
Abstract
The increasing rate of non-communicable diseases calls for early identification and intervention. Trained paramedical forces can cater to the healthcare needs on the prevention front. This opens the doors for social enterprises to address this social need in an economically sustainable way. The present research article discusses the unique health intervention ‘Santhwanam’, a collaborative effort of Kudumbashree, the State Livelihood Mission of Kerala, the State Bank of India and Health Action by the People. It addresses the rural people’s unmet health needs by creating a pool of trained paramedical professionals. At present, ‘Santhwanam’ has trained 356 women in paramedical services and reached nearly 3.41 lakh people’s lives in 14 districts of Kerala.
Background of the Sector
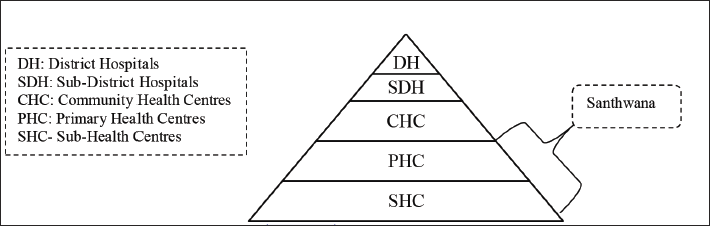
In India, the healthcare sector includes businesses that provide medical services, drugs, medical equipment, medical insurance and any other business involved in providing healthcare facilities to patients. In the World Health Organization ranking of world health systems, India ranks 112 (WHO, 2023). Regarding per capita healthcare spending, India spends over 6% of its GDP on healthcare (Ministry of Finance, Government of India, 2022). According to WHO, India has about 0.49 doctors and 0.80 beds for every 1,000 people in the country. The present healthcare system operates through district hospitals, sub-district hospitals, community health centres (CHC), primary health centres (PHC) and sub-health centres. Currently, 722 district hospitals, 4,833 CHCs, 24,049 PHCs and 148,366 sub-centres are insufficient for a country like India, where 54% of its population lives in rural areas (Karan et al., 2021; Ministry of Finance, Government of India, 2022; Suryavanshi et al., 2020).
India’s present healthcare system has evolved from the Bhore Committee report, 1946. The committee recommended a three-tiered healthcare system to provide preventive and curative healthcare in urban and rural areas. Placing health workers on government payrolls and limiting the need for private practitioners became the principle on which the current public healthcare systems were built. Such a system was assumed to ensure access to primary care by all individuals, irrespective of their socioeconomic status. However, the increased number of people and the lack of capacity of public health systems to provide access to quality care resulted in a simultaneous evolution of the private healthcare systems with a constant and gradual expansion of private healthcare services (Patel et al., 2022).
In India, the private sector is considered to have huge untapped potential. Despite being unregulated, expensive, inequitable, over-indulgent in clinical procedures and less transparent, it is perceived to be more efficient, better managed and easily accessible compared to its public counterparts (Vyas & Pandya, 2012). It is assumed that public/private partnerships would improve quality, efficiency, accountability, and accessibility and bring equity to the healthcare system. Advocates of the private sector argue that from the collaboration, both private and public sectors can gain from one another in terms of knowledge, skill, technology, physical resources, cost efficiency, management practices and even a makeover of their images (Hernandez-Aguado & Zaragoza, 2016). The partnership is expected to help the private sector deal with resource constraints by reducing their investments in expensive tertiary care services (Tyagi, 2014).
There is a growing agreement among experts from different sectors that social development is a joint responsibility of the state, private players and civil society. This model is popularly called ‘inclusive capitalism’ and is considered more sustainable than sheer corporate social activities (de Jong, 2021). However, the success of such a model heavily depends on the presence of trained human resources at the community level. The key to sustainable growth is empowering the left-behind grassroots communities by encouraging social entrepreneurs (Gupta et al., 2020). Social enterprises aim to improve society’s general welfare and apply market-based strategies to achieve a social purpose. Social entrepreneurs make society better, bringing positive changes by working on opportunities that others miss, improving existing systems, inventing new approaches and processes and creating new solutions (Gupta et al., 2020). Social entrepreneurs address social problems with an entrepreneurial mindset and skill set. In a country like India, where the public healthcare system is under-resourced and overburdened, there is an imperative need for social enterprises that can mobilise the resources to design innovative solutions for addressing the demand–supply gaps in the healthcare system (Bansal et al., 2019). ‘Aravind Eye Care Systems’ and ‘Narayana Hrudayalaya’ are glaring examples of initiatives that have done commendable work in the Indian healthcare system (Agarwal et al., 2018).
