
Abstract
Background
Children and adolescents with a history of developmental language disorder are at elevated risk of experiencing internalising and externalising symptoms. The existing literature suggests a link between developmental language disorder, bullying victimisation and low self-esteem, both of which are negatively associated with child and adolescent mental health more generally.
Aim
We examined the relationship between having a history of developmental language disorder and internalising and externalising symptoms in adolescence. We also tested whether bullying victimisation and self-esteem were associated with mental health outcomes, and whether they moderated the association between a history of developmental language disorder and psychological symptoms.
There is a robust association between language disorder 1 and poor psychosocial outcomes. This includes internalising (e.g. anxiety, depression) and externalising symptoms (e.g. conduct problems, attention difficulties) (Conti-Ramsden, Mok, Pickles, & Durkin, 2013; Snowling, Bishop, Stothard, Chipchase, & Kaplan, 2006). However, why language disorder is linked with poor mental health outcomes is unclear. Consideration of factors known to influence mental health in the broader population can provide some insights. For example, it is well recognised that the impact of life stressors may vary with age, and that males and females are vulnerable to different patterns of internalising and externalising symptoms (Gupta, 2016; Martel, 2013). However, a growing body of research has identified other factors relevant to mental health in individuals with developmental language disorder (DLD). van den Bedem, Dockrell, van Alphen, Kalicharan, and Rieffe (2016) noted that depressive symptoms in children with DLD could not be solely explained by the severity of their language difficulties; rather, this association was mediated by the use of maladaptive emotional regulation strategies. Botting, Durkin, Toseeb, Pickles, and Conti-Ramsden (2016) found that the association between language ability and emotional health in adults with a history of DLD was mediated by self-efficacy. In contrast, Forrest, Gibson, Halligan, and St Clair (2018) found adolescents who had a reported history of language difficulties and peer problems at age 7 were more likely to present with poorer emotional health at ages 7 and 14. This range of findings highlights the need for further investigation of factors underlying mental health for individuals with language disorder.
To this end, there is increasing evidence linking language disorder with bullying victimisation (van den Bedem et al., 2016) and low self-esteem (Botting et al., 2016), which have also been identified as risk factors for mental health difficulties in the broader child psychology literature (Sowislo & Orth, 2013). Furthermore, there is mounting evidence for a bi-directional association between bullying victimisation and low self-esteem, wherein individuals develop low self-esteem linked with bullying victimisation experiences, and individuals with low self-esteem are at increased risk of being bullied (van Geel, Goemans, Zwaanswijk, Gini, & Vedder, 2018). However, it is unknown whether these risk factors can explain mental health in the context of DLD. To the best of our knowledge, no studies have examined language disorder, bullying victimisation, self-esteem, and mental health in the same sample, which was the aim of the current study.
Mental health in the context of DLD
Difficulties with language have been variously described as “language disorder”, “language impairment”, “language difficulties” and “Specific Language Impairment” (SLI).
More recently, the term “language disorder” has been proposed to describe children with significant language difficulties that are likely to persist, with functional impact on social interaction and educational progress, while “developmental language disorder” (DLD) refers to language disorder with no known differentiating condition such as brain injury or autism (Bishop, Snowling, Thompson, & Greenhalgh, 2017). It is estimated that DLD affects approximately 7% of the population (Norbury et al., 2016).
Individuals with DLD are reportedly at increased risk of experiencing poor social, emotional and mental health outcomes, though additional factors affecting these outcomes as well as the age of onset of mental health symptoms in individuals with DLD are unclear (Conti-Ramsden & Botting, 2008; Lindsay & Dockrell, 2012; Snowling et al., 2006). Adolescence is generally a period of increased risk for any cohort, with most mental health disorders surfacing in adolescence (Clements-Nolle & Rivera, 2013). However, much of the research in DLD has explored mental health in younger age groups (Goh Kok Yew & O’Kearney, 2013, 2015; Levickis et al., 2018).
