
Abstract
Background and aims
Early diagnosis of autism spectrum disorder, while providing many benefits, also presents challenges. Accurately predicting symptom severity allows clinicians to confidently diagnose and assign the most appropriate intervention. Little available research predicts symptom severity in children with autism spectrum disorder who have not been exposed to significant levels of intervention.
Methods
The present file review study examined preverbal skills as predictors of symptom severity, approximately one year later, in a group of young children (18–64 months) with autism spectrum disorder (n = 199).
Results
Of the two core diagnostic features (social communicative deficits and restricted repetitive behaviors), social communicative skills best predicted symptom severity. Furthermore, social communicative gestures predicted symptom severity after age, adaptive behavior, restricted repetitive behaviors, and functional gestures had been accounted for.
Conclusions
Social communicative gestures are excellent predictors of future symptom severity independent of intervention effects in very young children with autism spectrum disorder.
Implications
Previously, the social aspect of gestures has been missing in the literature on language and symptom prediction in children with autism spectrum disorder. Careful attention to social communicative gestures in the future may help with early diagnosis and more accurate predictions of symptom and developmental trajectories.
Autism spectrum disorder (ASD) is a neurological condition marked by impaired social communication skills and restricted repetitive behaviors and interests. One of the best predictors of symptom severity and outcomes in children with ASD is language level at diagnosis or start of intervention (Luyster, Qiu, Lopez, & Lord, 2007; Turner, Stone, Pozdol, & Coonrod, 2006). As children are now diagnosed at earlier ages, we have the opportunity to look for early predictors of outcomes, such as specific preverbal skills. Children with ASD experience a delayed and atypical developmental trajectory in gesture use (Paparella, Stickes, Goods, Freeman, & Kasari, 2011) and deficits in imitation and person relatedness, all of which are intricately related to language development (Ingersoll & Meyer, 2011; Stone & Yoder, 2001). Thus the preverbal skills gestures and imitation, and person relatedness have potential to be early predictors of symptom severity in children with ASD. Moreover, the majority of research compares children pre and post intervention. As a result, we know very little about how earlier child factors are associated with later symptom presentation without the influence of intervention. Intervention is clearly confounded with development since outcomes are most often measured post intervention programs, which usually focus on improving the skills studied (Smith, Klorman, & Mruzek, 2015). The present study examines the predictive association of gesture use, imitation, and person relatedness for symptom severity outcomes in a group of children with ASD who have not been exposed to significant levels of intervention.
Diagnosis of ASD
Recent advancements in early diagnosis of ASD have highlighted the importance of better and earlier predictors of symptom severity. Typical age of diagnosis of ASD has now dropped from over five years to well below five years of age (Parner et al., 2011). Although more difficult, diagnosis may be made in children without severe developmental delays as young as 15 to 24 months of age (Barbaro & Dissanayake, 2012; Guthrie, Swineford, Nottke, & Wetherby, 2013). Earlier diagnosis has many advantages. Principally it allows earlier access to intervention, a factor well established in the research literature to predict more positive outcomes (Freeman & Perry, 2010; Perry et al., 2011). Nevertheless, early diagnosis presents clinical challenges, two of which are the ease of diagnosis and stability of symptom level within the diagnosis. It requires a well trained and experienced clinician with an excellent understanding of infant development to make a diagnosis of ASD in the early years. Thus, many clinicians feel more comfortable leaving a diagnosis of ASD to a later age, which is a strategy that is not in the child's best interest if the family is to access early intervention for the child (Flanagan, Perry, & Freeman, 2012).
