
Abstract
Introduction
Lactating physicians face considerable challenges in achieving lactation goals due to inflexible schedules and a lack of break time. While federal mandates have outlined the necessity of lactation breaks, the frequency and duration of breaks are unspecified. The objective of this study was to fill this gap by designing and implementing an outpatient neurology resident clinic schedule with protected lactation breaks, ensuring support and quality of trainees’ educational experience.
Methods
This quality improvement study began with developing a prototype schedule with input from lactating physicians, a lactation consultant, and neurology residency program leadership. Neurology residents and fellows with prior lactation experience were surveyed to determine if the proposed schedule would have fit their individual needs. The clinic schedule with protected lactation break time was then implemented, and lactating neurology residents were surveyed regarding their experience.
Results
Eleven previously lactating neurology residents and fellows who were surveyed about the proposed schedule agreed that the prototype schedule would suffice for their personal lactation needs. The clinic schedule was implemented for 5 neurology residents returning from maternity leave in 2022 to 2023, and 4 residents completed a survey of their experience. There was unanimous agreement that protected lactation breaks helped residents achieve their lactation goals and strongly benefited work/life balance and overall well-being. Despite this intervention, 75% of respondents stopped breastfeeding earlier than intended, and 100% of respondents experienced complications perceived to be related to inadequate pumping, such as diminished milk supply. Ongoing barriers to achieving breastfeeding goals included work interrupting lactation breaks, lack of lactation rooms, and lack of computer workstations in lactation rooms.
Conclusions
Inclusion of protected lactation breaks in outpatient clinic schedules helped neurology residents achieve their lactation goals as well as promoted work/life balance and overall well-being. However, more work is needed to address other barriers to achieving lactation goals.
Introduction
Lactation offers a myriad of benefits for both the mother and infant.
1
Lactation breaks were first federally mandated by the Patient Protection and Affordable Care Act in 2010, which states an employer shall provide (A) a reasonable break time for an employee to express breast milk for her nursing child for 1 year after the child's birth each time such employee has need to express the milk; and (B) a place, other than a bathroom, that is shielded from view and free from intrusion from coworkers and the public, which may be used by an employee to express breast milk.
2
The Providing Urgent Maternal Protections (PUMP) for Nursing Mothers Act expanded these requirements to apply to more workers and clarified that employees must be paid if they are working while expressing breast milk. 3
Although lactation break times have been legally protected since 2010, lack of time and schedule flexibility are commonly cited barriers to breastfeeding by lactating physicians.4–6 Limited workplace support has been shown to contribute to premature cessation of breastfeeding among residents. 7 Protected lactation breaks have larger economic benefits as well. Enhanced workplace lactation support is strongly associated with longer breastfeeding duration and job satisfaction. 8 Parents who are breastfeeding miss half as much work as parents of formula-fed infants due to reduction in infant illness. 9 Healthier infants also result in financial savings for the employer as a result of lower healthcare costs and higher employee retention. 10
Establishing a standard outpatient clinic schedule can help support lactating healthcare providers, but defining the exact frequency, duration, or timing is challenging due to individual needs. Additionally, a significant number of physicians are unfamiliar with the general time demands associated with lactation. 11 The development of a comprehensive action plan, including revision of the resident lactation policy and enhancement of faculty and resident education, was reported to foster a more supportive culture for lactation and contribute to the healthy development of the physician workforce. 12 The goal of this study was to design and qualitatively evaluate implementing a schedule for designated lactation breaks for neurology residents in an outpatient healthcare setting.
Methods
A clinic lactation schedule was designed with input from a lactation consultant, discussion with residency program leadership, and a survey of previously lactating neurology residents and fellows. Responses were recorded, and a schedule was proposed and approved by departmental leadership.
During the 2022 to 2023 academic year, the lactation schedule was implemented for the resident continuity clinic at the Department of Neurology, Mayo Clinic, United States. All residents or fellows who were lactating during this time frame were surveyed regarding their lactation goals and experience using the lactation schedule (survey provided in Supplementary File 1).
Standard Protocol Approvals, Registrations, and Patient Consents
This quality improvement study was conducted in accordance with the Standards for Quality Improvement Reporting Excellence in Education (SQUIRE-EDU in Supplementary File 2). This study was exempt from Mayo Clinic Institutional Review Board (IRB) approval. The nature of this study made it exempt from ethics committee review and formal informed consent.
Data Availability
Anonymized data not published within this article will be shared upon request from any qualified investigator.
