
Abstract
Objectives
Despite data showing many opportunities for emergency medicine (EM) physicians to practice in rural settings, only 8% of EM graduates are exposed to rural environments during training. 5 The authors of this study noted a curricular gap in their EM training program and developed a 4-week rural elective for PGY-2 and PGY-3 EM residents. While prior literature has focused on the logistics of a rural rotation and associated procedural experiences, to our knowledge, no previous studies have focused on resident perceptions of the rural experience or preparedness for a future career in rural EM. This qualitative study aimed to gain a rich understanding of the residents’ experiences and the impact of those experiences on the 2 study aims.
Methods
Between June 2019 and May 2020, upper-level residents (PGY-2/3) completing a rural EM rotation participated in semistructured interviews exploring their perceptions of a rural EM rotation, and data was analyzed using inductive thematic analysis. Codes were informed by social cognitive theory, and a constant comparative approach was applied, with data collection concluding upon reaching thematic saturation.
Results
Four overarching themes were established. Rural EM electives provide (1) understanding of differing patient presentations in a rural emergency department, (2) exposure to differing approaches to patient care when compared to academic settings, (3) appreciation of the transport logistics associated with transferring patients to higher level care, and (4) understanding of the perceived benefits of the rural experience on EM resident training and preparedness for rural EM practice.
Conclusion
Exposure to a rural EM elective provides residents with unique experiences on rural EM, which enhances a deeper understanding of care provided in a rural environment and leads to a sense of preparedness for practice in rural EM.
Introduction
In recent years, reports of an oversupply of nearly 8000 emergency physicians (EPs) have negatively impacted the specialty of emergency medicine (EM), including a direct insult to medical student recruitment into the specialty.1,2 This is likely in part due to concerns regarding the availability of attending physician positions in EM following completion of training. 1 Despite the projected oversupply of EM physicians, many career opportunities remain available for board certified EM physicians in rural emergency departments (ED)—with evidence demonstrating that there are fewer board-certified EM physicians in rural states. 3 Demographic work outlining the distribution of EPs nationally has demonstrated that only a small fraction of board certified EPs choose to practice in a rural setting—with 5.6% of all EP's practicing in a large rural county and 2.5% practicing in a small rural county in 2020. 4 Additionally, EM physicians practicing in these settings are older and closer to retirement age than their nonrural colleagues. 4 When considered altogether, the demographic data suggests that there will indeed be opportunities available for EM physicians in rural areas.
A challenge in preparing an EM workforce that can meet the rural EM staffing need is lack of exposure to rural EM training environments during training. Although the incidence of programs requiring a rural EM experience has increased from 5% to 24% over the past decade, recent literature demonstrates that there are still nearly half of EM programs surveyed that do not offer any form of rural EM experience.5,6 Most recently, lack of exposure to low resource settings in EM training has been identified as a potentially important area of focus, as the Accreditation Council for Graduate Medical Education (ACGME) residency review committee (RRC) for EM has proposed that all EM residents must complete 8 weeks of training in a low resource ED, with most rural environments meeting their definition of “low resource.” 7 Rural rotations expose EM resident physicians to a different practice environment compared to the traditional tertiary or quaternary referral centers where most EM residency programs are located. Although we hypothesize that residents exposed to the rural environment during training should be more prepared to work in a similar environment after graduation, there has been little prior work evaluating the impact of rural EM rotations on perceptions of the rural environment or preparedness for rural practice after graduation.
Reasons that graduates may not feel prepared to work in a rural ED after training are likely multifactorial. Prior authors have postulated that the increased need to transfer patients to higher levels of care and the difference in scope of practice in rural environments may cause EM residency graduates to feel unprepared and hesitant to practice in these environments without rural training. 8 Furthermore, literature demonstrates an increased likelihood of a graduate immediately entering rural practice if they have had exposure to the rural environment, which provides them with clinical experiences in working with limited resources and managing complex dispositions.6,9,10
Social cognitive learning theory (which we will later introduce as the conceptual framework for this study) emphasizes the strength of exposure to the environment as a significant contributor to learning. When residents are self-assessing their readiness for independent practice, it is entirely plausible that they lack confidence in the skills necessary to practice in a rural environment. Exposure to a rural EM environment would expectedly lead to an increased sense of self-efficacy and preparedness for rural EM practice.11–13
The authors of this study constructed a rural EM rotation to address this perceived curricular gap. The purpose of this study was 2-fold: (1) discover resident perceptions of the rural EM experience and (2) assess the potential impact of the experience on preparedness for a rural EM career. A qualitative approach was chosen to explore these 2 main questions, as it would allow the authors to gain a rich understanding of the participants lived experiences and share this understanding with the EM educational community.
