
Abstract
Introduction
: Structural competency is essential for teaching health professional students about the social and structural drivers of health (SSDoH) before they enter practice. While some curricula exist, most are classroom-based, and studies suggest that students also seek opportunities to practice these skills in clinical settings with real patients. This curriculum was developed to provide these opportunities.
Methods
: To address this, we developed the Structural Influence of Health Project, an innovative curriculum within the required third-year Family Medicine Clerkship on the Kansas City campus of the University of Kansas School of Medicine. The program combines didactic seminars, interprofessional home visits, and structured faculty-led debriefs, allowing students to apply structural competency in real-world clinical contexts. Medical students (n=125) completed pre- and post-surveys, and 90 students provided written responses on how to improve the training. This sample size was based on the students enrolled in the Family Medicine clerkship in the 2021-2022 academic year.
Results
: After being exposed to the curriculum, the students showed a significantly improved ability to identify social and structural contributors affecting patients’ health. Students reported experiential learning opportunities, such as patient home visits, as valuable for applying SSDoH concepts in real-world settings. They appreciated the inclusivity of the curriculum but suggested that it should be more patient- and community-centered. Many have advocated for a shift from problem identification to actionable solutions, with practical approaches integrated into clinical discussions. Expanding the curriculum to include topics such as gender-affirming care, rural health disparities, and insurance challenges was recommended. Future directions may include more deliberate faculty development to allow greater skill with these difficult topics.
Introduction
The structural competency framework has emerged as a key approach to teaching health disparities in health professions education. 1 It centers on understanding how structural factors—such as zoning laws, racism, economic policy, and political decisions—produce and sustain disparities across dimensions like race, geography, and gender. In health professions education, structural competency involves both recognizing structural disparities and actively working to address these in clinical practice.2-5 Proponents argue that structural competency enhances interprofessional collaboration and promotes health equity. 6
Despite growing interest, structural competency is still underrepresented in national medical education curricula. A recent review identified 30 examples of structural competency training across disciplines such as medicine, pharmacy, nursing, and social work; only about one-third were in undergraduate medical education, and most were classroom-based. 7 These curricula were positively received and showed improvements in learners’ understanding of structural factors affecting health. 5 However, many learners expressed distress at being made aware of structural contributors without corresponding clinical applications, calling for mentorship and real-world examples. Scholars have thus urged that structural competency training “move beyond the classroom” 3 and called for the development of new models to guide structural change in clinical practice. 1
Innovative methods—such as neighborhood tours, photovoice, community-engaged rotations, team-based learning, and case scenarios—offer promising directions. Training can be brief or longitudinal, yet integration into clinical learning environments is still limited. Although recent scoping reviews highlight simulation-based training, there is a notable lack of curricula that apply a structural competency framework in clinical settings.7-12 Structural competency is essential for health care providers, yet few learners are exposed to it in clinical training. To address this gap, the development and evaluation of structural competency curricula embedded in clinical learning environments is urgently needed and this was our goal.
Confronting social complexity and resulting health disparities can overwhelm students’ emotional capacity, sometimes producing discouragement and changes in empathy.13,14 Though there is some evidence that medical students experience distress when learning about SSDoH students would find SSDoH discouraging to a career in medicine than other aspects of a clinical clerkship. To address these concerns, we designed the Structural Influence on Health Project, an innovative curriculum to teach structural competency embedded in a required Family Medicine Clerkship on the Kansas City Campus of the University of Kansas School of Medicine. This curriculum included didactic seminars, interprofessional home visits, and structured faculty-led debriefings, providing students with opportunities to apply structural competency concepts in real-world clinical contexts. The home visits were interprofessional due to their integration in our Team-Based Teaching Clinic.
Methods
The University of Kansas School of Medicine is the only allopathic medical school in Kansas. Their mission is “to enhance the quality of life and serve our community through the discovery of knowledge, the education of health professionals and by improving the health of the public”. Most accepted students are from Kansas and are expected to serve Kansas, and there is an emphasis on primary care.
