
Abstract
Background
Burnout is prevalent among medical students due to the demanding, academically and emotionally intensive nature of medical education. It is a psychological condition arising from persistent work-related stress and personal factors. According to Erikson's model, social interactions, and relationships are vital for psychosocial growth. This study aimed to examine the relationship between psychosocial development and burnout among male and female medical students across different academic phases.
Methods
A cross-sectional analytical study was conducted at King Saud bin Abdulaziz University for Health Sciences in Jeddah from May to September 2022. Participants completed electronic surveys containing demographic data, the adapted student version of the Oldenburg Burnout Inventory to measure burnout, and the Psychosocial Inventory of Ego Strength - Short Form to assess psychosocial development. Pearson's correlation was used to examine the relationship between burnout and psychosocial development, and a one-way analysis of variance was used to compare differences across academic phases. A significance level of P < 0.05 with a 95% confidence interval was applied.
Results
The study included 315 students with a mean age of 20.33 years; 52.1% were in phase one. Female students (M = 43.50) reported significantly higher burnout levels than males (M = 40.58) (P < 0.001). No significant differences in burnout were found across phases. Male students scored higher in psychosocial development (M = 109.38) than females (M = 104.86) (P = 0.011). Psychosocial development was highest in phase three students (M = 110.14) compared to phase one (M = 104.91) and phase two (M = 108.97) (P = 0.036).
Conclusion
Psychosocial development is inversely related to burnout among medical students. Female students showed higher burnout, whereas male students and phase three students demonstrated higher psychosocial development. These findings highlight the importance of integrating emotional intelligence and psychosocial development training into medical curricula to support student well-being and reduce burnout risk.
Keywords
Introduction
Medical education is academically and emotionally demanding, making medical students more susceptible to psychological issues than the general population.1,2 Consequently, these students are often at increased risk for burnout. 3
In recent years, burnout among healthcare professionals has received significant research attention. 4 Studies report that 71% to 76.8% of medical students experience burnout. 3 Burnout is characterized by a loss of vitality and severe exhaustion due to insufficient resources, positive emotions, and support. 5 It is a psychological syndrome resulting from ongoing work-related stress and individual factors. The core features of burnout syndrome include emotional fatigue, depersonalization, and diminished professional satisfaction.6–8 While burnout can affect many occupations, it is especially common among those interacting extensively with the community, such as medical professionals. 9 Individual characteristics and factors like social support and workload can accelerate academic burnout.8,10,11
Although burnout is generally common among medical students, research is inconsistent on whether pre-clinical or clinical students experience it more. Some studies find that burnout is 29.7% higher among pre-clinical students, while others report higher rates in the clinical phases.3,12 Geographical differences also exist; for instance, students in the Middle East and Oceania show higher burnout rates than those on other continents. 3 A local study at Qassim University in Saudi Arabia found higher burnout in male students and higher depression in female students. 13
In Saudi Arabia, medical education is a 6-year undergraduate program that admits students after high school, typically at around 18 or 19 years old. The curriculum has three phases: the premedical year, focusing on foundational sciences and academic skills; the pre-clinical phase, emphasizing basic medical sciences through system-based and problem-based learning; and the clinical clerkship, which provides direct patient care and hands-on training in major specialties. Unlike graduate-entry programs in the United States and the United Kingdom, Saudi students begin medical training earlier. 14
In the last two decades, the number of medical schools in Saudi Arabia has grown from 5 to over 20. Curricula have shifted from traditional, discipline-based models to more innovative, problem-based, and community-focused approaches. Most students are Saudi nationals, as international enrollment is limited. Male and female students follow the same curriculum, typically on gender-segregated campuses. Public universities offer tuition-free education, thereby supporting students from varied socioeconomic backgrounds. These factors—early entry, expanding institutions, curriculum reforms, limited international diversity, and government funding—create a unique learning environment that can influence student stress and burnout. 14
Although burnout is often attributed to physical or mental stress, it may also be influenced by personality development. Erikson's theory of psychosocial development is a well-known and comprehensive framework that explains how social interactions and relationships shape human development.15,16 For example, his theory helps explain the formation of career identity. 17 According to Erikson, development involves resolving eight psychosocial stages across the lifespan.18,19 Each stage presents two opposing psychosocial tasks, one positive and one negative.15,20 Successfully managing these challenges leads to the acquisition of virtues, while failure can hinder future development and limit the acquisition of positive ego qualities. 18
The PIES-SF was developed and validated with Western populations. Its application in the Middle East may be affected by different cultural norms and gender roles. Therefore, when assessing psychosocial development among Saudi medical students, it is important to consider local cultural factors that shape ego strength.