Studies consistently indicate that the younger the child (Kasari, Gulsrad, Freeman, Paparella, & Hellmann, 2012; Virues-Ortega, Rodriguez, & Yu, 2013), the better the child's language (Stahmer, Akshoomoff, & Cunningham, 2011; Turner, Stone, Pozdol, & Coonrod, 2006) and cognitive skills (Flanagan et al., 2012; Howlin & Moss, 2012), and the milder the symptoms (Vivanti, Barbaro, Hudry, & Dissanayake, 2013) at diagnosis and subsequent intervention, the more positive the outcomes are expected to be. A deficit in social communicative language is one of the distinctive core features of ASD and as such, determining the earliest expression of social communication is important. There is a large body of developmental research outlining preverbal skills that can be reliably measured and can reliably predict future language abilities and are strongly associated with symptom severity and outcomes in ASD (Weismer & Kover, 2015; Yoder, Watson & Lambert, 2015). It is reasonable to hypothesize then that specific preverbal skills would predict not only later language ability but also later symptom level in children with ASD.
Preverbal skills
Preverbal children develop skills such as imitation and gesture use; skills that scaffold language learning (Bakeman & Adamson; 1984; Goldin-Meadow, 2014). Children with ASD are found to exhibit impaired imitation skills in general and spontaneous imitation in particular (Charman et al., 1997; Ingersoll, Shreibman, & Tran, 2003), and gesture at both a lower rate and later age than typically developing children (Wetherby, Watt, Morgan, & Shumway, 2007). Few studies have examined these preverbal skills as predictors of language development in children with ASD, and very few have examined these skills in the context of general outcomes or symptom severity in children with ASD. Predictors of milder symptom level over time include attaining first words by 24 months (Mayo, Chlebowski, Fein, & Eigsti, 2012), higher receptive language levels (Luyster, Lopez, & Lord, 2007), and better imitation (Luyster, Kadlec, Cater, & Tager-Flushberg, 2008; Sallows & Gaupner, 2005) and gesture abilities (Chawarska, Klin, Paul, Macari, & Vokmar, 2009; Kjellmer, Hedvall, Fernell, Gillberg, & Norrelgen, 2012).
Imitation
Imitation is fundamental to a number of skills that are intricately related to language learning. Imitation provides a vehicle for learning and sets the stage for reciprocity which is fundamental to communication (Landa, 2007). Imitation skills grow from simple copying of muscle movements to imitating a goal by form and function as the child progresses through the mastery of mimicry, emulation, and finally imitation (Elsner, 2007; Jones, 2014; Sevlever & Gillis, 2010). In effect, imitation becomes increasingly complex and symbolic in nature as children develop and their imitative acts become more social in purpose. Children with ASD demonstrate overall poor imitation skills and are more likely to imitate in a structured, elicited situation than an unstructured socially-driven context (Ingersoll, 2008; Ingersoll & Meyer, 2011; Rogers, Hepburn, Stackhouse, & Wehner, 2003) compared to typically developing children.
Gestures
In general, research findings demonstrate that gestures supplement, clarify, scaffold, and promote language development (Hall, Rumney, Holler, & Kidd, 2013). Infants typically develop an increasingly intricate combination of gestures and gaze or gestures and vocalizations before they produce words (Murillo & Belinchon, 2012). Furthermore, gestures are found to be related to expressive and receptive vocabulary development (Rowe, Ozcaliskan, & Goldin-Meadow, 2008) and to support the achievement of cognitive and linguistic milestones (Alibali & Goldin-Meadow, 1993). As such, use of gestures also follows a developmental pathway in infants that becomes increasingly complex, symbolic, and communicative in nature.
It is well established that children with ASD gesture at a lower rate than typically developing children and experience a delay in gesture development (Shumway & Wetherby, 2009), but children with ASD also demonstrate an atypical developmental trajectory for gesturing (Paparella et al., 2011). The gestures that appear the most affected, those that are delayed and out of sequence, are what we refer to as social communicative gestures, such as pointing to show, initiate engagement, and share interest. Gestures that function to regulate one's environment, get one's needs met, regulate behavior (Watson, Crais, Baranek, Dykstra, & Wilson, 2013) or seek help (Bruner, 1981) appear less affected. We refer to these as functional gestures. Furthermore, when children with ASD do gesture, they gesture significantly more to regulate the behavior of others than to interact in a social communicative manner. Typically developing children display the opposite pattern (Maljaars, Noens, Jansen, Scholte, & van Berckelaer-Onneset, 2011). Thus, in children with ASD, social communicative gestures not only develop late and out of sequence, but they also are underused if and when they do develop. Therefore, compared to functional gestures, social communicative gestures should be better predictors of language development and signify more favorable outcomes in children with ASD. Furthermore, imitation and gestural skills are intimately intertwined with a child's awareness and ability to relate to others. Relating to people, however, is unfortunately a part of the core deficits in ASD (American Psychiatric Association, 2014).
