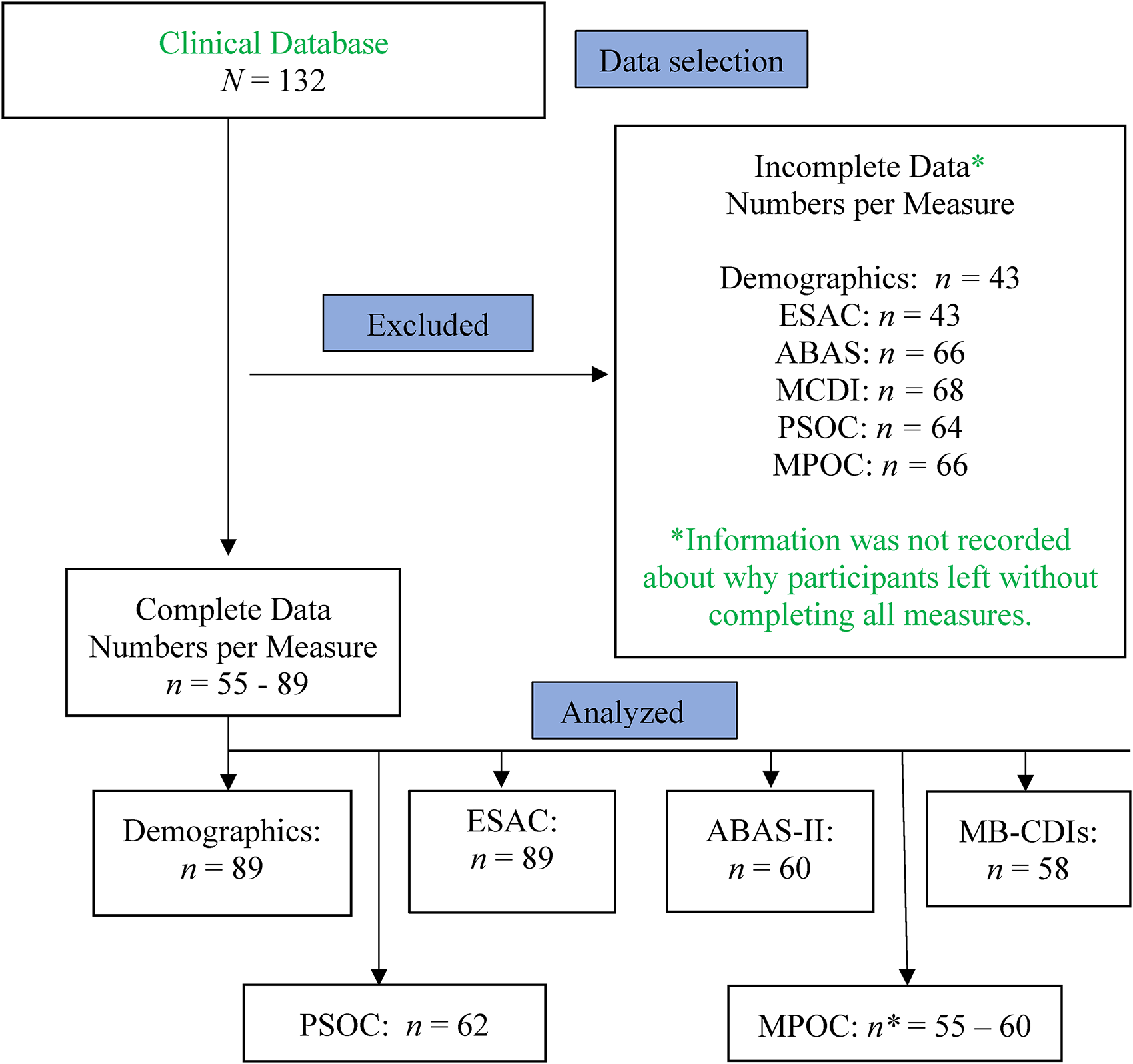
Numbers analyzed, per measure.
Of the 89 families with complete demographic data, 91% (n = 82) were two-parent and employed, 92% (n = 82) of the mothers had a college education or higher and 85% (n = 76) of the fathers had a college education or higher. Sixty-four percent (n = 57) identified English as their home language, 6% (n = 5) French, and 9% (n = 8) bilingual French and English. QuickStart families are representative of population proportions for education, employment, and languages of people in the greater Ottawa, Canada community (Statistics Canada, 2017).
