
Abstract
Background and aims
There is a paucity of literature investigating health-related quality of life in neurodevelopmental populations including children with developmental language disorders and children with autism spectrum disorder. Health-related quality of life in these two groups remains poorly understood. Furthermore, studies have typically relied on reports from caregivers and teachers rather than using self-report measures. The aim of the current study is to compare the levels and profiles of self-reported health-related quality of life of children with developmental language disorders and children with autism spectrum disorder.
Methods
Participants comprised 114 7-to-13-year-old children with developmental language disorders (n = 63) and children with autism spectrum disorder (n = 51) attending mainstream school. Self-reported health-related quality of life was measured using the KIDSCREEN-52. We also collected standardised measures of receptive language, autism spectrum disorder symptoms, nonverbal IQ and emotional and behavioural problems.
Results
Children with developmental language disorders reported health-related quality of life commensurate with normative ranges, except for 2 of the 10 dimensions; the Moods and Emotions domain and the Social acceptance/bullying domain, which were below norms. Children with autism spectrum disorder reported significantly lower health-related quality of life compared to norms and the developmental language disorders group. However, when the effects of non-verbal ability and language – on which the groups were not matched – were covaried most group differences fell to non-significance or disappeared. Child characteristics showed few associations with dimensions of health-related quality of life across groups.
Conclusions
Children with autism spectrum disorder may be particularly vulnerable to poorer health-related quality of life and the relevant professionals need to be aware of this. Children with developmental language disorders exhibit a profile of health-related quality of life more in-line with average ranges. However, certain domains warrant monitoring and may benefit from intervention. Many of the between-group differences in self-reported health-related quality of life disappeared when non-verbal and language ability were covaried, though neither of the covariates was systematically related to scores. Other within-child factors such as emotional understanding and competence should be explored in future studies.
Implications
Further research into child and contextual factors may elucidate risk or protective factors for health-related quality of life in children with neurodevelopmental disorders.
Keywords
It is well documented that children with developmental language disorders (DLDs) 1 and autism spectrum disorders (ASDs) are vulnerable to various difficulties beyond their immediate symptoms (Simonoff et al., 2013; Yew & O'Kearney, 2013). Together these may adversely impact on their well-being in numerous ways. Measuring Health-Related Quality of Life (HRQoL) in children with DLD and ASD provides an opportunity to comprehensively capture and compare how these children are functioning in everyday life. Although there are some shared areas of difficultly in children and young people with DLD and ASD (Williams, Botting, & Boucher, 2008) with both groups, for example, having more difficulties with communication than their typical peers; there are also areas of difference (notwithstanding the heterogeneity seen in both groups). Children and young people with ASD have greater difficulty in understanding emotions and internal states and also higher levels of rigid and routinised behaviours. Children and young people with DLD all have impaired language ability, which is also seen in some but not all children and young people with ASD. By comparing these two groups, this study aims to explore the impact of those with potentially reduced social communication skills as a result of structural language difficulties compared to those with broader pervasive social communication difficulties.
Children with ASD and DLD are at risk of behavioural, emotional and social difficulties. Many studies have found elevated or clinical levels of behavioural, emotional and social difficulties in samples of children with DLD when compared to a typically developing peers (Conti-Ramsden, 2013; Durkin & Conti-Ramsden, 2010; Lindsay & Dockrell, 2012; Lindsay, Dockrell, & Strand 2007; Yew & O'Kearney, 2013). Furthermore, research indicates a high prevalence of elevated clinically significant emotional and behavioural symptoms (Totsika, Hastings, Emerson, Lancaster, & Berridge, 2011) and co-occurring psychiatric conditions for children with ASD (Leyfer, Tager-Flusberg, Dowd, Tomblin, & Folstein 2008; Simonoff et al., 2008).
Social difficulties are consistently reported in research for children with DLD and ASD. Research indicates that children with DLD often have poorer social skills, less co-operative behavior (Brinton & Fujiki, 1999; Durkin & Conti-Ramsden, 2010) and have fewer and poorer quality friendships (Van den Bedem, Willems, Dockrell, Van Alphen, & Rieffe, 2019). When compared to typically developing peers, it is reported that children with ASD had fewer, shorter, lower quality and less mutual friendships (Petrina, Carter, & Stephenson, 2014) and significantly fewer friendships than other pupils with special educational needs (SEN) (Rowley et al., 2012). Alongside social difficulties, children with DLD and ASD are reportedly more vulnerable to bullying. Significantly more 11-year-olds with DLD self-reported risk of victimisation than peers (36% vs. 12%) (Conti-Ramsden & Botting, 2004; see also Knox & Conti-Ramsden, 2003; Lindsay, Dockrell, & Mackie, 2008; Redmond, 2011). For children with ASD, prevalence rates as high as 40–75% have been reported for being bullied (Batten, Corbett, Rosenblatt, Withers, & Yuille, 2006; Little, 2001; Rowley et al., 2012).