Person relatedness
The ability to relate to people is not frequently considered in language development in children with ASD. This ability is apparent when infants develop an awareness of goal directed behavior (Carpenter et al., 1998; Murillo & Belinchon, 2012). Such awareness of goal directed behavior is strongly enhanced by monitoring the gaze of self and others, which supports imitation, gesture, and joint attention (Carpenter, Pennington, & Rogers, 2002; Meltzoff, 2013; Mundy & Newell, 2007). These interconnected abilities emerge within the first six months of life and appear to be part of the foundation of social communication skills. The ability to imitate and develop other preverbal skills such as gesture use, must logically begin with the ability to relate to others (Stone & Yoder, 2001; Toth, Munson, Meltzoff, & Dawson, 2006). Clearly imitation, gesture use, and the ability to relate to others are interconnected in critical ways to support the acquisition of social communication skills. Since person relatedness is a deficit that is central to ASD and an important factor in the development of social communication, the severity of the deficit would necessarily impact the development of social communication skills and the presentation of symptom severity. It is reasonable to expect that these skills, imitation, gesture use, and person relatedness, would predict future communication skills and overall outcomes in children with ASD. This is in fact what research suggests.
Predictive nature of imitation, gestures, and person relatedness
Imitation and gesture use predict expressive and receptive language in typically developing children (Capone & McGregor, 2004; Carpenter et al., 1998; Charman et al., 2001; Murillo & Belinchon, 2012; Ozcaliskan & Goldin-Meadow, 2005) and in children with ASD (Luyster et al., 2008; Luyster et al., 2007a; Shumway & Wetherby, 2009; Stone & Yoder, 2001; Toth et al., 2006). Gesture use also predicts symptom severity (Chawarska et al., 2009; Kjellmer et al., 2012) and ASD diagnosis (Colgan et al., 2006). However, it is important to highlight that the gestures included in these studies are limited in number or include both social communicative and functional gestures without making a distinction between the two categories. Although Colgan and colleagues used gestures that they classified as socially interactive, they included gestures that could be considered noncommunicative and nonsocial in manner (e.g., dances) and they excluded gestures that were clearly social communicative (e.g., pointing to share interest). Conceptually, we define social communicative gestures as those used to initiate joint attention and those involved in imaginative play and turn taking interactions. Functional gestures would include help seeking and other gestures that are not symbolic in nature and do not require a partner in social interaction. We are thus able to encompass the intentions that Bruner (1981) outlines, while delineating between those that are social in nature and those that merely function to regulate one's environment.
Few studies have examined person relatedness, language development, and symptom severity or overall outcomes in children with ASD. The few that have however, found that children with a higher interest in or tolerance for interactions with others demonstrated better language and general communication skill development outcomes than those that did not (Darrou et al., 2010; Sallows & Graupner, 2005; Sherer & Schriebman, 2005).