There is significant variability in the terminology used to describe mental health outcomes in general, as well as for the DLD population. This complicates the process of determining mental health prognoses. For example, several studies have reported an increased risk of internalising disorders (Snowling et al., 2006), emotional regulation difficulties (Fujiki, Spackman, Brinton, & Hall, 2004), poor emotional health (Forrest et al., 2018), externalising symptoms (Conti-Ramsden et al., 2013), low self-esteem and poor social relationships (Wadman, Botting, Durkin, & Conti-Ramsden, 2011) for individuals with DLD. In the interest of clarity, the term “mental health” in this paper aligns with the definition put forward by the World Health Organization (2004), as “a state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community”. As such, “poor mental health outcomes” will be used to discuss symptomatology.
In their 2013 systematic review and meta-analysis, Goh Kok Yew and O’Kearney reported significantly increased prevalence and severity of emotional, behavioural and attention deficit hyperactivity problems for children and adolescents with language disorder compared to typically developing (TD) peers, and elevated risk of depression for children with language disorder. This is consistent with the findings of Conti-Ramsden and Botting (2008), and Botting et al. (2016), who also reported increased risk of depression and anxiety symptoms for adolescents with DLD. However, this is in contrast to the findings of Levickis et al. (2018) who investigated social–emotional and behavioural difficulties in a longitudinal community-based study, following children with and without language disorder between the ages of 4 and 7. Participants with language disorder presented with greater total difficulties than matched peers on a measure of social and emotional functioning at 4, 5 and 7 years, but the nature of some difficulties changed over time. Hyperactivity and conduct problems were consistently higher across all time points for children with language disorder, while peer problems were not reported at 7 years, and emotional problems were not reported at all. Levickis et al. (2018) acknowledged that the severity of language disorder might not have been comparable with those in other studies, which may explain the lack of association. Additionally, the focus of this research was the psychosocial wellbeing of 4–7 year olds, not the social/emotional outcomes of participants in adolescence. Given what we know about the emergence of mental health symptoms for adolescents, these results may not be reflective of participants’ lifelong mental health outcomes.
While the evidence for an association between language and mental health outcomes is robust, why the relationship exists is still unclear. Additionally, little research examines why some individuals with DLD present with internalising problems, others present with externalising problems, and others never present with poor mental health. Thus, consideration of other factors impacting individuals with DLD that have been linked with mental health outcomes is necessary to inform evidence-based assessment and intervention.
Risk factors for mental health in the context of DLD
A number of risk factors for mental health have been examined in the DLD population. These include self-efficacy (Botting et al., 2016), bullying victimisation (van den Bedem et al., 2016; Wadman et al., 2011), poor emotional knowledge (van den Bedem et al., 2016), parenting style (Aarne, Almkvist, Mothander, & Tallberg, 2013), self-esteem (Jerome, Fujiki, Brinton, & James, 2002; Marton, Abramoff, & Rosenzweig, 2004) and shyness (Durkin, Toseeb, Botting, Pickles, & Conti-Ramsden, 2017). While all are important considerations, self-esteem and bullying victimisation are two that have received particular attention.
Self-esteem refers to the value one places on oneself, based on self-evaluation and internalisation of others’ perceptions (Botting et al., 2016; Jerome et al., 2002). Low self-esteem has generally been linked to poor psychosocial outcomes, characterised by internalising and externalising symptoms, academic failure and/or dependence on welfare benefits (Jerome et al., 2002). In addition, research has established an increased risk of low self-esteem for children with various communication impairments (Capps, Sigman, & Yirmiya, 1995; Harter, Whitesell, & Junkin, 1998). The literature investigating self-esteem for children with DLD is less clear-cut. Jerome et al. (2002) investigated the self-esteem of children with DLD aged 6--13 years. Their findings indicated that the majority of the younger DLD sample (aged 6--9 years) scored within one standard deviation of TD peers. In contrast, those aged 10--13 years scored significantly lower than their peers on measures of scholastic competence, social acceptance and behaviour conduct. This provides empirical support for the theory that mental health symptoms may arise and/or increase as individuals approach adolescence (Clements-Nolle & Rivera, 2013). Marton et al. (2004) reported that children with DLD aged 7--10 years displayed low social self-esteem compared to matched controls, while academic self-esteem was comparable. More recently, Botting et al. (2016) and Durkin et al. (2017) reported a direct and significant association between adolescent language and global self-esteem in adulthood.