Lactation Schedule Development
To determine the frequency of lactation breaks, it is essential to consider the typical timing of return from parental leave, which is typically at 6 to 12 weeks after birth. Infants in this age range feed approximately 8 to 10 times per day.13,14 Other industries were benchmarked with mothers working for a major health insurance organization reporting 2 to 3 lactation breaks per 8 h workday. 15 A common lactation routine involves expressing milk upon waking, 3 lactation breaks at work, and additional sessions after returning home, before bed, and during the night until the baby can sleep through the night. Given that most outpatient healthcare providers work from 8 am to 5 pm, the schedule was designed to incorporate 3 lactation breaks per day. Providing 3 breaks rather than 2 allowed for more inclusive support of a broader range of lactation needs.
Determination of Lactation Break Duration
To determine the duration of breaks, we adhered to our institutional policy of 30 min lactation break time. This length of time is necessary for an individual to access a lactation room, set up pump equipment, express milk, store milk, clean pump equipment, and then return to work.
Determination of Lactation Break Timing Relative to Clinic Flow
To determine the timing of breaks relative to patient visits, program leadership determined that new patients (90 min slots) needed to be scheduled at the beginning of the time block to have adequate time for staffing. Neurology consults and return patients required less staffing therefore were scheduled for the second half of the time block.
Lactation Spaces
Dedicated lactation spaces were provided for residents in proximity to clinic spaces with options for reserving spaces or first-come, first-served basis. Lactation spaces were equipped with a medical-grade pump but did not include computers, and most rooms contained a phone. All spaces had a sink, with a separate spigot for hot water, a comfortable chair, and a movable table and were separate from restroom facilities.
Inclusion and Exclusion Criteria
The inclusion criteria are as follows: postgraduate trainees in neurology at Mayo Clinic, currently lactating at the time of enrollment, actively expressing breast milk via pumping, and able and willing to provide informed consent. Exclusion criteria include: not expressing breast milk by pumping during the study period.
Final Schedule and Feedback
The final clinic schedule had 30 min lactation breaks scheduled at 9:30 am, 12:15 pm, and 2:30 pm (Figure 1). Eleven neurology residents and fellows with personal experience lactating during residency were contacted via email regarding the proposed schedule soliciting feedback. The number of study participants was dependent on the number of lactating residents present at the time of the study, and all eligible residents were included to ensure ethical consideration.

Outpatient clinic schedule with lactation breaks for resident continuity clinic. This schedule includes lactation breaks during each clinic half-day, as well as at noon. Each lactation break is 30 minutes in duration.
Policy Dissemination
Announcements regarding the policy occurred at the all-resident program director meeting that occurs on a monthly basis, with dissemination of minutes to all residents. The program director announced the policy at a monthly faculty meeting. All staff supervising continuity clinic were notified of the changes. We found that with clear communication and knowledge of the resident needs, staffing of patients did not infringe on lactation time.
Data Analysis
Quantitative survey data were summarized descriptively using counts and percentages. Free-text responses were reviewed by the study team and grouped into broad themes to capture common experiences.
Results
Resident and Fellow Input on Proposed Schedule
Eleven neurology residents and fellows with personal experience lactating during residency were asked to provide feedback on the proposed clinic schedule, and all of them responded. There was 100% agreement that outpatient clinic days were challenging because of the lack of designated lactation time. All individuals agreed that the designed schedule had an adequate frequency and duration of lactation breaks for their individual needs.
Resident Participation
A total of 5 residents, including Adult and Child Neurology residents, used the clinic schedule with protected lactation break time in the 2022 to 2023 academic year. The survey was filled out by 80% of residents regarding their experience. Of the respondents, 75% were aged between 31 and 35 years, and 25% ranged between 36 and 40 years.
Outcomes
Table 1 summarizes the survey results. Of the respondents, 75% intended to breastfeed/pump for 12 months, and 25% had a goal of 18 to 24 months. Respondents actually breastfed/pumped for 10, 11, and 15 months, and one was still lactating at the time of the survey. All respondents who had stopped lactating indicated that they stopped earlier than they intended.
Survey Results.