Nearly half of the mothers (n = 44) reported prenatal complications (anemia, gestational diabetes, preterm labor, pre-eclampsia, bleeding, or multiple complications). Twenty-five percent (n = 22) of families reported preterm births for the toddler participant; delivery at 37 weeks or less. Ten percent (n = 9) of toddlers were born preterm or low birth weight (LBW; <2500 g), a higher preterm birth rate than the national average of 7% to 8%, and higher than the national LBW rate of 6% (Statistics Canada, 2016). The percentage of children delivered by Caesarean was 33.3% (n = 29), comparable to the national percentage of 27.2% (Matteis, 2015).
Toddlers
There were complete demographic data for 89 toddlers. They ranged in age from 12 to 39 months (M = 27.1, SD = 5.77) at the beginning of their participation. Seventy-four percent (n = 66) were boys, in keeping with current reports of a 3:1 male-to-female ratio for ASD diagnoses (Loomes et al., 2017). Sixty-three percent (n = 56) had one or more siblings; 24% (n = 21) had at least one sibling with ASD, and 27% (n = 24) had a sibling with health concerns, including ASD. Twenty-one percent (n = 19) of the toddlers had no other illnesses; 34% (n = 36) had ear infections and 45% (n = 40) had other types of childhood diseases or conditions (e.g., bronchitis, bronchiolitis, chicken pox, jaundice, croup, breathing difficulties, colds, pneumonia, flu, strep throat, or other infections).
Parents reported having concerns about their toddler's development between 2 and 27 months of age, with the most reported age being at 18 months (n = 27; 30%). Twelve months was the next most commonly reported age (n = 5; 16%). Communication and/or speech development were frequently the first concerns, but others were sensory issues, missed milestones, abnormal social interactions, behavior problems (including aggression), and attention difficulties. Three percent of families (n = 3) with an early diagnosis reported that the diagnosis itself was their primary concern.
Toddlers received screening and/or assessments for ASD from community-based pediatricians, registered psychologists, or a developmental pediatrician at a children's treatment center. Specific diagnostic and screening tools used were not recorded because we only required a positive indication of ASD risk at the entry for every child that enrolled; at enrollment, all toddlers received and screened positive on the ESAC (Wetherby et al., 2021). There was no difference in wait time to begin QuickStart for children who had not yet received an ASD diagnosis and those who had.
Of the 89 toddlers with demographic data, 59 (66%) had received an ASD diagnosis before enrolling. All of those 89 exited the program with a positive diagnosis. Toddlers’ diagnoses were received between the ages of 11 and 41 months of age (later ages indicate diagnosis after enrollment). The mean age of diagnosis was 24.8 months (SD = 6.48), earlier than most children in Canada who typically receive a diagnosis between 39 and 55 months of age, depending on their region (Ouellette-Kuntz et al., 2009). Families were asked to limit other therapies for their toddlers to <10 h per week while in QuickStart.
Demographic information for participants who had complete pre–post-data was compared to that of participants who did not have complete data. Chi-square tests indicate that they did not significantly differ on categorical variables of child sex (X2 (1, N = 132) = 2.28, p = .13), ethnicity (X2 (6, N = 131) = 7.67, p = .26), home language (X2 (10, N = 132) = 7.73, p = .66), maternal education level (X2 (4, N = 132) = 4.12, p = .39), or number of siblings in the home (X2 (5, N = 130) = 3.96, p = .56). Because cell counts were less than usually accepted minimums, we used caution interpreting the findings.
An independent samples t-test revealed that, on average, the ESAC scores of toddlers who had complete pre–post-data (M = 32.5, SD = 9.9) were not significantly different from those who did not (M = 35.1, SD = 11.2), t (87) = −1.13, p = .26, 95% CI [−7.2, 2.0]. They did not differ on the MPOC. We therefore have confidence that the sample represents our clinical population for the ESAC and the MPOC.
Differences were found between those with complete pre–post scores and those with only pre-QuickStart scores for the ABAS-II and the PSOC. Those with incomplete data had significantly lower scores than those with complete data on the pre-QuickStart ABAS-II practical composite score (t[123] = 2.04, p = .04; mean difference = 4.91, 95% CI 5 [0.15, 9.68]). This difference may indicate an unintended developmental advantage in QuickStart for the children with complete data. Additionally, Chi-square tests revealed a higher proportion of males to females in those with complete data when compared to those with incomplete data, for the ABAS-II (χ2 [1, N = 132] = 4.95; p = .03), and the PSOC (χ2 [1, N = 132] = 5.90; p = .02).