The Structural Influence of Health Project is an innovative curriculum to teach structural competency embedded in a required Family Medicine Clerkship on the Kansas City Campus of the University of Kansas School of Medicine. The curriculum was composed of three parts. First, students participated in didactic seminars during the first week of the clerkship (Appendix B). The purpose of the seminars was to introduce learners to important structural contributors of health concepts, discuss their influence with a faculty expert, and build a common language and framework. The seminar topics included insurance coverage, language isolation and interpreter ethics, climate change, systemic racism, and community resources. Attention was given to defining and discussing intergenerational policies, structural violence, structural vulnerability, naturalizing inequality, cultural competency, cultural humility, structural humility, and structural competency.
All students on the Kansas City campus participate in our Team-Based Teaching Clinic, in which interprofessional teams of students work together to evaluate patients and make their recommendations. As part of this clinical setting, the students completed an interprofessional home visit. Each team typically includes medical students, pharmacy students, a supervising physician, and a supervising pharmacy faculty. The team traveled to the patient’s home and neighborhood to provide care. Patients were referred by their Primary Care Physician within the Department of Family Medicine and Community Health. Many of these patients were also supported by a Community Health Worker. Physicians in the department who identified a transportation or mobility need during a visit in the office could refer their patient to receive a home visit. Patients consented to being cared for in their home by the interprofessional group of learners and preceptors. One to two medical students and one to two pharmacy students participated in each home visit. Each visit lasted approximately 20-60 minutes depending on the needs of the patient. Patients were seen for a variety of acute and chronic medical conditions, identical to medical needs that would be addressed in an outpatient clinic. These home visits took place in the context of a synchronous interprofessional clinic environment which allowed them to generalize the roles of their profession. Medical students routinely took the medical history and performed the physical exams while pharmacy learners took extensive medication history, even examining, with consent, the bottles of medicine the patient had in the household. Additionally, during the home visit, the student team worked with the patient to complete a social driver screener (Appendix C) and interviewed the patient about structural forces most impacting their health. 15
After the home visit, the student team helped to coordinate care with an interprofessional team that may have consisted of a community health worker, nurse, social worker, psychologist, and their attendings imbedded with in our Family Medicine Clinic. The student teams were then asked to complete two assignments. First, they worked with local and CDC open access geomaps to better characterize which structural forces may influence the patient’s health based on zip code. This interactive dataset is publicly available.14,16 Second, they worked together to build a solutions-based care plan to respond to the influence of structural contributors uncovered during their home visit (Appendix D).
Finally, at the end of their experience, student teams met in small groups to present their care plans. Through facilitated discussion, the students were asked to demonstrate their structural competency, knowledge, and skills. The faculty guided these discussions toward the learning objectives and the structural level. The five alternating faculty participating were experienced small group facilitators and members of the clinical team who participated in home visits. Each of the faculty had independently completed implicit bias training and small group facilitation faculty development. Additionally, the facilitating faculty had been deeply involved in the creation of this curriculum. The debrief allowed the students to consolidate their lived experiences, their clinical experiences, and classroom content.
The learning objectives for the curriculum were as follows.
At the end of the curriculum, the learner will be able to. • Apply what they have learned about structural and social contributors of health to a real patient’s care and to a population in which that patient lives. • Understand the root causes of illness. • Generate strategies for responding to the influence of structures in the clinic and community. • Build confidence caring for patients with medical and social complexity.
