
Abstract
Background
Weight stigma in healthcare settings is implicated in lower quality of care for higher-weight patients. Physicians’ implicit and explicit antifat bias can undermine rapport, reduce health education, and discourage preventive care, eroding patient trust and fueling healthcare avoidance. Because medical education shapes trainees’ attitudes through both formal curricula and hidden cultural norms, it represents a critical leverage point for stigma reduction. Yet most interventions are stand-alone workshops that remain separate from core content and have limited reach.
Methods
We conducted a grounded theory analysis of the preclerkship nutrition curriculum at a large US medical school to examine how weight stigma is embedded in core teaching. Fifteen pre-recorded lectures (10.2 h) delivered by 13 faculty members were independently reviewed by a multidisciplinary team of medical students and a faculty expert in weight stigma. Reviewers documented potential instances of stigma in structured memos. Through iterative coding and team consensus, we developed conceptual categories and integrated these into broader themes.
Results
Reviewers generated 123 memos capturing stigmatizing language, attitudes, and framing. Five themes emerged: (1) stigmatizing terminology and imagery; (2) assumptions about the controllability of weight; (3) judgments about the behavior and health of higher-weight patients; (4) overemphasis on weight as a marker of health; and (5) statements that reinforce socially constructed body ideals and moralize food and eating. We propose a literature-informed framework for educators: adopt neutral, precise language; challenge weight-based stereotypes; highlight multifactorial determinants of health; avoid reinforcing body ideals or moralizing food; and use content warnings for sensitive topics.
Conclusions
Early exposure to weight-normative messages in foundational curricula can perpetuate antifat bias in clinical practice. Integrating stigma-reduction strategies into core teaching offers a promising approach to dismantle structural weight stigma and promote equitable, person-centered care, and warrants evaluation.
Introduction
Weight stigma describes the negative attitudes and beliefs directed toward individuals with higher weights (ie, antifat bias), leading to inequitable treatment. Those who experience weight stigma, independent of body mass index (BMI), are at increased risk of depression, anxiety, social isolation, substance use, suicidal ideation, negative body image, binge eating, and exercise avoidance.1,2 In healthcare settings, weight stigma is implicated in lower quality of care for higher-weight patients. Physicians are known to have both implicit and explicit antifat bias, which can affect patient interactions. 1 For example, physicians have been shown to build less rapport with and provide less health education to higher-weight patients. 1 Additionally, higher-weight patients may receive fewer cancer screenings, further undermining care. 1 These experiences can erode patient-provider trust, contribute to nonadherence and healthcare avoidance, 3 and hinder effective treatment.1,4 Weight stigma in healthcare can also manifest in the physical environment (eg, design, seating, and equipment), clinical algorithms, and diagnostic criteria (eg, anorexia nervosa). 5
Medical education plays a formative role in shaping trainees’ beliefs about weight, through both formal curricula and the hidden curriculum of cultural norms and role modeling in classroom and clinical settings.6,7 Formal curricula remains largely weight-centric, emphasizing the diagnosis of “obesity” by BMI and training clinicians to counsel patients on weight loss, with little explicit attention to weight stigma or bias and their impact on patient care. 8 Weight stigma may also be perpetuated by educators themselves; nearly 40% of medical students report hearing derogatory remarks about higher-weight patients from their instructors. 9 Although many medical trainees enter medical school with implicit and explicit biases toward higher-weight individuals, they may be more receptive to new information than more established clinicians,1,10 making medical education a critical leverage point for reducing weight stigma.
Most weight stigma interventions in medical education have utilized adjunctive workshops and activities for trainees. 11 Although these efforts show promise in raising awareness and reducing self-reported stigma, 10 they are time-intensive and disconnected from core content, which ultimately limits their reach and sustainability. 12 Comprehensive stigma reduction efforts should go beyond supplementary programming 13 and address the stigma within the core curriculum, especially in foundational topics like nutrition. 5
Methods
This qualitative study used a grounded theory approach to inductively explore how weight stigma appears in preclerkship medical education. Grounded theory is a qualitative research method in which theory is generated inductively from systematic engagement with data.14,15 Analysis involves iterative coding, constant comparison, and team discussion to develop conceptual themes, which are then linked to existing literature.14,15
The analysis involved a detailed curricular review of the nutrition and metabolism curriculum at a large US medical school. Nutrition was selected given the frequent coverage of relevant topics (eg, weight, body size, and diet).14,15 Fifteen lectures totaling 10.2 h delivered by 13 medical school faculty were available as recorded videos. The lectures included topics such as Obesity and Satiety, Macronutrients, Nutrition and Population Health, Healthy Nutrition Counseling, Medical Weight Management, Bariatric Surgery, and a patient panel.
