
Abstract
Background and aim
Individuals with developmental language disorder have been found to exhibit increased emotional difficulties compared to their typically developed peers. However, the underlying pathways involved in this relationship are unclear. It may be that poor language leads to social exclusion, resulting in feelings of frustration and isolation. Additionally, previous research has focused on clinical samples or early childhood in population cohorts. Therefore, the current paper examines the mediating effect of childhood peer problems on poor emotional outcomes in adolescence using a population cohort.
Methods
Data from the Millennium Cohort Study were analysed at ages 5, 7 and 14. The risk of developmental language disorder group (children considered at risk of developing developmental language disorder based on parental report of difficulties or a score −1.5 standard deviation on Naming Vocabulary subtest at age 5) was compared to a general population group. A Sobel–Goodman test was used to examine the mediating effect of teacher-reported peer problems at age 7 on the association between language difficulties at age 5 and parent-reported emotional problems at age 7 and 14.
Results
Peer problems at age 7 accounted for approximately 14% of the effect of language difficulties at age 5 on emotional problems at age 7, and approximately 17% of the effect of language difficulties at age 5 on emotional problems at age 14.
Conclusions
This paper supports previous findings that children and adolescents with language difficulties are at increased risk for social and emotional problems as reported by their parents and teachers. Furthermore, the findings show that peer problems partially mediate the relationship between language difficulties and emotional problems, suggesting that better relationships with peers may offer some protection against poor mental health outcomes in adolescents at risk of developmental language disorder.
Implications
This paper adds to the literature that investigates the mechanisms involved in the relationship between developmental language disorder and increased emotional problems. Practitioners wishing to reduce risk of emotional difficulties in children with developmental language disorder may wish to reflect on what they can do to support a child to develop positive peer relationships.
Introduction
Language ability is a necessary skill for adaptive functioning. Not only do language skills help with reasoning and problem-solving abilities, they are also vital for communicating and socialising with others. Children with language difficulties, or who have developmental language disorder (DLD), 1 have been shown to have higher ratings of withdrawal (Beitchman et al., 1996; Hart, Fujiki, Brinton, & Hart, 2004; Maggio et al., 2014), increased feelings of anxiety and depression (Beitchman et al., 2001; Conti-Ramsden, Mok, Pickles, & Durkin, 2013; Voci, Beitchman, Brownlie, & Wilson, 2006) and lower self-esteem (Wadman, Durkin, & Conti-Ramsden, 2008) compared to typically developing (TD) peers. DLD affects approximately 7% of the population and manifests as a difficulty with receptive and/or expressive language that cannot be accounted for by any other hearing, oromotor impairment or global intellectual disability (Norbury et al., 2016). Associated emotional difficulties can persist throughout the life span (Clegg, Hollis, Mawhood, & Rutter, 2005). Additionally, there are high rates of previously undiagnosed language difficulties in samples of young people referred to child and adolescent mental health services (Cohen, Barwick, Horodezky, Vallance, & Im, 1998) and youth offenders (Hughes et al., 2017). Therefore, there is a clear need to unravel the close association between language difficulties and increased emotional problems.
Some gaps in the literature exist despite evidence of associations between language difficulties and poor emotional outcomes. For instance, research focuses on cross-sectional studies conducted in childhood, which does not account for the developmental pathways involved in the relationship (Yew & O’Kearney, 2013). Also, there is conflict surrounding the extent to which language ability is the strongest predictor of poor emotional outcomes. For example, some studies have shown that language ability predicts emotional problems in teacher reports but not parent reports (Lindsay, Dockrell, & Strand, 2007; Redmond & Rice, 1998, 2002) but this same pattern has not been found in other studies (Lindsay & Dockrell, 2012; Wadman, Botting, Durkin, & Conti-Ramsden, 2011). Additionally, some young people with DLD have no problems with emotional functioning (Snowling, Bishop, Stothard, Chipchase, & Kaplan, 2006) and a recent follow-up study on a cohort with DLD found that previously high levels of social anxiety at age 19 had dissipated by the age of 31 (Beitchman, Brownlie, & Bao, 2014). These inconsistencies in the direct relationship between language ability and emotional outcomes suggest that there may be mediating or third factors involved in the relationship between language difficulties and negative emotional outcomes, perhaps exacerbated by language difficulties but more directly related to the resulting emotional difficulties (Bakopoulou & Dockrell, 2016; Conti-Ramsden & Botting, 2008; Durkin, Toseeb, Botting, Pickles, & Conti-Ramsden, 2017).
One possibility is that poor language skills inhibit social functioning, which in turn increases risk of emotional problems (Redmond & Rice, 1998). It is clear that language plays an integral role in social functioning as the social skills required for effective interactions depend on strong verbal skills. Therefore, individuals with language difficulties may have particular difficulty with social interactions and exhibit poor social functioning. For example, observational studies demonstrate that children with DLD struggle to integrate into conversations and social situations (Brinton, Fujiki, Spencer, & Robinson, 1997). In turn, these social difficulties may lead to poor emotional outcomes as individuals experience loneliness and decreased social support. Consistent with this, children and adolescents with DLD report increased social stress (Wadman, Durkin, & Conti-Ramsden, 2011b) and higher levels of social anxiety (Voci et al., 2006) compared to their TD peers.
