
Abstract
Introduction
Trauma-informed care (TIC) is a critical yet underrepresented component of medical education, particularly in residency training. Despite high rates of trauma exposure in the United States, most physicians lack formal training in how to recognize and sensitively respond to patients with trauma histories. This study evaluates the impact of a hybrid educational intervention—including didactics and standardized patient (SP) scenarios—on internal medicine residents’ empathy and attitudes toward TIC.
Methods
Second-year internal medicine residents at a single academic institution participated in a structured TIC curriculum consisting of educational sessions followed by 3 Observed Structured Clinical Examinations (OSCEs) using SPs portraying trauma-related scenarios. Faculty provided formative feedback using structured checklists. Residents completed the Jefferson Scale of Empathy (JSE) and the Attitudes Related to Trauma-Informed Care (ARTIC) Scale at baseline, 3 months, and 6 months posttraining.
Results
Among 50 participating residents, survey response rates were 98%, 56%, and 58% at the 3 timepoints, respectively. Baseline scores were relatively high on both the JSE and ARTIC, with trends toward increased empathy and trauma-informed attitudes over time. While changes were not statistically significant, no decline was observed, suggesting a positive trajectory since other studies document a decline in empathy over residency training.
Conclusion
This study demonstrates the feasibility and potential benefit of integrating TIC training into residency education. Even among a cohort with high baseline empathy, participation in structured TIC education and OSCEs may support the maintenance and growth of trauma-informed communication skills. These findings support the inclusion of TIC as a formal component of graduate medical education and warrant further study in larger, longitudinal cohorts.
Keywords
Introduction
Trauma is nearly universal. Patients who have experienced violence or personal trauma, extending to structural and historical forms of trauma (ie, racism, discrimination, poverty, etc), often present with a wide range of physical, psychological, and behavioral manifestations. The prevalence of trauma in the United States, whether physical, sexual, emotional, or more subtle in nature, is both staggering and deeply consequential for the practice of medicine.1–4 National data suggest that approximately 61% of men and 51% of women report experiencing at least 1 traumatic event in their lifetime, and about 13 million Americans were living with posttraumatic stress disorder (PTSD) in 2020.5–8 Yet trauma extends beyond diagnosable PTSD, encompassing a range of experiences that can shape how individuals perceive and interact with the healthcare system. Trauma-informed care (TIC) operates on the premise that any patient may have experienced trauma and emphasizes the need to create a clinical environment that fosters safety, empowerment, and trust—especially in the inherently invasive context of medical care.
In this study, trauma is defined broadly to include any form of traumatic exposure, including adverse childhood experiences and other life-course stressors, and is not limited to formal psychiatric diagnoses such as acute stress disorder or PTSD, although these conditions may be encompassed. These effects are particularly pronounced when survivors lack adequate support during the grieving process or face limited access to social support systems. 9 When trauma remains unresolved or inadequately addressed, it is frequently associated with adverse health outcomes, including increased morbidity and mortality across multiple conditions, as well as reduced engagement with healthcare systems. While medical education has long emphasized the development of empathy in medical students, 10 even experienced physicians can find it challenging to care for patients with complex trauma histories. For resident physicians, these challenges are compounded by limited clinical experience and a lack of formal training in recognizing and responding to trauma. Residents may struggle to identify deeply rooted trauma, initiate sensitive conversations such as those involving intimate partner violence or the risks of firearm access, and connect patients to appropriate support resources.
In 2014, U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) developed a Trauma Informed Care (TIC) framework to help clinicians and health systems address these unmet needs through 6 principles: (1) safety; (2) trustworthiness and transparency; (3) peer support; (4) collaboration and mutuality; (5) empowerment, voice, and choice; and (6) acknowledgment of cultural, historical, and gender issues. 11 Informed by the Association of American Medical Colleges competency-based medical education, work has started in undergraduate medical education with the National Collaborative on Trauma-Informed Health Care Education and Research (TIHCER) forming a task force which developed of a validated set of TIC competencies.12–14 Traditional learning models such as didactics may not be sufficient. 15 Role-modeling from senior physicians, while it can be incredibly valuable, may be inconsistent and is difficult to assess in real time given the practical limitations of rotations and time for direct observation. Thus, incorporating hybrid educational models including didactics allowed by experiential learning and application of theoretical concepts to practice may be a more useful approach.
