
Abstract
Introduction
Medical professionalism may be defined operationally as an amalgamation of behaviours, attributes, and adherence to standards. Assessing professionalism is challenging due to its broad and contextual nature, but also due to ambiguity around expectations of students within a given scenario. This qualitative study explores the respective opinions of students and teaching faculty at UK medical schools as to what constitutes “adequate professionalism” at defined milestones during undergraduate medical education.
Methods
Fifteen key professionalism themes were identified from published regulatory guidance. Four behavioural descriptors were written for each theme, using the lens of Miller's Pyramid to describe how a medical student might progress from “novice” to “proficient” across 4 defined milestones of their undergraduate medical school career. Using an online survey, students and faculty at UK medical schools were invited to provide their opinions as to what constituted “adequate professionalism” at each milestone, with respect to each theme.
Results
Eight medical schools participated in the study. A total of 112 responses were received from 74 (66.1%) medical students and 38 (33.9%) faculty members. The data mapped students’ journeys from “novice” to “proficient” as they transited the respective milestones of entering medical school, first patient contact, regular patient contact, and graduation. Student and faculty respondents broadly agreed about what defined “adequate professionalism” at each milestone. However, faculty expressed higher expectations than students in 1 theme, while students had higher expectations than faculty for at least 1 milestone across 10 themes. In some themes, students were expected to perform above the “most novice” descriptor at the first milestone. In other themes, students were not expected to reach the “most proficient” descriptor by the final milestone.
Conclusions
This study benchmarks “adequate professionalism” for medical students at defined milestones in the undergraduate medical curriculum. Its insights provide opportunities for curriculum planning, granular assessment of professionalism, and raise several further research questions.
Introduction
Medical professionalism may be defined operationally as an amalgamation of behaviours, attributes, and adherence to standards. It forms part of a triad of skills necessary to function as a healthcare professional, namely: “clinical skills,” “adhering to contracts of employment,” and “professionalism.” 1 With this in mind, professionalism training at undergraduate medical school has become increasingly prominent in recent years. 2 The UK General Medical Council recognises “professionalism” as a key component of its Medical Licensing Examination, 3 the final checkpoint before a student is awarded a primary medical qualification from a UK medical school. As professionalism training becomes increasingly integrated into undergraduate medical curricula, the literature around its pedagogy and how it may be assessed has rapidly expanded.
Assessment is widely acknowledged to be a key component of any curriculum,4,5 but assessing professionalism is notoriously difficult. This reflects the broad variety and contextual nature of professionalism topics, a relative paucity of validated assessment tools, and ambiguity about the expected standards for a student tackling a specific scenario.
The literature pertaining to professionalism assessment describes a tendency towards using snapshot judgements and assessment tools, including longitudinal portfolios,6–8 Objective Structured Clinical Examination (OSCE) stations,9,10 reflective writing,2,6 and global rating scales. 11 Little detail is captured relating to student behaviours involved in this assessment process, and the specific definition of what is being assessed varies from highly detailed to single-word descriptors. 1 Such tools may not be externally validated or correlated with future performance. They also tend to focus on “avoiding poor conduct” rather than documenting progression on the student's journey. It is also important to highlight the subjective nature of “professionalism” assessment, and faculty members may “fail to fail” students. Many contributory factors to this have been mooted: self-doubt on the part of the assessor; anxiety about negative impact on the student's career trajectory; uncertainty about processes or whether they have been followed. 11 This creates challenges for educators, given that medical students are recognised to begin a journey of professional identity formation and growth early in their undergraduate studies. This dynamic process continues into the postgraduate space, involving change at the individual level and within communities of practice. 12 Snapshot and/or outcome based assessments may fail to capture the richness of a student's professional growth and the positive evolution of their professional identity; indeed, some would argue that assessing this journey requires alternative strategies that diverge from more traditional assessment practice, capturing the extent to which a student's normal behaviours align with assessment criteria, rather than evaluation of how the student performs in an exam situation. 13
For practical purposes, standards for healthcare professionals can be drawn from published regulatory guidance. In the UK, this is defined for doctors by Good Medical Practice, 14 while Achieving Good Medical Practice 15 and Outcomes for Graduates, 16 respectively define standards for medical schools and medical students. Collectively, these documents provide a standard for assessing professionalism at the point of graduation from medical school. However, it is less clear what standards should be expected of medical students as they progress through milestones of their undergraduate studies, for example, during the first months of study as a “novice,” at their first clinical encounter, and during regular clinical attachments until ultimately graduating as a “competent practitioner.” This study addresses this gap by exploring the incremental standards expected of undergraduate medical students as they progress through the curriculum. Specific milestones are identified, and the respective views of faculty and students are sought regarding how professionalism might be defined at each of these waypoints. The aim of the study is thus to benchmark student and faculty expectations of “adequate professionalism” at defined milestones of undergraduate medical education.