Given a situation where many people do not have access to primary healthcare facilities, there is a need to create a pool of trained personnel at the grassroots level who can cater for the healthcare needs of the communities. Any such entrepreneurial intervention needs to be analysed and replicated to create a multi-fold impact. Kudumbashree is one such initiative of the Government of Kerala to empower women socioeconomically. Its focus is on creating livelihoods for rural women in different sectors. Kudumbashree started initiatives to create healthcare services with qualified medical practitioners to fill the rural people’s health needs gap. The present research aimed to understand and analyse the business model of social enterprises in the healthcare sector initiated by the Kudumbashree. The present study aimed to understand the role of social enterprise in the healthcare sector.
Social Entrepreneurship
Social enterprises apply business solutions to social problems. They find innovative ways to address social problems and attain economic sustainability. They use business principles, market characteristics and traditional values of private sector responsiveness to the community to serve the public interest. Though social entrepreneurship has the elements of entrepreneurship, the difference lies in its understanding of social problems as an opportunity for bringing social change, and this is explicitly stated in its mission (Christensen et al., 2006; Dees 1998; Henderson et al., 2019; Teasdale et al., 2022; Vazquez-Maguirre & Portales, 2014). Creating social value by reducing any barrier obstructing the inclusion of any social group motivates social entrepreneurship (Austin & Seitanidi, 2012; Austin et al., 2006; Kay et al., 2016), rather than accumulating wealth. The social entrepreneur has a dual responsibility of creating social and economic value. They work under pressure to find economically viable solutions to address social problems sustainably (Dees, 2007; Defourny & Nyssens, 2008; Mair & Marti, 2006; Roy et al., 2014). They can address this tension through an effective business model. Hence, understanding the business model of social enterprises is the core of their success.
Business models identify the central elements that must be known and identified during their construction, analysis and development (Baldassarre et al., 2020; Bocken et al., 2014; Castro-Arce & Vanclay, 2020). These elements are related to the generation of wealth, the strategy and the operation that a company/enterprise has when operating in the market (Osterwalder et al., 2014; Teece, 2010). A business model contains three essential components: value creation/proposition, value delivery and value capture (Grassl, 2012; Osterwalder & Pigneur, 2010). The social business model is a tool which visualises how social enterprise generates social and economic value and how profits guarantee its operations and sustain the social enterprise in creating social impact (Morris et al., 2005; Osterwalder, 2004).
The business model includes an operational strategy and a resource strategy. The operational strategy includes the internal structure of the organisation, external collaborations and partnerships that are crucial for creating the intended impact (Roh, 2016). Resources strategy includes exploring how an organisation acquire resources for its operations. The business model is an instrument for social enterprises that describes how inputs are converted into outcomes and creates the desired social value (impact) and economic value (revenue).
Research Context
Non-communicable diseases (NCDs) are responsible for nearly 74% of all deaths globally. Each year, 17 million people die from an NCD (cardiovascular disease, cancer, chronic respiratory disease, diabetes and kidney disease) before age 70. NCD or chronic diseases tend to result from a combination of genetic, physiological, environmental and behavioural factors and develop over a long duration. So early detection, screening, treatment and palliative care can address the issue of NCD. Sustainable development goals (3.4) also stress the importance of preventing and treating premature mortality from NCD by 2030 (NITI Aayog, 2018; NSSO, 2019; WHO, 2019, 2023).
In India, the increasing number of lifestyle diseases and various contagious and fatal diseases are a significant concern in urban and rural areas. The household expenditure on health in India is in increasing trend. The rich people at least have knowledge about and accessibility to the available healthcare facilities. However, poor people who reside in rural areas have neither sufficient knowledge nor accessibility and affordability to avail of healthcare facilities. Lifestyle diseases can be prevented from becoming fatal if given early diagnosis and care. However, all people cannot visit hospitals for periodical check-ups. Most of the time, people are so busy with their daily work that they do not find time to visit the doctor until something severe happens. With increased lifestyle diseases in Kerala, visits to hospitals and clinics for periodical check-ups have become necessary for people experiencing poverty and the elite. In 2006, Kudumbashree developed one of its significant interventions in the healthcare sector through the ‘Santhwanam’ project to address this need. The Healthcare system in India is presented in the Figure 1.