To the best of our knowledge, no prior research has examined the relationship between psychosocial development and burnout among medical students. The study results will contribute to the literature on the local prevalence of burnout syndrome and psychosocial development, thereby aiding early detection and prevention. Therefore, the current study aims to investigate whether such a relationship exists among male and female medical students in phases 1, 2, and 3 at King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Jeddah Campus.
Methods
Study Design and Setting
An analytical cross-sectional study was conducted at KSAU-HS in Jeddah between May and September 2022. KSAU-HS is a governmental university specializing in health sciences. The study participants were recruited from the College of Medicine and the College of Science and Health Professions.
Out of 1990 invited medical students, 315 participated in the survey. All data were collected at a single time point to measure the relationship between burnout and psychosocial development for male and female students in phases 1, 2, and 3 during the 2021-2022 academic year. Each phase lasts two years: phase 1 is premedical, phase 2 is pre-clinical, and phase 3 is clinical. As medical education in Saudi Arabia is an undergraduate degree, Stream 2 students—those with prior bachelor's degrees—were excluded from the study.
Sampling Technique and Sample Size
This study employed quota sampling, a non-random sampling technique that involves selecting individuals with predefined characteristics and quotas to collect data. Quota sampling was selected to ensure proportional representation from each academic phase based on the actual population distribution. The sample size was calculated using the Raosoft online calculator 21 with a 5% margin of error and a 95% confidence level. The recommended minimum sample size was 323 from a total population of 1990 students. Based on the total number of students in the College of Science and Health Professions and the College of Medicine, 62% of the population are phase 1 students, 21% are phase 2 students, and 17% are phase 3 students. Hence, the required sample sizes for each phase were 202 students in phase 1, 67 in phase 2, and 54 in phase 3.
Data Collection Tool
The participants completed an online questionnaire-based survey, comprising two well-known scales, both of which have been approved for content and face validity. The first scale used was the adapted student version of the “Oldenburg Burnout Inventory (OLBI),” 22 which measures the risk of developing burnout. It consists of 16 statements, with each statement categorized into two dimensions: disengagement and exhaustion. Disengagement (items 1, 3, 6, 7, 9, 11, 13, and 15) refers to distancing students from their academic demands and to the endorsement of negative attitudes toward their courses and colleagues.22,23 For instance, one of the statements is “I always find new and interesting aspects in my studies.” Exhaustion (items 2, 4, 5, 8, 10, 12, 14, and 16) is characterized by extreme physical, emotional, and cognitive strain, such as the long-term effects of repeated exposure to academic demands.22,23 An example of an exhaustion statement is “ There are days when I feel tired before I arrive in class or start studying.” The distributed survey allowed participants to choose from 1 to 4 (1 = strongly agree, 2 = agree, 3 = disagree, 4 = strongly disagree). The scoring key for the OLBI was as follows: Items 1, 5, 7, 10, 13, 14, 15, and 16 were scored from 1-4, as in the distributed survey. Items 2, 3, 4, 6, 8, 9, 11, and 12 were scored in reverse (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree). 22
The second scale used was “The Psychosocial Inventory of Ego Strength - Short Form (PIES-SF),”
24