Another factor for consideration for adolescents with DLD is the nature of peer relationships and vulnerability to bullying victimisation (experiencing repeated, deliberate aggressive acts by a peer/s). Supportive friendships are associated with positive social and emotional outcomes, and are a protective factor against bullying victimisation (Alvord & Grados, 2005; Schwartz, Dodge, Pettit, & Bates, 2000). However, children with DLD are at risk of limited or poor peer relationships (Mok, Pickles, Durkin, & Conti-Ramsden, 2014), and of experiencing significantly more bullying victimisation than TD peers (Conti-Ramsden & Botting, 2004; Redmond, 2011; van den Bedem et al., 2016). Redmond (2011) reported significantly increased bullying victimisation experiences for participants with DLD, over and above those with ADHD (though prevalence in this group was still high). Bullying victimisation has been associated with serious psychological consequences, including increased risk of internalising symptoms, poor classroom attention and suicidal ideation (Redmond, 2011). For participants with DLD identified as at risk of depression at 16 and/or 17 years, increased experiences of bullying victimisation was associated with an elevated risk of depression at 17 years (Wadman et al., 2011). However, Wadman et al. (2011) asked a single question of participants regarding bullying victimisation and highlighted the need for further investigation using a more detailed measure. To the best of our knowledge, these findings have not been examined further. Given the potential negative outcomes of experiencing bullying victimisation and the preliminary evidence for its association with DLD, further investigation is crucial.
The current study
The current study aimed to examine the impact of early language disorder on adolescent mental health. We anticipated that a history of DLD would be associated with internalising and externalising symptoms, self-esteem and bullying victimisation. Specifically, we expected that adolescents with a history of DLD would report higher levels of internalising and externalising symptoms, lower self-esteem and more experiences of bullying victimisation as compared to TD peers. In addition, we aimed to test whether bullying victimisation and self-esteem moderated the association between DLD and mental health outcomes. We expected the association to be strengthened at high levels of bullying victimisation and low levels of self-esteem.
Methods
Ethical approval
The present study received ethical approval from the Curtin University Human Research and Ethics Committee (approval number HRE2016-0134).
Recruitment and participants
In total, 42 participants took part. Twenty participants with a history of DLD (aged 10–16 years; 10% female, 90% male) were recruited through four Language Development Centres (LDCs) across the North East Metropolitan Region. The LDC service model is unique to Western Australia; the Centres provide intensive intervention for children in Kindergarten (aged 3–4 years) to Year 2 (aged 6–7 years) whose language profiles are consistent with that of DLD. LDCs offer up to three years of school placement with a focus on developing oral language skills. In order to participate, adolescents were required to have attended an LDC for a minimum of one year. Thus, all participants in the history of DLD group had received at least one, and a maximum of three years, of intensive intervention in a specialised education context and were attending a mainstream school at the time of recruitment and data collection.
Referral to an LDC requires a comprehensive assessment: a thorough case history, assessment of the child’s oral language skills using standardised, norm-referenced tests and language sample analysis, and a developmental assessment by a paediatrician or psychologist. Therefore, all participants in the history of DLD group had early language abilities significantly below the average range, with demonstrated functional impact, and no other diagnosis that could better explain their language problems.
Recruitment took place through LDC mailing lists and/or via the school website. Interested families with children who met the criteria contacted the researcher directly for further details.
Additionally, 22 participants with no history of DLD or neurodevelopmental disorder (aged 10–16 years; 36.4% female, 63.6% male) were recruited through snowballing and social media advertising. All children and parents provided written consent prior to participating in the study and were given opportunity to have questions answered by the researchers.
Measures
A series of self-report and standardised measures were used to examine participants’ language skills, self-esteem, bullying victimisation experiences and screen their mental health. Self-report measures were conducted through interviewing with participants across both groups, using visual supports with all participants to ensure comprehension of stimulus items.