Healthcare in India.
Description of the Case
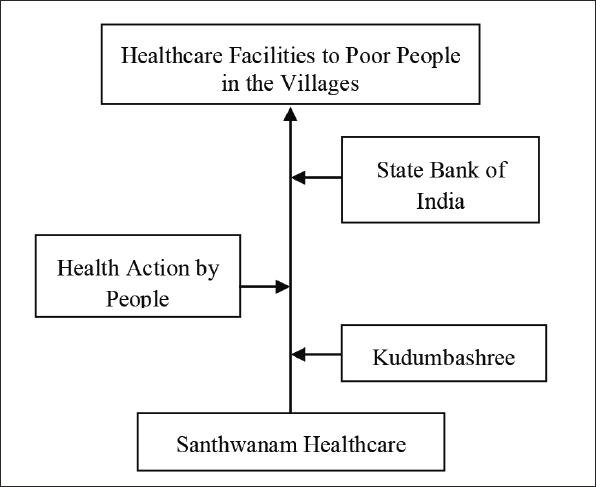
‘Santhwanam’ is a collaborative effort of Kudumbashree, Health Action by People (HAP), a not-for-profit health research organisation, and the State Bank of India (SBI), the funder. It is an individual micro-enterprise under the Yuvashree scheme of the Kudumbashree mission. Yuvashree scheme aimed to provide work to unemployed youth aged 18–45 below the poverty line. Under ‘Santhwanam’, women from Kudumbashree Neighbourhood Groups having education of up to intermediate (10 + 2) or graduating in science or youth with auxiliary and midwife courses or lab technicians or nurses are selected as volunteers. HAP conducts a seven-day training programme on technical inputs and personality development for the selected volunteers. The Santhwanam Healthcare stakeholders presented in the Figure 2.
Conceptualisation of the Enterprise.
Methodology
The present study is based on a single case study research design. An intrinsic case study is typically considered when the researcher is interested in learning about a unique phenomenon. The case chosen for this study is a unique initiative in its approach, that is, imparting training to 12th-grade science women pass-outs in basic paramedical services and equipping them to cater for the needs of rural populations, regular monitoring of health status, early diagnosis of critical illness and hassle-free and timely referral services. Such an initiative is very appreciable in a developing country like India, where there exists a considerable gap between the number of healthcare professionals and healthcare seekers. The importance of this model also derives from the fact that it is well accepted by the customers. The study is an effort to understand how a healthcare service model working on a minimalistic approach, that is, training to handle basic medical diagnostic equipment and recognising the early symptoms of critical lifestyle diseases, provides the maximum benefits (Yin, 1994). The data were collected from five major stakeholders: rural livelihood mission personnel; SBI, the funding agency; NGO, the knowledge partner; women voluntaries; and the customers. Primary data were collected through interviews.
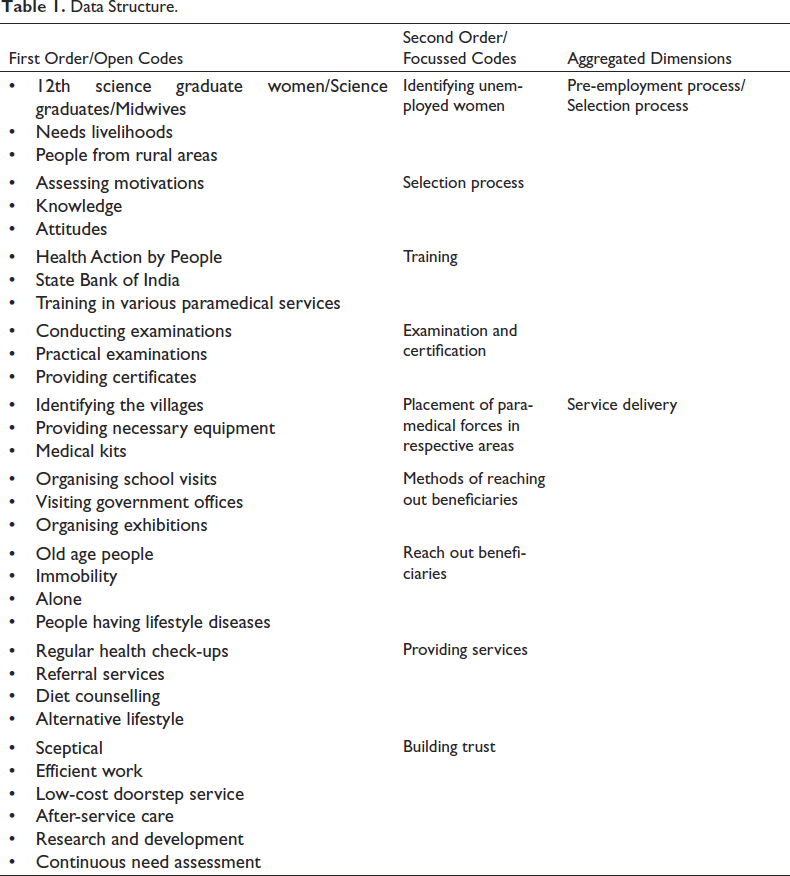
Data related to various information like year of establishment, number of employees and number of beneficiaries, paramedical staff training process, service delivery system and socioeconomic impact created by the enterprise were collected using a semi-structured interview schedule. All major stakeholders were interviewed through in-depth interviews for the data triangulation, observation method and document analysis were also done. From the qualitative data, the themes were generated at three levels. After the data transcription, the first-order codes were generated in the first level. More focused codes were defined at the second level, looking at the similarities and dissimilarities within the first order. Finally, the researchers arrived at the theoretical themes in the third level by aggregating the focused codes.
Data Analysis