Context
This exploratory, qualitative, convenience survey study was performed in the United Kingdom between November 2022 and June 2023. The reporting of this study conforms to the CROSS checklist 17 (see supplementary file 1).
Methods
The study used regulatory guidance 14 as a reference as to what defined “adequate professionalism” for qualified doctors from the point of graduation (Appendix A). The authors used their working experience of clinical medicine and undergraduate medical education to collate the 79 paragraphs of Good Medical Practice 14 into 15 broad theme headings (Table 1).
Professionalism themes.

The hierarchy of categories in Miller's Pyramid, namely knowledge, competence, performance, and action, 18 was used to create 4 behavioural descriptors within each of the themes (Appendix B). These were intended to describe a student's development from “novice” to “competent practitioner” with respect to each theme.
Face validity for the themes and behavioural descriptors was established through discussion with expert clinicians and educators at a local level and through wider discussion with the membership of the UK Council for Educators of Medical Professionalism (UKCEMP), the UK association for medical professionalism teachers, during their national conference.
Four milestones were chosen to represent identifiable waypoints of an undergraduate medical student journey (Table 2). These were intended to be recognisable across a wide range of undergraduate curricula.
Undergraduate medical education milestones.

An online survey (Appendix C and Appendix D) was created to gather participants’ opinions about what constituted “adequate professionalism” at each milestone. Specifically, participants were asked to specify which of the behavioural descriptors within each theme was “adequate” for a student at each milestone. Each question consisted of a description of the theme, with 4 behavioural descriptors (and a “not relevant” option). Participants were asked to indicate their preferred behavioural descriptor for each milestone. The survey was piloted with local colleagues with respect to its content and technical functionality.
Participants
Undergraduate medical students and faculty in UK medical schools were invited to participate in the study.
The authors used their professional networks and an electronic invitation distributed via UKCEMP to recruit UK medical schools to participate in the study. The authors also spoke at a UKCEMP conference about the proposed study. The invitation was sent to 89 teaching leads for professionalism and other senior academic staff across 40 UK medical schools. A total of 3 invitations to participate in the study were sent during the period November 2022-June 2023.
Participating medical schools were provided with study materials, including an electronic participant information leaflet, and survey links customised for their school. They were asked to invite their medical students and faculty to participate, providing them with the participant information leaflet and survey link. Medical students were defined as those currently enrolled in an undergraduate programme leading to the award of a primary medical qualification in the UK. Faculty were defined as teaching staff. The specific means of distributing this invitation and its internal promotion were at the discretion of each medical school, subject to the study's ethical approval framework. Individuals participated voluntarily and anonymously, with no prejudice to students’ grades or faculty career development. The first survey question asked participants to indicate their written consent to participate. This consent was recorded electronically as part of the dataset. Anyone not wishing to consent to participation was unable to proceed with the survey. The authors did not have access to the mailing lists used to distribute surveys within each medical school, and there are no publicly available lists of student and faculty numbers per school. This meant they were unaware of the total number of people invited to participate.