Internalising and externalising measure
The Strength and Difficulties Questionnaire (SDQ) is a psychometrically sound, evidence-based self-report instrument used to identify internalising and externalising symptoms for children aged 4;0–16;0 (α = .78–.85; Hawes & Dadds, 2004). While the SDQ has not yet been validated with a DLD population, there is preliminary evidence for its use (Conti-Ramsden et al., 2013; Helland, Helland, & Heimann, 2014). The questionnaire comprises five sub-scales, examining conduct problems, hyperactivity, peer problems, emotional symptoms, and prosocial behaviour. Each sub-scale has five items that ask the respondent to rate whether each item is (0) not true, (1) somewhat true or (2) certainly true for them (e.g. I worry a lot). The internalising score is calculated by summing the emotional and peer problems’ scales, and the externalising score by summing the conduct and hyperactivity scales. Both the internalising and externalising scores range from 0 to 20, and higher scores indicate increased symptoms. The SDQ total score ranges from 0 to 40 and is the sum of the internalising and externalising scores, measuring the overall risk of mental health symptoms. Both parent and child report versions of the SDQ are available (Hawes & Dadds, 2004). We used the self-report version of the SDQ, and it demonstrated adequate reliability for both internalising (α = .74) and externalising (α = .79) symptoms in our sample.
Bullying victimisation measure
The Social and Health Assessment Peer Victimisation Scale (SHAPV) is a nine-item self-report questionnaire that was used to measure bullying victimisation (Ruchkin, Schwab-Stone, & Vermeiren, 2004). Although the scale has not yet been validated with adolescents with DLD, it has demonstrated strong reliability with an adolescent sample in the US (α = .82; Maynard & Joseph, 2000) as well as in our own sample (α = .87). Participants were asked to report whether they had experienced the peer victimisation behaviour outlined in each item (0) never, (1) once, (2) two or three times or (3) four or more times in the past year (e.g. During this year, has anyone called you names or sworn at you?). All items were summed to generate a total score, ranging from 0 to 27. This score was standardised to ensure comparability between the age groups in the present study. Higher scores indicated increased bullying victimisation experiences.
Self-esteem measures
Harter’s (2012a, 2012b) Self-Perception scales include the Self-Perception Profile for Adolescents (SPPA) and Self-Perception Profile for Children (SPPC) and are self-report instruments measuring a range of self-perception constructs that contribute to a Global Self-Worth score. This score represents the average of six items pertaining to global self-worth and ranges from 1 to 4. Each survey item is scored between 1 and 4, where 4 represents the highest level of self-worth and 1 represents the lowest. Items were designed to follow a “structured alternative format” (Harter, 1982), where respondents are required to identify to what extent they associate with either end of a scale of behaviour or pattern of thought (e.g. Some kids often forget what they learn, but other kids can remember things easily). This format is reported to counterbalance the tendency for children to respond in a socially desirable way, thereby increasing the reliability of the results (Harter, 2012a, 2012b). The Global Self-Worth score was standardised to ensure comparability between the age groups in the present study. Harter’s scales have sound psychometric properties for community samples (SPPA: α = .80–.89; SPPC: α = .78–.87; Harter, 2012a, 2012b), and were found to be similarly reliable in our sample (SPPA: α = .76; SPPA α = .87). The scales have also been used to successfully measure self-esteem in a language-disordered sample (Jerome et al., 2002; Lindsay, Dockrell, & Palikara, 2010; Tomblin, 2008).
Language measure
The Clinical Evaluation of Language Fundamentals-4 (CELF-4) (Semel, Wiig, & Secord, 2006) is a widely used Australian-normed language measure with sound validity and reliability (reliability coefficients ≥.90 across language indicators) and provides Receptive, Expressive and Core language scores (the Core language score is an overall measure of language ability). Raw scores for each subtest are converted to scaled scores according to age norms, which are summed and converted to an overall standard score for the Core, Receptive and Expressive language scores. Scores that fell in the range of 1.5–2 standard deviations below the mean of the normative sample were classified as moderately low, and scores falling in the range of 2 or more standard deviations below the mean were classified as severely low, as per the test manual.