This underscores the urgent need to incorporate TIC education into residency training. TIC is an approach that requires healthcare professionals and systems to understand the full context of a patient's life, including past and present trauma, to deliver care that promotes healing and trust, placing a central emphasis on safety and the need to recognize and actively address the inherent power imbalance between clinicians and patients. It acknowledges that conventional models of care, while well-intentioned, may unintentionally retraumatize individuals by evoking feelings of disempowerment, distress, or silence—particularly among those with a history of trauma. These dynamics can lead to disengagement from both care and work, ultimately contributing to poorer outcomes for patients and increased strain on physicians and providers. Core elements of TIC include patient-centered communication, creating spaces where individuals can express their preferences and connect with others who share similar experiences, and critically re-evaluating institutional policies and clinical practices to reduce the risk of retraumatization.
Evidence has shown that integrating TIC into clinical care leads to improved health outcomes and stronger patient–physician relationships.16,17 Following the model of trauma-informed competencies for undergraduate medical education set out by Berman et al and to address this educational gap, a structured curriculum was developed for second-year internal medicine residents, combining didactic instruction with simulation-based training. 12 The curriculum includes 3 Observed Structured Clinical Examinations (OSCEs), utilizing standardized patients (SPs) trained to portray scenarios involving trauma-related presentations. This pilot focused on program development, emphasizes detailed curricular content, implementation strategies, and feasibility of integrating TIC education into residency training, with exploratory assessment of learner outcomes.
Methods
At Cooper University Hospital, all second-year (PGY-2) internal medicine residents are required to participate in an educational training in TIC. This training was given to 50 postgraduate year 2 (PGY-2) internal medicine residents for 2 consecutive years, 2022 to 2023. There were 23 residents participating in year 1 and 27 participating in year 2, out of 28 each year, as some residents were on vacation during the OSCE and training. Thus, the population represented a convenience sample with inclusion criteria being all PGY-2 internal medicine residents.
This pilot intervention prioritized comprehensive description of curricular content, instructional methods, and assessment processes to facilitate replication and adaptation by other residency programs. The trauma-informed training included two 60-min educational training sessions over 2 days, led by an expert in TIC. The sessions were a mix of didactic material, small group discussion, and opportunities for reflection with guided questions on applying the material. This was followed by a case-based, in-class experiential session for group learning in how to interact with patients with sensitive issues and then by 3 SP scenarios as part of an “Advanced Communication” OSCEs, each involving sensitive patient issues that must be addressed. The sequencing of didactics followed by OSCE-based experiential learning was deliberately chosen to reinforce application of TIC principles in clinically realistic scenarios.
The residents interacted with the SP for 20 min to allow sufficient time for the residents to build rapport and have a chance to uncover the history of trauma in that patient's presentation. Faculty who were also part of the internal medicine residency program observed the residents, completed a checklist of critical components of the interaction, and then shared feedback with the resident for 7 min. The SP also had 2 min to share their perspective of the interaction. The topics of these OSCEs were as follows:
Fatigue—a patient presents to an outpatient office with vague symptoms of fatigue. They have a history of recently losing a son to gun violence. Intimate partner violence—an LGBTQ patient presents with bruising but ostensibly wants to discuss an unrelated problem. PTSD—a veteran with a history of exposure to improvised explosive device explosion presents with signs of PTSD.
Following each encounter with the SP, the residents received feedback on their communication skills from both the trained SP and a faculty advisor. The faculty advisor used a structured checklist for evaluation and also provided formative recommendations for skill development.