With less exposure to social situations, children with DLD may have fewer opportunities to develop social skills and, as a result, fewer resources to draw on during social interactions (Crick & Dodge, 1994). Consequently, children may be missing out on learning social skills, such as conflict resolution skills, and instead resort to less adaptive responses such as physical aggression (Bakopoulou & Dockrell, 2016). An inability to solve problems using words may act as a further barrier to social functioning, as children avoid those who are too aggressive or emotional (Wolters, Knoors, Cillessen, & Verhoeven, 2013). Indeed, children with DLD receive more ‘dislike’ ratings than their age-matched peers in classroom rating studies (Andres-Roqueta, Adrian, Clemente, & Villanueva, 2016; Gertner, Rice, & Hadley, 1994). These findings are consistent with parent, teacher and self-reports of increased peer problems compared to TD peers (Conti-Ramsden et al., 2013; Mok, Pickles, Durkin, & Conti-Ramsden, 2014; St Clair, Pickles, Durkin, & Conti-Ramsden, 2011). Children and young people with DLD are also more prone to victimisation compared to their TD peers (Conti-Ramsden & Botting, 2004; Redmond, 2011), which could negatively impact their self-esteem and increase feelings of anxiety or depression (Hawker & Boulton, 2000), illustrating again the impact of social difficulties on the mental health of individuals with DLD. Incidents of bullying may also have a stronger impact on children and adolescents with DLD, with victimisation predicting behaviour problems in children with DLD but not in their TD counterparts (Knox & Conti-Ramsden, 2007). Although, there are contrasting reports of risk of victimisation in children and young adolescents with DLD, with some studies reporting similar rates to TD peers and those with learning disabilities (Lindsay, Dockrell, & Mackie, 2008).
Nevertheless, these cross-sectional studies do not fully explain the mechanisms involved in the relationship between DLD and emotional outcomes. Longitudinal studies on individuals with DLD have illustrated different trajectories of poor social functioning throughout development (Mok et al., 2014) with some finding that social difficulties tend to increase during adolescence (Lindsay & Dockrell, 2012; St Clair et al., 2011). This increase in peer problems could reflect the general increased complexity of peer relations in adolescence and the growing importance that friendships play in shaping self-esteem and emotional well-being by providing social support (Van Harmelen et al., 2017). Early difficulty in friendships and social functioning may snowball across development, potentially even relating more strongly to emotional problems due to the increasingly important role of language in the more complex friendships in adolescence. For example, St Clair et al. (2011) found impaired pragmatic (e.g. social) language skills predicted peer problems and emotional problems at age 11 and 16, while (Wadman et al., 2011) found that peer problems predicted concurrent depressive symptoms at age 16. Therefore, there is a need to examine these factors throughout childhood and adolescence in order to distinguish the pathways involved.
Current study
The current study analyses the pathways between early language difficulties at age 5 and later emotional difficulties at age 14 in a population cohort, the Millennium Cohort Study (MCS). Previous studies have found increased social and emotional problems in children and young people with a diagnosis of DLD from a clinical cohort, the Manchester Language Study (e.g. Conti-Ramsden et al., 2013; Mok et al., 2014; St Clair et al., 2011). As highlighted by a recent panel of experts in the field, it is important to examine whether these same patterns of negative outcomes are found in individuals with impaired language from a population cohort (Bishop, Snowling, Thompson, Greenhalgh, & consortium, 2016). There is evidence of associated emotional and behavioural problems from previous population studies of language difficulties, but outcomes are from young children aged four (Bretherton et al., 2014); five (Girard, Pingault, Doyle, Falissard, & Tremblay, 2016, 2017); six (Clegg, Law, Rush, Peters, & Roulstone, 2015) and seven years of age (Levickis et al., 2017). The current study is the first in the UK to use a longitudinal population approach from the age of 5–14 years focusing on children with language difficulties. Adolescence is a key period to study emotional outcomes due to the potential that emotional problems may develop into psychiatric disorders later in life (Jones, 2013). Therefore, it would be beneficial to examine whether, and how, language difficulties predict emotional and social problems throughout childhood and adolescence.
In addition to extending previous findings into adolescence, the current study will examine whether there is a mediating factor involved in the relationship, to provide more detailed understanding of the pathways between language difficulties at age 5 and later emotional difficulties at age 7 and 14. Specifically, we will examine the mediating effect of social functioning. Social functioning is an umbrella term and is defined in this paper as adaptive social interactions with others, such as quality and quantity of friendships, while difficulties in social functioning are reflected by experiences of peer problems and victimisation. Any group differences in different aspects of social functioning will be included in the mediation model in order to explain the relationship between language and emotional difficulties. A better understanding of how this relationship manifests may help speech and language therapists evaluate interventions to provide a more comprehensive approach that also examines current social functioning. Firstly, it is hypothesised that participants with a language difficulty at age 5 will experience higher rates of emotional difficulties than their age-matched peers at age 7 and 14, as evidenced by parent report on the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) and self-report on the Short Mood and Feelings Questionnaire (SMFQ; Angold et al., 1995). Secondly, participants with a language difficulty at age 5 are hypothesised to experience poorer social functioning at age 7 and 14 in comparison to their age-matched peers, as evidenced by higher reports of victimisation and increased rates of teacher-reported peer problems from the SDQ. Finally, social functioning is expected to mediate the relationship between early language difficulties and later emotional difficulties, with those with reports of poorer social functioning experiencing higher levels of emotional problems than their peers.
Method
Ethics
The original study received full ethical approval from the NHS Multi-Centre Research and Ethics Committee (MREC) at each wave (Connelly & Platt, 2014).
Participants
Participants were obtained from waves 1–6 of the MCS (University of London, 2018). This birth cohort follows children born between September 2000 and January 2002 at age 9 months, and 3, 5, 7, 11 and 14 years of age. The full sample size was 19,518 children. In total, 5256 individuals were excluded from this analysis (537 due to multiple births and 4719 due to missing risk of developmental language disorder (rDLD) status data). The current sample is 14,262 singletons. The sample was 46.8% female (n = 6675) (see Figure 1).