Research indicates children with ASD and DLD are also at increased risk of academic and attainment difficulties. Children with ASD or DLD are highly represented in the population of children identified with SEN in the UK. Children classified with ASD or DLD comprise approximately 30% of pupils with identified SEN in the UK (Department for Education, 2013; Lindsay, Ricketts, Peacey, Dockrell, & Charman, 2016). Children with DLD and ASD may be at risk of generalised poorer academic educational attainment, with difficulties across academic domains, including reading, writing and maths (Beitchman et al., 1996; Catts, Sittner Bridges, Little, & Tomblin 2008; Dockrell, Ricketts, Charman, & Lindsay, 2014; Estes, Rivera, Bryan, Cali, & Dawson, 2011; Griswold, Barnhill, Smith Myes, Hagiwara, & Simpson, 2002; Ricketts, Dockrell, Patel, Charman, & Lindsay, 2015).
Quality of life (QoL) is a measure of ‘an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’ (The World Health Organization, 1995, p. 1405). HRQoL refers to the impact of a health condition and treatment on an individual's QoL (Drotar, 2004). There is consensus that HRQoL is subjective, dynamic and multidimensional (Bakas et al., 2012). There is also agreement that it includes distinct physical, psychological and social domains, but there is heterogeneity in how these domains are labelled and subdivided (Feeney, Desha, Ziviani, & Nicholson, 2011).
Multiple models have been developed to apply a framework to HRQoL. A systematic review completed by Bakas et al. (2012) found that the most commonly used models were those developed by Wilson and Cleary (1995), Ferrans, Zerwic, Wilbur, and Larson (2005) and the World Health Organisation's International Classification of Functioning, Disability and Health (WHO IFC, 2001). Ferrans et al. (2005) extended Wilson and Cleary's (1995) model by explicitly acknowledging the influence of contextual factors on HRQoL. Both of the models developed by Ferrans et al. (2005) and the WHO ICF (2001) model focus on the impact of a condition and suggest bidirectional interactions between components and individual's condition and their environment. Children with DLD and ASD commonly have difficulties beyond their immediate symptoms. We therefore adopted the ICF model as it can be used to describe how these factors may interact with contextual elements (e.g. the school environment) to influence the impact of a DLD or ASD on functioning (Campbell & Skarakis-Doyle, 2007).
Recent studies have explored constructs such as well-being and HRQoL in children with DLD and ASD. Feeney, Desha Kahn, and Ziviani (2017) indicated that parental reports of concern about receptive language, for children aged 4–9, were negatively associated with HRQoL across all domains. They suggested that DLD is associated with reduced HRQoL, concluding that typically developing speech and language skills is a protective factor for HRQoL in children. Additionally, some studies suggest that children with DLD may experience significantly poorer HRQoL in social domains. Parents of three-year-old children with language delays reported significantly lower scores than typical children on social domains, in a shortened version of the TNO-AZL Pre-school children Quality of Life-questionnaire (TAPQOL) (van Agt et al., 2005). Another study found significantly lower psychosocial summary scores but no difference for physical scores on the Child Health Questionnaire Parent Form 28 (CHQPF28) for eight-year-olds with DLD compared to controls (Van Agt et al., 2011). In contrast, other studies have reported HRQoL in-line with normative ranges for young people with DLD. No significant difference in total self-reported HRQoL was found in 8- to 11-year-olds with DLD (Arkkila et al., 2011) or adolescents with a childhood diagnosis of DLD compared to typical peers (Arkkila et al., 2009). In summary, whilst some studies have reported lower HRQoL in children and young people with DLD compared to typical peers, others have reported no differences. Although it appears that parents and children differ in their reporting of impaired HRQoL, with parents reporting more impaired HRQoL in their children than children and young people do when self-reporting their own HRQoL. However, studies have varied in the use of self vs. proxy (parent) report and also by age of the sample making definitive conclusions about the profile of HRQoL in children with DLD difficult.
