
Abstract
Objective
To examine medical students’ perceptions of the nutrition education received and their ability to apply that knowledge in clinical settings.
Methods
This is a qualitative study using a structured survey with free responses to solicit the perspective of US medical students regarding their nutrition education. A national online survey was distributed by the American Academy of Pediatrics, Section on Pediatric Trainees. An expert committee in nutrition education evaluated and conducted a thematic analysis of the survey responses.
Results
Twenty-four surveys were completed (10 medical students and 14 pediatric interns). The survey revealed students were not satisfied with the nutrition education they received in several areas including nutritional recommendations for obesity and prediabetes/diabetes; nutritional needs during pregnancy, childhood, and adolescent age-related dietary recommendations; cultural influences on diet and eating habits; and food insecurity. Students also reported a lack of confidence in providing healthful nutrition counseling to adolescent patients and delivering culturally appropriate nutrition advice.
Conclusions
Survey responses revealed the need for improvements in several areas of nutrition curricula related to health and chronic disease management and suggest broader social determinants of health such as cultural influences on nutrition practices and food insecurity. The results of this survey provide unique insight into the medical student perspective on nutrition education and can inform the development of future medical school nutrition curriculums.
Introduction
Obesity is a serious public health issue in the United States 1 The prevalence of obesity, defined by body mass index (BMI) in children ages 2 to 19 years in the United States was 18.5%, or 13.7 million children, 2 and approximately 42.4% among American adults in 2017 to 2018. 3 The literature reports unhealthy diets are a risk factor for developing chronic diseases such as obesity, hypertension, and dyslipidemia. 4 This risk is present throughout the lifespan and can impact subsequent generations. 4
Several interventions aim to address obesity including community-based, school-based, work-based, family-based, and hospital-based interventions.1,5–7 Furthermore, food pharmacies have emerged to increase public access to healthy foods, offer coupons to alleviate financial barriers, and offer nutrition and culinary education. 8 Upstream approaches are also important to address this public health issue, such as increasing the nutrition education of future physicians preventing obesity, and managing obese patients.9–11
To address obesity as a serious public health issue and to inform the development of interventions addressing obesity, we need to look at the training of healthcare providers. Several studies highlight the need for improved nutrition education for healthcare providers. A national survey created by the Nutrition in Medicine Project at the University of North Carolina at Chapel Hill found only 9 medical schools consistently met the recommended 25 h of nutrition instruction. 11 Medical residents also demonstrate weaknesses in providing nutrition counseling to patients. 12 At a university-based internal medicine training program, 77% of the respondents agreed nutrition assessments were important during routine primary care visits, but only 14% felt adequately trained to provide nutrition counseling. 12 Among practicing providers, similar sentiments are felt. According to a scoping literature review, primary care doctors and nurses were more likely to provide nutrition counseling only when BMI was increasing, and the quality of that advice may be poor. 13
What is missing from prior studies examining nutrition education is the perspective of the learners themselves. Systematic reviews detail shortcomings in medical education including “poor integration of nutrition in the curricula,” “absence of priority for nutrition education,” “poor application of nutrition science to clinical practice,” and “poor collaboration with nutrition professionals.” 14 Our present qualitative study focuses on the medical student's perspective of the nutrition education they receive, especially surrounding pediatric care, and their ability to apply that knowledge in clinical settings. The overarching goal of this report is to enable medical educators to inform, shape, and improve nutrition curricula.
Methods
We conducted a qualitative study using a structured survey with free responses about nutrition education and delivered it electronically to US medical students. The target population/ inclusion group included fourth-year medical students and first-year pediatric residents who are members of the Section of Pediatric Trainees (SOPT) in the American Academy of Pediatrics. These groups were chosen as they can comment on the nutrition education received in the preclinical years of medical school and on their clinical clerkship experiences applying that knowledge and counseling to patient interactions. Responses from other groups of medical students such as first-, second-, or third-year students were excluded.