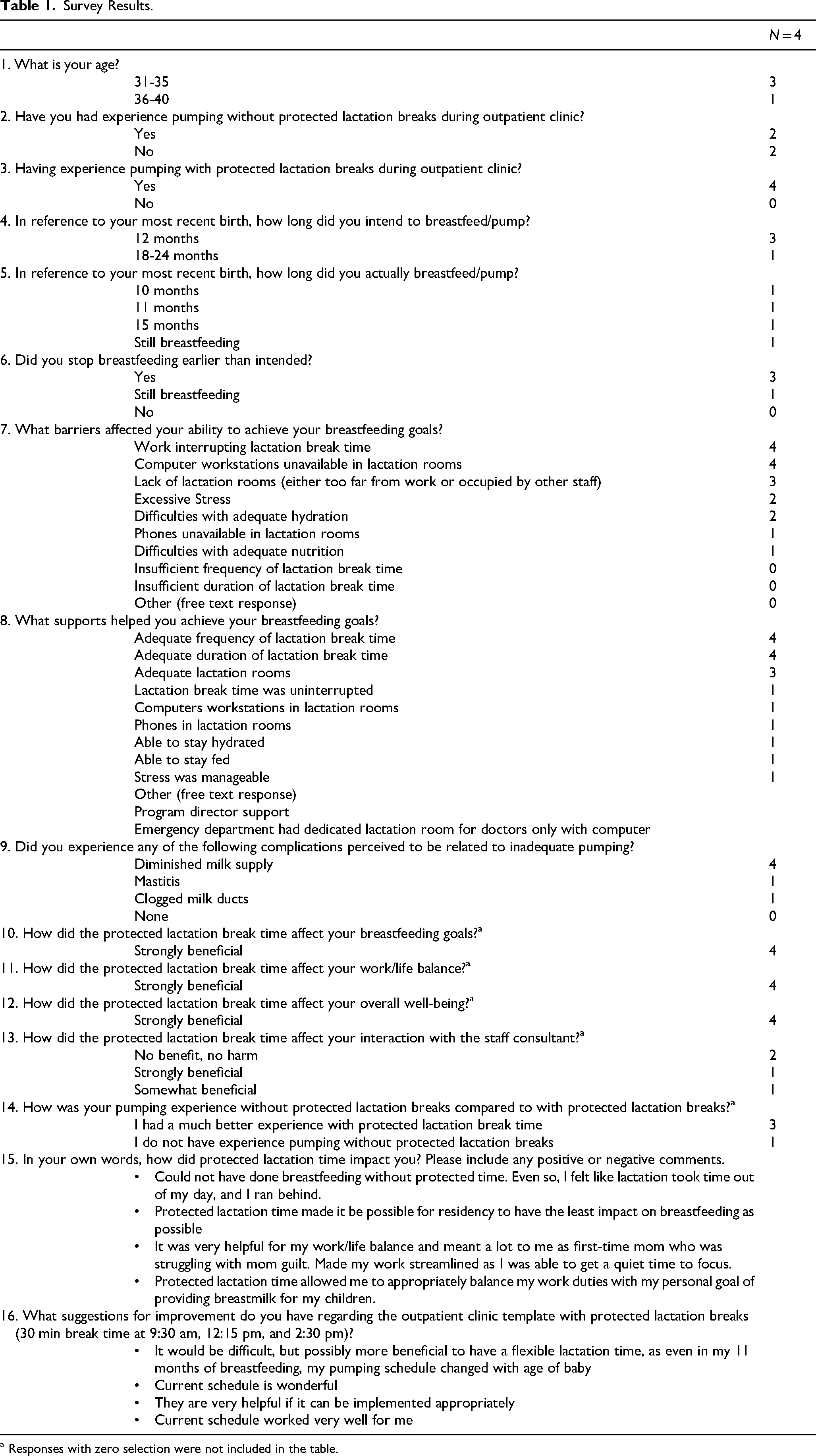
a Responses with zero selection were not included in the table.
When given a list of commonly cited barriers, none of the respondents indicated that insufficient frequency or duration of lactation break time affected their ability to achieve their lactation goals. All respondents indicated that work interrupting lactation break time and the unavailability of computer workstations in lactation rooms were barriers to their goals, and 75% of respondents indicated that a lack of lactation rooms was also a contributing factor. Other cited barriers included difficulties with adequate hydration and nutrition, excessive stress, and phones being unavailable in lactation rooms.
When given a list of factors that helped with achieving lactation goals, 100% of respondents indicated that adequate frequency and duration of lactation breaks, and 75% of respondents indicated that adequate lactation rooms were helpful. Additional supportive factors included uninterrupted lactation break time, computer workstation and phone availability, the ability to stay hydrated and nourished, and manageable levels of stress. Free text responses included program director support and that the emergency department had a dedicated lactation room for doctors only that included a computer workstation.
All respondents reported experiencing diminished milk supply, a common complication perceived to be related to inadequate pumping. One quarter of respondents reported mastitis and clogged milk ducts, which can also be health complications from inadequate pumping.
All respondents indicated that protected lactation break time strongly benefited their breastfeeding goals, work/life balance, and overall well-being. There was a mixed response, with 50% of respondents indicating that protected lactation breaks had a positive effect on their interaction with the staff consultant, and none reported the breaks harming their staff consultant interactions.
Free-text responses regarding their experience elicited overall positive themes, especially on work/life balance, as well as navigating the challenges of being a physician-parent. Specific commentary on the clinic schedule included a request for flexibility to change the schedule as lactation needs change.
Discussion
Based on this study, a 30 min lactation break located in the middle of a clinic half-day effectively eliminates one of the largest obstacles encountered by lactating healthcare providers. This schedule offers 3 lactation breaks per day for those requiring more frequent breaks and can be adjusted easily to adapt to other individual needs. This study has important implications, as this outpatient schedule with lactation breaks can be adopted by any organization.