Included materials consisted of all pre-recorded lectures focused on nutrition and metabolism that were offered as part of the preclerkship medical curriculum during January to February 2022, as well as a virtual patient panel recorded during the same curricular block. Excluded materials included lectures outside this curricular block, live sessions without recorded content, and curricular content not focused on nutrition or metabolism. Because this study reviewed the entirety of the available nutrition curriculum relevant to the research question, rather than sampling from a larger pool, a traditional sample size calculation or power analysis was not applicable. This comprehensive review enhanced qualitative rigor by encompassing the full scope of relevant instructional materials.
Analysis
The analytic process followed 4 grounded theory phases:14,15
Conceptual development (memo review) Category development (clustering and refining codes) Theoretical integration (organizing into conceptual themes) Contextualization (linking themes to existing literature)
To identify key concepts and patterns related to weight stigma, a review team consisting of 4 medical students with prior knowledge of weight stigma and one faculty member from the Department of Nutritional Sciences with expertise in weight stigma reviewed all 15 lectures. Stigma was defined as language, attitudes, or content that stereotyped, judged, or discriminated against individuals based on body size. Each lecture was independently reviewed by the faculty member and at least one medical student. Reviewers created analytic memos documenting potential instances of weight stigma. Each memo included a summary of the instance, a timestamp or slide number, and a reviewer-generated descriptive label to facilitate comparison across lectures and support conceptual development.
Three medical students independently reviewed each memo and developed preliminary categories characterizing the observed stigma. The full review team then adjudicated and refined the preliminary categories using an iterative process that involved reviewing content flags, identifying broad concepts, reviewing clarifying examples, revising/refining concepts, and aggregating the concepts into higher-order categories. Detailed category descriptions with specific examples observed within the curriculum were developed to integrate the emerging conceptual insights into coherent themes. To contextualize these findings, a literature review was performed to identify recommendations and guidelines aligned with observed themes, which then informed the development of possible strategies for reducing weight stigma.
Initial content review and conceptual development, including memo review, were conducted between July and August 2022. Subsequent analytic phases, including category development, theoretical integration, and contextualization, were conducted from September 2022 through April 2023.
This study did not involve human subjects. It analyzed recorded curricular content and did not link findings to individual faculty members. Permission to review the nutrition lectures was obtained from co-author Dr Cherry-Bukowiec, the nutrition sequence lead. Access to the video lectures was provided to student and faculty reviewers for the sole purpose of identifying weight-related content and developing recommendations to reduce weight stigma in medical education. No identifying information about individual faculty members was retained during coding or analysis, ensuring confidentiality. As the study did not involve human participants or identifiable private information, informed consent was not applicable and institutional review board approval was not required.
Results: Identified Themes of Weight Stigma
The lecture review process generated 123 memos that captured weight stigma in various forms, including overt weight stigma, messaging that may perpetuate stigma, imprecise, or oversimplified discussions of weight, and other concerns regarding the presentation of weight-related content. Through iterative review, 5 major themes emerged (Table 1):
Stigmatizing terminology and imagery; Assumptions regarding the controllability of weight; Judgments about the behavior and health status of higher-weight patients; Overemphasis on the role of weight in overall health; and Statements that uphold socially constructed body ideals and moralize food/eating.
Themes of Weight Stigma Identified in Curricular Content.