Survey creation and distribution
We created survey questions de novo (as no prior survey existed) using published nutrition survey data obtained from faculty instructors across US medical schools.11,15 The survey was piloted with 5 fourth-year medical students (11.5% of the total survey population) to assess the quality and clarity of questions. The Charles R. Drew University of Medicine and Science (CDU) Institutional Review Board approved the date collection as an exempt study (FWA00002736, Date of study 9/17/2019). The survey was submitted to the SOPT section manager for distribution. The SOPT is comprised of over 16,000 members who are medical students, resident physicians, and fellowship trainees. The survey was distributed via monthly “What's New” emails to SOPT members between September and November 2019 and between March and May 2020. Participation was by self-selection. Participants voluntarily opted to complete the survey by clicking on the survey link within the emails. After clicking on the survey link, participants were provided with the study background and information sheet informing them of the risks and benefits of participating and the approximate time of the survey (30 min) before being directed to another link to access the survey. Completion of the survey was considered as informed consent and this method of obtaining informed consent was approved by the CDU Institutional Review Board. The completed surveys were collected and managed using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Charles R. Drew University of Medicine and Science. 16 REDCap is a secure, web-based software platform designed to support data capture for research students, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads as to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
The survey consisted of 4 subject domains: educational history, nutrition education before medical school, nutrition education during medical school, and application of nutritional knowledge in clinical settings. Questions focused on nutritional competencies from the Society for Nutrition Education and Behavior related to obesity and its comorbidities, nutritional competencies through the life course from prenatal to adolescence, and nutritional competencies related to culture and food justice. Likert Scale questions with free responses were used and survey respondents were instructed to provide comments if not satisfied with the nutrition education received in the area being questioned. These free responses served as the basis for the qualitative study. The answers to the free responses were exported to an excel document for analysis.