Children with ASD experience poorer HRQoL across multiple domains. Eglison, Olafsdottir, Leosdottir, and Saemundsen (2017) compared HRQoL a sample of children between the ages of 8 and 17 years with a diagnosis of ASD to a sample of typically developing peers, using the Icelandic version of KIDSCREEN-27 self-report and proxy reports from parents. Their study found that overall children with ASD were reported by parents to have lower HRQoL across all domains, when compared to the control sample. A negative relationship between severity of autism symptoms and HRQoL has been demonstrated in a number of studies (Cohen & Studhalter, 2005; Kose et al., 2013; Kuhlthau et al. 2010, 2013). Some studies have also found that within samples of children and young people with ASD, higher levels of behavioural, emotional and social difficulties are associated with lower levels of HRQoL (Kuhlthau et al., 2010). Lastly, significantly lower scores on all Pediatric Quality of Life Inventory (PedsQL) domains were found for ASD youth with comorbid attention deficit/hyperactivity disorder (ADHD) symptoms compared to ASD alone (Sikora, Vora, Coury, & Rosenberg 2012). The majority of studies that have examined HRQoL in children and young people with ASD have found lower levels compared to typical peers.
Existing HRQoL research in DLD and ASD children has been limited by a number of factors. First, most samples have been drawn from clinical populations who may be representative only of those with higher levels of emotional and behavioural difficulties and findings of HRQoL in such samples might not be generalisable to the wider population of children and young people with DLD and ASD. Second, most studies have used parent ‘proxy’ report, in part due to concerns over the reliability and validity of child self-reports. However, significant disparity between parent and child report has been found in HRQoL studies which have used both, whereby parents tend to rate HRQoL significantly lower than children and young people do (Potvin, Snider, Prelock, Wood-Dauphinee, & Kehayia, 2015). This was further supported by research by Eglison et al. (2017), when comparing parent and child self-responses to KIDSCREEN-27. Their results indicated that parents of children with ASD reported lower HRQoL than was reported by their children, for physical well-being, psychological well-being, social support and peers and school environment.
The present study
The current study examined self-reported HRQoL in children with DLD and ASD in a sample ascertained from the same mainstream schools. We address the following questions:
What level of HRQoL do children with DLD and children with ASD in mainstream schools exhibit? Do their profiles differ? For each group are dimensions of HRQoL associated with child characteristics including age, language ability, non-verbal Intelligence (NVIQ), level of autistic symptoms or level of behavioural, emotional and social difficulties? Do these associations differ in children with DLD and children with ASD?
Method
Participants
Study participants comprised 114 primary and secondary school pupils who were between the ages of 7-to-13-year-olds with ASD (n = 51, 44 males, 7 females) or DLD (n = 63; 48 males, 15 females). These participants formed part of a larger sample (n = 157) enlisted in a UK research project called the Better Communication Research Programme (BCRP) (Dockrell, Lindsay, Law, & Roulstone, 2014). Only those children and young people aged seven years and above who were considered able to complete the self-report HRQoL measure are included in the current study. Participants were initially recruited from 74 mainstream schools across five Local Authorities in the South East of England. Children who had ASD or speech, language and communication needs (SLCN) recorded as a SEN with the Department for Education were recruited with parent and child informed consent and with school approval. Exclusion criteria included English not being spoken as a first language, hearing or untreated visual impairment. Prior to data collection, ethics approval was obtained from the University of Warwick Humanities and Social Science Ethics Committee, in line with the British Psychological Society guidelines.
Measures
HRQoL measure. The KIDSCREEN-52 (KIDSCREEN Group Europe, 2006) is a tool to measure HRQoL in 8-to-18-year-olds. It includes 52 items spread across 10 dimensions: Physical well-being, Psychological well-being, Moods and emotions, Self-perception, Autonomy, Parent relations/home life, Social support and peers, School environment, Social acceptance/bullying and Financial resources. Children are asked to self-rate items on a 5-point Likert-type scale considering the statement in the context of the past week. Each dimension produces an overall T score (M = 50, SD = 10) and higher scores reflect more positive HRQoL. The normative values are derived from a large population-based sample of children (N = 22,827; N = 1877 from the UK) from over 13 European countries (Ravens-Sieberer et al., 2005). Although three children were a few months younger than eight years (all were 93 months or older), we considered it appropriate to use the widely normed and well-established KIDSCREEN-52 measure.