Flow diagram of group allocation.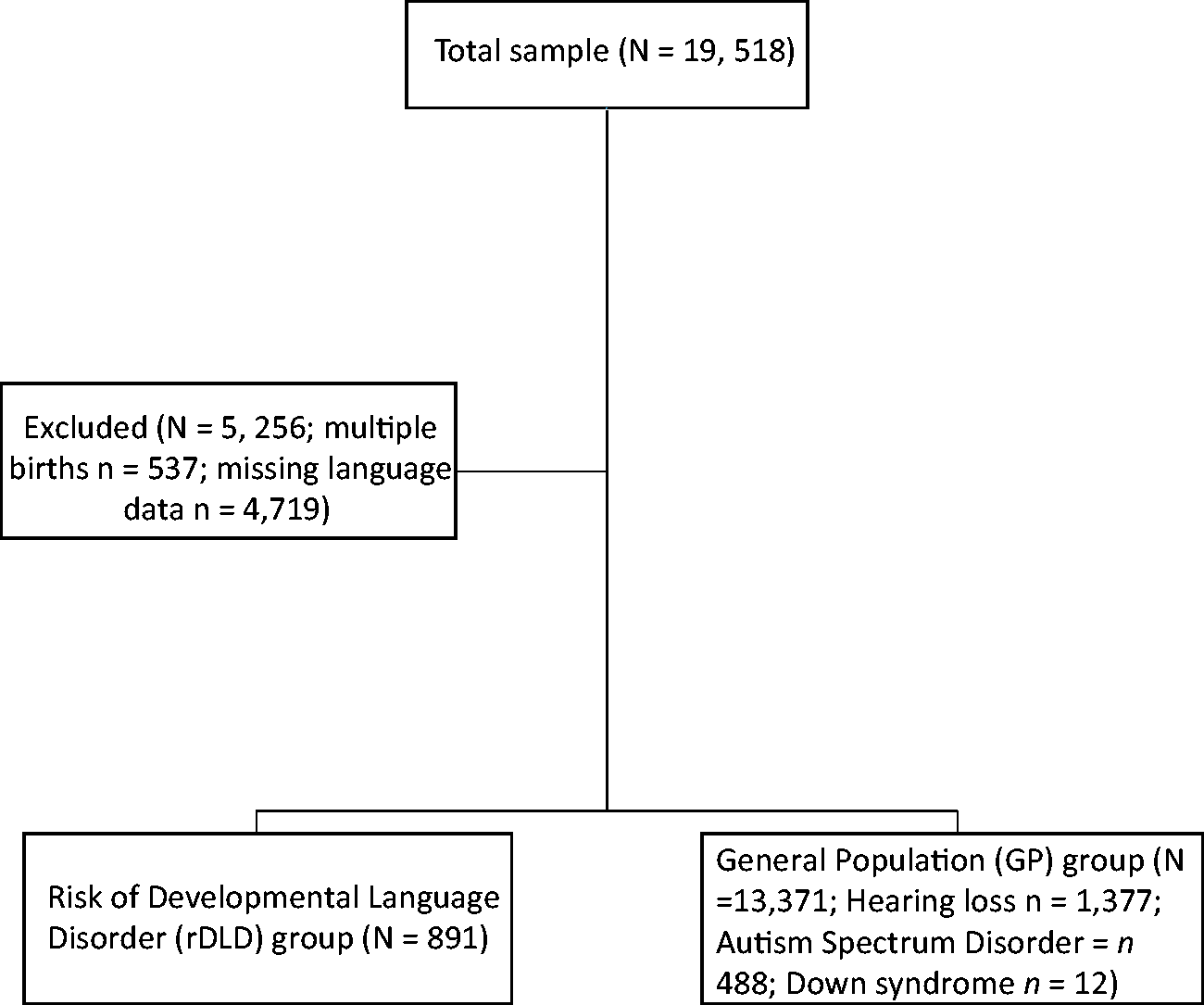
Measures
Risk of developmental language disorder (rDLD)
As recommended by recent literature (Bishop et al., 2016), we employ the term DLD to describe the group with receptive and/or expressive language difficulties at age 5 that cannot be accounted for by any other hearing or cognitive impairment. Consistent terminology enables researchers, parents and professionals to be on the same page when referring to children with significant language difficulties not otherwise explained by other conditions. However, it should be noted that, due to secondary data analysis, there was only one standardised measure of expressive language available and therefore there is no formal diagnosis of DLD in the sample. To this end, we created the ‘rDLD’ variable as a measure of children considered at risk of developing DLD. This was based on lower language ability as measured by parent report or a standardised test. Both measures were taken from the third wave of data collection at age 5, as children who have low language abilities by this age are likely to continue to have low language as they develop (McKean et al., 2017b). Bishop and McDonald (2009) note that the combination of measures from different sources provides a more comprehensive picture of language abilities. Children had to meet at least one of the following two criteria to be included in the rDLD group. Firstly, participants were included in the rDLD group if they received a positive response to the statements ‘Language developing slowly’ or ‘Doesn’t understand others’ from parent report at age 5 (n = 440). This provided a measure of functional language in everyday use. Participants were not included if parents endorsed items relating to speech or hearing problems, such as ‘S/he pronounces words poorly’, ‘S/he doesn’t hear well’ and ‘S/he stutters’. See Hughes, Sciberras, and Goldfeld (2016) for a similar measure of parental report of language difficulties relating to social and emotional problems. Secondly, participants were included if they scored 1.5 SD below the mean (T score of 35 or below) on the British Ability Scales (BAS) naming vocabulary subtest (n = 529) (Elliott, Smith, & McCulloch, 1997). This test provides a measure of expressive language ability, requiring participants to name pictures of objects and has a reliability coefficient of .65 at age 5 (Elliott et al., 1997). Reilly et al. (2014) recommend a cut point of more than 1.25 SD below the mean on language tasks. Given that there was only one standardised language test available in the current cohort, we have used the threshold of 1.5 SD below the mean to provide a conservative estimate of children at risk of DLD. This decision also follows Law, Rush, Anandan, Cox and Wood’s (2012) example of using a 1.5 SD cut point to define language impairment from the same population cohort. There were 78 children who met both criteria of parent report of language difficulties and low score on the naming vocabulary subtest. Both criteria of rDLD were administered to all parents and children.