Research team
An expert committee of 6 medical doctors and educators specializing in pediatrics and a nursing educator and epidemiologist (PhD) was convened to analyze the results of the survey. All members of the research team have experience with qualitative research methods.
Survey analysis
The expert committee read the open-ended responses individually, and then as a group, coded the free responses. Using an inductive content analysis approach, the expert committee identified 2 recurring categories: Medical student-identified barriers in nutrition curricula and medical student-identified needs in nutrition curricula. After the data was coded, the expert committee assigned the free responses to the 2 codes and conducted a thematic analysis across the 2 codes and survey topic areas. Two themes were identified: “barriers,” areas respondents identified as receiving limited or no education, and “needs,” based on respondents’ suggestions of how to improve their nutritional knowledge and competencies in the areas identified (Tables 3 and 4). The expert committee met as a group several times to discuss and refine the themes across each code and survey topic area until all members agreed that saturation was achieved, and the themes established accurately reflected the free responses of respondents.
Results
We received 43 total survey responses of which 39 surveys were complete and 4 surveys were incomplete. Of the 39 surveys that were complete, 24 surveys were from participants in the target population/inclusion group of Pediatric interns and fourth-year medical students and were analyzed for discussion. See the flowchart of surveys analyzed below Figure 1.
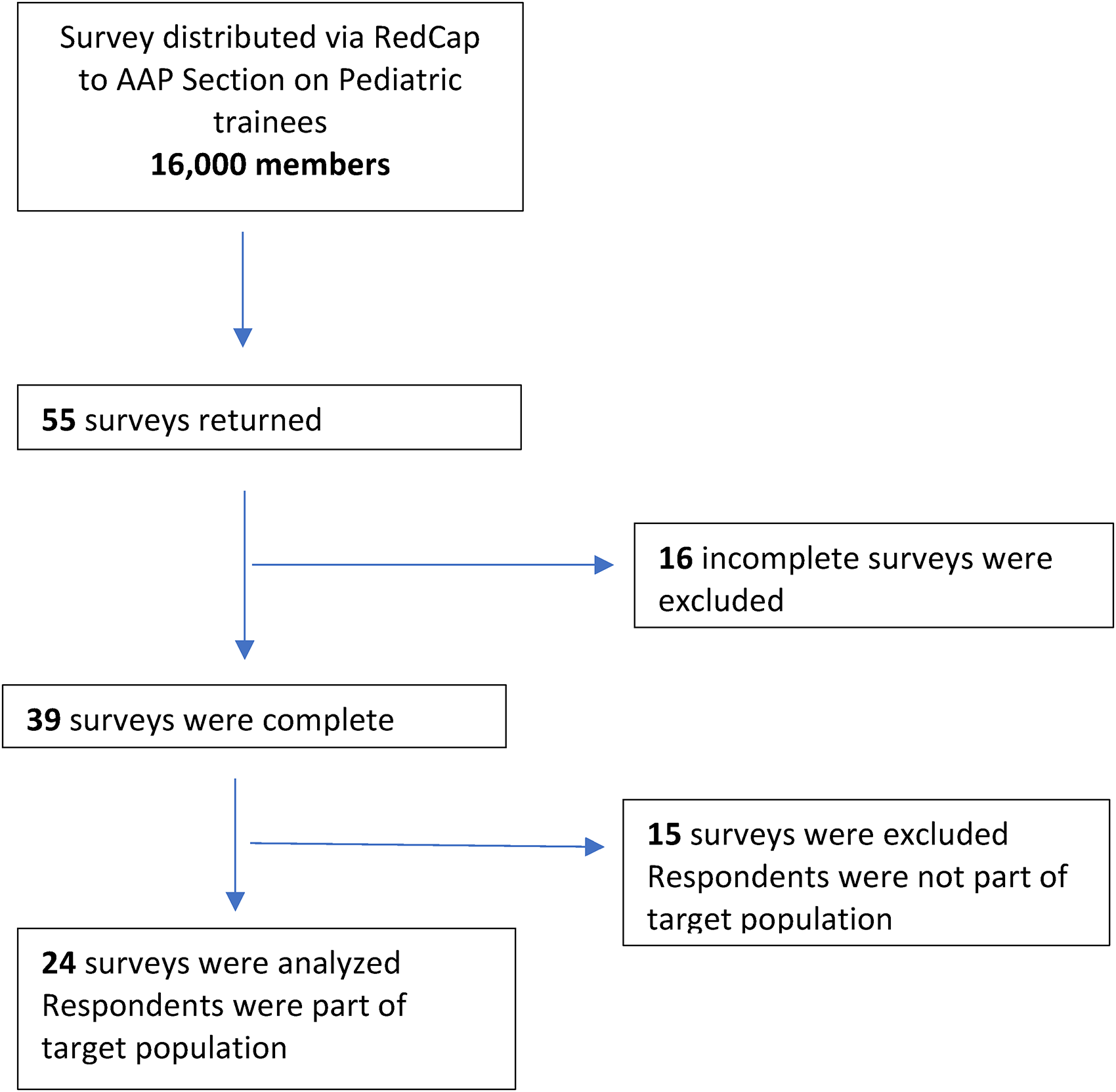
COREQ flow chart.
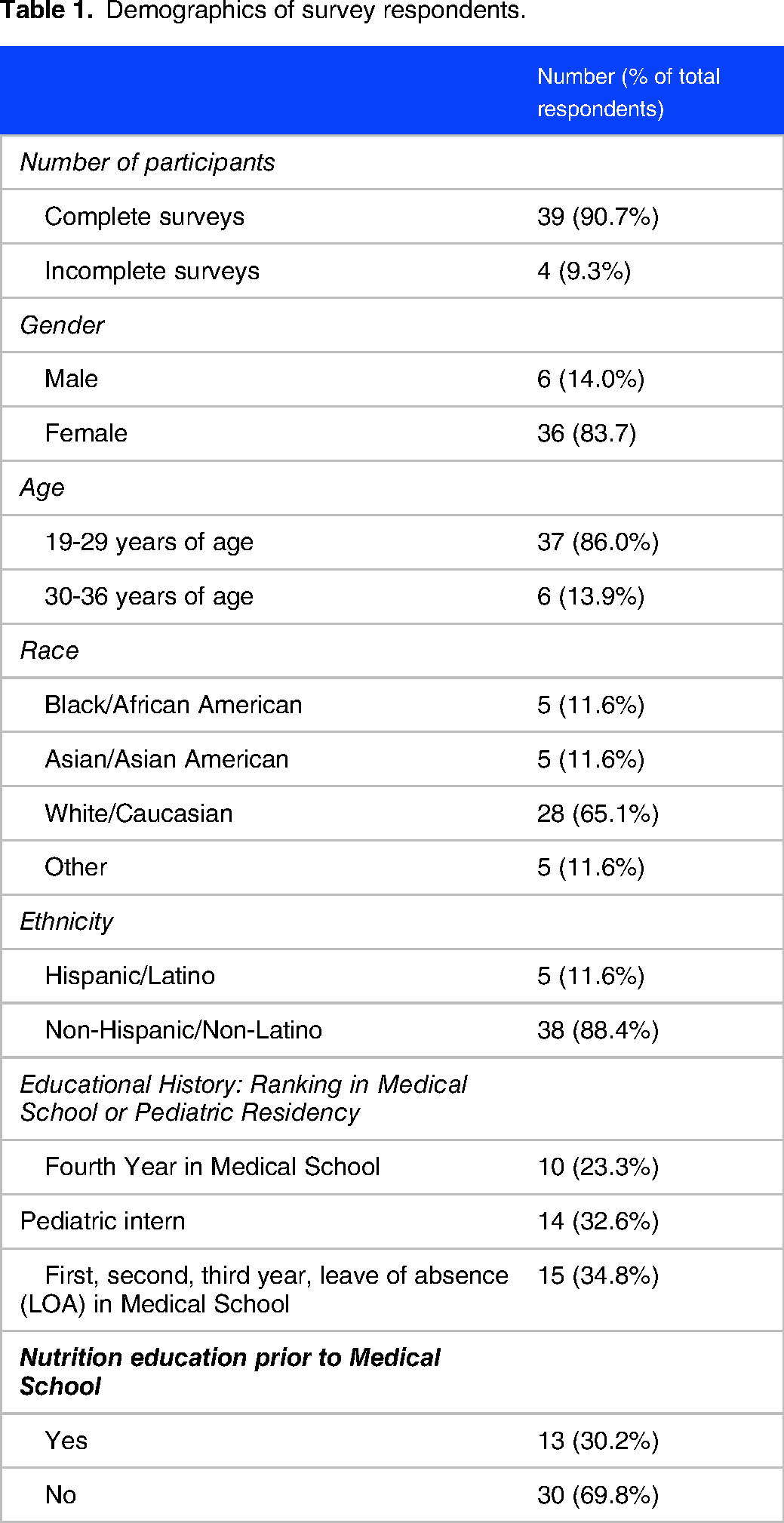
Table 1 shows the demographics of the study respondents. The majority of participants were female (84%), between 19 and 29 years of age (86%), self-identified as non-Hispanic Caucasian (65%), and had no prior nutrition education before medical school (70%). In addition, pediatric interns reflecting on their medical school nutrition curriculum made up a slightly higher percentage of participants (35%) compared to fourth-year medical students (26%).