Procedure
Data were collected by a certified, practising speech pathologist with several years’ experience administering assessments and intervention to children with DLD. Participants were interviewed by the researcher in a quiet room in their home. It was made clear to all participants that consent was completely voluntary, and adolescents were shown a visual schedule to support comprehension. Participants in both groups undertook a formal assessment of their language skills using the CELF-4 as well as the aforementioned series of self-report measures to examine their self-esteem, bullying victimisation experiences and mental health. Where participants had difficulty understanding the language in assessments, the researcher defined terms (as long as this did not compromise standardised protocols). At the end of the assessment, adolescent participants were provided with a movie voucher and parents with a report outlining their child’s language results. As per the ethically approved protocol, if participants’ SDQ scores fell in the High or Very High range (n = 2), their parents were contacted by a registered psychologist on the research team who provided further information about accessing support.
Data analyses
Data were analysed in three stages using SPSS 24 (IBM Corp., 2016). First, we examined the data for univariate and multivariate outliers, and a missing value analysis was conducted. One participant’s data point was missing completely at random on the bullying victimisation measure (SHAPV) [χ2(56) = 10.93, p > .99]. Therefore, this single data point was imputed using expectation maximisation. Second, the descriptive statistics were examined, disaggregated by DLD history, in order to ensure that the groups did not differ systematically on any sociodemographic variables. Correlations between DLD history, age, gender, language scores, internalising, externalising and total scores, bullying victimisation and self-esteem scores were also examined. Finally, associations between the history of DLD, self-esteem, bullying victimisation, and both internalising and externalising symptoms were tested in two hierarchical multivariate linear regressions. The first regression examined the SDQ internalising score as the dependent variable, and the second examined the SDQ externalising score as the dependent variable. Within each regression, two models were tested. History of DLD, bullying victimisation and self-esteem were entered simultaneously in Step 1. We then tested the history of DLD × bullying victimisation and history of DLD × self-esteem interactions in simple regression models, including only the relevant predictors and interaction term. Where the interactions were significant in the simple models, they were included in the final multivariate model (Step 2). All predictor variables were standardised and significant interactions were probed using simple slope analyses (Aiken, West, & Reno, 1991).
Results
Bivariate analyses
First, a series of bivariate correlation analyses were conducted. Participant data from both groups were compared on measures of language, mental health, bullying and self-esteem. Age and gender were also included in order to determine whether they were potential confounders and needed to be adjusted. Descriptive statistics and correlations between the variables of interest are summarised in Tables 1 and 2, respectively. As expected, adolescents with a history of DLD scored significantly lower on the language assessments. The groups did not differ significantly in terms of age [t(40) = .08, p = .934]. However, there was a significantly greater proportion of females in the group with no history of DLD as compared to the history of DLD group [χ2(1) = 4.01, p = .045].
Group means and standard deviations.
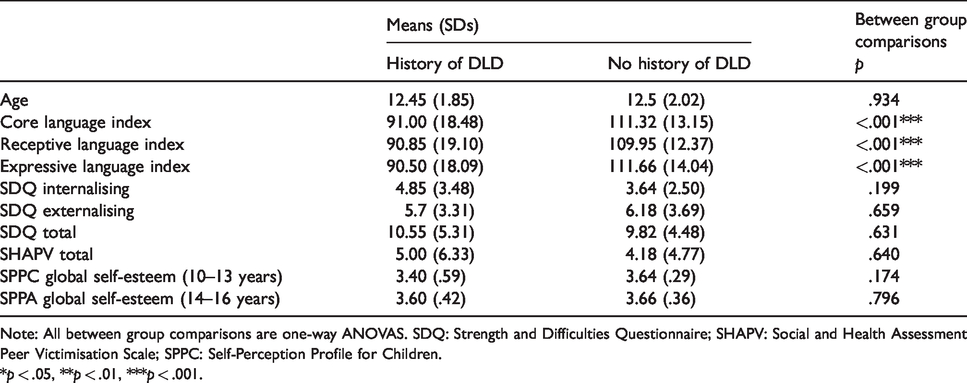
Note: All between group comparisons are one-way ANOVAS. SDQ: Strength and Difficulties Questionnaire; SHAPV: Social and Health Assessment Peer Victimisation Scale; SPPC: Self-Perception Profile for Children.*p < .05, **p < .01, ***p < .001.