This observational study was approved by Rowan University's Institutional Review Board (IRB, PRO-2022-62). The reporting of this study conforms to the STROBE statement for observational cohort studies (Supplement 1). While all residents participated in the TIC training and OSCE, participation in the survey was optional. Residents were offered written informed consent if they chose to participate in the pre- and posttests to evaluate their knowledge of TIC principles. Follow-up surveys were administered at 3 and 6 months to evaluate the continued use of TIC in clinical practice. All resident surveys were anonymous with no demographic details recorded to ensure no identifying information could link the surveys to later assessments or evaluations and to allow the residents to respond freely. Anonymous survey administration prevented within-subject matching across time points, necessitating aggregate (between-group) analysis of psychometric outcomes. To encourage participation, residents received a gift certificate for each completed survey. The assessment included 2 validated instruments: the Jefferson Scale of Empathy (JSE) and the Attitudes Related to Trauma-Informed Care (ARTIC) Scale.10,18 The JSE, a 20-item tool widely used in medical education, measures empathy in patient care using a 7-point Likert scale, with responses ranging from “strongly disagree” (1) to “strongly agree” (7). The JSE has demonstrated a stable multidimensional factor structure comprising Perspective Taking, Compassionate Care, and Standing in the Patient's Shoes, with confirmatory factor analysis supporting these subscales as distinct latent constructs within the measure. Research across multiple countries and versions of the JSE affirms the multidimensional structure, reinforcing that the 3 domains reflect valid subscales rather than artifacts of item grouping. The ARTIC Scale, designed to evaluate attitudes toward TIC, is available in multiple lengths; for simplicity, the 10-item version was selected, though 35- and 45-question surveys are available. Each item begins with “I believe…” and is similarly rated on a 7-point Likert scale. A response of 1 indicates not agreeing with the statement, while 7 indicates strongly agreeing. All surveys were administered via the Qualtrics platform through Rowan University for streamlined data collection.
Results
As expected for a pilot study not powered for definitive outcome comparisons and results are assessed in aggregate, results are presented to illustrate feasibility, response patterns, and preliminary trends rather than to establish causal effects.
Attitudes Related to Trauma-Informed Care (ARTIC) Scale
The study assessed TIC understanding and empathy levels of internal medicine residents using the ARTIC and JSE over 3 timepoints: before the training (T1), 3 months after the training (T2), and 6 months posttraining (T3).
Fifty students participated in the training and we received 49 responses at 1-month posttraining for the ARTIC Scale. Follow-up surveys were administered to the same cohort at 3 and 6 months; however, responses were collected anonymously and could not be linked longitudinally. At 3 months, 28 responses were received (56% response rate), and at 6 months, 29 responses were received (58% response rate).
Mean ARTIC scores were relatively high at 1 month (mean = 5.18) and demonstrated a modest increase at subsequent timepoints (range: 5.35-5.64). Although scores trended upward over time, the difference did not reach statistical significance. A Kruskal–Wallis 1-way analysis of variance by ranks was conducted to assess differences across the 3 independent samples and was not statistically significant (P = .170), indicating no statistically detectable change in TIC understanding across timepoints. The associated effect size (epsilon-squared) was small (ε2 = 0.034), indicating minimal variance in ARTIC scores attributable to time (Figure 1).

Jefferson empathy scale trend over time.
Jefferson Scale of Empathy (JSE)
Fifty students participated in the training and completed the baseline JSE, yielding a 100% response rate at time 1 (n = 50 of 50). Follow-up surveys were administered to the same cohort at 3 and 6 months; however, responses were collected anonymously and could not be linked longitudinally. At 3 months, 28 responses were received (56% response rate), and at 6 months, 20 responses were received (40% response rate) (Figure 2).