Methods
This study was conducted at a single EM residency program, based in a large, academic health system that is constructed in a hub-and-spoke model. Residents spend most of their training at the university-based academic ED. The department also manages the physician staffing for multiple community and rural EDs throughout the health system. The presence of board-certified EPs at several EDs through the system allowed the program to construct a 4-week rural EM elective experience for upper level (PGY2/3) EM residents to rotate through multiple rural ED's during the elective. Figure 1 illustrates the various rural locations available for residents to select from and the geographic proximity from the primary training site.

Rural sites available for EM residents to complete clinical shifts at during their rural EM elective and their geographic proximity to the primary training site (Site 1).
Theoretical and Conceptual Framework
This study utilized qualitative thematic analysis and was informed by social cognitive learning theory—a theoretical framework to investigate the construction of and perceptions of the resident experience. 11 Social cognitive theory posits that learning is a dynamic, collaborative interaction between the environment, the learner, and the content, with each component in that interaction creating a desired behavior. 11
Additionally, this research was performed from a constructivist paradigm—whereby the authors developed a rotation exposing EM residents to a new rural learning environment. Building on previous clinical exposures and knowledge obtained, this new rural exposure allows the learners to develop their own perceptions and knowledge frameworks related to rural EM. 11 Completing this qualitative study through a constructivist lens and incorporating social cognitive theory as the framework allowed the authors to gain a rich understanding of EM resident perceptions developed during a rural EM rotation and their preparedness for practice in a rural environment after graduation.
Researcher Characteristics and Reflexivity
This study was a collaborative effort between 2 EM faculty, CK and ES, and 1 nonphysician medical education faculty, AL. CK and ES are EM faculty physicians, with 25 years of combined EM program leadership experience. Their expertise in curriculum development and EM clinical practice shaped the rural EM elective design. Both CK and ES are West Virginia (WV) natives, the state where the study was conducted. ES is a native of one of the rural towns where residents rotated. AL, a nonphysician educator/researcher, specializes in qualitative methods and has significant knowledge and expertise in the practice of curricular development, teaching, and learner identity formation in the medical profession. All 3 are faculty at the research institution.
Context of the Study
The context for this study is a single site ACGME accredited, 3-year EM residency program, accepting 10 residents a year. The primary clinical training site is a large quaternary referral center in WV. This newly developed rural EM rotation is offered to trainees as a 1-month elective experience during either the PGY-2 or PGY-3 training year.
The rural rotation was facilitated by the previously described hub-and-spoke model of the department, making multiple rotation sites staffed by board certified EPs available for trainee experiences. Given that the ACGME requires ABEM certified physicians to supervise all trainee experiences, the institutional staffing model allowed the program to overcome this barrier, which has been cited by some as a barrier to the construction of similar rural EM rotations. 8
The study was conducted from June 2019 to May 2020, using a purposive sample of 7 EM residents who participated in the rotation and subsequently completed a semistructured narrative interview regarding the rural experience. Demographics of participants are illustrated in Table 1. This study period was chosen as it represented the time during which our program transitioned the rural experience from a single site opportunity to a multisite opportunity.
Demographic Information for EM Residents Completing Rural EM Rotation.
Data Collection, Processing, and Analysis
After consenting participants, the study utilized semistructured narrative interviews to gain a rich understanding of resident perceptions of the rural environment and how those lived experiences influenced their sense of preparedness for rural practice after residency graduation. Interview questions are available for further review in Appendix A. Interviews were recorded using podcast tools, transcripts were transcribed, anonymized, and analyzed using DedooseTM, a qualitative analysis software program which allowed multiple researchers to work with data simultaneously.