The QuickStart EI program
The Early Start Denver Model (ESDM; Rogers and Dawson (2010) is a 2-year program based on developmental and applied behavioral analytic principles, delivered by trained therapists and parents. It is designed to foster positive relationships between children and significant adults by enhancing parent–child interaction skills that optimize child learning (Franz & Dawson, 2019; Zhou et al., 2018). ESDM strategies include promoting sensitive parental responsiveness, turn-taking, following the child's lead, imitation, and progressive matching. These are important foundations for learning, verbal language development, and social communication development (Camarata, 2014; Sandbank et al., 2020; Schreibman et al., 2015; Wetherby et al., 2018). At least one meta-analysis of ESDM describes positive child effects (Fuller et al., 2020) and other evidence shows improved cognitive performance, language skills, and adaptive-behavior skills in some young children with ASD following ESDM (Dawson et al., 2010; Ryberg, 2015; Warren et al., 2011).
In the ensuing low-intensity parent-delivered ESDM (P-ESDM; Rogers et al., 2012), parents are coached to use the interactive principles associated with ESDM rather than the EI being therapist-delivered. Parents do not elicit or tally specific behavioral objectives in P-ESDM, instead, they learn to incorporate strategies fitting their child's unique needs, within typical activities. Reviews of parent-mediated EI, including P-ESDM (Rogers et al., 2012, 2019a, 2019b), have found effects on parent behaviors but less robust changes for children on standardized measures of verbal and nonverbal performance, or on ASD symptoms, especially in low-dose interventions (Sandbank et al., 2020; Wetherby et al., 2018). There is limited evidence that P-ESDM is associated with a reduction in autism symptom severity and gains in cognitive and adaptive skills (Weitlauf et al., 2022).
Quickstart adaptations for a hybrid approach
QuickStart is delivered to individual parent–child dyads at a community clinic in weekly, 1–1.5 h sessions. Seven weeks of individual sessions with the SLP and/or OT, and one home visit by a parent coach, were major adaptations to P-ESDM (Rogers et al., 2012). The additional eight sessions were provided before the 12 weeks of P-ESDM, for a total of 20 weeks in the program. Using P-ESDM methods and materials (Rogers et al., 2012), QuickStart coaches encourage parents to use strategies for responsive and child-centered interactions in play and other daily routines (Rogers et al., 2012, 2019b). As parents become increasingly competent using the strategies, they are able to provide consistent, positive, stimulation for their toddlers in most environments. With the adaptations, QuickStart is a hybrid approach, providing both parent-mediated intervention and therapist support.
At week 7, a 1 to 1.5 h P-ESDM evaluation and transfer to the parent coach session occurs with the SLP or OT and the family. This session achieves two important objectives for the parent–toddler dyads: (1) the opportunity to focus on domain-specific development goals and (2) the opportunity to create an inter- and multi-disciplinary family centered approach to the treatment plan. Table 1 presents an overview of the general structure for the first seven weeks’ sessions.
General structure of adaptations #1 (SLP) and #2 (OT): seven weeks in individual sessions with therapists, determined by the child's needs.

SLP: speech-language pathologists; OT: occupational therapist.
Note. aWeekly sessions may alternate between OT and SLP, or be focused more on one discipline, depending on the child's needs.
P-ESDM intervention sessions
During the last 12 weeks of QuickStart, P-ESDM strategies are introduced as instructed in the parent manual and according to each parent's progress (Rogers & Dawson, 2010; Rogers et al., 2012). P-ESDM involves guided practice for the parent and reflection on their interactions with their child when using the strategies. The manual is a resource guide for parents during the collaborative coaching process with a new topic each week. Topics are based on parent reports of successes and challenges during the week, the coach's observation of a parent's strategy used in the first activity of the session, and a reflective discussion between them about the interaction. The number of strategies and their order of introduction are determined collaboratively by the coach and parent and are responsive to individual needs. Coaches used either English or French in their sessions, depending on the preference of the family.
