
Abstract
Background and aims
Early play behaviors may provide important information regarding later-diagnosed developmental delays. Play behaviors of young children with autism spectrum disorder are restricted in diversity, frequency, and complexity. Most autism spectrum disorder research focuses on play in children over 18 months of age. This study examined three groups of infants (later diagnosed with autism spectrum disorder, later diagnosed with other developmental disorders, and typically developing) with the aims of: (1) describing the play behaviors of the three groups of infants at two time points (9–12 months and 15–18 months); (2) examining group differences in four hierarchical levels of play at both time points; (3) comparing groups with respect to the highest level of play achieved; and (4) determining if the highest level of play achieved by infants with autism spectrum disorder and other developmental delays correlated with later developmental outcomes.
Methods
The current study used longitudinal retrospective video analysis to examine object play behaviors of the three groups of infants (total n = 92) at two time points (time 1: 9–12 months of age, and time 2: 15–18 months of age). Coding of play behaviors was based on existing literature and distribution of data from the current study. Developmental outcomes examined were measured using the Vineland Adaptive Behavior Scales, Childhood Autism Rating Scale, and a non-verbal developmental quotient calculated using visual reception scores from the Mullen Scales for Early Learning.
Results
Results indicate group differences in play, with infants later diagnosed with autism spectrum disorder showing significantly less sophisticated play than those with typical development. In addition, modest but significant correlations were found between highest level of play achieved at time 1 (9–12 months) and time 2 (15–18 months) and later outcomes for the autism spectrum disorder group.
Conclusions and implications
Results suggest that examination of infant play behaviors is important for early screening and intervention planning to potentially mitigate effects on later developmental outcomes.
Introduction
Play is an integral component of development during early childhood, and a means by which typically-developing (TD) children explore, discover, and develop knowledge of their physical and social worlds (Naber et al., 2008; Vig, 2007). Furthermore, play is one of the primary means by which children build fundamental skills that facilitate development of language and social cognition throughout life (Lifter, Foster-Sanda, Arzamarski, & McClure, 2011). Along with those who have noted motor development (e.g. Iverson & Braddock, 2011; Leonard & Hill, 2014) and maternal responsiveness (Bornstein, Tamis-LeMonda, Hahn, & Haynes, 2008) as contributing factors to cognitive and language development, many researchers have documented a relationship between the development of play and language (e.g. Lewis, 2003; Vig, 2007). Infants at high risk for autism spectrum disorder (ASD) and those who later receive this diagnosis tend to exhibit early motor delays (Bhat, Landa, & Galloway, 2011; Leonard & Hill, 2014), and deficits in visual attention (Sacrey, Bryson, & Zwaigenbaum, 2013) and social attention (Bhat, Galloway, & Landa, 2010; Sahley & Panksepp, 1987), all of which have been related to cognitive and language delays. Further, children with ASD who are more adept at play exhibit fewer delays in development (Pierucci, Barber, Gilpin, Crisler, & Klinger, 2015). Because a child’s play can reflect multiple areas of development, analyzing quality of play, even in the first year of life, can reveal precursors to later cognitive, language, or other developmental delays (DDs) (Poon, Watson, Baranek, & Poe, 2012; Vig, 2007).
Developmental levels of object play
Object play is an early-emerging skill that coincides with a child’s development of the ability to create cognitive representations of events and objects in their environment (Frey & Kaiser, 2011). Developmental stages of object play generally involve: (1) sensorimotor or exploratory play, (2) relational play, (3) conventional or functional play, and (4) symbolic play (Libby, Powell, Messer, & Jordan, 1998; Naber et al., 2008). Although these stages are not purely hierarchical and mutually exclusive, play becomes more sophisticated over time, building on previous stages (Stagnitti, 2004). Most children exhibit a variety of play levels simultaneously, and return to earlier stages with new objects or toys.