The data collected were analyzed along the lines of a 6-phase reflexive thematic analysis (TA), following the systematic process for inductive TA, as suggested by Braun and Clarke.14,15 Once the data were collected, the authors immersed themselves into the datasets for the first phase of TA by reading and re-reading text and making notes on the initial impressions of the text. 16 Next, the authors coded using a multistep process beginning with inductive open coding of the data, representing the second phase of TA. Once the codebook was established, the authors moved to the third phase of TA. In the third phase, the authors collaborated on an iterative process whereby they constantly compared the initial 36 codes, reducing them into code clusters, until they were satisfied that thematic saturation was reached, as signified by no new information being identified from ongoing analysis. Once thematic saturation was achieved, the authors felt comfortable that the data analysis met established standards for rigor in the reporting of qualitative TA, and as such, no further interviews were conducted14,17
Phase 4 of TA required the researchers to collaboratively compare and contrast core properties and interconnected categories from groups of similar code clusters into initial themes. Visual mapping provided space for theme and subtheme development and revision. This process continued into phase 5 and 6—the refinement of themes and subthemes into the development, definition, and naming of 4 themes. Internal validity was established throughout steps 1-3. We conducted member checking with participants to confirm findings and refine key themes. The reporting of this study conforms to the standards for reporting qualitative research as outlined in the EQUATOR guidelines and the associated checklist is available for reference as Appendix B. 18 This study protocol was approved by the WV University Institutional Review Board (protocol #1906608011). Written informed consent was obtained from each participant prior to any interview being conducted in concordance with the approved IRB protocol referenced above.
Results
From the data collected, the authors aimed to establish themes to provide insight into understanding the 2 main aims of the study. The following 4 overarching themes regarding the rural EM elective experience emerged: (1) understanding of differing patient presentations in a rural ED, (2) exposure to differing approaches to patient care when compared to academic settings, (3) appreciation of the transport logistics associated with rural emergency care, and (4) understanding of the perceived benefits of the rural experience on EM resident training and preparedness for rural EM practice. Figure 2 illustrates how the experiences in the rural environment informed the resident perceptions of the rotation while also enhancing resident preparedness for a rural EM career. In the sections that follow, we outline each theme and explore how the subthemes illustrate the rural EM elective experience via the lived experience of the learner.