Demographics of survey respondents.
Fourth-year medical students and pediatric interns indicated they were satisfied or very satisfied with their curricula in nutritional recommendations for hypertension and breastfeeding recommendations for infants. Table 2 highlights that most students indicated they were neutral, dissatisfied, or very dissatisfied with nutritional recommendations for obesity, prediabetes/diabetes, and dyslipidemia; nutritional needs during pregnancy; solid food recommendations during infancy; childhood and adolescent age-related dietary recommendations; childhood and adolescent age-related parenting skills related to eating habits; childhood and adolescent media practices that influence eating behavior; cultural factors that influence diet and eating habits; food insecurity; and nutrition assistance programs for vulnerable populations.
Areas of nutrition education dissatisfaction for medical students.

Students also provided feedback about why they were dissatisfied or very dissatisfied. Table 3 highlights the nutritional topics identified by students who did not receive adequate coverage in the medical school curriculum.
Medical student-identified barriers in nutrition curricula.

Students also provided nutritional information they wished they had received before starting their medical school clinical rotations. Table 4 shows the nutritional education needs identified by students.
Medical student-identified needs in nutrition curricula.

Discussion
The results of the nutrition survey highlight the areas in nutrition education that medical students and pediatric interns deemed unsatisfactory. To the best of our knowledge, this is the first survey to provide this perspective. Furthermore, students identified important topics to address and future directions for inclusion in medical education. The topics identified emphasized the role of food as medicine and preventing illness, the role of nutrition throughout the life course, and the role nutrition plays in different cultures and populations.
Food as medicine and preventing illness (primary and secondary prevention)
Emerging research indicates nutrition interventions tailored to patients and their health conditions may be associated with improved health outcomes and decreased healthcare usage and costs. 17 This aligns well with precision nutrition, which is personalized nutrition focused on the individual, their DNA, dietary patterns, metabolic response to specific foods, and microbiome. 18 Nutrition education focused on patient health conditions is lacking. Our nutrition survey revealed medical students believe they received inadequate nutrition training on obesity, dyslipidemia, and prediabetes/diabetes. They identified gaps in their counseling skills to support patients and their families in these areas. This correlates with findings from international studies, which assessed students’ confidence in providing nutrition care and showed that some students were not confident to counsel patients and were not confident that patients would improve their eating behaviors after nutrition care.14,19,20 It was also found that students rarely recognized their role in obesity prevention and treatment and reported not feeling prepared to provide weight loss interventions for overweight and obese patients with health-related issues.21,22 In addition, more education on specific dietary recommendations for chronic medical conditions was identified. This information is timely as many medical schools are redesigning their curricula. 23 Furthermore, these findings align well with the “Food is Medicine” initiative that includes therapeutic meals, food pharmacies, and produce prescription programs. 17
Nutrition through the life course
The nutritional needs of children change from infancy to adolescence. Similarly, during pregnancy, adequate nutrition is important to meet the needs of the growing fetus. Our results suggest that students perceived insufficient education on dietary recommendations during pregnancy. The results of a systematic literature review showed that women do not receive adequate nutrition counseling during pregnancy. 24 While providers recognize the importance of nutrition education, barriers include lack of time, lack of resources, and lack of relevant training. 24 The results also suggest a need for age-related dietary recommendations and healthy eating practices, ie, restrictive eating and eating in front of the screen. These areas could be supported by understanding how parents and the home environment shape dietary and eating practices. 25
Nutrition, culture, and vulnerable populations
It is well-known culture influences the types of food, preparation of food, and frequency of certain foods people eat. 26 Students in the survey called for more education on the role cultural and societal norms have on food choices and eating behaviors as well as more practical strategies to support healthful adjustments to cultural diets.