P-ESDM sessions are consistent. The parent and child first engage in preferred play, allowing the coach to identify weekly progress and challenges. Then the coach invites discussions with the parent about the week's practice and, when necessary, suggests supplementary goals. Following the discussion, the coach introduces a new strategy and provides supplementary written information. Written material is provided for complete descriptions of each ESDM theme. The one-to-one coaching then focuses on how to embed each strategy into their child's play and other daily interactions, and how to integrate the new strategy with previous strategies (Rogers et al., 2012). Parents also learn to identify other activities and interactions for strategy practice, to encourage generalization.
Individual objectives for the parent–toddler dyads derive from SLP and OT consultations, parents' expression of their priority needs, and completed ESDM Curriculum Checklists (Rogers & Dawson, 2010). Goals are based on individual learning needs in developmental domains: (a) receptive, and (b) expressive, communication, (c) joint attention/social skills, (d) imitation, (e) cognition, (f) fine and gross motor skills, (g) behavior, and (h) personal independence. Manualized parent-friendly goals are presented in 4 to 6 steps. The coach helps the parent identify toys, games, and daily activities that best facilitate goal achievement, each week. At every session, the coach informally evaluates progress by observing dyad interactions and by discussing journal entries. Only when a parent has particular difficulty implementing a strategy do coaches actively intervene within the parent–toddler dyad.
Child measures
MB-CDIs raw scores in children with ASD are concurrently associated with communicative word use in language samples (Feldman et al., 2005). The MB-CDIs demonstrate agreement with other standardized measures and direct observation of behavior for expressive language in children with developmental delays (Heilmann et al., 2005).
Parent measures
Analytic plan
We were acutely cautious applying statistical tests, understanding the limitations of our post-hoc analyses of data taken from a clinical dataset and our one-group pre–post design. We took care not to risk assumptions beyond the simple data and so applied within-subject pre–post comparative analyses (i.e., paired samples t-tests) when appropriate. Data analyses occurred for between 55 and 66 toddlers and parents, depending on the measure. All measures were non-blinded parent-report measures. Raw or scaled scores were used to compute and compare simple within-subject means (uncorrected p-values). Since some families had pre- and post-scores on one measure but not others, the sample is not comparable across measures; we discuss findings measure by measure or subscale by subscale.
Results
Child measures
Early screening of autism and communication
ESAC data were available for 89 toddlers. The ESAC indicates significant red flags for ASD if a child between the ages of 12 to 17 months scores 20 or higher, or a child between the ages of 18 to 36 months scores 18 or higher. ESAC scores ranged from 6 to 60 (M = 34.06, SD = 10.72). The mean ESAC score for QuickStart toddlers aged 12 to 17 months was 33.6 (SD = 12.2), and 34.1 (SD = 10.7) for those aged 18 to 36 months. All 89 toddlers in the sample had received the ESAC and were screened at high risk for ASD.
Adaptive behavior assessment system-II
Pre- and post-intervention ABAS-II scores were available for 60 toddlers. Paired samples t-tests examined pre- to post-QuickStart changes in individual daily living domains and for four composite scores (general-adaptive, conceptual, social, and practical). We found significant changes in domains of communication, pre-academics, and self-care; and for general-adaptive and conceptual composite scores. Parents reported significantly improved functioning in areas that correspond to some clinical symptoms or concerns of ASD; namely, verbal and non-verbal communication, learning, and self-help or practical skills (Table 2).
Adaptive behavior assessment system (ABAS) scaled scores, pre- to post-QuickStart intervention.

Note. n = 60.
MacArthur-Bates communication development inventories
The MB-CDIs Words and Gestures form was administered at pre- and post-QuickStart interviews. Of 58 toddlers with pre- and post-intervention scores, 26% (n = 15) who were reported by parents not to respond to their name pre-QuickStart, did at post-QuickStart (X2 [1, N = 58] = 1.88, p = .17). Similarly, 12% (n = 7) who did not respond to “no–no” at pre-QuickStart did at post-QuickStart (X2 [1, N = 58] = 15.16, p < .001); 22% (n = 13) who did not respond to “there's mommy/daddy” at pre-QuickStart did at post-QuickStart (X2 [1, N = 58] = 3.49, p = .06); 81% (n = 47) who did not imitate at pre-QuickStart did at post-QuickStart (X2 [1, N = 58] = 8.68, p = .003); and 59% (n = 34) who did not label at pre-QuickStart did at post-QuickStart (X2 [1, N = 58] = 11.98, p = .001).
Raw scores on the vocabulary checklist from pre- to post-QuickStart were compared using paired samples t-tests. Mean scores for phrases understood, words understood, words understood and said, and total gesture use, increased significantly from pre- to post-QuickStart as is shown in Table 3.