Lactation breaks are federally mandated; however, employers leave the burden of scheduling changes to the lactating employee. This responsibility adds further work to an employee who is already managing significant changes to their lifestyle with a new infant, return to work after birth, and the common postpartum physical, mental, and emotional issues. Evidence demonstrates that lack of time and schedule flexibility are barriers frequently encountered by lactating physicians. 4
This schedule serves as a resource for employers to support lactating employees. Workplaces with supportive lactation policies have increased job satisfaction and employee retention. 8 Infants who are breastfed experience less illness compared to formula-fed infants, resulting in reduced parental absenteeism due to child illness and decreased healthcare costs.9,10 Our research demonstrates that outpatient clinic schedules with protected lactation breaks facilitates achievement of lactation goals and improved work/life balance.
As institutions develop more supportive parental leave policies, we offer this evidence-based schedule as a tool. 16 In addition to supported time, workplaces can further accommodate lactating healthcare providers by providing designated lactation rooms with a lockable door, a comfortable chair, an electrical outlet, and a flat surface for the breast pump and supplies. 14 Lactation rooms should also include a sink for handwashing and washing pump supplies, and a refrigerator for breast milk storage. Providers can multitask and continue providing patient care if a phone and computer workstation are included in lactation rooms. 17 Making lactation breaks flexible according to individual needs could also improve the effectiveness of these breaks.
Protected lactation time is one factor that can promote breastfeeding. This study also uncovered other barriers to breastfeeding that should be addressed to further support trainees and employees of healthcare institutions. Some of these barriers are inherent to medicine, such as stress levels, busy schedules, and ability to maintain adequate hydration and nutrition. Similarly, previous studies have reported that common barriers to breastfeeding among physicians, residents, and medical students include inadequate and inaccessible space, time constraints and inflexible scheduling, and limited colleague support. These barriers have been associated with low milk supply and early discontinuation of breastfeeding. 18
Educators and supervisors should also consider these and other needs of lactating individuals. While the lactation schedule had a strong positive impact on trainees, the high numbers of individuals who did not meet their lactation goals show that more work is needed in this area.
Limitations of this study include the small sample size and restriction to a single institution. A further limitation is that the number of participants was based on the availability of lactating residents, rather than a calculated sample size. Future directions include examining the effectiveness of this schedule for faculty members and providers at other institutions. This study was conducted in an outpatient setting; further research is needed to design lactation breaks for implementation in inpatient settings. Also, maternity leave policies vary considerably worldwide, which may limit the generalizability of our findings. Our results should be interpreted within the context of the United States, where maternity leave is often shorter than in many other countries.
Conclusions
In conclusion, implementation of a standard clinic schedule with designated lactation times ensures adherence with federal policy mandating lactation breaks while creating an inclusive and supportive culture that promotes the well-being of lactating healthcare providers. This approach is sustainable, adaptable to other clinical settings, and highlights the need for further evaluation across diverse institutions to assess long-term impact on both providers and patient care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251407378 - Supplemental material for Implementing a Clinic Schedule with Protected Lactation Break Time Helps Neurology Residents Achieve Lactation Goals
Supplemental material, sj-docx-1-mde-10.1177_23821205251407378 for Implementing a Clinic Schedule with Protected Lactation Break Time Helps Neurology Residents Achieve Lactation Goals by Deborah Setter, Molly Mustafa, Afrooz Feili and Elizabeth A Coon in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251407378 - Supplemental material for Implementing a Clinic Schedule with Protected Lactation Break Time Helps Neurology Residents Achieve Lactation Goals
Supplemental material, sj-docx-2-mde-10.1177_23821205251407378 for Implementing a Clinic Schedule with Protected Lactation Break Time Helps Neurology Residents Achieve Lactation Goals by Deborah Setter, Molly Mustafa, Afrooz Feili and Elizabeth A Coon in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
This study was exempt from Mayo Clinic Institutional Review Board (IRB) approval, as its nature did not require ethics committee review or formal informed consent.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Authors’ Contribution
DS, EAC, and MM contributed to conceptualization, data gathering, and performed data analysis. DS, EAC, MM, and AF were involved in writing the manuscript. All authors read and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared thefollowing potential conflicts of interest with respect to the research,authorship, and/or publication of this article: Dr. Deborah Setter reports no disclosures. Ms. Molly Mustafa is the owner of her own lactation consultation practice. She provided feedback on the clinic schedule and whether it would be suitable for lactating individuals. She did not directly interact with any of the participants as part of this study. Her information was not disseminated to the participants of this study. Dr. Afrooz Feili reports no disclosures. Dr. Elizabeth A. Coon reports no disclosures.
Availability of Data and Materials
Clinical Trial Number
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.