Researchers have increasingly used the MacArthur-Bates Communicative Development Inventory (CDI) to examine gestures and language and outcomes in ASD (e.g., Kjellmer et al., 2010; Luyster et al., 2007a). Luyster et al. (2007b) did not find gestures to be predictive of symptom severity; however, they examined gestures globally and as early and late gestures. Since Paparella et al. (2011) found that gestures that we would categorize as social-communicative gestures were delayed and out of sequence in ASD, studies that examine categories of early and late gestures in children with ASD would result in a mixture of functional and social-communicative gestures within those groups. This makes it unlikely that consistent associations would be found between gestures and symptom severity by examining gestures as they appear in typical chronological sequence or as a total gesture count. This highlights the need for a careful and fine grained examination of the role of implicitly learned social communicative gestures (Luyster et al., 2007b). The current study offers an opportunity to fill this gap in the existing research by examining the predictive nature of gesture use in a more finely nuanced manner.
The current study
The vast majority of researchers who examine predictors of outcome in children with ASD have restricted their analysis to children who have acquired words and been exposed to a significant level of intervention. No study that we are aware of has examined preverbal social communicative skills along with person relatedness in order to determine their contribution to later symptom severity in children with ASD who have not been exposed to significant levels of intervention. Furthermore, our analysis looks at some of the earliest behavioral manifestations of social communication skills—gestures that are socially driven and those that are not—and their ability to predict symptom severity. We hypothesized that of the two core symptoms of ASD, social communicative factors (i.e., imitation, gesture use, and person relatedness) would better predict symptom severity approximately one year later than restricted repetitive behaviors. It was also expected that gestures that are social communicative in nature would better predict symptom severity approximately one year later than gestures that are functional in purpose, even after controlling for factors identified by previous research as predictive of symptom outcomes (i.e., age, adaptive level, and restricted repetitive behaviors).
Methods
Participants
The present study consisted of a file review of children at a government funded urban intervention centre for autism in Ontario, Canada. The Research Ethics Board of the centre operates in accordance with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, the standards of the professions represented on the Board, the standards reflected in the bioethics literature, and personal and community values. The children whose files were reviewed had previously received a diagnosis of ASD by a community clinician and went through a screening process at the centre to confirm severity level and thus eligibility for intervention. For some children, particularly very young children or children who appear to be on the borderline between moderate and severe symptomatology, it was difficult to confirm severity level and they were rescreened approximately twelve months later. Files referred for rescreening were utilized in this study to examine symptom severity over time in children with minimal exposure to intervention.
Exclusion criteria
Children with significant medical comorbidities (e.g., Norrie disease, bilateral vision impairment, trisomy 21) or whose parents required the services of a translator for the interview were excluded. Parent reports are generally very reliable (Crais, Douglas, & Campbell, 2004); however, files that noted multiple examples of inconsistencies between clinical and parent reports and observations were excluded. That is to say, at both Time 1 and Time 2, when there was more than one measure that had a notation of “Questionable Validity” due to an inconsistency in reporting (e.g., reporting no expressive language on the CARS but reporting expressive language on the VABS), or a high degree of inconsistency between parent reports and observations during the clinical screening that are not resolved by a second screening at Time 1 (when this is the case it is also the practice of the Centre to complete a second screening involving the CARS in the community, such as a daycare centre or drop-in-play program) or Time 2, the decision was made to exclude the file. Approximately 10 files were excluded as a result.
Materials and procedure
At the screening appointment (Time 1), children were given measures of ASD diagnosis and symptom severity, adaptive behavior, and gesture skills. At rescreening (Time 2), measures of symptom severity and adaptive behavior were administered.
ASD diagnosis and symptom severity
The Childhood Autism Rating Scale, Second Edition (CARS-2; Schopler, Van Bourgeondien, Wellman, & Love, 2010) was used to rate severity of autism symptomatology. The CARS-2 provides a total score and a diagnostic description ranging from mild to severe. Concurrent validity with the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview—Revised) is reported to be between .77 and .79 (Vaughn, 2011) and .67, respectively (Saemundsen, Magnusson, Smari, & Sigurdardottir, 2003). Higher scores indicate higher symptom severity. The total score on the CARS-2 at Time 2 was used to represent symptom severity as an outcome variable.