which assesses psychosocial development by Erikson's eight ego strengths (hope, will, purpose, competence, fidelity, love, care, and wisdom) with 32 items. The short-form version of the PIES was chosen for its strong psychometric properties, reduced respondent burden, and established reliability in undergraduate and medical student populations worldwide. The distributed questionnaire's choices ranged from 5 (always) to 1 (never). The items were divided into positive and negative virtues. The positive statements were: (2, 3, 4, 6, 8, 10, 11, 12, 13, 16, 19, 21, 27, 30, 31, 32). For example, statement 2 is “In many ways, I have control over my future”. The negative statements were (1, 5, 7, 9, 14, 15, 17, 18, 20, 22, 23, 24, 25, 26, 28, 29). For example, “I find myself easily distracted even when I really need to finish a task.” The following formula was used for scoring: (summation of positive virtues - summation of negative virtues)
In addition to the OLBI and PIES-SF scales, the questionnaire includes questions on relevant demographics of medical students, including age, gender, and level of education. The full questionnaire is provided in the Supplemental material [see Additional file 1]
Statistical Analysis
Descriptive statistics were used to present counts, proportions (%), means, and standard deviations. To examine the association between burnout level and psychosocial development in medical students, a two-tailed t-test was followed by a Pearson correlation. One-way analysis of variance (ANOVA) was conducted to assess differences among the three phases of medical students in terms of psychosocial development and burnout. A correlation analysis was conducted to determine the linear relationship between burnout and psychosocial development, as well as their dimensions. The reliability of both scales, OLBI and PIES-SF, was confirmed using Cronbach's alpha coefficient. Data analysis was performed using Statistical Package for Social Sciences version 25. Statistical significance was set at P < 0.05. In addition to P-values, effect sizes (Cohen's d for t-tests, η2 for ANOVA, and r2 for correlations) were reported to indicate the magnitude and practical significance of the findings. All survey items were mandatory in the electronic form; therefore, no missing data were present in the dataset.
Ethical Considerations
A cross-sectional informed consent form was provided, and ethical approval was obtained from King Abdullah International Medical Research Center (Study protocol SP22J/019/02). Written informed consent was obtained from all participants prior to completing the survey. A study information sheet was provided with the questionnaire, stating that participation is voluntary and that respondents’ identities will not be collected or linked to their answers.
Reporting Guidelines
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25 A completed STROBE checklist is provided as a supplementary file [see Additional file 2].
Results
Demographics
A total of 1990 students were invited to participate in the survey, of whom 315 responded, yielding a response rate of 15.85%. The students’ ages ranged from 18 to 23 years, with a mean age of 20.33 years. Of the total respondents, 48.9% were male, and 51.1% were female. The response rates for the first, second, and third phases were 52.1%, 29.5%, and 18.4%, respectively (Table 1).
Characteristics of the Participants and Their Association with Burnout and Psychosocial Development Levels.

*P ≤ 0.05, **P ≤ 0.001
Correlation of the OLBI and PIES-SF Tools
The reliability of the OLBI (16 items) and PIES-SF (32 items) tools was confirmed with Cronbach's alphas of 0.864 and 0.803, respectively, indicating their suitability for use in the current research. The two scales were found to have a significant positive relationship between their domains, as well as between each domain and the total score. Specifically, the first domain of the burnout scale (exhaustion) showed a Pearson correlation (r) of 0.888 with the total burnout domains, with a significant P-value of <0.001. Similarly, the first domain of the psychosocial scale (hope) showed a correlation of r = 0.762 with the total psychosocial domains, with a statistically significant P-value of <0.001.