In total, 6.3% of the sample (N = 891) were included in the rDLD group at age 5, which is a conservative rate given the recent UK prevalence rate of 7.6% for DLD (Norbury et al., 2016). This is to be expected, given that only one standardised language subtest is used in the current study compared to the more comprehensive language assessments that are employed in Norbury et al.’s (2016) study and others in the literature. Analyses were rerun on separate groups with each inclusion criteria and a strikingly similar pattern of group differences were found for naming vocabulary and parent report individually (see Supplemental materials).
As we were interested in those with a primary language difficulty, children who met criteria for the rDLD group but were in a family environment where English was not spoken at least 50% of the time were dropped from the analysis (n = 320). Parent reports of additional support in the classroom and special educational needs were examined for evidence of Autism Spectrum Disorder (ASD) (n = 487), hearing difficulties (n = 1229) or Down Syndrome at age 7 and age 11 (n = 12) and participants were excluded when they met these criteria. No other reports of additional support or special educational needs related to global intellectual disability were reported in the rDLD group.
All individuals who did not meet criteria for the rDLD group were then entered into the general population (GP) comparison group, even if there was evidence of hearing problems, ASD or Down Syndrome. This is in line with recent recommendations for control groups with developmental disorders as outlined in Fombonne (2016). Of the total sample eligible for the study (after excluding multiple births and missing rDLD data), 93.7% were included in the GP group at age 5 (N = 13,371).
Emotional difficulties outcome
The SDQ (Goodman, 1997) was completed by the main respondent (predominantly the mother) at ages 7 and 14 years. This 25-item scale is comprised of five subscales (Emotional Symptoms, Conduct Problems, Hyperactivity, Peer Problems and Prosocial). Each item is rated on a scale of Very True, Somewhat True and Not True. Scores of 2, 1 or 0 are assigned to each rating. The SDQ has a test–retest reliability of .85 (Goodman, 1999). The scale of interest was the Emotional Symptoms subscale, which is comprised of five items. Total scores on this subtest can range from 0 to 10 with a higher score denoting more problems. UK population norms state that a score of 0–3 is ‘close to average’ while scores of 5–6 are ‘high’ and scores of 7–10 are ‘very high’.
The SMFQ (Angold et al., 1995) was completed by adolescents at age 14. The SMFQ consists of 13 statements that measure depressive thoughts and feelings over the last two weeks. Participants rate the items as either 0 Not true; 1 Sometimes true or 2 True, resulting in a total score ranging from 0 to 26. A higher score denotes increased feelings of depression. The SMFQ has a test–retest reliability of .85 (Angold et al., 1995) and has a moderate diagnostic accuracy (Area Under Curve (AUC) = .73) when compared to the Diagnostic Interview Schedule for Children (DISC) in a community sample of children aged 10–13 years (Rhew et al., 2010).
Social functioning
Social functioning measures were taken from the ‘Your Friends’ section of the MCS at age 7 and 14. Questions about number of best friends (Do you have any best/close friends?), victimisation (How often do other children hurt you or pick on you on purpose?) and bullying (How often do you hurt or pick on other children on purpose?) were included. The victimisation and bullying scales at age 7 used the terms All of the time, Some of the time and Never, while at age 14, the ratings were Most days, About once a week, About once a month, Every few months, Less often and Never. For ease of comparison, age 14 ratings were recoded into the same scales as the age 7 items. Thus, Most days and About once a week were recoded as All the time; About once a month and Every few months were recoded as Some of the time; and Less often and Never were recoded as Never. The question How happy are you with your friends? from the well-being grid in the ‘Personality and Well-being’ module at age 14 was also included as a predictor of social functioning. Participants rated their happiness on a scale of 1 Completely happy to 7 Not at all happy. The Peer Problems subscale from the teacher report of the SDQ administered at age 7 was also analysed as a measure of social functioning. This subscale consists of five items that are rated on a scale of Very True, Somewhat True and Not True. Scores of 2, 1 or 0 are assigned to each rating. Scores can range from 0 to 10 and two of the items are reverse scored so that a higher score denotes higher problems. For example, compared to UK population norms, a score of 0–2 is ‘close to average’, while a score of 5 is ‘high’ and a score of 6–10 reflects ‘very high’ peer problems.