Six items from the CARS-2 Time 1 were used to create two composite scores (of three items each) to represent the two core symptoms for ASD: Social Communicative Skills and Restricted Repetitive Behaviors. Since a number of items on the CARS-2 overlap between social communicative skills and restricted repetitive behaviors (e.g., listening response can be scored for responding to name and also sensory aversion), the number of items per composite was restricted to the nonoverlapping items. The Social Communication Skills Composite score was the average of the three items: Imitation, Nonverbal Communication (which includes gestures), and Relating to People. The Restricted Repetitive Behavior Composite score was the average of the three items: Body Use, Object Use, and Taste, Smell, and Touch.
Adaptive behavior
The Vineland Adaptive Behavior Scales, Second Edition, Survey Interview Form (VABS; Sparrow, Cicchetti, & Balla, 2005), a caregiver interview report, was used to measure adaptive functioning. Four domain standard scores (Communication, Daily Living Skills, Socialization, and Motor Skills) are provided. An adaptive behavior composite score was calculated from the sum of the domain scores. The adaptive behavior composite from Time 1 was used as a predictor variable in the second research question.
Gesture skills
The MacArthur-Bates Communicative Development Inventory: Words and Gestures (CDI; Fenson et al., 2007) were used to measure gesture skills. The gestures subsection, which contains 63 items, was recoded to distinguish between social communicative and functional gestures. Guided by the literature on language and gesture development (Alibali & Goldin-Meadow, 1993; Capone & McGregor, 2004; Ozcaliskan & Goldin-Meadow, 2005) we suggest that social communicative gestures require an understanding of symbols, are typically acquired by implicit learning or imitation, and require interaction with others (e.g., nods head yes, shakes head no). Gestures that may have a social context but are often explicitly taught were not included in this category. Waving goodbye, for example, is a gesture that parents typically explicitly teach and strongly and positively reward their child for engaging in (Jones, 2014). Functional gestures do not require an understanding of symbols, are used to regulate one's environment, and may be used in isolation without interaction with others (e.g. dances, eats with a spoon or fork).
Recoding of the gestures portion of the CDI identified 30 items as social communicative, 31 items as functional gestures, and 2 items as social communicative but commonly taught. Given the small number in the taught category, these items were dropped from the analysis and only the social communicative and functional gesture categories were utilized. Four of the five subcategories of the gesture items in the CDI are coded dichotomously (present or absent). In one subsection the coding is broken down to never, sometimes, and often. For this subcategory, the sometimes and often codes were collapsed into one (present) so that all subcategories were dichotomously coded. Proportion scores were calculated for each gesture category.
Reliability was confirmed, κ = .91, p < .001, for the recoding of the CDI gestures into social communicative and functional gesture categories before scoring of the current study data began. Discrepancies were resolved through discussion between the first and second author.
Procedure
All children identified for rescreening from 2000 to 2014 at two time points: initial screening (Time 1) and the rescreening approximately 12 months later (Time 2) were included in the present study (n = 199).
Results
Data screening
Data distributions were screened for univariate and multivariate normality, linearity, homogeneity of variances, and independence of observations and all assumptions were met with the exception of univariate normality for social communicative gestures, which was positively skewed. This was to be expected since many children in the group had few if any gestures. As a result, confidence intervals and standard errors based on 1000 bootstrap samples were applied to the regression analysis that utilized the social communicative gestures variable. Bootstrapping allows for an estimation of the property of the sampling distribution using the sample data, and a computation of robust estimates of the beta values and confidence intervals (Wright, London, & Field, 2011) despite the skewness of the one variable. Casewise diagnostics and Mahalanobis distance values identified two cases that were potential influential outliers. Parallel analyses were completed and results were equivalent with and without the outliers. Thus results were reported with the outliers included in the data.
Sample characteristics
Descriptive characteristics.

Symptom severity: CARS-2 total score; adaptive level: vineland adaptive behavior composite standard score; social communicative composite and restricted repetitive behaviors composite are based on the CARS; social communicative gestures and functional gestures are based on the communicative development inventory.
n = 199.
n = 186.
n = 150.