Burnout and Psychosocial Development Levels in Relation to Gender and Phases
The study employed an independent t-test to examine whether gender differences existed in burnout and psychosocial development. The results indicated that the mean burnout scores were 43.50 for males and 40.58 for females, while the mean psychosocial development scores were 109.38 for males and 104.86 for females (Table 1). The analysis revealed a highly significant difference in burnout levels, with females showing higher levels than males (P < 0.001), t (313) = 3.53, and Cohen's d = 0.40. Conversely, males scored significantly higher on the psychosocial development scale than females (P < 0.05), t (313) = 2.55, and Cohen's d = 0.29.
Regarding the academic phases, one-way ANOVA showed no significant difference in burnout levels across the three phases (P = 0.917). However, it revealed a significant difference in psychosocial development across the phases, F (2, 312) = 3.36, P = 0.036, and η2 = 0.021.
Post-hoc analysis was performed using the least significant difference test, which revealed significant differences between phase one and two (P = 0.046) and between phase one and three (P = 0.029), while no significant difference was found between phase two and three (Figure 1).

Comparison of burnout and psychosocial development scores by gender and academic phases. (a) Burnout levels of male and female participants, showing a significant difference in burnout levels with P < 0.001. (b) Psychosocial development scores of male and female participants, showing a significant difference with P < 0.05. (c) Psychosocial development scores across the academic phase, with a significant difference between the phases at P < 0.05.
Association Between Burnout and Psychosocial Development Levels
The statistical analysis revealed a moderately significant negative Pearson correlation (r = -0.552, P < 0.001) between burnout and psychosocial development, indicating an inverse relationship between the two variables explaining approximately 30% of shared variance (r2 = 0.30) (Figure 2).
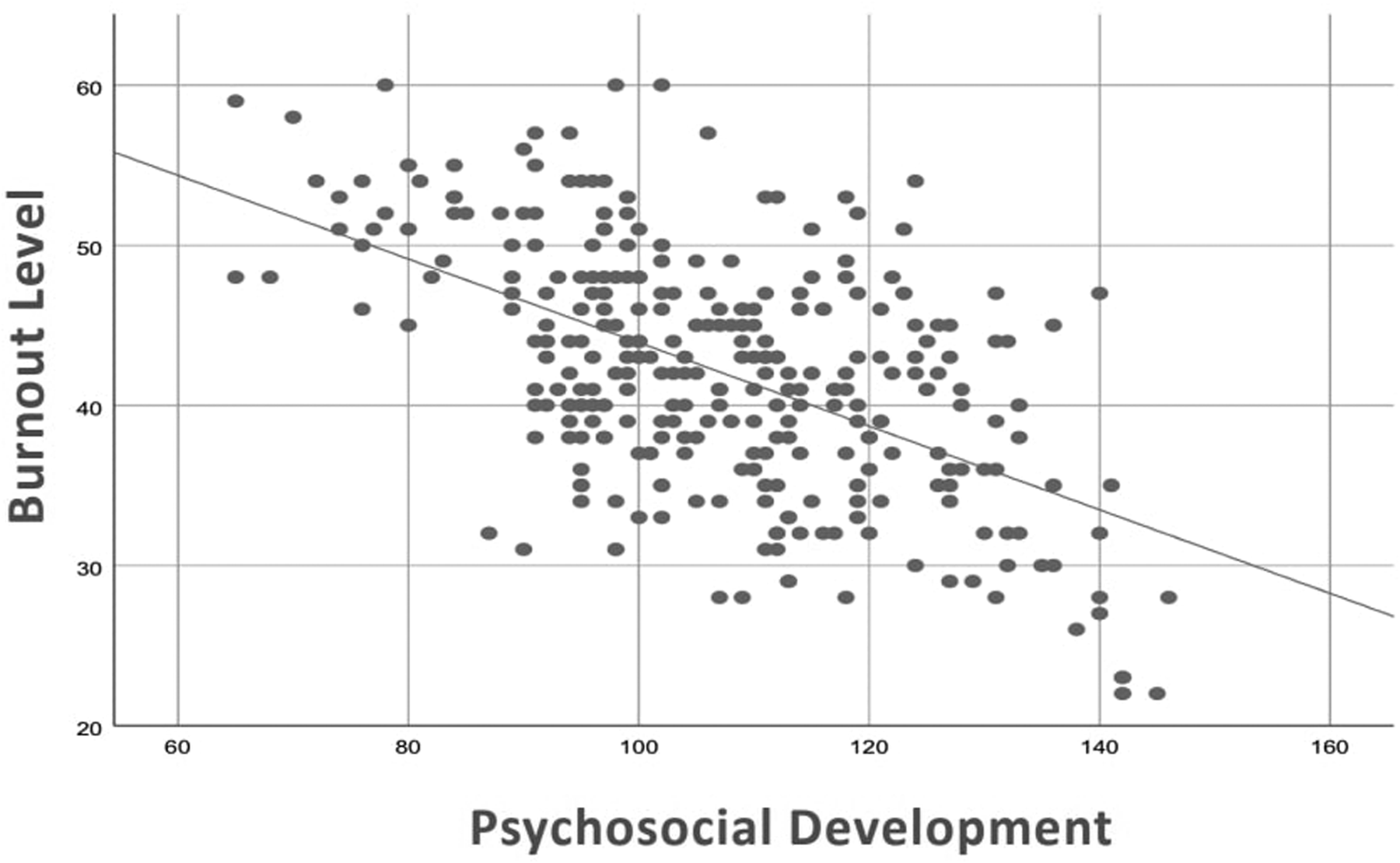
The association between psychosocial development and burnout level. The association between psychosocial development and burnout level was significant (P < 0.01, r = –0.552), indicating a negative correlation (R2 = 0.304).
Discussion
This study aimed to assess the relationship between psychosocial development and burnout among medical students at KSAU-HS, Jeddah campus. Burnout syndrome is a well-documented condition that negatively impacts medical students’ lives and academic performance. Multiple studies with various assessment methods have found that medical students’ burnout rates range from 10.3 to 76.8%. 