The data are analysed based on the data structure (Table 1); through data structure, two dimensions emerged, that is, the pre-employment process/selection process and service delivery of Santhwanam.
Data Structure.
Pre-employment Process/Selection Process
Pre-employment process/Selection process emerged from focused codes, that is, identifying unemployed women, the selection process of volunteers, training process of volunteers, training and examination and certification.
Identifying Unemployed Women
Women who completed their education up to intermediate (12th class)/graduated in science/youth with auxiliary and midwife courses/lab technicians or nurses are eligible to be selected as Santhwanam volunteers.
Selection Process
‘Kudumbashree’ district mission interviews to select the members based on their aptitude and personality and further provides them training on the designed seven-day module.
Training
The volunteers are trained to check people’s height, body weight, body mass index, body fat, blood pressure and blood glucose levels.
Examination and Certification
After completing the training programme, HAP conducts examinations to test the knowledge and skills gained by the trained people. The HAP provides certificates to practice; in addition, they monitor the performance of the selected people every six months.
Service Delivery
Service delivery emerged from focused codes, that is, placement of paramedical forces in respective areas, methods of reaching out beneficiaries, reaching out beneficiaries, providing services and building trust.
Placement of Paramedical Forces
The selected members get allotted to their respective residing panchayat. Efficient Santhwanam volunteers may get to serve more than one panchayat. There may be situations where a panchayat has more than one Santhwanam volunteer. It varies on the number of wards in the village. Panchayat provides this service through these Kudumbashree members who are Santhwanam volunteers. They are provided ID cards, a certificate from HAP and a white coat. In addition, the volunteers get access to 24-h technical support from HAP. The volunteers are given mobile phones and two wheelers so that they can be easily accessible to their patients. The field-level issues and queries are answered in a time-bound manner. The machines are calibrated once a year to ensure accurate readings. To analyse the performance of the volunteers, the Kudumbashree Mission conducts zonal meetings once every six months.
Methods of Reaching Out Beneficiaries
The Santhwanam volunteers visit individual households, schools and offices and organise exhibitions in their operated areas to reach beneficiaries.
Reach Out Beneficiaries
As the Santhwanam volunteers use digital equipment for checking blood pressure or blood sugar, which gives the result within 3–5 min. These volunteers get the service charges from the patient. In addition, they also visit offices and schools to cover the working individuals. They also participate in fairs and festivals where they get plenty of patients to carry out check-ups and earn a good amount of money. The major advantage of this scheme is that periodic check-ups give individuals a warning signal about their health status, enabling them to visit the hospital in time for further treatment.