Survey
The Online Surveys platform (Jisc) was used to create and host the surveys. Duplicate surveys were created for student and faculty respondents, respectively. While it was not technically possible to prevent multiple submissions by one individual, each survey collected basic, anonymous, demographic information. For student participants, this included their medical school and stage of training. For faculty participants, this included their background qualifications, their role in the context of medical education, and the frequency of student contact. This was considered important information to gather as the definition of “teaching faculty” could vary between institutions, including permanent university employees or clinicians who regularly taught students during clinical attachments, but who had no formal university affiliation.
Data was exported from Online Surveys for analysis using Microsoft Excel (Microsoft Corporation). Only the study authors had access to the data.
The data was analysed to determine student and faculty perspectives on “adequate professionalism” at each milestone and with respect to each theme.
Ethical approval was obtained from the University of Glasgow College of Medicine, Veterinary and Life Sciences Ethics Committee (reference 200220019).
Results
Eight medical schools participated in the study. A total of 112 responses were received from 74 (66.1%) medical students and 38 (33.9%) faculty members (Table 3).
Medical schools and participants.
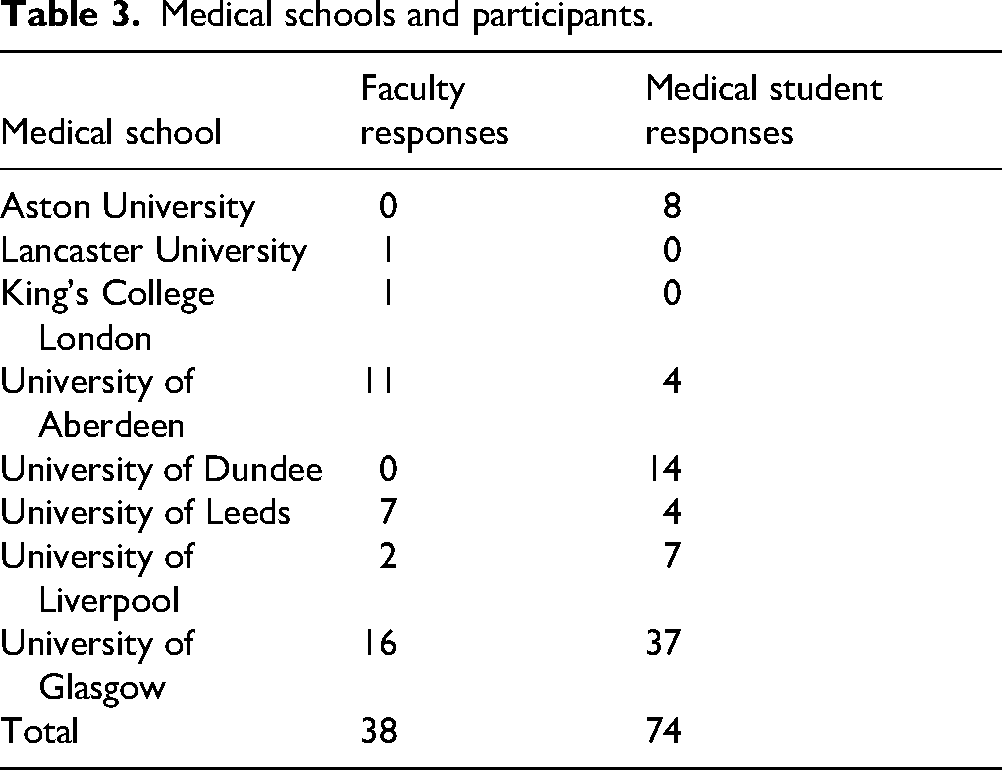
Medical student respondents were in fifth year (n = 5, 7%), fourth year (n = 31, 42%), third year (n = 12, 16.2%), second year (n = 11, 14.9%), first year (n = 9, 12.2%) or undertaking an intercalated [optional additional year of study] year (n = 6, 8.1%). Faculty respondents met students on a daily (n = 18, 47.3%), weekly (n = 13, 34.2%), fortnightly (n = 4, 10.5%), or monthly basis (n = 2, 5.2%). One response was excluded due to an ambiguous free-text response. Faculty had a primary medical degree (n = 33, 86.8%), biomedical science qualification (n = 2, 5.2%), or another unspecified qualification (n = 2, 5.2%).