Sensorimotor or exploratory play marks the earliest infant manipulations of an object (e.g. mouthing, banging), and serves as a means of gaining information about the physical world (Naber et al., 2008; Williams, 2003). Exploratory play is exemplified by simple actions on single objects. No functional relationship exists between the infant’s actions and the object; thus, actions are indiscriminate and repetitive. By exploring objects over time, infants begin to understand how they relate to one another (Williams, 2003), thereby transitioning into relational play. The association (e.g. nesting or taking apart) of similar or related objects characterizes this second stage of play, which also becomes gradually more sophisticated (Naber et al., 2008). Functional play appears around one year of age when a child manipulates objects in ways that are socially and functionally intended (Bigelow, MacLean, & Proctor, 2004). For example, a child may put a telephone to his ear, use play utensils, or push a toy car. During this stage, play remains pre-symbolic. The final stage is symbolic play, which begins between 18 and 24 months and becomes increasingly more sophisticated through the preschool years. Symbolic play involves pretense or complex play actions that incorporate items, attributes, or contexts not actually present, or the substitution of objects (Naber et al., 2008). This stage is an important outcome of the cognitive, language, social, and joint attention skills developed and refined during the earlier stages of play (Lewis, 2003; Stagnitti, 2004; Vig, 2007).
Object play in children with ASD
Research shows that young children with, and at high risk for, ASD are markedly different in their object play, compared to children who are TD or have other DDs (Mulligan & White, 2012; Naber et al., 2008; Pierucci et al., 2015). Children with ASD demonstrate more repetitive and stereotypical, and less varied, flexible, inventive, and social play (Baranek et al., 2005; Christensen et al., 2010; Stronach & Wetherby, 2014). They spend more time in exploratory play than children who are TD or have other DDs (Boucher, 1999; Williams, 2003), engaging in sensory stimulating activities, such as visual or tactile examination (Naber et al., 2008). They also generate fewer examples of relational play than children with typical development or Down syndrome (Libby et al., 1998). Libby et al. (1998) argue that preoccupation with sensorimotor play might suppress the emergence of functional and symbolic skills. Although children with ASD may play with objects functionally, this play tends to be less frequent, diverse, integrated, and complex than that of other children (Christensen et al., 2010). Moreover, symbolic play is the stage where most children with ASD struggle, often lacking the ability to develop original ideas for pretend play; thus, their play often seems rote and less spontaneous (Williams, Reddy, & Costall, 2001).
Very few studies exist describing the play of children with ASD during early infancy. In a retrospective video analysis (RVA) exploring object play at 9–12 months among infants later diagnosed with ASD, infants who were TD, and those with other DDs, Baranek et al. (2005) found no significant differences in engagement with objects or duration of exploratory play. However, only typically developing infants engaged in the higher level of functional play. Some researchers have studied object play of high-risk infant siblings of children with ASD and discovered less object manipulation (Mulligan & White, 2012), difficulty disengaging attention from objects (Sacrey et al., 2013), and more repetitive object manipulation (Elison et al., 2014). Others have found that fine motor and grasping delays of high-risk infants result in delays in object exploration (Libertus, Sheperd, Ross, & Landa, 2014). Play may inform assessment of the core features of ASD as well as development of effective early interventions (Pierucci et al., 2015; Poon et al., 2012); however, this field of inquiry is still in its infancy. Most children are diagnosed after two years of age (Steiner, Goldsmith, Snow, & Chawarska, 2012), thereby delaying early intervention; however, recent research points to subtle symptoms (including play deficits) of ASD in the first two years of life (Landa & Garret-Mayer, 2006; Maestro et al., 2005; Palomo, Belinchón, & Ozonoff, 2006).
Retrospective video analysis
Researchers have used both prospective and retrospective methods to analyze features that discriminate infants who go on to have ASD from those who do not. Prospective studies typically recruit infants at high familial risk for ASD, and although they allow researchers to study behaviors in a more controlled setting and in present-time, they are costly and time-consuming. Retrospective video analysis has been invaluable for analyzing ASD features in more heterogeneous samples with unknown genetic liability, and can provide information efficiently about developmental trajectories (Baranek et al., 2005; Clifford, Young, & Williamson, 2007; Maestro et al., 2005; Palomo et al., 2006; Saint-Georges et al., 2010).
Although RVA has some inherent limitations (e.g. lack of control over the quality and content of video footage; Clifford et al., 2007), researchers can gain additional controls by including rigorous methods of assessing participants, controlling for age in the videos, and developing systematic methods for obtaining, editing, and coding videos (Baranek, 1999; Maestro et al., 2005; Palomo et al., 2006). Analysis of home videos has strong ecological validity, offering observations of actions and the environment in ‘real life’ settings as opposed to contrived laboratory settings. A recent comparative analysis concluded that both retrospective and prospective methods are worthy tools for study of infant behavior (Saint-Georges et al., 2010).