Although the children in the sample were wait-listed for Intensive Behavioral Intervention, all were eligible for Applied Behavior Analysis (a less intensive form of therapy applicable to a broader age) and other intervention services, such as speech language therapy. A small percentage (13%) of the families in the sample reported that they had obtained therapy services through private agencies for at least a brief period before Time 2. A visual inspection of the data indicated only five of the children who were reported to be receiving therapy received more than 10 h of therapy per week and none were reported as receiving more than 18 h per week. Since it is the general consensus of the literature that a minimum of 20 h of therapy per week qualifies as intensive intervention (Gabriels, Hill, Pierce, Rogers, & Wehner, 2001; Freeman & Perry, 2010), the very small number of children receiving this therapy for an undetermined amount of time would not significantly affect the data.
As expected, the sample was predominantly male (n = 152; 76%) so independent t-tests were conducted to determine if there were sex differences on measures of symptom severity, adaptive behavior level, age, social communicative skills composite, restricted repetitive behaviors composite, and functional and social communicative gestures. Results of the t-tests indicated no significant sex differences on any of the measures.
Social communicative skills versus restricted repetitive behaviors
A standard multiple regression analysis was conducted to determine which of the two core symptoms of ASD at Time 1, social communicative skills or restricted repetitive behaviors, contributed the greatest unique variance to symptom severity at Time 2 (n = 199). A correlation analysis demonstrated that symptom severity at Time 2 was significantly related to social communicative skills and restricted repetitive behaviors (r (197) = .59 and .52, respectively, p < .001), and that social communicative skills was significantly correlated with restricted repetitive behaviors (r (197) = .54, p < .001). The overall regression model for the equation was significant, R2 = .41, R2adj = .40, F (2, 196) = 67.36, p < .001. This represents a large effect size. Both social communicative skills and restricted repetitive behaviors at Time 1 significantly predicted symptom severity at Time 2; however, social communicative skills accounted for more of the unique variance (14%), B = 1.94, t (196) = 6.76, p < .001, CI = 1.38–2.51, compared to restricted repetitive behaviors (5%), B = 1.16, t (196) = 4.26, p < .001, CI = .62–1.70.
To rule out the possibility that this finding reflects differences in correlations between social communicative skills and restrictive repetitive behaviors with symptom severity at Time 1, correlational analyses of these variables were considered at Time 1 only. Results demonstrated that social communicative skills and restricted repetitive behaviors at Time 1 were significantly related to symptom severity at Time 1, r (197) = .80 and .79, respectively, p < .001. These two correlations are not significantly different from each other, indicating that both social communicative skills and restricted repetitive behaviors are equally sensitive with respect to predicting symptom severity at Time 1.
Social communicative gestures vs. functional gestures
Zero order bivariate correlations for symptom severity, age, adaptive level, restricted repetitive behaviors, functional gestures, and social communicative gestures (n = 142).
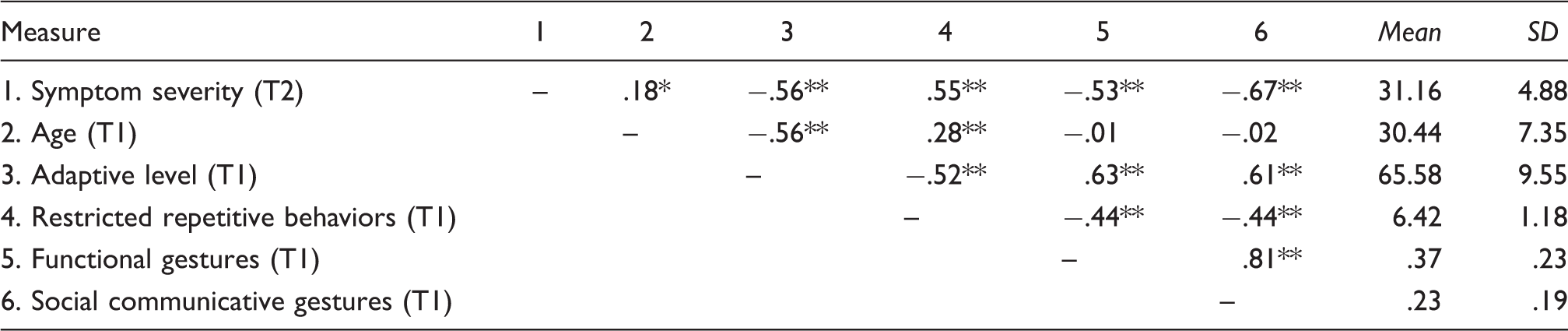
p < .05, ** p < .001.