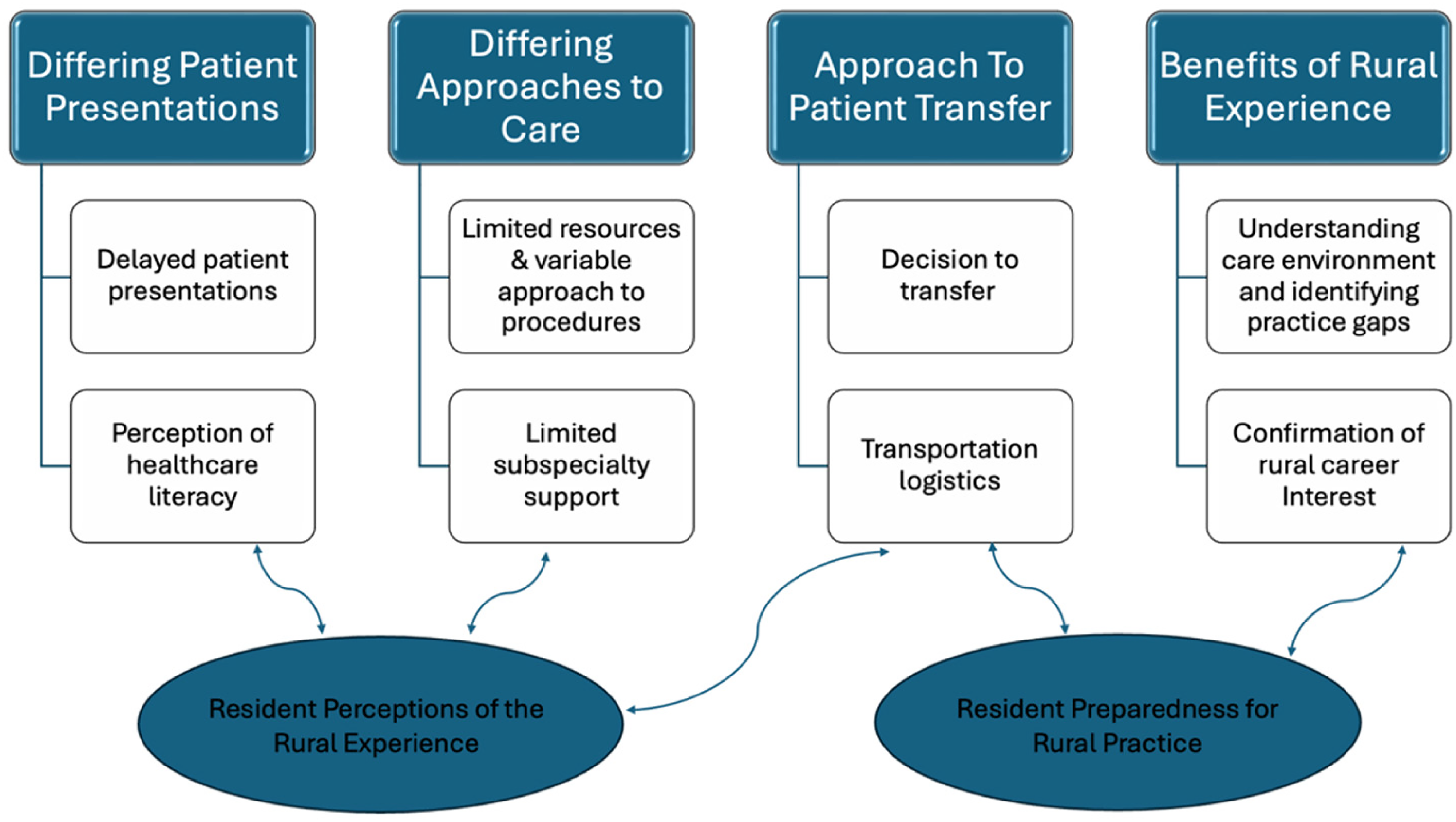
Illustration of the major themes and subthemes identified and how those themes relate to the 2 main study aims.
Theme 1: Understanding Differing Patient Presentations (Research Aim 1)
Participants in the rural EM elective noted that patients presenting to rural EM sites differed in both time frame for presentations, level of acuity, and patient's perceived understanding of their medical status/condition, when compared to experiences in the more traditional quaternary care setting. In general, patients were more loyal to the local community facility, presented later in course of illness, and overall, had less frequent contact with the healthcare system and a perceived lower healthcare literacy. Illustrative quotes supporting these themes and subthemes are outlined below.
Reflecting upon these lived experiences allowed the residents to describe the differences in patient presentations, health literacy, and loyalty to the community—which allowed the authors to understand resident perceptions of care provision in the rural environment.
Subtheme 1.1: Delayed Patient Presentation
The other thing from kind of the rural standpoint is I feel like rural folk tend to be really hearty and not wanting to come on into the Emergency Department unless they absolutely have to. They don’t like seeing a doctor unless they absolutely have to, and so I think the other extreme of that is seeing pathology that was kind of further developed. So, folks who had been sitting at home with a busted ankle for a couple of days, folks who had fallen days ago and now I still can’t walk four days later maybe now I should go see a doctor. You know that stuff typically you don’t see at Ruby [tertiary care setting]. Typically, people are more in touch with the academic center. They come here they’re more incline to be seen by a physician where I felt like that was not necessarily the case out there [in the rural setting].
I haven’t seen a doctor in 10, 20 years … I don’t know if I have high blood pressure, I have no IDEA if I have cholesterol. I’m just here because my chest hurts.’ So, I think that's a big part of the patients and their overall expectations for their visit, as they differ significantly.
Subtheme 1.2: Perception of Health Literacy
Regarding health literacy, participants noted that patients had less understanding of the complexity of their illness and the resources needed to care for them locally. Residents noted that although patients desired to stay at their local facility, given their loyalty to the community and local healthcare providers, there were times when their presentations necessitated a higher level of care. These situations required residents to carefully explain why a transfer was in the patient's best interest, which is a skill not frequently practiced in a quaternary medical center. This experience identified a knowledge gap for residents who have limited experiences in discussing the need for transfer to a higher level of care in hesitant patients.