Current study
To address a need for expanded characterization of object play among infants with ASD, the current study compared object play of infants who are TD, infants later diagnosed with other DDs (DD), and infants later diagnosed with ASD (ASD) at two time points (time 1: 9–12 months, and time 2: 15–18 months) using longitudinal RVA. The videotapes analyzed were collected as part of the Infant Behavior Project starting in the mid-1990s. This Infant Behavior Project was implemented in conjunction with various other research projects to establish a library of early home videos that could be used to study early symptoms of ASD and other DDs in comparison to behaviors of TD infants. The growing video library has been the source of data for other published studies (Baranek, 1999; Baranek et al., 2005; Watson, Crais, Baranek, Dykstra, & Wilson, 2013). The aims of the current study were to: (1) describe the play behaviors of the three groups of infants at both time points; (2) examine group differences in four hierarchical levels of play at both time points; (3) compare groups with respect to the highest level of play achieved; and (4) determine if the highest level of play achieved during infancy correlates with later developmental outcomes for the two groups of infants with developmental disorders (ASD and DD).
Methods
Participants and measures
Participants were recruited from two geographic regions (Midwest and Southeast) through varied methods (e.g. information booths, mailings, collaborations with clinics, university participant registries). All parents of participants reviewed and signed the Institutional Review Board’s approved informed consent prior to submitting family videos, and participants were assigned identification numbers to protect confidentiality. Participants were given information regarding the risks and benefits of participation in the study, and were ensured that all study procedures would be conducted in accordance with universal ethical principles.
Children were between 2 and 7 years of age at the time of recruitment and diagnostic/developmental assessment. Mean age in months at recruitment for each group was as follows: TD: 47 (SD = 4); DD: 51 (SD = 7); ASD: 54 (SD = 3). Home videos from the infancy period were included in the study if they contained codeable footage of the child in at least one of the two time points targeted (time 1: 9–12 months, time 2: 15–18 months). These age ranges were chosen as of central interest at the initial creation of the Infant Behavior Project video library. The rationale for focusing on these age ranges included the rapid developmental changes seen during these periods in many areas (including play behaviors), along with seminal findings that behavioral symptoms of ASD can emerge as early as the end of the first year of life, and are readily identified in many children by 18 months of age (Adrien et al., 1993; Gillberg et al., 1990; Osterling & Dawson, 1994). These two age ranges are especially appropriate for comparing play behaviors across diagnostic groups due to the emergence of functional and early symbolic play between the end of the first year and the middle of the second year of life (e.g. McCune, 1995). Participants (n = 92) met criteria for one of the three groups (TD, DD, ASD). Children in the TD group (n = 29) had no history of DD or learning/behavior problems, had not received therapy or special education, were not currently medicated for psychiatric, learning, or attention problems, and were functioning in the average or above range in cognition and adaptive behavior. Children in the DD group (n = 20) had significant delays based on scores obtained from group placement measures described below, scoring >2 standard deviations below the mean for overall cognitive functioning or one domain of development, or >1.5 standard deviations below the mean for two separate developmental domains (e.g. expressive language, fine motor). This group included children with idiopathic DDs (n = 9), genetic conditions associated with intellectual disabilities (e.g. Down syndrome) (n = 9), and children with delay associated with prematurity (n = 2). Children in the ASD group (n = 43) were diagnosed with Autistic Disorder according to DSM-IV-TR criteria (American Psychiatric Association, 2000) by a licensed professional. Diagnoses were confirmed using the Autism Diagnostic Interview-Revised (ADI-R; Lord, Rutter, & LeCouteur, 1994), the Autism Diagnostic Observation Scale (ADOS; Lord, Rutter, DiLavore, & Risi, 1999), and/or the Childhood Autism Rating Scales (CARS; Schopler, Reichler, & Renner, 1988). Research suggests that children who meet DSM-IV criteria for Autistic Disorder are likely to meet the revised DSM-V criteria for ASD (McPartland, Reichow, & Volkmar, 2012). Children with significant neuromotor, visual, or hearing impairments, and fragile X syndrome (due to high comorbidity with ASD) were excluded from all groups. Both the TD and DD groups were screened with the CARS to ensure they did not have significant symptoms of ASD and infants were excluded from these groups if they had a family history of ASD (first degree biological relative).