Statistical analysis
Data were analysed using Stata 14 (StataCorp, 2015) with the prefix svy to adjust for survey data, as recommended for the MCS (Ketende & Jones, 2011). The svy prefix accounts for sampling weights, cluster sampling and stratification of the survey design. This procedure also accounts for attrition or non-response rates and adjusts for the sampling design used in this cohort in order to provide accurate estimates for the underlying UK population (finite population correction factor (fpc)). Consequently, missing data were treated as missing at random due to attrition or non-response in each wave. Logistic regression was used to examine the influence of language difficulties at age 5 on the presence of best/close friends at age 7 and 14, while ordered logistic regression was used to examine the influence of language difficulties at age 5 on the remaining self-report social functioning measures at age 7 and 14. Odds ratio provide a comparable measure of the effect of these analyses. The SDQ subscales of Emotional Symptoms and Peer Problems were highly skewed, as was the SMFQ, therefore negative binomial regression was used to analyse the relationship between language difficulties at age 5 and each of the SDQ subscales at age 7 and 14 (Peer Problems and Emotional Symptoms) and the SMFQ at age 14. Confidence intervals provide a measure of the strength of the effect for these analyses, as it was not possible to provide effect sizes due to the combination of negative binomial regression with survey estimation techniques. Sex and poverty were covaried for in all analyses. Poverty was defined by the Organisation for Economic Cooperation and Development (OECD) as below 60% of the median income. A Sobel–Goodman test was used to analyse the mediating effect of social functioning at age 7 on the relationship between language difficulties at age 5 and emotional problems at age 7 and 14. The mediation between social functioning at age 7 and emotional problems at age 14 was then analysed while controlling for emotional problems at age 7. For all mediation analyses, the sgmediation command was used while controlling for OECD and gender.
Results
Demographics
Social functioning and emotional problems in risk of developmental language disorder (rDLD) group and general population (GP) group at age 7.
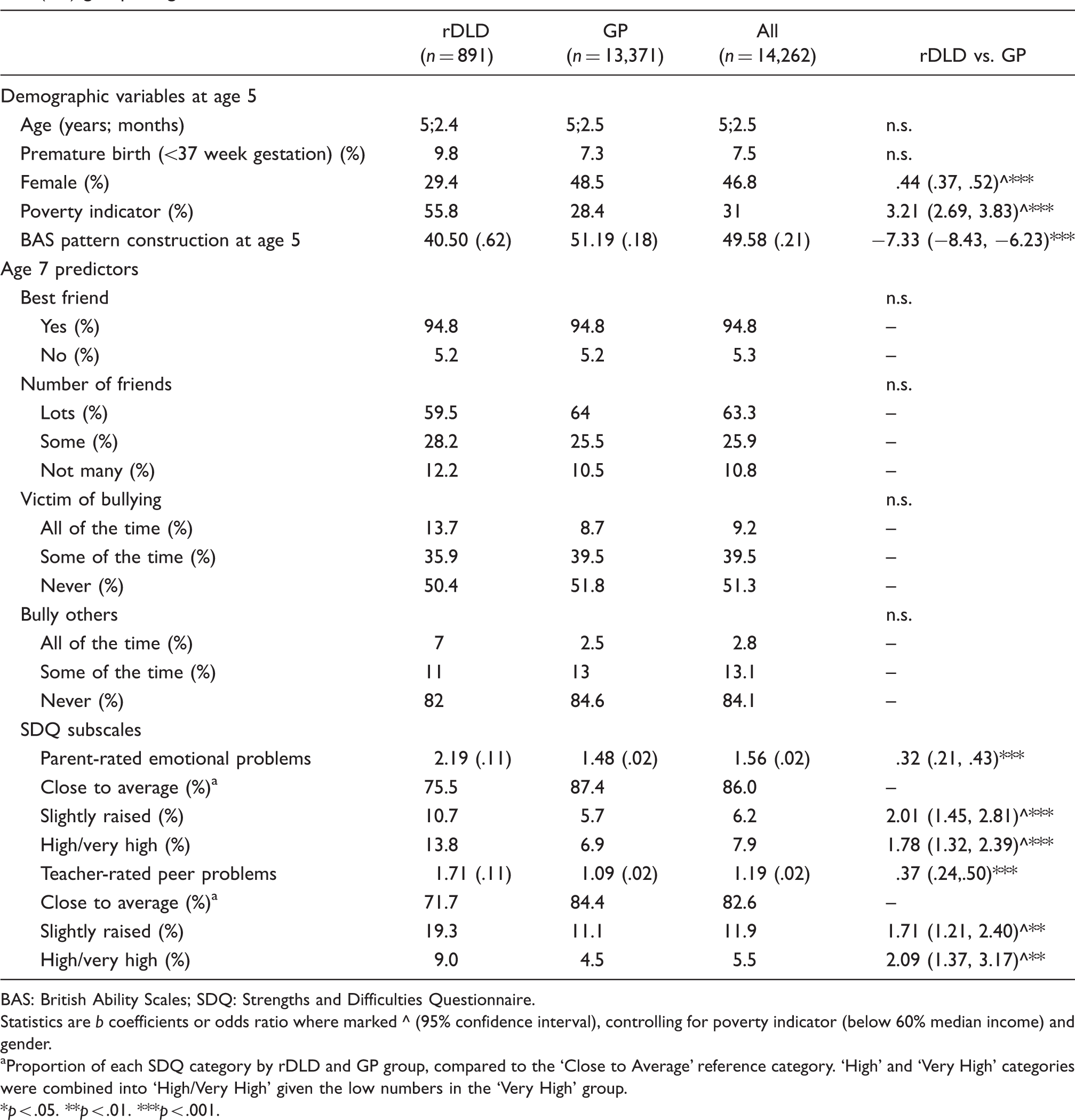
BAS: British Ability Scales; SDQ: Strengths and Difficulties Questionnaire.
Statistics are b coefficients or odds ratio where marked ^ (95% confidence interval), controlling for poverty indicator (below 60% median income) and gender.