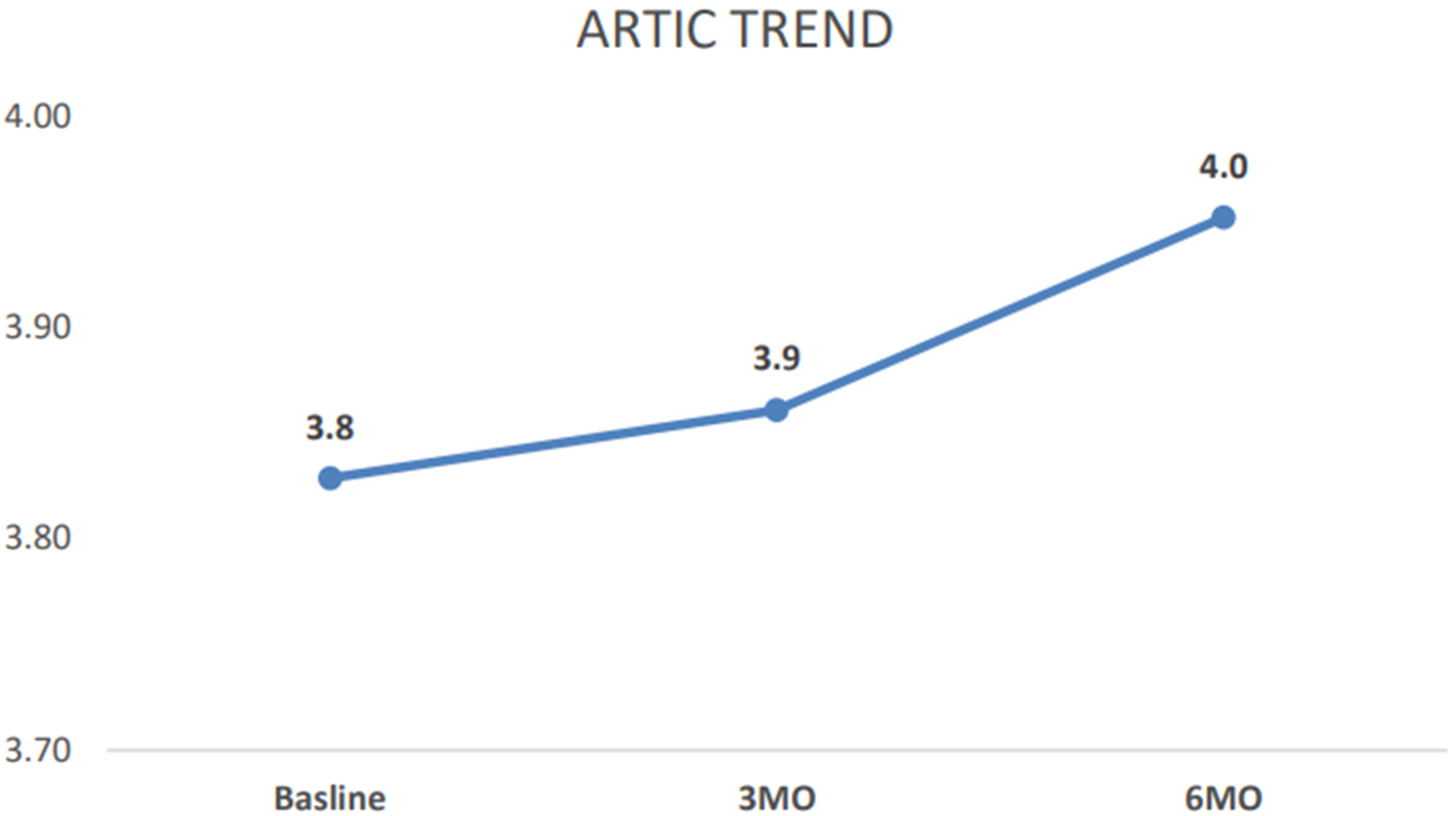
ARTIC scale trend over time. Abbreviation: ARTIC, Attitudes Related to Trauma-Informed Care.