Participant demographics – Frequency (%).

Video collection, editing, and coding procedures, and analyses
Number of participants with data at two time points.
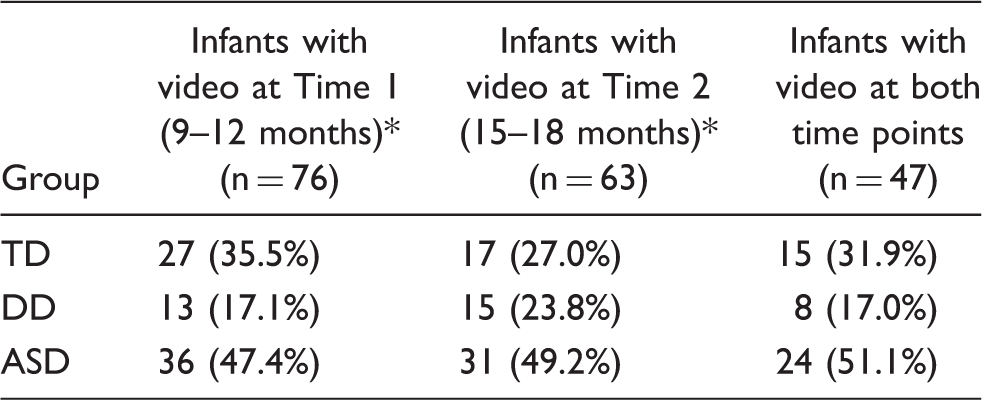
Overlap exists between these two subsets of participants, with 92 total participants.
Situations captured in the home videos were variable based on caregivers’ available footage and included special events (e.g. birthdays, vacations) and daily occupations (e.g. bath, meals, outdoor play, indoor play). An editor, blind to group status, selected cross-sections of situations available for each child for each of the two time points. Instructions to the editor were to select random scenes for each child based on maximum variation in the footage available across that age range (e.g. scenes from 9, 10, and 11 months vs. three scenes all at 10 months) and maximum variation in situational contexts (e.g. as many contexts as possible) per time point. For each age range, a maximum of two segments (5 minutes each) was edited and content coded for each child to examine comparability across groups with respect to the (a) average age per segment, (b) average number of people, (c) level of structure imposed on the child during interactions, and (d) level of physical activity restriction (see Baranek, 1999). Results of content coding comparisons across groups at each time point revealed no significant difference in: (a) mean age per segment at time 1 [F(2,66) = .39, p = .67] or time 2 [F(2,20) = .22, p = .80]; (b) mean number of people per segment at time 1 [F(2,66) = 2.52, p = .088] or time 2 [F(2,20) = .69, p = .89]; (c) mean level of imposed structure used in engaging the child in interaction at time 1 [F(2,66) = .52, p = .59] or time 2 [F(2,20) =.09, p = .91]; or mean amount of physical restriction at time 1 [F(2,66) = .06, p = .94] or time 2 [F(2,20) = .14, p = .87]. Contact the authors for the full content of the content coding manual.
Once videos were edited and content coded, they were provided to the behavioral coders (research assistants blind to group status) to complete the object play coding. For this study, object play was defined as the child’s physical interaction with inanimate entities in the environment for the primary purpose of playful engagement, sensorimotor exploration, and/or symbolic functions. Coding of play behaviors followed a manualized protocol (see Baranek et al., 2005) and used Observer 5.0 coding software (Noldus Information Technology). This coding protocol was chosen for the current study due to the correspondence between the two studies’ overall research questions (i.e. how do infants with ASD differ from those with DD and TD in their object play?) and the manualized (i.e. replicable) nature of the protocol’s procedures. The original coding hierarchy consisted of exploratory, relational, functional, and symbolic play levels, with two to four sublevels per play level. That hierarchy was adjusted for data analysis in the current study based on the distribution of object play data; however, all coding procedures were identical to those used in Baranek et al. (2005).
Four judgments were made in coding each behavior: (1) Is the child engaging with an object? (2) Is the child engaging in play with the object? (3) In what level of object play is the child engaging? and (4) Under what sublevel of object play does this behavior fall? In instances of co-occurring levels of play behaviors, the higher level was coded.