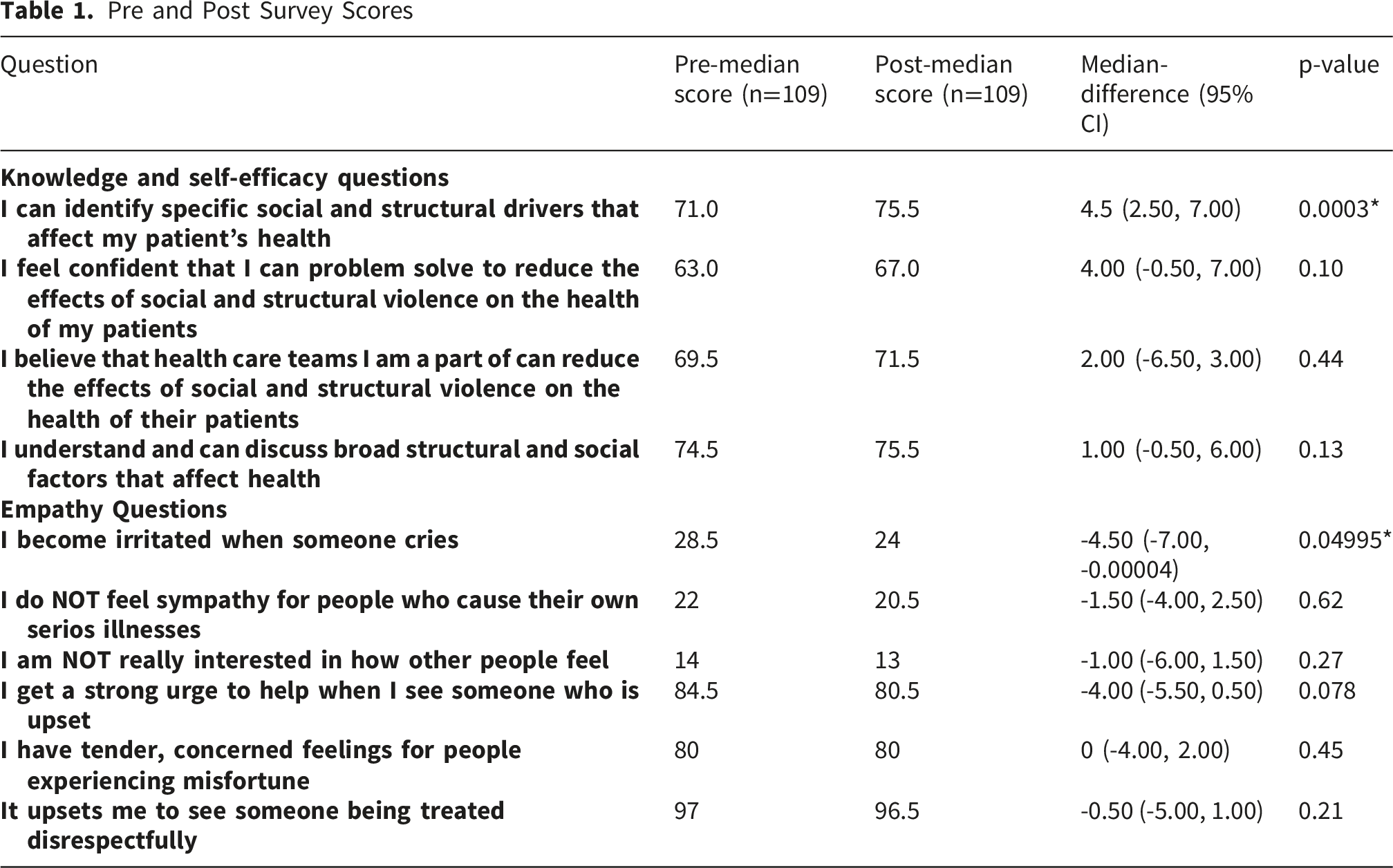
We measured changes in students’ empathy, skills, and confidence in identifying and managing patients’ social determinants of health (SSDoH) before and after the clerkship. Students also reflected on key aspects of the clerkship, identifying elements that promoted or hindered their learning and suggesting ways to enhance the experience. The study follows DoCTRINE guidelines (see Appendix C).
Data Collection and Analysis
Each student completed a pre-survey at the beginning of their clerkship and then a post-survey at the end of the clerkship, after their home visit encounters. The surveys were reviewed by the IRB and were waived as a component of the clerkship. These surveys included questions based on the Toronto Empathy Scale. 17 In the post survey, students were asked to select classes, assignments, and experiences from the Family Medicine clerkship that made them feel either “encouraged” or “discouraged” about becoming a physician.