Participants indicated the behavioural descriptor that reflected “adequate professionalism” at each milestone for each of the 15 themes. For analysis purposes, the behavioural descriptors were arbitrarily converted into a numerical score where “1”= most proficient behavioural descriptor and “4”=most novice behavioural descriptor within each theme. This enabled calculation of mean, median, and mode scores with respect to the chosen behavioural descriptor best reflecting each milestone within each theme (see supplementary file 2). Differences between faculty and student scores were calculated at each stage, arbitrarily assuming a numerical difference of ±0.5 to be sufficiently substantive (see supplementary file 2).
The data show that students are generally expected to follow a linear progression from a “novice” score (behavioural descriptors 4 or 3) to a “proficient” score (behavioural descriptors 2 or 1) as they transition through the milestones from entering medical school to graduation. Student participants felt that across 11 themes, behavioural descriptor 3 or better was expected from entry to medical school (milestone A). Faculty agreed with this for 9 themes. Faculty participants felt that achievement of behavioural descriptor 1 was not required by graduation (milestone D) for 3 themes. Student participants agreed with this for 1 of these themes.
Students and faculty broadly agreed about which behavioural descriptor represented “adequate professionalism” for any given milestone. However, in 10 themes, students had higher expectations than faculty for at least 1 milestone. The level of disagreement was by a factor of 1 behavioural descriptor, i.e. 1 level of Miller's pyramid. In theme 13, students felt behavioural descriptor 1 was applicable at every milestone, whereas faculty felt students should progress from behavioural descriptor 3 to behavioural descriptor 1 as they transitioned milestones A, B, and C. Faculty expectations exceeded those of students in theme 2. While students felt behavioural descriptor 3 was reasonable by milestone C, faculty felt students should have reached the higher level of performance of behavioural descriptor 2.
Discussion
This qualitative study explored the views of undergraduate medical students and teaching faculty at UK medical schools regarding what constitutes “adequate professionalism” at different milestones of the undergraduate curriculum. Behavioural descriptors based upon regulatory guidance and tethered to waypoints along students’ journeys enable detailed assessment of the emergence and maturation of medical student professionalism during their undergraduate career. The work establishes checkpoints for student progression throughout undergraduate training. This provides a basis for assessment strategies during undergraduate medical training, notwithstanding existing regulatory guidance that defines expected standards by the point of graduation. 14 It also highlights varying teaching priorities at different curricular stages and raises questions about medical school admissions criteria and the expected standards for newly graduated doctors.
The data was surprising in several respects. One might expect students to enter medical school as a novice in every regard, but this was not reflected in the results. Both student and faculty respondents felt that a more advanced level of proficiency was required in several areas at milestone A. These included English language skills, communication of student status, and the ability to maintain confidentiality. Some of these measures could be reflected in medical school admissions policies, but others may place unrealistic expectations on potential applicants. Further work should explore the potential influence of bias or prejudice on these expectations.
It was also unexpected that achieving the “most proficient” behavioural descriptor for each theme was not considered essential by milestone D (graduation from medical school). Even more surprising was that faculty held this view for 3 of the 15 themes, which directly reflect the regulatory definitions of fitness-to-practise at the point of graduation. Further work should explore this unanticipated finding in more depth.
Most surprising of all was the suggestion that slow progression through theme 2 (concerning addressing patients’ basic needs) was satisfactory, and not essential to have mastered by graduation. This may be at odds with the literature describing the benefits of junior health care worker roles for medical students. 19 It is feasible, however, that respondents were describing their perceptions of what currently happens, rather than aspirations for what should happen. This might reflect an understanding of the complexity presented by this apparently simple theme, but patients and the public might disagree with this finding.