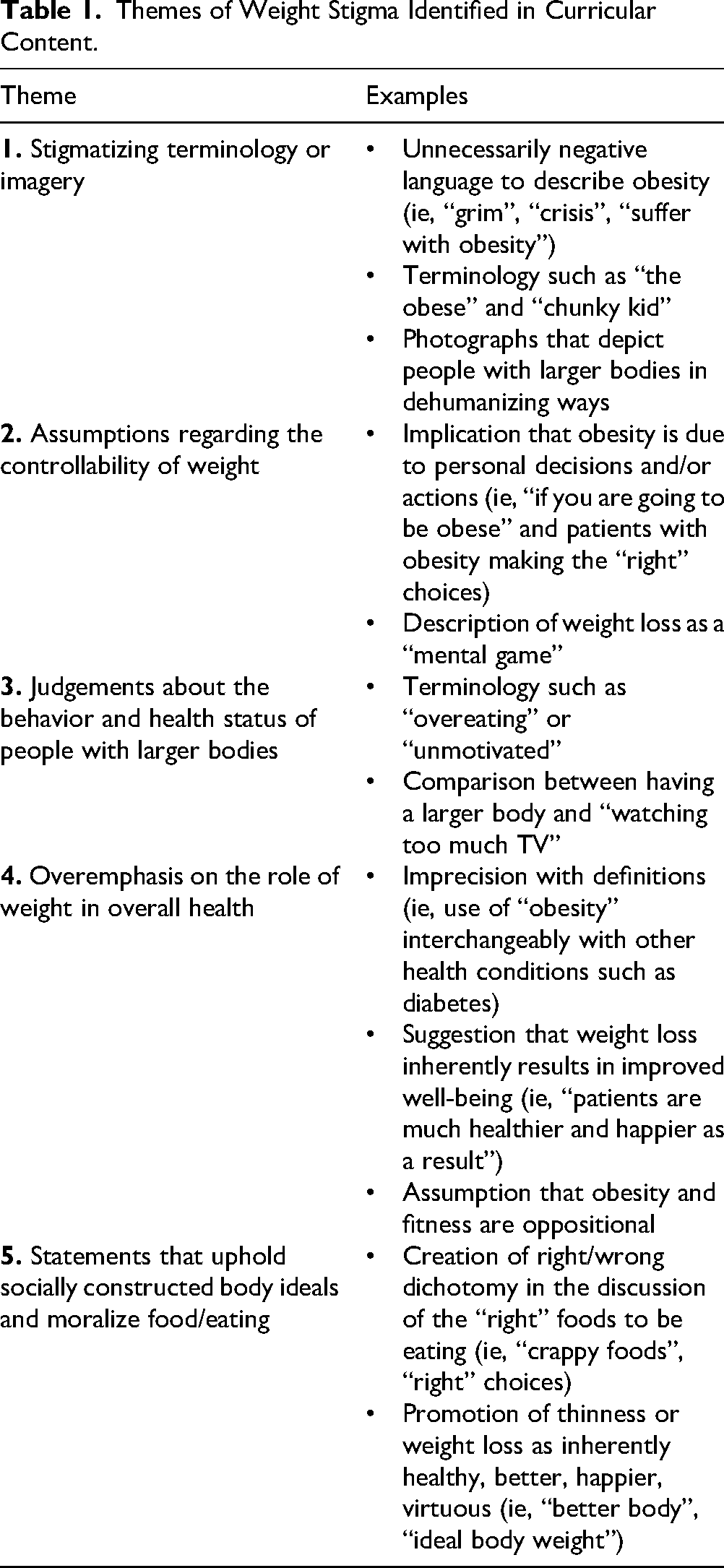
Collectively, these themes reflect weight-normative perspectives, which prioritize weight as a primary indicator of health and assume individual responsibility for weight, overlooking social, economic, and genetic contributors.8,16
Results: Framework for Change
To inform the development of a framework for reducing weight stigma in medical education, we conducted a targeted review of existing recommendations addressing weight stigma in medical training,6,11,17–19 as well as literature and guidelines related to weight-related terminology and imagery,13,20–23 and the science of weight regulation and weight controllability.24–27 This literature was explicitly linked to the conceptual themes generated through the grounded theory analysis to ensure that the resulting framework was both evidence-informed and practically relevant.