Um, I think as a provider you feel a little frustrated. Just because, I think a lot of it boils down to like medical knowledge and medical literacy of the patient. You know, like they think I am going to the hospital, right? Like the hospital is like this black box to people that can solve all of their problems, and especially if you’re local like it is “the hospital.”
So, I think they don’t realize all of the pieces and all of the kind of the background that makes a hospital good or functional or um, provide good care to patients. You just have to, you just kind of have to explain to the patient as best as you can, as simply as you can why it is in their best interest not that we’re trying to get rid of them, or that we are trying to push the problem onto someone else. That we are unable to take care of it because of the limited resources.
I don’t know. I feel like they haven’t been around doctors as much as the patients they do have all of the specialists at [the main academic site]. So, I guess those patients are used to seeing doctors and being in the healthcare systems, so they know more on the lingo, whereas you go to {rural EM site} and you know the same person has heart problems they don’t know how to communicate as well. History is a lot harder at the smaller places than it can be here I think.
Just in general, the patients didn’t want to go elsewhere. I think the patient have a trust in the local providers and saying you know if you’re recommending this, if you can do it, if you’re confident just do it.
I think people wait longer to present with their problems …, and then you see people who’ve waited 50 years for a mass in their abdomen, and they come in and you’re like wow you have full blown cancer. So, I think it is kind of both sides of the spectrum, but it all boils down to health literacy and access to care issues.
Theme 2: Differing Approaches to Patient Care During Rural Medicine Rotation (Research Aim 1)
Participants in the rural elective described the necessity for different approaches to patient care in rural environments, primarily given the differences in resource availability compared to quaternary centers. Participants largely viewed this differing approach to patient care as a positive educational experience that allowed them to function more autonomously and improvise when doing procedures in a resource limited environment.
Subtheme 2.1: Lack of Consultation Services and Working Without a Safety Net
There are a variety of factors identified as more limited in the rural setting, including but not limited to, consultant services, nursing support, and radiologic support. These limitations provide residents an opportunity to work without the safety net they are typically used to in a well-resourced quaternary center, making them primarily responsible for all aspects of patient care.
You know, if that was here at Ruby there would be the full emergency department team, a full trauma service team. I would be focusing pretty much on his airway, and pretty much everything from the neck up. the trauma team would be assessing from the neck down. Obviously, trauma wasn’t there. So, I have to do the full assessment on that. You know, make sure there's no other injuries. I have to come up with my plan for what imaging I want, because a lot of times here, trauma would take point on the imaging that they want. I can give them my recommendations of what I want here, but ultimately, they make the final decision.
Orthopedics is one that jumps to mind. A fracture where, at the Level 1 center, you would come in [to the ER], I would see you, and say, ‘yes, you have a fracture. I’m going to plan to do a sedation with an orthopedic provider that makes sure this is in perfect anatomical alignment. We’re going to get you this perfectly molded splint made out of plaster, you’ll go immediately upstairs, that splint will be cut off in 12 h, we’ll do surgery and fix your ankle.’ In a rural setting, thinking of a couple patients I had, it's ‘we’re going to get you to comfort, ability to go home, and we’re going to get you an orthopedist in a couple days. You’re not going to see one in the EM department.
Subtheme 2.2: Differing Approaches to Procedures Based on Availability of Equipment
Participants noted the need for improvisation with procedures, largely due to the facility being unfamiliar with certain procedures or lacking the prepackaged procedural tools usually available at the academic center. Some participants also noted the need for increased utilization and comfort with point-of-care ultrasound due to the lack of routine availability of other advanced imaging techniques.
Like doing a knee arthrocentesis didn’t have a long enough 18 gauge needle our hospital didn’t have one. So, I used a spinal needle, which is way longer, so your fulcrum is a lot different, but it works. You just have to have to use your resources. Creativity. Dr X was telling me a story where he had to improvise a Large-Bore chest tube system, because they had these things from the seventies, they didn’t have what he needed. So, he ultimately put in the chest tube but had to MacGyver some type of apparatus.
We couldn’t get a CT because of the situation we are in so, we jumped to more of a very, very thorough abdominal ultrasound, which we were able to do at bedside. Which a lot of times I would do an ultrasound here at Ruby, but not, not nearly to the extent that I had to do there. And so, the ultrasound was effective and showing concerns with their liver.