Student respondents had overall higher expectations than faculty respondents with respect to the behavioural descriptor required to be achieved across each milestone. This is perhaps unsurprising in the context of the literature describing medical students’ tendencies towards perfectionism: being overly critical of oneself can lead to burnout in students. 20 Attainment of many of the behavioural descriptors described in this study traditionally resides in the hidden curriculum, 2 and student expectations have not hitherto been explored in such detail. The insights provided here create opportunities for teaching faculty to openly discuss and rationalise expectations within their student cohorts, potentially reducing the risks of student distress and burnout.
Strengths and Limitations
There is wide variation between UK medical school curricula in terms of their construction and delivery. The milestones used in this study were chosen to reflect stages of training that were recognisable across institutions. It is acknowledged that alternative or additional milestones may be required by individual schools looking to implement these findings locally. The authors also recognise that some themes and behavioural descriptors may be difficult to evidence at some milestones, particularly for students at earlier stages of training. For example, themes addressing issues such as engaging in the provision of medical education may not be strictly relevant at milestone A (first day of medical school).
UK medical regulatory guidance 14 was used as the basis for this UK-based study. Postgraduate definitions of fitness-to-practise were used since the purpose of undergraduate medical curricula is ultimately to produce graduates who can meet this standard. The authors intended that each of the 15 themes derived from Good Medical Practice 14 would provide recognisable, practical reflections of this guidance that could also apply across professions and geographies. It is recognised that cultural factors, declinism (the tendency to view the past with disproportionate optimism and the future pessimistically), 21 and differences between health professional roles can influence how professionalism is perceived by staff, patients, and the public. Further work based upon updated UK regulatory guidance, 14 alternative professions’ regulatory guidance, and using frameworks focused specifically on undergraduate medical education15,16 will provide additional insights to the data presented here.
The “novice to expert” principles of Miller's pyramid 18 were used to construct the behavioural descriptors within each theme. The term “competent” rather than “expert” practitioner was used to describe behavioural descriptor 1 with respect to each theme, reflecting that “expert” might not be the most appropriate descriptor for a newly qualified medical graduate. Nonetheless, behavioural descriptor 1 was written to match the regulatory standard defined in Good Medical Practice. 14 Further work exploring the nature of “competence” versus “expertise” with respect to each theme would strengthen the findings and enrich the literature relating to the assessment of professionalism in medical undergraduate education and postgraduate practice.
The authors considered that each behavioural descriptor broadly represented typical student progression with respect to each theme. It is acknowledged, however, that these could benefit from further refinement with respect to some themes or milestones. For example, some schools might consider additional or alternative milestones to accommodate the needs of graduate entry programmes, or where groups of students from external institutions join the course at the commencement of clinical training. Different dimensions of progression are considered across the themes and descriptors; for example, theme 1 considers English language proficiency, while theme 2 compares awareness of, and ability to address, patients’ basic needs (Appendix B). These descriptors were contextual to each theme and written with pragmatism in mind; however, the authors acknowledge that mixing assessment constructs may reduce reliability, and further work is required to validate these measures.
The themes and behavioural descriptors were created based upon the authors’ considerable experience of clinical practice, medical education, and teaching professionalism. Face validity was established through local discussion, and separately with recognised professionalism education experts attending a national conference. Time and funding constraints limited efforts to formally pilot the themes, behavioural descriptors, and survey beyond this, which the authors acknowledge as a limitation of the study.
An online survey format was used to collect data. No funding or logistical support was available to support alternative means of data collection, such as focus groups or interviews, 22 which could have provided further insights. This is acknowledged as a limitation of the study. Small sample size and potential sampling bias are further limitations of the study. Efforts were made to engage with every UK medical school, although only 8 schools provided responses. This did include a spread of newer and more established schools located across Scotland and England, but it is acknowledged that a broader response would have provided strength to the study findings. Similarly, relatively low proportions of the total student and faculty numbers in each school provided responses. These numbers may reflect a more general difficulty that has been described anecdotally with engaging students and faculty with professionalism content at medical school.