Proportion of each SDQ category by rDLD and GP group, compared to the ‘Close to Average’ reference category. ‘High’ and ‘Very High’ categories were combined into ‘High/Very High’ given the low numbers in the ‘Very High’ group.
p < .05. **p < .01. ***p < .001.
Group difference in emotional problems
Social functioning and emotional problems in risk of developmental language disorder (rDLD) group and general population (GP) group at age 14.

SDQ: Strengths and Difficulties Questionnaire.
Statistics are b coefficients or odds ratio where marked ^ (95% confidence interval), controlling for poverty indicator (below 60% median income) and gender.
The scales for ‘Victim of bullying’ and ‘Bully others’ at age 14 were originally Most days, About once a week, About once a month, Every few months, Less often and Never but were recoded to remain consistent with the ratings at age 7.
Proportion of each SDQ category by rDLD and GP group, compared to the ‘Close to Average’ reference category. ‘High’ and ‘Very High’ categories were combined into ‘High/Very High’ given the low numbers in the ‘Very High’ group.
p < .05 **p < .01 ***p < .001
Group difference in social functioning
There was no significant group difference in self-reported social functioning at age 7. Approximately 95% of the rDLD group and the GP group stated that they had a best friend. However, at age 14, the number of individuals reporting that they had close friends differed significantly between the groups, b = .88, 95% CI (.41, 1.34), p < .001. Approximately 9% of the rDLD group reported having no close friends, compared to only 3% of the GP group. Nonetheless, when asked how happy they were with their friends, there was no significant difference between the rDLD group (M = 2.02, standard error (SE) = .07) and the GP group (M = 2.11, SE = .02), b = −.04, 95% CI (−.11, .04), p = .32.
There was no significant difference between the rDLD group and the GP group in overall experiences of bullying at either time point. There was no significant group difference in reports of being bullied at age 7, b = −.03, 95% CI (−.27, .21), p = .80, nor at age 14, b = −.23, 95% CI (−.57, .11), p = .19. Similarly, there was no significant group difference in reports of bullying others at age 7, b = −.01, 95% CI (−.29, .27), p = .96 nor at age 14, b = −.22, 95% CI (−.66, .21), p = .31.
At age 7, the rDLD group was rated by teachers as having significantly more peer problems, b = .37, 95% CI (.24, .50), p < .001. The majority of individuals were within the ‘Close to average’ category for both the rDLD group (71.7%) and the GP group (84.4%). Using the ‘Close to Average’ category as a reference point, logistic regression shows that being categorised as having ‘Slightly raised’ peer problems (OR = 1.71, 95% CI (1.21, 2.40), p < .01) or ‘High/Very High’ peer problems (OR = 2.09, 95% CI (1.37, 3.17), p < .01) is more likely for members of the rDLD group than the GP group.
Peer problems as a mediator for age 7 emotional problems
The association between language difficulties at age 5 and parent reported emotional problems at age 7 was partially mediated by teacher reported peer problems at age 7. Figure 2 illustrates that language difficulties at age 5 significantly predicted peer problems at age 7, b = .47, SE = .11, p < .001, and these peer problems were significantly related to concurrent emotional problems, b = .16, SE = .02, p < .001. The effect of language difficulties on emotional problems at age 7, b = .56, SE = .14, p < .001, was reduced after controlling for peer problems, b = .49, SE = .14, p < .001, consistent with partial mediation. A Sobel–Goodman, z = 3.9, SE = .02, p < .001, test found that approximately 14% of the relationship between language difficulties at age 5 and emotional problems at age 7 was mediated by peer problems at age 7.
Regression coefficients for the relationship between risk of developmental language disorder (rDLD) at age 5 and emotional problems at age 7 as mediated by peer problems at age 7. The regression coefficient for the effect of rDLD grouping on emotional problems after controlling for peer problems is shown in parentheses.
Peer problems as a mediator for age 14 emotional problems
The association between language difficulties at age 5 and emotional problems at age 14 was partially mediated by peer problems at age 7. Figure 3 illustrates that language difficulties at age 5 was a significant predictor of peer problems at age 7, b = .62, SE = .13, p < .001, and that peer problems at age 7 were a significant predictor of emotional problems at age 14, b = .17, SE = .02, p < .001. The effect of language difficulties on emotional problems at age 14, b = .62, SE = .19, p < .001, was significantly reduced after controlling for peer problems at age 7, b = .51, SE = .18, p < .01. This finding is consistent with partial mediation. A Sobel–Goodman test was used to analyse the mediating effect of peer problems, z = 3.92, p < .001, demonstrating that approximately 17% of the relationship between language difficulties at age 5 and emotional problems at age 14 was mediated by peer problems at age 7.
Regression coefficients for the relationship between risk of developmental language disorder (rDLD) at age 5 and emotional problems at age 14 as mediated by peer problems at age 7. The regression coefficient for the effect of rDLD grouping on emotional problems after controlling for peer problems is shown in parentheses.
However, when emotional problems at age 7 were controlled for, the relationship between language difficulties and emotional problems at age 14 was not significant, b = .28, SE = .19, p = .13 (see Figure 4). This result is unsurprising given previous research within the MCS has found that the increase in emotional difficulties between the rDLD and GP groups stays consistent across development (St Clair et al., under review).
Regression coefficients for the relationship between risk of developmental language disorder (rDLD) at age 5 and emotional problems at age 14 as mediated by peer problems at age 7, while controlling for emotional problems at age 7. The regression coefficient for the effect of rDLD grouping on emotional problems after controlling for peer problems is shown in parentheses.