Research assistants were trained in the coding schema and each reached a minimum of 80% reliability with the training protocol before coding participants’ videos. Twenty five percent of videos were assessed for interrater reliability. Interrater reliabilities were estimated using intraclass correlations (ICCs), which are similar to Cohen’s kappa calculated on squared differences between the chance-corrected agreements between coders. Although Cohen’s kappa assumes nominal level data, ICCs allow for the inherent ordering of categories (Banerjee, Capozzoli, McSweeney, & Sinha, 1999). This method can be applied to judgments obtained from multiple rater pairs (Bartko, 1966; Schuster, 2004) and is appropriate for judgments made on a continuum. Estimated interrater reliabilities were high, ranging from .81 to .99.
During coding, object play behaviors were originally categorized into two sublevels of exploratory play, two sublevels of relational play, four sublevels of functional play, and two sublevels of symbolic play (see Table 1 in Baranek et al., 2005 for detailed information about the original coding schema). However, preliminary analyses showed the majority of coded play behaviors falling under exploratory and relational play, while minimal occurrences of functional and symbolic play were observed across groups. Based on this distribution, the coded data for the current study were reorganized as follows: the two sublevels of exploratory play (i.e. indiscriminate play and simple manipulation) were treated as two of the four overall play levels based on the high numbers of these play actions in the coded data; relational play was treated as the third level and was not separated into sublevels; and due to rare occurrence of play actions coded as either functional or symbolic play, all sublevels of functional and symbolic play were collapsed into the fourth level of play. This reorganization of the data resulted in the following four play levels being examined for all analyses: (1) exploratory play: indiscriminate play (e.g. mouthing and banging objects); (2) exploratory play: simple manipulation (e.g. pushing a button or rolling a car); (3) relational play (taking toys apart and combining toys, such as with puzzles or shape sorters); and (4) functional and symbolic play (all sublevels combined, including using objects as intended and using objects in pretend play).
Data were analyzed for each study aim (see numbered aims at end of Introduction) using the following procedures, each of which is described in more detail in the Results section below to increase continuity between analysis description and results: (1) descriptive statistics; (2) ordered logistic regression (OLR) with follow-up exploratory descriptive statistics; (3) non-parametric Kruskal–Wallis one-way analysis of variance (ANOVA) with the Mann–Whitney follow-up comparisons; and (4) non-parametric Spearman’s rank-order correlations. Our examination of the potential impact of outliers on results of the analyses suggested stable multivariate model estimates and bivariate statistics robust against undue influence from univariate outliers and from clusters of univariate outliers.
Results
Time spent in object play
Total time in object play and proportion of time at each play level.

Group differences across play levels and time points
Ordered logistic regression was used to investigate differences in use of the play levels across groups and over time. OLR is appropriate for use with categorical dependent variables in which each category is sequentially ordered from low to high (Long & Freese, 2006). Obtaining valid parameter estimates with OLR requires that the assumption of proportional odds is not violated across model cut-points. We tested this assumption for all independent variables using the Brant test (Brant, 1990; Hosmer, Lemeshow, & Sturdivant, 2013). Findings from this procedure were insignificant, indicating that model assumptions were not violated. We also adjusted for the expected nonzero covariance among standard errors arising from repeated observations among study participants using a maximum likelihood estimation procedure (Huber, 1981; White, 1980). Multiple observations among study participants reflect treating each time point (age) of video as a unique observation, resulting in 139 observations for study analyses. The statistical software STATA, version 12, was used for these statistical analyses (STATA, 2012).
We assessed sample power available for multivariate procedures using POWERLOG, available from UCLA for STATA users (Philip B. Ender, Statistical Computing and Consulting, UCLA Academic Technology Services). Power analysis procedures allow estimates of the availability of study power based on sample size and study design to determine if sufficient sample size (power) is available for analysis. A conservative approach to specifying the power analysis was followed, including: defining cut-offs based on sample data (average play levels), threshold power levels at .80, with a significance criterion of 0.05, and assuming a one-tailed test. Findings indicated that our sample contained sufficient power, exceeding minimal sample size requirements. For example, POWERLOG results indicated 0.90 confidence with 130 cases. We exceeded this with our study design, which included 139 observations available for multivariate analyses.
Ordered logit results: Group differences in observed play levels.

Note: ns: not significant; CI: Confidence Interval; L: Left; R: Right.
p < 0.05.
p < 0.001.