Correlations between language ability, mental health, self-esteem, victimisation and potential confounders (age and gender).

CLI: Core language index; RLI: Receptive language index; ELI: Expressive language index.
*Correlation is significant at the 0.05 level (two-tailed).
**Correlation is significant at the 0.01 level (two-tailed).
***Correlation is significant at the 0.001 level (two-tailed).
Overall, the correlations were in the expected directions (Table 2). Consistent with the notion that DLD is likely to endure, a history of DLD was associated with poorer expressive and receptive scores on the current language assessment. Bullying victimisation and internalising symptoms were strongly and positively correlated [r(40) = 0.52, p = .001], and self-esteem and mental health were negatively correlated [r(40) = –.31, p = .045]. Unexpectedly, a history of DLD was not associated with either internalising or externalising symptoms in between group comparisons. History of DLD was not significantly associated with self-esteem. Regression analyses were conducted in the interest of exploratory investigation to determine how much a history of DLD, self-esteem and bullying predicted internalising and externalising symptoms.
Multivariate analyses
To test multivariate associations between the history of DLD, bullying victimisation and self-esteem, and both internalising and externalising symptoms, we conducted two hierarchical linear regressions. 2
Internalising symptoms
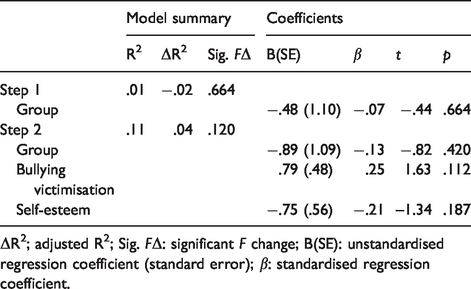
Step 1 accounted for a significant 35.5% of the variance in internalising symptoms [F(3,37) = 6.79, p = .001]. Neither the history of DLD nor self-esteem was significantly associated with internalising symptoms; however, bullying victimisation was positively associated with internalising symptoms. In simple regression models including only the relevant predictors and two-way interaction, the history of DLD×self-esteem interaction was not significant [β = .48, p = .433]. However, the history of DLD × bullying victimisation interaction was significant [β = 1.01, p = .019], and we therefore entered this into the full multivariate model to determine whether it remained significant. Step 2 accounted for a significant 38.7% of the variance in internalising symptoms [F(1,36) = 7.31, p < 0.001]. Bullying victimisation as well as the interaction between the history of DLD and bullying victimisation were both significant predictors in this model (see Table 3). Furthermore, given the difference in proportion of boys and girls across the DLD and comparison groups, we re-ran the full multivariate model adjusting for gender; bullying victimisation and the interaction between the history of DLD and bullying victimisation both remained significant (see Table 5 in Supplementary materials). In order to probe the interaction between the history of DLD and bullying victimisation, we conducted simple slope tests (Aiken et al., 1991). Internalising scores for individuals with and without a history of DLD were plotted at low (−1SD) and high (+1SD) levels of bullying victimisation (Figure 1). DLD was not associated with internalising symptoms at low levels of bullying victimisation [t(41) = –.67, p = .51]. However, there was a significant association between the history of DLD and internalising symptoms at high levels of bullying victimisation [t(41) = 2.52, p = .02].
Summary of hierarchical linear regression for internalising symptoms.

ΔR2: adjusted R2; Sig. FΔ: significant F change; B(SE): unstandardised regression coefficient (standard error); β: standardised regression coefficient. *p < .05, **p < .01, ***p<.001.

Interactions between bullying and group with regard to internalising symptoms.
Externalising symptoms
The results of the regression analyses indicated no significant relationships between the history of DLD, bullying victimisation, self-esteem and externalising symptoms (see Table 4). Neither the DLD×self-esteem nor the DLD×bullying victimisation interactions were significantly associated with externalising symptoms.