26 Psychosocial development was measured using the PIES, a tool grounded in Erikson's theory and designed to assess eight core ego strengths.24,27 Research in other undergraduate groups suggests male students have higher ego strength, 28 but studies in medical students are limited. Thus, other studies examining ego strength in health workers were also considered. For instance, ego strength is thought to contribute to the development of professional and ego identity. 29 Longitudinal studies in nursing students showed that ego identity fluctuated over time, while psychosocial maturity improved. 30 Similarly, Srivastava et al found that ego strength was highest in phase 3 medical students, supporting the current findings. 31
The study showed a significant negative correlation between psychosocial development and burnout. Lower psychosocial development scores were associated with a higher risk of burnout. Females had higher burnout and lower psychosocial development than males. While burnout did not differ across academic phases, phase 3 students had higher psychosocial development than phases 1 and 2, suggesting improvement with academic progression. Due to psychosocial stressors throughout their academic and training years, medical students are at risk of burnout. 32 As a result, several studies have investigated this phenomenon. In this study, burnout levels were higher among female students, consistent with previous reports. 33 Furthermore, one study showed that females were more exposed to childhood maltreatment and gender discrimination than males, which led to a greater prevalence of mental health disorders in females. 34 Moreover, Saudi women continue to uphold family life, requiring female students to put in extra effort to reach their objectives. This often involves dedicating more physical and mental energy to manage both academic demands and family responsibilities. 35 This may further explain females’ lower psychosocial development and higher burnout.
Beyond these sociocultural factors, psychological mechanisms may also help explain the gender gap. Impostor syndrome (IS), characterized by persistent self-doubt and difficulty internalizing success, is common among medical trainees. 36 Local data from Saudi Arabia demonstrate the prevalence of IS in medical trainees: 93.2% of surgical and medical residents in Makkah exhibited moderate to high impostor characteristics, 37 while 42.1% of medical students at King Saud University in Riyadh screened positive for IS. 38 These findings indicate that impostor-related cognitive and emotional patterns may affect how trainees evaluate their psychosocial strengths. This interpretation is further supported by international data. In a study of U.S. medical students, almost a quarter of male students and almost half of female students reported IS. 39 Since IS affects self-appraisal, it may therefore affect how students respond to ego-strength items in the PIES-SF.