Subtheme 2.3: Variable Approach to Psychiatric Patients
Participating residents found lack of access to psychiatric subspecialty care and placement support to be a significant challenge in caring for this patient population. Despite residents perceiving this as a challenge, the proposed RRC requirements for EM have cited primarily managing and dispositioning psychiatric patients as a potential gap in the standard EM curriculum.
6
The experiences outlined below demonstrate opportunities to care for psychiatric patients in a rural environment as an avenue through which programs can fill this training gap.
…Well psych here [the tertiary medical center] is easy right? We call psych and they come see them and determine what to do. At some of the rural places it's tough. Some places have teletype, which they have an iPad and psych can talk to the patient and give recommendations about where they should go, but it's still on you to make the referrals to like all these psych facilities around the state right? So, it's a lot more difficult, but they don’t see as many psych patients at the small facilities like they do here. So, that helps.
At [academic center], we kind of let psych deal with it the psych residents. But at the smaller [rural] hospitals it's kind of on you like what is their risk for kind of going through with it or do they need admitted or can they be safe to go home? So, that's a big thing of getting like a more detailed history, calling family, things like that besides saying oh you’re suicidal and then they just get plugged into the system and we forget about you right? So, it's different.
Theme 3: Approaches to Transferring Patients During Rural Medicine Rotation (Research Aims 1 and 2)
Given most EM rotations occur at academic medical centers where transfers are infrequent, EM residents typically lack experience or formal training in assessing criteria for and mode of transport to other facilities. 19 Residents completing the rural rotation learned how to make appropriate transfer decisions, including most appropriate modality for and timing of the transfer. Additionally, the rural experience provided frequent opportunities for residents to speak with accepting physicians and advocate appropriately for patient acceptance.
Subtheme 3.1: Decision to Transfer and Communication With Accepting Physicians
During the rural elective, residents learned how common chief complaints in EM, that would result in a straightforward admission at an academic center, require more complex decision making about transfer to a higher level of care due to lack of resources at the primary site.
…She had pretty bad COPD and pneumonia and she had an increasing oxygen requirement. She's looking ok now and he was like well we talked about she has a history of getting worse and we have no idea where this could go so felt better transferring her to another hospital because she looked ok now and would probably do fine there, but in case something would happen they wouldn’t have the capacity to take care of her. So, that's something that I had to think about. It's kind of is like the next steps.
So, the core workup stuff is all the same. You know so EKG, labs, and give them Aspirin and whatever. That can be done anywhere. At some of the smaller places the question is the availability of either inpatient care or specialty care and the logistics of making that happen. So, I think for example we had a chest pain lady at [rural site] who was kind of borderline. She wasn’t super high risk her heart score was maybe like 3 or 4. But, they only have one day a week that they have a provider that does stress test onsite, and that would’ve been 4 or 5 days later. So, the question is do you transfer said person? Are you truly concerned enough you want to transfer them to [larger community site] … So, at ruby you call, you admit for a chest pain rule out, and then it's taken care of and there's no logistics and there's no time and it's not really weighing risks and benefits as so much as it is as a slam dunk admission basically.
Subtheme 3.2: Transportation Logistics
Although exposure to EMS and medical command is a common program requirement for EM training, residents rotating at rural sites get a particularly nuanced look at the prehospital setting. In this setting, they are immersed in an environment where knowing more about the logistics of EMS crew capabilities, prioritizing multiple patients for transfer, and deciding what method of transfer will be utilized, are essential to rural EM practice. Although there is a paucity of prior literature evaluating the education of EM residents on interfacility transfers, the available studies have focused upon didactic curricular interventions rather than an immersive clinical experience.
18
When considered via the lens of social cognitive theory and constructivism, it stands to reason that when EM residents are actually placed in an environment where they are the sending physician rather than the receiving physician, this experience will allow them to create new knowledge frameworks around interfacility transfers and increase their perceived self-efficacy in this area.
So, what can an ACLS crew do as opposed to a critical care crew. So that was a learning experience. As we were discussing then being able to convey to the transfer facility and why that patient needs to be transferred. Why I am going to transfer them the way I am transferring them. So that was all very different than what I normally do.