The response data collected from the pre- and post-surveys were matched for each student. Each participant’s data and responses were coded with a unique study number, allowing researchers to link the data to information obtained from questionnaires and other study activities while maintaining student anonymity. To further protect privacy, no demographic information was collected, as the small size of the clerkship groups could make individuals easily identifiable by their demographics. All responses that could be identifiably matched from the pre- and post-surveys were included in the analysis. Any survey responses that could not be matched between the pre- or post-survey were excluded from the analysis. The questions from the post-survey about items that encouraged or discouraged the students from becoming a physician were evaluated by the frequency of each response. All respondents from the post-survey were included. The comparison of the pre and post-test scores from the surveys was performed using a Wilcoxon signed-rank test. The median difference was compared for all matched responses. Statistical significance was evaluated at the level of α=0.05. All statistical analyses were conducted using R version 4.4.1, and results were reported with corresponding p-values.
Categorization of Responses
The post-survey included the free-text question, “How can we make training about Social and Structural Drivers of Health (SSDoH) more effective or more inclusive?” Three team members independently reviewed and coded all the written responses to the question. The team met to discuss codes and reached a consensus on the codes. Coders then organized responses into common themes using an inductive approach.
Results
Pre and Post Survey Scores
On the post-survey, 125 medical students answered the question, “Were there any parts of the Family Medicine Curriculum that caused you to feel encouraged/discouraged about becoming a physician?” Students reported outpatient and inpatient clinical experience most often as encouraging aspects of the family medicine clerkship, followed by the patient home visits. Figure 1 is a