Providing Services
For providing onsite assistance, volunteers visit houses where immobile patients, aged persons, lonely elderly patients and persons having no one to address their health needs reside. They conduct blood sugar tests using a glucometer and measure the blood pressure level and body weight regularly. The patient is advised to contact the physician immediately if any abnormality is identified. They follow the best available medical facilities like sterilisation, disposable needles, swabs for blood collection from finger pricks, and test strips for glucose meter readings. The volunteer gets the fee paid by the patients for the service, and the patient gets the health status report regularly at their doorstep. This keeps the patients informed about their health condition. They also give awareness on how to prevent lifestyle diseases, and if anybody is already affected, they suggest a diet and alternative lifestyle. If there is no improvement in the person’s condition, volunteers refer the patient to the nearest government hospital located at Taluka, district, or primary healthcare centre. The patients pay small fees for the service rendered by the volunteers. A Santhwanam volunteer earns, on average, 15,000–25,000 rupees per month.
Building Trust
In the beginning, people were sceptical about the services provided by the Santhwanam volunteers as they did not have a medical degree from any medical institute or degree. However, with their efficient work, the volunteers proved people’s fear of being wrong. People started liking it as they could avail cheap service at their doorstep. It was developed to provide service to people experiencing poverty through awareness of how to prevent diseases and recommend the beneficiary a balanced diet. Santhwanam volunteers have now developed a customer base for immobile patients in public by participating in exhibitions and fairs and visiting schools and public offices.
After six months, Kudumbashree imparts performance improvement training to the volunteers. Presently, 300 women volunteers are on board and operating across the state. They envisage having at least one Santhwanam volunteer in every local self-government institution. Their dream has been turning into reality for the very last two years. It helps poor people by providing doorstep services at a nominal price. They save time and money, and at the same time, it creates livelihood opportunities. As the regional private laboratories charge high prices, the elite are also starting to benefit along with people experiencing poverty. It helps in empowering women by creating employment opportunities for them, which change their lives in a positive way. The trust and acceptability they had earned during the past years were reflected through their income. Mission calibration is conducted yearly, including training and meetings to convey people’s needs. Recent meetings raised the need for additional services such as urine tests, uric acid and blood group checks. The research centre is working on machines having all these facilities along with it, and they also assess the need before the inception of any services.
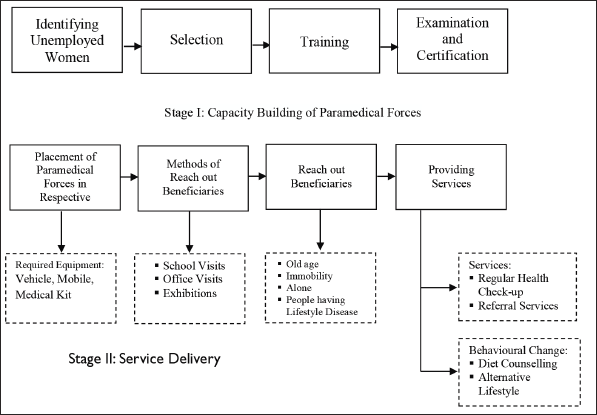
Figure 3 schematically presents the two dimensions and the interrelationship among the focussed codes.
Santhwanam Healthcare Service Delivery Process.
Santhwanam Business Model
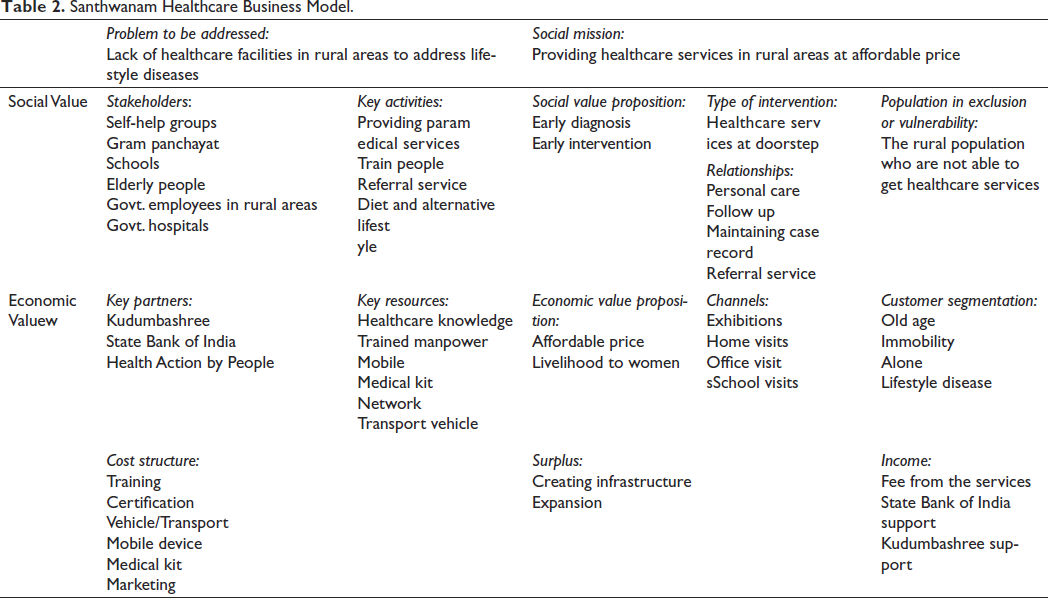
Generally, the business canvas model discusses key partners, key activities, key resources, value propositions, relationships, channels, market segmentation, cost structure and revenue streams. Such business canvass models effectively do not explain social enterprises as social enterprises are not solely guided by profit motives and are created to address social problems. Portales (2019) developed a business canvas model for social enterprises that discusses problems existing in the external world and the social mission of the social enterprise, stakeholders involved in the entrepreneurial activity, the value proposition including social value proposition, economic value proposition and interventions for excluded population. The model includes how enterprises utilise surplus, that is, profits of the enterprise. The business models give practitioners, students and prospective entrepreneurs a common language to communicate and understand the social businesses’ context, process, and outcome. Hence, the researchers have tried to put the data into an existing social business model (Table 2).