Although some individual JSE items demonstrated variation across timepoints, there was no statistically significant difference in overall JSE scores. A Kruskal–Wallis 1-way analysis of variance by ranks was conducted to assess differences across the 3 independent samples and was not statistically significant (H = 3.253, P = .14297). The associated effect size (epsilon-squared) was small (ε2 = 0.030), indicating minimal variance in empathy scores attributable to time.
Discussion
Educating resident physicians in TIC is essential to developing empathic, effective clinicians who can skillfully navigate sensitive interactions and recognize when trauma may be influencing patient behavior or engagement. Our study suggests that many residents began the training with a solid foundation in empathy and awareness of TIC principles. The pilot curriculum was intentionally designed to include to provide a foundation in TIC, successively reinforced through case-based scenarios and through interactions with SPs in OSCEs. Importantly, the primary contribution of this pilot study lies not in demonstrating statistically significant changes in empathy or trauma-informed attitudes, but in providing a detailed, implementation-ready description of a TIC curriculum that can be embedded within residency training. By outlining the educational content, SP scenarios, and feedback mechanisms, this study offers a practical framework for programs seeking to operationalize TIC competencies. It also provides preliminary evidence suggesting feasibility and potential value.
The absence of statistically significant change does not negate the relevance of the observed trends. The consistency of directional improvement across multiple measures in aggregate, despite high baseline scores and a limited sample size, suggests that the curriculum may help sustain and modestly enhance TIC-related competencies over time. With more appropriate longitudinal analytic approaches assessing within-individual differences, such as linear mixed-effects models that account for repeated measures and individual variability, and with reporting of effect sizes, future analyses may better characterize the magnitude and educational relevance of these changes. In this context, the current study provides early signals that structured TIC education is feasible within residency training and may hold promise for reinforcing empathic and trauma-informed practices, particularly when delivered longitudinally.
Several factors may have influenced these results. The host institution serves a predominantly low-income, socioeconomically disadvantaged population, and residents are frequently exposed to patients facing structural inequities and psychosocial adversity. This environment, combined with a residency curriculum that already emphasizes social justice and humanistic care, may have fostered higher initial empathy levels. Additionally, the affiliated medical school's focus on compassion, empathy, and trauma-informed principles likely contributed to shaping learners’ foundational values. These institutional strengths, while beneficial, may have limited the observable impact of a single intervention. To support the effectiveness and sustainability of the intervention, we also engaged program leadership in faculty development to ensure informed, consistent feedback to residents during SP encounters. Faculty in the internal medicine residency participated in the same 2 educational sessions. One of the authors (EC) shared articles on TIC and hosted a separate educational session as part of program leadership meetings. Faculty were also invited to provide feedback on the OSCE scenarios and on the evaluation checklists that would be used during the sessions. Integrating faculty in this way helps create a learning environment where TIC is reinforced through both formal instruction and real-time mentorship.