MacArthur–Bates communicative development inventories (MB-CDIs) raw scores pre- and post-intervention

Note. n = 58; *** p < .001.
Parent measures
Parental sense of competence
The PSOC scale has a raw score range from 16 to 96. We calculated algorithm scores where 1 = low self-confidence, 2 = moderate self-confidence, and 3 = high self-confidence. For 62 parents with PSOC pre- and post-QuickStart scores, significant changes were not observed. Parents reported less than moderate self-confidence in their parenting at both times (n = 62) as presented in Table 4.
Total parental sense of competence (PSOC) scale scores and algorithm pre- and post-intervention.

Note. n = 62.
Measure of processes of care
On average, parents felt “to a great extent” that they received the information, support, and care they needed while enrolled in QuickStart. These findings suggest that QuickStart is acceptably family centered. MPOC responses and ratings are presented in Table 5.
Measure of processes of care (MPOC) mean scale scores, post-intervention.

Note: aScores are scale scores as per the MPOC manual.
Discussion
Studying intervention and treatment delivery innovations in community settings via applied, exploratory, research will advance outcomes for families of young children with ASD. Embedded translational research in community settings could provide local practical solutions to challenges for best practice service delivery. This report presents comprehensive descriptions of a unique parent- and therapist-delivered hybrid EI, adapted for a community clinic, with encouraging findings. QuickStart aimed to provide toddlers with ASD a critical early start to foundational learning in their home community at a time when options for EI were scarce. Our clinical dataset presented an opportunity to study outcomes for toddlers with ASD and their parents.
Families were provided the QuickStart EI free of charge because of funding from the QuickStart-EI for Autism charity in Ottawa, Canada (QuickStart, 2021). QuickStart provided families with 20 weeks of an adapted version of the evidence-based P-ESDM EI (Dawson et al., 2010; Rogers et al., 2012). QuickStart began with seven individual sessions with OT and SLP clinicians followed by one home visit by the parent-coach before the 12 P-ESDM sessions began, resulting in a parent- and therapist-delivered hybrid approach (Landa, 2018). QuickStart chose to use P-ESDM curricula because it integrated ABA principles with a developmental, relationship-based approach, and it is manualized, structured, and comprehensive (Rogers & Dawson, 2010). QuickStart is child-focused and family centered. It is multi-disciplinary in parent consultations, collaborations, and goal setting. The emerging use of QuickStart strategies in natural environments by primary adult partners increases the likelihood of opportunities for generalized learning experiences for their toddlers which may result in important social–emotional and play skill development.
QuickStart provides supplemental practices that include: (a) a predictable structure for the coaching sessions, (b) a responsive team approach for collaboration with parents, (c) a high-intensity, low-dose, intervention; high intensity as parents become interventionists, (d) a required commitment from a parent to attend all sessions and participate in required minimum practice levels every day, and (e) elicited feedback from parents via journaling. Additionally, individualized goals, intervention steps, and methods intrinsic to P-ESDM are introduced and reinforced by the SLP and OT in their sessions, as they aim to encourage consistent engagement by each parent in learning experiences that are essential and positive for their toddler.
Our study of QuickStart's adapted hybrid EI is preliminary. We report the results of a one-group, pre–post, exploratory study of a community clinic application of an evidence-informed model. Our clinical evidence indicates acceptable practical effectiveness in this setting for a relatively low-dose treatment. We believe that our adaptations to P-ESDM prepared parents to better understand child development and early characteristics of ASD, and therefore to optimally use EI strategies at home. The first eight weeks in QuickStart may have provided valuable time for the treatment team and families to form trusting relationships and collaboratively establish individual goals. The contribution of multidisciplinary clinical expertise to goal setting and treatment collaboration may have helped parents fully engage as effective interventionists. Though the resource demand of adding clinician consultation must be considered, the possibility that these low-dose enhancements benefit child outcomes in parent-mediated EI models is worth considering in future investigations (Landa, 2018).
QuickStart becomes progressively intensive during the 12 weeks of parent coaching because parents become increasingly competent at embedding the intervention in daily living with their toddlers. Parents learn to scaffold their skills and become proficient social communication partners who enrich all interactions for optimal learning by their toddler, thereby generalizing the strategies. Assessing parents’ intervention dose and intensity outside of coached sessions will be important to objectively inform future practice.