Summary of hierarchical linear regression for externalising symptoms.
ΔR2; adjusted R2; Sig. FΔ: significant F change; B(SE): unstandardised regression coefficient (standard error); β: standardised regression coefficient.
Discussion
This study aimed to further explore the association between DLD and both internalising and externalising symptoms, and examine whether self-esteem and bullying victimisation moderated this association. Unexpectedly, having a history of DLD was not directly associated with bullying victimisation, self-esteem or either internalising or externalising symptoms in our sample. However, bullying victimisation did interact with the history of DLD in predicting internalising symptoms. Specifically, the history of DLD was associated with internalising symptoms, but only at high levels of bullying victimisation. These findings extend the research indicating higher prevalence of bullying victimisation for children with DLD than for TD peers (Conti-Ramsden & Botting, 2004; Redmond, 2011; van den Bedem et al., 2016). Our findings also align with those of Wadman et al. (2011), who reported that participants with DLD who were at increased risk of experiencing depression at 16 and/or 17 years remained at risk if they had experienced bullying victimisation at 16 years. The present study builds on these findings by examining internalising symptoms across a broader age group for adolescents with and without DLD.
Our findings also reflect the view put forward by Conti-Ramsden and Botting (2008); that children with a history of language disorder experience increased risk of emotional health difficulties, but this does not appear to relate directly to poor communication experiences. Rather, it is likely that other factors are at play (Conti-Ramsden & Botting, 2008; Goh Kok Yew & O’Kearney, 2013), as discussed in a recent meta-analysis conducted by Curtis, Frey, Watson, Hampton, and Roberts (2018) who also suggest that other “mechanisms” or factors are key in predicting mental health outcomes for the DLD population, in particular emotional regulation and executive functioning. Investigating the influence of such factors for individuals with DLD across the lifespan is key to identify patterns within participant profiles. Conti-Ramsden et al. (2018) indicate that generally, development in children with DLD is varied, as is the development of emotional difficulties and peer problems. In their longitudinal study, five distinct patterns of development were identified; participants varied as to the prevalence, severity and age of onset of emotional and peer problems throughout childhood and adolescence (Conti-Ramsden et al., 2018). Variability in developmental trajectories reflected the influence of a range of factors.
Interestingly, a history of DLD and externalising symptoms were not associated in the present study. It is possible that additional factors linked with externalising symptoms (e.g. family problems, academic achievement) may not have been pervasive for our participants at this stage in their lives (Hser et al., 2015; Vaillancourt, Brittain, McDougall, & Duku, 2013). These factors were not investigated in the present study, and further research is necessary into whether they may mediate or moderate any association between language and externalising symptoms. Externalising symptoms also tend to decline over the course of development, while internalising symptoms typically emerge as children enter pre-adolescence, which may help to explain the lack of association in the present study (Miner & Clarke-Stewart, 2008; Toumbourou, Williams, Letcher, Sanson, & Smart, 2011). Another key consideration is the influence of early language intervention on mental health. Where research populations have been drawn from psychological service providers, the prevalence of unidentified language impairment has been consistently high, up to 89% (Benner, Nelson, & Epsein, 2002; Hollo, Wehby, & Oliver, 2014). In such populations, access to oral language interventions has likely been limited or non-existent. Furthermore, the prevalence of mental health symptoms in individuals with identified DLD is also reportedly high; children with DLD are two times more likely to experience clinical levels of internalising and externalising symptoms (Goh Kok Yew & O’Kearney, 2013). Existing research has clearly established that evidence-informed early intervention is effective in improving language abilities for children with DLD (Spencer, 2018). However, there is very little literature examining mental health outcomes for children who have received early oral language intervention (Goldfeld et al., 2017). Our participants with a history of DLD were recruited from an early language intervention setting and had all spent at between one and three years in a specialist classroom with highly structured and intensive oral language support. Comparison of internalising and externalising symptoms for individuals with DLD who have and have not attended an early intervention setting is recommended, as well as investigation of oral language and social skills intervention in early childhood as a protective factor for individuals with DLD.