Regardless of later diagnosis, age (i.e. time point) was an important factor influencing level of play. After holding group membership constant, the odds of being classified in a higher versus lower level of play were 5.098 (p < 0.001) times greater among infants at time 2 (15–18 months) in comparison with those at time 1 (9–12 months), suggesting that regardless of group, significant gains in play levels were observed with increasing age.
To further examine the substantive impact of results presented in Table 4, we conducted a trend analysis of change in play level from time 1 (9–12 months) to time 2 (15–18 months) by group. Although some gains in play level were observed among all three groups, findings from this analysis indicated that higher levels of play were most pronounced in the TD group (z = 2.88; p < 0.001) and the ASD group showed the least amount of gain in play level (z = 3.22; p < 0.001). Consistent with findings presented in Table 4, trend analysis findings indicate that change in play level was not significantly different from time 1 to time 2 among those with DD (z = 0.16; p = 0.874).
Group differences in highest level of play
The highest level of play achieved across the two time points by each group was compared using non-parametric Kruskal–Wallis one-way ANOVA. Only infants who had video data at both time points (n = 47) were included. Results showed a significant group difference (χ2 = 6.306, p = .043). Mann–Whitney’s paired comparison U tests were used for post-hoc analysis, and indicated a statistically significant difference between the ASD and TD groups in their highest level of play across time points (U = 2.431, p = .015) with the TD group exhibiting more sophisticated play than the ASD group. Comparisons showed no significant difference between the ASD and DD groups (U = .567, p = .571) or between the TD and DD groups (U = 1.512, p = .131) in their highest level of play across time points. For further comparison, Figure 1 illustrates the percentage of infants in each group who exhibited each of the four play levels at each time point.
Percent of infants with data at both time points exhibiting each level of play.
Relationship between highest level of play and developmental outcomes
This analysis was restricted to the two disability groups (ASD and DD), excluding the TD group due to lack of variability in their outcome measures. To examine the highest level of play in infancy and its correlation to later developmental outcomes, we examined scores on the CARS (for ASD only, to examine correlation between early play behavior and later ASD symptom severity), VABS (overall and communication subscale), and NVDQ. These measures were chosen to represent outcomes across the areas of ASD symptomatology (for the ASD group), adaptive behavior, communication, and cognitive functioning. We hypothesized that lower play levels in infancy, presumably reflecting more repetitive actions, would be correlated with greater ASD symptom severity later in life; thus, we expected a negative correlation between CARS scores and highest level of play in the ASD group. We expected a positive correlation between highest level of play and developmental outcomes (i.e. VABS overall standard score, VABS communication subscale standard score, and NVDQ) in both the ASD and DD groups, and expected these relationships to be more apparent at time 2 than at time 1. Spearman’s rho results indicated that the highest level of play exhibited by the ASD group was significantly positively correlated with the group’s later VABS overall standard scores when examining the infants’ play at both time 1 (r = .297, p = .031) and time 2 (r = .332, p = .018). Although significant, it is important to note that these correlations were modest in size. For the ASD group, there was not a significant correlation between later VABS communication standard scores and highest level of play at time 1 (r = .258, p = .154) or time 2 (r = .167, p = .387) or later NVDQ and highest level of play at time 1 (r = .160, p = .162) or time 2 (r = .189, p = .121). For ASD symptoms in the ASD group, we found no significant correlation between CARS scores and highest level of play at time 1 (r = −.175, p = .140) or time 2 (r = −.033, p = .420). We did not find significant correlations for the DD group when looking at later VABS overall standard scores and highest level of play at time 1 (r = .192, p = .238) or time 2 (r = .065, p = .405), VABS communication standard scores and highest level of play at time 1 (r = .322, p = .284) or time 2 (r = .201, p = .473), or NVDQ and highest level of play at time 1 (r = −.206, p = .231) or time 2 (r = .291, p = .146).