graphic representation of student responses regarding whether aspects of the clerkship were encouraging or discouraging. The most selected discouraging elements of the clerkship were the insurance coverage seminar, inpatient service, and the systemic racism seminar. The structure of this question was intentionally a drop-down menu of choices rather than a Likert scale to suit broader curriculum evaluation goals for the clerkship leadership. Rather than the extent of the encouragement or distress, we were interested in the discrete count per educational exposure to better target future interventions. Distribution of student responses regarding encouraging and discouraging aspects of the clerkship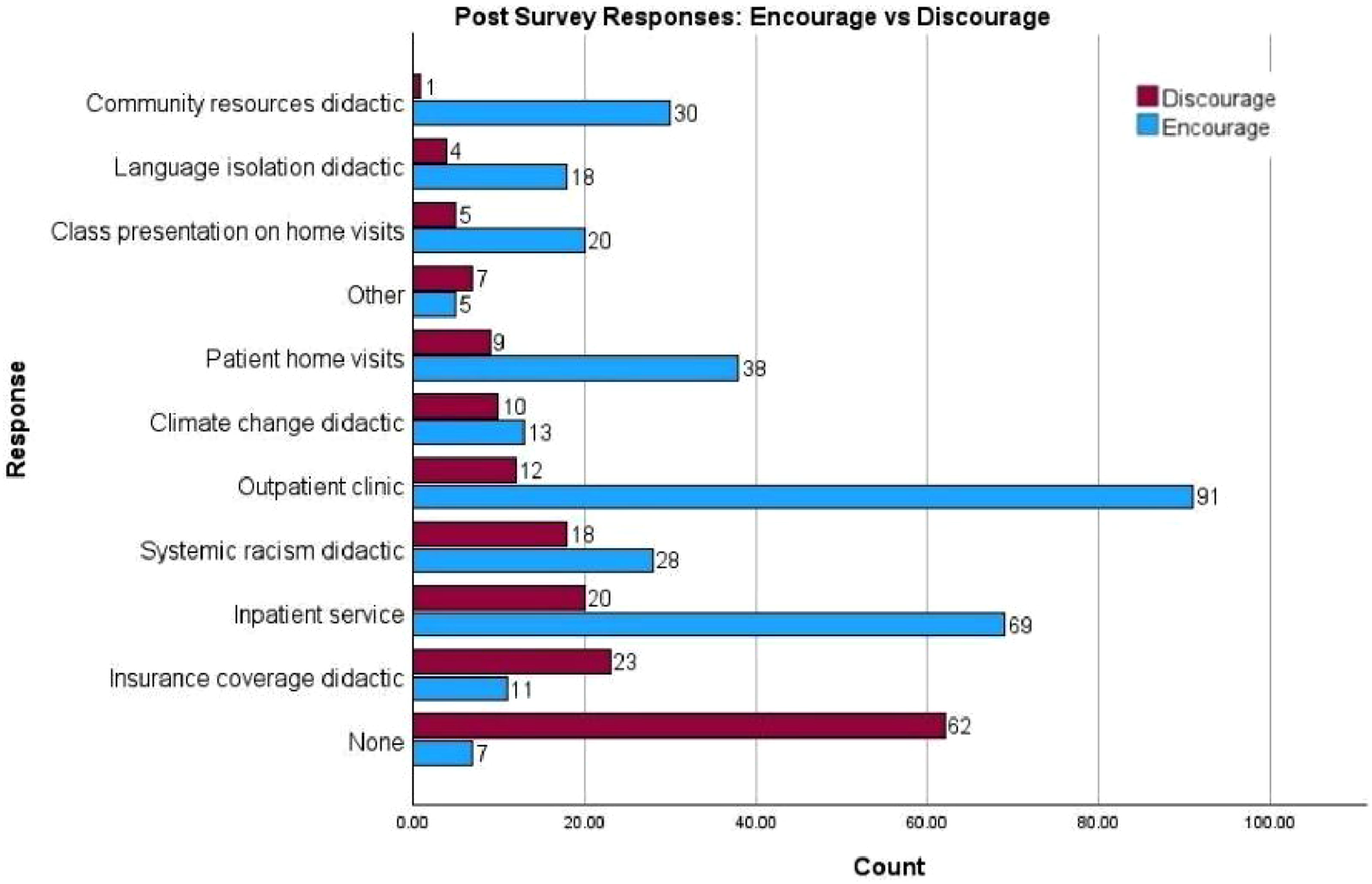
Student Perspectives on Making SSDoH Training More Effective and Inclusive
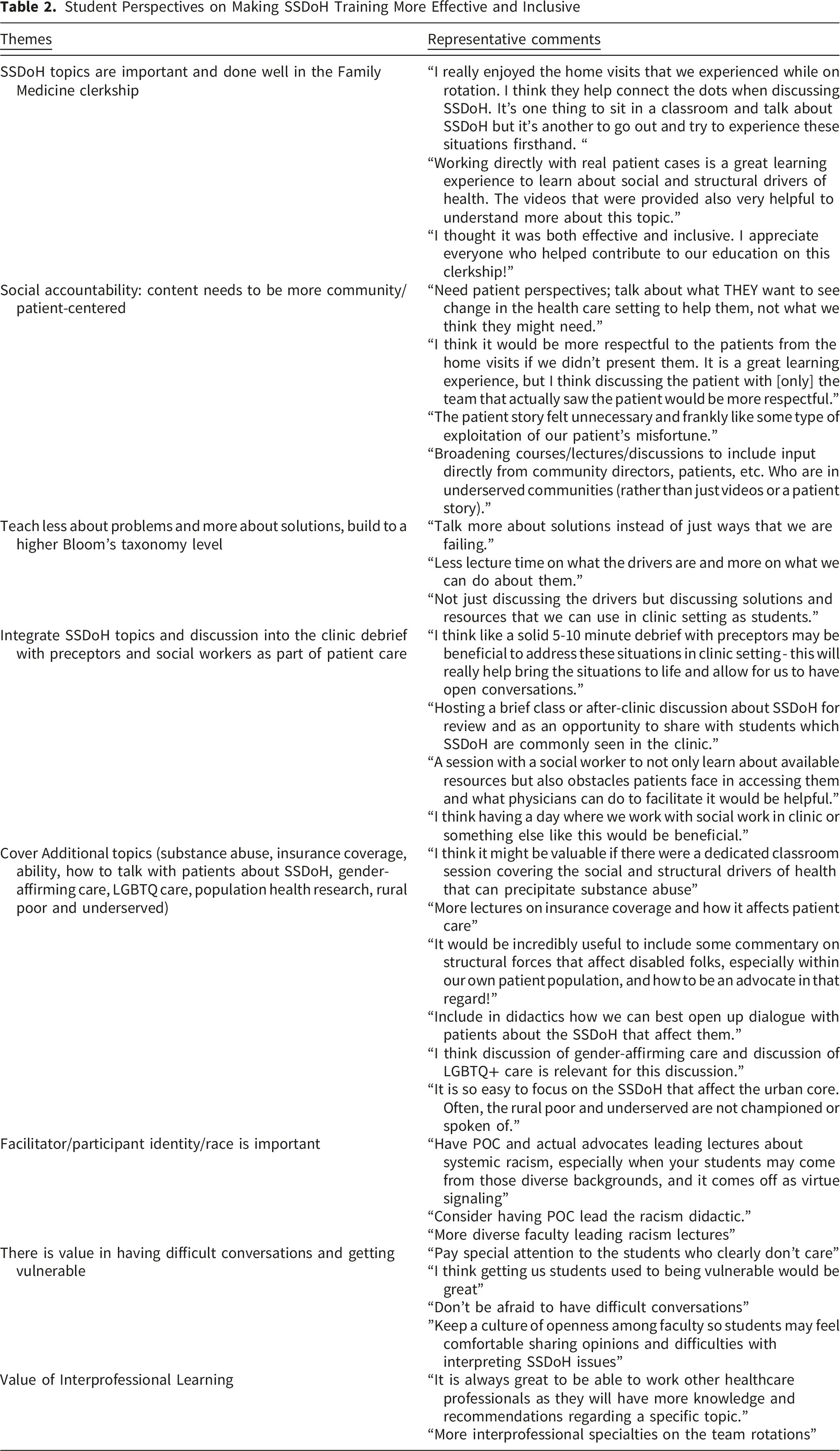
Students found that the integration of SSDoH topics in the Family Medicine clerkship was impactful. Hands-on experiences, such as home visits, were especially valuable for bridging classroom discussions with real-world applications. These opportunities allowed students to engage directly with patients and better understand SSDoH in context. Supplemental resources like patient cases and videos were also noted as effective learning tools. Overall, students described the clerkship as inclusive and well-supported by educators, contributing to a positive and enriching learning experience.
However, students expressed a need for the curriculum to be more community- and patient-centered. They emphasized the importance of including patient perspectives to better understand what changes patients themselves wish to see in healthcare. Concerns were raised about the potential exploitation of patients’ stories during presentations, suggesting that discussions should remain within the immediate care team to respect patient privacy. Students also recommended involving community leaders and individuals from underserved populations directly in lectures and discussions to provide a broader and more authentic perspective.