Non-verbal intelligence. NVIQ was assessed using the Matrices performance test from the British Ability Scales 2 (BAS-II) (Elliott, Smith, & McCulloch, 1997). The Matrices subtest produces an age standardized T scores (M = 50, SD = 10).
Language ability. Three language measures were completed. First, the Test for the Reception of Grammar (TROG-E) (Bishop, 2005). The TROG-E requires respondents to select one picture out of four options that is indicated by an orally delivered sentence. Sentences increase with grammatical complexity and the TROG-E is a test of receptive grammar. The TROG-E produces a standardised score (M = 100, SD = 15). Second, the British Picture Vocabulary Scale, 3rd edition (BPVS-3; Dunn, Dunn, & NFER, 2009). It asks participants to select the one picture out of four options that matches the orally presented word. It is a measure of receptive vocabulary. The BPVS-3 produces a standardised score (M = 100, SD = 15). Third, the Concepts and Following Directions (CFD) subtest from the Clinical Evaluation of Language Fundamental – 4th Edition (CELF-4 UK; Semel, Wiig, & Secord, 2006). The CFD subtest asks children to point to the object they were instructed to via oral direction and is a measure of receptive comprehension and memory. The CFD subscale produces a scaled score (M = 10, SD = 3). We selected receptive language ability as a recent meta-analysis has demonstrated that this is specifically association with later behavioural difficulties (Chow, Ekholm, & Coleman, 2018).
ASD symptoms. Teacher reported Social Responsiveness Scale (SRS: Constantino & Gruber, 2005) total scores were used to measure the level of ASD symptoms in all participants. The SRS is designed to measure the presence and extent of autism symptoms. The SRS contains three subscales: social awareness, social cognition and autistic mannerisms. Respondents are presented with items about autism symptoms across these domains and asked to rate the frequency of their occurrence on a 5-point scale. SRS scores are expressed as age standardized T scores (M = 50, SD = 10). In the present study, the total SRS difficulties composite was used to provide a continuous measure of symptom severity derived from the three subscales. Higher T scores reflect more severe autism symptoms.
Levels of behavioural, emotional and social difficulties. The level of behavioural, emotional and social difficulties was assessed using the teacher-reported Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997). The SDQ comprises five subscales: Hyperactivity, Conduct problems, Emotional symptoms and Peer problems, which together produce a Total difficulties score, plus Prosocial, which is a measure of positive behaviour. Each scale contains 5 items that are scored from 0 to 2, hence scale scores vary from 0 to 10, and the Total difficulties score varies from 0 to 40, with higher scores reflecting higher levels of behavioural, emotional and social difficulties.
Procedures
In order to identify pupils specifically with clinically relevant DLD symptoms, all the pupils with registered SLCN were screened. For the purpose of this study, pupils were identified as having a DLD if they scored at least one standard deviation below the normative mean on either the Word classes or Recalling sentences tests from the CELF-4 UK. To have ASD registered as their primary SEN, pupils will have at some point been formally diagnosed by a clinical professional based on International Classification of Diseases–Tenth Edition (ICD-10) (World Health Organization, 1993) or Diagnostic and Statistical Manual of Mental Disorders–Fourth edition (DSM-IV) (American Psychological Association, 2000) criteria.
Once the groups had been established, the participants undertook a series of measures assessing HRQoL and additional measures of language, cognition and academic achievement. The mean time this was completed after screening was 3.9 months.
Analysis
Data were analysed using Stata version 15.0, statistical software (StataCorp, 2017). T-tests were used to check for differences between participants with and without KIDSCREEN data. Descriptive statistics illustrated sample characteristics of DLD and ASD participants with KIDSCREEN data and comparative analysis was performed again using analyses of variance (ANOVAs). Cronbach's alphas were used to assess the internal consistency of the HRQoL instrument in school-age children with ASD and DLD. Mean group scores for all KIDSCREEN subscales for the ASD and DLD groups were compared using a multivariate analysis of variance (MANOVA) and then a series of follow-up ANOVAs examining group differences for each KIDSCREEN subscale, with the significance value adjusted for multiple comparisons (10 comparisons, p < .005). Since the two groups differed on NVIQ and language ability (see below) these were covaried and results are highlighted where group differences changed. Cohen's d was used as a measure of effect size throughout. The percentage of participants within each group exhibiting scores more than 1.5 SD below normative means (lowest 6.7%) was also calculated (Ravens-Sieberer et al., 2005). Pearson's correlation coefficients were used to investigate correlations between HRQoL dimensions and child characteristics. Due to the large number of correlations but also given the exploratory nature of this analysis significance was set at p < .01, in order to highlight potentially meaningful associations that could be further confirmed in future analyses with larger samples.