Our findings build upon existing literature, highlighting gaps in TIC preparedness among trainees.19–21 A 2017 study found that 83% of internal medicine residents underestimated the prevalence of trauma, and nearly one-third felt unprepared to respond to trauma disclosures. 22 Additionally, a national survey conducted through the Council of Academic Family Medicine Educational Research Alliance (CERA) found that only 27% of family medicine residency programs had TIC integrated into their curriculum, and even then, content was limited to fewer than 5 h. 23 More recent work from the National Collaborative on TIHCER task force developed a validated TIC competency set containing 43 competencies across the 8-physician competency reference set domains (Knowledge for practice, Patient care, Practice-based learning and improvement, Interpersonal and communication skills, Professionalism, Systems-based practice, Interprofessional collaboration, and Personal and professional development). 12 Pilot studies with workshops, electronic modules, and didactics serve as examples.24–27 Case-based role plays, patient interviews, and small-group discussions compliment these pedagogical structures. 28 Our study adds to this field by piloting a longitudinal educational intervention that combines didactics, SP-based OSCEs, and faculty engagement to strengthen TIC practices and empathetic communication among internal medicine residents.17,29,30
Several limitations should be acknowledged. First, this study was conducted at a single academic institution with a relatively small sample size, limiting statistical power and the ability to detect modest changes in empathy and trauma-informed attitudes. Second, although initial survey response rates were high, there was notable attrition at the 3- and 6-month follow-up time points, which may introduce response bias and limit the interpretation of longitudinal trends. Third, the study population represents a convenience sample of internal medicine residents within 1 residency program, which may limit generalizability to other institutions, specialties, or training environments with differing curricular emphases or patient populations. Additionally, baseline empathy and TIC scores were relatively high, raising the possibility of a ceiling effect that may have constrained measurable improvement. Fifth, to assuage resident concerns that the psychometrics would be used for personal evaluation purposes, all psychometrics were deidentified. While this may have allowed the residents to respond more freely, it did not permit linked assessment of the psychometrics over time, limiting direct conclusions of within-individual changes. Finally, outcomes were assessed using self-reported instruments rather than direct measures of clinical behavior or patient outcomes, which may not fully capture the real-world impact of the intervention. While validated surveys such as the JSE and ARTIC measures are widely used in medical education research, self-reported data primarily capture learner perceptions, awareness, and intent rather than observable clinical behaviors. As such, the current findings should be interpreted as indicators of educational impact, specifically increased reflection and engagement with trauma-informed principles, rather than evidence of improved communication or changes in patient–provider interactions. However, these limitations are consistent with the exploratory nature of a pilot study focused on curriculum development and feasibility rather than hypothesis testing.
Despite these limitations, our results suggest that TIC-focused education may support retention and growth of empathy over time among a cohort of residents. Future studies should examine the impact of repeated, longitudinal TIC interventions across larger cohorts and within individuals, and explore how such training influences not only resident knowledge and attitudes, but also patient outcomes and clinical behaviors.
Conclusion
As a pilot focused on curriculum development and implementation, this study provides a detailed, reproducible model for integrating TIC education into graduate medical education and supports further evaluation in larger, multi-institutional cohorts. Although statistically significant changes were not observed, the findings suggest that scaffolded TIC education may enhance resident awareness, reflection, and engagement with TIC principles. Given that outcomes were based on participant-reported measures, these results should be interpreted as indicators of educational impact rather than evidence of changes in clinical behavior or patient–provider relationships. Future studies incorporating objective behavioral assessments, patient-reported outcomes, within-resident outcomes, or multisite designs will be needed to evaluate whether increased awareness translates into sustained changes in clinical practice. As residency programs increasingly grapple with burnout, moral distress, and the demands of complex patient care, TIC offers a framework that benefits both patients and clinicians. Our findings set a foundation for future scholarship and curricular development, with the potential to meaningfully shape the next generation of trauma-informed physicians.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261437244 - Supplemental material for Educating for Empathy: A Simulation-Based Approach to Trauma-Informed Care in Residency Training
Supplemental material, sj-docx-1-mde-10.1177_23821205261437244 for Educating for Empathy: A Simulation-Based Approach to Trauma-Informed Care in Residency Training by Elizabeth Cerceo, Amir Davoodi, Krystal Hunter, Rachel Nash and Jeanna Mastrocinque in Journal of Medical Education and Curricular Development
Footnotes
Ethical Considerations
The study was approved by Rowan University's Institutional Review Board (IRB, PRO-2022-62).
Consent to Participate
Residents completed written informed consent if they chose to participate in the survey.
Authors Contributions
EC—conceptualization, writing—original draft, writing—review and editing, revisions, investigation, methodology, funding acquisition, and supervision; AD—writing—original draft; KH—data analysis and visualization; RN—project administration; JM—conceptualization, investigation, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported with funding from the Camden Health Research Initiative.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.