There were a couple of times we would have two patients that needed to go out at the same time and EMS would pick up one of them. And so, then you had to wait another 6 h in total for them to drop off and come back and everything then pick up the second patient.
You know, learning what is needed for a BLS transport, an ALS transport or calling life flight to send somebody? Also, having the discussions with the crews who are doing the transports themselves. When they come on and they say I don’t necessarily feel comfortable with all of this. It added another level of complexity. You’re not just handing off to the doctor who's upstairs you’re handing off to a doctor who's at another facility, and you’re handing off to the medical team who's going to be transporting them there.
Theme 4: Perceived Benefits of the Rural Experience on EM Training (Research Aim 2)
After completing the rural rotation, residents better understand the unique environment and resource limitations that define rural EM. Similar to our discussion around environmental exposure leading to an increased confidence in interfacility transfers in Subtheme 3.2, Theme 4 also demonstrates that once a resident immerses themselves in the rural environment, they are more confident in their ability to practice in a similar environment. While this may seem intuitive, this strongly relates to our underpinned framework of social cognitive theory and associated concept of self-efficacy. Through a social cognitive lens, learning is a dynamic interaction between the learner, the content, and the environment. Self-efficacy is the confidence to carry out the necessary course of action in a given situation. In totality, this theme suggests that through direct environmental exposure (social cognitive learning theory) and increased confidence in rural practice (self-efficacy), residents feel more prepared in a similar environment after this experience.11,12
The excerpts below are illustrative of the 2 subthemes elicited in this space.
Subtheme 4.1: Better Understanding of the Rural Care Environment and Identification of Practice Gaps
So, for example, a lot of times when I do an intubation here at Ruby I have respiratory right there. They immediately hook them up to the vent. They manage the patient on the vent. The patient goes to the ICU. I do very little vent management here in the ED. My first intubation at [rural site], the Respiratory Therapist who was completely capable of managing the vent turned to me and said what vent settings do you want? What do you want me to do? And I kind of had this blank face. It made me realize that I need to learn how to manage my vent settings a lot better. I need to know what I am thinking of and what I need. Because I may not necessarily have someone who is comfortable with setting that stuff up.
“So, what are you going to do?” “You going to fix it”? “You going to ship it”? “Here we are in the middle of nowhere!” “What's your call”? So, sending someone for a laceration like that, that is in our scope of practice to repair was exciting for me to do because, I don’t often get to do that repair. I don’t often get to figure out how am I going to do this? So, I got to do a nerve block of the ear. Which I haven’t been able to do before. Because normally ENT would do that.
Well, we had several intubations that I did where video wasn’t even available, so it was only direct. So, the equipment was slightly different. I didn’t have necessarily that back up as readily available. I’m sure if I needed it I could’ve gotten it eventually, but it wouldn’t have been nearly as quick. So, my reliance on that safety net wasn’t necessarily there. So, knowing how to do that procedure is something I do every day, but not having that specific equipment that level of comfort wasn’t there. So, definitely made me a little bit more nervous. Ultimately, I’m glad I got the experience because, that wasn’t the case for most of the hospitals where I went to. Where maybe they had video but, it wasn’t necessarily the equipment I was used to using or if I was able to get it, it was going to take time to get it. So, while I was confident in doing the procedures there were other challenges along the rotations that made it more difficult.
Subtheme 4.2: Resident Confirmation of Future Rural Career Interest
So, this was more of me kind of pushing my comfort levels and what I need to work on and what I need to practice with. So, I felt like this helped expose a lot of weaknesses that I have, and things that I need to work on.
I already had an idea, but this confirmed my idea to want to practice rural. The more that I’ve done it and the more that I’ve talked to all of these people at these outside hospitals I’ve considered staying on for a year or two here just because I have had such great experiences at all of these hospitals and everyone that I talk to just loves [residency program].
It confirmed my job choice. I probably should’ve done it before I signed the contract, but I had already signed the contract, but it confirmed, alright, I can do this, I like this.