Discussion
The aim of this paper was to examine the mediating effect of social functioning on the relationship between early language difficulties and later emotional difficulties in a population cohort. Again, it should be noted that the rDLD group in the current paper is not a clinically diagnosed sample and the variable is comprised of an expressive language measure and parent report of language difficulties. Therefore, results should be interpreted with caution when compared to clinical samples and studies using more in-depth language assessments. However, the participants in this group may be at risk of persistent DLD. As hypothesised, parent-reported emotional problems were significantly higher in the rDLD group compared to the GP group, but there was no group difference in self-reported emotional problems. Similarly, the prediction of poorer social functioning in the rDLD group compared to the GP group was partially supported; a significant group difference in teacher-reported peer problems was found but there were very few differences in self-reports of social functioning. Teacher-reported peer problems at age 7 partially mediated the relationship between language difficulties at age 5 and parent-reported emotional problems at ages 7 and 14. However, the relationship at age 14 was not significant after controlling for parent-reported emotional problems at age 7.
The findings support previous research with clinical samples (St Clair et al., 2011), suggesting that even in non-clinical groups children and adolescents who are at risk of developing DLD are more at risk for emotional difficulties, as there was a higher rate of parent-reported emotional problems in the rDLD group compared to the GP group at ages 7 and 14. Additionally, these findings extend previous community-based research that has focused on young children with language difficulties and found increased rates of behavioural problems but no group differences in emotional outcomes (Bretherton et al., 2014; Girard et al., 2016; Levickis et al., 2017; McKean et al., 2017a), highlighting that adolescence is a key time to study emotional difficulties. However, it is worth noting that the mean ratings from clinical samples are higher and a greater proportion reflect scores in the ‘High’ or ‘Very high’ category, although these scores are obtained from self- and teacher-reports, respectively (Conti-Ramsden et al., 2013; St Clair et al., 2011). Conversely, self-report of depressive symptoms from the SMFQ at age 14 was not significantly different between the groups, and in fact showed a trend for higher scores in the GP group compared to the rDLD group. These findings contradict previous studies that found increased emotional problems from both parent- and self-report (e.g. Conti-Ramsden & Botting, 2008; Wadman et al., 2011), and suggest that in non-clinical samples with participants who are at risk of DLD, depressive symptoms may not be associated with language difficulties, at least according to adolescents’ own reports at age 14.
Self-reports of social functioning were also similar between groups. There was no significant difference in the prevalence of victimisation between groups at either time point, supporting Lindsay, Dockrell and Mackie’s (2008) findings that demonstrated no difference in victimisation between groups of children with language difficulties, special educational needs or their TD peers. There was also no evidence of group differences on the other self-report measures of social functioning, except for a significantly lower number of close friends at age 14 in the rDLD group. However, the rate of close friends for both groups at age 14 was over 90%, similar to previous reports for adolescents (Wadman, Durkin, & Conti-Ramsden, 2011a). Importantly, despite the difference in number of friendships, both groups reported feeling satisfied with their friends, which contrasts previous reports of poorer quality friendships in DLD samples (Botting & Conti-Ramsden, 2008; Durkin & Conti-Ramsden, 2007). Social support has a strong association with mental health outcomes (Parker, Rubin, Erath, Wojslawowicz, & Buskirk, 2015) and the finding that rDLD group participants are able to develop close friendships despite their language difficulties may account for the lack of group difference in self-reported depressive symptoms.
In contrast to self-report suggesting intact social functioning, the rDLD group received higher ratings of peer problems from teacher-reported SDQ at age 7. The group difference in teacher-reported peer problems is consistent with previous literature from longitudinal clinical samples, but again is lower in severity (Mok et al., 2014; St Clair et al., 2011). Different patterns of findings according to the informant are also common in the literature. For example, Lindsay and Dockrell (2012) reported teacher ratings of peer problems in young people with DLD increasing from 12 to 16 years of age but self-reports of social functioning over the same period showed a more positive trend and were not significantly different from the norm. Lindsay, Dockrell and Strand (2007) also found different patterns of ratings between parent and teacher SDQs and suggested that context may play a role in teachers’ ratings, which may account for the discrepancy between teacher-ratings and self-report in the current study.
On the other hand, the lack of group difference in self-reported social problems may be due to young people at risk of DLD having lower expectations about social relationships and being more content with their social situation, whereas parents and teachers expect equivalent social skills and friendships in these children as they find in children with typical language development. This has been demonstrated in previous research that shows adolescents with DLD perceive themselves to have adequate social functioning, similar to their TD peers (Wadman et al., 2011b). It is important to remember that social cognition abilities are still developing during this period (Blakemore, 2008) and as children progress through adolescence, their perception of social and emotional problems may be influenced by the general increased complexity of peer relations and their importance in shaping self-esteem and emotional wellbeing (La Greca & Harrison, 2005). More research into this age range should be encouraged to give adolescents an opportunity to report their own experiences and allow for greater insight into these issues.
Finally, teacher-reported peer problems at age 7 were found to partially mediate the relationship between language difficulties at age 5 and parent-reported emotional problems at age 7 and age 14, supporting previous research that found peer problems predict concurrent depressive symptoms at age 16 (Wadman et al., 2011). These findings suggest that early language difficulties limit social interactions, leading to peer problems and increased emotional problems in both middle childhood and adolescence. Therefore, individuals with better relationships with peers may be somewhat protected from emotional problems even with substantial language difficulties. This should be considered by speech and language therapists as using a therapy approach that integrates language and social understanding may lead to an improvement in emotional outcomes.