Nonetheless, not all studies find consistent gender or age effects. Some studies reported contradictory findings, indicating no differences in burnout scores between genders. 40 In addition, no significant associations were found between students of different age groups, similar to the findings of two studies3,41 and contrary to one study. 42 The absence of a correlation between burnout and the phases may indicate that the demanding schedule, competitive environment, high stress levels, excessive workload, sleep deprivation, and peer pressure are prevalent throughout the entirety of medical education. 2 Variation in reported burnout rates may stem from different measurement instruments. There may also be cultural, social, and environmental factors that influence burnout in different circumstances. 2
Similarly, phase-related differences in burnout are inconsistent in the literature, which may reflect measurement or dimensional issues. The current study showed no significant difference in burnout levels across different educational phases. This finding aligns with other local studies, which showed that the academic year was not a straightforward risk factor for burnout.3,43 It is possible that there may be variation across the three dimensions of burnout, with one dimension higher than another across phases. For example, in a study conducted in Morocco, students showed a higher level of cynicism (or depersonalization) as medical education progressed. The level of cynicism was also found to be predicted by the learning phase, workload, meaningfulness and neuroticism. 44 This dilutes the overall level of burnout across phases and stresses the multi-dimensional nature of burnout. Furthermore, measurement timing may influence burnout levels, as short-term stressors (e.g. mid-semester demands, pre-exam period, or the beginning of exam week) can cause fluctuations that mask phase-related patterns. Therefore, future research may benefit from prospective, longitudinal designs to capture changes more accurately over time.
While previous research focused on the ego strength of healthcare students and other variables, the current study explores its relationship with burnout. The inverse relationship between the two variables could be explained by another confounding variable. To illustrate, a study found that elevated burnout and decreased psychosocial health among nurses caring for oncology patients are strongly associated with poor psychological resilience. 45 In tandem with the current findings, another study found that ego weakness was a predictor of burnout in HIV/AIDS healthcare workers. 46
Given these findings, addressing burnout through emotional intelligence and incorporating psychosocial training in medical curricula becomes essential. Recent studies suggest that implementing mental health and emotional intelligence courses, particularly for female students, can enhance coping strategies and reduce stress-related burnout. Promoting social support through peer interaction and regular communication with parents further strengthens resilience and overall well-being. 47 It is recommended that medical schools revise learning outcomes and enhance support services in response to burnout trends and psychosocial development patterns. Implementing counseling, mentorship programs, and anti-stigma initiatives can help foster a supportive environment. 48 Structured emotional intelligence workshops, faculty-student mentorship programs, reflective practice modules, and stress management approaches such as mindfulness and coping-skills training—as well as peer-support activities—can reinforce resilience and normalize help-seeking. These interventions can feasibly be integrated as short electives or co-curricular sessions, with sustainability ensured through collaboration with student wellness units and faculty mentors.
As for sample selection, it was considered best to exclude Stream 2 students from the current research for two reasons. Firstly, even though previous critiques of Markstrom's PIES scale did not find any conclusive connections between ego strength and age, the psychosocial obstacles to overcome in Erikson's stages of psychological development depend, in part, on a person's age. 17 Also, as previously explained, the medical year is highly correlated with the levels of burnout. The older, more experienced graduate medical students have been found to perceive and cope with stress differently from younger undergraduates. 49 Therefore, it was plausible to assume that age is a factor that might interfere with the result if not considered within the sample.