Hierarchical regression analysis predicting symptom severity (n = 142) [95% corrected and accelerated confidence intervals reported in parenthesis].

p < .05, **p < .01, ***p < .001
Discussion
This study examined the role of early social communicative skills as predictors of symptom severity in very young children with ASD who had not been exposed to significant levels of intervention. As hypothesized, results from the current study show that social communicative skills predict symptom severity, approximately one year later, better than the other core symptom of ASD, restricted repetitive behaviors. The second hypothesis, that social communicative gestures would predict symptom severity, approximately one year later, after age, adaptive behavior, restricted repetitive behaviors, and functional gestures had been accounted for, is also supported.
Social communicative skills and symptom severity
The current study is the first to compare early behavioral manifestations of social communicative skills to restricted repetitive behaviors as predictors of symptom severity in a large group of very young children with ASD without the confound of intervention effects. Our results are consistent with previous research that shows social engagement and social skills are more predictive of outcomes in individuals with ASD than restricted interests and repetitive behaviors (e.g., Smith et al., 2015; Szatmari et al., 2003). Our findings however, extend the literature by showing that very early social communicative skills predict symptom severity without the effects of intervention and may place children at risk for a more negative symptom trajectory. This has important clinical implications given the more salient nature of restricted repetitive behaviors compared to social communicative deficits. Our findings suggest that clinicians, educators, and family members should give specific attention to social communicative deficits for diagnosis and intervention planning. It is imperative that clinicians also recognize that the level of social communicative competency provides critical information with regard to present and future functioning of the child.
By distinguishing between social communicative and functional gestures the present study adds to the existing knowledge in particularly unique ways. Our findings are the first to show that social communicative gestures predict symptom severity of children with ASD even after age, adaptive level, restricted repetitive behaviors, and functional gestures are already accounted for. Unlike previous studies, which have found gestures to be one of several predictors of outcomes (e.g., Chawarska et al., 2009), the current results show that social communicative gestures are a critical predictor of symptom severity. By separating gestures into two categories: social communicative and functional, we show which aspect better reflects the language skills that are disregulated in ASD. In order to determine this, social communicative and functional gestures need to be distinguished, something that has not been considered prior to the present study. Furthermore, the fact that social communicative gestures are predictive after controlling for functional gestures suggests that the two aspects of gestures development are distinct and separate and that the lack of gesture use in children with autism is likely not related to motor difficulties but rather is the result of an underlying disruption in social communicative development. Responsiveness to the social aspect of gestures and the subsequent development of this social communicative tool is implicated. These findings lend further evidence to the proposal that the social impairments in autism drive the resulting communication impairments (Paul, Feurst, Ramsay, Chawarska, & Klin, 2011), thus increasing the severity of symptom presentation.
By considering the social communicative aspects of ASD, we are reminded of the importance of carefully examining all aspects of language development. Communication is more than producing words. Although most researchers realize this, they frequently rely on vocabulary counts to estimate expressive and receptive language. Vocabulary is a good predictor of language ability; nevertheless, it is neither the only nor the earliest predictor. Before typically developing children begin to use words, they actively communicate via gestures. It is important to be just as observant of children's preverbal skills as their early use of words. Our results suggest that careful attention to a child's use or lack of use of social communicative gestures on the part of clinicians is highly recommended. Moreover, we utilized a commonly used measure of communicative development in a novel manner that potentially allows clinicians to significantly improve the sensitivity of their diagnostic process. Our results support the use of measures that focus on early social communicative skills and highlight the importance of careful consideration of items that measure social communicative skills in screening, diagnostic, and intervention planning settings.