Discussion
Despite the 2020 EM workforce study suggestion that urban EM positions will likely be saturated in 2030, the study also reinforced that there would be ongoing need for EM physicians in the rural settings. 1 The same study inferred that there is an understandable hesitancy for new graduates to accept jobs in these areas that has not been well explored in previous literature. 1 This inference is likely multifactorial; however, it seems reasonable to assume that the lack of standardized rural EM training and preparedness for practice in these environments would be one of the plausible explanations. As outlined in our results, the elective rotation introduces residents to the unique challenges of the rural EM environment, better preparing them to care for patients in resource limited environments and potentially pursue a career in rural EM.
In February 2025, the EM RRC introduced proposed program requirement revisions mandating rotations in low resource environments with limited subspecialty backup, which will inevitably necessitate rural EM experiences for some programs. 6 Although not directly stated in the requirements, the RRC has implied that although most EM programs routinely expose trainees to large, well-resourced academic environments, trainees are not traditionally exposed to lower resource environments. The proposed educational benefits of these low resource experiences are that residents will be able to provide competent care in the absence of subspecialty services, assume the lead of longitudinal care on medically complex patients awaiting transfer, learn to improvise when standard equipment is not available, and become knowledgeable of the situations that will require transfer to a higher level of care, in addition to the logistics of executing the transfer.
Even though our training program has offered a well-structured, rural EM experience for many years, which well preceded the recently announced RRC requirement for low resource exposure for EM residents, the themes from our study incidentally align with the educational rationale for the low resource rotation proposed by the RRC. Our residents specifically cited that the rural experience exposed them to differing patient presentations, differing approaches to care and procedures in the absence of subspecialty resources, and familiarity with interfacility transfers—ultimately allowing them to feel more prepared for rural practice. Furthermore, our institution's hub-and-spoke model made the development of this rotation straightforward and removed many of the previously described barriers. Institutions with a similar organizational structure may seek to implement an analogous model to develop low resource rotations to meet this new ACGME requirement, as our model has successfully exposed residents to the differences in the rural environment and increased preparedness for practicing in a similar environment after training.
Limitations
This study utilized thematic analysis as a qualitative approach and thus was not designed to make statistical comparisons between groups. This qualitative study followed the principles for trustworthiness in publishing qualitative research, and satisfied the requirements for credibility, transferability, dependability, confirmability, and reflexivity.18,20
This was a single site study conducted at a program in a health system where development and implementation of a multisite rural experience was possible. The authors understand that the development of a similar experience in a dissimilar health system may be more challenging. Even if an identical rotation could not be constructed elsewhere, the understanding of the lived experiences of residents completing our rotation may be used to inform construction of a low resource environment rotation at another institution.
The aim of this study was to gain a rich understanding of the perspective of residents completing a rural EM experience. While our purposive sample only included resident perceptions from a single site, the authors still feel that a deep understanding of these resident's lived experiences is informative and valuable for program directors interested in setting up a similar rural experience for their trainees. This information is valuable and timely, particularly in light of the potential addition of a rural, low resource experience to the ACGME common program requirements.
Conclusion
Exposure to a rural EM elective provides residents with unique perceptions of rural EM. This arms them with knowledge relating to differences in patient presentations and overall care logistics, which may differ widely from more traditional academic training environments. Residents completing the rotation had an enhanced understanding of rural care and felt more prepared to transition from residency into a rural EM practice environment.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251405326 - Supplemental material for A Thematic Analysis Exploring the Impact of a Rural Emergency Medicine Rotation on Resident Perceptions of Care and Readiness for Rural Practice
Supplemental material, sj-docx-1-mde-10.1177_23821205251405326 for A Thematic Analysis Exploring the Impact of a Rural Emergency Medicine Rotation on Resident Perceptions of Care and Readiness for Rural Practice by Christopher S. Kiefer, Anna Lama and Erica B. Shaver in Journal of Medical Education and Curricular Development
Footnotes
Ethical Approval and Consent to Participate
This study protocol was approved by the West Virginia University Institutional Review Board (IRB) (Protocol No. 1906608011). Informed consent was obtained from each participant prior to any interview being conducted in concordance with the approved IRB protocol referenced above.
Author Contribution
CSK and EBS developed the novel rural EM rotation and partnered with AL to design this qualitative study, generate the interview questions, conceptual framework, and supporting educational theory. AL conducted the interviews with residents. All authors participated in data analysis and drafting and revising of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.