As expected, lower self-esteem was associated with poorer mental health for the whole sample in correlation analyses. This is consistent with the literature (Jerome et al., 2002; Steiger, Allemand, Robins, & Fend, 2014). However, in the present study, no significant associations between the history of DLD, psychosocial outcomes and self-esteem were found. One possible explanation for this unexpected finding is the variability in how self-esteem is defined as a construct in the literature. Our study focussed on self-esteem as a global construct, which has been linked with mental health outcomes in psychology literature and DLD research (Durkin et al., 2017; Millings, Black, Montgomery, Spears, & Stallard, 2012). However, where other studies have been powered to do so, self-esteem has been considered a multi-dimensional construct. Lindsay et al. (2010) examined self-esteem in a sample of 54 adolescents with language disorder and identified vulnerability to lower academic self-esteem at 16 years across the cohort and lower self-esteem in social and physical appearance domains for female participants. A similar approach was taken by Jerome et al. (2002) to investigating scholastic, social and behavioural self-esteem for adolescents with language disorder. Considering self-esteem as a multi-dimensional construct in research and practice may allow the specific needs of adolescents with DLD to be represented more clearly. However, an alternative explanation for the results of the present study may lie in the age of our participants. Durkin et al. (2017) indicated that language ability in adolescence was associated with self-esteem at 24 years for individuals with a history of DLD, and suggest that language skills in middle-adolescence may be a key factor affecting social confidence. Furthermore, these patterns were not as apparent where language ability at 17 years was examined as a potential factor affecting self-esteem and social confidence at 24 years (Durkin et al., 2017). This would suggest that the effects of having DLD in adolescence may become increasingly evident as the individual enters adulthood. Given that our participants were aged between 10 and 16 years, the full effects of experiencing language deficits in early childhood and adolescence may not be evident.
Limitations
The present study was conducted with a relatively small sample of participants, which may have affected power. Future research should attempt replication with a larger sample. Participants were also recruited by responding to an advert, which may be associated with a self-selection bias. In addition, participants’ mental health, self-esteem and experiences of bullying victimisation were measured using self-report tools, which, like all self-report measures, can be subjective. Replication with triangulation of the child’s self-report measure with parent and teacher reports is also recommended. Finally, while we attempted to account for possible weaknesses in working- and short-term memory through the use of visual supports, participants’ memory and processing skills were not assessed. This may be a relevant consideration in reviewing the results.
Implications for clinical practice
The findings of our study have a number of clinical implications. Speech language therapists have an important role to play in monitoring the psychosocial wellbeing of individuals with DLD. This responsibility has been recognised in the Speech Pathology Australia (2015), and in the Speech Pathology Australia (2018). Additionally, examining the impact of anti-bullying interventions on mental health for children and adolescents with DLD is recommended. Finally, further investigation into early and intensive language intervention as a protective factor for adolescent mental health should be prioritised.
Summary
Internalising and externalising symptoms can significantly impact all facets of an individual’s daily life. For adolescents with a history of DLD, the risk of experiencing internalising difficulties in adolescence was higher than for TD peers if they had also experienced more bullying victimisation. Given current focus on DLD theory and diagnostic criteria, a prime opportunity exists to promote awareness of the impact of early language impairment on social, emotional and mental health outcomes in adolescence. Speech language therapists have a crucial role to play in advocating for clients with DLD, monitoring their psychosocial wellbeing and encouraging further investigation into language and mental health.
Supplemental Material
DLI893313 Supplemental Material - Supplemental material for Mental health in adolescents with a history of developmental language disorder: The moderating effect of bullying victimisation
Supplemental material, DLI893313 Supplemental Material for Mental health in adolescents with a history of developmental language disorder: The moderating effect of bullying victimisation by Tina Kilpatrick, Suze Leitão and Mark Boyes in Autism & Developmental Language Impairments
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tina Kilpatrick worked as Support Officer Speech and Language at the North East Metropolitan Language Development Centre, March 2014–February 2019. The other authors did not have any conflict of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.