Future directions
Outcome studies report that many young children with ASD respond well to intervention; however, some make remarkable gains whereas others respond minimally (Sallows & Graupner, 2005; Smith et al., 2015). Exceptional responders are frequently children who display a greater tolerance for social interactions, even though they may exhibit high levels of restricted repetitive behaviors (Sherer & Schreibman, 2005). It is possible that social communicative skills may be good predictors of high versus low response to intervention in children with ASD; thus future studies examining factors associated with high and poor outcome would do well to include early social communicative skills, particularly social communicative gestures. Furthermore, children who show moderate response to therapy tend to have highly variable outcomes compared to children who respond well or poorly to therapy (Prichard, 2012; Weiss, 1999). Children who respond well to therapy show stable progress as a group and children who demonstrate low response to therapy progress at low rates as a group. In the moderate groups however; some children go on to progress at a rapid rate, some at a moderate rate, and others at a low rate. Thus, although high and low responding groups demonstrate a predictable trajectory, the medium responding groups tend to be highly variable. Perhaps the variability in outcomes found in this group is related to variability in development of gesture use by observational learning, intervention programs that target gesture use, or a combination of the early social communicative skills that this study has isolated (imitation, social communicative gestures and/or relating to people). Finally, it is important to determine if the type of response to intervention can be predicted by preverbal social communicative skills in order to support streaming children into the most appropriate intervention program for their specific needs.
Recent studies have demonstrated the feasibility of teaching gestures to typically developing toddlers (LeBarton, Goldin-Meadow, & Raudenbush, 2015) and to children with ASD (Ingersoll & Lalonde, 2010; Ingersoll, Lewis & Krowman, 2007) with significant improvement of language skill found in both groups. Given the association between gestures, language, and cognitive development, it would be prudent to evaluate gesture use in screening, diagnosing, and treating children with ASD, and to include teaching gesture use in intervention programs.
The children in the current study had ASD symptomology that ranged from mild to severe, indicating a fairly broad range of symptom levels. Nevertheless, it must be acknowledged that the sample of files for review was drawn from a group of children presenting for intensive intervention and initially diagnosed as having moderate to severe ASD. Therefore, including a sample with a full range of ASD presentation, for example all children who receive a diagnosis on the spectrum, independent of their eligibility for publicly funded intensive intervention, would potentially increase the generalizability of the findings. We also acknowledge that in the current study, a measure of general cognitive ability was not used. Although measures of adaptive ability are moderately correlated with cognitive functioning (Perry, Flanagan, Dunn Geier, & Freeman, 2009), it would be prudent to include a measure of overall cognitive functioning in future studies.
Chronological development of gesture use in typically developing children is now well documented in the literature (Hall et al., 2013; Stanfield, Williamson & Ozcaliskan, 2014). Given the disrupted developmental trajectory of gesture use in ASD, it is clear that a detailed longitudinal investigation of gesture development in children with ASD is necessary to have a nuanced item analysis of this skill for these children. In light of our findings, a better understanding of preverbal early manifestations of social communicative skills could provide crucial information for predicting developmental pathways and symptom severity in children with ASD.
Footnotes
Authors' note
This research was presented at the 2017 Annual Convention of the Canadian Psychological Association, Toronto, Ontario, Canada.
Acknowledgements
We are deeply grateful to, and would like to thank, Surrey Place Centre for allowing us to collect the data for this study. This paper was based on a Master's thesis submitted by J. Lobban-Shymko to the Department of Psychology at Trent University, Peterborough, Ontario.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.