Informed by the theme related to socially constructed body ideals and the moralization of food and eating, we also considered the potential impact of stigmatizing curricular content on medical students themselves. Prior research indicates that exposure to weight stigma may contribute to poorer wellbeing among medical students with higher body weights, 28 and may be particularly salient for students carrying varying degrees of traumatic stress related to prior weight-based experiences. 29
Based on this synthesis, we developed a preliminary framework to provide practical guidance for educators to foster a more inclusive and evidence-aligned learning environment for medical trainees. The framework includes 5 strategies (Table 2):
Strategies for Reducing Weight Stigma in Medical Education Curricula.

Discussion
The early exposure to weight stigma in medical education, as identified in this grounded theory analysis, presents a critical opportunity to reduce stigma and promote more inclusive practices. We identified 5 patterns of weight stigma that reinforce weight-normative perspectives. These findings closely parallel those of Olson et al, who described how medical education can introduce and perpetuate weight stigma. 6 Their work highlighted how teaching that frames body weight primarily as a biomedical characteristic reinforces a weight-normative view of health, a theme reflected in our findings on assumptions about the controllability of weight and on judgments about the behavior and health status of higher-weight patients. 6 Our analysis extends this perspective by showing how curricular statements that uphold socially constructed body ideals and moralize food and eating can deepen stigma. Similar to our study, the Olson et al noted that stigmatizing language is often modeled in case discussions of higher-weight patients and in teaching about weight-associated conditions, and that weight is inappropriately centered in treatment planning. 6 They also emphasized that individuals at higher weights are rarely recognized as a marginalized group.
Together, these studies underscore the need to shift toward a weight-inclusive approach, which defines health as more than body size, actively challenges weight stigma, and promotes person-centered care. Such an approach encourages learners to engage patients with respectful curiosity and nonjudgmental inquiry into each person's lived experience of body size and health. These efforts can help address structural stigma and foster stigma resistance among students.31,32 Importantly, meaningful change must extend beyond curricular content (eg, lectures and educational materials) to include medical educators themselves,7,33 and should not be confined to isolated programs that operate within an otherwise weight-normative institutional context. 13 Programs that support educators in recognizing and addressing bias have the potential to improve teaching practices and shift broader institutional norms. 1
The strengths of this study include a robust review of all lectures from an entire section of a curriculum, covering a breadth of topics related to nutrition and various lecturers. Additionally, multiple reviewers reviewed each lecture to help decrease personal bias. However, the analysis is limited by the scope of the reviewed curriculum. Including lectures from other medical schools and/or curricular areas (eg, cardiology and pediatrics) could have revealed different patterns of weight stigma.
Conclusion
Early exposure to weight stigma in medical education has lasting implications for patient care. This study highlights how weight stigma is embedded in a foundational curriculum and offers a practical, literature-informed framework for change. Through inclusive curricula and educator support, medical education can play a central role in dismantling weight stigma and promoting more equitable care. Future areas of study include examining the usability of these recommendations, their effectiveness in mediating curricular change, and their impact on medical student attitudes and behaviors. Ongoing evaluation, adaptation, and refinement of the proposed strategies will be essential to account for the evolving nature of medical education and shifting language practices.
Footnotes
Acknowledgments
The authors would like to thank Karri Grob, Ed.D. for her mentorship and guidance at the outset of this research and Paula Thompson, PhD for her insightful comments and editing.
Ethics
This study did not involve Human Subjects and thus Institutional Review was not required.
Consent
This study did not involve Human Subjects and thus did not involve obtaining informed consent.
Author's Contribution
AH was involved in conceptualization, methodology, formal analysis, writing—original draft, and project administration; RF in conceptualization, methodology, formal analysis, and writing—original draft; KE in formal analysis, writing—original draft, and writing—reviewing & editing; CM in formal analysis, writing—original draft, and writing—reviewing & editing; JRC-B in resources, writing—reviewing & editing, and supervision; and KRS in conceptualization, methodology, formal analysis, writing—original draft, and supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Reni Forer was supported by the Fogarty International Center of the National Institutes of Health under grant #D43TW009345 awarded to the Northern Pacific Global Health Fellows Program.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.