For the purpose of this study, scores on all three language measures were summarised into a composite measure of receptive language ability based on mean Z score. A single measure of ability was used to reduce the number of language variables to simplify analysis. This was justifiable based on the high correlations between the measures (BPVS and CELF-CFD, r = .56, BPVS and TROG-E, r = .58, CELF-CFD and TROG-E, r = .53; all p < .001). We selected receptive language ability as a recent meta-analysis has demonstrated that this is specifically association with later behavioural difficulties (Chow, Ekholm & Coleman, 2018).
Results
Participants with and without KIDSCREEN data
Of the 122 participants invited to complete the KIDSCREEN, 114 (93%) participants did so. Participants who completed the KIDSCREEN did not differ significantly from those who did not in age, NVIQ, language ability, SRS score or SDQ score (all p > .10). Details of this analysis are available from the corresponding author in request.
Participant characteristics.
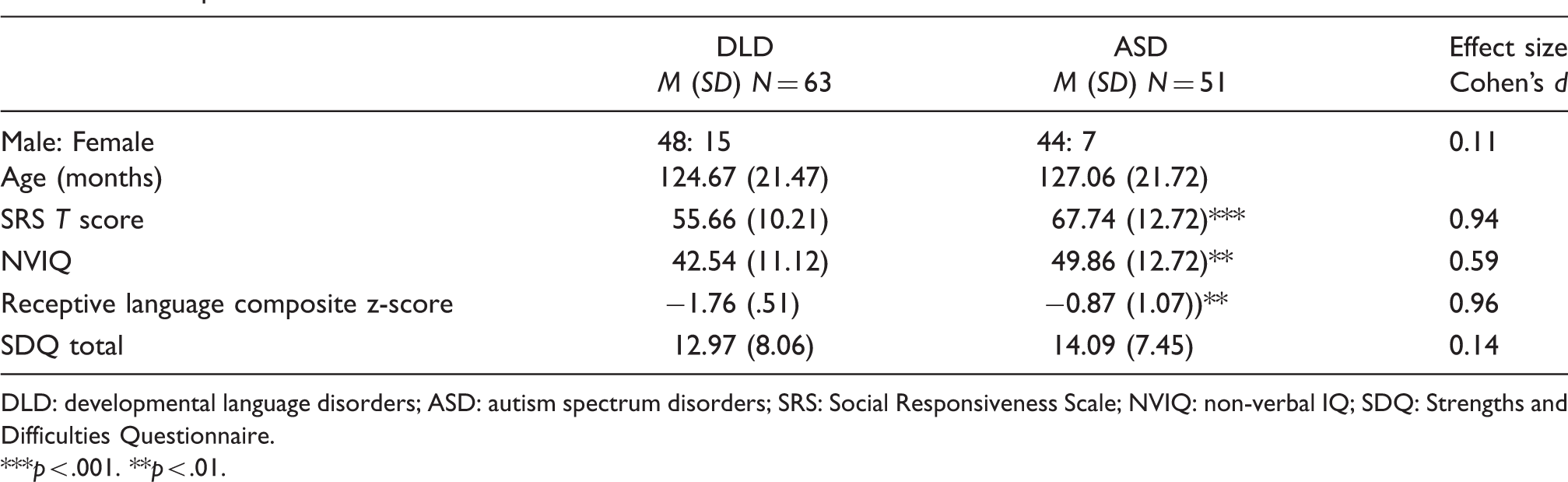
DLD: developmental language disorders; ASD: autism spectrum disorders; SRS: Social Responsiveness Scale; NVIQ: non-verbal IQ; SDQ: Strengths and Difficulties Questionnaire.