Santhwanam Healthcare Business Model.
Discussion
The major findings of the present research article can be summarised under the following points. The literature reveals that there exists a huge gap in the health service sector, more specifically in rural areas. The number of doctors, nurses and midwives per 10,000 in India is 6.5, which is relatively low compared to WHO’s standard of 44.5. Kerala, with 8.0, stands at a better position than the national average but is still far behind the WHO-prescribed standard. In the three-tier healthcare systems, the primary healthcare centre (for 20,000–30,000 population) and sub-health centre (3,000–5,000 population) operate at the village level (Ministry of Health and Family Welfare (MoHFW), 2017). As per WHO (2019), the ratio of community health workers to population is 1:500 in rural areas and 1:1,000 in urban areas and the ratio of nurses to population is 1:5,000. This indicates the dearth of medical professionals in India. This situation calls for training more workforces to meet the healthcare needs at the grassroots level. Santhwanam’s efforts to train the educated youth to meet such requirements at the grassroots and create livelihood opportunities for the educated youth.
Recent statistics show an increasing trend for non-communicable diseases, which can be addressed through early diagnosis, constant monitoring and healthy lifestyle practices. When it comes to prevention, paramedical personnel can play a significant role in the labour market. There are qualified unemployed youth whose skills and knowledge can be monetised by providing hands-on training and experience. So, we need institutions which can work on these issues. In this direction, ‘Santhwanam’ exemplifies a successful model. So far, they have trained more than 356 women volunteers working across 14 districts of the state.
Health-related problems can be preventive and curative. Curative health facilities require more health infrastructure, sophisticated technology, and a highly skilled workforce. However, preventive and early detection and intervention can be done with the paramedical workforce trained in simple diagnostic techniques and knowledge of human anatomy, risky health behaviours and alternative lifestyles. Considering the vast population burden and resource crunch, working on the preventive and early diagnosis front will be more helpful. At present, ’Santhwanam’ has reached nearly 3.41 lakh people’s lives.
Conclusion
Santhwanam healthcare caters to rural people’s health needs at an affordable price and trains the mid-level paramedical forces with the help of supporting agencies. It also creates livelihood opportunities for educated unemployed women below the poverty line. In a country like India, where many social problems exist, society needs innovations to break the vicious circle of social problems. Zahra et al. (2009) discussed social bricoleurs who address social problems using locally available resources to cater for the needs of the people. Santwanam addresses social problems and creates social value with available resources. In India, the healthcare expenditure of the government is increasing significantly, and individual expenditure is increasing by more than 20%–40% (NSSO and NHM). It shows the importance of healthcare in the country, but the public and the private sector alone cannot cater to people’s needs. We need a hybrid mixture of both in the form of social enterprises. Santhanam is a successful example of such a model. It fills the treatment gap and provides affordable healthcare to rural communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.