Discussion
Results of this study add to the existing literature on object play in children with ASD, specifically at 9–12 and 15–18 months of age. In addressing the first aim of the study, descriptive analyses of object play behaviors captured in home videos showed that, across groups, infants spent 20–33% of their time engaged in any type of object play across both time points analyzed in this study, with the vast majority of that time spent in exploratory play. In contrast to findings from the empirical review by Williams (2003), we did not find less exploratory behaviors for the ASD group compared to other groups, which is perhaps attributable to the less structured naturalistic (vs. lab-based experiments) nature of the videotaped contexts in the present study. Higher levels of play (i.e. relational and functional + symbolic) were observed at very low frequencies in the home videos. Even at 15–18 months, less than 50% of infants with TD or DD, and only 32% in the ASD group exhibited relational play. In slight contrast to findings from Christensen et al. (2010) that infants with and without high risk for ASD exhibited few symbolic play acts at 18 months of age (in a structured lab context), we noted that at 15–18 months, functional + symbolic play acts were exhibited by 41% of the TD group, but only by 13% of the DD group and 9% of the ASD group. These results point to the low frequency of high level play behaviors (i.e. relational or functional + symbolic) exhibited by infants in natural contexts, especially by infants with ASD and other DDs. Thus, although infants may be capable of higher levels of play than they typically choose to engage in, these more sophisticated behaviors may require more structured probes or specific object sets to be elicited in laboratory settings.
In addressing the second aim of the study, examining group differences across play levels and time points, findings from the OLR analysis indicate that infants later diagnosed with ASD do, in fact, exhibit significantly less high level play behavior (i.e. functional +symbolic being the highest category in this study) in both early (9–12 months) and later (15–18 months) infancy in comparison to their TD peers. However, infants later diagnosed with ASD were not found to be significantly different from those later diagnosed with other DDs in their use of the four levels of play examined across the age ranges in this study. Despite the ASD and DD groups exhibiting similar object play behaviors at 9–12 months, by 15–18 months, the DD group was statistically indistinguishable from the TD group, while the ASD group continued to lag significantly behind at this age. Reinforcing this finding, results related to the third aim of the study (i.e. comparing the highest level of play achieved by the three groups of infants across both time points) show the TD group exhibiting more sophisticated play than the ASD group, with no significant difference between the ASD and DD groups.
Further exploratory examination of patterns in play development provided insight into the complex nature of play development patterns among children with ASD relative to children with other DDs as well as children with typical development. The limited gains in play observed among children later diagnosed with ASD versus those with typical development are consistent with previous findings from studies of infant siblings of children with ASD. In one study that examined parent-reported behaviors at 12, 18, and 24 months, the absence of pretend play was one of the most useful markers in differentiating between children with ASD versus other DDs at 24 months, but did not significantly discriminate between these groups at 18 months (when many children in both groups failed to exhibit pretend play; Barbaro & Dissanayake, 2013). However, another study involving observations of play at 18 months found the specific subtypes of functional play observed contributed to distinguishing among infants who went on to be diagnosed with ASD versus other DD or no delay (Christensen et al., 2010).
The final study aim of examining possible correlations between highest level of play achieved and later developmental outcomes resulted in modest correlations between the highest level of play at 9–12 and 15–18 months by the ASD group and their later VABS standard scores. These results build upon the existing ASD literature (e.g. Stanley & Konstantareas, 2007) by suggesting that play behaviors exhibited in the first years of life may predict signs of future delays in some developmental domains. Given differences in measurement of play and developmental functioning between these two studies, the older ages of the participants in Stanley and Konstantareas compared to ours, and the concurrent correlational design of that earlier study versus the longitudinal design of the current study, it is unsurprising that we did not find that infant play predicted development in all the domains that correlated with symbolic play in the Stanley and Konstantareas study. For example, we did not find that highest level of infant play predicted later NVDQ, whereas they found concurrent correlations between symbolic play behaviors and nonverbal cognitive functioning. However, the lack of correlation between the highest level of play and later CARS scores in the ASD group is contrary to recent findings in another longitudinal study that showed lower levels of play in toddlers at high genetic risk for ASD at 22 months of age are associated with ASD symptom severity at 36 months of age (Campbell, Leezenbaum, Mahoney, Moore, & Brownell, 2016). It is possible that the play coding system used in the current study of home videos is a less sensitive measure of play than that used by Campbell et al. during laboratory-based sessions of parent–child play using a consistent set of toys. Additionally, even an age difference of a few months between 9 and 22 months of age can represent a time during which children typically show major progressions in object play development; thus, observing children at 22 months rather than 9–12 or 15–18 months may simply provide a better differentiation among infants and toddlers later diagnosed with ASD related to both their later developmental skills and their later ASD symptom severity.