***p < .001. **p < .01.
Levels and profiles of HRQoL
Mean T scores across the KIDSCREEN dimensions for the DLD and ASD group are shown in Table 2 and Figure 1. The mean Cronbach's alpha was .72 for the DLD group and .76 for the ASD group across dimensions. An omnibus MANOVA showed that the groups differed across the 10 KIDSCREEN subscales, F(1,105) = 3.55, p < .001. Follow-up ANOVAs showed significantly lower scores in the ASD group compared to the DLD group across the dimensions of Psychological well-being, F(1,112) = 8.49, p = .004, d = .53, Autonomy, F(1,112) = 23.03, p < .001, d = .83, Parent relations and home life, F(1,111) = 24.85, p < .001, d = .86, Financial resources, F(1,107) = 9.50, p = .003, Social support and peers, F(1, 109) = 13.45, p < .001, d = .66 and School Environment, F(1, 111) = 8.78, p = .004, d = .54. The DLD group had marginally but non-significantly higher scores than the ASD group on the Physical well-being, F(1, 112) = 3.54, p = .06, d .35 and Self-perception, F(1, 112) = 3.91, p = .05, d = .37 dimensions. There were no group differences on the Mood and emotions, F(1, 112) = 0.24, p = .63, d = .09 and Social acceptance/bullying scale, F(1, 110) = 0.48, p = .49, d = .13 dimensions. When NVIQ and language ability were entered into the ANOVAs only two significant group differences remained at our adjusted significance threshold of p < .005: The ASD group scored lower than the DLD group on the Autonomy (p = .001) and Parents/Home life (p < .001) subscales. There was only one marginal effect of NVIQ on the Self-perception subscale (p = .01), with the (median split 44 and below vs. 45 and above) participants with lower NVIQ scoring higher than the participants with higher NVIQ (50.32 (12.35) vs. 45.06 (9.66)).
Mean KIDSCREEN-52 T scores across each dimension for the DLD and ASD groups. *Error bars represent the standard error (SD/√N). Mean T scores across dimensions of the KIDSCREEN for the developmental language disorders (DLD) and autism spectrum disorders (ASD) groups and the proportion of each group scoring <1.5SD below the normative scores. ***p < .001. **p < .005.

Child characteristics and HRQoL
Correlations between KIDSCREEN dimensions and child characteristics for the developmental language disorders (DLD) and autism spectrum disorders (ASD) groups.

SDQ: Strengths and Difficulties Questionnaire; SRS: Social Responsiveness Scale; NVIQ: non-verbal Intelligence.
p < .01.
Discussion
The present study aimed to examine self-reported HRQoL in a sample of children and young people with ASD or DLD from UK mainstream schools. The findings indicated that children with DLD and children with ASD have somewhat different profiles of HRQoL. The DLD group self-reported scores in line with normative ranges across most subscales of the KIDSCREEN. However, lower scores (more than 1 SD below population norms) were reported on the Moods and emotions and Social acceptance and bullying dimensions. The ASD group reported significantly lower scores than the DLD group on 6 out of the 10 subscales (Psychological well-being, Autonomy, Parents/home life, Financial resources, Social support and peers and School environment) and in common with the DLD group had score more than 1 SD below the norms on the Moods and emotions and Social acceptance and bullying dimensions. However, many of these differences became non-significant when NVIQ and language ability, on which the two groups differed, were covaried, although the ASD group continued to report lower HRQoL than the DLD group on the Autonomy and Parents/Home life subscales. Some of the apparent group differences appear to be, at least in part, due to differences in intellectual and language abilities between the DLD and ASD groups. Within our study it is not possible to disentangle the extent to which cognitive and language abilities might be affecting how children and young people experience their lives from how they are able to access and report them on a questionnaire measure (even when read out loud to them). The effect of such factors should be explored in future studies.
The findings align with previous research that has investigated HRQoL in both groups separately. A longitudinal study found self-reported scores in the normative range on measures of wellbeing in DLD youth followed from 10 to 17 years (Lindsay & Dockrell, 2012). Normative self-reported HRQoL was found in a samples of 8-to 11-year-olds with DLD (Arkkila et al., 2011) and 12- to-16-year-olds with childhood diagnoses of DLD (Arkkila et al., 2009). The findings from the ASD group, confirm previous studies that have indicated poor HRQoL using both parent-report (Kuhlthau et al., 2010, 2013; Limbers, Heffer, & Varni, 2009) and self-report (Potvin et al., 2015; Tavernor, Barron, Rodgers, & Mcconachie, 2013). Some studies of adolescents with ASD have reported HRQoL in-line with normative ranges in some domains such as relationships with parents and school functioning (Clark, Magill-Evans, & Koning, 2014; Cottenceau et al., 2012).