Many students suggested shifting the focus from identifying problems to discussing actionable solutions. They felt that time spent describing contributors could be reduced, with greater emphasis placed on available resources and strategies to address these issues in clinical settings. Teaching practical approaches, such as using resources during patient care, would help elevate learning to higher levels of Bloom’s taxonomy.
Students also advocated integrating SSDoH discussions into clinic debriefs with preceptors and social workers. Brief post-clinic discussions could help contextualize the challenges faced by patients and facilitate meaningful conversations. Additionally, sessions with social workers to explore available resources and the obstacles patients face could further enrich students’ understanding of how to support patients effectively.
Students commented that the curriculum could also benefit from expanding its scope to include additional topics such as substance use disorders, insurance coverage, structural challenges faced by disabled individuals, gender-affirming care, LGBTQ+ health, rural health disparities, and population health research. Students highlighted the importance of equipping them with skills to engage patients in conversations about SSDoH while ensuring that diverse and underserved populations are adequately represented in the curriculum.
The identity and diversity of facilitators were also noted as significant. Students recommended having people of color (POC) lead discussions on systemic racism to ensure authenticity and relatability, particularly for students from diverse backgrounds. This approach would enhance the credibility and impact of discussions.
Finally, students acknowledged the value of fostering an environment where difficult conversations can occur. They stressed the importance of cultivating openness and vulnerability among both faculty and students to encourage dialogue and deeper understanding of SSDoH issues. They also recognized the benefits of interprofessional learning, noting that collaboration with other healthcare professionals during rotations enriched their learning experience and provided valuable insights.