Even though this study will contribute to the literature on burnout syndrome and psychosocial development in Saudi Arabia, which may assist in the early detection and prevention of burnout, it has some limitations. The first limitation of this study was the use of a cross-sectional design, which can determine statistical associations but not causal relationships. Second, the use of a self-administered questionnaire could introduce self-report bias. 50 Third, the low response rate (15.85%) may introduce response bias, as students who chose to participate may differ from those who didn’t, potentially affecting the representativeness of the findings. Fourth, conducting the study at a single institution and employing quota sampling, a non-random method that may introduce selection bias, limits the generalizability of the findings to the broader medical student population. Fifth, the PIES-SF instrument, which assesses psychosocial development, was originally developed and validated in Western populations. Cultural norms, gender roles, and sociocultural expectations in Saudi Arabia could influence how students interpret and respond to items measuring ego strength, potentially affecting the instrument's accuracy. Consequently, these cultural differences may limit the interpretability and generalizability of findings on psychosocial development.
Future research would benefit from a mixed-methods approach, incorporating quantitative evaluations and structured interviews or focus group discussions among male and female students across various academic phases. Descriptive information on the gender and phase-related patterns would also supplement the description with qualitative data. Furthermore, longitudinal, multi-institutional studies are needed to track psychosocial development and burnout trajectories over time, thereby increasing generalizability across Saudi medical schools.
Conclusion
The current study found an inverse relationship between psychosocial development and burnout. Furthermore, burnout levels were higher in female medical students. Regarding psychosocial development, it was higher in males. Regarding the academic phases, there was no significant difference in burnout levels, whereas psychosocial development was highest among students in the clinical years (phase 3). These findings underscore the importance of fostering a supportive learning environment that prioritizes student well-being. Implementing stress management programs and promoting emotional intelligence and psychosocial development may help reduce burnout and support healthier professional growth. Further studies are needed on a larger population.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205251414782 - Supplemental material for The Relationship Between Psychosocial Development and Burnout Among Medical Students in Jeddah, Saudi Arabia
Supplemental material, sj-pdf-1-mde-10.1177_23821205251414782 for The Relationship Between Psychosocial Development and Burnout Among Medical Students in Jeddah, Saudi Arabia by Taif Alkhatabi, Norah Alkahtani, Sultanah AlBoraie, Rahaf Sherbini, Amal Albaqami, Manar Alqahtani and Rania Zahid in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205251414782 - Supplemental material for The Relationship Between Psychosocial Development and Burnout Among Medical Students in Jeddah, Saudi Arabia
Supplemental material, sj-pdf-2-mde-10.1177_23821205251414782 for The Relationship Between Psychosocial Development and Burnout Among Medical Students in Jeddah, Saudi Arabia by Taif Alkhatabi, Norah Alkahtani, Sultanah AlBoraie, Rahaf Sherbini, Amal Albaqami, Manar Alqahtani and Rania Zahid in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to express our gratitude and appreciation to Prof. Alaa Althubaiti, Dr Muhammad Anwar Khan, and Prof. Anwar Borai for their assistance and support in revising and updating the statistical analysis and improving the quality of the manuscript.
Ethics Approval and Informed Consent
This study was approved by the King Abdullah International Medical Research Center (KAIMRC) institutional review board. (Study protocol SP22J/019/02). All responses were kept fully confidential with authorized access only. Informed consent was obtained from all study participants, and they were informed that no identifying information would be collected. The authors declare that it conforms to the Declaration of Helsinki.
Consent for Publication
Not applicable.
Authors’ Contributions
TA contributed to project administration, data collection, writing—original draft, and writing—review & editing. NA contributed to data collection, writing – original draft, writing – review & editing, visualization. SB contributed to data collection, analysis, writing—original draft, writing—review & editing, and visualization. RS contributed to data collection, writing—original draft, and writing—review & editing. AA contributed to data collection, writing—original draft, writing—review & editing, and visualization. MA contributed to data collection, writing—original draft, and writing—review & editing. RZ contributed to methodology, conceptualization, analysis, validation, and supervision. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to respondents’ confidentiality; however, they are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.