The lowest scores for both groups were seen on the Social acceptance and bullying and Moods and emotions scales. Scores were more than 1 SD below normative means, with over 40% of both groups scoring more than 1.5 SD below the norms, group differences between the DLD and ASD children did not reach significance and the effect sizes were very small. Low mean scores on the Social acceptance and bullying subscale (that includes items about being afraid of other children and being called names and bullied) reflect the heightened vulnerability to peer victimization seen in children with DLD and children with ASD (Knox & Conti-Ramsden, 2003; Rowley et al., 2012). The Moods and emotions dimension examines experiences of negative emotional symptoms such as stress, loneliness and insufficiency. Behavioural, emotional and social difficulties are common in DLD and ASD children and are consistent with these findings of self-reported mood and emotional difficulties (Charman, Ricketts, Dockrell, Lindsay, & Palikara, 2015; Yew & O'Kearney, 2013).
Both groups seem to be at risk of difficulties in these areas with considerable negative effects on well-being and these vulnerabilities need to be understood by practitioners who work with children with DLD and ASD. For the DLD group, generally good HRQoL across other dimensions may suggest that broadly they feel sufficiently supported and accepted in their current environments, or alternatively they experience difficulties but are not attuned to these. The scores on the School Environment scale (the highest for both groups) suggested good levels of HRQoL in their mainstream school environments. This supports previous positive self-report scores on school HRQoL dimensions in DLD and ASD children (Arkkila et al., 2011; Clark et al., 2014; Kuhlthau et al., 2010). Scores on the Self-perception scale are in line with research showing positive self-concept in youth with DLD (Lindsay & Dockrell, 2012) and highly rated self-image in adolescents with ASD (Cottenceau et al., 2012). However, with two exceptions (the Autonomy and Parents/Home life subscales) the between group differences in self-reported HRQoL disappeared when non-verbal and language ability – on which the groups were not matched – were covaried, though neither of the covariates was systematically related to scores on the KIDSCREEN. Other within-child factors, such as emotional understanding and competence, that may play a role in self-perception of QoL in young people with neurodevelopmental conditions but that were not measured in the present study should be explored in future studies.
Association with child characteristics
For both groups, the child characteristics investigated (age, NVIQ, language ability, severity of autism symptoms and levels of emotional and behavioural problems) showed few associations with HRQoL. Overall, only four (from 100 tested) correlations reached significance at p < .01, despite there being quite wide heterogeneity in child characteristics in our sample. For most associations the shared variance (r 2 ) was below 10%. We examined associations between these child characteristics and self-reported HRQoL because we anticipated that children with lower cognitive or language ability or higher levels of ASD symptoms or emotional and behavioural problems might report lower QoL. Broadly, this was not the case. However, the possible effects of these factors are complicated and may also directly relate to the child's ability to accurately access and report their own experiences. We did not collect proxy parental ratings alongside self-reported HRQoL and this might help disentangle these effects in future studies. It may also be the case that different aspects of children's functioning that we did not measure are associated with their HRQoL. For example, a recent study found that secondary difficulties in emotional competence in children with DLD make these children more vulnerable to victimization and warrant specific support and interventions (van den Bedem, Dockrell, van Alphenm Kalicharan, & Rieffe, 2018).
Only one association reached significance in the ASD group (Parents/home life and SDQ total problems score) and there was no association with age, NVIQ, language ability of ASD severity. One previous study reported a negative effect of age on all PedsQL domains (Kuhlthau et al., 2010). However, others have reported no association with age consistent with our findings (Kose et al., 2013), although our sample were mostly under age 13 years and future studies should examine HRQoL in adolescent samples of young people with ASD. In contrast to our findings, some previous studies have found significant negative associations between the severity of autism symptoms, levels of emotional and behavioural problems and HRQoL (Kose et al., 2013; Kuhlthau et al., 2010; Kuhlthau et al., 2013).