Lack of correlation between highest level of play and later VABS communication scores for either disability group at either time point is surprising given literature citing the relationship between play and language in young children (e.g. Ungerer & Sigman, 1981); however, the current study’s results in this area may be due to limited variability in play skills exhibited at these young ages (compared to studies of older children), limited variability in VABS communication scores in the ASD and DD groups, or perhaps the fact that other factors must be taken into account when examining the communication skills of older children. Finally, the overall lack of correlations between highest level of play and later cognitive and adaptive outcomes for the DD group at either time point may be due to the group’s small sample size, providing limited power and also potentially yielding unstable correlation coefficients. For example, we note that time 1 play correlated with NVDQ in a negative direction for the DD group, whereas time 2 play correlated in a positive direction, with both of these correlations being modest in magnitude and nonsignificant. Another potential factor influencing these results is the inclusion criteria for the DD group being more restricted than for the ASD group in terms of cognitive and adaptive skills, as the DD participants were required to evidence intellectual disability, while the ASD group had a broader range of cognitive and adaptive abilities. The magnitude of some of the nonsignificant correlations in the DD group’s analyses is similar to the magnitude of those seen in the ASD group’s analyses. This is likely due to the small sample size in the DD group; however, we suggest these results be interpreted with attention to this fact.
Conclusions
Findings from this study support those of others (e.g. Libby et al., 1998) who note that children with ASD exhibit restricted use of higher levels of play, and also add to the literature by demonstrating through direct observation of videotaped naturalistic contexts that this pattern occurs in infants prior to diagnosis. The findings further suggest support for the proposition that play is a means for early learning and development of fundamental skills needed for later adaptive growth in children with ASD. If development proceeds along a direct path, as proposed by Orr and Geva (2015), then derailment of early object play would be detrimental for the later development of symbolic play and other key domains. We acknowledge that other variables, such as motor and/or attention skills, may help explain the associations found in our study (cf. Bornstein, Hahn, & Wolke, 2013).
Together, findings from this study have implications for professionals and caregivers who may identify delays and seek to facilitate early play skills through early intervention services and evidence-based strategies. For infants, play is a key method for learning about the world. Their language and social cognitive development depends on their increasingly complex and flexible exploration of objects and people during play (Lifter et al., 2011). In collaboration with professionals (e.g. speech-language pathologists, educators, occupational therapists), caregivers of infants with, or at risk for, ASD may support their child’s development through structured interactions that facilitate play within their child’s zone of proximal development (i.e. what they can achieve with a modest amount of support). For example, a child exhibiting only simple manipulation of objects into their second year of life may benefit from interventions and supports that include modeling, structured teaching, and visual supports, among others, to expand their play to the next level. The hierarchy of play categories utilized in the current study provides a developmental framework for professionals and caregivers to consider in this process.
Limitations related to data ascertainment and coding were noted earlier and are consistent with the nature of retrospective data with smaller samples. Another specific limitation is the variation in group size due to challenges in recruiting participants who met the criteria for certain groups. Despite these limitations, the current study adds to the body of literature describing early play trajectories in children with ASD as well as DD in a naturalistic context, and presents a developmental play schema that can be utilized by researchers as well as professionals to facilitate study, identification, and remediation of delays in play development for children at risk for ASD. Future efforts to expand on this line of study may include analysis of qualitative differences in early play behaviors (e.g. diversity of exploratory play acts and unusual features), which may be important to developmental or diagnostic outcomes (Kirby, Boyd, Williams, Faldowski, & Baranek, 2017).
Footnotes
Acknowledgements
We thank the families whose participation made this study possible, and staff that collected data, edited videotapes, and coded and entered data. Finally, we acknowledge Don Trull for his software assistance, and the invaluable assistance of Michele Poe and Richard Faldowski with statistical analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Child Health and Human Development grant that provided support for participant recruitment through the Neurodevelopmental Disorders Research Center Autism Subject Registry at The University of North Carolina at Chapel Hill [grant #P30-HD03110]. This work was also supported in part by funding from the National Institute of Child Health and Human Development [grant #R01-HD42168] and Cure Autism Now Foundation (now merged with Autism Speaks), the Ireland Family Foundation, and a United States Department of Education Doctoral Leadership Training Grant [grant #H325D070011].