Discussion
Here we described the Structural Influence of Health Project, a longitudinal structural competency curriculum embedded in the University of Kansas School of Medicine’s Family Medicine Clerkship. The curriculum includes introductory seminars on structural contributors of health, interprofessional home visits with care coordination and solutions-based planning, and faculty-facilitated discussions to reinforce knowledge and provide feedback on structural competency skills. Our findings suggest that students found the integration of SSDoH topics impactful, with real-world, patient-centered experiences like home visits providing the most benefit.
Student Perspectives
The findings from the post-survey highlight key elements of the Family Medicine curriculum that influenced students’ perceptions of pursuing a career in medicine. Clinical experiences, both outpatient and inpatient, emerged as the most encouraging aspects, suggesting that direct patient interaction remains a cornerstone for fostering interest and enthusiasm in medicine. Notably, patient home visits were also a significant source of encouragement, underscoring the value students place on the opportunity to see the broader context of patients’ lives.
Conversely, certain didactic components of the curriculum were perceived as discouraging. The insurance coverage seminar, the systemic racism seminar, and inpatient service were the most frequently mentioned. These findings suggest a potential disconnect between the students’ expectations and the reality of the health insurance system in the United States. The discouraging response to the systemic racism seminar may reflect discomfort or a lack of engagement with the topic, highlighting the need to refine how such critical issues are addressed.
Student perspectives in this study underscore the importance of moving SSDoH education from the classroom to the bedside, with the clinical learning environment serving as a critical context for this work. While core faculty bring expertise in their respective fields and routinely address structural disparities in clinical practice, they often lack formal training in SSDoH and structural competency, as these topics were not part of their own medical education. Without targeted faculty development, they may struggle to effectively teach these concepts due to limited familiarity with the necessary language and frameworks.
Integration of Theory and Practice
Multiple national organizations emphasize physicians’ role in addressing social determinants of health (SDOH) and advocate integrating SDOH into all stages of medical education. 18
Framework Utilization
The 5 A’s framework—Awareness, Adjustment, Assistance, Alignment, and Advocacy—is one teaching model that provides a structured approach to integrating SDOH into undergraduate medical education. 19 It emphasizes recognizing patients’ social needs (Awareness), adapting clinical care to address these needs (Adjustment), connecting patients to relevant resources (Assistance), coordinating efforts with community and policy initiatives (Alignment), and promoting systemic changes to improve health equity (Advocacy). 20 By incorporating this framework, medical curricula can better prepare future physicians to address the broader social factors influencing patient health outcomes. The Structural Influence of Health Project described here aligns with the 5A’s framework by increasing awareness through seminars on structural and social contributors of health, enhancing assessment with home visits and data analysis, and helping by involving interprofessional teams to connect patients with resources. It also supports adjustment by guiding students to develop patient-centered care plans, though it does not explicitly address systemic workflow changes. While the project encourages students to recognize and respond to structural barriers, it lacks a strong emphasis on advocacy for long-term policy change or the strategies needed to advocate successfully.
Need for Faculty Development
Prior research by our team revealed that over half of family medicine clerkships do not teach structural competency or about the health consequences of systemic racism, despite student interest and institutional support. 21 Although increased faculty training hours were associated with the inclusion of education about the health implications of racism, causality remains unclear, further emphasizing the need for robust faculty development in systemic racism and structural competency. Our observations showed that faculty need to learn the necessary skills, constructs, and language alongside their students. Without this support, clinical teachers may experience the same feelings of distress and uncertainty that students report when engaging with complex SSDoH issues. This discomfort could hinder effective teaching and sustainability of the curriculum. These findings underline the importance of faculty development to ensure that clinical educators are equipped to lead these discussions as well as being able to incorporate these important concepts into a clinical setting. Developing these skills will ultimately enriching the educational experience and the quality of SSDoH instruction as well as providing this additional context needed to provide the best care for patients.