Students also identified gaps in knowledge about food insecurity and nutrition assistance programs. It is recognized that the economic resources of the family impact nutrition status. Food insecurity affected 13.9% of US households in 2018, and 7.1% of children in these households were food insecure. 27 Given the high prevalence of food insecurity, medical professionals need to feel confident about discussing available resources with families. Additionally, students voiced wanting more education on food insecurity and chronic diseases. A study conducted by the University of California showed that providing a nutrition course with an integrated hands-on teaching kitchen component to undergraduate students contributed to increased food literacy and associated reduction in food insecurity among the participants. 28 This nutrition course offered to UCLA health professional students and medical students during the 2019 to 2020 academic year used a blended approach to deliver educational nutrition content including in-class didactics, interactive hands-on cooking sessions, and a service-learning experience.23,28,29 This upstream approach to increasing food literacy benefits medical students and future patients.23,28,29
Lastly, students acknowledged the extremely problematic and common cultural issue of weight stigma. In the nutritional survey, students acknowledged the need to develop counseling skills sensitive to addressing weight in patients. There is overwhelming evidence of weight bias among medical students, physicians, and nurses. 30 More teaching in this area is critical given the physical and mental health issues obese individuals experience compounded by decreased health services utilization due to stigma experienced during health care visits. 31 Awareness of internal biases is important especially when counseling patients on sensitive topics, like weight. 32
Future directions
Four recommendations to improve nutrition education in medical school were identified from the survey results. The first is to include education on food as a form of medicine and prevention of chronic illnesses. The second is to include education on the nutritional needs of children along the life course including prenatally as nutritional needs change at each stage of development. The third is to increase students’ knowledge of specific cultural dietary practices and alternatives to address medical conditions that arise. Fourth is to increase students’ education on food justice including food insecurity and nutrition assistance programs.
Limitations
An identified limitation of this study is that the regional distribution of respondents was not part of the survey questionnaire and is unknown. This information would have been useful to determine if regional differences exist in satisfaction levels of the medical school nutrition curriculum. Lastly, most respondents were non-Hispanic Caucasian, limiting the diversity of perspectives obtained from the survey.
Conclusion
This study offers insight into medical students’ perspectives on the nutrition education received during medical school. Nutritional guidance is a core ingredient in the prevention and treatment of chronic illnesses such as obesity. As medical students learn about these illnesses, dietary and nutrition education should be integrated to improve their knowledge and counseling skills. Medical students must also be aware of the changing nutritional requirements along the life course to effectively counsel patients and families. Furthermore, knowledge of cultural dietary practices, and an understanding of the association between food insecurity and health and well-being is important. Additional studies should be conducted with a greater number of participants to determine the generalizability of the results and to gain greater insight into the needs and barriers related to medical student nutrition education and counseling.
Footnotes
Author Contributions
Shanika Boyce conceptualized the study, developed the survey, analyzed the data, prepared the first draft of the manuscript, and made revisions to the manuscript. Huan Dong assisted in developing the survey and uploading it to RedCap, analyzed the data, and revised the manuscript. Alma Guerrero and Wendelin Slusser assisted in developing the survey. Alma Guerrero, Cambria Garell, Catherine Carpenter, Christine Thang, and Wendelin Slusser all analyzed the data and revised the manuscript. All authors approved the final draft of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by a grant from the UniHealth Foundation (Grant #11-001282; Principal Investigator: Wendelin Slusser). Funding for recruitment purposes was made possible by the Semel Healthy Campus Initiative Center at UCLA. Shanika Boyce and the research reported in this article brief report were supported by NIH/NIMHD CRECD grant # G008070, NIH/NIMHD grant #U54MD007598 (formerly #U54RR026138), NIH/NCRR/NCATS grant #UL1TR000124, and NIH/NIMHD award #S21MD000103. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIMHD and NIH. The funder did not interfere with the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Ethical Approval
The Charles R. Drew University of Medicine and Science (CDU) Institutional Review Board approved the date collection as an exempt study (FWA00002736, Date of study: 9/17/2019). Completion of the survey was considered as informed consent and this method of obtaining informed consent was approved by the CDU Institutional Review Board.