Eliciting self-reported QoL in children with neurodevelopmental disorders
It should be acknowledged that there are potential pitfalls with using self-report to assess HRQoL in these populations. It is possible that due to their receptive language difficulties the DLD group may have experienced some difficulties reading and/or comprehending the questionnaire. In fact, 87% of the DLD group had the KIDSCREEN read aloud to them to facilitate self-report although it is possible that some comprehension difficulties occurred when listening to the items. It is also arguable that due to impairments with theory of mind and high levels of alexithymia in children with ASD (Ben Shalom et al., 2006; Berthoz & Hill, 2005; Gaigg & Bowler, 2008; Milosavljevic et al., 2016) the use of self-report to assess HRQoL in ASD children has limited reliability and validity. However, there is a growing literature indicating that ASD youth are capable of reflection on their affective states (Rieffe, Terwogt, & Stockmann, 2000; Shipman et al., 2011). There is evidence for the reliability and validity of self-report in this study. Mean Cronbach's alphas for both groups were acceptable (both > .70). Both the DLD and ASD groups produced a range of different scores across dimensions. This could be interpreted as evidence of their ability to distinguish between areas of HRQoL that are subjectively better or poorer. The pattern of observed results (overall good HRQoL in DLD populations and poorer HRQoL in ASD children) is largely consistent with the existing literature. Overall, it remains important to understand how children with neurodevelopmental disorders perceive their own HRQoL.
Limitations
The study has notable strengths. The response rate from participants invited to complete the KIDSCREEN was very high (93%) suggesting good acceptability. Thus, the observed results are representative of the original school sample. The sampling from mainstream schools is another strength of this study and should ensure generalisability to wider DLD and ASD populations. This also avoids the pitfall of comparing clinically ascertained groups of children with DLD and children with ASD who may differ from each other in numerous ways, thus providing a more ‘like for like’ comparison. However, the study also has a number of limitations. The level of autism symptoms and emotional and behavioural difficulties were based on teacher report measures. The lack of other informants (parent, clinician) is another limitation as children's behaviour may vary across contexts (home/in the community: Lindsay et al., 2007). Due to the exploratory nature of the study and the number of child characteristics that were being investigated, associations between SDQ subscales and HRQoL dimensions were not explored. Different effects of internalizing and externalizing symptoms on the HRQoL profile of ASD children have been found in previous studies (Kuhlthau et al., 2010). This study was also limited by the lack of investigation of environmental factors (familial, peer, support). Conceptual frameworks (Ferrans, Zerwic, Wilbur, & Larson, 2005) suggest that both individual (child) and environmental characteristics exert influence on HRQoL. The use of self-report to examine HRQoL is a strength. This is important due to the inherently subjective nature of the construct and the significant discrepancy that has been found between parent and child reports (Eglison et al., 2017; Potvin et al., 2015; Shipman, Sheldrick, & Perrin, 2011; Sheldrick, Neger, Shipman, & Perrin, 2012). However, using self-report meant that only children with sufficient language abilities were included in the study but this is the population of children with DLD and ASD in mainstream school provision in the UK. Future studies a multi-informant approach using parents, educational staff or even peers may be advantageous and provide the opportunity to triangulate evidence. Use of multiple respondents may also yield rich information about functioning across different contexts.
Conclusion
Our results suggest that children with DLD and ASD in mainstream schools experience somewhat different but also partly overlapping profiles of HRQoL. Children with DLD exhibit a profile of HRQoL more in-line with average ranges; whilst the ASD group reported significantly lower HRQoL across many dimensions. Both groups had very low scores in the domains of Mood and emotions (emotional wellbeing) and Social acceptance and bullying; highlighting their social vulnerability and need for support in these areas. However, when NVIQ and language ability were covaried only a few group differences remained, suggesting that the two groups' overall HRQoL are not so distinct from each other. The child characteristics investigated were largely unrelated to HRQoL for both groups suggesting that the profiles we identified were broadly representative of the whole sample. However, other factors which we have not captured in the present study may play a role in young people's experiences of life satisfaction or in their reporting of their experiences on self-report questionnaires and should be investigated in future studies. Professionals working with ASD children need to be aware of their vulnerability for lower HRQoL and of domains that may be problematic for both children with DLD and children with ASD. Further research into child and contextual factors may elucidate risk or protective factors for HRQoL in children with neurodevelopmental disorders.
Footnotes
Acknowledgements
We would like to acknowledge the support of all the students, their families and schools. We are also grateful to Nita Patel, Shona Kelly and Melissa Hollinworth for assistance with data collection and project planning.
Authors’ note
Catherine Coales and Natalie Heaney are joint first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.