Challenges Identified
Faculty of color often face “cultural taxation,” as they are disproportionately called upon to serve as on-the-spot racism experts, compounding their existing academic responsibilities. 22 This dynamic, exacerbated by the absence of White professors from such initiatives 23 , not only places additional burdens on faculty of color but also limits the breadth of students’ social justice education. Research highlights the importance of both empowered faculty of color and White allies in teaching about racism, as each brings unique contributions to students’ learning experiences. 24 While White professors taking active roles in race-related education face challenges such as the need for specialized preparation and self-reflection25,26,27-29 these difficulties differ significantly from the racial oppression often experienced by faculty of color, who may encounter hostility, exhaustion, and biased evaluations in response to their work. Addressing these systemic disparities requires a collective effort to ensure equity and effectiveness in teaching about racism. White professors may need time to reflect on their identity, privilege, and perspectives on racism before students can move beyond viewing their race as a barrier. However, this is challenging within the constraints of a two-hour didactic session on systemic racism. Further work is also needed to expand these concepts through the entire medilcal school curricula.
Recommendations for Improvement
This program represents a deliberate step toward “moving beyond the classroom” which has been found to be valuable to not only learners but educators. It leverages the clinical learning environment and supervising physicians as educators. Preliminary evaluation results indicate positive impacts on learners, though formal evaluation is needed to assess the full range of outcomes, including any unintended effects. In the future, there could be opportunities to more deliberately include patients as a part of the team, allowing them to function as educators from their vantage point.
Limitations
This was a sample of convenience. Only students who completed their Family Medicine clerkship on the Kansas City campus participated. This did not include students on the Wichita or Salina campuses or those who chose to complete their clerkship in a rural setting due to logistical constraints of the curriculum.
The curriculum’s effectiveness was not evaluated with a follow-up component to discuss the learners’ long-term understanding for future clinical practice.
The curriculum’s effectiveness was not evaluated with a follow-up component to assess learners’ long-term understanding or its impact on future clinical practice. Reliance on self-reported survey data may introduce bias, as students may provide socially desirable responses rather than an accurate reflection of their true experiences or attitudes. These surveys were collected in the company of overall curricular surveys required by the school of medicine, thus there may have been a component of survey fatigue or disinterest in providing robust narrative feedback.
Conclusion
In conclusion, this study demonstrates that while students recognize the value of learning about social determinants of health during their medical curriculum, they find it most beneficial to do this in the setting of patient care. This information should lead to increased inclusion of the social determinants of health in clinical learning settings. While this will be a challenge, it will lead to more competent physicians as well as better, more comprehensive care for our patients.
Supplemental Material
Supplemental Material - Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment
Supplemental Material for Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment by Kristina M. Bridges, Hannah Maxfield, Ashley Glissman, Kalee Kirmer-Voss, Kate Rampon, Wendi Born and Laurel B. Witt in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment
Supplemental Material for Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment by Kristina M. Bridges, Hannah Maxfield, Ashley Glissman, Kalee Kirmer-Voss, Kate Rampon, Wendi Born and Laurel B. Witt in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment
Supplemental Material for Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment by Kristina M. Bridges, Hannah Maxfield, Ashley Glissman, Kalee Kirmer-Voss, Kate Rampon, Wendi Born and Laurel B. Witt in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment
Supplemental Material for Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment by Kristina M. Bridges, Hannah Maxfield, Ashley Glissman, Kalee Kirmer-Voss, Kate Rampon, Wendi Born and Laurel B. Witt in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental Material - Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment
Supplemental Material for Bridging Classroom Learning and Clinical Practice: A model for teaching structural competency in the clinical learning environment by Kristina M. Bridges, Hannah Maxfield, Ashley Glissman, Kalee Kirmer-Voss, Kate Rampon, Wendi Born and Laurel B. Witt in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgements
Special thanks to Megan Soeken, RN, who assisted in finding appropriate patients for home visits and scheduling them.
Ethical Considerations
Study was submitted to The University of Kansas Medical Center IRB and was determined to be exempt, STUDY00149533.
Consent to Participate
Written informed consent was obtained from each participant who participated in the survey.
Consent for Publication
Not applicable; no identifying data was collected.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.