Though QuickStart parents were satisfied with the EI methods (MPOC) their self-reports of low–moderate confidence in their parenting competence (PSOC), an important aspect of emotional well-being, persisted over the 20 weeks. QuickStart did not have a direct focus on parenting competence, but our finding is noteworthy, given that parents’ contributions to, and their ad hoc reports of, their children's progress were positive; and that other studies have found improvements through parent training (Brian et al., 2022b; Iadarola et al., 2018). We posit that perhaps the PSOC, used as our sole measure of parent self-efficacy, could not identify all the complex aspects of our parents’ emotional experiences, to detect changes in their emotional well-being, over the 20 weeks (e.g., Karp et al., 2015; Wittkowski et al., 2017). Future studies should include a predetermined and clear plan to measure parent well-being which will help interpret our conundrum.
We did not measure parent stress though we know that participation in EI can disrupt family systems, beginning with the diagnosis. Parents of toddlers newly diagnosed with ASD experience very high levels of stress as they are faced with developmental and behavioral challenges (Nordahl-Hansen et al., 2018) and continuing high levels of stress can affect all aspects of their lives (Costa et al., 2017; Halstead et al., 2018). Since stress can negatively affect family functioning (Rovane et al., 2020; Stadnick et al., 2015; Weitlauf et al., 2022), a multifactorial model of evaluation may be required in future studies to examine, with validity, parenting self-efficacy, stress, mental health and the parent–child relationship relating to intervention outcomes in parent-mediated EI programs (Karst & Van Hecke, 2012). Perhaps more frequent repeated measures and especially, a delayed post-treatment measurement, when parents have become removed from performance demands and perceived judgments that are necessary for intervention, could more clearly demonstrate positive changes. Future studies with a planned focus on parents should help inform these hypotheses (Shalev et al., 2020).
Parent-mediated EI for children with ASD should have a strong basis in family centered care (Division for Early Childhood, 2014) where the well-being of the whole family is considered (Lindsey & Barry, 2018; Wetherby et al., 2018; Zwaigenbaum et al., 2015a). We deliberately cultivated a family focus in our adaptations, which may have influenced parents’ comfort with QuickStart procedures and resulted in their positive acceptance of the P-ESDM intervention with cascading benefits for the toddler (Lindsey & Barry, 2018).
Limitations
Though our parent report measures are completely acceptable in clinical settings, sole reliance on them for research is not considered adequately rigorous. Parent report measures introduce a risk of detection bias (Sandbank et al., 2020) that decreases our confidence in child outcome findings. Parent report is problematic to parent-mediated EI research because parents are the direct recipients of the intervention and their reports regarding development could be secondary to their increased sensitivity and responsivity through training. Future clinical evidence can be strengthened using RCT designs that control for child maturation and parental sensitivity, and by using diverse test batteries that include objective measures.
We did not measure parent treatment fidelity (FOT), nor track time in daily practice. Measuring parental FOT and practice time would enable correlation analyses between them and child outcomes. Moreover, because there was no randomization nor a control or comparison group, we could not demonstrate a correlation between QuickStart and the reported child outcomes, and obviously no causation. We therefore cannot claim that QuickStart is superior to or worse than another EI, or indeed, different than no intervention at all.
Toddlers with complete data for the ABAS-II had higher scores on the practical composite score at pre-QuickStart than those who did not have complete data. The toddlers with families who completed the post-ABAS-II may have started QuickStart with a developmental advantage that positively affected their post-ABAS-II outcomes. We did not track reasons for incomplete data. There were families who completed the intervention but did not complete all post-intervention measures. Families’ reasons for incomplete ABAS-II, as well as other measures, were not tracked. The lack of data to answer the question about developmental differences at the outset of QuickStart is a weakness of our convenience, post-hoc, clinical data analysis that will be remedied in a future study.
Though our population was diverse with respect to birth complications, it was skewed to the upper middle class and highly educated families in Canada's capital city. We cannot generalize findings to other or more diverse populations or locations. Future studies of QuickStart will include diverse demographics as well as birth situations.
Conclusions
This detailed clinical report with critical discussions of a preliminary applied research study is meant to add practical information to dialogues for ASD EI research. We hope to motivate other clinicians and administrators to conduct embedded translational research within their practices, ask important clinical questions, and find data-informed solutions about how to advance treatments for toddlers in their communities.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the QuickStart Early Intervention for Autism Registered Charity, Ottawa, Canada.