The data was amalgamated for analysis purposes, since the small number of responses from each school limited the ability to make formal statistical comparisons between institutions. There was broad agreement among faculty and student responses from different schools. Indeed, the study originally intended to use a Delphi approach; however, the results were sufficiently uniform that the authors considered further rounds of data collection to be unnecessary. Given the broad spread of respondents in terms of geography, institution, and career stage, the authors suggest the data are likely to be meaningful, but accept that respondents may not be truly representative of their respective groups. Moreover, the sampling strategy made it difficult to establish a response rate, as the total number of students and faculty invited to participate at each institution was unknown. The authors also recognise that a difference of ±0.5 was a somewhat arbitrary means of identifying “significant” differences between respondents; it is not asserted that this represents statistical significance in a positivist sense, in this qualitative study. This was deemed a reasonable measure of difference in the context of a small sample size for which formal statistical analysis was not feasible. Future work should seek to validate these findings using a larger, more tightly defined sample, informed by a power calculation that supports formal statistical analysis, and using additional means of data collection. More broadly, it remains to be seen whether medical students and teaching faculty can provide the most valid barometer of what constitutes “adequate professionalism” during the undergraduate medical course. Future work should explore the views of patients, the public, and other stakeholder groups.
Acknowledging the above limitations, these data provide the first insights into how detailed assessments of professionalism might be performed during medical students’ undergraduate journey. Crucially, the study provides language and behavioural descriptors that move beyond the reliance existing tools place upon global rating scales and binary measures. Further work includes embedding these behavioural descriptors at the appropriate stages of medical school assessment and exploring their impact on students’ professional journeys. This supports earlier calls for professionalism to be integrated into undergraduate medical curricula; for longitudinal professionalism assessment across undergraduate training; and for a change of emphasis away from “avoiding negatives,” toward “positive professionalism.”1,23,24
Benchmarks provided by this study inform future curriculum design and optimisation of which aspects of professionalism are taught at which stages of the undergraduate course. The data also support the development of a comprehensive professionalism assessment during students’ undergraduate careers. The behavioural descriptors focus on positive achievement and progression, rather than binary global assessment ratings or the avoidance of negative behaviours. This enables a roadmap to be created for individual students as their professional identities form and evolve. 25 This speaks to several recommendations made by the Ottawa working group on professionalism assessment. 26 For example, recommendations 2 and 3 describe the need for “defensible assessment approaches across the continuum of professional development” and to develop “clearly articulated and operationalizable definition[s]” for this purpose.
Conclusion
These data benchmark “adequate professionalism” from the perspectives of undergraduate medical students and teaching faculty across UK medical schools. These insights provide opportunities for curriculum planning, granular assessment of professionalism, and raise several questions deserving of further study. Undergraduate medical schools are encouraged to integrate this work into assessments of professionalism throughout the curriculum.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-1-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-2-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-3-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-4-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-5-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-6-mde-10.1177_23821205251408682 - Supplemental material for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study
Supplemental material, sj-docx-6-mde-10.1177_23821205251408682 for Benchmarking “Adequate Professionalism” During Undergraduate Medical Education: An Exploratory Survey Study by Alexandra M. Goodwin and Scott W. Oliver in Journal of Medical Education and Curricular Development
Footnotes
List of Abbreviations
Acknowledgments
The authors would like to acknowledge all study participants, UKCEMP, and colleagues in the NHS Lanarkshire medical education department.
The authors also thank Professor Al Dowie, University of Glasgow, for reviewing a draft of the manuscript.
Ethical Approval
Ethical approval was obtained from the University of Glasgow College of Veterinary and Life Sciences Ethics Committee (reference 200220019).
Consent to Participate
Participants were sent a participant information leaflet to read prior to completing the survey. Consent was recorded by each participant being required to explicitly acknowledge that they had read the leaflet and consented to participating in this study before providing data.
Authors’ Contributions
Both authors (AG and SO) made substantial contributions to the conception and design of the research, as well as analysis and interpretation of data. Both authors approved the submitted manuscript.
Contribution List
Both authors (AG and SO) made substantial contributions to the conception and design of the research, as well as analysis and interpretation of data. Both authors approved the submitted manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by the NHS Lanarkshire medical education department, which also employs both authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.