However, it should be noted that peer problems only partially mediated the relationship, suggesting that there are other factors involved. Indeed, when emotional problems at age 7 were controlled for, the relationship between language difficulties and emotional problems at age 14 was not significant. This suggests that emotional problems at age 7 have a much greater influence on the relationship between language and emotional problems at age 14 and warrants further research. As emotional problems tend to decrease or stabilise in later adolescence (St Clair et al., 2011, 2012), it would be interesting to examine whether this pattern holds true for the current population cohort when later waves of the MCS are released. Additionally, other predictors such as social cognition (Conti-Ramsden & Botting, 2008) or early emotion regulation problems could be examined.
This study has both strengths and limitations. Analysing a population cohort, such as the MCS, allows for a large sample to be investigated without the potential overestimation of mental health problems that may arise from using a clinical cohort (Girard et al., 2016). The fact that the current study has partially replicated previous findings through parent- and teacher report suggests that previous studies using clinical cohorts present a reliable picture of the emotional and social functioning of young people with DLD.
The longitudinal nature of the MCS also allows for different time points to be examined with a variety of informants. The SDQ is a standardised measure of social, emotional and behavioural functioning that is commonly used in the literature. The current study had access to both teacher report and parent report, which, along with self-report of social functioning and depressive feelings, allowed for a wider range of input into the child’s social and emotional functioning. Data collection was conducted at three time points, covering childhood and adolescence. Adolescence is under-researched in this area (Botting & Conti-Ramsden, 2008) and is a critical period to study when the risk for development of later psychiatric disorders is increased (Jones, 2013). Additionally, we used both parent report and a standardised test in the form of the BAS Naming Vocabulary subscale, which adds more weight to the rDLD grouping in the present study as performance on a singular test does not provide adequate information about whether the child has significant difficulties with language (Bishop & McDonald, 2009; Law, Rush, Schoon, & Parsons, 2009). Previous research using parent report of language difficulties has also found a positive relationship with social and emotional problems (Hughes et al., 2016). The distribution of 6.25% in the rDLD grouping was similar to the 7.58% prevalence of DLD found in a recent community study (Norbury et al., 2016) and similar patterns were found when the analyses were re-run with only parent report and BAS naming vocabulary as predictors, suggesting that the rDLD variable is an adequate measure of children who are at risk of developing DLD. Furthermore, the rDLD group appeared to fit the known risk factors for DLD, with a higher rate of males and a higher percentage of children below the poverty line (Tomblin et al., 1997). However, due to the nature of the cohort study it is impossible to determine whether all children included in this group would meet criteria for DLD if tested individually.
The GP control group used in this study was also a strength compared to previous research employing TD groups as comparison. A TD control group may hinder research by underestimating the level of emotional problems that are present in the comparison group and inflating the association between emotional problems and DLD by creating an artificially ‘clean’ group without any difficulties (Fombonne, 2016). In the current study, the only exclusion criteria believed to be of importance for the GP group was language difficulty, as the presence of other disorders is a better representation of the GP.
One clear limitation when analysing secondary data, particularly a large cohort such as the MCS, is the potential for high attrition rates. However, this was taken into account by using the svy prefix for survey data in Stata (StataCorp, 2015), to adjust for weighting and attrition in the different waves as recommended for the MCS (Ketende & Jones, 2011). Additionally, there is less control over variables in secondary data compared to designing a study from the very beginning. For example, there is no measure of teacher-rated peer problems at age 14 which would have been beneficial to compare to parent reports of emotional problems at age 14. Furthermore, there was no standardised measure of social functioning reported by the young people in the study. Finally, in a data set this large, small differences can be classed as significant and without a suitable measure of effect size it is important to bear this in mind when interpreting the results. However, ORs (which allow comparison across findings) and CIs are provided.
Conclusion
The rDLD group of children considered to be at risk of developing DLD was found to experience increased emotional and social difficulties compared to the GP group. However, these differences were noted by parents and teachers, but generally not by the children and adolescents themselves. Peer problems at age 7 were found to partially mediate the relationship between language difficulties at age 5 and emotional problems at age 14; however, this was not significant once emotional problems at 7 were controlled for. To the authors’ knowledge, this is the first time that peer problems have been examined as a mediating factor in the relationship between language difficulties and emotional problems in a population cohort. However, these results are not based on a comprehensive assessment of language difficulties and therefore should be interpreted with caution. It is important to obtain a better understanding of the underlying mechanisms involved in the relationship between DLD and emotional problems in order for the most appropriate support to be given. Analysing a protective factor such as social functioning is beneficial as these results could have an impact on interventions. For example, the Social Communication Intervention Project (Adams et al., 2012) has demonstrated improvements in parent-reported social communication problems. Further research on the MCS is encouraged to investigate the full impact of emotional problems at age 7 and whether the mediating effect of peer problems at age 7 remains in later adolescence and adulthood.
Supplemental Material
Supplemental material for A longitudinal analysis of early language difficulty and peer problems on later emotional difficulties in adolescence: Evidence from the Millennium Cohort Study
Supplemental material for A longitudinal analysis of early language difficulty and peer problems on later emotional difficulties in adolescence: Evidence from the Millennium Cohort Study by Claire L Forrest, Jenny L Gibson, Sarah L Halligan and Michelle C St Claira in Autism & Developmental Language Impairments
Footnotes
Acknowledgements
Our appreciation and thanks go to all participants and their families who participate in the MCS. We also acknowledge the time and effort of the MCS team at the Centre for Longitudinal Studies at the UCL Institute of Education, as well as the UK Data Service, in collating and making the data available for researchers. However, they bear no responsibility for the analysis or interpretation of these data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Note
Supplementary Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.